User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Once daily poziotinib shows efficacy in non–small cell lung cancer
Tumor reductions, stated lead author Robin Cornelissen, PhD, MD, Erasmus University, Rotterdam, the Netherlands, were seen in 88% of patients.
EGFR and HER2 exon 20 insertion mutations are rare subsets accounting for about 10% each of all mutations and 2%-4% each in NSCLC. “There is no approved therapy for either treatment-naive or previously treated NSCLC with HER2 exon 20 mutations,” Dr. Cornelissen said in a virtual oral presentation (abstract LBA46) on Sept. 18. While chemotherapy agents with or without checkpoint inhibitors and tyrosine kinase inhibitors (TKIs) are currently utilized, none are specific to exon 20 mutations, and historical response rates from mostly small uncontrolled studies vary widely from about 6.9%-35%, with median progression-free survival (PFS) ranging from 3 to 7 months. Poziotinib is a potent oral pan-HER TKI with activity in patients with EGFR or HER2 exon 20–mutated NSCLC.
Dr. Cornelissen presented preliminary safety and efficacy data from the phase 2 ZENITH20, a seven-cohort global clinical trial, specifically from cohort 4 (daily dosing) which included 48 HER2 exon 20 insertion NSCLC patients (median age, 60.5 years; female/male, 26/22) treated first-line with oral daily poziotinib (16 mg). The majority were White (75%), female (54%), and nonsmokers (69%) with an Eastern Cooperative Oncology Group performance status of 1 (65%).The primary endpoint was objective response rate evaluated centrally by an independent image review committee using RECIST 1.1 criteria.
All patients have experienced treatment-related adverse events (TRAEs) with 10% considered serious, and permanent discontinuation in 13%. About 83% of patients had dose interruptions and 76% had dose reductions. The most common adverse events were diarrhea (any grade, 83%; grade 3, 15%), rash (any grade, 69%; grade 3, 35%), stomatitis/mucosal inflammation (any grade, 81%; grade 3, 21%), and paronychia (any grade, 46%; grade 3 8%). Pneumonitis occurred in two patients (4%), with one grade 3 (2%). No grade 4/5 TRAEs were reported.
Discontinuations in 44 patients (92%), Dr. Cornelissen said, are attributed to death (5/10%), disease progression (30/63%), adverse events (1/2%), and other (8/17%), with treatment ongoing in 4 patients (8%).
The rate for the primary endpoint of ORR was 43.8% (n = 21) (95% confidence interval, 29.5%-58.8%).Tumor reductions have been observed in 42/48 patients (88%) with a median reduction of 35%. One complete response was reported (2.1%), with partial responses in 20 (41.7%), stable disease in 15 (31.3%), progressive disease in 7 (14.6%), and 5 (10.4%) not evaluable. The disease control rate was 75.0%.
Among secondary endpoints, median duration of response (DoR) was 5.4 months (range, 2.8 to >19.1), with 42% of patients having response duration greater than6 months and 24% greater than 12 months. Median PFS was 5.6 months (range, 0 to >20.2), with progression-free survival duration greater than6 months in 42% and duration greater than12 months in 26%.
Dr. Cornelissen concluded: “Poziotinib shows clinically meaningful efficacy for treatment-naive NSCLC HER2 exon 20 mutations with [daily] dosing.” The toxicity profile, he added, is manageable and in line with previous poziotinib studies and other second-generation EGFR TKIs.
Noting that improved tolerability and antitumor activity have been observed in the cohort 5 (8 mg b.i.d.) interim analysis, Dr. Cornelissen said that cohort 4 is ongoing with patients enrolling at 8-mg b.i.d. dosing.
HER2 mutations represents 1.7%-2.2% of NSCLC, with high-sequence homology with EGFR mutation, observed ESMO-appointed discussant Daniel S.W. Tan, PhD, National Cancer Center in Singapore. He pointed out that, while HER2 antibody drug conjugates and TKIs have gained approval in other cancer types (e.g., breast, gastric), currently no HER2 therapies are approved in NSCLC. Reviewing ZENITH20 findings (risk ratio, 43.8%; DoR, 5.4 months; PFS, 5.6 months), Dr. Tan stated that poziotinib is an active agent in HER2 mutated NSCLC. “One concern that remains for me is the safety profile that will require further evaluation in order to determine optimal dosing,” he said.
Potential combinations, he added, need to be explored to improve the durability of response. “Until we can properly characterize this and other important aspects such as CNS activity, we need to be cautious about transitioning to a frontline setting. Also, we do need to give due consideration to strategies to improve HER2 testing rates in order to expand on clinical experience. This argues for the importance of broad upfront next generation sequencing testing in NSCLC.”
The study was funded by Spectrum Pharmaceuticals. Other authors associated with the research disclosed full or part-time employment with Spectrum.
Tumor reductions, stated lead author Robin Cornelissen, PhD, MD, Erasmus University, Rotterdam, the Netherlands, were seen in 88% of patients.
EGFR and HER2 exon 20 insertion mutations are rare subsets accounting for about 10% each of all mutations and 2%-4% each in NSCLC. “There is no approved therapy for either treatment-naive or previously treated NSCLC with HER2 exon 20 mutations,” Dr. Cornelissen said in a virtual oral presentation (abstract LBA46) on Sept. 18. While chemotherapy agents with or without checkpoint inhibitors and tyrosine kinase inhibitors (TKIs) are currently utilized, none are specific to exon 20 mutations, and historical response rates from mostly small uncontrolled studies vary widely from about 6.9%-35%, with median progression-free survival (PFS) ranging from 3 to 7 months. Poziotinib is a potent oral pan-HER TKI with activity in patients with EGFR or HER2 exon 20–mutated NSCLC.
Dr. Cornelissen presented preliminary safety and efficacy data from the phase 2 ZENITH20, a seven-cohort global clinical trial, specifically from cohort 4 (daily dosing) which included 48 HER2 exon 20 insertion NSCLC patients (median age, 60.5 years; female/male, 26/22) treated first-line with oral daily poziotinib (16 mg). The majority were White (75%), female (54%), and nonsmokers (69%) with an Eastern Cooperative Oncology Group performance status of 1 (65%).The primary endpoint was objective response rate evaluated centrally by an independent image review committee using RECIST 1.1 criteria.
All patients have experienced treatment-related adverse events (TRAEs) with 10% considered serious, and permanent discontinuation in 13%. About 83% of patients had dose interruptions and 76% had dose reductions. The most common adverse events were diarrhea (any grade, 83%; grade 3, 15%), rash (any grade, 69%; grade 3, 35%), stomatitis/mucosal inflammation (any grade, 81%; grade 3, 21%), and paronychia (any grade, 46%; grade 3 8%). Pneumonitis occurred in two patients (4%), with one grade 3 (2%). No grade 4/5 TRAEs were reported.
Discontinuations in 44 patients (92%), Dr. Cornelissen said, are attributed to death (5/10%), disease progression (30/63%), adverse events (1/2%), and other (8/17%), with treatment ongoing in 4 patients (8%).
The rate for the primary endpoint of ORR was 43.8% (n = 21) (95% confidence interval, 29.5%-58.8%).Tumor reductions have been observed in 42/48 patients (88%) with a median reduction of 35%. One complete response was reported (2.1%), with partial responses in 20 (41.7%), stable disease in 15 (31.3%), progressive disease in 7 (14.6%), and 5 (10.4%) not evaluable. The disease control rate was 75.0%.
Among secondary endpoints, median duration of response (DoR) was 5.4 months (range, 2.8 to >19.1), with 42% of patients having response duration greater than6 months and 24% greater than 12 months. Median PFS was 5.6 months (range, 0 to >20.2), with progression-free survival duration greater than6 months in 42% and duration greater than12 months in 26%.
Dr. Cornelissen concluded: “Poziotinib shows clinically meaningful efficacy for treatment-naive NSCLC HER2 exon 20 mutations with [daily] dosing.” The toxicity profile, he added, is manageable and in line with previous poziotinib studies and other second-generation EGFR TKIs.
Noting that improved tolerability and antitumor activity have been observed in the cohort 5 (8 mg b.i.d.) interim analysis, Dr. Cornelissen said that cohort 4 is ongoing with patients enrolling at 8-mg b.i.d. dosing.
HER2 mutations represents 1.7%-2.2% of NSCLC, with high-sequence homology with EGFR mutation, observed ESMO-appointed discussant Daniel S.W. Tan, PhD, National Cancer Center in Singapore. He pointed out that, while HER2 antibody drug conjugates and TKIs have gained approval in other cancer types (e.g., breast, gastric), currently no HER2 therapies are approved in NSCLC. Reviewing ZENITH20 findings (risk ratio, 43.8%; DoR, 5.4 months; PFS, 5.6 months), Dr. Tan stated that poziotinib is an active agent in HER2 mutated NSCLC. “One concern that remains for me is the safety profile that will require further evaluation in order to determine optimal dosing,” he said.
Potential combinations, he added, need to be explored to improve the durability of response. “Until we can properly characterize this and other important aspects such as CNS activity, we need to be cautious about transitioning to a frontline setting. Also, we do need to give due consideration to strategies to improve HER2 testing rates in order to expand on clinical experience. This argues for the importance of broad upfront next generation sequencing testing in NSCLC.”
The study was funded by Spectrum Pharmaceuticals. Other authors associated with the research disclosed full or part-time employment with Spectrum.
Tumor reductions, stated lead author Robin Cornelissen, PhD, MD, Erasmus University, Rotterdam, the Netherlands, were seen in 88% of patients.
EGFR and HER2 exon 20 insertion mutations are rare subsets accounting for about 10% each of all mutations and 2%-4% each in NSCLC. “There is no approved therapy for either treatment-naive or previously treated NSCLC with HER2 exon 20 mutations,” Dr. Cornelissen said in a virtual oral presentation (abstract LBA46) on Sept. 18. While chemotherapy agents with or without checkpoint inhibitors and tyrosine kinase inhibitors (TKIs) are currently utilized, none are specific to exon 20 mutations, and historical response rates from mostly small uncontrolled studies vary widely from about 6.9%-35%, with median progression-free survival (PFS) ranging from 3 to 7 months. Poziotinib is a potent oral pan-HER TKI with activity in patients with EGFR or HER2 exon 20–mutated NSCLC.
Dr. Cornelissen presented preliminary safety and efficacy data from the phase 2 ZENITH20, a seven-cohort global clinical trial, specifically from cohort 4 (daily dosing) which included 48 HER2 exon 20 insertion NSCLC patients (median age, 60.5 years; female/male, 26/22) treated first-line with oral daily poziotinib (16 mg). The majority were White (75%), female (54%), and nonsmokers (69%) with an Eastern Cooperative Oncology Group performance status of 1 (65%).The primary endpoint was objective response rate evaluated centrally by an independent image review committee using RECIST 1.1 criteria.
All patients have experienced treatment-related adverse events (TRAEs) with 10% considered serious, and permanent discontinuation in 13%. About 83% of patients had dose interruptions and 76% had dose reductions. The most common adverse events were diarrhea (any grade, 83%; grade 3, 15%), rash (any grade, 69%; grade 3, 35%), stomatitis/mucosal inflammation (any grade, 81%; grade 3, 21%), and paronychia (any grade, 46%; grade 3 8%). Pneumonitis occurred in two patients (4%), with one grade 3 (2%). No grade 4/5 TRAEs were reported.
Discontinuations in 44 patients (92%), Dr. Cornelissen said, are attributed to death (5/10%), disease progression (30/63%), adverse events (1/2%), and other (8/17%), with treatment ongoing in 4 patients (8%).
The rate for the primary endpoint of ORR was 43.8% (n = 21) (95% confidence interval, 29.5%-58.8%).Tumor reductions have been observed in 42/48 patients (88%) with a median reduction of 35%. One complete response was reported (2.1%), with partial responses in 20 (41.7%), stable disease in 15 (31.3%), progressive disease in 7 (14.6%), and 5 (10.4%) not evaluable. The disease control rate was 75.0%.
Among secondary endpoints, median duration of response (DoR) was 5.4 months (range, 2.8 to >19.1), with 42% of patients having response duration greater than6 months and 24% greater than 12 months. Median PFS was 5.6 months (range, 0 to >20.2), with progression-free survival duration greater than6 months in 42% and duration greater than12 months in 26%.
Dr. Cornelissen concluded: “Poziotinib shows clinically meaningful efficacy for treatment-naive NSCLC HER2 exon 20 mutations with [daily] dosing.” The toxicity profile, he added, is manageable and in line with previous poziotinib studies and other second-generation EGFR TKIs.
Noting that improved tolerability and antitumor activity have been observed in the cohort 5 (8 mg b.i.d.) interim analysis, Dr. Cornelissen said that cohort 4 is ongoing with patients enrolling at 8-mg b.i.d. dosing.
HER2 mutations represents 1.7%-2.2% of NSCLC, with high-sequence homology with EGFR mutation, observed ESMO-appointed discussant Daniel S.W. Tan, PhD, National Cancer Center in Singapore. He pointed out that, while HER2 antibody drug conjugates and TKIs have gained approval in other cancer types (e.g., breast, gastric), currently no HER2 therapies are approved in NSCLC. Reviewing ZENITH20 findings (risk ratio, 43.8%; DoR, 5.4 months; PFS, 5.6 months), Dr. Tan stated that poziotinib is an active agent in HER2 mutated NSCLC. “One concern that remains for me is the safety profile that will require further evaluation in order to determine optimal dosing,” he said.
Potential combinations, he added, need to be explored to improve the durability of response. “Until we can properly characterize this and other important aspects such as CNS activity, we need to be cautious about transitioning to a frontline setting. Also, we do need to give due consideration to strategies to improve HER2 testing rates in order to expand on clinical experience. This argues for the importance of broad upfront next generation sequencing testing in NSCLC.”
The study was funded by Spectrum Pharmaceuticals. Other authors associated with the research disclosed full or part-time employment with Spectrum.
FROM ESMO 2021
Novel drug effective for essential tremor, but with significant side effects
new research suggests.
The phase 2 KINETIC trial involved patients with essential tremor. Among patients treated with SAGE-324 for 28 days, there was a statistically significant reduction in upper-limb tremors on day 29 – meeting the primary endpoint of the study.
However, moderate to severe treatment-emergent adverse events (TEAEs) led to many treatment and/or study discontinuations, the investigators reported.
The findings were presented at the International Congress of Parkinson’s Disease and Movement Disorders.
Mechanism of action
Essential tremor affects an estimated 6.4 million adults in the United States. Available drugs are not helpful for 30%-50% of these patients. No new drug for this condition has been approved by the Food and Drug Administration for the past 50 years. Of the several drugs used to treat essential tremor, propranolol is the only one that has been approved, according to the American Academy of Neurology.
Deficits in inhibitory signaling via the gamma-aminobutyric acid system may have a role in the pathophysiology of essential tremor because the GABAergic system is the major neuroinhibitory system in the brain.
SAGE-324 is a steroid-positive allosteric modulator of the GABAA receptor. It acts on the receptor distant from the neuronal synapse to enhance GABAergic (inhibitory) signaling.
In the phase 2 multicenter KINETIC trial, investigators enrolled 69 patients aged 18-80 years. The patients had moderate to severe essential tremor, as determined on the basis of their having a score of 10 or higher on item 4 of the Essential Tremor Rating Assessment Scale (TETRAS) on screening day and at baseline/day 1 of the trial.
Participants did not take medications for essential tremor during the 28-day washout period. They were randomly assigned in a 1:1 ratio to receive SAGE-324 60 mg (n = 34) or placebo (n = 35) once daily. Dose reductions were allowed.
The groups were reasonably matched for age (mean, 69.4 years for SAGE-324 vs. 64.7 years for placebo) and dominant hand (right, 85.3% for SAGE-324 vs. 88.6% for placebo). Women composed 35.3% of the drug group and 57.1% of the placebo group.
The primary endpoint of the trial was change from baseline for the active drug in comparison with placebo on day 29 (1 day after the final dose) for upper-limb tremor, as measured by item 4 of TETRAS. There was also a 2-week follow-up with assessments on day 42.
Primary endpoint met, high dropout rate
Baseline mean TETRAS Performance Subscale item 4 scores were 12.82 for the SAGE-324 group and 12.28 for the placebo group.
On day 29, the least squares mean difference from baseline was –2.31 with SAGE-324 (n = 21) versus –1.24 with placebo (n = 33; P = .049). There was no difference between the SAGE-324 and placebo groups on day 42.
“Their significant reduction in upper-limb tremor score at day 29 corresponds to a 36% reduction from baseline in tremor amplitude in patients receiving SAGE-324, compared with a 21% reduction in tremor amplitude in patients receiving a placebo,” said lead investigator Kemi Bankole, MBBCh, of Sage Therapeutics.
“A reduction in tremor amplitude of 36% is a clinically significant improvement for most patients with essential tremor. For patients with moderate-severe tremor, a 41% improvement would be clinically noticeable and appreciated,” said Helen Colquhoun, MBChB, vice president at Sage.
“We believe patients with more severe tremor, that is, a TETRAS score of greater than 12, represent the majority of [essential tremor] patients getting diagnosed and seeking treatment today,” Dr. Colquhoun said.
There was an even greater reduction in tremor amplitude for the subgroup of patients with more severe tremor at baseline, meaning those with a median TETRAS score of 12 or greater (–2.75 for SAGE-324 vs. –1.05 for placebo; P = .0066).
These figures represented a 41% reduction from baseline in tremor amplitude for the SAGE-324 group, versus an 18% reduction in the placebo group. Again, the effect had disappeared in comparison with placebo at the 2-week off-drug follow-up on day 42.
Tolerability of SAGE-324 was a major problem, leading to dose reductions, treatment discontinuations, and study discontinuations. Of the 34 patients who received SAGE-324, 13 dropped out of the study, compared with 2 of 35 patients who received placebo.
Most TEAEs were moderate or severe in the SAGE-324 group, whereas most were mild in the placebo group.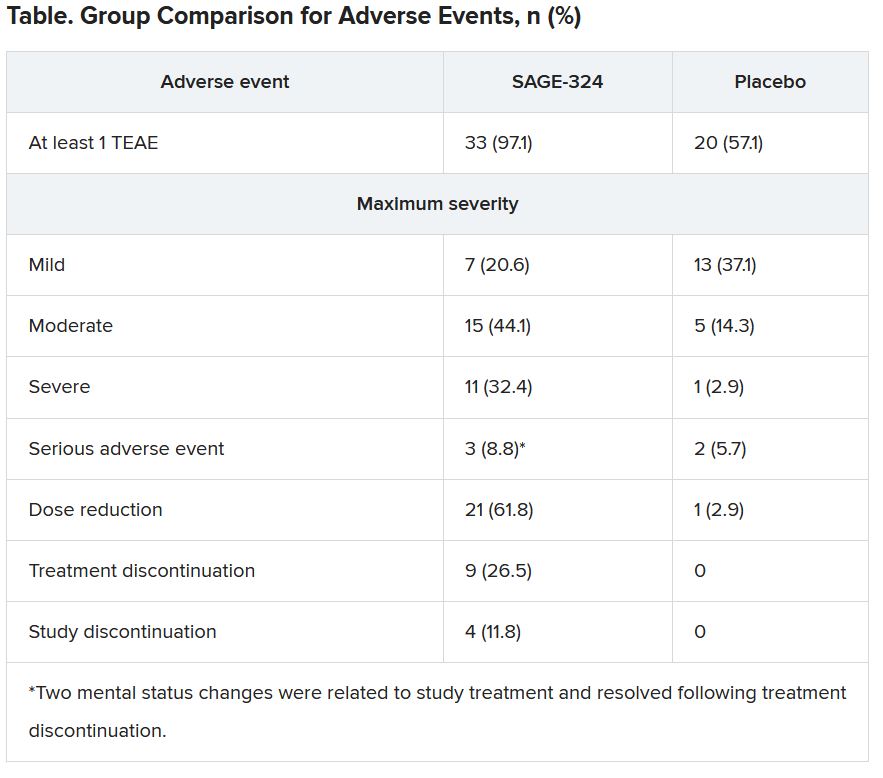
The most common TEAEs for participants who received SAGE-324 were somnolence (67.6%) and dizziness (38.2%), followed by balance problems, diplopia, dysarthria, and gait disturbance. In the placebo group, somnolence affected 5.7%, and dizziness affected 11.4%. There were no deaths in either group.
Dr. Colquhoun said these findings “are in line with our expectations for the 60-mg dose.”
More than one-third of the SAGE-324 group discontinued treatment before the end of the trial, and continuing treatment often required dose reductions. Only 24% completed the trial while taking the 60-mg dose; 15% completed the trial while taking 45 mg; and 24% did so while taking 30 mg.
Dr. Colquhoun noted that the company plans to initiate a phase 2b dose-ranging study later this year to optimize the dosing regimen with regard to tolerability and sustained tremor control.
No advantage over older drugs?
Commenting on the findings, Michele Tagliati, MD, director of the movement disorders program at Cedars-Sinai Medical Center, Los Angeles, said he had been aware of the study and was interested in seeing the results. However, he does not see an advantage with this drug, compared with what is already used for essential tremor.
“The response of people is not that different than when we treat them with the old barbiturates and benzodiazepines,” said Dr. Tagliati, who was not involved with the research.
He also noted the high rate of adverse events, particularly somnolence, and said that in his experience with current treatments, some patients prefer to live with their tremors rather than be sleepy and not thinking well.
Dr. Tagliati said he thinks use of SAGE-324 is going to be limited to patients who can tolerate it, “which was not that many.”
In addition, the trial was limited by its relatively small size, a “huge placebo effect,” and a high dropout rate in the active treatment arm, he concluded.
The study was funded by Sage Therapeutics and Biogen. Dr. Bankole and Dr. Calquhoun are employees of Sage. Dr. Tagliati reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
The phase 2 KINETIC trial involved patients with essential tremor. Among patients treated with SAGE-324 for 28 days, there was a statistically significant reduction in upper-limb tremors on day 29 – meeting the primary endpoint of the study.
However, moderate to severe treatment-emergent adverse events (TEAEs) led to many treatment and/or study discontinuations, the investigators reported.
The findings were presented at the International Congress of Parkinson’s Disease and Movement Disorders.
Mechanism of action
Essential tremor affects an estimated 6.4 million adults in the United States. Available drugs are not helpful for 30%-50% of these patients. No new drug for this condition has been approved by the Food and Drug Administration for the past 50 years. Of the several drugs used to treat essential tremor, propranolol is the only one that has been approved, according to the American Academy of Neurology.
Deficits in inhibitory signaling via the gamma-aminobutyric acid system may have a role in the pathophysiology of essential tremor because the GABAergic system is the major neuroinhibitory system in the brain.
SAGE-324 is a steroid-positive allosteric modulator of the GABAA receptor. It acts on the receptor distant from the neuronal synapse to enhance GABAergic (inhibitory) signaling.
In the phase 2 multicenter KINETIC trial, investigators enrolled 69 patients aged 18-80 years. The patients had moderate to severe essential tremor, as determined on the basis of their having a score of 10 or higher on item 4 of the Essential Tremor Rating Assessment Scale (TETRAS) on screening day and at baseline/day 1 of the trial.
Participants did not take medications for essential tremor during the 28-day washout period. They were randomly assigned in a 1:1 ratio to receive SAGE-324 60 mg (n = 34) or placebo (n = 35) once daily. Dose reductions were allowed.
The groups were reasonably matched for age (mean, 69.4 years for SAGE-324 vs. 64.7 years for placebo) and dominant hand (right, 85.3% for SAGE-324 vs. 88.6% for placebo). Women composed 35.3% of the drug group and 57.1% of the placebo group.
The primary endpoint of the trial was change from baseline for the active drug in comparison with placebo on day 29 (1 day after the final dose) for upper-limb tremor, as measured by item 4 of TETRAS. There was also a 2-week follow-up with assessments on day 42.
Primary endpoint met, high dropout rate
Baseline mean TETRAS Performance Subscale item 4 scores were 12.82 for the SAGE-324 group and 12.28 for the placebo group.
On day 29, the least squares mean difference from baseline was –2.31 with SAGE-324 (n = 21) versus –1.24 with placebo (n = 33; P = .049). There was no difference between the SAGE-324 and placebo groups on day 42.
“Their significant reduction in upper-limb tremor score at day 29 corresponds to a 36% reduction from baseline in tremor amplitude in patients receiving SAGE-324, compared with a 21% reduction in tremor amplitude in patients receiving a placebo,” said lead investigator Kemi Bankole, MBBCh, of Sage Therapeutics.
“A reduction in tremor amplitude of 36% is a clinically significant improvement for most patients with essential tremor. For patients with moderate-severe tremor, a 41% improvement would be clinically noticeable and appreciated,” said Helen Colquhoun, MBChB, vice president at Sage.
“We believe patients with more severe tremor, that is, a TETRAS score of greater than 12, represent the majority of [essential tremor] patients getting diagnosed and seeking treatment today,” Dr. Colquhoun said.
There was an even greater reduction in tremor amplitude for the subgroup of patients with more severe tremor at baseline, meaning those with a median TETRAS score of 12 or greater (–2.75 for SAGE-324 vs. –1.05 for placebo; P = .0066).
These figures represented a 41% reduction from baseline in tremor amplitude for the SAGE-324 group, versus an 18% reduction in the placebo group. Again, the effect had disappeared in comparison with placebo at the 2-week off-drug follow-up on day 42.
Tolerability of SAGE-324 was a major problem, leading to dose reductions, treatment discontinuations, and study discontinuations. Of the 34 patients who received SAGE-324, 13 dropped out of the study, compared with 2 of 35 patients who received placebo.
Most TEAEs were moderate or severe in the SAGE-324 group, whereas most were mild in the placebo group.
The most common TEAEs for participants who received SAGE-324 were somnolence (67.6%) and dizziness (38.2%), followed by balance problems, diplopia, dysarthria, and gait disturbance. In the placebo group, somnolence affected 5.7%, and dizziness affected 11.4%. There were no deaths in either group.
Dr. Colquhoun said these findings “are in line with our expectations for the 60-mg dose.”
More than one-third of the SAGE-324 group discontinued treatment before the end of the trial, and continuing treatment often required dose reductions. Only 24% completed the trial while taking the 60-mg dose; 15% completed the trial while taking 45 mg; and 24% did so while taking 30 mg.
Dr. Colquhoun noted that the company plans to initiate a phase 2b dose-ranging study later this year to optimize the dosing regimen with regard to tolerability and sustained tremor control.
No advantage over older drugs?
Commenting on the findings, Michele Tagliati, MD, director of the movement disorders program at Cedars-Sinai Medical Center, Los Angeles, said he had been aware of the study and was interested in seeing the results. However, he does not see an advantage with this drug, compared with what is already used for essential tremor.
“The response of people is not that different than when we treat them with the old barbiturates and benzodiazepines,” said Dr. Tagliati, who was not involved with the research.
He also noted the high rate of adverse events, particularly somnolence, and said that in his experience with current treatments, some patients prefer to live with their tremors rather than be sleepy and not thinking well.
Dr. Tagliati said he thinks use of SAGE-324 is going to be limited to patients who can tolerate it, “which was not that many.”
In addition, the trial was limited by its relatively small size, a “huge placebo effect,” and a high dropout rate in the active treatment arm, he concluded.
The study was funded by Sage Therapeutics and Biogen. Dr. Bankole and Dr. Calquhoun are employees of Sage. Dr. Tagliati reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
The phase 2 KINETIC trial involved patients with essential tremor. Among patients treated with SAGE-324 for 28 days, there was a statistically significant reduction in upper-limb tremors on day 29 – meeting the primary endpoint of the study.
However, moderate to severe treatment-emergent adverse events (TEAEs) led to many treatment and/or study discontinuations, the investigators reported.
The findings were presented at the International Congress of Parkinson’s Disease and Movement Disorders.
Mechanism of action
Essential tremor affects an estimated 6.4 million adults in the United States. Available drugs are not helpful for 30%-50% of these patients. No new drug for this condition has been approved by the Food and Drug Administration for the past 50 years. Of the several drugs used to treat essential tremor, propranolol is the only one that has been approved, according to the American Academy of Neurology.
Deficits in inhibitory signaling via the gamma-aminobutyric acid system may have a role in the pathophysiology of essential tremor because the GABAergic system is the major neuroinhibitory system in the brain.
SAGE-324 is a steroid-positive allosteric modulator of the GABAA receptor. It acts on the receptor distant from the neuronal synapse to enhance GABAergic (inhibitory) signaling.
In the phase 2 multicenter KINETIC trial, investigators enrolled 69 patients aged 18-80 years. The patients had moderate to severe essential tremor, as determined on the basis of their having a score of 10 or higher on item 4 of the Essential Tremor Rating Assessment Scale (TETRAS) on screening day and at baseline/day 1 of the trial.
Participants did not take medications for essential tremor during the 28-day washout period. They were randomly assigned in a 1:1 ratio to receive SAGE-324 60 mg (n = 34) or placebo (n = 35) once daily. Dose reductions were allowed.
The groups were reasonably matched for age (mean, 69.4 years for SAGE-324 vs. 64.7 years for placebo) and dominant hand (right, 85.3% for SAGE-324 vs. 88.6% for placebo). Women composed 35.3% of the drug group and 57.1% of the placebo group.
The primary endpoint of the trial was change from baseline for the active drug in comparison with placebo on day 29 (1 day after the final dose) for upper-limb tremor, as measured by item 4 of TETRAS. There was also a 2-week follow-up with assessments on day 42.
Primary endpoint met, high dropout rate
Baseline mean TETRAS Performance Subscale item 4 scores were 12.82 for the SAGE-324 group and 12.28 for the placebo group.
On day 29, the least squares mean difference from baseline was –2.31 with SAGE-324 (n = 21) versus –1.24 with placebo (n = 33; P = .049). There was no difference between the SAGE-324 and placebo groups on day 42.
“Their significant reduction in upper-limb tremor score at day 29 corresponds to a 36% reduction from baseline in tremor amplitude in patients receiving SAGE-324, compared with a 21% reduction in tremor amplitude in patients receiving a placebo,” said lead investigator Kemi Bankole, MBBCh, of Sage Therapeutics.
“A reduction in tremor amplitude of 36% is a clinically significant improvement for most patients with essential tremor. For patients with moderate-severe tremor, a 41% improvement would be clinically noticeable and appreciated,” said Helen Colquhoun, MBChB, vice president at Sage.
“We believe patients with more severe tremor, that is, a TETRAS score of greater than 12, represent the majority of [essential tremor] patients getting diagnosed and seeking treatment today,” Dr. Colquhoun said.
There was an even greater reduction in tremor amplitude for the subgroup of patients with more severe tremor at baseline, meaning those with a median TETRAS score of 12 or greater (–2.75 for SAGE-324 vs. –1.05 for placebo; P = .0066).
These figures represented a 41% reduction from baseline in tremor amplitude for the SAGE-324 group, versus an 18% reduction in the placebo group. Again, the effect had disappeared in comparison with placebo at the 2-week off-drug follow-up on day 42.
Tolerability of SAGE-324 was a major problem, leading to dose reductions, treatment discontinuations, and study discontinuations. Of the 34 patients who received SAGE-324, 13 dropped out of the study, compared with 2 of 35 patients who received placebo.
Most TEAEs were moderate or severe in the SAGE-324 group, whereas most were mild in the placebo group.
The most common TEAEs for participants who received SAGE-324 were somnolence (67.6%) and dizziness (38.2%), followed by balance problems, diplopia, dysarthria, and gait disturbance. In the placebo group, somnolence affected 5.7%, and dizziness affected 11.4%. There were no deaths in either group.
Dr. Colquhoun said these findings “are in line with our expectations for the 60-mg dose.”
More than one-third of the SAGE-324 group discontinued treatment before the end of the trial, and continuing treatment often required dose reductions. Only 24% completed the trial while taking the 60-mg dose; 15% completed the trial while taking 45 mg; and 24% did so while taking 30 mg.
Dr. Colquhoun noted that the company plans to initiate a phase 2b dose-ranging study later this year to optimize the dosing regimen with regard to tolerability and sustained tremor control.
No advantage over older drugs?
Commenting on the findings, Michele Tagliati, MD, director of the movement disorders program at Cedars-Sinai Medical Center, Los Angeles, said he had been aware of the study and was interested in seeing the results. However, he does not see an advantage with this drug, compared with what is already used for essential tremor.
“The response of people is not that different than when we treat them with the old barbiturates and benzodiazepines,” said Dr. Tagliati, who was not involved with the research.
He also noted the high rate of adverse events, particularly somnolence, and said that in his experience with current treatments, some patients prefer to live with their tremors rather than be sleepy and not thinking well.
Dr. Tagliati said he thinks use of SAGE-324 is going to be limited to patients who can tolerate it, “which was not that many.”
In addition, the trial was limited by its relatively small size, a “huge placebo effect,” and a high dropout rate in the active treatment arm, he concluded.
The study was funded by Sage Therapeutics and Biogen. Dr. Bankole and Dr. Calquhoun are employees of Sage. Dr. Tagliati reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM MDS VIRTUAL CONGRESS 2021
PCOS linked to menopausal urogenital symptoms but not hot flashes
Women with a history of polycystic ovary syndrome (PCOS) are more likely to experience somatic and urogenital symptoms post menopause, but they were no more likely to experience severe hot flashes than were other women with similar characteristics, according to research presented Sept. 24 at the hybrid annual meeting of the North American Menopause Society.
PCOS and vasomotor symptoms are each risk factors for cardiovascular disease, so researchers wanted to find out whether they were linked to one another, which might indicate that they are markers for the same underlying mechanisms that increase heart disease risk. The lack of an association, however, raises questions about how much each of these conditions might independently increase cardiovascular risk.
“Should we take a little more time to truly risk-assess these patients not just with their ASCVD risk score, but take into account that they have PCOS and they’re going through menopause, and how severe their hot flashes are?” asked Angie S. Lobo, MD, an internal medicine specialist at Mayo Clinic in Rochester, Minn., when she discussed her findings in an interview.
The association between PCOS and urogenital symptoms was surprising, Dr. Lobo said, but she said she suspects the reason for the finding may be the self-reported nature of the study.
“If you ask the question, you get the answer,” Dr. Lobo said. ”Are we just not asking the right questions to our patients? And should we be doing this more often? This is an exciting finding because there’s so much room to improve the clinical care of our patients.”
The researchers analyzed data from 3,308 women, ages 45-60, in a cross-sectional study from the Data Registry on the Experiences of Aging, Menopause, and Sexuality (DREAMS). The study occurred at Mayo Clinic locations between May 2015 and December 2019 in Rochester, Minn., in Scottsdale, Ariz., and in Jacksonville, Fla.
The women were an average 53 years old and were primarily White, educated, and postmenopausal. Among the 4.6% of women with a self-reported history of PCOS, 56% of them reported depression symptoms, compared to 42% of women without PCOS. Those with PCOS also had nearly twice the prevalence of obesity – 42% versus 22.5% among women without PCOS – and had a higher average overall score on the Menopause Rating Scale (17.7 vs. 14.7; P < .001).
Although women with PCOS initially had a greater burden of psychological symptoms on the same scale, that association disappeared after adjustment for menopause status, body mass index, depression, anxiety, and current use of hormone therapy. Even after adjustment, however, women with PCOS had higher average scores for somatic symptoms (6.7 vs. 5.6) and urogenital symptoms (5.2 vs. 4.3) than those of women without PCOS (P < .001).
Severe or very severe hot flashes were no more likely in women with a history of PCOS than in the other women in the study.
”The mechanisms underlying the correlation between PCOS and menopause symptoms in the psychological and urogenital symptom domains requires further study, although the well-known association between PCOS and mood disorders may explain the high psychological symptom burden in these women during the menopause transition,” the authors concluded.
Rachael B. Smith, DO, clinical assistant professor of ob.gyn. at the University of Arizona in Phoenix, said she was not surprised to see an association between PCOS and menopause symptoms overall, but she was surprised that PCOS did not correlate with severity of vasomotor symptoms. But Dr. Smith pointed out that the sample size of women with PCOS is fairly small (n = 151).
“Given that PCOS prevalence is about 6%-10%, I feel this association should be further studied to improve our counseling and treatment for this PCOS population,” Dr. Smith, who was not involved in the research, said in an interview. “The take-home message for physicians is improved patient-tailored counseling that takes into account patients’ prior medical history of PCOS.”
Although it will require more research to find out, Dr. Smith said she suspects that PCOS and vasomotor symptoms are additive risk factors for cardiovascular disease. She also noted that the study is limited by the homogeneity of the study population.
The research was funded by the National Institutes of Health. Dr. Lobo and Dr. Smith had no disclosures.
Women with a history of polycystic ovary syndrome (PCOS) are more likely to experience somatic and urogenital symptoms post menopause, but they were no more likely to experience severe hot flashes than were other women with similar characteristics, according to research presented Sept. 24 at the hybrid annual meeting of the North American Menopause Society.
PCOS and vasomotor symptoms are each risk factors for cardiovascular disease, so researchers wanted to find out whether they were linked to one another, which might indicate that they are markers for the same underlying mechanisms that increase heart disease risk. The lack of an association, however, raises questions about how much each of these conditions might independently increase cardiovascular risk.
“Should we take a little more time to truly risk-assess these patients not just with their ASCVD risk score, but take into account that they have PCOS and they’re going through menopause, and how severe their hot flashes are?” asked Angie S. Lobo, MD, an internal medicine specialist at Mayo Clinic in Rochester, Minn., when she discussed her findings in an interview.
The association between PCOS and urogenital symptoms was surprising, Dr. Lobo said, but she said she suspects the reason for the finding may be the self-reported nature of the study.
“If you ask the question, you get the answer,” Dr. Lobo said. ”Are we just not asking the right questions to our patients? And should we be doing this more often? This is an exciting finding because there’s so much room to improve the clinical care of our patients.”
The researchers analyzed data from 3,308 women, ages 45-60, in a cross-sectional study from the Data Registry on the Experiences of Aging, Menopause, and Sexuality (DREAMS). The study occurred at Mayo Clinic locations between May 2015 and December 2019 in Rochester, Minn., in Scottsdale, Ariz., and in Jacksonville, Fla.
The women were an average 53 years old and were primarily White, educated, and postmenopausal. Among the 4.6% of women with a self-reported history of PCOS, 56% of them reported depression symptoms, compared to 42% of women without PCOS. Those with PCOS also had nearly twice the prevalence of obesity – 42% versus 22.5% among women without PCOS – and had a higher average overall score on the Menopause Rating Scale (17.7 vs. 14.7; P < .001).
Although women with PCOS initially had a greater burden of psychological symptoms on the same scale, that association disappeared after adjustment for menopause status, body mass index, depression, anxiety, and current use of hormone therapy. Even after adjustment, however, women with PCOS had higher average scores for somatic symptoms (6.7 vs. 5.6) and urogenital symptoms (5.2 vs. 4.3) than those of women without PCOS (P < .001).
Severe or very severe hot flashes were no more likely in women with a history of PCOS than in the other women in the study.
”The mechanisms underlying the correlation between PCOS and menopause symptoms in the psychological and urogenital symptom domains requires further study, although the well-known association between PCOS and mood disorders may explain the high psychological symptom burden in these women during the menopause transition,” the authors concluded.
Rachael B. Smith, DO, clinical assistant professor of ob.gyn. at the University of Arizona in Phoenix, said she was not surprised to see an association between PCOS and menopause symptoms overall, but she was surprised that PCOS did not correlate with severity of vasomotor symptoms. But Dr. Smith pointed out that the sample size of women with PCOS is fairly small (n = 151).
“Given that PCOS prevalence is about 6%-10%, I feel this association should be further studied to improve our counseling and treatment for this PCOS population,” Dr. Smith, who was not involved in the research, said in an interview. “The take-home message for physicians is improved patient-tailored counseling that takes into account patients’ prior medical history of PCOS.”
Although it will require more research to find out, Dr. Smith said she suspects that PCOS and vasomotor symptoms are additive risk factors for cardiovascular disease. She also noted that the study is limited by the homogeneity of the study population.
The research was funded by the National Institutes of Health. Dr. Lobo and Dr. Smith had no disclosures.
Women with a history of polycystic ovary syndrome (PCOS) are more likely to experience somatic and urogenital symptoms post menopause, but they were no more likely to experience severe hot flashes than were other women with similar characteristics, according to research presented Sept. 24 at the hybrid annual meeting of the North American Menopause Society.
PCOS and vasomotor symptoms are each risk factors for cardiovascular disease, so researchers wanted to find out whether they were linked to one another, which might indicate that they are markers for the same underlying mechanisms that increase heart disease risk. The lack of an association, however, raises questions about how much each of these conditions might independently increase cardiovascular risk.
“Should we take a little more time to truly risk-assess these patients not just with their ASCVD risk score, but take into account that they have PCOS and they’re going through menopause, and how severe their hot flashes are?” asked Angie S. Lobo, MD, an internal medicine specialist at Mayo Clinic in Rochester, Minn., when she discussed her findings in an interview.
The association between PCOS and urogenital symptoms was surprising, Dr. Lobo said, but she said she suspects the reason for the finding may be the self-reported nature of the study.
“If you ask the question, you get the answer,” Dr. Lobo said. ”Are we just not asking the right questions to our patients? And should we be doing this more often? This is an exciting finding because there’s so much room to improve the clinical care of our patients.”
The researchers analyzed data from 3,308 women, ages 45-60, in a cross-sectional study from the Data Registry on the Experiences of Aging, Menopause, and Sexuality (DREAMS). The study occurred at Mayo Clinic locations between May 2015 and December 2019 in Rochester, Minn., in Scottsdale, Ariz., and in Jacksonville, Fla.
The women were an average 53 years old and were primarily White, educated, and postmenopausal. Among the 4.6% of women with a self-reported history of PCOS, 56% of them reported depression symptoms, compared to 42% of women without PCOS. Those with PCOS also had nearly twice the prevalence of obesity – 42% versus 22.5% among women without PCOS – and had a higher average overall score on the Menopause Rating Scale (17.7 vs. 14.7; P < .001).
Although women with PCOS initially had a greater burden of psychological symptoms on the same scale, that association disappeared after adjustment for menopause status, body mass index, depression, anxiety, and current use of hormone therapy. Even after adjustment, however, women with PCOS had higher average scores for somatic symptoms (6.7 vs. 5.6) and urogenital symptoms (5.2 vs. 4.3) than those of women without PCOS (P < .001).
Severe or very severe hot flashes were no more likely in women with a history of PCOS than in the other women in the study.
”The mechanisms underlying the correlation between PCOS and menopause symptoms in the psychological and urogenital symptom domains requires further study, although the well-known association between PCOS and mood disorders may explain the high psychological symptom burden in these women during the menopause transition,” the authors concluded.
Rachael B. Smith, DO, clinical assistant professor of ob.gyn. at the University of Arizona in Phoenix, said she was not surprised to see an association between PCOS and menopause symptoms overall, but she was surprised that PCOS did not correlate with severity of vasomotor symptoms. But Dr. Smith pointed out that the sample size of women with PCOS is fairly small (n = 151).
“Given that PCOS prevalence is about 6%-10%, I feel this association should be further studied to improve our counseling and treatment for this PCOS population,” Dr. Smith, who was not involved in the research, said in an interview. “The take-home message for physicians is improved patient-tailored counseling that takes into account patients’ prior medical history of PCOS.”
Although it will require more research to find out, Dr. Smith said she suspects that PCOS and vasomotor symptoms are additive risk factors for cardiovascular disease. She also noted that the study is limited by the homogeneity of the study population.
The research was funded by the National Institutes of Health. Dr. Lobo and Dr. Smith had no disclosures.
FROM NAMS 2021
Atezolizumab plus chemotherapy superior to best supportive care in early lung cancer
according to Enriqueta Felip, MD, the head of thoracic and head and neck cancer unit at Vall d’Hebron Institute of Oncology, Hospital, Barcelona.
IMpower010 is the first positive randomized phase 3 study to show significant disease-free survival (DFS) improvement with adjuvant cancer immunotherapy (atezolizumab, anti–programmed death–ligand 1, and platinum-based chemotherapy) in this population, Dr. Felip said in a presentation at the 2021 European Society for Medical Oncology Congress on Sept. 20 (abstract LBA9).
High unmet need
Up to 60% of patients with stage I-III NSCLC still experience disease relapse despite having received treatment, Dr. Felip said. IMpower010 included 1,280 patients who received up to four cycles of chemotherapy (cisplatin with pemetrexed, gemcitabine, docetaxel, or vinorelbine) after completely resected stage IB-IIIA NSCLC. Patients were randomized to open label to atezolizumab (1,200 mg every 21 days for 16 cycles or best supportive care (BSC). The primary endpoint of investigator-assessed DFS in the stage II-IIIA population (n = 1,005) was stratified according to three groups: PD-L1 tumor cells of at least 1% (stage II-IIIA), all-randomized (stage II-IIIA) and intention-to-treat (stage IB-IIIA).
Median disease-free survival in PD-L1 tumor cells of at least 1% was not estimated in the atezolizumab group and was 35.3 months in the BSC group (95% CI, 29.0 to NE). In the all-randomized group, median DFS was 42.3 months in the atezolizumab group (95% CI, 36.0 to NE) and 35.3 months in the BSC group (95% CI, 30.4-46.4) with a stratified hazard ratio of 0.79 (95% CI, 0.64-0.96; P = .02). In the intent-to-treat population, median DFS was not evaluable in the atezolizumab group and 37.2 months in the BSC group (95% CI, 31.6 to NE) with a hazard ratio of 0.81 (95% CI, 0.67-0.99; P = .04).
DFS hazard ratio 0.43 in TC ≥50% group
Looking at DFS by PD-L1 status in the population with and without known EGFR/ALK+ disease, Dr. Felip said that the hazard ratio for the tumor cells of at least 50% group (n = 229) was 0.43 (95% CI, 0.27-0.68), as compared with 0.87 (95% CI, 0.60-1.26) for the tumor cells 1%-49% group. With EGFR/ALK+ patients excluded, the respective HRs were similar (0.43/0.82). Considering DFS events including only disease recurrence, disease incidence was 29.4%/44.7% in the atezolizumab and BSC groups, respectively for those with PD-L1 tumor cells of at least 1%. The same pattern of atezolizumab benefit persisted in the all-randomized and intent-to-treat groups.
An assessment according to regions of relapse (locoregional only, distant only, locoregional and distant, CNS only, second primary lung) revealed no differences in the three groups. Analysis of time from randomization to relapse revealed regional differences in the PD-L1 tumor cells of at least 1% group with a median time to any relapse of 17.6 months in the atezolizumab group and 10.9 months in the BSC group. Time from randomization to relapse was generally similar for atezolizumab and best supportive care in the all randomized and intent-to-treat groups (about 11-12 months).
“The greatest magnitude of disease-free survival benefit was observed in the PD-L1 tumor cell of at least 50% population with a hazard ratio of 0.43,” Dr. Felip said. In a post hoc analysis excluding patients with known EFGR/ALK with NSCLC, she said that hazard ratios were numerically improved in most PD-L1 subgroups. Postrelapse cancer immunotherapies were used at a higher rate in the BSC arm of the trial. “Longer-term follow-up is warranted and may reveal differences in relapse patterns and treatment options.
Playing with the immune system
Benjamin Besse, MD, director of oncology and chair of the EORTC Lung Group at Paris-Saclay University, acknowledged the disease-free survival benefit with atezolizumab in IMpower010 and underscored that adjuvant immunotherapy has been changing treatment in resected cancers across tumor types (i.e., melanoma, renal cell carcinoma, NSCLC). He voiced some concerns, including the absence of benefit in PD-L1 less than 1%, pneumonectomy and EGFRmut/ALK+ patients, and generally the potential “when you play with the immune system for there to be a dark side too.” Dr. Besse said delayed side effects in 43.2% of patients , citing a recent report of chronic, mostly grade 1-2 immune-related adverse events following (>12 weeks after discontinuation) adjuvant anti–PD-1 therapy for high-risk resected melanoma. He mentioned, however, that the rate of second primary lung tumors in the atezolizumab group (1.4%) was lower than in the BSC group (2.6%), with generally similar rates between immuno- and nonimmunotherapies in melanoma and breast cancer trials.
“IMpower 010 is the first adjuvant study establishing immune checkpoint blockade as a new standard of care. We need to cure more, not to delay relapse,” he said. The optimal population for treatment is still yet to be defined, as is the best perioperative strategy, Dr. Besse added. “If approved I would prescribe adjuvant atezolizumab ... until I see the overall survival curves.”
IMpower010 was funded by–F. Hoffmann-La Roche. Dr. Felip disclosed numerous financial interests, including having received financial support from F. Hoffmann–La Roche, AstraZeneca, Amgen, and Merck, among other pharmaceutical companies.
according to Enriqueta Felip, MD, the head of thoracic and head and neck cancer unit at Vall d’Hebron Institute of Oncology, Hospital, Barcelona.
IMpower010 is the first positive randomized phase 3 study to show significant disease-free survival (DFS) improvement with adjuvant cancer immunotherapy (atezolizumab, anti–programmed death–ligand 1, and platinum-based chemotherapy) in this population, Dr. Felip said in a presentation at the 2021 European Society for Medical Oncology Congress on Sept. 20 (abstract LBA9).
High unmet need
Up to 60% of patients with stage I-III NSCLC still experience disease relapse despite having received treatment, Dr. Felip said. IMpower010 included 1,280 patients who received up to four cycles of chemotherapy (cisplatin with pemetrexed, gemcitabine, docetaxel, or vinorelbine) after completely resected stage IB-IIIA NSCLC. Patients were randomized to open label to atezolizumab (1,200 mg every 21 days for 16 cycles or best supportive care (BSC). The primary endpoint of investigator-assessed DFS in the stage II-IIIA population (n = 1,005) was stratified according to three groups: PD-L1 tumor cells of at least 1% (stage II-IIIA), all-randomized (stage II-IIIA) and intention-to-treat (stage IB-IIIA).
Median disease-free survival in PD-L1 tumor cells of at least 1% was not estimated in the atezolizumab group and was 35.3 months in the BSC group (95% CI, 29.0 to NE). In the all-randomized group, median DFS was 42.3 months in the atezolizumab group (95% CI, 36.0 to NE) and 35.3 months in the BSC group (95% CI, 30.4-46.4) with a stratified hazard ratio of 0.79 (95% CI, 0.64-0.96; P = .02). In the intent-to-treat population, median DFS was not evaluable in the atezolizumab group and 37.2 months in the BSC group (95% CI, 31.6 to NE) with a hazard ratio of 0.81 (95% CI, 0.67-0.99; P = .04).
DFS hazard ratio 0.43 in TC ≥50% group
Looking at DFS by PD-L1 status in the population with and without known EGFR/ALK+ disease, Dr. Felip said that the hazard ratio for the tumor cells of at least 50% group (n = 229) was 0.43 (95% CI, 0.27-0.68), as compared with 0.87 (95% CI, 0.60-1.26) for the tumor cells 1%-49% group. With EGFR/ALK+ patients excluded, the respective HRs were similar (0.43/0.82). Considering DFS events including only disease recurrence, disease incidence was 29.4%/44.7% in the atezolizumab and BSC groups, respectively for those with PD-L1 tumor cells of at least 1%. The same pattern of atezolizumab benefit persisted in the all-randomized and intent-to-treat groups.
An assessment according to regions of relapse (locoregional only, distant only, locoregional and distant, CNS only, second primary lung) revealed no differences in the three groups. Analysis of time from randomization to relapse revealed regional differences in the PD-L1 tumor cells of at least 1% group with a median time to any relapse of 17.6 months in the atezolizumab group and 10.9 months in the BSC group. Time from randomization to relapse was generally similar for atezolizumab and best supportive care in the all randomized and intent-to-treat groups (about 11-12 months).
“The greatest magnitude of disease-free survival benefit was observed in the PD-L1 tumor cell of at least 50% population with a hazard ratio of 0.43,” Dr. Felip said. In a post hoc analysis excluding patients with known EFGR/ALK with NSCLC, she said that hazard ratios were numerically improved in most PD-L1 subgroups. Postrelapse cancer immunotherapies were used at a higher rate in the BSC arm of the trial. “Longer-term follow-up is warranted and may reveal differences in relapse patterns and treatment options.
Playing with the immune system
Benjamin Besse, MD, director of oncology and chair of the EORTC Lung Group at Paris-Saclay University, acknowledged the disease-free survival benefit with atezolizumab in IMpower010 and underscored that adjuvant immunotherapy has been changing treatment in resected cancers across tumor types (i.e., melanoma, renal cell carcinoma, NSCLC). He voiced some concerns, including the absence of benefit in PD-L1 less than 1%, pneumonectomy and EGFRmut/ALK+ patients, and generally the potential “when you play with the immune system for there to be a dark side too.” Dr. Besse said delayed side effects in 43.2% of patients , citing a recent report of chronic, mostly grade 1-2 immune-related adverse events following (>12 weeks after discontinuation) adjuvant anti–PD-1 therapy for high-risk resected melanoma. He mentioned, however, that the rate of second primary lung tumors in the atezolizumab group (1.4%) was lower than in the BSC group (2.6%), with generally similar rates between immuno- and nonimmunotherapies in melanoma and breast cancer trials.
“IMpower 010 is the first adjuvant study establishing immune checkpoint blockade as a new standard of care. We need to cure more, not to delay relapse,” he said. The optimal population for treatment is still yet to be defined, as is the best perioperative strategy, Dr. Besse added. “If approved I would prescribe adjuvant atezolizumab ... until I see the overall survival curves.”
IMpower010 was funded by–F. Hoffmann-La Roche. Dr. Felip disclosed numerous financial interests, including having received financial support from F. Hoffmann–La Roche, AstraZeneca, Amgen, and Merck, among other pharmaceutical companies.
according to Enriqueta Felip, MD, the head of thoracic and head and neck cancer unit at Vall d’Hebron Institute of Oncology, Hospital, Barcelona.
IMpower010 is the first positive randomized phase 3 study to show significant disease-free survival (DFS) improvement with adjuvant cancer immunotherapy (atezolizumab, anti–programmed death–ligand 1, and platinum-based chemotherapy) in this population, Dr. Felip said in a presentation at the 2021 European Society for Medical Oncology Congress on Sept. 20 (abstract LBA9).
High unmet need
Up to 60% of patients with stage I-III NSCLC still experience disease relapse despite having received treatment, Dr. Felip said. IMpower010 included 1,280 patients who received up to four cycles of chemotherapy (cisplatin with pemetrexed, gemcitabine, docetaxel, or vinorelbine) after completely resected stage IB-IIIA NSCLC. Patients were randomized to open label to atezolizumab (1,200 mg every 21 days for 16 cycles or best supportive care (BSC). The primary endpoint of investigator-assessed DFS in the stage II-IIIA population (n = 1,005) was stratified according to three groups: PD-L1 tumor cells of at least 1% (stage II-IIIA), all-randomized (stage II-IIIA) and intention-to-treat (stage IB-IIIA).
Median disease-free survival in PD-L1 tumor cells of at least 1% was not estimated in the atezolizumab group and was 35.3 months in the BSC group (95% CI, 29.0 to NE). In the all-randomized group, median DFS was 42.3 months in the atezolizumab group (95% CI, 36.0 to NE) and 35.3 months in the BSC group (95% CI, 30.4-46.4) with a stratified hazard ratio of 0.79 (95% CI, 0.64-0.96; P = .02). In the intent-to-treat population, median DFS was not evaluable in the atezolizumab group and 37.2 months in the BSC group (95% CI, 31.6 to NE) with a hazard ratio of 0.81 (95% CI, 0.67-0.99; P = .04).
DFS hazard ratio 0.43 in TC ≥50% group
Looking at DFS by PD-L1 status in the population with and without known EGFR/ALK+ disease, Dr. Felip said that the hazard ratio for the tumor cells of at least 50% group (n = 229) was 0.43 (95% CI, 0.27-0.68), as compared with 0.87 (95% CI, 0.60-1.26) for the tumor cells 1%-49% group. With EGFR/ALK+ patients excluded, the respective HRs were similar (0.43/0.82). Considering DFS events including only disease recurrence, disease incidence was 29.4%/44.7% in the atezolizumab and BSC groups, respectively for those with PD-L1 tumor cells of at least 1%. The same pattern of atezolizumab benefit persisted in the all-randomized and intent-to-treat groups.
An assessment according to regions of relapse (locoregional only, distant only, locoregional and distant, CNS only, second primary lung) revealed no differences in the three groups. Analysis of time from randomization to relapse revealed regional differences in the PD-L1 tumor cells of at least 1% group with a median time to any relapse of 17.6 months in the atezolizumab group and 10.9 months in the BSC group. Time from randomization to relapse was generally similar for atezolizumab and best supportive care in the all randomized and intent-to-treat groups (about 11-12 months).
“The greatest magnitude of disease-free survival benefit was observed in the PD-L1 tumor cell of at least 50% population with a hazard ratio of 0.43,” Dr. Felip said. In a post hoc analysis excluding patients with known EFGR/ALK with NSCLC, she said that hazard ratios were numerically improved in most PD-L1 subgroups. Postrelapse cancer immunotherapies were used at a higher rate in the BSC arm of the trial. “Longer-term follow-up is warranted and may reveal differences in relapse patterns and treatment options.
Playing with the immune system
Benjamin Besse, MD, director of oncology and chair of the EORTC Lung Group at Paris-Saclay University, acknowledged the disease-free survival benefit with atezolizumab in IMpower010 and underscored that adjuvant immunotherapy has been changing treatment in resected cancers across tumor types (i.e., melanoma, renal cell carcinoma, NSCLC). He voiced some concerns, including the absence of benefit in PD-L1 less than 1%, pneumonectomy and EGFRmut/ALK+ patients, and generally the potential “when you play with the immune system for there to be a dark side too.” Dr. Besse said delayed side effects in 43.2% of patients , citing a recent report of chronic, mostly grade 1-2 immune-related adverse events following (>12 weeks after discontinuation) adjuvant anti–PD-1 therapy for high-risk resected melanoma. He mentioned, however, that the rate of second primary lung tumors in the atezolizumab group (1.4%) was lower than in the BSC group (2.6%), with generally similar rates between immuno- and nonimmunotherapies in melanoma and breast cancer trials.
“IMpower 010 is the first adjuvant study establishing immune checkpoint blockade as a new standard of care. We need to cure more, not to delay relapse,” he said. The optimal population for treatment is still yet to be defined, as is the best perioperative strategy, Dr. Besse added. “If approved I would prescribe adjuvant atezolizumab ... until I see the overall survival curves.”
IMpower010 was funded by–F. Hoffmann-La Roche. Dr. Felip disclosed numerous financial interests, including having received financial support from F. Hoffmann–La Roche, AstraZeneca, Amgen, and Merck, among other pharmaceutical companies.
FROM ESMO 2021
Study supports chemotherapy with immunotherapy for some never-smokers with lung cancer
Median overall survival was similar at 21.0 months and 22.1 months in 169 patients who received cancer immunotherapy plus chemotherapy and 351 who received cancer immunotherapy monotherapy, respectively (adjusted hazard ratio, 1.03). Median real-world progression-free survival (PFS) was also similar in the two groups (10.8 vs. 11.5 months; aHR, 1.04), Solange Peters, MD, reported at the 2021 European Society for Medical Oncology Congress on Sept. 17 (abstract VP2_2021).
However, in a small subgroup of 50 never-smokers, CIT plus chemotherapy showed significant and meaningful improvement in both overall survival and real-world progression-free survival, compared with CIT monotherapy, said Dr. Peters, ESMO president and professor and chair of medical oncology at the Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland.
The hazard ratios for overall survival and progression-free survival, after adjusting for baseline characteristics, were 0.50 and 0.40 in this subgroup, Dr. Peters said.
She and her colleagues reviewed data from the nationwide Flatiron Health Electronic Health Record–derived deidentified database for patients with metastatic nonsquamous NSCLC with a PD-L1 tumor proportion score at least 50% expression who initiated first-line CIT monotherapy or CIT plus chemotherapy between Oct. 24, 2016, and Feb. 28, 2019.
Median follow-up was 23.5 and 19.9 months in the monotherapy and combination therapy groups, respectively.
The findings are notable because “this is a very important scientific question, which by the way, is a daily question we have,” Dr. Peters said during a plenary debate session at the conference.
“One in four patients [with metastatic nonsquamous NSCLC has] this high PDL expression,” she explained, noting that both treatment approaches are commonly used in the first-line setting in this patient population.
The findings highlight the value of “well-conducted real-world evidence trials” in the absence of randomized trial results, she said.
Invited discussant Marina Chiara Garassino, MBBS, professor of medicine at the University of Chicago, also acknowledged the importance of the findings, noting the “multiple possibilities” for treatment selection in the metastatic nonsquamous NSCLC patient population.
Although patients with PD-L1 expression below 50% derive clear benefit from combination versus single-agent therapy, treatment selection for those with high PD-L1 expression is “very tricky and debatable,” she said.
For those with high PD-L1 expression, the choice is less clear and wrought with uncertainties – particularly for certain subgroups like never-smokers and those with PD-L1 expression over 90%, she said.
The findings reinforce those seen in prior meta-analyses and other clinical trials, particularly with respect to the role of smoking history when making treatment decisions.
“After these results and previous subgroup analyses, in my opinion, in [patients with] PD-L1 expression over 50%, we should consider the combination of chemotherapy and immunotherapy,” she said.
Conversely, findings from this study showing no difference in outcomes between the treatment approaches in patients with brain or liver metastases are based on small numbers and lack power for drawing any conclusions, she said. It also remains unclear whether there is a differential effect for women and those with PD-L1 expression over 90%, high tumor mutation burden, performance score greater than 2, and age over 75 years.
Both Dr. Garassino and Dr. Peters said they are looking to the INSIGNA trial, which is currently recruiting patients in the United States to evaluate the timing of pembrolizumab alone or with chemotherapy as first-line treatment and maintenance in NSCLC, to provide more clarification regarding the best treatment approaches.
This study was funded by F. Hoffmann–La Roche. Dr. Peters and Dr. Garassino each disclosed personal and/or institutional financial relationships with numerous pharmaceutical companies.
Median overall survival was similar at 21.0 months and 22.1 months in 169 patients who received cancer immunotherapy plus chemotherapy and 351 who received cancer immunotherapy monotherapy, respectively (adjusted hazard ratio, 1.03). Median real-world progression-free survival (PFS) was also similar in the two groups (10.8 vs. 11.5 months; aHR, 1.04), Solange Peters, MD, reported at the 2021 European Society for Medical Oncology Congress on Sept. 17 (abstract VP2_2021).
However, in a small subgroup of 50 never-smokers, CIT plus chemotherapy showed significant and meaningful improvement in both overall survival and real-world progression-free survival, compared with CIT monotherapy, said Dr. Peters, ESMO president and professor and chair of medical oncology at the Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland.
The hazard ratios for overall survival and progression-free survival, after adjusting for baseline characteristics, were 0.50 and 0.40 in this subgroup, Dr. Peters said.
She and her colleagues reviewed data from the nationwide Flatiron Health Electronic Health Record–derived deidentified database for patients with metastatic nonsquamous NSCLC with a PD-L1 tumor proportion score at least 50% expression who initiated first-line CIT monotherapy or CIT plus chemotherapy between Oct. 24, 2016, and Feb. 28, 2019.
Median follow-up was 23.5 and 19.9 months in the monotherapy and combination therapy groups, respectively.
The findings are notable because “this is a very important scientific question, which by the way, is a daily question we have,” Dr. Peters said during a plenary debate session at the conference.
“One in four patients [with metastatic nonsquamous NSCLC has] this high PDL expression,” she explained, noting that both treatment approaches are commonly used in the first-line setting in this patient population.
The findings highlight the value of “well-conducted real-world evidence trials” in the absence of randomized trial results, she said.
Invited discussant Marina Chiara Garassino, MBBS, professor of medicine at the University of Chicago, also acknowledged the importance of the findings, noting the “multiple possibilities” for treatment selection in the metastatic nonsquamous NSCLC patient population.
Although patients with PD-L1 expression below 50% derive clear benefit from combination versus single-agent therapy, treatment selection for those with high PD-L1 expression is “very tricky and debatable,” she said.
For those with high PD-L1 expression, the choice is less clear and wrought with uncertainties – particularly for certain subgroups like never-smokers and those with PD-L1 expression over 90%, she said.
The findings reinforce those seen in prior meta-analyses and other clinical trials, particularly with respect to the role of smoking history when making treatment decisions.
“After these results and previous subgroup analyses, in my opinion, in [patients with] PD-L1 expression over 50%, we should consider the combination of chemotherapy and immunotherapy,” she said.
Conversely, findings from this study showing no difference in outcomes between the treatment approaches in patients with brain or liver metastases are based on small numbers and lack power for drawing any conclusions, she said. It also remains unclear whether there is a differential effect for women and those with PD-L1 expression over 90%, high tumor mutation burden, performance score greater than 2, and age over 75 years.
Both Dr. Garassino and Dr. Peters said they are looking to the INSIGNA trial, which is currently recruiting patients in the United States to evaluate the timing of pembrolizumab alone or with chemotherapy as first-line treatment and maintenance in NSCLC, to provide more clarification regarding the best treatment approaches.
This study was funded by F. Hoffmann–La Roche. Dr. Peters and Dr. Garassino each disclosed personal and/or institutional financial relationships with numerous pharmaceutical companies.
Median overall survival was similar at 21.0 months and 22.1 months in 169 patients who received cancer immunotherapy plus chemotherapy and 351 who received cancer immunotherapy monotherapy, respectively (adjusted hazard ratio, 1.03). Median real-world progression-free survival (PFS) was also similar in the two groups (10.8 vs. 11.5 months; aHR, 1.04), Solange Peters, MD, reported at the 2021 European Society for Medical Oncology Congress on Sept. 17 (abstract VP2_2021).
However, in a small subgroup of 50 never-smokers, CIT plus chemotherapy showed significant and meaningful improvement in both overall survival and real-world progression-free survival, compared with CIT monotherapy, said Dr. Peters, ESMO president and professor and chair of medical oncology at the Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland.
The hazard ratios for overall survival and progression-free survival, after adjusting for baseline characteristics, were 0.50 and 0.40 in this subgroup, Dr. Peters said.
She and her colleagues reviewed data from the nationwide Flatiron Health Electronic Health Record–derived deidentified database for patients with metastatic nonsquamous NSCLC with a PD-L1 tumor proportion score at least 50% expression who initiated first-line CIT monotherapy or CIT plus chemotherapy between Oct. 24, 2016, and Feb. 28, 2019.
Median follow-up was 23.5 and 19.9 months in the monotherapy and combination therapy groups, respectively.
The findings are notable because “this is a very important scientific question, which by the way, is a daily question we have,” Dr. Peters said during a plenary debate session at the conference.
“One in four patients [with metastatic nonsquamous NSCLC has] this high PDL expression,” she explained, noting that both treatment approaches are commonly used in the first-line setting in this patient population.
The findings highlight the value of “well-conducted real-world evidence trials” in the absence of randomized trial results, she said.
Invited discussant Marina Chiara Garassino, MBBS, professor of medicine at the University of Chicago, also acknowledged the importance of the findings, noting the “multiple possibilities” for treatment selection in the metastatic nonsquamous NSCLC patient population.
Although patients with PD-L1 expression below 50% derive clear benefit from combination versus single-agent therapy, treatment selection for those with high PD-L1 expression is “very tricky and debatable,” she said.
For those with high PD-L1 expression, the choice is less clear and wrought with uncertainties – particularly for certain subgroups like never-smokers and those with PD-L1 expression over 90%, she said.
The findings reinforce those seen in prior meta-analyses and other clinical trials, particularly with respect to the role of smoking history when making treatment decisions.
“After these results and previous subgroup analyses, in my opinion, in [patients with] PD-L1 expression over 50%, we should consider the combination of chemotherapy and immunotherapy,” she said.
Conversely, findings from this study showing no difference in outcomes between the treatment approaches in patients with brain or liver metastases are based on small numbers and lack power for drawing any conclusions, she said. It also remains unclear whether there is a differential effect for women and those with PD-L1 expression over 90%, high tumor mutation burden, performance score greater than 2, and age over 75 years.
Both Dr. Garassino and Dr. Peters said they are looking to the INSIGNA trial, which is currently recruiting patients in the United States to evaluate the timing of pembrolizumab alone or with chemotherapy as first-line treatment and maintenance in NSCLC, to provide more clarification regarding the best treatment approaches.
This study was funded by F. Hoffmann–La Roche. Dr. Peters and Dr. Garassino each disclosed personal and/or institutional financial relationships with numerous pharmaceutical companies.
FROM ESMO 2021
Apple devices identify early Parkinson’s disease
, new research shows. Results from the WATCH-PD study show clear differences in a finger-tapping task in the Parkinson’s disease versus control group. The finger-tapping task also correlated with “traditional measures,” such as the Movement Disorder Society–Unified Parkinson’s Disease Rating Scale (MDS-UPDRS), investigators reported.
“And then the smartphone and smartwatch also showed differences in gait between groups,” said lead investigator Jamie Adams, MD, University of Rochester, New York.
The findings were presented at the International Congress of Parkinson’s Disease and Movement Disorders.
WATCH-PD
The 12-month WATCH-PD study included 132 individuals at 17 Parkinson’s Study Group sites, 82 with Parkinson’s disease and 50 controls.
Participants with Parkinson’s disease were untreated, were no more than 2 years out from diagnosis (mean disease duration, 10.0 ±7.3 months), and were in Hoehn and Yahr stage 1 or 2.
Apple Watches and iPhones were provided to participants, all of whom underwent in-clinic assessments at baseline and at months 1, 3, 6, 9, and 12. The assessments included motor and cognitive tasks using the devices, which contained motion sensors.
The phone also contained an app that could assess verbal, cognitive, and other abilities. Participants wore a set of inertial sensors (APDM Mobility Lab) while performing the MDS-UPDRS Part III motor examination.
In addition, there were biweekly at-home tasks. Questions and tests on the watch assessed symptoms of mood, fatigue, cognition, and falls as well as cognitive performance involving perceptual, verbal, visual spatial, and fine motor abilities. Both the watch and iPhone were used to gauge gait, balance, and tremor.
Ages of the participants were approximately the same in the Parkinson’s disease and control groups (63.3 years vs. 60.2 years, respectively), but male to female ratios differed between the groups. There were more men in the Parkinson’s disease cohort (56% men vs. 44% women) and more women in the control cohort (36% vs. 64%; P =.03).
Between-group differences
Results showed that MDS-UPDRS total scores and on all individual parts of the rating scale were significantly better for the control group (lower scores are better), as shown in the following table.
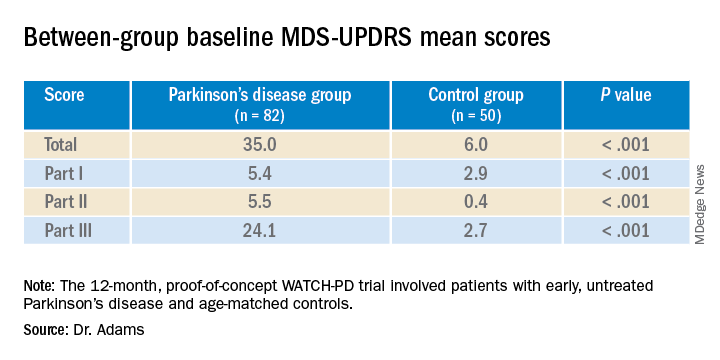
Similarly, the control group performed better than the Parkinson’s disease group on the Montreal Cognitive Assessment (MoCA), with higher scores showing better performance on the 0 to 30 scale (28.1 vs. 27.6, respectively).
Touchscreen assessments on the phone also showed group differences in a finger-tapping task, with more taps by the control group than by the Parkinson’s disease group. The difference was more pronounced when the dominant hand was used.
The median numbers of taps in 20 seconds for the dominant hand were 103.7 for the Parkinson’s disease cohort versus 131.9 for control cohort (P < .005); and for the nondominant hand the numbers of taps were 106.6 versus 122.1 (P < .05), respectively. The control group also scored better on tests of hand fine-motor control (P < .01) and on the mobile digit symbols modalities test (P < .05)
Measures of gait in a 1-minute walk test also showed group differences.
“The five gait measures that differed most were cadence, which is steps per minute, double support, arm swing amplitude, arm swing variation, and turn duration,” Dr. Adams said.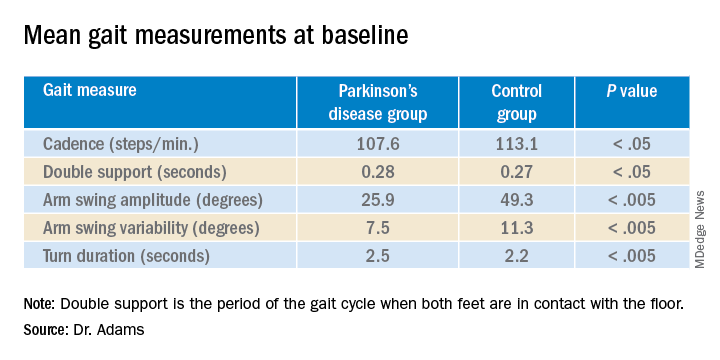
‘Tremendous interest’
Commenting on the findings, Ludy Shih, MD, MMSc, of Boston University, noted that in the future, devices such as the ones used in this study may help clinicians remotely monitor their patients’ Parkinson’s disease conditions and response to therapy.
That would “eliminate some of the transportation barrier for people with Parkinson’s disease,” said Dr. Shih, who was not involved with the research.
The devices can give objective measurements, reducing inter-rater variability in assessment of movements, she noted.
“I think there’s tremendous interest in using digital measures to pick up on subtle disease phenotypes earlier than a clinical diagnosis can be made,” Dr. Shih said.
She also referred to literature “going back a few decades” showing that finger tapping can be used as a pharmacodynamic measure of how well a patient’s dopaminergic medications are working, so the devices may be a way to remotely assess treatment efficacy and decide when it is time to make adjustments.
Dr. Shih said she thinks regulatory agencies are now open “to consider these as part of the totality of evidence that a therapeutic [device] might be working.”
Whether these would need to be professional grade and approved as medical devices or if patients could just buy smartwatches and smartphones to generate useful data is still a question, she said. Already, there are several Parkinson’s apps that the public can download to track symptoms, improve voice, provide exercises, find support groups or research studies, and more.
Dr. Shih predicted that the biweekly at-home tasks, as in the current protocol, could be a burden to some people. If only a segment of the population were willing to comply, it could call into question how generalizable the results were, she added.
“There’s even a prior publication showing that compliance rate really dropped like a rock,” she noted. However, for those people willing to perform the tasks on a regular schedule, the results could be valuable, Dr. Shih said.
Dr. Adams concurred, saying that she had received feedback from some of her study participants that the biweekly tasks were a bit much.
The study was supported by Biogen and Takeda Pharmaceuticals. Dr. Adams receives research support from Biogen. Dr. Shih has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows. Results from the WATCH-PD study show clear differences in a finger-tapping task in the Parkinson’s disease versus control group. The finger-tapping task also correlated with “traditional measures,” such as the Movement Disorder Society–Unified Parkinson’s Disease Rating Scale (MDS-UPDRS), investigators reported.
“And then the smartphone and smartwatch also showed differences in gait between groups,” said lead investigator Jamie Adams, MD, University of Rochester, New York.
The findings were presented at the International Congress of Parkinson’s Disease and Movement Disorders.
WATCH-PD
The 12-month WATCH-PD study included 132 individuals at 17 Parkinson’s Study Group sites, 82 with Parkinson’s disease and 50 controls.
Participants with Parkinson’s disease were untreated, were no more than 2 years out from diagnosis (mean disease duration, 10.0 ±7.3 months), and were in Hoehn and Yahr stage 1 or 2.
Apple Watches and iPhones were provided to participants, all of whom underwent in-clinic assessments at baseline and at months 1, 3, 6, 9, and 12. The assessments included motor and cognitive tasks using the devices, which contained motion sensors.
The phone also contained an app that could assess verbal, cognitive, and other abilities. Participants wore a set of inertial sensors (APDM Mobility Lab) while performing the MDS-UPDRS Part III motor examination.
In addition, there were biweekly at-home tasks. Questions and tests on the watch assessed symptoms of mood, fatigue, cognition, and falls as well as cognitive performance involving perceptual, verbal, visual spatial, and fine motor abilities. Both the watch and iPhone were used to gauge gait, balance, and tremor.
Ages of the participants were approximately the same in the Parkinson’s disease and control groups (63.3 years vs. 60.2 years, respectively), but male to female ratios differed between the groups. There were more men in the Parkinson’s disease cohort (56% men vs. 44% women) and more women in the control cohort (36% vs. 64%; P =.03).
Between-group differences
Results showed that MDS-UPDRS total scores and on all individual parts of the rating scale were significantly better for the control group (lower scores are better), as shown in the following table.
Similarly, the control group performed better than the Parkinson’s disease group on the Montreal Cognitive Assessment (MoCA), with higher scores showing better performance on the 0 to 30 scale (28.1 vs. 27.6, respectively).
Touchscreen assessments on the phone also showed group differences in a finger-tapping task, with more taps by the control group than by the Parkinson’s disease group. The difference was more pronounced when the dominant hand was used.
The median numbers of taps in 20 seconds for the dominant hand were 103.7 for the Parkinson’s disease cohort versus 131.9 for control cohort (P < .005); and for the nondominant hand the numbers of taps were 106.6 versus 122.1 (P < .05), respectively. The control group also scored better on tests of hand fine-motor control (P < .01) and on the mobile digit symbols modalities test (P < .05)
Measures of gait in a 1-minute walk test also showed group differences.
“The five gait measures that differed most were cadence, which is steps per minute, double support, arm swing amplitude, arm swing variation, and turn duration,” Dr. Adams said.
‘Tremendous interest’
Commenting on the findings, Ludy Shih, MD, MMSc, of Boston University, noted that in the future, devices such as the ones used in this study may help clinicians remotely monitor their patients’ Parkinson’s disease conditions and response to therapy.
That would “eliminate some of the transportation barrier for people with Parkinson’s disease,” said Dr. Shih, who was not involved with the research.
The devices can give objective measurements, reducing inter-rater variability in assessment of movements, she noted.
“I think there’s tremendous interest in using digital measures to pick up on subtle disease phenotypes earlier than a clinical diagnosis can be made,” Dr. Shih said.
She also referred to literature “going back a few decades” showing that finger tapping can be used as a pharmacodynamic measure of how well a patient’s dopaminergic medications are working, so the devices may be a way to remotely assess treatment efficacy and decide when it is time to make adjustments.
Dr. Shih said she thinks regulatory agencies are now open “to consider these as part of the totality of evidence that a therapeutic [device] might be working.”
Whether these would need to be professional grade and approved as medical devices or if patients could just buy smartwatches and smartphones to generate useful data is still a question, she said. Already, there are several Parkinson’s apps that the public can download to track symptoms, improve voice, provide exercises, find support groups or research studies, and more.
Dr. Shih predicted that the biweekly at-home tasks, as in the current protocol, could be a burden to some people. If only a segment of the population were willing to comply, it could call into question how generalizable the results were, she added.
“There’s even a prior publication showing that compliance rate really dropped like a rock,” she noted. However, for those people willing to perform the tasks on a regular schedule, the results could be valuable, Dr. Shih said.
Dr. Adams concurred, saying that she had received feedback from some of her study participants that the biweekly tasks were a bit much.
The study was supported by Biogen and Takeda Pharmaceuticals. Dr. Adams receives research support from Biogen. Dr. Shih has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows. Results from the WATCH-PD study show clear differences in a finger-tapping task in the Parkinson’s disease versus control group. The finger-tapping task also correlated with “traditional measures,” such as the Movement Disorder Society–Unified Parkinson’s Disease Rating Scale (MDS-UPDRS), investigators reported.
“And then the smartphone and smartwatch also showed differences in gait between groups,” said lead investigator Jamie Adams, MD, University of Rochester, New York.
The findings were presented at the International Congress of Parkinson’s Disease and Movement Disorders.
WATCH-PD
The 12-month WATCH-PD study included 132 individuals at 17 Parkinson’s Study Group sites, 82 with Parkinson’s disease and 50 controls.
Participants with Parkinson’s disease were untreated, were no more than 2 years out from diagnosis (mean disease duration, 10.0 ±7.3 months), and were in Hoehn and Yahr stage 1 or 2.
Apple Watches and iPhones were provided to participants, all of whom underwent in-clinic assessments at baseline and at months 1, 3, 6, 9, and 12. The assessments included motor and cognitive tasks using the devices, which contained motion sensors.
The phone also contained an app that could assess verbal, cognitive, and other abilities. Participants wore a set of inertial sensors (APDM Mobility Lab) while performing the MDS-UPDRS Part III motor examination.
In addition, there were biweekly at-home tasks. Questions and tests on the watch assessed symptoms of mood, fatigue, cognition, and falls as well as cognitive performance involving perceptual, verbal, visual spatial, and fine motor abilities. Both the watch and iPhone were used to gauge gait, balance, and tremor.
Ages of the participants were approximately the same in the Parkinson’s disease and control groups (63.3 years vs. 60.2 years, respectively), but male to female ratios differed between the groups. There were more men in the Parkinson’s disease cohort (56% men vs. 44% women) and more women in the control cohort (36% vs. 64%; P =.03).
Between-group differences
Results showed that MDS-UPDRS total scores and on all individual parts of the rating scale were significantly better for the control group (lower scores are better), as shown in the following table.
Similarly, the control group performed better than the Parkinson’s disease group on the Montreal Cognitive Assessment (MoCA), with higher scores showing better performance on the 0 to 30 scale (28.1 vs. 27.6, respectively).
Touchscreen assessments on the phone also showed group differences in a finger-tapping task, with more taps by the control group than by the Parkinson’s disease group. The difference was more pronounced when the dominant hand was used.
The median numbers of taps in 20 seconds for the dominant hand were 103.7 for the Parkinson’s disease cohort versus 131.9 for control cohort (P < .005); and for the nondominant hand the numbers of taps were 106.6 versus 122.1 (P < .05), respectively. The control group also scored better on tests of hand fine-motor control (P < .01) and on the mobile digit symbols modalities test (P < .05)
Measures of gait in a 1-minute walk test also showed group differences.
“The five gait measures that differed most were cadence, which is steps per minute, double support, arm swing amplitude, arm swing variation, and turn duration,” Dr. Adams said.
‘Tremendous interest’
Commenting on the findings, Ludy Shih, MD, MMSc, of Boston University, noted that in the future, devices such as the ones used in this study may help clinicians remotely monitor their patients’ Parkinson’s disease conditions and response to therapy.
That would “eliminate some of the transportation barrier for people with Parkinson’s disease,” said Dr. Shih, who was not involved with the research.
The devices can give objective measurements, reducing inter-rater variability in assessment of movements, she noted.
“I think there’s tremendous interest in using digital measures to pick up on subtle disease phenotypes earlier than a clinical diagnosis can be made,” Dr. Shih said.
She also referred to literature “going back a few decades” showing that finger tapping can be used as a pharmacodynamic measure of how well a patient’s dopaminergic medications are working, so the devices may be a way to remotely assess treatment efficacy and decide when it is time to make adjustments.
Dr. Shih said she thinks regulatory agencies are now open “to consider these as part of the totality of evidence that a therapeutic [device] might be working.”
Whether these would need to be professional grade and approved as medical devices or if patients could just buy smartwatches and smartphones to generate useful data is still a question, she said. Already, there are several Parkinson’s apps that the public can download to track symptoms, improve voice, provide exercises, find support groups or research studies, and more.
Dr. Shih predicted that the biweekly at-home tasks, as in the current protocol, could be a burden to some people. If only a segment of the population were willing to comply, it could call into question how generalizable the results were, she added.
“There’s even a prior publication showing that compliance rate really dropped like a rock,” she noted. However, for those people willing to perform the tasks on a regular schedule, the results could be valuable, Dr. Shih said.
Dr. Adams concurred, saying that she had received feedback from some of her study participants that the biweekly tasks were a bit much.
The study was supported by Biogen and Takeda Pharmaceuticals. Dr. Adams receives research support from Biogen. Dr. Shih has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM MDS VIRTUAL CONGRESS 2021
Updates to CDC’s STI guidelines relevant to midlife women too
Sexually transmitted infection rates have not increased as dramatically in older women as they have in women in their teens and 20s, but rates of chlamydia and gonorrhea in women over age 35 have seen a steady incline over the past decade, and syphilis rates have climbed steeply, according to data from the Centers for Disease Control and Prevention.
That makes the STI treatment guidelines released by the CDC in July even timelier for practitioners of menopause medicine, according to Michael S. Policar, MD, MPH, a professor emeritus of ob.gyn. and reproductive sciences at the University of California, San Francisco.
Dr. Policar discussed what clinicians need to know about STIs in midlife women at the hybrid annual meeting of the North American Menopause Society. Even the nomenclature change in the guidelines from “sexually transmitted diseases” to “sexually transmitted infections” is important “because they want to acknowledge the fact that a lot of the sexually transmitted infections that we’re treating are asymptomatic, are colonizations, and are not yet diseases,” Dr. Policar said. “We’re trying to be much more expansive in thinking about finding these infections before they actually start causing morbidity in the form of a disease.”
Sexual history
The primary guidelines update for taking sexual history is the recommendation to ask patients about their intentions regarding pregnancy. The “5 Ps” of sexual history are now Partners, Practices, Protection from STIs, Past history of STIs, and Pregnancy intention.
“There should be a sixth P that has to do with pleasure questions,” Policar added. “We ask all the time for patients that we see in the context of perimenopausal and menopausal services, ‘Are you satisfied with your sexual relationship with your partner?’ Hopefully that will make it into the CDC guidelines as the sixth P at some point, but for now, that’s aspirational.”
In asking about partners, instead of asking patients whether they have sex with men, women, or both, clinicians should ask first if the patient is having sex of any kind – oral, vaginal, or anal – with anyone. From there, providers should ask how many sex partners the patient has had, the gender(s) of the partners, and whether they or their partners have other sex partners, using more gender-inclusive language.
When asking about practices, in addition to asking about the type of sexual contact patients have had, additional questions include whether the patient met their partners online or through apps, whether they or any of their partners use drugs, and whether the patient has exchanged sex for any needs, such as money, housing, or drugs. The additional questions can identify those at higher risk for STIs.
After reviewing the CDC’s list of risk factors for gonorrhea and chlamydia screening, Dr. Policar shared the screening list from the California Department of Public Health, which he finds more helpful:
- History of gonorrhea, chlamydia, or pelvic inflammatory disease (PID) in the past 2 years.
- More than 1 sexual partner in the past year.
- New sexual partner within 90 days.
- Reason to believe that a sex partner has had other partners in the past year.
- Exchanging sex for drugs or money within the past year.
- Other factors identified locally, including prevalence of infection in the community.
STI screening guidelines
For those with a positive gonorrhea/chlamydia (GC/CT) screen, a nucleic acid amplification test (NAAT) vaginal swab is the preferred specimen source, and self-collection is fine for women of any age, Dr. Policar said. In addition, cis-women who received anal intercourse in the preceding year should consider undergoing a rectal GC/CT NAAT, and those who performed oral sex should consider a pharyngeal GC/CT NAAT, based on shared clinical decision-making. A rectal swab requires an insertion of 3-4 cm and a 360-degree twirl of the wrist, not the swab, to ensure you get a sample from the entire circumference. Pharyngeal samples require swabbing both tonsillar pillars while taking care for those who may gag.
For contact testing – asymptomatic people who have had a high-risk sexual exposure – providers should test for gonorrhea, chlamydia, HIV, and syphilis but not for herpes, high-risk HPV, hepatitis B, hepatitis C, or bacterial vaginosis. “Maybe we’ll do a screen for trichomoniasis, and maybe we’ll offer herpes type 2 serology or antibody screening,” Dr. Policar said. Providers should also ask patients requesting contact testing if they have been vaccinated for hepatitis B. If not, “the conversation should be how can we get you vaccinated for hepatitis B,” Dr. Policar said.
HIV screening only needs to occur once between the ages of 15 and 65 for low-risk people and then once annually (or more often if necessary) for those who have a sex partner with HIV, use injectable drugs, engage in commercial sex work, have a new sex partner with unknown HIV status, received care at an STD or TB clinic, or were in a correctional facility or homeless shelter.
Those at increased risk for syphilis include men who have sex with men, men under age 29, and anyone living with HIV or who has a history of incarceration or a history of commercial sex work. In addition, African Americans have the greatest risk for syphilis of racial/ethnic groups, followed by Hispanics. Most adults only require hepatitis C screening with anti-hep C antibody testing once in their lifetime. Periodic hepatitis C screening should occur for people who inject drugs. If the screening is positive, providers should conduct an RNA polymerase chain reaction (PCR) test to determine whether a chronic infection is present.
Trichomoniasis screening should occur annually in women living with HIV or in correctional facilities. Others to consider screening include people with new or multiple sex partners, a history of STIs, inconsistent condom use, a history of sex work, and intravenous drug use. Dr. Policar also noted that several new assays, including NAAT, PCR, and a rapid test, are available for trichomoniasis.
STI treatment guidelines
For women with mucoprurulent cervicitis, the cause could be chlamydia, gonorrhea, herpes, trichomonas, mycoplasma, or even progesterone from pregnancy or contraception, Dr. Policar said. The new preferred treatment is 100 mg of doxycycline. The alternative, albeit less preferred, treatment is 1 g azithromycin.
The preferred treatment for chlamydia is now 100 mg oral doxycycline twice daily, or doxycycline 200 mg delayed-release once daily, for 7 days. Alternative regimens include 1 g oral azithromycin in a single dose or 500 mg oral levofloxacin once daily for 7 days. The switch to recommending doxycycline over azithromycin is based on recent evidence showing that doxycycline has a slightly higher efficacy for urogenital chlamydia and a substantially higher efficacy for rectal chlamydia. In addition, an increasing proportion of gonorrheal infections have shown resistance to azithromycin, particularly beginning in 2014.
Preferred treatment of new, uncomplicated gonorrhea infections of the cervix, urethra, rectum, and pharynx is one 500-mg dose of ceftriaxone for those weighing under 150 kg and 1 g for those weighing 150 kg or more. If ceftriaxone is unavailable, the new alternative recommended treatment for gonorrhea is 800 mg cefixime. For pharyngeal gonorrhea only, the CDC recommends a test-of-cure 7-14 days after treatment.
For gonorrheal infections, the CDC also recommends treatment with doxycycline if chlamydia has not been excluded, but the agency no longer recommends dual therapy with azithromycin unless it’s used in place of doxycycline for those who are pregnant, have an allergy, or may not be compliant with a 7-day doxycycline regimen.
The preferred treatment for bacterial vaginosis has not changed. The new recommended regimen for trichomoniasis is 500 mg oral metronidazole for 7 days, with the alternative being a single 2-g dose of tinidazole. Male partners should receive 2 g oral metronidazole. The CDC also notes that patients taking metronidazole no longer need to abstain from alcohol during treatment.
”Another area where the guidelines changed is in their description of expedited partner therapy, which means that, when we find an index case who has gonorrhea or chlamydia, we always have a discussion with her about getting her partners treated,” Dr. Policar said. “The CDC was quite clear that the responsibility for discussing partner treatment rests with us as the diagnosing provider” since city and county health departments don’t have the time or resources for contact tracing these STIs.
The two main ways to treat partners are to have the patient bring their partner(s) to the appointment with them or to do patient-delivered partner therapy. Ideally, clinicians who dispense their own medications can give the patient enough drugs to give her partner(s) a complete dose as well. Otherwise, providers can prescribe extra doses in the index patients’ name or write prescriptions in the partner’s name.
“In every state of the union now, it is legal for you to to prescribe antibiotics for partners sight unseen, Dr. Policar said.
Margaret Sullivan, MD, an ob.gyn. from rural western North Carolina, noted during the Q&A that an obstacle to partner therapy at her practice has been cost, particularly since many of the men don’t have insurance.
“I have not heard before of prescribing the extra doses for partners under the patient’s name,” Dr. Sullivan said. “I’ve thought about doing it, but [was worried about] it potentially being fraudulent if that patient has Medicaid and we’re prescribing extra doses under her name, so how do you work around that?”
Dr. Policar acknowledged that barrier and recommended that patients use the website/app Goodrx.com to find discounts for out-of-pocket generic medications. He also noted the occasional obstacle of pharmacists balking at filling a double or triple dose.
“What we’ve been suggesting in that circumstance is to literally copy that part of the CDC guidelines, which explains expedited partner therapy or patient-delivered partner therapy and send that off to the pharmacist so they can see that it’s a national recommendation of the CDC,” Dr. Policar said.
Claudia Rodriguez, MD, an ob.gyn. who works at Sherman Hospital in Elgin, Ill., asked about the CDC recommendations for HPV vaccination in older women. Although the CDC permits women over age 26 to receive the HPV vaccine, the agency does not “make a solid recommendation to have this done, which oftentimes makes a big difference in whether or not health insurance will actually pay for vaccination in that circumstance,” Dr. Policar said.
Patients are welcome to request the vaccine after shared decision-making, but “we should never present this as something which is routine,” he said. For women in their 50s, for example, “there’s virtually no data about any additional degree of protection that you would get” from HPV vaccination, Dr. Policar said in response to a similar question from Tara Allmen, MD, an ob.gyn. in New York City. “If you ask me for my personal clinical opinion about it, I would say it’s not going to be worth it,” he said.
Dr Policar had no disclosures. Disclosures were unavailable for attendees who spoke.
Sexually transmitted infection rates have not increased as dramatically in older women as they have in women in their teens and 20s, but rates of chlamydia and gonorrhea in women over age 35 have seen a steady incline over the past decade, and syphilis rates have climbed steeply, according to data from the Centers for Disease Control and Prevention.
That makes the STI treatment guidelines released by the CDC in July even timelier for practitioners of menopause medicine, according to Michael S. Policar, MD, MPH, a professor emeritus of ob.gyn. and reproductive sciences at the University of California, San Francisco.
Dr. Policar discussed what clinicians need to know about STIs in midlife women at the hybrid annual meeting of the North American Menopause Society. Even the nomenclature change in the guidelines from “sexually transmitted diseases” to “sexually transmitted infections” is important “because they want to acknowledge the fact that a lot of the sexually transmitted infections that we’re treating are asymptomatic, are colonizations, and are not yet diseases,” Dr. Policar said. “We’re trying to be much more expansive in thinking about finding these infections before they actually start causing morbidity in the form of a disease.”
Sexual history
The primary guidelines update for taking sexual history is the recommendation to ask patients about their intentions regarding pregnancy. The “5 Ps” of sexual history are now Partners, Practices, Protection from STIs, Past history of STIs, and Pregnancy intention.
“There should be a sixth P that has to do with pleasure questions,” Policar added. “We ask all the time for patients that we see in the context of perimenopausal and menopausal services, ‘Are you satisfied with your sexual relationship with your partner?’ Hopefully that will make it into the CDC guidelines as the sixth P at some point, but for now, that’s aspirational.”
In asking about partners, instead of asking patients whether they have sex with men, women, or both, clinicians should ask first if the patient is having sex of any kind – oral, vaginal, or anal – with anyone. From there, providers should ask how many sex partners the patient has had, the gender(s) of the partners, and whether they or their partners have other sex partners, using more gender-inclusive language.
When asking about practices, in addition to asking about the type of sexual contact patients have had, additional questions include whether the patient met their partners online or through apps, whether they or any of their partners use drugs, and whether the patient has exchanged sex for any needs, such as money, housing, or drugs. The additional questions can identify those at higher risk for STIs.
After reviewing the CDC’s list of risk factors for gonorrhea and chlamydia screening, Dr. Policar shared the screening list from the California Department of Public Health, which he finds more helpful:
- History of gonorrhea, chlamydia, or pelvic inflammatory disease (PID) in the past 2 years.
- More than 1 sexual partner in the past year.
- New sexual partner within 90 days.
- Reason to believe that a sex partner has had other partners in the past year.
- Exchanging sex for drugs or money within the past year.
- Other factors identified locally, including prevalence of infection in the community.
STI screening guidelines
For those with a positive gonorrhea/chlamydia (GC/CT) screen, a nucleic acid amplification test (NAAT) vaginal swab is the preferred specimen source, and self-collection is fine for women of any age, Dr. Policar said. In addition, cis-women who received anal intercourse in the preceding year should consider undergoing a rectal GC/CT NAAT, and those who performed oral sex should consider a pharyngeal GC/CT NAAT, based on shared clinical decision-making. A rectal swab requires an insertion of 3-4 cm and a 360-degree twirl of the wrist, not the swab, to ensure you get a sample from the entire circumference. Pharyngeal samples require swabbing both tonsillar pillars while taking care for those who may gag.
For contact testing – asymptomatic people who have had a high-risk sexual exposure – providers should test for gonorrhea, chlamydia, HIV, and syphilis but not for herpes, high-risk HPV, hepatitis B, hepatitis C, or bacterial vaginosis. “Maybe we’ll do a screen for trichomoniasis, and maybe we’ll offer herpes type 2 serology or antibody screening,” Dr. Policar said. Providers should also ask patients requesting contact testing if they have been vaccinated for hepatitis B. If not, “the conversation should be how can we get you vaccinated for hepatitis B,” Dr. Policar said.
HIV screening only needs to occur once between the ages of 15 and 65 for low-risk people and then once annually (or more often if necessary) for those who have a sex partner with HIV, use injectable drugs, engage in commercial sex work, have a new sex partner with unknown HIV status, received care at an STD or TB clinic, or were in a correctional facility or homeless shelter.
Those at increased risk for syphilis include men who have sex with men, men under age 29, and anyone living with HIV or who has a history of incarceration or a history of commercial sex work. In addition, African Americans have the greatest risk for syphilis of racial/ethnic groups, followed by Hispanics. Most adults only require hepatitis C screening with anti-hep C antibody testing once in their lifetime. Periodic hepatitis C screening should occur for people who inject drugs. If the screening is positive, providers should conduct an RNA polymerase chain reaction (PCR) test to determine whether a chronic infection is present.
Trichomoniasis screening should occur annually in women living with HIV or in correctional facilities. Others to consider screening include people with new or multiple sex partners, a history of STIs, inconsistent condom use, a history of sex work, and intravenous drug use. Dr. Policar also noted that several new assays, including NAAT, PCR, and a rapid test, are available for trichomoniasis.
STI treatment guidelines
For women with mucoprurulent cervicitis, the cause could be chlamydia, gonorrhea, herpes, trichomonas, mycoplasma, or even progesterone from pregnancy or contraception, Dr. Policar said. The new preferred treatment is 100 mg of doxycycline. The alternative, albeit less preferred, treatment is 1 g azithromycin.
The preferred treatment for chlamydia is now 100 mg oral doxycycline twice daily, or doxycycline 200 mg delayed-release once daily, for 7 days. Alternative regimens include 1 g oral azithromycin in a single dose or 500 mg oral levofloxacin once daily for 7 days. The switch to recommending doxycycline over azithromycin is based on recent evidence showing that doxycycline has a slightly higher efficacy for urogenital chlamydia and a substantially higher efficacy for rectal chlamydia. In addition, an increasing proportion of gonorrheal infections have shown resistance to azithromycin, particularly beginning in 2014.
Preferred treatment of new, uncomplicated gonorrhea infections of the cervix, urethra, rectum, and pharynx is one 500-mg dose of ceftriaxone for those weighing under 150 kg and 1 g for those weighing 150 kg or more. If ceftriaxone is unavailable, the new alternative recommended treatment for gonorrhea is 800 mg cefixime. For pharyngeal gonorrhea only, the CDC recommends a test-of-cure 7-14 days after treatment.
For gonorrheal infections, the CDC also recommends treatment with doxycycline if chlamydia has not been excluded, but the agency no longer recommends dual therapy with azithromycin unless it’s used in place of doxycycline for those who are pregnant, have an allergy, or may not be compliant with a 7-day doxycycline regimen.
The preferred treatment for bacterial vaginosis has not changed. The new recommended regimen for trichomoniasis is 500 mg oral metronidazole for 7 days, with the alternative being a single 2-g dose of tinidazole. Male partners should receive 2 g oral metronidazole. The CDC also notes that patients taking metronidazole no longer need to abstain from alcohol during treatment.
”Another area where the guidelines changed is in their description of expedited partner therapy, which means that, when we find an index case who has gonorrhea or chlamydia, we always have a discussion with her about getting her partners treated,” Dr. Policar said. “The CDC was quite clear that the responsibility for discussing partner treatment rests with us as the diagnosing provider” since city and county health departments don’t have the time or resources for contact tracing these STIs.
The two main ways to treat partners are to have the patient bring their partner(s) to the appointment with them or to do patient-delivered partner therapy. Ideally, clinicians who dispense their own medications can give the patient enough drugs to give her partner(s) a complete dose as well. Otherwise, providers can prescribe extra doses in the index patients’ name or write prescriptions in the partner’s name.
“In every state of the union now, it is legal for you to to prescribe antibiotics for partners sight unseen, Dr. Policar said.
Margaret Sullivan, MD, an ob.gyn. from rural western North Carolina, noted during the Q&A that an obstacle to partner therapy at her practice has been cost, particularly since many of the men don’t have insurance.
“I have not heard before of prescribing the extra doses for partners under the patient’s name,” Dr. Sullivan said. “I’ve thought about doing it, but [was worried about] it potentially being fraudulent if that patient has Medicaid and we’re prescribing extra doses under her name, so how do you work around that?”
Dr. Policar acknowledged that barrier and recommended that patients use the website/app Goodrx.com to find discounts for out-of-pocket generic medications. He also noted the occasional obstacle of pharmacists balking at filling a double or triple dose.
“What we’ve been suggesting in that circumstance is to literally copy that part of the CDC guidelines, which explains expedited partner therapy or patient-delivered partner therapy and send that off to the pharmacist so they can see that it’s a national recommendation of the CDC,” Dr. Policar said.
Claudia Rodriguez, MD, an ob.gyn. who works at Sherman Hospital in Elgin, Ill., asked about the CDC recommendations for HPV vaccination in older women. Although the CDC permits women over age 26 to receive the HPV vaccine, the agency does not “make a solid recommendation to have this done, which oftentimes makes a big difference in whether or not health insurance will actually pay for vaccination in that circumstance,” Dr. Policar said.
Patients are welcome to request the vaccine after shared decision-making, but “we should never present this as something which is routine,” he said. For women in their 50s, for example, “there’s virtually no data about any additional degree of protection that you would get” from HPV vaccination, Dr. Policar said in response to a similar question from Tara Allmen, MD, an ob.gyn. in New York City. “If you ask me for my personal clinical opinion about it, I would say it’s not going to be worth it,” he said.
Dr Policar had no disclosures. Disclosures were unavailable for attendees who spoke.
Sexually transmitted infection rates have not increased as dramatically in older women as they have in women in their teens and 20s, but rates of chlamydia and gonorrhea in women over age 35 have seen a steady incline over the past decade, and syphilis rates have climbed steeply, according to data from the Centers for Disease Control and Prevention.
That makes the STI treatment guidelines released by the CDC in July even timelier for practitioners of menopause medicine, according to Michael S. Policar, MD, MPH, a professor emeritus of ob.gyn. and reproductive sciences at the University of California, San Francisco.
Dr. Policar discussed what clinicians need to know about STIs in midlife women at the hybrid annual meeting of the North American Menopause Society. Even the nomenclature change in the guidelines from “sexually transmitted diseases” to “sexually transmitted infections” is important “because they want to acknowledge the fact that a lot of the sexually transmitted infections that we’re treating are asymptomatic, are colonizations, and are not yet diseases,” Dr. Policar said. “We’re trying to be much more expansive in thinking about finding these infections before they actually start causing morbidity in the form of a disease.”
Sexual history
The primary guidelines update for taking sexual history is the recommendation to ask patients about their intentions regarding pregnancy. The “5 Ps” of sexual history are now Partners, Practices, Protection from STIs, Past history of STIs, and Pregnancy intention.
“There should be a sixth P that has to do with pleasure questions,” Policar added. “We ask all the time for patients that we see in the context of perimenopausal and menopausal services, ‘Are you satisfied with your sexual relationship with your partner?’ Hopefully that will make it into the CDC guidelines as the sixth P at some point, but for now, that’s aspirational.”
In asking about partners, instead of asking patients whether they have sex with men, women, or both, clinicians should ask first if the patient is having sex of any kind – oral, vaginal, or anal – with anyone. From there, providers should ask how many sex partners the patient has had, the gender(s) of the partners, and whether they or their partners have other sex partners, using more gender-inclusive language.
When asking about practices, in addition to asking about the type of sexual contact patients have had, additional questions include whether the patient met their partners online or through apps, whether they or any of their partners use drugs, and whether the patient has exchanged sex for any needs, such as money, housing, or drugs. The additional questions can identify those at higher risk for STIs.
After reviewing the CDC’s list of risk factors for gonorrhea and chlamydia screening, Dr. Policar shared the screening list from the California Department of Public Health, which he finds more helpful:
- History of gonorrhea, chlamydia, or pelvic inflammatory disease (PID) in the past 2 years.
- More than 1 sexual partner in the past year.
- New sexual partner within 90 days.
- Reason to believe that a sex partner has had other partners in the past year.
- Exchanging sex for drugs or money within the past year.
- Other factors identified locally, including prevalence of infection in the community.
STI screening guidelines
For those with a positive gonorrhea/chlamydia (GC/CT) screen, a nucleic acid amplification test (NAAT) vaginal swab is the preferred specimen source, and self-collection is fine for women of any age, Dr. Policar said. In addition, cis-women who received anal intercourse in the preceding year should consider undergoing a rectal GC/CT NAAT, and those who performed oral sex should consider a pharyngeal GC/CT NAAT, based on shared clinical decision-making. A rectal swab requires an insertion of 3-4 cm and a 360-degree twirl of the wrist, not the swab, to ensure you get a sample from the entire circumference. Pharyngeal samples require swabbing both tonsillar pillars while taking care for those who may gag.
For contact testing – asymptomatic people who have had a high-risk sexual exposure – providers should test for gonorrhea, chlamydia, HIV, and syphilis but not for herpes, high-risk HPV, hepatitis B, hepatitis C, or bacterial vaginosis. “Maybe we’ll do a screen for trichomoniasis, and maybe we’ll offer herpes type 2 serology or antibody screening,” Dr. Policar said. Providers should also ask patients requesting contact testing if they have been vaccinated for hepatitis B. If not, “the conversation should be how can we get you vaccinated for hepatitis B,” Dr. Policar said.
HIV screening only needs to occur once between the ages of 15 and 65 for low-risk people and then once annually (or more often if necessary) for those who have a sex partner with HIV, use injectable drugs, engage in commercial sex work, have a new sex partner with unknown HIV status, received care at an STD or TB clinic, or were in a correctional facility or homeless shelter.
Those at increased risk for syphilis include men who have sex with men, men under age 29, and anyone living with HIV or who has a history of incarceration or a history of commercial sex work. In addition, African Americans have the greatest risk for syphilis of racial/ethnic groups, followed by Hispanics. Most adults only require hepatitis C screening with anti-hep C antibody testing once in their lifetime. Periodic hepatitis C screening should occur for people who inject drugs. If the screening is positive, providers should conduct an RNA polymerase chain reaction (PCR) test to determine whether a chronic infection is present.
Trichomoniasis screening should occur annually in women living with HIV or in correctional facilities. Others to consider screening include people with new or multiple sex partners, a history of STIs, inconsistent condom use, a history of sex work, and intravenous drug use. Dr. Policar also noted that several new assays, including NAAT, PCR, and a rapid test, are available for trichomoniasis.
STI treatment guidelines
For women with mucoprurulent cervicitis, the cause could be chlamydia, gonorrhea, herpes, trichomonas, mycoplasma, or even progesterone from pregnancy or contraception, Dr. Policar said. The new preferred treatment is 100 mg of doxycycline. The alternative, albeit less preferred, treatment is 1 g azithromycin.
The preferred treatment for chlamydia is now 100 mg oral doxycycline twice daily, or doxycycline 200 mg delayed-release once daily, for 7 days. Alternative regimens include 1 g oral azithromycin in a single dose or 500 mg oral levofloxacin once daily for 7 days. The switch to recommending doxycycline over azithromycin is based on recent evidence showing that doxycycline has a slightly higher efficacy for urogenital chlamydia and a substantially higher efficacy for rectal chlamydia. In addition, an increasing proportion of gonorrheal infections have shown resistance to azithromycin, particularly beginning in 2014.
Preferred treatment of new, uncomplicated gonorrhea infections of the cervix, urethra, rectum, and pharynx is one 500-mg dose of ceftriaxone for those weighing under 150 kg and 1 g for those weighing 150 kg or more. If ceftriaxone is unavailable, the new alternative recommended treatment for gonorrhea is 800 mg cefixime. For pharyngeal gonorrhea only, the CDC recommends a test-of-cure 7-14 days after treatment.
For gonorrheal infections, the CDC also recommends treatment with doxycycline if chlamydia has not been excluded, but the agency no longer recommends dual therapy with azithromycin unless it’s used in place of doxycycline for those who are pregnant, have an allergy, or may not be compliant with a 7-day doxycycline regimen.
The preferred treatment for bacterial vaginosis has not changed. The new recommended regimen for trichomoniasis is 500 mg oral metronidazole for 7 days, with the alternative being a single 2-g dose of tinidazole. Male partners should receive 2 g oral metronidazole. The CDC also notes that patients taking metronidazole no longer need to abstain from alcohol during treatment.
”Another area where the guidelines changed is in their description of expedited partner therapy, which means that, when we find an index case who has gonorrhea or chlamydia, we always have a discussion with her about getting her partners treated,” Dr. Policar said. “The CDC was quite clear that the responsibility for discussing partner treatment rests with us as the diagnosing provider” since city and county health departments don’t have the time or resources for contact tracing these STIs.
The two main ways to treat partners are to have the patient bring their partner(s) to the appointment with them or to do patient-delivered partner therapy. Ideally, clinicians who dispense their own medications can give the patient enough drugs to give her partner(s) a complete dose as well. Otherwise, providers can prescribe extra doses in the index patients’ name or write prescriptions in the partner’s name.
“In every state of the union now, it is legal for you to to prescribe antibiotics for partners sight unseen, Dr. Policar said.
Margaret Sullivan, MD, an ob.gyn. from rural western North Carolina, noted during the Q&A that an obstacle to partner therapy at her practice has been cost, particularly since many of the men don’t have insurance.
“I have not heard before of prescribing the extra doses for partners under the patient’s name,” Dr. Sullivan said. “I’ve thought about doing it, but [was worried about] it potentially being fraudulent if that patient has Medicaid and we’re prescribing extra doses under her name, so how do you work around that?”
Dr. Policar acknowledged that barrier and recommended that patients use the website/app Goodrx.com to find discounts for out-of-pocket generic medications. He also noted the occasional obstacle of pharmacists balking at filling a double or triple dose.
“What we’ve been suggesting in that circumstance is to literally copy that part of the CDC guidelines, which explains expedited partner therapy or patient-delivered partner therapy and send that off to the pharmacist so they can see that it’s a national recommendation of the CDC,” Dr. Policar said.
Claudia Rodriguez, MD, an ob.gyn. who works at Sherman Hospital in Elgin, Ill., asked about the CDC recommendations for HPV vaccination in older women. Although the CDC permits women over age 26 to receive the HPV vaccine, the agency does not “make a solid recommendation to have this done, which oftentimes makes a big difference in whether or not health insurance will actually pay for vaccination in that circumstance,” Dr. Policar said.
Patients are welcome to request the vaccine after shared decision-making, but “we should never present this as something which is routine,” he said. For women in their 50s, for example, “there’s virtually no data about any additional degree of protection that you would get” from HPV vaccination, Dr. Policar said in response to a similar question from Tara Allmen, MD, an ob.gyn. in New York City. “If you ask me for my personal clinical opinion about it, I would say it’s not going to be worth it,” he said.
Dr Policar had no disclosures. Disclosures were unavailable for attendees who spoke.
FROM NAMS 2021
Outreach Finds Veterans Unaware of Service Connection
The US Department of Veterans Affairs (VA) Northeast Ohio Healthcare System has been eaching out directly by postal mail to hundreds of veterans with cancer who may have been exposed to Agent Orange or contaminated water at Camp Lejeune in North Carolina. Advocates say they’ve connected dozens to “service-connected” benefits that pay for 100% of the veterans’ care and can potentially provide support to their spouses after they pass away.
The details and outcomes of the outreach project were presented at the 2021 annual meeting of the Association of VA Hematology/Oncology (AVAHO) being held virtually and in person in Denver, Colorado, from September 24 to September 26, 2021.
“Once you get a devastating diagnosis like cancer, you’ve got enough going on in your head. You shouldn’t have to worry about what the next step is in the benefit process,” said VA Northeast Ohio Healthcare System outreach coordinator Willie J. Berry in an interview. “We want you to focus on your care and not have to worry about anything else.”
Agent Orange, made up of 2,3,7,8-tetrachlorodibenzo-p-dioxin, was used to defoliate forests and kill crops during the Vietnam War. Through “100% service connection” the VA fully covers benefits for certain cancers and other diseases for veterans who are considered to have been exposed to Agent Orange in Vietnam and elsewhere.
Veterans do not need to pay copays in these cases, Berry said, and care outside the VA may be fully funded once arrangements are made.
The VA also fully covers benefits for a similar list of diseases, also including some types of cancer, for veterans who are considered to have been exposed to a contaminated water supply at Camp Lejeune in the early 1980s.
Vietnam War veterans may not be aware of the Agent Orange benefits due to a negative perception of the VA, Berry said. “They were treated poorly [by the VA] and didn’t want to have anything to do with it.”
In the first phase of the project, the VA Northeast Ohio Healthcare System tried to reach potentially eligible veterans with both cancer and possible Agent Orange exposure via phone. Seventy veterans were referred to outreach coordinators, and 16 received 100% service connection after 6 months. The latter number later grew to 34.
“The most inefficient thing were doing was calling veterans one by one,” Berry said. “We felt a mailer would be more efficient in order to reach more people.”
For the second phase, in 2021, coordinators sent informational “Dear veteran” mailers to 427 veterans with cancer who may be eligible for special Agent Orange/Camp Lejeune benefits based on their service history.
The Agent Orange letters began this way: “Through a recent medical diagnosis, VA has identified you as possibly being impacted by a change in Agent Orange Exposure legislation.” The letters then list the eligible conditions, which as of 2021 now include bladder cancer, hyperthyroidism and parkinsonism.
The letters also note that “claims often enhance a veteran’s VA compensation and reduce their cost of care. Additionally, if a veteran were to succumb to a diagnosis that they were service connected for, their spouse might be able to receive both VA health care (until the age of Medicare eligibility) as well as financial benefits for the rest of their life.”
If veterans were terminally ill, the application process for the special benefits could be expedited, Berry said. The number of veterans who received 100% service connection in the second phase of the project was not provided.
No study funding is reported. Berry has no disclosures.
The US Department of Veterans Affairs (VA) Northeast Ohio Healthcare System has been eaching out directly by postal mail to hundreds of veterans with cancer who may have been exposed to Agent Orange or contaminated water at Camp Lejeune in North Carolina. Advocates say they’ve connected dozens to “service-connected” benefits that pay for 100% of the veterans’ care and can potentially provide support to their spouses after they pass away.
The details and outcomes of the outreach project were presented at the 2021 annual meeting of the Association of VA Hematology/Oncology (AVAHO) being held virtually and in person in Denver, Colorado, from September 24 to September 26, 2021.
“Once you get a devastating diagnosis like cancer, you’ve got enough going on in your head. You shouldn’t have to worry about what the next step is in the benefit process,” said VA Northeast Ohio Healthcare System outreach coordinator Willie J. Berry in an interview. “We want you to focus on your care and not have to worry about anything else.”
Agent Orange, made up of 2,3,7,8-tetrachlorodibenzo-p-dioxin, was used to defoliate forests and kill crops during the Vietnam War. Through “100% service connection” the VA fully covers benefits for certain cancers and other diseases for veterans who are considered to have been exposed to Agent Orange in Vietnam and elsewhere.
Veterans do not need to pay copays in these cases, Berry said, and care outside the VA may be fully funded once arrangements are made.
The VA also fully covers benefits for a similar list of diseases, also including some types of cancer, for veterans who are considered to have been exposed to a contaminated water supply at Camp Lejeune in the early 1980s.
Vietnam War veterans may not be aware of the Agent Orange benefits due to a negative perception of the VA, Berry said. “They were treated poorly [by the VA] and didn’t want to have anything to do with it.”
In the first phase of the project, the VA Northeast Ohio Healthcare System tried to reach potentially eligible veterans with both cancer and possible Agent Orange exposure via phone. Seventy veterans were referred to outreach coordinators, and 16 received 100% service connection after 6 months. The latter number later grew to 34.
“The most inefficient thing were doing was calling veterans one by one,” Berry said. “We felt a mailer would be more efficient in order to reach more people.”
For the second phase, in 2021, coordinators sent informational “Dear veteran” mailers to 427 veterans with cancer who may be eligible for special Agent Orange/Camp Lejeune benefits based on their service history.
The Agent Orange letters began this way: “Through a recent medical diagnosis, VA has identified you as possibly being impacted by a change in Agent Orange Exposure legislation.” The letters then list the eligible conditions, which as of 2021 now include bladder cancer, hyperthyroidism and parkinsonism.
The letters also note that “claims often enhance a veteran’s VA compensation and reduce their cost of care. Additionally, if a veteran were to succumb to a diagnosis that they were service connected for, their spouse might be able to receive both VA health care (until the age of Medicare eligibility) as well as financial benefits for the rest of their life.”
If veterans were terminally ill, the application process for the special benefits could be expedited, Berry said. The number of veterans who received 100% service connection in the second phase of the project was not provided.
No study funding is reported. Berry has no disclosures.
The US Department of Veterans Affairs (VA) Northeast Ohio Healthcare System has been eaching out directly by postal mail to hundreds of veterans with cancer who may have been exposed to Agent Orange or contaminated water at Camp Lejeune in North Carolina. Advocates say they’ve connected dozens to “service-connected” benefits that pay for 100% of the veterans’ care and can potentially provide support to their spouses after they pass away.
The details and outcomes of the outreach project were presented at the 2021 annual meeting of the Association of VA Hematology/Oncology (AVAHO) being held virtually and in person in Denver, Colorado, from September 24 to September 26, 2021.
“Once you get a devastating diagnosis like cancer, you’ve got enough going on in your head. You shouldn’t have to worry about what the next step is in the benefit process,” said VA Northeast Ohio Healthcare System outreach coordinator Willie J. Berry in an interview. “We want you to focus on your care and not have to worry about anything else.”
Agent Orange, made up of 2,3,7,8-tetrachlorodibenzo-p-dioxin, was used to defoliate forests and kill crops during the Vietnam War. Through “100% service connection” the VA fully covers benefits for certain cancers and other diseases for veterans who are considered to have been exposed to Agent Orange in Vietnam and elsewhere.
Veterans do not need to pay copays in these cases, Berry said, and care outside the VA may be fully funded once arrangements are made.
The VA also fully covers benefits for a similar list of diseases, also including some types of cancer, for veterans who are considered to have been exposed to a contaminated water supply at Camp Lejeune in the early 1980s.
Vietnam War veterans may not be aware of the Agent Orange benefits due to a negative perception of the VA, Berry said. “They were treated poorly [by the VA] and didn’t want to have anything to do with it.”
In the first phase of the project, the VA Northeast Ohio Healthcare System tried to reach potentially eligible veterans with both cancer and possible Agent Orange exposure via phone. Seventy veterans were referred to outreach coordinators, and 16 received 100% service connection after 6 months. The latter number later grew to 34.
“The most inefficient thing were doing was calling veterans one by one,” Berry said. “We felt a mailer would be more efficient in order to reach more people.”
For the second phase, in 2021, coordinators sent informational “Dear veteran” mailers to 427 veterans with cancer who may be eligible for special Agent Orange/Camp Lejeune benefits based on their service history.
The Agent Orange letters began this way: “Through a recent medical diagnosis, VA has identified you as possibly being impacted by a change in Agent Orange Exposure legislation.” The letters then list the eligible conditions, which as of 2021 now include bladder cancer, hyperthyroidism and parkinsonism.
The letters also note that “claims often enhance a veteran’s VA compensation and reduce their cost of care. Additionally, if a veteran were to succumb to a diagnosis that they were service connected for, their spouse might be able to receive both VA health care (until the age of Medicare eligibility) as well as financial benefits for the rest of their life.”
If veterans were terminally ill, the application process for the special benefits could be expedited, Berry said. The number of veterans who received 100% service connection in the second phase of the project was not provided.
No study funding is reported. Berry has no disclosures.
Duty to Assist: Assisting Veterans with Exposures to Hazardous Materials
Community outreach coordinators identified Veterans who were not aware of their entitlement to service-connected benefits. Veterans were also unaware of the importance of adding new presumptive diagnoses to their existing service connection and were unaware of new conditions that were added to the presumptive lists. Many Veterans, unaware of the Agent Orange/Camp Lejeune presumptive conditions, were paying out of pocket for their oncology care. A project was developed between community outreach and oncology to identify, and contact Veterans newly diagnosed with cancers on the presumptive list for Vietnam and Camp Lejeune. The goals for the project were to: Increase presumptive condition awareness, assist Veterans in navigating the VHA, VBA and VSC (Veteran Service Commission) and provide a VA resource for the Veterans for assistance. Oncology team reviewed the cancer registry each month and identified Veterans who served during the Vietnam Era or the Marine Corps and contacted them to screen for military history. If a Veteran met the time and location qualifications, the Veteran was referred to the community outreach coordinators. The coordinators then further screened the Veterans for eligibility, assisted the Veterans in initiating their claims applications and connected the Veterans with their local VSC. At the six month follow up, 74 Veterans had been referred to community outreach, and 16 Veterans had received 100% service connection. It is important to note, the benefits application process can take several months to complete under normal circumstances. Since implementation the project has been revised. The project team developed mailers to alert Veterans of: Potential benefits eligibility, importance for filing claims, contact information for their local VSC and contact information for VA Outreach for additional assistance. Informatics was recruited to assist with identifying Veterans who met the service criteria and providing their addresses. The Veterans identified were then sent mailers, which expedited the process, allowing the project team to reach more Veterans in a shorter timeframe. Since project initiation, 74 Veterans were contacted directly by outreach coordinators, 273 mailers have been sent to potentially eligible Veterans, and 34 have received 100% service connection to date. al center will continue this practice moving forward.
Community outreach coordinators identified Veterans who were not aware of their entitlement to service-connected benefits. Veterans were also unaware of the importance of adding new presumptive diagnoses to their existing service connection and were unaware of new conditions that were added to the presumptive lists. Many Veterans, unaware of the Agent Orange/Camp Lejeune presumptive conditions, were paying out of pocket for their oncology care. A project was developed between community outreach and oncology to identify, and contact Veterans newly diagnosed with cancers on the presumptive list for Vietnam and Camp Lejeune. The goals for the project were to: Increase presumptive condition awareness, assist Veterans in navigating the VHA, VBA and VSC (Veteran Service Commission) and provide a VA resource for the Veterans for assistance. Oncology team reviewed the cancer registry each month and identified Veterans who served during the Vietnam Era or the Marine Corps and contacted them to screen for military history. If a Veteran met the time and location qualifications, the Veteran was referred to the community outreach coordinators. The coordinators then further screened the Veterans for eligibility, assisted the Veterans in initiating their claims applications and connected the Veterans with their local VSC. At the six month follow up, 74 Veterans had been referred to community outreach, and 16 Veterans had received 100% service connection. It is important to note, the benefits application process can take several months to complete under normal circumstances. Since implementation the project has been revised. The project team developed mailers to alert Veterans of: Potential benefits eligibility, importance for filing claims, contact information for their local VSC and contact information for VA Outreach for additional assistance. Informatics was recruited to assist with identifying Veterans who met the service criteria and providing their addresses. The Veterans identified were then sent mailers, which expedited the process, allowing the project team to reach more Veterans in a shorter timeframe. Since project initiation, 74 Veterans were contacted directly by outreach coordinators, 273 mailers have been sent to potentially eligible Veterans, and 34 have received 100% service connection to date. al center will continue this practice moving forward.
Community outreach coordinators identified Veterans who were not aware of their entitlement to service-connected benefits. Veterans were also unaware of the importance of adding new presumptive diagnoses to their existing service connection and were unaware of new conditions that were added to the presumptive lists. Many Veterans, unaware of the Agent Orange/Camp Lejeune presumptive conditions, were paying out of pocket for their oncology care. A project was developed between community outreach and oncology to identify, and contact Veterans newly diagnosed with cancers on the presumptive list for Vietnam and Camp Lejeune. The goals for the project were to: Increase presumptive condition awareness, assist Veterans in navigating the VHA, VBA and VSC (Veteran Service Commission) and provide a VA resource for the Veterans for assistance. Oncology team reviewed the cancer registry each month and identified Veterans who served during the Vietnam Era or the Marine Corps and contacted them to screen for military history. If a Veteran met the time and location qualifications, the Veteran was referred to the community outreach coordinators. The coordinators then further screened the Veterans for eligibility, assisted the Veterans in initiating their claims applications and connected the Veterans with their local VSC. At the six month follow up, 74 Veterans had been referred to community outreach, and 16 Veterans had received 100% service connection. It is important to note, the benefits application process can take several months to complete under normal circumstances. Since implementation the project has been revised. The project team developed mailers to alert Veterans of: Potential benefits eligibility, importance for filing claims, contact information for their local VSC and contact information for VA Outreach for additional assistance. Informatics was recruited to assist with identifying Veterans who met the service criteria and providing their addresses. The Veterans identified were then sent mailers, which expedited the process, allowing the project team to reach more Veterans in a shorter timeframe. Since project initiation, 74 Veterans were contacted directly by outreach coordinators, 273 mailers have been sent to potentially eligible Veterans, and 34 have received 100% service connection to date. al center will continue this practice moving forward.
Should Geriatric Veterans Get Immunotherapy?
Patients in their 90s with cancer tolerated immunotherapy well with few serious adverse effects, and they lived for an average of 1.6 years after treatment, a small new study within the US Department of Veterans Affairs (VA) health system reports.
Only 6.3% of 48 patients who were treated with immune checkpoint inhibitors experienced the most severe types of side effects – grade III/IV events – and a total of 27% had any adverse effects, according to the report, which was presented at the 2021 annual meeting of the Association of VA Hematology/Oncology (AVAHO) being held virtually and inperson in Denver Colorado, September 24 to September 26, 2021.
“Our project should help give confidence to oncologists treating the elderly,” said Andrew Joseph Benefield, MD, a hematology/oncology fellow at Wake Forest Baptist Medical Center, in an interview. “Immunotherapy can be given safely and likely effectively in select individuals over the age of 90 with good performance status.”
Benefield and colleagues launched their study to gain insight into a little-studied area: How does cancer treatment affects nonagenarians? “I think many oncologists have been in a situation where they encounter an individual over the age of 90 years who has a good performance status, and they've wondered if immunotherapy would be helpful and safe, particularly given our knowledge of waning immune strength as people age,” he said.
The researchers retrospectively tracked patients with cancer who were at least 90 years old from 2016 to 2017 and were treated with immune checkpoint inhibitors. Most were fit or fairly fit with Eastern Cooperative Oncology Group (ECOG) physical performance scales of 0 or 1 (n = 26), and nearly all had cancer in stage IV (n = 42). Melanoma was the most common type of cancer (n = 19), followed by non-small-cell lung cancer (n = 15). Patients were treated with an average of 12.2 cycles.
“In general, we saw that treatment was well-tolerated,” Dr. Benefield said. “We also noted that a trend toward better long-term survival outcomes in individuals with very good performance status at the start of treatment. We hope to parse this out more as we add more data to our data-set, as the numbers are still too small for confident direct comparison.”
Dr. Benefield said he has treated a limited number of patients in their 90s who were highly physical fit for their age and “very eager” to be treated. “They wanted to do anything they could to maintain their lifestyle,” he said. “In my experience, aggressive supportive care and close monitoring for developing toxicities has been most helpful.”
The researchers don’t know the causes of death of many of the patients, and it’s not clear how they fared in their final days. Still, Dr. Benefield said, “extending someone's life by more than 1 year with relatively low risk of adverse effects is reasonable.”
Oncologist Melisa Wong, MD, MAS, of the University of California, San Francisco, reviewed the study and said in an interview that it “a valuable description of outcomes for nonagenarians receiving immunotherapy in the VA healthcare system.” As she noted, “many other studies of immunotherapy among older adults focus on patients aged 65 or 70 and older while very few focus on octogenarians or nonagenarians.”
The findings suggest that “it is important to move beyond chronological age and assess patients’ physiologic age through a geriatric assessment,” she said. “Geriatric assessment-derived risk scores have been shown to predict chemotherapy toxicity for older adults and research to develop similar tools for immunotherapy are ongoing.”
However, she cautioned that older patients may become suffer so much from the most common side effect of immunotherapy -- fatigue – that “their independence is at stake.”
“Some of these patient choose to stop immunotherapy because the side effects aren’t worth it anymore,” she said. “The challenge for oncologists is not knowing in advance which patients will fall into each of these categories.”
She added that her geriatric oncology research focuses on improving risk stratification for older adults, such as those who are at least 70 with lung adenocarcinoma.
Oncologist Grant R. Williams, MD, MSPH, director of the Cancer & Aging Program at the University of Alabama at Birmingham, agreed in an interview that comprehensive geriatric assessments are important to guide treatment in the oldest adults. “In addition, it is important to elicit the goals of treatment as well,” he said. “For older adults that are fit or at least pre-frail and desire aggressive treatment, immunotherapy is a very reasonable approach, particularly when patients are closely monitored for side effects.”
No study funding is reported. The authors report no disclosures. Dr. Wong discloses an immediate family member is an employee and stock holder of Genentech. Dr. Williams has no disclosures.
Patients in their 90s with cancer tolerated immunotherapy well with few serious adverse effects, and they lived for an average of 1.6 years after treatment, a small new study within the US Department of Veterans Affairs (VA) health system reports.
Only 6.3% of 48 patients who were treated with immune checkpoint inhibitors experienced the most severe types of side effects – grade III/IV events – and a total of 27% had any adverse effects, according to the report, which was presented at the 2021 annual meeting of the Association of VA Hematology/Oncology (AVAHO) being held virtually and inperson in Denver Colorado, September 24 to September 26, 2021.
“Our project should help give confidence to oncologists treating the elderly,” said Andrew Joseph Benefield, MD, a hematology/oncology fellow at Wake Forest Baptist Medical Center, in an interview. “Immunotherapy can be given safely and likely effectively in select individuals over the age of 90 with good performance status.”
Benefield and colleagues launched their study to gain insight into a little-studied area: How does cancer treatment affects nonagenarians? “I think many oncologists have been in a situation where they encounter an individual over the age of 90 years who has a good performance status, and they've wondered if immunotherapy would be helpful and safe, particularly given our knowledge of waning immune strength as people age,” he said.
The researchers retrospectively tracked patients with cancer who were at least 90 years old from 2016 to 2017 and were treated with immune checkpoint inhibitors. Most were fit or fairly fit with Eastern Cooperative Oncology Group (ECOG) physical performance scales of 0 or 1 (n = 26), and nearly all had cancer in stage IV (n = 42). Melanoma was the most common type of cancer (n = 19), followed by non-small-cell lung cancer (n = 15). Patients were treated with an average of 12.2 cycles.
“In general, we saw that treatment was well-tolerated,” Dr. Benefield said. “We also noted that a trend toward better long-term survival outcomes in individuals with very good performance status at the start of treatment. We hope to parse this out more as we add more data to our data-set, as the numbers are still too small for confident direct comparison.”
Dr. Benefield said he has treated a limited number of patients in their 90s who were highly physical fit for their age and “very eager” to be treated. “They wanted to do anything they could to maintain their lifestyle,” he said. “In my experience, aggressive supportive care and close monitoring for developing toxicities has been most helpful.”
The researchers don’t know the causes of death of many of the patients, and it’s not clear how they fared in their final days. Still, Dr. Benefield said, “extending someone's life by more than 1 year with relatively low risk of adverse effects is reasonable.”
Oncologist Melisa Wong, MD, MAS, of the University of California, San Francisco, reviewed the study and said in an interview that it “a valuable description of outcomes for nonagenarians receiving immunotherapy in the VA healthcare system.” As she noted, “many other studies of immunotherapy among older adults focus on patients aged 65 or 70 and older while very few focus on octogenarians or nonagenarians.”
The findings suggest that “it is important to move beyond chronological age and assess patients’ physiologic age through a geriatric assessment,” she said. “Geriatric assessment-derived risk scores have been shown to predict chemotherapy toxicity for older adults and research to develop similar tools for immunotherapy are ongoing.”
However, she cautioned that older patients may become suffer so much from the most common side effect of immunotherapy -- fatigue – that “their independence is at stake.”
“Some of these patient choose to stop immunotherapy because the side effects aren’t worth it anymore,” she said. “The challenge for oncologists is not knowing in advance which patients will fall into each of these categories.”
She added that her geriatric oncology research focuses on improving risk stratification for older adults, such as those who are at least 70 with lung adenocarcinoma.
Oncologist Grant R. Williams, MD, MSPH, director of the Cancer & Aging Program at the University of Alabama at Birmingham, agreed in an interview that comprehensive geriatric assessments are important to guide treatment in the oldest adults. “In addition, it is important to elicit the goals of treatment as well,” he said. “For older adults that are fit or at least pre-frail and desire aggressive treatment, immunotherapy is a very reasonable approach, particularly when patients are closely monitored for side effects.”
No study funding is reported. The authors report no disclosures. Dr. Wong discloses an immediate family member is an employee and stock holder of Genentech. Dr. Williams has no disclosures.
Patients in their 90s with cancer tolerated immunotherapy well with few serious adverse effects, and they lived for an average of 1.6 years after treatment, a small new study within the US Department of Veterans Affairs (VA) health system reports.
Only 6.3% of 48 patients who were treated with immune checkpoint inhibitors experienced the most severe types of side effects – grade III/IV events – and a total of 27% had any adverse effects, according to the report, which was presented at the 2021 annual meeting of the Association of VA Hematology/Oncology (AVAHO) being held virtually and inperson in Denver Colorado, September 24 to September 26, 2021.
“Our project should help give confidence to oncologists treating the elderly,” said Andrew Joseph Benefield, MD, a hematology/oncology fellow at Wake Forest Baptist Medical Center, in an interview. “Immunotherapy can be given safely and likely effectively in select individuals over the age of 90 with good performance status.”
Benefield and colleagues launched their study to gain insight into a little-studied area: How does cancer treatment affects nonagenarians? “I think many oncologists have been in a situation where they encounter an individual over the age of 90 years who has a good performance status, and they've wondered if immunotherapy would be helpful and safe, particularly given our knowledge of waning immune strength as people age,” he said.
The researchers retrospectively tracked patients with cancer who were at least 90 years old from 2016 to 2017 and were treated with immune checkpoint inhibitors. Most were fit or fairly fit with Eastern Cooperative Oncology Group (ECOG) physical performance scales of 0 or 1 (n = 26), and nearly all had cancer in stage IV (n = 42). Melanoma was the most common type of cancer (n = 19), followed by non-small-cell lung cancer (n = 15). Patients were treated with an average of 12.2 cycles.
“In general, we saw that treatment was well-tolerated,” Dr. Benefield said. “We also noted that a trend toward better long-term survival outcomes in individuals with very good performance status at the start of treatment. We hope to parse this out more as we add more data to our data-set, as the numbers are still too small for confident direct comparison.”
Dr. Benefield said he has treated a limited number of patients in their 90s who were highly physical fit for their age and “very eager” to be treated. “They wanted to do anything they could to maintain their lifestyle,” he said. “In my experience, aggressive supportive care and close monitoring for developing toxicities has been most helpful.”
The researchers don’t know the causes of death of many of the patients, and it’s not clear how they fared in their final days. Still, Dr. Benefield said, “extending someone's life by more than 1 year with relatively low risk of adverse effects is reasonable.”
Oncologist Melisa Wong, MD, MAS, of the University of California, San Francisco, reviewed the study and said in an interview that it “a valuable description of outcomes for nonagenarians receiving immunotherapy in the VA healthcare system.” As she noted, “many other studies of immunotherapy among older adults focus on patients aged 65 or 70 and older while very few focus on octogenarians or nonagenarians.”
The findings suggest that “it is important to move beyond chronological age and assess patients’ physiologic age through a geriatric assessment,” she said. “Geriatric assessment-derived risk scores have been shown to predict chemotherapy toxicity for older adults and research to develop similar tools for immunotherapy are ongoing.”
However, she cautioned that older patients may become suffer so much from the most common side effect of immunotherapy -- fatigue – that “their independence is at stake.”
“Some of these patient choose to stop immunotherapy because the side effects aren’t worth it anymore,” she said. “The challenge for oncologists is not knowing in advance which patients will fall into each of these categories.”
She added that her geriatric oncology research focuses on improving risk stratification for older adults, such as those who are at least 70 with lung adenocarcinoma.
Oncologist Grant R. Williams, MD, MSPH, director of the Cancer & Aging Program at the University of Alabama at Birmingham, agreed in an interview that comprehensive geriatric assessments are important to guide treatment in the oldest adults. “In addition, it is important to elicit the goals of treatment as well,” he said. “For older adults that are fit or at least pre-frail and desire aggressive treatment, immunotherapy is a very reasonable approach, particularly when patients are closely monitored for side effects.”
No study funding is reported. The authors report no disclosures. Dr. Wong discloses an immediate family member is an employee and stock holder of Genentech. Dr. Williams has no disclosures.