User login
Treating the jowl fat overhang with deoxycholic acid
Rejuvenation of the lower face often involves treatment of the submentum and the jowls. Energy-based devices such as lasers, radiofrequency, radiofrequency microneedling, CoolSculpting, and ultrasound have been used in the tightening of the neck and jowls.

However, the only noninvasive injectable treatment approved for the reduction of submental fat is deoxycholic acid (Kybella). The mechanism of action of deoxycholic acid has been documented as adipocyte lysis, followed by a local tissue response with neutrophil infiltration, septal thickening, neocollagenesis, and neovascularization within the subcutaneous layer, with no adverse changes in the dermis or epidermis. This treatment, which has a dose-dependent response, is highly effective for submental fat reduction and jaw contouring.

In my practice, I have found that multiple consecutive treatments with deoxycholic acid (an off-label use) are effective in permanently reducing the jowl overhang with minimal adverse effects.
Jowl fat is a common cause of sagging of the jowls, and there are few alternatives to treatment with surgery or liposuction. Jowl overhang results from multiple factors related to aging, including skeletal resorption, subcutaneous atrophy, superior and inferior fat pad compartment displacement, or mandibular septum dehiscence, which allows for the accumulation of fat pockets to migrate into the neck.

A prospective study published earlier this year describes results in 66 adults with excess jowl fat, who were treated with 2 mg/cm2 of deoxycholic acid. Injections were done in patients with “pinchable fat on the jawline” and “relatively” minimal skin laxity of 0.2 mL spaced approximately 1 cm apart or 0.1 mL spaced 0.5 cm-0.75 cm apart; the mean injection volume was 0.8 mL. After 6 months, 98% of the patients experienced improvement with a mean of 1.8 treatments. Common injection site adverse events included edema, numbness, tenderness, and bruising.
In my experience, injection volumes from 1.0 mL to 1.5 mL of deoxycholic acid can be used in each jowl with minimal adverse events if proper landmarks are followed. It is crucial that the correct patient is selected (one with minimal skin laxity), and that during injection, the fat and skin are pinched away from the underlying musculature and neurovascular structures to avoid injection near the marginal mandibular nerve. Volumes less than 1.0 mL have minimal visible improvements and will require more than 3-4 treatment sessions for optimal results.
. I often see a marked improvement in patients who present prominent marionette lines who have been unhappy with fillers in the lower face. Often, the marionette lines are a result of significant overhang from jowl fat and hyaluronic acid fillers are a temporary and often unsatisfactory treatment option. The use of deoxycholic acid in the treatment of the jowl fat is a highly effective option to minimize the appearance of marionette lines caused by displaced fat pockets in the aging lower face.
Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com . They had no relevant disclosures.
Rejuvenation of the lower face often involves treatment of the submentum and the jowls. Energy-based devices such as lasers, radiofrequency, radiofrequency microneedling, CoolSculpting, and ultrasound have been used in the tightening of the neck and jowls.
However, the only noninvasive injectable treatment approved for the reduction of submental fat is deoxycholic acid (Kybella). The mechanism of action of deoxycholic acid has been documented as adipocyte lysis, followed by a local tissue response with neutrophil infiltration, septal thickening, neocollagenesis, and neovascularization within the subcutaneous layer, with no adverse changes in the dermis or epidermis. This treatment, which has a dose-dependent response, is highly effective for submental fat reduction and jaw contouring.
In my practice, I have found that multiple consecutive treatments with deoxycholic acid (an off-label use) are effective in permanently reducing the jowl overhang with minimal adverse effects.
Jowl fat is a common cause of sagging of the jowls, and there are few alternatives to treatment with surgery or liposuction. Jowl overhang results from multiple factors related to aging, including skeletal resorption, subcutaneous atrophy, superior and inferior fat pad compartment displacement, or mandibular septum dehiscence, which allows for the accumulation of fat pockets to migrate into the neck.
A prospective study published earlier this year describes results in 66 adults with excess jowl fat, who were treated with 2 mg/cm2 of deoxycholic acid. Injections were done in patients with “pinchable fat on the jawline” and “relatively” minimal skin laxity of 0.2 mL spaced approximately 1 cm apart or 0.1 mL spaced 0.5 cm-0.75 cm apart; the mean injection volume was 0.8 mL. After 6 months, 98% of the patients experienced improvement with a mean of 1.8 treatments. Common injection site adverse events included edema, numbness, tenderness, and bruising.
In my experience, injection volumes from 1.0 mL to 1.5 mL of deoxycholic acid can be used in each jowl with minimal adverse events if proper landmarks are followed. It is crucial that the correct patient is selected (one with minimal skin laxity), and that during injection, the fat and skin are pinched away from the underlying musculature and neurovascular structures to avoid injection near the marginal mandibular nerve. Volumes less than 1.0 mL have minimal visible improvements and will require more than 3-4 treatment sessions for optimal results.
. I often see a marked improvement in patients who present prominent marionette lines who have been unhappy with fillers in the lower face. Often, the marionette lines are a result of significant overhang from jowl fat and hyaluronic acid fillers are a temporary and often unsatisfactory treatment option. The use of deoxycholic acid in the treatment of the jowl fat is a highly effective option to minimize the appearance of marionette lines caused by displaced fat pockets in the aging lower face.
Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com . They had no relevant disclosures.
Rejuvenation of the lower face often involves treatment of the submentum and the jowls. Energy-based devices such as lasers, radiofrequency, radiofrequency microneedling, CoolSculpting, and ultrasound have been used in the tightening of the neck and jowls.
However, the only noninvasive injectable treatment approved for the reduction of submental fat is deoxycholic acid (Kybella). The mechanism of action of deoxycholic acid has been documented as adipocyte lysis, followed by a local tissue response with neutrophil infiltration, septal thickening, neocollagenesis, and neovascularization within the subcutaneous layer, with no adverse changes in the dermis or epidermis. This treatment, which has a dose-dependent response, is highly effective for submental fat reduction and jaw contouring.
In my practice, I have found that multiple consecutive treatments with deoxycholic acid (an off-label use) are effective in permanently reducing the jowl overhang with minimal adverse effects.
Jowl fat is a common cause of sagging of the jowls, and there are few alternatives to treatment with surgery or liposuction. Jowl overhang results from multiple factors related to aging, including skeletal resorption, subcutaneous atrophy, superior and inferior fat pad compartment displacement, or mandibular septum dehiscence, which allows for the accumulation of fat pockets to migrate into the neck.
A prospective study published earlier this year describes results in 66 adults with excess jowl fat, who were treated with 2 mg/cm2 of deoxycholic acid. Injections were done in patients with “pinchable fat on the jawline” and “relatively” minimal skin laxity of 0.2 mL spaced approximately 1 cm apart or 0.1 mL spaced 0.5 cm-0.75 cm apart; the mean injection volume was 0.8 mL. After 6 months, 98% of the patients experienced improvement with a mean of 1.8 treatments. Common injection site adverse events included edema, numbness, tenderness, and bruising.
In my experience, injection volumes from 1.0 mL to 1.5 mL of deoxycholic acid can be used in each jowl with minimal adverse events if proper landmarks are followed. It is crucial that the correct patient is selected (one with minimal skin laxity), and that during injection, the fat and skin are pinched away from the underlying musculature and neurovascular structures to avoid injection near the marginal mandibular nerve. Volumes less than 1.0 mL have minimal visible improvements and will require more than 3-4 treatment sessions for optimal results.
. I often see a marked improvement in patients who present prominent marionette lines who have been unhappy with fillers in the lower face. Often, the marionette lines are a result of significant overhang from jowl fat and hyaluronic acid fillers are a temporary and often unsatisfactory treatment option. The use of deoxycholic acid in the treatment of the jowl fat is a highly effective option to minimize the appearance of marionette lines caused by displaced fat pockets in the aging lower face.
Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com . They had no relevant disclosures.
It’s not time to abandon routine screening mammography in average-risk women in their 40s
In the 1970s and early 1980s, population-based screening mammography was studied in numerous randomized control trials (RCTs), with the primary outcome of reduced breast cancer mortality. Although technology and the sensitivity of mammography in the 1980s was somewhat rudimentary compared with current screening, a meta-analysis of these RCTs demonstrated a clear mortality benefit for screening mammography.1 As a result, widespread population-based mammography was introduced in the mid-1980s in the United States and has become a standard for breast cancer screening.
Since that time, few RCTs of screening mammography versus observation have been conducted because of the ethical challenges of entering women into such studies as well as the difficulty and expense of long-term follow-up to measure the effect of screening on breast cancer mortality. Without ongoing RCTs of mammography, retrospective, observational, and computer simulation trials of the efficacy and harms of screening mammography have been conducted using proxy measures of mortality (such as stage at diagnosis), and some have questioned the overall benefit of screening mammography.2,3
To further complicate this controversy, some national guidelines have recommended against routinely recommending screening mammography for women aged 40 to 49 based on concerns that the harms (callbacks, benign breast biopsies, overdiagnosis) exceed the potential benefits (earlier diagnosis, possible decrease in needed treatments, reduced breast cancer mortality).4 This has resulted in a confusing morass of national recommendations with uncertainty regarding the question of whether to routinely offer screening mammography for women in their 40s at average risk for breast cancer.4-6
Recently, to address this question Duffy and colleagues conducted a large RCT of women in their 40s to evaluate the long-term effect of mammography on breast cancer mortality.7 Here, I review the study in depth and offer some guidance to clinicians and women struggling with screening decisions.
Breast cancer mortality significantly lower in the screening group
The RCT, known as the UK Age trial, was conducted in England, Wales, and Scotland and enrolled 160,921 women from 1990 through 1997.7 Women were randomly assigned in a 2:1 ratio to observation or annual screening mammogram beginning at age 39–41 until age 48. (In the United Kingdom, all women are screened starting at age 50.) Study enrollees were followed for a median of 22.8 years, and the primary outcome was breast cancer mortality.
The study results showed a 25% relative risk (RR) reduction in breast cancer mortality at 10 years of follow-up in the mammography group compared with the unscreened women (83 breast cancer deaths in the mammography group vs 219 in the observation group [RR, 0.75; 95% confidence interval (CI), 0.58–0.97; P = .029]). Based on the prevalence of breast cancer in women in their 40s, this 25% relative risk reduction translates into approximately 1 less death per 1,000 women who undergo routine screening in their 40s.
While there was no additional significant mortality reduction beyond 10 years of follow-up, as noted mammography is offered routinely starting at age 50 to all women in the United Kingdom. The authors concluded that “reducing the lower age limit for screening from 50 to 40 years [of age] could potentially reduce breast cancer mortality.”
Was overdiagnosis a concern? Another finding in this trial was related to overdiagnosis of breast cancer in the screened group. Overdiagnosis refers to mammographic-only diagnosis (that is, no clinical findings) of nonaggressive breast cancer, which would remain indolent and not harm the patient. The study results demonstrated essentially no overdiagnosis in women screened at age 40 compared with the unscreened group.
Continue to: Large trial, long follow-up are key strengths...
Large trial, long follow-up are key strengths
The UK Age trial’s primary strength is its study design: a large population-based RCT that included diverse participants with the critical study outcome for cancer screening (mortality). The study’s long-term follow-up is another key strength, since breast cancer mortality typically occurs 7 to 10 years after diagnosis. In addition, results were available for 99.9% of the women enrolled in the trial (that is, only 0.1% of women were lost to follow-up). Interestingly, the demonstrated mortality reduction with screening mammography for women in their 40s validates the mortality benefit demonstrated in other large RCTs of women in their 40s.1
Another strong point is that the study addresses the issue of whether screening women in their 40s results in overdiagnosis compared with women who start screening in their 50s. Further, this study validates a prior observational study that mammographic findings of nonprogressive cancers do not disappear, so nonaggressive cancers that present on mammography in women in their 40s still would be detected when women start screening in their 50s.8
Study limitations should be noted
The study has several limitations. For example, significant improvements have been made in breast cancer treatments that may mitigate against the positive impact of screening mammography. The impact of changed breast cancer management over the past 20 years could not be addressed with this study’s design since women would have been treated in the 1990s. In addition, substantial improvements have occurred in breast cancer screening standards (2 views vs the single view used in the study) and technology since the 1990s. Current mammography includes nearly uniform use of either digital mammography (DM) or digital breast tomosynthesis (DBT), both of which improve breast cancer detection for women in their 40s compared with the older film-screen technology. In addition, DBT reduces false-positive results by approximately 40%, resulting in fewer callbacks and biopsies. While improved cancer detection and reduced false-positive results are seen with DM and DBT, whether these technology improvements result in improved breast cancer mortality has not yet been sufficiently studied.
Perhaps the most important limitation in this study is that the women did not undergo routine risk assessment before trial entry to assure that they all were at “average risk.” As a result, both high- and average-risk women would have been included in this population-based trial. Without risk stratification, it remains uncertain whether the reduction in breast cancer mortality disproportionately exists within a high-risk subgroup (such as breast cancer gene mutation carriers).
Finally, the cost efficacy of routine screening mammography for women in their 40s was not evaluated in this study.
The UK Age trial in perspective
The good news is that there is the clear evidence that breast cancer mortality rates (deaths per 100,000) have decreased by about 40% over the past 50 years, likely due to improvements in breast cancer treatment and routine screening mammography.9 Breast cancer mortality reduction is particularly important because breast cancer remains the most common cancer and is the second leading cause of cancer death in women in the United States. In the past decade, considerable debate has arisen arguing whether this reduction in breast cancer mortality is due to improved treatments, routine screening mammography, or both. Authors of a retrospective trial in Australia, recently reviewed in OBG Management, suggested that the majority of improvement is due to improvements in treatment.3,10 However, as the authors pointed out, due to the trial’s retrospective design, causality only can be inferred. The current UK Age trial does add to the numerous prospective trials demonstrating mortality benefit for mammography in women in their 40s.11
What remains a challenge for clinicians, and for women struggling with the mammography question, is the absence of risk assessment in these long-term RCT trials as well as in the large retrospective database studies. Without risk stratification, these studies treated all the study population as “average risk.” Because breast cancer risk assessment is sporadically performed in clinical practice and there are no published RCTs of screening mammography in risk-assessed “average risk” women in their 40s, it remains uncertain whether the women benefiting from screening in their 40s are in a high-risk group or whether women of average risk in this age group also are benefiting from routine screening mammography.
Continue to: What’s next: Incorporate routine risk assessment into clinical practice...
What’s next: Incorporate routine risk assessment into clinical practice
It is not time to abandon screening mammography for all women in their 40s. Rather, routine risk assessment should be performed using one of many available validated or widely tested tools, a recommendation supported by the American College of Obstetricians and Gynecologists, the National Comprehensive Cancer Network, and the US Preventive Services Task Force.5,6,12
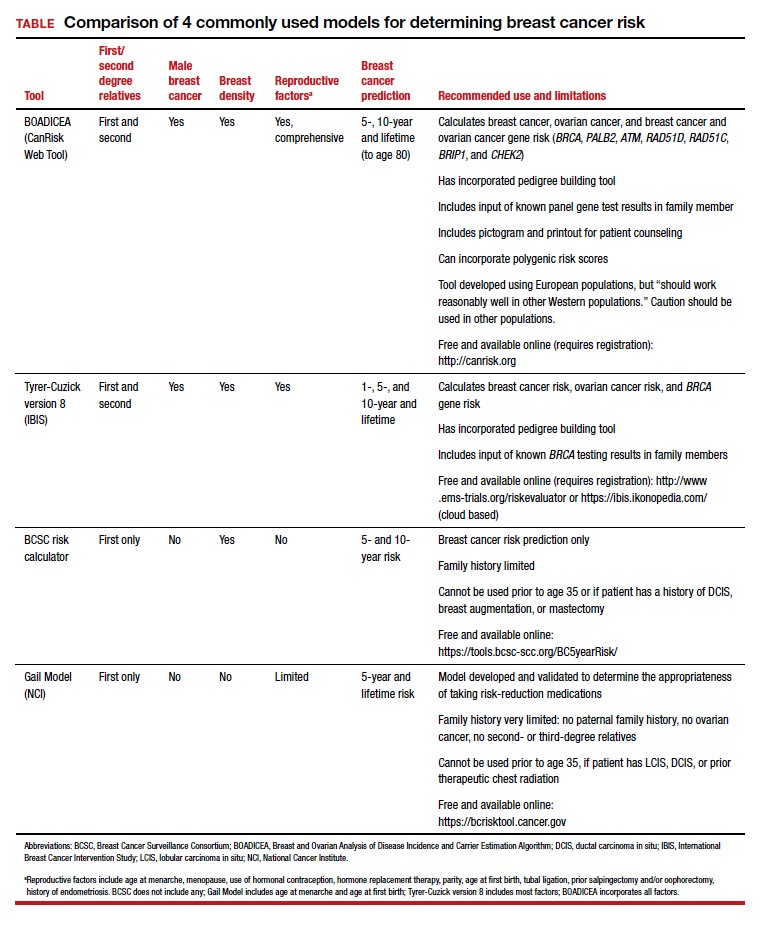
Ideally, these tools can be incorporated into an electronic health record and prepopulated using already available patient data (such as age, reproductive risk factors, current medications, breast density if available, and family history). Prepopulating available data into breast cancer risk calculators would allow clinicians to spend time on counseling women regarding breast cancer risk and appropriate screening methods. The TABLE provides a summary of useful breast cancer risk calculators and includes comments about their utility and significant limitations and benefits. In addition to breast cancer risk, the more comprehensive risk calculators (Tyrer-Cuzick and BOADICEA) allow calculation of ovarian cancer risk and gene mutation risk.
Routinely performing breast cancer risk assessment can guide discussions of screening mammography and can provide data for conducting a more individualized discussion on cancer genetic counseling and testing, risk reduction methods in high-risk women, and possible use of intensive breast cancer screening tools in identified high-risk women.
Ultimately, debating the question of whether all women should have routine breast cancer screening in their 40s should be passé. Ideally, all women should undergo breast cancer risk assessment in their 20s. Risk assessment results can then be used to guide the discussion of multiple potential interventions for women in their 40s (or earlier if appropriate), including routine screening mammography, cancer genetic counseling and testing in appropriate individuals, and intervention for women who are identified at high risk.
Absent breast cancer risk assessment, screening mammography still should be offered to women in their 40s, and the decision to proceed should be based on a discussion of risks, benefits, and the value the patient places on these factors.●
- Nelson HD, Fu R, Cantor A, et al. Effectiveness of breast cancer screening: systematic review and meta-analysis to update the 2009 US Preventive Services Task Force recommendation. Ann Intern Med. 2016;164:244-255.
- Bleyer A, Welch HG. Effect of three decades of screening mammography on breast-cancer incidence. N Engl J Med. 2012;367:1998-2005.
- Burton R, Stevenson C. Assessment of breast cancer mortality trends associated with mammographic screening and adjuvant therapy from 1986 to 2013 in the state of Victoria, Australia. JAMA Netw Open. 2020;3:e208249-e.
- Nelson HD, Cantor A, Humphrey L, et al. A systematic review to update the 2009 US Preventive Services Task Force recommendation. Evidence syntheses No. 124. AHRQ Publication No. 14-05201-EF-1. Rockville, MD: Agency for Healthcare Research and Quality; 2016.
- Bevers TB, Helvie M, Bonaccio E, et al. Breast cancer screening and diagnosis, version 3.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2018;16:1362-1389.
- ACOG Committee on Practice Bulletins–Gynecology. Breast cancer risk assessment and screening in average-risk women. Obstet Gynecol. 2017;130:e1-e16.
- Duffy SW, Vulkan D, Cuckle H, et al. Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): final results of a randomised, controlled trial. Lancet Oncol. 2020;21:1165-1172.
- Arleo EK, Monticciolo DL, Monsees B, et al. Persistent untreated screening-detected breast cancer: an argument against delaying screening or increasing the interval between screenings. J Am Coll Radiol. 2017;14:863-867.
- DeSantis CE, Ma J, Gaudet MM, et al. Breast cancer statistics, 2019. CA Cancer J Clin. 2019;69:438-451.
- Kaunitz AM. How effective is screening mammography for preventing breast cancer mortality? OBG Manag. 2020;32(8):17,49.
- Oeffinger KC, Fontham ET, Etzioni R, et al; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314:1599-1614.
- US Preventive Services Task Force; Owens DK, Davidson KW, Krist AH, et al. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer: US Preventive Services Task Force recommendation statement. JAMA. 2019;322:652-665.
Mark D. Pearlman, MD
Professor Emeritus (Active), Department of Obstetrics and Gynecology
Professor Emeritus (Active), Department of Surgery
Michigan Medicine
Ann Arbor, Michigan
The author reports no financial relationships relevant to this article.
Mark D. Pearlman, MD
Professor Emeritus (Active), Department of Obstetrics and Gynecology
Professor Emeritus (Active), Department of Surgery
Michigan Medicine
Ann Arbor, Michigan
The author reports no financial relationships relevant to this article.
Mark D. Pearlman, MD
Professor Emeritus (Active), Department of Obstetrics and Gynecology
Professor Emeritus (Active), Department of Surgery
Michigan Medicine
Ann Arbor, Michigan
The author reports no financial relationships relevant to this article.
In the 1970s and early 1980s, population-based screening mammography was studied in numerous randomized control trials (RCTs), with the primary outcome of reduced breast cancer mortality. Although technology and the sensitivity of mammography in the 1980s was somewhat rudimentary compared with current screening, a meta-analysis of these RCTs demonstrated a clear mortality benefit for screening mammography.1 As a result, widespread population-based mammography was introduced in the mid-1980s in the United States and has become a standard for breast cancer screening.
Since that time, few RCTs of screening mammography versus observation have been conducted because of the ethical challenges of entering women into such studies as well as the difficulty and expense of long-term follow-up to measure the effect of screening on breast cancer mortality. Without ongoing RCTs of mammography, retrospective, observational, and computer simulation trials of the efficacy and harms of screening mammography have been conducted using proxy measures of mortality (such as stage at diagnosis), and some have questioned the overall benefit of screening mammography.2,3
To further complicate this controversy, some national guidelines have recommended against routinely recommending screening mammography for women aged 40 to 49 based on concerns that the harms (callbacks, benign breast biopsies, overdiagnosis) exceed the potential benefits (earlier diagnosis, possible decrease in needed treatments, reduced breast cancer mortality).4 This has resulted in a confusing morass of national recommendations with uncertainty regarding the question of whether to routinely offer screening mammography for women in their 40s at average risk for breast cancer.4-6
Recently, to address this question Duffy and colleagues conducted a large RCT of women in their 40s to evaluate the long-term effect of mammography on breast cancer mortality.7 Here, I review the study in depth and offer some guidance to clinicians and women struggling with screening decisions.
Breast cancer mortality significantly lower in the screening group
The RCT, known as the UK Age trial, was conducted in England, Wales, and Scotland and enrolled 160,921 women from 1990 through 1997.7 Women were randomly assigned in a 2:1 ratio to observation or annual screening mammogram beginning at age 39–41 until age 48. (In the United Kingdom, all women are screened starting at age 50.) Study enrollees were followed for a median of 22.8 years, and the primary outcome was breast cancer mortality.
The study results showed a 25% relative risk (RR) reduction in breast cancer mortality at 10 years of follow-up in the mammography group compared with the unscreened women (83 breast cancer deaths in the mammography group vs 219 in the observation group [RR, 0.75; 95% confidence interval (CI), 0.58–0.97; P = .029]). Based on the prevalence of breast cancer in women in their 40s, this 25% relative risk reduction translates into approximately 1 less death per 1,000 women who undergo routine screening in their 40s.
While there was no additional significant mortality reduction beyond 10 years of follow-up, as noted mammography is offered routinely starting at age 50 to all women in the United Kingdom. The authors concluded that “reducing the lower age limit for screening from 50 to 40 years [of age] could potentially reduce breast cancer mortality.”
Was overdiagnosis a concern? Another finding in this trial was related to overdiagnosis of breast cancer in the screened group. Overdiagnosis refers to mammographic-only diagnosis (that is, no clinical findings) of nonaggressive breast cancer, which would remain indolent and not harm the patient. The study results demonstrated essentially no overdiagnosis in women screened at age 40 compared with the unscreened group.
Continue to: Large trial, long follow-up are key strengths...
Large trial, long follow-up are key strengths
The UK Age trial’s primary strength is its study design: a large population-based RCT that included diverse participants with the critical study outcome for cancer screening (mortality). The study’s long-term follow-up is another key strength, since breast cancer mortality typically occurs 7 to 10 years after diagnosis. In addition, results were available for 99.9% of the women enrolled in the trial (that is, only 0.1% of women were lost to follow-up). Interestingly, the demonstrated mortality reduction with screening mammography for women in their 40s validates the mortality benefit demonstrated in other large RCTs of women in their 40s.1
Another strong point is that the study addresses the issue of whether screening women in their 40s results in overdiagnosis compared with women who start screening in their 50s. Further, this study validates a prior observational study that mammographic findings of nonprogressive cancers do not disappear, so nonaggressive cancers that present on mammography in women in their 40s still would be detected when women start screening in their 50s.8
Study limitations should be noted
The study has several limitations. For example, significant improvements have been made in breast cancer treatments that may mitigate against the positive impact of screening mammography. The impact of changed breast cancer management over the past 20 years could not be addressed with this study’s design since women would have been treated in the 1990s. In addition, substantial improvements have occurred in breast cancer screening standards (2 views vs the single view used in the study) and technology since the 1990s. Current mammography includes nearly uniform use of either digital mammography (DM) or digital breast tomosynthesis (DBT), both of which improve breast cancer detection for women in their 40s compared with the older film-screen technology. In addition, DBT reduces false-positive results by approximately 40%, resulting in fewer callbacks and biopsies. While improved cancer detection and reduced false-positive results are seen with DM and DBT, whether these technology improvements result in improved breast cancer mortality has not yet been sufficiently studied.
Perhaps the most important limitation in this study is that the women did not undergo routine risk assessment before trial entry to assure that they all were at “average risk.” As a result, both high- and average-risk women would have been included in this population-based trial. Without risk stratification, it remains uncertain whether the reduction in breast cancer mortality disproportionately exists within a high-risk subgroup (such as breast cancer gene mutation carriers).
Finally, the cost efficacy of routine screening mammography for women in their 40s was not evaluated in this study.
The UK Age trial in perspective
The good news is that there is the clear evidence that breast cancer mortality rates (deaths per 100,000) have decreased by about 40% over the past 50 years, likely due to improvements in breast cancer treatment and routine screening mammography.9 Breast cancer mortality reduction is particularly important because breast cancer remains the most common cancer and is the second leading cause of cancer death in women in the United States. In the past decade, considerable debate has arisen arguing whether this reduction in breast cancer mortality is due to improved treatments, routine screening mammography, or both. Authors of a retrospective trial in Australia, recently reviewed in OBG Management, suggested that the majority of improvement is due to improvements in treatment.3,10 However, as the authors pointed out, due to the trial’s retrospective design, causality only can be inferred. The current UK Age trial does add to the numerous prospective trials demonstrating mortality benefit for mammography in women in their 40s.11
What remains a challenge for clinicians, and for women struggling with the mammography question, is the absence of risk assessment in these long-term RCT trials as well as in the large retrospective database studies. Without risk stratification, these studies treated all the study population as “average risk.” Because breast cancer risk assessment is sporadically performed in clinical practice and there are no published RCTs of screening mammography in risk-assessed “average risk” women in their 40s, it remains uncertain whether the women benefiting from screening in their 40s are in a high-risk group or whether women of average risk in this age group also are benefiting from routine screening mammography.
Continue to: What’s next: Incorporate routine risk assessment into clinical practice...
What’s next: Incorporate routine risk assessment into clinical practice
It is not time to abandon screening mammography for all women in their 40s. Rather, routine risk assessment should be performed using one of many available validated or widely tested tools, a recommendation supported by the American College of Obstetricians and Gynecologists, the National Comprehensive Cancer Network, and the US Preventive Services Task Force.5,6,12
Ideally, these tools can be incorporated into an electronic health record and prepopulated using already available patient data (such as age, reproductive risk factors, current medications, breast density if available, and family history). Prepopulating available data into breast cancer risk calculators would allow clinicians to spend time on counseling women regarding breast cancer risk and appropriate screening methods. The TABLE provides a summary of useful breast cancer risk calculators and includes comments about their utility and significant limitations and benefits. In addition to breast cancer risk, the more comprehensive risk calculators (Tyrer-Cuzick and BOADICEA) allow calculation of ovarian cancer risk and gene mutation risk.
Routinely performing breast cancer risk assessment can guide discussions of screening mammography and can provide data for conducting a more individualized discussion on cancer genetic counseling and testing, risk reduction methods in high-risk women, and possible use of intensive breast cancer screening tools in identified high-risk women.
Ultimately, debating the question of whether all women should have routine breast cancer screening in their 40s should be passé. Ideally, all women should undergo breast cancer risk assessment in their 20s. Risk assessment results can then be used to guide the discussion of multiple potential interventions for women in their 40s (or earlier if appropriate), including routine screening mammography, cancer genetic counseling and testing in appropriate individuals, and intervention for women who are identified at high risk.
Absent breast cancer risk assessment, screening mammography still should be offered to women in their 40s, and the decision to proceed should be based on a discussion of risks, benefits, and the value the patient places on these factors.●
In the 1970s and early 1980s, population-based screening mammography was studied in numerous randomized control trials (RCTs), with the primary outcome of reduced breast cancer mortality. Although technology and the sensitivity of mammography in the 1980s was somewhat rudimentary compared with current screening, a meta-analysis of these RCTs demonstrated a clear mortality benefit for screening mammography.1 As a result, widespread population-based mammography was introduced in the mid-1980s in the United States and has become a standard for breast cancer screening.
Since that time, few RCTs of screening mammography versus observation have been conducted because of the ethical challenges of entering women into such studies as well as the difficulty and expense of long-term follow-up to measure the effect of screening on breast cancer mortality. Without ongoing RCTs of mammography, retrospective, observational, and computer simulation trials of the efficacy and harms of screening mammography have been conducted using proxy measures of mortality (such as stage at diagnosis), and some have questioned the overall benefit of screening mammography.2,3
To further complicate this controversy, some national guidelines have recommended against routinely recommending screening mammography for women aged 40 to 49 based on concerns that the harms (callbacks, benign breast biopsies, overdiagnosis) exceed the potential benefits (earlier diagnosis, possible decrease in needed treatments, reduced breast cancer mortality).4 This has resulted in a confusing morass of national recommendations with uncertainty regarding the question of whether to routinely offer screening mammography for women in their 40s at average risk for breast cancer.4-6
Recently, to address this question Duffy and colleagues conducted a large RCT of women in their 40s to evaluate the long-term effect of mammography on breast cancer mortality.7 Here, I review the study in depth and offer some guidance to clinicians and women struggling with screening decisions.
Breast cancer mortality significantly lower in the screening group
The RCT, known as the UK Age trial, was conducted in England, Wales, and Scotland and enrolled 160,921 women from 1990 through 1997.7 Women were randomly assigned in a 2:1 ratio to observation or annual screening mammogram beginning at age 39–41 until age 48. (In the United Kingdom, all women are screened starting at age 50.) Study enrollees were followed for a median of 22.8 years, and the primary outcome was breast cancer mortality.
The study results showed a 25% relative risk (RR) reduction in breast cancer mortality at 10 years of follow-up in the mammography group compared with the unscreened women (83 breast cancer deaths in the mammography group vs 219 in the observation group [RR, 0.75; 95% confidence interval (CI), 0.58–0.97; P = .029]). Based on the prevalence of breast cancer in women in their 40s, this 25% relative risk reduction translates into approximately 1 less death per 1,000 women who undergo routine screening in their 40s.
While there was no additional significant mortality reduction beyond 10 years of follow-up, as noted mammography is offered routinely starting at age 50 to all women in the United Kingdom. The authors concluded that “reducing the lower age limit for screening from 50 to 40 years [of age] could potentially reduce breast cancer mortality.”
Was overdiagnosis a concern? Another finding in this trial was related to overdiagnosis of breast cancer in the screened group. Overdiagnosis refers to mammographic-only diagnosis (that is, no clinical findings) of nonaggressive breast cancer, which would remain indolent and not harm the patient. The study results demonstrated essentially no overdiagnosis in women screened at age 40 compared with the unscreened group.
Continue to: Large trial, long follow-up are key strengths...
Large trial, long follow-up are key strengths
The UK Age trial’s primary strength is its study design: a large population-based RCT that included diverse participants with the critical study outcome for cancer screening (mortality). The study’s long-term follow-up is another key strength, since breast cancer mortality typically occurs 7 to 10 years after diagnosis. In addition, results were available for 99.9% of the women enrolled in the trial (that is, only 0.1% of women were lost to follow-up). Interestingly, the demonstrated mortality reduction with screening mammography for women in their 40s validates the mortality benefit demonstrated in other large RCTs of women in their 40s.1
Another strong point is that the study addresses the issue of whether screening women in their 40s results in overdiagnosis compared with women who start screening in their 50s. Further, this study validates a prior observational study that mammographic findings of nonprogressive cancers do not disappear, so nonaggressive cancers that present on mammography in women in their 40s still would be detected when women start screening in their 50s.8
Study limitations should be noted
The study has several limitations. For example, significant improvements have been made in breast cancer treatments that may mitigate against the positive impact of screening mammography. The impact of changed breast cancer management over the past 20 years could not be addressed with this study’s design since women would have been treated in the 1990s. In addition, substantial improvements have occurred in breast cancer screening standards (2 views vs the single view used in the study) and technology since the 1990s. Current mammography includes nearly uniform use of either digital mammography (DM) or digital breast tomosynthesis (DBT), both of which improve breast cancer detection for women in their 40s compared with the older film-screen technology. In addition, DBT reduces false-positive results by approximately 40%, resulting in fewer callbacks and biopsies. While improved cancer detection and reduced false-positive results are seen with DM and DBT, whether these technology improvements result in improved breast cancer mortality has not yet been sufficiently studied.
Perhaps the most important limitation in this study is that the women did not undergo routine risk assessment before trial entry to assure that they all were at “average risk.” As a result, both high- and average-risk women would have been included in this population-based trial. Without risk stratification, it remains uncertain whether the reduction in breast cancer mortality disproportionately exists within a high-risk subgroup (such as breast cancer gene mutation carriers).
Finally, the cost efficacy of routine screening mammography for women in their 40s was not evaluated in this study.
The UK Age trial in perspective
The good news is that there is the clear evidence that breast cancer mortality rates (deaths per 100,000) have decreased by about 40% over the past 50 years, likely due to improvements in breast cancer treatment and routine screening mammography.9 Breast cancer mortality reduction is particularly important because breast cancer remains the most common cancer and is the second leading cause of cancer death in women in the United States. In the past decade, considerable debate has arisen arguing whether this reduction in breast cancer mortality is due to improved treatments, routine screening mammography, or both. Authors of a retrospective trial in Australia, recently reviewed in OBG Management, suggested that the majority of improvement is due to improvements in treatment.3,10 However, as the authors pointed out, due to the trial’s retrospective design, causality only can be inferred. The current UK Age trial does add to the numerous prospective trials demonstrating mortality benefit for mammography in women in their 40s.11
What remains a challenge for clinicians, and for women struggling with the mammography question, is the absence of risk assessment in these long-term RCT trials as well as in the large retrospective database studies. Without risk stratification, these studies treated all the study population as “average risk.” Because breast cancer risk assessment is sporadically performed in clinical practice and there are no published RCTs of screening mammography in risk-assessed “average risk” women in their 40s, it remains uncertain whether the women benefiting from screening in their 40s are in a high-risk group or whether women of average risk in this age group also are benefiting from routine screening mammography.
Continue to: What’s next: Incorporate routine risk assessment into clinical practice...
What’s next: Incorporate routine risk assessment into clinical practice
It is not time to abandon screening mammography for all women in their 40s. Rather, routine risk assessment should be performed using one of many available validated or widely tested tools, a recommendation supported by the American College of Obstetricians and Gynecologists, the National Comprehensive Cancer Network, and the US Preventive Services Task Force.5,6,12
Ideally, these tools can be incorporated into an electronic health record and prepopulated using already available patient data (such as age, reproductive risk factors, current medications, breast density if available, and family history). Prepopulating available data into breast cancer risk calculators would allow clinicians to spend time on counseling women regarding breast cancer risk and appropriate screening methods. The TABLE provides a summary of useful breast cancer risk calculators and includes comments about their utility and significant limitations and benefits. In addition to breast cancer risk, the more comprehensive risk calculators (Tyrer-Cuzick and BOADICEA) allow calculation of ovarian cancer risk and gene mutation risk.
Routinely performing breast cancer risk assessment can guide discussions of screening mammography and can provide data for conducting a more individualized discussion on cancer genetic counseling and testing, risk reduction methods in high-risk women, and possible use of intensive breast cancer screening tools in identified high-risk women.
Ultimately, debating the question of whether all women should have routine breast cancer screening in their 40s should be passé. Ideally, all women should undergo breast cancer risk assessment in their 20s. Risk assessment results can then be used to guide the discussion of multiple potential interventions for women in their 40s (or earlier if appropriate), including routine screening mammography, cancer genetic counseling and testing in appropriate individuals, and intervention for women who are identified at high risk.
Absent breast cancer risk assessment, screening mammography still should be offered to women in their 40s, and the decision to proceed should be based on a discussion of risks, benefits, and the value the patient places on these factors.●
- Nelson HD, Fu R, Cantor A, et al. Effectiveness of breast cancer screening: systematic review and meta-analysis to update the 2009 US Preventive Services Task Force recommendation. Ann Intern Med. 2016;164:244-255.
- Bleyer A, Welch HG. Effect of three decades of screening mammography on breast-cancer incidence. N Engl J Med. 2012;367:1998-2005.
- Burton R, Stevenson C. Assessment of breast cancer mortality trends associated with mammographic screening and adjuvant therapy from 1986 to 2013 in the state of Victoria, Australia. JAMA Netw Open. 2020;3:e208249-e.
- Nelson HD, Cantor A, Humphrey L, et al. A systematic review to update the 2009 US Preventive Services Task Force recommendation. Evidence syntheses No. 124. AHRQ Publication No. 14-05201-EF-1. Rockville, MD: Agency for Healthcare Research and Quality; 2016.
- Bevers TB, Helvie M, Bonaccio E, et al. Breast cancer screening and diagnosis, version 3.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2018;16:1362-1389.
- ACOG Committee on Practice Bulletins–Gynecology. Breast cancer risk assessment and screening in average-risk women. Obstet Gynecol. 2017;130:e1-e16.
- Duffy SW, Vulkan D, Cuckle H, et al. Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): final results of a randomised, controlled trial. Lancet Oncol. 2020;21:1165-1172.
- Arleo EK, Monticciolo DL, Monsees B, et al. Persistent untreated screening-detected breast cancer: an argument against delaying screening or increasing the interval between screenings. J Am Coll Radiol. 2017;14:863-867.
- DeSantis CE, Ma J, Gaudet MM, et al. Breast cancer statistics, 2019. CA Cancer J Clin. 2019;69:438-451.
- Kaunitz AM. How effective is screening mammography for preventing breast cancer mortality? OBG Manag. 2020;32(8):17,49.
- Oeffinger KC, Fontham ET, Etzioni R, et al; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314:1599-1614.
- US Preventive Services Task Force; Owens DK, Davidson KW, Krist AH, et al. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer: US Preventive Services Task Force recommendation statement. JAMA. 2019;322:652-665.
- Nelson HD, Fu R, Cantor A, et al. Effectiveness of breast cancer screening: systematic review and meta-analysis to update the 2009 US Preventive Services Task Force recommendation. Ann Intern Med. 2016;164:244-255.
- Bleyer A, Welch HG. Effect of three decades of screening mammography on breast-cancer incidence. N Engl J Med. 2012;367:1998-2005.
- Burton R, Stevenson C. Assessment of breast cancer mortality trends associated with mammographic screening and adjuvant therapy from 1986 to 2013 in the state of Victoria, Australia. JAMA Netw Open. 2020;3:e208249-e.
- Nelson HD, Cantor A, Humphrey L, et al. A systematic review to update the 2009 US Preventive Services Task Force recommendation. Evidence syntheses No. 124. AHRQ Publication No. 14-05201-EF-1. Rockville, MD: Agency for Healthcare Research and Quality; 2016.
- Bevers TB, Helvie M, Bonaccio E, et al. Breast cancer screening and diagnosis, version 3.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2018;16:1362-1389.
- ACOG Committee on Practice Bulletins–Gynecology. Breast cancer risk assessment and screening in average-risk women. Obstet Gynecol. 2017;130:e1-e16.
- Duffy SW, Vulkan D, Cuckle H, et al. Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): final results of a randomised, controlled trial. Lancet Oncol. 2020;21:1165-1172.
- Arleo EK, Monticciolo DL, Monsees B, et al. Persistent untreated screening-detected breast cancer: an argument against delaying screening or increasing the interval between screenings. J Am Coll Radiol. 2017;14:863-867.
- DeSantis CE, Ma J, Gaudet MM, et al. Breast cancer statistics, 2019. CA Cancer J Clin. 2019;69:438-451.
- Kaunitz AM. How effective is screening mammography for preventing breast cancer mortality? OBG Manag. 2020;32(8):17,49.
- Oeffinger KC, Fontham ET, Etzioni R, et al; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314:1599-1614.
- US Preventive Services Task Force; Owens DK, Davidson KW, Krist AH, et al. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer: US Preventive Services Task Force recommendation statement. JAMA. 2019;322:652-665.
Efforts to close the ‘AYA gap’ in lymphoma
In the 1970s, cancer survival was poor for young children and older adults in the United States, as shown by data published in the Journal of the National Cancer Institute.
Great progress has been made since the 1970s, but improvements in outcome have been less impressive for cancer patients aged 15-39 years, as shown by research published in Cancer.

Patients aged 15-39 years have been designated by the National Institutes of Health (NIH) as “adolescents and young adults (AYAs),” and the lag in survival benefit has been termed “the AYA gap.”
The AYA gap persists in lymphoma patients, and an expert panel recently outlined differences between lymphoma in AYAs and lymphoma in other age groups.
The experts spoke at a special session of the AACR Virtual Meeting: Advances in Malignant Lymphoma moderated by Somali M. Smith, MD, of the University of Chicago.
Factors that contribute to the AYA gap
About 89,000 AYAs are diagnosed with cancer each year in the United States, according to data from the National Cancer Institute (NCI). Lymphomas and thyroid cancer are the most common cancers among younger AYAs, aged 15-24 years.
In a report commissioned by the NIH in 2006, many factors contributing to the AYA gap were identified. Chief among them were:
- Limitations in access to care.
- Delayed diagnosis.
- Inconsistency in treatment and follow-up.
- Long-term toxicity (fertility, second malignancies, and cardiovascular disease).
These factors compromise health-related survival, even when cancer-specific survival is improved.
Panelist Kara Kelly, MD, of Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., noted that there are additional unique challenges for AYAs with cancer. These include:
- Pubertal changes.
- Developmental transition to independence.
- Societal impediments such as insurance coverage and disparities in access to specialized centers.
- Psychosocial factors such as health literacy and adherence to treatment and follow-up.
Focusing on lymphoma specifically, Dr. Kelly noted that lymphoma biology differs across the age spectrum and by race and ethnicity. Both tumor and host factors require further study, she said.
Clinical trial access for AYAs
Dr. Kelly emphasized that, unfortunately, clinical research participation is low among AYAs. A major impediment is that adult clinical trials historically required participants to be at least 18 years old.
In addition, there has not been a focused effort to educate AYAs about regulatory safeguards to ensure safety and the promise of enhanced benefit to them in NCI Cancer Trials Network (NCTN) trials. As a result, the refusal rate is high.
A multi-stakeholder workshop, convened in May 2016 by the American Society of Clinical Oncology and Friends of Cancer Research, outlined opportunities for expanding trial eligibility to include children younger than 18 years in first-in-human and other adult cancer clinical trials, enhancing their access to new agents, without compromising safety.
Recently, collaborative efforts between the adult and children’s NCTN research groups have included AYAs in studies addressing cancers that span the age spectrum, including lymphoma.
However, as Dr. Kelly noted, there are differences in AYA lymphoid malignancy types with a transition from more pediatric to more adult types.
Hodgkin lymphoma and primary mediastinal B-cell lymphoma
Panelist Lisa G. Roth, MD, of Weill Cornell Medicine, New York, reviewed the genomic landscape of Hodgkin lymphoma (HL) and primary mediastinal B-cell lymphoma (PMBCL).
Dr. Roth explained that both HL and PMBCL are derived from thymic B cells, predominantly affect the mediastinum, and are CD30-positive lymphomas. Both are characterized by upregulation of JAK/STAT and NF-kappaB as well as overexpression of PD-L1.
Dr. Roth noted that HL is challenging to sequence by standard methods because Reed Sternberg (HRS) cells represent less than 1% of the cellular infiltrate. Recurrently mutated genes in HL cluster by histologic subtype.
Whole-exome sequencing of HRS cells show loss of beta-2 microglobulin and MHC-1 expression, HLA-B, NF-kappaB signaling, and JAK-STAT signaling, according to data published in Blood Advances in 2019.
Dr. Roth’s lab performed immunohistochemistry on tissue microarrays in 145 cases of HL (unpublished data). Results showed that loss of beta-2 microglobulin is more common in younger HL patients. For other alterations, there were too few cases to know.
Dr. Roth’s lab is a member of a pediatric/AYA HL sequencing multi-institutional consortium that has been able to extract DNA and RNA from samples submitted for whole-exome sequencing. The consortium’s goal is to shed light on implications of other genomic alterations that may differ by age in HL patients.
Dr. Roth cited research showing that PMBCL shares molecular alterations similar to those of HL. Alterations in PMBCL suggest dysregulated cellular signaling and immune evasion mechanisms (e.g., deletions in MHC type 1 and 2, beta-2 microglobulin, JAK-STAT, and NF-kappaB mutations) that provide opportunities to study novel agents, according to data published in Blood in 2019.
By early 2021, the S1826 and ANHL1931 studies, which have no age restriction, will be available to AYA lymphoma patients with HL and PMBCL, respectively, Dr. Roth said.
Follicular lymphoma: Clinical features by age
Panelist Abner Louissaint Jr, MD, PhD, of Massachusetts General Hospital in Boston, discussed age-related differences in follicular lymphoma (FL).
He noted that FL typically presents at an advanced stage, with low- or high-grade histology. It is increasingly common in adults in their 50s and 60s, representing 20% of all lymphomas. FL is rare in children and AYAs.
Dr. Louissaint explained that the typical flow cytometric findings in FL are BCL2 translocations, occurring in up to 85%-90% of low-grade and 50% of high-grade cases. The t(14;18)(q32;q21) translocation juxtaposes BCL2 on 18q21 to regulatory sequences and enhances the expression of elements of the Ig heavy chain.
Malignant cells in FL patients express CD20, CD10, CD21, and BCL2 (in contrast to normal germinal centers) and overexpress BCL6 (in contrast to normal follicles), Dr. Louissaint noted. He said the Ki-67 proliferative index of the malignant cells is typically low.
Pediatric-type FL is rare, but case series show clinical, pathologic, and molecular features that are distinctive from adult FL, Dr. Louissaint explained.
He then discussed the features of pediatric-type FL in multiple domains. In the clinical domain, there is a male predilection, and stage tends to be low. There is frequent involvement of nodes of the head and neck region and rare involvement of internal lymph node chains.
Pathologically, the malignant cells appear high grade, with architectural effacement, expansile follicular pattern, large lymphocyte size, and an elevated proliferation index. In contrast to adult FL, malignant cells in pediatric-type FL lack aberrant BCL2 expression.
Most importantly, for pediatric-type FL, the prognosis is excellent with durable remissions after surgical excision, Dr. Louissaint said.
Follicular lymphoma: Molecular features by age
Because of the excellent prognosis in pediatric-type FL, it is important to assess whether young adults with FL have adult-type or pediatric-type lesions, Dr. Louissaint said.
He cited many studies showing differences in adult and pediatric-type FL. In adult FL, the mutational landscape is characterized by frequent chromatin-modifying mutations in genes such as CREBBP, KM22D, and EP300.
In contrast, in pediatric-type FL, there are frequent activating MAPK pathway mutations, including mutations in the negative regulatory domain of MAP2K1. These mutations are not seen in adult FL.
Dr. Louissaint noted that there may be mutations in epigenetic modifiers (CREBBP, TNFRSF14) in both adult and pediatric-type FL. However, CREBBP is very unusual in pediatric-type FL and common in adult FL. This suggests the alterations in pediatric-type FL do not simply represent an early stage of the same disease as adult FL.
Despite a high proliferating fraction and absence of BCL2/BCL6/IRF4 rearrangements in pediatric-type FL, the presence of these features was associated with dramatic difference in progression-free survival, according to research published in Blood in 2012.
A distinct entity
In 2016, the World Health Organization recognized pediatric-type FL as a distinct entity, with the following diagnostic criteria (published in Blood):
- At least partial effacement of nodal architecture, expansile follicles, intermediate-size blastoid cells, and no component of diffuse large B-cell lymphoma.
- Immunohistochemistry showing BCL6 positivity, BCL2 negativity or weak positivity, and a high proliferative fraction.
- Genomic studies showing no BCL2 amplification.
- Clinical features of nodal disease in the head and neck region, early clinical stage, age younger than 40 years, typically in a male with no internal nodes involved.
When FL occurs in AYAs, the diagnostic findings of pediatric-type FL suggest the patient will do well with conservative management (e.g., excision alone), Dr. Louissaint noted.
Two sizes do not fit all
The strategies that have improved cancer outcomes since the 1970s for children and older adults have been much less successful for AYAs with cancer.
As an oncologic community, we should not allow the AYA gap to persist. As always, the solutions are likely to involve focused clinical research, education, and communication. Effort will need to be targeted specifically to the AYA population.
Since health-related mortality is high even when cancer-specific outcomes improve, adopting and maintaining a healthy lifestyle must be a key part of the discussion with these young patients.
The biologic differences associated with AYA lymphomas demand participation in clinical trials.
Oncologists should vigorously support removing impediments to the participation of AYAs in prospective clinical trials, stratified (but unrestricted) by age, with careful analysis of patient-reported outcomes, late adverse effects, and biospecimen collection.
As Dr. Kelly noted in the question-and-answer period, the Children’s Oncology Group has an existing biobank of paraffin-embedded tumor samples, DNA from lymphoma specimens, plasma, and sera with clinically annotated data that can be given to investigators upon request and justification.
Going beyond eligibility for clinical trials
Unfortunately, we will likely find that broadening eligibility criteria is the “low-hanging fruit.” There are protocol-, patient-, and physician-related obstacles, according to a review published in Cancer in 2019.
Patient-related obstacles include fear of toxicity, uncertainty about placebos, a steep learning curve for health literacy, insurance-related impediments, and other access-related issues.
Discussions will need to be tailored to the AYA population. Frank, early conversations about fertility, sexuality, financial hardship, career advancement, work-life balance, and cognitive risks may not only facilitate treatment planning but also encourage the trust that is essential for patients to enroll in trials.
The investment in time, multidisciplinary staff and physician involvement, and potential delays in treatment initiation may be painful and inconvenient, but the benefits for long-term health outcomes and personal-professional relationships will be gratifying beyond measure.
Dr. Smith disclosed relationships with Genentech/Roche, Celgene, TGTX, Karyopharm, Janssen, and Bantem. Dr. Roth disclosed relationships with Janssen, ADC Therapeutics, and Celgene. Dr. Kelly and Dr. Louissaint had no financial relationships to disclose.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
In the 1970s, cancer survival was poor for young children and older adults in the United States, as shown by data published in the Journal of the National Cancer Institute.
Great progress has been made since the 1970s, but improvements in outcome have been less impressive for cancer patients aged 15-39 years, as shown by research published in Cancer.
Patients aged 15-39 years have been designated by the National Institutes of Health (NIH) as “adolescents and young adults (AYAs),” and the lag in survival benefit has been termed “the AYA gap.”
The AYA gap persists in lymphoma patients, and an expert panel recently outlined differences between lymphoma in AYAs and lymphoma in other age groups.
The experts spoke at a special session of the AACR Virtual Meeting: Advances in Malignant Lymphoma moderated by Somali M. Smith, MD, of the University of Chicago.
Factors that contribute to the AYA gap
About 89,000 AYAs are diagnosed with cancer each year in the United States, according to data from the National Cancer Institute (NCI). Lymphomas and thyroid cancer are the most common cancers among younger AYAs, aged 15-24 years.
In a report commissioned by the NIH in 2006, many factors contributing to the AYA gap were identified. Chief among them were:
- Limitations in access to care.
- Delayed diagnosis.
- Inconsistency in treatment and follow-up.
- Long-term toxicity (fertility, second malignancies, and cardiovascular disease).
These factors compromise health-related survival, even when cancer-specific survival is improved.
Panelist Kara Kelly, MD, of Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., noted that there are additional unique challenges for AYAs with cancer. These include:
- Pubertal changes.
- Developmental transition to independence.
- Societal impediments such as insurance coverage and disparities in access to specialized centers.
- Psychosocial factors such as health literacy and adherence to treatment and follow-up.
Focusing on lymphoma specifically, Dr. Kelly noted that lymphoma biology differs across the age spectrum and by race and ethnicity. Both tumor and host factors require further study, she said.
Clinical trial access for AYAs
Dr. Kelly emphasized that, unfortunately, clinical research participation is low among AYAs. A major impediment is that adult clinical trials historically required participants to be at least 18 years old.
In addition, there has not been a focused effort to educate AYAs about regulatory safeguards to ensure safety and the promise of enhanced benefit to them in NCI Cancer Trials Network (NCTN) trials. As a result, the refusal rate is high.
A multi-stakeholder workshop, convened in May 2016 by the American Society of Clinical Oncology and Friends of Cancer Research, outlined opportunities for expanding trial eligibility to include children younger than 18 years in first-in-human and other adult cancer clinical trials, enhancing their access to new agents, without compromising safety.
Recently, collaborative efforts between the adult and children’s NCTN research groups have included AYAs in studies addressing cancers that span the age spectrum, including lymphoma.
However, as Dr. Kelly noted, there are differences in AYA lymphoid malignancy types with a transition from more pediatric to more adult types.
Hodgkin lymphoma and primary mediastinal B-cell lymphoma
Panelist Lisa G. Roth, MD, of Weill Cornell Medicine, New York, reviewed the genomic landscape of Hodgkin lymphoma (HL) and primary mediastinal B-cell lymphoma (PMBCL).
Dr. Roth explained that both HL and PMBCL are derived from thymic B cells, predominantly affect the mediastinum, and are CD30-positive lymphomas. Both are characterized by upregulation of JAK/STAT and NF-kappaB as well as overexpression of PD-L1.
Dr. Roth noted that HL is challenging to sequence by standard methods because Reed Sternberg (HRS) cells represent less than 1% of the cellular infiltrate. Recurrently mutated genes in HL cluster by histologic subtype.
Whole-exome sequencing of HRS cells show loss of beta-2 microglobulin and MHC-1 expression, HLA-B, NF-kappaB signaling, and JAK-STAT signaling, according to data published in Blood Advances in 2019.
Dr. Roth’s lab performed immunohistochemistry on tissue microarrays in 145 cases of HL (unpublished data). Results showed that loss of beta-2 microglobulin is more common in younger HL patients. For other alterations, there were too few cases to know.
Dr. Roth’s lab is a member of a pediatric/AYA HL sequencing multi-institutional consortium that has been able to extract DNA and RNA from samples submitted for whole-exome sequencing. The consortium’s goal is to shed light on implications of other genomic alterations that may differ by age in HL patients.
Dr. Roth cited research showing that PMBCL shares molecular alterations similar to those of HL. Alterations in PMBCL suggest dysregulated cellular signaling and immune evasion mechanisms (e.g., deletions in MHC type 1 and 2, beta-2 microglobulin, JAK-STAT, and NF-kappaB mutations) that provide opportunities to study novel agents, according to data published in Blood in 2019.
By early 2021, the S1826 and ANHL1931 studies, which have no age restriction, will be available to AYA lymphoma patients with HL and PMBCL, respectively, Dr. Roth said.
Follicular lymphoma: Clinical features by age
Panelist Abner Louissaint Jr, MD, PhD, of Massachusetts General Hospital in Boston, discussed age-related differences in follicular lymphoma (FL).
He noted that FL typically presents at an advanced stage, with low- or high-grade histology. It is increasingly common in adults in their 50s and 60s, representing 20% of all lymphomas. FL is rare in children and AYAs.
Dr. Louissaint explained that the typical flow cytometric findings in FL are BCL2 translocations, occurring in up to 85%-90% of low-grade and 50% of high-grade cases. The t(14;18)(q32;q21) translocation juxtaposes BCL2 on 18q21 to regulatory sequences and enhances the expression of elements of the Ig heavy chain.
Malignant cells in FL patients express CD20, CD10, CD21, and BCL2 (in contrast to normal germinal centers) and overexpress BCL6 (in contrast to normal follicles), Dr. Louissaint noted. He said the Ki-67 proliferative index of the malignant cells is typically low.
Pediatric-type FL is rare, but case series show clinical, pathologic, and molecular features that are distinctive from adult FL, Dr. Louissaint explained.
He then discussed the features of pediatric-type FL in multiple domains. In the clinical domain, there is a male predilection, and stage tends to be low. There is frequent involvement of nodes of the head and neck region and rare involvement of internal lymph node chains.
Pathologically, the malignant cells appear high grade, with architectural effacement, expansile follicular pattern, large lymphocyte size, and an elevated proliferation index. In contrast to adult FL, malignant cells in pediatric-type FL lack aberrant BCL2 expression.
Most importantly, for pediatric-type FL, the prognosis is excellent with durable remissions after surgical excision, Dr. Louissaint said.
Follicular lymphoma: Molecular features by age
Because of the excellent prognosis in pediatric-type FL, it is important to assess whether young adults with FL have adult-type or pediatric-type lesions, Dr. Louissaint said.
He cited many studies showing differences in adult and pediatric-type FL. In adult FL, the mutational landscape is characterized by frequent chromatin-modifying mutations in genes such as CREBBP, KM22D, and EP300.
In contrast, in pediatric-type FL, there are frequent activating MAPK pathway mutations, including mutations in the negative regulatory domain of MAP2K1. These mutations are not seen in adult FL.
Dr. Louissaint noted that there may be mutations in epigenetic modifiers (CREBBP, TNFRSF14) in both adult and pediatric-type FL. However, CREBBP is very unusual in pediatric-type FL and common in adult FL. This suggests the alterations in pediatric-type FL do not simply represent an early stage of the same disease as adult FL.
Despite a high proliferating fraction and absence of BCL2/BCL6/IRF4 rearrangements in pediatric-type FL, the presence of these features was associated with dramatic difference in progression-free survival, according to research published in Blood in 2012.
A distinct entity
In 2016, the World Health Organization recognized pediatric-type FL as a distinct entity, with the following diagnostic criteria (published in Blood):
- At least partial effacement of nodal architecture, expansile follicles, intermediate-size blastoid cells, and no component of diffuse large B-cell lymphoma.
- Immunohistochemistry showing BCL6 positivity, BCL2 negativity or weak positivity, and a high proliferative fraction.
- Genomic studies showing no BCL2 amplification.
- Clinical features of nodal disease in the head and neck region, early clinical stage, age younger than 40 years, typically in a male with no internal nodes involved.
When FL occurs in AYAs, the diagnostic findings of pediatric-type FL suggest the patient will do well with conservative management (e.g., excision alone), Dr. Louissaint noted.
Two sizes do not fit all
The strategies that have improved cancer outcomes since the 1970s for children and older adults have been much less successful for AYAs with cancer.
As an oncologic community, we should not allow the AYA gap to persist. As always, the solutions are likely to involve focused clinical research, education, and communication. Effort will need to be targeted specifically to the AYA population.
Since health-related mortality is high even when cancer-specific outcomes improve, adopting and maintaining a healthy lifestyle must be a key part of the discussion with these young patients.
The biologic differences associated with AYA lymphomas demand participation in clinical trials.
Oncologists should vigorously support removing impediments to the participation of AYAs in prospective clinical trials, stratified (but unrestricted) by age, with careful analysis of patient-reported outcomes, late adverse effects, and biospecimen collection.
As Dr. Kelly noted in the question-and-answer period, the Children’s Oncology Group has an existing biobank of paraffin-embedded tumor samples, DNA from lymphoma specimens, plasma, and sera with clinically annotated data that can be given to investigators upon request and justification.
Going beyond eligibility for clinical trials
Unfortunately, we will likely find that broadening eligibility criteria is the “low-hanging fruit.” There are protocol-, patient-, and physician-related obstacles, according to a review published in Cancer in 2019.
Patient-related obstacles include fear of toxicity, uncertainty about placebos, a steep learning curve for health literacy, insurance-related impediments, and other access-related issues.
Discussions will need to be tailored to the AYA population. Frank, early conversations about fertility, sexuality, financial hardship, career advancement, work-life balance, and cognitive risks may not only facilitate treatment planning but also encourage the trust that is essential for patients to enroll in trials.
The investment in time, multidisciplinary staff and physician involvement, and potential delays in treatment initiation may be painful and inconvenient, but the benefits for long-term health outcomes and personal-professional relationships will be gratifying beyond measure.
Dr. Smith disclosed relationships with Genentech/Roche, Celgene, TGTX, Karyopharm, Janssen, and Bantem. Dr. Roth disclosed relationships with Janssen, ADC Therapeutics, and Celgene. Dr. Kelly and Dr. Louissaint had no financial relationships to disclose.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
In the 1970s, cancer survival was poor for young children and older adults in the United States, as shown by data published in the Journal of the National Cancer Institute.
Great progress has been made since the 1970s, but improvements in outcome have been less impressive for cancer patients aged 15-39 years, as shown by research published in Cancer.
Patients aged 15-39 years have been designated by the National Institutes of Health (NIH) as “adolescents and young adults (AYAs),” and the lag in survival benefit has been termed “the AYA gap.”
The AYA gap persists in lymphoma patients, and an expert panel recently outlined differences between lymphoma in AYAs and lymphoma in other age groups.
The experts spoke at a special session of the AACR Virtual Meeting: Advances in Malignant Lymphoma moderated by Somali M. Smith, MD, of the University of Chicago.
Factors that contribute to the AYA gap
About 89,000 AYAs are diagnosed with cancer each year in the United States, according to data from the National Cancer Institute (NCI). Lymphomas and thyroid cancer are the most common cancers among younger AYAs, aged 15-24 years.
In a report commissioned by the NIH in 2006, many factors contributing to the AYA gap were identified. Chief among them were:
- Limitations in access to care.
- Delayed diagnosis.
- Inconsistency in treatment and follow-up.
- Long-term toxicity (fertility, second malignancies, and cardiovascular disease).
These factors compromise health-related survival, even when cancer-specific survival is improved.
Panelist Kara Kelly, MD, of Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., noted that there are additional unique challenges for AYAs with cancer. These include:
- Pubertal changes.
- Developmental transition to independence.
- Societal impediments such as insurance coverage and disparities in access to specialized centers.
- Psychosocial factors such as health literacy and adherence to treatment and follow-up.
Focusing on lymphoma specifically, Dr. Kelly noted that lymphoma biology differs across the age spectrum and by race and ethnicity. Both tumor and host factors require further study, she said.
Clinical trial access for AYAs
Dr. Kelly emphasized that, unfortunately, clinical research participation is low among AYAs. A major impediment is that adult clinical trials historically required participants to be at least 18 years old.
In addition, there has not been a focused effort to educate AYAs about regulatory safeguards to ensure safety and the promise of enhanced benefit to them in NCI Cancer Trials Network (NCTN) trials. As a result, the refusal rate is high.
A multi-stakeholder workshop, convened in May 2016 by the American Society of Clinical Oncology and Friends of Cancer Research, outlined opportunities for expanding trial eligibility to include children younger than 18 years in first-in-human and other adult cancer clinical trials, enhancing their access to new agents, without compromising safety.
Recently, collaborative efforts between the adult and children’s NCTN research groups have included AYAs in studies addressing cancers that span the age spectrum, including lymphoma.
However, as Dr. Kelly noted, there are differences in AYA lymphoid malignancy types with a transition from more pediatric to more adult types.
Hodgkin lymphoma and primary mediastinal B-cell lymphoma
Panelist Lisa G. Roth, MD, of Weill Cornell Medicine, New York, reviewed the genomic landscape of Hodgkin lymphoma (HL) and primary mediastinal B-cell lymphoma (PMBCL).
Dr. Roth explained that both HL and PMBCL are derived from thymic B cells, predominantly affect the mediastinum, and are CD30-positive lymphomas. Both are characterized by upregulation of JAK/STAT and NF-kappaB as well as overexpression of PD-L1.
Dr. Roth noted that HL is challenging to sequence by standard methods because Reed Sternberg (HRS) cells represent less than 1% of the cellular infiltrate. Recurrently mutated genes in HL cluster by histologic subtype.
Whole-exome sequencing of HRS cells show loss of beta-2 microglobulin and MHC-1 expression, HLA-B, NF-kappaB signaling, and JAK-STAT signaling, according to data published in Blood Advances in 2019.
Dr. Roth’s lab performed immunohistochemistry on tissue microarrays in 145 cases of HL (unpublished data). Results showed that loss of beta-2 microglobulin is more common in younger HL patients. For other alterations, there were too few cases to know.
Dr. Roth’s lab is a member of a pediatric/AYA HL sequencing multi-institutional consortium that has been able to extract DNA and RNA from samples submitted for whole-exome sequencing. The consortium’s goal is to shed light on implications of other genomic alterations that may differ by age in HL patients.
Dr. Roth cited research showing that PMBCL shares molecular alterations similar to those of HL. Alterations in PMBCL suggest dysregulated cellular signaling and immune evasion mechanisms (e.g., deletions in MHC type 1 and 2, beta-2 microglobulin, JAK-STAT, and NF-kappaB mutations) that provide opportunities to study novel agents, according to data published in Blood in 2019.
By early 2021, the S1826 and ANHL1931 studies, which have no age restriction, will be available to AYA lymphoma patients with HL and PMBCL, respectively, Dr. Roth said.
Follicular lymphoma: Clinical features by age
Panelist Abner Louissaint Jr, MD, PhD, of Massachusetts General Hospital in Boston, discussed age-related differences in follicular lymphoma (FL).
He noted that FL typically presents at an advanced stage, with low- or high-grade histology. It is increasingly common in adults in their 50s and 60s, representing 20% of all lymphomas. FL is rare in children and AYAs.
Dr. Louissaint explained that the typical flow cytometric findings in FL are BCL2 translocations, occurring in up to 85%-90% of low-grade and 50% of high-grade cases. The t(14;18)(q32;q21) translocation juxtaposes BCL2 on 18q21 to regulatory sequences and enhances the expression of elements of the Ig heavy chain.
Malignant cells in FL patients express CD20, CD10, CD21, and BCL2 (in contrast to normal germinal centers) and overexpress BCL6 (in contrast to normal follicles), Dr. Louissaint noted. He said the Ki-67 proliferative index of the malignant cells is typically low.
Pediatric-type FL is rare, but case series show clinical, pathologic, and molecular features that are distinctive from adult FL, Dr. Louissaint explained.
He then discussed the features of pediatric-type FL in multiple domains. In the clinical domain, there is a male predilection, and stage tends to be low. There is frequent involvement of nodes of the head and neck region and rare involvement of internal lymph node chains.
Pathologically, the malignant cells appear high grade, with architectural effacement, expansile follicular pattern, large lymphocyte size, and an elevated proliferation index. In contrast to adult FL, malignant cells in pediatric-type FL lack aberrant BCL2 expression.
Most importantly, for pediatric-type FL, the prognosis is excellent with durable remissions after surgical excision, Dr. Louissaint said.
Follicular lymphoma: Molecular features by age
Because of the excellent prognosis in pediatric-type FL, it is important to assess whether young adults with FL have adult-type or pediatric-type lesions, Dr. Louissaint said.
He cited many studies showing differences in adult and pediatric-type FL. In adult FL, the mutational landscape is characterized by frequent chromatin-modifying mutations in genes such as CREBBP, KM22D, and EP300.
In contrast, in pediatric-type FL, there are frequent activating MAPK pathway mutations, including mutations in the negative regulatory domain of MAP2K1. These mutations are not seen in adult FL.
Dr. Louissaint noted that there may be mutations in epigenetic modifiers (CREBBP, TNFRSF14) in both adult and pediatric-type FL. However, CREBBP is very unusual in pediatric-type FL and common in adult FL. This suggests the alterations in pediatric-type FL do not simply represent an early stage of the same disease as adult FL.
Despite a high proliferating fraction and absence of BCL2/BCL6/IRF4 rearrangements in pediatric-type FL, the presence of these features was associated with dramatic difference in progression-free survival, according to research published in Blood in 2012.
A distinct entity
In 2016, the World Health Organization recognized pediatric-type FL as a distinct entity, with the following diagnostic criteria (published in Blood):
- At least partial effacement of nodal architecture, expansile follicles, intermediate-size blastoid cells, and no component of diffuse large B-cell lymphoma.
- Immunohistochemistry showing BCL6 positivity, BCL2 negativity or weak positivity, and a high proliferative fraction.
- Genomic studies showing no BCL2 amplification.
- Clinical features of nodal disease in the head and neck region, early clinical stage, age younger than 40 years, typically in a male with no internal nodes involved.
When FL occurs in AYAs, the diagnostic findings of pediatric-type FL suggest the patient will do well with conservative management (e.g., excision alone), Dr. Louissaint noted.
Two sizes do not fit all
The strategies that have improved cancer outcomes since the 1970s for children and older adults have been much less successful for AYAs with cancer.
As an oncologic community, we should not allow the AYA gap to persist. As always, the solutions are likely to involve focused clinical research, education, and communication. Effort will need to be targeted specifically to the AYA population.
Since health-related mortality is high even when cancer-specific outcomes improve, adopting and maintaining a healthy lifestyle must be a key part of the discussion with these young patients.
The biologic differences associated with AYA lymphomas demand participation in clinical trials.
Oncologists should vigorously support removing impediments to the participation of AYAs in prospective clinical trials, stratified (but unrestricted) by age, with careful analysis of patient-reported outcomes, late adverse effects, and biospecimen collection.
As Dr. Kelly noted in the question-and-answer period, the Children’s Oncology Group has an existing biobank of paraffin-embedded tumor samples, DNA from lymphoma specimens, plasma, and sera with clinically annotated data that can be given to investigators upon request and justification.
Going beyond eligibility for clinical trials
Unfortunately, we will likely find that broadening eligibility criteria is the “low-hanging fruit.” There are protocol-, patient-, and physician-related obstacles, according to a review published in Cancer in 2019.
Patient-related obstacles include fear of toxicity, uncertainty about placebos, a steep learning curve for health literacy, insurance-related impediments, and other access-related issues.
Discussions will need to be tailored to the AYA population. Frank, early conversations about fertility, sexuality, financial hardship, career advancement, work-life balance, and cognitive risks may not only facilitate treatment planning but also encourage the trust that is essential for patients to enroll in trials.
The investment in time, multidisciplinary staff and physician involvement, and potential delays in treatment initiation may be painful and inconvenient, but the benefits for long-term health outcomes and personal-professional relationships will be gratifying beyond measure.
Dr. Smith disclosed relationships with Genentech/Roche, Celgene, TGTX, Karyopharm, Janssen, and Bantem. Dr. Roth disclosed relationships with Janssen, ADC Therapeutics, and Celgene. Dr. Kelly and Dr. Louissaint had no financial relationships to disclose.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
FROM AACR ADVANCES IN MALIGNANT LYMPHOMA 2020
Conquering the stigma of getting mental health care
Last summer, back when people traveled, I had the pleasure of being in Amsterdam for Pride Week. With a half-million tourists, it was a colorful and costumed display of LGBTQ pride, and both the streets and canals had celebrations with food, drinks, music, and displays beyond anything I could describe.

It was all not that long ago that the American Psychiatric Association classified homosexuality as a psychiatric disorder. Now we have Pride celebrations, and I don’t think twice about mentioning my brother-in-law’s husband, or a female colleague’s wife, nor am I shocked when I hear that the children of my friends are in the process of gender transition. Obviously, the idea that people express both their gender and their sexuality in diverse ways is not accepted by everyone, but we’ve come a long way toward acceptance of people who were once stigmatized and pathologized. I’ll also point out that this shift occurred despite the fact that the gay community was affected by AIDS.
There are many other differences – and illnesses – that our society has come to either accept or sympathize with more graciously over time, and yet both mental illness and substance abuse disorders remain stigmatized and punished. To put it bluntly, we have done a terrible job of making these conditions acceptable illnesses to have, even though we have done a reasonably good job of offering effective treatments. Cancer no longer carries the stigma it once did, even though cancer is a leading cause of death, and the treatments are painful, toxic, and may include the loss of body parts and hair. But if you become ill with cancer, your friends bring casseroles (or perhaps rotisserie chickens), and if you’re hospitalized with bipolar disorder or check into a drug treatment center, you’re more likely to be the recipient of judgment and even scorn.
We have to fix this. We talk about the need to destigmatize mental illness and substance use disorders, and to make these illnesses more on par with other diseases. Maybe that is the wrong call: These disorders sometimes cause people to behave in disruptive, dangerous, and illegal ways that we don’t often see with other illnesses. Frankly psychotic people may be seen as “other,” they may smell bad, they may behave in bizarre ways, and they may be frightening. Their rare acts of violence have been publicized so much that “He’s mentally ill” is accepted by the public as a full explanation for why someone would commit a mass shooting. Depression can cause people to be irritable and unpleasant, and our society equates a lack of motivation with laziness. While people may have sympathy for the suicidal thoughts and feelings of others, completed suicide leaves behind devastated survivors. People with substance use problems may become belligerent or commit crimes to support their addictions. In 2018, over 10,500 people were killed by drivers who were impaired by alcohol. I’m not sure how we destigmatize these conditions, but commercials, billboards, and educational programs aren’t doing it.
Fears around treatment
Perhaps our efforts need to go toward destigmatizing treatment. It is shocking to me how resistant people are to getting help, or having others know they are getting help, when treatment often renders them free from the psychological agony or misbehaviors caused by their condition.
Since I work in an outpatient setting, I see people who have made it beyond the barrier of seeking help. Almost all of my patients are willing to try medications – there is self-selection among those who chose to see a psychiatrist as opposed to another type of psychotherapist. I also believe that direct-to-consumer advertising has helped normalize the use of psychotropic medications.
When it comes to getting a higher level of care, however, the conversations are so much harder. Many of my patients insist they will never be admitted to a psychiatric unit, and when I ask depressed people if they are having suicidal thoughts, some tell me they are afraid to let me know they are for fear I might hospitalize them. This fear of hospitalization is present in people who have never been in a hospital and have only media depictions or their imaginations to go by, but I also see this with patients who have previously been hospitalized and have emerged from their inpatient stays feeling much better. While we know that any type of hospitalization involves a loss of control, unpleasant moments, and sometimes painful procedures, I have never heard anyone say that, if they were to have a second heart attack, they would refuse an admission to the cardiac care unit.
Discussions about treatment for substance use are even more difficult. People with addictions often don’t want to abstain from the substance they are using, and this is an enormous hurdle. Beyond that, they don’t like the labels that come with acknowledging a problem – words like “junkie,” “addict,” “drunk,” and “alcoholic” are hard to escape.
People fear hospitalization for many reasons: They fear losing control, they don’t recognize that they have a problem, or they rationalize their psychosis or substance use as normal. Most of all, they fear what others will think of them and what repercussions this will have for their futures. Patients would rather continue in a state of agony and dysfunction when inpatient treatment would make them better faster. This is nothing short of tragic.
What can we do? The answer is “a lot.” We need to work harder to make the hospital experience a pleasant one for patients. Inpatient units need to be clean, safe places where patients are treated with kindness, dignity, and respect and activities are appropriate, interesting, and promote healing.
Maria, a Maryland attorney, told me about her experience with inpatient treatment. “I experienced my hospitalization as jailing and acutely felt the loss of liberty, especially in the ER, where I was confined to something I recognized from my time visiting incarcerated and detained people as a holding cell, complete with a uniformed guard. I was scared to engage in any kind of meaningful self-advocacy around leaving out of fear for my license to practice law and of lengthening my time as an inpatient. As a result, I found myself concentrating on getting out, and not on getting well. With the benefit of hindsight, I can say now that my hospitalization was a lost opportunity, and the coercive elements were barriers to accessing the treatment that I needed, both at the time and in the years following the hospitalization.”
We have too many policies in place where infractions are met with force, seclusion, and sometimes restraint, and we need to be more flexible with these policies. If a psychiatric unit requires lab work prior to admission and the patient refuses, should force be used in the emergency department if there is nothing to indicate that the patient’s health is in imminent danger? And if the hospital has a policy that all psychiatric patients must disrobe to be examined for preexisting scars or contraband – this is an admission standard for some hospitals, but not others – and the patient refuses, what then? Typically, inpatients are not allowed access to their cell phones or the Internet (for many good reasons), but patients find this very upsetting; might it make sense to allow periods where they can use devices with supervision? Hospitals often forbid smoking, and people with psychiatric disorders may smoke – while it is a wonderful health ideal, is it reasonable to forbid smoking for the course of a hospitalization?
We must work to get questions about psychiatric and substance use disorders removed from any job- or licensure-related forms. There is no reason to believe that people answer these forms truthfully or that including these questions protects the public in any way. What we do know is that people don’t seek help because they, like Maria, are afraid of the consequences of getting care. It doesn’t matter if a surgeon’s abilities are limited because he has episodes of hypoglycemia or past episodes of mania, and the only question on licensing forms should be about current conditions that impair the ability to work. Every district branch of the American Psychiatric Association should be actively speaking with their state professional licensing boards about the harm these questions do.
We need better treatments that have fewer side effects, and we need to acknowledge that, while getting help is the right thing to do, not everyone finds the right treatment with the first attempt and not everyone gets better. Our party line to those who feel suicidal has been “Get Help,” often with a phone number for the National Suicide Prevention Lifeline. While this is an important resource to have readily available, many of the people who die of suicide are already in active treatment. Our party line needs to change to “Get Help, and if it isn’t working, Get Different Help.” We want to be careful that our messaging does not foster a sense of hopelessness in those who have sought care and still suffer.
It’s good to talk about the potential benefits of treatment, but we don’t have enough beds and we don’t have enough mental health clinicians. There are states where psychiatric patients who have committed no crime are held in jail cells while they wait for beds to open – that we allow this is nothing short of a disgrace. The sickest patients with treatment-resistant conditions need access to the best care, and that access should not be limited by finances or networks. And while I’m here: We need our mental health professionals to spend their time working with patients, not computer screens, check boxes, and prior authorization protocols.
Finally, we need to work with the media to show positive and accurate depictions of psychiatric treatment as something that helps. We are still undoing the harm of Nurse Ratched and the depiction of electroconvulsive therapy in the 1975 film “One Flew Over the Cuckoo’s Nest,” and the current focus on mental illness and violence does nothing to help people feel comfortable seeking care.
I’ll end with one more thought from Maria: “Mental health professionals need to talk about hospitalization up front, no matter how uncomfortable, and encourage patients to think about hospitalization as a treatment option on a continuum before it is needed, so they are not approaching hospitalization as an abstract concept, often with a lot of fear and stigma attached to it, but rather as an option that they might explore in a fact-based way.”
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, both in Baltimore. She reported having nothing to disclose.
Last summer, back when people traveled, I had the pleasure of being in Amsterdam for Pride Week. With a half-million tourists, it was a colorful and costumed display of LGBTQ pride, and both the streets and canals had celebrations with food, drinks, music, and displays beyond anything I could describe.
It was all not that long ago that the American Psychiatric Association classified homosexuality as a psychiatric disorder. Now we have Pride celebrations, and I don’t think twice about mentioning my brother-in-law’s husband, or a female colleague’s wife, nor am I shocked when I hear that the children of my friends are in the process of gender transition. Obviously, the idea that people express both their gender and their sexuality in diverse ways is not accepted by everyone, but we’ve come a long way toward acceptance of people who were once stigmatized and pathologized. I’ll also point out that this shift occurred despite the fact that the gay community was affected by AIDS.
There are many other differences – and illnesses – that our society has come to either accept or sympathize with more graciously over time, and yet both mental illness and substance abuse disorders remain stigmatized and punished. To put it bluntly, we have done a terrible job of making these conditions acceptable illnesses to have, even though we have done a reasonably good job of offering effective treatments. Cancer no longer carries the stigma it once did, even though cancer is a leading cause of death, and the treatments are painful, toxic, and may include the loss of body parts and hair. But if you become ill with cancer, your friends bring casseroles (or perhaps rotisserie chickens), and if you’re hospitalized with bipolar disorder or check into a drug treatment center, you’re more likely to be the recipient of judgment and even scorn.
We have to fix this. We talk about the need to destigmatize mental illness and substance use disorders, and to make these illnesses more on par with other diseases. Maybe that is the wrong call: These disorders sometimes cause people to behave in disruptive, dangerous, and illegal ways that we don’t often see with other illnesses. Frankly psychotic people may be seen as “other,” they may smell bad, they may behave in bizarre ways, and they may be frightening. Their rare acts of violence have been publicized so much that “He’s mentally ill” is accepted by the public as a full explanation for why someone would commit a mass shooting. Depression can cause people to be irritable and unpleasant, and our society equates a lack of motivation with laziness. While people may have sympathy for the suicidal thoughts and feelings of others, completed suicide leaves behind devastated survivors. People with substance use problems may become belligerent or commit crimes to support their addictions. In 2018, over 10,500 people were killed by drivers who were impaired by alcohol. I’m not sure how we destigmatize these conditions, but commercials, billboards, and educational programs aren’t doing it.
Fears around treatment
Perhaps our efforts need to go toward destigmatizing treatment. It is shocking to me how resistant people are to getting help, or having others know they are getting help, when treatment often renders them free from the psychological agony or misbehaviors caused by their condition.
Since I work in an outpatient setting, I see people who have made it beyond the barrier of seeking help. Almost all of my patients are willing to try medications – there is self-selection among those who chose to see a psychiatrist as opposed to another type of psychotherapist. I also believe that direct-to-consumer advertising has helped normalize the use of psychotropic medications.
When it comes to getting a higher level of care, however, the conversations are so much harder. Many of my patients insist they will never be admitted to a psychiatric unit, and when I ask depressed people if they are having suicidal thoughts, some tell me they are afraid to let me know they are for fear I might hospitalize them. This fear of hospitalization is present in people who have never been in a hospital and have only media depictions or their imaginations to go by, but I also see this with patients who have previously been hospitalized and have emerged from their inpatient stays feeling much better. While we know that any type of hospitalization involves a loss of control, unpleasant moments, and sometimes painful procedures, I have never heard anyone say that, if they were to have a second heart attack, they would refuse an admission to the cardiac care unit.
Discussions about treatment for substance use are even more difficult. People with addictions often don’t want to abstain from the substance they are using, and this is an enormous hurdle. Beyond that, they don’t like the labels that come with acknowledging a problem – words like “junkie,” “addict,” “drunk,” and “alcoholic” are hard to escape.
People fear hospitalization for many reasons: They fear losing control, they don’t recognize that they have a problem, or they rationalize their psychosis or substance use as normal. Most of all, they fear what others will think of them and what repercussions this will have for their futures. Patients would rather continue in a state of agony and dysfunction when inpatient treatment would make them better faster. This is nothing short of tragic.
What can we do? The answer is “a lot.” We need to work harder to make the hospital experience a pleasant one for patients. Inpatient units need to be clean, safe places where patients are treated with kindness, dignity, and respect and activities are appropriate, interesting, and promote healing.
Maria, a Maryland attorney, told me about her experience with inpatient treatment. “I experienced my hospitalization as jailing and acutely felt the loss of liberty, especially in the ER, where I was confined to something I recognized from my time visiting incarcerated and detained people as a holding cell, complete with a uniformed guard. I was scared to engage in any kind of meaningful self-advocacy around leaving out of fear for my license to practice law and of lengthening my time as an inpatient. As a result, I found myself concentrating on getting out, and not on getting well. With the benefit of hindsight, I can say now that my hospitalization was a lost opportunity, and the coercive elements were barriers to accessing the treatment that I needed, both at the time and in the years following the hospitalization.”
We have too many policies in place where infractions are met with force, seclusion, and sometimes restraint, and we need to be more flexible with these policies. If a psychiatric unit requires lab work prior to admission and the patient refuses, should force be used in the emergency department if there is nothing to indicate that the patient’s health is in imminent danger? And if the hospital has a policy that all psychiatric patients must disrobe to be examined for preexisting scars or contraband – this is an admission standard for some hospitals, but not others – and the patient refuses, what then? Typically, inpatients are not allowed access to their cell phones or the Internet (for many good reasons), but patients find this very upsetting; might it make sense to allow periods where they can use devices with supervision? Hospitals often forbid smoking, and people with psychiatric disorders may smoke – while it is a wonderful health ideal, is it reasonable to forbid smoking for the course of a hospitalization?
We must work to get questions about psychiatric and substance use disorders removed from any job- or licensure-related forms. There is no reason to believe that people answer these forms truthfully or that including these questions protects the public in any way. What we do know is that people don’t seek help because they, like Maria, are afraid of the consequences of getting care. It doesn’t matter if a surgeon’s abilities are limited because he has episodes of hypoglycemia or past episodes of mania, and the only question on licensing forms should be about current conditions that impair the ability to work. Every district branch of the American Psychiatric Association should be actively speaking with their state professional licensing boards about the harm these questions do.
We need better treatments that have fewer side effects, and we need to acknowledge that, while getting help is the right thing to do, not everyone finds the right treatment with the first attempt and not everyone gets better. Our party line to those who feel suicidal has been “Get Help,” often with a phone number for the National Suicide Prevention Lifeline. While this is an important resource to have readily available, many of the people who die of suicide are already in active treatment. Our party line needs to change to “Get Help, and if it isn’t working, Get Different Help.” We want to be careful that our messaging does not foster a sense of hopelessness in those who have sought care and still suffer.
It’s good to talk about the potential benefits of treatment, but we don’t have enough beds and we don’t have enough mental health clinicians. There are states where psychiatric patients who have committed no crime are held in jail cells while they wait for beds to open – that we allow this is nothing short of a disgrace. The sickest patients with treatment-resistant conditions need access to the best care, and that access should not be limited by finances or networks. And while I’m here: We need our mental health professionals to spend their time working with patients, not computer screens, check boxes, and prior authorization protocols.
Finally, we need to work with the media to show positive and accurate depictions of psychiatric treatment as something that helps. We are still undoing the harm of Nurse Ratched and the depiction of electroconvulsive therapy in the 1975 film “One Flew Over the Cuckoo’s Nest,” and the current focus on mental illness and violence does nothing to help people feel comfortable seeking care.
I’ll end with one more thought from Maria: “Mental health professionals need to talk about hospitalization up front, no matter how uncomfortable, and encourage patients to think about hospitalization as a treatment option on a continuum before it is needed, so they are not approaching hospitalization as an abstract concept, often with a lot of fear and stigma attached to it, but rather as an option that they might explore in a fact-based way.”
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, both in Baltimore. She reported having nothing to disclose.
Last summer, back when people traveled, I had the pleasure of being in Amsterdam for Pride Week. With a half-million tourists, it was a colorful and costumed display of LGBTQ pride, and both the streets and canals had celebrations with food, drinks, music, and displays beyond anything I could describe.
It was all not that long ago that the American Psychiatric Association classified homosexuality as a psychiatric disorder. Now we have Pride celebrations, and I don’t think twice about mentioning my brother-in-law’s husband, or a female colleague’s wife, nor am I shocked when I hear that the children of my friends are in the process of gender transition. Obviously, the idea that people express both their gender and their sexuality in diverse ways is not accepted by everyone, but we’ve come a long way toward acceptance of people who were once stigmatized and pathologized. I’ll also point out that this shift occurred despite the fact that the gay community was affected by AIDS.
There are many other differences – and illnesses – that our society has come to either accept or sympathize with more graciously over time, and yet both mental illness and substance abuse disorders remain stigmatized and punished. To put it bluntly, we have done a terrible job of making these conditions acceptable illnesses to have, even though we have done a reasonably good job of offering effective treatments. Cancer no longer carries the stigma it once did, even though cancer is a leading cause of death, and the treatments are painful, toxic, and may include the loss of body parts and hair. But if you become ill with cancer, your friends bring casseroles (or perhaps rotisserie chickens), and if you’re hospitalized with bipolar disorder or check into a drug treatment center, you’re more likely to be the recipient of judgment and even scorn.
We have to fix this. We talk about the need to destigmatize mental illness and substance use disorders, and to make these illnesses more on par with other diseases. Maybe that is the wrong call: These disorders sometimes cause people to behave in disruptive, dangerous, and illegal ways that we don’t often see with other illnesses. Frankly psychotic people may be seen as “other,” they may smell bad, they may behave in bizarre ways, and they may be frightening. Their rare acts of violence have been publicized so much that “He’s mentally ill” is accepted by the public as a full explanation for why someone would commit a mass shooting. Depression can cause people to be irritable and unpleasant, and our society equates a lack of motivation with laziness. While people may have sympathy for the suicidal thoughts and feelings of others, completed suicide leaves behind devastated survivors. People with substance use problems may become belligerent or commit crimes to support their addictions. In 2018, over 10,500 people were killed by drivers who were impaired by alcohol. I’m not sure how we destigmatize these conditions, but commercials, billboards, and educational programs aren’t doing it.
Fears around treatment
Perhaps our efforts need to go toward destigmatizing treatment. It is shocking to me how resistant people are to getting help, or having others know they are getting help, when treatment often renders them free from the psychological agony or misbehaviors caused by their condition.
Since I work in an outpatient setting, I see people who have made it beyond the barrier of seeking help. Almost all of my patients are willing to try medications – there is self-selection among those who chose to see a psychiatrist as opposed to another type of psychotherapist. I also believe that direct-to-consumer advertising has helped normalize the use of psychotropic medications.
When it comes to getting a higher level of care, however, the conversations are so much harder. Many of my patients insist they will never be admitted to a psychiatric unit, and when I ask depressed people if they are having suicidal thoughts, some tell me they are afraid to let me know they are for fear I might hospitalize them. This fear of hospitalization is present in people who have never been in a hospital and have only media depictions or their imaginations to go by, but I also see this with patients who have previously been hospitalized and have emerged from their inpatient stays feeling much better. While we know that any type of hospitalization involves a loss of control, unpleasant moments, and sometimes painful procedures, I have never heard anyone say that, if they were to have a second heart attack, they would refuse an admission to the cardiac care unit.
Discussions about treatment for substance use are even more difficult. People with addictions often don’t want to abstain from the substance they are using, and this is an enormous hurdle. Beyond that, they don’t like the labels that come with acknowledging a problem – words like “junkie,” “addict,” “drunk,” and “alcoholic” are hard to escape.
People fear hospitalization for many reasons: They fear losing control, they don’t recognize that they have a problem, or they rationalize their psychosis or substance use as normal. Most of all, they fear what others will think of them and what repercussions this will have for their futures. Patients would rather continue in a state of agony and dysfunction when inpatient treatment would make them better faster. This is nothing short of tragic.
What can we do? The answer is “a lot.” We need to work harder to make the hospital experience a pleasant one for patients. Inpatient units need to be clean, safe places where patients are treated with kindness, dignity, and respect and activities are appropriate, interesting, and promote healing.
Maria, a Maryland attorney, told me about her experience with inpatient treatment. “I experienced my hospitalization as jailing and acutely felt the loss of liberty, especially in the ER, where I was confined to something I recognized from my time visiting incarcerated and detained people as a holding cell, complete with a uniformed guard. I was scared to engage in any kind of meaningful self-advocacy around leaving out of fear for my license to practice law and of lengthening my time as an inpatient. As a result, I found myself concentrating on getting out, and not on getting well. With the benefit of hindsight, I can say now that my hospitalization was a lost opportunity, and the coercive elements were barriers to accessing the treatment that I needed, both at the time and in the years following the hospitalization.”
We have too many policies in place where infractions are met with force, seclusion, and sometimes restraint, and we need to be more flexible with these policies. If a psychiatric unit requires lab work prior to admission and the patient refuses, should force be used in the emergency department if there is nothing to indicate that the patient’s health is in imminent danger? And if the hospital has a policy that all psychiatric patients must disrobe to be examined for preexisting scars or contraband – this is an admission standard for some hospitals, but not others – and the patient refuses, what then? Typically, inpatients are not allowed access to their cell phones or the Internet (for many good reasons), but patients find this very upsetting; might it make sense to allow periods where they can use devices with supervision? Hospitals often forbid smoking, and people with psychiatric disorders may smoke – while it is a wonderful health ideal, is it reasonable to forbid smoking for the course of a hospitalization?
We must work to get questions about psychiatric and substance use disorders removed from any job- or licensure-related forms. There is no reason to believe that people answer these forms truthfully or that including these questions protects the public in any way. What we do know is that people don’t seek help because they, like Maria, are afraid of the consequences of getting care. It doesn’t matter if a surgeon’s abilities are limited because he has episodes of hypoglycemia or past episodes of mania, and the only question on licensing forms should be about current conditions that impair the ability to work. Every district branch of the American Psychiatric Association should be actively speaking with their state professional licensing boards about the harm these questions do.
We need better treatments that have fewer side effects, and we need to acknowledge that, while getting help is the right thing to do, not everyone finds the right treatment with the first attempt and not everyone gets better. Our party line to those who feel suicidal has been “Get Help,” often with a phone number for the National Suicide Prevention Lifeline. While this is an important resource to have readily available, many of the people who die of suicide are already in active treatment. Our party line needs to change to “Get Help, and if it isn’t working, Get Different Help.” We want to be careful that our messaging does not foster a sense of hopelessness in those who have sought care and still suffer.
It’s good to talk about the potential benefits of treatment, but we don’t have enough beds and we don’t have enough mental health clinicians. There are states where psychiatric patients who have committed no crime are held in jail cells while they wait for beds to open – that we allow this is nothing short of a disgrace. The sickest patients with treatment-resistant conditions need access to the best care, and that access should not be limited by finances or networks. And while I’m here: We need our mental health professionals to spend their time working with patients, not computer screens, check boxes, and prior authorization protocols.
Finally, we need to work with the media to show positive and accurate depictions of psychiatric treatment as something that helps. We are still undoing the harm of Nurse Ratched and the depiction of electroconvulsive therapy in the 1975 film “One Flew Over the Cuckoo’s Nest,” and the current focus on mental illness and violence does nothing to help people feel comfortable seeking care.
I’ll end with one more thought from Maria: “Mental health professionals need to talk about hospitalization up front, no matter how uncomfortable, and encourage patients to think about hospitalization as a treatment option on a continuum before it is needed, so they are not approaching hospitalization as an abstract concept, often with a lot of fear and stigma attached to it, but rather as an option that they might explore in a fact-based way.”
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, both in Baltimore. She reported having nothing to disclose.
Caring for patients who experience stillbirth: Dos and don’ts
As a provider whose passion is helping women after stillbirth or neonatal loss, I get many transfers of women from their previous practice after a loss. Sometimes they transfer because they need a “fresh start,” but often, it is because they were let down by the practice – not by the medical care they received but by the emotional care and support and what was said or not said after the loss of the baby. A 2014 meta-analysis in the British Journal of Obstetrics and Gynaecology found that “Parents regarded contacts with health professionals as their central source of reassurance; but experiences often fell short of expectations.”1 I decided to conduct a survey via local and national support groups about what “loss parents” felt helpful or not helpful after the loss of a child. I purposely made these quotes the dominant part of this article, as I believe our patients are often our best teachers.
Inappropriate comments providers make
A very common theme among loss parents was how providers had made comments about how rare stillbirth is after it had just happened to them. Parents expressed that they felt this statistic kept them from getting the care that they needed prior to their loss and then they were told to not worry. Some example quotes include:
“ ‘This only happens to 1% of babies. Very rare.’ (It happened to our baby, and we have to live with this grief our whole lives. She is more than a statistic. She was our hopes, dreams, and future.)”
“I wish doctors didn’t wait to act based on statistics. There’s a lot of us in the 1% of unlikely occurrences.”
“For me, when my practice brushed off my feelings, I knew in my gut something was wrong. They said, ‘We need to wean you from worrying.’”
Another very common theme from parents included examples of helpful and not helpful care they received in the hospital.
Help parents make good memories

Many parents mentioned the importance of providing resources for after they go home. Most labor and delivery units have pregnancy loss services and have improved on the care they provide for loss families. One very common positive comment responded to the memories that nurses and providers helped them make after delivery. One parent said the following:
“While with baby and after loss, I think it’s really important to give ideas of what to do/experiences because the moments are so fleeting, and I needed someone to say, ‘You can dress him.’ ‘Let’s take pictures of his toes.’ ‘Save breast milk, etc.’”
“I appreciated the doctors and nurses who acknowledged my child, who looked at him and humanized him. One nurse even held him, which I still love her to this day for.”
“Explain things over, over, and over again, like you are explaining it to a child. I didn’t know what a cuddle cot was, and I didn’t use it because I didn’t understand.”
“Give suggestions and stress the importance of making memories. There are things I wish I did and now regret not doing. Taking pictures, handprints, lock of hair, giving the baby a bath.”
“For unknown losses give a full explanation of the autopsy and what it entails. Parents are making SO many decisions, and they need guidance.”
“Don’t shy away from it. It happened, and it is important to be human and compassionate. If you cannot do it, find someone else who can.”
“Ask to hold the baby and comment how beautiful the baby is. Treat the baby as if it were living.”
Don’t use the ‘silver lining’ theme
A common “don’t” in the hospital and postpartum is the “at least” and “silver lining” theme that is commonly expressed by providers. When I do my teaching sessions with a bereaved parents panel, we always stress that comforting words never begin with “at least.” We say a lot that there is no “silver lining” to a stillbirth. Dr. Brene Brown, in her TED talk on empathy, discussed that an empathic statement never starts with “at least.” However, this response is an all too common experience for women after stillbirth. Here are some examples from the Internet responses:
“‘The silver lining is you and your daughter have taught us so much.’ There is no silver lining, and her life was not for anyone’s easy path to learning lessons. She was wanted and loved.”
“What not to say: From a doctor, ‘You’re going to have lots more children.’ Anything along the lines of ‘at least you can get pregnant/have children’ is not OK.”
“As a teacher, ‘At least you are already a mother to your students.’ (I cannot even tell you how many times I’ve been told this. They already have mothers, and teaching a child 40 minutes once a week is not even close to being a mother to your own child.)”
“I felt it unhelpful for people to tell me how I should feel. I felt comments like ‘oh, you are young you can have another baby’ unhelpful.”
“Do not say, ‘you can have another, it wasn’t God’s plan, God wanted another angel, there is a reason for everything,’ etc.”
“The doctor who told me my baby was dead referred to him as a fetus. I was 38 weeks pregnant and did not refer to my baby as a fetus.”
Handling patient care after the loss
A huge portion of the response I received was regarding care from the practice where they delivered after the loss. These parents provided very important advice for any practice after a patient experiences a loss. Emotional support is vital for these patients. They also made it clear that topics such a medications and counseling should be frequently revisited.
“The care a patient receives after can really change their life – not physical care but emotional care. I truly believe I recovered well, and I am the person I am today because of my provider’s phone calls, suggestions for medications, support groups, and counseling. Don’t underestimate what simple phone calls can do. You don’t have to provide a solution or give advice, just listen.”
“Revisit conversations about medications. I have never taken anything in my entire life. In fact, I was very against it. Don’t be afraid to suggest medications time and time again if you think that it is the right plan. After 6 months, I said ‘yes’ to the medication, and it helped immensely.”
“My OB checking in with me constantly. Doctors offering compassionate and informative advice and encouragement. SUPPORT GROUPS. Star Legacy Foundation mentor!!! Klonopin! Psychologist!!”
“Also, I think it’s important for providers to continue to follow-up with patients even if they don’t seem receptive. Keep checking in. After losing your child you are in a fog. You don’t know quite what you need. But those calls, I promise you they mean something.”
When the patient returns to the office
The care received by a loss parent after returning to the office is challenging but so important. Some very careful steps can and must be made to help avoid emotionally harmful situations for the staff and patients. Offices need to make special accommodations and mark what happened clearly in the chart regarding the loss. When I have a mother coming in for a postpartum visit after a loss, I make sure she is the last patient of the day and try to bring her to our satellite offices where she can be the only patient there. Many parents made comments about carefully labeling what happened to the baby in the chart.
“Make sure it’s noted in the chart, and don’t AVOID talking about it. We like to have our baby brought up. Make sure staff knows the situation before entering the office so they don’t say something stupid (for example, ‘How is breast feeding going?’)”
“#1 don’t in my book: Not reading the patient’s chart and labels on it before seeing them if you’re not familiar with the patient. ... Nurses, techs and providers alike have assumed or asked “this is your first,” when clearly my chart lists “fetal death in utero.’”
“Many others have stated this, but having a BIG HUGE MASSIVE flag on our accounts and making sure ALL parts of the office are trained on this would be so incredibly helpful.”
“The nurse at my doctor’s office yesterday said, ‘Well, you’ve lost some weight since you were here last, so that’s good!’ My response was, ‘Well, losing a baby will do that.’”
“The follow-up appointment is awful. I went in heartbroken and angry and anxious. A phone call the day before acknowledging those feelings and reassuring me it was okay would have been nice.”
“At my first follow-up after my son died, I walked in, the receptionist pulled up my chart, saw I was there for my post-delivery appointment, and in the loudest, most cheery voice said, ‘Oooooooooh how’s he doing, how’s the baby?!’ It was awful telling her that he died, and I also felt terrible for all the pregnant woman in the waiting room who may have heard it.”
“When I was in emergency for a complication after birth, the only condolence a doctor from our previous practice gave was, ‘Well, that sucks’ (in regard to our daughter).”
Continuing care in the office
The care of women in the office immediately after loss and in years to come is a very important piece of the care they receive. In the same BJOG meta-analysis they found, “Parents frequently encountered professionals who were unaware of their history, through lack of access to/or reading of notes before a consultation. Dismissive attitudes to fears and concerns and insensitive and inappropriate comments sometimes resulted. These often remained with parents long after the event. In contrast, emotional wellbeing was enhanced when care providers demonstrated empathy, listened to concerns and committed to a collaborative and supportive relationship. Parents valued direct acknowledgment of the baby who had died, including using his or her name. Flexible antenatal care including extra appointments, routinely or on request, was also welcomed.”1 These findings were very similar to those reflected in the comments that I received.
“To the mother, there is no difference between a living baby and a stillborn baby. This stillborn baby is JUST AS MUCH a life to us. I’ve had four kids, and I can’t differentiate between how I feel about them.”
“Also, if staying with the same provider, ‘do’ ask what accommodations can be made moving forward. (For me I needed a different ultrasound tech and a different office for my ultrasounds in my subsequent pregnancies as I couldn’t go back there but wanted to stay with my same OB).”
“Don’t be afraid to ask about the child. I want people to know I like talking about my son, that he existed and how much love there was in his short but meaningful life.”
“Saying nothing is worse than saying you don’t know what to say and you are sorry.”
“Some moms love the rainbow baby term, and if they use it first, it’s fine to use it and encourage it and promote it. However, some moms do not like it because 1) they don’t like referring to their loss baby as a ‘storm.’ My baby was a BABY, and he was perfect and loved and I don’t like people referring to him as a storm. A storm is derogatory, [and] 2) the notion the subsequent baby makes everything okay is ridiculous. 3) Not everyone has another baby after a loss, so the ‘after every storm comes a rainbow’ phrase is stupid. It makes it seem like you can never be happy again unless you get a rainbow, and that is not true. 4) It’s a signal to the outside world that ‘everything’ is great and ok when in reality you can have grief, joy, sadness, happiness, pain, and hope all at the [same] time forever.”
Patients and their families who have lost their babies deserve our very best. No one grieves the same, and the differences in how our patients grieve must be respected. However, members of the loss community do have some common themes on responses that they appreciated or did not appreciate regarding their care. Most patients who deliver a stillborn baby or experience a neonatal death or pre-viable baby have had no time to prepare, and they are looking for our guidance and support. The more time we spend with them after diagnosis, during delivery, and after will be so appreciated. I hope some of these quotes ring true to many providers and that they either lead to attempts to change care or reinforce the amazing care providers are already providing. Being at our best when our patients are experiencing potentially the worst moments of their lives is our job as obstetrical providers. Our patients deserve the best care we can possibly provide. Hopefully, these suggestions from patients will help the care of future loss families.
Dr. Florescue is an ob.gyn. in private practice at Women Gynecology and Childbirth Associates in Rochester, N.Y. She delivers babies at Highland Hospital in Rochester. She has no relevant financial disclosures. Email her at obnews@mdedge.com.
Reference
1. BJOG. 2014 Jul; 121(8):943-50. doi: 10.1111/1471-0528.12656.
As a provider whose passion is helping women after stillbirth or neonatal loss, I get many transfers of women from their previous practice after a loss. Sometimes they transfer because they need a “fresh start,” but often, it is because they were let down by the practice – not by the medical care they received but by the emotional care and support and what was said or not said after the loss of the baby. A 2014 meta-analysis in the British Journal of Obstetrics and Gynaecology found that “Parents regarded contacts with health professionals as their central source of reassurance; but experiences often fell short of expectations.”1 I decided to conduct a survey via local and national support groups about what “loss parents” felt helpful or not helpful after the loss of a child. I purposely made these quotes the dominant part of this article, as I believe our patients are often our best teachers.
Inappropriate comments providers make
A very common theme among loss parents was how providers had made comments about how rare stillbirth is after it had just happened to them. Parents expressed that they felt this statistic kept them from getting the care that they needed prior to their loss and then they were told to not worry. Some example quotes include:
“ ‘This only happens to 1% of babies. Very rare.’ (It happened to our baby, and we have to live with this grief our whole lives. She is more than a statistic. She was our hopes, dreams, and future.)”
“I wish doctors didn’t wait to act based on statistics. There’s a lot of us in the 1% of unlikely occurrences.”
“For me, when my practice brushed off my feelings, I knew in my gut something was wrong. They said, ‘We need to wean you from worrying.’”
Another very common theme from parents included examples of helpful and not helpful care they received in the hospital.
Help parents make good memories
Many parents mentioned the importance of providing resources for after they go home. Most labor and delivery units have pregnancy loss services and have improved on the care they provide for loss families. One very common positive comment responded to the memories that nurses and providers helped them make after delivery. One parent said the following:
“While with baby and after loss, I think it’s really important to give ideas of what to do/experiences because the moments are so fleeting, and I needed someone to say, ‘You can dress him.’ ‘Let’s take pictures of his toes.’ ‘Save breast milk, etc.’”
“I appreciated the doctors and nurses who acknowledged my child, who looked at him and humanized him. One nurse even held him, which I still love her to this day for.”
“Explain things over, over, and over again, like you are explaining it to a child. I didn’t know what a cuddle cot was, and I didn’t use it because I didn’t understand.”
“Give suggestions and stress the importance of making memories. There are things I wish I did and now regret not doing. Taking pictures, handprints, lock of hair, giving the baby a bath.”
“For unknown losses give a full explanation of the autopsy and what it entails. Parents are making SO many decisions, and they need guidance.”
“Don’t shy away from it. It happened, and it is important to be human and compassionate. If you cannot do it, find someone else who can.”
“Ask to hold the baby and comment how beautiful the baby is. Treat the baby as if it were living.”
Don’t use the ‘silver lining’ theme
A common “don’t” in the hospital and postpartum is the “at least” and “silver lining” theme that is commonly expressed by providers. When I do my teaching sessions with a bereaved parents panel, we always stress that comforting words never begin with “at least.” We say a lot that there is no “silver lining” to a stillbirth. Dr. Brene Brown, in her TED talk on empathy, discussed that an empathic statement never starts with “at least.” However, this response is an all too common experience for women after stillbirth. Here are some examples from the Internet responses:
“‘The silver lining is you and your daughter have taught us so much.’ There is no silver lining, and her life was not for anyone’s easy path to learning lessons. She was wanted and loved.”
“What not to say: From a doctor, ‘You’re going to have lots more children.’ Anything along the lines of ‘at least you can get pregnant/have children’ is not OK.”
“As a teacher, ‘At least you are already a mother to your students.’ (I cannot even tell you how many times I’ve been told this. They already have mothers, and teaching a child 40 minutes once a week is not even close to being a mother to your own child.)”
“I felt it unhelpful for people to tell me how I should feel. I felt comments like ‘oh, you are young you can have another baby’ unhelpful.”
“Do not say, ‘you can have another, it wasn’t God’s plan, God wanted another angel, there is a reason for everything,’ etc.”
“The doctor who told me my baby was dead referred to him as a fetus. I was 38 weeks pregnant and did not refer to my baby as a fetus.”
Handling patient care after the loss
A huge portion of the response I received was regarding care from the practice where they delivered after the loss. These parents provided very important advice for any practice after a patient experiences a loss. Emotional support is vital for these patients. They also made it clear that topics such a medications and counseling should be frequently revisited.
“The care a patient receives after can really change their life – not physical care but emotional care. I truly believe I recovered well, and I am the person I am today because of my provider’s phone calls, suggestions for medications, support groups, and counseling. Don’t underestimate what simple phone calls can do. You don’t have to provide a solution or give advice, just listen.”
“Revisit conversations about medications. I have never taken anything in my entire life. In fact, I was very against it. Don’t be afraid to suggest medications time and time again if you think that it is the right plan. After 6 months, I said ‘yes’ to the medication, and it helped immensely.”
“My OB checking in with me constantly. Doctors offering compassionate and informative advice and encouragement. SUPPORT GROUPS. Star Legacy Foundation mentor!!! Klonopin! Psychologist!!”
“Also, I think it’s important for providers to continue to follow-up with patients even if they don’t seem receptive. Keep checking in. After losing your child you are in a fog. You don’t know quite what you need. But those calls, I promise you they mean something.”
When the patient returns to the office
The care received by a loss parent after returning to the office is challenging but so important. Some very careful steps can and must be made to help avoid emotionally harmful situations for the staff and patients. Offices need to make special accommodations and mark what happened clearly in the chart regarding the loss. When I have a mother coming in for a postpartum visit after a loss, I make sure she is the last patient of the day and try to bring her to our satellite offices where she can be the only patient there. Many parents made comments about carefully labeling what happened to the baby in the chart.
“Make sure it’s noted in the chart, and don’t AVOID talking about it. We like to have our baby brought up. Make sure staff knows the situation before entering the office so they don’t say something stupid (for example, ‘How is breast feeding going?’)”
“#1 don’t in my book: Not reading the patient’s chart and labels on it before seeing them if you’re not familiar with the patient. ... Nurses, techs and providers alike have assumed or asked “this is your first,” when clearly my chart lists “fetal death in utero.’”
“Many others have stated this, but having a BIG HUGE MASSIVE flag on our accounts and making sure ALL parts of the office are trained on this would be so incredibly helpful.”
“The nurse at my doctor’s office yesterday said, ‘Well, you’ve lost some weight since you were here last, so that’s good!’ My response was, ‘Well, losing a baby will do that.’”
“The follow-up appointment is awful. I went in heartbroken and angry and anxious. A phone call the day before acknowledging those feelings and reassuring me it was okay would have been nice.”
“At my first follow-up after my son died, I walked in, the receptionist pulled up my chart, saw I was there for my post-delivery appointment, and in the loudest, most cheery voice said, ‘Oooooooooh how’s he doing, how’s the baby?!’ It was awful telling her that he died, and I also felt terrible for all the pregnant woman in the waiting room who may have heard it.”
“When I was in emergency for a complication after birth, the only condolence a doctor from our previous practice gave was, ‘Well, that sucks’ (in regard to our daughter).”
Continuing care in the office
The care of women in the office immediately after loss and in years to come is a very important piece of the care they receive. In the same BJOG meta-analysis they found, “Parents frequently encountered professionals who were unaware of their history, through lack of access to/or reading of notes before a consultation. Dismissive attitudes to fears and concerns and insensitive and inappropriate comments sometimes resulted. These often remained with parents long after the event. In contrast, emotional wellbeing was enhanced when care providers demonstrated empathy, listened to concerns and committed to a collaborative and supportive relationship. Parents valued direct acknowledgment of the baby who had died, including using his or her name. Flexible antenatal care including extra appointments, routinely or on request, was also welcomed.”1 These findings were very similar to those reflected in the comments that I received.
“To the mother, there is no difference between a living baby and a stillborn baby. This stillborn baby is JUST AS MUCH a life to us. I’ve had four kids, and I can’t differentiate between how I feel about them.”
“Also, if staying with the same provider, ‘do’ ask what accommodations can be made moving forward. (For me I needed a different ultrasound tech and a different office for my ultrasounds in my subsequent pregnancies as I couldn’t go back there but wanted to stay with my same OB).”
“Don’t be afraid to ask about the child. I want people to know I like talking about my son, that he existed and how much love there was in his short but meaningful life.”
“Saying nothing is worse than saying you don’t know what to say and you are sorry.”
“Some moms love the rainbow baby term, and if they use it first, it’s fine to use it and encourage it and promote it. However, some moms do not like it because 1) they don’t like referring to their loss baby as a ‘storm.’ My baby was a BABY, and he was perfect and loved and I don’t like people referring to him as a storm. A storm is derogatory, [and] 2) the notion the subsequent baby makes everything okay is ridiculous. 3) Not everyone has another baby after a loss, so the ‘after every storm comes a rainbow’ phrase is stupid. It makes it seem like you can never be happy again unless you get a rainbow, and that is not true. 4) It’s a signal to the outside world that ‘everything’ is great and ok when in reality you can have grief, joy, sadness, happiness, pain, and hope all at the [same] time forever.”
Patients and their families who have lost their babies deserve our very best. No one grieves the same, and the differences in how our patients grieve must be respected. However, members of the loss community do have some common themes on responses that they appreciated or did not appreciate regarding their care. Most patients who deliver a stillborn baby or experience a neonatal death or pre-viable baby have had no time to prepare, and they are looking for our guidance and support. The more time we spend with them after diagnosis, during delivery, and after will be so appreciated. I hope some of these quotes ring true to many providers and that they either lead to attempts to change care or reinforce the amazing care providers are already providing. Being at our best when our patients are experiencing potentially the worst moments of their lives is our job as obstetrical providers. Our patients deserve the best care we can possibly provide. Hopefully, these suggestions from patients will help the care of future loss families.
Dr. Florescue is an ob.gyn. in private practice at Women Gynecology and Childbirth Associates in Rochester, N.Y. She delivers babies at Highland Hospital in Rochester. She has no relevant financial disclosures. Email her at obnews@mdedge.com.
Reference
1. BJOG. 2014 Jul; 121(8):943-50. doi: 10.1111/1471-0528.12656.
As a provider whose passion is helping women after stillbirth or neonatal loss, I get many transfers of women from their previous practice after a loss. Sometimes they transfer because they need a “fresh start,” but often, it is because they were let down by the practice – not by the medical care they received but by the emotional care and support and what was said or not said after the loss of the baby. A 2014 meta-analysis in the British Journal of Obstetrics and Gynaecology found that “Parents regarded contacts with health professionals as their central source of reassurance; but experiences often fell short of expectations.”1 I decided to conduct a survey via local and national support groups about what “loss parents” felt helpful or not helpful after the loss of a child. I purposely made these quotes the dominant part of this article, as I believe our patients are often our best teachers.
Inappropriate comments providers make
A very common theme among loss parents was how providers had made comments about how rare stillbirth is after it had just happened to them. Parents expressed that they felt this statistic kept them from getting the care that they needed prior to their loss and then they were told to not worry. Some example quotes include:
“ ‘This only happens to 1% of babies. Very rare.’ (It happened to our baby, and we have to live with this grief our whole lives. She is more than a statistic. She was our hopes, dreams, and future.)”
“I wish doctors didn’t wait to act based on statistics. There’s a lot of us in the 1% of unlikely occurrences.”
“For me, when my practice brushed off my feelings, I knew in my gut something was wrong. They said, ‘We need to wean you from worrying.’”
Another very common theme from parents included examples of helpful and not helpful care they received in the hospital.
Help parents make good memories
Many parents mentioned the importance of providing resources for after they go home. Most labor and delivery units have pregnancy loss services and have improved on the care they provide for loss families. One very common positive comment responded to the memories that nurses and providers helped them make after delivery. One parent said the following:
“While with baby and after loss, I think it’s really important to give ideas of what to do/experiences because the moments are so fleeting, and I needed someone to say, ‘You can dress him.’ ‘Let’s take pictures of his toes.’ ‘Save breast milk, etc.’”
“I appreciated the doctors and nurses who acknowledged my child, who looked at him and humanized him. One nurse even held him, which I still love her to this day for.”
“Explain things over, over, and over again, like you are explaining it to a child. I didn’t know what a cuddle cot was, and I didn’t use it because I didn’t understand.”
“Give suggestions and stress the importance of making memories. There are things I wish I did and now regret not doing. Taking pictures, handprints, lock of hair, giving the baby a bath.”
“For unknown losses give a full explanation of the autopsy and what it entails. Parents are making SO many decisions, and they need guidance.”
“Don’t shy away from it. It happened, and it is important to be human and compassionate. If you cannot do it, find someone else who can.”
“Ask to hold the baby and comment how beautiful the baby is. Treat the baby as if it were living.”
Don’t use the ‘silver lining’ theme
A common “don’t” in the hospital and postpartum is the “at least” and “silver lining” theme that is commonly expressed by providers. When I do my teaching sessions with a bereaved parents panel, we always stress that comforting words never begin with “at least.” We say a lot that there is no “silver lining” to a stillbirth. Dr. Brene Brown, in her TED talk on empathy, discussed that an empathic statement never starts with “at least.” However, this response is an all too common experience for women after stillbirth. Here are some examples from the Internet responses:
“‘The silver lining is you and your daughter have taught us so much.’ There is no silver lining, and her life was not for anyone’s easy path to learning lessons. She was wanted and loved.”
“What not to say: From a doctor, ‘You’re going to have lots more children.’ Anything along the lines of ‘at least you can get pregnant/have children’ is not OK.”
“As a teacher, ‘At least you are already a mother to your students.’ (I cannot even tell you how many times I’ve been told this. They already have mothers, and teaching a child 40 minutes once a week is not even close to being a mother to your own child.)”
“I felt it unhelpful for people to tell me how I should feel. I felt comments like ‘oh, you are young you can have another baby’ unhelpful.”
“Do not say, ‘you can have another, it wasn’t God’s plan, God wanted another angel, there is a reason for everything,’ etc.”
“The doctor who told me my baby was dead referred to him as a fetus. I was 38 weeks pregnant and did not refer to my baby as a fetus.”
Handling patient care after the loss
A huge portion of the response I received was regarding care from the practice where they delivered after the loss. These parents provided very important advice for any practice after a patient experiences a loss. Emotional support is vital for these patients. They also made it clear that topics such a medications and counseling should be frequently revisited.
“The care a patient receives after can really change their life – not physical care but emotional care. I truly believe I recovered well, and I am the person I am today because of my provider’s phone calls, suggestions for medications, support groups, and counseling. Don’t underestimate what simple phone calls can do. You don’t have to provide a solution or give advice, just listen.”
“Revisit conversations about medications. I have never taken anything in my entire life. In fact, I was very against it. Don’t be afraid to suggest medications time and time again if you think that it is the right plan. After 6 months, I said ‘yes’ to the medication, and it helped immensely.”
“My OB checking in with me constantly. Doctors offering compassionate and informative advice and encouragement. SUPPORT GROUPS. Star Legacy Foundation mentor!!! Klonopin! Psychologist!!”
“Also, I think it’s important for providers to continue to follow-up with patients even if they don’t seem receptive. Keep checking in. After losing your child you are in a fog. You don’t know quite what you need. But those calls, I promise you they mean something.”
When the patient returns to the office
The care received by a loss parent after returning to the office is challenging but so important. Some very careful steps can and must be made to help avoid emotionally harmful situations for the staff and patients. Offices need to make special accommodations and mark what happened clearly in the chart regarding the loss. When I have a mother coming in for a postpartum visit after a loss, I make sure she is the last patient of the day and try to bring her to our satellite offices where she can be the only patient there. Many parents made comments about carefully labeling what happened to the baby in the chart.
“Make sure it’s noted in the chart, and don’t AVOID talking about it. We like to have our baby brought up. Make sure staff knows the situation before entering the office so they don’t say something stupid (for example, ‘How is breast feeding going?’)”
“#1 don’t in my book: Not reading the patient’s chart and labels on it before seeing them if you’re not familiar with the patient. ... Nurses, techs and providers alike have assumed or asked “this is your first,” when clearly my chart lists “fetal death in utero.’”
“Many others have stated this, but having a BIG HUGE MASSIVE flag on our accounts and making sure ALL parts of the office are trained on this would be so incredibly helpful.”
“The nurse at my doctor’s office yesterday said, ‘Well, you’ve lost some weight since you were here last, so that’s good!’ My response was, ‘Well, losing a baby will do that.’”
“The follow-up appointment is awful. I went in heartbroken and angry and anxious. A phone call the day before acknowledging those feelings and reassuring me it was okay would have been nice.”
“At my first follow-up after my son died, I walked in, the receptionist pulled up my chart, saw I was there for my post-delivery appointment, and in the loudest, most cheery voice said, ‘Oooooooooh how’s he doing, how’s the baby?!’ It was awful telling her that he died, and I also felt terrible for all the pregnant woman in the waiting room who may have heard it.”
“When I was in emergency for a complication after birth, the only condolence a doctor from our previous practice gave was, ‘Well, that sucks’ (in regard to our daughter).”
Continuing care in the office
The care of women in the office immediately after loss and in years to come is a very important piece of the care they receive. In the same BJOG meta-analysis they found, “Parents frequently encountered professionals who were unaware of their history, through lack of access to/or reading of notes before a consultation. Dismissive attitudes to fears and concerns and insensitive and inappropriate comments sometimes resulted. These often remained with parents long after the event. In contrast, emotional wellbeing was enhanced when care providers demonstrated empathy, listened to concerns and committed to a collaborative and supportive relationship. Parents valued direct acknowledgment of the baby who had died, including using his or her name. Flexible antenatal care including extra appointments, routinely or on request, was also welcomed.”1 These findings were very similar to those reflected in the comments that I received.
“To the mother, there is no difference between a living baby and a stillborn baby. This stillborn baby is JUST AS MUCH a life to us. I’ve had four kids, and I can’t differentiate between how I feel about them.”
“Also, if staying with the same provider, ‘do’ ask what accommodations can be made moving forward. (For me I needed a different ultrasound tech and a different office for my ultrasounds in my subsequent pregnancies as I couldn’t go back there but wanted to stay with my same OB).”
“Don’t be afraid to ask about the child. I want people to know I like talking about my son, that he existed and how much love there was in his short but meaningful life.”
“Saying nothing is worse than saying you don’t know what to say and you are sorry.”
“Some moms love the rainbow baby term, and if they use it first, it’s fine to use it and encourage it and promote it. However, some moms do not like it because 1) they don’t like referring to their loss baby as a ‘storm.’ My baby was a BABY, and he was perfect and loved and I don’t like people referring to him as a storm. A storm is derogatory, [and] 2) the notion the subsequent baby makes everything okay is ridiculous. 3) Not everyone has another baby after a loss, so the ‘after every storm comes a rainbow’ phrase is stupid. It makes it seem like you can never be happy again unless you get a rainbow, and that is not true. 4) It’s a signal to the outside world that ‘everything’ is great and ok when in reality you can have grief, joy, sadness, happiness, pain, and hope all at the [same] time forever.”
Patients and their families who have lost their babies deserve our very best. No one grieves the same, and the differences in how our patients grieve must be respected. However, members of the loss community do have some common themes on responses that they appreciated or did not appreciate regarding their care. Most patients who deliver a stillborn baby or experience a neonatal death or pre-viable baby have had no time to prepare, and they are looking for our guidance and support. The more time we spend with them after diagnosis, during delivery, and after will be so appreciated. I hope some of these quotes ring true to many providers and that they either lead to attempts to change care or reinforce the amazing care providers are already providing. Being at our best when our patients are experiencing potentially the worst moments of their lives is our job as obstetrical providers. Our patients deserve the best care we can possibly provide. Hopefully, these suggestions from patients will help the care of future loss families.
Dr. Florescue is an ob.gyn. in private practice at Women Gynecology and Childbirth Associates in Rochester, N.Y. She delivers babies at Highland Hospital in Rochester. She has no relevant financial disclosures. Email her at obnews@mdedge.com.
Reference
1. BJOG. 2014 Jul; 121(8):943-50. doi: 10.1111/1471-0528.12656.
New Americans: Considerations for culturally collaborative care
Adam is a 14-year-old who presents for “behavioral concerns” as recommended by his teacher. He is in the eighth grade and is struggling academically and socially. He has intermittent outbursts and poor engagement with other children, and often refuses to do schoolwork. He is seen in the outpatient primary care clinic, usually with his mother and two older siblings, one of whom typically translates for his Arabic-speaking mother. Adam is bilingual, although he prefers Arabic. It is difficult to understand the presenting concern as Adam states that he is doing well and is unsure why the teacher would have made such a report. Mother notes that she does not see these behaviors at home either.
What must we consider? Are there potential barriers, alternate ways to engage, and what role may culture have?
There are many things to consider in the above case, including language barriers, nuanced interactions, and cultural expectations and norms. To understand the scope, statistics reveal that the United States leads the world in its immigrant population with about 44.8 million foreign-born persons in 2018, which accounts for approximately 13.7% of the U.S. population.1 In 2019, 30,000 refugees were resettled in the United States.2 In 2017, immigrant children made up 27% (19.6 million) of U.S. children, of which second-generation children (born in the United States to immigrant parents) were the vast majority at 16.7 million.3 Given this information, 
Culture is defined as a set of shared beliefs, norms, values, and behaviors exhibited by a group. Culture plays a role and impacts children in various ways throughout their development. Health care providers would benefit from aspiring to exude cultural humility – learning with and from patients and their families with openness, kindness, and a desire for collaboration. The provider also must consider a family’s history of migration as the response to migration may vary based on age, personal experiences, age at which migration occurred, language abilities, and amount of cultural engagement in the new country (i.e. acculturation).4,5
Cultural framework model
One example of a potential framework to use to engage within a cultural context includes the LEARN (Listen, Explain, Acknowledge, Recommend, Negotiate) model,6,7 which initially was developed to be used within a family medicine clinic. It includes the following:
Listen with sympathy and understanding to the patient’s perception of the problem. Try to understand their perspective of symptoms through considering their thoughts regarding etiology and treatment options.
Explain your perception of the problem. Have a dialogue about what you perceive is the likely cause based on a medical perspective.
Acknowledge and discuss the differences and similarities. Engage in open conversation while being cognizant that there may be similarities and differences in the perception you may have versus your patient’s perception. Try to find areas that can be engaged in and an alliance built upon, as well as respectfully and humbly addressing any concerns about potentially harmful patient understandings.
Recommend treatment. Present a treatment recommendation that considers both yours and the patient’s perspectives.
Negotiate agreement. Discuss, collaborate, and finalize a treatment plan that considers a biopsychosocial and spiritual/religious model of care that is patient-centered and personalized such that the main goal is optimal health and wellness for the patient/family.
The following are tips to consider in the life-long process of becoming more culturally aware:
- Be willing to learn with your patients and be thoughtful about your own feelings/thoughts/behaviors that may be positively or negatively impacting those interactions.
- Be aware of your own identity and what that may contribute to the clinical space.
- Recognize that you are not meant to know everything, but being open to the journey and learning process will go a long way.
- Try to shift the focus from paternalistic medicine to collaborative and patient-centered approaches.
The case at hand
In returning to our case and applying the LEARN model and cultural humility, we may be able to uncover more of the story. Adam is seen at a subsequent appointment, and you determine it best to obtain an in-person interpreter for this appointment. As you listen to the story, you learn that his father was killed early in Adam’s life, his mother has suffered from depression, and they moved here 3 years ago from a refugee camp, where most of their family continues to reside. He notes that at times he feels that he is back in that space and that he also feels frustrated. He is accustomed to doing well academically, but English has been difficult to learn.

You explain your understanding and acknowledge concerns for his past experiences playing a role, the importance of having community supports, and that learning a new language is challenging. You recommend that the school offer culturally appropriate interventions, trauma-informed assessments, and English-language opportunities. Adam and his mother note willingness to engage in this plan but would like to speak to their local religious leader as well.
Collaborating in a manner similar to this will likely build a therapeutic alliance between the patient, their family, and caretakers, thus leading to improved outcomes.
For further reading, consider AACAP Finding Mental Healthcare for Children of Immigrants and the American Academy of Pediatrics Providing Culturally Effective Care Toolkit.
Dr. Abdul-Karim, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
References
1. “Key findings about U.S. immigrants.” Pew Research Center, Washington, D.C. (2020)
2. “Key facts about refugees to the U.S.” Pew Research Center, Washington, D.C. (2019)
3. “Immigrant Children.” Child Trends, Bethesda, MD (2018).
4. Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry, 11th ed. (Philadelphia: Lippincott Williams & Wilkins, 2015, pp. 139-45).
5. Lewis’sChild and Adolescent Psychiatry: A Comprehensive Textbook, 5th ed. (Philadelphia: Lippincott Williams & Wilkins, 2017, pp. 111-22).
6. Berlin EA, Fowkes WA Jr.A teaching framework for cross-cultural health care. Application in family practice. West J Med 1983;139(6):934-8.
7. Paediatr Child Health. 2018 Feb;23(1):66-9.
Adam is a 14-year-old who presents for “behavioral concerns” as recommended by his teacher. He is in the eighth grade and is struggling academically and socially. He has intermittent outbursts and poor engagement with other children, and often refuses to do schoolwork. He is seen in the outpatient primary care clinic, usually with his mother and two older siblings, one of whom typically translates for his Arabic-speaking mother. Adam is bilingual, although he prefers Arabic. It is difficult to understand the presenting concern as Adam states that he is doing well and is unsure why the teacher would have made such a report. Mother notes that she does not see these behaviors at home either.
What must we consider? Are there potential barriers, alternate ways to engage, and what role may culture have?
There are many things to consider in the above case, including language barriers, nuanced interactions, and cultural expectations and norms. To understand the scope, statistics reveal that the United States leads the world in its immigrant population with about 44.8 million foreign-born persons in 2018, which accounts for approximately 13.7% of the U.S. population.1 In 2019, 30,000 refugees were resettled in the United States.2 In 2017, immigrant children made up 27% (19.6 million) of U.S. children, of which second-generation children (born in the United States to immigrant parents) were the vast majority at 16.7 million.3 Given this information,
Culture is defined as a set of shared beliefs, norms, values, and behaviors exhibited by a group. Culture plays a role and impacts children in various ways throughout their development. Health care providers would benefit from aspiring to exude cultural humility – learning with and from patients and their families with openness, kindness, and a desire for collaboration. The provider also must consider a family’s history of migration as the response to migration may vary based on age, personal experiences, age at which migration occurred, language abilities, and amount of cultural engagement in the new country (i.e. acculturation).4,5
Cultural framework model
One example of a potential framework to use to engage within a cultural context includes the LEARN (Listen, Explain, Acknowledge, Recommend, Negotiate) model,6,7 which initially was developed to be used within a family medicine clinic. It includes the following:
Listen with sympathy and understanding to the patient’s perception of the problem. Try to understand their perspective of symptoms through considering their thoughts regarding etiology and treatment options.
Explain your perception of the problem. Have a dialogue about what you perceive is the likely cause based on a medical perspective.
Acknowledge and discuss the differences and similarities. Engage in open conversation while being cognizant that there may be similarities and differences in the perception you may have versus your patient’s perception. Try to find areas that can be engaged in and an alliance built upon, as well as respectfully and humbly addressing any concerns about potentially harmful patient understandings.
Recommend treatment. Present a treatment recommendation that considers both yours and the patient’s perspectives.
Negotiate agreement. Discuss, collaborate, and finalize a treatment plan that considers a biopsychosocial and spiritual/religious model of care that is patient-centered and personalized such that the main goal is optimal health and wellness for the patient/family.
The following are tips to consider in the life-long process of becoming more culturally aware:
- Be willing to learn with your patients and be thoughtful about your own feelings/thoughts/behaviors that may be positively or negatively impacting those interactions.
- Be aware of your own identity and what that may contribute to the clinical space.
- Recognize that you are not meant to know everything, but being open to the journey and learning process will go a long way.
- Try to shift the focus from paternalistic medicine to collaborative and patient-centered approaches.
The case at hand
In returning to our case and applying the LEARN model and cultural humility, we may be able to uncover more of the story. Adam is seen at a subsequent appointment, and you determine it best to obtain an in-person interpreter for this appointment. As you listen to the story, you learn that his father was killed early in Adam’s life, his mother has suffered from depression, and they moved here 3 years ago from a refugee camp, where most of their family continues to reside. He notes that at times he feels that he is back in that space and that he also feels frustrated. He is accustomed to doing well academically, but English has been difficult to learn.
You explain your understanding and acknowledge concerns for his past experiences playing a role, the importance of having community supports, and that learning a new language is challenging. You recommend that the school offer culturally appropriate interventions, trauma-informed assessments, and English-language opportunities. Adam and his mother note willingness to engage in this plan but would like to speak to their local religious leader as well.
Collaborating in a manner similar to this will likely build a therapeutic alliance between the patient, their family, and caretakers, thus leading to improved outcomes.
For further reading, consider AACAP Finding Mental Healthcare for Children of Immigrants and the American Academy of Pediatrics Providing Culturally Effective Care Toolkit.
Dr. Abdul-Karim, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
References
1. “Key findings about U.S. immigrants.” Pew Research Center, Washington, D.C. (2020)
2. “Key facts about refugees to the U.S.” Pew Research Center, Washington, D.C. (2019)
3. “Immigrant Children.” Child Trends, Bethesda, MD (2018).
4. Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry, 11th ed. (Philadelphia: Lippincott Williams & Wilkins, 2015, pp. 139-45).
5. Lewis’sChild and Adolescent Psychiatry: A Comprehensive Textbook, 5th ed. (Philadelphia: Lippincott Williams & Wilkins, 2017, pp. 111-22).
6. Berlin EA, Fowkes WA Jr.A teaching framework for cross-cultural health care. Application in family practice. West J Med 1983;139(6):934-8.
7. Paediatr Child Health. 2018 Feb;23(1):66-9.
Adam is a 14-year-old who presents for “behavioral concerns” as recommended by his teacher. He is in the eighth grade and is struggling academically and socially. He has intermittent outbursts and poor engagement with other children, and often refuses to do schoolwork. He is seen in the outpatient primary care clinic, usually with his mother and two older siblings, one of whom typically translates for his Arabic-speaking mother. Adam is bilingual, although he prefers Arabic. It is difficult to understand the presenting concern as Adam states that he is doing well and is unsure why the teacher would have made such a report. Mother notes that she does not see these behaviors at home either.
What must we consider? Are there potential barriers, alternate ways to engage, and what role may culture have?
There are many things to consider in the above case, including language barriers, nuanced interactions, and cultural expectations and norms. To understand the scope, statistics reveal that the United States leads the world in its immigrant population with about 44.8 million foreign-born persons in 2018, which accounts for approximately 13.7% of the U.S. population.1 In 2019, 30,000 refugees were resettled in the United States.2 In 2017, immigrant children made up 27% (19.6 million) of U.S. children, of which second-generation children (born in the United States to immigrant parents) were the vast majority at 16.7 million.3 Given this information,
Culture is defined as a set of shared beliefs, norms, values, and behaviors exhibited by a group. Culture plays a role and impacts children in various ways throughout their development. Health care providers would benefit from aspiring to exude cultural humility – learning with and from patients and their families with openness, kindness, and a desire for collaboration. The provider also must consider a family’s history of migration as the response to migration may vary based on age, personal experiences, age at which migration occurred, language abilities, and amount of cultural engagement in the new country (i.e. acculturation).4,5
Cultural framework model
One example of a potential framework to use to engage within a cultural context includes the LEARN (Listen, Explain, Acknowledge, Recommend, Negotiate) model,6,7 which initially was developed to be used within a family medicine clinic. It includes the following:
Listen with sympathy and understanding to the patient’s perception of the problem. Try to understand their perspective of symptoms through considering their thoughts regarding etiology and treatment options.
Explain your perception of the problem. Have a dialogue about what you perceive is the likely cause based on a medical perspective.
Acknowledge and discuss the differences and similarities. Engage in open conversation while being cognizant that there may be similarities and differences in the perception you may have versus your patient’s perception. Try to find areas that can be engaged in and an alliance built upon, as well as respectfully and humbly addressing any concerns about potentially harmful patient understandings.
Recommend treatment. Present a treatment recommendation that considers both yours and the patient’s perspectives.
Negotiate agreement. Discuss, collaborate, and finalize a treatment plan that considers a biopsychosocial and spiritual/religious model of care that is patient-centered and personalized such that the main goal is optimal health and wellness for the patient/family.
The following are tips to consider in the life-long process of becoming more culturally aware:
- Be willing to learn with your patients and be thoughtful about your own feelings/thoughts/behaviors that may be positively or negatively impacting those interactions.
- Be aware of your own identity and what that may contribute to the clinical space.
- Recognize that you are not meant to know everything, but being open to the journey and learning process will go a long way.
- Try to shift the focus from paternalistic medicine to collaborative and patient-centered approaches.
The case at hand
In returning to our case and applying the LEARN model and cultural humility, we may be able to uncover more of the story. Adam is seen at a subsequent appointment, and you determine it best to obtain an in-person interpreter for this appointment. As you listen to the story, you learn that his father was killed early in Adam’s life, his mother has suffered from depression, and they moved here 3 years ago from a refugee camp, where most of their family continues to reside. He notes that at times he feels that he is back in that space and that he also feels frustrated. He is accustomed to doing well academically, but English has been difficult to learn.
You explain your understanding and acknowledge concerns for his past experiences playing a role, the importance of having community supports, and that learning a new language is challenging. You recommend that the school offer culturally appropriate interventions, trauma-informed assessments, and English-language opportunities. Adam and his mother note willingness to engage in this plan but would like to speak to their local religious leader as well.
Collaborating in a manner similar to this will likely build a therapeutic alliance between the patient, their family, and caretakers, thus leading to improved outcomes.
For further reading, consider AACAP Finding Mental Healthcare for Children of Immigrants and the American Academy of Pediatrics Providing Culturally Effective Care Toolkit.
Dr. Abdul-Karim, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
References
1. “Key findings about U.S. immigrants.” Pew Research Center, Washington, D.C. (2020)
2. “Key facts about refugees to the U.S.” Pew Research Center, Washington, D.C. (2019)
3. “Immigrant Children.” Child Trends, Bethesda, MD (2018).
4. Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry, 11th ed. (Philadelphia: Lippincott Williams & Wilkins, 2015, pp. 139-45).
5. Lewis’sChild and Adolescent Psychiatry: A Comprehensive Textbook, 5th ed. (Philadelphia: Lippincott Williams & Wilkins, 2017, pp. 111-22).
6. Berlin EA, Fowkes WA Jr.A teaching framework for cross-cultural health care. Application in family practice. West J Med 1983;139(6):934-8.
7. Paediatr Child Health. 2018 Feb;23(1):66-9.
A teen presents with a severe, tender rash on the extremities
“There’s rue for you, and here’s some for me; we may call it herb of grace o’ Sundays. O, you must wear your rue with a difference.”
— Ophelia in Hamlet by William Shakespeare
The patient was admitted to the hospital for IV fluids, pain control, and observation. The following day she admitted using the leaves of a plant on the trail as a bug repellent, as one time was taught by her grandfather. She rubbed some of the leaves on the brother as well. The grandfather shared some pictures of the bushes, and the plant was identified as Ruta graveolens.

The blisters were deroofed, cleaned with saline, and wrapped with triamcinolone ointment and petrolatum. The patient was also started on a prednisone taper and received analgesics for the severe pain.
Ruta graveolens also known as common rue or herb of grace, is an ornamental plant from the Rutaceae family. This plant is also used as a medicinal herb, condiment, and as an insect repellent. If ingested in large doses, it can cause severe abdominal pain and vomiting. It also can be hepatotoxic.
The herb contains furocumarines, such as 8-methoxypsoralen and 5-methoxypsoralen and furoquinoline alkaloids. These chemicals when exposed to UVA radiation cause cell injury and inflammation of the skin. This is considered a phototoxic reaction of the skin, compared with allergic reactions, such as poison ivy dermatitis, which need a prior sensitization to the allergen for the T cells to be activated and cause injury in the skin. Other common plants and fruits that can cause phytophotodermatitis include citrus fruits, figs, carrots, celery, parsnips, parsley, and other wildflowers like hogweed.

Depending on the degree of injury, the patients can be treated with topical corticosteroids, petrolatum wraps, and pain control. In severe cases like our patient, systemic prednisone may help stop the progression of the lesions and help with the inflammation. Skin hyperpigmentation after the initial injury may take months to clear, and some patient can develop scars.
The differential diagnosis should include severe bullous contact dermatitis like exposure to urushiol in poison ivy; second- and third-degree burns; severe medications reactions such Stevens-Johnson syndrome or toxic epidermal necrolysis, and inmunobullous diseases such as bullous lupus erythematosus, pemphigus vulgaris, or bullous pemphigoid. If there is no history of exposure or there are any other systemic symptoms, consider performing a skin biopsy of one of the lesions.
In this patient’s case, the history of exposure and skin findings helped the dermatologist on call make the right diagnosis.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at pdnews@mdedge.com.
References
J Burn Care Res. 2018 Oct 23;39(6):1064-6.
Dermatitis. 2007 Mar;18(1):52-5.
BMJ Case Rep. 2015 Dec 23;2015:bcr2015213388.
“There’s rue for you, and here’s some for me; we may call it herb of grace o’ Sundays. O, you must wear your rue with a difference.”
— Ophelia in Hamlet by William Shakespeare
The patient was admitted to the hospital for IV fluids, pain control, and observation. The following day she admitted using the leaves of a plant on the trail as a bug repellent, as one time was taught by her grandfather. She rubbed some of the leaves on the brother as well. The grandfather shared some pictures of the bushes, and the plant was identified as Ruta graveolens.
The blisters were deroofed, cleaned with saline, and wrapped with triamcinolone ointment and petrolatum. The patient was also started on a prednisone taper and received analgesics for the severe pain.
Ruta graveolens also known as common rue or herb of grace, is an ornamental plant from the Rutaceae family. This plant is also used as a medicinal herb, condiment, and as an insect repellent. If ingested in large doses, it can cause severe abdominal pain and vomiting. It also can be hepatotoxic.
The herb contains furocumarines, such as 8-methoxypsoralen and 5-methoxypsoralen and furoquinoline alkaloids. These chemicals when exposed to UVA radiation cause cell injury and inflammation of the skin. This is considered a phototoxic reaction of the skin, compared with allergic reactions, such as poison ivy dermatitis, which need a prior sensitization to the allergen for the T cells to be activated and cause injury in the skin. Other common plants and fruits that can cause phytophotodermatitis include citrus fruits, figs, carrots, celery, parsnips, parsley, and other wildflowers like hogweed.
Depending on the degree of injury, the patients can be treated with topical corticosteroids, petrolatum wraps, and pain control. In severe cases like our patient, systemic prednisone may help stop the progression of the lesions and help with the inflammation. Skin hyperpigmentation after the initial injury may take months to clear, and some patient can develop scars.
The differential diagnosis should include severe bullous contact dermatitis like exposure to urushiol in poison ivy; second- and third-degree burns; severe medications reactions such Stevens-Johnson syndrome or toxic epidermal necrolysis, and inmunobullous diseases such as bullous lupus erythematosus, pemphigus vulgaris, or bullous pemphigoid. If there is no history of exposure or there are any other systemic symptoms, consider performing a skin biopsy of one of the lesions.
In this patient’s case, the history of exposure and skin findings helped the dermatologist on call make the right diagnosis.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at pdnews@mdedge.com.
References
J Burn Care Res. 2018 Oct 23;39(6):1064-6.
Dermatitis. 2007 Mar;18(1):52-5.
BMJ Case Rep. 2015 Dec 23;2015:bcr2015213388.
“There’s rue for you, and here’s some for me; we may call it herb of grace o’ Sundays. O, you must wear your rue with a difference.”
— Ophelia in Hamlet by William Shakespeare
The patient was admitted to the hospital for IV fluids, pain control, and observation. The following day she admitted using the leaves of a plant on the trail as a bug repellent, as one time was taught by her grandfather. She rubbed some of the leaves on the brother as well. The grandfather shared some pictures of the bushes, and the plant was identified as Ruta graveolens.
The blisters were deroofed, cleaned with saline, and wrapped with triamcinolone ointment and petrolatum. The patient was also started on a prednisone taper and received analgesics for the severe pain.
Ruta graveolens also known as common rue or herb of grace, is an ornamental plant from the Rutaceae family. This plant is also used as a medicinal herb, condiment, and as an insect repellent. If ingested in large doses, it can cause severe abdominal pain and vomiting. It also can be hepatotoxic.
The herb contains furocumarines, such as 8-methoxypsoralen and 5-methoxypsoralen and furoquinoline alkaloids. These chemicals when exposed to UVA radiation cause cell injury and inflammation of the skin. This is considered a phototoxic reaction of the skin, compared with allergic reactions, such as poison ivy dermatitis, which need a prior sensitization to the allergen for the T cells to be activated and cause injury in the skin. Other common plants and fruits that can cause phytophotodermatitis include citrus fruits, figs, carrots, celery, parsnips, parsley, and other wildflowers like hogweed.
Depending on the degree of injury, the patients can be treated with topical corticosteroids, petrolatum wraps, and pain control. In severe cases like our patient, systemic prednisone may help stop the progression of the lesions and help with the inflammation. Skin hyperpigmentation after the initial injury may take months to clear, and some patient can develop scars.
The differential diagnosis should include severe bullous contact dermatitis like exposure to urushiol in poison ivy; second- and third-degree burns; severe medications reactions such Stevens-Johnson syndrome or toxic epidermal necrolysis, and inmunobullous diseases such as bullous lupus erythematosus, pemphigus vulgaris, or bullous pemphigoid. If there is no history of exposure or there are any other systemic symptoms, consider performing a skin biopsy of one of the lesions.
In this patient’s case, the history of exposure and skin findings helped the dermatologist on call make the right diagnosis.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at pdnews@mdedge.com.
References
J Burn Care Res. 2018 Oct 23;39(6):1064-6.
Dermatitis. 2007 Mar;18(1):52-5.
BMJ Case Rep. 2015 Dec 23;2015:bcr2015213388.

She started taking lithium for depression and anxiety 3 weeks prior to her developing the rash. She denies taking any other medications, supplements, or recreational drugs.
She denied any prior history of photosensitivity, no history of mouth ulcers, joint pain, muscle weakness, hair loss, or any other symptoms.
Besides her brother, there are no other affected family members, and no history of immune bullous disorders or other skin conditions.
On physical exam, the girl appears in a lot of pain and is uncomfortable. The skin is red and hot, and there are tense bullae on the neck, arms, and legs. There are no ocular or mucosal lesions.
The unsteady state
As the COVID-19 pandemic continues to chug along, some communities feel it slowing to a pace at which they might feel comfortable about a return to, if not quite “business as usual,” at least “business as sort of normal-ish.” They are ready to accept a level of disease that signals they have reached a steady state. However, in other communities, the virus has picked up speed and is threatening to overwhelm the medical infrastructure. If you are in one of those fortunate and skillfully managed states in which folks are beginning to talk seriously, but with little evidence, that it is time to return to normal, it is probably far too early.

Eons ago in pandemic terms, the World Health Organization in Thailand published a list of criteria to aid in determining when a community could consider lifting the limits that seemed to have been effective in halting transmission of the virus (“Transitioning to and maintaining a steady state of low-level or no transmission,” WHO, Thailand, 2020 Apr 18). While much more has been learned about the behavior of the virus since the spring of 2020, the criteria from the WHO in Thailand are worth considering.
Here is my summary of their criteria for returning to normalcy. First, virus transmission is controlled to the point that only sporadic cases and small clusters exist, and that all of these are traceable in origin. Second, health care and public health systems are in place with sufficient capacities to manage a shift from detection to treatment should the case load increase dramatically; this capacity should include detection, testing, isolation, and quarantine. Third, outbreaks in high-risk populations such as nursing homes have been minimized. Fourth, workplace prevention strategies are in place and have been demonstrated to be effective. Fifth, risk of imported cases is at manageable levels. Finally, communities are engaged.
It is hard to argue with the rationale behind each of these criteria. However, the United States is not Thailand, and just thinking about how this country would go about meeting those criteria provides a window into some of the reasons why we have done so poorly and will continue to be challenged in dealing with the pandemic.
First, notice that the criteria make no mention of a vaccine. One gets the sense that from the top down our country is banking too heavily on the effectiveness and widespread delivery of a vaccine. Even if and when a vaccine is developed and delivered, all of these criteria still must be met and kept in mind for a future pandemic.
Second, the criteria call for an effective health care system, but it is abundantly clear that the United States does not have a cohesive health care system and probably won’t for the foreseeable future. The best we can hope for is individual states cobbling together their own systems, which may in turn serve as examples for those states who haven’t had the foresight. We have had a public health system of sorts, but its credibility and effectiveness has been neutered to the point that again we must rely on each state’s ability to see through the haze and create it’s own systems for detection, testing, tracking, isolating, and quarantining – often with little help in materiel support from the federal government. The sliver of good news is that, after a bit of a stumbling start, detecting and limiting the importation of cases from abroad is being addressed.
We continue to hear and see evidence that there are segments of the population who are not engaged in the activities that we have learned are necessary to stabilize the pandemic. My sense is that those people represent a very small minority. But, it is probably large enough to make the route to a steady state on a national level long and painful. This unfortunately is to be expected in a country that was built on a framework of personal freedoms. The best you can hope for in achieving a steady state is to live in one of the states that seems to be achieving the fine balance between personal freedoms and the common good.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
As the COVID-19 pandemic continues to chug along, some communities feel it slowing to a pace at which they might feel comfortable about a return to, if not quite “business as usual,” at least “business as sort of normal-ish.” They are ready to accept a level of disease that signals they have reached a steady state. However, in other communities, the virus has picked up speed and is threatening to overwhelm the medical infrastructure. If you are in one of those fortunate and skillfully managed states in which folks are beginning to talk seriously, but with little evidence, that it is time to return to normal, it is probably far too early.
Eons ago in pandemic terms, the World Health Organization in Thailand published a list of criteria to aid in determining when a community could consider lifting the limits that seemed to have been effective in halting transmission of the virus (“Transitioning to and maintaining a steady state of low-level or no transmission,” WHO, Thailand, 2020 Apr 18). While much more has been learned about the behavior of the virus since the spring of 2020, the criteria from the WHO in Thailand are worth considering.
Here is my summary of their criteria for returning to normalcy. First, virus transmission is controlled to the point that only sporadic cases and small clusters exist, and that all of these are traceable in origin. Second, health care and public health systems are in place with sufficient capacities to manage a shift from detection to treatment should the case load increase dramatically; this capacity should include detection, testing, isolation, and quarantine. Third, outbreaks in high-risk populations such as nursing homes have been minimized. Fourth, workplace prevention strategies are in place and have been demonstrated to be effective. Fifth, risk of imported cases is at manageable levels. Finally, communities are engaged.
It is hard to argue with the rationale behind each of these criteria. However, the United States is not Thailand, and just thinking about how this country would go about meeting those criteria provides a window into some of the reasons why we have done so poorly and will continue to be challenged in dealing with the pandemic.
First, notice that the criteria make no mention of a vaccine. One gets the sense that from the top down our country is banking too heavily on the effectiveness and widespread delivery of a vaccine. Even if and when a vaccine is developed and delivered, all of these criteria still must be met and kept in mind for a future pandemic.
Second, the criteria call for an effective health care system, but it is abundantly clear that the United States does not have a cohesive health care system and probably won’t for the foreseeable future. The best we can hope for is individual states cobbling together their own systems, which may in turn serve as examples for those states who haven’t had the foresight. We have had a public health system of sorts, but its credibility and effectiveness has been neutered to the point that again we must rely on each state’s ability to see through the haze and create it’s own systems for detection, testing, tracking, isolating, and quarantining – often with little help in materiel support from the federal government. The sliver of good news is that, after a bit of a stumbling start, detecting and limiting the importation of cases from abroad is being addressed.
We continue to hear and see evidence that there are segments of the population who are not engaged in the activities that we have learned are necessary to stabilize the pandemic. My sense is that those people represent a very small minority. But, it is probably large enough to make the route to a steady state on a national level long and painful. This unfortunately is to be expected in a country that was built on a framework of personal freedoms. The best you can hope for in achieving a steady state is to live in one of the states that seems to be achieving the fine balance between personal freedoms and the common good.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
As the COVID-19 pandemic continues to chug along, some communities feel it slowing to a pace at which they might feel comfortable about a return to, if not quite “business as usual,” at least “business as sort of normal-ish.” They are ready to accept a level of disease that signals they have reached a steady state. However, in other communities, the virus has picked up speed and is threatening to overwhelm the medical infrastructure. If you are in one of those fortunate and skillfully managed states in which folks are beginning to talk seriously, but with little evidence, that it is time to return to normal, it is probably far too early.
Eons ago in pandemic terms, the World Health Organization in Thailand published a list of criteria to aid in determining when a community could consider lifting the limits that seemed to have been effective in halting transmission of the virus (“Transitioning to and maintaining a steady state of low-level or no transmission,” WHO, Thailand, 2020 Apr 18). While much more has been learned about the behavior of the virus since the spring of 2020, the criteria from the WHO in Thailand are worth considering.
Here is my summary of their criteria for returning to normalcy. First, virus transmission is controlled to the point that only sporadic cases and small clusters exist, and that all of these are traceable in origin. Second, health care and public health systems are in place with sufficient capacities to manage a shift from detection to treatment should the case load increase dramatically; this capacity should include detection, testing, isolation, and quarantine. Third, outbreaks in high-risk populations such as nursing homes have been minimized. Fourth, workplace prevention strategies are in place and have been demonstrated to be effective. Fifth, risk of imported cases is at manageable levels. Finally, communities are engaged.
It is hard to argue with the rationale behind each of these criteria. However, the United States is not Thailand, and just thinking about how this country would go about meeting those criteria provides a window into some of the reasons why we have done so poorly and will continue to be challenged in dealing with the pandemic.
First, notice that the criteria make no mention of a vaccine. One gets the sense that from the top down our country is banking too heavily on the effectiveness and widespread delivery of a vaccine. Even if and when a vaccine is developed and delivered, all of these criteria still must be met and kept in mind for a future pandemic.
Second, the criteria call for an effective health care system, but it is abundantly clear that the United States does not have a cohesive health care system and probably won’t for the foreseeable future. The best we can hope for is individual states cobbling together their own systems, which may in turn serve as examples for those states who haven’t had the foresight. We have had a public health system of sorts, but its credibility and effectiveness has been neutered to the point that again we must rely on each state’s ability to see through the haze and create it’s own systems for detection, testing, tracking, isolating, and quarantining – often with little help in materiel support from the federal government. The sliver of good news is that, after a bit of a stumbling start, detecting and limiting the importation of cases from abroad is being addressed.
We continue to hear and see evidence that there are segments of the population who are not engaged in the activities that we have learned are necessary to stabilize the pandemic. My sense is that those people represent a very small minority. But, it is probably large enough to make the route to a steady state on a national level long and painful. This unfortunately is to be expected in a country that was built on a framework of personal freedoms. The best you can hope for in achieving a steady state is to live in one of the states that seems to be achieving the fine balance between personal freedoms and the common good.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Mastering mask communicating
. For those specialties not accustomed to wearing a mask all day, it’s frustrating: How many times have you had to repeat yourself today? Or ask your patient to say something again? (Ain’t no one got time to repeat a third time how to do that prednisone taper). Worse, we’re losing important nonverbal cues that help us connect with our patients. How can we be understood when our faces are covered and 6 feet away?

Masks muffle both verbal and nonverbal communication. For soft-spoken or high-pitched speakers, the verbal effect is significant. In particular, masks make hearing consonants more difficult. They can make the “sh,” “th,” “f,” and “s” sounds difficult to distinguish. Typically, we’d use context and lip reading to boost the signal, but this fix is blocked (and the clear mouth-window masks are kinda creepy).
Masks also prevent us from seeing facial microexpressions, critical information when you are trying to connect with someone or to build trust. A randomized controlled trial published in 2013 indeed showed that doctors wearing a mask were perceived as less empathetic and had diminished relational continuity with patients as compared to doctors not wearing a mask. There are a few things we can do to help.
Speak more loudly is obvious advice. Loud talking has limitations though, as it can feel rude, and it blunts inflections, which add richness and emotion. (Shouting “THIS WILL ONLY HURT A LITTLE” seems a mixed message). More important than the volume is your choice of words. Try to use simple terms and short sentences. Pause between points. Hit your consonants harder.
It’s also important that you have their full attention and are giving yours. As much as possible, try to align squared up with patients. Facing your computer exacerbates the problem. Look them in their eyes and be sure they are connected with you before any complex or difficult conversations. Hearing-impaired patients are now sometimes leaving out their aids because it’s too uncomfortable to wear them with their mask. You might ask them to put them back in. Check in with patients and repeat back what you heard them say. This can help with clarity and with connecting. Use your face more: if you’ve ever acted on stage, this would be your on-stage face. Exaggerate your expressions so it’s a little easier for them to read you.
Lastly, there are apps such as Ava or Google Live Translator, which can transcribe your speech real time. You could then share your screen with the patient so they can read exactly what you’ve said.
Some of us are natural communicators. Even if you are not, you can mitigate some of our current challenges. I’ll admit, it’s been a bit easier for me than for others. Between my prominent eyebrows and Italian-American upbringing, I can express my way through pretty much any face covering. If you’d like to learn how to use your hands better, then just watch this little girl: https://youtu.be/Z5wAWyqDrnc.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
. For those specialties not accustomed to wearing a mask all day, it’s frustrating: How many times have you had to repeat yourself today? Or ask your patient to say something again? (Ain’t no one got time to repeat a third time how to do that prednisone taper). Worse, we’re losing important nonverbal cues that help us connect with our patients. How can we be understood when our faces are covered and 6 feet away?
Masks muffle both verbal and nonverbal communication. For soft-spoken or high-pitched speakers, the verbal effect is significant. In particular, masks make hearing consonants more difficult. They can make the “sh,” “th,” “f,” and “s” sounds difficult to distinguish. Typically, we’d use context and lip reading to boost the signal, but this fix is blocked (and the clear mouth-window masks are kinda creepy).
Masks also prevent us from seeing facial microexpressions, critical information when you are trying to connect with someone or to build trust. A randomized controlled trial published in 2013 indeed showed that doctors wearing a mask were perceived as less empathetic and had diminished relational continuity with patients as compared to doctors not wearing a mask. There are a few things we can do to help.
Speak more loudly is obvious advice. Loud talking has limitations though, as it can feel rude, and it blunts inflections, which add richness and emotion. (Shouting “THIS WILL ONLY HURT A LITTLE” seems a mixed message). More important than the volume is your choice of words. Try to use simple terms and short sentences. Pause between points. Hit your consonants harder.
It’s also important that you have their full attention and are giving yours. As much as possible, try to align squared up with patients. Facing your computer exacerbates the problem. Look them in their eyes and be sure they are connected with you before any complex or difficult conversations. Hearing-impaired patients are now sometimes leaving out their aids because it’s too uncomfortable to wear them with their mask. You might ask them to put them back in. Check in with patients and repeat back what you heard them say. This can help with clarity and with connecting. Use your face more: if you’ve ever acted on stage, this would be your on-stage face. Exaggerate your expressions so it’s a little easier for them to read you.
Lastly, there are apps such as Ava or Google Live Translator, which can transcribe your speech real time. You could then share your screen with the patient so they can read exactly what you’ve said.
Some of us are natural communicators. Even if you are not, you can mitigate some of our current challenges. I’ll admit, it’s been a bit easier for me than for others. Between my prominent eyebrows and Italian-American upbringing, I can express my way through pretty much any face covering. If you’d like to learn how to use your hands better, then just watch this little girl: https://youtu.be/Z5wAWyqDrnc.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
. For those specialties not accustomed to wearing a mask all day, it’s frustrating: How many times have you had to repeat yourself today? Or ask your patient to say something again? (Ain’t no one got time to repeat a third time how to do that prednisone taper). Worse, we’re losing important nonverbal cues that help us connect with our patients. How can we be understood when our faces are covered and 6 feet away?
Masks muffle both verbal and nonverbal communication. For soft-spoken or high-pitched speakers, the verbal effect is significant. In particular, masks make hearing consonants more difficult. They can make the “sh,” “th,” “f,” and “s” sounds difficult to distinguish. Typically, we’d use context and lip reading to boost the signal, but this fix is blocked (and the clear mouth-window masks are kinda creepy).
Masks also prevent us from seeing facial microexpressions, critical information when you are trying to connect with someone or to build trust. A randomized controlled trial published in 2013 indeed showed that doctors wearing a mask were perceived as less empathetic and had diminished relational continuity with patients as compared to doctors not wearing a mask. There are a few things we can do to help.
Speak more loudly is obvious advice. Loud talking has limitations though, as it can feel rude, and it blunts inflections, which add richness and emotion. (Shouting “THIS WILL ONLY HURT A LITTLE” seems a mixed message). More important than the volume is your choice of words. Try to use simple terms and short sentences. Pause between points. Hit your consonants harder.
It’s also important that you have their full attention and are giving yours. As much as possible, try to align squared up with patients. Facing your computer exacerbates the problem. Look them in their eyes and be sure they are connected with you before any complex or difficult conversations. Hearing-impaired patients are now sometimes leaving out their aids because it’s too uncomfortable to wear them with their mask. You might ask them to put them back in. Check in with patients and repeat back what you heard them say. This can help with clarity and with connecting. Use your face more: if you’ve ever acted on stage, this would be your on-stage face. Exaggerate your expressions so it’s a little easier for them to read you.
Lastly, there are apps such as Ava or Google Live Translator, which can transcribe your speech real time. You could then share your screen with the patient so they can read exactly what you’ve said.
Some of us are natural communicators. Even if you are not, you can mitigate some of our current challenges. I’ll admit, it’s been a bit easier for me than for others. Between my prominent eyebrows and Italian-American upbringing, I can express my way through pretty much any face covering. If you’d like to learn how to use your hands better, then just watch this little girl: https://youtu.be/Z5wAWyqDrnc.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Manners matter
Have you been surprised and impressed by a child who says after a visit, “Thank you, Doctor [Howard]”? While it may seem antiquated to teach such manners to children these days, there are several important benefits to this education.

Manners serve important functions in benefiting a person’s group with cohesiveness and the individuals themselves with acceptance in the group. Use of manners instantly suggests a more trustworthy person.
There are three main categories of manners: hygiene, courtesy, and cultural norm manners.
Hygiene manners, from using the toilet to refraining from picking one’s nose, have obvious health benefits of not spreading disease. Hygiene manners take time to teach, but parents are motivated and helped by natural reactions of disgust that even infants recognize.
Courtesy manners, on the other hand, are habits of self-control and good-faith behaviors that signal that one is putting the interests of others ahead of one’s own for the moment. Taking another’s comfort into account, basic to kindness and respect, does not require agreeing with or submitting to the other. Courtesy manners require a developing self-awareness (I can choose to act this way) and awareness of social status (I am not more important than everyone else) that begins in toddlerhood. Modeling manners around the child is the most important way to teach courtesy. Parents usually start actively teaching the child to say “please” and “thank you,” and show pride in this apparent “demonstration of appreciation” even when it is simply reinforced behavior at first. The delight of grandparents reinforces both the parents and children, and reflects manners as building tribe cohesiveness.
Good manners become a habit
Manners such as warm greetings, a firm handshake (before COVID-19), and prompt thanks are most believable when occurring promptly when appropriate – when they come from habit. This immediate reaction, a result of so-called “fast thinking,” develops when behaviors learned from “slow thinking” are instilled early and often until they are automatic. The other benefit of this overlearning is that the behavior then looks unambivalent; a lag of too many milliseconds makes the recipient doubt genuineness.
Parents often ask us how to handle their child‘s rude or disrespectful behavior. Praise for manners is a simple start. Toddlers and preschoolers are taught manners best by adult modeling, but also by reinforcement and praise for the basics: to say “Hello,” ask “Please,” and say “Thank you,” “Excuse me,” “You’re welcome,” or “Would you help me, please?” The behaviors also include avoiding raising one’s voice, suppressing interrupting, and apologizing when appropriate. Even shy children can learn eye contact by making a game of figuring out the other’s eye color. Shaming, yelling, and punishing for poor manners usually backfires because it shows disrespect of the child who will likely give this back.
Older children can be taught to offer other people the opportunity to go through a door first, to be first to select a seat, speak first and without interruption, or order first. There are daily opportunities for these manners of showing respect. Opening doors for others, or standing when a guest enters the room are more formal but still appreciated. Parents who use and expect courtesy manners with everyone – irrespective of gender, race, ethnicity, or role as a server versus professional – show that they value others and build antiracism.

School age is a time to learn to wait before speaking to consider whether what they say could be experienced as hurtful to the other person. This requires taking someone else’s point of view, an ability that emerges around age 6 years and can be promoted when parents review with their child “How would you feel if it were you?” Role playing common scenarios of how to behave and speak when seeing a person who looks or acts different is also effective. Avoiding interrupting may be more difficult for very talkative or impulsive children, especially those with ADHD. Practicing waiting for permission to speak by being handed a “talking stick” at the dinner table can be good practice for everyone.
Manners are a group asset
Beyond personal benefits, manners are the basis of a civil society. Cultural norm manners are particular to groups, helping members feel affiliated, as well as identifying those with different manners as “other.”
Teens are particularly likely to use a different code of behavior to fit in with a subgroup. This may be acceptable if restricted to within their group (such as swear words) or within certain agreed-upon limits with family members. But teens need to understand the value of learning, practicing, and using manners for their own, as well as their group’s and nation’s, well-being.
As a developmental-behavioral pediatrician, I have cared for many children with intellectual disabilities and autism spectrum disorder (ASD). Deficits in social interaction skills are a basic criterion for the diagnosis of ASD. Overtraining is especially needed for children with ASD whose mirror movements, social attention, and imitation are weak. For children with these conditions, making manners a strong habit takes more effort but is even more vital than for neurotypical children. Temple Grandin, a famous adult with ASD, has described how her mother taught her manners as a survival skill. She reports incorporating manners very consciously and methodically because they did not come naturally. Children with even rote social skills are liked better by peers and teachers, their atypical behaviors is better tolerated, and they get more positive feedback that encourages integration inside and outside the classroom. Manners may make the difference between being allowed in or expelled from classrooms, libraries, clubs, teams, or religious institutions. When it is time to get a job, social skills are the key factor for employment for these individuals and a significant help for neurotypical individuals as well. Failure to signal socially appropriate behavior can make a person appear threatening and has had the rare but tragic result of rough or fatal handling by police.
Has the teaching of manners waned? Perhaps, because, for some families, the child is being socialized mostly by nonfamily caregivers who have low use of manners. Some parents have made teaching manners a low priority or even resisted using manners themselves as inauthentic. This may reflect prioritizing a “laid-back” lifestyle and speaking crudely as a sign of independence, perhaps in reaction to lack of autonomy at work. Mastering the careful interactions developed over time to avoid invoking an aggressive response depend on direct feedback from reactions of the recipient. With so much of our communication done electronically, asynchronously, even anonymously, the usual feedback has been reduced. Practicing curses, insults, and put-downs online easily extends to in-person interactions without the perpetrator even noticing and are generally reinforced and repeated without parental supervision. Disrespectful behavior from community leaders also reduces the threshold for society.
When people are ignorant of or choose not to use manners they may be perceived as “other” and hostile. This may lead to distrust, dislike, and lowered ability to find the common ground needed for making decisions that benefit the greater society. Oliver Wendell Holmes said “Under bad manners ... lies very commonly an overestimate of our special individuality, as distinguished from our generic humanity (“The Professor at the Breakfast Table,” 1858). Working for major goals that benefit all of humanity is essential to survival in our highly interconnected world. Considering all of humanity is a difficult concept for children, and even for many adults, but it starts with using civil behavior at home, in school, and in one’s community.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
Have you been surprised and impressed by a child who says after a visit, “Thank you, Doctor [Howard]”? While it may seem antiquated to teach such manners to children these days, there are several important benefits to this education.
Manners serve important functions in benefiting a person’s group with cohesiveness and the individuals themselves with acceptance in the group. Use of manners instantly suggests a more trustworthy person.
There are three main categories of manners: hygiene, courtesy, and cultural norm manners.
Hygiene manners, from using the toilet to refraining from picking one’s nose, have obvious health benefits of not spreading disease. Hygiene manners take time to teach, but parents are motivated and helped by natural reactions of disgust that even infants recognize.
Courtesy manners, on the other hand, are habits of self-control and good-faith behaviors that signal that one is putting the interests of others ahead of one’s own for the moment. Taking another’s comfort into account, basic to kindness and respect, does not require agreeing with or submitting to the other. Courtesy manners require a developing self-awareness (I can choose to act this way) and awareness of social status (I am not more important than everyone else) that begins in toddlerhood. Modeling manners around the child is the most important way to teach courtesy. Parents usually start actively teaching the child to say “please” and “thank you,” and show pride in this apparent “demonstration of appreciation” even when it is simply reinforced behavior at first. The delight of grandparents reinforces both the parents and children, and reflects manners as building tribe cohesiveness.
Good manners become a habit
Manners such as warm greetings, a firm handshake (before COVID-19), and prompt thanks are most believable when occurring promptly when appropriate – when they come from habit. This immediate reaction, a result of so-called “fast thinking,” develops when behaviors learned from “slow thinking” are instilled early and often until they are automatic. The other benefit of this overlearning is that the behavior then looks unambivalent; a lag of too many milliseconds makes the recipient doubt genuineness.
Parents often ask us how to handle their child‘s rude or disrespectful behavior. Praise for manners is a simple start. Toddlers and preschoolers are taught manners best by adult modeling, but also by reinforcement and praise for the basics: to say “Hello,” ask “Please,” and say “Thank you,” “Excuse me,” “You’re welcome,” or “Would you help me, please?” The behaviors also include avoiding raising one’s voice, suppressing interrupting, and apologizing when appropriate. Even shy children can learn eye contact by making a game of figuring out the other’s eye color. Shaming, yelling, and punishing for poor manners usually backfires because it shows disrespect of the child who will likely give this back.
Older children can be taught to offer other people the opportunity to go through a door first, to be first to select a seat, speak first and without interruption, or order first. There are daily opportunities for these manners of showing respect. Opening doors for others, or standing when a guest enters the room are more formal but still appreciated. Parents who use and expect courtesy manners with everyone – irrespective of gender, race, ethnicity, or role as a server versus professional – show that they value others and build antiracism.
School age is a time to learn to wait before speaking to consider whether what they say could be experienced as hurtful to the other person. This requires taking someone else’s point of view, an ability that emerges around age 6 years and can be promoted when parents review with their child “How would you feel if it were you?” Role playing common scenarios of how to behave and speak when seeing a person who looks or acts different is also effective. Avoiding interrupting may be more difficult for very talkative or impulsive children, especially those with ADHD. Practicing waiting for permission to speak by being handed a “talking stick” at the dinner table can be good practice for everyone.
Manners are a group asset
Beyond personal benefits, manners are the basis of a civil society. Cultural norm manners are particular to groups, helping members feel affiliated, as well as identifying those with different manners as “other.”
Teens are particularly likely to use a different code of behavior to fit in with a subgroup. This may be acceptable if restricted to within their group (such as swear words) or within certain agreed-upon limits with family members. But teens need to understand the value of learning, practicing, and using manners for their own, as well as their group’s and nation’s, well-being.
As a developmental-behavioral pediatrician, I have cared for many children with intellectual disabilities and autism spectrum disorder (ASD). Deficits in social interaction skills are a basic criterion for the diagnosis of ASD. Overtraining is especially needed for children with ASD whose mirror movements, social attention, and imitation are weak. For children with these conditions, making manners a strong habit takes more effort but is even more vital than for neurotypical children. Temple Grandin, a famous adult with ASD, has described how her mother taught her manners as a survival skill. She reports incorporating manners very consciously and methodically because they did not come naturally. Children with even rote social skills are liked better by peers and teachers, their atypical behaviors is better tolerated, and they get more positive feedback that encourages integration inside and outside the classroom. Manners may make the difference between being allowed in or expelled from classrooms, libraries, clubs, teams, or religious institutions. When it is time to get a job, social skills are the key factor for employment for these individuals and a significant help for neurotypical individuals as well. Failure to signal socially appropriate behavior can make a person appear threatening and has had the rare but tragic result of rough or fatal handling by police.
Has the teaching of manners waned? Perhaps, because, for some families, the child is being socialized mostly by nonfamily caregivers who have low use of manners. Some parents have made teaching manners a low priority or even resisted using manners themselves as inauthentic. This may reflect prioritizing a “laid-back” lifestyle and speaking crudely as a sign of independence, perhaps in reaction to lack of autonomy at work. Mastering the careful interactions developed over time to avoid invoking an aggressive response depend on direct feedback from reactions of the recipient. With so much of our communication done electronically, asynchronously, even anonymously, the usual feedback has been reduced. Practicing curses, insults, and put-downs online easily extends to in-person interactions without the perpetrator even noticing and are generally reinforced and repeated without parental supervision. Disrespectful behavior from community leaders also reduces the threshold for society.
When people are ignorant of or choose not to use manners they may be perceived as “other” and hostile. This may lead to distrust, dislike, and lowered ability to find the common ground needed for making decisions that benefit the greater society. Oliver Wendell Holmes said “Under bad manners ... lies very commonly an overestimate of our special individuality, as distinguished from our generic humanity (“The Professor at the Breakfast Table,” 1858). Working for major goals that benefit all of humanity is essential to survival in our highly interconnected world. Considering all of humanity is a difficult concept for children, and even for many adults, but it starts with using civil behavior at home, in school, and in one’s community.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
Have you been surprised and impressed by a child who says after a visit, “Thank you, Doctor [Howard]”? While it may seem antiquated to teach such manners to children these days, there are several important benefits to this education.
Manners serve important functions in benefiting a person’s group with cohesiveness and the individuals themselves with acceptance in the group. Use of manners instantly suggests a more trustworthy person.
There are three main categories of manners: hygiene, courtesy, and cultural norm manners.
Hygiene manners, from using the toilet to refraining from picking one’s nose, have obvious health benefits of not spreading disease. Hygiene manners take time to teach, but parents are motivated and helped by natural reactions of disgust that even infants recognize.
Courtesy manners, on the other hand, are habits of self-control and good-faith behaviors that signal that one is putting the interests of others ahead of one’s own for the moment. Taking another’s comfort into account, basic to kindness and respect, does not require agreeing with or submitting to the other. Courtesy manners require a developing self-awareness (I can choose to act this way) and awareness of social status (I am not more important than everyone else) that begins in toddlerhood. Modeling manners around the child is the most important way to teach courtesy. Parents usually start actively teaching the child to say “please” and “thank you,” and show pride in this apparent “demonstration of appreciation” even when it is simply reinforced behavior at first. The delight of grandparents reinforces both the parents and children, and reflects manners as building tribe cohesiveness.
Good manners become a habit
Manners such as warm greetings, a firm handshake (before COVID-19), and prompt thanks are most believable when occurring promptly when appropriate – when they come from habit. This immediate reaction, a result of so-called “fast thinking,” develops when behaviors learned from “slow thinking” are instilled early and often until they are automatic. The other benefit of this overlearning is that the behavior then looks unambivalent; a lag of too many milliseconds makes the recipient doubt genuineness.
Parents often ask us how to handle their child‘s rude or disrespectful behavior. Praise for manners is a simple start. Toddlers and preschoolers are taught manners best by adult modeling, but also by reinforcement and praise for the basics: to say “Hello,” ask “Please,” and say “Thank you,” “Excuse me,” “You’re welcome,” or “Would you help me, please?” The behaviors also include avoiding raising one’s voice, suppressing interrupting, and apologizing when appropriate. Even shy children can learn eye contact by making a game of figuring out the other’s eye color. Shaming, yelling, and punishing for poor manners usually backfires because it shows disrespect of the child who will likely give this back.
Older children can be taught to offer other people the opportunity to go through a door first, to be first to select a seat, speak first and without interruption, or order first. There are daily opportunities for these manners of showing respect. Opening doors for others, or standing when a guest enters the room are more formal but still appreciated. Parents who use and expect courtesy manners with everyone – irrespective of gender, race, ethnicity, or role as a server versus professional – show that they value others and build antiracism.
School age is a time to learn to wait before speaking to consider whether what they say could be experienced as hurtful to the other person. This requires taking someone else’s point of view, an ability that emerges around age 6 years and can be promoted when parents review with their child “How would you feel if it were you?” Role playing common scenarios of how to behave and speak when seeing a person who looks or acts different is also effective. Avoiding interrupting may be more difficult for very talkative or impulsive children, especially those with ADHD. Practicing waiting for permission to speak by being handed a “talking stick” at the dinner table can be good practice for everyone.
Manners are a group asset
Beyond personal benefits, manners are the basis of a civil society. Cultural norm manners are particular to groups, helping members feel affiliated, as well as identifying those with different manners as “other.”
Teens are particularly likely to use a different code of behavior to fit in with a subgroup. This may be acceptable if restricted to within their group (such as swear words) or within certain agreed-upon limits with family members. But teens need to understand the value of learning, practicing, and using manners for their own, as well as their group’s and nation’s, well-being.
As a developmental-behavioral pediatrician, I have cared for many children with intellectual disabilities and autism spectrum disorder (ASD). Deficits in social interaction skills are a basic criterion for the diagnosis of ASD. Overtraining is especially needed for children with ASD whose mirror movements, social attention, and imitation are weak. For children with these conditions, making manners a strong habit takes more effort but is even more vital than for neurotypical children. Temple Grandin, a famous adult with ASD, has described how her mother taught her manners as a survival skill. She reports incorporating manners very consciously and methodically because they did not come naturally. Children with even rote social skills are liked better by peers and teachers, their atypical behaviors is better tolerated, and they get more positive feedback that encourages integration inside and outside the classroom. Manners may make the difference between being allowed in or expelled from classrooms, libraries, clubs, teams, or religious institutions. When it is time to get a job, social skills are the key factor for employment for these individuals and a significant help for neurotypical individuals as well. Failure to signal socially appropriate behavior can make a person appear threatening and has had the rare but tragic result of rough or fatal handling by police.
Has the teaching of manners waned? Perhaps, because, for some families, the child is being socialized mostly by nonfamily caregivers who have low use of manners. Some parents have made teaching manners a low priority or even resisted using manners themselves as inauthentic. This may reflect prioritizing a “laid-back” lifestyle and speaking crudely as a sign of independence, perhaps in reaction to lack of autonomy at work. Mastering the careful interactions developed over time to avoid invoking an aggressive response depend on direct feedback from reactions of the recipient. With so much of our communication done electronically, asynchronously, even anonymously, the usual feedback has been reduced. Practicing curses, insults, and put-downs online easily extends to in-person interactions without the perpetrator even noticing and are generally reinforced and repeated without parental supervision. Disrespectful behavior from community leaders also reduces the threshold for society.
When people are ignorant of or choose not to use manners they may be perceived as “other” and hostile. This may lead to distrust, dislike, and lowered ability to find the common ground needed for making decisions that benefit the greater society. Oliver Wendell Holmes said “Under bad manners ... lies very commonly an overestimate of our special individuality, as distinguished from our generic humanity (“The Professor at the Breakfast Table,” 1858). Working for major goals that benefit all of humanity is essential to survival in our highly interconnected world. Considering all of humanity is a difficult concept for children, and even for many adults, but it starts with using civil behavior at home, in school, and in one’s community.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.