User login
New guidelines on MRI use in patients with MS explained
MS affects approximately one million people in the United States. As family physicians, these guidelines are important to know, because we are often the ones who make the initial diagnosis of MS. Similarly, if we order the wrong imaging study, we can miss making an accurate diagnosis.

The new guidelines (MAGNIMS), which were sponsored by the Consortium of Multiple Sclerosis Centres, were published in August. The documents offers detailed guidance on the use of standardized MRI protocols as well as the use of IV gadolinium contrast agents, including in children and pregnant patients.
It is advised to use 3-D techniques (as opposed to two-dimensional) and it is noted that this is becoming more clinically available. Sagittal 3-D T2-weighted fluid-attenuated inversion recovery (FLAIR) is the core sequence considered for MS diagnosis and monitoring because of its high sensitivity. High-quality 2-D pulse sequences can be used alternatively when 3-D FLAIR is not available.
When 3 T scanners are not available, 1.5 T scanners are sufficient. However, 3 T scanners do have a higher detection rate for MS lesions. In evaluating the imaging, T2 lesion counts, gadolinium lesion counts, and interval changes should be reported.
The use of GBCAs (gadolinium-based contrast agents) is needed to diagnose MS and rule out other diseases. The time between injection of contrast should ideally be 10 minutes but no less than 5. Optic nerve MRI is recommended only in patients with atypical symptoms, such as new visual symptoms. Spinal cord MRI is also not routinely advised unless it is needed for prognosis.
When the initial MRI does not meet the full criteria of MS, brain MRI should be repeated every 6-12 months in suspected cases. The same modality should be used each time. After treatment is started, it is recommended to perform MRI without GBCAs for 3 months and annual follow ups. The use of GBCAs-free MRIs for routine follow up is a new recommendation compared to previous ones. However, if the use of GBCAs would change the management, then they should be utilized for monitoring.
The same imaging standards are recommended in pediatric patients. Spinal cord MRI should be utilized in kids with spinal cord symptoms or inconclusive brain MRI. Similar scan frequency is recommended as in adults. MRI is not contraindicated during pregnancy but should be decided on an individual basis. Standard protocols should be used as well as a magnetic field strength of 1.5 T. GBCAs should not be used during pregnancy. There are no limitations in the postpartum period.
The complete set of guidelines is quite extensive and adds to the previous guidelines published in 2017. They were first published in The Lancet Neurology.
While most of these patients will be referred to neurologists, as the primary care physician it is our responsibility to know all aspects of our patients’ diseases and treatments. While we may not be actively treating MS in these patients, we need to know their medications, how they interact with others, and how their disease is progressing
Additionally, we may be the ones asked to order MRIs for monitoring. It is imperative that we know the guidelines for how to do this.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.
MS affects approximately one million people in the United States. As family physicians, these guidelines are important to know, because we are often the ones who make the initial diagnosis of MS. Similarly, if we order the wrong imaging study, we can miss making an accurate diagnosis.
The new guidelines (MAGNIMS), which were sponsored by the Consortium of Multiple Sclerosis Centres, were published in August. The documents offers detailed guidance on the use of standardized MRI protocols as well as the use of IV gadolinium contrast agents, including in children and pregnant patients.
It is advised to use 3-D techniques (as opposed to two-dimensional) and it is noted that this is becoming more clinically available. Sagittal 3-D T2-weighted fluid-attenuated inversion recovery (FLAIR) is the core sequence considered for MS diagnosis and monitoring because of its high sensitivity. High-quality 2-D pulse sequences can be used alternatively when 3-D FLAIR is not available.
When 3 T scanners are not available, 1.5 T scanners are sufficient. However, 3 T scanners do have a higher detection rate for MS lesions. In evaluating the imaging, T2 lesion counts, gadolinium lesion counts, and interval changes should be reported.
The use of GBCAs (gadolinium-based contrast agents) is needed to diagnose MS and rule out other diseases. The time between injection of contrast should ideally be 10 minutes but no less than 5. Optic nerve MRI is recommended only in patients with atypical symptoms, such as new visual symptoms. Spinal cord MRI is also not routinely advised unless it is needed for prognosis.
When the initial MRI does not meet the full criteria of MS, brain MRI should be repeated every 6-12 months in suspected cases. The same modality should be used each time. After treatment is started, it is recommended to perform MRI without GBCAs for 3 months and annual follow ups. The use of GBCAs-free MRIs for routine follow up is a new recommendation compared to previous ones. However, if the use of GBCAs would change the management, then they should be utilized for monitoring.
The same imaging standards are recommended in pediatric patients. Spinal cord MRI should be utilized in kids with spinal cord symptoms or inconclusive brain MRI. Similar scan frequency is recommended as in adults. MRI is not contraindicated during pregnancy but should be decided on an individual basis. Standard protocols should be used as well as a magnetic field strength of 1.5 T. GBCAs should not be used during pregnancy. There are no limitations in the postpartum period.
The complete set of guidelines is quite extensive and adds to the previous guidelines published in 2017. They were first published in The Lancet Neurology.
While most of these patients will be referred to neurologists, as the primary care physician it is our responsibility to know all aspects of our patients’ diseases and treatments. While we may not be actively treating MS in these patients, we need to know their medications, how they interact with others, and how their disease is progressing
Additionally, we may be the ones asked to order MRIs for monitoring. It is imperative that we know the guidelines for how to do this.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.
MS affects approximately one million people in the United States. As family physicians, these guidelines are important to know, because we are often the ones who make the initial diagnosis of MS. Similarly, if we order the wrong imaging study, we can miss making an accurate diagnosis.
The new guidelines (MAGNIMS), which were sponsored by the Consortium of Multiple Sclerosis Centres, were published in August. The documents offers detailed guidance on the use of standardized MRI protocols as well as the use of IV gadolinium contrast agents, including in children and pregnant patients.
It is advised to use 3-D techniques (as opposed to two-dimensional) and it is noted that this is becoming more clinically available. Sagittal 3-D T2-weighted fluid-attenuated inversion recovery (FLAIR) is the core sequence considered for MS diagnosis and monitoring because of its high sensitivity. High-quality 2-D pulse sequences can be used alternatively when 3-D FLAIR is not available.
When 3 T scanners are not available, 1.5 T scanners are sufficient. However, 3 T scanners do have a higher detection rate for MS lesions. In evaluating the imaging, T2 lesion counts, gadolinium lesion counts, and interval changes should be reported.
The use of GBCAs (gadolinium-based contrast agents) is needed to diagnose MS and rule out other diseases. The time between injection of contrast should ideally be 10 minutes but no less than 5. Optic nerve MRI is recommended only in patients with atypical symptoms, such as new visual symptoms. Spinal cord MRI is also not routinely advised unless it is needed for prognosis.
When the initial MRI does not meet the full criteria of MS, brain MRI should be repeated every 6-12 months in suspected cases. The same modality should be used each time. After treatment is started, it is recommended to perform MRI without GBCAs for 3 months and annual follow ups. The use of GBCAs-free MRIs for routine follow up is a new recommendation compared to previous ones. However, if the use of GBCAs would change the management, then they should be utilized for monitoring.
The same imaging standards are recommended in pediatric patients. Spinal cord MRI should be utilized in kids with spinal cord symptoms or inconclusive brain MRI. Similar scan frequency is recommended as in adults. MRI is not contraindicated during pregnancy but should be decided on an individual basis. Standard protocols should be used as well as a magnetic field strength of 1.5 T. GBCAs should not be used during pregnancy. There are no limitations in the postpartum period.
The complete set of guidelines is quite extensive and adds to the previous guidelines published in 2017. They were first published in The Lancet Neurology.
While most of these patients will be referred to neurologists, as the primary care physician it is our responsibility to know all aspects of our patients’ diseases and treatments. While we may not be actively treating MS in these patients, we need to know their medications, how they interact with others, and how their disease is progressing
Additionally, we may be the ones asked to order MRIs for monitoring. It is imperative that we know the guidelines for how to do this.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.
Filling opioid prescriptions akin to a Sisyphean task
Pain management is a huge part of how we in palliative care help patients – and most of the time, I think we do it well, but in the regulatory environment of the opioid epidemic,
A patient – let’s call her Joan – calls me in distress. She is a 62-year-old woman with widespread metastatic breast cancer. Her pain is mainly due to bone metastases, but she also has discomfort due to the cancer’s invasion of the thin membranes that line her lungs and abdomen.
She was started on a combination opioid and acetaminophen tablet about 2 months ago by her oncologist, but is now requiring it around the clock, nearing the ceiling dose for this particular medication.
Given that her pain is escalating, Joan and I discuss starting a long-acting opioid to better manage the peak and trough effect of short-acting opioids, which can make a patient feel that the pain is relieved only for a few hours at a time, with sharp spikes throughout the day that mandate the next dose of short-acting opioid. This tethers the patient to the clock, having to take as many as six or eight doses of medication per day, and can be very disruptive to daily life.

I send an e-prescription for the same opioid Joan’s currently taking, but in a long-acting format that will slow-release over 8-10 hours, relieving her of the need to take a medication every 3-4 hours. I have learned over the years that nearly every long-acting opioid automatically generates a prior authorization request from the patient’s insurance company and so I immediately email our prior authorization team to submit to Joan’s insurance right away to avoid this extra delay.
Our prior authorization team is exceptionally responsive and submits these requests with urgency every time – they understand that cancer pain is a serious problem and we can’t wait 5 business days for answers. They are typically able to obtain an approved prior authorization for nearly every long-acting opioid I write within 24-48 hours.
But here’s where things go sideways.
First, the insurance company denies the prior authorization request, demanding that I revise the prescription from the long-acting version of the opioid she is currently taking to a cheaper, older opioid that she’s never tried before. In other words, they won’t cover the drug I requested without Joan first trying a completely different drug and failing it. This only makes sense for the insurance company’s bottom line – it makes no clinical sense at all. Why would I try a novel compound that Joan’s never had and one to which I have no idea how she’ll respond when I could keep her on the same compound knowing that she tolerates it just fine?
Past experience tells me insurance companies rarely budge on this, and appealing the decision would just introduce even more delay of care, so I begrudgingly change the prescription and send it again to the pharmacy. I message Joan to let her know that her insurance won’t cover my drug of choice and that we have to try this older one first.
A few hours later, Joan sends me a message: “My pharmacy says it’s going to take A WEEK to get the long-acting medicine!”
In the meantime, Joan has been using her short-acting opioid faster than anticipated because of her escalating pain – so she’s now running low on that as well.
I write for more of her short-acting opioid and e-script it to her pharmacy.
Within a few hours, we get another automatic response from her insurance that we’re going to need a prior authorization for additional short-acting opioid because she’s exceeded “quantity limitations,” which as far as I can tell is a completely arbitrary number not based on clinical evidence.
The prior auth team jumps on it and submits to override the quantity limit – successfully – and sends the override code to her pharmacy to reprocess the prescription.
But now the pharmacist tells Joan that they won’t fill the Rx anyway because it’s “too early.” They tell her that “state laws” prevent them from filling the scrip.
Is this true? I have no idea. I’m not an expert on California pharmacy law. All I know is that my patient is in pain and something needs to happen quickly.
I write for a second short-acting opioid – again a completely different compound. Ironically, this Rx goes through instantly without need for prior authorization. But now Joan has to switch to another new drug for no good medical reason.
If you’re still with me this far into the weeds, I’m grateful. In all it took a combined 4 hours of work (between myself and the prior auth team) to get two opioid Rx’s filled – and these were completely different medications than the ones I originally wrote for. I also had to move her prescriptions to the hospital’s pharmacy (another inconvenience for Joan and her family) so that she could get the medications in a timely manner. All this work to ensure that a single patient had adequate and timely pain relief and to prevent her from having to make an unnecessary visit to the emergency department for pain crisis.
This is just a regular day in outpatient palliative care in the era of the opioid epidemic.
The epidemic has caused tremendous pain and suffering for millions of people over the past 2 decades – namely those lost to opioid overdoses and their loved ones. And for the most part, tightening access to opioids for routine aches and pains among a relatively healthy population is not wrong, in my opinion, as long as those restrictions are based in good faith on robust evidence.
But the hidden cost of the Centers for Disease Control and Prevention’s 2016 opioid prescribing guidelines for nonmalignant pain, as well as the flurry of restrictive state laws they generated, is felt every day by patients with serious illness even though the guidelines were never meant to affect them. Patients with active cancer, receiving palliative care services, or at the end of life, were supposed to be exempted from these guidelines since good evidence supports the use of opioids in these populations.
Instead of preserving access to desperately needed pain medicine for those suffering with serious illness, states and insurers have aggressively sought to gatekeep opioids from everyone, resulting in stigma, delays, and needless suffering.
Several recent studies have revealed the effects of this gatekeeping on patients with cancer.
A qualitative study with 26 advanced cancer patients described the demoralization and stigma many patients felt when taking opioids, which they directly tied to media messaging around the opioid epidemic. Even when they reluctantly agreed to take opioids to treat cancer-related pain, there were systemic impediments to achieving adequate pain relief – similar to my experience with Joan – that were directly caused by insurance and pharmacy constraints.
Those of us who care for oncology patients also appear to be undertreating cancer-related pain. Another recent study that found the amount of opioid medications prescribed to an advanced cancer patient near the end of life dropped by 38% between 2007 and 2017. The authors suggest that a direct consequence of this decline in appropriate opioid prescribing is an observed 50% rise in emergency department visits over the same time period by cancer patients for pain-related reasons.
This makes sense – if patients aren’t routinely prescribed the opioids they need to manage their cancer-related pain; or, if the stigma against using opioids is so harsh that it causes patients to shun opioids; or, if there are so many system barriers in place to prevent patients from obtaining opioids in a timely manner – then patients’ pain will crescendo, leaving them with little alternative but to head to the emergency department.
This undertreatment is corroborated by another study that examined data from the Centers for Medicare & Medicaid Services Part D prescriber database between 2013 and 2017, finding that both oncologists and nononcologists prescribed about 21% fewer opioids to Medicare beneficiaries during that time, compared with the period prior to 2013.
Interestingly, the researchers also found that opioid prescribing by palliative care providers increased by 15% over the same period. On a positive note, this suggests the presence of a growing outpatient palliative care workforce. But it may also reflect growing unease among oncologists with the perceived liability for prescribing opioids and a desire to ask other specialists to take on this liability. At the same time, it may reflect the very real and ever-increasing administrative burden associated with prescribing opioids and the fact that busy oncologists may not have time to spend on this aspect of cancer care. Thus, as palliative care clinicians become more visible and numerous in the outpatient arena, oncologists may increasingly ask palliative care clinicians like myself to take this on.
The problem with this is that merely handing off the administrative burden to another clinician doesn’t address the underlying problem. Anecdotal evidence suggests (and my own experiences corroborate) this administrative burden can cause real harm. A survey of 1,000 physicians conducted by the American Medical Association in 2021 found that 93% of respondents reported a delay in patient care due to prior authorization burden and 34% of respondents reported that their patients had suffered a “serious adverse event” due to prior authorization requirements.
The CDC recently announced it will take steps to revise the 2016 opioid prescribing guidelines for chronic pain after hearing from members of the medical community as well as patients living with chronic pain about the harsh, unintended consequences of the guidelines. I can only hope that insurance companies will follow suit, revising their opioid prior authorization requirements to finally come into alignment with the rational, safe use of opioids in patients with advanced cancer. It’s too bad that any improvement in the future will be too late for the millions of patients who have suffered irreversible iatrogenic harms due to delays in achieving adequate pain relief.
Sarah F. D’Ambruoso, NP, is a palliative care nurse practitioner in Santa Monica, Calif.
Pain management is a huge part of how we in palliative care help patients – and most of the time, I think we do it well, but in the regulatory environment of the opioid epidemic,
A patient – let’s call her Joan – calls me in distress. She is a 62-year-old woman with widespread metastatic breast cancer. Her pain is mainly due to bone metastases, but she also has discomfort due to the cancer’s invasion of the thin membranes that line her lungs and abdomen.
She was started on a combination opioid and acetaminophen tablet about 2 months ago by her oncologist, but is now requiring it around the clock, nearing the ceiling dose for this particular medication.
Given that her pain is escalating, Joan and I discuss starting a long-acting opioid to better manage the peak and trough effect of short-acting opioids, which can make a patient feel that the pain is relieved only for a few hours at a time, with sharp spikes throughout the day that mandate the next dose of short-acting opioid. This tethers the patient to the clock, having to take as many as six or eight doses of medication per day, and can be very disruptive to daily life.
I send an e-prescription for the same opioid Joan’s currently taking, but in a long-acting format that will slow-release over 8-10 hours, relieving her of the need to take a medication every 3-4 hours. I have learned over the years that nearly every long-acting opioid automatically generates a prior authorization request from the patient’s insurance company and so I immediately email our prior authorization team to submit to Joan’s insurance right away to avoid this extra delay.
Our prior authorization team is exceptionally responsive and submits these requests with urgency every time – they understand that cancer pain is a serious problem and we can’t wait 5 business days for answers. They are typically able to obtain an approved prior authorization for nearly every long-acting opioid I write within 24-48 hours.
But here’s where things go sideways.
First, the insurance company denies the prior authorization request, demanding that I revise the prescription from the long-acting version of the opioid she is currently taking to a cheaper, older opioid that she’s never tried before. In other words, they won’t cover the drug I requested without Joan first trying a completely different drug and failing it. This only makes sense for the insurance company’s bottom line – it makes no clinical sense at all. Why would I try a novel compound that Joan’s never had and one to which I have no idea how she’ll respond when I could keep her on the same compound knowing that she tolerates it just fine?
Past experience tells me insurance companies rarely budge on this, and appealing the decision would just introduce even more delay of care, so I begrudgingly change the prescription and send it again to the pharmacy. I message Joan to let her know that her insurance won’t cover my drug of choice and that we have to try this older one first.
A few hours later, Joan sends me a message: “My pharmacy says it’s going to take A WEEK to get the long-acting medicine!”
In the meantime, Joan has been using her short-acting opioid faster than anticipated because of her escalating pain – so she’s now running low on that as well.
I write for more of her short-acting opioid and e-script it to her pharmacy.
Within a few hours, we get another automatic response from her insurance that we’re going to need a prior authorization for additional short-acting opioid because she’s exceeded “quantity limitations,” which as far as I can tell is a completely arbitrary number not based on clinical evidence.
The prior auth team jumps on it and submits to override the quantity limit – successfully – and sends the override code to her pharmacy to reprocess the prescription.
But now the pharmacist tells Joan that they won’t fill the Rx anyway because it’s “too early.” They tell her that “state laws” prevent them from filling the scrip.
Is this true? I have no idea. I’m not an expert on California pharmacy law. All I know is that my patient is in pain and something needs to happen quickly.
I write for a second short-acting opioid – again a completely different compound. Ironically, this Rx goes through instantly without need for prior authorization. But now Joan has to switch to another new drug for no good medical reason.
If you’re still with me this far into the weeds, I’m grateful. In all it took a combined 4 hours of work (between myself and the prior auth team) to get two opioid Rx’s filled – and these were completely different medications than the ones I originally wrote for. I also had to move her prescriptions to the hospital’s pharmacy (another inconvenience for Joan and her family) so that she could get the medications in a timely manner. All this work to ensure that a single patient had adequate and timely pain relief and to prevent her from having to make an unnecessary visit to the emergency department for pain crisis.
This is just a regular day in outpatient palliative care in the era of the opioid epidemic.
The epidemic has caused tremendous pain and suffering for millions of people over the past 2 decades – namely those lost to opioid overdoses and their loved ones. And for the most part, tightening access to opioids for routine aches and pains among a relatively healthy population is not wrong, in my opinion, as long as those restrictions are based in good faith on robust evidence.
But the hidden cost of the Centers for Disease Control and Prevention’s 2016 opioid prescribing guidelines for nonmalignant pain, as well as the flurry of restrictive state laws they generated, is felt every day by patients with serious illness even though the guidelines were never meant to affect them. Patients with active cancer, receiving palliative care services, or at the end of life, were supposed to be exempted from these guidelines since good evidence supports the use of opioids in these populations.
Instead of preserving access to desperately needed pain medicine for those suffering with serious illness, states and insurers have aggressively sought to gatekeep opioids from everyone, resulting in stigma, delays, and needless suffering.
Several recent studies have revealed the effects of this gatekeeping on patients with cancer.
A qualitative study with 26 advanced cancer patients described the demoralization and stigma many patients felt when taking opioids, which they directly tied to media messaging around the opioid epidemic. Even when they reluctantly agreed to take opioids to treat cancer-related pain, there were systemic impediments to achieving adequate pain relief – similar to my experience with Joan – that were directly caused by insurance and pharmacy constraints.
Those of us who care for oncology patients also appear to be undertreating cancer-related pain. Another recent study that found the amount of opioid medications prescribed to an advanced cancer patient near the end of life dropped by 38% between 2007 and 2017. The authors suggest that a direct consequence of this decline in appropriate opioid prescribing is an observed 50% rise in emergency department visits over the same time period by cancer patients for pain-related reasons.
This makes sense – if patients aren’t routinely prescribed the opioids they need to manage their cancer-related pain; or, if the stigma against using opioids is so harsh that it causes patients to shun opioids; or, if there are so many system barriers in place to prevent patients from obtaining opioids in a timely manner – then patients’ pain will crescendo, leaving them with little alternative but to head to the emergency department.
This undertreatment is corroborated by another study that examined data from the Centers for Medicare & Medicaid Services Part D prescriber database between 2013 and 2017, finding that both oncologists and nononcologists prescribed about 21% fewer opioids to Medicare beneficiaries during that time, compared with the period prior to 2013.
Interestingly, the researchers also found that opioid prescribing by palliative care providers increased by 15% over the same period. On a positive note, this suggests the presence of a growing outpatient palliative care workforce. But it may also reflect growing unease among oncologists with the perceived liability for prescribing opioids and a desire to ask other specialists to take on this liability. At the same time, it may reflect the very real and ever-increasing administrative burden associated with prescribing opioids and the fact that busy oncologists may not have time to spend on this aspect of cancer care. Thus, as palliative care clinicians become more visible and numerous in the outpatient arena, oncologists may increasingly ask palliative care clinicians like myself to take this on.
The problem with this is that merely handing off the administrative burden to another clinician doesn’t address the underlying problem. Anecdotal evidence suggests (and my own experiences corroborate) this administrative burden can cause real harm. A survey of 1,000 physicians conducted by the American Medical Association in 2021 found that 93% of respondents reported a delay in patient care due to prior authorization burden and 34% of respondents reported that their patients had suffered a “serious adverse event” due to prior authorization requirements.
The CDC recently announced it will take steps to revise the 2016 opioid prescribing guidelines for chronic pain after hearing from members of the medical community as well as patients living with chronic pain about the harsh, unintended consequences of the guidelines. I can only hope that insurance companies will follow suit, revising their opioid prior authorization requirements to finally come into alignment with the rational, safe use of opioids in patients with advanced cancer. It’s too bad that any improvement in the future will be too late for the millions of patients who have suffered irreversible iatrogenic harms due to delays in achieving adequate pain relief.
Sarah F. D’Ambruoso, NP, is a palliative care nurse practitioner in Santa Monica, Calif.
Pain management is a huge part of how we in palliative care help patients – and most of the time, I think we do it well, but in the regulatory environment of the opioid epidemic,
A patient – let’s call her Joan – calls me in distress. She is a 62-year-old woman with widespread metastatic breast cancer. Her pain is mainly due to bone metastases, but she also has discomfort due to the cancer’s invasion of the thin membranes that line her lungs and abdomen.
She was started on a combination opioid and acetaminophen tablet about 2 months ago by her oncologist, but is now requiring it around the clock, nearing the ceiling dose for this particular medication.
Given that her pain is escalating, Joan and I discuss starting a long-acting opioid to better manage the peak and trough effect of short-acting opioids, which can make a patient feel that the pain is relieved only for a few hours at a time, with sharp spikes throughout the day that mandate the next dose of short-acting opioid. This tethers the patient to the clock, having to take as many as six or eight doses of medication per day, and can be very disruptive to daily life.
I send an e-prescription for the same opioid Joan’s currently taking, but in a long-acting format that will slow-release over 8-10 hours, relieving her of the need to take a medication every 3-4 hours. I have learned over the years that nearly every long-acting opioid automatically generates a prior authorization request from the patient’s insurance company and so I immediately email our prior authorization team to submit to Joan’s insurance right away to avoid this extra delay.
Our prior authorization team is exceptionally responsive and submits these requests with urgency every time – they understand that cancer pain is a serious problem and we can’t wait 5 business days for answers. They are typically able to obtain an approved prior authorization for nearly every long-acting opioid I write within 24-48 hours.
But here’s where things go sideways.
First, the insurance company denies the prior authorization request, demanding that I revise the prescription from the long-acting version of the opioid she is currently taking to a cheaper, older opioid that she’s never tried before. In other words, they won’t cover the drug I requested without Joan first trying a completely different drug and failing it. This only makes sense for the insurance company’s bottom line – it makes no clinical sense at all. Why would I try a novel compound that Joan’s never had and one to which I have no idea how she’ll respond when I could keep her on the same compound knowing that she tolerates it just fine?
Past experience tells me insurance companies rarely budge on this, and appealing the decision would just introduce even more delay of care, so I begrudgingly change the prescription and send it again to the pharmacy. I message Joan to let her know that her insurance won’t cover my drug of choice and that we have to try this older one first.
A few hours later, Joan sends me a message: “My pharmacy says it’s going to take A WEEK to get the long-acting medicine!”
In the meantime, Joan has been using her short-acting opioid faster than anticipated because of her escalating pain – so she’s now running low on that as well.
I write for more of her short-acting opioid and e-script it to her pharmacy.
Within a few hours, we get another automatic response from her insurance that we’re going to need a prior authorization for additional short-acting opioid because she’s exceeded “quantity limitations,” which as far as I can tell is a completely arbitrary number not based on clinical evidence.
The prior auth team jumps on it and submits to override the quantity limit – successfully – and sends the override code to her pharmacy to reprocess the prescription.
But now the pharmacist tells Joan that they won’t fill the Rx anyway because it’s “too early.” They tell her that “state laws” prevent them from filling the scrip.
Is this true? I have no idea. I’m not an expert on California pharmacy law. All I know is that my patient is in pain and something needs to happen quickly.
I write for a second short-acting opioid – again a completely different compound. Ironically, this Rx goes through instantly without need for prior authorization. But now Joan has to switch to another new drug for no good medical reason.
If you’re still with me this far into the weeds, I’m grateful. In all it took a combined 4 hours of work (between myself and the prior auth team) to get two opioid Rx’s filled – and these were completely different medications than the ones I originally wrote for. I also had to move her prescriptions to the hospital’s pharmacy (another inconvenience for Joan and her family) so that she could get the medications in a timely manner. All this work to ensure that a single patient had adequate and timely pain relief and to prevent her from having to make an unnecessary visit to the emergency department for pain crisis.
This is just a regular day in outpatient palliative care in the era of the opioid epidemic.
The epidemic has caused tremendous pain and suffering for millions of people over the past 2 decades – namely those lost to opioid overdoses and their loved ones. And for the most part, tightening access to opioids for routine aches and pains among a relatively healthy population is not wrong, in my opinion, as long as those restrictions are based in good faith on robust evidence.
But the hidden cost of the Centers for Disease Control and Prevention’s 2016 opioid prescribing guidelines for nonmalignant pain, as well as the flurry of restrictive state laws they generated, is felt every day by patients with serious illness even though the guidelines were never meant to affect them. Patients with active cancer, receiving palliative care services, or at the end of life, were supposed to be exempted from these guidelines since good evidence supports the use of opioids in these populations.
Instead of preserving access to desperately needed pain medicine for those suffering with serious illness, states and insurers have aggressively sought to gatekeep opioids from everyone, resulting in stigma, delays, and needless suffering.
Several recent studies have revealed the effects of this gatekeeping on patients with cancer.
A qualitative study with 26 advanced cancer patients described the demoralization and stigma many patients felt when taking opioids, which they directly tied to media messaging around the opioid epidemic. Even when they reluctantly agreed to take opioids to treat cancer-related pain, there were systemic impediments to achieving adequate pain relief – similar to my experience with Joan – that were directly caused by insurance and pharmacy constraints.
Those of us who care for oncology patients also appear to be undertreating cancer-related pain. Another recent study that found the amount of opioid medications prescribed to an advanced cancer patient near the end of life dropped by 38% between 2007 and 2017. The authors suggest that a direct consequence of this decline in appropriate opioid prescribing is an observed 50% rise in emergency department visits over the same time period by cancer patients for pain-related reasons.
This makes sense – if patients aren’t routinely prescribed the opioids they need to manage their cancer-related pain; or, if the stigma against using opioids is so harsh that it causes patients to shun opioids; or, if there are so many system barriers in place to prevent patients from obtaining opioids in a timely manner – then patients’ pain will crescendo, leaving them with little alternative but to head to the emergency department.
This undertreatment is corroborated by another study that examined data from the Centers for Medicare & Medicaid Services Part D prescriber database between 2013 and 2017, finding that both oncologists and nononcologists prescribed about 21% fewer opioids to Medicare beneficiaries during that time, compared with the period prior to 2013.
Interestingly, the researchers also found that opioid prescribing by palliative care providers increased by 15% over the same period. On a positive note, this suggests the presence of a growing outpatient palliative care workforce. But it may also reflect growing unease among oncologists with the perceived liability for prescribing opioids and a desire to ask other specialists to take on this liability. At the same time, it may reflect the very real and ever-increasing administrative burden associated with prescribing opioids and the fact that busy oncologists may not have time to spend on this aspect of cancer care. Thus, as palliative care clinicians become more visible and numerous in the outpatient arena, oncologists may increasingly ask palliative care clinicians like myself to take this on.
The problem with this is that merely handing off the administrative burden to another clinician doesn’t address the underlying problem. Anecdotal evidence suggests (and my own experiences corroborate) this administrative burden can cause real harm. A survey of 1,000 physicians conducted by the American Medical Association in 2021 found that 93% of respondents reported a delay in patient care due to prior authorization burden and 34% of respondents reported that their patients had suffered a “serious adverse event” due to prior authorization requirements.
The CDC recently announced it will take steps to revise the 2016 opioid prescribing guidelines for chronic pain after hearing from members of the medical community as well as patients living with chronic pain about the harsh, unintended consequences of the guidelines. I can only hope that insurance companies will follow suit, revising their opioid prior authorization requirements to finally come into alignment with the rational, safe use of opioids in patients with advanced cancer. It’s too bad that any improvement in the future will be too late for the millions of patients who have suffered irreversible iatrogenic harms due to delays in achieving adequate pain relief.
Sarah F. D’Ambruoso, NP, is a palliative care nurse practitioner in Santa Monica, Calif.
Is family reunification our goal?
This has been an unfortunate, but not an atypical year, for the children in Maine whose lives have intersected with the state’s Department of Health and Human Services. In 2021, 25 children died of abuse and neglect or in homes with prior involvement with the child protective system. Four cases not included in that number are currently listed as homicides. At a recent legislative hearing the grandmother of one of those victims told her story to the lawmaker.
Her grandson was removed from his mother’s custody at 3 months of age after a 2-year-old sibling overdosed on methadone. Father and grandmother became his caregivers but when the father was arrested the child was returned to the mother’s custody by a judge despite the pleas of the child’s court-appointed guardian. The child eventually returned to the care of his paternal aunt and father, but when the father was arrested again the then 3-year-old was returned to his mother. Within months he was dead with multiple fractures, including to his spine and with internal and intracranial bleeding (Overton P. Maine’s child welfare system failed a 3-year old who died, grandmother tells lawmakers. 2022 Feb 11. Portland Press Herald).

The grandmother questioned the legislators why a vulnerable child would be returned to the care of a woman with such an extensive history of involvement with the Department of Health and Human Services. While there may have been errors of judgment on the part of department staff, in large part the answer lies in the system’s emphasis on reunification. Like apple pie, motherhood, and more recently fatherhood, have been viewed as something deserving of our unquestioning efforts to preserve.
This is not a recent trend. Some of the most frustrating cases over my 40 years of practice involved the failure of the courts and in some cases social workers to place a child’s welfare in the proper perspective as court schedules and custody decisions were made. Too often the reunification of “the family” seemed to trump the needs of the child. Fortunately, I’m unaware of any of my patients who died as the result of these untimely and poorly made decisions. However, many of my patients lived in unsettled conditions never sure what the next week would bring while the system focused on giving an adult whose life was a mess one more chance to demonstrate his or her ability to parent.
Of course, there are occasions in which child protective workers have been too hasty in pulling a child from his or her parents. But, in my experience those cases pale next to the number of times in which children were exposed to home environments that threatened their psychological health and development. Yes, there are bad foster homes. Many foster homes might do a better job if they were working in a system that put a higher value on the emotional needs and safety of the children in making its custody decisions.
We have a governor here in Maine who has worked hard to do the right thing during the pandemic and has made child health a focus. However, her recent proposed appropriations bill appears to continue the focus on reunification by funneling money into programs such as family reunion training and coaching as well as a parent mentorship program. Certainly, one can’t argue that these kind of programs might be helpful to some families. On the other hand, we can’t let these programs create the impression that an intact family is our primary goal. Not every family is repairable, at least on a time schedule compatible with the emotional and health needs of the children.
I wouldn’t be surprised to learn that many of you have experienced a similar frustration when decisions based on an unrealistic goal of family reunification have put your patients at risk.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
This has been an unfortunate, but not an atypical year, for the children in Maine whose lives have intersected with the state’s Department of Health and Human Services. In 2021, 25 children died of abuse and neglect or in homes with prior involvement with the child protective system. Four cases not included in that number are currently listed as homicides. At a recent legislative hearing the grandmother of one of those victims told her story to the lawmaker.
Her grandson was removed from his mother’s custody at 3 months of age after a 2-year-old sibling overdosed on methadone. Father and grandmother became his caregivers but when the father was arrested the child was returned to the mother’s custody by a judge despite the pleas of the child’s court-appointed guardian. The child eventually returned to the care of his paternal aunt and father, but when the father was arrested again the then 3-year-old was returned to his mother. Within months he was dead with multiple fractures, including to his spine and with internal and intracranial bleeding (Overton P. Maine’s child welfare system failed a 3-year old who died, grandmother tells lawmakers. 2022 Feb 11. Portland Press Herald).
The grandmother questioned the legislators why a vulnerable child would be returned to the care of a woman with such an extensive history of involvement with the Department of Health and Human Services. While there may have been errors of judgment on the part of department staff, in large part the answer lies in the system’s emphasis on reunification. Like apple pie, motherhood, and more recently fatherhood, have been viewed as something deserving of our unquestioning efforts to preserve.
This is not a recent trend. Some of the most frustrating cases over my 40 years of practice involved the failure of the courts and in some cases social workers to place a child’s welfare in the proper perspective as court schedules and custody decisions were made. Too often the reunification of “the family” seemed to trump the needs of the child. Fortunately, I’m unaware of any of my patients who died as the result of these untimely and poorly made decisions. However, many of my patients lived in unsettled conditions never sure what the next week would bring while the system focused on giving an adult whose life was a mess one more chance to demonstrate his or her ability to parent.
Of course, there are occasions in which child protective workers have been too hasty in pulling a child from his or her parents. But, in my experience those cases pale next to the number of times in which children were exposed to home environments that threatened their psychological health and development. Yes, there are bad foster homes. Many foster homes might do a better job if they were working in a system that put a higher value on the emotional needs and safety of the children in making its custody decisions.
We have a governor here in Maine who has worked hard to do the right thing during the pandemic and has made child health a focus. However, her recent proposed appropriations bill appears to continue the focus on reunification by funneling money into programs such as family reunion training and coaching as well as a parent mentorship program. Certainly, one can’t argue that these kind of programs might be helpful to some families. On the other hand, we can’t let these programs create the impression that an intact family is our primary goal. Not every family is repairable, at least on a time schedule compatible with the emotional and health needs of the children.
I wouldn’t be surprised to learn that many of you have experienced a similar frustration when decisions based on an unrealistic goal of family reunification have put your patients at risk.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
This has been an unfortunate, but not an atypical year, for the children in Maine whose lives have intersected with the state’s Department of Health and Human Services. In 2021, 25 children died of abuse and neglect or in homes with prior involvement with the child protective system. Four cases not included in that number are currently listed as homicides. At a recent legislative hearing the grandmother of one of those victims told her story to the lawmaker.
Her grandson was removed from his mother’s custody at 3 months of age after a 2-year-old sibling overdosed on methadone. Father and grandmother became his caregivers but when the father was arrested the child was returned to the mother’s custody by a judge despite the pleas of the child’s court-appointed guardian. The child eventually returned to the care of his paternal aunt and father, but when the father was arrested again the then 3-year-old was returned to his mother. Within months he was dead with multiple fractures, including to his spine and with internal and intracranial bleeding (Overton P. Maine’s child welfare system failed a 3-year old who died, grandmother tells lawmakers. 2022 Feb 11. Portland Press Herald).
The grandmother questioned the legislators why a vulnerable child would be returned to the care of a woman with such an extensive history of involvement with the Department of Health and Human Services. While there may have been errors of judgment on the part of department staff, in large part the answer lies in the system’s emphasis on reunification. Like apple pie, motherhood, and more recently fatherhood, have been viewed as something deserving of our unquestioning efforts to preserve.
This is not a recent trend. Some of the most frustrating cases over my 40 years of practice involved the failure of the courts and in some cases social workers to place a child’s welfare in the proper perspective as court schedules and custody decisions were made. Too often the reunification of “the family” seemed to trump the needs of the child. Fortunately, I’m unaware of any of my patients who died as the result of these untimely and poorly made decisions. However, many of my patients lived in unsettled conditions never sure what the next week would bring while the system focused on giving an adult whose life was a mess one more chance to demonstrate his or her ability to parent.
Of course, there are occasions in which child protective workers have been too hasty in pulling a child from his or her parents. But, in my experience those cases pale next to the number of times in which children were exposed to home environments that threatened their psychological health and development. Yes, there are bad foster homes. Many foster homes might do a better job if they were working in a system that put a higher value on the emotional needs and safety of the children in making its custody decisions.
We have a governor here in Maine who has worked hard to do the right thing during the pandemic and has made child health a focus. However, her recent proposed appropriations bill appears to continue the focus on reunification by funneling money into programs such as family reunion training and coaching as well as a parent mentorship program. Certainly, one can’t argue that these kind of programs might be helpful to some families. On the other hand, we can’t let these programs create the impression that an intact family is our primary goal. Not every family is repairable, at least on a time schedule compatible with the emotional and health needs of the children.
I wouldn’t be surprised to learn that many of you have experienced a similar frustration when decisions based on an unrealistic goal of family reunification have put your patients at risk.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
A-fib prevention, treatment, and screening: Where does the evidence lead us?
Atrial fibrillation (AF) is a common problem confronting family physicians. In this issue of JFP, we offer 2 articles about AF: one on prevention and one on treatment. Both provide evidence-based guidance to help you refine your care. But gaps remain. I’ll get to that in a bit.
Prevention. This month’s PURL1 discusses a randomized controlled trial (RCT) that enrolled moderate alcohol drinkers with AF.2 Compared to those who continued to drink moderately, those who reduced their alcohol consumption to 2 drinks per week had a significant reduction in recurrent AF (73% vs 53%), fewer hospitalizations (20% vs 9%), and less moderate or severe symptoms (32% vs 10%). Although previous studies of moderate alcohol consumption have shown positive effects on heart disease, this study and other more recent studies cast serious doubt on this assertion.3
Treatment. In their applied evidence article, Osayande and Sharma4 pose the question: When is catheter ablation a sound option for your patient with AF? They give us an excellent, evidence-based answer and remind us that we must focus on the treatment goals: to prevent stroke and to control symptoms. They recommend a stepwise approach, starting with rate control, progressing to rhythm control, and saving catheter ablation for resistant cases. In nearly all cases, anticoagulation to prevent stroke must be a part of treatment, with the exception of those with very low risk (so-called “lone atrial fibrillation”).
Screening. And what about screening for asymptomatic AF? The US Preventive Services Task Force recently reaffirmed its conclusion that there is insufficient evidence for screening for asymptomatic AF (a topic discussed in an online Practice Alert Brief5).6 Since wearable exercise-monitoring devices can detect heart arrhythmias (and are advertised for this purpose), a patient may present after receiving a notification about asymptomatic AF. What shall we do in these cases? The dilemma is that your patient will know she has a potentially dangerous condition, but there is no evidence that treating it will result in more benefit than harm.
A recently published study suggests that we should be very cautious in recommending treatment. In an RCT of patients ages 70 to 90 years, 1501 patients received an implantable loop recorder, while 4503 received routine health care; median follow-up was 64.5 months.7 Although more cases of AF were detected (32% in the monitored group vs 12% in the usual care group), and oral anticoagulation treatment was started more frequently (30% vs 13%, respectively), there was no significant difference in the proportion of patients who had a stroke or systemic arterial embolism (4.5% vs 5.6%).7 Until we have more data, reassurance seems to be the best recommendation for asymptomatic AF.
1. Thiel DJ, Marshall RC, Rogers TS. Alcohol abstinence reduces A-fib burden in drinkers. J Fam Pract. 2022;71:85-87.
2. Voskoboinik A, Kalman JM, De Silva A, et al. Alcohol abstinence in drinkers with atrial fibrillation. N Engl J Med. 2020;382:20-28. doi: 10.1056/NEJMoa1817591
3. Hoek AG, van Oort S, Mukamal KJ, et al. Alcohol consumption and cardiovascular disease risk: placing new data in context [published online ahead of print, 2022 Feb 7]. Curr Atheroscler Rep. doi: 10.1007/s11883-022-00992-1
4. Osayande AS, Sharma N. When is catheter ablation a sound option for your patient with A-fib? J Fam Pract. 2022;71:54-62.
5. Campos-Outcalt D. USPSTF releases updated guidance on asymptomatic A-fb. J Fam Pract. 2022;3. Accessed February 18, 2022. www.mdedge.com/familymedicine/article/251911/cardiology/uspstf-releases-updated-guidance-asymptomatic-fib
6. USPSTF. Screening for atrial fibrillation: US Preventive Services Task Force recommendation statement. JAMA. 2022;327:360-367. doi: 10.1001/jama.2021.23732
7. Svendsen JH, Diederichsen SZ, Hojberg S, et al. Implantable loop recorder detection of atrial fibrillation to prevent stroke (The LOOP Study): a randomised controlled trial. Lancet. 2021;398:1507-1516.
Editor-in-Chief
Editor-in-Chief
Editor-in-Chief
Atrial fibrillation (AF) is a common problem confronting family physicians. In this issue of JFP, we offer 2 articles about AF: one on prevention and one on treatment. Both provide evidence-based guidance to help you refine your care. But gaps remain. I’ll get to that in a bit.
Prevention. This month’s PURL1 discusses a randomized controlled trial (RCT) that enrolled moderate alcohol drinkers with AF.2 Compared to those who continued to drink moderately, those who reduced their alcohol consumption to 2 drinks per week had a significant reduction in recurrent AF (73% vs 53%), fewer hospitalizations (20% vs 9%), and less moderate or severe symptoms (32% vs 10%). Although previous studies of moderate alcohol consumption have shown positive effects on heart disease, this study and other more recent studies cast serious doubt on this assertion.3
Treatment. In their applied evidence article, Osayande and Sharma4 pose the question: When is catheter ablation a sound option for your patient with AF? They give us an excellent, evidence-based answer and remind us that we must focus on the treatment goals: to prevent stroke and to control symptoms. They recommend a stepwise approach, starting with rate control, progressing to rhythm control, and saving catheter ablation for resistant cases. In nearly all cases, anticoagulation to prevent stroke must be a part of treatment, with the exception of those with very low risk (so-called “lone atrial fibrillation”).
Screening. And what about screening for asymptomatic AF? The US Preventive Services Task Force recently reaffirmed its conclusion that there is insufficient evidence for screening for asymptomatic AF (a topic discussed in an online Practice Alert Brief5).6 Since wearable exercise-monitoring devices can detect heart arrhythmias (and are advertised for this purpose), a patient may present after receiving a notification about asymptomatic AF. What shall we do in these cases? The dilemma is that your patient will know she has a potentially dangerous condition, but there is no evidence that treating it will result in more benefit than harm.
A recently published study suggests that we should be very cautious in recommending treatment. In an RCT of patients ages 70 to 90 years, 1501 patients received an implantable loop recorder, while 4503 received routine health care; median follow-up was 64.5 months.7 Although more cases of AF were detected (32% in the monitored group vs 12% in the usual care group), and oral anticoagulation treatment was started more frequently (30% vs 13%, respectively), there was no significant difference in the proportion of patients who had a stroke or systemic arterial embolism (4.5% vs 5.6%).7 Until we have more data, reassurance seems to be the best recommendation for asymptomatic AF.
Atrial fibrillation (AF) is a common problem confronting family physicians. In this issue of JFP, we offer 2 articles about AF: one on prevention and one on treatment. Both provide evidence-based guidance to help you refine your care. But gaps remain. I’ll get to that in a bit.
Prevention. This month’s PURL1 discusses a randomized controlled trial (RCT) that enrolled moderate alcohol drinkers with AF.2 Compared to those who continued to drink moderately, those who reduced their alcohol consumption to 2 drinks per week had a significant reduction in recurrent AF (73% vs 53%), fewer hospitalizations (20% vs 9%), and less moderate or severe symptoms (32% vs 10%). Although previous studies of moderate alcohol consumption have shown positive effects on heart disease, this study and other more recent studies cast serious doubt on this assertion.3
Treatment. In their applied evidence article, Osayande and Sharma4 pose the question: When is catheter ablation a sound option for your patient with AF? They give us an excellent, evidence-based answer and remind us that we must focus on the treatment goals: to prevent stroke and to control symptoms. They recommend a stepwise approach, starting with rate control, progressing to rhythm control, and saving catheter ablation for resistant cases. In nearly all cases, anticoagulation to prevent stroke must be a part of treatment, with the exception of those with very low risk (so-called “lone atrial fibrillation”).
Screening. And what about screening for asymptomatic AF? The US Preventive Services Task Force recently reaffirmed its conclusion that there is insufficient evidence for screening for asymptomatic AF (a topic discussed in an online Practice Alert Brief5).6 Since wearable exercise-monitoring devices can detect heart arrhythmias (and are advertised for this purpose), a patient may present after receiving a notification about asymptomatic AF. What shall we do in these cases? The dilemma is that your patient will know she has a potentially dangerous condition, but there is no evidence that treating it will result in more benefit than harm.
A recently published study suggests that we should be very cautious in recommending treatment. In an RCT of patients ages 70 to 90 years, 1501 patients received an implantable loop recorder, while 4503 received routine health care; median follow-up was 64.5 months.7 Although more cases of AF were detected (32% in the monitored group vs 12% in the usual care group), and oral anticoagulation treatment was started more frequently (30% vs 13%, respectively), there was no significant difference in the proportion of patients who had a stroke or systemic arterial embolism (4.5% vs 5.6%).7 Until we have more data, reassurance seems to be the best recommendation for asymptomatic AF.
1. Thiel DJ, Marshall RC, Rogers TS. Alcohol abstinence reduces A-fib burden in drinkers. J Fam Pract. 2022;71:85-87.
2. Voskoboinik A, Kalman JM, De Silva A, et al. Alcohol abstinence in drinkers with atrial fibrillation. N Engl J Med. 2020;382:20-28. doi: 10.1056/NEJMoa1817591
3. Hoek AG, van Oort S, Mukamal KJ, et al. Alcohol consumption and cardiovascular disease risk: placing new data in context [published online ahead of print, 2022 Feb 7]. Curr Atheroscler Rep. doi: 10.1007/s11883-022-00992-1
4. Osayande AS, Sharma N. When is catheter ablation a sound option for your patient with A-fib? J Fam Pract. 2022;71:54-62.
5. Campos-Outcalt D. USPSTF releases updated guidance on asymptomatic A-fb. J Fam Pract. 2022;3. Accessed February 18, 2022. www.mdedge.com/familymedicine/article/251911/cardiology/uspstf-releases-updated-guidance-asymptomatic-fib
6. USPSTF. Screening for atrial fibrillation: US Preventive Services Task Force recommendation statement. JAMA. 2022;327:360-367. doi: 10.1001/jama.2021.23732
7. Svendsen JH, Diederichsen SZ, Hojberg S, et al. Implantable loop recorder detection of atrial fibrillation to prevent stroke (The LOOP Study): a randomised controlled trial. Lancet. 2021;398:1507-1516.
1. Thiel DJ, Marshall RC, Rogers TS. Alcohol abstinence reduces A-fib burden in drinkers. J Fam Pract. 2022;71:85-87.
2. Voskoboinik A, Kalman JM, De Silva A, et al. Alcohol abstinence in drinkers with atrial fibrillation. N Engl J Med. 2020;382:20-28. doi: 10.1056/NEJMoa1817591
3. Hoek AG, van Oort S, Mukamal KJ, et al. Alcohol consumption and cardiovascular disease risk: placing new data in context [published online ahead of print, 2022 Feb 7]. Curr Atheroscler Rep. doi: 10.1007/s11883-022-00992-1
4. Osayande AS, Sharma N. When is catheter ablation a sound option for your patient with A-fib? J Fam Pract. 2022;71:54-62.
5. Campos-Outcalt D. USPSTF releases updated guidance on asymptomatic A-fb. J Fam Pract. 2022;3. Accessed February 18, 2022. www.mdedge.com/familymedicine/article/251911/cardiology/uspstf-releases-updated-guidance-asymptomatic-fib
6. USPSTF. Screening for atrial fibrillation: US Preventive Services Task Force recommendation statement. JAMA. 2022;327:360-367. doi: 10.1001/jama.2021.23732
7. Svendsen JH, Diederichsen SZ, Hojberg S, et al. Implantable loop recorder detection of atrial fibrillation to prevent stroke (The LOOP Study): a randomised controlled trial. Lancet. 2021;398:1507-1516.
Let’s be more careful about the data—and commentary—we publish
In a recent letter to the editor, “25-hydroxyvitamin D concentration is key to analyzing vitamin D’s effects” (J Fam Pract. 2021;70:472), Dr. Grant links vitamin D supplementation with important health outcomes. He concludes that the positivity rate of SARS-CoV-2 was only 5.9% in people with higher concentrations of 25(OH)D vs 12.5% in those with lower concentrations. This is a flawed conclusion on the face of it, because the great confabulatory factor is behavior. Is it possible that those more likely to take supplemental vitamin D do so as a result of overall healthier lifestyles and choices (eg, vaccinations)? As health care representatives, we must be very careful about the data we publish and the commentary we attach to it, lest we advertise inadvertent follies. I see so much of that in our “peer-reviewed literature.”
I came to medicine as a chemist, and the rigors of peer review impressed upon the hard (fundamental) sciences are markedly different from those we “claim” adherence to in medicine. I find that some of the medical literature and study designs fall short of what would pass muster in the fundamental science industry. That is a shame! Such statements, as discussed here, have to be served for public consumption, and even to our colleagues, with a generous helping of skepticism and qualification.
RA Segal, MD, MPH
Gainesville, FL
In a recent letter to the editor, “25-hydroxyvitamin D concentration is key to analyzing vitamin D’s effects” (J Fam Pract. 2021;70:472), Dr. Grant links vitamin D supplementation with important health outcomes. He concludes that the positivity rate of SARS-CoV-2 was only 5.9% in people with higher concentrations of 25(OH)D vs 12.5% in those with lower concentrations. This is a flawed conclusion on the face of it, because the great confabulatory factor is behavior. Is it possible that those more likely to take supplemental vitamin D do so as a result of overall healthier lifestyles and choices (eg, vaccinations)? As health care representatives, we must be very careful about the data we publish and the commentary we attach to it, lest we advertise inadvertent follies. I see so much of that in our “peer-reviewed literature.”
I came to medicine as a chemist, and the rigors of peer review impressed upon the hard (fundamental) sciences are markedly different from those we “claim” adherence to in medicine. I find that some of the medical literature and study designs fall short of what would pass muster in the fundamental science industry. That is a shame! Such statements, as discussed here, have to be served for public consumption, and even to our colleagues, with a generous helping of skepticism and qualification.
RA Segal, MD, MPH
Gainesville, FL
In a recent letter to the editor, “25-hydroxyvitamin D concentration is key to analyzing vitamin D’s effects” (J Fam Pract. 2021;70:472), Dr. Grant links vitamin D supplementation with important health outcomes. He concludes that the positivity rate of SARS-CoV-2 was only 5.9% in people with higher concentrations of 25(OH)D vs 12.5% in those with lower concentrations. This is a flawed conclusion on the face of it, because the great confabulatory factor is behavior. Is it possible that those more likely to take supplemental vitamin D do so as a result of overall healthier lifestyles and choices (eg, vaccinations)? As health care representatives, we must be very careful about the data we publish and the commentary we attach to it, lest we advertise inadvertent follies. I see so much of that in our “peer-reviewed literature.”
I came to medicine as a chemist, and the rigors of peer review impressed upon the hard (fundamental) sciences are markedly different from those we “claim” adherence to in medicine. I find that some of the medical literature and study designs fall short of what would pass muster in the fundamental science industry. That is a shame! Such statements, as discussed here, have to be served for public consumption, and even to our colleagues, with a generous helping of skepticism and qualification.
RA Segal, MD, MPH
Gainesville, FL
Pandemic continues to exact a high toll on gastroenterologists’ well-being
The COVID-19 pandemic continues to take a toll on the happiness, wellness, and lifestyles of many segments of the population, but especially those in the health care field, including gastroenterologists.
The newly released Medscape Gastroenterologist Lifestyle, Happiness & Burnout Report 2022 explores gastroenterologists’ level of happiness in their personal and professional lives and how they maintain their mental and physical health.
Prior to the global pandemic, 8 in 10 (80%) gastroenterologists said they were “very” or “somewhat” happy outside of work, similar to physicians overall (81%).
But as the pandemic has worn on, feelings have shifted, and there are clear signs of stress and strain on those in the health care field.
Now, the percentage of gastroenterologists who say they are currently “very” or “somewhat” happy outside of work has dropped to 60%, about the same as physicians overall (59%).
Buried in paperwork
In 2021’s report, 42% of gastroenterologists reported burnout; that’s risen to 47% this year.
When it comes to burnout, gastroenterologists remain in the middle range of burned-out physicians.
Perhaps not surprising given the challenges of the COVID-19 pandemic, burnout rates are highest among emergency medicine and critical care specialists.
About half of gastroenterologists (52%) report being more burned out now than during the initial quarantine months of the pandemic, similar to physicians overall (55%). About 4 in 10 (39%) said their burnout was the same.
Female gastroenterologists report burnout at a greater rate than their male colleagues – 57% versus 46%.
“There’s no question that women have reported far more role strain during the pandemic than men,” said Carol A. Bernstein, MD, a psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at Albert Einstein College of Medicine, New York.
“Often women assumed more of the childcare and home-schooling responsibilities in their households. As [a] result, we know that more women dropped out of the workforce. Also, past studies indicate that women are more likely to report feelings of burnout than men,” Dr. Bernstein noted.
The volume of bureaucratic tasks is the main driver of gastroenterologist burnout, similar to that for physicians overall. Lack of respect from colleagues and more time devoted to electronic health records were also selected as major factors in this year’s report.
Gastroenterologists’ top ways to quell burnout are reducing their hours on the job (24%), changing workflow or staffing to ease their workload (23%), and taking advantage of meditation or other stress-reduction methods (18%) – similar to physicians overall.
Roughly one-third (34%) of gastroenterologists feel that their personality type contributes to their burnout, similar to physicians overall. Six in 10 gastroenterologists (60%) say burnout affects their relationships, similar to physicians overall (68%).
Seeking better work-life balance
More than half of gastroenterologists (57%) said they are willing to take a cut in pay in order to achieve a better work-life balance or have more free time – similar among physicians overall (55%).
About 16% of gastroenterologists reported clinical depression (severe depression lasting some time and not caused by grief), while 71% reported colloquial depression (feeling down, blue, sad).
About half (53%) of depressed gastroenterologists said their depression does not have an impact on relationships with patients.
Among those who saw an impact, the major behaviors they reported included being easily exasperated with patients (44%) and feeling less motivated to take patient notes carefully (20%).
To maintain well-being, gastroenterologists often choose to spend their time with their loved ones (59%), do the things they enjoy (58%), exercise (57%), get plenty of sleep (42%), and eat right (35%).
Perhaps not surprisingly, more gastroenterologists were happy with their work-life balance before the pandemic than now (70% vs. 44%). The same holds for physicians overall.
Before the pandemic, 22% of gastroenterologists reported being unhappy with their work-life balance. That has risen to 39% this year.
Most gastroenterologists are currently in a committed relationship, with 90% either married or living with a partner, a somewhat higher percentage than physicians overall (83%).
About 83% of gastroenterologists say they are in a “very good” or “good” marriage. This is down somewhat from the 2021 report (89%).
Nearly 6 in 10 gastroenterologists have partners who do not work in medicine. This is similar to the proportion among all physicians.
Findings from Medscape’s latest happiness, wellness, and lifestyle survey are based on 13,069 Medscape member physicians (61% male) practicing in the United States who completed an online survey conducted between June 29, 2021, and Sept. 26, 2021. Most respondents were between 35 and 64 years old.
A version of this article first appeared on Medscape.com.
The COVID-19 pandemic continues to take a toll on the happiness, wellness, and lifestyles of many segments of the population, but especially those in the health care field, including gastroenterologists.
The newly released Medscape Gastroenterologist Lifestyle, Happiness & Burnout Report 2022 explores gastroenterologists’ level of happiness in their personal and professional lives and how they maintain their mental and physical health.
Prior to the global pandemic, 8 in 10 (80%) gastroenterologists said they were “very” or “somewhat” happy outside of work, similar to physicians overall (81%).
But as the pandemic has worn on, feelings have shifted, and there are clear signs of stress and strain on those in the health care field.
Now, the percentage of gastroenterologists who say they are currently “very” or “somewhat” happy outside of work has dropped to 60%, about the same as physicians overall (59%).
Buried in paperwork
In 2021’s report, 42% of gastroenterologists reported burnout; that’s risen to 47% this year.
When it comes to burnout, gastroenterologists remain in the middle range of burned-out physicians.
Perhaps not surprising given the challenges of the COVID-19 pandemic, burnout rates are highest among emergency medicine and critical care specialists.
About half of gastroenterologists (52%) report being more burned out now than during the initial quarantine months of the pandemic, similar to physicians overall (55%). About 4 in 10 (39%) said their burnout was the same.
Female gastroenterologists report burnout at a greater rate than their male colleagues – 57% versus 46%.
“There’s no question that women have reported far more role strain during the pandemic than men,” said Carol A. Bernstein, MD, a psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at Albert Einstein College of Medicine, New York.
“Often women assumed more of the childcare and home-schooling responsibilities in their households. As [a] result, we know that more women dropped out of the workforce. Also, past studies indicate that women are more likely to report feelings of burnout than men,” Dr. Bernstein noted.
The volume of bureaucratic tasks is the main driver of gastroenterologist burnout, similar to that for physicians overall. Lack of respect from colleagues and more time devoted to electronic health records were also selected as major factors in this year’s report.
Gastroenterologists’ top ways to quell burnout are reducing their hours on the job (24%), changing workflow or staffing to ease their workload (23%), and taking advantage of meditation or other stress-reduction methods (18%) – similar to physicians overall.
Roughly one-third (34%) of gastroenterologists feel that their personality type contributes to their burnout, similar to physicians overall. Six in 10 gastroenterologists (60%) say burnout affects their relationships, similar to physicians overall (68%).
Seeking better work-life balance
More than half of gastroenterologists (57%) said they are willing to take a cut in pay in order to achieve a better work-life balance or have more free time – similar among physicians overall (55%).
About 16% of gastroenterologists reported clinical depression (severe depression lasting some time and not caused by grief), while 71% reported colloquial depression (feeling down, blue, sad).
About half (53%) of depressed gastroenterologists said their depression does not have an impact on relationships with patients.
Among those who saw an impact, the major behaviors they reported included being easily exasperated with patients (44%) and feeling less motivated to take patient notes carefully (20%).
To maintain well-being, gastroenterologists often choose to spend their time with their loved ones (59%), do the things they enjoy (58%), exercise (57%), get plenty of sleep (42%), and eat right (35%).
Perhaps not surprisingly, more gastroenterologists were happy with their work-life balance before the pandemic than now (70% vs. 44%). The same holds for physicians overall.
Before the pandemic, 22% of gastroenterologists reported being unhappy with their work-life balance. That has risen to 39% this year.
Most gastroenterologists are currently in a committed relationship, with 90% either married or living with a partner, a somewhat higher percentage than physicians overall (83%).
About 83% of gastroenterologists say they are in a “very good” or “good” marriage. This is down somewhat from the 2021 report (89%).
Nearly 6 in 10 gastroenterologists have partners who do not work in medicine. This is similar to the proportion among all physicians.
Findings from Medscape’s latest happiness, wellness, and lifestyle survey are based on 13,069 Medscape member physicians (61% male) practicing in the United States who completed an online survey conducted between June 29, 2021, and Sept. 26, 2021. Most respondents were between 35 and 64 years old.
A version of this article first appeared on Medscape.com.
The COVID-19 pandemic continues to take a toll on the happiness, wellness, and lifestyles of many segments of the population, but especially those in the health care field, including gastroenterologists.
The newly released Medscape Gastroenterologist Lifestyle, Happiness & Burnout Report 2022 explores gastroenterologists’ level of happiness in their personal and professional lives and how they maintain their mental and physical health.
Prior to the global pandemic, 8 in 10 (80%) gastroenterologists said they were “very” or “somewhat” happy outside of work, similar to physicians overall (81%).
But as the pandemic has worn on, feelings have shifted, and there are clear signs of stress and strain on those in the health care field.
Now, the percentage of gastroenterologists who say they are currently “very” or “somewhat” happy outside of work has dropped to 60%, about the same as physicians overall (59%).
Buried in paperwork
In 2021’s report, 42% of gastroenterologists reported burnout; that’s risen to 47% this year.
When it comes to burnout, gastroenterologists remain in the middle range of burned-out physicians.
Perhaps not surprising given the challenges of the COVID-19 pandemic, burnout rates are highest among emergency medicine and critical care specialists.
About half of gastroenterologists (52%) report being more burned out now than during the initial quarantine months of the pandemic, similar to physicians overall (55%). About 4 in 10 (39%) said their burnout was the same.
Female gastroenterologists report burnout at a greater rate than their male colleagues – 57% versus 46%.
“There’s no question that women have reported far more role strain during the pandemic than men,” said Carol A. Bernstein, MD, a psychiatrist at Montefiore Health System and professor and vice chair for faculty development and well-being at Albert Einstein College of Medicine, New York.
“Often women assumed more of the childcare and home-schooling responsibilities in their households. As [a] result, we know that more women dropped out of the workforce. Also, past studies indicate that women are more likely to report feelings of burnout than men,” Dr. Bernstein noted.
The volume of bureaucratic tasks is the main driver of gastroenterologist burnout, similar to that for physicians overall. Lack of respect from colleagues and more time devoted to electronic health records were also selected as major factors in this year’s report.
Gastroenterologists’ top ways to quell burnout are reducing their hours on the job (24%), changing workflow or staffing to ease their workload (23%), and taking advantage of meditation or other stress-reduction methods (18%) – similar to physicians overall.
Roughly one-third (34%) of gastroenterologists feel that their personality type contributes to their burnout, similar to physicians overall. Six in 10 gastroenterologists (60%) say burnout affects their relationships, similar to physicians overall (68%).
Seeking better work-life balance
More than half of gastroenterologists (57%) said they are willing to take a cut in pay in order to achieve a better work-life balance or have more free time – similar among physicians overall (55%).
About 16% of gastroenterologists reported clinical depression (severe depression lasting some time and not caused by grief), while 71% reported colloquial depression (feeling down, blue, sad).
About half (53%) of depressed gastroenterologists said their depression does not have an impact on relationships with patients.
Among those who saw an impact, the major behaviors they reported included being easily exasperated with patients (44%) and feeling less motivated to take patient notes carefully (20%).
To maintain well-being, gastroenterologists often choose to spend their time with their loved ones (59%), do the things they enjoy (58%), exercise (57%), get plenty of sleep (42%), and eat right (35%).
Perhaps not surprisingly, more gastroenterologists were happy with their work-life balance before the pandemic than now (70% vs. 44%). The same holds for physicians overall.
Before the pandemic, 22% of gastroenterologists reported being unhappy with their work-life balance. That has risen to 39% this year.
Most gastroenterologists are currently in a committed relationship, with 90% either married or living with a partner, a somewhat higher percentage than physicians overall (83%).
About 83% of gastroenterologists say they are in a “very good” or “good” marriage. This is down somewhat from the 2021 report (89%).
Nearly 6 in 10 gastroenterologists have partners who do not work in medicine. This is similar to the proportion among all physicians.
Findings from Medscape’s latest happiness, wellness, and lifestyle survey are based on 13,069 Medscape member physicians (61% male) practicing in the United States who completed an online survey conducted between June 29, 2021, and Sept. 26, 2021. Most respondents were between 35 and 64 years old.
A version of this article first appeared on Medscape.com.
Mental Health Pharmacists: Increasing Necessary Mental Health Service Delivery
The COVID-19 pandemic has significantly impacted mental health. Adolescents, adults, and health care professionals (HCPs) report worsening mental health outcomes since the pandemic.1-3 Anxiety rates have tripled, depression quadrupled, and substance and alcohol use also have increased.3 The World Health Organization (WHO) reported that during the COVID-19 pandemic, 93% of countries worldwide documented disruptions to mental health services.4 HCP shortages, worsened by the pandemic, have resulted in a mental health crisis. What can we do?
Over the past 20 years, pharmacists have assumed a more significant role in managing patients’ mental health conditions through multidisciplinary team engagement. Pharmacists’ training includes optimizing pharmacotherapy, identifying and managing adverse effects (AEs), improving medication adherence, and reducing unnecessary health care costs.5 Pharmacists have assumed pivotal roles in mental health management, including but not limited to screening, drug selection, medication management, and decision-making support for patients and HCPs. Pharmacist-provided services have led to improved medication therapy outcomes and patient satisfaction.6
According to the 2012 National Alliance on Mental Illness national survey, > 50% of patients treated for a mental health condition report having a strong relationship with their pharmacist.7 The US Department of Veterans Affairs (VA) has led the charge, engaging pharmacists in patient-oriented mental health care,including those specific to accessing mental health care (eg, fear of stigmatization).8 After obtaining a 4-year PharmD degree, psychiatric pharmacists receive additional postgraduate residency training (2 years) focused on direct patient care and then are eligible for board certification. There are about 2000 board-certified psychiatric pharmacists in the United States. Qualified psychiatric pharmacists, especially those in underresourced states, have increased the number of available patient-oriented mental health services.7 However, to continue expanding and improving access to care, we need more HCPs and pharmacists.
Mental health clinical pharmacy specialists (CPSs) within the VA work in a variety of settings, including but not limited to, the inpatient psychiatric unit; residential programs for posttraumatic stress disorder (PTSD) and substance misuse; as part of the Mental Health Intensive Case Management (MHICM) team; and in pain, telehealth, and other outpatient clinics. The VA’s mental health CPSs operate under an independent scope of practice (SOP) and manage a variety of mental health disorders. The SOP also allows pharmacists to independently manage medications for psychiatric conditions, request laboratory tests, and change therapy as needed based on patient response. The Table describes pharmacist-reported roles in a single VA facility in various mental health practice sites (eg, inpatient, outpatient, substance misuse). Pharmacist involvement in medication management with the interdisciplinary team improved symptoms, medication adherence, and reduced AEs for conditions such as depression.9
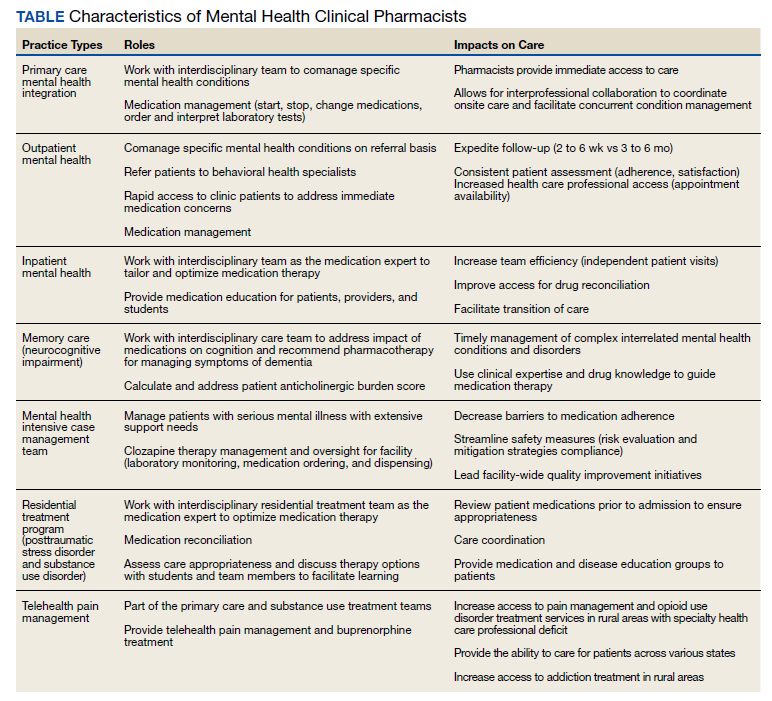
Within the VA, the outpatient mental health pharmacist works collaboratively with psychiatrists and HCPs to manage common psychiatric conditions on the phone and in person. VA pharmacists also are involved in the monitoring of patients on second-generation antipsychotics. Pharmacists assist with metabolic monitoring and assessing patients for movements disorders, using standardized rating scales. Pharmacists can manage complex psychiatric patients in collaboration with psychiatrists by providing medication management, laboratory test monitoring, medication counseling, and HCP referrals.
Pharmacists’ expertise is used in diverse ways in the VHA. At one facility, pharmacists functioned as interim prescribers when the facility experienced a turnover in behavioral health professionals. Pharmacists’ involvement decreased inappropriate use of psychiatric emergency services.10 VA pharmacists who manage patients’ mental health needs in primary care help achieve symptom improvement and medication adherence as well as lower referral rates for specialty mental health services.9 Pharmacist-managed electronic consult service provided a costs savings of about $40,000 a year.11
Pharmacists have shown that they can expand their roles. Pharmacists are versatile HCPs, currently working and collaborating with other HCPs in various settings to provide mental health services. Health care systems need to continue to use and expand the number of pharmacists. Including pharmacists in the primary and specialty care teams can increase access to care and improve health outcomes during the pandemic and beyond. The American Association of Colleges of Pharmacy in partnership with the American Medical Association established a resource to support and guide institutions interested in embedding pharmacists into different clinical sites.12 Opportunities for increased services by pharmacists can lead to improved outcomes, timely patient care, appropriate use of psychiatric medications and services, and cost savings.
Acknowledgments
We acknowledge the following Boise Veterans Affairs pharmacists: Paul Black, PharmD; Josh Gerving, PharmD; Kristin Helmboldt, PharmD; Samantha Patton, PharmD; Heather Walser, PharmD; and Andrea Winterswyk, PharmD, for contributing information about their practice roles and impact on patient care.
1. Panchal N, Kamal R. The implications of COVID-19 for mental health and substance use. Published February 10, 2021. Accessed February 8, 2022. https://www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use
2. How the pandemic has impacted teen mental health. National poll on children’s health. Published December 21, 2020. Accessed February 8, 2022. https://mottpoll.org/reports/how-pandemic-has-impacted-teen-mental-health
3. Substance Abuse and Mental Health Services Administration. A preliminary look at the mental health and substance use-related effects of the COVID-19 pandemic. Published May 2021. Accessed February 8, 2022. https://www.samhsa.gov/sites/default/files/dtac/mental-health-substance-use-effects-covid-pandemic-srb.pdf
4. World Health Organization. News release. COVID-19 disrupting mental health services in most countries, WHO survey. Published October 5, 2020. Accessed February 9, 2022. https://www.who.int/news/item/05-10-2020-covid-19-disrupting-mental-health-services-in-most-countries-who-survey
5. Avalere Health LLC. Exploring pharmacists’ role in a changing healthcare environment. Published May 2014. Accessed February 9, 2022. https://www.nacds.org/pdfs/comm/2014/pharmacist-role.pdf.
6. Silvia R. Collaborative treatment of depression by a psychiatric pharmacist integrated within a community health center primary care clinic. J Pharm Practice. 2016;29(3):270-341. doi:10.1177/0897190016645328
7. Caley C, Stimmel G. Characterizing the relationship between individuals with mental health conditions and community pharmacists. Published 2012. Accessed February 9, 2022. https://www.nami.org/About-NAMI/Publications-Reports/Survey-Reports/nami-cpnp-survey-report2012.pdf
8. Bovin MJ, Koenig CJ, Zamora KA, et al. Veterans’ experiences initiating VA-based mental health care. Psychol Serv. 2019;16(4):612-620. doi:10.1037/ser0000233
9. Herbert C, Winkler H. Impact of a clinical pharmacist–managed clinic in primary care mental health integration at a Veterans Affairs health system. Ment Health Clin. 2018;8(3):105-109. doi:10.9740/mhc.2018.05.105
10. Gibu M, Clark J, Gold J. Mental health pharmacists as interim prescribers. Ment Health Clin. 2018;7(3):111-115. doi:10.9740/mhc.2017.05.111
11. Herbert C, Winkler H, Moore TA. Outcomes of mental health pharmacist-managed electronic consults at a Veterans Affairs health care system. Ment Health Clin. 2018;7(3):131-136. doi:10.9740/mhc.2017.05.131
12. AACP. Embedding pharmacists into the practice. Accessed February 9, 2022. https://edhub.ama-assn.org/steps-forward/module/2702554
The COVID-19 pandemic has significantly impacted mental health. Adolescents, adults, and health care professionals (HCPs) report worsening mental health outcomes since the pandemic.1-3 Anxiety rates have tripled, depression quadrupled, and substance and alcohol use also have increased.3 The World Health Organization (WHO) reported that during the COVID-19 pandemic, 93% of countries worldwide documented disruptions to mental health services.4 HCP shortages, worsened by the pandemic, have resulted in a mental health crisis. What can we do?
Over the past 20 years, pharmacists have assumed a more significant role in managing patients’ mental health conditions through multidisciplinary team engagement. Pharmacists’ training includes optimizing pharmacotherapy, identifying and managing adverse effects (AEs), improving medication adherence, and reducing unnecessary health care costs.5 Pharmacists have assumed pivotal roles in mental health management, including but not limited to screening, drug selection, medication management, and decision-making support for patients and HCPs. Pharmacist-provided services have led to improved medication therapy outcomes and patient satisfaction.6
According to the 2012 National Alliance on Mental Illness national survey, > 50% of patients treated for a mental health condition report having a strong relationship with their pharmacist.7 The US Department of Veterans Affairs (VA) has led the charge, engaging pharmacists in patient-oriented mental health care,including those specific to accessing mental health care (eg, fear of stigmatization).8 After obtaining a 4-year PharmD degree, psychiatric pharmacists receive additional postgraduate residency training (2 years) focused on direct patient care and then are eligible for board certification. There are about 2000 board-certified psychiatric pharmacists in the United States. Qualified psychiatric pharmacists, especially those in underresourced states, have increased the number of available patient-oriented mental health services.7 However, to continue expanding and improving access to care, we need more HCPs and pharmacists.
Mental health clinical pharmacy specialists (CPSs) within the VA work in a variety of settings, including but not limited to, the inpatient psychiatric unit; residential programs for posttraumatic stress disorder (PTSD) and substance misuse; as part of the Mental Health Intensive Case Management (MHICM) team; and in pain, telehealth, and other outpatient clinics. The VA’s mental health CPSs operate under an independent scope of practice (SOP) and manage a variety of mental health disorders. The SOP also allows pharmacists to independently manage medications for psychiatric conditions, request laboratory tests, and change therapy as needed based on patient response. The Table describes pharmacist-reported roles in a single VA facility in various mental health practice sites (eg, inpatient, outpatient, substance misuse). Pharmacist involvement in medication management with the interdisciplinary team improved symptoms, medication adherence, and reduced AEs for conditions such as depression.9
Within the VA, the outpatient mental health pharmacist works collaboratively with psychiatrists and HCPs to manage common psychiatric conditions on the phone and in person. VA pharmacists also are involved in the monitoring of patients on second-generation antipsychotics. Pharmacists assist with metabolic monitoring and assessing patients for movements disorders, using standardized rating scales. Pharmacists can manage complex psychiatric patients in collaboration with psychiatrists by providing medication management, laboratory test monitoring, medication counseling, and HCP referrals.
Pharmacists’ expertise is used in diverse ways in the VHA. At one facility, pharmacists functioned as interim prescribers when the facility experienced a turnover in behavioral health professionals. Pharmacists’ involvement decreased inappropriate use of psychiatric emergency services.10 VA pharmacists who manage patients’ mental health needs in primary care help achieve symptom improvement and medication adherence as well as lower referral rates for specialty mental health services.9 Pharmacist-managed electronic consult service provided a costs savings of about $40,000 a year.11
Pharmacists have shown that they can expand their roles. Pharmacists are versatile HCPs, currently working and collaborating with other HCPs in various settings to provide mental health services. Health care systems need to continue to use and expand the number of pharmacists. Including pharmacists in the primary and specialty care teams can increase access to care and improve health outcomes during the pandemic and beyond. The American Association of Colleges of Pharmacy in partnership with the American Medical Association established a resource to support and guide institutions interested in embedding pharmacists into different clinical sites.12 Opportunities for increased services by pharmacists can lead to improved outcomes, timely patient care, appropriate use of psychiatric medications and services, and cost savings.
Acknowledgments
We acknowledge the following Boise Veterans Affairs pharmacists: Paul Black, PharmD; Josh Gerving, PharmD; Kristin Helmboldt, PharmD; Samantha Patton, PharmD; Heather Walser, PharmD; and Andrea Winterswyk, PharmD, for contributing information about their practice roles and impact on patient care.
The COVID-19 pandemic has significantly impacted mental health. Adolescents, adults, and health care professionals (HCPs) report worsening mental health outcomes since the pandemic.1-3 Anxiety rates have tripled, depression quadrupled, and substance and alcohol use also have increased.3 The World Health Organization (WHO) reported that during the COVID-19 pandemic, 93% of countries worldwide documented disruptions to mental health services.4 HCP shortages, worsened by the pandemic, have resulted in a mental health crisis. What can we do?
Over the past 20 years, pharmacists have assumed a more significant role in managing patients’ mental health conditions through multidisciplinary team engagement. Pharmacists’ training includes optimizing pharmacotherapy, identifying and managing adverse effects (AEs), improving medication adherence, and reducing unnecessary health care costs.5 Pharmacists have assumed pivotal roles in mental health management, including but not limited to screening, drug selection, medication management, and decision-making support for patients and HCPs. Pharmacist-provided services have led to improved medication therapy outcomes and patient satisfaction.6
According to the 2012 National Alliance on Mental Illness national survey, > 50% of patients treated for a mental health condition report having a strong relationship with their pharmacist.7 The US Department of Veterans Affairs (VA) has led the charge, engaging pharmacists in patient-oriented mental health care,including those specific to accessing mental health care (eg, fear of stigmatization).8 After obtaining a 4-year PharmD degree, psychiatric pharmacists receive additional postgraduate residency training (2 years) focused on direct patient care and then are eligible for board certification. There are about 2000 board-certified psychiatric pharmacists in the United States. Qualified psychiatric pharmacists, especially those in underresourced states, have increased the number of available patient-oriented mental health services.7 However, to continue expanding and improving access to care, we need more HCPs and pharmacists.
Mental health clinical pharmacy specialists (CPSs) within the VA work in a variety of settings, including but not limited to, the inpatient psychiatric unit; residential programs for posttraumatic stress disorder (PTSD) and substance misuse; as part of the Mental Health Intensive Case Management (MHICM) team; and in pain, telehealth, and other outpatient clinics. The VA’s mental health CPSs operate under an independent scope of practice (SOP) and manage a variety of mental health disorders. The SOP also allows pharmacists to independently manage medications for psychiatric conditions, request laboratory tests, and change therapy as needed based on patient response. The Table describes pharmacist-reported roles in a single VA facility in various mental health practice sites (eg, inpatient, outpatient, substance misuse). Pharmacist involvement in medication management with the interdisciplinary team improved symptoms, medication adherence, and reduced AEs for conditions such as depression.9
Within the VA, the outpatient mental health pharmacist works collaboratively with psychiatrists and HCPs to manage common psychiatric conditions on the phone and in person. VA pharmacists also are involved in the monitoring of patients on second-generation antipsychotics. Pharmacists assist with metabolic monitoring and assessing patients for movements disorders, using standardized rating scales. Pharmacists can manage complex psychiatric patients in collaboration with psychiatrists by providing medication management, laboratory test monitoring, medication counseling, and HCP referrals.
Pharmacists’ expertise is used in diverse ways in the VHA. At one facility, pharmacists functioned as interim prescribers when the facility experienced a turnover in behavioral health professionals. Pharmacists’ involvement decreased inappropriate use of psychiatric emergency services.10 VA pharmacists who manage patients’ mental health needs in primary care help achieve symptom improvement and medication adherence as well as lower referral rates for specialty mental health services.9 Pharmacist-managed electronic consult service provided a costs savings of about $40,000 a year.11
Pharmacists have shown that they can expand their roles. Pharmacists are versatile HCPs, currently working and collaborating with other HCPs in various settings to provide mental health services. Health care systems need to continue to use and expand the number of pharmacists. Including pharmacists in the primary and specialty care teams can increase access to care and improve health outcomes during the pandemic and beyond. The American Association of Colleges of Pharmacy in partnership with the American Medical Association established a resource to support and guide institutions interested in embedding pharmacists into different clinical sites.12 Opportunities for increased services by pharmacists can lead to improved outcomes, timely patient care, appropriate use of psychiatric medications and services, and cost savings.
Acknowledgments
We acknowledge the following Boise Veterans Affairs pharmacists: Paul Black, PharmD; Josh Gerving, PharmD; Kristin Helmboldt, PharmD; Samantha Patton, PharmD; Heather Walser, PharmD; and Andrea Winterswyk, PharmD, for contributing information about their practice roles and impact on patient care.
1. Panchal N, Kamal R. The implications of COVID-19 for mental health and substance use. Published February 10, 2021. Accessed February 8, 2022. https://www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use
2. How the pandemic has impacted teen mental health. National poll on children’s health. Published December 21, 2020. Accessed February 8, 2022. https://mottpoll.org/reports/how-pandemic-has-impacted-teen-mental-health
3. Substance Abuse and Mental Health Services Administration. A preliminary look at the mental health and substance use-related effects of the COVID-19 pandemic. Published May 2021. Accessed February 8, 2022. https://www.samhsa.gov/sites/default/files/dtac/mental-health-substance-use-effects-covid-pandemic-srb.pdf
4. World Health Organization. News release. COVID-19 disrupting mental health services in most countries, WHO survey. Published October 5, 2020. Accessed February 9, 2022. https://www.who.int/news/item/05-10-2020-covid-19-disrupting-mental-health-services-in-most-countries-who-survey
5. Avalere Health LLC. Exploring pharmacists’ role in a changing healthcare environment. Published May 2014. Accessed February 9, 2022. https://www.nacds.org/pdfs/comm/2014/pharmacist-role.pdf.
6. Silvia R. Collaborative treatment of depression by a psychiatric pharmacist integrated within a community health center primary care clinic. J Pharm Practice. 2016;29(3):270-341. doi:10.1177/0897190016645328
7. Caley C, Stimmel G. Characterizing the relationship between individuals with mental health conditions and community pharmacists. Published 2012. Accessed February 9, 2022. https://www.nami.org/About-NAMI/Publications-Reports/Survey-Reports/nami-cpnp-survey-report2012.pdf
8. Bovin MJ, Koenig CJ, Zamora KA, et al. Veterans’ experiences initiating VA-based mental health care. Psychol Serv. 2019;16(4):612-620. doi:10.1037/ser0000233
9. Herbert C, Winkler H. Impact of a clinical pharmacist–managed clinic in primary care mental health integration at a Veterans Affairs health system. Ment Health Clin. 2018;8(3):105-109. doi:10.9740/mhc.2018.05.105
10. Gibu M, Clark J, Gold J. Mental health pharmacists as interim prescribers. Ment Health Clin. 2018;7(3):111-115. doi:10.9740/mhc.2017.05.111
11. Herbert C, Winkler H, Moore TA. Outcomes of mental health pharmacist-managed electronic consults at a Veterans Affairs health care system. Ment Health Clin. 2018;7(3):131-136. doi:10.9740/mhc.2017.05.131
12. AACP. Embedding pharmacists into the practice. Accessed February 9, 2022. https://edhub.ama-assn.org/steps-forward/module/2702554
1. Panchal N, Kamal R. The implications of COVID-19 for mental health and substance use. Published February 10, 2021. Accessed February 8, 2022. https://www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use
2. How the pandemic has impacted teen mental health. National poll on children’s health. Published December 21, 2020. Accessed February 8, 2022. https://mottpoll.org/reports/how-pandemic-has-impacted-teen-mental-health
3. Substance Abuse and Mental Health Services Administration. A preliminary look at the mental health and substance use-related effects of the COVID-19 pandemic. Published May 2021. Accessed February 8, 2022. https://www.samhsa.gov/sites/default/files/dtac/mental-health-substance-use-effects-covid-pandemic-srb.pdf
4. World Health Organization. News release. COVID-19 disrupting mental health services in most countries, WHO survey. Published October 5, 2020. Accessed February 9, 2022. https://www.who.int/news/item/05-10-2020-covid-19-disrupting-mental-health-services-in-most-countries-who-survey
5. Avalere Health LLC. Exploring pharmacists’ role in a changing healthcare environment. Published May 2014. Accessed February 9, 2022. https://www.nacds.org/pdfs/comm/2014/pharmacist-role.pdf.
6. Silvia R. Collaborative treatment of depression by a psychiatric pharmacist integrated within a community health center primary care clinic. J Pharm Practice. 2016;29(3):270-341. doi:10.1177/0897190016645328
7. Caley C, Stimmel G. Characterizing the relationship between individuals with mental health conditions and community pharmacists. Published 2012. Accessed February 9, 2022. https://www.nami.org/About-NAMI/Publications-Reports/Survey-Reports/nami-cpnp-survey-report2012.pdf
8. Bovin MJ, Koenig CJ, Zamora KA, et al. Veterans’ experiences initiating VA-based mental health care. Psychol Serv. 2019;16(4):612-620. doi:10.1037/ser0000233
9. Herbert C, Winkler H. Impact of a clinical pharmacist–managed clinic in primary care mental health integration at a Veterans Affairs health system. Ment Health Clin. 2018;8(3):105-109. doi:10.9740/mhc.2018.05.105
10. Gibu M, Clark J, Gold J. Mental health pharmacists as interim prescribers. Ment Health Clin. 2018;7(3):111-115. doi:10.9740/mhc.2017.05.111
11. Herbert C, Winkler H, Moore TA. Outcomes of mental health pharmacist-managed electronic consults at a Veterans Affairs health care system. Ment Health Clin. 2018;7(3):131-136. doi:10.9740/mhc.2017.05.131
12. AACP. Embedding pharmacists into the practice. Accessed February 9, 2022. https://edhub.ama-assn.org/steps-forward/module/2702554
A Pioneer in Women’s Federal Practice
March is Women’s History Month. Many women have served in all branches of government health care over centuries and are worthy of celebrating. These nurses, physicians, pharmacists, and other allied health professionals devoted their time and talents, compassion, and competence to deliver and improve the care of wounded service members, disabled veterans, and the underresourced in our communities. To honor the collective contribution of women to federal practice in the Indian Health Service, Public Health Service Core, US Department of Veterans Affairs (VA) and the US Department of Defense, this column examines one pioneer in women’s federal practice—Margaret D. Craighill, MD—who epitomizes the spirit of the selfless dedication that generations of women have given to public service. Craighill is an ideal choice to represent this noble cadre of women as her career spanned active military duty, public health, and the Veterans Health Administration.
Craighill was a graduate of several of the finest institutions of medical training in the United States. Born in Southport, North Carolina, in 1898, she earned her undergraduate degree Phi Beta Kappa and master’s degree from the University of Wisconsin.2 She set her sights on becoming a physician at a period in American history when many prominent medical schools accepted few women. A marked exception—due to the fund raising and lobbying of influential women—was the prestigious Johns Hopkins University School of Medicine.3 She graduated in 1924 and held a postgraduate position at Yale Medical School. She then worked as a physiologist at a military arsenal, a pathologist, a general surgeon, and completed a residency in obstetrics and gynecology. This broad training gave her the diverse expertise she would need for her future work.4
Craighill came from a military family: Her father was a colonel in the engineering corps, and her grandfather rose to become chief engineer of the Army.5 Along with many of America’s best and brightest, Craighill left her successful medical career as dean of the Women’s Medical College of Pennsylvania to join the war effort. Author Alan G. Knight points out, more than in civilian medicine, gender stereotypes kept women from entering the military: Women were expected and accepted as nurses, not doctors.5 But in 1943 Congress passed and President Roosevelt signed the Sparkman-Johnson Bill, enabling women to enter the then all-male Army and Navy Medical Corps. Craighill took advantage of this opportunity and accepted an appointment to the Women’s Army Corps (WAC) as a major in 1943 at age 45 years, becoming the first woman physician to be commissioned an officer in the Army.
Major Craighill’s initial assignment was to the Office of the Surgeon General in the Preventive Medicine Division as the consultant for health and welfare of women. Here, she served as liaison to another innovation in women’s history in military medicine—the WAC. Journeying 56,000 miles to war zones in multiple countries, she assessed the health of 160,000 Army nurses and other staff whose focus was public health and infectious disease and hygiene. The history of women in medicine in and out of federal service is marked by overcoming innumerable biases and barriers. Craighill faced the prevailing presumption that women were unfit for military duty. In an early example of evidence-based medicine, she disproved this theory, showing that women were faring well doing hard jobs in tough environments.4
Their fortitude is more remarkable considering induction examinations for women during World War II were cursory and not tailored to address women’s health care needs. Based on her visits to WACs in theater and at home, Craighill observed recruits suffering from previously undiagnosed gynecologic and psychiatric conditions that adversely affected their health and function. She advocated for comprehensive standardized examinations that would detect many of these disorders.5
Craighill promoted other prejudices of her era. WAC command wanted to win public approval of women in the service and was concerned that lesbian relationships and “heterosexual promiscuity” would damage their public relations aims. They pressured Craighill to develop induction examinations that would screen lesbians and women with behavioral problems. She urged tolerance of homosexual behavior until it was proven.
Though clearly discriminatory and personally offensive to gay persons in federal service, we must recognize that only last year did the Pentagon move to overturn the prior administration’s prohibition against transgender persons serving in uniform.6 In this light Craighill, as the first female physician-leader in a 1940s military, adopted a relatively progressive stance.
Craighill rose to the rank of lieutenant colonel and received the Legion of Merit award for her exemplary wartime service. In 1945, she earned another first when she was appointed to be a consultant on the medical care of women veterans. For women veterans, gaining access to newly earned benefits and receiving appropriate care were serious problems that Craighill worked to solve. For many women veterans, those challenges remain, and Craighill’s legacy summons us to take up the charge to empower women in federal health professions to enhance the quality of care women veterans receive in all sectors of US medicine.
Critics and advocates agree that the VA still has a long way to go to achieve equity and excellence in our care for women veterans.7,8 Craighill’s position stands as a landmark in this effort. During her VA tenure, Craighill entered a residency in the first class of the Menninger School of Psychiatry in Topeka, Kansas, and completed psychoanalytic training. Her wartime experiences had convinced her of the need to provide high-quality mental health care to women veterans. She put her new psychosomatic knowledge and skills to use, serving as the chief of a women’s health clinic at the VA Hospital in Topeka and published several important scholarly papers.5,9Craighill went on to have a distinguished career in academic medicine, underscoring the long and valuable relationship of US medicine and the scholarly medical community. Once her psychiatric training was finished, she returned to private practice, ending her career as chief psychiatrist at Connecticut College for Women.
Craighill made a significant contribution to the role of women in federal practice. She was a visionary in her conviction that women, whether physicians, nurses, or other health care professionals, had the gifts and the grit to serve with distinction and valor and that their military service entitled them in war and peace to gender-sensitive health care. As the epigraph for this editorial shows, Craighill knew the path for women in federal practice or service while not easy is well worth treading. Her pioneering career can inspire all those women who today and in the future choose to follow in her footsteps.
1. Bellafaire J, Graf MH. Women Doctors in War. Texas A&M University Press; 2009:61.
2. Nuland SB. Doctors: The Biography of Medicine. Alfred A. Knopf; 1988:399-405.
3. Dr. Margaret D. Craighill, at 78, former dean of medical college. Obituary. New York Times, July 26, 1977. Accessed February 24, 2022. https://www.nytimes.com/1977/07/26/archives/dr-margaret-d-craighill-at-78-former-dean-of-medical-college.html
4. US Library of Medicine. Changing the face of medicine: Dr. Margaret D. Craighill. Updated June 03, 2015. Accessed February 23, 2022. https://cfmedicine.nlm.nih.gov/physicians/biography_72.html
5. Knight AG. Dr. Margaret D. Craighill, M.D. On Point. 2018;23(4):19-22. Accessed February 24, 2022. https://www.jstor.org/stable/26478427.
6. Wamsley L. Pentagon releases new policies enabling transgender people to serve in the military. Updated March 31, 2021. Accessed February 23, 2022. https://www.npr.org/2021/03/31/983118029/pentagon-releases-new-policies-enabling-transgender-people-to-serve-in-the-milit
7. Shane L. Is VA shortchanging women’s health programs. Military Times. Published February 28, 2019. Accessed February 24, 2022. https://www.militarytimes.com/news/pentagon-congress/2019/02/28/is-va-spending-enough-on-womens-health-programs
8. Marshall V, Stryczek KC, Haverhals L, et al. The focus they deserve: improving women veterans’ health care access. Womens Health Issues. 2021;31(4):399-407. doi:10.1016/j.whi.2020.12.011
9. Craighill MD. Psychiatric aspects of women serving in the Army. Am J Psychiatry. 1947;104(4):226-230. doi:10.1176/ajp.104.4.226
March is Women’s History Month. Many women have served in all branches of government health care over centuries and are worthy of celebrating. These nurses, physicians, pharmacists, and other allied health professionals devoted their time and talents, compassion, and competence to deliver and improve the care of wounded service members, disabled veterans, and the underresourced in our communities. To honor the collective contribution of women to federal practice in the Indian Health Service, Public Health Service Core, US Department of Veterans Affairs (VA) and the US Department of Defense, this column examines one pioneer in women’s federal practice—Margaret D. Craighill, MD—who epitomizes the spirit of the selfless dedication that generations of women have given to public service. Craighill is an ideal choice to represent this noble cadre of women as her career spanned active military duty, public health, and the Veterans Health Administration.
Craighill was a graduate of several of the finest institutions of medical training in the United States. Born in Southport, North Carolina, in 1898, she earned her undergraduate degree Phi Beta Kappa and master’s degree from the University of Wisconsin.2 She set her sights on becoming a physician at a period in American history when many prominent medical schools accepted few women. A marked exception—due to the fund raising and lobbying of influential women—was the prestigious Johns Hopkins University School of Medicine.3 She graduated in 1924 and held a postgraduate position at Yale Medical School. She then worked as a physiologist at a military arsenal, a pathologist, a general surgeon, and completed a residency in obstetrics and gynecology. This broad training gave her the diverse expertise she would need for her future work.4
Craighill came from a military family: Her father was a colonel in the engineering corps, and her grandfather rose to become chief engineer of the Army.5 Along with many of America’s best and brightest, Craighill left her successful medical career as dean of the Women’s Medical College of Pennsylvania to join the war effort. Author Alan G. Knight points out, more than in civilian medicine, gender stereotypes kept women from entering the military: Women were expected and accepted as nurses, not doctors.5 But in 1943 Congress passed and President Roosevelt signed the Sparkman-Johnson Bill, enabling women to enter the then all-male Army and Navy Medical Corps. Craighill took advantage of this opportunity and accepted an appointment to the Women’s Army Corps (WAC) as a major in 1943 at age 45 years, becoming the first woman physician to be commissioned an officer in the Army.
Major Craighill’s initial assignment was to the Office of the Surgeon General in the Preventive Medicine Division as the consultant for health and welfare of women. Here, she served as liaison to another innovation in women’s history in military medicine—the WAC. Journeying 56,000 miles to war zones in multiple countries, she assessed the health of 160,000 Army nurses and other staff whose focus was public health and infectious disease and hygiene. The history of women in medicine in and out of federal service is marked by overcoming innumerable biases and barriers. Craighill faced the prevailing presumption that women were unfit for military duty. In an early example of evidence-based medicine, she disproved this theory, showing that women were faring well doing hard jobs in tough environments.4
Their fortitude is more remarkable considering induction examinations for women during World War II were cursory and not tailored to address women’s health care needs. Based on her visits to WACs in theater and at home, Craighill observed recruits suffering from previously undiagnosed gynecologic and psychiatric conditions that adversely affected their health and function. She advocated for comprehensive standardized examinations that would detect many of these disorders.5
Craighill promoted other prejudices of her era. WAC command wanted to win public approval of women in the service and was concerned that lesbian relationships and “heterosexual promiscuity” would damage their public relations aims. They pressured Craighill to develop induction examinations that would screen lesbians and women with behavioral problems. She urged tolerance of homosexual behavior until it was proven.
Though clearly discriminatory and personally offensive to gay persons in federal service, we must recognize that only last year did the Pentagon move to overturn the prior administration’s prohibition against transgender persons serving in uniform.6 In this light Craighill, as the first female physician-leader in a 1940s military, adopted a relatively progressive stance.
Craighill rose to the rank of lieutenant colonel and received the Legion of Merit award for her exemplary wartime service. In 1945, she earned another first when she was appointed to be a consultant on the medical care of women veterans. For women veterans, gaining access to newly earned benefits and receiving appropriate care were serious problems that Craighill worked to solve. For many women veterans, those challenges remain, and Craighill’s legacy summons us to take up the charge to empower women in federal health professions to enhance the quality of care women veterans receive in all sectors of US medicine.
Critics and advocates agree that the VA still has a long way to go to achieve equity and excellence in our care for women veterans.7,8 Craighill’s position stands as a landmark in this effort. During her VA tenure, Craighill entered a residency in the first class of the Menninger School of Psychiatry in Topeka, Kansas, and completed psychoanalytic training. Her wartime experiences had convinced her of the need to provide high-quality mental health care to women veterans. She put her new psychosomatic knowledge and skills to use, serving as the chief of a women’s health clinic at the VA Hospital in Topeka and published several important scholarly papers.5,9Craighill went on to have a distinguished career in academic medicine, underscoring the long and valuable relationship of US medicine and the scholarly medical community. Once her psychiatric training was finished, she returned to private practice, ending her career as chief psychiatrist at Connecticut College for Women.
Craighill made a significant contribution to the role of women in federal practice. She was a visionary in her conviction that women, whether physicians, nurses, or other health care professionals, had the gifts and the grit to serve with distinction and valor and that their military service entitled them in war and peace to gender-sensitive health care. As the epigraph for this editorial shows, Craighill knew the path for women in federal practice or service while not easy is well worth treading. Her pioneering career can inspire all those women who today and in the future choose to follow in her footsteps.
March is Women’s History Month. Many women have served in all branches of government health care over centuries and are worthy of celebrating. These nurses, physicians, pharmacists, and other allied health professionals devoted their time and talents, compassion, and competence to deliver and improve the care of wounded service members, disabled veterans, and the underresourced in our communities. To honor the collective contribution of women to federal practice in the Indian Health Service, Public Health Service Core, US Department of Veterans Affairs (VA) and the US Department of Defense, this column examines one pioneer in women’s federal practice—Margaret D. Craighill, MD—who epitomizes the spirit of the selfless dedication that generations of women have given to public service. Craighill is an ideal choice to represent this noble cadre of women as her career spanned active military duty, public health, and the Veterans Health Administration.
Craighill was a graduate of several of the finest institutions of medical training in the United States. Born in Southport, North Carolina, in 1898, she earned her undergraduate degree Phi Beta Kappa and master’s degree from the University of Wisconsin.2 She set her sights on becoming a physician at a period in American history when many prominent medical schools accepted few women. A marked exception—due to the fund raising and lobbying of influential women—was the prestigious Johns Hopkins University School of Medicine.3 She graduated in 1924 and held a postgraduate position at Yale Medical School. She then worked as a physiologist at a military arsenal, a pathologist, a general surgeon, and completed a residency in obstetrics and gynecology. This broad training gave her the diverse expertise she would need for her future work.4
Craighill came from a military family: Her father was a colonel in the engineering corps, and her grandfather rose to become chief engineer of the Army.5 Along with many of America’s best and brightest, Craighill left her successful medical career as dean of the Women’s Medical College of Pennsylvania to join the war effort. Author Alan G. Knight points out, more than in civilian medicine, gender stereotypes kept women from entering the military: Women were expected and accepted as nurses, not doctors.5 But in 1943 Congress passed and President Roosevelt signed the Sparkman-Johnson Bill, enabling women to enter the then all-male Army and Navy Medical Corps. Craighill took advantage of this opportunity and accepted an appointment to the Women’s Army Corps (WAC) as a major in 1943 at age 45 years, becoming the first woman physician to be commissioned an officer in the Army.
Major Craighill’s initial assignment was to the Office of the Surgeon General in the Preventive Medicine Division as the consultant for health and welfare of women. Here, she served as liaison to another innovation in women’s history in military medicine—the WAC. Journeying 56,000 miles to war zones in multiple countries, she assessed the health of 160,000 Army nurses and other staff whose focus was public health and infectious disease and hygiene. The history of women in medicine in and out of federal service is marked by overcoming innumerable biases and barriers. Craighill faced the prevailing presumption that women were unfit for military duty. In an early example of evidence-based medicine, she disproved this theory, showing that women were faring well doing hard jobs in tough environments.4
Their fortitude is more remarkable considering induction examinations for women during World War II were cursory and not tailored to address women’s health care needs. Based on her visits to WACs in theater and at home, Craighill observed recruits suffering from previously undiagnosed gynecologic and psychiatric conditions that adversely affected their health and function. She advocated for comprehensive standardized examinations that would detect many of these disorders.5
Craighill promoted other prejudices of her era. WAC command wanted to win public approval of women in the service and was concerned that lesbian relationships and “heterosexual promiscuity” would damage their public relations aims. They pressured Craighill to develop induction examinations that would screen lesbians and women with behavioral problems. She urged tolerance of homosexual behavior until it was proven.
Though clearly discriminatory and personally offensive to gay persons in federal service, we must recognize that only last year did the Pentagon move to overturn the prior administration’s prohibition against transgender persons serving in uniform.6 In this light Craighill, as the first female physician-leader in a 1940s military, adopted a relatively progressive stance.
Craighill rose to the rank of lieutenant colonel and received the Legion of Merit award for her exemplary wartime service. In 1945, she earned another first when she was appointed to be a consultant on the medical care of women veterans. For women veterans, gaining access to newly earned benefits and receiving appropriate care were serious problems that Craighill worked to solve. For many women veterans, those challenges remain, and Craighill’s legacy summons us to take up the charge to empower women in federal health professions to enhance the quality of care women veterans receive in all sectors of US medicine.
Critics and advocates agree that the VA still has a long way to go to achieve equity and excellence in our care for women veterans.7,8 Craighill’s position stands as a landmark in this effort. During her VA tenure, Craighill entered a residency in the first class of the Menninger School of Psychiatry in Topeka, Kansas, and completed psychoanalytic training. Her wartime experiences had convinced her of the need to provide high-quality mental health care to women veterans. She put her new psychosomatic knowledge and skills to use, serving as the chief of a women’s health clinic at the VA Hospital in Topeka and published several important scholarly papers.5,9Craighill went on to have a distinguished career in academic medicine, underscoring the long and valuable relationship of US medicine and the scholarly medical community. Once her psychiatric training was finished, she returned to private practice, ending her career as chief psychiatrist at Connecticut College for Women.
Craighill made a significant contribution to the role of women in federal practice. She was a visionary in her conviction that women, whether physicians, nurses, or other health care professionals, had the gifts and the grit to serve with distinction and valor and that their military service entitled them in war and peace to gender-sensitive health care. As the epigraph for this editorial shows, Craighill knew the path for women in federal practice or service while not easy is well worth treading. Her pioneering career can inspire all those women who today and in the future choose to follow in her footsteps.
1. Bellafaire J, Graf MH. Women Doctors in War. Texas A&M University Press; 2009:61.
2. Nuland SB. Doctors: The Biography of Medicine. Alfred A. Knopf; 1988:399-405.
3. Dr. Margaret D. Craighill, at 78, former dean of medical college. Obituary. New York Times, July 26, 1977. Accessed February 24, 2022. https://www.nytimes.com/1977/07/26/archives/dr-margaret-d-craighill-at-78-former-dean-of-medical-college.html
4. US Library of Medicine. Changing the face of medicine: Dr. Margaret D. Craighill. Updated June 03, 2015. Accessed February 23, 2022. https://cfmedicine.nlm.nih.gov/physicians/biography_72.html
5. Knight AG. Dr. Margaret D. Craighill, M.D. On Point. 2018;23(4):19-22. Accessed February 24, 2022. https://www.jstor.org/stable/26478427.
6. Wamsley L. Pentagon releases new policies enabling transgender people to serve in the military. Updated March 31, 2021. Accessed February 23, 2022. https://www.npr.org/2021/03/31/983118029/pentagon-releases-new-policies-enabling-transgender-people-to-serve-in-the-milit
7. Shane L. Is VA shortchanging women’s health programs. Military Times. Published February 28, 2019. Accessed February 24, 2022. https://www.militarytimes.com/news/pentagon-congress/2019/02/28/is-va-spending-enough-on-womens-health-programs
8. Marshall V, Stryczek KC, Haverhals L, et al. The focus they deserve: improving women veterans’ health care access. Womens Health Issues. 2021;31(4):399-407. doi:10.1016/j.whi.2020.12.011
9. Craighill MD. Psychiatric aspects of women serving in the Army. Am J Psychiatry. 1947;104(4):226-230. doi:10.1176/ajp.104.4.226
1. Bellafaire J, Graf MH. Women Doctors in War. Texas A&M University Press; 2009:61.
2. Nuland SB. Doctors: The Biography of Medicine. Alfred A. Knopf; 1988:399-405.
3. Dr. Margaret D. Craighill, at 78, former dean of medical college. Obituary. New York Times, July 26, 1977. Accessed February 24, 2022. https://www.nytimes.com/1977/07/26/archives/dr-margaret-d-craighill-at-78-former-dean-of-medical-college.html
4. US Library of Medicine. Changing the face of medicine: Dr. Margaret D. Craighill. Updated June 03, 2015. Accessed February 23, 2022. https://cfmedicine.nlm.nih.gov/physicians/biography_72.html
5. Knight AG. Dr. Margaret D. Craighill, M.D. On Point. 2018;23(4):19-22. Accessed February 24, 2022. https://www.jstor.org/stable/26478427.
6. Wamsley L. Pentagon releases new policies enabling transgender people to serve in the military. Updated March 31, 2021. Accessed February 23, 2022. https://www.npr.org/2021/03/31/983118029/pentagon-releases-new-policies-enabling-transgender-people-to-serve-in-the-milit
7. Shane L. Is VA shortchanging women’s health programs. Military Times. Published February 28, 2019. Accessed February 24, 2022. https://www.militarytimes.com/news/pentagon-congress/2019/02/28/is-va-spending-enough-on-womens-health-programs
8. Marshall V, Stryczek KC, Haverhals L, et al. The focus they deserve: improving women veterans’ health care access. Womens Health Issues. 2021;31(4):399-407. doi:10.1016/j.whi.2020.12.011
9. Craighill MD. Psychiatric aspects of women serving in the Army. Am J Psychiatry. 1947;104(4):226-230. doi:10.1176/ajp.104.4.226
Is a progression-free survival benefit alone really worth $10,000 a month?
In the field of lung cancer, and more broadly in oncology, many of our biggest advances in 2021 have come as clinically meaningful improvements in surrogate endpoints – disease-free survival, progression-free survival, and sometimes even pathologic complete response rate.
I have historically been most compelled to consider new findings to be practice-changing when they improve overall survival or quality of life – the endpoints that translate to direct benefits for patients. However, I also feel it is appropriate to call surrogate endpoints practice-changing when they can predict improvements in overall survival or quality of life.
Take the PACIFIC trial, which assessed maintenance durvalumab after concurrent chemoradiation for unresectable stage III non–small cell lung cancer (NSCLC).
Back in 2017, I was initially unconvinced by the interim phase 3 data that were presented in a press release that highlighted the disease-free survival benefit. However, after examining additional data more closely, I saw the dramatic improvement in time to distant relapse or death was overwhelmingly likely to predict an improvement in overall survival – a benefit that the data subsequently bore out.
More recently, the disease-free survival results for adjuvant osimertinib in resected endothelial growth factor receptor mutation–positive NSCLC and adjuvant atezolizumab in resected programmed death-ligand 1–positive stage II-IIIA NSCLC have led to excitement about Food and Drug Administration approvals for these therapies. Although there is reason to be cautious about the likelihood of an overall survival benefit with either therapy – particularly for patients with low programmed death-ligand 1 who receive atezolizumab – I think that the results are promising enough to discuss these treatment options with appropriate patients.
Some argue, however, that overall survival is not necessarily a critical goal and that certain surrogate endpoints are inherently beneficial. Patients and oncologists may, for instance, view delaying disease progression as a win, even if overall survival remains the same.
I appreciate the view that favorable scan results are an achievement, even without a survival benefit. Patients appreciate the good news, and it is gratifying for us to deliver it. However, what remains unspoken is whether the benefit can be provided at a reasonable value given the financial costs associated with the new treatment.
In the United States, we consider the physician-patient relationship to be autonomous and even revered, but we conveniently ignore the fact that both are deciding on treatments that are funded by people who are not represented in the room. And in a health care system that fails to cover basic cancer care needs as well as other critical, high-value interventions for both the uninsured and underinsured, we should acknowledge that our decisions redirect limited resources from others.
Is it the best use of $10,000 per month for a new drug that improves disease-free survival but not overall survival?
At the same time, we also have to remain vigilant and reflect on whether we are echoing the marketing messages of the companies selling these treatments. Having recently watched the excellent Hulu series Dopesick, which realistically portrays the medical community’s egregious overuse of Oxycontin at the behest of Purdue Pharmaceuticals, it is striking to see how effectively the pharmaceutical industry can co-opt stakeholders. Very few physicians or patients have expertise in health care policy with broad societal perspective, yet subspecialists offer edicts as if society should dedicate unlimited resources first and foremost to our career focus or personal cause.
I certainly appreciate the appeal of surrogate endpoints in a world in which we hope to offer novel therapies to patients in a timely fashion. In the next few years, some of our most promising data in oncology will demand that we consider whether surrogate endpoints are practice-changing. We are facing a fundamental question: Are we using these surrogate endpoints to predict overall survival or quality of life or do these endpoints stand on their own as practice-changing metrics?
We need to acknowledge that our primary clinical focus is not the only one that deserves our attention, particularly when our treatment decisions are, in fact, spending other people’s money. We should be asking not whether we prefer to deliver good news after a scan, but whether that alone is enough to justify the high cost of a new treatment without an overall survival benefit.
Dr. West disclosed serving as a director, officer, partner, employee, adviser, consultant, or trustee for Ariad/Takeda, Bristol-Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, and Merck; serving as a speaker or a member of a speakers bureau for Ariad/Takeda, AstraZeneca, and Genentech/Roche; and receiving income from Eli Lilly. A version of this article first appeared on Medscape.com.
In the field of lung cancer, and more broadly in oncology, many of our biggest advances in 2021 have come as clinically meaningful improvements in surrogate endpoints – disease-free survival, progression-free survival, and sometimes even pathologic complete response rate.
I have historically been most compelled to consider new findings to be practice-changing when they improve overall survival or quality of life – the endpoints that translate to direct benefits for patients. However, I also feel it is appropriate to call surrogate endpoints practice-changing when they can predict improvements in overall survival or quality of life.
Take the PACIFIC trial, which assessed maintenance durvalumab after concurrent chemoradiation for unresectable stage III non–small cell lung cancer (NSCLC).
Back in 2017, I was initially unconvinced by the interim phase 3 data that were presented in a press release that highlighted the disease-free survival benefit. However, after examining additional data more closely, I saw the dramatic improvement in time to distant relapse or death was overwhelmingly likely to predict an improvement in overall survival – a benefit that the data subsequently bore out.
More recently, the disease-free survival results for adjuvant osimertinib in resected endothelial growth factor receptor mutation–positive NSCLC and adjuvant atezolizumab in resected programmed death-ligand 1–positive stage II-IIIA NSCLC have led to excitement about Food and Drug Administration approvals for these therapies. Although there is reason to be cautious about the likelihood of an overall survival benefit with either therapy – particularly for patients with low programmed death-ligand 1 who receive atezolizumab – I think that the results are promising enough to discuss these treatment options with appropriate patients.
Some argue, however, that overall survival is not necessarily a critical goal and that certain surrogate endpoints are inherently beneficial. Patients and oncologists may, for instance, view delaying disease progression as a win, even if overall survival remains the same.
I appreciate the view that favorable scan results are an achievement, even without a survival benefit. Patients appreciate the good news, and it is gratifying for us to deliver it. However, what remains unspoken is whether the benefit can be provided at a reasonable value given the financial costs associated with the new treatment.
In the United States, we consider the physician-patient relationship to be autonomous and even revered, but we conveniently ignore the fact that both are deciding on treatments that are funded by people who are not represented in the room. And in a health care system that fails to cover basic cancer care needs as well as other critical, high-value interventions for both the uninsured and underinsured, we should acknowledge that our decisions redirect limited resources from others.
Is it the best use of $10,000 per month for a new drug that improves disease-free survival but not overall survival?
At the same time, we also have to remain vigilant and reflect on whether we are echoing the marketing messages of the companies selling these treatments. Having recently watched the excellent Hulu series Dopesick, which realistically portrays the medical community’s egregious overuse of Oxycontin at the behest of Purdue Pharmaceuticals, it is striking to see how effectively the pharmaceutical industry can co-opt stakeholders. Very few physicians or patients have expertise in health care policy with broad societal perspective, yet subspecialists offer edicts as if society should dedicate unlimited resources first and foremost to our career focus or personal cause.
I certainly appreciate the appeal of surrogate endpoints in a world in which we hope to offer novel therapies to patients in a timely fashion. In the next few years, some of our most promising data in oncology will demand that we consider whether surrogate endpoints are practice-changing. We are facing a fundamental question: Are we using these surrogate endpoints to predict overall survival or quality of life or do these endpoints stand on their own as practice-changing metrics?
We need to acknowledge that our primary clinical focus is not the only one that deserves our attention, particularly when our treatment decisions are, in fact, spending other people’s money. We should be asking not whether we prefer to deliver good news after a scan, but whether that alone is enough to justify the high cost of a new treatment without an overall survival benefit.
Dr. West disclosed serving as a director, officer, partner, employee, adviser, consultant, or trustee for Ariad/Takeda, Bristol-Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, and Merck; serving as a speaker or a member of a speakers bureau for Ariad/Takeda, AstraZeneca, and Genentech/Roche; and receiving income from Eli Lilly. A version of this article first appeared on Medscape.com.
In the field of lung cancer, and more broadly in oncology, many of our biggest advances in 2021 have come as clinically meaningful improvements in surrogate endpoints – disease-free survival, progression-free survival, and sometimes even pathologic complete response rate.
I have historically been most compelled to consider new findings to be practice-changing when they improve overall survival or quality of life – the endpoints that translate to direct benefits for patients. However, I also feel it is appropriate to call surrogate endpoints practice-changing when they can predict improvements in overall survival or quality of life.
Take the PACIFIC trial, which assessed maintenance durvalumab after concurrent chemoradiation for unresectable stage III non–small cell lung cancer (NSCLC).
Back in 2017, I was initially unconvinced by the interim phase 3 data that were presented in a press release that highlighted the disease-free survival benefit. However, after examining additional data more closely, I saw the dramatic improvement in time to distant relapse or death was overwhelmingly likely to predict an improvement in overall survival – a benefit that the data subsequently bore out.
More recently, the disease-free survival results for adjuvant osimertinib in resected endothelial growth factor receptor mutation–positive NSCLC and adjuvant atezolizumab in resected programmed death-ligand 1–positive stage II-IIIA NSCLC have led to excitement about Food and Drug Administration approvals for these therapies. Although there is reason to be cautious about the likelihood of an overall survival benefit with either therapy – particularly for patients with low programmed death-ligand 1 who receive atezolizumab – I think that the results are promising enough to discuss these treatment options with appropriate patients.
Some argue, however, that overall survival is not necessarily a critical goal and that certain surrogate endpoints are inherently beneficial. Patients and oncologists may, for instance, view delaying disease progression as a win, even if overall survival remains the same.
I appreciate the view that favorable scan results are an achievement, even without a survival benefit. Patients appreciate the good news, and it is gratifying for us to deliver it. However, what remains unspoken is whether the benefit can be provided at a reasonable value given the financial costs associated with the new treatment.
In the United States, we consider the physician-patient relationship to be autonomous and even revered, but we conveniently ignore the fact that both are deciding on treatments that are funded by people who are not represented in the room. And in a health care system that fails to cover basic cancer care needs as well as other critical, high-value interventions for both the uninsured and underinsured, we should acknowledge that our decisions redirect limited resources from others.
Is it the best use of $10,000 per month for a new drug that improves disease-free survival but not overall survival?
At the same time, we also have to remain vigilant and reflect on whether we are echoing the marketing messages of the companies selling these treatments. Having recently watched the excellent Hulu series Dopesick, which realistically portrays the medical community’s egregious overuse of Oxycontin at the behest of Purdue Pharmaceuticals, it is striking to see how effectively the pharmaceutical industry can co-opt stakeholders. Very few physicians or patients have expertise in health care policy with broad societal perspective, yet subspecialists offer edicts as if society should dedicate unlimited resources first and foremost to our career focus or personal cause.
I certainly appreciate the appeal of surrogate endpoints in a world in which we hope to offer novel therapies to patients in a timely fashion. In the next few years, some of our most promising data in oncology will demand that we consider whether surrogate endpoints are practice-changing. We are facing a fundamental question: Are we using these surrogate endpoints to predict overall survival or quality of life or do these endpoints stand on their own as practice-changing metrics?
We need to acknowledge that our primary clinical focus is not the only one that deserves our attention, particularly when our treatment decisions are, in fact, spending other people’s money. We should be asking not whether we prefer to deliver good news after a scan, but whether that alone is enough to justify the high cost of a new treatment without an overall survival benefit.
Dr. West disclosed serving as a director, officer, partner, employee, adviser, consultant, or trustee for Ariad/Takeda, Bristol-Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, and Merck; serving as a speaker or a member of a speakers bureau for Ariad/Takeda, AstraZeneca, and Genentech/Roche; and receiving income from Eli Lilly. A version of this article first appeared on Medscape.com.