User login
Paid Parental Leave: Impact on Maternal Mental Health and Child Wellbeing
Maternal mental health has a profound impact on the health and wellbeing of the child. Since the onset of the pandemic, rates of postpartum depression have increased, affecting an estimated 1 in 5 women.1 Numerous studies show the impact of postpartum depression on the newborn child across multiple domains, from bonding to healthy weight gain to meeting developmental milestones.

While new medications are being studied and approved to specifically target postpartum depression, these treatments are inaccessible to many because of high costs and long wait lists. Beyond medication, structural changes such as paid parental leave have been shown to have a substantial impact on maternal mental health, thus impacting the health of children as well.
Implications for Mothers and Children
Psychiatric diagnoses such as postpartum depression are on the rise.1,2 This is likely attributable to a combination of factors, including increased isolation since the start of the pandemic, worsening health inequities across race and socioeconomic status, and difficulty accessing mental health care.3-5 The effect that postpartum depression has on the family is significant for the newborn as well as other children in the home.

Data suggest that postpartum depression impacts both the physical and mental health of the child. Infants of mothers with postpartum depression may experience challenges with weight gain, decreased breastfeeding, sleep disruptions, and delays in achieving developmental milestones.6-9 They may also show decreased maternal infant bonding, challenges with cognitive development including language and IQ, and increased risk of behavioral disturbances.10,11 These effects are likely attributable to a combination of factors, including decreased maternal responsiveness to infant cues.7,12 Many of these effects are mediated by the chronicity and severity of depressive symptoms, suggesting the importance of screening and treatment of postpartum depression.10,11 However, treatment for postpartum depression can be difficult to access, particularly given the increased level of need.
It is therefore critical to consider what structural interventions and policy changes can decrease the risk of developing postpartum depression. Data consistently show that access to paid parental leave improves maternal mental health outcomes. Among patients with access to parental leave, research shows that paid leave of longer duration, at least 2-3 months, is the most protective.13 Studies have identified decreased depressive symptoms, decreased stress, decreased use of mental health services, and decreased hospital admissions among women with longer parental leave.13 The positive effects of paid parental leave on maternal mental health can extend beyond the postpartum period, solidifying its impact on the long-term health outcomes of both mother and child.13
Advocacy Is Imperative
In 2024, the United States is the only high-income country, and one of only seven countries in the world, that does not guarantee access to paid parental leave. The Family Medical Leave Act is a 31-year-old federal law that requires some employers to provide unpaid leave to eligible employees. It is narrow in scope, and it excludes many low-wage workers and LGBTQ+ families. Thirteen states — California, Colorado, Connecticut, Delaware, Maine, Massachusetts, Maryland, Minnesota, New Jersey, New York, Oregon, Rhode Island, and Washington — as well as the District of Columbia, have enacted their own paid leave policies. However, there are no federal laws requiring access to paid parental leave. As of 2023, fewer than 30% of workers in the United States have access to paid parental leave, and only 16% of employees in the service industry have access to paid parental leave.14 This disproportionately affects families from lower income backgrounds, and further exacerbates socioeconomic, racial, and gender inequities. From a health systems lens, this increases risk of adverse maternal mental health outcomes among those who already have decreased access to mental health services, worsening health disparities.
Paid parental leave has strong public support across party lines, with polls showing the majority of Americans support comprehensive paid family and medical leave.15 Despite this, the United States has failed to enact legislation on this issue since 1993. Multiple attempts at expanding leave have not come to fruition. In the past year, both the house and the senate have announced bipartisan efforts to expand access to paid parental leave. However, legislative frameworks are still in early stages.
As physicians, it is crucial that we advocate for expanded access to paid parental leave. We must use our expertise to speak to the impact that paid parental leave can have on the mental and physical health of parents, children, and families. By advocating for paid parental leave, we can help create a more just and equitable healthcare system.
Dr. Shannon is a second-year psychiatry resident at University of California, Los Angeles. She attended Stanford University for her undergraduate degree and Dartmouth Geisel School of Medicine for medical school. Her interests include perinatal psychiatry, health systems research, and mental health policy advocacy. Dr. Richards is assistant clinical professor in the department of psychiatry and biobehavioral sciences; program director of the child and adolescent psychiatry fellowship; and associate medical director of the perinatal program at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
References
1. Wang Z et al. Mapping Global Prevalence of Depression Among Postpartum Women. Transl Psychiatry. 2021 Oct 20. doi: 10.1038/s41398-021-01663-6.
2. Iyengar U et al. One Year Into the Pandemic: A Systematic Review of Perinatal Mental Health Outcomes During COVID-19. Front Psychiatry. 2021 Jun 24. doi: 10.3389/fpsyt.2021.674194.
3. World Health Organization. Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact: Scientific Brief. 2022 Mar 2. www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1.
4. Masters GA et al. Impact of the COVID-19 Pandemic on Mental Health, Access to Care, and Health Disparities in the Perinatal Period. J Psychiatr Res. 2021 May. doi: 10.1016/j.jpsychires.2021.02.056.
5. Shuffrey LC et al. Improving Perinatal Maternal Mental Health Starts With Addressing Structural Inequities. JAMA Psychiatry. 2022 May 1. doi: 10.1001/jamapsychiatry.2022.0097.
6. Lubotzky-Gete S et al. Postpartum Depression and Infant Development Up to 24 months: A Nationwide Population-Based Study. J Affect Disord. 2021 Apr 15. doi: 10.1016/j.jad.2021.02.042.
7. Saharoy R et al. Postpartum Depression and Maternal Care: Exploring the Complex Effects on Mothers and Infants. Cureus. 2023 Jul 4. doi: 10.7759/cureus.41381..
8. Gress-Smith JL et al. Postpartum Depression Prevalence and Impact on Infant Health, Weight, and Sleep in Low-Income and Ethnic Minority Women and Infants. Matern Child Health J. 2012 May. doi: 10.1007/s10995-011-0812-y.
9. Kim S et al. The Impact of Antepartum Depression and Postpartum Depression on Exclusive Breastfeeding: A Systematic Review and Meta-Analysis. Clin Nurs Res. 2022 Jun. doi: 10.1177/10547738211053507.
10. Mirhosseini H et al. Cognitive Behavioral Development in Children Following Maternal Postpartum Depression: A Review Article. Electron Physician. 2015 Dec 20. doi: 10.19082/1673.
11. Grace SL et al. The Effect of Postpartum Depression on Child Cognitive Development and Behavior: A Review and Critical Analysis of the Literature. Arch Womens Ment Health. 2003 Nov. doi: 10.1007/s00737-003-0024-6.
12. Milgrom J et al. The Mediating Role of Maternal Responsiveness in Some Longer Term Effects of Postnatal Depression on Infant Development. Infant Behavior and Development. 2004 Sep 11. doi.org/10.1016/j.infbeh.2004.03.003.
13. Heshmati A et al. The Effect of Parental Leave on Parents’ Mental Health: A Systematic Review. Lancet Public Health. 2023 Jan. doi: 10.1016/S2468-2667(22)00311-5.
14. U.S. Bureau of Labor Statistics, What Data Does the BLS Publish on Family Leave? 2023 Sept 21. www.bls.gov/ebs/factsheets/family-leave-benefits-fact-sheet.htm.
15. Horowitz JM et al. Americans Widely Support Paid Family and Medical Leave, But Differ Over Specific Policies. Pew Research Center’s Social & Demographic Trends Project, Pew Research Center. 2017 Mar 23. www.pewresearch.org/social-trends/2017/03/23/americans-widely-support-paid-family-and-medical-leave-but-differ-over-specific-policies/.
Maternal mental health has a profound impact on the health and wellbeing of the child. Since the onset of the pandemic, rates of postpartum depression have increased, affecting an estimated 1 in 5 women.1 Numerous studies show the impact of postpartum depression on the newborn child across multiple domains, from bonding to healthy weight gain to meeting developmental milestones.
While new medications are being studied and approved to specifically target postpartum depression, these treatments are inaccessible to many because of high costs and long wait lists. Beyond medication, structural changes such as paid parental leave have been shown to have a substantial impact on maternal mental health, thus impacting the health of children as well.
Implications for Mothers and Children
Psychiatric diagnoses such as postpartum depression are on the rise.1,2 This is likely attributable to a combination of factors, including increased isolation since the start of the pandemic, worsening health inequities across race and socioeconomic status, and difficulty accessing mental health care.3-5 The effect that postpartum depression has on the family is significant for the newborn as well as other children in the home.
Data suggest that postpartum depression impacts both the physical and mental health of the child. Infants of mothers with postpartum depression may experience challenges with weight gain, decreased breastfeeding, sleep disruptions, and delays in achieving developmental milestones.6-9 They may also show decreased maternal infant bonding, challenges with cognitive development including language and IQ, and increased risk of behavioral disturbances.10,11 These effects are likely attributable to a combination of factors, including decreased maternal responsiveness to infant cues.7,12 Many of these effects are mediated by the chronicity and severity of depressive symptoms, suggesting the importance of screening and treatment of postpartum depression.10,11 However, treatment for postpartum depression can be difficult to access, particularly given the increased level of need.
It is therefore critical to consider what structural interventions and policy changes can decrease the risk of developing postpartum depression. Data consistently show that access to paid parental leave improves maternal mental health outcomes. Among patients with access to parental leave, research shows that paid leave of longer duration, at least 2-3 months, is the most protective.13 Studies have identified decreased depressive symptoms, decreased stress, decreased use of mental health services, and decreased hospital admissions among women with longer parental leave.13 The positive effects of paid parental leave on maternal mental health can extend beyond the postpartum period, solidifying its impact on the long-term health outcomes of both mother and child.13
Advocacy Is Imperative
In 2024, the United States is the only high-income country, and one of only seven countries in the world, that does not guarantee access to paid parental leave. The Family Medical Leave Act is a 31-year-old federal law that requires some employers to provide unpaid leave to eligible employees. It is narrow in scope, and it excludes many low-wage workers and LGBTQ+ families. Thirteen states — California, Colorado, Connecticut, Delaware, Maine, Massachusetts, Maryland, Minnesota, New Jersey, New York, Oregon, Rhode Island, and Washington — as well as the District of Columbia, have enacted their own paid leave policies. However, there are no federal laws requiring access to paid parental leave. As of 2023, fewer than 30% of workers in the United States have access to paid parental leave, and only 16% of employees in the service industry have access to paid parental leave.14 This disproportionately affects families from lower income backgrounds, and further exacerbates socioeconomic, racial, and gender inequities. From a health systems lens, this increases risk of adverse maternal mental health outcomes among those who already have decreased access to mental health services, worsening health disparities.
Paid parental leave has strong public support across party lines, with polls showing the majority of Americans support comprehensive paid family and medical leave.15 Despite this, the United States has failed to enact legislation on this issue since 1993. Multiple attempts at expanding leave have not come to fruition. In the past year, both the house and the senate have announced bipartisan efforts to expand access to paid parental leave. However, legislative frameworks are still in early stages.
As physicians, it is crucial that we advocate for expanded access to paid parental leave. We must use our expertise to speak to the impact that paid parental leave can have on the mental and physical health of parents, children, and families. By advocating for paid parental leave, we can help create a more just and equitable healthcare system.
Dr. Shannon is a second-year psychiatry resident at University of California, Los Angeles. She attended Stanford University for her undergraduate degree and Dartmouth Geisel School of Medicine for medical school. Her interests include perinatal psychiatry, health systems research, and mental health policy advocacy. Dr. Richards is assistant clinical professor in the department of psychiatry and biobehavioral sciences; program director of the child and adolescent psychiatry fellowship; and associate medical director of the perinatal program at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
References
1. Wang Z et al. Mapping Global Prevalence of Depression Among Postpartum Women. Transl Psychiatry. 2021 Oct 20. doi: 10.1038/s41398-021-01663-6.
2. Iyengar U et al. One Year Into the Pandemic: A Systematic Review of Perinatal Mental Health Outcomes During COVID-19. Front Psychiatry. 2021 Jun 24. doi: 10.3389/fpsyt.2021.674194.
3. World Health Organization. Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact: Scientific Brief. 2022 Mar 2. www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1.
4. Masters GA et al. Impact of the COVID-19 Pandemic on Mental Health, Access to Care, and Health Disparities in the Perinatal Period. J Psychiatr Res. 2021 May. doi: 10.1016/j.jpsychires.2021.02.056.
5. Shuffrey LC et al. Improving Perinatal Maternal Mental Health Starts With Addressing Structural Inequities. JAMA Psychiatry. 2022 May 1. doi: 10.1001/jamapsychiatry.2022.0097.
6. Lubotzky-Gete S et al. Postpartum Depression and Infant Development Up to 24 months: A Nationwide Population-Based Study. J Affect Disord. 2021 Apr 15. doi: 10.1016/j.jad.2021.02.042.
7. Saharoy R et al. Postpartum Depression and Maternal Care: Exploring the Complex Effects on Mothers and Infants. Cureus. 2023 Jul 4. doi: 10.7759/cureus.41381..
8. Gress-Smith JL et al. Postpartum Depression Prevalence and Impact on Infant Health, Weight, and Sleep in Low-Income and Ethnic Minority Women and Infants. Matern Child Health J. 2012 May. doi: 10.1007/s10995-011-0812-y.
9. Kim S et al. The Impact of Antepartum Depression and Postpartum Depression on Exclusive Breastfeeding: A Systematic Review and Meta-Analysis. Clin Nurs Res. 2022 Jun. doi: 10.1177/10547738211053507.
10. Mirhosseini H et al. Cognitive Behavioral Development in Children Following Maternal Postpartum Depression: A Review Article. Electron Physician. 2015 Dec 20. doi: 10.19082/1673.
11. Grace SL et al. The Effect of Postpartum Depression on Child Cognitive Development and Behavior: A Review and Critical Analysis of the Literature. Arch Womens Ment Health. 2003 Nov. doi: 10.1007/s00737-003-0024-6.
12. Milgrom J et al. The Mediating Role of Maternal Responsiveness in Some Longer Term Effects of Postnatal Depression on Infant Development. Infant Behavior and Development. 2004 Sep 11. doi.org/10.1016/j.infbeh.2004.03.003.
13. Heshmati A et al. The Effect of Parental Leave on Parents’ Mental Health: A Systematic Review. Lancet Public Health. 2023 Jan. doi: 10.1016/S2468-2667(22)00311-5.
14. U.S. Bureau of Labor Statistics, What Data Does the BLS Publish on Family Leave? 2023 Sept 21. www.bls.gov/ebs/factsheets/family-leave-benefits-fact-sheet.htm.
15. Horowitz JM et al. Americans Widely Support Paid Family and Medical Leave, But Differ Over Specific Policies. Pew Research Center’s Social & Demographic Trends Project, Pew Research Center. 2017 Mar 23. www.pewresearch.org/social-trends/2017/03/23/americans-widely-support-paid-family-and-medical-leave-but-differ-over-specific-policies/.
Maternal mental health has a profound impact on the health and wellbeing of the child. Since the onset of the pandemic, rates of postpartum depression have increased, affecting an estimated 1 in 5 women.1 Numerous studies show the impact of postpartum depression on the newborn child across multiple domains, from bonding to healthy weight gain to meeting developmental milestones.
While new medications are being studied and approved to specifically target postpartum depression, these treatments are inaccessible to many because of high costs and long wait lists. Beyond medication, structural changes such as paid parental leave have been shown to have a substantial impact on maternal mental health, thus impacting the health of children as well.
Implications for Mothers and Children
Psychiatric diagnoses such as postpartum depression are on the rise.1,2 This is likely attributable to a combination of factors, including increased isolation since the start of the pandemic, worsening health inequities across race and socioeconomic status, and difficulty accessing mental health care.3-5 The effect that postpartum depression has on the family is significant for the newborn as well as other children in the home.
Data suggest that postpartum depression impacts both the physical and mental health of the child. Infants of mothers with postpartum depression may experience challenges with weight gain, decreased breastfeeding, sleep disruptions, and delays in achieving developmental milestones.6-9 They may also show decreased maternal infant bonding, challenges with cognitive development including language and IQ, and increased risk of behavioral disturbances.10,11 These effects are likely attributable to a combination of factors, including decreased maternal responsiveness to infant cues.7,12 Many of these effects are mediated by the chronicity and severity of depressive symptoms, suggesting the importance of screening and treatment of postpartum depression.10,11 However, treatment for postpartum depression can be difficult to access, particularly given the increased level of need.
It is therefore critical to consider what structural interventions and policy changes can decrease the risk of developing postpartum depression. Data consistently show that access to paid parental leave improves maternal mental health outcomes. Among patients with access to parental leave, research shows that paid leave of longer duration, at least 2-3 months, is the most protective.13 Studies have identified decreased depressive symptoms, decreased stress, decreased use of mental health services, and decreased hospital admissions among women with longer parental leave.13 The positive effects of paid parental leave on maternal mental health can extend beyond the postpartum period, solidifying its impact on the long-term health outcomes of both mother and child.13
Advocacy Is Imperative
In 2024, the United States is the only high-income country, and one of only seven countries in the world, that does not guarantee access to paid parental leave. The Family Medical Leave Act is a 31-year-old federal law that requires some employers to provide unpaid leave to eligible employees. It is narrow in scope, and it excludes many low-wage workers and LGBTQ+ families. Thirteen states — California, Colorado, Connecticut, Delaware, Maine, Massachusetts, Maryland, Minnesota, New Jersey, New York, Oregon, Rhode Island, and Washington — as well as the District of Columbia, have enacted their own paid leave policies. However, there are no federal laws requiring access to paid parental leave. As of 2023, fewer than 30% of workers in the United States have access to paid parental leave, and only 16% of employees in the service industry have access to paid parental leave.14 This disproportionately affects families from lower income backgrounds, and further exacerbates socioeconomic, racial, and gender inequities. From a health systems lens, this increases risk of adverse maternal mental health outcomes among those who already have decreased access to mental health services, worsening health disparities.
Paid parental leave has strong public support across party lines, with polls showing the majority of Americans support comprehensive paid family and medical leave.15 Despite this, the United States has failed to enact legislation on this issue since 1993. Multiple attempts at expanding leave have not come to fruition. In the past year, both the house and the senate have announced bipartisan efforts to expand access to paid parental leave. However, legislative frameworks are still in early stages.
As physicians, it is crucial that we advocate for expanded access to paid parental leave. We must use our expertise to speak to the impact that paid parental leave can have on the mental and physical health of parents, children, and families. By advocating for paid parental leave, we can help create a more just and equitable healthcare system.
Dr. Shannon is a second-year psychiatry resident at University of California, Los Angeles. She attended Stanford University for her undergraduate degree and Dartmouth Geisel School of Medicine for medical school. Her interests include perinatal psychiatry, health systems research, and mental health policy advocacy. Dr. Richards is assistant clinical professor in the department of psychiatry and biobehavioral sciences; program director of the child and adolescent psychiatry fellowship; and associate medical director of the perinatal program at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
References
1. Wang Z et al. Mapping Global Prevalence of Depression Among Postpartum Women. Transl Psychiatry. 2021 Oct 20. doi: 10.1038/s41398-021-01663-6.
2. Iyengar U et al. One Year Into the Pandemic: A Systematic Review of Perinatal Mental Health Outcomes During COVID-19. Front Psychiatry. 2021 Jun 24. doi: 10.3389/fpsyt.2021.674194.
3. World Health Organization. Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact: Scientific Brief. 2022 Mar 2. www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1.
4. Masters GA et al. Impact of the COVID-19 Pandemic on Mental Health, Access to Care, and Health Disparities in the Perinatal Period. J Psychiatr Res. 2021 May. doi: 10.1016/j.jpsychires.2021.02.056.
5. Shuffrey LC et al. Improving Perinatal Maternal Mental Health Starts With Addressing Structural Inequities. JAMA Psychiatry. 2022 May 1. doi: 10.1001/jamapsychiatry.2022.0097.
6. Lubotzky-Gete S et al. Postpartum Depression and Infant Development Up to 24 months: A Nationwide Population-Based Study. J Affect Disord. 2021 Apr 15. doi: 10.1016/j.jad.2021.02.042.
7. Saharoy R et al. Postpartum Depression and Maternal Care: Exploring the Complex Effects on Mothers and Infants. Cureus. 2023 Jul 4. doi: 10.7759/cureus.41381..
8. Gress-Smith JL et al. Postpartum Depression Prevalence and Impact on Infant Health, Weight, and Sleep in Low-Income and Ethnic Minority Women and Infants. Matern Child Health J. 2012 May. doi: 10.1007/s10995-011-0812-y.
9. Kim S et al. The Impact of Antepartum Depression and Postpartum Depression on Exclusive Breastfeeding: A Systematic Review and Meta-Analysis. Clin Nurs Res. 2022 Jun. doi: 10.1177/10547738211053507.
10. Mirhosseini H et al. Cognitive Behavioral Development in Children Following Maternal Postpartum Depression: A Review Article. Electron Physician. 2015 Dec 20. doi: 10.19082/1673.
11. Grace SL et al. The Effect of Postpartum Depression on Child Cognitive Development and Behavior: A Review and Critical Analysis of the Literature. Arch Womens Ment Health. 2003 Nov. doi: 10.1007/s00737-003-0024-6.
12. Milgrom J et al. The Mediating Role of Maternal Responsiveness in Some Longer Term Effects of Postnatal Depression on Infant Development. Infant Behavior and Development. 2004 Sep 11. doi.org/10.1016/j.infbeh.2004.03.003.
13. Heshmati A et al. The Effect of Parental Leave on Parents’ Mental Health: A Systematic Review. Lancet Public Health. 2023 Jan. doi: 10.1016/S2468-2667(22)00311-5.
14. U.S. Bureau of Labor Statistics, What Data Does the BLS Publish on Family Leave? 2023 Sept 21. www.bls.gov/ebs/factsheets/family-leave-benefits-fact-sheet.htm.
15. Horowitz JM et al. Americans Widely Support Paid Family and Medical Leave, But Differ Over Specific Policies. Pew Research Center’s Social & Demographic Trends Project, Pew Research Center. 2017 Mar 23. www.pewresearch.org/social-trends/2017/03/23/americans-widely-support-paid-family-and-medical-leave-but-differ-over-specific-policies/.

New Research Dissects Transgenerational Obesity and Diabetes
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1).
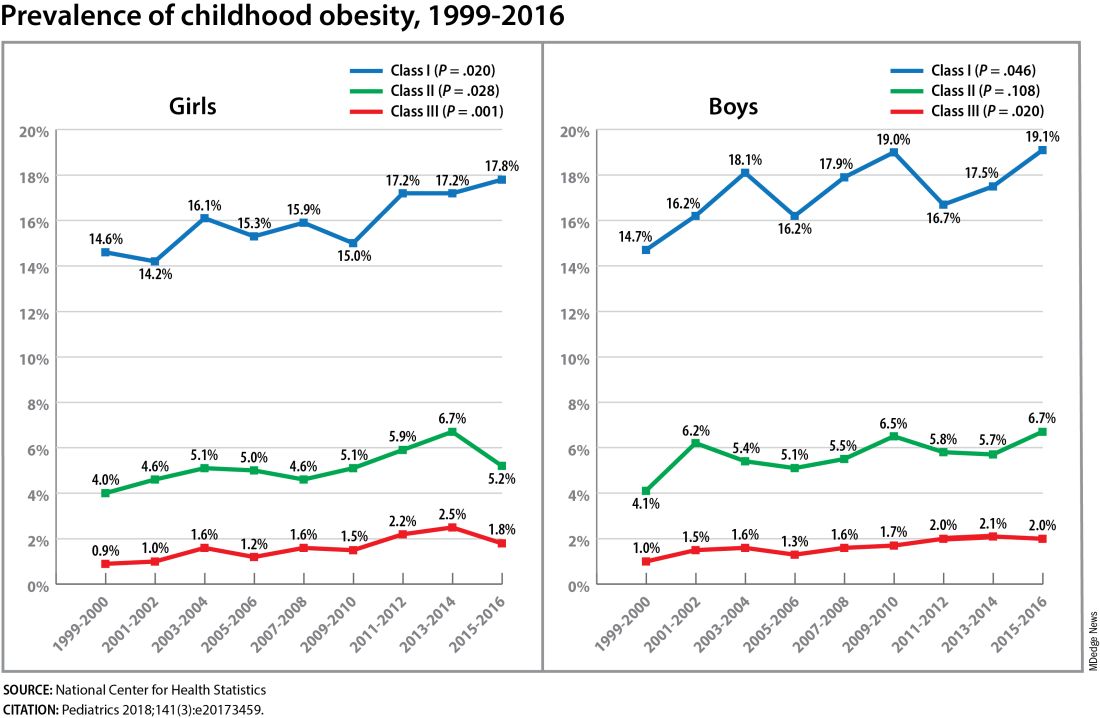
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1).
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1).
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FROM DPSG-NA 2023
Risk for Preterm Birth Stops Maternal RSV Vaccine Trial
A phase 3 trial of a maternal vaccine candidate for respiratory syncytial virus (RSV) has been stopped early because the risk for preterm births is higher in the candidate vaccine group than in the placebo group.
By the time enrollment was stopped on February 25, 2022 because of the safety signal of preterm birth, 5328 pregnant women had been vaccinated, about half of the intended 10,000 enrollees. Of these, 3557 received the candidate vaccine RSV prefusion F protein–based maternal vaccine, and another 1771 received a placebo.
Data from the trial, sponsored by GSK, were immediately made available when recruitment and vaccination were stopped, and investigation of the preterm birth risk followed. Results of that analysis, led by Ilse Dieussaert, IR, vice president for vaccine development at GSK in Wavre, Belgium, are published online on March 13 in The New England Journal of Medicine.
“We have discontinued our work on this RSV maternal candidate vaccine, and we are closing out all ongoing trials with the exception of the MAT-015 follow-on study to monitor subsequent pregnancies,” a GSK spokesperson said in an interview.
The trial was conducted in pregnant women aged 18-49 years to assess the efficacy and safety of the vaccine. The women were randomly assigned 2:1 to receive the candidate vaccine or placebo between 24 and 34 weeks’ gestation.
Preterm Births
The primary outcomes were any or severe medically assessed RSV-associated lower respiratory tract infection in infants from birth to 6 months and safety in infants from birth to 12 months.
According to the data, preterm birth occurred in 6.8% of the infants in the vaccine group and in 4.9% of those in the placebo group (relative risk [RR], 1.37; 95% CI, 1.08-1.74; P = .01). Neonatal death occurred in 0.4% in the vaccine group and 0.2% in the placebo group (RR, 2.16; 95% CI, 0.62-7.56; P = .23).
To date, only one RSV vaccine (Abrysvo, Pfizer) has been approved for use during pregnancy to protect infants from RSV-associated lower respiratory tract infection.
“It was a very big deal that this trial was stopped, and the new candidate won’t get approval.” said Aaron E. Glatt, MD, chair of the Department of Medicine and chief of Infectious Diseases and Hospital Epidemiologist at Mount Sinai South Nassau in Oceanside, New York.
Only One RSV Vaccine Approved in Pregnancy
Dr. Glatt pointed out the GSK vaccine is like the maternal vaccine that did get approved. “The data clearly show that there was a slight but increased risk in preterm labor,” Dr. Glatt said, “and while not as clearly shown, there was an increase in neonatal death in the group of very small numbers, but any neonatal death is of concern.”
The implications were disturbing, he added, “You’re giving this vaccine to prevent neonatal death.” Though the Pfizer vaccine that was granted approval had a very slight increase in premature birth, the risk wasn’t statistically significant, he pointed out, “and it showed similar benefits in preventing neonatal illness, which can be fatal.”
Dr. Glatt said that there is still a lingering concern with the approved vaccine, and he explained that most clinicians will give it closer to the end of the recommended time window of 34 weeks. “This way, even if there is a slight increase in premature term labor, you’re probably not going to have a serious outcome because the baby will be far enough along.”
A difference in the incidence of preterm birth between the experimental vaccine and placebo groups was predominantly found in low- and middle-income countries, according to Dieussaert’s team, “where approximately 50% of the trial population was enrolled and where the medical need for maternal RSV vaccines is the greatest.”
The RR was 1.56 (95% CI, 1.17-2.10) for low- and middle-income countries and 1.04 (95% CI, 0.68-1.58) for high-income countries.
“If a smaller percentage of participants from low- and middle-income countries had been enrolled in our trial, the RR for preterm birth in the vaccine group as compared with the placebo group might have been reduced in the overall trial population,” they reported.
The authors explained that the data do not reveal the cause of the higher risk for preterm birth in the vaccine group.
“We do not know what caused the signal,” the company’s spokesperson added. “GSK completed all the necessary steps of product development including preclinical toxicology studies and clinical studies in nonpregnant women prior to starting the studies in pregnant women. There were no safety signals identified in any of the earlier parts of the clinical testing. There have been no safety signals identified in the other phase 3 trials for this vaccine candidate.”
Researchers did not find a correlation between preterm births in the treatment vs control groups with gestational age at the time of vaccination or with particular vaccine clinical trial material lots, race, ethnicity, maternal smoking, alcohol consumption, body mass index, or time between study vaccination and delivery, the GSK spokesperson said.
The spokesperson noted that the halted vaccine is different from GSK’s currently approved adjuvanted RSV vaccine (Arexvy) for adults aged 60 years or older.
What’s Next for Other Vaccines
Maternal vaccines have been effective in preventing other diseases in infants, such as tetanus, influenza, and pertussis, but RSV is a very hard virus to make a vaccine for, Dr. Glatt shared.
The need is great to have more than one option for a maternal RSV vaccine, he added, to address any potential supply concerns.
“People have to realize how serious RSV can be in infants,” he said. “It can be a fatal disease. This can be a serious illness even in healthy children.”
A version of this article appeared on Medscape.com.
A phase 3 trial of a maternal vaccine candidate for respiratory syncytial virus (RSV) has been stopped early because the risk for preterm births is higher in the candidate vaccine group than in the placebo group.
By the time enrollment was stopped on February 25, 2022 because of the safety signal of preterm birth, 5328 pregnant women had been vaccinated, about half of the intended 10,000 enrollees. Of these, 3557 received the candidate vaccine RSV prefusion F protein–based maternal vaccine, and another 1771 received a placebo.
Data from the trial, sponsored by GSK, were immediately made available when recruitment and vaccination were stopped, and investigation of the preterm birth risk followed. Results of that analysis, led by Ilse Dieussaert, IR, vice president for vaccine development at GSK in Wavre, Belgium, are published online on March 13 in The New England Journal of Medicine.
“We have discontinued our work on this RSV maternal candidate vaccine, and we are closing out all ongoing trials with the exception of the MAT-015 follow-on study to monitor subsequent pregnancies,” a GSK spokesperson said in an interview.
The trial was conducted in pregnant women aged 18-49 years to assess the efficacy and safety of the vaccine. The women were randomly assigned 2:1 to receive the candidate vaccine or placebo between 24 and 34 weeks’ gestation.
Preterm Births
The primary outcomes were any or severe medically assessed RSV-associated lower respiratory tract infection in infants from birth to 6 months and safety in infants from birth to 12 months.
According to the data, preterm birth occurred in 6.8% of the infants in the vaccine group and in 4.9% of those in the placebo group (relative risk [RR], 1.37; 95% CI, 1.08-1.74; P = .01). Neonatal death occurred in 0.4% in the vaccine group and 0.2% in the placebo group (RR, 2.16; 95% CI, 0.62-7.56; P = .23).
To date, only one RSV vaccine (Abrysvo, Pfizer) has been approved for use during pregnancy to protect infants from RSV-associated lower respiratory tract infection.
“It was a very big deal that this trial was stopped, and the new candidate won’t get approval.” said Aaron E. Glatt, MD, chair of the Department of Medicine and chief of Infectious Diseases and Hospital Epidemiologist at Mount Sinai South Nassau in Oceanside, New York.
Only One RSV Vaccine Approved in Pregnancy
Dr. Glatt pointed out the GSK vaccine is like the maternal vaccine that did get approved. “The data clearly show that there was a slight but increased risk in preterm labor,” Dr. Glatt said, “and while not as clearly shown, there was an increase in neonatal death in the group of very small numbers, but any neonatal death is of concern.”
The implications were disturbing, he added, “You’re giving this vaccine to prevent neonatal death.” Though the Pfizer vaccine that was granted approval had a very slight increase in premature birth, the risk wasn’t statistically significant, he pointed out, “and it showed similar benefits in preventing neonatal illness, which can be fatal.”
Dr. Glatt said that there is still a lingering concern with the approved vaccine, and he explained that most clinicians will give it closer to the end of the recommended time window of 34 weeks. “This way, even if there is a slight increase in premature term labor, you’re probably not going to have a serious outcome because the baby will be far enough along.”
A difference in the incidence of preterm birth between the experimental vaccine and placebo groups was predominantly found in low- and middle-income countries, according to Dieussaert’s team, “where approximately 50% of the trial population was enrolled and where the medical need for maternal RSV vaccines is the greatest.”
The RR was 1.56 (95% CI, 1.17-2.10) for low- and middle-income countries and 1.04 (95% CI, 0.68-1.58) for high-income countries.
“If a smaller percentage of participants from low- and middle-income countries had been enrolled in our trial, the RR for preterm birth in the vaccine group as compared with the placebo group might have been reduced in the overall trial population,” they reported.
The authors explained that the data do not reveal the cause of the higher risk for preterm birth in the vaccine group.
“We do not know what caused the signal,” the company’s spokesperson added. “GSK completed all the necessary steps of product development including preclinical toxicology studies and clinical studies in nonpregnant women prior to starting the studies in pregnant women. There were no safety signals identified in any of the earlier parts of the clinical testing. There have been no safety signals identified in the other phase 3 trials for this vaccine candidate.”
Researchers did not find a correlation between preterm births in the treatment vs control groups with gestational age at the time of vaccination or with particular vaccine clinical trial material lots, race, ethnicity, maternal smoking, alcohol consumption, body mass index, or time between study vaccination and delivery, the GSK spokesperson said.
The spokesperson noted that the halted vaccine is different from GSK’s currently approved adjuvanted RSV vaccine (Arexvy) for adults aged 60 years or older.
What’s Next for Other Vaccines
Maternal vaccines have been effective in preventing other diseases in infants, such as tetanus, influenza, and pertussis, but RSV is a very hard virus to make a vaccine for, Dr. Glatt shared.
The need is great to have more than one option for a maternal RSV vaccine, he added, to address any potential supply concerns.
“People have to realize how serious RSV can be in infants,” he said. “It can be a fatal disease. This can be a serious illness even in healthy children.”
A version of this article appeared on Medscape.com.
A phase 3 trial of a maternal vaccine candidate for respiratory syncytial virus (RSV) has been stopped early because the risk for preterm births is higher in the candidate vaccine group than in the placebo group.
By the time enrollment was stopped on February 25, 2022 because of the safety signal of preterm birth, 5328 pregnant women had been vaccinated, about half of the intended 10,000 enrollees. Of these, 3557 received the candidate vaccine RSV prefusion F protein–based maternal vaccine, and another 1771 received a placebo.
Data from the trial, sponsored by GSK, were immediately made available when recruitment and vaccination were stopped, and investigation of the preterm birth risk followed. Results of that analysis, led by Ilse Dieussaert, IR, vice president for vaccine development at GSK in Wavre, Belgium, are published online on March 13 in The New England Journal of Medicine.
“We have discontinued our work on this RSV maternal candidate vaccine, and we are closing out all ongoing trials with the exception of the MAT-015 follow-on study to monitor subsequent pregnancies,” a GSK spokesperson said in an interview.
The trial was conducted in pregnant women aged 18-49 years to assess the efficacy and safety of the vaccine. The women were randomly assigned 2:1 to receive the candidate vaccine or placebo between 24 and 34 weeks’ gestation.
Preterm Births
The primary outcomes were any or severe medically assessed RSV-associated lower respiratory tract infection in infants from birth to 6 months and safety in infants from birth to 12 months.
According to the data, preterm birth occurred in 6.8% of the infants in the vaccine group and in 4.9% of those in the placebo group (relative risk [RR], 1.37; 95% CI, 1.08-1.74; P = .01). Neonatal death occurred in 0.4% in the vaccine group and 0.2% in the placebo group (RR, 2.16; 95% CI, 0.62-7.56; P = .23).
To date, only one RSV vaccine (Abrysvo, Pfizer) has been approved for use during pregnancy to protect infants from RSV-associated lower respiratory tract infection.
“It was a very big deal that this trial was stopped, and the new candidate won’t get approval.” said Aaron E. Glatt, MD, chair of the Department of Medicine and chief of Infectious Diseases and Hospital Epidemiologist at Mount Sinai South Nassau in Oceanside, New York.
Only One RSV Vaccine Approved in Pregnancy
Dr. Glatt pointed out the GSK vaccine is like the maternal vaccine that did get approved. “The data clearly show that there was a slight but increased risk in preterm labor,” Dr. Glatt said, “and while not as clearly shown, there was an increase in neonatal death in the group of very small numbers, but any neonatal death is of concern.”
The implications were disturbing, he added, “You’re giving this vaccine to prevent neonatal death.” Though the Pfizer vaccine that was granted approval had a very slight increase in premature birth, the risk wasn’t statistically significant, he pointed out, “and it showed similar benefits in preventing neonatal illness, which can be fatal.”
Dr. Glatt said that there is still a lingering concern with the approved vaccine, and he explained that most clinicians will give it closer to the end of the recommended time window of 34 weeks. “This way, even if there is a slight increase in premature term labor, you’re probably not going to have a serious outcome because the baby will be far enough along.”
A difference in the incidence of preterm birth between the experimental vaccine and placebo groups was predominantly found in low- and middle-income countries, according to Dieussaert’s team, “where approximately 50% of the trial population was enrolled and where the medical need for maternal RSV vaccines is the greatest.”
The RR was 1.56 (95% CI, 1.17-2.10) for low- and middle-income countries and 1.04 (95% CI, 0.68-1.58) for high-income countries.
“If a smaller percentage of participants from low- and middle-income countries had been enrolled in our trial, the RR for preterm birth in the vaccine group as compared with the placebo group might have been reduced in the overall trial population,” they reported.
The authors explained that the data do not reveal the cause of the higher risk for preterm birth in the vaccine group.
“We do not know what caused the signal,” the company’s spokesperson added. “GSK completed all the necessary steps of product development including preclinical toxicology studies and clinical studies in nonpregnant women prior to starting the studies in pregnant women. There were no safety signals identified in any of the earlier parts of the clinical testing. There have been no safety signals identified in the other phase 3 trials for this vaccine candidate.”
Researchers did not find a correlation between preterm births in the treatment vs control groups with gestational age at the time of vaccination or with particular vaccine clinical trial material lots, race, ethnicity, maternal smoking, alcohol consumption, body mass index, or time between study vaccination and delivery, the GSK spokesperson said.
The spokesperson noted that the halted vaccine is different from GSK’s currently approved adjuvanted RSV vaccine (Arexvy) for adults aged 60 years or older.
What’s Next for Other Vaccines
Maternal vaccines have been effective in preventing other diseases in infants, such as tetanus, influenza, and pertussis, but RSV is a very hard virus to make a vaccine for, Dr. Glatt shared.
The need is great to have more than one option for a maternal RSV vaccine, he added, to address any potential supply concerns.
“People have to realize how serious RSV can be in infants,” he said. “It can be a fatal disease. This can be a serious illness even in healthy children.”
A version of this article appeared on Medscape.com.
High Cesarean Rates Persist in Obesity Despite Standardized Protocols
NATIONAL HARBOR, MARYLAND — Implementation of a standardized induction of labor protocol had no significant effect on the rates of cesarean delivery in patients with obesity, based on data from more than 5000 individuals.
Previous research has shown that the risk for cesarean delivery increases by 5% with each 1-kg/m2 increase in body mass index (BMI) among nulliparous patients, said Melissa Riegel, MD, of the University of Pennsylvania, Philadelphia, in a presentation at the meeting sponsored by the Society for Maternal-Fetal Medicine. (abstract 82).
Research on the relationship between obesity and higher cesarean delivery rates “has been clouded by the inability to reduce variation in care,” Dr. Riegel said at the meeting sponsored by the Society for Maternal Fetal Medicine. Failed induction of labor (IOL) is a leading indicator for cesarean delivery, and cesarean delivery is 80% more likely in patients with obesity undergoing IOL than in normal-weight patients, Dr. Riegel said.
Possible explanations for these differences include provider factors such as variability in care management, conscious and unconscious biases, or physiologic differences in patients with obesity such as elevated hormones, differences in the labor curve, and higher doses of oxytocin and prostaglandins, Dr. Riegel said.
Dr. Riegel and colleagues hypothesized that differences in cesarean delivery rates would persist despite a standardized labor induction protocol, thereby supporting the effects of factors other than variations in care on increased cesarean delivery risk after IOL in patients with obesity.
The researchers reviewed data from two sites comparing 2-year periods before and after implementation of an IOL protocol from 2018 to 2022. The study population included nulliparous women with singleton pregnancies at term who underwent IOL with intact membranes and unfavorable cervices, and had a BMI of at least 30 kg/m2 at delivery. The preimplementation group (PRE) included 2480 individuals and the postimplementation group (POST) included 2651 individuals. Patients were divided into weight classes based on BMI: 30-34.9; 35-39.9; ≥40.
The standardized protocol consisted of active labor management with cervical exams, with an amniotomy by the time of the first exam with 4 cm or greater cervical dilation, and further intervention with medication such as oxytocin or an intrauterine pressure catheter if no cervical change was noted after 2 hours.
In a multivariate analysis, the overall cesarean delivery rate was 24.9% before the protocol implementation and 26.0% in the postimplementation group. There were no differences in the risk of cesarean delivery in any obesity class from the PRE to POST period.
In addition, no significant differences appeared in the secondary outcomes of duration of labor, maternal morbidity, or neonatal morbidity, Dr. Riegel said. Nonreassuring fetal heart rate tracing was the most common reason for cesarean delivery across all obesity classes and the PRE and POST groups.
Study limitations included the use of data from only two sites, but the results were strengthened by the large sample size, said Dr. Reigel. The results indicate that reducing variation in IOL management had no significant effect on the relationship between obesity and cesarean delivery and support underlying physiologic explanations, she said.
Making the Case for Physiology
“By standardizing induction practices, we were able to minimize differences in care and better answer why the increased cesarean delivery rate exists in this patient population,” Dr. Riegel said in an interview. The findings were in line with the primary hypothesis that standardized induction would not affect cesarean delivery rates in patients with obesity, she said. Instead, the findings support potential physiologic differences as “the driving force behind this relationship,” she added.
Looking ahead, “There is a role for translational work to investigate the specific biological changes in patients with obesity that might contribute to an increased risk of cesarean delivery and there is also a role for investigating the effectiveness of different labor induction interventions specifically in patients with obesity,” Dr. Riegel said.
Different Induction Protocols Needed for Obese Patients?
“Given that severe maternal morbidity and mortality are continuing to increase in the United States, this study is critical, as we know that both cesarean delivery and obesity are driving factors in increasing maternal morbidity,” said Marissa Platner, MD, a maternal-fetal medicine specialist at Emory University, Atlanta, Georgia, in an interview.
However, the novel takeaway message from the current study is that patients with obesity were more likely to require cesarean delivery even with a protocol in which variation in labor induction techniques are minimized, said Dr. Platner, who was not involved in the study. “This leads to the question of [whether] we should have different standards or protocols for our patients with obesity, as well as a need for clear counseling for these patients early on in pregnancy,” she said.
As for further research, “It would be interesting to see if the risk of cesarean delivery changed based on class of obesity, and the primary drivers of cesarean delivery in this study,” Dr. Platner said. “Additionally, it would be helpful to know how much pitocin was needed for patients, based on their BMI category, to achieve successful vaginal delivery,” she noted.
The study was supported by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Development. The researchers had no financial conflicts to disclose. Dr. Platner had no financial conflicts to disclose.
NATIONAL HARBOR, MARYLAND — Implementation of a standardized induction of labor protocol had no significant effect on the rates of cesarean delivery in patients with obesity, based on data from more than 5000 individuals.
Previous research has shown that the risk for cesarean delivery increases by 5% with each 1-kg/m2 increase in body mass index (BMI) among nulliparous patients, said Melissa Riegel, MD, of the University of Pennsylvania, Philadelphia, in a presentation at the meeting sponsored by the Society for Maternal-Fetal Medicine. (abstract 82).
Research on the relationship between obesity and higher cesarean delivery rates “has been clouded by the inability to reduce variation in care,” Dr. Riegel said at the meeting sponsored by the Society for Maternal Fetal Medicine. Failed induction of labor (IOL) is a leading indicator for cesarean delivery, and cesarean delivery is 80% more likely in patients with obesity undergoing IOL than in normal-weight patients, Dr. Riegel said.
Possible explanations for these differences include provider factors such as variability in care management, conscious and unconscious biases, or physiologic differences in patients with obesity such as elevated hormones, differences in the labor curve, and higher doses of oxytocin and prostaglandins, Dr. Riegel said.
Dr. Riegel and colleagues hypothesized that differences in cesarean delivery rates would persist despite a standardized labor induction protocol, thereby supporting the effects of factors other than variations in care on increased cesarean delivery risk after IOL in patients with obesity.
The researchers reviewed data from two sites comparing 2-year periods before and after implementation of an IOL protocol from 2018 to 2022. The study population included nulliparous women with singleton pregnancies at term who underwent IOL with intact membranes and unfavorable cervices, and had a BMI of at least 30 kg/m2 at delivery. The preimplementation group (PRE) included 2480 individuals and the postimplementation group (POST) included 2651 individuals. Patients were divided into weight classes based on BMI: 30-34.9; 35-39.9; ≥40.
The standardized protocol consisted of active labor management with cervical exams, with an amniotomy by the time of the first exam with 4 cm or greater cervical dilation, and further intervention with medication such as oxytocin or an intrauterine pressure catheter if no cervical change was noted after 2 hours.
In a multivariate analysis, the overall cesarean delivery rate was 24.9% before the protocol implementation and 26.0% in the postimplementation group. There were no differences in the risk of cesarean delivery in any obesity class from the PRE to POST period.
In addition, no significant differences appeared in the secondary outcomes of duration of labor, maternal morbidity, or neonatal morbidity, Dr. Riegel said. Nonreassuring fetal heart rate tracing was the most common reason for cesarean delivery across all obesity classes and the PRE and POST groups.
Study limitations included the use of data from only two sites, but the results were strengthened by the large sample size, said Dr. Reigel. The results indicate that reducing variation in IOL management had no significant effect on the relationship between obesity and cesarean delivery and support underlying physiologic explanations, she said.
Making the Case for Physiology
“By standardizing induction practices, we were able to minimize differences in care and better answer why the increased cesarean delivery rate exists in this patient population,” Dr. Riegel said in an interview. The findings were in line with the primary hypothesis that standardized induction would not affect cesarean delivery rates in patients with obesity, she said. Instead, the findings support potential physiologic differences as “the driving force behind this relationship,” she added.
Looking ahead, “There is a role for translational work to investigate the specific biological changes in patients with obesity that might contribute to an increased risk of cesarean delivery and there is also a role for investigating the effectiveness of different labor induction interventions specifically in patients with obesity,” Dr. Riegel said.
Different Induction Protocols Needed for Obese Patients?
“Given that severe maternal morbidity and mortality are continuing to increase in the United States, this study is critical, as we know that both cesarean delivery and obesity are driving factors in increasing maternal morbidity,” said Marissa Platner, MD, a maternal-fetal medicine specialist at Emory University, Atlanta, Georgia, in an interview.
However, the novel takeaway message from the current study is that patients with obesity were more likely to require cesarean delivery even with a protocol in which variation in labor induction techniques are minimized, said Dr. Platner, who was not involved in the study. “This leads to the question of [whether] we should have different standards or protocols for our patients with obesity, as well as a need for clear counseling for these patients early on in pregnancy,” she said.
As for further research, “It would be interesting to see if the risk of cesarean delivery changed based on class of obesity, and the primary drivers of cesarean delivery in this study,” Dr. Platner said. “Additionally, it would be helpful to know how much pitocin was needed for patients, based on their BMI category, to achieve successful vaginal delivery,” she noted.
The study was supported by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Development. The researchers had no financial conflicts to disclose. Dr. Platner had no financial conflicts to disclose.
NATIONAL HARBOR, MARYLAND — Implementation of a standardized induction of labor protocol had no significant effect on the rates of cesarean delivery in patients with obesity, based on data from more than 5000 individuals.
Previous research has shown that the risk for cesarean delivery increases by 5% with each 1-kg/m2 increase in body mass index (BMI) among nulliparous patients, said Melissa Riegel, MD, of the University of Pennsylvania, Philadelphia, in a presentation at the meeting sponsored by the Society for Maternal-Fetal Medicine. (abstract 82).
Research on the relationship between obesity and higher cesarean delivery rates “has been clouded by the inability to reduce variation in care,” Dr. Riegel said at the meeting sponsored by the Society for Maternal Fetal Medicine. Failed induction of labor (IOL) is a leading indicator for cesarean delivery, and cesarean delivery is 80% more likely in patients with obesity undergoing IOL than in normal-weight patients, Dr. Riegel said.
Possible explanations for these differences include provider factors such as variability in care management, conscious and unconscious biases, or physiologic differences in patients with obesity such as elevated hormones, differences in the labor curve, and higher doses of oxytocin and prostaglandins, Dr. Riegel said.
Dr. Riegel and colleagues hypothesized that differences in cesarean delivery rates would persist despite a standardized labor induction protocol, thereby supporting the effects of factors other than variations in care on increased cesarean delivery risk after IOL in patients with obesity.
The researchers reviewed data from two sites comparing 2-year periods before and after implementation of an IOL protocol from 2018 to 2022. The study population included nulliparous women with singleton pregnancies at term who underwent IOL with intact membranes and unfavorable cervices, and had a BMI of at least 30 kg/m2 at delivery. The preimplementation group (PRE) included 2480 individuals and the postimplementation group (POST) included 2651 individuals. Patients were divided into weight classes based on BMI: 30-34.9; 35-39.9; ≥40.
The standardized protocol consisted of active labor management with cervical exams, with an amniotomy by the time of the first exam with 4 cm or greater cervical dilation, and further intervention with medication such as oxytocin or an intrauterine pressure catheter if no cervical change was noted after 2 hours.
In a multivariate analysis, the overall cesarean delivery rate was 24.9% before the protocol implementation and 26.0% in the postimplementation group. There were no differences in the risk of cesarean delivery in any obesity class from the PRE to POST period.
In addition, no significant differences appeared in the secondary outcomes of duration of labor, maternal morbidity, or neonatal morbidity, Dr. Riegel said. Nonreassuring fetal heart rate tracing was the most common reason for cesarean delivery across all obesity classes and the PRE and POST groups.
Study limitations included the use of data from only two sites, but the results were strengthened by the large sample size, said Dr. Reigel. The results indicate that reducing variation in IOL management had no significant effect on the relationship between obesity and cesarean delivery and support underlying physiologic explanations, she said.
Making the Case for Physiology
“By standardizing induction practices, we were able to minimize differences in care and better answer why the increased cesarean delivery rate exists in this patient population,” Dr. Riegel said in an interview. The findings were in line with the primary hypothesis that standardized induction would not affect cesarean delivery rates in patients with obesity, she said. Instead, the findings support potential physiologic differences as “the driving force behind this relationship,” she added.
Looking ahead, “There is a role for translational work to investigate the specific biological changes in patients with obesity that might contribute to an increased risk of cesarean delivery and there is also a role for investigating the effectiveness of different labor induction interventions specifically in patients with obesity,” Dr. Riegel said.
Different Induction Protocols Needed for Obese Patients?
“Given that severe maternal morbidity and mortality are continuing to increase in the United States, this study is critical, as we know that both cesarean delivery and obesity are driving factors in increasing maternal morbidity,” said Marissa Platner, MD, a maternal-fetal medicine specialist at Emory University, Atlanta, Georgia, in an interview.
However, the novel takeaway message from the current study is that patients with obesity were more likely to require cesarean delivery even with a protocol in which variation in labor induction techniques are minimized, said Dr. Platner, who was not involved in the study. “This leads to the question of [whether] we should have different standards or protocols for our patients with obesity, as well as a need for clear counseling for these patients early on in pregnancy,” she said.
As for further research, “It would be interesting to see if the risk of cesarean delivery changed based on class of obesity, and the primary drivers of cesarean delivery in this study,” Dr. Platner said. “Additionally, it would be helpful to know how much pitocin was needed for patients, based on their BMI category, to achieve successful vaginal delivery,” she noted.
The study was supported by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Development. The researchers had no financial conflicts to disclose. Dr. Platner had no financial conflicts to disclose.
AT THE PREGNANCY MEETING
Skin Infections in Pregnant Women: Many Drugs Safe, but Not All
SAN DIEGO — . However, several drugs should be avoided or used with caution because of potential risks during pregnancy.
When treating bacterial infections in pregnant women, there are many options, “especially for the sort of short-term antibiotic use that we tend to use for treating infections,” said Jenny Murase, MD, of the Palo Alto Foundation Medical Group and the University of California San Francisco.

During a presentation on treating infections in pregnant patients, she made the following recommendations for treating pyogenic infections:
- Impetigo: First-line treatments are topical mupirocin, oral first-generation cephalosporins, and oral dicloxacillin.
- Cellulitis: Recommended treatments are oral or intravenous penicillin, oral first-generation cephalosporins, and oral dicloxacillin.
- Methicillin-resistant Staphylococcus aureus (MRSA): “Clindamycin is first-line, dependent on bacteria culture and sensitivities,” and because of its safety, “it’s a really good choice for a pregnant woman.” Dr. Murase said. However, be aware of potential inducible resistance and test for the erm gene, she said.
- Abscesses: Incision and drainage are recommended. “Whenever we’re managing a patient with a condition during pregnancy, we want to try to use nonmedications when possible,” Dr. Murase said. “No antibiotic is necessary unless the abscess is greater than 5 cm or if it’s greater than 2 cm with erythema around the abscess.”
- Tuberculosis: The best strategy is rifampin, but peripartum vitamin K prophylaxis for mother and fetus should be used, she said.
General Infections
With regard to antibiotics to treat general infections — for instance, if a patient with atopic dermatitis has a secondary skin infection — Dr. Murase recommended first-line oral antibiotic therapy with penicillin, first-generation cephalosporins, or dicloxacillin. For second-line therapy, erythromycin is the preferred macrolide over azithromycin and clarithromycin, she said.
She noted that there is an increased risk for atrial/ventricular septal defects and pyloric stenosis associated with the use of erythromycin when used during the first trimester of pregnancy. In addition, erythromycin estolate increases the risk of liver toxicity, while erythromycin base and erythromycin ethylsuccinate do not.
Sulfonamides are a second-line line choice up until the third trimester. If given to a patient in the first trimester, she said, “make sure that they are supplementing with folic acid efficiently, at least 0.5 mg a day.” During the peripartum period they are contraindicated, as they pose a risk for hemolytic anemia, hyperbilirubinemia, and kernicterus.
The combination drug trimethoprim/sulfamethoxazole is a second-line choice for complicated infections because of the associated risk for low birth weight and prematurity, Dr. Murase said.
Quinolones are also a second-line option during pregnancy she said, and ciprofloxacin and norfloxacin have been studied the most. “If you have to choose a quinolone for a complicated infection in pregnancy, those would be the quinolones of choice,” Dr. Murase said.
Considering the bad reputation of tetracyclines in pregnancy, dermatologists may be surprised to learn that they are considered a second-line therapy up to 14 weeks’ gestation, she said. After that time, however, they’re contraindicated because of bone growth inhibition, teeth discoloration, and maternal hepatitis.
Fungal Infections
As for fungal infections, clotrimazole is the first choice for topical treatment of tinea corporis, followed by miconazole and then ketoconazole, according to Dr. Murase. There are limited data for topical terbinafine, naftifine, and ciclopirox during pregnancy she noted, but they are likely safe.
There is also limited data about these drugs when used for topical treatment of candidiasis during pregnancy. Nystatin is safe, but less effective than other options, Dr. Murase said. Other options include clotrimazole, miconazole, and ketoconazole, which, in animals exposed to high doses, have not been associated with defects, and topical gentian violet (0.5%-1% solution), she noted.
For topical treatment of tinea versicolor during pregnancy, limited application of clotrimazole or miconazole is considered safe, and zinc pyrithione soap or topical benzoyl peroxide soap can be used for more widespread areas.
Dr. Murase recommended caution when using selenium sulfide since poisoning has been linked to miscarriages, she said. Limited application appears to be safe, “so make sure that the patient is using it on smaller body surface areas.”
As for systemic antifungal treatments, fluconazole, ketoconazole, and itraconazole should be avoided in pregnancy because of the risks of craniosynostosis, congenital heart defects, and skeletal anomalies, Dr. Murase said. However, she referred to a study that found no increased risk of congenital malformations with fluconazole during the first trimester, and a patient could be reassured if, for example, she was treated for a yeast infection before she knew she was pregnant, she said.
Griseofulvin is not recommended during pregnancy, but a 2020 study suggests that terbinafine is safe, she said. In that study, oral or topical terbinafine did not appear to be associated with an increased risk for spontaneous abortion or major malformations. “Certainly, we can wait until after the pregnancy to treat onychomycosis. But I have had situations that even in spite of regular topical therapy, pregnant patients needed to take some kind of oral agent” because of severe itching.
Viral Infections
For herpes simplex, acyclovir is the top choice, and famciclovir and valacyclovir (Valtrex) are likely safe, but daily prophylaxis is not recommended during pregnancy, Dr. Murase said.
Because of a lack of data, podofilox, cantharidin, and imiquimod for treating human papillomavirus (HPV) should be avoided, she said. Podophyllin is extremely dangerous in pregnancy and has been linked to maternal and fetal deaths, and malformations, and is contraindicated in pregnancy, she added.
Instead, liquid nitrogen is the treatment of choice for HPV in pregnant patients, she said.
Trichloracetic acid is the treatment of choice for condylomata acuminata, and squaric acid or intralesional Candida antigen injection for periungual verrucas can be used, she said, and limited applications of salicylic acid are considered safe.
Dr. Murase highlighted a 2014 paper that she coauthored on the safety of dermatologic medications during pregnancy, noting that an updated report will be published later this year.
Dr. Murase disclosed relationships with Regeneron and UCB (speaker), Sanofi/Regeneron and Bristol-Myers Squibb (advisory board), and UCB, AbbVie, and UpToDate (consulting).
A version of this article appeared on Medscape.com.
SAN DIEGO — . However, several drugs should be avoided or used with caution because of potential risks during pregnancy.
When treating bacterial infections in pregnant women, there are many options, “especially for the sort of short-term antibiotic use that we tend to use for treating infections,” said Jenny Murase, MD, of the Palo Alto Foundation Medical Group and the University of California San Francisco.
During a presentation on treating infections in pregnant patients, she made the following recommendations for treating pyogenic infections:
- Impetigo: First-line treatments are topical mupirocin, oral first-generation cephalosporins, and oral dicloxacillin.
- Cellulitis: Recommended treatments are oral or intravenous penicillin, oral first-generation cephalosporins, and oral dicloxacillin.
- Methicillin-resistant Staphylococcus aureus (MRSA): “Clindamycin is first-line, dependent on bacteria culture and sensitivities,” and because of its safety, “it’s a really good choice for a pregnant woman.” Dr. Murase said. However, be aware of potential inducible resistance and test for the erm gene, she said.
- Abscesses: Incision and drainage are recommended. “Whenever we’re managing a patient with a condition during pregnancy, we want to try to use nonmedications when possible,” Dr. Murase said. “No antibiotic is necessary unless the abscess is greater than 5 cm or if it’s greater than 2 cm with erythema around the abscess.”
- Tuberculosis: The best strategy is rifampin, but peripartum vitamin K prophylaxis for mother and fetus should be used, she said.
General Infections
With regard to antibiotics to treat general infections — for instance, if a patient with atopic dermatitis has a secondary skin infection — Dr. Murase recommended first-line oral antibiotic therapy with penicillin, first-generation cephalosporins, or dicloxacillin. For second-line therapy, erythromycin is the preferred macrolide over azithromycin and clarithromycin, she said.
She noted that there is an increased risk for atrial/ventricular septal defects and pyloric stenosis associated with the use of erythromycin when used during the first trimester of pregnancy. In addition, erythromycin estolate increases the risk of liver toxicity, while erythromycin base and erythromycin ethylsuccinate do not.
Sulfonamides are a second-line line choice up until the third trimester. If given to a patient in the first trimester, she said, “make sure that they are supplementing with folic acid efficiently, at least 0.5 mg a day.” During the peripartum period they are contraindicated, as they pose a risk for hemolytic anemia, hyperbilirubinemia, and kernicterus.
The combination drug trimethoprim/sulfamethoxazole is a second-line choice for complicated infections because of the associated risk for low birth weight and prematurity, Dr. Murase said.
Quinolones are also a second-line option during pregnancy she said, and ciprofloxacin and norfloxacin have been studied the most. “If you have to choose a quinolone for a complicated infection in pregnancy, those would be the quinolones of choice,” Dr. Murase said.
Considering the bad reputation of tetracyclines in pregnancy, dermatologists may be surprised to learn that they are considered a second-line therapy up to 14 weeks’ gestation, she said. After that time, however, they’re contraindicated because of bone growth inhibition, teeth discoloration, and maternal hepatitis.
Fungal Infections
As for fungal infections, clotrimazole is the first choice for topical treatment of tinea corporis, followed by miconazole and then ketoconazole, according to Dr. Murase. There are limited data for topical terbinafine, naftifine, and ciclopirox during pregnancy she noted, but they are likely safe.
There is also limited data about these drugs when used for topical treatment of candidiasis during pregnancy. Nystatin is safe, but less effective than other options, Dr. Murase said. Other options include clotrimazole, miconazole, and ketoconazole, which, in animals exposed to high doses, have not been associated with defects, and topical gentian violet (0.5%-1% solution), she noted.
For topical treatment of tinea versicolor during pregnancy, limited application of clotrimazole or miconazole is considered safe, and zinc pyrithione soap or topical benzoyl peroxide soap can be used for more widespread areas.
Dr. Murase recommended caution when using selenium sulfide since poisoning has been linked to miscarriages, she said. Limited application appears to be safe, “so make sure that the patient is using it on smaller body surface areas.”
As for systemic antifungal treatments, fluconazole, ketoconazole, and itraconazole should be avoided in pregnancy because of the risks of craniosynostosis, congenital heart defects, and skeletal anomalies, Dr. Murase said. However, she referred to a study that found no increased risk of congenital malformations with fluconazole during the first trimester, and a patient could be reassured if, for example, she was treated for a yeast infection before she knew she was pregnant, she said.
Griseofulvin is not recommended during pregnancy, but a 2020 study suggests that terbinafine is safe, she said. In that study, oral or topical terbinafine did not appear to be associated with an increased risk for spontaneous abortion or major malformations. “Certainly, we can wait until after the pregnancy to treat onychomycosis. But I have had situations that even in spite of regular topical therapy, pregnant patients needed to take some kind of oral agent” because of severe itching.
Viral Infections
For herpes simplex, acyclovir is the top choice, and famciclovir and valacyclovir (Valtrex) are likely safe, but daily prophylaxis is not recommended during pregnancy, Dr. Murase said.
Because of a lack of data, podofilox, cantharidin, and imiquimod for treating human papillomavirus (HPV) should be avoided, she said. Podophyllin is extremely dangerous in pregnancy and has been linked to maternal and fetal deaths, and malformations, and is contraindicated in pregnancy, she added.
Instead, liquid nitrogen is the treatment of choice for HPV in pregnant patients, she said.
Trichloracetic acid is the treatment of choice for condylomata acuminata, and squaric acid or intralesional Candida antigen injection for periungual verrucas can be used, she said, and limited applications of salicylic acid are considered safe.
Dr. Murase highlighted a 2014 paper that she coauthored on the safety of dermatologic medications during pregnancy, noting that an updated report will be published later this year.
Dr. Murase disclosed relationships with Regeneron and UCB (speaker), Sanofi/Regeneron and Bristol-Myers Squibb (advisory board), and UCB, AbbVie, and UpToDate (consulting).
A version of this article appeared on Medscape.com.
SAN DIEGO — . However, several drugs should be avoided or used with caution because of potential risks during pregnancy.
When treating bacterial infections in pregnant women, there are many options, “especially for the sort of short-term antibiotic use that we tend to use for treating infections,” said Jenny Murase, MD, of the Palo Alto Foundation Medical Group and the University of California San Francisco.
During a presentation on treating infections in pregnant patients, she made the following recommendations for treating pyogenic infections:
- Impetigo: First-line treatments are topical mupirocin, oral first-generation cephalosporins, and oral dicloxacillin.
- Cellulitis: Recommended treatments are oral or intravenous penicillin, oral first-generation cephalosporins, and oral dicloxacillin.
- Methicillin-resistant Staphylococcus aureus (MRSA): “Clindamycin is first-line, dependent on bacteria culture and sensitivities,” and because of its safety, “it’s a really good choice for a pregnant woman.” Dr. Murase said. However, be aware of potential inducible resistance and test for the erm gene, she said.
- Abscesses: Incision and drainage are recommended. “Whenever we’re managing a patient with a condition during pregnancy, we want to try to use nonmedications when possible,” Dr. Murase said. “No antibiotic is necessary unless the abscess is greater than 5 cm or if it’s greater than 2 cm with erythema around the abscess.”
- Tuberculosis: The best strategy is rifampin, but peripartum vitamin K prophylaxis for mother and fetus should be used, she said.
General Infections
With regard to antibiotics to treat general infections — for instance, if a patient with atopic dermatitis has a secondary skin infection — Dr. Murase recommended first-line oral antibiotic therapy with penicillin, first-generation cephalosporins, or dicloxacillin. For second-line therapy, erythromycin is the preferred macrolide over azithromycin and clarithromycin, she said.
She noted that there is an increased risk for atrial/ventricular septal defects and pyloric stenosis associated with the use of erythromycin when used during the first trimester of pregnancy. In addition, erythromycin estolate increases the risk of liver toxicity, while erythromycin base and erythromycin ethylsuccinate do not.
Sulfonamides are a second-line line choice up until the third trimester. If given to a patient in the first trimester, she said, “make sure that they are supplementing with folic acid efficiently, at least 0.5 mg a day.” During the peripartum period they are contraindicated, as they pose a risk for hemolytic anemia, hyperbilirubinemia, and kernicterus.
The combination drug trimethoprim/sulfamethoxazole is a second-line choice for complicated infections because of the associated risk for low birth weight and prematurity, Dr. Murase said.
Quinolones are also a second-line option during pregnancy she said, and ciprofloxacin and norfloxacin have been studied the most. “If you have to choose a quinolone for a complicated infection in pregnancy, those would be the quinolones of choice,” Dr. Murase said.
Considering the bad reputation of tetracyclines in pregnancy, dermatologists may be surprised to learn that they are considered a second-line therapy up to 14 weeks’ gestation, she said. After that time, however, they’re contraindicated because of bone growth inhibition, teeth discoloration, and maternal hepatitis.
Fungal Infections
As for fungal infections, clotrimazole is the first choice for topical treatment of tinea corporis, followed by miconazole and then ketoconazole, according to Dr. Murase. There are limited data for topical terbinafine, naftifine, and ciclopirox during pregnancy she noted, but they are likely safe.
There is also limited data about these drugs when used for topical treatment of candidiasis during pregnancy. Nystatin is safe, but less effective than other options, Dr. Murase said. Other options include clotrimazole, miconazole, and ketoconazole, which, in animals exposed to high doses, have not been associated with defects, and topical gentian violet (0.5%-1% solution), she noted.
For topical treatment of tinea versicolor during pregnancy, limited application of clotrimazole or miconazole is considered safe, and zinc pyrithione soap or topical benzoyl peroxide soap can be used for more widespread areas.
Dr. Murase recommended caution when using selenium sulfide since poisoning has been linked to miscarriages, she said. Limited application appears to be safe, “so make sure that the patient is using it on smaller body surface areas.”
As for systemic antifungal treatments, fluconazole, ketoconazole, and itraconazole should be avoided in pregnancy because of the risks of craniosynostosis, congenital heart defects, and skeletal anomalies, Dr. Murase said. However, she referred to a study that found no increased risk of congenital malformations with fluconazole during the first trimester, and a patient could be reassured if, for example, she was treated for a yeast infection before she knew she was pregnant, she said.
Griseofulvin is not recommended during pregnancy, but a 2020 study suggests that terbinafine is safe, she said. In that study, oral or topical terbinafine did not appear to be associated with an increased risk for spontaneous abortion or major malformations. “Certainly, we can wait until after the pregnancy to treat onychomycosis. But I have had situations that even in spite of regular topical therapy, pregnant patients needed to take some kind of oral agent” because of severe itching.
Viral Infections
For herpes simplex, acyclovir is the top choice, and famciclovir and valacyclovir (Valtrex) are likely safe, but daily prophylaxis is not recommended during pregnancy, Dr. Murase said.
Because of a lack of data, podofilox, cantharidin, and imiquimod for treating human papillomavirus (HPV) should be avoided, she said. Podophyllin is extremely dangerous in pregnancy and has been linked to maternal and fetal deaths, and malformations, and is contraindicated in pregnancy, she added.
Instead, liquid nitrogen is the treatment of choice for HPV in pregnant patients, she said.
Trichloracetic acid is the treatment of choice for condylomata acuminata, and squaric acid or intralesional Candida antigen injection for periungual verrucas can be used, she said, and limited applications of salicylic acid are considered safe.
Dr. Murase highlighted a 2014 paper that she coauthored on the safety of dermatologic medications during pregnancy, noting that an updated report will be published later this year.
Dr. Murase disclosed relationships with Regeneron and UCB (speaker), Sanofi/Regeneron and Bristol-Myers Squibb (advisory board), and UCB, AbbVie, and UpToDate (consulting).
A version of this article appeared on Medscape.com.
FROM AAD 2024
California Pushes to Expand the Universe of Abortion Care Providers
California’s efforts to expand access to abortion care are enabling more types of medical practitioners to perform certain abortion procedures — potentially a boon for patients in rural areas especially, but a source of concern for doctors’ groups that have long fought efforts to expand the role of non-physicians.
The latest move is a law that enables trained physician assistants, also known as physician associates, to perform first-trimester abortions without a supervising physician present. The measure, which passed last year and took effect Jan. 1, also lets PAs who have been disciplined or convicted solely for performing an abortion in a state where the practice is restricted apply for a license in California.
Physician assistants are now on par with nurse practitioners and certified nurse midwives trained in abortion care, who in 2022 won the ability to perform abortions without a doctor present.
The need for more abortion care practitioners is being driven by efforts in many states to gut abortion rights following the Supreme Court’s 2022 decision ending constitutional protection for the procedure. Thirty-one states have implemented abortion restrictions that range from cutting federal funding for abortion coverage to outright bans, according to the Guttmacher Institute, a research organization concerned with reproductive health.
With the new law, “there will be fewer barriers, and shorter wait times for this essential service,” said Jeremy Meis, president-elect of the California Academy of Physician Associates. While it is unclear how many of California’s 16,000 PAs will be trained in performing abortions, research shows that PAs are more likely than physicians to practice in rural areas where access to abortion is limited. More than 40% of counties in California lack clinics that provide abortion.
Comparing data from the first six months of 2020 with the same period in 2023, the number of abortions jumped from 77,030 to 92,600 a 20% increase as the state became a refuge for women seeking abortions. California has passed a suite of reproductive health laws to build in protections and increase access, and a dozen other states, including Oregon, Minnesota, and New York, have mounted similar efforts. Seventeen states, including California, now allow PAs to perform first-trimester abortions, according to the American Academy of Physician Associates.
There was little opposition to the new California law, with two physicians’ groups supporting it. But the American Medical Association, the country’s most powerful doctors’ lobby, has fought vigorously against what it calls “scope creep” — that is, changes that allow clinicians like PAs to do medical procedures independent of physicians.
“Our policy stance is the same on scope of practice expansion regardless of procedure,” noted Kelly Jakubek, the AMA’s media relations manager. The AMA’s website points to legislative victories in 2023, including striking down “legislation allowing physician assistants to practice independently without physician oversight,” in states including Arizona and New York. The AMA did not take a formal position on the California legislation. Its local chapter, the California Medical Association, took a neutral position on the legislation.
In preparation for the new law, one physician assistant at Planned Parenthood Pasadena & San Gabriel Valley began learning how to perform aspiration abortions — a procedure also known as dilation and curettage that uses gentle suction to end a pregnancy — at the end of last year. The PA, who requested anonymity due to concerns about safety, said that with abortion restrictions in place around the country, “I just think it’s really important to be able to provide a comfortable, safe, and very effective way to terminate a pregnancy for patients.”
She is now one of six PAs and midwives at her clinic who can offer aspiration abortions. To reach competency, she participated in 50 procedures and learned how to administer medication that eases pain and anxiety. Such conscious sedation, as it is known, is frequently used for first-trimester abortions. Now she, like any other advanced practice clinician who has obtained skills in performing abortions, can train her peers — another feature of the new law.
The length of time for training and the number of procedures to reach competency varies based on a practitioner’s previous experience.
“It’s encouraging this cross-profession training and collaborations, which is really important when we’re looking at increasing access to essential services,” said Jessica Dieseldorff, senior program manager of abortion services at Planned Parenthood Mar Monte in Santa Cruz.
In December, California committed $18 million to help accelerate training in abortion and reproductive care for practitioners, including PAs, through the Reproductive Health Care Access Initiative.
Dieseldorff, a nurse practitioner who trains other advanced-practice clinicians in abortion care, said that rural communities, in particular, will reap the benefits since many rely solely on physician assistants and other allied clinicians.
Reflecting on her career, she said much has changed since she became a nurse 25 years ago. At that time, she worked only as support staff to doctors providing abortions.
“When I began, medication abortions did not exist in this country,” she said, referring to the practice of using two drugs often prescribed to induce abortions. “It’s been gratifying to be able to progress and become a provider myself, provide non-stigmatizing and compassionate and safe care to patients; and now, at this stage in my career to be training others to do the same.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
California’s efforts to expand access to abortion care are enabling more types of medical practitioners to perform certain abortion procedures — potentially a boon for patients in rural areas especially, but a source of concern for doctors’ groups that have long fought efforts to expand the role of non-physicians.
The latest move is a law that enables trained physician assistants, also known as physician associates, to perform first-trimester abortions without a supervising physician present. The measure, which passed last year and took effect Jan. 1, also lets PAs who have been disciplined or convicted solely for performing an abortion in a state where the practice is restricted apply for a license in California.
Physician assistants are now on par with nurse practitioners and certified nurse midwives trained in abortion care, who in 2022 won the ability to perform abortions without a doctor present.
The need for more abortion care practitioners is being driven by efforts in many states to gut abortion rights following the Supreme Court’s 2022 decision ending constitutional protection for the procedure. Thirty-one states have implemented abortion restrictions that range from cutting federal funding for abortion coverage to outright bans, according to the Guttmacher Institute, a research organization concerned with reproductive health.
With the new law, “there will be fewer barriers, and shorter wait times for this essential service,” said Jeremy Meis, president-elect of the California Academy of Physician Associates. While it is unclear how many of California’s 16,000 PAs will be trained in performing abortions, research shows that PAs are more likely than physicians to practice in rural areas where access to abortion is limited. More than 40% of counties in California lack clinics that provide abortion.
Comparing data from the first six months of 2020 with the same period in 2023, the number of abortions jumped from 77,030 to 92,600 a 20% increase as the state became a refuge for women seeking abortions. California has passed a suite of reproductive health laws to build in protections and increase access, and a dozen other states, including Oregon, Minnesota, and New York, have mounted similar efforts. Seventeen states, including California, now allow PAs to perform first-trimester abortions, according to the American Academy of Physician Associates.
There was little opposition to the new California law, with two physicians’ groups supporting it. But the American Medical Association, the country’s most powerful doctors’ lobby, has fought vigorously against what it calls “scope creep” — that is, changes that allow clinicians like PAs to do medical procedures independent of physicians.
“Our policy stance is the same on scope of practice expansion regardless of procedure,” noted Kelly Jakubek, the AMA’s media relations manager. The AMA’s website points to legislative victories in 2023, including striking down “legislation allowing physician assistants to practice independently without physician oversight,” in states including Arizona and New York. The AMA did not take a formal position on the California legislation. Its local chapter, the California Medical Association, took a neutral position on the legislation.
In preparation for the new law, one physician assistant at Planned Parenthood Pasadena & San Gabriel Valley began learning how to perform aspiration abortions — a procedure also known as dilation and curettage that uses gentle suction to end a pregnancy — at the end of last year. The PA, who requested anonymity due to concerns about safety, said that with abortion restrictions in place around the country, “I just think it’s really important to be able to provide a comfortable, safe, and very effective way to terminate a pregnancy for patients.”
She is now one of six PAs and midwives at her clinic who can offer aspiration abortions. To reach competency, she participated in 50 procedures and learned how to administer medication that eases pain and anxiety. Such conscious sedation, as it is known, is frequently used for first-trimester abortions. Now she, like any other advanced practice clinician who has obtained skills in performing abortions, can train her peers — another feature of the new law.
The length of time for training and the number of procedures to reach competency varies based on a practitioner’s previous experience.
“It’s encouraging this cross-profession training and collaborations, which is really important when we’re looking at increasing access to essential services,” said Jessica Dieseldorff, senior program manager of abortion services at Planned Parenthood Mar Monte in Santa Cruz.
In December, California committed $18 million to help accelerate training in abortion and reproductive care for practitioners, including PAs, through the Reproductive Health Care Access Initiative.
Dieseldorff, a nurse practitioner who trains other advanced-practice clinicians in abortion care, said that rural communities, in particular, will reap the benefits since many rely solely on physician assistants and other allied clinicians.
Reflecting on her career, she said much has changed since she became a nurse 25 years ago. At that time, she worked only as support staff to doctors providing abortions.
“When I began, medication abortions did not exist in this country,” she said, referring to the practice of using two drugs often prescribed to induce abortions. “It’s been gratifying to be able to progress and become a provider myself, provide non-stigmatizing and compassionate and safe care to patients; and now, at this stage in my career to be training others to do the same.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
California’s efforts to expand access to abortion care are enabling more types of medical practitioners to perform certain abortion procedures — potentially a boon for patients in rural areas especially, but a source of concern for doctors’ groups that have long fought efforts to expand the role of non-physicians.
The latest move is a law that enables trained physician assistants, also known as physician associates, to perform first-trimester abortions without a supervising physician present. The measure, which passed last year and took effect Jan. 1, also lets PAs who have been disciplined or convicted solely for performing an abortion in a state where the practice is restricted apply for a license in California.
Physician assistants are now on par with nurse practitioners and certified nurse midwives trained in abortion care, who in 2022 won the ability to perform abortions without a doctor present.
The need for more abortion care practitioners is being driven by efforts in many states to gut abortion rights following the Supreme Court’s 2022 decision ending constitutional protection for the procedure. Thirty-one states have implemented abortion restrictions that range from cutting federal funding for abortion coverage to outright bans, according to the Guttmacher Institute, a research organization concerned with reproductive health.
With the new law, “there will be fewer barriers, and shorter wait times for this essential service,” said Jeremy Meis, president-elect of the California Academy of Physician Associates. While it is unclear how many of California’s 16,000 PAs will be trained in performing abortions, research shows that PAs are more likely than physicians to practice in rural areas where access to abortion is limited. More than 40% of counties in California lack clinics that provide abortion.
Comparing data from the first six months of 2020 with the same period in 2023, the number of abortions jumped from 77,030 to 92,600 a 20% increase as the state became a refuge for women seeking abortions. California has passed a suite of reproductive health laws to build in protections and increase access, and a dozen other states, including Oregon, Minnesota, and New York, have mounted similar efforts. Seventeen states, including California, now allow PAs to perform first-trimester abortions, according to the American Academy of Physician Associates.
There was little opposition to the new California law, with two physicians’ groups supporting it. But the American Medical Association, the country’s most powerful doctors’ lobby, has fought vigorously against what it calls “scope creep” — that is, changes that allow clinicians like PAs to do medical procedures independent of physicians.
“Our policy stance is the same on scope of practice expansion regardless of procedure,” noted Kelly Jakubek, the AMA’s media relations manager. The AMA’s website points to legislative victories in 2023, including striking down “legislation allowing physician assistants to practice independently without physician oversight,” in states including Arizona and New York. The AMA did not take a formal position on the California legislation. Its local chapter, the California Medical Association, took a neutral position on the legislation.
In preparation for the new law, one physician assistant at Planned Parenthood Pasadena & San Gabriel Valley began learning how to perform aspiration abortions — a procedure also known as dilation and curettage that uses gentle suction to end a pregnancy — at the end of last year. The PA, who requested anonymity due to concerns about safety, said that with abortion restrictions in place around the country, “I just think it’s really important to be able to provide a comfortable, safe, and very effective way to terminate a pregnancy for patients.”
She is now one of six PAs and midwives at her clinic who can offer aspiration abortions. To reach competency, she participated in 50 procedures and learned how to administer medication that eases pain and anxiety. Such conscious sedation, as it is known, is frequently used for first-trimester abortions. Now she, like any other advanced practice clinician who has obtained skills in performing abortions, can train her peers — another feature of the new law.
The length of time for training and the number of procedures to reach competency varies based on a practitioner’s previous experience.
“It’s encouraging this cross-profession training and collaborations, which is really important when we’re looking at increasing access to essential services,” said Jessica Dieseldorff, senior program manager of abortion services at Planned Parenthood Mar Monte in Santa Cruz.
In December, California committed $18 million to help accelerate training in abortion and reproductive care for practitioners, including PAs, through the Reproductive Health Care Access Initiative.
Dieseldorff, a nurse practitioner who trains other advanced-practice clinicians in abortion care, said that rural communities, in particular, will reap the benefits since many rely solely on physician assistants and other allied clinicians.
Reflecting on her career, she said much has changed since she became a nurse 25 years ago. At that time, she worked only as support staff to doctors providing abortions.
“When I began, medication abortions did not exist in this country,” she said, referring to the practice of using two drugs often prescribed to induce abortions. “It’s been gratifying to be able to progress and become a provider myself, provide non-stigmatizing and compassionate and safe care to patients; and now, at this stage in my career to be training others to do the same.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
FDA Removes Harmful Chemicals From Food Packaging
Issued on February 28, 2024, “this means the major source of dietary exposure to PFAS from food packaging like fast-food wrappers, microwave popcorn bags, take-out paperboard containers, and pet food bags is being eliminated,” the FDA said in a statement.
In 2020, the FDA had secured commitments from manufacturers to stop selling products containing PFAS used in the food packaging for grease-proofing. “Today’s announcement marks the fulfillment of these voluntary commitments,” according to the agency.
PFAS, a class of thousands of chemicals also called “forever chemicals” are widely used in consumer and industrial products. People may be exposed via contaminated food packaging (although perhaps no longer in the United States) or occupationally. Studies have found that some PFAS disrupt hormones including estrogen and testosterone, whereas others may impair thyroid function.
Endocrine Society Report Sounds the Alarm About PFAS and Others
The FDA’s announcement came just 2 days after the Endocrine Society issued a new alarm about the human health dangers from environmental EDCs including PFAS in a report covering the latest science.
“Endocrine disrupting chemicals” are individual substances or mixtures that can interfere with natural hormonal function, leading to disease or even death. Many are ubiquitous in the modern environment and contribute to a wide range of human diseases.
The new report Endocrine Disrupting Chemicals: Threats to Human Health was issued jointly with the International Pollutants Elimination Network (IPEN), a global advocacy organization. It’s an update to the Endocrine Society’s 2015 report, providing new data on the endocrine-disrupting substances previously covered and adding four EDCs not discussed in that document: Pesticides, plastics, PFAS, and children’s products containing arsenic.
At a briefing held during the United Nations Environment Assembly meeting in Nairobi, Kenya, last week, the new report’s lead author Andrea C. Gore, PhD, of the University of Texas at Austin, noted, “A well-established body of scientific research indicates that endocrine-disrupting chemicals that are part of our daily lives are making us more susceptible to reproductive disorders, cancer, diabetes, obesity, heart disease, and other serious health conditions.”
Added Dr. Gore, who is also a member of the Endocrine Society’s Board of Directors, “These chemicals pose particularly serious risks to pregnant women and children. Now is the time for the UN Environment Assembly and other global policymakers to take action to address this threat to public health.”
While the science has been emerging rapidly, global and national chemical control policies haven’t kept up, the authors said. Of particular concern is that EDCs behave differently from other chemicals in many ways, including that even very low-dose exposures can pose health threats, but policies thus far haven’t dealt with that aspect.
Moreover, “the effects of low doses cannot be predicted by the effects observed at high doses. This means there may be no safe dose for exposure to EDCs,” according to the report.
Exposures can come from household products, including furniture, toys, and food packages, as well as electronics building materials and cosmetics. These chemicals are also in the outdoor environment, via pesticides, air pollution, and industrial waste.
“IPEN and the Endocrine Society call for chemical regulations based on the most modern scientific understanding of how hormones act and how EDCs can perturb these actions. We work to educate policy makers in global, regional, and national government assemblies and help ensure that regulations correlate with current scientific understanding,” they said in the report.
New Data on Four Classes of EDCs
Chapters of the report summarized the latest information about the science of EDCs and their links to endocrine disease and real-world exposure. It included a special section about “EDCs throughout the plastics life cycle” and a summary of the links between EDCs and climate change.
The report reviewed three pesticides, including the world’s most heavily applied herbicide, glycophosphate. Exposures can occur directly from the air, water, dust, and food residues. Recent data linked glycophosphate to adverse reproductive health outcomes.
Two toxic plastic chemicals, phthalates and bisphenols, are present in personal care products, among others. Emerging evidence links them with impaired neurodevelopment, leading to impaired cognitive function, learning, attention, and impulsivity.
Arsenic has long been linked to human health conditions including cancer, but more recent evidence finds it can disrupt multiple endocrine systems and lead to metabolic conditions including diabetes, reproductive dysfunction, and cardiovascular and neurocognitive conditions.
The special section about plastics noted that they are made from fossil fuels and chemicals, including many toxic substances that are known or suspected EDCs. People who live near plastic production facilities or waste dumps may be at greatest risk, but anyone can be exposed using any plastic product. Plastic waste disposal is increasingly problematic and often foisted on lower- and middle-income countries.
‘Additional Education and Awareness-Raising Among Stakeholders Remain Necessary’
Policies aimed at reducing human health risks from EDCs have included the 2022 Plastics Treaty, a resolution adopted by 175 countries at the United Nations Environmental Assembly that “may be a significant step toward global control of plastics and elimination of threats from exposures to EDCs in plastics,” the report said.
The authors added, “While significant progress has been made in recent years connecting scientific advances on EDCs with health-protective policies, additional education and awareness-raising among stakeholders remain necessary to achieve a safer and more sustainable environment that minimizes exposure to these harmful chemicals.”
The document was produced with financial contributions from the Government of Sweden, the Tides Foundation, Passport Foundation, and other donors.
A version of this article appeared on Medscape.com.
Issued on February 28, 2024, “this means the major source of dietary exposure to PFAS from food packaging like fast-food wrappers, microwave popcorn bags, take-out paperboard containers, and pet food bags is being eliminated,” the FDA said in a statement.
In 2020, the FDA had secured commitments from manufacturers to stop selling products containing PFAS used in the food packaging for grease-proofing. “Today’s announcement marks the fulfillment of these voluntary commitments,” according to the agency.
PFAS, a class of thousands of chemicals also called “forever chemicals” are widely used in consumer and industrial products. People may be exposed via contaminated food packaging (although perhaps no longer in the United States) or occupationally. Studies have found that some PFAS disrupt hormones including estrogen and testosterone, whereas others may impair thyroid function.
Endocrine Society Report Sounds the Alarm About PFAS and Others
The FDA’s announcement came just 2 days after the Endocrine Society issued a new alarm about the human health dangers from environmental EDCs including PFAS in a report covering the latest science.
“Endocrine disrupting chemicals” are individual substances or mixtures that can interfere with natural hormonal function, leading to disease or even death. Many are ubiquitous in the modern environment and contribute to a wide range of human diseases.
The new report Endocrine Disrupting Chemicals: Threats to Human Health was issued jointly with the International Pollutants Elimination Network (IPEN), a global advocacy organization. It’s an update to the Endocrine Society’s 2015 report, providing new data on the endocrine-disrupting substances previously covered and adding four EDCs not discussed in that document: Pesticides, plastics, PFAS, and children’s products containing arsenic.
At a briefing held during the United Nations Environment Assembly meeting in Nairobi, Kenya, last week, the new report’s lead author Andrea C. Gore, PhD, of the University of Texas at Austin, noted, “A well-established body of scientific research indicates that endocrine-disrupting chemicals that are part of our daily lives are making us more susceptible to reproductive disorders, cancer, diabetes, obesity, heart disease, and other serious health conditions.”
Added Dr. Gore, who is also a member of the Endocrine Society’s Board of Directors, “These chemicals pose particularly serious risks to pregnant women and children. Now is the time for the UN Environment Assembly and other global policymakers to take action to address this threat to public health.”
While the science has been emerging rapidly, global and national chemical control policies haven’t kept up, the authors said. Of particular concern is that EDCs behave differently from other chemicals in many ways, including that even very low-dose exposures can pose health threats, but policies thus far haven’t dealt with that aspect.
Moreover, “the effects of low doses cannot be predicted by the effects observed at high doses. This means there may be no safe dose for exposure to EDCs,” according to the report.
Exposures can come from household products, including furniture, toys, and food packages, as well as electronics building materials and cosmetics. These chemicals are also in the outdoor environment, via pesticides, air pollution, and industrial waste.
“IPEN and the Endocrine Society call for chemical regulations based on the most modern scientific understanding of how hormones act and how EDCs can perturb these actions. We work to educate policy makers in global, regional, and national government assemblies and help ensure that regulations correlate with current scientific understanding,” they said in the report.
New Data on Four Classes of EDCs
Chapters of the report summarized the latest information about the science of EDCs and their links to endocrine disease and real-world exposure. It included a special section about “EDCs throughout the plastics life cycle” and a summary of the links between EDCs and climate change.
The report reviewed three pesticides, including the world’s most heavily applied herbicide, glycophosphate. Exposures can occur directly from the air, water, dust, and food residues. Recent data linked glycophosphate to adverse reproductive health outcomes.
Two toxic plastic chemicals, phthalates and bisphenols, are present in personal care products, among others. Emerging evidence links them with impaired neurodevelopment, leading to impaired cognitive function, learning, attention, and impulsivity.
Arsenic has long been linked to human health conditions including cancer, but more recent evidence finds it can disrupt multiple endocrine systems and lead to metabolic conditions including diabetes, reproductive dysfunction, and cardiovascular and neurocognitive conditions.
The special section about plastics noted that they are made from fossil fuels and chemicals, including many toxic substances that are known or suspected EDCs. People who live near plastic production facilities or waste dumps may be at greatest risk, but anyone can be exposed using any plastic product. Plastic waste disposal is increasingly problematic and often foisted on lower- and middle-income countries.
‘Additional Education and Awareness-Raising Among Stakeholders Remain Necessary’
Policies aimed at reducing human health risks from EDCs have included the 2022 Plastics Treaty, a resolution adopted by 175 countries at the United Nations Environmental Assembly that “may be a significant step toward global control of plastics and elimination of threats from exposures to EDCs in plastics,” the report said.
The authors added, “While significant progress has been made in recent years connecting scientific advances on EDCs with health-protective policies, additional education and awareness-raising among stakeholders remain necessary to achieve a safer and more sustainable environment that minimizes exposure to these harmful chemicals.”
The document was produced with financial contributions from the Government of Sweden, the Tides Foundation, Passport Foundation, and other donors.
A version of this article appeared on Medscape.com.
Issued on February 28, 2024, “this means the major source of dietary exposure to PFAS from food packaging like fast-food wrappers, microwave popcorn bags, take-out paperboard containers, and pet food bags is being eliminated,” the FDA said in a statement.
In 2020, the FDA had secured commitments from manufacturers to stop selling products containing PFAS used in the food packaging for grease-proofing. “Today’s announcement marks the fulfillment of these voluntary commitments,” according to the agency.
PFAS, a class of thousands of chemicals also called “forever chemicals” are widely used in consumer and industrial products. People may be exposed via contaminated food packaging (although perhaps no longer in the United States) or occupationally. Studies have found that some PFAS disrupt hormones including estrogen and testosterone, whereas others may impair thyroid function.
Endocrine Society Report Sounds the Alarm About PFAS and Others
The FDA’s announcement came just 2 days after the Endocrine Society issued a new alarm about the human health dangers from environmental EDCs including PFAS in a report covering the latest science.
“Endocrine disrupting chemicals” are individual substances or mixtures that can interfere with natural hormonal function, leading to disease or even death. Many are ubiquitous in the modern environment and contribute to a wide range of human diseases.
The new report Endocrine Disrupting Chemicals: Threats to Human Health was issued jointly with the International Pollutants Elimination Network (IPEN), a global advocacy organization. It’s an update to the Endocrine Society’s 2015 report, providing new data on the endocrine-disrupting substances previously covered and adding four EDCs not discussed in that document: Pesticides, plastics, PFAS, and children’s products containing arsenic.
At a briefing held during the United Nations Environment Assembly meeting in Nairobi, Kenya, last week, the new report’s lead author Andrea C. Gore, PhD, of the University of Texas at Austin, noted, “A well-established body of scientific research indicates that endocrine-disrupting chemicals that are part of our daily lives are making us more susceptible to reproductive disorders, cancer, diabetes, obesity, heart disease, and other serious health conditions.”
Added Dr. Gore, who is also a member of the Endocrine Society’s Board of Directors, “These chemicals pose particularly serious risks to pregnant women and children. Now is the time for the UN Environment Assembly and other global policymakers to take action to address this threat to public health.”
While the science has been emerging rapidly, global and national chemical control policies haven’t kept up, the authors said. Of particular concern is that EDCs behave differently from other chemicals in many ways, including that even very low-dose exposures can pose health threats, but policies thus far haven’t dealt with that aspect.
Moreover, “the effects of low doses cannot be predicted by the effects observed at high doses. This means there may be no safe dose for exposure to EDCs,” according to the report.
Exposures can come from household products, including furniture, toys, and food packages, as well as electronics building materials and cosmetics. These chemicals are also in the outdoor environment, via pesticides, air pollution, and industrial waste.
“IPEN and the Endocrine Society call for chemical regulations based on the most modern scientific understanding of how hormones act and how EDCs can perturb these actions. We work to educate policy makers in global, regional, and national government assemblies and help ensure that regulations correlate with current scientific understanding,” they said in the report.
New Data on Four Classes of EDCs
Chapters of the report summarized the latest information about the science of EDCs and their links to endocrine disease and real-world exposure. It included a special section about “EDCs throughout the plastics life cycle” and a summary of the links between EDCs and climate change.
The report reviewed three pesticides, including the world’s most heavily applied herbicide, glycophosphate. Exposures can occur directly from the air, water, dust, and food residues. Recent data linked glycophosphate to adverse reproductive health outcomes.
Two toxic plastic chemicals, phthalates and bisphenols, are present in personal care products, among others. Emerging evidence links them with impaired neurodevelopment, leading to impaired cognitive function, learning, attention, and impulsivity.
Arsenic has long been linked to human health conditions including cancer, but more recent evidence finds it can disrupt multiple endocrine systems and lead to metabolic conditions including diabetes, reproductive dysfunction, and cardiovascular and neurocognitive conditions.
The special section about plastics noted that they are made from fossil fuels and chemicals, including many toxic substances that are known or suspected EDCs. People who live near plastic production facilities or waste dumps may be at greatest risk, but anyone can be exposed using any plastic product. Plastic waste disposal is increasingly problematic and often foisted on lower- and middle-income countries.
‘Additional Education and Awareness-Raising Among Stakeholders Remain Necessary’
Policies aimed at reducing human health risks from EDCs have included the 2022 Plastics Treaty, a resolution adopted by 175 countries at the United Nations Environmental Assembly that “may be a significant step toward global control of plastics and elimination of threats from exposures to EDCs in plastics,” the report said.
The authors added, “While significant progress has been made in recent years connecting scientific advances on EDCs with health-protective policies, additional education and awareness-raising among stakeholders remain necessary to achieve a safer and more sustainable environment that minimizes exposure to these harmful chemicals.”
The document was produced with financial contributions from the Government of Sweden, the Tides Foundation, Passport Foundation, and other donors.
A version of this article appeared on Medscape.com.
Conservative management results in no greater morbidity than other alternatives after placenta accreta
NATIONAL HARBOR, MARYLAND — Rates of maternal morbidity in individuals with placenta accreta were similar with alternative strategies to cesarean hysterectomy regardless of the severity of the condition, based on data from 60 individuals.
Currently, the recommended management strategy for placenta accreta spectrum (PAS) is a cesarean hysterectomy, but data are lacking on alternative strategies, especially for individuals wishing to keep their uterus and potentially preserve fertility, Farah H. Amro, MD, of the University of Texas Health Science Center at Houston McGovern Medical School said in a presentation at the Pregnancy Meeting (abstract 70).
Alternative options are being studied worldwide, including delayed hysterectomy (typically performed at 4-6 weeks postpartum), Dr. Amro said at the meeting, which was sponsored by the Society for Maternal-Fetal Medicine.
At UT Houston, delayed hysterectomy is performed for more aggressive PAS that involves parametrial invasion, and the placenta left in situ until resorption/passage for those wishing to keep their uterus, Dr. Amro said in an interview.
In a cohort study at UT Houston, a level IV academic center, Dr. Amro and colleagues evaluated outcomes in 60 individuals with suspected PAS who were given three management options after extensive counseling. Of these, 29 opted for a cesarean hysterectomy (CH); 16 opted for delayed interval hysterectomy (IH) performed 4-6 weeks after delivery; and 15 individuals with a preference for uterine preservation were assigned to conservative management.
The study occurred between January 2020 and July 2023. The primary outcome was composite maternal morbidity, which was further divided into composite acute morbidity (within 24 hours from cesarean delivery or hysterectomy) and composite delayed morbidity (24 hours or more postoperatively). Secondary outcomes included total estimated blood loss, need for blood transfusion, unplanned hospital readmission, and pathology diagnosis.
Overall maternal morbidity rates were 55%, 56%, and 53% in the CH, IH, and CM groups, respectively, although those who were planned for IH and CM had more severe PAS.
The planned procedure was performed in 90% of the CH patients. Approximately 20% of patients in the IH and CM groups underwent unplanned procedures. No cases of sepsis or maternal death occurred, and uterine infection rates were 0%, 6%, and 13% in the CH, IH, and CM groups, respectively.
Patients in the CM and IH groups were significantly less likely to require blood transfusions than those in the CH group. In addition, composite delayed morbidity (24 hours or more after surgery) was similar among the groups, with rates of 31%, 38%, and 33% for CH, IH, and CM, respectively (P = .94). These results are important, given the concerns regarding leaving a placenta in situ after cesarean delivery, said Dr. Amro.
The findings were limited by several factors including the use of data from a single site, the lack of randomization, patient compliance, and cost effectiveness. However, the results were strengthened by the diverse population and comparison of novel approaches that aren’t frequently utilized In the United States, as well as the large volume of PAS cases treated in a relatively short time frame, Dr. Amro said.
More Options Empower Mothers
Overall, the results support the use of delayed hysterectomy and conservative management as safe alternatives to cesarean hysterectomy, especially in those with severe PAS (opting for IH Instead of CH) and those seeking to preserve the uterus (CM), Dr. Amro said. However, these alternative options can be offered only to patients who can engage in frequent postpartum follow-up and live close to the hospital; with the CM group, resorption/passage of the placenta may take as long as 6 months in some cases, she explained.
The greatest concerns with leaving the placenta in place in PAS patients are the risk of infection or subsequent hemorrhage, Dr. Amro said in an interview. However, the current study showed that the infection rate was not as high as anticipated, and the frequency of unplanned procedures occurred in only 20%, which should alleviate some of these concerns, she said.
“We have completed 28 cases of conservative management since 2015, four have gone on to successful pregnancy with no cases of PAS in the subsequent pregnancies,” Dr. Amro said. Conservative management gives mothers another option, she added. “Moms feel empowered by being given a choice, especially for those that want to keep their uterus for fertility or religious/cultural considerations, and many opt for CM.”
The next step is to take the conservative management strategy to larger groups at other centers to replicate the results in other locations, said Dr. Amro. “Also, we are looking at the utility of other interventions such as uterine artery embolization and performing delayed dilation and curettage to help with passage of the placenta in those opting for CM.”
Study Supports Safety of Conservative Management
“There are patients that may want to preserve their reproductive organs in the face of an accreta (such as for religious, cultural, and personal reasons), and this study helps address some of the safety considerations with conservative approaches,” Corrina M. Oxford-Horrey, MD, a maternal-fetal medicine specialist at Weill Cornell Medicine, New York, said in an interview.
“I was surprised that there was not a lot of infectious morbidity (such as sepsis) in the cohorts; that was helpful to see,” said Dr. Oxford-Horrey, who served as a moderator for the session in which the study was presented.
Based on the study findings, “nontraditional approaches to placenta accreta spectrum management may be reasonable, given similar overall postoperative composite morbidity between the groups,” she said.
As for additional research, replicating the study in a multicenter fashion would add to the generalizability of the findings, Dr. Oxford-Horrey said.
The study received no outside funding. The researchers and Dr. Oxford-Horrey had no financial conflicts to disclose.
NATIONAL HARBOR, MARYLAND — Rates of maternal morbidity in individuals with placenta accreta were similar with alternative strategies to cesarean hysterectomy regardless of the severity of the condition, based on data from 60 individuals.
Currently, the recommended management strategy for placenta accreta spectrum (PAS) is a cesarean hysterectomy, but data are lacking on alternative strategies, especially for individuals wishing to keep their uterus and potentially preserve fertility, Farah H. Amro, MD, of the University of Texas Health Science Center at Houston McGovern Medical School said in a presentation at the Pregnancy Meeting (abstract 70).
Alternative options are being studied worldwide, including delayed hysterectomy (typically performed at 4-6 weeks postpartum), Dr. Amro said at the meeting, which was sponsored by the Society for Maternal-Fetal Medicine.
At UT Houston, delayed hysterectomy is performed for more aggressive PAS that involves parametrial invasion, and the placenta left in situ until resorption/passage for those wishing to keep their uterus, Dr. Amro said in an interview.
In a cohort study at UT Houston, a level IV academic center, Dr. Amro and colleagues evaluated outcomes in 60 individuals with suspected PAS who were given three management options after extensive counseling. Of these, 29 opted for a cesarean hysterectomy (CH); 16 opted for delayed interval hysterectomy (IH) performed 4-6 weeks after delivery; and 15 individuals with a preference for uterine preservation were assigned to conservative management.
The study occurred between January 2020 and July 2023. The primary outcome was composite maternal morbidity, which was further divided into composite acute morbidity (within 24 hours from cesarean delivery or hysterectomy) and composite delayed morbidity (24 hours or more postoperatively). Secondary outcomes included total estimated blood loss, need for blood transfusion, unplanned hospital readmission, and pathology diagnosis.
Overall maternal morbidity rates were 55%, 56%, and 53% in the CH, IH, and CM groups, respectively, although those who were planned for IH and CM had more severe PAS.
The planned procedure was performed in 90% of the CH patients. Approximately 20% of patients in the IH and CM groups underwent unplanned procedures. No cases of sepsis or maternal death occurred, and uterine infection rates were 0%, 6%, and 13% in the CH, IH, and CM groups, respectively.
Patients in the CM and IH groups were significantly less likely to require blood transfusions than those in the CH group. In addition, composite delayed morbidity (24 hours or more after surgery) was similar among the groups, with rates of 31%, 38%, and 33% for CH, IH, and CM, respectively (P = .94). These results are important, given the concerns regarding leaving a placenta in situ after cesarean delivery, said Dr. Amro.
The findings were limited by several factors including the use of data from a single site, the lack of randomization, patient compliance, and cost effectiveness. However, the results were strengthened by the diverse population and comparison of novel approaches that aren’t frequently utilized In the United States, as well as the large volume of PAS cases treated in a relatively short time frame, Dr. Amro said.
More Options Empower Mothers
Overall, the results support the use of delayed hysterectomy and conservative management as safe alternatives to cesarean hysterectomy, especially in those with severe PAS (opting for IH Instead of CH) and those seeking to preserve the uterus (CM), Dr. Amro said. However, these alternative options can be offered only to patients who can engage in frequent postpartum follow-up and live close to the hospital; with the CM group, resorption/passage of the placenta may take as long as 6 months in some cases, she explained.
The greatest concerns with leaving the placenta in place in PAS patients are the risk of infection or subsequent hemorrhage, Dr. Amro said in an interview. However, the current study showed that the infection rate was not as high as anticipated, and the frequency of unplanned procedures occurred in only 20%, which should alleviate some of these concerns, she said.
“We have completed 28 cases of conservative management since 2015, four have gone on to successful pregnancy with no cases of PAS in the subsequent pregnancies,” Dr. Amro said. Conservative management gives mothers another option, she added. “Moms feel empowered by being given a choice, especially for those that want to keep their uterus for fertility or religious/cultural considerations, and many opt for CM.”
The next step is to take the conservative management strategy to larger groups at other centers to replicate the results in other locations, said Dr. Amro. “Also, we are looking at the utility of other interventions such as uterine artery embolization and performing delayed dilation and curettage to help with passage of the placenta in those opting for CM.”
Study Supports Safety of Conservative Management
“There are patients that may want to preserve their reproductive organs in the face of an accreta (such as for religious, cultural, and personal reasons), and this study helps address some of the safety considerations with conservative approaches,” Corrina M. Oxford-Horrey, MD, a maternal-fetal medicine specialist at Weill Cornell Medicine, New York, said in an interview.
“I was surprised that there was not a lot of infectious morbidity (such as sepsis) in the cohorts; that was helpful to see,” said Dr. Oxford-Horrey, who served as a moderator for the session in which the study was presented.
Based on the study findings, “nontraditional approaches to placenta accreta spectrum management may be reasonable, given similar overall postoperative composite morbidity between the groups,” she said.
As for additional research, replicating the study in a multicenter fashion would add to the generalizability of the findings, Dr. Oxford-Horrey said.
The study received no outside funding. The researchers and Dr. Oxford-Horrey had no financial conflicts to disclose.
NATIONAL HARBOR, MARYLAND — Rates of maternal morbidity in individuals with placenta accreta were similar with alternative strategies to cesarean hysterectomy regardless of the severity of the condition, based on data from 60 individuals.
Currently, the recommended management strategy for placenta accreta spectrum (PAS) is a cesarean hysterectomy, but data are lacking on alternative strategies, especially for individuals wishing to keep their uterus and potentially preserve fertility, Farah H. Amro, MD, of the University of Texas Health Science Center at Houston McGovern Medical School said in a presentation at the Pregnancy Meeting (abstract 70).
Alternative options are being studied worldwide, including delayed hysterectomy (typically performed at 4-6 weeks postpartum), Dr. Amro said at the meeting, which was sponsored by the Society for Maternal-Fetal Medicine.
At UT Houston, delayed hysterectomy is performed for more aggressive PAS that involves parametrial invasion, and the placenta left in situ until resorption/passage for those wishing to keep their uterus, Dr. Amro said in an interview.
In a cohort study at UT Houston, a level IV academic center, Dr. Amro and colleagues evaluated outcomes in 60 individuals with suspected PAS who were given three management options after extensive counseling. Of these, 29 opted for a cesarean hysterectomy (CH); 16 opted for delayed interval hysterectomy (IH) performed 4-6 weeks after delivery; and 15 individuals with a preference for uterine preservation were assigned to conservative management.
The study occurred between January 2020 and July 2023. The primary outcome was composite maternal morbidity, which was further divided into composite acute morbidity (within 24 hours from cesarean delivery or hysterectomy) and composite delayed morbidity (24 hours or more postoperatively). Secondary outcomes included total estimated blood loss, need for blood transfusion, unplanned hospital readmission, and pathology diagnosis.
Overall maternal morbidity rates were 55%, 56%, and 53% in the CH, IH, and CM groups, respectively, although those who were planned for IH and CM had more severe PAS.
The planned procedure was performed in 90% of the CH patients. Approximately 20% of patients in the IH and CM groups underwent unplanned procedures. No cases of sepsis or maternal death occurred, and uterine infection rates were 0%, 6%, and 13% in the CH, IH, and CM groups, respectively.
Patients in the CM and IH groups were significantly less likely to require blood transfusions than those in the CH group. In addition, composite delayed morbidity (24 hours or more after surgery) was similar among the groups, with rates of 31%, 38%, and 33% for CH, IH, and CM, respectively (P = .94). These results are important, given the concerns regarding leaving a placenta in situ after cesarean delivery, said Dr. Amro.
The findings were limited by several factors including the use of data from a single site, the lack of randomization, patient compliance, and cost effectiveness. However, the results were strengthened by the diverse population and comparison of novel approaches that aren’t frequently utilized In the United States, as well as the large volume of PAS cases treated in a relatively short time frame, Dr. Amro said.
More Options Empower Mothers
Overall, the results support the use of delayed hysterectomy and conservative management as safe alternatives to cesarean hysterectomy, especially in those with severe PAS (opting for IH Instead of CH) and those seeking to preserve the uterus (CM), Dr. Amro said. However, these alternative options can be offered only to patients who can engage in frequent postpartum follow-up and live close to the hospital; with the CM group, resorption/passage of the placenta may take as long as 6 months in some cases, she explained.
The greatest concerns with leaving the placenta in place in PAS patients are the risk of infection or subsequent hemorrhage, Dr. Amro said in an interview. However, the current study showed that the infection rate was not as high as anticipated, and the frequency of unplanned procedures occurred in only 20%, which should alleviate some of these concerns, she said.
“We have completed 28 cases of conservative management since 2015, four have gone on to successful pregnancy with no cases of PAS in the subsequent pregnancies,” Dr. Amro said. Conservative management gives mothers another option, she added. “Moms feel empowered by being given a choice, especially for those that want to keep their uterus for fertility or religious/cultural considerations, and many opt for CM.”
The next step is to take the conservative management strategy to larger groups at other centers to replicate the results in other locations, said Dr. Amro. “Also, we are looking at the utility of other interventions such as uterine artery embolization and performing delayed dilation and curettage to help with passage of the placenta in those opting for CM.”
Study Supports Safety of Conservative Management
“There are patients that may want to preserve their reproductive organs in the face of an accreta (such as for religious, cultural, and personal reasons), and this study helps address some of the safety considerations with conservative approaches,” Corrina M. Oxford-Horrey, MD, a maternal-fetal medicine specialist at Weill Cornell Medicine, New York, said in an interview.
“I was surprised that there was not a lot of infectious morbidity (such as sepsis) in the cohorts; that was helpful to see,” said Dr. Oxford-Horrey, who served as a moderator for the session in which the study was presented.
Based on the study findings, “nontraditional approaches to placenta accreta spectrum management may be reasonable, given similar overall postoperative composite morbidity between the groups,” she said.
As for additional research, replicating the study in a multicenter fashion would add to the generalizability of the findings, Dr. Oxford-Horrey said.
The study received no outside funding. The researchers and Dr. Oxford-Horrey had no financial conflicts to disclose.
AT THE PREGNANCY MEETING
AHA: Urgent Need To Reduce Maternal Postpartum CVD Risk
Complications during pregnancy may be a wake-up call pointing to a higher risk for cardiovascular (CVD) and other diseases later in life. Therefore, the postpartum and interpregnancy periods are opportune windows for reducing CVD susceptibility and providing preventive care, especially for mothers with a history of adverse pregnancy outcomes (APOs). To that end, the American Heart Association recently released a scientific statement in Circulation outlining pregnancy-related CVD risks and reviewing evidence for preventive lifestyle strategies based on the AHA’s Life’s Essential 8 recommendations.
The Life’s Essential 8 encompass healthy eating, sleeping, and activity patterns; controlling weight, blood pressure, cholesterol, and blood sugar; and avoiding tobacco use.
“The motivation behind this statement was that complications in pregnancy are becoming more common and we now have more understanding that these serve as important risk factors for heart disease later in life,” said Jennifer Lewey, MD, MPH, director of the Penn Women’s Cardiovascular Health Program and an assistant professor of medicine at the University of Pennsylvania Perelman School of Medicine in Philadelphia.

“These risk factors are underrecognized and underappreciated. Clinicians don’t feel comfortable counseling their patients about how to reduce their cardiovascular disease risk,” Dr. Lewey, chair of the AHA writing group, said in an interview.
“So we thought this was the perfect time to highlight what we know and don’t know about how to care for this population,” she said.
APOs predispose mothers to heart disease and other long-term complications, including heart failure, stroke, chronic kidney disease, and vascular dementia. “Pregnancy is a significant stress on the body, and APOs such as preeclampsia can lead to vascular changes in the blood vessels and structural changes to the heart that can persist long term,” Dr. Lewey explained. Reduced maternal physical activity and unshed weight can compound the problem.
Varying by race and ethnicity, the proportion of mothers experiencing pregnancy complications, such as high blood pressure, gestational diabetes, and/or preterm birth is estimated at 10%-20%, the statement authors noted. These complications may serve as a wake-up call to young mothers.
The AHA panel believes that identifying at-risk women at younger ages will enable prevention through lifestyle changes and timely treatment. Little is known, however about what specific care may best reduce long-term CVD risk in women who had pregnancy complications, Dr. Lewey said. While randomized clinical trials have yet to evaluate the effects of postpartum interventions on CVD outcomes, the need for strategies supported by rigorous evidence is clear. “In particular, the fourth trimester, defined as the 12 weeks after delivery, is an optimal time to engage postpartum individuals in care to reduce maternal morbidity and improve care transitions,” the AHA group wrote.
An earlier AHA statement in 2021 recommended frequent cardiac risk factor screening in the first year postpartum at 6 and 12 weeks and again at 6 and 12 months, with appropriate transition from postpartum to longitudinal primary care around the 8- to 12-week mark.
Among the current statement’s findings: High blood pressure is the most prevalent cardiovascular condition during pregnancy, and the last two decades have seen a 25% increase in preeclampsia.
Hypertension during pregnancy carries a two- to fourfold higher risk of chronic hypertension within 2-7 years.
Women with one or more APOs experience heart attack and stroke at younger ages. Commenting on the statement but not involved in it, internist Natalie A. Cameron, MD, a primary and preventive care physician at Northwestern Medicine in Chicago, said, “This statement will be very helpful for physicians from a primary care perspective, especially since in internal medicine we don’t standardly receive education in cardiovascular health in the context of pregnancy and the first year postpartum.”

Dr. Cameron also noted that new research suggests the mother’s cardiovascular health during pregnancy can affect the child’s health through adolescence. “There’s a potential intergenerational effect and there may even be some programming and changes to the offspring in utero related to maternal lifestyle factors.”
While the postpartum period would seem like an opportune time to piggyback postpartum visits with infant wellness checkups, “the fact is that, in the U.S., many mothers are lost to care after delivery,” Dr. Lewey said. “But it’s essential to ensure transition to postpartum care.”
According to Dr. Cameron, physicians should be aware of the risk factor data and educate their pregnant and postpartum patients about reducing risk factors. “As I like to say, ‘If you’re going to take care of others, you need to take care of yourself first.’ ” While this statement may be a good starting point, future trials are needed to improve screening for subclinical CVD in individuals with APOs before symptom onset, the statement authors wrote.
This scientific statement was prepared on behalf of the American Heart Association. Dr. Lewey and several coauthors reported research funding from various agencies within the National Institutes of Health. Dr. Brown reported research funding from a cy-près court settlement with Wyeth. Dr. Cameron had no competing interests relevant to her comments.
Complications during pregnancy may be a wake-up call pointing to a higher risk for cardiovascular (CVD) and other diseases later in life. Therefore, the postpartum and interpregnancy periods are opportune windows for reducing CVD susceptibility and providing preventive care, especially for mothers with a history of adverse pregnancy outcomes (APOs). To that end, the American Heart Association recently released a scientific statement in Circulation outlining pregnancy-related CVD risks and reviewing evidence for preventive lifestyle strategies based on the AHA’s Life’s Essential 8 recommendations.
The Life’s Essential 8 encompass healthy eating, sleeping, and activity patterns; controlling weight, blood pressure, cholesterol, and blood sugar; and avoiding tobacco use.
“The motivation behind this statement was that complications in pregnancy are becoming more common and we now have more understanding that these serve as important risk factors for heart disease later in life,” said Jennifer Lewey, MD, MPH, director of the Penn Women’s Cardiovascular Health Program and an assistant professor of medicine at the University of Pennsylvania Perelman School of Medicine in Philadelphia.
“These risk factors are underrecognized and underappreciated. Clinicians don’t feel comfortable counseling their patients about how to reduce their cardiovascular disease risk,” Dr. Lewey, chair of the AHA writing group, said in an interview.
“So we thought this was the perfect time to highlight what we know and don’t know about how to care for this population,” she said.
APOs predispose mothers to heart disease and other long-term complications, including heart failure, stroke, chronic kidney disease, and vascular dementia. “Pregnancy is a significant stress on the body, and APOs such as preeclampsia can lead to vascular changes in the blood vessels and structural changes to the heart that can persist long term,” Dr. Lewey explained. Reduced maternal physical activity and unshed weight can compound the problem.
Varying by race and ethnicity, the proportion of mothers experiencing pregnancy complications, such as high blood pressure, gestational diabetes, and/or preterm birth is estimated at 10%-20%, the statement authors noted. These complications may serve as a wake-up call to young mothers.
The AHA panel believes that identifying at-risk women at younger ages will enable prevention through lifestyle changes and timely treatment. Little is known, however about what specific care may best reduce long-term CVD risk in women who had pregnancy complications, Dr. Lewey said. While randomized clinical trials have yet to evaluate the effects of postpartum interventions on CVD outcomes, the need for strategies supported by rigorous evidence is clear. “In particular, the fourth trimester, defined as the 12 weeks after delivery, is an optimal time to engage postpartum individuals in care to reduce maternal morbidity and improve care transitions,” the AHA group wrote.
An earlier AHA statement in 2021 recommended frequent cardiac risk factor screening in the first year postpartum at 6 and 12 weeks and again at 6 and 12 months, with appropriate transition from postpartum to longitudinal primary care around the 8- to 12-week mark.
Among the current statement’s findings: High blood pressure is the most prevalent cardiovascular condition during pregnancy, and the last two decades have seen a 25% increase in preeclampsia.
Hypertension during pregnancy carries a two- to fourfold higher risk of chronic hypertension within 2-7 years.
Women with one or more APOs experience heart attack and stroke at younger ages. Commenting on the statement but not involved in it, internist Natalie A. Cameron, MD, a primary and preventive care physician at Northwestern Medicine in Chicago, said, “This statement will be very helpful for physicians from a primary care perspective, especially since in internal medicine we don’t standardly receive education in cardiovascular health in the context of pregnancy and the first year postpartum.”
Dr. Cameron also noted that new research suggests the mother’s cardiovascular health during pregnancy can affect the child’s health through adolescence. “There’s a potential intergenerational effect and there may even be some programming and changes to the offspring in utero related to maternal lifestyle factors.”
While the postpartum period would seem like an opportune time to piggyback postpartum visits with infant wellness checkups, “the fact is that, in the U.S., many mothers are lost to care after delivery,” Dr. Lewey said. “But it’s essential to ensure transition to postpartum care.”
According to Dr. Cameron, physicians should be aware of the risk factor data and educate their pregnant and postpartum patients about reducing risk factors. “As I like to say, ‘If you’re going to take care of others, you need to take care of yourself first.’ ” While this statement may be a good starting point, future trials are needed to improve screening for subclinical CVD in individuals with APOs before symptom onset, the statement authors wrote.
This scientific statement was prepared on behalf of the American Heart Association. Dr. Lewey and several coauthors reported research funding from various agencies within the National Institutes of Health. Dr. Brown reported research funding from a cy-près court settlement with Wyeth. Dr. Cameron had no competing interests relevant to her comments.
Complications during pregnancy may be a wake-up call pointing to a higher risk for cardiovascular (CVD) and other diseases later in life. Therefore, the postpartum and interpregnancy periods are opportune windows for reducing CVD susceptibility and providing preventive care, especially for mothers with a history of adverse pregnancy outcomes (APOs). To that end, the American Heart Association recently released a scientific statement in Circulation outlining pregnancy-related CVD risks and reviewing evidence for preventive lifestyle strategies based on the AHA’s Life’s Essential 8 recommendations.
The Life’s Essential 8 encompass healthy eating, sleeping, and activity patterns; controlling weight, blood pressure, cholesterol, and blood sugar; and avoiding tobacco use.
“The motivation behind this statement was that complications in pregnancy are becoming more common and we now have more understanding that these serve as important risk factors for heart disease later in life,” said Jennifer Lewey, MD, MPH, director of the Penn Women’s Cardiovascular Health Program and an assistant professor of medicine at the University of Pennsylvania Perelman School of Medicine in Philadelphia.
“These risk factors are underrecognized and underappreciated. Clinicians don’t feel comfortable counseling their patients about how to reduce their cardiovascular disease risk,” Dr. Lewey, chair of the AHA writing group, said in an interview.
“So we thought this was the perfect time to highlight what we know and don’t know about how to care for this population,” she said.
APOs predispose mothers to heart disease and other long-term complications, including heart failure, stroke, chronic kidney disease, and vascular dementia. “Pregnancy is a significant stress on the body, and APOs such as preeclampsia can lead to vascular changes in the blood vessels and structural changes to the heart that can persist long term,” Dr. Lewey explained. Reduced maternal physical activity and unshed weight can compound the problem.
Varying by race and ethnicity, the proportion of mothers experiencing pregnancy complications, such as high blood pressure, gestational diabetes, and/or preterm birth is estimated at 10%-20%, the statement authors noted. These complications may serve as a wake-up call to young mothers.
The AHA panel believes that identifying at-risk women at younger ages will enable prevention through lifestyle changes and timely treatment. Little is known, however about what specific care may best reduce long-term CVD risk in women who had pregnancy complications, Dr. Lewey said. While randomized clinical trials have yet to evaluate the effects of postpartum interventions on CVD outcomes, the need for strategies supported by rigorous evidence is clear. “In particular, the fourth trimester, defined as the 12 weeks after delivery, is an optimal time to engage postpartum individuals in care to reduce maternal morbidity and improve care transitions,” the AHA group wrote.
An earlier AHA statement in 2021 recommended frequent cardiac risk factor screening in the first year postpartum at 6 and 12 weeks and again at 6 and 12 months, with appropriate transition from postpartum to longitudinal primary care around the 8- to 12-week mark.
Among the current statement’s findings: High blood pressure is the most prevalent cardiovascular condition during pregnancy, and the last two decades have seen a 25% increase in preeclampsia.
Hypertension during pregnancy carries a two- to fourfold higher risk of chronic hypertension within 2-7 years.
Women with one or more APOs experience heart attack and stroke at younger ages. Commenting on the statement but not involved in it, internist Natalie A. Cameron, MD, a primary and preventive care physician at Northwestern Medicine in Chicago, said, “This statement will be very helpful for physicians from a primary care perspective, especially since in internal medicine we don’t standardly receive education in cardiovascular health in the context of pregnancy and the first year postpartum.”
Dr. Cameron also noted that new research suggests the mother’s cardiovascular health during pregnancy can affect the child’s health through adolescence. “There’s a potential intergenerational effect and there may even be some programming and changes to the offspring in utero related to maternal lifestyle factors.”
While the postpartum period would seem like an opportune time to piggyback postpartum visits with infant wellness checkups, “the fact is that, in the U.S., many mothers are lost to care after delivery,” Dr. Lewey said. “But it’s essential to ensure transition to postpartum care.”
According to Dr. Cameron, physicians should be aware of the risk factor data and educate their pregnant and postpartum patients about reducing risk factors. “As I like to say, ‘If you’re going to take care of others, you need to take care of yourself first.’ ” While this statement may be a good starting point, future trials are needed to improve screening for subclinical CVD in individuals with APOs before symptom onset, the statement authors wrote.
This scientific statement was prepared on behalf of the American Heart Association. Dr. Lewey and several coauthors reported research funding from various agencies within the National Institutes of Health. Dr. Brown reported research funding from a cy-près court settlement with Wyeth. Dr. Cameron had no competing interests relevant to her comments.
FROM CIRCULATION
Obesity’s Effect on Neonatal Outcomes Is Dose Dependent
TOPLINE:
Higher body mass index (BMI) at the start of pregnancy is associated with increased risk for adverse maternal outcomes, including preeclampsia, and neonatal complications, such as respiratory distress syndrome (RDS), in a dose-dependent manner, new research shows.
METHODOLOGY:
- Researchers conducted a retrospective study of 58,497 singleton pregnancies delivered at an urban hospital between 2013 and 2021.
- They focused on pregnancies delivered between 24 and 42 weeks of gestation, for which information about BMI at the first prenatal visit was available.
- 21.1% of mothers had class I , 9.3% had class II obesity, and 6% had class III obesity.
TAKEAWAY:
- Obesity was associated with a dose-dependent increase in cesarean deliveries (27% of deliveries without obesity vs 46% of deliveries with class III obesity).
- Severe preeclampsia occurred in 8% of mothers without obesity and in 19% of mothers with class III obesity.
- Infants born to mothers with class III obesity were more likely than were infants born to mothers without obesity to have RDS, with a relative risk (RR) of 2.66.
- With class II obesity, the RR was 1.77. With class I obesity, the RR was 1.3.
- Obesity also was associated with increased risk for grade III-IV (RR), 4.58 for class III obesity) and (RR, 3.76).
IN PRACTICE:
“Infants born to patients with higher classes of obesity have significant associated morbidity including a 2 to 4 times increased risk of neonatal acidosis, grades III-IV intraventricular hemorrhage, sepsis, and RDS,” the researchers reported.
SOURCE:
Sara I. Jones, MD, with University of Texas Southwestern Medical Center in Dallas, presented the study on February 14 at the 2024 Pregnancy Meeting of the Society for Maternal-Fetal Medicine, in National Harbor, Maryland.
DISCLOSURES:
The researchers had no conflicts of interest to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Higher body mass index (BMI) at the start of pregnancy is associated with increased risk for adverse maternal outcomes, including preeclampsia, and neonatal complications, such as respiratory distress syndrome (RDS), in a dose-dependent manner, new research shows.
METHODOLOGY:
- Researchers conducted a retrospective study of 58,497 singleton pregnancies delivered at an urban hospital between 2013 and 2021.
- They focused on pregnancies delivered between 24 and 42 weeks of gestation, for which information about BMI at the first prenatal visit was available.
- 21.1% of mothers had class I , 9.3% had class II obesity, and 6% had class III obesity.
TAKEAWAY:
- Obesity was associated with a dose-dependent increase in cesarean deliveries (27% of deliveries without obesity vs 46% of deliveries with class III obesity).
- Severe preeclampsia occurred in 8% of mothers without obesity and in 19% of mothers with class III obesity.
- Infants born to mothers with class III obesity were more likely than were infants born to mothers without obesity to have RDS, with a relative risk (RR) of 2.66.
- With class II obesity, the RR was 1.77. With class I obesity, the RR was 1.3.
- Obesity also was associated with increased risk for grade III-IV (RR), 4.58 for class III obesity) and (RR, 3.76).
IN PRACTICE:
“Infants born to patients with higher classes of obesity have significant associated morbidity including a 2 to 4 times increased risk of neonatal acidosis, grades III-IV intraventricular hemorrhage, sepsis, and RDS,” the researchers reported.
SOURCE:
Sara I. Jones, MD, with University of Texas Southwestern Medical Center in Dallas, presented the study on February 14 at the 2024 Pregnancy Meeting of the Society for Maternal-Fetal Medicine, in National Harbor, Maryland.
DISCLOSURES:
The researchers had no conflicts of interest to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Higher body mass index (BMI) at the start of pregnancy is associated with increased risk for adverse maternal outcomes, including preeclampsia, and neonatal complications, such as respiratory distress syndrome (RDS), in a dose-dependent manner, new research shows.
METHODOLOGY:
- Researchers conducted a retrospective study of 58,497 singleton pregnancies delivered at an urban hospital between 2013 and 2021.
- They focused on pregnancies delivered between 24 and 42 weeks of gestation, for which information about BMI at the first prenatal visit was available.
- 21.1% of mothers had class I , 9.3% had class II obesity, and 6% had class III obesity.
TAKEAWAY:
- Obesity was associated with a dose-dependent increase in cesarean deliveries (27% of deliveries without obesity vs 46% of deliveries with class III obesity).
- Severe preeclampsia occurred in 8% of mothers without obesity and in 19% of mothers with class III obesity.
- Infants born to mothers with class III obesity were more likely than were infants born to mothers without obesity to have RDS, with a relative risk (RR) of 2.66.
- With class II obesity, the RR was 1.77. With class I obesity, the RR was 1.3.
- Obesity also was associated with increased risk for grade III-IV (RR), 4.58 for class III obesity) and (RR, 3.76).
IN PRACTICE:
“Infants born to patients with higher classes of obesity have significant associated morbidity including a 2 to 4 times increased risk of neonatal acidosis, grades III-IV intraventricular hemorrhage, sepsis, and RDS,” the researchers reported.
SOURCE:
Sara I. Jones, MD, with University of Texas Southwestern Medical Center in Dallas, presented the study on February 14 at the 2024 Pregnancy Meeting of the Society for Maternal-Fetal Medicine, in National Harbor, Maryland.
DISCLOSURES:
The researchers had no conflicts of interest to disclose.
A version of this article appeared on Medscape.com.