User login
New Research Dissects Transgenerational Obesity and Diabetes
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
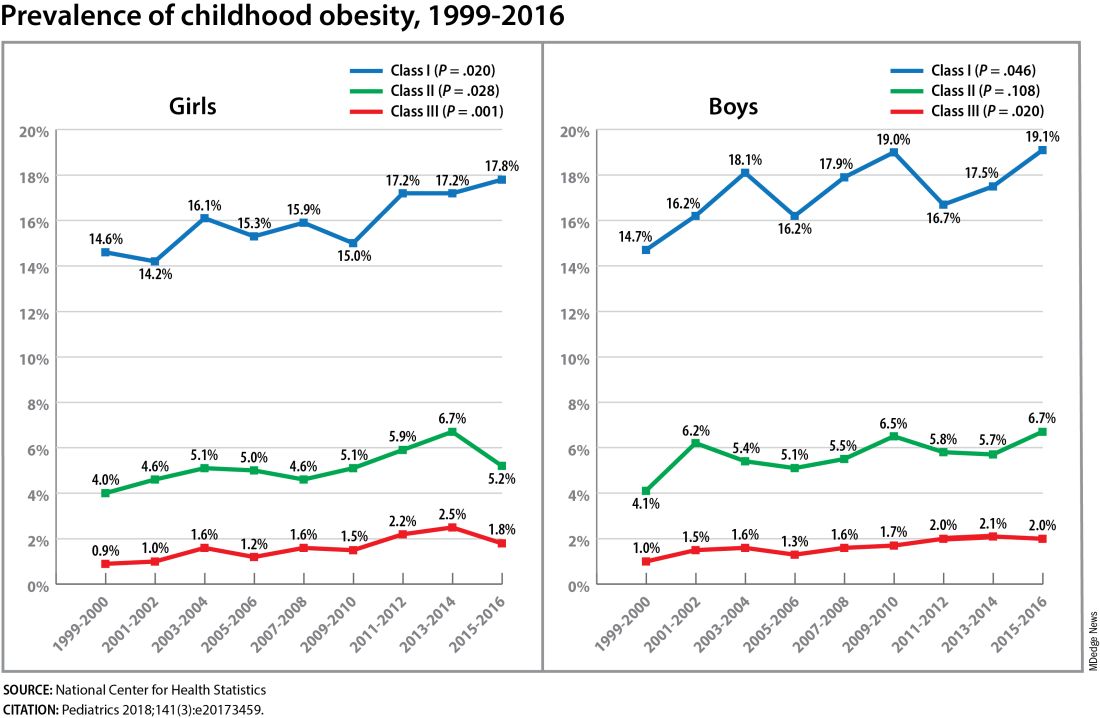
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1).
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1).
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FAIRFAX, VIRGINIA — Nearly 30 years ago, in a 1995 paper, the British physician-epidemiologist David Barker, MD, PhD, wrote about his fetal origins hypothesis — the idea that programs to address fetal undernutrition and low birth weight produced later coronary heart disease (BMJ 1995;311:171-4).
His hypothesis and subsequent research led to the concept of adult diseases of fetal origins, which today extends beyond low birth weight and implicates the in utero environment as a significant determinant of risk for adverse childhood and adult metabolic outcomes and for major chronic diseases, including diabetes and obesity. Studies have shown that the offspring of pregnant mothers with diabetes have a higher risk of developing obesity and diabetes themselves.
“It’s a whole discipline [of research],” E. Albert Reece, MD, PhD, MBA, of the University of Maryland School of Medicine (UMSOM), said in an interview. “But what we’ve never quite understood is the ‘how’ and ‘why’? What are the mechanisms driving the fetal origins of such adverse outcomes in offspring?
At the biennial meeting of the Diabetes in Pregnancy Study Group of North America (DPSG), investigators described studies underway that are digging deeper into the associations between the intrauterine milieu and longer-term offspring health — and that are searching for biological and molecular processes that may be involved.
The studies are like “branches of the Barker hypothesis,” said Dr. Reece, former dean of UMSOM and current director of the UMSOM Center for Advanced Research Training and Innovation, who co-organized the DPSG meeting. “They’re taking the hypothesis and dissecting it by asking, for instance, it is possible that transgenerational obesity may align with the Barker hypothesis? Is it possible that it involves epigenetics regulation? Could we find biomarkers?”
The need for a better understanding of the fetal origins framework — and its subsequent transgenerational impact — is urgent. From 2000 to 2018, the prevalence of childhood obesity increased from 14.7% to 19.2% (a 31% increase) and the prevalence of severe childhood obesity rose from 3.9% to 6.1% (a 56% increase), according to data from the U.S. National Health and Nutrition Examination Survey (Obes Facts. 2022;15[4]:560-9).
Children aged 2-5 years have had an especially sharp increase in obesity (Pediatrics 2018;141[3]:e20173459), Christine Wey Hockett, PhD, of the University of South Dakota School of Medicine, said at the DPSG meeting (Figure 1).
Also notable, she said, is that one-quarter of today’s pediatric diabetes cases are type 2 diabetes, which “is significant as there is a higher prevalence of early complications and comorbidities in youth with type 2 diabetes compared to type 1 diabetes.”
Moreover, recent projections estimate that 57% of today’s children will be obese at 35 years of age (N Engl J Med. 2017;377[22]:2145-53) and that 45% will have diabetes or prediabetes by 2030 (Popul Health Manag. 2017;20[1]:6-12), said Dr. Hockett, assistant professor in the university’s department of pediatrics. An investigator of the Exploring Perinatal Outcomes Among Children (EPOCH) study, which looked at gestational diabetes (GDM) and offspring cardiometabolic risks, she said more chronic disease “at increasingly younger ages [points toward] prebirth influences.”
She noted that there are critical periods postnatally — such as infancy and puberty — that can “impact or further shift the trajectory of chronic disease.” The developmental origins theory posits that life events and biological and environmental processes during the lifespan can modify the effects of intrauterine exposures.
The transgenerational implications “are clear,” she said. “As the number of reproductive-aged individuals with chronic diseases rises, the number of exposed offspring also rises ... It leads to a vicious cycle.”
Deeper Dives Into Associations, Potential Mechanisms
The EPOCH prospective cohort study with which Dr. Hockett was involved gave her a front-seat view of the transgenerational adverse effects of in utero exposure to hyperglycemia. The study recruited ethnically diverse maternal/child dyads from the Kaiser Permanente of Colorado perinatal database from 1992 to 2002 and assessed 418 offspring at two points — a mean age of 10.5 years and 16.5 years — for fasting blood glucose, adiposity, and diet and physical activity. The second visit also involved an oral glucose tolerance test.
The 77 offspring who had been exposed in utero to GDM had a homeostatic model assessment of insulin resistance (HOMA-IR) that was 18% higher, a 19% lower Matsuda index, and a 9% greater HOMA of β-cell function (HOMA-β) than the 341 offspring whose mothers did not have diabetes. Each 5-kg/m2 increase in prepregnancy body mass index predicted increased insulin resistance, but there was no combined effect of both maternal obesity and diabetes in utero.
Exposed offspring had a higher BMI and increased adiposity, but when BMI was controlled for in the analysis of metabolic outcomes, maternal diabetes was still associated with 12% higher HOMA-IR and a 17% lower Matsuda index. “So [the metabolic outcomes] are a direct effect of maternal diabetes,” Dr. Hockett said at the DPSG meeting, noting the fetal overnutrition hypothesis in which maternal glucose, but not maternal insulin, freely passes through the placenta, promoting growth and adiposity in the fetus.
[The EPOCH results on metabolic outcomes and offspring adiposity were published in 2017 and 2019, respectively (Diabet Med. 2017;34:1392-9; Diabetologia. 2019;62:2017-24). In 2020, EPOCH researchers reported sex-specific effects on cardiovascular outcomes, with GDM exposure associated with higher total and LDL cholesterol in girls and higher systolic blood pressure in boys (Pediatr Obes. 2020;15[5]:e12611).]
Now, a new longitudinal cohort study underway in Phoenix, is taking a deeper dive, trying to pinpoint what exactly influences childhood obesity and metabolic risk by following Hispanic and American Indian maternal/child dyads from pregnancy until 18 years postpartum. Researchers are looking not only at associations between maternal risk factors (pregnancy BMI, gestational weight gain, and diabetes in pregnancy) and offspring BMI, adiposity, and growth patterns, but also how various factors during pregnancy — clinical, genetic, lifestyle, biochemical — ”may mediate the associations,” said lead investigator Madhumita Sinha, MD.
“We need a better understanding at the molecular level of the biological processes that lead to obesity in children and that cause metabolic dysfunction,” said Dr. Sinha, who heads the Diabetes Epidemiology and Clinical Research Section of the of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) branch in Phoenix.
The populations being enrolled in the ETCHED study (for Early Tracking of Childhood Health Determinants) are at especially high risk of childhood obesity and metabolic dysfunction. Research conducted decades ago by the NIDDK in Phoenix showed that approximately 50% of Pima Indian children from diabetic pregnancies develop type 2 diabetes by age 25 (N Engl J Med. 1983;308:242-5). Years later, to tease out possible genetic factors, researchers compared siblings born before and after their mother was found to have type 2 diabetes, and found significantly higher rates of diabetes in those born after the mother’s diagnosis, affirming the role of in utero toxicity (Diabetes 2000;49:2208-11).
In the new study, the researchers will look at adipokines and inflammatory biomarkers in the mothers and offspring in addition to traditional anthropometric and glycemic measures. They’ll analyze placental tissue, breast milk, and the gut microbiome longitudinally, and they’ll lean heavily on genomics/epigenomics, proteomics, and metabolomics. “There’s potential,” Dr. Sinha said, “to develop a more accurate predictive and prognostic model of childhood obesity.”
The researchers also will study the role of family, socioeconomics, and environmental factors in influencing child growth patterns and they’ll look at neurodevelopment in infancy and childhood. As of October 2023, almost 80 pregnant women, most with obesity and almost one-third with type 2 diabetes, had enrolled in the study. Over the next several years, the study aims to enroll 750 dyads.
The Timing of In Utero Exposure
Shelley Ehrlich, MD, ScD, MPH, of the University of Cincinnati and Cincinnati Children’s Hospital Medical Center, is aiming, meanwhile, to learn how the timing of in utero exposure to hyperglycemia predicts specific metabolic and cardiovascular morbidities in the adult offspring of diabetic mothers.
“While we know that exposure to maternal diabetes, regardless of type, increases the risk of obesity, insulin resistance, diabetes, renal compromise, and cardiovascular disease in the offspring, there is little known about the level and timing of hyperglycemic exposure during fetal development that triggers these adverse outcomes,” said Dr. Ehrlich. A goal, she said, is to identify gestational profiles that predict phenotypes of offspring at risk for morbidity in later life.
She and other investigators with the TEAM (Transgenerational Effect on Adult Morbidity) study have recruited over 170 offspring of mothers who participated in the Diabetes in Pregnancy Program Project Grant (PPG) at the University of Cincinnati Medical Center from 1978 to 1995 — a landmark study that demonstrated the effect of strict glucose control in reducing major congenital malformations.
The women in the PPG study had frequent glucose monitoring (up to 6-8 times a day) throughout their pregnancies, and now, their recruited offspring, who are up to 43 years of age, are being assessed for obesity, diabetes/metabolic health, cardiovascular disease/cardiac and peripheral vascular structure and function, and other outcomes including those that may be amenable to secondary prevention (J Diabetes Res. Nov 1;2021:6590431).
Preliminary findings from over 170 offspring recruited between 2017 and 2022 suggest that in utero exposure to dysglycemia (as measured by standard deviations of glycohemoglobin) in the third trimester appears to increase the risk of morbid obesity in adulthood, while exposure to dysglycemia in the first trimester increases the risk of impaired glucose tolerance. The risk of B-cell dysfunction, meanwhile, appears to be linked to dysglycemia in the first and third trimesters — particularly the first — Dr. Ehrlich reported.
Cognitive outcomes in offspring have also been assessed and here it appears that dysglycemia in the third trimester is linked to worse scores on the Wechsler Abbreviated Scale of Intelligence (WASI-II), said Katherine Bowers, PhD, MPH, a TEAM study coinvestigator, also of Cincinnati Children’s Hospital Medical Center.
“We’ve already observed [an association between] diabetes in pregnancy and cognition in early childhood and through adolescence, but [the question has been] does this association persist into adulthood?” she said.
Preliminary analyses of 104 offspring show no statistically significant associations between maternal dysglycemia in the first or second trimesters and offspring cognition, but “consistent inverse associations between maternal glycohemoglobin in the third trimester across two [WASI-II] subscales and composite measures of cognition,” Dr. Bowers said.
Their analysis adjusted for a variety of factors, including maternal age, prepregnancy and first trimester BMI, race, family history of diabetes, and diabetes severity/macrovascular complications.
Back In The Laboratory
At the other end of the research spectrum, basic research scientists are also investigating the mechanisms and sequelae of in utero hyperglycemia and other injuries, including congenital malformations, placental adaptive responses and fetal programming. Researchers are asking, for instance, what does placental metabolic reprogramming entail? What role do placental extracellular vesicles play in GDM? Can we alter the in utero environment and thus improve the short and long-term fetal/infant outcomes?
Animal research done at the UMSOM Center for Birth Defects Research, led by Dr. Reece and Peixin Yang, PhD, suggests that “a good portion of in utero injury is due to epigenetics,” Dr. Reece said in the interview. “We’ve shown that under conditions of hyperglycemia, for example, genetic regulation and genetic function can be altered.”
Through in vivo research, they have also shown that antioxidants or membrane stabilizers such as arachidonic acid or myo-inositol, or experimental inhibitors to certain pro-apoptotic intermediates, can individually or collectively result in reduced malformations. “It is highly likely that understanding the biological impact of various altered in utero environments, and then modifying or reversing those environments, will result in short and long-term outcome improvements similar to those shown with congenital malformations,” Dr. Reece said.
FROM DPSG-NA 2023
Glycemic control in pregnancy: The role of CGM for T1D and T2D, and intrapartum management
WASHINGTON — Continuous glucose monitoring (CGM) is widely used during pregnancy for individuals with type 1 diabetes — with pregnancy-specific target metrics now chosen and benefits on perinatal outcomes demonstrated — but more research is needed to elucidate its role in the growing population of pregnant people with type 2 diabetes and gestational diabetes (GDM). And overall, there are still “many more questions unanswered about CGM use in pregnancy than what we have answered,” Celeste Durnwald, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
There’s much to learn about how to best interpret “the detailed and complex data that CGM provides,” and what targets in addition to time in range (TIR) are most important, said Dr. Durnwald, director of the perinatal diabetes program and associate professor of ob.gyn. at the Hospital of the University of Pennsylvania, Philadelphia, in a presentation on CGM.
Among other questions are whether fasting glucose is “as important in the era of CGM,” and whether there should be different glycemic targets for nocturnal versus daytime TIR, she said. Moreover, questions justifiably remain about whether the TIR targets for type 1 diabetes in pregnancy are indeed optimal, she said in a discussion period.
Ongoing research is looking at whether CGM can motivate and guide patients with GDM through diet and lifestyle changes such that “we can see changes in amounts of medication we use,” Dr. Durnwald noted in her presentation. “There’s a whole breadth of research looking at whether CGM can help predict diagnosis of GDM, large for gestational age, or preeclampsia, and what are the targets.”
Maternal hypoglycemia during pregnancy — a time when strict glycemic control is recommended to reduce the risk of congenital malformations and other fetal and neonatal morbidity — remains a concern in type 1 diabetes, even with widespread use of CGM in this population, said Barak Rosenn, MD, during a presentation on glycemic control in type 1 diabetes.
A pilot study of a newly designed pregnancy-specific closed-loop insulin delivery system, published last year (Diabetes Care. 2023;46:1425-31), has offered the first “really encouraging information about the ability to use our most up-to-date technology to help our type 1 patients maintain strict control and at the same time decrease their risk of severe hypoglycemia,” said Dr. Rosenn, a maternal-fetal medicine specialist at the Jersey City Medical Center, Jersey City, New Jersey.
Guidance for tight intrapartum glucose control, meanwhile, has been backed by little evidence, said Michal Fishel Bartal, MD, MS, and some recent studies and reviews have shown little to no effect of such tight control on neonatal hypoglycemia, which is the aim of the guidance.
“We need to reexamine current recommendations,” said Dr. Bartal, assistant professor in the division of maternal-fetal medicine at the University of Texas Health Science Center, Houston, during a presentation on intrapartum care. “There’s very limited evidence-based data for the way we manage people with diabetes [during labor and delivery].”
The Knowns And Unknowns of CGM in Pregnancy
The multicenter, international CONCEPTT trial (Continuous Glucose Monitoring in Pregnant Women With Type 1 Diabetes), published in 2017, was the first trial to demonstrate improvements in perinatal outcomes, and it “brought CGM to the forefront in terms of widespread use,” Dr. Durnwald said.
The trial randomized more than 300 patients with type 1 diabetes who were pregnant or planning pregnancy (both users of insulin pumps and users of multiple insulin injections) to continuous, real-time CGM in addition to finger-stick glucose monitoring, or standard finger-stick glucose tests alone. In addition to small improvements in A1c and 7% more TIR (without an increase in hypoglycemia), pregnant CGM users had reductions in large-for-gestational age (LGA) births (53% vs 69%, P = .0489), neonatal intensive care admissions lasting more than 24 hours, and severe neonatal hypoglycemia.
Numbers needed to treat to prevent adverse outcomes in the CONCEPTT trial were six for LGA, six for NICU admission, and eight for neonatal hypoglycemia.
Data from the CONCEPTT trial featured prominently in the development of consensus recommendations for CGM targets in pregnancy by an international expert panel endorsed by the American Diabetes Association. In its 2019 report, the group recommended a target range of 63-140 mg/dL for type 1 and type 2 diabetes during pregnancy (compared with 70-180 mg/dL outside of pregnancy), and a TIR > 70% for pregnant people with type 1 diabetes. (Targets for time below range and time above range are also defined for type 1.)
More data are needed, the group said, in order to recommend TIR targets for type 2 diabetes in pregnancy or GDM (Diabetes Care. 2019;42:1593-603). “Many argue,” Dr. Durnwald said, “that there could be more stringent targets for those at less risk for [maternal] hypoglycemia, especially our GDM population.”
There’s a question of whether even higher TIR would further improve perinatal outcomes, she said, “or will we reach a threshold where higher TIR doesn’t get us a [further] reduction in LGA or preeclampsia.”
And while TIR is “certainly our buzzword,” lower mean glucose levels have also been associated with a lower risk of LGA and other adverse neonatal outcomes. A 2019 retrospective study from Sweden, for instance, analyzed patterns of CGM data from 186 pregnant women with type 1 diabetes and found significant associations between elevated mean glucose levels (in the second and third trimesters) and both LGA and an adverse neonatal composite outcome (Diabetologia. 2019;62:1143-53).
Elevated TIR was also associated with LGA, but “mean glucose had the strongest association with the rate of LGA,” Dr. Durnwald said.
Similarly, a 2020 subanalysis of the CONCEPTT trial data found that a higher mean glucose at both 24 and 34 weeks of gestation was significantly associated with a greater risk of LGA (Diabetes Care. 2020;43:1178-84), and a smaller 2015 analysis of data from two randomized controlled trials of CGM in pregnant women with type 1 and type 2 diabetes found this association in trimesters 2 and 3 (Diabetes Care. 2015;38;1319-25).
The ADA’s Standards of Care in Diabetes (Diabetes Care. 2024;47:S282-S294) endorse CGM as an adjunctive tool in pregnancy — not as a replacement for all traditional blood glucose monitoring — and advise that the use of CGM-reported mean glucose is superior to the use of estimated A1c, glucose management indicator, and other calculations to estimate A1c. Changes occur in pregnancy, Dr. Durnwald pointed out. “Most experts will identify a [target] mean glucose < 120 mg/dL in those with type 1, but there’s potential to have a mean glucose closer to 100 in certainly our patients with GDM and some of our patients with type 2,” she said. To a lesser extent, researchers have also looked at the effect of CMG-reported glycemic variability on outcomes such as LGA, with at least two studies finding some association, and there has been some research on nocturnal glucose and LGA, Dr. Durnwald said. CGM “gives us the opportunity,” she said, “to think about nocturnal glucose as a possible target” for further optimizing diabetes management during pregnancy.
CGM in Type 2, GDM
CGM in type 2 diabetes in pregnancy was addressed in a recently published systematic review and meta-analysis, which found only three qualifying randomized controlled trials and concluded that CGM use was not associated with improvements in perinatal outcomes, as assessed by LGA and preeclampsia (Am J Obstet Gynecol MFM. 2023;5:100969). “It’s very limited by the small sample size and the fact that most [patients] were using intermittent CGM,” Dr. Durnwald said. “It highlights how important it is to perform larger studies with continuous CGM.”
While the 2024 ADA standards say there are insufficient data to support the use of CGM in all patients with type 2 diabetes or GDM — and that the decision should be individualized “based on treatment regimen, circumstance, preferences, and needs” — real-world access to CGM for type 2, and even a bit for GDM, is improving, she said.
Some insurers require patients to be on insulin, but the trends are such that “we certainly talk about CGM to all our patients with type 2 diabetes and even our patients with GDM,” Dr. Durnwald said in a later interview. “CGMs are being advertised so we definitely have people who ask about them upon diagnosis, and we try to make it work for them.”
Is Preventing Maternal Hypoglycemia Possible?
Advancements in technology and pharmacology aimed at optimizing glycemic control — increased adoption of CGM, the use of insulin pump therapy, and the use of more rapid insulin analogs — appear to have had little to no impact on rates of severe maternal hypoglycemia in type 1 diabetes in pregnancy, said Dr. Rosenn, referring to several published studies.
The CONCEPTT study in type 1 diabetes, for instance, “gave us the best data we have on the use of CGM,” but differences in the percentage of patients with severe hypoglycemia and the total number of severe hypoglycemia episodes were basically the same whether patients used CGM or not, he said.
Closed-loop insulin delivery systems have been found in nonpregnant patients with type 1 diabetes to “be helpful in keeping people in range and also possibly [decreasing nocturnal hypoglycemia],” but the systems are not approved for use in pregnancy. “There’s not enough data on use in pregnancy, but probably more important, the algorithms used in the closed-loop systems are not directed to the targets we consider ideal for pregnancy,” Dr. Rosenn said.
In a pilot study of a closed-loop delivery system customized for pregnancies complicated by type 1 diabetes, 10 pregnant women were recruited at 14-32 weeks and, after a 1- to 2-week run-in period using a regular CGM-augmented pump, they used the closed-loop system targeting a daytime glucose of 80-110 mg/dL and nocturnal glucose of 80-100 mg/dL.
Mean TIR (a target range of 63-140 mg/dL) increased from 65% during the run-in period to 79% on the closed-loop system, and there were significant decreases in both time above range and time in the hypoglycemic ranges of < 63 mg/dL and < 54 mg/dL. Hypoglycemic events per week (defined as < 54 mg/dL for over 15 minutes) decreased from 4 to 0.7 (Diabetes Care. 2023;46:1425-31).
The investigators are continuing their research, and there are currently two randomized controlled trials underway examining use of closed-loop systems designed for pregnancy, said Dr. Rosenn, who was involved in feasibility research leading up to the pilot study. “So I’m hopeful we’ll see some encouraging information in the future.”
Maternal hypoglycemia during pregnancy is more common in type 1 diabetes, but it also affects pregnancies complicated by type 2 diabetes and GDM. In addition to the strict glycemic control imposed to improve maternal and fetal outcomes, pregnancy itself plays a role.
Research several decades ago from the Diabetes in Pregnancy Program Project, a prospective cohort in Cincinnati which Dr. Rosenn co-led, documented impaired counterregulatory physiology in pregnancy. Even in nondiabetic patients, there are declines in secretion of glucagon and growth hormone in response to hypoglycemia, for instance. In patients with type 1 diabetes, the diminishment in counterregulatory response is more severe.
Rethinking Intrapartum Care
Guidance for tight blood glucose control during labor and delivery for insulin-treated individuals — as reflected in the American College of Obstetricians and Gynecologists Practice Bulletin No. 201 on Pregestational Diabetes and in recommendations from the United Kingdom’s National Institute for Health and Care Excellence (NICE) — is based on small case series and overall “poor-quality” evidence that more recent research has failed to back up, Dr. Bartal said.
A systematic review published in 2018, for example, concluded there is a paucity of high-quality data supporting the association of glucose during labor and delivery with neonatal hypoglycemia in pregnancies complicated by diabetes (Diabet Med. 2018;35:173-83). And in a subsequent retrospective cohort study of pregnant women with type 1/type 2/GDM and their neonates, the same investigators reported no difference in the target glucose in labor between those with and without neonatal hypotension, after adjustment for important neonatal factors such as LGA and preterm delivery (Diabet Med. 2020;37:138-46).
Also exemplifying the body of research, Dr. Bartal said, is another single-center retrospective study published in 2020 that evaluated outcomes in the years before and after the institution of a formal intrapartum insulin regimen (a standardized protocol for titration of insulin and glucose infusions) for women with pregestational or gestational diabetes. The protocol was associated with improved maternal glucose control, but an increased frequency of neonatal hypoglycemia (Obstet Gynecol. 2020;136:411-6).
Her own group at the University of Texas in Houston looked retrospectively at 233 insulin-treated pregnancies complicated by type 2 diabetes and found no significant difference in the rate of neonatal hypoglycemia between those placed on a drip and those who were not, Dr. Bartal said. Over 40% of the newborns had hypoglycemia; it occurred irrespective of the route of delivery as well (J Matern Fetal Neonatal Med. 2022;35:7445-51).
Only two published randomized controlled trials have evaluated blood sugar control in labor, she said. The first, published in 2006, compared a continuous insulin drip with a rotation of glucose and non–glucose-containing fluids in insulin-requiring diabetes and found no differences in maternal blood glucose (the primary outcome) and a similar risk of neonatal hypoglycemia (Am J Obstet Gynecol. 2006;195;1095-9).
The second RCT, published in 2019, evaluated tight versus liberalized control (60-100 mg/dL, checking every hour, versus 60-120 mg/dL, checking every 4 hours) in laboring women with GDM. The first neonatal blood glucose level was similar in both groups, while the mean neonatal blood glucose level in the first 24 hours of life was lower with tight control (54 vs 58 mg/dL, P = .49) (Obstet Gynecol. 2019;133:1171-7). Findings from a new RCT conducted at the University of Texas in Houston of usual care versus more permissive glucose control will be presented at the SMFM Pregnancy Meeting in February 2024, she said.
Neonatal hypoglycemia is associated with increased risk of NICU admission, “but it’s also associated with possible long-term developmental deficit,” Dr. Bartal said, with the risk highest in children exposed to severe, recurrent, or clinically undetected hypoglycemia. Research has documented significantly increased risks of low executive function and visual motor function, for instance, in children who experienced neonatal hypoglycemia.
The risk of neonatal hypoglycemia has been linked to a variety of factors outside of the intrapartum period such as diabetes control and weight gain during pregnancy, neonatal birth weight/LGA, neonatal adiposity, gestational age at delivery, maternal body mass index, smoking, and diabetes control prior to pregnancy, Dr. Bartal noted. Also challenging is the reality that neonatal hypoglycemia as a research outcome is not standardized; definitions have varied across studies.
Tight intrapartum control comes with “costs,” from close monitoring of labor to increased resource utilization, and it may affect the labor experience/satisfaction, Dr. Bartal said. “But furthermore,” she said, “there are studies coming out, especially in the anesthesiology journals, that show there may be possible harm,” such as the risk of maternal and neonatal hyponatremia, and maternal hypoglycemia. A 2016 editorial in Anaesthesia (2016;71:750) describes these concerns, she noted.
“I do think we need to rethink our current recommendations,” she said.
Dr. Durnwald reported serving on the Dexcom GDM advisory board and receiving funding from United Health Group and the Helmsley Charitable Trust. Dr. Bartal and Dr. Rosenn reported no conflicts of interest.
WASHINGTON — Continuous glucose monitoring (CGM) is widely used during pregnancy for individuals with type 1 diabetes — with pregnancy-specific target metrics now chosen and benefits on perinatal outcomes demonstrated — but more research is needed to elucidate its role in the growing population of pregnant people with type 2 diabetes and gestational diabetes (GDM). And overall, there are still “many more questions unanswered about CGM use in pregnancy than what we have answered,” Celeste Durnwald, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
There’s much to learn about how to best interpret “the detailed and complex data that CGM provides,” and what targets in addition to time in range (TIR) are most important, said Dr. Durnwald, director of the perinatal diabetes program and associate professor of ob.gyn. at the Hospital of the University of Pennsylvania, Philadelphia, in a presentation on CGM.
Among other questions are whether fasting glucose is “as important in the era of CGM,” and whether there should be different glycemic targets for nocturnal versus daytime TIR, she said. Moreover, questions justifiably remain about whether the TIR targets for type 1 diabetes in pregnancy are indeed optimal, she said in a discussion period.
Ongoing research is looking at whether CGM can motivate and guide patients with GDM through diet and lifestyle changes such that “we can see changes in amounts of medication we use,” Dr. Durnwald noted in her presentation. “There’s a whole breadth of research looking at whether CGM can help predict diagnosis of GDM, large for gestational age, or preeclampsia, and what are the targets.”
Maternal hypoglycemia during pregnancy — a time when strict glycemic control is recommended to reduce the risk of congenital malformations and other fetal and neonatal morbidity — remains a concern in type 1 diabetes, even with widespread use of CGM in this population, said Barak Rosenn, MD, during a presentation on glycemic control in type 1 diabetes.
A pilot study of a newly designed pregnancy-specific closed-loop insulin delivery system, published last year (Diabetes Care. 2023;46:1425-31), has offered the first “really encouraging information about the ability to use our most up-to-date technology to help our type 1 patients maintain strict control and at the same time decrease their risk of severe hypoglycemia,” said Dr. Rosenn, a maternal-fetal medicine specialist at the Jersey City Medical Center, Jersey City, New Jersey.
Guidance for tight intrapartum glucose control, meanwhile, has been backed by little evidence, said Michal Fishel Bartal, MD, MS, and some recent studies and reviews have shown little to no effect of such tight control on neonatal hypoglycemia, which is the aim of the guidance.
“We need to reexamine current recommendations,” said Dr. Bartal, assistant professor in the division of maternal-fetal medicine at the University of Texas Health Science Center, Houston, during a presentation on intrapartum care. “There’s very limited evidence-based data for the way we manage people with diabetes [during labor and delivery].”
The Knowns And Unknowns of CGM in Pregnancy
The multicenter, international CONCEPTT trial (Continuous Glucose Monitoring in Pregnant Women With Type 1 Diabetes), published in 2017, was the first trial to demonstrate improvements in perinatal outcomes, and it “brought CGM to the forefront in terms of widespread use,” Dr. Durnwald said.
The trial randomized more than 300 patients with type 1 diabetes who were pregnant or planning pregnancy (both users of insulin pumps and users of multiple insulin injections) to continuous, real-time CGM in addition to finger-stick glucose monitoring, or standard finger-stick glucose tests alone. In addition to small improvements in A1c and 7% more TIR (without an increase in hypoglycemia), pregnant CGM users had reductions in large-for-gestational age (LGA) births (53% vs 69%, P = .0489), neonatal intensive care admissions lasting more than 24 hours, and severe neonatal hypoglycemia.
Numbers needed to treat to prevent adverse outcomes in the CONCEPTT trial were six for LGA, six for NICU admission, and eight for neonatal hypoglycemia.
Data from the CONCEPTT trial featured prominently in the development of consensus recommendations for CGM targets in pregnancy by an international expert panel endorsed by the American Diabetes Association. In its 2019 report, the group recommended a target range of 63-140 mg/dL for type 1 and type 2 diabetes during pregnancy (compared with 70-180 mg/dL outside of pregnancy), and a TIR > 70% for pregnant people with type 1 diabetes. (Targets for time below range and time above range are also defined for type 1.)
More data are needed, the group said, in order to recommend TIR targets for type 2 diabetes in pregnancy or GDM (Diabetes Care. 2019;42:1593-603). “Many argue,” Dr. Durnwald said, “that there could be more stringent targets for those at less risk for [maternal] hypoglycemia, especially our GDM population.”
There’s a question of whether even higher TIR would further improve perinatal outcomes, she said, “or will we reach a threshold where higher TIR doesn’t get us a [further] reduction in LGA or preeclampsia.”
And while TIR is “certainly our buzzword,” lower mean glucose levels have also been associated with a lower risk of LGA and other adverse neonatal outcomes. A 2019 retrospective study from Sweden, for instance, analyzed patterns of CGM data from 186 pregnant women with type 1 diabetes and found significant associations between elevated mean glucose levels (in the second and third trimesters) and both LGA and an adverse neonatal composite outcome (Diabetologia. 2019;62:1143-53).
Elevated TIR was also associated with LGA, but “mean glucose had the strongest association with the rate of LGA,” Dr. Durnwald said.
Similarly, a 2020 subanalysis of the CONCEPTT trial data found that a higher mean glucose at both 24 and 34 weeks of gestation was significantly associated with a greater risk of LGA (Diabetes Care. 2020;43:1178-84), and a smaller 2015 analysis of data from two randomized controlled trials of CGM in pregnant women with type 1 and type 2 diabetes found this association in trimesters 2 and 3 (Diabetes Care. 2015;38;1319-25).
The ADA’s Standards of Care in Diabetes (Diabetes Care. 2024;47:S282-S294) endorse CGM as an adjunctive tool in pregnancy — not as a replacement for all traditional blood glucose monitoring — and advise that the use of CGM-reported mean glucose is superior to the use of estimated A1c, glucose management indicator, and other calculations to estimate A1c. Changes occur in pregnancy, Dr. Durnwald pointed out. “Most experts will identify a [target] mean glucose < 120 mg/dL in those with type 1, but there’s potential to have a mean glucose closer to 100 in certainly our patients with GDM and some of our patients with type 2,” she said. To a lesser extent, researchers have also looked at the effect of CMG-reported glycemic variability on outcomes such as LGA, with at least two studies finding some association, and there has been some research on nocturnal glucose and LGA, Dr. Durnwald said. CGM “gives us the opportunity,” she said, “to think about nocturnal glucose as a possible target” for further optimizing diabetes management during pregnancy.
CGM in Type 2, GDM
CGM in type 2 diabetes in pregnancy was addressed in a recently published systematic review and meta-analysis, which found only three qualifying randomized controlled trials and concluded that CGM use was not associated with improvements in perinatal outcomes, as assessed by LGA and preeclampsia (Am J Obstet Gynecol MFM. 2023;5:100969). “It’s very limited by the small sample size and the fact that most [patients] were using intermittent CGM,” Dr. Durnwald said. “It highlights how important it is to perform larger studies with continuous CGM.”
While the 2024 ADA standards say there are insufficient data to support the use of CGM in all patients with type 2 diabetes or GDM — and that the decision should be individualized “based on treatment regimen, circumstance, preferences, and needs” — real-world access to CGM for type 2, and even a bit for GDM, is improving, she said.
Some insurers require patients to be on insulin, but the trends are such that “we certainly talk about CGM to all our patients with type 2 diabetes and even our patients with GDM,” Dr. Durnwald said in a later interview. “CGMs are being advertised so we definitely have people who ask about them upon diagnosis, and we try to make it work for them.”
Is Preventing Maternal Hypoglycemia Possible?
Advancements in technology and pharmacology aimed at optimizing glycemic control — increased adoption of CGM, the use of insulin pump therapy, and the use of more rapid insulin analogs — appear to have had little to no impact on rates of severe maternal hypoglycemia in type 1 diabetes in pregnancy, said Dr. Rosenn, referring to several published studies.
The CONCEPTT study in type 1 diabetes, for instance, “gave us the best data we have on the use of CGM,” but differences in the percentage of patients with severe hypoglycemia and the total number of severe hypoglycemia episodes were basically the same whether patients used CGM or not, he said.
Closed-loop insulin delivery systems have been found in nonpregnant patients with type 1 diabetes to “be helpful in keeping people in range and also possibly [decreasing nocturnal hypoglycemia],” but the systems are not approved for use in pregnancy. “There’s not enough data on use in pregnancy, but probably more important, the algorithms used in the closed-loop systems are not directed to the targets we consider ideal for pregnancy,” Dr. Rosenn said.
In a pilot study of a closed-loop delivery system customized for pregnancies complicated by type 1 diabetes, 10 pregnant women were recruited at 14-32 weeks and, after a 1- to 2-week run-in period using a regular CGM-augmented pump, they used the closed-loop system targeting a daytime glucose of 80-110 mg/dL and nocturnal glucose of 80-100 mg/dL.
Mean TIR (a target range of 63-140 mg/dL) increased from 65% during the run-in period to 79% on the closed-loop system, and there were significant decreases in both time above range and time in the hypoglycemic ranges of < 63 mg/dL and < 54 mg/dL. Hypoglycemic events per week (defined as < 54 mg/dL for over 15 minutes) decreased from 4 to 0.7 (Diabetes Care. 2023;46:1425-31).
The investigators are continuing their research, and there are currently two randomized controlled trials underway examining use of closed-loop systems designed for pregnancy, said Dr. Rosenn, who was involved in feasibility research leading up to the pilot study. “So I’m hopeful we’ll see some encouraging information in the future.”
Maternal hypoglycemia during pregnancy is more common in type 1 diabetes, but it also affects pregnancies complicated by type 2 diabetes and GDM. In addition to the strict glycemic control imposed to improve maternal and fetal outcomes, pregnancy itself plays a role.
Research several decades ago from the Diabetes in Pregnancy Program Project, a prospective cohort in Cincinnati which Dr. Rosenn co-led, documented impaired counterregulatory physiology in pregnancy. Even in nondiabetic patients, there are declines in secretion of glucagon and growth hormone in response to hypoglycemia, for instance. In patients with type 1 diabetes, the diminishment in counterregulatory response is more severe.
Rethinking Intrapartum Care
Guidance for tight blood glucose control during labor and delivery for insulin-treated individuals — as reflected in the American College of Obstetricians and Gynecologists Practice Bulletin No. 201 on Pregestational Diabetes and in recommendations from the United Kingdom’s National Institute for Health and Care Excellence (NICE) — is based on small case series and overall “poor-quality” evidence that more recent research has failed to back up, Dr. Bartal said.
A systematic review published in 2018, for example, concluded there is a paucity of high-quality data supporting the association of glucose during labor and delivery with neonatal hypoglycemia in pregnancies complicated by diabetes (Diabet Med. 2018;35:173-83). And in a subsequent retrospective cohort study of pregnant women with type 1/type 2/GDM and their neonates, the same investigators reported no difference in the target glucose in labor between those with and without neonatal hypotension, after adjustment for important neonatal factors such as LGA and preterm delivery (Diabet Med. 2020;37:138-46).
Also exemplifying the body of research, Dr. Bartal said, is another single-center retrospective study published in 2020 that evaluated outcomes in the years before and after the institution of a formal intrapartum insulin regimen (a standardized protocol for titration of insulin and glucose infusions) for women with pregestational or gestational diabetes. The protocol was associated with improved maternal glucose control, but an increased frequency of neonatal hypoglycemia (Obstet Gynecol. 2020;136:411-6).
Her own group at the University of Texas in Houston looked retrospectively at 233 insulin-treated pregnancies complicated by type 2 diabetes and found no significant difference in the rate of neonatal hypoglycemia between those placed on a drip and those who were not, Dr. Bartal said. Over 40% of the newborns had hypoglycemia; it occurred irrespective of the route of delivery as well (J Matern Fetal Neonatal Med. 2022;35:7445-51).
Only two published randomized controlled trials have evaluated blood sugar control in labor, she said. The first, published in 2006, compared a continuous insulin drip with a rotation of glucose and non–glucose-containing fluids in insulin-requiring diabetes and found no differences in maternal blood glucose (the primary outcome) and a similar risk of neonatal hypoglycemia (Am J Obstet Gynecol. 2006;195;1095-9).
The second RCT, published in 2019, evaluated tight versus liberalized control (60-100 mg/dL, checking every hour, versus 60-120 mg/dL, checking every 4 hours) in laboring women with GDM. The first neonatal blood glucose level was similar in both groups, while the mean neonatal blood glucose level in the first 24 hours of life was lower with tight control (54 vs 58 mg/dL, P = .49) (Obstet Gynecol. 2019;133:1171-7). Findings from a new RCT conducted at the University of Texas in Houston of usual care versus more permissive glucose control will be presented at the SMFM Pregnancy Meeting in February 2024, she said.
Neonatal hypoglycemia is associated with increased risk of NICU admission, “but it’s also associated with possible long-term developmental deficit,” Dr. Bartal said, with the risk highest in children exposed to severe, recurrent, or clinically undetected hypoglycemia. Research has documented significantly increased risks of low executive function and visual motor function, for instance, in children who experienced neonatal hypoglycemia.
The risk of neonatal hypoglycemia has been linked to a variety of factors outside of the intrapartum period such as diabetes control and weight gain during pregnancy, neonatal birth weight/LGA, neonatal adiposity, gestational age at delivery, maternal body mass index, smoking, and diabetes control prior to pregnancy, Dr. Bartal noted. Also challenging is the reality that neonatal hypoglycemia as a research outcome is not standardized; definitions have varied across studies.
Tight intrapartum control comes with “costs,” from close monitoring of labor to increased resource utilization, and it may affect the labor experience/satisfaction, Dr. Bartal said. “But furthermore,” she said, “there are studies coming out, especially in the anesthesiology journals, that show there may be possible harm,” such as the risk of maternal and neonatal hyponatremia, and maternal hypoglycemia. A 2016 editorial in Anaesthesia (2016;71:750) describes these concerns, she noted.
“I do think we need to rethink our current recommendations,” she said.
Dr. Durnwald reported serving on the Dexcom GDM advisory board and receiving funding from United Health Group and the Helmsley Charitable Trust. Dr. Bartal and Dr. Rosenn reported no conflicts of interest.
WASHINGTON — Continuous glucose monitoring (CGM) is widely used during pregnancy for individuals with type 1 diabetes — with pregnancy-specific target metrics now chosen and benefits on perinatal outcomes demonstrated — but more research is needed to elucidate its role in the growing population of pregnant people with type 2 diabetes and gestational diabetes (GDM). And overall, there are still “many more questions unanswered about CGM use in pregnancy than what we have answered,” Celeste Durnwald, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
There’s much to learn about how to best interpret “the detailed and complex data that CGM provides,” and what targets in addition to time in range (TIR) are most important, said Dr. Durnwald, director of the perinatal diabetes program and associate professor of ob.gyn. at the Hospital of the University of Pennsylvania, Philadelphia, in a presentation on CGM.
Among other questions are whether fasting glucose is “as important in the era of CGM,” and whether there should be different glycemic targets for nocturnal versus daytime TIR, she said. Moreover, questions justifiably remain about whether the TIR targets for type 1 diabetes in pregnancy are indeed optimal, she said in a discussion period.
Ongoing research is looking at whether CGM can motivate and guide patients with GDM through diet and lifestyle changes such that “we can see changes in amounts of medication we use,” Dr. Durnwald noted in her presentation. “There’s a whole breadth of research looking at whether CGM can help predict diagnosis of GDM, large for gestational age, or preeclampsia, and what are the targets.”
Maternal hypoglycemia during pregnancy — a time when strict glycemic control is recommended to reduce the risk of congenital malformations and other fetal and neonatal morbidity — remains a concern in type 1 diabetes, even with widespread use of CGM in this population, said Barak Rosenn, MD, during a presentation on glycemic control in type 1 diabetes.
A pilot study of a newly designed pregnancy-specific closed-loop insulin delivery system, published last year (Diabetes Care. 2023;46:1425-31), has offered the first “really encouraging information about the ability to use our most up-to-date technology to help our type 1 patients maintain strict control and at the same time decrease their risk of severe hypoglycemia,” said Dr. Rosenn, a maternal-fetal medicine specialist at the Jersey City Medical Center, Jersey City, New Jersey.
Guidance for tight intrapartum glucose control, meanwhile, has been backed by little evidence, said Michal Fishel Bartal, MD, MS, and some recent studies and reviews have shown little to no effect of such tight control on neonatal hypoglycemia, which is the aim of the guidance.
“We need to reexamine current recommendations,” said Dr. Bartal, assistant professor in the division of maternal-fetal medicine at the University of Texas Health Science Center, Houston, during a presentation on intrapartum care. “There’s very limited evidence-based data for the way we manage people with diabetes [during labor and delivery].”
The Knowns And Unknowns of CGM in Pregnancy
The multicenter, international CONCEPTT trial (Continuous Glucose Monitoring in Pregnant Women With Type 1 Diabetes), published in 2017, was the first trial to demonstrate improvements in perinatal outcomes, and it “brought CGM to the forefront in terms of widespread use,” Dr. Durnwald said.
The trial randomized more than 300 patients with type 1 diabetes who were pregnant or planning pregnancy (both users of insulin pumps and users of multiple insulin injections) to continuous, real-time CGM in addition to finger-stick glucose monitoring, or standard finger-stick glucose tests alone. In addition to small improvements in A1c and 7% more TIR (without an increase in hypoglycemia), pregnant CGM users had reductions in large-for-gestational age (LGA) births (53% vs 69%, P = .0489), neonatal intensive care admissions lasting more than 24 hours, and severe neonatal hypoglycemia.
Numbers needed to treat to prevent adverse outcomes in the CONCEPTT trial were six for LGA, six for NICU admission, and eight for neonatal hypoglycemia.
Data from the CONCEPTT trial featured prominently in the development of consensus recommendations for CGM targets in pregnancy by an international expert panel endorsed by the American Diabetes Association. In its 2019 report, the group recommended a target range of 63-140 mg/dL for type 1 and type 2 diabetes during pregnancy (compared with 70-180 mg/dL outside of pregnancy), and a TIR > 70% for pregnant people with type 1 diabetes. (Targets for time below range and time above range are also defined for type 1.)
More data are needed, the group said, in order to recommend TIR targets for type 2 diabetes in pregnancy or GDM (Diabetes Care. 2019;42:1593-603). “Many argue,” Dr. Durnwald said, “that there could be more stringent targets for those at less risk for [maternal] hypoglycemia, especially our GDM population.”
There’s a question of whether even higher TIR would further improve perinatal outcomes, she said, “or will we reach a threshold where higher TIR doesn’t get us a [further] reduction in LGA or preeclampsia.”
And while TIR is “certainly our buzzword,” lower mean glucose levels have also been associated with a lower risk of LGA and other adverse neonatal outcomes. A 2019 retrospective study from Sweden, for instance, analyzed patterns of CGM data from 186 pregnant women with type 1 diabetes and found significant associations between elevated mean glucose levels (in the second and third trimesters) and both LGA and an adverse neonatal composite outcome (Diabetologia. 2019;62:1143-53).
Elevated TIR was also associated with LGA, but “mean glucose had the strongest association with the rate of LGA,” Dr. Durnwald said.
Similarly, a 2020 subanalysis of the CONCEPTT trial data found that a higher mean glucose at both 24 and 34 weeks of gestation was significantly associated with a greater risk of LGA (Diabetes Care. 2020;43:1178-84), and a smaller 2015 analysis of data from two randomized controlled trials of CGM in pregnant women with type 1 and type 2 diabetes found this association in trimesters 2 and 3 (Diabetes Care. 2015;38;1319-25).
The ADA’s Standards of Care in Diabetes (Diabetes Care. 2024;47:S282-S294) endorse CGM as an adjunctive tool in pregnancy — not as a replacement for all traditional blood glucose monitoring — and advise that the use of CGM-reported mean glucose is superior to the use of estimated A1c, glucose management indicator, and other calculations to estimate A1c. Changes occur in pregnancy, Dr. Durnwald pointed out. “Most experts will identify a [target] mean glucose < 120 mg/dL in those with type 1, but there’s potential to have a mean glucose closer to 100 in certainly our patients with GDM and some of our patients with type 2,” she said. To a lesser extent, researchers have also looked at the effect of CMG-reported glycemic variability on outcomes such as LGA, with at least two studies finding some association, and there has been some research on nocturnal glucose and LGA, Dr. Durnwald said. CGM “gives us the opportunity,” she said, “to think about nocturnal glucose as a possible target” for further optimizing diabetes management during pregnancy.
CGM in Type 2, GDM
CGM in type 2 diabetes in pregnancy was addressed in a recently published systematic review and meta-analysis, which found only three qualifying randomized controlled trials and concluded that CGM use was not associated with improvements in perinatal outcomes, as assessed by LGA and preeclampsia (Am J Obstet Gynecol MFM. 2023;5:100969). “It’s very limited by the small sample size and the fact that most [patients] were using intermittent CGM,” Dr. Durnwald said. “It highlights how important it is to perform larger studies with continuous CGM.”
While the 2024 ADA standards say there are insufficient data to support the use of CGM in all patients with type 2 diabetes or GDM — and that the decision should be individualized “based on treatment regimen, circumstance, preferences, and needs” — real-world access to CGM for type 2, and even a bit for GDM, is improving, she said.
Some insurers require patients to be on insulin, but the trends are such that “we certainly talk about CGM to all our patients with type 2 diabetes and even our patients with GDM,” Dr. Durnwald said in a later interview. “CGMs are being advertised so we definitely have people who ask about them upon diagnosis, and we try to make it work for them.”
Is Preventing Maternal Hypoglycemia Possible?
Advancements in technology and pharmacology aimed at optimizing glycemic control — increased adoption of CGM, the use of insulin pump therapy, and the use of more rapid insulin analogs — appear to have had little to no impact on rates of severe maternal hypoglycemia in type 1 diabetes in pregnancy, said Dr. Rosenn, referring to several published studies.
The CONCEPTT study in type 1 diabetes, for instance, “gave us the best data we have on the use of CGM,” but differences in the percentage of patients with severe hypoglycemia and the total number of severe hypoglycemia episodes were basically the same whether patients used CGM or not, he said.
Closed-loop insulin delivery systems have been found in nonpregnant patients with type 1 diabetes to “be helpful in keeping people in range and also possibly [decreasing nocturnal hypoglycemia],” but the systems are not approved for use in pregnancy. “There’s not enough data on use in pregnancy, but probably more important, the algorithms used in the closed-loop systems are not directed to the targets we consider ideal for pregnancy,” Dr. Rosenn said.
In a pilot study of a closed-loop delivery system customized for pregnancies complicated by type 1 diabetes, 10 pregnant women were recruited at 14-32 weeks and, after a 1- to 2-week run-in period using a regular CGM-augmented pump, they used the closed-loop system targeting a daytime glucose of 80-110 mg/dL and nocturnal glucose of 80-100 mg/dL.
Mean TIR (a target range of 63-140 mg/dL) increased from 65% during the run-in period to 79% on the closed-loop system, and there were significant decreases in both time above range and time in the hypoglycemic ranges of < 63 mg/dL and < 54 mg/dL. Hypoglycemic events per week (defined as < 54 mg/dL for over 15 minutes) decreased from 4 to 0.7 (Diabetes Care. 2023;46:1425-31).
The investigators are continuing their research, and there are currently two randomized controlled trials underway examining use of closed-loop systems designed for pregnancy, said Dr. Rosenn, who was involved in feasibility research leading up to the pilot study. “So I’m hopeful we’ll see some encouraging information in the future.”
Maternal hypoglycemia during pregnancy is more common in type 1 diabetes, but it also affects pregnancies complicated by type 2 diabetes and GDM. In addition to the strict glycemic control imposed to improve maternal and fetal outcomes, pregnancy itself plays a role.
Research several decades ago from the Diabetes in Pregnancy Program Project, a prospective cohort in Cincinnati which Dr. Rosenn co-led, documented impaired counterregulatory physiology in pregnancy. Even in nondiabetic patients, there are declines in secretion of glucagon and growth hormone in response to hypoglycemia, for instance. In patients with type 1 diabetes, the diminishment in counterregulatory response is more severe.
Rethinking Intrapartum Care
Guidance for tight blood glucose control during labor and delivery for insulin-treated individuals — as reflected in the American College of Obstetricians and Gynecologists Practice Bulletin No. 201 on Pregestational Diabetes and in recommendations from the United Kingdom’s National Institute for Health and Care Excellence (NICE) — is based on small case series and overall “poor-quality” evidence that more recent research has failed to back up, Dr. Bartal said.
A systematic review published in 2018, for example, concluded there is a paucity of high-quality data supporting the association of glucose during labor and delivery with neonatal hypoglycemia in pregnancies complicated by diabetes (Diabet Med. 2018;35:173-83). And in a subsequent retrospective cohort study of pregnant women with type 1/type 2/GDM and their neonates, the same investigators reported no difference in the target glucose in labor between those with and without neonatal hypotension, after adjustment for important neonatal factors such as LGA and preterm delivery (Diabet Med. 2020;37:138-46).
Also exemplifying the body of research, Dr. Bartal said, is another single-center retrospective study published in 2020 that evaluated outcomes in the years before and after the institution of a formal intrapartum insulin regimen (a standardized protocol for titration of insulin and glucose infusions) for women with pregestational or gestational diabetes. The protocol was associated with improved maternal glucose control, but an increased frequency of neonatal hypoglycemia (Obstet Gynecol. 2020;136:411-6).
Her own group at the University of Texas in Houston looked retrospectively at 233 insulin-treated pregnancies complicated by type 2 diabetes and found no significant difference in the rate of neonatal hypoglycemia between those placed on a drip and those who were not, Dr. Bartal said. Over 40% of the newborns had hypoglycemia; it occurred irrespective of the route of delivery as well (J Matern Fetal Neonatal Med. 2022;35:7445-51).
Only two published randomized controlled trials have evaluated blood sugar control in labor, she said. The first, published in 2006, compared a continuous insulin drip with a rotation of glucose and non–glucose-containing fluids in insulin-requiring diabetes and found no differences in maternal blood glucose (the primary outcome) and a similar risk of neonatal hypoglycemia (Am J Obstet Gynecol. 2006;195;1095-9).
The second RCT, published in 2019, evaluated tight versus liberalized control (60-100 mg/dL, checking every hour, versus 60-120 mg/dL, checking every 4 hours) in laboring women with GDM. The first neonatal blood glucose level was similar in both groups, while the mean neonatal blood glucose level in the first 24 hours of life was lower with tight control (54 vs 58 mg/dL, P = .49) (Obstet Gynecol. 2019;133:1171-7). Findings from a new RCT conducted at the University of Texas in Houston of usual care versus more permissive glucose control will be presented at the SMFM Pregnancy Meeting in February 2024, she said.
Neonatal hypoglycemia is associated with increased risk of NICU admission, “but it’s also associated with possible long-term developmental deficit,” Dr. Bartal said, with the risk highest in children exposed to severe, recurrent, or clinically undetected hypoglycemia. Research has documented significantly increased risks of low executive function and visual motor function, for instance, in children who experienced neonatal hypoglycemia.
The risk of neonatal hypoglycemia has been linked to a variety of factors outside of the intrapartum period such as diabetes control and weight gain during pregnancy, neonatal birth weight/LGA, neonatal adiposity, gestational age at delivery, maternal body mass index, smoking, and diabetes control prior to pregnancy, Dr. Bartal noted. Also challenging is the reality that neonatal hypoglycemia as a research outcome is not standardized; definitions have varied across studies.
Tight intrapartum control comes with “costs,” from close monitoring of labor to increased resource utilization, and it may affect the labor experience/satisfaction, Dr. Bartal said. “But furthermore,” she said, “there are studies coming out, especially in the anesthesiology journals, that show there may be possible harm,” such as the risk of maternal and neonatal hyponatremia, and maternal hypoglycemia. A 2016 editorial in Anaesthesia (2016;71:750) describes these concerns, she noted.
“I do think we need to rethink our current recommendations,” she said.
Dr. Durnwald reported serving on the Dexcom GDM advisory board and receiving funding from United Health Group and the Helmsley Charitable Trust. Dr. Bartal and Dr. Rosenn reported no conflicts of interest.
FROM DPSG-NA 2024
Gestational Diabetes Treatment Moves Forward With Uncertainty And Hope
FAIRFAX, VIRGINIA — , but researchers at the biennial meeting of the Diabetes in Pregnancy Study Group of North America expressed hope for more clarity in the near future and the ability to someday individualize treatment to account for what is increasingly viewed as a heterogeneous condition.
Until studies in 2015 and 2018 cast doubt on glyburide, “we used to have 80% [of our GDM patients] on glyburide, and 20% on insulin,” Maisa Feghali, MD, of the University of Pittsburgh, said during a discussion period. “Now we have 95% on insulin and 5% on oral hypoglycemics. I rely on insulin because I don’t have a better option, and I rely on research efforts [underway to provide better options]” in the future.
The American College of Obstetricians and Gynecologists recommends insulin as the preferred first-line pharmacologic therapy for GDM when pharmacologic therapy is needed, with metformin as an option when patients decline or cannot safely use insulin. Glyburide, ACOG said in its 2018 practice bulletin on GDM (Obstet Gynecol. 2018;131[2]:e49-64), should not be recommended as a first-line pharmacologic therapy.
The Society of Maternal-Fetal Medicine, on the other hand, has accepted metformin as a “reasonable and safe” first-line alternative to insulin — while recognizing that half of women will still require insulin to achieve glycemic control — and does not rule out consideration of glyburide. In its 2018 statement on the pharmacologic treatment of GDM, the society said that the evidence of benefit of one oral agent over another remains limited.
“When you have dueling guidelines, it means the data are not that clear,” George Saade, MD, professor and chair of obstetrics and gynecology at the Eastern Virginia School of Medicine, Norfolk, said in a presentation on GDM. An upcoming $12 million multicenter study to be led by the Ohio State University College of Medicine — coined the DECIDE trial — should provide clarity, he said.
The trial, funded by the Patient-Centered Outcomes Research Institute, which funds comparative clinical effectiveness research designed to be broadly applicable to practice, will enroll and randomize over 1500 pregnant individuals with GDM to either oral metformin or insulin and will follow mothers and children until 2 years after delivery.
The study’s primary and secondary hypotheses, respectively, are that metformin is not inferior to insulin in reducing a composite adverse neonatal outcome (large for gestational age, neonatal hypoglycemia and/or hyperbilirubemia) and that metformin does not result in increased child body mass index at 2 years, compared with insulin. It will also look at patient-reported factors associated with metformin use compared to insulin use — factors that “are important ... to enable clinical implementation of study findings,” said Dr. Saade, who played a role in designing the study over the past several years.
The study will take a pragmatic, real-world approach by ensuring racial and ethnic, socioeconomic, urban and rural, and geographic diversity at both large academic and community-based sites across the United States.
The trial, to be led by Mark Landon, MD, and Kartik Venkatesh, MD, PhD, of Ohio State University, will be the first large trial in the United States to both directly compare the ability of oral hypoglycemics and insulin to prevent GDM-associated pregnancy complications, and to follow children for 2 years, Dr. Saade said. “Prior research was either outside the United States, not randomized, not adequately powered, or had no long-term child follow-up,” he added after the meeting.
The State Of Knowledge About Oral Hypoglycemics
The trial was envisioned several years ago as a three-arm comparative trial including the sulfonylurea glyburide, but data published in recent years has increasingly “not favored” glyburide, and many providers “have stopped using it,” Dr. Saade said during and after the meeting. At this point, “it would not be useful to include it” in a pragmatic trial, he said.
Glyburide became the number one agent after a seminal trial published in 2000 (N Engl J Med. 2000;343:1134-8) showed equivalent glycemic control in about 400 women with GDM who were randomized to receive insulin or glyburide. While the trial was not powered to evaluate other outcomes, there were no significant differences in neonatal complications.
In 2015, a large retrospective population-based study (JAMA Pediatr. 2015;169[5]:452-8) of more than 9,000 women with GDM showed higher risks of neonatal intensive care admission, neonatal hypoglycemia, and large-for-gestational age with glyburide compared with insulin. “It prompted a pause in thinking,” Dr. Saade recalled at the DPSG meeting. After that, several meta-analyses/systematic reviews compared the two treatments, showing varying and sometimes conflicting degrees of difference in neonatal outcomes.
In 2018, a French noninferiority randomized controlled trial (JAMA 2018;319[17]:1773-80) did not show that glyburide is not inferior to insulin in the prevention of perinatal outcomes (macrosomia, neonatal hypoglycemia, and hyperbilirubinemia). “If you add this trial to the systematic reviews, it would probably would shift more in favor of insulin,” Dr. Saade said, noting that the trial’s supplementary data included a higher rate of maternal hypoglycemia with glyburide. “I feel personally now, with all the data, that glyburide is inferior to insulin.”
A 2021 network meta-analysis (BMC Endocr Disord. 2021;21:199) that looked at glycemic control and neonatal outcomes in GDM treated with glyburide, metformin, or insulin, also offers valuable insight, Dr. Saade said. The meta-analysis used a Bayesian framework and presents results as a ranking estimated probability of a treatment being the best or worst — or in between — for different outcomes (glycemic control and neonatal outcomes), which “is one of the best ways to look at data these days,” he said.
“It tells us how likely [it is for one agent] to be better than others. Will it work most of the time? More than 60% of the time?” Dr. Saade explained. For example, the analysis “tell us that for large for gestational age, glyburide has a 94% chance of being the worst, metformin has an 80% change of being the best, and insulin a 76% chance of being in between.”
Overall, the 2021 analysis suggests that “glyburide is the most likely to be worst in most outcomes and that there is equipoise between metformin and insulin,” he said.
Meta-analyses of pharmacologic treatment of GDM have been challenged, he said, by inconsistent reporting in trials of GDM diagnostic criteria, severity of hyperglycemia, and small sample sizes (and wide confidence intervals). Criteria for supplemental insulin are also often “unclear” in trials, Dr. Saade said, as is involvement of social determinants of health and the “care package” enveloping pharmacologic interventions.
Dr. Saade, Dr. Landon, and other researchers have also lamented over the years that there is limited long-term follow-up of exposed offspring.
The Challenge of Heterogeneity
In another presentation on GDM, Maisa Feghali, MD, MS, emphasized that GDM is a heterogeneous condition, with clinical hyperglycemia not capturing individual variation in underlying physiologic processes. A 2016 study (Diabetes Care. 2016;39[6]:1052-5) assessing insulin sensitivity and secretion in 800-plus women at 24-30 weeks’ gestation found that about 50% of those with GDM had predominant insulin resistance, 30% had predominant insulin secretion deficit, and 20% were mixed.
Those with predominant insulin resistance had higher BMI, higher fasting glucose, larger infants, and greater risk of GDM-associated adverse outcomes, “suggesting that the risk is not universal or equivalent,” said Dr. Feghali, assistant professor in the department of obstetrics, gynecology and reproductive sciences at the University of Pittsburgh and the UPCM Magee-Women’s Hospital.
A 2019 multicenter European study (Diabetologia. 2019;62[11]:2118-28) found an even higher proportion of GDM involving predominant insulin resistance and, similarly, a greater risk of adverse pregnancy outcomes in these women than in insulin-sensitive women with GDM, “again suggesting that there’s probably some benefit to looking deeper at physiology to understand individual risk,” she said.
Research published decades ago showed that insulin sensitivity decreases by over 50% during pregnancy, and “what we’ve come to recognize is there [can be] insulin secretion deficiency that’s not able to surmount or overcome the insulin resistance that develops during advanced gestation,” she said. “We need to think not at the population level but at the individual level.”
Dr. Feghali is leading the MATCh-GDM (Metabolic Analysis for Treatment Choice in GDM) study, which has been randomizing women to receive either usual, unmatched treatment or treatment matched to GDM mechanism — metformin for predominant insulin resistance, glyburide, or insulin for predominant insulin secretion defects, and one of the three for combined mechanisms. Data are not available yet.
There is still more to be learned about the pharmacologic effects of oral hypoglycemics, she noted, pointing to a 2020 study (Clin Pharmacol Ther. 2020;107[6]:1362-72) that randomized women to glyburide, metformin, or glyburide/metformin combination therapy and measured insulin sensitivity, beta-cell responsivity, and disposition index. (The latter describes the overall metabolic state and is a product of insulin sensitivity and total beta-cell responsivity.)
“Somewhat surprisingly, they found metformin performed better than glyburide,” shifting the overall disposition index closer to normal, Dr. Feghali said. “But not surprisingly, they found the combination worked best.”
Total beta-cell responsivity occurred in 56% of the glyburide group and 74% of the combination group. Improvements in insulin sensitivity occurred in 84% of the metformin group and 74% of the combination group. Surprisingly, there was “a decrease in first-phase insulin secretion” with glyburide, noted Dr. Feghali — a finding that means “the glyburide story has turned out to be a little more complicated.” With metformin, there was a positive change in insulin secretion as well as insulin sensitivity.
The authors’ conclusion, she noted, “is that there’s potential in thinking about metformin first, as the primary treatment, and then adding glyburide after that.”
Future Use Of Incretin Mimetics, and Intensive Targets in Overweight/Obesity
Dr. Feghali wonders whether incretin hormone mimetics — such as glucagonlike peptide–1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP) — could play a future role in GDM treatment, helping to increase insulin secretion.
She is currently recruiting for a pilot study on the pharmacokinetics and pharmacodynamics in GDM of exenatide, a FDA-approved GLP-1 agonist that has been shown not to cross the placenta and that should, research suggests, lower the risk of maternal hypoglycemia and limit the risk of excessive fetal growth, “overcoming some of the concerns we have with glyburide,” Dr. Feghali said.
A recent study of the gut-generated incretin response during an oral glucose tolerance test in pregnant women with and without GDM showed that post-load GLP-1 and GIP were higher in women with GDM, and that the GLP-1 secretion was associated with insulin secretion only in those with GDM (J Clin Endocrinol Metab. 2022;107(6):e2425-30). “In those with normal OGTT, insulin secretion was independent of GLP-1,” she said. “This study suggests there’s a potential role for incretin mimetics in GDM.”
Also regarding the individualization of GDM treatment, patients who are overweight or obese in the prepregnancy setting and have gestational diabetes represent a different phenotype, she noted, with higher fasting and postprandial blood glucose compared to normal-weight counterparts despite higher doses of medication.
“After controlling for gestational weight gain and glycemic control, we see there’s an independent effect of prepregnancy obesity specifically for an increased risk of macrosomia, preterm birth, and hypertensive disorders of pregnancy,” said Dr. Feghali, referring to a 2015 retrospective study of GDM and obesity (Obstet Gynecol. 2015;126:316-25). “It suggests that we might think about redrawing the line, not on diagnosis and screening but on treatment.”
The randomized, controlled Intensive Glycemic Targets in Overweight and Obese Women with Gestational Diabetes Mellitus (iGDM) trial, is now recruiting at multiple centers, including at Dr. Feghali’s University of Pittsburgh, and will investigate the effect of intensive glycemic targets (fasting < 90 mg/dL, 1-hour postprandial < 120 mg/dL) versus standard glycemic targets (fasting < 95 mg/dL, 1-hour postprandial < 140 mg/dL), she said.
In another presentation on GDM, Monica Longo, MD, PhD, of the Inova Health System in Fairfax, Va., said researchers are also looking at whether nutritional supplements such as myo-inositol can reduce the risk of adverse pregnancy outcomes in GDM, and whether probiotics can improve insulin sensitivity in some patients.
Data on newer insulin analogs in pregnancy are lacking, she noted. “Preliminary data has shown no malformations in infants, but there is some increase in hypoglycemia-related admissions to the NICU,” she said. “It’s worth it [to research more].”
FAIRFAX, VIRGINIA — , but researchers at the biennial meeting of the Diabetes in Pregnancy Study Group of North America expressed hope for more clarity in the near future and the ability to someday individualize treatment to account for what is increasingly viewed as a heterogeneous condition.
Until studies in 2015 and 2018 cast doubt on glyburide, “we used to have 80% [of our GDM patients] on glyburide, and 20% on insulin,” Maisa Feghali, MD, of the University of Pittsburgh, said during a discussion period. “Now we have 95% on insulin and 5% on oral hypoglycemics. I rely on insulin because I don’t have a better option, and I rely on research efforts [underway to provide better options]” in the future.
The American College of Obstetricians and Gynecologists recommends insulin as the preferred first-line pharmacologic therapy for GDM when pharmacologic therapy is needed, with metformin as an option when patients decline or cannot safely use insulin. Glyburide, ACOG said in its 2018 practice bulletin on GDM (Obstet Gynecol. 2018;131[2]:e49-64), should not be recommended as a first-line pharmacologic therapy.
The Society of Maternal-Fetal Medicine, on the other hand, has accepted metformin as a “reasonable and safe” first-line alternative to insulin — while recognizing that half of women will still require insulin to achieve glycemic control — and does not rule out consideration of glyburide. In its 2018 statement on the pharmacologic treatment of GDM, the society said that the evidence of benefit of one oral agent over another remains limited.
“When you have dueling guidelines, it means the data are not that clear,” George Saade, MD, professor and chair of obstetrics and gynecology at the Eastern Virginia School of Medicine, Norfolk, said in a presentation on GDM. An upcoming $12 million multicenter study to be led by the Ohio State University College of Medicine — coined the DECIDE trial — should provide clarity, he said.
The trial, funded by the Patient-Centered Outcomes Research Institute, which funds comparative clinical effectiveness research designed to be broadly applicable to practice, will enroll and randomize over 1500 pregnant individuals with GDM to either oral metformin or insulin and will follow mothers and children until 2 years after delivery.
The study’s primary and secondary hypotheses, respectively, are that metformin is not inferior to insulin in reducing a composite adverse neonatal outcome (large for gestational age, neonatal hypoglycemia and/or hyperbilirubemia) and that metformin does not result in increased child body mass index at 2 years, compared with insulin. It will also look at patient-reported factors associated with metformin use compared to insulin use — factors that “are important ... to enable clinical implementation of study findings,” said Dr. Saade, who played a role in designing the study over the past several years.
The study will take a pragmatic, real-world approach by ensuring racial and ethnic, socioeconomic, urban and rural, and geographic diversity at both large academic and community-based sites across the United States.
The trial, to be led by Mark Landon, MD, and Kartik Venkatesh, MD, PhD, of Ohio State University, will be the first large trial in the United States to both directly compare the ability of oral hypoglycemics and insulin to prevent GDM-associated pregnancy complications, and to follow children for 2 years, Dr. Saade said. “Prior research was either outside the United States, not randomized, not adequately powered, or had no long-term child follow-up,” he added after the meeting.
The State Of Knowledge About Oral Hypoglycemics
The trial was envisioned several years ago as a three-arm comparative trial including the sulfonylurea glyburide, but data published in recent years has increasingly “not favored” glyburide, and many providers “have stopped using it,” Dr. Saade said during and after the meeting. At this point, “it would not be useful to include it” in a pragmatic trial, he said.
Glyburide became the number one agent after a seminal trial published in 2000 (N Engl J Med. 2000;343:1134-8) showed equivalent glycemic control in about 400 women with GDM who were randomized to receive insulin or glyburide. While the trial was not powered to evaluate other outcomes, there were no significant differences in neonatal complications.
In 2015, a large retrospective population-based study (JAMA Pediatr. 2015;169[5]:452-8) of more than 9,000 women with GDM showed higher risks of neonatal intensive care admission, neonatal hypoglycemia, and large-for-gestational age with glyburide compared with insulin. “It prompted a pause in thinking,” Dr. Saade recalled at the DPSG meeting. After that, several meta-analyses/systematic reviews compared the two treatments, showing varying and sometimes conflicting degrees of difference in neonatal outcomes.
In 2018, a French noninferiority randomized controlled trial (JAMA 2018;319[17]:1773-80) did not show that glyburide is not inferior to insulin in the prevention of perinatal outcomes (macrosomia, neonatal hypoglycemia, and hyperbilirubinemia). “If you add this trial to the systematic reviews, it would probably would shift more in favor of insulin,” Dr. Saade said, noting that the trial’s supplementary data included a higher rate of maternal hypoglycemia with glyburide. “I feel personally now, with all the data, that glyburide is inferior to insulin.”
A 2021 network meta-analysis (BMC Endocr Disord. 2021;21:199) that looked at glycemic control and neonatal outcomes in GDM treated with glyburide, metformin, or insulin, also offers valuable insight, Dr. Saade said. The meta-analysis used a Bayesian framework and presents results as a ranking estimated probability of a treatment being the best or worst — or in between — for different outcomes (glycemic control and neonatal outcomes), which “is one of the best ways to look at data these days,” he said.
“It tells us how likely [it is for one agent] to be better than others. Will it work most of the time? More than 60% of the time?” Dr. Saade explained. For example, the analysis “tell us that for large for gestational age, glyburide has a 94% chance of being the worst, metformin has an 80% change of being the best, and insulin a 76% chance of being in between.”
Overall, the 2021 analysis suggests that “glyburide is the most likely to be worst in most outcomes and that there is equipoise between metformin and insulin,” he said.
Meta-analyses of pharmacologic treatment of GDM have been challenged, he said, by inconsistent reporting in trials of GDM diagnostic criteria, severity of hyperglycemia, and small sample sizes (and wide confidence intervals). Criteria for supplemental insulin are also often “unclear” in trials, Dr. Saade said, as is involvement of social determinants of health and the “care package” enveloping pharmacologic interventions.
Dr. Saade, Dr. Landon, and other researchers have also lamented over the years that there is limited long-term follow-up of exposed offspring.
The Challenge of Heterogeneity
In another presentation on GDM, Maisa Feghali, MD, MS, emphasized that GDM is a heterogeneous condition, with clinical hyperglycemia not capturing individual variation in underlying physiologic processes. A 2016 study (Diabetes Care. 2016;39[6]:1052-5) assessing insulin sensitivity and secretion in 800-plus women at 24-30 weeks’ gestation found that about 50% of those with GDM had predominant insulin resistance, 30% had predominant insulin secretion deficit, and 20% were mixed.
Those with predominant insulin resistance had higher BMI, higher fasting glucose, larger infants, and greater risk of GDM-associated adverse outcomes, “suggesting that the risk is not universal or equivalent,” said Dr. Feghali, assistant professor in the department of obstetrics, gynecology and reproductive sciences at the University of Pittsburgh and the UPCM Magee-Women’s Hospital.
A 2019 multicenter European study (Diabetologia. 2019;62[11]:2118-28) found an even higher proportion of GDM involving predominant insulin resistance and, similarly, a greater risk of adverse pregnancy outcomes in these women than in insulin-sensitive women with GDM, “again suggesting that there’s probably some benefit to looking deeper at physiology to understand individual risk,” she said.
Research published decades ago showed that insulin sensitivity decreases by over 50% during pregnancy, and “what we’ve come to recognize is there [can be] insulin secretion deficiency that’s not able to surmount or overcome the insulin resistance that develops during advanced gestation,” she said. “We need to think not at the population level but at the individual level.”
Dr. Feghali is leading the MATCh-GDM (Metabolic Analysis for Treatment Choice in GDM) study, which has been randomizing women to receive either usual, unmatched treatment or treatment matched to GDM mechanism — metformin for predominant insulin resistance, glyburide, or insulin for predominant insulin secretion defects, and one of the three for combined mechanisms. Data are not available yet.
There is still more to be learned about the pharmacologic effects of oral hypoglycemics, she noted, pointing to a 2020 study (Clin Pharmacol Ther. 2020;107[6]:1362-72) that randomized women to glyburide, metformin, or glyburide/metformin combination therapy and measured insulin sensitivity, beta-cell responsivity, and disposition index. (The latter describes the overall metabolic state and is a product of insulin sensitivity and total beta-cell responsivity.)
“Somewhat surprisingly, they found metformin performed better than glyburide,” shifting the overall disposition index closer to normal, Dr. Feghali said. “But not surprisingly, they found the combination worked best.”
Total beta-cell responsivity occurred in 56% of the glyburide group and 74% of the combination group. Improvements in insulin sensitivity occurred in 84% of the metformin group and 74% of the combination group. Surprisingly, there was “a decrease in first-phase insulin secretion” with glyburide, noted Dr. Feghali — a finding that means “the glyburide story has turned out to be a little more complicated.” With metformin, there was a positive change in insulin secretion as well as insulin sensitivity.
The authors’ conclusion, she noted, “is that there’s potential in thinking about metformin first, as the primary treatment, and then adding glyburide after that.”
Future Use Of Incretin Mimetics, and Intensive Targets in Overweight/Obesity
Dr. Feghali wonders whether incretin hormone mimetics — such as glucagonlike peptide–1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP) — could play a future role in GDM treatment, helping to increase insulin secretion.
She is currently recruiting for a pilot study on the pharmacokinetics and pharmacodynamics in GDM of exenatide, a FDA-approved GLP-1 agonist that has been shown not to cross the placenta and that should, research suggests, lower the risk of maternal hypoglycemia and limit the risk of excessive fetal growth, “overcoming some of the concerns we have with glyburide,” Dr. Feghali said.
A recent study of the gut-generated incretin response during an oral glucose tolerance test in pregnant women with and without GDM showed that post-load GLP-1 and GIP were higher in women with GDM, and that the GLP-1 secretion was associated with insulin secretion only in those with GDM (J Clin Endocrinol Metab. 2022;107(6):e2425-30). “In those with normal OGTT, insulin secretion was independent of GLP-1,” she said. “This study suggests there’s a potential role for incretin mimetics in GDM.”
Also regarding the individualization of GDM treatment, patients who are overweight or obese in the prepregnancy setting and have gestational diabetes represent a different phenotype, she noted, with higher fasting and postprandial blood glucose compared to normal-weight counterparts despite higher doses of medication.
“After controlling for gestational weight gain and glycemic control, we see there’s an independent effect of prepregnancy obesity specifically for an increased risk of macrosomia, preterm birth, and hypertensive disorders of pregnancy,” said Dr. Feghali, referring to a 2015 retrospective study of GDM and obesity (Obstet Gynecol. 2015;126:316-25). “It suggests that we might think about redrawing the line, not on diagnosis and screening but on treatment.”
The randomized, controlled Intensive Glycemic Targets in Overweight and Obese Women with Gestational Diabetes Mellitus (iGDM) trial, is now recruiting at multiple centers, including at Dr. Feghali’s University of Pittsburgh, and will investigate the effect of intensive glycemic targets (fasting < 90 mg/dL, 1-hour postprandial < 120 mg/dL) versus standard glycemic targets (fasting < 95 mg/dL, 1-hour postprandial < 140 mg/dL), she said.
In another presentation on GDM, Monica Longo, MD, PhD, of the Inova Health System in Fairfax, Va., said researchers are also looking at whether nutritional supplements such as myo-inositol can reduce the risk of adverse pregnancy outcomes in GDM, and whether probiotics can improve insulin sensitivity in some patients.
Data on newer insulin analogs in pregnancy are lacking, she noted. “Preliminary data has shown no malformations in infants, but there is some increase in hypoglycemia-related admissions to the NICU,” she said. “It’s worth it [to research more].”
FAIRFAX, VIRGINIA — , but researchers at the biennial meeting of the Diabetes in Pregnancy Study Group of North America expressed hope for more clarity in the near future and the ability to someday individualize treatment to account for what is increasingly viewed as a heterogeneous condition.
Until studies in 2015 and 2018 cast doubt on glyburide, “we used to have 80% [of our GDM patients] on glyburide, and 20% on insulin,” Maisa Feghali, MD, of the University of Pittsburgh, said during a discussion period. “Now we have 95% on insulin and 5% on oral hypoglycemics. I rely on insulin because I don’t have a better option, and I rely on research efforts [underway to provide better options]” in the future.
The American College of Obstetricians and Gynecologists recommends insulin as the preferred first-line pharmacologic therapy for GDM when pharmacologic therapy is needed, with metformin as an option when patients decline or cannot safely use insulin. Glyburide, ACOG said in its 2018 practice bulletin on GDM (Obstet Gynecol. 2018;131[2]:e49-64), should not be recommended as a first-line pharmacologic therapy.
The Society of Maternal-Fetal Medicine, on the other hand, has accepted metformin as a “reasonable and safe” first-line alternative to insulin — while recognizing that half of women will still require insulin to achieve glycemic control — and does not rule out consideration of glyburide. In its 2018 statement on the pharmacologic treatment of GDM, the society said that the evidence of benefit of one oral agent over another remains limited.
“When you have dueling guidelines, it means the data are not that clear,” George Saade, MD, professor and chair of obstetrics and gynecology at the Eastern Virginia School of Medicine, Norfolk, said in a presentation on GDM. An upcoming $12 million multicenter study to be led by the Ohio State University College of Medicine — coined the DECIDE trial — should provide clarity, he said.
The trial, funded by the Patient-Centered Outcomes Research Institute, which funds comparative clinical effectiveness research designed to be broadly applicable to practice, will enroll and randomize over 1500 pregnant individuals with GDM to either oral metformin or insulin and will follow mothers and children until 2 years after delivery.
The study’s primary and secondary hypotheses, respectively, are that metformin is not inferior to insulin in reducing a composite adverse neonatal outcome (large for gestational age, neonatal hypoglycemia and/or hyperbilirubemia) and that metformin does not result in increased child body mass index at 2 years, compared with insulin. It will also look at patient-reported factors associated with metformin use compared to insulin use — factors that “are important ... to enable clinical implementation of study findings,” said Dr. Saade, who played a role in designing the study over the past several years.
The study will take a pragmatic, real-world approach by ensuring racial and ethnic, socioeconomic, urban and rural, and geographic diversity at both large academic and community-based sites across the United States.
The trial, to be led by Mark Landon, MD, and Kartik Venkatesh, MD, PhD, of Ohio State University, will be the first large trial in the United States to both directly compare the ability of oral hypoglycemics and insulin to prevent GDM-associated pregnancy complications, and to follow children for 2 years, Dr. Saade said. “Prior research was either outside the United States, not randomized, not adequately powered, or had no long-term child follow-up,” he added after the meeting.
The State Of Knowledge About Oral Hypoglycemics
The trial was envisioned several years ago as a three-arm comparative trial including the sulfonylurea glyburide, but data published in recent years has increasingly “not favored” glyburide, and many providers “have stopped using it,” Dr. Saade said during and after the meeting. At this point, “it would not be useful to include it” in a pragmatic trial, he said.
Glyburide became the number one agent after a seminal trial published in 2000 (N Engl J Med. 2000;343:1134-8) showed equivalent glycemic control in about 400 women with GDM who were randomized to receive insulin or glyburide. While the trial was not powered to evaluate other outcomes, there were no significant differences in neonatal complications.
In 2015, a large retrospective population-based study (JAMA Pediatr. 2015;169[5]:452-8) of more than 9,000 women with GDM showed higher risks of neonatal intensive care admission, neonatal hypoglycemia, and large-for-gestational age with glyburide compared with insulin. “It prompted a pause in thinking,” Dr. Saade recalled at the DPSG meeting. After that, several meta-analyses/systematic reviews compared the two treatments, showing varying and sometimes conflicting degrees of difference in neonatal outcomes.
In 2018, a French noninferiority randomized controlled trial (JAMA 2018;319[17]:1773-80) did not show that glyburide is not inferior to insulin in the prevention of perinatal outcomes (macrosomia, neonatal hypoglycemia, and hyperbilirubinemia). “If you add this trial to the systematic reviews, it would probably would shift more in favor of insulin,” Dr. Saade said, noting that the trial’s supplementary data included a higher rate of maternal hypoglycemia with glyburide. “I feel personally now, with all the data, that glyburide is inferior to insulin.”
A 2021 network meta-analysis (BMC Endocr Disord. 2021;21:199) that looked at glycemic control and neonatal outcomes in GDM treated with glyburide, metformin, or insulin, also offers valuable insight, Dr. Saade said. The meta-analysis used a Bayesian framework and presents results as a ranking estimated probability of a treatment being the best or worst — or in between — for different outcomes (glycemic control and neonatal outcomes), which “is one of the best ways to look at data these days,” he said.
“It tells us how likely [it is for one agent] to be better than others. Will it work most of the time? More than 60% of the time?” Dr. Saade explained. For example, the analysis “tell us that for large for gestational age, glyburide has a 94% chance of being the worst, metformin has an 80% change of being the best, and insulin a 76% chance of being in between.”
Overall, the 2021 analysis suggests that “glyburide is the most likely to be worst in most outcomes and that there is equipoise between metformin and insulin,” he said.
Meta-analyses of pharmacologic treatment of GDM have been challenged, he said, by inconsistent reporting in trials of GDM diagnostic criteria, severity of hyperglycemia, and small sample sizes (and wide confidence intervals). Criteria for supplemental insulin are also often “unclear” in trials, Dr. Saade said, as is involvement of social determinants of health and the “care package” enveloping pharmacologic interventions.
Dr. Saade, Dr. Landon, and other researchers have also lamented over the years that there is limited long-term follow-up of exposed offspring.
The Challenge of Heterogeneity
In another presentation on GDM, Maisa Feghali, MD, MS, emphasized that GDM is a heterogeneous condition, with clinical hyperglycemia not capturing individual variation in underlying physiologic processes. A 2016 study (Diabetes Care. 2016;39[6]:1052-5) assessing insulin sensitivity and secretion in 800-plus women at 24-30 weeks’ gestation found that about 50% of those with GDM had predominant insulin resistance, 30% had predominant insulin secretion deficit, and 20% were mixed.
Those with predominant insulin resistance had higher BMI, higher fasting glucose, larger infants, and greater risk of GDM-associated adverse outcomes, “suggesting that the risk is not universal or equivalent,” said Dr. Feghali, assistant professor in the department of obstetrics, gynecology and reproductive sciences at the University of Pittsburgh and the UPCM Magee-Women’s Hospital.
A 2019 multicenter European study (Diabetologia. 2019;62[11]:2118-28) found an even higher proportion of GDM involving predominant insulin resistance and, similarly, a greater risk of adverse pregnancy outcomes in these women than in insulin-sensitive women with GDM, “again suggesting that there’s probably some benefit to looking deeper at physiology to understand individual risk,” she said.
Research published decades ago showed that insulin sensitivity decreases by over 50% during pregnancy, and “what we’ve come to recognize is there [can be] insulin secretion deficiency that’s not able to surmount or overcome the insulin resistance that develops during advanced gestation,” she said. “We need to think not at the population level but at the individual level.”
Dr. Feghali is leading the MATCh-GDM (Metabolic Analysis for Treatment Choice in GDM) study, which has been randomizing women to receive either usual, unmatched treatment or treatment matched to GDM mechanism — metformin for predominant insulin resistance, glyburide, or insulin for predominant insulin secretion defects, and one of the three for combined mechanisms. Data are not available yet.
There is still more to be learned about the pharmacologic effects of oral hypoglycemics, she noted, pointing to a 2020 study (Clin Pharmacol Ther. 2020;107[6]:1362-72) that randomized women to glyburide, metformin, or glyburide/metformin combination therapy and measured insulin sensitivity, beta-cell responsivity, and disposition index. (The latter describes the overall metabolic state and is a product of insulin sensitivity and total beta-cell responsivity.)
“Somewhat surprisingly, they found metformin performed better than glyburide,” shifting the overall disposition index closer to normal, Dr. Feghali said. “But not surprisingly, they found the combination worked best.”
Total beta-cell responsivity occurred in 56% of the glyburide group and 74% of the combination group. Improvements in insulin sensitivity occurred in 84% of the metformin group and 74% of the combination group. Surprisingly, there was “a decrease in first-phase insulin secretion” with glyburide, noted Dr. Feghali — a finding that means “the glyburide story has turned out to be a little more complicated.” With metformin, there was a positive change in insulin secretion as well as insulin sensitivity.
The authors’ conclusion, she noted, “is that there’s potential in thinking about metformin first, as the primary treatment, and then adding glyburide after that.”
Future Use Of Incretin Mimetics, and Intensive Targets in Overweight/Obesity
Dr. Feghali wonders whether incretin hormone mimetics — such as glucagonlike peptide–1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP) — could play a future role in GDM treatment, helping to increase insulin secretion.
She is currently recruiting for a pilot study on the pharmacokinetics and pharmacodynamics in GDM of exenatide, a FDA-approved GLP-1 agonist that has been shown not to cross the placenta and that should, research suggests, lower the risk of maternal hypoglycemia and limit the risk of excessive fetal growth, “overcoming some of the concerns we have with glyburide,” Dr. Feghali said.
A recent study of the gut-generated incretin response during an oral glucose tolerance test in pregnant women with and without GDM showed that post-load GLP-1 and GIP were higher in women with GDM, and that the GLP-1 secretion was associated with insulin secretion only in those with GDM (J Clin Endocrinol Metab. 2022;107(6):e2425-30). “In those with normal OGTT, insulin secretion was independent of GLP-1,” she said. “This study suggests there’s a potential role for incretin mimetics in GDM.”
Also regarding the individualization of GDM treatment, patients who are overweight or obese in the prepregnancy setting and have gestational diabetes represent a different phenotype, she noted, with higher fasting and postprandial blood glucose compared to normal-weight counterparts despite higher doses of medication.
“After controlling for gestational weight gain and glycemic control, we see there’s an independent effect of prepregnancy obesity specifically for an increased risk of macrosomia, preterm birth, and hypertensive disorders of pregnancy,” said Dr. Feghali, referring to a 2015 retrospective study of GDM and obesity (Obstet Gynecol. 2015;126:316-25). “It suggests that we might think about redrawing the line, not on diagnosis and screening but on treatment.”
The randomized, controlled Intensive Glycemic Targets in Overweight and Obese Women with Gestational Diabetes Mellitus (iGDM) trial, is now recruiting at multiple centers, including at Dr. Feghali’s University of Pittsburgh, and will investigate the effect of intensive glycemic targets (fasting < 90 mg/dL, 1-hour postprandial < 120 mg/dL) versus standard glycemic targets (fasting < 95 mg/dL, 1-hour postprandial < 140 mg/dL), she said.
In another presentation on GDM, Monica Longo, MD, PhD, of the Inova Health System in Fairfax, Va., said researchers are also looking at whether nutritional supplements such as myo-inositol can reduce the risk of adverse pregnancy outcomes in GDM, and whether probiotics can improve insulin sensitivity in some patients.
Data on newer insulin analogs in pregnancy are lacking, she noted. “Preliminary data has shown no malformations in infants, but there is some increase in hypoglycemia-related admissions to the NICU,” she said. “It’s worth it [to research more].”
FROM DPSG-NA 2023
The Knowns and Unknowns About Delivery Timing in Diabetes
FAIRFAX, VIRGINIA — The lack of data on optimal timing of delivery for pregnancies complicated by diabetes remains a major challenge in obstetrics — one with considerable implications given the high and rising prevalence of pregestational and gestational diabetes, Katherine Laughon Grantz, MD, MS, of the National Institute of Child Health and Human Development, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“While 39-40 weeks might be ideal for low-risk pregnancies, the optimal timing for pregnancies with complications [like diabetes] is unknown,” said Dr. Grantz, a senior investigator in the NICHD’s epidemiology branch.
The percentage of mothers with gestational diabetes mellitus (GDM) increased from 6% in 2016 to 8% in 2021, according to the most recent data from the National Vital Statistics System of the Centers for Disease Control and Prevention (MMWR Morb Mortal Wkly Rep. 2023;72:16). Meanwhile, the prevalence of prepregnancy obesity, which raises the risk of gestational and type 2 diabetes, was 29% in 2019; this represents an 11% increase from 2015 (NCHS Data Brief. 2020;392:1-8) and has occurred across all maternal ages, races, ethnic groups, and educational levels, she said.
“The reason clinicians deliver pregnancies with diabetes earlier is because there’s a decreased risk of macrosomia, shoulder dystocia, and stillbirth. And these risks need to be balanced with the increased risk of neonatal morbidity and mortality associated with earlier delivery,” said Dr. Grantz, who noted during her talk that delivery timing also appears to influence long-term neurodevelopmental outcomes. “Yet despite [diabetes in pregnancy] being so common, there is complete uncertainty about when to deliver.”
ACOG Recommendations, Randomized Trials (New And Old)
The American College of Obstetricians and Gynecologists, in a Committee Opinion on Medically Indicated Late-Preterm and Early-Term Deliveries, published in collaboration with the Society of Maternal-Fetal Medicine, offers recommendations based on the type of diabetes and the level of control. For instance, the suggested delivery timing for well-controlled GDM is full term (39 0/7 to 40 6/7 weeks of gestation), while the recommendation for poorly controlled diabetes is individualized late preterm/early term management (Obstet Gynecol. 2021;138:e35-9).
In defining and evaluating control, she noted, “the clinical focus is on glucose, but there are likely other important parameters that are not taken into account ... which [could be] important when considering the timing of delivery.” Potentially important factors include estimated fetal weight, fetal growth velocity, lipids, and amino acids, she said.
ACOG’s recommendations are based mainly on retrospective data, Dr. Grantz said. Only two randomized controlled trials have investigated the timing of delivery in the context of diabetes, and both focused on cesarean section and were “generally underpowered to study neonatal outcomes,” she said.
The first RCT, published in 1993, enrolled 200 women with uncomplicated insulin-requiring diabetes (187 with GDM and 13 with pregestational diabetes) at 38 weeks of gestation, and compared active induction of labor within 5 days to expectant management. There was no significant difference in the cesarean delivery rate (the primary outcome), but rates of macrosomia and large for gestational age were higher in the expectant management group (27% vs. 15%, P = .05, and 23% vs. 10%, P = .02, respectively). Shoulder dystocia occurred in three deliveries, each of which was expectantly managed (Am J Obstet Gynecol. 1993;169[3]:611-5). Notably, the study included “only women with excellent glucose control,” Dr. Grantz said.
The second RCT, published in 2017 by a group in Italy, enrolled 425 patients with GDM (diagnosed by the International Association of Diabetes and Pregnancy Study Groups criteria) between week 38 and week 39 of gestation and similarly randomized them to induction of labor or expectant management. No difference in cesarean delivery was found (BJOG. 2017;124[4]:669-77). Induction of labor was associated with a higher risk of hyperbilirubinemia, and there was a trend toward a decreased risk of macrosomia, but again, the study was underpowered to detect differences in most outcomes, she said. (The study also was stopped early because of an inability to recruit, she noted.)
Dr. Grantz is currently recruiting for a randomized trial aimed at determining the optimal time between 37 and 39 weeks to initiate delivery — the time when neonatal morbidity and perinatal mortality risk is the lowest – for uncontrolled GDM-complicated pregnancies. The trial is designed to recruit up to 3,450 pregnant women with uncontrolled GDM and randomize the timing of their delivery (NCT05515744).
Those who are eligible for the study but do not consent to participate in randomization for delivery will be asked about chart review only (an estimated additional 3,000). The SPAN TIME study will also assess newborn development and behavior outcomes, as well as anthropometric measures, as secondary outcomes. An exploratory analysis will look for clinical, nonclinical or biochemical factors that could be helpful in optimizing delivery timing.
What Retrospective Studies Reveal
Factors that may influence the timing of delivery include the duration of neonatal exposure to hyperglycemia/hyperinsulinemia (pregestational vs. gestational diabetes), the level of diabetes control, and comorbidities (e.g. maternal renal disease or chronic hypertension). However, research “investigating how these factors influence morbidity and the timing of delivery is limited,” said Dr. Grantz.
Overall, it has been difficult through retrospective studies, she said, to investigate neonatal morbidity in diabetic pregnancies and tease apart the relative effects of diabetes as a precursor for early delivery and prematurity itself. Among the studies suggesting an independent risk of diabetes is a retrospective study focusing on neonatal respiratory morbidity — “one of the most common adverse outcomes associated with diabetes.”
The study, an analysis of the Consortium on Safe Labor study (an electronic medical record study of more than 220,000 singleton pregnancies), stratified morbidity by the probability of delivering at term (≥ 37 weeks). GDM and pregestational diabetes complicated 5.1% and 1.5% of the pregnancies, respectively, and were found to be associated with increased risks of neonatal respiratory morbidity compared to women without diabetes — regardless of the probability of delivering at term.
However, these associations were stronger with a higher probability of delivering at term, which suggests that the neonatal respiratory morbidity associated with diabetes is not fully explained by a greater propensity for prematurity (Am J Perinatol. 2017;34[11]:1160-8).
In addition, the rates of all neonatal respiratory morbidities and mortality were higher for pregestational diabetes compared with gestational diabetes, said Dr. Grantz, a senior author of the study. (Morbidities included neonatal intensive care unit admission, transient tachypnea of newborn, apnea, respiratory distress syndrome, mechanical ventilation, and stillbirth.)
The pathophysiology of diabetes and neonatal respiratory morbidity is “not fully known,” she said. It is believed that fetal hyperinsulinemia may cause delayed pulmonary maturation and there is evidence from animal studies that insulin decreases the incorporation of glucose and fatty acids into phospholipid phosphatidylglycerol. Indirect effects stem from the physiologic immaturity of earlier delivery and a higher cesarean delivery rate in pregnancies complicated by diabetes, Dr. Grantz said.
Among other retrospective studies was a population-based study from Canada (2004-2014), published in 2020, of large numbers of women with all types of diabetes and a comparison group of over 2.5 million without diabetes. For maternal morbidity/mortality, there were no significant differences by gestational age between iatrogenic delivery and expectant management among any form of diabetes. But for neonatal morbidity and mortality, the study found differences.
In women with gestational diabetes, iatrogenic delivery was associated with increased risk of neonatal morbidity/mortality at 36 and 37 weeks’ gestation and with decreased risk at weeks 38-40. Increased risk with iatrogenic delivery was also found for women with type 1 and type 2 diabetes at weeks 36 and 37 (Acta Obstet Gynecol Scand. 2020;99[3]:341-9).
Another retrospective study using California vital statistics (1997-2006) examined rates of stillbirth and infant death in women with GDM by gestational age at delivery (Am J Obstet Gynecol. 2012;206[4]:309.e1-e7). The 190,000-plus women with GDM had elevated risk of stillbirth at each gestational age compared to those without GDM, but “the [excess] risk for GDM was lowest at 38 weeks and again at 40 weeks,” Dr. Grantz said. The investigators concluded, she said, “that the risk of expectant management exceeded that of delivery at 38 weeks and beyond.”
Dr. Grantz reported no disclosures.
FAIRFAX, VIRGINIA — The lack of data on optimal timing of delivery for pregnancies complicated by diabetes remains a major challenge in obstetrics — one with considerable implications given the high and rising prevalence of pregestational and gestational diabetes, Katherine Laughon Grantz, MD, MS, of the National Institute of Child Health and Human Development, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“While 39-40 weeks might be ideal for low-risk pregnancies, the optimal timing for pregnancies with complications [like diabetes] is unknown,” said Dr. Grantz, a senior investigator in the NICHD’s epidemiology branch.
The percentage of mothers with gestational diabetes mellitus (GDM) increased from 6% in 2016 to 8% in 2021, according to the most recent data from the National Vital Statistics System of the Centers for Disease Control and Prevention (MMWR Morb Mortal Wkly Rep. 2023;72:16). Meanwhile, the prevalence of prepregnancy obesity, which raises the risk of gestational and type 2 diabetes, was 29% in 2019; this represents an 11% increase from 2015 (NCHS Data Brief. 2020;392:1-8) and has occurred across all maternal ages, races, ethnic groups, and educational levels, she said.
“The reason clinicians deliver pregnancies with diabetes earlier is because there’s a decreased risk of macrosomia, shoulder dystocia, and stillbirth. And these risks need to be balanced with the increased risk of neonatal morbidity and mortality associated with earlier delivery,” said Dr. Grantz, who noted during her talk that delivery timing also appears to influence long-term neurodevelopmental outcomes. “Yet despite [diabetes in pregnancy] being so common, there is complete uncertainty about when to deliver.”
ACOG Recommendations, Randomized Trials (New And Old)
The American College of Obstetricians and Gynecologists, in a Committee Opinion on Medically Indicated Late-Preterm and Early-Term Deliveries, published in collaboration with the Society of Maternal-Fetal Medicine, offers recommendations based on the type of diabetes and the level of control. For instance, the suggested delivery timing for well-controlled GDM is full term (39 0/7 to 40 6/7 weeks of gestation), while the recommendation for poorly controlled diabetes is individualized late preterm/early term management (Obstet Gynecol. 2021;138:e35-9).
In defining and evaluating control, she noted, “the clinical focus is on glucose, but there are likely other important parameters that are not taken into account ... which [could be] important when considering the timing of delivery.” Potentially important factors include estimated fetal weight, fetal growth velocity, lipids, and amino acids, she said.
ACOG’s recommendations are based mainly on retrospective data, Dr. Grantz said. Only two randomized controlled trials have investigated the timing of delivery in the context of diabetes, and both focused on cesarean section and were “generally underpowered to study neonatal outcomes,” she said.
The first RCT, published in 1993, enrolled 200 women with uncomplicated insulin-requiring diabetes (187 with GDM and 13 with pregestational diabetes) at 38 weeks of gestation, and compared active induction of labor within 5 days to expectant management. There was no significant difference in the cesarean delivery rate (the primary outcome), but rates of macrosomia and large for gestational age were higher in the expectant management group (27% vs. 15%, P = .05, and 23% vs. 10%, P = .02, respectively). Shoulder dystocia occurred in three deliveries, each of which was expectantly managed (Am J Obstet Gynecol. 1993;169[3]:611-5). Notably, the study included “only women with excellent glucose control,” Dr. Grantz said.
The second RCT, published in 2017 by a group in Italy, enrolled 425 patients with GDM (diagnosed by the International Association of Diabetes and Pregnancy Study Groups criteria) between week 38 and week 39 of gestation and similarly randomized them to induction of labor or expectant management. No difference in cesarean delivery was found (BJOG. 2017;124[4]:669-77). Induction of labor was associated with a higher risk of hyperbilirubinemia, and there was a trend toward a decreased risk of macrosomia, but again, the study was underpowered to detect differences in most outcomes, she said. (The study also was stopped early because of an inability to recruit, she noted.)
Dr. Grantz is currently recruiting for a randomized trial aimed at determining the optimal time between 37 and 39 weeks to initiate delivery — the time when neonatal morbidity and perinatal mortality risk is the lowest – for uncontrolled GDM-complicated pregnancies. The trial is designed to recruit up to 3,450 pregnant women with uncontrolled GDM and randomize the timing of their delivery (NCT05515744).
Those who are eligible for the study but do not consent to participate in randomization for delivery will be asked about chart review only (an estimated additional 3,000). The SPAN TIME study will also assess newborn development and behavior outcomes, as well as anthropometric measures, as secondary outcomes. An exploratory analysis will look for clinical, nonclinical or biochemical factors that could be helpful in optimizing delivery timing.
What Retrospective Studies Reveal
Factors that may influence the timing of delivery include the duration of neonatal exposure to hyperglycemia/hyperinsulinemia (pregestational vs. gestational diabetes), the level of diabetes control, and comorbidities (e.g. maternal renal disease or chronic hypertension). However, research “investigating how these factors influence morbidity and the timing of delivery is limited,” said Dr. Grantz.
Overall, it has been difficult through retrospective studies, she said, to investigate neonatal morbidity in diabetic pregnancies and tease apart the relative effects of diabetes as a precursor for early delivery and prematurity itself. Among the studies suggesting an independent risk of diabetes is a retrospective study focusing on neonatal respiratory morbidity — “one of the most common adverse outcomes associated with diabetes.”
The study, an analysis of the Consortium on Safe Labor study (an electronic medical record study of more than 220,000 singleton pregnancies), stratified morbidity by the probability of delivering at term (≥ 37 weeks). GDM and pregestational diabetes complicated 5.1% and 1.5% of the pregnancies, respectively, and were found to be associated with increased risks of neonatal respiratory morbidity compared to women without diabetes — regardless of the probability of delivering at term.
However, these associations were stronger with a higher probability of delivering at term, which suggests that the neonatal respiratory morbidity associated with diabetes is not fully explained by a greater propensity for prematurity (Am J Perinatol. 2017;34[11]:1160-8).
In addition, the rates of all neonatal respiratory morbidities and mortality were higher for pregestational diabetes compared with gestational diabetes, said Dr. Grantz, a senior author of the study. (Morbidities included neonatal intensive care unit admission, transient tachypnea of newborn, apnea, respiratory distress syndrome, mechanical ventilation, and stillbirth.)
The pathophysiology of diabetes and neonatal respiratory morbidity is “not fully known,” she said. It is believed that fetal hyperinsulinemia may cause delayed pulmonary maturation and there is evidence from animal studies that insulin decreases the incorporation of glucose and fatty acids into phospholipid phosphatidylglycerol. Indirect effects stem from the physiologic immaturity of earlier delivery and a higher cesarean delivery rate in pregnancies complicated by diabetes, Dr. Grantz said.
Among other retrospective studies was a population-based study from Canada (2004-2014), published in 2020, of large numbers of women with all types of diabetes and a comparison group of over 2.5 million without diabetes. For maternal morbidity/mortality, there were no significant differences by gestational age between iatrogenic delivery and expectant management among any form of diabetes. But for neonatal morbidity and mortality, the study found differences.
In women with gestational diabetes, iatrogenic delivery was associated with increased risk of neonatal morbidity/mortality at 36 and 37 weeks’ gestation and with decreased risk at weeks 38-40. Increased risk with iatrogenic delivery was also found for women with type 1 and type 2 diabetes at weeks 36 and 37 (Acta Obstet Gynecol Scand. 2020;99[3]:341-9).
Another retrospective study using California vital statistics (1997-2006) examined rates of stillbirth and infant death in women with GDM by gestational age at delivery (Am J Obstet Gynecol. 2012;206[4]:309.e1-e7). The 190,000-plus women with GDM had elevated risk of stillbirth at each gestational age compared to those without GDM, but “the [excess] risk for GDM was lowest at 38 weeks and again at 40 weeks,” Dr. Grantz said. The investigators concluded, she said, “that the risk of expectant management exceeded that of delivery at 38 weeks and beyond.”
Dr. Grantz reported no disclosures.
FAIRFAX, VIRGINIA — The lack of data on optimal timing of delivery for pregnancies complicated by diabetes remains a major challenge in obstetrics — one with considerable implications given the high and rising prevalence of pregestational and gestational diabetes, Katherine Laughon Grantz, MD, MS, of the National Institute of Child Health and Human Development, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“While 39-40 weeks might be ideal for low-risk pregnancies, the optimal timing for pregnancies with complications [like diabetes] is unknown,” said Dr. Grantz, a senior investigator in the NICHD’s epidemiology branch.
The percentage of mothers with gestational diabetes mellitus (GDM) increased from 6% in 2016 to 8% in 2021, according to the most recent data from the National Vital Statistics System of the Centers for Disease Control and Prevention (MMWR Morb Mortal Wkly Rep. 2023;72:16). Meanwhile, the prevalence of prepregnancy obesity, which raises the risk of gestational and type 2 diabetes, was 29% in 2019; this represents an 11% increase from 2015 (NCHS Data Brief. 2020;392:1-8) and has occurred across all maternal ages, races, ethnic groups, and educational levels, she said.
“The reason clinicians deliver pregnancies with diabetes earlier is because there’s a decreased risk of macrosomia, shoulder dystocia, and stillbirth. And these risks need to be balanced with the increased risk of neonatal morbidity and mortality associated with earlier delivery,” said Dr. Grantz, who noted during her talk that delivery timing also appears to influence long-term neurodevelopmental outcomes. “Yet despite [diabetes in pregnancy] being so common, there is complete uncertainty about when to deliver.”
ACOG Recommendations, Randomized Trials (New And Old)
The American College of Obstetricians and Gynecologists, in a Committee Opinion on Medically Indicated Late-Preterm and Early-Term Deliveries, published in collaboration with the Society of Maternal-Fetal Medicine, offers recommendations based on the type of diabetes and the level of control. For instance, the suggested delivery timing for well-controlled GDM is full term (39 0/7 to 40 6/7 weeks of gestation), while the recommendation for poorly controlled diabetes is individualized late preterm/early term management (Obstet Gynecol. 2021;138:e35-9).
In defining and evaluating control, she noted, “the clinical focus is on glucose, but there are likely other important parameters that are not taken into account ... which [could be] important when considering the timing of delivery.” Potentially important factors include estimated fetal weight, fetal growth velocity, lipids, and amino acids, she said.
ACOG’s recommendations are based mainly on retrospective data, Dr. Grantz said. Only two randomized controlled trials have investigated the timing of delivery in the context of diabetes, and both focused on cesarean section and were “generally underpowered to study neonatal outcomes,” she said.
The first RCT, published in 1993, enrolled 200 women with uncomplicated insulin-requiring diabetes (187 with GDM and 13 with pregestational diabetes) at 38 weeks of gestation, and compared active induction of labor within 5 days to expectant management. There was no significant difference in the cesarean delivery rate (the primary outcome), but rates of macrosomia and large for gestational age were higher in the expectant management group (27% vs. 15%, P = .05, and 23% vs. 10%, P = .02, respectively). Shoulder dystocia occurred in three deliveries, each of which was expectantly managed (Am J Obstet Gynecol. 1993;169[3]:611-5). Notably, the study included “only women with excellent glucose control,” Dr. Grantz said.
The second RCT, published in 2017 by a group in Italy, enrolled 425 patients with GDM (diagnosed by the International Association of Diabetes and Pregnancy Study Groups criteria) between week 38 and week 39 of gestation and similarly randomized them to induction of labor or expectant management. No difference in cesarean delivery was found (BJOG. 2017;124[4]:669-77). Induction of labor was associated with a higher risk of hyperbilirubinemia, and there was a trend toward a decreased risk of macrosomia, but again, the study was underpowered to detect differences in most outcomes, she said. (The study also was stopped early because of an inability to recruit, she noted.)
Dr. Grantz is currently recruiting for a randomized trial aimed at determining the optimal time between 37 and 39 weeks to initiate delivery — the time when neonatal morbidity and perinatal mortality risk is the lowest – for uncontrolled GDM-complicated pregnancies. The trial is designed to recruit up to 3,450 pregnant women with uncontrolled GDM and randomize the timing of their delivery (NCT05515744).
Those who are eligible for the study but do not consent to participate in randomization for delivery will be asked about chart review only (an estimated additional 3,000). The SPAN TIME study will also assess newborn development and behavior outcomes, as well as anthropometric measures, as secondary outcomes. An exploratory analysis will look for clinical, nonclinical or biochemical factors that could be helpful in optimizing delivery timing.
What Retrospective Studies Reveal
Factors that may influence the timing of delivery include the duration of neonatal exposure to hyperglycemia/hyperinsulinemia (pregestational vs. gestational diabetes), the level of diabetes control, and comorbidities (e.g. maternal renal disease or chronic hypertension). However, research “investigating how these factors influence morbidity and the timing of delivery is limited,” said Dr. Grantz.
Overall, it has been difficult through retrospective studies, she said, to investigate neonatal morbidity in diabetic pregnancies and tease apart the relative effects of diabetes as a precursor for early delivery and prematurity itself. Among the studies suggesting an independent risk of diabetes is a retrospective study focusing on neonatal respiratory morbidity — “one of the most common adverse outcomes associated with diabetes.”
The study, an analysis of the Consortium on Safe Labor study (an electronic medical record study of more than 220,000 singleton pregnancies), stratified morbidity by the probability of delivering at term (≥ 37 weeks). GDM and pregestational diabetes complicated 5.1% and 1.5% of the pregnancies, respectively, and were found to be associated with increased risks of neonatal respiratory morbidity compared to women without diabetes — regardless of the probability of delivering at term.
However, these associations were stronger with a higher probability of delivering at term, which suggests that the neonatal respiratory morbidity associated with diabetes is not fully explained by a greater propensity for prematurity (Am J Perinatol. 2017;34[11]:1160-8).
In addition, the rates of all neonatal respiratory morbidities and mortality were higher for pregestational diabetes compared with gestational diabetes, said Dr. Grantz, a senior author of the study. (Morbidities included neonatal intensive care unit admission, transient tachypnea of newborn, apnea, respiratory distress syndrome, mechanical ventilation, and stillbirth.)
The pathophysiology of diabetes and neonatal respiratory morbidity is “not fully known,” she said. It is believed that fetal hyperinsulinemia may cause delayed pulmonary maturation and there is evidence from animal studies that insulin decreases the incorporation of glucose and fatty acids into phospholipid phosphatidylglycerol. Indirect effects stem from the physiologic immaturity of earlier delivery and a higher cesarean delivery rate in pregnancies complicated by diabetes, Dr. Grantz said.
Among other retrospective studies was a population-based study from Canada (2004-2014), published in 2020, of large numbers of women with all types of diabetes and a comparison group of over 2.5 million without diabetes. For maternal morbidity/mortality, there were no significant differences by gestational age between iatrogenic delivery and expectant management among any form of diabetes. But for neonatal morbidity and mortality, the study found differences.
In women with gestational diabetes, iatrogenic delivery was associated with increased risk of neonatal morbidity/mortality at 36 and 37 weeks’ gestation and with decreased risk at weeks 38-40. Increased risk with iatrogenic delivery was also found for women with type 1 and type 2 diabetes at weeks 36 and 37 (Acta Obstet Gynecol Scand. 2020;99[3]:341-9).
Another retrospective study using California vital statistics (1997-2006) examined rates of stillbirth and infant death in women with GDM by gestational age at delivery (Am J Obstet Gynecol. 2012;206[4]:309.e1-e7). The 190,000-plus women with GDM had elevated risk of stillbirth at each gestational age compared to those without GDM, but “the [excess] risk for GDM was lowest at 38 weeks and again at 40 weeks,” Dr. Grantz said. The investigators concluded, she said, “that the risk of expectant management exceeded that of delivery at 38 weeks and beyond.”
Dr. Grantz reported no disclosures.
FROM DPSG-NA 2023