User login
Heart failure readmission-reducing device debuts slowly
In an era when rehospitalization of patients with heart failure for episodes of acute decompensation has become a top target for reduction in the U.S. health care system via Medicare’s Readmissions Reduction Program CardioMEMS looks like the tool that every U.S. health care system and medical center has dreamed of having.
A wireless and battery-less implanted device, CardioMEMS guides management of stage III heart failure patients by allowing daily monitoring of patients’ pulmonary-artery pressure (PAP). Using these measures to fine-tune patient treatment with diuretics and vasodilators led to a statistically significant and clinically meaningful 37% relative reduction in heart failure rehospitalizations over an average 15-month follow-up, based on results from CardioMEMS’ pivotal U.S. trial as well as from subsequent secondary analyses. All-cause mortality was reduced and patients’ quality of life improved. And device-driven therapy yielded these benefits equally well in patients with either preserved or reduced left ventricular function as well as in a variety of other subgroups including patients with cardiac resynchronization devices or implantable cardioverter defibrillators, chronic obstructive pulmonary disease, chronic kidney disease, atrial fibrillation, pulmonary hypertension, or a history of myocardial infarction.
Yet in the first year after CardioMEMS received Food and Drug Administration approval and came onto the U.S. market, the device has taken a strikingly slow path into routine heart failure practice, according to heart failure cardiologists at several U.S. centers. A representative of St. Jude, the company that markets CardioMEMS, saidin July that sales of the device during the first half of 2015 had involved more than 200 U.S. customers and slightly surpassed earlier expectations, and the company now anticipated full 2015 sales to run roughly 25% ahead of projections made at the start of this year. Despite that, the company’s second quarter report acknowledged the challenges that CardioMEMS faced during its first year on the U.S. market.
Numbers show a slow rollout
“I belong to a consortium of academic heart failure physicians who come from many of the major U.S. academic medical centers, and a recent straw poll of the members showed that close to no one was using it [CardioMEMS] on a regular basis, and the majority said they were not yet using it at all or in the process of starting their program,” said Dr. Javed Butler, a heart failure specialist who is professor of medicine, chief of cardiology, and codirector of the Stony Brook (N.Y.) University Heart Center.

At Stony Brook, no heart failure patient had received the device as of July 2015, although Dr. Butler said that his program’s use of CardioMEMS will probably start soon. Cardiologists at a handful of other U.S. centers report similarly slow starts.
At Massachusetts General Hospital (MGH) in Boston not a single patient has received CardioMEMS, though the heart failure staff there hopes to soon launch pilot use in 10 patients, said Dr. Kimberly A. Parks, associate director of the resynchronization and advanced cardiac therapeutics program. At the University of Colorado Hospital in Aurora, three patients have received the device since their first implant in the late winter, and the program is now on track to place devices in another one or two patients each month, said Dr. Natasha L. Altman, a cardiologist who heads the center’s CardioMEMS program. At Brigham and Women’s Hospital in Boston, which participated in the CHAMPION (CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients) pivotal trial that led to CardioMEMS approval, so far a “handful, fewer than 10 patients” received the device since marketing began, said Dr. Akshay S. Desai, associate director of Brigham Cardiovascular Consultants. Even at Ohio State’s Wexner Medical Center in Columbus, the program run by Dr. William T. Abraham, coprincipal investigator for CHAMPION, a relatively modest number of roughly 50 patients had received CardioMEMS in routine practice since the first patient received a device there in June 2014 following the FDA’s approval, Dr. Abraham said in an interview.

Contrasting with this level of use is the substantial number of patients who meet the CHAMPION enrollment criteria of New York Heart Association class III heart failure and a heart failure hospitalization within the prior year. Experts estimate that throughout the United States this group must number at least a half-million patients, and at the level of individual medical centers that provide advanced heart failure care, the numbers likely reach several hundred patients at each site.
Several challenges slow CardioMEMS implantation
Why such a slow start for what seems to be such an attractive device that clinicians uniformly praise for having a strong evidence base in CHAMPION and a compelling medical rationale? The answer seems multifactorial, including the need to convince skeptical hospital administrators and insurance payers to provide and pay for the device and follow-up care, a requirement to ramp up the patient-monitoring and management infrastructure, and the challenge of transitioning a relatively complex therapeutic formula from a successful clinical trial model into routine care.
“If this was a pill that you could prescribe to patients at hospital discharge, people would jump on it. But CardioMEMS is not as simple as prescribing a pill. There are a lot of logistical issues that make it very difficult,” said Stony Brook’s Dr. Butler in an interview.
This sentiment was shared not only by other cardiologists but also by St. Jude itself, as a company spokesman itemized several challenges the company encountered once it began trying to sell CardioMEMS commercially. “Developing the market for CardioMEMS will continue to take time,” said the St. Jude staffer during a July webcast on the company’s second-quarter 2015 performance. CardioMEMS’ sales were affected by the need to educate multiple constituencies, satisfy new-technology review committees, address reimbursement, access capital budgets, and create consensus among disparate stakeholders, the webcast said. In addition, the early St. Jude experience selling CardioMEMS showed that once a new customer signs a contract, “we find that customers tend to introduce CardioMEMS ... [on] a pilot basis to gain experience with the technology and the reimbursement process.”

First is the challenge of selling a hospital’s administrative leadership on making an upfront capital investment in CardioMEMS equipment, giving the green light to performing procedures that just about break even relative to reimbursement, and then waiting to recoup the initial expenditure and perhaps make some money in the long term by avoiding readmissions and cutting lengths of stay. According to an analysis run by Dr. Parks of MGH, based on the CHAMPION results, for every 10 patients managed using CardioMEMS for 6 months, a center could expect to prevent nearly 15 patient-days in the hospital.
“Our administration is in support, but skeptical; I think that’s why it’s been slow to start,” said Dr. Parks. “The biggest limitation is the upfront cost of the device, and it’s not clear that the reimbursement will allow you to break even” when putting in devices, she said in an interview. “You could justify this by saying you’ll reduce hospitalizations, but the first impression from our administrators was that we were already doing a pretty good job limiting rehospitalizations so why do we need to add this?” The MGH leadership and clinicians eventually agreed on a plan to start the program with 10 implants and then analyze the results to decide if it makes sense to continue. Dr. Parks said she and her colleagues hope to have their first 10 patients implanted with a CardioMEMS before the end of this year.
Another hurdle at MGH was setting up the infrastructure so that a nurse could monitor patients and set in motion the alerts and treatment changes designed to normalize PAP normalized when it falls out of the target range. “It’s a lot of work to put the system in place to manage the devices,” Dr. Parks noted.
Dr. Butler echoed both these challenges. “You need to convince the hospital administrators and make a case based on the cost savings [later on during ongoing management] rather than positive revenue when you do the procedure. If you can expect future cost savings it’s a viable case to make, but a more difficult case to make,” he said. “You also take on the liability of monitoring patients” long term. “If you can follow several hundred patients there may be enough [follow-up] interventions to pay the salaries of staff ” who monitor the patients, but it is very difficult if you have a nurse who is monitoring five patients,” he said. Another issue complicating the economics is that the physicians who supervise monitoring are mostly not the same ones who performed the CardioMEMS placement procedure and received the procedure’s reimbursement. “These are the system barriers that are out there,” Dr. Butler said.
Dr. Altman in Colorado faced a different challenge. “We had good buy-in from our administration. Everyone is interested in reducing rehospitalizations so the administrators were very supportive. The major roadblock has been insurers. Medicare covers it, but so far Colorado Medicaid and several private insurers do not,” Dr. Altman said in an interview. The inconsistent pattern of insurance coverage has already meant that some heart failure patients in her program who were good clinical candidates for CardioMEMS could not receive the device. “I’ve had at least six or seven good candidates, but only three received the device because of insurance reimbursement issues,” she said.
But Dr. Altman expressed optimism that the coverage situation would improve as more programs start using CarioMEMS and insurers grow more familiar with daily PAP monitoring of heart failure patients. She noted that a new CardioMEMS program will soon start at a second Denver-based medical center, and she expressed confidence that ongoing pressure from physicians and administrators at both institutions will change the mind of officials at Colorado’s Medicaid program to provide reimbursement, and once that happens she expects the private insurers will change their policies as well.
To Dr. Abraham at Ohio State, one of the developers of the concept of using an implanted PAP monitor to guide management of heart failure patients, CardioMEMS slow take off is not surprising. “It provides physicians with daily information on a patient’s hemodynamics, which is something they never had before except in the catheterization laboratory, intensive care unit or cardiac care unit. Managing patients based on hemodynamics even in the absence of worsening signs and symptoms is a paradigm shift. It takes time to adopt new things.” He noted that most hospitals and health systems already have in place case managers or nurse navigators who run systems that have relied on the insensitive parameters of signs, symptoms, and patients’ weights. The same infrastructure should be able to fairly easily switch to focusing instead on PAP, said Dr. Abraham, professor and director of cardiovascular medicine at Wexner Medical Center.
He acknowledged that the upfront capital cost required to start a CardioMEMS program can poses a financial barrier at many U.S. centers, but once that start-up price is paid the actual implantation into each patient comes close to breaking even with existing reimbursements and the system should eventually result in a return on the investment in the form of reduced readmissions and keeping patients stable, he said. Dr. Abraham suggested that the possibility also exists that maintaining better stability in patients with class III heart failure and preventing episodes of acute decompensation through better-titrated fluid-volume control could produce a long-term change in the natural history of these patients, whose disease historically has been marked by progression to class IV heart failure and the eventual need for a left ventricular assist device, heart transplant, and death. Although this potential impact of refined treatment based on daily PAP monitoring remains to be proven, a secondary analysis from CHAMPION showing a 57% relative reduction in all-cause mortality over an average of 17 months of follow-up that Dr. Abraham reported at the American College of Cardiology annual meeting in March
The hurdle of routine practice
Transitioning CardioMEMS from its successful research track record to everyday clinical practice may pose the trickiest barrier of all. The consensus among heart failure experts seems to be that the best approach to do this successfully is to start slow, focus on the most rational patients within the broad enrollment criteria used in CHAMPION, and then gradually expand from that presuming the first wave of results from routine use at a particular site look similar to those from the trial.

“The next big question for PAP monitoring is can we replicate the trial’s success in routine practice? Can this be scaled up?” said Dr. Desai from Brigham and Women’s. “We’re still learning how to identify the right patients, the ones who’ll benefit,”
“The two types of patients we are primarily implanting now are those with classic class III heart failure who were hospitalized during the past 12 months and now are hospitalized again and are right in front of us. They are the lowest-hanging fruit because they are in the hospital today,” said Dr. Abraham. “The second group are the patients who come into the clinic complaining about their symptoms. What we are not yet doing is calling in all patients” with stage III heart failure and a history of at least one hospitalization.”
Other groups are taking a much more selective approach. Dr. Altman and her colleagues in Denver are only targeting patients who have been hospitalized at least twice within the past year, and more specifically patients recently rehospitalized within 30 days of their prior hospitalization. They are also focusing on patients expected to have a high level of compliance with the daily data-collection demands of PAP monitoring and the need to regularly adjust their medication dosages after receiving call backs from their clinicians. This criteria means that they are ruling out patients with a history of substance abuse, she said.
She also noted the need to tailor the target PAP to the specific clinical status of individual patients. Patients with mitral regurgitation, for example, will have a higher “normal” diastolic PAP and hence require a somewhat different target for stability maintenance. “You need to understand each patient’s baseline pressures and adjust their medications based on that,” Dr. Altman said.
“In real life patients tend to be older and sicker, so their benefit may be even greater than what was seen in CHAMPION, but perhaps the results will also be diluted because of comorbidities like renal failure or chronic obstructive pulmonary disease,” said Dr. Butler, although post hoc subanalyses of CHAMPION data showed that these comorbidities did not blunt the positive impact of PAP-guided treatment. “I don’t know if I’ll be successful in selecting the right patients, and whether my interventions in real life will produce the same good outcomes” seen in CHAMPION. “We’ll select patients who are close to the CHAMPION criteria, but not patients on dialysis [who were excluded from CHAMPION]; we’ll select patients with a modest degree of comorbidity and reasonable expected survival,” Dr. Butler said.
“If you had a drug that reduced rehospitalization rates it would be pretty clear how to proceed, but in this case it is not the device that reduces readmissions, it just gives you data and you need to act on the data,” Dr. Butler added. He acknowledged that the CHAMPION investigators used a relatively simple, straightforward management algorithm for patients whose PAP fell out of the target range, such as a diastolic PAP greater than 20 mm Hg or less than 8 mm Hg. The first management step is to raise or reduce the patient’s diuretic dosage, and if that fails to quickly normalize PAP the next step is to adjust the vasodilator dosage.
Managing patients in CHAMPION was “not totally an art” but neither was it “totally a science,” Dr. Butler said. Managing patients based on daily data collected using a CardioMEMS device will “require a little finesse,” he said. “It’s not straight science.”
Programs that have already used PAP monitoring on a routine basis, like those in Denver and at Brigham and Women’s, consider their experience too small in size and short in duration to draw any substantive conclusions regarding their success compared with the CHAMPION results. But Dr. Abraham, whose program has now placed CardioMEMS routinely in a few dozen patients and followed them for as long as a year, said that in his center’s patients the device and management system has produced outcomes that roughly match what he saw in the pivotal trial.
“The ongoing concern is that what was achieved in the CHAMPION trial may not be what is achieved in routine practice,” said Dr. Desai. The care that patients received in the trial is “a little of a black box,” he said, and during the FDA’s approval process some reviewers raised concerns that patients in the active-treatment arm simply received more intensive surveillance, although this concern eventually resolved. “There is not a lot of skepticism” among clinicians about this treatment, but there is uncertainly about exactly whom are the best patients to treat and whether their responses be as good as in CHAMPION, Dr. Desai said in an interview.
“The proof [of efficacy] will be in each individual center’s experience” using CardioMEMS, Dr. Altman said.
CHAMPION was initially funded by CardioMEMS, which then was acquired by St. Jude which is the company marketing the CardioMEMS device and associated hardware. Dr. Butler said that he had no current relevant disclosures, although in the past he had been a consultant to CardioMEMS (prior to its acquisition by St. Jude). Dr. Parks and Dr. Altman had no disclosures. Dr. Desai has been a consultant to and has received honoraria as a speaker on behalf of CardioMEMS and St. Jude. Dr. Abraham has been a consultant to CardioMEMS and St. Jude, was co-principal investigator on the CHAMPION trial, and is the principal investigator on a new St. Jude-funded trial studying CardioMEMS.
On Twitter @mitchelzoler
In an era when rehospitalization of patients with heart failure for episodes of acute decompensation has become a top target for reduction in the U.S. health care system via Medicare’s Readmissions Reduction Program CardioMEMS looks like the tool that every U.S. health care system and medical center has dreamed of having.
A wireless and battery-less implanted device, CardioMEMS guides management of stage III heart failure patients by allowing daily monitoring of patients’ pulmonary-artery pressure (PAP). Using these measures to fine-tune patient treatment with diuretics and vasodilators led to a statistically significant and clinically meaningful 37% relative reduction in heart failure rehospitalizations over an average 15-month follow-up, based on results from CardioMEMS’ pivotal U.S. trial as well as from subsequent secondary analyses. All-cause mortality was reduced and patients’ quality of life improved. And device-driven therapy yielded these benefits equally well in patients with either preserved or reduced left ventricular function as well as in a variety of other subgroups including patients with cardiac resynchronization devices or implantable cardioverter defibrillators, chronic obstructive pulmonary disease, chronic kidney disease, atrial fibrillation, pulmonary hypertension, or a history of myocardial infarction.
Yet in the first year after CardioMEMS received Food and Drug Administration approval and came onto the U.S. market, the device has taken a strikingly slow path into routine heart failure practice, according to heart failure cardiologists at several U.S. centers. A representative of St. Jude, the company that markets CardioMEMS, saidin July that sales of the device during the first half of 2015 had involved more than 200 U.S. customers and slightly surpassed earlier expectations, and the company now anticipated full 2015 sales to run roughly 25% ahead of projections made at the start of this year. Despite that, the company’s second quarter report acknowledged the challenges that CardioMEMS faced during its first year on the U.S. market.
Numbers show a slow rollout
“I belong to a consortium of academic heart failure physicians who come from many of the major U.S. academic medical centers, and a recent straw poll of the members showed that close to no one was using it [CardioMEMS] on a regular basis, and the majority said they were not yet using it at all or in the process of starting their program,” said Dr. Javed Butler, a heart failure specialist who is professor of medicine, chief of cardiology, and codirector of the Stony Brook (N.Y.) University Heart Center.
At Stony Brook, no heart failure patient had received the device as of July 2015, although Dr. Butler said that his program’s use of CardioMEMS will probably start soon. Cardiologists at a handful of other U.S. centers report similarly slow starts.
At Massachusetts General Hospital (MGH) in Boston not a single patient has received CardioMEMS, though the heart failure staff there hopes to soon launch pilot use in 10 patients, said Dr. Kimberly A. Parks, associate director of the resynchronization and advanced cardiac therapeutics program. At the University of Colorado Hospital in Aurora, three patients have received the device since their first implant in the late winter, and the program is now on track to place devices in another one or two patients each month, said Dr. Natasha L. Altman, a cardiologist who heads the center’s CardioMEMS program. At Brigham and Women’s Hospital in Boston, which participated in the CHAMPION (CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients) pivotal trial that led to CardioMEMS approval, so far a “handful, fewer than 10 patients” received the device since marketing began, said Dr. Akshay S. Desai, associate director of Brigham Cardiovascular Consultants. Even at Ohio State’s Wexner Medical Center in Columbus, the program run by Dr. William T. Abraham, coprincipal investigator for CHAMPION, a relatively modest number of roughly 50 patients had received CardioMEMS in routine practice since the first patient received a device there in June 2014 following the FDA’s approval, Dr. Abraham said in an interview.
Contrasting with this level of use is the substantial number of patients who meet the CHAMPION enrollment criteria of New York Heart Association class III heart failure and a heart failure hospitalization within the prior year. Experts estimate that throughout the United States this group must number at least a half-million patients, and at the level of individual medical centers that provide advanced heart failure care, the numbers likely reach several hundred patients at each site.
Several challenges slow CardioMEMS implantation
Why such a slow start for what seems to be such an attractive device that clinicians uniformly praise for having a strong evidence base in CHAMPION and a compelling medical rationale? The answer seems multifactorial, including the need to convince skeptical hospital administrators and insurance payers to provide and pay for the device and follow-up care, a requirement to ramp up the patient-monitoring and management infrastructure, and the challenge of transitioning a relatively complex therapeutic formula from a successful clinical trial model into routine care.
“If this was a pill that you could prescribe to patients at hospital discharge, people would jump on it. But CardioMEMS is not as simple as prescribing a pill. There are a lot of logistical issues that make it very difficult,” said Stony Brook’s Dr. Butler in an interview.
This sentiment was shared not only by other cardiologists but also by St. Jude itself, as a company spokesman itemized several challenges the company encountered once it began trying to sell CardioMEMS commercially. “Developing the market for CardioMEMS will continue to take time,” said the St. Jude staffer during a July webcast on the company’s second-quarter 2015 performance. CardioMEMS’ sales were affected by the need to educate multiple constituencies, satisfy new-technology review committees, address reimbursement, access capital budgets, and create consensus among disparate stakeholders, the webcast said. In addition, the early St. Jude experience selling CardioMEMS showed that once a new customer signs a contract, “we find that customers tend to introduce CardioMEMS ... [on] a pilot basis to gain experience with the technology and the reimbursement process.”
First is the challenge of selling a hospital’s administrative leadership on making an upfront capital investment in CardioMEMS equipment, giving the green light to performing procedures that just about break even relative to reimbursement, and then waiting to recoup the initial expenditure and perhaps make some money in the long term by avoiding readmissions and cutting lengths of stay. According to an analysis run by Dr. Parks of MGH, based on the CHAMPION results, for every 10 patients managed using CardioMEMS for 6 months, a center could expect to prevent nearly 15 patient-days in the hospital.
“Our administration is in support, but skeptical; I think that’s why it’s been slow to start,” said Dr. Parks. “The biggest limitation is the upfront cost of the device, and it’s not clear that the reimbursement will allow you to break even” when putting in devices, she said in an interview. “You could justify this by saying you’ll reduce hospitalizations, but the first impression from our administrators was that we were already doing a pretty good job limiting rehospitalizations so why do we need to add this?” The MGH leadership and clinicians eventually agreed on a plan to start the program with 10 implants and then analyze the results to decide if it makes sense to continue. Dr. Parks said she and her colleagues hope to have their first 10 patients implanted with a CardioMEMS before the end of this year.
Another hurdle at MGH was setting up the infrastructure so that a nurse could monitor patients and set in motion the alerts and treatment changes designed to normalize PAP normalized when it falls out of the target range. “It’s a lot of work to put the system in place to manage the devices,” Dr. Parks noted.
Dr. Butler echoed both these challenges. “You need to convince the hospital administrators and make a case based on the cost savings [later on during ongoing management] rather than positive revenue when you do the procedure. If you can expect future cost savings it’s a viable case to make, but a more difficult case to make,” he said. “You also take on the liability of monitoring patients” long term. “If you can follow several hundred patients there may be enough [follow-up] interventions to pay the salaries of staff ” who monitor the patients, but it is very difficult if you have a nurse who is monitoring five patients,” he said. Another issue complicating the economics is that the physicians who supervise monitoring are mostly not the same ones who performed the CardioMEMS placement procedure and received the procedure’s reimbursement. “These are the system barriers that are out there,” Dr. Butler said.
Dr. Altman in Colorado faced a different challenge. “We had good buy-in from our administration. Everyone is interested in reducing rehospitalizations so the administrators were very supportive. The major roadblock has been insurers. Medicare covers it, but so far Colorado Medicaid and several private insurers do not,” Dr. Altman said in an interview. The inconsistent pattern of insurance coverage has already meant that some heart failure patients in her program who were good clinical candidates for CardioMEMS could not receive the device. “I’ve had at least six or seven good candidates, but only three received the device because of insurance reimbursement issues,” she said.
But Dr. Altman expressed optimism that the coverage situation would improve as more programs start using CarioMEMS and insurers grow more familiar with daily PAP monitoring of heart failure patients. She noted that a new CardioMEMS program will soon start at a second Denver-based medical center, and she expressed confidence that ongoing pressure from physicians and administrators at both institutions will change the mind of officials at Colorado’s Medicaid program to provide reimbursement, and once that happens she expects the private insurers will change their policies as well.
To Dr. Abraham at Ohio State, one of the developers of the concept of using an implanted PAP monitor to guide management of heart failure patients, CardioMEMS slow take off is not surprising. “It provides physicians with daily information on a patient’s hemodynamics, which is something they never had before except in the catheterization laboratory, intensive care unit or cardiac care unit. Managing patients based on hemodynamics even in the absence of worsening signs and symptoms is a paradigm shift. It takes time to adopt new things.” He noted that most hospitals and health systems already have in place case managers or nurse navigators who run systems that have relied on the insensitive parameters of signs, symptoms, and patients’ weights. The same infrastructure should be able to fairly easily switch to focusing instead on PAP, said Dr. Abraham, professor and director of cardiovascular medicine at Wexner Medical Center.
He acknowledged that the upfront capital cost required to start a CardioMEMS program can poses a financial barrier at many U.S. centers, but once that start-up price is paid the actual implantation into each patient comes close to breaking even with existing reimbursements and the system should eventually result in a return on the investment in the form of reduced readmissions and keeping patients stable, he said. Dr. Abraham suggested that the possibility also exists that maintaining better stability in patients with class III heart failure and preventing episodes of acute decompensation through better-titrated fluid-volume control could produce a long-term change in the natural history of these patients, whose disease historically has been marked by progression to class IV heart failure and the eventual need for a left ventricular assist device, heart transplant, and death. Although this potential impact of refined treatment based on daily PAP monitoring remains to be proven, a secondary analysis from CHAMPION showing a 57% relative reduction in all-cause mortality over an average of 17 months of follow-up that Dr. Abraham reported at the American College of Cardiology annual meeting in March
The hurdle of routine practice
Transitioning CardioMEMS from its successful research track record to everyday clinical practice may pose the trickiest barrier of all. The consensus among heart failure experts seems to be that the best approach to do this successfully is to start slow, focus on the most rational patients within the broad enrollment criteria used in CHAMPION, and then gradually expand from that presuming the first wave of results from routine use at a particular site look similar to those from the trial.
“The next big question for PAP monitoring is can we replicate the trial’s success in routine practice? Can this be scaled up?” said Dr. Desai from Brigham and Women’s. “We’re still learning how to identify the right patients, the ones who’ll benefit,”
“The two types of patients we are primarily implanting now are those with classic class III heart failure who were hospitalized during the past 12 months and now are hospitalized again and are right in front of us. They are the lowest-hanging fruit because they are in the hospital today,” said Dr. Abraham. “The second group are the patients who come into the clinic complaining about their symptoms. What we are not yet doing is calling in all patients” with stage III heart failure and a history of at least one hospitalization.”
Other groups are taking a much more selective approach. Dr. Altman and her colleagues in Denver are only targeting patients who have been hospitalized at least twice within the past year, and more specifically patients recently rehospitalized within 30 days of their prior hospitalization. They are also focusing on patients expected to have a high level of compliance with the daily data-collection demands of PAP monitoring and the need to regularly adjust their medication dosages after receiving call backs from their clinicians. This criteria means that they are ruling out patients with a history of substance abuse, she said.
She also noted the need to tailor the target PAP to the specific clinical status of individual patients. Patients with mitral regurgitation, for example, will have a higher “normal” diastolic PAP and hence require a somewhat different target for stability maintenance. “You need to understand each patient’s baseline pressures and adjust their medications based on that,” Dr. Altman said.
“In real life patients tend to be older and sicker, so their benefit may be even greater than what was seen in CHAMPION, but perhaps the results will also be diluted because of comorbidities like renal failure or chronic obstructive pulmonary disease,” said Dr. Butler, although post hoc subanalyses of CHAMPION data showed that these comorbidities did not blunt the positive impact of PAP-guided treatment. “I don’t know if I’ll be successful in selecting the right patients, and whether my interventions in real life will produce the same good outcomes” seen in CHAMPION. “We’ll select patients who are close to the CHAMPION criteria, but not patients on dialysis [who were excluded from CHAMPION]; we’ll select patients with a modest degree of comorbidity and reasonable expected survival,” Dr. Butler said.
“If you had a drug that reduced rehospitalization rates it would be pretty clear how to proceed, but in this case it is not the device that reduces readmissions, it just gives you data and you need to act on the data,” Dr. Butler added. He acknowledged that the CHAMPION investigators used a relatively simple, straightforward management algorithm for patients whose PAP fell out of the target range, such as a diastolic PAP greater than 20 mm Hg or less than 8 mm Hg. The first management step is to raise or reduce the patient’s diuretic dosage, and if that fails to quickly normalize PAP the next step is to adjust the vasodilator dosage.
Managing patients in CHAMPION was “not totally an art” but neither was it “totally a science,” Dr. Butler said. Managing patients based on daily data collected using a CardioMEMS device will “require a little finesse,” he said. “It’s not straight science.”
Programs that have already used PAP monitoring on a routine basis, like those in Denver and at Brigham and Women’s, consider their experience too small in size and short in duration to draw any substantive conclusions regarding their success compared with the CHAMPION results. But Dr. Abraham, whose program has now placed CardioMEMS routinely in a few dozen patients and followed them for as long as a year, said that in his center’s patients the device and management system has produced outcomes that roughly match what he saw in the pivotal trial.
“The ongoing concern is that what was achieved in the CHAMPION trial may not be what is achieved in routine practice,” said Dr. Desai. The care that patients received in the trial is “a little of a black box,” he said, and during the FDA’s approval process some reviewers raised concerns that patients in the active-treatment arm simply received more intensive surveillance, although this concern eventually resolved. “There is not a lot of skepticism” among clinicians about this treatment, but there is uncertainly about exactly whom are the best patients to treat and whether their responses be as good as in CHAMPION, Dr. Desai said in an interview.
“The proof [of efficacy] will be in each individual center’s experience” using CardioMEMS, Dr. Altman said.
CHAMPION was initially funded by CardioMEMS, which then was acquired by St. Jude which is the company marketing the CardioMEMS device and associated hardware. Dr. Butler said that he had no current relevant disclosures, although in the past he had been a consultant to CardioMEMS (prior to its acquisition by St. Jude). Dr. Parks and Dr. Altman had no disclosures. Dr. Desai has been a consultant to and has received honoraria as a speaker on behalf of CardioMEMS and St. Jude. Dr. Abraham has been a consultant to CardioMEMS and St. Jude, was co-principal investigator on the CHAMPION trial, and is the principal investigator on a new St. Jude-funded trial studying CardioMEMS.
On Twitter @mitchelzoler
In an era when rehospitalization of patients with heart failure for episodes of acute decompensation has become a top target for reduction in the U.S. health care system via Medicare’s Readmissions Reduction Program CardioMEMS looks like the tool that every U.S. health care system and medical center has dreamed of having.
A wireless and battery-less implanted device, CardioMEMS guides management of stage III heart failure patients by allowing daily monitoring of patients’ pulmonary-artery pressure (PAP). Using these measures to fine-tune patient treatment with diuretics and vasodilators led to a statistically significant and clinically meaningful 37% relative reduction in heart failure rehospitalizations over an average 15-month follow-up, based on results from CardioMEMS’ pivotal U.S. trial as well as from subsequent secondary analyses. All-cause mortality was reduced and patients’ quality of life improved. And device-driven therapy yielded these benefits equally well in patients with either preserved or reduced left ventricular function as well as in a variety of other subgroups including patients with cardiac resynchronization devices or implantable cardioverter defibrillators, chronic obstructive pulmonary disease, chronic kidney disease, atrial fibrillation, pulmonary hypertension, or a history of myocardial infarction.
Yet in the first year after CardioMEMS received Food and Drug Administration approval and came onto the U.S. market, the device has taken a strikingly slow path into routine heart failure practice, according to heart failure cardiologists at several U.S. centers. A representative of St. Jude, the company that markets CardioMEMS, saidin July that sales of the device during the first half of 2015 had involved more than 200 U.S. customers and slightly surpassed earlier expectations, and the company now anticipated full 2015 sales to run roughly 25% ahead of projections made at the start of this year. Despite that, the company’s second quarter report acknowledged the challenges that CardioMEMS faced during its first year on the U.S. market.
Numbers show a slow rollout
“I belong to a consortium of academic heart failure physicians who come from many of the major U.S. academic medical centers, and a recent straw poll of the members showed that close to no one was using it [CardioMEMS] on a regular basis, and the majority said they were not yet using it at all or in the process of starting their program,” said Dr. Javed Butler, a heart failure specialist who is professor of medicine, chief of cardiology, and codirector of the Stony Brook (N.Y.) University Heart Center.
At Stony Brook, no heart failure patient had received the device as of July 2015, although Dr. Butler said that his program’s use of CardioMEMS will probably start soon. Cardiologists at a handful of other U.S. centers report similarly slow starts.
At Massachusetts General Hospital (MGH) in Boston not a single patient has received CardioMEMS, though the heart failure staff there hopes to soon launch pilot use in 10 patients, said Dr. Kimberly A. Parks, associate director of the resynchronization and advanced cardiac therapeutics program. At the University of Colorado Hospital in Aurora, three patients have received the device since their first implant in the late winter, and the program is now on track to place devices in another one or two patients each month, said Dr. Natasha L. Altman, a cardiologist who heads the center’s CardioMEMS program. At Brigham and Women’s Hospital in Boston, which participated in the CHAMPION (CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients) pivotal trial that led to CardioMEMS approval, so far a “handful, fewer than 10 patients” received the device since marketing began, said Dr. Akshay S. Desai, associate director of Brigham Cardiovascular Consultants. Even at Ohio State’s Wexner Medical Center in Columbus, the program run by Dr. William T. Abraham, coprincipal investigator for CHAMPION, a relatively modest number of roughly 50 patients had received CardioMEMS in routine practice since the first patient received a device there in June 2014 following the FDA’s approval, Dr. Abraham said in an interview.
Contrasting with this level of use is the substantial number of patients who meet the CHAMPION enrollment criteria of New York Heart Association class III heart failure and a heart failure hospitalization within the prior year. Experts estimate that throughout the United States this group must number at least a half-million patients, and at the level of individual medical centers that provide advanced heart failure care, the numbers likely reach several hundred patients at each site.
Several challenges slow CardioMEMS implantation
Why such a slow start for what seems to be such an attractive device that clinicians uniformly praise for having a strong evidence base in CHAMPION and a compelling medical rationale? The answer seems multifactorial, including the need to convince skeptical hospital administrators and insurance payers to provide and pay for the device and follow-up care, a requirement to ramp up the patient-monitoring and management infrastructure, and the challenge of transitioning a relatively complex therapeutic formula from a successful clinical trial model into routine care.
“If this was a pill that you could prescribe to patients at hospital discharge, people would jump on it. But CardioMEMS is not as simple as prescribing a pill. There are a lot of logistical issues that make it very difficult,” said Stony Brook’s Dr. Butler in an interview.
This sentiment was shared not only by other cardiologists but also by St. Jude itself, as a company spokesman itemized several challenges the company encountered once it began trying to sell CardioMEMS commercially. “Developing the market for CardioMEMS will continue to take time,” said the St. Jude staffer during a July webcast on the company’s second-quarter 2015 performance. CardioMEMS’ sales were affected by the need to educate multiple constituencies, satisfy new-technology review committees, address reimbursement, access capital budgets, and create consensus among disparate stakeholders, the webcast said. In addition, the early St. Jude experience selling CardioMEMS showed that once a new customer signs a contract, “we find that customers tend to introduce CardioMEMS ... [on] a pilot basis to gain experience with the technology and the reimbursement process.”
First is the challenge of selling a hospital’s administrative leadership on making an upfront capital investment in CardioMEMS equipment, giving the green light to performing procedures that just about break even relative to reimbursement, and then waiting to recoup the initial expenditure and perhaps make some money in the long term by avoiding readmissions and cutting lengths of stay. According to an analysis run by Dr. Parks of MGH, based on the CHAMPION results, for every 10 patients managed using CardioMEMS for 6 months, a center could expect to prevent nearly 15 patient-days in the hospital.
“Our administration is in support, but skeptical; I think that’s why it’s been slow to start,” said Dr. Parks. “The biggest limitation is the upfront cost of the device, and it’s not clear that the reimbursement will allow you to break even” when putting in devices, she said in an interview. “You could justify this by saying you’ll reduce hospitalizations, but the first impression from our administrators was that we were already doing a pretty good job limiting rehospitalizations so why do we need to add this?” The MGH leadership and clinicians eventually agreed on a plan to start the program with 10 implants and then analyze the results to decide if it makes sense to continue. Dr. Parks said she and her colleagues hope to have their first 10 patients implanted with a CardioMEMS before the end of this year.
Another hurdle at MGH was setting up the infrastructure so that a nurse could monitor patients and set in motion the alerts and treatment changes designed to normalize PAP normalized when it falls out of the target range. “It’s a lot of work to put the system in place to manage the devices,” Dr. Parks noted.
Dr. Butler echoed both these challenges. “You need to convince the hospital administrators and make a case based on the cost savings [later on during ongoing management] rather than positive revenue when you do the procedure. If you can expect future cost savings it’s a viable case to make, but a more difficult case to make,” he said. “You also take on the liability of monitoring patients” long term. “If you can follow several hundred patients there may be enough [follow-up] interventions to pay the salaries of staff ” who monitor the patients, but it is very difficult if you have a nurse who is monitoring five patients,” he said. Another issue complicating the economics is that the physicians who supervise monitoring are mostly not the same ones who performed the CardioMEMS placement procedure and received the procedure’s reimbursement. “These are the system barriers that are out there,” Dr. Butler said.
Dr. Altman in Colorado faced a different challenge. “We had good buy-in from our administration. Everyone is interested in reducing rehospitalizations so the administrators were very supportive. The major roadblock has been insurers. Medicare covers it, but so far Colorado Medicaid and several private insurers do not,” Dr. Altman said in an interview. The inconsistent pattern of insurance coverage has already meant that some heart failure patients in her program who were good clinical candidates for CardioMEMS could not receive the device. “I’ve had at least six or seven good candidates, but only three received the device because of insurance reimbursement issues,” she said.
But Dr. Altman expressed optimism that the coverage situation would improve as more programs start using CarioMEMS and insurers grow more familiar with daily PAP monitoring of heart failure patients. She noted that a new CardioMEMS program will soon start at a second Denver-based medical center, and she expressed confidence that ongoing pressure from physicians and administrators at both institutions will change the mind of officials at Colorado’s Medicaid program to provide reimbursement, and once that happens she expects the private insurers will change their policies as well.
To Dr. Abraham at Ohio State, one of the developers of the concept of using an implanted PAP monitor to guide management of heart failure patients, CardioMEMS slow take off is not surprising. “It provides physicians with daily information on a patient’s hemodynamics, which is something they never had before except in the catheterization laboratory, intensive care unit or cardiac care unit. Managing patients based on hemodynamics even in the absence of worsening signs and symptoms is a paradigm shift. It takes time to adopt new things.” He noted that most hospitals and health systems already have in place case managers or nurse navigators who run systems that have relied on the insensitive parameters of signs, symptoms, and patients’ weights. The same infrastructure should be able to fairly easily switch to focusing instead on PAP, said Dr. Abraham, professor and director of cardiovascular medicine at Wexner Medical Center.
He acknowledged that the upfront capital cost required to start a CardioMEMS program can poses a financial barrier at many U.S. centers, but once that start-up price is paid the actual implantation into each patient comes close to breaking even with existing reimbursements and the system should eventually result in a return on the investment in the form of reduced readmissions and keeping patients stable, he said. Dr. Abraham suggested that the possibility also exists that maintaining better stability in patients with class III heart failure and preventing episodes of acute decompensation through better-titrated fluid-volume control could produce a long-term change in the natural history of these patients, whose disease historically has been marked by progression to class IV heart failure and the eventual need for a left ventricular assist device, heart transplant, and death. Although this potential impact of refined treatment based on daily PAP monitoring remains to be proven, a secondary analysis from CHAMPION showing a 57% relative reduction in all-cause mortality over an average of 17 months of follow-up that Dr. Abraham reported at the American College of Cardiology annual meeting in March
The hurdle of routine practice
Transitioning CardioMEMS from its successful research track record to everyday clinical practice may pose the trickiest barrier of all. The consensus among heart failure experts seems to be that the best approach to do this successfully is to start slow, focus on the most rational patients within the broad enrollment criteria used in CHAMPION, and then gradually expand from that presuming the first wave of results from routine use at a particular site look similar to those from the trial.
“The next big question for PAP monitoring is can we replicate the trial’s success in routine practice? Can this be scaled up?” said Dr. Desai from Brigham and Women’s. “We’re still learning how to identify the right patients, the ones who’ll benefit,”
“The two types of patients we are primarily implanting now are those with classic class III heart failure who were hospitalized during the past 12 months and now are hospitalized again and are right in front of us. They are the lowest-hanging fruit because they are in the hospital today,” said Dr. Abraham. “The second group are the patients who come into the clinic complaining about their symptoms. What we are not yet doing is calling in all patients” with stage III heart failure and a history of at least one hospitalization.”
Other groups are taking a much more selective approach. Dr. Altman and her colleagues in Denver are only targeting patients who have been hospitalized at least twice within the past year, and more specifically patients recently rehospitalized within 30 days of their prior hospitalization. They are also focusing on patients expected to have a high level of compliance with the daily data-collection demands of PAP monitoring and the need to regularly adjust their medication dosages after receiving call backs from their clinicians. This criteria means that they are ruling out patients with a history of substance abuse, she said.
She also noted the need to tailor the target PAP to the specific clinical status of individual patients. Patients with mitral regurgitation, for example, will have a higher “normal” diastolic PAP and hence require a somewhat different target for stability maintenance. “You need to understand each patient’s baseline pressures and adjust their medications based on that,” Dr. Altman said.
“In real life patients tend to be older and sicker, so their benefit may be even greater than what was seen in CHAMPION, but perhaps the results will also be diluted because of comorbidities like renal failure or chronic obstructive pulmonary disease,” said Dr. Butler, although post hoc subanalyses of CHAMPION data showed that these comorbidities did not blunt the positive impact of PAP-guided treatment. “I don’t know if I’ll be successful in selecting the right patients, and whether my interventions in real life will produce the same good outcomes” seen in CHAMPION. “We’ll select patients who are close to the CHAMPION criteria, but not patients on dialysis [who were excluded from CHAMPION]; we’ll select patients with a modest degree of comorbidity and reasonable expected survival,” Dr. Butler said.
“If you had a drug that reduced rehospitalization rates it would be pretty clear how to proceed, but in this case it is not the device that reduces readmissions, it just gives you data and you need to act on the data,” Dr. Butler added. He acknowledged that the CHAMPION investigators used a relatively simple, straightforward management algorithm for patients whose PAP fell out of the target range, such as a diastolic PAP greater than 20 mm Hg or less than 8 mm Hg. The first management step is to raise or reduce the patient’s diuretic dosage, and if that fails to quickly normalize PAP the next step is to adjust the vasodilator dosage.
Managing patients in CHAMPION was “not totally an art” but neither was it “totally a science,” Dr. Butler said. Managing patients based on daily data collected using a CardioMEMS device will “require a little finesse,” he said. “It’s not straight science.”
Programs that have already used PAP monitoring on a routine basis, like those in Denver and at Brigham and Women’s, consider their experience too small in size and short in duration to draw any substantive conclusions regarding their success compared with the CHAMPION results. But Dr. Abraham, whose program has now placed CardioMEMS routinely in a few dozen patients and followed them for as long as a year, said that in his center’s patients the device and management system has produced outcomes that roughly match what he saw in the pivotal trial.
“The ongoing concern is that what was achieved in the CHAMPION trial may not be what is achieved in routine practice,” said Dr. Desai. The care that patients received in the trial is “a little of a black box,” he said, and during the FDA’s approval process some reviewers raised concerns that patients in the active-treatment arm simply received more intensive surveillance, although this concern eventually resolved. “There is not a lot of skepticism” among clinicians about this treatment, but there is uncertainly about exactly whom are the best patients to treat and whether their responses be as good as in CHAMPION, Dr. Desai said in an interview.
“The proof [of efficacy] will be in each individual center’s experience” using CardioMEMS, Dr. Altman said.
CHAMPION was initially funded by CardioMEMS, which then was acquired by St. Jude which is the company marketing the CardioMEMS device and associated hardware. Dr. Butler said that he had no current relevant disclosures, although in the past he had been a consultant to CardioMEMS (prior to its acquisition by St. Jude). Dr. Parks and Dr. Altman had no disclosures. Dr. Desai has been a consultant to and has received honoraria as a speaker on behalf of CardioMEMS and St. Jude. Dr. Abraham has been a consultant to CardioMEMS and St. Jude, was co-principal investigator on the CHAMPION trial, and is the principal investigator on a new St. Jude-funded trial studying CardioMEMS.
On Twitter @mitchelzoler

VIDEO: Hospitalized heart failure patients susceptible to C. difficile
LONDON – U.S. patients hospitalized for heart failure and treated with antibiotics during their hospital stay had an increased rate both for developing Clostridium difficile infection and dying from it, based on nationwide data collected from nearly six million patients.
“Heart failure was an independent risk factor” in multivariate analyses that controlled for demographic factors as well as for several comorbidities of heart failure, Dr. Petra Mamic said in a video interview at the annual congress of the European Society of Cardiology.
She and her associates used data collected by the National Inpatient Sample during 2012 in more than 5.8 million U.S. hospitalized patients who received antibiotic treatment for a urinary tract infection, pneumonia, or sepsis. They compared the rate of subsequent infection with C. difficile in the roughly 1.4 million of these patients who had heart failure and the nearly 4.5 million without heart failure. In a multivariate analysis heart failure patients were 13% more likely to develop C. difficile infection compared with patients without heart failure. In a second multivariate analysis that focused just on patients with heart failure those who had become infected by C. difficile were 81% more likely to die in hospital compared with heart failure patients without this type of infection.
“Heart failure patients are frequently hospitalized and have a lot of bacterial infections, and so receive treatment with a lot of antibiotics,” said Dr. Mamic, an internal medicine physician at Stanford (Calif.) University. “What is important is that C. difficile infection is preventable. Our ultimate goal is to prevent C. difficile in these patients who have such high morbidity and mortality,”
Dr. Mamic had no disclosures.
On Twitter @mitchelzoler
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LONDON – U.S. patients hospitalized for heart failure and treated with antibiotics during their hospital stay had an increased rate both for developing Clostridium difficile infection and dying from it, based on nationwide data collected from nearly six million patients.
“Heart failure was an independent risk factor” in multivariate analyses that controlled for demographic factors as well as for several comorbidities of heart failure, Dr. Petra Mamic said in a video interview at the annual congress of the European Society of Cardiology.
She and her associates used data collected by the National Inpatient Sample during 2012 in more than 5.8 million U.S. hospitalized patients who received antibiotic treatment for a urinary tract infection, pneumonia, or sepsis. They compared the rate of subsequent infection with C. difficile in the roughly 1.4 million of these patients who had heart failure and the nearly 4.5 million without heart failure. In a multivariate analysis heart failure patients were 13% more likely to develop C. difficile infection compared with patients without heart failure. In a second multivariate analysis that focused just on patients with heart failure those who had become infected by C. difficile were 81% more likely to die in hospital compared with heart failure patients without this type of infection.
“Heart failure patients are frequently hospitalized and have a lot of bacterial infections, and so receive treatment with a lot of antibiotics,” said Dr. Mamic, an internal medicine physician at Stanford (Calif.) University. “What is important is that C. difficile infection is preventable. Our ultimate goal is to prevent C. difficile in these patients who have such high morbidity and mortality,”
Dr. Mamic had no disclosures.
On Twitter @mitchelzoler
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LONDON – U.S. patients hospitalized for heart failure and treated with antibiotics during their hospital stay had an increased rate both for developing Clostridium difficile infection and dying from it, based on nationwide data collected from nearly six million patients.
“Heart failure was an independent risk factor” in multivariate analyses that controlled for demographic factors as well as for several comorbidities of heart failure, Dr. Petra Mamic said in a video interview at the annual congress of the European Society of Cardiology.
She and her associates used data collected by the National Inpatient Sample during 2012 in more than 5.8 million U.S. hospitalized patients who received antibiotic treatment for a urinary tract infection, pneumonia, or sepsis. They compared the rate of subsequent infection with C. difficile in the roughly 1.4 million of these patients who had heart failure and the nearly 4.5 million without heart failure. In a multivariate analysis heart failure patients were 13% more likely to develop C. difficile infection compared with patients without heart failure. In a second multivariate analysis that focused just on patients with heart failure those who had become infected by C. difficile were 81% more likely to die in hospital compared with heart failure patients without this type of infection.
“Heart failure patients are frequently hospitalized and have a lot of bacterial infections, and so receive treatment with a lot of antibiotics,” said Dr. Mamic, an internal medicine physician at Stanford (Calif.) University. “What is important is that C. difficile infection is preventable. Our ultimate goal is to prevent C. difficile in these patients who have such high morbidity and mortality,”
Dr. Mamic had no disclosures.
On Twitter @mitchelzoler
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE ESC CONGRESS 2015

ESC: Cyclosporine intervention failed to benefit STEMI patients
Intravenous administration of cyclosporine just before percutaneous coronary intervention was not associated with a reduced risk of adverse outcomes at 1 year in a study of patients who underwent the procedure after experiencing an acute anterior ST-segment elevation myocardial infarction.
Findings from the multicenter, randomized study, known as the Does Cyclosporine Improve Clinical Outcome in ST Elevation Myocardial Infarction Patients (CIRCUS) trial, were presented at the annual congress of the European Society of Cardiology and published simultaneously in the New England Journal of Medicine (doi: 10.1056/NEJMoa1505489).
For the phase 3 trial, Dr. Michel Ovize and associates investigated whether a single intravenous dose of cyclosporine, administered just before PCI, would improve clinical outcomes and prevent left adverse left ventricular modeling at 1 year in patients with anterior STEMI.
“Growing evidence from experimental studies and small-size proof-of-concept clinical trials shows that reperfusion injury contributes greatly to the final infarct size,” the researchers wrote. “Preclinical studies indicate that the opening of the mitochondrial permeability transition pore (PTP) in the inner mitochondrial membrane plays a major role in reperfusion injury. Either genetic or pharmacologic inhibition of cyclophilin D, a major component of the PTP, reduces the severity of myocardial reperfusion injury.”
Dr. Ovize of the Clinical Investigation Center of Lyon, France, and his associates chose to test cyclosporine, a pharmacologic inhibitor of cyclophilin D, after a phase 2 trial conducted by the same researchers found that administration of cyclosporine immediately before PCI reduced the myocardial infarct size in patients with STEMI. In CIRCUS, which was conducted from April 2011 through February 2014 at 42 hospitals in three countries, 475 patients with an acute anterior STEMI who were undergoing PCI within 12 hours of symptom onset received IV cyclosporine at a dose of 2.5 mg/kg of body weight, while 495 patients received placebo. The primary outcome was a composite of death from any cause, worsening of heart failure during initial hospitalization, rehospitalization for heart failure, or adverse left ventricular remodeling at 1 year.
At baseline, the mean age of patients was 60 years, 82% were men, and their mean body mass index was 27 kg/m2. One year of follow-up data was available for 395 patients in the cyclosporine group and 396 in the placebo group. The researchers found no significant differences between the two groups in the proportion who experienced a primary outcome event (59% in the cyclosporine group vs. 58% in the control group) or in the rate of all-cause mortality (7.1% vs. 6.6%).
There were also no differences between groups in the rate of initial worsening of heart failure or rehospitalization for heart failure at 1 year (22.8% vs. 22.7%). In addition, a similar proportion of patients in both groups experienced adverse left ventricular remodeling (42.8% vs. 40.7%).
“One important limitation of this trial is that we included in the primary outcome the nonclinical outcome of adverse left ventricular remodeling, which accounted for a substantial proportion of the primary outcome rate,” the researchers wrote. “Left ventricular remodeling is a surrogate outcome – one that was not successfully measured in 17.4% of the trial participants. However, in secondary analyses, no beneficial effect of cyclosporine was detected on any of the hard clinical outcomes.”
They went on to note that nearly one of four patients in CIRCUS died or was hospitalized for heart failure, “a reminder of the substantial residual risk in this population and the persistent room for improvement in the medical treatment of high-risk patients with STEMI. The results of this trial do not challenge the concept that reperfusion injury is clinically important. Recent phase 2 trials that have used either ischemic or pharmacologic postconditioning suggest that interventions applied at the time of reperfusion can limit infarct size and improve functional recovery. Their effect on clinical outcome remains to be determined in phase 3 studies.”
The study was supported by grants from the French Ministry of Health and Research National Program and NeuroVive Pharmaceutical. Dr. Ovize disclosed that he is a consultant for NueroVive Pharmaceutical.
Why, despite the promising experimental and clinical data, did cyclosporine have no effect on clinical outcomes? Several factors may be considered. First, although the experimental data supporting the cardioprotective effect of cyclosporine are extensive, not all the studies have been positive. The clinical evidence in favor of a cardioprotective effect is limited to one study in this patient group. Another study involving patients with STEMI who were treated with thrombolysis showed no effect with cyclosporine.
Second, the use of an increase in left ventricular end-diastolic volume as one of the primary outcomes has to be queried. This outcome, for which data were missing in 17% of patients, is not a clinical one but a surrogate marker of adverse left ventricular modeling.
Finally, the use of CicloMulsion (NeuroVive Pharmaceutical), a new formulation of cyclosporine that was used in this study, instead of Sandimmune (Novartis), which was used in the original study by Piot et al., may have contributed to the neutral results.
CicloMulsion contains a lipid emulsion carrier vehicle, thereby avoiding the risk of anaphylaxis that has been associated with Sandimmune, which uses an ethanol and polyoxyethylated castor oil (Cremophor EL) carrier vehicle.
Although the results of the CIRCUS study are disappointing, they do not disprove the existence or clinical significance of myocardial reperfusion injury, because it appears that the formulation of cyclosporine used in the study might not have been effective at preventing myocardial reperfusion injury. If the benefits of PTP inhibition are to be harnessed, more specific inhibitors will need to be discovered. Therefore, the search to find an effective therapy for preventing myocardial reperfusion injury and improving clinical outcomes in patients with reperfused STEMI should continue.
Dr. Derek J. Hausenloy and Derek M. Yellon, D.Sc., are with the Hatter Cardiovascular Institute, University College London, and the National Institute of Health Research University College London Hospitals Biomedical Research Centre. Both reported having no financial disclosures. This text was extracted from an editorial that appeared online Aug. 30, 2015 in the New England Journal of Medicine (doi: 10.1056/NEJMe1509718).
Why, despite the promising experimental and clinical data, did cyclosporine have no effect on clinical outcomes? Several factors may be considered. First, although the experimental data supporting the cardioprotective effect of cyclosporine are extensive, not all the studies have been positive. The clinical evidence in favor of a cardioprotective effect is limited to one study in this patient group. Another study involving patients with STEMI who were treated with thrombolysis showed no effect with cyclosporine.
Second, the use of an increase in left ventricular end-diastolic volume as one of the primary outcomes has to be queried. This outcome, for which data were missing in 17% of patients, is not a clinical one but a surrogate marker of adverse left ventricular modeling.
Finally, the use of CicloMulsion (NeuroVive Pharmaceutical), a new formulation of cyclosporine that was used in this study, instead of Sandimmune (Novartis), which was used in the original study by Piot et al., may have contributed to the neutral results.
CicloMulsion contains a lipid emulsion carrier vehicle, thereby avoiding the risk of anaphylaxis that has been associated with Sandimmune, which uses an ethanol and polyoxyethylated castor oil (Cremophor EL) carrier vehicle.
Although the results of the CIRCUS study are disappointing, they do not disprove the existence or clinical significance of myocardial reperfusion injury, because it appears that the formulation of cyclosporine used in the study might not have been effective at preventing myocardial reperfusion injury. If the benefits of PTP inhibition are to be harnessed, more specific inhibitors will need to be discovered. Therefore, the search to find an effective therapy for preventing myocardial reperfusion injury and improving clinical outcomes in patients with reperfused STEMI should continue.
Dr. Derek J. Hausenloy and Derek M. Yellon, D.Sc., are with the Hatter Cardiovascular Institute, University College London, and the National Institute of Health Research University College London Hospitals Biomedical Research Centre. Both reported having no financial disclosures. This text was extracted from an editorial that appeared online Aug. 30, 2015 in the New England Journal of Medicine (doi: 10.1056/NEJMe1509718).
Why, despite the promising experimental and clinical data, did cyclosporine have no effect on clinical outcomes? Several factors may be considered. First, although the experimental data supporting the cardioprotective effect of cyclosporine are extensive, not all the studies have been positive. The clinical evidence in favor of a cardioprotective effect is limited to one study in this patient group. Another study involving patients with STEMI who were treated with thrombolysis showed no effect with cyclosporine.
Second, the use of an increase in left ventricular end-diastolic volume as one of the primary outcomes has to be queried. This outcome, for which data were missing in 17% of patients, is not a clinical one but a surrogate marker of adverse left ventricular modeling.
Finally, the use of CicloMulsion (NeuroVive Pharmaceutical), a new formulation of cyclosporine that was used in this study, instead of Sandimmune (Novartis), which was used in the original study by Piot et al., may have contributed to the neutral results.
CicloMulsion contains a lipid emulsion carrier vehicle, thereby avoiding the risk of anaphylaxis that has been associated with Sandimmune, which uses an ethanol and polyoxyethylated castor oil (Cremophor EL) carrier vehicle.
Although the results of the CIRCUS study are disappointing, they do not disprove the existence or clinical significance of myocardial reperfusion injury, because it appears that the formulation of cyclosporine used in the study might not have been effective at preventing myocardial reperfusion injury. If the benefits of PTP inhibition are to be harnessed, more specific inhibitors will need to be discovered. Therefore, the search to find an effective therapy for preventing myocardial reperfusion injury and improving clinical outcomes in patients with reperfused STEMI should continue.
Dr. Derek J. Hausenloy and Derek M. Yellon, D.Sc., are with the Hatter Cardiovascular Institute, University College London, and the National Institute of Health Research University College London Hospitals Biomedical Research Centre. Both reported having no financial disclosures. This text was extracted from an editorial that appeared online Aug. 30, 2015 in the New England Journal of Medicine (doi: 10.1056/NEJMe1509718).
Intravenous administration of cyclosporine just before percutaneous coronary intervention was not associated with a reduced risk of adverse outcomes at 1 year in a study of patients who underwent the procedure after experiencing an acute anterior ST-segment elevation myocardial infarction.
Findings from the multicenter, randomized study, known as the Does Cyclosporine Improve Clinical Outcome in ST Elevation Myocardial Infarction Patients (CIRCUS) trial, were presented at the annual congress of the European Society of Cardiology and published simultaneously in the New England Journal of Medicine (doi: 10.1056/NEJMoa1505489).
For the phase 3 trial, Dr. Michel Ovize and associates investigated whether a single intravenous dose of cyclosporine, administered just before PCI, would improve clinical outcomes and prevent left adverse left ventricular modeling at 1 year in patients with anterior STEMI.
“Growing evidence from experimental studies and small-size proof-of-concept clinical trials shows that reperfusion injury contributes greatly to the final infarct size,” the researchers wrote. “Preclinical studies indicate that the opening of the mitochondrial permeability transition pore (PTP) in the inner mitochondrial membrane plays a major role in reperfusion injury. Either genetic or pharmacologic inhibition of cyclophilin D, a major component of the PTP, reduces the severity of myocardial reperfusion injury.”
Dr. Ovize of the Clinical Investigation Center of Lyon, France, and his associates chose to test cyclosporine, a pharmacologic inhibitor of cyclophilin D, after a phase 2 trial conducted by the same researchers found that administration of cyclosporine immediately before PCI reduced the myocardial infarct size in patients with STEMI. In CIRCUS, which was conducted from April 2011 through February 2014 at 42 hospitals in three countries, 475 patients with an acute anterior STEMI who were undergoing PCI within 12 hours of symptom onset received IV cyclosporine at a dose of 2.5 mg/kg of body weight, while 495 patients received placebo. The primary outcome was a composite of death from any cause, worsening of heart failure during initial hospitalization, rehospitalization for heart failure, or adverse left ventricular remodeling at 1 year.
At baseline, the mean age of patients was 60 years, 82% were men, and their mean body mass index was 27 kg/m2. One year of follow-up data was available for 395 patients in the cyclosporine group and 396 in the placebo group. The researchers found no significant differences between the two groups in the proportion who experienced a primary outcome event (59% in the cyclosporine group vs. 58% in the control group) or in the rate of all-cause mortality (7.1% vs. 6.6%).
There were also no differences between groups in the rate of initial worsening of heart failure or rehospitalization for heart failure at 1 year (22.8% vs. 22.7%). In addition, a similar proportion of patients in both groups experienced adverse left ventricular remodeling (42.8% vs. 40.7%).
“One important limitation of this trial is that we included in the primary outcome the nonclinical outcome of adverse left ventricular remodeling, which accounted for a substantial proportion of the primary outcome rate,” the researchers wrote. “Left ventricular remodeling is a surrogate outcome – one that was not successfully measured in 17.4% of the trial participants. However, in secondary analyses, no beneficial effect of cyclosporine was detected on any of the hard clinical outcomes.”
They went on to note that nearly one of four patients in CIRCUS died or was hospitalized for heart failure, “a reminder of the substantial residual risk in this population and the persistent room for improvement in the medical treatment of high-risk patients with STEMI. The results of this trial do not challenge the concept that reperfusion injury is clinically important. Recent phase 2 trials that have used either ischemic or pharmacologic postconditioning suggest that interventions applied at the time of reperfusion can limit infarct size and improve functional recovery. Their effect on clinical outcome remains to be determined in phase 3 studies.”
The study was supported by grants from the French Ministry of Health and Research National Program and NeuroVive Pharmaceutical. Dr. Ovize disclosed that he is a consultant for NueroVive Pharmaceutical.
Intravenous administration of cyclosporine just before percutaneous coronary intervention was not associated with a reduced risk of adverse outcomes at 1 year in a study of patients who underwent the procedure after experiencing an acute anterior ST-segment elevation myocardial infarction.
Findings from the multicenter, randomized study, known as the Does Cyclosporine Improve Clinical Outcome in ST Elevation Myocardial Infarction Patients (CIRCUS) trial, were presented at the annual congress of the European Society of Cardiology and published simultaneously in the New England Journal of Medicine (doi: 10.1056/NEJMoa1505489).
For the phase 3 trial, Dr. Michel Ovize and associates investigated whether a single intravenous dose of cyclosporine, administered just before PCI, would improve clinical outcomes and prevent left adverse left ventricular modeling at 1 year in patients with anterior STEMI.
“Growing evidence from experimental studies and small-size proof-of-concept clinical trials shows that reperfusion injury contributes greatly to the final infarct size,” the researchers wrote. “Preclinical studies indicate that the opening of the mitochondrial permeability transition pore (PTP) in the inner mitochondrial membrane plays a major role in reperfusion injury. Either genetic or pharmacologic inhibition of cyclophilin D, a major component of the PTP, reduces the severity of myocardial reperfusion injury.”
Dr. Ovize of the Clinical Investigation Center of Lyon, France, and his associates chose to test cyclosporine, a pharmacologic inhibitor of cyclophilin D, after a phase 2 trial conducted by the same researchers found that administration of cyclosporine immediately before PCI reduced the myocardial infarct size in patients with STEMI. In CIRCUS, which was conducted from April 2011 through February 2014 at 42 hospitals in three countries, 475 patients with an acute anterior STEMI who were undergoing PCI within 12 hours of symptom onset received IV cyclosporine at a dose of 2.5 mg/kg of body weight, while 495 patients received placebo. The primary outcome was a composite of death from any cause, worsening of heart failure during initial hospitalization, rehospitalization for heart failure, or adverse left ventricular remodeling at 1 year.
At baseline, the mean age of patients was 60 years, 82% were men, and their mean body mass index was 27 kg/m2. One year of follow-up data was available for 395 patients in the cyclosporine group and 396 in the placebo group. The researchers found no significant differences between the two groups in the proportion who experienced a primary outcome event (59% in the cyclosporine group vs. 58% in the control group) or in the rate of all-cause mortality (7.1% vs. 6.6%).
There were also no differences between groups in the rate of initial worsening of heart failure or rehospitalization for heart failure at 1 year (22.8% vs. 22.7%). In addition, a similar proportion of patients in both groups experienced adverse left ventricular remodeling (42.8% vs. 40.7%).
“One important limitation of this trial is that we included in the primary outcome the nonclinical outcome of adverse left ventricular remodeling, which accounted for a substantial proportion of the primary outcome rate,” the researchers wrote. “Left ventricular remodeling is a surrogate outcome – one that was not successfully measured in 17.4% of the trial participants. However, in secondary analyses, no beneficial effect of cyclosporine was detected on any of the hard clinical outcomes.”
They went on to note that nearly one of four patients in CIRCUS died or was hospitalized for heart failure, “a reminder of the substantial residual risk in this population and the persistent room for improvement in the medical treatment of high-risk patients with STEMI. The results of this trial do not challenge the concept that reperfusion injury is clinically important. Recent phase 2 trials that have used either ischemic or pharmacologic postconditioning suggest that interventions applied at the time of reperfusion can limit infarct size and improve functional recovery. Their effect on clinical outcome remains to be determined in phase 3 studies.”
The study was supported by grants from the French Ministry of Health and Research National Program and NeuroVive Pharmaceutical. Dr. Ovize disclosed that he is a consultant for NueroVive Pharmaceutical.
FROM THE ESC CONGRESS 2015
Key clinical point: Cyclosporine administration prior to PCI did not benefit STEMI patients.
Major finding: There were no significant differences between intervention and control groups in the proportion who experienced a primary outcome event (59% in the cyclosporine group vs. 58% in the control group).
Data source: A randomized, placebo-controlled trial of 970 patients with an acute anterior ST-segment elevation myocardial infarction who were undergoing percutaneous coronary intervention within 12 hours after symptom onset.
Disclosures: The study was supported by grants from the French Ministry of Health and Research National Program and NeuroVive Pharmaceutical. Dr. Ovize disclosed that he is a consultant for NueroVive Pharmaceutical.
First-line ambrisentan plus tadalafil halved PAH events
First-line combination therapy with ambrisentan and tadalafil cut the rate of clinical events in pulmonary arterial hypertension (PAH) by half, compared with monotherapy using either drug, in an international phase 3-4 clinical trial reported online Aug. 27 in the New England Journal of Medicine.
Ambrisentan, a selective endothelin-A-receptor antagonist, and tadalafil, a phosphodiesterase type 5 inhibitor, target different intracellular pathways known to have dysfunctional signaling in PAH, so researchers expected them to have an additive effect when combined. The study findings support the rationale of targeting multiple affected pathways early in the course of PAH, rather than following the traditional approach of sequentially adding newer agents to established background therapy, said Dr. Nazzareno Galie of the department of experimental, diagnostic, and specialty medicine, University of Bologna (Italy), and his associates.

The 4-year, industry-sponsored trial involved 500 adults treated at 120 medical centers in 14 countries for PAH with World Health Organization functional class II or III symptoms. It included patients whose disorder was idiopathic; hereditary; or associated with connective tissue disease, drugs or toxins, stable HIV infection, or repaired congenital heart defects.
The mean age of participants was 54.4 years, and 78% were women. The mean pulmonary artery pressure was 48.7 mm Hg, and mean 6-minute walk distance was 353 m at baseline. A total of 253 patients were randomly assigned to receive oral, once-daily combination therapy, 126 to receive ambrisentan plus placebo, and 121 to receive tadalafil plus placebo. They were assessed at monthly intervals during the 24-week treatment period and were allowed to continue therapy indefinitely. The mean duration of use of the study medication was 517 days. Patients were followed up a final time 1 month after taking their last dose of study medication.
The primary efficacy endpoint was the first event of clinical failure, which was a composite of death, hospitalization for worsening PAH, disease progression, or unsatisfactory long-term treatment response. Only 18% of the combination-therapy group reached this endpoint, compared with 34% of the ambrisentan group, 28% of the tadalafil group, and 31% of the pooled-monotherapy group. The hazard ratios for the primary endpoint were 0.50 for the combination therapy versus pooled monotherapy, 0.48 for combination therapy versus ambrisentan alone, and 0.53 for combination therapy versus tadalafil alone.
This treatment benefit was mainly driven by one component of the combined endpoint: The rate of hospitalization for worsening PAH was three times higher with the two monotherapies (12%) than with combination therapy (4%). Improvement in the secondary endpoints of change in N-terminal pro–brain natriuretic peptide level, the percentage of participants with a satisfactory treatment response, and change in 6-minute walk distance all significantly favored the combination therapy, Dr. Galie and his associates said (N Engl J Med. 2015 Aug 27. doi: 10.1056/NEJMoa1413687).It is important to note, however, that “despite improvements in a variety of factors with combination therapy, we found no significant difference in WHO functional class among the study groups at week 24,” they wrote.
The combination of ambrisentan and tadalafil produced more adverse effects than either monotherapy, but the rate of discontinuation of a study drug and the rate of serious adverse events were similar across the three study groups. The most frequent adverse effects were peripheral edema, headache, nasal congestion, and anemia.
The AMBITION study was funded by Gilead Sciences and GlaxoSmithKline, which designed the trial, collected and analyzed the data, and wrote the report in conjunction with the authors. Gilead Sciences, GlaxoSmithKline, and Eli Lilly provided the study drugs. Dr. Galie reported receiving grants and personal fees from GlaxoSmithKline, Actelion, Bayer, and Pfizer; his associates reported ties to numerous industry sources.
First-line combination therapy with ambrisentan and tadalafil cut the rate of clinical events in pulmonary arterial hypertension (PAH) by half, compared with monotherapy using either drug, in an international phase 3-4 clinical trial reported online Aug. 27 in the New England Journal of Medicine.
Ambrisentan, a selective endothelin-A-receptor antagonist, and tadalafil, a phosphodiesterase type 5 inhibitor, target different intracellular pathways known to have dysfunctional signaling in PAH, so researchers expected them to have an additive effect when combined. The study findings support the rationale of targeting multiple affected pathways early in the course of PAH, rather than following the traditional approach of sequentially adding newer agents to established background therapy, said Dr. Nazzareno Galie of the department of experimental, diagnostic, and specialty medicine, University of Bologna (Italy), and his associates.
The 4-year, industry-sponsored trial involved 500 adults treated at 120 medical centers in 14 countries for PAH with World Health Organization functional class II or III symptoms. It included patients whose disorder was idiopathic; hereditary; or associated with connective tissue disease, drugs or toxins, stable HIV infection, or repaired congenital heart defects.
The mean age of participants was 54.4 years, and 78% were women. The mean pulmonary artery pressure was 48.7 mm Hg, and mean 6-minute walk distance was 353 m at baseline. A total of 253 patients were randomly assigned to receive oral, once-daily combination therapy, 126 to receive ambrisentan plus placebo, and 121 to receive tadalafil plus placebo. They were assessed at monthly intervals during the 24-week treatment period and were allowed to continue therapy indefinitely. The mean duration of use of the study medication was 517 days. Patients were followed up a final time 1 month after taking their last dose of study medication.
The primary efficacy endpoint was the first event of clinical failure, which was a composite of death, hospitalization for worsening PAH, disease progression, or unsatisfactory long-term treatment response. Only 18% of the combination-therapy group reached this endpoint, compared with 34% of the ambrisentan group, 28% of the tadalafil group, and 31% of the pooled-monotherapy group. The hazard ratios for the primary endpoint were 0.50 for the combination therapy versus pooled monotherapy, 0.48 for combination therapy versus ambrisentan alone, and 0.53 for combination therapy versus tadalafil alone.
This treatment benefit was mainly driven by one component of the combined endpoint: The rate of hospitalization for worsening PAH was three times higher with the two monotherapies (12%) than with combination therapy (4%). Improvement in the secondary endpoints of change in N-terminal pro–brain natriuretic peptide level, the percentage of participants with a satisfactory treatment response, and change in 6-minute walk distance all significantly favored the combination therapy, Dr. Galie and his associates said (N Engl J Med. 2015 Aug 27. doi: 10.1056/NEJMoa1413687).It is important to note, however, that “despite improvements in a variety of factors with combination therapy, we found no significant difference in WHO functional class among the study groups at week 24,” they wrote.
The combination of ambrisentan and tadalafil produced more adverse effects than either monotherapy, but the rate of discontinuation of a study drug and the rate of serious adverse events were similar across the three study groups. The most frequent adverse effects were peripheral edema, headache, nasal congestion, and anemia.
The AMBITION study was funded by Gilead Sciences and GlaxoSmithKline, which designed the trial, collected and analyzed the data, and wrote the report in conjunction with the authors. Gilead Sciences, GlaxoSmithKline, and Eli Lilly provided the study drugs. Dr. Galie reported receiving grants and personal fees from GlaxoSmithKline, Actelion, Bayer, and Pfizer; his associates reported ties to numerous industry sources.
First-line combination therapy with ambrisentan and tadalafil cut the rate of clinical events in pulmonary arterial hypertension (PAH) by half, compared with monotherapy using either drug, in an international phase 3-4 clinical trial reported online Aug. 27 in the New England Journal of Medicine.
Ambrisentan, a selective endothelin-A-receptor antagonist, and tadalafil, a phosphodiesterase type 5 inhibitor, target different intracellular pathways known to have dysfunctional signaling in PAH, so researchers expected them to have an additive effect when combined. The study findings support the rationale of targeting multiple affected pathways early in the course of PAH, rather than following the traditional approach of sequentially adding newer agents to established background therapy, said Dr. Nazzareno Galie of the department of experimental, diagnostic, and specialty medicine, University of Bologna (Italy), and his associates.
The 4-year, industry-sponsored trial involved 500 adults treated at 120 medical centers in 14 countries for PAH with World Health Organization functional class II or III symptoms. It included patients whose disorder was idiopathic; hereditary; or associated with connective tissue disease, drugs or toxins, stable HIV infection, or repaired congenital heart defects.
The mean age of participants was 54.4 years, and 78% were women. The mean pulmonary artery pressure was 48.7 mm Hg, and mean 6-minute walk distance was 353 m at baseline. A total of 253 patients were randomly assigned to receive oral, once-daily combination therapy, 126 to receive ambrisentan plus placebo, and 121 to receive tadalafil plus placebo. They were assessed at monthly intervals during the 24-week treatment period and were allowed to continue therapy indefinitely. The mean duration of use of the study medication was 517 days. Patients were followed up a final time 1 month after taking their last dose of study medication.
The primary efficacy endpoint was the first event of clinical failure, which was a composite of death, hospitalization for worsening PAH, disease progression, or unsatisfactory long-term treatment response. Only 18% of the combination-therapy group reached this endpoint, compared with 34% of the ambrisentan group, 28% of the tadalafil group, and 31% of the pooled-monotherapy group. The hazard ratios for the primary endpoint were 0.50 for the combination therapy versus pooled monotherapy, 0.48 for combination therapy versus ambrisentan alone, and 0.53 for combination therapy versus tadalafil alone.
This treatment benefit was mainly driven by one component of the combined endpoint: The rate of hospitalization for worsening PAH was three times higher with the two monotherapies (12%) than with combination therapy (4%). Improvement in the secondary endpoints of change in N-terminal pro–brain natriuretic peptide level, the percentage of participants with a satisfactory treatment response, and change in 6-minute walk distance all significantly favored the combination therapy, Dr. Galie and his associates said (N Engl J Med. 2015 Aug 27. doi: 10.1056/NEJMoa1413687).It is important to note, however, that “despite improvements in a variety of factors with combination therapy, we found no significant difference in WHO functional class among the study groups at week 24,” they wrote.
The combination of ambrisentan and tadalafil produced more adverse effects than either monotherapy, but the rate of discontinuation of a study drug and the rate of serious adverse events were similar across the three study groups. The most frequent adverse effects were peripheral edema, headache, nasal congestion, and anemia.
The AMBITION study was funded by Gilead Sciences and GlaxoSmithKline, which designed the trial, collected and analyzed the data, and wrote the report in conjunction with the authors. Gilead Sciences, GlaxoSmithKline, and Eli Lilly provided the study drugs. Dr. Galie reported receiving grants and personal fees from GlaxoSmithKline, Actelion, Bayer, and Pfizer; his associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: First-line combination therapy with ambrisentan plus tadalafil cut the rate of clinical events in pulmonary arterial hypertension by half, compared with either monotherapy.
Major finding: Only 18% of the combination-therapy group reached the primary efficacy endpoint of clinical failure, compared with 34% of the ambrisentan group, 28% of the tadalafil group, and 31% of the pooled-monotherapy group.
Data source: An international, randomized, double-blind phase 3-4 clinical trial involving 500 men and women with previously untreated PAH.
Disclosures: The AMBITION study was funded by Gilead Sciences and GlaxoSmithKline, which designed the trial, collected and analyzed the data, and wrote the report in conjunction with the authors. Gilead Sciences, GlaxoSmithKline, and Eli Lilly provided the study drugs. Dr. Galie reported receiving grants and personal fees from GlaxoSmithKline, Actelion, Bayer, and Pfizer; his associates reported ties to numerous industry sources.

ICDs in the elderly
There has been a spate of recent publications dealing with the lack of implantable cardioverter-defibrillator implantations in the elderly. The most recent indicates that only 8% of patients over age 75 years who have experienced a non–ST-segment elevation myocardial infarction (NSTEMI) or STEMI receive an ICD largely due to the restriction of implantation within 40 days of the incident infarction because of the delayed repair of ventricular function after an MI and the uncertainty of ejection fraction measurements during this period. That article indicates that despite this delay, patients who receive an ICD had an improved survival over the subsequent 2 years, compared with those who did not (JAMA. 2015;313[24]:2433-40). Some of my octogenarian friends might question whether improved survival and the prevention of sudden death is a benefit at that age.
An accompanying editorial suggests that a closer follow-up of these patients is warranted in order to improve the rate of implantation in those patients who are discharged so that they do not “fall through the cracks” and are lost to follow-up (JAMA. 2015:313[24]:2429-30).
Although there has been a tapering off of the explosive use of ICDs in the United States, almost a quarter million devices were implanted between 2010 and 2011 (Heart Rhythm. 2013 Apr;10[4]:e59-65). The U.S. number is roughly four times that of Western Europe. Primary prevention was the reason for implantation in 73.8%, and half of the implantations were in patients over 65; 29% were in the 70-79 age group, and 14% were octogenarians. A history of New York Heart Association class II-IV heart failure was present in 82% and a myocardial infarction in 49%.
There are of course other reasons why the elderly may not receive an ICD. The most frequent are the presence of concomitant diseases like stroke, cancer, and chronic renal disease. However, many elderly do not wish to have their survival tied to a device that they have no control over. Some may view sudden death as an acceptable mortality outcome considering other alternatives. Certainly, adverse lifestyle changes at advanced age may be a reason for the reluctance to choose an ICD.
The application of our new technologies like ICDs, catheter-implanted aortic valves, and mini–left ventricular assist devices have been remarkably successful and have brought lifesaving interventions to thousands of patients. Their relative ease of application has led to a casualness in regard to appropriateness in patients with concomitant diseases, and particularly in the elderly.
The definition of who is elderly has changed dramatically in clinical trials from the mid–20th century when those studies excluded patients over 65. In today’s world, the definition of the elderly has become a slippery slope, as there is no age limit and the inclusion of octogenarians is not unusual. The observation that elderly postinfarction patients with decreased ejection fraction can experience improved survival needs to be evaluated in the light of important considerations of current and expected quality of life in individual patients, as well as their own mortality expectations.
Most of the studies examining implantation rates, extensively analyze the effect of comorbidity and cost benefit of implantation. They rarely deal with how quality of life of the patient and their own mortality expectation impacts on the decision for ICD implantation. Once implanted, removal of the device is often impossible and when possible, as with an ICD, raise important and difficult ethical questions for patient, family, and doctor.
For those of us who are octogenarians and treat octogenarians, these issues are first and foremost in the decision process. The decision to use these devices for the relatively short-term benefit may become an onerous burden for the very elderly whose future quality of life can become abruptly abbreviated by the aging process. Easy exodus from life by sudden death may unfortunately be prolonged by an ICD.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
There has been a spate of recent publications dealing with the lack of implantable cardioverter-defibrillator implantations in the elderly. The most recent indicates that only 8% of patients over age 75 years who have experienced a non–ST-segment elevation myocardial infarction (NSTEMI) or STEMI receive an ICD largely due to the restriction of implantation within 40 days of the incident infarction because of the delayed repair of ventricular function after an MI and the uncertainty of ejection fraction measurements during this period. That article indicates that despite this delay, patients who receive an ICD had an improved survival over the subsequent 2 years, compared with those who did not (JAMA. 2015;313[24]:2433-40). Some of my octogenarian friends might question whether improved survival and the prevention of sudden death is a benefit at that age.
An accompanying editorial suggests that a closer follow-up of these patients is warranted in order to improve the rate of implantation in those patients who are discharged so that they do not “fall through the cracks” and are lost to follow-up (JAMA. 2015:313[24]:2429-30).
Although there has been a tapering off of the explosive use of ICDs in the United States, almost a quarter million devices were implanted between 2010 and 2011 (Heart Rhythm. 2013 Apr;10[4]:e59-65). The U.S. number is roughly four times that of Western Europe. Primary prevention was the reason for implantation in 73.8%, and half of the implantations were in patients over 65; 29% were in the 70-79 age group, and 14% were octogenarians. A history of New York Heart Association class II-IV heart failure was present in 82% and a myocardial infarction in 49%.
There are of course other reasons why the elderly may not receive an ICD. The most frequent are the presence of concomitant diseases like stroke, cancer, and chronic renal disease. However, many elderly do not wish to have their survival tied to a device that they have no control over. Some may view sudden death as an acceptable mortality outcome considering other alternatives. Certainly, adverse lifestyle changes at advanced age may be a reason for the reluctance to choose an ICD.
The application of our new technologies like ICDs, catheter-implanted aortic valves, and mini–left ventricular assist devices have been remarkably successful and have brought lifesaving interventions to thousands of patients. Their relative ease of application has led to a casualness in regard to appropriateness in patients with concomitant diseases, and particularly in the elderly.
The definition of who is elderly has changed dramatically in clinical trials from the mid–20th century when those studies excluded patients over 65. In today’s world, the definition of the elderly has become a slippery slope, as there is no age limit and the inclusion of octogenarians is not unusual. The observation that elderly postinfarction patients with decreased ejection fraction can experience improved survival needs to be evaluated in the light of important considerations of current and expected quality of life in individual patients, as well as their own mortality expectations.
Most of the studies examining implantation rates, extensively analyze the effect of comorbidity and cost benefit of implantation. They rarely deal with how quality of life of the patient and their own mortality expectation impacts on the decision for ICD implantation. Once implanted, removal of the device is often impossible and when possible, as with an ICD, raise important and difficult ethical questions for patient, family, and doctor.
For those of us who are octogenarians and treat octogenarians, these issues are first and foremost in the decision process. The decision to use these devices for the relatively short-term benefit may become an onerous burden for the very elderly whose future quality of life can become abruptly abbreviated by the aging process. Easy exodus from life by sudden death may unfortunately be prolonged by an ICD.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
There has been a spate of recent publications dealing with the lack of implantable cardioverter-defibrillator implantations in the elderly. The most recent indicates that only 8% of patients over age 75 years who have experienced a non–ST-segment elevation myocardial infarction (NSTEMI) or STEMI receive an ICD largely due to the restriction of implantation within 40 days of the incident infarction because of the delayed repair of ventricular function after an MI and the uncertainty of ejection fraction measurements during this period. That article indicates that despite this delay, patients who receive an ICD had an improved survival over the subsequent 2 years, compared with those who did not (JAMA. 2015;313[24]:2433-40). Some of my octogenarian friends might question whether improved survival and the prevention of sudden death is a benefit at that age.
An accompanying editorial suggests that a closer follow-up of these patients is warranted in order to improve the rate of implantation in those patients who are discharged so that they do not “fall through the cracks” and are lost to follow-up (JAMA. 2015:313[24]:2429-30).
Although there has been a tapering off of the explosive use of ICDs in the United States, almost a quarter million devices were implanted between 2010 and 2011 (Heart Rhythm. 2013 Apr;10[4]:e59-65). The U.S. number is roughly four times that of Western Europe. Primary prevention was the reason for implantation in 73.8%, and half of the implantations were in patients over 65; 29% were in the 70-79 age group, and 14% were octogenarians. A history of New York Heart Association class II-IV heart failure was present in 82% and a myocardial infarction in 49%.
There are of course other reasons why the elderly may not receive an ICD. The most frequent are the presence of concomitant diseases like stroke, cancer, and chronic renal disease. However, many elderly do not wish to have their survival tied to a device that they have no control over. Some may view sudden death as an acceptable mortality outcome considering other alternatives. Certainly, adverse lifestyle changes at advanced age may be a reason for the reluctance to choose an ICD.
The application of our new technologies like ICDs, catheter-implanted aortic valves, and mini–left ventricular assist devices have been remarkably successful and have brought lifesaving interventions to thousands of patients. Their relative ease of application has led to a casualness in regard to appropriateness in patients with concomitant diseases, and particularly in the elderly.
The definition of who is elderly has changed dramatically in clinical trials from the mid–20th century when those studies excluded patients over 65. In today’s world, the definition of the elderly has become a slippery slope, as there is no age limit and the inclusion of octogenarians is not unusual. The observation that elderly postinfarction patients with decreased ejection fraction can experience improved survival needs to be evaluated in the light of important considerations of current and expected quality of life in individual patients, as well as their own mortality expectations.
Most of the studies examining implantation rates, extensively analyze the effect of comorbidity and cost benefit of implantation. They rarely deal with how quality of life of the patient and their own mortality expectation impacts on the decision for ICD implantation. Once implanted, removal of the device is often impossible and when possible, as with an ICD, raise important and difficult ethical questions for patient, family, and doctor.
For those of us who are octogenarians and treat octogenarians, these issues are first and foremost in the decision process. The decision to use these devices for the relatively short-term benefit may become an onerous burden for the very elderly whose future quality of life can become abruptly abbreviated by the aging process. Easy exodus from life by sudden death may unfortunately be prolonged by an ICD.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
U-shaped link between physical activity and heart failure
A longitudinal cohort study shows a U-shaped relationship between total physical activity and heart failure risk in men.
The 15-year study of 33,012 men, average age 60 years at baseline, showed that those who engaged in the highest levels and intensity of total physical activity had a 31% greater risk of heart failure than did those in the median activity category.

However, men who undertook the lowest levels of physical activity had up to a 69% greater risk of heart failure compared to the median activity group, according to the results, published online Aug. 12 in JACC: Heart Failure.
“The U-shaped relationship between exercise levels and the likelihood of subsequent heart failure is a unique finding and will stimulate further research in the important field of prevention,” said Dr. Christopher O’Connor, editor-in-chief of JACC: Heart Failure, who was not involved in the study.
The questionnaire-based study involved of 3,609 heart failure events, which included 3,190 first events of heart failure hospitalizations and 419 deaths from heart failure.
The study authors assigned intensity scores – defined as metabolic equivalents (MET) hours/day – to each type of physical activity, then calculated a total daily physical activity score for each individual by multiplying the intensity scores by reported duration of each activity.
Watching TV, reading, and sleep were assigned the lowest intensity MET scores, walking or bicycling were in the mid-range, and exercise was assigned the highest MET scores.
Walking or bicycling at least 20 minutes a day were associated with the greatest reductions in the risk of heart failure – 21% – compared to not walking or biking, and this type and level of activity was linked to an 8-month delay in the onset of heart failure among those who engaged in it.
The investigators also found no differences between the two groups in terms of age or education level, and the exclusion of study participants who developed heart failure in the 3 first years of follow-up did not impact results.
“When examining long-term behavior regarding walking or biking and HF [heart failure] risk, the results suggested that more recent active behavior in this PA [physical activity] domain may be more important for HF protection than past PA levels,” wrote Dr. Iffat Rahman and colleagues at the Karolinska Institute, Stockholm.
Exercising for more than 1 hour per week was linked with a 14% reduction in risk, but work occupation, household work, and physical inactivity did not affect heart failure risk (JACC Heart Fail. 2015 Aug 12. doi:10.1016/j.jchf.2015.05.006).
While previous studies have shown that lower levels of physical activity increase the risk of heart failure, the authors said this was the first to show an increase in risk among individuals who undertake very high levels of physical activity.
“It is possible that substantial increase of pumping of blood by the heart could damage the cardiac muscle fibers causing damage in the myocardium,” the authors wrote.
“Moreover, adverse cardiovascular outcomes could potentially be attributed to increased oxidative stress, arterial stiffness, and coronary artery calcification.”
A similar study looking at the relationship between physical activity and heart failure in women did not find an increased risk with very high levels of physical activity, suggesting a differential effect between men and women.
There were no conflicts of interest declared.
This study reminds us that we still know relatively little about how variations in physical activity and exercise “dose” might impact disease onset, and further information is needed about whether or not exercise and physical activity confer different levels of immunity based on the type and volume of exercise, as well as race, gender, and the presence of comorbidities.
However, for the vast majority of the patients we counsel about exercise and disease prevention, recommending the current exercise guidelines of 150 minutes or more of moderate intensity exercise per week is prudent.
Dr. Steven J. Keteyian and Dr. Clinton A. Brawner are from the division of cardiovascular medicine at Henry Ford Hospital, Detroit. These comments are taken from an editorial (JACC Heart Fail. 2015 Aug 12. doi:10.1016/j.jchf.2015.06.002). No conflicts of interest were declared.
This study reminds us that we still know relatively little about how variations in physical activity and exercise “dose” might impact disease onset, and further information is needed about whether or not exercise and physical activity confer different levels of immunity based on the type and volume of exercise, as well as race, gender, and the presence of comorbidities.
However, for the vast majority of the patients we counsel about exercise and disease prevention, recommending the current exercise guidelines of 150 minutes or more of moderate intensity exercise per week is prudent.
Dr. Steven J. Keteyian and Dr. Clinton A. Brawner are from the division of cardiovascular medicine at Henry Ford Hospital, Detroit. These comments are taken from an editorial (JACC Heart Fail. 2015 Aug 12. doi:10.1016/j.jchf.2015.06.002). No conflicts of interest were declared.
This study reminds us that we still know relatively little about how variations in physical activity and exercise “dose” might impact disease onset, and further information is needed about whether or not exercise and physical activity confer different levels of immunity based on the type and volume of exercise, as well as race, gender, and the presence of comorbidities.
However, for the vast majority of the patients we counsel about exercise and disease prevention, recommending the current exercise guidelines of 150 minutes or more of moderate intensity exercise per week is prudent.
Dr. Steven J. Keteyian and Dr. Clinton A. Brawner are from the division of cardiovascular medicine at Henry Ford Hospital, Detroit. These comments are taken from an editorial (JACC Heart Fail. 2015 Aug 12. doi:10.1016/j.jchf.2015.06.002). No conflicts of interest were declared.
A longitudinal cohort study shows a U-shaped relationship between total physical activity and heart failure risk in men.
The 15-year study of 33,012 men, average age 60 years at baseline, showed that those who engaged in the highest levels and intensity of total physical activity had a 31% greater risk of heart failure than did those in the median activity category.
However, men who undertook the lowest levels of physical activity had up to a 69% greater risk of heart failure compared to the median activity group, according to the results, published online Aug. 12 in JACC: Heart Failure.
“The U-shaped relationship between exercise levels and the likelihood of subsequent heart failure is a unique finding and will stimulate further research in the important field of prevention,” said Dr. Christopher O’Connor, editor-in-chief of JACC: Heart Failure, who was not involved in the study.
The questionnaire-based study involved of 3,609 heart failure events, which included 3,190 first events of heart failure hospitalizations and 419 deaths from heart failure.
The study authors assigned intensity scores – defined as metabolic equivalents (MET) hours/day – to each type of physical activity, then calculated a total daily physical activity score for each individual by multiplying the intensity scores by reported duration of each activity.
Watching TV, reading, and sleep were assigned the lowest intensity MET scores, walking or bicycling were in the mid-range, and exercise was assigned the highest MET scores.
Walking or bicycling at least 20 minutes a day were associated with the greatest reductions in the risk of heart failure – 21% – compared to not walking or biking, and this type and level of activity was linked to an 8-month delay in the onset of heart failure among those who engaged in it.
The investigators also found no differences between the two groups in terms of age or education level, and the exclusion of study participants who developed heart failure in the 3 first years of follow-up did not impact results.
“When examining long-term behavior regarding walking or biking and HF [heart failure] risk, the results suggested that more recent active behavior in this PA [physical activity] domain may be more important for HF protection than past PA levels,” wrote Dr. Iffat Rahman and colleagues at the Karolinska Institute, Stockholm.
Exercising for more than 1 hour per week was linked with a 14% reduction in risk, but work occupation, household work, and physical inactivity did not affect heart failure risk (JACC Heart Fail. 2015 Aug 12. doi:10.1016/j.jchf.2015.05.006).
While previous studies have shown that lower levels of physical activity increase the risk of heart failure, the authors said this was the first to show an increase in risk among individuals who undertake very high levels of physical activity.
“It is possible that substantial increase of pumping of blood by the heart could damage the cardiac muscle fibers causing damage in the myocardium,” the authors wrote.
“Moreover, adverse cardiovascular outcomes could potentially be attributed to increased oxidative stress, arterial stiffness, and coronary artery calcification.”
A similar study looking at the relationship between physical activity and heart failure in women did not find an increased risk with very high levels of physical activity, suggesting a differential effect between men and women.
There were no conflicts of interest declared.
A longitudinal cohort study shows a U-shaped relationship between total physical activity and heart failure risk in men.
The 15-year study of 33,012 men, average age 60 years at baseline, showed that those who engaged in the highest levels and intensity of total physical activity had a 31% greater risk of heart failure than did those in the median activity category.
However, men who undertook the lowest levels of physical activity had up to a 69% greater risk of heart failure compared to the median activity group, according to the results, published online Aug. 12 in JACC: Heart Failure.
“The U-shaped relationship between exercise levels and the likelihood of subsequent heart failure is a unique finding and will stimulate further research in the important field of prevention,” said Dr. Christopher O’Connor, editor-in-chief of JACC: Heart Failure, who was not involved in the study.
The questionnaire-based study involved of 3,609 heart failure events, which included 3,190 first events of heart failure hospitalizations and 419 deaths from heart failure.
The study authors assigned intensity scores – defined as metabolic equivalents (MET) hours/day – to each type of physical activity, then calculated a total daily physical activity score for each individual by multiplying the intensity scores by reported duration of each activity.
Watching TV, reading, and sleep were assigned the lowest intensity MET scores, walking or bicycling were in the mid-range, and exercise was assigned the highest MET scores.
Walking or bicycling at least 20 minutes a day were associated with the greatest reductions in the risk of heart failure – 21% – compared to not walking or biking, and this type and level of activity was linked to an 8-month delay in the onset of heart failure among those who engaged in it.
The investigators also found no differences between the two groups in terms of age or education level, and the exclusion of study participants who developed heart failure in the 3 first years of follow-up did not impact results.
“When examining long-term behavior regarding walking or biking and HF [heart failure] risk, the results suggested that more recent active behavior in this PA [physical activity] domain may be more important for HF protection than past PA levels,” wrote Dr. Iffat Rahman and colleagues at the Karolinska Institute, Stockholm.
Exercising for more than 1 hour per week was linked with a 14% reduction in risk, but work occupation, household work, and physical inactivity did not affect heart failure risk (JACC Heart Fail. 2015 Aug 12. doi:10.1016/j.jchf.2015.05.006).
While previous studies have shown that lower levels of physical activity increase the risk of heart failure, the authors said this was the first to show an increase in risk among individuals who undertake very high levels of physical activity.
“It is possible that substantial increase of pumping of blood by the heart could damage the cardiac muscle fibers causing damage in the myocardium,” the authors wrote.
“Moreover, adverse cardiovascular outcomes could potentially be attributed to increased oxidative stress, arterial stiffness, and coronary artery calcification.”
A similar study looking at the relationship between physical activity and heart failure in women did not find an increased risk with very high levels of physical activity, suggesting a differential effect between men and women.
There were no conflicts of interest declared.
FROM JACC: HEART FAILURE
Key clinical point: A study has found a U-shaped association between total physical activity and heart failure risk in men.
Major finding: Men who engaged in the highest levels and intensity of total physical activity had a 31% greater risk of heart failure than did those in the median activity category.
Data source: A longitudinal cohort study of 33,012 men.
Disclosures: There were no conflicts of interest declared.

High troponin T level doubles CVD risk
An abnormal troponin T level of 14 ng/L or higher, as measured using a high-sensitivity assay, doubles the risk of cardiovascular events and death among patients who have stable ischemic heart disease and type 2 diabetes, according to a report published online Aug. 13 in the New England Journal of Medicine.
Moreover, an increase of more than 25% in troponin T level during the course of 1 year predicts a worse outcome than do stable or decreasing troponin T levels in this patient population, significantly increasing the rates of death from cardiovascular causes, MI, or stroke. These findings “raise the possibility that serial measurements of troponin concentration may improve its prognostic value, and that persistently elevated and increasing troponin concentrations may be the best predictor of adverse outcomes,” said Dr. Brendan M. Everett of the divisions of cardiovascular medicine and preventive medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston.
These findings have particular significance because the prevalence of elevated troponin T was fully 40% in this study, noted Dr. Everett and his associates.
To examine the possible relationship between elevated troponin T and adverse cardiovascular outcomes in patients who had both stable ischemic heart disease and diabetes, the investigators performed a post hoc analysis of data gathered in the Bypass Angioplasty Revascularization Investigation in Type 2 Diabetes (BARI 2D) clinical trial, which compared outcomes between patients who underwent preventive percutaneous coronary intervention or CABG plus intensive medical therapy against those who received intensive medical therapy alone.
For their ancillary study, Dr. Everett and his colleagues focused on 2,285 of these participants who had high-sensitivity assays to measure very low cardiac troponin levels in plasma samples and who were followed for a mean of 5 years. At baseline, 897 (40%) of these patients had troponin T levels of 14 ng/L or higher, the current cutoff point for both men and women.
The 5-year incidence of the composite outcome of death from cardiovascular causes, MI, or stroke was 27.1% in patients with elevated troponin T at baseline, compared with 12.9% in those with normal troponin T. The between-groups differences in each of the individual components of this composite outcome were of similar magnitude, as were the between-group differences in the secondary outcomes of death from any cause and heart failure (N Engl J Med. 2015 Aug 13 [doi:10.1056/NEJMoa1415921]).
This association remained robust after the data were adjusted to account for numerous potentially confounding factors such as traditional CV risk factors, a history of MI, a history of heart failure, the severity of diabetes, glomerular filtration rate, ECG abnormalities, the number of coronary lesions, and the presence of an abnormal ejection fraction.
In a further analysis that divided patients into five groups according to their troponin T levels, adverse event rates were substantially higher than average only in the highest two categories: 14.0-23.0 ng/L and 23.0 ng/L and higher.
In another analysis, the investigators assessed outcomes in a subgroup of 1,984 participants who underwent troponin T testing both at baseline and 1 year later. Patients whose levels increased by more than 25% during that year – about 7% of this subgroup – showed significantly increased risk of all adverse outcomes, compared with patients whose troponin T levels either remained stable or decreased.
Prompt revascularization via percutaneous coronary intervention or coronary artery bypass surgery did not lower the risk of any adverse outcomes in patients who had elevated troponin T. It is therefore crucial that the troponin T assay, already in widespread use, not be used to justify revascularization procedures, the researchers wrote. At least on the basis of this study’s findings, such procedures appear to offer little benefit, they noted.
The National Heart, Lung, and Blood Institute, the National Institute of Diabetes and Digestive and Kidney Diseases, and Roche Diagnostics supported the study. Dr. Everett reported ties with Roche, Novartis, and Genzyme; his associates reported ties to numerous industry sources.
The findings of this study add to the accumulating data that suggest cardiac troponin testing may become routine for risk stratification across the entire spectrum of ischemic heart disease.
However, it is important to note that interpreting elevations in troponin T is a challenge in patients who have kidney impairment, because the problem may impair renal clearance of troponin. In addition, kidney disease may be a concomitant risk factor for ongoing subclinical thrombosis, which could be one of the pathological mechanisms underlying troponin elevation in patients with stable ischemic heart disease.
Chiara Melloni, M.D., and Matthew T. Roe, M.D., are at Duke Clinical Research Institute, Durham, N.C. Their financial disclosures are available at NEJM.org. Dr. Melloni and Dr. Roe made these remarks in an editorial accompanying Dr. Everett’s report (N Engl J Med. 2015 Aug 13 [doi:10.1056/NEJMe1506298]).
The findings of this study add to the accumulating data that suggest cardiac troponin testing may become routine for risk stratification across the entire spectrum of ischemic heart disease.
However, it is important to note that interpreting elevations in troponin T is a challenge in patients who have kidney impairment, because the problem may impair renal clearance of troponin. In addition, kidney disease may be a concomitant risk factor for ongoing subclinical thrombosis, which could be one of the pathological mechanisms underlying troponin elevation in patients with stable ischemic heart disease.
Chiara Melloni, M.D., and Matthew T. Roe, M.D., are at Duke Clinical Research Institute, Durham, N.C. Their financial disclosures are available at NEJM.org. Dr. Melloni and Dr. Roe made these remarks in an editorial accompanying Dr. Everett’s report (N Engl J Med. 2015 Aug 13 [doi:10.1056/NEJMe1506298]).
The findings of this study add to the accumulating data that suggest cardiac troponin testing may become routine for risk stratification across the entire spectrum of ischemic heart disease.
However, it is important to note that interpreting elevations in troponin T is a challenge in patients who have kidney impairment, because the problem may impair renal clearance of troponin. In addition, kidney disease may be a concomitant risk factor for ongoing subclinical thrombosis, which could be one of the pathological mechanisms underlying troponin elevation in patients with stable ischemic heart disease.
Chiara Melloni, M.D., and Matthew T. Roe, M.D., are at Duke Clinical Research Institute, Durham, N.C. Their financial disclosures are available at NEJM.org. Dr. Melloni and Dr. Roe made these remarks in an editorial accompanying Dr. Everett’s report (N Engl J Med. 2015 Aug 13 [doi:10.1056/NEJMe1506298]).
An abnormal troponin T level of 14 ng/L or higher, as measured using a high-sensitivity assay, doubles the risk of cardiovascular events and death among patients who have stable ischemic heart disease and type 2 diabetes, according to a report published online Aug. 13 in the New England Journal of Medicine.
Moreover, an increase of more than 25% in troponin T level during the course of 1 year predicts a worse outcome than do stable or decreasing troponin T levels in this patient population, significantly increasing the rates of death from cardiovascular causes, MI, or stroke. These findings “raise the possibility that serial measurements of troponin concentration may improve its prognostic value, and that persistently elevated and increasing troponin concentrations may be the best predictor of adverse outcomes,” said Dr. Brendan M. Everett of the divisions of cardiovascular medicine and preventive medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston.
These findings have particular significance because the prevalence of elevated troponin T was fully 40% in this study, noted Dr. Everett and his associates.
To examine the possible relationship between elevated troponin T and adverse cardiovascular outcomes in patients who had both stable ischemic heart disease and diabetes, the investigators performed a post hoc analysis of data gathered in the Bypass Angioplasty Revascularization Investigation in Type 2 Diabetes (BARI 2D) clinical trial, which compared outcomes between patients who underwent preventive percutaneous coronary intervention or CABG plus intensive medical therapy against those who received intensive medical therapy alone.
For their ancillary study, Dr. Everett and his colleagues focused on 2,285 of these participants who had high-sensitivity assays to measure very low cardiac troponin levels in plasma samples and who were followed for a mean of 5 years. At baseline, 897 (40%) of these patients had troponin T levels of 14 ng/L or higher, the current cutoff point for both men and women.
The 5-year incidence of the composite outcome of death from cardiovascular causes, MI, or stroke was 27.1% in patients with elevated troponin T at baseline, compared with 12.9% in those with normal troponin T. The between-groups differences in each of the individual components of this composite outcome were of similar magnitude, as were the between-group differences in the secondary outcomes of death from any cause and heart failure (N Engl J Med. 2015 Aug 13 [doi:10.1056/NEJMoa1415921]).
This association remained robust after the data were adjusted to account for numerous potentially confounding factors such as traditional CV risk factors, a history of MI, a history of heart failure, the severity of diabetes, glomerular filtration rate, ECG abnormalities, the number of coronary lesions, and the presence of an abnormal ejection fraction.
In a further analysis that divided patients into five groups according to their troponin T levels, adverse event rates were substantially higher than average only in the highest two categories: 14.0-23.0 ng/L and 23.0 ng/L and higher.
In another analysis, the investigators assessed outcomes in a subgroup of 1,984 participants who underwent troponin T testing both at baseline and 1 year later. Patients whose levels increased by more than 25% during that year – about 7% of this subgroup – showed significantly increased risk of all adverse outcomes, compared with patients whose troponin T levels either remained stable or decreased.
Prompt revascularization via percutaneous coronary intervention or coronary artery bypass surgery did not lower the risk of any adverse outcomes in patients who had elevated troponin T. It is therefore crucial that the troponin T assay, already in widespread use, not be used to justify revascularization procedures, the researchers wrote. At least on the basis of this study’s findings, such procedures appear to offer little benefit, they noted.
The National Heart, Lung, and Blood Institute, the National Institute of Diabetes and Digestive and Kidney Diseases, and Roche Diagnostics supported the study. Dr. Everett reported ties with Roche, Novartis, and Genzyme; his associates reported ties to numerous industry sources.
An abnormal troponin T level of 14 ng/L or higher, as measured using a high-sensitivity assay, doubles the risk of cardiovascular events and death among patients who have stable ischemic heart disease and type 2 diabetes, according to a report published online Aug. 13 in the New England Journal of Medicine.
Moreover, an increase of more than 25% in troponin T level during the course of 1 year predicts a worse outcome than do stable or decreasing troponin T levels in this patient population, significantly increasing the rates of death from cardiovascular causes, MI, or stroke. These findings “raise the possibility that serial measurements of troponin concentration may improve its prognostic value, and that persistently elevated and increasing troponin concentrations may be the best predictor of adverse outcomes,” said Dr. Brendan M. Everett of the divisions of cardiovascular medicine and preventive medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston.
These findings have particular significance because the prevalence of elevated troponin T was fully 40% in this study, noted Dr. Everett and his associates.
To examine the possible relationship between elevated troponin T and adverse cardiovascular outcomes in patients who had both stable ischemic heart disease and diabetes, the investigators performed a post hoc analysis of data gathered in the Bypass Angioplasty Revascularization Investigation in Type 2 Diabetes (BARI 2D) clinical trial, which compared outcomes between patients who underwent preventive percutaneous coronary intervention or CABG plus intensive medical therapy against those who received intensive medical therapy alone.
For their ancillary study, Dr. Everett and his colleagues focused on 2,285 of these participants who had high-sensitivity assays to measure very low cardiac troponin levels in plasma samples and who were followed for a mean of 5 years. At baseline, 897 (40%) of these patients had troponin T levels of 14 ng/L or higher, the current cutoff point for both men and women.
The 5-year incidence of the composite outcome of death from cardiovascular causes, MI, or stroke was 27.1% in patients with elevated troponin T at baseline, compared with 12.9% in those with normal troponin T. The between-groups differences in each of the individual components of this composite outcome were of similar magnitude, as were the between-group differences in the secondary outcomes of death from any cause and heart failure (N Engl J Med. 2015 Aug 13 [doi:10.1056/NEJMoa1415921]).
This association remained robust after the data were adjusted to account for numerous potentially confounding factors such as traditional CV risk factors, a history of MI, a history of heart failure, the severity of diabetes, glomerular filtration rate, ECG abnormalities, the number of coronary lesions, and the presence of an abnormal ejection fraction.
In a further analysis that divided patients into five groups according to their troponin T levels, adverse event rates were substantially higher than average only in the highest two categories: 14.0-23.0 ng/L and 23.0 ng/L and higher.
In another analysis, the investigators assessed outcomes in a subgroup of 1,984 participants who underwent troponin T testing both at baseline and 1 year later. Patients whose levels increased by more than 25% during that year – about 7% of this subgroup – showed significantly increased risk of all adverse outcomes, compared with patients whose troponin T levels either remained stable or decreased.
Prompt revascularization via percutaneous coronary intervention or coronary artery bypass surgery did not lower the risk of any adverse outcomes in patients who had elevated troponin T. It is therefore crucial that the troponin T assay, already in widespread use, not be used to justify revascularization procedures, the researchers wrote. At least on the basis of this study’s findings, such procedures appear to offer little benefit, they noted.
The National Heart, Lung, and Blood Institute, the National Institute of Diabetes and Digestive and Kidney Diseases, and Roche Diagnostics supported the study. Dr. Everett reported ties with Roche, Novartis, and Genzyme; his associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Troponin T levels of 14 ng/L or higher double the risk of CVD events and death in patients with stable ischemic heart disease and concomitant type 2 diabetes.
Major finding: The 5-year incidence of the composite outcome of death from cardiovascular causes, MI, or stroke was 27.1% in patients with elevated troponin T at baseline, compared with 12.9% in those with normal troponin T.
Data source: A post hoc analysis of data in the Bypass Angioplasty Revascularization Type 2 Diabetes (BARI 2D) trial of 2,285 participants who were followed for 5 years.
Disclosures: The National Heart, Lung, and Blood Institute, the National Institute of Diabetes and Digestive and Kidney Diseases, and Roche Diagnostics supported the study. Dr. Everett reported ties with Roche, Novartis, and Genzyme; his associates reported ties to numerous industry sources.
Inpatient mortality down for high-volume conditions
Inpatient mortality for pneumonia, acute MI, heart failure, and stroke each fell significantly from 2002 to 2012, the Agency for Healthcare Research and Quality reported.
Over that period, mortality among adults hospitalized with pneumonia went from 65 per 1,000 admissions to 35.8 per 1,000 for a drop of 45% – largest of the four high-volume conditions. Corresponding declines for the others were 41% for acute MI, 29% for heart failure, and 27% for stroke, the AHRQ noted.

Since “death following discharge from a hospital is not reflected in these data,” the report said, measures of inpatient mortality “can reflect both improvements in health care and shifts in where end-of-life care takes place over time.”
The estimates in the report are based on data from the Nationwide Inpatient Sample (2002-2011) and State Inpatient Databases (2012).
Inpatient mortality for pneumonia, acute MI, heart failure, and stroke each fell significantly from 2002 to 2012, the Agency for Healthcare Research and Quality reported.
Over that period, mortality among adults hospitalized with pneumonia went from 65 per 1,000 admissions to 35.8 per 1,000 for a drop of 45% – largest of the four high-volume conditions. Corresponding declines for the others were 41% for acute MI, 29% for heart failure, and 27% for stroke, the AHRQ noted.
Since “death following discharge from a hospital is not reflected in these data,” the report said, measures of inpatient mortality “can reflect both improvements in health care and shifts in where end-of-life care takes place over time.”
The estimates in the report are based on data from the Nationwide Inpatient Sample (2002-2011) and State Inpatient Databases (2012).
Inpatient mortality for pneumonia, acute MI, heart failure, and stroke each fell significantly from 2002 to 2012, the Agency for Healthcare Research and Quality reported.
Over that period, mortality among adults hospitalized with pneumonia went from 65 per 1,000 admissions to 35.8 per 1,000 for a drop of 45% – largest of the four high-volume conditions. Corresponding declines for the others were 41% for acute MI, 29% for heart failure, and 27% for stroke, the AHRQ noted.
Since “death following discharge from a hospital is not reflected in these data,” the report said, measures of inpatient mortality “can reflect both improvements in health care and shifts in where end-of-life care takes place over time.”
The estimates in the report are based on data from the Nationwide Inpatient Sample (2002-2011) and State Inpatient Databases (2012).
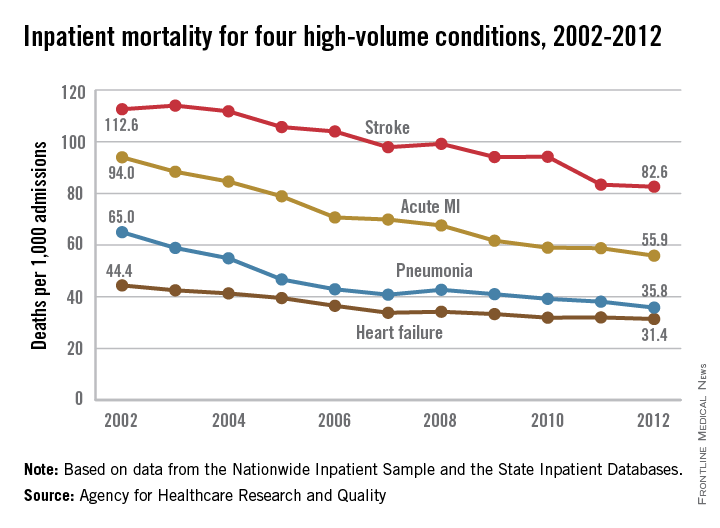
LVEF improvements over time in ICD recipients tied to lower mortality
In the one-quarter of heart failure patients who receive an implantable cardioverter defibrillator for primary prevention and whose left ventricular ejection fraction improves more than 35%, both mortality and appropriate ICD shocks are decreased, according to a report published online July 27 in Journal of the American College of Cardiology.
This raises the question of whether such patients’ risk for sudden cardiac death still warrants replacement of the ICD generator years later, especially among those whose devices have never needed to deliver a shock, said Yiyi Zhang, Ph.D., of the Welch Center for Prevention, Epidemiology, and Clinical Research, Johns Hopkins University, Baltimore, and her associates.

To examine this issue, the investigators analyzed data from PROSE-ICD (Prospective Observational Study of Implantable Cardioverter-Defibrillators), in which patients with systolic heart failure received primary-prevention ICDs at four U.S. cardiology centers after an initial LVEF assessment. For their study, Dr. Zhang and her associates focused on 538 of these study participants whose LVEF was reassessed at least once during roughly 5 years of follow-up.
About 57% of the study subjects were white and 70% were men. The average age at baseline was 59 years.
LVEF improved after ICD implantation in 215 (40%) of the participants, including 134 patients (25%) in whom it improved to greater than 35%. These patients were at significantly reduced risk of all-cause mortality and of requiring ICD shocks, compared with patients whose LVEF was either unchanged (47%) or decreased (13%) after ICD implantation, the investigators said. In a Cox regression model adjusted for age, sex, race, baseline LVEF, and stratified by enrollment center, the hazard ratio for all-cause mortality was 0.31, and that for an appropriate shock was 0.33 (J. Am. Coll. Cardiol. 2015 July 27 [doi:10.1016/j.jacc.2015.05.057]).
The mode of death could not be determined in many cases because records were unreliable for patients who died out of hospital, so the researchers couldn’t examine any association between LVEF changes and cardiac-specific mortality.
These study results are consistent with those of several previous studies, Dr. Zhang and her associates noted.
“Findings from our study indicate that repeated LVEF assessment after ICD implantation can provide additional prognostic information and may also allow for more informed decision making regarding ICD generator replacement, especially in patients whose LVEF improved significantly,” they said.
Further studies in larger populations that have more frequent LVEF reassessments are needed to establish whether ICD generator replacement has a positive or negative impact on this patient population, and to better guide clinicians in deciding whether ICD generator replacement should be deferred in individual patients, the investigators added.
Dr. Zhang and colleagues have conducted a meticulous analysis and made an important contribution to a critical area of patient care.
However, even though the findings were consistent with those of previous studies and even though this is the largest series of ICD recipients with improved LVEF done to date, it included only 134 such patients. These are small numbers, and the results should be interpreted with caution.
The essential question for physicians – helping patients decide if the benefit of continued ICD therapy is worth the risk – requires longer-term follow-up in a considerably larger study population.
Dr. Kristen K. Patton is in the division of cardiology at the University of Washington, Seattle. She reported having no relevant financial disclosures. Dr. Patton made these remarks in an editorial comment accompanying Dr. Zhang’s report (J. Am. Coll. Cardiol. 2015 July 27 [doi:10.1016/j.jacc.2015.06.015]).
Dr. Zhang and colleagues have conducted a meticulous analysis and made an important contribution to a critical area of patient care.
However, even though the findings were consistent with those of previous studies and even though this is the largest series of ICD recipients with improved LVEF done to date, it included only 134 such patients. These are small numbers, and the results should be interpreted with caution.
The essential question for physicians – helping patients decide if the benefit of continued ICD therapy is worth the risk – requires longer-term follow-up in a considerably larger study population.
Dr. Kristen K. Patton is in the division of cardiology at the University of Washington, Seattle. She reported having no relevant financial disclosures. Dr. Patton made these remarks in an editorial comment accompanying Dr. Zhang’s report (J. Am. Coll. Cardiol. 2015 July 27 [doi:10.1016/j.jacc.2015.06.015]).
Dr. Zhang and colleagues have conducted a meticulous analysis and made an important contribution to a critical area of patient care.
However, even though the findings were consistent with those of previous studies and even though this is the largest series of ICD recipients with improved LVEF done to date, it included only 134 such patients. These are small numbers, and the results should be interpreted with caution.
The essential question for physicians – helping patients decide if the benefit of continued ICD therapy is worth the risk – requires longer-term follow-up in a considerably larger study population.
Dr. Kristen K. Patton is in the division of cardiology at the University of Washington, Seattle. She reported having no relevant financial disclosures. Dr. Patton made these remarks in an editorial comment accompanying Dr. Zhang’s report (J. Am. Coll. Cardiol. 2015 July 27 [doi:10.1016/j.jacc.2015.06.015]).
In the one-quarter of heart failure patients who receive an implantable cardioverter defibrillator for primary prevention and whose left ventricular ejection fraction improves more than 35%, both mortality and appropriate ICD shocks are decreased, according to a report published online July 27 in Journal of the American College of Cardiology.
This raises the question of whether such patients’ risk for sudden cardiac death still warrants replacement of the ICD generator years later, especially among those whose devices have never needed to deliver a shock, said Yiyi Zhang, Ph.D., of the Welch Center for Prevention, Epidemiology, and Clinical Research, Johns Hopkins University, Baltimore, and her associates.
To examine this issue, the investigators analyzed data from PROSE-ICD (Prospective Observational Study of Implantable Cardioverter-Defibrillators), in which patients with systolic heart failure received primary-prevention ICDs at four U.S. cardiology centers after an initial LVEF assessment. For their study, Dr. Zhang and her associates focused on 538 of these study participants whose LVEF was reassessed at least once during roughly 5 years of follow-up.
About 57% of the study subjects were white and 70% were men. The average age at baseline was 59 years.
LVEF improved after ICD implantation in 215 (40%) of the participants, including 134 patients (25%) in whom it improved to greater than 35%. These patients were at significantly reduced risk of all-cause mortality and of requiring ICD shocks, compared with patients whose LVEF was either unchanged (47%) or decreased (13%) after ICD implantation, the investigators said. In a Cox regression model adjusted for age, sex, race, baseline LVEF, and stratified by enrollment center, the hazard ratio for all-cause mortality was 0.31, and that for an appropriate shock was 0.33 (J. Am. Coll. Cardiol. 2015 July 27 [doi:10.1016/j.jacc.2015.05.057]).
The mode of death could not be determined in many cases because records were unreliable for patients who died out of hospital, so the researchers couldn’t examine any association between LVEF changes and cardiac-specific mortality.
These study results are consistent with those of several previous studies, Dr. Zhang and her associates noted.
“Findings from our study indicate that repeated LVEF assessment after ICD implantation can provide additional prognostic information and may also allow for more informed decision making regarding ICD generator replacement, especially in patients whose LVEF improved significantly,” they said.
Further studies in larger populations that have more frequent LVEF reassessments are needed to establish whether ICD generator replacement has a positive or negative impact on this patient population, and to better guide clinicians in deciding whether ICD generator replacement should be deferred in individual patients, the investigators added.
In the one-quarter of heart failure patients who receive an implantable cardioverter defibrillator for primary prevention and whose left ventricular ejection fraction improves more than 35%, both mortality and appropriate ICD shocks are decreased, according to a report published online July 27 in Journal of the American College of Cardiology.
This raises the question of whether such patients’ risk for sudden cardiac death still warrants replacement of the ICD generator years later, especially among those whose devices have never needed to deliver a shock, said Yiyi Zhang, Ph.D., of the Welch Center for Prevention, Epidemiology, and Clinical Research, Johns Hopkins University, Baltimore, and her associates.
To examine this issue, the investigators analyzed data from PROSE-ICD (Prospective Observational Study of Implantable Cardioverter-Defibrillators), in which patients with systolic heart failure received primary-prevention ICDs at four U.S. cardiology centers after an initial LVEF assessment. For their study, Dr. Zhang and her associates focused on 538 of these study participants whose LVEF was reassessed at least once during roughly 5 years of follow-up.
About 57% of the study subjects were white and 70% were men. The average age at baseline was 59 years.
LVEF improved after ICD implantation in 215 (40%) of the participants, including 134 patients (25%) in whom it improved to greater than 35%. These patients were at significantly reduced risk of all-cause mortality and of requiring ICD shocks, compared with patients whose LVEF was either unchanged (47%) or decreased (13%) after ICD implantation, the investigators said. In a Cox regression model adjusted for age, sex, race, baseline LVEF, and stratified by enrollment center, the hazard ratio for all-cause mortality was 0.31, and that for an appropriate shock was 0.33 (J. Am. Coll. Cardiol. 2015 July 27 [doi:10.1016/j.jacc.2015.05.057]).
The mode of death could not be determined in many cases because records were unreliable for patients who died out of hospital, so the researchers couldn’t examine any association between LVEF changes and cardiac-specific mortality.
These study results are consistent with those of several previous studies, Dr. Zhang and her associates noted.
“Findings from our study indicate that repeated LVEF assessment after ICD implantation can provide additional prognostic information and may also allow for more informed decision making regarding ICD generator replacement, especially in patients whose LVEF improved significantly,” they said.
Further studies in larger populations that have more frequent LVEF reassessments are needed to establish whether ICD generator replacement has a positive or negative impact on this patient population, and to better guide clinicians in deciding whether ICD generator replacement should be deferred in individual patients, the investigators added.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Key clinical point: LVEF improves to greater than 35% in about a quarter of patients with heart failure who receive ICDs for primary prevention, and that change is associated with lower mortality and fewer inappropriate shocks.
Major finding: In HF patients whose LVEF improved after ICD implantation (40%), all-cause mortality and appropriate shocks were reduced by nearly 70%.
Data source: A secondary analysis of data from PROSE-ICD, a multicenter prospective observational study in 538 HF patients with ICDs whose LVEF was assessed at least once during 10 years of follow-up.
Disclosures: This study was supported by the Donald W. Reynolds Foundation and the National Institutes of Health. Dr. Zhang reported having no relevant financial disclosures; Dr. Zhang’s associates reported ties to Medtronic, Boston Scientific, Biotronik, and St. Jude Medical.

Patiromer cuts potassium in diabetic CKD with hyperkalemia
Patiromer, an orally administered potassium-binding polymer, significantly decreased serum potassium in adults who had diabetic kidney disease with hyperkalemia in a phase II study funded by and conducted with the manufacturer.
Patiromer consists of tiny, smooth beads in a liquid suspension and works by binding potassium throughout the GI tract, allowing it to be excreted in the feces. After preliminary studies demonstrated the agent’s usefulness in reducing hyperkalemia for up to 12 weeks in high-risk patients, researchers performed this open-label, uncontrolled trial to determine optimal dosing and to assess its longer-term safety. The findings were reported online July 14 in JAMA.
All four doses of patiromer studied significantly reduced serum potassium, beginning within 48 hours of the initial dose and continuing through all 52 weeks of treatment. The proportion of patients whose potassium levels reached target range at all scheduled visits ranged from 83% to 93% in those who had mild hyperkalemia at baseline and from 77% to 95% in those who had moderate hyperkalemia at baseline. Hyperkalemia quickly reappeared when patiromer treatment ended, reverting to baseline levels, wrote Dr. George L. Bakris of the ASH Comprehensive Hypertension Center, division of endocrinology, diabetes, and metabolism, University of Chicago, and his associates.
Study participants were 222 white patients with mild and 84 with moderate hyperkalemia (mean age, 66 years). All had type 2 diabetes and hypertension, and approximately one-third had heart failure; 65% had stage 3 and 22% had stage 4 chronic kidney disease (CKD), All were taking an ACE inhibitor, an angiotensin II receptor blocker, or both, with or without spironolactone. At 48 medical centers in five European countries, they were randomly assigned to receive one of four doses of patiromer that could be titrated up or down as needed for 4 weeks. Patients then entered an 8-week treatment phase, after which they continued maintenance therapy for a further 40 weeks (JAMA 2015 July 14 [doi:10.1001/jama.2015.7446]).
The optimal doses of patiromer were found to be the two lowest doses assessed in this study, 8.4 g daily and 16.8 g daily, which significantly decreased serum potassium without provoking hypokalemia. These doses will now be tested in a phase III study.
The most frequent treatment-related adverse events in the phase II study were nonsevere hypomagnesemia (7.2%), constipation (4.6%), and diarrhea (2.7%). A total of 28 patients (9.2%) developed at least one adverse event prompting them to discontinue patiromer, including worsening of CKD (which was considered unrelated to treatment), hypokalemia (5 patients), and one hypertensive crisis (also unrelated to treatment). No dose-related edema was noted, and there were no clinically relevant changes in serum calcium or phosphate levels.
The findings of Bakris et al. have the potential to fundamentally change the current treatment approach for hyperkalemia.
Relypsa, the manufacturer of patiromer, filed a New Drug Application with the Food and Drug Administration, and the agent will likely be approved for use in the United States by the end of October. The FDA should consider mandating a sizable postmarketing trial and safety surveillance program to clearly establish the agent’s safety and effectiveness for the hard endpoints that patients care about: halting the progression of chronic kidney disease and thus deferring dialysis, and improving heart failure. Otherwise the manufacturer may not be motivated to conduct such crucial trials, especially if it could instead spend those dollars on marketing and company-directed contract research.
Wolfgang C. Winkelmayer, M.D., Sc.D., is in the nephrology section at Baylor University, Houston, and is an associate editor at JAMA. He reported serving as an adviser or consultant to Amgen, AstraZeneca, Bayer, Keryx, Medgenics, Medtronic, Mitsubishi Tanabe, and Rockwell Pharma. Dr. Winkelmayer made these remarks in an editorial accompanying Dr. Bakris’ report (JAMA 2015 July 14;314:129-30).
The findings of Bakris et al. have the potential to fundamentally change the current treatment approach for hyperkalemia.
Relypsa, the manufacturer of patiromer, filed a New Drug Application with the Food and Drug Administration, and the agent will likely be approved for use in the United States by the end of October. The FDA should consider mandating a sizable postmarketing trial and safety surveillance program to clearly establish the agent’s safety and effectiveness for the hard endpoints that patients care about: halting the progression of chronic kidney disease and thus deferring dialysis, and improving heart failure. Otherwise the manufacturer may not be motivated to conduct such crucial trials, especially if it could instead spend those dollars on marketing and company-directed contract research.
Wolfgang C. Winkelmayer, M.D., Sc.D., is in the nephrology section at Baylor University, Houston, and is an associate editor at JAMA. He reported serving as an adviser or consultant to Amgen, AstraZeneca, Bayer, Keryx, Medgenics, Medtronic, Mitsubishi Tanabe, and Rockwell Pharma. Dr. Winkelmayer made these remarks in an editorial accompanying Dr. Bakris’ report (JAMA 2015 July 14;314:129-30).
The findings of Bakris et al. have the potential to fundamentally change the current treatment approach for hyperkalemia.
Relypsa, the manufacturer of patiromer, filed a New Drug Application with the Food and Drug Administration, and the agent will likely be approved for use in the United States by the end of October. The FDA should consider mandating a sizable postmarketing trial and safety surveillance program to clearly establish the agent’s safety and effectiveness for the hard endpoints that patients care about: halting the progression of chronic kidney disease and thus deferring dialysis, and improving heart failure. Otherwise the manufacturer may not be motivated to conduct such crucial trials, especially if it could instead spend those dollars on marketing and company-directed contract research.
Wolfgang C. Winkelmayer, M.D., Sc.D., is in the nephrology section at Baylor University, Houston, and is an associate editor at JAMA. He reported serving as an adviser or consultant to Amgen, AstraZeneca, Bayer, Keryx, Medgenics, Medtronic, Mitsubishi Tanabe, and Rockwell Pharma. Dr. Winkelmayer made these remarks in an editorial accompanying Dr. Bakris’ report (JAMA 2015 July 14;314:129-30).
Patiromer, an orally administered potassium-binding polymer, significantly decreased serum potassium in adults who had diabetic kidney disease with hyperkalemia in a phase II study funded by and conducted with the manufacturer.
Patiromer consists of tiny, smooth beads in a liquid suspension and works by binding potassium throughout the GI tract, allowing it to be excreted in the feces. After preliminary studies demonstrated the agent’s usefulness in reducing hyperkalemia for up to 12 weeks in high-risk patients, researchers performed this open-label, uncontrolled trial to determine optimal dosing and to assess its longer-term safety. The findings were reported online July 14 in JAMA.
All four doses of patiromer studied significantly reduced serum potassium, beginning within 48 hours of the initial dose and continuing through all 52 weeks of treatment. The proportion of patients whose potassium levels reached target range at all scheduled visits ranged from 83% to 93% in those who had mild hyperkalemia at baseline and from 77% to 95% in those who had moderate hyperkalemia at baseline. Hyperkalemia quickly reappeared when patiromer treatment ended, reverting to baseline levels, wrote Dr. George L. Bakris of the ASH Comprehensive Hypertension Center, division of endocrinology, diabetes, and metabolism, University of Chicago, and his associates.
Study participants were 222 white patients with mild and 84 with moderate hyperkalemia (mean age, 66 years). All had type 2 diabetes and hypertension, and approximately one-third had heart failure; 65% had stage 3 and 22% had stage 4 chronic kidney disease (CKD), All were taking an ACE inhibitor, an angiotensin II receptor blocker, or both, with or without spironolactone. At 48 medical centers in five European countries, they were randomly assigned to receive one of four doses of patiromer that could be titrated up or down as needed for 4 weeks. Patients then entered an 8-week treatment phase, after which they continued maintenance therapy for a further 40 weeks (JAMA 2015 July 14 [doi:10.1001/jama.2015.7446]).
The optimal doses of patiromer were found to be the two lowest doses assessed in this study, 8.4 g daily and 16.8 g daily, which significantly decreased serum potassium without provoking hypokalemia. These doses will now be tested in a phase III study.
The most frequent treatment-related adverse events in the phase II study were nonsevere hypomagnesemia (7.2%), constipation (4.6%), and diarrhea (2.7%). A total of 28 patients (9.2%) developed at least one adverse event prompting them to discontinue patiromer, including worsening of CKD (which was considered unrelated to treatment), hypokalemia (5 patients), and one hypertensive crisis (also unrelated to treatment). No dose-related edema was noted, and there were no clinically relevant changes in serum calcium or phosphate levels.
Patiromer, an orally administered potassium-binding polymer, significantly decreased serum potassium in adults who had diabetic kidney disease with hyperkalemia in a phase II study funded by and conducted with the manufacturer.
Patiromer consists of tiny, smooth beads in a liquid suspension and works by binding potassium throughout the GI tract, allowing it to be excreted in the feces. After preliminary studies demonstrated the agent’s usefulness in reducing hyperkalemia for up to 12 weeks in high-risk patients, researchers performed this open-label, uncontrolled trial to determine optimal dosing and to assess its longer-term safety. The findings were reported online July 14 in JAMA.
All four doses of patiromer studied significantly reduced serum potassium, beginning within 48 hours of the initial dose and continuing through all 52 weeks of treatment. The proportion of patients whose potassium levels reached target range at all scheduled visits ranged from 83% to 93% in those who had mild hyperkalemia at baseline and from 77% to 95% in those who had moderate hyperkalemia at baseline. Hyperkalemia quickly reappeared when patiromer treatment ended, reverting to baseline levels, wrote Dr. George L. Bakris of the ASH Comprehensive Hypertension Center, division of endocrinology, diabetes, and metabolism, University of Chicago, and his associates.
Study participants were 222 white patients with mild and 84 with moderate hyperkalemia (mean age, 66 years). All had type 2 diabetes and hypertension, and approximately one-third had heart failure; 65% had stage 3 and 22% had stage 4 chronic kidney disease (CKD), All were taking an ACE inhibitor, an angiotensin II receptor blocker, or both, with or without spironolactone. At 48 medical centers in five European countries, they were randomly assigned to receive one of four doses of patiromer that could be titrated up or down as needed for 4 weeks. Patients then entered an 8-week treatment phase, after which they continued maintenance therapy for a further 40 weeks (JAMA 2015 July 14 [doi:10.1001/jama.2015.7446]).
The optimal doses of patiromer were found to be the two lowest doses assessed in this study, 8.4 g daily and 16.8 g daily, which significantly decreased serum potassium without provoking hypokalemia. These doses will now be tested in a phase III study.
The most frequent treatment-related adverse events in the phase II study were nonsevere hypomagnesemia (7.2%), constipation (4.6%), and diarrhea (2.7%). A total of 28 patients (9.2%) developed at least one adverse event prompting them to discontinue patiromer, including worsening of CKD (which was considered unrelated to treatment), hypokalemia (5 patients), and one hypertensive crisis (also unrelated to treatment). No dose-related edema was noted, and there were no clinically relevant changes in serum calcium or phosphate levels.
FROM JAMA
Key clinical point: The oral potassium-binding polymer patiromer decreased serum potassium in patients who had diabetic kidney disease with hyperkalemia.
Major finding: The proportion of patients whose potassium levels remained within target range throughout 1 year of treatment was 83%-93% in those who had mild hyperkalemia at baseline and 77%-95% in those who had moderate hyperkalemia at baseline.
Data source: A multicenter open-label, noncontrolled phase II, randomized trial involving 306 adults with diabetic kidney disease and mild to moderate hyperkalemia treated for 1 year.
Disclosures: This study was funded by Relypsa, maker of patiromer. Relypsa also was involved in designing and conducting the study; collecting, analyzing, and interpreting the data; and preparing the manuscript. Dr. Bakris reported receiving personal fees from AbbVie, Takeda. Medtronic, Relypsa, Janssen, Daiichi-Sankyo, Novartis, and Bayer, as well as grants from Takeda. His associates reported ties to numerous industry sources.