User login
Patients with blood cancers underutilize palliative care
I used to attend the Supportive Care in Oncology Symposium every year, but to my dismay, the American Society for Clinical Oncology stopped hosting the symposium a few years ago. Instead, ASCO now incorporates palliative care research fully into its annual meeting which was held in early June in Chicago. Being integrated into the annual meeting means greater exposure to a broader audience that may not otherwise see this work. In this column, I highlight some presentations that stood out to me.
Palliative care studies for patients with hematologic malignancies
There continues to be low uptake of outpatient palliative care services among patients with hematologic malignancies. Fortunately, there are efforts underway to study the impact of integrating early palliative care into the routine care of hematology patients. In a study presented by Mazie Tsang, MD, a clinical fellow at the University of California, San Francisco, researchers embedded a palliative care nurse practitioner in a hematology clinic and studied the impact this single NP had over 4 years of integration. They found that patients were less likely to be hospitalized or visit the emergency department after integrating the NP. They also found that advance directives were more likely to be completed following NP integration. The results were limited by small sample size and lack of a true control group, but generally trended toward significance when compared with historical controls.

Other studies highlighted the relatively high symptom burden among patients with hematologic malignancies, such as myeloma, leukemia, and lymphoma. In a study presented by Sarah E. Monick, MD, of the University of Chicago, researchers found that, among adolescents and young adults with hematologic malignancies seen in a clinic where a palliative care provider was embedded, symptom burden was high across the board regardless of where patients were in their disease trajectory or their demographic characteristics. Due to the presence of high symptom burden among adolescents and young adults, the authors suggest that patients undergo screening at every visit and that supportive care be incorporated throughout the patient’s journey.
Kyle Fitzgibbon of the Princess Margaret Cancer Centre in Toronto shared details of an ongoing multicenter, randomized, controlled, phase 3 trial designed to evaluate the effect of a novel psychosocial/palliative care intervention for patients with acute leukemia hospitalized for induction chemotherapy. The intervention will consist of 8 weeks of psychological support as well as access to palliative care for physical symptoms. Participants will be randomized to receive either intervention or standard of care at the beginning of their hospitalization. Researchers plan to study the impact of the intervention on physical and psychological symptom severity, quality of life, and patient satisfaction at multiple time points. It will be exciting to see the results of this study given that there are very few research clinical trials examining early palliative care with patients who have hematologic malignancies.
Trends in palliative care integration with oncology care
One key trend that I am elated to see is the integration of palliative care throughout the entire patient journey. A secondary analysis of oncology practice data from the National Cancer Institute Community Oncology Research Program found that more than three-quarters of outpatient oncology practices surveyed in 2015 have integrated palliative care inpatient and outpatient services. 36% said they had an outpatient palliative care clinic. More availability of services typically translates to better access to care and improved outcomes for patients, so it is always nice to see these quality metrics continue to move in a positive direction. The analysis was presented by Tiffany M. Statler, PA, of Atrium Health Wake Forest Baptist, Winston Salem, N.C.
It turns out that patients are also advocating for integrated palliative care. A unique qualitative project brought together patient advocates from several countries to hold a moderated discussion about quality of life and treatment side effects. The advocates focused on the importance of maintaining independence with activities of daily living as a significant quality of life goal, particularly as treatments tend to cause cumulative mental and physical fatigue. They highlighted the importance of palliative care for helping achieve quality of life goals, especially in latter part of the disease trajectory. The project was presented by Paul Wheatley-Price, MD, of the Ottawa Hospital Cancer Centre, University of Ottawa.
In 2010, a study by Temel and colleagues was published, finding that patients with metastatic non–small cell lung cancer who received palliative care early had significant improvements in quality of life and mood as compared with patients who received standard care. It was a landmark study and is frequently cited. The Temel group reports on the planning process for a new randomized controlled trial of palliative care with metastatic lung cancer patients who have targetable mutations. With next generation sequencing of tumor tissue, many patients with metastatic lung cancer are identified at diagnosis as having a targetable mutation. As such, they may receive a targeted therapy as first-line treatment instead of traditional chemotherapy. This has lengthened survival considerably, but the disease remains incurable and ultimately fatal, and the trajectory can resemble a roller-coaster ride.
In this new randomized controlled trial, patients in the experimental arm will receive four monthly visits with a palliative care clinician who is specially trained to help patients manage the uncertainties of prolonged illness. The researchers plan to evaluate patients’ distress levels and prognostic awareness, as well as evidence of advance care planning in the chart.
And, a study presented by Roberto Enrique Ochoa Planchart, MD, of Chen Medical Centers, Miami, found that when primary care providers used declines in functional status as a trigger for referring advanced cancer patients to palliative care, those patients were less likely to be admitted to the hospital near the end of life, translating to an 86% cost savings. This study reiterated the importance of partnering with a patient’s nononcologic providers, that is, primary care and palliative care clinicians to improve outcomes at the end of life.
Use of technology in palliative care
Numerous studies were reported on innovative uses of technology for various functions relevant to palliative care. They included everything from capturing patient-reported outcomes through patient-facing smartphone apps, to using artificial intelligence and/or machine learning to build prognostication tools and to generate earlier referrals to palliative care. There were presentations on the use of online tools to assist with and document goals of care conversations.
As a clinician who is always looking for new ways to capture patient symptom information and motivate patients to engage in advance care planning, I am excited about the prospect of using some of these tools in real time.
Ms. D’Ambruoso is a hospice and palliative care nurse practitioner for UCLA Health Cancer Care, Santa Monica, Calif.
I used to attend the Supportive Care in Oncology Symposium every year, but to my dismay, the American Society for Clinical Oncology stopped hosting the symposium a few years ago. Instead, ASCO now incorporates palliative care research fully into its annual meeting which was held in early June in Chicago. Being integrated into the annual meeting means greater exposure to a broader audience that may not otherwise see this work. In this column, I highlight some presentations that stood out to me.
Palliative care studies for patients with hematologic malignancies
There continues to be low uptake of outpatient palliative care services among patients with hematologic malignancies. Fortunately, there are efforts underway to study the impact of integrating early palliative care into the routine care of hematology patients. In a study presented by Mazie Tsang, MD, a clinical fellow at the University of California, San Francisco, researchers embedded a palliative care nurse practitioner in a hematology clinic and studied the impact this single NP had over 4 years of integration. They found that patients were less likely to be hospitalized or visit the emergency department after integrating the NP. They also found that advance directives were more likely to be completed following NP integration. The results were limited by small sample size and lack of a true control group, but generally trended toward significance when compared with historical controls.
Other studies highlighted the relatively high symptom burden among patients with hematologic malignancies, such as myeloma, leukemia, and lymphoma. In a study presented by Sarah E. Monick, MD, of the University of Chicago, researchers found that, among adolescents and young adults with hematologic malignancies seen in a clinic where a palliative care provider was embedded, symptom burden was high across the board regardless of where patients were in their disease trajectory or their demographic characteristics. Due to the presence of high symptom burden among adolescents and young adults, the authors suggest that patients undergo screening at every visit and that supportive care be incorporated throughout the patient’s journey.
Kyle Fitzgibbon of the Princess Margaret Cancer Centre in Toronto shared details of an ongoing multicenter, randomized, controlled, phase 3 trial designed to evaluate the effect of a novel psychosocial/palliative care intervention for patients with acute leukemia hospitalized for induction chemotherapy. The intervention will consist of 8 weeks of psychological support as well as access to palliative care for physical symptoms. Participants will be randomized to receive either intervention or standard of care at the beginning of their hospitalization. Researchers plan to study the impact of the intervention on physical and psychological symptom severity, quality of life, and patient satisfaction at multiple time points. It will be exciting to see the results of this study given that there are very few research clinical trials examining early palliative care with patients who have hematologic malignancies.
Trends in palliative care integration with oncology care
One key trend that I am elated to see is the integration of palliative care throughout the entire patient journey. A secondary analysis of oncology practice data from the National Cancer Institute Community Oncology Research Program found that more than three-quarters of outpatient oncology practices surveyed in 2015 have integrated palliative care inpatient and outpatient services. 36% said they had an outpatient palliative care clinic. More availability of services typically translates to better access to care and improved outcomes for patients, so it is always nice to see these quality metrics continue to move in a positive direction. The analysis was presented by Tiffany M. Statler, PA, of Atrium Health Wake Forest Baptist, Winston Salem, N.C.
It turns out that patients are also advocating for integrated palliative care. A unique qualitative project brought together patient advocates from several countries to hold a moderated discussion about quality of life and treatment side effects. The advocates focused on the importance of maintaining independence with activities of daily living as a significant quality of life goal, particularly as treatments tend to cause cumulative mental and physical fatigue. They highlighted the importance of palliative care for helping achieve quality of life goals, especially in latter part of the disease trajectory. The project was presented by Paul Wheatley-Price, MD, of the Ottawa Hospital Cancer Centre, University of Ottawa.
In 2010, a study by Temel and colleagues was published, finding that patients with metastatic non–small cell lung cancer who received palliative care early had significant improvements in quality of life and mood as compared with patients who received standard care. It was a landmark study and is frequently cited. The Temel group reports on the planning process for a new randomized controlled trial of palliative care with metastatic lung cancer patients who have targetable mutations. With next generation sequencing of tumor tissue, many patients with metastatic lung cancer are identified at diagnosis as having a targetable mutation. As such, they may receive a targeted therapy as first-line treatment instead of traditional chemotherapy. This has lengthened survival considerably, but the disease remains incurable and ultimately fatal, and the trajectory can resemble a roller-coaster ride.
In this new randomized controlled trial, patients in the experimental arm will receive four monthly visits with a palliative care clinician who is specially trained to help patients manage the uncertainties of prolonged illness. The researchers plan to evaluate patients’ distress levels and prognostic awareness, as well as evidence of advance care planning in the chart.
And, a study presented by Roberto Enrique Ochoa Planchart, MD, of Chen Medical Centers, Miami, found that when primary care providers used declines in functional status as a trigger for referring advanced cancer patients to palliative care, those patients were less likely to be admitted to the hospital near the end of life, translating to an 86% cost savings. This study reiterated the importance of partnering with a patient’s nononcologic providers, that is, primary care and palliative care clinicians to improve outcomes at the end of life.
Use of technology in palliative care
Numerous studies were reported on innovative uses of technology for various functions relevant to palliative care. They included everything from capturing patient-reported outcomes through patient-facing smartphone apps, to using artificial intelligence and/or machine learning to build prognostication tools and to generate earlier referrals to palliative care. There were presentations on the use of online tools to assist with and document goals of care conversations.
As a clinician who is always looking for new ways to capture patient symptom information and motivate patients to engage in advance care planning, I am excited about the prospect of using some of these tools in real time.
Ms. D’Ambruoso is a hospice and palliative care nurse practitioner for UCLA Health Cancer Care, Santa Monica, Calif.
I used to attend the Supportive Care in Oncology Symposium every year, but to my dismay, the American Society for Clinical Oncology stopped hosting the symposium a few years ago. Instead, ASCO now incorporates palliative care research fully into its annual meeting which was held in early June in Chicago. Being integrated into the annual meeting means greater exposure to a broader audience that may not otherwise see this work. In this column, I highlight some presentations that stood out to me.
Palliative care studies for patients with hematologic malignancies
There continues to be low uptake of outpatient palliative care services among patients with hematologic malignancies. Fortunately, there are efforts underway to study the impact of integrating early palliative care into the routine care of hematology patients. In a study presented by Mazie Tsang, MD, a clinical fellow at the University of California, San Francisco, researchers embedded a palliative care nurse practitioner in a hematology clinic and studied the impact this single NP had over 4 years of integration. They found that patients were less likely to be hospitalized or visit the emergency department after integrating the NP. They also found that advance directives were more likely to be completed following NP integration. The results were limited by small sample size and lack of a true control group, but generally trended toward significance when compared with historical controls.
Other studies highlighted the relatively high symptom burden among patients with hematologic malignancies, such as myeloma, leukemia, and lymphoma. In a study presented by Sarah E. Monick, MD, of the University of Chicago, researchers found that, among adolescents and young adults with hematologic malignancies seen in a clinic where a palliative care provider was embedded, symptom burden was high across the board regardless of where patients were in their disease trajectory or their demographic characteristics. Due to the presence of high symptom burden among adolescents and young adults, the authors suggest that patients undergo screening at every visit and that supportive care be incorporated throughout the patient’s journey.
Kyle Fitzgibbon of the Princess Margaret Cancer Centre in Toronto shared details of an ongoing multicenter, randomized, controlled, phase 3 trial designed to evaluate the effect of a novel psychosocial/palliative care intervention for patients with acute leukemia hospitalized for induction chemotherapy. The intervention will consist of 8 weeks of psychological support as well as access to palliative care for physical symptoms. Participants will be randomized to receive either intervention or standard of care at the beginning of their hospitalization. Researchers plan to study the impact of the intervention on physical and psychological symptom severity, quality of life, and patient satisfaction at multiple time points. It will be exciting to see the results of this study given that there are very few research clinical trials examining early palliative care with patients who have hematologic malignancies.
Trends in palliative care integration with oncology care
One key trend that I am elated to see is the integration of palliative care throughout the entire patient journey. A secondary analysis of oncology practice data from the National Cancer Institute Community Oncology Research Program found that more than three-quarters of outpatient oncology practices surveyed in 2015 have integrated palliative care inpatient and outpatient services. 36% said they had an outpatient palliative care clinic. More availability of services typically translates to better access to care and improved outcomes for patients, so it is always nice to see these quality metrics continue to move in a positive direction. The analysis was presented by Tiffany M. Statler, PA, of Atrium Health Wake Forest Baptist, Winston Salem, N.C.
It turns out that patients are also advocating for integrated palliative care. A unique qualitative project brought together patient advocates from several countries to hold a moderated discussion about quality of life and treatment side effects. The advocates focused on the importance of maintaining independence with activities of daily living as a significant quality of life goal, particularly as treatments tend to cause cumulative mental and physical fatigue. They highlighted the importance of palliative care for helping achieve quality of life goals, especially in latter part of the disease trajectory. The project was presented by Paul Wheatley-Price, MD, of the Ottawa Hospital Cancer Centre, University of Ottawa.
In 2010, a study by Temel and colleagues was published, finding that patients with metastatic non–small cell lung cancer who received palliative care early had significant improvements in quality of life and mood as compared with patients who received standard care. It was a landmark study and is frequently cited. The Temel group reports on the planning process for a new randomized controlled trial of palliative care with metastatic lung cancer patients who have targetable mutations. With next generation sequencing of tumor tissue, many patients with metastatic lung cancer are identified at diagnosis as having a targetable mutation. As such, they may receive a targeted therapy as first-line treatment instead of traditional chemotherapy. This has lengthened survival considerably, but the disease remains incurable and ultimately fatal, and the trajectory can resemble a roller-coaster ride.
In this new randomized controlled trial, patients in the experimental arm will receive four monthly visits with a palliative care clinician who is specially trained to help patients manage the uncertainties of prolonged illness. The researchers plan to evaluate patients’ distress levels and prognostic awareness, as well as evidence of advance care planning in the chart.
And, a study presented by Roberto Enrique Ochoa Planchart, MD, of Chen Medical Centers, Miami, found that when primary care providers used declines in functional status as a trigger for referring advanced cancer patients to palliative care, those patients were less likely to be admitted to the hospital near the end of life, translating to an 86% cost savings. This study reiterated the importance of partnering with a patient’s nononcologic providers, that is, primary care and palliative care clinicians to improve outcomes at the end of life.
Use of technology in palliative care
Numerous studies were reported on innovative uses of technology for various functions relevant to palliative care. They included everything from capturing patient-reported outcomes through patient-facing smartphone apps, to using artificial intelligence and/or machine learning to build prognostication tools and to generate earlier referrals to palliative care. There were presentations on the use of online tools to assist with and document goals of care conversations.
As a clinician who is always looking for new ways to capture patient symptom information and motivate patients to engage in advance care planning, I am excited about the prospect of using some of these tools in real time.
Ms. D’Ambruoso is a hospice and palliative care nurse practitioner for UCLA Health Cancer Care, Santa Monica, Calif.
FROM ASCO 2022
Updated AHA/ASA guideline changes care for spontaneous intracerebral hemorrhage
Many strategies widely considered “standard care” for managing spontaneous intracerebral hemorrhage (ICH) are not as effective as previously thought and are no longer recommended in updated guidelines from the American Heart Association/American Stroke Association (ASA).
Compression stockings, antiseizure medication, and steroid treatment are among the treatments with uncertain effectiveness, the writing group says.
The 2022 Guideline for the Management of Patients With Spontaneous ICH was published online in Stroke. The 80-page document contains major changes and refinements to the 2015 guideline on ICH management.
“Advances have been made in an array of fields related to ICH, including the organization of regional health care systems, reversal of the negative effects of blood thinners, minimally invasive surgical procedures, and the underlying disease in small blood vessels,” Steven M. Greenberg, MD, PhD, chair of the guideline writing group with Harvard Medical School and Massachusetts General Hospital, both in Boston, said in a news release.
“We’ve updated sections across the board. There’s probably no area that went untouched with some tweaking and new evidence added that led to some changes in level of evidence or strength of a recommendation,” Dr. Greenberg added in an interview with this news organization.
“Each section comes with knowledge gaps, and it wasn’t hard to come up with knowledge gaps in every section,” Dr. Greenberg acknowledged.
Time-honored treatments no more?
Among the key updates are changes to some “time-honored” treatments that continue to be used with some “regularity” for patients with ICH, yet appear to confer either no benefit or harm, Dr. Greenberg said.
For example, for emergency or critical care treatment of ICH, prophylactic corticosteroids or continuous hyperosmolar therapy is not recommended, because it appears to have no benefit for outcome, while use of platelet transfusions outside the setting of emergency surgery or severe thrombocytopenia appears to worsen outcome, the authors say.
Use of graduated knee- or thigh-high compression stockings alone is not an effective prophylactic therapy for prevention of deep vein thrombosis (DVT). Instead, intermittent pneumatic compression (IPC) starting on the day of diagnosis is now recommended for DVT prophylaxis.
“This is an area where we still have a lot of exploration to do. It is unclear whether even specialized compression devices reduce the risks of deep vein thrombosis or improve the overall health of people with a brain bleed,” Dr. Greenberg said in the release.
The new guidance advises against use of antiseizure or antidepressant medications for ICH patients in whom there is no evidence of seizures or depression.
In clinical trials, antiseizure medication did not contribute to improvements in functionality or long-term seizure control, and the use of antidepressants increased the chance of bone fractures, the authors say.
The guideline also provides updated recommendations for acute reversal of anticoagulation after ICH. It highlights the use of protein complex concentrate for reversal of vitamin K antagonists, such as warfarin; idarucizumab for reversal of the thrombin inhibitor dabigatran; and andexanet alfa for reversal of factor Xa inhibitors, such as rivaroxaban, apixaban, and edoxaban.
For acute blood pressure lowering after mild to moderate ICH, treatment regimens that limit blood pressure variability and achieve smooth, sustained blood pressure control appear to reduce hematoma expansion and yield better functional outcome, the guideline says.
It also notes that minimally invasive approaches for hematoma evacuation, compared with medical management alone‚ have been shown to reduce mortality.
For patients with cerebellar hemorrhage, indications for immediate surgical evacuation with or without an external ventricular drain to reduce mortality now include larger volume (> 15 mL) in addition to previously recommended indications of neurologic deterioration, brainstem compression, and hydrocephalus, the authors note.
However, a “major knowledge gap is whether we can improve functional outcome with hematoma evacuation,” Dr. Greenberg said.
Multidisciplinary care
For rehabilitation after ICH, the guideline reinforces the importance of having a multidisciplinary team to develop a comprehensive plan for recovery.
Starting rehabilitation activities such as stretching and functional task training may be considered 24 to 48 hours following mild or moderate ICH. However, early aggressive mobilization within the first 24 hours has been linked to an increased risk of death within 14 days after an ICH, the guideline says.
Knowledge gaps include how soon it’s safe to return to work, drive, and participate in other social engagements. Recommendations on sexual activity and exercise levels that are safe after a stroke are also needed.
“People need additional help with these lifestyle changes, whether it’s moving around more, curbing their alcohol use, or eating healthier foods. This all happens after they leave the hospital, and we need to be sure we are empowering families with the information they may need to be properly supportive,” Dr. Greenberg says in the release.
The guideline points to the patient’s home caregiver as a “key and sometimes overlooked” member of the care team. It recommends psychosocial education, practical support, and training for the caregiver to improve the patient’s balance, activity level, and overall quality of life.
Opportunity for prevention?
The guideline also suggests there may be an opportunity to prevent ICH in some people through neuroimaging markers.
While neuroimaging is not routinely performed as a part of risk stratification for primary ICH risk, damage to small blood vessels that is associated with ICH may be evident on MRI that could signal future ICH risk, the guideline says.
“We added to the guidelines for the first time a section on mostly imaging markers of risk for having a first-ever hemorrhage,” Dr. Greenberg said in an interview.
“We don’t make any recommendations as to how to act on these markers because there is a knowledge gap. The hope is that we’ll see growth in our ability to predict first-ever hemorrhage and be able to do things to prevent first-ever hemorrhage,” he said.
“We believe the wide range of knowledge set forth in the new guideline will translate into meaningful improvements in ICH care,” Dr. Greenberg adds in the release.
The updated guideline has been endorsed by the American Association of Neurological Surgeons and Congress of Neurological Surgeons, the Society of Vascular and Interventional Neurology, and the Neurocritical Care Society. The American Academy of Neurology has affirmed the value of this statement as an educational tool for neurologists.
This research had no commercial funding. Dr. Greenberg has disclosed no relevant financial relationships. A complete list of disclosures for the guideline group is available with the original article.
A version of this article first appeared on Medscape.com.
Many strategies widely considered “standard care” for managing spontaneous intracerebral hemorrhage (ICH) are not as effective as previously thought and are no longer recommended in updated guidelines from the American Heart Association/American Stroke Association (ASA).
Compression stockings, antiseizure medication, and steroid treatment are among the treatments with uncertain effectiveness, the writing group says.
The 2022 Guideline for the Management of Patients With Spontaneous ICH was published online in Stroke. The 80-page document contains major changes and refinements to the 2015 guideline on ICH management.
“Advances have been made in an array of fields related to ICH, including the organization of regional health care systems, reversal of the negative effects of blood thinners, minimally invasive surgical procedures, and the underlying disease in small blood vessels,” Steven M. Greenberg, MD, PhD, chair of the guideline writing group with Harvard Medical School and Massachusetts General Hospital, both in Boston, said in a news release.
“We’ve updated sections across the board. There’s probably no area that went untouched with some tweaking and new evidence added that led to some changes in level of evidence or strength of a recommendation,” Dr. Greenberg added in an interview with this news organization.
“Each section comes with knowledge gaps, and it wasn’t hard to come up with knowledge gaps in every section,” Dr. Greenberg acknowledged.
Time-honored treatments no more?
Among the key updates are changes to some “time-honored” treatments that continue to be used with some “regularity” for patients with ICH, yet appear to confer either no benefit or harm, Dr. Greenberg said.
For example, for emergency or critical care treatment of ICH, prophylactic corticosteroids or continuous hyperosmolar therapy is not recommended, because it appears to have no benefit for outcome, while use of platelet transfusions outside the setting of emergency surgery or severe thrombocytopenia appears to worsen outcome, the authors say.
Use of graduated knee- or thigh-high compression stockings alone is not an effective prophylactic therapy for prevention of deep vein thrombosis (DVT). Instead, intermittent pneumatic compression (IPC) starting on the day of diagnosis is now recommended for DVT prophylaxis.
“This is an area where we still have a lot of exploration to do. It is unclear whether even specialized compression devices reduce the risks of deep vein thrombosis or improve the overall health of people with a brain bleed,” Dr. Greenberg said in the release.
The new guidance advises against use of antiseizure or antidepressant medications for ICH patients in whom there is no evidence of seizures or depression.
In clinical trials, antiseizure medication did not contribute to improvements in functionality or long-term seizure control, and the use of antidepressants increased the chance of bone fractures, the authors say.
The guideline also provides updated recommendations for acute reversal of anticoagulation after ICH. It highlights the use of protein complex concentrate for reversal of vitamin K antagonists, such as warfarin; idarucizumab for reversal of the thrombin inhibitor dabigatran; and andexanet alfa for reversal of factor Xa inhibitors, such as rivaroxaban, apixaban, and edoxaban.
For acute blood pressure lowering after mild to moderate ICH, treatment regimens that limit blood pressure variability and achieve smooth, sustained blood pressure control appear to reduce hematoma expansion and yield better functional outcome, the guideline says.
It also notes that minimally invasive approaches for hematoma evacuation, compared with medical management alone‚ have been shown to reduce mortality.
For patients with cerebellar hemorrhage, indications for immediate surgical evacuation with or without an external ventricular drain to reduce mortality now include larger volume (> 15 mL) in addition to previously recommended indications of neurologic deterioration, brainstem compression, and hydrocephalus, the authors note.
However, a “major knowledge gap is whether we can improve functional outcome with hematoma evacuation,” Dr. Greenberg said.
Multidisciplinary care
For rehabilitation after ICH, the guideline reinforces the importance of having a multidisciplinary team to develop a comprehensive plan for recovery.
Starting rehabilitation activities such as stretching and functional task training may be considered 24 to 48 hours following mild or moderate ICH. However, early aggressive mobilization within the first 24 hours has been linked to an increased risk of death within 14 days after an ICH, the guideline says.
Knowledge gaps include how soon it’s safe to return to work, drive, and participate in other social engagements. Recommendations on sexual activity and exercise levels that are safe after a stroke are also needed.
“People need additional help with these lifestyle changes, whether it’s moving around more, curbing their alcohol use, or eating healthier foods. This all happens after they leave the hospital, and we need to be sure we are empowering families with the information they may need to be properly supportive,” Dr. Greenberg says in the release.
The guideline points to the patient’s home caregiver as a “key and sometimes overlooked” member of the care team. It recommends psychosocial education, practical support, and training for the caregiver to improve the patient’s balance, activity level, and overall quality of life.
Opportunity for prevention?
The guideline also suggests there may be an opportunity to prevent ICH in some people through neuroimaging markers.
While neuroimaging is not routinely performed as a part of risk stratification for primary ICH risk, damage to small blood vessels that is associated with ICH may be evident on MRI that could signal future ICH risk, the guideline says.
“We added to the guidelines for the first time a section on mostly imaging markers of risk for having a first-ever hemorrhage,” Dr. Greenberg said in an interview.
“We don’t make any recommendations as to how to act on these markers because there is a knowledge gap. The hope is that we’ll see growth in our ability to predict first-ever hemorrhage and be able to do things to prevent first-ever hemorrhage,” he said.
“We believe the wide range of knowledge set forth in the new guideline will translate into meaningful improvements in ICH care,” Dr. Greenberg adds in the release.
The updated guideline has been endorsed by the American Association of Neurological Surgeons and Congress of Neurological Surgeons, the Society of Vascular and Interventional Neurology, and the Neurocritical Care Society. The American Academy of Neurology has affirmed the value of this statement as an educational tool for neurologists.
This research had no commercial funding. Dr. Greenberg has disclosed no relevant financial relationships. A complete list of disclosures for the guideline group is available with the original article.
A version of this article first appeared on Medscape.com.
Many strategies widely considered “standard care” for managing spontaneous intracerebral hemorrhage (ICH) are not as effective as previously thought and are no longer recommended in updated guidelines from the American Heart Association/American Stroke Association (ASA).
Compression stockings, antiseizure medication, and steroid treatment are among the treatments with uncertain effectiveness, the writing group says.
The 2022 Guideline for the Management of Patients With Spontaneous ICH was published online in Stroke. The 80-page document contains major changes and refinements to the 2015 guideline on ICH management.
“Advances have been made in an array of fields related to ICH, including the organization of regional health care systems, reversal of the negative effects of blood thinners, minimally invasive surgical procedures, and the underlying disease in small blood vessels,” Steven M. Greenberg, MD, PhD, chair of the guideline writing group with Harvard Medical School and Massachusetts General Hospital, both in Boston, said in a news release.
“We’ve updated sections across the board. There’s probably no area that went untouched with some tweaking and new evidence added that led to some changes in level of evidence or strength of a recommendation,” Dr. Greenberg added in an interview with this news organization.
“Each section comes with knowledge gaps, and it wasn’t hard to come up with knowledge gaps in every section,” Dr. Greenberg acknowledged.
Time-honored treatments no more?
Among the key updates are changes to some “time-honored” treatments that continue to be used with some “regularity” for patients with ICH, yet appear to confer either no benefit or harm, Dr. Greenberg said.
For example, for emergency or critical care treatment of ICH, prophylactic corticosteroids or continuous hyperosmolar therapy is not recommended, because it appears to have no benefit for outcome, while use of platelet transfusions outside the setting of emergency surgery or severe thrombocytopenia appears to worsen outcome, the authors say.
Use of graduated knee- or thigh-high compression stockings alone is not an effective prophylactic therapy for prevention of deep vein thrombosis (DVT). Instead, intermittent pneumatic compression (IPC) starting on the day of diagnosis is now recommended for DVT prophylaxis.
“This is an area where we still have a lot of exploration to do. It is unclear whether even specialized compression devices reduce the risks of deep vein thrombosis or improve the overall health of people with a brain bleed,” Dr. Greenberg said in the release.
The new guidance advises against use of antiseizure or antidepressant medications for ICH patients in whom there is no evidence of seizures or depression.
In clinical trials, antiseizure medication did not contribute to improvements in functionality or long-term seizure control, and the use of antidepressants increased the chance of bone fractures, the authors say.
The guideline also provides updated recommendations for acute reversal of anticoagulation after ICH. It highlights the use of protein complex concentrate for reversal of vitamin K antagonists, such as warfarin; idarucizumab for reversal of the thrombin inhibitor dabigatran; and andexanet alfa for reversal of factor Xa inhibitors, such as rivaroxaban, apixaban, and edoxaban.
For acute blood pressure lowering after mild to moderate ICH, treatment regimens that limit blood pressure variability and achieve smooth, sustained blood pressure control appear to reduce hematoma expansion and yield better functional outcome, the guideline says.
It also notes that minimally invasive approaches for hematoma evacuation, compared with medical management alone‚ have been shown to reduce mortality.
For patients with cerebellar hemorrhage, indications for immediate surgical evacuation with or without an external ventricular drain to reduce mortality now include larger volume (> 15 mL) in addition to previously recommended indications of neurologic deterioration, brainstem compression, and hydrocephalus, the authors note.
However, a “major knowledge gap is whether we can improve functional outcome with hematoma evacuation,” Dr. Greenberg said.
Multidisciplinary care
For rehabilitation after ICH, the guideline reinforces the importance of having a multidisciplinary team to develop a comprehensive plan for recovery.
Starting rehabilitation activities such as stretching and functional task training may be considered 24 to 48 hours following mild or moderate ICH. However, early aggressive mobilization within the first 24 hours has been linked to an increased risk of death within 14 days after an ICH, the guideline says.
Knowledge gaps include how soon it’s safe to return to work, drive, and participate in other social engagements. Recommendations on sexual activity and exercise levels that are safe after a stroke are also needed.
“People need additional help with these lifestyle changes, whether it’s moving around more, curbing their alcohol use, or eating healthier foods. This all happens after they leave the hospital, and we need to be sure we are empowering families with the information they may need to be properly supportive,” Dr. Greenberg says in the release.
The guideline points to the patient’s home caregiver as a “key and sometimes overlooked” member of the care team. It recommends psychosocial education, practical support, and training for the caregiver to improve the patient’s balance, activity level, and overall quality of life.
Opportunity for prevention?
The guideline also suggests there may be an opportunity to prevent ICH in some people through neuroimaging markers.
While neuroimaging is not routinely performed as a part of risk stratification for primary ICH risk, damage to small blood vessels that is associated with ICH may be evident on MRI that could signal future ICH risk, the guideline says.
“We added to the guidelines for the first time a section on mostly imaging markers of risk for having a first-ever hemorrhage,” Dr. Greenberg said in an interview.
“We don’t make any recommendations as to how to act on these markers because there is a knowledge gap. The hope is that we’ll see growth in our ability to predict first-ever hemorrhage and be able to do things to prevent first-ever hemorrhage,” he said.
“We believe the wide range of knowledge set forth in the new guideline will translate into meaningful improvements in ICH care,” Dr. Greenberg adds in the release.
The updated guideline has been endorsed by the American Association of Neurological Surgeons and Congress of Neurological Surgeons, the Society of Vascular and Interventional Neurology, and the Neurocritical Care Society. The American Academy of Neurology has affirmed the value of this statement as an educational tool for neurologists.
This research had no commercial funding. Dr. Greenberg has disclosed no relevant financial relationships. A complete list of disclosures for the guideline group is available with the original article.
A version of this article first appeared on Medscape.com.
Cancer patients unaware of their increased thrombosis risk
It is up to their physician to discuss this with them.
This link is explained by the authors of an article in Cancer Treatment and Research Communications that reports results of a survey carried out by the European Cancer Patient Coalition (ECPC). “The aim of this pan-European patient survey was to assess patient awareness and knowledge about cancer-associated thrombosis (CAT), including risk factors, signs and symptoms, and interventions, to better prevent and treat CAT,” write the authors. “The idea was to create a sort of starting point for subsequent communication and information strategies and for comparing the results of any action taken in this area,” they add.
A roundtable discussion that included oncology healthcare professionals, policymakers, and patient advocates was convened to discuss and review the evidence regarding their ongoing concerns of excessive CAT-associated morbidity and mortality, as well as patients’ desire for greater CAT awareness.
“These discussions demonstrated that very little change had occurred over the years and that greater knowledge about CAT was still needed across the spectrum of healthcare practitioners and patients, particularly regarding primary and secondary prevention of thrombosis,” the authors write.
It was from this starting point that the idea for the pan-European survey was born. The ECPC, widely viewed as the “unified voice of cancer patients across Europe,” led the survey. This survey spanned six countries (France, Germany, Greece, Italy, United Kingdom, and Spain) and involved 1,365 patients and caregivers. The ECPC survey result was originally released at World Thrombosis Day in late 2018.
In an interview, Anna Falanga, MD, the main author of the article and professor of hematology at the University of Milan-Bicocca, Italy, reviewed the results and explained how to improve knowledge of CAT among patients with cancer.
“Data support that up to 20% of patients with cancer will experience venous thromboembolism (VTE), which is approximately 4–5 times higher than the general population,” said Dr. Falanga, who is also chief of the department of immunohematology and transfusion medicine and the Thrombosis and Hemostasis Center at the Hospital Papa Giovanni XXIII, in Bergamo, Italy.
“We have known about the link between thrombosis and cancer since the 19th century, but it has taken until midway through the last century for our level of understanding and awareness of the problem to reach its current level. Initially, this was limited to fundamental research, with large advances in our understanding of the mechanisms of the link between the two; it has only been more recently that we have had clinical studies that have piqued the interest of healthcare professionals, who were previously uninterested in the topic,” she said.
Poor understanding
One piece of data stands out from the European survey: Nearly three quarters of respondents (72%) said that before taking part in the survey, they were not aware that people with cancer have a higher-than-normal risk of developing thrombosis. “We asked participants to rate their overall understanding of CAT on a scale of 1 (low) to 10 (high), with the average (mean) score obtained being 4.1. Only 21% of patients gave a rating of 7 or above (high understanding). The average rating was very similar in the different countries surveyed,” write the authors. They note that the survey also assessed how much participants had learned about the topic from their physicians.
Approximately 35% of patients were made aware of CAT either immediately before or at the time of their cancer diagnosis. Of particular concern, one quarter (26%) of respondents (the largest proportion) noted that they first became aware of CAT when they suffered a blood clot. The average rating was very similar in the different countries surveyed. “Let us not forget that cancer and cancer treatments themselves cause a number of side effects, some of which can be very serious, so in some ways, a clot might be seen as a minor problem. Yet, in reality, it isn’t. It is a significant cause of death and disease in cancer patients,” said Dr. Falanga.
When discussing prevention, most respondents (87%) said they were aware that taking a walk could reduce their risk. Slightly fewer were aware that stopping smoking could reduce their risk (75%), and even fewer were aware that keeping hydrated (63%) and stretching their legs (55%) could reduce their risk.
Symptoms of CAT appeared to be relatively well known; 73% of survey participants indicated that they were aware that swelling in the foot, ankle, or leg could be a sign of DVT, and 71% indicated that shortness of breath could be a sign of pulmonary embolism (PE). “Other symptoms, however, were less well known, with just over half (57%) of participants being aware that pain, cramping, and tenderness could be a sign of DVT. About one third (33%) knew that irregular heartbeat could be a sign of PE. These results varied between countries,” according to the authors.
The survey highlighted that just over a third of respondents said that they were currently using anticoagulants, although almost all (96%) knew that anticoagulants could be used to effectively treat thrombosis. Only 41% of those using anticoagulants said they had been told about any possible side effects.
The Italian situation
The report containing the full results of the European survey goes even further, since, in addition to its overall results, it also gives information about individual countries.
The data from Italy, which are based on 246 persons, show that only 27% of patients and caregivers were aware of the increased risk of thrombosis after a cancer diagnosis. This figure is in line with the overall results of the survey, although the average score of the 10-point scale was lower for the Italy cohort (3.3/10 vs 4.1/10).
The results are more variable in terms of knowledge of risk factors. Most respondents (89%) said that they were aware of the risks related to inactivity. Just over half (52%), however, said that they were aware of the risks related to radiotherapy. Nevertheless, 75% of participants knew about the risks relating to cancer surgery and chemotherapy. “To all intents and purposes, all types of cancer drug can significantly affect the risk of developing a clot. And this is also the case for more modern types of treatment, such as immunotherapy,” said Dr. Falanga.
Most respondents reported that they got information about cancer-associated thrombosis verbally, usually from their hospital doctor (11%). Some respondents (6%) said that they found out about it from their own research, usually online. Almost 1 in 4 patients (24%) in Italy said that they first became aware of CAT when they suffered a blood clot. Answers to questions about knowledge of symptoms show that 58% of Italian patients and caregivers know that swelling of the lower limbs can be a symptom of DVT, and the same percentage knows that shortness of breath might indicate PE.
In terms of preventive action, the picture in Italy is somewhat variable: 74% of participants were aware of the importance of walking, but far fewer knew about the need to stop smoking (57%) and stretch the legs (35%). Of the 41% of Italians who were also taking an anticoagulant drug, 53% said that they knew about the possible side effects of such medication.
Which way forward?
“The high rate of CAT suggests that, despite the clinical evidence and clear guideline recommendations for patients with cancer, CAT prevention and recognition remain low among healthcare professionals,” the authors write.
The results of the ECPC survey further confirm those of previous studies, highlighting patients’ lack of knowledge about CAT and the need for more in-depth discussions between physician and patient.
So, what can be done? As highlighted by previous studies, “patients’ experiences are an education in themselves, particularly for the oncology care team,” the authors write. “Once the patient has a thrombosis, the opportunity for thrombosis prevention, which should be the most crucial focus of the care clinics (surgical, oncology, and palliative care), is gone,” they add.
“Oncology professionals, as well as other members of the patient’s care team (eg, internists, surgeons, nurses), need to perform better, at every stage of the patient’s cancer pathway, to ensure patients are aware of CAT and their individual risk to develop a blood clot,” said Dr. Falanga. She explained that in this group, it is the general practitioner who is the first contact. “These professionals are on the front line of the battle; they are among the first healthcare workers given the chance to suspect a clot and should, therefore, be fully aware of the increased risk in oncology patients,” she reiterated.
Experts agree on the fact that a multidisciplinary approach is of utmost importance in this context: the different roles in the team must be clear. “It is also fundamental to establish who does what in terms of educating and informing the patient,” said Dr. Falanga.
The researchers also put forward an example of a successful initiative: the Venous Thromboembolism Prevention in the Ambulatory Cancer Clinic (VTE-PACC) program. The initiative was developed by experts from the University of Vermont and was described in a recent article in JCO Oncology Practice.
Numerous resources are available online to help physicians talk to their patients and explain the risks linked to CAT along the continuum of cancer care. Among them is a resource titled, “Cancer Associated Thrombosis (CAT): Be Clot Conscious,” which can be found on the ECPC’s website.
“We have a collective responsibility using the ECPC patient survey as a baseline to inform patients with cancer on how to identify signs and symptoms of CAT to enable faster diagnosis and treatment,” the authors conclude.
This article was translated from Univadis Italy.
It is up to their physician to discuss this with them.
This link is explained by the authors of an article in Cancer Treatment and Research Communications that reports results of a survey carried out by the European Cancer Patient Coalition (ECPC). “The aim of this pan-European patient survey was to assess patient awareness and knowledge about cancer-associated thrombosis (CAT), including risk factors, signs and symptoms, and interventions, to better prevent and treat CAT,” write the authors. “The idea was to create a sort of starting point for subsequent communication and information strategies and for comparing the results of any action taken in this area,” they add.
A roundtable discussion that included oncology healthcare professionals, policymakers, and patient advocates was convened to discuss and review the evidence regarding their ongoing concerns of excessive CAT-associated morbidity and mortality, as well as patients’ desire for greater CAT awareness.
“These discussions demonstrated that very little change had occurred over the years and that greater knowledge about CAT was still needed across the spectrum of healthcare practitioners and patients, particularly regarding primary and secondary prevention of thrombosis,” the authors write.
It was from this starting point that the idea for the pan-European survey was born. The ECPC, widely viewed as the “unified voice of cancer patients across Europe,” led the survey. This survey spanned six countries (France, Germany, Greece, Italy, United Kingdom, and Spain) and involved 1,365 patients and caregivers. The ECPC survey result was originally released at World Thrombosis Day in late 2018.
In an interview, Anna Falanga, MD, the main author of the article and professor of hematology at the University of Milan-Bicocca, Italy, reviewed the results and explained how to improve knowledge of CAT among patients with cancer.
“Data support that up to 20% of patients with cancer will experience venous thromboembolism (VTE), which is approximately 4–5 times higher than the general population,” said Dr. Falanga, who is also chief of the department of immunohematology and transfusion medicine and the Thrombosis and Hemostasis Center at the Hospital Papa Giovanni XXIII, in Bergamo, Italy.
“We have known about the link between thrombosis and cancer since the 19th century, but it has taken until midway through the last century for our level of understanding and awareness of the problem to reach its current level. Initially, this was limited to fundamental research, with large advances in our understanding of the mechanisms of the link between the two; it has only been more recently that we have had clinical studies that have piqued the interest of healthcare professionals, who were previously uninterested in the topic,” she said.
Poor understanding
One piece of data stands out from the European survey: Nearly three quarters of respondents (72%) said that before taking part in the survey, they were not aware that people with cancer have a higher-than-normal risk of developing thrombosis. “We asked participants to rate their overall understanding of CAT on a scale of 1 (low) to 10 (high), with the average (mean) score obtained being 4.1. Only 21% of patients gave a rating of 7 or above (high understanding). The average rating was very similar in the different countries surveyed,” write the authors. They note that the survey also assessed how much participants had learned about the topic from their physicians.
Approximately 35% of patients were made aware of CAT either immediately before or at the time of their cancer diagnosis. Of particular concern, one quarter (26%) of respondents (the largest proportion) noted that they first became aware of CAT when they suffered a blood clot. The average rating was very similar in the different countries surveyed. “Let us not forget that cancer and cancer treatments themselves cause a number of side effects, some of which can be very serious, so in some ways, a clot might be seen as a minor problem. Yet, in reality, it isn’t. It is a significant cause of death and disease in cancer patients,” said Dr. Falanga.
When discussing prevention, most respondents (87%) said they were aware that taking a walk could reduce their risk. Slightly fewer were aware that stopping smoking could reduce their risk (75%), and even fewer were aware that keeping hydrated (63%) and stretching their legs (55%) could reduce their risk.
Symptoms of CAT appeared to be relatively well known; 73% of survey participants indicated that they were aware that swelling in the foot, ankle, or leg could be a sign of DVT, and 71% indicated that shortness of breath could be a sign of pulmonary embolism (PE). “Other symptoms, however, were less well known, with just over half (57%) of participants being aware that pain, cramping, and tenderness could be a sign of DVT. About one third (33%) knew that irregular heartbeat could be a sign of PE. These results varied between countries,” according to the authors.
The survey highlighted that just over a third of respondents said that they were currently using anticoagulants, although almost all (96%) knew that anticoagulants could be used to effectively treat thrombosis. Only 41% of those using anticoagulants said they had been told about any possible side effects.
The Italian situation
The report containing the full results of the European survey goes even further, since, in addition to its overall results, it also gives information about individual countries.
The data from Italy, which are based on 246 persons, show that only 27% of patients and caregivers were aware of the increased risk of thrombosis after a cancer diagnosis. This figure is in line with the overall results of the survey, although the average score of the 10-point scale was lower for the Italy cohort (3.3/10 vs 4.1/10).
The results are more variable in terms of knowledge of risk factors. Most respondents (89%) said that they were aware of the risks related to inactivity. Just over half (52%), however, said that they were aware of the risks related to radiotherapy. Nevertheless, 75% of participants knew about the risks relating to cancer surgery and chemotherapy. “To all intents and purposes, all types of cancer drug can significantly affect the risk of developing a clot. And this is also the case for more modern types of treatment, such as immunotherapy,” said Dr. Falanga.
Most respondents reported that they got information about cancer-associated thrombosis verbally, usually from their hospital doctor (11%). Some respondents (6%) said that they found out about it from their own research, usually online. Almost 1 in 4 patients (24%) in Italy said that they first became aware of CAT when they suffered a blood clot. Answers to questions about knowledge of symptoms show that 58% of Italian patients and caregivers know that swelling of the lower limbs can be a symptom of DVT, and the same percentage knows that shortness of breath might indicate PE.
In terms of preventive action, the picture in Italy is somewhat variable: 74% of participants were aware of the importance of walking, but far fewer knew about the need to stop smoking (57%) and stretch the legs (35%). Of the 41% of Italians who were also taking an anticoagulant drug, 53% said that they knew about the possible side effects of such medication.
Which way forward?
“The high rate of CAT suggests that, despite the clinical evidence and clear guideline recommendations for patients with cancer, CAT prevention and recognition remain low among healthcare professionals,” the authors write.
The results of the ECPC survey further confirm those of previous studies, highlighting patients’ lack of knowledge about CAT and the need for more in-depth discussions between physician and patient.
So, what can be done? As highlighted by previous studies, “patients’ experiences are an education in themselves, particularly for the oncology care team,” the authors write. “Once the patient has a thrombosis, the opportunity for thrombosis prevention, which should be the most crucial focus of the care clinics (surgical, oncology, and palliative care), is gone,” they add.
“Oncology professionals, as well as other members of the patient’s care team (eg, internists, surgeons, nurses), need to perform better, at every stage of the patient’s cancer pathway, to ensure patients are aware of CAT and their individual risk to develop a blood clot,” said Dr. Falanga. She explained that in this group, it is the general practitioner who is the first contact. “These professionals are on the front line of the battle; they are among the first healthcare workers given the chance to suspect a clot and should, therefore, be fully aware of the increased risk in oncology patients,” she reiterated.
Experts agree on the fact that a multidisciplinary approach is of utmost importance in this context: the different roles in the team must be clear. “It is also fundamental to establish who does what in terms of educating and informing the patient,” said Dr. Falanga.
The researchers also put forward an example of a successful initiative: the Venous Thromboembolism Prevention in the Ambulatory Cancer Clinic (VTE-PACC) program. The initiative was developed by experts from the University of Vermont and was described in a recent article in JCO Oncology Practice.
Numerous resources are available online to help physicians talk to their patients and explain the risks linked to CAT along the continuum of cancer care. Among them is a resource titled, “Cancer Associated Thrombosis (CAT): Be Clot Conscious,” which can be found on the ECPC’s website.
“We have a collective responsibility using the ECPC patient survey as a baseline to inform patients with cancer on how to identify signs and symptoms of CAT to enable faster diagnosis and treatment,” the authors conclude.
This article was translated from Univadis Italy.
It is up to their physician to discuss this with them.
This link is explained by the authors of an article in Cancer Treatment and Research Communications that reports results of a survey carried out by the European Cancer Patient Coalition (ECPC). “The aim of this pan-European patient survey was to assess patient awareness and knowledge about cancer-associated thrombosis (CAT), including risk factors, signs and symptoms, and interventions, to better prevent and treat CAT,” write the authors. “The idea was to create a sort of starting point for subsequent communication and information strategies and for comparing the results of any action taken in this area,” they add.
A roundtable discussion that included oncology healthcare professionals, policymakers, and patient advocates was convened to discuss and review the evidence regarding their ongoing concerns of excessive CAT-associated morbidity and mortality, as well as patients’ desire for greater CAT awareness.
“These discussions demonstrated that very little change had occurred over the years and that greater knowledge about CAT was still needed across the spectrum of healthcare practitioners and patients, particularly regarding primary and secondary prevention of thrombosis,” the authors write.
It was from this starting point that the idea for the pan-European survey was born. The ECPC, widely viewed as the “unified voice of cancer patients across Europe,” led the survey. This survey spanned six countries (France, Germany, Greece, Italy, United Kingdom, and Spain) and involved 1,365 patients and caregivers. The ECPC survey result was originally released at World Thrombosis Day in late 2018.
In an interview, Anna Falanga, MD, the main author of the article and professor of hematology at the University of Milan-Bicocca, Italy, reviewed the results and explained how to improve knowledge of CAT among patients with cancer.
“Data support that up to 20% of patients with cancer will experience venous thromboembolism (VTE), which is approximately 4–5 times higher than the general population,” said Dr. Falanga, who is also chief of the department of immunohematology and transfusion medicine and the Thrombosis and Hemostasis Center at the Hospital Papa Giovanni XXIII, in Bergamo, Italy.
“We have known about the link between thrombosis and cancer since the 19th century, but it has taken until midway through the last century for our level of understanding and awareness of the problem to reach its current level. Initially, this was limited to fundamental research, with large advances in our understanding of the mechanisms of the link between the two; it has only been more recently that we have had clinical studies that have piqued the interest of healthcare professionals, who were previously uninterested in the topic,” she said.
Poor understanding
One piece of data stands out from the European survey: Nearly three quarters of respondents (72%) said that before taking part in the survey, they were not aware that people with cancer have a higher-than-normal risk of developing thrombosis. “We asked participants to rate their overall understanding of CAT on a scale of 1 (low) to 10 (high), with the average (mean) score obtained being 4.1. Only 21% of patients gave a rating of 7 or above (high understanding). The average rating was very similar in the different countries surveyed,” write the authors. They note that the survey also assessed how much participants had learned about the topic from their physicians.
Approximately 35% of patients were made aware of CAT either immediately before or at the time of their cancer diagnosis. Of particular concern, one quarter (26%) of respondents (the largest proportion) noted that they first became aware of CAT when they suffered a blood clot. The average rating was very similar in the different countries surveyed. “Let us not forget that cancer and cancer treatments themselves cause a number of side effects, some of which can be very serious, so in some ways, a clot might be seen as a minor problem. Yet, in reality, it isn’t. It is a significant cause of death and disease in cancer patients,” said Dr. Falanga.
When discussing prevention, most respondents (87%) said they were aware that taking a walk could reduce their risk. Slightly fewer were aware that stopping smoking could reduce their risk (75%), and even fewer were aware that keeping hydrated (63%) and stretching their legs (55%) could reduce their risk.
Symptoms of CAT appeared to be relatively well known; 73% of survey participants indicated that they were aware that swelling in the foot, ankle, or leg could be a sign of DVT, and 71% indicated that shortness of breath could be a sign of pulmonary embolism (PE). “Other symptoms, however, were less well known, with just over half (57%) of participants being aware that pain, cramping, and tenderness could be a sign of DVT. About one third (33%) knew that irregular heartbeat could be a sign of PE. These results varied between countries,” according to the authors.
The survey highlighted that just over a third of respondents said that they were currently using anticoagulants, although almost all (96%) knew that anticoagulants could be used to effectively treat thrombosis. Only 41% of those using anticoagulants said they had been told about any possible side effects.
The Italian situation
The report containing the full results of the European survey goes even further, since, in addition to its overall results, it also gives information about individual countries.
The data from Italy, which are based on 246 persons, show that only 27% of patients and caregivers were aware of the increased risk of thrombosis after a cancer diagnosis. This figure is in line with the overall results of the survey, although the average score of the 10-point scale was lower for the Italy cohort (3.3/10 vs 4.1/10).
The results are more variable in terms of knowledge of risk factors. Most respondents (89%) said that they were aware of the risks related to inactivity. Just over half (52%), however, said that they were aware of the risks related to radiotherapy. Nevertheless, 75% of participants knew about the risks relating to cancer surgery and chemotherapy. “To all intents and purposes, all types of cancer drug can significantly affect the risk of developing a clot. And this is also the case for more modern types of treatment, such as immunotherapy,” said Dr. Falanga.
Most respondents reported that they got information about cancer-associated thrombosis verbally, usually from their hospital doctor (11%). Some respondents (6%) said that they found out about it from their own research, usually online. Almost 1 in 4 patients (24%) in Italy said that they first became aware of CAT when they suffered a blood clot. Answers to questions about knowledge of symptoms show that 58% of Italian patients and caregivers know that swelling of the lower limbs can be a symptom of DVT, and the same percentage knows that shortness of breath might indicate PE.
In terms of preventive action, the picture in Italy is somewhat variable: 74% of participants were aware of the importance of walking, but far fewer knew about the need to stop smoking (57%) and stretch the legs (35%). Of the 41% of Italians who were also taking an anticoagulant drug, 53% said that they knew about the possible side effects of such medication.
Which way forward?
“The high rate of CAT suggests that, despite the clinical evidence and clear guideline recommendations for patients with cancer, CAT prevention and recognition remain low among healthcare professionals,” the authors write.
The results of the ECPC survey further confirm those of previous studies, highlighting patients’ lack of knowledge about CAT and the need for more in-depth discussions between physician and patient.
So, what can be done? As highlighted by previous studies, “patients’ experiences are an education in themselves, particularly for the oncology care team,” the authors write. “Once the patient has a thrombosis, the opportunity for thrombosis prevention, which should be the most crucial focus of the care clinics (surgical, oncology, and palliative care), is gone,” they add.
“Oncology professionals, as well as other members of the patient’s care team (eg, internists, surgeons, nurses), need to perform better, at every stage of the patient’s cancer pathway, to ensure patients are aware of CAT and their individual risk to develop a blood clot,” said Dr. Falanga. She explained that in this group, it is the general practitioner who is the first contact. “These professionals are on the front line of the battle; they are among the first healthcare workers given the chance to suspect a clot and should, therefore, be fully aware of the increased risk in oncology patients,” she reiterated.
Experts agree on the fact that a multidisciplinary approach is of utmost importance in this context: the different roles in the team must be clear. “It is also fundamental to establish who does what in terms of educating and informing the patient,” said Dr. Falanga.
The researchers also put forward an example of a successful initiative: the Venous Thromboembolism Prevention in the Ambulatory Cancer Clinic (VTE-PACC) program. The initiative was developed by experts from the University of Vermont and was described in a recent article in JCO Oncology Practice.
Numerous resources are available online to help physicians talk to their patients and explain the risks linked to CAT along the continuum of cancer care. Among them is a resource titled, “Cancer Associated Thrombosis (CAT): Be Clot Conscious,” which can be found on the ECPC’s website.
“We have a collective responsibility using the ECPC patient survey as a baseline to inform patients with cancer on how to identify signs and symptoms of CAT to enable faster diagnosis and treatment,” the authors conclude.
This article was translated from Univadis Italy.
FROM CANCER TREATMENT AND RESEARCH COMMUNICATIONS
Novel COVID-19 vaccine could fill the void for patients with blood cancers
according to study results presented at the annual meeting of the American Association for Cancer Research.
The phase 1/2 trial included 54 patients with a B-cell deficiency (mean age, 63 years; 28% female): 4 had congenital B-cell deficiency and 50 had a blood cancer (lymphocytic leukemia or lymphoma). T-cell immune responses were observed in 86% of patients 28 days after vaccination with a single CoVac-1 dose. The potency of CoVac-1–induced T-cell responses exceeded those seen typically with B cell–deficient patient responses after mRNA vaccine treatment and were comparable with those seen among nonimmunocompromised COVID-19 patients.
In the majority of individuals, currently approved SARS-CoV-2 vaccines induce a robust immune response, however, their efficacy, has been shown to be decreased among individuals who are immunocompromised. Patients treated for hematologic cancers, in particular, receive treatment regimens that damage healthy immune cells, particularly B cells, said Juliane Walz, MD, the study’s senior author and professor of medicine at University Hospital Tübingen (Germany).
“In the clinic, we see many cancer patients who do not mount sufficient humoral immune responses after vaccination with available SARS-CoV-2 vaccines,” Dr. Walz said. “These patients are at a high risk for a severe course of COVID-19.”
B-cell deficiency, she stated, can be compensated for by enhancing T-cell responses against SARS-CoV-2, which can then combat infections in the absence of neutralizing antibodies.
In a prior study of CoVac-1 among 36 adults without immune deficiency, the vaccine elicited T-cell responses that were still robust 3 months post vaccination, and that included responses against omicron and other key SARS-CoV-2 variants.
While mRNA-based or adenoviral vector-based vaccines are limited to the spike protein and are thus prone to loss of activity because of viral mutations, CoVac-1–induced T-cell immunity is far more intense and broader, Dr. Walz said.
CoVac-1 is a peptide vaccine that is injected directly rather than being encoded via mRNA and targets different viral components. It would not be given, however, to healthy, immunocompetent adults because it is important for them to have both B-cell antibody and T-cell response.
The patients with B-cell deficiency recruited for the study were given a single dose of CoVac-1 and assessed for safety and immunogenicity until day 56. Prior vaccinations with an approved SARS-CoV-2 vaccine had failed to elicit a humoral response in 87% of the subjects.
“Our vaccine does not induce antibody responses,” Dr. Walz said. “However, it could be used to induce broad T-cell responses as a complementary or additive vaccine for elderly adults. In the elderly, antibody responses decline very, very fast after vaccination.”
Dr. Walz said that CoVac-1 could find application in various syndromes associated with congenital B-cell deficiencies, in autoimmune diseases such as rheumatoid arthritis and multiple sclerosis, or diseases treated with rituximab or other B cell–depleting therapies (for example, ofatumumab, blinatumomab, or chimeric antigen receptor T cells), and in transplant patients.
A phase 3 study of CoVac-1 versus placebo is under discussion and would require about 300-500 subjects, Dr. Walz said.
“CoVac-1 is designed to induce broad and long-lasting SARS-CoV-2 T-cell immunity, even in individuals who have impaired ability to mount sufficient immunity from a currently approved vaccine, and thus protect these high-risk patients from a severe course of COVID-19,” Dr. Walz said.
“Having an option for these patients is just critical – so this is significant work,” said Ana Maria Lopez, MD, MPH, of the Sidney Kimmel Cancer Center–Jefferson Health, Philadelphia.
Limitations of this study included the small sample size with low racial and ethnic diversity, Dr. Walz stated.
Funding was provided by the Ministry of Science, Research and the Arts of the state of Baden-Württemberg; the Federal Ministry of Research and Education in Germany; the German Research Foundation under Germany’s Excellence Strategy; and the Clinical Cooperation Unit Translational Immunology at University Hospital Tübingen. Dr. Walz holds the CoVac-1 patent.
according to study results presented at the annual meeting of the American Association for Cancer Research.
The phase 1/2 trial included 54 patients with a B-cell deficiency (mean age, 63 years; 28% female): 4 had congenital B-cell deficiency and 50 had a blood cancer (lymphocytic leukemia or lymphoma). T-cell immune responses were observed in 86% of patients 28 days after vaccination with a single CoVac-1 dose. The potency of CoVac-1–induced T-cell responses exceeded those seen typically with B cell–deficient patient responses after mRNA vaccine treatment and were comparable with those seen among nonimmunocompromised COVID-19 patients.
In the majority of individuals, currently approved SARS-CoV-2 vaccines induce a robust immune response, however, their efficacy, has been shown to be decreased among individuals who are immunocompromised. Patients treated for hematologic cancers, in particular, receive treatment regimens that damage healthy immune cells, particularly B cells, said Juliane Walz, MD, the study’s senior author and professor of medicine at University Hospital Tübingen (Germany).
“In the clinic, we see many cancer patients who do not mount sufficient humoral immune responses after vaccination with available SARS-CoV-2 vaccines,” Dr. Walz said. “These patients are at a high risk for a severe course of COVID-19.”
B-cell deficiency, she stated, can be compensated for by enhancing T-cell responses against SARS-CoV-2, which can then combat infections in the absence of neutralizing antibodies.
In a prior study of CoVac-1 among 36 adults without immune deficiency, the vaccine elicited T-cell responses that were still robust 3 months post vaccination, and that included responses against omicron and other key SARS-CoV-2 variants.
While mRNA-based or adenoviral vector-based vaccines are limited to the spike protein and are thus prone to loss of activity because of viral mutations, CoVac-1–induced T-cell immunity is far more intense and broader, Dr. Walz said.
CoVac-1 is a peptide vaccine that is injected directly rather than being encoded via mRNA and targets different viral components. It would not be given, however, to healthy, immunocompetent adults because it is important for them to have both B-cell antibody and T-cell response.
The patients with B-cell deficiency recruited for the study were given a single dose of CoVac-1 and assessed for safety and immunogenicity until day 56. Prior vaccinations with an approved SARS-CoV-2 vaccine had failed to elicit a humoral response in 87% of the subjects.
“Our vaccine does not induce antibody responses,” Dr. Walz said. “However, it could be used to induce broad T-cell responses as a complementary or additive vaccine for elderly adults. In the elderly, antibody responses decline very, very fast after vaccination.”
Dr. Walz said that CoVac-1 could find application in various syndromes associated with congenital B-cell deficiencies, in autoimmune diseases such as rheumatoid arthritis and multiple sclerosis, or diseases treated with rituximab or other B cell–depleting therapies (for example, ofatumumab, blinatumomab, or chimeric antigen receptor T cells), and in transplant patients.
A phase 3 study of CoVac-1 versus placebo is under discussion and would require about 300-500 subjects, Dr. Walz said.
“CoVac-1 is designed to induce broad and long-lasting SARS-CoV-2 T-cell immunity, even in individuals who have impaired ability to mount sufficient immunity from a currently approved vaccine, and thus protect these high-risk patients from a severe course of COVID-19,” Dr. Walz said.
“Having an option for these patients is just critical – so this is significant work,” said Ana Maria Lopez, MD, MPH, of the Sidney Kimmel Cancer Center–Jefferson Health, Philadelphia.
Limitations of this study included the small sample size with low racial and ethnic diversity, Dr. Walz stated.
Funding was provided by the Ministry of Science, Research and the Arts of the state of Baden-Württemberg; the Federal Ministry of Research and Education in Germany; the German Research Foundation under Germany’s Excellence Strategy; and the Clinical Cooperation Unit Translational Immunology at University Hospital Tübingen. Dr. Walz holds the CoVac-1 patent.
according to study results presented at the annual meeting of the American Association for Cancer Research.
The phase 1/2 trial included 54 patients with a B-cell deficiency (mean age, 63 years; 28% female): 4 had congenital B-cell deficiency and 50 had a blood cancer (lymphocytic leukemia or lymphoma). T-cell immune responses were observed in 86% of patients 28 days after vaccination with a single CoVac-1 dose. The potency of CoVac-1–induced T-cell responses exceeded those seen typically with B cell–deficient patient responses after mRNA vaccine treatment and were comparable with those seen among nonimmunocompromised COVID-19 patients.
In the majority of individuals, currently approved SARS-CoV-2 vaccines induce a robust immune response, however, their efficacy, has been shown to be decreased among individuals who are immunocompromised. Patients treated for hematologic cancers, in particular, receive treatment regimens that damage healthy immune cells, particularly B cells, said Juliane Walz, MD, the study’s senior author and professor of medicine at University Hospital Tübingen (Germany).
“In the clinic, we see many cancer patients who do not mount sufficient humoral immune responses after vaccination with available SARS-CoV-2 vaccines,” Dr. Walz said. “These patients are at a high risk for a severe course of COVID-19.”
B-cell deficiency, she stated, can be compensated for by enhancing T-cell responses against SARS-CoV-2, which can then combat infections in the absence of neutralizing antibodies.
In a prior study of CoVac-1 among 36 adults without immune deficiency, the vaccine elicited T-cell responses that were still robust 3 months post vaccination, and that included responses against omicron and other key SARS-CoV-2 variants.
While mRNA-based or adenoviral vector-based vaccines are limited to the spike protein and are thus prone to loss of activity because of viral mutations, CoVac-1–induced T-cell immunity is far more intense and broader, Dr. Walz said.
CoVac-1 is a peptide vaccine that is injected directly rather than being encoded via mRNA and targets different viral components. It would not be given, however, to healthy, immunocompetent adults because it is important for them to have both B-cell antibody and T-cell response.
The patients with B-cell deficiency recruited for the study were given a single dose of CoVac-1 and assessed for safety and immunogenicity until day 56. Prior vaccinations with an approved SARS-CoV-2 vaccine had failed to elicit a humoral response in 87% of the subjects.
“Our vaccine does not induce antibody responses,” Dr. Walz said. “However, it could be used to induce broad T-cell responses as a complementary or additive vaccine for elderly adults. In the elderly, antibody responses decline very, very fast after vaccination.”
Dr. Walz said that CoVac-1 could find application in various syndromes associated with congenital B-cell deficiencies, in autoimmune diseases such as rheumatoid arthritis and multiple sclerosis, or diseases treated with rituximab or other B cell–depleting therapies (for example, ofatumumab, blinatumomab, or chimeric antigen receptor T cells), and in transplant patients.
A phase 3 study of CoVac-1 versus placebo is under discussion and would require about 300-500 subjects, Dr. Walz said.
“CoVac-1 is designed to induce broad and long-lasting SARS-CoV-2 T-cell immunity, even in individuals who have impaired ability to mount sufficient immunity from a currently approved vaccine, and thus protect these high-risk patients from a severe course of COVID-19,” Dr. Walz said.
“Having an option for these patients is just critical – so this is significant work,” said Ana Maria Lopez, MD, MPH, of the Sidney Kimmel Cancer Center–Jefferson Health, Philadelphia.
Limitations of this study included the small sample size with low racial and ethnic diversity, Dr. Walz stated.
Funding was provided by the Ministry of Science, Research and the Arts of the state of Baden-Württemberg; the Federal Ministry of Research and Education in Germany; the German Research Foundation under Germany’s Excellence Strategy; and the Clinical Cooperation Unit Translational Immunology at University Hospital Tübingen. Dr. Walz holds the CoVac-1 patent.
FROM AACR 2022
Rapper sings about living with sickle cell disease
MANCHESTER, ENGLAND – A London-based rapper known for his gospel-inspired music has now given a voice to patients with sickle cell disease. He is using one of his music videos to raise awareness and educate health care professionals about living with the condition.
One important aim of the video, he says, is to help educate health care professionals, some of whom have not come across this condition, he explained at a session during the annual meeting of the British Society for Haematology, held recently in Manchester, England.
“It’s kind of frustrating to feel like your safe space, when you’re in front of doctors and nurses and paramedics who are supposed to know what it is and react with treatment, [and they] don’t know what it is,” Mr. Gaspar said.
He recalled an occasion in which he was experiencing a crisis, and his wife called for an ambulance. The paramedics arrived and his wife asked them for “gas and air and morphine, and they were, like, no, we don’t want to give that to him.” She tried to explain that he has sickle cell disease, but the paramedics had not heard of the condition and were suspicious that the request for morphine was a sign of drug addiction.
Mr. Gaspar expressed his frustration over “constantly having to prove that you have something serious enough to need the treatment you are asking for.”
At the meeting, Mr. Gaspar was talking on the stage with hematologist Dr. Stephen Hibbs from Barts Health NHS Trust, London.
Mr. Gaspar explained that it took years before he eventually reached “a point where I understood that it’s something that affects me and affects many other people, and I didn’t want to hide it any more.”
Sickle cell disease, which occurs primarily in people of Afro-Caribbean background, is a taboo subject in his community, Mr. Gaspar elaborated in an interview.
The condition has been associated with a great deal of stigma, with young sufferers traditionally seen as “demonically possessed,” he commented.
“So there was always a shameful aspect around it when it came to African families speaking about it, especially back in Africa.”
But after his parents came to the United Kingdom, he was able to “do his research and understand that it’s just genetics.”
This knowledge, Mr. Gaspar said, “takes away the spiritual aspect” and allows people to “have the conversation about sickle cell with potential partners” and ask them to find out their genotype, which in turn helps to “break down the barriers and the stigma.”
Mr. Gaspar emphasizes that there is much more work still to do.
In the video, he appeals to the Black community to make blood donations.
He said that something that “haunts” him is that currently, only 1% of Black people in the United Kingdom give blood, “so I really want the song to move my community to take a step forward and make that difference.”
He has been in contact with NHS Blood and Transplant, which provides blood and transplantation service to the National Health Service. They “really liked” the song, Mr. Gaspar said, and helped him get access to a hospital ward in University College Hospital, London, for the video.
“I really wanted to make a video that made people uncomfortable when watching it,” he said. It shows him hospitalized for pain and breathlessness and recalling having to use a Zimmer frame at the age of 25.
“This is a side of sickle cell that normally people don’t know,” he said.
Since releasing the song and the video, Mr. Gaspar says he has been contacted by many fellow patients. They have told him that he is now their “voice”; when they are asked how the condition affects them, “they can show someone the Hidden Pain video and say: This is how it feels.”
Clinicians have also approached him, asking if they can show his video to illustrate to patients and their families how having the condition may affect their lives.
Preventable deaths
At the meeting, Dr. Hibbs highlighted the 2021 report No One’s Listening, which was issued by the Sickle Cell Society following an inquiry into avoidable deaths and failures of care for sickle cell patients.
The inquiry, published by an All-Party Parliamentary group, found “serious care failings” in acute services and evidence of attitudes underpinned by racism. There was evidence of substandard care for sickle cell patients who were admitted to general wards or to hospital accident and emergency departments, as well as low awareness of the condition among health care professionals.
The report noted that the care failings have led to patient deaths, some which could have been prevented, and that there have been many “near misses.”
Many patients with sickle cell disease said they are “not being listened to” or are not being understood, especially during that vulnerable period when they are “in a crisis.”
Mr. Gaspar said that the report, and also the deaths, really struck a chord with him and many in his community. “We felt like that was us. ... We’ve all been in that same position where we’ve been misunderstood and not heard by nurses, doctors, or paramedics.”
He emphasized the need for awareness of the condition and the need for timely treatment. Just 3 weeks ago, Mr. Gaspar attended the funeral of one of his friends who is in the Hidden Pain video, a fellow sickle cell disease patient, who died at 30 years of age.
Ignorance about the condition ‘all too common’
The lack of awareness about sickle cell disease, even among health care professionals, is “all too common,” says Dr. Subarna Chakravorty, consultant pediatric hematologist, King’s College Hospital, London.
Even in London, where there is a large Black community and the teaching hospitals have world-class expertise, patients with sickle cell disease are “still facing a lot of problems with knowledge” among health care professionals, she said in an interview.
“Often people are having to speak for their own condition; which is fine, except that sometimes they are not believed,” she commented.
“On the one hand, you rely on the patient to provide information about their disease, and then when you receive it, you don’t do anything about it. So [they’re] between a rock and a hard place.”
Why are sickle cell patients treated in this way?
For Dr. Chakravorty, there is “a lot to be said about racism and disparities” in treating patients “as morphine-seekers, opiate addicts, even in children.”
“So we really need to improve the knowledge and perceptions among nonspecialist staff,” she said, “and even among specialists.”
Mr. Gaspar aims to help with this effort and hopes that his song and video will be useful to health care professionals. Sickle cell disease “needs to be spoken about,” and more doctors and nurses need to “know what it is,” he said.
He said it is a relief to encounter health care professionals who are knowledgeable about his condition. There have been times when he has been “having a crisis at home, calling the ambulance, and the paramedic comes and says: ‘Mr. Gaspar, you have sickle cell...we believe that you usually have gas and air and morphine, is that correct?’”
“That gives me a sense of peace, to know that I don’t have to fight my case or convince someone I have sickle cell, and I need to start treatment. They already know.”
No relevant financial relationships have been disclosed.
A version of this article first appeared on Medscape.com.
MANCHESTER, ENGLAND – A London-based rapper known for his gospel-inspired music has now given a voice to patients with sickle cell disease. He is using one of his music videos to raise awareness and educate health care professionals about living with the condition.
One important aim of the video, he says, is to help educate health care professionals, some of whom have not come across this condition, he explained at a session during the annual meeting of the British Society for Haematology, held recently in Manchester, England.
“It’s kind of frustrating to feel like your safe space, when you’re in front of doctors and nurses and paramedics who are supposed to know what it is and react with treatment, [and they] don’t know what it is,” Mr. Gaspar said.
He recalled an occasion in which he was experiencing a crisis, and his wife called for an ambulance. The paramedics arrived and his wife asked them for “gas and air and morphine, and they were, like, no, we don’t want to give that to him.” She tried to explain that he has sickle cell disease, but the paramedics had not heard of the condition and were suspicious that the request for morphine was a sign of drug addiction.
Mr. Gaspar expressed his frustration over “constantly having to prove that you have something serious enough to need the treatment you are asking for.”
At the meeting, Mr. Gaspar was talking on the stage with hematologist Dr. Stephen Hibbs from Barts Health NHS Trust, London.
Mr. Gaspar explained that it took years before he eventually reached “a point where I understood that it’s something that affects me and affects many other people, and I didn’t want to hide it any more.”
Sickle cell disease, which occurs primarily in people of Afro-Caribbean background, is a taboo subject in his community, Mr. Gaspar elaborated in an interview.
The condition has been associated with a great deal of stigma, with young sufferers traditionally seen as “demonically possessed,” he commented.
“So there was always a shameful aspect around it when it came to African families speaking about it, especially back in Africa.”
But after his parents came to the United Kingdom, he was able to “do his research and understand that it’s just genetics.”
This knowledge, Mr. Gaspar said, “takes away the spiritual aspect” and allows people to “have the conversation about sickle cell with potential partners” and ask them to find out their genotype, which in turn helps to “break down the barriers and the stigma.”
Mr. Gaspar emphasizes that there is much more work still to do.
In the video, he appeals to the Black community to make blood donations.
He said that something that “haunts” him is that currently, only 1% of Black people in the United Kingdom give blood, “so I really want the song to move my community to take a step forward and make that difference.”
He has been in contact with NHS Blood and Transplant, which provides blood and transplantation service to the National Health Service. They “really liked” the song, Mr. Gaspar said, and helped him get access to a hospital ward in University College Hospital, London, for the video.
“I really wanted to make a video that made people uncomfortable when watching it,” he said. It shows him hospitalized for pain and breathlessness and recalling having to use a Zimmer frame at the age of 25.
“This is a side of sickle cell that normally people don’t know,” he said.
Since releasing the song and the video, Mr. Gaspar says he has been contacted by many fellow patients. They have told him that he is now their “voice”; when they are asked how the condition affects them, “they can show someone the Hidden Pain video and say: This is how it feels.”
Clinicians have also approached him, asking if they can show his video to illustrate to patients and their families how having the condition may affect their lives.
Preventable deaths
At the meeting, Dr. Hibbs highlighted the 2021 report No One’s Listening, which was issued by the Sickle Cell Society following an inquiry into avoidable deaths and failures of care for sickle cell patients.
The inquiry, published by an All-Party Parliamentary group, found “serious care failings” in acute services and evidence of attitudes underpinned by racism. There was evidence of substandard care for sickle cell patients who were admitted to general wards or to hospital accident and emergency departments, as well as low awareness of the condition among health care professionals.
The report noted that the care failings have led to patient deaths, some which could have been prevented, and that there have been many “near misses.”
Many patients with sickle cell disease said they are “not being listened to” or are not being understood, especially during that vulnerable period when they are “in a crisis.”
Mr. Gaspar said that the report, and also the deaths, really struck a chord with him and many in his community. “We felt like that was us. ... We’ve all been in that same position where we’ve been misunderstood and not heard by nurses, doctors, or paramedics.”
He emphasized the need for awareness of the condition and the need for timely treatment. Just 3 weeks ago, Mr. Gaspar attended the funeral of one of his friends who is in the Hidden Pain video, a fellow sickle cell disease patient, who died at 30 years of age.
Ignorance about the condition ‘all too common’
The lack of awareness about sickle cell disease, even among health care professionals, is “all too common,” says Dr. Subarna Chakravorty, consultant pediatric hematologist, King’s College Hospital, London.
Even in London, where there is a large Black community and the teaching hospitals have world-class expertise, patients with sickle cell disease are “still facing a lot of problems with knowledge” among health care professionals, she said in an interview.
“Often people are having to speak for their own condition; which is fine, except that sometimes they are not believed,” she commented.
“On the one hand, you rely on the patient to provide information about their disease, and then when you receive it, you don’t do anything about it. So [they’re] between a rock and a hard place.”
Why are sickle cell patients treated in this way?
For Dr. Chakravorty, there is “a lot to be said about racism and disparities” in treating patients “as morphine-seekers, opiate addicts, even in children.”
“So we really need to improve the knowledge and perceptions among nonspecialist staff,” she said, “and even among specialists.”
Mr. Gaspar aims to help with this effort and hopes that his song and video will be useful to health care professionals. Sickle cell disease “needs to be spoken about,” and more doctors and nurses need to “know what it is,” he said.
He said it is a relief to encounter health care professionals who are knowledgeable about his condition. There have been times when he has been “having a crisis at home, calling the ambulance, and the paramedic comes and says: ‘Mr. Gaspar, you have sickle cell...we believe that you usually have gas and air and morphine, is that correct?’”
“That gives me a sense of peace, to know that I don’t have to fight my case or convince someone I have sickle cell, and I need to start treatment. They already know.”
No relevant financial relationships have been disclosed.
A version of this article first appeared on Medscape.com.
MANCHESTER, ENGLAND – A London-based rapper known for his gospel-inspired music has now given a voice to patients with sickle cell disease. He is using one of his music videos to raise awareness and educate health care professionals about living with the condition.
One important aim of the video, he says, is to help educate health care professionals, some of whom have not come across this condition, he explained at a session during the annual meeting of the British Society for Haematology, held recently in Manchester, England.
“It’s kind of frustrating to feel like your safe space, when you’re in front of doctors and nurses and paramedics who are supposed to know what it is and react with treatment, [and they] don’t know what it is,” Mr. Gaspar said.
He recalled an occasion in which he was experiencing a crisis, and his wife called for an ambulance. The paramedics arrived and his wife asked them for “gas and air and morphine, and they were, like, no, we don’t want to give that to him.” She tried to explain that he has sickle cell disease, but the paramedics had not heard of the condition and were suspicious that the request for morphine was a sign of drug addiction.
Mr. Gaspar expressed his frustration over “constantly having to prove that you have something serious enough to need the treatment you are asking for.”
At the meeting, Mr. Gaspar was talking on the stage with hematologist Dr. Stephen Hibbs from Barts Health NHS Trust, London.
Mr. Gaspar explained that it took years before he eventually reached “a point where I understood that it’s something that affects me and affects many other people, and I didn’t want to hide it any more.”
Sickle cell disease, which occurs primarily in people of Afro-Caribbean background, is a taboo subject in his community, Mr. Gaspar elaborated in an interview.
The condition has been associated with a great deal of stigma, with young sufferers traditionally seen as “demonically possessed,” he commented.
“So there was always a shameful aspect around it when it came to African families speaking about it, especially back in Africa.”
But after his parents came to the United Kingdom, he was able to “do his research and understand that it’s just genetics.”
This knowledge, Mr. Gaspar said, “takes away the spiritual aspect” and allows people to “have the conversation about sickle cell with potential partners” and ask them to find out their genotype, which in turn helps to “break down the barriers and the stigma.”
Mr. Gaspar emphasizes that there is much more work still to do.
In the video, he appeals to the Black community to make blood donations.
He said that something that “haunts” him is that currently, only 1% of Black people in the United Kingdom give blood, “so I really want the song to move my community to take a step forward and make that difference.”
He has been in contact with NHS Blood and Transplant, which provides blood and transplantation service to the National Health Service. They “really liked” the song, Mr. Gaspar said, and helped him get access to a hospital ward in University College Hospital, London, for the video.
“I really wanted to make a video that made people uncomfortable when watching it,” he said. It shows him hospitalized for pain and breathlessness and recalling having to use a Zimmer frame at the age of 25.
“This is a side of sickle cell that normally people don’t know,” he said.
Since releasing the song and the video, Mr. Gaspar says he has been contacted by many fellow patients. They have told him that he is now their “voice”; when they are asked how the condition affects them, “they can show someone the Hidden Pain video and say: This is how it feels.”
Clinicians have also approached him, asking if they can show his video to illustrate to patients and their families how having the condition may affect their lives.
Preventable deaths
At the meeting, Dr. Hibbs highlighted the 2021 report No One’s Listening, which was issued by the Sickle Cell Society following an inquiry into avoidable deaths and failures of care for sickle cell patients.
The inquiry, published by an All-Party Parliamentary group, found “serious care failings” in acute services and evidence of attitudes underpinned by racism. There was evidence of substandard care for sickle cell patients who were admitted to general wards or to hospital accident and emergency departments, as well as low awareness of the condition among health care professionals.
The report noted that the care failings have led to patient deaths, some which could have been prevented, and that there have been many “near misses.”
Many patients with sickle cell disease said they are “not being listened to” or are not being understood, especially during that vulnerable period when they are “in a crisis.”
Mr. Gaspar said that the report, and also the deaths, really struck a chord with him and many in his community. “We felt like that was us. ... We’ve all been in that same position where we’ve been misunderstood and not heard by nurses, doctors, or paramedics.”
He emphasized the need for awareness of the condition and the need for timely treatment. Just 3 weeks ago, Mr. Gaspar attended the funeral of one of his friends who is in the Hidden Pain video, a fellow sickle cell disease patient, who died at 30 years of age.
Ignorance about the condition ‘all too common’
The lack of awareness about sickle cell disease, even among health care professionals, is “all too common,” says Dr. Subarna Chakravorty, consultant pediatric hematologist, King’s College Hospital, London.
Even in London, where there is a large Black community and the teaching hospitals have world-class expertise, patients with sickle cell disease are “still facing a lot of problems with knowledge” among health care professionals, she said in an interview.
“Often people are having to speak for their own condition; which is fine, except that sometimes they are not believed,” she commented.
“On the one hand, you rely on the patient to provide information about their disease, and then when you receive it, you don’t do anything about it. So [they’re] between a rock and a hard place.”
Why are sickle cell patients treated in this way?
For Dr. Chakravorty, there is “a lot to be said about racism and disparities” in treating patients “as morphine-seekers, opiate addicts, even in children.”
“So we really need to improve the knowledge and perceptions among nonspecialist staff,” she said, “and even among specialists.”
Mr. Gaspar aims to help with this effort and hopes that his song and video will be useful to health care professionals. Sickle cell disease “needs to be spoken about,” and more doctors and nurses need to “know what it is,” he said.
He said it is a relief to encounter health care professionals who are knowledgeable about his condition. There have been times when he has been “having a crisis at home, calling the ambulance, and the paramedic comes and says: ‘Mr. Gaspar, you have sickle cell...we believe that you usually have gas and air and morphine, is that correct?’”
“That gives me a sense of peace, to know that I don’t have to fight my case or convince someone I have sickle cell, and I need to start treatment. They already know.”
No relevant financial relationships have been disclosed.
A version of this article first appeared on Medscape.com.
Some leukemias detectable up to 16 years before diagnosis?
Previous analyses showed that monoclonal B-cell lymphocytosis (MBL), a CLL precursor state, has been detected up to 6 years before CLL diagnosis, the investigators explained, noting that “[a]nother prognostically relevant immunogenetic feature of CLL concerns the stereotype of the B-cell receptor immunoglobulins (BcR IG).”
“Indeed, distinct stereotyped subsets can be defined by the expression of shared sequence motifs and are associated with particular presentation and outcomes,” P. Martijn Kolijn, PhD, a researcher in the department of immunology at Erasmus Medical Center, Rotterdam, the Netherlands, and colleagues wrote in a brief report published online in Blood. In an effort to “gain insight into the composition of the BcR IG repertoire during the early stages of CLL,” the investigators utilized next-generation sequencing to analyze 124 blood samples taken from healthy individuals up to 22 years before they received a diagnosis of CLL or small lymphocytic leukemia (SLL). An additional 118 matched control samples were also analyzed.
Study subjects were participants in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort.
“First, unsurprisingly, we observed a significant difference in the frequency of the dominant clonotype in CLL patients versus controls with a median frequency of 54.9%, compared to only 0.38% in controls,” they wrote.
Among 28 patients whose lymphocyte counts were measured at baseline, 10 showed evidence of lymphocytosis up to 8 years before CLL diagnosis.
This suggests undiagnosed instances of high-count MBL (cases with a cell count above 0.5x 109 cells/L, which can progress to CLL) or asymptomatic CLL, they explained.
“In contrast, next-generation sequencing results showed detectable skewing of the IGH gene repertoire in 21/28 patients up to 15 years before CLL diagnosis, often in the absence of elevated lymphocyte counts,” they wrote. “Remarkably, some patients with CLL requiring treatment and clinical transformation to an aggressive B-cell lymphoma displayed considerable skewing in the IGH gene repertoire even 16 years before CLL diagnosis.”
Patients with a prediagnostic IGHV-unmutated dominant clonotype had significantly shorter overall survival after CLL diagnosis than did those with an IGHV-mutated clonotype, they noted.
“Furthermore, at early timepoints (>10 years before diagnosis), patients with a high dominant clonotype frequency were more likely to be IGHV mutated, whereas closer to diagnosis this tendency was lost, indicating that the prediagnostic phase may be even longer than 16 years for [mutated] CLL patients,” they added.
The investigators also found that:
- Twenty-five patients carried stereotyped BcR IG up to 17 years prior to CLL diagnosis, and of these, 10 clonotypes were assigned to minor subsets and 15 to major CLL subsets. Among the latter, 14 of the 15 belonged to high-risk subsets, and most of those showed a trend for faster disease evolution.
- High frequency of the dominant clonotype was evident in samples obtained less than 6 years before diagnosis, whereas high-risk stereotyped clonotypes found longer before diagnosis (as early as 16 years) tended to have a lower dominant clonotype frequency (<20% of IGH gene repertoire)
- The stereotyped BcR IG matched the clonotype at diagnosis for both patients with diagnostic material.
- No stereotyped subsets were identified among the dominant clonotypes of the healthy controls.
“To our knowledge, the dynamics of the emergence of biclonality in an MBL patient and subsequent progression to CLL have never been captured in such a convincing manner,” they noted.
The findings “extend current knowledge on the evolution of the IGH repertoire prior to CLL diagnosis, highlighting that even high-risk CLL subtypes may display a prolonged indolent preclinical stage,” they added, speculating that “somatic genetic aberrations, (auto)stimulation, epigenetic and/or microenvironmental influences are required for the transformation into overt CLL.”
The investigators also noted that since the observed skewing in the IGH gene repertoire often occurs prior to B-cell lymphocytosis, they consider the findings “a novel extension to the characterization of MBL.”
“Further studies may prove invaluable in the clinical distinction between ‘progressing’ MBL versus ‘stable’ MBL. Notwithstanding the above, we emphasize that early detection is only warranted if it provides clear benefits to patient care,” they concluded.
In a related commentary, Gerald Marti, MD, PhD, of the National Heart, Lung, and Blood Institute, emphasized that the findings “represent the earliest detection of a clonotypic precursor cell for CLL.” .
They also raise new questions and point to new directions for research, Dr. Marti noted.
“Where do we go from here? CLL has a long evolutionary history in which early branching may start as an oligoclonal process (antigen stimulation) and include driver mutations,” he wrote. “A long-term analysis of the B-cell repertoire in familial CLL might shed light on this process. Further clarification of the mechanisms of age-related immune senescence is also of interest.”
The study authors and Dr. Marti reported having no competing financial interests.
Previous analyses showed that monoclonal B-cell lymphocytosis (MBL), a CLL precursor state, has been detected up to 6 years before CLL diagnosis, the investigators explained, noting that “[a]nother prognostically relevant immunogenetic feature of CLL concerns the stereotype of the B-cell receptor immunoglobulins (BcR IG).”
“Indeed, distinct stereotyped subsets can be defined by the expression of shared sequence motifs and are associated with particular presentation and outcomes,” P. Martijn Kolijn, PhD, a researcher in the department of immunology at Erasmus Medical Center, Rotterdam, the Netherlands, and colleagues wrote in a brief report published online in Blood. In an effort to “gain insight into the composition of the BcR IG repertoire during the early stages of CLL,” the investigators utilized next-generation sequencing to analyze 124 blood samples taken from healthy individuals up to 22 years before they received a diagnosis of CLL or small lymphocytic leukemia (SLL). An additional 118 matched control samples were also analyzed.
Study subjects were participants in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort.
“First, unsurprisingly, we observed a significant difference in the frequency of the dominant clonotype in CLL patients versus controls with a median frequency of 54.9%, compared to only 0.38% in controls,” they wrote.
Among 28 patients whose lymphocyte counts were measured at baseline, 10 showed evidence of lymphocytosis up to 8 years before CLL diagnosis.
This suggests undiagnosed instances of high-count MBL (cases with a cell count above 0.5x 109 cells/L, which can progress to CLL) or asymptomatic CLL, they explained.
“In contrast, next-generation sequencing results showed detectable skewing of the IGH gene repertoire in 21/28 patients up to 15 years before CLL diagnosis, often in the absence of elevated lymphocyte counts,” they wrote. “Remarkably, some patients with CLL requiring treatment and clinical transformation to an aggressive B-cell lymphoma displayed considerable skewing in the IGH gene repertoire even 16 years before CLL diagnosis.”
Patients with a prediagnostic IGHV-unmutated dominant clonotype had significantly shorter overall survival after CLL diagnosis than did those with an IGHV-mutated clonotype, they noted.
“Furthermore, at early timepoints (>10 years before diagnosis), patients with a high dominant clonotype frequency were more likely to be IGHV mutated, whereas closer to diagnosis this tendency was lost, indicating that the prediagnostic phase may be even longer than 16 years for [mutated] CLL patients,” they added.
The investigators also found that:
- Twenty-five patients carried stereotyped BcR IG up to 17 years prior to CLL diagnosis, and of these, 10 clonotypes were assigned to minor subsets and 15 to major CLL subsets. Among the latter, 14 of the 15 belonged to high-risk subsets, and most of those showed a trend for faster disease evolution.
- High frequency of the dominant clonotype was evident in samples obtained less than 6 years before diagnosis, whereas high-risk stereotyped clonotypes found longer before diagnosis (as early as 16 years) tended to have a lower dominant clonotype frequency (<20% of IGH gene repertoire)
- The stereotyped BcR IG matched the clonotype at diagnosis for both patients with diagnostic material.
- No stereotyped subsets were identified among the dominant clonotypes of the healthy controls.
“To our knowledge, the dynamics of the emergence of biclonality in an MBL patient and subsequent progression to CLL have never been captured in such a convincing manner,” they noted.
The findings “extend current knowledge on the evolution of the IGH repertoire prior to CLL diagnosis, highlighting that even high-risk CLL subtypes may display a prolonged indolent preclinical stage,” they added, speculating that “somatic genetic aberrations, (auto)stimulation, epigenetic and/or microenvironmental influences are required for the transformation into overt CLL.”
The investigators also noted that since the observed skewing in the IGH gene repertoire often occurs prior to B-cell lymphocytosis, they consider the findings “a novel extension to the characterization of MBL.”
“Further studies may prove invaluable in the clinical distinction between ‘progressing’ MBL versus ‘stable’ MBL. Notwithstanding the above, we emphasize that early detection is only warranted if it provides clear benefits to patient care,” they concluded.
In a related commentary, Gerald Marti, MD, PhD, of the National Heart, Lung, and Blood Institute, emphasized that the findings “represent the earliest detection of a clonotypic precursor cell for CLL.” .
They also raise new questions and point to new directions for research, Dr. Marti noted.
“Where do we go from here? CLL has a long evolutionary history in which early branching may start as an oligoclonal process (antigen stimulation) and include driver mutations,” he wrote. “A long-term analysis of the B-cell repertoire in familial CLL might shed light on this process. Further clarification of the mechanisms of age-related immune senescence is also of interest.”
The study authors and Dr. Marti reported having no competing financial interests.
Previous analyses showed that monoclonal B-cell lymphocytosis (MBL), a CLL precursor state, has been detected up to 6 years before CLL diagnosis, the investigators explained, noting that “[a]nother prognostically relevant immunogenetic feature of CLL concerns the stereotype of the B-cell receptor immunoglobulins (BcR IG).”
“Indeed, distinct stereotyped subsets can be defined by the expression of shared sequence motifs and are associated with particular presentation and outcomes,” P. Martijn Kolijn, PhD, a researcher in the department of immunology at Erasmus Medical Center, Rotterdam, the Netherlands, and colleagues wrote in a brief report published online in Blood. In an effort to “gain insight into the composition of the BcR IG repertoire during the early stages of CLL,” the investigators utilized next-generation sequencing to analyze 124 blood samples taken from healthy individuals up to 22 years before they received a diagnosis of CLL or small lymphocytic leukemia (SLL). An additional 118 matched control samples were also analyzed.
Study subjects were participants in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort.
“First, unsurprisingly, we observed a significant difference in the frequency of the dominant clonotype in CLL patients versus controls with a median frequency of 54.9%, compared to only 0.38% in controls,” they wrote.
Among 28 patients whose lymphocyte counts were measured at baseline, 10 showed evidence of lymphocytosis up to 8 years before CLL diagnosis.
This suggests undiagnosed instances of high-count MBL (cases with a cell count above 0.5x 109 cells/L, which can progress to CLL) or asymptomatic CLL, they explained.
“In contrast, next-generation sequencing results showed detectable skewing of the IGH gene repertoire in 21/28 patients up to 15 years before CLL diagnosis, often in the absence of elevated lymphocyte counts,” they wrote. “Remarkably, some patients with CLL requiring treatment and clinical transformation to an aggressive B-cell lymphoma displayed considerable skewing in the IGH gene repertoire even 16 years before CLL diagnosis.”
Patients with a prediagnostic IGHV-unmutated dominant clonotype had significantly shorter overall survival after CLL diagnosis than did those with an IGHV-mutated clonotype, they noted.
“Furthermore, at early timepoints (>10 years before diagnosis), patients with a high dominant clonotype frequency were more likely to be IGHV mutated, whereas closer to diagnosis this tendency was lost, indicating that the prediagnostic phase may be even longer than 16 years for [mutated] CLL patients,” they added.
The investigators also found that:
- Twenty-five patients carried stereotyped BcR IG up to 17 years prior to CLL diagnosis, and of these, 10 clonotypes were assigned to minor subsets and 15 to major CLL subsets. Among the latter, 14 of the 15 belonged to high-risk subsets, and most of those showed a trend for faster disease evolution.
- High frequency of the dominant clonotype was evident in samples obtained less than 6 years before diagnosis, whereas high-risk stereotyped clonotypes found longer before diagnosis (as early as 16 years) tended to have a lower dominant clonotype frequency (<20% of IGH gene repertoire)
- The stereotyped BcR IG matched the clonotype at diagnosis for both patients with diagnostic material.
- No stereotyped subsets were identified among the dominant clonotypes of the healthy controls.
“To our knowledge, the dynamics of the emergence of biclonality in an MBL patient and subsequent progression to CLL have never been captured in such a convincing manner,” they noted.
The findings “extend current knowledge on the evolution of the IGH repertoire prior to CLL diagnosis, highlighting that even high-risk CLL subtypes may display a prolonged indolent preclinical stage,” they added, speculating that “somatic genetic aberrations, (auto)stimulation, epigenetic and/or microenvironmental influences are required for the transformation into overt CLL.”
The investigators also noted that since the observed skewing in the IGH gene repertoire often occurs prior to B-cell lymphocytosis, they consider the findings “a novel extension to the characterization of MBL.”
“Further studies may prove invaluable in the clinical distinction between ‘progressing’ MBL versus ‘stable’ MBL. Notwithstanding the above, we emphasize that early detection is only warranted if it provides clear benefits to patient care,” they concluded.
In a related commentary, Gerald Marti, MD, PhD, of the National Heart, Lung, and Blood Institute, emphasized that the findings “represent the earliest detection of a clonotypic precursor cell for CLL.” .
They also raise new questions and point to new directions for research, Dr. Marti noted.
“Where do we go from here? CLL has a long evolutionary history in which early branching may start as an oligoclonal process (antigen stimulation) and include driver mutations,” he wrote. “A long-term analysis of the B-cell repertoire in familial CLL might shed light on this process. Further clarification of the mechanisms of age-related immune senescence is also of interest.”
The study authors and Dr. Marti reported having no competing financial interests.
FROM BLOOD
Cancer Data Trends 2022
Federal Practitioner, in collaboration with the Association of VA Hematology/Oncology (AVAHO), present the 2022 edition of Cancer Data Trends (click to view the digital edition). This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.

In this issue:
- Exposure-Related Cancers
- Cancer in Women
- Genitourinary Cancers
- Gastrointestinal Cancers
- Telehealth in Oncology
- Precision Oncology
- Palliative and Hospice Care
- Alcohol and Cancer
- Lung Cancer
- Oropharyngeal Cancer
- Hematologic Cancers
Federal Practitioner and AVAHO would like to thank the following experts for their contributions to this issue:
Anita Aggarwal, DO, PhD; Sara Ahmed, PhD; Katherine Faricy-Anderson, MD; Apar Kishor Ganti, MD, MS; Solomon A Graf, MD; Kate Hendricks Thomas, PhD; Michael Kelley, MD; Mark Klein, MD, Gina McWhirter, MSN, MBA, RN; Bruce Montgomery, MD; Vida Almario Passero, MD, MBA; Thomas D Rodgers, MD; Vlad C Sandulache, MD, PhD; David H Wang, MD, PhD.
Federal Practitioner, in collaboration with the Association of VA Hematology/Oncology (AVAHO), present the 2022 edition of Cancer Data Trends (click to view the digital edition). This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.
In this issue:
- Exposure-Related Cancers
- Cancer in Women
- Genitourinary Cancers
- Gastrointestinal Cancers
- Telehealth in Oncology
- Precision Oncology
- Palliative and Hospice Care
- Alcohol and Cancer
- Lung Cancer
- Oropharyngeal Cancer
- Hematologic Cancers
Federal Practitioner and AVAHO would like to thank the following experts for their contributions to this issue:
Anita Aggarwal, DO, PhD; Sara Ahmed, PhD; Katherine Faricy-Anderson, MD; Apar Kishor Ganti, MD, MS; Solomon A Graf, MD; Kate Hendricks Thomas, PhD; Michael Kelley, MD; Mark Klein, MD, Gina McWhirter, MSN, MBA, RN; Bruce Montgomery, MD; Vida Almario Passero, MD, MBA; Thomas D Rodgers, MD; Vlad C Sandulache, MD, PhD; David H Wang, MD, PhD.
Federal Practitioner, in collaboration with the Association of VA Hematology/Oncology (AVAHO), present the 2022 edition of Cancer Data Trends (click to view the digital edition). This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.
In this issue:
- Exposure-Related Cancers
- Cancer in Women
- Genitourinary Cancers
- Gastrointestinal Cancers
- Telehealth in Oncology
- Precision Oncology
- Palliative and Hospice Care
- Alcohol and Cancer
- Lung Cancer
- Oropharyngeal Cancer
- Hematologic Cancers
Federal Practitioner and AVAHO would like to thank the following experts for their contributions to this issue:
Anita Aggarwal, DO, PhD; Sara Ahmed, PhD; Katherine Faricy-Anderson, MD; Apar Kishor Ganti, MD, MS; Solomon A Graf, MD; Kate Hendricks Thomas, PhD; Michael Kelley, MD; Mark Klein, MD, Gina McWhirter, MSN, MBA, RN; Bruce Montgomery, MD; Vida Almario Passero, MD, MBA; Thomas D Rodgers, MD; Vlad C Sandulache, MD, PhD; David H Wang, MD, PhD.

First-line CAR T-cell therapy could help cure some lymphomas
Results of the phase 2 ZUMA-12 trial suggest that axicabtagene ciloleucel (axi-cel), a chimeric antigen receptor (CAR) T-cell therapy approved to treat certain types of lymphoma, also shows promise as a treatment for another group of lymphoma patients – those with high-risk large B-cell lymphoma (LBCL) who failed two rounds of standard chemoimmunotherapy. In fact, a study author said, first-line treatment with this therapy could help usher some patients toward a cure.
The results appeared March 21, 2022, in Nature Medicine.
“The high efficacy with manageable safety profile suggest that further evaluation of axi-cel in first-line setting in patients with high-risk LBCL is warranted in a randomized, phase 3 trial comparing it to standard chemoimmunotherapy,” study lead author Sattva S. Neelapu, MD, of the University of Texas MD Anderson Cancer Center, Houston, said in an interview.
According to Dr. Neelapu, “patients with high-risk LBCL include those with high-intermediate or high International Prognostic Index score and those with certain molecular subtypes such as double- or triple-hit lymphoma. These patients have lower response rates and lower progression-free and overall survival with standard chemoimmunotherapy.”
Treatment of these patients can be especially challenging because they are underrepresented in clinical research, hematologist Michael Dickinson, MBBS, of the Peter MacCallum Cancer Center in Melbourne, said in an interview. “They often have disease that requires urgent treatment, so there is no time to recruit them into trials. A feature of ZUMA-12 is that it allowed patients to be recruited after short exposure to chemotherapy, which means that higher-risk patients could successfully be recruited into the trial.”
Axi-cel is already Food and Drug Administration approved for treatment of relapsed or refractory LBCL after 2 or more lines of systemic therapy plus relapsed or refractory follicular lymphoma, also after two or more lines of systemic therapy, Dr. Neelapu said.
For this study, researchers administered the treatment to 40 subjects with high-risk disease from 2019-2020 (median age, 61 years; 68% male; 95% at disease stage III or IV).
The researchers reported that 78% of 37 patients in the primary efficacy analysis reached complete response rate (95% confidence interval, 62-90); the median time to first complete response rate was 30 days (range, 27-207). About 89% of these subjects reached the secondary endpoint of objective response rate (95% CI, 75-97); the median time to first objective response was 29 days (range, 27-207).
At a median follow-up of 15.9 months, 73% were still in objective response.
“This is quite remarkable,” Dr. Neelapu said. “The durability of more than 70% is far higher than what would be expected with standard chemoimmunotherapy in these patients – under 40% durability with standard chemoimmunotherapy. Also, axi-cel induces durable responses in about 40% of patients in second- and third-line setting. However, when used as part of first-line therapy in this study, durable responses were observed in more than 70% of patients, suggesting that the efficacy of axi-cel may be much higher when used in first-line setting.”
Dr. Neelapu added: “Although the follow-up is short, it is highly likely that the majority of the patients with ongoing response beyond 1 year will likely be cured of their lymphoma.”
As for side effects, no treatment-related grade 5 events occurred, but 18 patients (45%) experienced serious adverse events. Grade 3 or higher cytokine release syndrome occurred in three patients (8%) and nine experienced neurologic events (23%).
“The majority of the higher-grade adverse events observed were due to cytopenias, which were expected due to the conditioning therapy,” Dr. Neelapu said. “Such cytopenias would also have been expected if these patients had received standard chemoimmunotherapy.”
Six patients (15%) died, 4 of progressive disease after going forward to other therapies.
As for cost, Dr. Neelapu said it should be similar to that of axi-cel as an FDA-approved third-line therapy. Axi-cel is highly expensive. Research has suggested that CAR T-cell therapy can boost costs beyond standard chemotherapy by $350,000-$490,000 with gains of 2-8 years of life (J Med Econ. Jan-Dec 2021;24[1]:458-68).
The study was funded by Kite. The authors reported various disclosures.
Results of the phase 2 ZUMA-12 trial suggest that axicabtagene ciloleucel (axi-cel), a chimeric antigen receptor (CAR) T-cell therapy approved to treat certain types of lymphoma, also shows promise as a treatment for another group of lymphoma patients – those with high-risk large B-cell lymphoma (LBCL) who failed two rounds of standard chemoimmunotherapy. In fact, a study author said, first-line treatment with this therapy could help usher some patients toward a cure.
The results appeared March 21, 2022, in Nature Medicine.
“The high efficacy with manageable safety profile suggest that further evaluation of axi-cel in first-line setting in patients with high-risk LBCL is warranted in a randomized, phase 3 trial comparing it to standard chemoimmunotherapy,” study lead author Sattva S. Neelapu, MD, of the University of Texas MD Anderson Cancer Center, Houston, said in an interview.
According to Dr. Neelapu, “patients with high-risk LBCL include those with high-intermediate or high International Prognostic Index score and those with certain molecular subtypes such as double- or triple-hit lymphoma. These patients have lower response rates and lower progression-free and overall survival with standard chemoimmunotherapy.”
Treatment of these patients can be especially challenging because they are underrepresented in clinical research, hematologist Michael Dickinson, MBBS, of the Peter MacCallum Cancer Center in Melbourne, said in an interview. “They often have disease that requires urgent treatment, so there is no time to recruit them into trials. A feature of ZUMA-12 is that it allowed patients to be recruited after short exposure to chemotherapy, which means that higher-risk patients could successfully be recruited into the trial.”
Axi-cel is already Food and Drug Administration approved for treatment of relapsed or refractory LBCL after 2 or more lines of systemic therapy plus relapsed or refractory follicular lymphoma, also after two or more lines of systemic therapy, Dr. Neelapu said.
For this study, researchers administered the treatment to 40 subjects with high-risk disease from 2019-2020 (median age, 61 years; 68% male; 95% at disease stage III or IV).
The researchers reported that 78% of 37 patients in the primary efficacy analysis reached complete response rate (95% confidence interval, 62-90); the median time to first complete response rate was 30 days (range, 27-207). About 89% of these subjects reached the secondary endpoint of objective response rate (95% CI, 75-97); the median time to first objective response was 29 days (range, 27-207).
At a median follow-up of 15.9 months, 73% were still in objective response.
“This is quite remarkable,” Dr. Neelapu said. “The durability of more than 70% is far higher than what would be expected with standard chemoimmunotherapy in these patients – under 40% durability with standard chemoimmunotherapy. Also, axi-cel induces durable responses in about 40% of patients in second- and third-line setting. However, when used as part of first-line therapy in this study, durable responses were observed in more than 70% of patients, suggesting that the efficacy of axi-cel may be much higher when used in first-line setting.”
Dr. Neelapu added: “Although the follow-up is short, it is highly likely that the majority of the patients with ongoing response beyond 1 year will likely be cured of their lymphoma.”
As for side effects, no treatment-related grade 5 events occurred, but 18 patients (45%) experienced serious adverse events. Grade 3 or higher cytokine release syndrome occurred in three patients (8%) and nine experienced neurologic events (23%).
“The majority of the higher-grade adverse events observed were due to cytopenias, which were expected due to the conditioning therapy,” Dr. Neelapu said. “Such cytopenias would also have been expected if these patients had received standard chemoimmunotherapy.”
Six patients (15%) died, 4 of progressive disease after going forward to other therapies.
As for cost, Dr. Neelapu said it should be similar to that of axi-cel as an FDA-approved third-line therapy. Axi-cel is highly expensive. Research has suggested that CAR T-cell therapy can boost costs beyond standard chemotherapy by $350,000-$490,000 with gains of 2-8 years of life (J Med Econ. Jan-Dec 2021;24[1]:458-68).
The study was funded by Kite. The authors reported various disclosures.
Results of the phase 2 ZUMA-12 trial suggest that axicabtagene ciloleucel (axi-cel), a chimeric antigen receptor (CAR) T-cell therapy approved to treat certain types of lymphoma, also shows promise as a treatment for another group of lymphoma patients – those with high-risk large B-cell lymphoma (LBCL) who failed two rounds of standard chemoimmunotherapy. In fact, a study author said, first-line treatment with this therapy could help usher some patients toward a cure.
The results appeared March 21, 2022, in Nature Medicine.
“The high efficacy with manageable safety profile suggest that further evaluation of axi-cel in first-line setting in patients with high-risk LBCL is warranted in a randomized, phase 3 trial comparing it to standard chemoimmunotherapy,” study lead author Sattva S. Neelapu, MD, of the University of Texas MD Anderson Cancer Center, Houston, said in an interview.
According to Dr. Neelapu, “patients with high-risk LBCL include those with high-intermediate or high International Prognostic Index score and those with certain molecular subtypes such as double- or triple-hit lymphoma. These patients have lower response rates and lower progression-free and overall survival with standard chemoimmunotherapy.”
Treatment of these patients can be especially challenging because they are underrepresented in clinical research, hematologist Michael Dickinson, MBBS, of the Peter MacCallum Cancer Center in Melbourne, said in an interview. “They often have disease that requires urgent treatment, so there is no time to recruit them into trials. A feature of ZUMA-12 is that it allowed patients to be recruited after short exposure to chemotherapy, which means that higher-risk patients could successfully be recruited into the trial.”
Axi-cel is already Food and Drug Administration approved for treatment of relapsed or refractory LBCL after 2 or more lines of systemic therapy plus relapsed or refractory follicular lymphoma, also after two or more lines of systemic therapy, Dr. Neelapu said.
For this study, researchers administered the treatment to 40 subjects with high-risk disease from 2019-2020 (median age, 61 years; 68% male; 95% at disease stage III or IV).
The researchers reported that 78% of 37 patients in the primary efficacy analysis reached complete response rate (95% confidence interval, 62-90); the median time to first complete response rate was 30 days (range, 27-207). About 89% of these subjects reached the secondary endpoint of objective response rate (95% CI, 75-97); the median time to first objective response was 29 days (range, 27-207).
At a median follow-up of 15.9 months, 73% were still in objective response.
“This is quite remarkable,” Dr. Neelapu said. “The durability of more than 70% is far higher than what would be expected with standard chemoimmunotherapy in these patients – under 40% durability with standard chemoimmunotherapy. Also, axi-cel induces durable responses in about 40% of patients in second- and third-line setting. However, when used as part of first-line therapy in this study, durable responses were observed in more than 70% of patients, suggesting that the efficacy of axi-cel may be much higher when used in first-line setting.”
Dr. Neelapu added: “Although the follow-up is short, it is highly likely that the majority of the patients with ongoing response beyond 1 year will likely be cured of their lymphoma.”
As for side effects, no treatment-related grade 5 events occurred, but 18 patients (45%) experienced serious adverse events. Grade 3 or higher cytokine release syndrome occurred in three patients (8%) and nine experienced neurologic events (23%).
“The majority of the higher-grade adverse events observed were due to cytopenias, which were expected due to the conditioning therapy,” Dr. Neelapu said. “Such cytopenias would also have been expected if these patients had received standard chemoimmunotherapy.”
Six patients (15%) died, 4 of progressive disease after going forward to other therapies.
As for cost, Dr. Neelapu said it should be similar to that of axi-cel as an FDA-approved third-line therapy. Axi-cel is highly expensive. Research has suggested that CAR T-cell therapy can boost costs beyond standard chemotherapy by $350,000-$490,000 with gains of 2-8 years of life (J Med Econ. Jan-Dec 2021;24[1]:458-68).
The study was funded by Kite. The authors reported various disclosures.
FROM NATURE MEDICINE
Eating olive oil may slow CLL disease progression
Olive oil is a major component of the Mediterranean diet, and olive phenols have been shown to convey antioxidant, anti-inflammatory, anticancer, neuroprotective, and antidiabetic effects by modulating various molecular pathways, Andrea Paola Rojas Gil, PhD, of the University of Peloponnese, Tripoli, Greece, and colleagues wrote.
In most patients, CLL is incurable, but those at the early stages do not need immediate therapy and may benefit from an intervention to prevent disease progression, the authors wrote. Previous research suggested that dietary intervention exerts a salutary effect on early CLL, and in vitro studies suggested that oleocanthal, a component of extra virgin olive oil, induced anticancer activity.
In a study published in Frontiers in Oncology, the researchers enrolled adults with early stage CLL who had not undergone chemotherapy or other treatment. All patients adhered to a Mediterranean-style diet.
After a washout period of 9-12 months, the researchers randomized 22 patients to extra virgin olive oil high in oleocanthal and oleacein (high OC/OL-EVOO). Patients in the intervention group consumed 40 mL/day of high OC/OL-EVOO before meals. Their average age was 71 years; 10 were women and 12 were men.
The primary outcomes included changes in hematological, biochemical, and apoptotic markers. After 6 months, patients in the intervention group showed a statistically significant reduction in white blood cells and lymphocyte count, compared with measurements taken 3 months before the intervention. The WBC decrease was greatest among patients with the highest WBC levels at baseline.
As for biochemical markers, the researchers observed a significant decrease in glucose levels during the intervention, but no significant effects on metabolic indexes or renal function.
After 3 months and also after 6 months of the olive oil intervention, patients showed a significant increase in the apoptotic markers ccK18 and Apo1-Fas (P ≤ .05 for both), as well as an increase in the cell cycle negative regulator p21. The dietary intervention also was associated with significant decreases in expression of the antiapoptotic protein survivin and in cyclin D, a positive cell cycle regulator protein.
Further, patients who had a high ccK18 level at baseline showed a significantly greater increase in ccK18 after the intervention, compared with those with lower ccK18 at baseline (P = .001).
Notably, “a negative correlation of the WBC at the end of the dietary intervention with the fluctuation of the protein expression of the apoptotic marker ccK18 (final – initial) was observed,” the researchers wrote in their discussion.
The study findings were limited by several factors including the small sample size, short intervention time, and pilot design, the researchers said. Other limitations include the possible effect of other unmeasured properties of olive oil.
However, the results reflect previous studies showing the benefits of a Mediterranean-type diet, and they represent the first clinical trial to indicate possible beneficial effects from oleocanthal and oleacein on the progression of CLL. Therefore, the authors concluded, the study is worthy of a large, multicenter trial.
Pilot data merit more research
In an interview, corresponding author Prokopios Magiatis, PhD, noted that CLL is “the most commonly diagnosed adult leukemia in Western countries and is responsible for about one in four cases of all leukemias.” CLL remains incurable in most patients, and ways to delay disease progression are needed.
“Oleocanthal is the active ingredient of early harvest olive oil with proven anticancer activities in vitro and in vivo,” Dr. Magiatis explained. “For this reason, it was a unique challenge to investigate the anticancer activity of this compound for the first time in humans through the dietary consumption of specifically selected olive oil.” He expressed surprise at the beneficial effects of high-oleocanthal olive oil, not only to the white blood cells, but also to glucose levels.
“It seems that oleocanthal can activate mechanisms related to the apoptosis of cancer cells, and also mechanisms related to blood glucose regulation without affecting any normal cells of the body,” he said. “All anticancer drugs usually have severe side effects, however the administration of 25 mg of oleocanthal through the dietary consumption of olive oil did not present any harmful effects for at least 6 months of everyday use.
“The addition of naturally produced high-oleocanthal olive oil in the diet of early-stage CLL patients at a dose of three tablespoons per day [40 mL] is a practice that may lower the cancerous white blood cells of the patients without any risk,” said Dr. Magiatis. “High-oleocanthal early-harvest olive oil has been consumed for centuries, and may be the key of longevity of several Mediterranean populations.
“In our study, the number of the white blood cells returned back to the number it was one year before the initiation of the study; this clearly shows that it could be a significant factor for the delay of the progress of the disease,” he said.
The current trial was a pilot study in one hospital with only 22 patients for 6 months, said Dr. Magiatis. “We are currently preparing the expansion of the study to other hospitals and other countries, and we aim to include at least 100 patients for at least 1 year, to validate the already-obtained beneficial results.”
The clinical trial is supported by the nonprofit organization World Olive Center for Health, he added.
The current study received no outside funding. The researchers had no financial conflicts to disclose.
Olive oil is a major component of the Mediterranean diet, and olive phenols have been shown to convey antioxidant, anti-inflammatory, anticancer, neuroprotective, and antidiabetic effects by modulating various molecular pathways, Andrea Paola Rojas Gil, PhD, of the University of Peloponnese, Tripoli, Greece, and colleagues wrote.
In most patients, CLL is incurable, but those at the early stages do not need immediate therapy and may benefit from an intervention to prevent disease progression, the authors wrote. Previous research suggested that dietary intervention exerts a salutary effect on early CLL, and in vitro studies suggested that oleocanthal, a component of extra virgin olive oil, induced anticancer activity.
In a study published in Frontiers in Oncology, the researchers enrolled adults with early stage CLL who had not undergone chemotherapy or other treatment. All patients adhered to a Mediterranean-style diet.
After a washout period of 9-12 months, the researchers randomized 22 patients to extra virgin olive oil high in oleocanthal and oleacein (high OC/OL-EVOO). Patients in the intervention group consumed 40 mL/day of high OC/OL-EVOO before meals. Their average age was 71 years; 10 were women and 12 were men.
The primary outcomes included changes in hematological, biochemical, and apoptotic markers. After 6 months, patients in the intervention group showed a statistically significant reduction in white blood cells and lymphocyte count, compared with measurements taken 3 months before the intervention. The WBC decrease was greatest among patients with the highest WBC levels at baseline.
As for biochemical markers, the researchers observed a significant decrease in glucose levels during the intervention, but no significant effects on metabolic indexes or renal function.
After 3 months and also after 6 months of the olive oil intervention, patients showed a significant increase in the apoptotic markers ccK18 and Apo1-Fas (P ≤ .05 for both), as well as an increase in the cell cycle negative regulator p21. The dietary intervention also was associated with significant decreases in expression of the antiapoptotic protein survivin and in cyclin D, a positive cell cycle regulator protein.
Further, patients who had a high ccK18 level at baseline showed a significantly greater increase in ccK18 after the intervention, compared with those with lower ccK18 at baseline (P = .001).
Notably, “a negative correlation of the WBC at the end of the dietary intervention with the fluctuation of the protein expression of the apoptotic marker ccK18 (final – initial) was observed,” the researchers wrote in their discussion.
The study findings were limited by several factors including the small sample size, short intervention time, and pilot design, the researchers said. Other limitations include the possible effect of other unmeasured properties of olive oil.
However, the results reflect previous studies showing the benefits of a Mediterranean-type diet, and they represent the first clinical trial to indicate possible beneficial effects from oleocanthal and oleacein on the progression of CLL. Therefore, the authors concluded, the study is worthy of a large, multicenter trial.
Pilot data merit more research
In an interview, corresponding author Prokopios Magiatis, PhD, noted that CLL is “the most commonly diagnosed adult leukemia in Western countries and is responsible for about one in four cases of all leukemias.” CLL remains incurable in most patients, and ways to delay disease progression are needed.
“Oleocanthal is the active ingredient of early harvest olive oil with proven anticancer activities in vitro and in vivo,” Dr. Magiatis explained. “For this reason, it was a unique challenge to investigate the anticancer activity of this compound for the first time in humans through the dietary consumption of specifically selected olive oil.” He expressed surprise at the beneficial effects of high-oleocanthal olive oil, not only to the white blood cells, but also to glucose levels.
“It seems that oleocanthal can activate mechanisms related to the apoptosis of cancer cells, and also mechanisms related to blood glucose regulation without affecting any normal cells of the body,” he said. “All anticancer drugs usually have severe side effects, however the administration of 25 mg of oleocanthal through the dietary consumption of olive oil did not present any harmful effects for at least 6 months of everyday use.
“The addition of naturally produced high-oleocanthal olive oil in the diet of early-stage CLL patients at a dose of three tablespoons per day [40 mL] is a practice that may lower the cancerous white blood cells of the patients without any risk,” said Dr. Magiatis. “High-oleocanthal early-harvest olive oil has been consumed for centuries, and may be the key of longevity of several Mediterranean populations.
“In our study, the number of the white blood cells returned back to the number it was one year before the initiation of the study; this clearly shows that it could be a significant factor for the delay of the progress of the disease,” he said.
The current trial was a pilot study in one hospital with only 22 patients for 6 months, said Dr. Magiatis. “We are currently preparing the expansion of the study to other hospitals and other countries, and we aim to include at least 100 patients for at least 1 year, to validate the already-obtained beneficial results.”
The clinical trial is supported by the nonprofit organization World Olive Center for Health, he added.
The current study received no outside funding. The researchers had no financial conflicts to disclose.
Olive oil is a major component of the Mediterranean diet, and olive phenols have been shown to convey antioxidant, anti-inflammatory, anticancer, neuroprotective, and antidiabetic effects by modulating various molecular pathways, Andrea Paola Rojas Gil, PhD, of the University of Peloponnese, Tripoli, Greece, and colleagues wrote.
In most patients, CLL is incurable, but those at the early stages do not need immediate therapy and may benefit from an intervention to prevent disease progression, the authors wrote. Previous research suggested that dietary intervention exerts a salutary effect on early CLL, and in vitro studies suggested that oleocanthal, a component of extra virgin olive oil, induced anticancer activity.
In a study published in Frontiers in Oncology, the researchers enrolled adults with early stage CLL who had not undergone chemotherapy or other treatment. All patients adhered to a Mediterranean-style diet.
After a washout period of 9-12 months, the researchers randomized 22 patients to extra virgin olive oil high in oleocanthal and oleacein (high OC/OL-EVOO). Patients in the intervention group consumed 40 mL/day of high OC/OL-EVOO before meals. Their average age was 71 years; 10 were women and 12 were men.
The primary outcomes included changes in hematological, biochemical, and apoptotic markers. After 6 months, patients in the intervention group showed a statistically significant reduction in white blood cells and lymphocyte count, compared with measurements taken 3 months before the intervention. The WBC decrease was greatest among patients with the highest WBC levels at baseline.
As for biochemical markers, the researchers observed a significant decrease in glucose levels during the intervention, but no significant effects on metabolic indexes or renal function.
After 3 months and also after 6 months of the olive oil intervention, patients showed a significant increase in the apoptotic markers ccK18 and Apo1-Fas (P ≤ .05 for both), as well as an increase in the cell cycle negative regulator p21. The dietary intervention also was associated with significant decreases in expression of the antiapoptotic protein survivin and in cyclin D, a positive cell cycle regulator protein.
Further, patients who had a high ccK18 level at baseline showed a significantly greater increase in ccK18 after the intervention, compared with those with lower ccK18 at baseline (P = .001).
Notably, “a negative correlation of the WBC at the end of the dietary intervention with the fluctuation of the protein expression of the apoptotic marker ccK18 (final – initial) was observed,” the researchers wrote in their discussion.
The study findings were limited by several factors including the small sample size, short intervention time, and pilot design, the researchers said. Other limitations include the possible effect of other unmeasured properties of olive oil.
However, the results reflect previous studies showing the benefits of a Mediterranean-type diet, and they represent the first clinical trial to indicate possible beneficial effects from oleocanthal and oleacein on the progression of CLL. Therefore, the authors concluded, the study is worthy of a large, multicenter trial.
Pilot data merit more research
In an interview, corresponding author Prokopios Magiatis, PhD, noted that CLL is “the most commonly diagnosed adult leukemia in Western countries and is responsible for about one in four cases of all leukemias.” CLL remains incurable in most patients, and ways to delay disease progression are needed.
“Oleocanthal is the active ingredient of early harvest olive oil with proven anticancer activities in vitro and in vivo,” Dr. Magiatis explained. “For this reason, it was a unique challenge to investigate the anticancer activity of this compound for the first time in humans through the dietary consumption of specifically selected olive oil.” He expressed surprise at the beneficial effects of high-oleocanthal olive oil, not only to the white blood cells, but also to glucose levels.
“It seems that oleocanthal can activate mechanisms related to the apoptosis of cancer cells, and also mechanisms related to blood glucose regulation without affecting any normal cells of the body,” he said. “All anticancer drugs usually have severe side effects, however the administration of 25 mg of oleocanthal through the dietary consumption of olive oil did not present any harmful effects for at least 6 months of everyday use.
“The addition of naturally produced high-oleocanthal olive oil in the diet of early-stage CLL patients at a dose of three tablespoons per day [40 mL] is a practice that may lower the cancerous white blood cells of the patients without any risk,” said Dr. Magiatis. “High-oleocanthal early-harvest olive oil has been consumed for centuries, and may be the key of longevity of several Mediterranean populations.
“In our study, the number of the white blood cells returned back to the number it was one year before the initiation of the study; this clearly shows that it could be a significant factor for the delay of the progress of the disease,” he said.
The current trial was a pilot study in one hospital with only 22 patients for 6 months, said Dr. Magiatis. “We are currently preparing the expansion of the study to other hospitals and other countries, and we aim to include at least 100 patients for at least 1 year, to validate the already-obtained beneficial results.”
The clinical trial is supported by the nonprofit organization World Olive Center for Health, he added.
The current study received no outside funding. The researchers had no financial conflicts to disclose.
FROM FRONTIERS IN ONCOLOGY
A Practical and Cost-Effective Approach to the Diagnosis of Heparin-Induced Thrombocytopenia: A Single-Center Quality Improvement Study
From the Veterans Affairs Ann Arbor Healthcare System Medicine Service (Dr. Cusick), University of Michigan College of Pharmacy, Clinical Pharmacy Service, Michigan Medicine (Dr. Hanigan), Department of Internal Medicine Clinical Experience and Quality, Michigan Medicine (Linda Bashaw), Department of Internal Medicine, University of Michigan Medical School, Ann Arbor, MI (Dr. Heidemann), and the Operational Excellence Department, Sparrow Health System, Lansing, MI (Matthew Johnson).
Abstract
Background: Diagnosis of heparin-induced thrombocytopenia (HIT) requires completion of an enzyme-linked immunosorbent assay (ELISA)–based heparin-platelet factor 4 (PF4) antibody test. If this test is negative, HIT is excluded. If positive, a serotonin-release assay (SRA) test is indicated. The SRA is expensive and sometimes inappropriately ordered despite negative PF4 results, leading to unnecessary treatment with argatroban while awaiting SRA results.
Objectives: The primary objectives of this project were to reduce unnecessary SRA testing and argatroban utilization in patients with suspected HIT.
Methods: The authors implemented an intervention at a tertiary care academic hospital in November 2017 targeting patients hospitalized with suspected HIT. The intervention was controlled at the level of the laboratory and prevented ordering of SRA tests in the absence of a positive PF4 test. The number of SRA tests performed and argatroban bags administered were identified retrospectively via chart review before the intervention (January 2016 to November 2017) and post intervention (December 2017 to March 2020). Associated costs were calculated based on institutional SRA testing cost as well as the average wholesale price of argatroban.
Results: SRA testing decreased from an average of 3.7 SRA results per 1000 admissions before the intervention to an average of 0.6 results per 1000 admissions post intervention. The number of 50-mL argatroban bags used per 1000 admissions decreased from 18.8 prior to the intervention to 14.3 post intervention. Total estimated cost savings per 1000 admissions was $2361.20.
Conclusion: An evidence-based testing strategy for HIT can be effectively implemented at the level of the laboratory. This approach led to reductions in SRA testing and argatroban utilization with resultant cost savings.
Keywords: HIT, argatroban, anticoagulation, serotonin-release assay.
Thrombocytopenia is a common finding in hospitalized patients.1,2 Heparin-induced thrombocytopenia (HIT) is one of the many potential causes of thrombocytopenia in hospitalized patients and occurs when antibodies to the heparin-platelet factor 4 (PF4) complex develop after heparin exposure. This triggers a cascade of events, leading to platelet activation, platelet consumption, and thrombosis. While HIT is relatively rare, occurring in 0.3% to 0.5% of critically ill patients, many patients will be tested to rule out this potentially life-threatening cause of thrombocytopenia.3
The diagnosis of HIT utilizes a combination of both clinical suspicion and laboratory testing.4 The 4T score (Table) was developed to evaluate the clinical probability of HIT and involves assessing the degree and timing of thrombocytopenia, the presence or absence of thrombosis, and other potential causes of the thrombocytopenia.5 The 4T score is designed to be utilized to identify patients who require laboratory testing for HIT; however, it has low inter-rater agreement in patients undergoing evaluation for HIT,6 and, in our experience, completion of this scoring is time-consuming.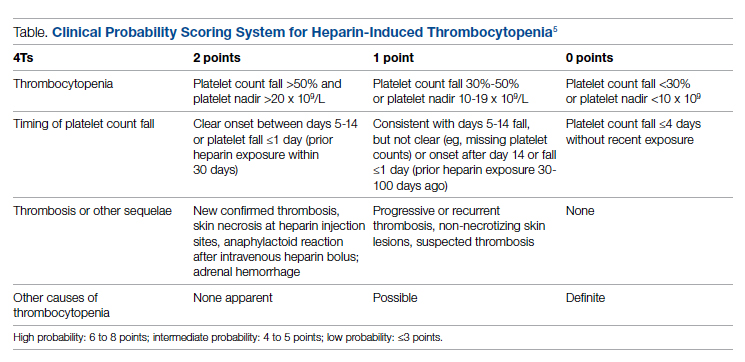
The enzyme-linked immunosorbent assay (ELISA) is a commonly used laboratory test to diagnose HIT that detects antibodies to the heparin-PF4 complex utilizing optical density (OD) units. When using an OD cutoff of 0.400, ELISA PF4 (PF4) tests have a sensitivity of 99.6%, but poor specificity at 69.3%.7 When the PF4 antibody test is positive with an OD ≥0.400, then a functional test is used to determine whether the antibodies detected will activate platelets. The serotonin-release assay (SRA) is a functional test that measures 14C-labeled serotonin release from donor platelets when mixed with patient serum or plasma containing HIT antibodies. In the correct clinical context, a positive ELISA PF4 antibody test along with a positive SRA is diagnostic of HIT.8
The process of diagnosing HIT in a timely and cost-effective manner is dependent on the clinician’s experience in diagnosing HIT as well as access to the laboratory testing necessary to confirm the diagnosis. PF4 antibody tests are time-consuming and not always available daily and/or are not available onsite. The SRA requires access to donor platelets and specialized radioactivity counting equipment, making it available only at particular centers.
The treatment of HIT is more straightforward and involves stopping all heparin products and starting a nonheparin anticoagulant. The direct thrombin inhibitor argatroban is one of the standard nonheparin anticoagulants used in patients with suspected HIT.4 While it is expensive, its short half-life and lack of renal clearance make it ideal for treatment of hospitalized patients with suspected HIT, many of whom need frequent procedures and/or have renal disease.
At our academic tertiary care center, we performed a retrospective analysis that showed inappropriate ordering of diagnostic HIT testing as well as unnecessary use of argatroban even when there was low suspicion for HIT based on laboratory findings. The aim of our project was to reduce unnecessary HIT testing and argatroban utilization without overburdening providers or interfering with established workflows.
Methods
Setting
The University of Michigan (UM) hospital is a 1000-bed tertiary care center in Ann Arbor, Michigan. The UM guidelines reflect evidence-based guidelines for the diagnosis and treatment of HIT.4 In 2016 the UM guidelines for laboratory testing included sending the PF4 antibody test first when there was clinical suspicion of HIT. The SRA was to be sent separately only when the PF4 returned positive (OD ≥ 0.400). Standard guidelines at UM also included switching patients with suspected HIT from heparin to a nonheparin anticoagulant and stopping all heparin products while awaiting the SRA results. The direct thrombin inhibitor argatroban is utilized at UM and monitored with anti-IIa levels. University of Michigan Hospital utilizes the Immucor PF4 IgG ELISA for detecting heparin-associated antibodies.9 In 2016, this PF4 test was performed in the UM onsite laboratory Monday through Friday. At UM the SRA is performed off site, with a turnaround time of 3 to 5 business days.
Baseline Data
We retrospectively reviewed PF4 and SRA testing as well as argatroban usage from December 2016 to May 2017. Despite the institutional guidelines, providers were sending PF4 and SRA simultaneously as soon as HIT was suspected; 62% of PF4 tests were ordered simultaneously with the SRA, but only 8% of these PF4 tests were positive with an OD ≥0.400. Of those patients with negative PF4 testing, argatroban was continued until the SRA returned negative, leading to many days of unnecessary argatroban usage. An informal survey of the anticoagulation pharmacists revealed that many recommended discontinuing argatroban when the PF4 test was negative, but providers routinely did not feel comfortable with this approach. This suggested many providers misunderstood the performance characteristics of the PF4 test.
Intervention
Our team consisted of hematology and internal medicine faculty, pharmacists, coagulation laboratory personnel, and quality improvement specialists. We designed and implemented an intervention in November 2017 focused on controlling the ordering of the SRA test. We chose to focus on this step due to the excellent sensitivity of the PF4 test with a cutoff of OD <0.400 and the significant expense of the SRA test. Under direction of the Coagulation Laboratory Director, a standard operating procedure was developed where the coagulation laboratory personnel did not send out the SRA until a positive PF4 test (OD ≥ 0.400) was reported. If the PF4 was negative, the SRA was canceled and the ordering provider received notification of the cancelled test via the electronic medical record, accompanied by education about HIT testing (Figure 1). In addition, the lab increased the availability of PF4 testing from 5 days to 7 days a week so there were no delays in tests ordered on Fridays or weekends.
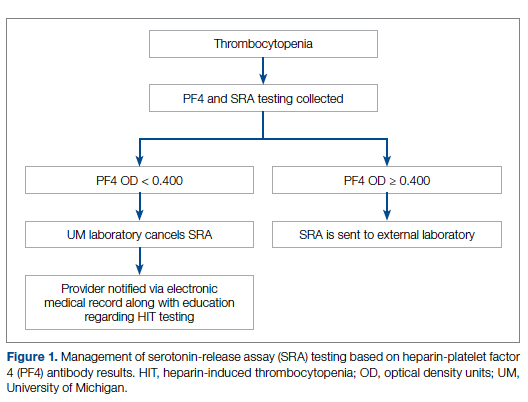
Outcomes
Our primary goals were to decrease both SRA testing and argatroban use. Secondarily, we examined the cost-effectiveness of this intervention. We hypothesized that controlling the SRA testing at the laboratory level would decrease both SRA testing and argatroban use.
Data Collection
Pre- and postintervention data were collected retrospectively. Pre-intervention data were from January 2016 through November 2017, and postintervention data were from December 2017 through March 2020. The number of SRA tests performed were identified retrospectively via review of electronic ordering records. All patients who had a hospital admission after January 1, 2016, were included. These patients were filtered to include only those who had a result for an SRA test. In order to calculate cost-savings, we identified both the number of SRA tests ordered retrospectively as well as patients who had both an SRA resulted and had been administered argatroban. Cost-savings were calculated based on our institutional cost of $357 per SRA test.
At our institution, argatroban is supplied in 50-mL bags; therefore, we utilized the number of bags to identify argatroban usage. Savings were calculated using the average wholesale price (AWP) of $292.50 per 50-mL bag. The amounts billed or collected for the SRA testing or argatroban treatment were not collected. Costs were estimated using only direct costs to the institution. Safety data were not collected. As the intent of our project was a quality improvement activity, this project did not require institutional review board regulation per our institutional guidance.
Results
During the pre-intervention period, the average number of admissions (adults and children) at UM was 5863 per month. Post intervention there was an average of 5842 admissions per month. A total of 1192 PF4 tests were ordered before the intervention and 1148 were ordered post intervention. Prior to the intervention, 481 SRA tests were completed, while post intervention 105 were completed. Serotonin-release testing decreased from an average of 3.7 SRA results per 1000 admissions during the pre-intervention period to an average of 0.6 per 1000 admissions post intervention (Figure 2). Cost-savings were $1045 per 1000 admissions.
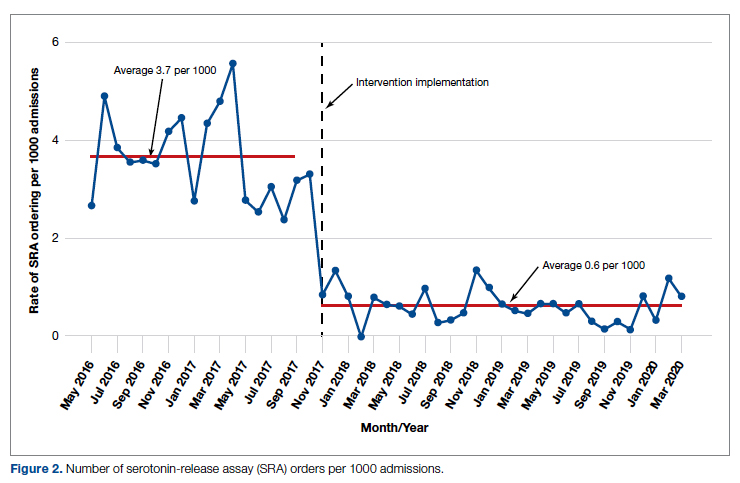
During the pre-intervention period, 2539 bags of argatroban were used, while 2337 bags were used post intervention. The number of 50-mL argatroban bags used per 1000 admissions decreased from 18.8 before the intervention to 14.3 post intervention. Cost-savings were $1316.20 per 1000 admissions. Figure 3 illustrates the monthly argatroban utilization per 1000 admissions during each quarter from January 2016 through March 2020.
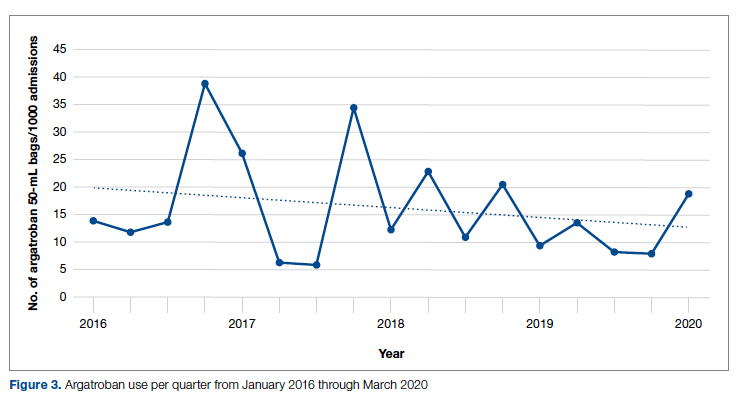
Discussion
We designed and implemented an evidence-based strategy for HIT at our academic institution which led to a decrease in unnecessary SRA testing and argatroban utilization, with associated cost savings. By focusing on a single point of intervention at the laboratory level where SRA tests were held and canceled if the PF4 test was negative, we helped offload the decision-making from the provider while simultaneously providing just-in-time education to the provider. This intervention was designed with input from multiple stakeholders, including physicians, quality improvement specialists, pharmacists, and coagulation laboratory personnel.
Serotonin-release testing dramatically decreased post intervention even though a similar number of PF4 tests were performed before and after the intervention. This suggests that the decrease in SRA testing was a direct consequence of our intervention. Post intervention the number of completed SRA tests was 9% of the number of PF4 tests sent. This is consistent with our baseline pre-intervention data showing that only 8% of all PF4 tests sent were positive.
While the absolute number of argatroban bags utilized did not dramatically decrease after the intervention, the quarterly rate did, particularly after 2018. Given that argatroban data were only drawn from patients with a concurrent SRA test, this decrease is clearly from decreased usage in patients with suspected HIT. We suspect the decrease occurred because argatroban was not being continued while awaiting an SRA test in patients with a negative PF4 test. Decreasing the utilization of argatroban not only saved money but also reduced days of exposure to argatroban. While we do not have data regarding adverse events related to argatroban prior to the intervention, it is logical to conclude that reducing unnecessary exposure to argatroban reduces the risk of adverse events related to bleeding. Future studies would ideally address specific safety outcome metrics such as adverse events, bleeding risk, or missed diagnoses of HIT.
Our institutional guidelines for the diagnosis of HIT are evidence-based and helpful but are rarely followed by busy inpatient providers. Controlling the utilization of the SRA at the laboratory level had several advantages. First, removing SRA decision-making from providers who are not experts in the diagnosis of HIT guaranteed adherence to evidence-based guidelines. Second, pharmacists could safely recommend discontinuing argatroban when the PF4 test was negative as there was no SRA pending. Third, with cancellation at the laboratory level there was no need to further burden providers with yet another alert in the electronic health record. Fourth, just-in-time education was provided to the providers with justification for why the SRA test was canceled. Last, ruling out HIT within 24 hours with the PF4 test alone allowed providers to evaluate patients for other causes of thrombocytopenia much earlier than the 3 to 5 business days before the SRA results returned.
A limitation of this study is that it was conducted at a single center. Our approach is also limited by the lack of universal applicability. At our institution we are fortunate to have PF4 testing available in our coagulation laboratory 7 days a week. In addition, the coagulation laboratory controls sending the SRA to the reference laboratory. The specific intervention of controlling the SRA testing is therefore applicable only to institutions similar to ours; however, the concept of removing control of specialized testing from the provider is not unique. Inpatient thrombophilia testing has been a successful target of this approach.11-13 While electronic alerts and education of individual providers can also be effective initially, the effectiveness of these interventions has been repeatedly shown to wane over time.14-16
Conclusion
At our institution we were able to implement practical, evidence-based testing for HIT by implementing control over SRA testing at the level of the laboratory. This approach led to decreased argatroban utilization and cost savings.
Corresponding author: Alice Cusick, MD; LTC Charles S Kettles VA Medical Center, 2215 Fuller Road, Ann Arbor, MI 48105; mccoyag@med.umich.edu
Disclosures: None reported.
doi: 10.12788/jcom.0087
1. Fountain E, Arepally GM. Thrombocytopenia in hospitalized non-ICU patients. Blood. 2015;126(23):1060. doi:10.1182/blood.v126.23.1060.1060
2. Hui P, Cook DJ, Lim W, Fraser GA, Arnold DM. The frequency and clinical significance of thrombocytopenia complicating critical illness: a systematic review. Chest. 2011;139(2):271-278. doi:10.1378/chest.10-2243
3. Warkentin TE. Heparin-induced thrombocytopenia. Curr Opin Crit Care. 2015;21(6):576-585. doi:10.1097/MCC.0000000000000259
4. Cuker A, Arepally GM, Chong BH, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: heparin-induced thrombocytopenia. Blood Adv. 2018;2(22):3360-3392. doi:10.1182/bloodadvances.2018024489
5. Cuker A, Gimotty PA, Crowther MA, Warkentin TE. Predictive value of the 4Ts scoring system for heparin-induced thrombocytopenia: a systematic review and meta-analysis. Blood. 2012;120(20):4160-4167. doi:10.1182/blood-2012-07-443051
6. Northam KA, Parker WF, Chen S-L, et al. Evaluation of 4Ts score inter-rater agreement in patients undergoing evaluation for heparin-induced thrombocytopenia. Blood Coagul Fibrinolysis. 2021;32(5):328-334. doi:10.1097/MBC.0000000000001042
7. Raschke RA, Curry SC, Warkentin TE, Gerkin RD. Improving clinical interpretation of the anti-platelet factor 4/heparin enzyme-linked immunosorbent assay for the diagnosis of heparin-induced thrombocytopenia through the use of receiver operating characteristic analysis, stratum-specific likelihood ratios, and Bayes theorem. Chest. 2013;144(4):1269-1275. doi:10.1378/chest.12-2712
8. Warkentin TE, Arnold DM, Nazi I, Kelton JG. The platelet serotonin-release assay. Am J Hematol. 2015;90(6):564-572. doi:10.1002/ajh.24006
9. Use IFOR, Contents TOF. LIFECODES ® PF4 IgG assay:1-9.
10. Ancker JS, Edwards A, Nosal S, Hauser D, Mauer E, Kaushal R. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med Inform Decis Mak. 2017;17(1):1-9. doi:10.1186/s12911-017-0430-8
11. O’Connor N, Carter-Johnson R. Effective screening of pathology tests controls costs: thrombophilia testing. J Clin Pathol. 2006;59(5):556. doi:10.1136/jcp.2005.030700
12. Lim MY, Greenberg CS. Inpatient thrombophilia testing: Impact of healthcare system technology and targeted clinician education on changing practice patterns. Vasc Med (United Kingdom). 2018;23(1):78-79. doi:10.1177/1358863X17742509
13. Cox JL, Shunkwiler SM, Koepsell SA. Requirement for a pathologist’s second signature limits inappropriate inpatient thrombophilia testing. Lab Med. 2017;48(4):367-371. doi:10.1093/labmed/lmx040
14. Kwang H, Mou E, Richman I, et al. Thrombophilia testing in the inpatient setting: impact of an educational intervention. BMC Med Inform Decis Mak. 2019;19(1):167. doi:10.1186/s12911-019-0889-6
15. Shah T, Patel-Teague S, Kroupa L, Meyer AND, Singh H. Impact of a national QI programme on reducing electronic health record notifications to clinicians. BMJ Qual Saf. 2019;28(1):10-14. doi:10.1136/bmjqs-2017-007447
16. Singh H, Spitzmueller C, Petersen NJ, Sawhney MK, Sittig DF. Information overload and missed test results in electronic health record-based settings. JAMA Intern Med. 2013;173(8):702-704. doi:10.1001/2013.jamainternmed.61
From the Veterans Affairs Ann Arbor Healthcare System Medicine Service (Dr. Cusick), University of Michigan College of Pharmacy, Clinical Pharmacy Service, Michigan Medicine (Dr. Hanigan), Department of Internal Medicine Clinical Experience and Quality, Michigan Medicine (Linda Bashaw), Department of Internal Medicine, University of Michigan Medical School, Ann Arbor, MI (Dr. Heidemann), and the Operational Excellence Department, Sparrow Health System, Lansing, MI (Matthew Johnson).
Abstract
Background: Diagnosis of heparin-induced thrombocytopenia (HIT) requires completion of an enzyme-linked immunosorbent assay (ELISA)–based heparin-platelet factor 4 (PF4) antibody test. If this test is negative, HIT is excluded. If positive, a serotonin-release assay (SRA) test is indicated. The SRA is expensive and sometimes inappropriately ordered despite negative PF4 results, leading to unnecessary treatment with argatroban while awaiting SRA results.
Objectives: The primary objectives of this project were to reduce unnecessary SRA testing and argatroban utilization in patients with suspected HIT.
Methods: The authors implemented an intervention at a tertiary care academic hospital in November 2017 targeting patients hospitalized with suspected HIT. The intervention was controlled at the level of the laboratory and prevented ordering of SRA tests in the absence of a positive PF4 test. The number of SRA tests performed and argatroban bags administered were identified retrospectively via chart review before the intervention (January 2016 to November 2017) and post intervention (December 2017 to March 2020). Associated costs were calculated based on institutional SRA testing cost as well as the average wholesale price of argatroban.
Results: SRA testing decreased from an average of 3.7 SRA results per 1000 admissions before the intervention to an average of 0.6 results per 1000 admissions post intervention. The number of 50-mL argatroban bags used per 1000 admissions decreased from 18.8 prior to the intervention to 14.3 post intervention. Total estimated cost savings per 1000 admissions was $2361.20.
Conclusion: An evidence-based testing strategy for HIT can be effectively implemented at the level of the laboratory. This approach led to reductions in SRA testing and argatroban utilization with resultant cost savings.
Keywords: HIT, argatroban, anticoagulation, serotonin-release assay.
Thrombocytopenia is a common finding in hospitalized patients.1,2 Heparin-induced thrombocytopenia (HIT) is one of the many potential causes of thrombocytopenia in hospitalized patients and occurs when antibodies to the heparin-platelet factor 4 (PF4) complex develop after heparin exposure. This triggers a cascade of events, leading to platelet activation, platelet consumption, and thrombosis. While HIT is relatively rare, occurring in 0.3% to 0.5% of critically ill patients, many patients will be tested to rule out this potentially life-threatening cause of thrombocytopenia.3
The diagnosis of HIT utilizes a combination of both clinical suspicion and laboratory testing.4 The 4T score (Table) was developed to evaluate the clinical probability of HIT and involves assessing the degree and timing of thrombocytopenia, the presence or absence of thrombosis, and other potential causes of the thrombocytopenia.5 The 4T score is designed to be utilized to identify patients who require laboratory testing for HIT; however, it has low inter-rater agreement in patients undergoing evaluation for HIT,6 and, in our experience, completion of this scoring is time-consuming.
The enzyme-linked immunosorbent assay (ELISA) is a commonly used laboratory test to diagnose HIT that detects antibodies to the heparin-PF4 complex utilizing optical density (OD) units. When using an OD cutoff of 0.400, ELISA PF4 (PF4) tests have a sensitivity of 99.6%, but poor specificity at 69.3%.7 When the PF4 antibody test is positive with an OD ≥0.400, then a functional test is used to determine whether the antibodies detected will activate platelets. The serotonin-release assay (SRA) is a functional test that measures 14C-labeled serotonin release from donor platelets when mixed with patient serum or plasma containing HIT antibodies. In the correct clinical context, a positive ELISA PF4 antibody test along with a positive SRA is diagnostic of HIT.8
The process of diagnosing HIT in a timely and cost-effective manner is dependent on the clinician’s experience in diagnosing HIT as well as access to the laboratory testing necessary to confirm the diagnosis. PF4 antibody tests are time-consuming and not always available daily and/or are not available onsite. The SRA requires access to donor platelets and specialized radioactivity counting equipment, making it available only at particular centers.
The treatment of HIT is more straightforward and involves stopping all heparin products and starting a nonheparin anticoagulant. The direct thrombin inhibitor argatroban is one of the standard nonheparin anticoagulants used in patients with suspected HIT.4 While it is expensive, its short half-life and lack of renal clearance make it ideal for treatment of hospitalized patients with suspected HIT, many of whom need frequent procedures and/or have renal disease.
At our academic tertiary care center, we performed a retrospective analysis that showed inappropriate ordering of diagnostic HIT testing as well as unnecessary use of argatroban even when there was low suspicion for HIT based on laboratory findings. The aim of our project was to reduce unnecessary HIT testing and argatroban utilization without overburdening providers or interfering with established workflows.
Methods
Setting
The University of Michigan (UM) hospital is a 1000-bed tertiary care center in Ann Arbor, Michigan. The UM guidelines reflect evidence-based guidelines for the diagnosis and treatment of HIT.4 In 2016 the UM guidelines for laboratory testing included sending the PF4 antibody test first when there was clinical suspicion of HIT. The SRA was to be sent separately only when the PF4 returned positive (OD ≥ 0.400). Standard guidelines at UM also included switching patients with suspected HIT from heparin to a nonheparin anticoagulant and stopping all heparin products while awaiting the SRA results. The direct thrombin inhibitor argatroban is utilized at UM and monitored with anti-IIa levels. University of Michigan Hospital utilizes the Immucor PF4 IgG ELISA for detecting heparin-associated antibodies.9 In 2016, this PF4 test was performed in the UM onsite laboratory Monday through Friday. At UM the SRA is performed off site, with a turnaround time of 3 to 5 business days.
Baseline Data
We retrospectively reviewed PF4 and SRA testing as well as argatroban usage from December 2016 to May 2017. Despite the institutional guidelines, providers were sending PF4 and SRA simultaneously as soon as HIT was suspected; 62% of PF4 tests were ordered simultaneously with the SRA, but only 8% of these PF4 tests were positive with an OD ≥0.400. Of those patients with negative PF4 testing, argatroban was continued until the SRA returned negative, leading to many days of unnecessary argatroban usage. An informal survey of the anticoagulation pharmacists revealed that many recommended discontinuing argatroban when the PF4 test was negative, but providers routinely did not feel comfortable with this approach. This suggested many providers misunderstood the performance characteristics of the PF4 test.
Intervention
Our team consisted of hematology and internal medicine faculty, pharmacists, coagulation laboratory personnel, and quality improvement specialists. We designed and implemented an intervention in November 2017 focused on controlling the ordering of the SRA test. We chose to focus on this step due to the excellent sensitivity of the PF4 test with a cutoff of OD <0.400 and the significant expense of the SRA test. Under direction of the Coagulation Laboratory Director, a standard operating procedure was developed where the coagulation laboratory personnel did not send out the SRA until a positive PF4 test (OD ≥ 0.400) was reported. If the PF4 was negative, the SRA was canceled and the ordering provider received notification of the cancelled test via the electronic medical record, accompanied by education about HIT testing (Figure 1). In addition, the lab increased the availability of PF4 testing from 5 days to 7 days a week so there were no delays in tests ordered on Fridays or weekends.
Outcomes
Our primary goals were to decrease both SRA testing and argatroban use. Secondarily, we examined the cost-effectiveness of this intervention. We hypothesized that controlling the SRA testing at the laboratory level would decrease both SRA testing and argatroban use.
Data Collection
Pre- and postintervention data were collected retrospectively. Pre-intervention data were from January 2016 through November 2017, and postintervention data were from December 2017 through March 2020. The number of SRA tests performed were identified retrospectively via review of electronic ordering records. All patients who had a hospital admission after January 1, 2016, were included. These patients were filtered to include only those who had a result for an SRA test. In order to calculate cost-savings, we identified both the number of SRA tests ordered retrospectively as well as patients who had both an SRA resulted and had been administered argatroban. Cost-savings were calculated based on our institutional cost of $357 per SRA test.
At our institution, argatroban is supplied in 50-mL bags; therefore, we utilized the number of bags to identify argatroban usage. Savings were calculated using the average wholesale price (AWP) of $292.50 per 50-mL bag. The amounts billed or collected for the SRA testing or argatroban treatment were not collected. Costs were estimated using only direct costs to the institution. Safety data were not collected. As the intent of our project was a quality improvement activity, this project did not require institutional review board regulation per our institutional guidance.
Results
During the pre-intervention period, the average number of admissions (adults and children) at UM was 5863 per month. Post intervention there was an average of 5842 admissions per month. A total of 1192 PF4 tests were ordered before the intervention and 1148 were ordered post intervention. Prior to the intervention, 481 SRA tests were completed, while post intervention 105 were completed. Serotonin-release testing decreased from an average of 3.7 SRA results per 1000 admissions during the pre-intervention period to an average of 0.6 per 1000 admissions post intervention (Figure 2). Cost-savings were $1045 per 1000 admissions.
During the pre-intervention period, 2539 bags of argatroban were used, while 2337 bags were used post intervention. The number of 50-mL argatroban bags used per 1000 admissions decreased from 18.8 before the intervention to 14.3 post intervention. Cost-savings were $1316.20 per 1000 admissions. Figure 3 illustrates the monthly argatroban utilization per 1000 admissions during each quarter from January 2016 through March 2020.
Discussion
We designed and implemented an evidence-based strategy for HIT at our academic institution which led to a decrease in unnecessary SRA testing and argatroban utilization, with associated cost savings. By focusing on a single point of intervention at the laboratory level where SRA tests were held and canceled if the PF4 test was negative, we helped offload the decision-making from the provider while simultaneously providing just-in-time education to the provider. This intervention was designed with input from multiple stakeholders, including physicians, quality improvement specialists, pharmacists, and coagulation laboratory personnel.
Serotonin-release testing dramatically decreased post intervention even though a similar number of PF4 tests were performed before and after the intervention. This suggests that the decrease in SRA testing was a direct consequence of our intervention. Post intervention the number of completed SRA tests was 9% of the number of PF4 tests sent. This is consistent with our baseline pre-intervention data showing that only 8% of all PF4 tests sent were positive.
While the absolute number of argatroban bags utilized did not dramatically decrease after the intervention, the quarterly rate did, particularly after 2018. Given that argatroban data were only drawn from patients with a concurrent SRA test, this decrease is clearly from decreased usage in patients with suspected HIT. We suspect the decrease occurred because argatroban was not being continued while awaiting an SRA test in patients with a negative PF4 test. Decreasing the utilization of argatroban not only saved money but also reduced days of exposure to argatroban. While we do not have data regarding adverse events related to argatroban prior to the intervention, it is logical to conclude that reducing unnecessary exposure to argatroban reduces the risk of adverse events related to bleeding. Future studies would ideally address specific safety outcome metrics such as adverse events, bleeding risk, or missed diagnoses of HIT.
Our institutional guidelines for the diagnosis of HIT are evidence-based and helpful but are rarely followed by busy inpatient providers. Controlling the utilization of the SRA at the laboratory level had several advantages. First, removing SRA decision-making from providers who are not experts in the diagnosis of HIT guaranteed adherence to evidence-based guidelines. Second, pharmacists could safely recommend discontinuing argatroban when the PF4 test was negative as there was no SRA pending. Third, with cancellation at the laboratory level there was no need to further burden providers with yet another alert in the electronic health record. Fourth, just-in-time education was provided to the providers with justification for why the SRA test was canceled. Last, ruling out HIT within 24 hours with the PF4 test alone allowed providers to evaluate patients for other causes of thrombocytopenia much earlier than the 3 to 5 business days before the SRA results returned.
A limitation of this study is that it was conducted at a single center. Our approach is also limited by the lack of universal applicability. At our institution we are fortunate to have PF4 testing available in our coagulation laboratory 7 days a week. In addition, the coagulation laboratory controls sending the SRA to the reference laboratory. The specific intervention of controlling the SRA testing is therefore applicable only to institutions similar to ours; however, the concept of removing control of specialized testing from the provider is not unique. Inpatient thrombophilia testing has been a successful target of this approach.11-13 While electronic alerts and education of individual providers can also be effective initially, the effectiveness of these interventions has been repeatedly shown to wane over time.14-16
Conclusion
At our institution we were able to implement practical, evidence-based testing for HIT by implementing control over SRA testing at the level of the laboratory. This approach led to decreased argatroban utilization and cost savings.
Corresponding author: Alice Cusick, MD; LTC Charles S Kettles VA Medical Center, 2215 Fuller Road, Ann Arbor, MI 48105; mccoyag@med.umich.edu
Disclosures: None reported.
doi: 10.12788/jcom.0087
From the Veterans Affairs Ann Arbor Healthcare System Medicine Service (Dr. Cusick), University of Michigan College of Pharmacy, Clinical Pharmacy Service, Michigan Medicine (Dr. Hanigan), Department of Internal Medicine Clinical Experience and Quality, Michigan Medicine (Linda Bashaw), Department of Internal Medicine, University of Michigan Medical School, Ann Arbor, MI (Dr. Heidemann), and the Operational Excellence Department, Sparrow Health System, Lansing, MI (Matthew Johnson).
Abstract
Background: Diagnosis of heparin-induced thrombocytopenia (HIT) requires completion of an enzyme-linked immunosorbent assay (ELISA)–based heparin-platelet factor 4 (PF4) antibody test. If this test is negative, HIT is excluded. If positive, a serotonin-release assay (SRA) test is indicated. The SRA is expensive and sometimes inappropriately ordered despite negative PF4 results, leading to unnecessary treatment with argatroban while awaiting SRA results.
Objectives: The primary objectives of this project were to reduce unnecessary SRA testing and argatroban utilization in patients with suspected HIT.
Methods: The authors implemented an intervention at a tertiary care academic hospital in November 2017 targeting patients hospitalized with suspected HIT. The intervention was controlled at the level of the laboratory and prevented ordering of SRA tests in the absence of a positive PF4 test. The number of SRA tests performed and argatroban bags administered were identified retrospectively via chart review before the intervention (January 2016 to November 2017) and post intervention (December 2017 to March 2020). Associated costs were calculated based on institutional SRA testing cost as well as the average wholesale price of argatroban.
Results: SRA testing decreased from an average of 3.7 SRA results per 1000 admissions before the intervention to an average of 0.6 results per 1000 admissions post intervention. The number of 50-mL argatroban bags used per 1000 admissions decreased from 18.8 prior to the intervention to 14.3 post intervention. Total estimated cost savings per 1000 admissions was $2361.20.
Conclusion: An evidence-based testing strategy for HIT can be effectively implemented at the level of the laboratory. This approach led to reductions in SRA testing and argatroban utilization with resultant cost savings.
Keywords: HIT, argatroban, anticoagulation, serotonin-release assay.
Thrombocytopenia is a common finding in hospitalized patients.1,2 Heparin-induced thrombocytopenia (HIT) is one of the many potential causes of thrombocytopenia in hospitalized patients and occurs when antibodies to the heparin-platelet factor 4 (PF4) complex develop after heparin exposure. This triggers a cascade of events, leading to platelet activation, platelet consumption, and thrombosis. While HIT is relatively rare, occurring in 0.3% to 0.5% of critically ill patients, many patients will be tested to rule out this potentially life-threatening cause of thrombocytopenia.3
The diagnosis of HIT utilizes a combination of both clinical suspicion and laboratory testing.4 The 4T score (Table) was developed to evaluate the clinical probability of HIT and involves assessing the degree and timing of thrombocytopenia, the presence or absence of thrombosis, and other potential causes of the thrombocytopenia.5 The 4T score is designed to be utilized to identify patients who require laboratory testing for HIT; however, it has low inter-rater agreement in patients undergoing evaluation for HIT,6 and, in our experience, completion of this scoring is time-consuming.
The enzyme-linked immunosorbent assay (ELISA) is a commonly used laboratory test to diagnose HIT that detects antibodies to the heparin-PF4 complex utilizing optical density (OD) units. When using an OD cutoff of 0.400, ELISA PF4 (PF4) tests have a sensitivity of 99.6%, but poor specificity at 69.3%.7 When the PF4 antibody test is positive with an OD ≥0.400, then a functional test is used to determine whether the antibodies detected will activate platelets. The serotonin-release assay (SRA) is a functional test that measures 14C-labeled serotonin release from donor platelets when mixed with patient serum or plasma containing HIT antibodies. In the correct clinical context, a positive ELISA PF4 antibody test along with a positive SRA is diagnostic of HIT.8
The process of diagnosing HIT in a timely and cost-effective manner is dependent on the clinician’s experience in diagnosing HIT as well as access to the laboratory testing necessary to confirm the diagnosis. PF4 antibody tests are time-consuming and not always available daily and/or are not available onsite. The SRA requires access to donor platelets and specialized radioactivity counting equipment, making it available only at particular centers.
The treatment of HIT is more straightforward and involves stopping all heparin products and starting a nonheparin anticoagulant. The direct thrombin inhibitor argatroban is one of the standard nonheparin anticoagulants used in patients with suspected HIT.4 While it is expensive, its short half-life and lack of renal clearance make it ideal for treatment of hospitalized patients with suspected HIT, many of whom need frequent procedures and/or have renal disease.
At our academic tertiary care center, we performed a retrospective analysis that showed inappropriate ordering of diagnostic HIT testing as well as unnecessary use of argatroban even when there was low suspicion for HIT based on laboratory findings. The aim of our project was to reduce unnecessary HIT testing and argatroban utilization without overburdening providers or interfering with established workflows.
Methods
Setting
The University of Michigan (UM) hospital is a 1000-bed tertiary care center in Ann Arbor, Michigan. The UM guidelines reflect evidence-based guidelines for the diagnosis and treatment of HIT.4 In 2016 the UM guidelines for laboratory testing included sending the PF4 antibody test first when there was clinical suspicion of HIT. The SRA was to be sent separately only when the PF4 returned positive (OD ≥ 0.400). Standard guidelines at UM also included switching patients with suspected HIT from heparin to a nonheparin anticoagulant and stopping all heparin products while awaiting the SRA results. The direct thrombin inhibitor argatroban is utilized at UM and monitored with anti-IIa levels. University of Michigan Hospital utilizes the Immucor PF4 IgG ELISA for detecting heparin-associated antibodies.9 In 2016, this PF4 test was performed in the UM onsite laboratory Monday through Friday. At UM the SRA is performed off site, with a turnaround time of 3 to 5 business days.
Baseline Data
We retrospectively reviewed PF4 and SRA testing as well as argatroban usage from December 2016 to May 2017. Despite the institutional guidelines, providers were sending PF4 and SRA simultaneously as soon as HIT was suspected; 62% of PF4 tests were ordered simultaneously with the SRA, but only 8% of these PF4 tests were positive with an OD ≥0.400. Of those patients with negative PF4 testing, argatroban was continued until the SRA returned negative, leading to many days of unnecessary argatroban usage. An informal survey of the anticoagulation pharmacists revealed that many recommended discontinuing argatroban when the PF4 test was negative, but providers routinely did not feel comfortable with this approach. This suggested many providers misunderstood the performance characteristics of the PF4 test.
Intervention
Our team consisted of hematology and internal medicine faculty, pharmacists, coagulation laboratory personnel, and quality improvement specialists. We designed and implemented an intervention in November 2017 focused on controlling the ordering of the SRA test. We chose to focus on this step due to the excellent sensitivity of the PF4 test with a cutoff of OD <0.400 and the significant expense of the SRA test. Under direction of the Coagulation Laboratory Director, a standard operating procedure was developed where the coagulation laboratory personnel did not send out the SRA until a positive PF4 test (OD ≥ 0.400) was reported. If the PF4 was negative, the SRA was canceled and the ordering provider received notification of the cancelled test via the electronic medical record, accompanied by education about HIT testing (Figure 1). In addition, the lab increased the availability of PF4 testing from 5 days to 7 days a week so there were no delays in tests ordered on Fridays or weekends.
Outcomes
Our primary goals were to decrease both SRA testing and argatroban use. Secondarily, we examined the cost-effectiveness of this intervention. We hypothesized that controlling the SRA testing at the laboratory level would decrease both SRA testing and argatroban use.
Data Collection
Pre- and postintervention data were collected retrospectively. Pre-intervention data were from January 2016 through November 2017, and postintervention data were from December 2017 through March 2020. The number of SRA tests performed were identified retrospectively via review of electronic ordering records. All patients who had a hospital admission after January 1, 2016, were included. These patients were filtered to include only those who had a result for an SRA test. In order to calculate cost-savings, we identified both the number of SRA tests ordered retrospectively as well as patients who had both an SRA resulted and had been administered argatroban. Cost-savings were calculated based on our institutional cost of $357 per SRA test.
At our institution, argatroban is supplied in 50-mL bags; therefore, we utilized the number of bags to identify argatroban usage. Savings were calculated using the average wholesale price (AWP) of $292.50 per 50-mL bag. The amounts billed or collected for the SRA testing or argatroban treatment were not collected. Costs were estimated using only direct costs to the institution. Safety data were not collected. As the intent of our project was a quality improvement activity, this project did not require institutional review board regulation per our institutional guidance.
Results
During the pre-intervention period, the average number of admissions (adults and children) at UM was 5863 per month. Post intervention there was an average of 5842 admissions per month. A total of 1192 PF4 tests were ordered before the intervention and 1148 were ordered post intervention. Prior to the intervention, 481 SRA tests were completed, while post intervention 105 were completed. Serotonin-release testing decreased from an average of 3.7 SRA results per 1000 admissions during the pre-intervention period to an average of 0.6 per 1000 admissions post intervention (Figure 2). Cost-savings were $1045 per 1000 admissions.
During the pre-intervention period, 2539 bags of argatroban were used, while 2337 bags were used post intervention. The number of 50-mL argatroban bags used per 1000 admissions decreased from 18.8 before the intervention to 14.3 post intervention. Cost-savings were $1316.20 per 1000 admissions. Figure 3 illustrates the monthly argatroban utilization per 1000 admissions during each quarter from January 2016 through March 2020.
Discussion
We designed and implemented an evidence-based strategy for HIT at our academic institution which led to a decrease in unnecessary SRA testing and argatroban utilization, with associated cost savings. By focusing on a single point of intervention at the laboratory level where SRA tests were held and canceled if the PF4 test was negative, we helped offload the decision-making from the provider while simultaneously providing just-in-time education to the provider. This intervention was designed with input from multiple stakeholders, including physicians, quality improvement specialists, pharmacists, and coagulation laboratory personnel.
Serotonin-release testing dramatically decreased post intervention even though a similar number of PF4 tests were performed before and after the intervention. This suggests that the decrease in SRA testing was a direct consequence of our intervention. Post intervention the number of completed SRA tests was 9% of the number of PF4 tests sent. This is consistent with our baseline pre-intervention data showing that only 8% of all PF4 tests sent were positive.
While the absolute number of argatroban bags utilized did not dramatically decrease after the intervention, the quarterly rate did, particularly after 2018. Given that argatroban data were only drawn from patients with a concurrent SRA test, this decrease is clearly from decreased usage in patients with suspected HIT. We suspect the decrease occurred because argatroban was not being continued while awaiting an SRA test in patients with a negative PF4 test. Decreasing the utilization of argatroban not only saved money but also reduced days of exposure to argatroban. While we do not have data regarding adverse events related to argatroban prior to the intervention, it is logical to conclude that reducing unnecessary exposure to argatroban reduces the risk of adverse events related to bleeding. Future studies would ideally address specific safety outcome metrics such as adverse events, bleeding risk, or missed diagnoses of HIT.
Our institutional guidelines for the diagnosis of HIT are evidence-based and helpful but are rarely followed by busy inpatient providers. Controlling the utilization of the SRA at the laboratory level had several advantages. First, removing SRA decision-making from providers who are not experts in the diagnosis of HIT guaranteed adherence to evidence-based guidelines. Second, pharmacists could safely recommend discontinuing argatroban when the PF4 test was negative as there was no SRA pending. Third, with cancellation at the laboratory level there was no need to further burden providers with yet another alert in the electronic health record. Fourth, just-in-time education was provided to the providers with justification for why the SRA test was canceled. Last, ruling out HIT within 24 hours with the PF4 test alone allowed providers to evaluate patients for other causes of thrombocytopenia much earlier than the 3 to 5 business days before the SRA results returned.
A limitation of this study is that it was conducted at a single center. Our approach is also limited by the lack of universal applicability. At our institution we are fortunate to have PF4 testing available in our coagulation laboratory 7 days a week. In addition, the coagulation laboratory controls sending the SRA to the reference laboratory. The specific intervention of controlling the SRA testing is therefore applicable only to institutions similar to ours; however, the concept of removing control of specialized testing from the provider is not unique. Inpatient thrombophilia testing has been a successful target of this approach.11-13 While electronic alerts and education of individual providers can also be effective initially, the effectiveness of these interventions has been repeatedly shown to wane over time.14-16
Conclusion
At our institution we were able to implement practical, evidence-based testing for HIT by implementing control over SRA testing at the level of the laboratory. This approach led to decreased argatroban utilization and cost savings.
Corresponding author: Alice Cusick, MD; LTC Charles S Kettles VA Medical Center, 2215 Fuller Road, Ann Arbor, MI 48105; mccoyag@med.umich.edu
Disclosures: None reported.
doi: 10.12788/jcom.0087
1. Fountain E, Arepally GM. Thrombocytopenia in hospitalized non-ICU patients. Blood. 2015;126(23):1060. doi:10.1182/blood.v126.23.1060.1060
2. Hui P, Cook DJ, Lim W, Fraser GA, Arnold DM. The frequency and clinical significance of thrombocytopenia complicating critical illness: a systematic review. Chest. 2011;139(2):271-278. doi:10.1378/chest.10-2243
3. Warkentin TE. Heparin-induced thrombocytopenia. Curr Opin Crit Care. 2015;21(6):576-585. doi:10.1097/MCC.0000000000000259
4. Cuker A, Arepally GM, Chong BH, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: heparin-induced thrombocytopenia. Blood Adv. 2018;2(22):3360-3392. doi:10.1182/bloodadvances.2018024489
5. Cuker A, Gimotty PA, Crowther MA, Warkentin TE. Predictive value of the 4Ts scoring system for heparin-induced thrombocytopenia: a systematic review and meta-analysis. Blood. 2012;120(20):4160-4167. doi:10.1182/blood-2012-07-443051
6. Northam KA, Parker WF, Chen S-L, et al. Evaluation of 4Ts score inter-rater agreement in patients undergoing evaluation for heparin-induced thrombocytopenia. Blood Coagul Fibrinolysis. 2021;32(5):328-334. doi:10.1097/MBC.0000000000001042
7. Raschke RA, Curry SC, Warkentin TE, Gerkin RD. Improving clinical interpretation of the anti-platelet factor 4/heparin enzyme-linked immunosorbent assay for the diagnosis of heparin-induced thrombocytopenia through the use of receiver operating characteristic analysis, stratum-specific likelihood ratios, and Bayes theorem. Chest. 2013;144(4):1269-1275. doi:10.1378/chest.12-2712
8. Warkentin TE, Arnold DM, Nazi I, Kelton JG. The platelet serotonin-release assay. Am J Hematol. 2015;90(6):564-572. doi:10.1002/ajh.24006
9. Use IFOR, Contents TOF. LIFECODES ® PF4 IgG assay:1-9.
10. Ancker JS, Edwards A, Nosal S, Hauser D, Mauer E, Kaushal R. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med Inform Decis Mak. 2017;17(1):1-9. doi:10.1186/s12911-017-0430-8
11. O’Connor N, Carter-Johnson R. Effective screening of pathology tests controls costs: thrombophilia testing. J Clin Pathol. 2006;59(5):556. doi:10.1136/jcp.2005.030700
12. Lim MY, Greenberg CS. Inpatient thrombophilia testing: Impact of healthcare system technology and targeted clinician education on changing practice patterns. Vasc Med (United Kingdom). 2018;23(1):78-79. doi:10.1177/1358863X17742509
13. Cox JL, Shunkwiler SM, Koepsell SA. Requirement for a pathologist’s second signature limits inappropriate inpatient thrombophilia testing. Lab Med. 2017;48(4):367-371. doi:10.1093/labmed/lmx040
14. Kwang H, Mou E, Richman I, et al. Thrombophilia testing in the inpatient setting: impact of an educational intervention. BMC Med Inform Decis Mak. 2019;19(1):167. doi:10.1186/s12911-019-0889-6
15. Shah T, Patel-Teague S, Kroupa L, Meyer AND, Singh H. Impact of a national QI programme on reducing electronic health record notifications to clinicians. BMJ Qual Saf. 2019;28(1):10-14. doi:10.1136/bmjqs-2017-007447
16. Singh H, Spitzmueller C, Petersen NJ, Sawhney MK, Sittig DF. Information overload and missed test results in electronic health record-based settings. JAMA Intern Med. 2013;173(8):702-704. doi:10.1001/2013.jamainternmed.61
1. Fountain E, Arepally GM. Thrombocytopenia in hospitalized non-ICU patients. Blood. 2015;126(23):1060. doi:10.1182/blood.v126.23.1060.1060
2. Hui P, Cook DJ, Lim W, Fraser GA, Arnold DM. The frequency and clinical significance of thrombocytopenia complicating critical illness: a systematic review. Chest. 2011;139(2):271-278. doi:10.1378/chest.10-2243
3. Warkentin TE. Heparin-induced thrombocytopenia. Curr Opin Crit Care. 2015;21(6):576-585. doi:10.1097/MCC.0000000000000259
4. Cuker A, Arepally GM, Chong BH, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: heparin-induced thrombocytopenia. Blood Adv. 2018;2(22):3360-3392. doi:10.1182/bloodadvances.2018024489
5. Cuker A, Gimotty PA, Crowther MA, Warkentin TE. Predictive value of the 4Ts scoring system for heparin-induced thrombocytopenia: a systematic review and meta-analysis. Blood. 2012;120(20):4160-4167. doi:10.1182/blood-2012-07-443051
6. Northam KA, Parker WF, Chen S-L, et al. Evaluation of 4Ts score inter-rater agreement in patients undergoing evaluation for heparin-induced thrombocytopenia. Blood Coagul Fibrinolysis. 2021;32(5):328-334. doi:10.1097/MBC.0000000000001042
7. Raschke RA, Curry SC, Warkentin TE, Gerkin RD. Improving clinical interpretation of the anti-platelet factor 4/heparin enzyme-linked immunosorbent assay for the diagnosis of heparin-induced thrombocytopenia through the use of receiver operating characteristic analysis, stratum-specific likelihood ratios, and Bayes theorem. Chest. 2013;144(4):1269-1275. doi:10.1378/chest.12-2712
8. Warkentin TE, Arnold DM, Nazi I, Kelton JG. The platelet serotonin-release assay. Am J Hematol. 2015;90(6):564-572. doi:10.1002/ajh.24006
9. Use IFOR, Contents TOF. LIFECODES ® PF4 IgG assay:1-9.
10. Ancker JS, Edwards A, Nosal S, Hauser D, Mauer E, Kaushal R. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med Inform Decis Mak. 2017;17(1):1-9. doi:10.1186/s12911-017-0430-8
11. O’Connor N, Carter-Johnson R. Effective screening of pathology tests controls costs: thrombophilia testing. J Clin Pathol. 2006;59(5):556. doi:10.1136/jcp.2005.030700
12. Lim MY, Greenberg CS. Inpatient thrombophilia testing: Impact of healthcare system technology and targeted clinician education on changing practice patterns. Vasc Med (United Kingdom). 2018;23(1):78-79. doi:10.1177/1358863X17742509
13. Cox JL, Shunkwiler SM, Koepsell SA. Requirement for a pathologist’s second signature limits inappropriate inpatient thrombophilia testing. Lab Med. 2017;48(4):367-371. doi:10.1093/labmed/lmx040
14. Kwang H, Mou E, Richman I, et al. Thrombophilia testing in the inpatient setting: impact of an educational intervention. BMC Med Inform Decis Mak. 2019;19(1):167. doi:10.1186/s12911-019-0889-6
15. Shah T, Patel-Teague S, Kroupa L, Meyer AND, Singh H. Impact of a national QI programme on reducing electronic health record notifications to clinicians. BMJ Qual Saf. 2019;28(1):10-14. doi:10.1136/bmjqs-2017-007447
16. Singh H, Spitzmueller C, Petersen NJ, Sawhney MK, Sittig DF. Information overload and missed test results in electronic health record-based settings. JAMA Intern Med. 2013;173(8):702-704. doi:10.1001/2013.jamainternmed.61