User login
Hematocrit, White Blood Cells, and Thrombotic Events in the Veteran Population With Polycythemia Vera
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
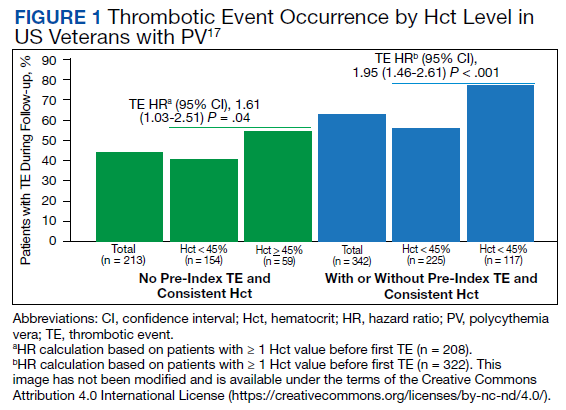
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
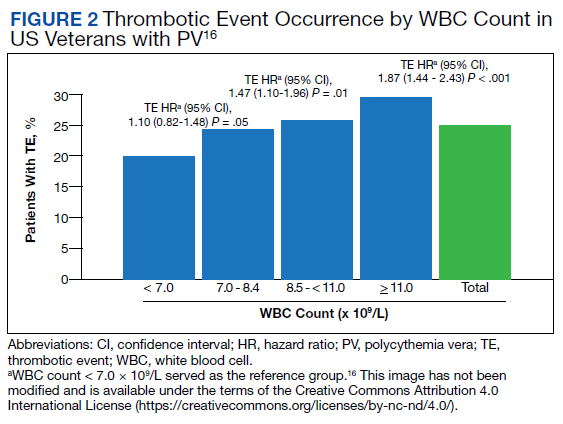
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891
Rare pediatric cancers persist 63 years after nuclear accident
Chernobyl. Fukushima. Three Mile Island.
The world knows these names all too well because of accidents there: complete or partial meltdowns of nuclear reactors that released massive amounts of cancer-causing radiation into the air, soil, and water.
The Santa Susana Field Lab is far less well-known, but no less infamous for what took place at this former rocket engine and nuclear energy test site just 28 miles northwest of downtown Los Angeles.
In July 1959, an accident involving one of 10 experimental nuclear reactors at the SSFL site released a cloud of harmful radiation and toxic chemicals over the surrounding area, including Simi Valley, San Gabriel Valley, Chatsworth, and Canoga Park. The small reactor had no containment vessel.
This accident resulted in a release of radioactive iodine estimated to be as much as 250 times that of the partial meltdown that would occur 2 decades later at Three Mile Island, a much larger commercial reactor that had a containment vessel.
Decades-long cover-up
In 1959, the public knew nothing about what happened at the site.
According to John Pace, then an employee at SSFL, the accident was covered up. Mr. Pace recounted the cover-up in the documentary “In the Dark of the Valley,” which first aired in November 2021 on MSNBC.
In fact, the accident at SSFL remained under wraps for 2 decades, according to Daniel Hirsch, former director of the Program on Environmental and Nuclear Policy at the University of California, Santa Cruz, and now president of Committee to Bridge the Gap, a nuclear policy nongovernmental organization.
“Students working with me while I was teaching at UCLA in 1979 uncovered these Atomic Energy Commission reports from Atomics International,” he said in an interview. “We had to order the documents from the annex to the UCLA Engineering Library. They were stored offsite, and it took a few days, and when we got them, we opened them up, and there were these fold-out photographs of the fuel [rods]. As we folded out the photographs further, we saw one photo with an arrow labeled ‘longitudinal cracks,’ and then other arrows showing other kinds of cracks, and then another arrow labeled ‘melted blob.’ ”
Mr. Hirsch and his students found that other accidents had occurred at SSFL, including a fuel fabrication system that leached plutonium, fires in a “hot” lab where irradiated nuclear fuel from around the United States was handled, and open-air burn pits where radioactive and toxic chemical wastes were illegally torched.
According to the Committee to Bridge the Gap, when the 2,800-acre SSFL site was being developed under the name Rocketdyne by aircraft maker North American Aviation, the area was sparsely populated, with nearly as many grazing animals as people in its hills and valleys.
North American Aviation later became part of Rockwell International, which in turn sold its aerospace and defense business units to the Boeing Company in 1996. Boeing, now in charge of the site and the cleanup efforts, is doing everything in its power to shirk or diminish its responsibility, Mr. Hirsch and other critics say.
Parents against SSFL
Today, more than 150,000 people live within 5 miles of SSFL, and more than half a million live within 10 miles.
Melissa Bumstead is one of those residents. She and her family live 3.7 miles from the Santa Susana site. When her toddler Grace was diagnosed with a rare form of leukemia in 2014, doctors told Ms. Bumstead there were no known links between her daughter’s cancer and environmental contamination.
But during Grace’s treatment at Children’s Hospital Los Angeles, her mother began meeting other parents who lived near her and had children facing equally rare cancers.
Lauren Hammersley, whose daughter Hazel was diagnosed with a rare brain tumor called neuroblastoma at age 2, lived about 10 miles from Ms. Bumstead on the other side of a mountain and just over 4 miles from SSFL.
On her street alone, Ms. Bumstead discovered three cases of pediatric cancer, including two children in adjacent homes who had the same rare brain tumor as Hazel Hammersley.
As Ms. Bumstead told Los Angeles National Public Radio station KCRW in 2021, “I started to panic because I knew that childhood cancer is extremely rare. There’s only 15,000 new cases every year out of 72 million children in America. So, the chance of knowing your neighbors, especially at an internationally renowned hospital like Children’s Hospital Los Angeles – we knew something wasn’t right.”
After a relapse of her tumor, Hazel died in 2018, a few months after her seventh birthday.
Cancer clusters
Hoping to understand why their kids were getting so sick, Ms. Bumstead and the other parents formed a Facebook group. They plotted their homes on Google Maps and found that they all lived within roughly 10 miles of one another. It would take another year for them to realize that the SSFL site was at the center of the circle.
Once they realized that being close to SSFL could be their common thread, Ms. Bumstead and parents in her group began to gradually piece together the story, linking unusual or unexplained illnesses in their families to potential radiation or toxic chemical exposures from the lab.
“What really convinced me that this was absolutely a problem was when I learned about the epidemiological study by Dr. Hal Morgenstern that found that residents living within 2 miles of the Santa Susana Field Lab actually had a 60% higher cancer incidence rate and that over 1,500 workers have been diagnosed with cancer just from the Santa Susana Field Lab,” she told KCRW.
In 2015, Ms. Bumstead and other parents formed Parents Against Santa Susana Field Lab to hold SSFL site owner Boeing accountable for radiologic and toxic contamination and to ensure that Boeing cleans the site and surrounding areas. The group “seeks to reduce, to the greatest extent possible, the number of local families who have to hear the words, ‘Your child has cancer.’ ”
No longer quite so rare
Dr. Morgenstern, now retired from the University of Michigan, declined to be interviewed for this article. But as he and colleagues reported to the Centers for Disease Control and Prevention’s Agency for Toxic Substances and Disease Registry in 2007, there were strong signs of a link between contamination of the site and cancer.
The researchers compared cancer rates of adults living within 2 miles and 2-5 miles from SSFL with those of adults living more than 5 miles away, in Ventura and Los Angeles counties. They found that from 1988 through 1995, residents living within 2 miles of SSFL had a 60% higher rate of cancers than the control group. These included cancers of the thyroid, oral and nasal cavities, pharynx, larynx, esophagus, and bladder, as well as blood cancers such as leukemia, lymphoma, and multiple myeloma.
In separate studies, the investigators found higher rates of certain cancers among workers at SSFL who were exposed to radiation and to hydrazine, a chemical in rocket fuel.
In an interview, Dr. Saro Armenian, a pediatric hematologist-oncologist who was not involved in the studies, said the 60% increase in cancer incidence, which translated into a 1.6-fold increase in risk, merits more investigation.
“In epidemiologic studies, a 1.6-fold risk is actually a pretty strong signal because typically, most signals that you get are somewhere around 1.1- to 1.2-fold increased risk,” noted Dr. Armenian, a specialist in pediatric cancer survivorship and outcomes at City of Hope National Medical Center in Duarte, Calif.
However, Dr. Thomas Mack, former director of the Los Angeles County Cancer Surveillance Program, contends that there is insufficient evidence to support a direct link between the 1959 reactor accident and recent incident cancers. Dr. Mack is currently a professor of preventive medicine and pathology at the University of Southern California in Los Angeles.
“I have evaluated concerns about local excesses of cancer at least 100 times, usually from county residents, but for a while I represented the CDC and the California cancer registry,” Dr. Mack said, in response to an emailed request for comment.
“So far I have seen no evidence of carcinogenic radionucleotides or chemical carcinogens from Santa Susana found in any meaningful amount in any nearby community, but if someone has such evidence that would constitute evidence, that needs a response,” Dr. Mack added.
Boeing and California
Boeing has said problems at SSFL were not responsible for the high cancer rates among children in the community.
In April 2007, in a statement opposing a bill before the California State Legislature that would compel Boeing to pay for SSFL site cleanup, the company said that “in contrast to the accusations made against The Boeing Company that falsely claim increased cancer rates in the communities surrounding SSFL, a recent study conducted by the University of Michigan School of Public Health just concluded the opposite.”
Yet as Dr. Morgenstern wrote in 2007 to California state Sen. Joe Simitian, then chair of the Committee on Environmental Quality: “For the period 1996 through 2002, we found that the incidence rate of thyroid cancer was more than 60% greater among residents living within 2 miles of SSFL than for residents living more than 5 miles from SSFL. The magnitude and consistency of the thyroid finding for both periods is especially provocative because of evidence from other studies linking thyroid cancer with environmental exposures originating at SSFL and found in the surrounding communities.”
Boeing chose to ignore the results and instead focused on the methods used in the study, where the authors acknowledged that they measured distance from the site rather than environmental exposures and thus could not conclusively link excess cancer rates to exposures arising from SSFL.
But Dr. Morgenstern emphasized the conclusion of the report: “Despite the methodologic limitations of this study, the findings suggest there may be elevated incidence rates of certain cancers near SSFL that have been linked in previous studies with hazardous substances used at Rocketdyne, some of which have been observed or projected to exist offsite.”
Failure to come clean
In 2008, a law that set standards for cleanup of the site was passed. But the law was overturned in 2014 after a legal challenge by Boeing.
That left in place a 2007 order of consent between Boeing, NASA, the U.S. Department of Energy, and the California Department of Toxic Substances Control (DTSC) that required cleanup of SSFL to a much less stringent standard.
As of last year, Boeing and DTSC had begun confidential, nonbinding agreements regarding the 2007 order of consent, according to Parents Against SSFL.
Among the contaminants lingering at the site are radioactive particles, chemical compounds, heavy metals, and polluted water.
“In fact, over 300 contaminants of concern have been found at the site, and they are refusing to clean it,” Mr. Hirsch said. “This company releases large amounts of carcinogens, and perhaps significant numbers of people get sick with cancer, and the company doesn’t go to prison. They get more federal contracts.”
A version of this article first appeared on WebMD.com.
April 20, 2022 – Editor’s note: This article has been updated to include an interview with Dr. Thomas Mack, former director of the Los Angeles County Cancer Surveillance Program, who contends that there is insufficient evidence to support a direct link between the 1959 reactor accident and recent incident cancers.
Chernobyl. Fukushima. Three Mile Island.
The world knows these names all too well because of accidents there: complete or partial meltdowns of nuclear reactors that released massive amounts of cancer-causing radiation into the air, soil, and water.
The Santa Susana Field Lab is far less well-known, but no less infamous for what took place at this former rocket engine and nuclear energy test site just 28 miles northwest of downtown Los Angeles.
In July 1959, an accident involving one of 10 experimental nuclear reactors at the SSFL site released a cloud of harmful radiation and toxic chemicals over the surrounding area, including Simi Valley, San Gabriel Valley, Chatsworth, and Canoga Park. The small reactor had no containment vessel.
This accident resulted in a release of radioactive iodine estimated to be as much as 250 times that of the partial meltdown that would occur 2 decades later at Three Mile Island, a much larger commercial reactor that had a containment vessel.
Decades-long cover-up
In 1959, the public knew nothing about what happened at the site.
According to John Pace, then an employee at SSFL, the accident was covered up. Mr. Pace recounted the cover-up in the documentary “In the Dark of the Valley,” which first aired in November 2021 on MSNBC.
In fact, the accident at SSFL remained under wraps for 2 decades, according to Daniel Hirsch, former director of the Program on Environmental and Nuclear Policy at the University of California, Santa Cruz, and now president of Committee to Bridge the Gap, a nuclear policy nongovernmental organization.
“Students working with me while I was teaching at UCLA in 1979 uncovered these Atomic Energy Commission reports from Atomics International,” he said in an interview. “We had to order the documents from the annex to the UCLA Engineering Library. They were stored offsite, and it took a few days, and when we got them, we opened them up, and there were these fold-out photographs of the fuel [rods]. As we folded out the photographs further, we saw one photo with an arrow labeled ‘longitudinal cracks,’ and then other arrows showing other kinds of cracks, and then another arrow labeled ‘melted blob.’ ”
Mr. Hirsch and his students found that other accidents had occurred at SSFL, including a fuel fabrication system that leached plutonium, fires in a “hot” lab where irradiated nuclear fuel from around the United States was handled, and open-air burn pits where radioactive and toxic chemical wastes were illegally torched.
According to the Committee to Bridge the Gap, when the 2,800-acre SSFL site was being developed under the name Rocketdyne by aircraft maker North American Aviation, the area was sparsely populated, with nearly as many grazing animals as people in its hills and valleys.
North American Aviation later became part of Rockwell International, which in turn sold its aerospace and defense business units to the Boeing Company in 1996. Boeing, now in charge of the site and the cleanup efforts, is doing everything in its power to shirk or diminish its responsibility, Mr. Hirsch and other critics say.
Parents against SSFL
Today, more than 150,000 people live within 5 miles of SSFL, and more than half a million live within 10 miles.
Melissa Bumstead is one of those residents. She and her family live 3.7 miles from the Santa Susana site. When her toddler Grace was diagnosed with a rare form of leukemia in 2014, doctors told Ms. Bumstead there were no known links between her daughter’s cancer and environmental contamination.
But during Grace’s treatment at Children’s Hospital Los Angeles, her mother began meeting other parents who lived near her and had children facing equally rare cancers.
Lauren Hammersley, whose daughter Hazel was diagnosed with a rare brain tumor called neuroblastoma at age 2, lived about 10 miles from Ms. Bumstead on the other side of a mountain and just over 4 miles from SSFL.
On her street alone, Ms. Bumstead discovered three cases of pediatric cancer, including two children in adjacent homes who had the same rare brain tumor as Hazel Hammersley.
As Ms. Bumstead told Los Angeles National Public Radio station KCRW in 2021, “I started to panic because I knew that childhood cancer is extremely rare. There’s only 15,000 new cases every year out of 72 million children in America. So, the chance of knowing your neighbors, especially at an internationally renowned hospital like Children’s Hospital Los Angeles – we knew something wasn’t right.”
After a relapse of her tumor, Hazel died in 2018, a few months after her seventh birthday.
Cancer clusters
Hoping to understand why their kids were getting so sick, Ms. Bumstead and the other parents formed a Facebook group. They plotted their homes on Google Maps and found that they all lived within roughly 10 miles of one another. It would take another year for them to realize that the SSFL site was at the center of the circle.
Once they realized that being close to SSFL could be their common thread, Ms. Bumstead and parents in her group began to gradually piece together the story, linking unusual or unexplained illnesses in their families to potential radiation or toxic chemical exposures from the lab.
“What really convinced me that this was absolutely a problem was when I learned about the epidemiological study by Dr. Hal Morgenstern that found that residents living within 2 miles of the Santa Susana Field Lab actually had a 60% higher cancer incidence rate and that over 1,500 workers have been diagnosed with cancer just from the Santa Susana Field Lab,” she told KCRW.
In 2015, Ms. Bumstead and other parents formed Parents Against Santa Susana Field Lab to hold SSFL site owner Boeing accountable for radiologic and toxic contamination and to ensure that Boeing cleans the site and surrounding areas. The group “seeks to reduce, to the greatest extent possible, the number of local families who have to hear the words, ‘Your child has cancer.’ ”
No longer quite so rare
Dr. Morgenstern, now retired from the University of Michigan, declined to be interviewed for this article. But as he and colleagues reported to the Centers for Disease Control and Prevention’s Agency for Toxic Substances and Disease Registry in 2007, there were strong signs of a link between contamination of the site and cancer.
The researchers compared cancer rates of adults living within 2 miles and 2-5 miles from SSFL with those of adults living more than 5 miles away, in Ventura and Los Angeles counties. They found that from 1988 through 1995, residents living within 2 miles of SSFL had a 60% higher rate of cancers than the control group. These included cancers of the thyroid, oral and nasal cavities, pharynx, larynx, esophagus, and bladder, as well as blood cancers such as leukemia, lymphoma, and multiple myeloma.
In separate studies, the investigators found higher rates of certain cancers among workers at SSFL who were exposed to radiation and to hydrazine, a chemical in rocket fuel.
In an interview, Dr. Saro Armenian, a pediatric hematologist-oncologist who was not involved in the studies, said the 60% increase in cancer incidence, which translated into a 1.6-fold increase in risk, merits more investigation.
“In epidemiologic studies, a 1.6-fold risk is actually a pretty strong signal because typically, most signals that you get are somewhere around 1.1- to 1.2-fold increased risk,” noted Dr. Armenian, a specialist in pediatric cancer survivorship and outcomes at City of Hope National Medical Center in Duarte, Calif.
However, Dr. Thomas Mack, former director of the Los Angeles County Cancer Surveillance Program, contends that there is insufficient evidence to support a direct link between the 1959 reactor accident and recent incident cancers. Dr. Mack is currently a professor of preventive medicine and pathology at the University of Southern California in Los Angeles.
“I have evaluated concerns about local excesses of cancer at least 100 times, usually from county residents, but for a while I represented the CDC and the California cancer registry,” Dr. Mack said, in response to an emailed request for comment.
“So far I have seen no evidence of carcinogenic radionucleotides or chemical carcinogens from Santa Susana found in any meaningful amount in any nearby community, but if someone has such evidence that would constitute evidence, that needs a response,” Dr. Mack added.
Boeing and California
Boeing has said problems at SSFL were not responsible for the high cancer rates among children in the community.
In April 2007, in a statement opposing a bill before the California State Legislature that would compel Boeing to pay for SSFL site cleanup, the company said that “in contrast to the accusations made against The Boeing Company that falsely claim increased cancer rates in the communities surrounding SSFL, a recent study conducted by the University of Michigan School of Public Health just concluded the opposite.”
Yet as Dr. Morgenstern wrote in 2007 to California state Sen. Joe Simitian, then chair of the Committee on Environmental Quality: “For the period 1996 through 2002, we found that the incidence rate of thyroid cancer was more than 60% greater among residents living within 2 miles of SSFL than for residents living more than 5 miles from SSFL. The magnitude and consistency of the thyroid finding for both periods is especially provocative because of evidence from other studies linking thyroid cancer with environmental exposures originating at SSFL and found in the surrounding communities.”
Boeing chose to ignore the results and instead focused on the methods used in the study, where the authors acknowledged that they measured distance from the site rather than environmental exposures and thus could not conclusively link excess cancer rates to exposures arising from SSFL.
But Dr. Morgenstern emphasized the conclusion of the report: “Despite the methodologic limitations of this study, the findings suggest there may be elevated incidence rates of certain cancers near SSFL that have been linked in previous studies with hazardous substances used at Rocketdyne, some of which have been observed or projected to exist offsite.”
Failure to come clean
In 2008, a law that set standards for cleanup of the site was passed. But the law was overturned in 2014 after a legal challenge by Boeing.
That left in place a 2007 order of consent between Boeing, NASA, the U.S. Department of Energy, and the California Department of Toxic Substances Control (DTSC) that required cleanup of SSFL to a much less stringent standard.
As of last year, Boeing and DTSC had begun confidential, nonbinding agreements regarding the 2007 order of consent, according to Parents Against SSFL.
Among the contaminants lingering at the site are radioactive particles, chemical compounds, heavy metals, and polluted water.
“In fact, over 300 contaminants of concern have been found at the site, and they are refusing to clean it,” Mr. Hirsch said. “This company releases large amounts of carcinogens, and perhaps significant numbers of people get sick with cancer, and the company doesn’t go to prison. They get more federal contracts.”
A version of this article first appeared on WebMD.com.
April 20, 2022 – Editor’s note: This article has been updated to include an interview with Dr. Thomas Mack, former director of the Los Angeles County Cancer Surveillance Program, who contends that there is insufficient evidence to support a direct link between the 1959 reactor accident and recent incident cancers.
Chernobyl. Fukushima. Three Mile Island.
The world knows these names all too well because of accidents there: complete or partial meltdowns of nuclear reactors that released massive amounts of cancer-causing radiation into the air, soil, and water.
The Santa Susana Field Lab is far less well-known, but no less infamous for what took place at this former rocket engine and nuclear energy test site just 28 miles northwest of downtown Los Angeles.
In July 1959, an accident involving one of 10 experimental nuclear reactors at the SSFL site released a cloud of harmful radiation and toxic chemicals over the surrounding area, including Simi Valley, San Gabriel Valley, Chatsworth, and Canoga Park. The small reactor had no containment vessel.
This accident resulted in a release of radioactive iodine estimated to be as much as 250 times that of the partial meltdown that would occur 2 decades later at Three Mile Island, a much larger commercial reactor that had a containment vessel.
Decades-long cover-up
In 1959, the public knew nothing about what happened at the site.
According to John Pace, then an employee at SSFL, the accident was covered up. Mr. Pace recounted the cover-up in the documentary “In the Dark of the Valley,” which first aired in November 2021 on MSNBC.
In fact, the accident at SSFL remained under wraps for 2 decades, according to Daniel Hirsch, former director of the Program on Environmental and Nuclear Policy at the University of California, Santa Cruz, and now president of Committee to Bridge the Gap, a nuclear policy nongovernmental organization.
“Students working with me while I was teaching at UCLA in 1979 uncovered these Atomic Energy Commission reports from Atomics International,” he said in an interview. “We had to order the documents from the annex to the UCLA Engineering Library. They were stored offsite, and it took a few days, and when we got them, we opened them up, and there were these fold-out photographs of the fuel [rods]. As we folded out the photographs further, we saw one photo with an arrow labeled ‘longitudinal cracks,’ and then other arrows showing other kinds of cracks, and then another arrow labeled ‘melted blob.’ ”
Mr. Hirsch and his students found that other accidents had occurred at SSFL, including a fuel fabrication system that leached plutonium, fires in a “hot” lab where irradiated nuclear fuel from around the United States was handled, and open-air burn pits where radioactive and toxic chemical wastes were illegally torched.
According to the Committee to Bridge the Gap, when the 2,800-acre SSFL site was being developed under the name Rocketdyne by aircraft maker North American Aviation, the area was sparsely populated, with nearly as many grazing animals as people in its hills and valleys.
North American Aviation later became part of Rockwell International, which in turn sold its aerospace and defense business units to the Boeing Company in 1996. Boeing, now in charge of the site and the cleanup efforts, is doing everything in its power to shirk or diminish its responsibility, Mr. Hirsch and other critics say.
Parents against SSFL
Today, more than 150,000 people live within 5 miles of SSFL, and more than half a million live within 10 miles.
Melissa Bumstead is one of those residents. She and her family live 3.7 miles from the Santa Susana site. When her toddler Grace was diagnosed with a rare form of leukemia in 2014, doctors told Ms. Bumstead there were no known links between her daughter’s cancer and environmental contamination.
But during Grace’s treatment at Children’s Hospital Los Angeles, her mother began meeting other parents who lived near her and had children facing equally rare cancers.
Lauren Hammersley, whose daughter Hazel was diagnosed with a rare brain tumor called neuroblastoma at age 2, lived about 10 miles from Ms. Bumstead on the other side of a mountain and just over 4 miles from SSFL.
On her street alone, Ms. Bumstead discovered three cases of pediatric cancer, including two children in adjacent homes who had the same rare brain tumor as Hazel Hammersley.
As Ms. Bumstead told Los Angeles National Public Radio station KCRW in 2021, “I started to panic because I knew that childhood cancer is extremely rare. There’s only 15,000 new cases every year out of 72 million children in America. So, the chance of knowing your neighbors, especially at an internationally renowned hospital like Children’s Hospital Los Angeles – we knew something wasn’t right.”
After a relapse of her tumor, Hazel died in 2018, a few months after her seventh birthday.
Cancer clusters
Hoping to understand why their kids were getting so sick, Ms. Bumstead and the other parents formed a Facebook group. They plotted their homes on Google Maps and found that they all lived within roughly 10 miles of one another. It would take another year for them to realize that the SSFL site was at the center of the circle.
Once they realized that being close to SSFL could be their common thread, Ms. Bumstead and parents in her group began to gradually piece together the story, linking unusual or unexplained illnesses in their families to potential radiation or toxic chemical exposures from the lab.
“What really convinced me that this was absolutely a problem was when I learned about the epidemiological study by Dr. Hal Morgenstern that found that residents living within 2 miles of the Santa Susana Field Lab actually had a 60% higher cancer incidence rate and that over 1,500 workers have been diagnosed with cancer just from the Santa Susana Field Lab,” she told KCRW.
In 2015, Ms. Bumstead and other parents formed Parents Against Santa Susana Field Lab to hold SSFL site owner Boeing accountable for radiologic and toxic contamination and to ensure that Boeing cleans the site and surrounding areas. The group “seeks to reduce, to the greatest extent possible, the number of local families who have to hear the words, ‘Your child has cancer.’ ”
No longer quite so rare
Dr. Morgenstern, now retired from the University of Michigan, declined to be interviewed for this article. But as he and colleagues reported to the Centers for Disease Control and Prevention’s Agency for Toxic Substances and Disease Registry in 2007, there were strong signs of a link between contamination of the site and cancer.
The researchers compared cancer rates of adults living within 2 miles and 2-5 miles from SSFL with those of adults living more than 5 miles away, in Ventura and Los Angeles counties. They found that from 1988 through 1995, residents living within 2 miles of SSFL had a 60% higher rate of cancers than the control group. These included cancers of the thyroid, oral and nasal cavities, pharynx, larynx, esophagus, and bladder, as well as blood cancers such as leukemia, lymphoma, and multiple myeloma.
In separate studies, the investigators found higher rates of certain cancers among workers at SSFL who were exposed to radiation and to hydrazine, a chemical in rocket fuel.
In an interview, Dr. Saro Armenian, a pediatric hematologist-oncologist who was not involved in the studies, said the 60% increase in cancer incidence, which translated into a 1.6-fold increase in risk, merits more investigation.
“In epidemiologic studies, a 1.6-fold risk is actually a pretty strong signal because typically, most signals that you get are somewhere around 1.1- to 1.2-fold increased risk,” noted Dr. Armenian, a specialist in pediatric cancer survivorship and outcomes at City of Hope National Medical Center in Duarte, Calif.
However, Dr. Thomas Mack, former director of the Los Angeles County Cancer Surveillance Program, contends that there is insufficient evidence to support a direct link between the 1959 reactor accident and recent incident cancers. Dr. Mack is currently a professor of preventive medicine and pathology at the University of Southern California in Los Angeles.
“I have evaluated concerns about local excesses of cancer at least 100 times, usually from county residents, but for a while I represented the CDC and the California cancer registry,” Dr. Mack said, in response to an emailed request for comment.
“So far I have seen no evidence of carcinogenic radionucleotides or chemical carcinogens from Santa Susana found in any meaningful amount in any nearby community, but if someone has such evidence that would constitute evidence, that needs a response,” Dr. Mack added.
Boeing and California
Boeing has said problems at SSFL were not responsible for the high cancer rates among children in the community.
In April 2007, in a statement opposing a bill before the California State Legislature that would compel Boeing to pay for SSFL site cleanup, the company said that “in contrast to the accusations made against The Boeing Company that falsely claim increased cancer rates in the communities surrounding SSFL, a recent study conducted by the University of Michigan School of Public Health just concluded the opposite.”
Yet as Dr. Morgenstern wrote in 2007 to California state Sen. Joe Simitian, then chair of the Committee on Environmental Quality: “For the period 1996 through 2002, we found that the incidence rate of thyroid cancer was more than 60% greater among residents living within 2 miles of SSFL than for residents living more than 5 miles from SSFL. The magnitude and consistency of the thyroid finding for both periods is especially provocative because of evidence from other studies linking thyroid cancer with environmental exposures originating at SSFL and found in the surrounding communities.”
Boeing chose to ignore the results and instead focused on the methods used in the study, where the authors acknowledged that they measured distance from the site rather than environmental exposures and thus could not conclusively link excess cancer rates to exposures arising from SSFL.
But Dr. Morgenstern emphasized the conclusion of the report: “Despite the methodologic limitations of this study, the findings suggest there may be elevated incidence rates of certain cancers near SSFL that have been linked in previous studies with hazardous substances used at Rocketdyne, some of which have been observed or projected to exist offsite.”
Failure to come clean
In 2008, a law that set standards for cleanup of the site was passed. But the law was overturned in 2014 after a legal challenge by Boeing.
That left in place a 2007 order of consent between Boeing, NASA, the U.S. Department of Energy, and the California Department of Toxic Substances Control (DTSC) that required cleanup of SSFL to a much less stringent standard.
As of last year, Boeing and DTSC had begun confidential, nonbinding agreements regarding the 2007 order of consent, according to Parents Against SSFL.
Among the contaminants lingering at the site are radioactive particles, chemical compounds, heavy metals, and polluted water.
“In fact, over 300 contaminants of concern have been found at the site, and they are refusing to clean it,” Mr. Hirsch said. “This company releases large amounts of carcinogens, and perhaps significant numbers of people get sick with cancer, and the company doesn’t go to prison. They get more federal contracts.”
A version of this article first appeared on WebMD.com.
April 20, 2022 – Editor’s note: This article has been updated to include an interview with Dr. Thomas Mack, former director of the Los Angeles County Cancer Surveillance Program, who contends that there is insufficient evidence to support a direct link between the 1959 reactor accident and recent incident cancers.
Complex link between gut microbiome and immunotherapy response in advanced melanoma
A large-scale than previously thought.
Overall, researchers identified a panel of species, including Roseburia spp. and Akkermansia muciniphila, associated with responses to ICI therapy. However, no single species was a “fully consistent biomarker” across the studies, the authors explain.
This “machine learning analysis confirmed the link between the microbiome and overall response rates (ORRs) and progression-free survival (PFS) with ICIs but also revealed limited reproducibility of microbiome-based signatures across cohorts,” Karla A. Lee, PhD, a clinical research fellow at King’s College London, and colleagues report. The results suggest that “the microbiome is predictive of response in some, but not all, cohorts.”
The findings were published online Feb. 28 in Nature Medicine.
Despite recent advances in targeted therapies for melanoma, less than half of the those who receive a single-agent ICI respond, and those who receive combination ICI therapy often suffer from severe drug toxicity problems. That is why finding patients more likely to respond to a single-agent ICI has become a priority.
Previous studies have identified the gut microbiome as “a potential biomarker of response, as well as a therapeutic target” in melanoma and other malignancies, but “little consensus exists on which microbiome characteristics are associated with treatment responses in the human setting,” the authors explain.
To further clarify the microbiome–immunotherapy relationship, the researchers performed metagenomic sequencing of stool samples collected from 165 ICI-naive patients with unresectable stage III or IV cutaneous melanoma from 5 observational cohorts in the Netherlands, United Kingdom, and Spain. These data were integrated with 147 samples from publicly available datasets.
First, the authors highlighted the variability in findings across these observational studies. For instance, they analyzed stool samples from one UK-based observational study of patients with melanoma (PRIMM-UK) and found a small but statistically significant difference in the microbiome composition of immunotherapy responders versus nonresponders (P = .05) but did not find such an association in a parallel study in the Netherlands (PRIMM-NL, P = .61).
The investigators also explored biomarkers of response across different cohorts and found several standouts. In trials using ORR as an endpoint, two uncultivated Roseburia species (CAG:182 and CAG:471) were associated with responses to ICIs. For patients with available PFS data, Phascolarctobacterium succinatutens and Lactobacillus vaginalis were “enriched in responders” across 7 datasets and significant in 3 of the 8 meta-analysis approaches. A muciniphila and Dorea formicigenerans were also associated with ORR and PFS at 12 months in several meta-analyses.
However, “no single bacterium was a fully consistent biomarker of response across all datasets,” the authors wrote.
Still, the findings could have important implications for the more than 50% of patients with advanced melanoma who don’t respond to single-agent ICI therapy.
“Our study shows that studying the microbiome is important to improve and personalize immunotherapy treatments for melanoma,” study coauthor Nicola Segata, PhD, principal investigator in the Laboratory of Computational Metagenomics, University of Trento, Italy, said in a press release. “However, it also suggests that because of the person-to-person variability of the gut microbiome, even larger studies must be carried out to understand the specific gut microbial features that are more likely to lead to a positive response to immunotherapy.”
Coauthor Tim Spector, PhD, head of the Department of Twin Research & Genetic Epidemiology at King’s College London, added that “the ultimate goal is to identify which specific features of the microbiome are directly influencing the clinical benefits of immunotherapy to exploit these features in new personalized approaches to support cancer immunotherapy.”
In the meantime, he said, “this study highlights the potential impact of good diet and gut health on chances of survival in patients undergoing immunotherapy.”
This study was coordinated by King’s College London, CIBIO Department of the University of Trento and European Institute of Oncology in Italy, and the University of Groningen in the Netherlands, and was funded by the Seerave Foundation. Dr. Lee, Dr. Segata, and Dr. Spector have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A large-scale than previously thought.
Overall, researchers identified a panel of species, including Roseburia spp. and Akkermansia muciniphila, associated with responses to ICI therapy. However, no single species was a “fully consistent biomarker” across the studies, the authors explain.
This “machine learning analysis confirmed the link between the microbiome and overall response rates (ORRs) and progression-free survival (PFS) with ICIs but also revealed limited reproducibility of microbiome-based signatures across cohorts,” Karla A. Lee, PhD, a clinical research fellow at King’s College London, and colleagues report. The results suggest that “the microbiome is predictive of response in some, but not all, cohorts.”
The findings were published online Feb. 28 in Nature Medicine.
Despite recent advances in targeted therapies for melanoma, less than half of the those who receive a single-agent ICI respond, and those who receive combination ICI therapy often suffer from severe drug toxicity problems. That is why finding patients more likely to respond to a single-agent ICI has become a priority.
Previous studies have identified the gut microbiome as “a potential biomarker of response, as well as a therapeutic target” in melanoma and other malignancies, but “little consensus exists on which microbiome characteristics are associated with treatment responses in the human setting,” the authors explain.
To further clarify the microbiome–immunotherapy relationship, the researchers performed metagenomic sequencing of stool samples collected from 165 ICI-naive patients with unresectable stage III or IV cutaneous melanoma from 5 observational cohorts in the Netherlands, United Kingdom, and Spain. These data were integrated with 147 samples from publicly available datasets.
First, the authors highlighted the variability in findings across these observational studies. For instance, they analyzed stool samples from one UK-based observational study of patients with melanoma (PRIMM-UK) and found a small but statistically significant difference in the microbiome composition of immunotherapy responders versus nonresponders (P = .05) but did not find such an association in a parallel study in the Netherlands (PRIMM-NL, P = .61).
The investigators also explored biomarkers of response across different cohorts and found several standouts. In trials using ORR as an endpoint, two uncultivated Roseburia species (CAG:182 and CAG:471) were associated with responses to ICIs. For patients with available PFS data, Phascolarctobacterium succinatutens and Lactobacillus vaginalis were “enriched in responders” across 7 datasets and significant in 3 of the 8 meta-analysis approaches. A muciniphila and Dorea formicigenerans were also associated with ORR and PFS at 12 months in several meta-analyses.
However, “no single bacterium was a fully consistent biomarker of response across all datasets,” the authors wrote.
Still, the findings could have important implications for the more than 50% of patients with advanced melanoma who don’t respond to single-agent ICI therapy.
“Our study shows that studying the microbiome is important to improve and personalize immunotherapy treatments for melanoma,” study coauthor Nicola Segata, PhD, principal investigator in the Laboratory of Computational Metagenomics, University of Trento, Italy, said in a press release. “However, it also suggests that because of the person-to-person variability of the gut microbiome, even larger studies must be carried out to understand the specific gut microbial features that are more likely to lead to a positive response to immunotherapy.”
Coauthor Tim Spector, PhD, head of the Department of Twin Research & Genetic Epidemiology at King’s College London, added that “the ultimate goal is to identify which specific features of the microbiome are directly influencing the clinical benefits of immunotherapy to exploit these features in new personalized approaches to support cancer immunotherapy.”
In the meantime, he said, “this study highlights the potential impact of good diet and gut health on chances of survival in patients undergoing immunotherapy.”
This study was coordinated by King’s College London, CIBIO Department of the University of Trento and European Institute of Oncology in Italy, and the University of Groningen in the Netherlands, and was funded by the Seerave Foundation. Dr. Lee, Dr. Segata, and Dr. Spector have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A large-scale than previously thought.
Overall, researchers identified a panel of species, including Roseburia spp. and Akkermansia muciniphila, associated with responses to ICI therapy. However, no single species was a “fully consistent biomarker” across the studies, the authors explain.
This “machine learning analysis confirmed the link between the microbiome and overall response rates (ORRs) and progression-free survival (PFS) with ICIs but also revealed limited reproducibility of microbiome-based signatures across cohorts,” Karla A. Lee, PhD, a clinical research fellow at King’s College London, and colleagues report. The results suggest that “the microbiome is predictive of response in some, but not all, cohorts.”
The findings were published online Feb. 28 in Nature Medicine.
Despite recent advances in targeted therapies for melanoma, less than half of the those who receive a single-agent ICI respond, and those who receive combination ICI therapy often suffer from severe drug toxicity problems. That is why finding patients more likely to respond to a single-agent ICI has become a priority.
Previous studies have identified the gut microbiome as “a potential biomarker of response, as well as a therapeutic target” in melanoma and other malignancies, but “little consensus exists on which microbiome characteristics are associated with treatment responses in the human setting,” the authors explain.
To further clarify the microbiome–immunotherapy relationship, the researchers performed metagenomic sequencing of stool samples collected from 165 ICI-naive patients with unresectable stage III or IV cutaneous melanoma from 5 observational cohorts in the Netherlands, United Kingdom, and Spain. These data were integrated with 147 samples from publicly available datasets.
First, the authors highlighted the variability in findings across these observational studies. For instance, they analyzed stool samples from one UK-based observational study of patients with melanoma (PRIMM-UK) and found a small but statistically significant difference in the microbiome composition of immunotherapy responders versus nonresponders (P = .05) but did not find such an association in a parallel study in the Netherlands (PRIMM-NL, P = .61).
The investigators also explored biomarkers of response across different cohorts and found several standouts. In trials using ORR as an endpoint, two uncultivated Roseburia species (CAG:182 and CAG:471) were associated with responses to ICIs. For patients with available PFS data, Phascolarctobacterium succinatutens and Lactobacillus vaginalis were “enriched in responders” across 7 datasets and significant in 3 of the 8 meta-analysis approaches. A muciniphila and Dorea formicigenerans were also associated with ORR and PFS at 12 months in several meta-analyses.
However, “no single bacterium was a fully consistent biomarker of response across all datasets,” the authors wrote.
Still, the findings could have important implications for the more than 50% of patients with advanced melanoma who don’t respond to single-agent ICI therapy.
“Our study shows that studying the microbiome is important to improve and personalize immunotherapy treatments for melanoma,” study coauthor Nicola Segata, PhD, principal investigator in the Laboratory of Computational Metagenomics, University of Trento, Italy, said in a press release. “However, it also suggests that because of the person-to-person variability of the gut microbiome, even larger studies must be carried out to understand the specific gut microbial features that are more likely to lead to a positive response to immunotherapy.”
Coauthor Tim Spector, PhD, head of the Department of Twin Research & Genetic Epidemiology at King’s College London, added that “the ultimate goal is to identify which specific features of the microbiome are directly influencing the clinical benefits of immunotherapy to exploit these features in new personalized approaches to support cancer immunotherapy.”
In the meantime, he said, “this study highlights the potential impact of good diet and gut health on chances of survival in patients undergoing immunotherapy.”
This study was coordinated by King’s College London, CIBIO Department of the University of Trento and European Institute of Oncology in Italy, and the University of Groningen in the Netherlands, and was funded by the Seerave Foundation. Dr. Lee, Dr. Segata, and Dr. Spector have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA approves new CAR T-cell treatment for multiple myeloma
A new treatment option for patients with refractory/relapsed multiple myeloma who have already tried four or more therapies has been approved by the U.S. Food and Drug Administration.
There are already two other therapies on the market that target BCMA – another CAR T cell, idecabtagene vicleucel (Abecma), which was approved by the FDA in March 2021, and a drug conjugate, belantamab mafodotin (Blenrep), which was approved in August 2020.
The approval of cilta-cel was based on clinical data from the CARTITUDE-1 study, which were initially presented in December 2020 at the annual meeting of the American Society of Hematology, as reported at the time by this news organization.
The trial involved 97 patients with relapsed/refractory multiple myeloma who had already received a median of six previous treatments (range, three to 18), including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody.
“The treatment journey for the majority of patients living with multiple myeloma is a relentless cycle of remission and relapse, with fewer patients achieving a deep response as they progress through later lines of therapy,” commented Sundar Jagannath, MBBS, professor of medicine, hematology, and medical oncology at Mount Sinai, who was a principal investigator on the pivotal study.
“That is why I have been really excited about the results from the CARTITUDE-1 study, which has demonstrated that cilta-cel can provide deep and durable responses and long-term treatment-free intervals, even in this heavily pretreated multiple myeloma patient population,” he said.
“Today’s approval of Carvykti helps address a great unmet need for these patients,” he commented in a press release from the manufacturer.
Like other CAR T-cell therapies, ciltacabtagene autoleucel is a one-time treatment. It involves collecting blood from the patient, extracting T cells, genetically engineering them, then transfusing them back to the patient, who in the meantime has undergone conditioning.
The results from CARTITUDE-1 show that this one-time treatment resulted in deep and durable responses.
The overall response rate was 98%, and the majority of patients (78%) achieved a stringent complete response, in which physicians are unable to observe any signs or symptoms of disease via imaging or other tests after treatment.
At a median of 18 months’ follow-up, the median duration of response was 21.8 months.
“The responses in the CARTITUDE-1 study showed durability over time and resulted in the majority of heavily pretreated patients achieving deep responses after 18-month follow-up,” commented Mr. Jagannath.
“The approval of cilta-cel provides physicians an immunotherapy treatment option that offers patients an opportunity to be free from anti-myeloma therapies for a period of time,” he added.
As with other CAR T-cell therapies, there were serious side effects, and these products are available only through restricted programs under a risk evaluation and mitigation strategy.
The product information for Cartykti includes a boxed warning that mentions cytokine release syndrome (CRS), immune effector cell–associated neurotoxicity syndrome, parkinsonism, Guillain-Barré syndrome, hemophagocytic lymphohistiocytosis/macrophage activation syndrome, and prolonged and/or recurrent cytopenias.
The most common adverse reactions (reported in greater than or equal to 20% of patients) are pyrexia, CRS, hypogammaglobulinemia, hypotension, musculoskeletal pain, fatigue, infections–pathogens unspecified, cough, chills, diarrhea, nausea, encephalopathy, decreased appetite, upper respiratory tract infection, headache, tachycardia, dizziness, dyspnea, edema, viral infections, coagulopathy, constipation, and vomiting.
A version of this article first appeared on Medscape.com.
A new treatment option for patients with refractory/relapsed multiple myeloma who have already tried four or more therapies has been approved by the U.S. Food and Drug Administration.
There are already two other therapies on the market that target BCMA – another CAR T cell, idecabtagene vicleucel (Abecma), which was approved by the FDA in March 2021, and a drug conjugate, belantamab mafodotin (Blenrep), which was approved in August 2020.
The approval of cilta-cel was based on clinical data from the CARTITUDE-1 study, which were initially presented in December 2020 at the annual meeting of the American Society of Hematology, as reported at the time by this news organization.
The trial involved 97 patients with relapsed/refractory multiple myeloma who had already received a median of six previous treatments (range, three to 18), including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody.
“The treatment journey for the majority of patients living with multiple myeloma is a relentless cycle of remission and relapse, with fewer patients achieving a deep response as they progress through later lines of therapy,” commented Sundar Jagannath, MBBS, professor of medicine, hematology, and medical oncology at Mount Sinai, who was a principal investigator on the pivotal study.
“That is why I have been really excited about the results from the CARTITUDE-1 study, which has demonstrated that cilta-cel can provide deep and durable responses and long-term treatment-free intervals, even in this heavily pretreated multiple myeloma patient population,” he said.
“Today’s approval of Carvykti helps address a great unmet need for these patients,” he commented in a press release from the manufacturer.
Like other CAR T-cell therapies, ciltacabtagene autoleucel is a one-time treatment. It involves collecting blood from the patient, extracting T cells, genetically engineering them, then transfusing them back to the patient, who in the meantime has undergone conditioning.
The results from CARTITUDE-1 show that this one-time treatment resulted in deep and durable responses.
The overall response rate was 98%, and the majority of patients (78%) achieved a stringent complete response, in which physicians are unable to observe any signs or symptoms of disease via imaging or other tests after treatment.
At a median of 18 months’ follow-up, the median duration of response was 21.8 months.
“The responses in the CARTITUDE-1 study showed durability over time and resulted in the majority of heavily pretreated patients achieving deep responses after 18-month follow-up,” commented Mr. Jagannath.
“The approval of cilta-cel provides physicians an immunotherapy treatment option that offers patients an opportunity to be free from anti-myeloma therapies for a period of time,” he added.
As with other CAR T-cell therapies, there were serious side effects, and these products are available only through restricted programs under a risk evaluation and mitigation strategy.
The product information for Cartykti includes a boxed warning that mentions cytokine release syndrome (CRS), immune effector cell–associated neurotoxicity syndrome, parkinsonism, Guillain-Barré syndrome, hemophagocytic lymphohistiocytosis/macrophage activation syndrome, and prolonged and/or recurrent cytopenias.
The most common adverse reactions (reported in greater than or equal to 20% of patients) are pyrexia, CRS, hypogammaglobulinemia, hypotension, musculoskeletal pain, fatigue, infections–pathogens unspecified, cough, chills, diarrhea, nausea, encephalopathy, decreased appetite, upper respiratory tract infection, headache, tachycardia, dizziness, dyspnea, edema, viral infections, coagulopathy, constipation, and vomiting.
A version of this article first appeared on Medscape.com.
A new treatment option for patients with refractory/relapsed multiple myeloma who have already tried four or more therapies has been approved by the U.S. Food and Drug Administration.
There are already two other therapies on the market that target BCMA – another CAR T cell, idecabtagene vicleucel (Abecma), which was approved by the FDA in March 2021, and a drug conjugate, belantamab mafodotin (Blenrep), which was approved in August 2020.
The approval of cilta-cel was based on clinical data from the CARTITUDE-1 study, which were initially presented in December 2020 at the annual meeting of the American Society of Hematology, as reported at the time by this news organization.
The trial involved 97 patients with relapsed/refractory multiple myeloma who had already received a median of six previous treatments (range, three to 18), including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody.
“The treatment journey for the majority of patients living with multiple myeloma is a relentless cycle of remission and relapse, with fewer patients achieving a deep response as they progress through later lines of therapy,” commented Sundar Jagannath, MBBS, professor of medicine, hematology, and medical oncology at Mount Sinai, who was a principal investigator on the pivotal study.
“That is why I have been really excited about the results from the CARTITUDE-1 study, which has demonstrated that cilta-cel can provide deep and durable responses and long-term treatment-free intervals, even in this heavily pretreated multiple myeloma patient population,” he said.
“Today’s approval of Carvykti helps address a great unmet need for these patients,” he commented in a press release from the manufacturer.
Like other CAR T-cell therapies, ciltacabtagene autoleucel is a one-time treatment. It involves collecting blood from the patient, extracting T cells, genetically engineering them, then transfusing them back to the patient, who in the meantime has undergone conditioning.
The results from CARTITUDE-1 show that this one-time treatment resulted in deep and durable responses.
The overall response rate was 98%, and the majority of patients (78%) achieved a stringent complete response, in which physicians are unable to observe any signs or symptoms of disease via imaging or other tests after treatment.
At a median of 18 months’ follow-up, the median duration of response was 21.8 months.
“The responses in the CARTITUDE-1 study showed durability over time and resulted in the majority of heavily pretreated patients achieving deep responses after 18-month follow-up,” commented Mr. Jagannath.
“The approval of cilta-cel provides physicians an immunotherapy treatment option that offers patients an opportunity to be free from anti-myeloma therapies for a period of time,” he added.
As with other CAR T-cell therapies, there were serious side effects, and these products are available only through restricted programs under a risk evaluation and mitigation strategy.
The product information for Cartykti includes a boxed warning that mentions cytokine release syndrome (CRS), immune effector cell–associated neurotoxicity syndrome, parkinsonism, Guillain-Barré syndrome, hemophagocytic lymphohistiocytosis/macrophage activation syndrome, and prolonged and/or recurrent cytopenias.
The most common adverse reactions (reported in greater than or equal to 20% of patients) are pyrexia, CRS, hypogammaglobulinemia, hypotension, musculoskeletal pain, fatigue, infections–pathogens unspecified, cough, chills, diarrhea, nausea, encephalopathy, decreased appetite, upper respiratory tract infection, headache, tachycardia, dizziness, dyspnea, edema, viral infections, coagulopathy, constipation, and vomiting.
A version of this article first appeared on Medscape.com.
More exercise for people with hemophilia, experts advise
Clinicians should do more to encourage people with hemophilia to undertake regular physical activity and sporting activities, a panel of Italian experts has advised.
they wrote in a consensus paper published in Blood Transfusion.
Physical activity is not only recommended by the World Federation of Hemophilia for people with this bleeding disorder, but also recommended for everyone, depending on their age, by the World Health Organization.
People with hemophilia “are not exempt” from the WHO recommendations, noted Dr. Chiara Biasoli of the unit of transfusion medicine and Centre for Inherited Bleeding Disorders, Maurizio Bufalini Hospital in Cesena, Italy, and fellow expert panel members.
MEMO expert consensus project
To help clinicians decide when and how to recommend physical exercise to people with hemophilia, Dr. Biasoli and colleagues initiated the MEMO (Movement for Persons With Haemophilia) expert consensus project. The aim was to offer some clear practical guidance for routine practice.
The project began with a core group of 11 hemophilia experts meeting virtually in early 2020 because of the COVID-19 pandemic. The MEMO scientific committee, as they became known, formulated a set of consensus statements which they then put before members of the Italian Association of Hemophilia Centres, asking them to vote online on their level of agreement with each statement.
A modified Delphi approach was used to reach a consensus, with statements that scored 7 or higher on a 9-point rating scale moving forward into the next round of voting. A total of three voting rounds was made, which took into account the views of 40 experts, overall.
Overview of the MEMO consensus statements
The MEMO consensus statements cover three topic areas: the first four statements focus on the impact of hemophilia on movement, the next three give physical activity recommendations, and the final three look at choice and management of sporting activities.
Regarding the impact of hemophilia on movement, Dr. Biasoli and colleagues noted that “overweight and obesity are an increasing problem in PwH” and, due to their known association with poor physical health, urgently need to be addressed.
Perhaps “insufficient education by hematologists and other invoiced specialists” is at play, they suggested. Importantly, in children, “parents’ fears with consequent overprotection” may be contributing factors.
Not only is movement beneficial for improving joint function, they stated, but it’s also crucial to improving bone density and reducing the risk of joint bleeds.
Even people with inhibitors should be encouraged to be active more regularly, the expert panel said. This should of course be done with “particular caution and monitoring of the effectiveness of prophylaxis for the prevention of acute bleeding events, so that physical activity is conducted safely.”
The panel’s recommendations on sporting activities include the advice to work in a multidisciplinary team that involves hematologists, musculoskeletal specialists and specialists in sports medicine, with the latter helping decide on what sporting activity might be most appropriate. They also suggest that participation in sport should be encouraged from a young age, noting that the Canadian Hemophilia Society has issued some good tips in that regard.
Alongside the recommendations the MEMO expert panel has created four “pyramids of movement” to help clinicians visualize and discuss the recommendations with their patients.
“Physical activity can be considered as a low price intervention that can prevent/reduce the occurrence of chronic diseases and should be further encouraged,” Dr. Biasoli and fellow MEMO expert panel members concluded.
The members of the MEMO expert panel disclosed multiple financial ties with pharmaceutical companies, but none are relevant to the recommendations they made.
Clinicians should do more to encourage people with hemophilia to undertake regular physical activity and sporting activities, a panel of Italian experts has advised.
they wrote in a consensus paper published in Blood Transfusion.
Physical activity is not only recommended by the World Federation of Hemophilia for people with this bleeding disorder, but also recommended for everyone, depending on their age, by the World Health Organization.
People with hemophilia “are not exempt” from the WHO recommendations, noted Dr. Chiara Biasoli of the unit of transfusion medicine and Centre for Inherited Bleeding Disorders, Maurizio Bufalini Hospital in Cesena, Italy, and fellow expert panel members.
MEMO expert consensus project
To help clinicians decide when and how to recommend physical exercise to people with hemophilia, Dr. Biasoli and colleagues initiated the MEMO (Movement for Persons With Haemophilia) expert consensus project. The aim was to offer some clear practical guidance for routine practice.
The project began with a core group of 11 hemophilia experts meeting virtually in early 2020 because of the COVID-19 pandemic. The MEMO scientific committee, as they became known, formulated a set of consensus statements which they then put before members of the Italian Association of Hemophilia Centres, asking them to vote online on their level of agreement with each statement.
A modified Delphi approach was used to reach a consensus, with statements that scored 7 or higher on a 9-point rating scale moving forward into the next round of voting. A total of three voting rounds was made, which took into account the views of 40 experts, overall.
Overview of the MEMO consensus statements
The MEMO consensus statements cover three topic areas: the first four statements focus on the impact of hemophilia on movement, the next three give physical activity recommendations, and the final three look at choice and management of sporting activities.
Regarding the impact of hemophilia on movement, Dr. Biasoli and colleagues noted that “overweight and obesity are an increasing problem in PwH” and, due to their known association with poor physical health, urgently need to be addressed.
Perhaps “insufficient education by hematologists and other invoiced specialists” is at play, they suggested. Importantly, in children, “parents’ fears with consequent overprotection” may be contributing factors.
Not only is movement beneficial for improving joint function, they stated, but it’s also crucial to improving bone density and reducing the risk of joint bleeds.
Even people with inhibitors should be encouraged to be active more regularly, the expert panel said. This should of course be done with “particular caution and monitoring of the effectiveness of prophylaxis for the prevention of acute bleeding events, so that physical activity is conducted safely.”
The panel’s recommendations on sporting activities include the advice to work in a multidisciplinary team that involves hematologists, musculoskeletal specialists and specialists in sports medicine, with the latter helping decide on what sporting activity might be most appropriate. They also suggest that participation in sport should be encouraged from a young age, noting that the Canadian Hemophilia Society has issued some good tips in that regard.
Alongside the recommendations the MEMO expert panel has created four “pyramids of movement” to help clinicians visualize and discuss the recommendations with their patients.
“Physical activity can be considered as a low price intervention that can prevent/reduce the occurrence of chronic diseases and should be further encouraged,” Dr. Biasoli and fellow MEMO expert panel members concluded.
The members of the MEMO expert panel disclosed multiple financial ties with pharmaceutical companies, but none are relevant to the recommendations they made.
Clinicians should do more to encourage people with hemophilia to undertake regular physical activity and sporting activities, a panel of Italian experts has advised.
they wrote in a consensus paper published in Blood Transfusion.
Physical activity is not only recommended by the World Federation of Hemophilia for people with this bleeding disorder, but also recommended for everyone, depending on their age, by the World Health Organization.
People with hemophilia “are not exempt” from the WHO recommendations, noted Dr. Chiara Biasoli of the unit of transfusion medicine and Centre for Inherited Bleeding Disorders, Maurizio Bufalini Hospital in Cesena, Italy, and fellow expert panel members.
MEMO expert consensus project
To help clinicians decide when and how to recommend physical exercise to people with hemophilia, Dr. Biasoli and colleagues initiated the MEMO (Movement for Persons With Haemophilia) expert consensus project. The aim was to offer some clear practical guidance for routine practice.
The project began with a core group of 11 hemophilia experts meeting virtually in early 2020 because of the COVID-19 pandemic. The MEMO scientific committee, as they became known, formulated a set of consensus statements which they then put before members of the Italian Association of Hemophilia Centres, asking them to vote online on their level of agreement with each statement.
A modified Delphi approach was used to reach a consensus, with statements that scored 7 or higher on a 9-point rating scale moving forward into the next round of voting. A total of three voting rounds was made, which took into account the views of 40 experts, overall.
Overview of the MEMO consensus statements
The MEMO consensus statements cover three topic areas: the first four statements focus on the impact of hemophilia on movement, the next three give physical activity recommendations, and the final three look at choice and management of sporting activities.
Regarding the impact of hemophilia on movement, Dr. Biasoli and colleagues noted that “overweight and obesity are an increasing problem in PwH” and, due to their known association with poor physical health, urgently need to be addressed.
Perhaps “insufficient education by hematologists and other invoiced specialists” is at play, they suggested. Importantly, in children, “parents’ fears with consequent overprotection” may be contributing factors.
Not only is movement beneficial for improving joint function, they stated, but it’s also crucial to improving bone density and reducing the risk of joint bleeds.
Even people with inhibitors should be encouraged to be active more regularly, the expert panel said. This should of course be done with “particular caution and monitoring of the effectiveness of prophylaxis for the prevention of acute bleeding events, so that physical activity is conducted safely.”
The panel’s recommendations on sporting activities include the advice to work in a multidisciplinary team that involves hematologists, musculoskeletal specialists and specialists in sports medicine, with the latter helping decide on what sporting activity might be most appropriate. They also suggest that participation in sport should be encouraged from a young age, noting that the Canadian Hemophilia Society has issued some good tips in that regard.
Alongside the recommendations the MEMO expert panel has created four “pyramids of movement” to help clinicians visualize and discuss the recommendations with their patients.
“Physical activity can be considered as a low price intervention that can prevent/reduce the occurrence of chronic diseases and should be further encouraged,” Dr. Biasoli and fellow MEMO expert panel members concluded.
The members of the MEMO expert panel disclosed multiple financial ties with pharmaceutical companies, but none are relevant to the recommendations they made.
FROM BLOOD TRANSFUSION
Pediatrics group stresses benefits of vitamin K shots for infants
After the American Academy of Pediatrics (AAP) began recommending vitamin K shots for newborns in 1961, infant bleeding as a result of vitamin K deficiency plummeted. The life-threatening disorder is so rare that some parents now question the need for injections to safeguard against it.
The situation amounts to “a failure of our success,” Ivan Hand, MD, a coauthor of a new AAP statement on vitamin K, told this news organization. Much like diseases that can be prevented with vaccines, vitamin K deficiency bleeding isn’t top of mind for parents. “It’s not something they’re aware of or afraid of,” he said.
In 2019, however, the AAP listed public education about the importance of the shots in its 10 most important priorities.
The policy update urges clinicians to bone up on the benefits and perceived risks of vitamin K deficiency, which is essential for clotting, and to “strongly advocate” for the shot in discussions with parents who may get competing messages from their social circles, the internet, and other health care professionals.
Dr. Hand, director of neonatology at NYC Health + Hospitals Kings County, Brooklyn, said clinicians walk a line between educating and alienating parents who favor natural birth processes. “We’re hoping that by talking to the families and answering their questions and explaining the risks, parents will accept vitamin K as a necessary treatment for their babies,” he said.
Vitamin K does not easily pass through the placenta and is not plentiful in breast milk, the preferred nutrition source for newborns. It takes months for babies to build their stores through food and gut bacteria.
Infants who do not receive vitamin K at birth are 81 times more likely to develop late-onset vitamin K deficiency bleeding, which occurs a week to 6 months after birth, according to the Centers for Disease Control and Prevention. One in five babies with the disorder dies, and about half have bleeding in the skull that can lead to brain damage.
New dosing for premature infants
The AAP’s new statement, published in the journal Pediatrics, reaffirms the administration of a 1-mg intramuscular dose for infants weighing more than 1,500 grams, or about 3 lb 5 oz, within 6 hours of birth. For premature infants who weigh less, the guidance recommends an intramuscular dose of 0.3 to 0.5 mg/kg.
The group notes that oral preparations of vitamin K have proven less effective because of malabsorption and challenges with adhering to dosing regimens.
The document also warns that breastfed babies can experience vitamin K deficiency bleeding even if they have received the shot, because concentration of vitamin K often wanes before a baby starts eating solid food. The disorder “should be considered when evaluating bleeding in the first 6 months of life, even in infants who received prophylaxis, and especially in exclusively breastfed infants,” it states.
Accounts of parental refusals date back to 2013, when the CDC reported four cases of deficiency bleeding in Tennessee. The infants’ parents said they declined vitamin K because they worried about increased risk of leukemia, thought the injection was unnecessary, or wanted to minimize the baby’s exposure to “toxins.” Leukemia concern stemmed from a 1992 report linking vitamin K to childhood cancer, an association that did not hold up in subsequent studies.
More recent research has documented parental concerns about preservatives and injection pain as well as distrust of medical and public health authorities. Some parents have been accused of neglect for refusing to allow their babies to receive the shots.
Phoebe Danziger, MD, a pediatrician and writer in rural Michigan who has studied parental refusal of standard-of-care interventions, called the document a “welcome update” to the AAP’s last statement on the topic, in 2003. She told this news organization that lower dosing for premature infants may reassure some vitamin K–hesitant parents who worry about one-size-fits-all dosing.
But Dr. Danziger added that “evidence is lacking to support the claim that pediatricians can really move the needle on parental hesitancy and refusal simply through better listening and more persuasive counseling.” She said the AAP should do more to address “the broader social climate of mistrust and misinformation” that fuels refusal.
Dr. Hand and Dr. Danziger have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
After the American Academy of Pediatrics (AAP) began recommending vitamin K shots for newborns in 1961, infant bleeding as a result of vitamin K deficiency plummeted. The life-threatening disorder is so rare that some parents now question the need for injections to safeguard against it.
The situation amounts to “a failure of our success,” Ivan Hand, MD, a coauthor of a new AAP statement on vitamin K, told this news organization. Much like diseases that can be prevented with vaccines, vitamin K deficiency bleeding isn’t top of mind for parents. “It’s not something they’re aware of or afraid of,” he said.
In 2019, however, the AAP listed public education about the importance of the shots in its 10 most important priorities.
The policy update urges clinicians to bone up on the benefits and perceived risks of vitamin K deficiency, which is essential for clotting, and to “strongly advocate” for the shot in discussions with parents who may get competing messages from their social circles, the internet, and other health care professionals.
Dr. Hand, director of neonatology at NYC Health + Hospitals Kings County, Brooklyn, said clinicians walk a line between educating and alienating parents who favor natural birth processes. “We’re hoping that by talking to the families and answering their questions and explaining the risks, parents will accept vitamin K as a necessary treatment for their babies,” he said.
Vitamin K does not easily pass through the placenta and is not plentiful in breast milk, the preferred nutrition source for newborns. It takes months for babies to build their stores through food and gut bacteria.
Infants who do not receive vitamin K at birth are 81 times more likely to develop late-onset vitamin K deficiency bleeding, which occurs a week to 6 months after birth, according to the Centers for Disease Control and Prevention. One in five babies with the disorder dies, and about half have bleeding in the skull that can lead to brain damage.
New dosing for premature infants
The AAP’s new statement, published in the journal Pediatrics, reaffirms the administration of a 1-mg intramuscular dose for infants weighing more than 1,500 grams, or about 3 lb 5 oz, within 6 hours of birth. For premature infants who weigh less, the guidance recommends an intramuscular dose of 0.3 to 0.5 mg/kg.
The group notes that oral preparations of vitamin K have proven less effective because of malabsorption and challenges with adhering to dosing regimens.
The document also warns that breastfed babies can experience vitamin K deficiency bleeding even if they have received the shot, because concentration of vitamin K often wanes before a baby starts eating solid food. The disorder “should be considered when evaluating bleeding in the first 6 months of life, even in infants who received prophylaxis, and especially in exclusively breastfed infants,” it states.
Accounts of parental refusals date back to 2013, when the CDC reported four cases of deficiency bleeding in Tennessee. The infants’ parents said they declined vitamin K because they worried about increased risk of leukemia, thought the injection was unnecessary, or wanted to minimize the baby’s exposure to “toxins.” Leukemia concern stemmed from a 1992 report linking vitamin K to childhood cancer, an association that did not hold up in subsequent studies.
More recent research has documented parental concerns about preservatives and injection pain as well as distrust of medical and public health authorities. Some parents have been accused of neglect for refusing to allow their babies to receive the shots.
Phoebe Danziger, MD, a pediatrician and writer in rural Michigan who has studied parental refusal of standard-of-care interventions, called the document a “welcome update” to the AAP’s last statement on the topic, in 2003. She told this news organization that lower dosing for premature infants may reassure some vitamin K–hesitant parents who worry about one-size-fits-all dosing.
But Dr. Danziger added that “evidence is lacking to support the claim that pediatricians can really move the needle on parental hesitancy and refusal simply through better listening and more persuasive counseling.” She said the AAP should do more to address “the broader social climate of mistrust and misinformation” that fuels refusal.
Dr. Hand and Dr. Danziger have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
After the American Academy of Pediatrics (AAP) began recommending vitamin K shots for newborns in 1961, infant bleeding as a result of vitamin K deficiency plummeted. The life-threatening disorder is so rare that some parents now question the need for injections to safeguard against it.
The situation amounts to “a failure of our success,” Ivan Hand, MD, a coauthor of a new AAP statement on vitamin K, told this news organization. Much like diseases that can be prevented with vaccines, vitamin K deficiency bleeding isn’t top of mind for parents. “It’s not something they’re aware of or afraid of,” he said.
In 2019, however, the AAP listed public education about the importance of the shots in its 10 most important priorities.
The policy update urges clinicians to bone up on the benefits and perceived risks of vitamin K deficiency, which is essential for clotting, and to “strongly advocate” for the shot in discussions with parents who may get competing messages from their social circles, the internet, and other health care professionals.
Dr. Hand, director of neonatology at NYC Health + Hospitals Kings County, Brooklyn, said clinicians walk a line between educating and alienating parents who favor natural birth processes. “We’re hoping that by talking to the families and answering their questions and explaining the risks, parents will accept vitamin K as a necessary treatment for their babies,” he said.
Vitamin K does not easily pass through the placenta and is not plentiful in breast milk, the preferred nutrition source for newborns. It takes months for babies to build their stores through food and gut bacteria.
Infants who do not receive vitamin K at birth are 81 times more likely to develop late-onset vitamin K deficiency bleeding, which occurs a week to 6 months after birth, according to the Centers for Disease Control and Prevention. One in five babies with the disorder dies, and about half have bleeding in the skull that can lead to brain damage.
New dosing for premature infants
The AAP’s new statement, published in the journal Pediatrics, reaffirms the administration of a 1-mg intramuscular dose for infants weighing more than 1,500 grams, or about 3 lb 5 oz, within 6 hours of birth. For premature infants who weigh less, the guidance recommends an intramuscular dose of 0.3 to 0.5 mg/kg.
The group notes that oral preparations of vitamin K have proven less effective because of malabsorption and challenges with adhering to dosing regimens.
The document also warns that breastfed babies can experience vitamin K deficiency bleeding even if they have received the shot, because concentration of vitamin K often wanes before a baby starts eating solid food. The disorder “should be considered when evaluating bleeding in the first 6 months of life, even in infants who received prophylaxis, and especially in exclusively breastfed infants,” it states.
Accounts of parental refusals date back to 2013, when the CDC reported four cases of deficiency bleeding in Tennessee. The infants’ parents said they declined vitamin K because they worried about increased risk of leukemia, thought the injection was unnecessary, or wanted to minimize the baby’s exposure to “toxins.” Leukemia concern stemmed from a 1992 report linking vitamin K to childhood cancer, an association that did not hold up in subsequent studies.
More recent research has documented parental concerns about preservatives and injection pain as well as distrust of medical and public health authorities. Some parents have been accused of neglect for refusing to allow their babies to receive the shots.
Phoebe Danziger, MD, a pediatrician and writer in rural Michigan who has studied parental refusal of standard-of-care interventions, called the document a “welcome update” to the AAP’s last statement on the topic, in 2003. She told this news organization that lower dosing for premature infants may reassure some vitamin K–hesitant parents who worry about one-size-fits-all dosing.
But Dr. Danziger added that “evidence is lacking to support the claim that pediatricians can really move the needle on parental hesitancy and refusal simply through better listening and more persuasive counseling.” She said the AAP should do more to address “the broader social climate of mistrust and misinformation” that fuels refusal.
Dr. Hand and Dr. Danziger have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Post–COVID vaccine AHA cases raise eyebrows in Italy
“The overall number of cases observed does not allow ... any definitive conclusion over a possible causal relationship between SARS-CoV-2 vaccination and AHA, which would need more epidemiological and pharmacovigilance data about suspected vaccine-related adverse events,” Maria Cristina Leone, MD, of Azienda USL-IRCCS di Reggio Emilia (Italy), and colleagues reported online on Jan. 19, 2022, in a letter to the editors of Thrombosis Research.
The cases, observed in Reggio Emilia during the first 8 months of the vaccination campaign, occurred following receipt of mRNA BNT162b2 (Pfizer-BioNTech) vaccine. The AHA patients included two men and two women who ranged in age from 67 to 86 years.
During this time frame, 235,597 people received at least one dose of BNT162b2 vaccine, the authors noted.
In the 5 years prior, from January 2016 to December 2020, only zero to two cases of AHA were observed each year, totaling five cases, or 1.9 cases per million people/year. These numbers are in line with the estimated incidence of the disease, the researchers noted, adding that “it should nonetheless be underlined that vaccination benefits exceed potential side effects and play a central role in individual and public health to effectively protect people from COVID-19 and stop the pandemic.”
However, they also wrote that the “unusual observation of four cases of a rare disease during the first months of the vaccination campaign in our province could be of interest and could sensitize health care personnel toward a possible complication of SARS-CoV-2 immunization.”
AHA is a rare autoimmune disease caused by neutralizing autoantibodies against coagulation factor VIII. It is mainly associated with malignancy, autoimmune diseases, certain medications, and postnatal status.
“Sporadic AHA cases have been reported in association with infectious diseases or vaccinations,” the author noted, adding that associations between the BNT162b2 vaccine immune complications, including AHA, have also been reported by other authors.
Three of the four case patients in Reggio Emilia had “at least one common clinical association of AHA,” they found, suggesting that these associations could “reflect susceptibility to autoimmunity potentially triggered by vaccination.”
“Case four died due to complications from sepsis after being treated with steroid and rituximab, whereas the first three cases underwent clinical and laboratory remission after immunosuppressive therapy, and no relapse has been observed during follow-up, as in the other two cases reported: This could suggest a more favorable prognosis in respect to other non–vaccine-associated cases, but longer-term data are definitely needed,” they concluded.
The authors reported having no disclosures.
“The overall number of cases observed does not allow ... any definitive conclusion over a possible causal relationship between SARS-CoV-2 vaccination and AHA, which would need more epidemiological and pharmacovigilance data about suspected vaccine-related adverse events,” Maria Cristina Leone, MD, of Azienda USL-IRCCS di Reggio Emilia (Italy), and colleagues reported online on Jan. 19, 2022, in a letter to the editors of Thrombosis Research.
The cases, observed in Reggio Emilia during the first 8 months of the vaccination campaign, occurred following receipt of mRNA BNT162b2 (Pfizer-BioNTech) vaccine. The AHA patients included two men and two women who ranged in age from 67 to 86 years.
During this time frame, 235,597 people received at least one dose of BNT162b2 vaccine, the authors noted.
In the 5 years prior, from January 2016 to December 2020, only zero to two cases of AHA were observed each year, totaling five cases, or 1.9 cases per million people/year. These numbers are in line with the estimated incidence of the disease, the researchers noted, adding that “it should nonetheless be underlined that vaccination benefits exceed potential side effects and play a central role in individual and public health to effectively protect people from COVID-19 and stop the pandemic.”
However, they also wrote that the “unusual observation of four cases of a rare disease during the first months of the vaccination campaign in our province could be of interest and could sensitize health care personnel toward a possible complication of SARS-CoV-2 immunization.”
AHA is a rare autoimmune disease caused by neutralizing autoantibodies against coagulation factor VIII. It is mainly associated with malignancy, autoimmune diseases, certain medications, and postnatal status.
“Sporadic AHA cases have been reported in association with infectious diseases or vaccinations,” the author noted, adding that associations between the BNT162b2 vaccine immune complications, including AHA, have also been reported by other authors.
Three of the four case patients in Reggio Emilia had “at least one common clinical association of AHA,” they found, suggesting that these associations could “reflect susceptibility to autoimmunity potentially triggered by vaccination.”
“Case four died due to complications from sepsis after being treated with steroid and rituximab, whereas the first three cases underwent clinical and laboratory remission after immunosuppressive therapy, and no relapse has been observed during follow-up, as in the other two cases reported: This could suggest a more favorable prognosis in respect to other non–vaccine-associated cases, but longer-term data are definitely needed,” they concluded.
The authors reported having no disclosures.
“The overall number of cases observed does not allow ... any definitive conclusion over a possible causal relationship between SARS-CoV-2 vaccination and AHA, which would need more epidemiological and pharmacovigilance data about suspected vaccine-related adverse events,” Maria Cristina Leone, MD, of Azienda USL-IRCCS di Reggio Emilia (Italy), and colleagues reported online on Jan. 19, 2022, in a letter to the editors of Thrombosis Research.
The cases, observed in Reggio Emilia during the first 8 months of the vaccination campaign, occurred following receipt of mRNA BNT162b2 (Pfizer-BioNTech) vaccine. The AHA patients included two men and two women who ranged in age from 67 to 86 years.
During this time frame, 235,597 people received at least one dose of BNT162b2 vaccine, the authors noted.
In the 5 years prior, from January 2016 to December 2020, only zero to two cases of AHA were observed each year, totaling five cases, or 1.9 cases per million people/year. These numbers are in line with the estimated incidence of the disease, the researchers noted, adding that “it should nonetheless be underlined that vaccination benefits exceed potential side effects and play a central role in individual and public health to effectively protect people from COVID-19 and stop the pandemic.”
However, they also wrote that the “unusual observation of four cases of a rare disease during the first months of the vaccination campaign in our province could be of interest and could sensitize health care personnel toward a possible complication of SARS-CoV-2 immunization.”
AHA is a rare autoimmune disease caused by neutralizing autoantibodies against coagulation factor VIII. It is mainly associated with malignancy, autoimmune diseases, certain medications, and postnatal status.
“Sporadic AHA cases have been reported in association with infectious diseases or vaccinations,” the author noted, adding that associations between the BNT162b2 vaccine immune complications, including AHA, have also been reported by other authors.
Three of the four case patients in Reggio Emilia had “at least one common clinical association of AHA,” they found, suggesting that these associations could “reflect susceptibility to autoimmunity potentially triggered by vaccination.”
“Case four died due to complications from sepsis after being treated with steroid and rituximab, whereas the first three cases underwent clinical and laboratory remission after immunosuppressive therapy, and no relapse has been observed during follow-up, as in the other two cases reported: This could suggest a more favorable prognosis in respect to other non–vaccine-associated cases, but longer-term data are definitely needed,” they concluded.
The authors reported having no disclosures.
FROM THROMBOSIS RESEARCH
Endometriosis not linked with preterm birth, new study finds
These new findings, which were published online in JAMA Network Open, suggest that changing monitoring strategies to prevent preterm birth for women with the disease may not be necessary.
The research team, led by Louis Marcellin, MD, PhD, with the department of obstetrics and gynecology at Université de Paris, also found that disease phenotype or whether the preterm birth was induced or spontaneous did not appear to alter the result.
Those results differ from previous research. Data on the phenotypes and their link with preterm birth have been scarce, but previous studies have shown the risk for preterm birth is more pronounced in women who have deep endometriosis than in women with ovarian endometriosis.
Dr. Marcellin said in an interview that “little is known about the impact of endometriosis on obstetric outcomes. In contrast to previous studies, we reported no differences in the risk for preterm delivery between women with endometriosis (34 of 470 [7.2%]) and those without endometriosis (53 of 881 [6.0%]), even when adjusted for multiple factors.”
The authors accounted for mother’s age, body mass index before pregnancy, birth country, number of times the woman had given birth, previous cesarean delivery, and history of preterm birth. After adjusting for potential confounders, endometriosis was not associated with preterm birth (adjusted odds ratio, 1.07; 95% confidence interval, 0.64-1.77).
The researchers found no differences among preterm births based on a mother’s endometriosis phenotype. Those phenotypes include Isolated superficial peritoneal endometriosis, ovarian endometrioma, and deep endometriosis.
“Monitoring pregnancy beyond the normal protocols or changing management strategies may not be warranted in cases of endometriosis,” Dr. Marcellin said.
More research on endometriosis’ potential link to birth outcomes is needed.
An expert not involved with the study said the new paper highlights important new avenues of research but should not be seen as the final word on the connection between endometriosis and preterm birth.
Of the 1,351 study participants (mean age, 32.9 years) who had a singleton delivery after 22 weeks’ gestation, 470 were assigned to the endometriosis group, and 881 were assigned to the control group.
The authors concluded that “pregnant women with endometriosis should not be considered to have an exceptionally high risk for preterm birth. However, further studies are needed to examine the potential for other adverse perinatal outcomes or specific but rare complications.”
Daniela Carusi, MD, said the difficulty with the study’s design is that “premature birth is not one problem or one disease.”
Many very different problems can all end with premature birth. Sometimes it’s an infection or inflammation or bleeding in the uterus or hypertension in the mother, for example, and all those things can lead to a preterm birth, she explained.
“This study inherently lumps all those things together,” said Dr. Carusi, who is director of surgical obstetrics and placental abnormalities in the department of obstetrics and gynecology at Brigham and Women’s Hospital, Boston. “It’s quite possible endometriosis can have a big impact in one of those areas and no impact in the other areas, but the study design wouldn’t be able to pick that up.”
Editorialists: Results challenge findings of previous studies
In an accompanying commentary, Liisu Saavalainen, MD, PhD, and Oskari Heikinheimo, MD, PhD, both with the department of obstetrics and gynecology, Helsinki University Hospital, wrote that several previous studies have suggested that women with endometriosis have a slightly higher risk for preterm birth.
Those studies were mostly retrospective and differed in the way they classified endometriosis and the way they selected patients, the editorialists write. Also, most women in these studies typically had subfertility, they added.
The study by Dr. Marcellin and colleagues differs from previous related research in that was prospective and assessed the risk for preterm delivery in women both with endometriosis and those without endometriosis from several maternity centers in France. The women with endometriosis were classified according to the severity of their disease.
The editorialists wrote: “The novel results by Marcellin et al. challenge the findings of most previous studies on this topic. These results are valuable and comforting. However, they are also likely to trigger new studies on the pregnancy risks associated with different types of endometriosis. That is good news.”
Dr. Carusi said the study was well done and included a notably large size. Further complimenting the research, she said it’s important to talk about this little-discussed pregnancy complication. There’s been much more focus for women with endometriosis and their physicians on getting pregnant and on talking about the length of their term.
The study leaves some things unanswered.
The study was funded by research grants from the French Ministry of Health and was sponsored by the Département de la Recherche Clinique et du Développement de l’Assistance Publique–Hôpitaux de Paris. Dr. Carusi reported no relevant financial relationships. One study coauthor reported receiving personal fees from Bioserinity and Ferring outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
These new findings, which were published online in JAMA Network Open, suggest that changing monitoring strategies to prevent preterm birth for women with the disease may not be necessary.
The research team, led by Louis Marcellin, MD, PhD, with the department of obstetrics and gynecology at Université de Paris, also found that disease phenotype or whether the preterm birth was induced or spontaneous did not appear to alter the result.
Those results differ from previous research. Data on the phenotypes and their link with preterm birth have been scarce, but previous studies have shown the risk for preterm birth is more pronounced in women who have deep endometriosis than in women with ovarian endometriosis.
Dr. Marcellin said in an interview that “little is known about the impact of endometriosis on obstetric outcomes. In contrast to previous studies, we reported no differences in the risk for preterm delivery between women with endometriosis (34 of 470 [7.2%]) and those without endometriosis (53 of 881 [6.0%]), even when adjusted for multiple factors.”
The authors accounted for mother’s age, body mass index before pregnancy, birth country, number of times the woman had given birth, previous cesarean delivery, and history of preterm birth. After adjusting for potential confounders, endometriosis was not associated with preterm birth (adjusted odds ratio, 1.07; 95% confidence interval, 0.64-1.77).
The researchers found no differences among preterm births based on a mother’s endometriosis phenotype. Those phenotypes include Isolated superficial peritoneal endometriosis, ovarian endometrioma, and deep endometriosis.
“Monitoring pregnancy beyond the normal protocols or changing management strategies may not be warranted in cases of endometriosis,” Dr. Marcellin said.
More research on endometriosis’ potential link to birth outcomes is needed.
An expert not involved with the study said the new paper highlights important new avenues of research but should not be seen as the final word on the connection between endometriosis and preterm birth.
Of the 1,351 study participants (mean age, 32.9 years) who had a singleton delivery after 22 weeks’ gestation, 470 were assigned to the endometriosis group, and 881 were assigned to the control group.
The authors concluded that “pregnant women with endometriosis should not be considered to have an exceptionally high risk for preterm birth. However, further studies are needed to examine the potential for other adverse perinatal outcomes or specific but rare complications.”
Daniela Carusi, MD, said the difficulty with the study’s design is that “premature birth is not one problem or one disease.”
Many very different problems can all end with premature birth. Sometimes it’s an infection or inflammation or bleeding in the uterus or hypertension in the mother, for example, and all those things can lead to a preterm birth, she explained.
“This study inherently lumps all those things together,” said Dr. Carusi, who is director of surgical obstetrics and placental abnormalities in the department of obstetrics and gynecology at Brigham and Women’s Hospital, Boston. “It’s quite possible endometriosis can have a big impact in one of those areas and no impact in the other areas, but the study design wouldn’t be able to pick that up.”
Editorialists: Results challenge findings of previous studies
In an accompanying commentary, Liisu Saavalainen, MD, PhD, and Oskari Heikinheimo, MD, PhD, both with the department of obstetrics and gynecology, Helsinki University Hospital, wrote that several previous studies have suggested that women with endometriosis have a slightly higher risk for preterm birth.
Those studies were mostly retrospective and differed in the way they classified endometriosis and the way they selected patients, the editorialists write. Also, most women in these studies typically had subfertility, they added.
The study by Dr. Marcellin and colleagues differs from previous related research in that was prospective and assessed the risk for preterm delivery in women both with endometriosis and those without endometriosis from several maternity centers in France. The women with endometriosis were classified according to the severity of their disease.
The editorialists wrote: “The novel results by Marcellin et al. challenge the findings of most previous studies on this topic. These results are valuable and comforting. However, they are also likely to trigger new studies on the pregnancy risks associated with different types of endometriosis. That is good news.”
Dr. Carusi said the study was well done and included a notably large size. Further complimenting the research, she said it’s important to talk about this little-discussed pregnancy complication. There’s been much more focus for women with endometriosis and their physicians on getting pregnant and on talking about the length of their term.
The study leaves some things unanswered.
The study was funded by research grants from the French Ministry of Health and was sponsored by the Département de la Recherche Clinique et du Développement de l’Assistance Publique–Hôpitaux de Paris. Dr. Carusi reported no relevant financial relationships. One study coauthor reported receiving personal fees from Bioserinity and Ferring outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
These new findings, which were published online in JAMA Network Open, suggest that changing monitoring strategies to prevent preterm birth for women with the disease may not be necessary.
The research team, led by Louis Marcellin, MD, PhD, with the department of obstetrics and gynecology at Université de Paris, also found that disease phenotype or whether the preterm birth was induced or spontaneous did not appear to alter the result.
Those results differ from previous research. Data on the phenotypes and their link with preterm birth have been scarce, but previous studies have shown the risk for preterm birth is more pronounced in women who have deep endometriosis than in women with ovarian endometriosis.
Dr. Marcellin said in an interview that “little is known about the impact of endometriosis on obstetric outcomes. In contrast to previous studies, we reported no differences in the risk for preterm delivery between women with endometriosis (34 of 470 [7.2%]) and those without endometriosis (53 of 881 [6.0%]), even when adjusted for multiple factors.”
The authors accounted for mother’s age, body mass index before pregnancy, birth country, number of times the woman had given birth, previous cesarean delivery, and history of preterm birth. After adjusting for potential confounders, endometriosis was not associated with preterm birth (adjusted odds ratio, 1.07; 95% confidence interval, 0.64-1.77).
The researchers found no differences among preterm births based on a mother’s endometriosis phenotype. Those phenotypes include Isolated superficial peritoneal endometriosis, ovarian endometrioma, and deep endometriosis.
“Monitoring pregnancy beyond the normal protocols or changing management strategies may not be warranted in cases of endometriosis,” Dr. Marcellin said.
More research on endometriosis’ potential link to birth outcomes is needed.
An expert not involved with the study said the new paper highlights important new avenues of research but should not be seen as the final word on the connection between endometriosis and preterm birth.
Of the 1,351 study participants (mean age, 32.9 years) who had a singleton delivery after 22 weeks’ gestation, 470 were assigned to the endometriosis group, and 881 were assigned to the control group.
The authors concluded that “pregnant women with endometriosis should not be considered to have an exceptionally high risk for preterm birth. However, further studies are needed to examine the potential for other adverse perinatal outcomes or specific but rare complications.”
Daniela Carusi, MD, said the difficulty with the study’s design is that “premature birth is not one problem or one disease.”
Many very different problems can all end with premature birth. Sometimes it’s an infection or inflammation or bleeding in the uterus or hypertension in the mother, for example, and all those things can lead to a preterm birth, she explained.
“This study inherently lumps all those things together,” said Dr. Carusi, who is director of surgical obstetrics and placental abnormalities in the department of obstetrics and gynecology at Brigham and Women’s Hospital, Boston. “It’s quite possible endometriosis can have a big impact in one of those areas and no impact in the other areas, but the study design wouldn’t be able to pick that up.”
Editorialists: Results challenge findings of previous studies
In an accompanying commentary, Liisu Saavalainen, MD, PhD, and Oskari Heikinheimo, MD, PhD, both with the department of obstetrics and gynecology, Helsinki University Hospital, wrote that several previous studies have suggested that women with endometriosis have a slightly higher risk for preterm birth.
Those studies were mostly retrospective and differed in the way they classified endometriosis and the way they selected patients, the editorialists write. Also, most women in these studies typically had subfertility, they added.
The study by Dr. Marcellin and colleagues differs from previous related research in that was prospective and assessed the risk for preterm delivery in women both with endometriosis and those without endometriosis from several maternity centers in France. The women with endometriosis were classified according to the severity of their disease.
The editorialists wrote: “The novel results by Marcellin et al. challenge the findings of most previous studies on this topic. These results are valuable and comforting. However, they are also likely to trigger new studies on the pregnancy risks associated with different types of endometriosis. That is good news.”
Dr. Carusi said the study was well done and included a notably large size. Further complimenting the research, she said it’s important to talk about this little-discussed pregnancy complication. There’s been much more focus for women with endometriosis and their physicians on getting pregnant and on talking about the length of their term.
The study leaves some things unanswered.
The study was funded by research grants from the French Ministry of Health and was sponsored by the Département de la Recherche Clinique et du Développement de l’Assistance Publique–Hôpitaux de Paris. Dr. Carusi reported no relevant financial relationships. One study coauthor reported receiving personal fees from Bioserinity and Ferring outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Stopping venetoclax treatment early reduces CLL survival outcomes
“There’s not a lot of awareness about the fact that you’re probably better off not permanently discontinuing treatment,” Anthony R. Mato, first author of the research published in Haematologica, said in an interview.

“Instead, attempting dose reductions with later resumption to complete the planned schedule for treatment probably could improve outcomes,” said Dr. Mato, who is director of the CLL Program at Memorial Sloan Kettering Cancer Center in New York.
Venetoclax, a potent B-cell lymphoma-2 (BCL2) inhibitor, provides a novel, chemotherapy-free treatment option for first-line and r/r CLL. While its safety profile is manageable, treatment interruptions are very common, and premature discontinuations are reported in about a third of patients, often because of adverse events.
Lacking data on the effects of those interruptions on survival outcomes, Dr. Mato and colleagues conducted a post hoc analysis of the phase 3 MURANO trial. In this open-label study, treatment with six cycles of venetoclax in combination with rituximab followed by venetoclax once daily for a total of 2 years showed superior progression-free survival, compared with six cycles of bendamustine plus rituximab in patients with r/r CLL (P < .0001).
The current analysis involved 194 intention-to-treat patients from the trial’s venetoclax arm, among whom 140 (72%) completed 2 years of therapy, and 54 (28%) prematurely discontinued treatment. The most common reasons for discontinuation were adverse events (53.7%) and disease progression (22.2%).
Among those with early discontinuation for any reason except disease progression, the rate of progression-free survival was significantly inferior, compared with those who completed the treatment (hazard ratio, 5.98; P < .0001), as was the rate or discontinuation caused specifically by adverse events, which most commonly involved neutropenia or thrombocytopenia (HR, 5.82; P < .0001).
Those who discontinued had a mean duration of venetoclax therapy of 11.3 months, compared with 24.4 months for all patients. For each additional month of venetoclax therapy, there was a significantly lower risk of a progression-free survival event (P = .0263) and of an overall survival event (P < .0001).
The treatment interruption rate was much higher, at 69% (134), involving neutropenia in 43% (84) of instances and requiring dose reductions in 23% (45) of cases.
However, in contrast to permanent discontinuations, the temporary interruptions and dose reductions had no significant effect on progression-free or overall survival, regardless of the duration.
“Improved progression-free and overall survival were associated with greater cumulative venetoclax treatment exposure,” the authors wrote.
“The results of these analyses highlight the importance of appropriately managing treatment modifications to ensure optimal outcomes for patients receiving targeted treatment for CLL,” they said.
Key measures including “better supportive care, use of growth factors, and more aggressive strategies for dose reduction could potentially help to improve or decrease the number of patients discontinuing due to an adverse event,” Dr. Mato added.“We can’t say definitively because this is not a randomized study – it’s a retrospective analysis from a randomized study – but those measures likely could have a positive impact on patient outcomes.”
The study received support from Genentech and AbbVie. Dr. Mato reported consulting or other relationships with AbbVie, AstraZeneca, Celgene, DTRM, Genentech, Janssen, Loxo, PCYC, Sunesis, and TG Therapeutics.
“There’s not a lot of awareness about the fact that you’re probably better off not permanently discontinuing treatment,” Anthony R. Mato, first author of the research published in Haematologica, said in an interview.
“Instead, attempting dose reductions with later resumption to complete the planned schedule for treatment probably could improve outcomes,” said Dr. Mato, who is director of the CLL Program at Memorial Sloan Kettering Cancer Center in New York.
Venetoclax, a potent B-cell lymphoma-2 (BCL2) inhibitor, provides a novel, chemotherapy-free treatment option for first-line and r/r CLL. While its safety profile is manageable, treatment interruptions are very common, and premature discontinuations are reported in about a third of patients, often because of adverse events.
Lacking data on the effects of those interruptions on survival outcomes, Dr. Mato and colleagues conducted a post hoc analysis of the phase 3 MURANO trial. In this open-label study, treatment with six cycles of venetoclax in combination with rituximab followed by venetoclax once daily for a total of 2 years showed superior progression-free survival, compared with six cycles of bendamustine plus rituximab in patients with r/r CLL (P < .0001).
The current analysis involved 194 intention-to-treat patients from the trial’s venetoclax arm, among whom 140 (72%) completed 2 years of therapy, and 54 (28%) prematurely discontinued treatment. The most common reasons for discontinuation were adverse events (53.7%) and disease progression (22.2%).
Among those with early discontinuation for any reason except disease progression, the rate of progression-free survival was significantly inferior, compared with those who completed the treatment (hazard ratio, 5.98; P < .0001), as was the rate or discontinuation caused specifically by adverse events, which most commonly involved neutropenia or thrombocytopenia (HR, 5.82; P < .0001).
Those who discontinued had a mean duration of venetoclax therapy of 11.3 months, compared with 24.4 months for all patients. For each additional month of venetoclax therapy, there was a significantly lower risk of a progression-free survival event (P = .0263) and of an overall survival event (P < .0001).
The treatment interruption rate was much higher, at 69% (134), involving neutropenia in 43% (84) of instances and requiring dose reductions in 23% (45) of cases.
However, in contrast to permanent discontinuations, the temporary interruptions and dose reductions had no significant effect on progression-free or overall survival, regardless of the duration.
“Improved progression-free and overall survival were associated with greater cumulative venetoclax treatment exposure,” the authors wrote.
“The results of these analyses highlight the importance of appropriately managing treatment modifications to ensure optimal outcomes for patients receiving targeted treatment for CLL,” they said.
Key measures including “better supportive care, use of growth factors, and more aggressive strategies for dose reduction could potentially help to improve or decrease the number of patients discontinuing due to an adverse event,” Dr. Mato added.“We can’t say definitively because this is not a randomized study – it’s a retrospective analysis from a randomized study – but those measures likely could have a positive impact on patient outcomes.”
The study received support from Genentech and AbbVie. Dr. Mato reported consulting or other relationships with AbbVie, AstraZeneca, Celgene, DTRM, Genentech, Janssen, Loxo, PCYC, Sunesis, and TG Therapeutics.
“There’s not a lot of awareness about the fact that you’re probably better off not permanently discontinuing treatment,” Anthony R. Mato, first author of the research published in Haematologica, said in an interview.
“Instead, attempting dose reductions with later resumption to complete the planned schedule for treatment probably could improve outcomes,” said Dr. Mato, who is director of the CLL Program at Memorial Sloan Kettering Cancer Center in New York.
Venetoclax, a potent B-cell lymphoma-2 (BCL2) inhibitor, provides a novel, chemotherapy-free treatment option for first-line and r/r CLL. While its safety profile is manageable, treatment interruptions are very common, and premature discontinuations are reported in about a third of patients, often because of adverse events.
Lacking data on the effects of those interruptions on survival outcomes, Dr. Mato and colleagues conducted a post hoc analysis of the phase 3 MURANO trial. In this open-label study, treatment with six cycles of venetoclax in combination with rituximab followed by venetoclax once daily for a total of 2 years showed superior progression-free survival, compared with six cycles of bendamustine plus rituximab in patients with r/r CLL (P < .0001).
The current analysis involved 194 intention-to-treat patients from the trial’s venetoclax arm, among whom 140 (72%) completed 2 years of therapy, and 54 (28%) prematurely discontinued treatment. The most common reasons for discontinuation were adverse events (53.7%) and disease progression (22.2%).
Among those with early discontinuation for any reason except disease progression, the rate of progression-free survival was significantly inferior, compared with those who completed the treatment (hazard ratio, 5.98; P < .0001), as was the rate or discontinuation caused specifically by adverse events, which most commonly involved neutropenia or thrombocytopenia (HR, 5.82; P < .0001).
Those who discontinued had a mean duration of venetoclax therapy of 11.3 months, compared with 24.4 months for all patients. For each additional month of venetoclax therapy, there was a significantly lower risk of a progression-free survival event (P = .0263) and of an overall survival event (P < .0001).
The treatment interruption rate was much higher, at 69% (134), involving neutropenia in 43% (84) of instances and requiring dose reductions in 23% (45) of cases.
However, in contrast to permanent discontinuations, the temporary interruptions and dose reductions had no significant effect on progression-free or overall survival, regardless of the duration.
“Improved progression-free and overall survival were associated with greater cumulative venetoclax treatment exposure,” the authors wrote.
“The results of these analyses highlight the importance of appropriately managing treatment modifications to ensure optimal outcomes for patients receiving targeted treatment for CLL,” they said.
Key measures including “better supportive care, use of growth factors, and more aggressive strategies for dose reduction could potentially help to improve or decrease the number of patients discontinuing due to an adverse event,” Dr. Mato added.“We can’t say definitively because this is not a randomized study – it’s a retrospective analysis from a randomized study – but those measures likely could have a positive impact on patient outcomes.”
The study received support from Genentech and AbbVie. Dr. Mato reported consulting or other relationships with AbbVie, AstraZeneca, Celgene, DTRM, Genentech, Janssen, Loxo, PCYC, Sunesis, and TG Therapeutics.
Prophylactic meds may prevent cesarean bleeding
Methylergonovine is often used to control severe bleeding immediately after cesarean deliveries. But a new study suggests that the ergot alkaloid agent could benefit these women if administered before delivery, researchers from the University of Iowa Hospitals, Iowa City, reported in the January edition of the American Journal of Obstetrics and Gynecology. The data were presented Feb. 4 at the 2022 virtual Pregnancy Meeting of the Society of Maternal-Fetal Medicine.
The findings have prompted the institution to begin administering prophylactic methylergonovine in addition to oxytocin at the time of cesarean deliveries, according to the researchers.
“The addition of prophylactic methylergonovine improved uterine tone, decreased the requirement of additional uterotonic agents, decreased the risk of postpartum hemorrhage, and decreased the need for blood transfusions,” lead author Nicole Masse, MD, assistant professor of maternal-fetal medicine at the University of Iowa, said in an interview.
Abnormal uterine tone is the leading cause of postpartum hemorrhage, Dr. Masse said. “Satisfactory uterine tone following delivery is essential. This study found a decreased need for blood transfusions in patients who received prophylactic methylergonovine. Given the risks of blood transfusions, which can include disease transmission and allergic reactions, transfusions should be avoided whenever possible.”
Conducted between June 2019 and February 2021, the single-center, randomized controlled trial of 160 women undergoing an intrapartum cesarean birth is the largest of its kind to date, Dr. Masse said. Women received either intravenous oxytocin at a dose of 300 mU per minute plus 1 mL of intramuscular normal saline (n = 80) or intravenous oxytocin at a dose of 300 mU per minute plus 0.2 mg (1 mL) of intramuscular methylergonovine (n = 80).
Women who received prophylactic methylergonovine required significantly less additional uterotonic agents than those who received oxytocin alone (20% vs. 55%; relative risk, 0.36; 95% confidence interval 0.22-0.59), according to the researchers. Those receiving methylergonovine were more likely to experience improved uterine tone (80% vs. 41.2%; RR, 1.94; 95% CI, 1.46-2.56), a lower incidence of postpartum hemorrhage (35% vs. 58.8%; RR, 0.6; 95% CI, 0.42-0.85), decreased need for a blood transfusion (5% vs. 22.5%; RR, 0.22; 95% CI, 0.08-0.63), and lower mean quantitative blood loss (996 mL vs. 1,315 mL; P = .004), they reported.
“As the majority of postpartum hemorrhages are preventable, this study is clinically relevant and can serve to decrease the morbidity associated with postpartum hemorrhage,” Dr. Masse said.
Jennifer Choi, DO, clinical assistant professor of maternal-fetal medicine at Stony Brook University Hospital, New York, said the Iowa team’s results are contrary to prior studies showing no benefit with simultaneous use of oxytocin and ergot alkaloids.
“It would be interesting to see long-term benefits across a diverse population,” she said. “But as methylergonovine is a known contraindication to hypertensive and cardiovascular disorders, including pre-eclampsia, patients would have to be carefully screened.”
Kecia Gaither, MD, MPH, associate professor of clinical obstetrics and gynecology at Weill Cornell Medicine, New York, called the study “a novel idea, but more research and higher numbers are needed for a substantive conclusion.”
Additional studies should look at variables such as the number of prior cesarean deliveries, body mass index, presence of uterine myomas, presence of abnormal placentation (placenta accreta, increta, percreta), and presence of multiple gestation, said Dr. Gaither, who also is director of perinatal services at NYC Health + Hospitals/Lincoln.
“Methergine [methylergonovine] use is contraindicated in women with hypertension/pre-eclampsia spectrum, mitral valve prolapse, history of coronary artery disease, and liver pathology,” she noted.
The researchers reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Methylergonovine is often used to control severe bleeding immediately after cesarean deliveries. But a new study suggests that the ergot alkaloid agent could benefit these women if administered before delivery, researchers from the University of Iowa Hospitals, Iowa City, reported in the January edition of the American Journal of Obstetrics and Gynecology. The data were presented Feb. 4 at the 2022 virtual Pregnancy Meeting of the Society of Maternal-Fetal Medicine.
The findings have prompted the institution to begin administering prophylactic methylergonovine in addition to oxytocin at the time of cesarean deliveries, according to the researchers.
“The addition of prophylactic methylergonovine improved uterine tone, decreased the requirement of additional uterotonic agents, decreased the risk of postpartum hemorrhage, and decreased the need for blood transfusions,” lead author Nicole Masse, MD, assistant professor of maternal-fetal medicine at the University of Iowa, said in an interview.
Abnormal uterine tone is the leading cause of postpartum hemorrhage, Dr. Masse said. “Satisfactory uterine tone following delivery is essential. This study found a decreased need for blood transfusions in patients who received prophylactic methylergonovine. Given the risks of blood transfusions, which can include disease transmission and allergic reactions, transfusions should be avoided whenever possible.”
Conducted between June 2019 and February 2021, the single-center, randomized controlled trial of 160 women undergoing an intrapartum cesarean birth is the largest of its kind to date, Dr. Masse said. Women received either intravenous oxytocin at a dose of 300 mU per minute plus 1 mL of intramuscular normal saline (n = 80) or intravenous oxytocin at a dose of 300 mU per minute plus 0.2 mg (1 mL) of intramuscular methylergonovine (n = 80).
Women who received prophylactic methylergonovine required significantly less additional uterotonic agents than those who received oxytocin alone (20% vs. 55%; relative risk, 0.36; 95% confidence interval 0.22-0.59), according to the researchers. Those receiving methylergonovine were more likely to experience improved uterine tone (80% vs. 41.2%; RR, 1.94; 95% CI, 1.46-2.56), a lower incidence of postpartum hemorrhage (35% vs. 58.8%; RR, 0.6; 95% CI, 0.42-0.85), decreased need for a blood transfusion (5% vs. 22.5%; RR, 0.22; 95% CI, 0.08-0.63), and lower mean quantitative blood loss (996 mL vs. 1,315 mL; P = .004), they reported.
“As the majority of postpartum hemorrhages are preventable, this study is clinically relevant and can serve to decrease the morbidity associated with postpartum hemorrhage,” Dr. Masse said.
Jennifer Choi, DO, clinical assistant professor of maternal-fetal medicine at Stony Brook University Hospital, New York, said the Iowa team’s results are contrary to prior studies showing no benefit with simultaneous use of oxytocin and ergot alkaloids.
“It would be interesting to see long-term benefits across a diverse population,” she said. “But as methylergonovine is a known contraindication to hypertensive and cardiovascular disorders, including pre-eclampsia, patients would have to be carefully screened.”
Kecia Gaither, MD, MPH, associate professor of clinical obstetrics and gynecology at Weill Cornell Medicine, New York, called the study “a novel idea, but more research and higher numbers are needed for a substantive conclusion.”
Additional studies should look at variables such as the number of prior cesarean deliveries, body mass index, presence of uterine myomas, presence of abnormal placentation (placenta accreta, increta, percreta), and presence of multiple gestation, said Dr. Gaither, who also is director of perinatal services at NYC Health + Hospitals/Lincoln.
“Methergine [methylergonovine] use is contraindicated in women with hypertension/pre-eclampsia spectrum, mitral valve prolapse, history of coronary artery disease, and liver pathology,” she noted.
The researchers reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Methylergonovine is often used to control severe bleeding immediately after cesarean deliveries. But a new study suggests that the ergot alkaloid agent could benefit these women if administered before delivery, researchers from the University of Iowa Hospitals, Iowa City, reported in the January edition of the American Journal of Obstetrics and Gynecology. The data were presented Feb. 4 at the 2022 virtual Pregnancy Meeting of the Society of Maternal-Fetal Medicine.
The findings have prompted the institution to begin administering prophylactic methylergonovine in addition to oxytocin at the time of cesarean deliveries, according to the researchers.
“The addition of prophylactic methylergonovine improved uterine tone, decreased the requirement of additional uterotonic agents, decreased the risk of postpartum hemorrhage, and decreased the need for blood transfusions,” lead author Nicole Masse, MD, assistant professor of maternal-fetal medicine at the University of Iowa, said in an interview.
Abnormal uterine tone is the leading cause of postpartum hemorrhage, Dr. Masse said. “Satisfactory uterine tone following delivery is essential. This study found a decreased need for blood transfusions in patients who received prophylactic methylergonovine. Given the risks of blood transfusions, which can include disease transmission and allergic reactions, transfusions should be avoided whenever possible.”
Conducted between June 2019 and February 2021, the single-center, randomized controlled trial of 160 women undergoing an intrapartum cesarean birth is the largest of its kind to date, Dr. Masse said. Women received either intravenous oxytocin at a dose of 300 mU per minute plus 1 mL of intramuscular normal saline (n = 80) or intravenous oxytocin at a dose of 300 mU per minute plus 0.2 mg (1 mL) of intramuscular methylergonovine (n = 80).
Women who received prophylactic methylergonovine required significantly less additional uterotonic agents than those who received oxytocin alone (20% vs. 55%; relative risk, 0.36; 95% confidence interval 0.22-0.59), according to the researchers. Those receiving methylergonovine were more likely to experience improved uterine tone (80% vs. 41.2%; RR, 1.94; 95% CI, 1.46-2.56), a lower incidence of postpartum hemorrhage (35% vs. 58.8%; RR, 0.6; 95% CI, 0.42-0.85), decreased need for a blood transfusion (5% vs. 22.5%; RR, 0.22; 95% CI, 0.08-0.63), and lower mean quantitative blood loss (996 mL vs. 1,315 mL; P = .004), they reported.
“As the majority of postpartum hemorrhages are preventable, this study is clinically relevant and can serve to decrease the morbidity associated with postpartum hemorrhage,” Dr. Masse said.
Jennifer Choi, DO, clinical assistant professor of maternal-fetal medicine at Stony Brook University Hospital, New York, said the Iowa team’s results are contrary to prior studies showing no benefit with simultaneous use of oxytocin and ergot alkaloids.
“It would be interesting to see long-term benefits across a diverse population,” she said. “But as methylergonovine is a known contraindication to hypertensive and cardiovascular disorders, including pre-eclampsia, patients would have to be carefully screened.”
Kecia Gaither, MD, MPH, associate professor of clinical obstetrics and gynecology at Weill Cornell Medicine, New York, called the study “a novel idea, but more research and higher numbers are needed for a substantive conclusion.”
Additional studies should look at variables such as the number of prior cesarean deliveries, body mass index, presence of uterine myomas, presence of abnormal placentation (placenta accreta, increta, percreta), and presence of multiple gestation, said Dr. Gaither, who also is director of perinatal services at NYC Health + Hospitals/Lincoln.
“Methergine [methylergonovine] use is contraindicated in women with hypertension/pre-eclampsia spectrum, mitral valve prolapse, history of coronary artery disease, and liver pathology,” she noted.
The researchers reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.