User login
The ABIM sends a follow-up letter
A month ago the American Board of Internal Medicine sent a letter to diplomates saying they “got it wrong,” referring to the process of maintenance of certification or MOC, that the board required. They acknowledged that “parts of the new program are not meeting the needs of physicians like yourself.” Some of the things they proposed include changing the content of the Internal Medicine recertification exam to be “more reflective of what physicians in practice are doing,” with a promise that subspecialty recertification exams will follow suit. They also talk about “new and more flexible ways ... to demonstrate ... medical knowledge,” likely making room for the continuing medical education or CME credits that state licensures require.
While the letter was evidence that physician grievances were being heard, it was widely criticized for not having gone far enough. Questions remained about the financial and time cost of certification, the relevance of the exam, and the motivation of the board.
Well, the ABIM has written us again. Except it’s still not saying much. They simply say that they have been listening to feedback, and they list some points about what they’ve been hearing and are presumably going to take into consideration. In summary, they are recognizing that the while we all agree that we need a way for physicians to keep up on their medical knowledge, there is “a shared sense that defining ‘keeping up’ is the work of the whole community, including physicians, specialty societies, patient groups, and health care institutions.”
They proceed to outline what they’ve heard and will presumably consider, including the suggestion that the recertification exam be eliminated completely, and that CME units count toward recertification. Like I said, they didn’t say much. But this is promising. Particularly telling is the part where they acknowledge that the job of defining ‘keeping up’ does not fall solely on, as a friend put it, people that sit in their ivory towers and are removed from the daily grind of patient care.
Apropos of all this, I recently got my first 10 points toward MOC by taking a 30-question exam posted by the American College of Rheumatology. Each question comes with a list of references that you can review should you need or want to. To my great surprise, one of the references was in German. So what does that tell you about the people writing the questions and the process they use? What does that tell you about the validity of the questions as a measure of my competence and ability to treat people?
Exams like the boards are a measure of test-taking skills and retention, neither one of which is a true measure of what a capable, competent physician should be. The ABIM is imposing on us an onerous and ill-conceived tool, one that most physicians agree is irrelevant. I am glad this conversation is happening, because frankly the process was enough to make me want to quit being a doctor.
Dr. Chan practices rheumatology in Pawtucket, R.I.
A month ago the American Board of Internal Medicine sent a letter to diplomates saying they “got it wrong,” referring to the process of maintenance of certification or MOC, that the board required. They acknowledged that “parts of the new program are not meeting the needs of physicians like yourself.” Some of the things they proposed include changing the content of the Internal Medicine recertification exam to be “more reflective of what physicians in practice are doing,” with a promise that subspecialty recertification exams will follow suit. They also talk about “new and more flexible ways ... to demonstrate ... medical knowledge,” likely making room for the continuing medical education or CME credits that state licensures require.
While the letter was evidence that physician grievances were being heard, it was widely criticized for not having gone far enough. Questions remained about the financial and time cost of certification, the relevance of the exam, and the motivation of the board.
Well, the ABIM has written us again. Except it’s still not saying much. They simply say that they have been listening to feedback, and they list some points about what they’ve been hearing and are presumably going to take into consideration. In summary, they are recognizing that the while we all agree that we need a way for physicians to keep up on their medical knowledge, there is “a shared sense that defining ‘keeping up’ is the work of the whole community, including physicians, specialty societies, patient groups, and health care institutions.”
They proceed to outline what they’ve heard and will presumably consider, including the suggestion that the recertification exam be eliminated completely, and that CME units count toward recertification. Like I said, they didn’t say much. But this is promising. Particularly telling is the part where they acknowledge that the job of defining ‘keeping up’ does not fall solely on, as a friend put it, people that sit in their ivory towers and are removed from the daily grind of patient care.
Apropos of all this, I recently got my first 10 points toward MOC by taking a 30-question exam posted by the American College of Rheumatology. Each question comes with a list of references that you can review should you need or want to. To my great surprise, one of the references was in German. So what does that tell you about the people writing the questions and the process they use? What does that tell you about the validity of the questions as a measure of my competence and ability to treat people?
Exams like the boards are a measure of test-taking skills and retention, neither one of which is a true measure of what a capable, competent physician should be. The ABIM is imposing on us an onerous and ill-conceived tool, one that most physicians agree is irrelevant. I am glad this conversation is happening, because frankly the process was enough to make me want to quit being a doctor.
Dr. Chan practices rheumatology in Pawtucket, R.I.
A month ago the American Board of Internal Medicine sent a letter to diplomates saying they “got it wrong,” referring to the process of maintenance of certification or MOC, that the board required. They acknowledged that “parts of the new program are not meeting the needs of physicians like yourself.” Some of the things they proposed include changing the content of the Internal Medicine recertification exam to be “more reflective of what physicians in practice are doing,” with a promise that subspecialty recertification exams will follow suit. They also talk about “new and more flexible ways ... to demonstrate ... medical knowledge,” likely making room for the continuing medical education or CME credits that state licensures require.
While the letter was evidence that physician grievances were being heard, it was widely criticized for not having gone far enough. Questions remained about the financial and time cost of certification, the relevance of the exam, and the motivation of the board.
Well, the ABIM has written us again. Except it’s still not saying much. They simply say that they have been listening to feedback, and they list some points about what they’ve been hearing and are presumably going to take into consideration. In summary, they are recognizing that the while we all agree that we need a way for physicians to keep up on their medical knowledge, there is “a shared sense that defining ‘keeping up’ is the work of the whole community, including physicians, specialty societies, patient groups, and health care institutions.”
They proceed to outline what they’ve heard and will presumably consider, including the suggestion that the recertification exam be eliminated completely, and that CME units count toward recertification. Like I said, they didn’t say much. But this is promising. Particularly telling is the part where they acknowledge that the job of defining ‘keeping up’ does not fall solely on, as a friend put it, people that sit in their ivory towers and are removed from the daily grind of patient care.
Apropos of all this, I recently got my first 10 points toward MOC by taking a 30-question exam posted by the American College of Rheumatology. Each question comes with a list of references that you can review should you need or want to. To my great surprise, one of the references was in German. So what does that tell you about the people writing the questions and the process they use? What does that tell you about the validity of the questions as a measure of my competence and ability to treat people?
Exams like the boards are a measure of test-taking skills and retention, neither one of which is a true measure of what a capable, competent physician should be. The ABIM is imposing on us an onerous and ill-conceived tool, one that most physicians agree is irrelevant. I am glad this conversation is happening, because frankly the process was enough to make me want to quit being a doctor.
Dr. Chan practices rheumatology in Pawtucket, R.I.

Cardiologists honor a fallen colleague
It’s extremely unusual for a cardiologist or cardiac surgeon to die in the line of duty, but that tragedy occurred last January in Boston when the enraged son of a patient mortally shot Dr. Michael J. Davidson while he was on the job as director of endovascular cardiac surgery at Brigham and Women’s Hospital in Boston.
Dr. Davidson had been an active coinvestigator in the PARTNER study since it began in 2007 to make the first direct comparison of a transcatheter aortic valve replacement (TAVR) system against aortic-valve replacement with conventional heart surgery.
Because of Dr. Davidson’s long and active involvement with the PARTNER trial, his colleagues decided to dedicate the study’s 5-year follow-up findings to him, making the announcement during the first public release of the 5-year results in mid-March at the annual meeting of the American College of Cardiology.

“On behalf of the PARTNER team, we would like to dedicate this study – the 5-year outcomes – to Mike Davidson,” said Dr. Michael J. Mack as he finished his podium presentation of the report.
Preceding Dr. Mack’s talk, the session began with brief remarks about Dr. Davidson from Dr. Martin B. Leon, coleader of the PARTNER trial, and then the airing of a 6-minute video featuring several of Dr. Davidson’s colleagues recalling his unique career and accomplishments.
Notable in their comments was the outline they provided of the unusual training and career path Dr. Davidson forged for himself, based on his remarkably prescient realization a decade or more ago that the future of cardiology and cardiac surgery lay in fusing the two into a hybrid discipline.
Dr. Davidson’s colleagues cited the training he undertook to become both a fully qualified cardiac surgeon and a skilled interventional cardiologist, turning himself into an embodiment of the “heart team.” Several in the video called him “visionary” for recognizing this fusion as an important step toward the future of treating heart disease.
The poignancy of the moment did not stop there.
After the video ended and before Dr. Mack delivered the session’s first talk, ACC president Dr. Patrick T. O’Gara presented a posthumous distinguished-service award from the ACC to Dr. Davidson – with Dr. O’Gara handing the award to the fallen surgeon’s parents, including his father, Dr. Robert M. Davidson, a long-time ACC fellow and former clinical chief of cardiology at Cedars-Sinai Medical Center in Los Angeles.
Following the award, Dr. Athena Poppas, chair of the meeting’s program committee and cochair for the latebreaker session on heart valve replacement, stressed that the entire session was dedicated to honor Dr. Michael Davidson.
Perhaps most moving of all were the small white buttons that Dr. O’Gara, Dr. Davidson’s parents, and others wore on their lapels during the session, featuring a blue heart and the initials MJD. It combined for an affecting tribute to someone who had played a central role in transforming heart-valve replacement and then was murdered for doing this work.
On Twitter @mitchelzoler
It’s extremely unusual for a cardiologist or cardiac surgeon to die in the line of duty, but that tragedy occurred last January in Boston when the enraged son of a patient mortally shot Dr. Michael J. Davidson while he was on the job as director of endovascular cardiac surgery at Brigham and Women’s Hospital in Boston.
Dr. Davidson had been an active coinvestigator in the PARTNER study since it began in 2007 to make the first direct comparison of a transcatheter aortic valve replacement (TAVR) system against aortic-valve replacement with conventional heart surgery.
Because of Dr. Davidson’s long and active involvement with the PARTNER trial, his colleagues decided to dedicate the study’s 5-year follow-up findings to him, making the announcement during the first public release of the 5-year results in mid-March at the annual meeting of the American College of Cardiology.
“On behalf of the PARTNER team, we would like to dedicate this study – the 5-year outcomes – to Mike Davidson,” said Dr. Michael J. Mack as he finished his podium presentation of the report.
Preceding Dr. Mack’s talk, the session began with brief remarks about Dr. Davidson from Dr. Martin B. Leon, coleader of the PARTNER trial, and then the airing of a 6-minute video featuring several of Dr. Davidson’s colleagues recalling his unique career and accomplishments.
Notable in their comments was the outline they provided of the unusual training and career path Dr. Davidson forged for himself, based on his remarkably prescient realization a decade or more ago that the future of cardiology and cardiac surgery lay in fusing the two into a hybrid discipline.
Dr. Davidson’s colleagues cited the training he undertook to become both a fully qualified cardiac surgeon and a skilled interventional cardiologist, turning himself into an embodiment of the “heart team.” Several in the video called him “visionary” for recognizing this fusion as an important step toward the future of treating heart disease.
The poignancy of the moment did not stop there.
After the video ended and before Dr. Mack delivered the session’s first talk, ACC president Dr. Patrick T. O’Gara presented a posthumous distinguished-service award from the ACC to Dr. Davidson – with Dr. O’Gara handing the award to the fallen surgeon’s parents, including his father, Dr. Robert M. Davidson, a long-time ACC fellow and former clinical chief of cardiology at Cedars-Sinai Medical Center in Los Angeles.
Following the award, Dr. Athena Poppas, chair of the meeting’s program committee and cochair for the latebreaker session on heart valve replacement, stressed that the entire session was dedicated to honor Dr. Michael Davidson.
Perhaps most moving of all were the small white buttons that Dr. O’Gara, Dr. Davidson’s parents, and others wore on their lapels during the session, featuring a blue heart and the initials MJD. It combined for an affecting tribute to someone who had played a central role in transforming heart-valve replacement and then was murdered for doing this work.
On Twitter @mitchelzoler
It’s extremely unusual for a cardiologist or cardiac surgeon to die in the line of duty, but that tragedy occurred last January in Boston when the enraged son of a patient mortally shot Dr. Michael J. Davidson while he was on the job as director of endovascular cardiac surgery at Brigham and Women’s Hospital in Boston.
Dr. Davidson had been an active coinvestigator in the PARTNER study since it began in 2007 to make the first direct comparison of a transcatheter aortic valve replacement (TAVR) system against aortic-valve replacement with conventional heart surgery.
Because of Dr. Davidson’s long and active involvement with the PARTNER trial, his colleagues decided to dedicate the study’s 5-year follow-up findings to him, making the announcement during the first public release of the 5-year results in mid-March at the annual meeting of the American College of Cardiology.
“On behalf of the PARTNER team, we would like to dedicate this study – the 5-year outcomes – to Mike Davidson,” said Dr. Michael J. Mack as he finished his podium presentation of the report.
Preceding Dr. Mack’s talk, the session began with brief remarks about Dr. Davidson from Dr. Martin B. Leon, coleader of the PARTNER trial, and then the airing of a 6-minute video featuring several of Dr. Davidson’s colleagues recalling his unique career and accomplishments.
Notable in their comments was the outline they provided of the unusual training and career path Dr. Davidson forged for himself, based on his remarkably prescient realization a decade or more ago that the future of cardiology and cardiac surgery lay in fusing the two into a hybrid discipline.
Dr. Davidson’s colleagues cited the training he undertook to become both a fully qualified cardiac surgeon and a skilled interventional cardiologist, turning himself into an embodiment of the “heart team.” Several in the video called him “visionary” for recognizing this fusion as an important step toward the future of treating heart disease.
The poignancy of the moment did not stop there.
After the video ended and before Dr. Mack delivered the session’s first talk, ACC president Dr. Patrick T. O’Gara presented a posthumous distinguished-service award from the ACC to Dr. Davidson – with Dr. O’Gara handing the award to the fallen surgeon’s parents, including his father, Dr. Robert M. Davidson, a long-time ACC fellow and former clinical chief of cardiology at Cedars-Sinai Medical Center in Los Angeles.
Following the award, Dr. Athena Poppas, chair of the meeting’s program committee and cochair for the latebreaker session on heart valve replacement, stressed that the entire session was dedicated to honor Dr. Michael Davidson.
Perhaps most moving of all were the small white buttons that Dr. O’Gara, Dr. Davidson’s parents, and others wore on their lapels during the session, featuring a blue heart and the initials MJD. It combined for an affecting tribute to someone who had played a central role in transforming heart-valve replacement and then was murdered for doing this work.
On Twitter @mitchelzoler

Was mental illness a factor in the Germanwings crash?
Earlier this week, an airplane headed from Barcelona to Dusseldorf crashed into the French Alps, leaving 150 people dead. The black box recorder indicated that the copilot was left alone in the cockpit, the pilot was locked out and attempted to gain re-entry, and the flight was reprogrammed to cruise at an altitude of 100 feet, causing the plane to crash after an 8-minute descent. The evidence indicates a deliberate action on the part of the 27-year-old co-pilot, Andreas Lubitz.
With nothing to point to terrorism at this point, the investigation will include the question of whether or not the copilot suffered from a mental illness as a way of explaining his unexplainable actions. In short, was this a combination mass murder/suicide? Was there any way to predict that such an atrocity might happen? Are there measures that can be taken to ensure that it doesn’t happen again?

In the United States, treatment with any psychotropic medication has been a reason to ground a pilot permanently. In April 2010, the Federal Aviation Administration’s rules changed such that a pilot could fly if he’d been treated for mild to moderate depression with a selective serotonin reuptake inhibitor after 12 months. At that time, the FAA announced a 6-month amnesty period where a pilot could come forward about a diagnosis of depression that he had not previously felt comfortable disclosing. Presumably, other countries also have rules that ground pilots for mental illness.
So far, some reports in the media indicate that the copilot was not obviously suffering from a psychiatric disorder; all those who have been interviewed for these reports have expressed shock that Lubitz might have deliberately crashed the plane.
There also has been speculation in the media that a break in the copilot’s training 6 years ago was due to depression, and the mother of a school mate reportedly said that Lubitz had been treated for depression. Finally, investigators found a doctor’s note excusing Lubitz from work. At this point, the Wall Street Journal is reporting that he was being treated for depression. Apparently, he had shredded the note and flew on Tuesday, despite the written work excuse.
Still, all discussion of the copilot’s mental state is purely speculation. The media is noted for sensationalist reporting – and in efforts to get information out quickly, the details are often confused or simply wrong, sometimes to a remarkable extent. We don’t know if the work excuse was written by a psychiatrist or another type of physician; we don’t know if it was for a psychiatric condition, cancer, or simply strep throat.
What we’ve been told is that a copilot who was cleared to fly did so despite a work excuse from a physician, he did not disclose this condition to his employer, and he crashed a plane killing 150 people.
We might assume that the pilot suffered from some type of psychic distress – whether he met criteria for a mental disorder or not, it’s not normal to kill 150 people. If the pilot did have a history of depression and was being treated at the time of this week’s flight, then we may be left with a very unsatisfactory answer.
The anti-psychiatry activists will say that psychotropic medications caused Lubitz to crash the plane. Psychiatrists will be left with no great answer with such a scenario and will be left to say that whatever treatment he was receiving, it wasn’t enough. Certainly, the physician who told Lubitz to take off from work was right: He didn’t belong in a cockpit that day. Presumably, that physician would have done more had he been aware that the patient was about to commit a mass murder.
If the copilot does have a history of depression, but his current work excuse was for an unrelated condition, we might wonder if an untreated recurrence of depression played some role in his actions. One might speculate that the copilot could have been afraid to seek care at this time, perhaps because of a fear that he would lose his vocation.
Still, major depression can hardly explain such an act, and it is unfortunate that the press has already begun to run headlines linking this man’s alleged psychiatric diagnosis to a catastrophic mass murder. Somehow, “mental illness” gets used as an endpoint explanation for why such things happen; and short of a severe psychotic delusional system, it’s a very unsatisfying answer for an unprecedented act of violence.
The facts will unfold and perhaps we’ll learn a little more. We’ll find out what condition the copilot was being treated for and whether there were other stresses going on in his personal life. But people get depressed, take antidepressants, and deal with stress all the time.
It’s possible, if not likely, that we’ll never understand why this copilot decided to end the lives of so many people along with his own.
Dr. Miller is a coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work (Baltimore: The Johns Hopkins University, 2011).
Earlier this week, an airplane headed from Barcelona to Dusseldorf crashed into the French Alps, leaving 150 people dead. The black box recorder indicated that the copilot was left alone in the cockpit, the pilot was locked out and attempted to gain re-entry, and the flight was reprogrammed to cruise at an altitude of 100 feet, causing the plane to crash after an 8-minute descent. The evidence indicates a deliberate action on the part of the 27-year-old co-pilot, Andreas Lubitz.
With nothing to point to terrorism at this point, the investigation will include the question of whether or not the copilot suffered from a mental illness as a way of explaining his unexplainable actions. In short, was this a combination mass murder/suicide? Was there any way to predict that such an atrocity might happen? Are there measures that can be taken to ensure that it doesn’t happen again?
In the United States, treatment with any psychotropic medication has been a reason to ground a pilot permanently. In April 2010, the Federal Aviation Administration’s rules changed such that a pilot could fly if he’d been treated for mild to moderate depression with a selective serotonin reuptake inhibitor after 12 months. At that time, the FAA announced a 6-month amnesty period where a pilot could come forward about a diagnosis of depression that he had not previously felt comfortable disclosing. Presumably, other countries also have rules that ground pilots for mental illness.
So far, some reports in the media indicate that the copilot was not obviously suffering from a psychiatric disorder; all those who have been interviewed for these reports have expressed shock that Lubitz might have deliberately crashed the plane.
There also has been speculation in the media that a break in the copilot’s training 6 years ago was due to depression, and the mother of a school mate reportedly said that Lubitz had been treated for depression. Finally, investigators found a doctor’s note excusing Lubitz from work. At this point, the Wall Street Journal is reporting that he was being treated for depression. Apparently, he had shredded the note and flew on Tuesday, despite the written work excuse.
Still, all discussion of the copilot’s mental state is purely speculation. The media is noted for sensationalist reporting – and in efforts to get information out quickly, the details are often confused or simply wrong, sometimes to a remarkable extent. We don’t know if the work excuse was written by a psychiatrist or another type of physician; we don’t know if it was for a psychiatric condition, cancer, or simply strep throat.
What we’ve been told is that a copilot who was cleared to fly did so despite a work excuse from a physician, he did not disclose this condition to his employer, and he crashed a plane killing 150 people.
We might assume that the pilot suffered from some type of psychic distress – whether he met criteria for a mental disorder or not, it’s not normal to kill 150 people. If the pilot did have a history of depression and was being treated at the time of this week’s flight, then we may be left with a very unsatisfactory answer.
The anti-psychiatry activists will say that psychotropic medications caused Lubitz to crash the plane. Psychiatrists will be left with no great answer with such a scenario and will be left to say that whatever treatment he was receiving, it wasn’t enough. Certainly, the physician who told Lubitz to take off from work was right: He didn’t belong in a cockpit that day. Presumably, that physician would have done more had he been aware that the patient was about to commit a mass murder.
If the copilot does have a history of depression, but his current work excuse was for an unrelated condition, we might wonder if an untreated recurrence of depression played some role in his actions. One might speculate that the copilot could have been afraid to seek care at this time, perhaps because of a fear that he would lose his vocation.
Still, major depression can hardly explain such an act, and it is unfortunate that the press has already begun to run headlines linking this man’s alleged psychiatric diagnosis to a catastrophic mass murder. Somehow, “mental illness” gets used as an endpoint explanation for why such things happen; and short of a severe psychotic delusional system, it’s a very unsatisfying answer for an unprecedented act of violence.
The facts will unfold and perhaps we’ll learn a little more. We’ll find out what condition the copilot was being treated for and whether there were other stresses going on in his personal life. But people get depressed, take antidepressants, and deal with stress all the time.
It’s possible, if not likely, that we’ll never understand why this copilot decided to end the lives of so many people along with his own.
Dr. Miller is a coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work (Baltimore: The Johns Hopkins University, 2011).
Earlier this week, an airplane headed from Barcelona to Dusseldorf crashed into the French Alps, leaving 150 people dead. The black box recorder indicated that the copilot was left alone in the cockpit, the pilot was locked out and attempted to gain re-entry, and the flight was reprogrammed to cruise at an altitude of 100 feet, causing the plane to crash after an 8-minute descent. The evidence indicates a deliberate action on the part of the 27-year-old co-pilot, Andreas Lubitz.
With nothing to point to terrorism at this point, the investigation will include the question of whether or not the copilot suffered from a mental illness as a way of explaining his unexplainable actions. In short, was this a combination mass murder/suicide? Was there any way to predict that such an atrocity might happen? Are there measures that can be taken to ensure that it doesn’t happen again?
In the United States, treatment with any psychotropic medication has been a reason to ground a pilot permanently. In April 2010, the Federal Aviation Administration’s rules changed such that a pilot could fly if he’d been treated for mild to moderate depression with a selective serotonin reuptake inhibitor after 12 months. At that time, the FAA announced a 6-month amnesty period where a pilot could come forward about a diagnosis of depression that he had not previously felt comfortable disclosing. Presumably, other countries also have rules that ground pilots for mental illness.
So far, some reports in the media indicate that the copilot was not obviously suffering from a psychiatric disorder; all those who have been interviewed for these reports have expressed shock that Lubitz might have deliberately crashed the plane.
There also has been speculation in the media that a break in the copilot’s training 6 years ago was due to depression, and the mother of a school mate reportedly said that Lubitz had been treated for depression. Finally, investigators found a doctor’s note excusing Lubitz from work. At this point, the Wall Street Journal is reporting that he was being treated for depression. Apparently, he had shredded the note and flew on Tuesday, despite the written work excuse.
Still, all discussion of the copilot’s mental state is purely speculation. The media is noted for sensationalist reporting – and in efforts to get information out quickly, the details are often confused or simply wrong, sometimes to a remarkable extent. We don’t know if the work excuse was written by a psychiatrist or another type of physician; we don’t know if it was for a psychiatric condition, cancer, or simply strep throat.
What we’ve been told is that a copilot who was cleared to fly did so despite a work excuse from a physician, he did not disclose this condition to his employer, and he crashed a plane killing 150 people.
We might assume that the pilot suffered from some type of psychic distress – whether he met criteria for a mental disorder or not, it’s not normal to kill 150 people. If the pilot did have a history of depression and was being treated at the time of this week’s flight, then we may be left with a very unsatisfactory answer.
The anti-psychiatry activists will say that psychotropic medications caused Lubitz to crash the plane. Psychiatrists will be left with no great answer with such a scenario and will be left to say that whatever treatment he was receiving, it wasn’t enough. Certainly, the physician who told Lubitz to take off from work was right: He didn’t belong in a cockpit that day. Presumably, that physician would have done more had he been aware that the patient was about to commit a mass murder.
If the copilot does have a history of depression, but his current work excuse was for an unrelated condition, we might wonder if an untreated recurrence of depression played some role in his actions. One might speculate that the copilot could have been afraid to seek care at this time, perhaps because of a fear that he would lose his vocation.
Still, major depression can hardly explain such an act, and it is unfortunate that the press has already begun to run headlines linking this man’s alleged psychiatric diagnosis to a catastrophic mass murder. Somehow, “mental illness” gets used as an endpoint explanation for why such things happen; and short of a severe psychotic delusional system, it’s a very unsatisfying answer for an unprecedented act of violence.
The facts will unfold and perhaps we’ll learn a little more. We’ll find out what condition the copilot was being treated for and whether there were other stresses going on in his personal life. But people get depressed, take antidepressants, and deal with stress all the time.
It’s possible, if not likely, that we’ll never understand why this copilot decided to end the lives of so many people along with his own.
Dr. Miller is a coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work (Baltimore: The Johns Hopkins University, 2011).

Too little time and too many worries for social media
I’m not on Facebook, either professionally or personally.
My office doesn’t have a Twitter account.
In fact, my only nod to social media at all is a rarely updated LinkedIn page, which is really just a public CV.
Why, in this age of connectedness, do I hide from these things? One reason is time. There isn’t much of it in the course of a day. Between my practice (patients, dictations, forms, returning calls, reviewing tests, rinse, wash, repeat), my family (wife, kids, dogs, house), and all the other things that make up a day (driving, finances, bathing, sleep), I don’t have much extra time. I really have no desire to see what others had for breakfast, look at pictures of a distant cousin’s kids, or have an online political argument with in-laws.
Another reason is privacy. Most patients are good people, but there are scary ones, too. I don’t want them knowing my kids’ names, or what school they go to, or seeing their pictures. In this age trying to have a degree of personal privacy is hard enough. I don’t want to make it any easier for someone looking to cause trouble.
I have nothing against my patients. I like the majority of them. But I don’t want to be online friends with them, either. Practicing objective medicine requires a degree of emotional distance, and I don’t want to do anything to shorten that. Social media connections with someone may also clue you into their personal and political beliefs, and, as I’ve said before, I think knowing those about patients (and them knowing mine) can only make the relationship difficult.
And the last is from a medical-legal view. The definition of what constitutes medical advice seems to be quite vague, and I worry anything I innocuously post or tweet could be taken to mean that I had an established treating medical relationship with someone or that my malpractice carrier could raise my rates by saying I was doing online medicine.
There’s also the simple fact that anything can be interpreted in any way. I worry that something I might put up could be used against me in court. Let’s say a patient dies while I’m on vacation, and the family decides to sue. Pictures of me relaxing with my kids on the trip could be used to make me look like an uncaring, callous doctor, even if I had no idea what was going on back home.
I’ll keep my somewhat under-the-radar personal existence as it is. Others may feel I’m missing out on the wonders of the social age, but I’m happy with keeping my home life just that – at home.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m not on Facebook, either professionally or personally.
My office doesn’t have a Twitter account.
In fact, my only nod to social media at all is a rarely updated LinkedIn page, which is really just a public CV.
Why, in this age of connectedness, do I hide from these things? One reason is time. There isn’t much of it in the course of a day. Between my practice (patients, dictations, forms, returning calls, reviewing tests, rinse, wash, repeat), my family (wife, kids, dogs, house), and all the other things that make up a day (driving, finances, bathing, sleep), I don’t have much extra time. I really have no desire to see what others had for breakfast, look at pictures of a distant cousin’s kids, or have an online political argument with in-laws.
Another reason is privacy. Most patients are good people, but there are scary ones, too. I don’t want them knowing my kids’ names, or what school they go to, or seeing their pictures. In this age trying to have a degree of personal privacy is hard enough. I don’t want to make it any easier for someone looking to cause trouble.
I have nothing against my patients. I like the majority of them. But I don’t want to be online friends with them, either. Practicing objective medicine requires a degree of emotional distance, and I don’t want to do anything to shorten that. Social media connections with someone may also clue you into their personal and political beliefs, and, as I’ve said before, I think knowing those about patients (and them knowing mine) can only make the relationship difficult.
And the last is from a medical-legal view. The definition of what constitutes medical advice seems to be quite vague, and I worry anything I innocuously post or tweet could be taken to mean that I had an established treating medical relationship with someone or that my malpractice carrier could raise my rates by saying I was doing online medicine.
There’s also the simple fact that anything can be interpreted in any way. I worry that something I might put up could be used against me in court. Let’s say a patient dies while I’m on vacation, and the family decides to sue. Pictures of me relaxing with my kids on the trip could be used to make me look like an uncaring, callous doctor, even if I had no idea what was going on back home.
I’ll keep my somewhat under-the-radar personal existence as it is. Others may feel I’m missing out on the wonders of the social age, but I’m happy with keeping my home life just that – at home.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m not on Facebook, either professionally or personally.
My office doesn’t have a Twitter account.
In fact, my only nod to social media at all is a rarely updated LinkedIn page, which is really just a public CV.
Why, in this age of connectedness, do I hide from these things? One reason is time. There isn’t much of it in the course of a day. Between my practice (patients, dictations, forms, returning calls, reviewing tests, rinse, wash, repeat), my family (wife, kids, dogs, house), and all the other things that make up a day (driving, finances, bathing, sleep), I don’t have much extra time. I really have no desire to see what others had for breakfast, look at pictures of a distant cousin’s kids, or have an online political argument with in-laws.
Another reason is privacy. Most patients are good people, but there are scary ones, too. I don’t want them knowing my kids’ names, or what school they go to, or seeing their pictures. In this age trying to have a degree of personal privacy is hard enough. I don’t want to make it any easier for someone looking to cause trouble.
I have nothing against my patients. I like the majority of them. But I don’t want to be online friends with them, either. Practicing objective medicine requires a degree of emotional distance, and I don’t want to do anything to shorten that. Social media connections with someone may also clue you into their personal and political beliefs, and, as I’ve said before, I think knowing those about patients (and them knowing mine) can only make the relationship difficult.
And the last is from a medical-legal view. The definition of what constitutes medical advice seems to be quite vague, and I worry anything I innocuously post or tweet could be taken to mean that I had an established treating medical relationship with someone or that my malpractice carrier could raise my rates by saying I was doing online medicine.
There’s also the simple fact that anything can be interpreted in any way. I worry that something I might put up could be used against me in court. Let’s say a patient dies while I’m on vacation, and the family decides to sue. Pictures of me relaxing with my kids on the trip could be used to make me look like an uncaring, callous doctor, even if I had no idea what was going on back home.
I’ll keep my somewhat under-the-radar personal existence as it is. Others may feel I’m missing out on the wonders of the social age, but I’m happy with keeping my home life just that – at home.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.

It's All About the Spit!
Remember eighth grade, when you were taught the correlation between pH and saliva? You learned that testing saliva provides information on whether the mouth is an acidic, basic, or neutral environment. But did you ever suspect then that saliva would become a formidable instrument for medical diagnosis, health, and research?
It’s true, friends and colleagues: Spit is the latest, greatest trend in health care! This important physiologic fluid, which contains a highly complex assortment of substances, is rapidly gaining notice as a diagnostic tool. Don’t believe it? Read on!
The oral cavity, according to Dr. Jack Dillenberg, the inaugural dean of the Arizona School of Dentistry and Oral Health (ASDOH), “is the gateway and window into health in our body. The signs of nutritional deficiencies, general infections, and systemic diseases that affect the entire body may first become apparent in the oral cavity via lesions or other oral problems. Saliva plays a significant role in maintaining oral health and has a strong correlation to tooth decay.”1
Yes, we’ve known for a while that an adequate amount of saliva serves as a pH buffer; when plaque pH drops below 5.5, dental caries can occur. But according to researchers at The Johns Hopkins University’s Center for Interdisciplinary Salivary Bioscience Research (yes, a research center dedicated to spit!), saliva holds a wealth of data that is easily collected and economically analyzed and may be a key to many mysteries of human biology and genetics, as well as a helpful tool to combat disease. “There’s lots of potential in exploring what’s in saliva,” according to Dr. Doug Granger, the center’s director and a psychoneuroendocrinologist (what a mouthful—pun intended!) at Arizona State University.2
Saliva in the mouth forms a thin film that protects against dental caries, erosion, attrition, abrasion, periodontal diseases, candidiasis, and abrasive mucosal lesions. Studies suggest saliva may be useful in detecting heart disease, acid reflux, and diabetes; it is already being used for rapid HIV testing.3-5 Researchers have also reported encouraging results in the use of saliva for the diagnosis of autoimmune disorders, breast cancer, oral cancers, gum disease, and cardiovascular, endocrine, and infectious diseases.6,7
Is saliva screening the new "blood test"?
So is saliva screening the new “blood test”? Blood testing, performed as an aid to diagnosis, has its drawbacks: Samples are often uncomfortable to obtain, a lab visit may be necessary, and processing takes time. Finding a reasonable alternative would be beneficial, but there are several steps to such a process.
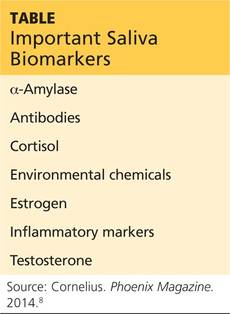
The capacity to monitor health status, disease onset and progression, and treatment outcomes through noninvasive means is a goal in health care promotion and delivery. For this to occur, three things must happen: first, specific biomarkers associated with a health or disease state must be established; second, a noninvasive manner to detect and monitor those biomarkers must be developed; and third, a mechanism to differentiate between the results is needed. Dr. Granger’s team has been studying the possibilities for several years now. Some of the key biomarkers measurable via saliva are listed in the Table below.8
Meanwhile, Dr. Tony Hashemian and colleagues at the ASDOH have developed a diagnostic tool based on pH. The purpose of their pH of Oral Health (pH2OH) initiative is to deliver new technology for pH saliva testing.9 This innovation uses a mobile phone application to capture time-sensitive data and to communicate with a server (in compliance with HIPAA regulations, of course).
Next page: Saliva-testing examination tool >>
A saliva-testing examination tool is used by the dental team to educate patients, inform preventive treatment planning, and assist with proper selection of dental materials to initiate changes in the patient’s oral hygiene. Dental teams measure saliva pH with test strips—the litmus paper we used even as kids in school. It is simply a strip of colored paper that, when soaked in sample saliva, turns a different color depending on the pH level. The color scale ranges from red (indicating a strong acidic state [pH < 3]) to dark blue or purple (indicating a strong alkaline state [pH > 11]).
The free iPhone or Android app developed by Dr. Hashemian’s team is designed to capture the pH value for a patient. The app can manually set the value, or you can take a picture of a test strip and auto-calculate the pH using color-coding analysis. Once set, the app will allow you to save the data and track improvements to oral pH over time.9
With improvements in immunology, microbiology, and biochemistry, salivary testing—in both research and clinical settings—may prove to be an applied and reliable means of recognizing oral signs of systemic illness and exposure to risk factors.10 Salivary diagnostics will be the next great breakthrough in improving the general health of the public. Stay tuned.
What are your thoughts about how “spit” could be applied clinically? Contact me at PAEditor@frontlinemedcom.com.
REFERENCES
1. Personal communication. February 17, 2015.
2. Walker AK. Researchers eye saliva for patient testing. Baltimore Sun. May 23, 2012.
3. Devi TJ. Saliva: a potential diagnostic tool. J Dental Med Sci. 2014;13(2):52-57.
4. Giannobile WV, Beikler T, Kinney JS, et al. Saliva as a diagnostic tool for periodontal disease: current state and future directions. Periodontol 2000. 2009;50:52-64.
5. Gopinath VK, Arzreanne AR. Saliva as a diagnostic tool for assessment of dental caries. Arch Orofacial Sci. 2006;1:57-59.
6. Streckfus CF, Bigler LR. Salivary glands and saliva: saliva as a diagnostic fluid. Oral Dis. 2002;8:69-76.
7. Lee JM, Garon E, Wong DR. Salivary diagnostics. Orthod Cranioffac Res. 2009;12:206211.
8. Cornelius K. Spit, polished. Phoenix Magazine. November 2014; 38.
9. AT Still University, Arizona School of Dentistry and Oral Health. pH2OH. www.ph2oh.com/apps/. Accessed March 21, 2015.
10. Lawrence HP. Salivary markers of systemic disease: noninvasive diagnosis of disease and monitoring of general health. J Can Dent Assoc. 2002;68(3):170-174.
Remember eighth grade, when you were taught the correlation between pH and saliva? You learned that testing saliva provides information on whether the mouth is an acidic, basic, or neutral environment. But did you ever suspect then that saliva would become a formidable instrument for medical diagnosis, health, and research?
It’s true, friends and colleagues: Spit is the latest, greatest trend in health care! This important physiologic fluid, which contains a highly complex assortment of substances, is rapidly gaining notice as a diagnostic tool. Don’t believe it? Read on!
The oral cavity, according to Dr. Jack Dillenberg, the inaugural dean of the Arizona School of Dentistry and Oral Health (ASDOH), “is the gateway and window into health in our body. The signs of nutritional deficiencies, general infections, and systemic diseases that affect the entire body may first become apparent in the oral cavity via lesions or other oral problems. Saliva plays a significant role in maintaining oral health and has a strong correlation to tooth decay.”1
Yes, we’ve known for a while that an adequate amount of saliva serves as a pH buffer; when plaque pH drops below 5.5, dental caries can occur. But according to researchers at The Johns Hopkins University’s Center for Interdisciplinary Salivary Bioscience Research (yes, a research center dedicated to spit!), saliva holds a wealth of data that is easily collected and economically analyzed and may be a key to many mysteries of human biology and genetics, as well as a helpful tool to combat disease. “There’s lots of potential in exploring what’s in saliva,” according to Dr. Doug Granger, the center’s director and a psychoneuroendocrinologist (what a mouthful—pun intended!) at Arizona State University.2
Saliva in the mouth forms a thin film that protects against dental caries, erosion, attrition, abrasion, periodontal diseases, candidiasis, and abrasive mucosal lesions. Studies suggest saliva may be useful in detecting heart disease, acid reflux, and diabetes; it is already being used for rapid HIV testing.3-5 Researchers have also reported encouraging results in the use of saliva for the diagnosis of autoimmune disorders, breast cancer, oral cancers, gum disease, and cardiovascular, endocrine, and infectious diseases.6,7
Is saliva screening the new "blood test"?
So is saliva screening the new “blood test”? Blood testing, performed as an aid to diagnosis, has its drawbacks: Samples are often uncomfortable to obtain, a lab visit may be necessary, and processing takes time. Finding a reasonable alternative would be beneficial, but there are several steps to such a process.
The capacity to monitor health status, disease onset and progression, and treatment outcomes through noninvasive means is a goal in health care promotion and delivery. For this to occur, three things must happen: first, specific biomarkers associated with a health or disease state must be established; second, a noninvasive manner to detect and monitor those biomarkers must be developed; and third, a mechanism to differentiate between the results is needed. Dr. Granger’s team has been studying the possibilities for several years now. Some of the key biomarkers measurable via saliva are listed in the Table below.8
Meanwhile, Dr. Tony Hashemian and colleagues at the ASDOH have developed a diagnostic tool based on pH. The purpose of their pH of Oral Health (pH2OH) initiative is to deliver new technology for pH saliva testing.9 This innovation uses a mobile phone application to capture time-sensitive data and to communicate with a server (in compliance with HIPAA regulations, of course).
Next page: Saliva-testing examination tool >>
A saliva-testing examination tool is used by the dental team to educate patients, inform preventive treatment planning, and assist with proper selection of dental materials to initiate changes in the patient’s oral hygiene. Dental teams measure saliva pH with test strips—the litmus paper we used even as kids in school. It is simply a strip of colored paper that, when soaked in sample saliva, turns a different color depending on the pH level. The color scale ranges from red (indicating a strong acidic state [pH < 3]) to dark blue or purple (indicating a strong alkaline state [pH > 11]).
The free iPhone or Android app developed by Dr. Hashemian’s team is designed to capture the pH value for a patient. The app can manually set the value, or you can take a picture of a test strip and auto-calculate the pH using color-coding analysis. Once set, the app will allow you to save the data and track improvements to oral pH over time.9
With improvements in immunology, microbiology, and biochemistry, salivary testing—in both research and clinical settings—may prove to be an applied and reliable means of recognizing oral signs of systemic illness and exposure to risk factors.10 Salivary diagnostics will be the next great breakthrough in improving the general health of the public. Stay tuned.
What are your thoughts about how “spit” could be applied clinically? Contact me at PAEditor@frontlinemedcom.com.
REFERENCES
1. Personal communication. February 17, 2015.
2. Walker AK. Researchers eye saliva for patient testing. Baltimore Sun. May 23, 2012.
3. Devi TJ. Saliva: a potential diagnostic tool. J Dental Med Sci. 2014;13(2):52-57.
4. Giannobile WV, Beikler T, Kinney JS, et al. Saliva as a diagnostic tool for periodontal disease: current state and future directions. Periodontol 2000. 2009;50:52-64.
5. Gopinath VK, Arzreanne AR. Saliva as a diagnostic tool for assessment of dental caries. Arch Orofacial Sci. 2006;1:57-59.
6. Streckfus CF, Bigler LR. Salivary glands and saliva: saliva as a diagnostic fluid. Oral Dis. 2002;8:69-76.
7. Lee JM, Garon E, Wong DR. Salivary diagnostics. Orthod Cranioffac Res. 2009;12:206211.
8. Cornelius K. Spit, polished. Phoenix Magazine. November 2014; 38.
9. AT Still University, Arizona School of Dentistry and Oral Health. pH2OH. www.ph2oh.com/apps/. Accessed March 21, 2015.
10. Lawrence HP. Salivary markers of systemic disease: noninvasive diagnosis of disease and monitoring of general health. J Can Dent Assoc. 2002;68(3):170-174.
Remember eighth grade, when you were taught the correlation between pH and saliva? You learned that testing saliva provides information on whether the mouth is an acidic, basic, or neutral environment. But did you ever suspect then that saliva would become a formidable instrument for medical diagnosis, health, and research?
It’s true, friends and colleagues: Spit is the latest, greatest trend in health care! This important physiologic fluid, which contains a highly complex assortment of substances, is rapidly gaining notice as a diagnostic tool. Don’t believe it? Read on!
The oral cavity, according to Dr. Jack Dillenberg, the inaugural dean of the Arizona School of Dentistry and Oral Health (ASDOH), “is the gateway and window into health in our body. The signs of nutritional deficiencies, general infections, and systemic diseases that affect the entire body may first become apparent in the oral cavity via lesions or other oral problems. Saliva plays a significant role in maintaining oral health and has a strong correlation to tooth decay.”1
Yes, we’ve known for a while that an adequate amount of saliva serves as a pH buffer; when plaque pH drops below 5.5, dental caries can occur. But according to researchers at The Johns Hopkins University’s Center for Interdisciplinary Salivary Bioscience Research (yes, a research center dedicated to spit!), saliva holds a wealth of data that is easily collected and economically analyzed and may be a key to many mysteries of human biology and genetics, as well as a helpful tool to combat disease. “There’s lots of potential in exploring what’s in saliva,” according to Dr. Doug Granger, the center’s director and a psychoneuroendocrinologist (what a mouthful—pun intended!) at Arizona State University.2
Saliva in the mouth forms a thin film that protects against dental caries, erosion, attrition, abrasion, periodontal diseases, candidiasis, and abrasive mucosal lesions. Studies suggest saliva may be useful in detecting heart disease, acid reflux, and diabetes; it is already being used for rapid HIV testing.3-5 Researchers have also reported encouraging results in the use of saliva for the diagnosis of autoimmune disorders, breast cancer, oral cancers, gum disease, and cardiovascular, endocrine, and infectious diseases.6,7
Is saliva screening the new "blood test"?
So is saliva screening the new “blood test”? Blood testing, performed as an aid to diagnosis, has its drawbacks: Samples are often uncomfortable to obtain, a lab visit may be necessary, and processing takes time. Finding a reasonable alternative would be beneficial, but there are several steps to such a process.
The capacity to monitor health status, disease onset and progression, and treatment outcomes through noninvasive means is a goal in health care promotion and delivery. For this to occur, three things must happen: first, specific biomarkers associated with a health or disease state must be established; second, a noninvasive manner to detect and monitor those biomarkers must be developed; and third, a mechanism to differentiate between the results is needed. Dr. Granger’s team has been studying the possibilities for several years now. Some of the key biomarkers measurable via saliva are listed in the Table below.8
Meanwhile, Dr. Tony Hashemian and colleagues at the ASDOH have developed a diagnostic tool based on pH. The purpose of their pH of Oral Health (pH2OH) initiative is to deliver new technology for pH saliva testing.9 This innovation uses a mobile phone application to capture time-sensitive data and to communicate with a server (in compliance with HIPAA regulations, of course).
Next page: Saliva-testing examination tool >>
A saliva-testing examination tool is used by the dental team to educate patients, inform preventive treatment planning, and assist with proper selection of dental materials to initiate changes in the patient’s oral hygiene. Dental teams measure saliva pH with test strips—the litmus paper we used even as kids in school. It is simply a strip of colored paper that, when soaked in sample saliva, turns a different color depending on the pH level. The color scale ranges from red (indicating a strong acidic state [pH < 3]) to dark blue or purple (indicating a strong alkaline state [pH > 11]).
The free iPhone or Android app developed by Dr. Hashemian’s team is designed to capture the pH value for a patient. The app can manually set the value, or you can take a picture of a test strip and auto-calculate the pH using color-coding analysis. Once set, the app will allow you to save the data and track improvements to oral pH over time.9
With improvements in immunology, microbiology, and biochemistry, salivary testing—in both research and clinical settings—may prove to be an applied and reliable means of recognizing oral signs of systemic illness and exposure to risk factors.10 Salivary diagnostics will be the next great breakthrough in improving the general health of the public. Stay tuned.
What are your thoughts about how “spit” could be applied clinically? Contact me at PAEditor@frontlinemedcom.com.
REFERENCES
1. Personal communication. February 17, 2015.
2. Walker AK. Researchers eye saliva for patient testing. Baltimore Sun. May 23, 2012.
3. Devi TJ. Saliva: a potential diagnostic tool. J Dental Med Sci. 2014;13(2):52-57.
4. Giannobile WV, Beikler T, Kinney JS, et al. Saliva as a diagnostic tool for periodontal disease: current state and future directions. Periodontol 2000. 2009;50:52-64.
5. Gopinath VK, Arzreanne AR. Saliva as a diagnostic tool for assessment of dental caries. Arch Orofacial Sci. 2006;1:57-59.
6. Streckfus CF, Bigler LR. Salivary glands and saliva: saliva as a diagnostic fluid. Oral Dis. 2002;8:69-76.
7. Lee JM, Garon E, Wong DR. Salivary diagnostics. Orthod Cranioffac Res. 2009;12:206211.
8. Cornelius K. Spit, polished. Phoenix Magazine. November 2014; 38.
9. AT Still University, Arizona School of Dentistry and Oral Health. pH2OH. www.ph2oh.com/apps/. Accessed March 21, 2015.
10. Lawrence HP. Salivary markers of systemic disease: noninvasive diagnosis of disease and monitoring of general health. J Can Dent Assoc. 2002;68(3):170-174.
Poison plants
After a long, cold, snowy winter, I actually cheered at the first site of a purple crocus emerging from my front yard. Spring brings with it warmer weather, outdoor sports, blooming flowers, and trees full of leaves. Unfortunately, it also brings some less-desirable plants with it as well, such as poison ivy, poison oak, and poison sumac. As your patients happily emerge from their houses to play outside, some will inevitably end up in your offices itching and uncomfortable from contact dermatitis. As many as 50% of people who come in contact with these plants will have a reaction.
As with most illnesses, prevention is the best cure. Once a child (or adult, for that matter) has been exposed to poison ivy, oak, or sumac, from the genus Toxicodendron, the best you can do is try and relieve symptoms until the dermatitis resolves on its own.

The first step in prevention is recognition. The old adage, “Leaves of three, let them be” – describing three leaflets, often with small black dots, arising from a reddish stem – is generally accurate; however, there are some exceptions to this rule depending on the type of plant (particularly poison sumac) and geographic location. If you aren’t already aware of the species in your area, it is worth spending a few minutes researching what types of plants are common locally (www.cdc.gov/niosh/topics/plants).
Avoiding all contact with these plants is best; long pants, shirt sleeves, and gloves help avoid exposure, but this is often not practical for a child playing outside, and urushiol (the allergenic substance on the surface of these plants) adheres to clothes, and pets, and other things. … If known or potential exposure has happened, it is best to wash all areas of your skin as soon as possible, particularly focusing on hands and under your fingernails. There are a variety of products such as Tecnu, Zanfel, and Goop Hand Cleaner, which are effective at preventing reactions after exposure has occurred (and, in the case of Zanfel, can also relieve symptoms if a reaction occurs); however, these products can be pricey and not always on hand when you need them. Topical dish washing soap has been found in one study to be an effective alternative (Dial Ultra Dish washing Soap [no longer available] was the product used, but any surfactant-based dish washing detergent is likely effective).*
However, speaking from experience, even the best efforts to avoid or minimize exposure are not always successful. Symptoms usually occur within the first 4 days of exposure, with lesions cropping up at different times depending on the location and type of skin and intensity of exposure to urushiol. Lesions are typically very itchy and can be plaques, papules, vesicles, or bullae. It is commonly believed that the lesions can be “spread” through contact with the fluid inside these vesicles or other parts of the lesions; however, this is not in fact true. This misperception likely stems from the fact, as noted, that the lesions do appear at different times after exposure to the plant, which can make it seem as if they are spreading from one site to another. Reactions can peak anywhere from 1 day to 2 weeks after exposure and can last for several weeks. Again, speaking from experience, this is a long time to be itchy and uncomfortable, especially for young children, so management of symptoms is very important.
There are many strategies and commercial products that can help reduce itching and irritation. First, it is important to keep the skin clean and not to cause breaks in the skin through itching, hard as that may be, in order to avoid bacterial superinfection. Gentle interventions such as oatmeal baths or cool wet compresses may be helpful; swimming may also provide relief. Topical medications can play a role – topical corticosteroids, particularly higher dose, can be helpful in relief of symptoms. Calamine lotion, products containing menthol, and topical astringents are other effective options. Oral antihistamines are not terribly effective, as the itching is not caused by histamine, however, the sedating effects can help patients get some rest at night. For severe cases, oral corticosteroids are sometimes used, but care must be taken to give a long enough course to avoid rebound. And, perhaps most importantly, provide reassurance that this will get better eventually! As with most things in pediatrics, preventative measures and supportive care are key to making sure your patients enjoy their spring and summer without too much discomfort!
Dr. Beers is an assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, Washington. She is chair of the American Academy of Pediatrics Committee on Residency Scholarships and immediate past president of the District of Columbia chapter of the American Academy of Pediatrics. E-mail Dr. Beers at pdnews@frontlinemedcom.com.
* This story was updated 3/26/2015.
After a long, cold, snowy winter, I actually cheered at the first site of a purple crocus emerging from my front yard. Spring brings with it warmer weather, outdoor sports, blooming flowers, and trees full of leaves. Unfortunately, it also brings some less-desirable plants with it as well, such as poison ivy, poison oak, and poison sumac. As your patients happily emerge from their houses to play outside, some will inevitably end up in your offices itching and uncomfortable from contact dermatitis. As many as 50% of people who come in contact with these plants will have a reaction.
As with most illnesses, prevention is the best cure. Once a child (or adult, for that matter) has been exposed to poison ivy, oak, or sumac, from the genus Toxicodendron, the best you can do is try and relieve symptoms until the dermatitis resolves on its own.
The first step in prevention is recognition. The old adage, “Leaves of three, let them be” – describing three leaflets, often with small black dots, arising from a reddish stem – is generally accurate; however, there are some exceptions to this rule depending on the type of plant (particularly poison sumac) and geographic location. If you aren’t already aware of the species in your area, it is worth spending a few minutes researching what types of plants are common locally (www.cdc.gov/niosh/topics/plants).
Avoiding all contact with these plants is best; long pants, shirt sleeves, and gloves help avoid exposure, but this is often not practical for a child playing outside, and urushiol (the allergenic substance on the surface of these plants) adheres to clothes, and pets, and other things. … If known or potential exposure has happened, it is best to wash all areas of your skin as soon as possible, particularly focusing on hands and under your fingernails. There are a variety of products such as Tecnu, Zanfel, and Goop Hand Cleaner, which are effective at preventing reactions after exposure has occurred (and, in the case of Zanfel, can also relieve symptoms if a reaction occurs); however, these products can be pricey and not always on hand when you need them. Topical dish washing soap has been found in one study to be an effective alternative (Dial Ultra Dish washing Soap [no longer available] was the product used, but any surfactant-based dish washing detergent is likely effective).*
However, speaking from experience, even the best efforts to avoid or minimize exposure are not always successful. Symptoms usually occur within the first 4 days of exposure, with lesions cropping up at different times depending on the location and type of skin and intensity of exposure to urushiol. Lesions are typically very itchy and can be plaques, papules, vesicles, or bullae. It is commonly believed that the lesions can be “spread” through contact with the fluid inside these vesicles or other parts of the lesions; however, this is not in fact true. This misperception likely stems from the fact, as noted, that the lesions do appear at different times after exposure to the plant, which can make it seem as if they are spreading from one site to another. Reactions can peak anywhere from 1 day to 2 weeks after exposure and can last for several weeks. Again, speaking from experience, this is a long time to be itchy and uncomfortable, especially for young children, so management of symptoms is very important.
There are many strategies and commercial products that can help reduce itching and irritation. First, it is important to keep the skin clean and not to cause breaks in the skin through itching, hard as that may be, in order to avoid bacterial superinfection. Gentle interventions such as oatmeal baths or cool wet compresses may be helpful; swimming may also provide relief. Topical medications can play a role – topical corticosteroids, particularly higher dose, can be helpful in relief of symptoms. Calamine lotion, products containing menthol, and topical astringents are other effective options. Oral antihistamines are not terribly effective, as the itching is not caused by histamine, however, the sedating effects can help patients get some rest at night. For severe cases, oral corticosteroids are sometimes used, but care must be taken to give a long enough course to avoid rebound. And, perhaps most importantly, provide reassurance that this will get better eventually! As with most things in pediatrics, preventative measures and supportive care are key to making sure your patients enjoy their spring and summer without too much discomfort!
Dr. Beers is an assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, Washington. She is chair of the American Academy of Pediatrics Committee on Residency Scholarships and immediate past president of the District of Columbia chapter of the American Academy of Pediatrics. E-mail Dr. Beers at pdnews@frontlinemedcom.com.
* This story was updated 3/26/2015.
After a long, cold, snowy winter, I actually cheered at the first site of a purple crocus emerging from my front yard. Spring brings with it warmer weather, outdoor sports, blooming flowers, and trees full of leaves. Unfortunately, it also brings some less-desirable plants with it as well, such as poison ivy, poison oak, and poison sumac. As your patients happily emerge from their houses to play outside, some will inevitably end up in your offices itching and uncomfortable from contact dermatitis. As many as 50% of people who come in contact with these plants will have a reaction.
As with most illnesses, prevention is the best cure. Once a child (or adult, for that matter) has been exposed to poison ivy, oak, or sumac, from the genus Toxicodendron, the best you can do is try and relieve symptoms until the dermatitis resolves on its own.
The first step in prevention is recognition. The old adage, “Leaves of three, let them be” – describing three leaflets, often with small black dots, arising from a reddish stem – is generally accurate; however, there are some exceptions to this rule depending on the type of plant (particularly poison sumac) and geographic location. If you aren’t already aware of the species in your area, it is worth spending a few minutes researching what types of plants are common locally (www.cdc.gov/niosh/topics/plants).
Avoiding all contact with these plants is best; long pants, shirt sleeves, and gloves help avoid exposure, but this is often not practical for a child playing outside, and urushiol (the allergenic substance on the surface of these plants) adheres to clothes, and pets, and other things. … If known or potential exposure has happened, it is best to wash all areas of your skin as soon as possible, particularly focusing on hands and under your fingernails. There are a variety of products such as Tecnu, Zanfel, and Goop Hand Cleaner, which are effective at preventing reactions after exposure has occurred (and, in the case of Zanfel, can also relieve symptoms if a reaction occurs); however, these products can be pricey and not always on hand when you need them. Topical dish washing soap has been found in one study to be an effective alternative (Dial Ultra Dish washing Soap [no longer available] was the product used, but any surfactant-based dish washing detergent is likely effective).*
However, speaking from experience, even the best efforts to avoid or minimize exposure are not always successful. Symptoms usually occur within the first 4 days of exposure, with lesions cropping up at different times depending on the location and type of skin and intensity of exposure to urushiol. Lesions are typically very itchy and can be plaques, papules, vesicles, or bullae. It is commonly believed that the lesions can be “spread” through contact with the fluid inside these vesicles or other parts of the lesions; however, this is not in fact true. This misperception likely stems from the fact, as noted, that the lesions do appear at different times after exposure to the plant, which can make it seem as if they are spreading from one site to another. Reactions can peak anywhere from 1 day to 2 weeks after exposure and can last for several weeks. Again, speaking from experience, this is a long time to be itchy and uncomfortable, especially for young children, so management of symptoms is very important.
There are many strategies and commercial products that can help reduce itching and irritation. First, it is important to keep the skin clean and not to cause breaks in the skin through itching, hard as that may be, in order to avoid bacterial superinfection. Gentle interventions such as oatmeal baths or cool wet compresses may be helpful; swimming may also provide relief. Topical medications can play a role – topical corticosteroids, particularly higher dose, can be helpful in relief of symptoms. Calamine lotion, products containing menthol, and topical astringents are other effective options. Oral antihistamines are not terribly effective, as the itching is not caused by histamine, however, the sedating effects can help patients get some rest at night. For severe cases, oral corticosteroids are sometimes used, but care must be taken to give a long enough course to avoid rebound. And, perhaps most importantly, provide reassurance that this will get better eventually! As with most things in pediatrics, preventative measures and supportive care are key to making sure your patients enjoy their spring and summer without too much discomfort!
Dr. Beers is an assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, Washington. She is chair of the American Academy of Pediatrics Committee on Residency Scholarships and immediate past president of the District of Columbia chapter of the American Academy of Pediatrics. E-mail Dr. Beers at pdnews@frontlinemedcom.com.
* This story was updated 3/26/2015.

How I responded to a nonvaccinating parent
Practicing pediatrics in California, where the measles outbreak occurred at Disneyland in December, has been an interesting experience. Suddenly, families are calling in a panic, wondering if their kids have had the vaccine, if they need the second one, if they should go to Disneyland with their infant or at all. This also seemed to me the perfect opportunity to again broach the benefit of vaccines with one of the few nonvaccinating families in my practice.

“So, has this measles outbreak made you reconsider vaccinating the kids with the MMR vaccine?” I asked my patient’s mother. “Actually, it has reinforced my beliefs,” she replied. “How is that?” I questioned. “Well, the more I read the Vaccine Adverse Event Reporting System (VAERS) reports, the more I realize that more people actually have died from the MMR vaccine than from measles in the past 10 years.” Having not reviewed the VAERS reports myself, I could not really argue intelligently, so I replied, “I’m not aware of that being true, and I will have to review the information and get back to you.”
The following is my response to her.
Dear nonvaccinating parent,
I wanted to follow up our discussion about immunizations from your visit last week. As a physician, my first duty to my patients is to first, do no harm. When you expressed your concerns regarding the VAERS data and said how more deaths were occurring from immunizations than from the measles virus itself, I felt a need to further investigate.
I reviewed the information, specifically deaths reported that were associated with the MMR vaccine on the Centers for Disease Control and Prevention VAERS website (wonder.cdc.gov/vaers.html). As you are aware, this site has been open since June of 1990 and everyone, health providers as well as parents, can report an adverse event following any vaccine at any point in time. The report yielded 65 events with regards to death and MMR vaccine over the past 25 years. Of the 65 reports, 4 of them were repeat reports of the same person, 18 had other causes that could explain death aside from the vaccine, such as leukemia diagnosed the same day, and some were associated with the vaccine, but no direct cause.
The death rate from measles has declined in recent years. According to the CDC web site, prior to the vaccine being available in 1963, in the United States alone, there were 500 deaths per year and some 4,000 cases of encephalitis. In the year 2000, the United States eliminated measles from the country (no cases in over 12 months). The last documented death from measles in the United States was in 2005, according to the CDC. This is in large part due to our vaccination rates. Worldwide, according to the World Health Organization web site, there were still 145,700 deaths in 2013.
It is interesting to me how two people can look at the same data and come to such different conclusions. You see the deaths reported on VAERS as so many deaths caused by the vaccine, and I see how many lives have been saved by vaccinating. According to the CDC data, about 85% of children are being immunized. We can extrapolate that at least 85 million children have been vaccinated in the past 25 years, and only 65 deaths have been reported to VAERS. So the death rate from measles is 1/500 and the death rate from vaccines is 1/1,000,000.
You also must keep in mind that as more and more people choose not to vaccinate, the benefit of the herd immunity your children are experiencing right now will be lost and the rate of deaths will climb again.
Sincerely,
Nazzi Mojibi, M.D.
Dr. Mojibi practices pediatrics in Fresno, Calif. She said that she had no relevant financial disclosures. E-mail her at pdnews@frontlinemedcom.com.
Practicing pediatrics in California, where the measles outbreak occurred at Disneyland in December, has been an interesting experience. Suddenly, families are calling in a panic, wondering if their kids have had the vaccine, if they need the second one, if they should go to Disneyland with their infant or at all. This also seemed to me the perfect opportunity to again broach the benefit of vaccines with one of the few nonvaccinating families in my practice.
“So, has this measles outbreak made you reconsider vaccinating the kids with the MMR vaccine?” I asked my patient’s mother. “Actually, it has reinforced my beliefs,” she replied. “How is that?” I questioned. “Well, the more I read the Vaccine Adverse Event Reporting System (VAERS) reports, the more I realize that more people actually have died from the MMR vaccine than from measles in the past 10 years.” Having not reviewed the VAERS reports myself, I could not really argue intelligently, so I replied, “I’m not aware of that being true, and I will have to review the information and get back to you.”
The following is my response to her.
Dear nonvaccinating parent,
I wanted to follow up our discussion about immunizations from your visit last week. As a physician, my first duty to my patients is to first, do no harm. When you expressed your concerns regarding the VAERS data and said how more deaths were occurring from immunizations than from the measles virus itself, I felt a need to further investigate.
I reviewed the information, specifically deaths reported that were associated with the MMR vaccine on the Centers for Disease Control and Prevention VAERS website (wonder.cdc.gov/vaers.html). As you are aware, this site has been open since June of 1990 and everyone, health providers as well as parents, can report an adverse event following any vaccine at any point in time. The report yielded 65 events with regards to death and MMR vaccine over the past 25 years. Of the 65 reports, 4 of them were repeat reports of the same person, 18 had other causes that could explain death aside from the vaccine, such as leukemia diagnosed the same day, and some were associated with the vaccine, but no direct cause.
The death rate from measles has declined in recent years. According to the CDC web site, prior to the vaccine being available in 1963, in the United States alone, there were 500 deaths per year and some 4,000 cases of encephalitis. In the year 2000, the United States eliminated measles from the country (no cases in over 12 months). The last documented death from measles in the United States was in 2005, according to the CDC. This is in large part due to our vaccination rates. Worldwide, according to the World Health Organization web site, there were still 145,700 deaths in 2013.
It is interesting to me how two people can look at the same data and come to such different conclusions. You see the deaths reported on VAERS as so many deaths caused by the vaccine, and I see how many lives have been saved by vaccinating. According to the CDC data, about 85% of children are being immunized. We can extrapolate that at least 85 million children have been vaccinated in the past 25 years, and only 65 deaths have been reported to VAERS. So the death rate from measles is 1/500 and the death rate from vaccines is 1/1,000,000.
You also must keep in mind that as more and more people choose not to vaccinate, the benefit of the herd immunity your children are experiencing right now will be lost and the rate of deaths will climb again.
Sincerely,
Nazzi Mojibi, M.D.
Dr. Mojibi practices pediatrics in Fresno, Calif. She said that she had no relevant financial disclosures. E-mail her at pdnews@frontlinemedcom.com.
Practicing pediatrics in California, where the measles outbreak occurred at Disneyland in December, has been an interesting experience. Suddenly, families are calling in a panic, wondering if their kids have had the vaccine, if they need the second one, if they should go to Disneyland with their infant or at all. This also seemed to me the perfect opportunity to again broach the benefit of vaccines with one of the few nonvaccinating families in my practice.
“So, has this measles outbreak made you reconsider vaccinating the kids with the MMR vaccine?” I asked my patient’s mother. “Actually, it has reinforced my beliefs,” she replied. “How is that?” I questioned. “Well, the more I read the Vaccine Adverse Event Reporting System (VAERS) reports, the more I realize that more people actually have died from the MMR vaccine than from measles in the past 10 years.” Having not reviewed the VAERS reports myself, I could not really argue intelligently, so I replied, “I’m not aware of that being true, and I will have to review the information and get back to you.”
The following is my response to her.
Dear nonvaccinating parent,
I wanted to follow up our discussion about immunizations from your visit last week. As a physician, my first duty to my patients is to first, do no harm. When you expressed your concerns regarding the VAERS data and said how more deaths were occurring from immunizations than from the measles virus itself, I felt a need to further investigate.
I reviewed the information, specifically deaths reported that were associated with the MMR vaccine on the Centers for Disease Control and Prevention VAERS website (wonder.cdc.gov/vaers.html). As you are aware, this site has been open since June of 1990 and everyone, health providers as well as parents, can report an adverse event following any vaccine at any point in time. The report yielded 65 events with regards to death and MMR vaccine over the past 25 years. Of the 65 reports, 4 of them were repeat reports of the same person, 18 had other causes that could explain death aside from the vaccine, such as leukemia diagnosed the same day, and some were associated with the vaccine, but no direct cause.
The death rate from measles has declined in recent years. According to the CDC web site, prior to the vaccine being available in 1963, in the United States alone, there were 500 deaths per year and some 4,000 cases of encephalitis. In the year 2000, the United States eliminated measles from the country (no cases in over 12 months). The last documented death from measles in the United States was in 2005, according to the CDC. This is in large part due to our vaccination rates. Worldwide, according to the World Health Organization web site, there were still 145,700 deaths in 2013.
It is interesting to me how two people can look at the same data and come to such different conclusions. You see the deaths reported on VAERS as so many deaths caused by the vaccine, and I see how many lives have been saved by vaccinating. According to the CDC data, about 85% of children are being immunized. We can extrapolate that at least 85 million children have been vaccinated in the past 25 years, and only 65 deaths have been reported to VAERS. So the death rate from measles is 1/500 and the death rate from vaccines is 1/1,000,000.
You also must keep in mind that as more and more people choose not to vaccinate, the benefit of the herd immunity your children are experiencing right now will be lost and the rate of deaths will climb again.
Sincerely,
Nazzi Mojibi, M.D.
Dr. Mojibi practices pediatrics in Fresno, Calif. She said that she had no relevant financial disclosures. E-mail her at pdnews@frontlinemedcom.com.

Dos and don’ts for handling common sling complications
Large-scale randomized trials have not only documented the efficacy of minimally invasive midurethral slings for stress urinary continence, they have also provided more adequate data on the incidence of complications. In practice, meanwhile, we are seeing more complications as the number of midurethral sling placements increases.
Often times, complications can be significantly more impactful than the original urinary incontinence. It is important to take the complications of sling placement seriously. Let patients know that their symptoms matter, and that there are ways to manage complications.
With more long-term data and experience, we have learned more about what to do, and what not to do, to prevent, diagnose, and manage the complications associated with midurethral slings. Here is my approach to the complications most commonly encountered, including bladder perforation, voiding dysfunction, erosion, pain, and recurrent stress urinary incontinence.

I will not address vascular injury in this article, but certainly, this is a surgical emergency that needs to be handled as such. As described in the February 2015 edition of Master Class on midurethral sling technique, accurate visualization toward the ipsilateral shoulder during needle passage is an essential part of preventing vascular injuries during retropubic sling placement.
Bladder perforation
Bladder perforation has consistently been shown to be significantly more common with retropubic slings than with transobturator slings. Reported incidence has ranged from 0.8% to 34% for tension-free vaginal tape (TVT) procedures, with the higher rates seen mainly in teaching institutions. Most commonly, the reported incidence is less than 10%.
Bladder perforation has no effect on the efficacy of the treatment, and no apparent long-term consequences, as long as the injury is identified. Especially with a retropubic sling, cystoscopy should be performed after both needles are placed but prior to advancing the needles all the way through the retropubic space. Simply withdrawing a needle will cause little bladder injury while retracting deployed mesh is significantly more consequential.
I recommend filling the bladder to approximately 300 cc, or to the point where you can see evidence of full distension such as flattened urethral orifices. This confirms that the bladder is under enough distension to preclude any mucosal wrinkles or folds that can hide a trocar injury.
The first step upon recognition of a perforation is to stay calm. In the vast majority of cases, simply withdrawing the needle, replacing it, and verifying correct replacement will prevent any long-term consequences. On the other hand, you must be fully alert to the possibility that the needle wandered away from the pubic bone, and consequently may have entered a space such as the peritoneum. Suspicion for visceral injury should be increased.
Resist the temptation to replace the needle more laterally. This course correction is often an unhelpful instinct, because a more lateral replacement will not move the needle farther from the bladder; it will instead bring it closer to the iliac vessels. Vascular injuries resulting from the surgeon’s attempts at needle replacement are unfortunate, as a minor complication becomes a major one. The key is to be as distal as possible – as close to the pubic bone as possible – and not to replace the needles more laterally.
Postoperative drainage for 1-2 days may be considered, but there is nothing in the literature to require this, and many surgeons do not employ any sort of extra catheterization after surgery where perforation has been observed.
Voiding dysfunction
Some degree of voiding dysfunction is not uncommon in the short term, but when a patient is still unable to void normally or completely after several days, an evaluation is warranted. As with bladder perforation, reported incidence of voiding dysfunction has varied widely, from 2% to 45% with the newer midurethral slings. Generally, the need for surgical revision is about 2%.
There are two reasons for urinary retention: Insufficient contraction force in the bladder or too much resistance. If retention persists beyond a week – in the 7-10 day postop time period – I assess whether the problem is resulting from too much obstruction from the sling, some form of hypotonic bladder, other surgery performed in conjunction with sling placement, medications, or something else.
Difficulty in passing a small urethra catheter in the office may indicate excessive obstruction, for instance, and there may be indications on vaginal examination or through cystoscopy that the sling is too tight. A midurethral “speed bump,” or elevation at the midpoint, with either catheterization or the scope is consistent with over-correction.
Do not dilate or pull down on the sling with any kind of urethra dilator. The sling is more robust than the urethral mucosa, and we now appreciate that this practice is associated with urethral erosion.
If the problem is deemed to be excessive obstruction or over-resistance, and it is fewer than 10 days postop, the patient may be offered a minor revision; the original incision is reopened, the sling material is identified, and the sling arms (lateral to the urethra) are grasped with clamps. Gentle downward traction can loosen the sling.
The sling should be grasped laterally and not at the midpoint; some sling materials will stretch and fracture where the force is applied. A little bit of gentle downward traction (3-5 mm) will often give you the needed amount of space for relieving some of the obstruction.
Beyond 10 days postop, tissue in-growth makes such a sling adjustment difficult, if not impossible. At this point, I recommend transecting the entire sling in the midline.There is differing opinion about whether a portion of the mesh should be resected; I believe that such a resection is usually unnecessary, and that a simple midline release procedure is the best approach.
A study we performed more than a decade ago on surgical release of TVT showed that persistent post-TVT voiding dysfunction can be successfully managed with a simple midline release. Of 1,175 women who underwent TVT placement for stress urinary incontinence and/or intrinsic sphincter deficiency, 23 (1.9%) had persistent voiding dysfunction. All cases of impaired emptying were completely resolved with a release of the tape, and the majority remained cured in terms of their continence or went from “cured” to “improved” over baseline. Three patients (13%) had recurrence of stress incontinence (Obstet. Gynecol. 2002;100:898-902).
We used to wait longer before revising the sling out of fear of losing the entire benefit of the sling. As it turns out, a simple midline release (leaving most, if not all, of the mesh in place) is usually just enough to treat the new complaint while still providing enough lateral support so that the patient retains most or all of the continence achieved with the sling.
Complaints of de novo urge incontinence, or overactive bladder, should be taken seriously. Urge incontinence has even more significant associations with depression and poor quality of life than stress incontinence. In the absence of retention, usual first-line therapies for overactive bladder can be employed, including anticholinergic medications, behavioral therapies, and physical therapy. Failing these interventions, my assessment for this complaint will be similar to that for retention; I’ll look for evidence of too much resistance, such as difficulty in passing a catheter, a “speed bump” cystoscopically, or an elevated pDet on pressure-flow studies, for instance.
If any of these are present, I usually offer sling release first. If, on the other hand, there is no evidence of over resistance in a patient who has de novo urge incontinence or overactive bladder and is refractory to conservative measures, a trial of sacral neuromodulation or botox injections is considered the next step.
Erosion
Erosion remains a difficult complication to understand. Long-term follow-up data show that it occurs after 3%-4% of sling placements, rather than 1% as originally believed. Data are inconsistent, but there probably is a slightly higher incidence of vaginal erosion with a transobturator sling, given more contact between the sling and the anterior vaginal wall.
There are hints in the literature that erosion may be related to technique – perhaps to the depth of dissection during surgery – but this is difficult to quantify. Moreover, many of the reported cases of erosion occur several years, or longer, after surgery. It is hard to blame surgical technique for such delayed erosion.
As we’ve seen with previous generations of mesh, there does not appear to be any window of time after which erosion is no longer a risk. We need to recognize that there is a medium- and long-term risk of erosion and appreciate its presenting symptoms: Recurrent urinary tract infection, pain with voiding, urgency, urinary incontinence, and microscopic hematuria of new onset.
Prevention may well entail preoperative estrogenization. The science looking at the effect of estrogen on sling placement is becoming more robust. While there are uncertainties, I believe that studies likely will show that topical estrogen in the preoperative and perioperative phases plays an important role in preventing erosion from occurring. Personally, I am using it much more than I was 10 years ago.
I like the convenience of the Vagifem tablet (Novo Nordisk Inc., Plainsboro, N.J.), and am reassured by data on systemic absorption with the 10-mcg dose, but any vaginal cream or compounded suppository can be used. I usually advise 4-6 weeks of preoperative preparation, with nightly use for 2 weeks followed by 2-3 nights per week thereafter. Smoking is also a likely risk factor. Data are not entirely consistent, but I believe we should provide counseling and encourage smoking cessation before the implant of mesh.
Management is dependent on when the erosion occurs or is recognized. When erosion occurs within 6 weeks post operatively, primary repair is an option. When erosion is detected after the 6-week window and is causing symptoms, a conservative trim of bristles poking through the vaginal mucosa is worth a try. I do not advise more than one such conservative trim, however, as repeated attempts and series of small resections can make the sling exceedingly difficult to remove if more complete resection is ultimately needed. After one unsuccessful trim, I usually remove the whole sling belly, or most of the vaginal part of the sling.
For slings made of type 1 macroporous mesh, resection of the retropubic or transobturator portions of the mesh usually is not required. In the more rare situation where those pelvic areas of the mesh are associated with pain, I favor a laparoscopic approach to the retropubic space to facilitate minimally invasive removal.
Postop pain, sling failure
Groin pain, or thigh pain, sometimes occurs after placement of a transobturator sling. As I discussed in the previous Master Class on midurethral sling technique, I have seen a significant decrease in groin pain in my patients – without any reduction in benefit – with the use of a shorter transobturator sling that does not leave mesh in the adductor compartment of the thigh and groin.
For persistent groin pain, I favor the use of trigger point injection. Sometimes one injection will impact the inflammatory cycle such that the patient derives long-term benefit. At other times, the trigger point injection will serve as a diagnostic; if pain returns after a period of benefit, I am inclined to resect that part of the mesh.
Pain inside the pelvis, especially on the pelvic sidewall (obturator or puborectalis complex) usually is related to mechanical tension. In my experience, this type of discomfort is slightly more likely to occur with the transobturator slings, which penetrate through the muscular pelvic sidewall and lead to more fibrosis and scar tissue formation.
In most cases of pain and discomfort, attempting to reproduce the patient’s symptoms by putting tension on particular parts of the sling during the office exam helps guide management. If I find that palpating or putting the sling on tension recreates her complaints, and conservative injections have provided temporary or inadequate relief, I usually advocate resecting the vaginal portion of the mesh to relieve that tension.
In cases of recurrent stress urinary incontinence (when the sling has failed), a TVT or repeat TVT is often warranted. The TVT sling has been demonstrated to work after nearly every other previous kind of anti-incontinence procedure, even after a previous retropubic sling. There is little data on mesh removal in such cases. I believe that unless a previously placed but failed sling is causing symptoms, there is no need to resect it. Mesh removal is significantly more traumatic than mesh placement, and in most cases it is not necessary.
Dr. Rardin reported that he has no relevant financial disclosures.
Large-scale randomized trials have not only documented the efficacy of minimally invasive midurethral slings for stress urinary continence, they have also provided more adequate data on the incidence of complications. In practice, meanwhile, we are seeing more complications as the number of midurethral sling placements increases.
Often times, complications can be significantly more impactful than the original urinary incontinence. It is important to take the complications of sling placement seriously. Let patients know that their symptoms matter, and that there are ways to manage complications.
With more long-term data and experience, we have learned more about what to do, and what not to do, to prevent, diagnose, and manage the complications associated with midurethral slings. Here is my approach to the complications most commonly encountered, including bladder perforation, voiding dysfunction, erosion, pain, and recurrent stress urinary incontinence.
I will not address vascular injury in this article, but certainly, this is a surgical emergency that needs to be handled as such. As described in the February 2015 edition of Master Class on midurethral sling technique, accurate visualization toward the ipsilateral shoulder during needle passage is an essential part of preventing vascular injuries during retropubic sling placement.
Bladder perforation
Bladder perforation has consistently been shown to be significantly more common with retropubic slings than with transobturator slings. Reported incidence has ranged from 0.8% to 34% for tension-free vaginal tape (TVT) procedures, with the higher rates seen mainly in teaching institutions. Most commonly, the reported incidence is less than 10%.
Bladder perforation has no effect on the efficacy of the treatment, and no apparent long-term consequences, as long as the injury is identified. Especially with a retropubic sling, cystoscopy should be performed after both needles are placed but prior to advancing the needles all the way through the retropubic space. Simply withdrawing a needle will cause little bladder injury while retracting deployed mesh is significantly more consequential.
I recommend filling the bladder to approximately 300 cc, or to the point where you can see evidence of full distension such as flattened urethral orifices. This confirms that the bladder is under enough distension to preclude any mucosal wrinkles or folds that can hide a trocar injury.
The first step upon recognition of a perforation is to stay calm. In the vast majority of cases, simply withdrawing the needle, replacing it, and verifying correct replacement will prevent any long-term consequences. On the other hand, you must be fully alert to the possibility that the needle wandered away from the pubic bone, and consequently may have entered a space such as the peritoneum. Suspicion for visceral injury should be increased.
Resist the temptation to replace the needle more laterally. This course correction is often an unhelpful instinct, because a more lateral replacement will not move the needle farther from the bladder; it will instead bring it closer to the iliac vessels. Vascular injuries resulting from the surgeon’s attempts at needle replacement are unfortunate, as a minor complication becomes a major one. The key is to be as distal as possible – as close to the pubic bone as possible – and not to replace the needles more laterally.
Postoperative drainage for 1-2 days may be considered, but there is nothing in the literature to require this, and many surgeons do not employ any sort of extra catheterization after surgery where perforation has been observed.
Voiding dysfunction
Some degree of voiding dysfunction is not uncommon in the short term, but when a patient is still unable to void normally or completely after several days, an evaluation is warranted. As with bladder perforation, reported incidence of voiding dysfunction has varied widely, from 2% to 45% with the newer midurethral slings. Generally, the need for surgical revision is about 2%.
There are two reasons for urinary retention: Insufficient contraction force in the bladder or too much resistance. If retention persists beyond a week – in the 7-10 day postop time period – I assess whether the problem is resulting from too much obstruction from the sling, some form of hypotonic bladder, other surgery performed in conjunction with sling placement, medications, or something else.
Difficulty in passing a small urethra catheter in the office may indicate excessive obstruction, for instance, and there may be indications on vaginal examination or through cystoscopy that the sling is too tight. A midurethral “speed bump,” or elevation at the midpoint, with either catheterization or the scope is consistent with over-correction.
Do not dilate or pull down on the sling with any kind of urethra dilator. The sling is more robust than the urethral mucosa, and we now appreciate that this practice is associated with urethral erosion.
If the problem is deemed to be excessive obstruction or over-resistance, and it is fewer than 10 days postop, the patient may be offered a minor revision; the original incision is reopened, the sling material is identified, and the sling arms (lateral to the urethra) are grasped with clamps. Gentle downward traction can loosen the sling.
The sling should be grasped laterally and not at the midpoint; some sling materials will stretch and fracture where the force is applied. A little bit of gentle downward traction (3-5 mm) will often give you the needed amount of space for relieving some of the obstruction.
Beyond 10 days postop, tissue in-growth makes such a sling adjustment difficult, if not impossible. At this point, I recommend transecting the entire sling in the midline.There is differing opinion about whether a portion of the mesh should be resected; I believe that such a resection is usually unnecessary, and that a simple midline release procedure is the best approach.
A study we performed more than a decade ago on surgical release of TVT showed that persistent post-TVT voiding dysfunction can be successfully managed with a simple midline release. Of 1,175 women who underwent TVT placement for stress urinary incontinence and/or intrinsic sphincter deficiency, 23 (1.9%) had persistent voiding dysfunction. All cases of impaired emptying were completely resolved with a release of the tape, and the majority remained cured in terms of their continence or went from “cured” to “improved” over baseline. Three patients (13%) had recurrence of stress incontinence (Obstet. Gynecol. 2002;100:898-902).
We used to wait longer before revising the sling out of fear of losing the entire benefit of the sling. As it turns out, a simple midline release (leaving most, if not all, of the mesh in place) is usually just enough to treat the new complaint while still providing enough lateral support so that the patient retains most or all of the continence achieved with the sling.
Complaints of de novo urge incontinence, or overactive bladder, should be taken seriously. Urge incontinence has even more significant associations with depression and poor quality of life than stress incontinence. In the absence of retention, usual first-line therapies for overactive bladder can be employed, including anticholinergic medications, behavioral therapies, and physical therapy. Failing these interventions, my assessment for this complaint will be similar to that for retention; I’ll look for evidence of too much resistance, such as difficulty in passing a catheter, a “speed bump” cystoscopically, or an elevated pDet on pressure-flow studies, for instance.
If any of these are present, I usually offer sling release first. If, on the other hand, there is no evidence of over resistance in a patient who has de novo urge incontinence or overactive bladder and is refractory to conservative measures, a trial of sacral neuromodulation or botox injections is considered the next step.
Erosion
Erosion remains a difficult complication to understand. Long-term follow-up data show that it occurs after 3%-4% of sling placements, rather than 1% as originally believed. Data are inconsistent, but there probably is a slightly higher incidence of vaginal erosion with a transobturator sling, given more contact between the sling and the anterior vaginal wall.
There are hints in the literature that erosion may be related to technique – perhaps to the depth of dissection during surgery – but this is difficult to quantify. Moreover, many of the reported cases of erosion occur several years, or longer, after surgery. It is hard to blame surgical technique for such delayed erosion.
As we’ve seen with previous generations of mesh, there does not appear to be any window of time after which erosion is no longer a risk. We need to recognize that there is a medium- and long-term risk of erosion and appreciate its presenting symptoms: Recurrent urinary tract infection, pain with voiding, urgency, urinary incontinence, and microscopic hematuria of new onset.
Prevention may well entail preoperative estrogenization. The science looking at the effect of estrogen on sling placement is becoming more robust. While there are uncertainties, I believe that studies likely will show that topical estrogen in the preoperative and perioperative phases plays an important role in preventing erosion from occurring. Personally, I am using it much more than I was 10 years ago.
I like the convenience of the Vagifem tablet (Novo Nordisk Inc., Plainsboro, N.J.), and am reassured by data on systemic absorption with the 10-mcg dose, but any vaginal cream or compounded suppository can be used. I usually advise 4-6 weeks of preoperative preparation, with nightly use for 2 weeks followed by 2-3 nights per week thereafter. Smoking is also a likely risk factor. Data are not entirely consistent, but I believe we should provide counseling and encourage smoking cessation before the implant of mesh.
Management is dependent on when the erosion occurs or is recognized. When erosion occurs within 6 weeks post operatively, primary repair is an option. When erosion is detected after the 6-week window and is causing symptoms, a conservative trim of bristles poking through the vaginal mucosa is worth a try. I do not advise more than one such conservative trim, however, as repeated attempts and series of small resections can make the sling exceedingly difficult to remove if more complete resection is ultimately needed. After one unsuccessful trim, I usually remove the whole sling belly, or most of the vaginal part of the sling.
For slings made of type 1 macroporous mesh, resection of the retropubic or transobturator portions of the mesh usually is not required. In the more rare situation where those pelvic areas of the mesh are associated with pain, I favor a laparoscopic approach to the retropubic space to facilitate minimally invasive removal.
Postop pain, sling failure
Groin pain, or thigh pain, sometimes occurs after placement of a transobturator sling. As I discussed in the previous Master Class on midurethral sling technique, I have seen a significant decrease in groin pain in my patients – without any reduction in benefit – with the use of a shorter transobturator sling that does not leave mesh in the adductor compartment of the thigh and groin.
For persistent groin pain, I favor the use of trigger point injection. Sometimes one injection will impact the inflammatory cycle such that the patient derives long-term benefit. At other times, the trigger point injection will serve as a diagnostic; if pain returns after a period of benefit, I am inclined to resect that part of the mesh.
Pain inside the pelvis, especially on the pelvic sidewall (obturator or puborectalis complex) usually is related to mechanical tension. In my experience, this type of discomfort is slightly more likely to occur with the transobturator slings, which penetrate through the muscular pelvic sidewall and lead to more fibrosis and scar tissue formation.
In most cases of pain and discomfort, attempting to reproduce the patient’s symptoms by putting tension on particular parts of the sling during the office exam helps guide management. If I find that palpating or putting the sling on tension recreates her complaints, and conservative injections have provided temporary or inadequate relief, I usually advocate resecting the vaginal portion of the mesh to relieve that tension.
In cases of recurrent stress urinary incontinence (when the sling has failed), a TVT or repeat TVT is often warranted. The TVT sling has been demonstrated to work after nearly every other previous kind of anti-incontinence procedure, even after a previous retropubic sling. There is little data on mesh removal in such cases. I believe that unless a previously placed but failed sling is causing symptoms, there is no need to resect it. Mesh removal is significantly more traumatic than mesh placement, and in most cases it is not necessary.
Dr. Rardin reported that he has no relevant financial disclosures.
Large-scale randomized trials have not only documented the efficacy of minimally invasive midurethral slings for stress urinary continence, they have also provided more adequate data on the incidence of complications. In practice, meanwhile, we are seeing more complications as the number of midurethral sling placements increases.
Often times, complications can be significantly more impactful than the original urinary incontinence. It is important to take the complications of sling placement seriously. Let patients know that their symptoms matter, and that there are ways to manage complications.
With more long-term data and experience, we have learned more about what to do, and what not to do, to prevent, diagnose, and manage the complications associated with midurethral slings. Here is my approach to the complications most commonly encountered, including bladder perforation, voiding dysfunction, erosion, pain, and recurrent stress urinary incontinence.
I will not address vascular injury in this article, but certainly, this is a surgical emergency that needs to be handled as such. As described in the February 2015 edition of Master Class on midurethral sling technique, accurate visualization toward the ipsilateral shoulder during needle passage is an essential part of preventing vascular injuries during retropubic sling placement.
Bladder perforation
Bladder perforation has consistently been shown to be significantly more common with retropubic slings than with transobturator slings. Reported incidence has ranged from 0.8% to 34% for tension-free vaginal tape (TVT) procedures, with the higher rates seen mainly in teaching institutions. Most commonly, the reported incidence is less than 10%.
Bladder perforation has no effect on the efficacy of the treatment, and no apparent long-term consequences, as long as the injury is identified. Especially with a retropubic sling, cystoscopy should be performed after both needles are placed but prior to advancing the needles all the way through the retropubic space. Simply withdrawing a needle will cause little bladder injury while retracting deployed mesh is significantly more consequential.
I recommend filling the bladder to approximately 300 cc, or to the point where you can see evidence of full distension such as flattened urethral orifices. This confirms that the bladder is under enough distension to preclude any mucosal wrinkles or folds that can hide a trocar injury.
The first step upon recognition of a perforation is to stay calm. In the vast majority of cases, simply withdrawing the needle, replacing it, and verifying correct replacement will prevent any long-term consequences. On the other hand, you must be fully alert to the possibility that the needle wandered away from the pubic bone, and consequently may have entered a space such as the peritoneum. Suspicion for visceral injury should be increased.
Resist the temptation to replace the needle more laterally. This course correction is often an unhelpful instinct, because a more lateral replacement will not move the needle farther from the bladder; it will instead bring it closer to the iliac vessels. Vascular injuries resulting from the surgeon’s attempts at needle replacement are unfortunate, as a minor complication becomes a major one. The key is to be as distal as possible – as close to the pubic bone as possible – and not to replace the needles more laterally.
Postoperative drainage for 1-2 days may be considered, but there is nothing in the literature to require this, and many surgeons do not employ any sort of extra catheterization after surgery where perforation has been observed.
Voiding dysfunction
Some degree of voiding dysfunction is not uncommon in the short term, but when a patient is still unable to void normally or completely after several days, an evaluation is warranted. As with bladder perforation, reported incidence of voiding dysfunction has varied widely, from 2% to 45% with the newer midurethral slings. Generally, the need for surgical revision is about 2%.
There are two reasons for urinary retention: Insufficient contraction force in the bladder or too much resistance. If retention persists beyond a week – in the 7-10 day postop time period – I assess whether the problem is resulting from too much obstruction from the sling, some form of hypotonic bladder, other surgery performed in conjunction with sling placement, medications, or something else.
Difficulty in passing a small urethra catheter in the office may indicate excessive obstruction, for instance, and there may be indications on vaginal examination or through cystoscopy that the sling is too tight. A midurethral “speed bump,” or elevation at the midpoint, with either catheterization or the scope is consistent with over-correction.
Do not dilate or pull down on the sling with any kind of urethra dilator. The sling is more robust than the urethral mucosa, and we now appreciate that this practice is associated with urethral erosion.
If the problem is deemed to be excessive obstruction or over-resistance, and it is fewer than 10 days postop, the patient may be offered a minor revision; the original incision is reopened, the sling material is identified, and the sling arms (lateral to the urethra) are grasped with clamps. Gentle downward traction can loosen the sling.
The sling should be grasped laterally and not at the midpoint; some sling materials will stretch and fracture where the force is applied. A little bit of gentle downward traction (3-5 mm) will often give you the needed amount of space for relieving some of the obstruction.
Beyond 10 days postop, tissue in-growth makes such a sling adjustment difficult, if not impossible. At this point, I recommend transecting the entire sling in the midline.There is differing opinion about whether a portion of the mesh should be resected; I believe that such a resection is usually unnecessary, and that a simple midline release procedure is the best approach.
A study we performed more than a decade ago on surgical release of TVT showed that persistent post-TVT voiding dysfunction can be successfully managed with a simple midline release. Of 1,175 women who underwent TVT placement for stress urinary incontinence and/or intrinsic sphincter deficiency, 23 (1.9%) had persistent voiding dysfunction. All cases of impaired emptying were completely resolved with a release of the tape, and the majority remained cured in terms of their continence or went from “cured” to “improved” over baseline. Three patients (13%) had recurrence of stress incontinence (Obstet. Gynecol. 2002;100:898-902).
We used to wait longer before revising the sling out of fear of losing the entire benefit of the sling. As it turns out, a simple midline release (leaving most, if not all, of the mesh in place) is usually just enough to treat the new complaint while still providing enough lateral support so that the patient retains most or all of the continence achieved with the sling.
Complaints of de novo urge incontinence, or overactive bladder, should be taken seriously. Urge incontinence has even more significant associations with depression and poor quality of life than stress incontinence. In the absence of retention, usual first-line therapies for overactive bladder can be employed, including anticholinergic medications, behavioral therapies, and physical therapy. Failing these interventions, my assessment for this complaint will be similar to that for retention; I’ll look for evidence of too much resistance, such as difficulty in passing a catheter, a “speed bump” cystoscopically, or an elevated pDet on pressure-flow studies, for instance.
If any of these are present, I usually offer sling release first. If, on the other hand, there is no evidence of over resistance in a patient who has de novo urge incontinence or overactive bladder and is refractory to conservative measures, a trial of sacral neuromodulation or botox injections is considered the next step.
Erosion
Erosion remains a difficult complication to understand. Long-term follow-up data show that it occurs after 3%-4% of sling placements, rather than 1% as originally believed. Data are inconsistent, but there probably is a slightly higher incidence of vaginal erosion with a transobturator sling, given more contact between the sling and the anterior vaginal wall.
There are hints in the literature that erosion may be related to technique – perhaps to the depth of dissection during surgery – but this is difficult to quantify. Moreover, many of the reported cases of erosion occur several years, or longer, after surgery. It is hard to blame surgical technique for such delayed erosion.
As we’ve seen with previous generations of mesh, there does not appear to be any window of time after which erosion is no longer a risk. We need to recognize that there is a medium- and long-term risk of erosion and appreciate its presenting symptoms: Recurrent urinary tract infection, pain with voiding, urgency, urinary incontinence, and microscopic hematuria of new onset.
Prevention may well entail preoperative estrogenization. The science looking at the effect of estrogen on sling placement is becoming more robust. While there are uncertainties, I believe that studies likely will show that topical estrogen in the preoperative and perioperative phases plays an important role in preventing erosion from occurring. Personally, I am using it much more than I was 10 years ago.
I like the convenience of the Vagifem tablet (Novo Nordisk Inc., Plainsboro, N.J.), and am reassured by data on systemic absorption with the 10-mcg dose, but any vaginal cream or compounded suppository can be used. I usually advise 4-6 weeks of preoperative preparation, with nightly use for 2 weeks followed by 2-3 nights per week thereafter. Smoking is also a likely risk factor. Data are not entirely consistent, but I believe we should provide counseling and encourage smoking cessation before the implant of mesh.
Management is dependent on when the erosion occurs or is recognized. When erosion occurs within 6 weeks post operatively, primary repair is an option. When erosion is detected after the 6-week window and is causing symptoms, a conservative trim of bristles poking through the vaginal mucosa is worth a try. I do not advise more than one such conservative trim, however, as repeated attempts and series of small resections can make the sling exceedingly difficult to remove if more complete resection is ultimately needed. After one unsuccessful trim, I usually remove the whole sling belly, or most of the vaginal part of the sling.
For slings made of type 1 macroporous mesh, resection of the retropubic or transobturator portions of the mesh usually is not required. In the more rare situation where those pelvic areas of the mesh are associated with pain, I favor a laparoscopic approach to the retropubic space to facilitate minimally invasive removal.
Postop pain, sling failure
Groin pain, or thigh pain, sometimes occurs after placement of a transobturator sling. As I discussed in the previous Master Class on midurethral sling technique, I have seen a significant decrease in groin pain in my patients – without any reduction in benefit – with the use of a shorter transobturator sling that does not leave mesh in the adductor compartment of the thigh and groin.
For persistent groin pain, I favor the use of trigger point injection. Sometimes one injection will impact the inflammatory cycle such that the patient derives long-term benefit. At other times, the trigger point injection will serve as a diagnostic; if pain returns after a period of benefit, I am inclined to resect that part of the mesh.
Pain inside the pelvis, especially on the pelvic sidewall (obturator or puborectalis complex) usually is related to mechanical tension. In my experience, this type of discomfort is slightly more likely to occur with the transobturator slings, which penetrate through the muscular pelvic sidewall and lead to more fibrosis and scar tissue formation.
In most cases of pain and discomfort, attempting to reproduce the patient’s symptoms by putting tension on particular parts of the sling during the office exam helps guide management. If I find that palpating or putting the sling on tension recreates her complaints, and conservative injections have provided temporary or inadequate relief, I usually advocate resecting the vaginal portion of the mesh to relieve that tension.
In cases of recurrent stress urinary incontinence (when the sling has failed), a TVT or repeat TVT is often warranted. The TVT sling has been demonstrated to work after nearly every other previous kind of anti-incontinence procedure, even after a previous retropubic sling. There is little data on mesh removal in such cases. I believe that unless a previously placed but failed sling is causing symptoms, there is no need to resect it. Mesh removal is significantly more traumatic than mesh placement, and in most cases it is not necessary.
Dr. Rardin reported that he has no relevant financial disclosures.

Tackling midurethral sling complications
Over the past 2 decades, midurethral slings, both via a retropubic and a transobturator approach have become the first-line therapy for the surgical correction of female stress urinary incontinence. Not only are cure rates excellent for both techniques, but the incidence of complications are low.
Intraoperatively, major concerns include vascular lesions, nerve injuries, and injuries to the bowel. More minor concerns are related to the bladder.

Perioperative complications include retropubic hematoma, blood loss, urinary tract infection, and spondylitis. Postoperative risks include transient versus permanent urinary retention, vaginal versus urethral erosion, de novo urgency, bladder erosion, and urethral obstruction.
In this edition of Master Class in gynecologic surgery, I am pleased to solicit the help of Dr. Charles Rardin, who will make recommendations regarding the management of some of the most common complications related to midurethral sling procedures.
Dr. Rardin is the director of the Robotic Surgery Program at Women & Infants Hospital of Rhode Island, in Providence; a surgeon in Women & Infants’ division of urogynecology and Reconstructive Pelvic Surgery; and is the director of the hospital’s fellowship urogynecology and reconstructive pelvic surgery.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; the director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller is a consultant and on the speaker’s bureau for Ethicon.
Over the past 2 decades, midurethral slings, both via a retropubic and a transobturator approach have become the first-line therapy for the surgical correction of female stress urinary incontinence. Not only are cure rates excellent for both techniques, but the incidence of complications are low.
Intraoperatively, major concerns include vascular lesions, nerve injuries, and injuries to the bowel. More minor concerns are related to the bladder.
Perioperative complications include retropubic hematoma, blood loss, urinary tract infection, and spondylitis. Postoperative risks include transient versus permanent urinary retention, vaginal versus urethral erosion, de novo urgency, bladder erosion, and urethral obstruction.
In this edition of Master Class in gynecologic surgery, I am pleased to solicit the help of Dr. Charles Rardin, who will make recommendations regarding the management of some of the most common complications related to midurethral sling procedures.
Dr. Rardin is the director of the Robotic Surgery Program at Women & Infants Hospital of Rhode Island, in Providence; a surgeon in Women & Infants’ division of urogynecology and Reconstructive Pelvic Surgery; and is the director of the hospital’s fellowship urogynecology and reconstructive pelvic surgery.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; the director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller is a consultant and on the speaker’s bureau for Ethicon.
Over the past 2 decades, midurethral slings, both via a retropubic and a transobturator approach have become the first-line therapy for the surgical correction of female stress urinary incontinence. Not only are cure rates excellent for both techniques, but the incidence of complications are low.
Intraoperatively, major concerns include vascular lesions, nerve injuries, and injuries to the bowel. More minor concerns are related to the bladder.
Perioperative complications include retropubic hematoma, blood loss, urinary tract infection, and spondylitis. Postoperative risks include transient versus permanent urinary retention, vaginal versus urethral erosion, de novo urgency, bladder erosion, and urethral obstruction.
In this edition of Master Class in gynecologic surgery, I am pleased to solicit the help of Dr. Charles Rardin, who will make recommendations regarding the management of some of the most common complications related to midurethral sling procedures.
Dr. Rardin is the director of the Robotic Surgery Program at Women & Infants Hospital of Rhode Island, in Providence; a surgeon in Women & Infants’ division of urogynecology and Reconstructive Pelvic Surgery; and is the director of the hospital’s fellowship urogynecology and reconstructive pelvic surgery.
Dr. Miller is clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; the director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill.; and the medical editor of this column, Master Class. Dr. Miller is a consultant and on the speaker’s bureau for Ethicon.

The Value of National and Hospital Registries
Following Dr. Sarmiento’s commentary, “Orthopedic Registries: Second Thoughts,” we agree that it is important and appropriate to question the value of any new additions to the orthopedic field, and registries are no exception. We thank Dr. Sarmiento for his comments on the viability of registries and the need for continued critical evaluation. Before joint registries, however, we had to rely on small-cohort analyses to assess outcomes and complications. Now, national and hospital registries, specifically joint registries, may be an invaluable source of information for orthopedic surgeons, patients, health care administrators, regulators, and implant suppliers.1,2
Contrary to Dr. Sarmiento’s belief that registry data results are likely to have been reported in the literature, it is difficult to refute the value of recent years’ registry data in helping surgeons shape their practice. For example, according to Lewallen and Etkin,3 the National Joint Registry of England and Wales information has provided orthopedic surgeons with crucial findings regarding the outcomes of metal-on-metal hip arthroplasties. Using the England and Wales registry data from more than 400,000 primary total hip arthroplasties, Smith and colleagues4 noted that metal-on-metal stemmed articulations led to poor implant survival, particularly in young women with large-diameter heads, and indicated these articulations should not be used. Australian registry data on metal-on-metal devices and reports of failure rates up to 11%5 led one manufacturer to recall its implants.6 In addition, the Norwegian Arthroplasty Register evaluated survival rates and reasons for revision for 7 types of cemented primary total knee arthroplasty (TKA) between 1994 and 2009.7 Data on more than 17,000 primary TKAs allowed Plate and colleagues8 to confidently determine that aseptic loosening was related to certain TKA designs. Using registry information, they identified patients at risk for dislocation in total hip arthroplasty and concluded that large-diameter femoral head articulations could reduce dislocation rates.
Obtaining such large cohorts of patients in individual studies is not only difficult but highly unlikely. Unlike registry data, these studies are often impractical in evaluating factors of low incidence, such as revision rates, as it is often difficult to find significant differences in small populations.9 Furthermore, these controlled trials homogenize patients—using exclusion and inclusion criteria to eliminate potential confounders—and thus poorly represent the heterogeneity of a typical hospital’s patient population.10 Although the literature may indeed have alluded to such complications, only a database as extensive as a registry can allow us to fully comprehend the outcomes of particular implants and devices.
Dr. Sarmiento points to the AO Swiss Fracture Registry as being of little benefit and raises the concern that the American Joint Replacement Registry (AJRR) may follow with the same results. However, realizing a registry’s benefits may take time and the gradual accumulation of data. Supporting this, Hübschle and colleagues11 recently used AO Swiss Fracture Registry data to validate use of balloon kyphoplasty for vertebral compression fractures and concluded that the technique is safe and effective in reducing pain—thus possibly providing the federal office with the evidence needed for reimbursement for this intervention. Therefore, this registry is now providing useful information.
We can never truly know the veracity of participating surgeons, but it is naïve to assume that this issue arises only vis-à-vis registries. If we were to debate the ethical and professional standards of colleagues in our field, such questions could extend to all studies performed, even peer-reviewed studies. Therefore, we do not think this is reason to exclude the patient data and outcomes found in registries. We must emphasize that ultimately registry data are often most useful in highlighting trends and determining triggers for further study rather than in arriving at conclusions.1 In particular, registry data may be used in cohort studies that evaluate the risk factors for and incidence of certain outcomes. Focused higher-level interventional studies can then follow the trends observed.1 However, registry data are also valuable on their own, when higher-level, randomized controlled trials may be impractical or unethical.12
Dr. Sarmiento refers to corrupt relationships between companies and orthopedists as “representing a widespread loss of professionalism in our ranks.” Despite a US Justice Department investigation into these relationships, only a few doctors were found to have had inappropriate relationships.13 In addition, the investigation and prosecution of companies led to an agreement requiring federal monitoring and new corporate compliance procedures, which should ensure stricter adherence to regulations.14 We do not believe this should undermine the value of registries and the work that has been contributed by thousands of surgeons hoping to improve the field of orthopedics. In addition, concerns about the influence of well-known individuals may be better directed at individual institution–based research, particularly as these specific authors also often have conflicts of interest that may skew the presentation of results. The strength of registry data is in providing collective data and large samples from a multitude of surgeons rather than from just high-volume surgeons, and therefore registry data provide a better overall picture of patients and their procedures.15 Furthermore, trends observed in national registries in countries such as New Zealand16 may aid in effectively reducing the revision rate, possibly up to 10%.17 If a US national joint registry is marginally as effective, then we may see considerable savings for our health care services.17,18
We wholeheartedly agree that a yearly review of registries may be constructive. Dr. Sarmiento suggests an annual publication summarizing peer-reviewed articles and the opportunity for orthopedists to decide for themselves what treatments to choose based on reports from independent investigators. Although this sounds feasible, it would be difficult to decide which articles should be selected as pertinent for this type of publication. Any selection would be biased, and not all studies with high-level evidence are necessarily important or relevant. Therefore, selecting what is most appropriate to cite is not without its difficulties. We appreciate that there are problems in standardizing data reporting among registries. However, to improve interregistry collaboration, the US Food and Drug Administration is sponsoring the International Consortium of Orthopaedic Registries (ICOR) to facilitate data presentation.19 ICOR aims to increase cooperation, standardize analyses, and improve reporting, which will only strengthen the data available to us. Such efforts will ultimately enhance coordination and international collaboration among registries.15 In addition, incorporating patient-reported outcomes into our national registry will aid in quantifying arthroplasty outcomes from the patient’s perspective and will continue to improve total joint arthroplasties.20
Overall, this debate is useful and highly relevant in highlighting potential issues with registries. Although registries are not without their flaws, like all aspects of orthopedics they are ever evolving, and they must be continually modified and improved. However, disregard for the potential value of AJRR, which has benefits for orthopedists and patients alike, is premature. Once again, we thank Dr. Sarmiento for starting this discussion, which will allow us to continue to evaluate and improve our registries.
1. Konan S, Haddad FS. Joint registries: a Ptolemaic model of data interpretation? Bone Joint J Br. 2013;95(12):1585-1586.
2. Banerjee S, Cafri G, Isaacs AJ, et al. A distributed health data network analysis of survival outcomes: the International Consortium of Orthopaedic Registries perspective. J Bone Joint Surg Am. 2014;96(suppl 1):7-11.
3. Lewallen DG, Etkin CD. The need for a national total joint registry. Orthop Nurs. 2013;32(1):4-5.
4. Smith AJ, Dieppe P, Vernon K, Porter M, Blom AW; National Joint Registry of England and Wales. Failure rates of stemmed metal-on-metal hip replacements: analysis of data from the National Joint Registry of England and Wales. Lancet. 2012;379(9822):1199-1204.
5. de Steiger RN, Hang JR, Miller LN, Graves SE, Davidson DC. Five-year results of the ASR XL Acetabular System and the ASR Hip Resurfacing System: an analysis from the Australian Orthopaedic Association National Joint Replacement Registry. J Bone Joint Surg Am. 2011;93(24):2287-2293.
6. Hug KT, Watters TS, Vail TP, Bolognesi MP. The withdrawn ASR™ THA and hip resurfacing systems: how have our patients fared over 1 to 6 years? Clin Orthop. 2013;471(2):430-438.
7. Gøthesen O, Espehaug B, Havelin L, et al. Survival rates and causes of revision in cemented primary total knee replacement: a report from the Norwegian Arthroplasty Register 1994–2009. Bone Joint J Br. 2013;95(5):636-642.
8. Plate JF, Seyler TM, Stroh DA, Issa K, Akbar M, Mont MA. Risk of dislocation using large- vs. small-diameter femoral heads in total hip arthroplasty. BMC Res Notes. 2012;5:553.
9. Daruwalla ZJ, Wong KL, Pillay KR, Leong KM, Murphy DP. Does ageing Singapore need an electronic database of hip fracture patients? The value and role of a national joint registry and an electronic database of intertrochanteric and femoral neck fractures. Singapore Med J. 2014;55(5):287-288.
10. Rasmussen JV, Olsen BS, Fevang BT, et al. A review of national shoulder and elbow joint replacement registries. J Shoulder Elbow Surg. 2012;21(10):1328-1335.
11. Hübschle L, Borgström F, Olafsson G, et al. Real-life results of balloon kyphoplasty for vertebral compression fractures from the SWISSspine registry. Spine J. 2014;14(9):2063-2077.
12. Ahn H, Court-Brown CM, McQueen MM, Schemitsch EH. The use of hospital registries in orthopaedic surgery. J Bone Joint Surg Am. 2009;91(suppl 3):68-72.
13. Youngstrom N. Swept up in major medical device case, physician pays $650,000 to settle kickback charges. AIS Health Business Daily. May 3, 2010.
14. Five companies in hip and knee replacement industry avoid prosecution by agreeing to compliance rules and monitoring [press release]. US Department of Justice website. http://www.justice.gov/usao/nj/Press/files/pdffiles/Older/hips0927.rel.pdf. Published September 27, 2007. Accessed February 19, 2015.
15. Namba RS, Inacio MC, Paxton EW, Robertsson O, Graves SE. The role of registry data in the evaluation of mobile-bearing total knee arthroplasty. J Bone Joint Surg Am. 2011;93(suppl 3):48-50.
16. Insull PJ, Cobbett H, Frampton CM, Munro JT. The use of a lipped acetabular liner decreases the rate of revision for instability after total hip replacement: a study using data from the New Zealand Joint Registry. Bone Joint J Br. 2014;96(7):884-888.
17. Rankin EA. AJRR: becoming a national US joint registry. Orthopedics. 2013;36(3):175-176.
18. American Joint Replacement Registry website. https://teamwork.aaos.org/ajrr/SitePages/About%20Us.aspx. Accessed February 19, 2015.
19. International Consortium of Orthopaedic Registries website. http://www.icor-initiative.org. Accessed February 19, 2015.
20. Franklin PD, Harrold L, Ayers DC. Incorporating patient-reported outcomes in total joint arthroplasty registries: challenges and opportunities. Clin Orthop. 2013;471(11):3482-3488.
Following Dr. Sarmiento’s commentary, “Orthopedic Registries: Second Thoughts,” we agree that it is important and appropriate to question the value of any new additions to the orthopedic field, and registries are no exception. We thank Dr. Sarmiento for his comments on the viability of registries and the need for continued critical evaluation. Before joint registries, however, we had to rely on small-cohort analyses to assess outcomes and complications. Now, national and hospital registries, specifically joint registries, may be an invaluable source of information for orthopedic surgeons, patients, health care administrators, regulators, and implant suppliers.1,2
Contrary to Dr. Sarmiento’s belief that registry data results are likely to have been reported in the literature, it is difficult to refute the value of recent years’ registry data in helping surgeons shape their practice. For example, according to Lewallen and Etkin,3 the National Joint Registry of England and Wales information has provided orthopedic surgeons with crucial findings regarding the outcomes of metal-on-metal hip arthroplasties. Using the England and Wales registry data from more than 400,000 primary total hip arthroplasties, Smith and colleagues4 noted that metal-on-metal stemmed articulations led to poor implant survival, particularly in young women with large-diameter heads, and indicated these articulations should not be used. Australian registry data on metal-on-metal devices and reports of failure rates up to 11%5 led one manufacturer to recall its implants.6 In addition, the Norwegian Arthroplasty Register evaluated survival rates and reasons for revision for 7 types of cemented primary total knee arthroplasty (TKA) between 1994 and 2009.7 Data on more than 17,000 primary TKAs allowed Plate and colleagues8 to confidently determine that aseptic loosening was related to certain TKA designs. Using registry information, they identified patients at risk for dislocation in total hip arthroplasty and concluded that large-diameter femoral head articulations could reduce dislocation rates.
Obtaining such large cohorts of patients in individual studies is not only difficult but highly unlikely. Unlike registry data, these studies are often impractical in evaluating factors of low incidence, such as revision rates, as it is often difficult to find significant differences in small populations.9 Furthermore, these controlled trials homogenize patients—using exclusion and inclusion criteria to eliminate potential confounders—and thus poorly represent the heterogeneity of a typical hospital’s patient population.10 Although the literature may indeed have alluded to such complications, only a database as extensive as a registry can allow us to fully comprehend the outcomes of particular implants and devices.
Dr. Sarmiento points to the AO Swiss Fracture Registry as being of little benefit and raises the concern that the American Joint Replacement Registry (AJRR) may follow with the same results. However, realizing a registry’s benefits may take time and the gradual accumulation of data. Supporting this, Hübschle and colleagues11 recently used AO Swiss Fracture Registry data to validate use of balloon kyphoplasty for vertebral compression fractures and concluded that the technique is safe and effective in reducing pain—thus possibly providing the federal office with the evidence needed for reimbursement for this intervention. Therefore, this registry is now providing useful information.
We can never truly know the veracity of participating surgeons, but it is naïve to assume that this issue arises only vis-à-vis registries. If we were to debate the ethical and professional standards of colleagues in our field, such questions could extend to all studies performed, even peer-reviewed studies. Therefore, we do not think this is reason to exclude the patient data and outcomes found in registries. We must emphasize that ultimately registry data are often most useful in highlighting trends and determining triggers for further study rather than in arriving at conclusions.1 In particular, registry data may be used in cohort studies that evaluate the risk factors for and incidence of certain outcomes. Focused higher-level interventional studies can then follow the trends observed.1 However, registry data are also valuable on their own, when higher-level, randomized controlled trials may be impractical or unethical.12
Dr. Sarmiento refers to corrupt relationships between companies and orthopedists as “representing a widespread loss of professionalism in our ranks.” Despite a US Justice Department investigation into these relationships, only a few doctors were found to have had inappropriate relationships.13 In addition, the investigation and prosecution of companies led to an agreement requiring federal monitoring and new corporate compliance procedures, which should ensure stricter adherence to regulations.14 We do not believe this should undermine the value of registries and the work that has been contributed by thousands of surgeons hoping to improve the field of orthopedics. In addition, concerns about the influence of well-known individuals may be better directed at individual institution–based research, particularly as these specific authors also often have conflicts of interest that may skew the presentation of results. The strength of registry data is in providing collective data and large samples from a multitude of surgeons rather than from just high-volume surgeons, and therefore registry data provide a better overall picture of patients and their procedures.15 Furthermore, trends observed in national registries in countries such as New Zealand16 may aid in effectively reducing the revision rate, possibly up to 10%.17 If a US national joint registry is marginally as effective, then we may see considerable savings for our health care services.17,18
We wholeheartedly agree that a yearly review of registries may be constructive. Dr. Sarmiento suggests an annual publication summarizing peer-reviewed articles and the opportunity for orthopedists to decide for themselves what treatments to choose based on reports from independent investigators. Although this sounds feasible, it would be difficult to decide which articles should be selected as pertinent for this type of publication. Any selection would be biased, and not all studies with high-level evidence are necessarily important or relevant. Therefore, selecting what is most appropriate to cite is not without its difficulties. We appreciate that there are problems in standardizing data reporting among registries. However, to improve interregistry collaboration, the US Food and Drug Administration is sponsoring the International Consortium of Orthopaedic Registries (ICOR) to facilitate data presentation.19 ICOR aims to increase cooperation, standardize analyses, and improve reporting, which will only strengthen the data available to us. Such efforts will ultimately enhance coordination and international collaboration among registries.15 In addition, incorporating patient-reported outcomes into our national registry will aid in quantifying arthroplasty outcomes from the patient’s perspective and will continue to improve total joint arthroplasties.20
Overall, this debate is useful and highly relevant in highlighting potential issues with registries. Although registries are not without their flaws, like all aspects of orthopedics they are ever evolving, and they must be continually modified and improved. However, disregard for the potential value of AJRR, which has benefits for orthopedists and patients alike, is premature. Once again, we thank Dr. Sarmiento for starting this discussion, which will allow us to continue to evaluate and improve our registries.
Following Dr. Sarmiento’s commentary, “Orthopedic Registries: Second Thoughts,” we agree that it is important and appropriate to question the value of any new additions to the orthopedic field, and registries are no exception. We thank Dr. Sarmiento for his comments on the viability of registries and the need for continued critical evaluation. Before joint registries, however, we had to rely on small-cohort analyses to assess outcomes and complications. Now, national and hospital registries, specifically joint registries, may be an invaluable source of information for orthopedic surgeons, patients, health care administrators, regulators, and implant suppliers.1,2
Contrary to Dr. Sarmiento’s belief that registry data results are likely to have been reported in the literature, it is difficult to refute the value of recent years’ registry data in helping surgeons shape their practice. For example, according to Lewallen and Etkin,3 the National Joint Registry of England and Wales information has provided orthopedic surgeons with crucial findings regarding the outcomes of metal-on-metal hip arthroplasties. Using the England and Wales registry data from more than 400,000 primary total hip arthroplasties, Smith and colleagues4 noted that metal-on-metal stemmed articulations led to poor implant survival, particularly in young women with large-diameter heads, and indicated these articulations should not be used. Australian registry data on metal-on-metal devices and reports of failure rates up to 11%5 led one manufacturer to recall its implants.6 In addition, the Norwegian Arthroplasty Register evaluated survival rates and reasons for revision for 7 types of cemented primary total knee arthroplasty (TKA) between 1994 and 2009.7 Data on more than 17,000 primary TKAs allowed Plate and colleagues8 to confidently determine that aseptic loosening was related to certain TKA designs. Using registry information, they identified patients at risk for dislocation in total hip arthroplasty and concluded that large-diameter femoral head articulations could reduce dislocation rates.
Obtaining such large cohorts of patients in individual studies is not only difficult but highly unlikely. Unlike registry data, these studies are often impractical in evaluating factors of low incidence, such as revision rates, as it is often difficult to find significant differences in small populations.9 Furthermore, these controlled trials homogenize patients—using exclusion and inclusion criteria to eliminate potential confounders—and thus poorly represent the heterogeneity of a typical hospital’s patient population.10 Although the literature may indeed have alluded to such complications, only a database as extensive as a registry can allow us to fully comprehend the outcomes of particular implants and devices.
Dr. Sarmiento points to the AO Swiss Fracture Registry as being of little benefit and raises the concern that the American Joint Replacement Registry (AJRR) may follow with the same results. However, realizing a registry’s benefits may take time and the gradual accumulation of data. Supporting this, Hübschle and colleagues11 recently used AO Swiss Fracture Registry data to validate use of balloon kyphoplasty for vertebral compression fractures and concluded that the technique is safe and effective in reducing pain—thus possibly providing the federal office with the evidence needed for reimbursement for this intervention. Therefore, this registry is now providing useful information.
We can never truly know the veracity of participating surgeons, but it is naïve to assume that this issue arises only vis-à-vis registries. If we were to debate the ethical and professional standards of colleagues in our field, such questions could extend to all studies performed, even peer-reviewed studies. Therefore, we do not think this is reason to exclude the patient data and outcomes found in registries. We must emphasize that ultimately registry data are often most useful in highlighting trends and determining triggers for further study rather than in arriving at conclusions.1 In particular, registry data may be used in cohort studies that evaluate the risk factors for and incidence of certain outcomes. Focused higher-level interventional studies can then follow the trends observed.1 However, registry data are also valuable on their own, when higher-level, randomized controlled trials may be impractical or unethical.12
Dr. Sarmiento refers to corrupt relationships between companies and orthopedists as “representing a widespread loss of professionalism in our ranks.” Despite a US Justice Department investigation into these relationships, only a few doctors were found to have had inappropriate relationships.13 In addition, the investigation and prosecution of companies led to an agreement requiring federal monitoring and new corporate compliance procedures, which should ensure stricter adherence to regulations.14 We do not believe this should undermine the value of registries and the work that has been contributed by thousands of surgeons hoping to improve the field of orthopedics. In addition, concerns about the influence of well-known individuals may be better directed at individual institution–based research, particularly as these specific authors also often have conflicts of interest that may skew the presentation of results. The strength of registry data is in providing collective data and large samples from a multitude of surgeons rather than from just high-volume surgeons, and therefore registry data provide a better overall picture of patients and their procedures.15 Furthermore, trends observed in national registries in countries such as New Zealand16 may aid in effectively reducing the revision rate, possibly up to 10%.17 If a US national joint registry is marginally as effective, then we may see considerable savings for our health care services.17,18
We wholeheartedly agree that a yearly review of registries may be constructive. Dr. Sarmiento suggests an annual publication summarizing peer-reviewed articles and the opportunity for orthopedists to decide for themselves what treatments to choose based on reports from independent investigators. Although this sounds feasible, it would be difficult to decide which articles should be selected as pertinent for this type of publication. Any selection would be biased, and not all studies with high-level evidence are necessarily important or relevant. Therefore, selecting what is most appropriate to cite is not without its difficulties. We appreciate that there are problems in standardizing data reporting among registries. However, to improve interregistry collaboration, the US Food and Drug Administration is sponsoring the International Consortium of Orthopaedic Registries (ICOR) to facilitate data presentation.19 ICOR aims to increase cooperation, standardize analyses, and improve reporting, which will only strengthen the data available to us. Such efforts will ultimately enhance coordination and international collaboration among registries.15 In addition, incorporating patient-reported outcomes into our national registry will aid in quantifying arthroplasty outcomes from the patient’s perspective and will continue to improve total joint arthroplasties.20
Overall, this debate is useful and highly relevant in highlighting potential issues with registries. Although registries are not without their flaws, like all aspects of orthopedics they are ever evolving, and they must be continually modified and improved. However, disregard for the potential value of AJRR, which has benefits for orthopedists and patients alike, is premature. Once again, we thank Dr. Sarmiento for starting this discussion, which will allow us to continue to evaluate and improve our registries.
1. Konan S, Haddad FS. Joint registries: a Ptolemaic model of data interpretation? Bone Joint J Br. 2013;95(12):1585-1586.
2. Banerjee S, Cafri G, Isaacs AJ, et al. A distributed health data network analysis of survival outcomes: the International Consortium of Orthopaedic Registries perspective. J Bone Joint Surg Am. 2014;96(suppl 1):7-11.
3. Lewallen DG, Etkin CD. The need for a national total joint registry. Orthop Nurs. 2013;32(1):4-5.
4. Smith AJ, Dieppe P, Vernon K, Porter M, Blom AW; National Joint Registry of England and Wales. Failure rates of stemmed metal-on-metal hip replacements: analysis of data from the National Joint Registry of England and Wales. Lancet. 2012;379(9822):1199-1204.
5. de Steiger RN, Hang JR, Miller LN, Graves SE, Davidson DC. Five-year results of the ASR XL Acetabular System and the ASR Hip Resurfacing System: an analysis from the Australian Orthopaedic Association National Joint Replacement Registry. J Bone Joint Surg Am. 2011;93(24):2287-2293.
6. Hug KT, Watters TS, Vail TP, Bolognesi MP. The withdrawn ASR™ THA and hip resurfacing systems: how have our patients fared over 1 to 6 years? Clin Orthop. 2013;471(2):430-438.
7. Gøthesen O, Espehaug B, Havelin L, et al. Survival rates and causes of revision in cemented primary total knee replacement: a report from the Norwegian Arthroplasty Register 1994–2009. Bone Joint J Br. 2013;95(5):636-642.
8. Plate JF, Seyler TM, Stroh DA, Issa K, Akbar M, Mont MA. Risk of dislocation using large- vs. small-diameter femoral heads in total hip arthroplasty. BMC Res Notes. 2012;5:553.
9. Daruwalla ZJ, Wong KL, Pillay KR, Leong KM, Murphy DP. Does ageing Singapore need an electronic database of hip fracture patients? The value and role of a national joint registry and an electronic database of intertrochanteric and femoral neck fractures. Singapore Med J. 2014;55(5):287-288.
10. Rasmussen JV, Olsen BS, Fevang BT, et al. A review of national shoulder and elbow joint replacement registries. J Shoulder Elbow Surg. 2012;21(10):1328-1335.
11. Hübschle L, Borgström F, Olafsson G, et al. Real-life results of balloon kyphoplasty for vertebral compression fractures from the SWISSspine registry. Spine J. 2014;14(9):2063-2077.
12. Ahn H, Court-Brown CM, McQueen MM, Schemitsch EH. The use of hospital registries in orthopaedic surgery. J Bone Joint Surg Am. 2009;91(suppl 3):68-72.
13. Youngstrom N. Swept up in major medical device case, physician pays $650,000 to settle kickback charges. AIS Health Business Daily. May 3, 2010.
14. Five companies in hip and knee replacement industry avoid prosecution by agreeing to compliance rules and monitoring [press release]. US Department of Justice website. http://www.justice.gov/usao/nj/Press/files/pdffiles/Older/hips0927.rel.pdf. Published September 27, 2007. Accessed February 19, 2015.
15. Namba RS, Inacio MC, Paxton EW, Robertsson O, Graves SE. The role of registry data in the evaluation of mobile-bearing total knee arthroplasty. J Bone Joint Surg Am. 2011;93(suppl 3):48-50.
16. Insull PJ, Cobbett H, Frampton CM, Munro JT. The use of a lipped acetabular liner decreases the rate of revision for instability after total hip replacement: a study using data from the New Zealand Joint Registry. Bone Joint J Br. 2014;96(7):884-888.
17. Rankin EA. AJRR: becoming a national US joint registry. Orthopedics. 2013;36(3):175-176.
18. American Joint Replacement Registry website. https://teamwork.aaos.org/ajrr/SitePages/About%20Us.aspx. Accessed February 19, 2015.
19. International Consortium of Orthopaedic Registries website. http://www.icor-initiative.org. Accessed February 19, 2015.
20. Franklin PD, Harrold L, Ayers DC. Incorporating patient-reported outcomes in total joint arthroplasty registries: challenges and opportunities. Clin Orthop. 2013;471(11):3482-3488.
1. Konan S, Haddad FS. Joint registries: a Ptolemaic model of data interpretation? Bone Joint J Br. 2013;95(12):1585-1586.
2. Banerjee S, Cafri G, Isaacs AJ, et al. A distributed health data network analysis of survival outcomes: the International Consortium of Orthopaedic Registries perspective. J Bone Joint Surg Am. 2014;96(suppl 1):7-11.
3. Lewallen DG, Etkin CD. The need for a national total joint registry. Orthop Nurs. 2013;32(1):4-5.
4. Smith AJ, Dieppe P, Vernon K, Porter M, Blom AW; National Joint Registry of England and Wales. Failure rates of stemmed metal-on-metal hip replacements: analysis of data from the National Joint Registry of England and Wales. Lancet. 2012;379(9822):1199-1204.
5. de Steiger RN, Hang JR, Miller LN, Graves SE, Davidson DC. Five-year results of the ASR XL Acetabular System and the ASR Hip Resurfacing System: an analysis from the Australian Orthopaedic Association National Joint Replacement Registry. J Bone Joint Surg Am. 2011;93(24):2287-2293.
6. Hug KT, Watters TS, Vail TP, Bolognesi MP. The withdrawn ASR™ THA and hip resurfacing systems: how have our patients fared over 1 to 6 years? Clin Orthop. 2013;471(2):430-438.
7. Gøthesen O, Espehaug B, Havelin L, et al. Survival rates and causes of revision in cemented primary total knee replacement: a report from the Norwegian Arthroplasty Register 1994–2009. Bone Joint J Br. 2013;95(5):636-642.
8. Plate JF, Seyler TM, Stroh DA, Issa K, Akbar M, Mont MA. Risk of dislocation using large- vs. small-diameter femoral heads in total hip arthroplasty. BMC Res Notes. 2012;5:553.
9. Daruwalla ZJ, Wong KL, Pillay KR, Leong KM, Murphy DP. Does ageing Singapore need an electronic database of hip fracture patients? The value and role of a national joint registry and an electronic database of intertrochanteric and femoral neck fractures. Singapore Med J. 2014;55(5):287-288.
10. Rasmussen JV, Olsen BS, Fevang BT, et al. A review of national shoulder and elbow joint replacement registries. J Shoulder Elbow Surg. 2012;21(10):1328-1335.
11. Hübschle L, Borgström F, Olafsson G, et al. Real-life results of balloon kyphoplasty for vertebral compression fractures from the SWISSspine registry. Spine J. 2014;14(9):2063-2077.
12. Ahn H, Court-Brown CM, McQueen MM, Schemitsch EH. The use of hospital registries in orthopaedic surgery. J Bone Joint Surg Am. 2009;91(suppl 3):68-72.
13. Youngstrom N. Swept up in major medical device case, physician pays $650,000 to settle kickback charges. AIS Health Business Daily. May 3, 2010.
14. Five companies in hip and knee replacement industry avoid prosecution by agreeing to compliance rules and monitoring [press release]. US Department of Justice website. http://www.justice.gov/usao/nj/Press/files/pdffiles/Older/hips0927.rel.pdf. Published September 27, 2007. Accessed February 19, 2015.
15. Namba RS, Inacio MC, Paxton EW, Robertsson O, Graves SE. The role of registry data in the evaluation of mobile-bearing total knee arthroplasty. J Bone Joint Surg Am. 2011;93(suppl 3):48-50.
16. Insull PJ, Cobbett H, Frampton CM, Munro JT. The use of a lipped acetabular liner decreases the rate of revision for instability after total hip replacement: a study using data from the New Zealand Joint Registry. Bone Joint J Br. 2014;96(7):884-888.
17. Rankin EA. AJRR: becoming a national US joint registry. Orthopedics. 2013;36(3):175-176.
18. American Joint Replacement Registry website. https://teamwork.aaos.org/ajrr/SitePages/About%20Us.aspx. Accessed February 19, 2015.
19. International Consortium of Orthopaedic Registries website. http://www.icor-initiative.org. Accessed February 19, 2015.
20. Franklin PD, Harrold L, Ayers DC. Incorporating patient-reported outcomes in total joint arthroplasty registries: challenges and opportunities. Clin Orthop. 2013;471(11):3482-3488.