User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
First-line bevacizumab-osimertinib disappoint in EGFR-mutant NSCLC
Median progression-free survival (PFS) was 20.2 months in 61 patients in the osimertinib monotherapy arm and 22.1 months in 61 patients in the combination treatment arm (hazard ratio, 0.862), Hirotsugu Kenmotsu, MD, PhD, reported at the 2021 Congress of the European Society for Medical Oncology Sept. 18 (abstract LBA44).
“The study did not meet the primary endpoint,” said Dr. Kenmotsu of Shizuoka Cancer Center, Nagaizumi, Japan. “One-year progression-free survival was 63.7% and 73.8%, respectively.
However, subgroup analyses showed a trend toward improved PFS with combination bevacizumab and osimertinib in ever-smokers (HR, 0.481) and patients with Del19 mutations (HR, 0.622), he said.
Bevacizumab was also associated with a significant reduction in the risk of pneumonitis, an interstitial lung disease (ILD): Pneumonitis occurred in 18.3% of patients in the combination therapy arm, compared with 3.3% in the osimertinib monotherapy arm.
Study participants were untreated patients with advanced nonsquamous NSCLC harboring an EGFR-sensitizing mutation – either Del19 or L858R – without symptomatic brain metastases. They were enrolled between January 2018 and September 2018 and randomized to receive 80 mg of osimertinib daily, either alone or with 15 mg/kg of bevacizumab every 3 weeks.
The objective response rate was 82% in the combination therapy arm and 86% in osimertinib monotherapy arm, Dr. Kenmotsu said, adding that overall survival data are not yet mature.
Grade 3-4 adverse events occurred in 34 patients (56%) in the combination therapy arm and in 29 patients (48%) in the osimertinib monotherapy arm, he noted.
Osimertinib, a third-generation EGFR tyrosine kinase inhibitor has been a standard first-line treatment for NSCLC harboring activating EGFR mutations, he explained, noting that prior studies have shown promise for improved PFS with the addition of antivascular endothelial growth factor inhibitors to first-generation EGFR TKIs in this population.
Although the current study failed to show efficacy of the combination therapy versus osimertinib monotherapy for improving PFS in nonsquamous NSCLC harboring EGFR mutation, ever-smokers and patients with exon 19 deletions might benefit from the combination therapy as first-line treatment, and the combination might also reduce the risk of osimertinib-related pneumonitis, Dr. Kenmotsu said.
The study is among those that address “really important questions in lung cancer today,” said invited discussant Natasha B. Leighl, MD, professor of medicine at the University of Toronto’s Princess Margaret Cancer Center.
“I certainly agree with the authors that this study is a negative trial and bevacizumab does not improve PFS over the standard of osimertinib alone,” she said, acknowledging that the study is the first randomized comparison of the two treatment approaches in the first-line setting. She also agreed with the authors that the subgroup findings are intriguing.
“But ... what is the biomarker?” she asked, referring to the “very interesting” finding of a possible bevacizumab benefit among ever-smokers. “I’m looking forward to more correlative studies to help define this further.”
The novel finding of a significantly reduced risk of pneumonitis with the addition of bevacizumab, on the other hand, is “extremely exciting,” she said, explaining that the combination therapy approach could “perhaps [be used] as a potential therapy for patients with TKI-induced ILD and no other options, or those at very high risk of ILD, for example, perhaps, post immunotherapy or in high-risk populations.”
This study was funded by AstraZeneca. Dr. Kenmotsu and Dr. Leigh each disclosed financial relationships with numerous pharmaceutical companies.
This article was updated Sept. 24, 2021.
Median progression-free survival (PFS) was 20.2 months in 61 patients in the osimertinib monotherapy arm and 22.1 months in 61 patients in the combination treatment arm (hazard ratio, 0.862), Hirotsugu Kenmotsu, MD, PhD, reported at the 2021 Congress of the European Society for Medical Oncology Sept. 18 (abstract LBA44).
“The study did not meet the primary endpoint,” said Dr. Kenmotsu of Shizuoka Cancer Center, Nagaizumi, Japan. “One-year progression-free survival was 63.7% and 73.8%, respectively.
However, subgroup analyses showed a trend toward improved PFS with combination bevacizumab and osimertinib in ever-smokers (HR, 0.481) and patients with Del19 mutations (HR, 0.622), he said.
Bevacizumab was also associated with a significant reduction in the risk of pneumonitis, an interstitial lung disease (ILD): Pneumonitis occurred in 18.3% of patients in the combination therapy arm, compared with 3.3% in the osimertinib monotherapy arm.
Study participants were untreated patients with advanced nonsquamous NSCLC harboring an EGFR-sensitizing mutation – either Del19 or L858R – without symptomatic brain metastases. They were enrolled between January 2018 and September 2018 and randomized to receive 80 mg of osimertinib daily, either alone or with 15 mg/kg of bevacizumab every 3 weeks.
The objective response rate was 82% in the combination therapy arm and 86% in osimertinib monotherapy arm, Dr. Kenmotsu said, adding that overall survival data are not yet mature.
Grade 3-4 adverse events occurred in 34 patients (56%) in the combination therapy arm and in 29 patients (48%) in the osimertinib monotherapy arm, he noted.
Osimertinib, a third-generation EGFR tyrosine kinase inhibitor has been a standard first-line treatment for NSCLC harboring activating EGFR mutations, he explained, noting that prior studies have shown promise for improved PFS with the addition of antivascular endothelial growth factor inhibitors to first-generation EGFR TKIs in this population.
Although the current study failed to show efficacy of the combination therapy versus osimertinib monotherapy for improving PFS in nonsquamous NSCLC harboring EGFR mutation, ever-smokers and patients with exon 19 deletions might benefit from the combination therapy as first-line treatment, and the combination might also reduce the risk of osimertinib-related pneumonitis, Dr. Kenmotsu said.
The study is among those that address “really important questions in lung cancer today,” said invited discussant Natasha B. Leighl, MD, professor of medicine at the University of Toronto’s Princess Margaret Cancer Center.
“I certainly agree with the authors that this study is a negative trial and bevacizumab does not improve PFS over the standard of osimertinib alone,” she said, acknowledging that the study is the first randomized comparison of the two treatment approaches in the first-line setting. She also agreed with the authors that the subgroup findings are intriguing.
“But ... what is the biomarker?” she asked, referring to the “very interesting” finding of a possible bevacizumab benefit among ever-smokers. “I’m looking forward to more correlative studies to help define this further.”
The novel finding of a significantly reduced risk of pneumonitis with the addition of bevacizumab, on the other hand, is “extremely exciting,” she said, explaining that the combination therapy approach could “perhaps [be used] as a potential therapy for patients with TKI-induced ILD and no other options, or those at very high risk of ILD, for example, perhaps, post immunotherapy or in high-risk populations.”
This study was funded by AstraZeneca. Dr. Kenmotsu and Dr. Leigh each disclosed financial relationships with numerous pharmaceutical companies.
This article was updated Sept. 24, 2021.
Median progression-free survival (PFS) was 20.2 months in 61 patients in the osimertinib monotherapy arm and 22.1 months in 61 patients in the combination treatment arm (hazard ratio, 0.862), Hirotsugu Kenmotsu, MD, PhD, reported at the 2021 Congress of the European Society for Medical Oncology Sept. 18 (abstract LBA44).
“The study did not meet the primary endpoint,” said Dr. Kenmotsu of Shizuoka Cancer Center, Nagaizumi, Japan. “One-year progression-free survival was 63.7% and 73.8%, respectively.
However, subgroup analyses showed a trend toward improved PFS with combination bevacizumab and osimertinib in ever-smokers (HR, 0.481) and patients with Del19 mutations (HR, 0.622), he said.
Bevacizumab was also associated with a significant reduction in the risk of pneumonitis, an interstitial lung disease (ILD): Pneumonitis occurred in 18.3% of patients in the combination therapy arm, compared with 3.3% in the osimertinib monotherapy arm.
Study participants were untreated patients with advanced nonsquamous NSCLC harboring an EGFR-sensitizing mutation – either Del19 or L858R – without symptomatic brain metastases. They were enrolled between January 2018 and September 2018 and randomized to receive 80 mg of osimertinib daily, either alone or with 15 mg/kg of bevacizumab every 3 weeks.
The objective response rate was 82% in the combination therapy arm and 86% in osimertinib monotherapy arm, Dr. Kenmotsu said, adding that overall survival data are not yet mature.
Grade 3-4 adverse events occurred in 34 patients (56%) in the combination therapy arm and in 29 patients (48%) in the osimertinib monotherapy arm, he noted.
Osimertinib, a third-generation EGFR tyrosine kinase inhibitor has been a standard first-line treatment for NSCLC harboring activating EGFR mutations, he explained, noting that prior studies have shown promise for improved PFS with the addition of antivascular endothelial growth factor inhibitors to first-generation EGFR TKIs in this population.
Although the current study failed to show efficacy of the combination therapy versus osimertinib monotherapy for improving PFS in nonsquamous NSCLC harboring EGFR mutation, ever-smokers and patients with exon 19 deletions might benefit from the combination therapy as first-line treatment, and the combination might also reduce the risk of osimertinib-related pneumonitis, Dr. Kenmotsu said.
The study is among those that address “really important questions in lung cancer today,” said invited discussant Natasha B. Leighl, MD, professor of medicine at the University of Toronto’s Princess Margaret Cancer Center.
“I certainly agree with the authors that this study is a negative trial and bevacizumab does not improve PFS over the standard of osimertinib alone,” she said, acknowledging that the study is the first randomized comparison of the two treatment approaches in the first-line setting. She also agreed with the authors that the subgroup findings are intriguing.
“But ... what is the biomarker?” she asked, referring to the “very interesting” finding of a possible bevacizumab benefit among ever-smokers. “I’m looking forward to more correlative studies to help define this further.”
The novel finding of a significantly reduced risk of pneumonitis with the addition of bevacizumab, on the other hand, is “extremely exciting,” she said, explaining that the combination therapy approach could “perhaps [be used] as a potential therapy for patients with TKI-induced ILD and no other options, or those at very high risk of ILD, for example, perhaps, post immunotherapy or in high-risk populations.”
This study was funded by AstraZeneca. Dr. Kenmotsu and Dr. Leigh each disclosed financial relationships with numerous pharmaceutical companies.
This article was updated Sept. 24, 2021.
FROM ESMO 2021
Combination treatment shows promise for men with advanced prostate cancer
The findings were specific to patients not yet been treated with chemotherapy and whose tumors were positive for homologous recombination deficiency (HRD). However, for patients whose tumors were negative for HRD, the clinical activity was limited, said Daniel P. Petrylak, MD, Yale University, New Haven, Conn., and lead investigator for the study called CheckMate 9KD (NCT03338790) .
The patients who were included in all CheckMate 9KD cohorts had no prior treatment with targeted T-cell co-stimulation or immune checkpoint pathways. They had metastatic castrate resistant prostate cancer with documented disease progression, ECOG performance status of 0-1, and tissue available for HRD testing.
Dr. Petrylak offered an updated analysis of cohort A2 with 71 patients (median age 73 years), all of whom had received 1-2 prior new hormonal therapies in the pre-chemotherapy setting. Patients who had received prior PARP inhibitors were ineligible, as were those who refused chemotherapy treatment.
ORR/PSA RR primary endpoints
Patients received nivolumab and rucaparib, nivolumab at 480 mg (q4 weeks up to 2 years) and rucaparib at 600 mg b.i.d., until disease progression or unacceptable toxicity. Objective response rate and PSA response rate (PSA-RR) were the primary endpoint, with overall survival as a secondary endpoint, along with time to objective response, duration of objective response, time to PSA progression, safety, and radiographic progression-free survival.
Median follow-up was 17.5 months with median treatment duration of 4.6 months in the nivolumab group and 5.5 months for rucaparib. At the time of the final database lock in March 2021, 65 patients (91.5%) had discontinued treatment, most often for disease progression (n = 43; 60.6%) or study drug toxicity (n = 8; 11.3%). Four patients (5.6%) remained on treatment.
Better responses for HRD and BRCA 1/2 positive
Stratifying response outcomes showed higher rates for patients who were HRD positive and BRCA1/2 positive for confirmed objective response rate (HRD+ 25.0%, BRCA 1/2+ 33.3%, HRD-/not evaluable 5.3%, all patients 15.4%) and for PSA response (HRD+ 41.9%, BRCA 1/2+ 84.6%, HRD-/not evaluable 14.3%, all patients 27.3%). Partial response rates were 33.3% for BRCA 1/2, 25.0% for HRD positive, 5.3% for HRD- and 15.4% for all patients. Radiographic progression-free survival was longer in the HRD positive group at a median of 10.9 months (95% CI 6.7-12.0), compared with 5.6 months (3.7-9.1) in the HRD-/not evaluable group. Overall survival was similar in the HRD negative group/not evaluable group at 19.0 months (8.2-22.1) and the HRD positive group at 22.7 months (14.1-NE).
Safety profile as expected
Treatment-related adverse events were reported for most patients (64/71, 90.1%), with grade 3-4 events in about half (50.7%). The most common event was grade 1-2 nausea (40.8%), with anemia at 32.4% and alanine aminotransferase (ALT) increases and fatigue both at 28.2%. Adverse events led to discontinuation in 23.9% of patients, with anemia and increased ALT leading both at 4.2%. Grade 3-4 adverse events led to discontinuation in 15.5% of patients. Investigators reported no treatment-related deaths. “The safety profile of nivolumab plus rucaparib was as expected based on the individual components with no new safety signals,” Dr. Petrylak said.
Longer follow-up is needed, Dr. Petrylak added, to better characterize the clinical benefits of adding nivolumab to rucaparib for this population.
Discussion moderator Guilia Baciarello, MD, Milan, asked how much nivolumab added to the rucaparib benefit. Dr. Petrylak responded, “We really can’t determine how much it’s adding because the single-agent data, particularly with the checkpoints, is generally very low. I can’t recall any published data with nivolumab as a single agent, but for example with pembrolizumab or atezolizumab in unselected patients it’s 5%-10%. So, we really can’t tell how much nivolumab added in the BRCA positive patients.”
Dr. Baciarello asked, “Will there be a nivolumab versus rucaparib trial in HRD positive patients?”
“I think that’s something that needs to be considered. I think we may also want to consider doing a broader phase II in that group of patients to really nail down the signal. That’s under discussion,” Dr. Petrylak said.
The study was funded by Bristol Myers Squibb. Dr. Petrylak disclosed numerous financial interests including personal and consulting fees.
This article was updated Sept. 24, 2021.
The findings were specific to patients not yet been treated with chemotherapy and whose tumors were positive for homologous recombination deficiency (HRD). However, for patients whose tumors were negative for HRD, the clinical activity was limited, said Daniel P. Petrylak, MD, Yale University, New Haven, Conn., and lead investigator for the study called CheckMate 9KD (NCT03338790) .
The patients who were included in all CheckMate 9KD cohorts had no prior treatment with targeted T-cell co-stimulation or immune checkpoint pathways. They had metastatic castrate resistant prostate cancer with documented disease progression, ECOG performance status of 0-1, and tissue available for HRD testing.
Dr. Petrylak offered an updated analysis of cohort A2 with 71 patients (median age 73 years), all of whom had received 1-2 prior new hormonal therapies in the pre-chemotherapy setting. Patients who had received prior PARP inhibitors were ineligible, as were those who refused chemotherapy treatment.
ORR/PSA RR primary endpoints
Patients received nivolumab and rucaparib, nivolumab at 480 mg (q4 weeks up to 2 years) and rucaparib at 600 mg b.i.d., until disease progression or unacceptable toxicity. Objective response rate and PSA response rate (PSA-RR) were the primary endpoint, with overall survival as a secondary endpoint, along with time to objective response, duration of objective response, time to PSA progression, safety, and radiographic progression-free survival.
Median follow-up was 17.5 months with median treatment duration of 4.6 months in the nivolumab group and 5.5 months for rucaparib. At the time of the final database lock in March 2021, 65 patients (91.5%) had discontinued treatment, most often for disease progression (n = 43; 60.6%) or study drug toxicity (n = 8; 11.3%). Four patients (5.6%) remained on treatment.
Better responses for HRD and BRCA 1/2 positive
Stratifying response outcomes showed higher rates for patients who were HRD positive and BRCA1/2 positive for confirmed objective response rate (HRD+ 25.0%, BRCA 1/2+ 33.3%, HRD-/not evaluable 5.3%, all patients 15.4%) and for PSA response (HRD+ 41.9%, BRCA 1/2+ 84.6%, HRD-/not evaluable 14.3%, all patients 27.3%). Partial response rates were 33.3% for BRCA 1/2, 25.0% for HRD positive, 5.3% for HRD- and 15.4% for all patients. Radiographic progression-free survival was longer in the HRD positive group at a median of 10.9 months (95% CI 6.7-12.0), compared with 5.6 months (3.7-9.1) in the HRD-/not evaluable group. Overall survival was similar in the HRD negative group/not evaluable group at 19.0 months (8.2-22.1) and the HRD positive group at 22.7 months (14.1-NE).
Safety profile as expected
Treatment-related adverse events were reported for most patients (64/71, 90.1%), with grade 3-4 events in about half (50.7%). The most common event was grade 1-2 nausea (40.8%), with anemia at 32.4% and alanine aminotransferase (ALT) increases and fatigue both at 28.2%. Adverse events led to discontinuation in 23.9% of patients, with anemia and increased ALT leading both at 4.2%. Grade 3-4 adverse events led to discontinuation in 15.5% of patients. Investigators reported no treatment-related deaths. “The safety profile of nivolumab plus rucaparib was as expected based on the individual components with no new safety signals,” Dr. Petrylak said.
Longer follow-up is needed, Dr. Petrylak added, to better characterize the clinical benefits of adding nivolumab to rucaparib for this population.
Discussion moderator Guilia Baciarello, MD, Milan, asked how much nivolumab added to the rucaparib benefit. Dr. Petrylak responded, “We really can’t determine how much it’s adding because the single-agent data, particularly with the checkpoints, is generally very low. I can’t recall any published data with nivolumab as a single agent, but for example with pembrolizumab or atezolizumab in unselected patients it’s 5%-10%. So, we really can’t tell how much nivolumab added in the BRCA positive patients.”
Dr. Baciarello asked, “Will there be a nivolumab versus rucaparib trial in HRD positive patients?”
“I think that’s something that needs to be considered. I think we may also want to consider doing a broader phase II in that group of patients to really nail down the signal. That’s under discussion,” Dr. Petrylak said.
The study was funded by Bristol Myers Squibb. Dr. Petrylak disclosed numerous financial interests including personal and consulting fees.
This article was updated Sept. 24, 2021.
The findings were specific to patients not yet been treated with chemotherapy and whose tumors were positive for homologous recombination deficiency (HRD). However, for patients whose tumors were negative for HRD, the clinical activity was limited, said Daniel P. Petrylak, MD, Yale University, New Haven, Conn., and lead investigator for the study called CheckMate 9KD (NCT03338790) .
The patients who were included in all CheckMate 9KD cohorts had no prior treatment with targeted T-cell co-stimulation or immune checkpoint pathways. They had metastatic castrate resistant prostate cancer with documented disease progression, ECOG performance status of 0-1, and tissue available for HRD testing.
Dr. Petrylak offered an updated analysis of cohort A2 with 71 patients (median age 73 years), all of whom had received 1-2 prior new hormonal therapies in the pre-chemotherapy setting. Patients who had received prior PARP inhibitors were ineligible, as were those who refused chemotherapy treatment.
ORR/PSA RR primary endpoints
Patients received nivolumab and rucaparib, nivolumab at 480 mg (q4 weeks up to 2 years) and rucaparib at 600 mg b.i.d., until disease progression or unacceptable toxicity. Objective response rate and PSA response rate (PSA-RR) were the primary endpoint, with overall survival as a secondary endpoint, along with time to objective response, duration of objective response, time to PSA progression, safety, and radiographic progression-free survival.
Median follow-up was 17.5 months with median treatment duration of 4.6 months in the nivolumab group and 5.5 months for rucaparib. At the time of the final database lock in March 2021, 65 patients (91.5%) had discontinued treatment, most often for disease progression (n = 43; 60.6%) or study drug toxicity (n = 8; 11.3%). Four patients (5.6%) remained on treatment.
Better responses for HRD and BRCA 1/2 positive
Stratifying response outcomes showed higher rates for patients who were HRD positive and BRCA1/2 positive for confirmed objective response rate (HRD+ 25.0%, BRCA 1/2+ 33.3%, HRD-/not evaluable 5.3%, all patients 15.4%) and for PSA response (HRD+ 41.9%, BRCA 1/2+ 84.6%, HRD-/not evaluable 14.3%, all patients 27.3%). Partial response rates were 33.3% for BRCA 1/2, 25.0% for HRD positive, 5.3% for HRD- and 15.4% for all patients. Radiographic progression-free survival was longer in the HRD positive group at a median of 10.9 months (95% CI 6.7-12.0), compared with 5.6 months (3.7-9.1) in the HRD-/not evaluable group. Overall survival was similar in the HRD negative group/not evaluable group at 19.0 months (8.2-22.1) and the HRD positive group at 22.7 months (14.1-NE).
Safety profile as expected
Treatment-related adverse events were reported for most patients (64/71, 90.1%), with grade 3-4 events in about half (50.7%). The most common event was grade 1-2 nausea (40.8%), with anemia at 32.4% and alanine aminotransferase (ALT) increases and fatigue both at 28.2%. Adverse events led to discontinuation in 23.9% of patients, with anemia and increased ALT leading both at 4.2%. Grade 3-4 adverse events led to discontinuation in 15.5% of patients. Investigators reported no treatment-related deaths. “The safety profile of nivolumab plus rucaparib was as expected based on the individual components with no new safety signals,” Dr. Petrylak said.
Longer follow-up is needed, Dr. Petrylak added, to better characterize the clinical benefits of adding nivolumab to rucaparib for this population.
Discussion moderator Guilia Baciarello, MD, Milan, asked how much nivolumab added to the rucaparib benefit. Dr. Petrylak responded, “We really can’t determine how much it’s adding because the single-agent data, particularly with the checkpoints, is generally very low. I can’t recall any published data with nivolumab as a single agent, but for example with pembrolizumab or atezolizumab in unselected patients it’s 5%-10%. So, we really can’t tell how much nivolumab added in the BRCA positive patients.”
Dr. Baciarello asked, “Will there be a nivolumab versus rucaparib trial in HRD positive patients?”
“I think that’s something that needs to be considered. I think we may also want to consider doing a broader phase II in that group of patients to really nail down the signal. That’s under discussion,” Dr. Petrylak said.
The study was funded by Bristol Myers Squibb. Dr. Petrylak disclosed numerous financial interests including personal and consulting fees.
This article was updated Sept. 24, 2021.
FROM ESMO 2021
Early vs. late TNFi switch in AS patients associated with different risk factors
Older age, higher subjective disease activity, and exercising for more than 120 minutes per week were three factors linked to patients with ankylosing spondylitis (AS) who switched from their original tumor necrosis factor inhibitor (TNFi) treatment within 2 years in a U.S.-based study.

Data from the Prospective Study of Outcomes in Ankylosing Spondylitis (PSOAS) also found that higher levels of inflammation, but not radiographic disease, were linked to patients changing from one TNFi to another, or to an interleukin (IL)-17 inhibitor or Janus kinase (JAK) inhibitor.
“Different factors were associated in AS patients who switch from their initial TNF inhibitor to another TNF inhibitor, IL-17 inhibitor, or JAK inhibitor within 2 years versus after 2 years of treatment,” John D. Reveille, MD, professor and vice chair of rheumatology and clinical immunogenetics with McGovern Medical School at UTHealth Houston, said at the 12th International Congress on Spondyloarthritides.
“We’re currently looking at different approaches to analyzing these data. And, certainly, this needs need to be looked at in other cohorts,” Dr. Reveille said.
PSOAS is a prospective observational cohort study that has been looking at predictors of AS severity for almost 20 years. Started in 2002, the study has routinely collected a whole host of data on various demographic and disease-related factors.
The reasoning behind the current analysis of PSOAS data was that a relatively recent study based on a commercial claims database had found that many patients with AS do not remain on their initial TNFi 2 years after initiation. So, Dr. Reveille and associates decided to look at the factors that could be influencing whether patients who started a TNFi would remain on their original drug in the PSOAS cohort.
In all, 533 patients from the PSOAS cohort who had at least 2 years of follow-up were included in the analysis. The majority (n = 496) were treated with a TNFi, 34 had received an IL-17 inhibitor, and 3 had received a JAK inhibitor.
Of the 496 patients treated with a TNFi, almost 70% (n = 344) persisted with this treatment for the duration of the study. Of those that switched to another TNFi or IL-17 or JAK inhibitor treatment, 20% (n = 101) did so within 2 years and the remaining 10% (n = 51) after 2 years.
Multinominal logistic regression modeling revealed a number of different factors that were associated with switching within 2 years versus switching after 2 years.
Compared to patients who persisted with treatment throughout the study period, patients who switched from their original TNFi within 2 years were more likely to be older (odds ratio [OR], 2.0 for ≥ 40 vs. < 40 years; P = .002), have a higher Bath Ankylosing Spondyloarthritis Disease Activity Index (BASDAI) score at baseline (OR, 1.73 for ≥ 4 vs. < 4; P = .03), higher C-reactive protein levels (OR, 1.94 for ≥ 0.8 mg/dL vs. < 0.8 mg/dL, P = .004), and greater weekly duration of exercise (OR, 1.95 for ≥ 120 minutes per week vs. < 120; P <.001).
Switchers also were less likely to have severe radiographic disease at baseline, as determined by the modified Stoke Ankylosing Spondylitis Spinal Score (mSASSS, OR, 0.63; P = .03), and less likely to be current smokers (OR, 0.69; P < .001).
Factors associated with switching after 2 years versus persisting with treatment were higher baseline BASDAI (OR, 2.31; P = .01), exercising more than 120 minutes per week (OR, 1.66; P = .03), and having more comorbidities (OR, 1.63 for ≥ 2 vs. < 2, P = .04).
However, patients who switched after 2 years were less likely to be depressed (OR, 0.35; P = .002) or to have a longer baseline disease duration (OR, 0.27 for ≥ 20 years vs. < 20 years P < .001).
The association observed between switching within 2 years and lower likelihood of currently smoking was a “little bit puzzling,” one delegate said after Dr. Reveille’s presentation. “The opposite has been shown in the literature, and current smokers seem to be refractory to TNF inhibitor therapy,” the delegate observed.
“I was confounded when I saw the data,” Dr. Reveille acknowledged. Because this was an observational study, this finding needs more investigation, he agreed. “Interestingly, we have seen this negative association with some other parameters, too,” he added.
The HLA-B27 carrier and radiographic status were carefully checked, so there should not be a problem with the diagnosis, Dr. Reveille reassured. Further analyses of the findings are now warranted.
Funding for the study was provided by the U.S. Department of Health and Human Services, the National Institutes of Health, and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Additional funding was received from the Spondyloarthritis Association of America and Eli Lilly.
Dr. Reveille made no personal disclosures; a coauthor of the abstract was an employee of Eli Lilly.
Older age, higher subjective disease activity, and exercising for more than 120 minutes per week were three factors linked to patients with ankylosing spondylitis (AS) who switched from their original tumor necrosis factor inhibitor (TNFi) treatment within 2 years in a U.S.-based study.
Data from the Prospective Study of Outcomes in Ankylosing Spondylitis (PSOAS) also found that higher levels of inflammation, but not radiographic disease, were linked to patients changing from one TNFi to another, or to an interleukin (IL)-17 inhibitor or Janus kinase (JAK) inhibitor.
“Different factors were associated in AS patients who switch from their initial TNF inhibitor to another TNF inhibitor, IL-17 inhibitor, or JAK inhibitor within 2 years versus after 2 years of treatment,” John D. Reveille, MD, professor and vice chair of rheumatology and clinical immunogenetics with McGovern Medical School at UTHealth Houston, said at the 12th International Congress on Spondyloarthritides.
“We’re currently looking at different approaches to analyzing these data. And, certainly, this needs need to be looked at in other cohorts,” Dr. Reveille said.
PSOAS is a prospective observational cohort study that has been looking at predictors of AS severity for almost 20 years. Started in 2002, the study has routinely collected a whole host of data on various demographic and disease-related factors.
The reasoning behind the current analysis of PSOAS data was that a relatively recent study based on a commercial claims database had found that many patients with AS do not remain on their initial TNFi 2 years after initiation. So, Dr. Reveille and associates decided to look at the factors that could be influencing whether patients who started a TNFi would remain on their original drug in the PSOAS cohort.
In all, 533 patients from the PSOAS cohort who had at least 2 years of follow-up were included in the analysis. The majority (n = 496) were treated with a TNFi, 34 had received an IL-17 inhibitor, and 3 had received a JAK inhibitor.
Of the 496 patients treated with a TNFi, almost 70% (n = 344) persisted with this treatment for the duration of the study. Of those that switched to another TNFi or IL-17 or JAK inhibitor treatment, 20% (n = 101) did so within 2 years and the remaining 10% (n = 51) after 2 years.
Multinominal logistic regression modeling revealed a number of different factors that were associated with switching within 2 years versus switching after 2 years.
Compared to patients who persisted with treatment throughout the study period, patients who switched from their original TNFi within 2 years were more likely to be older (odds ratio [OR], 2.0 for ≥ 40 vs. < 40 years; P = .002), have a higher Bath Ankylosing Spondyloarthritis Disease Activity Index (BASDAI) score at baseline (OR, 1.73 for ≥ 4 vs. < 4; P = .03), higher C-reactive protein levels (OR, 1.94 for ≥ 0.8 mg/dL vs. < 0.8 mg/dL, P = .004), and greater weekly duration of exercise (OR, 1.95 for ≥ 120 minutes per week vs. < 120; P <.001).
Switchers also were less likely to have severe radiographic disease at baseline, as determined by the modified Stoke Ankylosing Spondylitis Spinal Score (mSASSS, OR, 0.63; P = .03), and less likely to be current smokers (OR, 0.69; P < .001).
Factors associated with switching after 2 years versus persisting with treatment were higher baseline BASDAI (OR, 2.31; P = .01), exercising more than 120 minutes per week (OR, 1.66; P = .03), and having more comorbidities (OR, 1.63 for ≥ 2 vs. < 2, P = .04).
However, patients who switched after 2 years were less likely to be depressed (OR, 0.35; P = .002) or to have a longer baseline disease duration (OR, 0.27 for ≥ 20 years vs. < 20 years P < .001).
The association observed between switching within 2 years and lower likelihood of currently smoking was a “little bit puzzling,” one delegate said after Dr. Reveille’s presentation. “The opposite has been shown in the literature, and current smokers seem to be refractory to TNF inhibitor therapy,” the delegate observed.
“I was confounded when I saw the data,” Dr. Reveille acknowledged. Because this was an observational study, this finding needs more investigation, he agreed. “Interestingly, we have seen this negative association with some other parameters, too,” he added.
The HLA-B27 carrier and radiographic status were carefully checked, so there should not be a problem with the diagnosis, Dr. Reveille reassured. Further analyses of the findings are now warranted.
Funding for the study was provided by the U.S. Department of Health and Human Services, the National Institutes of Health, and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Additional funding was received from the Spondyloarthritis Association of America and Eli Lilly.
Dr. Reveille made no personal disclosures; a coauthor of the abstract was an employee of Eli Lilly.
Older age, higher subjective disease activity, and exercising for more than 120 minutes per week were three factors linked to patients with ankylosing spondylitis (AS) who switched from their original tumor necrosis factor inhibitor (TNFi) treatment within 2 years in a U.S.-based study.
Data from the Prospective Study of Outcomes in Ankylosing Spondylitis (PSOAS) also found that higher levels of inflammation, but not radiographic disease, were linked to patients changing from one TNFi to another, or to an interleukin (IL)-17 inhibitor or Janus kinase (JAK) inhibitor.
“Different factors were associated in AS patients who switch from their initial TNF inhibitor to another TNF inhibitor, IL-17 inhibitor, or JAK inhibitor within 2 years versus after 2 years of treatment,” John D. Reveille, MD, professor and vice chair of rheumatology and clinical immunogenetics with McGovern Medical School at UTHealth Houston, said at the 12th International Congress on Spondyloarthritides.
“We’re currently looking at different approaches to analyzing these data. And, certainly, this needs need to be looked at in other cohorts,” Dr. Reveille said.
PSOAS is a prospective observational cohort study that has been looking at predictors of AS severity for almost 20 years. Started in 2002, the study has routinely collected a whole host of data on various demographic and disease-related factors.
The reasoning behind the current analysis of PSOAS data was that a relatively recent study based on a commercial claims database had found that many patients with AS do not remain on their initial TNFi 2 years after initiation. So, Dr. Reveille and associates decided to look at the factors that could be influencing whether patients who started a TNFi would remain on their original drug in the PSOAS cohort.
In all, 533 patients from the PSOAS cohort who had at least 2 years of follow-up were included in the analysis. The majority (n = 496) were treated with a TNFi, 34 had received an IL-17 inhibitor, and 3 had received a JAK inhibitor.
Of the 496 patients treated with a TNFi, almost 70% (n = 344) persisted with this treatment for the duration of the study. Of those that switched to another TNFi or IL-17 or JAK inhibitor treatment, 20% (n = 101) did so within 2 years and the remaining 10% (n = 51) after 2 years.
Multinominal logistic regression modeling revealed a number of different factors that were associated with switching within 2 years versus switching after 2 years.
Compared to patients who persisted with treatment throughout the study period, patients who switched from their original TNFi within 2 years were more likely to be older (odds ratio [OR], 2.0 for ≥ 40 vs. < 40 years; P = .002), have a higher Bath Ankylosing Spondyloarthritis Disease Activity Index (BASDAI) score at baseline (OR, 1.73 for ≥ 4 vs. < 4; P = .03), higher C-reactive protein levels (OR, 1.94 for ≥ 0.8 mg/dL vs. < 0.8 mg/dL, P = .004), and greater weekly duration of exercise (OR, 1.95 for ≥ 120 minutes per week vs. < 120; P <.001).
Switchers also were less likely to have severe radiographic disease at baseline, as determined by the modified Stoke Ankylosing Spondylitis Spinal Score (mSASSS, OR, 0.63; P = .03), and less likely to be current smokers (OR, 0.69; P < .001).
Factors associated with switching after 2 years versus persisting with treatment were higher baseline BASDAI (OR, 2.31; P = .01), exercising more than 120 minutes per week (OR, 1.66; P = .03), and having more comorbidities (OR, 1.63 for ≥ 2 vs. < 2, P = .04).
However, patients who switched after 2 years were less likely to be depressed (OR, 0.35; P = .002) or to have a longer baseline disease duration (OR, 0.27 for ≥ 20 years vs. < 20 years P < .001).
The association observed between switching within 2 years and lower likelihood of currently smoking was a “little bit puzzling,” one delegate said after Dr. Reveille’s presentation. “The opposite has been shown in the literature, and current smokers seem to be refractory to TNF inhibitor therapy,” the delegate observed.
“I was confounded when I saw the data,” Dr. Reveille acknowledged. Because this was an observational study, this finding needs more investigation, he agreed. “Interestingly, we have seen this negative association with some other parameters, too,” he added.
The HLA-B27 carrier and radiographic status were carefully checked, so there should not be a problem with the diagnosis, Dr. Reveille reassured. Further analyses of the findings are now warranted.
Funding for the study was provided by the U.S. Department of Health and Human Services, the National Institutes of Health, and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Additional funding was received from the Spondyloarthritis Association of America and Eli Lilly.
Dr. Reveille made no personal disclosures; a coauthor of the abstract was an employee of Eli Lilly.
FROM THE 2021 SPA CONGRESS
EASD: Precision in diabetes management and impact of COVID-19
The annual meeting of the European Association for the Study of Diabetes 2021 will delve into individualized approaches in diabetes management, particularly with regard to tailoring drug therapy for type 2 diabetes and management of type 1 diabetes.

The virtual meeting, taking place Sept. 28 to Oct. 1 in Central European Summer Time, will feature results from TriMASTER (a three-way cross-over trial of precision medicine strategy of second-/third-line therapy in type 2 diabetes), new subgroup analyses from the GRADE (Glycemia Reduction Approaches in Diabetes: A Comparative Effectiveness) study, the final version of a consensus statement on type 1 diabetes management, and new data on the dual incretin agonist tirzepatide, as well as much more.
“I’m a strong believer in personalization. I don’t think the big blockbuster [drugs] will serve the entire community with diabetes. Even in type 1 diabetes, there’s evidence of heterogeneity. ... We need a better way to identify individual needs. I think that’s where we’re going. ... It’s one of the themes of the conference,” EASD President Stefano Del Prato, MD, professor of endocrinology at the University of Pisa (Italy), told this news organization.
He noted that EASD and the American Diabetes Association have recently teamed up with other organizations to form the Precision Medicine in Diabetes Initiative
As would be expected, the meeting will also feature numerous presentations on the COVID-19 pandemic, including studies looking at how people with COVID-19 and diabetes have fared; how the pandemic has affected diabetes care; and the still unclear impact of SARS-CoV-2 on pancreatic beta cells and whether, in some instances, it triggers new-onset diabetes.
New data from previously reported trials
There will be new data from several previously reported trials focusing on specific groups of patients with type 2 diabetes. One is the EMPEROR-Preserved study of empagliflozin (Jardiance) in individuals with heart failure and preserved ejection fraction. Initially presented in August 2021 at the annual congress of the European Society of Cardiology, the new data will focus on patient subpopulations, efficacy endpoints, and safety in patients with and without diabetes. A companion study, EMPEROR-Reduced, in those with heart failure and reduced ejection fraction, was presented at the ESC Congress in August 2020.
New findings will also be presented from the DAPA-CKD study of dapagliflozin (Farxiga) in patients with chronic kidney disease. The study was stopped early in March 2020 because of overwhelming efficacy of the drug in preventing CKD. Now, the data will be analyzed in terms of metabolic, nephrology, and cardiology parameters.
And from FIDELIO-DKD and FIGARO-DKD, trials of the nonsteroidal mineralocorticoid receptor antagonist finerenone (Kerendia), new data will also focus on a variety of subgroups of individuals with type 2 diabetes and chronic kidney disease.
“Our goal is to cover most aspects of what’s happening in the type 2 diabetes field,” EASD Honorary Secretary Mikael Rydén, MD, PhD, professor and senior consultant in endocrinology at the Karolinska Institute and Karolinska University Hospital, Stockholm, said in an interview.
Dr. Rydén, who chairs the meeting’s scientific program committee, added: “We can only focus on so much every year but we try to be active and changing from year to year. I’m convinced that a clinician or translational researcher will definitely have a number of very interesting symposia to follow and learn new things. If you follow all of these things, you will know a lot about what’s cooking in the diabetes world.”
Consensus on type 1 diabetes management: Special considerations
Both Dr. Del Prato and Dr. Rydén cited presentation of the new type 1 diabetes ADA/EASD consensus report as among the most clinically important of the conference. Initially presented in draft form at the ADA Scientific Sessions in June 2021, the document aims to move away from routinely applying principles derived from studies of patients with type 2 diabetes to those with type 1 diabetes, an autoimmune disease with unique characteristics.
The final version of the document is expected to include information on goals of therapy, glycemic targets, prevention and management of hypoglycemia and diabetic ketoacidosis, psychosocial care, and special populations, among other issues. It is also expected to include a section dedicated to adjunctive treatments beyond insulin, including metformin, pramlintide, glucagonlike peptide–1 agonists, and sodium-glucose cotransporter 2 inhibitors for certain patients.
Dr. Del Prato noted, “From a clinical point of view, this is quite an important step that two major organizations came together recommending some strategies for treating type 2 diabetes ... It really deals with a big problem and tries to provide the tools for improving homogenization of the treatment of type 1 diabetes across the different health systems.”
And Dr. Rydén commented: “I think it’s really important to have, since there’s been so much focus on type 2 diabetes for the last few years, and to have the ADA and EASD getting together and actually write this.”
But Dr. Rydén also pointed out that outcomes data are much more conclusive for drugs in type 2 diabetes to inform international guidelines, whereas “this is much more difficult to demonstrate with type 1 diabetes. With a new pump or [continuous glucose monitor (CGM)] you might show a reduction in [hemoglobin] A1c of X percent or X mmol/mol or hypoglycemia events, but it’s much harder to show improvements in hard outcomes like deaths and cardiovascular events. I’m really looking forward to having this presented.”
Diabetes in 2021: It’s personal
Several meeting sessions will specifically address precision medicine approaches, including the TriMASTER study, which aims to identify subgroups of patients with type 2 diabetes who respond well or poorly to particular drugs based on clinical characteristics so that treatments can be better targeted to individuals. In total, 600 patients with type 2 diabetes and suboptimal glycemic control with metformin were randomized to a dipeptidyl peptidase–4 inhibitor, an SGLT2 inhibitor, or thiazolidinedione (TZD).
According to Dr. Rydén, “The TriMASTER final results will be interesting. TZDs still have a place. ... You can’t give them to people with heart failure, but I think like a carpenter you have to have many tools in your toolbox. And I still think that there are some individuals who respond well to pioglitazone. [The study findings] could be influential, depending on the results.”
An EASD/ADA symposium entitled “Optimizing diabetes diagnosis, prevention, and care: Is precision medicine the answer?” will offer three distinct perspectives, with one speaker arguing it’s the future of diabetes medicine, another that it isn’t, and a third explaining that “the devil is in the details.”
The Diabetologia symposium will focus on a related concept: The use of artificial intelligence in diabetes research and care, with particular application to glucose control, neuropathy, and wound healing.
And during the 36th Camillo Golgi Lecture, kidney disease expert H.J. Lambers Heerspink, PhD, of the University of Groningen (the Netherlands), will speak about personalizing treatment for patients with type 2 diabetes, arguing that “the mean is meaningless.”
Next-generation incretin therapy: Is weight loss the treatment?
New data will continue the buzz from the ADA meeting surrounding tirzepatide, the dual GLP-1 receptor agonist and glucose-dependent insulinotropic polypeptide agent.
A session will add new data from SURPASS-3 CGM, looking at the effect of the drug captured by continuous glucose monitoring in patients with type 2 diabetes; SURPASS-3 MRI, examining the effect of the drug on liver fat content and abdominal adipose tissue; and SURPASS-4, investigating efficacy and safety of tirzepatide once-weekly versus insulin glargine in patients with type 2 diabetes and increased cardiovascular risk.
The drug is notable for its dramatic reductions in both A1c and weight, although questions remain about the incidence of gastrointestinal side effects and effects on long-term cardiovascular and renal outcomes.
Dr. Rydén commented: “Given its effects on A1c and body weight, we would expect a positive result, but one never knows. It’s at least safe, that’s for sure. I think this mode of action is extremely interesting.”
Dr. Del Prato noted that tirzepatide could also “open up a new area of intervention for type 1 diabetes. The initial data were promising. ... It’s worth keeping an eye on.”
A related symposium will address the future of incretin-based treatments overall, while the EASD-Lancet symposium will examine whether the treatment of obesity is the «future» of diabetes treatment.
COVID-19, hypoglycemia, bone, and much more
As always, there’s much more on the agenda. Other noteworthy sessions include those addressing hypoglycemia management; a joint EASD/European Society of Endocrinology session on diabetes and bone; a debate about whether women with diabetes are at higher cardiovascular risk than men; and in-hospital management of hyperglycemia.
A new feature of the meeting will be a daily roundup/wrap-up, where members of the program committee and speakers will summarize the day’s highlights. And another feature, “EASD e-Learning,” has been expanded to include more clinical topics around insulin use, nonalcoholic fatty liver disease, obesity, and neuropathy.
Overall, Dr. Del Prato said, “it’s a very populated program, with more than 700 presenters, 162 invited symposia speakers, and 53 chairs. It’s covering widely different areas from basic to clinical research. ... It’s a lot of stuff going on.”
Both Dr. Rydén and Dr. Del Prato have disclosures with multiple manufacturers of diabetes-related products.
A version of this article first appeared on Medscape.com.
The annual meeting of the European Association for the Study of Diabetes 2021 will delve into individualized approaches in diabetes management, particularly with regard to tailoring drug therapy for type 2 diabetes and management of type 1 diabetes.
The virtual meeting, taking place Sept. 28 to Oct. 1 in Central European Summer Time, will feature results from TriMASTER (a three-way cross-over trial of precision medicine strategy of second-/third-line therapy in type 2 diabetes), new subgroup analyses from the GRADE (Glycemia Reduction Approaches in Diabetes: A Comparative Effectiveness) study, the final version of a consensus statement on type 1 diabetes management, and new data on the dual incretin agonist tirzepatide, as well as much more.
“I’m a strong believer in personalization. I don’t think the big blockbuster [drugs] will serve the entire community with diabetes. Even in type 1 diabetes, there’s evidence of heterogeneity. ... We need a better way to identify individual needs. I think that’s where we’re going. ... It’s one of the themes of the conference,” EASD President Stefano Del Prato, MD, professor of endocrinology at the University of Pisa (Italy), told this news organization.
He noted that EASD and the American Diabetes Association have recently teamed up with other organizations to form the Precision Medicine in Diabetes Initiative
As would be expected, the meeting will also feature numerous presentations on the COVID-19 pandemic, including studies looking at how people with COVID-19 and diabetes have fared; how the pandemic has affected diabetes care; and the still unclear impact of SARS-CoV-2 on pancreatic beta cells and whether, in some instances, it triggers new-onset diabetes.
New data from previously reported trials
There will be new data from several previously reported trials focusing on specific groups of patients with type 2 diabetes. One is the EMPEROR-Preserved study of empagliflozin (Jardiance) in individuals with heart failure and preserved ejection fraction. Initially presented in August 2021 at the annual congress of the European Society of Cardiology, the new data will focus on patient subpopulations, efficacy endpoints, and safety in patients with and without diabetes. A companion study, EMPEROR-Reduced, in those with heart failure and reduced ejection fraction, was presented at the ESC Congress in August 2020.
New findings will also be presented from the DAPA-CKD study of dapagliflozin (Farxiga) in patients with chronic kidney disease. The study was stopped early in March 2020 because of overwhelming efficacy of the drug in preventing CKD. Now, the data will be analyzed in terms of metabolic, nephrology, and cardiology parameters.
And from FIDELIO-DKD and FIGARO-DKD, trials of the nonsteroidal mineralocorticoid receptor antagonist finerenone (Kerendia), new data will also focus on a variety of subgroups of individuals with type 2 diabetes and chronic kidney disease.
“Our goal is to cover most aspects of what’s happening in the type 2 diabetes field,” EASD Honorary Secretary Mikael Rydén, MD, PhD, professor and senior consultant in endocrinology at the Karolinska Institute and Karolinska University Hospital, Stockholm, said in an interview.
Dr. Rydén, who chairs the meeting’s scientific program committee, added: “We can only focus on so much every year but we try to be active and changing from year to year. I’m convinced that a clinician or translational researcher will definitely have a number of very interesting symposia to follow and learn new things. If you follow all of these things, you will know a lot about what’s cooking in the diabetes world.”
Consensus on type 1 diabetes management: Special considerations
Both Dr. Del Prato and Dr. Rydén cited presentation of the new type 1 diabetes ADA/EASD consensus report as among the most clinically important of the conference. Initially presented in draft form at the ADA Scientific Sessions in June 2021, the document aims to move away from routinely applying principles derived from studies of patients with type 2 diabetes to those with type 1 diabetes, an autoimmune disease with unique characteristics.
The final version of the document is expected to include information on goals of therapy, glycemic targets, prevention and management of hypoglycemia and diabetic ketoacidosis, psychosocial care, and special populations, among other issues. It is also expected to include a section dedicated to adjunctive treatments beyond insulin, including metformin, pramlintide, glucagonlike peptide–1 agonists, and sodium-glucose cotransporter 2 inhibitors for certain patients.
Dr. Del Prato noted, “From a clinical point of view, this is quite an important step that two major organizations came together recommending some strategies for treating type 2 diabetes ... It really deals with a big problem and tries to provide the tools for improving homogenization of the treatment of type 1 diabetes across the different health systems.”
And Dr. Rydén commented: “I think it’s really important to have, since there’s been so much focus on type 2 diabetes for the last few years, and to have the ADA and EASD getting together and actually write this.”
But Dr. Rydén also pointed out that outcomes data are much more conclusive for drugs in type 2 diabetes to inform international guidelines, whereas “this is much more difficult to demonstrate with type 1 diabetes. With a new pump or [continuous glucose monitor (CGM)] you might show a reduction in [hemoglobin] A1c of X percent or X mmol/mol or hypoglycemia events, but it’s much harder to show improvements in hard outcomes like deaths and cardiovascular events. I’m really looking forward to having this presented.”
Diabetes in 2021: It’s personal
Several meeting sessions will specifically address precision medicine approaches, including the TriMASTER study, which aims to identify subgroups of patients with type 2 diabetes who respond well or poorly to particular drugs based on clinical characteristics so that treatments can be better targeted to individuals. In total, 600 patients with type 2 diabetes and suboptimal glycemic control with metformin were randomized to a dipeptidyl peptidase–4 inhibitor, an SGLT2 inhibitor, or thiazolidinedione (TZD).
According to Dr. Rydén, “The TriMASTER final results will be interesting. TZDs still have a place. ... You can’t give them to people with heart failure, but I think like a carpenter you have to have many tools in your toolbox. And I still think that there are some individuals who respond well to pioglitazone. [The study findings] could be influential, depending on the results.”
An EASD/ADA symposium entitled “Optimizing diabetes diagnosis, prevention, and care: Is precision medicine the answer?” will offer three distinct perspectives, with one speaker arguing it’s the future of diabetes medicine, another that it isn’t, and a third explaining that “the devil is in the details.”
The Diabetologia symposium will focus on a related concept: The use of artificial intelligence in diabetes research and care, with particular application to glucose control, neuropathy, and wound healing.
And during the 36th Camillo Golgi Lecture, kidney disease expert H.J. Lambers Heerspink, PhD, of the University of Groningen (the Netherlands), will speak about personalizing treatment for patients with type 2 diabetes, arguing that “the mean is meaningless.”
Next-generation incretin therapy: Is weight loss the treatment?
New data will continue the buzz from the ADA meeting surrounding tirzepatide, the dual GLP-1 receptor agonist and glucose-dependent insulinotropic polypeptide agent.
A session will add new data from SURPASS-3 CGM, looking at the effect of the drug captured by continuous glucose monitoring in patients with type 2 diabetes; SURPASS-3 MRI, examining the effect of the drug on liver fat content and abdominal adipose tissue; and SURPASS-4, investigating efficacy and safety of tirzepatide once-weekly versus insulin glargine in patients with type 2 diabetes and increased cardiovascular risk.
The drug is notable for its dramatic reductions in both A1c and weight, although questions remain about the incidence of gastrointestinal side effects and effects on long-term cardiovascular and renal outcomes.
Dr. Rydén commented: “Given its effects on A1c and body weight, we would expect a positive result, but one never knows. It’s at least safe, that’s for sure. I think this mode of action is extremely interesting.”
Dr. Del Prato noted that tirzepatide could also “open up a new area of intervention for type 1 diabetes. The initial data were promising. ... It’s worth keeping an eye on.”
A related symposium will address the future of incretin-based treatments overall, while the EASD-Lancet symposium will examine whether the treatment of obesity is the «future» of diabetes treatment.
COVID-19, hypoglycemia, bone, and much more
As always, there’s much more on the agenda. Other noteworthy sessions include those addressing hypoglycemia management; a joint EASD/European Society of Endocrinology session on diabetes and bone; a debate about whether women with diabetes are at higher cardiovascular risk than men; and in-hospital management of hyperglycemia.
A new feature of the meeting will be a daily roundup/wrap-up, where members of the program committee and speakers will summarize the day’s highlights. And another feature, “EASD e-Learning,” has been expanded to include more clinical topics around insulin use, nonalcoholic fatty liver disease, obesity, and neuropathy.
Overall, Dr. Del Prato said, “it’s a very populated program, with more than 700 presenters, 162 invited symposia speakers, and 53 chairs. It’s covering widely different areas from basic to clinical research. ... It’s a lot of stuff going on.”
Both Dr. Rydén and Dr. Del Prato have disclosures with multiple manufacturers of diabetes-related products.
A version of this article first appeared on Medscape.com.
The annual meeting of the European Association for the Study of Diabetes 2021 will delve into individualized approaches in diabetes management, particularly with regard to tailoring drug therapy for type 2 diabetes and management of type 1 diabetes.
The virtual meeting, taking place Sept. 28 to Oct. 1 in Central European Summer Time, will feature results from TriMASTER (a three-way cross-over trial of precision medicine strategy of second-/third-line therapy in type 2 diabetes), new subgroup analyses from the GRADE (Glycemia Reduction Approaches in Diabetes: A Comparative Effectiveness) study, the final version of a consensus statement on type 1 diabetes management, and new data on the dual incretin agonist tirzepatide, as well as much more.
“I’m a strong believer in personalization. I don’t think the big blockbuster [drugs] will serve the entire community with diabetes. Even in type 1 diabetes, there’s evidence of heterogeneity. ... We need a better way to identify individual needs. I think that’s where we’re going. ... It’s one of the themes of the conference,” EASD President Stefano Del Prato, MD, professor of endocrinology at the University of Pisa (Italy), told this news organization.
He noted that EASD and the American Diabetes Association have recently teamed up with other organizations to form the Precision Medicine in Diabetes Initiative
As would be expected, the meeting will also feature numerous presentations on the COVID-19 pandemic, including studies looking at how people with COVID-19 and diabetes have fared; how the pandemic has affected diabetes care; and the still unclear impact of SARS-CoV-2 on pancreatic beta cells and whether, in some instances, it triggers new-onset diabetes.
New data from previously reported trials
There will be new data from several previously reported trials focusing on specific groups of patients with type 2 diabetes. One is the EMPEROR-Preserved study of empagliflozin (Jardiance) in individuals with heart failure and preserved ejection fraction. Initially presented in August 2021 at the annual congress of the European Society of Cardiology, the new data will focus on patient subpopulations, efficacy endpoints, and safety in patients with and without diabetes. A companion study, EMPEROR-Reduced, in those with heart failure and reduced ejection fraction, was presented at the ESC Congress in August 2020.
New findings will also be presented from the DAPA-CKD study of dapagliflozin (Farxiga) in patients with chronic kidney disease. The study was stopped early in March 2020 because of overwhelming efficacy of the drug in preventing CKD. Now, the data will be analyzed in terms of metabolic, nephrology, and cardiology parameters.
And from FIDELIO-DKD and FIGARO-DKD, trials of the nonsteroidal mineralocorticoid receptor antagonist finerenone (Kerendia), new data will also focus on a variety of subgroups of individuals with type 2 diabetes and chronic kidney disease.
“Our goal is to cover most aspects of what’s happening in the type 2 diabetes field,” EASD Honorary Secretary Mikael Rydén, MD, PhD, professor and senior consultant in endocrinology at the Karolinska Institute and Karolinska University Hospital, Stockholm, said in an interview.
Dr. Rydén, who chairs the meeting’s scientific program committee, added: “We can only focus on so much every year but we try to be active and changing from year to year. I’m convinced that a clinician or translational researcher will definitely have a number of very interesting symposia to follow and learn new things. If you follow all of these things, you will know a lot about what’s cooking in the diabetes world.”
Consensus on type 1 diabetes management: Special considerations
Both Dr. Del Prato and Dr. Rydén cited presentation of the new type 1 diabetes ADA/EASD consensus report as among the most clinically important of the conference. Initially presented in draft form at the ADA Scientific Sessions in June 2021, the document aims to move away from routinely applying principles derived from studies of patients with type 2 diabetes to those with type 1 diabetes, an autoimmune disease with unique characteristics.
The final version of the document is expected to include information on goals of therapy, glycemic targets, prevention and management of hypoglycemia and diabetic ketoacidosis, psychosocial care, and special populations, among other issues. It is also expected to include a section dedicated to adjunctive treatments beyond insulin, including metformin, pramlintide, glucagonlike peptide–1 agonists, and sodium-glucose cotransporter 2 inhibitors for certain patients.
Dr. Del Prato noted, “From a clinical point of view, this is quite an important step that two major organizations came together recommending some strategies for treating type 2 diabetes ... It really deals with a big problem and tries to provide the tools for improving homogenization of the treatment of type 1 diabetes across the different health systems.”
And Dr. Rydén commented: “I think it’s really important to have, since there’s been so much focus on type 2 diabetes for the last few years, and to have the ADA and EASD getting together and actually write this.”
But Dr. Rydén also pointed out that outcomes data are much more conclusive for drugs in type 2 diabetes to inform international guidelines, whereas “this is much more difficult to demonstrate with type 1 diabetes. With a new pump or [continuous glucose monitor (CGM)] you might show a reduction in [hemoglobin] A1c of X percent or X mmol/mol or hypoglycemia events, but it’s much harder to show improvements in hard outcomes like deaths and cardiovascular events. I’m really looking forward to having this presented.”
Diabetes in 2021: It’s personal
Several meeting sessions will specifically address precision medicine approaches, including the TriMASTER study, which aims to identify subgroups of patients with type 2 diabetes who respond well or poorly to particular drugs based on clinical characteristics so that treatments can be better targeted to individuals. In total, 600 patients with type 2 diabetes and suboptimal glycemic control with metformin were randomized to a dipeptidyl peptidase–4 inhibitor, an SGLT2 inhibitor, or thiazolidinedione (TZD).
According to Dr. Rydén, “The TriMASTER final results will be interesting. TZDs still have a place. ... You can’t give them to people with heart failure, but I think like a carpenter you have to have many tools in your toolbox. And I still think that there are some individuals who respond well to pioglitazone. [The study findings] could be influential, depending on the results.”
An EASD/ADA symposium entitled “Optimizing diabetes diagnosis, prevention, and care: Is precision medicine the answer?” will offer three distinct perspectives, with one speaker arguing it’s the future of diabetes medicine, another that it isn’t, and a third explaining that “the devil is in the details.”
The Diabetologia symposium will focus on a related concept: The use of artificial intelligence in diabetes research and care, with particular application to glucose control, neuropathy, and wound healing.
And during the 36th Camillo Golgi Lecture, kidney disease expert H.J. Lambers Heerspink, PhD, of the University of Groningen (the Netherlands), will speak about personalizing treatment for patients with type 2 diabetes, arguing that “the mean is meaningless.”
Next-generation incretin therapy: Is weight loss the treatment?
New data will continue the buzz from the ADA meeting surrounding tirzepatide, the dual GLP-1 receptor agonist and glucose-dependent insulinotropic polypeptide agent.
A session will add new data from SURPASS-3 CGM, looking at the effect of the drug captured by continuous glucose monitoring in patients with type 2 diabetes; SURPASS-3 MRI, examining the effect of the drug on liver fat content and abdominal adipose tissue; and SURPASS-4, investigating efficacy and safety of tirzepatide once-weekly versus insulin glargine in patients with type 2 diabetes and increased cardiovascular risk.
The drug is notable for its dramatic reductions in both A1c and weight, although questions remain about the incidence of gastrointestinal side effects and effects on long-term cardiovascular and renal outcomes.
Dr. Rydén commented: “Given its effects on A1c and body weight, we would expect a positive result, but one never knows. It’s at least safe, that’s for sure. I think this mode of action is extremely interesting.”
Dr. Del Prato noted that tirzepatide could also “open up a new area of intervention for type 1 diabetes. The initial data were promising. ... It’s worth keeping an eye on.”
A related symposium will address the future of incretin-based treatments overall, while the EASD-Lancet symposium will examine whether the treatment of obesity is the «future» of diabetes treatment.
COVID-19, hypoglycemia, bone, and much more
As always, there’s much more on the agenda. Other noteworthy sessions include those addressing hypoglycemia management; a joint EASD/European Society of Endocrinology session on diabetes and bone; a debate about whether women with diabetes are at higher cardiovascular risk than men; and in-hospital management of hyperglycemia.
A new feature of the meeting will be a daily roundup/wrap-up, where members of the program committee and speakers will summarize the day’s highlights. And another feature, “EASD e-Learning,” has been expanded to include more clinical topics around insulin use, nonalcoholic fatty liver disease, obesity, and neuropathy.
Overall, Dr. Del Prato said, “it’s a very populated program, with more than 700 presenters, 162 invited symposia speakers, and 53 chairs. It’s covering widely different areas from basic to clinical research. ... It’s a lot of stuff going on.”
Both Dr. Rydén and Dr. Del Prato have disclosures with multiple manufacturers of diabetes-related products.
A version of this article first appeared on Medscape.com.
Long COVID appears to ‘impair’ survival in cancer patients
More than one in six cancer patients experience long-term sequelae following SARS-CoV-2 infection, placing them at increased risk of discontinuing their cancer treatment or dying, according to European registry data.
Given the “high lethality” of COVID-19 in cancer patients and the risk for long-term complications following infection in the general population, Alessio Cortellini, MD, a consultant medical oncologist at Hammersmith Hospital and Imperial College London, and colleagues wanted to explore the “prevalence and clinical significance of COVID-19 sequelae in cancer patients and their oncological continuity of care.”
Dr. Cortellini presented the OnCovid registry research on Sept. 21 at the 2021 European Society for Medical Oncology Congress. He reported that overall, the data suggest that post–COVID-19 complications may “impair” patients’ cancer survival as well as their cancer care.
The OnCovid registry data showed that the 15% of cancer patients who had long-term COVID-19 complications were 76% more likely to die than those without sequelae. Cancer patients with COVID-19 sequelae were significantly more likely to permanently stop taking their systemic anticancer therapy, and they were more than 3.5 times more likely to die than those who continued their treatment as planned. In terms of long-term complications, almost half of patients experienced dyspnea, and two-fifths reported chronic fatigue.
“This data confirms the need to continue to prioritize cancer patients,” Antonio Passaro, MD, PhD, division of thoracic oncology, European Institute of Oncology IRCCS, Milan, commented in a press release. “In the fight against the pandemic, it is of the utmost importance that we do not neglect to study and understand the curves of cancer incidence and mortality.”
Invited to discuss the results, Anne-Marie C. Dingemans, MD, PhD, a pulmonologist and professor of thoracic oncology at Erasmus Medical Center, Rotterdam, the Netherlands, said COVID-19 remains a “very important” issue for cancer patients.
Interestingly, Dr. Dingemans noted that COVID-19 sequelae in patients with cancer appear to occur slightly less frequently, compared with estimates in the general population – which range from 13% to 60% – though patients with cancer tend to have more respiratory problems.
However, Dr. Dingemans added, the difficulty with comparing sequelae rates between cancer patients and the general population is that cancer patients “probably already have a lot of symptoms” associated with long COVID, such as dyspnea and fatigue, and may not be aware that they are experiencing COVID sequelae.
The registry results
To investigate the long-term impact of COVID-19 on survival and continuity of care, the team examined data from the OnCovid registry, which was established at the beginning of the pandemic to study consecutive patients aged 18 years and older with confirmed SARS-CoV-2 infection and a history of solid or hematologic malignancies.
At the data cutoff on March 1, 2021, the registry included 35 institutions in six European countries. The institutions collected information on patient demographics and comorbidities, cancer history, anticancer therapy, COVID-19 investigations, and COVID-19–specific therapies.
For the current analysis, the team included 1,557 of 2,634 patients who had undergone a clinical reassessment after recovering from COVID-19. Information sufficient to conduct multivariate analysis was available for 840 of these patients.
About half of the patients were younger than 60 years, and just over half were women. The most common cancer diagnoses were breast cancer (23.4%), gastrointestinal tumors (16.5%), gynecologic/genitourinary tumors (19.3%), and hematologic cancers (14.1%), with even distribution between local/locoregional and advanced disease.
The median interval between COVID-19 recovery and reassessment was 44 days, and the mean post–COVID-19 follow-up period was 128 days.
About 15% of patients experienced at least one long-term sequela from COVID-19. The most common were dyspnea/shortness of breath (49.6%), fatigue (41.0%), chronic cough (33.8%), and other respiratory complications (10.7%).
Dr. Cortellini noted that cancer patients who experienced sequelae were more likely to be male, aged 65 years or older, to have at least two comorbidities, and to have a history of smoking. In addition, cancer patients who experienced long-term complications were significantly more likely to have had COVID-19 complications, to have required COVID-19 therapy, and to have been hospitalized for the disease.
Factoring in gender, age, comorbidity burden, primary tumor, stage, receipt of anticancer and anti–COVID-19 therapy, COVID-19 complications, and hospitalization, the team found that COVID-19 sequelae were independently associated with an increased risk for death (hazard ratio, 1.76).
Further analysis of patterns of systemic anticancer therapy in 471 patients revealed that 14.8% of COVID-19 survivors permanently discontinued therapy and that a dose or regimen adjustment occurred for 37.8%.
Patients who permanently discontinued anticancer therapy were more likely to be former or current smokers, to have had COVID-19 complications or been hospitalized for COVID-19, and to have had COVID-19 sequelae at reassessment. The investigators found no association between permanent discontinuation of therapy and cancer disease stage.
Dr. Cortellini and colleagues reported that permanent cessation of systemic anticancer therapy was associated with an increased risk for death. A change in dose or regimen did not affect survival.
The most common reason for stopping therapy permanently was deterioration of the patient’s performance status (61.3%), followed by disease progression (29.0%). Dose or regimen adjustments typically occurred to avoid immune suppression (50.0%), hospitalization (25.8%), and intravenous drug administration (19.1%).
Dr. Cortellini concluded his presentation by highlighting the importance of increasing awareness of long COVID in patients with cancer as well as early treatment of COVID-19 sequelae to improve patient outcomes.
The study was funded by the Imperial College Biomedical Research Center. Dr. Cortellini has relationships with MSD, Bristol-Myers Squibb, Roche, Novartis, AstraZeneca, Astellas, and Sun Pharma. Dr. Dingemans has relationships with Roche, Eli Lilly, Boehringer Ingelheim, AstraZeneca, Jansen, Chiesi, Amgen, Pfizer, Bayer, Takeda, Pharmamar, and Sanofi.
A version of this article first appeared on Medscape.com.
More than one in six cancer patients experience long-term sequelae following SARS-CoV-2 infection, placing them at increased risk of discontinuing their cancer treatment or dying, according to European registry data.
Given the “high lethality” of COVID-19 in cancer patients and the risk for long-term complications following infection in the general population, Alessio Cortellini, MD, a consultant medical oncologist at Hammersmith Hospital and Imperial College London, and colleagues wanted to explore the “prevalence and clinical significance of COVID-19 sequelae in cancer patients and their oncological continuity of care.”
Dr. Cortellini presented the OnCovid registry research on Sept. 21 at the 2021 European Society for Medical Oncology Congress. He reported that overall, the data suggest that post–COVID-19 complications may “impair” patients’ cancer survival as well as their cancer care.
The OnCovid registry data showed that the 15% of cancer patients who had long-term COVID-19 complications were 76% more likely to die than those without sequelae. Cancer patients with COVID-19 sequelae were significantly more likely to permanently stop taking their systemic anticancer therapy, and they were more than 3.5 times more likely to die than those who continued their treatment as planned. In terms of long-term complications, almost half of patients experienced dyspnea, and two-fifths reported chronic fatigue.
“This data confirms the need to continue to prioritize cancer patients,” Antonio Passaro, MD, PhD, division of thoracic oncology, European Institute of Oncology IRCCS, Milan, commented in a press release. “In the fight against the pandemic, it is of the utmost importance that we do not neglect to study and understand the curves of cancer incidence and mortality.”
Invited to discuss the results, Anne-Marie C. Dingemans, MD, PhD, a pulmonologist and professor of thoracic oncology at Erasmus Medical Center, Rotterdam, the Netherlands, said COVID-19 remains a “very important” issue for cancer patients.
Interestingly, Dr. Dingemans noted that COVID-19 sequelae in patients with cancer appear to occur slightly less frequently, compared with estimates in the general population – which range from 13% to 60% – though patients with cancer tend to have more respiratory problems.
However, Dr. Dingemans added, the difficulty with comparing sequelae rates between cancer patients and the general population is that cancer patients “probably already have a lot of symptoms” associated with long COVID, such as dyspnea and fatigue, and may not be aware that they are experiencing COVID sequelae.
The registry results
To investigate the long-term impact of COVID-19 on survival and continuity of care, the team examined data from the OnCovid registry, which was established at the beginning of the pandemic to study consecutive patients aged 18 years and older with confirmed SARS-CoV-2 infection and a history of solid or hematologic malignancies.
At the data cutoff on March 1, 2021, the registry included 35 institutions in six European countries. The institutions collected information on patient demographics and comorbidities, cancer history, anticancer therapy, COVID-19 investigations, and COVID-19–specific therapies.
For the current analysis, the team included 1,557 of 2,634 patients who had undergone a clinical reassessment after recovering from COVID-19. Information sufficient to conduct multivariate analysis was available for 840 of these patients.
About half of the patients were younger than 60 years, and just over half were women. The most common cancer diagnoses were breast cancer (23.4%), gastrointestinal tumors (16.5%), gynecologic/genitourinary tumors (19.3%), and hematologic cancers (14.1%), with even distribution between local/locoregional and advanced disease.
The median interval between COVID-19 recovery and reassessment was 44 days, and the mean post–COVID-19 follow-up period was 128 days.
About 15% of patients experienced at least one long-term sequela from COVID-19. The most common were dyspnea/shortness of breath (49.6%), fatigue (41.0%), chronic cough (33.8%), and other respiratory complications (10.7%).
Dr. Cortellini noted that cancer patients who experienced sequelae were more likely to be male, aged 65 years or older, to have at least two comorbidities, and to have a history of smoking. In addition, cancer patients who experienced long-term complications were significantly more likely to have had COVID-19 complications, to have required COVID-19 therapy, and to have been hospitalized for the disease.
Factoring in gender, age, comorbidity burden, primary tumor, stage, receipt of anticancer and anti–COVID-19 therapy, COVID-19 complications, and hospitalization, the team found that COVID-19 sequelae were independently associated with an increased risk for death (hazard ratio, 1.76).
Further analysis of patterns of systemic anticancer therapy in 471 patients revealed that 14.8% of COVID-19 survivors permanently discontinued therapy and that a dose or regimen adjustment occurred for 37.8%.
Patients who permanently discontinued anticancer therapy were more likely to be former or current smokers, to have had COVID-19 complications or been hospitalized for COVID-19, and to have had COVID-19 sequelae at reassessment. The investigators found no association between permanent discontinuation of therapy and cancer disease stage.
Dr. Cortellini and colleagues reported that permanent cessation of systemic anticancer therapy was associated with an increased risk for death. A change in dose or regimen did not affect survival.
The most common reason for stopping therapy permanently was deterioration of the patient’s performance status (61.3%), followed by disease progression (29.0%). Dose or regimen adjustments typically occurred to avoid immune suppression (50.0%), hospitalization (25.8%), and intravenous drug administration (19.1%).
Dr. Cortellini concluded his presentation by highlighting the importance of increasing awareness of long COVID in patients with cancer as well as early treatment of COVID-19 sequelae to improve patient outcomes.
The study was funded by the Imperial College Biomedical Research Center. Dr. Cortellini has relationships with MSD, Bristol-Myers Squibb, Roche, Novartis, AstraZeneca, Astellas, and Sun Pharma. Dr. Dingemans has relationships with Roche, Eli Lilly, Boehringer Ingelheim, AstraZeneca, Jansen, Chiesi, Amgen, Pfizer, Bayer, Takeda, Pharmamar, and Sanofi.
A version of this article first appeared on Medscape.com.
More than one in six cancer patients experience long-term sequelae following SARS-CoV-2 infection, placing them at increased risk of discontinuing their cancer treatment or dying, according to European registry data.
Given the “high lethality” of COVID-19 in cancer patients and the risk for long-term complications following infection in the general population, Alessio Cortellini, MD, a consultant medical oncologist at Hammersmith Hospital and Imperial College London, and colleagues wanted to explore the “prevalence and clinical significance of COVID-19 sequelae in cancer patients and their oncological continuity of care.”
Dr. Cortellini presented the OnCovid registry research on Sept. 21 at the 2021 European Society for Medical Oncology Congress. He reported that overall, the data suggest that post–COVID-19 complications may “impair” patients’ cancer survival as well as their cancer care.
The OnCovid registry data showed that the 15% of cancer patients who had long-term COVID-19 complications were 76% more likely to die than those without sequelae. Cancer patients with COVID-19 sequelae were significantly more likely to permanently stop taking their systemic anticancer therapy, and they were more than 3.5 times more likely to die than those who continued their treatment as planned. In terms of long-term complications, almost half of patients experienced dyspnea, and two-fifths reported chronic fatigue.
“This data confirms the need to continue to prioritize cancer patients,” Antonio Passaro, MD, PhD, division of thoracic oncology, European Institute of Oncology IRCCS, Milan, commented in a press release. “In the fight against the pandemic, it is of the utmost importance that we do not neglect to study and understand the curves of cancer incidence and mortality.”
Invited to discuss the results, Anne-Marie C. Dingemans, MD, PhD, a pulmonologist and professor of thoracic oncology at Erasmus Medical Center, Rotterdam, the Netherlands, said COVID-19 remains a “very important” issue for cancer patients.
Interestingly, Dr. Dingemans noted that COVID-19 sequelae in patients with cancer appear to occur slightly less frequently, compared with estimates in the general population – which range from 13% to 60% – though patients with cancer tend to have more respiratory problems.
However, Dr. Dingemans added, the difficulty with comparing sequelae rates between cancer patients and the general population is that cancer patients “probably already have a lot of symptoms” associated with long COVID, such as dyspnea and fatigue, and may not be aware that they are experiencing COVID sequelae.
The registry results
To investigate the long-term impact of COVID-19 on survival and continuity of care, the team examined data from the OnCovid registry, which was established at the beginning of the pandemic to study consecutive patients aged 18 years and older with confirmed SARS-CoV-2 infection and a history of solid or hematologic malignancies.
At the data cutoff on March 1, 2021, the registry included 35 institutions in six European countries. The institutions collected information on patient demographics and comorbidities, cancer history, anticancer therapy, COVID-19 investigations, and COVID-19–specific therapies.
For the current analysis, the team included 1,557 of 2,634 patients who had undergone a clinical reassessment after recovering from COVID-19. Information sufficient to conduct multivariate analysis was available for 840 of these patients.
About half of the patients were younger than 60 years, and just over half were women. The most common cancer diagnoses were breast cancer (23.4%), gastrointestinal tumors (16.5%), gynecologic/genitourinary tumors (19.3%), and hematologic cancers (14.1%), with even distribution between local/locoregional and advanced disease.
The median interval between COVID-19 recovery and reassessment was 44 days, and the mean post–COVID-19 follow-up period was 128 days.
About 15% of patients experienced at least one long-term sequela from COVID-19. The most common were dyspnea/shortness of breath (49.6%), fatigue (41.0%), chronic cough (33.8%), and other respiratory complications (10.7%).
Dr. Cortellini noted that cancer patients who experienced sequelae were more likely to be male, aged 65 years or older, to have at least two comorbidities, and to have a history of smoking. In addition, cancer patients who experienced long-term complications were significantly more likely to have had COVID-19 complications, to have required COVID-19 therapy, and to have been hospitalized for the disease.
Factoring in gender, age, comorbidity burden, primary tumor, stage, receipt of anticancer and anti–COVID-19 therapy, COVID-19 complications, and hospitalization, the team found that COVID-19 sequelae were independently associated with an increased risk for death (hazard ratio, 1.76).
Further analysis of patterns of systemic anticancer therapy in 471 patients revealed that 14.8% of COVID-19 survivors permanently discontinued therapy and that a dose or regimen adjustment occurred for 37.8%.
Patients who permanently discontinued anticancer therapy were more likely to be former or current smokers, to have had COVID-19 complications or been hospitalized for COVID-19, and to have had COVID-19 sequelae at reassessment. The investigators found no association between permanent discontinuation of therapy and cancer disease stage.
Dr. Cortellini and colleagues reported that permanent cessation of systemic anticancer therapy was associated with an increased risk for death. A change in dose or regimen did not affect survival.
The most common reason for stopping therapy permanently was deterioration of the patient’s performance status (61.3%), followed by disease progression (29.0%). Dose or regimen adjustments typically occurred to avoid immune suppression (50.0%), hospitalization (25.8%), and intravenous drug administration (19.1%).
Dr. Cortellini concluded his presentation by highlighting the importance of increasing awareness of long COVID in patients with cancer as well as early treatment of COVID-19 sequelae to improve patient outcomes.
The study was funded by the Imperial College Biomedical Research Center. Dr. Cortellini has relationships with MSD, Bristol-Myers Squibb, Roche, Novartis, AstraZeneca, Astellas, and Sun Pharma. Dr. Dingemans has relationships with Roche, Eli Lilly, Boehringer Ingelheim, AstraZeneca, Jansen, Chiesi, Amgen, Pfizer, Bayer, Takeda, Pharmamar, and Sanofi.
A version of this article first appeared on Medscape.com.
Remdesivir sharply cuts COVID hospitalization risk, Gilead says
Remdesivir (Veklury, Gilead) was found to reduce some COVID-19 patients’ risk of hospitalization by 87% in a phase 3 trial, the drug’s manufacturer announced Sept. 22 in a press release.
The randomized, double-blind, placebo-controlled trial evaluated the efficacy and safety of a 3-day course of intravenous remdesivir in an analysis of 562 nonhospitalized patients at high risk for disease progression.
Remdesivir demonstrated a statistically significant 87% reduction in risk for COVID-19–related hospitalization or all-cause death by Day 28 (0.7% [2/279]) compared with placebo (5.3% [15/283]) P = .008. Participants were assigned 1:1 to remdesivir or the placebo group.
Researchers also found an 81% reduction in risk for the composite secondary endpoint – medical visits due to COVID-19 or all-cause death by Day 28. Only 1.6% had COVID-19 medical visits ([4/246]) compared with those in the placebo group (8.3% [21/252]) P = .002. No deaths were observed in either arm by Day 28.
“These latest data show remdesivir’s potential to help high-risk patients recover before they get sicker and stay out of the hospital altogether,” coauthor Robert L. Gottlieb, MD, PhD, from Baylor University Medical Center, Houston, said in the press release.
Remdesivir is the only drug approved by the U.S. Food and Drug Administration for hospitalized COVID-19 patients at least 12 years old. Its treatment of nonhospitalized patients with 3 days of dosing is investigational, and the safety and efficacy for this use and dosing duration have not been established or approved by any regulatory agency, the Gilead press release notes.
The patients in this study were considered high-risk for disease progression based on comorbidities – commonly obesity, hypertension, and diabetes – and age, but had not recently been hospitalized due to COVID-19.
A third of the participants were at least 60 years old. Participants in the study must have received a positive diagnosis within 4 days of starting treatment and experienced symptoms for 7 days or less.
Use of remdesivir controversial
Results from the Adaptive COVID-19 Treatment Trial (ACTT-1) showed remdesivir was superior to placebo in shortening time to recovery in adults hospitalized with COVID-19 with evidence of lower respiratory tract infection.
However, a large trial of more than 11,000 people in 30 countries, sponsored by the World Health Organization, did not show any benefit for the drug in reducing COVID deaths.
The WHO has conditionally recommended against using remdesivir in hospitalized patients, regardless of disease severity, “as there is currently no evidence that remdesivir improves survival and other outcomes in these patients.”
The drug also is given intravenously, and this study tested three infusions over 3 days, a difficult treatment for nonhospitalized patients.
The study results were released ahead of IDWeek, where the late-breaking abstract will be presented at the virtual conference in full at the end of next week.
A version of this article first appeared on Medscape.com.
Remdesivir (Veklury, Gilead) was found to reduce some COVID-19 patients’ risk of hospitalization by 87% in a phase 3 trial, the drug’s manufacturer announced Sept. 22 in a press release.
The randomized, double-blind, placebo-controlled trial evaluated the efficacy and safety of a 3-day course of intravenous remdesivir in an analysis of 562 nonhospitalized patients at high risk for disease progression.
Remdesivir demonstrated a statistically significant 87% reduction in risk for COVID-19–related hospitalization or all-cause death by Day 28 (0.7% [2/279]) compared with placebo (5.3% [15/283]) P = .008. Participants were assigned 1:1 to remdesivir or the placebo group.
Researchers also found an 81% reduction in risk for the composite secondary endpoint – medical visits due to COVID-19 or all-cause death by Day 28. Only 1.6% had COVID-19 medical visits ([4/246]) compared with those in the placebo group (8.3% [21/252]) P = .002. No deaths were observed in either arm by Day 28.
“These latest data show remdesivir’s potential to help high-risk patients recover before they get sicker and stay out of the hospital altogether,” coauthor Robert L. Gottlieb, MD, PhD, from Baylor University Medical Center, Houston, said in the press release.
Remdesivir is the only drug approved by the U.S. Food and Drug Administration for hospitalized COVID-19 patients at least 12 years old. Its treatment of nonhospitalized patients with 3 days of dosing is investigational, and the safety and efficacy for this use and dosing duration have not been established or approved by any regulatory agency, the Gilead press release notes.
The patients in this study were considered high-risk for disease progression based on comorbidities – commonly obesity, hypertension, and diabetes – and age, but had not recently been hospitalized due to COVID-19.
A third of the participants were at least 60 years old. Participants in the study must have received a positive diagnosis within 4 days of starting treatment and experienced symptoms for 7 days or less.
Use of remdesivir controversial
Results from the Adaptive COVID-19 Treatment Trial (ACTT-1) showed remdesivir was superior to placebo in shortening time to recovery in adults hospitalized with COVID-19 with evidence of lower respiratory tract infection.
However, a large trial of more than 11,000 people in 30 countries, sponsored by the World Health Organization, did not show any benefit for the drug in reducing COVID deaths.
The WHO has conditionally recommended against using remdesivir in hospitalized patients, regardless of disease severity, “as there is currently no evidence that remdesivir improves survival and other outcomes in these patients.”
The drug also is given intravenously, and this study tested three infusions over 3 days, a difficult treatment for nonhospitalized patients.
The study results were released ahead of IDWeek, where the late-breaking abstract will be presented at the virtual conference in full at the end of next week.
A version of this article first appeared on Medscape.com.
Remdesivir (Veklury, Gilead) was found to reduce some COVID-19 patients’ risk of hospitalization by 87% in a phase 3 trial, the drug’s manufacturer announced Sept. 22 in a press release.
The randomized, double-blind, placebo-controlled trial evaluated the efficacy and safety of a 3-day course of intravenous remdesivir in an analysis of 562 nonhospitalized patients at high risk for disease progression.
Remdesivir demonstrated a statistically significant 87% reduction in risk for COVID-19–related hospitalization or all-cause death by Day 28 (0.7% [2/279]) compared with placebo (5.3% [15/283]) P = .008. Participants were assigned 1:1 to remdesivir or the placebo group.
Researchers also found an 81% reduction in risk for the composite secondary endpoint – medical visits due to COVID-19 or all-cause death by Day 28. Only 1.6% had COVID-19 medical visits ([4/246]) compared with those in the placebo group (8.3% [21/252]) P = .002. No deaths were observed in either arm by Day 28.
“These latest data show remdesivir’s potential to help high-risk patients recover before they get sicker and stay out of the hospital altogether,” coauthor Robert L. Gottlieb, MD, PhD, from Baylor University Medical Center, Houston, said in the press release.
Remdesivir is the only drug approved by the U.S. Food and Drug Administration for hospitalized COVID-19 patients at least 12 years old. Its treatment of nonhospitalized patients with 3 days of dosing is investigational, and the safety and efficacy for this use and dosing duration have not been established or approved by any regulatory agency, the Gilead press release notes.
The patients in this study were considered high-risk for disease progression based on comorbidities – commonly obesity, hypertension, and diabetes – and age, but had not recently been hospitalized due to COVID-19.
A third of the participants were at least 60 years old. Participants in the study must have received a positive diagnosis within 4 days of starting treatment and experienced symptoms for 7 days or less.
Use of remdesivir controversial
Results from the Adaptive COVID-19 Treatment Trial (ACTT-1) showed remdesivir was superior to placebo in shortening time to recovery in adults hospitalized with COVID-19 with evidence of lower respiratory tract infection.
However, a large trial of more than 11,000 people in 30 countries, sponsored by the World Health Organization, did not show any benefit for the drug in reducing COVID deaths.
The WHO has conditionally recommended against using remdesivir in hospitalized patients, regardless of disease severity, “as there is currently no evidence that remdesivir improves survival and other outcomes in these patients.”
The drug also is given intravenously, and this study tested three infusions over 3 days, a difficult treatment for nonhospitalized patients.
The study results were released ahead of IDWeek, where the late-breaking abstract will be presented at the virtual conference in full at the end of next week.
A version of this article first appeared on Medscape.com.
Rare hematologic malignancy may first present to a dermatologist
in about 80% of cases.
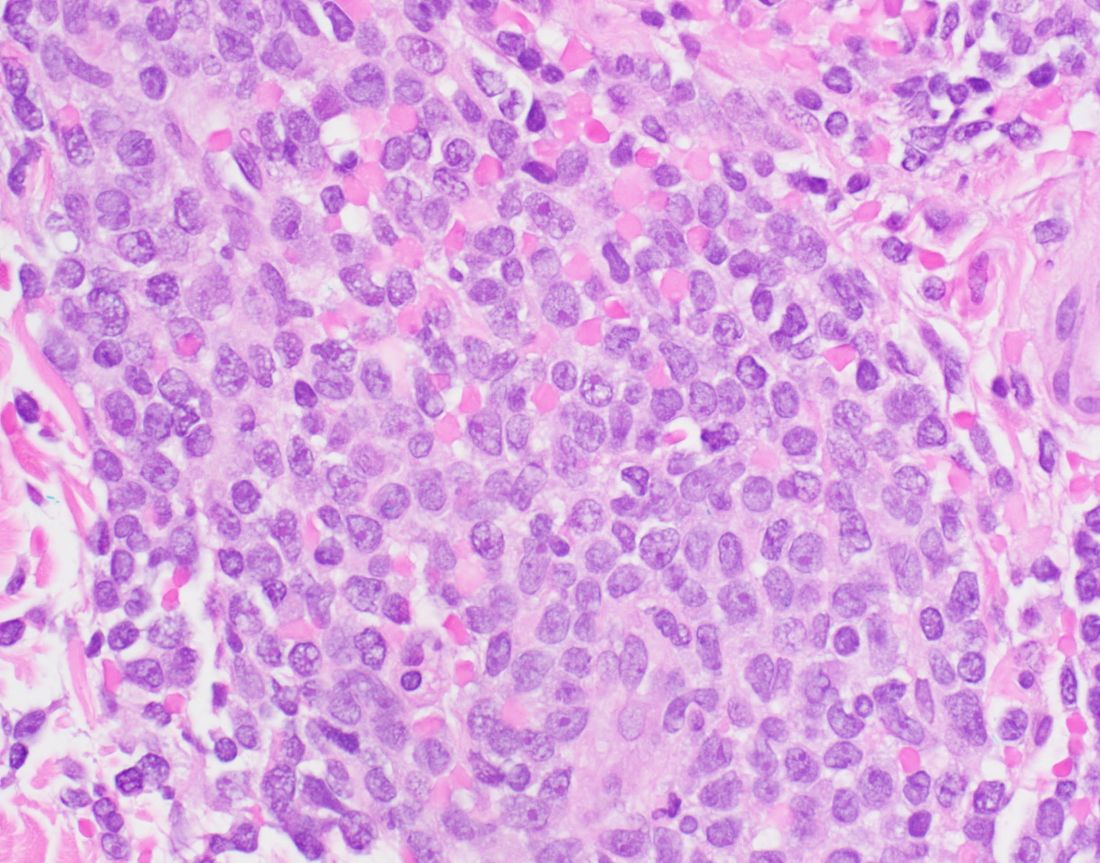
“You won’t see blastic plasmacytoid dendritic cell neoplasm listed on our primary cutaneous lymphoma classifications because it’s not technically a primary cutaneous disease,” Brittney K. DeClerck, MD, said during the annual meeting of the Pacific Dermatologic Association. “It’s a systemic disease that has secondary cutaneous manifestations. That’s a very important distinction to make, in terms of not missing the underlying disease associated with what might be commonly first seen on the skin.”

BPDCN is a malignancy of plasmacytoid dendritic cells, which capture, process, and present antigen, and allow the remainder of the immune system to be activated. “They are mainly derived from the myeloid cell lineage, and possibly from the lymphoid line in a subset of cases,” said Dr. DeClerck, associate professor of clinical pathology and dermatology at the University of Southern California, Los Angeles. “They secrete high levels of type I interferons, which is important for antiviral immunity, but they can also be implicated in severe systemic inflammatory diseases, such as systemic lupus erythematosus and systemic sclerosis.”
BPDCN involves the skin in about 80% of cases, she added, “but invariably at some point it involves the bone marrow and has an acute leukemic presentation, whether or not it happens concurrently with what we see on the skin as dermatologists. We also see variable involvement of the peripheral blood, lymph nodes, and the central nervous system.”
The classification of BPDCN has changed over time based on evolving immunohistochemical markers and technologies. For example, in 1995 it was called agranular CD4+ NK cell leukemia, in 2001 it was called blastic NK-cell lymphoma, in 2005 it was called CD4+/CD56+ hematodermic neoplasm, and in 2008 it was called BPDCN (AML subset). In 2016 it became classified as its own entity: BPDCN.
Because of changing nomenclature, the true incidence of the disease is unknown, but according to the best available literature, 75% of cases occur in men and the median age is between 60 and 70 years, “but all ages can be affected,” Dr. DeClerck said. “Cases seem to come in clusters. Our most recent cluster has been in our pediatric population. At Children’s Hospital Los Angeles, we’ve had three cases in the last couple of years. To me, that was a bit unusual.”
She added that 10%-20% of patients will have either a history of, or will develop another, hematologic malignancy, such as myelodysplastic syndrome (MDS), chronic myelogenous leukemia (CML), or acute myelogenous leukemia (AML).
The general prognosis of BPDCN is poor, and the mean time from onset of lesions to an actual diagnosis is about 6.2 months, which underscores the importance of early diagnosis, Dr. DeClerck said. “There can be some nondescript solitary lesions that patients can present with, so don’t hesitate to biopsy.” The median overall survival is less than 20 months, but patients under 60 years of age have a slightly better prognosis.
Clinical presentation
Clinically, the malignancy presents with variable involvement of the skin, bone marrow, lymph nodes, peripheral blood, and central nervous system. “Patients may have one or all of these,” she said. Because 80% of patients have skin lesions, “dermatologists should be aware of this entity in order to communicate with our pathologists to understand that maybe one biopsy isn’t enough. Several biopsies may be required.”
The most common dermatologic presentation of BPDCN is erythematous to deeply violaceous nodules. Other patients may present with infiltrated ecchymotic plaques or petechial to hyperpigmented macules, patches, and plaques. Biopsy reveals a diffusely infiltrated dermis of markedly atypical large cells, but occasionally can be more subtle. “Early lesions may only be perivascular in nature, so going on high power on anything that looks atypical on low power is important in these cases,” Dr. DeClerck said.
The recommended histochemical stains for suspected BPDCN include CD123, CD4, and CD56. “We need to have other stains to rule out other things, such as negative stains that are going to exclude other T cell and B cell processes, and Merkel cell carcinoma, which can express CD56. We also want to have another confirmatory stain because other things can express CD123, CD4, and CD56. Commonly we use TCL1 or TCF4.”
The differential diagnosis of cutaneous findings includes leukemia cutis, mycosis fungoides, NK/T-cell lymphoma, and cutaneous gamma-delta T-cell lymphoma, while the differential diagnosis of biopsy findings includes AML, acute lymphoblastic leukemia, and NK/T-cell lymphoma.
Treatment of BPDCN
Historically, BPDCN was treated with multiagent high-dose chemotherapy. “Patients would frequently respond early but would relapse quickly, progress, and have a poor outcome,” Dr. DeClerck said. Now, first-line therapy is tagraxofusp-erzs (Elzonris) or multiagent chemotherapy based on where the patient is in the course of disease. Tagraxofusp-erzs is an IL-3 conjugated diphtheria toxic fusion protein which binds to CD123, which was approved by the Food and Drug Administration in 2018 for treating BPDCN. After that initial therapy, it is determined whether the patient has a complete response or failed response, she said. “If they have a complete response, they frequently go on to bone marrow transplantation, which is the only curative therapy at this point for these patients.”
According to Dr. DeClerck, an anti-BCL-2 therapy, venetoclax, can be used for patients with BPDCN as well. National Comprehensive Cancer Network (NCCN) guidelines for the treatment of BPDCN can be found on the NCCN website.
Dr. DeClerck emphasized the importance of reviewing biopsy results with a hematopathologist, “because there are complex leukemias that are beyond what dermatopathologists have been trained in.” Once a patient is diagnosed with BPDCN, she recommends rapid referral to a large center for treatment and possible bone marrow transplantation.
Dr. DeClerck disclosed that she is an adviser for tagraxofusp-erzs manufacturer Stemline Therapeutics.
in about 80% of cases.
“You won’t see blastic plasmacytoid dendritic cell neoplasm listed on our primary cutaneous lymphoma classifications because it’s not technically a primary cutaneous disease,” Brittney K. DeClerck, MD, said during the annual meeting of the Pacific Dermatologic Association. “It’s a systemic disease that has secondary cutaneous manifestations. That’s a very important distinction to make, in terms of not missing the underlying disease associated with what might be commonly first seen on the skin.”
BPDCN is a malignancy of plasmacytoid dendritic cells, which capture, process, and present antigen, and allow the remainder of the immune system to be activated. “They are mainly derived from the myeloid cell lineage, and possibly from the lymphoid line in a subset of cases,” said Dr. DeClerck, associate professor of clinical pathology and dermatology at the University of Southern California, Los Angeles. “They secrete high levels of type I interferons, which is important for antiviral immunity, but they can also be implicated in severe systemic inflammatory diseases, such as systemic lupus erythematosus and systemic sclerosis.”
BPDCN involves the skin in about 80% of cases, she added, “but invariably at some point it involves the bone marrow and has an acute leukemic presentation, whether or not it happens concurrently with what we see on the skin as dermatologists. We also see variable involvement of the peripheral blood, lymph nodes, and the central nervous system.”
The classification of BPDCN has changed over time based on evolving immunohistochemical markers and technologies. For example, in 1995 it was called agranular CD4+ NK cell leukemia, in 2001 it was called blastic NK-cell lymphoma, in 2005 it was called CD4+/CD56+ hematodermic neoplasm, and in 2008 it was called BPDCN (AML subset). In 2016 it became classified as its own entity: BPDCN.
Because of changing nomenclature, the true incidence of the disease is unknown, but according to the best available literature, 75% of cases occur in men and the median age is between 60 and 70 years, “but all ages can be affected,” Dr. DeClerck said. “Cases seem to come in clusters. Our most recent cluster has been in our pediatric population. At Children’s Hospital Los Angeles, we’ve had three cases in the last couple of years. To me, that was a bit unusual.”
She added that 10%-20% of patients will have either a history of, or will develop another, hematologic malignancy, such as myelodysplastic syndrome (MDS), chronic myelogenous leukemia (CML), or acute myelogenous leukemia (AML).
The general prognosis of BPDCN is poor, and the mean time from onset of lesions to an actual diagnosis is about 6.2 months, which underscores the importance of early diagnosis, Dr. DeClerck said. “There can be some nondescript solitary lesions that patients can present with, so don’t hesitate to biopsy.” The median overall survival is less than 20 months, but patients under 60 years of age have a slightly better prognosis.
Clinical presentation
Clinically, the malignancy presents with variable involvement of the skin, bone marrow, lymph nodes, peripheral blood, and central nervous system. “Patients may have one or all of these,” she said. Because 80% of patients have skin lesions, “dermatologists should be aware of this entity in order to communicate with our pathologists to understand that maybe one biopsy isn’t enough. Several biopsies may be required.”
The most common dermatologic presentation of BPDCN is erythematous to deeply violaceous nodules. Other patients may present with infiltrated ecchymotic plaques or petechial to hyperpigmented macules, patches, and plaques. Biopsy reveals a diffusely infiltrated dermis of markedly atypical large cells, but occasionally can be more subtle. “Early lesions may only be perivascular in nature, so going on high power on anything that looks atypical on low power is important in these cases,” Dr. DeClerck said.
The recommended histochemical stains for suspected BPDCN include CD123, CD4, and CD56. “We need to have other stains to rule out other things, such as negative stains that are going to exclude other T cell and B cell processes, and Merkel cell carcinoma, which can express CD56. We also want to have another confirmatory stain because other things can express CD123, CD4, and CD56. Commonly we use TCL1 or TCF4.”
The differential diagnosis of cutaneous findings includes leukemia cutis, mycosis fungoides, NK/T-cell lymphoma, and cutaneous gamma-delta T-cell lymphoma, while the differential diagnosis of biopsy findings includes AML, acute lymphoblastic leukemia, and NK/T-cell lymphoma.
Treatment of BPDCN
Historically, BPDCN was treated with multiagent high-dose chemotherapy. “Patients would frequently respond early but would relapse quickly, progress, and have a poor outcome,” Dr. DeClerck said. Now, first-line therapy is tagraxofusp-erzs (Elzonris) or multiagent chemotherapy based on where the patient is in the course of disease. Tagraxofusp-erzs is an IL-3 conjugated diphtheria toxic fusion protein which binds to CD123, which was approved by the Food and Drug Administration in 2018 for treating BPDCN. After that initial therapy, it is determined whether the patient has a complete response or failed response, she said. “If they have a complete response, they frequently go on to bone marrow transplantation, which is the only curative therapy at this point for these patients.”
According to Dr. DeClerck, an anti-BCL-2 therapy, venetoclax, can be used for patients with BPDCN as well. National Comprehensive Cancer Network (NCCN) guidelines for the treatment of BPDCN can be found on the NCCN website.
Dr. DeClerck emphasized the importance of reviewing biopsy results with a hematopathologist, “because there are complex leukemias that are beyond what dermatopathologists have been trained in.” Once a patient is diagnosed with BPDCN, she recommends rapid referral to a large center for treatment and possible bone marrow transplantation.
Dr. DeClerck disclosed that she is an adviser for tagraxofusp-erzs manufacturer Stemline Therapeutics.
in about 80% of cases.
“You won’t see blastic plasmacytoid dendritic cell neoplasm listed on our primary cutaneous lymphoma classifications because it’s not technically a primary cutaneous disease,” Brittney K. DeClerck, MD, said during the annual meeting of the Pacific Dermatologic Association. “It’s a systemic disease that has secondary cutaneous manifestations. That’s a very important distinction to make, in terms of not missing the underlying disease associated with what might be commonly first seen on the skin.”
BPDCN is a malignancy of plasmacytoid dendritic cells, which capture, process, and present antigen, and allow the remainder of the immune system to be activated. “They are mainly derived from the myeloid cell lineage, and possibly from the lymphoid line in a subset of cases,” said Dr. DeClerck, associate professor of clinical pathology and dermatology at the University of Southern California, Los Angeles. “They secrete high levels of type I interferons, which is important for antiviral immunity, but they can also be implicated in severe systemic inflammatory diseases, such as systemic lupus erythematosus and systemic sclerosis.”
BPDCN involves the skin in about 80% of cases, she added, “but invariably at some point it involves the bone marrow and has an acute leukemic presentation, whether or not it happens concurrently with what we see on the skin as dermatologists. We also see variable involvement of the peripheral blood, lymph nodes, and the central nervous system.”
The classification of BPDCN has changed over time based on evolving immunohistochemical markers and technologies. For example, in 1995 it was called agranular CD4+ NK cell leukemia, in 2001 it was called blastic NK-cell lymphoma, in 2005 it was called CD4+/CD56+ hematodermic neoplasm, and in 2008 it was called BPDCN (AML subset). In 2016 it became classified as its own entity: BPDCN.
Because of changing nomenclature, the true incidence of the disease is unknown, but according to the best available literature, 75% of cases occur in men and the median age is between 60 and 70 years, “but all ages can be affected,” Dr. DeClerck said. “Cases seem to come in clusters. Our most recent cluster has been in our pediatric population. At Children’s Hospital Los Angeles, we’ve had three cases in the last couple of years. To me, that was a bit unusual.”
She added that 10%-20% of patients will have either a history of, or will develop another, hematologic malignancy, such as myelodysplastic syndrome (MDS), chronic myelogenous leukemia (CML), or acute myelogenous leukemia (AML).
The general prognosis of BPDCN is poor, and the mean time from onset of lesions to an actual diagnosis is about 6.2 months, which underscores the importance of early diagnosis, Dr. DeClerck said. “There can be some nondescript solitary lesions that patients can present with, so don’t hesitate to biopsy.” The median overall survival is less than 20 months, but patients under 60 years of age have a slightly better prognosis.
Clinical presentation
Clinically, the malignancy presents with variable involvement of the skin, bone marrow, lymph nodes, peripheral blood, and central nervous system. “Patients may have one or all of these,” she said. Because 80% of patients have skin lesions, “dermatologists should be aware of this entity in order to communicate with our pathologists to understand that maybe one biopsy isn’t enough. Several biopsies may be required.”
The most common dermatologic presentation of BPDCN is erythematous to deeply violaceous nodules. Other patients may present with infiltrated ecchymotic plaques or petechial to hyperpigmented macules, patches, and plaques. Biopsy reveals a diffusely infiltrated dermis of markedly atypical large cells, but occasionally can be more subtle. “Early lesions may only be perivascular in nature, so going on high power on anything that looks atypical on low power is important in these cases,” Dr. DeClerck said.
The recommended histochemical stains for suspected BPDCN include CD123, CD4, and CD56. “We need to have other stains to rule out other things, such as negative stains that are going to exclude other T cell and B cell processes, and Merkel cell carcinoma, which can express CD56. We also want to have another confirmatory stain because other things can express CD123, CD4, and CD56. Commonly we use TCL1 or TCF4.”
The differential diagnosis of cutaneous findings includes leukemia cutis, mycosis fungoides, NK/T-cell lymphoma, and cutaneous gamma-delta T-cell lymphoma, while the differential diagnosis of biopsy findings includes AML, acute lymphoblastic leukemia, and NK/T-cell lymphoma.
Treatment of BPDCN
Historically, BPDCN was treated with multiagent high-dose chemotherapy. “Patients would frequently respond early but would relapse quickly, progress, and have a poor outcome,” Dr. DeClerck said. Now, first-line therapy is tagraxofusp-erzs (Elzonris) or multiagent chemotherapy based on where the patient is in the course of disease. Tagraxofusp-erzs is an IL-3 conjugated diphtheria toxic fusion protein which binds to CD123, which was approved by the Food and Drug Administration in 2018 for treating BPDCN. After that initial therapy, it is determined whether the patient has a complete response or failed response, she said. “If they have a complete response, they frequently go on to bone marrow transplantation, which is the only curative therapy at this point for these patients.”
According to Dr. DeClerck, an anti-BCL-2 therapy, venetoclax, can be used for patients with BPDCN as well. National Comprehensive Cancer Network (NCCN) guidelines for the treatment of BPDCN can be found on the NCCN website.
Dr. DeClerck emphasized the importance of reviewing biopsy results with a hematopathologist, “because there are complex leukemias that are beyond what dermatopathologists have been trained in.” Once a patient is diagnosed with BPDCN, she recommends rapid referral to a large center for treatment and possible bone marrow transplantation.
Dr. DeClerck disclosed that she is an adviser for tagraxofusp-erzs manufacturer Stemline Therapeutics.
FROM PDA 2021
Study identifies pandemic-related stressor in Parkinson’s disease
a team of researchers in the Netherlands reported, but they also identified meaningful targets for intervention.

Lisanne Dommershuijsen, MSc, a PhD candidate and researcher in epidemiology at the Erasmus University Medical Center in Rotterdam, the Netherlands, reported on a cross-sectional study of 833 participants with Parkinson’s disease in the PRIME-NL study at the International Congress of Parkinson’s Disease and Movement Disorders. The average age of participants was 70.2 and 38% were women.
“We studied targeted hypothetical interventions on COVID-19 stressors in people with Parkinson’s disease,” Ms. Dommershuijsen said. “This disruption in normal life caused considerable psychological stress in community-dwelling individuals. People with Parkinson’s disease might be especially vulnerable to this stress.
“For instance, because reduced levels of physical activity have worsened symptoms or because people with Parkinson’s often have difficulty with flexible [adaptations] to drastic and rapid changes in daily routines, such as those introduced by the COVID-19 pandemic, previous studies found that COVID-19 worsened depression and anxiety symptoms and reduced quality of life (QOL) in people with Parkinson’s disease,” Ms. Dommershuijsen said.
Hence, the goal of the study was to identify the most vulnerable subgroups in the Parkinson’s population and to suggest potential interventions to ameliorate these impacts, she said.
The study focused on eight different stressors that emerged in the pandemic: access to care, medicine and nursing services; loss of social contact; canceled social events; tension or conflict in the home; inability to perform physical activity or relax; and COVID-19 symptoms. The outcomes of interest were depression, as measured with the Beck Depression Inventory (BDI); anxiety, as measured with the Spielberger State-Trait Anxiety Inventory (STAI); and QOL, with the Parkinson’s Disease Quality of Life Questionnaire. The aggregate resulted in a scale of 0-40, with the mean stressor score in the study being 9.6, Ms. Dommershuijsen said.
The BDI and STAI scores for social stressors – loss of social contacts, social events canceled and tension or conflict at home – exceeded those for the so-called care stressors – problems accessing care, medication or nursing – she said, although all eight stressors yielded higher BDI and STAI scores across the board.
Vulnerable subgroups
“When we looked at vulnerable subgroups of people with Parkinson’s disease, we found more pronounced associations between the COVID-19 stress and mental health in women, in highly educated participants, and in participants with advanced Parkinson’s disease,” Ms. Dommershuijsen said. The impact on women and people with advanced disease is explainable, Ms. Dommershuijsen added in an interview; the former because depressive symptoms are more common in women, and the latter because loss of access to care impacts mental wellness.
“The finding that social stressors were more related to anxiety in highly educated people was surprising to us, given that depression in general is more common in people with a lower education,” she said in an interview. “One previous study of the general population suggested this might be related to expectations about available resources, but this findings and the possible explanation warrants further investigation.”
When the study stratified for coping strategies, the COVID-19 stressors had a smaller effect on depressive and anxiety symptoms in Parkinson’s disease patients prone to confrontive coping and planful problem solving, she said. “Whereas, we observed a larger effect of these stressors in people who are prone to using distancing or seeking social support as coping mechanisms,” Ms. Dommershuijsen said.
The researchers also created a model of a hypothetical 50% reduction in COVID-19 stressors among all study participants, but the effect wasn’t clinically relevant, Ms. Dommershuijsen said. However, in people with advanced Parkinson’s disease – that is, with an Movement Disorder Society–Unified Parkinson Disease Rating Scale score above median – the effect was clinically relevant in all outcomes.
The potential interventions the study identified were telemedicine via virtual consultations to alleviate care stressors, and virtual support groups and online classes to address social stressors. “However, a more personalized approach is needed to target tension or conflict at home, which was the most important social stressor influencing depression and anxiety symptoms in our study,” she said. “Social work can play an important role here.”
Asked to comment on the study, Roy Alcalay, MD, professor of neurology at Columbia University Irving Medical Center in New York, said in an interview that the findings align with his research on the impact of COVID-19 and related restrictions on people with Parkinson’s disease.
“The pandemic has affected people in different ways,” he said. “Initially very acutely, people just didn’t have access to doctors. There was also the acute question in movement disorders, but also in other diseases where the people with Parkinson’s disease are going to have the worse outcome when they have COVID-19.” Dr. Alcalay authored two recent papers on the impact of COVID-19 in people with Parkinson’s disease.
“Then we see that, in addition to that question, there’s the question of even if they don’t have COVID-19, just the social distancing and the lack of access to health care, and specifically to physical and occupational therapy and other services, can be quite damaging,” he said.
What’s commendable about the study, he said, was that it just doesn’t highlight the problem. “They’re also highlighting potential solutions, that planful problem solving and coping strategies can be helpful to people.”
Neither Ms. Dommershuijsen nor Dr. Alcalay have any relevant relationships to disclose.
a team of researchers in the Netherlands reported, but they also identified meaningful targets for intervention.
Lisanne Dommershuijsen, MSc, a PhD candidate and researcher in epidemiology at the Erasmus University Medical Center in Rotterdam, the Netherlands, reported on a cross-sectional study of 833 participants with Parkinson’s disease in the PRIME-NL study at the International Congress of Parkinson’s Disease and Movement Disorders. The average age of participants was 70.2 and 38% were women.
“We studied targeted hypothetical interventions on COVID-19 stressors in people with Parkinson’s disease,” Ms. Dommershuijsen said. “This disruption in normal life caused considerable psychological stress in community-dwelling individuals. People with Parkinson’s disease might be especially vulnerable to this stress.
“For instance, because reduced levels of physical activity have worsened symptoms or because people with Parkinson’s often have difficulty with flexible [adaptations] to drastic and rapid changes in daily routines, such as those introduced by the COVID-19 pandemic, previous studies found that COVID-19 worsened depression and anxiety symptoms and reduced quality of life (QOL) in people with Parkinson’s disease,” Ms. Dommershuijsen said.
Hence, the goal of the study was to identify the most vulnerable subgroups in the Parkinson’s population and to suggest potential interventions to ameliorate these impacts, she said.
The study focused on eight different stressors that emerged in the pandemic: access to care, medicine and nursing services; loss of social contact; canceled social events; tension or conflict in the home; inability to perform physical activity or relax; and COVID-19 symptoms. The outcomes of interest were depression, as measured with the Beck Depression Inventory (BDI); anxiety, as measured with the Spielberger State-Trait Anxiety Inventory (STAI); and QOL, with the Parkinson’s Disease Quality of Life Questionnaire. The aggregate resulted in a scale of 0-40, with the mean stressor score in the study being 9.6, Ms. Dommershuijsen said.
The BDI and STAI scores for social stressors – loss of social contacts, social events canceled and tension or conflict at home – exceeded those for the so-called care stressors – problems accessing care, medication or nursing – she said, although all eight stressors yielded higher BDI and STAI scores across the board.
Vulnerable subgroups
“When we looked at vulnerable subgroups of people with Parkinson’s disease, we found more pronounced associations between the COVID-19 stress and mental health in women, in highly educated participants, and in participants with advanced Parkinson’s disease,” Ms. Dommershuijsen said. The impact on women and people with advanced disease is explainable, Ms. Dommershuijsen added in an interview; the former because depressive symptoms are more common in women, and the latter because loss of access to care impacts mental wellness.
“The finding that social stressors were more related to anxiety in highly educated people was surprising to us, given that depression in general is more common in people with a lower education,” she said in an interview. “One previous study of the general population suggested this might be related to expectations about available resources, but this findings and the possible explanation warrants further investigation.”
When the study stratified for coping strategies, the COVID-19 stressors had a smaller effect on depressive and anxiety symptoms in Parkinson’s disease patients prone to confrontive coping and planful problem solving, she said. “Whereas, we observed a larger effect of these stressors in people who are prone to using distancing or seeking social support as coping mechanisms,” Ms. Dommershuijsen said.
The researchers also created a model of a hypothetical 50% reduction in COVID-19 stressors among all study participants, but the effect wasn’t clinically relevant, Ms. Dommershuijsen said. However, in people with advanced Parkinson’s disease – that is, with an Movement Disorder Society–Unified Parkinson Disease Rating Scale score above median – the effect was clinically relevant in all outcomes.
The potential interventions the study identified were telemedicine via virtual consultations to alleviate care stressors, and virtual support groups and online classes to address social stressors. “However, a more personalized approach is needed to target tension or conflict at home, which was the most important social stressor influencing depression and anxiety symptoms in our study,” she said. “Social work can play an important role here.”
Asked to comment on the study, Roy Alcalay, MD, professor of neurology at Columbia University Irving Medical Center in New York, said in an interview that the findings align with his research on the impact of COVID-19 and related restrictions on people with Parkinson’s disease.
“The pandemic has affected people in different ways,” he said. “Initially very acutely, people just didn’t have access to doctors. There was also the acute question in movement disorders, but also in other diseases where the people with Parkinson’s disease are going to have the worse outcome when they have COVID-19.” Dr. Alcalay authored two recent papers on the impact of COVID-19 in people with Parkinson’s disease.
“Then we see that, in addition to that question, there’s the question of even if they don’t have COVID-19, just the social distancing and the lack of access to health care, and specifically to physical and occupational therapy and other services, can be quite damaging,” he said.
What’s commendable about the study, he said, was that it just doesn’t highlight the problem. “They’re also highlighting potential solutions, that planful problem solving and coping strategies can be helpful to people.”
Neither Ms. Dommershuijsen nor Dr. Alcalay have any relevant relationships to disclose.
a team of researchers in the Netherlands reported, but they also identified meaningful targets for intervention.
Lisanne Dommershuijsen, MSc, a PhD candidate and researcher in epidemiology at the Erasmus University Medical Center in Rotterdam, the Netherlands, reported on a cross-sectional study of 833 participants with Parkinson’s disease in the PRIME-NL study at the International Congress of Parkinson’s Disease and Movement Disorders. The average age of participants was 70.2 and 38% were women.
“We studied targeted hypothetical interventions on COVID-19 stressors in people with Parkinson’s disease,” Ms. Dommershuijsen said. “This disruption in normal life caused considerable psychological stress in community-dwelling individuals. People with Parkinson’s disease might be especially vulnerable to this stress.
“For instance, because reduced levels of physical activity have worsened symptoms or because people with Parkinson’s often have difficulty with flexible [adaptations] to drastic and rapid changes in daily routines, such as those introduced by the COVID-19 pandemic, previous studies found that COVID-19 worsened depression and anxiety symptoms and reduced quality of life (QOL) in people with Parkinson’s disease,” Ms. Dommershuijsen said.
Hence, the goal of the study was to identify the most vulnerable subgroups in the Parkinson’s population and to suggest potential interventions to ameliorate these impacts, she said.
The study focused on eight different stressors that emerged in the pandemic: access to care, medicine and nursing services; loss of social contact; canceled social events; tension or conflict in the home; inability to perform physical activity or relax; and COVID-19 symptoms. The outcomes of interest were depression, as measured with the Beck Depression Inventory (BDI); anxiety, as measured with the Spielberger State-Trait Anxiety Inventory (STAI); and QOL, with the Parkinson’s Disease Quality of Life Questionnaire. The aggregate resulted in a scale of 0-40, with the mean stressor score in the study being 9.6, Ms. Dommershuijsen said.
The BDI and STAI scores for social stressors – loss of social contacts, social events canceled and tension or conflict at home – exceeded those for the so-called care stressors – problems accessing care, medication or nursing – she said, although all eight stressors yielded higher BDI and STAI scores across the board.
Vulnerable subgroups
“When we looked at vulnerable subgroups of people with Parkinson’s disease, we found more pronounced associations between the COVID-19 stress and mental health in women, in highly educated participants, and in participants with advanced Parkinson’s disease,” Ms. Dommershuijsen said. The impact on women and people with advanced disease is explainable, Ms. Dommershuijsen added in an interview; the former because depressive symptoms are more common in women, and the latter because loss of access to care impacts mental wellness.
“The finding that social stressors were more related to anxiety in highly educated people was surprising to us, given that depression in general is more common in people with a lower education,” she said in an interview. “One previous study of the general population suggested this might be related to expectations about available resources, but this findings and the possible explanation warrants further investigation.”
When the study stratified for coping strategies, the COVID-19 stressors had a smaller effect on depressive and anxiety symptoms in Parkinson’s disease patients prone to confrontive coping and planful problem solving, she said. “Whereas, we observed a larger effect of these stressors in people who are prone to using distancing or seeking social support as coping mechanisms,” Ms. Dommershuijsen said.
The researchers also created a model of a hypothetical 50% reduction in COVID-19 stressors among all study participants, but the effect wasn’t clinically relevant, Ms. Dommershuijsen said. However, in people with advanced Parkinson’s disease – that is, with an Movement Disorder Society–Unified Parkinson Disease Rating Scale score above median – the effect was clinically relevant in all outcomes.
The potential interventions the study identified were telemedicine via virtual consultations to alleviate care stressors, and virtual support groups and online classes to address social stressors. “However, a more personalized approach is needed to target tension or conflict at home, which was the most important social stressor influencing depression and anxiety symptoms in our study,” she said. “Social work can play an important role here.”
Asked to comment on the study, Roy Alcalay, MD, professor of neurology at Columbia University Irving Medical Center in New York, said in an interview that the findings align with his research on the impact of COVID-19 and related restrictions on people with Parkinson’s disease.
“The pandemic has affected people in different ways,” he said. “Initially very acutely, people just didn’t have access to doctors. There was also the acute question in movement disorders, but also in other diseases where the people with Parkinson’s disease are going to have the worse outcome when they have COVID-19.” Dr. Alcalay authored two recent papers on the impact of COVID-19 in people with Parkinson’s disease.
“Then we see that, in addition to that question, there’s the question of even if they don’t have COVID-19, just the social distancing and the lack of access to health care, and specifically to physical and occupational therapy and other services, can be quite damaging,” he said.
What’s commendable about the study, he said, was that it just doesn’t highlight the problem. “They’re also highlighting potential solutions, that planful problem solving and coping strategies can be helpful to people.”
Neither Ms. Dommershuijsen nor Dr. Alcalay have any relevant relationships to disclose.
FROM MDS VIRTUAL CONGRESS 2021
Sexual assault in women tied to increased stroke, dementia risk
Traumatic experiences, especially sexual assault, may put women at greater risk for poor brain health.
In the Ms Brain study, middle-aged women with trauma exposure had a greater volume of white matter hyperintensities (WMHs) than those without trauma. In addition, the differences persisted even after adjusting for depressive or post-traumatic stress symptoms.
WMHs are “an important indicator of small vessel disease in the brain and have been linked to future stroke risk, dementia risk, and mortality,” lead investigator Rebecca Thurston, PhD, from the University of Pittsburgh, told this news organization.
“What I take from this is, really, that sexual assault has implications for women’s health, far beyond exclusively mental health outcomes, but also for their cardiovascular health, as we have shown in other work and for their stroke and dementia risk as we are seeing in the present work,” Dr. Thurston added.
The study was presented at the North American Menopause Society (NAMS) Annual Meeting in Washington, D.C., and has been accepted for publication in the journal Brain Imaging and Behavior.
Beyond the usual suspects
As part of the study, 145 women (mean age, 59 years) free of clinical cardiovascular disease, stroke, or dementia provided their medical history, including history of traumatic experiences, depression, and post-traumatic stress disorder and underwent magnetic resonance brain imaging for WMHs.
More than two-thirds (68%) of the women reported at least one trauma, most commonly sexual assault (23%).
In multivariate analysis, women with trauma exposure had greater WMH volume than women without trauma (P = .01), with sexual assault most strongly associated with greater WMH volume (P = .02).
The associations persisted after adjusting for depressive or post-traumatic stress symptoms.
“A history of sexual assault was particularly related to white matter hyperintensities in the parietal lobe, and these kinds of white matter hyperintensities have been linked to Alzheimer’s disease in a fairly pronounced way,” Dr. Thurston said.
“When we think about risk factors for stroke, dementia, we need to think beyond exclusively our usual suspects and also think about women [who experienced] psychological trauma and experienced sexual assault in particular. So ask about it and consider it part of your screening regimen,” she added.
‘Burgeoning’ literature
Commenting on the findings, Charles Nemeroff, MD, PhD, professor and chair, department of psychiatry and behavioral sciences, Dell Medical School, University of Texas at Austin, and director of its Institute for Early Life Adversity Research, said the research adds to the “burgeoning literature on the long term neurobiological consequences of trauma and more specifically, sexual abuse, on brain imaging measures.”
“Our group and others reported several years ago that patients with mood disorders, more specifically bipolar disorder and major depression, had higher rates of WMH than matched controls. Those older studies did not control for a history of early life adversity such as childhood maltreatment,” Dr. Nemeroff said.
“In addition to this finding of increased WMH in subjects exposed to trauma is a very large literature documenting other central nervous system (CNS) changes in this population, including cortical thinning in certain brain areas and clearly an emerging finding that different forms of childhood maltreatment are associated with quite distinct structural brain alterations in adulthood,” he noted.
The study was supported by grants from the National Institutes of Health. Dr. Thurston and Dr. Nemeroff have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Traumatic experiences, especially sexual assault, may put women at greater risk for poor brain health.
In the Ms Brain study, middle-aged women with trauma exposure had a greater volume of white matter hyperintensities (WMHs) than those without trauma. In addition, the differences persisted even after adjusting for depressive or post-traumatic stress symptoms.
WMHs are “an important indicator of small vessel disease in the brain and have been linked to future stroke risk, dementia risk, and mortality,” lead investigator Rebecca Thurston, PhD, from the University of Pittsburgh, told this news organization.
“What I take from this is, really, that sexual assault has implications for women’s health, far beyond exclusively mental health outcomes, but also for their cardiovascular health, as we have shown in other work and for their stroke and dementia risk as we are seeing in the present work,” Dr. Thurston added.
The study was presented at the North American Menopause Society (NAMS) Annual Meeting in Washington, D.C., and has been accepted for publication in the journal Brain Imaging and Behavior.
Beyond the usual suspects
As part of the study, 145 women (mean age, 59 years) free of clinical cardiovascular disease, stroke, or dementia provided their medical history, including history of traumatic experiences, depression, and post-traumatic stress disorder and underwent magnetic resonance brain imaging for WMHs.
More than two-thirds (68%) of the women reported at least one trauma, most commonly sexual assault (23%).
In multivariate analysis, women with trauma exposure had greater WMH volume than women without trauma (P = .01), with sexual assault most strongly associated with greater WMH volume (P = .02).
The associations persisted after adjusting for depressive or post-traumatic stress symptoms.
“A history of sexual assault was particularly related to white matter hyperintensities in the parietal lobe, and these kinds of white matter hyperintensities have been linked to Alzheimer’s disease in a fairly pronounced way,” Dr. Thurston said.
“When we think about risk factors for stroke, dementia, we need to think beyond exclusively our usual suspects and also think about women [who experienced] psychological trauma and experienced sexual assault in particular. So ask about it and consider it part of your screening regimen,” she added.
‘Burgeoning’ literature
Commenting on the findings, Charles Nemeroff, MD, PhD, professor and chair, department of psychiatry and behavioral sciences, Dell Medical School, University of Texas at Austin, and director of its Institute for Early Life Adversity Research, said the research adds to the “burgeoning literature on the long term neurobiological consequences of trauma and more specifically, sexual abuse, on brain imaging measures.”
“Our group and others reported several years ago that patients with mood disorders, more specifically bipolar disorder and major depression, had higher rates of WMH than matched controls. Those older studies did not control for a history of early life adversity such as childhood maltreatment,” Dr. Nemeroff said.
“In addition to this finding of increased WMH in subjects exposed to trauma is a very large literature documenting other central nervous system (CNS) changes in this population, including cortical thinning in certain brain areas and clearly an emerging finding that different forms of childhood maltreatment are associated with quite distinct structural brain alterations in adulthood,” he noted.
The study was supported by grants from the National Institutes of Health. Dr. Thurston and Dr. Nemeroff have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Traumatic experiences, especially sexual assault, may put women at greater risk for poor brain health.
In the Ms Brain study, middle-aged women with trauma exposure had a greater volume of white matter hyperintensities (WMHs) than those without trauma. In addition, the differences persisted even after adjusting for depressive or post-traumatic stress symptoms.
WMHs are “an important indicator of small vessel disease in the brain and have been linked to future stroke risk, dementia risk, and mortality,” lead investigator Rebecca Thurston, PhD, from the University of Pittsburgh, told this news organization.
“What I take from this is, really, that sexual assault has implications for women’s health, far beyond exclusively mental health outcomes, but also for their cardiovascular health, as we have shown in other work and for their stroke and dementia risk as we are seeing in the present work,” Dr. Thurston added.
The study was presented at the North American Menopause Society (NAMS) Annual Meeting in Washington, D.C., and has been accepted for publication in the journal Brain Imaging and Behavior.
Beyond the usual suspects
As part of the study, 145 women (mean age, 59 years) free of clinical cardiovascular disease, stroke, or dementia provided their medical history, including history of traumatic experiences, depression, and post-traumatic stress disorder and underwent magnetic resonance brain imaging for WMHs.
More than two-thirds (68%) of the women reported at least one trauma, most commonly sexual assault (23%).
In multivariate analysis, women with trauma exposure had greater WMH volume than women without trauma (P = .01), with sexual assault most strongly associated with greater WMH volume (P = .02).
The associations persisted after adjusting for depressive or post-traumatic stress symptoms.
“A history of sexual assault was particularly related to white matter hyperintensities in the parietal lobe, and these kinds of white matter hyperintensities have been linked to Alzheimer’s disease in a fairly pronounced way,” Dr. Thurston said.
“When we think about risk factors for stroke, dementia, we need to think beyond exclusively our usual suspects and also think about women [who experienced] psychological trauma and experienced sexual assault in particular. So ask about it and consider it part of your screening regimen,” she added.
‘Burgeoning’ literature
Commenting on the findings, Charles Nemeroff, MD, PhD, professor and chair, department of psychiatry and behavioral sciences, Dell Medical School, University of Texas at Austin, and director of its Institute for Early Life Adversity Research, said the research adds to the “burgeoning literature on the long term neurobiological consequences of trauma and more specifically, sexual abuse, on brain imaging measures.”
“Our group and others reported several years ago that patients with mood disorders, more specifically bipolar disorder and major depression, had higher rates of WMH than matched controls. Those older studies did not control for a history of early life adversity such as childhood maltreatment,” Dr. Nemeroff said.
“In addition to this finding of increased WMH in subjects exposed to trauma is a very large literature documenting other central nervous system (CNS) changes in this population, including cortical thinning in certain brain areas and clearly an emerging finding that different forms of childhood maltreatment are associated with quite distinct structural brain alterations in adulthood,” he noted.
The study was supported by grants from the National Institutes of Health. Dr. Thurston and Dr. Nemeroff have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigative botulinum toxin formulation shows prolonged effect
, according to results of a phase 3 clinical trial presented at the virtual International Congress of Parkinson’s Disease and Movement Disorders.

The ASPEN-1 trial evaluated 301 patients with moderate to severe cervical dystonia for up to 36 weeks and found that those receiving two doses of DaxibotulinumtoxinA, known as DAXI, versus placebo improved their scores on the Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS), said Joseph Jankovic, MD, professor of neurology and director of the Parkinson’s Disease Center and Movement Disorders Clinic at Baylor College of Medicine in Houston.
“Botulinum neurotoxin is clearly the treatment of choice for cervical dystonia,” Dr. Jankovic said in an interview. “While the majority of patients obtain satisfactory benefit from BoNT injections, some experience adverse effects such as neck weakness and difficulty swallowing.” Another limitation of BoNT is that its effects wear off after about 3 months or less and patients have to be re-injected, he said.
“This is why I am quite encouraged by the results of the DAXI study that suggest that this formulation of BoNT (type A) may have a longer response and relatively few side effects,” he said.
Patients in the study were randomized 1:3:3 to placebo, DAXI 125U or DAXI 250U. The average TWSTRS score upon enrollment was 43.3. The placebo group had a mean ± standard error TWSTRS improvement of 4.3 ± 1.8 at 4 or 6 weeks, while the treatment groups had mean ± SE improvements of 12.7 ± 1.3 for 125U and 10.9 ± 1.2 for 250U (P = .0006 vs. placebo). They translate into improvements of 12%, 31%, and 27% for the placebo and low- and high-dose treatment groups, respectively.
“Even though paradoxically it seems the high-dose group did slightly less well than the low-dose group, there was no difference between the two groups,” Dr. Jankovic said in the presentation.
The median duration of benefit was 24 weeks in the low-dose group and 20.3 weeks in the high-dose group.
The treatment groups demonstrated similar benefit compared with placebo in TWSTRS subscales for disease severity, disability, and pain, Dr. Jankovic said. “The majority of the patients had little better, moderately better, or very much better from the botulinum toxin injection with respect to clinical global impression of change and patient global impression of change,” he said.
Likewise, both the Clinician Global Impression of Change (CGIC) and Patient Global Impression of Change (PGIC) demonstrated improvement versus placebo: 77.6% and 76.9% in the 125U and 250U doses versus 45.7% for the former; and 71.2% and 73.1% versus 41.3% for the latter.
Side effects “were remarkably minimal,” Dr. Jankovic said, “but I want to call attention to the low frequency of neck weakness or dysphagia in comparison with other studies of botulinum toxin in cervical dystonia.” The rates of dysphagia were 1.6% and 3.9% in the 125U and 250U treatment groups, respectively. Sixteen of the 255 patients in the treatment groups reported muscular weakness or musculoskeletal pain, and seven had dysphagia.
The rate of dysphagia after injection is noteworthy, said David Charles, MD, professor and vice chair of neurology at Vanderbilt University in Nashville, Tenn., who was not involved in the research. “The one thing we worry about most in people with cervical dystonia are swallowing and choking – dysphagia – and the numbers are very modest: 2 out of 127 in the 125U dose and 5 of 130 in the 250U dose,” he said. “That’s a very low rate of that adverse event.”
The duration of action for both doses is “rather remarkable,” Dr. Charles said. “With the other formulations, my patients are coming back every 12 weeks for treatment; the BoNT helps so much that [these] patients make their appointments every 3 months for as far out as they can,” he said. “This could potentially mean two or three trips a year as opposed to four trips a year.”
The trial was funded by Revance Therapeutics. Dr. Jankovic is an investigator for Revance, and three coauthors are employees of Revance. Dr. Charles is a consultant to the company.
, according to results of a phase 3 clinical trial presented at the virtual International Congress of Parkinson’s Disease and Movement Disorders.
The ASPEN-1 trial evaluated 301 patients with moderate to severe cervical dystonia for up to 36 weeks and found that those receiving two doses of DaxibotulinumtoxinA, known as DAXI, versus placebo improved their scores on the Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS), said Joseph Jankovic, MD, professor of neurology and director of the Parkinson’s Disease Center and Movement Disorders Clinic at Baylor College of Medicine in Houston.
“Botulinum neurotoxin is clearly the treatment of choice for cervical dystonia,” Dr. Jankovic said in an interview. “While the majority of patients obtain satisfactory benefit from BoNT injections, some experience adverse effects such as neck weakness and difficulty swallowing.” Another limitation of BoNT is that its effects wear off after about 3 months or less and patients have to be re-injected, he said.
“This is why I am quite encouraged by the results of the DAXI study that suggest that this formulation of BoNT (type A) may have a longer response and relatively few side effects,” he said.
Patients in the study were randomized 1:3:3 to placebo, DAXI 125U or DAXI 250U. The average TWSTRS score upon enrollment was 43.3. The placebo group had a mean ± standard error TWSTRS improvement of 4.3 ± 1.8 at 4 or 6 weeks, while the treatment groups had mean ± SE improvements of 12.7 ± 1.3 for 125U and 10.9 ± 1.2 for 250U (P = .0006 vs. placebo). They translate into improvements of 12%, 31%, and 27% for the placebo and low- and high-dose treatment groups, respectively.
“Even though paradoxically it seems the high-dose group did slightly less well than the low-dose group, there was no difference between the two groups,” Dr. Jankovic said in the presentation.
The median duration of benefit was 24 weeks in the low-dose group and 20.3 weeks in the high-dose group.
The treatment groups demonstrated similar benefit compared with placebo in TWSTRS subscales for disease severity, disability, and pain, Dr. Jankovic said. “The majority of the patients had little better, moderately better, or very much better from the botulinum toxin injection with respect to clinical global impression of change and patient global impression of change,” he said.
Likewise, both the Clinician Global Impression of Change (CGIC) and Patient Global Impression of Change (PGIC) demonstrated improvement versus placebo: 77.6% and 76.9% in the 125U and 250U doses versus 45.7% for the former; and 71.2% and 73.1% versus 41.3% for the latter.
Side effects “were remarkably minimal,” Dr. Jankovic said, “but I want to call attention to the low frequency of neck weakness or dysphagia in comparison with other studies of botulinum toxin in cervical dystonia.” The rates of dysphagia were 1.6% and 3.9% in the 125U and 250U treatment groups, respectively. Sixteen of the 255 patients in the treatment groups reported muscular weakness or musculoskeletal pain, and seven had dysphagia.
The rate of dysphagia after injection is noteworthy, said David Charles, MD, professor and vice chair of neurology at Vanderbilt University in Nashville, Tenn., who was not involved in the research. “The one thing we worry about most in people with cervical dystonia are swallowing and choking – dysphagia – and the numbers are very modest: 2 out of 127 in the 125U dose and 5 of 130 in the 250U dose,” he said. “That’s a very low rate of that adverse event.”
The duration of action for both doses is “rather remarkable,” Dr. Charles said. “With the other formulations, my patients are coming back every 12 weeks for treatment; the BoNT helps so much that [these] patients make their appointments every 3 months for as far out as they can,” he said. “This could potentially mean two or three trips a year as opposed to four trips a year.”
The trial was funded by Revance Therapeutics. Dr. Jankovic is an investigator for Revance, and three coauthors are employees of Revance. Dr. Charles is a consultant to the company.
, according to results of a phase 3 clinical trial presented at the virtual International Congress of Parkinson’s Disease and Movement Disorders.
The ASPEN-1 trial evaluated 301 patients with moderate to severe cervical dystonia for up to 36 weeks and found that those receiving two doses of DaxibotulinumtoxinA, known as DAXI, versus placebo improved their scores on the Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS), said Joseph Jankovic, MD, professor of neurology and director of the Parkinson’s Disease Center and Movement Disorders Clinic at Baylor College of Medicine in Houston.
“Botulinum neurotoxin is clearly the treatment of choice for cervical dystonia,” Dr. Jankovic said in an interview. “While the majority of patients obtain satisfactory benefit from BoNT injections, some experience adverse effects such as neck weakness and difficulty swallowing.” Another limitation of BoNT is that its effects wear off after about 3 months or less and patients have to be re-injected, he said.
“This is why I am quite encouraged by the results of the DAXI study that suggest that this formulation of BoNT (type A) may have a longer response and relatively few side effects,” he said.
Patients in the study were randomized 1:3:3 to placebo, DAXI 125U or DAXI 250U. The average TWSTRS score upon enrollment was 43.3. The placebo group had a mean ± standard error TWSTRS improvement of 4.3 ± 1.8 at 4 or 6 weeks, while the treatment groups had mean ± SE improvements of 12.7 ± 1.3 for 125U and 10.9 ± 1.2 for 250U (P = .0006 vs. placebo). They translate into improvements of 12%, 31%, and 27% for the placebo and low- and high-dose treatment groups, respectively.
“Even though paradoxically it seems the high-dose group did slightly less well than the low-dose group, there was no difference between the two groups,” Dr. Jankovic said in the presentation.
The median duration of benefit was 24 weeks in the low-dose group and 20.3 weeks in the high-dose group.
The treatment groups demonstrated similar benefit compared with placebo in TWSTRS subscales for disease severity, disability, and pain, Dr. Jankovic said. “The majority of the patients had little better, moderately better, or very much better from the botulinum toxin injection with respect to clinical global impression of change and patient global impression of change,” he said.
Likewise, both the Clinician Global Impression of Change (CGIC) and Patient Global Impression of Change (PGIC) demonstrated improvement versus placebo: 77.6% and 76.9% in the 125U and 250U doses versus 45.7% for the former; and 71.2% and 73.1% versus 41.3% for the latter.
Side effects “were remarkably minimal,” Dr. Jankovic said, “but I want to call attention to the low frequency of neck weakness or dysphagia in comparison with other studies of botulinum toxin in cervical dystonia.” The rates of dysphagia were 1.6% and 3.9% in the 125U and 250U treatment groups, respectively. Sixteen of the 255 patients in the treatment groups reported muscular weakness or musculoskeletal pain, and seven had dysphagia.
The rate of dysphagia after injection is noteworthy, said David Charles, MD, professor and vice chair of neurology at Vanderbilt University in Nashville, Tenn., who was not involved in the research. “The one thing we worry about most in people with cervical dystonia are swallowing and choking – dysphagia – and the numbers are very modest: 2 out of 127 in the 125U dose and 5 of 130 in the 250U dose,” he said. “That’s a very low rate of that adverse event.”
The duration of action for both doses is “rather remarkable,” Dr. Charles said. “With the other formulations, my patients are coming back every 12 weeks for treatment; the BoNT helps so much that [these] patients make their appointments every 3 months for as far out as they can,” he said. “This could potentially mean two or three trips a year as opposed to four trips a year.”
The trial was funded by Revance Therapeutics. Dr. Jankovic is an investigator for Revance, and three coauthors are employees of Revance. Dr. Charles is a consultant to the company.
FROM MDS VIRTUAL CONGRESS 2021