User login
Rethinking the management of labor
Over the last 50 years, we have witnessed some incredible advancements that have vastly improved maternal and fetal outcomes, even in the face of the most complex obstetrical dilemmas. As our practice and the research continues to evolve, it is increasingly important that we carefully review our practice standards to ensure that every woman and her baby receives the most up-to-date medical care.
This month’s Master Class highlights a critical area of obstetrics where the convergence of technology, clinical observation, and research stimulated a change in practice guidelines: the use of the labor curve to monitor normal versus abnormal labor. Until quite recently, ob.gyns. had based labor criteria on the “Friedman Curve,” first established in the mid-1950s, and supported by other smaller and less comprehensive studies. This work was adopted by the American College of Obstetricians and Gynecologists.

For more than half a century, we used these parameters to determine if a woman had entered active-phase arrest, and to make the very important decision of whether to perform a cesarean section. However, work in the early 2000s strongly suggested that the old criteria no longer applied to the full course of labor in contemporary patients (Am J Obstet Gynecol. 2002 Oct;187[4]:824-8). A 2010 comprehensive study showed that we needed to consider a new approach to labor management (Am J Obstet Gynecol. 2010 Oct;203[4]:326.e1-326.e10).
It may seem incredible that it took such a long time to update our thinking about what constitutes normal versus abnormal labor progression. However, we must keep in mind that many studies supported the original labor curve, and advanced tools to assess fetal health during labor were just being developed. The first commercially available fetal heart rate monitor would not be produced until 1968, and debates about the utility of these devices would continue into the early 1990s.
Additionally, our patient population has changed. As we have discussed in previous columns, the incidence and severity of other chronic conditions, such as diabetes and obesity, has increased significantly and deeply impacted labor progression.
Just as technology has advanced and our patients’ needs have changed, so, too, must our practice standards. We have invited Dr. Alison G. Cahill, associate professor and chief of the division of maternal-fetal medicine in the department of obstetrics and gynecology at Washington University, St. Louis, to discuss the importance and implications of the new labor curve.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
Over the last 50 years, we have witnessed some incredible advancements that have vastly improved maternal and fetal outcomes, even in the face of the most complex obstetrical dilemmas. As our practice and the research continues to evolve, it is increasingly important that we carefully review our practice standards to ensure that every woman and her baby receives the most up-to-date medical care.
This month’s Master Class highlights a critical area of obstetrics where the convergence of technology, clinical observation, and research stimulated a change in practice guidelines: the use of the labor curve to monitor normal versus abnormal labor. Until quite recently, ob.gyns. had based labor criteria on the “Friedman Curve,” first established in the mid-1950s, and supported by other smaller and less comprehensive studies. This work was adopted by the American College of Obstetricians and Gynecologists.
For more than half a century, we used these parameters to determine if a woman had entered active-phase arrest, and to make the very important decision of whether to perform a cesarean section. However, work in the early 2000s strongly suggested that the old criteria no longer applied to the full course of labor in contemporary patients (Am J Obstet Gynecol. 2002 Oct;187[4]:824-8). A 2010 comprehensive study showed that we needed to consider a new approach to labor management (Am J Obstet Gynecol. 2010 Oct;203[4]:326.e1-326.e10).
It may seem incredible that it took such a long time to update our thinking about what constitutes normal versus abnormal labor progression. However, we must keep in mind that many studies supported the original labor curve, and advanced tools to assess fetal health during labor were just being developed. The first commercially available fetal heart rate monitor would not be produced until 1968, and debates about the utility of these devices would continue into the early 1990s.
Additionally, our patient population has changed. As we have discussed in previous columns, the incidence and severity of other chronic conditions, such as diabetes and obesity, has increased significantly and deeply impacted labor progression.
Just as technology has advanced and our patients’ needs have changed, so, too, must our practice standards. We have invited Dr. Alison G. Cahill, associate professor and chief of the division of maternal-fetal medicine in the department of obstetrics and gynecology at Washington University, St. Louis, to discuss the importance and implications of the new labor curve.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
Over the last 50 years, we have witnessed some incredible advancements that have vastly improved maternal and fetal outcomes, even in the face of the most complex obstetrical dilemmas. As our practice and the research continues to evolve, it is increasingly important that we carefully review our practice standards to ensure that every woman and her baby receives the most up-to-date medical care.
This month’s Master Class highlights a critical area of obstetrics where the convergence of technology, clinical observation, and research stimulated a change in practice guidelines: the use of the labor curve to monitor normal versus abnormal labor. Until quite recently, ob.gyns. had based labor criteria on the “Friedman Curve,” first established in the mid-1950s, and supported by other smaller and less comprehensive studies. This work was adopted by the American College of Obstetricians and Gynecologists.
For more than half a century, we used these parameters to determine if a woman had entered active-phase arrest, and to make the very important decision of whether to perform a cesarean section. However, work in the early 2000s strongly suggested that the old criteria no longer applied to the full course of labor in contemporary patients (Am J Obstet Gynecol. 2002 Oct;187[4]:824-8). A 2010 comprehensive study showed that we needed to consider a new approach to labor management (Am J Obstet Gynecol. 2010 Oct;203[4]:326.e1-326.e10).
It may seem incredible that it took such a long time to update our thinking about what constitutes normal versus abnormal labor progression. However, we must keep in mind that many studies supported the original labor curve, and advanced tools to assess fetal health during labor were just being developed. The first commercially available fetal heart rate monitor would not be produced until 1968, and debates about the utility of these devices would continue into the early 1990s.
Additionally, our patient population has changed. As we have discussed in previous columns, the incidence and severity of other chronic conditions, such as diabetes and obesity, has increased significantly and deeply impacted labor progression.
Just as technology has advanced and our patients’ needs have changed, so, too, must our practice standards. We have invited Dr. Alison G. Cahill, associate professor and chief of the division of maternal-fetal medicine in the department of obstetrics and gynecology at Washington University, St. Louis, to discuss the importance and implications of the new labor curve.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.

Infection control is everyone’s responsibility
Big things come in small packages, very small – so small they may even be invisible to the naked eye. Take for instance a huge infection causing multiorgan system failure, disseminated intravascular coagulation, even septic shock refractory to high-dose pressors. This catastrophe may be the end result of exposure to tiny pathogenic microbes that can take down an otherwise healthy 300-pound man, tout suite!
Microorganisms are everywhere. We can’t live without them, but we can’t live with certain ones either. Unless you live in a bubble you are going to be exposed to countless bacteria each and every day. They are in the air we breathe, the water we drink, the beds we sleep in. While it is a given that we all will be continuously exposed to bacteria, having a well-considered strategy to curtail the spread of disease can dramatically decrease the risk that we, our families, and our patients are needlessly exposed to potentially life-threatening organisms.

We all know we are to wash our hands on the way in, and out, of patients’ rooms. This practice is our front line of defense against the spread of numerous potentially lethal diseases. Yet, many clinicians, as well as ancillary hospital personnel, repeatedly fail to abide by this rule, thinking that ‘this one time won’t hurt anything.’ Whether it’s the nurse who rushes into a patient’s room to stop a beeping IV pole or the doctor who eyes a family member in the room and makes a beeline to discuss the discharge plan, all of us have been guilty of entering or leaving a patient’s room without following appropriate infection control standards.
Or, how many times have you followed the protocol meticulously, at least initially, and removed your gown and gloves and washed your hands on your way out the door when the patient remembers another question, or asks you to hand him something that leads to more contact with him or his surroundings? You already washed your hands once, so must you really do it again? After all, what is the likelihood that you pick up (or pass along) any germs anyway? Sometimes, more than we realize. Something as simple as handing a patient his nurses’ call button can expose us to enough C. difficile spores to cause infection in us or others we come into contact with unwittingly. So wash those hands, and wash them again if you touch anything in a patient’s room, even if it is not the patient himself.
Direct observation (AKA “Secret Santas”) can provide invaluable information about adherence to hand hygiene among health care workers and providing feedback is key. This can be unit based, group based, and even provider based. Once collected, this information should be used to drive changes in behavior, which could be punitive or positive; each hospital should decide how to best use its data.
Visitor contact is another important issue and not everyone agrees on how to enforce, or whether to even try to enforce, infection control procedures. The Society for Healthcare Epidemiology of America (SHEA) has several helpful pocket guidelines to address this and other infection control issues. For instance, the society recommends that hospitals consider adopting guidelines to minimize horizontal transmission by visitors, though these guidelines should be feasible to enforce. Factors such as the specific organism and its potential to cause harm are important to consider when developing these guidelines. For instance, the spouse of a patient admitted with influenza has likely already been exposed, and postexposure prophylaxis may be more feasible to her than wearing an uncomfortable mask during an 8-hour hospital visit.
A pharmacy stewardship program is another invaluable infection control tool. With this model, a group of pharmacists, under the direction of an infectious disease specialist, reviews culture results daily and makes recommendations to the physician regarding narrowing antibiotic coverage. I greatly appreciate receiving calls to notify me that the final culture results are in long before I would have actually seen them myself. This allows me to adjust antibiotics in a timely fashion, thus reducing the emergence of drug-resistant organisms or precipitating an unnecessary case of C. difficile.
In addition, written guidelines should be established for indwelling catheters, both urinary and venous. The indication for continued use should be reassessed daily; a computer alert that requires a response is very helpful, as is a call from the friendly floor nurse asking, “Does this patient really still need his catheter?”
Infection control is everyone’s responsibility and we all need to work together toward this common goal.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.
Big things come in small packages, very small – so small they may even be invisible to the naked eye. Take for instance a huge infection causing multiorgan system failure, disseminated intravascular coagulation, even septic shock refractory to high-dose pressors. This catastrophe may be the end result of exposure to tiny pathogenic microbes that can take down an otherwise healthy 300-pound man, tout suite!
Microorganisms are everywhere. We can’t live without them, but we can’t live with certain ones either. Unless you live in a bubble you are going to be exposed to countless bacteria each and every day. They are in the air we breathe, the water we drink, the beds we sleep in. While it is a given that we all will be continuously exposed to bacteria, having a well-considered strategy to curtail the spread of disease can dramatically decrease the risk that we, our families, and our patients are needlessly exposed to potentially life-threatening organisms.
We all know we are to wash our hands on the way in, and out, of patients’ rooms. This practice is our front line of defense against the spread of numerous potentially lethal diseases. Yet, many clinicians, as well as ancillary hospital personnel, repeatedly fail to abide by this rule, thinking that ‘this one time won’t hurt anything.’ Whether it’s the nurse who rushes into a patient’s room to stop a beeping IV pole or the doctor who eyes a family member in the room and makes a beeline to discuss the discharge plan, all of us have been guilty of entering or leaving a patient’s room without following appropriate infection control standards.
Or, how many times have you followed the protocol meticulously, at least initially, and removed your gown and gloves and washed your hands on your way out the door when the patient remembers another question, or asks you to hand him something that leads to more contact with him or his surroundings? You already washed your hands once, so must you really do it again? After all, what is the likelihood that you pick up (or pass along) any germs anyway? Sometimes, more than we realize. Something as simple as handing a patient his nurses’ call button can expose us to enough C. difficile spores to cause infection in us or others we come into contact with unwittingly. So wash those hands, and wash them again if you touch anything in a patient’s room, even if it is not the patient himself.
Direct observation (AKA “Secret Santas”) can provide invaluable information about adherence to hand hygiene among health care workers and providing feedback is key. This can be unit based, group based, and even provider based. Once collected, this information should be used to drive changes in behavior, which could be punitive or positive; each hospital should decide how to best use its data.
Visitor contact is another important issue and not everyone agrees on how to enforce, or whether to even try to enforce, infection control procedures. The Society for Healthcare Epidemiology of America (SHEA) has several helpful pocket guidelines to address this and other infection control issues. For instance, the society recommends that hospitals consider adopting guidelines to minimize horizontal transmission by visitors, though these guidelines should be feasible to enforce. Factors such as the specific organism and its potential to cause harm are important to consider when developing these guidelines. For instance, the spouse of a patient admitted with influenza has likely already been exposed, and postexposure prophylaxis may be more feasible to her than wearing an uncomfortable mask during an 8-hour hospital visit.
A pharmacy stewardship program is another invaluable infection control tool. With this model, a group of pharmacists, under the direction of an infectious disease specialist, reviews culture results daily and makes recommendations to the physician regarding narrowing antibiotic coverage. I greatly appreciate receiving calls to notify me that the final culture results are in long before I would have actually seen them myself. This allows me to adjust antibiotics in a timely fashion, thus reducing the emergence of drug-resistant organisms or precipitating an unnecessary case of C. difficile.
In addition, written guidelines should be established for indwelling catheters, both urinary and venous. The indication for continued use should be reassessed daily; a computer alert that requires a response is very helpful, as is a call from the friendly floor nurse asking, “Does this patient really still need his catheter?”
Infection control is everyone’s responsibility and we all need to work together toward this common goal.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.
Big things come in small packages, very small – so small they may even be invisible to the naked eye. Take for instance a huge infection causing multiorgan system failure, disseminated intravascular coagulation, even septic shock refractory to high-dose pressors. This catastrophe may be the end result of exposure to tiny pathogenic microbes that can take down an otherwise healthy 300-pound man, tout suite!
Microorganisms are everywhere. We can’t live without them, but we can’t live with certain ones either. Unless you live in a bubble you are going to be exposed to countless bacteria each and every day. They are in the air we breathe, the water we drink, the beds we sleep in. While it is a given that we all will be continuously exposed to bacteria, having a well-considered strategy to curtail the spread of disease can dramatically decrease the risk that we, our families, and our patients are needlessly exposed to potentially life-threatening organisms.
We all know we are to wash our hands on the way in, and out, of patients’ rooms. This practice is our front line of defense against the spread of numerous potentially lethal diseases. Yet, many clinicians, as well as ancillary hospital personnel, repeatedly fail to abide by this rule, thinking that ‘this one time won’t hurt anything.’ Whether it’s the nurse who rushes into a patient’s room to stop a beeping IV pole or the doctor who eyes a family member in the room and makes a beeline to discuss the discharge plan, all of us have been guilty of entering or leaving a patient’s room without following appropriate infection control standards.
Or, how many times have you followed the protocol meticulously, at least initially, and removed your gown and gloves and washed your hands on your way out the door when the patient remembers another question, or asks you to hand him something that leads to more contact with him or his surroundings? You already washed your hands once, so must you really do it again? After all, what is the likelihood that you pick up (or pass along) any germs anyway? Sometimes, more than we realize. Something as simple as handing a patient his nurses’ call button can expose us to enough C. difficile spores to cause infection in us or others we come into contact with unwittingly. So wash those hands, and wash them again if you touch anything in a patient’s room, even if it is not the patient himself.
Direct observation (AKA “Secret Santas”) can provide invaluable information about adherence to hand hygiene among health care workers and providing feedback is key. This can be unit based, group based, and even provider based. Once collected, this information should be used to drive changes in behavior, which could be punitive or positive; each hospital should decide how to best use its data.
Visitor contact is another important issue and not everyone agrees on how to enforce, or whether to even try to enforce, infection control procedures. The Society for Healthcare Epidemiology of America (SHEA) has several helpful pocket guidelines to address this and other infection control issues. For instance, the society recommends that hospitals consider adopting guidelines to minimize horizontal transmission by visitors, though these guidelines should be feasible to enforce. Factors such as the specific organism and its potential to cause harm are important to consider when developing these guidelines. For instance, the spouse of a patient admitted with influenza has likely already been exposed, and postexposure prophylaxis may be more feasible to her than wearing an uncomfortable mask during an 8-hour hospital visit.
A pharmacy stewardship program is another invaluable infection control tool. With this model, a group of pharmacists, under the direction of an infectious disease specialist, reviews culture results daily and makes recommendations to the physician regarding narrowing antibiotic coverage. I greatly appreciate receiving calls to notify me that the final culture results are in long before I would have actually seen them myself. This allows me to adjust antibiotics in a timely fashion, thus reducing the emergence of drug-resistant organisms or precipitating an unnecessary case of C. difficile.
In addition, written guidelines should be established for indwelling catheters, both urinary and venous. The indication for continued use should be reassessed daily; a computer alert that requires a response is very helpful, as is a call from the friendly floor nurse asking, “Does this patient really still need his catheter?”
Infection control is everyone’s responsibility and we all need to work together toward this common goal.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.

Sorrows hidden in plain sight
“The greatest hazard of all, losing one’s self, can occur very quietly in the world, as if it were nothing at all. No other loss can occur so quietly”
—Søren Kierkegaard
In our interactions with patients we often focus on the medical issue at hand, forgetting the other dimensions of our patients’ lives. Yet these invisible dimensions can have a huge impact on their humanity. I humbly submit that it can be profoundly meaningful, for them and for us, if we paid close attention.

1. JV has rheumatoid arthritis. He is not the most compliant, and I had not seen him in over a year. He was well controlled on Enbrel.
He came to the office one day last week to make an appointment. We gave him one for the next day, but he missed the appointment. When he finally came a week later, I got the real story. He had gotten arrested.
The day he came into my office to ask for an appointment after a prolonged absence, it was because his insurance was denying coverage for his Enbrel. His next stop, after making his appointment, was to the Social Security office to try to sort out his coverage. When asked about whether or not he needed special accommodations, he made a point to mention his hearing loss. However, the person ultimately assigned to help him was not a native English speaker. This made for a very confusing and loud exchange that led to a heated argument with security. It ended with him being led out of the office in handcuffs, and spending the night in jail.
2. Tyler has inflammatory arthritis. He received his diagnosis in Arizona 5 years ago. He was stable on Plaquenil when I met him a year ago, and I only see him every 6 months.
On our third visit, I noticed he had gained weight. He attributed this to the discontinuation of his Dexedrine, in the interest of adjusting his medications for bipolar disorder. I couldn’t remember our second visit very well, but he apologized profusely for having been “lit.” He apparently was so manic that it drove his family crazy. In an effort to get him to take medications for the problem, his sister said: “It’s like living with Vincent van Gogh, except now we have meds for it.”
Now he takes his medications. As a result, his body feels foreign. In the summer, he ran around the backyard all day and night constructing an obstacle course for his dog that he knew he would never get right. Now he is lucky if he gets a few days a week of productive work on his art. He feels dulled; he is not as quick-witted. It is sad, but, he says, this is what society expects of him.
3. Judy is in her mid-70s. That’s not old these days, but she is somewhat crippled by her rheumatoid arthritis. She lived in Manhattan with her husband and enjoyed the city immensely. After her husband passed away, she managed to live in her Manhattan apartment independently for a little bit, but after suffering a fall, she let her children move her to Rhode Island to be closer to them. She has struggled to find her own apartment with amenities that will allow her to remain independent. For the past 3 years she has been in an assisted living facility.
She is so unhappy there. She doesn’t like forced interactions, doesn’t like to gossip, doesn’t like when her neighbors behave like they’re in middle school. It has taken 3 years for the people around her to finally respect her desire to be left alone, to spend her time reading and listening to the opera rather than engaging in idle chitchat that does not interest her at all.
Dr. Chan practices rheumatology in Pawtucket, R.I.
“The greatest hazard of all, losing one’s self, can occur very quietly in the world, as if it were nothing at all. No other loss can occur so quietly”
—Søren Kierkegaard
In our interactions with patients we often focus on the medical issue at hand, forgetting the other dimensions of our patients’ lives. Yet these invisible dimensions can have a huge impact on their humanity. I humbly submit that it can be profoundly meaningful, for them and for us, if we paid close attention.
1. JV has rheumatoid arthritis. He is not the most compliant, and I had not seen him in over a year. He was well controlled on Enbrel.
He came to the office one day last week to make an appointment. We gave him one for the next day, but he missed the appointment. When he finally came a week later, I got the real story. He had gotten arrested.
The day he came into my office to ask for an appointment after a prolonged absence, it was because his insurance was denying coverage for his Enbrel. His next stop, after making his appointment, was to the Social Security office to try to sort out his coverage. When asked about whether or not he needed special accommodations, he made a point to mention his hearing loss. However, the person ultimately assigned to help him was not a native English speaker. This made for a very confusing and loud exchange that led to a heated argument with security. It ended with him being led out of the office in handcuffs, and spending the night in jail.
2. Tyler has inflammatory arthritis. He received his diagnosis in Arizona 5 years ago. He was stable on Plaquenil when I met him a year ago, and I only see him every 6 months.
On our third visit, I noticed he had gained weight. He attributed this to the discontinuation of his Dexedrine, in the interest of adjusting his medications for bipolar disorder. I couldn’t remember our second visit very well, but he apologized profusely for having been “lit.” He apparently was so manic that it drove his family crazy. In an effort to get him to take medications for the problem, his sister said: “It’s like living with Vincent van Gogh, except now we have meds for it.”
Now he takes his medications. As a result, his body feels foreign. In the summer, he ran around the backyard all day and night constructing an obstacle course for his dog that he knew he would never get right. Now he is lucky if he gets a few days a week of productive work on his art. He feels dulled; he is not as quick-witted. It is sad, but, he says, this is what society expects of him.
3. Judy is in her mid-70s. That’s not old these days, but she is somewhat crippled by her rheumatoid arthritis. She lived in Manhattan with her husband and enjoyed the city immensely. After her husband passed away, she managed to live in her Manhattan apartment independently for a little bit, but after suffering a fall, she let her children move her to Rhode Island to be closer to them. She has struggled to find her own apartment with amenities that will allow her to remain independent. For the past 3 years she has been in an assisted living facility.
She is so unhappy there. She doesn’t like forced interactions, doesn’t like to gossip, doesn’t like when her neighbors behave like they’re in middle school. It has taken 3 years for the people around her to finally respect her desire to be left alone, to spend her time reading and listening to the opera rather than engaging in idle chitchat that does not interest her at all.
Dr. Chan practices rheumatology in Pawtucket, R.I.
“The greatest hazard of all, losing one’s self, can occur very quietly in the world, as if it were nothing at all. No other loss can occur so quietly”
—Søren Kierkegaard
In our interactions with patients we often focus on the medical issue at hand, forgetting the other dimensions of our patients’ lives. Yet these invisible dimensions can have a huge impact on their humanity. I humbly submit that it can be profoundly meaningful, for them and for us, if we paid close attention.
1. JV has rheumatoid arthritis. He is not the most compliant, and I had not seen him in over a year. He was well controlled on Enbrel.
He came to the office one day last week to make an appointment. We gave him one for the next day, but he missed the appointment. When he finally came a week later, I got the real story. He had gotten arrested.
The day he came into my office to ask for an appointment after a prolonged absence, it was because his insurance was denying coverage for his Enbrel. His next stop, after making his appointment, was to the Social Security office to try to sort out his coverage. When asked about whether or not he needed special accommodations, he made a point to mention his hearing loss. However, the person ultimately assigned to help him was not a native English speaker. This made for a very confusing and loud exchange that led to a heated argument with security. It ended with him being led out of the office in handcuffs, and spending the night in jail.
2. Tyler has inflammatory arthritis. He received his diagnosis in Arizona 5 years ago. He was stable on Plaquenil when I met him a year ago, and I only see him every 6 months.
On our third visit, I noticed he had gained weight. He attributed this to the discontinuation of his Dexedrine, in the interest of adjusting his medications for bipolar disorder. I couldn’t remember our second visit very well, but he apologized profusely for having been “lit.” He apparently was so manic that it drove his family crazy. In an effort to get him to take medications for the problem, his sister said: “It’s like living with Vincent van Gogh, except now we have meds for it.”
Now he takes his medications. As a result, his body feels foreign. In the summer, he ran around the backyard all day and night constructing an obstacle course for his dog that he knew he would never get right. Now he is lucky if he gets a few days a week of productive work on his art. He feels dulled; he is not as quick-witted. It is sad, but, he says, this is what society expects of him.
3. Judy is in her mid-70s. That’s not old these days, but she is somewhat crippled by her rheumatoid arthritis. She lived in Manhattan with her husband and enjoyed the city immensely. After her husband passed away, she managed to live in her Manhattan apartment independently for a little bit, but after suffering a fall, she let her children move her to Rhode Island to be closer to them. She has struggled to find her own apartment with amenities that will allow her to remain independent. For the past 3 years she has been in an assisted living facility.
She is so unhappy there. She doesn’t like forced interactions, doesn’t like to gossip, doesn’t like when her neighbors behave like they’re in middle school. It has taken 3 years for the people around her to finally respect her desire to be left alone, to spend her time reading and listening to the opera rather than engaging in idle chitchat that does not interest her at all.
Dr. Chan practices rheumatology in Pawtucket, R.I.

#payattention
Social media consumes the attention of the majority of teens. It is a place to express yourself, flirt, intimidate, and keep them up to date with the latest happenings in the social circles. But, teens are using social media for much more.

Instagram, a social media site comprising photographs followed by comments, is one of the most common sites used by teens. They post everything from the meal they are eating to the new love in their life and everything in between.
A hashtag is a type of label or metadata tag used on social networks and microblogging services, which makes it easier for users to find messages with a specific theme or content. Users create hashtags by placing the hash character # (the number sign) in front of a word or unspaced phrase, either in the main text of a message or at the end. Searching for that hashtag will then present each message that has been tagged with it.1 Although teens seem to prefer simple phrases, these hashtags are used to link users to what many refer to as “Secret Society.”
For example, if a teen girl was “cutting” or interested in connecting with other teens that cut, putting #cat would link her to several social communities with the related topic. Similarly, #selfharm was the initial term used to connect to this secret society. When that was shut down by the social media site, it resurfaced as #selfharmmm2.
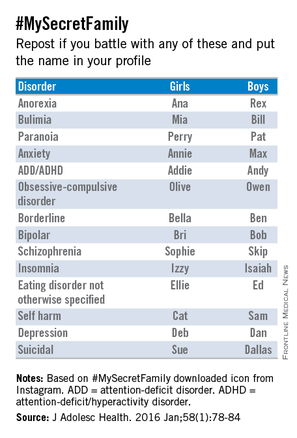
#MySecretFamily is a very popular hashtag that connects teens struggling with a variety of mental illnesses. Teens are instructed to put various names in their profile to identify which mental illness they are battling. For example, depression would be identified as “DEB” for a girl and “DAN” for a boy. The chart below lists various disorders.2
Nonsuicidal self-injury (NSSI) or deliberate destruction of one’s body in the absence of suicidal intent3 is most common in the middle school ages, and exposure to peer NSSI may increase the risk of engaging these behaviors.2,4 Although distinct from suicidal behaviors, there is a comorbidity between them. The normalization of these behaviors through social media and acceptance into the this “Secret Society” can only augment the risk of NSSI.
Parents not only need to be educated about the importance of monitoring their children’s social media but also about what to look for that may be a sign that something more serious is going on with them.
Although we hear so much of the negative impact of social media, it also can be a tool for early intervention.
References
1. Oxford English Dictionary, definition of “hashtag.”
2. J Adolesc Health. 2016 Jan;58(1):78-84.
4. Dev Psychol. 2006 May;42(3):407-17.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
Social media consumes the attention of the majority of teens. It is a place to express yourself, flirt, intimidate, and keep them up to date with the latest happenings in the social circles. But, teens are using social media for much more.
Instagram, a social media site comprising photographs followed by comments, is one of the most common sites used by teens. They post everything from the meal they are eating to the new love in their life and everything in between.
A hashtag is a type of label or metadata tag used on social networks and microblogging services, which makes it easier for users to find messages with a specific theme or content. Users create hashtags by placing the hash character # (the number sign) in front of a word or unspaced phrase, either in the main text of a message or at the end. Searching for that hashtag will then present each message that has been tagged with it.1 Although teens seem to prefer simple phrases, these hashtags are used to link users to what many refer to as “Secret Society.”
For example, if a teen girl was “cutting” or interested in connecting with other teens that cut, putting #cat would link her to several social communities with the related topic. Similarly, #selfharm was the initial term used to connect to this secret society. When that was shut down by the social media site, it resurfaced as #selfharmmm2.
#MySecretFamily is a very popular hashtag that connects teens struggling with a variety of mental illnesses. Teens are instructed to put various names in their profile to identify which mental illness they are battling. For example, depression would be identified as “DEB” for a girl and “DAN” for a boy. The chart below lists various disorders.2
Nonsuicidal self-injury (NSSI) or deliberate destruction of one’s body in the absence of suicidal intent3 is most common in the middle school ages, and exposure to peer NSSI may increase the risk of engaging these behaviors.2,4 Although distinct from suicidal behaviors, there is a comorbidity between them. The normalization of these behaviors through social media and acceptance into the this “Secret Society” can only augment the risk of NSSI.
Parents not only need to be educated about the importance of monitoring their children’s social media but also about what to look for that may be a sign that something more serious is going on with them.
Although we hear so much of the negative impact of social media, it also can be a tool for early intervention.
References
1. Oxford English Dictionary, definition of “hashtag.”
2. J Adolesc Health. 2016 Jan;58(1):78-84.
4. Dev Psychol. 2006 May;42(3):407-17.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
Social media consumes the attention of the majority of teens. It is a place to express yourself, flirt, intimidate, and keep them up to date with the latest happenings in the social circles. But, teens are using social media for much more.
Instagram, a social media site comprising photographs followed by comments, is one of the most common sites used by teens. They post everything from the meal they are eating to the new love in their life and everything in between.
A hashtag is a type of label or metadata tag used on social networks and microblogging services, which makes it easier for users to find messages with a specific theme or content. Users create hashtags by placing the hash character # (the number sign) in front of a word or unspaced phrase, either in the main text of a message or at the end. Searching for that hashtag will then present each message that has been tagged with it.1 Although teens seem to prefer simple phrases, these hashtags are used to link users to what many refer to as “Secret Society.”
For example, if a teen girl was “cutting” or interested in connecting with other teens that cut, putting #cat would link her to several social communities with the related topic. Similarly, #selfharm was the initial term used to connect to this secret society. When that was shut down by the social media site, it resurfaced as #selfharmmm2.
#MySecretFamily is a very popular hashtag that connects teens struggling with a variety of mental illnesses. Teens are instructed to put various names in their profile to identify which mental illness they are battling. For example, depression would be identified as “DEB” for a girl and “DAN” for a boy. The chart below lists various disorders.2
Nonsuicidal self-injury (NSSI) or deliberate destruction of one’s body in the absence of suicidal intent3 is most common in the middle school ages, and exposure to peer NSSI may increase the risk of engaging these behaviors.2,4 Although distinct from suicidal behaviors, there is a comorbidity between them. The normalization of these behaviors through social media and acceptance into the this “Secret Society” can only augment the risk of NSSI.
Parents not only need to be educated about the importance of monitoring their children’s social media but also about what to look for that may be a sign that something more serious is going on with them.
Although we hear so much of the negative impact of social media, it also can be a tool for early intervention.
References
1. Oxford English Dictionary, definition of “hashtag.”
2. J Adolesc Health. 2016 Jan;58(1):78-84.
4. Dev Psychol. 2006 May;42(3):407-17.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.

Treating influenza: A guide to antiviral safety in pregnancy
Oseltamivir and zanamivir are competitive inhibitors for the neuraminidase enzyme for the influenza virus. They block the surface receptor enzyme and prevent release of virus from the host cell, thus limiting propagation of the infection. These medications can be given as prophylaxis after exposure to influenza or can be given therapeutically for a suspected or confirmed infection. Oseltamivir is recommended for treatment of suspected or confirmed influenza infection in the special population of pregnant women, as the risk for complications of influenza is increased in this group.
Safety evidence
However, there are limited data on the safety and efficacy of the neuraminidase inhibitors in pregnancy. With respect to safety, there have been seven publications in the literature addressing the risk for major birth defects following treatment or prophylaxis with one or both of these products, with the majority of the published data relating to oseltamivir exposure.

In a review by Tanaka et al. in 2009, 90 pregnancies treated therapeutically with oseltamivir in the first trimester were reported to two teratogen information services in Japan; one major birth defect (1.1%) was reported (CMAJ. 2009 Jul 7;181[1-2]:55-8). A year later, Greer et al. published a retrospective chart review at a Texas hospital between 2003 and 2008. During that period, 137 pregnancies that involved a pharmacy record of dispensing of oseltamivir were identified. Of these, 18 were dispensed in the first trimester, and none were linked to a major birth defect outcome (Obstet Gynecol. 2010 Apr;115[4]:711-6).
A 2011 record linkage study in Sweden identified 86 pregnant women for whom oseltamivir (n=81) or zanamivir had been prescribed. Of these, four were linked to a major birth defect in the infant; however, only one of the four prescriptions had been filled in the first trimester (Pharmacoepidemiol Drug Saf. 2011 Oct;20[10]:1030-4). In 2013, Saito et al. reported on a case series gathered from 157 obstetric facilities in Japan. Among 156 infants born to women exposed to oseltamivir in the first trimester, 2 (1.3%) were reported to have a major congenital anomaly; there were no congenital malformations reported in the 15 first-trimester exposures to zanamivir (Am J Obstet Gynecol. 2013 Aug;209[2[:130.e1-9).
In 2014, a teratogen information service in the United Kingdom reported on eight first-trimester exposures to oseltamivir and 37 to zanamivir, with no major birth defects noted in either group (BJOG. 2014 Jun;121[7]:901-6). Additionally, a French prescription database study identified 49 pregnancies thought to be exposed to oseltamivir in the first trimester with one reported congenital anomaly (BJOG. 2014 Jun;121[7]:895-900).
Finally, the manufacturer of oseltamivir published a summary of pregnancies from global pharmacovigilance data accumulated through spontaneous reports and other studies between 2000 and 2012 (Pharmacoepidemiol Drug Saf. 2014 Oct;23[10]:1035-42). Outcomes were available for 1,875 infants. Among these, 81 (4.3%) had major birth defects. However, following case review, the authors indicated that only 11 of the defects (occurring in 9 infants) were biologically plausible based on the timing of the exposure to oseltamivir.
Efficacy examined
With respect to efficacy, two small studies have addressed the pharmacokinetics of oseltamivir in pregnancy to determine if the recommended dosages for nonpregnant individuals are appropriate for pregnancy.
In the earlier of the two studies, Greer et al. looked at the pharmacokinetics of oseltamivir in 30 pregnant women, 10 in each of the three trimesters, who were taking 75 mg of the drug either once or twice daily. Maternal samples were drawn before and after the first dose of oseltamivir. They found little evidence of differences across the three trimesters and concluded that the parent drug values were in the pharmacologic range for clinical efficacy (Am J Obstet Gynecol. 2011 Jun;204[6 Suppl 1]:S89-93).
In contrast, Pillai et al. enrolled a small sample of women being treated with oseltamivir; they evaluated pharmacokinetics for the active metabolite of oseltamivir following 48 or more hours of treatment in 29 pregnant and 35 nonpregnant women (Br J Clin Pharmacol. 2015 Nov;80[5]:1042-50). Significantly lower levels of the active metabolite were noted in the pregnant women, compared with nonpregnant women. The authors suggested that the physiologic changes of pregnancy, correlated with increased renal clearance, produced an approximate 30% lower exposure to the drug in the pregnant state. While they were not able to relate this to maternal or infant outcomes, this finding suggested that further work is needed to determine if dosing recommendations should be adjusted in pregnancy.
The current recommendation is that pregnant women or women within 2 weeks post partum be given oseltamivir for treatment of suspected or confirmed influenza regardless of trimester of pregnancy. The limited safety data that are currently available have not suggested an increased risk for major birth defects following treatment with this product. However, the data are sparse for oseltamivir and even more so for zanamivir. Larger studies focused on these treatments are needed.
Dr. Chambers is professor of pediatrics and director of clinical research at Rady Children’s Hospital, and associate director of the Clinical and Translational Research Institute at the University of California, San Diego. She is director of MotherToBaby California, past president of the Organization of Teratology Information Specialists, and past president of the Teratology Society. She reported having no financial disclosures relevant to this column, but has received research funding Roche-Genentech and GlaxoSmithKline unrelated to antiviral medications. Email her at obnews@frontlinemedcom.com.
Oseltamivir and zanamivir are competitive inhibitors for the neuraminidase enzyme for the influenza virus. They block the surface receptor enzyme and prevent release of virus from the host cell, thus limiting propagation of the infection. These medications can be given as prophylaxis after exposure to influenza or can be given therapeutically for a suspected or confirmed infection. Oseltamivir is recommended for treatment of suspected or confirmed influenza infection in the special population of pregnant women, as the risk for complications of influenza is increased in this group.
Safety evidence
However, there are limited data on the safety and efficacy of the neuraminidase inhibitors in pregnancy. With respect to safety, there have been seven publications in the literature addressing the risk for major birth defects following treatment or prophylaxis with one or both of these products, with the majority of the published data relating to oseltamivir exposure.
In a review by Tanaka et al. in 2009, 90 pregnancies treated therapeutically with oseltamivir in the first trimester were reported to two teratogen information services in Japan; one major birth defect (1.1%) was reported (CMAJ. 2009 Jul 7;181[1-2]:55-8). A year later, Greer et al. published a retrospective chart review at a Texas hospital between 2003 and 2008. During that period, 137 pregnancies that involved a pharmacy record of dispensing of oseltamivir were identified. Of these, 18 were dispensed in the first trimester, and none were linked to a major birth defect outcome (Obstet Gynecol. 2010 Apr;115[4]:711-6).
A 2011 record linkage study in Sweden identified 86 pregnant women for whom oseltamivir (n=81) or zanamivir had been prescribed. Of these, four were linked to a major birth defect in the infant; however, only one of the four prescriptions had been filled in the first trimester (Pharmacoepidemiol Drug Saf. 2011 Oct;20[10]:1030-4). In 2013, Saito et al. reported on a case series gathered from 157 obstetric facilities in Japan. Among 156 infants born to women exposed to oseltamivir in the first trimester, 2 (1.3%) were reported to have a major congenital anomaly; there were no congenital malformations reported in the 15 first-trimester exposures to zanamivir (Am J Obstet Gynecol. 2013 Aug;209[2[:130.e1-9).
In 2014, a teratogen information service in the United Kingdom reported on eight first-trimester exposures to oseltamivir and 37 to zanamivir, with no major birth defects noted in either group (BJOG. 2014 Jun;121[7]:901-6). Additionally, a French prescription database study identified 49 pregnancies thought to be exposed to oseltamivir in the first trimester with one reported congenital anomaly (BJOG. 2014 Jun;121[7]:895-900).
Finally, the manufacturer of oseltamivir published a summary of pregnancies from global pharmacovigilance data accumulated through spontaneous reports and other studies between 2000 and 2012 (Pharmacoepidemiol Drug Saf. 2014 Oct;23[10]:1035-42). Outcomes were available for 1,875 infants. Among these, 81 (4.3%) had major birth defects. However, following case review, the authors indicated that only 11 of the defects (occurring in 9 infants) were biologically plausible based on the timing of the exposure to oseltamivir.
Efficacy examined
With respect to efficacy, two small studies have addressed the pharmacokinetics of oseltamivir in pregnancy to determine if the recommended dosages for nonpregnant individuals are appropriate for pregnancy.
In the earlier of the two studies, Greer et al. looked at the pharmacokinetics of oseltamivir in 30 pregnant women, 10 in each of the three trimesters, who were taking 75 mg of the drug either once or twice daily. Maternal samples were drawn before and after the first dose of oseltamivir. They found little evidence of differences across the three trimesters and concluded that the parent drug values were in the pharmacologic range for clinical efficacy (Am J Obstet Gynecol. 2011 Jun;204[6 Suppl 1]:S89-93).
In contrast, Pillai et al. enrolled a small sample of women being treated with oseltamivir; they evaluated pharmacokinetics for the active metabolite of oseltamivir following 48 or more hours of treatment in 29 pregnant and 35 nonpregnant women (Br J Clin Pharmacol. 2015 Nov;80[5]:1042-50). Significantly lower levels of the active metabolite were noted in the pregnant women, compared with nonpregnant women. The authors suggested that the physiologic changes of pregnancy, correlated with increased renal clearance, produced an approximate 30% lower exposure to the drug in the pregnant state. While they were not able to relate this to maternal or infant outcomes, this finding suggested that further work is needed to determine if dosing recommendations should be adjusted in pregnancy.
The current recommendation is that pregnant women or women within 2 weeks post partum be given oseltamivir for treatment of suspected or confirmed influenza regardless of trimester of pregnancy. The limited safety data that are currently available have not suggested an increased risk for major birth defects following treatment with this product. However, the data are sparse for oseltamivir and even more so for zanamivir. Larger studies focused on these treatments are needed.
Dr. Chambers is professor of pediatrics and director of clinical research at Rady Children’s Hospital, and associate director of the Clinical and Translational Research Institute at the University of California, San Diego. She is director of MotherToBaby California, past president of the Organization of Teratology Information Specialists, and past president of the Teratology Society. She reported having no financial disclosures relevant to this column, but has received research funding Roche-Genentech and GlaxoSmithKline unrelated to antiviral medications. Email her at obnews@frontlinemedcom.com.
Oseltamivir and zanamivir are competitive inhibitors for the neuraminidase enzyme for the influenza virus. They block the surface receptor enzyme and prevent release of virus from the host cell, thus limiting propagation of the infection. These medications can be given as prophylaxis after exposure to influenza or can be given therapeutically for a suspected or confirmed infection. Oseltamivir is recommended for treatment of suspected or confirmed influenza infection in the special population of pregnant women, as the risk for complications of influenza is increased in this group.
Safety evidence
However, there are limited data on the safety and efficacy of the neuraminidase inhibitors in pregnancy. With respect to safety, there have been seven publications in the literature addressing the risk for major birth defects following treatment or prophylaxis with one or both of these products, with the majority of the published data relating to oseltamivir exposure.
In a review by Tanaka et al. in 2009, 90 pregnancies treated therapeutically with oseltamivir in the first trimester were reported to two teratogen information services in Japan; one major birth defect (1.1%) was reported (CMAJ. 2009 Jul 7;181[1-2]:55-8). A year later, Greer et al. published a retrospective chart review at a Texas hospital between 2003 and 2008. During that period, 137 pregnancies that involved a pharmacy record of dispensing of oseltamivir were identified. Of these, 18 were dispensed in the first trimester, and none were linked to a major birth defect outcome (Obstet Gynecol. 2010 Apr;115[4]:711-6).
A 2011 record linkage study in Sweden identified 86 pregnant women for whom oseltamivir (n=81) or zanamivir had been prescribed. Of these, four were linked to a major birth defect in the infant; however, only one of the four prescriptions had been filled in the first trimester (Pharmacoepidemiol Drug Saf. 2011 Oct;20[10]:1030-4). In 2013, Saito et al. reported on a case series gathered from 157 obstetric facilities in Japan. Among 156 infants born to women exposed to oseltamivir in the first trimester, 2 (1.3%) were reported to have a major congenital anomaly; there were no congenital malformations reported in the 15 first-trimester exposures to zanamivir (Am J Obstet Gynecol. 2013 Aug;209[2[:130.e1-9).
In 2014, a teratogen information service in the United Kingdom reported on eight first-trimester exposures to oseltamivir and 37 to zanamivir, with no major birth defects noted in either group (BJOG. 2014 Jun;121[7]:901-6). Additionally, a French prescription database study identified 49 pregnancies thought to be exposed to oseltamivir in the first trimester with one reported congenital anomaly (BJOG. 2014 Jun;121[7]:895-900).
Finally, the manufacturer of oseltamivir published a summary of pregnancies from global pharmacovigilance data accumulated through spontaneous reports and other studies between 2000 and 2012 (Pharmacoepidemiol Drug Saf. 2014 Oct;23[10]:1035-42). Outcomes were available for 1,875 infants. Among these, 81 (4.3%) had major birth defects. However, following case review, the authors indicated that only 11 of the defects (occurring in 9 infants) were biologically plausible based on the timing of the exposure to oseltamivir.
Efficacy examined
With respect to efficacy, two small studies have addressed the pharmacokinetics of oseltamivir in pregnancy to determine if the recommended dosages for nonpregnant individuals are appropriate for pregnancy.
In the earlier of the two studies, Greer et al. looked at the pharmacokinetics of oseltamivir in 30 pregnant women, 10 in each of the three trimesters, who were taking 75 mg of the drug either once or twice daily. Maternal samples were drawn before and after the first dose of oseltamivir. They found little evidence of differences across the three trimesters and concluded that the parent drug values were in the pharmacologic range for clinical efficacy (Am J Obstet Gynecol. 2011 Jun;204[6 Suppl 1]:S89-93).
In contrast, Pillai et al. enrolled a small sample of women being treated with oseltamivir; they evaluated pharmacokinetics for the active metabolite of oseltamivir following 48 or more hours of treatment in 29 pregnant and 35 nonpregnant women (Br J Clin Pharmacol. 2015 Nov;80[5]:1042-50). Significantly lower levels of the active metabolite were noted in the pregnant women, compared with nonpregnant women. The authors suggested that the physiologic changes of pregnancy, correlated with increased renal clearance, produced an approximate 30% lower exposure to the drug in the pregnant state. While they were not able to relate this to maternal or infant outcomes, this finding suggested that further work is needed to determine if dosing recommendations should be adjusted in pregnancy.
The current recommendation is that pregnant women or women within 2 weeks post partum be given oseltamivir for treatment of suspected or confirmed influenza regardless of trimester of pregnancy. The limited safety data that are currently available have not suggested an increased risk for major birth defects following treatment with this product. However, the data are sparse for oseltamivir and even more so for zanamivir. Larger studies focused on these treatments are needed.
Dr. Chambers is professor of pediatrics and director of clinical research at Rady Children’s Hospital, and associate director of the Clinical and Translational Research Institute at the University of California, San Diego. She is director of MotherToBaby California, past president of the Organization of Teratology Information Specialists, and past president of the Teratology Society. She reported having no financial disclosures relevant to this column, but has received research funding Roche-Genentech and GlaxoSmithKline unrelated to antiviral medications. Email her at obnews@frontlinemedcom.com.

‘We need to protect the brain’ Addressing the growing problem of chronic traumatic encephalopathy
The National Football League (NFL) had its highest concussion tally last year: 182 such injuries reported1 in the 2014-2015 regular season. The true rate of concussion in the NFL is likely higher, as a result of multiple factors (fear of “letting the team [or the coach] down,” fear of retaliation from team owners,2 etc.).
To simply call a head injury a “concussion” is a disservice to players and their family: Any blow to the head, severe or otherwise, has the potential to cause microvascular disruption in the brain; repeated blows to the head undoubtedly cause further damage.
In reality, a “concussion” is a mild traumatic brain injury (mTBI). With repeated blows, an mTBI can lead to chronic traumatic encephalopathy (CTE). In 2015, eighty-seven of 91 brains from autopsied former NFL players displayed some stage of CTE.3
Pathophysiology and presentation
CTE comprises 4 histological stages; Stage 4 is the most advanced. Alzheimer’s disease (AD) and CTE display similarities, which suggests a separate classification of CTE-AD; the presence of amyloid β plaques correlates with (1) more severe hyperphosphorylated tau (pTau) pathology and (2) advanced stages of the disease and clinical presentations. Death tends to occur 10 years earlier in CTE-AD than in AD, suggesting that repetitive mTBI might change the deposition and accumulation of amyloid β plaques, and even accelerate the aging process in the brain.4
Symptoms. The case series by Omalu et al4 (which inspired the 2015 motion picture Concussion) and the case series presented by McKee et al5 described severe psychiatric symptoms associated with CTE:
- decreased speed of information processing
- increase in religiosity
- lack of insight
- poor judgment
- involvement in illegal activities
- substance abuse
- indiscretion
- verbal and physical abuse
- problems with interpersonal relationships
- isolation
- restlessness and hyperactivity
- somatic complaints.
The 2 groups of researchers also noted hopelessness, social phobia, anxiety, agitation, mania, labile mood, insomnia, explosivity, and suicidal ideation, attempt, and completion.4,5
By Stage 4, all affected patients are symptomatic. Cognitive impairment is severe; many are described as having “severe memory loss with dementia,”5 “profound” inattention and loss of concentration,5 and dysarthria. Paranoia may develop. Mood symptoms can be severe: Approximately 31% of subjects studied have contemplated suicide; of those, 26% had “suicidal tendencies” and 14% completed suicide.5
Two distinct types of CTE progression are apparent:
- patients who display cognitive deficits first; they progress to dementia but live longer
- patients who display mood and behavioral symptoms first; they tend to be younger, more violent, depressed, and explosive.6
CTE cannot be diagnosed with imaging. There are, however, a few positron emission tomography (PET) ligands for pTau that show promise:
- [F-18]FDDNP, which consistently identifies pTau deposits in brains in which CTE is clinically suspected, in the same distribution of pTau neurofibrillary tangles on autopsy.
- [11C]DPA-713, which detected TBI-related inflammation of neurons in 9 former NFL players in whom CTE was suspected based on the clinical presentation.
- PiB amyloid ligand, under investigation for use in PET neuroimaging.7
Casualties
In January 2016 alone, at least 3 former NFL players were found to have CTE posthumously.
Earl Morrall. Former quarterback who had a 21-year NFL career. Official cause of death in 2014 at age 79 was recorded as “complications of Parkinson’s disease.” In 2016, Stage-4 CTE was discovered on autopsy.8
Ken Stabler. Former quarterback for several NFL teams over 15 seasons. Died of colon cancer at age 69 in 2015. On autopsy, was found to have Stage-3 CTE.9
Tyler Sash. Former University of Iowa and New York Giants football player. Died in September 2015 at age 27 of an apparent drug overdose; posthumously, determined to have Stage-2 CTE. His family reported memory loss, minor fits of rage, confusion, inattention, lack of focus, and chronic pain.
Sash’s mother said, “My son knew something was wrong, but he couldn’t express it. He was such a good person, and it’s sad that he struggled so with this—not knowing where to go with it. Now it makes sense.”10 Sash played 16 years of football in all, sustaining at least 5 concussions. (“If you’ve played football, you know there are often other incidents [of head trauma],” Sash’s father said.10)
Cultural and medical mindsets about contact sports
In the United States, children as young as age 5, with a low weight limit of 35 pounds, routinely are introduced to football.11 Reports of 5 high school players dying from football-related injury in the 2014 season, and 3 deaths in the 2015 season, led a St. Louis, Missouri, area school district to defund their football program entirely. The district’s 2015 homecoming game was a soccer match; students and parents seemed to embrace the change.12
On its face, soccer seems a good alternative to football. When children are instructed to “head” the ball, however, concern arises about CTE: Mild CTE changes have been reported in 2 young soccer players, and late-stage CTE changes were seen in a retired soccer player with dementia.13
Perhaps most disturbing is that players who develop symptoms of CTE, or are at risk, are unlikely to seek psychiatric help. We, as psychiatric clinicians, must be diligent about questioning young patients about their extracurricular activities. It is not enough to simply ask about a history of head trauma: Ask patients about any blow to the head, and don’t limit your questioning to whether they sustained a “concussion” during practice or play.
When speaking with adult and geriatric patients, ask about a history of playing interscholastic or collegiate contact sports, such as football, hockey, and soccer.
Is the solution to better shield the head?
That is not a solution: Helmets and other protective headgear appear to be insufficient to protect the brain from traumatic injury. Perhaps keeping children from engaging in violent sports that put them at high risk of CTE later is the preventive approach that merits the most attention.
1. Blackstone J. NFL tackles alarming increase in concussions. CBS News. http://www.cbsnews.com/news/nfl-studying-how-to-tackle-alarming-increase-in-concussions. Published February 2, 2016. Accessed February 3, 2016.
2. McNamee M, Partridge B, Anderson L. Concussion ethics and sports medicine. Clin Sports Med. 2015;35(2):257-267.
3. Abreu MA, Cromartie FJ, Spradley BD; United States Sports Academy. Chronic traumatic encephalopathy (CTE) and former National Football League player suicides. The Sport Journal. http://thesportjournal.org/article/chronic-traumatic-encephalopathy-cte-and-former-national-football-league-player-suicides. Published January 29, 2016. Accessed January 29, 2016.
4. Omalu B, Bailes J, Hamilton RL, et al. Emerging histomorphologic phenotypes of chronic traumatic encephalopathy in american athletes. Neurosurgery. 2011;69(1):173-183; discussion 183.
5. McKee AC, Stern RA, Nowinski CJ, et al. The spectrum of disease in chronic traumatic encephalopathy. Brain. 2013;136(pt 1):43-64.
6. Stern RA, Daneshvar DH, Baugh CM, et al. Clinical presentation of chronic traumatic encephalopathy. Neurology. 2013;81(13):1122-1129.
7. Eisenmenger LB, Huo EJ, Hoffman JM, et al. Advances in PET imaging of degenerative, cerebrovascular, and traumatic causes of dementia. Semin Nucl Med. 2016;46(1):57-87.
8. Jackson B. Report: former Miami Dolphins QB Earl Morrall had brain disease CTE. Miami Herald. http://www.miamiherald.com/sports/nfl/miami-dolphins/article58794523.html. Published February 5, 2016. Accessed February 6, 2016.
9. Fantz A. Ex-NFL player Ken Stabler had concussion disease CTE, doctor says. CNN. http://www.cnn.com/2016/02/03/health/ken-stabler-cte. Updated February 4, 2016. Accessed February 9, 2016.
10. Pennington B. C.T.E. is found in an Ex-Giant Tyler Sash, who died at 27. The New York Times. http://www.nytimes.com/2016/01/27/sports/football/former-giants-safety-tyler-sash-found-to-have-cte.html?_r=0. Published January 26, 2016. Accessed January 27, 2016.
11. Pop Warner Little Scholars, Inc. Ages and weights for tackle football programs. http://www.popwarner.com/football/footballstructure.htm. Accessed February 5, 2016.
12. Fowler L. No football for homecoming? No problem at Maplewood-Richmond Heights High. St. Louis Post Dispatch. http://www.stltoday.com/news/local/education/no-football-for-homecoming-no-problem-at-maplewood-richmond-heights/article_cc8dc31b-5097-5114-ba9b-9b3584f478b9.html. Published October 9, 2015. Accessed February 3, 2016.
13. Hales C, Neill S, Gearing M, et al. Late-stage CTE pathology in a retired soccer player with dementia. Neurology. 2014;83(24):2307-2309. doi: 10.1212/WNL.0000000000001081.
The National Football League (NFL) had its highest concussion tally last year: 182 such injuries reported1 in the 2014-2015 regular season. The true rate of concussion in the NFL is likely higher, as a result of multiple factors (fear of “letting the team [or the coach] down,” fear of retaliation from team owners,2 etc.).
To simply call a head injury a “concussion” is a disservice to players and their family: Any blow to the head, severe or otherwise, has the potential to cause microvascular disruption in the brain; repeated blows to the head undoubtedly cause further damage.
In reality, a “concussion” is a mild traumatic brain injury (mTBI). With repeated blows, an mTBI can lead to chronic traumatic encephalopathy (CTE). In 2015, eighty-seven of 91 brains from autopsied former NFL players displayed some stage of CTE.3
Pathophysiology and presentation
CTE comprises 4 histological stages; Stage 4 is the most advanced. Alzheimer’s disease (AD) and CTE display similarities, which suggests a separate classification of CTE-AD; the presence of amyloid β plaques correlates with (1) more severe hyperphosphorylated tau (pTau) pathology and (2) advanced stages of the disease and clinical presentations. Death tends to occur 10 years earlier in CTE-AD than in AD, suggesting that repetitive mTBI might change the deposition and accumulation of amyloid β plaques, and even accelerate the aging process in the brain.4
Symptoms. The case series by Omalu et al4 (which inspired the 2015 motion picture Concussion) and the case series presented by McKee et al5 described severe psychiatric symptoms associated with CTE:
- decreased speed of information processing
- increase in religiosity
- lack of insight
- poor judgment
- involvement in illegal activities
- substance abuse
- indiscretion
- verbal and physical abuse
- problems with interpersonal relationships
- isolation
- restlessness and hyperactivity
- somatic complaints.
The 2 groups of researchers also noted hopelessness, social phobia, anxiety, agitation, mania, labile mood, insomnia, explosivity, and suicidal ideation, attempt, and completion.4,5
By Stage 4, all affected patients are symptomatic. Cognitive impairment is severe; many are described as having “severe memory loss with dementia,”5 “profound” inattention and loss of concentration,5 and dysarthria. Paranoia may develop. Mood symptoms can be severe: Approximately 31% of subjects studied have contemplated suicide; of those, 26% had “suicidal tendencies” and 14% completed suicide.5
Two distinct types of CTE progression are apparent:
- patients who display cognitive deficits first; they progress to dementia but live longer
- patients who display mood and behavioral symptoms first; they tend to be younger, more violent, depressed, and explosive.6
CTE cannot be diagnosed with imaging. There are, however, a few positron emission tomography (PET) ligands for pTau that show promise:
- [F-18]FDDNP, which consistently identifies pTau deposits in brains in which CTE is clinically suspected, in the same distribution of pTau neurofibrillary tangles on autopsy.
- [11C]DPA-713, which detected TBI-related inflammation of neurons in 9 former NFL players in whom CTE was suspected based on the clinical presentation.
- PiB amyloid ligand, under investigation for use in PET neuroimaging.7
Casualties
In January 2016 alone, at least 3 former NFL players were found to have CTE posthumously.
Earl Morrall. Former quarterback who had a 21-year NFL career. Official cause of death in 2014 at age 79 was recorded as “complications of Parkinson’s disease.” In 2016, Stage-4 CTE was discovered on autopsy.8
Ken Stabler. Former quarterback for several NFL teams over 15 seasons. Died of colon cancer at age 69 in 2015. On autopsy, was found to have Stage-3 CTE.9
Tyler Sash. Former University of Iowa and New York Giants football player. Died in September 2015 at age 27 of an apparent drug overdose; posthumously, determined to have Stage-2 CTE. His family reported memory loss, minor fits of rage, confusion, inattention, lack of focus, and chronic pain.
Sash’s mother said, “My son knew something was wrong, but he couldn’t express it. He was such a good person, and it’s sad that he struggled so with this—not knowing where to go with it. Now it makes sense.”10 Sash played 16 years of football in all, sustaining at least 5 concussions. (“If you’ve played football, you know there are often other incidents [of head trauma],” Sash’s father said.10)
Cultural and medical mindsets about contact sports
In the United States, children as young as age 5, with a low weight limit of 35 pounds, routinely are introduced to football.11 Reports of 5 high school players dying from football-related injury in the 2014 season, and 3 deaths in the 2015 season, led a St. Louis, Missouri, area school district to defund their football program entirely. The district’s 2015 homecoming game was a soccer match; students and parents seemed to embrace the change.12
On its face, soccer seems a good alternative to football. When children are instructed to “head” the ball, however, concern arises about CTE: Mild CTE changes have been reported in 2 young soccer players, and late-stage CTE changes were seen in a retired soccer player with dementia.13
Perhaps most disturbing is that players who develop symptoms of CTE, or are at risk, are unlikely to seek psychiatric help. We, as psychiatric clinicians, must be diligent about questioning young patients about their extracurricular activities. It is not enough to simply ask about a history of head trauma: Ask patients about any blow to the head, and don’t limit your questioning to whether they sustained a “concussion” during practice or play.
When speaking with adult and geriatric patients, ask about a history of playing interscholastic or collegiate contact sports, such as football, hockey, and soccer.
Is the solution to better shield the head?
That is not a solution: Helmets and other protective headgear appear to be insufficient to protect the brain from traumatic injury. Perhaps keeping children from engaging in violent sports that put them at high risk of CTE later is the preventive approach that merits the most attention.
The National Football League (NFL) had its highest concussion tally last year: 182 such injuries reported1 in the 2014-2015 regular season. The true rate of concussion in the NFL is likely higher, as a result of multiple factors (fear of “letting the team [or the coach] down,” fear of retaliation from team owners,2 etc.).
To simply call a head injury a “concussion” is a disservice to players and their family: Any blow to the head, severe or otherwise, has the potential to cause microvascular disruption in the brain; repeated blows to the head undoubtedly cause further damage.
In reality, a “concussion” is a mild traumatic brain injury (mTBI). With repeated blows, an mTBI can lead to chronic traumatic encephalopathy (CTE). In 2015, eighty-seven of 91 brains from autopsied former NFL players displayed some stage of CTE.3
Pathophysiology and presentation
CTE comprises 4 histological stages; Stage 4 is the most advanced. Alzheimer’s disease (AD) and CTE display similarities, which suggests a separate classification of CTE-AD; the presence of amyloid β plaques correlates with (1) more severe hyperphosphorylated tau (pTau) pathology and (2) advanced stages of the disease and clinical presentations. Death tends to occur 10 years earlier in CTE-AD than in AD, suggesting that repetitive mTBI might change the deposition and accumulation of amyloid β plaques, and even accelerate the aging process in the brain.4
Symptoms. The case series by Omalu et al4 (which inspired the 2015 motion picture Concussion) and the case series presented by McKee et al5 described severe psychiatric symptoms associated with CTE:
- decreased speed of information processing
- increase in religiosity
- lack of insight
- poor judgment
- involvement in illegal activities
- substance abuse
- indiscretion
- verbal and physical abuse
- problems with interpersonal relationships
- isolation
- restlessness and hyperactivity
- somatic complaints.
The 2 groups of researchers also noted hopelessness, social phobia, anxiety, agitation, mania, labile mood, insomnia, explosivity, and suicidal ideation, attempt, and completion.4,5
By Stage 4, all affected patients are symptomatic. Cognitive impairment is severe; many are described as having “severe memory loss with dementia,”5 “profound” inattention and loss of concentration,5 and dysarthria. Paranoia may develop. Mood symptoms can be severe: Approximately 31% of subjects studied have contemplated suicide; of those, 26% had “suicidal tendencies” and 14% completed suicide.5
Two distinct types of CTE progression are apparent:
- patients who display cognitive deficits first; they progress to dementia but live longer
- patients who display mood and behavioral symptoms first; they tend to be younger, more violent, depressed, and explosive.6
CTE cannot be diagnosed with imaging. There are, however, a few positron emission tomography (PET) ligands for pTau that show promise:
- [F-18]FDDNP, which consistently identifies pTau deposits in brains in which CTE is clinically suspected, in the same distribution of pTau neurofibrillary tangles on autopsy.
- [11C]DPA-713, which detected TBI-related inflammation of neurons in 9 former NFL players in whom CTE was suspected based on the clinical presentation.
- PiB amyloid ligand, under investigation for use in PET neuroimaging.7
Casualties
In January 2016 alone, at least 3 former NFL players were found to have CTE posthumously.
Earl Morrall. Former quarterback who had a 21-year NFL career. Official cause of death in 2014 at age 79 was recorded as “complications of Parkinson’s disease.” In 2016, Stage-4 CTE was discovered on autopsy.8
Ken Stabler. Former quarterback for several NFL teams over 15 seasons. Died of colon cancer at age 69 in 2015. On autopsy, was found to have Stage-3 CTE.9
Tyler Sash. Former University of Iowa and New York Giants football player. Died in September 2015 at age 27 of an apparent drug overdose; posthumously, determined to have Stage-2 CTE. His family reported memory loss, minor fits of rage, confusion, inattention, lack of focus, and chronic pain.
Sash’s mother said, “My son knew something was wrong, but he couldn’t express it. He was such a good person, and it’s sad that he struggled so with this—not knowing where to go with it. Now it makes sense.”10 Sash played 16 years of football in all, sustaining at least 5 concussions. (“If you’ve played football, you know there are often other incidents [of head trauma],” Sash’s father said.10)
Cultural and medical mindsets about contact sports
In the United States, children as young as age 5, with a low weight limit of 35 pounds, routinely are introduced to football.11 Reports of 5 high school players dying from football-related injury in the 2014 season, and 3 deaths in the 2015 season, led a St. Louis, Missouri, area school district to defund their football program entirely. The district’s 2015 homecoming game was a soccer match; students and parents seemed to embrace the change.12
On its face, soccer seems a good alternative to football. When children are instructed to “head” the ball, however, concern arises about CTE: Mild CTE changes have been reported in 2 young soccer players, and late-stage CTE changes were seen in a retired soccer player with dementia.13
Perhaps most disturbing is that players who develop symptoms of CTE, or are at risk, are unlikely to seek psychiatric help. We, as psychiatric clinicians, must be diligent about questioning young patients about their extracurricular activities. It is not enough to simply ask about a history of head trauma: Ask patients about any blow to the head, and don’t limit your questioning to whether they sustained a “concussion” during practice or play.
When speaking with adult and geriatric patients, ask about a history of playing interscholastic or collegiate contact sports, such as football, hockey, and soccer.
Is the solution to better shield the head?
That is not a solution: Helmets and other protective headgear appear to be insufficient to protect the brain from traumatic injury. Perhaps keeping children from engaging in violent sports that put them at high risk of CTE later is the preventive approach that merits the most attention.
1. Blackstone J. NFL tackles alarming increase in concussions. CBS News. http://www.cbsnews.com/news/nfl-studying-how-to-tackle-alarming-increase-in-concussions. Published February 2, 2016. Accessed February 3, 2016.
2. McNamee M, Partridge B, Anderson L. Concussion ethics and sports medicine. Clin Sports Med. 2015;35(2):257-267.
3. Abreu MA, Cromartie FJ, Spradley BD; United States Sports Academy. Chronic traumatic encephalopathy (CTE) and former National Football League player suicides. The Sport Journal. http://thesportjournal.org/article/chronic-traumatic-encephalopathy-cte-and-former-national-football-league-player-suicides. Published January 29, 2016. Accessed January 29, 2016.
4. Omalu B, Bailes J, Hamilton RL, et al. Emerging histomorphologic phenotypes of chronic traumatic encephalopathy in american athletes. Neurosurgery. 2011;69(1):173-183; discussion 183.
5. McKee AC, Stern RA, Nowinski CJ, et al. The spectrum of disease in chronic traumatic encephalopathy. Brain. 2013;136(pt 1):43-64.
6. Stern RA, Daneshvar DH, Baugh CM, et al. Clinical presentation of chronic traumatic encephalopathy. Neurology. 2013;81(13):1122-1129.
7. Eisenmenger LB, Huo EJ, Hoffman JM, et al. Advances in PET imaging of degenerative, cerebrovascular, and traumatic causes of dementia. Semin Nucl Med. 2016;46(1):57-87.
8. Jackson B. Report: former Miami Dolphins QB Earl Morrall had brain disease CTE. Miami Herald. http://www.miamiherald.com/sports/nfl/miami-dolphins/article58794523.html. Published February 5, 2016. Accessed February 6, 2016.
9. Fantz A. Ex-NFL player Ken Stabler had concussion disease CTE, doctor says. CNN. http://www.cnn.com/2016/02/03/health/ken-stabler-cte. Updated February 4, 2016. Accessed February 9, 2016.
10. Pennington B. C.T.E. is found in an Ex-Giant Tyler Sash, who died at 27. The New York Times. http://www.nytimes.com/2016/01/27/sports/football/former-giants-safety-tyler-sash-found-to-have-cte.html?_r=0. Published January 26, 2016. Accessed January 27, 2016.
11. Pop Warner Little Scholars, Inc. Ages and weights for tackle football programs. http://www.popwarner.com/football/footballstructure.htm. Accessed February 5, 2016.
12. Fowler L. No football for homecoming? No problem at Maplewood-Richmond Heights High. St. Louis Post Dispatch. http://www.stltoday.com/news/local/education/no-football-for-homecoming-no-problem-at-maplewood-richmond-heights/article_cc8dc31b-5097-5114-ba9b-9b3584f478b9.html. Published October 9, 2015. Accessed February 3, 2016.
13. Hales C, Neill S, Gearing M, et al. Late-stage CTE pathology in a retired soccer player with dementia. Neurology. 2014;83(24):2307-2309. doi: 10.1212/WNL.0000000000001081.
1. Blackstone J. NFL tackles alarming increase in concussions. CBS News. http://www.cbsnews.com/news/nfl-studying-how-to-tackle-alarming-increase-in-concussions. Published February 2, 2016. Accessed February 3, 2016.
2. McNamee M, Partridge B, Anderson L. Concussion ethics and sports medicine. Clin Sports Med. 2015;35(2):257-267.
3. Abreu MA, Cromartie FJ, Spradley BD; United States Sports Academy. Chronic traumatic encephalopathy (CTE) and former National Football League player suicides. The Sport Journal. http://thesportjournal.org/article/chronic-traumatic-encephalopathy-cte-and-former-national-football-league-player-suicides. Published January 29, 2016. Accessed January 29, 2016.
4. Omalu B, Bailes J, Hamilton RL, et al. Emerging histomorphologic phenotypes of chronic traumatic encephalopathy in american athletes. Neurosurgery. 2011;69(1):173-183; discussion 183.
5. McKee AC, Stern RA, Nowinski CJ, et al. The spectrum of disease in chronic traumatic encephalopathy. Brain. 2013;136(pt 1):43-64.
6. Stern RA, Daneshvar DH, Baugh CM, et al. Clinical presentation of chronic traumatic encephalopathy. Neurology. 2013;81(13):1122-1129.
7. Eisenmenger LB, Huo EJ, Hoffman JM, et al. Advances in PET imaging of degenerative, cerebrovascular, and traumatic causes of dementia. Semin Nucl Med. 2016;46(1):57-87.
8. Jackson B. Report: former Miami Dolphins QB Earl Morrall had brain disease CTE. Miami Herald. http://www.miamiherald.com/sports/nfl/miami-dolphins/article58794523.html. Published February 5, 2016. Accessed February 6, 2016.
9. Fantz A. Ex-NFL player Ken Stabler had concussion disease CTE, doctor says. CNN. http://www.cnn.com/2016/02/03/health/ken-stabler-cte. Updated February 4, 2016. Accessed February 9, 2016.
10. Pennington B. C.T.E. is found in an Ex-Giant Tyler Sash, who died at 27. The New York Times. http://www.nytimes.com/2016/01/27/sports/football/former-giants-safety-tyler-sash-found-to-have-cte.html?_r=0. Published January 26, 2016. Accessed January 27, 2016.
11. Pop Warner Little Scholars, Inc. Ages and weights for tackle football programs. http://www.popwarner.com/football/footballstructure.htm. Accessed February 5, 2016.
12. Fowler L. No football for homecoming? No problem at Maplewood-Richmond Heights High. St. Louis Post Dispatch. http://www.stltoday.com/news/local/education/no-football-for-homecoming-no-problem-at-maplewood-richmond-heights/article_cc8dc31b-5097-5114-ba9b-9b3584f478b9.html. Published October 9, 2015. Accessed February 3, 2016.
13. Hales C, Neill S, Gearing M, et al. Late-stage CTE pathology in a retired soccer player with dementia. Neurology. 2014;83(24):2307-2309. doi: 10.1212/WNL.0000000000001081.

We are not ‘psychiatrists’; 'The beauty of the asylum’; Challenges with false-positive urine drug screens
We are not ‘psychiatrists’
I found Dr. Nasrallah’s editorial regarding the future developments in psychiatry interesting (Do you practice sophisticated psychiatry? 10 Proposed foundations of advanced care, From the Editor, Current Psychiatry. August 2015 p. 12-13). As a young psychiatrist in private practice, I understand why the title “psychiatrist” was initially adopted. I am sure that many of my colleagues agree that the word “psyche” is an abstract, confusing concept: How can we claim to treat something that is not part of known human anatomy?
Nevertheless, we need to clarify the specific nature of our work, namely: the diagnosis and treatment of diseases of the brain, considering other medical causes that can present or exacerbate brain nosology, while providing guidance to modify behavior, thus improving the functional, social, and overall lifestyle of our patients.
We need to change our title to what we really are—encephalopathologists, not psychiatrists!
Marios Efstathiou, MD
Psychiatrist, Private Practice
Member, Cyprus Psychiatric Association
Cyprus
'The beauty of the asylum’
I appreciate Dr. Nasrallah’s metaphor of closing asylums to psychosocial abruptio placentae (Needed: A biopsychosocial ‘therapeutic placenta’ for people with schizophrenia, Current Psychiatry. October 2015 pp. 16,19-20). His proposed components of a therapeutic placenta are supported by evidence-based practice and compassion. I wrote a poem about my feelings about this editorial.
Asylum
I inherited an asylum by profession
where past lives listen
when I console a grief stricken heart
watch when medicines are given.
There are names, dates, and why
scribbled on walls begging for closures.
Around me are kindling, plastic
wasting brains waiting for answers.
Where are the lives that belong to them?
Some were sent home alone
others with loved ones, to foster homes.
They had twins, farmed corn, caught
catfish, carved decoys, built roads,
stargazed away from here.
I cried, stumbled when they slept
under bridges, get mugged, homeless
called from morgues, in jail, sent here.
Like a pendulum of serenity, despair
I vacillated from talking to silence
writing then putting away my
prescriptions.
Exhausted I remember past lives
that chattered once with joy and grief.
That is the beauty of the asylum
I inherited this chain of custody
today, I am one among them.
E. Leynes Bautista, MD
Psychiatrist
Lower Shore Clinic
Wicomico Health Department
Salisbury, Maryland
Challenges with false-positive urine drug screens
Drs. Jeffrey Pawlowski’s and Vicki L. Ellingrod’s article, “Urine drug screens: When might a test be false-positive?” (Savvy Psychopharmacology, Current Psychiatry. October 2015 p. 17,22-24), not only was of high clinical relevance, but it also hinted at another issue of crucial importance: namely, not prematurely dismissing a patient’s reports that he (she) has been abstaining from a drug. It is easy for providers to become jaded and assume that patients, particularly those with a history of substance use, are not being truthful when their self-reported abstinence contradicts laboratory results.
I hope that this article encourages us to become intimately familiar with the specifics of the urine drug screens we employ in practice. We owe it to our patients to do so.
Monifa S. Seawell, MD
Assistant Professor of Psychiatry
Morehouse School of Medicine
Atlanta, Georgia
In the article, “Urine drug screens: When might a test be false-positive?”, it was noted that false positives in immunoassays are rare, but that those involving opiates and amphetamines were more common than cocaine-metabolite and cannabinoid false positives. In the Table, the authors noted that dextromethorphan, diphenhydramine, fluoroquinolones, poppy seeds and oil, and rifampin can trigger a false-positive result for opiates.
The importance of false-positive opiate screens cannot be overemphasized, in light of the epidemic of opioid use disorder—especially among clinicians working in a treatment program. Some of the challenging aspects about treating patients with opioid use disorder are:
- high prevalence of the disorder
- diversion of existing medication-assisted treatments (ie, buprenorphine), compliance with treatment
- urine drug monitoring.
The article addressed urine drug screening, particularly cross-reactivity of the different drugs. With buprenorphine treatment, cross-reactivity of the buprenorphine screening assays varies, depending on which assay is being used. In a study comparing the new Lin-Zhi urine buprenorphine enzyme immunoassay (EIA) with the well-known Microgenics cloned enzyme donor immunoassay, investigators concluded that the latter assay generated a higher percentage of opioid cross-reactivity than the former, and that there also was interference from structurally unrelated drugs (ie, chloroquine and hydroxychloroquine).1 The EIA assay demonstrated more highly specific and sensitive detection of buprenorphine, without opioid cross-reactivity.
In a study2 that examined cross-reactivity of naloxone with oxycodone immunoassays, researchers proposed that urine samples with a high naloxone concentration produced higher cross-reactivity with oxycodone. They proposed that such high naloxone concentrations could occur in adulterated or substituted urine when patients have attempted to dissolve buprenorphine in the urine sample to provide the appearance of compliance. The authors mentioned that typical total urine naloxone concentrations are usually quite low for standard buprenorphine formulations, because of their low bioavailability when taken orally. The clinical recommendation in the article states that it is good practice to confirm positive screens with gas chromatography–mass spectrometry tests.
Adegboyega Oyemade, MD, FAPA
Addiction Psychiatrist
Maryland Treatment Centers, Inc.
Baltimore, Maryland
References
1. Melanson SE, Snyder ML, Jarolim P, et al. A new highly specific buprenorphine immunoassay for monitoring buprenorphine compliance and abuse. J Anal Toxicol. 2012;36(3):201-206.
2. Jenkins AJ, Poirier JG 3rd, Juhascik MP. Cross-reactivity of naloxone with oxycodone immunoassays: implications for individuals taking Suboxone. Clin Chem. 2009;55(7):1434-1436.
We are not ‘psychiatrists’
I found Dr. Nasrallah’s editorial regarding the future developments in psychiatry interesting (Do you practice sophisticated psychiatry? 10 Proposed foundations of advanced care, From the Editor, Current Psychiatry. August 2015 p. 12-13). As a young psychiatrist in private practice, I understand why the title “psychiatrist” was initially adopted. I am sure that many of my colleagues agree that the word “psyche” is an abstract, confusing concept: How can we claim to treat something that is not part of known human anatomy?
Nevertheless, we need to clarify the specific nature of our work, namely: the diagnosis and treatment of diseases of the brain, considering other medical causes that can present or exacerbate brain nosology, while providing guidance to modify behavior, thus improving the functional, social, and overall lifestyle of our patients.
We need to change our title to what we really are—encephalopathologists, not psychiatrists!
Marios Efstathiou, MD
Psychiatrist, Private Practice
Member, Cyprus Psychiatric Association
Cyprus
'The beauty of the asylum’
I appreciate Dr. Nasrallah’s metaphor of closing asylums to psychosocial abruptio placentae (Needed: A biopsychosocial ‘therapeutic placenta’ for people with schizophrenia, Current Psychiatry. October 2015 pp. 16,19-20). His proposed components of a therapeutic placenta are supported by evidence-based practice and compassion. I wrote a poem about my feelings about this editorial.
Asylum
I inherited an asylum by profession
where past lives listen
when I console a grief stricken heart
watch when medicines are given.
There are names, dates, and why
scribbled on walls begging for closures.
Around me are kindling, plastic
wasting brains waiting for answers.
Where are the lives that belong to them?
Some were sent home alone
others with loved ones, to foster homes.
They had twins, farmed corn, caught
catfish, carved decoys, built roads,
stargazed away from here.
I cried, stumbled when they slept
under bridges, get mugged, homeless
called from morgues, in jail, sent here.
Like a pendulum of serenity, despair
I vacillated from talking to silence
writing then putting away my
prescriptions.
Exhausted I remember past lives
that chattered once with joy and grief.
That is the beauty of the asylum
I inherited this chain of custody
today, I am one among them.
E. Leynes Bautista, MD
Psychiatrist
Lower Shore Clinic
Wicomico Health Department
Salisbury, Maryland
Challenges with false-positive urine drug screens
Drs. Jeffrey Pawlowski’s and Vicki L. Ellingrod’s article, “Urine drug screens: When might a test be false-positive?” (Savvy Psychopharmacology, Current Psychiatry. October 2015 p. 17,22-24), not only was of high clinical relevance, but it also hinted at another issue of crucial importance: namely, not prematurely dismissing a patient’s reports that he (she) has been abstaining from a drug. It is easy for providers to become jaded and assume that patients, particularly those with a history of substance use, are not being truthful when their self-reported abstinence contradicts laboratory results.
I hope that this article encourages us to become intimately familiar with the specifics of the urine drug screens we employ in practice. We owe it to our patients to do so.
Monifa S. Seawell, MD
Assistant Professor of Psychiatry
Morehouse School of Medicine
Atlanta, Georgia
In the article, “Urine drug screens: When might a test be false-positive?”, it was noted that false positives in immunoassays are rare, but that those involving opiates and amphetamines were more common than cocaine-metabolite and cannabinoid false positives. In the Table, the authors noted that dextromethorphan, diphenhydramine, fluoroquinolones, poppy seeds and oil, and rifampin can trigger a false-positive result for opiates.
The importance of false-positive opiate screens cannot be overemphasized, in light of the epidemic of opioid use disorder—especially among clinicians working in a treatment program. Some of the challenging aspects about treating patients with opioid use disorder are:
- high prevalence of the disorder
- diversion of existing medication-assisted treatments (ie, buprenorphine), compliance with treatment
- urine drug monitoring.
The article addressed urine drug screening, particularly cross-reactivity of the different drugs. With buprenorphine treatment, cross-reactivity of the buprenorphine screening assays varies, depending on which assay is being used. In a study comparing the new Lin-Zhi urine buprenorphine enzyme immunoassay (EIA) with the well-known Microgenics cloned enzyme donor immunoassay, investigators concluded that the latter assay generated a higher percentage of opioid cross-reactivity than the former, and that there also was interference from structurally unrelated drugs (ie, chloroquine and hydroxychloroquine).1 The EIA assay demonstrated more highly specific and sensitive detection of buprenorphine, without opioid cross-reactivity.
In a study2 that examined cross-reactivity of naloxone with oxycodone immunoassays, researchers proposed that urine samples with a high naloxone concentration produced higher cross-reactivity with oxycodone. They proposed that such high naloxone concentrations could occur in adulterated or substituted urine when patients have attempted to dissolve buprenorphine in the urine sample to provide the appearance of compliance. The authors mentioned that typical total urine naloxone concentrations are usually quite low for standard buprenorphine formulations, because of their low bioavailability when taken orally. The clinical recommendation in the article states that it is good practice to confirm positive screens with gas chromatography–mass spectrometry tests.
Adegboyega Oyemade, MD, FAPA
Addiction Psychiatrist
Maryland Treatment Centers, Inc.
Baltimore, Maryland
References
1. Melanson SE, Snyder ML, Jarolim P, et al. A new highly specific buprenorphine immunoassay for monitoring buprenorphine compliance and abuse. J Anal Toxicol. 2012;36(3):201-206.
2. Jenkins AJ, Poirier JG 3rd, Juhascik MP. Cross-reactivity of naloxone with oxycodone immunoassays: implications for individuals taking Suboxone. Clin Chem. 2009;55(7):1434-1436.
We are not ‘psychiatrists’
I found Dr. Nasrallah’s editorial regarding the future developments in psychiatry interesting (Do you practice sophisticated psychiatry? 10 Proposed foundations of advanced care, From the Editor, Current Psychiatry. August 2015 p. 12-13). As a young psychiatrist in private practice, I understand why the title “psychiatrist” was initially adopted. I am sure that many of my colleagues agree that the word “psyche” is an abstract, confusing concept: How can we claim to treat something that is not part of known human anatomy?
Nevertheless, we need to clarify the specific nature of our work, namely: the diagnosis and treatment of diseases of the brain, considering other medical causes that can present or exacerbate brain nosology, while providing guidance to modify behavior, thus improving the functional, social, and overall lifestyle of our patients.
We need to change our title to what we really are—encephalopathologists, not psychiatrists!
Marios Efstathiou, MD
Psychiatrist, Private Practice
Member, Cyprus Psychiatric Association
Cyprus
'The beauty of the asylum’
I appreciate Dr. Nasrallah’s metaphor of closing asylums to psychosocial abruptio placentae (Needed: A biopsychosocial ‘therapeutic placenta’ for people with schizophrenia, Current Psychiatry. October 2015 pp. 16,19-20). His proposed components of a therapeutic placenta are supported by evidence-based practice and compassion. I wrote a poem about my feelings about this editorial.
Asylum
I inherited an asylum by profession
where past lives listen
when I console a grief stricken heart
watch when medicines are given.
There are names, dates, and why
scribbled on walls begging for closures.
Around me are kindling, plastic
wasting brains waiting for answers.
Where are the lives that belong to them?
Some were sent home alone
others with loved ones, to foster homes.
They had twins, farmed corn, caught
catfish, carved decoys, built roads,
stargazed away from here.
I cried, stumbled when they slept
under bridges, get mugged, homeless
called from morgues, in jail, sent here.
Like a pendulum of serenity, despair
I vacillated from talking to silence
writing then putting away my
prescriptions.
Exhausted I remember past lives
that chattered once with joy and grief.
That is the beauty of the asylum
I inherited this chain of custody
today, I am one among them.
E. Leynes Bautista, MD
Psychiatrist
Lower Shore Clinic
Wicomico Health Department
Salisbury, Maryland
Challenges with false-positive urine drug screens
Drs. Jeffrey Pawlowski’s and Vicki L. Ellingrod’s article, “Urine drug screens: When might a test be false-positive?” (Savvy Psychopharmacology, Current Psychiatry. October 2015 p. 17,22-24), not only was of high clinical relevance, but it also hinted at another issue of crucial importance: namely, not prematurely dismissing a patient’s reports that he (she) has been abstaining from a drug. It is easy for providers to become jaded and assume that patients, particularly those with a history of substance use, are not being truthful when their self-reported abstinence contradicts laboratory results.
I hope that this article encourages us to become intimately familiar with the specifics of the urine drug screens we employ in practice. We owe it to our patients to do so.
Monifa S. Seawell, MD
Assistant Professor of Psychiatry
Morehouse School of Medicine
Atlanta, Georgia
In the article, “Urine drug screens: When might a test be false-positive?”, it was noted that false positives in immunoassays are rare, but that those involving opiates and amphetamines were more common than cocaine-metabolite and cannabinoid false positives. In the Table, the authors noted that dextromethorphan, diphenhydramine, fluoroquinolones, poppy seeds and oil, and rifampin can trigger a false-positive result for opiates.
The importance of false-positive opiate screens cannot be overemphasized, in light of the epidemic of opioid use disorder—especially among clinicians working in a treatment program. Some of the challenging aspects about treating patients with opioid use disorder are:
- high prevalence of the disorder
- diversion of existing medication-assisted treatments (ie, buprenorphine), compliance with treatment
- urine drug monitoring.
The article addressed urine drug screening, particularly cross-reactivity of the different drugs. With buprenorphine treatment, cross-reactivity of the buprenorphine screening assays varies, depending on which assay is being used. In a study comparing the new Lin-Zhi urine buprenorphine enzyme immunoassay (EIA) with the well-known Microgenics cloned enzyme donor immunoassay, investigators concluded that the latter assay generated a higher percentage of opioid cross-reactivity than the former, and that there also was interference from structurally unrelated drugs (ie, chloroquine and hydroxychloroquine).1 The EIA assay demonstrated more highly specific and sensitive detection of buprenorphine, without opioid cross-reactivity.
In a study2 that examined cross-reactivity of naloxone with oxycodone immunoassays, researchers proposed that urine samples with a high naloxone concentration produced higher cross-reactivity with oxycodone. They proposed that such high naloxone concentrations could occur in adulterated or substituted urine when patients have attempted to dissolve buprenorphine in the urine sample to provide the appearance of compliance. The authors mentioned that typical total urine naloxone concentrations are usually quite low for standard buprenorphine formulations, because of their low bioavailability when taken orally. The clinical recommendation in the article states that it is good practice to confirm positive screens with gas chromatography–mass spectrometry tests.
Adegboyega Oyemade, MD, FAPA
Addiction Psychiatrist
Maryland Treatment Centers, Inc.
Baltimore, Maryland
References
1. Melanson SE, Snyder ML, Jarolim P, et al. A new highly specific buprenorphine immunoassay for monitoring buprenorphine compliance and abuse. J Anal Toxicol. 2012;36(3):201-206.
2. Jenkins AJ, Poirier JG 3rd, Juhascik MP. Cross-reactivity of naloxone with oxycodone immunoassays: implications for individuals taking Suboxone. Clin Chem. 2009;55(7):1434-1436.

Zika virus a great unknown, but let’s stick to the facts
Much has rightly been written about the Zika virus in the last few months, yet still we see a number of misunderstandings, rumors, and fears about potential risk, being propagated widely through the media.
Each day brings new developments and expert opinion on the subject, but also, more speculation and subterfuge, with prophylactic advice varying from travel bans, mosquito repellents, contraception, and even abstention from pregnancy.

A crucial factor amplifying this trend, and perhaps the elephant in the room, is the impending 2016 Rio Summer Olympic games. With the world’s eye soon to be focused on Brazil, there is clearly a demand from governments, companies, and other interested parties to ensure they safeguard their respective populations as best they can. Unfortunately, this also means we have seen a number of them act too hastily in their assessment of the risks presented by the Zika virus.
So, what are the risks? Well, we know for sure that there is no vaccine, and it is unlikely we will see one developed this year. But the risk to adults and healthy individuals is still relatively small, as symptoms of Zika virus infection are comparable with the common cold – and certainly not life threatening or even highly infectious in the way prior tropical diseases from Africa, like Ebola, have been. In fact, Zika remained an “unsexy” and largely forgotten virus until we saw the recent probable linkages with microcephaly.
The greatest risk currently recognized is clearly to women who are pregnant or are planning to be pregnant in the near future, and at this point, we believe the risk is probably greatest in the first trimester. This is obviously a major challenge for the domestic populations of Latin America, especially when it is at present unclear whether there is any risk in asymptomatic cases of Zika. From the information we have, and until a fuller understanding of the virus risk is known, it appears that the strongest link of microcephaly presents in cases in which patients have shown symptoms; however, 25% of the mothers of babies with microcephaly remain without any symptoms. And this is, of course, a situation made even more complex by the religious elements of society in South America, where contraception remains enshrouded in cultural stigma and abortion is illegal in many countries – even in those with cases of known prebirth microcephaly.
With no vaccine on the horizon and no cure or effective treatment once infected, clearly, the only viable preventive technique is to cut the spread of the virus. In this case, we must look to reduce the vectors of this disease – namely the Aedes aegypti mosquito. This particular type of Aedes mosquito is prominent throughout tropical regions – namely much of Latin America, South Asia, around the Gulf coast, and in isolated pockets near the Black Sea in Europe. In terms of the virus and the regions in which it has been found, most cases appear in the Latin American mainland, the Caribbean, and Cape Verde – although it may be just a matter of time before it spreads into the Aedes aegypti mosquito’s other habitats within Africa and even Asia. And, of course, it is essential we continue to investigate how viable a vector other species of the Aedes mosquito may be.
Despite these concerns, the risk in terms of the 2016 Olympics, especially for traveling populations, remains low – with the notable exception of pregnant women. In fact, the U.S. Centers for Disease Control and Prevention recommends that any travelers who are pregnant (at any stage/trimester) or planning to become pregnant, should avoid traveling to areas with Zika virus outbreaks. If they cannot avoid travel or if people live in areas where Zika virus transmission is known to occur, meticulous efforts to avoid mosquito bites during both daytime and nighttime hours must be adhered to. While it may sound a rather low-tech solution for modern health care, pregnant women in Zika-affected areas should wear protective clothing, apply a U.S. Environmental Protection Agency–approved insect repellent, and sleep in a screened room or under a mosquito net. However, it is also important to note that the Aedes aegypti mosquitoes predominantly bite during the day, especially around dawn and dusk, and therefore the correct timing and use of mosquito repellents and other personal protection measures are essential.
One final important point to emphasize is that contraception for travelers during the Rio Olympics, and when they return home, is another area of vigilance. By this, we mean both men and women, as evidence suggests Zika may be able to survive in semen for up to 1 month after infection – some reports even suggest cases of Zika remaining in semen for several months. However, the advice remains the same, if you were symptomless, then 1 month of condom use after your return will be enough to mitigate the risk of infection to a sexual partner, and 6 months after return for those who have symptoms.
The obvious unknown is the symptomless cases: Can the virus remain transmissible after the return of an athlete or visitor to the games? This is a crucial point and helps explain where there are still a number of misunderstandings. While in Brazil’s population there are some symptomless cases, people from abroad with no prior exposure to Zika virus (and therefore no resistance), would certainly have some symptoms. This remains true for both North Americans and Europeans, and so they are at no risk of further spreading the virus 1 month after their return from Brazil – should they not present any symptoms.
In one recent case of overkill, Kenya threatened to boycott the Summer Games entirely on safety grounds, a move clearly based on no identifiable scientific evidence, as the risk for athletes alone remains very low and fundamentally manageable. Conversely, the other controversial advice I have recently seen stems from the World Health Organization itself – which suggested women in Latin America should not put off pregnancy for fear of Zika. But until more information is known, and the RNA is properly analyzed or a vaccine becomes available, this is not a position I can yet support. We need to fully understand the risks of Zika virus infection, and there is still a long way to go.
Prof. Dr. Eskild Petersen is a member of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) study group for Infections in Travellers and Migrants (ESGITM) as well as a professor of tropical medicine at Aarhus University Hospital, Denmark, and senior consultant of infectious diseases at the Royal Hospital, Muscat, Oman. He has undertaken work on infectious diseases, clinical immunology, and tropical and travel medicine. His recent research focuses on the rapid spread of Zika virus in the Americas and the implications for the 2016 Rio Olympic Games.
Much has rightly been written about the Zika virus in the last few months, yet still we see a number of misunderstandings, rumors, and fears about potential risk, being propagated widely through the media.
Each day brings new developments and expert opinion on the subject, but also, more speculation and subterfuge, with prophylactic advice varying from travel bans, mosquito repellents, contraception, and even abstention from pregnancy.
A crucial factor amplifying this trend, and perhaps the elephant in the room, is the impending 2016 Rio Summer Olympic games. With the world’s eye soon to be focused on Brazil, there is clearly a demand from governments, companies, and other interested parties to ensure they safeguard their respective populations as best they can. Unfortunately, this also means we have seen a number of them act too hastily in their assessment of the risks presented by the Zika virus.
So, what are the risks? Well, we know for sure that there is no vaccine, and it is unlikely we will see one developed this year. But the risk to adults and healthy individuals is still relatively small, as symptoms of Zika virus infection are comparable with the common cold – and certainly not life threatening or even highly infectious in the way prior tropical diseases from Africa, like Ebola, have been. In fact, Zika remained an “unsexy” and largely forgotten virus until we saw the recent probable linkages with microcephaly.
The greatest risk currently recognized is clearly to women who are pregnant or are planning to be pregnant in the near future, and at this point, we believe the risk is probably greatest in the first trimester. This is obviously a major challenge for the domestic populations of Latin America, especially when it is at present unclear whether there is any risk in asymptomatic cases of Zika. From the information we have, and until a fuller understanding of the virus risk is known, it appears that the strongest link of microcephaly presents in cases in which patients have shown symptoms; however, 25% of the mothers of babies with microcephaly remain without any symptoms. And this is, of course, a situation made even more complex by the religious elements of society in South America, where contraception remains enshrouded in cultural stigma and abortion is illegal in many countries – even in those with cases of known prebirth microcephaly.
With no vaccine on the horizon and no cure or effective treatment once infected, clearly, the only viable preventive technique is to cut the spread of the virus. In this case, we must look to reduce the vectors of this disease – namely the Aedes aegypti mosquito. This particular type of Aedes mosquito is prominent throughout tropical regions – namely much of Latin America, South Asia, around the Gulf coast, and in isolated pockets near the Black Sea in Europe. In terms of the virus and the regions in which it has been found, most cases appear in the Latin American mainland, the Caribbean, and Cape Verde – although it may be just a matter of time before it spreads into the Aedes aegypti mosquito’s other habitats within Africa and even Asia. And, of course, it is essential we continue to investigate how viable a vector other species of the Aedes mosquito may be.
Despite these concerns, the risk in terms of the 2016 Olympics, especially for traveling populations, remains low – with the notable exception of pregnant women. In fact, the U.S. Centers for Disease Control and Prevention recommends that any travelers who are pregnant (at any stage/trimester) or planning to become pregnant, should avoid traveling to areas with Zika virus outbreaks. If they cannot avoid travel or if people live in areas where Zika virus transmission is known to occur, meticulous efforts to avoid mosquito bites during both daytime and nighttime hours must be adhered to. While it may sound a rather low-tech solution for modern health care, pregnant women in Zika-affected areas should wear protective clothing, apply a U.S. Environmental Protection Agency–approved insect repellent, and sleep in a screened room or under a mosquito net. However, it is also important to note that the Aedes aegypti mosquitoes predominantly bite during the day, especially around dawn and dusk, and therefore the correct timing and use of mosquito repellents and other personal protection measures are essential.
One final important point to emphasize is that contraception for travelers during the Rio Olympics, and when they return home, is another area of vigilance. By this, we mean both men and women, as evidence suggests Zika may be able to survive in semen for up to 1 month after infection – some reports even suggest cases of Zika remaining in semen for several months. However, the advice remains the same, if you were symptomless, then 1 month of condom use after your return will be enough to mitigate the risk of infection to a sexual partner, and 6 months after return for those who have symptoms.
The obvious unknown is the symptomless cases: Can the virus remain transmissible after the return of an athlete or visitor to the games? This is a crucial point and helps explain where there are still a number of misunderstandings. While in Brazil’s population there are some symptomless cases, people from abroad with no prior exposure to Zika virus (and therefore no resistance), would certainly have some symptoms. This remains true for both North Americans and Europeans, and so they are at no risk of further spreading the virus 1 month after their return from Brazil – should they not present any symptoms.
In one recent case of overkill, Kenya threatened to boycott the Summer Games entirely on safety grounds, a move clearly based on no identifiable scientific evidence, as the risk for athletes alone remains very low and fundamentally manageable. Conversely, the other controversial advice I have recently seen stems from the World Health Organization itself – which suggested women in Latin America should not put off pregnancy for fear of Zika. But until more information is known, and the RNA is properly analyzed or a vaccine becomes available, this is not a position I can yet support. We need to fully understand the risks of Zika virus infection, and there is still a long way to go.
Prof. Dr. Eskild Petersen is a member of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) study group for Infections in Travellers and Migrants (ESGITM) as well as a professor of tropical medicine at Aarhus University Hospital, Denmark, and senior consultant of infectious diseases at the Royal Hospital, Muscat, Oman. He has undertaken work on infectious diseases, clinical immunology, and tropical and travel medicine. His recent research focuses on the rapid spread of Zika virus in the Americas and the implications for the 2016 Rio Olympic Games.
Much has rightly been written about the Zika virus in the last few months, yet still we see a number of misunderstandings, rumors, and fears about potential risk, being propagated widely through the media.
Each day brings new developments and expert opinion on the subject, but also, more speculation and subterfuge, with prophylactic advice varying from travel bans, mosquito repellents, contraception, and even abstention from pregnancy.
A crucial factor amplifying this trend, and perhaps the elephant in the room, is the impending 2016 Rio Summer Olympic games. With the world’s eye soon to be focused on Brazil, there is clearly a demand from governments, companies, and other interested parties to ensure they safeguard their respective populations as best they can. Unfortunately, this also means we have seen a number of them act too hastily in their assessment of the risks presented by the Zika virus.
So, what are the risks? Well, we know for sure that there is no vaccine, and it is unlikely we will see one developed this year. But the risk to adults and healthy individuals is still relatively small, as symptoms of Zika virus infection are comparable with the common cold – and certainly not life threatening or even highly infectious in the way prior tropical diseases from Africa, like Ebola, have been. In fact, Zika remained an “unsexy” and largely forgotten virus until we saw the recent probable linkages with microcephaly.
The greatest risk currently recognized is clearly to women who are pregnant or are planning to be pregnant in the near future, and at this point, we believe the risk is probably greatest in the first trimester. This is obviously a major challenge for the domestic populations of Latin America, especially when it is at present unclear whether there is any risk in asymptomatic cases of Zika. From the information we have, and until a fuller understanding of the virus risk is known, it appears that the strongest link of microcephaly presents in cases in which patients have shown symptoms; however, 25% of the mothers of babies with microcephaly remain without any symptoms. And this is, of course, a situation made even more complex by the religious elements of society in South America, where contraception remains enshrouded in cultural stigma and abortion is illegal in many countries – even in those with cases of known prebirth microcephaly.
With no vaccine on the horizon and no cure or effective treatment once infected, clearly, the only viable preventive technique is to cut the spread of the virus. In this case, we must look to reduce the vectors of this disease – namely the Aedes aegypti mosquito. This particular type of Aedes mosquito is prominent throughout tropical regions – namely much of Latin America, South Asia, around the Gulf coast, and in isolated pockets near the Black Sea in Europe. In terms of the virus and the regions in which it has been found, most cases appear in the Latin American mainland, the Caribbean, and Cape Verde – although it may be just a matter of time before it spreads into the Aedes aegypti mosquito’s other habitats within Africa and even Asia. And, of course, it is essential we continue to investigate how viable a vector other species of the Aedes mosquito may be.
Despite these concerns, the risk in terms of the 2016 Olympics, especially for traveling populations, remains low – with the notable exception of pregnant women. In fact, the U.S. Centers for Disease Control and Prevention recommends that any travelers who are pregnant (at any stage/trimester) or planning to become pregnant, should avoid traveling to areas with Zika virus outbreaks. If they cannot avoid travel or if people live in areas where Zika virus transmission is known to occur, meticulous efforts to avoid mosquito bites during both daytime and nighttime hours must be adhered to. While it may sound a rather low-tech solution for modern health care, pregnant women in Zika-affected areas should wear protective clothing, apply a U.S. Environmental Protection Agency–approved insect repellent, and sleep in a screened room or under a mosquito net. However, it is also important to note that the Aedes aegypti mosquitoes predominantly bite during the day, especially around dawn and dusk, and therefore the correct timing and use of mosquito repellents and other personal protection measures are essential.
One final important point to emphasize is that contraception for travelers during the Rio Olympics, and when they return home, is another area of vigilance. By this, we mean both men and women, as evidence suggests Zika may be able to survive in semen for up to 1 month after infection – some reports even suggest cases of Zika remaining in semen for several months. However, the advice remains the same, if you were symptomless, then 1 month of condom use after your return will be enough to mitigate the risk of infection to a sexual partner, and 6 months after return for those who have symptoms.
The obvious unknown is the symptomless cases: Can the virus remain transmissible after the return of an athlete or visitor to the games? This is a crucial point and helps explain where there are still a number of misunderstandings. While in Brazil’s population there are some symptomless cases, people from abroad with no prior exposure to Zika virus (and therefore no resistance), would certainly have some symptoms. This remains true for both North Americans and Europeans, and so they are at no risk of further spreading the virus 1 month after their return from Brazil – should they not present any symptoms.
In one recent case of overkill, Kenya threatened to boycott the Summer Games entirely on safety grounds, a move clearly based on no identifiable scientific evidence, as the risk for athletes alone remains very low and fundamentally manageable. Conversely, the other controversial advice I have recently seen stems from the World Health Organization itself – which suggested women in Latin America should not put off pregnancy for fear of Zika. But until more information is known, and the RNA is properly analyzed or a vaccine becomes available, this is not a position I can yet support. We need to fully understand the risks of Zika virus infection, and there is still a long way to go.
Prof. Dr. Eskild Petersen is a member of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) study group for Infections in Travellers and Migrants (ESGITM) as well as a professor of tropical medicine at Aarhus University Hospital, Denmark, and senior consultant of infectious diseases at the Royal Hospital, Muscat, Oman. He has undertaken work on infectious diseases, clinical immunology, and tropical and travel medicine. His recent research focuses on the rapid spread of Zika virus in the Americas and the implications for the 2016 Rio Olympic Games.

Optimizing Outcomes of Total Joint Arthroplasty Under the Comprehensive Care for Joint Replacement
On July 9, 2015, the Centers for Medicare and Medicaid Services announced the Comprehensive Care for Joint Replacement model, which aims to improve coordination of the whole episode of care for total hip and knee replacement.1 At stake is the fact that hip and knee replacements are the most common inpatient procedures among Medicare beneficiaries, costing over $7 billion in 20141 and projected to grow to $50 billion by 2030.2 Under Medicare’s new initiative, hospitals and physicians are held accountable for the quality and cost of care delivered from the time of surgery through 90 days after discharge. For the first time in the history of our profession, large-scale reimbursement is based on outcomes and value rather than fee-for-service. As a result, a hospital can either earn a reward or be held liable for added expenses related to events such as prolonged hospitalization, readmissions, and complications.
How can we optimize outcomes for total joint arthroplasty (TJA) patients in this era of Medicare (r)evolution? A good outcome starts with good patient selection. Numerous studies have been published on patient-related risk factors for postoperative TJA complications including obesity, congestive heart failure, lung disease, and depression.3,4 The risks and benefits of TJA should be carefully weighed in high-risk patients and surgery delayed until appropriate medical optimization has been achieved. Following the famous saying, “Good surgeons know how to operate, better surgeons know when to operate, and the best surgeons know when not to operate,” one cannot overemphasize the need for an objective assessment of the likelihood of patient outcome weighed against patient risk factors.
Moderating patient expectation is another crucial component given the changing demographics of our country. Patients seeking TJA today are younger, more obese, and better educated; live longer; and have higher expectations.5 Unrealistic expectations can have a profound impact on surgical outcomes, leading to frustration, dissatisfaction, and unnecessary resource utilization. For example, despite alleviating pain and restoring function in a severely degenerative joint, TJA does not necessarily translate to weight loss. There is currently conflicting evidence on this topic,6-8 and the expectation of weight loss after TJA cannot be supported. There is also a paucity of data regarding return to athletic activity after TJA and the effect of athletic activity on TJA survivorship.9 Communication and transparency are needed to moderate unrealistic expectations before surgery, outlining clear and achievable goals.
Clinical pathways for TJA have seen tremendous improvements in the past decade with the advent of multimodal analgesia, rapid recovery programs, use of spinal and regional anesthesia, and evidence-based guidelines for prevention of venous thromboembolic disease. Adequate pain control is critical to recovery. In a prospective, randomized controlled trial, Lamplot and colleagues10 showed that the use of multimodal analgesia correlated with improved pain scores, decreased narcotic usage, faster functional recovery, and higher patient satisfaction after total knee arthroplasty (TKA). In another study, Quack and colleagues11 performed a systematic review of the literature on fast-track rehabilitation and found that it reduced both inpatient length of stay and costs after TKA. With respect to anesthetic choice, Pugely and colleagues12 reviewed a national database of 14,052 cases of primary TKA and found that patients with multiple comorbidities were at higher risk of complications after general anesthesia when compared with spinal anesthesia. We should continue to invest in safer and more effective modalities for pain control and functional recovery.
Last but not least, in today’s era of Medicare’s Comprehensive Care for Joint Replacement, the role of low-volume orthopedic surgeons performing TJA deserves special mention. Over the next few years, we could likely see a decline in the role of low-volume surgeons in favor of high-volume surgeons. While most orthopedic surgeons are comfortable doing primary TJA, failed cases and complications are frequently referred to larger centers, which may create frustration among patients owing to fragmentation of care. The economic pressures related to bundled payments could further influence this transition. Given the lack of a widespread, long-standing national joint registry, the incidence of failed TJA performed by low-volume orthopedic surgeons compared with high-volume orthopedic surgeons is unknown. However, multiple studies have shown surgeon volume to be associated with lower rates of complication, mortality, readmission, reoperation, and discharge to postacute facilities.13-16 As hospitals assume further financial risk, considerable data on physician performance will undoubtedly be gathered and leveraged. Time and data will determine the value of this transition of care.
Today, more than ever, we are challenged to provide efficient, high-quality, patient-centered care. As our nation grapples with reforming a broken health care system, initiatives like the Comprehensive Care for Joint Replacement will continue to emerge in the future. Orthopedic surgeons are the gatekeepers of the system and therefore hold significant responsibility to patients and society. Ensuring good outcomes should be a top priority not just from a financial standpoint, but as a moral obligation. We shall continue to be leaders in the face of challenges, using innovation and integrity to produce the best results and advance our profession.
1. Comprehensive Care for Joint Replacement model. Centers for Medicare and Medicaid Services website. https://innovation.cms.gov/initiatives/cjr. Updated December 21, 2015. Accessed December 30, 2015.
2. Wilson NA, Schneller ES, Montgomery K, Bozic KJ. Hip and knee implants: current trends and policy considerations. Health Aff. 2008;27(6):1587-1598.
3. Bozic KJ, Lau E, Ong K, et al. Risk factors for early revision after primary total hip arthroplasty in Medicare patients. Clin Orthop Relat Res. 2014;472(2):449-454.
4. Bozic KJ, Lau E, Ong K, et al. Risk factors for early revision after primary TKA in Medicare patients. Clin Orthop Relat Res. 2014;472(1):232-237.
5. Mason JB. The new demands by patients in the modern era of total joint arthroplasty: a point of view. Clin Orthop Relat Res. 2008;466(1):146-152.
6. Riddle DL, Singh JA, Harmsen WS, Schleck CD, Lewallen DG. Clinically important body weight gain following knee arthroplasty: a five-year comparative cohort study. Arthritis Care Res. 2013;65(5):669-677.
7. Zeni JA Jr, Snyder-Mackler L. Most patients gain weight in the 2 years after total knee arthroplasty: comparison to a healthy control group. Osteoarthritis Cartilage. 2010;18(4):510-514.
8. Ast MP, Abdel MP, Lee YY, Lyman S, Ruel AV, Westrich GH. Weight changes after total hip or knee arthroplasty: prevalence, predictors, and effects on outcomes. J Bone Joint Surg Am. 2015;97(11):911-919.
9. Healy WL, Sharma S, Schwartz B, Iorio R. Athletic activity after total joint arthroplasty. J Bone Joint Surg Am. 2008;90(10):2245-2252.
10. Lamplot JD, Wagner ER, Manning DW. Multimodal pain management in total knee arthroplasty: a prospective randomized controlled trial. J Arthroplasty. 2014;29(2):329-334.
11. Quack V, Ippendorf AV, Betsch M, et al. Multidisciplinary rehabilitation and fast-track rehabilitation after knee replacement: faster, better, cheaper? A survey and systematic review of literature [in German]. Rehabilitation (Stuttg). 2015;54(4):245-251.
12. Pugely AJ, Martin CT, Gao Y, Mendoza-Lattes S, Callaghan JJ. Differences in short-term complications between spinal and general anesthesia for primary total knee arthroplasty. J Bone Joint Surg Am. 2013;95(3):193-199.
13. Katz JN, Losina E, Barrett J, et al. Association between hospital and surgeon procedure volume and outcomes of total hip replacement in the United States medicare population. J Bone Joint Surg Am. 2001;83(11):1622-1629.
14. Manley M, Ong K, Lau E, Kurtz SM. Effect of volume on total hip arthroplasty revision rates in the United States Medicare population. J Bone Joint Surg Am. 2008;90(11):2446-2451.
15. Bozic KJ, Maselli J, Pekow PS, Lindenauer PK, Vail TP, Auerbach AD. The influence of procedure volumes and standardization of care on quality and efficiency in total joint replacement surgery. J Bone Joint Surg Am. 2010;92(16):2643-2652.
16. Lau RL, Perruccio AV, Gandhi R, Mahomed NN. The role of surgeon volume on patient outcome in total knee arthroplasty: a systematic review of the literature. BMC Musculoskelet Disord. 2012;13:250.
On July 9, 2015, the Centers for Medicare and Medicaid Services announced the Comprehensive Care for Joint Replacement model, which aims to improve coordination of the whole episode of care for total hip and knee replacement.1 At stake is the fact that hip and knee replacements are the most common inpatient procedures among Medicare beneficiaries, costing over $7 billion in 20141 and projected to grow to $50 billion by 2030.2 Under Medicare’s new initiative, hospitals and physicians are held accountable for the quality and cost of care delivered from the time of surgery through 90 days after discharge. For the first time in the history of our profession, large-scale reimbursement is based on outcomes and value rather than fee-for-service. As a result, a hospital can either earn a reward or be held liable for added expenses related to events such as prolonged hospitalization, readmissions, and complications.
How can we optimize outcomes for total joint arthroplasty (TJA) patients in this era of Medicare (r)evolution? A good outcome starts with good patient selection. Numerous studies have been published on patient-related risk factors for postoperative TJA complications including obesity, congestive heart failure, lung disease, and depression.3,4 The risks and benefits of TJA should be carefully weighed in high-risk patients and surgery delayed until appropriate medical optimization has been achieved. Following the famous saying, “Good surgeons know how to operate, better surgeons know when to operate, and the best surgeons know when not to operate,” one cannot overemphasize the need for an objective assessment of the likelihood of patient outcome weighed against patient risk factors.
Moderating patient expectation is another crucial component given the changing demographics of our country. Patients seeking TJA today are younger, more obese, and better educated; live longer; and have higher expectations.5 Unrealistic expectations can have a profound impact on surgical outcomes, leading to frustration, dissatisfaction, and unnecessary resource utilization. For example, despite alleviating pain and restoring function in a severely degenerative joint, TJA does not necessarily translate to weight loss. There is currently conflicting evidence on this topic,6-8 and the expectation of weight loss after TJA cannot be supported. There is also a paucity of data regarding return to athletic activity after TJA and the effect of athletic activity on TJA survivorship.9 Communication and transparency are needed to moderate unrealistic expectations before surgery, outlining clear and achievable goals.
Clinical pathways for TJA have seen tremendous improvements in the past decade with the advent of multimodal analgesia, rapid recovery programs, use of spinal and regional anesthesia, and evidence-based guidelines for prevention of venous thromboembolic disease. Adequate pain control is critical to recovery. In a prospective, randomized controlled trial, Lamplot and colleagues10 showed that the use of multimodal analgesia correlated with improved pain scores, decreased narcotic usage, faster functional recovery, and higher patient satisfaction after total knee arthroplasty (TKA). In another study, Quack and colleagues11 performed a systematic review of the literature on fast-track rehabilitation and found that it reduced both inpatient length of stay and costs after TKA. With respect to anesthetic choice, Pugely and colleagues12 reviewed a national database of 14,052 cases of primary TKA and found that patients with multiple comorbidities were at higher risk of complications after general anesthesia when compared with spinal anesthesia. We should continue to invest in safer and more effective modalities for pain control and functional recovery.
Last but not least, in today’s era of Medicare’s Comprehensive Care for Joint Replacement, the role of low-volume orthopedic surgeons performing TJA deserves special mention. Over the next few years, we could likely see a decline in the role of low-volume surgeons in favor of high-volume surgeons. While most orthopedic surgeons are comfortable doing primary TJA, failed cases and complications are frequently referred to larger centers, which may create frustration among patients owing to fragmentation of care. The economic pressures related to bundled payments could further influence this transition. Given the lack of a widespread, long-standing national joint registry, the incidence of failed TJA performed by low-volume orthopedic surgeons compared with high-volume orthopedic surgeons is unknown. However, multiple studies have shown surgeon volume to be associated with lower rates of complication, mortality, readmission, reoperation, and discharge to postacute facilities.13-16 As hospitals assume further financial risk, considerable data on physician performance will undoubtedly be gathered and leveraged. Time and data will determine the value of this transition of care.
Today, more than ever, we are challenged to provide efficient, high-quality, patient-centered care. As our nation grapples with reforming a broken health care system, initiatives like the Comprehensive Care for Joint Replacement will continue to emerge in the future. Orthopedic surgeons are the gatekeepers of the system and therefore hold significant responsibility to patients and society. Ensuring good outcomes should be a top priority not just from a financial standpoint, but as a moral obligation. We shall continue to be leaders in the face of challenges, using innovation and integrity to produce the best results and advance our profession.
On July 9, 2015, the Centers for Medicare and Medicaid Services announced the Comprehensive Care for Joint Replacement model, which aims to improve coordination of the whole episode of care for total hip and knee replacement.1 At stake is the fact that hip and knee replacements are the most common inpatient procedures among Medicare beneficiaries, costing over $7 billion in 20141 and projected to grow to $50 billion by 2030.2 Under Medicare’s new initiative, hospitals and physicians are held accountable for the quality and cost of care delivered from the time of surgery through 90 days after discharge. For the first time in the history of our profession, large-scale reimbursement is based on outcomes and value rather than fee-for-service. As a result, a hospital can either earn a reward or be held liable for added expenses related to events such as prolonged hospitalization, readmissions, and complications.
How can we optimize outcomes for total joint arthroplasty (TJA) patients in this era of Medicare (r)evolution? A good outcome starts with good patient selection. Numerous studies have been published on patient-related risk factors for postoperative TJA complications including obesity, congestive heart failure, lung disease, and depression.3,4 The risks and benefits of TJA should be carefully weighed in high-risk patients and surgery delayed until appropriate medical optimization has been achieved. Following the famous saying, “Good surgeons know how to operate, better surgeons know when to operate, and the best surgeons know when not to operate,” one cannot overemphasize the need for an objective assessment of the likelihood of patient outcome weighed against patient risk factors.
Moderating patient expectation is another crucial component given the changing demographics of our country. Patients seeking TJA today are younger, more obese, and better educated; live longer; and have higher expectations.5 Unrealistic expectations can have a profound impact on surgical outcomes, leading to frustration, dissatisfaction, and unnecessary resource utilization. For example, despite alleviating pain and restoring function in a severely degenerative joint, TJA does not necessarily translate to weight loss. There is currently conflicting evidence on this topic,6-8 and the expectation of weight loss after TJA cannot be supported. There is also a paucity of data regarding return to athletic activity after TJA and the effect of athletic activity on TJA survivorship.9 Communication and transparency are needed to moderate unrealistic expectations before surgery, outlining clear and achievable goals.
Clinical pathways for TJA have seen tremendous improvements in the past decade with the advent of multimodal analgesia, rapid recovery programs, use of spinal and regional anesthesia, and evidence-based guidelines for prevention of venous thromboembolic disease. Adequate pain control is critical to recovery. In a prospective, randomized controlled trial, Lamplot and colleagues10 showed that the use of multimodal analgesia correlated with improved pain scores, decreased narcotic usage, faster functional recovery, and higher patient satisfaction after total knee arthroplasty (TKA). In another study, Quack and colleagues11 performed a systematic review of the literature on fast-track rehabilitation and found that it reduced both inpatient length of stay and costs after TKA. With respect to anesthetic choice, Pugely and colleagues12 reviewed a national database of 14,052 cases of primary TKA and found that patients with multiple comorbidities were at higher risk of complications after general anesthesia when compared with spinal anesthesia. We should continue to invest in safer and more effective modalities for pain control and functional recovery.
Last but not least, in today’s era of Medicare’s Comprehensive Care for Joint Replacement, the role of low-volume orthopedic surgeons performing TJA deserves special mention. Over the next few years, we could likely see a decline in the role of low-volume surgeons in favor of high-volume surgeons. While most orthopedic surgeons are comfortable doing primary TJA, failed cases and complications are frequently referred to larger centers, which may create frustration among patients owing to fragmentation of care. The economic pressures related to bundled payments could further influence this transition. Given the lack of a widespread, long-standing national joint registry, the incidence of failed TJA performed by low-volume orthopedic surgeons compared with high-volume orthopedic surgeons is unknown. However, multiple studies have shown surgeon volume to be associated with lower rates of complication, mortality, readmission, reoperation, and discharge to postacute facilities.13-16 As hospitals assume further financial risk, considerable data on physician performance will undoubtedly be gathered and leveraged. Time and data will determine the value of this transition of care.
Today, more than ever, we are challenged to provide efficient, high-quality, patient-centered care. As our nation grapples with reforming a broken health care system, initiatives like the Comprehensive Care for Joint Replacement will continue to emerge in the future. Orthopedic surgeons are the gatekeepers of the system and therefore hold significant responsibility to patients and society. Ensuring good outcomes should be a top priority not just from a financial standpoint, but as a moral obligation. We shall continue to be leaders in the face of challenges, using innovation and integrity to produce the best results and advance our profession.
1. Comprehensive Care for Joint Replacement model. Centers for Medicare and Medicaid Services website. https://innovation.cms.gov/initiatives/cjr. Updated December 21, 2015. Accessed December 30, 2015.
2. Wilson NA, Schneller ES, Montgomery K, Bozic KJ. Hip and knee implants: current trends and policy considerations. Health Aff. 2008;27(6):1587-1598.
3. Bozic KJ, Lau E, Ong K, et al. Risk factors for early revision after primary total hip arthroplasty in Medicare patients. Clin Orthop Relat Res. 2014;472(2):449-454.
4. Bozic KJ, Lau E, Ong K, et al. Risk factors for early revision after primary TKA in Medicare patients. Clin Orthop Relat Res. 2014;472(1):232-237.
5. Mason JB. The new demands by patients in the modern era of total joint arthroplasty: a point of view. Clin Orthop Relat Res. 2008;466(1):146-152.
6. Riddle DL, Singh JA, Harmsen WS, Schleck CD, Lewallen DG. Clinically important body weight gain following knee arthroplasty: a five-year comparative cohort study. Arthritis Care Res. 2013;65(5):669-677.
7. Zeni JA Jr, Snyder-Mackler L. Most patients gain weight in the 2 years after total knee arthroplasty: comparison to a healthy control group. Osteoarthritis Cartilage. 2010;18(4):510-514.
8. Ast MP, Abdel MP, Lee YY, Lyman S, Ruel AV, Westrich GH. Weight changes after total hip or knee arthroplasty: prevalence, predictors, and effects on outcomes. J Bone Joint Surg Am. 2015;97(11):911-919.
9. Healy WL, Sharma S, Schwartz B, Iorio R. Athletic activity after total joint arthroplasty. J Bone Joint Surg Am. 2008;90(10):2245-2252.
10. Lamplot JD, Wagner ER, Manning DW. Multimodal pain management in total knee arthroplasty: a prospective randomized controlled trial. J Arthroplasty. 2014;29(2):329-334.
11. Quack V, Ippendorf AV, Betsch M, et al. Multidisciplinary rehabilitation and fast-track rehabilitation after knee replacement: faster, better, cheaper? A survey and systematic review of literature [in German]. Rehabilitation (Stuttg). 2015;54(4):245-251.
12. Pugely AJ, Martin CT, Gao Y, Mendoza-Lattes S, Callaghan JJ. Differences in short-term complications between spinal and general anesthesia for primary total knee arthroplasty. J Bone Joint Surg Am. 2013;95(3):193-199.
13. Katz JN, Losina E, Barrett J, et al. Association between hospital and surgeon procedure volume and outcomes of total hip replacement in the United States medicare population. J Bone Joint Surg Am. 2001;83(11):1622-1629.
14. Manley M, Ong K, Lau E, Kurtz SM. Effect of volume on total hip arthroplasty revision rates in the United States Medicare population. J Bone Joint Surg Am. 2008;90(11):2446-2451.
15. Bozic KJ, Maselli J, Pekow PS, Lindenauer PK, Vail TP, Auerbach AD. The influence of procedure volumes and standardization of care on quality and efficiency in total joint replacement surgery. J Bone Joint Surg Am. 2010;92(16):2643-2652.
16. Lau RL, Perruccio AV, Gandhi R, Mahomed NN. The role of surgeon volume on patient outcome in total knee arthroplasty: a systematic review of the literature. BMC Musculoskelet Disord. 2012;13:250.
1. Comprehensive Care for Joint Replacement model. Centers for Medicare and Medicaid Services website. https://innovation.cms.gov/initiatives/cjr. Updated December 21, 2015. Accessed December 30, 2015.
2. Wilson NA, Schneller ES, Montgomery K, Bozic KJ. Hip and knee implants: current trends and policy considerations. Health Aff. 2008;27(6):1587-1598.
3. Bozic KJ, Lau E, Ong K, et al. Risk factors for early revision after primary total hip arthroplasty in Medicare patients. Clin Orthop Relat Res. 2014;472(2):449-454.
4. Bozic KJ, Lau E, Ong K, et al. Risk factors for early revision after primary TKA in Medicare patients. Clin Orthop Relat Res. 2014;472(1):232-237.
5. Mason JB. The new demands by patients in the modern era of total joint arthroplasty: a point of view. Clin Orthop Relat Res. 2008;466(1):146-152.
6. Riddle DL, Singh JA, Harmsen WS, Schleck CD, Lewallen DG. Clinically important body weight gain following knee arthroplasty: a five-year comparative cohort study. Arthritis Care Res. 2013;65(5):669-677.
7. Zeni JA Jr, Snyder-Mackler L. Most patients gain weight in the 2 years after total knee arthroplasty: comparison to a healthy control group. Osteoarthritis Cartilage. 2010;18(4):510-514.
8. Ast MP, Abdel MP, Lee YY, Lyman S, Ruel AV, Westrich GH. Weight changes after total hip or knee arthroplasty: prevalence, predictors, and effects on outcomes. J Bone Joint Surg Am. 2015;97(11):911-919.
9. Healy WL, Sharma S, Schwartz B, Iorio R. Athletic activity after total joint arthroplasty. J Bone Joint Surg Am. 2008;90(10):2245-2252.
10. Lamplot JD, Wagner ER, Manning DW. Multimodal pain management in total knee arthroplasty: a prospective randomized controlled trial. J Arthroplasty. 2014;29(2):329-334.
11. Quack V, Ippendorf AV, Betsch M, et al. Multidisciplinary rehabilitation and fast-track rehabilitation after knee replacement: faster, better, cheaper? A survey and systematic review of literature [in German]. Rehabilitation (Stuttg). 2015;54(4):245-251.
12. Pugely AJ, Martin CT, Gao Y, Mendoza-Lattes S, Callaghan JJ. Differences in short-term complications between spinal and general anesthesia for primary total knee arthroplasty. J Bone Joint Surg Am. 2013;95(3):193-199.
13. Katz JN, Losina E, Barrett J, et al. Association between hospital and surgeon procedure volume and outcomes of total hip replacement in the United States medicare population. J Bone Joint Surg Am. 2001;83(11):1622-1629.
14. Manley M, Ong K, Lau E, Kurtz SM. Effect of volume on total hip arthroplasty revision rates in the United States Medicare population. J Bone Joint Surg Am. 2008;90(11):2446-2451.
15. Bozic KJ, Maselli J, Pekow PS, Lindenauer PK, Vail TP, Auerbach AD. The influence of procedure volumes and standardization of care on quality and efficiency in total joint replacement surgery. J Bone Joint Surg Am. 2010;92(16):2643-2652.
16. Lau RL, Perruccio AV, Gandhi R, Mahomed NN. The role of surgeon volume on patient outcome in total knee arthroplasty: a systematic review of the literature. BMC Musculoskelet Disord. 2012;13:250.
Editorial Board Biographies
Asheesh Bedi, MD
Deputy Editor-in-Chief

Dr. Bedi is the Harold and Helen W. Gehring Professor of Orthopaedic Surgery; chief of sports medicine and shoulder surgery at the University of Michigan and MedSport program; team physician for the University of Michigan Athletic Department and the Detroit Lions; and consultant for the NBA, NFL, and NHL Players Associations. He completed his undergraduate training at Northwestern University, where he graduated Summa Cum Laude. He graduated from the University of Michigan Medical School with AOA recognition, and completed his residency training in orthopaedic surgery at the University of Michigan. He completed a 2-year fellowship in sports medicine and shoulder surgery at the Hospital for Special Surgery and Weill Cornell Medical College in New York. His research interests include shoulder, elbow, knee, and hip injuries in athletes.
Joshua S. Dines, MD
Deputy Editor-in-Chief

Dr. Dines is an orthopedic surgeon specializing in sports medicine at the Hospital for Special Surgery in New York; associate professor of orthopedic surgery at Weill Cornell Medical College; assistant team physician for the NY Mets; sports medicine consultant for the NY Rangers; and consultant for the LA Dodgers and LI Ducks. He attended Dartmouth as an undergraduate, completed medical school at Cornell, and completed his residency at the Hospital for Special Surgery. He also completed a sports medicine fellowship at Kerlan-Jobe Orthopaedic Clinic in Los Angeles, California, where he worked as part of the medical staff for the LA Dodgers and the LA Lakers. Previously he served as head team physician for the United States Davis Cup Tennis Team. He is a member of American Academy of Orthopaedic Surgeons, American Shoulder and Elbow Surgeons, The Council on Sports Medicine, The Interurban Orthopedic Association, the American Orthopedic Association, Arthroscopy Association of North America (AANA), and the American Orthopaedic Society for Sports Medicine.
Shane J. Nho, MD, MS
Deputy Editor-in-Chief

Dr. Nho is the director of the Hip Preservation Center, co-head of the Hip Study Group, and assistant professor, Department of Orthopedic Surgery, Division of Sports Medicine at Rush University Medical Center in Chicago, Illinois; and team physician for the Chicago White Sox. He graduated from Northwestern University and enrolled in the MD/MS program at Rush Medical College and the Graduate College of Rush University. He completed his surgical internship at New York Presbyterian Hospital of Weill Cornell Medical College, and completed his residency in orthopedic surgery at the Hospital for Special Surgery in New York. He completed his fellowship in sports medicine at Rush University Medical Center in Chicago, Illinois, where he was the recipient of the Herodicus Society Traveling Fellowship. His research interests include hip, shoulder, and knee reconstruction.
Robin V. West, MD
Deputy Editor-in-Chief

Dr. West is the chairman of sports medicine at Inova Health System; lead team physician for the Washington Nationals; and associate professor at Georgetown University Medical Center and Virginia Commonwealth University School of Medicine in Virginia. She attended Johns Hopkins University as an undergraduate, and completed medical school and an orthopedic surgery residency at George Washington University. Previously, she served as a team physician for the Pittsburgh Steelers; head team physician for the University of Pittsburgh Men’s Basketball team; head team physician for Carnegie Mellon University; and was a former member of the NFL Physician’s Society. She currently is an active member of American Academy of Orthopaedic Surgeons (AAOS), American Orthopaedic Society for Sports Medicine (AOSSM), Major League Baseball Team Physicians Society, and Arthroscopy Association of North America (AANA).
Lisa A. Fortier, DVM, PhD, DACVS
Associate Editor for Translation Science and Animal Research

Dr. Fortier is professor of surgery at Cornell University in Ithaca, New York; board-certified equine surgeon with practices at Cornell University and Ruffian Center in Elmont, New York; vice president of the International Veterinary Regenerative Medicine Society; faculty director of the Cornell Equine Park; staff surgeon at Cornell Ruffian Equine Specialists in Long Island, New York; and executive board (treasurer) of the International Cartilage Repair Society (ICRS). She received her DVM from Colorado State University, and completed her PhD and surgical residency training at Cornell University. She has received the Jacques Lemans Award from the ICRS, the New Investigator Research Award from the ORS, the Pfizer Research Award for Research Excellence from Cornell University, and was elected as a Distinguished Graduate from Drayton High School. She was also the first veterinarian to be elected as president of the ICRS. Her research interests include osteoarthritis, biologics, cartilage repair, and tendonosis.
Alan M. Hirahara, MD, FRCSC
Associate Editor for Sports Medicine/Ultrasound and Biologics

Dr. Hirahara is an orthopaedic surgeon specializing in sports medicine. He runs a private practice in Sacramento, CA. He speaks and teaches nationally and internationally, and does research on arthroscopic shoulder and knee surgery, orthobiologics, and the use of ultrasound. He is board-certified in orthopaedic surgery and orthopaedic sports medicine in the U.S. and Canada. He is the medical director and team physician for California State University, Sacramento Athletics; and head team physician for the Sacramento River Cats. He has been the team physician for the NCAA championships and Olympic Trials in Sacramento since 2001. He did his fellowship training in orthopaedic sports medicine at the University of Toronto. He completed his residency training in orthopaedic surgery in French at l’Université de Montréal. He attended medical school at UCSF and completed his BS in Kinesiology at UCLA with College Honors, Departmental Honors, Phi Beta Kappa, and graduated Magna Cum Laude.
Thay Q. Lee, PhD
Associate Editor for Biomechanics

Dr. Lee is the director and senior research career scientist at VA Long Beach Healthcare System; professor and vice chair for research in the Department of Orthopaedic Surgery; and professor in the Department of Biomedical Engineering at the University of California, Irvine. He received his undergraduate degree in Bioengineering and his Master of Science degree in applied mechanics from the University of California, San Diego. He completed his doctorate degree in biomaterials at Gothenburg University in Sweden. He was elected Fellow for the American Society of Mechanical Engineers (ASME) and the American Institute for Medical and Biological Engineering (AIMBE). He is also an elected member of the American Shoulder and Elbow Surgeons (ASES), Orthopaedic Research Society (ORS), American Society of Biomechanics (ASB), California Orthopaedic Association (COA), Society for Biomaterials (SFB), Biomedical Engineering Society (BMES), and American Orthopaedic Society for Sports Medicine (AOSSM). His research interests include joint biomechanics, shoulder, and knee.
Raffy Mirzayan, MD
Associate Editor for Biologics

Dr. Mirzayan is a board-certified orthopedic surgeon with a subspecialty in sports medicine at Kaiser Permanente in Baldwin Park, California; and founder and director of the Advanced Concepts course held in Las Vegas. He received his Bachelor of Science degree from University of California, Los Angeles (UCLA) and graduated from the Keck School of Medicine of University of Southern California (USC) with AOA Honors. He completed his residency at the Los Angeles County/USC Medical Center, and his fellowship at the Kerlan-Jobe Orthopedic Clinic. He belongs to several orthopedic and sports medicine societies, and was chosen as an American Academy of Orthopaedic Surgeons (AAOS) Leadership Fellow and an American Orthopaedic Society for Sports Medicine (AOSSM) Traveling Fellow. His research interests include shoulder, elbow, knee, cartilage reconstruction, osteotomies, meniscal transplantation, and orthobiologics.
Asheesh Bedi, MD
Deputy Editor-in-Chief
Dr. Bedi is the Harold and Helen W. Gehring Professor of Orthopaedic Surgery; chief of sports medicine and shoulder surgery at the University of Michigan and MedSport program; team physician for the University of Michigan Athletic Department and the Detroit Lions; and consultant for the NBA, NFL, and NHL Players Associations. He completed his undergraduate training at Northwestern University, where he graduated Summa Cum Laude. He graduated from the University of Michigan Medical School with AOA recognition, and completed his residency training in orthopaedic surgery at the University of Michigan. He completed a 2-year fellowship in sports medicine and shoulder surgery at the Hospital for Special Surgery and Weill Cornell Medical College in New York. His research interests include shoulder, elbow, knee, and hip injuries in athletes.
Joshua S. Dines, MD
Deputy Editor-in-Chief
Dr. Dines is an orthopedic surgeon specializing in sports medicine at the Hospital for Special Surgery in New York; associate professor of orthopedic surgery at Weill Cornell Medical College; assistant team physician for the NY Mets; sports medicine consultant for the NY Rangers; and consultant for the LA Dodgers and LI Ducks. He attended Dartmouth as an undergraduate, completed medical school at Cornell, and completed his residency at the Hospital for Special Surgery. He also completed a sports medicine fellowship at Kerlan-Jobe Orthopaedic Clinic in Los Angeles, California, where he worked as part of the medical staff for the LA Dodgers and the LA Lakers. Previously he served as head team physician for the United States Davis Cup Tennis Team. He is a member of American Academy of Orthopaedic Surgeons, American Shoulder and Elbow Surgeons, The Council on Sports Medicine, The Interurban Orthopedic Association, the American Orthopedic Association, Arthroscopy Association of North America (AANA), and the American Orthopaedic Society for Sports Medicine.
Shane J. Nho, MD, MS
Deputy Editor-in-Chief
Dr. Nho is the director of the Hip Preservation Center, co-head of the Hip Study Group, and assistant professor, Department of Orthopedic Surgery, Division of Sports Medicine at Rush University Medical Center in Chicago, Illinois; and team physician for the Chicago White Sox. He graduated from Northwestern University and enrolled in the MD/MS program at Rush Medical College and the Graduate College of Rush University. He completed his surgical internship at New York Presbyterian Hospital of Weill Cornell Medical College, and completed his residency in orthopedic surgery at the Hospital for Special Surgery in New York. He completed his fellowship in sports medicine at Rush University Medical Center in Chicago, Illinois, where he was the recipient of the Herodicus Society Traveling Fellowship. His research interests include hip, shoulder, and knee reconstruction.
Robin V. West, MD
Deputy Editor-in-Chief
Dr. West is the chairman of sports medicine at Inova Health System; lead team physician for the Washington Nationals; and associate professor at Georgetown University Medical Center and Virginia Commonwealth University School of Medicine in Virginia. She attended Johns Hopkins University as an undergraduate, and completed medical school and an orthopedic surgery residency at George Washington University. Previously, she served as a team physician for the Pittsburgh Steelers; head team physician for the University of Pittsburgh Men’s Basketball team; head team physician for Carnegie Mellon University; and was a former member of the NFL Physician’s Society. She currently is an active member of American Academy of Orthopaedic Surgeons (AAOS), American Orthopaedic Society for Sports Medicine (AOSSM), Major League Baseball Team Physicians Society, and Arthroscopy Association of North America (AANA).
Lisa A. Fortier, DVM, PhD, DACVS
Associate Editor for Translation Science and Animal Research
Dr. Fortier is professor of surgery at Cornell University in Ithaca, New York; board-certified equine surgeon with practices at Cornell University and Ruffian Center in Elmont, New York; vice president of the International Veterinary Regenerative Medicine Society; faculty director of the Cornell Equine Park; staff surgeon at Cornell Ruffian Equine Specialists in Long Island, New York; and executive board (treasurer) of the International Cartilage Repair Society (ICRS). She received her DVM from Colorado State University, and completed her PhD and surgical residency training at Cornell University. She has received the Jacques Lemans Award from the ICRS, the New Investigator Research Award from the ORS, the Pfizer Research Award for Research Excellence from Cornell University, and was elected as a Distinguished Graduate from Drayton High School. She was also the first veterinarian to be elected as president of the ICRS. Her research interests include osteoarthritis, biologics, cartilage repair, and tendonosis.
Alan M. Hirahara, MD, FRCSC
Associate Editor for Sports Medicine/Ultrasound and Biologics
Dr. Hirahara is an orthopaedic surgeon specializing in sports medicine. He runs a private practice in Sacramento, CA. He speaks and teaches nationally and internationally, and does research on arthroscopic shoulder and knee surgery, orthobiologics, and the use of ultrasound. He is board-certified in orthopaedic surgery and orthopaedic sports medicine in the U.S. and Canada. He is the medical director and team physician for California State University, Sacramento Athletics; and head team physician for the Sacramento River Cats. He has been the team physician for the NCAA championships and Olympic Trials in Sacramento since 2001. He did his fellowship training in orthopaedic sports medicine at the University of Toronto. He completed his residency training in orthopaedic surgery in French at l’Université de Montréal. He attended medical school at UCSF and completed his BS in Kinesiology at UCLA with College Honors, Departmental Honors, Phi Beta Kappa, and graduated Magna Cum Laude.
Thay Q. Lee, PhD
Associate Editor for Biomechanics
Dr. Lee is the director and senior research career scientist at VA Long Beach Healthcare System; professor and vice chair for research in the Department of Orthopaedic Surgery; and professor in the Department of Biomedical Engineering at the University of California, Irvine. He received his undergraduate degree in Bioengineering and his Master of Science degree in applied mechanics from the University of California, San Diego. He completed his doctorate degree in biomaterials at Gothenburg University in Sweden. He was elected Fellow for the American Society of Mechanical Engineers (ASME) and the American Institute for Medical and Biological Engineering (AIMBE). He is also an elected member of the American Shoulder and Elbow Surgeons (ASES), Orthopaedic Research Society (ORS), American Society of Biomechanics (ASB), California Orthopaedic Association (COA), Society for Biomaterials (SFB), Biomedical Engineering Society (BMES), and American Orthopaedic Society for Sports Medicine (AOSSM). His research interests include joint biomechanics, shoulder, and knee.
Raffy Mirzayan, MD
Associate Editor for Biologics
Dr. Mirzayan is a board-certified orthopedic surgeon with a subspecialty in sports medicine at Kaiser Permanente in Baldwin Park, California; and founder and director of the Advanced Concepts course held in Las Vegas. He received his Bachelor of Science degree from University of California, Los Angeles (UCLA) and graduated from the Keck School of Medicine of University of Southern California (USC) with AOA Honors. He completed his residency at the Los Angeles County/USC Medical Center, and his fellowship at the Kerlan-Jobe Orthopedic Clinic. He belongs to several orthopedic and sports medicine societies, and was chosen as an American Academy of Orthopaedic Surgeons (AAOS) Leadership Fellow and an American Orthopaedic Society for Sports Medicine (AOSSM) Traveling Fellow. His research interests include shoulder, elbow, knee, cartilage reconstruction, osteotomies, meniscal transplantation, and orthobiologics.
Asheesh Bedi, MD
Deputy Editor-in-Chief
Dr. Bedi is the Harold and Helen W. Gehring Professor of Orthopaedic Surgery; chief of sports medicine and shoulder surgery at the University of Michigan and MedSport program; team physician for the University of Michigan Athletic Department and the Detroit Lions; and consultant for the NBA, NFL, and NHL Players Associations. He completed his undergraduate training at Northwestern University, where he graduated Summa Cum Laude. He graduated from the University of Michigan Medical School with AOA recognition, and completed his residency training in orthopaedic surgery at the University of Michigan. He completed a 2-year fellowship in sports medicine and shoulder surgery at the Hospital for Special Surgery and Weill Cornell Medical College in New York. His research interests include shoulder, elbow, knee, and hip injuries in athletes.
Joshua S. Dines, MD
Deputy Editor-in-Chief
Dr. Dines is an orthopedic surgeon specializing in sports medicine at the Hospital for Special Surgery in New York; associate professor of orthopedic surgery at Weill Cornell Medical College; assistant team physician for the NY Mets; sports medicine consultant for the NY Rangers; and consultant for the LA Dodgers and LI Ducks. He attended Dartmouth as an undergraduate, completed medical school at Cornell, and completed his residency at the Hospital for Special Surgery. He also completed a sports medicine fellowship at Kerlan-Jobe Orthopaedic Clinic in Los Angeles, California, where he worked as part of the medical staff for the LA Dodgers and the LA Lakers. Previously he served as head team physician for the United States Davis Cup Tennis Team. He is a member of American Academy of Orthopaedic Surgeons, American Shoulder and Elbow Surgeons, The Council on Sports Medicine, The Interurban Orthopedic Association, the American Orthopedic Association, Arthroscopy Association of North America (AANA), and the American Orthopaedic Society for Sports Medicine.
Shane J. Nho, MD, MS
Deputy Editor-in-Chief
Dr. Nho is the director of the Hip Preservation Center, co-head of the Hip Study Group, and assistant professor, Department of Orthopedic Surgery, Division of Sports Medicine at Rush University Medical Center in Chicago, Illinois; and team physician for the Chicago White Sox. He graduated from Northwestern University and enrolled in the MD/MS program at Rush Medical College and the Graduate College of Rush University. He completed his surgical internship at New York Presbyterian Hospital of Weill Cornell Medical College, and completed his residency in orthopedic surgery at the Hospital for Special Surgery in New York. He completed his fellowship in sports medicine at Rush University Medical Center in Chicago, Illinois, where he was the recipient of the Herodicus Society Traveling Fellowship. His research interests include hip, shoulder, and knee reconstruction.
Robin V. West, MD
Deputy Editor-in-Chief
Dr. West is the chairman of sports medicine at Inova Health System; lead team physician for the Washington Nationals; and associate professor at Georgetown University Medical Center and Virginia Commonwealth University School of Medicine in Virginia. She attended Johns Hopkins University as an undergraduate, and completed medical school and an orthopedic surgery residency at George Washington University. Previously, she served as a team physician for the Pittsburgh Steelers; head team physician for the University of Pittsburgh Men’s Basketball team; head team physician for Carnegie Mellon University; and was a former member of the NFL Physician’s Society. She currently is an active member of American Academy of Orthopaedic Surgeons (AAOS), American Orthopaedic Society for Sports Medicine (AOSSM), Major League Baseball Team Physicians Society, and Arthroscopy Association of North America (AANA).
Lisa A. Fortier, DVM, PhD, DACVS
Associate Editor for Translation Science and Animal Research
Dr. Fortier is professor of surgery at Cornell University in Ithaca, New York; board-certified equine surgeon with practices at Cornell University and Ruffian Center in Elmont, New York; vice president of the International Veterinary Regenerative Medicine Society; faculty director of the Cornell Equine Park; staff surgeon at Cornell Ruffian Equine Specialists in Long Island, New York; and executive board (treasurer) of the International Cartilage Repair Society (ICRS). She received her DVM from Colorado State University, and completed her PhD and surgical residency training at Cornell University. She has received the Jacques Lemans Award from the ICRS, the New Investigator Research Award from the ORS, the Pfizer Research Award for Research Excellence from Cornell University, and was elected as a Distinguished Graduate from Drayton High School. She was also the first veterinarian to be elected as president of the ICRS. Her research interests include osteoarthritis, biologics, cartilage repair, and tendonosis.
Alan M. Hirahara, MD, FRCSC
Associate Editor for Sports Medicine/Ultrasound and Biologics
Dr. Hirahara is an orthopaedic surgeon specializing in sports medicine. He runs a private practice in Sacramento, CA. He speaks and teaches nationally and internationally, and does research on arthroscopic shoulder and knee surgery, orthobiologics, and the use of ultrasound. He is board-certified in orthopaedic surgery and orthopaedic sports medicine in the U.S. and Canada. He is the medical director and team physician for California State University, Sacramento Athletics; and head team physician for the Sacramento River Cats. He has been the team physician for the NCAA championships and Olympic Trials in Sacramento since 2001. He did his fellowship training in orthopaedic sports medicine at the University of Toronto. He completed his residency training in orthopaedic surgery in French at l’Université de Montréal. He attended medical school at UCSF and completed his BS in Kinesiology at UCLA with College Honors, Departmental Honors, Phi Beta Kappa, and graduated Magna Cum Laude.
Thay Q. Lee, PhD
Associate Editor for Biomechanics
Dr. Lee is the director and senior research career scientist at VA Long Beach Healthcare System; professor and vice chair for research in the Department of Orthopaedic Surgery; and professor in the Department of Biomedical Engineering at the University of California, Irvine. He received his undergraduate degree in Bioengineering and his Master of Science degree in applied mechanics from the University of California, San Diego. He completed his doctorate degree in biomaterials at Gothenburg University in Sweden. He was elected Fellow for the American Society of Mechanical Engineers (ASME) and the American Institute for Medical and Biological Engineering (AIMBE). He is also an elected member of the American Shoulder and Elbow Surgeons (ASES), Orthopaedic Research Society (ORS), American Society of Biomechanics (ASB), California Orthopaedic Association (COA), Society for Biomaterials (SFB), Biomedical Engineering Society (BMES), and American Orthopaedic Society for Sports Medicine (AOSSM). His research interests include joint biomechanics, shoulder, and knee.
Raffy Mirzayan, MD
Associate Editor for Biologics
Dr. Mirzayan is a board-certified orthopedic surgeon with a subspecialty in sports medicine at Kaiser Permanente in Baldwin Park, California; and founder and director of the Advanced Concepts course held in Las Vegas. He received his Bachelor of Science degree from University of California, Los Angeles (UCLA) and graduated from the Keck School of Medicine of University of Southern California (USC) with AOA Honors. He completed his residency at the Los Angeles County/USC Medical Center, and his fellowship at the Kerlan-Jobe Orthopedic Clinic. He belongs to several orthopedic and sports medicine societies, and was chosen as an American Academy of Orthopaedic Surgeons (AAOS) Leadership Fellow and an American Orthopaedic Society for Sports Medicine (AOSSM) Traveling Fellow. His research interests include shoulder, elbow, knee, cartilage reconstruction, osteotomies, meniscal transplantation, and orthobiologics.