User login
Learning a growth mindset
“Turns out smarter kids are made, not born.” The headline of the article leapt off the computer screen. Although I realize that it has limits when it comes to dissuading vaccine refusers, I believe that education is a critical element in the success of individuals and the societies they inhabit. However, I must admit to a bias based on my observations that, in general, cognitive skill is inherited. This is an opinion I suspect I share with most folks. You can understand why the article I discovered describing a recent study by several Harvard-based researchers caught my attention.
The study involved 33 mothers and their 1-year-old children. The researchers found that infants whose mothers were stressed and had a “fixed mindset” had lower brain activity than the infants of stressed mothers who held a “growth mindset.” You may be on top of the education literature but I had to do some heavy Googling to learn what was up with growth and fixed mindsets. Was this just a new riff on the whole mindfulness thing?

I quickly learned that in 2006 Carol Dweck, PhD, a psychologist now at Stanford, published a book titled “Mindset” (New York: Penguin Random House) in which she described individuals with a “fixed mindset” who believe that their personality or intelligence will not change over time. On the other hand, individuals with a “growth mindset” view their intelligence and personality as malleable. Her observations have spread across the education and self-help literature like a wildfire that has somehow been roaring along under my radar. I guess I have noticed a subtle change in emphasis when I hear some parents and educators praising a child’s effort in situations in which I might have expected them to say, “You’re so smart.” But, in general I have been clueless.
My initial impression was that this mindset stuff was just coining new buzz words to differentiate optimists from pessimists. But, here I am again revealing a fixed mindset bias. I probably should have said that someone demonstrating a growth mindset approach is “exercising optimism” instead of implying that they were simply born with a sunny disposition.
The growth mindset revolution has not been without skeptics and critics, which is not surprising because educators have a history of jumping on bandwagons before all the wheels have been completely tightened. However, the mindset approach does have some merit, especially for individuals in the center of the bell-shaped curve. We all know of individuals who have failed to meet or have exceeded what would seem to be rational expectations. It is likely that the degree to which a growth mindset approach was applied may be the explanation.
Which brings me to the question of whether we as pediatricians should be more careful of how we choose our words when talking to patients and parents. If the results of the study that alerted me to the growth mindset are reproducible, maybe we should be spending more time with new parents (all of whom are stressed by definition), helping them discover ways in which they can improve the situation they find themselves in by praising them for their efforts at parenting.
Should we be modeling growth mindset language by using it when we interact with our patients? For example, not just complimenting a child on the acquisition of a skill but adding that we were even more impressed by the effort required to acquire it. When we hear a parent clearly expressing a fixed mindset in describing their child should we correct them on the spot or make an appointment to discuss how adopting a growth mindset might help their child meet or exceed his or her potential?
Most smart children may be born that way, but there are always opportunities for improvement, and our patients and their parents need to believe that.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
“Turns out smarter kids are made, not born.” The headline of the article leapt off the computer screen. Although I realize that it has limits when it comes to dissuading vaccine refusers, I believe that education is a critical element in the success of individuals and the societies they inhabit. However, I must admit to a bias based on my observations that, in general, cognitive skill is inherited. This is an opinion I suspect I share with most folks. You can understand why the article I discovered describing a recent study by several Harvard-based researchers caught my attention.
The study involved 33 mothers and their 1-year-old children. The researchers found that infants whose mothers were stressed and had a “fixed mindset” had lower brain activity than the infants of stressed mothers who held a “growth mindset.” You may be on top of the education literature but I had to do some heavy Googling to learn what was up with growth and fixed mindsets. Was this just a new riff on the whole mindfulness thing?
I quickly learned that in 2006 Carol Dweck, PhD, a psychologist now at Stanford, published a book titled “Mindset” (New York: Penguin Random House) in which she described individuals with a “fixed mindset” who believe that their personality or intelligence will not change over time. On the other hand, individuals with a “growth mindset” view their intelligence and personality as malleable. Her observations have spread across the education and self-help literature like a wildfire that has somehow been roaring along under my radar. I guess I have noticed a subtle change in emphasis when I hear some parents and educators praising a child’s effort in situations in which I might have expected them to say, “You’re so smart.” But, in general I have been clueless.
My initial impression was that this mindset stuff was just coining new buzz words to differentiate optimists from pessimists. But, here I am again revealing a fixed mindset bias. I probably should have said that someone demonstrating a growth mindset approach is “exercising optimism” instead of implying that they were simply born with a sunny disposition.
The growth mindset revolution has not been without skeptics and critics, which is not surprising because educators have a history of jumping on bandwagons before all the wheels have been completely tightened. However, the mindset approach does have some merit, especially for individuals in the center of the bell-shaped curve. We all know of individuals who have failed to meet or have exceeded what would seem to be rational expectations. It is likely that the degree to which a growth mindset approach was applied may be the explanation.
Which brings me to the question of whether we as pediatricians should be more careful of how we choose our words when talking to patients and parents. If the results of the study that alerted me to the growth mindset are reproducible, maybe we should be spending more time with new parents (all of whom are stressed by definition), helping them discover ways in which they can improve the situation they find themselves in by praising them for their efforts at parenting.
Should we be modeling growth mindset language by using it when we interact with our patients? For example, not just complimenting a child on the acquisition of a skill but adding that we were even more impressed by the effort required to acquire it. When we hear a parent clearly expressing a fixed mindset in describing their child should we correct them on the spot or make an appointment to discuss how adopting a growth mindset might help their child meet or exceed his or her potential?
Most smart children may be born that way, but there are always opportunities for improvement, and our patients and their parents need to believe that.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
“Turns out smarter kids are made, not born.” The headline of the article leapt off the computer screen. Although I realize that it has limits when it comes to dissuading vaccine refusers, I believe that education is a critical element in the success of individuals and the societies they inhabit. However, I must admit to a bias based on my observations that, in general, cognitive skill is inherited. This is an opinion I suspect I share with most folks. You can understand why the article I discovered describing a recent study by several Harvard-based researchers caught my attention.
The study involved 33 mothers and their 1-year-old children. The researchers found that infants whose mothers were stressed and had a “fixed mindset” had lower brain activity than the infants of stressed mothers who held a “growth mindset.” You may be on top of the education literature but I had to do some heavy Googling to learn what was up with growth and fixed mindsets. Was this just a new riff on the whole mindfulness thing?
I quickly learned that in 2006 Carol Dweck, PhD, a psychologist now at Stanford, published a book titled “Mindset” (New York: Penguin Random House) in which she described individuals with a “fixed mindset” who believe that their personality or intelligence will not change over time. On the other hand, individuals with a “growth mindset” view their intelligence and personality as malleable. Her observations have spread across the education and self-help literature like a wildfire that has somehow been roaring along under my radar. I guess I have noticed a subtle change in emphasis when I hear some parents and educators praising a child’s effort in situations in which I might have expected them to say, “You’re so smart.” But, in general I have been clueless.
My initial impression was that this mindset stuff was just coining new buzz words to differentiate optimists from pessimists. But, here I am again revealing a fixed mindset bias. I probably should have said that someone demonstrating a growth mindset approach is “exercising optimism” instead of implying that they were simply born with a sunny disposition.
The growth mindset revolution has not been without skeptics and critics, which is not surprising because educators have a history of jumping on bandwagons before all the wheels have been completely tightened. However, the mindset approach does have some merit, especially for individuals in the center of the bell-shaped curve. We all know of individuals who have failed to meet or have exceeded what would seem to be rational expectations. It is likely that the degree to which a growth mindset approach was applied may be the explanation.
Which brings me to the question of whether we as pediatricians should be more careful of how we choose our words when talking to patients and parents. If the results of the study that alerted me to the growth mindset are reproducible, maybe we should be spending more time with new parents (all of whom are stressed by definition), helping them discover ways in which they can improve the situation they find themselves in by praising them for their efforts at parenting.
Should we be modeling growth mindset language by using it when we interact with our patients? For example, not just complimenting a child on the acquisition of a skill but adding that we were even more impressed by the effort required to acquire it. When we hear a parent clearly expressing a fixed mindset in describing their child should we correct them on the spot or make an appointment to discuss how adopting a growth mindset might help their child meet or exceed his or her potential?
Most smart children may be born that way, but there are always opportunities for improvement, and our patients and their parents need to believe that.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Easing dementia caregiver burden, addressing interpersonal violence
The number of people with dementia globally is expected to reach 74.7 million by 2030 and 131.5 million by 2050.1 Because dementia is progressive, many patients will exhibit severe symptoms termed behavioral crises. Deteriorating interpersonal conduct and escalating antisocial acts result in an acquired sociopathy.2 Increasing cognitive impairment causes these patients to misunderstand intimate care and perceive it as a threat, often resulting in outbursts of violence against their caregivers.3
Available studies (TABLE4-17) make evident the incidence of interpersonal violence experienced by caregivers secondary to aggressive acts by patients with dementia. This violence ranges from verbal abuse, including racial slurs, to physical abuse—sometimes resulting in significant physical injury. Aggressive behavior by patients with dementia, resulting in violence towards their caregivers or partners, stems from progressive cognitive decline, which can make optimal care difficult. Such episodes may also impair the psychological and physical well-being of caregivers, increasing their risk of depression, anxiety, and even post-traumatic stress disorder (PTSD).18 The extent of the impact is also determined by the interpretation of the abuse by the caregivers themselves. One study suggested that the perception of aggressive or violent behavior as “normal” by a caregiver reduced the overall negative effect of the interactions.7Our review emphasizes the unintended burden that can fall to caregivers of patients with dementia. We also address the role of primary care providers (PCPs) in identifying these instances of violence and intervening appropriately by providing safety strategies, education, resources, and support.

CASE
A 67-year-old man with a medical history of PTSD with depression, type 2 diabetes, alcohol use disorder/dependence, hypertension, and obstructive sleep apnea was brought to his PCP by his wife. She said he had recently been unable to keep appointment times, pay bills, or take his usual medications, venlafaxine and bupropion. She also said his PTSD symptoms had worsened. He was sleeping 12 to 14 hours per day and was increasingly irritable. The patient denied any concerns or changes in his behavior.
The PCP administered a Saint Louis University Mental Status (SLUMS) examination to screen for cognitive impairment.19 The patient scored 14/30 (less than 20 is indicative of dementia). He was unable to complete a simple math problem, recall any items from a list of 5, count in reverse, draw a clock correctly, or recall a full story. Throughout the exam, the patient demonstrated minimal effort and was often only able to complete a task after further prompting by the examiner.

A computed tomography scan of the head revealed no signs of hemorrhage or damage. Thyroid-stimulating hormone levels and vitamin B12 levels were normal. A rapid plasma reagin test result was negative. The patient was given a diagnosis of Alzheimer disease. Donepezil was added to the patient’s medications, starting at 5 mg and then increased to 10 mg. His wife began to assist him with his tasks of daily living. His mood improved, and his wife noted he began to remember his appointments and take his medications with assistance.

However, the patient’s irritability continued to escalate. He grew paranoid and accused his wife of mismanaging their money. This pattern steadily worsened over the course of 6 months. The situation escalated until one day the patient’s wife called a mental health hotline reporting that her husband was holding her hostage and threatening to kill her with a gun. He told her, “I can do something to you, and they won’t even find a fingernail. It doesn’t have to be with a gun either.” She was counseled to try to stay calm to avoid aggravating the situation and to go to a safe place and stay there until help arrived.
His memory had worsened to the point that he could not recall any events from the previous 2 years. He was paranoid about anyone entering his home and would not allow his deteriorating roof to be repaired or his yard to be maintained. He did not shower for weeks at a time. He slept holding a rifle and accused his wife of embezzlement.
Continue to: The patient was evaluated...
The patient was evaluated by another specialist, who assessed his SLUMS score to be 18/30. He increased the patient’s donepezil dose, initiated a bupropion taper, and added sertraline to the regimen. The PCP spoke to the patient’s wife regarding options for her safety including leaving the home, hiding firearms, and calling the police in cases of interpersonal violence. The wife said she did not want to pursue these options. She expressed worry that he might be harmed if he was uncooperative with the police and said there was no one except her to take care of him.
Caregivers struggle to care for their loved ones
Instances of personal violence lead to shock, astonishment, heartbreak, and fear. Anticipation of a recurrence of violence causes many partners and caregivers to feel exhausted, because there is minimal hope for any chance of improvement. There are a few exceptions, however, as our case will show. In addition to emotional exhaustion, there is also a never-ending sense of self-doubt, leading many caregivers to question their ability to handle their family member.20,21 Over time, this leads to caregiver burnout, leaving them unable to understand their family member’s aggression. The sudden loss of caregiver control in dealing with the patient may also result in the family member exhibiting behavioral changes reflecting emotional trauma. For caregivers who do not live with the patient, they may choose to make fewer or shorter visits—or not visit at all—because they fear being abused.7,22
Caregivers of patients with dementia often feel helpless and powerless once abrupt and drastic changes in personality lead to some form of interpersonal violence. Additionally, caregivers with a poor health status are more likely to have lower physical function and experience greater caregiving stress overall.23 Other factors increasing stress are longer years of caregiving and the severity of a patient’s dementia and functional impairment.23
Interventions to reduce caregiver burden
Many studies have assessed the role of different interventions to reduce caregiver burden, such as teaching them problem-solving skills, increasing their knowledge of dementia, recommending social resources, providing emotional support, changing caregiver perceptions of the care situation, introducing coping strategies, relying on strengths and experiences in caregiving, help-seeking, and engaging in activity programs.24-28 For Hispanic caregivers, a structured and self-paced online telenovela format has been effective in improving care and relieving caregiver stress.29 Online positive emotion regulators helped in significantly improving quality of life and physical health in the caregivers.30 In this last intervention, caregivers had 6 online sessions with a facilitator who taught them emotional regulation skills that included: noticing positive events, capitalizing on them, and feeling gratitude; practicing mindfulness; doing a positive reappraisal; acknowledging personal strengths and setting attainable goals; and performing acts of kindness. Empowerment programs have also shown significant improvement in the well-being of caregivers.31
Caregivers may reject support.
Continue to: These practical tips can help
These practical tips can help
Based on our review of the literature, we recommend offering the following supports to caregivers:
- Counsel caregivers early on in a patient’s dementia that behavior changes are likely and may be unpredictable. Explain that dementia can involve changes to personality and behavior as well as memory difficulties.33,34
- Describe resources for support, such as day programs for senior adults, insurance coverage for caregiver respite programs, and the Alzheimer’s Association (www.alz.org/). Encourage caregivers to seek general medical and mental health care for themselves. Caregivers should have opportunities and support to discuss their experiences and to be appropriately trained for the challenge of caring for a family member with dementia.35
- Encourage disclosure about abrupt changes in the patient’s behavior. This invites families to discuss issues with you and may make them more comfortable with such conversations.
- Involve ancillary services (eg, social worker) to plan for a higher level of care well in advance of it becoming necessary.
- Discuss safety strategies for the caregiver, including when it is appropriate to alter a patient’s set routines such as bedtimes and mealtimes.33,34
- Discuss when and how to involve law enforcement, if necessary.33,34 Emphasize the importance of removing firearms from the home as a safety measure. Although federal laws do not explicitly prohibit possession of arms by patients with neurologic damage, a few states mention “organic brain syndrome” or “dementia” as conditions prohibiting use or possession of firearms.36
- Suggest, as feasible, nonpharmacologic aids for the patient such as massage therapy, animal-assisted therapy, personalized interventions, music therapy, and light therapy.37 Prescribe medications to the patient to aid in behavior modification when appropriate.
- Screen caregivers and family members for signs of interpersonal violence. Take notice of changes in caregiver behavior or irregularity in attending follow-up appointments.
CASE
Over the next month, the patient’s symptoms further deteriorated. His PCP recommended hospitalization, but the patient and his wife declined. Magnetic resonance imaging of the patient’s brain revealed severe confluent and patchy regions of white matter and T2 signal hyperintensity, consistent with chronic microvascular ischemic disease. An old, small, left parietal lobe infarct was also noted.
One month later, the patient presented to the emergency department. His symptoms were largely unchanged, but his wife indicated that she could no longer live at home due to burnout. The patient’s medications were adjusted, but he was not admitted for inpatient care. His wife said they needed help at home, but the patient opposed the idea any time that it was mentioned.
A few weeks later, the patient presented for outpatient follow-up. He was delusional, believing that the government was compelling citizens to take sertraline in order to harm their mental health. He had also begun viewing online pornography in front of his wife and attempting to remove all of his money from the bank. He was prescribed aripiprazole 15 mg, and his symptoms began to improve. Soon after, however, he threatened to kill his grandson, then took all his Lasix pills (a 7-day supply) simultaneously. The patient denied that this was a suicide attempt.
Over the course of the next month, the patient began to report hearing voices. A neuropsychological evaluation confirmed a diagnosis of dementia with psychiatric symptoms due to neurologic injury. The patient was referred to a geriatric psychiatrist and continued to be managed medically. He was assigned a multidisciplinary team comprising palliative care, social work, and care management to assist in his care and provide support to the family. His behavior improved.
Continue to: At the time of this publication...
At the time of this publication, the patient’s irritability and paranoia had subsided and he had made no further threats to his family. He has allowed a home health aide into the house and has agreed to have his roof repaired. His wife still lives with him and assists him with activities of daily living.
Interprofessional teams are key
Caregiver burnout increases the risk of patient neglect or abuse, as individuals who have been the targets of aggressive behavior are more likely to leave demented patients unattended.8,16,23 Although tools are available to screen caregivers for depression and burnout, an important step forward would be to develop an interprofessional team to aid in identifying and closely following high-risk patient–caregiver groups. This continual and varied assessment of psychosocial stressors could help prevent the development of violent interactions. These teams would allow integration with the primary health care system by frequent and effective shared communication of knowledge, development of goals, and shared decision-making.38 Setting expectations, providing support, and discussing safety strategies can improve the health and welfare of caregivers and patients with dementia alike.
CORRESPONDENCE
Abu Baker Sheikh, MD, MSC 10-5550, 1 University of New Mexico, Albuquerque, NM 87131; absheikh@salud.unm.edu.
1. Wu YT, Beiser AS, Breteler MMB, et al. The changing prevalence and incidence of dementia over time - current evidence. Nat Rev Neurol. 2017;13:327-339.
2. Cipriani G, Borin G, Vedovello M, et al. Sociopathic behavior and dementia. Acta Neurol Belg. 2013;113:111-115.
3. Cipriani G, Lucetti C, Danti S, et al. Violent and criminal manifestations in dementia patients. Geriatr Gerontol Int. 2016;16:541-549.
4. Skovdahl K, Kihlgren AL, Kihlgren M. Different attitudes when handling aggressive behaviour in dementia—narratives from two caregiver groups. Aging Ment Health. 2003;7:277-286.
5. Kristiansen L, Hellzén O, Asplund K. Swedish assistant nurses’ experiences of job satisfaction when caring for persons suffering from dementia and behavioural disturbances. An interview study. Int J Qualitat Stud Health Well-being. 2006;1:245-256.
6. Wharton TC, Ford BK. What is known about dementia care recipient violence and aggression against caregivers? J Gerontol Soc Work. 2014;57:460-477.
7. Ostaszkiewicz J, Lakhan P, O’Connell B, et al. Ongoing challenges responding to behavioural and psychological symptoms of dementia. Int Nurs Rev. 2015;62:506-516.
8. Kim J, De Bellis AM, Xiao LD. The experience of paid family-care workers of people with dementia in South Korea. Asian Nurs Res (Korean Soc Nurs Sci). 2018;12:34-41.
9. Band-Winterstein T, Avieli H. Women coping with a partner’s dementia-related violence: a qualitative study. J Nurs Scholarsh. 2019; 51:368-379.
10. Munkejord MC, Stefansdottir OA, Sveinbjarnardottir EK. Who cares for the carer? The suffering, struggles and unmet needs of older women caring for husbands living with cognitive decline. Int Pract Devel J. 2020;10:1-11.
11. Seidel D, Thyrian JR. Burden of caring for people with dementia - comparing family caregivers and professional caregivers. A descriptive study. J Multidiscip Healthc. 2019;12:655-663.
12. Tang W, Friedman DB, Kannaley K, et al. Experiences of caregivers by care recipient’s health condition: a study of caregivers for Alzheimer’s disease and related dementias versus other chronic conditions. Geriatr Nurs. 2019;40:181-184.
13. Benbow SM, Bhattacharyya S, Kingston P. Older adults and violence: an analysis of domestic homicide reviews in England involving adults over 60 years of age. Ageing Soc. 2018;39:1097-1121.
14. Herron RV, Wrathall MA. Putting responsive behaviours in place: examining how formal and informal carers understand the actions of people with dementia. Soc Sci Med. 2018;204:9-15.
15. Herron RV, Rosenberg MW. Responding to aggression and reactive behaviours in the home. Dementia (London). 2019;18:1328-1340.
16. Spencer D, Funk LM, Herron RV, et al. Fear, defensive strategies and caring for cognitively impaired family members. J Gerontol Soc Work. 2019;62:67-85.
17. Skovdahl K, Kihlgren AL, Kihlgren M. Dementia and aggressiveness: stimulated recall interviews with caregivers after video-recorded interactions. J Clin Nurs. 2004;13:515-525.
18. Needham I, Abderhalden C, Halfens RJ, et al. Non-somatic effects of patient aggression on nurses: a systematic review. J Adv Nurs. 2005;49:283-296.
19. Tariq SH, Tumosa N, Chibnall JT, et al. The Saint Louis University Mental Status (SLUMS) Examination for detecting mild cognitive impairment and dementia is more sensitive than the Mini-Mental Status Examination (MMSE) - a pilot study. Am J Geriatr Psych. 2006;14:900-910.
20. Janzen S, Zecevic AA, Kloseck M, et al. Managing agitation using nonpharmacological interventions for seniors with dementia. Am J Alzheimers Dis Other Demen. 2013;28:524-532.
21. Zeller A, Dassen T, Kok G, et al. Nursing home caregivers’ explanations for and coping strategies with residents’ aggression: a qualitative study. J Clin Nurs. 2011;20:2469-2478.
22. Alzheimer’s Society. Fix dementia care: homecare. Accessed December 28, 2021. https://www.alzheimers.org.uk/sites/default/files/migrate/downloads/fix_dementia_care_homecare_report.pdf
23. von Känel R, Mausbach BT, Dimsdale JE, et al. Refining caregiver vulnerability for clinical practice: determinants of self-rated health in spousal dementia caregivers. BMC Geriatr. 2019;19:18.
24. Chen HM, Huang MF, Yeh YC, et al. Effectiveness of coping strategies intervention on caregiver burden among caregivers of elderly patients with dementia. Psychogeriatrics. 2015; 15:20-25.
25. Wawrziczny E, Larochette C, Papo D, et al. A customized intervention for dementia caregivers: a quasi-experimental design. J Aging Health. 2019;31:1172-1195.
26. Gitlin LN, Piersol CV, Hodgson N, et al. Reducing neuropsychiatric symptoms in persons with dementia and associated burden in family caregivers using tailored activities: Design and methods of a randomized clinical trial. Contemp Clin Trials. 2016;49:92-102.
27. de Oliveira AM, Radanovic M, Homem de Mello PC, et al. An intervention to reduce neuropsychiatric symptoms and caregiver burden in dementia: preliminary results from a randomized trial of the tailored activity program-outpatient version. Int J Geriatr Psychiatry. 2019;34:1301-1307.
28. Livingston G, Barber J, Rapaport P, et al. Clinical effectiveness of a manual based coping strategy programme (START, STrAtegies for RelaTives) in promoting the mental health of carers of family members with dementia: pragmatic randomised controlled trial. BMJ. 2013;347:f6276.
29. Kajiyama B, Fernandez G, Carter EA, et al. Helping Hispanic dementia caregivers cope with stress using technology-based resources. Clin Gerontol. 2018;41:209-216.
30. Moskowitz JT, Cheung EO, Snowberg KE, et al. Randomized controlled trial of a facilitated online positive emotion regulation intervention for dementia caregivers. Health Psychol. 2019;38:391-402.
31. Yoon HK, Kim GS. An empowerment program for family caregivers of people with dementia. Public Health Nurs. 2020;37:222-233.
32. Zwingmann I, Dreier-Wolfgramm A, Esser A, et al. Why do family dementia caregivers reject caregiver support services? Analyzing types of rejection and associated health-impairments in a cluster-randomized controlled intervention trial. BMC Health Serv Res. 2020;20:121.
33. Nybakken S, Strandås M, Bondas T. Caregivers’ perceptions of aggressive behaviour in nursing home residents living with dementia: A meta-ethnography. J Adv Nurs. 2018;74:2713-2726.
34. Nakaishi L, Moss H, Weinstein M, et al. Exploring workplace violence among home care workers in a consumer-driven home health care program. Workplace Health Saf. 2013;61:441-450.
35. Medical Advisory Secretariat. Caregiver- and patient-directed interventions for dementia: an evidence-based analysis. Ont Health Technol Assess Ser. 2008;8:1-98.
36. Betz ME, McCourt AD, Vernick JS, et al. Firearms and dementia: clinical considerations. Ann Intern Med. 2018;169:47-49.
37. Leng M, Zhao Y, Wang Z. Comparative efficacy of non-pharmacological interventions on agitation in people with dementia: a systematic review and Bayesian network meta-analysis. Int J Nurs Stud. 2020;102:103489.
38. Morgan S, Pullon S, McKinlay E. Observation of interprofessional collaborative practice in primary care teams: an integrative literature review. Int J Nurs Stud. 2015;52:1217-1230.
The number of people with dementia globally is expected to reach 74.7 million by 2030 and 131.5 million by 2050.1 Because dementia is progressive, many patients will exhibit severe symptoms termed behavioral crises. Deteriorating interpersonal conduct and escalating antisocial acts result in an acquired sociopathy.2 Increasing cognitive impairment causes these patients to misunderstand intimate care and perceive it as a threat, often resulting in outbursts of violence against their caregivers.3
Available studies (TABLE4-17) make evident the incidence of interpersonal violence experienced by caregivers secondary to aggressive acts by patients with dementia. This violence ranges from verbal abuse, including racial slurs, to physical abuse—sometimes resulting in significant physical injury. Aggressive behavior by patients with dementia, resulting in violence towards their caregivers or partners, stems from progressive cognitive decline, which can make optimal care difficult. Such episodes may also impair the psychological and physical well-being of caregivers, increasing their risk of depression, anxiety, and even post-traumatic stress disorder (PTSD).18 The extent of the impact is also determined by the interpretation of the abuse by the caregivers themselves. One study suggested that the perception of aggressive or violent behavior as “normal” by a caregiver reduced the overall negative effect of the interactions.7Our review emphasizes the unintended burden that can fall to caregivers of patients with dementia. We also address the role of primary care providers (PCPs) in identifying these instances of violence and intervening appropriately by providing safety strategies, education, resources, and support.
CASE
A 67-year-old man with a medical history of PTSD with depression, type 2 diabetes, alcohol use disorder/dependence, hypertension, and obstructive sleep apnea was brought to his PCP by his wife. She said he had recently been unable to keep appointment times, pay bills, or take his usual medications, venlafaxine and bupropion. She also said his PTSD symptoms had worsened. He was sleeping 12 to 14 hours per day and was increasingly irritable. The patient denied any concerns or changes in his behavior.
The PCP administered a Saint Louis University Mental Status (SLUMS) examination to screen for cognitive impairment.19 The patient scored 14/30 (less than 20 is indicative of dementia). He was unable to complete a simple math problem, recall any items from a list of 5, count in reverse, draw a clock correctly, or recall a full story. Throughout the exam, the patient demonstrated minimal effort and was often only able to complete a task after further prompting by the examiner.
A computed tomography scan of the head revealed no signs of hemorrhage or damage. Thyroid-stimulating hormone levels and vitamin B12 levels were normal. A rapid plasma reagin test result was negative. The patient was given a diagnosis of Alzheimer disease. Donepezil was added to the patient’s medications, starting at 5 mg and then increased to 10 mg. His wife began to assist him with his tasks of daily living. His mood improved, and his wife noted he began to remember his appointments and take his medications with assistance.
However, the patient’s irritability continued to escalate. He grew paranoid and accused his wife of mismanaging their money. This pattern steadily worsened over the course of 6 months. The situation escalated until one day the patient’s wife called a mental health hotline reporting that her husband was holding her hostage and threatening to kill her with a gun. He told her, “I can do something to you, and they won’t even find a fingernail. It doesn’t have to be with a gun either.” She was counseled to try to stay calm to avoid aggravating the situation and to go to a safe place and stay there until help arrived.
His memory had worsened to the point that he could not recall any events from the previous 2 years. He was paranoid about anyone entering his home and would not allow his deteriorating roof to be repaired or his yard to be maintained. He did not shower for weeks at a time. He slept holding a rifle and accused his wife of embezzlement.
Continue to: The patient was evaluated...
The patient was evaluated by another specialist, who assessed his SLUMS score to be 18/30. He increased the patient’s donepezil dose, initiated a bupropion taper, and added sertraline to the regimen. The PCP spoke to the patient’s wife regarding options for her safety including leaving the home, hiding firearms, and calling the police in cases of interpersonal violence. The wife said she did not want to pursue these options. She expressed worry that he might be harmed if he was uncooperative with the police and said there was no one except her to take care of him.
Caregivers struggle to care for their loved ones
Instances of personal violence lead to shock, astonishment, heartbreak, and fear. Anticipation of a recurrence of violence causes many partners and caregivers to feel exhausted, because there is minimal hope for any chance of improvement. There are a few exceptions, however, as our case will show. In addition to emotional exhaustion, there is also a never-ending sense of self-doubt, leading many caregivers to question their ability to handle their family member.20,21 Over time, this leads to caregiver burnout, leaving them unable to understand their family member’s aggression. The sudden loss of caregiver control in dealing with the patient may also result in the family member exhibiting behavioral changes reflecting emotional trauma. For caregivers who do not live with the patient, they may choose to make fewer or shorter visits—or not visit at all—because they fear being abused.7,22
Caregivers of patients with dementia often feel helpless and powerless once abrupt and drastic changes in personality lead to some form of interpersonal violence. Additionally, caregivers with a poor health status are more likely to have lower physical function and experience greater caregiving stress overall.23 Other factors increasing stress are longer years of caregiving and the severity of a patient’s dementia and functional impairment.23
Interventions to reduce caregiver burden
Many studies have assessed the role of different interventions to reduce caregiver burden, such as teaching them problem-solving skills, increasing their knowledge of dementia, recommending social resources, providing emotional support, changing caregiver perceptions of the care situation, introducing coping strategies, relying on strengths and experiences in caregiving, help-seeking, and engaging in activity programs.24-28 For Hispanic caregivers, a structured and self-paced online telenovela format has been effective in improving care and relieving caregiver stress.29 Online positive emotion regulators helped in significantly improving quality of life and physical health in the caregivers.30 In this last intervention, caregivers had 6 online sessions with a facilitator who taught them emotional regulation skills that included: noticing positive events, capitalizing on them, and feeling gratitude; practicing mindfulness; doing a positive reappraisal; acknowledging personal strengths and setting attainable goals; and performing acts of kindness. Empowerment programs have also shown significant improvement in the well-being of caregivers.31
Caregivers may reject support.
Continue to: These practical tips can help
These practical tips can help
Based on our review of the literature, we recommend offering the following supports to caregivers:
- Counsel caregivers early on in a patient’s dementia that behavior changes are likely and may be unpredictable. Explain that dementia can involve changes to personality and behavior as well as memory difficulties.33,34
- Describe resources for support, such as day programs for senior adults, insurance coverage for caregiver respite programs, and the Alzheimer’s Association (www.alz.org/). Encourage caregivers to seek general medical and mental health care for themselves. Caregivers should have opportunities and support to discuss their experiences and to be appropriately trained for the challenge of caring for a family member with dementia.35
- Encourage disclosure about abrupt changes in the patient’s behavior. This invites families to discuss issues with you and may make them more comfortable with such conversations.
- Involve ancillary services (eg, social worker) to plan for a higher level of care well in advance of it becoming necessary.
- Discuss safety strategies for the caregiver, including when it is appropriate to alter a patient’s set routines such as bedtimes and mealtimes.33,34
- Discuss when and how to involve law enforcement, if necessary.33,34 Emphasize the importance of removing firearms from the home as a safety measure. Although federal laws do not explicitly prohibit possession of arms by patients with neurologic damage, a few states mention “organic brain syndrome” or “dementia” as conditions prohibiting use or possession of firearms.36
- Suggest, as feasible, nonpharmacologic aids for the patient such as massage therapy, animal-assisted therapy, personalized interventions, music therapy, and light therapy.37 Prescribe medications to the patient to aid in behavior modification when appropriate.
- Screen caregivers and family members for signs of interpersonal violence. Take notice of changes in caregiver behavior or irregularity in attending follow-up appointments.
CASE
Over the next month, the patient’s symptoms further deteriorated. His PCP recommended hospitalization, but the patient and his wife declined. Magnetic resonance imaging of the patient’s brain revealed severe confluent and patchy regions of white matter and T2 signal hyperintensity, consistent with chronic microvascular ischemic disease. An old, small, left parietal lobe infarct was also noted.
One month later, the patient presented to the emergency department. His symptoms were largely unchanged, but his wife indicated that she could no longer live at home due to burnout. The patient’s medications were adjusted, but he was not admitted for inpatient care. His wife said they needed help at home, but the patient opposed the idea any time that it was mentioned.
A few weeks later, the patient presented for outpatient follow-up. He was delusional, believing that the government was compelling citizens to take sertraline in order to harm their mental health. He had also begun viewing online pornography in front of his wife and attempting to remove all of his money from the bank. He was prescribed aripiprazole 15 mg, and his symptoms began to improve. Soon after, however, he threatened to kill his grandson, then took all his Lasix pills (a 7-day supply) simultaneously. The patient denied that this was a suicide attempt.
Over the course of the next month, the patient began to report hearing voices. A neuropsychological evaluation confirmed a diagnosis of dementia with psychiatric symptoms due to neurologic injury. The patient was referred to a geriatric psychiatrist and continued to be managed medically. He was assigned a multidisciplinary team comprising palliative care, social work, and care management to assist in his care and provide support to the family. His behavior improved.
Continue to: At the time of this publication...
At the time of this publication, the patient’s irritability and paranoia had subsided and he had made no further threats to his family. He has allowed a home health aide into the house and has agreed to have his roof repaired. His wife still lives with him and assists him with activities of daily living.
Interprofessional teams are key
Caregiver burnout increases the risk of patient neglect or abuse, as individuals who have been the targets of aggressive behavior are more likely to leave demented patients unattended.8,16,23 Although tools are available to screen caregivers for depression and burnout, an important step forward would be to develop an interprofessional team to aid in identifying and closely following high-risk patient–caregiver groups. This continual and varied assessment of psychosocial stressors could help prevent the development of violent interactions. These teams would allow integration with the primary health care system by frequent and effective shared communication of knowledge, development of goals, and shared decision-making.38 Setting expectations, providing support, and discussing safety strategies can improve the health and welfare of caregivers and patients with dementia alike.
CORRESPONDENCE
Abu Baker Sheikh, MD, MSC 10-5550, 1 University of New Mexico, Albuquerque, NM 87131; absheikh@salud.unm.edu.
The number of people with dementia globally is expected to reach 74.7 million by 2030 and 131.5 million by 2050.1 Because dementia is progressive, many patients will exhibit severe symptoms termed behavioral crises. Deteriorating interpersonal conduct and escalating antisocial acts result in an acquired sociopathy.2 Increasing cognitive impairment causes these patients to misunderstand intimate care and perceive it as a threat, often resulting in outbursts of violence against their caregivers.3
Available studies (TABLE4-17) make evident the incidence of interpersonal violence experienced by caregivers secondary to aggressive acts by patients with dementia. This violence ranges from verbal abuse, including racial slurs, to physical abuse—sometimes resulting in significant physical injury. Aggressive behavior by patients with dementia, resulting in violence towards their caregivers or partners, stems from progressive cognitive decline, which can make optimal care difficult. Such episodes may also impair the psychological and physical well-being of caregivers, increasing their risk of depression, anxiety, and even post-traumatic stress disorder (PTSD).18 The extent of the impact is also determined by the interpretation of the abuse by the caregivers themselves. One study suggested that the perception of aggressive or violent behavior as “normal” by a caregiver reduced the overall negative effect of the interactions.7Our review emphasizes the unintended burden that can fall to caregivers of patients with dementia. We also address the role of primary care providers (PCPs) in identifying these instances of violence and intervening appropriately by providing safety strategies, education, resources, and support.
CASE
A 67-year-old man with a medical history of PTSD with depression, type 2 diabetes, alcohol use disorder/dependence, hypertension, and obstructive sleep apnea was brought to his PCP by his wife. She said he had recently been unable to keep appointment times, pay bills, or take his usual medications, venlafaxine and bupropion. She also said his PTSD symptoms had worsened. He was sleeping 12 to 14 hours per day and was increasingly irritable. The patient denied any concerns or changes in his behavior.
The PCP administered a Saint Louis University Mental Status (SLUMS) examination to screen for cognitive impairment.19 The patient scored 14/30 (less than 20 is indicative of dementia). He was unable to complete a simple math problem, recall any items from a list of 5, count in reverse, draw a clock correctly, or recall a full story. Throughout the exam, the patient demonstrated minimal effort and was often only able to complete a task after further prompting by the examiner.
A computed tomography scan of the head revealed no signs of hemorrhage or damage. Thyroid-stimulating hormone levels and vitamin B12 levels were normal. A rapid plasma reagin test result was negative. The patient was given a diagnosis of Alzheimer disease. Donepezil was added to the patient’s medications, starting at 5 mg and then increased to 10 mg. His wife began to assist him with his tasks of daily living. His mood improved, and his wife noted he began to remember his appointments and take his medications with assistance.
However, the patient’s irritability continued to escalate. He grew paranoid and accused his wife of mismanaging their money. This pattern steadily worsened over the course of 6 months. The situation escalated until one day the patient’s wife called a mental health hotline reporting that her husband was holding her hostage and threatening to kill her with a gun. He told her, “I can do something to you, and they won’t even find a fingernail. It doesn’t have to be with a gun either.” She was counseled to try to stay calm to avoid aggravating the situation and to go to a safe place and stay there until help arrived.
His memory had worsened to the point that he could not recall any events from the previous 2 years. He was paranoid about anyone entering his home and would not allow his deteriorating roof to be repaired or his yard to be maintained. He did not shower for weeks at a time. He slept holding a rifle and accused his wife of embezzlement.
Continue to: The patient was evaluated...
The patient was evaluated by another specialist, who assessed his SLUMS score to be 18/30. He increased the patient’s donepezil dose, initiated a bupropion taper, and added sertraline to the regimen. The PCP spoke to the patient’s wife regarding options for her safety including leaving the home, hiding firearms, and calling the police in cases of interpersonal violence. The wife said she did not want to pursue these options. She expressed worry that he might be harmed if he was uncooperative with the police and said there was no one except her to take care of him.
Caregivers struggle to care for their loved ones
Instances of personal violence lead to shock, astonishment, heartbreak, and fear. Anticipation of a recurrence of violence causes many partners and caregivers to feel exhausted, because there is minimal hope for any chance of improvement. There are a few exceptions, however, as our case will show. In addition to emotional exhaustion, there is also a never-ending sense of self-doubt, leading many caregivers to question their ability to handle their family member.20,21 Over time, this leads to caregiver burnout, leaving them unable to understand their family member’s aggression. The sudden loss of caregiver control in dealing with the patient may also result in the family member exhibiting behavioral changes reflecting emotional trauma. For caregivers who do not live with the patient, they may choose to make fewer or shorter visits—or not visit at all—because they fear being abused.7,22
Caregivers of patients with dementia often feel helpless and powerless once abrupt and drastic changes in personality lead to some form of interpersonal violence. Additionally, caregivers with a poor health status are more likely to have lower physical function and experience greater caregiving stress overall.23 Other factors increasing stress are longer years of caregiving and the severity of a patient’s dementia and functional impairment.23
Interventions to reduce caregiver burden
Many studies have assessed the role of different interventions to reduce caregiver burden, such as teaching them problem-solving skills, increasing their knowledge of dementia, recommending social resources, providing emotional support, changing caregiver perceptions of the care situation, introducing coping strategies, relying on strengths and experiences in caregiving, help-seeking, and engaging in activity programs.24-28 For Hispanic caregivers, a structured and self-paced online telenovela format has been effective in improving care and relieving caregiver stress.29 Online positive emotion regulators helped in significantly improving quality of life and physical health in the caregivers.30 In this last intervention, caregivers had 6 online sessions with a facilitator who taught them emotional regulation skills that included: noticing positive events, capitalizing on them, and feeling gratitude; practicing mindfulness; doing a positive reappraisal; acknowledging personal strengths and setting attainable goals; and performing acts of kindness. Empowerment programs have also shown significant improvement in the well-being of caregivers.31
Caregivers may reject support.
Continue to: These practical tips can help
These practical tips can help
Based on our review of the literature, we recommend offering the following supports to caregivers:
- Counsel caregivers early on in a patient’s dementia that behavior changes are likely and may be unpredictable. Explain that dementia can involve changes to personality and behavior as well as memory difficulties.33,34
- Describe resources for support, such as day programs for senior adults, insurance coverage for caregiver respite programs, and the Alzheimer’s Association (www.alz.org/). Encourage caregivers to seek general medical and mental health care for themselves. Caregivers should have opportunities and support to discuss their experiences and to be appropriately trained for the challenge of caring for a family member with dementia.35
- Encourage disclosure about abrupt changes in the patient’s behavior. This invites families to discuss issues with you and may make them more comfortable with such conversations.
- Involve ancillary services (eg, social worker) to plan for a higher level of care well in advance of it becoming necessary.
- Discuss safety strategies for the caregiver, including when it is appropriate to alter a patient’s set routines such as bedtimes and mealtimes.33,34
- Discuss when and how to involve law enforcement, if necessary.33,34 Emphasize the importance of removing firearms from the home as a safety measure. Although federal laws do not explicitly prohibit possession of arms by patients with neurologic damage, a few states mention “organic brain syndrome” or “dementia” as conditions prohibiting use or possession of firearms.36
- Suggest, as feasible, nonpharmacologic aids for the patient such as massage therapy, animal-assisted therapy, personalized interventions, music therapy, and light therapy.37 Prescribe medications to the patient to aid in behavior modification when appropriate.
- Screen caregivers and family members for signs of interpersonal violence. Take notice of changes in caregiver behavior or irregularity in attending follow-up appointments.
CASE
Over the next month, the patient’s symptoms further deteriorated. His PCP recommended hospitalization, but the patient and his wife declined. Magnetic resonance imaging of the patient’s brain revealed severe confluent and patchy regions of white matter and T2 signal hyperintensity, consistent with chronic microvascular ischemic disease. An old, small, left parietal lobe infarct was also noted.
One month later, the patient presented to the emergency department. His symptoms were largely unchanged, but his wife indicated that she could no longer live at home due to burnout. The patient’s medications were adjusted, but he was not admitted for inpatient care. His wife said they needed help at home, but the patient opposed the idea any time that it was mentioned.
A few weeks later, the patient presented for outpatient follow-up. He was delusional, believing that the government was compelling citizens to take sertraline in order to harm their mental health. He had also begun viewing online pornography in front of his wife and attempting to remove all of his money from the bank. He was prescribed aripiprazole 15 mg, and his symptoms began to improve. Soon after, however, he threatened to kill his grandson, then took all his Lasix pills (a 7-day supply) simultaneously. The patient denied that this was a suicide attempt.
Over the course of the next month, the patient began to report hearing voices. A neuropsychological evaluation confirmed a diagnosis of dementia with psychiatric symptoms due to neurologic injury. The patient was referred to a geriatric psychiatrist and continued to be managed medically. He was assigned a multidisciplinary team comprising palliative care, social work, and care management to assist in his care and provide support to the family. His behavior improved.
Continue to: At the time of this publication...
At the time of this publication, the patient’s irritability and paranoia had subsided and he had made no further threats to his family. He has allowed a home health aide into the house and has agreed to have his roof repaired. His wife still lives with him and assists him with activities of daily living.
Interprofessional teams are key
Caregiver burnout increases the risk of patient neglect or abuse, as individuals who have been the targets of aggressive behavior are more likely to leave demented patients unattended.8,16,23 Although tools are available to screen caregivers for depression and burnout, an important step forward would be to develop an interprofessional team to aid in identifying and closely following high-risk patient–caregiver groups. This continual and varied assessment of psychosocial stressors could help prevent the development of violent interactions. These teams would allow integration with the primary health care system by frequent and effective shared communication of knowledge, development of goals, and shared decision-making.38 Setting expectations, providing support, and discussing safety strategies can improve the health and welfare of caregivers and patients with dementia alike.
CORRESPONDENCE
Abu Baker Sheikh, MD, MSC 10-5550, 1 University of New Mexico, Albuquerque, NM 87131; absheikh@salud.unm.edu.
1. Wu YT, Beiser AS, Breteler MMB, et al. The changing prevalence and incidence of dementia over time - current evidence. Nat Rev Neurol. 2017;13:327-339.
2. Cipriani G, Borin G, Vedovello M, et al. Sociopathic behavior and dementia. Acta Neurol Belg. 2013;113:111-115.
3. Cipriani G, Lucetti C, Danti S, et al. Violent and criminal manifestations in dementia patients. Geriatr Gerontol Int. 2016;16:541-549.
4. Skovdahl K, Kihlgren AL, Kihlgren M. Different attitudes when handling aggressive behaviour in dementia—narratives from two caregiver groups. Aging Ment Health. 2003;7:277-286.
5. Kristiansen L, Hellzén O, Asplund K. Swedish assistant nurses’ experiences of job satisfaction when caring for persons suffering from dementia and behavioural disturbances. An interview study. Int J Qualitat Stud Health Well-being. 2006;1:245-256.
6. Wharton TC, Ford BK. What is known about dementia care recipient violence and aggression against caregivers? J Gerontol Soc Work. 2014;57:460-477.
7. Ostaszkiewicz J, Lakhan P, O’Connell B, et al. Ongoing challenges responding to behavioural and psychological symptoms of dementia. Int Nurs Rev. 2015;62:506-516.
8. Kim J, De Bellis AM, Xiao LD. The experience of paid family-care workers of people with dementia in South Korea. Asian Nurs Res (Korean Soc Nurs Sci). 2018;12:34-41.
9. Band-Winterstein T, Avieli H. Women coping with a partner’s dementia-related violence: a qualitative study. J Nurs Scholarsh. 2019; 51:368-379.
10. Munkejord MC, Stefansdottir OA, Sveinbjarnardottir EK. Who cares for the carer? The suffering, struggles and unmet needs of older women caring for husbands living with cognitive decline. Int Pract Devel J. 2020;10:1-11.
11. Seidel D, Thyrian JR. Burden of caring for people with dementia - comparing family caregivers and professional caregivers. A descriptive study. J Multidiscip Healthc. 2019;12:655-663.
12. Tang W, Friedman DB, Kannaley K, et al. Experiences of caregivers by care recipient’s health condition: a study of caregivers for Alzheimer’s disease and related dementias versus other chronic conditions. Geriatr Nurs. 2019;40:181-184.
13. Benbow SM, Bhattacharyya S, Kingston P. Older adults and violence: an analysis of domestic homicide reviews in England involving adults over 60 years of age. Ageing Soc. 2018;39:1097-1121.
14. Herron RV, Wrathall MA. Putting responsive behaviours in place: examining how formal and informal carers understand the actions of people with dementia. Soc Sci Med. 2018;204:9-15.
15. Herron RV, Rosenberg MW. Responding to aggression and reactive behaviours in the home. Dementia (London). 2019;18:1328-1340.
16. Spencer D, Funk LM, Herron RV, et al. Fear, defensive strategies and caring for cognitively impaired family members. J Gerontol Soc Work. 2019;62:67-85.
17. Skovdahl K, Kihlgren AL, Kihlgren M. Dementia and aggressiveness: stimulated recall interviews with caregivers after video-recorded interactions. J Clin Nurs. 2004;13:515-525.
18. Needham I, Abderhalden C, Halfens RJ, et al. Non-somatic effects of patient aggression on nurses: a systematic review. J Adv Nurs. 2005;49:283-296.
19. Tariq SH, Tumosa N, Chibnall JT, et al. The Saint Louis University Mental Status (SLUMS) Examination for detecting mild cognitive impairment and dementia is more sensitive than the Mini-Mental Status Examination (MMSE) - a pilot study. Am J Geriatr Psych. 2006;14:900-910.
20. Janzen S, Zecevic AA, Kloseck M, et al. Managing agitation using nonpharmacological interventions for seniors with dementia. Am J Alzheimers Dis Other Demen. 2013;28:524-532.
21. Zeller A, Dassen T, Kok G, et al. Nursing home caregivers’ explanations for and coping strategies with residents’ aggression: a qualitative study. J Clin Nurs. 2011;20:2469-2478.
22. Alzheimer’s Society. Fix dementia care: homecare. Accessed December 28, 2021. https://www.alzheimers.org.uk/sites/default/files/migrate/downloads/fix_dementia_care_homecare_report.pdf
23. von Känel R, Mausbach BT, Dimsdale JE, et al. Refining caregiver vulnerability for clinical practice: determinants of self-rated health in spousal dementia caregivers. BMC Geriatr. 2019;19:18.
24. Chen HM, Huang MF, Yeh YC, et al. Effectiveness of coping strategies intervention on caregiver burden among caregivers of elderly patients with dementia. Psychogeriatrics. 2015; 15:20-25.
25. Wawrziczny E, Larochette C, Papo D, et al. A customized intervention for dementia caregivers: a quasi-experimental design. J Aging Health. 2019;31:1172-1195.
26. Gitlin LN, Piersol CV, Hodgson N, et al. Reducing neuropsychiatric symptoms in persons with dementia and associated burden in family caregivers using tailored activities: Design and methods of a randomized clinical trial. Contemp Clin Trials. 2016;49:92-102.
27. de Oliveira AM, Radanovic M, Homem de Mello PC, et al. An intervention to reduce neuropsychiatric symptoms and caregiver burden in dementia: preliminary results from a randomized trial of the tailored activity program-outpatient version. Int J Geriatr Psychiatry. 2019;34:1301-1307.
28. Livingston G, Barber J, Rapaport P, et al. Clinical effectiveness of a manual based coping strategy programme (START, STrAtegies for RelaTives) in promoting the mental health of carers of family members with dementia: pragmatic randomised controlled trial. BMJ. 2013;347:f6276.
29. Kajiyama B, Fernandez G, Carter EA, et al. Helping Hispanic dementia caregivers cope with stress using technology-based resources. Clin Gerontol. 2018;41:209-216.
30. Moskowitz JT, Cheung EO, Snowberg KE, et al. Randomized controlled trial of a facilitated online positive emotion regulation intervention for dementia caregivers. Health Psychol. 2019;38:391-402.
31. Yoon HK, Kim GS. An empowerment program for family caregivers of people with dementia. Public Health Nurs. 2020;37:222-233.
32. Zwingmann I, Dreier-Wolfgramm A, Esser A, et al. Why do family dementia caregivers reject caregiver support services? Analyzing types of rejection and associated health-impairments in a cluster-randomized controlled intervention trial. BMC Health Serv Res. 2020;20:121.
33. Nybakken S, Strandås M, Bondas T. Caregivers’ perceptions of aggressive behaviour in nursing home residents living with dementia: A meta-ethnography. J Adv Nurs. 2018;74:2713-2726.
34. Nakaishi L, Moss H, Weinstein M, et al. Exploring workplace violence among home care workers in a consumer-driven home health care program. Workplace Health Saf. 2013;61:441-450.
35. Medical Advisory Secretariat. Caregiver- and patient-directed interventions for dementia: an evidence-based analysis. Ont Health Technol Assess Ser. 2008;8:1-98.
36. Betz ME, McCourt AD, Vernick JS, et al. Firearms and dementia: clinical considerations. Ann Intern Med. 2018;169:47-49.
37. Leng M, Zhao Y, Wang Z. Comparative efficacy of non-pharmacological interventions on agitation in people with dementia: a systematic review and Bayesian network meta-analysis. Int J Nurs Stud. 2020;102:103489.
38. Morgan S, Pullon S, McKinlay E. Observation of interprofessional collaborative practice in primary care teams: an integrative literature review. Int J Nurs Stud. 2015;52:1217-1230.
1. Wu YT, Beiser AS, Breteler MMB, et al. The changing prevalence and incidence of dementia over time - current evidence. Nat Rev Neurol. 2017;13:327-339.
2. Cipriani G, Borin G, Vedovello M, et al. Sociopathic behavior and dementia. Acta Neurol Belg. 2013;113:111-115.
3. Cipriani G, Lucetti C, Danti S, et al. Violent and criminal manifestations in dementia patients. Geriatr Gerontol Int. 2016;16:541-549.
4. Skovdahl K, Kihlgren AL, Kihlgren M. Different attitudes when handling aggressive behaviour in dementia—narratives from two caregiver groups. Aging Ment Health. 2003;7:277-286.
5. Kristiansen L, Hellzén O, Asplund K. Swedish assistant nurses’ experiences of job satisfaction when caring for persons suffering from dementia and behavioural disturbances. An interview study. Int J Qualitat Stud Health Well-being. 2006;1:245-256.
6. Wharton TC, Ford BK. What is known about dementia care recipient violence and aggression against caregivers? J Gerontol Soc Work. 2014;57:460-477.
7. Ostaszkiewicz J, Lakhan P, O’Connell B, et al. Ongoing challenges responding to behavioural and psychological symptoms of dementia. Int Nurs Rev. 2015;62:506-516.
8. Kim J, De Bellis AM, Xiao LD. The experience of paid family-care workers of people with dementia in South Korea. Asian Nurs Res (Korean Soc Nurs Sci). 2018;12:34-41.
9. Band-Winterstein T, Avieli H. Women coping with a partner’s dementia-related violence: a qualitative study. J Nurs Scholarsh. 2019; 51:368-379.
10. Munkejord MC, Stefansdottir OA, Sveinbjarnardottir EK. Who cares for the carer? The suffering, struggles and unmet needs of older women caring for husbands living with cognitive decline. Int Pract Devel J. 2020;10:1-11.
11. Seidel D, Thyrian JR. Burden of caring for people with dementia - comparing family caregivers and professional caregivers. A descriptive study. J Multidiscip Healthc. 2019;12:655-663.
12. Tang W, Friedman DB, Kannaley K, et al. Experiences of caregivers by care recipient’s health condition: a study of caregivers for Alzheimer’s disease and related dementias versus other chronic conditions. Geriatr Nurs. 2019;40:181-184.
13. Benbow SM, Bhattacharyya S, Kingston P. Older adults and violence: an analysis of domestic homicide reviews in England involving adults over 60 years of age. Ageing Soc. 2018;39:1097-1121.
14. Herron RV, Wrathall MA. Putting responsive behaviours in place: examining how formal and informal carers understand the actions of people with dementia. Soc Sci Med. 2018;204:9-15.
15. Herron RV, Rosenberg MW. Responding to aggression and reactive behaviours in the home. Dementia (London). 2019;18:1328-1340.
16. Spencer D, Funk LM, Herron RV, et al. Fear, defensive strategies and caring for cognitively impaired family members. J Gerontol Soc Work. 2019;62:67-85.
17. Skovdahl K, Kihlgren AL, Kihlgren M. Dementia and aggressiveness: stimulated recall interviews with caregivers after video-recorded interactions. J Clin Nurs. 2004;13:515-525.
18. Needham I, Abderhalden C, Halfens RJ, et al. Non-somatic effects of patient aggression on nurses: a systematic review. J Adv Nurs. 2005;49:283-296.
19. Tariq SH, Tumosa N, Chibnall JT, et al. The Saint Louis University Mental Status (SLUMS) Examination for detecting mild cognitive impairment and dementia is more sensitive than the Mini-Mental Status Examination (MMSE) - a pilot study. Am J Geriatr Psych. 2006;14:900-910.
20. Janzen S, Zecevic AA, Kloseck M, et al. Managing agitation using nonpharmacological interventions for seniors with dementia. Am J Alzheimers Dis Other Demen. 2013;28:524-532.
21. Zeller A, Dassen T, Kok G, et al. Nursing home caregivers’ explanations for and coping strategies with residents’ aggression: a qualitative study. J Clin Nurs. 2011;20:2469-2478.
22. Alzheimer’s Society. Fix dementia care: homecare. Accessed December 28, 2021. https://www.alzheimers.org.uk/sites/default/files/migrate/downloads/fix_dementia_care_homecare_report.pdf
23. von Känel R, Mausbach BT, Dimsdale JE, et al. Refining caregiver vulnerability for clinical practice: determinants of self-rated health in spousal dementia caregivers. BMC Geriatr. 2019;19:18.
24. Chen HM, Huang MF, Yeh YC, et al. Effectiveness of coping strategies intervention on caregiver burden among caregivers of elderly patients with dementia. Psychogeriatrics. 2015; 15:20-25.
25. Wawrziczny E, Larochette C, Papo D, et al. A customized intervention for dementia caregivers: a quasi-experimental design. J Aging Health. 2019;31:1172-1195.
26. Gitlin LN, Piersol CV, Hodgson N, et al. Reducing neuropsychiatric symptoms in persons with dementia and associated burden in family caregivers using tailored activities: Design and methods of a randomized clinical trial. Contemp Clin Trials. 2016;49:92-102.
27. de Oliveira AM, Radanovic M, Homem de Mello PC, et al. An intervention to reduce neuropsychiatric symptoms and caregiver burden in dementia: preliminary results from a randomized trial of the tailored activity program-outpatient version. Int J Geriatr Psychiatry. 2019;34:1301-1307.
28. Livingston G, Barber J, Rapaport P, et al. Clinical effectiveness of a manual based coping strategy programme (START, STrAtegies for RelaTives) in promoting the mental health of carers of family members with dementia: pragmatic randomised controlled trial. BMJ. 2013;347:f6276.
29. Kajiyama B, Fernandez G, Carter EA, et al. Helping Hispanic dementia caregivers cope with stress using technology-based resources. Clin Gerontol. 2018;41:209-216.
30. Moskowitz JT, Cheung EO, Snowberg KE, et al. Randomized controlled trial of a facilitated online positive emotion regulation intervention for dementia caregivers. Health Psychol. 2019;38:391-402.
31. Yoon HK, Kim GS. An empowerment program for family caregivers of people with dementia. Public Health Nurs. 2020;37:222-233.
32. Zwingmann I, Dreier-Wolfgramm A, Esser A, et al. Why do family dementia caregivers reject caregiver support services? Analyzing types of rejection and associated health-impairments in a cluster-randomized controlled intervention trial. BMC Health Serv Res. 2020;20:121.
33. Nybakken S, Strandås M, Bondas T. Caregivers’ perceptions of aggressive behaviour in nursing home residents living with dementia: A meta-ethnography. J Adv Nurs. 2018;74:2713-2726.
34. Nakaishi L, Moss H, Weinstein M, et al. Exploring workplace violence among home care workers in a consumer-driven home health care program. Workplace Health Saf. 2013;61:441-450.
35. Medical Advisory Secretariat. Caregiver- and patient-directed interventions for dementia: an evidence-based analysis. Ont Health Technol Assess Ser. 2008;8:1-98.
36. Betz ME, McCourt AD, Vernick JS, et al. Firearms and dementia: clinical considerations. Ann Intern Med. 2018;169:47-49.
37. Leng M, Zhao Y, Wang Z. Comparative efficacy of non-pharmacological interventions on agitation in people with dementia: a systematic review and Bayesian network meta-analysis. Int J Nurs Stud. 2020;102:103489.
38. Morgan S, Pullon S, McKinlay E. Observation of interprofessional collaborative practice in primary care teams: an integrative literature review. Int J Nurs Stud. 2015;52:1217-1230.
PRACTICE RECOMMENDATIONS
› Screen caregivers and family members of patients with dementia for signs of interpersonal violence. C
› Counsel caregivers early on that behavior changes in patients with dementia are likely and may be unpredictable. C
› Discuss safety strategies for the caregiver, including when it is appropriate to alter routines such as bedtimes and meals. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series

Siblings of people with bipolar disorder have higher cancer risk
, according to new research from Taiwan.
“To our knowledge, our study is the first to report an increased overall cancer risk as well as increased risks of breast and ectodermal cancer among the unaffected siblings aged < 50 years of patients with bipolar disorder,” Ya-Mei Bai, MD, PhD, of National Yang-Ming University, Taipei, Taiwan, and colleagues write in an article published online in the International Journal of Cancer.
Most, but not all, previous studies have shown a link between bipolar disorder and cancer. Whether the elevated risk of malignancy extends to family members without the mental health condition has not been elucidated.
To investigate, the researchers turned to the National Health Insurance Research Database of Taiwan. They identified 25,356 individuals diagnosed with bipolar disorder by a psychiatrist between 1996 and 2010 and the same number of unaffected siblings, as well as more than 100,000 age-, sex-, income-, and residence-matched controls without severe mental illness.
Compared with the control group, people with bipolar disorder (odds ratio, 1.22) and their unaffected siblings (OR, 1.17) both had a higher risk of developing malignant cancer of any kind. The researchers also found that both groups were at higher risk for breast cancer, with odds ratios of 1.98 in individuals with bipolar disorder and 1.73 in their unaffected siblings.
However, the risk of skin cancer was only high in people with bipolar disorder (OR, 2.70) and not in their siblings (OR, 0.62). And conversely, the risk of kidney cancer was significantly increased in unaffected siblings (OR, 2.45) but not in people with bipolar disorder (OR, 0.47).
When stratified by the embryonic developmental layer from which tumors had originated – ectodermal, mesodermal, or endodermal – the authors observed a significantly increased risk for only ectodermal cancers. In addition, only people under age 50 in both groups (OR, 1.90 for those with bipolar disorder; OR, 1.65 for siblings) were more likely to develop an ectodermal cancer, especially of the breast, compared with the control group. The risks remained elevated after excluding breast cancer but were no longer significant.
When stratified by age, the risk of developing any cancer in both groups also only appeared to be greater for those under age 50 (OR, 1.34 in people with bipolar disorder; OR, 1.32 in siblings) compared with those aged 50 and over (OR, 0.97 and 0.99, respectively). The authors highlighted these figures in the supplemental data set but did not discuss it further in the study beyond a brief mention that “younger patients with bipolar disorder and younger unaffected siblings (< 50 years), but not older ones (≥ 50 years), were more likely to develop any malignancy during the follow-up than matched controls.”
“This paper essentially finds what we have found in our previous work – that people with bipolar disorder have a greater risk of cancer,” said Michael Berk, MBBCh, PhD, a professor of psychiatry at the Deakin University School of Medicine in Geelong, Australia, who published a systematic review and meta-analysis last spring on cancer risk and the role of lithium treatment in bipolar disorder.
“The interesting finding in our work,” Dr. Berk told this news organization, “is that this risk is attenuated by use of lithium but not other agents.”
The Taiwanese researchers propose a “biopsychosocial explanation” for their results, noting that both the nervous system and the breast and skin develop from the ectoderm, and that cancer risk factors such as smoking and obesity are more common in people with bipolar disorder and their unaffected siblings.
“The findings,” they write, “imply a genetic overlap in neurodevelopment and malignancy pathogenesis and may encourage clinicians to closely monitor patients with bipolar disorder and their unaffected siblings for cancer warning signs.”
The authors, however, caution that their study needs validation and had several limitations, including lack of adjustment for drug treatment and lifestyle and environmental factors.
“Our findings may persuade clinicians and researchers to reevaluate the cancer risk among the unaffected siblings of patients with schizophrenia and bipolar disorder because these two severe mental disorders may have a common biopsychosocial pathophysiology,” the team writes.
The study was supported by a grant from Taipei Veterans General Hospital, Yen Tjing Ling Medical Foundation, and the Ministry of Science and Technology, Taiwan.
A version of this article first appeared on Medscape.com.
, according to new research from Taiwan.
“To our knowledge, our study is the first to report an increased overall cancer risk as well as increased risks of breast and ectodermal cancer among the unaffected siblings aged < 50 years of patients with bipolar disorder,” Ya-Mei Bai, MD, PhD, of National Yang-Ming University, Taipei, Taiwan, and colleagues write in an article published online in the International Journal of Cancer.
Most, but not all, previous studies have shown a link between bipolar disorder and cancer. Whether the elevated risk of malignancy extends to family members without the mental health condition has not been elucidated.
To investigate, the researchers turned to the National Health Insurance Research Database of Taiwan. They identified 25,356 individuals diagnosed with bipolar disorder by a psychiatrist between 1996 and 2010 and the same number of unaffected siblings, as well as more than 100,000 age-, sex-, income-, and residence-matched controls without severe mental illness.
Compared with the control group, people with bipolar disorder (odds ratio, 1.22) and their unaffected siblings (OR, 1.17) both had a higher risk of developing malignant cancer of any kind. The researchers also found that both groups were at higher risk for breast cancer, with odds ratios of 1.98 in individuals with bipolar disorder and 1.73 in their unaffected siblings.
However, the risk of skin cancer was only high in people with bipolar disorder (OR, 2.70) and not in their siblings (OR, 0.62). And conversely, the risk of kidney cancer was significantly increased in unaffected siblings (OR, 2.45) but not in people with bipolar disorder (OR, 0.47).
When stratified by the embryonic developmental layer from which tumors had originated – ectodermal, mesodermal, or endodermal – the authors observed a significantly increased risk for only ectodermal cancers. In addition, only people under age 50 in both groups (OR, 1.90 for those with bipolar disorder; OR, 1.65 for siblings) were more likely to develop an ectodermal cancer, especially of the breast, compared with the control group. The risks remained elevated after excluding breast cancer but were no longer significant.
When stratified by age, the risk of developing any cancer in both groups also only appeared to be greater for those under age 50 (OR, 1.34 in people with bipolar disorder; OR, 1.32 in siblings) compared with those aged 50 and over (OR, 0.97 and 0.99, respectively). The authors highlighted these figures in the supplemental data set but did not discuss it further in the study beyond a brief mention that “younger patients with bipolar disorder and younger unaffected siblings (< 50 years), but not older ones (≥ 50 years), were more likely to develop any malignancy during the follow-up than matched controls.”
“This paper essentially finds what we have found in our previous work – that people with bipolar disorder have a greater risk of cancer,” said Michael Berk, MBBCh, PhD, a professor of psychiatry at the Deakin University School of Medicine in Geelong, Australia, who published a systematic review and meta-analysis last spring on cancer risk and the role of lithium treatment in bipolar disorder.
“The interesting finding in our work,” Dr. Berk told this news organization, “is that this risk is attenuated by use of lithium but not other agents.”
The Taiwanese researchers propose a “biopsychosocial explanation” for their results, noting that both the nervous system and the breast and skin develop from the ectoderm, and that cancer risk factors such as smoking and obesity are more common in people with bipolar disorder and their unaffected siblings.
“The findings,” they write, “imply a genetic overlap in neurodevelopment and malignancy pathogenesis and may encourage clinicians to closely monitor patients with bipolar disorder and their unaffected siblings for cancer warning signs.”
The authors, however, caution that their study needs validation and had several limitations, including lack of adjustment for drug treatment and lifestyle and environmental factors.
“Our findings may persuade clinicians and researchers to reevaluate the cancer risk among the unaffected siblings of patients with schizophrenia and bipolar disorder because these two severe mental disorders may have a common biopsychosocial pathophysiology,” the team writes.
The study was supported by a grant from Taipei Veterans General Hospital, Yen Tjing Ling Medical Foundation, and the Ministry of Science and Technology, Taiwan.
A version of this article first appeared on Medscape.com.
, according to new research from Taiwan.
“To our knowledge, our study is the first to report an increased overall cancer risk as well as increased risks of breast and ectodermal cancer among the unaffected siblings aged < 50 years of patients with bipolar disorder,” Ya-Mei Bai, MD, PhD, of National Yang-Ming University, Taipei, Taiwan, and colleagues write in an article published online in the International Journal of Cancer.
Most, but not all, previous studies have shown a link between bipolar disorder and cancer. Whether the elevated risk of malignancy extends to family members without the mental health condition has not been elucidated.
To investigate, the researchers turned to the National Health Insurance Research Database of Taiwan. They identified 25,356 individuals diagnosed with bipolar disorder by a psychiatrist between 1996 and 2010 and the same number of unaffected siblings, as well as more than 100,000 age-, sex-, income-, and residence-matched controls without severe mental illness.
Compared with the control group, people with bipolar disorder (odds ratio, 1.22) and their unaffected siblings (OR, 1.17) both had a higher risk of developing malignant cancer of any kind. The researchers also found that both groups were at higher risk for breast cancer, with odds ratios of 1.98 in individuals with bipolar disorder and 1.73 in their unaffected siblings.
However, the risk of skin cancer was only high in people with bipolar disorder (OR, 2.70) and not in their siblings (OR, 0.62). And conversely, the risk of kidney cancer was significantly increased in unaffected siblings (OR, 2.45) but not in people with bipolar disorder (OR, 0.47).
When stratified by the embryonic developmental layer from which tumors had originated – ectodermal, mesodermal, or endodermal – the authors observed a significantly increased risk for only ectodermal cancers. In addition, only people under age 50 in both groups (OR, 1.90 for those with bipolar disorder; OR, 1.65 for siblings) were more likely to develop an ectodermal cancer, especially of the breast, compared with the control group. The risks remained elevated after excluding breast cancer but were no longer significant.
When stratified by age, the risk of developing any cancer in both groups also only appeared to be greater for those under age 50 (OR, 1.34 in people with bipolar disorder; OR, 1.32 in siblings) compared with those aged 50 and over (OR, 0.97 and 0.99, respectively). The authors highlighted these figures in the supplemental data set but did not discuss it further in the study beyond a brief mention that “younger patients with bipolar disorder and younger unaffected siblings (< 50 years), but not older ones (≥ 50 years), were more likely to develop any malignancy during the follow-up than matched controls.”
“This paper essentially finds what we have found in our previous work – that people with bipolar disorder have a greater risk of cancer,” said Michael Berk, MBBCh, PhD, a professor of psychiatry at the Deakin University School of Medicine in Geelong, Australia, who published a systematic review and meta-analysis last spring on cancer risk and the role of lithium treatment in bipolar disorder.
“The interesting finding in our work,” Dr. Berk told this news organization, “is that this risk is attenuated by use of lithium but not other agents.”
The Taiwanese researchers propose a “biopsychosocial explanation” for their results, noting that both the nervous system and the breast and skin develop from the ectoderm, and that cancer risk factors such as smoking and obesity are more common in people with bipolar disorder and their unaffected siblings.
“The findings,” they write, “imply a genetic overlap in neurodevelopment and malignancy pathogenesis and may encourage clinicians to closely monitor patients with bipolar disorder and their unaffected siblings for cancer warning signs.”
The authors, however, caution that their study needs validation and had several limitations, including lack of adjustment for drug treatment and lifestyle and environmental factors.
“Our findings may persuade clinicians and researchers to reevaluate the cancer risk among the unaffected siblings of patients with schizophrenia and bipolar disorder because these two severe mental disorders may have a common biopsychosocial pathophysiology,” the team writes.
The study was supported by a grant from Taipei Veterans General Hospital, Yen Tjing Ling Medical Foundation, and the Ministry of Science and Technology, Taiwan.
A version of this article first appeared on Medscape.com.
FROM INTERNATIONAL JOURNAL OF CANCER
Novel biomarker found for Alzheimer’s disease
The study covered in this summary was published in medRxiv.org as a preprint and has not yet been peer reviewed.
Key takeaways
- Estimated beta-amyloid (Aβ42) cellular uptake can be more than two times greater in AD patients compared to cognitively normal subjects. A less pronounced yet increased uptake rate was also observed in patients with late-onset mild cognitive impairment (MCI). This increased uptake may prove to be a key mechanism defining age-related AD progression.
- The increased cellular amyloid uptake in AD and LMCI may lead to quicker disease progression, but early-onset MCI may result from increased production of toxic amyloid metabolites.
Why this matters
- Additional biomarkers for AD could greatly aid diagnosis and course prediction, as they are currently limited to PET scan analysis of amyloid plaque deposits and concentration of Aβ42 in cerebrospinal fluid (CSF).
- Amyloid deposits found by PET have a positive correlation with AD diagnosis. In contrast, CSF-Aβ42 and AD diagnosis or cognitive decline are negatively correlated. Normal cognition (NC) is associated with higher CSF beta-amyloid levels, but previous research has not explained why CSF-Aβ42 levels can be equivalent in patients with NC but high amyloid load and patients with AD and low amyloid load.
Study design
- The authors of this retrospective study used anonymized data obtained from the Alzheimer’s’s Disease Neuroimaging Initiative (ADNI). ADNI’s goal has been to test whether serial MRI scans, PET scans, biomarkers, and clinical/neuropsychological assessment can be combined to measure the progression of MCI and AD.
- Study subjects had either an AD diagnosis or NC and were divided into two groups: low amyloid load and high amyloid load. The fraction of patients with an AD diagnosis was calculated as a function of CSF-Aβ42.
- Calculations and statistical comparisons were performed using Microsoft Excel and custom-written C++ programs.
Key results
- The lowest levels of CSF-Aβ42 correlated with the highest percentage of AD-diagnosed patients, estimated to be 27% in subjects with low amyloid deposit density and 65% in those with high deposit density.
- The relationship between CSF-Aβ42 levels and amyloid load can be described using a simple mathematical model: Amyloid concentration in the interstitial cells is equal to the synthesis rate divided by the density of amyloid deposits plus the sum of the rate of amyloid removal through the CSF and the cellular amyloid uptake rate.
- AD and late-onset MCI patients had a significantly higher amyloid removal rate compared to NC subjects.
- Early-onset MCI patients had Aβ42 turnover similar to that of NC subjects, pointing to a different underlying mechanism such as enzymatic disbalance.
Limitations
- The model used to explain amyloid exchange between the interstitial space and the CSF is oversimplified; the actual process is more complex.
- Synthesis and uptake rates of Aβ42 vary throughout areas of the brain. The model assumes a homogeneous distribution within the interstitial compartment.
Study disclosures
- Research reported in this publication was not supported by any external funding. Data collection and sharing for this project were funded by ADNI.
A version of this article first appeared on Medscape.com.
The study covered in this summary was published in medRxiv.org as a preprint and has not yet been peer reviewed.
Key takeaways
- Estimated beta-amyloid (Aβ42) cellular uptake can be more than two times greater in AD patients compared to cognitively normal subjects. A less pronounced yet increased uptake rate was also observed in patients with late-onset mild cognitive impairment (MCI). This increased uptake may prove to be a key mechanism defining age-related AD progression.
- The increased cellular amyloid uptake in AD and LMCI may lead to quicker disease progression, but early-onset MCI may result from increased production of toxic amyloid metabolites.
Why this matters
- Additional biomarkers for AD could greatly aid diagnosis and course prediction, as they are currently limited to PET scan analysis of amyloid plaque deposits and concentration of Aβ42 in cerebrospinal fluid (CSF).
- Amyloid deposits found by PET have a positive correlation with AD diagnosis. In contrast, CSF-Aβ42 and AD diagnosis or cognitive decline are negatively correlated. Normal cognition (NC) is associated with higher CSF beta-amyloid levels, but previous research has not explained why CSF-Aβ42 levels can be equivalent in patients with NC but high amyloid load and patients with AD and low amyloid load.
Study design
- The authors of this retrospective study used anonymized data obtained from the Alzheimer’s’s Disease Neuroimaging Initiative (ADNI). ADNI’s goal has been to test whether serial MRI scans, PET scans, biomarkers, and clinical/neuropsychological assessment can be combined to measure the progression of MCI and AD.
- Study subjects had either an AD diagnosis or NC and were divided into two groups: low amyloid load and high amyloid load. The fraction of patients with an AD diagnosis was calculated as a function of CSF-Aβ42.
- Calculations and statistical comparisons were performed using Microsoft Excel and custom-written C++ programs.
Key results
- The lowest levels of CSF-Aβ42 correlated with the highest percentage of AD-diagnosed patients, estimated to be 27% in subjects with low amyloid deposit density and 65% in those with high deposit density.
- The relationship between CSF-Aβ42 levels and amyloid load can be described using a simple mathematical model: Amyloid concentration in the interstitial cells is equal to the synthesis rate divided by the density of amyloid deposits plus the sum of the rate of amyloid removal through the CSF and the cellular amyloid uptake rate.
- AD and late-onset MCI patients had a significantly higher amyloid removal rate compared to NC subjects.
- Early-onset MCI patients had Aβ42 turnover similar to that of NC subjects, pointing to a different underlying mechanism such as enzymatic disbalance.
Limitations
- The model used to explain amyloid exchange between the interstitial space and the CSF is oversimplified; the actual process is more complex.
- Synthesis and uptake rates of Aβ42 vary throughout areas of the brain. The model assumes a homogeneous distribution within the interstitial compartment.
Study disclosures
- Research reported in this publication was not supported by any external funding. Data collection and sharing for this project were funded by ADNI.
A version of this article first appeared on Medscape.com.
The study covered in this summary was published in medRxiv.org as a preprint and has not yet been peer reviewed.
Key takeaways
- Estimated beta-amyloid (Aβ42) cellular uptake can be more than two times greater in AD patients compared to cognitively normal subjects. A less pronounced yet increased uptake rate was also observed in patients with late-onset mild cognitive impairment (MCI). This increased uptake may prove to be a key mechanism defining age-related AD progression.
- The increased cellular amyloid uptake in AD and LMCI may lead to quicker disease progression, but early-onset MCI may result from increased production of toxic amyloid metabolites.
Why this matters
- Additional biomarkers for AD could greatly aid diagnosis and course prediction, as they are currently limited to PET scan analysis of amyloid plaque deposits and concentration of Aβ42 in cerebrospinal fluid (CSF).
- Amyloid deposits found by PET have a positive correlation with AD diagnosis. In contrast, CSF-Aβ42 and AD diagnosis or cognitive decline are negatively correlated. Normal cognition (NC) is associated with higher CSF beta-amyloid levels, but previous research has not explained why CSF-Aβ42 levels can be equivalent in patients with NC but high amyloid load and patients with AD and low amyloid load.
Study design
- The authors of this retrospective study used anonymized data obtained from the Alzheimer’s’s Disease Neuroimaging Initiative (ADNI). ADNI’s goal has been to test whether serial MRI scans, PET scans, biomarkers, and clinical/neuropsychological assessment can be combined to measure the progression of MCI and AD.
- Study subjects had either an AD diagnosis or NC and were divided into two groups: low amyloid load and high amyloid load. The fraction of patients with an AD diagnosis was calculated as a function of CSF-Aβ42.
- Calculations and statistical comparisons were performed using Microsoft Excel and custom-written C++ programs.
Key results
- The lowest levels of CSF-Aβ42 correlated with the highest percentage of AD-diagnosed patients, estimated to be 27% in subjects with low amyloid deposit density and 65% in those with high deposit density.
- The relationship between CSF-Aβ42 levels and amyloid load can be described using a simple mathematical model: Amyloid concentration in the interstitial cells is equal to the synthesis rate divided by the density of amyloid deposits plus the sum of the rate of amyloid removal through the CSF and the cellular amyloid uptake rate.
- AD and late-onset MCI patients had a significantly higher amyloid removal rate compared to NC subjects.
- Early-onset MCI patients had Aβ42 turnover similar to that of NC subjects, pointing to a different underlying mechanism such as enzymatic disbalance.
Limitations
- The model used to explain amyloid exchange between the interstitial space and the CSF is oversimplified; the actual process is more complex.
- Synthesis and uptake rates of Aβ42 vary throughout areas of the brain. The model assumes a homogeneous distribution within the interstitial compartment.
Study disclosures
- Research reported in this publication was not supported by any external funding. Data collection and sharing for this project were funded by ADNI.
A version of this article first appeared on Medscape.com.
Did a switch to a generic antidepressant cause relapse?
Dramatic increase in driving high after cannabis legislation
Since Canada legalized marijuana in 2018, there has been a dramatic increase in the number of individuals driving while high, new research shows.
Investigators studied over 4,000 drivers treated after a motor vehicle collision in British Columbia trauma centers and found that, before cannabis was legalized, a THC level greater than 0 ng/mL in the blood was present in roughly 10% of drivers. After the drug was legalized this percentage increased to 18%. The percentages of injured drivers with at least 2 ng/mL, the Canadian legal limit, and at least 5 ng/mL more than doubled.

“It’s concerning that we’re seeing such a dramatic increase,” study investigator Jeffrey Brubacher, MD, associate professor, department of emergency medicine, University of British Columbia, Vancouver, said in a press release.
“There are serious risks associated with driving after cannabis use and our findings suggest more [work] is needed to deter this dangerous behavior in light of legalization,” he said.
The study was published online Jan. 12 in the New England Journal of Medicine.
Impact of legalization?
The investigators note that the Canadian government introduced a law aiming to prevent cannabis-impaired driving by establishing penalties and criminal charges for drivers found with a whole-blood THC level of 2 ng/mL, with more severe penalties for those with a THC level of greater than 5 ng/mL or greater than 2.5 ng/mL combined with a blood alcohol level of .05%.
Cannabis use is “associated with cognitive deficits and psychomotor impairment, and there is evidence that it increases the risk of motor vehicle crashes, especially at higher THC levels,” they noted.
“I’m an emergency physician at Vancouver General Hospital’s trauma center. We’ve been measuring drug levels in injured drivers since 2013 here in British Columbia and, in particular, we’ve been measuring THC levels,” Dr. Brubacher said in an interview. “We thought it would be interesting and important to see what would happen after legalization.”
The investigators studied 4,339 drivers – 3,550 whose accident took place before legalization of cannabis, and 789 after legalization – who had been moderately injured in a motor vehicle collision and presented to four British Columbia trauma centers between January 2013 and March 2020.
said Dr. Brubacher. Drivers included in the study had excess blood remaining after the clinical testing had been completed, which was then used for drug analysis.
Insufficient laws
After legalization there was an increased prevalence of drivers with a THC level greater than 0 ng/mL, a TCH level of at least 2 ng/mL, and a THC level of at least 5 ng/mL.
The largest increases in a THC level of at least 2 ng/mL were in drivers 50 years of age or older and among male drivers (adjusted prevalence ratio, 5.18; 95% confidence interval, 2.49-10.78 and aPR, 2.44; 95% CI, 1.60-3.74, respectively).
“There were no significant changes in the prevalence of drivers testing positive for alcohol,” the authors reported.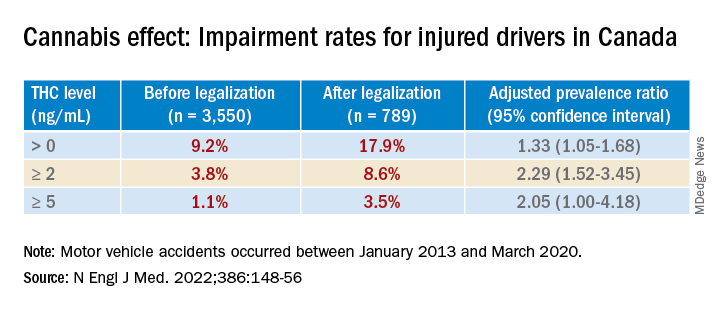
Dr. Brubacher said the evidence suggests these new laws “are not enough to stop everyone from driving after using cannabis.”
The findings have implications for clinicians and patients and for policymakers, he said. “My moderately conservative recommendations are that, if you are going to smoke cannabis, wait at least 4 hours after smoking before you drive. Edibles last longer, and patients should wait least 8 hours after ingesting [edibles] before driving. And of course, if you continue to feel the effects of the THC, you should avoid driving altogether until the time has elapsed and you no longer feel any effects.”
Dr. Brubacher hopes policy makers will use the study’s findings to “design public information campaigns and enforcement measures that encourage drivers, especially older drivers, to separate cannabis use from driving.”
Additionally, “policy makers shouldn’t lose sight of drinking and driving because that’s an even bigger problem than the risk of driving under the influence of cannabis.”
Focus on older adults
In a comment, Anees Bahji, MD, an International Collaborative Addiction Medicine research fellow at the British Columbia Centre on Substance Use, called the study “interesting and relevant.”
He raised several questions regarding the “correlation between the level of a substance in a person’s system and the degree of impairment.” For example, “does the same level of THC in the blood affect us all the same way? And to what extent do the levels detected at the time of the analysis correlate with the level in the person’s system at the time of driving?”
An additional consideration “is for individuals with cannabis use disorder and for those who have developed tolerance to the psychoactive effects of THC: Does it affect their driving skills in the same way as someone who is cannabis naive?” asked Dr. Bahji, a clinical assistant professor at the University of Calgary (Alta.) who was not involved with the study.
Also commenting, Eric Sevigny, PhD, associate professor of criminal justice and criminology at Georgia State University, Atlanta, described it as a “well-designed study that adds yet another data point for considering appropriate road safety policy responses alongside ongoing cannabis liberalization.”
However, the findings “cannot say much about whether cannabis legalization leads to an increase in cannabis-impaired driving, because current research finds little correlation between biological THC concentrations and driving performance,” said Dr. Sevigny, who was not involved with the study.
The finding of “higher THC prevalence among older adults is also relevant for road safety, as this population has a number of concomitant risk factors, such as cognitive decline and prescription drug use,” Dr. Sevigny added.
The study was supported by the Canadian Institutes of Health Research. Dr. Brubacher and Dr. Sevigny disclosed no relevant financial relationships. Dr. Bahji reported receiving research funding from the Canadian Institutes of Health Research, the Calgary Health Trust, the American Psychiatric Association, NIDA, and the University of Calgary.
A version of this article first appeared on Medscape.com.
Since Canada legalized marijuana in 2018, there has been a dramatic increase in the number of individuals driving while high, new research shows.
Investigators studied over 4,000 drivers treated after a motor vehicle collision in British Columbia trauma centers and found that, before cannabis was legalized, a THC level greater than 0 ng/mL in the blood was present in roughly 10% of drivers. After the drug was legalized this percentage increased to 18%. The percentages of injured drivers with at least 2 ng/mL, the Canadian legal limit, and at least 5 ng/mL more than doubled.
“It’s concerning that we’re seeing such a dramatic increase,” study investigator Jeffrey Brubacher, MD, associate professor, department of emergency medicine, University of British Columbia, Vancouver, said in a press release.
“There are serious risks associated with driving after cannabis use and our findings suggest more [work] is needed to deter this dangerous behavior in light of legalization,” he said.
The study was published online Jan. 12 in the New England Journal of Medicine.
Impact of legalization?
The investigators note that the Canadian government introduced a law aiming to prevent cannabis-impaired driving by establishing penalties and criminal charges for drivers found with a whole-blood THC level of 2 ng/mL, with more severe penalties for those with a THC level of greater than 5 ng/mL or greater than 2.5 ng/mL combined with a blood alcohol level of .05%.
Cannabis use is “associated with cognitive deficits and psychomotor impairment, and there is evidence that it increases the risk of motor vehicle crashes, especially at higher THC levels,” they noted.
“I’m an emergency physician at Vancouver General Hospital’s trauma center. We’ve been measuring drug levels in injured drivers since 2013 here in British Columbia and, in particular, we’ve been measuring THC levels,” Dr. Brubacher said in an interview. “We thought it would be interesting and important to see what would happen after legalization.”
The investigators studied 4,339 drivers – 3,550 whose accident took place before legalization of cannabis, and 789 after legalization – who had been moderately injured in a motor vehicle collision and presented to four British Columbia trauma centers between January 2013 and March 2020.
said Dr. Brubacher. Drivers included in the study had excess blood remaining after the clinical testing had been completed, which was then used for drug analysis.
Insufficient laws
After legalization there was an increased prevalence of drivers with a THC level greater than 0 ng/mL, a TCH level of at least 2 ng/mL, and a THC level of at least 5 ng/mL.
The largest increases in a THC level of at least 2 ng/mL were in drivers 50 years of age or older and among male drivers (adjusted prevalence ratio, 5.18; 95% confidence interval, 2.49-10.78 and aPR, 2.44; 95% CI, 1.60-3.74, respectively).
“There were no significant changes in the prevalence of drivers testing positive for alcohol,” the authors reported.
Dr. Brubacher said the evidence suggests these new laws “are not enough to stop everyone from driving after using cannabis.”
The findings have implications for clinicians and patients and for policymakers, he said. “My moderately conservative recommendations are that, if you are going to smoke cannabis, wait at least 4 hours after smoking before you drive. Edibles last longer, and patients should wait least 8 hours after ingesting [edibles] before driving. And of course, if you continue to feel the effects of the THC, you should avoid driving altogether until the time has elapsed and you no longer feel any effects.”
Dr. Brubacher hopes policy makers will use the study’s findings to “design public information campaigns and enforcement measures that encourage drivers, especially older drivers, to separate cannabis use from driving.”
Additionally, “policy makers shouldn’t lose sight of drinking and driving because that’s an even bigger problem than the risk of driving under the influence of cannabis.”
Focus on older adults
In a comment, Anees Bahji, MD, an International Collaborative Addiction Medicine research fellow at the British Columbia Centre on Substance Use, called the study “interesting and relevant.”
He raised several questions regarding the “correlation between the level of a substance in a person’s system and the degree of impairment.” For example, “does the same level of THC in the blood affect us all the same way? And to what extent do the levels detected at the time of the analysis correlate with the level in the person’s system at the time of driving?”
An additional consideration “is for individuals with cannabis use disorder and for those who have developed tolerance to the psychoactive effects of THC: Does it affect their driving skills in the same way as someone who is cannabis naive?” asked Dr. Bahji, a clinical assistant professor at the University of Calgary (Alta.) who was not involved with the study.
Also commenting, Eric Sevigny, PhD, associate professor of criminal justice and criminology at Georgia State University, Atlanta, described it as a “well-designed study that adds yet another data point for considering appropriate road safety policy responses alongside ongoing cannabis liberalization.”
However, the findings “cannot say much about whether cannabis legalization leads to an increase in cannabis-impaired driving, because current research finds little correlation between biological THC concentrations and driving performance,” said Dr. Sevigny, who was not involved with the study.
The finding of “higher THC prevalence among older adults is also relevant for road safety, as this population has a number of concomitant risk factors, such as cognitive decline and prescription drug use,” Dr. Sevigny added.
The study was supported by the Canadian Institutes of Health Research. Dr. Brubacher and Dr. Sevigny disclosed no relevant financial relationships. Dr. Bahji reported receiving research funding from the Canadian Institutes of Health Research, the Calgary Health Trust, the American Psychiatric Association, NIDA, and the University of Calgary.
A version of this article first appeared on Medscape.com.
Since Canada legalized marijuana in 2018, there has been a dramatic increase in the number of individuals driving while high, new research shows.
Investigators studied over 4,000 drivers treated after a motor vehicle collision in British Columbia trauma centers and found that, before cannabis was legalized, a THC level greater than 0 ng/mL in the blood was present in roughly 10% of drivers. After the drug was legalized this percentage increased to 18%. The percentages of injured drivers with at least 2 ng/mL, the Canadian legal limit, and at least 5 ng/mL more than doubled.
“It’s concerning that we’re seeing such a dramatic increase,” study investigator Jeffrey Brubacher, MD, associate professor, department of emergency medicine, University of British Columbia, Vancouver, said in a press release.
“There are serious risks associated with driving after cannabis use and our findings suggest more [work] is needed to deter this dangerous behavior in light of legalization,” he said.
The study was published online Jan. 12 in the New England Journal of Medicine.
Impact of legalization?
The investigators note that the Canadian government introduced a law aiming to prevent cannabis-impaired driving by establishing penalties and criminal charges for drivers found with a whole-blood THC level of 2 ng/mL, with more severe penalties for those with a THC level of greater than 5 ng/mL or greater than 2.5 ng/mL combined with a blood alcohol level of .05%.
Cannabis use is “associated with cognitive deficits and psychomotor impairment, and there is evidence that it increases the risk of motor vehicle crashes, especially at higher THC levels,” they noted.
“I’m an emergency physician at Vancouver General Hospital’s trauma center. We’ve been measuring drug levels in injured drivers since 2013 here in British Columbia and, in particular, we’ve been measuring THC levels,” Dr. Brubacher said in an interview. “We thought it would be interesting and important to see what would happen after legalization.”
The investigators studied 4,339 drivers – 3,550 whose accident took place before legalization of cannabis, and 789 after legalization – who had been moderately injured in a motor vehicle collision and presented to four British Columbia trauma centers between January 2013 and March 2020.
said Dr. Brubacher. Drivers included in the study had excess blood remaining after the clinical testing had been completed, which was then used for drug analysis.
Insufficient laws
After legalization there was an increased prevalence of drivers with a THC level greater than 0 ng/mL, a TCH level of at least 2 ng/mL, and a THC level of at least 5 ng/mL.
The largest increases in a THC level of at least 2 ng/mL were in drivers 50 years of age or older and among male drivers (adjusted prevalence ratio, 5.18; 95% confidence interval, 2.49-10.78 and aPR, 2.44; 95% CI, 1.60-3.74, respectively).
“There were no significant changes in the prevalence of drivers testing positive for alcohol,” the authors reported.
Dr. Brubacher said the evidence suggests these new laws “are not enough to stop everyone from driving after using cannabis.”
The findings have implications for clinicians and patients and for policymakers, he said. “My moderately conservative recommendations are that, if you are going to smoke cannabis, wait at least 4 hours after smoking before you drive. Edibles last longer, and patients should wait least 8 hours after ingesting [edibles] before driving. And of course, if you continue to feel the effects of the THC, you should avoid driving altogether until the time has elapsed and you no longer feel any effects.”
Dr. Brubacher hopes policy makers will use the study’s findings to “design public information campaigns and enforcement measures that encourage drivers, especially older drivers, to separate cannabis use from driving.”
Additionally, “policy makers shouldn’t lose sight of drinking and driving because that’s an even bigger problem than the risk of driving under the influence of cannabis.”
Focus on older adults
In a comment, Anees Bahji, MD, an International Collaborative Addiction Medicine research fellow at the British Columbia Centre on Substance Use, called the study “interesting and relevant.”
He raised several questions regarding the “correlation between the level of a substance in a person’s system and the degree of impairment.” For example, “does the same level of THC in the blood affect us all the same way? And to what extent do the levels detected at the time of the analysis correlate with the level in the person’s system at the time of driving?”
An additional consideration “is for individuals with cannabis use disorder and for those who have developed tolerance to the psychoactive effects of THC: Does it affect their driving skills in the same way as someone who is cannabis naive?” asked Dr. Bahji, a clinical assistant professor at the University of Calgary (Alta.) who was not involved with the study.
Also commenting, Eric Sevigny, PhD, associate professor of criminal justice and criminology at Georgia State University, Atlanta, described it as a “well-designed study that adds yet another data point for considering appropriate road safety policy responses alongside ongoing cannabis liberalization.”
However, the findings “cannot say much about whether cannabis legalization leads to an increase in cannabis-impaired driving, because current research finds little correlation between biological THC concentrations and driving performance,” said Dr. Sevigny, who was not involved with the study.
The finding of “higher THC prevalence among older adults is also relevant for road safety, as this population has a number of concomitant risk factors, such as cognitive decline and prescription drug use,” Dr. Sevigny added.
The study was supported by the Canadian Institutes of Health Research. Dr. Brubacher and Dr. Sevigny disclosed no relevant financial relationships. Dr. Bahji reported receiving research funding from the Canadian Institutes of Health Research, the Calgary Health Trust, the American Psychiatric Association, NIDA, and the University of Calgary.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Psychiatry resident’s viral posts reveal his own mental health battle
First-year psychiatry resident Jake Goodman, MD, knew he was taking a chance when he opened up on his popular social media platforms about his personal mental health battle. He mulled over the decision for several weeks before deciding to take the plunge.

As he voiced recently on his TikTok page, his biggest social media fanbase, with 1.3 million followers, it felt freeing to get his personal struggle off his chest.
“I’m a doctor in training, and most doctors would advise me not to post this,” the 29-year-old from Miami said in the video last month, which garnered 1.2 million views on TikTok alone. “They would say it’s risky for my career. But I didn’t join the medical field to continue the toxic status quo. I’m part of a new generation of health care professionals that are not afraid to be vulnerable and talk about mental health.”
“Dr. Jake,” as he calls himself on social media, admitted he was a physician who treats mental illness and also takes medication for it. “It felt good to say that. And by the way, I’m proud of it,” he said in the TikTok post.
A champion of mental health throughout the pandemic, Dr. Goodman called attention to the illness in the medical field. In a message on Instagram, he stated, “Opening up about your mental health as a medical professional, especially as a doctor who treats mental illness, can be taboo ... So here’s me leading by example.”
He also cited statistics on the challenge: “1 in 2 people will be diagnosed with a mental health illness at some point in their life. Yet many of us will never take medication that can help correct the chemical imbalance in our brains due to medication stigma: the fear that taking medications for our mental health somehow makes us weak.”
Mental health remains an issue among residents. Nearly 70% of residents polled by Medscape in its 2021 Residents Lifestyle & Happiness Report said they strongly or somewhat agree there’s a stigma against seeking mental health help. And nearly half, or 47% of those polled, said they sometimes (36%) or always/most of the time (11%) were depressed. The latter category rose in the past year.
Dr. Goodman told this news organization that he became passionate about mental health when he lost a college friend to suicide. “It really exposed the stigma” of mental health, he said. “I always knew it was there, but it took me seeing someone lose his life and [asking] why didn’t he feel comfortable talking to us, and why didn’t I feel comfortable talking to him?”
Stress of medical training
The decision to pursue psychiatry as his specialty came after a rotation in a clinic for people struggling with substance use disorders. “I was enthralled to see people change their life ... just by mental health care.” It’s why he went into medicine, he tells this news organization. “I always wanted to be in a field to help people [before they hit] rock bottom, when no one else could be there for them.”
Dr. Goodman’s personal battle with mental health didn’t arise until he started residency. “I was not really myself.” He said he felt numb and burned out. “I was not getting as much enjoyment out of things.” A friend pointed out that he might be depressed, so he went to see a therapist and then a psychiatrist and started on medication. “It had a profound impact on how I felt.”
Still, it took a while before Dr. Goodman was comfortable sharing his story with the 1.6 million followers he had already built across his social media platforms.
“I started on social media in 2020 with the goal of advocating for mental health and inspiring future doctors.” He said the message seemed to resonate with people struggling during the early part of the pandemic. On his social media accounts, he also talks about medical school, residency, and being a health care provider. His fiancé is also a resident doctor, in internal medicine.
Dr. Goodman is also trying to create a more realistic image of doctors than the superheroes he believed they were growing up. He wants those who grow up wanting to be doctors and who look up to him to see him as a human being with vulnerabilities, such as mental health.
“You can be a doctor and have mental health issues. Seeking treatment for mental health makes you a better doctor, and for other health care workers suffering in the midst of the pandemic, I want to let them know they are not alone.”
He pointed to the statistic that doctors have one of the highest suicide rates of any professions. “It’s better to talk about that in the early stages of training.”
Students, residents, or attending physicians who have mental health challenges shouldn’t allow their symptoms to go untreated, Dr. Goodman added. “Holding in all the stress and anxiety and feelings in a very traumatic field may be dangerous. ”
One of his goals is to campaign for the removal of a question on state medical licensing forms requiring doctors to report any mental health diagnosis. It’s why doctors may be afraid to admit that they are struggling. “I’m still here. It didn’t ruin my career.”
Doctors who seek treatment for mental health are theoretically protected under the Americans With Disabilities Act from being refused a license on the basis of that diagnosis. Dr. Goodman hopes to advocate at the state level to reduce discrimination and increase accessibility for doctors to seek mental health care.
Still, Dr. Goodman concedes he was initially fearful of the repercussions. “I opened up about it because this post could save lives. I was doing what I believed in.”
So if he runs into barriers to receive his medical license because of his admission, “that’s a serious problem,” he said. “There is already a shortage of doctors. We’ll see what happens in a few years. I am not the only one who will answer ‘yes’ to having sought treatment for a mental illness. The questions do not really need to be there.”
A version of this article first appeared on Medscape.com.
First-year psychiatry resident Jake Goodman, MD, knew he was taking a chance when he opened up on his popular social media platforms about his personal mental health battle. He mulled over the decision for several weeks before deciding to take the plunge.
As he voiced recently on his TikTok page, his biggest social media fanbase, with 1.3 million followers, it felt freeing to get his personal struggle off his chest.
“I’m a doctor in training, and most doctors would advise me not to post this,” the 29-year-old from Miami said in the video last month, which garnered 1.2 million views on TikTok alone. “They would say it’s risky for my career. But I didn’t join the medical field to continue the toxic status quo. I’m part of a new generation of health care professionals that are not afraid to be vulnerable and talk about mental health.”
“Dr. Jake,” as he calls himself on social media, admitted he was a physician who treats mental illness and also takes medication for it. “It felt good to say that. And by the way, I’m proud of it,” he said in the TikTok post.
A champion of mental health throughout the pandemic, Dr. Goodman called attention to the illness in the medical field. In a message on Instagram, he stated, “Opening up about your mental health as a medical professional, especially as a doctor who treats mental illness, can be taboo ... So here’s me leading by example.”
He also cited statistics on the challenge: “1 in 2 people will be diagnosed with a mental health illness at some point in their life. Yet many of us will never take medication that can help correct the chemical imbalance in our brains due to medication stigma: the fear that taking medications for our mental health somehow makes us weak.”
Mental health remains an issue among residents. Nearly 70% of residents polled by Medscape in its 2021 Residents Lifestyle & Happiness Report said they strongly or somewhat agree there’s a stigma against seeking mental health help. And nearly half, or 47% of those polled, said they sometimes (36%) or always/most of the time (11%) were depressed. The latter category rose in the past year.
Dr. Goodman told this news organization that he became passionate about mental health when he lost a college friend to suicide. “It really exposed the stigma” of mental health, he said. “I always knew it was there, but it took me seeing someone lose his life and [asking] why didn’t he feel comfortable talking to us, and why didn’t I feel comfortable talking to him?”
Stress of medical training
The decision to pursue psychiatry as his specialty came after a rotation in a clinic for people struggling with substance use disorders. “I was enthralled to see people change their life ... just by mental health care.” It’s why he went into medicine, he tells this news organization. “I always wanted to be in a field to help people [before they hit] rock bottom, when no one else could be there for them.”
Dr. Goodman’s personal battle with mental health didn’t arise until he started residency. “I was not really myself.” He said he felt numb and burned out. “I was not getting as much enjoyment out of things.” A friend pointed out that he might be depressed, so he went to see a therapist and then a psychiatrist and started on medication. “It had a profound impact on how I felt.”
Still, it took a while before Dr. Goodman was comfortable sharing his story with the 1.6 million followers he had already built across his social media platforms.
“I started on social media in 2020 with the goal of advocating for mental health and inspiring future doctors.” He said the message seemed to resonate with people struggling during the early part of the pandemic. On his social media accounts, he also talks about medical school, residency, and being a health care provider. His fiancé is also a resident doctor, in internal medicine.
Dr. Goodman is also trying to create a more realistic image of doctors than the superheroes he believed they were growing up. He wants those who grow up wanting to be doctors and who look up to him to see him as a human being with vulnerabilities, such as mental health.
“You can be a doctor and have mental health issues. Seeking treatment for mental health makes you a better doctor, and for other health care workers suffering in the midst of the pandemic, I want to let them know they are not alone.”
He pointed to the statistic that doctors have one of the highest suicide rates of any professions. “It’s better to talk about that in the early stages of training.”
Students, residents, or attending physicians who have mental health challenges shouldn’t allow their symptoms to go untreated, Dr. Goodman added. “Holding in all the stress and anxiety and feelings in a very traumatic field may be dangerous. ”
One of his goals is to campaign for the removal of a question on state medical licensing forms requiring doctors to report any mental health diagnosis. It’s why doctors may be afraid to admit that they are struggling. “I’m still here. It didn’t ruin my career.”
Doctors who seek treatment for mental health are theoretically protected under the Americans With Disabilities Act from being refused a license on the basis of that diagnosis. Dr. Goodman hopes to advocate at the state level to reduce discrimination and increase accessibility for doctors to seek mental health care.
Still, Dr. Goodman concedes he was initially fearful of the repercussions. “I opened up about it because this post could save lives. I was doing what I believed in.”
So if he runs into barriers to receive his medical license because of his admission, “that’s a serious problem,” he said. “There is already a shortage of doctors. We’ll see what happens in a few years. I am not the only one who will answer ‘yes’ to having sought treatment for a mental illness. The questions do not really need to be there.”
A version of this article first appeared on Medscape.com.
First-year psychiatry resident Jake Goodman, MD, knew he was taking a chance when he opened up on his popular social media platforms about his personal mental health battle. He mulled over the decision for several weeks before deciding to take the plunge.
As he voiced recently on his TikTok page, his biggest social media fanbase, with 1.3 million followers, it felt freeing to get his personal struggle off his chest.
“I’m a doctor in training, and most doctors would advise me not to post this,” the 29-year-old from Miami said in the video last month, which garnered 1.2 million views on TikTok alone. “They would say it’s risky for my career. But I didn’t join the medical field to continue the toxic status quo. I’m part of a new generation of health care professionals that are not afraid to be vulnerable and talk about mental health.”
“Dr. Jake,” as he calls himself on social media, admitted he was a physician who treats mental illness and also takes medication for it. “It felt good to say that. And by the way, I’m proud of it,” he said in the TikTok post.
A champion of mental health throughout the pandemic, Dr. Goodman called attention to the illness in the medical field. In a message on Instagram, he stated, “Opening up about your mental health as a medical professional, especially as a doctor who treats mental illness, can be taboo ... So here’s me leading by example.”
He also cited statistics on the challenge: “1 in 2 people will be diagnosed with a mental health illness at some point in their life. Yet many of us will never take medication that can help correct the chemical imbalance in our brains due to medication stigma: the fear that taking medications for our mental health somehow makes us weak.”
Mental health remains an issue among residents. Nearly 70% of residents polled by Medscape in its 2021 Residents Lifestyle & Happiness Report said they strongly or somewhat agree there’s a stigma against seeking mental health help. And nearly half, or 47% of those polled, said they sometimes (36%) or always/most of the time (11%) were depressed. The latter category rose in the past year.
Dr. Goodman told this news organization that he became passionate about mental health when he lost a college friend to suicide. “It really exposed the stigma” of mental health, he said. “I always knew it was there, but it took me seeing someone lose his life and [asking] why didn’t he feel comfortable talking to us, and why didn’t I feel comfortable talking to him?”
Stress of medical training
The decision to pursue psychiatry as his specialty came after a rotation in a clinic for people struggling with substance use disorders. “I was enthralled to see people change their life ... just by mental health care.” It’s why he went into medicine, he tells this news organization. “I always wanted to be in a field to help people [before they hit] rock bottom, when no one else could be there for them.”
Dr. Goodman’s personal battle with mental health didn’t arise until he started residency. “I was not really myself.” He said he felt numb and burned out. “I was not getting as much enjoyment out of things.” A friend pointed out that he might be depressed, so he went to see a therapist and then a psychiatrist and started on medication. “It had a profound impact on how I felt.”
Still, it took a while before Dr. Goodman was comfortable sharing his story with the 1.6 million followers he had already built across his social media platforms.
“I started on social media in 2020 with the goal of advocating for mental health and inspiring future doctors.” He said the message seemed to resonate with people struggling during the early part of the pandemic. On his social media accounts, he also talks about medical school, residency, and being a health care provider. His fiancé is also a resident doctor, in internal medicine.
Dr. Goodman is also trying to create a more realistic image of doctors than the superheroes he believed they were growing up. He wants those who grow up wanting to be doctors and who look up to him to see him as a human being with vulnerabilities, such as mental health.
“You can be a doctor and have mental health issues. Seeking treatment for mental health makes you a better doctor, and for other health care workers suffering in the midst of the pandemic, I want to let them know they are not alone.”
He pointed to the statistic that doctors have one of the highest suicide rates of any professions. “It’s better to talk about that in the early stages of training.”
Students, residents, or attending physicians who have mental health challenges shouldn’t allow their symptoms to go untreated, Dr. Goodman added. “Holding in all the stress and anxiety and feelings in a very traumatic field may be dangerous. ”
One of his goals is to campaign for the removal of a question on state medical licensing forms requiring doctors to report any mental health diagnosis. It’s why doctors may be afraid to admit that they are struggling. “I’m still here. It didn’t ruin my career.”
Doctors who seek treatment for mental health are theoretically protected under the Americans With Disabilities Act from being refused a license on the basis of that diagnosis. Dr. Goodman hopes to advocate at the state level to reduce discrimination and increase accessibility for doctors to seek mental health care.
Still, Dr. Goodman concedes he was initially fearful of the repercussions. “I opened up about it because this post could save lives. I was doing what I believed in.”
So if he runs into barriers to receive his medical license because of his admission, “that’s a serious problem,” he said. “There is already a shortage of doctors. We’ll see what happens in a few years. I am not the only one who will answer ‘yes’ to having sought treatment for a mental illness. The questions do not really need to be there.”
A version of this article first appeared on Medscape.com.
Mental health problems in kids linked with school closures
Behavior problems, anxiety, and depression in youths were associated with these individuals participating in remote schooling during broader social lockdowns in a new study.
The systematic review, which was published in JAMA Pediatrics on Jan. 18, 2022, was based on data from 36 studies from 11 countries on mental health, physical health, and well-being in children and adolescents aged 0-18 years. The total population included 79,781 children and 18,028 parents or caregivers. The studies reflected the first wave of pandemic school closures and lockdowns from February to July 2020, with the duration of school closure ranging from 1 week to 3 months.
“There are strong theoretical reasons to suggest that school closures may have contributed to a considerable proportion of the harms identified here, particularly mental health harms, through reduction in social contacts with peers and teachers,” Russell Viner, PhD, of UCL Great Ormond St Institute of Child Health, London, and colleagues wrote in their paper.
The researchers included 9 longitudinal pre-post studies, 5 cohort studies, 21 cross-sectional studies, and 1 modeling study in their analysis. Overall, approximately one-third of the studies (36%) were considered high quality, and approximately two-thirds (64%) of the studies were published in journals. Twenty-five of the reports analyzed focused on mental health and well-being.
Schools provide not only education, but also services including meals, health care, and health supplies. Schools also serve as a safety net and source of social support for children, the researchers noted.
The losses children may have experienced during school closures occurred during a time when more than 167,000 children younger than 18 years lost a parent or caregiver to COVID-19, according to a recent report titled “Hidden Pain” by researchers at the University of Pennsylvania, Nemours Children’s Health, and the COVID Collaborative. Although not addressed in the current study, school closures would prevent bereaved children from receiving social-emotional support from friends and teachers. This crisis of loss also prompted the American Academy of Pediatrics to issue a National State of Emergency in Children’s Mental Health in October 2021.
New study results
These studies identified associations between school closures during broader lockdowns and increased emotional and behavioral problems, as well as increased restlessness and inattention. Across these studies, 18%-60% of children and adolescents scored higher than the risk thresholds for diagnoses of distress, especially depressive symptoms and anxiety.
Although two studies showed no significant association with suicide in response to school closures during lockdowns, three studies suggested increased use of screen time, two studies reported increased social media use, and six studies reported lower levels of physical activity.
Three studies of child abuse showed decreases in notifications during lockdowns, likely driven by lack of referrals from schools, the authors noted. A total of 10 studies on sleep and 5 studies on diet showed inconsistent evidence of harm during the specific period of school closures and social lockdowns.
“The contrast of rises in distress with decreases in presentations suggests that there was an escalation of unmet mental health need during lockdowns in already vulnerable children and adolescents,” the researchers wrote. “More troubling still is evidence of a reduction in the ability of the health and social care systems to protect children in many countries, as shown by the large falls in child protection referrals seen in high-quality cohort studies.”
‘Study presents concrete assessments rather than speculation’
“Concerns have been widely expressed in the lay media and beyond that school closures could negatively impact the mental and physical health of children and adolescents,” M. Susan Jay, MD, of the Medical College of Wisconsin, Milwaukee, said in an interview. “The authors presented a narrative synthesis summarizing available evidence for the first wave of COVID-19 on school closures during the broader social lockdown occurring during this period.”
The “importance” of this research is that “it is not a single convenience sample study, but a systematic review from 11 countries including the United States, United Kingdom, China, and Turkey, among others, and that the quality of the information was graded,” Dr. Jay said. “Although not a meta-analysis, the study presents concrete assessments rather than speculation and overviews its limitations so that the clinician can weigh this information. Importantly, the authors excluded closure of schools with transmission of infection.
“Clearly, school lockdowns as a measure of controlling infectious disease needs balance with potential of negative health behaviors in children and adolescents. Ongoing prospective longitudinal studies are needed as sequential waves of the pandemic continue,” she emphasized.
“Clinically, this study highlights the need for clinicians to consider [asking] about the impact of school closures and remote versus hybrid versus in-person education [as part of their] patients and families question inventory,” Dr. Jay said. “Also, the use of depression inventories can be offered to youth to assess their mental health state at a visit, either via telemedicine or in person, and ideally at sequential visits for a more in-depth assessment.”
Schools play key role in social and emotional development
“It was important to conduct this study now, because this current time is unprecedented,” Peter L. Loper Jr., MD, of the University of South Carolina, Columbia, said in an interview. “We know based on evolutionary biology, anthropology, and developmental psychology, among other disciplines, that meaningful interpersonal interactions embedded in the context of community are vital to supporting human well-being.

“In our current time, the primary framework of community for our children is the school setting; it is the predominant space where they engage in the interpersonal interactions necessary for developing resilience, their sense of purpose, belonging, and fidelity,” he emphasized.
“Rarely in the course of human existence have kids been removed from the broader context of community to this extent and for this duration,” Dr. Loper said. “This study capitalizes on this unprecedented moment to begin to further understand how compromises in our sociocultural infrastructure of community, like school closures and lockdowns, may manifest as mental health problems in children and adolescents. More importantly, it contributes to the exploration of potential unintended consequences of our current infection control measures so we can adapt to support the overall well-being of our children in this ‘new normal.’ ”
Dr. Loper added that he was not surprised by the new study’s findings.
“We were already seeing a decline in pediatric mental health and overall well-being in the years preceding COVID-19 because of the ‘isolation epidemic’ involving many of the factors that this study explored,” he said. “I think this review further illustrates the vital necessity of community to support the health and well-being of humans, and specifically children and adolescents.”
From a clinical standpoint, “we need to be intentional and consistent in balancing infection control measures with our kids’ fundamental psychosocial needs,” Dr. Loper said.
“We need to recognize that, when children and adolescents are isolated from community, their fundamental psychosocial needs go unmet,” he emphasized. “If children and adolescents cannot access the meaningful interpersonal interactions necessary for resilience, then they cannot overcome or navigate distress. They will exhibit the avoidance and withdrawal behaviors that accumulate to manifest as adverse mental health symptoms like anxiety and depression.
“Additional research is needed to further explore how compromises in the psychosocial infrastructure of community manifest as downstream symptom indicators such as anxiety and depression,” which are often manifestations of unmet needs, Dr. Loper said.
Limitations and strengths, according to authors
The findings were limited by several factors, including a lack of examination of school closures’ effects on mental health independent of broader social lockdowns, according to the researchers. Other limitations included the authors potentially having missed studies, inclusion of cross-sectional studies with relatively weak evidence, potential bias from studies using parent reports, and a focus on the first COVID-19 wave, during which many school closures were of limited duration. Also, the researchers said they did not include studies focused on particular groups, such as children with learning difficulties or autism.
The use of large databases from education as well as health care in studies analyzed were strengths of the new research, they said. The investigators received no outside funding for their study. The researchers, Dr. Jay, and Dr. Loper had no financial conflicts to disclose. Dr. Jay serves on the editorial advisory board of Pediatric News.
Behavior problems, anxiety, and depression in youths were associated with these individuals participating in remote schooling during broader social lockdowns in a new study.
The systematic review, which was published in JAMA Pediatrics on Jan. 18, 2022, was based on data from 36 studies from 11 countries on mental health, physical health, and well-being in children and adolescents aged 0-18 years. The total population included 79,781 children and 18,028 parents or caregivers. The studies reflected the first wave of pandemic school closures and lockdowns from February to July 2020, with the duration of school closure ranging from 1 week to 3 months.
“There are strong theoretical reasons to suggest that school closures may have contributed to a considerable proportion of the harms identified here, particularly mental health harms, through reduction in social contacts with peers and teachers,” Russell Viner, PhD, of UCL Great Ormond St Institute of Child Health, London, and colleagues wrote in their paper.
The researchers included 9 longitudinal pre-post studies, 5 cohort studies, 21 cross-sectional studies, and 1 modeling study in their analysis. Overall, approximately one-third of the studies (36%) were considered high quality, and approximately two-thirds (64%) of the studies were published in journals. Twenty-five of the reports analyzed focused on mental health and well-being.
Schools provide not only education, but also services including meals, health care, and health supplies. Schools also serve as a safety net and source of social support for children, the researchers noted.
The losses children may have experienced during school closures occurred during a time when more than 167,000 children younger than 18 years lost a parent or caregiver to COVID-19, according to a recent report titled “Hidden Pain” by researchers at the University of Pennsylvania, Nemours Children’s Health, and the COVID Collaborative. Although not addressed in the current study, school closures would prevent bereaved children from receiving social-emotional support from friends and teachers. This crisis of loss also prompted the American Academy of Pediatrics to issue a National State of Emergency in Children’s Mental Health in October 2021.
New study results
These studies identified associations between school closures during broader lockdowns and increased emotional and behavioral problems, as well as increased restlessness and inattention. Across these studies, 18%-60% of children and adolescents scored higher than the risk thresholds for diagnoses of distress, especially depressive symptoms and anxiety.
Although two studies showed no significant association with suicide in response to school closures during lockdowns, three studies suggested increased use of screen time, two studies reported increased social media use, and six studies reported lower levels of physical activity.
Three studies of child abuse showed decreases in notifications during lockdowns, likely driven by lack of referrals from schools, the authors noted. A total of 10 studies on sleep and 5 studies on diet showed inconsistent evidence of harm during the specific period of school closures and social lockdowns.
“The contrast of rises in distress with decreases in presentations suggests that there was an escalation of unmet mental health need during lockdowns in already vulnerable children and adolescents,” the researchers wrote. “More troubling still is evidence of a reduction in the ability of the health and social care systems to protect children in many countries, as shown by the large falls in child protection referrals seen in high-quality cohort studies.”
‘Study presents concrete assessments rather than speculation’
“Concerns have been widely expressed in the lay media and beyond that school closures could negatively impact the mental and physical health of children and adolescents,” M. Susan Jay, MD, of the Medical College of Wisconsin, Milwaukee, said in an interview. “The authors presented a narrative synthesis summarizing available evidence for the first wave of COVID-19 on school closures during the broader social lockdown occurring during this period.”
The “importance” of this research is that “it is not a single convenience sample study, but a systematic review from 11 countries including the United States, United Kingdom, China, and Turkey, among others, and that the quality of the information was graded,” Dr. Jay said. “Although not a meta-analysis, the study presents concrete assessments rather than speculation and overviews its limitations so that the clinician can weigh this information. Importantly, the authors excluded closure of schools with transmission of infection.
“Clearly, school lockdowns as a measure of controlling infectious disease needs balance with potential of negative health behaviors in children and adolescents. Ongoing prospective longitudinal studies are needed as sequential waves of the pandemic continue,” she emphasized.
“Clinically, this study highlights the need for clinicians to consider [asking] about the impact of school closures and remote versus hybrid versus in-person education [as part of their] patients and families question inventory,” Dr. Jay said. “Also, the use of depression inventories can be offered to youth to assess their mental health state at a visit, either via telemedicine or in person, and ideally at sequential visits for a more in-depth assessment.”
Schools play key role in social and emotional development
“It was important to conduct this study now, because this current time is unprecedented,” Peter L. Loper Jr., MD, of the University of South Carolina, Columbia, said in an interview. “We know based on evolutionary biology, anthropology, and developmental psychology, among other disciplines, that meaningful interpersonal interactions embedded in the context of community are vital to supporting human well-being.
“In our current time, the primary framework of community for our children is the school setting; it is the predominant space where they engage in the interpersonal interactions necessary for developing resilience, their sense of purpose, belonging, and fidelity,” he emphasized.
“Rarely in the course of human existence have kids been removed from the broader context of community to this extent and for this duration,” Dr. Loper said. “This study capitalizes on this unprecedented moment to begin to further understand how compromises in our sociocultural infrastructure of community, like school closures and lockdowns, may manifest as mental health problems in children and adolescents. More importantly, it contributes to the exploration of potential unintended consequences of our current infection control measures so we can adapt to support the overall well-being of our children in this ‘new normal.’ ”
Dr. Loper added that he was not surprised by the new study’s findings.
“We were already seeing a decline in pediatric mental health and overall well-being in the years preceding COVID-19 because of the ‘isolation epidemic’ involving many of the factors that this study explored,” he said. “I think this review further illustrates the vital necessity of community to support the health and well-being of humans, and specifically children and adolescents.”
From a clinical standpoint, “we need to be intentional and consistent in balancing infection control measures with our kids’ fundamental psychosocial needs,” Dr. Loper said.
“We need to recognize that, when children and adolescents are isolated from community, their fundamental psychosocial needs go unmet,” he emphasized. “If children and adolescents cannot access the meaningful interpersonal interactions necessary for resilience, then they cannot overcome or navigate distress. They will exhibit the avoidance and withdrawal behaviors that accumulate to manifest as adverse mental health symptoms like anxiety and depression.
“Additional research is needed to further explore how compromises in the psychosocial infrastructure of community manifest as downstream symptom indicators such as anxiety and depression,” which are often manifestations of unmet needs, Dr. Loper said.
Limitations and strengths, according to authors
The findings were limited by several factors, including a lack of examination of school closures’ effects on mental health independent of broader social lockdowns, according to the researchers. Other limitations included the authors potentially having missed studies, inclusion of cross-sectional studies with relatively weak evidence, potential bias from studies using parent reports, and a focus on the first COVID-19 wave, during which many school closures were of limited duration. Also, the researchers said they did not include studies focused on particular groups, such as children with learning difficulties or autism.
The use of large databases from education as well as health care in studies analyzed were strengths of the new research, they said. The investigators received no outside funding for their study. The researchers, Dr. Jay, and Dr. Loper had no financial conflicts to disclose. Dr. Jay serves on the editorial advisory board of Pediatric News.
Behavior problems, anxiety, and depression in youths were associated with these individuals participating in remote schooling during broader social lockdowns in a new study.
The systematic review, which was published in JAMA Pediatrics on Jan. 18, 2022, was based on data from 36 studies from 11 countries on mental health, physical health, and well-being in children and adolescents aged 0-18 years. The total population included 79,781 children and 18,028 parents or caregivers. The studies reflected the first wave of pandemic school closures and lockdowns from February to July 2020, with the duration of school closure ranging from 1 week to 3 months.
“There are strong theoretical reasons to suggest that school closures may have contributed to a considerable proportion of the harms identified here, particularly mental health harms, through reduction in social contacts with peers and teachers,” Russell Viner, PhD, of UCL Great Ormond St Institute of Child Health, London, and colleagues wrote in their paper.
The researchers included 9 longitudinal pre-post studies, 5 cohort studies, 21 cross-sectional studies, and 1 modeling study in their analysis. Overall, approximately one-third of the studies (36%) were considered high quality, and approximately two-thirds (64%) of the studies were published in journals. Twenty-five of the reports analyzed focused on mental health and well-being.
Schools provide not only education, but also services including meals, health care, and health supplies. Schools also serve as a safety net and source of social support for children, the researchers noted.
The losses children may have experienced during school closures occurred during a time when more than 167,000 children younger than 18 years lost a parent or caregiver to COVID-19, according to a recent report titled “Hidden Pain” by researchers at the University of Pennsylvania, Nemours Children’s Health, and the COVID Collaborative. Although not addressed in the current study, school closures would prevent bereaved children from receiving social-emotional support from friends and teachers. This crisis of loss also prompted the American Academy of Pediatrics to issue a National State of Emergency in Children’s Mental Health in October 2021.
New study results
These studies identified associations between school closures during broader lockdowns and increased emotional and behavioral problems, as well as increased restlessness and inattention. Across these studies, 18%-60% of children and adolescents scored higher than the risk thresholds for diagnoses of distress, especially depressive symptoms and anxiety.
Although two studies showed no significant association with suicide in response to school closures during lockdowns, three studies suggested increased use of screen time, two studies reported increased social media use, and six studies reported lower levels of physical activity.
Three studies of child abuse showed decreases in notifications during lockdowns, likely driven by lack of referrals from schools, the authors noted. A total of 10 studies on sleep and 5 studies on diet showed inconsistent evidence of harm during the specific period of school closures and social lockdowns.
“The contrast of rises in distress with decreases in presentations suggests that there was an escalation of unmet mental health need during lockdowns in already vulnerable children and adolescents,” the researchers wrote. “More troubling still is evidence of a reduction in the ability of the health and social care systems to protect children in many countries, as shown by the large falls in child protection referrals seen in high-quality cohort studies.”
‘Study presents concrete assessments rather than speculation’
“Concerns have been widely expressed in the lay media and beyond that school closures could negatively impact the mental and physical health of children and adolescents,” M. Susan Jay, MD, of the Medical College of Wisconsin, Milwaukee, said in an interview. “The authors presented a narrative synthesis summarizing available evidence for the first wave of COVID-19 on school closures during the broader social lockdown occurring during this period.”
The “importance” of this research is that “it is not a single convenience sample study, but a systematic review from 11 countries including the United States, United Kingdom, China, and Turkey, among others, and that the quality of the information was graded,” Dr. Jay said. “Although not a meta-analysis, the study presents concrete assessments rather than speculation and overviews its limitations so that the clinician can weigh this information. Importantly, the authors excluded closure of schools with transmission of infection.
“Clearly, school lockdowns as a measure of controlling infectious disease needs balance with potential of negative health behaviors in children and adolescents. Ongoing prospective longitudinal studies are needed as sequential waves of the pandemic continue,” she emphasized.
“Clinically, this study highlights the need for clinicians to consider [asking] about the impact of school closures and remote versus hybrid versus in-person education [as part of their] patients and families question inventory,” Dr. Jay said. “Also, the use of depression inventories can be offered to youth to assess their mental health state at a visit, either via telemedicine or in person, and ideally at sequential visits for a more in-depth assessment.”
Schools play key role in social and emotional development
“It was important to conduct this study now, because this current time is unprecedented,” Peter L. Loper Jr., MD, of the University of South Carolina, Columbia, said in an interview. “We know based on evolutionary biology, anthropology, and developmental psychology, among other disciplines, that meaningful interpersonal interactions embedded in the context of community are vital to supporting human well-being.
“In our current time, the primary framework of community for our children is the school setting; it is the predominant space where they engage in the interpersonal interactions necessary for developing resilience, their sense of purpose, belonging, and fidelity,” he emphasized.
“Rarely in the course of human existence have kids been removed from the broader context of community to this extent and for this duration,” Dr. Loper said. “This study capitalizes on this unprecedented moment to begin to further understand how compromises in our sociocultural infrastructure of community, like school closures and lockdowns, may manifest as mental health problems in children and adolescents. More importantly, it contributes to the exploration of potential unintended consequences of our current infection control measures so we can adapt to support the overall well-being of our children in this ‘new normal.’ ”
Dr. Loper added that he was not surprised by the new study’s findings.
“We were already seeing a decline in pediatric mental health and overall well-being in the years preceding COVID-19 because of the ‘isolation epidemic’ involving many of the factors that this study explored,” he said. “I think this review further illustrates the vital necessity of community to support the health and well-being of humans, and specifically children and adolescents.”
From a clinical standpoint, “we need to be intentional and consistent in balancing infection control measures with our kids’ fundamental psychosocial needs,” Dr. Loper said.
“We need to recognize that, when children and adolescents are isolated from community, their fundamental psychosocial needs go unmet,” he emphasized. “If children and adolescents cannot access the meaningful interpersonal interactions necessary for resilience, then they cannot overcome or navigate distress. They will exhibit the avoidance and withdrawal behaviors that accumulate to manifest as adverse mental health symptoms like anxiety and depression.
“Additional research is needed to further explore how compromises in the psychosocial infrastructure of community manifest as downstream symptom indicators such as anxiety and depression,” which are often manifestations of unmet needs, Dr. Loper said.
Limitations and strengths, according to authors
The findings were limited by several factors, including a lack of examination of school closures’ effects on mental health independent of broader social lockdowns, according to the researchers. Other limitations included the authors potentially having missed studies, inclusion of cross-sectional studies with relatively weak evidence, potential bias from studies using parent reports, and a focus on the first COVID-19 wave, during which many school closures were of limited duration. Also, the researchers said they did not include studies focused on particular groups, such as children with learning difficulties or autism.
The use of large databases from education as well as health care in studies analyzed were strengths of the new research, they said. The investigators received no outside funding for their study. The researchers, Dr. Jay, and Dr. Loper had no financial conflicts to disclose. Dr. Jay serves on the editorial advisory board of Pediatric News.
FROM JAMA PEDIATRICS
Preschool boys’ behaviors traced back to moms’ thyroid hormones
Pregnant women’s thyroid hormone trajectories (levels in the first, second, and third trimester) may predict whether their male offspring are aggressive or withdrawn at age 4.
Certain maternal thyroid hormone trajectories were associated with problem behaviors in preschool boys in a study of close to 2,000 mother-child pairs in China.
The researchers identified low, moderate, and high thyroid-stimulating hormone (TSH) and free thyroxine (FT4) trajectories.

Most women had a low TSH trajectory and moderate FT4 trajectory, which the researchers deemed to be reference (normal) trajectories.
The children’s primary caregiver (parent or grandparent) completed an extensive questionnaire about their child’s behavior at age 4.
The 4-year-old boys whose mothers had a high TSH trajectory during pregnancy were more likely to be withdrawn and to externalize problems (odds ratio, 2.01 and 2.69, respectively).
Boys whose mothers had a high FT4 trajectory during pregnancy were more likely to be anxious/depressed (OR, 2.22).
And boys whose mothers had a moderate TSH trajectory or low FT4 trajectory were more likely to show aggressive behavior (OR, 3.76 and 4.17, respectively), compared with boys whose mothers had normal TSH and FT4 trajectories, after adjusting for potential confounders.
However, there was no association between abnormal maternal thyroid hormone trajectories and behavior problems in 4-year-old girls.
The study by Peixuan Li, BM, and colleagues was published online Jan. 6 in the Journal of Clinical Endocrinology & Metabolism.
‘Study supports monitoring thyroid function in pregnancy’
“Our findings highlight the significance of close monitoring and management of maternal thyroid function during pregnancy,” senior author Kun Huang, PhD, said in a press release from the Endocrine Society.
“This research presents a new perspective in early intervention of children’s emotional and behavioral problems,” added Dr. Huang, from Anhui Medical University, Hefei, China.
The results add to a growing body of literature about a controversial link between maternal thyroid hormones in pregnancy, when the fetal brain is developing, and subsequent behavior in preschool children, Caroline T. Nguyen, MD, who was not involved with this research, commented in an email.
“Some studies show an association between thyroid levels and behavioral outcomes, others not,” added Dr. Nguyen, assistant professor of clinical medicine, Keck School of Medicine, University of Southern California, Los Angeles. And “some studies have found sex-specific associations with maternal thyroid levels and neurocognitive/behavioral outcomes, others have not.”
Women considering pregnancy should be evaluated for possible thyroid disease, she continued. Currently, no universal screening mandates exist for thyroid disease in pregnancy, but the 2017 American Thyroid Association guidelines do recommend screening women at risk for thyroid dysfunction.
“I think screening for thyroid peroxidase antibody (TPOAb) positivity is helpful in women desiring pregnancy,” Dr. Nguyen continued, “because we know that patients with TPOAb positivity are at increased risk for miscarriage and have a blunted response to the increased demands of pregnancy for thyroid hormone production.”
TPOAb positivity is also associated with the increased risk of postpartum and long-term thyroid dysfunction.
This current study, Dr. Nguyen summarized, “adds to a growing body of research of the relationship of thyroid hormone levels and neurocognitive outcomes [in offspring] and supports the monitoring of thyroid disease in pregnancy.”
“However, we do not have sufficient data to demonstrate the benefits of intervention with levothyroxine treatment,” she noted.
Nevertheless, the lack of positive data does not suggest there is no theoretical benefit of intervention, she said, as such studies are very challenging to do.
“Physicians can help reduce stress and anxiety in patients desiring pregnancy by [recommending] preconception counseling, screening patients at risk for thyroid disease, and optimizing thyroid hormone levels before and during pregnancy,” according to Dr. Nguyen.
Maternal TSH and FT4 trajectories and preschoolers’ behaviors
Previous studies have reported that during pregnancy, maternal subclinical hypothyroidism (elevated TSH with normal FT4) as well as isolated hypothyroxinemia (decreased FT4 with normal TSH) are associated with adverse maternal and child outcomes, including preterm delivery and low birth weight.
However, most studies have not determined maternal thyroid hormone levels in different trimesters.
Researchers recruited pregnant women going for their first antenatal checkup at the Ma’anshan Maternal and Child Health Hospital in China from May 2013 to September 2014 and identified 1,860 mother-child pairs.
They determined maternal thyroid hormone levels from blood samples taken during the first, second, and third trimester: on average, gestational week 10, 25, and 34, respectively.
The researchers found that TSH levels increased somewhat from trimester 1 to trimester 2 and then decreased slightly in trimester 3. Most women (68%) had a low TSH trajectory, 28% had a moderate TSH trajectory, and 4% had a high TSH trajectory.
FT4 levels dropped sharply from trimester 1 to trimester 2 and then increased somewhat in trimester 3. About half of the women (52%) had a moderate FT4 trajectory, 33% had a low FT4 trajectory, and 15% had a high FT4 trajectory.
Most women (96.5%) had a low and stable TPOAb level, and the rest (3.5%) had high and decreasing TPOAb levels.
When the children in the study were 4 years old, their main caregiver (parent or grandparent) completed the 100-question Achenbach Child Behavior checklist to identify whether the child often, sometimes, or never displayed three internalizing problem behaviors (emotionally reactive, anxious/depressed, or withdrawn) and/or two externalizing problem behaviors (attention problems or aggressive behavior).
Study limitations, more research needed
It is not clear why the associations between maternal hormones and offspring behavior were only seen in boys. Perhaps male fetuses are more sensitive than female fetuses to changing maternal thyroid hormone levels in pregnancy, the researchers speculate.
They acknowledge that study limitations include there were few children with aggressive behavior, so the confidence interval for the association of the moderate TSH trajectory with aggressive behavior was very wide.
In addition, evaluation of children’s behavior by caregivers was subjective. Also, the researchers did not have information about iodine levels, and low iodine levels can impair child brain development.
And there may have been residual confounders that researchers did not account for, such as differences in family upbringing, parental marital status, and the mother’s exposure to endocrine disruptors.
Therefore, further research is needed.
The study was supported by grants from the National Natural Science Foundation of China, the University Synergy Innovation Program of Anhui Province, the Sci-Tech Basic Resources Research Program of China, the National Key Research and Development Program, the Chinese Academy of Medical Sciences, and the Research Fund of Anhui Institute of Translational Medicine. The researchers and Dr. Nguyen have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Pregnant women’s thyroid hormone trajectories (levels in the first, second, and third trimester) may predict whether their male offspring are aggressive or withdrawn at age 4.
Certain maternal thyroid hormone trajectories were associated with problem behaviors in preschool boys in a study of close to 2,000 mother-child pairs in China.
The researchers identified low, moderate, and high thyroid-stimulating hormone (TSH) and free thyroxine (FT4) trajectories.
Most women had a low TSH trajectory and moderate FT4 trajectory, which the researchers deemed to be reference (normal) trajectories.
The children’s primary caregiver (parent or grandparent) completed an extensive questionnaire about their child’s behavior at age 4.
The 4-year-old boys whose mothers had a high TSH trajectory during pregnancy were more likely to be withdrawn and to externalize problems (odds ratio, 2.01 and 2.69, respectively).
Boys whose mothers had a high FT4 trajectory during pregnancy were more likely to be anxious/depressed (OR, 2.22).
And boys whose mothers had a moderate TSH trajectory or low FT4 trajectory were more likely to show aggressive behavior (OR, 3.76 and 4.17, respectively), compared with boys whose mothers had normal TSH and FT4 trajectories, after adjusting for potential confounders.
However, there was no association between abnormal maternal thyroid hormone trajectories and behavior problems in 4-year-old girls.
The study by Peixuan Li, BM, and colleagues was published online Jan. 6 in the Journal of Clinical Endocrinology & Metabolism.
‘Study supports monitoring thyroid function in pregnancy’
“Our findings highlight the significance of close monitoring and management of maternal thyroid function during pregnancy,” senior author Kun Huang, PhD, said in a press release from the Endocrine Society.
“This research presents a new perspective in early intervention of children’s emotional and behavioral problems,” added Dr. Huang, from Anhui Medical University, Hefei, China.
The results add to a growing body of literature about a controversial link between maternal thyroid hormones in pregnancy, when the fetal brain is developing, and subsequent behavior in preschool children, Caroline T. Nguyen, MD, who was not involved with this research, commented in an email.
“Some studies show an association between thyroid levels and behavioral outcomes, others not,” added Dr. Nguyen, assistant professor of clinical medicine, Keck School of Medicine, University of Southern California, Los Angeles. And “some studies have found sex-specific associations with maternal thyroid levels and neurocognitive/behavioral outcomes, others have not.”
Women considering pregnancy should be evaluated for possible thyroid disease, she continued. Currently, no universal screening mandates exist for thyroid disease in pregnancy, but the 2017 American Thyroid Association guidelines do recommend screening women at risk for thyroid dysfunction.
“I think screening for thyroid peroxidase antibody (TPOAb) positivity is helpful in women desiring pregnancy,” Dr. Nguyen continued, “because we know that patients with TPOAb positivity are at increased risk for miscarriage and have a blunted response to the increased demands of pregnancy for thyroid hormone production.”
TPOAb positivity is also associated with the increased risk of postpartum and long-term thyroid dysfunction.
This current study, Dr. Nguyen summarized, “adds to a growing body of research of the relationship of thyroid hormone levels and neurocognitive outcomes [in offspring] and supports the monitoring of thyroid disease in pregnancy.”
“However, we do not have sufficient data to demonstrate the benefits of intervention with levothyroxine treatment,” she noted.
Nevertheless, the lack of positive data does not suggest there is no theoretical benefit of intervention, she said, as such studies are very challenging to do.
“Physicians can help reduce stress and anxiety in patients desiring pregnancy by [recommending] preconception counseling, screening patients at risk for thyroid disease, and optimizing thyroid hormone levels before and during pregnancy,” according to Dr. Nguyen.
Maternal TSH and FT4 trajectories and preschoolers’ behaviors
Previous studies have reported that during pregnancy, maternal subclinical hypothyroidism (elevated TSH with normal FT4) as well as isolated hypothyroxinemia (decreased FT4 with normal TSH) are associated with adverse maternal and child outcomes, including preterm delivery and low birth weight.
However, most studies have not determined maternal thyroid hormone levels in different trimesters.
Researchers recruited pregnant women going for their first antenatal checkup at the Ma’anshan Maternal and Child Health Hospital in China from May 2013 to September 2014 and identified 1,860 mother-child pairs.
They determined maternal thyroid hormone levels from blood samples taken during the first, second, and third trimester: on average, gestational week 10, 25, and 34, respectively.
The researchers found that TSH levels increased somewhat from trimester 1 to trimester 2 and then decreased slightly in trimester 3. Most women (68%) had a low TSH trajectory, 28% had a moderate TSH trajectory, and 4% had a high TSH trajectory.
FT4 levels dropped sharply from trimester 1 to trimester 2 and then increased somewhat in trimester 3. About half of the women (52%) had a moderate FT4 trajectory, 33% had a low FT4 trajectory, and 15% had a high FT4 trajectory.
Most women (96.5%) had a low and stable TPOAb level, and the rest (3.5%) had high and decreasing TPOAb levels.
When the children in the study were 4 years old, their main caregiver (parent or grandparent) completed the 100-question Achenbach Child Behavior checklist to identify whether the child often, sometimes, or never displayed three internalizing problem behaviors (emotionally reactive, anxious/depressed, or withdrawn) and/or two externalizing problem behaviors (attention problems or aggressive behavior).
Study limitations, more research needed
It is not clear why the associations between maternal hormones and offspring behavior were only seen in boys. Perhaps male fetuses are more sensitive than female fetuses to changing maternal thyroid hormone levels in pregnancy, the researchers speculate.
They acknowledge that study limitations include there were few children with aggressive behavior, so the confidence interval for the association of the moderate TSH trajectory with aggressive behavior was very wide.
In addition, evaluation of children’s behavior by caregivers was subjective. Also, the researchers did not have information about iodine levels, and low iodine levels can impair child brain development.
And there may have been residual confounders that researchers did not account for, such as differences in family upbringing, parental marital status, and the mother’s exposure to endocrine disruptors.
Therefore, further research is needed.
The study was supported by grants from the National Natural Science Foundation of China, the University Synergy Innovation Program of Anhui Province, the Sci-Tech Basic Resources Research Program of China, the National Key Research and Development Program, the Chinese Academy of Medical Sciences, and the Research Fund of Anhui Institute of Translational Medicine. The researchers and Dr. Nguyen have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Pregnant women’s thyroid hormone trajectories (levels in the first, second, and third trimester) may predict whether their male offspring are aggressive or withdrawn at age 4.
Certain maternal thyroid hormone trajectories were associated with problem behaviors in preschool boys in a study of close to 2,000 mother-child pairs in China.
The researchers identified low, moderate, and high thyroid-stimulating hormone (TSH) and free thyroxine (FT4) trajectories.
Most women had a low TSH trajectory and moderate FT4 trajectory, which the researchers deemed to be reference (normal) trajectories.
The children’s primary caregiver (parent or grandparent) completed an extensive questionnaire about their child’s behavior at age 4.
The 4-year-old boys whose mothers had a high TSH trajectory during pregnancy were more likely to be withdrawn and to externalize problems (odds ratio, 2.01 and 2.69, respectively).
Boys whose mothers had a high FT4 trajectory during pregnancy were more likely to be anxious/depressed (OR, 2.22).
And boys whose mothers had a moderate TSH trajectory or low FT4 trajectory were more likely to show aggressive behavior (OR, 3.76 and 4.17, respectively), compared with boys whose mothers had normal TSH and FT4 trajectories, after adjusting for potential confounders.
However, there was no association between abnormal maternal thyroid hormone trajectories and behavior problems in 4-year-old girls.
The study by Peixuan Li, BM, and colleagues was published online Jan. 6 in the Journal of Clinical Endocrinology & Metabolism.
‘Study supports monitoring thyroid function in pregnancy’
“Our findings highlight the significance of close monitoring and management of maternal thyroid function during pregnancy,” senior author Kun Huang, PhD, said in a press release from the Endocrine Society.
“This research presents a new perspective in early intervention of children’s emotional and behavioral problems,” added Dr. Huang, from Anhui Medical University, Hefei, China.
The results add to a growing body of literature about a controversial link between maternal thyroid hormones in pregnancy, when the fetal brain is developing, and subsequent behavior in preschool children, Caroline T. Nguyen, MD, who was not involved with this research, commented in an email.
“Some studies show an association between thyroid levels and behavioral outcomes, others not,” added Dr. Nguyen, assistant professor of clinical medicine, Keck School of Medicine, University of Southern California, Los Angeles. And “some studies have found sex-specific associations with maternal thyroid levels and neurocognitive/behavioral outcomes, others have not.”
Women considering pregnancy should be evaluated for possible thyroid disease, she continued. Currently, no universal screening mandates exist for thyroid disease in pregnancy, but the 2017 American Thyroid Association guidelines do recommend screening women at risk for thyroid dysfunction.
“I think screening for thyroid peroxidase antibody (TPOAb) positivity is helpful in women desiring pregnancy,” Dr. Nguyen continued, “because we know that patients with TPOAb positivity are at increased risk for miscarriage and have a blunted response to the increased demands of pregnancy for thyroid hormone production.”
TPOAb positivity is also associated with the increased risk of postpartum and long-term thyroid dysfunction.
This current study, Dr. Nguyen summarized, “adds to a growing body of research of the relationship of thyroid hormone levels and neurocognitive outcomes [in offspring] and supports the monitoring of thyroid disease in pregnancy.”
“However, we do not have sufficient data to demonstrate the benefits of intervention with levothyroxine treatment,” she noted.
Nevertheless, the lack of positive data does not suggest there is no theoretical benefit of intervention, she said, as such studies are very challenging to do.
“Physicians can help reduce stress and anxiety in patients desiring pregnancy by [recommending] preconception counseling, screening patients at risk for thyroid disease, and optimizing thyroid hormone levels before and during pregnancy,” according to Dr. Nguyen.
Maternal TSH and FT4 trajectories and preschoolers’ behaviors
Previous studies have reported that during pregnancy, maternal subclinical hypothyroidism (elevated TSH with normal FT4) as well as isolated hypothyroxinemia (decreased FT4 with normal TSH) are associated with adverse maternal and child outcomes, including preterm delivery and low birth weight.
However, most studies have not determined maternal thyroid hormone levels in different trimesters.
Researchers recruited pregnant women going for their first antenatal checkup at the Ma’anshan Maternal and Child Health Hospital in China from May 2013 to September 2014 and identified 1,860 mother-child pairs.
They determined maternal thyroid hormone levels from blood samples taken during the first, second, and third trimester: on average, gestational week 10, 25, and 34, respectively.
The researchers found that TSH levels increased somewhat from trimester 1 to trimester 2 and then decreased slightly in trimester 3. Most women (68%) had a low TSH trajectory, 28% had a moderate TSH trajectory, and 4% had a high TSH trajectory.
FT4 levels dropped sharply from trimester 1 to trimester 2 and then increased somewhat in trimester 3. About half of the women (52%) had a moderate FT4 trajectory, 33% had a low FT4 trajectory, and 15% had a high FT4 trajectory.
Most women (96.5%) had a low and stable TPOAb level, and the rest (3.5%) had high and decreasing TPOAb levels.
When the children in the study were 4 years old, their main caregiver (parent or grandparent) completed the 100-question Achenbach Child Behavior checklist to identify whether the child often, sometimes, or never displayed three internalizing problem behaviors (emotionally reactive, anxious/depressed, or withdrawn) and/or two externalizing problem behaviors (attention problems or aggressive behavior).
Study limitations, more research needed
It is not clear why the associations between maternal hormones and offspring behavior were only seen in boys. Perhaps male fetuses are more sensitive than female fetuses to changing maternal thyroid hormone levels in pregnancy, the researchers speculate.
They acknowledge that study limitations include there were few children with aggressive behavior, so the confidence interval for the association of the moderate TSH trajectory with aggressive behavior was very wide.
In addition, evaluation of children’s behavior by caregivers was subjective. Also, the researchers did not have information about iodine levels, and low iodine levels can impair child brain development.
And there may have been residual confounders that researchers did not account for, such as differences in family upbringing, parental marital status, and the mother’s exposure to endocrine disruptors.
Therefore, further research is needed.
The study was supported by grants from the National Natural Science Foundation of China, the University Synergy Innovation Program of Anhui Province, the Sci-Tech Basic Resources Research Program of China, the National Key Research and Development Program, the Chinese Academy of Medical Sciences, and the Research Fund of Anhui Institute of Translational Medicine. The researchers and Dr. Nguyen have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM
Antidepressants: Is less more?
When it comes to antidepressant prescribing, less may be more, new research suggests.
A new review suggests antidepressants are overprescribed and that the efficacy of these agents is questionable, leading researchers to recommend that, when physicians prescribe these medications, it should be for shorter periods.
“Antidepressants have never been shown to have a clinically significant difference from placebo in the treatment of depression,” study co\investigator Mark Horowitz, GDPsych, PhD, division of psychiatry, University College London, said in an interview.
He added antidepressants “exert profound adverse effects on the body and brain” and can be difficult to stop because of physical dependence that occurs when the brain adapts to them.
“The best way to take people off these drugs is to do so gradually enough that the unpleasant effects are minimized and in a way that means the reductions in dose get smaller and smaller as the total dose gets lower,” Dr. Horowitz said.
However, at least one expert urged caution in interpreting the review’s findings.
“The reality is that millions of people do benefit from these medications, and this review minimizes those benefits,” Philip Muskin, MD, chief of consultation-liaison for psychiatry and professor of psychiatry, Columbia University Medical Center and New York–Presbyterian Hospital, said when approached for comment.
The findings were published online Dec. 20, 2021, in the Drug and Therapeutics Bulletin.
Personal experience
Prescribing of newer-generation antidepressants, such as SSRIs and serotonin and norepinephrine reuptake inhibitors (SNRIs), is increasing, with an estimated one in six adults in the United Kingdom receiving at least one prescription in 2019-2020, the investigators noted.
Dr. Horowitz noted a personal motivation for conducting the review. “As well as being an academic psychiatrist, I’m also a patient who has been prescribed antidepressants since age 21, when my mood was poor, due to life circumstances.”
The antidepressant “didn’t have particularly helpful effects,” but Dr. Horowitz continued taking it for 18 years. “I was told it was helpful and internalized that message. I came to understand that much of the information around antidepressants came from the drug companies that manufactured them or from academics paid by these companies.”
Dr. Horowitz is currently discontinuing his medication – a tapering process now in its third year. He said he has come to realize, in retrospect, that symptoms not initially attributed to the drug, such as fatigue, impaired concentration, and impaired memory, have improved since reducing the medication.
“That experience sensitized me to look for these symptoms in my patients and I see them; but most of my patients were told by their doctors that the cause of those problems was the depression or anxiety itself and not the drug,” he said.
Dr. Horowitz collaborated with Michael Wilcock, DTB, Pharmacy, Royal Cornwall Hospitals, NHS Trust, Truro, England, in conducting the review “to provide an independent assessment of benefits and harms of antidepressants.”
“Much of the evidence of the efficacy of antidepressants comes from randomized placebo-controlled trials,” Dr. Horowitz said. Several meta-analyses of these studies showed a difference of about two points between the agent and the placebo on the Hamilton Depression Rating Scale (HAM-D).
“Although this might be statistically significant, it does not meet the threshold for a clinical significance – those aren’t the same thing,” Dr. Horowitz said. Some analyses suggest that a “minimally clinically important difference” on the HAM-D would range from 3 to 6 points.
The findings in adolescents and children are “even less convincing,” the investigators noted, citing a Cochrane review.
“This is especially concerning because the number of children and adolescents being treated with antidepressants is rapidly increasing,” Dr. Horowitz said.
Additionally, the short duration of most trials, typically 6-12 weeks, is “largely uninformative for the clinical treatment of depression.”
Relapse or withdrawal?
The researchers reviewed the adverse effects of long-term antidepressant use, including daytime sleepiness, dry mouth, profuse sweating, weight gain, sexual dysfunction, restlessness, and feeling “foggy or detached.”
“Antidepressants have toxic effects on the brain and cause brain damage when they artificially increase serotonin and modify brain chemistry, which is why people become sick for years after stopping,” Dr. Horowitz said. “When the drug is reduced or stopped, the brain has difficulty dealing with the sudden drop in neurotransmitters, and withdrawal symptoms result, similar to stopping caffeine, nicotine, or opioids.”
He added it is not necessarily the original condition of depression or anxiety that is recurring but rather withdrawal, which can last for months or even years after medication discontinuation.
“Unfortunately, doctors have been taught that there are minimal withdrawal symptoms, euphemized as ‘discontinuation symptoms,’ and so when patients have reported withdrawal symptoms, they have been told it is a return of their underlying condition,” Dr. Horowitz said.
“This has led to many patients being incorrectly told that they need to get back on their antidepressants,” he added.
He likened this approach to “telling people that the need to continue smoking because when they stop, they get more anxiety.” Rather, the “correct response would be that they simply need to taper off the antidepressant more carefully,” he said.
Helpful in the short term
Patients should be informed prior to initiation of antidepressant treatment about the risk of withdrawal effects if they stop the drug, the investigators advise. They reference the Royal College of Psychiatrists’ updated guidance, which recommends slow tapering over a period long enough to mitigate withdrawal symptoms to “tolerable levels.”
The guidance suggests that patients start with a small “test reduction.” Withdrawal symptoms should be monitored for the following 2-4 weeks, using a symptom checklist such as the Discontinuation Emergent Signs and Symptoms Scale, with subsequent reductions based on the tolerability of the process.
Gradual dose reductions and very small final doses may necessitate the use of formulations of medication other than those commonly available in tablet forms, the researchers noted. During the tapering process, patients may benefit from increased psychosocial support.
Dr. Horowitz noted that antidepressants can be helpful on a short-term basis, and likened their use to the use of a cast to stabilize a broken arm.
“It’s useful for a short period. But if you leave someone in a plastic cast permanently, their arm will shrivel and you will disable them. These drugs should be prescribed minimally, and for the shortest possible period of time,” he said.
Dr. Horowitz recommended the recent draft National Institute for Health and Care Excellence depression guidance that recommends multiple other options beyond antidepressants, including cognitive-behavioral therapy, problem solving, counseling, and exercise.
Lack of balance
Dr. Muskin commented that the review is helpful in guiding clinicians on how to approach tapering of antidepressants and making patients aware of discontinuation symptoms.
However, “a lot of people will read this who need treatment, but they won’t get treated because they’ll take away the message that ‘drugs don’t work,’ ” he said.
“As it is, there is already stigma and prejudice toward psychiatric illness and using medications for treatment,” said Dr. Muskin, who was not involved with the research.
The current review “isn’t balanced, in terms of the efficacy of these drugs – both for the spectrum of depressive disorders and for panic or anxiety disorder. And there is nowhere that the authors say these drugs help people,” he added.
Moreover, the investigators’ assertion that long-term use of antidepressants causes harm is incorrect, he said.
“Yes, there are ongoing side effects that impose a burden, but that’s not the same as harm. And while the side effects are sometimes burdensome, ongoing depression is also terribly burdensome,” Dr. Muskin concluded.
Dr. Horowitz, Dr. Wilcock, and Dr. Muskin have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
When it comes to antidepressant prescribing, less may be more, new research suggests.
A new review suggests antidepressants are overprescribed and that the efficacy of these agents is questionable, leading researchers to recommend that, when physicians prescribe these medications, it should be for shorter periods.
“Antidepressants have never been shown to have a clinically significant difference from placebo in the treatment of depression,” study co\investigator Mark Horowitz, GDPsych, PhD, division of psychiatry, University College London, said in an interview.
He added antidepressants “exert profound adverse effects on the body and brain” and can be difficult to stop because of physical dependence that occurs when the brain adapts to them.
“The best way to take people off these drugs is to do so gradually enough that the unpleasant effects are minimized and in a way that means the reductions in dose get smaller and smaller as the total dose gets lower,” Dr. Horowitz said.
However, at least one expert urged caution in interpreting the review’s findings.
“The reality is that millions of people do benefit from these medications, and this review minimizes those benefits,” Philip Muskin, MD, chief of consultation-liaison for psychiatry and professor of psychiatry, Columbia University Medical Center and New York–Presbyterian Hospital, said when approached for comment.
The findings were published online Dec. 20, 2021, in the Drug and Therapeutics Bulletin.
Personal experience
Prescribing of newer-generation antidepressants, such as SSRIs and serotonin and norepinephrine reuptake inhibitors (SNRIs), is increasing, with an estimated one in six adults in the United Kingdom receiving at least one prescription in 2019-2020, the investigators noted.
Dr. Horowitz noted a personal motivation for conducting the review. “As well as being an academic psychiatrist, I’m also a patient who has been prescribed antidepressants since age 21, when my mood was poor, due to life circumstances.”
The antidepressant “didn’t have particularly helpful effects,” but Dr. Horowitz continued taking it for 18 years. “I was told it was helpful and internalized that message. I came to understand that much of the information around antidepressants came from the drug companies that manufactured them or from academics paid by these companies.”
Dr. Horowitz is currently discontinuing his medication – a tapering process now in its third year. He said he has come to realize, in retrospect, that symptoms not initially attributed to the drug, such as fatigue, impaired concentration, and impaired memory, have improved since reducing the medication.
“That experience sensitized me to look for these symptoms in my patients and I see them; but most of my patients were told by their doctors that the cause of those problems was the depression or anxiety itself and not the drug,” he said.
Dr. Horowitz collaborated with Michael Wilcock, DTB, Pharmacy, Royal Cornwall Hospitals, NHS Trust, Truro, England, in conducting the review “to provide an independent assessment of benefits and harms of antidepressants.”
“Much of the evidence of the efficacy of antidepressants comes from randomized placebo-controlled trials,” Dr. Horowitz said. Several meta-analyses of these studies showed a difference of about two points between the agent and the placebo on the Hamilton Depression Rating Scale (HAM-D).
“Although this might be statistically significant, it does not meet the threshold for a clinical significance – those aren’t the same thing,” Dr. Horowitz said. Some analyses suggest that a “minimally clinically important difference” on the HAM-D would range from 3 to 6 points.
The findings in adolescents and children are “even less convincing,” the investigators noted, citing a Cochrane review.
“This is especially concerning because the number of children and adolescents being treated with antidepressants is rapidly increasing,” Dr. Horowitz said.
Additionally, the short duration of most trials, typically 6-12 weeks, is “largely uninformative for the clinical treatment of depression.”
Relapse or withdrawal?
The researchers reviewed the adverse effects of long-term antidepressant use, including daytime sleepiness, dry mouth, profuse sweating, weight gain, sexual dysfunction, restlessness, and feeling “foggy or detached.”
“Antidepressants have toxic effects on the brain and cause brain damage when they artificially increase serotonin and modify brain chemistry, which is why people become sick for years after stopping,” Dr. Horowitz said. “When the drug is reduced or stopped, the brain has difficulty dealing with the sudden drop in neurotransmitters, and withdrawal symptoms result, similar to stopping caffeine, nicotine, or opioids.”
He added it is not necessarily the original condition of depression or anxiety that is recurring but rather withdrawal, which can last for months or even years after medication discontinuation.
“Unfortunately, doctors have been taught that there are minimal withdrawal symptoms, euphemized as ‘discontinuation symptoms,’ and so when patients have reported withdrawal symptoms, they have been told it is a return of their underlying condition,” Dr. Horowitz said.
“This has led to many patients being incorrectly told that they need to get back on their antidepressants,” he added.
He likened this approach to “telling people that the need to continue smoking because when they stop, they get more anxiety.” Rather, the “correct response would be that they simply need to taper off the antidepressant more carefully,” he said.
Helpful in the short term
Patients should be informed prior to initiation of antidepressant treatment about the risk of withdrawal effects if they stop the drug, the investigators advise. They reference the Royal College of Psychiatrists’ updated guidance, which recommends slow tapering over a period long enough to mitigate withdrawal symptoms to “tolerable levels.”
The guidance suggests that patients start with a small “test reduction.” Withdrawal symptoms should be monitored for the following 2-4 weeks, using a symptom checklist such as the Discontinuation Emergent Signs and Symptoms Scale, with subsequent reductions based on the tolerability of the process.
Gradual dose reductions and very small final doses may necessitate the use of formulations of medication other than those commonly available in tablet forms, the researchers noted. During the tapering process, patients may benefit from increased psychosocial support.
Dr. Horowitz noted that antidepressants can be helpful on a short-term basis, and likened their use to the use of a cast to stabilize a broken arm.
“It’s useful for a short period. But if you leave someone in a plastic cast permanently, their arm will shrivel and you will disable them. These drugs should be prescribed minimally, and for the shortest possible period of time,” he said.
Dr. Horowitz recommended the recent draft National Institute for Health and Care Excellence depression guidance that recommends multiple other options beyond antidepressants, including cognitive-behavioral therapy, problem solving, counseling, and exercise.
Lack of balance
Dr. Muskin commented that the review is helpful in guiding clinicians on how to approach tapering of antidepressants and making patients aware of discontinuation symptoms.
However, “a lot of people will read this who need treatment, but they won’t get treated because they’ll take away the message that ‘drugs don’t work,’ ” he said.
“As it is, there is already stigma and prejudice toward psychiatric illness and using medications for treatment,” said Dr. Muskin, who was not involved with the research.
The current review “isn’t balanced, in terms of the efficacy of these drugs – both for the spectrum of depressive disorders and for panic or anxiety disorder. And there is nowhere that the authors say these drugs help people,” he added.
Moreover, the investigators’ assertion that long-term use of antidepressants causes harm is incorrect, he said.
“Yes, there are ongoing side effects that impose a burden, but that’s not the same as harm. And while the side effects are sometimes burdensome, ongoing depression is also terribly burdensome,” Dr. Muskin concluded.
Dr. Horowitz, Dr. Wilcock, and Dr. Muskin have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
When it comes to antidepressant prescribing, less may be more, new research suggests.
A new review suggests antidepressants are overprescribed and that the efficacy of these agents is questionable, leading researchers to recommend that, when physicians prescribe these medications, it should be for shorter periods.
“Antidepressants have never been shown to have a clinically significant difference from placebo in the treatment of depression,” study co\investigator Mark Horowitz, GDPsych, PhD, division of psychiatry, University College London, said in an interview.
He added antidepressants “exert profound adverse effects on the body and brain” and can be difficult to stop because of physical dependence that occurs when the brain adapts to them.
“The best way to take people off these drugs is to do so gradually enough that the unpleasant effects are minimized and in a way that means the reductions in dose get smaller and smaller as the total dose gets lower,” Dr. Horowitz said.
However, at least one expert urged caution in interpreting the review’s findings.
“The reality is that millions of people do benefit from these medications, and this review minimizes those benefits,” Philip Muskin, MD, chief of consultation-liaison for psychiatry and professor of psychiatry, Columbia University Medical Center and New York–Presbyterian Hospital, said when approached for comment.
The findings were published online Dec. 20, 2021, in the Drug and Therapeutics Bulletin.
Personal experience
Prescribing of newer-generation antidepressants, such as SSRIs and serotonin and norepinephrine reuptake inhibitors (SNRIs), is increasing, with an estimated one in six adults in the United Kingdom receiving at least one prescription in 2019-2020, the investigators noted.
Dr. Horowitz noted a personal motivation for conducting the review. “As well as being an academic psychiatrist, I’m also a patient who has been prescribed antidepressants since age 21, when my mood was poor, due to life circumstances.”
The antidepressant “didn’t have particularly helpful effects,” but Dr. Horowitz continued taking it for 18 years. “I was told it was helpful and internalized that message. I came to understand that much of the information around antidepressants came from the drug companies that manufactured them or from academics paid by these companies.”
Dr. Horowitz is currently discontinuing his medication – a tapering process now in its third year. He said he has come to realize, in retrospect, that symptoms not initially attributed to the drug, such as fatigue, impaired concentration, and impaired memory, have improved since reducing the medication.
“That experience sensitized me to look for these symptoms in my patients and I see them; but most of my patients were told by their doctors that the cause of those problems was the depression or anxiety itself and not the drug,” he said.
Dr. Horowitz collaborated with Michael Wilcock, DTB, Pharmacy, Royal Cornwall Hospitals, NHS Trust, Truro, England, in conducting the review “to provide an independent assessment of benefits and harms of antidepressants.”
“Much of the evidence of the efficacy of antidepressants comes from randomized placebo-controlled trials,” Dr. Horowitz said. Several meta-analyses of these studies showed a difference of about two points between the agent and the placebo on the Hamilton Depression Rating Scale (HAM-D).
“Although this might be statistically significant, it does not meet the threshold for a clinical significance – those aren’t the same thing,” Dr. Horowitz said. Some analyses suggest that a “minimally clinically important difference” on the HAM-D would range from 3 to 6 points.
The findings in adolescents and children are “even less convincing,” the investigators noted, citing a Cochrane review.
“This is especially concerning because the number of children and adolescents being treated with antidepressants is rapidly increasing,” Dr. Horowitz said.
Additionally, the short duration of most trials, typically 6-12 weeks, is “largely uninformative for the clinical treatment of depression.”
Relapse or withdrawal?
The researchers reviewed the adverse effects of long-term antidepressant use, including daytime sleepiness, dry mouth, profuse sweating, weight gain, sexual dysfunction, restlessness, and feeling “foggy or detached.”
“Antidepressants have toxic effects on the brain and cause brain damage when they artificially increase serotonin and modify brain chemistry, which is why people become sick for years after stopping,” Dr. Horowitz said. “When the drug is reduced or stopped, the brain has difficulty dealing with the sudden drop in neurotransmitters, and withdrawal symptoms result, similar to stopping caffeine, nicotine, or opioids.”
He added it is not necessarily the original condition of depression or anxiety that is recurring but rather withdrawal, which can last for months or even years after medication discontinuation.
“Unfortunately, doctors have been taught that there are minimal withdrawal symptoms, euphemized as ‘discontinuation symptoms,’ and so when patients have reported withdrawal symptoms, they have been told it is a return of their underlying condition,” Dr. Horowitz said.
“This has led to many patients being incorrectly told that they need to get back on their antidepressants,” he added.
He likened this approach to “telling people that the need to continue smoking because when they stop, they get more anxiety.” Rather, the “correct response would be that they simply need to taper off the antidepressant more carefully,” he said.
Helpful in the short term
Patients should be informed prior to initiation of antidepressant treatment about the risk of withdrawal effects if they stop the drug, the investigators advise. They reference the Royal College of Psychiatrists’ updated guidance, which recommends slow tapering over a period long enough to mitigate withdrawal symptoms to “tolerable levels.”
The guidance suggests that patients start with a small “test reduction.” Withdrawal symptoms should be monitored for the following 2-4 weeks, using a symptom checklist such as the Discontinuation Emergent Signs and Symptoms Scale, with subsequent reductions based on the tolerability of the process.
Gradual dose reductions and very small final doses may necessitate the use of formulations of medication other than those commonly available in tablet forms, the researchers noted. During the tapering process, patients may benefit from increased psychosocial support.
Dr. Horowitz noted that antidepressants can be helpful on a short-term basis, and likened their use to the use of a cast to stabilize a broken arm.
“It’s useful for a short period. But if you leave someone in a plastic cast permanently, their arm will shrivel and you will disable them. These drugs should be prescribed minimally, and for the shortest possible period of time,” he said.
Dr. Horowitz recommended the recent draft National Institute for Health and Care Excellence depression guidance that recommends multiple other options beyond antidepressants, including cognitive-behavioral therapy, problem solving, counseling, and exercise.
Lack of balance
Dr. Muskin commented that the review is helpful in guiding clinicians on how to approach tapering of antidepressants and making patients aware of discontinuation symptoms.
However, “a lot of people will read this who need treatment, but they won’t get treated because they’ll take away the message that ‘drugs don’t work,’ ” he said.
“As it is, there is already stigma and prejudice toward psychiatric illness and using medications for treatment,” said Dr. Muskin, who was not involved with the research.
The current review “isn’t balanced, in terms of the efficacy of these drugs – both for the spectrum of depressive disorders and for panic or anxiety disorder. And there is nowhere that the authors say these drugs help people,” he added.
Moreover, the investigators’ assertion that long-term use of antidepressants causes harm is incorrect, he said.
“Yes, there are ongoing side effects that impose a burden, but that’s not the same as harm. And while the side effects are sometimes burdensome, ongoing depression is also terribly burdensome,” Dr. Muskin concluded.
Dr. Horowitz, Dr. Wilcock, and Dr. Muskin have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE DRUG AND THERAPEUTICS BULLETIN