User login
Immunotherapy Cost-Effectiveness Varies By Cancer Type
Immunotherapy Cost-Effectiveness Varies By Cancer Type
TOPLINE:
A systematic review of 69 economic evaluations revealed that adjuvant immunotherapy was cost-effective in 58% of studies, with higher Quality-Adjusted Life-Year gains reported in 91% of cases. Cost-effectiveness varied significantly by cancer type, treatment strategy, and healthcare system context, with industry-funded studies more likely to report favorable outcomes.
METHODOLOGY:
- Multiple phase 3 trials have shown improved survival and reduced recurrence with adjuvant immunotherapy in various cancers. But the high cost of immunotherapy treatments, often exceeding $100,000 per patient, has raised questions about their economic value and affordability across different healthcare systems.
- Researchers conducted a systematic review of 69 economic evaluations published between January 2015 and January 2025, focusing on adjuvant immunotherapy across various cancer types.
- Analysis included studies from PubMed, Embase, Scopus, Web of Science, and Cochrane Library, with most evaluations conducted in the US (26 studies) and China (20 studies).
- Quality assessment utilized the Criteria for Health Economic Quality Evaluation tool, evaluating 48 attributes across methodologic and reporting quality dimensions.
- Markov modeling dominated the analytical approach (46 studies [67%]), with EuroQol Five-Dimensions being the most commonly used health utility instrument (56 studies [81%]).
TAKEAWAY:
- Of 69 studies analyzed, 58% concluded that adjuvant immunotherapy was cost-effective, with stronger evidence in non-small cell lung cancer and melanoma, particularly in early-stage and high-risk populations.
- Industry-funded studies more frequently reported cost-effective outcomes (17 of 20 studies [85%]) than nonindustry funded studies (13 of 28 studies [46%]).
- Higher Quality-Adjusted Life-Year/Life-Year gains were consistently reported in the adjuvant immunotherapy group (63 studies [91%]), especially for non-small cell lung cancer and combination regimens.
- Cost-effectiveness results varied significantly by cancer type, model assumptions, drug pricing, funding organizations, and country-specific willingness-to-pay thresholds.
IN PRACTICE:
“From a policy standpoint, the findings of this systematic review support the use of structured, context-specific health technology assessment frameworks to evaluate adjuvant immunotherapies. For health systems under financial constraints, prioritizing subgroups with the highest absolute benefit may be a viable approach to ensure sustainable access,” the authors of the review wrote.
SOURCE:
The systematic review was led by Rashidul Alam Mahumud, PhD, MCncrSc, MPH, MSc, Health Economics and Health Technology Assessment Unit, National Health and Medical Research Council Clinical Trials Centre, The University of Sydney in Camperdown, Australia. It was published online on January 22 in JAMA Oncology.
LIMITATIONS:
The methodologic heterogeneity across studies presents a significant limitation, with variations in time horizons, discounting methods, survival data extrapolation, and health utility measurements affecting result comparability. Geographic distribution primarily focused on high-income countries, limiting generalizability to low- and middle-income settings. Few evaluations incorporated adaptive pricing schemes or managed entry agreements that increasingly influence clinical reimbursement decisions.
DISCLOSURES:
Mahumud had full access to all study data and takes responsibility for data integrity and analysis accuracy. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A systematic review of 69 economic evaluations revealed that adjuvant immunotherapy was cost-effective in 58% of studies, with higher Quality-Adjusted Life-Year gains reported in 91% of cases. Cost-effectiveness varied significantly by cancer type, treatment strategy, and healthcare system context, with industry-funded studies more likely to report favorable outcomes.
METHODOLOGY:
- Multiple phase 3 trials have shown improved survival and reduced recurrence with adjuvant immunotherapy in various cancers. But the high cost of immunotherapy treatments, often exceeding $100,000 per patient, has raised questions about their economic value and affordability across different healthcare systems.
- Researchers conducted a systematic review of 69 economic evaluations published between January 2015 and January 2025, focusing on adjuvant immunotherapy across various cancer types.
- Analysis included studies from PubMed, Embase, Scopus, Web of Science, and Cochrane Library, with most evaluations conducted in the US (26 studies) and China (20 studies).
- Quality assessment utilized the Criteria for Health Economic Quality Evaluation tool, evaluating 48 attributes across methodologic and reporting quality dimensions.
- Markov modeling dominated the analytical approach (46 studies [67%]), with EuroQol Five-Dimensions being the most commonly used health utility instrument (56 studies [81%]).
TAKEAWAY:
- Of 69 studies analyzed, 58% concluded that adjuvant immunotherapy was cost-effective, with stronger evidence in non-small cell lung cancer and melanoma, particularly in early-stage and high-risk populations.
- Industry-funded studies more frequently reported cost-effective outcomes (17 of 20 studies [85%]) than nonindustry funded studies (13 of 28 studies [46%]).
- Higher Quality-Adjusted Life-Year/Life-Year gains were consistently reported in the adjuvant immunotherapy group (63 studies [91%]), especially for non-small cell lung cancer and combination regimens.
- Cost-effectiveness results varied significantly by cancer type, model assumptions, drug pricing, funding organizations, and country-specific willingness-to-pay thresholds.
IN PRACTICE:
“From a policy standpoint, the findings of this systematic review support the use of structured, context-specific health technology assessment frameworks to evaluate adjuvant immunotherapies. For health systems under financial constraints, prioritizing subgroups with the highest absolute benefit may be a viable approach to ensure sustainable access,” the authors of the review wrote.
SOURCE:
The systematic review was led by Rashidul Alam Mahumud, PhD, MCncrSc, MPH, MSc, Health Economics and Health Technology Assessment Unit, National Health and Medical Research Council Clinical Trials Centre, The University of Sydney in Camperdown, Australia. It was published online on January 22 in JAMA Oncology.
LIMITATIONS:
The methodologic heterogeneity across studies presents a significant limitation, with variations in time horizons, discounting methods, survival data extrapolation, and health utility measurements affecting result comparability. Geographic distribution primarily focused on high-income countries, limiting generalizability to low- and middle-income settings. Few evaluations incorporated adaptive pricing schemes or managed entry agreements that increasingly influence clinical reimbursement decisions.
DISCLOSURES:
Mahumud had full access to all study data and takes responsibility for data integrity and analysis accuracy. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A systematic review of 69 economic evaluations revealed that adjuvant immunotherapy was cost-effective in 58% of studies, with higher Quality-Adjusted Life-Year gains reported in 91% of cases. Cost-effectiveness varied significantly by cancer type, treatment strategy, and healthcare system context, with industry-funded studies more likely to report favorable outcomes.
METHODOLOGY:
- Multiple phase 3 trials have shown improved survival and reduced recurrence with adjuvant immunotherapy in various cancers. But the high cost of immunotherapy treatments, often exceeding $100,000 per patient, has raised questions about their economic value and affordability across different healthcare systems.
- Researchers conducted a systematic review of 69 economic evaluations published between January 2015 and January 2025, focusing on adjuvant immunotherapy across various cancer types.
- Analysis included studies from PubMed, Embase, Scopus, Web of Science, and Cochrane Library, with most evaluations conducted in the US (26 studies) and China (20 studies).
- Quality assessment utilized the Criteria for Health Economic Quality Evaluation tool, evaluating 48 attributes across methodologic and reporting quality dimensions.
- Markov modeling dominated the analytical approach (46 studies [67%]), with EuroQol Five-Dimensions being the most commonly used health utility instrument (56 studies [81%]).
TAKEAWAY:
- Of 69 studies analyzed, 58% concluded that adjuvant immunotherapy was cost-effective, with stronger evidence in non-small cell lung cancer and melanoma, particularly in early-stage and high-risk populations.
- Industry-funded studies more frequently reported cost-effective outcomes (17 of 20 studies [85%]) than nonindustry funded studies (13 of 28 studies [46%]).
- Higher Quality-Adjusted Life-Year/Life-Year gains were consistently reported in the adjuvant immunotherapy group (63 studies [91%]), especially for non-small cell lung cancer and combination regimens.
- Cost-effectiveness results varied significantly by cancer type, model assumptions, drug pricing, funding organizations, and country-specific willingness-to-pay thresholds.
IN PRACTICE:
“From a policy standpoint, the findings of this systematic review support the use of structured, context-specific health technology assessment frameworks to evaluate adjuvant immunotherapies. For health systems under financial constraints, prioritizing subgroups with the highest absolute benefit may be a viable approach to ensure sustainable access,” the authors of the review wrote.
SOURCE:
The systematic review was led by Rashidul Alam Mahumud, PhD, MCncrSc, MPH, MSc, Health Economics and Health Technology Assessment Unit, National Health and Medical Research Council Clinical Trials Centre, The University of Sydney in Camperdown, Australia. It was published online on January 22 in JAMA Oncology.
LIMITATIONS:
The methodologic heterogeneity across studies presents a significant limitation, with variations in time horizons, discounting methods, survival data extrapolation, and health utility measurements affecting result comparability. Geographic distribution primarily focused on high-income countries, limiting generalizability to low- and middle-income settings. Few evaluations incorporated adaptive pricing schemes or managed entry agreements that increasingly influence clinical reimbursement decisions.
DISCLOSURES:
Mahumud had full access to all study data and takes responsibility for data integrity and analysis accuracy. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Immunotherapy Cost-Effectiveness Varies By Cancer Type
Immunotherapy Cost-Effectiveness Varies By Cancer Type
When Does Spleen Size Signal Cancer Risk?
When Does Spleen Size Signal Cancer Risk?
TOPLINE:
Spleen volume larger than the 99th percentile was associated with an 11-fold increased risk for hematologic cancer compared with normal volumes, with 5-year risks as high as 46% among men aged 70 years or older. Significant risks for cirrhosis and liver cancer were also seen.
METHODOLOGY:
- Splenomegaly is often detected incidentally during imaging, but guidelines vary as to the threshold that should prompt evaluation — ranging from a spleen length of 120 mm to 150 mm. However, up to 21% of healthy individuals have spleen lengths > 120 mm, which could lead to unnecessary follow-up of low-risk patients.
- Researchers used data from two general population cohorts to evaluate the relative and absolute risks for hematologic cancer and liver disease (two common causes of spleen enlargement) among individuals with incidentally detected splenomegaly. They included 8459 Danish adults (57% female; median age, 61 years) and 38,607 UK adults (51.9% female; median age, 65 years) who underwent CT or MRI scans as part of study procedures.
- Spleen length and volume measurements were available from the Danish cohort, while only spleen volume was available from the UK group.
- Participants were followed for a median of 5 years after imaging to assess the incidence of hematologic cancers (both cohorts) and cirrhosis and liver cancer (UK cohort only). Hazard ratios were adjusted for age, sex, smoking status, alcohol consumption, comorbidities, and C-reactive protein levels.
TAKEAWAY:
- In the Danish cohort, the relative risk for any hematologic cancer was significantly increased among individuals with spleen lengths above the 99th percentile (≥ 135 mm) compared with those with spleen lengths in the 26th-74th percentile (hazard ratio [HR], 5.11; P < .001). Among individuals with a spleen length ≥ 140 mm, absolute 5-year risks reached 23% for men aged 70 years or older and 12% for women in that age group.
- Risks were even more pronounced for Danish adults with a spleen volume above the 99th percentile — > 433 mL. Relative to the 26th-74th percentile, their risk for any hematologic cancer was 11-fold higher (HR, 11.08; P < .001). Among people with a spleen volume ≥ 500 mL, 5-year risks reached 46% for men aged 70 years or older and 27% for women in that age group.
- Findings were similar in the UK cohort. Among individuals with a spleen volume above the 99th percentile (> 386 mL), the risk for hematologic cancer increased nearly 12-fold (HR, 11.82; P < .001). With a spleen volume ≥ 500 mL, 5-year risks reached 21% for men aged 70 years or older and 18% for women in that age group. Relative risks were also elevated — by 1.55-2.94 — among individuals in the 75th-99th percentile (199 mL-386 mL).
- The risks for liver disease began to rise substantially at a spleen volume ≥ 400 mL. Absolute 5-year risks for cirrhosis reached 10.8% for men and 9.3% for women aged 70 years or older with a spleen volume ≥ 500 mL. For liver cancer, 5-year risks reached 3.2% and 1.2% for men and women in that age group with a spleen volume ≥ 400 mL.
IN PRACTICE:
“To our knowledge, no previous studies have examined risk of hematologic cancers by spleen length or volume in incidentally detected splenomegaly,” the authors of the study wrote. “Risk was moderately increased at spleen length of 130-139 mm or spleen volume of 400-499 mL, where diagnostic workup may be considered, and more pronounced at spleen length of 140 mm or greater or spleen volume of 500 mL or greater, supporting that diagnostic workup may likely be relevant.”
They stressed, however, that the study participants were asymptomatic, and the underlying reason for imaging should always be considered.
SOURCE:
The study, led by Jens Helby, MD, PhD, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark, was published online in JAMA Oncology.
DISCLOSURES:
The study was funded by the Danish Cancer Society, the Boserup Foundation, Copenhagen University Hospital – Rigshospitalet, and Sanofi A/S. Helby reported having financial relationships with Sanofi and Disc Medicine. Additional disclosures are available in the full article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Spleen volume larger than the 99th percentile was associated with an 11-fold increased risk for hematologic cancer compared with normal volumes, with 5-year risks as high as 46% among men aged 70 years or older. Significant risks for cirrhosis and liver cancer were also seen.
METHODOLOGY:
- Splenomegaly is often detected incidentally during imaging, but guidelines vary as to the threshold that should prompt evaluation — ranging from a spleen length of 120 mm to 150 mm. However, up to 21% of healthy individuals have spleen lengths > 120 mm, which could lead to unnecessary follow-up of low-risk patients.
- Researchers used data from two general population cohorts to evaluate the relative and absolute risks for hematologic cancer and liver disease (two common causes of spleen enlargement) among individuals with incidentally detected splenomegaly. They included 8459 Danish adults (57% female; median age, 61 years) and 38,607 UK adults (51.9% female; median age, 65 years) who underwent CT or MRI scans as part of study procedures.
- Spleen length and volume measurements were available from the Danish cohort, while only spleen volume was available from the UK group.
- Participants were followed for a median of 5 years after imaging to assess the incidence of hematologic cancers (both cohorts) and cirrhosis and liver cancer (UK cohort only). Hazard ratios were adjusted for age, sex, smoking status, alcohol consumption, comorbidities, and C-reactive protein levels.
TAKEAWAY:
- In the Danish cohort, the relative risk for any hematologic cancer was significantly increased among individuals with spleen lengths above the 99th percentile (≥ 135 mm) compared with those with spleen lengths in the 26th-74th percentile (hazard ratio [HR], 5.11; P < .001). Among individuals with a spleen length ≥ 140 mm, absolute 5-year risks reached 23% for men aged 70 years or older and 12% for women in that age group.
- Risks were even more pronounced for Danish adults with a spleen volume above the 99th percentile — > 433 mL. Relative to the 26th-74th percentile, their risk for any hematologic cancer was 11-fold higher (HR, 11.08; P < .001). Among people with a spleen volume ≥ 500 mL, 5-year risks reached 46% for men aged 70 years or older and 27% for women in that age group.
- Findings were similar in the UK cohort. Among individuals with a spleen volume above the 99th percentile (> 386 mL), the risk for hematologic cancer increased nearly 12-fold (HR, 11.82; P < .001). With a spleen volume ≥ 500 mL, 5-year risks reached 21% for men aged 70 years or older and 18% for women in that age group. Relative risks were also elevated — by 1.55-2.94 — among individuals in the 75th-99th percentile (199 mL-386 mL).
- The risks for liver disease began to rise substantially at a spleen volume ≥ 400 mL. Absolute 5-year risks for cirrhosis reached 10.8% for men and 9.3% for women aged 70 years or older with a spleen volume ≥ 500 mL. For liver cancer, 5-year risks reached 3.2% and 1.2% for men and women in that age group with a spleen volume ≥ 400 mL.
IN PRACTICE:
“To our knowledge, no previous studies have examined risk of hematologic cancers by spleen length or volume in incidentally detected splenomegaly,” the authors of the study wrote. “Risk was moderately increased at spleen length of 130-139 mm or spleen volume of 400-499 mL, where diagnostic workup may be considered, and more pronounced at spleen length of 140 mm or greater or spleen volume of 500 mL or greater, supporting that diagnostic workup may likely be relevant.”
They stressed, however, that the study participants were asymptomatic, and the underlying reason for imaging should always be considered.
SOURCE:
The study, led by Jens Helby, MD, PhD, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark, was published online in JAMA Oncology.
DISCLOSURES:
The study was funded by the Danish Cancer Society, the Boserup Foundation, Copenhagen University Hospital – Rigshospitalet, and Sanofi A/S. Helby reported having financial relationships with Sanofi and Disc Medicine. Additional disclosures are available in the full article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Spleen volume larger than the 99th percentile was associated with an 11-fold increased risk for hematologic cancer compared with normal volumes, with 5-year risks as high as 46% among men aged 70 years or older. Significant risks for cirrhosis and liver cancer were also seen.
METHODOLOGY:
- Splenomegaly is often detected incidentally during imaging, but guidelines vary as to the threshold that should prompt evaluation — ranging from a spleen length of 120 mm to 150 mm. However, up to 21% of healthy individuals have spleen lengths > 120 mm, which could lead to unnecessary follow-up of low-risk patients.
- Researchers used data from two general population cohorts to evaluate the relative and absolute risks for hematologic cancer and liver disease (two common causes of spleen enlargement) among individuals with incidentally detected splenomegaly. They included 8459 Danish adults (57% female; median age, 61 years) and 38,607 UK adults (51.9% female; median age, 65 years) who underwent CT or MRI scans as part of study procedures.
- Spleen length and volume measurements were available from the Danish cohort, while only spleen volume was available from the UK group.
- Participants were followed for a median of 5 years after imaging to assess the incidence of hematologic cancers (both cohorts) and cirrhosis and liver cancer (UK cohort only). Hazard ratios were adjusted for age, sex, smoking status, alcohol consumption, comorbidities, and C-reactive protein levels.
TAKEAWAY:
- In the Danish cohort, the relative risk for any hematologic cancer was significantly increased among individuals with spleen lengths above the 99th percentile (≥ 135 mm) compared with those with spleen lengths in the 26th-74th percentile (hazard ratio [HR], 5.11; P < .001). Among individuals with a spleen length ≥ 140 mm, absolute 5-year risks reached 23% for men aged 70 years or older and 12% for women in that age group.
- Risks were even more pronounced for Danish adults with a spleen volume above the 99th percentile — > 433 mL. Relative to the 26th-74th percentile, their risk for any hematologic cancer was 11-fold higher (HR, 11.08; P < .001). Among people with a spleen volume ≥ 500 mL, 5-year risks reached 46% for men aged 70 years or older and 27% for women in that age group.
- Findings were similar in the UK cohort. Among individuals with a spleen volume above the 99th percentile (> 386 mL), the risk for hematologic cancer increased nearly 12-fold (HR, 11.82; P < .001). With a spleen volume ≥ 500 mL, 5-year risks reached 21% for men aged 70 years or older and 18% for women in that age group. Relative risks were also elevated — by 1.55-2.94 — among individuals in the 75th-99th percentile (199 mL-386 mL).
- The risks for liver disease began to rise substantially at a spleen volume ≥ 400 mL. Absolute 5-year risks for cirrhosis reached 10.8% for men and 9.3% for women aged 70 years or older with a spleen volume ≥ 500 mL. For liver cancer, 5-year risks reached 3.2% and 1.2% for men and women in that age group with a spleen volume ≥ 400 mL.
IN PRACTICE:
“To our knowledge, no previous studies have examined risk of hematologic cancers by spleen length or volume in incidentally detected splenomegaly,” the authors of the study wrote. “Risk was moderately increased at spleen length of 130-139 mm or spleen volume of 400-499 mL, where diagnostic workup may be considered, and more pronounced at spleen length of 140 mm or greater or spleen volume of 500 mL or greater, supporting that diagnostic workup may likely be relevant.”
They stressed, however, that the study participants were asymptomatic, and the underlying reason for imaging should always be considered.
SOURCE:
The study, led by Jens Helby, MD, PhD, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark, was published online in JAMA Oncology.
DISCLOSURES:
The study was funded by the Danish Cancer Society, the Boserup Foundation, Copenhagen University Hospital – Rigshospitalet, and Sanofi A/S. Helby reported having financial relationships with Sanofi and Disc Medicine. Additional disclosures are available in the full article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
When Does Spleen Size Signal Cancer Risk?
When Does Spleen Size Signal Cancer Risk?
Over 1 Million Cancer Screenings at Risk With Recent Medicaid Changes
Over 1 Million Cancer Screenings at Risk With Recent Medicaid Changes
Tightened Medicaid eligibility rules under the 2025 Budget Reconciliation Bill could result in more than 1 million missed cancer screenings within 2 years and over 150 avoidable cancer deaths, new findings suggested.
“Clinicians should be genuinely concerned,” corresponding author Adrian Diaz, MD, MPH, a surgical oncology fellow at the University of Chicago, Chicago, told Medscape Medical News. “These projections suggest that Medicaid eligibility restrictions are likely to translate into delayed diagnoses, more advanced disease at presentation, and worse outcomes.”
The new law, which significantly reduces federal Medicaid funding, introduces mandatory work or community-engagement requirements for working-age adults as well as more frequent recertification starting in 2027.
In the study, a Research Letter published online on January 8 in JAMA Oncology, Diaz and Sarah Shubeck, MD, also from the University of Chicago, drew on data from Arkansas to model how these 2025 federal Medicaid eligibility restrictions could lead to loss of Medicaid coverage and consequently missed cancer screenings, especially in states that expanded Medicaid.
Diaz and Shubeck then paired coverage losses with state-level self-reported screening prevalences and estimated incident breast, colorectal, and lung cancers using 2-year risks.
In the first 2 years after implementation, the researchers predicted that 7.5 million adults (range, 5.0-10.8 million) will lose Medicaid coverage due to the new provisions.
This coverage loss will lead to an estimated 405,706 missed mammograms, 679,745 missed colorectal screenings, and 67,213 missed lung cancer screenings.
As a result, 1055 breast cancers, 748 colorectal cancers, and 538 lung cancers will go undetected, with excess deaths totaling 155 — 70 for breast, 50 for colorectal, and 35 for lung cancers.
Predicted missed screenings and related cancer outcomes varied considerably by state, with missed screening rates generally lower in states that didn’t expand Medicaid.
“Importantly, our estimates focus on missed screening and do not account for patients already undergoing cancer treatment whose coverage could be interrupted, meaning the real-world impact is likely larger,” Diaz said.
Farhad Islami, MD, PhD, senior scientific director of Cancer Disparity Research at the American Cancer Society, said the estimated coverage losses are “consistent with the number” — 7.8 million — “estimated by the nonpartisan Congressional Budget Office.”
Islami also stressed that the harm caused by the new restrictions would be “far greater” than what the study reports, with coverage losses leading to delays in care seeking for cancer symptoms of all kinds “and consequently, delayed diagnosis for many more cancer cases.”
“Moreover,” he added, “the restrictions can reduce the utilization of preventive care (eg, counselling and pharmacotherapy for smoking cessation among people who smoke, counselling for reducing weight, and so on) and receipt of guideline-concordant cancer treatments among those who will lose Medicaid coverage.”
In Diaz’ view, clinicians can help mitigate the adverse effects of the new provisions.
“For example, proactively identifying patients at risk of coverage loss, engaging financial counselors and social workers early, and connecting uninsured or underinsured patients to safety-net screening and treatment programs,” he said. “At a systems level, clinicians also have an important role in documenting and communicating these downstream clinical consequences to health systems and policymakers.”
A version of this article first appeared on Medscape.com.
Tightened Medicaid eligibility rules under the 2025 Budget Reconciliation Bill could result in more than 1 million missed cancer screenings within 2 years and over 150 avoidable cancer deaths, new findings suggested.
“Clinicians should be genuinely concerned,” corresponding author Adrian Diaz, MD, MPH, a surgical oncology fellow at the University of Chicago, Chicago, told Medscape Medical News. “These projections suggest that Medicaid eligibility restrictions are likely to translate into delayed diagnoses, more advanced disease at presentation, and worse outcomes.”
The new law, which significantly reduces federal Medicaid funding, introduces mandatory work or community-engagement requirements for working-age adults as well as more frequent recertification starting in 2027.
In the study, a Research Letter published online on January 8 in JAMA Oncology, Diaz and Sarah Shubeck, MD, also from the University of Chicago, drew on data from Arkansas to model how these 2025 federal Medicaid eligibility restrictions could lead to loss of Medicaid coverage and consequently missed cancer screenings, especially in states that expanded Medicaid.
Diaz and Shubeck then paired coverage losses with state-level self-reported screening prevalences and estimated incident breast, colorectal, and lung cancers using 2-year risks.
In the first 2 years after implementation, the researchers predicted that 7.5 million adults (range, 5.0-10.8 million) will lose Medicaid coverage due to the new provisions.
This coverage loss will lead to an estimated 405,706 missed mammograms, 679,745 missed colorectal screenings, and 67,213 missed lung cancer screenings.
As a result, 1055 breast cancers, 748 colorectal cancers, and 538 lung cancers will go undetected, with excess deaths totaling 155 — 70 for breast, 50 for colorectal, and 35 for lung cancers.
Predicted missed screenings and related cancer outcomes varied considerably by state, with missed screening rates generally lower in states that didn’t expand Medicaid.
“Importantly, our estimates focus on missed screening and do not account for patients already undergoing cancer treatment whose coverage could be interrupted, meaning the real-world impact is likely larger,” Diaz said.
Farhad Islami, MD, PhD, senior scientific director of Cancer Disparity Research at the American Cancer Society, said the estimated coverage losses are “consistent with the number” — 7.8 million — “estimated by the nonpartisan Congressional Budget Office.”
Islami also stressed that the harm caused by the new restrictions would be “far greater” than what the study reports, with coverage losses leading to delays in care seeking for cancer symptoms of all kinds “and consequently, delayed diagnosis for many more cancer cases.”
“Moreover,” he added, “the restrictions can reduce the utilization of preventive care (eg, counselling and pharmacotherapy for smoking cessation among people who smoke, counselling for reducing weight, and so on) and receipt of guideline-concordant cancer treatments among those who will lose Medicaid coverage.”
In Diaz’ view, clinicians can help mitigate the adverse effects of the new provisions.
“For example, proactively identifying patients at risk of coverage loss, engaging financial counselors and social workers early, and connecting uninsured or underinsured patients to safety-net screening and treatment programs,” he said. “At a systems level, clinicians also have an important role in documenting and communicating these downstream clinical consequences to health systems and policymakers.”
A version of this article first appeared on Medscape.com.
Tightened Medicaid eligibility rules under the 2025 Budget Reconciliation Bill could result in more than 1 million missed cancer screenings within 2 years and over 150 avoidable cancer deaths, new findings suggested.
“Clinicians should be genuinely concerned,” corresponding author Adrian Diaz, MD, MPH, a surgical oncology fellow at the University of Chicago, Chicago, told Medscape Medical News. “These projections suggest that Medicaid eligibility restrictions are likely to translate into delayed diagnoses, more advanced disease at presentation, and worse outcomes.”
The new law, which significantly reduces federal Medicaid funding, introduces mandatory work or community-engagement requirements for working-age adults as well as more frequent recertification starting in 2027.
In the study, a Research Letter published online on January 8 in JAMA Oncology, Diaz and Sarah Shubeck, MD, also from the University of Chicago, drew on data from Arkansas to model how these 2025 federal Medicaid eligibility restrictions could lead to loss of Medicaid coverage and consequently missed cancer screenings, especially in states that expanded Medicaid.
Diaz and Shubeck then paired coverage losses with state-level self-reported screening prevalences and estimated incident breast, colorectal, and lung cancers using 2-year risks.
In the first 2 years after implementation, the researchers predicted that 7.5 million adults (range, 5.0-10.8 million) will lose Medicaid coverage due to the new provisions.
This coverage loss will lead to an estimated 405,706 missed mammograms, 679,745 missed colorectal screenings, and 67,213 missed lung cancer screenings.
As a result, 1055 breast cancers, 748 colorectal cancers, and 538 lung cancers will go undetected, with excess deaths totaling 155 — 70 for breast, 50 for colorectal, and 35 for lung cancers.
Predicted missed screenings and related cancer outcomes varied considerably by state, with missed screening rates generally lower in states that didn’t expand Medicaid.
“Importantly, our estimates focus on missed screening and do not account for patients already undergoing cancer treatment whose coverage could be interrupted, meaning the real-world impact is likely larger,” Diaz said.
Farhad Islami, MD, PhD, senior scientific director of Cancer Disparity Research at the American Cancer Society, said the estimated coverage losses are “consistent with the number” — 7.8 million — “estimated by the nonpartisan Congressional Budget Office.”
Islami also stressed that the harm caused by the new restrictions would be “far greater” than what the study reports, with coverage losses leading to delays in care seeking for cancer symptoms of all kinds “and consequently, delayed diagnosis for many more cancer cases.”
“Moreover,” he added, “the restrictions can reduce the utilization of preventive care (eg, counselling and pharmacotherapy for smoking cessation among people who smoke, counselling for reducing weight, and so on) and receipt of guideline-concordant cancer treatments among those who will lose Medicaid coverage.”
In Diaz’ view, clinicians can help mitigate the adverse effects of the new provisions.
“For example, proactively identifying patients at risk of coverage loss, engaging financial counselors and social workers early, and connecting uninsured or underinsured patients to safety-net screening and treatment programs,” he said. “At a systems level, clinicians also have an important role in documenting and communicating these downstream clinical consequences to health systems and policymakers.”
A version of this article first appeared on Medscape.com.
Over 1 Million Cancer Screenings at Risk With Recent Medicaid Changes
Over 1 Million Cancer Screenings at Risk With Recent Medicaid Changes
Cannabis May Ease Symptoms in Advanced Pancreatic Cancer
Cannabis May Ease Symptoms in Advanced Pancreatic Cancer
TOPLINE:
A randomized trial of 32 patients with advanced pancreatic cancer found that early access to medical cannabis patients' symptom burden, with minimal side effects.
METHODOLOGY:
- Patients with pancreatic cancer commonly experience moderate-to-severe pain, nausea, insomnia, and other symptoms that significantly affect their quality of life. Current management approaches are insufficient. Preliminary evidence suggests that medical cannabis has efficacy against multiple cancer-related symptoms, but high-quality data remain limited due to regulatory barriers.
- Researchers conducted a pilot randomized, waitlist-controlled trial involving 32 patients (median age, 71 years) with newly diagnosed locally advanced or metastatic pancreatic adenocarcinoma and at least one burdensome symptom.
- Patients were randomly assigned in a 1:1 ratio to early (0-8 weeks) or delayed (9-16 weeks) cannabis intervention through the Minnesota Medical Cannabis Program, which provided cannabis products and education in how to use them.
- Primary outcomes focused on feasibility, while secondary outcomes examined acceptability, changes in symptom burden, and quality of life in exploratory efficacy analyses.
TAKEAWAY:
- At baseline, patients reported a substantial moderate-to-severe symptom burden — most commonly insomnia (85%), pain (77%), and appetite loss (69%); 10 patients (31%) were using opioids.
- The study met all of its feasibility metrics, with 74% of the patients meeting enrollment eligibility and 81% complying with their random assignment. Patients in the arm with early cannabis access typically picked up their products 3 days after starting chemotherapy. Most used tablets or other oral cannabis formulations.
- At 8 weeks, patients in the early-access arm experienced numerically higher rates of improvement in pain (44% vs 20%; P = .35), appetite (56% vs 30%; P = .37), and insomnia (67% vs 30%; P = .18), as well as a reduction in opioid use. Their rates of potential cannabis side effects, including dry mouth, dizziness, and concentration problems, were lower compared with the waitlist group — possibly, the authors noted, due to their education to “start low, go slow.”
- Patients made a median of two trips to a cannabis dispensary during the study period, and most said that using cannabis was “easy” and “practical.”
IN PRACTICE:
“Early access to medical cannabis was associated with improvement in certain symptoms, such as insomnia, with minimal harms,” the authors wrote, adding that the research design offers a model collaboration between investigators and state cannabis programs.
“The encouraging preliminary efficacy and safety of cannabis in managing symptoms supports further exploration," they concluded.
SOURCE:
The study was led by Dylan Zylla, MD, MS, of HealthPartners Institute, Cancer Research Center, Minneapolis, Minnesota. It was presented on January 9 at the ASCO Gastrointestinal Cancers Symposium 2026 and simultaneously published in JCO Oncology Practice.
LIMITATIONS:
The trial was small and the 8-week primary study period precluded conclusions about longer-term benefits and safety. Generalizability may be limited as the trial was conducted in a single state with a predominantly urban and White patient population. Additionally, heterogeneity in state cannabis programs and laws may limit national applicability.
DISCLOSURES:
The study was supported by philanthropic support to the HealthPartners Cancer Research Center. Cannabis products were provided by Vireo Health (GreenGoods, Minnesota). Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A randomized trial of 32 patients with advanced pancreatic cancer found that early access to medical cannabis patients' symptom burden, with minimal side effects.
METHODOLOGY:
- Patients with pancreatic cancer commonly experience moderate-to-severe pain, nausea, insomnia, and other symptoms that significantly affect their quality of life. Current management approaches are insufficient. Preliminary evidence suggests that medical cannabis has efficacy against multiple cancer-related symptoms, but high-quality data remain limited due to regulatory barriers.
- Researchers conducted a pilot randomized, waitlist-controlled trial involving 32 patients (median age, 71 years) with newly diagnosed locally advanced or metastatic pancreatic adenocarcinoma and at least one burdensome symptom.
- Patients were randomly assigned in a 1:1 ratio to early (0-8 weeks) or delayed (9-16 weeks) cannabis intervention through the Minnesota Medical Cannabis Program, which provided cannabis products and education in how to use them.
- Primary outcomes focused on feasibility, while secondary outcomes examined acceptability, changes in symptom burden, and quality of life in exploratory efficacy analyses.
TAKEAWAY:
- At baseline, patients reported a substantial moderate-to-severe symptom burden — most commonly insomnia (85%), pain (77%), and appetite loss (69%); 10 patients (31%) were using opioids.
- The study met all of its feasibility metrics, with 74% of the patients meeting enrollment eligibility and 81% complying with their random assignment. Patients in the arm with early cannabis access typically picked up their products 3 days after starting chemotherapy. Most used tablets or other oral cannabis formulations.
- At 8 weeks, patients in the early-access arm experienced numerically higher rates of improvement in pain (44% vs 20%; P = .35), appetite (56% vs 30%; P = .37), and insomnia (67% vs 30%; P = .18), as well as a reduction in opioid use. Their rates of potential cannabis side effects, including dry mouth, dizziness, and concentration problems, were lower compared with the waitlist group — possibly, the authors noted, due to their education to “start low, go slow.”
- Patients made a median of two trips to a cannabis dispensary during the study period, and most said that using cannabis was “easy” and “practical.”
IN PRACTICE:
“Early access to medical cannabis was associated with improvement in certain symptoms, such as insomnia, with minimal harms,” the authors wrote, adding that the research design offers a model collaboration between investigators and state cannabis programs.
“The encouraging preliminary efficacy and safety of cannabis in managing symptoms supports further exploration," they concluded.
SOURCE:
The study was led by Dylan Zylla, MD, MS, of HealthPartners Institute, Cancer Research Center, Minneapolis, Minnesota. It was presented on January 9 at the ASCO Gastrointestinal Cancers Symposium 2026 and simultaneously published in JCO Oncology Practice.
LIMITATIONS:
The trial was small and the 8-week primary study period precluded conclusions about longer-term benefits and safety. Generalizability may be limited as the trial was conducted in a single state with a predominantly urban and White patient population. Additionally, heterogeneity in state cannabis programs and laws may limit national applicability.
DISCLOSURES:
The study was supported by philanthropic support to the HealthPartners Cancer Research Center. Cannabis products were provided by Vireo Health (GreenGoods, Minnesota). Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A randomized trial of 32 patients with advanced pancreatic cancer found that early access to medical cannabis patients' symptom burden, with minimal side effects.
METHODOLOGY:
- Patients with pancreatic cancer commonly experience moderate-to-severe pain, nausea, insomnia, and other symptoms that significantly affect their quality of life. Current management approaches are insufficient. Preliminary evidence suggests that medical cannabis has efficacy against multiple cancer-related symptoms, but high-quality data remain limited due to regulatory barriers.
- Researchers conducted a pilot randomized, waitlist-controlled trial involving 32 patients (median age, 71 years) with newly diagnosed locally advanced or metastatic pancreatic adenocarcinoma and at least one burdensome symptom.
- Patients were randomly assigned in a 1:1 ratio to early (0-8 weeks) or delayed (9-16 weeks) cannabis intervention through the Minnesota Medical Cannabis Program, which provided cannabis products and education in how to use them.
- Primary outcomes focused on feasibility, while secondary outcomes examined acceptability, changes in symptom burden, and quality of life in exploratory efficacy analyses.
TAKEAWAY:
- At baseline, patients reported a substantial moderate-to-severe symptom burden — most commonly insomnia (85%), pain (77%), and appetite loss (69%); 10 patients (31%) were using opioids.
- The study met all of its feasibility metrics, with 74% of the patients meeting enrollment eligibility and 81% complying with their random assignment. Patients in the arm with early cannabis access typically picked up their products 3 days after starting chemotherapy. Most used tablets or other oral cannabis formulations.
- At 8 weeks, patients in the early-access arm experienced numerically higher rates of improvement in pain (44% vs 20%; P = .35), appetite (56% vs 30%; P = .37), and insomnia (67% vs 30%; P = .18), as well as a reduction in opioid use. Their rates of potential cannabis side effects, including dry mouth, dizziness, and concentration problems, were lower compared with the waitlist group — possibly, the authors noted, due to their education to “start low, go slow.”
- Patients made a median of two trips to a cannabis dispensary during the study period, and most said that using cannabis was “easy” and “practical.”
IN PRACTICE:
“Early access to medical cannabis was associated with improvement in certain symptoms, such as insomnia, with minimal harms,” the authors wrote, adding that the research design offers a model collaboration between investigators and state cannabis programs.
“The encouraging preliminary efficacy and safety of cannabis in managing symptoms supports further exploration," they concluded.
SOURCE:
The study was led by Dylan Zylla, MD, MS, of HealthPartners Institute, Cancer Research Center, Minneapolis, Minnesota. It was presented on January 9 at the ASCO Gastrointestinal Cancers Symposium 2026 and simultaneously published in JCO Oncology Practice.
LIMITATIONS:
The trial was small and the 8-week primary study period precluded conclusions about longer-term benefits and safety. Generalizability may be limited as the trial was conducted in a single state with a predominantly urban and White patient population. Additionally, heterogeneity in state cannabis programs and laws may limit national applicability.
DISCLOSURES:
The study was supported by philanthropic support to the HealthPartners Cancer Research Center. Cannabis products were provided by Vireo Health (GreenGoods, Minnesota). Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Cannabis May Ease Symptoms in Advanced Pancreatic Cancer
Cannabis May Ease Symptoms in Advanced Pancreatic Cancer
Home Screening Cost-Effective for Anal Cancer
Home Screening Cost-Effective for Anal Cancer
TOPLINE:
A recent analysis suggested that home-based screening for anal cancer is a cost-effective way to increase screening compared to clinic-based screening. The study found that a home-based approach led to higher participation rates (89.2% vs 74.2% for a clinic-based approach) among sexual and gender minority individuals and was cost-effective, costing $25.19 per additional individual screened when accounting for both direct and indirect costs and $132.36 per additional individual screened when only accounting for direct medical costs.
METHODOLOGY:
- Anal cancer screening is recommended for high-risk populations, such as sexual and gender minority individuals. However, it's unclear how cost-effective home-based self-sampling is compared to clinic-based screening.
- Researchers conducted an economic evaluation using data from a randomized clinical trial that included 240 sexual and gender minority individuals in Milwaukee from January 2020 to August 2022.
- Participants, aged ≥ 25 years, were randomized to either home-based self-sampling or clinic-based screening.
- Researchers evaluated direct home-based screening costs from the trial, and sourced clinic-based costs from the Medicare reimbursement schedule. Travel and time costs were determined from participant self-reports.
- The primary outcome was the incremental cost-effectiveness ratio (ICER), which was the additional cost needed to increase screening participation by one person. The researchers calculated ICERs from both a healthcare payer and societal perspective. The healthcare perspective included only direct medical costs and the societal perspective accounted for direct medical costs as well as indirect time and travel costs.
TAKEAWAY:
- Home-based screening led to higher participation rates than clinic-based screening—89.2% vs 74.2%—with 107 participants completing home-based screening compared with 89 participants doing clinic-based screening.
- The cost per participant was $64.18 for home-based screening and $60.40 for clinic-based screening from the societal perspective, and $61.91 for home-based screening and $42.06 for clinic-based screening from the healthcare payer perspective.
- With home-based screening, the ICER per additional screened participant was $25.19 from a societal perspective and $132.36 from a healthcare payer perspective.
- From the societal perspective, the probability that home-based screening was cost-effective compared with clinic-based screening was nearly 50% at a willingness-to-pay threshold of $25 and 99.99% at a threshold of $100. From the healthcare perspective, the probability was 3.8% at a threshold of $100 and 90.9% at a threshold of $200.
IN PRACTICE:
"These findings suggest that home-based screening promises to be a cost-effective option to enhance anal cancer screening participation," the study authors concluded.
SOURCE:
The study, led by Haluk Damgacioglu, PhD, Department of Public Health Sciences, Medical University of South Carolina in Charleston, South Carolina, was published online in JAMA Network Open.
LIMITATIONS:
The study was conducted in an urban setting where proximity to clinics may reduce structural barriers, potentially limiting generalizability to rural areas where longer travel distances and limited clinician availability could affect participation rates. The analysis did not include downstream steps such as follow-up clinic visits, confirmatory testing, treatment of precancerous lesions, or cancer prevention outcomes. While home-based screening participants were required to visit clinics for digital anal rectal examination to exclude prevalent anal cancer, these follow-up visit costs were not included in the cost-effectiveness analysis.
DISCLOSURES:
Elizabeth Chiao, PhD, reported receiving grants from the National Institutes of Health during the study. Jennifer S. Smith, PhD, MPH, disclosed receiving personal fees from Hologic, Inc., and materials for research purposes from Rovers Medical Devices. Ashish A. Deshmukh, PhD, MPH, reported receiving personal fees from Value Analytics Lab. Alan G. Nyitray, PhD, reported receiving grants from the National Cancer Institute and test kits from Copan Diagnostics.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A recent analysis suggested that home-based screening for anal cancer is a cost-effective way to increase screening compared to clinic-based screening. The study found that a home-based approach led to higher participation rates (89.2% vs 74.2% for a clinic-based approach) among sexual and gender minority individuals and was cost-effective, costing $25.19 per additional individual screened when accounting for both direct and indirect costs and $132.36 per additional individual screened when only accounting for direct medical costs.
METHODOLOGY:
- Anal cancer screening is recommended for high-risk populations, such as sexual and gender minority individuals. However, it's unclear how cost-effective home-based self-sampling is compared to clinic-based screening.
- Researchers conducted an economic evaluation using data from a randomized clinical trial that included 240 sexual and gender minority individuals in Milwaukee from January 2020 to August 2022.
- Participants, aged ≥ 25 years, were randomized to either home-based self-sampling or clinic-based screening.
- Researchers evaluated direct home-based screening costs from the trial, and sourced clinic-based costs from the Medicare reimbursement schedule. Travel and time costs were determined from participant self-reports.
- The primary outcome was the incremental cost-effectiveness ratio (ICER), which was the additional cost needed to increase screening participation by one person. The researchers calculated ICERs from both a healthcare payer and societal perspective. The healthcare perspective included only direct medical costs and the societal perspective accounted for direct medical costs as well as indirect time and travel costs.
TAKEAWAY:
- Home-based screening led to higher participation rates than clinic-based screening—89.2% vs 74.2%—with 107 participants completing home-based screening compared with 89 participants doing clinic-based screening.
- The cost per participant was $64.18 for home-based screening and $60.40 for clinic-based screening from the societal perspective, and $61.91 for home-based screening and $42.06 for clinic-based screening from the healthcare payer perspective.
- With home-based screening, the ICER per additional screened participant was $25.19 from a societal perspective and $132.36 from a healthcare payer perspective.
- From the societal perspective, the probability that home-based screening was cost-effective compared with clinic-based screening was nearly 50% at a willingness-to-pay threshold of $25 and 99.99% at a threshold of $100. From the healthcare perspective, the probability was 3.8% at a threshold of $100 and 90.9% at a threshold of $200.
IN PRACTICE:
"These findings suggest that home-based screening promises to be a cost-effective option to enhance anal cancer screening participation," the study authors concluded.
SOURCE:
The study, led by Haluk Damgacioglu, PhD, Department of Public Health Sciences, Medical University of South Carolina in Charleston, South Carolina, was published online in JAMA Network Open.
LIMITATIONS:
The study was conducted in an urban setting where proximity to clinics may reduce structural barriers, potentially limiting generalizability to rural areas where longer travel distances and limited clinician availability could affect participation rates. The analysis did not include downstream steps such as follow-up clinic visits, confirmatory testing, treatment of precancerous lesions, or cancer prevention outcomes. While home-based screening participants were required to visit clinics for digital anal rectal examination to exclude prevalent anal cancer, these follow-up visit costs were not included in the cost-effectiveness analysis.
DISCLOSURES:
Elizabeth Chiao, PhD, reported receiving grants from the National Institutes of Health during the study. Jennifer S. Smith, PhD, MPH, disclosed receiving personal fees from Hologic, Inc., and materials for research purposes from Rovers Medical Devices. Ashish A. Deshmukh, PhD, MPH, reported receiving personal fees from Value Analytics Lab. Alan G. Nyitray, PhD, reported receiving grants from the National Cancer Institute and test kits from Copan Diagnostics.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A recent analysis suggested that home-based screening for anal cancer is a cost-effective way to increase screening compared to clinic-based screening. The study found that a home-based approach led to higher participation rates (89.2% vs 74.2% for a clinic-based approach) among sexual and gender minority individuals and was cost-effective, costing $25.19 per additional individual screened when accounting for both direct and indirect costs and $132.36 per additional individual screened when only accounting for direct medical costs.
METHODOLOGY:
- Anal cancer screening is recommended for high-risk populations, such as sexual and gender minority individuals. However, it's unclear how cost-effective home-based self-sampling is compared to clinic-based screening.
- Researchers conducted an economic evaluation using data from a randomized clinical trial that included 240 sexual and gender minority individuals in Milwaukee from January 2020 to August 2022.
- Participants, aged ≥ 25 years, were randomized to either home-based self-sampling or clinic-based screening.
- Researchers evaluated direct home-based screening costs from the trial, and sourced clinic-based costs from the Medicare reimbursement schedule. Travel and time costs were determined from participant self-reports.
- The primary outcome was the incremental cost-effectiveness ratio (ICER), which was the additional cost needed to increase screening participation by one person. The researchers calculated ICERs from both a healthcare payer and societal perspective. The healthcare perspective included only direct medical costs and the societal perspective accounted for direct medical costs as well as indirect time and travel costs.
TAKEAWAY:
- Home-based screening led to higher participation rates than clinic-based screening—89.2% vs 74.2%—with 107 participants completing home-based screening compared with 89 participants doing clinic-based screening.
- The cost per participant was $64.18 for home-based screening and $60.40 for clinic-based screening from the societal perspective, and $61.91 for home-based screening and $42.06 for clinic-based screening from the healthcare payer perspective.
- With home-based screening, the ICER per additional screened participant was $25.19 from a societal perspective and $132.36 from a healthcare payer perspective.
- From the societal perspective, the probability that home-based screening was cost-effective compared with clinic-based screening was nearly 50% at a willingness-to-pay threshold of $25 and 99.99% at a threshold of $100. From the healthcare perspective, the probability was 3.8% at a threshold of $100 and 90.9% at a threshold of $200.
IN PRACTICE:
"These findings suggest that home-based screening promises to be a cost-effective option to enhance anal cancer screening participation," the study authors concluded.
SOURCE:
The study, led by Haluk Damgacioglu, PhD, Department of Public Health Sciences, Medical University of South Carolina in Charleston, South Carolina, was published online in JAMA Network Open.
LIMITATIONS:
The study was conducted in an urban setting where proximity to clinics may reduce structural barriers, potentially limiting generalizability to rural areas where longer travel distances and limited clinician availability could affect participation rates. The analysis did not include downstream steps such as follow-up clinic visits, confirmatory testing, treatment of precancerous lesions, or cancer prevention outcomes. While home-based screening participants were required to visit clinics for digital anal rectal examination to exclude prevalent anal cancer, these follow-up visit costs were not included in the cost-effectiveness analysis.
DISCLOSURES:
Elizabeth Chiao, PhD, reported receiving grants from the National Institutes of Health during the study. Jennifer S. Smith, PhD, MPH, disclosed receiving personal fees from Hologic, Inc., and materials for research purposes from Rovers Medical Devices. Ashish A. Deshmukh, PhD, MPH, reported receiving personal fees from Value Analytics Lab. Alan G. Nyitray, PhD, reported receiving grants from the National Cancer Institute and test kits from Copan Diagnostics.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Home Screening Cost-Effective for Anal Cancer
Home Screening Cost-Effective for Anal Cancer
Simple Steps: Walking May Ease Colorectal Cancer Fatigue
Simple Steps: Walking May Ease Colorectal Cancer Fatigue
Regular physical activity—especially walking—may improve fatigue and boost quality of life for people with nonmetastatic colorectal cancer during the first 2 years after diagnosis, according to research presented at ASCO Gastrointestinal Cancers Symposium 2026.
The study, which tracked over 1700 patients with colorectal cancer, found that those with nonmetastatic disease who walked for exercise 6-12 months after their diagnosis showed significant improvement in their fatigue scores over time. Their quality-of-life ratings rose in tandem.
The findings suggest that simple, sustained movement may play a meaningful role in long-term survivorship care, lead investigator Louisa Liu, MD, of Cedars-Sinai Medical Center in Los Angeles, said during a press briefing.
“Fatigue is one of the most common and debilitating symptoms our patients experience, often long after treatment ends,” Liu noted.
The new data, she said, show that an accessible form of exercise, especially when maintained over time, “can make a real difference in how patients feel and function during recovery.”
Joel Saltzman, MD, an ASCO expert in gastrointestinal cancers based at Taussig Cancer Center, Cleveland Clinic, Cleveland, agreed.
This is a “super-important study for all of us in the cancer community,” Saltzman told the briefing, especially in light of the CHALLENGE trial.
That study demonstrated that a structured exercise program can actually improve overall survival for patients with early-stage colon cancer who completed surgery and adjuvant chemotherapy.
“When you couple that with how patients feel, it really begs the question: Are we as a society doing enough cancer rehabilitation?” Saltzman said. “Everyone’s familiar with cardiac rehab, but oncologic rehabilitation is really something that really should be thought about in the future.”
Among long-term colorectal cancer survivors, nearly 40% continue to experience moderate-to-severe fatigue years after treatment — a challenge that affects functional recovery, daily activity, and quality of life.
“Yet,” Liu said, “our toolbox of effective interventions remains limited.”
Growing evidence supports physical activity as a nonpharmacologic approach for managing cancer-related fatigue. The mechanisms, Liu noted, may be multiple and include reductions in systemic inflammation, preserved muscle mass, better sleep quality and improvements in psychological stress.
In fact, current clinical guidelines recommend physical activity as part of survivorship care, but some key questions remain unanswered, Liu said.
“We still don’t fully understand when during recovery activity is most beneficial, what types of activity are best for different patients, or how these effects play out in real-world longitudinal settings, especially in colorectal cancer survivors,” she explained.
To address some of those gaps, Liu and colleagues analyzed data from 1718 patients with colorectal cancer (mean age, 67 years; 48% women) enrolled in the International ColoCare prospective cohort study. Nearly 1 in 5 had metastatic disease at diagnosis.
Physical activity was assessed at baseline and at 6, 12, and 24 months after diagnosis using a validated questionnaire. Participants’ total number of metabolic equivalent of task (MET) minutes per week — a measurement of energy spent during physical activity — were calculated for walking, moderate activities, and vigorous activities.
Total physical activity was categorized as low (fewer than 600 MET min/wk), moderate (600-3000 MET min/wk), or high (over 3000 MET min/wk).
Cancer-related fatigue and quality of life were measured using the European Organization for Research and Treatment of Cancer QLQ-C30 scale.
Overall, patients who were more physically active reported less fatigue and better quality of life as they moved further into recovery. And walking, Liu said, showed the “clearest and most consistent” association with these improved outcomes.
Among patients with nonmetastatic disease, those who reported regular walking 6-12 months after diagnosis showed significantly lower fatigue and higher quality-of-life scores over 2 years. Fatigue scores in this group improved steadily with time, from 32.5 at diagnosis to 29 at 12 months post-diagnosis and 26.8 at 24 months post-diagnosis.
Patients with metastatic disease also showed reductions in fatigue scores — from 40.7 at diagnosis to 37.1 at 12 months and 36.4 at 24 months — although those differences did not reach statistical significance.
Liu pointed out that patients with metastatic disease, not surprisingly, reported greater fatigue and poorer quality of life across all time points vs those with early-stage disease.
So, she said, “we don’t yet have strong evidence that physical activity changes the fatigue trajectory in the long run for metastatic patients. But this is an area where more targeted research is really needed.”
Looking at patterns of physical activity, the researchers found that activity levels at the time of diagnosis did not reliably predict long-term fatigue and quality-of-life outcomes. Instead, a patient’s activity level maintained between diagnosis and 1 year follow-up was a predictor of better outcomes.
“Short-term increases in physical activity didn’t seem to make a meaningful difference,” Liu said. “This suggests that when it comes to managing cancer-related fatigue, the key is to build steady, lasting habits that patients can stick with throughout their recovery.”
The study had no commercial funding. Liu and Saltzman had no disclosures.
A version of this article first appeared on Medscape.com.
Regular physical activity—especially walking—may improve fatigue and boost quality of life for people with nonmetastatic colorectal cancer during the first 2 years after diagnosis, according to research presented at ASCO Gastrointestinal Cancers Symposium 2026.
The study, which tracked over 1700 patients with colorectal cancer, found that those with nonmetastatic disease who walked for exercise 6-12 months after their diagnosis showed significant improvement in their fatigue scores over time. Their quality-of-life ratings rose in tandem.
The findings suggest that simple, sustained movement may play a meaningful role in long-term survivorship care, lead investigator Louisa Liu, MD, of Cedars-Sinai Medical Center in Los Angeles, said during a press briefing.
“Fatigue is one of the most common and debilitating symptoms our patients experience, often long after treatment ends,” Liu noted.
The new data, she said, show that an accessible form of exercise, especially when maintained over time, “can make a real difference in how patients feel and function during recovery.”
Joel Saltzman, MD, an ASCO expert in gastrointestinal cancers based at Taussig Cancer Center, Cleveland Clinic, Cleveland, agreed.
This is a “super-important study for all of us in the cancer community,” Saltzman told the briefing, especially in light of the CHALLENGE trial.
That study demonstrated that a structured exercise program can actually improve overall survival for patients with early-stage colon cancer who completed surgery and adjuvant chemotherapy.
“When you couple that with how patients feel, it really begs the question: Are we as a society doing enough cancer rehabilitation?” Saltzman said. “Everyone’s familiar with cardiac rehab, but oncologic rehabilitation is really something that really should be thought about in the future.”
Among long-term colorectal cancer survivors, nearly 40% continue to experience moderate-to-severe fatigue years after treatment — a challenge that affects functional recovery, daily activity, and quality of life.
“Yet,” Liu said, “our toolbox of effective interventions remains limited.”
Growing evidence supports physical activity as a nonpharmacologic approach for managing cancer-related fatigue. The mechanisms, Liu noted, may be multiple and include reductions in systemic inflammation, preserved muscle mass, better sleep quality and improvements in psychological stress.
In fact, current clinical guidelines recommend physical activity as part of survivorship care, but some key questions remain unanswered, Liu said.
“We still don’t fully understand when during recovery activity is most beneficial, what types of activity are best for different patients, or how these effects play out in real-world longitudinal settings, especially in colorectal cancer survivors,” she explained.
To address some of those gaps, Liu and colleagues analyzed data from 1718 patients with colorectal cancer (mean age, 67 years; 48% women) enrolled in the International ColoCare prospective cohort study. Nearly 1 in 5 had metastatic disease at diagnosis.
Physical activity was assessed at baseline and at 6, 12, and 24 months after diagnosis using a validated questionnaire. Participants’ total number of metabolic equivalent of task (MET) minutes per week — a measurement of energy spent during physical activity — were calculated for walking, moderate activities, and vigorous activities.
Total physical activity was categorized as low (fewer than 600 MET min/wk), moderate (600-3000 MET min/wk), or high (over 3000 MET min/wk).
Cancer-related fatigue and quality of life were measured using the European Organization for Research and Treatment of Cancer QLQ-C30 scale.
Overall, patients who were more physically active reported less fatigue and better quality of life as they moved further into recovery. And walking, Liu said, showed the “clearest and most consistent” association with these improved outcomes.
Among patients with nonmetastatic disease, those who reported regular walking 6-12 months after diagnosis showed significantly lower fatigue and higher quality-of-life scores over 2 years. Fatigue scores in this group improved steadily with time, from 32.5 at diagnosis to 29 at 12 months post-diagnosis and 26.8 at 24 months post-diagnosis.
Patients with metastatic disease also showed reductions in fatigue scores — from 40.7 at diagnosis to 37.1 at 12 months and 36.4 at 24 months — although those differences did not reach statistical significance.
Liu pointed out that patients with metastatic disease, not surprisingly, reported greater fatigue and poorer quality of life across all time points vs those with early-stage disease.
So, she said, “we don’t yet have strong evidence that physical activity changes the fatigue trajectory in the long run for metastatic patients. But this is an area where more targeted research is really needed.”
Looking at patterns of physical activity, the researchers found that activity levels at the time of diagnosis did not reliably predict long-term fatigue and quality-of-life outcomes. Instead, a patient’s activity level maintained between diagnosis and 1 year follow-up was a predictor of better outcomes.
“Short-term increases in physical activity didn’t seem to make a meaningful difference,” Liu said. “This suggests that when it comes to managing cancer-related fatigue, the key is to build steady, lasting habits that patients can stick with throughout their recovery.”
The study had no commercial funding. Liu and Saltzman had no disclosures.
A version of this article first appeared on Medscape.com.
Regular physical activity—especially walking—may improve fatigue and boost quality of life for people with nonmetastatic colorectal cancer during the first 2 years after diagnosis, according to research presented at ASCO Gastrointestinal Cancers Symposium 2026.
The study, which tracked over 1700 patients with colorectal cancer, found that those with nonmetastatic disease who walked for exercise 6-12 months after their diagnosis showed significant improvement in their fatigue scores over time. Their quality-of-life ratings rose in tandem.
The findings suggest that simple, sustained movement may play a meaningful role in long-term survivorship care, lead investigator Louisa Liu, MD, of Cedars-Sinai Medical Center in Los Angeles, said during a press briefing.
“Fatigue is one of the most common and debilitating symptoms our patients experience, often long after treatment ends,” Liu noted.
The new data, she said, show that an accessible form of exercise, especially when maintained over time, “can make a real difference in how patients feel and function during recovery.”
Joel Saltzman, MD, an ASCO expert in gastrointestinal cancers based at Taussig Cancer Center, Cleveland Clinic, Cleveland, agreed.
This is a “super-important study for all of us in the cancer community,” Saltzman told the briefing, especially in light of the CHALLENGE trial.
That study demonstrated that a structured exercise program can actually improve overall survival for patients with early-stage colon cancer who completed surgery and adjuvant chemotherapy.
“When you couple that with how patients feel, it really begs the question: Are we as a society doing enough cancer rehabilitation?” Saltzman said. “Everyone’s familiar with cardiac rehab, but oncologic rehabilitation is really something that really should be thought about in the future.”
Among long-term colorectal cancer survivors, nearly 40% continue to experience moderate-to-severe fatigue years after treatment — a challenge that affects functional recovery, daily activity, and quality of life.
“Yet,” Liu said, “our toolbox of effective interventions remains limited.”
Growing evidence supports physical activity as a nonpharmacologic approach for managing cancer-related fatigue. The mechanisms, Liu noted, may be multiple and include reductions in systemic inflammation, preserved muscle mass, better sleep quality and improvements in psychological stress.
In fact, current clinical guidelines recommend physical activity as part of survivorship care, but some key questions remain unanswered, Liu said.
“We still don’t fully understand when during recovery activity is most beneficial, what types of activity are best for different patients, or how these effects play out in real-world longitudinal settings, especially in colorectal cancer survivors,” she explained.
To address some of those gaps, Liu and colleagues analyzed data from 1718 patients with colorectal cancer (mean age, 67 years; 48% women) enrolled in the International ColoCare prospective cohort study. Nearly 1 in 5 had metastatic disease at diagnosis.
Physical activity was assessed at baseline and at 6, 12, and 24 months after diagnosis using a validated questionnaire. Participants’ total number of metabolic equivalent of task (MET) minutes per week — a measurement of energy spent during physical activity — were calculated for walking, moderate activities, and vigorous activities.
Total physical activity was categorized as low (fewer than 600 MET min/wk), moderate (600-3000 MET min/wk), or high (over 3000 MET min/wk).
Cancer-related fatigue and quality of life were measured using the European Organization for Research and Treatment of Cancer QLQ-C30 scale.
Overall, patients who were more physically active reported less fatigue and better quality of life as they moved further into recovery. And walking, Liu said, showed the “clearest and most consistent” association with these improved outcomes.
Among patients with nonmetastatic disease, those who reported regular walking 6-12 months after diagnosis showed significantly lower fatigue and higher quality-of-life scores over 2 years. Fatigue scores in this group improved steadily with time, from 32.5 at diagnosis to 29 at 12 months post-diagnosis and 26.8 at 24 months post-diagnosis.
Patients with metastatic disease also showed reductions in fatigue scores — from 40.7 at diagnosis to 37.1 at 12 months and 36.4 at 24 months — although those differences did not reach statistical significance.
Liu pointed out that patients with metastatic disease, not surprisingly, reported greater fatigue and poorer quality of life across all time points vs those with early-stage disease.
So, she said, “we don’t yet have strong evidence that physical activity changes the fatigue trajectory in the long run for metastatic patients. But this is an area where more targeted research is really needed.”
Looking at patterns of physical activity, the researchers found that activity levels at the time of diagnosis did not reliably predict long-term fatigue and quality-of-life outcomes. Instead, a patient’s activity level maintained between diagnosis and 1 year follow-up was a predictor of better outcomes.
“Short-term increases in physical activity didn’t seem to make a meaningful difference,” Liu said. “This suggests that when it comes to managing cancer-related fatigue, the key is to build steady, lasting habits that patients can stick with throughout their recovery.”
The study had no commercial funding. Liu and Saltzman had no disclosures.
A version of this article first appeared on Medscape.com.
Simple Steps: Walking May Ease Colorectal Cancer Fatigue
Simple Steps: Walking May Ease Colorectal Cancer Fatigue
Rural Cancer Survivors Are More Likely to Have Chronic Pain
TOPLINE:
Rural cancer survivors experience significantly higher rates of chronic pain at 43.0% than those among urban survivors at 33.5%. Even after controlling for demographics and health conditions, rural residents showed 21% higher odds of experiencing chronic pain.
METHODOLOGY:
- Chronic pain prevalence among cancer survivors is twice that of the general US population and is associated with numerous negative outcomes. Rural residence is frequently linked to debilitating long-term survivorship effects, and current data lack information on whether chronic pain disparity exists specifically for rural cancer survivors.
- Researchers pooled data from the 2019–2021 and 2023 National Health Interview Survey, a cross–sectional survey conducted by the National Center for Health Statistics.
- Analysis included 5542 adult cancer survivors diagnosed within the previous 5 years, with 51.6% female participants and 48.4% male participants.
- Chronic pain was defined as pain experienced on most or all days over the past 3 months, following National Center for Health Statistics conventions.
- Rural residence classification was based on noncore or nonmetropolitan counties using the modified National Center for Health Statistics Urban–Rural Classification Scheme for Counties.
TAKEAWAY:
- Rural cancer survivors showed significantly higher odds of experiencing chronic pain compared with urban survivors (odds ratio [OR], 1.21; 95% CI, 1.01-1.45).
- Rural survivors were more likely to be non–Hispanic White, have less than a 4-year college degree, have an income below 200% of the federal poverty level, and have slightly more chronic health conditions.
- Having an income below 100% of the federal poverty level was associated with doubled odds of chronic pain (OR, 2.07; 95% CI, 1.54-2.77) compared with having an income at least four times the federal poverty level.
- Each additional health condition increased the odds of experiencing chronic pain by 32% (OR, 1.32; 95% CI, 1.26-1.39).
IN PRACTICE:
“Policymakers and health systems should work to close this gap by increasing the availability of pain management resources for rural cancer survivors. Approaches could include innovative payment models for integrative medicine in rural areas or supporting rural clinician access to pain specialists,” the authors of the study wrote.
SOURCE:
This study was led by Hyojin Choi, PhD, Department of Family Medicine, The Robert Larner MD College of Medicine, University of Vermont in Burlington, Vermont. It was published online in JAMA Network Open.
LIMITATIONS:
The authors note that the cross–sectional design of the study and limited information on individual respondents’ use of multimodal pain treatment options constrain the interpretation of findings.
DISCLOSURES:
The authors did not report any relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Rural cancer survivors experience significantly higher rates of chronic pain at 43.0% than those among urban survivors at 33.5%. Even after controlling for demographics and health conditions, rural residents showed 21% higher odds of experiencing chronic pain.
METHODOLOGY:
- Chronic pain prevalence among cancer survivors is twice that of the general US population and is associated with numerous negative outcomes. Rural residence is frequently linked to debilitating long-term survivorship effects, and current data lack information on whether chronic pain disparity exists specifically for rural cancer survivors.
- Researchers pooled data from the 2019–2021 and 2023 National Health Interview Survey, a cross–sectional survey conducted by the National Center for Health Statistics.
- Analysis included 5542 adult cancer survivors diagnosed within the previous 5 years, with 51.6% female participants and 48.4% male participants.
- Chronic pain was defined as pain experienced on most or all days over the past 3 months, following National Center for Health Statistics conventions.
- Rural residence classification was based on noncore or nonmetropolitan counties using the modified National Center for Health Statistics Urban–Rural Classification Scheme for Counties.
TAKEAWAY:
- Rural cancer survivors showed significantly higher odds of experiencing chronic pain compared with urban survivors (odds ratio [OR], 1.21; 95% CI, 1.01-1.45).
- Rural survivors were more likely to be non–Hispanic White, have less than a 4-year college degree, have an income below 200% of the federal poverty level, and have slightly more chronic health conditions.
- Having an income below 100% of the federal poverty level was associated with doubled odds of chronic pain (OR, 2.07; 95% CI, 1.54-2.77) compared with having an income at least four times the federal poverty level.
- Each additional health condition increased the odds of experiencing chronic pain by 32% (OR, 1.32; 95% CI, 1.26-1.39).
IN PRACTICE:
“Policymakers and health systems should work to close this gap by increasing the availability of pain management resources for rural cancer survivors. Approaches could include innovative payment models for integrative medicine in rural areas or supporting rural clinician access to pain specialists,” the authors of the study wrote.
SOURCE:
This study was led by Hyojin Choi, PhD, Department of Family Medicine, The Robert Larner MD College of Medicine, University of Vermont in Burlington, Vermont. It was published online in JAMA Network Open.
LIMITATIONS:
The authors note that the cross–sectional design of the study and limited information on individual respondents’ use of multimodal pain treatment options constrain the interpretation of findings.
DISCLOSURES:
The authors did not report any relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Rural cancer survivors experience significantly higher rates of chronic pain at 43.0% than those among urban survivors at 33.5%. Even after controlling for demographics and health conditions, rural residents showed 21% higher odds of experiencing chronic pain.
METHODOLOGY:
- Chronic pain prevalence among cancer survivors is twice that of the general US population and is associated with numerous negative outcomes. Rural residence is frequently linked to debilitating long-term survivorship effects, and current data lack information on whether chronic pain disparity exists specifically for rural cancer survivors.
- Researchers pooled data from the 2019–2021 and 2023 National Health Interview Survey, a cross–sectional survey conducted by the National Center for Health Statistics.
- Analysis included 5542 adult cancer survivors diagnosed within the previous 5 years, with 51.6% female participants and 48.4% male participants.
- Chronic pain was defined as pain experienced on most or all days over the past 3 months, following National Center for Health Statistics conventions.
- Rural residence classification was based on noncore or nonmetropolitan counties using the modified National Center for Health Statistics Urban–Rural Classification Scheme for Counties.
TAKEAWAY:
- Rural cancer survivors showed significantly higher odds of experiencing chronic pain compared with urban survivors (odds ratio [OR], 1.21; 95% CI, 1.01-1.45).
- Rural survivors were more likely to be non–Hispanic White, have less than a 4-year college degree, have an income below 200% of the federal poverty level, and have slightly more chronic health conditions.
- Having an income below 100% of the federal poverty level was associated with doubled odds of chronic pain (OR, 2.07; 95% CI, 1.54-2.77) compared with having an income at least four times the federal poverty level.
- Each additional health condition increased the odds of experiencing chronic pain by 32% (OR, 1.32; 95% CI, 1.26-1.39).
IN PRACTICE:
“Policymakers and health systems should work to close this gap by increasing the availability of pain management resources for rural cancer survivors. Approaches could include innovative payment models for integrative medicine in rural areas or supporting rural clinician access to pain specialists,” the authors of the study wrote.
SOURCE:
This study was led by Hyojin Choi, PhD, Department of Family Medicine, The Robert Larner MD College of Medicine, University of Vermont in Burlington, Vermont. It was published online in JAMA Network Open.
LIMITATIONS:
The authors note that the cross–sectional design of the study and limited information on individual respondents’ use of multimodal pain treatment options constrain the interpretation of findings.
DISCLOSURES:
The authors did not report any relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
NICE Endorses Chemo-Free First-Line Options for EGFR NSCLC
NICE Endorses Chemo-Free First-Line Options for EGFR NSCLC
The National Institute for Health and Care Excellence (NICE) has recommended amivantamab (Rybrevant) plus lazertinib (Lazcluze) as a first-line option for adults with previously untreated advanced non–small-cell lung cancer (NSCLC) harboring epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 L858R substitution mutations.
In final draft guidance, NICE said the combination therapy should be funded by the NHS in England for eligible patients when it is the most appropriate option. Around 1115 people are expected to benefit.
Lung cancer is the third most common cancer and the leading cause of cancer mortality in the UK. It accounted for 10% of all new cancer diagnoses and 20% of cancer deaths in 2020. Approximately 31,000 people received NSCLC diagnoses in England in 2021, comprising 91% of all lung cancer cases. EGFR mutation-positive NSCLC is more common in women, non-smokers, and individuals from Asian ethnic backgrounds.
Welcoming the decision, Virginia Harrison, research trustee, EGFR+ UK, said, “This is a meaningful advance for patients and their families facing this diagnosis. [It] provides something the EGFR community urgently needs: more choice in first-line treatment.”
How Practice May Shift
The recommendation adds an alternative to existing standards, including osimertinib monotherapy or osimertinib plus pemetrexed/platinum-based chemotherapy. Clinical specialists noted that no single standard care exists for this patient group.
Younger patients and those willing to accept greater side effects may choose between amivantamab plus lazertinib or osimertinib plus chemotherapy. Patients older than 80 years might prefer osimertinib monotherapy due to adverse event considerations.
Mechanism of Action and Clinical Evidence
Amivantamab is a bispecific antibody that simultaneously binds EGFR and mesenchymal-epithelial transition receptors, blocking downstream signaling pathways that drive tumor growth and promoting immune-mediated cancer cell killing. Lazertinib is an oral third-generation EGFR TKI that selectively inhibits mutant EGFR signaling. Together, the agents provides complementary suppression of EGFR-driven tumour growth and resistance mechanisms.
The NICE recommendation is supported by results from the phase 3 MARIPOSA trial, which met its primary endpoint of progression-free survival (PFS). Treatment with amivantamab plus lazertinib significantly prolonged median PFS to 23.7 months compared with 16.6 months with osimertinib. The combination also demonstrated a significant improvement in overall survival, reducing the risk for death by 25% vs osimertinib. Median OS was not reached in the combination arm and was 36.7 months with osimertinib.
The most common adverse reactions with the combination included rash, nail toxicity, hypoalbuminaemia, hepatotoxicity, and stomatitis.
A Medicines and Healthcare products Regulatory Agency-approved subcutaneous formulation of amivantamab, authorized after the committee’s initial meeting, may further improve tolerability and convenience. Administration-related reactions occurred in 63% of patients with the intravenous formulation vs 14% with the subcutaneous formulation. Clinicians expect subcutaneous dosing to replace intravenous use in practice.
Dosing, Access, and Implementation
Amivantamab is administered every 2 weeks, either intravenously or subcutaneously. Lazertinib is taken as a daily oral tablet.
Rybrevant costs £1079 for a 350-mg per 7-mL vial. Lazcluze is priced at £4128.50 for 56 x 80-mg tablets and £6192.75 for 28 x 240-mg tablets. Confidential NHS discounts are available through simple patient access schemes.
Integrated care boards, NHS England, and local authorities must implement the guidance within 90 days of publication. For drugs receiving positive draft recommendations for routine commissioning, interim funding becomes accessible from the Cancer Drugs Fund budget starting from the point of marketing authorisation or publication of draft guidance.
The National Institute for Health and Care Excellence (NICE) has recommended amivantamab (Rybrevant) plus lazertinib (Lazcluze) as a first-line option for adults with previously untreated advanced non–small-cell lung cancer (NSCLC) harboring epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 L858R substitution mutations.
In final draft guidance, NICE said the combination therapy should be funded by the NHS in England for eligible patients when it is the most appropriate option. Around 1115 people are expected to benefit.
Lung cancer is the third most common cancer and the leading cause of cancer mortality in the UK. It accounted for 10% of all new cancer diagnoses and 20% of cancer deaths in 2020. Approximately 31,000 people received NSCLC diagnoses in England in 2021, comprising 91% of all lung cancer cases. EGFR mutation-positive NSCLC is more common in women, non-smokers, and individuals from Asian ethnic backgrounds.
Welcoming the decision, Virginia Harrison, research trustee, EGFR+ UK, said, “This is a meaningful advance for patients and their families facing this diagnosis. [It] provides something the EGFR community urgently needs: more choice in first-line treatment.”
How Practice May Shift
The recommendation adds an alternative to existing standards, including osimertinib monotherapy or osimertinib plus pemetrexed/platinum-based chemotherapy. Clinical specialists noted that no single standard care exists for this patient group.
Younger patients and those willing to accept greater side effects may choose between amivantamab plus lazertinib or osimertinib plus chemotherapy. Patients older than 80 years might prefer osimertinib monotherapy due to adverse event considerations.
Mechanism of Action and Clinical Evidence
Amivantamab is a bispecific antibody that simultaneously binds EGFR and mesenchymal-epithelial transition receptors, blocking downstream signaling pathways that drive tumor growth and promoting immune-mediated cancer cell killing. Lazertinib is an oral third-generation EGFR TKI that selectively inhibits mutant EGFR signaling. Together, the agents provides complementary suppression of EGFR-driven tumour growth and resistance mechanisms.
The NICE recommendation is supported by results from the phase 3 MARIPOSA trial, which met its primary endpoint of progression-free survival (PFS). Treatment with amivantamab plus lazertinib significantly prolonged median PFS to 23.7 months compared with 16.6 months with osimertinib. The combination also demonstrated a significant improvement in overall survival, reducing the risk for death by 25% vs osimertinib. Median OS was not reached in the combination arm and was 36.7 months with osimertinib.
The most common adverse reactions with the combination included rash, nail toxicity, hypoalbuminaemia, hepatotoxicity, and stomatitis.
A Medicines and Healthcare products Regulatory Agency-approved subcutaneous formulation of amivantamab, authorized after the committee’s initial meeting, may further improve tolerability and convenience. Administration-related reactions occurred in 63% of patients with the intravenous formulation vs 14% with the subcutaneous formulation. Clinicians expect subcutaneous dosing to replace intravenous use in practice.
Dosing, Access, and Implementation
Amivantamab is administered every 2 weeks, either intravenously or subcutaneously. Lazertinib is taken as a daily oral tablet.
Rybrevant costs £1079 for a 350-mg per 7-mL vial. Lazcluze is priced at £4128.50 for 56 x 80-mg tablets and £6192.75 for 28 x 240-mg tablets. Confidential NHS discounts are available through simple patient access schemes.
Integrated care boards, NHS England, and local authorities must implement the guidance within 90 days of publication. For drugs receiving positive draft recommendations for routine commissioning, interim funding becomes accessible from the Cancer Drugs Fund budget starting from the point of marketing authorisation or publication of draft guidance.
The National Institute for Health and Care Excellence (NICE) has recommended amivantamab (Rybrevant) plus lazertinib (Lazcluze) as a first-line option for adults with previously untreated advanced non–small-cell lung cancer (NSCLC) harboring epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 L858R substitution mutations.
In final draft guidance, NICE said the combination therapy should be funded by the NHS in England for eligible patients when it is the most appropriate option. Around 1115 people are expected to benefit.
Lung cancer is the third most common cancer and the leading cause of cancer mortality in the UK. It accounted for 10% of all new cancer diagnoses and 20% of cancer deaths in 2020. Approximately 31,000 people received NSCLC diagnoses in England in 2021, comprising 91% of all lung cancer cases. EGFR mutation-positive NSCLC is more common in women, non-smokers, and individuals from Asian ethnic backgrounds.
Welcoming the decision, Virginia Harrison, research trustee, EGFR+ UK, said, “This is a meaningful advance for patients and their families facing this diagnosis. [It] provides something the EGFR community urgently needs: more choice in first-line treatment.”
How Practice May Shift
The recommendation adds an alternative to existing standards, including osimertinib monotherapy or osimertinib plus pemetrexed/platinum-based chemotherapy. Clinical specialists noted that no single standard care exists for this patient group.
Younger patients and those willing to accept greater side effects may choose between amivantamab plus lazertinib or osimertinib plus chemotherapy. Patients older than 80 years might prefer osimertinib monotherapy due to adverse event considerations.
Mechanism of Action and Clinical Evidence
Amivantamab is a bispecific antibody that simultaneously binds EGFR and mesenchymal-epithelial transition receptors, blocking downstream signaling pathways that drive tumor growth and promoting immune-mediated cancer cell killing. Lazertinib is an oral third-generation EGFR TKI that selectively inhibits mutant EGFR signaling. Together, the agents provides complementary suppression of EGFR-driven tumour growth and resistance mechanisms.
The NICE recommendation is supported by results from the phase 3 MARIPOSA trial, which met its primary endpoint of progression-free survival (PFS). Treatment with amivantamab plus lazertinib significantly prolonged median PFS to 23.7 months compared with 16.6 months with osimertinib. The combination also demonstrated a significant improvement in overall survival, reducing the risk for death by 25% vs osimertinib. Median OS was not reached in the combination arm and was 36.7 months with osimertinib.
The most common adverse reactions with the combination included rash, nail toxicity, hypoalbuminaemia, hepatotoxicity, and stomatitis.
A Medicines and Healthcare products Regulatory Agency-approved subcutaneous formulation of amivantamab, authorized after the committee’s initial meeting, may further improve tolerability and convenience. Administration-related reactions occurred in 63% of patients with the intravenous formulation vs 14% with the subcutaneous formulation. Clinicians expect subcutaneous dosing to replace intravenous use in practice.
Dosing, Access, and Implementation
Amivantamab is administered every 2 weeks, either intravenously or subcutaneously. Lazertinib is taken as a daily oral tablet.
Rybrevant costs £1079 for a 350-mg per 7-mL vial. Lazcluze is priced at £4128.50 for 56 x 80-mg tablets and £6192.75 for 28 x 240-mg tablets. Confidential NHS discounts are available through simple patient access schemes.
Integrated care boards, NHS England, and local authorities must implement the guidance within 90 days of publication. For drugs receiving positive draft recommendations for routine commissioning, interim funding becomes accessible from the Cancer Drugs Fund budget starting from the point of marketing authorisation or publication of draft guidance.
NICE Endorses Chemo-Free First-Line Options for EGFR NSCLC
NICE Endorses Chemo-Free First-Line Options for EGFR NSCLC
Turning the Cancer Research Problem Into an Opportunity
Turning the Cancer Research Problem Into an Opportunity
The War on Cancer, declared by President Richard Nixon some 50 years ago, has been canceled during the second Trump administration in 2025 — so saith The New York Times Sunday magazine cover story on September 14, 2025. This war seems now to be best described as "The War on Cancer Research."
To our horror and disbelief, we've witnessed the slow but persistent drift of much of the United States citizenry away from science and the sudden and severe movement of the US government to crush much medical research. But it is not as if we were not warned.
In August 2024, on these pages and without political bias, I urged Medscape readers to pay attention to Project 2025. A great deal of what we as a population are now experiencing was laid out as a carefully constructed plan.
What is surprising is the cruel ruthlessness of the "move fast and break things" approach, taken with little apparent concern about the resultant human tragedies (workforce and patients) and no clear care about the resulting fallout. As we've now learned, destroying something as grand as our cancer research enterprise can be accomplished very quickly. Rebuilding it is certain to be slow and difficult and perhaps can never be accomplished.
In this new anti-science, anti-research, and anti-researcher reality, what can we now do?
First and foremost, we must recognize that the war on cancer is not over. Cancer is not canceled, even if much of the US government's research effort/funding has been. Those of us in medicine and public health often speak in quantification of causes of death of our populations. As such, I'll remind Medscape readers that cancer afflicts some 20 million humans worldwide each year, killing nearly 10 million. Although two-thirds of Americans diagnosed with a potentially lethal malignancy are cured, cancer still kills roughly 600,000 Americans each year. Cancer has been the second most frequent cause of death of Americans for 75 years.
Being inevitable and immutable, death itself is not the enemy. We all die. Disease, disability, pain, and human suffering are the real enemies of us all. Cancer maims, pains, diabetes, and torments some 20 million humans worldwide each year. That is a huge humanitarian problem that should be recognized by individuals of all creeds and backgrounds.
With this depletion of our domestic government basic and applied cancer research program, what can we do?
- Think globally and look to the international scientific research enterprises — relying on them, much as they have relied on us.
- Defend the universal importance of reliable and available literature on medical science.
- Continue to translate and apply the vast amount of available published research in clinical practice and publish the results.
- Urge private industries to expand their research budgets into areas of study that may not produce quickly tangible positive bottom-line results.
- Remind the Secretary of the Department of Health and Human Services (for whom chronic diseases seem paramount) that cancer is the second leading American chronic disease by morbidity.
- Redouble efforts of cancer prevention, especially urging the FDA to ban combustible tobacco and strive more diligently to decrease obesity.
- Appeal to our vast philanthropic universe to increase its funding of nonprofit organizations active in the cancer investigation, diagnosis, and management space.
One such 501c3 organization is California-based Cancer Commons. (Disclosure: I named it in 2010 and serve as its editor in chief).
A commons is a space shared by a community to use for the common interest. As we originally envisioned it, a cancer commons is an open access internet location where individuals and organizations (eg, corporations, universities, government agencies, philanthropies) will voluntarily share their data to work together to defeat the common enemy of humans: cancer.
On September 8, 2025, Cancer Commons was the 15th annual Lundberg Institute Lecturer at the Commonwealth Club of California in San Francisco. At the lecture, Cancer Commons founder (and long-term survivor of metastatic malignant melanoma), Jay Martin "Martin" Tenenbaum, PhD, spoke of the need for a cancer commons and the founder's vision. Emma Shtivelman, PhD, the long-time compassionate chief scientist, described some of the thousands of patients with advanced cancer that she has helped — all free of charge. And newly named CEO Clifford Reid, MBA, PhD, used his entrepreneurial prowess to envision an ambitious future.
Cancer Commons has always focused on patients with cancer who are beyond standards of curative care. As Cancer Commons evolves, it anticipates focusing on patients with cancer who are beyond National Comprehensive Cancer Network Guidelines. The organization intends to greatly expand its 1000 patients per year with "high touch" engagement with PhD clinical scientists to many thousands by including artificial intelligence. It plans to extend its N-of-One approach to create new knowledge — especially regarding the hundreds of drugs that are FDA-approved for use in treating cancer but have not been further assessed for the utility in actually treating patients with cancer.
The war on cancer is not over. It remains a persistent foe that causes immense disability, pain, and human suffering. With government support depleted, the burden now shifts to the private sector and philanthropic organizations, such as Cancer Commons, to serve as the new vital infrastructure in the fight for a cure. Now, we must redouble our efforts to ensure that these research endeavors are supported if the US government will not do its part.
A version of this article first appeared on Medscape.com.
The War on Cancer, declared by President Richard Nixon some 50 years ago, has been canceled during the second Trump administration in 2025 — so saith The New York Times Sunday magazine cover story on September 14, 2025. This war seems now to be best described as "The War on Cancer Research."
To our horror and disbelief, we've witnessed the slow but persistent drift of much of the United States citizenry away from science and the sudden and severe movement of the US government to crush much medical research. But it is not as if we were not warned.
In August 2024, on these pages and without political bias, I urged Medscape readers to pay attention to Project 2025. A great deal of what we as a population are now experiencing was laid out as a carefully constructed plan.
What is surprising is the cruel ruthlessness of the "move fast and break things" approach, taken with little apparent concern about the resultant human tragedies (workforce and patients) and no clear care about the resulting fallout. As we've now learned, destroying something as grand as our cancer research enterprise can be accomplished very quickly. Rebuilding it is certain to be slow and difficult and perhaps can never be accomplished.
In this new anti-science, anti-research, and anti-researcher reality, what can we now do?
First and foremost, we must recognize that the war on cancer is not over. Cancer is not canceled, even if much of the US government's research effort/funding has been. Those of us in medicine and public health often speak in quantification of causes of death of our populations. As such, I'll remind Medscape readers that cancer afflicts some 20 million humans worldwide each year, killing nearly 10 million. Although two-thirds of Americans diagnosed with a potentially lethal malignancy are cured, cancer still kills roughly 600,000 Americans each year. Cancer has been the second most frequent cause of death of Americans for 75 years.
Being inevitable and immutable, death itself is not the enemy. We all die. Disease, disability, pain, and human suffering are the real enemies of us all. Cancer maims, pains, diabetes, and torments some 20 million humans worldwide each year. That is a huge humanitarian problem that should be recognized by individuals of all creeds and backgrounds.
With this depletion of our domestic government basic and applied cancer research program, what can we do?
- Think globally and look to the international scientific research enterprises — relying on them, much as they have relied on us.
- Defend the universal importance of reliable and available literature on medical science.
- Continue to translate and apply the vast amount of available published research in clinical practice and publish the results.
- Urge private industries to expand their research budgets into areas of study that may not produce quickly tangible positive bottom-line results.
- Remind the Secretary of the Department of Health and Human Services (for whom chronic diseases seem paramount) that cancer is the second leading American chronic disease by morbidity.
- Redouble efforts of cancer prevention, especially urging the FDA to ban combustible tobacco and strive more diligently to decrease obesity.
- Appeal to our vast philanthropic universe to increase its funding of nonprofit organizations active in the cancer investigation, diagnosis, and management space.
One such 501c3 organization is California-based Cancer Commons. (Disclosure: I named it in 2010 and serve as its editor in chief).
A commons is a space shared by a community to use for the common interest. As we originally envisioned it, a cancer commons is an open access internet location where individuals and organizations (eg, corporations, universities, government agencies, philanthropies) will voluntarily share their data to work together to defeat the common enemy of humans: cancer.
On September 8, 2025, Cancer Commons was the 15th annual Lundberg Institute Lecturer at the Commonwealth Club of California in San Francisco. At the lecture, Cancer Commons founder (and long-term survivor of metastatic malignant melanoma), Jay Martin "Martin" Tenenbaum, PhD, spoke of the need for a cancer commons and the founder's vision. Emma Shtivelman, PhD, the long-time compassionate chief scientist, described some of the thousands of patients with advanced cancer that she has helped — all free of charge. And newly named CEO Clifford Reid, MBA, PhD, used his entrepreneurial prowess to envision an ambitious future.
Cancer Commons has always focused on patients with cancer who are beyond standards of curative care. As Cancer Commons evolves, it anticipates focusing on patients with cancer who are beyond National Comprehensive Cancer Network Guidelines. The organization intends to greatly expand its 1000 patients per year with "high touch" engagement with PhD clinical scientists to many thousands by including artificial intelligence. It plans to extend its N-of-One approach to create new knowledge — especially regarding the hundreds of drugs that are FDA-approved for use in treating cancer but have not been further assessed for the utility in actually treating patients with cancer.
The war on cancer is not over. It remains a persistent foe that causes immense disability, pain, and human suffering. With government support depleted, the burden now shifts to the private sector and philanthropic organizations, such as Cancer Commons, to serve as the new vital infrastructure in the fight for a cure. Now, we must redouble our efforts to ensure that these research endeavors are supported if the US government will not do its part.
A version of this article first appeared on Medscape.com.
The War on Cancer, declared by President Richard Nixon some 50 years ago, has been canceled during the second Trump administration in 2025 — so saith The New York Times Sunday magazine cover story on September 14, 2025. This war seems now to be best described as "The War on Cancer Research."
To our horror and disbelief, we've witnessed the slow but persistent drift of much of the United States citizenry away from science and the sudden and severe movement of the US government to crush much medical research. But it is not as if we were not warned.
In August 2024, on these pages and without political bias, I urged Medscape readers to pay attention to Project 2025. A great deal of what we as a population are now experiencing was laid out as a carefully constructed plan.
What is surprising is the cruel ruthlessness of the "move fast and break things" approach, taken with little apparent concern about the resultant human tragedies (workforce and patients) and no clear care about the resulting fallout. As we've now learned, destroying something as grand as our cancer research enterprise can be accomplished very quickly. Rebuilding it is certain to be slow and difficult and perhaps can never be accomplished.
In this new anti-science, anti-research, and anti-researcher reality, what can we now do?
First and foremost, we must recognize that the war on cancer is not over. Cancer is not canceled, even if much of the US government's research effort/funding has been. Those of us in medicine and public health often speak in quantification of causes of death of our populations. As such, I'll remind Medscape readers that cancer afflicts some 20 million humans worldwide each year, killing nearly 10 million. Although two-thirds of Americans diagnosed with a potentially lethal malignancy are cured, cancer still kills roughly 600,000 Americans each year. Cancer has been the second most frequent cause of death of Americans for 75 years.
Being inevitable and immutable, death itself is not the enemy. We all die. Disease, disability, pain, and human suffering are the real enemies of us all. Cancer maims, pains, diabetes, and torments some 20 million humans worldwide each year. That is a huge humanitarian problem that should be recognized by individuals of all creeds and backgrounds.
With this depletion of our domestic government basic and applied cancer research program, what can we do?
- Think globally and look to the international scientific research enterprises — relying on them, much as they have relied on us.
- Defend the universal importance of reliable and available literature on medical science.
- Continue to translate and apply the vast amount of available published research in clinical practice and publish the results.
- Urge private industries to expand their research budgets into areas of study that may not produce quickly tangible positive bottom-line results.
- Remind the Secretary of the Department of Health and Human Services (for whom chronic diseases seem paramount) that cancer is the second leading American chronic disease by morbidity.
- Redouble efforts of cancer prevention, especially urging the FDA to ban combustible tobacco and strive more diligently to decrease obesity.
- Appeal to our vast philanthropic universe to increase its funding of nonprofit organizations active in the cancer investigation, diagnosis, and management space.
One such 501c3 organization is California-based Cancer Commons. (Disclosure: I named it in 2010 and serve as its editor in chief).
A commons is a space shared by a community to use for the common interest. As we originally envisioned it, a cancer commons is an open access internet location where individuals and organizations (eg, corporations, universities, government agencies, philanthropies) will voluntarily share their data to work together to defeat the common enemy of humans: cancer.
On September 8, 2025, Cancer Commons was the 15th annual Lundberg Institute Lecturer at the Commonwealth Club of California in San Francisco. At the lecture, Cancer Commons founder (and long-term survivor of metastatic malignant melanoma), Jay Martin "Martin" Tenenbaum, PhD, spoke of the need for a cancer commons and the founder's vision. Emma Shtivelman, PhD, the long-time compassionate chief scientist, described some of the thousands of patients with advanced cancer that she has helped — all free of charge. And newly named CEO Clifford Reid, MBA, PhD, used his entrepreneurial prowess to envision an ambitious future.
Cancer Commons has always focused on patients with cancer who are beyond standards of curative care. As Cancer Commons evolves, it anticipates focusing on patients with cancer who are beyond National Comprehensive Cancer Network Guidelines. The organization intends to greatly expand its 1000 patients per year with "high touch" engagement with PhD clinical scientists to many thousands by including artificial intelligence. It plans to extend its N-of-One approach to create new knowledge — especially regarding the hundreds of drugs that are FDA-approved for use in treating cancer but have not been further assessed for the utility in actually treating patients with cancer.
The war on cancer is not over. It remains a persistent foe that causes immense disability, pain, and human suffering. With government support depleted, the burden now shifts to the private sector and philanthropic organizations, such as Cancer Commons, to serve as the new vital infrastructure in the fight for a cure. Now, we must redouble our efforts to ensure that these research endeavors are supported if the US government will not do its part.
A version of this article first appeared on Medscape.com.
Turning the Cancer Research Problem Into an Opportunity
Turning the Cancer Research Problem Into an Opportunity

Impact of Retroactive Application of Updated Surveillance Guidelines on Endoscopy Center Capacity at a Large VA Health Care System
Impact of Retroactive Application of Updated Surveillance Guidelines on Endoscopy Center Capacity at a Large VA Health Care System
In 2020, the US Multi-Society Task Force (USMSTF) on Colorectal Cancer (CRC) increased the recommended colon polyp surveillance interval for 1 to 2 subcentimeter tubular adenomas from 5 to 10 years to 7 to 10 years.1 This change was prompted by emerging research indicating that rates of CRC and advanced neoplasia among patients with a history of only 1 to 2 subcentimeter tubular adenomas are lower than initially estimated.2,3 This extension provides an opportunity to increase endoscopy capacity and improve access to colonoscopies by retroactively applying the 2020 guidelines to surveillance interval recommendations made before their introduction. For example, based on the updated guidelines, patients previously recommended to undergo colon polyp surveillance colonoscopy 5 years after an index colonoscopy could extend their surveillance interval by 2 to 5 years. Increasing endoscopic capacity could address the growing demand for colonoscopies from new screening guidelines that reduced the age of initial CRC screening from 50 years to 45 years and the backlog of procedures due to COVID-19 restrictions.4
As part of a project to increase endoscopic capacity at the US Department of Veterans Affairs (VA) Pittsburgh Healthcare System (VAPHS), this study assessed the potential impact of retroactively applying the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity. These results may be informative for other VA and private-sector health care systems seeking to identify strategies to improve endoscopy capacity.
Methods
VAPHS is an integrated health care system in the Veterans Health Administration (VHA) serving 85,000 patients across 8 health care institutions in Pennsylvania, Ohio, and West Virginia. VAPHS manages colorectal screening recommendations for patients receiving medical care in the health care system regardless of whether their prior colonoscopy was performed at VAPHS or external facilities. The VA maintains a national CRC screening and surveillance electronic medical record reminder that prompts health care practitioners to order colon polyp surveillance based on interval recommendations from the index colonoscopy. This study reviewed all patients from the VAPHS panel with a reminder to undergo colonoscopy for screening for CRC or surveillance of colon polyps within 12 months from September 1, 2022.
Among patients with a reminder, 3 investigators reviewed index colonoscopy and pathology reports to identify CRC risk category, colonoscopy indication, procedural quality, and recommended repeat colonoscopy interval. Per the USMSTF guidelines, patients with incomplete colonoscopy or pathology records, high-risk indications (ie, personal history of inflammatory bowel disease, personal history of CRC, or family history of CRC), or inadequate bowel preparation (Boston Bowel Preparation Score < 6) were excluded. Additionally, patients who had CRC screening or surveillance discontinued due to age or comorbidities, had completed a subsequent follow-up colonoscopy, or were deceased at the time of review were excluded.
Retroactive Interval Reclassification
Among eligible patients, this study compared the repeat colonoscopy interval recommended by the prior endoscopist with those from the 2020 USMSTF guidelines. In cases where the interval was documented as a range of years, the lower end was considered the recommendation. Similarly, the lower end of the range from the 2020 USMSTF guidelines was used for the reclassified surveillance interval. Years extended per patient were quantified relative to September 1, 2023 (ie, 1 year after the review date). For example, if the index colonoscopy was completed on September 1, 2016, the initial surveillance recommendation was 5 years, and the reclassified recommendation was 7 years, the interval extension beyond September 1, 2023, was 0 years.
Furthermore, because index surveillance recommendations are not always guideline concordant, the years extended per patient were calculated by harmonizing the index endoscopist’s recommendations with the guidelines at the time of the index colonoscopy.5 For example, if the index colonoscopy was completed on September 1, 2018, and the endoscopist recommended a 5-year follow-up for a patient with average risk for CRC, adequate bowel preparation, and no colorectal polyps, that patient is eligible to extend their colonoscopy to September 1, 2028, based on guideline recommendations at the time of index endoscopy recommending that the next colonoscopy occur in 10 years. In this analysis the 2012 USMSTF guidelines were applied to all index colonoscopies completed in 2021 or earlier to allow time for adoption of the 2020 guidelines.
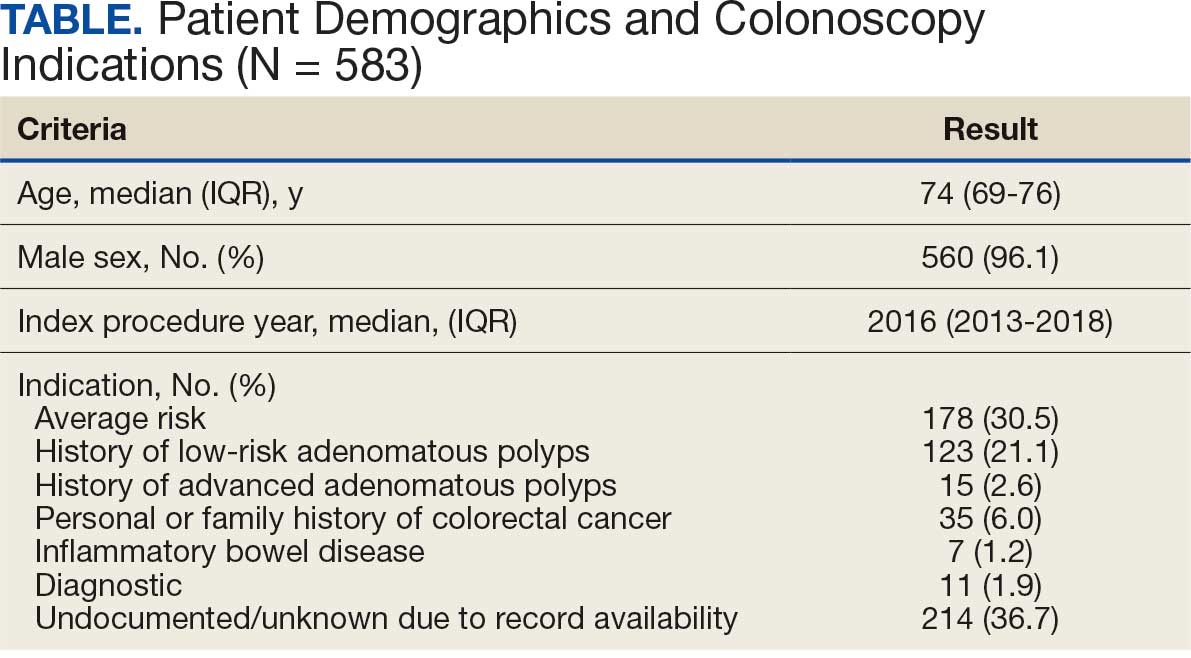
This project fulfilled a facility mandate to increase capacity to conduct endoscopic procedures. Institutional review board approval was not required by VAPHS policy relating to clinical operations projects. Approval for publication of clinical operations activity was obtained from the VAPHS facility director.
Results
Within 1 year of the September 1, 2022, review date, 637 patients receiving care at VAPHS had clinical reminders for an upcoming colonoscopy. Of these, 54 (8.4%) were already up to date or were deceased at the time of review. Of the 583 eligible patients, 96% were male, the median age was 74 years, the median index colonoscopy year was 2016, and 178 (30.5%) had an average-risk CRC screening indication at the index colonoscopy (Table).
Of the 583 patients due for colonoscopy, 331 (56.7%) had both colonoscopy and pathology reports available. The majority of those with incomplete records had the index colonoscopy completed outside VAPHS. Among these patients, 222 (67.0%) had adequate bowel preparation. Of those with adequate bowel preparation, 43 were not eligible for interval extension because of high-risk conditions and 13 were not eligible because there was no index surveillance interval recommendation from the index endoscopist. Of the patients due for colonoscopy, 166 (28.4%) were potentially eligible for surveillance interval extension (Figure).
Sixty-five (39.2%) of the 166 patients had 1 to 2 subcentimeter tubular adenomas on their index colonoscopy. Sixty-two patients were eligible for interval extension to 7 years, but this only resulted in ≥ 1 year of extension beyond the review date for 36 (6% of all 583 patients due for colonoscopy). The 36 patients were extended 63 years. By harmonizing the index endoscopists’ surveillance interval recommendation with the guideline at the time of the index colonoscopy, 29 additional patients could have their colonoscopy extended by ≥ 1 year. Harmonization extended colonoscopy intervals by 93 years. Retroactively applying the 2020 USMSTF polyp surveillance guidelines and harmonizing recommendations to guidelines extended the time of index colonoscopy by 153 years.
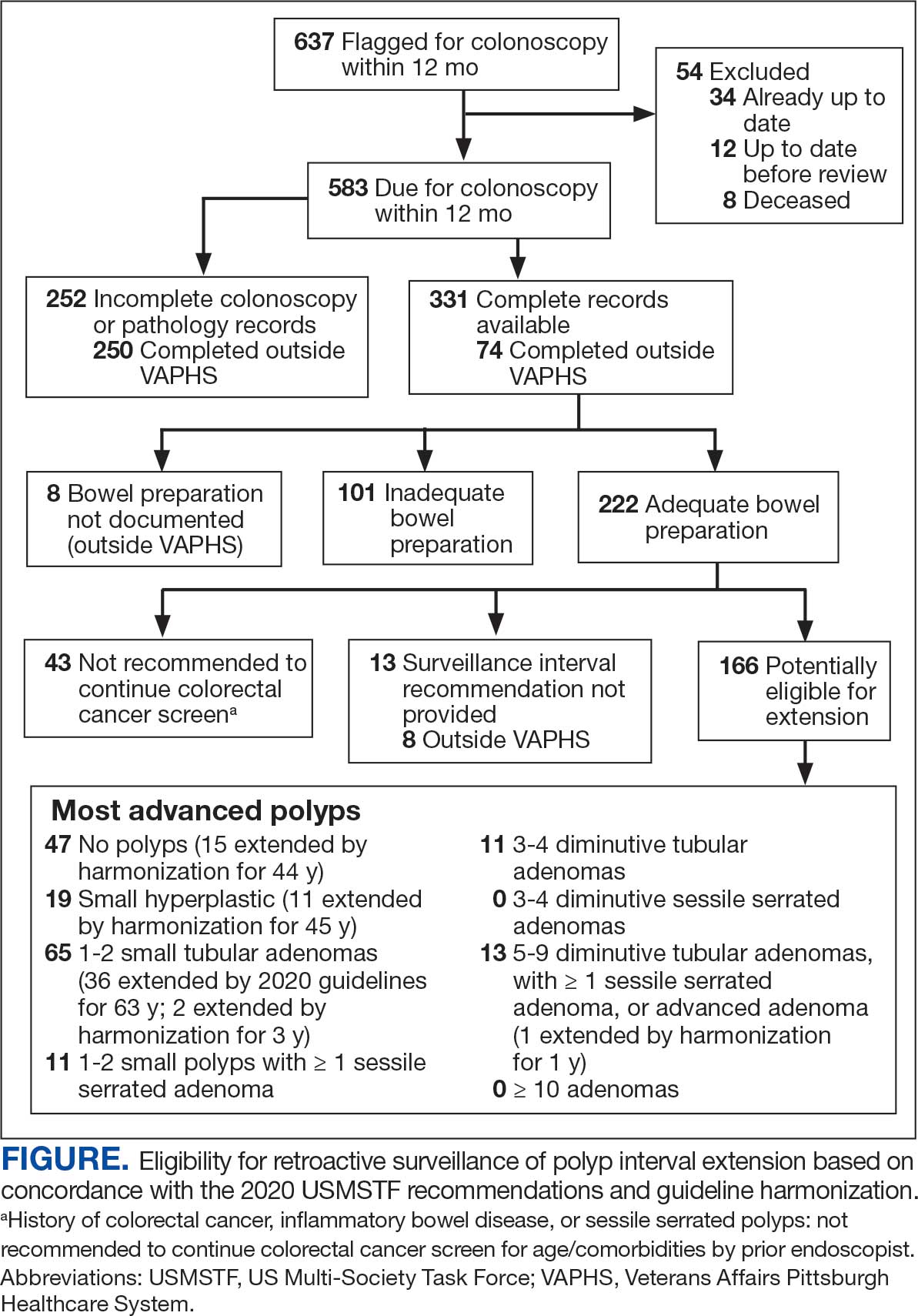
Discussion
With retroactive application of the 2020 USMSTF polyp surveillance guidelines, 6% of patients due for an upcoming colonoscopy could extend their follow-up by ≥ 1 year by extending the surveillance interval for 1 to 2 subcentimeter tubular adenomas to 7 years. An additional 5% of patients could extend their interval by harmonizing the index endoscopist’s interval recommendation with polyp surveillance guidelines at the time of the index colonoscopy. These findings are consistent with the results of 2 studies that demonstrated that about 14% of patients due for colonoscopy could have their interval extended.6,7 The current study enhances those insights by separating the contribution of 2020 USMSTF polyp surveillance guidelines from the contribution of harmonizing surveillance intervals with guidelines for other polyp histologies. This study found that there is an opportunity to improve endoscopic capacity by harmonizing recommendations with guidelines. This complements a 2023 study showing that even when knowledgeable about guidelines, clinicians do not necessarily follow recommendations.8 While this and previous research have identified that 11% to 14% of patients are eligible for extension, these individuals would also have to be willing to have their polyp surveillance intervals extended for there to be a real-world impact on endoscopic capacity. A 2024 study found that only 19% to 37% of patients with 1 to 2 small tubular adenomas were willing to have polyps surveillance interval extension.9 This suggests the actual effect on capacity may be even lower than reported.
Limitations
The overall impact of the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity was blunted by the high prevalence of incomplete index colonoscopy records among the study population. Without data on bowel preparation quality or procedure indications, this study could not assess whether 43% of patients were eligible for surveillance interval extension. Most index colonoscopies with incomplete documentation were completed at community-care gastroenterology facilities. This high rate of incomplete documentation is likely generalizable to other VA health care systems—especially in the era of the Veterans Access, Choice, and Accountability Act of 2014, which increased veteran access to non-VA community care.10 Veterans due for colon polyp surveillance colonoscopies are more likely to have had their prior colonoscopy in community care compared with prior eras.11 Furthermore, because the VHA is among the most established integrated health care systems offering primary and subspecialty care in the US, private sector health care systems may have even greater rates of care fragmentation for longitudinal CRC screening and colon polyp surveillance, as these systems have only begun to regionally integrate recently.12,13
Another limitation is that nearly one-third of the individuals with documentation had inadequate bowel preparation for surveillance recommendations. This results in shorter surveillance follow-up colonoscopies and increases downstream demand for future colonoscopies. The low yield of extending colon polyp surveillance interval in this study emphasizes that improved efforts to obtain colonoscopy and pathology reports from community care, right-sizing the colon polyp surveillance intervals recommended by endoscopists, and improving quality of bowel preparation could have downstream health care system benefits in the future. These efforts could increase colonoscopy capacity at VA health care systems, thereby shortening colonoscopy wait times, decreasing fragmentation of care, and increasing the number of veterans who receive high-quality colonoscopies at VA health care systems.14
Conclusions
Eleven percent of patients in this study due for a colonoscopy could extend their follow-up by ≥ 1 year. About half of these extensions were directly due to the 2020 USMSTF polyp surveillance interval extension for 1 to 2 subcentimeter tubular adenomas. The rest resulted from harmonizing recommendations with guidelines at the time of the procedure. To determine whether retroactively applying polyp surveillance guidelines to follow-up interval recommendations will result in improved endoscopic capacity, health care system administrators should consider the degree of CRC screening care fragmentation in their patient population. Greater long-term gains in endoscopic capacity may be achieved by proactively supporting endoscopists in making guideline-concordant screening recommendations at the time of colonoscopy.
Gupta S, Lieberman D, Anderson JC, et al. Recommendations for follow-up after colonoscopy and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2020;91:463-485. doi:10.1016/j.gie.2020.01.014
Dubé C, Yakubu M, McCurdy BR, et al. Risk of advanced adenoma, colorectal cancer, and colorectal cancer mortality in people with low-risk adenomas at baseline colonoscopy: a systematic review and meta-analysis. Am J Gastroenterol. 2017;112:1790-1801. doi:10.1038/ajg.2017.360
Click B, Pinsky PF, Hickey T, Doroudi M, Shoen RE. Association of colonoscopy adenoma findings with long-term colorectal cancer incidence. JAMA. 2018;319:2021-2031. doi:10.1001/jama.2018.5809
US Preventive Services Task Force, Davidson KW, Barry MJ, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325:1965-1977. doi:10.1001/jama.2021.6238
Djinbachian R, Dubé AJ, Durand M, et al. Adherence to post-polypectomy surveillance guidelines: a systematic review and meta-analysis. Endoscopy. 2019;51:673-683. doi:10.1055/a-0865-2082
Gawron AJ, Kaltenbach T, Dominitz JA. The impact of the coronavirus disease-19 pandemic on access to endoscopy procedures in the VA healthcare system. Gastroenterology. 2020;159:1216-1220.e1. doi:10.1053/j.gastro.2020.07.033
Xiao AH, Chang SY, Stevoff CG, Komanduri S, Pandolfino JE, Keswani RN. Adoption of multi-society guidelines facilitates value-based reduction in screening and surveillance colonoscopy volume during COVID-19 pandemic. Dig Dis Sci. 2021;66:2578-2584. doi:10.1007/s10620-020-06539-1
Dong J, Wang LF, Ardolino E, Feuerstein JD. Real-world compliance with the 2020 U.S. Multi-Society Task Force on Colorectal Cancer polypectomy surveillance guidelines: an observational study. Gastrointest Endosc. 2023;97:350-356.e3. doi:10.1016/j.gie.2022.08.020
Lee JK, Koripella PC, Jensen CD, et al. Randomized trial of patient outreach approaches to de-implement outdated colonoscopy surveillance intervals. Clin Gastroenterol Hepatol. 2024;22:1315-1322.e7. doi:10.1016/j.cgh.2023.12.027
Veterans Access, Choice, and Accountability Act of 2014, HR 3230, 113th Cong (2014). Accessed September 8, 2025. https://www.congress.gov/bill/113th-congress/house-bill/3230
Dueker JM, Khalid A. Performance of the Veterans Choice Program for improving access to colonoscopy at a tertiary VA facility. Fed Pract. 2020;37:224-228.
Oliver A. The Veterans Health Administration: an American success story? Milbank Q. 2007;85:5-35. doi:10.1111/j.1468-0009.2007.00475.x
Furukawa MF, Machta RM, Barrett KA, et al. Landscape of health systems in the United States. Med Care Res Rev. 2020;77:357-366. doi:10.1177/1077558718823130
Petros V, Tsambikos E, Madhoun M, Tierney WM. Impact of community referral on colonoscopy quality metrics in a Veterans Affairs Medical Center. Clin Transl Gastroenterol. 2022;13:e00460. doi:10.14309/ctg.0000000000000460
In 2020, the US Multi-Society Task Force (USMSTF) on Colorectal Cancer (CRC) increased the recommended colon polyp surveillance interval for 1 to 2 subcentimeter tubular adenomas from 5 to 10 years to 7 to 10 years.1 This change was prompted by emerging research indicating that rates of CRC and advanced neoplasia among patients with a history of only 1 to 2 subcentimeter tubular adenomas are lower than initially estimated.2,3 This extension provides an opportunity to increase endoscopy capacity and improve access to colonoscopies by retroactively applying the 2020 guidelines to surveillance interval recommendations made before their introduction. For example, based on the updated guidelines, patients previously recommended to undergo colon polyp surveillance colonoscopy 5 years after an index colonoscopy could extend their surveillance interval by 2 to 5 years. Increasing endoscopic capacity could address the growing demand for colonoscopies from new screening guidelines that reduced the age of initial CRC screening from 50 years to 45 years and the backlog of procedures due to COVID-19 restrictions.4
As part of a project to increase endoscopic capacity at the US Department of Veterans Affairs (VA) Pittsburgh Healthcare System (VAPHS), this study assessed the potential impact of retroactively applying the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity. These results may be informative for other VA and private-sector health care systems seeking to identify strategies to improve endoscopy capacity.
Methods
VAPHS is an integrated health care system in the Veterans Health Administration (VHA) serving 85,000 patients across 8 health care institutions in Pennsylvania, Ohio, and West Virginia. VAPHS manages colorectal screening recommendations for patients receiving medical care in the health care system regardless of whether their prior colonoscopy was performed at VAPHS or external facilities. The VA maintains a national CRC screening and surveillance electronic medical record reminder that prompts health care practitioners to order colon polyp surveillance based on interval recommendations from the index colonoscopy. This study reviewed all patients from the VAPHS panel with a reminder to undergo colonoscopy for screening for CRC or surveillance of colon polyps within 12 months from September 1, 2022.
Among patients with a reminder, 3 investigators reviewed index colonoscopy and pathology reports to identify CRC risk category, colonoscopy indication, procedural quality, and recommended repeat colonoscopy interval. Per the USMSTF guidelines, patients with incomplete colonoscopy or pathology records, high-risk indications (ie, personal history of inflammatory bowel disease, personal history of CRC, or family history of CRC), or inadequate bowel preparation (Boston Bowel Preparation Score < 6) were excluded. Additionally, patients who had CRC screening or surveillance discontinued due to age or comorbidities, had completed a subsequent follow-up colonoscopy, or were deceased at the time of review were excluded.
Retroactive Interval Reclassification
Among eligible patients, this study compared the repeat colonoscopy interval recommended by the prior endoscopist with those from the 2020 USMSTF guidelines. In cases where the interval was documented as a range of years, the lower end was considered the recommendation. Similarly, the lower end of the range from the 2020 USMSTF guidelines was used for the reclassified surveillance interval. Years extended per patient were quantified relative to September 1, 2023 (ie, 1 year after the review date). For example, if the index colonoscopy was completed on September 1, 2016, the initial surveillance recommendation was 5 years, and the reclassified recommendation was 7 years, the interval extension beyond September 1, 2023, was 0 years.
Furthermore, because index surveillance recommendations are not always guideline concordant, the years extended per patient were calculated by harmonizing the index endoscopist’s recommendations with the guidelines at the time of the index colonoscopy.5 For example, if the index colonoscopy was completed on September 1, 2018, and the endoscopist recommended a 5-year follow-up for a patient with average risk for CRC, adequate bowel preparation, and no colorectal polyps, that patient is eligible to extend their colonoscopy to September 1, 2028, based on guideline recommendations at the time of index endoscopy recommending that the next colonoscopy occur in 10 years. In this analysis the 2012 USMSTF guidelines were applied to all index colonoscopies completed in 2021 or earlier to allow time for adoption of the 2020 guidelines.
This project fulfilled a facility mandate to increase capacity to conduct endoscopic procedures. Institutional review board approval was not required by VAPHS policy relating to clinical operations projects. Approval for publication of clinical operations activity was obtained from the VAPHS facility director.
Results
Within 1 year of the September 1, 2022, review date, 637 patients receiving care at VAPHS had clinical reminders for an upcoming colonoscopy. Of these, 54 (8.4%) were already up to date or were deceased at the time of review. Of the 583 eligible patients, 96% were male, the median age was 74 years, the median index colonoscopy year was 2016, and 178 (30.5%) had an average-risk CRC screening indication at the index colonoscopy (Table).
Of the 583 patients due for colonoscopy, 331 (56.7%) had both colonoscopy and pathology reports available. The majority of those with incomplete records had the index colonoscopy completed outside VAPHS. Among these patients, 222 (67.0%) had adequate bowel preparation. Of those with adequate bowel preparation, 43 were not eligible for interval extension because of high-risk conditions and 13 were not eligible because there was no index surveillance interval recommendation from the index endoscopist. Of the patients due for colonoscopy, 166 (28.4%) were potentially eligible for surveillance interval extension (Figure).
Sixty-five (39.2%) of the 166 patients had 1 to 2 subcentimeter tubular adenomas on their index colonoscopy. Sixty-two patients were eligible for interval extension to 7 years, but this only resulted in ≥ 1 year of extension beyond the review date for 36 (6% of all 583 patients due for colonoscopy). The 36 patients were extended 63 years. By harmonizing the index endoscopists’ surveillance interval recommendation with the guideline at the time of the index colonoscopy, 29 additional patients could have their colonoscopy extended by ≥ 1 year. Harmonization extended colonoscopy intervals by 93 years. Retroactively applying the 2020 USMSTF polyp surveillance guidelines and harmonizing recommendations to guidelines extended the time of index colonoscopy by 153 years.
Discussion
With retroactive application of the 2020 USMSTF polyp surveillance guidelines, 6% of patients due for an upcoming colonoscopy could extend their follow-up by ≥ 1 year by extending the surveillance interval for 1 to 2 subcentimeter tubular adenomas to 7 years. An additional 5% of patients could extend their interval by harmonizing the index endoscopist’s interval recommendation with polyp surveillance guidelines at the time of the index colonoscopy. These findings are consistent with the results of 2 studies that demonstrated that about 14% of patients due for colonoscopy could have their interval extended.6,7 The current study enhances those insights by separating the contribution of 2020 USMSTF polyp surveillance guidelines from the contribution of harmonizing surveillance intervals with guidelines for other polyp histologies. This study found that there is an opportunity to improve endoscopic capacity by harmonizing recommendations with guidelines. This complements a 2023 study showing that even when knowledgeable about guidelines, clinicians do not necessarily follow recommendations.8 While this and previous research have identified that 11% to 14% of patients are eligible for extension, these individuals would also have to be willing to have their polyp surveillance intervals extended for there to be a real-world impact on endoscopic capacity. A 2024 study found that only 19% to 37% of patients with 1 to 2 small tubular adenomas were willing to have polyps surveillance interval extension.9 This suggests the actual effect on capacity may be even lower than reported.
Limitations
The overall impact of the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity was blunted by the high prevalence of incomplete index colonoscopy records among the study population. Without data on bowel preparation quality or procedure indications, this study could not assess whether 43% of patients were eligible for surveillance interval extension. Most index colonoscopies with incomplete documentation were completed at community-care gastroenterology facilities. This high rate of incomplete documentation is likely generalizable to other VA health care systems—especially in the era of the Veterans Access, Choice, and Accountability Act of 2014, which increased veteran access to non-VA community care.10 Veterans due for colon polyp surveillance colonoscopies are more likely to have had their prior colonoscopy in community care compared with prior eras.11 Furthermore, because the VHA is among the most established integrated health care systems offering primary and subspecialty care in the US, private sector health care systems may have even greater rates of care fragmentation for longitudinal CRC screening and colon polyp surveillance, as these systems have only begun to regionally integrate recently.12,13
Another limitation is that nearly one-third of the individuals with documentation had inadequate bowel preparation for surveillance recommendations. This results in shorter surveillance follow-up colonoscopies and increases downstream demand for future colonoscopies. The low yield of extending colon polyp surveillance interval in this study emphasizes that improved efforts to obtain colonoscopy and pathology reports from community care, right-sizing the colon polyp surveillance intervals recommended by endoscopists, and improving quality of bowel preparation could have downstream health care system benefits in the future. These efforts could increase colonoscopy capacity at VA health care systems, thereby shortening colonoscopy wait times, decreasing fragmentation of care, and increasing the number of veterans who receive high-quality colonoscopies at VA health care systems.14
Conclusions
Eleven percent of patients in this study due for a colonoscopy could extend their follow-up by ≥ 1 year. About half of these extensions were directly due to the 2020 USMSTF polyp surveillance interval extension for 1 to 2 subcentimeter tubular adenomas. The rest resulted from harmonizing recommendations with guidelines at the time of the procedure. To determine whether retroactively applying polyp surveillance guidelines to follow-up interval recommendations will result in improved endoscopic capacity, health care system administrators should consider the degree of CRC screening care fragmentation in their patient population. Greater long-term gains in endoscopic capacity may be achieved by proactively supporting endoscopists in making guideline-concordant screening recommendations at the time of colonoscopy.
In 2020, the US Multi-Society Task Force (USMSTF) on Colorectal Cancer (CRC) increased the recommended colon polyp surveillance interval for 1 to 2 subcentimeter tubular adenomas from 5 to 10 years to 7 to 10 years.1 This change was prompted by emerging research indicating that rates of CRC and advanced neoplasia among patients with a history of only 1 to 2 subcentimeter tubular adenomas are lower than initially estimated.2,3 This extension provides an opportunity to increase endoscopy capacity and improve access to colonoscopies by retroactively applying the 2020 guidelines to surveillance interval recommendations made before their introduction. For example, based on the updated guidelines, patients previously recommended to undergo colon polyp surveillance colonoscopy 5 years after an index colonoscopy could extend their surveillance interval by 2 to 5 years. Increasing endoscopic capacity could address the growing demand for colonoscopies from new screening guidelines that reduced the age of initial CRC screening from 50 years to 45 years and the backlog of procedures due to COVID-19 restrictions.4
As part of a project to increase endoscopic capacity at the US Department of Veterans Affairs (VA) Pittsburgh Healthcare System (VAPHS), this study assessed the potential impact of retroactively applying the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity. These results may be informative for other VA and private-sector health care systems seeking to identify strategies to improve endoscopy capacity.
Methods
VAPHS is an integrated health care system in the Veterans Health Administration (VHA) serving 85,000 patients across 8 health care institutions in Pennsylvania, Ohio, and West Virginia. VAPHS manages colorectal screening recommendations for patients receiving medical care in the health care system regardless of whether their prior colonoscopy was performed at VAPHS or external facilities. The VA maintains a national CRC screening and surveillance electronic medical record reminder that prompts health care practitioners to order colon polyp surveillance based on interval recommendations from the index colonoscopy. This study reviewed all patients from the VAPHS panel with a reminder to undergo colonoscopy for screening for CRC or surveillance of colon polyps within 12 months from September 1, 2022.
Among patients with a reminder, 3 investigators reviewed index colonoscopy and pathology reports to identify CRC risk category, colonoscopy indication, procedural quality, and recommended repeat colonoscopy interval. Per the USMSTF guidelines, patients with incomplete colonoscopy or pathology records, high-risk indications (ie, personal history of inflammatory bowel disease, personal history of CRC, or family history of CRC), or inadequate bowel preparation (Boston Bowel Preparation Score < 6) were excluded. Additionally, patients who had CRC screening or surveillance discontinued due to age or comorbidities, had completed a subsequent follow-up colonoscopy, or were deceased at the time of review were excluded.
Retroactive Interval Reclassification
Among eligible patients, this study compared the repeat colonoscopy interval recommended by the prior endoscopist with those from the 2020 USMSTF guidelines. In cases where the interval was documented as a range of years, the lower end was considered the recommendation. Similarly, the lower end of the range from the 2020 USMSTF guidelines was used for the reclassified surveillance interval. Years extended per patient were quantified relative to September 1, 2023 (ie, 1 year after the review date). For example, if the index colonoscopy was completed on September 1, 2016, the initial surveillance recommendation was 5 years, and the reclassified recommendation was 7 years, the interval extension beyond September 1, 2023, was 0 years.
Furthermore, because index surveillance recommendations are not always guideline concordant, the years extended per patient were calculated by harmonizing the index endoscopist’s recommendations with the guidelines at the time of the index colonoscopy.5 For example, if the index colonoscopy was completed on September 1, 2018, and the endoscopist recommended a 5-year follow-up for a patient with average risk for CRC, adequate bowel preparation, and no colorectal polyps, that patient is eligible to extend their colonoscopy to September 1, 2028, based on guideline recommendations at the time of index endoscopy recommending that the next colonoscopy occur in 10 years. In this analysis the 2012 USMSTF guidelines were applied to all index colonoscopies completed in 2021 or earlier to allow time for adoption of the 2020 guidelines.
This project fulfilled a facility mandate to increase capacity to conduct endoscopic procedures. Institutional review board approval was not required by VAPHS policy relating to clinical operations projects. Approval for publication of clinical operations activity was obtained from the VAPHS facility director.
Results
Within 1 year of the September 1, 2022, review date, 637 patients receiving care at VAPHS had clinical reminders for an upcoming colonoscopy. Of these, 54 (8.4%) were already up to date or were deceased at the time of review. Of the 583 eligible patients, 96% were male, the median age was 74 years, the median index colonoscopy year was 2016, and 178 (30.5%) had an average-risk CRC screening indication at the index colonoscopy (Table).
Of the 583 patients due for colonoscopy, 331 (56.7%) had both colonoscopy and pathology reports available. The majority of those with incomplete records had the index colonoscopy completed outside VAPHS. Among these patients, 222 (67.0%) had adequate bowel preparation. Of those with adequate bowel preparation, 43 were not eligible for interval extension because of high-risk conditions and 13 were not eligible because there was no index surveillance interval recommendation from the index endoscopist. Of the patients due for colonoscopy, 166 (28.4%) were potentially eligible for surveillance interval extension (Figure).
Sixty-five (39.2%) of the 166 patients had 1 to 2 subcentimeter tubular adenomas on their index colonoscopy. Sixty-two patients were eligible for interval extension to 7 years, but this only resulted in ≥ 1 year of extension beyond the review date for 36 (6% of all 583 patients due for colonoscopy). The 36 patients were extended 63 years. By harmonizing the index endoscopists’ surveillance interval recommendation with the guideline at the time of the index colonoscopy, 29 additional patients could have their colonoscopy extended by ≥ 1 year. Harmonization extended colonoscopy intervals by 93 years. Retroactively applying the 2020 USMSTF polyp surveillance guidelines and harmonizing recommendations to guidelines extended the time of index colonoscopy by 153 years.
Discussion
With retroactive application of the 2020 USMSTF polyp surveillance guidelines, 6% of patients due for an upcoming colonoscopy could extend their follow-up by ≥ 1 year by extending the surveillance interval for 1 to 2 subcentimeter tubular adenomas to 7 years. An additional 5% of patients could extend their interval by harmonizing the index endoscopist’s interval recommendation with polyp surveillance guidelines at the time of the index colonoscopy. These findings are consistent with the results of 2 studies that demonstrated that about 14% of patients due for colonoscopy could have their interval extended.6,7 The current study enhances those insights by separating the contribution of 2020 USMSTF polyp surveillance guidelines from the contribution of harmonizing surveillance intervals with guidelines for other polyp histologies. This study found that there is an opportunity to improve endoscopic capacity by harmonizing recommendations with guidelines. This complements a 2023 study showing that even when knowledgeable about guidelines, clinicians do not necessarily follow recommendations.8 While this and previous research have identified that 11% to 14% of patients are eligible for extension, these individuals would also have to be willing to have their polyp surveillance intervals extended for there to be a real-world impact on endoscopic capacity. A 2024 study found that only 19% to 37% of patients with 1 to 2 small tubular adenomas were willing to have polyps surveillance interval extension.9 This suggests the actual effect on capacity may be even lower than reported.
Limitations
The overall impact of the 2020 USMSTF polyp surveillance guidelines on endoscopic capacity was blunted by the high prevalence of incomplete index colonoscopy records among the study population. Without data on bowel preparation quality or procedure indications, this study could not assess whether 43% of patients were eligible for surveillance interval extension. Most index colonoscopies with incomplete documentation were completed at community-care gastroenterology facilities. This high rate of incomplete documentation is likely generalizable to other VA health care systems—especially in the era of the Veterans Access, Choice, and Accountability Act of 2014, which increased veteran access to non-VA community care.10 Veterans due for colon polyp surveillance colonoscopies are more likely to have had their prior colonoscopy in community care compared with prior eras.11 Furthermore, because the VHA is among the most established integrated health care systems offering primary and subspecialty care in the US, private sector health care systems may have even greater rates of care fragmentation for longitudinal CRC screening and colon polyp surveillance, as these systems have only begun to regionally integrate recently.12,13
Another limitation is that nearly one-third of the individuals with documentation had inadequate bowel preparation for surveillance recommendations. This results in shorter surveillance follow-up colonoscopies and increases downstream demand for future colonoscopies. The low yield of extending colon polyp surveillance interval in this study emphasizes that improved efforts to obtain colonoscopy and pathology reports from community care, right-sizing the colon polyp surveillance intervals recommended by endoscopists, and improving quality of bowel preparation could have downstream health care system benefits in the future. These efforts could increase colonoscopy capacity at VA health care systems, thereby shortening colonoscopy wait times, decreasing fragmentation of care, and increasing the number of veterans who receive high-quality colonoscopies at VA health care systems.14
Conclusions
Eleven percent of patients in this study due for a colonoscopy could extend their follow-up by ≥ 1 year. About half of these extensions were directly due to the 2020 USMSTF polyp surveillance interval extension for 1 to 2 subcentimeter tubular adenomas. The rest resulted from harmonizing recommendations with guidelines at the time of the procedure. To determine whether retroactively applying polyp surveillance guidelines to follow-up interval recommendations will result in improved endoscopic capacity, health care system administrators should consider the degree of CRC screening care fragmentation in their patient population. Greater long-term gains in endoscopic capacity may be achieved by proactively supporting endoscopists in making guideline-concordant screening recommendations at the time of colonoscopy.
Gupta S, Lieberman D, Anderson JC, et al. Recommendations for follow-up after colonoscopy and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2020;91:463-485. doi:10.1016/j.gie.2020.01.014
Dubé C, Yakubu M, McCurdy BR, et al. Risk of advanced adenoma, colorectal cancer, and colorectal cancer mortality in people with low-risk adenomas at baseline colonoscopy: a systematic review and meta-analysis. Am J Gastroenterol. 2017;112:1790-1801. doi:10.1038/ajg.2017.360
Click B, Pinsky PF, Hickey T, Doroudi M, Shoen RE. Association of colonoscopy adenoma findings with long-term colorectal cancer incidence. JAMA. 2018;319:2021-2031. doi:10.1001/jama.2018.5809
US Preventive Services Task Force, Davidson KW, Barry MJ, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325:1965-1977. doi:10.1001/jama.2021.6238
Djinbachian R, Dubé AJ, Durand M, et al. Adherence to post-polypectomy surveillance guidelines: a systematic review and meta-analysis. Endoscopy. 2019;51:673-683. doi:10.1055/a-0865-2082
Gawron AJ, Kaltenbach T, Dominitz JA. The impact of the coronavirus disease-19 pandemic on access to endoscopy procedures in the VA healthcare system. Gastroenterology. 2020;159:1216-1220.e1. doi:10.1053/j.gastro.2020.07.033
Xiao AH, Chang SY, Stevoff CG, Komanduri S, Pandolfino JE, Keswani RN. Adoption of multi-society guidelines facilitates value-based reduction in screening and surveillance colonoscopy volume during COVID-19 pandemic. Dig Dis Sci. 2021;66:2578-2584. doi:10.1007/s10620-020-06539-1
Dong J, Wang LF, Ardolino E, Feuerstein JD. Real-world compliance with the 2020 U.S. Multi-Society Task Force on Colorectal Cancer polypectomy surveillance guidelines: an observational study. Gastrointest Endosc. 2023;97:350-356.e3. doi:10.1016/j.gie.2022.08.020
Lee JK, Koripella PC, Jensen CD, et al. Randomized trial of patient outreach approaches to de-implement outdated colonoscopy surveillance intervals. Clin Gastroenterol Hepatol. 2024;22:1315-1322.e7. doi:10.1016/j.cgh.2023.12.027
Veterans Access, Choice, and Accountability Act of 2014, HR 3230, 113th Cong (2014). Accessed September 8, 2025. https://www.congress.gov/bill/113th-congress/house-bill/3230
Dueker JM, Khalid A. Performance of the Veterans Choice Program for improving access to colonoscopy at a tertiary VA facility. Fed Pract. 2020;37:224-228.
Oliver A. The Veterans Health Administration: an American success story? Milbank Q. 2007;85:5-35. doi:10.1111/j.1468-0009.2007.00475.x
Furukawa MF, Machta RM, Barrett KA, et al. Landscape of health systems in the United States. Med Care Res Rev. 2020;77:357-366. doi:10.1177/1077558718823130
Petros V, Tsambikos E, Madhoun M, Tierney WM. Impact of community referral on colonoscopy quality metrics in a Veterans Affairs Medical Center. Clin Transl Gastroenterol. 2022;13:e00460. doi:10.14309/ctg.0000000000000460
Gupta S, Lieberman D, Anderson JC, et al. Recommendations for follow-up after colonoscopy and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2020;91:463-485. doi:10.1016/j.gie.2020.01.014
Dubé C, Yakubu M, McCurdy BR, et al. Risk of advanced adenoma, colorectal cancer, and colorectal cancer mortality in people with low-risk adenomas at baseline colonoscopy: a systematic review and meta-analysis. Am J Gastroenterol. 2017;112:1790-1801. doi:10.1038/ajg.2017.360
Click B, Pinsky PF, Hickey T, Doroudi M, Shoen RE. Association of colonoscopy adenoma findings with long-term colorectal cancer incidence. JAMA. 2018;319:2021-2031. doi:10.1001/jama.2018.5809
US Preventive Services Task Force, Davidson KW, Barry MJ, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325:1965-1977. doi:10.1001/jama.2021.6238
Djinbachian R, Dubé AJ, Durand M, et al. Adherence to post-polypectomy surveillance guidelines: a systematic review and meta-analysis. Endoscopy. 2019;51:673-683. doi:10.1055/a-0865-2082
Gawron AJ, Kaltenbach T, Dominitz JA. The impact of the coronavirus disease-19 pandemic on access to endoscopy procedures in the VA healthcare system. Gastroenterology. 2020;159:1216-1220.e1. doi:10.1053/j.gastro.2020.07.033
Xiao AH, Chang SY, Stevoff CG, Komanduri S, Pandolfino JE, Keswani RN. Adoption of multi-society guidelines facilitates value-based reduction in screening and surveillance colonoscopy volume during COVID-19 pandemic. Dig Dis Sci. 2021;66:2578-2584. doi:10.1007/s10620-020-06539-1
Dong J, Wang LF, Ardolino E, Feuerstein JD. Real-world compliance with the 2020 U.S. Multi-Society Task Force on Colorectal Cancer polypectomy surveillance guidelines: an observational study. Gastrointest Endosc. 2023;97:350-356.e3. doi:10.1016/j.gie.2022.08.020
Lee JK, Koripella PC, Jensen CD, et al. Randomized trial of patient outreach approaches to de-implement outdated colonoscopy surveillance intervals. Clin Gastroenterol Hepatol. 2024;22:1315-1322.e7. doi:10.1016/j.cgh.2023.12.027
Veterans Access, Choice, and Accountability Act of 2014, HR 3230, 113th Cong (2014). Accessed September 8, 2025. https://www.congress.gov/bill/113th-congress/house-bill/3230
Dueker JM, Khalid A. Performance of the Veterans Choice Program for improving access to colonoscopy at a tertiary VA facility. Fed Pract. 2020;37:224-228.
Oliver A. The Veterans Health Administration: an American success story? Milbank Q. 2007;85:5-35. doi:10.1111/j.1468-0009.2007.00475.x
Furukawa MF, Machta RM, Barrett KA, et al. Landscape of health systems in the United States. Med Care Res Rev. 2020;77:357-366. doi:10.1177/1077558718823130
Petros V, Tsambikos E, Madhoun M, Tierney WM. Impact of community referral on colonoscopy quality metrics in a Veterans Affairs Medical Center. Clin Transl Gastroenterol. 2022;13:e00460. doi:10.14309/ctg.0000000000000460
Impact of Retroactive Application of Updated Surveillance Guidelines on Endoscopy Center Capacity at a Large VA Health Care System
Impact of Retroactive Application of Updated Surveillance Guidelines on Endoscopy Center Capacity at a Large VA Health Care System
