User login
Returning to competition
As we continue to stumble around trying to find our way out of the COVID-19 pandemic, it has become clear that the journey has been a never-ending continuum of exercises in risk/benefit assessment. The population always has sorted itself into a bell-shaped curve from those who are risk averse to those who revel in risk taking. And, of course, with a paucity of facts on which we can base our assessment of risk, the discussion often shifts to our gut feelings about the benefits.

When faced with the question of when it is time for children to return to in-person schooling, there seems to be reasonably good agreement about the benefits of face-to-face learning. The level of risk is still to be determined.
When it comes to the issue of when to return to competitive school sports, the risks are equally indeterminate but there is less agreement on the benefits. This lack of uniformity reflects a long-standing dichotomy between those parents and students with a passion for competitive sports and those who see them as nonessential. This existential tug-of-war has gone on in almost every school system I am aware of when the school budget comes up for a vote.
The debate about a return to competitive sports on a collegiate and professional level unfortunately is colored by enormous revenues from media contracts, which means that high school and middle schools can’t look to what are essentially businesses for guidance. The delay created confusion, fluctuating angst and disappointment, but the end product made some sense. Volleyball (indoor) and football were indefinitely delayed. Heavy breathing between competitors separated by a couple of feet and protected only by a flimsy net or helmet cage seems like a risk not worth taking – at least until we have more information.
Other sports were allowed to start with restrictions based on existing social distancing mandates which include no locker rooms and no fans. Some rules such as no throw-ins for soccer didn’t make sense given what we are learning about the virus. But, for the most part, the compromises should result in a chance to reap the benefits of competition for the students whose families are willing to expose them to the yet to be fully determined risks.

There has been some grumbling from parents who see the no-fans mandate as a step too far. Until we know more about the risk of group gatherings outdoors, having no fans, including parents and grandparents, makes sense. In fact, to me it is a step long overdue and a rare sliver of silver lining to the pandemic. Competitive youth sports are for the kids. They are not meant to be entertainment events. Too often children are exposed to parental pressure (voiced and unvoiced) about their “performance” on the field. Neither my younger sister nor I can remember our parents going to any of my away football games in high school or any of my lacrosse games in college. I never felt the loss.
Will I miss watching my grandchildren compete? Of course I will miss it badly. However, giving kids some space to learn and enjoy the competition for itself in an atmosphere free of parental over-involvement will be a breath of fresh air. Something we need badly during this pandemic.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
As we continue to stumble around trying to find our way out of the COVID-19 pandemic, it has become clear that the journey has been a never-ending continuum of exercises in risk/benefit assessment. The population always has sorted itself into a bell-shaped curve from those who are risk averse to those who revel in risk taking. And, of course, with a paucity of facts on which we can base our assessment of risk, the discussion often shifts to our gut feelings about the benefits.
When faced with the question of when it is time for children to return to in-person schooling, there seems to be reasonably good agreement about the benefits of face-to-face learning. The level of risk is still to be determined.
When it comes to the issue of when to return to competitive school sports, the risks are equally indeterminate but there is less agreement on the benefits. This lack of uniformity reflects a long-standing dichotomy between those parents and students with a passion for competitive sports and those who see them as nonessential. This existential tug-of-war has gone on in almost every school system I am aware of when the school budget comes up for a vote.
The debate about a return to competitive sports on a collegiate and professional level unfortunately is colored by enormous revenues from media contracts, which means that high school and middle schools can’t look to what are essentially businesses for guidance. The delay created confusion, fluctuating angst and disappointment, but the end product made some sense. Volleyball (indoor) and football were indefinitely delayed. Heavy breathing between competitors separated by a couple of feet and protected only by a flimsy net or helmet cage seems like a risk not worth taking – at least until we have more information.
Other sports were allowed to start with restrictions based on existing social distancing mandates which include no locker rooms and no fans. Some rules such as no throw-ins for soccer didn’t make sense given what we are learning about the virus. But, for the most part, the compromises should result in a chance to reap the benefits of competition for the students whose families are willing to expose them to the yet to be fully determined risks.
There has been some grumbling from parents who see the no-fans mandate as a step too far. Until we know more about the risk of group gatherings outdoors, having no fans, including parents and grandparents, makes sense. In fact, to me it is a step long overdue and a rare sliver of silver lining to the pandemic. Competitive youth sports are for the kids. They are not meant to be entertainment events. Too often children are exposed to parental pressure (voiced and unvoiced) about their “performance” on the field. Neither my younger sister nor I can remember our parents going to any of my away football games in high school or any of my lacrosse games in college. I never felt the loss.
Will I miss watching my grandchildren compete? Of course I will miss it badly. However, giving kids some space to learn and enjoy the competition for itself in an atmosphere free of parental over-involvement will be a breath of fresh air. Something we need badly during this pandemic.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
As we continue to stumble around trying to find our way out of the COVID-19 pandemic, it has become clear that the journey has been a never-ending continuum of exercises in risk/benefit assessment. The population always has sorted itself into a bell-shaped curve from those who are risk averse to those who revel in risk taking. And, of course, with a paucity of facts on which we can base our assessment of risk, the discussion often shifts to our gut feelings about the benefits.
When faced with the question of when it is time for children to return to in-person schooling, there seems to be reasonably good agreement about the benefits of face-to-face learning. The level of risk is still to be determined.
When it comes to the issue of when to return to competitive school sports, the risks are equally indeterminate but there is less agreement on the benefits. This lack of uniformity reflects a long-standing dichotomy between those parents and students with a passion for competitive sports and those who see them as nonessential. This existential tug-of-war has gone on in almost every school system I am aware of when the school budget comes up for a vote.
The debate about a return to competitive sports on a collegiate and professional level unfortunately is colored by enormous revenues from media contracts, which means that high school and middle schools can’t look to what are essentially businesses for guidance. The delay created confusion, fluctuating angst and disappointment, but the end product made some sense. Volleyball (indoor) and football were indefinitely delayed. Heavy breathing between competitors separated by a couple of feet and protected only by a flimsy net or helmet cage seems like a risk not worth taking – at least until we have more information.
Other sports were allowed to start with restrictions based on existing social distancing mandates which include no locker rooms and no fans. Some rules such as no throw-ins for soccer didn’t make sense given what we are learning about the virus. But, for the most part, the compromises should result in a chance to reap the benefits of competition for the students whose families are willing to expose them to the yet to be fully determined risks.
There has been some grumbling from parents who see the no-fans mandate as a step too far. Until we know more about the risk of group gatherings outdoors, having no fans, including parents and grandparents, makes sense. In fact, to me it is a step long overdue and a rare sliver of silver lining to the pandemic. Competitive youth sports are for the kids. They are not meant to be entertainment events. Too often children are exposed to parental pressure (voiced and unvoiced) about their “performance” on the field. Neither my younger sister nor I can remember our parents going to any of my away football games in high school or any of my lacrosse games in college. I never felt the loss.
Will I miss watching my grandchildren compete? Of course I will miss it badly. However, giving kids some space to learn and enjoy the competition for itself in an atmosphere free of parental over-involvement will be a breath of fresh air. Something we need badly during this pandemic.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Is depression contagious?
I previously wrote a column in which I discussed the possible relationship between television viewing and the risk of developing depression. In that column I mentioned that, while there is widespread suspicion that depression may have a genetic component, I was unaware of any strong evidence that this is the case. This week I encountered another study in the American Journal of Psychiatry that suggests that the environment in which a child is raised can play a significant role in whether he or she will develop depression.

All of the children in the study had been born to families in which at least one biological parent had been diagnosed with major depression. There were nearly 700 full sibships and 2,600 half sibships studied. The researchers found that children who had been adopted away and raised in families that had been selected for having high-quality childrearing standards were significantly less likely to develop depression (23% for full siblings, 19% for half siblings) than their siblings who had remained in the home of their biological parents. It is interesting that this protective effect of the adoptive home “disappeared when an adoptive parent or stepsibling had major depression or the adoptive home was disrupted by parental death or divorce.”
It is unlikely that this study ever will be replicated because of the unique manner in which these Swedish adoptions were managed and recorded. However, and probably even more of an influence than genetics.
Are you surprised by the results of this study? Or, like me, have you always suspected that a child growing up in a household with a depressed, missing, or divorced parent was at increased risk of becoming depressed, particularly they had a genetic vulnerability? How will you change your approach to families with a depressed parent or ones that are navigating through the stormy waters of even an amicable divorce? Will you be more diligent about screening children in these families for depression? Should the agencies that are responsible for managing adoption and foster home placement include this new information in their screening criteria?
It would be very interesting to see a similar study performed using families in which a biological parent had been diagnosed with anxiety or an attention-deficit disorder. Could it mean that we should be considering depression and these conditions as contagious disorders? The results from such studies might help provide clarity to why we are seeing more children with mental health complaints. They might explain why pediatricians are seeing an increasing frequency of mental health complaints in our offices. It may not be too far-fetched to use epidemiologic terms when we are talking about depression, anxiety, and ADHD. Should we be considering these conditions to be contagious under certain circumstances?
Since the human genome has been sequenced I sense that our attention has become overfocused on using what we are learning about our DNA to explain what makes us sick. It may be time to swing the pendulum back a few degrees and remind ourselves of the power of the family environment.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
I previously wrote a column in which I discussed the possible relationship between television viewing and the risk of developing depression. In that column I mentioned that, while there is widespread suspicion that depression may have a genetic component, I was unaware of any strong evidence that this is the case. This week I encountered another study in the American Journal of Psychiatry that suggests that the environment in which a child is raised can play a significant role in whether he or she will develop depression.
All of the children in the study had been born to families in which at least one biological parent had been diagnosed with major depression. There were nearly 700 full sibships and 2,600 half sibships studied. The researchers found that children who had been adopted away and raised in families that had been selected for having high-quality childrearing standards were significantly less likely to develop depression (23% for full siblings, 19% for half siblings) than their siblings who had remained in the home of their biological parents. It is interesting that this protective effect of the adoptive home “disappeared when an adoptive parent or stepsibling had major depression or the adoptive home was disrupted by parental death or divorce.”
It is unlikely that this study ever will be replicated because of the unique manner in which these Swedish adoptions were managed and recorded. However, and probably even more of an influence than genetics.
Are you surprised by the results of this study? Or, like me, have you always suspected that a child growing up in a household with a depressed, missing, or divorced parent was at increased risk of becoming depressed, particularly they had a genetic vulnerability? How will you change your approach to families with a depressed parent or ones that are navigating through the stormy waters of even an amicable divorce? Will you be more diligent about screening children in these families for depression? Should the agencies that are responsible for managing adoption and foster home placement include this new information in their screening criteria?
It would be very interesting to see a similar study performed using families in which a biological parent had been diagnosed with anxiety or an attention-deficit disorder. Could it mean that we should be considering depression and these conditions as contagious disorders? The results from such studies might help provide clarity to why we are seeing more children with mental health complaints. They might explain why pediatricians are seeing an increasing frequency of mental health complaints in our offices. It may not be too far-fetched to use epidemiologic terms when we are talking about depression, anxiety, and ADHD. Should we be considering these conditions to be contagious under certain circumstances?
Since the human genome has been sequenced I sense that our attention has become overfocused on using what we are learning about our DNA to explain what makes us sick. It may be time to swing the pendulum back a few degrees and remind ourselves of the power of the family environment.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
I previously wrote a column in which I discussed the possible relationship between television viewing and the risk of developing depression. In that column I mentioned that, while there is widespread suspicion that depression may have a genetic component, I was unaware of any strong evidence that this is the case. This week I encountered another study in the American Journal of Psychiatry that suggests that the environment in which a child is raised can play a significant role in whether he or she will develop depression.
All of the children in the study had been born to families in which at least one biological parent had been diagnosed with major depression. There were nearly 700 full sibships and 2,600 half sibships studied. The researchers found that children who had been adopted away and raised in families that had been selected for having high-quality childrearing standards were significantly less likely to develop depression (23% for full siblings, 19% for half siblings) than their siblings who had remained in the home of their biological parents. It is interesting that this protective effect of the adoptive home “disappeared when an adoptive parent or stepsibling had major depression or the adoptive home was disrupted by parental death or divorce.”
It is unlikely that this study ever will be replicated because of the unique manner in which these Swedish adoptions were managed and recorded. However, and probably even more of an influence than genetics.
Are you surprised by the results of this study? Or, like me, have you always suspected that a child growing up in a household with a depressed, missing, or divorced parent was at increased risk of becoming depressed, particularly they had a genetic vulnerability? How will you change your approach to families with a depressed parent or ones that are navigating through the stormy waters of even an amicable divorce? Will you be more diligent about screening children in these families for depression? Should the agencies that are responsible for managing adoption and foster home placement include this new information in their screening criteria?
It would be very interesting to see a similar study performed using families in which a biological parent had been diagnosed with anxiety or an attention-deficit disorder. Could it mean that we should be considering depression and these conditions as contagious disorders? The results from such studies might help provide clarity to why we are seeing more children with mental health complaints. They might explain why pediatricians are seeing an increasing frequency of mental health complaints in our offices. It may not be too far-fetched to use epidemiologic terms when we are talking about depression, anxiety, and ADHD. Should we be considering these conditions to be contagious under certain circumstances?
Since the human genome has been sequenced I sense that our attention has become overfocused on using what we are learning about our DNA to explain what makes us sick. It may be time to swing the pendulum back a few degrees and remind ourselves of the power of the family environment.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Full-time, part-time, FTE: Know the differences
The wholesale to them. While rules vary from state to state, some generalizations can be made.

Even the definitions of full-time and part-time vary. For instance, under the Affordable Care Act (ACA), full time means working at least 30 hours per week. Under the Families First Coronavirus Response Act (FFCRA), it is 40 hours.
Full-time equivalent (FTE) is a concept designed to document a part-time workforce in terms of full-time employment, by taking the total hours worked by all part-time employees and dividing by the full-time schedule. Of course, the ACA and the Paycheck Protection Program (PPP) calculate that number differently: The ACA requires you to total all the hours worked by part-time employees per month, and divide by 120. For the PPP, you divide the total part-time hours per week by 40, and round to the nearest tenth. (You can also use a simplified method that assigns a 1.0 for employees who work 40 hours or more per week and 0.5 for those who work fewer; whichever method you choose, you must apply it consistently on all PPP forms.)
FTEs are important for the purposes of the ACA because employers with 50 or more full-timers plus FTEs must offer health coverage to their full-timers and dependents. But most private practitioners need an accurate FTE total to deal with the PPP: If staffing levels weren’t maintained after you received a PPP loan, your loan forgiveness amount may be reduced. Staffing levels are determined by comparing the average number of full-timers plus FTEs during the “covered period” to either the period from Feb. 15 through June 30, 2019, or Jan. 1 through Feb. 28, 2020.
The PPP aside, FTEs have created confusion over when an employee is entitled to overtime pay. Under federal law, overtime is due whenever an employee works more than 40 hours per week; up to 40 hours, the regular wage is paid. (There are exemptions, and a few states use a daily number.) For example, if a part-timer receiving $900 per week for a 30-hour workweek works more than 30 hours, the hours from 30 to 40 would be compensated at their normal wage of $30 per hour ($900 ÷ 30). If the employee worked more than 40 hours, you would pay overtime (in this case $45 per hour, $30 x 1.5) for the hours in excess of 40.
To address a few other employment questions that I am frequently asked:
Under the FFCRA, you must provide both full- and part-time employees with emergency paid sick leave (EPSL) if they’re unable to work from your office or their home because of illness attributable to COVID-19, quarantine, or caring for a sick family member or child whose school is closed. Full-time employees are entitled to up to 80 hours of EPSL, and part-timers an average of what they work every 2 weeks. Some states have their own laws independent from the FFCRA. Check your state or local laws.
- Some states require you to provide meal and rest breaks to both full- and part-time employees. In California, for example, employers must provide a 30-minute meal break after no more than 5 hours of work, unless the total workday is less than 6 hours and both employers and employees consent to waive breaks. California also requires rest breaks after every 4 hours worked. Check the laws in your state.
- You must include part-time employees in a 401(k) retirement plan if they work at least 1,000 hours in a year, which is about 20 hours per week. That rule is changing in 2021 to 500 hours for employees older than 21. There are state-run retirement programs in California, Connecticut, New Jersey, Washington, and Oregon, among other states. Check your state law for details.
- If you offer paid vacations to full-time employees, you do not have to do the same for part-timers. (In fact, there is no requirement in most states to offer vacation time at all.) My office does offer it to part-time employees on a pro rata basis, as do many others in my area. Again, check your state law.
As always, consult with your attorney if it’s not clear which rules apply in your specific situation.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no relevant disclosures related to the topic of this column. Write to him at dermnews@mdedge.com.
The wholesale to them. While rules vary from state to state, some generalizations can be made.
Even the definitions of full-time and part-time vary. For instance, under the Affordable Care Act (ACA), full time means working at least 30 hours per week. Under the Families First Coronavirus Response Act (FFCRA), it is 40 hours.
Full-time equivalent (FTE) is a concept designed to document a part-time workforce in terms of full-time employment, by taking the total hours worked by all part-time employees and dividing by the full-time schedule. Of course, the ACA and the Paycheck Protection Program (PPP) calculate that number differently: The ACA requires you to total all the hours worked by part-time employees per month, and divide by 120. For the PPP, you divide the total part-time hours per week by 40, and round to the nearest tenth. (You can also use a simplified method that assigns a 1.0 for employees who work 40 hours or more per week and 0.5 for those who work fewer; whichever method you choose, you must apply it consistently on all PPP forms.)
FTEs are important for the purposes of the ACA because employers with 50 or more full-timers plus FTEs must offer health coverage to their full-timers and dependents. But most private practitioners need an accurate FTE total to deal with the PPP: If staffing levels weren’t maintained after you received a PPP loan, your loan forgiveness amount may be reduced. Staffing levels are determined by comparing the average number of full-timers plus FTEs during the “covered period” to either the period from Feb. 15 through June 30, 2019, or Jan. 1 through Feb. 28, 2020.
The PPP aside, FTEs have created confusion over when an employee is entitled to overtime pay. Under federal law, overtime is due whenever an employee works more than 40 hours per week; up to 40 hours, the regular wage is paid. (There are exemptions, and a few states use a daily number.) For example, if a part-timer receiving $900 per week for a 30-hour workweek works more than 30 hours, the hours from 30 to 40 would be compensated at their normal wage of $30 per hour ($900 ÷ 30). If the employee worked more than 40 hours, you would pay overtime (in this case $45 per hour, $30 x 1.5) for the hours in excess of 40.
To address a few other employment questions that I am frequently asked:
Under the FFCRA, you must provide both full- and part-time employees with emergency paid sick leave (EPSL) if they’re unable to work from your office or their home because of illness attributable to COVID-19, quarantine, or caring for a sick family member or child whose school is closed. Full-time employees are entitled to up to 80 hours of EPSL, and part-timers an average of what they work every 2 weeks. Some states have their own laws independent from the FFCRA. Check your state or local laws.
- Some states require you to provide meal and rest breaks to both full- and part-time employees. In California, for example, employers must provide a 30-minute meal break after no more than 5 hours of work, unless the total workday is less than 6 hours and both employers and employees consent to waive breaks. California also requires rest breaks after every 4 hours worked. Check the laws in your state.
- You must include part-time employees in a 401(k) retirement plan if they work at least 1,000 hours in a year, which is about 20 hours per week. That rule is changing in 2021 to 500 hours for employees older than 21. There are state-run retirement programs in California, Connecticut, New Jersey, Washington, and Oregon, among other states. Check your state law for details.
- If you offer paid vacations to full-time employees, you do not have to do the same for part-timers. (In fact, there is no requirement in most states to offer vacation time at all.) My office does offer it to part-time employees on a pro rata basis, as do many others in my area. Again, check your state law.
As always, consult with your attorney if it’s not clear which rules apply in your specific situation.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no relevant disclosures related to the topic of this column. Write to him at dermnews@mdedge.com.
The wholesale to them. While rules vary from state to state, some generalizations can be made.
Even the definitions of full-time and part-time vary. For instance, under the Affordable Care Act (ACA), full time means working at least 30 hours per week. Under the Families First Coronavirus Response Act (FFCRA), it is 40 hours.
Full-time equivalent (FTE) is a concept designed to document a part-time workforce in terms of full-time employment, by taking the total hours worked by all part-time employees and dividing by the full-time schedule. Of course, the ACA and the Paycheck Protection Program (PPP) calculate that number differently: The ACA requires you to total all the hours worked by part-time employees per month, and divide by 120. For the PPP, you divide the total part-time hours per week by 40, and round to the nearest tenth. (You can also use a simplified method that assigns a 1.0 for employees who work 40 hours or more per week and 0.5 for those who work fewer; whichever method you choose, you must apply it consistently on all PPP forms.)
FTEs are important for the purposes of the ACA because employers with 50 or more full-timers plus FTEs must offer health coverage to their full-timers and dependents. But most private practitioners need an accurate FTE total to deal with the PPP: If staffing levels weren’t maintained after you received a PPP loan, your loan forgiveness amount may be reduced. Staffing levels are determined by comparing the average number of full-timers plus FTEs during the “covered period” to either the period from Feb. 15 through June 30, 2019, or Jan. 1 through Feb. 28, 2020.
The PPP aside, FTEs have created confusion over when an employee is entitled to overtime pay. Under federal law, overtime is due whenever an employee works more than 40 hours per week; up to 40 hours, the regular wage is paid. (There are exemptions, and a few states use a daily number.) For example, if a part-timer receiving $900 per week for a 30-hour workweek works more than 30 hours, the hours from 30 to 40 would be compensated at their normal wage of $30 per hour ($900 ÷ 30). If the employee worked more than 40 hours, you would pay overtime (in this case $45 per hour, $30 x 1.5) for the hours in excess of 40.
To address a few other employment questions that I am frequently asked:
Under the FFCRA, you must provide both full- and part-time employees with emergency paid sick leave (EPSL) if they’re unable to work from your office or their home because of illness attributable to COVID-19, quarantine, or caring for a sick family member or child whose school is closed. Full-time employees are entitled to up to 80 hours of EPSL, and part-timers an average of what they work every 2 weeks. Some states have their own laws independent from the FFCRA. Check your state or local laws.
- Some states require you to provide meal and rest breaks to both full- and part-time employees. In California, for example, employers must provide a 30-minute meal break after no more than 5 hours of work, unless the total workday is less than 6 hours and both employers and employees consent to waive breaks. California also requires rest breaks after every 4 hours worked. Check the laws in your state.
- You must include part-time employees in a 401(k) retirement plan if they work at least 1,000 hours in a year, which is about 20 hours per week. That rule is changing in 2021 to 500 hours for employees older than 21. There are state-run retirement programs in California, Connecticut, New Jersey, Washington, and Oregon, among other states. Check your state law for details.
- If you offer paid vacations to full-time employees, you do not have to do the same for part-timers. (In fact, there is no requirement in most states to offer vacation time at all.) My office does offer it to part-time employees on a pro rata basis, as do many others in my area. Again, check your state law.
As always, consult with your attorney if it’s not clear which rules apply in your specific situation.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no relevant disclosures related to the topic of this column. Write to him at dermnews@mdedge.com.

COVID-19 and the superspreaders: Teens
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.

According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.
According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.
According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Please stop using the adjective “elective” to describe the important health services ObGyns provide
During the April 2020 peak of patient admissions to our hospital caused by coronavirus disease 2019 (COVID-19), we severely limited the number of surgical procedures performed to conserve health system resources. During this stressful time, some administrators and physicians began categorizing operations for cancer as "elective" procedures that could be postponed for months. Personally, I think the use of elective to describe cancer surgery is not optimal, even during a pandemic. In reality, the surgeries for patients with cancer were being postponed to ensure that services were available for patients with severe and critical COVID-19 disease, not because the surgeries were "elective." The health system leaders were making the rational decision to prioritize the needs of patients with COVID-19 infections over the needs of patients with cancer. However, they were using an inappropriate description of the rationale for postponing the surgery for patients with cancer—an intellectual short-cut.
This experience prompted me to explore all the medical interventions commonly described as elective. Surprisingly, among medical specialists, obstetricians excel in using the adjective elective to describe our important work. For example, in the medical record we commonly use terms such as “elective induction of labor,” “elective cesarean delivery” (CD) and “elective termination of pregnancy.” I believe it would advance our field if obstetricians stopped using the term elective to describe the important health services we provide.
Stop using the term “elective induction of labor”
Ghartey and Macones recently advocated for all obstetricians to stop using the term elective when describing induction of labor.1 The ARRIVE trial (A Randomized Trial of Induction vs Expectant Management)2 demonstrated that, among nulliparous women at 39 weeks’ gestation, induction of labor resulted in a lower CD rate than expectant management (18.6% vs 22.2%, respectively; relative risk, 0.84; 95% confidence interval [CI], 0.76-0.93). These findings indicate that induction of labor is not elective because it provides a clear health benefit over the alternative of expectant management. Given current expert guidance, induction of labor prior to 39 weeks’ gestation must be based on an accepted medical indication and provide a health benefit; hence, these inductions are medically indicated. Similarly, since induction of labor at 39 weeks’ gestation also provides a clear health benefit it is also medically indicated and not “elective.” Ghartey and Macones conclude1:
"The words we choose to
describe medical interventions
matter. They send a message
to patients, physicians, nurses,
and hospital administrators.
When the term 'elective' is applied to a medical intervention,
it implies that it is not really
necessary. That is certainly not
the case when it comes to 39-
week nulliparous induction. The
ARRIVE trial provides grade A
(good and consistent) evidence
that labor induction provided
benefit with no harm to women
and their infants. These inductions are not 'elective'."
An alternative descriptor is “medically indicated” induction.
Continue to: Stop using the term “elective cesarean delivery”...
Stop using the term “elective cesarean delivery”
I recently searched PubMed for publications using the key words, “elective cesarean delivery,” and more than 7,000 publications were identified by the National Library of Medicine. “Elective cesarean delivery” is clearly an important term used by obstetrical authorities. What do we mean by elective CD?
At 39 weeks’ gestation, a low-risk nulliparous pregnant woman has a limited number of options:
- induction of labor
- expectant management awaiting the onset of labor
- scheduled CD before the onset of labor.
For a low-risk pregnant woman at 39 weeks’ gestation, the American College of Obstetricians and Gynecologists recommends vaginal delivery because it best balances the risks and benefits for the woman and newborn.3 When a low-risk nulliparous pregnant woman asks a clinician about a scheduled CD, we are trained to thoroughly explore the reasons for the woman’s request, including her intellectual, fact-based, concerns about labor and vaginal birth and her emotional reaction to the thought of a vaginal or cesarean birth. In this situation the clinician will provide information about the risks and benefits of vaginal versus CD. In the vast majority of situations, the pregnant woman will agree to attempting vaginal delivery. In one study of 458,767 births, only 0.2% of women choose a “maternal request cesarean delivery.”4
After thorough counseling, if a woman and her clinician jointly agree to schedule a primary CD it will be the result of hours of intensive discussion, not an imprudent and hasty decision. In this case, the delivery is best characterized as a “maternal request cesarean delivery,” not an “elective” CD.
Stop using the terms “elective termination of pregnancy” and “elective abortion”
Janiak and Goldberg have advocated for the elimination of the phrase elective abortion.5 They write5:
"Support for abortion varies
depending on the reason for
the abortion—whether it is
'elective' or 'indicated.' In the
case of abortion, these terms
generally differentiate between
women seeking abortion for
reasons of maternal or fetal
health (an 'indicated abortion')
defined in contrast to women
seeking abortion for other
reasons (an 'elective abortion').
We argue that such a distinction is impossible to operationalize in a just manner. The use
of the phrase 'elective abortion'
promotes the institutionalization of a false hierarchy of need
among abortion patients."
My experience is that pregnant women never seek an abortion based on whimsy. Most pregnant women who consider an abortion struggle greatly with the choice, using reason and judgment to arrive at their final decision. The choice to seek an abortion is always a difficult one, influenced by a constellation of hard facts that impact the woman’s life. Using the term elective to describe an abortion implies a moral judgment and stigmatizes the choice to have an abortion. Janiak and Goldberg conclude by recommending the elimination of the phrase 'elective abortion' in favor of the phrase “induced abortion.”5
Continue to: Time for change...
Time for change
Shockingly, in searching the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD10), the word elective is most commonly used in the context of health services provided to pregnant women, including: elective induction of labor (Z34.90), elective cesarean delivery (O82), elective termination of pregnancy (Z33.2), and elective fetal reduction (Z031.30X0). In ICD10, other specialties do not describe the scope of their health services with the adjective elective.
There are many definitions and interpretations of elective. The most benign use of the word in the context of surgery is to contrast procedures that can be scheduled in the future with those that need to be performed urgently. In this context elective only refers to the timing, not the medical necessity, of the procedure. By contrast, describing a procedure as elective may signal that it is not medically necessary and is being performed based on the capricious preference of the patient or physician. Given the confusion and misunderstanding that may be caused by describing our important health services as “elective,” I hope that we can permanently sunset use of the term. ●
- Ghartey J, Macones GA. 39-week nulliparous inductions are not elective. Am J Obstet Gynecol. 2020;222:519-520.
- Grobman WA, Rice MM, Reddy UM, et al. Labor induction versus expectant management in low-risk nulliparous women. N Engl J Med. 2018;379:513-523.
- ACOG Committee Opinion No 761: cesarean delivery on maternal request. Obstet Gynecol. 2019;133.e73-e77.
- Gossman GL, Joesch JM, Tanfer K. Trends in maternal request cesarean delivery from 1991 to 2004. Obstet Gynecol. 2006;108:1506-1516.
- Janiak E, Goldberg AB. Eliminating the phrase “elective abortion”: why language matters. Contraception. 2016;93:89-92.

Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair Emeritus, Obstetrics and Gynecology
Brigham and Women’s Hospital
Boston, Massachusetts
Kate Macy Ladd Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair Emeritus, Obstetrics and Gynecology
Brigham and Women’s Hospital
Boston, Massachusetts
Kate Macy Ladd Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG Management
Chair Emeritus, Obstetrics and Gynecology
Brigham and Women’s Hospital
Boston, Massachusetts
Kate Macy Ladd Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Dr. Barbieri reports no financial relationships relevant to this article.
During the April 2020 peak of patient admissions to our hospital caused by coronavirus disease 2019 (COVID-19), we severely limited the number of surgical procedures performed to conserve health system resources. During this stressful time, some administrators and physicians began categorizing operations for cancer as "elective" procedures that could be postponed for months. Personally, I think the use of elective to describe cancer surgery is not optimal, even during a pandemic. In reality, the surgeries for patients with cancer were being postponed to ensure that services were available for patients with severe and critical COVID-19 disease, not because the surgeries were "elective." The health system leaders were making the rational decision to prioritize the needs of patients with COVID-19 infections over the needs of patients with cancer. However, they were using an inappropriate description of the rationale for postponing the surgery for patients with cancer—an intellectual short-cut.
This experience prompted me to explore all the medical interventions commonly described as elective. Surprisingly, among medical specialists, obstetricians excel in using the adjective elective to describe our important work. For example, in the medical record we commonly use terms such as “elective induction of labor,” “elective cesarean delivery” (CD) and “elective termination of pregnancy.” I believe it would advance our field if obstetricians stopped using the term elective to describe the important health services we provide.
Stop using the term “elective induction of labor”
Ghartey and Macones recently advocated for all obstetricians to stop using the term elective when describing induction of labor.1 The ARRIVE trial (A Randomized Trial of Induction vs Expectant Management)2 demonstrated that, among nulliparous women at 39 weeks’ gestation, induction of labor resulted in a lower CD rate than expectant management (18.6% vs 22.2%, respectively; relative risk, 0.84; 95% confidence interval [CI], 0.76-0.93). These findings indicate that induction of labor is not elective because it provides a clear health benefit over the alternative of expectant management. Given current expert guidance, induction of labor prior to 39 weeks’ gestation must be based on an accepted medical indication and provide a health benefit; hence, these inductions are medically indicated. Similarly, since induction of labor at 39 weeks’ gestation also provides a clear health benefit it is also medically indicated and not “elective.” Ghartey and Macones conclude1:
"The words we choose to
describe medical interventions
matter. They send a message
to patients, physicians, nurses,
and hospital administrators.
When the term 'elective' is applied to a medical intervention,
it implies that it is not really
necessary. That is certainly not
the case when it comes to 39-
week nulliparous induction. The
ARRIVE trial provides grade A
(good and consistent) evidence
that labor induction provided
benefit with no harm to women
and their infants. These inductions are not 'elective'."
An alternative descriptor is “medically indicated” induction.
Continue to: Stop using the term “elective cesarean delivery”...
Stop using the term “elective cesarean delivery”
I recently searched PubMed for publications using the key words, “elective cesarean delivery,” and more than 7,000 publications were identified by the National Library of Medicine. “Elective cesarean delivery” is clearly an important term used by obstetrical authorities. What do we mean by elective CD?
At 39 weeks’ gestation, a low-risk nulliparous pregnant woman has a limited number of options:
- induction of labor
- expectant management awaiting the onset of labor
- scheduled CD before the onset of labor.
For a low-risk pregnant woman at 39 weeks’ gestation, the American College of Obstetricians and Gynecologists recommends vaginal delivery because it best balances the risks and benefits for the woman and newborn.3 When a low-risk nulliparous pregnant woman asks a clinician about a scheduled CD, we are trained to thoroughly explore the reasons for the woman’s request, including her intellectual, fact-based, concerns about labor and vaginal birth and her emotional reaction to the thought of a vaginal or cesarean birth. In this situation the clinician will provide information about the risks and benefits of vaginal versus CD. In the vast majority of situations, the pregnant woman will agree to attempting vaginal delivery. In one study of 458,767 births, only 0.2% of women choose a “maternal request cesarean delivery.”4
After thorough counseling, if a woman and her clinician jointly agree to schedule a primary CD it will be the result of hours of intensive discussion, not an imprudent and hasty decision. In this case, the delivery is best characterized as a “maternal request cesarean delivery,” not an “elective” CD.
Stop using the terms “elective termination of pregnancy” and “elective abortion”
Janiak and Goldberg have advocated for the elimination of the phrase elective abortion.5 They write5:
"Support for abortion varies
depending on the reason for
the abortion—whether it is
'elective' or 'indicated.' In the
case of abortion, these terms
generally differentiate between
women seeking abortion for
reasons of maternal or fetal
health (an 'indicated abortion')
defined in contrast to women
seeking abortion for other
reasons (an 'elective abortion').
We argue that such a distinction is impossible to operationalize in a just manner. The use
of the phrase 'elective abortion'
promotes the institutionalization of a false hierarchy of need
among abortion patients."
My experience is that pregnant women never seek an abortion based on whimsy. Most pregnant women who consider an abortion struggle greatly with the choice, using reason and judgment to arrive at their final decision. The choice to seek an abortion is always a difficult one, influenced by a constellation of hard facts that impact the woman’s life. Using the term elective to describe an abortion implies a moral judgment and stigmatizes the choice to have an abortion. Janiak and Goldberg conclude by recommending the elimination of the phrase 'elective abortion' in favor of the phrase “induced abortion.”5
Continue to: Time for change...
Time for change
Shockingly, in searching the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD10), the word elective is most commonly used in the context of health services provided to pregnant women, including: elective induction of labor (Z34.90), elective cesarean delivery (O82), elective termination of pregnancy (Z33.2), and elective fetal reduction (Z031.30X0). In ICD10, other specialties do not describe the scope of their health services with the adjective elective.
There are many definitions and interpretations of elective. The most benign use of the word in the context of surgery is to contrast procedures that can be scheduled in the future with those that need to be performed urgently. In this context elective only refers to the timing, not the medical necessity, of the procedure. By contrast, describing a procedure as elective may signal that it is not medically necessary and is being performed based on the capricious preference of the patient or physician. Given the confusion and misunderstanding that may be caused by describing our important health services as “elective,” I hope that we can permanently sunset use of the term. ●
During the April 2020 peak of patient admissions to our hospital caused by coronavirus disease 2019 (COVID-19), we severely limited the number of surgical procedures performed to conserve health system resources. During this stressful time, some administrators and physicians began categorizing operations for cancer as "elective" procedures that could be postponed for months. Personally, I think the use of elective to describe cancer surgery is not optimal, even during a pandemic. In reality, the surgeries for patients with cancer were being postponed to ensure that services were available for patients with severe and critical COVID-19 disease, not because the surgeries were "elective." The health system leaders were making the rational decision to prioritize the needs of patients with COVID-19 infections over the needs of patients with cancer. However, they were using an inappropriate description of the rationale for postponing the surgery for patients with cancer—an intellectual short-cut.
This experience prompted me to explore all the medical interventions commonly described as elective. Surprisingly, among medical specialists, obstetricians excel in using the adjective elective to describe our important work. For example, in the medical record we commonly use terms such as “elective induction of labor,” “elective cesarean delivery” (CD) and “elective termination of pregnancy.” I believe it would advance our field if obstetricians stopped using the term elective to describe the important health services we provide.
Stop using the term “elective induction of labor”
Ghartey and Macones recently advocated for all obstetricians to stop using the term elective when describing induction of labor.1 The ARRIVE trial (A Randomized Trial of Induction vs Expectant Management)2 demonstrated that, among nulliparous women at 39 weeks’ gestation, induction of labor resulted in a lower CD rate than expectant management (18.6% vs 22.2%, respectively; relative risk, 0.84; 95% confidence interval [CI], 0.76-0.93). These findings indicate that induction of labor is not elective because it provides a clear health benefit over the alternative of expectant management. Given current expert guidance, induction of labor prior to 39 weeks’ gestation must be based on an accepted medical indication and provide a health benefit; hence, these inductions are medically indicated. Similarly, since induction of labor at 39 weeks’ gestation also provides a clear health benefit it is also medically indicated and not “elective.” Ghartey and Macones conclude1:
"The words we choose to
describe medical interventions
matter. They send a message
to patients, physicians, nurses,
and hospital administrators.
When the term 'elective' is applied to a medical intervention,
it implies that it is not really
necessary. That is certainly not
the case when it comes to 39-
week nulliparous induction. The
ARRIVE trial provides grade A
(good and consistent) evidence
that labor induction provided
benefit with no harm to women
and their infants. These inductions are not 'elective'."
An alternative descriptor is “medically indicated” induction.
Continue to: Stop using the term “elective cesarean delivery”...
Stop using the term “elective cesarean delivery”
I recently searched PubMed for publications using the key words, “elective cesarean delivery,” and more than 7,000 publications were identified by the National Library of Medicine. “Elective cesarean delivery” is clearly an important term used by obstetrical authorities. What do we mean by elective CD?
At 39 weeks’ gestation, a low-risk nulliparous pregnant woman has a limited number of options:
- induction of labor
- expectant management awaiting the onset of labor
- scheduled CD before the onset of labor.
For a low-risk pregnant woman at 39 weeks’ gestation, the American College of Obstetricians and Gynecologists recommends vaginal delivery because it best balances the risks and benefits for the woman and newborn.3 When a low-risk nulliparous pregnant woman asks a clinician about a scheduled CD, we are trained to thoroughly explore the reasons for the woman’s request, including her intellectual, fact-based, concerns about labor and vaginal birth and her emotional reaction to the thought of a vaginal or cesarean birth. In this situation the clinician will provide information about the risks and benefits of vaginal versus CD. In the vast majority of situations, the pregnant woman will agree to attempting vaginal delivery. In one study of 458,767 births, only 0.2% of women choose a “maternal request cesarean delivery.”4
After thorough counseling, if a woman and her clinician jointly agree to schedule a primary CD it will be the result of hours of intensive discussion, not an imprudent and hasty decision. In this case, the delivery is best characterized as a “maternal request cesarean delivery,” not an “elective” CD.
Stop using the terms “elective termination of pregnancy” and “elective abortion”
Janiak and Goldberg have advocated for the elimination of the phrase elective abortion.5 They write5:
"Support for abortion varies
depending on the reason for
the abortion—whether it is
'elective' or 'indicated.' In the
case of abortion, these terms
generally differentiate between
women seeking abortion for
reasons of maternal or fetal
health (an 'indicated abortion')
defined in contrast to women
seeking abortion for other
reasons (an 'elective abortion').
We argue that such a distinction is impossible to operationalize in a just manner. The use
of the phrase 'elective abortion'
promotes the institutionalization of a false hierarchy of need
among abortion patients."
My experience is that pregnant women never seek an abortion based on whimsy. Most pregnant women who consider an abortion struggle greatly with the choice, using reason and judgment to arrive at their final decision. The choice to seek an abortion is always a difficult one, influenced by a constellation of hard facts that impact the woman’s life. Using the term elective to describe an abortion implies a moral judgment and stigmatizes the choice to have an abortion. Janiak and Goldberg conclude by recommending the elimination of the phrase 'elective abortion' in favor of the phrase “induced abortion.”5
Continue to: Time for change...
Time for change
Shockingly, in searching the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD10), the word elective is most commonly used in the context of health services provided to pregnant women, including: elective induction of labor (Z34.90), elective cesarean delivery (O82), elective termination of pregnancy (Z33.2), and elective fetal reduction (Z031.30X0). In ICD10, other specialties do not describe the scope of their health services with the adjective elective.
There are many definitions and interpretations of elective. The most benign use of the word in the context of surgery is to contrast procedures that can be scheduled in the future with those that need to be performed urgently. In this context elective only refers to the timing, not the medical necessity, of the procedure. By contrast, describing a procedure as elective may signal that it is not medically necessary and is being performed based on the capricious preference of the patient or physician. Given the confusion and misunderstanding that may be caused by describing our important health services as “elective,” I hope that we can permanently sunset use of the term. ●
- Ghartey J, Macones GA. 39-week nulliparous inductions are not elective. Am J Obstet Gynecol. 2020;222:519-520.
- Grobman WA, Rice MM, Reddy UM, et al. Labor induction versus expectant management in low-risk nulliparous women. N Engl J Med. 2018;379:513-523.
- ACOG Committee Opinion No 761: cesarean delivery on maternal request. Obstet Gynecol. 2019;133.e73-e77.
- Gossman GL, Joesch JM, Tanfer K. Trends in maternal request cesarean delivery from 1991 to 2004. Obstet Gynecol. 2006;108:1506-1516.
- Janiak E, Goldberg AB. Eliminating the phrase “elective abortion”: why language matters. Contraception. 2016;93:89-92.
- Ghartey J, Macones GA. 39-week nulliparous inductions are not elective. Am J Obstet Gynecol. 2020;222:519-520.
- Grobman WA, Rice MM, Reddy UM, et al. Labor induction versus expectant management in low-risk nulliparous women. N Engl J Med. 2018;379:513-523.
- ACOG Committee Opinion No 761: cesarean delivery on maternal request. Obstet Gynecol. 2019;133.e73-e77.
- Gossman GL, Joesch JM, Tanfer K. Trends in maternal request cesarean delivery from 1991 to 2004. Obstet Gynecol. 2006;108:1506-1516.
- Janiak E, Goldberg AB. Eliminating the phrase “elective abortion”: why language matters. Contraception. 2016;93:89-92.
A conversation on mental health and cancer
Editor’s Note: This transcript from the October 7 episode of Psychcast and the October 8 episode of Blood & Cancer has been edited for clarity.
David Henry, MD: Welcome to this episode of Blood And Cancer. I’m your host, Dr. David Henry, and I’m joined today by another host in the MDedge family, Dr. Lorenzo Norris, who is the host of MDedge Psychcast on MDedge.com or wherever you get your podcasts. He is associate dean of student affairs and administration at the George Washington School of Medicine in Washington, DC. Dr. Norris, thank you so much for taking the time to do this today.

Lorenzo Norris, MD: Dr. Henry, thank you so very much. It’s always great to participate with the MDedge family and do a collaborative podcast, so I’m really looking forward to it.
Dr. Henry: I know you wrote a really nice article on cognitive behavioral therapy (CBT) in breast cancer patients (Psychiatr Ann. 2011;41(9):439-42). So could you talk a bit about that -- what did you do, and what did you find using CBT for breast cancer patients?
Dr. Norris: CBT in a nutshell -- how you think influences greatly your emotions, which influences your behavior. Very simple and very powerful. With breast cancer, as an example, patients are dealing with a great deal of stress. They are literally fighting for their lives.

So there are going to be various thoughts associated with that...One of the uses of CBT when working with patients is to help them think about and work with adaptive thoughts that are going to help them effectively cope as well as problem solve. So for instance, in regard to breast cancer, one of the first things that you’re going to want to do is just to think about, one, helping the patient understand where they’re at, because it’s going to be a shock level type of thing.
Make sure that they don’t have unnecessary or problematic distortions, whether it’s about the treatment, the prognosis, or what they themselves are capable of. And those three areas become actually rather important. Now with a diagnosis of cancer, a number of patients are going to have a period of adjustment. One of the first things that we’re thinking about is where do our patients fit along a continuum of distress.
They could be having an adjustment disorder or none whatsoever, just normal mood or an adjustment disorder with depressed mood. They could actually be in the midst of a unipolar depression. They could have a mood disorder secondary to the effects of the cancer itself. That would be more applicable to brain cancer or pancreatic cancer. Or they could have another category of mood disorder, such as a substance abuse mood disorder. But CBT is a very useful intervention, regardless of whether a person is having a normal syndrome of distress with a very challenging diagnosis or if they’re suffering from full-on psychiatric symptomatology such as a major depressive disorder.
Dr. Henry: In my practice I see a couple of things relevant to that discussion. I’ve always felt fear of the unknown is the worst fear, and fear of the known really helps you.
Medical students say to me sometimes, you just told this patient the same thing three times. They asked you the same thing three times. Well, I say, watch their eyes. Because as their eyes drift off, they’re thinking about their family, their financials, life and death. We’ve got to bring them on back because they’re afraid and not focused. I, in my amateur way, try and bring them back to the discussion to focus on what’s going on, what’s known, and how will we address it.
Interestingly, very rarely do I get, “So how long am I going to live?” You know, you see that in movies and Hollywood, and the doctor says six months, and it’s right on the button. I rarely get that question, because I think they’re afraid of the answer. If I do, I say, “Well, therapy works. You’ll do better and live on. If therapy doesn’t work, we got a problem, and it can be mortal”-- so they wouldn’t believe me if I just tiptoed around that-- but we have a second through-line. “I can always help you, win or lose.” So is that the similar way you approach those kinds of conversations?
Dr. Norris: Absolutely, Dr. Henry. I love how you described it in regard to that willingness, and I love how you described it to the medical students. A lot of being a physician or a healer is just that willingness to stay in a place with a patient and just repeat back the same thing in a different way until we make sure that they’ve heard it and we’ve heard it. And I think that’s very important.
But to get back to that “you have six months to live” type of thing. I actually find that patients actually do-- in my experience, do not immediately go there.
Dr. Henry: Agree. Agree.
Dr. Norris: There is the concept of...I wouldn’t even call that denial. But just that ability to focus on what is immediate. There are some aspects of protective denial. People intrinsically know how much information they need to focus on and deal with at the moment. Why focus on something that is outside of their control? Actually, when I see people jumping to conclusions like that, or catastrophizing, that’s a cognitive distortion. Black and white thinking is another cognitive distortion, as well as maladaptive denial, where you just kind of deny reality. Not discussing prognosis immediately--I would consider that focusing. Denying that you have cancer--that’s problematic denial to say the least.
Dr. Henry: Whole different problem.
Dr. Norris: I agree with you. I find that patients do not immediately jump to that in terms of prognosis or things of that nature. But their oncologist can do a great deal and actually level the distress just by doing what you did right there. Speaking with your patient three or four more times, repeating the same information, not using jargon, but also not sugarcoating anything, but giving what’s needed to get to the next step. And that’s probably what I think is one of the things that I focus on in therapy a lot. Let’s level the distress. Let’s focus on what’s needed to get to the next step and let’s not do anything that, if you’re not in a unipolar depression or major depression, could further exacerbate you developing it. So let’s stay focused on the treatment. And I find that a number of patients rally behind that.
Dr. Henry: Very well put, very well discussed. And we will have on our web page, the reference for the CBT article.
Dr. Norris: If you’re referring to the reference that was in an issue of “Psychiatric Annals,” that was a number of years ago. Because the actual reference you’re referring to (Psychiatr Ann. 2011;41(9):439-42) was part of a themed issue that I guest edited. It was called Cancer and Depression, and all the articles in there were focused on cancer. At that time, I was actually working with the American Cancer Society in regards to developing cancer survivorship guidelines.
Dr. Henry: So as we record this, of course, it’s the COVID era, and we’re taking care of patients with cancer who have to deal with the cancer and deal with themselves, family, and what’s happening in the world. I have found much more anxiety, much more depression than I’m used to seeing. Because they’re coming to see me, am I going to give it to them? Coming into the office, will they get it getting upstairs in our treatment area? So what are you seeing? And how are you handling taking care of patients with cancer in this time?
Dr. Norris: I hope everyone out there that’s listening is safe and well, and I hope your families are safe and well. The COVID pandemic has really unleashed something on the world as well as society that people have not seen basically since the Spanish Flu. But whether you’ve been through the AIDS epidemic or anything like that, you’ve never seen this.
So what are we seeing out there? We’re seeing that, definitively, more anxiety and depression across the board. We know that with the data now that’s been coming out that we are seeing an increase in anxiety and depression in the general population. The data in regard to cancer patients is limited, but we can start with what we know, and from that we can extrapolate and say that we would expect to see an increase in depression and anxiety.
We know that in cancer patients, depending on what study you look at, there’s going to be anywhere from a 0% to 38% prevalence of major depressive disorder and a 0% to 58% prevalence of any depressive spectrum disorder. Depending on the study, it’s going to level out somewhere around a 15% to 22% prevalence rate, regardless of cancer, of depressive symptoms. That’s usually across other medical conditions. Now the general rate of depression in a population is 6.6% with a 12-month prevalence. And the lifetime is 16.6%. So the take-home point is, with cancer, you have a two to four times greater risk of developing depression, whether you had it or not.
There’s a couple of reasons why we might be seeing an increase in depression and anxiety in this COVID era. One is isolation and lack of control. Due to quarantining and social isolation, our patients’ relationships with their oncologists can absolutely positively be disrupted. That is a very anxiety- and depression-inducing situation. One of the themes that came out of the survivorship literature when patients actually transition out of active treatment, one of the most distressing things for them, was the loss of their treatment team and their oncology provider. It almost can’t be said or overestimated the impact that the treatment team and a primary oncologist has on a patient’s life. I just wanted to make sure the audience realized that.
For your patients, you really, really, really are exceedingly important to them, as you are very much aware of that, but to levels you may or may not fully appreciate. So one of the things that COVID does, not only is it this deadly virus that our patients have to worry about in terms of it taking their life, as well as delaying treatment. It separates them from the people that have become paramount in their life, which for a number of folks is their oncology treatment team.
So when we take all of that into account, particularly isolation and loneliness, fragmentation, as well as any type of economic difficulties, that can be resulting due to the COVID-19 pandemic, you would absolutely suspect and predict that anxiety and depression in our patients would definitively increase. And a big part of that is them not being able to connect, certainly with others, but it’s [also] definitely their treatment team.
Dr. Henry: It’s been a stress on all of us, our caregivers as well as care receivers. And then back to putting on our regular oncology/hematology hats, seeing patients when COVID isn’t around. I remember a study long ago, maybe back when I was in training. I think it came out of Memorial Sloan Kettering.
It’s that fully 50% of our active advanced cancer patients are clinically depressed to the point where we should be considering intervention/medication. And if that’s still true, I’m a terrible doctor, because I am not recognizing and prescribing for that. Can you comment on how much depression and anxiety are in the average advanced cancer patient? And should we go after that in treatment?
Dr. Norris: When we’re talking about the advanced cancer patient, I definitely feel as though we should be screening as well as treating. Now as I mentioned before, in regards to the prevalence of depression or depressive spectrum disorders, it can be anywhere from 0% to 58%. In advanced stage cancer, you certainly are going to be thinking that risk is going to be high, probably anywhere from 25% to 33% or maybe even up to 50% of our patients can be suffering from symptoms of depression.
So when we’re talking about treating or referring, a big question you want to ask yourself is, what screening instrument are you using for depression? Some people argue just simply asking a patient whether they’re depressed or not would be perfectly acceptable. That is provided that you have enough time to do it, and you have enough time to follow up and you are pretty standardized with your approach.
However, clinicians just miss it. That’s well established and evidence-based. Clinicians just miss it. What I would recommend that folks consider doing is using the Patient Health Questionnaire, the two-question version called the PHQ-2 and the PHQ-9, the nine-question version. The PHQ-2 is actually a very good screening tool in regards to detecting depression. It has very good sensitivity and specificity.
And that’s going to allow you to actually think about or to screen for patients that you’re going to need to refer for treatment. So if you have a patient with advanced cancer, as an example, and you use the PHQ-2 or PHQ-9, then that’s going to give you a very evidence-based avenue in which to refer for treatment. Now you may be asking yourself, maybe I don’t want to use a PHQ-2 or 9, or I’m in a community practice or a private practice, I just don’t have the bandwidth to process this.
So I want to go off of just my own patient interaction. What are things that I can cue on?
With a patient with cancer, there’s going to be roughly four things that we’re considering in terms of depressive spectrum disorders: Adjustment disorder with depressed mood, major depression, a mood disorder due to cancer itself, or substance-induced mood disorder.
For our audience I want you to concentrate on right now on adjustment disorder with depressed mood and major depression. Now when you look at the evidence, there are roughly nine things that some people like to think about in regard to depressive symptoms to key on. For all of us as health practitioners, these are the things I would like for you to focus on in particular:
1. Non-adherence with treatment for cancer.
2. Impairment of their social or occupational function.
3. Your patient becomes demoralized when they start to lose a little bit of confidence or hope.
When you have those three things, or any one of them, in an advanced stage of cancer, with or without a PHQ screening, you need to really think about how you’re going to refer this patient for treatment. So we can break this down into three different types of interventions. One, the biggest thing, is just to ask, “How are you feeling? What is your mood? Are you suffering from a clinical depression?” You know, take a little bit of inspiration from Dr. Henry. Just give it to people straight and just ask. That’s the biggest thing people don’t do. They don’t ask.
The next thing, if you want to use an evidence-based scale, use a PHQ-2...You would have to follow up, but you-- rather you’re practicing solo or in a group practice or whether you have, your nurse or PA -- they generally assist with that.
And then the third thing is, when you’re interacting with the patient, look for those three things that I talked about: Non-adherence with treatment, impairment of social or occupational function, and then demoralization.
And then the final thing I want to focus on, because you can’t talk about depression without talking about suicide or really significant distress. Obviously, you can ask and you should ask about suicide if that is in your wheelhouse, but to be perfectly frank, most oncologists are not going to-- or most people outside of psychiatrists aren’t going to necessarily just routinely ask that question.
But here’s what I would say. It’s an old one but it’s a good one: Listen to that little voice. Listen to that little voice, all right? Depending on the evidence that you look at, a lot of detecting suicide can be aided by a clinician listening to their own gut instincts. What I mean by that is, you feel a sense of distress. You feel a sense of lack of connection. You find yourself [saying], “Wait a minute, why do I want to call that patient and checkup? Why do I want to reach out?”
When you start to feel like this, you need to listen. More importantly, you need to stop and then you need to make sure that that patient has a referral in place.
Dr. Henry: So they’re just tuning out so badly, you’re really losing the connection, and that’s when your little voice talks to you.
Dr. Norris: Exactly. Well said, Dr. Henry. Well said.
Dr. Henry: In my long career, drug abuse, narcotics, and suicide have been extremely rare. I can think of one patient who was a drug abuser with cancer, or it turned out she was a drug abuser before she had cancer. And then suicide, really quite rare. I’m sure they occur, and we have to watch for them, as you say, but fortunately I’ve not seen that so much. Thanks to your comments, I want to be sure I’m watching and looking.
And the PHQ-2 and -9, I’m sure, with so many of us having electronic medical records, you can simply Google while you’re talking to the patient for those two questionnaires and say, oh, you know, how about you answer these two questions, these nine questions, and see how many points the patient gets and worry about referral or even medication yourself if it looks like an antidepressant is in order.
Dr. Norris: Absolutely. Absolutely.
Dr. Henry: Well, I think we’ve covered an awful lot of ground. I really want to thank you. Any get-away thoughts? We worry about the cognitive behavioral therapy. We worry about it, and we should listen to it and do it.
Practicing in the COVID era is stressful for all of us. I told Dr. Norris at the outset, if I broke down and started baring my soul, he wouldn’t be surprised. Fortunately, I’ve kept it together while talking to a psychiatrist.
And finally watch for clinically significant depression, either by your own questions, which you’ve outlined, or the PHQ-2 and -9.
Really appreciate your thoughts today. Lorenzo, thanks so much for taking the time to do this today.
To hear the entire conversation, go to mdedge.com/podcasts or listen wherever you find your podcasts. David Henry, MD, is a clinical professor of medicine at the University of Pennsylvania and vice chairman of the department of medicine at Pennsylvania Hospital in Philadelphia. He is editor in chief of MDedge Hematology-Oncology and the host of the Blood & Cancer podcast. Dr. Henry reported being on the advisory board for Amgen, AMAG Pharmaceuticals, and Pharmacosmos. He reported institutional funding from the National Institutes of Health and FibroGen.
Lorenzo Norris, MD, is host of the MDedge Psychcast, editor in chief of MDedge Psychiatry, and assistant professor of psychiatry and behavioral sciences at George Washington University, Washington. He also serves as assistant dean of student affairs at the university, and medical director of psychiatric and behavioral sciences at GWU Hospital. Dr. Lorenzo Norris has no conflicts.
Editor’s Note: This transcript from the October 7 episode of Psychcast and the October 8 episode of Blood & Cancer has been edited for clarity.
David Henry, MD: Welcome to this episode of Blood And Cancer. I’m your host, Dr. David Henry, and I’m joined today by another host in the MDedge family, Dr. Lorenzo Norris, who is the host of MDedge Psychcast on MDedge.com or wherever you get your podcasts. He is associate dean of student affairs and administration at the George Washington School of Medicine in Washington, DC. Dr. Norris, thank you so much for taking the time to do this today.
Lorenzo Norris, MD: Dr. Henry, thank you so very much. It’s always great to participate with the MDedge family and do a collaborative podcast, so I’m really looking forward to it.
Dr. Henry: I know you wrote a really nice article on cognitive behavioral therapy (CBT) in breast cancer patients (Psychiatr Ann. 2011;41(9):439-42). So could you talk a bit about that -- what did you do, and what did you find using CBT for breast cancer patients?
Dr. Norris: CBT in a nutshell -- how you think influences greatly your emotions, which influences your behavior. Very simple and very powerful. With breast cancer, as an example, patients are dealing with a great deal of stress. They are literally fighting for their lives.
So there are going to be various thoughts associated with that...One of the uses of CBT when working with patients is to help them think about and work with adaptive thoughts that are going to help them effectively cope as well as problem solve. So for instance, in regard to breast cancer, one of the first things that you’re going to want to do is just to think about, one, helping the patient understand where they’re at, because it’s going to be a shock level type of thing.
Make sure that they don’t have unnecessary or problematic distortions, whether it’s about the treatment, the prognosis, or what they themselves are capable of. And those three areas become actually rather important. Now with a diagnosis of cancer, a number of patients are going to have a period of adjustment. One of the first things that we’re thinking about is where do our patients fit along a continuum of distress.
They could be having an adjustment disorder or none whatsoever, just normal mood or an adjustment disorder with depressed mood. They could actually be in the midst of a unipolar depression. They could have a mood disorder secondary to the effects of the cancer itself. That would be more applicable to brain cancer or pancreatic cancer. Or they could have another category of mood disorder, such as a substance abuse mood disorder. But CBT is a very useful intervention, regardless of whether a person is having a normal syndrome of distress with a very challenging diagnosis or if they’re suffering from full-on psychiatric symptomatology such as a major depressive disorder.
Dr. Henry: In my practice I see a couple of things relevant to that discussion. I’ve always felt fear of the unknown is the worst fear, and fear of the known really helps you.
Medical students say to me sometimes, you just told this patient the same thing three times. They asked you the same thing three times. Well, I say, watch their eyes. Because as their eyes drift off, they’re thinking about their family, their financials, life and death. We’ve got to bring them on back because they’re afraid and not focused. I, in my amateur way, try and bring them back to the discussion to focus on what’s going on, what’s known, and how will we address it.
Interestingly, very rarely do I get, “So how long am I going to live?” You know, you see that in movies and Hollywood, and the doctor says six months, and it’s right on the button. I rarely get that question, because I think they’re afraid of the answer. If I do, I say, “Well, therapy works. You’ll do better and live on. If therapy doesn’t work, we got a problem, and it can be mortal”-- so they wouldn’t believe me if I just tiptoed around that-- but we have a second through-line. “I can always help you, win or lose.” So is that the similar way you approach those kinds of conversations?
Dr. Norris: Absolutely, Dr. Henry. I love how you described it in regard to that willingness, and I love how you described it to the medical students. A lot of being a physician or a healer is just that willingness to stay in a place with a patient and just repeat back the same thing in a different way until we make sure that they’ve heard it and we’ve heard it. And I think that’s very important.
But to get back to that “you have six months to live” type of thing. I actually find that patients actually do-- in my experience, do not immediately go there.
Dr. Henry: Agree. Agree.
Dr. Norris: There is the concept of...I wouldn’t even call that denial. But just that ability to focus on what is immediate. There are some aspects of protective denial. People intrinsically know how much information they need to focus on and deal with at the moment. Why focus on something that is outside of their control? Actually, when I see people jumping to conclusions like that, or catastrophizing, that’s a cognitive distortion. Black and white thinking is another cognitive distortion, as well as maladaptive denial, where you just kind of deny reality. Not discussing prognosis immediately--I would consider that focusing. Denying that you have cancer--that’s problematic denial to say the least.
Dr. Henry: Whole different problem.
Dr. Norris: I agree with you. I find that patients do not immediately jump to that in terms of prognosis or things of that nature. But their oncologist can do a great deal and actually level the distress just by doing what you did right there. Speaking with your patient three or four more times, repeating the same information, not using jargon, but also not sugarcoating anything, but giving what’s needed to get to the next step. And that’s probably what I think is one of the things that I focus on in therapy a lot. Let’s level the distress. Let’s focus on what’s needed to get to the next step and let’s not do anything that, if you’re not in a unipolar depression or major depression, could further exacerbate you developing it. So let’s stay focused on the treatment. And I find that a number of patients rally behind that.
Dr. Henry: Very well put, very well discussed. And we will have on our web page, the reference for the CBT article.
Dr. Norris: If you’re referring to the reference that was in an issue of “Psychiatric Annals,” that was a number of years ago. Because the actual reference you’re referring to (Psychiatr Ann. 2011;41(9):439-42) was part of a themed issue that I guest edited. It was called Cancer and Depression, and all the articles in there were focused on cancer. At that time, I was actually working with the American Cancer Society in regards to developing cancer survivorship guidelines.
Dr. Henry: So as we record this, of course, it’s the COVID era, and we’re taking care of patients with cancer who have to deal with the cancer and deal with themselves, family, and what’s happening in the world. I have found much more anxiety, much more depression than I’m used to seeing. Because they’re coming to see me, am I going to give it to them? Coming into the office, will they get it getting upstairs in our treatment area? So what are you seeing? And how are you handling taking care of patients with cancer in this time?
Dr. Norris: I hope everyone out there that’s listening is safe and well, and I hope your families are safe and well. The COVID pandemic has really unleashed something on the world as well as society that people have not seen basically since the Spanish Flu. But whether you’ve been through the AIDS epidemic or anything like that, you’ve never seen this.
So what are we seeing out there? We’re seeing that, definitively, more anxiety and depression across the board. We know that with the data now that’s been coming out that we are seeing an increase in anxiety and depression in the general population. The data in regard to cancer patients is limited, but we can start with what we know, and from that we can extrapolate and say that we would expect to see an increase in depression and anxiety.
We know that in cancer patients, depending on what study you look at, there’s going to be anywhere from a 0% to 38% prevalence of major depressive disorder and a 0% to 58% prevalence of any depressive spectrum disorder. Depending on the study, it’s going to level out somewhere around a 15% to 22% prevalence rate, regardless of cancer, of depressive symptoms. That’s usually across other medical conditions. Now the general rate of depression in a population is 6.6% with a 12-month prevalence. And the lifetime is 16.6%. So the take-home point is, with cancer, you have a two to four times greater risk of developing depression, whether you had it or not.
There’s a couple of reasons why we might be seeing an increase in depression and anxiety in this COVID era. One is isolation and lack of control. Due to quarantining and social isolation, our patients’ relationships with their oncologists can absolutely positively be disrupted. That is a very anxiety- and depression-inducing situation. One of the themes that came out of the survivorship literature when patients actually transition out of active treatment, one of the most distressing things for them, was the loss of their treatment team and their oncology provider. It almost can’t be said or overestimated the impact that the treatment team and a primary oncologist has on a patient’s life. I just wanted to make sure the audience realized that.
For your patients, you really, really, really are exceedingly important to them, as you are very much aware of that, but to levels you may or may not fully appreciate. So one of the things that COVID does, not only is it this deadly virus that our patients have to worry about in terms of it taking their life, as well as delaying treatment. It separates them from the people that have become paramount in their life, which for a number of folks is their oncology treatment team.
So when we take all of that into account, particularly isolation and loneliness, fragmentation, as well as any type of economic difficulties, that can be resulting due to the COVID-19 pandemic, you would absolutely suspect and predict that anxiety and depression in our patients would definitively increase. And a big part of that is them not being able to connect, certainly with others, but it’s [also] definitely their treatment team.
Dr. Henry: It’s been a stress on all of us, our caregivers as well as care receivers. And then back to putting on our regular oncology/hematology hats, seeing patients when COVID isn’t around. I remember a study long ago, maybe back when I was in training. I think it came out of Memorial Sloan Kettering.
It’s that fully 50% of our active advanced cancer patients are clinically depressed to the point where we should be considering intervention/medication. And if that’s still true, I’m a terrible doctor, because I am not recognizing and prescribing for that. Can you comment on how much depression and anxiety are in the average advanced cancer patient? And should we go after that in treatment?
Dr. Norris: When we’re talking about the advanced cancer patient, I definitely feel as though we should be screening as well as treating. Now as I mentioned before, in regards to the prevalence of depression or depressive spectrum disorders, it can be anywhere from 0% to 58%. In advanced stage cancer, you certainly are going to be thinking that risk is going to be high, probably anywhere from 25% to 33% or maybe even up to 50% of our patients can be suffering from symptoms of depression.
So when we’re talking about treating or referring, a big question you want to ask yourself is, what screening instrument are you using for depression? Some people argue just simply asking a patient whether they’re depressed or not would be perfectly acceptable. That is provided that you have enough time to do it, and you have enough time to follow up and you are pretty standardized with your approach.
However, clinicians just miss it. That’s well established and evidence-based. Clinicians just miss it. What I would recommend that folks consider doing is using the Patient Health Questionnaire, the two-question version called the PHQ-2 and the PHQ-9, the nine-question version. The PHQ-2 is actually a very good screening tool in regards to detecting depression. It has very good sensitivity and specificity.
And that’s going to allow you to actually think about or to screen for patients that you’re going to need to refer for treatment. So if you have a patient with advanced cancer, as an example, and you use the PHQ-2 or PHQ-9, then that’s going to give you a very evidence-based avenue in which to refer for treatment. Now you may be asking yourself, maybe I don’t want to use a PHQ-2 or 9, or I’m in a community practice or a private practice, I just don’t have the bandwidth to process this.
So I want to go off of just my own patient interaction. What are things that I can cue on?
With a patient with cancer, there’s going to be roughly four things that we’re considering in terms of depressive spectrum disorders: Adjustment disorder with depressed mood, major depression, a mood disorder due to cancer itself, or substance-induced mood disorder.
For our audience I want you to concentrate on right now on adjustment disorder with depressed mood and major depression. Now when you look at the evidence, there are roughly nine things that some people like to think about in regard to depressive symptoms to key on. For all of us as health practitioners, these are the things I would like for you to focus on in particular:
1. Non-adherence with treatment for cancer.
2. Impairment of their social or occupational function.
3. Your patient becomes demoralized when they start to lose a little bit of confidence or hope.
When you have those three things, or any one of them, in an advanced stage of cancer, with or without a PHQ screening, you need to really think about how you’re going to refer this patient for treatment. So we can break this down into three different types of interventions. One, the biggest thing, is just to ask, “How are you feeling? What is your mood? Are you suffering from a clinical depression?” You know, take a little bit of inspiration from Dr. Henry. Just give it to people straight and just ask. That’s the biggest thing people don’t do. They don’t ask.
The next thing, if you want to use an evidence-based scale, use a PHQ-2...You would have to follow up, but you-- rather you’re practicing solo or in a group practice or whether you have, your nurse or PA -- they generally assist with that.
And then the third thing is, when you’re interacting with the patient, look for those three things that I talked about: Non-adherence with treatment, impairment of social or occupational function, and then demoralization.
And then the final thing I want to focus on, because you can’t talk about depression without talking about suicide or really significant distress. Obviously, you can ask and you should ask about suicide if that is in your wheelhouse, but to be perfectly frank, most oncologists are not going to-- or most people outside of psychiatrists aren’t going to necessarily just routinely ask that question.
But here’s what I would say. It’s an old one but it’s a good one: Listen to that little voice. Listen to that little voice, all right? Depending on the evidence that you look at, a lot of detecting suicide can be aided by a clinician listening to their own gut instincts. What I mean by that is, you feel a sense of distress. You feel a sense of lack of connection. You find yourself [saying], “Wait a minute, why do I want to call that patient and checkup? Why do I want to reach out?”
When you start to feel like this, you need to listen. More importantly, you need to stop and then you need to make sure that that patient has a referral in place.
Dr. Henry: So they’re just tuning out so badly, you’re really losing the connection, and that’s when your little voice talks to you.
Dr. Norris: Exactly. Well said, Dr. Henry. Well said.
Dr. Henry: In my long career, drug abuse, narcotics, and suicide have been extremely rare. I can think of one patient who was a drug abuser with cancer, or it turned out she was a drug abuser before she had cancer. And then suicide, really quite rare. I’m sure they occur, and we have to watch for them, as you say, but fortunately I’ve not seen that so much. Thanks to your comments, I want to be sure I’m watching and looking.
And the PHQ-2 and -9, I’m sure, with so many of us having electronic medical records, you can simply Google while you’re talking to the patient for those two questionnaires and say, oh, you know, how about you answer these two questions, these nine questions, and see how many points the patient gets and worry about referral or even medication yourself if it looks like an antidepressant is in order.
Dr. Norris: Absolutely. Absolutely.
Dr. Henry: Well, I think we’ve covered an awful lot of ground. I really want to thank you. Any get-away thoughts? We worry about the cognitive behavioral therapy. We worry about it, and we should listen to it and do it.
Practicing in the COVID era is stressful for all of us. I told Dr. Norris at the outset, if I broke down and started baring my soul, he wouldn’t be surprised. Fortunately, I’ve kept it together while talking to a psychiatrist.
And finally watch for clinically significant depression, either by your own questions, which you’ve outlined, or the PHQ-2 and -9.
Really appreciate your thoughts today. Lorenzo, thanks so much for taking the time to do this today.
To hear the entire conversation, go to mdedge.com/podcasts or listen wherever you find your podcasts. David Henry, MD, is a clinical professor of medicine at the University of Pennsylvania and vice chairman of the department of medicine at Pennsylvania Hospital in Philadelphia. He is editor in chief of MDedge Hematology-Oncology and the host of the Blood & Cancer podcast. Dr. Henry reported being on the advisory board for Amgen, AMAG Pharmaceuticals, and Pharmacosmos. He reported institutional funding from the National Institutes of Health and FibroGen.
Lorenzo Norris, MD, is host of the MDedge Psychcast, editor in chief of MDedge Psychiatry, and assistant professor of psychiatry and behavioral sciences at George Washington University, Washington. He also serves as assistant dean of student affairs at the university, and medical director of psychiatric and behavioral sciences at GWU Hospital. Dr. Lorenzo Norris has no conflicts.
Editor’s Note: This transcript from the October 7 episode of Psychcast and the October 8 episode of Blood & Cancer has been edited for clarity.
David Henry, MD: Welcome to this episode of Blood And Cancer. I’m your host, Dr. David Henry, and I’m joined today by another host in the MDedge family, Dr. Lorenzo Norris, who is the host of MDedge Psychcast on MDedge.com or wherever you get your podcasts. He is associate dean of student affairs and administration at the George Washington School of Medicine in Washington, DC. Dr. Norris, thank you so much for taking the time to do this today.
Lorenzo Norris, MD: Dr. Henry, thank you so very much. It’s always great to participate with the MDedge family and do a collaborative podcast, so I’m really looking forward to it.
Dr. Henry: I know you wrote a really nice article on cognitive behavioral therapy (CBT) in breast cancer patients (Psychiatr Ann. 2011;41(9):439-42). So could you talk a bit about that -- what did you do, and what did you find using CBT for breast cancer patients?
Dr. Norris: CBT in a nutshell -- how you think influences greatly your emotions, which influences your behavior. Very simple and very powerful. With breast cancer, as an example, patients are dealing with a great deal of stress. They are literally fighting for their lives.
So there are going to be various thoughts associated with that...One of the uses of CBT when working with patients is to help them think about and work with adaptive thoughts that are going to help them effectively cope as well as problem solve. So for instance, in regard to breast cancer, one of the first things that you’re going to want to do is just to think about, one, helping the patient understand where they’re at, because it’s going to be a shock level type of thing.
Make sure that they don’t have unnecessary or problematic distortions, whether it’s about the treatment, the prognosis, or what they themselves are capable of. And those three areas become actually rather important. Now with a diagnosis of cancer, a number of patients are going to have a period of adjustment. One of the first things that we’re thinking about is where do our patients fit along a continuum of distress.
They could be having an adjustment disorder or none whatsoever, just normal mood or an adjustment disorder with depressed mood. They could actually be in the midst of a unipolar depression. They could have a mood disorder secondary to the effects of the cancer itself. That would be more applicable to brain cancer or pancreatic cancer. Or they could have another category of mood disorder, such as a substance abuse mood disorder. But CBT is a very useful intervention, regardless of whether a person is having a normal syndrome of distress with a very challenging diagnosis or if they’re suffering from full-on psychiatric symptomatology such as a major depressive disorder.
Dr. Henry: In my practice I see a couple of things relevant to that discussion. I’ve always felt fear of the unknown is the worst fear, and fear of the known really helps you.
Medical students say to me sometimes, you just told this patient the same thing three times. They asked you the same thing three times. Well, I say, watch their eyes. Because as their eyes drift off, they’re thinking about their family, their financials, life and death. We’ve got to bring them on back because they’re afraid and not focused. I, in my amateur way, try and bring them back to the discussion to focus on what’s going on, what’s known, and how will we address it.
Interestingly, very rarely do I get, “So how long am I going to live?” You know, you see that in movies and Hollywood, and the doctor says six months, and it’s right on the button. I rarely get that question, because I think they’re afraid of the answer. If I do, I say, “Well, therapy works. You’ll do better and live on. If therapy doesn’t work, we got a problem, and it can be mortal”-- so they wouldn’t believe me if I just tiptoed around that-- but we have a second through-line. “I can always help you, win or lose.” So is that the similar way you approach those kinds of conversations?
Dr. Norris: Absolutely, Dr. Henry. I love how you described it in regard to that willingness, and I love how you described it to the medical students. A lot of being a physician or a healer is just that willingness to stay in a place with a patient and just repeat back the same thing in a different way until we make sure that they’ve heard it and we’ve heard it. And I think that’s very important.
But to get back to that “you have six months to live” type of thing. I actually find that patients actually do-- in my experience, do not immediately go there.
Dr. Henry: Agree. Agree.
Dr. Norris: There is the concept of...I wouldn’t even call that denial. But just that ability to focus on what is immediate. There are some aspects of protective denial. People intrinsically know how much information they need to focus on and deal with at the moment. Why focus on something that is outside of their control? Actually, when I see people jumping to conclusions like that, or catastrophizing, that’s a cognitive distortion. Black and white thinking is another cognitive distortion, as well as maladaptive denial, where you just kind of deny reality. Not discussing prognosis immediately--I would consider that focusing. Denying that you have cancer--that’s problematic denial to say the least.
Dr. Henry: Whole different problem.
Dr. Norris: I agree with you. I find that patients do not immediately jump to that in terms of prognosis or things of that nature. But their oncologist can do a great deal and actually level the distress just by doing what you did right there. Speaking with your patient three or four more times, repeating the same information, not using jargon, but also not sugarcoating anything, but giving what’s needed to get to the next step. And that’s probably what I think is one of the things that I focus on in therapy a lot. Let’s level the distress. Let’s focus on what’s needed to get to the next step and let’s not do anything that, if you’re not in a unipolar depression or major depression, could further exacerbate you developing it. So let’s stay focused on the treatment. And I find that a number of patients rally behind that.
Dr. Henry: Very well put, very well discussed. And we will have on our web page, the reference for the CBT article.
Dr. Norris: If you’re referring to the reference that was in an issue of “Psychiatric Annals,” that was a number of years ago. Because the actual reference you’re referring to (Psychiatr Ann. 2011;41(9):439-42) was part of a themed issue that I guest edited. It was called Cancer and Depression, and all the articles in there were focused on cancer. At that time, I was actually working with the American Cancer Society in regards to developing cancer survivorship guidelines.
Dr. Henry: So as we record this, of course, it’s the COVID era, and we’re taking care of patients with cancer who have to deal with the cancer and deal with themselves, family, and what’s happening in the world. I have found much more anxiety, much more depression than I’m used to seeing. Because they’re coming to see me, am I going to give it to them? Coming into the office, will they get it getting upstairs in our treatment area? So what are you seeing? And how are you handling taking care of patients with cancer in this time?
Dr. Norris: I hope everyone out there that’s listening is safe and well, and I hope your families are safe and well. The COVID pandemic has really unleashed something on the world as well as society that people have not seen basically since the Spanish Flu. But whether you’ve been through the AIDS epidemic or anything like that, you’ve never seen this.
So what are we seeing out there? We’re seeing that, definitively, more anxiety and depression across the board. We know that with the data now that’s been coming out that we are seeing an increase in anxiety and depression in the general population. The data in regard to cancer patients is limited, but we can start with what we know, and from that we can extrapolate and say that we would expect to see an increase in depression and anxiety.
We know that in cancer patients, depending on what study you look at, there’s going to be anywhere from a 0% to 38% prevalence of major depressive disorder and a 0% to 58% prevalence of any depressive spectrum disorder. Depending on the study, it’s going to level out somewhere around a 15% to 22% prevalence rate, regardless of cancer, of depressive symptoms. That’s usually across other medical conditions. Now the general rate of depression in a population is 6.6% with a 12-month prevalence. And the lifetime is 16.6%. So the take-home point is, with cancer, you have a two to four times greater risk of developing depression, whether you had it or not.
There’s a couple of reasons why we might be seeing an increase in depression and anxiety in this COVID era. One is isolation and lack of control. Due to quarantining and social isolation, our patients’ relationships with their oncologists can absolutely positively be disrupted. That is a very anxiety- and depression-inducing situation. One of the themes that came out of the survivorship literature when patients actually transition out of active treatment, one of the most distressing things for them, was the loss of their treatment team and their oncology provider. It almost can’t be said or overestimated the impact that the treatment team and a primary oncologist has on a patient’s life. I just wanted to make sure the audience realized that.
For your patients, you really, really, really are exceedingly important to them, as you are very much aware of that, but to levels you may or may not fully appreciate. So one of the things that COVID does, not only is it this deadly virus that our patients have to worry about in terms of it taking their life, as well as delaying treatment. It separates them from the people that have become paramount in their life, which for a number of folks is their oncology treatment team.
So when we take all of that into account, particularly isolation and loneliness, fragmentation, as well as any type of economic difficulties, that can be resulting due to the COVID-19 pandemic, you would absolutely suspect and predict that anxiety and depression in our patients would definitively increase. And a big part of that is them not being able to connect, certainly with others, but it’s [also] definitely their treatment team.
Dr. Henry: It’s been a stress on all of us, our caregivers as well as care receivers. And then back to putting on our regular oncology/hematology hats, seeing patients when COVID isn’t around. I remember a study long ago, maybe back when I was in training. I think it came out of Memorial Sloan Kettering.
It’s that fully 50% of our active advanced cancer patients are clinically depressed to the point where we should be considering intervention/medication. And if that’s still true, I’m a terrible doctor, because I am not recognizing and prescribing for that. Can you comment on how much depression and anxiety are in the average advanced cancer patient? And should we go after that in treatment?
Dr. Norris: When we’re talking about the advanced cancer patient, I definitely feel as though we should be screening as well as treating. Now as I mentioned before, in regards to the prevalence of depression or depressive spectrum disorders, it can be anywhere from 0% to 58%. In advanced stage cancer, you certainly are going to be thinking that risk is going to be high, probably anywhere from 25% to 33% or maybe even up to 50% of our patients can be suffering from symptoms of depression.
So when we’re talking about treating or referring, a big question you want to ask yourself is, what screening instrument are you using for depression? Some people argue just simply asking a patient whether they’re depressed or not would be perfectly acceptable. That is provided that you have enough time to do it, and you have enough time to follow up and you are pretty standardized with your approach.
However, clinicians just miss it. That’s well established and evidence-based. Clinicians just miss it. What I would recommend that folks consider doing is using the Patient Health Questionnaire, the two-question version called the PHQ-2 and the PHQ-9, the nine-question version. The PHQ-2 is actually a very good screening tool in regards to detecting depression. It has very good sensitivity and specificity.
And that’s going to allow you to actually think about or to screen for patients that you’re going to need to refer for treatment. So if you have a patient with advanced cancer, as an example, and you use the PHQ-2 or PHQ-9, then that’s going to give you a very evidence-based avenue in which to refer for treatment. Now you may be asking yourself, maybe I don’t want to use a PHQ-2 or 9, or I’m in a community practice or a private practice, I just don’t have the bandwidth to process this.
So I want to go off of just my own patient interaction. What are things that I can cue on?
With a patient with cancer, there’s going to be roughly four things that we’re considering in terms of depressive spectrum disorders: Adjustment disorder with depressed mood, major depression, a mood disorder due to cancer itself, or substance-induced mood disorder.
For our audience I want you to concentrate on right now on adjustment disorder with depressed mood and major depression. Now when you look at the evidence, there are roughly nine things that some people like to think about in regard to depressive symptoms to key on. For all of us as health practitioners, these are the things I would like for you to focus on in particular:
1. Non-adherence with treatment for cancer.
2. Impairment of their social or occupational function.
3. Your patient becomes demoralized when they start to lose a little bit of confidence or hope.
When you have those three things, or any one of them, in an advanced stage of cancer, with or without a PHQ screening, you need to really think about how you’re going to refer this patient for treatment. So we can break this down into three different types of interventions. One, the biggest thing, is just to ask, “How are you feeling? What is your mood? Are you suffering from a clinical depression?” You know, take a little bit of inspiration from Dr. Henry. Just give it to people straight and just ask. That’s the biggest thing people don’t do. They don’t ask.
The next thing, if you want to use an evidence-based scale, use a PHQ-2...You would have to follow up, but you-- rather you’re practicing solo or in a group practice or whether you have, your nurse or PA -- they generally assist with that.
And then the third thing is, when you’re interacting with the patient, look for those three things that I talked about: Non-adherence with treatment, impairment of social or occupational function, and then demoralization.
And then the final thing I want to focus on, because you can’t talk about depression without talking about suicide or really significant distress. Obviously, you can ask and you should ask about suicide if that is in your wheelhouse, but to be perfectly frank, most oncologists are not going to-- or most people outside of psychiatrists aren’t going to necessarily just routinely ask that question.
But here’s what I would say. It’s an old one but it’s a good one: Listen to that little voice. Listen to that little voice, all right? Depending on the evidence that you look at, a lot of detecting suicide can be aided by a clinician listening to their own gut instincts. What I mean by that is, you feel a sense of distress. You feel a sense of lack of connection. You find yourself [saying], “Wait a minute, why do I want to call that patient and checkup? Why do I want to reach out?”
When you start to feel like this, you need to listen. More importantly, you need to stop and then you need to make sure that that patient has a referral in place.
Dr. Henry: So they’re just tuning out so badly, you’re really losing the connection, and that’s when your little voice talks to you.
Dr. Norris: Exactly. Well said, Dr. Henry. Well said.
Dr. Henry: In my long career, drug abuse, narcotics, and suicide have been extremely rare. I can think of one patient who was a drug abuser with cancer, or it turned out she was a drug abuser before she had cancer. And then suicide, really quite rare. I’m sure they occur, and we have to watch for them, as you say, but fortunately I’ve not seen that so much. Thanks to your comments, I want to be sure I’m watching and looking.
And the PHQ-2 and -9, I’m sure, with so many of us having electronic medical records, you can simply Google while you’re talking to the patient for those two questionnaires and say, oh, you know, how about you answer these two questions, these nine questions, and see how many points the patient gets and worry about referral or even medication yourself if it looks like an antidepressant is in order.
Dr. Norris: Absolutely. Absolutely.
Dr. Henry: Well, I think we’ve covered an awful lot of ground. I really want to thank you. Any get-away thoughts? We worry about the cognitive behavioral therapy. We worry about it, and we should listen to it and do it.
Practicing in the COVID era is stressful for all of us. I told Dr. Norris at the outset, if I broke down and started baring my soul, he wouldn’t be surprised. Fortunately, I’ve kept it together while talking to a psychiatrist.
And finally watch for clinically significant depression, either by your own questions, which you’ve outlined, or the PHQ-2 and -9.
Really appreciate your thoughts today. Lorenzo, thanks so much for taking the time to do this today.
To hear the entire conversation, go to mdedge.com/podcasts or listen wherever you find your podcasts. David Henry, MD, is a clinical professor of medicine at the University of Pennsylvania and vice chairman of the department of medicine at Pennsylvania Hospital in Philadelphia. He is editor in chief of MDedge Hematology-Oncology and the host of the Blood & Cancer podcast. Dr. Henry reported being on the advisory board for Amgen, AMAG Pharmaceuticals, and Pharmacosmos. He reported institutional funding from the National Institutes of Health and FibroGen.
Lorenzo Norris, MD, is host of the MDedge Psychcast, editor in chief of MDedge Psychiatry, and assistant professor of psychiatry and behavioral sciences at George Washington University, Washington. He also serves as assistant dean of student affairs at the university, and medical director of psychiatric and behavioral sciences at GWU Hospital. Dr. Lorenzo Norris has no conflicts.
Everything I want to tell my adult ADHD patients during the pandemic
An ADHD brain thrives with daily routines, and requires spontaneity and challenge to remain engaged in work, academics, relationships, and even leisure activities. ADHD is a performance issue and not one of intellectual understanding. It is not a problem of knowing what to do, but rather, difficulty doing it.

The COVID-19 pandemic has led to the loss of structure, with many parents working out of their homes alongside their children engaged in virtual learning. There has been a significant loss of impromptu events, since all activities outside of the house require proper planning and safety precautions.
To help normalize the struggles of the adult patient with ADHD during the pandemic, when others’ coping strategies do not work for their ADHD brains.
Adult ADHD is a misnomer – and not just a disorder of inattention and hyperactivity
A better name for this often misconstrued disorder is inconsistent attention and motivation disorder with internal or external hyperactivity/impulsivity.
An ADHD brain vacillates between inattention and hyperfocus. It is not uncommon for individuals with ADHD to lose interest in a new television series when they become hyperfocused on finding the best pandemic-friendly toy for their 5-year-olds, which inevitably turns into a 3-hour Google rabbit-hole search.
These same individuals with ADHD may have low motivation for mundane household chores but become highly motivated when their nonessential Amazon purchases arrive. They may even go as far as pulling an all-nighter to have an electric toy jeep built and ready for the youngster by morning.
Adults with ADHD can also exhibit hyperactive symptoms, such as physical restlessness with fidgeting, and an internal restlessness with anxious and repetitive thoughts that affect their ability to unwind, relax, and even sleep. Impulsivity in adults with ADHD can present as rushing through tasks that one finds uninteresting or unimportant, interrupting others on a Zoom work call, or impulse buying an expensive hot tub instead of a more affordable on their spouse agreed to.
ADHD is a risk factor for contracting COVID-19
Untreated ADHD can increase one’s risk of contracting COVID-19. Israeli researchers published a study in the Journal of Attention Disorders showing that individuals with ADHD are 52% more likely to test positive for COVID-19, compared with those without ADHD, because of risk-taking behaviors, impulsivity, and carelessness. However, individuals whose ADHD symptoms are treated with stimulant medication do not increase their risk of contracting COVID-19, the researchers wrote.
ADHD might be noticed in family members
ADHD is a neurodevelopmental disorder that affects the development of the brain. We know that structural, functional, and chemical differences affect our patients’ ability to regulate attention, motivation, impulses, and emotions. ADHD tends to run in families and is highly genetic. Since spending more time with family members during the pandemic, patients might even recognize ADHD symptoms in siblings, children, and one or both of parents. A child who has ADHD has a 25% chance of having a parent with ADHD.
Strengths and attributes are related to ADHD
Your ability to thrive in new, stressful, and challenging situations is an ADHD attribute that will be beneficial during the pandemic. Creativity, great problem-solving skills, and ability to be flexible will be admired and helpful to our patients with ADHD and others during these uncertain times.
Those with ADHD might be highly sensitive to their environments
As previously mentioned, ADHD is a misnomer and not just a disorder of inattention but also too much attention. Unfortunately, this hyperfocused attention is usually on the wrong things. Those with ADHD might find it difficult to filter and process sensory information correctly and, therefore, can be easily distracted by auditory, visual, tactile, and olfactory stimuli. The change to working at home during the pandemic might make it hard to ignore children’s voices, the uncomfortable new mask bought after losing yet another mask over the weekend, and the smell of cookies emanating from the kitchen. This increased sensitivity may affect one’s emotions.
Heightened emotions are expected during the pandemic and even more so among adults with ADHD. The inability of adults with ADHD to properly filter information can also affect emotional stimuli. These intense emotions, coupled with impulsive behaviors, can cause disagreements with partners, lack of patience with children, and conflict with colleagues. When individuals with ADHD feel attacked or invalidated, they can become emotionally dysregulated and “vomit” their pent up feelings.
ADHD may affect interpersonal relationships
ADHD symptoms of inattention and impulsivity can affect the ability to connect with friends and family. When one is easily distracted by the pandemic’s chaos, it is harder to be mindful and emotionally and physically connected to one’s partner, which also disrupts their sex life and intimacy.
ADHD sensory integration issues can make people sensitive to particular touches, smells, and sensory information. A gentle touch from one’s partner might be annoying during the pandemic, since other senses may already be overstimulated by the loud sounds of children screaming, the visual and auditory distractions of a neighbor mowing the lawn, and the sun beating down because one forgot to get blinds in the home office before the pandemic.
These minor distractions that are usually insignificant to a non-ADHD brain can profoundly affect an ADHD brain since one must use valuable energy to tune out these unwanted disturbances.
Your brain uses a different motivational system than a non-ADHD brain
You have a deficiency in the neurotransmitter dopamine, which affects your motivational system. Your motivational system is based on what you find interesting, challenging, new, exciting, and urgent. Your non-ADHD partner, family members, friends, and colleagues motivate and accomplish their daily tasks differently from you and most likely use a system based on rewards and consequences.
Do not be surprised if you notice that your motivation is diminished during the pandemic because of less novelty and excitement in your life. The coronavirus’s chronic importance level may make everything else in your life not as essential and, therefore, less urgent, which indirectly also lowers your motivation.
Your non-ADHD partner may see that you can focus, prioritize, initiate, and complete tasks when you “choose” to, and confuse your inconsistent behaviors as being within your control. However, this lack of motivation for things that do not pique your interest, challenge you, and are not urgent is not voluntary. It is caused by a lack of neural connections in the area of the brain that controls motivation.
You can still have ADHD even though you were not diagnosed as a child or adolescent
Your symptoms of ADHD may not affect your level of functioning until you go away to college, obtain your first job, marry your partner, start a family, or even until a global pandemic alters every aspect of your daily life.
It is, therefore, never too late to get assessed and treated for ADHD. Stimulants are the first line of treatment for adult ADHD. Nonstimulants may also be prescribed if you do not tolerate the side effects of stimulants or have a history of certain medical conditions. These options include some antidepressants and high blood pressure medicines. Sometimes, just identifying the deficits of those with ADHD and how they may affect their performance at work, school, and interpersonal relationships can help the person living with ADHD. Many other any nonmedication types of effective treatment are available for adults with ADHD, including therapy, executive skills, and mindfulness training.
- ADHD focused cognitive-behavioral therapy can help one change your distorted, negative, and irrational thoughts about themselves, others, and situations and replace them with more realistic and rational thoughts that allow for helpful and adaptive behaviors.
- Executive skills training is a type of ADHD treatment that focuses on developing effective systems, routines, improving time management, organization, planning, productivity, and emotional self-regulation.
- Mindfulness meditation training is an additional treatment for adult ADHD. Mindfulness training teaches skills to focus on the present moment and become aware of one’s thoughts, emotions, and actions without judgment. The goal is to learn to accept your ADHD deficits and all that is out of your control while remaining mindful of your ADHD strengths and focusing on the daily choices within your control.
Silver linings of the pandemic
Numerous underserved and rural geographic areas lack adequate psychiatric care. Many primary care physicians and even some psychiatrists are uncomfortable diagnosing and treating attentional disorders because of a lack of proper training in medical school and fear related to the fact that the first-line treatment for adult ADHD is a controlled substance.
In response to the pandemic, the expansion of telepsychiatry services, state waivers that allow clinicians to practice across state lines, exemptions that enable the prescribing of controlled substances without an in-person medical evaluation, and the acceptance of employees working from home during the COVID-19 pandemic have increased the accessibility of adult ADHD psychiatric assessments and treatment.
It is hoped that when the COVID-19 pandemic is behind us, many of the benefits that have emerged, such as the growth of telepsychiatry, changes in state licensure and prescriber regulations, and reduced work commutes will continue into our postpandemic lives.
Dr. Abraham is a psychiatrist in private practice in Philadelphia. She has no disclosures.
An ADHD brain thrives with daily routines, and requires spontaneity and challenge to remain engaged in work, academics, relationships, and even leisure activities. ADHD is a performance issue and not one of intellectual understanding. It is not a problem of knowing what to do, but rather, difficulty doing it.
The COVID-19 pandemic has led to the loss of structure, with many parents working out of their homes alongside their children engaged in virtual learning. There has been a significant loss of impromptu events, since all activities outside of the house require proper planning and safety precautions.
To help normalize the struggles of the adult patient with ADHD during the pandemic, when others’ coping strategies do not work for their ADHD brains.
Adult ADHD is a misnomer – and not just a disorder of inattention and hyperactivity
A better name for this often misconstrued disorder is inconsistent attention and motivation disorder with internal or external hyperactivity/impulsivity.
An ADHD brain vacillates between inattention and hyperfocus. It is not uncommon for individuals with ADHD to lose interest in a new television series when they become hyperfocused on finding the best pandemic-friendly toy for their 5-year-olds, which inevitably turns into a 3-hour Google rabbit-hole search.
These same individuals with ADHD may have low motivation for mundane household chores but become highly motivated when their nonessential Amazon purchases arrive. They may even go as far as pulling an all-nighter to have an electric toy jeep built and ready for the youngster by morning.
Adults with ADHD can also exhibit hyperactive symptoms, such as physical restlessness with fidgeting, and an internal restlessness with anxious and repetitive thoughts that affect their ability to unwind, relax, and even sleep. Impulsivity in adults with ADHD can present as rushing through tasks that one finds uninteresting or unimportant, interrupting others on a Zoom work call, or impulse buying an expensive hot tub instead of a more affordable on their spouse agreed to.
ADHD is a risk factor for contracting COVID-19
Untreated ADHD can increase one’s risk of contracting COVID-19. Israeli researchers published a study in the Journal of Attention Disorders showing that individuals with ADHD are 52% more likely to test positive for COVID-19, compared with those without ADHD, because of risk-taking behaviors, impulsivity, and carelessness. However, individuals whose ADHD symptoms are treated with stimulant medication do not increase their risk of contracting COVID-19, the researchers wrote.
ADHD might be noticed in family members
ADHD is a neurodevelopmental disorder that affects the development of the brain. We know that structural, functional, and chemical differences affect our patients’ ability to regulate attention, motivation, impulses, and emotions. ADHD tends to run in families and is highly genetic. Since spending more time with family members during the pandemic, patients might even recognize ADHD symptoms in siblings, children, and one or both of parents. A child who has ADHD has a 25% chance of having a parent with ADHD.
Strengths and attributes are related to ADHD
Your ability to thrive in new, stressful, and challenging situations is an ADHD attribute that will be beneficial during the pandemic. Creativity, great problem-solving skills, and ability to be flexible will be admired and helpful to our patients with ADHD and others during these uncertain times.
Those with ADHD might be highly sensitive to their environments
As previously mentioned, ADHD is a misnomer and not just a disorder of inattention but also too much attention. Unfortunately, this hyperfocused attention is usually on the wrong things. Those with ADHD might find it difficult to filter and process sensory information correctly and, therefore, can be easily distracted by auditory, visual, tactile, and olfactory stimuli. The change to working at home during the pandemic might make it hard to ignore children’s voices, the uncomfortable new mask bought after losing yet another mask over the weekend, and the smell of cookies emanating from the kitchen. This increased sensitivity may affect one’s emotions.
Heightened emotions are expected during the pandemic and even more so among adults with ADHD. The inability of adults with ADHD to properly filter information can also affect emotional stimuli. These intense emotions, coupled with impulsive behaviors, can cause disagreements with partners, lack of patience with children, and conflict with colleagues. When individuals with ADHD feel attacked or invalidated, they can become emotionally dysregulated and “vomit” their pent up feelings.
ADHD may affect interpersonal relationships
ADHD symptoms of inattention and impulsivity can affect the ability to connect with friends and family. When one is easily distracted by the pandemic’s chaos, it is harder to be mindful and emotionally and physically connected to one’s partner, which also disrupts their sex life and intimacy.
ADHD sensory integration issues can make people sensitive to particular touches, smells, and sensory information. A gentle touch from one’s partner might be annoying during the pandemic, since other senses may already be overstimulated by the loud sounds of children screaming, the visual and auditory distractions of a neighbor mowing the lawn, and the sun beating down because one forgot to get blinds in the home office before the pandemic.
These minor distractions that are usually insignificant to a non-ADHD brain can profoundly affect an ADHD brain since one must use valuable energy to tune out these unwanted disturbances.
Your brain uses a different motivational system than a non-ADHD brain
You have a deficiency in the neurotransmitter dopamine, which affects your motivational system. Your motivational system is based on what you find interesting, challenging, new, exciting, and urgent. Your non-ADHD partner, family members, friends, and colleagues motivate and accomplish their daily tasks differently from you and most likely use a system based on rewards and consequences.
Do not be surprised if you notice that your motivation is diminished during the pandemic because of less novelty and excitement in your life. The coronavirus’s chronic importance level may make everything else in your life not as essential and, therefore, less urgent, which indirectly also lowers your motivation.
Your non-ADHD partner may see that you can focus, prioritize, initiate, and complete tasks when you “choose” to, and confuse your inconsistent behaviors as being within your control. However, this lack of motivation for things that do not pique your interest, challenge you, and are not urgent is not voluntary. It is caused by a lack of neural connections in the area of the brain that controls motivation.
You can still have ADHD even though you were not diagnosed as a child or adolescent
Your symptoms of ADHD may not affect your level of functioning until you go away to college, obtain your first job, marry your partner, start a family, or even until a global pandemic alters every aspect of your daily life.
It is, therefore, never too late to get assessed and treated for ADHD. Stimulants are the first line of treatment for adult ADHD. Nonstimulants may also be prescribed if you do not tolerate the side effects of stimulants or have a history of certain medical conditions. These options include some antidepressants and high blood pressure medicines. Sometimes, just identifying the deficits of those with ADHD and how they may affect their performance at work, school, and interpersonal relationships can help the person living with ADHD. Many other any nonmedication types of effective treatment are available for adults with ADHD, including therapy, executive skills, and mindfulness training.
- ADHD focused cognitive-behavioral therapy can help one change your distorted, negative, and irrational thoughts about themselves, others, and situations and replace them with more realistic and rational thoughts that allow for helpful and adaptive behaviors.
- Executive skills training is a type of ADHD treatment that focuses on developing effective systems, routines, improving time management, organization, planning, productivity, and emotional self-regulation.
- Mindfulness meditation training is an additional treatment for adult ADHD. Mindfulness training teaches skills to focus on the present moment and become aware of one’s thoughts, emotions, and actions without judgment. The goal is to learn to accept your ADHD deficits and all that is out of your control while remaining mindful of your ADHD strengths and focusing on the daily choices within your control.
Silver linings of the pandemic
Numerous underserved and rural geographic areas lack adequate psychiatric care. Many primary care physicians and even some psychiatrists are uncomfortable diagnosing and treating attentional disorders because of a lack of proper training in medical school and fear related to the fact that the first-line treatment for adult ADHD is a controlled substance.
In response to the pandemic, the expansion of telepsychiatry services, state waivers that allow clinicians to practice across state lines, exemptions that enable the prescribing of controlled substances without an in-person medical evaluation, and the acceptance of employees working from home during the COVID-19 pandemic have increased the accessibility of adult ADHD psychiatric assessments and treatment.
It is hoped that when the COVID-19 pandemic is behind us, many of the benefits that have emerged, such as the growth of telepsychiatry, changes in state licensure and prescriber regulations, and reduced work commutes will continue into our postpandemic lives.
Dr. Abraham is a psychiatrist in private practice in Philadelphia. She has no disclosures.
An ADHD brain thrives with daily routines, and requires spontaneity and challenge to remain engaged in work, academics, relationships, and even leisure activities. ADHD is a performance issue and not one of intellectual understanding. It is not a problem of knowing what to do, but rather, difficulty doing it.
The COVID-19 pandemic has led to the loss of structure, with many parents working out of their homes alongside their children engaged in virtual learning. There has been a significant loss of impromptu events, since all activities outside of the house require proper planning and safety precautions.
To help normalize the struggles of the adult patient with ADHD during the pandemic, when others’ coping strategies do not work for their ADHD brains.
Adult ADHD is a misnomer – and not just a disorder of inattention and hyperactivity
A better name for this often misconstrued disorder is inconsistent attention and motivation disorder with internal or external hyperactivity/impulsivity.
An ADHD brain vacillates between inattention and hyperfocus. It is not uncommon for individuals with ADHD to lose interest in a new television series when they become hyperfocused on finding the best pandemic-friendly toy for their 5-year-olds, which inevitably turns into a 3-hour Google rabbit-hole search.
These same individuals with ADHD may have low motivation for mundane household chores but become highly motivated when their nonessential Amazon purchases arrive. They may even go as far as pulling an all-nighter to have an electric toy jeep built and ready for the youngster by morning.
Adults with ADHD can also exhibit hyperactive symptoms, such as physical restlessness with fidgeting, and an internal restlessness with anxious and repetitive thoughts that affect their ability to unwind, relax, and even sleep. Impulsivity in adults with ADHD can present as rushing through tasks that one finds uninteresting or unimportant, interrupting others on a Zoom work call, or impulse buying an expensive hot tub instead of a more affordable on their spouse agreed to.
ADHD is a risk factor for contracting COVID-19
Untreated ADHD can increase one’s risk of contracting COVID-19. Israeli researchers published a study in the Journal of Attention Disorders showing that individuals with ADHD are 52% more likely to test positive for COVID-19, compared with those without ADHD, because of risk-taking behaviors, impulsivity, and carelessness. However, individuals whose ADHD symptoms are treated with stimulant medication do not increase their risk of contracting COVID-19, the researchers wrote.
ADHD might be noticed in family members
ADHD is a neurodevelopmental disorder that affects the development of the brain. We know that structural, functional, and chemical differences affect our patients’ ability to regulate attention, motivation, impulses, and emotions. ADHD tends to run in families and is highly genetic. Since spending more time with family members during the pandemic, patients might even recognize ADHD symptoms in siblings, children, and one or both of parents. A child who has ADHD has a 25% chance of having a parent with ADHD.
Strengths and attributes are related to ADHD
Your ability to thrive in new, stressful, and challenging situations is an ADHD attribute that will be beneficial during the pandemic. Creativity, great problem-solving skills, and ability to be flexible will be admired and helpful to our patients with ADHD and others during these uncertain times.
Those with ADHD might be highly sensitive to their environments
As previously mentioned, ADHD is a misnomer and not just a disorder of inattention but also too much attention. Unfortunately, this hyperfocused attention is usually on the wrong things. Those with ADHD might find it difficult to filter and process sensory information correctly and, therefore, can be easily distracted by auditory, visual, tactile, and olfactory stimuli. The change to working at home during the pandemic might make it hard to ignore children’s voices, the uncomfortable new mask bought after losing yet another mask over the weekend, and the smell of cookies emanating from the kitchen. This increased sensitivity may affect one’s emotions.
Heightened emotions are expected during the pandemic and even more so among adults with ADHD. The inability of adults with ADHD to properly filter information can also affect emotional stimuli. These intense emotions, coupled with impulsive behaviors, can cause disagreements with partners, lack of patience with children, and conflict with colleagues. When individuals with ADHD feel attacked or invalidated, they can become emotionally dysregulated and “vomit” their pent up feelings.
ADHD may affect interpersonal relationships
ADHD symptoms of inattention and impulsivity can affect the ability to connect with friends and family. When one is easily distracted by the pandemic’s chaos, it is harder to be mindful and emotionally and physically connected to one’s partner, which also disrupts their sex life and intimacy.
ADHD sensory integration issues can make people sensitive to particular touches, smells, and sensory information. A gentle touch from one’s partner might be annoying during the pandemic, since other senses may already be overstimulated by the loud sounds of children screaming, the visual and auditory distractions of a neighbor mowing the lawn, and the sun beating down because one forgot to get blinds in the home office before the pandemic.
These minor distractions that are usually insignificant to a non-ADHD brain can profoundly affect an ADHD brain since one must use valuable energy to tune out these unwanted disturbances.
Your brain uses a different motivational system than a non-ADHD brain
You have a deficiency in the neurotransmitter dopamine, which affects your motivational system. Your motivational system is based on what you find interesting, challenging, new, exciting, and urgent. Your non-ADHD partner, family members, friends, and colleagues motivate and accomplish their daily tasks differently from you and most likely use a system based on rewards and consequences.
Do not be surprised if you notice that your motivation is diminished during the pandemic because of less novelty and excitement in your life. The coronavirus’s chronic importance level may make everything else in your life not as essential and, therefore, less urgent, which indirectly also lowers your motivation.
Your non-ADHD partner may see that you can focus, prioritize, initiate, and complete tasks when you “choose” to, and confuse your inconsistent behaviors as being within your control. However, this lack of motivation for things that do not pique your interest, challenge you, and are not urgent is not voluntary. It is caused by a lack of neural connections in the area of the brain that controls motivation.
You can still have ADHD even though you were not diagnosed as a child or adolescent
Your symptoms of ADHD may not affect your level of functioning until you go away to college, obtain your first job, marry your partner, start a family, or even until a global pandemic alters every aspect of your daily life.
It is, therefore, never too late to get assessed and treated for ADHD. Stimulants are the first line of treatment for adult ADHD. Nonstimulants may also be prescribed if you do not tolerate the side effects of stimulants or have a history of certain medical conditions. These options include some antidepressants and high blood pressure medicines. Sometimes, just identifying the deficits of those with ADHD and how they may affect their performance at work, school, and interpersonal relationships can help the person living with ADHD. Many other any nonmedication types of effective treatment are available for adults with ADHD, including therapy, executive skills, and mindfulness training.
- ADHD focused cognitive-behavioral therapy can help one change your distorted, negative, and irrational thoughts about themselves, others, and situations and replace them with more realistic and rational thoughts that allow for helpful and adaptive behaviors.
- Executive skills training is a type of ADHD treatment that focuses on developing effective systems, routines, improving time management, organization, planning, productivity, and emotional self-regulation.
- Mindfulness meditation training is an additional treatment for adult ADHD. Mindfulness training teaches skills to focus on the present moment and become aware of one’s thoughts, emotions, and actions without judgment. The goal is to learn to accept your ADHD deficits and all that is out of your control while remaining mindful of your ADHD strengths and focusing on the daily choices within your control.
Silver linings of the pandemic
Numerous underserved and rural geographic areas lack adequate psychiatric care. Many primary care physicians and even some psychiatrists are uncomfortable diagnosing and treating attentional disorders because of a lack of proper training in medical school and fear related to the fact that the first-line treatment for adult ADHD is a controlled substance.
In response to the pandemic, the expansion of telepsychiatry services, state waivers that allow clinicians to practice across state lines, exemptions that enable the prescribing of controlled substances without an in-person medical evaluation, and the acceptance of employees working from home during the COVID-19 pandemic have increased the accessibility of adult ADHD psychiatric assessments and treatment.
It is hoped that when the COVID-19 pandemic is behind us, many of the benefits that have emerged, such as the growth of telepsychiatry, changes in state licensure and prescriber regulations, and reduced work commutes will continue into our postpandemic lives.
Dr. Abraham is a psychiatrist in private practice in Philadelphia. She has no disclosures.
Practicing cognitive techniques can help athletes reach optimal performance
Successful athletes exhibit positive mental health. This mental health is directly related to athletic success and high levels of performance.1 Mental skills are as important as natural physical ability and mechanical skills in the sport of tennis.
Research has shown that tennis is 85% mental and that players spend 80% of their time on the court handling emotions. Some players look good in practice when they are not under pressure but cannot win matches (they have the physical skill level to win) because they cannot handle their own emotions during the duress of a match. They are affected by anger, fear, stress, poor concentration, and other internal elements that interfere with their ability to perform at an optimal level. Competitors may also be affected by external factors such as the sun, wind, an opponent, and so on, and may use these situations as an excuse not to win.
Players normally practice physical skills but rarely practice cognitive techniques. Regardless of level of play – pro, collegiate, junior, or club – practicing mental skills will greatly improve the players’ arsenal of weapons, giving them an edge in matches and making them the best players they can be. Mental health professionals also can use these strategies to help motivate athletes who compete in other sports – and in other competitive endeavors.
Visualization is the formation of a mental image of something of your choice. Visualization imagery techniques can be used by players to calm themselves before playing a match so their emotions are not wasted on trying to quiet the minds and quell stress. Implementing the following visualization techniques will reduce a player’s anxiety during the match, allowing the player to direct energy toward optimal mental and physical performance on the court.
In advance of a match, encourage the player to learn and analyze the opponent’s strengths and weaknesses by watching the opponent play and/or from asking others. The night before the scheduled match, get the player to imagine how they will play points against their competitor. Play into the opponents’ vulnerabilities or first play to their strengths to expose shortcomings and – then attack their weakness. For example, if an opponent has a weak backhand, first play to the opponent’s forehand and, when the opponent is vulnerable, go into his backhand to get a short or weak ball – and attack. The following are specific strategies that mental health professionals who work with athletes can use to help them perform optimally.
Using visualization, shadowing
Visualize the correct way to hit a tennis stroke and repeat it over and over in your mind. On a tennis court or where ever you have adequate space, shadow a stroke by using a racket and repetitively performing the actual stroke without hitting a ball. At home, practice relaxation and deep breathing techniques at night before going to sleep. Put yourself in a relaxed state and visualize repetitively striking the ball correctly. The next time you actually hit the stroke, you will produce a better shot.
Focusing on, staying in the here and now
The “here” means to focus on what is happening on your own court, not what is happening on the court next to you. Players may be affected by external factors, such as the sun, wind, and their opponent and may use these conditions or situations as an excuse if they do not win. Ignore background chatter and distractions, and be a horse with blinders. Be responsible for yourself and your own actions; manage what you can and realize that you cannot control the weather or actions of your opponent.
The “now” refers to staying present and focusing only on the current point. Do not think of past mistakes. If you are winning a match, do not think about celebrating while the match is still in play. If you are losing, do not start to write a script of excuses why you lost the match. Instead, just concentrate on the present, point by point. Focusing will allow you to understand what is true and important in the here and now. Focusing will help alleviate stress and better equip you to make quick decisions and be clear about your intended actions.
Set realistic and achievable goals
It is always good to have goals and dreams; however, you as a player must understand the realities of your current level of play. Know your level; don’t be grandiose and think you are able to beat Rafael Nadal. Having an unrealistic attitude will result in frustration and poor performance during a match. Instead, set achievable, and realistic short- and long-term goals for yourself, which will aid in your overall tennis development. After the match is over, reflect upon and evaluate the points – and your overall performance.
Don’t devalue yourself if you lose a match. Do not feel too low from a loss or too high from a win. When you have a match loss, use it as an opportunity to learn from your mistakes and to improve by working on your weaknesses in future practice until you feel confident enough to use your new skills in a tournament.
Stay positive
Do not tie up your self-esteem as a person with your match outcome; in otherwords, separate feelings of self-worth from your match results. Cultivate an optimistic attitude and talk positively to yourself, strive to improve, and maintain positive self-esteem in practice and in matches. During practice, allocate 110% effort, and focus on the process, not the outcome. Arrange your practice matches so that one-third of them are against players of your same level, one-third against players worse than you, and one-third against players better than yourself.
Deal with adversity
It is important to be able to deal with external pressures going on in your life such as conflicts related to family, peers, school, work, and relationships. Deal with and manage this discord before your match so you can maintain control of your emotions and can give 100% effort on the court.
Learn mental techniques
Many athletes may have difficulty teaching themselves cognitive skills and would benefit from a few sessions with a sports psychologist/psychiatrist to understand and learn the techniques. Once the tactics are understood and learned, players can apply them to training and ultimately to their tournament arsenal, allowing them to play to their ultimate potential.
References
1. Morgan WP. Selected psychological factors limiting performance: A mental health model. In Clarke DH and Eckert HM (eds.), Limits of Human Performance. Champaign, Ill.: Human Kinetics Publishers, 1985.
Dr. Cohen had a private practice in psychiatry for more than 35 years. He is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University in Philadelphia. Dr. Cohen has been a nationally ranked tennis player from age 12 to the present and served as captain of the tennis team at the University of Pennsylvania, Philadelphia. Dr. Cohen, who was ranked No. 1 in tennis in the middle states section and in the country in various categories and times, was inducted into the Philadelphia Jewish Sports Hall of Fame in 2012. Dr. Cohen has no conflicts of interest.
Ms. Cohen, Dr. Cohen’s daughter, was No. 1 ranked in the United States in junior tennis and No. 4 in the world. In addition, Ms. Cohen was ranked among the top 100 players in the world by the professional World Tennis Association. She also was the No. 2 college player in United States, and an All-American at the University of Miami. She holds a master’s in sports psychology, and presently works as a sports psychologist and tennis professional in Philadelphia. Ms. Cohen has no conflicts of interest.
Successful athletes exhibit positive mental health. This mental health is directly related to athletic success and high levels of performance.1 Mental skills are as important as natural physical ability and mechanical skills in the sport of tennis.
Research has shown that tennis is 85% mental and that players spend 80% of their time on the court handling emotions. Some players look good in practice when they are not under pressure but cannot win matches (they have the physical skill level to win) because they cannot handle their own emotions during the duress of a match. They are affected by anger, fear, stress, poor concentration, and other internal elements that interfere with their ability to perform at an optimal level. Competitors may also be affected by external factors such as the sun, wind, an opponent, and so on, and may use these situations as an excuse not to win.
Players normally practice physical skills but rarely practice cognitive techniques. Regardless of level of play – pro, collegiate, junior, or club – practicing mental skills will greatly improve the players’ arsenal of weapons, giving them an edge in matches and making them the best players they can be. Mental health professionals also can use these strategies to help motivate athletes who compete in other sports – and in other competitive endeavors.
Visualization is the formation of a mental image of something of your choice. Visualization imagery techniques can be used by players to calm themselves before playing a match so their emotions are not wasted on trying to quiet the minds and quell stress. Implementing the following visualization techniques will reduce a player’s anxiety during the match, allowing the player to direct energy toward optimal mental and physical performance on the court.
In advance of a match, encourage the player to learn and analyze the opponent’s strengths and weaknesses by watching the opponent play and/or from asking others. The night before the scheduled match, get the player to imagine how they will play points against their competitor. Play into the opponents’ vulnerabilities or first play to their strengths to expose shortcomings and – then attack their weakness. For example, if an opponent has a weak backhand, first play to the opponent’s forehand and, when the opponent is vulnerable, go into his backhand to get a short or weak ball – and attack. The following are specific strategies that mental health professionals who work with athletes can use to help them perform optimally.
Using visualization, shadowing
Visualize the correct way to hit a tennis stroke and repeat it over and over in your mind. On a tennis court or where ever you have adequate space, shadow a stroke by using a racket and repetitively performing the actual stroke without hitting a ball. At home, practice relaxation and deep breathing techniques at night before going to sleep. Put yourself in a relaxed state and visualize repetitively striking the ball correctly. The next time you actually hit the stroke, you will produce a better shot.
Focusing on, staying in the here and now
The “here” means to focus on what is happening on your own court, not what is happening on the court next to you. Players may be affected by external factors, such as the sun, wind, and their opponent and may use these conditions or situations as an excuse if they do not win. Ignore background chatter and distractions, and be a horse with blinders. Be responsible for yourself and your own actions; manage what you can and realize that you cannot control the weather or actions of your opponent.
The “now” refers to staying present and focusing only on the current point. Do not think of past mistakes. If you are winning a match, do not think about celebrating while the match is still in play. If you are losing, do not start to write a script of excuses why you lost the match. Instead, just concentrate on the present, point by point. Focusing will allow you to understand what is true and important in the here and now. Focusing will help alleviate stress and better equip you to make quick decisions and be clear about your intended actions.
Set realistic and achievable goals
It is always good to have goals and dreams; however, you as a player must understand the realities of your current level of play. Know your level; don’t be grandiose and think you are able to beat Rafael Nadal. Having an unrealistic attitude will result in frustration and poor performance during a match. Instead, set achievable, and realistic short- and long-term goals for yourself, which will aid in your overall tennis development. After the match is over, reflect upon and evaluate the points – and your overall performance.
Don’t devalue yourself if you lose a match. Do not feel too low from a loss or too high from a win. When you have a match loss, use it as an opportunity to learn from your mistakes and to improve by working on your weaknesses in future practice until you feel confident enough to use your new skills in a tournament.
Stay positive
Do not tie up your self-esteem as a person with your match outcome; in otherwords, separate feelings of self-worth from your match results. Cultivate an optimistic attitude and talk positively to yourself, strive to improve, and maintain positive self-esteem in practice and in matches. During practice, allocate 110% effort, and focus on the process, not the outcome. Arrange your practice matches so that one-third of them are against players of your same level, one-third against players worse than you, and one-third against players better than yourself.
Deal with adversity
It is important to be able to deal with external pressures going on in your life such as conflicts related to family, peers, school, work, and relationships. Deal with and manage this discord before your match so you can maintain control of your emotions and can give 100% effort on the court.
Learn mental techniques
Many athletes may have difficulty teaching themselves cognitive skills and would benefit from a few sessions with a sports psychologist/psychiatrist to understand and learn the techniques. Once the tactics are understood and learned, players can apply them to training and ultimately to their tournament arsenal, allowing them to play to their ultimate potential.
References
1. Morgan WP. Selected psychological factors limiting performance: A mental health model. In Clarke DH and Eckert HM (eds.), Limits of Human Performance. Champaign, Ill.: Human Kinetics Publishers, 1985.
Dr. Cohen had a private practice in psychiatry for more than 35 years. He is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University in Philadelphia. Dr. Cohen has been a nationally ranked tennis player from age 12 to the present and served as captain of the tennis team at the University of Pennsylvania, Philadelphia. Dr. Cohen, who was ranked No. 1 in tennis in the middle states section and in the country in various categories and times, was inducted into the Philadelphia Jewish Sports Hall of Fame in 2012. Dr. Cohen has no conflicts of interest.
Ms. Cohen, Dr. Cohen’s daughter, was No. 1 ranked in the United States in junior tennis and No. 4 in the world. In addition, Ms. Cohen was ranked among the top 100 players in the world by the professional World Tennis Association. She also was the No. 2 college player in United States, and an All-American at the University of Miami. She holds a master’s in sports psychology, and presently works as a sports psychologist and tennis professional in Philadelphia. Ms. Cohen has no conflicts of interest.
Successful athletes exhibit positive mental health. This mental health is directly related to athletic success and high levels of performance.1 Mental skills are as important as natural physical ability and mechanical skills in the sport of tennis.
Research has shown that tennis is 85% mental and that players spend 80% of their time on the court handling emotions. Some players look good in practice when they are not under pressure but cannot win matches (they have the physical skill level to win) because they cannot handle their own emotions during the duress of a match. They are affected by anger, fear, stress, poor concentration, and other internal elements that interfere with their ability to perform at an optimal level. Competitors may also be affected by external factors such as the sun, wind, an opponent, and so on, and may use these situations as an excuse not to win.
Players normally practice physical skills but rarely practice cognitive techniques. Regardless of level of play – pro, collegiate, junior, or club – practicing mental skills will greatly improve the players’ arsenal of weapons, giving them an edge in matches and making them the best players they can be. Mental health professionals also can use these strategies to help motivate athletes who compete in other sports – and in other competitive endeavors.
Visualization is the formation of a mental image of something of your choice. Visualization imagery techniques can be used by players to calm themselves before playing a match so their emotions are not wasted on trying to quiet the minds and quell stress. Implementing the following visualization techniques will reduce a player’s anxiety during the match, allowing the player to direct energy toward optimal mental and physical performance on the court.
In advance of a match, encourage the player to learn and analyze the opponent’s strengths and weaknesses by watching the opponent play and/or from asking others. The night before the scheduled match, get the player to imagine how they will play points against their competitor. Play into the opponents’ vulnerabilities or first play to their strengths to expose shortcomings and – then attack their weakness. For example, if an opponent has a weak backhand, first play to the opponent’s forehand and, when the opponent is vulnerable, go into his backhand to get a short or weak ball – and attack. The following are specific strategies that mental health professionals who work with athletes can use to help them perform optimally.
Using visualization, shadowing
Visualize the correct way to hit a tennis stroke and repeat it over and over in your mind. On a tennis court or where ever you have adequate space, shadow a stroke by using a racket and repetitively performing the actual stroke without hitting a ball. At home, practice relaxation and deep breathing techniques at night before going to sleep. Put yourself in a relaxed state and visualize repetitively striking the ball correctly. The next time you actually hit the stroke, you will produce a better shot.
Focusing on, staying in the here and now
The “here” means to focus on what is happening on your own court, not what is happening on the court next to you. Players may be affected by external factors, such as the sun, wind, and their opponent and may use these conditions or situations as an excuse if they do not win. Ignore background chatter and distractions, and be a horse with blinders. Be responsible for yourself and your own actions; manage what you can and realize that you cannot control the weather or actions of your opponent.
The “now” refers to staying present and focusing only on the current point. Do not think of past mistakes. If you are winning a match, do not think about celebrating while the match is still in play. If you are losing, do not start to write a script of excuses why you lost the match. Instead, just concentrate on the present, point by point. Focusing will allow you to understand what is true and important in the here and now. Focusing will help alleviate stress and better equip you to make quick decisions and be clear about your intended actions.
Set realistic and achievable goals
It is always good to have goals and dreams; however, you as a player must understand the realities of your current level of play. Know your level; don’t be grandiose and think you are able to beat Rafael Nadal. Having an unrealistic attitude will result in frustration and poor performance during a match. Instead, set achievable, and realistic short- and long-term goals for yourself, which will aid in your overall tennis development. After the match is over, reflect upon and evaluate the points – and your overall performance.
Don’t devalue yourself if you lose a match. Do not feel too low from a loss or too high from a win. When you have a match loss, use it as an opportunity to learn from your mistakes and to improve by working on your weaknesses in future practice until you feel confident enough to use your new skills in a tournament.
Stay positive
Do not tie up your self-esteem as a person with your match outcome; in otherwords, separate feelings of self-worth from your match results. Cultivate an optimistic attitude and talk positively to yourself, strive to improve, and maintain positive self-esteem in practice and in matches. During practice, allocate 110% effort, and focus on the process, not the outcome. Arrange your practice matches so that one-third of them are against players of your same level, one-third against players worse than you, and one-third against players better than yourself.
Deal with adversity
It is important to be able to deal with external pressures going on in your life such as conflicts related to family, peers, school, work, and relationships. Deal with and manage this discord before your match so you can maintain control of your emotions and can give 100% effort on the court.
Learn mental techniques
Many athletes may have difficulty teaching themselves cognitive skills and would benefit from a few sessions with a sports psychologist/psychiatrist to understand and learn the techniques. Once the tactics are understood and learned, players can apply them to training and ultimately to their tournament arsenal, allowing them to play to their ultimate potential.
References
1. Morgan WP. Selected psychological factors limiting performance: A mental health model. In Clarke DH and Eckert HM (eds.), Limits of Human Performance. Champaign, Ill.: Human Kinetics Publishers, 1985.
Dr. Cohen had a private practice in psychiatry for more than 35 years. He is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University in Philadelphia. Dr. Cohen has been a nationally ranked tennis player from age 12 to the present and served as captain of the tennis team at the University of Pennsylvania, Philadelphia. Dr. Cohen, who was ranked No. 1 in tennis in the middle states section and in the country in various categories and times, was inducted into the Philadelphia Jewish Sports Hall of Fame in 2012. Dr. Cohen has no conflicts of interest.
Ms. Cohen, Dr. Cohen’s daughter, was No. 1 ranked in the United States in junior tennis and No. 4 in the world. In addition, Ms. Cohen was ranked among the top 100 players in the world by the professional World Tennis Association. She also was the No. 2 college player in United States, and an All-American at the University of Miami. She holds a master’s in sports psychology, and presently works as a sports psychologist and tennis professional in Philadelphia. Ms. Cohen has no conflicts of interest.
The Other Pandemic: Addiction
May 20 of this plague year, Reuters reported the death of a 32-year-old Florida nurse who had worked tirelessly to treat patients with COVID-19.1 The presumption is that, like so many selfless health care providers (HCPs), this nurse was exposed to and then sadly succumbed to the virus. That presumption would be wrong: COVID-19 did not take his young life. The other pandemic—addiction— did. Bereaved friends and family reported that the nurse had been in recovery from opioid use disorder (OUD) before the onslaught of the public health crisis. The chronicle of his relapse is instructive for the devastating effect COVID-19 has had on persons struggling with addiction, even those like the nurse who was in sustained remission from OUD with a bright future.
Many of the themes are familiar to HCPs and have been the subject of prior columns in this COVID-19 series. The nurse experienced acute stress symptoms, such as nightmares from the repeated crises of sick and dying patients in the intensive care unit where he worked.2 Like so many other HCPs, while he was desperately trying to save others, he also worried about having sufficient access to appropriate personal protective equipment (PPE).
Most relevant to this column, the caregiver was unable to access his primary source of support for his sobriety—attendance at 12-step meetings. Social distancing, which is one of the only proven means we have of reducing transmission of the virus, has had unintended consequences. Although many have found virtual connections rewarding, this nurse needed the curtailed face-to-face contact. The courage that had led him to volunteer for hazardous duty unwontedly resulted in his estrangement: Friends feared that he would expose them to the virus, and he worried that he would expose his family to danger. As in the 1918 flu pandemic, the humans we depend on for reality testing and companionship have been cruelly transformed into potential vectors of the virus.3
Isolation is the worst of all possible counselors as the great Spanish philosopher of alienation Miguel de Unamuno has argued. The deceptive promise of a rapid deliverance from anxiety and pain that substances of abuse proffer apparently led the nurse back to opioids. The virtue of being clean permitted the dirty drug to take advantage of the nurses’ reduced physiologic tolerance to opioids. It is suspected but not confirmed that he fatally overdosed alone in his car.
This Florida nurse is an especially tragic example of a terrible phenomenon being repeated all over the country. And the epidemic of substance use disorders (SUDs) related to COVID-19 is not confined to the US; there are similar reports from other afflicted nations, making addiction truly the other pandemic.4 The Centers for Disease Control and Prevention reported that 13.3% of American adults have started or increased their substance use as a means of managing the negative emotions associated with the pandemic.5 Also from March to May 2020, researchers in Baltimore found a 17.6% increase in suspected overdoses in counties advising social distancing and/or mandating stay at home orders.5
These data reinforce a well-known maxim in the addiction community that “addiction is a disease of isolation.”6-8 The burden of the lockdown falls harder on many of the patients we treat in the federal health care system whose other mental and physical health conditions, including chronic pain, depression, and posttraumatic stress disorder already placed them at elevated risk of SUDs.9 Director of the National Institute of Drug Abuse Nora Volkow, MD, recently traced the well-known arc from isolation to increased use of drugs and alcohol.10 Isolation is stressful and amplifies negative thoughts, dysphoria, and fearful emotions, which are recognized triggers for the use of substances of abuse. The usually available means of coping with craving, and in many cases withdrawal, such as prescribed medications, visits to therapists, participation in support groups are either not available or much more difficult to access.10 Nor are those without a current or even historical SUD immune to the psychosocial pressures of the pandemic: Isolation also constitutes a risk for the development of de novo addiction particularly among already marginalized groups, such as the elderly and disabled.
The federal government has initiated several important measures to reduce the adverse impact of isolation on persons with SUDs. The Drug Enforcement Administration is exempting qualified practitioners of medication-assisted treatment from the in-person evaluation that is usually required for the prescription of controlled substances, including buprenorphine. This exemption applies to both established patient prescriptions for buprenorphine and new buprenorphine patient prescriptions.11 These and other administrative contingencies at the federal government level can assist persons with OUD to continue to receive medicationassisted treatment.
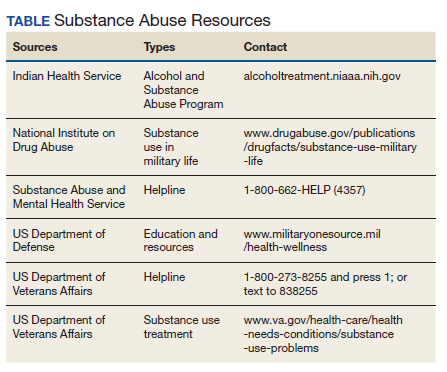
As individual clinicians in federal practice, we alone cannot engineer such major policy accommodations in response to COVID-19, yet we can still make a difference in the lives of our patients. We can focus a few minutes of our telehealth interactions on checking in with patients who have a history or a current SUD. We can remember to use evidence-based screens for these patients and those with other risk factors to detect drug or alcohol use before it becomes a disorder. And we can identify and refer not only patients but also our beleaguered colleagues who feel alone at sea—to the many lifelines our agencies have cast into what other commentators have referred to as a Perfect Storm of COVID-19 and the opioid crisis (Table).12
1. Borter G. A nurse struggled with COVID-19 trauma. He was found dead in his car. Reuters. May 20, 2020. https:// www.reuters.com/article/us-health-coronavirus-nurse -death-insigh/a-nurse-struggled-with-covid-19-trauma-he -was-found-dead-in-his-car-idUSKBN22W1JD Accessed September 15, 2020.
2. Geppert CMA. The duty to care and its exceptions in a pandemic. Fed Pract. 2020;37(5):210-211.
3. Kim NY. How the 1918 pandemic frayed social bonds. The Atlantic. March 31, 2020. https://www.theatlantic.com /family/archive/2020/03/coronavirus-loneliness-and-mistrust -1918-flu-pandemic-quarantine/609163. Accessed September 18, 2020.
4. Jemberie WB, Stewart Williams J, Eriksson M, et al. Substance use disorders and COVID-19: multi-faceted problems which require multi-pronged solutions. Front Psychiatry. 2020;11:714. Published 2020 Jul 21. doi:10.3389/fpsyt.2020.00714
5. Alter A, Yeager C. COVID-19 impact on US national overdose crises. http://www.odmap.org/Content/docs/news/2020 /ODMAP-Report-June-2020.pdf. Published May 2020. Accessed September 18, 2020.
6. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1049-1057. Published 2020 Aug 14. doi:10.15585/mmwr.mm6932a1
7. Grinspoon P. A tale of two epidemics: when COVID-19 and opioid addiction collide. https://www.health.harvard.edu /blog/a-tale-of-two-epidemics-when-covid-19-and-opioid -addiction-collide-2020042019569. Published April 20, 2020. Accessed September 16, 2020
8. Bebinger M. Addiction is “a disease of isolation”—so pandemic puts recovery at risk. https://khn.org/news/addiction -is-a-disease-of-isolation-so-pandemic-puts-recovery-at-risk. Published March 30, 2020. Accessed September 23, 2020.
9. National Institute of Drug Abuse. Substance abuse and military life. DrugFacts. https://www.drugabuse.gov/publications /drugfacts/substance-use-military-life. Published October 2019. Accessed September 16, 2020.
10. Volkow ND. Collision of the COVID-19 and addiction epidemics. Ann Intern Med. 2020;173(1):61-62. doi:10.7326/M20-1212
11. Substance Abuse and Mental Health Administration. FAQS: Provision of methadone and buprenorphine for the treatment of opioid use disorder in the COVID-19 emergency. https:// www.samhsa.gov/sites/default/files/faqs-for-oud-prescribing -and-dispensing.pdf. Updated April 21, 2020. Accessed September 22, 2020.
12. Spagnolo PA, Montemitro C, Leggio L. New challenges in addiction medicine: COVID-19 infection in patients with alcohol and substance usedisorders-the perfect storm. Am J Psychiatry. 2020;177(9):805-807. doi:10.1176/appi. ajp.2020.20040417
May 20 of this plague year, Reuters reported the death of a 32-year-old Florida nurse who had worked tirelessly to treat patients with COVID-19.1 The presumption is that, like so many selfless health care providers (HCPs), this nurse was exposed to and then sadly succumbed to the virus. That presumption would be wrong: COVID-19 did not take his young life. The other pandemic—addiction— did. Bereaved friends and family reported that the nurse had been in recovery from opioid use disorder (OUD) before the onslaught of the public health crisis. The chronicle of his relapse is instructive for the devastating effect COVID-19 has had on persons struggling with addiction, even those like the nurse who was in sustained remission from OUD with a bright future.
Many of the themes are familiar to HCPs and have been the subject of prior columns in this COVID-19 series. The nurse experienced acute stress symptoms, such as nightmares from the repeated crises of sick and dying patients in the intensive care unit where he worked.2 Like so many other HCPs, while he was desperately trying to save others, he also worried about having sufficient access to appropriate personal protective equipment (PPE).
Most relevant to this column, the caregiver was unable to access his primary source of support for his sobriety—attendance at 12-step meetings. Social distancing, which is one of the only proven means we have of reducing transmission of the virus, has had unintended consequences. Although many have found virtual connections rewarding, this nurse needed the curtailed face-to-face contact. The courage that had led him to volunteer for hazardous duty unwontedly resulted in his estrangement: Friends feared that he would expose them to the virus, and he worried that he would expose his family to danger. As in the 1918 flu pandemic, the humans we depend on for reality testing and companionship have been cruelly transformed into potential vectors of the virus.3
Isolation is the worst of all possible counselors as the great Spanish philosopher of alienation Miguel de Unamuno has argued. The deceptive promise of a rapid deliverance from anxiety and pain that substances of abuse proffer apparently led the nurse back to opioids. The virtue of being clean permitted the dirty drug to take advantage of the nurses’ reduced physiologic tolerance to opioids. It is suspected but not confirmed that he fatally overdosed alone in his car.
This Florida nurse is an especially tragic example of a terrible phenomenon being repeated all over the country. And the epidemic of substance use disorders (SUDs) related to COVID-19 is not confined to the US; there are similar reports from other afflicted nations, making addiction truly the other pandemic.4 The Centers for Disease Control and Prevention reported that 13.3% of American adults have started or increased their substance use as a means of managing the negative emotions associated with the pandemic.5 Also from March to May 2020, researchers in Baltimore found a 17.6% increase in suspected overdoses in counties advising social distancing and/or mandating stay at home orders.5
These data reinforce a well-known maxim in the addiction community that “addiction is a disease of isolation.”6-8 The burden of the lockdown falls harder on many of the patients we treat in the federal health care system whose other mental and physical health conditions, including chronic pain, depression, and posttraumatic stress disorder already placed them at elevated risk of SUDs.9 Director of the National Institute of Drug Abuse Nora Volkow, MD, recently traced the well-known arc from isolation to increased use of drugs and alcohol.10 Isolation is stressful and amplifies negative thoughts, dysphoria, and fearful emotions, which are recognized triggers for the use of substances of abuse. The usually available means of coping with craving, and in many cases withdrawal, such as prescribed medications, visits to therapists, participation in support groups are either not available or much more difficult to access.10 Nor are those without a current or even historical SUD immune to the psychosocial pressures of the pandemic: Isolation also constitutes a risk for the development of de novo addiction particularly among already marginalized groups, such as the elderly and disabled.
The federal government has initiated several important measures to reduce the adverse impact of isolation on persons with SUDs. The Drug Enforcement Administration is exempting qualified practitioners of medication-assisted treatment from the in-person evaluation that is usually required for the prescription of controlled substances, including buprenorphine. This exemption applies to both established patient prescriptions for buprenorphine and new buprenorphine patient prescriptions.11 These and other administrative contingencies at the federal government level can assist persons with OUD to continue to receive medicationassisted treatment.
As individual clinicians in federal practice, we alone cannot engineer such major policy accommodations in response to COVID-19, yet we can still make a difference in the lives of our patients. We can focus a few minutes of our telehealth interactions on checking in with patients who have a history or a current SUD. We can remember to use evidence-based screens for these patients and those with other risk factors to detect drug or alcohol use before it becomes a disorder. And we can identify and refer not only patients but also our beleaguered colleagues who feel alone at sea—to the many lifelines our agencies have cast into what other commentators have referred to as a Perfect Storm of COVID-19 and the opioid crisis (Table).12
May 20 of this plague year, Reuters reported the death of a 32-year-old Florida nurse who had worked tirelessly to treat patients with COVID-19.1 The presumption is that, like so many selfless health care providers (HCPs), this nurse was exposed to and then sadly succumbed to the virus. That presumption would be wrong: COVID-19 did not take his young life. The other pandemic—addiction— did. Bereaved friends and family reported that the nurse had been in recovery from opioid use disorder (OUD) before the onslaught of the public health crisis. The chronicle of his relapse is instructive for the devastating effect COVID-19 has had on persons struggling with addiction, even those like the nurse who was in sustained remission from OUD with a bright future.
Many of the themes are familiar to HCPs and have been the subject of prior columns in this COVID-19 series. The nurse experienced acute stress symptoms, such as nightmares from the repeated crises of sick and dying patients in the intensive care unit where he worked.2 Like so many other HCPs, while he was desperately trying to save others, he also worried about having sufficient access to appropriate personal protective equipment (PPE).
Most relevant to this column, the caregiver was unable to access his primary source of support for his sobriety—attendance at 12-step meetings. Social distancing, which is one of the only proven means we have of reducing transmission of the virus, has had unintended consequences. Although many have found virtual connections rewarding, this nurse needed the curtailed face-to-face contact. The courage that had led him to volunteer for hazardous duty unwontedly resulted in his estrangement: Friends feared that he would expose them to the virus, and he worried that he would expose his family to danger. As in the 1918 flu pandemic, the humans we depend on for reality testing and companionship have been cruelly transformed into potential vectors of the virus.3
Isolation is the worst of all possible counselors as the great Spanish philosopher of alienation Miguel de Unamuno has argued. The deceptive promise of a rapid deliverance from anxiety and pain that substances of abuse proffer apparently led the nurse back to opioids. The virtue of being clean permitted the dirty drug to take advantage of the nurses’ reduced physiologic tolerance to opioids. It is suspected but not confirmed that he fatally overdosed alone in his car.
This Florida nurse is an especially tragic example of a terrible phenomenon being repeated all over the country. And the epidemic of substance use disorders (SUDs) related to COVID-19 is not confined to the US; there are similar reports from other afflicted nations, making addiction truly the other pandemic.4 The Centers for Disease Control and Prevention reported that 13.3% of American adults have started or increased their substance use as a means of managing the negative emotions associated with the pandemic.5 Also from March to May 2020, researchers in Baltimore found a 17.6% increase in suspected overdoses in counties advising social distancing and/or mandating stay at home orders.5
These data reinforce a well-known maxim in the addiction community that “addiction is a disease of isolation.”6-8 The burden of the lockdown falls harder on many of the patients we treat in the federal health care system whose other mental and physical health conditions, including chronic pain, depression, and posttraumatic stress disorder already placed them at elevated risk of SUDs.9 Director of the National Institute of Drug Abuse Nora Volkow, MD, recently traced the well-known arc from isolation to increased use of drugs and alcohol.10 Isolation is stressful and amplifies negative thoughts, dysphoria, and fearful emotions, which are recognized triggers for the use of substances of abuse. The usually available means of coping with craving, and in many cases withdrawal, such as prescribed medications, visits to therapists, participation in support groups are either not available or much more difficult to access.10 Nor are those without a current or even historical SUD immune to the psychosocial pressures of the pandemic: Isolation also constitutes a risk for the development of de novo addiction particularly among already marginalized groups, such as the elderly and disabled.
The federal government has initiated several important measures to reduce the adverse impact of isolation on persons with SUDs. The Drug Enforcement Administration is exempting qualified practitioners of medication-assisted treatment from the in-person evaluation that is usually required for the prescription of controlled substances, including buprenorphine. This exemption applies to both established patient prescriptions for buprenorphine and new buprenorphine patient prescriptions.11 These and other administrative contingencies at the federal government level can assist persons with OUD to continue to receive medicationassisted treatment.
As individual clinicians in federal practice, we alone cannot engineer such major policy accommodations in response to COVID-19, yet we can still make a difference in the lives of our patients. We can focus a few minutes of our telehealth interactions on checking in with patients who have a history or a current SUD. We can remember to use evidence-based screens for these patients and those with other risk factors to detect drug or alcohol use before it becomes a disorder. And we can identify and refer not only patients but also our beleaguered colleagues who feel alone at sea—to the many lifelines our agencies have cast into what other commentators have referred to as a Perfect Storm of COVID-19 and the opioid crisis (Table).12
1. Borter G. A nurse struggled with COVID-19 trauma. He was found dead in his car. Reuters. May 20, 2020. https:// www.reuters.com/article/us-health-coronavirus-nurse -death-insigh/a-nurse-struggled-with-covid-19-trauma-he -was-found-dead-in-his-car-idUSKBN22W1JD Accessed September 15, 2020.
2. Geppert CMA. The duty to care and its exceptions in a pandemic. Fed Pract. 2020;37(5):210-211.
3. Kim NY. How the 1918 pandemic frayed social bonds. The Atlantic. March 31, 2020. https://www.theatlantic.com /family/archive/2020/03/coronavirus-loneliness-and-mistrust -1918-flu-pandemic-quarantine/609163. Accessed September 18, 2020.
4. Jemberie WB, Stewart Williams J, Eriksson M, et al. Substance use disorders and COVID-19: multi-faceted problems which require multi-pronged solutions. Front Psychiatry. 2020;11:714. Published 2020 Jul 21. doi:10.3389/fpsyt.2020.00714
5. Alter A, Yeager C. COVID-19 impact on US national overdose crises. http://www.odmap.org/Content/docs/news/2020 /ODMAP-Report-June-2020.pdf. Published May 2020. Accessed September 18, 2020.
6. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1049-1057. Published 2020 Aug 14. doi:10.15585/mmwr.mm6932a1
7. Grinspoon P. A tale of two epidemics: when COVID-19 and opioid addiction collide. https://www.health.harvard.edu /blog/a-tale-of-two-epidemics-when-covid-19-and-opioid -addiction-collide-2020042019569. Published April 20, 2020. Accessed September 16, 2020
8. Bebinger M. Addiction is “a disease of isolation”—so pandemic puts recovery at risk. https://khn.org/news/addiction -is-a-disease-of-isolation-so-pandemic-puts-recovery-at-risk. Published March 30, 2020. Accessed September 23, 2020.
9. National Institute of Drug Abuse. Substance abuse and military life. DrugFacts. https://www.drugabuse.gov/publications /drugfacts/substance-use-military-life. Published October 2019. Accessed September 16, 2020.
10. Volkow ND. Collision of the COVID-19 and addiction epidemics. Ann Intern Med. 2020;173(1):61-62. doi:10.7326/M20-1212
11. Substance Abuse and Mental Health Administration. FAQS: Provision of methadone and buprenorphine for the treatment of opioid use disorder in the COVID-19 emergency. https:// www.samhsa.gov/sites/default/files/faqs-for-oud-prescribing -and-dispensing.pdf. Updated April 21, 2020. Accessed September 22, 2020.
12. Spagnolo PA, Montemitro C, Leggio L. New challenges in addiction medicine: COVID-19 infection in patients with alcohol and substance usedisorders-the perfect storm. Am J Psychiatry. 2020;177(9):805-807. doi:10.1176/appi. ajp.2020.20040417
1. Borter G. A nurse struggled with COVID-19 trauma. He was found dead in his car. Reuters. May 20, 2020. https:// www.reuters.com/article/us-health-coronavirus-nurse -death-insigh/a-nurse-struggled-with-covid-19-trauma-he -was-found-dead-in-his-car-idUSKBN22W1JD Accessed September 15, 2020.
2. Geppert CMA. The duty to care and its exceptions in a pandemic. Fed Pract. 2020;37(5):210-211.
3. Kim NY. How the 1918 pandemic frayed social bonds. The Atlantic. March 31, 2020. https://www.theatlantic.com /family/archive/2020/03/coronavirus-loneliness-and-mistrust -1918-flu-pandemic-quarantine/609163. Accessed September 18, 2020.
4. Jemberie WB, Stewart Williams J, Eriksson M, et al. Substance use disorders and COVID-19: multi-faceted problems which require multi-pronged solutions. Front Psychiatry. 2020;11:714. Published 2020 Jul 21. doi:10.3389/fpsyt.2020.00714
5. Alter A, Yeager C. COVID-19 impact on US national overdose crises. http://www.odmap.org/Content/docs/news/2020 /ODMAP-Report-June-2020.pdf. Published May 2020. Accessed September 18, 2020.
6. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1049-1057. Published 2020 Aug 14. doi:10.15585/mmwr.mm6932a1
7. Grinspoon P. A tale of two epidemics: when COVID-19 and opioid addiction collide. https://www.health.harvard.edu /blog/a-tale-of-two-epidemics-when-covid-19-and-opioid -addiction-collide-2020042019569. Published April 20, 2020. Accessed September 16, 2020
8. Bebinger M. Addiction is “a disease of isolation”—so pandemic puts recovery at risk. https://khn.org/news/addiction -is-a-disease-of-isolation-so-pandemic-puts-recovery-at-risk. Published March 30, 2020. Accessed September 23, 2020.
9. National Institute of Drug Abuse. Substance abuse and military life. DrugFacts. https://www.drugabuse.gov/publications /drugfacts/substance-use-military-life. Published October 2019. Accessed September 16, 2020.
10. Volkow ND. Collision of the COVID-19 and addiction epidemics. Ann Intern Med. 2020;173(1):61-62. doi:10.7326/M20-1212
11. Substance Abuse and Mental Health Administration. FAQS: Provision of methadone and buprenorphine for the treatment of opioid use disorder in the COVID-19 emergency. https:// www.samhsa.gov/sites/default/files/faqs-for-oud-prescribing -and-dispensing.pdf. Updated April 21, 2020. Accessed September 22, 2020.
12. Spagnolo PA, Montemitro C, Leggio L. New challenges in addiction medicine: COVID-19 infection in patients with alcohol and substance usedisorders-the perfect storm. Am J Psychiatry. 2020;177(9):805-807. doi:10.1176/appi. ajp.2020.20040417
