User login
FDA approves first generics of pregabalin

The generics were approved to manage neuropathic pain associated with diabetic peripheral neuropathy, postherpetic neuralgia, and fibromyalgia, as well as neuropathic pain associated with spinal cord injury, and as an adjunctive therapy for the treatment of partial-onset seizures in patients aged 17 years and older. Approvals were granted to Alembic Pharmaceuticals, Alkem Laboratories, Amneal Pharmaceuticals, Dr. Reddy’s Laboratories, InvaGen Pharmaceuticals, MSN Laboratories, Rising Pharmaceuticals, Sciegen Pharmaceuticals, and Teva Pharmaceuticals.
The most common adverse events associated with pregabalin include dizziness, somnolence, dry mouth, swelling, blurred vision, weight gain, and abnormal thinking. Pregabalin must be dispensed with a patient Medication Guide containing a guide to the drug’s uses and risks. Angioedema, hypersensitivity reactions, increased seizure frequency, increased suicidal behavior, and peripheral edema are all possible.
“Today’s approval of the first generics for pregabalin, a widely used medication, is another example of the FDA’s long-standing commitment to advance patient access to lower-cost, high-quality generic medicines,” Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in a press release.
The generics were approved to manage neuropathic pain associated with diabetic peripheral neuropathy, postherpetic neuralgia, and fibromyalgia, as well as neuropathic pain associated with spinal cord injury, and as an adjunctive therapy for the treatment of partial-onset seizures in patients aged 17 years and older. Approvals were granted to Alembic Pharmaceuticals, Alkem Laboratories, Amneal Pharmaceuticals, Dr. Reddy’s Laboratories, InvaGen Pharmaceuticals, MSN Laboratories, Rising Pharmaceuticals, Sciegen Pharmaceuticals, and Teva Pharmaceuticals.
The most common adverse events associated with pregabalin include dizziness, somnolence, dry mouth, swelling, blurred vision, weight gain, and abnormal thinking. Pregabalin must be dispensed with a patient Medication Guide containing a guide to the drug’s uses and risks. Angioedema, hypersensitivity reactions, increased seizure frequency, increased suicidal behavior, and peripheral edema are all possible.
“Today’s approval of the first generics for pregabalin, a widely used medication, is another example of the FDA’s long-standing commitment to advance patient access to lower-cost, high-quality generic medicines,” Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in a press release.
The generics were approved to manage neuropathic pain associated with diabetic peripheral neuropathy, postherpetic neuralgia, and fibromyalgia, as well as neuropathic pain associated with spinal cord injury, and as an adjunctive therapy for the treatment of partial-onset seizures in patients aged 17 years and older. Approvals were granted to Alembic Pharmaceuticals, Alkem Laboratories, Amneal Pharmaceuticals, Dr. Reddy’s Laboratories, InvaGen Pharmaceuticals, MSN Laboratories, Rising Pharmaceuticals, Sciegen Pharmaceuticals, and Teva Pharmaceuticals.
The most common adverse events associated with pregabalin include dizziness, somnolence, dry mouth, swelling, blurred vision, weight gain, and abnormal thinking. Pregabalin must be dispensed with a patient Medication Guide containing a guide to the drug’s uses and risks. Angioedema, hypersensitivity reactions, increased seizure frequency, increased suicidal behavior, and peripheral edema are all possible.
“Today’s approval of the first generics for pregabalin, a widely used medication, is another example of the FDA’s long-standing commitment to advance patient access to lower-cost, high-quality generic medicines,” Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in a press release.
FDA declines dapagliflozin indication as adjunct for type 1 diabetes
The Food and Drug Administration has rejected AstraZeneca’s supplemental New Drug Application for the sodium-glucose cotransporter 2 inhibitor dapagliflozin (Farxiga) as an adjunct treatment to insulin in adult patients with type 1 diabetes.
The company said in a press statement that the FDA had issued a complete response letter regarding the application. No reason was given for the decision, but the company said it would work with the agency to discuss the next steps.
The once-daily therapy has been approved as both a monotherapy and combination therapy, as an adjunct to diet and exercise, for improving glycemic control in adults with type 2 diabetes who cannot achieve control with insulin alone. It also has additional demonstrated benefits of weight loss and reduction in blood pressure.
On March 25, 2019, the drug received its first approval for treatment of patients with type 1 diabetes when the European Commission gave it the green light for use in patients with a body mass index of 27 kg/m2 or more when insulin alone does not provide adequate glycemic control. Japan followed a few days later with its approval of the sodium-glucose cotransporter 2 inhibitor, also for type 1 disease in adults.
The approvals for type 1 diabetes in the European Union and Japan were based on data from the phase 3 DEPICT (Dapagliflozin Evaluation in Patients With Inadequately Controlled Type 1 Diabetes) trial program (DEPICT-1 and DEPICT-2), which showed that 5 mg dapagliflozin, taken daily as an oral adjunct to insulin in patients with hard-to-control type 1 disease, reduced blood glucose levels from baseline (the primary endpoint). Secondary endpoints – reductions in weight and total daily insulin use – were also achieved.
Dapagliflozin’s safety profile in the trials in patients with type 1 diabetes was consistent with that established in patients with type 2 disease. However, there was a higher number of cases of diabetic ketoacidosis events in patients who received dapagliflozin. Diabetic ketoacidosis is a known complication for adults with type 1 diabetes and is more prevalent in patients with type 1 disease than in those with type 2.
The Food and Drug Administration has rejected AstraZeneca’s supplemental New Drug Application for the sodium-glucose cotransporter 2 inhibitor dapagliflozin (Farxiga) as an adjunct treatment to insulin in adult patients with type 1 diabetes.
The company said in a press statement that the FDA had issued a complete response letter regarding the application. No reason was given for the decision, but the company said it would work with the agency to discuss the next steps.
The once-daily therapy has been approved as both a monotherapy and combination therapy, as an adjunct to diet and exercise, for improving glycemic control in adults with type 2 diabetes who cannot achieve control with insulin alone. It also has additional demonstrated benefits of weight loss and reduction in blood pressure.
On March 25, 2019, the drug received its first approval for treatment of patients with type 1 diabetes when the European Commission gave it the green light for use in patients with a body mass index of 27 kg/m2 or more when insulin alone does not provide adequate glycemic control. Japan followed a few days later with its approval of the sodium-glucose cotransporter 2 inhibitor, also for type 1 disease in adults.
The approvals for type 1 diabetes in the European Union and Japan were based on data from the phase 3 DEPICT (Dapagliflozin Evaluation in Patients With Inadequately Controlled Type 1 Diabetes) trial program (DEPICT-1 and DEPICT-2), which showed that 5 mg dapagliflozin, taken daily as an oral adjunct to insulin in patients with hard-to-control type 1 disease, reduced blood glucose levels from baseline (the primary endpoint). Secondary endpoints – reductions in weight and total daily insulin use – were also achieved.
Dapagliflozin’s safety profile in the trials in patients with type 1 diabetes was consistent with that established in patients with type 2 disease. However, there was a higher number of cases of diabetic ketoacidosis events in patients who received dapagliflozin. Diabetic ketoacidosis is a known complication for adults with type 1 diabetes and is more prevalent in patients with type 1 disease than in those with type 2.
The Food and Drug Administration has rejected AstraZeneca’s supplemental New Drug Application for the sodium-glucose cotransporter 2 inhibitor dapagliflozin (Farxiga) as an adjunct treatment to insulin in adult patients with type 1 diabetes.
The company said in a press statement that the FDA had issued a complete response letter regarding the application. No reason was given for the decision, but the company said it would work with the agency to discuss the next steps.
The once-daily therapy has been approved as both a monotherapy and combination therapy, as an adjunct to diet and exercise, for improving glycemic control in adults with type 2 diabetes who cannot achieve control with insulin alone. It also has additional demonstrated benefits of weight loss and reduction in blood pressure.
On March 25, 2019, the drug received its first approval for treatment of patients with type 1 diabetes when the European Commission gave it the green light for use in patients with a body mass index of 27 kg/m2 or more when insulin alone does not provide adequate glycemic control. Japan followed a few days later with its approval of the sodium-glucose cotransporter 2 inhibitor, also for type 1 disease in adults.
The approvals for type 1 diabetes in the European Union and Japan were based on data from the phase 3 DEPICT (Dapagliflozin Evaluation in Patients With Inadequately Controlled Type 1 Diabetes) trial program (DEPICT-1 and DEPICT-2), which showed that 5 mg dapagliflozin, taken daily as an oral adjunct to insulin in patients with hard-to-control type 1 disease, reduced blood glucose levels from baseline (the primary endpoint). Secondary endpoints – reductions in weight and total daily insulin use – were also achieved.
Dapagliflozin’s safety profile in the trials in patients with type 1 diabetes was consistent with that established in patients with type 2 disease. However, there was a higher number of cases of diabetic ketoacidosis events in patients who received dapagliflozin. Diabetic ketoacidosis is a known complication for adults with type 1 diabetes and is more prevalent in patients with type 1 disease than in those with type 2.
FDA approves Recarbrio for cUTI, cIAI treatment in adults
The Recarbrio is a three-drug combo injection containing imipenem/cilastatin, an antibiotic previously approved by the FDA, and relebactam, a beta-lactamase inhibitor.

The efficacy of Recarbrio was supported by data on the efficacy of imipenem/cilastatin in the treatment of cUTI and cIAI and by in vitro studies and animal models of infection with treatment by relebactam. The safety was assessed in a pair of clinical studies, one that assessed cUTI patients and another that assessed cIAI patients.
The most common adverse events reported were nausea, diarrhea, headache, fever, and increased liver enzymes. Treatment with Recarbrio is not recommended in patients taking ganciclovir, valproic acid, or divalproex sodium because there is an increased risk of seizures, according to the FDA.
“The FDA remains focused on facilitating the development of safe and effective new antibacterial drugs to give patients more options to fight serious infections. It is important that the use of Recarbrio be reserved for situations when there are limited or no alternative antibacterial drugs for treating a patient’s infection,” Ed Cox, MD, MPH, director for the Office of Antimicrobial Products in FDA’s Center for Drug Evaluation and Research, said in the press release.
Find the full press release on the FDA website.
The Recarbrio is a three-drug combo injection containing imipenem/cilastatin, an antibiotic previously approved by the FDA, and relebactam, a beta-lactamase inhibitor.
The efficacy of Recarbrio was supported by data on the efficacy of imipenem/cilastatin in the treatment of cUTI and cIAI and by in vitro studies and animal models of infection with treatment by relebactam. The safety was assessed in a pair of clinical studies, one that assessed cUTI patients and another that assessed cIAI patients.
The most common adverse events reported were nausea, diarrhea, headache, fever, and increased liver enzymes. Treatment with Recarbrio is not recommended in patients taking ganciclovir, valproic acid, or divalproex sodium because there is an increased risk of seizures, according to the FDA.
“The FDA remains focused on facilitating the development of safe and effective new antibacterial drugs to give patients more options to fight serious infections. It is important that the use of Recarbrio be reserved for situations when there are limited or no alternative antibacterial drugs for treating a patient’s infection,” Ed Cox, MD, MPH, director for the Office of Antimicrobial Products in FDA’s Center for Drug Evaluation and Research, said in the press release.
Find the full press release on the FDA website.
The Recarbrio is a three-drug combo injection containing imipenem/cilastatin, an antibiotic previously approved by the FDA, and relebactam, a beta-lactamase inhibitor.
The efficacy of Recarbrio was supported by data on the efficacy of imipenem/cilastatin in the treatment of cUTI and cIAI and by in vitro studies and animal models of infection with treatment by relebactam. The safety was assessed in a pair of clinical studies, one that assessed cUTI patients and another that assessed cIAI patients.
The most common adverse events reported were nausea, diarrhea, headache, fever, and increased liver enzymes. Treatment with Recarbrio is not recommended in patients taking ganciclovir, valproic acid, or divalproex sodium because there is an increased risk of seizures, according to the FDA.
“The FDA remains focused on facilitating the development of safe and effective new antibacterial drugs to give patients more options to fight serious infections. It is important that the use of Recarbrio be reserved for situations when there are limited or no alternative antibacterial drugs for treating a patient’s infection,” Ed Cox, MD, MPH, director for the Office of Antimicrobial Products in FDA’s Center for Drug Evaluation and Research, said in the press release.
Find the full press release on the FDA website.
FDA approves Gadavist for evaluation of supra-aortic, renal artery disease
The Food and Drug Administration has approved gadobutrol (Gadavist) injections, for use in conjunction with magnetic resonance angiography (MRA), to evaluate known or suspected supra-aortic or renal artery disease in adult and pediatric patients.

Approval was based on a pair of open-label, phase 3 studies in which the efficacy of gadobutrol was assessed, based on visualization and performance for distinguishing between normal and abnormal anatomy. MRA with gadobutrol improved visualization by 88%-98%, compared with unenhanced MRA, in which visualization was improved by 24%-82%. Sensitivity and specificity were noninferior to unenhanced MRA.
Gadobutrol was previously indicated for use in diagnostic MRI in both adults and children to detect areas with disrupted blood-brain barrier and/or abnormal vascularity of the central nervous system, and for MRI of the breast to assess the presence and extent of malignant breast disease. The safety profile in the two current trials matched data previously gathered, with the most common adverse events including headache, nausea, and dizziness.
“Until now, no contrast agents were FDA approved for use with MRA of the supra-aortic arteries. With FDA’s action, radiologists now have an approved MRA contrast agent to help visualize supra-aortic arteries in patients with known or suspected supra-aortic arterial disease, including conditions such as prior stroke or transient ischemic attack,” Elias Melhem, MD, chair of the department of diagnostic radiology and nuclear medicine at the University of Maryland, Baltimore, said in the press release.
Find the full release on the Bayer website.
The Food and Drug Administration has approved gadobutrol (Gadavist) injections, for use in conjunction with magnetic resonance angiography (MRA), to evaluate known or suspected supra-aortic or renal artery disease in adult and pediatric patients.
Approval was based on a pair of open-label, phase 3 studies in which the efficacy of gadobutrol was assessed, based on visualization and performance for distinguishing between normal and abnormal anatomy. MRA with gadobutrol improved visualization by 88%-98%, compared with unenhanced MRA, in which visualization was improved by 24%-82%. Sensitivity and specificity were noninferior to unenhanced MRA.
Gadobutrol was previously indicated for use in diagnostic MRI in both adults and children to detect areas with disrupted blood-brain barrier and/or abnormal vascularity of the central nervous system, and for MRI of the breast to assess the presence and extent of malignant breast disease. The safety profile in the two current trials matched data previously gathered, with the most common adverse events including headache, nausea, and dizziness.
“Until now, no contrast agents were FDA approved for use with MRA of the supra-aortic arteries. With FDA’s action, radiologists now have an approved MRA contrast agent to help visualize supra-aortic arteries in patients with known or suspected supra-aortic arterial disease, including conditions such as prior stroke or transient ischemic attack,” Elias Melhem, MD, chair of the department of diagnostic radiology and nuclear medicine at the University of Maryland, Baltimore, said in the press release.
Find the full release on the Bayer website.
The Food and Drug Administration has approved gadobutrol (Gadavist) injections, for use in conjunction with magnetic resonance angiography (MRA), to evaluate known or suspected supra-aortic or renal artery disease in adult and pediatric patients.
Approval was based on a pair of open-label, phase 3 studies in which the efficacy of gadobutrol was assessed, based on visualization and performance for distinguishing between normal and abnormal anatomy. MRA with gadobutrol improved visualization by 88%-98%, compared with unenhanced MRA, in which visualization was improved by 24%-82%. Sensitivity and specificity were noninferior to unenhanced MRA.
Gadobutrol was previously indicated for use in diagnostic MRI in both adults and children to detect areas with disrupted blood-brain barrier and/or abnormal vascularity of the central nervous system, and for MRI of the breast to assess the presence and extent of malignant breast disease. The safety profile in the two current trials matched data previously gathered, with the most common adverse events including headache, nausea, and dizziness.
“Until now, no contrast agents were FDA approved for use with MRA of the supra-aortic arteries. With FDA’s action, radiologists now have an approved MRA contrast agent to help visualize supra-aortic arteries in patients with known or suspected supra-aortic arterial disease, including conditions such as prior stroke or transient ischemic attack,” Elias Melhem, MD, chair of the department of diagnostic radiology and nuclear medicine at the University of Maryland, Baltimore, said in the press release.
Find the full release on the Bayer website.
FDA pushes for more diversity in clinical trials in draft guidance
Officials at the Food and Drug Administration have issued draft guidance aimed at increasing the diversity of clinical trial populations, including adding children and adolescents earlier in drug development and making trial participation less burdensome for patients.
Despite efforts to enroll clinical trial participants who better reflect a real-world population, “challenges to participation in clinical trials remain, and certain groups continue to be unnecessarily underrepresented in many clinical trials,” the FDA noted in the document’s introduction.
The FDA noted that these challenges could have a significant impact on trial outcomes.
For example, the failure to include complex patients in a clinical trial “may lead to a failure to discover important safety information about the use of the investigational drug in patients who will take the drug after approval.”
In its draft recommendations, the FDA calls on trial sponsors to conduct a closer examination of exclusion criteria and to make it as narrow as possible; consider whether criteria from phase 2 studies, which are restrictive but often transferred to phase 3 protocols, can be eliminated or modified; and consider including children and adolescents when appropriate.
Recommendations related to trial design include characterizing early on the drug metabolism and clearance across populations that may metabolize or clear the drug differently, such as elderly or patients with liver or kidney dysfunction. The agency also called on trial sponsors to use “adaptive clinical trials,” which allow for prespecified trial design changes during the trial, and an early pediatric development program.
Another set of draft recommendations relates to ensuring trial participation is less burdensome for patients by reducing the frequency of study visits and making participants more aware of reimbursement for travel and lodging associated with the trial.
Additionally, the agency is recommending that trial sponsors adopt enrollment and retention practices that enhance inclusiveness, such as ensuring that trial sites include geographic locations with a higher concentration of racial and ethnic minority patients, and holding recruitment events on nights and weekends and in nonclinical locations.
Finally, the FDA issued a set of recommendations to trial sponsors aimed at broadening eligibility criteria when evaluating drugs intended for the treatment of rare diseases. In those trials, the FDA recommended reenrolling participants from early-phase trials in later-phase trials if it can be done safely.
“Because rare diseases often affect small, geographically dispersed patient populations with disease-related travel limitations, special efforts may be necessary to enroll and retain these participants to ensure that a broad spectrum of the patient population is represented,” the agency stated.
At first blush, the draft recommendations are being greeted with a positive response.

“We certainly need more diversity in clinical trial populations, so I think anything that FDA can say that will help encourage that is a good thing,” Richard Schilsky, MD, senior vice president and chief medical officer at the American Society of Clinical Oncology, said in an interview, noting that this new guidance builds off the work that ASCO and Friends of Cancer Research did with the FDA on previous efforts to expand clinical trial populations.
“I think that this new guidance, as best as I can tell, builds off of that, generalizes it across all therapeutic areas and goes a little bit beyond eligibility criteria to other features of clinical trials that may be impediments to patient participation and thereby limit the diversity of the populations in the studies,” he added.
That said, Dr. Schilsky said he welcomed the draft document as a step toward getting broader participation from patients who are more representative of the ultimate users of these treatments.
“All people who could potentially benefit from the trial should have the opportunity to participate as long as it’s safe for them to do so, and they should not be excluded based upon some of these arbitrary structural things,” he said.
“More importantly, we need data on how these new interventions perform in the patients who are seen and treated by doctors every day. We don’t want data just on patients who have no comorbid illnesses, patients who are otherwise perfectly well, patients who could run a marathon before they go to the doctor’s office. Those are generally not the patients that most doctors are seeing. If they are not represented in the trial population, then we are left with having to extrapolate from the trial data to a population for whom there is no information on how to use the treatment,” he added.
Public comments on the draft document are due on Aug. 6.
Officials at the Food and Drug Administration have issued draft guidance aimed at increasing the diversity of clinical trial populations, including adding children and adolescents earlier in drug development and making trial participation less burdensome for patients.
Despite efforts to enroll clinical trial participants who better reflect a real-world population, “challenges to participation in clinical trials remain, and certain groups continue to be unnecessarily underrepresented in many clinical trials,” the FDA noted in the document’s introduction.
The FDA noted that these challenges could have a significant impact on trial outcomes.
For example, the failure to include complex patients in a clinical trial “may lead to a failure to discover important safety information about the use of the investigational drug in patients who will take the drug after approval.”
In its draft recommendations, the FDA calls on trial sponsors to conduct a closer examination of exclusion criteria and to make it as narrow as possible; consider whether criteria from phase 2 studies, which are restrictive but often transferred to phase 3 protocols, can be eliminated or modified; and consider including children and adolescents when appropriate.
Recommendations related to trial design include characterizing early on the drug metabolism and clearance across populations that may metabolize or clear the drug differently, such as elderly or patients with liver or kidney dysfunction. The agency also called on trial sponsors to use “adaptive clinical trials,” which allow for prespecified trial design changes during the trial, and an early pediatric development program.
Another set of draft recommendations relates to ensuring trial participation is less burdensome for patients by reducing the frequency of study visits and making participants more aware of reimbursement for travel and lodging associated with the trial.
Additionally, the agency is recommending that trial sponsors adopt enrollment and retention practices that enhance inclusiveness, such as ensuring that trial sites include geographic locations with a higher concentration of racial and ethnic minority patients, and holding recruitment events on nights and weekends and in nonclinical locations.
Finally, the FDA issued a set of recommendations to trial sponsors aimed at broadening eligibility criteria when evaluating drugs intended for the treatment of rare diseases. In those trials, the FDA recommended reenrolling participants from early-phase trials in later-phase trials if it can be done safely.
“Because rare diseases often affect small, geographically dispersed patient populations with disease-related travel limitations, special efforts may be necessary to enroll and retain these participants to ensure that a broad spectrum of the patient population is represented,” the agency stated.
At first blush, the draft recommendations are being greeted with a positive response.
“We certainly need more diversity in clinical trial populations, so I think anything that FDA can say that will help encourage that is a good thing,” Richard Schilsky, MD, senior vice president and chief medical officer at the American Society of Clinical Oncology, said in an interview, noting that this new guidance builds off the work that ASCO and Friends of Cancer Research did with the FDA on previous efforts to expand clinical trial populations.
“I think that this new guidance, as best as I can tell, builds off of that, generalizes it across all therapeutic areas and goes a little bit beyond eligibility criteria to other features of clinical trials that may be impediments to patient participation and thereby limit the diversity of the populations in the studies,” he added.
That said, Dr. Schilsky said he welcomed the draft document as a step toward getting broader participation from patients who are more representative of the ultimate users of these treatments.
“All people who could potentially benefit from the trial should have the opportunity to participate as long as it’s safe for them to do so, and they should not be excluded based upon some of these arbitrary structural things,” he said.
“More importantly, we need data on how these new interventions perform in the patients who are seen and treated by doctors every day. We don’t want data just on patients who have no comorbid illnesses, patients who are otherwise perfectly well, patients who could run a marathon before they go to the doctor’s office. Those are generally not the patients that most doctors are seeing. If they are not represented in the trial population, then we are left with having to extrapolate from the trial data to a population for whom there is no information on how to use the treatment,” he added.
Public comments on the draft document are due on Aug. 6.
Officials at the Food and Drug Administration have issued draft guidance aimed at increasing the diversity of clinical trial populations, including adding children and adolescents earlier in drug development and making trial participation less burdensome for patients.
Despite efforts to enroll clinical trial participants who better reflect a real-world population, “challenges to participation in clinical trials remain, and certain groups continue to be unnecessarily underrepresented in many clinical trials,” the FDA noted in the document’s introduction.
The FDA noted that these challenges could have a significant impact on trial outcomes.
For example, the failure to include complex patients in a clinical trial “may lead to a failure to discover important safety information about the use of the investigational drug in patients who will take the drug after approval.”
In its draft recommendations, the FDA calls on trial sponsors to conduct a closer examination of exclusion criteria and to make it as narrow as possible; consider whether criteria from phase 2 studies, which are restrictive but often transferred to phase 3 protocols, can be eliminated or modified; and consider including children and adolescents when appropriate.
Recommendations related to trial design include characterizing early on the drug metabolism and clearance across populations that may metabolize or clear the drug differently, such as elderly or patients with liver or kidney dysfunction. The agency also called on trial sponsors to use “adaptive clinical trials,” which allow for prespecified trial design changes during the trial, and an early pediatric development program.
Another set of draft recommendations relates to ensuring trial participation is less burdensome for patients by reducing the frequency of study visits and making participants more aware of reimbursement for travel and lodging associated with the trial.
Additionally, the agency is recommending that trial sponsors adopt enrollment and retention practices that enhance inclusiveness, such as ensuring that trial sites include geographic locations with a higher concentration of racial and ethnic minority patients, and holding recruitment events on nights and weekends and in nonclinical locations.
Finally, the FDA issued a set of recommendations to trial sponsors aimed at broadening eligibility criteria when evaluating drugs intended for the treatment of rare diseases. In those trials, the FDA recommended reenrolling participants from early-phase trials in later-phase trials if it can be done safely.
“Because rare diseases often affect small, geographically dispersed patient populations with disease-related travel limitations, special efforts may be necessary to enroll and retain these participants to ensure that a broad spectrum of the patient population is represented,” the agency stated.
At first blush, the draft recommendations are being greeted with a positive response.
“We certainly need more diversity in clinical trial populations, so I think anything that FDA can say that will help encourage that is a good thing,” Richard Schilsky, MD, senior vice president and chief medical officer at the American Society of Clinical Oncology, said in an interview, noting that this new guidance builds off the work that ASCO and Friends of Cancer Research did with the FDA on previous efforts to expand clinical trial populations.
“I think that this new guidance, as best as I can tell, builds off of that, generalizes it across all therapeutic areas and goes a little bit beyond eligibility criteria to other features of clinical trials that may be impediments to patient participation and thereby limit the diversity of the populations in the studies,” he added.
That said, Dr. Schilsky said he welcomed the draft document as a step toward getting broader participation from patients who are more representative of the ultimate users of these treatments.
“All people who could potentially benefit from the trial should have the opportunity to participate as long as it’s safe for them to do so, and they should not be excluded based upon some of these arbitrary structural things,” he said.
“More importantly, we need data on how these new interventions perform in the patients who are seen and treated by doctors every day. We don’t want data just on patients who have no comorbid illnesses, patients who are otherwise perfectly well, patients who could run a marathon before they go to the doctor’s office. Those are generally not the patients that most doctors are seeing. If they are not represented in the trial population, then we are left with having to extrapolate from the trial data to a population for whom there is no information on how to use the treatment,” he added.
Public comments on the draft document are due on Aug. 6.
CDC: Look for early symptoms of acute flaccid myelitis, report suspected cases
the CDC said in a telebriefing.
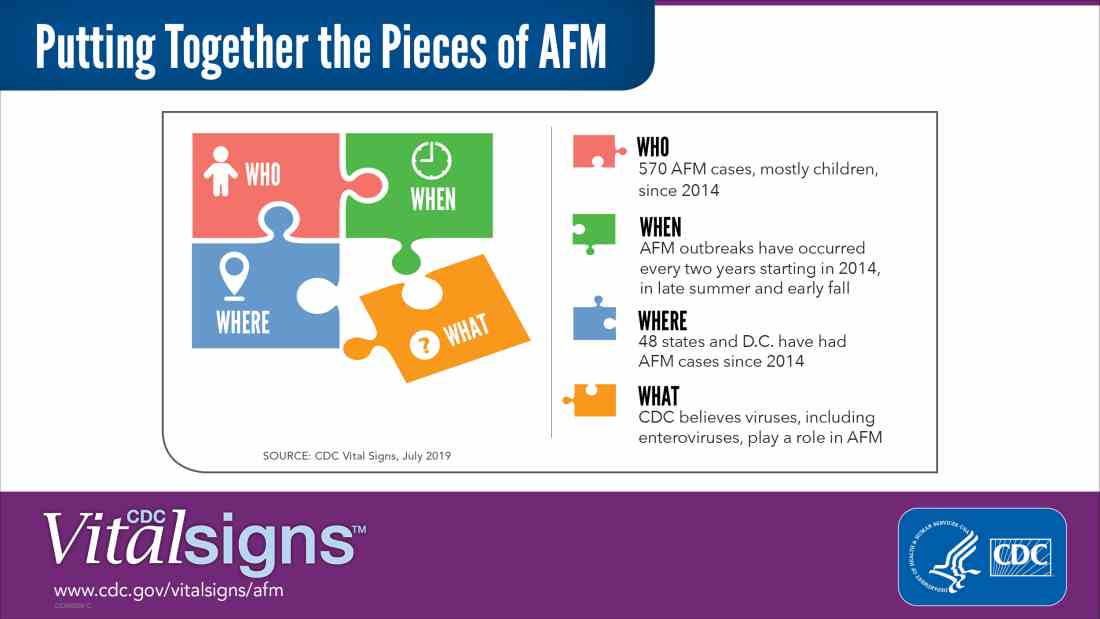
Acute flaccid myelitis (AFM) is defined as acute, flaccid muscle weakness that occurs less than 1 week after a fever or respiratory illness. Viruses, including enterovirus, are believed to play a role in AFM, but the cause still is unknown. The disease appears mostly in children, and the average age of a patient diagnosed with AFM is 5 years.
“Doctors and other clinicians in the United States play a critical role,” Anne Schuchat, MD, principal deputy director of the Centers for Disease Control and Prevention, said in the telebriefing. “We ask for your help with early recognition of patients with AFM symptoms, prompt specimen collection for testing, and immediate reporting of suspected AFM cases to health departments.”
While there is no proven treatment for AFM, early diagnosis is critical to getting patients the best care possible, according to a Vital Signs report released today. This means that clinicians should not wait for the CDC’s case definition before diagnosis, the CDC said.
“When specimens are collected as soon as possible after symptom onset, we have a better chance of understanding the causes of AFM, these recurrent outbreaks, and developing a diagnostic test,” Dr. Schuchat said. “Rapid reporting also helps us to identify and respond to outbreaks early and alert other clinicians and the public.”
AFM appears to follow a seasonal and biennial pattern, with the number of cases increasing mainly in the late summer and early fall. As the season approaches where AFM cases increase, CDC is asking clinicians to look out for patients with suspected AFM so cases can be reported as early as possible.
Since the CDC began tracking AFM, the number of cases has risen every 2 years. In 2018, there were 233 cases in 41 states, the highest number of reported cases since the CDC began tracking AFM following an outbreak in 2014, according to a Vital Signs report. Overall, there have been 570 cases of AFM reported in 48 states and the District of Columbia since 2014.
There is yet to be a confirmatory test for AFM, but clinicians should obtain cerebrospinal fluid, serum, stool and nasopharyngeal swab from patients with suspected AFM as soon as possible, followed by an MRI. AFM has unique MRI features , such as gray matter involvement, that can help distinguish it from other diseases characterized by acute weakness.
In the Vital Signs report, which examined AFM in 2018, 92% of confirmed cases had respiratory symptoms or fever, and 42% of confirmed cases had upper limb involvement. The median time from limb weakness to hospitalization was 1 day, and time from weakness to MRI was 2 days. Cases were reported to the CDC a median of 18 days from onset of limb weakness, but time to reporting ranged between 18 days and 36 days, said Tom Clark, MD, MPH, deputy director of the division of viral diseases at CDC.
“This delay hampers our ability to understand the causes AFM,” he said. “We believe that recognizing AFM early is critical and can lead to better patient management.”
In lieu of a diagnostic test for AFM, clinicians should make management decisions through review of patient symptoms, exam findings, MRI, other test results, and in consulting with neurology experts. The Transverse Myelitis Association also has created a support portal for 24/7 physician consultation in AFM cases.
SOURCE: Lopez A et al. MMWR Morb Mortal Wkly Rep. 2019;68:1-7 .
the CDC said in a telebriefing.
Acute flaccid myelitis (AFM) is defined as acute, flaccid muscle weakness that occurs less than 1 week after a fever or respiratory illness. Viruses, including enterovirus, are believed to play a role in AFM, but the cause still is unknown. The disease appears mostly in children, and the average age of a patient diagnosed with AFM is 5 years.
“Doctors and other clinicians in the United States play a critical role,” Anne Schuchat, MD, principal deputy director of the Centers for Disease Control and Prevention, said in the telebriefing. “We ask for your help with early recognition of patients with AFM symptoms, prompt specimen collection for testing, and immediate reporting of suspected AFM cases to health departments.”
While there is no proven treatment for AFM, early diagnosis is critical to getting patients the best care possible, according to a Vital Signs report released today. This means that clinicians should not wait for the CDC’s case definition before diagnosis, the CDC said.
“When specimens are collected as soon as possible after symptom onset, we have a better chance of understanding the causes of AFM, these recurrent outbreaks, and developing a diagnostic test,” Dr. Schuchat said. “Rapid reporting also helps us to identify and respond to outbreaks early and alert other clinicians and the public.”
AFM appears to follow a seasonal and biennial pattern, with the number of cases increasing mainly in the late summer and early fall. As the season approaches where AFM cases increase, CDC is asking clinicians to look out for patients with suspected AFM so cases can be reported as early as possible.
Since the CDC began tracking AFM, the number of cases has risen every 2 years. In 2018, there were 233 cases in 41 states, the highest number of reported cases since the CDC began tracking AFM following an outbreak in 2014, according to a Vital Signs report. Overall, there have been 570 cases of AFM reported in 48 states and the District of Columbia since 2014.
There is yet to be a confirmatory test for AFM, but clinicians should obtain cerebrospinal fluid, serum, stool and nasopharyngeal swab from patients with suspected AFM as soon as possible, followed by an MRI. AFM has unique MRI features , such as gray matter involvement, that can help distinguish it from other diseases characterized by acute weakness.
In the Vital Signs report, which examined AFM in 2018, 92% of confirmed cases had respiratory symptoms or fever, and 42% of confirmed cases had upper limb involvement. The median time from limb weakness to hospitalization was 1 day, and time from weakness to MRI was 2 days. Cases were reported to the CDC a median of 18 days from onset of limb weakness, but time to reporting ranged between 18 days and 36 days, said Tom Clark, MD, MPH, deputy director of the division of viral diseases at CDC.
“This delay hampers our ability to understand the causes AFM,” he said. “We believe that recognizing AFM early is critical and can lead to better patient management.”
In lieu of a diagnostic test for AFM, clinicians should make management decisions through review of patient symptoms, exam findings, MRI, other test results, and in consulting with neurology experts. The Transverse Myelitis Association also has created a support portal for 24/7 physician consultation in AFM cases.
SOURCE: Lopez A et al. MMWR Morb Mortal Wkly Rep. 2019;68:1-7 .
the CDC said in a telebriefing.
Acute flaccid myelitis (AFM) is defined as acute, flaccid muscle weakness that occurs less than 1 week after a fever or respiratory illness. Viruses, including enterovirus, are believed to play a role in AFM, but the cause still is unknown. The disease appears mostly in children, and the average age of a patient diagnosed with AFM is 5 years.
“Doctors and other clinicians in the United States play a critical role,” Anne Schuchat, MD, principal deputy director of the Centers for Disease Control and Prevention, said in the telebriefing. “We ask for your help with early recognition of patients with AFM symptoms, prompt specimen collection for testing, and immediate reporting of suspected AFM cases to health departments.”
While there is no proven treatment for AFM, early diagnosis is critical to getting patients the best care possible, according to a Vital Signs report released today. This means that clinicians should not wait for the CDC’s case definition before diagnosis, the CDC said.
“When specimens are collected as soon as possible after symptom onset, we have a better chance of understanding the causes of AFM, these recurrent outbreaks, and developing a diagnostic test,” Dr. Schuchat said. “Rapid reporting also helps us to identify and respond to outbreaks early and alert other clinicians and the public.”
AFM appears to follow a seasonal and biennial pattern, with the number of cases increasing mainly in the late summer and early fall. As the season approaches where AFM cases increase, CDC is asking clinicians to look out for patients with suspected AFM so cases can be reported as early as possible.
Since the CDC began tracking AFM, the number of cases has risen every 2 years. In 2018, there were 233 cases in 41 states, the highest number of reported cases since the CDC began tracking AFM following an outbreak in 2014, according to a Vital Signs report. Overall, there have been 570 cases of AFM reported in 48 states and the District of Columbia since 2014.
There is yet to be a confirmatory test for AFM, but clinicians should obtain cerebrospinal fluid, serum, stool and nasopharyngeal swab from patients with suspected AFM as soon as possible, followed by an MRI. AFM has unique MRI features , such as gray matter involvement, that can help distinguish it from other diseases characterized by acute weakness.
In the Vital Signs report, which examined AFM in 2018, 92% of confirmed cases had respiratory symptoms or fever, and 42% of confirmed cases had upper limb involvement. The median time from limb weakness to hospitalization was 1 day, and time from weakness to MRI was 2 days. Cases were reported to the CDC a median of 18 days from onset of limb weakness, but time to reporting ranged between 18 days and 36 days, said Tom Clark, MD, MPH, deputy director of the division of viral diseases at CDC.
“This delay hampers our ability to understand the causes AFM,” he said. “We believe that recognizing AFM early is critical and can lead to better patient management.”
In lieu of a diagnostic test for AFM, clinicians should make management decisions through review of patient symptoms, exam findings, MRI, other test results, and in consulting with neurology experts. The Transverse Myelitis Association also has created a support portal for 24/7 physician consultation in AFM cases.
SOURCE: Lopez A et al. MMWR Morb Mortal Wkly Rep. 2019;68:1-7 .
NEWS FROM THE FDA/CDC
FDA approves Xpovio for relapsed/refractory multiple myeloma
The oral therapy was approved for patients who have received at least four prior therapies and whose disease is resistant to several other forms of treatment, including at least two proteasome inhibitors, at least two immunomodulatory agents, and an anti-CD38 monoclonal antibody, according to the FDA.
The approval provides a “treatment option for patients with multiple myeloma with no (other) available therapy,” said Richard Pazdur, MD, director of the FDA Oncology Center of Excellence and acting director of the Office of Hematology and Oncology Products in the FDA Center for Drug Evaluation and Research.
The approval was based on a study that included 83 patients with RRMM who had an overall response rate of 25.3% to Xpovio in combination with dexamethasone.
“The median time to first response was 4 weeks, with a range of 1-10 weeks. The median duration of response was 3.8 months. The efficacy evaluation was supported by additional information from an ongoing, randomized trial in patients with multiple myeloma,” according to the statement.
Common side effects seen in patients taking Xpovio in combination with dexamethasone include leukopenia, neutropenia, thrombocytopenia, and anemia. Patients also reported vomiting, nausea, fatigue, diarrhea, fever, decreased appetite and weight, constipation, upper respiratory tract infections, and hyponatremia.
Patients taking Xpovio should be monitored for low blood counts, platelets, and sodium levels, and should avoid other medications that may cause dizziness or confusion. Patients’ hydration status, blood counts, and other medications should be optimized to avoid dizziness or confusion. Females of reproductive age and males with a female partner of reproductive potential must use effective contraception during treatment with Xpovio. Women who are pregnant or breastfeeding should not take Xpovio.
Xpovio must be dispensed with a patient Medication Guide that describes important information about the drug’s uses and risks.
Xpovio in combination with dexamethasone was granted accelerated approval, and further clinical trials are required to verify and describe the drug’s clinical benefit.
The FDA granted the approval of Xpovio to Karyopharm Therapeutics.
The oral therapy was approved for patients who have received at least four prior therapies and whose disease is resistant to several other forms of treatment, including at least two proteasome inhibitors, at least two immunomodulatory agents, and an anti-CD38 monoclonal antibody, according to the FDA.
The approval provides a “treatment option for patients with multiple myeloma with no (other) available therapy,” said Richard Pazdur, MD, director of the FDA Oncology Center of Excellence and acting director of the Office of Hematology and Oncology Products in the FDA Center for Drug Evaluation and Research.
The approval was based on a study that included 83 patients with RRMM who had an overall response rate of 25.3% to Xpovio in combination with dexamethasone.
“The median time to first response was 4 weeks, with a range of 1-10 weeks. The median duration of response was 3.8 months. The efficacy evaluation was supported by additional information from an ongoing, randomized trial in patients with multiple myeloma,” according to the statement.
Common side effects seen in patients taking Xpovio in combination with dexamethasone include leukopenia, neutropenia, thrombocytopenia, and anemia. Patients also reported vomiting, nausea, fatigue, diarrhea, fever, decreased appetite and weight, constipation, upper respiratory tract infections, and hyponatremia.
Patients taking Xpovio should be monitored for low blood counts, platelets, and sodium levels, and should avoid other medications that may cause dizziness or confusion. Patients’ hydration status, blood counts, and other medications should be optimized to avoid dizziness or confusion. Females of reproductive age and males with a female partner of reproductive potential must use effective contraception during treatment with Xpovio. Women who are pregnant or breastfeeding should not take Xpovio.
Xpovio must be dispensed with a patient Medication Guide that describes important information about the drug’s uses and risks.
Xpovio in combination with dexamethasone was granted accelerated approval, and further clinical trials are required to verify and describe the drug’s clinical benefit.
The FDA granted the approval of Xpovio to Karyopharm Therapeutics.
The oral therapy was approved for patients who have received at least four prior therapies and whose disease is resistant to several other forms of treatment, including at least two proteasome inhibitors, at least two immunomodulatory agents, and an anti-CD38 monoclonal antibody, according to the FDA.
The approval provides a “treatment option for patients with multiple myeloma with no (other) available therapy,” said Richard Pazdur, MD, director of the FDA Oncology Center of Excellence and acting director of the Office of Hematology and Oncology Products in the FDA Center for Drug Evaluation and Research.
The approval was based on a study that included 83 patients with RRMM who had an overall response rate of 25.3% to Xpovio in combination with dexamethasone.
“The median time to first response was 4 weeks, with a range of 1-10 weeks. The median duration of response was 3.8 months. The efficacy evaluation was supported by additional information from an ongoing, randomized trial in patients with multiple myeloma,” according to the statement.
Common side effects seen in patients taking Xpovio in combination with dexamethasone include leukopenia, neutropenia, thrombocytopenia, and anemia. Patients also reported vomiting, nausea, fatigue, diarrhea, fever, decreased appetite and weight, constipation, upper respiratory tract infections, and hyponatremia.
Patients taking Xpovio should be monitored for low blood counts, platelets, and sodium levels, and should avoid other medications that may cause dizziness or confusion. Patients’ hydration status, blood counts, and other medications should be optimized to avoid dizziness or confusion. Females of reproductive age and males with a female partner of reproductive potential must use effective contraception during treatment with Xpovio. Women who are pregnant or breastfeeding should not take Xpovio.
Xpovio must be dispensed with a patient Medication Guide that describes important information about the drug’s uses and risks.
Xpovio in combination with dexamethasone was granted accelerated approval, and further clinical trials are required to verify and describe the drug’s clinical benefit.
The FDA granted the approval of Xpovio to Karyopharm Therapeutics.
FDA approves bevacizumab-bvzr for several cancers
The Food and Drug Administration has approved bevacizumab-bvzr (Zirabev) – a biosimilar to bevacizumab (Avastin) – for the treatment of five cancers: metastatic colorectal cancer (mCRC); unresectable, locally advanced, recurrent or metastatic non-squamous non–small cell lung cancer (NSCLC); recurrent glioblastoma; metastatic renal cell carcinoma (RCC); and persistent, recurrent or metastatic cervical cancer.
![]()
Approval was based on “review of a comprehensive data package which demonstrated biosimilarity of [bevacizumab-bvzr] to the reference product,” Pfizer said in a statement announcing the approval.
Bevacizumab-bvzr is the second bevacizumab biosimilar to be approved, following approval of Amgen’s bevacizumab-awwb (Mvasi) in 2017.
Warnings and precautions with the biosimilars, as with bevacizumab, include serious and sometimes fatal gastrointestinal perforation, surgery and wound healing complications, and sometimes serious and fatal hemorrhage.
The most common adverse events observed in bevacizumab patients are epistaxis, headache, hypertension, rhinitis, proteinuria, taste alteration, dry skin, rectal hemorrhage, lacrimation disorder, back pain, and exfoliative dermatitis.
Specific indications for the biosimilar are as follows:
Metastatic colorectal cancer
Bevacizumab-bvzr, in combination with intravenous fluorouracil-based chemotherapy, is indicated for the first- or second-line treatment of patients with mCRC.
Bevacizumab-bvzr, in combination with fluoropyrimidine-irinotecan or fluoropyrimidine-oxaliplatin–based chemotherapy, is indicated for the second-line treatment of patients with mCRC who have progressed on a first-line bevacizumab product–containing regimen.
Bevacizumab-bvzr is not indicated for adjuvant treatment of colon cancer.
First-line nonsquamous non–small cell lung cancer
Bevacizumab-bvzr, in combination with carboplatin and paclitaxel, is indicated for the first-line treatment of patients with unresectable, locally advanced, recurrent or metastatic NSCLC.
Recurrent glioblastoma
Bevacizumab-bvzr is indicated for the treatment of recurrent glioblastoma in adults.
Metastatic renal cell carcinoma
Bevacizumab-bvzr, in combination with interferon alfa, is indicated for the treatment of metastatic RCC.
Persistent, recurrent, or metastatic cervical cancer
Bevacizumab-bvzr, in combination with paclitaxel and cisplatin or paclitaxel and topotecan, is indicated for the treatment of patients with persistent, recurrent, or metastatic cervical cancer.
Complete prescribing information can be found on the FDA website.
The Food and Drug Administration has approved bevacizumab-bvzr (Zirabev) – a biosimilar to bevacizumab (Avastin) – for the treatment of five cancers: metastatic colorectal cancer (mCRC); unresectable, locally advanced, recurrent or metastatic non-squamous non–small cell lung cancer (NSCLC); recurrent glioblastoma; metastatic renal cell carcinoma (RCC); and persistent, recurrent or metastatic cervical cancer.
![]()
Approval was based on “review of a comprehensive data package which demonstrated biosimilarity of [bevacizumab-bvzr] to the reference product,” Pfizer said in a statement announcing the approval.
Bevacizumab-bvzr is the second bevacizumab biosimilar to be approved, following approval of Amgen’s bevacizumab-awwb (Mvasi) in 2017.
Warnings and precautions with the biosimilars, as with bevacizumab, include serious and sometimes fatal gastrointestinal perforation, surgery and wound healing complications, and sometimes serious and fatal hemorrhage.
The most common adverse events observed in bevacizumab patients are epistaxis, headache, hypertension, rhinitis, proteinuria, taste alteration, dry skin, rectal hemorrhage, lacrimation disorder, back pain, and exfoliative dermatitis.
Specific indications for the biosimilar are as follows:
Metastatic colorectal cancer
Bevacizumab-bvzr, in combination with intravenous fluorouracil-based chemotherapy, is indicated for the first- or second-line treatment of patients with mCRC.
Bevacizumab-bvzr, in combination with fluoropyrimidine-irinotecan or fluoropyrimidine-oxaliplatin–based chemotherapy, is indicated for the second-line treatment of patients with mCRC who have progressed on a first-line bevacizumab product–containing regimen.
Bevacizumab-bvzr is not indicated for adjuvant treatment of colon cancer.
First-line nonsquamous non–small cell lung cancer
Bevacizumab-bvzr, in combination with carboplatin and paclitaxel, is indicated for the first-line treatment of patients with unresectable, locally advanced, recurrent or metastatic NSCLC.
Recurrent glioblastoma
Bevacizumab-bvzr is indicated for the treatment of recurrent glioblastoma in adults.
Metastatic renal cell carcinoma
Bevacizumab-bvzr, in combination with interferon alfa, is indicated for the treatment of metastatic RCC.
Persistent, recurrent, or metastatic cervical cancer
Bevacizumab-bvzr, in combination with paclitaxel and cisplatin or paclitaxel and topotecan, is indicated for the treatment of patients with persistent, recurrent, or metastatic cervical cancer.
Complete prescribing information can be found on the FDA website.
The Food and Drug Administration has approved bevacizumab-bvzr (Zirabev) – a biosimilar to bevacizumab (Avastin) – for the treatment of five cancers: metastatic colorectal cancer (mCRC); unresectable, locally advanced, recurrent or metastatic non-squamous non–small cell lung cancer (NSCLC); recurrent glioblastoma; metastatic renal cell carcinoma (RCC); and persistent, recurrent or metastatic cervical cancer.
![]()
Approval was based on “review of a comprehensive data package which demonstrated biosimilarity of [bevacizumab-bvzr] to the reference product,” Pfizer said in a statement announcing the approval.
Bevacizumab-bvzr is the second bevacizumab biosimilar to be approved, following approval of Amgen’s bevacizumab-awwb (Mvasi) in 2017.
Warnings and precautions with the biosimilars, as with bevacizumab, include serious and sometimes fatal gastrointestinal perforation, surgery and wound healing complications, and sometimes serious and fatal hemorrhage.
The most common adverse events observed in bevacizumab patients are epistaxis, headache, hypertension, rhinitis, proteinuria, taste alteration, dry skin, rectal hemorrhage, lacrimation disorder, back pain, and exfoliative dermatitis.
Specific indications for the biosimilar are as follows:
Metastatic colorectal cancer
Bevacizumab-bvzr, in combination with intravenous fluorouracil-based chemotherapy, is indicated for the first- or second-line treatment of patients with mCRC.
Bevacizumab-bvzr, in combination with fluoropyrimidine-irinotecan or fluoropyrimidine-oxaliplatin–based chemotherapy, is indicated for the second-line treatment of patients with mCRC who have progressed on a first-line bevacizumab product–containing regimen.
Bevacizumab-bvzr is not indicated for adjuvant treatment of colon cancer.
First-line nonsquamous non–small cell lung cancer
Bevacizumab-bvzr, in combination with carboplatin and paclitaxel, is indicated for the first-line treatment of patients with unresectable, locally advanced, recurrent or metastatic NSCLC.
Recurrent glioblastoma
Bevacizumab-bvzr is indicated for the treatment of recurrent glioblastoma in adults.
Metastatic renal cell carcinoma
Bevacizumab-bvzr, in combination with interferon alfa, is indicated for the treatment of metastatic RCC.
Persistent, recurrent, or metastatic cervical cancer
Bevacizumab-bvzr, in combination with paclitaxel and cisplatin or paclitaxel and topotecan, is indicated for the treatment of patients with persistent, recurrent, or metastatic cervical cancer.
Complete prescribing information can be found on the FDA website.
Daratumumab wins new indication for newly diagnosed myeloma patients
Janssen’s daratumumab (Darzalex) has picked up a sixth adult multiple myeloma indication, this time in combination with lenalidomide (Revlimid) and dexamethasone in newly diagnosed patients ineligible for autologous stem cell transplants.
The phase 3 MAIA trial found that 97 of 368 patients (26.4%) treated with the combination – dubbed DRd – progressed or died at a median follow-up of 28 months, versus 143 of 269 (38.8%) treated with lenalidomide and dexamethasone alone (Rd). An estimated 55.6% of patients on lenalidomide and dexamethasone, versus 70.6% with the daratumumab add-on, were alive without progression at 30 months (N Engl J Med. 2019 May 30;380[22]:2104-15).
Previously approved indications for daratumumab include relapsed or refractory disease after at least one other therapy; and combination treatment with bortezomib, melphalan, and prednisone, also in newly diagnosed patients who are ineligible for transplant.
The most common grade 3 and 4 adverse events reported in the MAIA trial were neutropenia (50.0% for the DRd group versus 35.3% for the Rd group), anemia (11.8% vs. 19.7%), lymphopenia (15.1% vs. 10.7%), and pneumonia (13.7% vs. 7.9%).
Janssen’s daratumumab (Darzalex) has picked up a sixth adult multiple myeloma indication, this time in combination with lenalidomide (Revlimid) and dexamethasone in newly diagnosed patients ineligible for autologous stem cell transplants.
The phase 3 MAIA trial found that 97 of 368 patients (26.4%) treated with the combination – dubbed DRd – progressed or died at a median follow-up of 28 months, versus 143 of 269 (38.8%) treated with lenalidomide and dexamethasone alone (Rd). An estimated 55.6% of patients on lenalidomide and dexamethasone, versus 70.6% with the daratumumab add-on, were alive without progression at 30 months (N Engl J Med. 2019 May 30;380[22]:2104-15).
Previously approved indications for daratumumab include relapsed or refractory disease after at least one other therapy; and combination treatment with bortezomib, melphalan, and prednisone, also in newly diagnosed patients who are ineligible for transplant.
The most common grade 3 and 4 adverse events reported in the MAIA trial were neutropenia (50.0% for the DRd group versus 35.3% for the Rd group), anemia (11.8% vs. 19.7%), lymphopenia (15.1% vs. 10.7%), and pneumonia (13.7% vs. 7.9%).
Janssen’s daratumumab (Darzalex) has picked up a sixth adult multiple myeloma indication, this time in combination with lenalidomide (Revlimid) and dexamethasone in newly diagnosed patients ineligible for autologous stem cell transplants.
The phase 3 MAIA trial found that 97 of 368 patients (26.4%) treated with the combination – dubbed DRd – progressed or died at a median follow-up of 28 months, versus 143 of 269 (38.8%) treated with lenalidomide and dexamethasone alone (Rd). An estimated 55.6% of patients on lenalidomide and dexamethasone, versus 70.6% with the daratumumab add-on, were alive without progression at 30 months (N Engl J Med. 2019 May 30;380[22]:2104-15).
Previously approved indications for daratumumab include relapsed or refractory disease after at least one other therapy; and combination treatment with bortezomib, melphalan, and prednisone, also in newly diagnosed patients who are ineligible for transplant.
The most common grade 3 and 4 adverse events reported in the MAIA trial were neutropenia (50.0% for the DRd group versus 35.3% for the Rd group), anemia (11.8% vs. 19.7%), lymphopenia (15.1% vs. 10.7%), and pneumonia (13.7% vs. 7.9%).
Cryptosporidiosis infections spike during summer swim season
Outbreaks of cryptosporidiosis increased in the United States by an average of 13% each year between 2009 and 2017, based on data from the Centers for Disease Control and Prevention.
In a study published in the CDC’s Morbidity and Mortality Weekly Report, researchers reviewed data from 444 reported outbreaks submitted to the CDC’s National Outbreak Reporting System totaling 7,465 cases, including 287 hospitalizations and one death.
The outbreaks during this period were most commonly associated with pools and water parks (35%), exposure to cattle (15%), and child care settings (13%). Another 3% of outbreaks were associated with drinking unpasteurized milk or apple cider. An outbreak was defined as two or more cases linked to a common source.
The profuse, watery diarrhea associated with infection from the cryptosporidium parasite can last for 3 weeks in healthy individuals and can cause life-threatening malnutrition in the immunocompromised, wrote Radhika Gharpure, DVM, of the CDC’s National Center for Emerging and Zoonotic Infectious Diseases, and colleagues.
The overall number of outbreaks peaked during July and August each year; the number associated with pools and water parks peaked between June and August, the number associated with cattle peaked between March and May, and the number associated with child care settings peaked between July and September.
The results were limited by several factors including likely underestimation of the number of outbreaks, the use of multipathogen testing panels that could have inflated the number of outbreaks, and the variation in the ability of jurisdictions to detect, investigate, and report outbreaks, the researchers noted. CryptoNet, a molecularly-based surveillance system, has shown potential to track disease transmission, they said.
However, primary prevention is important to prevent the spread of disease, and strategies include refraining from swimming when one has diarrhea and for 2 weeks after resolution of diarrhea, not sending children to child care when they have diarrhea, and washing hands thoroughly after contact with animals, the researchers said.
“If a cryptosporidiosis outbreak occurs, substantial decontamination measures are needed, including hyperchlorinating public treated recreational water venues (e.g., swimming pools at a hotel, apartment complex, or water park) and using hydrogen peroxide to disinfect surfaces in child care settings to inactivate Cryptosporidium oocysts,” they emphasized.
The researchers had no financial conflicts to disclose.
SOURCE: Gharpure R et al. MMWR. 2019 June 28. 68:568-72.
Outbreaks of cryptosporidiosis increased in the United States by an average of 13% each year between 2009 and 2017, based on data from the Centers for Disease Control and Prevention.
In a study published in the CDC’s Morbidity and Mortality Weekly Report, researchers reviewed data from 444 reported outbreaks submitted to the CDC’s National Outbreak Reporting System totaling 7,465 cases, including 287 hospitalizations and one death.
The outbreaks during this period were most commonly associated with pools and water parks (35%), exposure to cattle (15%), and child care settings (13%). Another 3% of outbreaks were associated with drinking unpasteurized milk or apple cider. An outbreak was defined as two or more cases linked to a common source.
The profuse, watery diarrhea associated with infection from the cryptosporidium parasite can last for 3 weeks in healthy individuals and can cause life-threatening malnutrition in the immunocompromised, wrote Radhika Gharpure, DVM, of the CDC’s National Center for Emerging and Zoonotic Infectious Diseases, and colleagues.
The overall number of outbreaks peaked during July and August each year; the number associated with pools and water parks peaked between June and August, the number associated with cattle peaked between March and May, and the number associated with child care settings peaked between July and September.
The results were limited by several factors including likely underestimation of the number of outbreaks, the use of multipathogen testing panels that could have inflated the number of outbreaks, and the variation in the ability of jurisdictions to detect, investigate, and report outbreaks, the researchers noted. CryptoNet, a molecularly-based surveillance system, has shown potential to track disease transmission, they said.
However, primary prevention is important to prevent the spread of disease, and strategies include refraining from swimming when one has diarrhea and for 2 weeks after resolution of diarrhea, not sending children to child care when they have diarrhea, and washing hands thoroughly after contact with animals, the researchers said.
“If a cryptosporidiosis outbreak occurs, substantial decontamination measures are needed, including hyperchlorinating public treated recreational water venues (e.g., swimming pools at a hotel, apartment complex, or water park) and using hydrogen peroxide to disinfect surfaces in child care settings to inactivate Cryptosporidium oocysts,” they emphasized.
The researchers had no financial conflicts to disclose.
SOURCE: Gharpure R et al. MMWR. 2019 June 28. 68:568-72.
Outbreaks of cryptosporidiosis increased in the United States by an average of 13% each year between 2009 and 2017, based on data from the Centers for Disease Control and Prevention.
In a study published in the CDC’s Morbidity and Mortality Weekly Report, researchers reviewed data from 444 reported outbreaks submitted to the CDC’s National Outbreak Reporting System totaling 7,465 cases, including 287 hospitalizations and one death.
The outbreaks during this period were most commonly associated with pools and water parks (35%), exposure to cattle (15%), and child care settings (13%). Another 3% of outbreaks were associated with drinking unpasteurized milk or apple cider. An outbreak was defined as two or more cases linked to a common source.
The profuse, watery diarrhea associated with infection from the cryptosporidium parasite can last for 3 weeks in healthy individuals and can cause life-threatening malnutrition in the immunocompromised, wrote Radhika Gharpure, DVM, of the CDC’s National Center for Emerging and Zoonotic Infectious Diseases, and colleagues.
The overall number of outbreaks peaked during July and August each year; the number associated with pools and water parks peaked between June and August, the number associated with cattle peaked between March and May, and the number associated with child care settings peaked between July and September.
The results were limited by several factors including likely underestimation of the number of outbreaks, the use of multipathogen testing panels that could have inflated the number of outbreaks, and the variation in the ability of jurisdictions to detect, investigate, and report outbreaks, the researchers noted. CryptoNet, a molecularly-based surveillance system, has shown potential to track disease transmission, they said.
However, primary prevention is important to prevent the spread of disease, and strategies include refraining from swimming when one has diarrhea and for 2 weeks after resolution of diarrhea, not sending children to child care when they have diarrhea, and washing hands thoroughly after contact with animals, the researchers said.
“If a cryptosporidiosis outbreak occurs, substantial decontamination measures are needed, including hyperchlorinating public treated recreational water venues (e.g., swimming pools at a hotel, apartment complex, or water park) and using hydrogen peroxide to disinfect surfaces in child care settings to inactivate Cryptosporidium oocysts,” they emphasized.
The researchers had no financial conflicts to disclose.
SOURCE: Gharpure R et al. MMWR. 2019 June 28. 68:568-72.
FROM MMWR