User login
Giving anesthesiologists what they want: How to write a useful preoperative consult
The ideal preoperative medical consultation (consult) is useful to the whole surgical team, ensures maximal patient readiness for surgery, and promotes optimal perioperative care of the patient. Too often, however, consults are ignored or, even worse, set the stage for legal problems. This article identifies problems frequently seen in preoperative consults, particularly from the perspective of anesthesiologists, and gives guidance to those who write consults—hospitalists, internists, cardiologists, and other medical consultants—on providing the information that is most needed by those who use them.
A WIDE RANGE OF END USERS
Anesthesiologists are most often the primary users of the information in preoperative consults, but many other members of the surgical and perioperative team benefit from a well-developed consult, including surgeons, intensivists, nurses, and pain management specialists. Most important, patients stand to benefit, as a good consult helps to ensure that the full breadth of relevant patient-specific information is brought to bear to anticipate potential difficulties and promote optimal care.
Purpose of a consult is in the eye of the beholder
The literature on medical consults in the perioperative arena is scant. The only fairly recent assessment of physician attitudes toward the role of consults was reported by Katz et al in 1998.1 These researchers surveyed attitudes about the various perceived purposes of preoperative cardiology consults, and received rather different responses from anesthesiologists, cardiologists, and surgeons.
There was consensus among all three specialties that two particular functions of a consult are important:
- Treating an inadequately managed cardiac condition before surgery
- Providing data to use in anesthetic management.
Additionally, all three specialties deemed the suggestion of intraoperative treatment modalities to be reasonably important when such suggestions were specifically included in the consult request, although anesthesiologists assigned less importance to this function.1
In contrast, anesthesiologists considered suggestions about intraoperative treatment generally unimportant when not specifically requested, and they viewed suggestions of intraoperative monitoring and advice on the safest type of anesthesia as even less important. Anesthesiologists also deemed “clearing the patient for surgery” as an unimportant function of the consult. Cardiologists rated all of these functions as more important than anesthesiologists did and in some cases as considerably more important. To many of the survey questions, surgeons responded that a specific purpose of a consult was “neither important nor unimportant.”1 That may be because the surgeon’s purpose in obtaining the consult is often simply to address the concerns of the anesthesiologist, who might otherwise delay or cancel a needed surgery.
Consult deficiencies: Vagueness, illegibility, dictating anesthetic choice
The survey by Katz et al also assessed each specialty’s perceptions of the most common deficiencies of preoperative cardiology consults. The deficiencies deemed most common were failure to give specific facts, illegible handwriting, and attempts to dictate the type of anesthesia to be used. Anesthesiologists considered each of the deficiencies assessed as occurring more commonly than their cardiologist or surgeon colleagues did.1
The requester–user disconnect
The differing perceptions of preoperative consults by anesthesiologists and surgeons underscore a fundamental problem: the primary requesters of consults (surgeons) are different from the primary users of consults (anesthesiologists).
Ideally, preoperative consults should be requested by anesthesiologists. Unless and until the ordering of consults changes on a wide scale, however, our advice is for consultants to ask the anesthesiologist what he or she needs to know, in addition to any questions directed to the requesting surgeon. Communication between the surgeon and anesthesiologist should be encouraged as much as possible, and consultants should keep both the anesthesiologist and surgeon in mind when writing consult notes.
A final end user: The plaintiff’s attorney
It is wise to keep in mind one more potential user of your consult: a plaintiff’s attorney. A poorly written consult may benefit plaintiffs’ lawyers. Consults should never give absolute instructions; it is better to use such phrases as “Strongly consider…” or “The current literature strongly suggests…” Otherwise, the surgical team is placed in an awkward position if it does not follow your recommendations, even if for good reason. If a certain recommendation absolutely must be followed, then direct oral communication from the consultant to the attending anesthesiologist (or surgeon) is best.
CONSIDER THE PRIMARY USER: WHAT ANESTHESIOLOGISTS ALREADY KNOW
For the purpose of preoperative consults, it is helpful to think of anesthesiologists as experts in acute medical care. Their 4-year training consists of the following:
- 1 year of internship, often in medicine, including 6 months of basic patient care in the ward or clinic (the last time they will manage chronic disease)
- 4 months in the intensive care unit (ICU) and 1 month in the recovery room, which yields solid intensivist training
- 3 months in pain management, covering acute and chronic pain and regional blocks
- ~24 months in the operating room, often devoted to care of complex problems in surgical subspecialties (obstetric, pediatric, neurologic, cardiothoracic, vascular)
- 1 month of preoperative screening and consultations (a recent requirement).
An optional fifth year may be spent in a subspecialty.
Since the large part of anesthesiologists’ training is in acute care, they generally do not need advice about the acute treatment of any ailment. Consults should not advise anesthesiologists on subjects in which they have considerable expertise. They already have well-established ideas about addressing hypertension, myocardial ischemia, heart failure, arrhythmias (unless unusual therapies are needed), bronchospasm, glucose levels, and pain in the operating room, so they are apt to ignore advice on such topics.
There are several additional topics in which anesthesiologists have considerable expertise and do not need guidance in consults:
- Choice of anesthetic type and its impact on outcome
- Choice of invasive or noninvasive monitoring for any comorbidity and operation
- Postoperative patient disposition (ie, whether to send a patient home, to the postanesthesia care unit, to the ICU, or to a step-down unit)
- Impact of optimizing organ function on perioperative outcome
- Cardiovascular and respiratory physiology
- Pharmacology of intravenous agents.
WHAT ANESTHESIOLOGISTS MAY NOT KNOW―AND NEED FROM CONSULTANTS
How to manage chronic diseases
Follow-up care (eg, for poorly controlled diabetes or hypertension) often can wait until after the operation, and a consultant’s opinion about that is appreciated. It is especially helpful to know that the patient will be followed without the surgeon or anesthesiologist having to arrange for it.
New evidence-based guidance from the literature
One case when recommendations on acute medical management should be provided is when they involve new information from the literature—ie, important data or guidelines published within the prior 5 years or so. It can take time for new information and recommendations to reach all clinicians even within a single specialty. Moreover, important information, such as on the perioperative use of beta-blockers and statins, is not necessarily published in the anesthesiology literature. It is critical to relay information such as the recent recommendation not to withdraw statins prior to surgery, as the current editions of most anesthesiology textbooks have incorrect information suggesting discontinuation. Thus, consultants should include pertinent recent data and guideline recommendations, especially if they go against previous dogma.
Rare diseases, blood disorders, other special cases
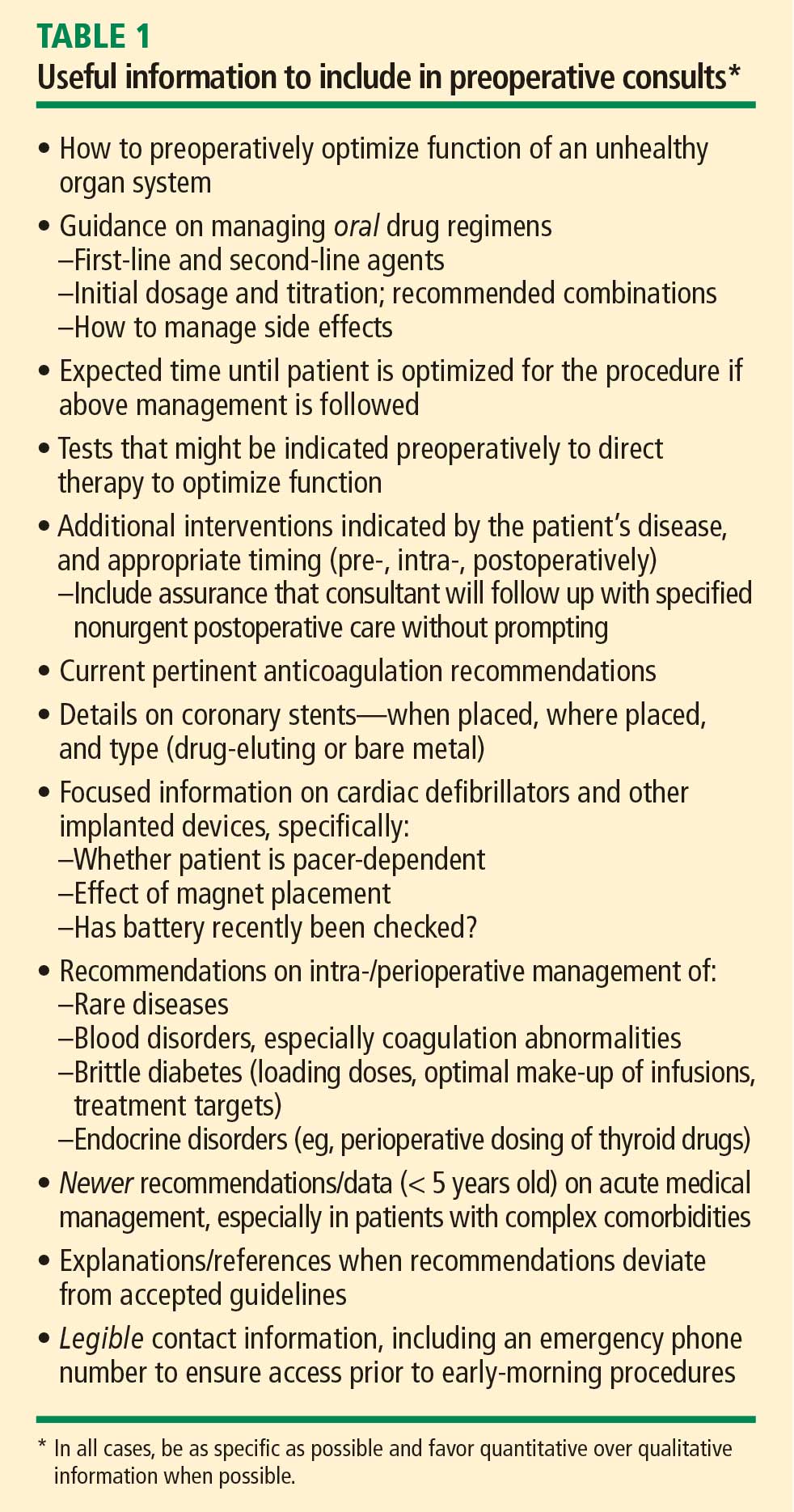
As outlined in Table 1, advice on perioperative management is appreciated for patients with rare diseases, coagulation disorders or other blood disorders, and brittle diabetes and other endocrine disorders, as most anesthesiologists are not intimately familiar with these conditions. Anesthesiologists also need, but often do not get, basic details on coronary stents and other implanted devices (see Table 1), as well as guidance on the latest anticoagulation recommendations, with which it is difficult to keep up to date.
A sensitivity to audience and context
It is always appropriate to ask the surgeon requesting a consult—and the anesthesiologist assigned to the case, if known—what he or she wants to know from the consult. If guidance on specific cases is impractical, it is appropriate to ask the chair of the anesthesiology department, or several anesthesiologists collectively, for general guidance on what they look for from preoperative consults.
Anesthesiologists, like consultants, comprise a broad range of people, and it is always important to be sensitive to context. Generalists who work mainly on healthy patients or in a community setting may have forgotten some of their training in acute medicine and are more likely to appreciate advice on intraoperative care. On the other hand, an anesthesiologist who trained in a cardiothoracic subspecialty fellowship, who routinely deals with issues such as left ventricular assist devices and heart transplants, would not benefit from such advice.
WHAT A CONSULT SHOULD―AND SHOULD NOT―BE
The above advice can be distilled into a few principles:
- A consult is an opportunity for the medical consultant to provide helpful management suggestions to the operative team.
- A fundamental objective of a consult is to optimize a patient’s underlying disease before it is compounded by the insult of surgery.
- The purpose of a consult is never to “clear” a patient for surgery. Whether or not to proceed to surgery is a question for the anesthesiologist, surgeon, and patient to decide after weighing the risks and benefits once the patient’s comorbidities are optimally managed. The consult is an important contributing factor to this decision, but it should never be the mechanism of the decision. Though the note from the surgeon requesting a consult may routinely be written as, “Clear the patient for surgery,” consultants should recognize this for what it is—the surgeon’s attempt to avoid having the anesthesiologist cancel the operation—and refrain from weighing in on “clearance” one way or the other.
CASE STUDY: CARDIAC CONSULT REQUESTED BEFORE FEM-POP BYPASS SURGERY
Cardiovascular problems are the most common reasons for requesting preoperative consults. The following case illustrates a typical scenario for a cardiac consult request and presents examples of good and bad notes requesting consults and good and bad consults written in response.
The case
A 47-year-old man is scheduled for femoral-popliteal bypass surgery. His medical history is significant for diabetes, a myocardial infarction (MI) 3 years ago followed by placement of a stent, and a limited ability to assess exercise tolerance. Evidence of an anteroseptal MI is present on 12-lead electrocardiography. His medications include metoprolol 25 mg twice daily and an oral hypoglycemic agent. His blood pressure is 152/89 mm Hg, heart rate 81 beats per minute, respiratory rate 14 breaths per minute, and arterial oxygen saturation 96% on room air.
The consult request: Bad and good examples
A bad consult request in this case would be, “Clear the patient for surgery.” Although this type of request is routinely written, it is routinely useless.
For this complex surgery with significant fluid requirements, a much better consult request would include several specific requests and questions and might read as follows:
—Please evaluate patient’s post-MI therapy for his CAD. Is further therapy required to optimize CAD treatment?
—Do his blood pressure or diabetic regimens need modification? If so, can this be done postoperatively?
—Please evaluate patient’s myocardial function in light of a lack of info on exercise tolerance. Is an echo indicated?
—Are other tests, therapies, or interventions warranted pre- or postoperatively?
Example of a bad consult
A poorly written consult in a case like this may:
- Include a brief history repeating facts that are already known and noting that “the patient is at his baseline without obvious ischemia.”
- State that the patient is cleared for “spinal” anesthesia. “Clearing a patient for anesthesia” is useless to begin with, but clearing for a certain type of anesthesia places the anesthesiologist in a terrible medicolegal position if general anesthesia turns out to be needed. Moreover, there are no proven major outcome differences related to the type of anesthetic chosen.
- Recommend that “a pulmonary artery catheter might be indicated to monitor hemodynamics.” Besides the fact that such catheters probably do more harm than good, such a recommendation is unnecessary since the anesthesiologist is already expert in managing perioperative care.
- Recommend that “the anesthesia team should monitor the patient carefully in the perioperative arena for hypoxia and hypotension.” Qualitative advice, such as “avoid hypoxia, hypotension, and tachycardia,” is not useful, but quantitative information, such as “during ischemic stress testing, the patient exhibited ischemia when his heart rate went to 142,” can be very helpful.
- State that the patient be sent to the ICU following surgery. Mandating an ICU stay in advance makes no sense unless the operation itself demands ICU care, which is the call of the surgeon and anesthesiologist anyway.
A consult like this doesn’t tell the perioperative team anything that it didn’t already know. Such a consult not only is unhelpful but also actually creates more work since much of the advice needs to be “undone” lest a lawyer see the chart and it not be clear why the consultant’s recommendations were not followed.
Example of a good consult
In contrast, a good consult for this case would involve:
- A detailed history examining the potential for silent ischemia associated with the diabetes, as well as the relationship of the hypertension and beta-blocker therapy to episodes of ischemia. The level of ischemia should be clearly categorized. If it cannot be determined, this should be noted; if it can be determined only that the ischemia is not New York Heart Association class III or IV, note this as well (the perioperative outcomes literature suggests that no preoperative ischemia testing is needed with class I or II angina).
- Guidance on blood pressure optimization in light of the relative urgency of the procedure. Blood pressure need not be normalized preoperatively in this case, but if the operation were totally elective and the consultant felt it could make a difference, it would be appropriate to suggest that blood pressure be optimized beforehand.
- A recommendation on whether and when to change the beta-blocker dosage. If the dosage needs to be increased, the anesthesiologist will want to know how many doses are needed to reach a new steady state. Joint guidelines from the American College of Cardiology (ACC) and American Heart Association (AHA)2 recommend 7 to 30 days, but this time frame is unrealistic in this setting, so more practical advice would be appreciated. A good consult notes any deviation from established guidelines, however, and explains the rationale for such deviation.
- Evaluation of the myocardium at risk. This is especially important with left main disease, as it influences the decision whether to test or intervene versus proceeding with careful beta-blocker titration.
- Evaluation of myocardial function and, if appropriate, a therapy suggestion for optimization.
- Notation of the heart rate or blood pressure thresholds at which ischemia develops if a stress test is performed.
GOOD GUIDANCE FROM THE ACC/AHA GUIDELINES
Our advice here is broadly consistent with the aforementioned 2007 ACC/AHA guidelines on perioperative cardiovascular evaluation for noncardiac surgery.2 The following observation on cardiac evaluations from these guidelines applies to preoperative consults in general:
The purpose of preoperative evaluation is not to give medical clearance but rather to perform an evaluation of the patient’s current medical status; make recommendations concerning the evaluation, management, and risk of cardiac problems over the entire perioperative period; and provide a clinical risk profile that [can be used] in making treatment decisions that may influence short- and long-term cardiac outcomes.2
These guidelines contain a good description of the ideal preoperative evaluation and consult in a short section (Section II, “General Approach to the Patient”)2 that is worthy of wide dissemination.
DISCUSSION
Question from the audience: Many consults are written more for the surgical team than for the anesthesiologists, hence advice such as managing intraoperative diabetes. Isn’t that appropriate?
Dr. Lubarsky: There are a variety of users of the information in a consult note. I focused on the anesthesiologist, but certainly the surgical staff and house staff would benefit from suggestions about postoperative management. However, they would not benefit from suggestions on intraoperative management; surgeons simply do not need this information and the anesthesiologist will have his or her own regimen. But if there is a specific type of insulin infusion that’s been shown to be best in the specific patient at hand, then detailing that obviously is beneficial.
Question from the audience: We all agree that communication is key, but how does the consultant reach the anesthesiologist to find out what he or she wants to know when the anesthesiologist isn’t usually assigned to the case until a day before surgery?
Dr. Lubarsky: If no anesthesiologist is yet assigned to a case, the consultant can discuss the case with the chief of the anesthesiology department. The discussion should be documented in the note. But it’s important that the system be changed so that anesthesiologists are assigned to cases well in advance. I instituted such a policy at my previous hospital. Many hospitals schedule surgeries 3 months in advance, and many anesthesiology departments have schedules made at least 1 month and often 2 to 3 months in advance. The department could assign a specific anesthesiologist to a future scheduled case with ease.
Question from the audience: How do anesthesiologists educate all the various people we rely on for consults when we can’t get them in one place at one time?
Dr. Lubarsky: It’s a challenge. I try many things, such as going to cardiology rounds, but there are always new people coming through. A good monograph or a set of guidelines with examples would help. If each specialty educates the other and speaks at each other’s conferences more often, that should help. Anesthesiologists would benefit from hearing about the challenges medical consultants face; we may not be doing all we can to optimize perioperative care. There’s room for improvement through communication on both sides. I should also emphasize that we’re all trying to do the right thing. Doctors try to be accommodating, but that doesn’t always make for good decisions. Recently a consultant in my hospital did a preoperative stress test on a patient who didn’t need one. When I asked why, he said, “Because the surgeon asked me to.”
Question from the audience: But don’t you agree that many anesthesiologists would like to see that negative stress test, even if a stress test is not indicated by the guidelines? Cardiologists know that the anesthesiologists are often looking for that on the morning of surgery.
Dr. Lubarsky: The point is that physicians should be responsible for what they have expertise in. When I am asked to intubate a patient, my response as an expert in intubation might be, “Actually, he doesn’t need to be intubated right now.” In the case of this unnecessary stress test, the cardiologist probably should have called the surgeon and said, “It’s really not indicated because the patient had a negative stress test 2 years ago, there’s been no change in symptoms and no angina since then, and he operates well above 4 metabolic equivalents. There’s a clear-cut reason not to do it.” If the surgeon still wanted the test done just to be reassured, that’s simply a poor use of society’s resources. We depend on experts to identify the tests that are indicated to evaluate a patient’s disease and not just do tests for the sake of doing them.
- Katz RI, Barnhart JM, Ho G, et al. A survey on the intended purposes and perceived utility of preoperative cardiology consultations. Anesth Analg 1998; 87:830–836.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2007; 116:e418–e499.
The ideal preoperative medical consultation (consult) is useful to the whole surgical team, ensures maximal patient readiness for surgery, and promotes optimal perioperative care of the patient. Too often, however, consults are ignored or, even worse, set the stage for legal problems. This article identifies problems frequently seen in preoperative consults, particularly from the perspective of anesthesiologists, and gives guidance to those who write consults—hospitalists, internists, cardiologists, and other medical consultants—on providing the information that is most needed by those who use them.
A WIDE RANGE OF END USERS
Anesthesiologists are most often the primary users of the information in preoperative consults, but many other members of the surgical and perioperative team benefit from a well-developed consult, including surgeons, intensivists, nurses, and pain management specialists. Most important, patients stand to benefit, as a good consult helps to ensure that the full breadth of relevant patient-specific information is brought to bear to anticipate potential difficulties and promote optimal care.
Purpose of a consult is in the eye of the beholder
The literature on medical consults in the perioperative arena is scant. The only fairly recent assessment of physician attitudes toward the role of consults was reported by Katz et al in 1998.1 These researchers surveyed attitudes about the various perceived purposes of preoperative cardiology consults, and received rather different responses from anesthesiologists, cardiologists, and surgeons.
There was consensus among all three specialties that two particular functions of a consult are important:
- Treating an inadequately managed cardiac condition before surgery
- Providing data to use in anesthetic management.
Additionally, all three specialties deemed the suggestion of intraoperative treatment modalities to be reasonably important when such suggestions were specifically included in the consult request, although anesthesiologists assigned less importance to this function.1
In contrast, anesthesiologists considered suggestions about intraoperative treatment generally unimportant when not specifically requested, and they viewed suggestions of intraoperative monitoring and advice on the safest type of anesthesia as even less important. Anesthesiologists also deemed “clearing the patient for surgery” as an unimportant function of the consult. Cardiologists rated all of these functions as more important than anesthesiologists did and in some cases as considerably more important. To many of the survey questions, surgeons responded that a specific purpose of a consult was “neither important nor unimportant.”1 That may be because the surgeon’s purpose in obtaining the consult is often simply to address the concerns of the anesthesiologist, who might otherwise delay or cancel a needed surgery.
Consult deficiencies: Vagueness, illegibility, dictating anesthetic choice
The survey by Katz et al also assessed each specialty’s perceptions of the most common deficiencies of preoperative cardiology consults. The deficiencies deemed most common were failure to give specific facts, illegible handwriting, and attempts to dictate the type of anesthesia to be used. Anesthesiologists considered each of the deficiencies assessed as occurring more commonly than their cardiologist or surgeon colleagues did.1
The requester–user disconnect
The differing perceptions of preoperative consults by anesthesiologists and surgeons underscore a fundamental problem: the primary requesters of consults (surgeons) are different from the primary users of consults (anesthesiologists).
Ideally, preoperative consults should be requested by anesthesiologists. Unless and until the ordering of consults changes on a wide scale, however, our advice is for consultants to ask the anesthesiologist what he or she needs to know, in addition to any questions directed to the requesting surgeon. Communication between the surgeon and anesthesiologist should be encouraged as much as possible, and consultants should keep both the anesthesiologist and surgeon in mind when writing consult notes.
A final end user: The plaintiff’s attorney
It is wise to keep in mind one more potential user of your consult: a plaintiff’s attorney. A poorly written consult may benefit plaintiffs’ lawyers. Consults should never give absolute instructions; it is better to use such phrases as “Strongly consider…” or “The current literature strongly suggests…” Otherwise, the surgical team is placed in an awkward position if it does not follow your recommendations, even if for good reason. If a certain recommendation absolutely must be followed, then direct oral communication from the consultant to the attending anesthesiologist (or surgeon) is best.
CONSIDER THE PRIMARY USER: WHAT ANESTHESIOLOGISTS ALREADY KNOW
For the purpose of preoperative consults, it is helpful to think of anesthesiologists as experts in acute medical care. Their 4-year training consists of the following:
- 1 year of internship, often in medicine, including 6 months of basic patient care in the ward or clinic (the last time they will manage chronic disease)
- 4 months in the intensive care unit (ICU) and 1 month in the recovery room, which yields solid intensivist training
- 3 months in pain management, covering acute and chronic pain and regional blocks
- ~24 months in the operating room, often devoted to care of complex problems in surgical subspecialties (obstetric, pediatric, neurologic, cardiothoracic, vascular)
- 1 month of preoperative screening and consultations (a recent requirement).
An optional fifth year may be spent in a subspecialty.
Since the large part of anesthesiologists’ training is in acute care, they generally do not need advice about the acute treatment of any ailment. Consults should not advise anesthesiologists on subjects in which they have considerable expertise. They already have well-established ideas about addressing hypertension, myocardial ischemia, heart failure, arrhythmias (unless unusual therapies are needed), bronchospasm, glucose levels, and pain in the operating room, so they are apt to ignore advice on such topics.
There are several additional topics in which anesthesiologists have considerable expertise and do not need guidance in consults:
- Choice of anesthetic type and its impact on outcome
- Choice of invasive or noninvasive monitoring for any comorbidity and operation
- Postoperative patient disposition (ie, whether to send a patient home, to the postanesthesia care unit, to the ICU, or to a step-down unit)
- Impact of optimizing organ function on perioperative outcome
- Cardiovascular and respiratory physiology
- Pharmacology of intravenous agents.
WHAT ANESTHESIOLOGISTS MAY NOT KNOW―AND NEED FROM CONSULTANTS
How to manage chronic diseases
Follow-up care (eg, for poorly controlled diabetes or hypertension) often can wait until after the operation, and a consultant’s opinion about that is appreciated. It is especially helpful to know that the patient will be followed without the surgeon or anesthesiologist having to arrange for it.
New evidence-based guidance from the literature
One case when recommendations on acute medical management should be provided is when they involve new information from the literature—ie, important data or guidelines published within the prior 5 years or so. It can take time for new information and recommendations to reach all clinicians even within a single specialty. Moreover, important information, such as on the perioperative use of beta-blockers and statins, is not necessarily published in the anesthesiology literature. It is critical to relay information such as the recent recommendation not to withdraw statins prior to surgery, as the current editions of most anesthesiology textbooks have incorrect information suggesting discontinuation. Thus, consultants should include pertinent recent data and guideline recommendations, especially if they go against previous dogma.
Rare diseases, blood disorders, other special cases
As outlined in Table 1, advice on perioperative management is appreciated for patients with rare diseases, coagulation disorders or other blood disorders, and brittle diabetes and other endocrine disorders, as most anesthesiologists are not intimately familiar with these conditions. Anesthesiologists also need, but often do not get, basic details on coronary stents and other implanted devices (see Table 1), as well as guidance on the latest anticoagulation recommendations, with which it is difficult to keep up to date.
A sensitivity to audience and context
It is always appropriate to ask the surgeon requesting a consult—and the anesthesiologist assigned to the case, if known—what he or she wants to know from the consult. If guidance on specific cases is impractical, it is appropriate to ask the chair of the anesthesiology department, or several anesthesiologists collectively, for general guidance on what they look for from preoperative consults.
Anesthesiologists, like consultants, comprise a broad range of people, and it is always important to be sensitive to context. Generalists who work mainly on healthy patients or in a community setting may have forgotten some of their training in acute medicine and are more likely to appreciate advice on intraoperative care. On the other hand, an anesthesiologist who trained in a cardiothoracic subspecialty fellowship, who routinely deals with issues such as left ventricular assist devices and heart transplants, would not benefit from such advice.
WHAT A CONSULT SHOULD―AND SHOULD NOT―BE
The above advice can be distilled into a few principles:
- A consult is an opportunity for the medical consultant to provide helpful management suggestions to the operative team.
- A fundamental objective of a consult is to optimize a patient’s underlying disease before it is compounded by the insult of surgery.
- The purpose of a consult is never to “clear” a patient for surgery. Whether or not to proceed to surgery is a question for the anesthesiologist, surgeon, and patient to decide after weighing the risks and benefits once the patient’s comorbidities are optimally managed. The consult is an important contributing factor to this decision, but it should never be the mechanism of the decision. Though the note from the surgeon requesting a consult may routinely be written as, “Clear the patient for surgery,” consultants should recognize this for what it is—the surgeon’s attempt to avoid having the anesthesiologist cancel the operation—and refrain from weighing in on “clearance” one way or the other.
CASE STUDY: CARDIAC CONSULT REQUESTED BEFORE FEM-POP BYPASS SURGERY
Cardiovascular problems are the most common reasons for requesting preoperative consults. The following case illustrates a typical scenario for a cardiac consult request and presents examples of good and bad notes requesting consults and good and bad consults written in response.
The case
A 47-year-old man is scheduled for femoral-popliteal bypass surgery. His medical history is significant for diabetes, a myocardial infarction (MI) 3 years ago followed by placement of a stent, and a limited ability to assess exercise tolerance. Evidence of an anteroseptal MI is present on 12-lead electrocardiography. His medications include metoprolol 25 mg twice daily and an oral hypoglycemic agent. His blood pressure is 152/89 mm Hg, heart rate 81 beats per minute, respiratory rate 14 breaths per minute, and arterial oxygen saturation 96% on room air.
The consult request: Bad and good examples
A bad consult request in this case would be, “Clear the patient for surgery.” Although this type of request is routinely written, it is routinely useless.
For this complex surgery with significant fluid requirements, a much better consult request would include several specific requests and questions and might read as follows:
—Please evaluate patient’s post-MI therapy for his CAD. Is further therapy required to optimize CAD treatment?
—Do his blood pressure or diabetic regimens need modification? If so, can this be done postoperatively?
—Please evaluate patient’s myocardial function in light of a lack of info on exercise tolerance. Is an echo indicated?
—Are other tests, therapies, or interventions warranted pre- or postoperatively?
Example of a bad consult
A poorly written consult in a case like this may:
- Include a brief history repeating facts that are already known and noting that “the patient is at his baseline without obvious ischemia.”
- State that the patient is cleared for “spinal” anesthesia. “Clearing a patient for anesthesia” is useless to begin with, but clearing for a certain type of anesthesia places the anesthesiologist in a terrible medicolegal position if general anesthesia turns out to be needed. Moreover, there are no proven major outcome differences related to the type of anesthetic chosen.
- Recommend that “a pulmonary artery catheter might be indicated to monitor hemodynamics.” Besides the fact that such catheters probably do more harm than good, such a recommendation is unnecessary since the anesthesiologist is already expert in managing perioperative care.
- Recommend that “the anesthesia team should monitor the patient carefully in the perioperative arena for hypoxia and hypotension.” Qualitative advice, such as “avoid hypoxia, hypotension, and tachycardia,” is not useful, but quantitative information, such as “during ischemic stress testing, the patient exhibited ischemia when his heart rate went to 142,” can be very helpful.
- State that the patient be sent to the ICU following surgery. Mandating an ICU stay in advance makes no sense unless the operation itself demands ICU care, which is the call of the surgeon and anesthesiologist anyway.
A consult like this doesn’t tell the perioperative team anything that it didn’t already know. Such a consult not only is unhelpful but also actually creates more work since much of the advice needs to be “undone” lest a lawyer see the chart and it not be clear why the consultant’s recommendations were not followed.
Example of a good consult
In contrast, a good consult for this case would involve:
- A detailed history examining the potential for silent ischemia associated with the diabetes, as well as the relationship of the hypertension and beta-blocker therapy to episodes of ischemia. The level of ischemia should be clearly categorized. If it cannot be determined, this should be noted; if it can be determined only that the ischemia is not New York Heart Association class III or IV, note this as well (the perioperative outcomes literature suggests that no preoperative ischemia testing is needed with class I or II angina).
- Guidance on blood pressure optimization in light of the relative urgency of the procedure. Blood pressure need not be normalized preoperatively in this case, but if the operation were totally elective and the consultant felt it could make a difference, it would be appropriate to suggest that blood pressure be optimized beforehand.
- A recommendation on whether and when to change the beta-blocker dosage. If the dosage needs to be increased, the anesthesiologist will want to know how many doses are needed to reach a new steady state. Joint guidelines from the American College of Cardiology (ACC) and American Heart Association (AHA)2 recommend 7 to 30 days, but this time frame is unrealistic in this setting, so more practical advice would be appreciated. A good consult notes any deviation from established guidelines, however, and explains the rationale for such deviation.
- Evaluation of the myocardium at risk. This is especially important with left main disease, as it influences the decision whether to test or intervene versus proceeding with careful beta-blocker titration.
- Evaluation of myocardial function and, if appropriate, a therapy suggestion for optimization.
- Notation of the heart rate or blood pressure thresholds at which ischemia develops if a stress test is performed.
GOOD GUIDANCE FROM THE ACC/AHA GUIDELINES
Our advice here is broadly consistent with the aforementioned 2007 ACC/AHA guidelines on perioperative cardiovascular evaluation for noncardiac surgery.2 The following observation on cardiac evaluations from these guidelines applies to preoperative consults in general:
The purpose of preoperative evaluation is not to give medical clearance but rather to perform an evaluation of the patient’s current medical status; make recommendations concerning the evaluation, management, and risk of cardiac problems over the entire perioperative period; and provide a clinical risk profile that [can be used] in making treatment decisions that may influence short- and long-term cardiac outcomes.2
These guidelines contain a good description of the ideal preoperative evaluation and consult in a short section (Section II, “General Approach to the Patient”)2 that is worthy of wide dissemination.
DISCUSSION
Question from the audience: Many consults are written more for the surgical team than for the anesthesiologists, hence advice such as managing intraoperative diabetes. Isn’t that appropriate?
Dr. Lubarsky: There are a variety of users of the information in a consult note. I focused on the anesthesiologist, but certainly the surgical staff and house staff would benefit from suggestions about postoperative management. However, they would not benefit from suggestions on intraoperative management; surgeons simply do not need this information and the anesthesiologist will have his or her own regimen. But if there is a specific type of insulin infusion that’s been shown to be best in the specific patient at hand, then detailing that obviously is beneficial.
Question from the audience: We all agree that communication is key, but how does the consultant reach the anesthesiologist to find out what he or she wants to know when the anesthesiologist isn’t usually assigned to the case until a day before surgery?
Dr. Lubarsky: If no anesthesiologist is yet assigned to a case, the consultant can discuss the case with the chief of the anesthesiology department. The discussion should be documented in the note. But it’s important that the system be changed so that anesthesiologists are assigned to cases well in advance. I instituted such a policy at my previous hospital. Many hospitals schedule surgeries 3 months in advance, and many anesthesiology departments have schedules made at least 1 month and often 2 to 3 months in advance. The department could assign a specific anesthesiologist to a future scheduled case with ease.
Question from the audience: How do anesthesiologists educate all the various people we rely on for consults when we can’t get them in one place at one time?
Dr. Lubarsky: It’s a challenge. I try many things, such as going to cardiology rounds, but there are always new people coming through. A good monograph or a set of guidelines with examples would help. If each specialty educates the other and speaks at each other’s conferences more often, that should help. Anesthesiologists would benefit from hearing about the challenges medical consultants face; we may not be doing all we can to optimize perioperative care. There’s room for improvement through communication on both sides. I should also emphasize that we’re all trying to do the right thing. Doctors try to be accommodating, but that doesn’t always make for good decisions. Recently a consultant in my hospital did a preoperative stress test on a patient who didn’t need one. When I asked why, he said, “Because the surgeon asked me to.”
Question from the audience: But don’t you agree that many anesthesiologists would like to see that negative stress test, even if a stress test is not indicated by the guidelines? Cardiologists know that the anesthesiologists are often looking for that on the morning of surgery.
Dr. Lubarsky: The point is that physicians should be responsible for what they have expertise in. When I am asked to intubate a patient, my response as an expert in intubation might be, “Actually, he doesn’t need to be intubated right now.” In the case of this unnecessary stress test, the cardiologist probably should have called the surgeon and said, “It’s really not indicated because the patient had a negative stress test 2 years ago, there’s been no change in symptoms and no angina since then, and he operates well above 4 metabolic equivalents. There’s a clear-cut reason not to do it.” If the surgeon still wanted the test done just to be reassured, that’s simply a poor use of society’s resources. We depend on experts to identify the tests that are indicated to evaluate a patient’s disease and not just do tests for the sake of doing them.
The ideal preoperative medical consultation (consult) is useful to the whole surgical team, ensures maximal patient readiness for surgery, and promotes optimal perioperative care of the patient. Too often, however, consults are ignored or, even worse, set the stage for legal problems. This article identifies problems frequently seen in preoperative consults, particularly from the perspective of anesthesiologists, and gives guidance to those who write consults—hospitalists, internists, cardiologists, and other medical consultants—on providing the information that is most needed by those who use them.
A WIDE RANGE OF END USERS
Anesthesiologists are most often the primary users of the information in preoperative consults, but many other members of the surgical and perioperative team benefit from a well-developed consult, including surgeons, intensivists, nurses, and pain management specialists. Most important, patients stand to benefit, as a good consult helps to ensure that the full breadth of relevant patient-specific information is brought to bear to anticipate potential difficulties and promote optimal care.
Purpose of a consult is in the eye of the beholder
The literature on medical consults in the perioperative arena is scant. The only fairly recent assessment of physician attitudes toward the role of consults was reported by Katz et al in 1998.1 These researchers surveyed attitudes about the various perceived purposes of preoperative cardiology consults, and received rather different responses from anesthesiologists, cardiologists, and surgeons.
There was consensus among all three specialties that two particular functions of a consult are important:
- Treating an inadequately managed cardiac condition before surgery
- Providing data to use in anesthetic management.
Additionally, all three specialties deemed the suggestion of intraoperative treatment modalities to be reasonably important when such suggestions were specifically included in the consult request, although anesthesiologists assigned less importance to this function.1
In contrast, anesthesiologists considered suggestions about intraoperative treatment generally unimportant when not specifically requested, and they viewed suggestions of intraoperative monitoring and advice on the safest type of anesthesia as even less important. Anesthesiologists also deemed “clearing the patient for surgery” as an unimportant function of the consult. Cardiologists rated all of these functions as more important than anesthesiologists did and in some cases as considerably more important. To many of the survey questions, surgeons responded that a specific purpose of a consult was “neither important nor unimportant.”1 That may be because the surgeon’s purpose in obtaining the consult is often simply to address the concerns of the anesthesiologist, who might otherwise delay or cancel a needed surgery.
Consult deficiencies: Vagueness, illegibility, dictating anesthetic choice
The survey by Katz et al also assessed each specialty’s perceptions of the most common deficiencies of preoperative cardiology consults. The deficiencies deemed most common were failure to give specific facts, illegible handwriting, and attempts to dictate the type of anesthesia to be used. Anesthesiologists considered each of the deficiencies assessed as occurring more commonly than their cardiologist or surgeon colleagues did.1
The requester–user disconnect
The differing perceptions of preoperative consults by anesthesiologists and surgeons underscore a fundamental problem: the primary requesters of consults (surgeons) are different from the primary users of consults (anesthesiologists).
Ideally, preoperative consults should be requested by anesthesiologists. Unless and until the ordering of consults changes on a wide scale, however, our advice is for consultants to ask the anesthesiologist what he or she needs to know, in addition to any questions directed to the requesting surgeon. Communication between the surgeon and anesthesiologist should be encouraged as much as possible, and consultants should keep both the anesthesiologist and surgeon in mind when writing consult notes.
A final end user: The plaintiff’s attorney
It is wise to keep in mind one more potential user of your consult: a plaintiff’s attorney. A poorly written consult may benefit plaintiffs’ lawyers. Consults should never give absolute instructions; it is better to use such phrases as “Strongly consider…” or “The current literature strongly suggests…” Otherwise, the surgical team is placed in an awkward position if it does not follow your recommendations, even if for good reason. If a certain recommendation absolutely must be followed, then direct oral communication from the consultant to the attending anesthesiologist (or surgeon) is best.
CONSIDER THE PRIMARY USER: WHAT ANESTHESIOLOGISTS ALREADY KNOW
For the purpose of preoperative consults, it is helpful to think of anesthesiologists as experts in acute medical care. Their 4-year training consists of the following:
- 1 year of internship, often in medicine, including 6 months of basic patient care in the ward or clinic (the last time they will manage chronic disease)
- 4 months in the intensive care unit (ICU) and 1 month in the recovery room, which yields solid intensivist training
- 3 months in pain management, covering acute and chronic pain and regional blocks
- ~24 months in the operating room, often devoted to care of complex problems in surgical subspecialties (obstetric, pediatric, neurologic, cardiothoracic, vascular)
- 1 month of preoperative screening and consultations (a recent requirement).
An optional fifth year may be spent in a subspecialty.
Since the large part of anesthesiologists’ training is in acute care, they generally do not need advice about the acute treatment of any ailment. Consults should not advise anesthesiologists on subjects in which they have considerable expertise. They already have well-established ideas about addressing hypertension, myocardial ischemia, heart failure, arrhythmias (unless unusual therapies are needed), bronchospasm, glucose levels, and pain in the operating room, so they are apt to ignore advice on such topics.
There are several additional topics in which anesthesiologists have considerable expertise and do not need guidance in consults:
- Choice of anesthetic type and its impact on outcome
- Choice of invasive or noninvasive monitoring for any comorbidity and operation
- Postoperative patient disposition (ie, whether to send a patient home, to the postanesthesia care unit, to the ICU, or to a step-down unit)
- Impact of optimizing organ function on perioperative outcome
- Cardiovascular and respiratory physiology
- Pharmacology of intravenous agents.
WHAT ANESTHESIOLOGISTS MAY NOT KNOW―AND NEED FROM CONSULTANTS
How to manage chronic diseases
Follow-up care (eg, for poorly controlled diabetes or hypertension) often can wait until after the operation, and a consultant’s opinion about that is appreciated. It is especially helpful to know that the patient will be followed without the surgeon or anesthesiologist having to arrange for it.
New evidence-based guidance from the literature
One case when recommendations on acute medical management should be provided is when they involve new information from the literature—ie, important data or guidelines published within the prior 5 years or so. It can take time for new information and recommendations to reach all clinicians even within a single specialty. Moreover, important information, such as on the perioperative use of beta-blockers and statins, is not necessarily published in the anesthesiology literature. It is critical to relay information such as the recent recommendation not to withdraw statins prior to surgery, as the current editions of most anesthesiology textbooks have incorrect information suggesting discontinuation. Thus, consultants should include pertinent recent data and guideline recommendations, especially if they go against previous dogma.
Rare diseases, blood disorders, other special cases
As outlined in Table 1, advice on perioperative management is appreciated for patients with rare diseases, coagulation disorders or other blood disorders, and brittle diabetes and other endocrine disorders, as most anesthesiologists are not intimately familiar with these conditions. Anesthesiologists also need, but often do not get, basic details on coronary stents and other implanted devices (see Table 1), as well as guidance on the latest anticoagulation recommendations, with which it is difficult to keep up to date.
A sensitivity to audience and context
It is always appropriate to ask the surgeon requesting a consult—and the anesthesiologist assigned to the case, if known—what he or she wants to know from the consult. If guidance on specific cases is impractical, it is appropriate to ask the chair of the anesthesiology department, or several anesthesiologists collectively, for general guidance on what they look for from preoperative consults.
Anesthesiologists, like consultants, comprise a broad range of people, and it is always important to be sensitive to context. Generalists who work mainly on healthy patients or in a community setting may have forgotten some of their training in acute medicine and are more likely to appreciate advice on intraoperative care. On the other hand, an anesthesiologist who trained in a cardiothoracic subspecialty fellowship, who routinely deals with issues such as left ventricular assist devices and heart transplants, would not benefit from such advice.
WHAT A CONSULT SHOULD―AND SHOULD NOT―BE
The above advice can be distilled into a few principles:
- A consult is an opportunity for the medical consultant to provide helpful management suggestions to the operative team.
- A fundamental objective of a consult is to optimize a patient’s underlying disease before it is compounded by the insult of surgery.
- The purpose of a consult is never to “clear” a patient for surgery. Whether or not to proceed to surgery is a question for the anesthesiologist, surgeon, and patient to decide after weighing the risks and benefits once the patient’s comorbidities are optimally managed. The consult is an important contributing factor to this decision, but it should never be the mechanism of the decision. Though the note from the surgeon requesting a consult may routinely be written as, “Clear the patient for surgery,” consultants should recognize this for what it is—the surgeon’s attempt to avoid having the anesthesiologist cancel the operation—and refrain from weighing in on “clearance” one way or the other.
CASE STUDY: CARDIAC CONSULT REQUESTED BEFORE FEM-POP BYPASS SURGERY
Cardiovascular problems are the most common reasons for requesting preoperative consults. The following case illustrates a typical scenario for a cardiac consult request and presents examples of good and bad notes requesting consults and good and bad consults written in response.
The case
A 47-year-old man is scheduled for femoral-popliteal bypass surgery. His medical history is significant for diabetes, a myocardial infarction (MI) 3 years ago followed by placement of a stent, and a limited ability to assess exercise tolerance. Evidence of an anteroseptal MI is present on 12-lead electrocardiography. His medications include metoprolol 25 mg twice daily and an oral hypoglycemic agent. His blood pressure is 152/89 mm Hg, heart rate 81 beats per minute, respiratory rate 14 breaths per minute, and arterial oxygen saturation 96% on room air.
The consult request: Bad and good examples
A bad consult request in this case would be, “Clear the patient for surgery.” Although this type of request is routinely written, it is routinely useless.
For this complex surgery with significant fluid requirements, a much better consult request would include several specific requests and questions and might read as follows:
—Please evaluate patient’s post-MI therapy for his CAD. Is further therapy required to optimize CAD treatment?
—Do his blood pressure or diabetic regimens need modification? If so, can this be done postoperatively?
—Please evaluate patient’s myocardial function in light of a lack of info on exercise tolerance. Is an echo indicated?
—Are other tests, therapies, or interventions warranted pre- or postoperatively?
Example of a bad consult
A poorly written consult in a case like this may:
- Include a brief history repeating facts that are already known and noting that “the patient is at his baseline without obvious ischemia.”
- State that the patient is cleared for “spinal” anesthesia. “Clearing a patient for anesthesia” is useless to begin with, but clearing for a certain type of anesthesia places the anesthesiologist in a terrible medicolegal position if general anesthesia turns out to be needed. Moreover, there are no proven major outcome differences related to the type of anesthetic chosen.
- Recommend that “a pulmonary artery catheter might be indicated to monitor hemodynamics.” Besides the fact that such catheters probably do more harm than good, such a recommendation is unnecessary since the anesthesiologist is already expert in managing perioperative care.
- Recommend that “the anesthesia team should monitor the patient carefully in the perioperative arena for hypoxia and hypotension.” Qualitative advice, such as “avoid hypoxia, hypotension, and tachycardia,” is not useful, but quantitative information, such as “during ischemic stress testing, the patient exhibited ischemia when his heart rate went to 142,” can be very helpful.
- State that the patient be sent to the ICU following surgery. Mandating an ICU stay in advance makes no sense unless the operation itself demands ICU care, which is the call of the surgeon and anesthesiologist anyway.
A consult like this doesn’t tell the perioperative team anything that it didn’t already know. Such a consult not only is unhelpful but also actually creates more work since much of the advice needs to be “undone” lest a lawyer see the chart and it not be clear why the consultant’s recommendations were not followed.
Example of a good consult
In contrast, a good consult for this case would involve:
- A detailed history examining the potential for silent ischemia associated with the diabetes, as well as the relationship of the hypertension and beta-blocker therapy to episodes of ischemia. The level of ischemia should be clearly categorized. If it cannot be determined, this should be noted; if it can be determined only that the ischemia is not New York Heart Association class III or IV, note this as well (the perioperative outcomes literature suggests that no preoperative ischemia testing is needed with class I or II angina).
- Guidance on blood pressure optimization in light of the relative urgency of the procedure. Blood pressure need not be normalized preoperatively in this case, but if the operation were totally elective and the consultant felt it could make a difference, it would be appropriate to suggest that blood pressure be optimized beforehand.
- A recommendation on whether and when to change the beta-blocker dosage. If the dosage needs to be increased, the anesthesiologist will want to know how many doses are needed to reach a new steady state. Joint guidelines from the American College of Cardiology (ACC) and American Heart Association (AHA)2 recommend 7 to 30 days, but this time frame is unrealistic in this setting, so more practical advice would be appreciated. A good consult notes any deviation from established guidelines, however, and explains the rationale for such deviation.
- Evaluation of the myocardium at risk. This is especially important with left main disease, as it influences the decision whether to test or intervene versus proceeding with careful beta-blocker titration.
- Evaluation of myocardial function and, if appropriate, a therapy suggestion for optimization.
- Notation of the heart rate or blood pressure thresholds at which ischemia develops if a stress test is performed.
GOOD GUIDANCE FROM THE ACC/AHA GUIDELINES
Our advice here is broadly consistent with the aforementioned 2007 ACC/AHA guidelines on perioperative cardiovascular evaluation for noncardiac surgery.2 The following observation on cardiac evaluations from these guidelines applies to preoperative consults in general:
The purpose of preoperative evaluation is not to give medical clearance but rather to perform an evaluation of the patient’s current medical status; make recommendations concerning the evaluation, management, and risk of cardiac problems over the entire perioperative period; and provide a clinical risk profile that [can be used] in making treatment decisions that may influence short- and long-term cardiac outcomes.2
These guidelines contain a good description of the ideal preoperative evaluation and consult in a short section (Section II, “General Approach to the Patient”)2 that is worthy of wide dissemination.
DISCUSSION
Question from the audience: Many consults are written more for the surgical team than for the anesthesiologists, hence advice such as managing intraoperative diabetes. Isn’t that appropriate?
Dr. Lubarsky: There are a variety of users of the information in a consult note. I focused on the anesthesiologist, but certainly the surgical staff and house staff would benefit from suggestions about postoperative management. However, they would not benefit from suggestions on intraoperative management; surgeons simply do not need this information and the anesthesiologist will have his or her own regimen. But if there is a specific type of insulin infusion that’s been shown to be best in the specific patient at hand, then detailing that obviously is beneficial.
Question from the audience: We all agree that communication is key, but how does the consultant reach the anesthesiologist to find out what he or she wants to know when the anesthesiologist isn’t usually assigned to the case until a day before surgery?
Dr. Lubarsky: If no anesthesiologist is yet assigned to a case, the consultant can discuss the case with the chief of the anesthesiology department. The discussion should be documented in the note. But it’s important that the system be changed so that anesthesiologists are assigned to cases well in advance. I instituted such a policy at my previous hospital. Many hospitals schedule surgeries 3 months in advance, and many anesthesiology departments have schedules made at least 1 month and often 2 to 3 months in advance. The department could assign a specific anesthesiologist to a future scheduled case with ease.
Question from the audience: How do anesthesiologists educate all the various people we rely on for consults when we can’t get them in one place at one time?
Dr. Lubarsky: It’s a challenge. I try many things, such as going to cardiology rounds, but there are always new people coming through. A good monograph or a set of guidelines with examples would help. If each specialty educates the other and speaks at each other’s conferences more often, that should help. Anesthesiologists would benefit from hearing about the challenges medical consultants face; we may not be doing all we can to optimize perioperative care. There’s room for improvement through communication on both sides. I should also emphasize that we’re all trying to do the right thing. Doctors try to be accommodating, but that doesn’t always make for good decisions. Recently a consultant in my hospital did a preoperative stress test on a patient who didn’t need one. When I asked why, he said, “Because the surgeon asked me to.”
Question from the audience: But don’t you agree that many anesthesiologists would like to see that negative stress test, even if a stress test is not indicated by the guidelines? Cardiologists know that the anesthesiologists are often looking for that on the morning of surgery.
Dr. Lubarsky: The point is that physicians should be responsible for what they have expertise in. When I am asked to intubate a patient, my response as an expert in intubation might be, “Actually, he doesn’t need to be intubated right now.” In the case of this unnecessary stress test, the cardiologist probably should have called the surgeon and said, “It’s really not indicated because the patient had a negative stress test 2 years ago, there’s been no change in symptoms and no angina since then, and he operates well above 4 metabolic equivalents. There’s a clear-cut reason not to do it.” If the surgeon still wanted the test done just to be reassured, that’s simply a poor use of society’s resources. We depend on experts to identify the tests that are indicated to evaluate a patient’s disease and not just do tests for the sake of doing them.
- Katz RI, Barnhart JM, Ho G, et al. A survey on the intended purposes and perceived utility of preoperative cardiology consultations. Anesth Analg 1998; 87:830–836.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2007; 116:e418–e499.
- Katz RI, Barnhart JM, Ho G, et al. A survey on the intended purposes and perceived utility of preoperative cardiology consultations. Anesth Analg 1998; 87:830–836.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2007; 116:e418–e499.
KEY POINTS
- Consults that provide pertinent quantitative data about the patient are helpful—eg, the heart rate at which ischemia was exhibited during stress testing and the degree of ischemia.
- Anesthesiologists do not need assistance with managing intravenous drugs (with the exception of unusual agents), but they can use specific guidance on managing oral medications pre- and postoperatively to best achieve optimization and steady-state concentrations.
- Pertinent recent information (< 5 years old) from the nonanesthesiology literature should be provided.
- Medical consultants should arrange for follow-up care for patients with active conditions not addressed by the surgery.
- Absolute recommendations should be avoided in a consult: the surgical team may have good reason not to follow them, and legal repercussions could ensue. The words “consider” or “strongly consider” usually suffice, except where there is an absolute standard of care.
Perioperative management of warfarin and antiplatelet therapy
Perioperative management of surgical patients who require temporary discontinuation of vitamin K antagonists (warfarin) or antiplatelet drugs is complicated. The risk of a thrombotic event during interruption of anticoagulant or antiplatelet therapy must be weighed against the risk of bleeding when such therapy is used in close proximity to a surgical procedure. This balancing of risks is guided by the patient’s individual risk for thromboembolism or bleeding and underlying conditions such as the presence of a mechanical heart valve or a coronary stent.
High-profile adverse events have made anticoagulant and antiplatelet management one of the most highly litigated aspects of perioperative medicine. Moreover, there is a paucity of randomized clinical trial data and definitive guidelines to address the perioperative needs of patients on antithrombotic therapy. Treatment protocols vary depending on many underlying factors, such as the presence of mechanical heart valves, comorbidities, stent type and location, patient age and medical history, and type of surgical procedure. While recent attention has focused on genetic variations that result in higher or lower sensitivity to warfarin in some patients, routine genetic testing for warfarin sensitivity is controversial and not part of widespread practice at this time.
The first portion of this article explores key issues and principles in the perioperative management of surgical patients on warfarin therapy, and the second portion does the same for surgical patients on antiplatelet therapy.
ACCP RECOMMENDATIONS FOR PERIOPERATIVE ANTICOAGULANT MANAGEMENT
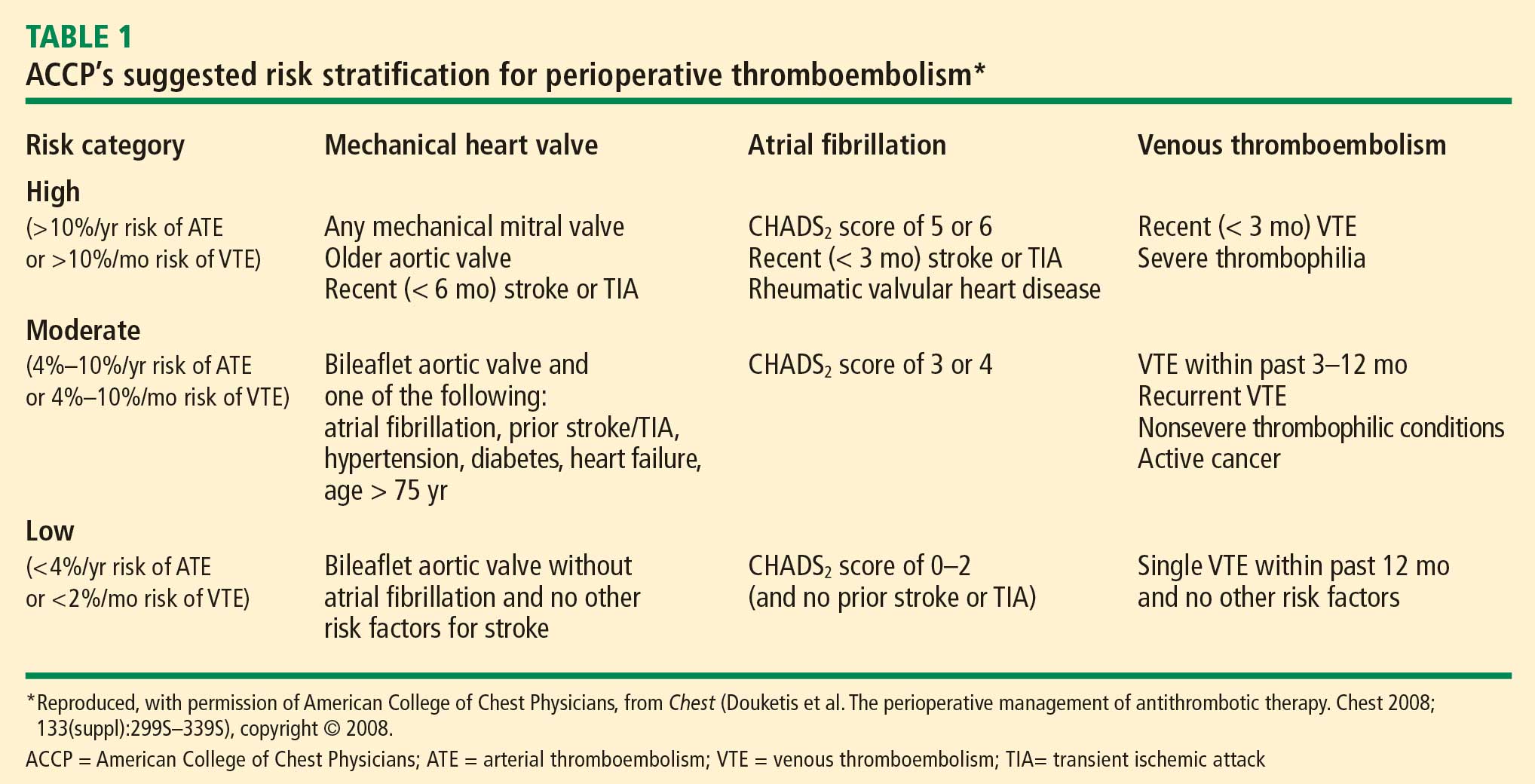
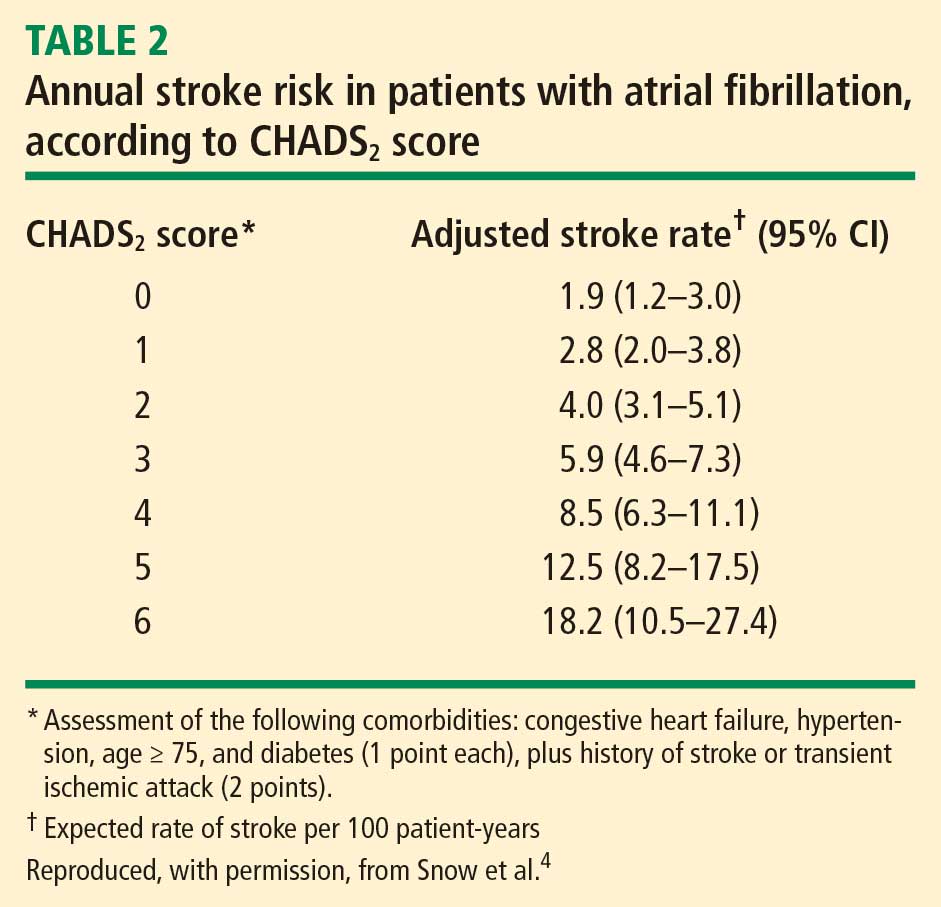
Patients with mechanical valves who are at high risk for perioperative thromboembolism include those with any mechanical mitral valve, an older valve, or a history of stroke or transient ischemic attack (TIA). Patients with atrial fibrillation who are at high risk include those with a recent stroke or TIA, rheumatic valvular heart disease, or a CHADS2 score of 5 or 6. (The CHADS2 scoring system assigns one point each for a history of congestive heart failure, hypertension, age greater than 75 years, or diabetes, and two points for history of stroke or TIA.) Patients with a history of VTE within the prior 3 months are also considered high risk.
Bridging anticoagulation (bridge therapy)—ie, the temporary use of intravenous unfractionated heparin (IV UFH) or low-molecular-weight heparin (LMWH) prior to surgery—is central to the ACCP’s recommendations for perioperative management in patients on long-term anticoagulant therapy. Key ACCP recommendations1 for these patients, according to their risk for thromboembolism (Table 1), are as follows:
- High risk—bridging anticoagulation with therapeutic-dose subcutaneous LMWH or IV UFH
- Moderate risk—bridging anticoagulation with therapeutic-dose subcutaneous LMWH, therapeutic-dose IV UFH, or low-dose subcutaneous LMWH
- Low risk—bridging anticoagulation with low-dose subcutaneous LMWH or no bridging.
ASSESSING RISKS: DETERMINING WHETHER TO BRIDGE
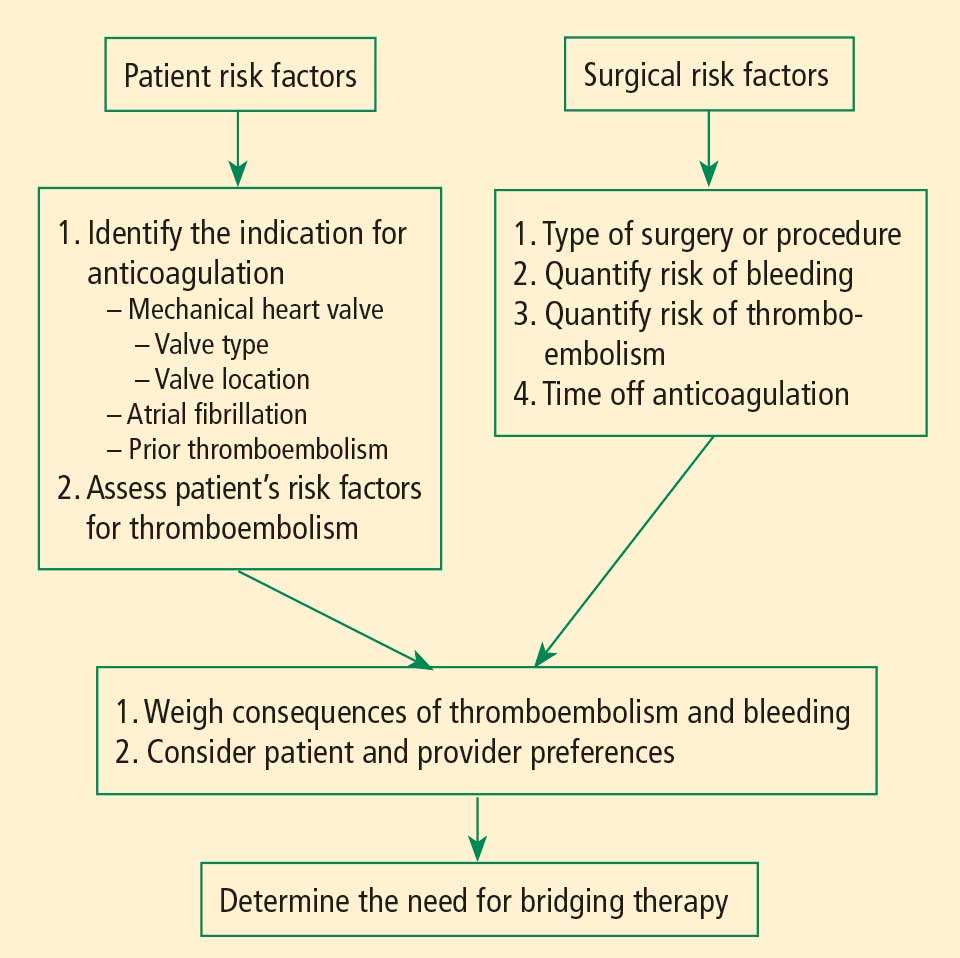
Patient-specific risk factors
Patient risk factors include the indication for anticoagulation, as detailed above, as well as other individual risks for thromboembolism, as discussed in the article by Michota on preventing VTE on page S45 of this supplement.
If anticoagulation is indicated because the patient has a mechanical heart valve, the valve type and position must be considered because these factors affect thromboembolic risk, as reflected in Table 1. For instance, the risk of thromboembolism is greater when the valve is in the mitral position than in the aortic position, and is also greater with an older caged-ball valve than with a newer-generation bileaflet valve.3
Procedure-related risk factors
Surgical risks factors include the type of surgery and its associated risks of bleeding and thromboembolism, as well as the expected time that anticoagulation will be interrupted. Estimating thromboembolic risk is complicated, however, and reliable results are generally not achieved with simplistic calculations or formulas. Such calculations tend not to appropriately account for the hypercoagulable state induced by surgery itself, as the risk of VTE is estimated to be 100 times greater during the perioperative period than in the nonoperative setting, owing to increased levels of plasminogen activator inhibitor-1. Moreover, multiple studies have demonstrated increases in coagulation factors that suggest that a “rebound hypercoagulability” may occur shortly after discontinuation of oral anticoagulant therapy.5–8
Net benefit vs risk in trials of bridge therapy
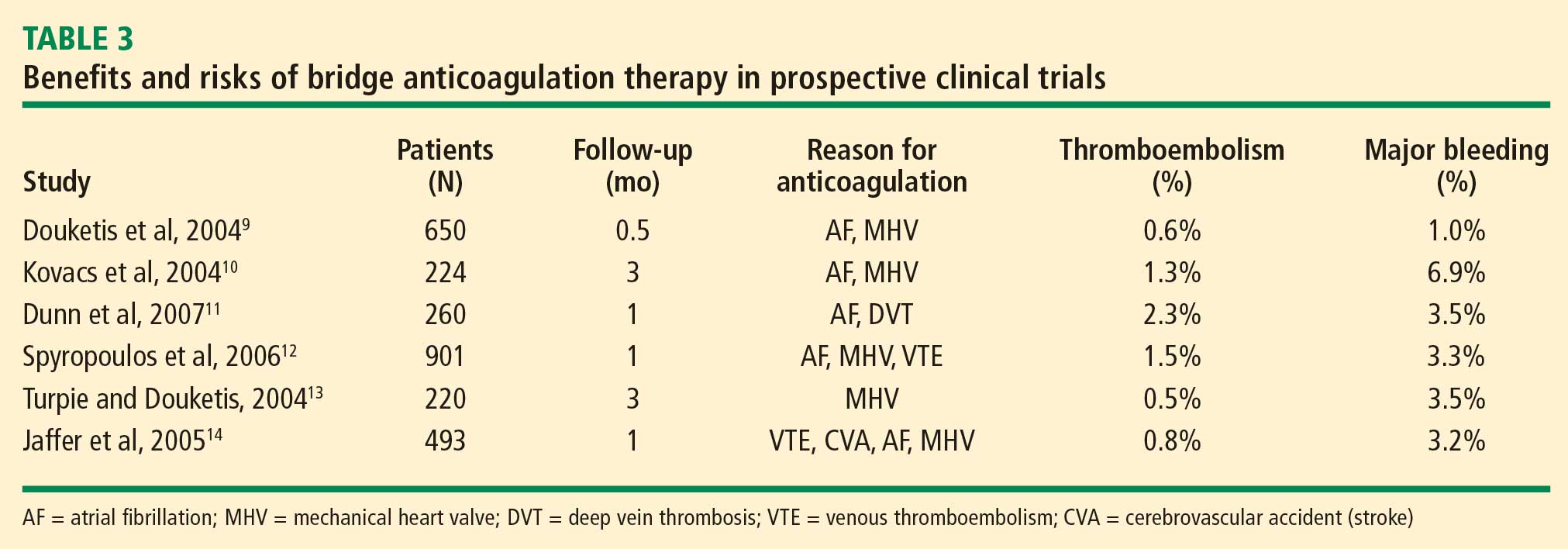
In an analysis of data from observational studies, Kearon and Hirsh estimated the relative risk reduction for thromboembolism with bridge therapy to be 66% to 80%, depending on the indication for anticoagulation.8 Thus, if a patient’s risk of developing thromboembolism is 1.5%, bridge therapy reduces the risk to 0.5% or less.
Weigh relative consequences of an event with the patient
Determining whether and how to initiate bridge therapy ultimately depends on the consequences of an event. Recurrent VTE is fatal in 5% to 10% of cases,15 and arterial thromboembolism is fatal in 20% of cases and causes permanent disability in at least 50% of cases.16 While 9% to 13% of major bleeding events are fatal, bleeding rarely causes permanent disability.17 Thus, whereas a patient who bleeds can be resuscitated, a patient who develops a thromboembolism may be permanently disabled. These considerations should be shared with the patient, and patient preference should factor into the management strategy. Though the risk of bleeding with anticoagulation may be much higher than the risk of stroke without it, many patients will be more concerned about stroke risk.
CHOICE OF AGENT FOR BRIDGE THERAPY
LMWH appears to offer cost advantage over UFH
For cost reasons, managed care organizations often recommend LMWH, which can be administered subcutaneously in outpatient settings, over IV UFH administered in the hospital. A retrospective analysis of medical costs from the 1990s in a managed care organization found that bridge therapy with LMWH prior to elective surgery cost an average of $13,114 less per patient (in total cost of care) than did bridge therapy with UFH.18
LMWH safety issues in valve patients are a myth
Clinical outcomes were not statistically significantly different for patients receiving LMWH or UFH in the above study.18 Nevertheless, there is a widely held notion that LMWH is not safe to use as bridge therapy for patients with mechanical heart valves. Recent prospective bridge studies do not support that view, demonstrating that LMWH used as bridge therapy is associated with low risks for thromboembolism and major bleeding even in patients with mechanical valves.9,10,12–14 In contrast, recent data on the use of IV UFH for bridging is minimal, with most bridge studies dating to the 1970s. Accordingly, the latest ACCP guidelines for perioperative management of patients on antithrombotic therapy recommend therapeutic-dose LMWH over IV UFH for bridge therapy, including in patients with mechanical heart valves.1 Likewise, 2006 guidelines from the American College of Cardiology and American Heart Association on management of patients with valvular heart disease endorse LMWH as an option for bridge therapy.19
A PRACTICAL APPROACH TO BRIDGE THERAPY
A bridge therapy protocol for patients receiving warfarin has been successfully used at the Cleveland Clinic, where I previously practiced. Essentials of the protocol20 are summarized here, followed by commentary that draws on additional sources.
Before surgery
- Discontinue warfarin 5 days before surgery (ie, hold four doses) if the preoperative international normalized ratio (INR) is 2 to 3, and 6 days before surgery (hold five doses) if the INR is 3 to 4.5.
- For bridge therapy, start LMWH (enoxaparin 1 mg/kg or dalteparin 100 IU/kg subcutaneously every 12 hours) beginning 36 hours after the last dose of warfarin.
- Give the last dose of LMWH approximately 24 hours prior to surgery.
After surgery
- For minor surgery, reinitiate LMWH at full dose approximately 24 hours after surgery. For major surgery and for patients at high risk of bleeding, consider using prophylactic doses on the first two postoperative days.
- Discuss the timing of anticoagulant reinitiation with the surgeon.
- Restart warfarin at preoperative dose 1 day after surgery.
- Order daily prothrombin time/INR tests until the patient is discharged and periodically after discharge until the INR is within the therapeutic range.
- Order a complete blood cell count with platelets on days 3 and 7.
- Discontinue LMWH when the INR is between 2 and 3 for 2 consecutive days.
Additionally, the plan should be discussed in advance with the patient, surgeon, and anesthesiologist, along with the risks and benefits associated with LMWH. The patient should receive written instructions for self-administration and information about signs and symptoms of bleeding and thromboembolism.
When to stop warfarin
Warfarin should be discontinued far enough in advance of surgery to achieve a preoperative target INR of less than 1.2.21 Patients with an initial INR of 2 to 3 tend to achieve that target after discontinuation of warfarin for about 5 days (four doses). A longer wait (6 days, or five doses) is necessary for patients with an initial INR of 3 to 4. Age is associated with a slower rate of decrease in the INR, and there is wide interpatient variation. The INR should always be checked prior to surgery.21
Warfarin need not be stopped for all procedures
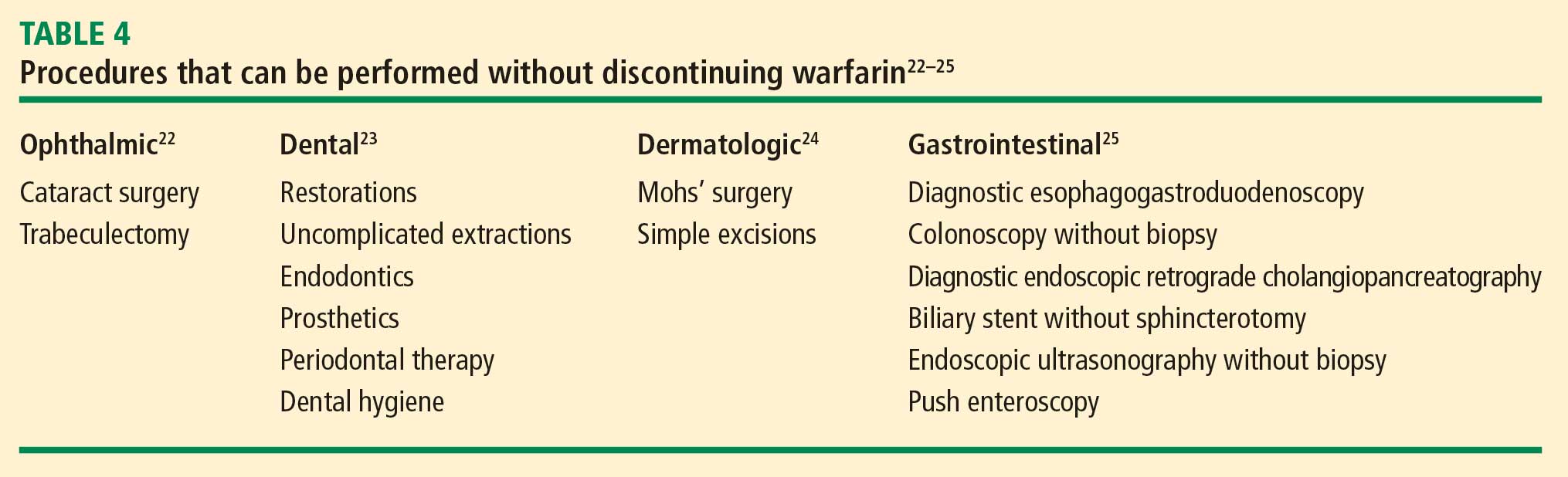
If warfarin is stopped for minor procedures, bridging may be counterproductive
At the same time, a recent prospective observational study evaluated the effects of brief (≤ 5 days) interruption of warfarin among more than 1,000 patients undergoing minor outpatient procedures and found low rates of both thromboembolism (0.7%) and major bleeding (0.6%).27 The risk of major bleeding was significantly higher among the small proportion of patients who received bridge therapy with UFH or LMWH. The study concluded that interrupting warfarin for 5 days or less for minor outpatient procedures carries a low risk of thromboembolism and that the risk of clinically significant bleeding should be weighed before bridge therapy is considered in this setting.
When to stop bridge therapy preoperatively
Bridge therapy with LMWH is commonly discontinued 12 hours before surgery, but it is preferable to discontinue 24 hours before surgery. In a study of preoperative anticoagulant activity in 80 patients, LMWH (enoxaparin 1 mg/kg) was administered twice daily and discontinued the night before surgery.28 Blood anti–factor Xa levels were measured shortly before surgery, at which time 68% of patients still had therapeutic levels of anti–Xa. This suggests that discontinuing LMWH too close to the time of surgery can increase the risk of bleeding.
Consistent with these findings, consensus guidelines from the American Society of Regional Anesthesia and Pain Medicine (ASRA) recommend that needle placement for regional anesthesia take place 12 hours after the last dose of LMWH if prophylactic dosing is used and 24 hours after the last dose of LMWH if therapeutic dosing is used (ie, ≥ 1 mg/kg of enoxaparin every 12 hours).29
Dosing and timing of postoperative bridge therapy
Postoperative use of full-dose bridge therapy is associated with increased risks of bleeding, according to a multicenter study of approximately 500 patients who received various doses of UFH or LMWH for bridge therapy.14 Patients who received full-dose LMWH or UFH after surgery had a fivefold to sixfold increase in the incidence of major bleeding compared with patients who received prophylactic doses. The study centers that frequently used full-dose bridge protocols were four times as likely to report major bleeding events. In light of these findings, waiting a couple of days after surgery to initiate full-dose bridge therapy is recommended, and prophylactic dosing may be considered in the interim.
The ASRA consensus guidelines recommend that indwelling catheters be removed prior to postoperative reinitiation of twice-daily dosing of LMWH. The first dose of LMWH should be given no sooner than 2 hours after catheter removal. Once-daily dosing of LMWH (European dosing) is acceptable under the ASRA guidelines, but the first dose should be given 6 to 8 hours after surgery and the second dose no sooner than 24 hours later. The guidelines state that once-daily (but not twice-daily) LMWH dosing is acceptable in patients with indwelling catheters; neurological status should be monitored in these patients, and the catheter should be removed 12 to 24 hours after the last dose of LMWH.29
PERIOPERATIVE MANAGEMENT OF ANTIPLATELET THERAPY: TYPE OF AGENT MATTERS
Unlike the considerations with warfarin, the timing of preoperative discontinuation of antiplatelet therapy in patients undergoing noncardiac surgery depends on the type of agent used and its pharmacokinetic actions. Commonly used antiplatelet drugs include aspirin, the thienopyridine agent clopidogrel, and nonsteroidal anti-inflammatory drugs (NSAIDs).
Aspirin works by irreversibly inhibiting platelet cyclooxygenase. The circulating platelet pool is replaced every 7 to 10 days, so aspirin therapy should be discontinued 7 to 10 days before surgery.1
NSAIDs reversibly inhibit platelet cyclooxygenase. Knowing whether a patient is using short- or long-acting NSAIDs is important for determining when to discontinue therapy. For a short-acting NSAID such as ibuprofen, discontinuation 24 hours before surgery may be adequate to normalize platelet function.1,30
Thienopyridines inhibit adenosine diphosphate receptor–mediated platelet activation and aggregation. Short-acting thienopyridines may be discontinued 24 hours before surgery, but long-acting agents such as clopidogrel should be stopped 7 days prior to surgery (including when used with aspirin as dual antiplatelet therapy),1 although some outcomes data suggest that 5 days may be sufficient.31
All of these agents should be resumed as soon as adequate hemostasis is achieved after surgery. The ACCP guidelines on perioperative management of antithrombotic therapy recommend resumption of aspirin at the usual maintenance dose the day after surgery, but they make no specific recommendations on when to resume other antiplatelet drugs.1
ANTIPLATELET THERAPY: SPECIAL CONSIDERATIONS IN PATIENTS WITH STENTS
Patients who are on antiplatelet therapy because they have a coronary stent merit special consideration due to the high risk of thrombosis if therapy is interrupted. The risk of stent thrombosis is especially elevated in the postoperative period, particularly if surgery follows soon after stent placement.
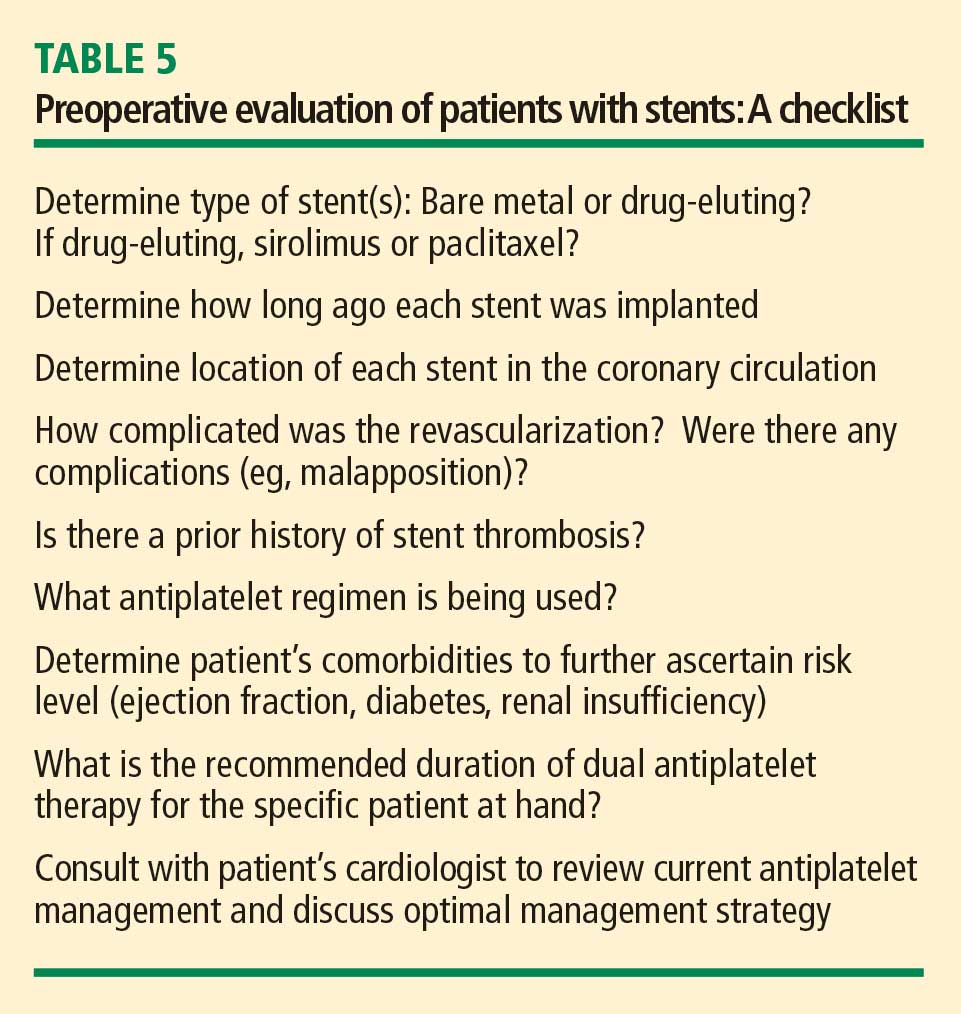
- Relative risks and benefits of stopping versus continuing antiplatelet therapy
- Identification of patients at high risk for a perioperative event after cessation of antiplatelet therapy
- Identification of patients at high risk of bleeding.
Bleeding vs stent thrombosis: Consider relative consequences
The risk of bleeding varies by individual patient. No laboratory tests are available to determine individual bleeding risk, but the risk of perioperative bleeding increases when two or more antiplatelet agents are used, as in dual antiplatelet therapy with aspirin and clopidogrel.31
When balancing risks of bleeding versus thrombotic events, the relative consequences of each event again must be considered. Bleeding is rarely life-threatening in comparison with the potential consequences of stent thrombosis. In a prospective observational study of 2,229 patients who received drug-eluting stents, 29 (1.3%) developed stent thrombosis during 9-month follow-up.32 Among these patients, 20 (69%) had a nonfatal myocardial infarction and 13 (45%) died. The most significant independent risk factor for stent thrombosis was premature discontinuation of antiplatelet therapy (hazard ratio = 89.78 [95% CI, 29.90–260.60]; P < .001). Other independent risk factors included renal failure, bifurcation lesions, diabetes, and low ejection fraction.
Premature interruption of antiplatelet therapy: Why it matters
Abrupt discontinuation of antiplatelet therapy can lead to a rebound effect marked by an inflammatory prothrombotic state, increased platelet adhesion and aggregation, and excessive thromboxane A2 activity. Surgery further increases the prothrombotic and inflammatory state, which, combined with incompletely endothelialized drug-eluting stents, can lead to stent thrombosis and, consequently, myocardial infarction and/or death.33
Timing of surgery after stenting: Getting it right
The US Food and Drug Administration recommends that dual antiplatelet therapy be continued for at least 3 months after placement of a sirolimus-eluting stent and at least 6 months after placement of a paclitaxel-eluting stent. Recent data suggest, however, that this duration of antiplatelet therapy may not be sufficient and that at least 1 year of therapy may be needed.34
A recent joint science advisory from the American College of Cardiology (ACC) and the American Heart Association (AHA) emphasizes the importance of educating providers about the “potentially catastrophic” risks of premature stopping of thienopyridine therapy in patients with coronary stents.34 In addition to recommendations in this joint advisory, the ACC and AHA issued updated guidelines in 2007 on perioperative cardiovascular evaluation and care for noncardiac surgery.35 Below is a summary of recommendations on the timing of surgery following stenting in light of these and other sources:
- Following placement of a bare metal stent, elective and nonurgent procedures should be delayed for at least 1 month, according to the ACC/AHA joint advisory,34 or at least 6 weeks, according to the ACC/AHA guidelines.35 Newer data suggest that the optimal interval for delay is likely to be 3 months.36,37
- For patients with recent (< 6 weeks) bare metal stent placement who require urgent surgery, dual antiplatelet therapy should be continued during the perioperative period.1
- Following placement of a drug-eluting stent, elective and nonurgent procedures should be delayed for at least 12 months.34,35
- For patients with recent drug-eluting stent placement in whom surgery cannot be delayed, dual antiplatelet therapy should be continued without interruption if the stent was placed within the prior 6 months.1,35 If the stent was placed more than 6 months before urgent surgery, aspirin should be continued without interruption (at ≥ 81 mg/day) and clopidogrel should be continued until 5 days before surgery and resumed as soon as possible after surgery (at a loading dose of 300 mg followed by 75 mg/day). If the surgeon is comfortable continuing dual antiplatelet therapy in a patient whose stent was placed 6 to 12 months earlier, that course should be considered.1
It is important to note that the ACC/AHA joint advisory34 and other documents have medicolegal implications, so delaying nonurgent surgery for the periods recommended is the most prudent approach.
CONCLUSIONS
Perioperative management of anticoagulant and antiplatelet therapy is complicated by the paucity of randomized clinical trial data and the risk for serious adverse events. The underlying indications for anticoagulant and antiplatelet therapy vary widely, so the best approach to perioperative management is to involve all members of the health care team—hospitalist, surgeon, cardiologist, and anesthesiologist, together with the patient—to ensure that care is individualized and all relevant considerations are accounted for. Patient and surgical risks can be identified and quantified to some extent, but patients often have greater concerns about the risk of stroke than the risk of bleeding. Ideally, nonemergency surgeries should be scheduled to allow enough time to thoroughly plan the management protocol, reducing risks for bleeding and thrombotic events as much as possible.
DISCUSSION
Question from the audience: If a patient’s INR is 1.3 or 1.4, rather than the recommended 1.2, is it necessary to cancel a planned epidural?
Dr. Jaffer: It depends on how comfortable the surgeon or anesthesiologist is with the INR level. Generally, an INR less than 1.5 is probably acceptable, but it depends on the procedure. For a craniotomy, for example, 1.2 is recommended.
Question from the audience: Is it necessary to use anti–Xa levels to guide bridge therapy when administering LMWH or UFH in a patient with a mechanical heart valve?
Dr. Jaffer: It’s not generally necessary, except for pregnant women. For most patients, doses are calculated as milligrams of LMWH per kilogram body weight or as International Units of LMWH per kilogram.
Question from the audience: You mentioned medicolegal disputes arising from adverse events associated with bridge therapy, drug discontinuation, or related issues. Who has final responsibility for making decisions about discontinuation of antiplatelet therapy, for example?
Dr. Jaffer: I don’t know if it ultimately comes down to just one person. Several physicians should be involved in the decision, and communication protocols within an institution should be very clear. It’s important to make certain everyone involved in the decision is reviewing the same literature. The final decision has to be something everyone involved can accept and support.
- Douketis JD, Berger PB, Dunn AS, et al. The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133(suppl 6):299S–339S.
- du Breuil AL, Umland EM. Outpatient management of anticoagulation therapy. Am Fam Physician 2007; 75:1031–1042.
- Cannegieter SC, Rosendaal FR, Briët E. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Circulation 1994; 89:635–641.
- Snow V, Weiss KB, LeFevre M, et al. Management of newly detected atrial fibrillation: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Intern Med 2003; 139:1009–1017.
- Genewein U, Haeberli A, Straub PW, Beer JH. Rebound after cessation of oral anticoagulant therapy: the biochemical evidence. Br J Haematol 1996; 92:479–485.
- Grip L, Blombäck M, Schulman S. Hypercoagulable state and thromboembolism following warfarin withdrawal in post-myocardial-infarction patients. Eur Heart J 1991; 12:1225–1233.
- Palareti G, Legnani C, Guazzaloca G, et al. Activation of blood coagulation after abrupt or stepwise withdrawal of oral anticoagulants: a prospective study. Thromb Haemost 1994; 72:222–226.
- Kearon C, Hirsh J. Management of anticoagulation before and after elective surgery. N Engl J Med 1997; 336:1506–1511.
- Douketis JD, Johnson JA, Turpie AG. Low-molecular-weight heparin as bridging anticoagulation during interruption of warfarin: assessment of a standardized periprocedural anticoagulation regimen. Arch Intern Med 2004; 164:1319–1326.
- Kovacs MJ, Kearon C, Rodger M, et al. Single-arm study of bridging therapy with low-molecular-weight heparin for patients at risk of arterial embolism who require temporary interruption of warfarin. Circulation 2004; 110:1658–1663.
- Dunn AS, Spyropoulos AC, Turpie AG. Bridging therapy in patients on long-term oral anticoagulants who require surgery: the Prospective Peri-operative Enoxaparin Cohort Trial (PROSPECT). J Thromb Haemost 2007; 5:2211–2218.
- Spyropoulos AC, Turpie AG, Dunn AS, et al. Clinical outcomes with unfractionated heparin or low-molecular-weight heparin as bridging therapy in patients on long-term oral anticoagulants: the REGIMEN registry. J Thromb Haemost 2006; 4:1246–1252.
- Turpie AG, Douketis JD. Enoxaparin is effective and safe as bridging anticoagulation in patients with a mechanical prosthetic heart valve who require temporary interruption of warfarin because of surgery or an invasive procedure. Blood 2004:202s. Abstract 703.
- Jaffer AK, Brotman DJ, White RH. The perioperative and periprocedural management of warfarin: the PPMW study. J Thromb Haemost 2005; 3(suppl 1). Abstract OR309.
- Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann Intern Med 2003; 139:893–900.
- Schulman S, Rhedin AS, Lindmarker P, et al. A comparison of six weeks with six months of oral anticoagulant therapy after a first episode of venous thromboembolism: duration of Anticoagulation Trial Study Group. N Engl J Med 1995; 332:1661–1665.
- Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation: analysis of pooled data from five randomized controlled trials. Arch Intern Med 1994; 154:1449–1457.
- Spyropoulos AC, Frost FJ, Hurley JS, Roberts M. Costs and clinical outcomes associated with low-molecular-weight heparin vs unfractionated heparin for perioperative bridging in patients receiving long-term oral anticoagulant therapy. Chest 2004; 125:1642–1650.
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. Circulation 2006; 114:e84–e231.
- Jaffer AK, Brotman DJ, Chukwumerjie N. When patients on warfarin need surgery. Cleve Clin J Med 2003; 70:973–984.
- White RH, McKittrick T, Hutchinson R, Twitchell J. Temporary discontinuation of warfarin therapy: changes in the international normalized ratio. Ann Intern Med 1995; 122:40–42.
- Konstantatos A. Anticoagulation and cataract surgery: a review of the current literature. Anaesth Intensive Care 2001; 29:11–18.
- Weibert RT. Oral anticoagulant therapy in patients undergoing dental surgery. Clin Pharm 1992; 11:857–864.
- Billingsley EM, Maloney ME. Intraoperative and postoperative bleeding problems in patients taking warfarin, aspirin, and nonsteroidal antiinflammatory agents: a prospective study. Dermatol Surg 1997; 23:381–383.
- Kadakia SC, Angueira CE, Ward JA, Moore M. Gastrointestinal endoscopy in patients taking antiplatelet agents and anticoagulants: survey of ASGE members: American Society for Gastrointestinal Endoscopy. Gastrointest Endosc 1996; 44:309–316.
- Dunn AS, Turpie AG. Perioperative management of patients receiving oral anticoagulants: a systematic review. Arch Intern Med 2003; 163:901–908.
- Garcia DA, Regan S, Henault LE, et al. Risk of thromboembolism with short-term interruption of warfarin therapy. Arch Intern Med 2008; 168:63–69.
- O’Donnell MJ, Kearon C, Johnson J, et al. Brief communication: preoperative anticoagulant activity after bridging low-molecular-weight heparin for temporary interruption of warfarin. Ann Intern Med 2007; 146:184–187.
- Horlocker TT, Wedel DJ, Benzon H, et al. Regional anesthesia in the anticoagulated patient: defining the risks (the second ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation). Reg Anesth Pain Med 2003; 28:172–197.
- Goldenberg NA, Jacobson L, Manco-Johnson MJ. Brief communication: duration of platelet dysfunction after a 7-day course of ibuprofen. Ann Intern Med 2005; 142:506–509.
- Lecompte T, Hardy JF. Antiplatelet agents and perioperative bleeding. Can J Anaesth 2006; 53(suppl 6):S103–S112.
- Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005; 293:2126–2130.
- Newsome LT, Weller RS, Gerancher JC, Kutcher MA, Royster RL. Coronary artery stents: II. Perioperative considerations and management. Anesth Analg 2008; 107:570–590.
- Grines CL, Bonow RO, Casey DE Jr, et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. Circulation 2007; 115:813–818.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines [published correction appears in J Am Coll Cardiol 2008; 52:794–797]. J Am Coll Cardiol 2007; 50:1707–1732.
- Brichon PY, Boitet P, Dujon A, et al. Perioperative in-stent thrombosis after lung resection performed within 3 months of coronary stenting. Eur J Cardiothorac Surg 2006; 30:793–796.
- Nuttall GA, Brown MJ, Stombaugh JW, et al. Time and cardiac risk of surgery after bare-metal stent percutaneous coronary intervention. Anesthesiology 2008; 109:588–595.
Perioperative management of surgical patients who require temporary discontinuation of vitamin K antagonists (warfarin) or antiplatelet drugs is complicated. The risk of a thrombotic event during interruption of anticoagulant or antiplatelet therapy must be weighed against the risk of bleeding when such therapy is used in close proximity to a surgical procedure. This balancing of risks is guided by the patient’s individual risk for thromboembolism or bleeding and underlying conditions such as the presence of a mechanical heart valve or a coronary stent.
High-profile adverse events have made anticoagulant and antiplatelet management one of the most highly litigated aspects of perioperative medicine. Moreover, there is a paucity of randomized clinical trial data and definitive guidelines to address the perioperative needs of patients on antithrombotic therapy. Treatment protocols vary depending on many underlying factors, such as the presence of mechanical heart valves, comorbidities, stent type and location, patient age and medical history, and type of surgical procedure. While recent attention has focused on genetic variations that result in higher or lower sensitivity to warfarin in some patients, routine genetic testing for warfarin sensitivity is controversial and not part of widespread practice at this time.
The first portion of this article explores key issues and principles in the perioperative management of surgical patients on warfarin therapy, and the second portion does the same for surgical patients on antiplatelet therapy.
ACCP RECOMMENDATIONS FOR PERIOPERATIVE ANTICOAGULANT MANAGEMENT
Patients with mechanical valves who are at high risk for perioperative thromboembolism include those with any mechanical mitral valve, an older valve, or a history of stroke or transient ischemic attack (TIA). Patients with atrial fibrillation who are at high risk include those with a recent stroke or TIA, rheumatic valvular heart disease, or a CHADS2 score of 5 or 6. (The CHADS2 scoring system assigns one point each for a history of congestive heart failure, hypertension, age greater than 75 years, or diabetes, and two points for history of stroke or TIA.) Patients with a history of VTE within the prior 3 months are also considered high risk.
Bridging anticoagulation (bridge therapy)—ie, the temporary use of intravenous unfractionated heparin (IV UFH) or low-molecular-weight heparin (LMWH) prior to surgery—is central to the ACCP’s recommendations for perioperative management in patients on long-term anticoagulant therapy. Key ACCP recommendations1 for these patients, according to their risk for thromboembolism (Table 1), are as follows:
- High risk—bridging anticoagulation with therapeutic-dose subcutaneous LMWH or IV UFH
- Moderate risk—bridging anticoagulation with therapeutic-dose subcutaneous LMWH, therapeutic-dose IV UFH, or low-dose subcutaneous LMWH
- Low risk—bridging anticoagulation with low-dose subcutaneous LMWH or no bridging.
ASSESSING RISKS: DETERMINING WHETHER TO BRIDGE
Patient-specific risk factors
Patient risk factors include the indication for anticoagulation, as detailed above, as well as other individual risks for thromboembolism, as discussed in the article by Michota on preventing VTE on page S45 of this supplement.
If anticoagulation is indicated because the patient has a mechanical heart valve, the valve type and position must be considered because these factors affect thromboembolic risk, as reflected in Table 1. For instance, the risk of thromboembolism is greater when the valve is in the mitral position than in the aortic position, and is also greater with an older caged-ball valve than with a newer-generation bileaflet valve.3
Procedure-related risk factors
Surgical risks factors include the type of surgery and its associated risks of bleeding and thromboembolism, as well as the expected time that anticoagulation will be interrupted. Estimating thromboembolic risk is complicated, however, and reliable results are generally not achieved with simplistic calculations or formulas. Such calculations tend not to appropriately account for the hypercoagulable state induced by surgery itself, as the risk of VTE is estimated to be 100 times greater during the perioperative period than in the nonoperative setting, owing to increased levels of plasminogen activator inhibitor-1. Moreover, multiple studies have demonstrated increases in coagulation factors that suggest that a “rebound hypercoagulability” may occur shortly after discontinuation of oral anticoagulant therapy.5–8
Net benefit vs risk in trials of bridge therapy
In an analysis of data from observational studies, Kearon and Hirsh estimated the relative risk reduction for thromboembolism with bridge therapy to be 66% to 80%, depending on the indication for anticoagulation.8 Thus, if a patient’s risk of developing thromboembolism is 1.5%, bridge therapy reduces the risk to 0.5% or less.
Weigh relative consequences of an event with the patient
Determining whether and how to initiate bridge therapy ultimately depends on the consequences of an event. Recurrent VTE is fatal in 5% to 10% of cases,15 and arterial thromboembolism is fatal in 20% of cases and causes permanent disability in at least 50% of cases.16 While 9% to 13% of major bleeding events are fatal, bleeding rarely causes permanent disability.17 Thus, whereas a patient who bleeds can be resuscitated, a patient who develops a thromboembolism may be permanently disabled. These considerations should be shared with the patient, and patient preference should factor into the management strategy. Though the risk of bleeding with anticoagulation may be much higher than the risk of stroke without it, many patients will be more concerned about stroke risk.
CHOICE OF AGENT FOR BRIDGE THERAPY
LMWH appears to offer cost advantage over UFH
For cost reasons, managed care organizations often recommend LMWH, which can be administered subcutaneously in outpatient settings, over IV UFH administered in the hospital. A retrospective analysis of medical costs from the 1990s in a managed care organization found that bridge therapy with LMWH prior to elective surgery cost an average of $13,114 less per patient (in total cost of care) than did bridge therapy with UFH.18
LMWH safety issues in valve patients are a myth
Clinical outcomes were not statistically significantly different for patients receiving LMWH or UFH in the above study.18 Nevertheless, there is a widely held notion that LMWH is not safe to use as bridge therapy for patients with mechanical heart valves. Recent prospective bridge studies do not support that view, demonstrating that LMWH used as bridge therapy is associated with low risks for thromboembolism and major bleeding even in patients with mechanical valves.9,10,12–14 In contrast, recent data on the use of IV UFH for bridging is minimal, with most bridge studies dating to the 1970s. Accordingly, the latest ACCP guidelines for perioperative management of patients on antithrombotic therapy recommend therapeutic-dose LMWH over IV UFH for bridge therapy, including in patients with mechanical heart valves.1 Likewise, 2006 guidelines from the American College of Cardiology and American Heart Association on management of patients with valvular heart disease endorse LMWH as an option for bridge therapy.19
A PRACTICAL APPROACH TO BRIDGE THERAPY
A bridge therapy protocol for patients receiving warfarin has been successfully used at the Cleveland Clinic, where I previously practiced. Essentials of the protocol20 are summarized here, followed by commentary that draws on additional sources.
Before surgery
- Discontinue warfarin 5 days before surgery (ie, hold four doses) if the preoperative international normalized ratio (INR) is 2 to 3, and 6 days before surgery (hold five doses) if the INR is 3 to 4.5.
- For bridge therapy, start LMWH (enoxaparin 1 mg/kg or dalteparin 100 IU/kg subcutaneously every 12 hours) beginning 36 hours after the last dose of warfarin.
- Give the last dose of LMWH approximately 24 hours prior to surgery.
After surgery
- For minor surgery, reinitiate LMWH at full dose approximately 24 hours after surgery. For major surgery and for patients at high risk of bleeding, consider using prophylactic doses on the first two postoperative days.
- Discuss the timing of anticoagulant reinitiation with the surgeon.
- Restart warfarin at preoperative dose 1 day after surgery.
- Order daily prothrombin time/INR tests until the patient is discharged and periodically after discharge until the INR is within the therapeutic range.
- Order a complete blood cell count with platelets on days 3 and 7.
- Discontinue LMWH when the INR is between 2 and 3 for 2 consecutive days.
Additionally, the plan should be discussed in advance with the patient, surgeon, and anesthesiologist, along with the risks and benefits associated with LMWH. The patient should receive written instructions for self-administration and information about signs and symptoms of bleeding and thromboembolism.
When to stop warfarin
Warfarin should be discontinued far enough in advance of surgery to achieve a preoperative target INR of less than 1.2.21 Patients with an initial INR of 2 to 3 tend to achieve that target after discontinuation of warfarin for about 5 days (four doses). A longer wait (6 days, or five doses) is necessary for patients with an initial INR of 3 to 4. Age is associated with a slower rate of decrease in the INR, and there is wide interpatient variation. The INR should always be checked prior to surgery.21
Warfarin need not be stopped for all procedures
If warfarin is stopped for minor procedures, bridging may be counterproductive
At the same time, a recent prospective observational study evaluated the effects of brief (≤ 5 days) interruption of warfarin among more than 1,000 patients undergoing minor outpatient procedures and found low rates of both thromboembolism (0.7%) and major bleeding (0.6%).27 The risk of major bleeding was significantly higher among the small proportion of patients who received bridge therapy with UFH or LMWH. The study concluded that interrupting warfarin for 5 days or less for minor outpatient procedures carries a low risk of thromboembolism and that the risk of clinically significant bleeding should be weighed before bridge therapy is considered in this setting.
When to stop bridge therapy preoperatively
Bridge therapy with LMWH is commonly discontinued 12 hours before surgery, but it is preferable to discontinue 24 hours before surgery. In a study of preoperative anticoagulant activity in 80 patients, LMWH (enoxaparin 1 mg/kg) was administered twice daily and discontinued the night before surgery.28 Blood anti–factor Xa levels were measured shortly before surgery, at which time 68% of patients still had therapeutic levels of anti–Xa. This suggests that discontinuing LMWH too close to the time of surgery can increase the risk of bleeding.
Consistent with these findings, consensus guidelines from the American Society of Regional Anesthesia and Pain Medicine (ASRA) recommend that needle placement for regional anesthesia take place 12 hours after the last dose of LMWH if prophylactic dosing is used and 24 hours after the last dose of LMWH if therapeutic dosing is used (ie, ≥ 1 mg/kg of enoxaparin every 12 hours).29
Dosing and timing of postoperative bridge therapy
Postoperative use of full-dose bridge therapy is associated with increased risks of bleeding, according to a multicenter study of approximately 500 patients who received various doses of UFH or LMWH for bridge therapy.14 Patients who received full-dose LMWH or UFH after surgery had a fivefold to sixfold increase in the incidence of major bleeding compared with patients who received prophylactic doses. The study centers that frequently used full-dose bridge protocols were four times as likely to report major bleeding events. In light of these findings, waiting a couple of days after surgery to initiate full-dose bridge therapy is recommended, and prophylactic dosing may be considered in the interim.
The ASRA consensus guidelines recommend that indwelling catheters be removed prior to postoperative reinitiation of twice-daily dosing of LMWH. The first dose of LMWH should be given no sooner than 2 hours after catheter removal. Once-daily dosing of LMWH (European dosing) is acceptable under the ASRA guidelines, but the first dose should be given 6 to 8 hours after surgery and the second dose no sooner than 24 hours later. The guidelines state that once-daily (but not twice-daily) LMWH dosing is acceptable in patients with indwelling catheters; neurological status should be monitored in these patients, and the catheter should be removed 12 to 24 hours after the last dose of LMWH.29
PERIOPERATIVE MANAGEMENT OF ANTIPLATELET THERAPY: TYPE OF AGENT MATTERS
Unlike the considerations with warfarin, the timing of preoperative discontinuation of antiplatelet therapy in patients undergoing noncardiac surgery depends on the type of agent used and its pharmacokinetic actions. Commonly used antiplatelet drugs include aspirin, the thienopyridine agent clopidogrel, and nonsteroidal anti-inflammatory drugs (NSAIDs).
Aspirin works by irreversibly inhibiting platelet cyclooxygenase. The circulating platelet pool is replaced every 7 to 10 days, so aspirin therapy should be discontinued 7 to 10 days before surgery.1
NSAIDs reversibly inhibit platelet cyclooxygenase. Knowing whether a patient is using short- or long-acting NSAIDs is important for determining when to discontinue therapy. For a short-acting NSAID such as ibuprofen, discontinuation 24 hours before surgery may be adequate to normalize platelet function.1,30
Thienopyridines inhibit adenosine diphosphate receptor–mediated platelet activation and aggregation. Short-acting thienopyridines may be discontinued 24 hours before surgery, but long-acting agents such as clopidogrel should be stopped 7 days prior to surgery (including when used with aspirin as dual antiplatelet therapy),1 although some outcomes data suggest that 5 days may be sufficient.31
All of these agents should be resumed as soon as adequate hemostasis is achieved after surgery. The ACCP guidelines on perioperative management of antithrombotic therapy recommend resumption of aspirin at the usual maintenance dose the day after surgery, but they make no specific recommendations on when to resume other antiplatelet drugs.1
ANTIPLATELET THERAPY: SPECIAL CONSIDERATIONS IN PATIENTS WITH STENTS
Patients who are on antiplatelet therapy because they have a coronary stent merit special consideration due to the high risk of thrombosis if therapy is interrupted. The risk of stent thrombosis is especially elevated in the postoperative period, particularly if surgery follows soon after stent placement.
- Relative risks and benefits of stopping versus continuing antiplatelet therapy
- Identification of patients at high risk for a perioperative event after cessation of antiplatelet therapy
- Identification of patients at high risk of bleeding.
Bleeding vs stent thrombosis: Consider relative consequences
The risk of bleeding varies by individual patient. No laboratory tests are available to determine individual bleeding risk, but the risk of perioperative bleeding increases when two or more antiplatelet agents are used, as in dual antiplatelet therapy with aspirin and clopidogrel.31
When balancing risks of bleeding versus thrombotic events, the relative consequences of each event again must be considered. Bleeding is rarely life-threatening in comparison with the potential consequences of stent thrombosis. In a prospective observational study of 2,229 patients who received drug-eluting stents, 29 (1.3%) developed stent thrombosis during 9-month follow-up.32 Among these patients, 20 (69%) had a nonfatal myocardial infarction and 13 (45%) died. The most significant independent risk factor for stent thrombosis was premature discontinuation of antiplatelet therapy (hazard ratio = 89.78 [95% CI, 29.90–260.60]; P < .001). Other independent risk factors included renal failure, bifurcation lesions, diabetes, and low ejection fraction.
Premature interruption of antiplatelet therapy: Why it matters
Abrupt discontinuation of antiplatelet therapy can lead to a rebound effect marked by an inflammatory prothrombotic state, increased platelet adhesion and aggregation, and excessive thromboxane A2 activity. Surgery further increases the prothrombotic and inflammatory state, which, combined with incompletely endothelialized drug-eluting stents, can lead to stent thrombosis and, consequently, myocardial infarction and/or death.33
Timing of surgery after stenting: Getting it right
The US Food and Drug Administration recommends that dual antiplatelet therapy be continued for at least 3 months after placement of a sirolimus-eluting stent and at least 6 months after placement of a paclitaxel-eluting stent. Recent data suggest, however, that this duration of antiplatelet therapy may not be sufficient and that at least 1 year of therapy may be needed.34
A recent joint science advisory from the American College of Cardiology (ACC) and the American Heart Association (AHA) emphasizes the importance of educating providers about the “potentially catastrophic” risks of premature stopping of thienopyridine therapy in patients with coronary stents.34 In addition to recommendations in this joint advisory, the ACC and AHA issued updated guidelines in 2007 on perioperative cardiovascular evaluation and care for noncardiac surgery.35 Below is a summary of recommendations on the timing of surgery following stenting in light of these and other sources:
- Following placement of a bare metal stent, elective and nonurgent procedures should be delayed for at least 1 month, according to the ACC/AHA joint advisory,34 or at least 6 weeks, according to the ACC/AHA guidelines.35 Newer data suggest that the optimal interval for delay is likely to be 3 months.36,37
- For patients with recent (< 6 weeks) bare metal stent placement who require urgent surgery, dual antiplatelet therapy should be continued during the perioperative period.1
- Following placement of a drug-eluting stent, elective and nonurgent procedures should be delayed for at least 12 months.34,35
- For patients with recent drug-eluting stent placement in whom surgery cannot be delayed, dual antiplatelet therapy should be continued without interruption if the stent was placed within the prior 6 months.1,35 If the stent was placed more than 6 months before urgent surgery, aspirin should be continued without interruption (at ≥ 81 mg/day) and clopidogrel should be continued until 5 days before surgery and resumed as soon as possible after surgery (at a loading dose of 300 mg followed by 75 mg/day). If the surgeon is comfortable continuing dual antiplatelet therapy in a patient whose stent was placed 6 to 12 months earlier, that course should be considered.1
It is important to note that the ACC/AHA joint advisory34 and other documents have medicolegal implications, so delaying nonurgent surgery for the periods recommended is the most prudent approach.
CONCLUSIONS
Perioperative management of anticoagulant and antiplatelet therapy is complicated by the paucity of randomized clinical trial data and the risk for serious adverse events. The underlying indications for anticoagulant and antiplatelet therapy vary widely, so the best approach to perioperative management is to involve all members of the health care team—hospitalist, surgeon, cardiologist, and anesthesiologist, together with the patient—to ensure that care is individualized and all relevant considerations are accounted for. Patient and surgical risks can be identified and quantified to some extent, but patients often have greater concerns about the risk of stroke than the risk of bleeding. Ideally, nonemergency surgeries should be scheduled to allow enough time to thoroughly plan the management protocol, reducing risks for bleeding and thrombotic events as much as possible.
DISCUSSION
Question from the audience: If a patient’s INR is 1.3 or 1.4, rather than the recommended 1.2, is it necessary to cancel a planned epidural?
Dr. Jaffer: It depends on how comfortable the surgeon or anesthesiologist is with the INR level. Generally, an INR less than 1.5 is probably acceptable, but it depends on the procedure. For a craniotomy, for example, 1.2 is recommended.
Question from the audience: Is it necessary to use anti–Xa levels to guide bridge therapy when administering LMWH or UFH in a patient with a mechanical heart valve?
Dr. Jaffer: It’s not generally necessary, except for pregnant women. For most patients, doses are calculated as milligrams of LMWH per kilogram body weight or as International Units of LMWH per kilogram.
Question from the audience: You mentioned medicolegal disputes arising from adverse events associated with bridge therapy, drug discontinuation, or related issues. Who has final responsibility for making decisions about discontinuation of antiplatelet therapy, for example?
Dr. Jaffer: I don’t know if it ultimately comes down to just one person. Several physicians should be involved in the decision, and communication protocols within an institution should be very clear. It’s important to make certain everyone involved in the decision is reviewing the same literature. The final decision has to be something everyone involved can accept and support.
Perioperative management of surgical patients who require temporary discontinuation of vitamin K antagonists (warfarin) or antiplatelet drugs is complicated. The risk of a thrombotic event during interruption of anticoagulant or antiplatelet therapy must be weighed against the risk of bleeding when such therapy is used in close proximity to a surgical procedure. This balancing of risks is guided by the patient’s individual risk for thromboembolism or bleeding and underlying conditions such as the presence of a mechanical heart valve or a coronary stent.
High-profile adverse events have made anticoagulant and antiplatelet management one of the most highly litigated aspects of perioperative medicine. Moreover, there is a paucity of randomized clinical trial data and definitive guidelines to address the perioperative needs of patients on antithrombotic therapy. Treatment protocols vary depending on many underlying factors, such as the presence of mechanical heart valves, comorbidities, stent type and location, patient age and medical history, and type of surgical procedure. While recent attention has focused on genetic variations that result in higher or lower sensitivity to warfarin in some patients, routine genetic testing for warfarin sensitivity is controversial and not part of widespread practice at this time.
The first portion of this article explores key issues and principles in the perioperative management of surgical patients on warfarin therapy, and the second portion does the same for surgical patients on antiplatelet therapy.
ACCP RECOMMENDATIONS FOR PERIOPERATIVE ANTICOAGULANT MANAGEMENT
Patients with mechanical valves who are at high risk for perioperative thromboembolism include those with any mechanical mitral valve, an older valve, or a history of stroke or transient ischemic attack (TIA). Patients with atrial fibrillation who are at high risk include those with a recent stroke or TIA, rheumatic valvular heart disease, or a CHADS2 score of 5 or 6. (The CHADS2 scoring system assigns one point each for a history of congestive heart failure, hypertension, age greater than 75 years, or diabetes, and two points for history of stroke or TIA.) Patients with a history of VTE within the prior 3 months are also considered high risk.
Bridging anticoagulation (bridge therapy)—ie, the temporary use of intravenous unfractionated heparin (IV UFH) or low-molecular-weight heparin (LMWH) prior to surgery—is central to the ACCP’s recommendations for perioperative management in patients on long-term anticoagulant therapy. Key ACCP recommendations1 for these patients, according to their risk for thromboembolism (Table 1), are as follows:
- High risk—bridging anticoagulation with therapeutic-dose subcutaneous LMWH or IV UFH
- Moderate risk—bridging anticoagulation with therapeutic-dose subcutaneous LMWH, therapeutic-dose IV UFH, or low-dose subcutaneous LMWH
- Low risk—bridging anticoagulation with low-dose subcutaneous LMWH or no bridging.
ASSESSING RISKS: DETERMINING WHETHER TO BRIDGE
Patient-specific risk factors
Patient risk factors include the indication for anticoagulation, as detailed above, as well as other individual risks for thromboembolism, as discussed in the article by Michota on preventing VTE on page S45 of this supplement.
If anticoagulation is indicated because the patient has a mechanical heart valve, the valve type and position must be considered because these factors affect thromboembolic risk, as reflected in Table 1. For instance, the risk of thromboembolism is greater when the valve is in the mitral position than in the aortic position, and is also greater with an older caged-ball valve than with a newer-generation bileaflet valve.3
Procedure-related risk factors
Surgical risks factors include the type of surgery and its associated risks of bleeding and thromboembolism, as well as the expected time that anticoagulation will be interrupted. Estimating thromboembolic risk is complicated, however, and reliable results are generally not achieved with simplistic calculations or formulas. Such calculations tend not to appropriately account for the hypercoagulable state induced by surgery itself, as the risk of VTE is estimated to be 100 times greater during the perioperative period than in the nonoperative setting, owing to increased levels of plasminogen activator inhibitor-1. Moreover, multiple studies have demonstrated increases in coagulation factors that suggest that a “rebound hypercoagulability” may occur shortly after discontinuation of oral anticoagulant therapy.5–8
Net benefit vs risk in trials of bridge therapy
In an analysis of data from observational studies, Kearon and Hirsh estimated the relative risk reduction for thromboembolism with bridge therapy to be 66% to 80%, depending on the indication for anticoagulation.8 Thus, if a patient’s risk of developing thromboembolism is 1.5%, bridge therapy reduces the risk to 0.5% or less.
Weigh relative consequences of an event with the patient
Determining whether and how to initiate bridge therapy ultimately depends on the consequences of an event. Recurrent VTE is fatal in 5% to 10% of cases,15 and arterial thromboembolism is fatal in 20% of cases and causes permanent disability in at least 50% of cases.16 While 9% to 13% of major bleeding events are fatal, bleeding rarely causes permanent disability.17 Thus, whereas a patient who bleeds can be resuscitated, a patient who develops a thromboembolism may be permanently disabled. These considerations should be shared with the patient, and patient preference should factor into the management strategy. Though the risk of bleeding with anticoagulation may be much higher than the risk of stroke without it, many patients will be more concerned about stroke risk.
CHOICE OF AGENT FOR BRIDGE THERAPY
LMWH appears to offer cost advantage over UFH
For cost reasons, managed care organizations often recommend LMWH, which can be administered subcutaneously in outpatient settings, over IV UFH administered in the hospital. A retrospective analysis of medical costs from the 1990s in a managed care organization found that bridge therapy with LMWH prior to elective surgery cost an average of $13,114 less per patient (in total cost of care) than did bridge therapy with UFH.18
LMWH safety issues in valve patients are a myth
Clinical outcomes were not statistically significantly different for patients receiving LMWH or UFH in the above study.18 Nevertheless, there is a widely held notion that LMWH is not safe to use as bridge therapy for patients with mechanical heart valves. Recent prospective bridge studies do not support that view, demonstrating that LMWH used as bridge therapy is associated with low risks for thromboembolism and major bleeding even in patients with mechanical valves.9,10,12–14 In contrast, recent data on the use of IV UFH for bridging is minimal, with most bridge studies dating to the 1970s. Accordingly, the latest ACCP guidelines for perioperative management of patients on antithrombotic therapy recommend therapeutic-dose LMWH over IV UFH for bridge therapy, including in patients with mechanical heart valves.1 Likewise, 2006 guidelines from the American College of Cardiology and American Heart Association on management of patients with valvular heart disease endorse LMWH as an option for bridge therapy.19
A PRACTICAL APPROACH TO BRIDGE THERAPY
A bridge therapy protocol for patients receiving warfarin has been successfully used at the Cleveland Clinic, where I previously practiced. Essentials of the protocol20 are summarized here, followed by commentary that draws on additional sources.
Before surgery
- Discontinue warfarin 5 days before surgery (ie, hold four doses) if the preoperative international normalized ratio (INR) is 2 to 3, and 6 days before surgery (hold five doses) if the INR is 3 to 4.5.
- For bridge therapy, start LMWH (enoxaparin 1 mg/kg or dalteparin 100 IU/kg subcutaneously every 12 hours) beginning 36 hours after the last dose of warfarin.
- Give the last dose of LMWH approximately 24 hours prior to surgery.
After surgery
- For minor surgery, reinitiate LMWH at full dose approximately 24 hours after surgery. For major surgery and for patients at high risk of bleeding, consider using prophylactic doses on the first two postoperative days.
- Discuss the timing of anticoagulant reinitiation with the surgeon.
- Restart warfarin at preoperative dose 1 day after surgery.
- Order daily prothrombin time/INR tests until the patient is discharged and periodically after discharge until the INR is within the therapeutic range.
- Order a complete blood cell count with platelets on days 3 and 7.
- Discontinue LMWH when the INR is between 2 and 3 for 2 consecutive days.
Additionally, the plan should be discussed in advance with the patient, surgeon, and anesthesiologist, along with the risks and benefits associated with LMWH. The patient should receive written instructions for self-administration and information about signs and symptoms of bleeding and thromboembolism.
When to stop warfarin
Warfarin should be discontinued far enough in advance of surgery to achieve a preoperative target INR of less than 1.2.21 Patients with an initial INR of 2 to 3 tend to achieve that target after discontinuation of warfarin for about 5 days (four doses). A longer wait (6 days, or five doses) is necessary for patients with an initial INR of 3 to 4. Age is associated with a slower rate of decrease in the INR, and there is wide interpatient variation. The INR should always be checked prior to surgery.21
Warfarin need not be stopped for all procedures
If warfarin is stopped for minor procedures, bridging may be counterproductive
At the same time, a recent prospective observational study evaluated the effects of brief (≤ 5 days) interruption of warfarin among more than 1,000 patients undergoing minor outpatient procedures and found low rates of both thromboembolism (0.7%) and major bleeding (0.6%).27 The risk of major bleeding was significantly higher among the small proportion of patients who received bridge therapy with UFH or LMWH. The study concluded that interrupting warfarin for 5 days or less for minor outpatient procedures carries a low risk of thromboembolism and that the risk of clinically significant bleeding should be weighed before bridge therapy is considered in this setting.
When to stop bridge therapy preoperatively
Bridge therapy with LMWH is commonly discontinued 12 hours before surgery, but it is preferable to discontinue 24 hours before surgery. In a study of preoperative anticoagulant activity in 80 patients, LMWH (enoxaparin 1 mg/kg) was administered twice daily and discontinued the night before surgery.28 Blood anti–factor Xa levels were measured shortly before surgery, at which time 68% of patients still had therapeutic levels of anti–Xa. This suggests that discontinuing LMWH too close to the time of surgery can increase the risk of bleeding.
Consistent with these findings, consensus guidelines from the American Society of Regional Anesthesia and Pain Medicine (ASRA) recommend that needle placement for regional anesthesia take place 12 hours after the last dose of LMWH if prophylactic dosing is used and 24 hours after the last dose of LMWH if therapeutic dosing is used (ie, ≥ 1 mg/kg of enoxaparin every 12 hours).29
Dosing and timing of postoperative bridge therapy
Postoperative use of full-dose bridge therapy is associated with increased risks of bleeding, according to a multicenter study of approximately 500 patients who received various doses of UFH or LMWH for bridge therapy.14 Patients who received full-dose LMWH or UFH after surgery had a fivefold to sixfold increase in the incidence of major bleeding compared with patients who received prophylactic doses. The study centers that frequently used full-dose bridge protocols were four times as likely to report major bleeding events. In light of these findings, waiting a couple of days after surgery to initiate full-dose bridge therapy is recommended, and prophylactic dosing may be considered in the interim.
The ASRA consensus guidelines recommend that indwelling catheters be removed prior to postoperative reinitiation of twice-daily dosing of LMWH. The first dose of LMWH should be given no sooner than 2 hours after catheter removal. Once-daily dosing of LMWH (European dosing) is acceptable under the ASRA guidelines, but the first dose should be given 6 to 8 hours after surgery and the second dose no sooner than 24 hours later. The guidelines state that once-daily (but not twice-daily) LMWH dosing is acceptable in patients with indwelling catheters; neurological status should be monitored in these patients, and the catheter should be removed 12 to 24 hours after the last dose of LMWH.29
PERIOPERATIVE MANAGEMENT OF ANTIPLATELET THERAPY: TYPE OF AGENT MATTERS
Unlike the considerations with warfarin, the timing of preoperative discontinuation of antiplatelet therapy in patients undergoing noncardiac surgery depends on the type of agent used and its pharmacokinetic actions. Commonly used antiplatelet drugs include aspirin, the thienopyridine agent clopidogrel, and nonsteroidal anti-inflammatory drugs (NSAIDs).
Aspirin works by irreversibly inhibiting platelet cyclooxygenase. The circulating platelet pool is replaced every 7 to 10 days, so aspirin therapy should be discontinued 7 to 10 days before surgery.1
NSAIDs reversibly inhibit platelet cyclooxygenase. Knowing whether a patient is using short- or long-acting NSAIDs is important for determining when to discontinue therapy. For a short-acting NSAID such as ibuprofen, discontinuation 24 hours before surgery may be adequate to normalize platelet function.1,30
Thienopyridines inhibit adenosine diphosphate receptor–mediated platelet activation and aggregation. Short-acting thienopyridines may be discontinued 24 hours before surgery, but long-acting agents such as clopidogrel should be stopped 7 days prior to surgery (including when used with aspirin as dual antiplatelet therapy),1 although some outcomes data suggest that 5 days may be sufficient.31
All of these agents should be resumed as soon as adequate hemostasis is achieved after surgery. The ACCP guidelines on perioperative management of antithrombotic therapy recommend resumption of aspirin at the usual maintenance dose the day after surgery, but they make no specific recommendations on when to resume other antiplatelet drugs.1
ANTIPLATELET THERAPY: SPECIAL CONSIDERATIONS IN PATIENTS WITH STENTS
Patients who are on antiplatelet therapy because they have a coronary stent merit special consideration due to the high risk of thrombosis if therapy is interrupted. The risk of stent thrombosis is especially elevated in the postoperative period, particularly if surgery follows soon after stent placement.
- Relative risks and benefits of stopping versus continuing antiplatelet therapy
- Identification of patients at high risk for a perioperative event after cessation of antiplatelet therapy
- Identification of patients at high risk of bleeding.
Bleeding vs stent thrombosis: Consider relative consequences
The risk of bleeding varies by individual patient. No laboratory tests are available to determine individual bleeding risk, but the risk of perioperative bleeding increases when two or more antiplatelet agents are used, as in dual antiplatelet therapy with aspirin and clopidogrel.31
When balancing risks of bleeding versus thrombotic events, the relative consequences of each event again must be considered. Bleeding is rarely life-threatening in comparison with the potential consequences of stent thrombosis. In a prospective observational study of 2,229 patients who received drug-eluting stents, 29 (1.3%) developed stent thrombosis during 9-month follow-up.32 Among these patients, 20 (69%) had a nonfatal myocardial infarction and 13 (45%) died. The most significant independent risk factor for stent thrombosis was premature discontinuation of antiplatelet therapy (hazard ratio = 89.78 [95% CI, 29.90–260.60]; P < .001). Other independent risk factors included renal failure, bifurcation lesions, diabetes, and low ejection fraction.
Premature interruption of antiplatelet therapy: Why it matters
Abrupt discontinuation of antiplatelet therapy can lead to a rebound effect marked by an inflammatory prothrombotic state, increased platelet adhesion and aggregation, and excessive thromboxane A2 activity. Surgery further increases the prothrombotic and inflammatory state, which, combined with incompletely endothelialized drug-eluting stents, can lead to stent thrombosis and, consequently, myocardial infarction and/or death.33
Timing of surgery after stenting: Getting it right
The US Food and Drug Administration recommends that dual antiplatelet therapy be continued for at least 3 months after placement of a sirolimus-eluting stent and at least 6 months after placement of a paclitaxel-eluting stent. Recent data suggest, however, that this duration of antiplatelet therapy may not be sufficient and that at least 1 year of therapy may be needed.34
A recent joint science advisory from the American College of Cardiology (ACC) and the American Heart Association (AHA) emphasizes the importance of educating providers about the “potentially catastrophic” risks of premature stopping of thienopyridine therapy in patients with coronary stents.34 In addition to recommendations in this joint advisory, the ACC and AHA issued updated guidelines in 2007 on perioperative cardiovascular evaluation and care for noncardiac surgery.35 Below is a summary of recommendations on the timing of surgery following stenting in light of these and other sources:
- Following placement of a bare metal stent, elective and nonurgent procedures should be delayed for at least 1 month, according to the ACC/AHA joint advisory,34 or at least 6 weeks, according to the ACC/AHA guidelines.35 Newer data suggest that the optimal interval for delay is likely to be 3 months.36,37
- For patients with recent (< 6 weeks) bare metal stent placement who require urgent surgery, dual antiplatelet therapy should be continued during the perioperative period.1
- Following placement of a drug-eluting stent, elective and nonurgent procedures should be delayed for at least 12 months.34,35
- For patients with recent drug-eluting stent placement in whom surgery cannot be delayed, dual antiplatelet therapy should be continued without interruption if the stent was placed within the prior 6 months.1,35 If the stent was placed more than 6 months before urgent surgery, aspirin should be continued without interruption (at ≥ 81 mg/day) and clopidogrel should be continued until 5 days before surgery and resumed as soon as possible after surgery (at a loading dose of 300 mg followed by 75 mg/day). If the surgeon is comfortable continuing dual antiplatelet therapy in a patient whose stent was placed 6 to 12 months earlier, that course should be considered.1
It is important to note that the ACC/AHA joint advisory34 and other documents have medicolegal implications, so delaying nonurgent surgery for the periods recommended is the most prudent approach.
CONCLUSIONS
Perioperative management of anticoagulant and antiplatelet therapy is complicated by the paucity of randomized clinical trial data and the risk for serious adverse events. The underlying indications for anticoagulant and antiplatelet therapy vary widely, so the best approach to perioperative management is to involve all members of the health care team—hospitalist, surgeon, cardiologist, and anesthesiologist, together with the patient—to ensure that care is individualized and all relevant considerations are accounted for. Patient and surgical risks can be identified and quantified to some extent, but patients often have greater concerns about the risk of stroke than the risk of bleeding. Ideally, nonemergency surgeries should be scheduled to allow enough time to thoroughly plan the management protocol, reducing risks for bleeding and thrombotic events as much as possible.
DISCUSSION
Question from the audience: If a patient’s INR is 1.3 or 1.4, rather than the recommended 1.2, is it necessary to cancel a planned epidural?
Dr. Jaffer: It depends on how comfortable the surgeon or anesthesiologist is with the INR level. Generally, an INR less than 1.5 is probably acceptable, but it depends on the procedure. For a craniotomy, for example, 1.2 is recommended.
Question from the audience: Is it necessary to use anti–Xa levels to guide bridge therapy when administering LMWH or UFH in a patient with a mechanical heart valve?
Dr. Jaffer: It’s not generally necessary, except for pregnant women. For most patients, doses are calculated as milligrams of LMWH per kilogram body weight or as International Units of LMWH per kilogram.
Question from the audience: You mentioned medicolegal disputes arising from adverse events associated with bridge therapy, drug discontinuation, or related issues. Who has final responsibility for making decisions about discontinuation of antiplatelet therapy, for example?
Dr. Jaffer: I don’t know if it ultimately comes down to just one person. Several physicians should be involved in the decision, and communication protocols within an institution should be very clear. It’s important to make certain everyone involved in the decision is reviewing the same literature. The final decision has to be something everyone involved can accept and support.
- Douketis JD, Berger PB, Dunn AS, et al. The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133(suppl 6):299S–339S.
- du Breuil AL, Umland EM. Outpatient management of anticoagulation therapy. Am Fam Physician 2007; 75:1031–1042.
- Cannegieter SC, Rosendaal FR, Briët E. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Circulation 1994; 89:635–641.
- Snow V, Weiss KB, LeFevre M, et al. Management of newly detected atrial fibrillation: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Intern Med 2003; 139:1009–1017.
- Genewein U, Haeberli A, Straub PW, Beer JH. Rebound after cessation of oral anticoagulant therapy: the biochemical evidence. Br J Haematol 1996; 92:479–485.
- Grip L, Blombäck M, Schulman S. Hypercoagulable state and thromboembolism following warfarin withdrawal in post-myocardial-infarction patients. Eur Heart J 1991; 12:1225–1233.
- Palareti G, Legnani C, Guazzaloca G, et al. Activation of blood coagulation after abrupt or stepwise withdrawal of oral anticoagulants: a prospective study. Thromb Haemost 1994; 72:222–226.
- Kearon C, Hirsh J. Management of anticoagulation before and after elective surgery. N Engl J Med 1997; 336:1506–1511.
- Douketis JD, Johnson JA, Turpie AG. Low-molecular-weight heparin as bridging anticoagulation during interruption of warfarin: assessment of a standardized periprocedural anticoagulation regimen. Arch Intern Med 2004; 164:1319–1326.
- Kovacs MJ, Kearon C, Rodger M, et al. Single-arm study of bridging therapy with low-molecular-weight heparin for patients at risk of arterial embolism who require temporary interruption of warfarin. Circulation 2004; 110:1658–1663.
- Dunn AS, Spyropoulos AC, Turpie AG. Bridging therapy in patients on long-term oral anticoagulants who require surgery: the Prospective Peri-operative Enoxaparin Cohort Trial (PROSPECT). J Thromb Haemost 2007; 5:2211–2218.
- Spyropoulos AC, Turpie AG, Dunn AS, et al. Clinical outcomes with unfractionated heparin or low-molecular-weight heparin as bridging therapy in patients on long-term oral anticoagulants: the REGIMEN registry. J Thromb Haemost 2006; 4:1246–1252.
- Turpie AG, Douketis JD. Enoxaparin is effective and safe as bridging anticoagulation in patients with a mechanical prosthetic heart valve who require temporary interruption of warfarin because of surgery or an invasive procedure. Blood 2004:202s. Abstract 703.
- Jaffer AK, Brotman DJ, White RH. The perioperative and periprocedural management of warfarin: the PPMW study. J Thromb Haemost 2005; 3(suppl 1). Abstract OR309.
- Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann Intern Med 2003; 139:893–900.
- Schulman S, Rhedin AS, Lindmarker P, et al. A comparison of six weeks with six months of oral anticoagulant therapy after a first episode of venous thromboembolism: duration of Anticoagulation Trial Study Group. N Engl J Med 1995; 332:1661–1665.
- Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation: analysis of pooled data from five randomized controlled trials. Arch Intern Med 1994; 154:1449–1457.
- Spyropoulos AC, Frost FJ, Hurley JS, Roberts M. Costs and clinical outcomes associated with low-molecular-weight heparin vs unfractionated heparin for perioperative bridging in patients receiving long-term oral anticoagulant therapy. Chest 2004; 125:1642–1650.
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. Circulation 2006; 114:e84–e231.
- Jaffer AK, Brotman DJ, Chukwumerjie N. When patients on warfarin need surgery. Cleve Clin J Med 2003; 70:973–984.
- White RH, McKittrick T, Hutchinson R, Twitchell J. Temporary discontinuation of warfarin therapy: changes in the international normalized ratio. Ann Intern Med 1995; 122:40–42.
- Konstantatos A. Anticoagulation and cataract surgery: a review of the current literature. Anaesth Intensive Care 2001; 29:11–18.
- Weibert RT. Oral anticoagulant therapy in patients undergoing dental surgery. Clin Pharm 1992; 11:857–864.
- Billingsley EM, Maloney ME. Intraoperative and postoperative bleeding problems in patients taking warfarin, aspirin, and nonsteroidal antiinflammatory agents: a prospective study. Dermatol Surg 1997; 23:381–383.
- Kadakia SC, Angueira CE, Ward JA, Moore M. Gastrointestinal endoscopy in patients taking antiplatelet agents and anticoagulants: survey of ASGE members: American Society for Gastrointestinal Endoscopy. Gastrointest Endosc 1996; 44:309–316.
- Dunn AS, Turpie AG. Perioperative management of patients receiving oral anticoagulants: a systematic review. Arch Intern Med 2003; 163:901–908.
- Garcia DA, Regan S, Henault LE, et al. Risk of thromboembolism with short-term interruption of warfarin therapy. Arch Intern Med 2008; 168:63–69.
- O’Donnell MJ, Kearon C, Johnson J, et al. Brief communication: preoperative anticoagulant activity after bridging low-molecular-weight heparin for temporary interruption of warfarin. Ann Intern Med 2007; 146:184–187.
- Horlocker TT, Wedel DJ, Benzon H, et al. Regional anesthesia in the anticoagulated patient: defining the risks (the second ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation). Reg Anesth Pain Med 2003; 28:172–197.
- Goldenberg NA, Jacobson L, Manco-Johnson MJ. Brief communication: duration of platelet dysfunction after a 7-day course of ibuprofen. Ann Intern Med 2005; 142:506–509.
- Lecompte T, Hardy JF. Antiplatelet agents and perioperative bleeding. Can J Anaesth 2006; 53(suppl 6):S103–S112.
- Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005; 293:2126–2130.
- Newsome LT, Weller RS, Gerancher JC, Kutcher MA, Royster RL. Coronary artery stents: II. Perioperative considerations and management. Anesth Analg 2008; 107:570–590.
- Grines CL, Bonow RO, Casey DE Jr, et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. Circulation 2007; 115:813–818.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines [published correction appears in J Am Coll Cardiol 2008; 52:794–797]. J Am Coll Cardiol 2007; 50:1707–1732.
- Brichon PY, Boitet P, Dujon A, et al. Perioperative in-stent thrombosis after lung resection performed within 3 months of coronary stenting. Eur J Cardiothorac Surg 2006; 30:793–796.
- Nuttall GA, Brown MJ, Stombaugh JW, et al. Time and cardiac risk of surgery after bare-metal stent percutaneous coronary intervention. Anesthesiology 2008; 109:588–595.
- Douketis JD, Berger PB, Dunn AS, et al. The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133(suppl 6):299S–339S.
- du Breuil AL, Umland EM. Outpatient management of anticoagulation therapy. Am Fam Physician 2007; 75:1031–1042.
- Cannegieter SC, Rosendaal FR, Briët E. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Circulation 1994; 89:635–641.
- Snow V, Weiss KB, LeFevre M, et al. Management of newly detected atrial fibrillation: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Intern Med 2003; 139:1009–1017.
- Genewein U, Haeberli A, Straub PW, Beer JH. Rebound after cessation of oral anticoagulant therapy: the biochemical evidence. Br J Haematol 1996; 92:479–485.
- Grip L, Blombäck M, Schulman S. Hypercoagulable state and thromboembolism following warfarin withdrawal in post-myocardial-infarction patients. Eur Heart J 1991; 12:1225–1233.
- Palareti G, Legnani C, Guazzaloca G, et al. Activation of blood coagulation after abrupt or stepwise withdrawal of oral anticoagulants: a prospective study. Thromb Haemost 1994; 72:222–226.
- Kearon C, Hirsh J. Management of anticoagulation before and after elective surgery. N Engl J Med 1997; 336:1506–1511.
- Douketis JD, Johnson JA, Turpie AG. Low-molecular-weight heparin as bridging anticoagulation during interruption of warfarin: assessment of a standardized periprocedural anticoagulation regimen. Arch Intern Med 2004; 164:1319–1326.
- Kovacs MJ, Kearon C, Rodger M, et al. Single-arm study of bridging therapy with low-molecular-weight heparin for patients at risk of arterial embolism who require temporary interruption of warfarin. Circulation 2004; 110:1658–1663.
- Dunn AS, Spyropoulos AC, Turpie AG. Bridging therapy in patients on long-term oral anticoagulants who require surgery: the Prospective Peri-operative Enoxaparin Cohort Trial (PROSPECT). J Thromb Haemost 2007; 5:2211–2218.
- Spyropoulos AC, Turpie AG, Dunn AS, et al. Clinical outcomes with unfractionated heparin or low-molecular-weight heparin as bridging therapy in patients on long-term oral anticoagulants: the REGIMEN registry. J Thromb Haemost 2006; 4:1246–1252.
- Turpie AG, Douketis JD. Enoxaparin is effective and safe as bridging anticoagulation in patients with a mechanical prosthetic heart valve who require temporary interruption of warfarin because of surgery or an invasive procedure. Blood 2004:202s. Abstract 703.
- Jaffer AK, Brotman DJ, White RH. The perioperative and periprocedural management of warfarin: the PPMW study. J Thromb Haemost 2005; 3(suppl 1). Abstract OR309.
- Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann Intern Med 2003; 139:893–900.
- Schulman S, Rhedin AS, Lindmarker P, et al. A comparison of six weeks with six months of oral anticoagulant therapy after a first episode of venous thromboembolism: duration of Anticoagulation Trial Study Group. N Engl J Med 1995; 332:1661–1665.
- Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation: analysis of pooled data from five randomized controlled trials. Arch Intern Med 1994; 154:1449–1457.
- Spyropoulos AC, Frost FJ, Hurley JS, Roberts M. Costs and clinical outcomes associated with low-molecular-weight heparin vs unfractionated heparin for perioperative bridging in patients receiving long-term oral anticoagulant therapy. Chest 2004; 125:1642–1650.
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. Circulation 2006; 114:e84–e231.
- Jaffer AK, Brotman DJ, Chukwumerjie N. When patients on warfarin need surgery. Cleve Clin J Med 2003; 70:973–984.
- White RH, McKittrick T, Hutchinson R, Twitchell J. Temporary discontinuation of warfarin therapy: changes in the international normalized ratio. Ann Intern Med 1995; 122:40–42.
- Konstantatos A. Anticoagulation and cataract surgery: a review of the current literature. Anaesth Intensive Care 2001; 29:11–18.
- Weibert RT. Oral anticoagulant therapy in patients undergoing dental surgery. Clin Pharm 1992; 11:857–864.
- Billingsley EM, Maloney ME. Intraoperative and postoperative bleeding problems in patients taking warfarin, aspirin, and nonsteroidal antiinflammatory agents: a prospective study. Dermatol Surg 1997; 23:381–383.
- Kadakia SC, Angueira CE, Ward JA, Moore M. Gastrointestinal endoscopy in patients taking antiplatelet agents and anticoagulants: survey of ASGE members: American Society for Gastrointestinal Endoscopy. Gastrointest Endosc 1996; 44:309–316.
- Dunn AS, Turpie AG. Perioperative management of patients receiving oral anticoagulants: a systematic review. Arch Intern Med 2003; 163:901–908.
- Garcia DA, Regan S, Henault LE, et al. Risk of thromboembolism with short-term interruption of warfarin therapy. Arch Intern Med 2008; 168:63–69.
- O’Donnell MJ, Kearon C, Johnson J, et al. Brief communication: preoperative anticoagulant activity after bridging low-molecular-weight heparin for temporary interruption of warfarin. Ann Intern Med 2007; 146:184–187.
- Horlocker TT, Wedel DJ, Benzon H, et al. Regional anesthesia in the anticoagulated patient: defining the risks (the second ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation). Reg Anesth Pain Med 2003; 28:172–197.
- Goldenberg NA, Jacobson L, Manco-Johnson MJ. Brief communication: duration of platelet dysfunction after a 7-day course of ibuprofen. Ann Intern Med 2005; 142:506–509.
- Lecompte T, Hardy JF. Antiplatelet agents and perioperative bleeding. Can J Anaesth 2006; 53(suppl 6):S103–S112.
- Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005; 293:2126–2130.
- Newsome LT, Weller RS, Gerancher JC, Kutcher MA, Royster RL. Coronary artery stents: II. Perioperative considerations and management. Anesth Analg 2008; 107:570–590.
- Grines CL, Bonow RO, Casey DE Jr, et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. Circulation 2007; 115:813–818.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines [published correction appears in J Am Coll Cardiol 2008; 52:794–797]. J Am Coll Cardiol 2007; 50:1707–1732.
- Brichon PY, Boitet P, Dujon A, et al. Perioperative in-stent thrombosis after lung resection performed within 3 months of coronary stenting. Eur J Cardiothorac Surg 2006; 30:793–796.
- Nuttall GA, Brown MJ, Stombaugh JW, et al. Time and cardiac risk of surgery after bare-metal stent percutaneous coronary intervention. Anesthesiology 2008; 109:588–595.
KEY POINTS
- Determining when and how to use bridge anticoagulation therapy depends on the patient’s risk for thromboembolism, which is in turn based on the indication for warfarin—ie, a mechanical heart valve, atrial fibrillation, or prior venous thromboembolism.
- Factor patient preference into whether and how to use bridge therapy: many patients are more concerned about stroke risk than bleeding risk, regardless of the relative frequency of these events.
- Anticoagulation with warfarin often does not need to be interrupted for patients undergoing minor surgery, such as some ophthalmic, dental, dermatologic, and gastrointestinal procedures.
- Premature discontinuation of antiplatelet therapy in surgical patients with recent coronary stent placement significantly raises the risk of catastrophic perioperative stent thrombosis.
Prevention of venous thromboembolism after surgery
Most surgical patients who require hospitalization should be considered at high risk for venous thromboembolism (VTE) and be given appropriate prophylaxis. For lower-risk procedures such as knee arthroscopy, prophylaxis is needed for those with individual risk factors such as morbid obesity, limited mobility after surgery, or a history of deep vein thrombosis (DVT) or malignancy. Too often, however, prophylaxis is not provided appropriately or not given at all.
This review surveys the essentials of perioperative VTE prophylaxis and important new developments in the field, which include the 2008 release of new evidence-based clinical practice guidelines on antithrombotic and thrombolytic therapy from the American College of Chest Physicians (ACCP). This 8th edition of the guidelines updates the previous edition, published in 2004, and includes a section by Geerts et al devoted to VTE prevention.1 Other major guidelines are also discussed, as are developments in VTE-related quality measurement, management of special patient populations (those with renal impairment or morbid obesity), and emerging therapies for VTE prophylaxis.
IMPETUS FOR QUALITY IMPROVEMENT IN VTE
A new seriousness about VTE quality measures
The 8th edition of the ACCP guidelines recommends that every hospital develop a formal, active strategy to consistently identify medical and surgical patients at risk for VTE and to prevent VTE occurrence.1 Although prior editions of the ACCP guidelines have made this recommendation for more than 2 decades, fewer than 1 in 10 acute care hospitals had any such strategy in place as recently as 5 years ago. Now, however, most US hospitals have implemented such a strategy, thanks to the growing national emphasis on health care quality measurement in recent years.
The Surgical Care Improvement Project (SCIP) has been at the forefront of this recent quality measures movement. SCIP, a joint project of the American Medical Association and federal government agencies, set a goal to reduce surgical complications in the United States by 25% from 2005 to 2010.2 Two SCIP process measures relate to improving VTE prophylaxis2,3:
- The proportion of surgical patients for whom recommended VTE prophylaxis is ordered
- The proportion of surgical patients who actually receive appropriate VTE prophylaxis within 24 hours before or after surgery.
The Joint Commission and the National Quality Forum recently endorsed these two SCIP performance measures for perioperative VTE prophylaxis along with several others relating to VTE treatment.
CMS raises the stakes with reimbursement restrictions
More significantly, the federal government’s Centers for Medicare and Medicaid Services (CMS) will soon refuse to reimburse for hospital treatment of a primary diagnosis of DVT or pulmonary embolism (PE) following recent (within 30 days) total hip or knee arthroplasty. Effective October 1, 2009, a primary VTE diagnosis following these joint replacement procedures will be added to CMS’ current list of “never events,” or hospital-acquired conditions for which CMS will not provide reimbursement because they are considered the result of preventable medical errors. (Notably, treatment of DVT or PE as a secondary diagnosis will still be reimbursed—for example, if a joint replacement patient develops nosocomial pneumonia, is transferred to the intensive care unit, and then develops VTE.) This addition of DVT and PE to the list is highly controversial since these events sometimes develop even if prophylactic therapy is appropriate and aggressive.
Strategies to promote best practices
In the update for the new 8th edition of its guidelines, the ACCP added recommendations on specific ways for hospitals to identify patients at high risk for VTE and ensure that they receive appropriate prophylaxis. These include the use of computer decision-support systems, preprinted orders, and periodic audit and feedback.1
Researchers at Brigham and Women’s Hospital evaluated the effectiveness of a computer alert system for notifying physicians of newly hospitalized patients at risk for DVT who were not receiving prevention therapy within the first 24 hours of hospital admission.4 These patients presumably “fell through the cracks” and warranted prophylaxis but were otherwise not recognized by the health care team. Risk was determined by a scoring system based on multiple variables, including malignancy, previous DVT or PE, hypercoagulability, major surgery, advanced age, obesity, ordered bed rest, and treatment with hormone replacement therapy or oral contraceptives. Study physicians had to acknowledge having received the alert but could choose whether or not to order VTE prophylaxis. Prophylaxis was used in considerably more patients from the intervention group than from a control group of high-risk patients whose physicians did not receive alerts (34% vs 14%, respectively); accordingly, the risk of a symptomatic DVT or PE event at 90 days was reduced by 41% in the intervention group.
Despite this evidence of improved practice under the alert system, the study begs the question of why the percentage of patients at risk for VTE who were given prophylaxis was still so low (34%), demonstrating how much progress in improving practice remains to be achieved.
PROPHYLAXIS STRATEGIES: MATCHING THERAPY TO RISK
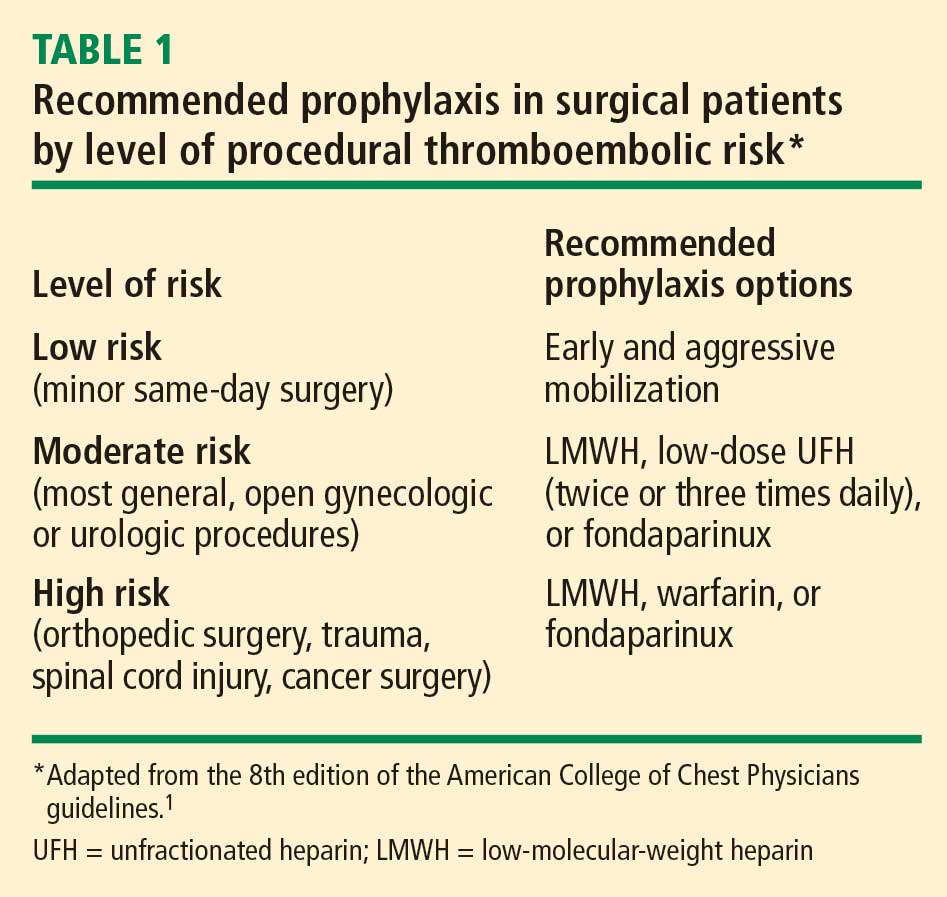
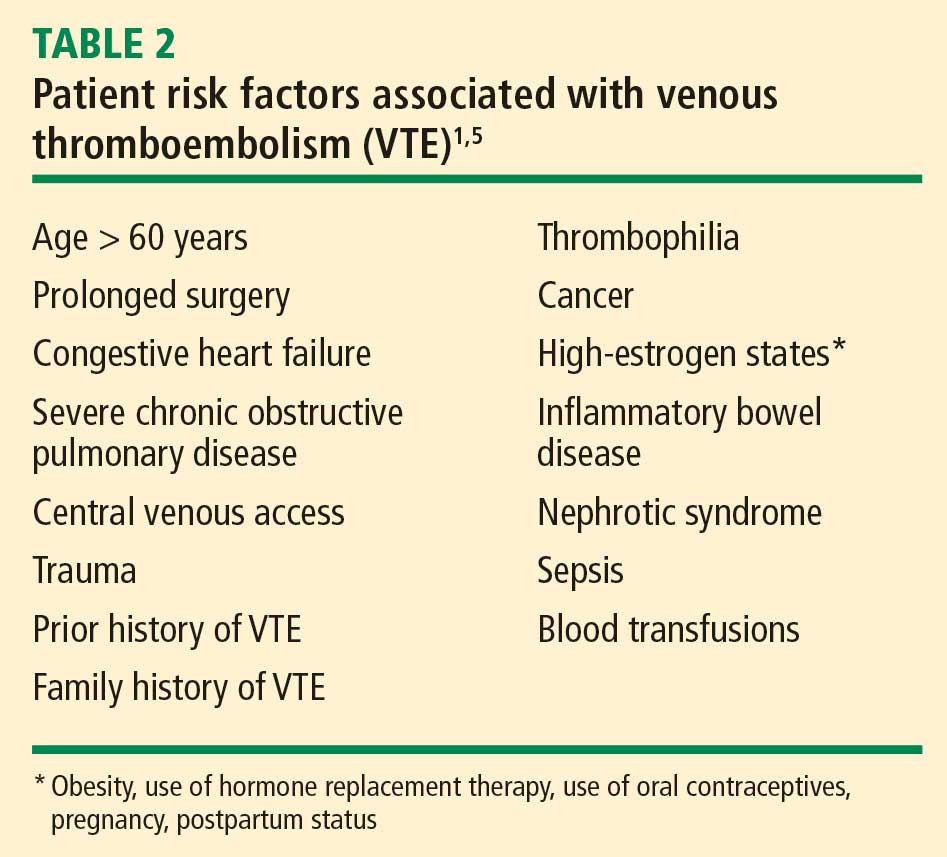
NONPHARMACOLOGIC PROPHYLAXIS STRATEGIES
Does ambulation prevent DVT?
Although it is commonly accepted that walking prevents DVT, this has never been directly tested. Walking may simply be a marker of health, and healthy people are less prone to develop thromboses. We have almost no evidence to show that forcing an unhealthy person to walk helps prevent DVT. Early ambulation offers many benefits and should be encouraged, but it should not be considered DVT prophylaxis; it is simply good hospital care.
Mechanical devices: Adherence is key
Amaragiri and Lees conducted a systematic literature review of randomized controlled trials evaluating the effectiveness of graduated compression stockings (elastic stockings) for preventing DVT in various groups of hospitalized patients.6 The analysis demonstrated a statistically significant reduction in DVT incidence with graduated compression stockings compared with control both among the nine trials in which stockings were used alone (odds ratio = 0.34) and among the seven trials in which stockings were used in addition to another method of thromboprophylaxis (odds ratio = 0.24). Although benefit was demonstrated, many of the trials in this review involved patients undergoing gynecologic surgery and date from the 1970s and 1980s (when obesity was less prevalent), so the applicability of their results today may be limited.
The 8th edition of the ACCP guidelines recommends that mechanical methods of VTE prophylaxis be used primarily in patients who are at high risk of bleeding and that careful attention be directed to ensuring their proper use and optimal adherence.1 The latter point about adherence cannot be emphasized enough, as graduated compression stockings and other mechanical devices have been shown not to be effective unless they are worn at least 18 to 20 hours a day. This degree of adherence is difficult to achieve, as it can severely limit patient mobility and leave patients susceptible to development of pressure ulcers.
Mechanical compression should be initiated prior to induction of anesthesia and continue intraoperatively and then into the postanesthesia care unit. Orders for use of mechanical devices should include instructions in the patient’s medical chart specifying how—and for how many hours per day—they are to be worn. Not doing so leaves the physician vulnerable to litigation, especially as the ACCP guidelines include language on optimal adherence to these devices (“they should be removed for only a short time each day when the patient is actually walking or for bathing”1).
Continuous external compression therapy
Newer mechanical device options include a continuous external compression therapy system that allows patients to be mobile while wearing it and provides rhythmic compression that results in good peak venous flows. Ideally such a device could be put on the patient preoperatively and worn during surgery, throughout the hospital stay, and even at home during recovery. Anecdotally, however, I see patients turn these new devices off at the side of the bed just as often as they do with traditional devices.
Vena caval interruption
Vena caval interruption involves placement of a retrievable vena cava filter before surgery and removal some time later; it offers the potential for VTE prophylaxis in patients who could not tolerate even minor amounts of bleeding, such as certain trauma patients. The Eastern Association for the Surgery of Trauma has put forth a consensus recommendation to consider vena caval interruption in high-risk trauma patients who cannot receive pharmacologic prophylaxis.7 A randomized trial evaluating the usefulness of vena caval interruption for patients undergoing surgery is needed. For now, this intervention should be regarded as experimental and considered only on a highly individualized basis.
PHARMACOLOGIC PROPHYLAXIS
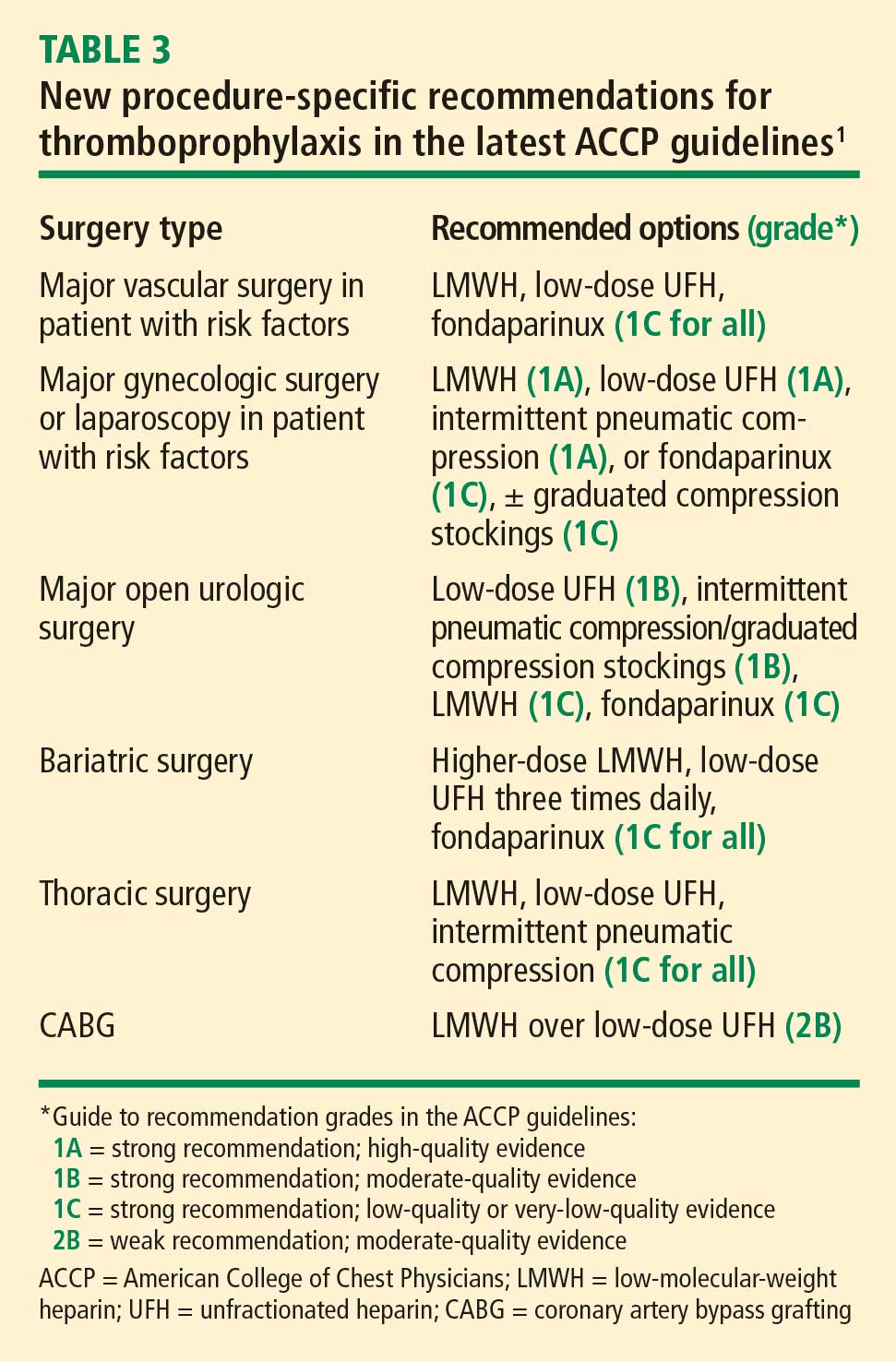
Timing of initiation
Pharmacologic VTE prophylaxis generally should begin 8 to 24 hours postoperatively. Of course, adequate hemostasis is required before initiation, and the net risk/benefit tradeoff with regard to timing of anticoagulant initiation has still not been well studied in many surgical patient populations.
Extended prophylaxis
In the update for the 8th edition of its guidelines, the ACCP added an explicit recommendation for extended outpatient prophylaxis with low-molecular-weight heparin (LMWH) for up to 28 days postoperatively in selected high-risk patients undergoing general or gynecologic surgery, including those with cancer or a history of VTE.1 This recommendation was based largely on studies of extended prophylaxis in patients with cancer undergoing colorectal surgery.8
Increased appreciation of the value of extended VTE prophylaxis after discharge is linked to a growing recognition that DVT and PE episodes in the community setting are often related to a recent hospital stay for either medical illness or surgery. A population-based study found that 59% of all community cases of a first lifetime VTE event in residents of Olmsted County, Minn., over a 15-year period could be linked to current or recent (< 30 days) hospitalization or nursing home residence.9 A similar population-based study in the Worcester, Mass., area found that three-fourths of all VTE events in a 3-year period occurred in the outpatient setting.10 Among patients with these outpatient VTE events, a large proportion had undergone surgery (23%) or hospitalization (37%) in the prior 3 months; among those, 67% experienced their VTE within 1 month of their time in the hospital.
These findings are no surprise, since surgery induces a hypercoagulable state that, when combined with individual risk factors such as obesity, old age, or poor heart function, cannot be assumed to return to baseline on postoperative day 4 or 5 just because the patient is being discharged.
Orthopedic surgery
For patients undergoing major orthopedic procedures, the ACCP guidelines recommend against routine screening for VTE with Doppler ultrasonography before discharge if the patient is asymptomatic.1 Such screening is not considered cost-effective because asymptomatic clots often are found, for which treatment is uncertain, and proximal clots may be missed, giving a false sense of security.
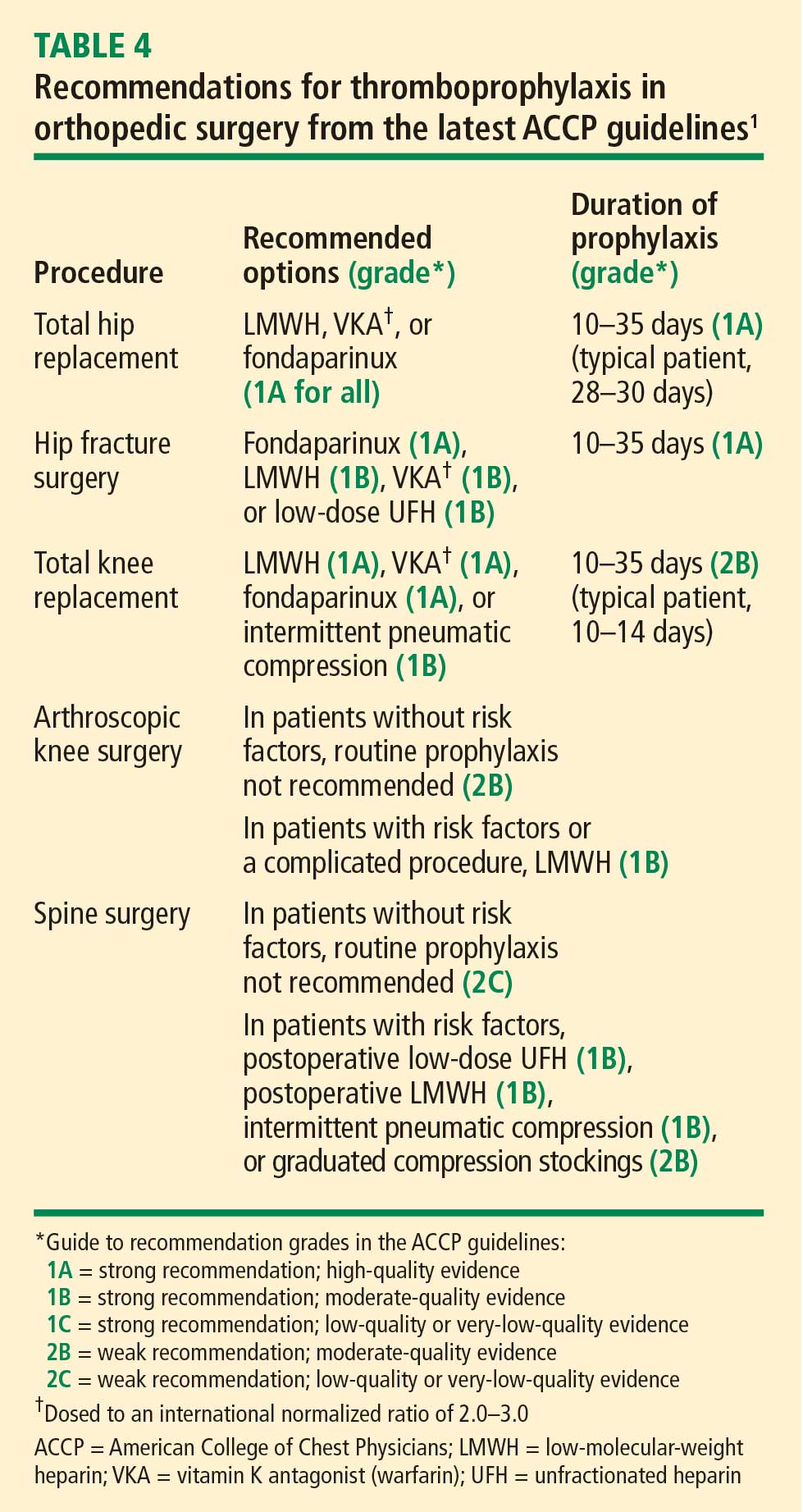
New to the ACCP guidelines in the 8th edition is the recommendation that patients undergoing knee arthroscopy who have risk factors for VTE (or whose procedure is complicated) should receive 1 week of prophylaxis with LMWH.1 Also new are recommendations for patients with risk factors undergoing single- or multilevel laminectomy (Table 4).
Recommendations unchanged in neurosurgery, spinal injury, trauma, burns
Recommendations for neurosurgery remain unchanged from the prior (2004) edition of the ACCP guidelines and are still based on the 2000 meta-analysis by Iorio and Agnelli of LMWH prophylaxis in neurosurgery cases.11 In the United States, the standard is overwhelmingly to use mechanical devices for thromboprophylaxis in neurosurgery, even for patients with cancer.
For prophylaxis in surgical patients with spinal cord injury, multisystem trauma, or burns, LMWH is predominantly used, and the ACCP recommendations are unchanged from 2004.
Drug-specific considerations
LMWH vs vitamin K antagonist. Although vitamin K antagonists (warfarin) still appear in the latest ACCP recommendations,1 LMWH is preferable. A 2004 meta-analysis of studies comparing vitamin K antagonists with LMWH for prophylaxis in patients undergoing orthopedic surgery found that vitamin K antagonists were associated with more episodes of total DVT (relative risk [RR] = 1.51; 95% CI, 1.27–1.79) and proximal DVT (RR = 1.51; 95% CI, 1.04–2.17) compared with LMWH.12 No difference was found in rates of wound hematoma or major bleeding. This finding of inferiority for vitamin K antagonists came despite the likelihood that warfarin was more often administered correctly (ie, with dose adjustment to achieve an international normalized ratio [INR] of 2.0 to 3.0 within 72 hours after surgery) in the studies in this analysis than it is in real-world practice.
Fondaparinux. The indirect factor Xa–specific inhibitor fondaparinux has had a surprisingly limited clinical adoption despite having been widely studied and found to be safe and effective. This is likely attributable in part to its 17-hour half-life, which raises concerns that it may take 3 days for its effects to stop if a patient begins to bleed. Large phase 3 studies have found fondaparinux to be equivalent to LMWH in VTE prevention after hip replacement, marginally superior to LMWH after knee replacement, and superior to LMWH following hip fracture repair.13 Fondaparinux was associated with an increase in bleeding events and instances of transfusion requirement, but only in one of the studies, which was in the setting of knee replacement surgery.14
Aspirin not recommended by ACCP. Although aspirin reduces the risk of VTE, practice guidelines from both the ACCP1 and the International Union of Angiology15 contain no recommendation for its use as prophylaxis because it is considered less effective and more risky than other therapies. In contrast, clinical practice guidelines from the American Academy of Orthopaedic Surgeons suggest that aspirin is reasonable for VTE prophylaxis.16 The varying recommendations reflect differences in perspective among these different specialties.
Aspirin has the advantages of ease of use and low cost, but it is clearly not the best evidence-based approach for VTE prophylaxis. The only recent randomized trial evidence in support of aspirin comes from the Pulmonary Embolism Prevention trial, a study with a flawed design involving more than 13,000 patients undergoing surgery for hip fracture or elective arthroplasty in five countries.17 Patients were randomized to receive aspirin 160 mg daily or placebo for 35 days along with any other prophylaxis deemed necessary (an important potential confounder). Aspirin was associated with an absolute reduction in symptomatic events of less than 1% relative to placebo, and no benefit was observed within the first week. The best results with aspirin were among patients with hip fracture. No benefit was shown among patients undergoing hip arthroplasty or knee arthroplasty; in those groups, both the aspirin and placebo recipients were also treated with LMWH. An absolute increase in rates of wound bleeding (0.6% increase) and gastrointestinal bleeding (1.0% increase) was observed in the aspirin group. The absolute increase in complications was greater than the absolute reduction in episodes of symptomatic DVT: for every episode of symptomatic DVT averted, one wound bleed and 10 gastrointestinal bleeds occurred.
SPECIAL PATIENT POPULATIONS
Renal impairment
The 8th edition of the ACCP guidelines recommends that renal function be kept in mind when considering LMWH, fondaparinux, and other antithrombotic drugs that are cleared by the kidneys. Fondaparinux and LMWH can bioaccumulate in patients with renal insufficiency, who have a higher risk of bleeding to begin with, thereby compounding the risk. Options for patients with renal compromise include avoiding drugs that bioaccumulate, using a lower dosage, and monitoring the drug level or anticoagulant effect.1
Fondaparinux is explicitly contraindicated in patients with low body weight (< 50 kg) or renal impairment (creatinine clearance < 30 mL/min). Renal function should be assessed periodically in any patients receiving the drug.18
I also would not use fondaparinux or LMWH in patients with rapidly changing renal function. For patients with chronic, stable renal impairment, one can reduce the dose of LMWH empirically; one LMWH, enoxaparin, has specific dosing guidelines in its package insert (one-third reduction in dose), but this option does not hold for patients with rapidly changing renal function.19
Obesity
The 8th edition of the ACCP guidelines recommends weight-based dosing of thromboprophylactic agents in obese patients. The guidelines particularly recommend that patients undergoing inpatient bariatric surgery be given higher doses of LMWH or unfractionated heparin.1,20
Frederiksen et al measured the anticoagulant effect of a single fixed dose of a LMWH (using anti-factor Xa heparin activity levels) and found that it was dependent on body weight.21 This suggests that fixed doses that are effective in normal-weight patients may have no detectable anti-coagulant effect in patients with very high body weight.
Weight-based dosing: mounting nonprospective evidence. Weight-based dosage adjustment for the morbidly obese has not been directly studied in a prospective, randomized fashion. A nonrandomized study by Scholten et al compared two regimens of enoxaparin (30 mg twice daily vs 40 mg twice daily) among 481 obese patients undergoing bariatric surgery; each regimen was used along with mechanical thromboprophylaxis.22 They found that the higher-dose regimen was associated with significantly fewer postoperative DVT complications (0.6% vs 5.4%; P < .01) without an increase in bleeding complications.
Separately, Shepherd et al used weight-adjusted doses of unfractionated heparin (started on the evening of surgery) to achieve subtherapeutic peak anti–factor Xa heparin activity levels of 0.11 to 0.25 IU/mL in a series of 700 patients undergoing laparoscopic gastric bypass surgery.23 The resulting doses were greater than those in traditional fixed-rate protocols, but rates of bleeding and VTE events were low and comparable to those reported in patients receiving standard doses.
Don’t rule out multimodal approaches. Multimodal prophylaxis can also be used in obese patients and need not be abandoned as a result of size considerations. For instance, two intermittent compression therapy devices can be pieced together with a Velcro binder if a single device is too small to be worn.
EMERGING ANTICOAGULANT OPTIONS
For many years, unfractionated heparin was the only available parenteral anticoagulant. While heparin has broad anticoagulant properties, it also has well-established limitations, including the need for parenteral delivery, recent problems related to contamination (it is derived from pig intestines), and of course heparin-induced thrombocytopenia (HIT). HIT is an immune-mediated form of platelet activation that can lead to widespread thrombosis throughout the body. It is more commonly associated with venous thrombosis, but arterial events with limb-threatening ischemia may also occur. LMWH is associated with a reduced risk of HIT, but LMWH does not avoid the risk entirely.
Beyond the issue of avoiding HIT, newer anticoagulant therapies are being developed with the aim of oral administration and more targeted inhibition of coagulation factors IIa (thrombin) and Xa.24
Oral direct thrombin inhibitors
One of the two most promising classes of emerging anticoagulants is the direct thrombin inhibitors, most of which are being developed for oral administration. There were high hopes for the initial compound in this class, ximelagatran, but it was abandoned about 5 years ago because of hepatotoxicity.
Dabigatran is the direct thrombin inhibitor furthest along in development today. Currently approved in Europe for prevention of VTE in patients undergoing total hip or knee replacement surgery, dabigatran is likely to be available soon in the United States. It is administered orally, has a rapid onset of action (< 1 hour), and has a predictable anticoagulant response that requires no monitoring.24 Because dabigatran is excreted essentially unchanged by the kidneys and may bioaccumulate, it should not be used in patients with renal impairment or rapidly changing renal function.
In phase 3 clinical trials for VTE prevention in knee replacement surgery, dabigatran was at least as effective as enoxaparin 40 mg once daily and had a comparable safety profile,25 but it was slightly less effective than enoxaparin 30 mg twice daily.26 In a phase 3 trial in patients undergoing hip replacement surgery, dabigatran was equivalent in efficacy and safety to enoxaparin 40 mg once daily.27
Oral direct factor Xa inhibitors
A key rationale for direct inhibition of factor Xa is that it results in inhibition of thrombin production on the activated platelet. Whereas fondaparinux is an indirect inhibitor of factor Xa, direct factor Xa inhibitors offer an advantage in that they inhibit factor Xa within the prothrombinase complex, which occurs on the surface of a platelet and is the main site for thrombin development (very little thrombin is actually produced on endothelial cells). Recall the adage that “thrombin begets more thrombin”: it activates not only platelets but the intrinsic and extrinsic pathways.28
Factor Xa may be a better target than thrombin for a number of other reasons:
- Factor Xa is believed to have few functions (compared with thrombin) outside of coagulation
- In vitro studies show that factor Xa has a wider therapeutic window than thrombin, which translates to greater separation between drug levels that will confer efficacy and bleeding
- Thrombin inhibitors are associated with rebound thrombin generation (there is no evidence of this with factor Xa inhibitors)
- The efficacy of heparin-based anticoagulants improves as selectivity for factor Xa increases (unfractionated heparin is less effective than LMWH, which is less effective than fondaparinux).
Two direct factor Xa inhibitors—both administered orally—are far along in development, as detailed below.
Apixaban has shown promise, but the phase 3 ADVANCE-1 study of apixaban for VTE prevention in patients undergoing knee surgery did not meet statistical criteria for noninferiority compared with enoxaparin 30 mg twice daily.29 This prompted a delay in regulatory filings for apixaban in the United States, and the drug’s prospects for approval for VTE prevention may be unclear until release of results from two other comparative phase 3 trials with enoxaparin in 2009 and 2010.
Rivaroxaban is more likely to become clinically available soon, in light of recent results from the phase 3 RECORD4 trial demonstrating that it was significantly superior to enoxaparin 30 mg twice daily in preventing VTE following knee replacement surgery with comparable rates of major bleeding.30
DISCUSSION
Question from the audience: Some surgeons in my hospital prescribe warfarin immediately after surgery without a bridge of LMWH. Is that appropriate?
Dr. Michota: Warfarin is an option for prophylaxis in orthopedic surgery, beginning on the day of surgery. It could even be started the day before surgery, but the dose should be monitored to achieve an INR between 2.0 and 3.0 within 72 hours of the procedure. If the INR is not in this optimum range, prophylactic doses of LMWH can be given until it is therapeutic.
Follow-up question: In practice, do you actually encourage INR monitoring? Usually we just put patients on a certain dose without monitoring. When we do check the INR, it’s usually 1.4 or 1.5.
Dr. Michota: Warfarin was shown to be effective in reducing VTE risk in orthopedic surgery with dose adjustment based on INR monitoring. On that basis, warfarin remains in the guideline recommendations. Unmonitored, warfarin has not been shown to reduce risk, so to give it that way would not be evidence-based.
Question from the audience: I work with several plastic surgeons who use compression stockings intraoperatively because they’ve heard of several patients who developed a PE during surgery. Is there any benefit to using compression stockings for 2 to 3 hours and then sending the patient home?
Dr. Michota: I don’t know. Theoretically, a device that is on and working before induction may reduce stasis.
The plastic surgery societies do have guidelines. Risk depends on the type of plastic surgery procedure; for example, risk probably increases due to inflammation in procedures that involve scraping the fat pads.
This is an area where we don’t have much data. These patients may be at risk, but we don’t know the best way to mitigate it. It is important that risks be discussed with patients in the informed-consent process and be documented. If the surgeon thinks it is reasonable to give pharmacologic prophylaxis after surgery, I wouldn’t hesitate to do that, but any form of bleeding in the setting of plastic surgery is catastrophic because it defeats the reason for which the surgery was done in the first place.
Question from the audience: How do the guidelines address being aggressive with pharmacologic thromboprophylaxis when a patient is already taking dual antiplatelet therapy?
Dr. Michota: For patients with an indication for VTE prophylaxis in a setting for which there is a specific strategy, the ACCP guidelines recommend that they be put on that regimen whether they are on antiplatelet agents or not. For example, consider a high-risk patient having colorectal surgery who should get unfractionated heparin or LMWH postoperatively and who is currently taking clopidogrel and aspirin. There is no evidence that the dual aspirin–clopidogrel therapy alone is effective in decreasing the risk of DVT. However, we do know that if we add on additional agents, the risk of bleeding is increased. The guidelines consider risk and benefit, and they recommend adding the agents that we know work to prevent DVT.
Question from the audience: You briefly mentioned prophylaxis for knee arthroscopy, which is the most frequently performed orthopedic procedure. Do these recommendations apply to all patients undergoing knee arthroscopy?
Dr. Michota: No. Prophylaxis is indicated only for patients with what the ACCP considers to be additional risk factors for thrombosis. They didn’t specify which risk factors, but good indications for prophylaxis would include morbid obesity, limited mobility after the procedure, a personal history of DVT, features of stasis noted on physical examination, stasis dermatitis (or other features that could indicate prior thrombosis), advanced age, and malignancy. If a patient undergoing knee arthroscopy has other nonmodifiable risk factors, you should also think about prophylaxis. But the vast majority of patients do not need it.
Question from the audience: I’m an academic hospitalist who works closely with orthopedic surgeons. Certain surgeons will only use aspirin for prophylaxis, and it is nonnegotiable. Where does that leave me from a medicolegal standpoint? Our model is to follow ACCP recommendations, but these orthopedic surgeons still use only aspirin.
Dr. Michota: You must do everything you can to come to a consensus with your surgeon colleagues. If you are uncomfortable, as a group you must say to the surgeons, “We are uncomfortable. This is how we view the data. How do you view the data?” If they answer, “We’re doing it because it’s easy, and the American Academy of Orthopaedic Surgeons says we can do it,” I don’t have a good response. But it is more likely that their use of aspirin is based on their own observations; they may not see many clots. Of course, the problem with observational data is that the numbers are not large and they are not generated in a randomized and prospective fashion. Perhaps you can come to some middle ground, but you could always make the difficult choice and say, “I’m just not going to follow your patients.”
- Geerts WH, Bergqvist D, Pineo GF, et al; American College of Chest Physicians. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133:381S–453S.
- Medicare Quality Improvement Community (MedQIC) Web site. http://www.medqic.org. Accessed June 1, 2009.
- Surgical Care Improvement Project (SCIP). Colorado Foundation for Medical Care Web site. http://www.cfmc.org/hospital/hospital_scip.htm. Accessed June 1, 2009.
- Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med 2005; 352:969–977.
- Anderson FA Jr, Spencer FA. Risk factors for venous thromboembolism. Circulation 2003; 107:I-9–I-16.
- Amaragiri SV, Lees TA. Elastic compression stockings for prevention of deep vein thrombosis. Cochrane Database Syst Rev 2000; (3):CD001484.
- Rogers FB, Cipolle MD, Velmahos G, et al. Practice management guidelines for the prevention of venous thromboembolism in trauma patients: the EAST Practice Management Work Group. J Trauma 2002; 53:142–164.
- Bergqvist D, Agnelli G, Cohen AT, et al. Duration of prophylaxis against venous thromboembolism with enoxaparin after surgery for cancer. N Engl J Med 2002; 346:975–980.
- Heit JA, O’Fallon WM, Petterson TM, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med 2002; 162:1245–1248.
- Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med 2007; 167:1471–1475.
- Iorio A, Agnelli G. Low-molecular-weight and unfractionated heparin for prevention of venous thromboembolism in neurosurgery: a meta-analysis. Arch Intern Med 2000; 160:2327–2332.
- Mismetti P, Laporte S, Zufferey P, et al. Prevention of venous thromboembolism in orthopedic surgery with vitamin K antagonists: a meta-analysis. J Thromb Haemost 2004; 2:1058–1070.
- Turpie AG, Bauer KA, Eriksson BI, Lassen MR. Fondaparinux vs enoxaparin for the prevention of venous thromboembolism in major orthopedic surgery: a meta-analysis of 4 randomized double-blind studies. Arch Intern Med 2002; 162:1833–1840.
- Bauer KA, Eriksson BI, Lassen MR, Turpie AG; Steering Committee of the Pentasaccharide in Major Knee Surgery Study. Fondaparinux compared with enoxaparin for the prevention of venous thromboembolism after elective major knee surgery. N Engl J Med 2001; 345:1305–1310.
- Cardiovascular Disease Educational and Research Trust; Cyprus Cardiovascular Disease Educational and Research Trust; European Venous Forum; International Surgical Thrombosis Forum; International Union of Angiology; Union Internationale de Phlébologie. Prevention and treatment of venous thromboembolism. International Consensus Statement (guidelines according to scientific evidence). Int Angiol 2006; 25:101–161.
- American Academy of Orthopaedic Surgeons clinical guideline on prevention of symptomatic pulmonary embolism in patients undergoing total hip or knee arthroplasty. http://www.aaos.org/research/guidelines/PE_summary.pdf. Accessed June 5, 2009.
- Prevention of pulmonary embolism and deep vein thrombosis with low dose aspirin: Pulmonary Embolism Prevention (PEP) trial. Lancet 2000; 355:1295-1302.
- Arixtra injection [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2008.
- Sanderink GJ, Guimart C, Jariwala N, et al. Enoxaparin pharmacokinetics and pharmacodynamics in renal impairment. J Am Coll Cardiol 2001; 37(suppl A):229A. Abstract.
- Hirsh J, Bauer KA, Donati MB, et al; American College of Chest Physicians. Parenteral anticoagulants: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) [published correction appears in Chest 2008; 134:473]. Chest 2008; 133:141S–159S.
- Frederiksen SG, Hedenbro JL, Norgren L. Enoxaparin effect depends on body-weight and current doses may be inadequate in obese patients. Br J Surg 2003; 90:547–548.
- Scholten DJ, Hoedema RM, Scholten SE. A comparison of two different prophylactic dose regimens of low molecular weight heparin in bariatric surgery. Obes Surg 2002; 12:19–24.
- Shepherd MF, Rosborough TK, Schwartz ML. Heparin thromboprophylaxis in gastric bypass surgery. Obes Surg 2003; 13:249–253.
- Weitz JI, Bates SM. New anticoagulants. J Thromb Haemost 2005; 3:1843–1853.
- Eriksson BI, Dahl OE, Rosencher N, et al. Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the RE-MODEL randomized trial. J Thromb Haemost 2007; 5:2178–2185.
- RE-MOBILIZE Writing Committee, Ginsberg JS, Davidson BL, et al. Oral thrombin inhibitor dabigatran etexilate vs North American enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgery. J Arthroplasty 2009; 24:1–9.
- Eriksson BI, Dahl OE, Rosencher N, et al; RE-NOVATE Study Group. Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: a randomised, double-blind, non-inferiority trial [published correction appears in Lancet 2007; 370:2004]. Lancet 2007: 370:949–956.
- Hoffman M, Monroe DM 3rd, Roberts HR. Activated factor VII activates factors IX and X on the surface of activated platelets: thoughts on the mechanism of action of high-dose activated factor VII. Blood Coagul Fibrinolysis 1998; 9(suppl 1):S61–S65.
- Bristol-Myers Squibb and Pfizer provide update on apixaban clinical development program [press release]. New York, NY: August 27, 2008.
- Turpie AG, Lassen MR, Davidson BL, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4): a randomised trial. Lancet 2009; 373:1673–1680.
Most surgical patients who require hospitalization should be considered at high risk for venous thromboembolism (VTE) and be given appropriate prophylaxis. For lower-risk procedures such as knee arthroscopy, prophylaxis is needed for those with individual risk factors such as morbid obesity, limited mobility after surgery, or a history of deep vein thrombosis (DVT) or malignancy. Too often, however, prophylaxis is not provided appropriately or not given at all.
This review surveys the essentials of perioperative VTE prophylaxis and important new developments in the field, which include the 2008 release of new evidence-based clinical practice guidelines on antithrombotic and thrombolytic therapy from the American College of Chest Physicians (ACCP). This 8th edition of the guidelines updates the previous edition, published in 2004, and includes a section by Geerts et al devoted to VTE prevention.1 Other major guidelines are also discussed, as are developments in VTE-related quality measurement, management of special patient populations (those with renal impairment or morbid obesity), and emerging therapies for VTE prophylaxis.
IMPETUS FOR QUALITY IMPROVEMENT IN VTE
A new seriousness about VTE quality measures
The 8th edition of the ACCP guidelines recommends that every hospital develop a formal, active strategy to consistently identify medical and surgical patients at risk for VTE and to prevent VTE occurrence.1 Although prior editions of the ACCP guidelines have made this recommendation for more than 2 decades, fewer than 1 in 10 acute care hospitals had any such strategy in place as recently as 5 years ago. Now, however, most US hospitals have implemented such a strategy, thanks to the growing national emphasis on health care quality measurement in recent years.
The Surgical Care Improvement Project (SCIP) has been at the forefront of this recent quality measures movement. SCIP, a joint project of the American Medical Association and federal government agencies, set a goal to reduce surgical complications in the United States by 25% from 2005 to 2010.2 Two SCIP process measures relate to improving VTE prophylaxis2,3:
- The proportion of surgical patients for whom recommended VTE prophylaxis is ordered
- The proportion of surgical patients who actually receive appropriate VTE prophylaxis within 24 hours before or after surgery.
The Joint Commission and the National Quality Forum recently endorsed these two SCIP performance measures for perioperative VTE prophylaxis along with several others relating to VTE treatment.
CMS raises the stakes with reimbursement restrictions
More significantly, the federal government’s Centers for Medicare and Medicaid Services (CMS) will soon refuse to reimburse for hospital treatment of a primary diagnosis of DVT or pulmonary embolism (PE) following recent (within 30 days) total hip or knee arthroplasty. Effective October 1, 2009, a primary VTE diagnosis following these joint replacement procedures will be added to CMS’ current list of “never events,” or hospital-acquired conditions for which CMS will not provide reimbursement because they are considered the result of preventable medical errors. (Notably, treatment of DVT or PE as a secondary diagnosis will still be reimbursed—for example, if a joint replacement patient develops nosocomial pneumonia, is transferred to the intensive care unit, and then develops VTE.) This addition of DVT and PE to the list is highly controversial since these events sometimes develop even if prophylactic therapy is appropriate and aggressive.
Strategies to promote best practices
In the update for the new 8th edition of its guidelines, the ACCP added recommendations on specific ways for hospitals to identify patients at high risk for VTE and ensure that they receive appropriate prophylaxis. These include the use of computer decision-support systems, preprinted orders, and periodic audit and feedback.1
Researchers at Brigham and Women’s Hospital evaluated the effectiveness of a computer alert system for notifying physicians of newly hospitalized patients at risk for DVT who were not receiving prevention therapy within the first 24 hours of hospital admission.4 These patients presumably “fell through the cracks” and warranted prophylaxis but were otherwise not recognized by the health care team. Risk was determined by a scoring system based on multiple variables, including malignancy, previous DVT or PE, hypercoagulability, major surgery, advanced age, obesity, ordered bed rest, and treatment with hormone replacement therapy or oral contraceptives. Study physicians had to acknowledge having received the alert but could choose whether or not to order VTE prophylaxis. Prophylaxis was used in considerably more patients from the intervention group than from a control group of high-risk patients whose physicians did not receive alerts (34% vs 14%, respectively); accordingly, the risk of a symptomatic DVT or PE event at 90 days was reduced by 41% in the intervention group.
Despite this evidence of improved practice under the alert system, the study begs the question of why the percentage of patients at risk for VTE who were given prophylaxis was still so low (34%), demonstrating how much progress in improving practice remains to be achieved.
PROPHYLAXIS STRATEGIES: MATCHING THERAPY TO RISK
NONPHARMACOLOGIC PROPHYLAXIS STRATEGIES
Does ambulation prevent DVT?
Although it is commonly accepted that walking prevents DVT, this has never been directly tested. Walking may simply be a marker of health, and healthy people are less prone to develop thromboses. We have almost no evidence to show that forcing an unhealthy person to walk helps prevent DVT. Early ambulation offers many benefits and should be encouraged, but it should not be considered DVT prophylaxis; it is simply good hospital care.
Mechanical devices: Adherence is key
Amaragiri and Lees conducted a systematic literature review of randomized controlled trials evaluating the effectiveness of graduated compression stockings (elastic stockings) for preventing DVT in various groups of hospitalized patients.6 The analysis demonstrated a statistically significant reduction in DVT incidence with graduated compression stockings compared with control both among the nine trials in which stockings were used alone (odds ratio = 0.34) and among the seven trials in which stockings were used in addition to another method of thromboprophylaxis (odds ratio = 0.24). Although benefit was demonstrated, many of the trials in this review involved patients undergoing gynecologic surgery and date from the 1970s and 1980s (when obesity was less prevalent), so the applicability of their results today may be limited.
The 8th edition of the ACCP guidelines recommends that mechanical methods of VTE prophylaxis be used primarily in patients who are at high risk of bleeding and that careful attention be directed to ensuring their proper use and optimal adherence.1 The latter point about adherence cannot be emphasized enough, as graduated compression stockings and other mechanical devices have been shown not to be effective unless they are worn at least 18 to 20 hours a day. This degree of adherence is difficult to achieve, as it can severely limit patient mobility and leave patients susceptible to development of pressure ulcers.
Mechanical compression should be initiated prior to induction of anesthesia and continue intraoperatively and then into the postanesthesia care unit. Orders for use of mechanical devices should include instructions in the patient’s medical chart specifying how—and for how many hours per day—they are to be worn. Not doing so leaves the physician vulnerable to litigation, especially as the ACCP guidelines include language on optimal adherence to these devices (“they should be removed for only a short time each day when the patient is actually walking or for bathing”1).
Continuous external compression therapy
Newer mechanical device options include a continuous external compression therapy system that allows patients to be mobile while wearing it and provides rhythmic compression that results in good peak venous flows. Ideally such a device could be put on the patient preoperatively and worn during surgery, throughout the hospital stay, and even at home during recovery. Anecdotally, however, I see patients turn these new devices off at the side of the bed just as often as they do with traditional devices.
Vena caval interruption
Vena caval interruption involves placement of a retrievable vena cava filter before surgery and removal some time later; it offers the potential for VTE prophylaxis in patients who could not tolerate even minor amounts of bleeding, such as certain trauma patients. The Eastern Association for the Surgery of Trauma has put forth a consensus recommendation to consider vena caval interruption in high-risk trauma patients who cannot receive pharmacologic prophylaxis.7 A randomized trial evaluating the usefulness of vena caval interruption for patients undergoing surgery is needed. For now, this intervention should be regarded as experimental and considered only on a highly individualized basis.
PHARMACOLOGIC PROPHYLAXIS
Timing of initiation
Pharmacologic VTE prophylaxis generally should begin 8 to 24 hours postoperatively. Of course, adequate hemostasis is required before initiation, and the net risk/benefit tradeoff with regard to timing of anticoagulant initiation has still not been well studied in many surgical patient populations.
Extended prophylaxis
In the update for the 8th edition of its guidelines, the ACCP added an explicit recommendation for extended outpatient prophylaxis with low-molecular-weight heparin (LMWH) for up to 28 days postoperatively in selected high-risk patients undergoing general or gynecologic surgery, including those with cancer or a history of VTE.1 This recommendation was based largely on studies of extended prophylaxis in patients with cancer undergoing colorectal surgery.8
Increased appreciation of the value of extended VTE prophylaxis after discharge is linked to a growing recognition that DVT and PE episodes in the community setting are often related to a recent hospital stay for either medical illness or surgery. A population-based study found that 59% of all community cases of a first lifetime VTE event in residents of Olmsted County, Minn., over a 15-year period could be linked to current or recent (< 30 days) hospitalization or nursing home residence.9 A similar population-based study in the Worcester, Mass., area found that three-fourths of all VTE events in a 3-year period occurred in the outpatient setting.10 Among patients with these outpatient VTE events, a large proportion had undergone surgery (23%) or hospitalization (37%) in the prior 3 months; among those, 67% experienced their VTE within 1 month of their time in the hospital.
These findings are no surprise, since surgery induces a hypercoagulable state that, when combined with individual risk factors such as obesity, old age, or poor heart function, cannot be assumed to return to baseline on postoperative day 4 or 5 just because the patient is being discharged.
Orthopedic surgery
For patients undergoing major orthopedic procedures, the ACCP guidelines recommend against routine screening for VTE with Doppler ultrasonography before discharge if the patient is asymptomatic.1 Such screening is not considered cost-effective because asymptomatic clots often are found, for which treatment is uncertain, and proximal clots may be missed, giving a false sense of security.
New to the ACCP guidelines in the 8th edition is the recommendation that patients undergoing knee arthroscopy who have risk factors for VTE (or whose procedure is complicated) should receive 1 week of prophylaxis with LMWH.1 Also new are recommendations for patients with risk factors undergoing single- or multilevel laminectomy (Table 4).
Recommendations unchanged in neurosurgery, spinal injury, trauma, burns
Recommendations for neurosurgery remain unchanged from the prior (2004) edition of the ACCP guidelines and are still based on the 2000 meta-analysis by Iorio and Agnelli of LMWH prophylaxis in neurosurgery cases.11 In the United States, the standard is overwhelmingly to use mechanical devices for thromboprophylaxis in neurosurgery, even for patients with cancer.
For prophylaxis in surgical patients with spinal cord injury, multisystem trauma, or burns, LMWH is predominantly used, and the ACCP recommendations are unchanged from 2004.
Drug-specific considerations
LMWH vs vitamin K antagonist. Although vitamin K antagonists (warfarin) still appear in the latest ACCP recommendations,1 LMWH is preferable. A 2004 meta-analysis of studies comparing vitamin K antagonists with LMWH for prophylaxis in patients undergoing orthopedic surgery found that vitamin K antagonists were associated with more episodes of total DVT (relative risk [RR] = 1.51; 95% CI, 1.27–1.79) and proximal DVT (RR = 1.51; 95% CI, 1.04–2.17) compared with LMWH.12 No difference was found in rates of wound hematoma or major bleeding. This finding of inferiority for vitamin K antagonists came despite the likelihood that warfarin was more often administered correctly (ie, with dose adjustment to achieve an international normalized ratio [INR] of 2.0 to 3.0 within 72 hours after surgery) in the studies in this analysis than it is in real-world practice.
Fondaparinux. The indirect factor Xa–specific inhibitor fondaparinux has had a surprisingly limited clinical adoption despite having been widely studied and found to be safe and effective. This is likely attributable in part to its 17-hour half-life, which raises concerns that it may take 3 days for its effects to stop if a patient begins to bleed. Large phase 3 studies have found fondaparinux to be equivalent to LMWH in VTE prevention after hip replacement, marginally superior to LMWH after knee replacement, and superior to LMWH following hip fracture repair.13 Fondaparinux was associated with an increase in bleeding events and instances of transfusion requirement, but only in one of the studies, which was in the setting of knee replacement surgery.14
Aspirin not recommended by ACCP. Although aspirin reduces the risk of VTE, practice guidelines from both the ACCP1 and the International Union of Angiology15 contain no recommendation for its use as prophylaxis because it is considered less effective and more risky than other therapies. In contrast, clinical practice guidelines from the American Academy of Orthopaedic Surgeons suggest that aspirin is reasonable for VTE prophylaxis.16 The varying recommendations reflect differences in perspective among these different specialties.
Aspirin has the advantages of ease of use and low cost, but it is clearly not the best evidence-based approach for VTE prophylaxis. The only recent randomized trial evidence in support of aspirin comes from the Pulmonary Embolism Prevention trial, a study with a flawed design involving more than 13,000 patients undergoing surgery for hip fracture or elective arthroplasty in five countries.17 Patients were randomized to receive aspirin 160 mg daily or placebo for 35 days along with any other prophylaxis deemed necessary (an important potential confounder). Aspirin was associated with an absolute reduction in symptomatic events of less than 1% relative to placebo, and no benefit was observed within the first week. The best results with aspirin were among patients with hip fracture. No benefit was shown among patients undergoing hip arthroplasty or knee arthroplasty; in those groups, both the aspirin and placebo recipients were also treated with LMWH. An absolute increase in rates of wound bleeding (0.6% increase) and gastrointestinal bleeding (1.0% increase) was observed in the aspirin group. The absolute increase in complications was greater than the absolute reduction in episodes of symptomatic DVT: for every episode of symptomatic DVT averted, one wound bleed and 10 gastrointestinal bleeds occurred.
SPECIAL PATIENT POPULATIONS
Renal impairment
The 8th edition of the ACCP guidelines recommends that renal function be kept in mind when considering LMWH, fondaparinux, and other antithrombotic drugs that are cleared by the kidneys. Fondaparinux and LMWH can bioaccumulate in patients with renal insufficiency, who have a higher risk of bleeding to begin with, thereby compounding the risk. Options for patients with renal compromise include avoiding drugs that bioaccumulate, using a lower dosage, and monitoring the drug level or anticoagulant effect.1
Fondaparinux is explicitly contraindicated in patients with low body weight (< 50 kg) or renal impairment (creatinine clearance < 30 mL/min). Renal function should be assessed periodically in any patients receiving the drug.18
I also would not use fondaparinux or LMWH in patients with rapidly changing renal function. For patients with chronic, stable renal impairment, one can reduce the dose of LMWH empirically; one LMWH, enoxaparin, has specific dosing guidelines in its package insert (one-third reduction in dose), but this option does not hold for patients with rapidly changing renal function.19
Obesity
The 8th edition of the ACCP guidelines recommends weight-based dosing of thromboprophylactic agents in obese patients. The guidelines particularly recommend that patients undergoing inpatient bariatric surgery be given higher doses of LMWH or unfractionated heparin.1,20
Frederiksen et al measured the anticoagulant effect of a single fixed dose of a LMWH (using anti-factor Xa heparin activity levels) and found that it was dependent on body weight.21 This suggests that fixed doses that are effective in normal-weight patients may have no detectable anti-coagulant effect in patients with very high body weight.
Weight-based dosing: mounting nonprospective evidence. Weight-based dosage adjustment for the morbidly obese has not been directly studied in a prospective, randomized fashion. A nonrandomized study by Scholten et al compared two regimens of enoxaparin (30 mg twice daily vs 40 mg twice daily) among 481 obese patients undergoing bariatric surgery; each regimen was used along with mechanical thromboprophylaxis.22 They found that the higher-dose regimen was associated with significantly fewer postoperative DVT complications (0.6% vs 5.4%; P < .01) without an increase in bleeding complications.
Separately, Shepherd et al used weight-adjusted doses of unfractionated heparin (started on the evening of surgery) to achieve subtherapeutic peak anti–factor Xa heparin activity levels of 0.11 to 0.25 IU/mL in a series of 700 patients undergoing laparoscopic gastric bypass surgery.23 The resulting doses were greater than those in traditional fixed-rate protocols, but rates of bleeding and VTE events were low and comparable to those reported in patients receiving standard doses.
Don’t rule out multimodal approaches. Multimodal prophylaxis can also be used in obese patients and need not be abandoned as a result of size considerations. For instance, two intermittent compression therapy devices can be pieced together with a Velcro binder if a single device is too small to be worn.
EMERGING ANTICOAGULANT OPTIONS
For many years, unfractionated heparin was the only available parenteral anticoagulant. While heparin has broad anticoagulant properties, it also has well-established limitations, including the need for parenteral delivery, recent problems related to contamination (it is derived from pig intestines), and of course heparin-induced thrombocytopenia (HIT). HIT is an immune-mediated form of platelet activation that can lead to widespread thrombosis throughout the body. It is more commonly associated with venous thrombosis, but arterial events with limb-threatening ischemia may also occur. LMWH is associated with a reduced risk of HIT, but LMWH does not avoid the risk entirely.
Beyond the issue of avoiding HIT, newer anticoagulant therapies are being developed with the aim of oral administration and more targeted inhibition of coagulation factors IIa (thrombin) and Xa.24
Oral direct thrombin inhibitors
One of the two most promising classes of emerging anticoagulants is the direct thrombin inhibitors, most of which are being developed for oral administration. There were high hopes for the initial compound in this class, ximelagatran, but it was abandoned about 5 years ago because of hepatotoxicity.
Dabigatran is the direct thrombin inhibitor furthest along in development today. Currently approved in Europe for prevention of VTE in patients undergoing total hip or knee replacement surgery, dabigatran is likely to be available soon in the United States. It is administered orally, has a rapid onset of action (< 1 hour), and has a predictable anticoagulant response that requires no monitoring.24 Because dabigatran is excreted essentially unchanged by the kidneys and may bioaccumulate, it should not be used in patients with renal impairment or rapidly changing renal function.
In phase 3 clinical trials for VTE prevention in knee replacement surgery, dabigatran was at least as effective as enoxaparin 40 mg once daily and had a comparable safety profile,25 but it was slightly less effective than enoxaparin 30 mg twice daily.26 In a phase 3 trial in patients undergoing hip replacement surgery, dabigatran was equivalent in efficacy and safety to enoxaparin 40 mg once daily.27
Oral direct factor Xa inhibitors
A key rationale for direct inhibition of factor Xa is that it results in inhibition of thrombin production on the activated platelet. Whereas fondaparinux is an indirect inhibitor of factor Xa, direct factor Xa inhibitors offer an advantage in that they inhibit factor Xa within the prothrombinase complex, which occurs on the surface of a platelet and is the main site for thrombin development (very little thrombin is actually produced on endothelial cells). Recall the adage that “thrombin begets more thrombin”: it activates not only platelets but the intrinsic and extrinsic pathways.28
Factor Xa may be a better target than thrombin for a number of other reasons:
- Factor Xa is believed to have few functions (compared with thrombin) outside of coagulation
- In vitro studies show that factor Xa has a wider therapeutic window than thrombin, which translates to greater separation between drug levels that will confer efficacy and bleeding
- Thrombin inhibitors are associated with rebound thrombin generation (there is no evidence of this with factor Xa inhibitors)
- The efficacy of heparin-based anticoagulants improves as selectivity for factor Xa increases (unfractionated heparin is less effective than LMWH, which is less effective than fondaparinux).
Two direct factor Xa inhibitors—both administered orally—are far along in development, as detailed below.
Apixaban has shown promise, but the phase 3 ADVANCE-1 study of apixaban for VTE prevention in patients undergoing knee surgery did not meet statistical criteria for noninferiority compared with enoxaparin 30 mg twice daily.29 This prompted a delay in regulatory filings for apixaban in the United States, and the drug’s prospects for approval for VTE prevention may be unclear until release of results from two other comparative phase 3 trials with enoxaparin in 2009 and 2010.
Rivaroxaban is more likely to become clinically available soon, in light of recent results from the phase 3 RECORD4 trial demonstrating that it was significantly superior to enoxaparin 30 mg twice daily in preventing VTE following knee replacement surgery with comparable rates of major bleeding.30
DISCUSSION
Question from the audience: Some surgeons in my hospital prescribe warfarin immediately after surgery without a bridge of LMWH. Is that appropriate?
Dr. Michota: Warfarin is an option for prophylaxis in orthopedic surgery, beginning on the day of surgery. It could even be started the day before surgery, but the dose should be monitored to achieve an INR between 2.0 and 3.0 within 72 hours of the procedure. If the INR is not in this optimum range, prophylactic doses of LMWH can be given until it is therapeutic.
Follow-up question: In practice, do you actually encourage INR monitoring? Usually we just put patients on a certain dose without monitoring. When we do check the INR, it’s usually 1.4 or 1.5.
Dr. Michota: Warfarin was shown to be effective in reducing VTE risk in orthopedic surgery with dose adjustment based on INR monitoring. On that basis, warfarin remains in the guideline recommendations. Unmonitored, warfarin has not been shown to reduce risk, so to give it that way would not be evidence-based.
Question from the audience: I work with several plastic surgeons who use compression stockings intraoperatively because they’ve heard of several patients who developed a PE during surgery. Is there any benefit to using compression stockings for 2 to 3 hours and then sending the patient home?
Dr. Michota: I don’t know. Theoretically, a device that is on and working before induction may reduce stasis.
The plastic surgery societies do have guidelines. Risk depends on the type of plastic surgery procedure; for example, risk probably increases due to inflammation in procedures that involve scraping the fat pads.
This is an area where we don’t have much data. These patients may be at risk, but we don’t know the best way to mitigate it. It is important that risks be discussed with patients in the informed-consent process and be documented. If the surgeon thinks it is reasonable to give pharmacologic prophylaxis after surgery, I wouldn’t hesitate to do that, but any form of bleeding in the setting of plastic surgery is catastrophic because it defeats the reason for which the surgery was done in the first place.
Question from the audience: How do the guidelines address being aggressive with pharmacologic thromboprophylaxis when a patient is already taking dual antiplatelet therapy?
Dr. Michota: For patients with an indication for VTE prophylaxis in a setting for which there is a specific strategy, the ACCP guidelines recommend that they be put on that regimen whether they are on antiplatelet agents or not. For example, consider a high-risk patient having colorectal surgery who should get unfractionated heparin or LMWH postoperatively and who is currently taking clopidogrel and aspirin. There is no evidence that the dual aspirin–clopidogrel therapy alone is effective in decreasing the risk of DVT. However, we do know that if we add on additional agents, the risk of bleeding is increased. The guidelines consider risk and benefit, and they recommend adding the agents that we know work to prevent DVT.
Question from the audience: You briefly mentioned prophylaxis for knee arthroscopy, which is the most frequently performed orthopedic procedure. Do these recommendations apply to all patients undergoing knee arthroscopy?
Dr. Michota: No. Prophylaxis is indicated only for patients with what the ACCP considers to be additional risk factors for thrombosis. They didn’t specify which risk factors, but good indications for prophylaxis would include morbid obesity, limited mobility after the procedure, a personal history of DVT, features of stasis noted on physical examination, stasis dermatitis (or other features that could indicate prior thrombosis), advanced age, and malignancy. If a patient undergoing knee arthroscopy has other nonmodifiable risk factors, you should also think about prophylaxis. But the vast majority of patients do not need it.
Question from the audience: I’m an academic hospitalist who works closely with orthopedic surgeons. Certain surgeons will only use aspirin for prophylaxis, and it is nonnegotiable. Where does that leave me from a medicolegal standpoint? Our model is to follow ACCP recommendations, but these orthopedic surgeons still use only aspirin.
Dr. Michota: You must do everything you can to come to a consensus with your surgeon colleagues. If you are uncomfortable, as a group you must say to the surgeons, “We are uncomfortable. This is how we view the data. How do you view the data?” If they answer, “We’re doing it because it’s easy, and the American Academy of Orthopaedic Surgeons says we can do it,” I don’t have a good response. But it is more likely that their use of aspirin is based on their own observations; they may not see many clots. Of course, the problem with observational data is that the numbers are not large and they are not generated in a randomized and prospective fashion. Perhaps you can come to some middle ground, but you could always make the difficult choice and say, “I’m just not going to follow your patients.”
Most surgical patients who require hospitalization should be considered at high risk for venous thromboembolism (VTE) and be given appropriate prophylaxis. For lower-risk procedures such as knee arthroscopy, prophylaxis is needed for those with individual risk factors such as morbid obesity, limited mobility after surgery, or a history of deep vein thrombosis (DVT) or malignancy. Too often, however, prophylaxis is not provided appropriately or not given at all.
This review surveys the essentials of perioperative VTE prophylaxis and important new developments in the field, which include the 2008 release of new evidence-based clinical practice guidelines on antithrombotic and thrombolytic therapy from the American College of Chest Physicians (ACCP). This 8th edition of the guidelines updates the previous edition, published in 2004, and includes a section by Geerts et al devoted to VTE prevention.1 Other major guidelines are also discussed, as are developments in VTE-related quality measurement, management of special patient populations (those with renal impairment or morbid obesity), and emerging therapies for VTE prophylaxis.
IMPETUS FOR QUALITY IMPROVEMENT IN VTE
A new seriousness about VTE quality measures
The 8th edition of the ACCP guidelines recommends that every hospital develop a formal, active strategy to consistently identify medical and surgical patients at risk for VTE and to prevent VTE occurrence.1 Although prior editions of the ACCP guidelines have made this recommendation for more than 2 decades, fewer than 1 in 10 acute care hospitals had any such strategy in place as recently as 5 years ago. Now, however, most US hospitals have implemented such a strategy, thanks to the growing national emphasis on health care quality measurement in recent years.
The Surgical Care Improvement Project (SCIP) has been at the forefront of this recent quality measures movement. SCIP, a joint project of the American Medical Association and federal government agencies, set a goal to reduce surgical complications in the United States by 25% from 2005 to 2010.2 Two SCIP process measures relate to improving VTE prophylaxis2,3:
- The proportion of surgical patients for whom recommended VTE prophylaxis is ordered
- The proportion of surgical patients who actually receive appropriate VTE prophylaxis within 24 hours before or after surgery.
The Joint Commission and the National Quality Forum recently endorsed these two SCIP performance measures for perioperative VTE prophylaxis along with several others relating to VTE treatment.
CMS raises the stakes with reimbursement restrictions
More significantly, the federal government’s Centers for Medicare and Medicaid Services (CMS) will soon refuse to reimburse for hospital treatment of a primary diagnosis of DVT or pulmonary embolism (PE) following recent (within 30 days) total hip or knee arthroplasty. Effective October 1, 2009, a primary VTE diagnosis following these joint replacement procedures will be added to CMS’ current list of “never events,” or hospital-acquired conditions for which CMS will not provide reimbursement because they are considered the result of preventable medical errors. (Notably, treatment of DVT or PE as a secondary diagnosis will still be reimbursed—for example, if a joint replacement patient develops nosocomial pneumonia, is transferred to the intensive care unit, and then develops VTE.) This addition of DVT and PE to the list is highly controversial since these events sometimes develop even if prophylactic therapy is appropriate and aggressive.
Strategies to promote best practices
In the update for the new 8th edition of its guidelines, the ACCP added recommendations on specific ways for hospitals to identify patients at high risk for VTE and ensure that they receive appropriate prophylaxis. These include the use of computer decision-support systems, preprinted orders, and periodic audit and feedback.1
Researchers at Brigham and Women’s Hospital evaluated the effectiveness of a computer alert system for notifying physicians of newly hospitalized patients at risk for DVT who were not receiving prevention therapy within the first 24 hours of hospital admission.4 These patients presumably “fell through the cracks” and warranted prophylaxis but were otherwise not recognized by the health care team. Risk was determined by a scoring system based on multiple variables, including malignancy, previous DVT or PE, hypercoagulability, major surgery, advanced age, obesity, ordered bed rest, and treatment with hormone replacement therapy or oral contraceptives. Study physicians had to acknowledge having received the alert but could choose whether or not to order VTE prophylaxis. Prophylaxis was used in considerably more patients from the intervention group than from a control group of high-risk patients whose physicians did not receive alerts (34% vs 14%, respectively); accordingly, the risk of a symptomatic DVT or PE event at 90 days was reduced by 41% in the intervention group.
Despite this evidence of improved practice under the alert system, the study begs the question of why the percentage of patients at risk for VTE who were given prophylaxis was still so low (34%), demonstrating how much progress in improving practice remains to be achieved.
PROPHYLAXIS STRATEGIES: MATCHING THERAPY TO RISK
NONPHARMACOLOGIC PROPHYLAXIS STRATEGIES
Does ambulation prevent DVT?
Although it is commonly accepted that walking prevents DVT, this has never been directly tested. Walking may simply be a marker of health, and healthy people are less prone to develop thromboses. We have almost no evidence to show that forcing an unhealthy person to walk helps prevent DVT. Early ambulation offers many benefits and should be encouraged, but it should not be considered DVT prophylaxis; it is simply good hospital care.
Mechanical devices: Adherence is key
Amaragiri and Lees conducted a systematic literature review of randomized controlled trials evaluating the effectiveness of graduated compression stockings (elastic stockings) for preventing DVT in various groups of hospitalized patients.6 The analysis demonstrated a statistically significant reduction in DVT incidence with graduated compression stockings compared with control both among the nine trials in which stockings were used alone (odds ratio = 0.34) and among the seven trials in which stockings were used in addition to another method of thromboprophylaxis (odds ratio = 0.24). Although benefit was demonstrated, many of the trials in this review involved patients undergoing gynecologic surgery and date from the 1970s and 1980s (when obesity was less prevalent), so the applicability of their results today may be limited.
The 8th edition of the ACCP guidelines recommends that mechanical methods of VTE prophylaxis be used primarily in patients who are at high risk of bleeding and that careful attention be directed to ensuring their proper use and optimal adherence.1 The latter point about adherence cannot be emphasized enough, as graduated compression stockings and other mechanical devices have been shown not to be effective unless they are worn at least 18 to 20 hours a day. This degree of adherence is difficult to achieve, as it can severely limit patient mobility and leave patients susceptible to development of pressure ulcers.
Mechanical compression should be initiated prior to induction of anesthesia and continue intraoperatively and then into the postanesthesia care unit. Orders for use of mechanical devices should include instructions in the patient’s medical chart specifying how—and for how many hours per day—they are to be worn. Not doing so leaves the physician vulnerable to litigation, especially as the ACCP guidelines include language on optimal adherence to these devices (“they should be removed for only a short time each day when the patient is actually walking or for bathing”1).
Continuous external compression therapy
Newer mechanical device options include a continuous external compression therapy system that allows patients to be mobile while wearing it and provides rhythmic compression that results in good peak venous flows. Ideally such a device could be put on the patient preoperatively and worn during surgery, throughout the hospital stay, and even at home during recovery. Anecdotally, however, I see patients turn these new devices off at the side of the bed just as often as they do with traditional devices.
Vena caval interruption
Vena caval interruption involves placement of a retrievable vena cava filter before surgery and removal some time later; it offers the potential for VTE prophylaxis in patients who could not tolerate even minor amounts of bleeding, such as certain trauma patients. The Eastern Association for the Surgery of Trauma has put forth a consensus recommendation to consider vena caval interruption in high-risk trauma patients who cannot receive pharmacologic prophylaxis.7 A randomized trial evaluating the usefulness of vena caval interruption for patients undergoing surgery is needed. For now, this intervention should be regarded as experimental and considered only on a highly individualized basis.
PHARMACOLOGIC PROPHYLAXIS
Timing of initiation
Pharmacologic VTE prophylaxis generally should begin 8 to 24 hours postoperatively. Of course, adequate hemostasis is required before initiation, and the net risk/benefit tradeoff with regard to timing of anticoagulant initiation has still not been well studied in many surgical patient populations.
Extended prophylaxis
In the update for the 8th edition of its guidelines, the ACCP added an explicit recommendation for extended outpatient prophylaxis with low-molecular-weight heparin (LMWH) for up to 28 days postoperatively in selected high-risk patients undergoing general or gynecologic surgery, including those with cancer or a history of VTE.1 This recommendation was based largely on studies of extended prophylaxis in patients with cancer undergoing colorectal surgery.8
Increased appreciation of the value of extended VTE prophylaxis after discharge is linked to a growing recognition that DVT and PE episodes in the community setting are often related to a recent hospital stay for either medical illness or surgery. A population-based study found that 59% of all community cases of a first lifetime VTE event in residents of Olmsted County, Minn., over a 15-year period could be linked to current or recent (< 30 days) hospitalization or nursing home residence.9 A similar population-based study in the Worcester, Mass., area found that three-fourths of all VTE events in a 3-year period occurred in the outpatient setting.10 Among patients with these outpatient VTE events, a large proportion had undergone surgery (23%) or hospitalization (37%) in the prior 3 months; among those, 67% experienced their VTE within 1 month of their time in the hospital.
These findings are no surprise, since surgery induces a hypercoagulable state that, when combined with individual risk factors such as obesity, old age, or poor heart function, cannot be assumed to return to baseline on postoperative day 4 or 5 just because the patient is being discharged.
Orthopedic surgery
For patients undergoing major orthopedic procedures, the ACCP guidelines recommend against routine screening for VTE with Doppler ultrasonography before discharge if the patient is asymptomatic.1 Such screening is not considered cost-effective because asymptomatic clots often are found, for which treatment is uncertain, and proximal clots may be missed, giving a false sense of security.
New to the ACCP guidelines in the 8th edition is the recommendation that patients undergoing knee arthroscopy who have risk factors for VTE (or whose procedure is complicated) should receive 1 week of prophylaxis with LMWH.1 Also new are recommendations for patients with risk factors undergoing single- or multilevel laminectomy (Table 4).
Recommendations unchanged in neurosurgery, spinal injury, trauma, burns
Recommendations for neurosurgery remain unchanged from the prior (2004) edition of the ACCP guidelines and are still based on the 2000 meta-analysis by Iorio and Agnelli of LMWH prophylaxis in neurosurgery cases.11 In the United States, the standard is overwhelmingly to use mechanical devices for thromboprophylaxis in neurosurgery, even for patients with cancer.
For prophylaxis in surgical patients with spinal cord injury, multisystem trauma, or burns, LMWH is predominantly used, and the ACCP recommendations are unchanged from 2004.
Drug-specific considerations
LMWH vs vitamin K antagonist. Although vitamin K antagonists (warfarin) still appear in the latest ACCP recommendations,1 LMWH is preferable. A 2004 meta-analysis of studies comparing vitamin K antagonists with LMWH for prophylaxis in patients undergoing orthopedic surgery found that vitamin K antagonists were associated with more episodes of total DVT (relative risk [RR] = 1.51; 95% CI, 1.27–1.79) and proximal DVT (RR = 1.51; 95% CI, 1.04–2.17) compared with LMWH.12 No difference was found in rates of wound hematoma or major bleeding. This finding of inferiority for vitamin K antagonists came despite the likelihood that warfarin was more often administered correctly (ie, with dose adjustment to achieve an international normalized ratio [INR] of 2.0 to 3.0 within 72 hours after surgery) in the studies in this analysis than it is in real-world practice.
Fondaparinux. The indirect factor Xa–specific inhibitor fondaparinux has had a surprisingly limited clinical adoption despite having been widely studied and found to be safe and effective. This is likely attributable in part to its 17-hour half-life, which raises concerns that it may take 3 days for its effects to stop if a patient begins to bleed. Large phase 3 studies have found fondaparinux to be equivalent to LMWH in VTE prevention after hip replacement, marginally superior to LMWH after knee replacement, and superior to LMWH following hip fracture repair.13 Fondaparinux was associated with an increase in bleeding events and instances of transfusion requirement, but only in one of the studies, which was in the setting of knee replacement surgery.14
Aspirin not recommended by ACCP. Although aspirin reduces the risk of VTE, practice guidelines from both the ACCP1 and the International Union of Angiology15 contain no recommendation for its use as prophylaxis because it is considered less effective and more risky than other therapies. In contrast, clinical practice guidelines from the American Academy of Orthopaedic Surgeons suggest that aspirin is reasonable for VTE prophylaxis.16 The varying recommendations reflect differences in perspective among these different specialties.
Aspirin has the advantages of ease of use and low cost, but it is clearly not the best evidence-based approach for VTE prophylaxis. The only recent randomized trial evidence in support of aspirin comes from the Pulmonary Embolism Prevention trial, a study with a flawed design involving more than 13,000 patients undergoing surgery for hip fracture or elective arthroplasty in five countries.17 Patients were randomized to receive aspirin 160 mg daily or placebo for 35 days along with any other prophylaxis deemed necessary (an important potential confounder). Aspirin was associated with an absolute reduction in symptomatic events of less than 1% relative to placebo, and no benefit was observed within the first week. The best results with aspirin were among patients with hip fracture. No benefit was shown among patients undergoing hip arthroplasty or knee arthroplasty; in those groups, both the aspirin and placebo recipients were also treated with LMWH. An absolute increase in rates of wound bleeding (0.6% increase) and gastrointestinal bleeding (1.0% increase) was observed in the aspirin group. The absolute increase in complications was greater than the absolute reduction in episodes of symptomatic DVT: for every episode of symptomatic DVT averted, one wound bleed and 10 gastrointestinal bleeds occurred.
SPECIAL PATIENT POPULATIONS
Renal impairment
The 8th edition of the ACCP guidelines recommends that renal function be kept in mind when considering LMWH, fondaparinux, and other antithrombotic drugs that are cleared by the kidneys. Fondaparinux and LMWH can bioaccumulate in patients with renal insufficiency, who have a higher risk of bleeding to begin with, thereby compounding the risk. Options for patients with renal compromise include avoiding drugs that bioaccumulate, using a lower dosage, and monitoring the drug level or anticoagulant effect.1
Fondaparinux is explicitly contraindicated in patients with low body weight (< 50 kg) or renal impairment (creatinine clearance < 30 mL/min). Renal function should be assessed periodically in any patients receiving the drug.18
I also would not use fondaparinux or LMWH in patients with rapidly changing renal function. For patients with chronic, stable renal impairment, one can reduce the dose of LMWH empirically; one LMWH, enoxaparin, has specific dosing guidelines in its package insert (one-third reduction in dose), but this option does not hold for patients with rapidly changing renal function.19
Obesity
The 8th edition of the ACCP guidelines recommends weight-based dosing of thromboprophylactic agents in obese patients. The guidelines particularly recommend that patients undergoing inpatient bariatric surgery be given higher doses of LMWH or unfractionated heparin.1,20
Frederiksen et al measured the anticoagulant effect of a single fixed dose of a LMWH (using anti-factor Xa heparin activity levels) and found that it was dependent on body weight.21 This suggests that fixed doses that are effective in normal-weight patients may have no detectable anti-coagulant effect in patients with very high body weight.
Weight-based dosing: mounting nonprospective evidence. Weight-based dosage adjustment for the morbidly obese has not been directly studied in a prospective, randomized fashion. A nonrandomized study by Scholten et al compared two regimens of enoxaparin (30 mg twice daily vs 40 mg twice daily) among 481 obese patients undergoing bariatric surgery; each regimen was used along with mechanical thromboprophylaxis.22 They found that the higher-dose regimen was associated with significantly fewer postoperative DVT complications (0.6% vs 5.4%; P < .01) without an increase in bleeding complications.
Separately, Shepherd et al used weight-adjusted doses of unfractionated heparin (started on the evening of surgery) to achieve subtherapeutic peak anti–factor Xa heparin activity levels of 0.11 to 0.25 IU/mL in a series of 700 patients undergoing laparoscopic gastric bypass surgery.23 The resulting doses were greater than those in traditional fixed-rate protocols, but rates of bleeding and VTE events were low and comparable to those reported in patients receiving standard doses.
Don’t rule out multimodal approaches. Multimodal prophylaxis can also be used in obese patients and need not be abandoned as a result of size considerations. For instance, two intermittent compression therapy devices can be pieced together with a Velcro binder if a single device is too small to be worn.
EMERGING ANTICOAGULANT OPTIONS
For many years, unfractionated heparin was the only available parenteral anticoagulant. While heparin has broad anticoagulant properties, it also has well-established limitations, including the need for parenteral delivery, recent problems related to contamination (it is derived from pig intestines), and of course heparin-induced thrombocytopenia (HIT). HIT is an immune-mediated form of platelet activation that can lead to widespread thrombosis throughout the body. It is more commonly associated with venous thrombosis, but arterial events with limb-threatening ischemia may also occur. LMWH is associated with a reduced risk of HIT, but LMWH does not avoid the risk entirely.
Beyond the issue of avoiding HIT, newer anticoagulant therapies are being developed with the aim of oral administration and more targeted inhibition of coagulation factors IIa (thrombin) and Xa.24
Oral direct thrombin inhibitors
One of the two most promising classes of emerging anticoagulants is the direct thrombin inhibitors, most of which are being developed for oral administration. There were high hopes for the initial compound in this class, ximelagatran, but it was abandoned about 5 years ago because of hepatotoxicity.
Dabigatran is the direct thrombin inhibitor furthest along in development today. Currently approved in Europe for prevention of VTE in patients undergoing total hip or knee replacement surgery, dabigatran is likely to be available soon in the United States. It is administered orally, has a rapid onset of action (< 1 hour), and has a predictable anticoagulant response that requires no monitoring.24 Because dabigatran is excreted essentially unchanged by the kidneys and may bioaccumulate, it should not be used in patients with renal impairment or rapidly changing renal function.
In phase 3 clinical trials for VTE prevention in knee replacement surgery, dabigatran was at least as effective as enoxaparin 40 mg once daily and had a comparable safety profile,25 but it was slightly less effective than enoxaparin 30 mg twice daily.26 In a phase 3 trial in patients undergoing hip replacement surgery, dabigatran was equivalent in efficacy and safety to enoxaparin 40 mg once daily.27
Oral direct factor Xa inhibitors
A key rationale for direct inhibition of factor Xa is that it results in inhibition of thrombin production on the activated platelet. Whereas fondaparinux is an indirect inhibitor of factor Xa, direct factor Xa inhibitors offer an advantage in that they inhibit factor Xa within the prothrombinase complex, which occurs on the surface of a platelet and is the main site for thrombin development (very little thrombin is actually produced on endothelial cells). Recall the adage that “thrombin begets more thrombin”: it activates not only platelets but the intrinsic and extrinsic pathways.28
Factor Xa may be a better target than thrombin for a number of other reasons:
- Factor Xa is believed to have few functions (compared with thrombin) outside of coagulation
- In vitro studies show that factor Xa has a wider therapeutic window than thrombin, which translates to greater separation between drug levels that will confer efficacy and bleeding
- Thrombin inhibitors are associated with rebound thrombin generation (there is no evidence of this with factor Xa inhibitors)
- The efficacy of heparin-based anticoagulants improves as selectivity for factor Xa increases (unfractionated heparin is less effective than LMWH, which is less effective than fondaparinux).
Two direct factor Xa inhibitors—both administered orally—are far along in development, as detailed below.
Apixaban has shown promise, but the phase 3 ADVANCE-1 study of apixaban for VTE prevention in patients undergoing knee surgery did not meet statistical criteria for noninferiority compared with enoxaparin 30 mg twice daily.29 This prompted a delay in regulatory filings for apixaban in the United States, and the drug’s prospects for approval for VTE prevention may be unclear until release of results from two other comparative phase 3 trials with enoxaparin in 2009 and 2010.
Rivaroxaban is more likely to become clinically available soon, in light of recent results from the phase 3 RECORD4 trial demonstrating that it was significantly superior to enoxaparin 30 mg twice daily in preventing VTE following knee replacement surgery with comparable rates of major bleeding.30
DISCUSSION
Question from the audience: Some surgeons in my hospital prescribe warfarin immediately after surgery without a bridge of LMWH. Is that appropriate?
Dr. Michota: Warfarin is an option for prophylaxis in orthopedic surgery, beginning on the day of surgery. It could even be started the day before surgery, but the dose should be monitored to achieve an INR between 2.0 and 3.0 within 72 hours of the procedure. If the INR is not in this optimum range, prophylactic doses of LMWH can be given until it is therapeutic.
Follow-up question: In practice, do you actually encourage INR monitoring? Usually we just put patients on a certain dose without monitoring. When we do check the INR, it’s usually 1.4 or 1.5.
Dr. Michota: Warfarin was shown to be effective in reducing VTE risk in orthopedic surgery with dose adjustment based on INR monitoring. On that basis, warfarin remains in the guideline recommendations. Unmonitored, warfarin has not been shown to reduce risk, so to give it that way would not be evidence-based.
Question from the audience: I work with several plastic surgeons who use compression stockings intraoperatively because they’ve heard of several patients who developed a PE during surgery. Is there any benefit to using compression stockings for 2 to 3 hours and then sending the patient home?
Dr. Michota: I don’t know. Theoretically, a device that is on and working before induction may reduce stasis.
The plastic surgery societies do have guidelines. Risk depends on the type of plastic surgery procedure; for example, risk probably increases due to inflammation in procedures that involve scraping the fat pads.
This is an area where we don’t have much data. These patients may be at risk, but we don’t know the best way to mitigate it. It is important that risks be discussed with patients in the informed-consent process and be documented. If the surgeon thinks it is reasonable to give pharmacologic prophylaxis after surgery, I wouldn’t hesitate to do that, but any form of bleeding in the setting of plastic surgery is catastrophic because it defeats the reason for which the surgery was done in the first place.
Question from the audience: How do the guidelines address being aggressive with pharmacologic thromboprophylaxis when a patient is already taking dual antiplatelet therapy?
Dr. Michota: For patients with an indication for VTE prophylaxis in a setting for which there is a specific strategy, the ACCP guidelines recommend that they be put on that regimen whether they are on antiplatelet agents or not. For example, consider a high-risk patient having colorectal surgery who should get unfractionated heparin or LMWH postoperatively and who is currently taking clopidogrel and aspirin. There is no evidence that the dual aspirin–clopidogrel therapy alone is effective in decreasing the risk of DVT. However, we do know that if we add on additional agents, the risk of bleeding is increased. The guidelines consider risk and benefit, and they recommend adding the agents that we know work to prevent DVT.
Question from the audience: You briefly mentioned prophylaxis for knee arthroscopy, which is the most frequently performed orthopedic procedure. Do these recommendations apply to all patients undergoing knee arthroscopy?
Dr. Michota: No. Prophylaxis is indicated only for patients with what the ACCP considers to be additional risk factors for thrombosis. They didn’t specify which risk factors, but good indications for prophylaxis would include morbid obesity, limited mobility after the procedure, a personal history of DVT, features of stasis noted on physical examination, stasis dermatitis (or other features that could indicate prior thrombosis), advanced age, and malignancy. If a patient undergoing knee arthroscopy has other nonmodifiable risk factors, you should also think about prophylaxis. But the vast majority of patients do not need it.
Question from the audience: I’m an academic hospitalist who works closely with orthopedic surgeons. Certain surgeons will only use aspirin for prophylaxis, and it is nonnegotiable. Where does that leave me from a medicolegal standpoint? Our model is to follow ACCP recommendations, but these orthopedic surgeons still use only aspirin.
Dr. Michota: You must do everything you can to come to a consensus with your surgeon colleagues. If you are uncomfortable, as a group you must say to the surgeons, “We are uncomfortable. This is how we view the data. How do you view the data?” If they answer, “We’re doing it because it’s easy, and the American Academy of Orthopaedic Surgeons says we can do it,” I don’t have a good response. But it is more likely that their use of aspirin is based on their own observations; they may not see many clots. Of course, the problem with observational data is that the numbers are not large and they are not generated in a randomized and prospective fashion. Perhaps you can come to some middle ground, but you could always make the difficult choice and say, “I’m just not going to follow your patients.”
- Geerts WH, Bergqvist D, Pineo GF, et al; American College of Chest Physicians. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133:381S–453S.
- Medicare Quality Improvement Community (MedQIC) Web site. http://www.medqic.org. Accessed June 1, 2009.
- Surgical Care Improvement Project (SCIP). Colorado Foundation for Medical Care Web site. http://www.cfmc.org/hospital/hospital_scip.htm. Accessed June 1, 2009.
- Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med 2005; 352:969–977.
- Anderson FA Jr, Spencer FA. Risk factors for venous thromboembolism. Circulation 2003; 107:I-9–I-16.
- Amaragiri SV, Lees TA. Elastic compression stockings for prevention of deep vein thrombosis. Cochrane Database Syst Rev 2000; (3):CD001484.
- Rogers FB, Cipolle MD, Velmahos G, et al. Practice management guidelines for the prevention of venous thromboembolism in trauma patients: the EAST Practice Management Work Group. J Trauma 2002; 53:142–164.
- Bergqvist D, Agnelli G, Cohen AT, et al. Duration of prophylaxis against venous thromboembolism with enoxaparin after surgery for cancer. N Engl J Med 2002; 346:975–980.
- Heit JA, O’Fallon WM, Petterson TM, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med 2002; 162:1245–1248.
- Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med 2007; 167:1471–1475.
- Iorio A, Agnelli G. Low-molecular-weight and unfractionated heparin for prevention of venous thromboembolism in neurosurgery: a meta-analysis. Arch Intern Med 2000; 160:2327–2332.
- Mismetti P, Laporte S, Zufferey P, et al. Prevention of venous thromboembolism in orthopedic surgery with vitamin K antagonists: a meta-analysis. J Thromb Haemost 2004; 2:1058–1070.
- Turpie AG, Bauer KA, Eriksson BI, Lassen MR. Fondaparinux vs enoxaparin for the prevention of venous thromboembolism in major orthopedic surgery: a meta-analysis of 4 randomized double-blind studies. Arch Intern Med 2002; 162:1833–1840.
- Bauer KA, Eriksson BI, Lassen MR, Turpie AG; Steering Committee of the Pentasaccharide in Major Knee Surgery Study. Fondaparinux compared with enoxaparin for the prevention of venous thromboembolism after elective major knee surgery. N Engl J Med 2001; 345:1305–1310.
- Cardiovascular Disease Educational and Research Trust; Cyprus Cardiovascular Disease Educational and Research Trust; European Venous Forum; International Surgical Thrombosis Forum; International Union of Angiology; Union Internationale de Phlébologie. Prevention and treatment of venous thromboembolism. International Consensus Statement (guidelines according to scientific evidence). Int Angiol 2006; 25:101–161.
- American Academy of Orthopaedic Surgeons clinical guideline on prevention of symptomatic pulmonary embolism in patients undergoing total hip or knee arthroplasty. http://www.aaos.org/research/guidelines/PE_summary.pdf. Accessed June 5, 2009.
- Prevention of pulmonary embolism and deep vein thrombosis with low dose aspirin: Pulmonary Embolism Prevention (PEP) trial. Lancet 2000; 355:1295-1302.
- Arixtra injection [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2008.
- Sanderink GJ, Guimart C, Jariwala N, et al. Enoxaparin pharmacokinetics and pharmacodynamics in renal impairment. J Am Coll Cardiol 2001; 37(suppl A):229A. Abstract.
- Hirsh J, Bauer KA, Donati MB, et al; American College of Chest Physicians. Parenteral anticoagulants: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) [published correction appears in Chest 2008; 134:473]. Chest 2008; 133:141S–159S.
- Frederiksen SG, Hedenbro JL, Norgren L. Enoxaparin effect depends on body-weight and current doses may be inadequate in obese patients. Br J Surg 2003; 90:547–548.
- Scholten DJ, Hoedema RM, Scholten SE. A comparison of two different prophylactic dose regimens of low molecular weight heparin in bariatric surgery. Obes Surg 2002; 12:19–24.
- Shepherd MF, Rosborough TK, Schwartz ML. Heparin thromboprophylaxis in gastric bypass surgery. Obes Surg 2003; 13:249–253.
- Weitz JI, Bates SM. New anticoagulants. J Thromb Haemost 2005; 3:1843–1853.
- Eriksson BI, Dahl OE, Rosencher N, et al. Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the RE-MODEL randomized trial. J Thromb Haemost 2007; 5:2178–2185.
- RE-MOBILIZE Writing Committee, Ginsberg JS, Davidson BL, et al. Oral thrombin inhibitor dabigatran etexilate vs North American enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgery. J Arthroplasty 2009; 24:1–9.
- Eriksson BI, Dahl OE, Rosencher N, et al; RE-NOVATE Study Group. Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: a randomised, double-blind, non-inferiority trial [published correction appears in Lancet 2007; 370:2004]. Lancet 2007: 370:949–956.
- Hoffman M, Monroe DM 3rd, Roberts HR. Activated factor VII activates factors IX and X on the surface of activated platelets: thoughts on the mechanism of action of high-dose activated factor VII. Blood Coagul Fibrinolysis 1998; 9(suppl 1):S61–S65.
- Bristol-Myers Squibb and Pfizer provide update on apixaban clinical development program [press release]. New York, NY: August 27, 2008.
- Turpie AG, Lassen MR, Davidson BL, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4): a randomised trial. Lancet 2009; 373:1673–1680.
- Geerts WH, Bergqvist D, Pineo GF, et al; American College of Chest Physicians. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133:381S–453S.
- Medicare Quality Improvement Community (MedQIC) Web site. http://www.medqic.org. Accessed June 1, 2009.
- Surgical Care Improvement Project (SCIP). Colorado Foundation for Medical Care Web site. http://www.cfmc.org/hospital/hospital_scip.htm. Accessed June 1, 2009.
- Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med 2005; 352:969–977.
- Anderson FA Jr, Spencer FA. Risk factors for venous thromboembolism. Circulation 2003; 107:I-9–I-16.
- Amaragiri SV, Lees TA. Elastic compression stockings for prevention of deep vein thrombosis. Cochrane Database Syst Rev 2000; (3):CD001484.
- Rogers FB, Cipolle MD, Velmahos G, et al. Practice management guidelines for the prevention of venous thromboembolism in trauma patients: the EAST Practice Management Work Group. J Trauma 2002; 53:142–164.
- Bergqvist D, Agnelli G, Cohen AT, et al. Duration of prophylaxis against venous thromboembolism with enoxaparin after surgery for cancer. N Engl J Med 2002; 346:975–980.
- Heit JA, O’Fallon WM, Petterson TM, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med 2002; 162:1245–1248.
- Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med 2007; 167:1471–1475.
- Iorio A, Agnelli G. Low-molecular-weight and unfractionated heparin for prevention of venous thromboembolism in neurosurgery: a meta-analysis. Arch Intern Med 2000; 160:2327–2332.
- Mismetti P, Laporte S, Zufferey P, et al. Prevention of venous thromboembolism in orthopedic surgery with vitamin K antagonists: a meta-analysis. J Thromb Haemost 2004; 2:1058–1070.
- Turpie AG, Bauer KA, Eriksson BI, Lassen MR. Fondaparinux vs enoxaparin for the prevention of venous thromboembolism in major orthopedic surgery: a meta-analysis of 4 randomized double-blind studies. Arch Intern Med 2002; 162:1833–1840.
- Bauer KA, Eriksson BI, Lassen MR, Turpie AG; Steering Committee of the Pentasaccharide in Major Knee Surgery Study. Fondaparinux compared with enoxaparin for the prevention of venous thromboembolism after elective major knee surgery. N Engl J Med 2001; 345:1305–1310.
- Cardiovascular Disease Educational and Research Trust; Cyprus Cardiovascular Disease Educational and Research Trust; European Venous Forum; International Surgical Thrombosis Forum; International Union of Angiology; Union Internationale de Phlébologie. Prevention and treatment of venous thromboembolism. International Consensus Statement (guidelines according to scientific evidence). Int Angiol 2006; 25:101–161.
- American Academy of Orthopaedic Surgeons clinical guideline on prevention of symptomatic pulmonary embolism in patients undergoing total hip or knee arthroplasty. http://www.aaos.org/research/guidelines/PE_summary.pdf. Accessed June 5, 2009.
- Prevention of pulmonary embolism and deep vein thrombosis with low dose aspirin: Pulmonary Embolism Prevention (PEP) trial. Lancet 2000; 355:1295-1302.
- Arixtra injection [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2008.
- Sanderink GJ, Guimart C, Jariwala N, et al. Enoxaparin pharmacokinetics and pharmacodynamics in renal impairment. J Am Coll Cardiol 2001; 37(suppl A):229A. Abstract.
- Hirsh J, Bauer KA, Donati MB, et al; American College of Chest Physicians. Parenteral anticoagulants: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) [published correction appears in Chest 2008; 134:473]. Chest 2008; 133:141S–159S.
- Frederiksen SG, Hedenbro JL, Norgren L. Enoxaparin effect depends on body-weight and current doses may be inadequate in obese patients. Br J Surg 2003; 90:547–548.
- Scholten DJ, Hoedema RM, Scholten SE. A comparison of two different prophylactic dose regimens of low molecular weight heparin in bariatric surgery. Obes Surg 2002; 12:19–24.
- Shepherd MF, Rosborough TK, Schwartz ML. Heparin thromboprophylaxis in gastric bypass surgery. Obes Surg 2003; 13:249–253.
- Weitz JI, Bates SM. New anticoagulants. J Thromb Haemost 2005; 3:1843–1853.
- Eriksson BI, Dahl OE, Rosencher N, et al. Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the RE-MODEL randomized trial. J Thromb Haemost 2007; 5:2178–2185.
- RE-MOBILIZE Writing Committee, Ginsberg JS, Davidson BL, et al. Oral thrombin inhibitor dabigatran etexilate vs North American enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgery. J Arthroplasty 2009; 24:1–9.
- Eriksson BI, Dahl OE, Rosencher N, et al; RE-NOVATE Study Group. Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: a randomised, double-blind, non-inferiority trial [published correction appears in Lancet 2007; 370:2004]. Lancet 2007: 370:949–956.
- Hoffman M, Monroe DM 3rd, Roberts HR. Activated factor VII activates factors IX and X on the surface of activated platelets: thoughts on the mechanism of action of high-dose activated factor VII. Blood Coagul Fibrinolysis 1998; 9(suppl 1):S61–S65.
- Bristol-Myers Squibb and Pfizer provide update on apixaban clinical development program [press release]. New York, NY: August 27, 2008.
- Turpie AG, Lassen MR, Davidson BL, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4): a randomised trial. Lancet 2009; 373:1673–1680.
KEY POINTS
- Effective October 1, 2009, the Centers for Medicare and Medicaid Services is refusing to reimburse for hospital treatment of a primary diagnosis of deep vein thrombosis or pulmonary embolism following recent (within 30 days) hip or knee replacement surgery.
- Mechanical methods of thromboprophylaxis are not effective unless used for at least 18 to 20 hours a day.
- The latest ACCP guidelines recommend extended pharmacologic VTE prophylaxis for up to 28 days in select high-risk patients undergoing general or gynecologic surgery. Extended prophylaxis of varying duration is recommended for patients undergoing major orthopedic procedures.
- Aspirin alone is not recommended for perioperative VTE prophylaxis in any patient group by the ACCP or the International Union of Angiology.
- Patients with renal impairment have fewer anticoagulant options and may require dose adjustment. Weight-based dosing appears to be safe and effective for obese surgical patients.
- New selective and orally administered direct thrombin inhibitors and oral direct factor Xa inhibitors may soon be available for perioperative VTE prophylaxis.
Perioperative management of diabetes: Translating evidence into practice
Diabetes confers an increased risk of perioperative morbidity and mortality, mostly from infection and cardiovascular events. It is not unusual for surgical patients with diabetes to have a number of comorbidities or underlying chronic vascular complications that put them at risk for cardiovascular events or an infectious complication. Silent ischemia, coronary artery disease, and autonomic neuropathy are common among patients with diabetes, and each can contribute to perioperative morbidity and mortality. These are important considerations since nearly one-fifth of surgical patients have diabetes and since a person with diabetes has a 50% risk of undergoing surgery at some point in his or her lifetime.1
This article reviews the preoperative evaluation of patients with diabetes, discusses the relation between glycemic control and perioperative outcomes, and examines targets and strategies for glycemic control in patients with type 1 and type 2 diabetes throughout the perioperative period.
PREOPERATIVE EVALUATION
The preoperative evaluation must consider first and foremost the status of the patient’s diabetes and his or her surgical risk factors. Also important are the characteristics of the procedure to be performed, the method of anesthesia to be used, and select laboratory values.
Diabetes status
The type of diabetes and its treatment must be considered. Type 1 diabetes requires continuous insulin therapy to prevent ketoacidosis; patients with type 2 diabetes are usually treated with oral medications with or without insulin. Baseline control of blood glucose is a predictor of morbidity following surgery. Hypoglycemia is associated with increased morbidity in the inpatient setting, so a history of severe hypoglycemic events or of difficulty recognizing hypoglycemia (hypoglycemia unawareness) should be elicited in the preoperative evaluation. Complications of diabetes and other comorbidities also must be evaluated, along with their treatments.
Surgical risk factors
Patients with diabetes have surgical risk factors specific to their health—namely, cardiovascular risk factors that may or may not have been previously diagnosed. Patients with diabetes may have silent ischemia, atypical manifestations of coronary ischemia, or underlying cardiomyopathy. Many patients with type 2 diabetes have hypertension, which may complicate perioperative management. Other common surgical risk factors in this population include obesity, chronic kidney disease, and undiagnosed autonomic dysfunction, which may compromise hemodynamic stability in the perioperative period. Additionally, patients with long-standing diabetes experience reductions in pulmonary function (eg, forced expiratory volume, peak expiratory flow, and diffusion capacity for carbon monoxide) related to disease duration and vascular injury,2 which may complicate weaning from ventilatory support.
Characteristics of the procedure and anesthetic
Both surgery and anesthesia may induce an increase in levels of stress hormones (epinephrine, cortisol, growth hormone) and inflammatory cytokines (interleukin-6 and tumor necrosis factor–alpha), resulting in insulin resistance and impaired insulin secretion (even among patients who present with adequate insulin secretion). These in turn contribute to lipolysis and protein catabolism, leading to hyperglycemia and, if a patient is severely insulin deficient, ketoacidosis. Other factors that particularly affect insulin resistance and secretion include cardiovascular bypass surgery, sepsis, the need for total parenteral nutrition, and steroid therapy.
The characteristics of the surgical procedure, including the type of surgery as well as its urgency, duration, and timing (morning vs later in the day), are important in planning for perioperative glycemic management. For example, a short, minor procedure may require only observation, whereas more extensive procedures warrant periodic monitoring and active glycemic management with insulin infusions.
The type of anesthesia should also be considered. Compared with epidural anesthesia, general anesthesia is associated with greater stimulation of the sympathetic nervous system and increased catecholamine levels, resulting in more pronounced hyperglycemia.3
Preoperative tests
Preoperative testing and laboratory evaluation should include, at minimum, an electrocardiogram, a basic metabolic panel to assess renal function, electrolyte levels, and hemoglobin A1c measurement. For low-risk procedures in patients with adequate exercise tolerance, no diagnostic tests might be needed. In any case, knowledge of the hemoglobin A1c level may help not only to classify perioperative risk but also to determine postoperative care, including the choice of antiglycemic medications at discharge.
IMPORTANCE OF GLYCEMIC CONTROL
Preoperative glycemic control has a significant impact on the risk of infectious complications—including pneumonia, wound infection, urinary tract infection, and sepsis—in patients with diabetes across a variety of surgical procedures.4 Similarly, postoperative glycemic control—to a mean blood glucose level less than 200 mg/dL in the immediate postoperative period—significantly reduces the incidence of deep sternal wound infection after open heart surgery.5
Among patients undergoing cardiothoracic surgery, both cardiac-related and overall mortality are greater with increasing postoperative blood glucose levels, although a cause-and-effect relationship has not been established.6
Glycemic control matters regardless of diabetes status
Hyperglycemia affects mortality regardless of diabetes status. In a study of 779 consecutive patients admitted for acute myocardial infarction, mortality at 180 days was highly associated with hyperglycemia on admission independent of a history of diabetes; the highest mortality was among hyperglycemic patients without previously known diabetes.7 Similarly, a large study of glycemic control in intensive care unit (ICU) patients receiving insulin found that mortality in nondiabetic patients increased with median glucose level and was higher than mortality in diabetic patients.8 These findings suggest a need for vigilance in the perioperative and critical care management of all patients with hyperglycemia, regardless of preadmission diabetes diagnosis, as they carry significant morbidity and mortality risk.
GLYCEMIC CONTROL IN THE CRITICALLY ILL: SOME SUPPORT FOR A MODIFIED TARGET, BUT VIGILANCE FOR HYPOGLYCEMIA NEEDED
The landmark study by Van den Berghe et al of intensive insulin therapy in surgical ICU patients demonstrated significant reductions in morbidity and mortality when glucose levels were controlled aggressively (80 to 110 mg/dL; average, 103 mg/dL) compared with conventional control (180 to 200 mg/dL).9 The benefit of intensive glycemic control was evident on outcomes such as the occurrence of sepsis, need for dialysis, need for blood transfusion, and development of acute polyneuropathy. Intensive insulin therapy was also associated with cost savings compared with conventional insulin therapy in mechanically ventilated patients.10
However, a number of subsequent studies have clearly shown that as blood glucose levels approach normoglycemia, the risks of hypoglycemia, especially severe hypoglycemia, can offset the benefits of tight blood glucose control.
A follow-up study by Ven den Berghe et al in a medical ICU failed to show a mortality benefit from tight glycemic control, though patients in the intensive control arm experienced less renal injury, faster weaning from ventilation, and earlier discharge from the ICU and hospital.11
The recent NICE-SUGAR study of aggressive glucose control in the ICU randomized patients to a target blood glucose of 81 to 108 mg/dL (intensive group) or 180 mg/dL or less (control group).12 At study’s end, the groups’ mean blood glucose levels were 115 mg/dL and 144 mg/dL, respectively, while rates of severe hypoglycemia (blood glucose < 40 mg/dL) were 6.8% and 0.5%, respectively. Mortality rates were higher in the intensive therapy group (27.5%) than in the control group (24.9%), driven by severe hypoglycemic events. Notably, blood glucose monitoring in this and other studies was conducted at a frequency of anywhere between 1 and 4 hours.
The conclusions of the available data would support, for the time being, a modified glycemic target in critically ill patients, with strict avoidance of severe hypoglycemia. The recent consensus statement from the American Association of Clinical Endocrinologists and the American Diabetes Association recommends using insulin therapy if blood glucose levels exceed 180 mg/dL, with target glucose levels less than 180 mg/dL in critically ill patients and less than 140 mg/dL in non–critically ill patients.13 Development and implementation of safer insulin infusion algorithms and more frequent and accurate blood glucose monitoring in this setting should enable us to achieve better glycemic targets with lower risk.
ELEMENTS OF PHYSIOLOGIC INSULIN REPLACEMENT
In hospitalized patients with hyperglycemia, three different components of insulin replacement require management1:
Basal insulin replacement consists of a long-acting insulin preparation administered regardless of the patient’s oral intake status, with the premise of matching hepatic (endogenous) glucose production
Prandial insulin replacement requires a rapid-acting insulin preparation given to cover nutritional needs
Supplemental (or correction) insulin replacement requires a rapid-acting preparation (usually the same insulin type as for prandial coverage) to correct blood glucose values that exceed predetermined glycemic targets.
For most patients, basal insulin replacement might be appropriate preoperatively to control fasting glucose, whereas during surgery, especially if prolonged or high risk, an intravenous (IV) insulin drip is the most effective means of glucose control. The postoperative transition from the IV insulin drip usually involves basal insulin replacement plus supplemental rapid-acting insulin. Prandial or nutritional insulin should be started once the patient begins to receive nutrition (oral, enteral, or hyperalimentation).
GOALS OF PERIOPERATIVE GLYCEMIC CONTROL
Perioperative glycemic management has several key objectives:
- Avoidance of clinically significant hyper- or hypoglycemia
- Maintenance of electrolyte and fluid balance
- Prevention of ketoacidosis, which is imperative in patients with type 1 diabetes, who require insulin at all times
- Achievement of specific glycemic targets, as discussed above—ie, less than 180 mg/dL in critically ill patients and less than 140 mg/dL in stable patients.13
Strategies differ across the perioperative timeline
Strategies for perioperative glycemic control differ before, during, and after surgery, as summarized immediately below and detailed in the following sections.
Preoperatively, glycemia should be stabilized, typically with subcutaneous insulin, if there is enough time to do so. For patients who have not previously been on insulin, placing them on an insulin supplemental scale to correct glycemia to desired targets might be a first step. In the setting of hyperglycemia, these patients may also be started on a low dose of basal insulin, with preference given to basal insulin analogs, given their consistent and relatively peakless action profile and lower risk of hypoglycemia. A starting dose of 0.2 to 0.4 U/kg is appropriate and carries a low risk of hypoglycemia. For patients already using insulin on an outpatient basis, continuing their basal insulin dose, possibly at a reduced dosage (25% less), together with supplemental-scale insulin coverage, should stabilize blood glucose levels. For patients on combination insulin or premixed insulin types, the basal insulin dose for preoperative management can be estimated by taking the patient’s usual total daily dose and delivering 40% to 50% of that dose as a basal insulin analog injection. Clearly, a supplemental scale should be implemented along with basal insulin replacement.
Intraoperatively, switching to IV insulin may be appropriate for stabilizing glycemia, depending on the type of surgery. A number of IV insulin protocols have been proposed, although no consistent comparisons of efficacy or safety among these protocols have been published.
Postoperatively, patients eventually should be transitioned from IV to subcutaneous insulin when glycemic control stabilizes. This transition may be complicated for many reasons. Oral intake may be inconsistent. The surgery and surrounding environment can induce stressors, promote susceptibility to infection, and increase insulin resistance. Additionally, some patients may be on hyperalimentation. Specific instructions for the transition from IV to subcutaneous insulin are covered later in this article.
PREOPERATIVE GLYCEMIC MANAGEMENT
In patients with type 2 diabetes, oral agents pose certain safety risks and should be discontinued prior to surgery.
Sulfonylureas may induce hypoglycemia in patients who are placed on NPO (“nothing by mouth”) orders and should be held in patients who are fasting.
Metformin can induce lactic acidosis if kidney function declines and should be withheld 1 to 2 days before planned surgery if a need for IV contrast is anticipated or the procedure could potentially lead to hemodynamic instability and reduced renal perfusion.
Thiazolidinediones may cause fluid retention that can complicate the postoperative period; they can be discontinued several days prior to a planned surgery.
GLP-1 agonists, such as exenatide, can slow gastric motility and potentially delay gastrointestinal recovery after major surgery; they should be held the day of surgery.
DPP-4 inhibitors (incretin enhancers), such as sitagliptin, do not have significant side effects and, if need be, can be continued. Because incretin therapies act via a glucose-dependent mechanism, they are unlikely to cause hypoglycemia, even in a patient whose oral intake is held or delayed. On the other hand, since their effect is mostly in reducing postprandial glycemia, there may be little need to use them in a patient who is NPO.
Patients with type 1 diabetes must continue basal insulin replacement preoperatively (0.2 to 0.3 U/kg/day of a long-acting insulin). Patients with type 2 diabetes may benefit from basal insulin replacement, as previously noted.
Supplemental insulin scales are used to correct hyperglycemia regardless of a patient’s oral intake status. They can be individualized based on the estimated total daily insulin dose and require glycemic targets to be established. Fingerstick glucose monitoring should be done every 4 to 6 hours in a patient who is NPO, and supplemental-scale insulin should be used to correct glucose values that exceed target. For supplemental-scale coverage, rapid-acting insulin analogs have a shorter duration of action than human regular insulin and may be given subcutaneously every 4 to 6 hours, whereas regular insulin should not be given more often than every 6 hours to correct hyperglycemia. These differences in action duration should be kept in mind to minimize the potential for insulin stacking.
INTRAOPERATIVE GLYCEMIC MANAGEMENT
Procedure length is an important determinant
Strategies for intraoperative glucose management vary according to the length of the procedure.
For minor, short procedures, the preoperative glucose management orders may be continued.
For longer, more complex procedures, a switch to an IV insulin drip is safe and allows rapid adjustments in dosing and plasma glucose levels. Ideally, IV insulin is started prior to the procedure so that the glucose level is stable once the patient arrives in the operating room. Given the logistics of IV insulin management, including the need for frequent monitoring (hourly) and dose adjustments, this type of treatment should be reserved for environments with adequate numbers of trained staff.
IV regular insulin is therapy of choice
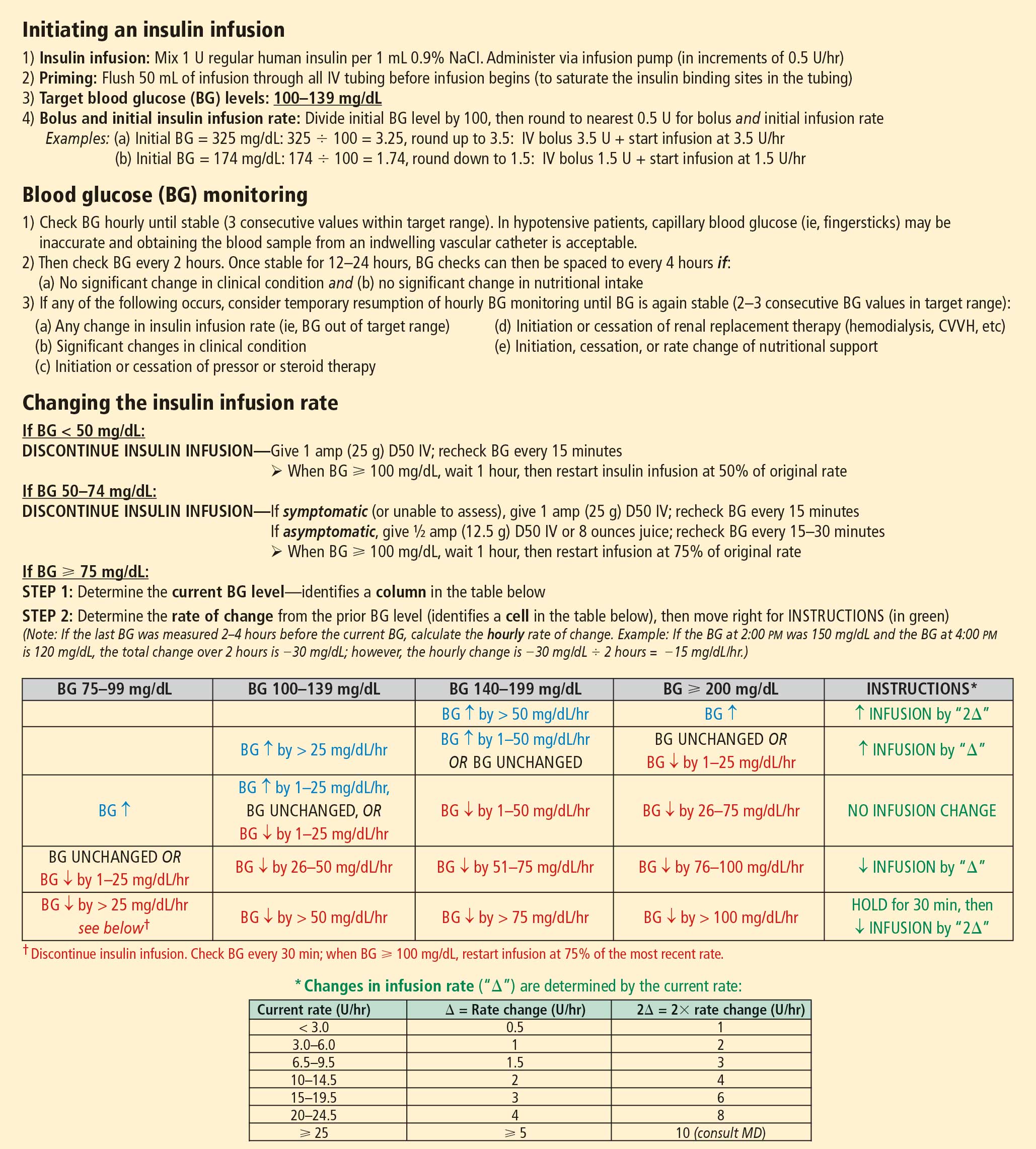
Several different algorithms for IV regular insulin therapy are in use. Some are static, such as those of Markovitz et al14 and Stockton et al,15 while others are dynamic (ie, doses are self-adjusted based on changes in blood glucose level), such as the “Yale protocol” of Goldberg et al (Figure 1).16
POSTOPERATIVE GLYCEMIC MANAGEMENT
Start subcutaneous transition before stopping IV drip
Transitioning from IV to subcutaneous insulin is often complicated. Nonoral nutrition options (ie, parenteral nutrition or enteral supplementation) must be considered. As noted, insulin must be replaced according to physiologic needs, which requires that a long-acting basal insulin be used regardless of oral intake status, a rapid-acting insulin be given to cover prandial or nutritional needs, and supplemental rapid-acting insulin be used to correct hyperglycemia.
In the transition from IV insulin, basal insulin replacement can begin at any time. I recommend starting the transition from IV to subcutaneous insulin about 12 to 24 hours before discontinuing the insulin drip. In type 1 diabetes, this transition ensures basal insulin coverage and minimizes the risk of developing ketones and ketoacidosis. In type 2 diabetes, it can ensure a more stable transition and better glycemic control.
Determining the basal insulin dose
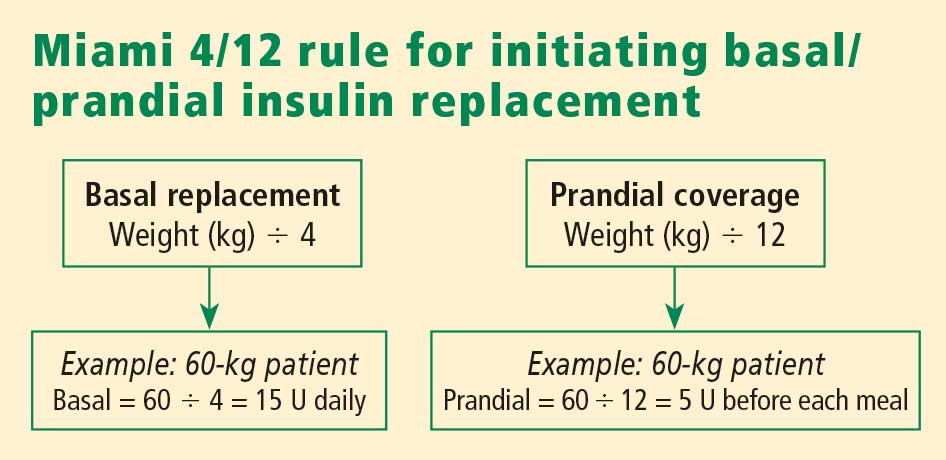
Switching to subcutaneous supplemental insulin
Instructions must be given for switching to subcutaneous supplemental doses of insulin. Glycemic targets, generally from less than 130 to 150 mg/dL, must be established, as must the frequency of fingerstick testing:
- If the patient is being fed enterally or parenterally, fingerstick testing is recommended every 4 to 6 hours if a rapid-acting insulin analog is used and every 6 hours if regular insulin is used.
- If the patient is eating, fingerstick testing should be performed before meals and at bedtime.
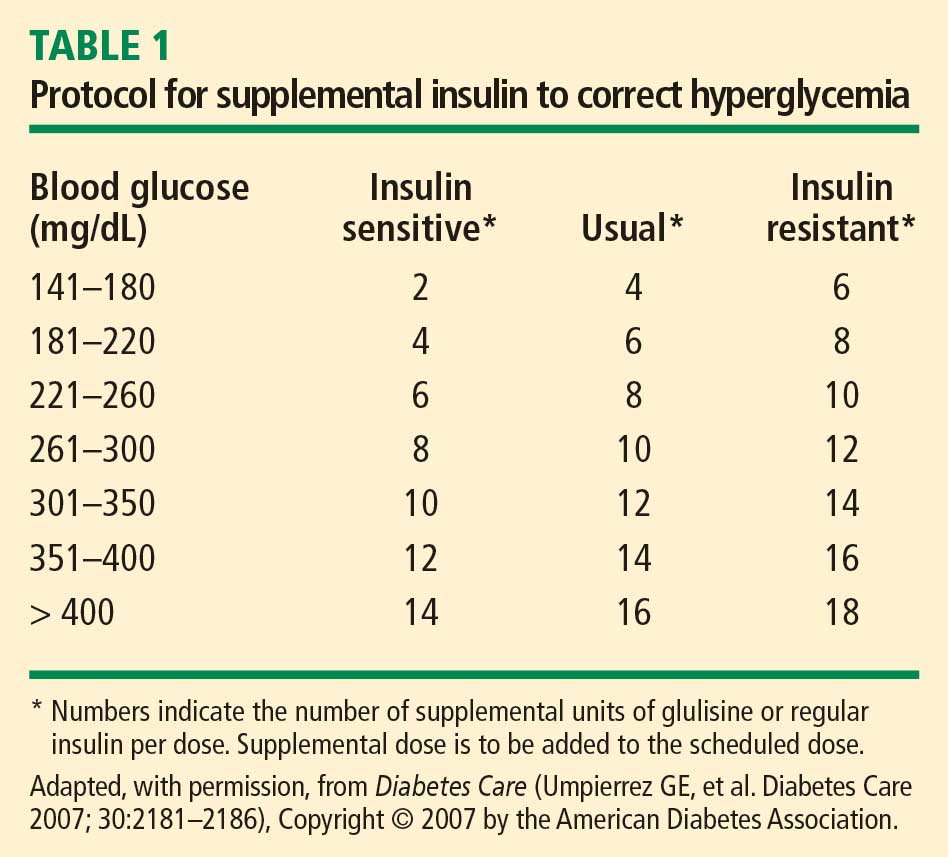
Covering nutritional requirements
Nutrition-related insulin needs depend on the type of caloric intake prescribed:
In patients receiving total parenteral nutrition (TPN), start 1 U of regular insulin (placed in the bag) for every 10 to 15 g of dextrose in the TPN mixture.
In patients receiving enteral nutrition, use regular insulin every 6 hours or a rapid-acting insulin analog every 4 hours. Start 1 U of insulin subcutaneously for every 10 to 15 g of delivered carbohydrates. For example, if a patient is receiving 10 g of carbohydrates per hour, a rapid-acting analog given at a dose of 4 U every 4 hours (1 U per 10 g of carbohydrates) should adequately cover enteral feedings. For any bolus feedings, give the injection as a full bolus 15 to 20 minutes in advance, based on the carbohydrate content of the feeding.
In patients who are eating, use regular insulin or a rapid-acting insulin analog before meals. Again, start 1 U of insulin subcutaneously for every 10 to 15 g of carbohydrates, or use the prandial portion of the Miami 4/12 rule (Figure 2). For example, in a 60-kg patient one would start with 5 U (60 ÷ 12) of a rapid-acting insulin before each meal.
Basal/bolus replacement outperforms supplemental-scale regular insulin
Use of a basal/bolus insulin regimen appears to be more beneficial than supplemental-scale regular insulin in hospitalized patients with type 2 diabetes, according to a recent randomized trial comparing the two approaches in 130 such patients with blood glucose levels greater than 140 mg/dL.17 In the group randomized to basal/bolus insulin, the starting total daily dose was 0.4 to 0.5 U/kg/day, with half the dose given as basal insulin (insulin glargine) once daily and half given as a rapid-acting insulin analog (glulisine) in fixed doses before every meal. A rapid-acting analog was used for supplemental insulin in the basal/bolus regimen. By study’s end, patients in the basal/bolus group were receiving a higher total daily insulin dose than those in the supplemental-scale group (mean of 42 U/day vs 13 U/day).
Mean daily blood glucose levels were 27 mg/dL lower, on average, in patients who received basal/bolus therapy compared with the supplemental-scale group, yet there was no difference between groups in the risk of hypoglycemia. More patients randomized to basal/bolus therapy achieved the glycemic goal of less than 140 mg/dL (66% vs 38%). Fourteen percent of patients assigned to supplemental-scale insulin had values persistently greater than 240 mg/dL and had to be switched to the basal/bolus regimen.17
SUMMARY
Perioperative glycemic control can reduce morbidity, particularly the incidence of infectious complications, in surgical patients, even in those without diagnosed diabetes. Optimal management of glycemia in the perioperative period involves applying principles of physiologic insulin replacement. Postoperatively, the transition from IV to subcutaneous insulin can be achieved through the use of basal insulin for coverage of fasting insulin needs, regardless of the patient’s feeding status, and the use of rapid-acting insulin to cover hyperglycemia and nutritional needs. Management of hospitalized patients exclusively with supplemental-scale regular insulin should be abandoned.
DISCUSSION
Question from the audience: As an attending physician in a preoperative clinic I’m never sure what to do with NPH insulin the morning of surgery. What guidance can you give?
Dr. Meneghini: NPH is a peaking basal insulin, and the peak can induce hypoglycemia in a patient who is NPO. If we have the opportunity, we try to switch patients previously receiving insulin therapy to a long-acting basal insulin analog, which has a much flatter action profile and is safer in the fasting state. If there is no opportunity for switching, we instruct the patient to take two-thirds of his or her usual morning dose of insulin and we initiate a D5 drip when the patient arrives at the hospital.
Question from the audience: How do you handle perioperative insulin in patients on insulin pumps?
Dr. Meneghini: The pumps provide a subcutaneous basal insulin infusion, which should, if set correctly, maintain stable blood glucose levels when the patient is NPO. Supplemental doses of insulin to correct hyperglycemia can be delivered via the usual subcutaneous practice with a syringe or insulin pen. If you are uncomfortable with pump function, or if the pump insertion site interferes with the surgery site, simply replace the 24-hour basal amount delivered via pump with an injection of glargine or detemir divided into twice-daily injections. Correct hyperglycemia with supplemental-scale insulin as per usual protocol.
Question from the audience: The manufacturer of insulin glargine makes no recommendations for its use the night before or morning of surgery. What do you recommend?
Dr. Meneghini: It depends on whether the glargine is dosed appropriately. Most patients with type 2 diabetes require 0.4 to 0.6 U/kg/day of a long-acting insulin. If they’re on much more, they may be overdosed, and I would cut the basal dose by about half. Otherwise, 75% to 100% of the usual basal amount is appropriate. In type 1 diabetes, the usual replacement dose of basal insulin is 0.2 to 0.3 U/kg/day. If a patient is in this range, the basal insulin can be continued. Patients who experience hypoglycemia, or a substantial fall in blood glucose if meals are skipped or delayed, may be getting too much basal insulin and might benefit from a dose reduction when placed on NPO status.
Question from the audience: Metformin has a black-box warning advising that it be stopped at least 48 hours before surgery, but patients often come to surgery having taken metformin within the prior 12 to 24 hours. How should we manage such patients coming for elective surgery?
Dr. Meneghini: Metformin is cleared exclusively by the kidneys; its accumulation as a result of impaired kidney function (eg, due to hemodynamic instability or radiology studies using IV iodine) can result in increased lactic acid production by the liver and lactic acidosis. A patient who has taken metformin within the prior 48 hours but doesn’t have a risk of hemodynamic dysfunction is at low risk of lactic acidosis if hydrated appropriately. There’s not much choice if a patient needs urgent surgery and has recently taken metformin; in that case, just ensure maintenance of adequate glomerular filtration via fluid repletion to clear the drug.
Question from the audience: What’s the evidence for tight glycemic control or any type of glycemic control in patients undergoing outpatient surgery or “same-day” patients who will be admitted to a regular surgical floor? Also, what would you consider maximal glucose values for a patient going into elective surgery?
Dr. Meneghini: I haven’t seen any guidelines for glycemic control in patients undergoing outpatient surgery. If a patient has poor glycemic control coming into surgery, even for a minor procedure, the risk of an infectious complication may be increased. Keeping blood glucose below 180 mg/dL and avoiding electrolyte imbalances is likely sufficient in such patients. On the second question, if it’s an elective procedure and can be delayed a few hours, you can certainly institute IV insulin therapy to correct hyperglycemia rapidly—just ensure adequate replacement of fluids since the patient may have had volume depletion or dehydration as a result of the preceding osmotic diuresis. Once glycemic control is improved (blood glucose < 180–200 mg/dL), the patient can proceed to surgery.
Question from the audience: What are your recommendations for resuming oral diabetes medications after surgery?
Dr. Meneghini: Once patients are tolerating their meals and being considered for discharge, you may want to resume their oral medications, assuming their admission hemoglobin A1c levels were near goal. If glycemic control was inadequate preoperatively, this may be a good opportunity to adjust their prior regimen to more appropriate therapy. In some cases, this might include some form of insulin, either basal therapy or basal and supplemental insulin.
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care 2004; 27:553–591.
- Kaparianos A, Argyropoulou E, Sampsonas F, et al. Pulmonary complications in diabetes mellitus. Chron Respir Dis 2008; 5:101–108.
- Grigoleit HG. Anesthesia and blood glucose. Acta Diabetologica 1973; 10:569–574.
- Dronge AS, Perkal MF, Kancir S, et al. Long-term glycemic control and postoperative infectious complications. Arch Surg 2006; 141:375–380.
- Zerr KJ, Furnary AP, Grunkemeier GL, Bookin S, Kanhere V, Starr A. Glucose control lowers the risk of wound infection in diabetics after open heart operations. Ann Thorac Surg 1997; 63:356–361.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg 2003; 125:1007–10021.
- Ainla T, Baburin A, Tessalu R, et al. The association between hyperglycaemia on admission and 180-day mortality in acute myocardial infarction patients with and without diabetes. Diabet Med 2005; 22:1321–1325.
- Rady MY, Johnson DJ, Patel BM, et al. Influence of individual characteristics on outcome of glycemic control in intensive care unit patients with or without diabetes mellitus. Mayo Clin Proc 2005; 80:1558–1567.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med 2001; 345:1359–1367.
- Van den Berghe G, Wouters PJ, Kesteloot K, Hilleman DE. Analysis of healthcare resource utilization with intensive insulin therapy in critically ill patients. Crit Care Med 2006; 34:612–616.
- Van den Berghe G, Wawilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. New Engl J Med 2006; 354:449–461.
- NICE-SUGAR Study Investigators. Intensive vs conventional glucose control in critically ill patients. N Engl J Med 2009; 360:1283–1297.
- Moghissi ES, Korytowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Endocr Pract 2009; 15:353–369.
- Markovitz LJ, Wiechmann RJ, Harris N, et al. Description and evaluation of a glycemic management protocol for patients with diabetes undergoing heart surgery. Endocr Pract 2002; 8:10–18.
- Stockton L, Baird M, Cook CB, et al. Development and implementation of evidence-based guidelines for IV insulin: a statewide collaborative approach. Insulin 2008; 3:67–77.
- Goldberg PA, Siegel MD, Sherwin RS, et al. Implementation of a safe and effective insulin infusion protocol in a medical intensive care unit. Diabetes Care 2004; 27:461–467.
- Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care 2007; 30:2181–2186.
Diabetes confers an increased risk of perioperative morbidity and mortality, mostly from infection and cardiovascular events. It is not unusual for surgical patients with diabetes to have a number of comorbidities or underlying chronic vascular complications that put them at risk for cardiovascular events or an infectious complication. Silent ischemia, coronary artery disease, and autonomic neuropathy are common among patients with diabetes, and each can contribute to perioperative morbidity and mortality. These are important considerations since nearly one-fifth of surgical patients have diabetes and since a person with diabetes has a 50% risk of undergoing surgery at some point in his or her lifetime.1
This article reviews the preoperative evaluation of patients with diabetes, discusses the relation between glycemic control and perioperative outcomes, and examines targets and strategies for glycemic control in patients with type 1 and type 2 diabetes throughout the perioperative period.
PREOPERATIVE EVALUATION
The preoperative evaluation must consider first and foremost the status of the patient’s diabetes and his or her surgical risk factors. Also important are the characteristics of the procedure to be performed, the method of anesthesia to be used, and select laboratory values.
Diabetes status
The type of diabetes and its treatment must be considered. Type 1 diabetes requires continuous insulin therapy to prevent ketoacidosis; patients with type 2 diabetes are usually treated with oral medications with or without insulin. Baseline control of blood glucose is a predictor of morbidity following surgery. Hypoglycemia is associated with increased morbidity in the inpatient setting, so a history of severe hypoglycemic events or of difficulty recognizing hypoglycemia (hypoglycemia unawareness) should be elicited in the preoperative evaluation. Complications of diabetes and other comorbidities also must be evaluated, along with their treatments.
Surgical risk factors
Patients with diabetes have surgical risk factors specific to their health—namely, cardiovascular risk factors that may or may not have been previously diagnosed. Patients with diabetes may have silent ischemia, atypical manifestations of coronary ischemia, or underlying cardiomyopathy. Many patients with type 2 diabetes have hypertension, which may complicate perioperative management. Other common surgical risk factors in this population include obesity, chronic kidney disease, and undiagnosed autonomic dysfunction, which may compromise hemodynamic stability in the perioperative period. Additionally, patients with long-standing diabetes experience reductions in pulmonary function (eg, forced expiratory volume, peak expiratory flow, and diffusion capacity for carbon monoxide) related to disease duration and vascular injury,2 which may complicate weaning from ventilatory support.
Characteristics of the procedure and anesthetic
Both surgery and anesthesia may induce an increase in levels of stress hormones (epinephrine, cortisol, growth hormone) and inflammatory cytokines (interleukin-6 and tumor necrosis factor–alpha), resulting in insulin resistance and impaired insulin secretion (even among patients who present with adequate insulin secretion). These in turn contribute to lipolysis and protein catabolism, leading to hyperglycemia and, if a patient is severely insulin deficient, ketoacidosis. Other factors that particularly affect insulin resistance and secretion include cardiovascular bypass surgery, sepsis, the need for total parenteral nutrition, and steroid therapy.
The characteristics of the surgical procedure, including the type of surgery as well as its urgency, duration, and timing (morning vs later in the day), are important in planning for perioperative glycemic management. For example, a short, minor procedure may require only observation, whereas more extensive procedures warrant periodic monitoring and active glycemic management with insulin infusions.
The type of anesthesia should also be considered. Compared with epidural anesthesia, general anesthesia is associated with greater stimulation of the sympathetic nervous system and increased catecholamine levels, resulting in more pronounced hyperglycemia.3
Preoperative tests
Preoperative testing and laboratory evaluation should include, at minimum, an electrocardiogram, a basic metabolic panel to assess renal function, electrolyte levels, and hemoglobin A1c measurement. For low-risk procedures in patients with adequate exercise tolerance, no diagnostic tests might be needed. In any case, knowledge of the hemoglobin A1c level may help not only to classify perioperative risk but also to determine postoperative care, including the choice of antiglycemic medications at discharge.
IMPORTANCE OF GLYCEMIC CONTROL
Preoperative glycemic control has a significant impact on the risk of infectious complications—including pneumonia, wound infection, urinary tract infection, and sepsis—in patients with diabetes across a variety of surgical procedures.4 Similarly, postoperative glycemic control—to a mean blood glucose level less than 200 mg/dL in the immediate postoperative period—significantly reduces the incidence of deep sternal wound infection after open heart surgery.5
Among patients undergoing cardiothoracic surgery, both cardiac-related and overall mortality are greater with increasing postoperative blood glucose levels, although a cause-and-effect relationship has not been established.6
Glycemic control matters regardless of diabetes status
Hyperglycemia affects mortality regardless of diabetes status. In a study of 779 consecutive patients admitted for acute myocardial infarction, mortality at 180 days was highly associated with hyperglycemia on admission independent of a history of diabetes; the highest mortality was among hyperglycemic patients without previously known diabetes.7 Similarly, a large study of glycemic control in intensive care unit (ICU) patients receiving insulin found that mortality in nondiabetic patients increased with median glucose level and was higher than mortality in diabetic patients.8 These findings suggest a need for vigilance in the perioperative and critical care management of all patients with hyperglycemia, regardless of preadmission diabetes diagnosis, as they carry significant morbidity and mortality risk.
GLYCEMIC CONTROL IN THE CRITICALLY ILL: SOME SUPPORT FOR A MODIFIED TARGET, BUT VIGILANCE FOR HYPOGLYCEMIA NEEDED
The landmark study by Van den Berghe et al of intensive insulin therapy in surgical ICU patients demonstrated significant reductions in morbidity and mortality when glucose levels were controlled aggressively (80 to 110 mg/dL; average, 103 mg/dL) compared with conventional control (180 to 200 mg/dL).9 The benefit of intensive glycemic control was evident on outcomes such as the occurrence of sepsis, need for dialysis, need for blood transfusion, and development of acute polyneuropathy. Intensive insulin therapy was also associated with cost savings compared with conventional insulin therapy in mechanically ventilated patients.10
However, a number of subsequent studies have clearly shown that as blood glucose levels approach normoglycemia, the risks of hypoglycemia, especially severe hypoglycemia, can offset the benefits of tight blood glucose control.
A follow-up study by Ven den Berghe et al in a medical ICU failed to show a mortality benefit from tight glycemic control, though patients in the intensive control arm experienced less renal injury, faster weaning from ventilation, and earlier discharge from the ICU and hospital.11
The recent NICE-SUGAR study of aggressive glucose control in the ICU randomized patients to a target blood glucose of 81 to 108 mg/dL (intensive group) or 180 mg/dL or less (control group).12 At study’s end, the groups’ mean blood glucose levels were 115 mg/dL and 144 mg/dL, respectively, while rates of severe hypoglycemia (blood glucose < 40 mg/dL) were 6.8% and 0.5%, respectively. Mortality rates were higher in the intensive therapy group (27.5%) than in the control group (24.9%), driven by severe hypoglycemic events. Notably, blood glucose monitoring in this and other studies was conducted at a frequency of anywhere between 1 and 4 hours.
The conclusions of the available data would support, for the time being, a modified glycemic target in critically ill patients, with strict avoidance of severe hypoglycemia. The recent consensus statement from the American Association of Clinical Endocrinologists and the American Diabetes Association recommends using insulin therapy if blood glucose levels exceed 180 mg/dL, with target glucose levels less than 180 mg/dL in critically ill patients and less than 140 mg/dL in non–critically ill patients.13 Development and implementation of safer insulin infusion algorithms and more frequent and accurate blood glucose monitoring in this setting should enable us to achieve better glycemic targets with lower risk.
ELEMENTS OF PHYSIOLOGIC INSULIN REPLACEMENT
In hospitalized patients with hyperglycemia, three different components of insulin replacement require management1:
Basal insulin replacement consists of a long-acting insulin preparation administered regardless of the patient’s oral intake status, with the premise of matching hepatic (endogenous) glucose production
Prandial insulin replacement requires a rapid-acting insulin preparation given to cover nutritional needs
Supplemental (or correction) insulin replacement requires a rapid-acting preparation (usually the same insulin type as for prandial coverage) to correct blood glucose values that exceed predetermined glycemic targets.
For most patients, basal insulin replacement might be appropriate preoperatively to control fasting glucose, whereas during surgery, especially if prolonged or high risk, an intravenous (IV) insulin drip is the most effective means of glucose control. The postoperative transition from the IV insulin drip usually involves basal insulin replacement plus supplemental rapid-acting insulin. Prandial or nutritional insulin should be started once the patient begins to receive nutrition (oral, enteral, or hyperalimentation).
GOALS OF PERIOPERATIVE GLYCEMIC CONTROL
Perioperative glycemic management has several key objectives:
- Avoidance of clinically significant hyper- or hypoglycemia
- Maintenance of electrolyte and fluid balance
- Prevention of ketoacidosis, which is imperative in patients with type 1 diabetes, who require insulin at all times
- Achievement of specific glycemic targets, as discussed above—ie, less than 180 mg/dL in critically ill patients and less than 140 mg/dL in stable patients.13
Strategies differ across the perioperative timeline
Strategies for perioperative glycemic control differ before, during, and after surgery, as summarized immediately below and detailed in the following sections.
Preoperatively, glycemia should be stabilized, typically with subcutaneous insulin, if there is enough time to do so. For patients who have not previously been on insulin, placing them on an insulin supplemental scale to correct glycemia to desired targets might be a first step. In the setting of hyperglycemia, these patients may also be started on a low dose of basal insulin, with preference given to basal insulin analogs, given their consistent and relatively peakless action profile and lower risk of hypoglycemia. A starting dose of 0.2 to 0.4 U/kg is appropriate and carries a low risk of hypoglycemia. For patients already using insulin on an outpatient basis, continuing their basal insulin dose, possibly at a reduced dosage (25% less), together with supplemental-scale insulin coverage, should stabilize blood glucose levels. For patients on combination insulin or premixed insulin types, the basal insulin dose for preoperative management can be estimated by taking the patient’s usual total daily dose and delivering 40% to 50% of that dose as a basal insulin analog injection. Clearly, a supplemental scale should be implemented along with basal insulin replacement.
Intraoperatively, switching to IV insulin may be appropriate for stabilizing glycemia, depending on the type of surgery. A number of IV insulin protocols have been proposed, although no consistent comparisons of efficacy or safety among these protocols have been published.
Postoperatively, patients eventually should be transitioned from IV to subcutaneous insulin when glycemic control stabilizes. This transition may be complicated for many reasons. Oral intake may be inconsistent. The surgery and surrounding environment can induce stressors, promote susceptibility to infection, and increase insulin resistance. Additionally, some patients may be on hyperalimentation. Specific instructions for the transition from IV to subcutaneous insulin are covered later in this article.
PREOPERATIVE GLYCEMIC MANAGEMENT
In patients with type 2 diabetes, oral agents pose certain safety risks and should be discontinued prior to surgery.
Sulfonylureas may induce hypoglycemia in patients who are placed on NPO (“nothing by mouth”) orders and should be held in patients who are fasting.
Metformin can induce lactic acidosis if kidney function declines and should be withheld 1 to 2 days before planned surgery if a need for IV contrast is anticipated or the procedure could potentially lead to hemodynamic instability and reduced renal perfusion.
Thiazolidinediones may cause fluid retention that can complicate the postoperative period; they can be discontinued several days prior to a planned surgery.
GLP-1 agonists, such as exenatide, can slow gastric motility and potentially delay gastrointestinal recovery after major surgery; they should be held the day of surgery.
DPP-4 inhibitors (incretin enhancers), such as sitagliptin, do not have significant side effects and, if need be, can be continued. Because incretin therapies act via a glucose-dependent mechanism, they are unlikely to cause hypoglycemia, even in a patient whose oral intake is held or delayed. On the other hand, since their effect is mostly in reducing postprandial glycemia, there may be little need to use them in a patient who is NPO.
Patients with type 1 diabetes must continue basal insulin replacement preoperatively (0.2 to 0.3 U/kg/day of a long-acting insulin). Patients with type 2 diabetes may benefit from basal insulin replacement, as previously noted.
Supplemental insulin scales are used to correct hyperglycemia regardless of a patient’s oral intake status. They can be individualized based on the estimated total daily insulin dose and require glycemic targets to be established. Fingerstick glucose monitoring should be done every 4 to 6 hours in a patient who is NPO, and supplemental-scale insulin should be used to correct glucose values that exceed target. For supplemental-scale coverage, rapid-acting insulin analogs have a shorter duration of action than human regular insulin and may be given subcutaneously every 4 to 6 hours, whereas regular insulin should not be given more often than every 6 hours to correct hyperglycemia. These differences in action duration should be kept in mind to minimize the potential for insulin stacking.
INTRAOPERATIVE GLYCEMIC MANAGEMENT
Procedure length is an important determinant
Strategies for intraoperative glucose management vary according to the length of the procedure.
For minor, short procedures, the preoperative glucose management orders may be continued.
For longer, more complex procedures, a switch to an IV insulin drip is safe and allows rapid adjustments in dosing and plasma glucose levels. Ideally, IV insulin is started prior to the procedure so that the glucose level is stable once the patient arrives in the operating room. Given the logistics of IV insulin management, including the need for frequent monitoring (hourly) and dose adjustments, this type of treatment should be reserved for environments with adequate numbers of trained staff.
IV regular insulin is therapy of choice
Several different algorithms for IV regular insulin therapy are in use. Some are static, such as those of Markovitz et al14 and Stockton et al,15 while others are dynamic (ie, doses are self-adjusted based on changes in blood glucose level), such as the “Yale protocol” of Goldberg et al (Figure 1).16
POSTOPERATIVE GLYCEMIC MANAGEMENT
Start subcutaneous transition before stopping IV drip
Transitioning from IV to subcutaneous insulin is often complicated. Nonoral nutrition options (ie, parenteral nutrition or enteral supplementation) must be considered. As noted, insulin must be replaced according to physiologic needs, which requires that a long-acting basal insulin be used regardless of oral intake status, a rapid-acting insulin be given to cover prandial or nutritional needs, and supplemental rapid-acting insulin be used to correct hyperglycemia.
In the transition from IV insulin, basal insulin replacement can begin at any time. I recommend starting the transition from IV to subcutaneous insulin about 12 to 24 hours before discontinuing the insulin drip. In type 1 diabetes, this transition ensures basal insulin coverage and minimizes the risk of developing ketones and ketoacidosis. In type 2 diabetes, it can ensure a more stable transition and better glycemic control.
Determining the basal insulin dose
Switching to subcutaneous supplemental insulin
Instructions must be given for switching to subcutaneous supplemental doses of insulin. Glycemic targets, generally from less than 130 to 150 mg/dL, must be established, as must the frequency of fingerstick testing:
- If the patient is being fed enterally or parenterally, fingerstick testing is recommended every 4 to 6 hours if a rapid-acting insulin analog is used and every 6 hours if regular insulin is used.
- If the patient is eating, fingerstick testing should be performed before meals and at bedtime.
Covering nutritional requirements
Nutrition-related insulin needs depend on the type of caloric intake prescribed:
In patients receiving total parenteral nutrition (TPN), start 1 U of regular insulin (placed in the bag) for every 10 to 15 g of dextrose in the TPN mixture.
In patients receiving enteral nutrition, use regular insulin every 6 hours or a rapid-acting insulin analog every 4 hours. Start 1 U of insulin subcutaneously for every 10 to 15 g of delivered carbohydrates. For example, if a patient is receiving 10 g of carbohydrates per hour, a rapid-acting analog given at a dose of 4 U every 4 hours (1 U per 10 g of carbohydrates) should adequately cover enteral feedings. For any bolus feedings, give the injection as a full bolus 15 to 20 minutes in advance, based on the carbohydrate content of the feeding.
In patients who are eating, use regular insulin or a rapid-acting insulin analog before meals. Again, start 1 U of insulin subcutaneously for every 10 to 15 g of carbohydrates, or use the prandial portion of the Miami 4/12 rule (Figure 2). For example, in a 60-kg patient one would start with 5 U (60 ÷ 12) of a rapid-acting insulin before each meal.
Basal/bolus replacement outperforms supplemental-scale regular insulin
Use of a basal/bolus insulin regimen appears to be more beneficial than supplemental-scale regular insulin in hospitalized patients with type 2 diabetes, according to a recent randomized trial comparing the two approaches in 130 such patients with blood glucose levels greater than 140 mg/dL.17 In the group randomized to basal/bolus insulin, the starting total daily dose was 0.4 to 0.5 U/kg/day, with half the dose given as basal insulin (insulin glargine) once daily and half given as a rapid-acting insulin analog (glulisine) in fixed doses before every meal. A rapid-acting analog was used for supplemental insulin in the basal/bolus regimen. By study’s end, patients in the basal/bolus group were receiving a higher total daily insulin dose than those in the supplemental-scale group (mean of 42 U/day vs 13 U/day).
Mean daily blood glucose levels were 27 mg/dL lower, on average, in patients who received basal/bolus therapy compared with the supplemental-scale group, yet there was no difference between groups in the risk of hypoglycemia. More patients randomized to basal/bolus therapy achieved the glycemic goal of less than 140 mg/dL (66% vs 38%). Fourteen percent of patients assigned to supplemental-scale insulin had values persistently greater than 240 mg/dL and had to be switched to the basal/bolus regimen.17
SUMMARY
Perioperative glycemic control can reduce morbidity, particularly the incidence of infectious complications, in surgical patients, even in those without diagnosed diabetes. Optimal management of glycemia in the perioperative period involves applying principles of physiologic insulin replacement. Postoperatively, the transition from IV to subcutaneous insulin can be achieved through the use of basal insulin for coverage of fasting insulin needs, regardless of the patient’s feeding status, and the use of rapid-acting insulin to cover hyperglycemia and nutritional needs. Management of hospitalized patients exclusively with supplemental-scale regular insulin should be abandoned.
DISCUSSION
Question from the audience: As an attending physician in a preoperative clinic I’m never sure what to do with NPH insulin the morning of surgery. What guidance can you give?
Dr. Meneghini: NPH is a peaking basal insulin, and the peak can induce hypoglycemia in a patient who is NPO. If we have the opportunity, we try to switch patients previously receiving insulin therapy to a long-acting basal insulin analog, which has a much flatter action profile and is safer in the fasting state. If there is no opportunity for switching, we instruct the patient to take two-thirds of his or her usual morning dose of insulin and we initiate a D5 drip when the patient arrives at the hospital.
Question from the audience: How do you handle perioperative insulin in patients on insulin pumps?
Dr. Meneghini: The pumps provide a subcutaneous basal insulin infusion, which should, if set correctly, maintain stable blood glucose levels when the patient is NPO. Supplemental doses of insulin to correct hyperglycemia can be delivered via the usual subcutaneous practice with a syringe or insulin pen. If you are uncomfortable with pump function, or if the pump insertion site interferes with the surgery site, simply replace the 24-hour basal amount delivered via pump with an injection of glargine or detemir divided into twice-daily injections. Correct hyperglycemia with supplemental-scale insulin as per usual protocol.
Question from the audience: The manufacturer of insulin glargine makes no recommendations for its use the night before or morning of surgery. What do you recommend?
Dr. Meneghini: It depends on whether the glargine is dosed appropriately. Most patients with type 2 diabetes require 0.4 to 0.6 U/kg/day of a long-acting insulin. If they’re on much more, they may be overdosed, and I would cut the basal dose by about half. Otherwise, 75% to 100% of the usual basal amount is appropriate. In type 1 diabetes, the usual replacement dose of basal insulin is 0.2 to 0.3 U/kg/day. If a patient is in this range, the basal insulin can be continued. Patients who experience hypoglycemia, or a substantial fall in blood glucose if meals are skipped or delayed, may be getting too much basal insulin and might benefit from a dose reduction when placed on NPO status.
Question from the audience: Metformin has a black-box warning advising that it be stopped at least 48 hours before surgery, but patients often come to surgery having taken metformin within the prior 12 to 24 hours. How should we manage such patients coming for elective surgery?
Dr. Meneghini: Metformin is cleared exclusively by the kidneys; its accumulation as a result of impaired kidney function (eg, due to hemodynamic instability or radiology studies using IV iodine) can result in increased lactic acid production by the liver and lactic acidosis. A patient who has taken metformin within the prior 48 hours but doesn’t have a risk of hemodynamic dysfunction is at low risk of lactic acidosis if hydrated appropriately. There’s not much choice if a patient needs urgent surgery and has recently taken metformin; in that case, just ensure maintenance of adequate glomerular filtration via fluid repletion to clear the drug.
Question from the audience: What’s the evidence for tight glycemic control or any type of glycemic control in patients undergoing outpatient surgery or “same-day” patients who will be admitted to a regular surgical floor? Also, what would you consider maximal glucose values for a patient going into elective surgery?
Dr. Meneghini: I haven’t seen any guidelines for glycemic control in patients undergoing outpatient surgery. If a patient has poor glycemic control coming into surgery, even for a minor procedure, the risk of an infectious complication may be increased. Keeping blood glucose below 180 mg/dL and avoiding electrolyte imbalances is likely sufficient in such patients. On the second question, if it’s an elective procedure and can be delayed a few hours, you can certainly institute IV insulin therapy to correct hyperglycemia rapidly—just ensure adequate replacement of fluids since the patient may have had volume depletion or dehydration as a result of the preceding osmotic diuresis. Once glycemic control is improved (blood glucose < 180–200 mg/dL), the patient can proceed to surgery.
Question from the audience: What are your recommendations for resuming oral diabetes medications after surgery?
Dr. Meneghini: Once patients are tolerating their meals and being considered for discharge, you may want to resume their oral medications, assuming their admission hemoglobin A1c levels were near goal. If glycemic control was inadequate preoperatively, this may be a good opportunity to adjust their prior regimen to more appropriate therapy. In some cases, this might include some form of insulin, either basal therapy or basal and supplemental insulin.
Diabetes confers an increased risk of perioperative morbidity and mortality, mostly from infection and cardiovascular events. It is not unusual for surgical patients with diabetes to have a number of comorbidities or underlying chronic vascular complications that put them at risk for cardiovascular events or an infectious complication. Silent ischemia, coronary artery disease, and autonomic neuropathy are common among patients with diabetes, and each can contribute to perioperative morbidity and mortality. These are important considerations since nearly one-fifth of surgical patients have diabetes and since a person with diabetes has a 50% risk of undergoing surgery at some point in his or her lifetime.1
This article reviews the preoperative evaluation of patients with diabetes, discusses the relation between glycemic control and perioperative outcomes, and examines targets and strategies for glycemic control in patients with type 1 and type 2 diabetes throughout the perioperative period.
PREOPERATIVE EVALUATION
The preoperative evaluation must consider first and foremost the status of the patient’s diabetes and his or her surgical risk factors. Also important are the characteristics of the procedure to be performed, the method of anesthesia to be used, and select laboratory values.
Diabetes status
The type of diabetes and its treatment must be considered. Type 1 diabetes requires continuous insulin therapy to prevent ketoacidosis; patients with type 2 diabetes are usually treated with oral medications with or without insulin. Baseline control of blood glucose is a predictor of morbidity following surgery. Hypoglycemia is associated with increased morbidity in the inpatient setting, so a history of severe hypoglycemic events or of difficulty recognizing hypoglycemia (hypoglycemia unawareness) should be elicited in the preoperative evaluation. Complications of diabetes and other comorbidities also must be evaluated, along with their treatments.
Surgical risk factors
Patients with diabetes have surgical risk factors specific to their health—namely, cardiovascular risk factors that may or may not have been previously diagnosed. Patients with diabetes may have silent ischemia, atypical manifestations of coronary ischemia, or underlying cardiomyopathy. Many patients with type 2 diabetes have hypertension, which may complicate perioperative management. Other common surgical risk factors in this population include obesity, chronic kidney disease, and undiagnosed autonomic dysfunction, which may compromise hemodynamic stability in the perioperative period. Additionally, patients with long-standing diabetes experience reductions in pulmonary function (eg, forced expiratory volume, peak expiratory flow, and diffusion capacity for carbon monoxide) related to disease duration and vascular injury,2 which may complicate weaning from ventilatory support.
Characteristics of the procedure and anesthetic
Both surgery and anesthesia may induce an increase in levels of stress hormones (epinephrine, cortisol, growth hormone) and inflammatory cytokines (interleukin-6 and tumor necrosis factor–alpha), resulting in insulin resistance and impaired insulin secretion (even among patients who present with adequate insulin secretion). These in turn contribute to lipolysis and protein catabolism, leading to hyperglycemia and, if a patient is severely insulin deficient, ketoacidosis. Other factors that particularly affect insulin resistance and secretion include cardiovascular bypass surgery, sepsis, the need for total parenteral nutrition, and steroid therapy.
The characteristics of the surgical procedure, including the type of surgery as well as its urgency, duration, and timing (morning vs later in the day), are important in planning for perioperative glycemic management. For example, a short, minor procedure may require only observation, whereas more extensive procedures warrant periodic monitoring and active glycemic management with insulin infusions.
The type of anesthesia should also be considered. Compared with epidural anesthesia, general anesthesia is associated with greater stimulation of the sympathetic nervous system and increased catecholamine levels, resulting in more pronounced hyperglycemia.3
Preoperative tests
Preoperative testing and laboratory evaluation should include, at minimum, an electrocardiogram, a basic metabolic panel to assess renal function, electrolyte levels, and hemoglobin A1c measurement. For low-risk procedures in patients with adequate exercise tolerance, no diagnostic tests might be needed. In any case, knowledge of the hemoglobin A1c level may help not only to classify perioperative risk but also to determine postoperative care, including the choice of antiglycemic medications at discharge.
IMPORTANCE OF GLYCEMIC CONTROL
Preoperative glycemic control has a significant impact on the risk of infectious complications—including pneumonia, wound infection, urinary tract infection, and sepsis—in patients with diabetes across a variety of surgical procedures.4 Similarly, postoperative glycemic control—to a mean blood glucose level less than 200 mg/dL in the immediate postoperative period—significantly reduces the incidence of deep sternal wound infection after open heart surgery.5
Among patients undergoing cardiothoracic surgery, both cardiac-related and overall mortality are greater with increasing postoperative blood glucose levels, although a cause-and-effect relationship has not been established.6
Glycemic control matters regardless of diabetes status
Hyperglycemia affects mortality regardless of diabetes status. In a study of 779 consecutive patients admitted for acute myocardial infarction, mortality at 180 days was highly associated with hyperglycemia on admission independent of a history of diabetes; the highest mortality was among hyperglycemic patients without previously known diabetes.7 Similarly, a large study of glycemic control in intensive care unit (ICU) patients receiving insulin found that mortality in nondiabetic patients increased with median glucose level and was higher than mortality in diabetic patients.8 These findings suggest a need for vigilance in the perioperative and critical care management of all patients with hyperglycemia, regardless of preadmission diabetes diagnosis, as they carry significant morbidity and mortality risk.
GLYCEMIC CONTROL IN THE CRITICALLY ILL: SOME SUPPORT FOR A MODIFIED TARGET, BUT VIGILANCE FOR HYPOGLYCEMIA NEEDED
The landmark study by Van den Berghe et al of intensive insulin therapy in surgical ICU patients demonstrated significant reductions in morbidity and mortality when glucose levels were controlled aggressively (80 to 110 mg/dL; average, 103 mg/dL) compared with conventional control (180 to 200 mg/dL).9 The benefit of intensive glycemic control was evident on outcomes such as the occurrence of sepsis, need for dialysis, need for blood transfusion, and development of acute polyneuropathy. Intensive insulin therapy was also associated with cost savings compared with conventional insulin therapy in mechanically ventilated patients.10
However, a number of subsequent studies have clearly shown that as blood glucose levels approach normoglycemia, the risks of hypoglycemia, especially severe hypoglycemia, can offset the benefits of tight blood glucose control.
A follow-up study by Ven den Berghe et al in a medical ICU failed to show a mortality benefit from tight glycemic control, though patients in the intensive control arm experienced less renal injury, faster weaning from ventilation, and earlier discharge from the ICU and hospital.11
The recent NICE-SUGAR study of aggressive glucose control in the ICU randomized patients to a target blood glucose of 81 to 108 mg/dL (intensive group) or 180 mg/dL or less (control group).12 At study’s end, the groups’ mean blood glucose levels were 115 mg/dL and 144 mg/dL, respectively, while rates of severe hypoglycemia (blood glucose < 40 mg/dL) were 6.8% and 0.5%, respectively. Mortality rates were higher in the intensive therapy group (27.5%) than in the control group (24.9%), driven by severe hypoglycemic events. Notably, blood glucose monitoring in this and other studies was conducted at a frequency of anywhere between 1 and 4 hours.
The conclusions of the available data would support, for the time being, a modified glycemic target in critically ill patients, with strict avoidance of severe hypoglycemia. The recent consensus statement from the American Association of Clinical Endocrinologists and the American Diabetes Association recommends using insulin therapy if blood glucose levels exceed 180 mg/dL, with target glucose levels less than 180 mg/dL in critically ill patients and less than 140 mg/dL in non–critically ill patients.13 Development and implementation of safer insulin infusion algorithms and more frequent and accurate blood glucose monitoring in this setting should enable us to achieve better glycemic targets with lower risk.
ELEMENTS OF PHYSIOLOGIC INSULIN REPLACEMENT
In hospitalized patients with hyperglycemia, three different components of insulin replacement require management1:
Basal insulin replacement consists of a long-acting insulin preparation administered regardless of the patient’s oral intake status, with the premise of matching hepatic (endogenous) glucose production
Prandial insulin replacement requires a rapid-acting insulin preparation given to cover nutritional needs
Supplemental (or correction) insulin replacement requires a rapid-acting preparation (usually the same insulin type as for prandial coverage) to correct blood glucose values that exceed predetermined glycemic targets.
For most patients, basal insulin replacement might be appropriate preoperatively to control fasting glucose, whereas during surgery, especially if prolonged or high risk, an intravenous (IV) insulin drip is the most effective means of glucose control. The postoperative transition from the IV insulin drip usually involves basal insulin replacement plus supplemental rapid-acting insulin. Prandial or nutritional insulin should be started once the patient begins to receive nutrition (oral, enteral, or hyperalimentation).
GOALS OF PERIOPERATIVE GLYCEMIC CONTROL
Perioperative glycemic management has several key objectives:
- Avoidance of clinically significant hyper- or hypoglycemia
- Maintenance of electrolyte and fluid balance
- Prevention of ketoacidosis, which is imperative in patients with type 1 diabetes, who require insulin at all times
- Achievement of specific glycemic targets, as discussed above—ie, less than 180 mg/dL in critically ill patients and less than 140 mg/dL in stable patients.13
Strategies differ across the perioperative timeline
Strategies for perioperative glycemic control differ before, during, and after surgery, as summarized immediately below and detailed in the following sections.
Preoperatively, glycemia should be stabilized, typically with subcutaneous insulin, if there is enough time to do so. For patients who have not previously been on insulin, placing them on an insulin supplemental scale to correct glycemia to desired targets might be a first step. In the setting of hyperglycemia, these patients may also be started on a low dose of basal insulin, with preference given to basal insulin analogs, given their consistent and relatively peakless action profile and lower risk of hypoglycemia. A starting dose of 0.2 to 0.4 U/kg is appropriate and carries a low risk of hypoglycemia. For patients already using insulin on an outpatient basis, continuing their basal insulin dose, possibly at a reduced dosage (25% less), together with supplemental-scale insulin coverage, should stabilize blood glucose levels. For patients on combination insulin or premixed insulin types, the basal insulin dose for preoperative management can be estimated by taking the patient’s usual total daily dose and delivering 40% to 50% of that dose as a basal insulin analog injection. Clearly, a supplemental scale should be implemented along with basal insulin replacement.
Intraoperatively, switching to IV insulin may be appropriate for stabilizing glycemia, depending on the type of surgery. A number of IV insulin protocols have been proposed, although no consistent comparisons of efficacy or safety among these protocols have been published.
Postoperatively, patients eventually should be transitioned from IV to subcutaneous insulin when glycemic control stabilizes. This transition may be complicated for many reasons. Oral intake may be inconsistent. The surgery and surrounding environment can induce stressors, promote susceptibility to infection, and increase insulin resistance. Additionally, some patients may be on hyperalimentation. Specific instructions for the transition from IV to subcutaneous insulin are covered later in this article.
PREOPERATIVE GLYCEMIC MANAGEMENT
In patients with type 2 diabetes, oral agents pose certain safety risks and should be discontinued prior to surgery.
Sulfonylureas may induce hypoglycemia in patients who are placed on NPO (“nothing by mouth”) orders and should be held in patients who are fasting.
Metformin can induce lactic acidosis if kidney function declines and should be withheld 1 to 2 days before planned surgery if a need for IV contrast is anticipated or the procedure could potentially lead to hemodynamic instability and reduced renal perfusion.
Thiazolidinediones may cause fluid retention that can complicate the postoperative period; they can be discontinued several days prior to a planned surgery.
GLP-1 agonists, such as exenatide, can slow gastric motility and potentially delay gastrointestinal recovery after major surgery; they should be held the day of surgery.
DPP-4 inhibitors (incretin enhancers), such as sitagliptin, do not have significant side effects and, if need be, can be continued. Because incretin therapies act via a glucose-dependent mechanism, they are unlikely to cause hypoglycemia, even in a patient whose oral intake is held or delayed. On the other hand, since their effect is mostly in reducing postprandial glycemia, there may be little need to use them in a patient who is NPO.
Patients with type 1 diabetes must continue basal insulin replacement preoperatively (0.2 to 0.3 U/kg/day of a long-acting insulin). Patients with type 2 diabetes may benefit from basal insulin replacement, as previously noted.
Supplemental insulin scales are used to correct hyperglycemia regardless of a patient’s oral intake status. They can be individualized based on the estimated total daily insulin dose and require glycemic targets to be established. Fingerstick glucose monitoring should be done every 4 to 6 hours in a patient who is NPO, and supplemental-scale insulin should be used to correct glucose values that exceed target. For supplemental-scale coverage, rapid-acting insulin analogs have a shorter duration of action than human regular insulin and may be given subcutaneously every 4 to 6 hours, whereas regular insulin should not be given more often than every 6 hours to correct hyperglycemia. These differences in action duration should be kept in mind to minimize the potential for insulin stacking.
INTRAOPERATIVE GLYCEMIC MANAGEMENT
Procedure length is an important determinant
Strategies for intraoperative glucose management vary according to the length of the procedure.
For minor, short procedures, the preoperative glucose management orders may be continued.
For longer, more complex procedures, a switch to an IV insulin drip is safe and allows rapid adjustments in dosing and plasma glucose levels. Ideally, IV insulin is started prior to the procedure so that the glucose level is stable once the patient arrives in the operating room. Given the logistics of IV insulin management, including the need for frequent monitoring (hourly) and dose adjustments, this type of treatment should be reserved for environments with adequate numbers of trained staff.
IV regular insulin is therapy of choice
Several different algorithms for IV regular insulin therapy are in use. Some are static, such as those of Markovitz et al14 and Stockton et al,15 while others are dynamic (ie, doses are self-adjusted based on changes in blood glucose level), such as the “Yale protocol” of Goldberg et al (Figure 1).16
POSTOPERATIVE GLYCEMIC MANAGEMENT
Start subcutaneous transition before stopping IV drip
Transitioning from IV to subcutaneous insulin is often complicated. Nonoral nutrition options (ie, parenteral nutrition or enteral supplementation) must be considered. As noted, insulin must be replaced according to physiologic needs, which requires that a long-acting basal insulin be used regardless of oral intake status, a rapid-acting insulin be given to cover prandial or nutritional needs, and supplemental rapid-acting insulin be used to correct hyperglycemia.
In the transition from IV insulin, basal insulin replacement can begin at any time. I recommend starting the transition from IV to subcutaneous insulin about 12 to 24 hours before discontinuing the insulin drip. In type 1 diabetes, this transition ensures basal insulin coverage and minimizes the risk of developing ketones and ketoacidosis. In type 2 diabetes, it can ensure a more stable transition and better glycemic control.
Determining the basal insulin dose
Switching to subcutaneous supplemental insulin
Instructions must be given for switching to subcutaneous supplemental doses of insulin. Glycemic targets, generally from less than 130 to 150 mg/dL, must be established, as must the frequency of fingerstick testing:
- If the patient is being fed enterally or parenterally, fingerstick testing is recommended every 4 to 6 hours if a rapid-acting insulin analog is used and every 6 hours if regular insulin is used.
- If the patient is eating, fingerstick testing should be performed before meals and at bedtime.
Covering nutritional requirements
Nutrition-related insulin needs depend on the type of caloric intake prescribed:
In patients receiving total parenteral nutrition (TPN), start 1 U of regular insulin (placed in the bag) for every 10 to 15 g of dextrose in the TPN mixture.
In patients receiving enteral nutrition, use regular insulin every 6 hours or a rapid-acting insulin analog every 4 hours. Start 1 U of insulin subcutaneously for every 10 to 15 g of delivered carbohydrates. For example, if a patient is receiving 10 g of carbohydrates per hour, a rapid-acting analog given at a dose of 4 U every 4 hours (1 U per 10 g of carbohydrates) should adequately cover enteral feedings. For any bolus feedings, give the injection as a full bolus 15 to 20 minutes in advance, based on the carbohydrate content of the feeding.
In patients who are eating, use regular insulin or a rapid-acting insulin analog before meals. Again, start 1 U of insulin subcutaneously for every 10 to 15 g of carbohydrates, or use the prandial portion of the Miami 4/12 rule (Figure 2). For example, in a 60-kg patient one would start with 5 U (60 ÷ 12) of a rapid-acting insulin before each meal.
Basal/bolus replacement outperforms supplemental-scale regular insulin
Use of a basal/bolus insulin regimen appears to be more beneficial than supplemental-scale regular insulin in hospitalized patients with type 2 diabetes, according to a recent randomized trial comparing the two approaches in 130 such patients with blood glucose levels greater than 140 mg/dL.17 In the group randomized to basal/bolus insulin, the starting total daily dose was 0.4 to 0.5 U/kg/day, with half the dose given as basal insulin (insulin glargine) once daily and half given as a rapid-acting insulin analog (glulisine) in fixed doses before every meal. A rapid-acting analog was used for supplemental insulin in the basal/bolus regimen. By study’s end, patients in the basal/bolus group were receiving a higher total daily insulin dose than those in the supplemental-scale group (mean of 42 U/day vs 13 U/day).
Mean daily blood glucose levels were 27 mg/dL lower, on average, in patients who received basal/bolus therapy compared with the supplemental-scale group, yet there was no difference between groups in the risk of hypoglycemia. More patients randomized to basal/bolus therapy achieved the glycemic goal of less than 140 mg/dL (66% vs 38%). Fourteen percent of patients assigned to supplemental-scale insulin had values persistently greater than 240 mg/dL and had to be switched to the basal/bolus regimen.17
SUMMARY
Perioperative glycemic control can reduce morbidity, particularly the incidence of infectious complications, in surgical patients, even in those without diagnosed diabetes. Optimal management of glycemia in the perioperative period involves applying principles of physiologic insulin replacement. Postoperatively, the transition from IV to subcutaneous insulin can be achieved through the use of basal insulin for coverage of fasting insulin needs, regardless of the patient’s feeding status, and the use of rapid-acting insulin to cover hyperglycemia and nutritional needs. Management of hospitalized patients exclusively with supplemental-scale regular insulin should be abandoned.
DISCUSSION
Question from the audience: As an attending physician in a preoperative clinic I’m never sure what to do with NPH insulin the morning of surgery. What guidance can you give?
Dr. Meneghini: NPH is a peaking basal insulin, and the peak can induce hypoglycemia in a patient who is NPO. If we have the opportunity, we try to switch patients previously receiving insulin therapy to a long-acting basal insulin analog, which has a much flatter action profile and is safer in the fasting state. If there is no opportunity for switching, we instruct the patient to take two-thirds of his or her usual morning dose of insulin and we initiate a D5 drip when the patient arrives at the hospital.
Question from the audience: How do you handle perioperative insulin in patients on insulin pumps?
Dr. Meneghini: The pumps provide a subcutaneous basal insulin infusion, which should, if set correctly, maintain stable blood glucose levels when the patient is NPO. Supplemental doses of insulin to correct hyperglycemia can be delivered via the usual subcutaneous practice with a syringe or insulin pen. If you are uncomfortable with pump function, or if the pump insertion site interferes with the surgery site, simply replace the 24-hour basal amount delivered via pump with an injection of glargine or detemir divided into twice-daily injections. Correct hyperglycemia with supplemental-scale insulin as per usual protocol.
Question from the audience: The manufacturer of insulin glargine makes no recommendations for its use the night before or morning of surgery. What do you recommend?
Dr. Meneghini: It depends on whether the glargine is dosed appropriately. Most patients with type 2 diabetes require 0.4 to 0.6 U/kg/day of a long-acting insulin. If they’re on much more, they may be overdosed, and I would cut the basal dose by about half. Otherwise, 75% to 100% of the usual basal amount is appropriate. In type 1 diabetes, the usual replacement dose of basal insulin is 0.2 to 0.3 U/kg/day. If a patient is in this range, the basal insulin can be continued. Patients who experience hypoglycemia, or a substantial fall in blood glucose if meals are skipped or delayed, may be getting too much basal insulin and might benefit from a dose reduction when placed on NPO status.
Question from the audience: Metformin has a black-box warning advising that it be stopped at least 48 hours before surgery, but patients often come to surgery having taken metformin within the prior 12 to 24 hours. How should we manage such patients coming for elective surgery?
Dr. Meneghini: Metformin is cleared exclusively by the kidneys; its accumulation as a result of impaired kidney function (eg, due to hemodynamic instability or radiology studies using IV iodine) can result in increased lactic acid production by the liver and lactic acidosis. A patient who has taken metformin within the prior 48 hours but doesn’t have a risk of hemodynamic dysfunction is at low risk of lactic acidosis if hydrated appropriately. There’s not much choice if a patient needs urgent surgery and has recently taken metformin; in that case, just ensure maintenance of adequate glomerular filtration via fluid repletion to clear the drug.
Question from the audience: What’s the evidence for tight glycemic control or any type of glycemic control in patients undergoing outpatient surgery or “same-day” patients who will be admitted to a regular surgical floor? Also, what would you consider maximal glucose values for a patient going into elective surgery?
Dr. Meneghini: I haven’t seen any guidelines for glycemic control in patients undergoing outpatient surgery. If a patient has poor glycemic control coming into surgery, even for a minor procedure, the risk of an infectious complication may be increased. Keeping blood glucose below 180 mg/dL and avoiding electrolyte imbalances is likely sufficient in such patients. On the second question, if it’s an elective procedure and can be delayed a few hours, you can certainly institute IV insulin therapy to correct hyperglycemia rapidly—just ensure adequate replacement of fluids since the patient may have had volume depletion or dehydration as a result of the preceding osmotic diuresis. Once glycemic control is improved (blood glucose < 180–200 mg/dL), the patient can proceed to surgery.
Question from the audience: What are your recommendations for resuming oral diabetes medications after surgery?
Dr. Meneghini: Once patients are tolerating their meals and being considered for discharge, you may want to resume their oral medications, assuming their admission hemoglobin A1c levels were near goal. If glycemic control was inadequate preoperatively, this may be a good opportunity to adjust their prior regimen to more appropriate therapy. In some cases, this might include some form of insulin, either basal therapy or basal and supplemental insulin.
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care 2004; 27:553–591.
- Kaparianos A, Argyropoulou E, Sampsonas F, et al. Pulmonary complications in diabetes mellitus. Chron Respir Dis 2008; 5:101–108.
- Grigoleit HG. Anesthesia and blood glucose. Acta Diabetologica 1973; 10:569–574.
- Dronge AS, Perkal MF, Kancir S, et al. Long-term glycemic control and postoperative infectious complications. Arch Surg 2006; 141:375–380.
- Zerr KJ, Furnary AP, Grunkemeier GL, Bookin S, Kanhere V, Starr A. Glucose control lowers the risk of wound infection in diabetics after open heart operations. Ann Thorac Surg 1997; 63:356–361.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg 2003; 125:1007–10021.
- Ainla T, Baburin A, Tessalu R, et al. The association between hyperglycaemia on admission and 180-day mortality in acute myocardial infarction patients with and without diabetes. Diabet Med 2005; 22:1321–1325.
- Rady MY, Johnson DJ, Patel BM, et al. Influence of individual characteristics on outcome of glycemic control in intensive care unit patients with or without diabetes mellitus. Mayo Clin Proc 2005; 80:1558–1567.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med 2001; 345:1359–1367.
- Van den Berghe G, Wouters PJ, Kesteloot K, Hilleman DE. Analysis of healthcare resource utilization with intensive insulin therapy in critically ill patients. Crit Care Med 2006; 34:612–616.
- Van den Berghe G, Wawilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. New Engl J Med 2006; 354:449–461.
- NICE-SUGAR Study Investigators. Intensive vs conventional glucose control in critically ill patients. N Engl J Med 2009; 360:1283–1297.
- Moghissi ES, Korytowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Endocr Pract 2009; 15:353–369.
- Markovitz LJ, Wiechmann RJ, Harris N, et al. Description and evaluation of a glycemic management protocol for patients with diabetes undergoing heart surgery. Endocr Pract 2002; 8:10–18.
- Stockton L, Baird M, Cook CB, et al. Development and implementation of evidence-based guidelines for IV insulin: a statewide collaborative approach. Insulin 2008; 3:67–77.
- Goldberg PA, Siegel MD, Sherwin RS, et al. Implementation of a safe and effective insulin infusion protocol in a medical intensive care unit. Diabetes Care 2004; 27:461–467.
- Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care 2007; 30:2181–2186.
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care 2004; 27:553–591.
- Kaparianos A, Argyropoulou E, Sampsonas F, et al. Pulmonary complications in diabetes mellitus. Chron Respir Dis 2008; 5:101–108.
- Grigoleit HG. Anesthesia and blood glucose. Acta Diabetologica 1973; 10:569–574.
- Dronge AS, Perkal MF, Kancir S, et al. Long-term glycemic control and postoperative infectious complications. Arch Surg 2006; 141:375–380.
- Zerr KJ, Furnary AP, Grunkemeier GL, Bookin S, Kanhere V, Starr A. Glucose control lowers the risk of wound infection in diabetics after open heart operations. Ann Thorac Surg 1997; 63:356–361.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg 2003; 125:1007–10021.
- Ainla T, Baburin A, Tessalu R, et al. The association between hyperglycaemia on admission and 180-day mortality in acute myocardial infarction patients with and without diabetes. Diabet Med 2005; 22:1321–1325.
- Rady MY, Johnson DJ, Patel BM, et al. Influence of individual characteristics on outcome of glycemic control in intensive care unit patients with or without diabetes mellitus. Mayo Clin Proc 2005; 80:1558–1567.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med 2001; 345:1359–1367.
- Van den Berghe G, Wouters PJ, Kesteloot K, Hilleman DE. Analysis of healthcare resource utilization with intensive insulin therapy in critically ill patients. Crit Care Med 2006; 34:612–616.
- Van den Berghe G, Wawilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. New Engl J Med 2006; 354:449–461.
- NICE-SUGAR Study Investigators. Intensive vs conventional glucose control in critically ill patients. N Engl J Med 2009; 360:1283–1297.
- Moghissi ES, Korytowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Endocr Pract 2009; 15:353–369.
- Markovitz LJ, Wiechmann RJ, Harris N, et al. Description and evaluation of a glycemic management protocol for patients with diabetes undergoing heart surgery. Endocr Pract 2002; 8:10–18.
- Stockton L, Baird M, Cook CB, et al. Development and implementation of evidence-based guidelines for IV insulin: a statewide collaborative approach. Insulin 2008; 3:67–77.
- Goldberg PA, Siegel MD, Sherwin RS, et al. Implementation of a safe and effective insulin infusion protocol in a medical intensive care unit. Diabetes Care 2004; 27:461–467.
- Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care 2007; 30:2181–2186.
KEY POINTS
- Surgery and anesthesia can induce hormonal and inflammatory stressors that increase the risk of complications in patients with diabetes.
- Elevated blood glucose levels are associated with worse outcomes in surgical patients, even among those not diagnosed with diabetes.
- The perioperative glycemic target in critically ill patients is 140 to 180 mg/dL. Evidence for a target in patients who are not critically ill is less robust, though fasting levels less than 140 mg/dL and random levels less than 180 mg/dL are appropriate.
- Postoperative nutrition-related insulin needs vary by nutrition type (parenteral or enteral), but ideally all regimens should incorporate a basal/bolus approach to insulin replacement.
Postoperative pulmonary complications: An update on risk assessment and reduction
Although pulmonary complications are not as well studied as cardiac complications in the postoperative setting, they are just as common following noncardiac surgery and are even more costly. It is worthwhile to identify surgical patients most at risk of postoperative pulmonary complications and take measures known to mitigate risk. This paper discusses important risk factors to identify during a preoperative pulmonary evaluation and then focuses on recent advances in strategies for reducing postoperative pulmonary complications. Teaching questions are included throughout, along with the rationale behind their answers.
POSTOPERATIVE PULMONARY COMPLICATIONS: WHAT ARE WE TRYING TO PREVENT AND WHY?
The definition of postoperative pulmonary complications is more variable and less intuitive than that of cardiac complications. Cardiac complications—postoperative myocardial infarction, cardiac death, and pulmonary edema—are more consistently defined and measured in clinical trials. Studies of postoperative pulmonary complications often group together pneumonia, respiratory failure, atelectasis, bronchospasm, and exacerbation of chronic obstructive pulmonary disease (COPD), making it more difficult to individually evaluate risk factors for different outcomes.
There are several reasons why it is important to consider pulmonary risk when evaluating patients preoperatively:
Pulmonary complications are as common as cardiac complications following noncardiac surgery. For example, in a secondary analysis of the cohort of noncardiac surgical patients used to validate the Revised Cardiac Risk Index,1 Fleischmann et al found that the incidence of pulmonary complications (2.7%) was highly comparable to that of cardiac complications (2.5%).2
Respiratory failure is a marker of ill health and predicts further complications. Postoperative respiratory failure (often defined as the need for ventilation for more than 48 hours after surgery) is an extremely morbid event. Johnson et al compared the outcomes of patients with and without respiratory failure as a complication of surgery.3 Among patients with respiratory failure, 26% died within 30 days, 6% had a myocardial infarction, 35% developed pneumonia, 10% developed acute renal failure, and 3% developed a deep vein thrombosis or pulmonary embolism; in contrast, rates of each of these events were lower than 2% among patients without respiratory failure.
Pulmonary complications are expensive and require lengthy hospitalization. The National Surgical Quality Improvement Program (NSQIP) compared hospitalization costs and length of stay among patients with various postoperative complications.4 Among infectious, cardiovascular, venous thromboembolic, and pulmonary complications, pulmonary complications were by far the most costly and, along with venous thromboembolic complications, required the longest mean hospital stay.
For these reasons, identifying patients at risk for pulmonary complications and developing a strategy to reduce the risk is clearly worthwhile.
IDENTIFYING RISK FOR PULMONARY COMPLICATIONS
Question: Which of the following is the most important risk factor for postoperative pulmonary complications?
A. High-risk surgical site
B. General anesthesia
C. COPD
D. Obesity
The correct answer is A. Pulmonary complications differ from cardiac complications in an important way: procedure-related factors are more predictive of pulmonary complications than are patient-related factors. Even healthy patients undergoing high-risk surgery are at risk for pulmonary complications. As for the other answer choices, general anesthesia and COPD are risk factors but are not as important as surgical site, and obesity has not been shown to be a risk factor at all.
Take-home points from the 2006 ACP guideline
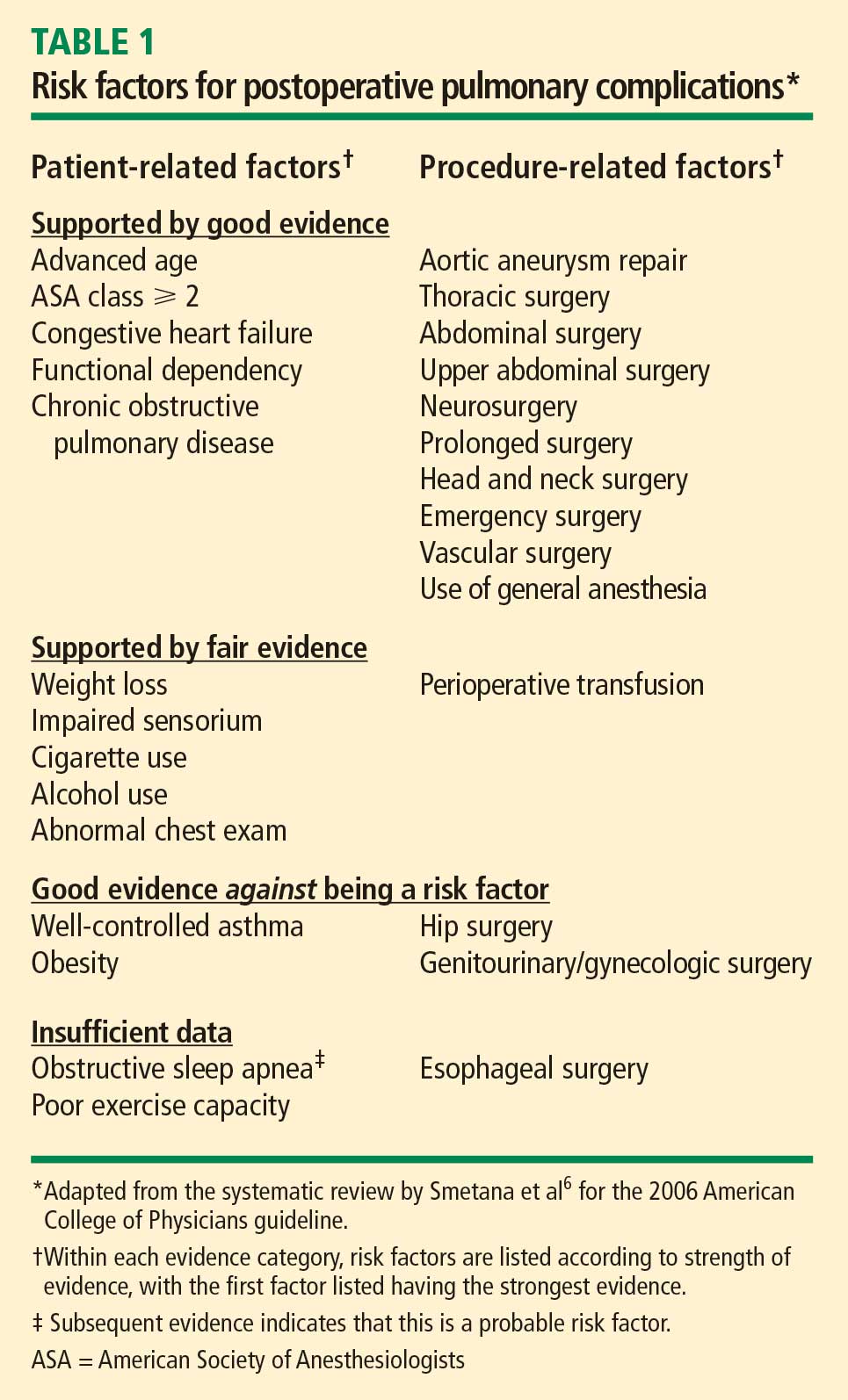
Patient-related risk factors. As noted in Table 1, the most important patient-related risk factors identified in the ACP guideline are increasing age and increasing American Society of Anesthesiologists (ASA) classification of comorbidity.
The effect of advanced age becomes particularly notable around age 60 years and escalates from there. This effect of age differs from that for cardiac complications, for which age drops out as a risk factor after adjustment for other diseases and risk factors. For pulmonary complications, in contrast, even older patients who are healthy are at increased risk.
The ASA classification is a general index of overall morbidity that ranges from class 1 (normal healthy patient) to class 5 (moribund patient who is not expected to survive without the operation).
Notably, COPD and smoking were only minor risk factors in the ACP analysis.
Procedure-related risk factors. Surgical site was found to be the most important of any of the patient- or procedure-related risk factors. The closer the incision is to the diaphragm, the greater the risk for pulmonary complications. Aortic, thoracic, and abdominal procedures carry the highest risk (Table 1), and among abdominal procedures, upper abdominal surgery (eg, cholecystectomy) is riskier than lower abdominal surgery (eg, gynecologic).
Other procedure-related risk factors identified were emergency surgery, surgery lasting more than 3 hours, use of general anesthesia, and multiple transfusions (Table 1).
Newly identified risk factors
Question: Which of the following has recently been identified as a risk factor for postoperative pulmonary complications?
A. Epidural anesthesia
B. Insulin-treated diabetes
C. Obstructive sleep apnea
D. Immobility
The correct answer is C. There is no evidence that epidural anesthesia or insulin-treated diabetes are risk factors. Immobility seems intuitively correct but has not emerged as a risk factor among high-quality studies in the literature.
Obstructive sleep apnea. The role of obstructive sleep apnea was unclear prior to publication of new data in the last couple of years. Hwang et al enrolled 172 patients who were soon to have elective surgery and had at least two of four clinical features of obstructive sleep apnea (snoring, daytime somnolence, witnessed apnea event, or crowded oropharynx).8 Patients underwent nocturnal oximetry before surgery and were divided into two groups based on number of desaturation episodes per hour. Patients with five or more desaturations had markedly higher rates of postoperative respiratory complications (8 complications among 98 patients) than did patients with fewer than five desaturations (1 complication among 74 patients). The presence of five or more desaturations was also associated with higher rates of cardiac, gastrointestinal, and bleeding complications. Though this was a small study, its results suggest a significant association between obstructive sleep apnea and pulmonary complications.
The issue of whether to screen patients for obstructive sleep apnea before major noncardiac surgery is still unresolved.
Pulmonary hypertension has also been identified as a risk factor in recent years with the publication of two studies that estimated its impact on morbidity and mortality after major noncardiac surgery.9,10 One of the studies, a retrospective database review, found a 28% incidence of respiratory failure among 145 surgical patients with pulmonary hypertension.9 In the other study, a prospective case-control trial, respiratory failure occurred in 21% of patients with pulmonary hypertension compared with only 3% of matched controls.10 In the case-control study, pulmonary hypertension was also associated with significantly elevated rates of heart failure and in-hospital death.
The results of these studies do not support preoperative screening for undiagnosed pulmonary hypertension, but they do underscore the need to recognize established pulmonary hypertension as an important risk factor for postoperative complications.
AN UPDATED INDEX FOR RESPIRATORY FAILURE
Several years ago, investigators from the Veterans Affairs Medical Centers developed a respiratory failure index using a design similar to those of well-established indices for cardiac risk.11 The same group also developed a separate risk index for pneumonia.12
This respiratory failure index was recently updated3 to reflect experience from private and academic hospitals, making the results more generally applicable. The researchers evaluated data from 180,000 patients undergoing major general or vascular surgery (defined according to the NSQIP) over a 3-year period. Respiratory failure was defined as requiring at least 48 hours of ventilation or unplanned reintubation.
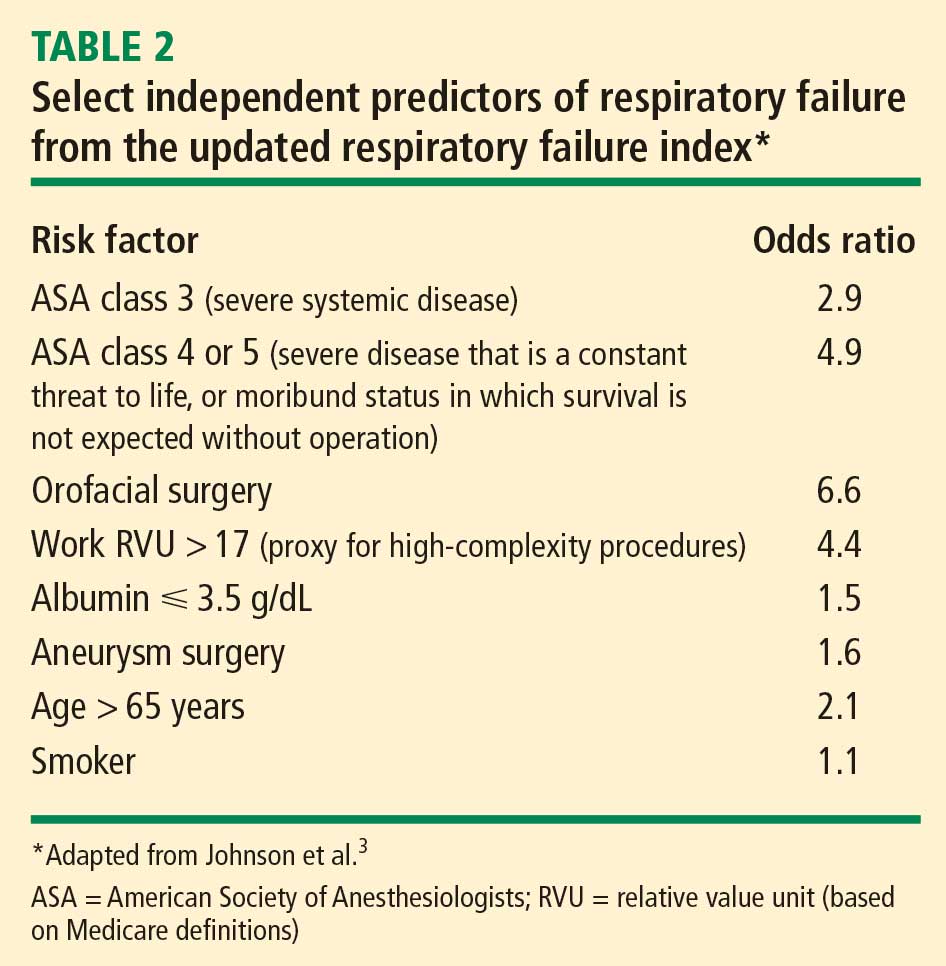
Comparison and contrast with the ACP guideline
Question: How does the updated respiratory failure index differ most significantly from the 2006 ACP guideline?
A. New index places greater emphasis on ASA class
B. New index offers a simplified weighted point scheme
C. New index ranks low albumin as a less important risk factor
D. New index attributes low risk to cigarette use
The correct answer is C: low albumin is a minor risk factor in the respiratory failure index, whereas it was one of the single most important predictors in the ACP guideline. As for the other answer choices, the new index places about the same emphasis on ASA class and cigarette use as does the ACP guideline, and it does not offer a simplified approach, as it incorporates 28 different factors.
Overall, most risk factors were similar in the updated respiratory failure index and the ACP guideline, but the index differs in several important ways:
- The index assigns less risk to low albumin, functional dependence, and congestive heart failure
- The index assigns greater risk to orofacial surgery
- The index identifies several new risk factors—high-complexity surgery, preoperative sepsis, ascites, and hypernatremia (serum sodium > 145 mmol/L).
STRATEGIES FOR RISK REDUCTION
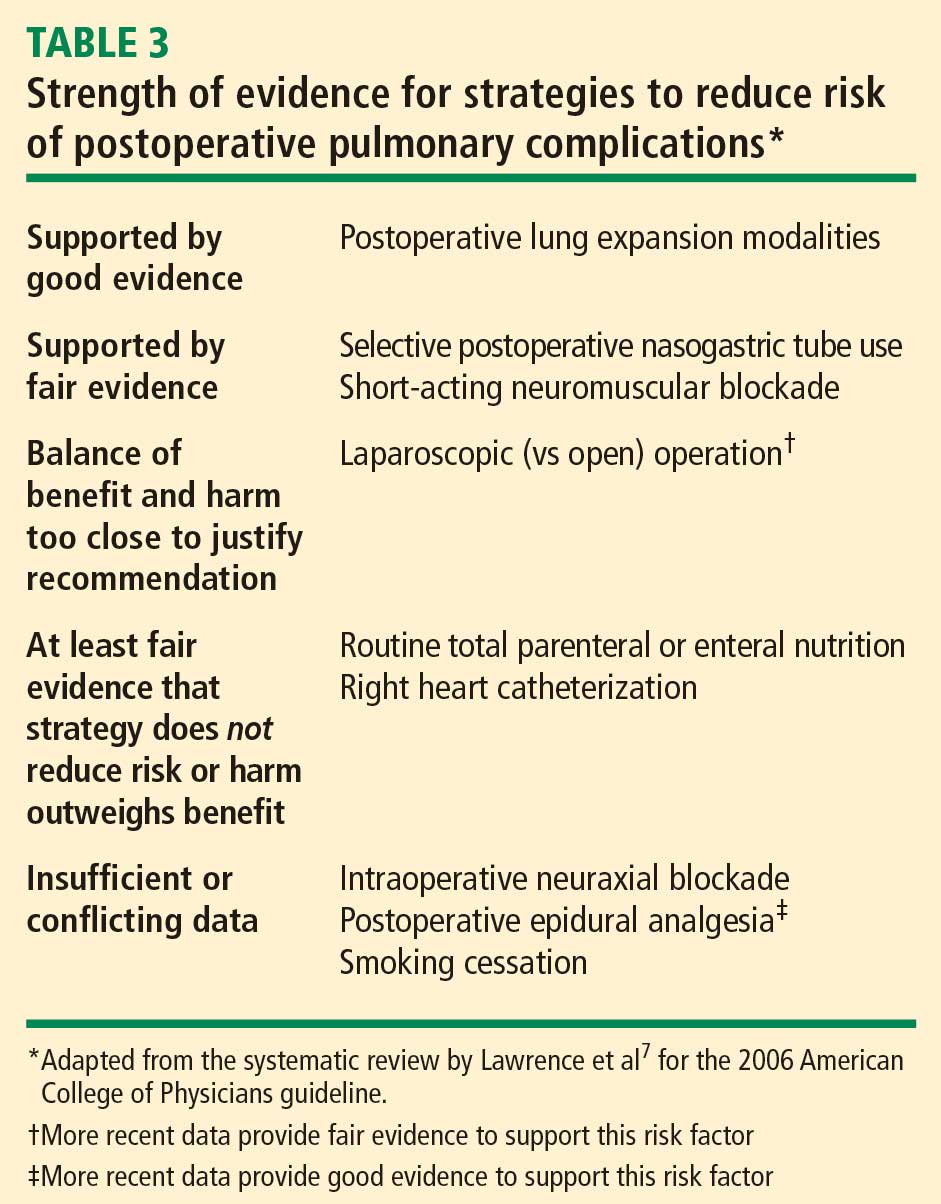
Postoperative CPAP: Good option when exercise ability is limited
Among the postoperative lung expansion modalities, continuous positive airway pressure (CPAP) is particularly useful for patients who are unable to perform deep breathing or incentive spirometry exercises. A recent systematic literature review identified nine randomized controlled trials of CPAP vs standard therapy in a total of 654 patients undergoing abdominal surgery.13 Meta-analysis of these studies showed that CPAP was associated with significant reductions in the risk of overall postoperative pulmonary complications (odds ratio [OR] = 0.66; 95% CI, 0.52–0.85), atelectasis (OR = 0.75; 95% CI, 0.58–0.97), and pneumonia (OR = 0.33; 95% CI, 0.14–0.75) relative to standard therapy.
Use nasogastric tubes selectively
Nasogastric tubes can be used either routinely following abdominal surgery or only in select patients—eg, those who have symptomatic abdominal distention or nausea. The difference is important since nasogastric tubes may potentially increase the risk of aspiration and thus lead to a pulmonary complication. Nelson et al conducted a meta-analysis of 24 studies that compared routine nasogastric tube use in abdominal surgery with selective use based on symptoms or abdominal distention.14 They found that routine use was associated with a significant increase in postoperative pulmonary complications (OR = 1.45; 95% CI, 1.08–1.93) relative to selective use, without achieving any of its intended goals.
Laparoscopic vs open surgery: Evidence begins to follow intuition
Intuitively, it seems that laparoscopic procedures should reduce risk for postoperative pulmonary complications compared with open surgical procedures, as they are associated with less postoperative pain, which should facilitate deep breathing and improve postoperative lung volumes. Nevertheless, evidence for whether laparoscopic surgery reduces the risk of pulmonary complications has been mixed until recently.
In 2008, however, Weller and Rosati published an analysis of a nationally representative database of 19,156 patients who underwent bariatric surgery in 2005.15 After adjusting for comorbidities, they found that the rate of postoperative pulmonary complications was nearly double if patients underwent open surgery as opposed to laparoscopic surgery (OR = 1.92; 95% CI, 1.54–2.38). Open surgery was also associated with significantly higher rates of sepsis, cardiovascular events, and reoperation compared with laparoscopic procedures. This study suggests that choosing laparoscopic procedures is another strategy that may reduce pulmonary complication rates, at least in the setting of bariatric surgery.
Postoperative thoracic epidural analgesia
Question: Thoracic epidural analgesia reduces rates of which of the following?
A. Pneumonia following abdominal aortic aneurysm repair
B. Pulmonary complications following coronary bypass surgery
C. Respiratory failure following abdominal surgery
D. All of the above
The correct answer is D. Thoracic epidural analgesia is another important strategy for reducing postoperative pulmonary complications, as demonstrated by a 2007 systematic literature review by Liu and Wu.16 Their analysis showed that rates of pneumonia, respiratory failure, and pulmonary complications overall were reduced by approximately one-third to more than one-half with the use of postoperative thoracic epidural analgesia in patients undergoing aortic aneurysm repair, coronary bypass surgery, and abdominal surgery.
Smoking cessation: The jury is still out
Whether preoperative cigarette cessation reduces pulmonary complication rates has been controversial over the past decade. Early reports showed that among patients who smoke, those who quit shortly before surgery actually had higher complication rates than patients who continued to smoke. The most reasonable explanation seems to be that many patients who stop smoking report increased coughing and sputum production for the first month or two. Selection bias also may have played a role in these findings.
More recently, two randomized trials studied the impact of perioperative smoking intervention programs involving counseling and nicotine replacement.17,18 Unfortunately, both studies primarily studied patients undergoing low-risk procedures and were insufficiently powered to show a difference in pulmonary complication rates. The question of whether smoking cessation is an effective strategy to reduce postoperative pulmonary risk remains unanswered.
Preoperative intensive lung expansion: A promising new intervention
While the effectiveness of postoperative lung expansion techniques is undisputed,7 preoperative lung expansion—also known as inspiratory muscle training—has only recently been investigated. Hulzebos et al randomized 279 patients undergoing coronary artery bypass graft surgery who were at high risk for developing pulmonary complications to either usual care or inspiratory muscle training.19 The latter intervention involved 20 minutes per day of incentive spirometry, active breathing, and forced expiration techniques for at least 2 weeks prior to surgery. Rates of high-grade postoperative pulmonary complications were cut in half (OR = 0.52; 95% CI, 0.30–0.92) and rates of pneumonia were reduced by 60% (OR = 0.40; 95% CI, 0.19–0.84) in patients who received inspiratory muscle training relative to the usual-care group.
In clinical practice, preoperative inspiratory muscle training can be done in a chest physical therapy outpatient setting or a pulmonary rehabilitation clinic in the hospital.
SUMMARY
There have been a number of significant recent developments in the perioperative management of pulmonary complications:
- Obstructive sleep apnea has been confirmed as a risk factor, and pulmonary hypertension has emerged as a novel risk factor.
- An updated respiratory failure index has emerged as a useful research tool to identify high-risk patients and to ensure uniform risk stratification in future research.
- Evidence has mounted for the effectiveness of several risk-reduction strategies, including the use of laparoscopic procedures for bariatric surgery; selective use of nasogastric tubes; postoperative thoracic epidural analgesia; and intensive preoperative inspiratory muscle training.
DISCUSSION
Question from the audience: I do preoperative evaluations in an orthopedic ambulatory surgery center. Our surgeons often tell me, “Just order preoperative pulmonary function tests,” or, “Get a blood gas.” How should I respond?
Dr. Smetana: This is an area of some controversy, but in general, spirometry does not add much to a preoperative risk assessment that is based on a history and physical exam. Usually if the spirometry is abnormal, it will not be a surprise after careful clinical assessment. Arterial blood gases have no role in routine preoperative assessment.
Question from the audience: A chest x-ray is often requested preoperatively, but is it a necessary study?
Dr. Smetana: The data for preoperative chest x-rays are fairly poor and don’t allow us to assess whether they accurately predict complication rates. Most studies on chest x-rays have looked at how they affect preoperative management—eg, whether they change the anesthesia or even the surgery—and have shown that preoperative management changes in only about 1% to 2% of cases. So the chest x-ray is a fairly low-yield test in this setting.
One could argue that a preoperative chest x-ray might provide a baseline for postoperative comparison, but actually it is not usually helpful in this regard. Having a baseline does not make it easier to correctly diagnose pneumonia postoperatively, for example. Abnormal chest x-rays correlate with higher risk, but most patients with abnormal films would be suspected of being at higher risk anyway based on findings from the clinical assessment.
Question from the audience: Many primary care doctors in my hospital screen patients for pulmonary hypertension, but this raises the question of what to do with any information gained. What do you tell patients? Anesthesiologists?
Dr. Smetana: I don’t recommend preoperative screening for pulmonary hypertension unless there is some specific clinical reason to look for it. We don’t know if the perioperative risks that I described for patients with diagnosed or symptomatic pulmonary hypertension would also apply to patients with unrecognized, asymptomatic pulmonary hypertension that happened to be identified by screening.
Patients with pulmonary hypertension are at very high risk, especially for respiratory failure. But we don’t have any risk-reduction strategies specific to these patients, although I would recommend applying the general risk-reduction strategies that I discussed.
Question from the audience: I saw a man at my high-risk preoperative clinic who scored normally on a 6-minute walk test but then was found sound asleep when I was ready to see him a little while later. I suspected he had undiagnosed sleep apnea, and therefore had an increased risk of postoperative pulmonary complications, but what evidence would I have to delay his surgery to diagnose the sleep apnea and stabilize him on CPAP?
Dr. Smetana: For a patient with clinically suspected but undiagnosed sleep apnea, we have some evidence that the diagnosis should be pursued before surgery is performed.8 If the surgery were elective, it would be appropriate to have the patient evaluated and, if obstructive sleep apnea were diagnosed, treated in the customary way with CPAP. For patients who are hospitalized after surgery, CPAP can be continued as soon as possible in the hospital.
I would not have made this recommendation a few years ago, but now the evidence is more compelling. However, at this point I would not recommend routine preoperative screening of all patients for sleep apnea. Ongoing research is looking at this question.
Follow-up question: How long should surgery be delayed to optimize the patient on CPAP?
Dr. Smetana: Risk for postoperative respiratory failure is reduced very quickly after initiating CPAP therapy. A week would probably be sufficient, but there are no good data to specifically address that question.
Question from the audience: What about patients with asthma who are undergoing surgery—which ones benefit from stress-level steroids and preoperative nebulizer therapy?
Dr. Smetana: Surprisingly, asthma—if well controlled—is not a risk factor for postoperative pulmonary complications. Patients within 80% of their predicted or personal best peak flow appear to have a risk similar to that of patients without asthma. For patients with uncontrolled or poorly controlled asthma, the general rule is the same as for patients with COPD: treat them the same as if they weren’t having surgery. If a patient with asthma has a clinical indication for corticosteroids based on his or her condition, give corticosteroids whether or not surgery is planned. Corticosteroids are safe and do not raise the risk of postoperative wound complications. But we have no evidence to support routine use of steroids for all patients with asthma simply because elective surgery is planned.
Follow-up question: Do you optimize poorly controlled patients with oral prednisone for several days preoperatively, or do you use a stress protocol?
Dr. Smetana: For a patient whom you would normally treat with an outpatient course of prednisone, you should do just that. For a patient with an exacerbation severe enough to require admission for intravenous steroids and inhaled nebulizer therapy, then you should use that strategy. If the surgery is elective, it should be delayed until the patient is at his or her personal best.
- Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999; 100:1043–1049.
- Fleischmann KE, Goldman L, Young B, et al. Association between cardiac and noncardiac complications in patients undergoing noncardiac surgery: outcomes and effects on length of stay. Am J Med 2003; 115:515–520.
- Johnson RG, Arozullah AM, Neumayer L, et al. Multivariable predictors of postoperative respiratory failure after general and vascular surgery: results from the Patient Safety in Surgery Study. J Am Coll Surg 2007; 204:1188–1198.
- Dimick JB, Chen SL, Taheri PA, et al. Hospital costs associated with surgical complications: a report from the private-sector National Surgical Quality Improvement Program. J Am Coll Surg 2004; 199:531–537.
- Qaseem A, Snow V, Fitterman N, et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med 2006; 144:575–580.
- Smetana GW, Lawrence VA, Cornell JE. Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006; 144:581–595.
- Lawrence VA, Cornell JE, Smetana GW; American College of Physicians. Strategies to reduce postoperative pulmonary complications after noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006; 144:596–608.
- Hwang D, Shakir N, Limann B, et al. Association of sleep-disordered breathing with postoperative complications. Chest 2008; 133:1128–1134.
- Ramakrishna G, Sprung J, Ravi BS, et al. Impact of pulmonary hypertension on the outcomes of noncardiac surgery: predictors of perioperative morbidity and mortality. J Am Coll Cardiol 2005; 45:1691–1699.
- Lai HC, Lai HC, Wang KY, Lee WL, Ting CT, Liu TJ. Severe pulmonary hypertension complicates postoperative outcome of noncardiac surgery. Br J Anaesth 2007; 99:184–190.
- Arozullah AM, Daley J, Henderson WG, Khuri SF. Multifactorial risk index for predicting postoperative respiratory failure in men after major noncardiac surgery. The National Veterans Administration Surgical Quality Improvement Program. Ann Surg 2000; 232:242–253.
- Arozullah AM, Khuri SF, Henderson WG, et al. Development and validation of a multifactorial risk index for predicting postoperative pneumonia after major noncardiac surgery. Ann Intern Med 2001; 135:847–857.
- Ferreyra GP, Baussano I, Squadrone V, et al. Continuous positive airway pressure for treatment of respiratory complications after abdominal surgery: a systematic review and meta-analysis. Ann Surg 2008; 247:617–626.
- Nelson R, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominal surgery. Cochrane Database Syst Rev 2007; Jul 18 (3):CD004929.
- Weller WE, Rosati C. Comparing outcomes of laparoscopic versus open bariatric surgery. Ann Surg 2008; 248:10–15.
- Liu SS, Wu CL. Effect of postoperative analgesia on major postoperative complications: a systematic update of the evidence. Anesth Analg 2007; 104:689–702.
- Møller AM, Villebro N, Pedersen T, Tønnesen H. Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet 2002; 359:114–117.
- Lindström D, Sadr Azodi O, Wladis A, et al. Effects of a perioperative smoking cessation intervention on postoperative complications: a randomized trial. Ann Surg 2008; 248:739–745.
- Hulzebos EH, Helders PJ, Favié NJ, et al. Preoperative intensive inspiratory muscle training to prevent postoperative pulmonary complications in high-risk patients undergoing CABG surgery: a randomized clinical trial. JAMA 2006; 296:1851–1857.
Although pulmonary complications are not as well studied as cardiac complications in the postoperative setting, they are just as common following noncardiac surgery and are even more costly. It is worthwhile to identify surgical patients most at risk of postoperative pulmonary complications and take measures known to mitigate risk. This paper discusses important risk factors to identify during a preoperative pulmonary evaluation and then focuses on recent advances in strategies for reducing postoperative pulmonary complications. Teaching questions are included throughout, along with the rationale behind their answers.
POSTOPERATIVE PULMONARY COMPLICATIONS: WHAT ARE WE TRYING TO PREVENT AND WHY?
The definition of postoperative pulmonary complications is more variable and less intuitive than that of cardiac complications. Cardiac complications—postoperative myocardial infarction, cardiac death, and pulmonary edema—are more consistently defined and measured in clinical trials. Studies of postoperative pulmonary complications often group together pneumonia, respiratory failure, atelectasis, bronchospasm, and exacerbation of chronic obstructive pulmonary disease (COPD), making it more difficult to individually evaluate risk factors for different outcomes.
There are several reasons why it is important to consider pulmonary risk when evaluating patients preoperatively:
Pulmonary complications are as common as cardiac complications following noncardiac surgery. For example, in a secondary analysis of the cohort of noncardiac surgical patients used to validate the Revised Cardiac Risk Index,1 Fleischmann et al found that the incidence of pulmonary complications (2.7%) was highly comparable to that of cardiac complications (2.5%).2
Respiratory failure is a marker of ill health and predicts further complications. Postoperative respiratory failure (often defined as the need for ventilation for more than 48 hours after surgery) is an extremely morbid event. Johnson et al compared the outcomes of patients with and without respiratory failure as a complication of surgery.3 Among patients with respiratory failure, 26% died within 30 days, 6% had a myocardial infarction, 35% developed pneumonia, 10% developed acute renal failure, and 3% developed a deep vein thrombosis or pulmonary embolism; in contrast, rates of each of these events were lower than 2% among patients without respiratory failure.
Pulmonary complications are expensive and require lengthy hospitalization. The National Surgical Quality Improvement Program (NSQIP) compared hospitalization costs and length of stay among patients with various postoperative complications.4 Among infectious, cardiovascular, venous thromboembolic, and pulmonary complications, pulmonary complications were by far the most costly and, along with venous thromboembolic complications, required the longest mean hospital stay.
For these reasons, identifying patients at risk for pulmonary complications and developing a strategy to reduce the risk is clearly worthwhile.
IDENTIFYING RISK FOR PULMONARY COMPLICATIONS
Question: Which of the following is the most important risk factor for postoperative pulmonary complications?
A. High-risk surgical site
B. General anesthesia
C. COPD
D. Obesity
The correct answer is A. Pulmonary complications differ from cardiac complications in an important way: procedure-related factors are more predictive of pulmonary complications than are patient-related factors. Even healthy patients undergoing high-risk surgery are at risk for pulmonary complications. As for the other answer choices, general anesthesia and COPD are risk factors but are not as important as surgical site, and obesity has not been shown to be a risk factor at all.
Take-home points from the 2006 ACP guideline
Patient-related risk factors. As noted in Table 1, the most important patient-related risk factors identified in the ACP guideline are increasing age and increasing American Society of Anesthesiologists (ASA) classification of comorbidity.
The effect of advanced age becomes particularly notable around age 60 years and escalates from there. This effect of age differs from that for cardiac complications, for which age drops out as a risk factor after adjustment for other diseases and risk factors. For pulmonary complications, in contrast, even older patients who are healthy are at increased risk.
The ASA classification is a general index of overall morbidity that ranges from class 1 (normal healthy patient) to class 5 (moribund patient who is not expected to survive without the operation).
Notably, COPD and smoking were only minor risk factors in the ACP analysis.
Procedure-related risk factors. Surgical site was found to be the most important of any of the patient- or procedure-related risk factors. The closer the incision is to the diaphragm, the greater the risk for pulmonary complications. Aortic, thoracic, and abdominal procedures carry the highest risk (Table 1), and among abdominal procedures, upper abdominal surgery (eg, cholecystectomy) is riskier than lower abdominal surgery (eg, gynecologic).
Other procedure-related risk factors identified were emergency surgery, surgery lasting more than 3 hours, use of general anesthesia, and multiple transfusions (Table 1).
Newly identified risk factors
Question: Which of the following has recently been identified as a risk factor for postoperative pulmonary complications?
A. Epidural anesthesia
B. Insulin-treated diabetes
C. Obstructive sleep apnea
D. Immobility
The correct answer is C. There is no evidence that epidural anesthesia or insulin-treated diabetes are risk factors. Immobility seems intuitively correct but has not emerged as a risk factor among high-quality studies in the literature.
Obstructive sleep apnea. The role of obstructive sleep apnea was unclear prior to publication of new data in the last couple of years. Hwang et al enrolled 172 patients who were soon to have elective surgery and had at least two of four clinical features of obstructive sleep apnea (snoring, daytime somnolence, witnessed apnea event, or crowded oropharynx).8 Patients underwent nocturnal oximetry before surgery and were divided into two groups based on number of desaturation episodes per hour. Patients with five or more desaturations had markedly higher rates of postoperative respiratory complications (8 complications among 98 patients) than did patients with fewer than five desaturations (1 complication among 74 patients). The presence of five or more desaturations was also associated with higher rates of cardiac, gastrointestinal, and bleeding complications. Though this was a small study, its results suggest a significant association between obstructive sleep apnea and pulmonary complications.
The issue of whether to screen patients for obstructive sleep apnea before major noncardiac surgery is still unresolved.
Pulmonary hypertension has also been identified as a risk factor in recent years with the publication of two studies that estimated its impact on morbidity and mortality after major noncardiac surgery.9,10 One of the studies, a retrospective database review, found a 28% incidence of respiratory failure among 145 surgical patients with pulmonary hypertension.9 In the other study, a prospective case-control trial, respiratory failure occurred in 21% of patients with pulmonary hypertension compared with only 3% of matched controls.10 In the case-control study, pulmonary hypertension was also associated with significantly elevated rates of heart failure and in-hospital death.
The results of these studies do not support preoperative screening for undiagnosed pulmonary hypertension, but they do underscore the need to recognize established pulmonary hypertension as an important risk factor for postoperative complications.
AN UPDATED INDEX FOR RESPIRATORY FAILURE
Several years ago, investigators from the Veterans Affairs Medical Centers developed a respiratory failure index using a design similar to those of well-established indices for cardiac risk.11 The same group also developed a separate risk index for pneumonia.12
This respiratory failure index was recently updated3 to reflect experience from private and academic hospitals, making the results more generally applicable. The researchers evaluated data from 180,000 patients undergoing major general or vascular surgery (defined according to the NSQIP) over a 3-year period. Respiratory failure was defined as requiring at least 48 hours of ventilation or unplanned reintubation.
Comparison and contrast with the ACP guideline
Question: How does the updated respiratory failure index differ most significantly from the 2006 ACP guideline?
A. New index places greater emphasis on ASA class
B. New index offers a simplified weighted point scheme
C. New index ranks low albumin as a less important risk factor
D. New index attributes low risk to cigarette use
The correct answer is C: low albumin is a minor risk factor in the respiratory failure index, whereas it was one of the single most important predictors in the ACP guideline. As for the other answer choices, the new index places about the same emphasis on ASA class and cigarette use as does the ACP guideline, and it does not offer a simplified approach, as it incorporates 28 different factors.
Overall, most risk factors were similar in the updated respiratory failure index and the ACP guideline, but the index differs in several important ways:
- The index assigns less risk to low albumin, functional dependence, and congestive heart failure
- The index assigns greater risk to orofacial surgery
- The index identifies several new risk factors—high-complexity surgery, preoperative sepsis, ascites, and hypernatremia (serum sodium > 145 mmol/L).
STRATEGIES FOR RISK REDUCTION
Postoperative CPAP: Good option when exercise ability is limited
Among the postoperative lung expansion modalities, continuous positive airway pressure (CPAP) is particularly useful for patients who are unable to perform deep breathing or incentive spirometry exercises. A recent systematic literature review identified nine randomized controlled trials of CPAP vs standard therapy in a total of 654 patients undergoing abdominal surgery.13 Meta-analysis of these studies showed that CPAP was associated with significant reductions in the risk of overall postoperative pulmonary complications (odds ratio [OR] = 0.66; 95% CI, 0.52–0.85), atelectasis (OR = 0.75; 95% CI, 0.58–0.97), and pneumonia (OR = 0.33; 95% CI, 0.14–0.75) relative to standard therapy.
Use nasogastric tubes selectively
Nasogastric tubes can be used either routinely following abdominal surgery or only in select patients—eg, those who have symptomatic abdominal distention or nausea. The difference is important since nasogastric tubes may potentially increase the risk of aspiration and thus lead to a pulmonary complication. Nelson et al conducted a meta-analysis of 24 studies that compared routine nasogastric tube use in abdominal surgery with selective use based on symptoms or abdominal distention.14 They found that routine use was associated with a significant increase in postoperative pulmonary complications (OR = 1.45; 95% CI, 1.08–1.93) relative to selective use, without achieving any of its intended goals.
Laparoscopic vs open surgery: Evidence begins to follow intuition
Intuitively, it seems that laparoscopic procedures should reduce risk for postoperative pulmonary complications compared with open surgical procedures, as they are associated with less postoperative pain, which should facilitate deep breathing and improve postoperative lung volumes. Nevertheless, evidence for whether laparoscopic surgery reduces the risk of pulmonary complications has been mixed until recently.
In 2008, however, Weller and Rosati published an analysis of a nationally representative database of 19,156 patients who underwent bariatric surgery in 2005.15 After adjusting for comorbidities, they found that the rate of postoperative pulmonary complications was nearly double if patients underwent open surgery as opposed to laparoscopic surgery (OR = 1.92; 95% CI, 1.54–2.38). Open surgery was also associated with significantly higher rates of sepsis, cardiovascular events, and reoperation compared with laparoscopic procedures. This study suggests that choosing laparoscopic procedures is another strategy that may reduce pulmonary complication rates, at least in the setting of bariatric surgery.
Postoperative thoracic epidural analgesia
Question: Thoracic epidural analgesia reduces rates of which of the following?
A. Pneumonia following abdominal aortic aneurysm repair
B. Pulmonary complications following coronary bypass surgery
C. Respiratory failure following abdominal surgery
D. All of the above
The correct answer is D. Thoracic epidural analgesia is another important strategy for reducing postoperative pulmonary complications, as demonstrated by a 2007 systematic literature review by Liu and Wu.16 Their analysis showed that rates of pneumonia, respiratory failure, and pulmonary complications overall were reduced by approximately one-third to more than one-half with the use of postoperative thoracic epidural analgesia in patients undergoing aortic aneurysm repair, coronary bypass surgery, and abdominal surgery.
Smoking cessation: The jury is still out
Whether preoperative cigarette cessation reduces pulmonary complication rates has been controversial over the past decade. Early reports showed that among patients who smoke, those who quit shortly before surgery actually had higher complication rates than patients who continued to smoke. The most reasonable explanation seems to be that many patients who stop smoking report increased coughing and sputum production for the first month or two. Selection bias also may have played a role in these findings.
More recently, two randomized trials studied the impact of perioperative smoking intervention programs involving counseling and nicotine replacement.17,18 Unfortunately, both studies primarily studied patients undergoing low-risk procedures and were insufficiently powered to show a difference in pulmonary complication rates. The question of whether smoking cessation is an effective strategy to reduce postoperative pulmonary risk remains unanswered.
Preoperative intensive lung expansion: A promising new intervention
While the effectiveness of postoperative lung expansion techniques is undisputed,7 preoperative lung expansion—also known as inspiratory muscle training—has only recently been investigated. Hulzebos et al randomized 279 patients undergoing coronary artery bypass graft surgery who were at high risk for developing pulmonary complications to either usual care or inspiratory muscle training.19 The latter intervention involved 20 minutes per day of incentive spirometry, active breathing, and forced expiration techniques for at least 2 weeks prior to surgery. Rates of high-grade postoperative pulmonary complications were cut in half (OR = 0.52; 95% CI, 0.30–0.92) and rates of pneumonia were reduced by 60% (OR = 0.40; 95% CI, 0.19–0.84) in patients who received inspiratory muscle training relative to the usual-care group.
In clinical practice, preoperative inspiratory muscle training can be done in a chest physical therapy outpatient setting or a pulmonary rehabilitation clinic in the hospital.
SUMMARY
There have been a number of significant recent developments in the perioperative management of pulmonary complications:
- Obstructive sleep apnea has been confirmed as a risk factor, and pulmonary hypertension has emerged as a novel risk factor.
- An updated respiratory failure index has emerged as a useful research tool to identify high-risk patients and to ensure uniform risk stratification in future research.
- Evidence has mounted for the effectiveness of several risk-reduction strategies, including the use of laparoscopic procedures for bariatric surgery; selective use of nasogastric tubes; postoperative thoracic epidural analgesia; and intensive preoperative inspiratory muscle training.
DISCUSSION
Question from the audience: I do preoperative evaluations in an orthopedic ambulatory surgery center. Our surgeons often tell me, “Just order preoperative pulmonary function tests,” or, “Get a blood gas.” How should I respond?
Dr. Smetana: This is an area of some controversy, but in general, spirometry does not add much to a preoperative risk assessment that is based on a history and physical exam. Usually if the spirometry is abnormal, it will not be a surprise after careful clinical assessment. Arterial blood gases have no role in routine preoperative assessment.
Question from the audience: A chest x-ray is often requested preoperatively, but is it a necessary study?
Dr. Smetana: The data for preoperative chest x-rays are fairly poor and don’t allow us to assess whether they accurately predict complication rates. Most studies on chest x-rays have looked at how they affect preoperative management—eg, whether they change the anesthesia or even the surgery—and have shown that preoperative management changes in only about 1% to 2% of cases. So the chest x-ray is a fairly low-yield test in this setting.
One could argue that a preoperative chest x-ray might provide a baseline for postoperative comparison, but actually it is not usually helpful in this regard. Having a baseline does not make it easier to correctly diagnose pneumonia postoperatively, for example. Abnormal chest x-rays correlate with higher risk, but most patients with abnormal films would be suspected of being at higher risk anyway based on findings from the clinical assessment.
Question from the audience: Many primary care doctors in my hospital screen patients for pulmonary hypertension, but this raises the question of what to do with any information gained. What do you tell patients? Anesthesiologists?
Dr. Smetana: I don’t recommend preoperative screening for pulmonary hypertension unless there is some specific clinical reason to look for it. We don’t know if the perioperative risks that I described for patients with diagnosed or symptomatic pulmonary hypertension would also apply to patients with unrecognized, asymptomatic pulmonary hypertension that happened to be identified by screening.
Patients with pulmonary hypertension are at very high risk, especially for respiratory failure. But we don’t have any risk-reduction strategies specific to these patients, although I would recommend applying the general risk-reduction strategies that I discussed.
Question from the audience: I saw a man at my high-risk preoperative clinic who scored normally on a 6-minute walk test but then was found sound asleep when I was ready to see him a little while later. I suspected he had undiagnosed sleep apnea, and therefore had an increased risk of postoperative pulmonary complications, but what evidence would I have to delay his surgery to diagnose the sleep apnea and stabilize him on CPAP?
Dr. Smetana: For a patient with clinically suspected but undiagnosed sleep apnea, we have some evidence that the diagnosis should be pursued before surgery is performed.8 If the surgery were elective, it would be appropriate to have the patient evaluated and, if obstructive sleep apnea were diagnosed, treated in the customary way with CPAP. For patients who are hospitalized after surgery, CPAP can be continued as soon as possible in the hospital.
I would not have made this recommendation a few years ago, but now the evidence is more compelling. However, at this point I would not recommend routine preoperative screening of all patients for sleep apnea. Ongoing research is looking at this question.
Follow-up question: How long should surgery be delayed to optimize the patient on CPAP?
Dr. Smetana: Risk for postoperative respiratory failure is reduced very quickly after initiating CPAP therapy. A week would probably be sufficient, but there are no good data to specifically address that question.
Question from the audience: What about patients with asthma who are undergoing surgery—which ones benefit from stress-level steroids and preoperative nebulizer therapy?
Dr. Smetana: Surprisingly, asthma—if well controlled—is not a risk factor for postoperative pulmonary complications. Patients within 80% of their predicted or personal best peak flow appear to have a risk similar to that of patients without asthma. For patients with uncontrolled or poorly controlled asthma, the general rule is the same as for patients with COPD: treat them the same as if they weren’t having surgery. If a patient with asthma has a clinical indication for corticosteroids based on his or her condition, give corticosteroids whether or not surgery is planned. Corticosteroids are safe and do not raise the risk of postoperative wound complications. But we have no evidence to support routine use of steroids for all patients with asthma simply because elective surgery is planned.
Follow-up question: Do you optimize poorly controlled patients with oral prednisone for several days preoperatively, or do you use a stress protocol?
Dr. Smetana: For a patient whom you would normally treat with an outpatient course of prednisone, you should do just that. For a patient with an exacerbation severe enough to require admission for intravenous steroids and inhaled nebulizer therapy, then you should use that strategy. If the surgery is elective, it should be delayed until the patient is at his or her personal best.
Although pulmonary complications are not as well studied as cardiac complications in the postoperative setting, they are just as common following noncardiac surgery and are even more costly. It is worthwhile to identify surgical patients most at risk of postoperative pulmonary complications and take measures known to mitigate risk. This paper discusses important risk factors to identify during a preoperative pulmonary evaluation and then focuses on recent advances in strategies for reducing postoperative pulmonary complications. Teaching questions are included throughout, along with the rationale behind their answers.
POSTOPERATIVE PULMONARY COMPLICATIONS: WHAT ARE WE TRYING TO PREVENT AND WHY?
The definition of postoperative pulmonary complications is more variable and less intuitive than that of cardiac complications. Cardiac complications—postoperative myocardial infarction, cardiac death, and pulmonary edema—are more consistently defined and measured in clinical trials. Studies of postoperative pulmonary complications often group together pneumonia, respiratory failure, atelectasis, bronchospasm, and exacerbation of chronic obstructive pulmonary disease (COPD), making it more difficult to individually evaluate risk factors for different outcomes.
There are several reasons why it is important to consider pulmonary risk when evaluating patients preoperatively:
Pulmonary complications are as common as cardiac complications following noncardiac surgery. For example, in a secondary analysis of the cohort of noncardiac surgical patients used to validate the Revised Cardiac Risk Index,1 Fleischmann et al found that the incidence of pulmonary complications (2.7%) was highly comparable to that of cardiac complications (2.5%).2
Respiratory failure is a marker of ill health and predicts further complications. Postoperative respiratory failure (often defined as the need for ventilation for more than 48 hours after surgery) is an extremely morbid event. Johnson et al compared the outcomes of patients with and without respiratory failure as a complication of surgery.3 Among patients with respiratory failure, 26% died within 30 days, 6% had a myocardial infarction, 35% developed pneumonia, 10% developed acute renal failure, and 3% developed a deep vein thrombosis or pulmonary embolism; in contrast, rates of each of these events were lower than 2% among patients without respiratory failure.
Pulmonary complications are expensive and require lengthy hospitalization. The National Surgical Quality Improvement Program (NSQIP) compared hospitalization costs and length of stay among patients with various postoperative complications.4 Among infectious, cardiovascular, venous thromboembolic, and pulmonary complications, pulmonary complications were by far the most costly and, along with venous thromboembolic complications, required the longest mean hospital stay.
For these reasons, identifying patients at risk for pulmonary complications and developing a strategy to reduce the risk is clearly worthwhile.
IDENTIFYING RISK FOR PULMONARY COMPLICATIONS
Question: Which of the following is the most important risk factor for postoperative pulmonary complications?
A. High-risk surgical site
B. General anesthesia
C. COPD
D. Obesity
The correct answer is A. Pulmonary complications differ from cardiac complications in an important way: procedure-related factors are more predictive of pulmonary complications than are patient-related factors. Even healthy patients undergoing high-risk surgery are at risk for pulmonary complications. As for the other answer choices, general anesthesia and COPD are risk factors but are not as important as surgical site, and obesity has not been shown to be a risk factor at all.
Take-home points from the 2006 ACP guideline
Patient-related risk factors. As noted in Table 1, the most important patient-related risk factors identified in the ACP guideline are increasing age and increasing American Society of Anesthesiologists (ASA) classification of comorbidity.
The effect of advanced age becomes particularly notable around age 60 years and escalates from there. This effect of age differs from that for cardiac complications, for which age drops out as a risk factor after adjustment for other diseases and risk factors. For pulmonary complications, in contrast, even older patients who are healthy are at increased risk.
The ASA classification is a general index of overall morbidity that ranges from class 1 (normal healthy patient) to class 5 (moribund patient who is not expected to survive without the operation).
Notably, COPD and smoking were only minor risk factors in the ACP analysis.
Procedure-related risk factors. Surgical site was found to be the most important of any of the patient- or procedure-related risk factors. The closer the incision is to the diaphragm, the greater the risk for pulmonary complications. Aortic, thoracic, and abdominal procedures carry the highest risk (Table 1), and among abdominal procedures, upper abdominal surgery (eg, cholecystectomy) is riskier than lower abdominal surgery (eg, gynecologic).
Other procedure-related risk factors identified were emergency surgery, surgery lasting more than 3 hours, use of general anesthesia, and multiple transfusions (Table 1).
Newly identified risk factors
Question: Which of the following has recently been identified as a risk factor for postoperative pulmonary complications?
A. Epidural anesthesia
B. Insulin-treated diabetes
C. Obstructive sleep apnea
D. Immobility
The correct answer is C. There is no evidence that epidural anesthesia or insulin-treated diabetes are risk factors. Immobility seems intuitively correct but has not emerged as a risk factor among high-quality studies in the literature.
Obstructive sleep apnea. The role of obstructive sleep apnea was unclear prior to publication of new data in the last couple of years. Hwang et al enrolled 172 patients who were soon to have elective surgery and had at least two of four clinical features of obstructive sleep apnea (snoring, daytime somnolence, witnessed apnea event, or crowded oropharynx).8 Patients underwent nocturnal oximetry before surgery and were divided into two groups based on number of desaturation episodes per hour. Patients with five or more desaturations had markedly higher rates of postoperative respiratory complications (8 complications among 98 patients) than did patients with fewer than five desaturations (1 complication among 74 patients). The presence of five or more desaturations was also associated with higher rates of cardiac, gastrointestinal, and bleeding complications. Though this was a small study, its results suggest a significant association between obstructive sleep apnea and pulmonary complications.
The issue of whether to screen patients for obstructive sleep apnea before major noncardiac surgery is still unresolved.
Pulmonary hypertension has also been identified as a risk factor in recent years with the publication of two studies that estimated its impact on morbidity and mortality after major noncardiac surgery.9,10 One of the studies, a retrospective database review, found a 28% incidence of respiratory failure among 145 surgical patients with pulmonary hypertension.9 In the other study, a prospective case-control trial, respiratory failure occurred in 21% of patients with pulmonary hypertension compared with only 3% of matched controls.10 In the case-control study, pulmonary hypertension was also associated with significantly elevated rates of heart failure and in-hospital death.
The results of these studies do not support preoperative screening for undiagnosed pulmonary hypertension, but they do underscore the need to recognize established pulmonary hypertension as an important risk factor for postoperative complications.
AN UPDATED INDEX FOR RESPIRATORY FAILURE
Several years ago, investigators from the Veterans Affairs Medical Centers developed a respiratory failure index using a design similar to those of well-established indices for cardiac risk.11 The same group also developed a separate risk index for pneumonia.12
This respiratory failure index was recently updated3 to reflect experience from private and academic hospitals, making the results more generally applicable. The researchers evaluated data from 180,000 patients undergoing major general or vascular surgery (defined according to the NSQIP) over a 3-year period. Respiratory failure was defined as requiring at least 48 hours of ventilation or unplanned reintubation.
Comparison and contrast with the ACP guideline
Question: How does the updated respiratory failure index differ most significantly from the 2006 ACP guideline?
A. New index places greater emphasis on ASA class
B. New index offers a simplified weighted point scheme
C. New index ranks low albumin as a less important risk factor
D. New index attributes low risk to cigarette use
The correct answer is C: low albumin is a minor risk factor in the respiratory failure index, whereas it was one of the single most important predictors in the ACP guideline. As for the other answer choices, the new index places about the same emphasis on ASA class and cigarette use as does the ACP guideline, and it does not offer a simplified approach, as it incorporates 28 different factors.
Overall, most risk factors were similar in the updated respiratory failure index and the ACP guideline, but the index differs in several important ways:
- The index assigns less risk to low albumin, functional dependence, and congestive heart failure
- The index assigns greater risk to orofacial surgery
- The index identifies several new risk factors—high-complexity surgery, preoperative sepsis, ascites, and hypernatremia (serum sodium > 145 mmol/L).
STRATEGIES FOR RISK REDUCTION
Postoperative CPAP: Good option when exercise ability is limited
Among the postoperative lung expansion modalities, continuous positive airway pressure (CPAP) is particularly useful for patients who are unable to perform deep breathing or incentive spirometry exercises. A recent systematic literature review identified nine randomized controlled trials of CPAP vs standard therapy in a total of 654 patients undergoing abdominal surgery.13 Meta-analysis of these studies showed that CPAP was associated with significant reductions in the risk of overall postoperative pulmonary complications (odds ratio [OR] = 0.66; 95% CI, 0.52–0.85), atelectasis (OR = 0.75; 95% CI, 0.58–0.97), and pneumonia (OR = 0.33; 95% CI, 0.14–0.75) relative to standard therapy.
Use nasogastric tubes selectively
Nasogastric tubes can be used either routinely following abdominal surgery or only in select patients—eg, those who have symptomatic abdominal distention or nausea. The difference is important since nasogastric tubes may potentially increase the risk of aspiration and thus lead to a pulmonary complication. Nelson et al conducted a meta-analysis of 24 studies that compared routine nasogastric tube use in abdominal surgery with selective use based on symptoms or abdominal distention.14 They found that routine use was associated with a significant increase in postoperative pulmonary complications (OR = 1.45; 95% CI, 1.08–1.93) relative to selective use, without achieving any of its intended goals.
Laparoscopic vs open surgery: Evidence begins to follow intuition
Intuitively, it seems that laparoscopic procedures should reduce risk for postoperative pulmonary complications compared with open surgical procedures, as they are associated with less postoperative pain, which should facilitate deep breathing and improve postoperative lung volumes. Nevertheless, evidence for whether laparoscopic surgery reduces the risk of pulmonary complications has been mixed until recently.
In 2008, however, Weller and Rosati published an analysis of a nationally representative database of 19,156 patients who underwent bariatric surgery in 2005.15 After adjusting for comorbidities, they found that the rate of postoperative pulmonary complications was nearly double if patients underwent open surgery as opposed to laparoscopic surgery (OR = 1.92; 95% CI, 1.54–2.38). Open surgery was also associated with significantly higher rates of sepsis, cardiovascular events, and reoperation compared with laparoscopic procedures. This study suggests that choosing laparoscopic procedures is another strategy that may reduce pulmonary complication rates, at least in the setting of bariatric surgery.
Postoperative thoracic epidural analgesia
Question: Thoracic epidural analgesia reduces rates of which of the following?
A. Pneumonia following abdominal aortic aneurysm repair
B. Pulmonary complications following coronary bypass surgery
C. Respiratory failure following abdominal surgery
D. All of the above
The correct answer is D. Thoracic epidural analgesia is another important strategy for reducing postoperative pulmonary complications, as demonstrated by a 2007 systematic literature review by Liu and Wu.16 Their analysis showed that rates of pneumonia, respiratory failure, and pulmonary complications overall were reduced by approximately one-third to more than one-half with the use of postoperative thoracic epidural analgesia in patients undergoing aortic aneurysm repair, coronary bypass surgery, and abdominal surgery.
Smoking cessation: The jury is still out
Whether preoperative cigarette cessation reduces pulmonary complication rates has been controversial over the past decade. Early reports showed that among patients who smoke, those who quit shortly before surgery actually had higher complication rates than patients who continued to smoke. The most reasonable explanation seems to be that many patients who stop smoking report increased coughing and sputum production for the first month or two. Selection bias also may have played a role in these findings.
More recently, two randomized trials studied the impact of perioperative smoking intervention programs involving counseling and nicotine replacement.17,18 Unfortunately, both studies primarily studied patients undergoing low-risk procedures and were insufficiently powered to show a difference in pulmonary complication rates. The question of whether smoking cessation is an effective strategy to reduce postoperative pulmonary risk remains unanswered.
Preoperative intensive lung expansion: A promising new intervention
While the effectiveness of postoperative lung expansion techniques is undisputed,7 preoperative lung expansion—also known as inspiratory muscle training—has only recently been investigated. Hulzebos et al randomized 279 patients undergoing coronary artery bypass graft surgery who were at high risk for developing pulmonary complications to either usual care or inspiratory muscle training.19 The latter intervention involved 20 minutes per day of incentive spirometry, active breathing, and forced expiration techniques for at least 2 weeks prior to surgery. Rates of high-grade postoperative pulmonary complications were cut in half (OR = 0.52; 95% CI, 0.30–0.92) and rates of pneumonia were reduced by 60% (OR = 0.40; 95% CI, 0.19–0.84) in patients who received inspiratory muscle training relative to the usual-care group.
In clinical practice, preoperative inspiratory muscle training can be done in a chest physical therapy outpatient setting or a pulmonary rehabilitation clinic in the hospital.
SUMMARY
There have been a number of significant recent developments in the perioperative management of pulmonary complications:
- Obstructive sleep apnea has been confirmed as a risk factor, and pulmonary hypertension has emerged as a novel risk factor.
- An updated respiratory failure index has emerged as a useful research tool to identify high-risk patients and to ensure uniform risk stratification in future research.
- Evidence has mounted for the effectiveness of several risk-reduction strategies, including the use of laparoscopic procedures for bariatric surgery; selective use of nasogastric tubes; postoperative thoracic epidural analgesia; and intensive preoperative inspiratory muscle training.
DISCUSSION
Question from the audience: I do preoperative evaluations in an orthopedic ambulatory surgery center. Our surgeons often tell me, “Just order preoperative pulmonary function tests,” or, “Get a blood gas.” How should I respond?
Dr. Smetana: This is an area of some controversy, but in general, spirometry does not add much to a preoperative risk assessment that is based on a history and physical exam. Usually if the spirometry is abnormal, it will not be a surprise after careful clinical assessment. Arterial blood gases have no role in routine preoperative assessment.
Question from the audience: A chest x-ray is often requested preoperatively, but is it a necessary study?
Dr. Smetana: The data for preoperative chest x-rays are fairly poor and don’t allow us to assess whether they accurately predict complication rates. Most studies on chest x-rays have looked at how they affect preoperative management—eg, whether they change the anesthesia or even the surgery—and have shown that preoperative management changes in only about 1% to 2% of cases. So the chest x-ray is a fairly low-yield test in this setting.
One could argue that a preoperative chest x-ray might provide a baseline for postoperative comparison, but actually it is not usually helpful in this regard. Having a baseline does not make it easier to correctly diagnose pneumonia postoperatively, for example. Abnormal chest x-rays correlate with higher risk, but most patients with abnormal films would be suspected of being at higher risk anyway based on findings from the clinical assessment.
Question from the audience: Many primary care doctors in my hospital screen patients for pulmonary hypertension, but this raises the question of what to do with any information gained. What do you tell patients? Anesthesiologists?
Dr. Smetana: I don’t recommend preoperative screening for pulmonary hypertension unless there is some specific clinical reason to look for it. We don’t know if the perioperative risks that I described for patients with diagnosed or symptomatic pulmonary hypertension would also apply to patients with unrecognized, asymptomatic pulmonary hypertension that happened to be identified by screening.
Patients with pulmonary hypertension are at very high risk, especially for respiratory failure. But we don’t have any risk-reduction strategies specific to these patients, although I would recommend applying the general risk-reduction strategies that I discussed.
Question from the audience: I saw a man at my high-risk preoperative clinic who scored normally on a 6-minute walk test but then was found sound asleep when I was ready to see him a little while later. I suspected he had undiagnosed sleep apnea, and therefore had an increased risk of postoperative pulmonary complications, but what evidence would I have to delay his surgery to diagnose the sleep apnea and stabilize him on CPAP?
Dr. Smetana: For a patient with clinically suspected but undiagnosed sleep apnea, we have some evidence that the diagnosis should be pursued before surgery is performed.8 If the surgery were elective, it would be appropriate to have the patient evaluated and, if obstructive sleep apnea were diagnosed, treated in the customary way with CPAP. For patients who are hospitalized after surgery, CPAP can be continued as soon as possible in the hospital.
I would not have made this recommendation a few years ago, but now the evidence is more compelling. However, at this point I would not recommend routine preoperative screening of all patients for sleep apnea. Ongoing research is looking at this question.
Follow-up question: How long should surgery be delayed to optimize the patient on CPAP?
Dr. Smetana: Risk for postoperative respiratory failure is reduced very quickly after initiating CPAP therapy. A week would probably be sufficient, but there are no good data to specifically address that question.
Question from the audience: What about patients with asthma who are undergoing surgery—which ones benefit from stress-level steroids and preoperative nebulizer therapy?
Dr. Smetana: Surprisingly, asthma—if well controlled—is not a risk factor for postoperative pulmonary complications. Patients within 80% of their predicted or personal best peak flow appear to have a risk similar to that of patients without asthma. For patients with uncontrolled or poorly controlled asthma, the general rule is the same as for patients with COPD: treat them the same as if they weren’t having surgery. If a patient with asthma has a clinical indication for corticosteroids based on his or her condition, give corticosteroids whether or not surgery is planned. Corticosteroids are safe and do not raise the risk of postoperative wound complications. But we have no evidence to support routine use of steroids for all patients with asthma simply because elective surgery is planned.
Follow-up question: Do you optimize poorly controlled patients with oral prednisone for several days preoperatively, or do you use a stress protocol?
Dr. Smetana: For a patient whom you would normally treat with an outpatient course of prednisone, you should do just that. For a patient with an exacerbation severe enough to require admission for intravenous steroids and inhaled nebulizer therapy, then you should use that strategy. If the surgery is elective, it should be delayed until the patient is at his or her personal best.
- Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999; 100:1043–1049.
- Fleischmann KE, Goldman L, Young B, et al. Association between cardiac and noncardiac complications in patients undergoing noncardiac surgery: outcomes and effects on length of stay. Am J Med 2003; 115:515–520.
- Johnson RG, Arozullah AM, Neumayer L, et al. Multivariable predictors of postoperative respiratory failure after general and vascular surgery: results from the Patient Safety in Surgery Study. J Am Coll Surg 2007; 204:1188–1198.
- Dimick JB, Chen SL, Taheri PA, et al. Hospital costs associated with surgical complications: a report from the private-sector National Surgical Quality Improvement Program. J Am Coll Surg 2004; 199:531–537.
- Qaseem A, Snow V, Fitterman N, et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med 2006; 144:575–580.
- Smetana GW, Lawrence VA, Cornell JE. Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006; 144:581–595.
- Lawrence VA, Cornell JE, Smetana GW; American College of Physicians. Strategies to reduce postoperative pulmonary complications after noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006; 144:596–608.
- Hwang D, Shakir N, Limann B, et al. Association of sleep-disordered breathing with postoperative complications. Chest 2008; 133:1128–1134.
- Ramakrishna G, Sprung J, Ravi BS, et al. Impact of pulmonary hypertension on the outcomes of noncardiac surgery: predictors of perioperative morbidity and mortality. J Am Coll Cardiol 2005; 45:1691–1699.
- Lai HC, Lai HC, Wang KY, Lee WL, Ting CT, Liu TJ. Severe pulmonary hypertension complicates postoperative outcome of noncardiac surgery. Br J Anaesth 2007; 99:184–190.
- Arozullah AM, Daley J, Henderson WG, Khuri SF. Multifactorial risk index for predicting postoperative respiratory failure in men after major noncardiac surgery. The National Veterans Administration Surgical Quality Improvement Program. Ann Surg 2000; 232:242–253.
- Arozullah AM, Khuri SF, Henderson WG, et al. Development and validation of a multifactorial risk index for predicting postoperative pneumonia after major noncardiac surgery. Ann Intern Med 2001; 135:847–857.
- Ferreyra GP, Baussano I, Squadrone V, et al. Continuous positive airway pressure for treatment of respiratory complications after abdominal surgery: a systematic review and meta-analysis. Ann Surg 2008; 247:617–626.
- Nelson R, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominal surgery. Cochrane Database Syst Rev 2007; Jul 18 (3):CD004929.
- Weller WE, Rosati C. Comparing outcomes of laparoscopic versus open bariatric surgery. Ann Surg 2008; 248:10–15.
- Liu SS, Wu CL. Effect of postoperative analgesia on major postoperative complications: a systematic update of the evidence. Anesth Analg 2007; 104:689–702.
- Møller AM, Villebro N, Pedersen T, Tønnesen H. Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet 2002; 359:114–117.
- Lindström D, Sadr Azodi O, Wladis A, et al. Effects of a perioperative smoking cessation intervention on postoperative complications: a randomized trial. Ann Surg 2008; 248:739–745.
- Hulzebos EH, Helders PJ, Favié NJ, et al. Preoperative intensive inspiratory muscle training to prevent postoperative pulmonary complications in high-risk patients undergoing CABG surgery: a randomized clinical trial. JAMA 2006; 296:1851–1857.
- Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999; 100:1043–1049.
- Fleischmann KE, Goldman L, Young B, et al. Association between cardiac and noncardiac complications in patients undergoing noncardiac surgery: outcomes and effects on length of stay. Am J Med 2003; 115:515–520.
- Johnson RG, Arozullah AM, Neumayer L, et al. Multivariable predictors of postoperative respiratory failure after general and vascular surgery: results from the Patient Safety in Surgery Study. J Am Coll Surg 2007; 204:1188–1198.
- Dimick JB, Chen SL, Taheri PA, et al. Hospital costs associated with surgical complications: a report from the private-sector National Surgical Quality Improvement Program. J Am Coll Surg 2004; 199:531–537.
- Qaseem A, Snow V, Fitterman N, et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med 2006; 144:575–580.
- Smetana GW, Lawrence VA, Cornell JE. Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006; 144:581–595.
- Lawrence VA, Cornell JE, Smetana GW; American College of Physicians. Strategies to reduce postoperative pulmonary complications after noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006; 144:596–608.
- Hwang D, Shakir N, Limann B, et al. Association of sleep-disordered breathing with postoperative complications. Chest 2008; 133:1128–1134.
- Ramakrishna G, Sprung J, Ravi BS, et al. Impact of pulmonary hypertension on the outcomes of noncardiac surgery: predictors of perioperative morbidity and mortality. J Am Coll Cardiol 2005; 45:1691–1699.
- Lai HC, Lai HC, Wang KY, Lee WL, Ting CT, Liu TJ. Severe pulmonary hypertension complicates postoperative outcome of noncardiac surgery. Br J Anaesth 2007; 99:184–190.
- Arozullah AM, Daley J, Henderson WG, Khuri SF. Multifactorial risk index for predicting postoperative respiratory failure in men after major noncardiac surgery. The National Veterans Administration Surgical Quality Improvement Program. Ann Surg 2000; 232:242–253.
- Arozullah AM, Khuri SF, Henderson WG, et al. Development and validation of a multifactorial risk index for predicting postoperative pneumonia after major noncardiac surgery. Ann Intern Med 2001; 135:847–857.
- Ferreyra GP, Baussano I, Squadrone V, et al. Continuous positive airway pressure for treatment of respiratory complications after abdominal surgery: a systematic review and meta-analysis. Ann Surg 2008; 247:617–626.
- Nelson R, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominal surgery. Cochrane Database Syst Rev 2007; Jul 18 (3):CD004929.
- Weller WE, Rosati C. Comparing outcomes of laparoscopic versus open bariatric surgery. Ann Surg 2008; 248:10–15.
- Liu SS, Wu CL. Effect of postoperative analgesia on major postoperative complications: a systematic update of the evidence. Anesth Analg 2007; 104:689–702.
- Møller AM, Villebro N, Pedersen T, Tønnesen H. Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet 2002; 359:114–117.
- Lindström D, Sadr Azodi O, Wladis A, et al. Effects of a perioperative smoking cessation intervention on postoperative complications: a randomized trial. Ann Surg 2008; 248:739–745.
- Hulzebos EH, Helders PJ, Favié NJ, et al. Preoperative intensive inspiratory muscle training to prevent postoperative pulmonary complications in high-risk patients undergoing CABG surgery: a randomized clinical trial. JAMA 2006; 296:1851–1857.
KEY POINTS
- Pulmonary complications are as common as cardiac complications following noncardiac surgery.
- Surgical site is the most important predictor of risk for postoperative pulmonary complications: aortic, thoracic, and upper abdominal surgeries are high-risk procedures, even in healthy patients.
- Obstructive sleep apnea and pulmonary hypertension have recently been identified as risk factors, but the limited available evidence does not support preoperative screening for these conditions in patients without symptoms.
- Postoperative continuous positive airway pressure therapy is effective for reducing pulmonary complications in patients who are unable to perform deep breathing or incentive spirometry exercises.
- The jury is out on whether smoking cessation shortly before surgery lowers risk for postoperative pulmonary complications.
Postoperative gastrointestinal tract dysfunction: An overview of causes and management strategies
Tolerance of an enteral diet is one of the fundamental components of postoperative wellness, along with the ability to mobilize freely without supplemental oxygen and a readiness to be discharged home as soon as possible. Accordingly, postoperative gastrointestinal (GI) tract dysfunction is best defined as intolerance of an enteral diet after having been tolerant of one preoperatively. I prefer the term postoperative GI tract dysfunction over postoperative ileus, as ileus is ill defined, covering a wide spectrum of clinical signs and having a range of published incidences so broad (5%–100%) that it defies useful discussion.
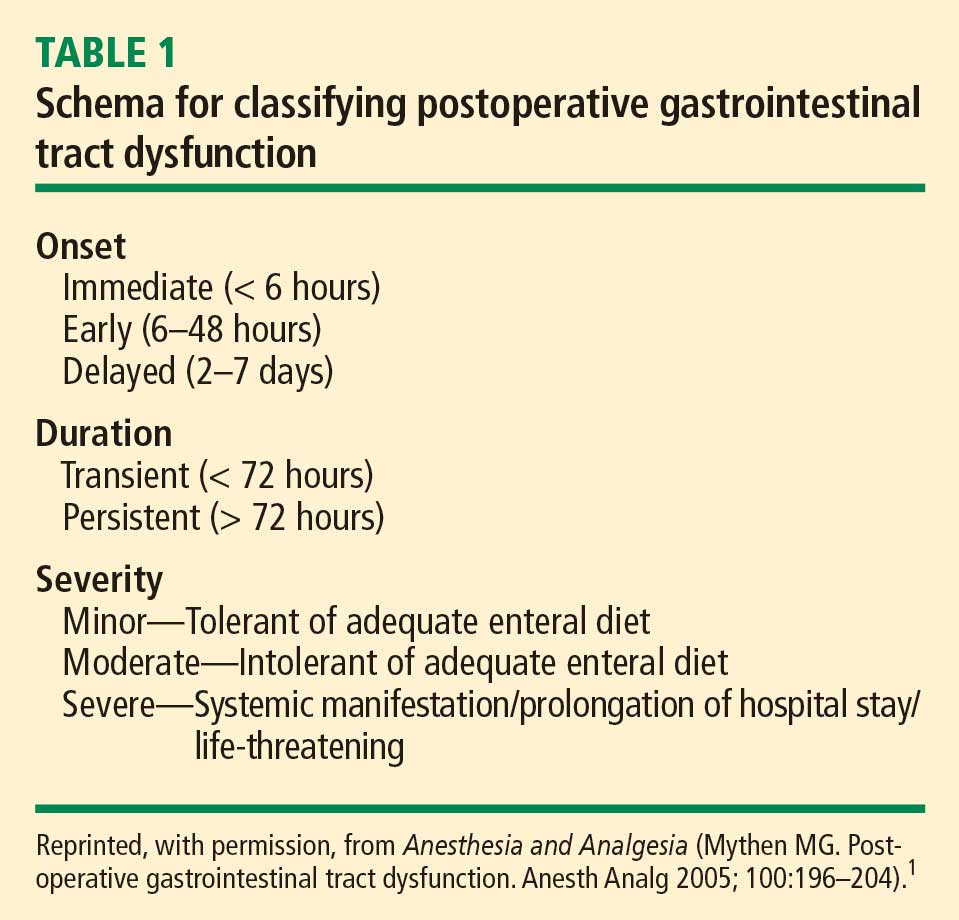
GI DYSFUNCTION: A COMMON POSTOPERATIVE MORBIDITY
Postoperative GI tract dysfunction is common, as illustrated by a large prospective cohort study at Duke University Medical Center3 that used the Postoperative Morbidity Survey (which has since been validated4) to document complications following major noncardiac surgery (ie, anticipated duration > 2 hours and anticipated blood loss > 500 mL). Hospital discharge was delayed in 27% of the study’s 438 patients as a result of a postoperative complication, and GI dysfunction was the most common type of complication overall and on postoperative days 5, 8, and 15. Episodes of GI dysfunction ranged from intolerance of an enteral diet to ischemic gut resulting in multiple organ failure.3
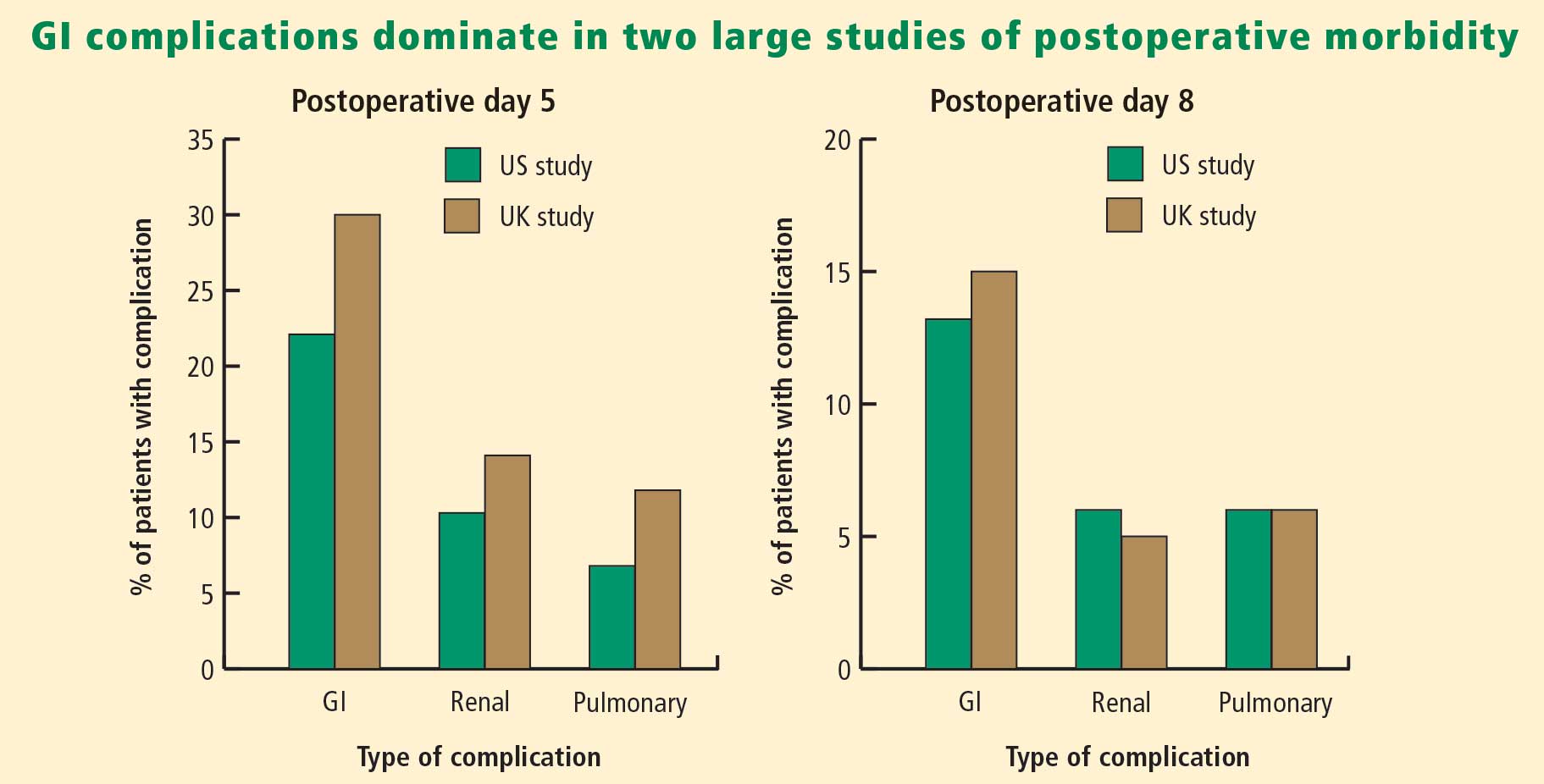
A MULTIFACTORIAL PATHOGENESIS
The pathophysiology of postoperative GI tract dysfunction can be ischemic, metabolic, toxic, neurogenic, myogenic, pharmacologic, or mechanical.
It is important to recognize that in many cases no single factor explains the whole story behind postsurgical GI tract dysfunction, and none of these factors is an ipso facto cause of such dysfunction. For instance, a “mechanical” pathogenesis refers to any manipulation of the gut that causes an inflammatory response in the gut’s various layers, resulting in injury.5,6 However, GI tract dysfunction commonly occurs after operations (including laparoscopic procedures) in which the gut was not handled at all. Similarly, in terms of a pharmacologic pathophysiology, while opioids can affect GI propulsion and cause constipation,7,8 avoidance of opioid use does not ensure prevention of GI tract dysfunction. Moreover, opioid abusers do not generally exhibit intolerance of enteral nutrition.
A common mechanism that is often ignored is perioperative gut ischemia resulting in low-grade injury. Low-grade hypovolemia can cause loss of perfusion to the tip of the microvillus, triggering apoptosis and potentially necrosis, which typically requires about 3 days for recovery. An experiment among 6 healthy volunteers who underwent elective hemorrhage (25% of blood volume removed) over 1 hour demonstrated that gastric tonometry was an earlier indicator of hypovolemia than were commonly measured hemodynamic variables such as invasive blood pressure, stroke volume, heart rate, and lactate and arterial blood gas measurements.9
FLUID LOADING AIDS GI RECOVERY
A targeted increase of intravascular volume and global blood flow perioperatively has been shown repeatedly to improve surgical outcome.10–24 In clinical trials, the most common intervention to achieve the predetermined hemodynamic goal has been fluid loading. Overall, targeted increases in perioperative global blood flow have been associated with reduced mortality,25 with the presumed mechanism being maintenance of end-organ perfusion.
The role of end-organ perfusion maintenance was confirmed in a controlled study of 60 patients undergoing cardiac surgery in which perioperative fluid loading (with colloid) maintained gut perfusion as measured by gastric tonometry, whereas a control group had a reproducible reduction in gut perfusion.15 Fluid loading was associated with a significant reduction in the incidence of gut mucosal hypoperfusion—from 56% to 7%—and significant reductions in the incidence of minor and major complications, mean days in the hospital, and mean days in the intensive care unit.
Fluid type matters
The type of intraoperative fluid loading is a factor in postoperative recovery.
Colloid vs crystalloid. Moretti et al found that colloid (6% hetastarch in saline or 6% hetastarch in balanced salt) was superior to crystalloid (lactated Ringer’s solution) in preventing nausea, severe pain, vomiting, periorbital edema, and double vision postoperatively (P < .05 for all) despite comparable hemodynamic profiles.26
Ringer’s vs normal saline. Williams et al compared intravenous lactated Ringer’s solution with normal saline (0.9% sodium chloride) in a randomized study of healthy volunteers.27 The group that received normal saline demonstrated central nervous system changes and a much higher incidence of abdominal discomfort, a finding consistent with the toxic properties of chlorine to the gut.
Balanced electrolyte solutions vs saline-based fluids. Wilkes et al compared crystalloid and colloid solutions with physiologically balanced electrolyte formulations (Hextend) against saline-based fluids (Hespan) in elderly surgical patients.28 They found that balanced electrolyte solutions were superior in improving gastric mucosal perfusion and preventing hyperchloremic metabolic acidosis. As a result of a reduction in GI tract perfusion, postoperative vomiting was more frequent in the group receiving saline-based fluids.
Evidence for Doppler-guided fluid management
Use of esophageal Doppler ultrasonography to guide fluid administration intraoperatively is fairly common in the United Kingdom and is based on randomized controlled trials showing that Doppler-guided colloid administration to maximize stroke volume reduces morbidity and length of hospital stay in surgical patients. In one government-supported study of 128 colorectal resection patients, Doppler-guided small boluses of colloid increased stroke volume, cardiac output, and oxygen delivery compared with conventional (central venous pressure–based) fluid management.29 Gut function improved significantly faster with Doppler-guided fluid management as evidenced by a more rapid return of flatus, opening of bowels, and achievement of a full diet, and by faster discharge from the hospital. The incidence of GI complications was reduced from 45.3% in the conventional management group to 14.1% in the Doppler group. The relative risk of GI tract dysfunction was 5.3 times higher with conventional management.
OTHER STRATEGIES TO REDUCE POSTOPERATIVE GI DYSFUNCTION
In addition to fluid loading, a number of other methods have been studied in an attempt to reduce the incidence of postoperative GI tract dysfunction.
Epidural neostigmine: Improvement in some measures
Epidural neostigmine was compared with saline control in a randomized study of 45 patients scheduled for abdominal aortic surgery.30 Time to first bowel sounds and time to first flatus were significantly shorter in the neostigmine group, but time to first defecation and the incidence of postoperative complications were similar between the groups.
Laxatives speed return of GI function
In a study of 53 women undergoing fast-track hysterectomy, recovery of GI tract function was faster in those randomized to receive laxatives (magnesium oxide and disodium phosphate) starting 6 hours postoperatively compared with those receiving placebo.31 Median time to first defecation was reduced from 69 hours in the placebo group to 45 hours in the laxative group (P < .0001), and postoperative hospitalization was shortened by a median of 1 day in the laxative group. There were no significant between-group differences in pain scores, postoperative nausea and vomiting, or the use of morphine or antiemetics.
Fentanyl reduces gastric myoelectrical activity
Intravenous administration of the opioid fentanyl significantly reduced gastric myoelectrical activity in an uncontrolled study of 20 patients undergoing elective surgery, but wide variation in effect was observed among patients.32 There was no correlation between the myoelectrical outcome and the presence of polymorphisms of the mu-opioid receptor gene.
Systemic lidocaine accelerates return of bowel function
Perioperative administration of systemic lidocaine, given as a 1.5-mg/kg bolus followed by continuous infusion at 2 mg/min, accelerated the return of bowel function and shortened the length of hospital stay compared with placebo in a randomized study of 60 colorectal surgery patients.33
Early oral feeding cuts length of stay
A recent meta-analysis of randomized trials found that early oral intake of fluids and food after major abdominal gynecologic surgery was associated with an increased risk of nausea but a reduced length of hospital stay.34 The authors recommended an individualized approach to early feeding, and called for cost-effectiveness and patient satisfaction studies.
Mosapride improves gastric emptying
Mosapride is a 5-HT4 agonist that has been shown to improve gastric emptying in a randomized controlled study of 40 patients undergoing laparoscopic colectomy.35 Time to first postoperative bowel movement, time to maximal gastric emptying rate, and postoperative hospital stay were all significantly shorter in patients receiving mosapride versus control. Mosapride is not currently approved for marketing in the United States.
Mu-opioid antagonists: Some show promise, others don’t
Mu-opioid receptor antagonists have been developed primarily to reverse opioid-induced bowel dysfunction. Commercially available drugs in this class include alvimopan, methylnaltrexone, nalbuphine, and naloxone. A recent meta-analysis of 23 randomized controlled studies of these agents for opioid-induced bowel dysfunction concluded that alvimopan and methylnaltrexone were superior to placebo but that evidence was insufficient for the safety or efficacy of naloxone and nalbuphine.36
Nasogastric decompression: Usually more harm than benefit
Prophylactic nasogastric decompression is an intervention devoid of evidence. A meta-analysis of 33 studies encompassing 5,240 patients randomized to routine nasogastric tube placement, selective nasogastric tube use, or no nasogastric tube placement after abdominal surgery found no advantage to routine nasogastric tube use.37 In fact, patients not receiving routine tube placement had a significantly earlier return of bowel function and a significant decrease in pulmonary complications. The incidence of anastomotic leak was not different among the groups. Routine tube use was associated with a lower incidence of vomiting but more patient discomfort. The clear conclusion is that, in most situations, elective placement of a nasogastric tube only causes harm.
Chewing gum: A simple intervention that works
In a recent meta-analysis of five randomized controlled trials, the simple intervention of gum chewing after colorectal surgery significantly accelerated the time to flatus and time to defecation, and was associated with a nonsignificant trend toward a shorter postoperative hospital stay.38
CONCLUSIONS ON MANAGEMENT
Traditional measures intended to reduce the incidence of postoperative GI tract dysfunction—administration of prokinetic drugs, placement of nasogastric tubes, avoidance of food and fluids—are not beneficial and are often harmful. Administration of targeted amounts of fluid to optimize ventricular filling and end-organ perfusion has repeatedly been demonstrated to improve outcomes, particularly those related to GI tract perfusion and function. Administration of larger volumes of colloid, to achieve predetermined increases in stroke volume, improves gut perfusion and reduces the incidence of GI tract dysfunction.
Many simple, inexpensive, and readily available strategies for preventing or reversing postoperative GI tract dysfunction have some degree of evidence-based support and should be considered. I would recommend a multimodal approach that includes a limited surgical incision, regional local anesthesia without use of opioids, immediate postoperative mobilization, early enteral feeding, and postoperative gum chewing.1 Such an approach promises to reduce GI tract dysfunction and other postoperative complications as well as to shorten hospital stay.
DISCUSSION
Question from the audience: You mentioned the selective use of nasogastric tubes. In which patients would you use them?
Dr. Mythen: For upper GI surgeries—esophagectomy, for example—a nasogastric tube is inevitable. Beyond that, the specific indications for tube placement are very limited. At our institution, we no longer place nasogastric tubes following the vast majority of GI tract operations, with esophagectomy being the exception.
Question from the audience: Would you comment on the selective contribution of thoracic epidural analgesia with respect to early feeding after abdominal or colon surgery?
Dr. Mythen: If you’re an enthusiast for thoracic epidurals, you can present the literature in a way that definitively demonstrates a huge advantage to thoracic epidurals. When they work well for the individual, they are fantastic, but you must have a very effective team and system to deliver success to the whole patient population. At our institution the failure rate 20 to 24 hours postoperatively is about 50%.
Question from the audience: I’m an internist and I’ve never heard of the esophageal Doppler-directed fluid bolus protocol—or of anyone using colloids at all. Is that something that is generally practiced in the United States?
Dr. Mythen: Some institutions are practicing goal-directed fluid management now. If you measure stroke volume and give small boluses of colloid, you need a lot less fluid to achieve a higher intravascular volume and goal. At our institution, we’ve repackaged it as “goal-directed fluid restriction” to gain acceptance among surgeons. Uptake has been slower in the United States, though studies here have reinforced the message and been supported by editorials. Guessing about fluids, which we’ve done historically, is not very smart. One thing that differentiates an anesthesiologist from an anesthetic technician is the ability to give goal-directed fluid therapy. The ability to act in a targeted fashion makes it possible to achieve an appropriate physiological goal, but it is more difficult.
Question from the audience: In terms of maintenance fluids and chloride toxicity, is there an alternative to D5 half-normal saline for maintenance fluid?
Dr. Mythen: We don’t have a very good postoperative maintenance fluid; D5 half-normal with some potassium is probably as good as it gets at present. I emphasize getting patients to drink as quickly as possible. If they’re not drinking (not using the GI tract), they need a very high level of physician input because fluid balance is rocket science. The GI tract is very clever. Once patients are drinking and eating, they’re fine, but if they still have an intravenous line in, close attention is required.
Question from the audience: Would you use lactated Ringer’s solution in a patient who is just not eating or drinking?
Dr. Mythen: I do, actually. I tend to mix it in with some D5 half-normal saline because lactated Ringer’s is a great solution. The body can use the lactate to make sugar if necessary. The brain is one of the few organs that will metabolize lactate.
Follow-up question: Would you use it at a lower rate to prevent volume overload?
Dr. Mythen: Yes, at 60 mL/hr. The important thing is that if intravenous fluids are still required, the patient needs to be in a fairly supervised, high-dependency environment. You must address the real issue: Why aren’t they drinking? If the patient is not drinking postoperatively, someone’s done a bad job or there is something that needs fixing.
Question from audience: In the operating room, do you have a preference between albumin and a high-molecular-weight hetastarch like Hextend?
Dr. Mythen: Europe is slightly different in its choice of colloids. We’ve pretty much abandoned the high-molecular-weight starches. We do not use albumin at our institution for cost reasons, and we can’t find any evidence to support its use. We would have to close one intensive care unit bed to be able to afford using albumin. We use low-molecular-weight hydroxyethyl starches, which I believe are now coming into the United States. They have no major coagulation effect.
- Mythen MG. Postoperative gastrointestinal tract dysfunction. Anesth Analg 2005; 100:196–204.
- Gan TJ, Meyer T, Apfel CC, et al. Consensus guidelines for managing postoperative nausea and vomiting. Anesth Analg 2003; 97:62–71.
- Bennett-Guerrero E, Welsby I, Dunn TJ, et al. The use of a postoperative morbidity survey to evaluate patients with prolonged hospitalization after routine, moderate-risk, elective surgery. Anesth Analg 1999; 89:514–519.
- Grocott MP, Browne JP, Van der Meulen J, et al. The Postoperative Morbidity Survey was validated and used to describe morbidity after major surgery. J Clin Epidemiol 2007; 60:919–928.
- Kalff JC, Schraut WH, Simmons RL, Bauer AJ. Surgical manipulation of the gut elicits an intestinal muscularis inflammatory response resulting in postsurgical ileus. Ann Surg 1998; 228:652–663.
- Schwarz NT, Beer-Stolz D, Simmons RL, Bauer AJ. Pathogenesis of paralytic ileus: intestinal manipulation opens a transient pathway between the intestinal lumen and the leukocytic infiltrate of the jejunal muscularis. Ann Surg 2002; 235:31–40.
- Manara L, Bianchetti A. The central and peripheral influences of opioids on gastrointestinal propulsion. Annu Rev Pharmacol Toxicol 1985; 25:249–273.
- Manara L, Bianchi G, Ferretti P, Tavani A. Inhibition of gastrointestinal transit by morphine in rats results primarily from direct drug action on gut opioid sites. J Pharmacol Exp Ther 1986; 237:945–949.
- Hamilton-Davies C, Mythen MG, Salmon JB, et al. Comparison of commonly used clinical indicators of hypovolaemia with gastrointestinal tonometry. Intensive Care Med 1997; 23:276–281.
- Bender JS, Smith-Meek MA, Jones CE. Routine pulmonary artery catheterization does not reduce morbidity and mortality of elective vascular surgery: results of a prospective, randomized trial. Ann Surg 1997; 226:229–237.
- Berlauk JF, Abrams JH, Gilmour IJ, et al. Preoperative optimization of cardiovascular hemodynamics improves outcome in peripheral vascular surgery: a prospective, randomized clinical trial. Ann Surg 1991; 214:289–299.
- Boyd O, Grounds RM, Bennett ED. A randomized clinical trial of the effect of deliberate perioperative increase of oxygen delivery on mortality in high-risk surgical patients. JAMA 1993; 270:2699–2707.
- Gan TJ, Soppitt A, Maroof M, et al. Goal-directed intraoperative fluid administration reduces length of hospital stay after major surgery. Anesthesiology 2002; 97:820–826.
- Lobo SM, Salgado PF, Castillo VG, et al. Effects of maximizing oxygen delivery on morbidity and mortality in high-risk surgical patients. Crit Care Med 2000; 28:3396–3404.
- Mythen MG, Webb AR. Perioperative plasma volume expansion reduces the incidence of gut mucosal hypoperfusion during cardiac surgery. Arch Surg 1995; 130:423–429.
- Pölönen P, Ruokonen E, Hippeläinen M, Pöyhönen M, Takala J. A prospective, randomized study of goal-oriented hemodynamic therapy in cardiac surgical patients. Anesth Analg 2000; 90:1052–1059.
- Sandham JD, Hull RD, Brant RF, et al. A randomized, controlled trial of the use of pulmonary-artery catheters in high-risk surgical patients. N Engl J Med 2003; 348:5–14.
- Shoemaker WC, Appel PL, Kram HB, Nathan RC, Thompson JL. Multicomponent noninvasive physiologic monitoring of circulatory function. Crit Care Med 1988; 16:482–490.
- Sinclair S, James S, Singer M. Intraoperative intravascular volume optimisation and length of hospital stay after repair of proximal femoral fracture: randomised controlled trial. BMJ 1997; 315:909–912.
- Ueno S, Tanabe G, Yamada H, et al. Response of patients with cirrhosis who have undergone partial hepatectomy to treatment aimed at achieving supranormal oxygen delivery and consumption. Surgery 1998; 123:278–286.
- Valentine RJ, Duke ML, Inman MH, et al. Effectiveness of pulmonary artery catheters in aortic surgery: a randomized trial. J Vasc Surg 1998; 27:203–212.
- Venn R, Steele A, Richardson P, Poloniecki J, Grounds M, Newman P. Randomized controlled trial to investigate influence of the fluid challenge on duration of hospital stay and perioperative morbidity in patients with hip fractures. Br J Anaesth 2002; 88:65–71.
- Wilson J, Woods I, Fawcett J, et al. Reducing the risk of major elective surgery: randomised controlled trial of preoperative optimisation of oxygen delivery. BMJ 1999; 318:1099–1103.
- Ziegler DW, Wright JG, Choban PS, Flancbaum L. A prospective randomized trial of preoperative “optimization” of cardiac function in patients undergoing elective peripheral vascular surgery. Surgery 1997; 122:584–592.
- Grocott MPW, Hamilton MA, Bennett ED, Harrison D, Rowan K. Perioperative increase in global blood flow to explicit defined goals and outcomes following surgery. Cochrane Database Syst Rev 2006; 2:CD004082. doi:10.1002/14651858.CD004082.pub4.
- Moretti EW, Robertson KM, El-Moalem H, Gan TJ. Intraoperative colloid administration reduces postoperative nausea and vomiting and improves postoperative outcomes compared with crystalloid administration. Anesth Analg 2003; 96:611–617.
- Williams EL, Hildebrand KL, McCormick SA, Bedel MJ. The effect of intravenous lactated Ringer’s solution versus 0.9% sodium chloride solution on serum osmolality in human volunteers. Anesth Analg 1999; 88:999–1003.
- Wilkes NJ, Woolf R, Mutch M, et al. The effects of balanced versus saline-based hetastarch and crystalloid solutions on acid-base and electrolyte status and gastric mucosal perfusion in elderly surgical patients. Anesth Analg 2001; 93:811–816.
- Wakeling HG, McFall MR, Jenkins CS, et al. Intraoperative oesophageal Doppler guided fluid management shortens postoperative hospital stay after major bowel surgery. Br J Anaesth 2005; 95:634–642.
- Caliskan E, Turkoz A, Sener M, et al. A prospective randomized double-blind study to determine the effect of thoracic epidural neostigmine on postoperative ileus after abdominal aortic surgery. Anesth Analg 2008; 106:959–964.
- Hansen CT, Sørensen M, Møller C, Ottesen B, Kehlet H. Effect of laxatives on gastrointestinal functional recovery in fast-track hysterectomy: a double-blind, placebo-controlled randomized study. Am J Obstet Gynecol 2007; 196:311.e1–311.e7.
- Walldén J, Lindberg G, Sandin M, Thörn SE, Wattwil M. Effects of fentanyl on gastric myoelectrical activity: a possible association with polymorphisms of the mu-opioid receptor gene? Acta Anaesthesiol Scand 2008; 52:708–715.
- Herroeder S, Pecher S, Schönherr ME, et al. Systemic lidocaine shortens length of hospital stay after colorectal surgery: a double-blinded, randomized, placebo-controlled trial. Ann Surg 2007; 246:192–200.
- Charoenkwan K, Phillipson G, Vutyavanich T. Early versus delayed oral fluids and food for reducing complications after major abdominal gynaecologic surgery. Cochrane Database Syst Rev 2007; 4:CD004508. doi:10.1002/14651858.CD004508.pub3.
- Narita K, Tsunoda A, Takenaka K, et al. Effect of mosapride on recovery of intestinal motility after hand-assisted laparoscopic colectomy for carcinoma. Dis Colon Rectum 2008; 51:1692–1695.
- McNicol ED, Boyce D, Schumann R, Carr DB. Mu-opioid antagonists for opioid-induced bowel dysfunction. Cochrane Database Syst Rev 2008; 2:CD006332. doi:10.1002/14651858.CD006332.pub2.
- Nelson RL, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominal surgery. Cochrane Database Syst Rev 2007; 3:CD004929. doi:10.1002/14651858.CD004929.pub3.
- de Castro SM, van den Esschert JW, van Heek NT, et al. A systematic review of the efficacy of gum chewing for the amelioration of postoperative ileus. Dig Surg 2008; 25:39–45.
Tolerance of an enteral diet is one of the fundamental components of postoperative wellness, along with the ability to mobilize freely without supplemental oxygen and a readiness to be discharged home as soon as possible. Accordingly, postoperative gastrointestinal (GI) tract dysfunction is best defined as intolerance of an enteral diet after having been tolerant of one preoperatively. I prefer the term postoperative GI tract dysfunction over postoperative ileus, as ileus is ill defined, covering a wide spectrum of clinical signs and having a range of published incidences so broad (5%–100%) that it defies useful discussion.
GI DYSFUNCTION: A COMMON POSTOPERATIVE MORBIDITY
Postoperative GI tract dysfunction is common, as illustrated by a large prospective cohort study at Duke University Medical Center3 that used the Postoperative Morbidity Survey (which has since been validated4) to document complications following major noncardiac surgery (ie, anticipated duration > 2 hours and anticipated blood loss > 500 mL). Hospital discharge was delayed in 27% of the study’s 438 patients as a result of a postoperative complication, and GI dysfunction was the most common type of complication overall and on postoperative days 5, 8, and 15. Episodes of GI dysfunction ranged from intolerance of an enteral diet to ischemic gut resulting in multiple organ failure.3
A MULTIFACTORIAL PATHOGENESIS
The pathophysiology of postoperative GI tract dysfunction can be ischemic, metabolic, toxic, neurogenic, myogenic, pharmacologic, or mechanical.
It is important to recognize that in many cases no single factor explains the whole story behind postsurgical GI tract dysfunction, and none of these factors is an ipso facto cause of such dysfunction. For instance, a “mechanical” pathogenesis refers to any manipulation of the gut that causes an inflammatory response in the gut’s various layers, resulting in injury.5,6 However, GI tract dysfunction commonly occurs after operations (including laparoscopic procedures) in which the gut was not handled at all. Similarly, in terms of a pharmacologic pathophysiology, while opioids can affect GI propulsion and cause constipation,7,8 avoidance of opioid use does not ensure prevention of GI tract dysfunction. Moreover, opioid abusers do not generally exhibit intolerance of enteral nutrition.
A common mechanism that is often ignored is perioperative gut ischemia resulting in low-grade injury. Low-grade hypovolemia can cause loss of perfusion to the tip of the microvillus, triggering apoptosis and potentially necrosis, which typically requires about 3 days for recovery. An experiment among 6 healthy volunteers who underwent elective hemorrhage (25% of blood volume removed) over 1 hour demonstrated that gastric tonometry was an earlier indicator of hypovolemia than were commonly measured hemodynamic variables such as invasive blood pressure, stroke volume, heart rate, and lactate and arterial blood gas measurements.9
FLUID LOADING AIDS GI RECOVERY
A targeted increase of intravascular volume and global blood flow perioperatively has been shown repeatedly to improve surgical outcome.10–24 In clinical trials, the most common intervention to achieve the predetermined hemodynamic goal has been fluid loading. Overall, targeted increases in perioperative global blood flow have been associated with reduced mortality,25 with the presumed mechanism being maintenance of end-organ perfusion.
The role of end-organ perfusion maintenance was confirmed in a controlled study of 60 patients undergoing cardiac surgery in which perioperative fluid loading (with colloid) maintained gut perfusion as measured by gastric tonometry, whereas a control group had a reproducible reduction in gut perfusion.15 Fluid loading was associated with a significant reduction in the incidence of gut mucosal hypoperfusion—from 56% to 7%—and significant reductions in the incidence of minor and major complications, mean days in the hospital, and mean days in the intensive care unit.
Fluid type matters
The type of intraoperative fluid loading is a factor in postoperative recovery.
Colloid vs crystalloid. Moretti et al found that colloid (6% hetastarch in saline or 6% hetastarch in balanced salt) was superior to crystalloid (lactated Ringer’s solution) in preventing nausea, severe pain, vomiting, periorbital edema, and double vision postoperatively (P < .05 for all) despite comparable hemodynamic profiles.26
Ringer’s vs normal saline. Williams et al compared intravenous lactated Ringer’s solution with normal saline (0.9% sodium chloride) in a randomized study of healthy volunteers.27 The group that received normal saline demonstrated central nervous system changes and a much higher incidence of abdominal discomfort, a finding consistent with the toxic properties of chlorine to the gut.
Balanced electrolyte solutions vs saline-based fluids. Wilkes et al compared crystalloid and colloid solutions with physiologically balanced electrolyte formulations (Hextend) against saline-based fluids (Hespan) in elderly surgical patients.28 They found that balanced electrolyte solutions were superior in improving gastric mucosal perfusion and preventing hyperchloremic metabolic acidosis. As a result of a reduction in GI tract perfusion, postoperative vomiting was more frequent in the group receiving saline-based fluids.
Evidence for Doppler-guided fluid management
Use of esophageal Doppler ultrasonography to guide fluid administration intraoperatively is fairly common in the United Kingdom and is based on randomized controlled trials showing that Doppler-guided colloid administration to maximize stroke volume reduces morbidity and length of hospital stay in surgical patients. In one government-supported study of 128 colorectal resection patients, Doppler-guided small boluses of colloid increased stroke volume, cardiac output, and oxygen delivery compared with conventional (central venous pressure–based) fluid management.29 Gut function improved significantly faster with Doppler-guided fluid management as evidenced by a more rapid return of flatus, opening of bowels, and achievement of a full diet, and by faster discharge from the hospital. The incidence of GI complications was reduced from 45.3% in the conventional management group to 14.1% in the Doppler group. The relative risk of GI tract dysfunction was 5.3 times higher with conventional management.
OTHER STRATEGIES TO REDUCE POSTOPERATIVE GI DYSFUNCTION
In addition to fluid loading, a number of other methods have been studied in an attempt to reduce the incidence of postoperative GI tract dysfunction.
Epidural neostigmine: Improvement in some measures
Epidural neostigmine was compared with saline control in a randomized study of 45 patients scheduled for abdominal aortic surgery.30 Time to first bowel sounds and time to first flatus were significantly shorter in the neostigmine group, but time to first defecation and the incidence of postoperative complications were similar between the groups.
Laxatives speed return of GI function
In a study of 53 women undergoing fast-track hysterectomy, recovery of GI tract function was faster in those randomized to receive laxatives (magnesium oxide and disodium phosphate) starting 6 hours postoperatively compared with those receiving placebo.31 Median time to first defecation was reduced from 69 hours in the placebo group to 45 hours in the laxative group (P < .0001), and postoperative hospitalization was shortened by a median of 1 day in the laxative group. There were no significant between-group differences in pain scores, postoperative nausea and vomiting, or the use of morphine or antiemetics.
Fentanyl reduces gastric myoelectrical activity
Intravenous administration of the opioid fentanyl significantly reduced gastric myoelectrical activity in an uncontrolled study of 20 patients undergoing elective surgery, but wide variation in effect was observed among patients.32 There was no correlation between the myoelectrical outcome and the presence of polymorphisms of the mu-opioid receptor gene.
Systemic lidocaine accelerates return of bowel function
Perioperative administration of systemic lidocaine, given as a 1.5-mg/kg bolus followed by continuous infusion at 2 mg/min, accelerated the return of bowel function and shortened the length of hospital stay compared with placebo in a randomized study of 60 colorectal surgery patients.33
Early oral feeding cuts length of stay
A recent meta-analysis of randomized trials found that early oral intake of fluids and food after major abdominal gynecologic surgery was associated with an increased risk of nausea but a reduced length of hospital stay.34 The authors recommended an individualized approach to early feeding, and called for cost-effectiveness and patient satisfaction studies.
Mosapride improves gastric emptying
Mosapride is a 5-HT4 agonist that has been shown to improve gastric emptying in a randomized controlled study of 40 patients undergoing laparoscopic colectomy.35 Time to first postoperative bowel movement, time to maximal gastric emptying rate, and postoperative hospital stay were all significantly shorter in patients receiving mosapride versus control. Mosapride is not currently approved for marketing in the United States.
Mu-opioid antagonists: Some show promise, others don’t
Mu-opioid receptor antagonists have been developed primarily to reverse opioid-induced bowel dysfunction. Commercially available drugs in this class include alvimopan, methylnaltrexone, nalbuphine, and naloxone. A recent meta-analysis of 23 randomized controlled studies of these agents for opioid-induced bowel dysfunction concluded that alvimopan and methylnaltrexone were superior to placebo but that evidence was insufficient for the safety or efficacy of naloxone and nalbuphine.36
Nasogastric decompression: Usually more harm than benefit
Prophylactic nasogastric decompression is an intervention devoid of evidence. A meta-analysis of 33 studies encompassing 5,240 patients randomized to routine nasogastric tube placement, selective nasogastric tube use, or no nasogastric tube placement after abdominal surgery found no advantage to routine nasogastric tube use.37 In fact, patients not receiving routine tube placement had a significantly earlier return of bowel function and a significant decrease in pulmonary complications. The incidence of anastomotic leak was not different among the groups. Routine tube use was associated with a lower incidence of vomiting but more patient discomfort. The clear conclusion is that, in most situations, elective placement of a nasogastric tube only causes harm.
Chewing gum: A simple intervention that works
In a recent meta-analysis of five randomized controlled trials, the simple intervention of gum chewing after colorectal surgery significantly accelerated the time to flatus and time to defecation, and was associated with a nonsignificant trend toward a shorter postoperative hospital stay.38
CONCLUSIONS ON MANAGEMENT
Traditional measures intended to reduce the incidence of postoperative GI tract dysfunction—administration of prokinetic drugs, placement of nasogastric tubes, avoidance of food and fluids—are not beneficial and are often harmful. Administration of targeted amounts of fluid to optimize ventricular filling and end-organ perfusion has repeatedly been demonstrated to improve outcomes, particularly those related to GI tract perfusion and function. Administration of larger volumes of colloid, to achieve predetermined increases in stroke volume, improves gut perfusion and reduces the incidence of GI tract dysfunction.
Many simple, inexpensive, and readily available strategies for preventing or reversing postoperative GI tract dysfunction have some degree of evidence-based support and should be considered. I would recommend a multimodal approach that includes a limited surgical incision, regional local anesthesia without use of opioids, immediate postoperative mobilization, early enteral feeding, and postoperative gum chewing.1 Such an approach promises to reduce GI tract dysfunction and other postoperative complications as well as to shorten hospital stay.
DISCUSSION
Question from the audience: You mentioned the selective use of nasogastric tubes. In which patients would you use them?
Dr. Mythen: For upper GI surgeries—esophagectomy, for example—a nasogastric tube is inevitable. Beyond that, the specific indications for tube placement are very limited. At our institution, we no longer place nasogastric tubes following the vast majority of GI tract operations, with esophagectomy being the exception.
Question from the audience: Would you comment on the selective contribution of thoracic epidural analgesia with respect to early feeding after abdominal or colon surgery?
Dr. Mythen: If you’re an enthusiast for thoracic epidurals, you can present the literature in a way that definitively demonstrates a huge advantage to thoracic epidurals. When they work well for the individual, they are fantastic, but you must have a very effective team and system to deliver success to the whole patient population. At our institution the failure rate 20 to 24 hours postoperatively is about 50%.
Question from the audience: I’m an internist and I’ve never heard of the esophageal Doppler-directed fluid bolus protocol—or of anyone using colloids at all. Is that something that is generally practiced in the United States?
Dr. Mythen: Some institutions are practicing goal-directed fluid management now. If you measure stroke volume and give small boluses of colloid, you need a lot less fluid to achieve a higher intravascular volume and goal. At our institution, we’ve repackaged it as “goal-directed fluid restriction” to gain acceptance among surgeons. Uptake has been slower in the United States, though studies here have reinforced the message and been supported by editorials. Guessing about fluids, which we’ve done historically, is not very smart. One thing that differentiates an anesthesiologist from an anesthetic technician is the ability to give goal-directed fluid therapy. The ability to act in a targeted fashion makes it possible to achieve an appropriate physiological goal, but it is more difficult.
Question from the audience: In terms of maintenance fluids and chloride toxicity, is there an alternative to D5 half-normal saline for maintenance fluid?
Dr. Mythen: We don’t have a very good postoperative maintenance fluid; D5 half-normal with some potassium is probably as good as it gets at present. I emphasize getting patients to drink as quickly as possible. If they’re not drinking (not using the GI tract), they need a very high level of physician input because fluid balance is rocket science. The GI tract is very clever. Once patients are drinking and eating, they’re fine, but if they still have an intravenous line in, close attention is required.
Question from the audience: Would you use lactated Ringer’s solution in a patient who is just not eating or drinking?
Dr. Mythen: I do, actually. I tend to mix it in with some D5 half-normal saline because lactated Ringer’s is a great solution. The body can use the lactate to make sugar if necessary. The brain is one of the few organs that will metabolize lactate.
Follow-up question: Would you use it at a lower rate to prevent volume overload?
Dr. Mythen: Yes, at 60 mL/hr. The important thing is that if intravenous fluids are still required, the patient needs to be in a fairly supervised, high-dependency environment. You must address the real issue: Why aren’t they drinking? If the patient is not drinking postoperatively, someone’s done a bad job or there is something that needs fixing.
Question from audience: In the operating room, do you have a preference between albumin and a high-molecular-weight hetastarch like Hextend?
Dr. Mythen: Europe is slightly different in its choice of colloids. We’ve pretty much abandoned the high-molecular-weight starches. We do not use albumin at our institution for cost reasons, and we can’t find any evidence to support its use. We would have to close one intensive care unit bed to be able to afford using albumin. We use low-molecular-weight hydroxyethyl starches, which I believe are now coming into the United States. They have no major coagulation effect.
Tolerance of an enteral diet is one of the fundamental components of postoperative wellness, along with the ability to mobilize freely without supplemental oxygen and a readiness to be discharged home as soon as possible. Accordingly, postoperative gastrointestinal (GI) tract dysfunction is best defined as intolerance of an enteral diet after having been tolerant of one preoperatively. I prefer the term postoperative GI tract dysfunction over postoperative ileus, as ileus is ill defined, covering a wide spectrum of clinical signs and having a range of published incidences so broad (5%–100%) that it defies useful discussion.
GI DYSFUNCTION: A COMMON POSTOPERATIVE MORBIDITY
Postoperative GI tract dysfunction is common, as illustrated by a large prospective cohort study at Duke University Medical Center3 that used the Postoperative Morbidity Survey (which has since been validated4) to document complications following major noncardiac surgery (ie, anticipated duration > 2 hours and anticipated blood loss > 500 mL). Hospital discharge was delayed in 27% of the study’s 438 patients as a result of a postoperative complication, and GI dysfunction was the most common type of complication overall and on postoperative days 5, 8, and 15. Episodes of GI dysfunction ranged from intolerance of an enteral diet to ischemic gut resulting in multiple organ failure.3
A MULTIFACTORIAL PATHOGENESIS
The pathophysiology of postoperative GI tract dysfunction can be ischemic, metabolic, toxic, neurogenic, myogenic, pharmacologic, or mechanical.
It is important to recognize that in many cases no single factor explains the whole story behind postsurgical GI tract dysfunction, and none of these factors is an ipso facto cause of such dysfunction. For instance, a “mechanical” pathogenesis refers to any manipulation of the gut that causes an inflammatory response in the gut’s various layers, resulting in injury.5,6 However, GI tract dysfunction commonly occurs after operations (including laparoscopic procedures) in which the gut was not handled at all. Similarly, in terms of a pharmacologic pathophysiology, while opioids can affect GI propulsion and cause constipation,7,8 avoidance of opioid use does not ensure prevention of GI tract dysfunction. Moreover, opioid abusers do not generally exhibit intolerance of enteral nutrition.
A common mechanism that is often ignored is perioperative gut ischemia resulting in low-grade injury. Low-grade hypovolemia can cause loss of perfusion to the tip of the microvillus, triggering apoptosis and potentially necrosis, which typically requires about 3 days for recovery. An experiment among 6 healthy volunteers who underwent elective hemorrhage (25% of blood volume removed) over 1 hour demonstrated that gastric tonometry was an earlier indicator of hypovolemia than were commonly measured hemodynamic variables such as invasive blood pressure, stroke volume, heart rate, and lactate and arterial blood gas measurements.9
FLUID LOADING AIDS GI RECOVERY
A targeted increase of intravascular volume and global blood flow perioperatively has been shown repeatedly to improve surgical outcome.10–24 In clinical trials, the most common intervention to achieve the predetermined hemodynamic goal has been fluid loading. Overall, targeted increases in perioperative global blood flow have been associated with reduced mortality,25 with the presumed mechanism being maintenance of end-organ perfusion.
The role of end-organ perfusion maintenance was confirmed in a controlled study of 60 patients undergoing cardiac surgery in which perioperative fluid loading (with colloid) maintained gut perfusion as measured by gastric tonometry, whereas a control group had a reproducible reduction in gut perfusion.15 Fluid loading was associated with a significant reduction in the incidence of gut mucosal hypoperfusion—from 56% to 7%—and significant reductions in the incidence of minor and major complications, mean days in the hospital, and mean days in the intensive care unit.
Fluid type matters
The type of intraoperative fluid loading is a factor in postoperative recovery.
Colloid vs crystalloid. Moretti et al found that colloid (6% hetastarch in saline or 6% hetastarch in balanced salt) was superior to crystalloid (lactated Ringer’s solution) in preventing nausea, severe pain, vomiting, periorbital edema, and double vision postoperatively (P < .05 for all) despite comparable hemodynamic profiles.26
Ringer’s vs normal saline. Williams et al compared intravenous lactated Ringer’s solution with normal saline (0.9% sodium chloride) in a randomized study of healthy volunteers.27 The group that received normal saline demonstrated central nervous system changes and a much higher incidence of abdominal discomfort, a finding consistent with the toxic properties of chlorine to the gut.
Balanced electrolyte solutions vs saline-based fluids. Wilkes et al compared crystalloid and colloid solutions with physiologically balanced electrolyte formulations (Hextend) against saline-based fluids (Hespan) in elderly surgical patients.28 They found that balanced electrolyte solutions were superior in improving gastric mucosal perfusion and preventing hyperchloremic metabolic acidosis. As a result of a reduction in GI tract perfusion, postoperative vomiting was more frequent in the group receiving saline-based fluids.
Evidence for Doppler-guided fluid management
Use of esophageal Doppler ultrasonography to guide fluid administration intraoperatively is fairly common in the United Kingdom and is based on randomized controlled trials showing that Doppler-guided colloid administration to maximize stroke volume reduces morbidity and length of hospital stay in surgical patients. In one government-supported study of 128 colorectal resection patients, Doppler-guided small boluses of colloid increased stroke volume, cardiac output, and oxygen delivery compared with conventional (central venous pressure–based) fluid management.29 Gut function improved significantly faster with Doppler-guided fluid management as evidenced by a more rapid return of flatus, opening of bowels, and achievement of a full diet, and by faster discharge from the hospital. The incidence of GI complications was reduced from 45.3% in the conventional management group to 14.1% in the Doppler group. The relative risk of GI tract dysfunction was 5.3 times higher with conventional management.
OTHER STRATEGIES TO REDUCE POSTOPERATIVE GI DYSFUNCTION
In addition to fluid loading, a number of other methods have been studied in an attempt to reduce the incidence of postoperative GI tract dysfunction.
Epidural neostigmine: Improvement in some measures
Epidural neostigmine was compared with saline control in a randomized study of 45 patients scheduled for abdominal aortic surgery.30 Time to first bowel sounds and time to first flatus were significantly shorter in the neostigmine group, but time to first defecation and the incidence of postoperative complications were similar between the groups.
Laxatives speed return of GI function
In a study of 53 women undergoing fast-track hysterectomy, recovery of GI tract function was faster in those randomized to receive laxatives (magnesium oxide and disodium phosphate) starting 6 hours postoperatively compared with those receiving placebo.31 Median time to first defecation was reduced from 69 hours in the placebo group to 45 hours in the laxative group (P < .0001), and postoperative hospitalization was shortened by a median of 1 day in the laxative group. There were no significant between-group differences in pain scores, postoperative nausea and vomiting, or the use of morphine or antiemetics.
Fentanyl reduces gastric myoelectrical activity
Intravenous administration of the opioid fentanyl significantly reduced gastric myoelectrical activity in an uncontrolled study of 20 patients undergoing elective surgery, but wide variation in effect was observed among patients.32 There was no correlation between the myoelectrical outcome and the presence of polymorphisms of the mu-opioid receptor gene.
Systemic lidocaine accelerates return of bowel function
Perioperative administration of systemic lidocaine, given as a 1.5-mg/kg bolus followed by continuous infusion at 2 mg/min, accelerated the return of bowel function and shortened the length of hospital stay compared with placebo in a randomized study of 60 colorectal surgery patients.33
Early oral feeding cuts length of stay
A recent meta-analysis of randomized trials found that early oral intake of fluids and food after major abdominal gynecologic surgery was associated with an increased risk of nausea but a reduced length of hospital stay.34 The authors recommended an individualized approach to early feeding, and called for cost-effectiveness and patient satisfaction studies.
Mosapride improves gastric emptying
Mosapride is a 5-HT4 agonist that has been shown to improve gastric emptying in a randomized controlled study of 40 patients undergoing laparoscopic colectomy.35 Time to first postoperative bowel movement, time to maximal gastric emptying rate, and postoperative hospital stay were all significantly shorter in patients receiving mosapride versus control. Mosapride is not currently approved for marketing in the United States.
Mu-opioid antagonists: Some show promise, others don’t
Mu-opioid receptor antagonists have been developed primarily to reverse opioid-induced bowel dysfunction. Commercially available drugs in this class include alvimopan, methylnaltrexone, nalbuphine, and naloxone. A recent meta-analysis of 23 randomized controlled studies of these agents for opioid-induced bowel dysfunction concluded that alvimopan and methylnaltrexone were superior to placebo but that evidence was insufficient for the safety or efficacy of naloxone and nalbuphine.36
Nasogastric decompression: Usually more harm than benefit
Prophylactic nasogastric decompression is an intervention devoid of evidence. A meta-analysis of 33 studies encompassing 5,240 patients randomized to routine nasogastric tube placement, selective nasogastric tube use, or no nasogastric tube placement after abdominal surgery found no advantage to routine nasogastric tube use.37 In fact, patients not receiving routine tube placement had a significantly earlier return of bowel function and a significant decrease in pulmonary complications. The incidence of anastomotic leak was not different among the groups. Routine tube use was associated with a lower incidence of vomiting but more patient discomfort. The clear conclusion is that, in most situations, elective placement of a nasogastric tube only causes harm.
Chewing gum: A simple intervention that works
In a recent meta-analysis of five randomized controlled trials, the simple intervention of gum chewing after colorectal surgery significantly accelerated the time to flatus and time to defecation, and was associated with a nonsignificant trend toward a shorter postoperative hospital stay.38
CONCLUSIONS ON MANAGEMENT
Traditional measures intended to reduce the incidence of postoperative GI tract dysfunction—administration of prokinetic drugs, placement of nasogastric tubes, avoidance of food and fluids—are not beneficial and are often harmful. Administration of targeted amounts of fluid to optimize ventricular filling and end-organ perfusion has repeatedly been demonstrated to improve outcomes, particularly those related to GI tract perfusion and function. Administration of larger volumes of colloid, to achieve predetermined increases in stroke volume, improves gut perfusion and reduces the incidence of GI tract dysfunction.
Many simple, inexpensive, and readily available strategies for preventing or reversing postoperative GI tract dysfunction have some degree of evidence-based support and should be considered. I would recommend a multimodal approach that includes a limited surgical incision, regional local anesthesia without use of opioids, immediate postoperative mobilization, early enteral feeding, and postoperative gum chewing.1 Such an approach promises to reduce GI tract dysfunction and other postoperative complications as well as to shorten hospital stay.
DISCUSSION
Question from the audience: You mentioned the selective use of nasogastric tubes. In which patients would you use them?
Dr. Mythen: For upper GI surgeries—esophagectomy, for example—a nasogastric tube is inevitable. Beyond that, the specific indications for tube placement are very limited. At our institution, we no longer place nasogastric tubes following the vast majority of GI tract operations, with esophagectomy being the exception.
Question from the audience: Would you comment on the selective contribution of thoracic epidural analgesia with respect to early feeding after abdominal or colon surgery?
Dr. Mythen: If you’re an enthusiast for thoracic epidurals, you can present the literature in a way that definitively demonstrates a huge advantage to thoracic epidurals. When they work well for the individual, they are fantastic, but you must have a very effective team and system to deliver success to the whole patient population. At our institution the failure rate 20 to 24 hours postoperatively is about 50%.
Question from the audience: I’m an internist and I’ve never heard of the esophageal Doppler-directed fluid bolus protocol—or of anyone using colloids at all. Is that something that is generally practiced in the United States?
Dr. Mythen: Some institutions are practicing goal-directed fluid management now. If you measure stroke volume and give small boluses of colloid, you need a lot less fluid to achieve a higher intravascular volume and goal. At our institution, we’ve repackaged it as “goal-directed fluid restriction” to gain acceptance among surgeons. Uptake has been slower in the United States, though studies here have reinforced the message and been supported by editorials. Guessing about fluids, which we’ve done historically, is not very smart. One thing that differentiates an anesthesiologist from an anesthetic technician is the ability to give goal-directed fluid therapy. The ability to act in a targeted fashion makes it possible to achieve an appropriate physiological goal, but it is more difficult.
Question from the audience: In terms of maintenance fluids and chloride toxicity, is there an alternative to D5 half-normal saline for maintenance fluid?
Dr. Mythen: We don’t have a very good postoperative maintenance fluid; D5 half-normal with some potassium is probably as good as it gets at present. I emphasize getting patients to drink as quickly as possible. If they’re not drinking (not using the GI tract), they need a very high level of physician input because fluid balance is rocket science. The GI tract is very clever. Once patients are drinking and eating, they’re fine, but if they still have an intravenous line in, close attention is required.
Question from the audience: Would you use lactated Ringer’s solution in a patient who is just not eating or drinking?
Dr. Mythen: I do, actually. I tend to mix it in with some D5 half-normal saline because lactated Ringer’s is a great solution. The body can use the lactate to make sugar if necessary. The brain is one of the few organs that will metabolize lactate.
Follow-up question: Would you use it at a lower rate to prevent volume overload?
Dr. Mythen: Yes, at 60 mL/hr. The important thing is that if intravenous fluids are still required, the patient needs to be in a fairly supervised, high-dependency environment. You must address the real issue: Why aren’t they drinking? If the patient is not drinking postoperatively, someone’s done a bad job or there is something that needs fixing.
Question from audience: In the operating room, do you have a preference between albumin and a high-molecular-weight hetastarch like Hextend?
Dr. Mythen: Europe is slightly different in its choice of colloids. We’ve pretty much abandoned the high-molecular-weight starches. We do not use albumin at our institution for cost reasons, and we can’t find any evidence to support its use. We would have to close one intensive care unit bed to be able to afford using albumin. We use low-molecular-weight hydroxyethyl starches, which I believe are now coming into the United States. They have no major coagulation effect.
- Mythen MG. Postoperative gastrointestinal tract dysfunction. Anesth Analg 2005; 100:196–204.
- Gan TJ, Meyer T, Apfel CC, et al. Consensus guidelines for managing postoperative nausea and vomiting. Anesth Analg 2003; 97:62–71.
- Bennett-Guerrero E, Welsby I, Dunn TJ, et al. The use of a postoperative morbidity survey to evaluate patients with prolonged hospitalization after routine, moderate-risk, elective surgery. Anesth Analg 1999; 89:514–519.
- Grocott MP, Browne JP, Van der Meulen J, et al. The Postoperative Morbidity Survey was validated and used to describe morbidity after major surgery. J Clin Epidemiol 2007; 60:919–928.
- Kalff JC, Schraut WH, Simmons RL, Bauer AJ. Surgical manipulation of the gut elicits an intestinal muscularis inflammatory response resulting in postsurgical ileus. Ann Surg 1998; 228:652–663.
- Schwarz NT, Beer-Stolz D, Simmons RL, Bauer AJ. Pathogenesis of paralytic ileus: intestinal manipulation opens a transient pathway between the intestinal lumen and the leukocytic infiltrate of the jejunal muscularis. Ann Surg 2002; 235:31–40.
- Manara L, Bianchetti A. The central and peripheral influences of opioids on gastrointestinal propulsion. Annu Rev Pharmacol Toxicol 1985; 25:249–273.
- Manara L, Bianchi G, Ferretti P, Tavani A. Inhibition of gastrointestinal transit by morphine in rats results primarily from direct drug action on gut opioid sites. J Pharmacol Exp Ther 1986; 237:945–949.
- Hamilton-Davies C, Mythen MG, Salmon JB, et al. Comparison of commonly used clinical indicators of hypovolaemia with gastrointestinal tonometry. Intensive Care Med 1997; 23:276–281.
- Bender JS, Smith-Meek MA, Jones CE. Routine pulmonary artery catheterization does not reduce morbidity and mortality of elective vascular surgery: results of a prospective, randomized trial. Ann Surg 1997; 226:229–237.
- Berlauk JF, Abrams JH, Gilmour IJ, et al. Preoperative optimization of cardiovascular hemodynamics improves outcome in peripheral vascular surgery: a prospective, randomized clinical trial. Ann Surg 1991; 214:289–299.
- Boyd O, Grounds RM, Bennett ED. A randomized clinical trial of the effect of deliberate perioperative increase of oxygen delivery on mortality in high-risk surgical patients. JAMA 1993; 270:2699–2707.
- Gan TJ, Soppitt A, Maroof M, et al. Goal-directed intraoperative fluid administration reduces length of hospital stay after major surgery. Anesthesiology 2002; 97:820–826.
- Lobo SM, Salgado PF, Castillo VG, et al. Effects of maximizing oxygen delivery on morbidity and mortality in high-risk surgical patients. Crit Care Med 2000; 28:3396–3404.
- Mythen MG, Webb AR. Perioperative plasma volume expansion reduces the incidence of gut mucosal hypoperfusion during cardiac surgery. Arch Surg 1995; 130:423–429.
- Pölönen P, Ruokonen E, Hippeläinen M, Pöyhönen M, Takala J. A prospective, randomized study of goal-oriented hemodynamic therapy in cardiac surgical patients. Anesth Analg 2000; 90:1052–1059.
- Sandham JD, Hull RD, Brant RF, et al. A randomized, controlled trial of the use of pulmonary-artery catheters in high-risk surgical patients. N Engl J Med 2003; 348:5–14.
- Shoemaker WC, Appel PL, Kram HB, Nathan RC, Thompson JL. Multicomponent noninvasive physiologic monitoring of circulatory function. Crit Care Med 1988; 16:482–490.
- Sinclair S, James S, Singer M. Intraoperative intravascular volume optimisation and length of hospital stay after repair of proximal femoral fracture: randomised controlled trial. BMJ 1997; 315:909–912.
- Ueno S, Tanabe G, Yamada H, et al. Response of patients with cirrhosis who have undergone partial hepatectomy to treatment aimed at achieving supranormal oxygen delivery and consumption. Surgery 1998; 123:278–286.
- Valentine RJ, Duke ML, Inman MH, et al. Effectiveness of pulmonary artery catheters in aortic surgery: a randomized trial. J Vasc Surg 1998; 27:203–212.
- Venn R, Steele A, Richardson P, Poloniecki J, Grounds M, Newman P. Randomized controlled trial to investigate influence of the fluid challenge on duration of hospital stay and perioperative morbidity in patients with hip fractures. Br J Anaesth 2002; 88:65–71.
- Wilson J, Woods I, Fawcett J, et al. Reducing the risk of major elective surgery: randomised controlled trial of preoperative optimisation of oxygen delivery. BMJ 1999; 318:1099–1103.
- Ziegler DW, Wright JG, Choban PS, Flancbaum L. A prospective randomized trial of preoperative “optimization” of cardiac function in patients undergoing elective peripheral vascular surgery. Surgery 1997; 122:584–592.
- Grocott MPW, Hamilton MA, Bennett ED, Harrison D, Rowan K. Perioperative increase in global blood flow to explicit defined goals and outcomes following surgery. Cochrane Database Syst Rev 2006; 2:CD004082. doi:10.1002/14651858.CD004082.pub4.
- Moretti EW, Robertson KM, El-Moalem H, Gan TJ. Intraoperative colloid administration reduces postoperative nausea and vomiting and improves postoperative outcomes compared with crystalloid administration. Anesth Analg 2003; 96:611–617.
- Williams EL, Hildebrand KL, McCormick SA, Bedel MJ. The effect of intravenous lactated Ringer’s solution versus 0.9% sodium chloride solution on serum osmolality in human volunteers. Anesth Analg 1999; 88:999–1003.
- Wilkes NJ, Woolf R, Mutch M, et al. The effects of balanced versus saline-based hetastarch and crystalloid solutions on acid-base and electrolyte status and gastric mucosal perfusion in elderly surgical patients. Anesth Analg 2001; 93:811–816.
- Wakeling HG, McFall MR, Jenkins CS, et al. Intraoperative oesophageal Doppler guided fluid management shortens postoperative hospital stay after major bowel surgery. Br J Anaesth 2005; 95:634–642.
- Caliskan E, Turkoz A, Sener M, et al. A prospective randomized double-blind study to determine the effect of thoracic epidural neostigmine on postoperative ileus after abdominal aortic surgery. Anesth Analg 2008; 106:959–964.
- Hansen CT, Sørensen M, Møller C, Ottesen B, Kehlet H. Effect of laxatives on gastrointestinal functional recovery in fast-track hysterectomy: a double-blind, placebo-controlled randomized study. Am J Obstet Gynecol 2007; 196:311.e1–311.e7.
- Walldén J, Lindberg G, Sandin M, Thörn SE, Wattwil M. Effects of fentanyl on gastric myoelectrical activity: a possible association with polymorphisms of the mu-opioid receptor gene? Acta Anaesthesiol Scand 2008; 52:708–715.
- Herroeder S, Pecher S, Schönherr ME, et al. Systemic lidocaine shortens length of hospital stay after colorectal surgery: a double-blinded, randomized, placebo-controlled trial. Ann Surg 2007; 246:192–200.
- Charoenkwan K, Phillipson G, Vutyavanich T. Early versus delayed oral fluids and food for reducing complications after major abdominal gynaecologic surgery. Cochrane Database Syst Rev 2007; 4:CD004508. doi:10.1002/14651858.CD004508.pub3.
- Narita K, Tsunoda A, Takenaka K, et al. Effect of mosapride on recovery of intestinal motility after hand-assisted laparoscopic colectomy for carcinoma. Dis Colon Rectum 2008; 51:1692–1695.
- McNicol ED, Boyce D, Schumann R, Carr DB. Mu-opioid antagonists for opioid-induced bowel dysfunction. Cochrane Database Syst Rev 2008; 2:CD006332. doi:10.1002/14651858.CD006332.pub2.
- Nelson RL, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominal surgery. Cochrane Database Syst Rev 2007; 3:CD004929. doi:10.1002/14651858.CD004929.pub3.
- de Castro SM, van den Esschert JW, van Heek NT, et al. A systematic review of the efficacy of gum chewing for the amelioration of postoperative ileus. Dig Surg 2008; 25:39–45.
- Mythen MG. Postoperative gastrointestinal tract dysfunction. Anesth Analg 2005; 100:196–204.
- Gan TJ, Meyer T, Apfel CC, et al. Consensus guidelines for managing postoperative nausea and vomiting. Anesth Analg 2003; 97:62–71.
- Bennett-Guerrero E, Welsby I, Dunn TJ, et al. The use of a postoperative morbidity survey to evaluate patients with prolonged hospitalization after routine, moderate-risk, elective surgery. Anesth Analg 1999; 89:514–519.
- Grocott MP, Browne JP, Van der Meulen J, et al. The Postoperative Morbidity Survey was validated and used to describe morbidity after major surgery. J Clin Epidemiol 2007; 60:919–928.
- Kalff JC, Schraut WH, Simmons RL, Bauer AJ. Surgical manipulation of the gut elicits an intestinal muscularis inflammatory response resulting in postsurgical ileus. Ann Surg 1998; 228:652–663.
- Schwarz NT, Beer-Stolz D, Simmons RL, Bauer AJ. Pathogenesis of paralytic ileus: intestinal manipulation opens a transient pathway between the intestinal lumen and the leukocytic infiltrate of the jejunal muscularis. Ann Surg 2002; 235:31–40.
- Manara L, Bianchetti A. The central and peripheral influences of opioids on gastrointestinal propulsion. Annu Rev Pharmacol Toxicol 1985; 25:249–273.
- Manara L, Bianchi G, Ferretti P, Tavani A. Inhibition of gastrointestinal transit by morphine in rats results primarily from direct drug action on gut opioid sites. J Pharmacol Exp Ther 1986; 237:945–949.
- Hamilton-Davies C, Mythen MG, Salmon JB, et al. Comparison of commonly used clinical indicators of hypovolaemia with gastrointestinal tonometry. Intensive Care Med 1997; 23:276–281.
- Bender JS, Smith-Meek MA, Jones CE. Routine pulmonary artery catheterization does not reduce morbidity and mortality of elective vascular surgery: results of a prospective, randomized trial. Ann Surg 1997; 226:229–237.
- Berlauk JF, Abrams JH, Gilmour IJ, et al. Preoperative optimization of cardiovascular hemodynamics improves outcome in peripheral vascular surgery: a prospective, randomized clinical trial. Ann Surg 1991; 214:289–299.
- Boyd O, Grounds RM, Bennett ED. A randomized clinical trial of the effect of deliberate perioperative increase of oxygen delivery on mortality in high-risk surgical patients. JAMA 1993; 270:2699–2707.
- Gan TJ, Soppitt A, Maroof M, et al. Goal-directed intraoperative fluid administration reduces length of hospital stay after major surgery. Anesthesiology 2002; 97:820–826.
- Lobo SM, Salgado PF, Castillo VG, et al. Effects of maximizing oxygen delivery on morbidity and mortality in high-risk surgical patients. Crit Care Med 2000; 28:3396–3404.
- Mythen MG, Webb AR. Perioperative plasma volume expansion reduces the incidence of gut mucosal hypoperfusion during cardiac surgery. Arch Surg 1995; 130:423–429.
- Pölönen P, Ruokonen E, Hippeläinen M, Pöyhönen M, Takala J. A prospective, randomized study of goal-oriented hemodynamic therapy in cardiac surgical patients. Anesth Analg 2000; 90:1052–1059.
- Sandham JD, Hull RD, Brant RF, et al. A randomized, controlled trial of the use of pulmonary-artery catheters in high-risk surgical patients. N Engl J Med 2003; 348:5–14.
- Shoemaker WC, Appel PL, Kram HB, Nathan RC, Thompson JL. Multicomponent noninvasive physiologic monitoring of circulatory function. Crit Care Med 1988; 16:482–490.
- Sinclair S, James S, Singer M. Intraoperative intravascular volume optimisation and length of hospital stay after repair of proximal femoral fracture: randomised controlled trial. BMJ 1997; 315:909–912.
- Ueno S, Tanabe G, Yamada H, et al. Response of patients with cirrhosis who have undergone partial hepatectomy to treatment aimed at achieving supranormal oxygen delivery and consumption. Surgery 1998; 123:278–286.
- Valentine RJ, Duke ML, Inman MH, et al. Effectiveness of pulmonary artery catheters in aortic surgery: a randomized trial. J Vasc Surg 1998; 27:203–212.
- Venn R, Steele A, Richardson P, Poloniecki J, Grounds M, Newman P. Randomized controlled trial to investigate influence of the fluid challenge on duration of hospital stay and perioperative morbidity in patients with hip fractures. Br J Anaesth 2002; 88:65–71.
- Wilson J, Woods I, Fawcett J, et al. Reducing the risk of major elective surgery: randomised controlled trial of preoperative optimisation of oxygen delivery. BMJ 1999; 318:1099–1103.
- Ziegler DW, Wright JG, Choban PS, Flancbaum L. A prospective randomized trial of preoperative “optimization” of cardiac function in patients undergoing elective peripheral vascular surgery. Surgery 1997; 122:584–592.
- Grocott MPW, Hamilton MA, Bennett ED, Harrison D, Rowan K. Perioperative increase in global blood flow to explicit defined goals and outcomes following surgery. Cochrane Database Syst Rev 2006; 2:CD004082. doi:10.1002/14651858.CD004082.pub4.
- Moretti EW, Robertson KM, El-Moalem H, Gan TJ. Intraoperative colloid administration reduces postoperative nausea and vomiting and improves postoperative outcomes compared with crystalloid administration. Anesth Analg 2003; 96:611–617.
- Williams EL, Hildebrand KL, McCormick SA, Bedel MJ. The effect of intravenous lactated Ringer’s solution versus 0.9% sodium chloride solution on serum osmolality in human volunteers. Anesth Analg 1999; 88:999–1003.
- Wilkes NJ, Woolf R, Mutch M, et al. The effects of balanced versus saline-based hetastarch and crystalloid solutions on acid-base and electrolyte status and gastric mucosal perfusion in elderly surgical patients. Anesth Analg 2001; 93:811–816.
- Wakeling HG, McFall MR, Jenkins CS, et al. Intraoperative oesophageal Doppler guided fluid management shortens postoperative hospital stay after major bowel surgery. Br J Anaesth 2005; 95:634–642.
- Caliskan E, Turkoz A, Sener M, et al. A prospective randomized double-blind study to determine the effect of thoracic epidural neostigmine on postoperative ileus after abdominal aortic surgery. Anesth Analg 2008; 106:959–964.
- Hansen CT, Sørensen M, Møller C, Ottesen B, Kehlet H. Effect of laxatives on gastrointestinal functional recovery in fast-track hysterectomy: a double-blind, placebo-controlled randomized study. Am J Obstet Gynecol 2007; 196:311.e1–311.e7.
- Walldén J, Lindberg G, Sandin M, Thörn SE, Wattwil M. Effects of fentanyl on gastric myoelectrical activity: a possible association with polymorphisms of the mu-opioid receptor gene? Acta Anaesthesiol Scand 2008; 52:708–715.
- Herroeder S, Pecher S, Schönherr ME, et al. Systemic lidocaine shortens length of hospital stay after colorectal surgery: a double-blinded, randomized, placebo-controlled trial. Ann Surg 2007; 246:192–200.
- Charoenkwan K, Phillipson G, Vutyavanich T. Early versus delayed oral fluids and food for reducing complications after major abdominal gynaecologic surgery. Cochrane Database Syst Rev 2007; 4:CD004508. doi:10.1002/14651858.CD004508.pub3.
- Narita K, Tsunoda A, Takenaka K, et al. Effect of mosapride on recovery of intestinal motility after hand-assisted laparoscopic colectomy for carcinoma. Dis Colon Rectum 2008; 51:1692–1695.
- McNicol ED, Boyce D, Schumann R, Carr DB. Mu-opioid antagonists for opioid-induced bowel dysfunction. Cochrane Database Syst Rev 2008; 2:CD006332. doi:10.1002/14651858.CD006332.pub2.
- Nelson RL, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominal surgery. Cochrane Database Syst Rev 2007; 3:CD004929. doi:10.1002/14651858.CD004929.pub3.
- de Castro SM, van den Esschert JW, van Heek NT, et al. A systematic review of the efficacy of gum chewing for the amelioration of postoperative ileus. Dig Surg 2008; 25:39–45.
KEY POINTS
- GI tract dysfunction is the most common type of postoperative morbidity and frequently delays hospital discharge.
- Low-grade hypovolemia leading to gut ischemia is a common but neglected mechanism of postoperative GI tract dysfunction.
- Administration of colloid to achieve target levels of cardiac output improves gut perfusion and lowers the incidence of GI tract dysfunction.
- Doppler-guided fluid management reduces GI morbidity and length of hospital stay in surgical patients.
Case studies in perioperative management: Challenges, controversies, and common ground
CASE 1: RADICAL PROSTATECTOMY IN A MAN WITH ACUTE DEEP VEIN THROMBOSIS
A 69-year-old man is seen in the preoperative clinic 1 week before a scheduled radical prostatectomy. He has been diagnosed with femoral deep vein thrombosis (DVT) following a complaint of calf soreness.
Question 1.1: How would you treat him for his DVT?
A. Intravenous (IV) unfractionated heparin (UFH)
B. Low-molecular-weight heparin (LMWH)
C. Inferior vena cava (IVC) filter
D. Combination of pharmacologic therapy and then an IVC filter
Dr. Steven L. Cohn: The latest edition of the American College of Chest Physicians (ACCP) evidence-based guidelines on antithrombotic therapy recommends the use of therapeutic-dose subcutaneous LMWH over IV UFH for initial treatment of acute DVT in the outpatient or inpatient setting.1 Additionally, indications for an IVC filter include the prevention of pulmonary embolism (PE) in a patient with DVT who requires full-dose anticoagulation but cannot receive it, as would be the case here if the patient proceeds with surgery as scheduled. So if surgery will be postponed, the best option is LMWH; if surgery will not be postponed, the best answer is a combination of pharmacologic therapy with low-dose LMWH and an IVC filter, preferably a retrievable one.2
Question 1.2: You recommend postponing surgery, but the patient is worried about metastatic disease. For how long should surgery be postponed?
A. 2 weeks
B. 1 month
C. 2 months
D. 3 months
E. 6 months
Dr. Cohn: In the absence of anticoagulation therapy, the risk of venous thromboembolism (VTE) is approximately 40% (~1% per day) during the first month following an acute VTE and then declines markedly, to approximately 10%, during the second and third months following the acute event.3 Therefore, I would suggest that the patient wait at least 1 month after an acute DVT before undergoing surgery.
Dr. BobbieJean Sweitzer: This patient is in a hypercoagulable state, and the surgery itself will induce excess hypercoagulability. With a femoral DVT already present, his risk of VTE or PE is likely to be greater than 1% per day during the first month. If he does develop a PE, it may potentially be fatal.
Question 1.3: According to the patient, the surgeon and the internist discussed options, but the surgeon “doesn’t believe in filters” and the patient doesn’t want to postpone the procedure, despite your recommendation. Two weeks later he shows up for surgery having stopped his LMWH 3 days before. What would you do?
A. Cancel the surgery and restart full-dose LMWH
B. Proceed with prophylactic-dose LMWH
C. Proceed after giving a full therapeutic dose
D. Insert a filter and give DVT prophylaxis
Dr. Cohn: A bridging protocol should have been discussed with the surgeon and anesthesiologist before the procedure. Therapeutic levels of LMWH persist as long as 18 hours after discontinuation; therefore, the ACCP recommends interrupting LMWH 24 hours before surgery.4
Dr. Sweitzer: The lack of a bridging protocol in this case created a problem. The patient was afraid to continue anticoagulation after hearing the internist and surgeon disagree about the plan, and thus stopped it entirely, and he did not want to delay surgery because he was fearful of metastasis. The surgeon was adamant that IVC filters don’t work. The internist was concerned that the patient was at high risk for a PE. Even though the documented risk of postponing radical prostatectomy for a short time is inconsequential, I was convinced that the patient would not believe this if metastasis were to develop in the future.
Question 1.4: How would you have managed his anticoagulation perioperatively?
A. Stop LMWH 12 hours before surgery and restart at full dose 12 to 24 hours after surgery
B. Stop LMWH 24 hours before surgery and restart at full dose 24 hours after surgery
C. Stop LMWH 24 hours before surgery and restart prophylactic dosing 12 to 24 hours after surgery, and then full-dose LMWH in 48 to 72 hours
D. Stop LMWH 24 hours before surgery and restart at full dose 72 hours after surgery
Dr. Cohn: The correct timing for stopping LMWH is 24 hours before surgery. As for how to resume anticoagulation in patients at high risk for VTE or those undergoing major surgery, the latest ACCP guidelines recommend the following4:
- Reinitiation of anticoagulation 12 to 24 hours postoperatively, assuming adequate hemostasis in patients not at high risk for bleeding
- Use of a prophylactic dose or no anticoagulation for up to 72 hours if the patient is at high risk for bleeding.
These recommendations are a departure from previous practice, in which we routinely restarted anticoagulation 6 to 12 hours postoperatively.
Dr. Sweitzer: According to guidelines from the American Society of Regional Anesthesia and Pain Medicine (ASRA),5 if twice-daily LMWH is stopped 24 hours ahead of time (as long as patients have normal renal function), it is safe to perform epidural or spinal anesthesia, if either is an option. If full-dose UFH is used, the partial thromboplastin time (PTT) is monitored and central neuraxial blockade may be done if the PTT is in the normal range, which typically is 2 to 6 hours after UFH is stopped.
Additionally, the platelet count should be checked every 3 days postoperatively while the patient is on UFH or LMWH. It may be just as important to monitor the platelet count preoperatively if the patient has been on UFH or LMWH for an extended duration, especially if a central neuraxial anesthetic technique is planned.
Dr. Cohn: The reason for monitoring the platelet count is the potential for heparin-induced thrombocytopenia in patients on UFH. I recently encountered a patient who developed postoperative heparin-induced thrombocytopenia with thrombosis while on LMWH, which is relatively uncommon compared with UFH.
Case resolution
After much discussion of the risk of a significant PE with the patient, family, urologist, and vascular surgeon, it is decided that a temporary IVC filter will be placed in the operating room immediately after induction of general anesthesia and before the prostatectomy. The operation is delayed about 1 hour to allow this option. The patient is successfully treated and has the IVC filter removed 1 month postoperatively.
CASE 2: RADICAL CYSTECTOMY IN ELDERLY MAN WITH CARDIAC RISK FACTORS
A 78-year-old obese Russian-speaking man is seen in the preoperative clinic prior to a scheduled radical cystectomy for highly invasive bladder cancer. He is a poor historian and argues with the several family members accompanying him, but it is determined that his medical history includes hypertension, diabetes mellitus, a myocardial infarction (MI) 5 years previously (in Russia), and stable angina that is determined to be class II.
He had no previous work-up and no electrocardiogram (ECG). His medications are aspirin, metoprolol, and metformin. His blood pressure is 190/100 mm Hg, heart rate 90 beats per minute, and body mass index 32. On examination, there is no murmur, S3 gallop, or rales. His blood glucose is 220 mg/dL, and his creatinine is slightly elevated (1.4 mg/dL). ECG verifies a prior MI.
Question 2.1: Which of the following additional tests should be ordered preoperatively?
A. Hemoglobin (Hb) A1c
B. Lipid profile
C. Both
D. Neither
Dr. Sweitzer: Because the surgery is not elective, no immediate benefit would be achieved by ordering either an HbA1c or a lipid profile. However, if you view the preoperative evaluation as an opportunity to manage risk factors over the long term, then it may be a good idea to order the lipid profile because this patient has rarely engaged the health care system. Likewise, the HbA1c can be ordered to set in place his long-term management. Sometimes we focus on the preoperative visit only in the context of the surgery, but if a test or intervention is appropriate and needed for long-term management, then it is appropriate to do now.
Dr. Cohn: There is no evidence to support using the preoperative HbA1c to alter management decisions. I would not postpone surgery based on the HbA1c value, as I would if his glucose level were 600 mg/dL. Most of the studies that have assessed postoperative complications based on preoperative HbA1c did not control for postoperative glucose levels. The incidence of complications varies based on the type of complication and the type of surgery.
Similarly, I would not use lipid values to guide management of this patient. Studies suggest that perioperative statin therapy may reduce postoperative morbidity and mortality in patients undergoing vascular surgery (see article by Poldermans on page S79 of this supplement), but our patient already has indications for a statin—a remote MI and diabetes—independent of what his lipid values are.
Question 2.2: How would you manage his elevated blood pressure (190/100 mm Hg)?
A. Discontinue metoprolol and start a different antihypertensive drug
B. Increase the metoprolol dose
C. Continue metoprolol and add a second drug
D. Observe him on his current regimen
Dr. Cohn: I would increase the dose of metoprolol and consider adding another drug, in view of his heart rate (90 beats per minute) and his cardiac status. Beta-blocker therapy should not be discontinued because doing so in the perioperative period is associated with an increased risk of adverse events such as cardiac death and MI.
Dr. Sweitzer: I would push up the metoprolol a bit to reduce the heart rate, knowing that beta-blockers are probably not the most efficacious antihypertensive agents. I would caution against starting an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB) because he is scheduled to undergo a fairly significant procedure with expected blood loss and fluid shifts, and either of those agents in combination with a beta-blocker would be challenging to manage on the day of surgery.
Question 2.3: How would you manage his metformin perioperatively?
A. Discontinue it 48 hours preoperatively
B. Discontinue it 24 hours preoperatively
C. Withhold it on the morning of surgery
D. Continue it on the morning of surgery
Dr. Sweitzer: We routinely advise patients to hold all their oral diabetes medications the morning of surgery, primarily because many anesthesiologists are uncertain about the differing risks of hypoglycemia associated with the various oral agents.
Most of us will never see a patient who has lactic acidosis from metformin use. A systematic literature review and analysis found no increase in the risk of lactic acidosis with metformin compared with other oral hypoglycemics,6 so fear of lactic acidosis is not a valid reason to discontinue metformin. In fact, I think it is inappropriate to ever postpone or cancel surgery simply because the patient inadvertently took metformin on the morning of surgery. Some may argue that patients with renal insufficiency are at higher risk of lactic acidosis from metformin use on the morning of surgery, but keep in mind that renal insufficiency is a relative contraindication to metformin use in the first place. Unless the patient is scheduled for a bilateral nephrectomy, his or her renal function is not going to be acutely reduced enough to enable a morning dose of metformin to cause lactic acidosis.
Dr. Cohn: Additionally, in a recent study of patients undergoing coronary artery bypass graft surgery (CABG), there was no increased risk of in-hospital morbidity or mortality in patients who received metformin on the morning of surgery,7 although I typically stop it 24 hours before major surgery.
Question 2.4: With respect to statin therapy, which course would you choose preoperatively?
A. Start a statin at a low dose
B. Start a statin at an intermediate dose
C. Start a statin at a high dose
D. Do not start a statin
Dr. Cohn: The answer to this question is not clear cut. The reason not to start a prophylactic statin would be the lack of evidence of benefit in patients undergoing noncardiac, nonvascular surgery, although there is evidence of potential benefit in patients undergoing vascular surgery.* The arguments in favor of starting a statin are that this patient has independent indications for a statin and the planned surgery is a high-risk procedure.
(* Editor’s note: In the time since this summit, results of the DECREASE-IV trial were published [Dunkelgrun et al, Ann Surg 2009; 249:921–926], showing a statisically nonsignificant trend toward improved outcomes at 30 days with fluvastatin in intermediate-risk patients undergoing noncardiovascular surgery.)
In cohort studies, perioperative death rates have been lower in statin recipients than in those not taking a statin.8 In the Dutch Echographic Cardiac Risk Evaluation Applying Stress Echo III (DECREASE III), which randomized noncardiac vascular surgery patients to perioperative fluvastatin or placebo, rates of MI and the composite end point of nonfatal MI or cardiovascular death were significantly lower in the statin group than in the placebo group.9
Question 2.5: Which of the following cardiac tests would you order preoperatively?
A. Exercise ECG
B. Dobutamine stress echocardiogram
C. Dipyridamole nuclear imaging
D. Coronary angiography
E. No further cardiac testing
Dr. Cohn: I wouldn’t do any cardiac testing since this patient needs surgery for his malignancy and the results of any testing would be highly unlikely to change management, in terms of canceling the surgery. This approach is consistent with the 2007 guidelines on perioperative cardiovascular evaluation for noncardiac surgery issued by the American College of Cardiology (ACC) and the American Heart Association (AHA).10
Dr. Sweitzer: I would differ on this question. This patient has not been evaluated adequately for his coronary artery disease. He has poor functional capacity that complicates assessment of his symptoms. He also has diabetes, so he is more likely to have silent myocardial ischemia. At age 78, he is understandably concerned about his survival: radical cystectomy is a major operation associated with significant blood loss, fluid shifts, and a long-term recuperative state. In this case, a cardiac evaluation may change management, not in terms of considering coronary revascularization before the surgery, but in terms of affecting the assessment of his chance of surviving this major operation, his life span following the operation, and his quality of life. For example, a highly positive dobutamine stress echocardiogram or certain wall motion abnormalities would suggest that he might not be protected even by optimal perioperative medical management.
Question 2.6: Which of the following would you do preoperatively to assess pulmonary risk?
A. Obtain pulmonary function tests
B. Order a sleep study
C. Both
D. Neither
Dr. Sweitzer: There is no evidence supporting routine pulmonary function tests for patients undergoing procedures other than lung resection. If obstructive sleep apnea were suspected, I would order a sleep study only if I had access to one quickly to avoid delaying the surgery. Cancer surgery should never be delayed to get a sleep study. However, if this patient were seen in the primary care clinic, I would order a sleep study and, if indicated, put him on continuous positive airway pressure (CPAP). Whether or not preoperative CPAP makes a difference hasn’t been shown. No randomized controlled trials have been conducted, but there are some suggestions that the risks of ischemia and atrial arrhythmias in patients with known coronary artery disease can be reduced with CPAP. It is not always easy to initiate CPAP postoperatively because the number of CPAP machines is limited and titration by a respiratory technician is required, which is typically done in a sleep lab.
How the case was actually managed
Neither an HbA1c measurement nor a lipid profile was ordered preoperatively, for lack of supportive evidence. The patient was continued on his beta-blocker and the dosage was increased sufficiently to control his blood pressure and heart rate. Metformin was continued, and statin therapy was begun preoperatively in light of the patient’s independent indications for it and the high-risk nature of the procedure. Stress testing was not ordered, in light of the lack of indication, given the patient’s stable angina. The patient refused a sleep study. The operation was lengthy and involved significant blood loss. The patient had a complicated postoperative course and ultimately died from multiorgan failure.
CASE 3: OPERATIONS OF VARIABLE RISK IN ELDERLY MAN WITH ACTIVE CARDIAC CONDITION
Scenario A: A 75-year-old man with diabetes, class III angina, and Q waves in inferior leads on his ECG is scheduled for elective femoropopliteal bypass surgery. His medications include isosorbide mononitrate (120 mg), amlodipine (10 mg), metoprolol controlled release (100 mg), atorvastatin (80 mg), insulin, and aspirin (81 mg). His heart rate is 64 beats per minute, blood pressure is controlled at 120/80 mm Hg, low-density lipoprotein cholesterol is 80 mg/dL, and creatinine is 1.5 μmol/L.
Scenario B: Consider the same patient undergoing elective cholecystectomy instead of a femoropopliteal bypass.
Scenario C: Consider the same patient scheduled for a cystoscopy instead of the other procedures. He had one episode of gross hematuria 1 week ago that resolved. Work-up by his urologist included a urinalysis and culture that were normal, cytology that was negative for malignancy, and a sonogram and computed tomography scan that were both negative. He has had no further bleeding and is not anemic. The urologist wants to do the cystoscopy for the sake of completeness.
Question 3.1: What would be your preoperative course of action in the above scenarios?
A. Order a dobutamine stress echocardiogram
B. Order nuclear imaging with dipyridamole or adenosine
C. Order coronary angiography
D. Order a resting two-dimensional echocardiogram
E. Continue his current medications and send to surgery with no further testing
Dr. Cohn: This is a man with an active cardiac condition and class III angina, which is considered severe angina in the ACC/AHA 2007 guidelines on perioperative cardiac evaluation and care.10 The guidelines’ recommendation is to delay surgery for further evaluation and treatment. He is already on maximal medical therapy, which has failed to control his symptoms. He has poor exercise capacity. The only difference among the case scenarios is a variation in surgical risk.
This patient has independent indications for coronary angiography regardless of whether or not he’s undergoing surgery. He deserves evaluation for possible revascularization to improve his quality of life and symptoms.
I would send the patient to the catheterization lab in every one of these instances, with the possible exception of the cystoscopy scenario, where one could argue that revascularization with stenting would require antiplatelet therapy that might increase the bleeding risk, and also that the antiplatelet therapy would have to be interrupted for the cystoscopy, potentially increasing thrombotic risk.
Dr. Sweitzer: I disagree. The ACC/AHA 2007 guidelines do not recommend going directly to catheterization but rather recommend delaying surgery for further evaluation and treatment.10 We must ask whether this patient is truly receiving optimal medical management. After all, he is not on an ACE inhibitor or an ARB.
We must also consider whether the surgery is truly elective. In the first scenario, if he has peripheral vascular disease, he is likely to develop gangrene and have a further decrease in exercise capacity, which reduces his functional ability and increases his risk of comorbid conditions. He is at significant risk of developing worsening renal insufficiency or renal failure if he undergoes angiography. Coronary revascularization will delay treatment of his peripheral vascular disease. The Coronary Artery Revascularization Prophylaxis (CARP) trial showed no benefit of coronary revascularization relative to medical management in patients undergoing vascular surgery,11 as is planned for this patient. I believe one must balance two competing risks and have an in-depth discussion with the patient.
In the second scenario, not treating gallstones or preventing cholelithiasis poses more risk to the health of this diabetic patient than does elective surgery if he needs a cholecystectomy. Emergency surgery, especially for acute cholecystitis, also significantly increases the risk of a cardiac event.
In the third scenario, the cystoscopy may uncover bladder cancer, which may be adversely affected by a delay of surgery. Regardless, the patient had gross hematuria and would be at risk for further bleeding should he undergo stenting with the requisite antiplatelet therapy.
Catheterization is not normally recommended unless CABG or stenting is being considered, yet I have seen no data that either of these procedures prolongs life except in very limited circumstances such as left main disease treated with bypass grafting. Though it is true that CABG reduces the incidence and severity of angina, it does not modify the physiologic cause of angina but rather may result in symptom improvement by damaging somatic nerve fibers to the heart. Putting a stent in this patient would be like applying a bandage: his symptoms will likely recur if he does not receive optimal medical management.
In a 2007 science advisory, several major medical societies cautioned against percutaneous coronary intervention (PCI) with drug-eluting stent placement in patients expected to undergo noncardiac surgery that would require interruption of antiplatelet therapy in the following 12 months (and against PCI with bare metal stent placement in patients undergoing such surgery in the following 4 to 6 weeks).12 Therefore, I would not recommend catheterization for a patient whose noncardiac disease is likely to require surgery in the very near future, as is the case in each of the surgical scenarios above. One could consider noninvasive stress testing, which would be a safer approach and would almost certainly identify either significant stenosis of the left main coronary artery or three-vessel disease, which would be the only possible reasons to recommend CABG. I don’t believe there is any role for PCI for this patient.
Dr. Cohn: I argue for symptom relief even if it doesn’t prolong life. This patient cannot walk across the room without having symptoms despite taking multiple medications. I think he deserves a chance at revascularization if the angiogram shows he has a stenosis amenable to it, but I agree that a drug-eluting stent should not be placed if we know that he will undergo surgery within a few months.
CASE 4: VENTRAL HERNIA REPAIR IN A MIDDLE-AGED WOMAN
A 60-year-old woman is scheduled for ventral hernia repair. Her medical history is unremarkable, with the exception of hypertension. She denies any bleeding problems and had no complications after a laparoscopic cholecystectomy 10 years ago. She has no family history of bleeding disorders.
Question 4.1: Would you order a prothrombin time (PT)/partial thromboplastin time (PTT)?
A. Yes
B. No
Dr. Cohn: I would not.
Dr. Sweitzer: I agree.
Question 4.2: Although not requested, a PT/PTT was ordered anyway. The PT is normal (12.2 sec/12 sec) and the PTT is abnormal (40 sec/25 sec). What is the most likely cause of the PTT abnormality?
A. Laboratory error
B. Factor VII deficiency
C. Factor IX deficiency
D. Factor XI deficiency
E. Factor XII deficiency
Dr. Cohn: The most likely cause is a sample with insufficient blood in the tube. The test wasn’t indicated in the first place, but now it must be done again.
Question 4.3: The PTT is repeated and remains abnormal: 42 sec/25 sec. Mixing studies correct the abnormality to 29 sec/25 sec. Based on this information, what is the most likely cause of the PTT abnormality?
A. Laboratory error
B. Lupus anticoagulant
C. Prekallikrein factor deficiency
D. Factor XII deficiency
Dr. Cohn: This is not a case of lupus anticoagulant because the abnormal PTT was corrected by the mixing study. Causes of a prolonged PTT include deficiencies of factors XII, XI, and IX, so factor XII deficiency is the most likely explanation, though a deficiency higher up the coagulation cascade (ie, prekallikrein factor deficiency) is possible. In the absence of any personal or family bleeding history, it is unlikely to be a deficiency of factors VII or IX (the hemophiliac) or of factor XI, so a deficiency of factor XII or one of the prekallikrein factors is more likely.
Dr. Sweitzer: A mixing study is indeed the appropriate first step. It is ordered from the lab and involves mixing the patient’s blood with normal plasma and incubating the mixture. If the mixture corrects the PTT result, as was the case with this patient, it indicates a coagulation factor deficiency in the patient’s blood; if it doesn’t correct, that should prompt evaluation for lupus anticoagulant or the presence of some other protein or hormone that’s prolonging the PTT.
Question 4.4: How would you manage this patient perioperatively?
A. Fresh frozen plasma
B. Platelet transfusion
C. Cryoprecipitate
D. Factor VII
E. No treatment necessary
Dr. Cohn: No treatment is necessary. Factor XII deficiency does not cause bleeding, regardless of the PTT. Factor XI deficiency is associated with bleeding, but usually there is a family history or a personal history of bleeding with surgery.
Screening coagulation studies are not usually indicated in a patient without a personal or family history of bleeding, liver disease, alcohol or drug use, or current anticoagulant therapy. Such studies are usually normal in such patients, and when they are not, it’s usually because of a lab error or a disease (hypercoagulable state) or factor deficiency that does not cause bleeding
Dr. Sweitzer: However, if the PTT is prolonged, the cause should be identified, because if the patient is sent to the operating room without an explanation for the prolongation, the perioperative team might think the patient has a bleeding problem and use fresh frozen plasma too readily. Fresh frozen plasma is not appropriate for everyone and may actually make a potentially hypercoagulable state worse.
DISCUSSION
Question from the audience: It was said that use of ACE inhibitors and ARBs should be avoided around the time of surgery. I’ve done an extensive literature search and found minimal to no evidence to support this practice. To the contrary, I found fairly good evidence to indicate that heart failure can be exacerbated significantly and acutely, as early as within 24 hours, when patients are taken off their ACE inhibitor or ARB. I would like your viewpoint on this basic pathology in perioperative medicine.
Dr. Cohn: The literature on the use of ACE inhibitors or ARBs prior to noncardiac surgery consists of five studies with fewer than 500 patients in total, as recently reviewed by Rosenman et al.13 Although there was no excess of death or MI associated with taking these medications on the morning of surgery, they did increase the need for fluid and pressors.
Dr. Sweitzer: Patients with hypertension have bigger variations of blood pressure, both hypo- and hypertension, in the perioperative period. For this reason, it was standard of care 30 years ago to stop all antihypertensive drugs, including beta-blockers, preoperatively. We soon found that although this practice prevented many episodes of hypotension, it increased the occurrence of perioperative hypertension and the likelihood of cardiac events. It then became standard of care to always continue antihypertensive drugs on the morning of surgery. In the late 1980s and early 1990s, several studies showed that ACE inhibitors and ARBs were associated with a more profound drop in blood pressure upon induction of general anesthesia compared with other antihypertensives.
The usual ways we treat drops in blood pressure—with phenylephrine and ephedrine—are not very effective in treating hypotension associated with general anesthesia in patients taking ACE inhibitors or ARBs. Vasopressin is effective in treating refractory hypotension during surgery, but anesthesiologists don’t use it often. Reducing the doses of induction agents is another means of attenuating the hypotension induced by ACE inhibitors and ARBs.
We should not routinely stop ACE inhibitors and ARBs on the day of surgery, particularly in patients being treated for heart failure, angina, or a prior MI. My bias is to selectively hold ACE inhibitors and ARBs on the morning of surgery in patients who are undergoing a significant operation with a high likelihood of hypotension, have well-controlled preoperative blood pressure, are taking multiple antihypertensive agents, and do not have heart failure. Otherwise, patients should continue their ACE inhibitors and ARBs on the morning of surgery, and the anesthesiologist should be prepared for significant hypotension upon induction of anesthesia, alter anesthesia induction doses accordingly, have vasopressin handy, and avoid the temptation to treat hypotension with fluids or repeated doses of phenylephrine and ephedrine. The previous comment about concerns with ACE inhibitors and ARBs was in the context of initiating new therapies in the immediate preoperative period.
Question from the audience: Urinalysis is ordered for many patients undergoing orthopedic surgery, and invariably some bacteriuria is found. Can you comment on the value of urinalysis and subsequent treatment of abnormal results?
Dr. Cohn: I believe you should never order a urinalysis in an asymptomatic patient, with the exception of patients undergoing procedures that involve genitourinary or gynecologic instrumentation. Ordering a urinalysis before joint replacement has been promoted in the orthopedic literature on the theoretical grounds that bacteria might somehow seed and colonize the joint. Orthopedic surgeons like to do it, but I disregard their requests for it.
Dr. Sweitzer: One study showed that we’d need to spend $1.5 million on screening urinalysis for asymptomatic patients scheduled for joint replacement surgery in order to prevent one joint infection.14
Dr. Cohn: Also, patients are going to get their one dose of cephalosporin before surgery anyway, and that will probably knock out any bacteria that would be found on urinalysis.
Question from the audience: Can you clarify how the 2007 ACC/AHA perioperative guidelines define an active cardiac condition? The patient in your third case report had class III angina, or angina with less than usual activities, but nothing was presented to suggest that his symptoms were unstable. I would suggest that despite his class III symptoms, his angina was stable, and I would have continued down the algorithm rather than defining his cardiac condition as active and considering an intervention.
Dr. Cohn: An active cardiac condition is defined by the ACC as unstable coronary syndromes, which include acute (within the prior 7 days) or recent (within the prior 30 days) MI, unstable angina, and severe (class III or IV) angina.
- Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ. Antithrombotic therapy for venous thromboembolic disease. American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest 2008; 133(6 suppl):454S–545S.
- Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest 2008; 133(6 suppl):381S–453S.
- Kearon C, Hirsh J. Management of anticoagulation before and after elective surgery. N Engl J Med 1997; 336:1506–1511.
- Douketis JD, Berger PB, Dunn AS, et al. The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest 2008; 133(6 suppl):299S–339S.
- Horlocker TT, Wedel DJ, Benzon H, et al. Regional anesthesia in the anticoagulated patient: defining the risks (the second ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation). Regional Anesthesia & Pain Medicine. 2003; 28:172–197. Available at: http://www.asra.com/consensus-statements/2.html. Accessed May 11, 2009.
- Salpeter S, Gryeber E, Pasternak G, Salpeter E. Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus. Cochrane Syst Rev 2006; (1):CD002967.
- Duncan AI, Koch CG, Xu M, et al. Recent metformin ingestion does not increase in-hospital morbidity or mortality after cardiac surgery. Anesth Analg 2007; 104:42–50.
- Kapoor AS, Kanji H, Buckingham J, Devereaux PJ, McAlister FA. Strength of evidence for perioperative use of statins to reduce cardiovascular risk: systematic review of controlled studies. BMJ 2006; 333:1149.
- Poldermans D. Fluvastatin XL use is associated with improved cardiac outcome after major vascular surgery: results from a randomized placebo controlled trial. Presented at: European Society of Cardiology Congress 2008; September 1, 2008; Munich, Germany.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery. J Am Coll Cardiol 2007; 50:e159–e242.
- McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med 2004; 351:2795–2804.
- Grines CL, Bonow RO, Casey DE Jr, et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. Circulation 2007; 115:813–818.
- Rosenman DJ, McDonald FS, Ebbert JO, Erwin PJ, LaBella M, Montori VM. Clinical consequences of withholding versus administering renin-agiotensin-aldosterone system antagonists in the preoperative period. J Hosp Med 2008; 3:319–325.
- Lawrence VA, Gafni A, Gross M. The unproven utility of the preoperative urinalysis: economic evaluation. J Clin Epidemiol 1989; 42:1185–1192.
CASE 1: RADICAL PROSTATECTOMY IN A MAN WITH ACUTE DEEP VEIN THROMBOSIS
A 69-year-old man is seen in the preoperative clinic 1 week before a scheduled radical prostatectomy. He has been diagnosed with femoral deep vein thrombosis (DVT) following a complaint of calf soreness.
Question 1.1: How would you treat him for his DVT?
A. Intravenous (IV) unfractionated heparin (UFH)
B. Low-molecular-weight heparin (LMWH)
C. Inferior vena cava (IVC) filter
D. Combination of pharmacologic therapy and then an IVC filter
Dr. Steven L. Cohn: The latest edition of the American College of Chest Physicians (ACCP) evidence-based guidelines on antithrombotic therapy recommends the use of therapeutic-dose subcutaneous LMWH over IV UFH for initial treatment of acute DVT in the outpatient or inpatient setting.1 Additionally, indications for an IVC filter include the prevention of pulmonary embolism (PE) in a patient with DVT who requires full-dose anticoagulation but cannot receive it, as would be the case here if the patient proceeds with surgery as scheduled. So if surgery will be postponed, the best option is LMWH; if surgery will not be postponed, the best answer is a combination of pharmacologic therapy with low-dose LMWH and an IVC filter, preferably a retrievable one.2
Question 1.2: You recommend postponing surgery, but the patient is worried about metastatic disease. For how long should surgery be postponed?
A. 2 weeks
B. 1 month
C. 2 months
D. 3 months
E. 6 months
Dr. Cohn: In the absence of anticoagulation therapy, the risk of venous thromboembolism (VTE) is approximately 40% (~1% per day) during the first month following an acute VTE and then declines markedly, to approximately 10%, during the second and third months following the acute event.3 Therefore, I would suggest that the patient wait at least 1 month after an acute DVT before undergoing surgery.
Dr. BobbieJean Sweitzer: This patient is in a hypercoagulable state, and the surgery itself will induce excess hypercoagulability. With a femoral DVT already present, his risk of VTE or PE is likely to be greater than 1% per day during the first month. If he does develop a PE, it may potentially be fatal.
Question 1.3: According to the patient, the surgeon and the internist discussed options, but the surgeon “doesn’t believe in filters” and the patient doesn’t want to postpone the procedure, despite your recommendation. Two weeks later he shows up for surgery having stopped his LMWH 3 days before. What would you do?
A. Cancel the surgery and restart full-dose LMWH
B. Proceed with prophylactic-dose LMWH
C. Proceed after giving a full therapeutic dose
D. Insert a filter and give DVT prophylaxis
Dr. Cohn: A bridging protocol should have been discussed with the surgeon and anesthesiologist before the procedure. Therapeutic levels of LMWH persist as long as 18 hours after discontinuation; therefore, the ACCP recommends interrupting LMWH 24 hours before surgery.4
Dr. Sweitzer: The lack of a bridging protocol in this case created a problem. The patient was afraid to continue anticoagulation after hearing the internist and surgeon disagree about the plan, and thus stopped it entirely, and he did not want to delay surgery because he was fearful of metastasis. The surgeon was adamant that IVC filters don’t work. The internist was concerned that the patient was at high risk for a PE. Even though the documented risk of postponing radical prostatectomy for a short time is inconsequential, I was convinced that the patient would not believe this if metastasis were to develop in the future.
Question 1.4: How would you have managed his anticoagulation perioperatively?
A. Stop LMWH 12 hours before surgery and restart at full dose 12 to 24 hours after surgery
B. Stop LMWH 24 hours before surgery and restart at full dose 24 hours after surgery
C. Stop LMWH 24 hours before surgery and restart prophylactic dosing 12 to 24 hours after surgery, and then full-dose LMWH in 48 to 72 hours
D. Stop LMWH 24 hours before surgery and restart at full dose 72 hours after surgery
Dr. Cohn: The correct timing for stopping LMWH is 24 hours before surgery. As for how to resume anticoagulation in patients at high risk for VTE or those undergoing major surgery, the latest ACCP guidelines recommend the following4:
- Reinitiation of anticoagulation 12 to 24 hours postoperatively, assuming adequate hemostasis in patients not at high risk for bleeding
- Use of a prophylactic dose or no anticoagulation for up to 72 hours if the patient is at high risk for bleeding.
These recommendations are a departure from previous practice, in which we routinely restarted anticoagulation 6 to 12 hours postoperatively.
Dr. Sweitzer: According to guidelines from the American Society of Regional Anesthesia and Pain Medicine (ASRA),5 if twice-daily LMWH is stopped 24 hours ahead of time (as long as patients have normal renal function), it is safe to perform epidural or spinal anesthesia, if either is an option. If full-dose UFH is used, the partial thromboplastin time (PTT) is monitored and central neuraxial blockade may be done if the PTT is in the normal range, which typically is 2 to 6 hours after UFH is stopped.
Additionally, the platelet count should be checked every 3 days postoperatively while the patient is on UFH or LMWH. It may be just as important to monitor the platelet count preoperatively if the patient has been on UFH or LMWH for an extended duration, especially if a central neuraxial anesthetic technique is planned.
Dr. Cohn: The reason for monitoring the platelet count is the potential for heparin-induced thrombocytopenia in patients on UFH. I recently encountered a patient who developed postoperative heparin-induced thrombocytopenia with thrombosis while on LMWH, which is relatively uncommon compared with UFH.
Case resolution
After much discussion of the risk of a significant PE with the patient, family, urologist, and vascular surgeon, it is decided that a temporary IVC filter will be placed in the operating room immediately after induction of general anesthesia and before the prostatectomy. The operation is delayed about 1 hour to allow this option. The patient is successfully treated and has the IVC filter removed 1 month postoperatively.
CASE 2: RADICAL CYSTECTOMY IN ELDERLY MAN WITH CARDIAC RISK FACTORS
A 78-year-old obese Russian-speaking man is seen in the preoperative clinic prior to a scheduled radical cystectomy for highly invasive bladder cancer. He is a poor historian and argues with the several family members accompanying him, but it is determined that his medical history includes hypertension, diabetes mellitus, a myocardial infarction (MI) 5 years previously (in Russia), and stable angina that is determined to be class II.
He had no previous work-up and no electrocardiogram (ECG). His medications are aspirin, metoprolol, and metformin. His blood pressure is 190/100 mm Hg, heart rate 90 beats per minute, and body mass index 32. On examination, there is no murmur, S3 gallop, or rales. His blood glucose is 220 mg/dL, and his creatinine is slightly elevated (1.4 mg/dL). ECG verifies a prior MI.
Question 2.1: Which of the following additional tests should be ordered preoperatively?
A. Hemoglobin (Hb) A1c
B. Lipid profile
C. Both
D. Neither
Dr. Sweitzer: Because the surgery is not elective, no immediate benefit would be achieved by ordering either an HbA1c or a lipid profile. However, if you view the preoperative evaluation as an opportunity to manage risk factors over the long term, then it may be a good idea to order the lipid profile because this patient has rarely engaged the health care system. Likewise, the HbA1c can be ordered to set in place his long-term management. Sometimes we focus on the preoperative visit only in the context of the surgery, but if a test or intervention is appropriate and needed for long-term management, then it is appropriate to do now.
Dr. Cohn: There is no evidence to support using the preoperative HbA1c to alter management decisions. I would not postpone surgery based on the HbA1c value, as I would if his glucose level were 600 mg/dL. Most of the studies that have assessed postoperative complications based on preoperative HbA1c did not control for postoperative glucose levels. The incidence of complications varies based on the type of complication and the type of surgery.
Similarly, I would not use lipid values to guide management of this patient. Studies suggest that perioperative statin therapy may reduce postoperative morbidity and mortality in patients undergoing vascular surgery (see article by Poldermans on page S79 of this supplement), but our patient already has indications for a statin—a remote MI and diabetes—independent of what his lipid values are.
Question 2.2: How would you manage his elevated blood pressure (190/100 mm Hg)?
A. Discontinue metoprolol and start a different antihypertensive drug
B. Increase the metoprolol dose
C. Continue metoprolol and add a second drug
D. Observe him on his current regimen
Dr. Cohn: I would increase the dose of metoprolol and consider adding another drug, in view of his heart rate (90 beats per minute) and his cardiac status. Beta-blocker therapy should not be discontinued because doing so in the perioperative period is associated with an increased risk of adverse events such as cardiac death and MI.
Dr. Sweitzer: I would push up the metoprolol a bit to reduce the heart rate, knowing that beta-blockers are probably not the most efficacious antihypertensive agents. I would caution against starting an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB) because he is scheduled to undergo a fairly significant procedure with expected blood loss and fluid shifts, and either of those agents in combination with a beta-blocker would be challenging to manage on the day of surgery.
Question 2.3: How would you manage his metformin perioperatively?
A. Discontinue it 48 hours preoperatively
B. Discontinue it 24 hours preoperatively
C. Withhold it on the morning of surgery
D. Continue it on the morning of surgery
Dr. Sweitzer: We routinely advise patients to hold all their oral diabetes medications the morning of surgery, primarily because many anesthesiologists are uncertain about the differing risks of hypoglycemia associated with the various oral agents.
Most of us will never see a patient who has lactic acidosis from metformin use. A systematic literature review and analysis found no increase in the risk of lactic acidosis with metformin compared with other oral hypoglycemics,6 so fear of lactic acidosis is not a valid reason to discontinue metformin. In fact, I think it is inappropriate to ever postpone or cancel surgery simply because the patient inadvertently took metformin on the morning of surgery. Some may argue that patients with renal insufficiency are at higher risk of lactic acidosis from metformin use on the morning of surgery, but keep in mind that renal insufficiency is a relative contraindication to metformin use in the first place. Unless the patient is scheduled for a bilateral nephrectomy, his or her renal function is not going to be acutely reduced enough to enable a morning dose of metformin to cause lactic acidosis.
Dr. Cohn: Additionally, in a recent study of patients undergoing coronary artery bypass graft surgery (CABG), there was no increased risk of in-hospital morbidity or mortality in patients who received metformin on the morning of surgery,7 although I typically stop it 24 hours before major surgery.
Question 2.4: With respect to statin therapy, which course would you choose preoperatively?
A. Start a statin at a low dose
B. Start a statin at an intermediate dose
C. Start a statin at a high dose
D. Do not start a statin
Dr. Cohn: The answer to this question is not clear cut. The reason not to start a prophylactic statin would be the lack of evidence of benefit in patients undergoing noncardiac, nonvascular surgery, although there is evidence of potential benefit in patients undergoing vascular surgery.* The arguments in favor of starting a statin are that this patient has independent indications for a statin and the planned surgery is a high-risk procedure.
(* Editor’s note: In the time since this summit, results of the DECREASE-IV trial were published [Dunkelgrun et al, Ann Surg 2009; 249:921–926], showing a statisically nonsignificant trend toward improved outcomes at 30 days with fluvastatin in intermediate-risk patients undergoing noncardiovascular surgery.)
In cohort studies, perioperative death rates have been lower in statin recipients than in those not taking a statin.8 In the Dutch Echographic Cardiac Risk Evaluation Applying Stress Echo III (DECREASE III), which randomized noncardiac vascular surgery patients to perioperative fluvastatin or placebo, rates of MI and the composite end point of nonfatal MI or cardiovascular death were significantly lower in the statin group than in the placebo group.9
Question 2.5: Which of the following cardiac tests would you order preoperatively?
A. Exercise ECG
B. Dobutamine stress echocardiogram
C. Dipyridamole nuclear imaging
D. Coronary angiography
E. No further cardiac testing
Dr. Cohn: I wouldn’t do any cardiac testing since this patient needs surgery for his malignancy and the results of any testing would be highly unlikely to change management, in terms of canceling the surgery. This approach is consistent with the 2007 guidelines on perioperative cardiovascular evaluation for noncardiac surgery issued by the American College of Cardiology (ACC) and the American Heart Association (AHA).10
Dr. Sweitzer: I would differ on this question. This patient has not been evaluated adequately for his coronary artery disease. He has poor functional capacity that complicates assessment of his symptoms. He also has diabetes, so he is more likely to have silent myocardial ischemia. At age 78, he is understandably concerned about his survival: radical cystectomy is a major operation associated with significant blood loss, fluid shifts, and a long-term recuperative state. In this case, a cardiac evaluation may change management, not in terms of considering coronary revascularization before the surgery, but in terms of affecting the assessment of his chance of surviving this major operation, his life span following the operation, and his quality of life. For example, a highly positive dobutamine stress echocardiogram or certain wall motion abnormalities would suggest that he might not be protected even by optimal perioperative medical management.
Question 2.6: Which of the following would you do preoperatively to assess pulmonary risk?
A. Obtain pulmonary function tests
B. Order a sleep study
C. Both
D. Neither
Dr. Sweitzer: There is no evidence supporting routine pulmonary function tests for patients undergoing procedures other than lung resection. If obstructive sleep apnea were suspected, I would order a sleep study only if I had access to one quickly to avoid delaying the surgery. Cancer surgery should never be delayed to get a sleep study. However, if this patient were seen in the primary care clinic, I would order a sleep study and, if indicated, put him on continuous positive airway pressure (CPAP). Whether or not preoperative CPAP makes a difference hasn’t been shown. No randomized controlled trials have been conducted, but there are some suggestions that the risks of ischemia and atrial arrhythmias in patients with known coronary artery disease can be reduced with CPAP. It is not always easy to initiate CPAP postoperatively because the number of CPAP machines is limited and titration by a respiratory technician is required, which is typically done in a sleep lab.
How the case was actually managed
Neither an HbA1c measurement nor a lipid profile was ordered preoperatively, for lack of supportive evidence. The patient was continued on his beta-blocker and the dosage was increased sufficiently to control his blood pressure and heart rate. Metformin was continued, and statin therapy was begun preoperatively in light of the patient’s independent indications for it and the high-risk nature of the procedure. Stress testing was not ordered, in light of the lack of indication, given the patient’s stable angina. The patient refused a sleep study. The operation was lengthy and involved significant blood loss. The patient had a complicated postoperative course and ultimately died from multiorgan failure.
CASE 3: OPERATIONS OF VARIABLE RISK IN ELDERLY MAN WITH ACTIVE CARDIAC CONDITION
Scenario A: A 75-year-old man with diabetes, class III angina, and Q waves in inferior leads on his ECG is scheduled for elective femoropopliteal bypass surgery. His medications include isosorbide mononitrate (120 mg), amlodipine (10 mg), metoprolol controlled release (100 mg), atorvastatin (80 mg), insulin, and aspirin (81 mg). His heart rate is 64 beats per minute, blood pressure is controlled at 120/80 mm Hg, low-density lipoprotein cholesterol is 80 mg/dL, and creatinine is 1.5 μmol/L.
Scenario B: Consider the same patient undergoing elective cholecystectomy instead of a femoropopliteal bypass.
Scenario C: Consider the same patient scheduled for a cystoscopy instead of the other procedures. He had one episode of gross hematuria 1 week ago that resolved. Work-up by his urologist included a urinalysis and culture that were normal, cytology that was negative for malignancy, and a sonogram and computed tomography scan that were both negative. He has had no further bleeding and is not anemic. The urologist wants to do the cystoscopy for the sake of completeness.
Question 3.1: What would be your preoperative course of action in the above scenarios?
A. Order a dobutamine stress echocardiogram
B. Order nuclear imaging with dipyridamole or adenosine
C. Order coronary angiography
D. Order a resting two-dimensional echocardiogram
E. Continue his current medications and send to surgery with no further testing
Dr. Cohn: This is a man with an active cardiac condition and class III angina, which is considered severe angina in the ACC/AHA 2007 guidelines on perioperative cardiac evaluation and care.10 The guidelines’ recommendation is to delay surgery for further evaluation and treatment. He is already on maximal medical therapy, which has failed to control his symptoms. He has poor exercise capacity. The only difference among the case scenarios is a variation in surgical risk.
This patient has independent indications for coronary angiography regardless of whether or not he’s undergoing surgery. He deserves evaluation for possible revascularization to improve his quality of life and symptoms.
I would send the patient to the catheterization lab in every one of these instances, with the possible exception of the cystoscopy scenario, where one could argue that revascularization with stenting would require antiplatelet therapy that might increase the bleeding risk, and also that the antiplatelet therapy would have to be interrupted for the cystoscopy, potentially increasing thrombotic risk.
Dr. Sweitzer: I disagree. The ACC/AHA 2007 guidelines do not recommend going directly to catheterization but rather recommend delaying surgery for further evaluation and treatment.10 We must ask whether this patient is truly receiving optimal medical management. After all, he is not on an ACE inhibitor or an ARB.
We must also consider whether the surgery is truly elective. In the first scenario, if he has peripheral vascular disease, he is likely to develop gangrene and have a further decrease in exercise capacity, which reduces his functional ability and increases his risk of comorbid conditions. He is at significant risk of developing worsening renal insufficiency or renal failure if he undergoes angiography. Coronary revascularization will delay treatment of his peripheral vascular disease. The Coronary Artery Revascularization Prophylaxis (CARP) trial showed no benefit of coronary revascularization relative to medical management in patients undergoing vascular surgery,11 as is planned for this patient. I believe one must balance two competing risks and have an in-depth discussion with the patient.
In the second scenario, not treating gallstones or preventing cholelithiasis poses more risk to the health of this diabetic patient than does elective surgery if he needs a cholecystectomy. Emergency surgery, especially for acute cholecystitis, also significantly increases the risk of a cardiac event.
In the third scenario, the cystoscopy may uncover bladder cancer, which may be adversely affected by a delay of surgery. Regardless, the patient had gross hematuria and would be at risk for further bleeding should he undergo stenting with the requisite antiplatelet therapy.
Catheterization is not normally recommended unless CABG or stenting is being considered, yet I have seen no data that either of these procedures prolongs life except in very limited circumstances such as left main disease treated with bypass grafting. Though it is true that CABG reduces the incidence and severity of angina, it does not modify the physiologic cause of angina but rather may result in symptom improvement by damaging somatic nerve fibers to the heart. Putting a stent in this patient would be like applying a bandage: his symptoms will likely recur if he does not receive optimal medical management.
In a 2007 science advisory, several major medical societies cautioned against percutaneous coronary intervention (PCI) with drug-eluting stent placement in patients expected to undergo noncardiac surgery that would require interruption of antiplatelet therapy in the following 12 months (and against PCI with bare metal stent placement in patients undergoing such surgery in the following 4 to 6 weeks).12 Therefore, I would not recommend catheterization for a patient whose noncardiac disease is likely to require surgery in the very near future, as is the case in each of the surgical scenarios above. One could consider noninvasive stress testing, which would be a safer approach and would almost certainly identify either significant stenosis of the left main coronary artery or three-vessel disease, which would be the only possible reasons to recommend CABG. I don’t believe there is any role for PCI for this patient.
Dr. Cohn: I argue for symptom relief even if it doesn’t prolong life. This patient cannot walk across the room without having symptoms despite taking multiple medications. I think he deserves a chance at revascularization if the angiogram shows he has a stenosis amenable to it, but I agree that a drug-eluting stent should not be placed if we know that he will undergo surgery within a few months.
CASE 4: VENTRAL HERNIA REPAIR IN A MIDDLE-AGED WOMAN
A 60-year-old woman is scheduled for ventral hernia repair. Her medical history is unremarkable, with the exception of hypertension. She denies any bleeding problems and had no complications after a laparoscopic cholecystectomy 10 years ago. She has no family history of bleeding disorders.
Question 4.1: Would you order a prothrombin time (PT)/partial thromboplastin time (PTT)?
A. Yes
B. No
Dr. Cohn: I would not.
Dr. Sweitzer: I agree.
Question 4.2: Although not requested, a PT/PTT was ordered anyway. The PT is normal (12.2 sec/12 sec) and the PTT is abnormal (40 sec/25 sec). What is the most likely cause of the PTT abnormality?
A. Laboratory error
B. Factor VII deficiency
C. Factor IX deficiency
D. Factor XI deficiency
E. Factor XII deficiency
Dr. Cohn: The most likely cause is a sample with insufficient blood in the tube. The test wasn’t indicated in the first place, but now it must be done again.
Question 4.3: The PTT is repeated and remains abnormal: 42 sec/25 sec. Mixing studies correct the abnormality to 29 sec/25 sec. Based on this information, what is the most likely cause of the PTT abnormality?
A. Laboratory error
B. Lupus anticoagulant
C. Prekallikrein factor deficiency
D. Factor XII deficiency
Dr. Cohn: This is not a case of lupus anticoagulant because the abnormal PTT was corrected by the mixing study. Causes of a prolonged PTT include deficiencies of factors XII, XI, and IX, so factor XII deficiency is the most likely explanation, though a deficiency higher up the coagulation cascade (ie, prekallikrein factor deficiency) is possible. In the absence of any personal or family bleeding history, it is unlikely to be a deficiency of factors VII or IX (the hemophiliac) or of factor XI, so a deficiency of factor XII or one of the prekallikrein factors is more likely.
Dr. Sweitzer: A mixing study is indeed the appropriate first step. It is ordered from the lab and involves mixing the patient’s blood with normal plasma and incubating the mixture. If the mixture corrects the PTT result, as was the case with this patient, it indicates a coagulation factor deficiency in the patient’s blood; if it doesn’t correct, that should prompt evaluation for lupus anticoagulant or the presence of some other protein or hormone that’s prolonging the PTT.
Question 4.4: How would you manage this patient perioperatively?
A. Fresh frozen plasma
B. Platelet transfusion
C. Cryoprecipitate
D. Factor VII
E. No treatment necessary
Dr. Cohn: No treatment is necessary. Factor XII deficiency does not cause bleeding, regardless of the PTT. Factor XI deficiency is associated with bleeding, but usually there is a family history or a personal history of bleeding with surgery.
Screening coagulation studies are not usually indicated in a patient without a personal or family history of bleeding, liver disease, alcohol or drug use, or current anticoagulant therapy. Such studies are usually normal in such patients, and when they are not, it’s usually because of a lab error or a disease (hypercoagulable state) or factor deficiency that does not cause bleeding
Dr. Sweitzer: However, if the PTT is prolonged, the cause should be identified, because if the patient is sent to the operating room without an explanation for the prolongation, the perioperative team might think the patient has a bleeding problem and use fresh frozen plasma too readily. Fresh frozen plasma is not appropriate for everyone and may actually make a potentially hypercoagulable state worse.
DISCUSSION
Question from the audience: It was said that use of ACE inhibitors and ARBs should be avoided around the time of surgery. I’ve done an extensive literature search and found minimal to no evidence to support this practice. To the contrary, I found fairly good evidence to indicate that heart failure can be exacerbated significantly and acutely, as early as within 24 hours, when patients are taken off their ACE inhibitor or ARB. I would like your viewpoint on this basic pathology in perioperative medicine.
Dr. Cohn: The literature on the use of ACE inhibitors or ARBs prior to noncardiac surgery consists of five studies with fewer than 500 patients in total, as recently reviewed by Rosenman et al.13 Although there was no excess of death or MI associated with taking these medications on the morning of surgery, they did increase the need for fluid and pressors.
Dr. Sweitzer: Patients with hypertension have bigger variations of blood pressure, both hypo- and hypertension, in the perioperative period. For this reason, it was standard of care 30 years ago to stop all antihypertensive drugs, including beta-blockers, preoperatively. We soon found that although this practice prevented many episodes of hypotension, it increased the occurrence of perioperative hypertension and the likelihood of cardiac events. It then became standard of care to always continue antihypertensive drugs on the morning of surgery. In the late 1980s and early 1990s, several studies showed that ACE inhibitors and ARBs were associated with a more profound drop in blood pressure upon induction of general anesthesia compared with other antihypertensives.
The usual ways we treat drops in blood pressure—with phenylephrine and ephedrine—are not very effective in treating hypotension associated with general anesthesia in patients taking ACE inhibitors or ARBs. Vasopressin is effective in treating refractory hypotension during surgery, but anesthesiologists don’t use it often. Reducing the doses of induction agents is another means of attenuating the hypotension induced by ACE inhibitors and ARBs.
We should not routinely stop ACE inhibitors and ARBs on the day of surgery, particularly in patients being treated for heart failure, angina, or a prior MI. My bias is to selectively hold ACE inhibitors and ARBs on the morning of surgery in patients who are undergoing a significant operation with a high likelihood of hypotension, have well-controlled preoperative blood pressure, are taking multiple antihypertensive agents, and do not have heart failure. Otherwise, patients should continue their ACE inhibitors and ARBs on the morning of surgery, and the anesthesiologist should be prepared for significant hypotension upon induction of anesthesia, alter anesthesia induction doses accordingly, have vasopressin handy, and avoid the temptation to treat hypotension with fluids or repeated doses of phenylephrine and ephedrine. The previous comment about concerns with ACE inhibitors and ARBs was in the context of initiating new therapies in the immediate preoperative period.
Question from the audience: Urinalysis is ordered for many patients undergoing orthopedic surgery, and invariably some bacteriuria is found. Can you comment on the value of urinalysis and subsequent treatment of abnormal results?
Dr. Cohn: I believe you should never order a urinalysis in an asymptomatic patient, with the exception of patients undergoing procedures that involve genitourinary or gynecologic instrumentation. Ordering a urinalysis before joint replacement has been promoted in the orthopedic literature on the theoretical grounds that bacteria might somehow seed and colonize the joint. Orthopedic surgeons like to do it, but I disregard their requests for it.
Dr. Sweitzer: One study showed that we’d need to spend $1.5 million on screening urinalysis for asymptomatic patients scheduled for joint replacement surgery in order to prevent one joint infection.14
Dr. Cohn: Also, patients are going to get their one dose of cephalosporin before surgery anyway, and that will probably knock out any bacteria that would be found on urinalysis.
Question from the audience: Can you clarify how the 2007 ACC/AHA perioperative guidelines define an active cardiac condition? The patient in your third case report had class III angina, or angina with less than usual activities, but nothing was presented to suggest that his symptoms were unstable. I would suggest that despite his class III symptoms, his angina was stable, and I would have continued down the algorithm rather than defining his cardiac condition as active and considering an intervention.
Dr. Cohn: An active cardiac condition is defined by the ACC as unstable coronary syndromes, which include acute (within the prior 7 days) or recent (within the prior 30 days) MI, unstable angina, and severe (class III or IV) angina.
CASE 1: RADICAL PROSTATECTOMY IN A MAN WITH ACUTE DEEP VEIN THROMBOSIS
A 69-year-old man is seen in the preoperative clinic 1 week before a scheduled radical prostatectomy. He has been diagnosed with femoral deep vein thrombosis (DVT) following a complaint of calf soreness.
Question 1.1: How would you treat him for his DVT?
A. Intravenous (IV) unfractionated heparin (UFH)
B. Low-molecular-weight heparin (LMWH)
C. Inferior vena cava (IVC) filter
D. Combination of pharmacologic therapy and then an IVC filter
Dr. Steven L. Cohn: The latest edition of the American College of Chest Physicians (ACCP) evidence-based guidelines on antithrombotic therapy recommends the use of therapeutic-dose subcutaneous LMWH over IV UFH for initial treatment of acute DVT in the outpatient or inpatient setting.1 Additionally, indications for an IVC filter include the prevention of pulmonary embolism (PE) in a patient with DVT who requires full-dose anticoagulation but cannot receive it, as would be the case here if the patient proceeds with surgery as scheduled. So if surgery will be postponed, the best option is LMWH; if surgery will not be postponed, the best answer is a combination of pharmacologic therapy with low-dose LMWH and an IVC filter, preferably a retrievable one.2
Question 1.2: You recommend postponing surgery, but the patient is worried about metastatic disease. For how long should surgery be postponed?
A. 2 weeks
B. 1 month
C. 2 months
D. 3 months
E. 6 months
Dr. Cohn: In the absence of anticoagulation therapy, the risk of venous thromboembolism (VTE) is approximately 40% (~1% per day) during the first month following an acute VTE and then declines markedly, to approximately 10%, during the second and third months following the acute event.3 Therefore, I would suggest that the patient wait at least 1 month after an acute DVT before undergoing surgery.
Dr. BobbieJean Sweitzer: This patient is in a hypercoagulable state, and the surgery itself will induce excess hypercoagulability. With a femoral DVT already present, his risk of VTE or PE is likely to be greater than 1% per day during the first month. If he does develop a PE, it may potentially be fatal.
Question 1.3: According to the patient, the surgeon and the internist discussed options, but the surgeon “doesn’t believe in filters” and the patient doesn’t want to postpone the procedure, despite your recommendation. Two weeks later he shows up for surgery having stopped his LMWH 3 days before. What would you do?
A. Cancel the surgery and restart full-dose LMWH
B. Proceed with prophylactic-dose LMWH
C. Proceed after giving a full therapeutic dose
D. Insert a filter and give DVT prophylaxis
Dr. Cohn: A bridging protocol should have been discussed with the surgeon and anesthesiologist before the procedure. Therapeutic levels of LMWH persist as long as 18 hours after discontinuation; therefore, the ACCP recommends interrupting LMWH 24 hours before surgery.4
Dr. Sweitzer: The lack of a bridging protocol in this case created a problem. The patient was afraid to continue anticoagulation after hearing the internist and surgeon disagree about the plan, and thus stopped it entirely, and he did not want to delay surgery because he was fearful of metastasis. The surgeon was adamant that IVC filters don’t work. The internist was concerned that the patient was at high risk for a PE. Even though the documented risk of postponing radical prostatectomy for a short time is inconsequential, I was convinced that the patient would not believe this if metastasis were to develop in the future.
Question 1.4: How would you have managed his anticoagulation perioperatively?
A. Stop LMWH 12 hours before surgery and restart at full dose 12 to 24 hours after surgery
B. Stop LMWH 24 hours before surgery and restart at full dose 24 hours after surgery
C. Stop LMWH 24 hours before surgery and restart prophylactic dosing 12 to 24 hours after surgery, and then full-dose LMWH in 48 to 72 hours
D. Stop LMWH 24 hours before surgery and restart at full dose 72 hours after surgery
Dr. Cohn: The correct timing for stopping LMWH is 24 hours before surgery. As for how to resume anticoagulation in patients at high risk for VTE or those undergoing major surgery, the latest ACCP guidelines recommend the following4:
- Reinitiation of anticoagulation 12 to 24 hours postoperatively, assuming adequate hemostasis in patients not at high risk for bleeding
- Use of a prophylactic dose or no anticoagulation for up to 72 hours if the patient is at high risk for bleeding.
These recommendations are a departure from previous practice, in which we routinely restarted anticoagulation 6 to 12 hours postoperatively.
Dr. Sweitzer: According to guidelines from the American Society of Regional Anesthesia and Pain Medicine (ASRA),5 if twice-daily LMWH is stopped 24 hours ahead of time (as long as patients have normal renal function), it is safe to perform epidural or spinal anesthesia, if either is an option. If full-dose UFH is used, the partial thromboplastin time (PTT) is monitored and central neuraxial blockade may be done if the PTT is in the normal range, which typically is 2 to 6 hours after UFH is stopped.
Additionally, the platelet count should be checked every 3 days postoperatively while the patient is on UFH or LMWH. It may be just as important to monitor the platelet count preoperatively if the patient has been on UFH or LMWH for an extended duration, especially if a central neuraxial anesthetic technique is planned.
Dr. Cohn: The reason for monitoring the platelet count is the potential for heparin-induced thrombocytopenia in patients on UFH. I recently encountered a patient who developed postoperative heparin-induced thrombocytopenia with thrombosis while on LMWH, which is relatively uncommon compared with UFH.
Case resolution
After much discussion of the risk of a significant PE with the patient, family, urologist, and vascular surgeon, it is decided that a temporary IVC filter will be placed in the operating room immediately after induction of general anesthesia and before the prostatectomy. The operation is delayed about 1 hour to allow this option. The patient is successfully treated and has the IVC filter removed 1 month postoperatively.
CASE 2: RADICAL CYSTECTOMY IN ELDERLY MAN WITH CARDIAC RISK FACTORS
A 78-year-old obese Russian-speaking man is seen in the preoperative clinic prior to a scheduled radical cystectomy for highly invasive bladder cancer. He is a poor historian and argues with the several family members accompanying him, but it is determined that his medical history includes hypertension, diabetes mellitus, a myocardial infarction (MI) 5 years previously (in Russia), and stable angina that is determined to be class II.
He had no previous work-up and no electrocardiogram (ECG). His medications are aspirin, metoprolol, and metformin. His blood pressure is 190/100 mm Hg, heart rate 90 beats per minute, and body mass index 32. On examination, there is no murmur, S3 gallop, or rales. His blood glucose is 220 mg/dL, and his creatinine is slightly elevated (1.4 mg/dL). ECG verifies a prior MI.
Question 2.1: Which of the following additional tests should be ordered preoperatively?
A. Hemoglobin (Hb) A1c
B. Lipid profile
C. Both
D. Neither
Dr. Sweitzer: Because the surgery is not elective, no immediate benefit would be achieved by ordering either an HbA1c or a lipid profile. However, if you view the preoperative evaluation as an opportunity to manage risk factors over the long term, then it may be a good idea to order the lipid profile because this patient has rarely engaged the health care system. Likewise, the HbA1c can be ordered to set in place his long-term management. Sometimes we focus on the preoperative visit only in the context of the surgery, but if a test or intervention is appropriate and needed for long-term management, then it is appropriate to do now.
Dr. Cohn: There is no evidence to support using the preoperative HbA1c to alter management decisions. I would not postpone surgery based on the HbA1c value, as I would if his glucose level were 600 mg/dL. Most of the studies that have assessed postoperative complications based on preoperative HbA1c did not control for postoperative glucose levels. The incidence of complications varies based on the type of complication and the type of surgery.
Similarly, I would not use lipid values to guide management of this patient. Studies suggest that perioperative statin therapy may reduce postoperative morbidity and mortality in patients undergoing vascular surgery (see article by Poldermans on page S79 of this supplement), but our patient already has indications for a statin—a remote MI and diabetes—independent of what his lipid values are.
Question 2.2: How would you manage his elevated blood pressure (190/100 mm Hg)?
A. Discontinue metoprolol and start a different antihypertensive drug
B. Increase the metoprolol dose
C. Continue metoprolol and add a second drug
D. Observe him on his current regimen
Dr. Cohn: I would increase the dose of metoprolol and consider adding another drug, in view of his heart rate (90 beats per minute) and his cardiac status. Beta-blocker therapy should not be discontinued because doing so in the perioperative period is associated with an increased risk of adverse events such as cardiac death and MI.
Dr. Sweitzer: I would push up the metoprolol a bit to reduce the heart rate, knowing that beta-blockers are probably not the most efficacious antihypertensive agents. I would caution against starting an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB) because he is scheduled to undergo a fairly significant procedure with expected blood loss and fluid shifts, and either of those agents in combination with a beta-blocker would be challenging to manage on the day of surgery.
Question 2.3: How would you manage his metformin perioperatively?
A. Discontinue it 48 hours preoperatively
B. Discontinue it 24 hours preoperatively
C. Withhold it on the morning of surgery
D. Continue it on the morning of surgery
Dr. Sweitzer: We routinely advise patients to hold all their oral diabetes medications the morning of surgery, primarily because many anesthesiologists are uncertain about the differing risks of hypoglycemia associated with the various oral agents.
Most of us will never see a patient who has lactic acidosis from metformin use. A systematic literature review and analysis found no increase in the risk of lactic acidosis with metformin compared with other oral hypoglycemics,6 so fear of lactic acidosis is not a valid reason to discontinue metformin. In fact, I think it is inappropriate to ever postpone or cancel surgery simply because the patient inadvertently took metformin on the morning of surgery. Some may argue that patients with renal insufficiency are at higher risk of lactic acidosis from metformin use on the morning of surgery, but keep in mind that renal insufficiency is a relative contraindication to metformin use in the first place. Unless the patient is scheduled for a bilateral nephrectomy, his or her renal function is not going to be acutely reduced enough to enable a morning dose of metformin to cause lactic acidosis.
Dr. Cohn: Additionally, in a recent study of patients undergoing coronary artery bypass graft surgery (CABG), there was no increased risk of in-hospital morbidity or mortality in patients who received metformin on the morning of surgery,7 although I typically stop it 24 hours before major surgery.
Question 2.4: With respect to statin therapy, which course would you choose preoperatively?
A. Start a statin at a low dose
B. Start a statin at an intermediate dose
C. Start a statin at a high dose
D. Do not start a statin
Dr. Cohn: The answer to this question is not clear cut. The reason not to start a prophylactic statin would be the lack of evidence of benefit in patients undergoing noncardiac, nonvascular surgery, although there is evidence of potential benefit in patients undergoing vascular surgery.* The arguments in favor of starting a statin are that this patient has independent indications for a statin and the planned surgery is a high-risk procedure.
(* Editor’s note: In the time since this summit, results of the DECREASE-IV trial were published [Dunkelgrun et al, Ann Surg 2009; 249:921–926], showing a statisically nonsignificant trend toward improved outcomes at 30 days with fluvastatin in intermediate-risk patients undergoing noncardiovascular surgery.)
In cohort studies, perioperative death rates have been lower in statin recipients than in those not taking a statin.8 In the Dutch Echographic Cardiac Risk Evaluation Applying Stress Echo III (DECREASE III), which randomized noncardiac vascular surgery patients to perioperative fluvastatin or placebo, rates of MI and the composite end point of nonfatal MI or cardiovascular death were significantly lower in the statin group than in the placebo group.9
Question 2.5: Which of the following cardiac tests would you order preoperatively?
A. Exercise ECG
B. Dobutamine stress echocardiogram
C. Dipyridamole nuclear imaging
D. Coronary angiography
E. No further cardiac testing
Dr. Cohn: I wouldn’t do any cardiac testing since this patient needs surgery for his malignancy and the results of any testing would be highly unlikely to change management, in terms of canceling the surgery. This approach is consistent with the 2007 guidelines on perioperative cardiovascular evaluation for noncardiac surgery issued by the American College of Cardiology (ACC) and the American Heart Association (AHA).10
Dr. Sweitzer: I would differ on this question. This patient has not been evaluated adequately for his coronary artery disease. He has poor functional capacity that complicates assessment of his symptoms. He also has diabetes, so he is more likely to have silent myocardial ischemia. At age 78, he is understandably concerned about his survival: radical cystectomy is a major operation associated with significant blood loss, fluid shifts, and a long-term recuperative state. In this case, a cardiac evaluation may change management, not in terms of considering coronary revascularization before the surgery, but in terms of affecting the assessment of his chance of surviving this major operation, his life span following the operation, and his quality of life. For example, a highly positive dobutamine stress echocardiogram or certain wall motion abnormalities would suggest that he might not be protected even by optimal perioperative medical management.
Question 2.6: Which of the following would you do preoperatively to assess pulmonary risk?
A. Obtain pulmonary function tests
B. Order a sleep study
C. Both
D. Neither
Dr. Sweitzer: There is no evidence supporting routine pulmonary function tests for patients undergoing procedures other than lung resection. If obstructive sleep apnea were suspected, I would order a sleep study only if I had access to one quickly to avoid delaying the surgery. Cancer surgery should never be delayed to get a sleep study. However, if this patient were seen in the primary care clinic, I would order a sleep study and, if indicated, put him on continuous positive airway pressure (CPAP). Whether or not preoperative CPAP makes a difference hasn’t been shown. No randomized controlled trials have been conducted, but there are some suggestions that the risks of ischemia and atrial arrhythmias in patients with known coronary artery disease can be reduced with CPAP. It is not always easy to initiate CPAP postoperatively because the number of CPAP machines is limited and titration by a respiratory technician is required, which is typically done in a sleep lab.
How the case was actually managed
Neither an HbA1c measurement nor a lipid profile was ordered preoperatively, for lack of supportive evidence. The patient was continued on his beta-blocker and the dosage was increased sufficiently to control his blood pressure and heart rate. Metformin was continued, and statin therapy was begun preoperatively in light of the patient’s independent indications for it and the high-risk nature of the procedure. Stress testing was not ordered, in light of the lack of indication, given the patient’s stable angina. The patient refused a sleep study. The operation was lengthy and involved significant blood loss. The patient had a complicated postoperative course and ultimately died from multiorgan failure.
CASE 3: OPERATIONS OF VARIABLE RISK IN ELDERLY MAN WITH ACTIVE CARDIAC CONDITION
Scenario A: A 75-year-old man with diabetes, class III angina, and Q waves in inferior leads on his ECG is scheduled for elective femoropopliteal bypass surgery. His medications include isosorbide mononitrate (120 mg), amlodipine (10 mg), metoprolol controlled release (100 mg), atorvastatin (80 mg), insulin, and aspirin (81 mg). His heart rate is 64 beats per minute, blood pressure is controlled at 120/80 mm Hg, low-density lipoprotein cholesterol is 80 mg/dL, and creatinine is 1.5 μmol/L.
Scenario B: Consider the same patient undergoing elective cholecystectomy instead of a femoropopliteal bypass.
Scenario C: Consider the same patient scheduled for a cystoscopy instead of the other procedures. He had one episode of gross hematuria 1 week ago that resolved. Work-up by his urologist included a urinalysis and culture that were normal, cytology that was negative for malignancy, and a sonogram and computed tomography scan that were both negative. He has had no further bleeding and is not anemic. The urologist wants to do the cystoscopy for the sake of completeness.
Question 3.1: What would be your preoperative course of action in the above scenarios?
A. Order a dobutamine stress echocardiogram
B. Order nuclear imaging with dipyridamole or adenosine
C. Order coronary angiography
D. Order a resting two-dimensional echocardiogram
E. Continue his current medications and send to surgery with no further testing
Dr. Cohn: This is a man with an active cardiac condition and class III angina, which is considered severe angina in the ACC/AHA 2007 guidelines on perioperative cardiac evaluation and care.10 The guidelines’ recommendation is to delay surgery for further evaluation and treatment. He is already on maximal medical therapy, which has failed to control his symptoms. He has poor exercise capacity. The only difference among the case scenarios is a variation in surgical risk.
This patient has independent indications for coronary angiography regardless of whether or not he’s undergoing surgery. He deserves evaluation for possible revascularization to improve his quality of life and symptoms.
I would send the patient to the catheterization lab in every one of these instances, with the possible exception of the cystoscopy scenario, where one could argue that revascularization with stenting would require antiplatelet therapy that might increase the bleeding risk, and also that the antiplatelet therapy would have to be interrupted for the cystoscopy, potentially increasing thrombotic risk.
Dr. Sweitzer: I disagree. The ACC/AHA 2007 guidelines do not recommend going directly to catheterization but rather recommend delaying surgery for further evaluation and treatment.10 We must ask whether this patient is truly receiving optimal medical management. After all, he is not on an ACE inhibitor or an ARB.
We must also consider whether the surgery is truly elective. In the first scenario, if he has peripheral vascular disease, he is likely to develop gangrene and have a further decrease in exercise capacity, which reduces his functional ability and increases his risk of comorbid conditions. He is at significant risk of developing worsening renal insufficiency or renal failure if he undergoes angiography. Coronary revascularization will delay treatment of his peripheral vascular disease. The Coronary Artery Revascularization Prophylaxis (CARP) trial showed no benefit of coronary revascularization relative to medical management in patients undergoing vascular surgery,11 as is planned for this patient. I believe one must balance two competing risks and have an in-depth discussion with the patient.
In the second scenario, not treating gallstones or preventing cholelithiasis poses more risk to the health of this diabetic patient than does elective surgery if he needs a cholecystectomy. Emergency surgery, especially for acute cholecystitis, also significantly increases the risk of a cardiac event.
In the third scenario, the cystoscopy may uncover bladder cancer, which may be adversely affected by a delay of surgery. Regardless, the patient had gross hematuria and would be at risk for further bleeding should he undergo stenting with the requisite antiplatelet therapy.
Catheterization is not normally recommended unless CABG or stenting is being considered, yet I have seen no data that either of these procedures prolongs life except in very limited circumstances such as left main disease treated with bypass grafting. Though it is true that CABG reduces the incidence and severity of angina, it does not modify the physiologic cause of angina but rather may result in symptom improvement by damaging somatic nerve fibers to the heart. Putting a stent in this patient would be like applying a bandage: his symptoms will likely recur if he does not receive optimal medical management.
In a 2007 science advisory, several major medical societies cautioned against percutaneous coronary intervention (PCI) with drug-eluting stent placement in patients expected to undergo noncardiac surgery that would require interruption of antiplatelet therapy in the following 12 months (and against PCI with bare metal stent placement in patients undergoing such surgery in the following 4 to 6 weeks).12 Therefore, I would not recommend catheterization for a patient whose noncardiac disease is likely to require surgery in the very near future, as is the case in each of the surgical scenarios above. One could consider noninvasive stress testing, which would be a safer approach and would almost certainly identify either significant stenosis of the left main coronary artery or three-vessel disease, which would be the only possible reasons to recommend CABG. I don’t believe there is any role for PCI for this patient.
Dr. Cohn: I argue for symptom relief even if it doesn’t prolong life. This patient cannot walk across the room without having symptoms despite taking multiple medications. I think he deserves a chance at revascularization if the angiogram shows he has a stenosis amenable to it, but I agree that a drug-eluting stent should not be placed if we know that he will undergo surgery within a few months.
CASE 4: VENTRAL HERNIA REPAIR IN A MIDDLE-AGED WOMAN
A 60-year-old woman is scheduled for ventral hernia repair. Her medical history is unremarkable, with the exception of hypertension. She denies any bleeding problems and had no complications after a laparoscopic cholecystectomy 10 years ago. She has no family history of bleeding disorders.
Question 4.1: Would you order a prothrombin time (PT)/partial thromboplastin time (PTT)?
A. Yes
B. No
Dr. Cohn: I would not.
Dr. Sweitzer: I agree.
Question 4.2: Although not requested, a PT/PTT was ordered anyway. The PT is normal (12.2 sec/12 sec) and the PTT is abnormal (40 sec/25 sec). What is the most likely cause of the PTT abnormality?
A. Laboratory error
B. Factor VII deficiency
C. Factor IX deficiency
D. Factor XI deficiency
E. Factor XII deficiency
Dr. Cohn: The most likely cause is a sample with insufficient blood in the tube. The test wasn’t indicated in the first place, but now it must be done again.
Question 4.3: The PTT is repeated and remains abnormal: 42 sec/25 sec. Mixing studies correct the abnormality to 29 sec/25 sec. Based on this information, what is the most likely cause of the PTT abnormality?
A. Laboratory error
B. Lupus anticoagulant
C. Prekallikrein factor deficiency
D. Factor XII deficiency
Dr. Cohn: This is not a case of lupus anticoagulant because the abnormal PTT was corrected by the mixing study. Causes of a prolonged PTT include deficiencies of factors XII, XI, and IX, so factor XII deficiency is the most likely explanation, though a deficiency higher up the coagulation cascade (ie, prekallikrein factor deficiency) is possible. In the absence of any personal or family bleeding history, it is unlikely to be a deficiency of factors VII or IX (the hemophiliac) or of factor XI, so a deficiency of factor XII or one of the prekallikrein factors is more likely.
Dr. Sweitzer: A mixing study is indeed the appropriate first step. It is ordered from the lab and involves mixing the patient’s blood with normal plasma and incubating the mixture. If the mixture corrects the PTT result, as was the case with this patient, it indicates a coagulation factor deficiency in the patient’s blood; if it doesn’t correct, that should prompt evaluation for lupus anticoagulant or the presence of some other protein or hormone that’s prolonging the PTT.
Question 4.4: How would you manage this patient perioperatively?
A. Fresh frozen plasma
B. Platelet transfusion
C. Cryoprecipitate
D. Factor VII
E. No treatment necessary
Dr. Cohn: No treatment is necessary. Factor XII deficiency does not cause bleeding, regardless of the PTT. Factor XI deficiency is associated with bleeding, but usually there is a family history or a personal history of bleeding with surgery.
Screening coagulation studies are not usually indicated in a patient without a personal or family history of bleeding, liver disease, alcohol or drug use, or current anticoagulant therapy. Such studies are usually normal in such patients, and when they are not, it’s usually because of a lab error or a disease (hypercoagulable state) or factor deficiency that does not cause bleeding
Dr. Sweitzer: However, if the PTT is prolonged, the cause should be identified, because if the patient is sent to the operating room without an explanation for the prolongation, the perioperative team might think the patient has a bleeding problem and use fresh frozen plasma too readily. Fresh frozen plasma is not appropriate for everyone and may actually make a potentially hypercoagulable state worse.
DISCUSSION
Question from the audience: It was said that use of ACE inhibitors and ARBs should be avoided around the time of surgery. I’ve done an extensive literature search and found minimal to no evidence to support this practice. To the contrary, I found fairly good evidence to indicate that heart failure can be exacerbated significantly and acutely, as early as within 24 hours, when patients are taken off their ACE inhibitor or ARB. I would like your viewpoint on this basic pathology in perioperative medicine.
Dr. Cohn: The literature on the use of ACE inhibitors or ARBs prior to noncardiac surgery consists of five studies with fewer than 500 patients in total, as recently reviewed by Rosenman et al.13 Although there was no excess of death or MI associated with taking these medications on the morning of surgery, they did increase the need for fluid and pressors.
Dr. Sweitzer: Patients with hypertension have bigger variations of blood pressure, both hypo- and hypertension, in the perioperative period. For this reason, it was standard of care 30 years ago to stop all antihypertensive drugs, including beta-blockers, preoperatively. We soon found that although this practice prevented many episodes of hypotension, it increased the occurrence of perioperative hypertension and the likelihood of cardiac events. It then became standard of care to always continue antihypertensive drugs on the morning of surgery. In the late 1980s and early 1990s, several studies showed that ACE inhibitors and ARBs were associated with a more profound drop in blood pressure upon induction of general anesthesia compared with other antihypertensives.
The usual ways we treat drops in blood pressure—with phenylephrine and ephedrine—are not very effective in treating hypotension associated with general anesthesia in patients taking ACE inhibitors or ARBs. Vasopressin is effective in treating refractory hypotension during surgery, but anesthesiologists don’t use it often. Reducing the doses of induction agents is another means of attenuating the hypotension induced by ACE inhibitors and ARBs.
We should not routinely stop ACE inhibitors and ARBs on the day of surgery, particularly in patients being treated for heart failure, angina, or a prior MI. My bias is to selectively hold ACE inhibitors and ARBs on the morning of surgery in patients who are undergoing a significant operation with a high likelihood of hypotension, have well-controlled preoperative blood pressure, are taking multiple antihypertensive agents, and do not have heart failure. Otherwise, patients should continue their ACE inhibitors and ARBs on the morning of surgery, and the anesthesiologist should be prepared for significant hypotension upon induction of anesthesia, alter anesthesia induction doses accordingly, have vasopressin handy, and avoid the temptation to treat hypotension with fluids or repeated doses of phenylephrine and ephedrine. The previous comment about concerns with ACE inhibitors and ARBs was in the context of initiating new therapies in the immediate preoperative period.
Question from the audience: Urinalysis is ordered for many patients undergoing orthopedic surgery, and invariably some bacteriuria is found. Can you comment on the value of urinalysis and subsequent treatment of abnormal results?
Dr. Cohn: I believe you should never order a urinalysis in an asymptomatic patient, with the exception of patients undergoing procedures that involve genitourinary or gynecologic instrumentation. Ordering a urinalysis before joint replacement has been promoted in the orthopedic literature on the theoretical grounds that bacteria might somehow seed and colonize the joint. Orthopedic surgeons like to do it, but I disregard their requests for it.
Dr. Sweitzer: One study showed that we’d need to spend $1.5 million on screening urinalysis for asymptomatic patients scheduled for joint replacement surgery in order to prevent one joint infection.14
Dr. Cohn: Also, patients are going to get their one dose of cephalosporin before surgery anyway, and that will probably knock out any bacteria that would be found on urinalysis.
Question from the audience: Can you clarify how the 2007 ACC/AHA perioperative guidelines define an active cardiac condition? The patient in your third case report had class III angina, or angina with less than usual activities, but nothing was presented to suggest that his symptoms were unstable. I would suggest that despite his class III symptoms, his angina was stable, and I would have continued down the algorithm rather than defining his cardiac condition as active and considering an intervention.
Dr. Cohn: An active cardiac condition is defined by the ACC as unstable coronary syndromes, which include acute (within the prior 7 days) or recent (within the prior 30 days) MI, unstable angina, and severe (class III or IV) angina.
- Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ. Antithrombotic therapy for venous thromboembolic disease. American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest 2008; 133(6 suppl):454S–545S.
- Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest 2008; 133(6 suppl):381S–453S.
- Kearon C, Hirsh J. Management of anticoagulation before and after elective surgery. N Engl J Med 1997; 336:1506–1511.
- Douketis JD, Berger PB, Dunn AS, et al. The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest 2008; 133(6 suppl):299S–339S.
- Horlocker TT, Wedel DJ, Benzon H, et al. Regional anesthesia in the anticoagulated patient: defining the risks (the second ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation). Regional Anesthesia & Pain Medicine. 2003; 28:172–197. Available at: http://www.asra.com/consensus-statements/2.html. Accessed May 11, 2009.
- Salpeter S, Gryeber E, Pasternak G, Salpeter E. Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus. Cochrane Syst Rev 2006; (1):CD002967.
- Duncan AI, Koch CG, Xu M, et al. Recent metformin ingestion does not increase in-hospital morbidity or mortality after cardiac surgery. Anesth Analg 2007; 104:42–50.
- Kapoor AS, Kanji H, Buckingham J, Devereaux PJ, McAlister FA. Strength of evidence for perioperative use of statins to reduce cardiovascular risk: systematic review of controlled studies. BMJ 2006; 333:1149.
- Poldermans D. Fluvastatin XL use is associated with improved cardiac outcome after major vascular surgery: results from a randomized placebo controlled trial. Presented at: European Society of Cardiology Congress 2008; September 1, 2008; Munich, Germany.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery. J Am Coll Cardiol 2007; 50:e159–e242.
- McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med 2004; 351:2795–2804.
- Grines CL, Bonow RO, Casey DE Jr, et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. Circulation 2007; 115:813–818.
- Rosenman DJ, McDonald FS, Ebbert JO, Erwin PJ, LaBella M, Montori VM. Clinical consequences of withholding versus administering renin-agiotensin-aldosterone system antagonists in the preoperative period. J Hosp Med 2008; 3:319–325.
- Lawrence VA, Gafni A, Gross M. The unproven utility of the preoperative urinalysis: economic evaluation. J Clin Epidemiol 1989; 42:1185–1192.
- Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ. Antithrombotic therapy for venous thromboembolic disease. American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest 2008; 133(6 suppl):454S–545S.
- Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest 2008; 133(6 suppl):381S–453S.
- Kearon C, Hirsh J. Management of anticoagulation before and after elective surgery. N Engl J Med 1997; 336:1506–1511.
- Douketis JD, Berger PB, Dunn AS, et al. The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest 2008; 133(6 suppl):299S–339S.
- Horlocker TT, Wedel DJ, Benzon H, et al. Regional anesthesia in the anticoagulated patient: defining the risks (the second ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation). Regional Anesthesia & Pain Medicine. 2003; 28:172–197. Available at: http://www.asra.com/consensus-statements/2.html. Accessed May 11, 2009.
- Salpeter S, Gryeber E, Pasternak G, Salpeter E. Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus. Cochrane Syst Rev 2006; (1):CD002967.
- Duncan AI, Koch CG, Xu M, et al. Recent metformin ingestion does not increase in-hospital morbidity or mortality after cardiac surgery. Anesth Analg 2007; 104:42–50.
- Kapoor AS, Kanji H, Buckingham J, Devereaux PJ, McAlister FA. Strength of evidence for perioperative use of statins to reduce cardiovascular risk: systematic review of controlled studies. BMJ 2006; 333:1149.
- Poldermans D. Fluvastatin XL use is associated with improved cardiac outcome after major vascular surgery: results from a randomized placebo controlled trial. Presented at: European Society of Cardiology Congress 2008; September 1, 2008; Munich, Germany.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery. J Am Coll Cardiol 2007; 50:e159–e242.
- McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med 2004; 351:2795–2804.
- Grines CL, Bonow RO, Casey DE Jr, et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. Circulation 2007; 115:813–818.
- Rosenman DJ, McDonald FS, Ebbert JO, Erwin PJ, LaBella M, Montori VM. Clinical consequences of withholding versus administering renin-agiotensin-aldosterone system antagonists in the preoperative period. J Hosp Med 2008; 3:319–325.
- Lawrence VA, Gafni A, Gross M. The unproven utility of the preoperative urinalysis: economic evaluation. J Clin Epidemiol 1989; 42:1185–1192.
Statins and noncardiac surgery: Current evidence and practical considerations
Current uncertainty over the best approach for preventing fatal perioperative myocardial infarction (MI) lies in our inability, despite sophisticated testing methods, to detect unstable coronary plaque prior to surgery. Unstable plaque can be present in patients with coronary lumina that appear normal on coronary angiography. Therefore, reliance on medical therapy to blunt inflammation is currently the best practice for minimizing the risk that unstable plaque poses.
Perioperative use of statins is a cornerstone of such therapy. This article briefly reviews the rationale for perioperative statin use in the setting of noncardiac surgery, presents the latest evidence on the clinical effects of perioperative statin use, and considers the potential role for statins in promoting recovery from acute kidney injury after vascular surgery.
FATAL MI: ORIGINS AND APPROACHES TO RISK REDUCTION
Fatal perioperative MI has two potential origins.1,2 One is a culprit coronary plaque that fissures and ruptures, causing a cascade of thrombogenic events (hemorrhage and thrombosis) inside the vessel wall, culminating in an MI. Less often, fatal perioperative MI results from long-lasting myocardial ischemia (a demand/supply mismatch of oxygen), typically as a consequence of a fixed coronary stenosis.
In nearly half of patients with fatal MI, coronary inflammation is a key contributor. In the perioperative setting, surgical stress induces the release of inflammatory cytokines that disrupt smooth muscle cells in the endothelium and contribute to disruption of a nonobstructing coronary plaque, predisposing to acute thrombus formation.
Risk reduction depends on pathophysiology
Strategies for minimizing the risk of perioperative MI depend on the pathophysiology involved. In the case of oxygen demand/supply mismatch as a result of flow-limiting stenosis, a beta-blocker and coronary revascularization, if possible, may be useful.
In the more common case of unstable plaque, a multifactorial strategy appears optimal, involving the following:
- Statin therapy to reduce coronary inflammation
- Aspirin to blunt the prothrombotic milieu postoperatively
- Chronic low-dose beta-blockade to decrease myocardial oxygen demand or inhibit plaque rupture.
A particular role for statins
Ridker et al found that patients with an acute coronary syndrome who experience a decline in high-sensitivity C-reactive protein (hsCRP) level after treatment with a statin have improved clinical outcomes compared with those whose hsCRP level remains high, regardless of their resultant low-density lipoprotein (LDL) cholesterol level.3
Among surgical patients, those most at risk for poor cardiovascular outcomes are those who undergo vascular surgery. In Europe, the cardiovascular death rate in such patients is approximately 2%.4
Retrospective cohort data and data from randomized clinical trials have demonstrated reductions in perioperative cardiac complications with statin use in patients undergoing various types of noncardiac vascular surgery.5–9 In light of these data, my colleagues and I recently undertook a prospective study to examine the effect of perioperative statin use on cardiovascular complications in patients undergoing vascular surgery.10 Key details and findings are surveyed in the following section.
DECREASE III: PROSPECTIVE EVIDENCE FOR ISCHEMIC BENEFIT FROM PERIOPERATIVE STATINS
The Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echo III (DECREASE III) was conducted at a single center (Erasmus Medical Center, Rotterdam, the Netherlands) in a randomized, double-blind, placebo-controlled manner.10
Patients and study design
The study population included 497 statin-naïve patients who were scheduled for one of four noncardiac vascular surgical procedures (repair or revascularization for abdominal aortic aneurysm, abdominal aortic stenosis, lower limb arterial stenosis, or carotid artery stenosis). Patients with unstable coronary artery disease or left main disease were excluded.
Patients were randomized to placebo or extended-release fluvastatin (80 mg/day) starting on the day of randomization, which was a median of 37 days before surgery. Treatment was continued until 30 days after surgery.
Extended-release fluvastatin was chosen because its long half-life permits a bridge to the early postoperative period, during which oral medications are not permitted in patients undergoing high-risk vascular surgery.
The primary end point was the occurrence of myocardial ischemia as assessed by three methods:
- Holter monitoring during the first 72 postoperative hours
- Measurement of troponin T on days 1, 3, 7, and 30
- Additional electrocardiographic recordings on days 7 and 30.
The secondary end point was a composite of cardiovascular death and nonfatal MI during the first 30 postoperative days.
Baseline characteristics were similar between the two randomized groups, with a median age approaching 66 years. About three-fourths of the patients were male, one-fourth had a history of MI, one-fourth had angina pectoris, one-fifth had diabetes mellitus, and nearly 30% had a history of cerebrovascular accident or transient ischemic attack.
All patients were being treated with a beta-blocker, about 60% with antiplatelet therapy, more than one-fourth with anticoagulant therapy, nearly half with either an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, and more than one-fourth with diuretics. There were no significant differences between the groups in the proportion of patients on each of these therapies.
Results: Reductions in inflammatory markers
Baseline levels of hsCRP and interleukin-6 (IL-6) were comparable between the groups. In patients randomized to placebo, the hsCRP level increased by 3%, from a median of 5.80 mg/L at randomization to 6.00 mg/L immediately prior to surgery. In contrast, the hsCRP level in patients randomized to extended-release fluvastatin decreased by 21%, from a median of 5.93 mg/L to 4.66 mg/L. The between-group difference in the change in hsCRP level was statistically significant (P < .001). There was also a significantly greater reduction from baseline in median level of IL-6 among fluvastatin recipients compared with placebo recipients (–33% vs –4%; P < .001).
The specificity of hsCRP for cardiac inflammation is not yet known, but measures of hsCRP and IL-6 can provide a fingerprint of inflammatory activity prior to surgery. Other inflammatory and noninflammatory markers are being investigated to better identify (prior to surgery) those high-risk patients most likely to benefit from perioperative statin use.
Results: Favorable effect on clinical end points
The incidence of the primary end point—myocardial ischemia 30 days after surgery—was significantly lower in the patients randomized to extended-release fluvastatin compared with placebo (10.9% vs 18.9%; P = .016), as was the incidence of the secondary end point of cardiovascular death or nonfatal MI (4.8% vs 10.1%; P = .039).
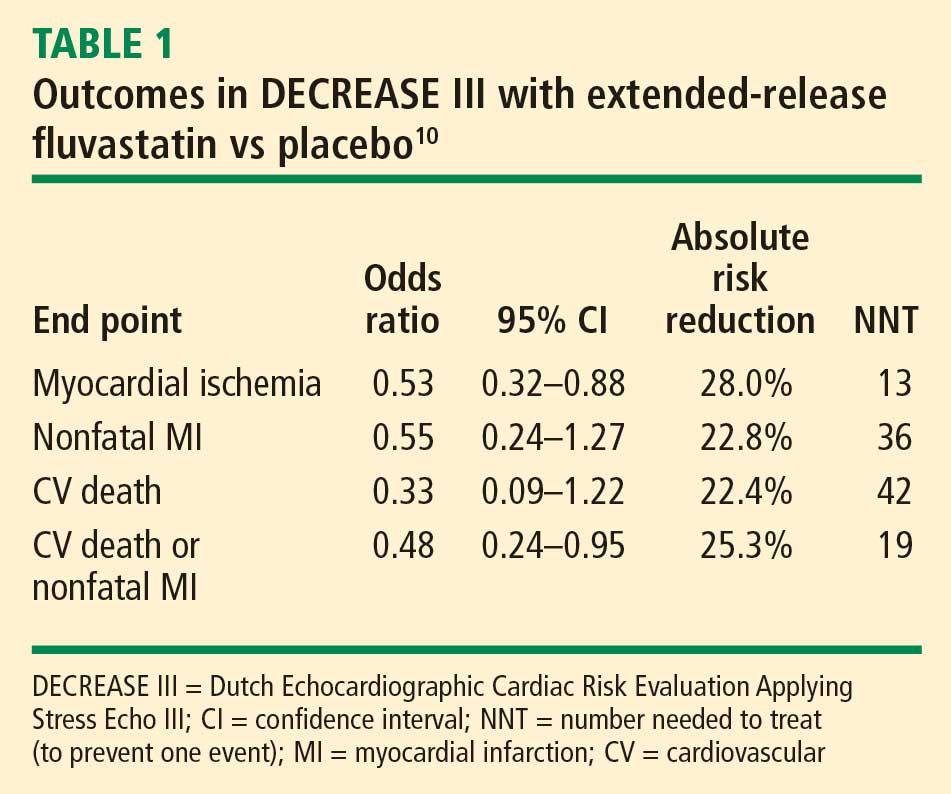
Safety: No effects on liver function or evidence of increased myopathy
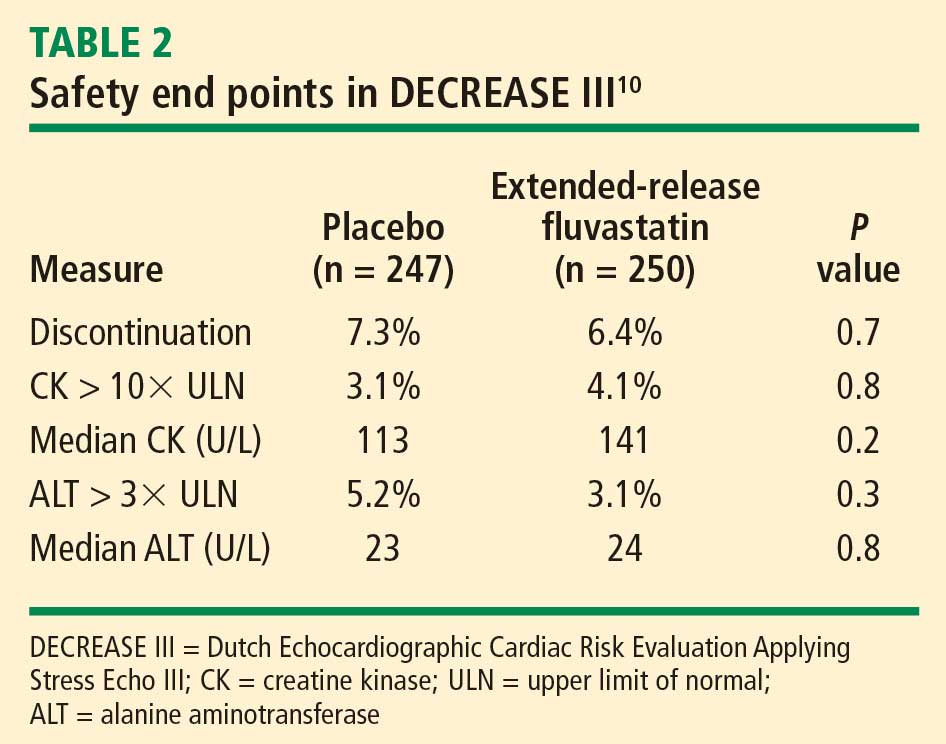
We concluded that initiation of therapy with a long-acting statin should be considered in statin-naïve patients undergoing vascular surgery.
PERIOPERATIVE STATIN USE: PRACTICAL CONSIDERATIONS
Inflammation, not cholesterol, should be the target
The optimal statin choice and the target level of LDL cholesterol immediately prior to surgery remain controversial. It may be that the more potent statins induce more side effects during surgery, but any such claim is speculative since no comparative studies exist. Regardless, the purpose of perioperative statin use should be reduction of the inflammatory stress response to surgery, with the long-term goal being achievement of recommended target lipid levels.
In particular, patients with peripheral arterial disease should have a statin initiated prior to high-risk vascular surgery (if they are not already receiving one), to increase the odds of recovering renal function after surgery (see section below) and to improve long-term outcomes.
Who are the best candidates?
Patients with multiple cardiac risk factors represent an especially high-risk group that benefits the most from statin therapy prior to vascular surgery, as they are likely to have more extensive disease and more extensive inflammation in the coronary artery tree.
Given the low incidence of side effects associated with statins, initiating a statin in patients with multiple cardiac risk factors who are undergoing intermediate-risk surgery may seem appropriate, but no data from large randomized trials are available to support this practice. Caution is in order when extrapolating data from studies conducted in the high-risk vascular surgery context to other surgical settings, since statins may pose hidden side effects such as liver dysfunction and myopathy, which may be missed in patients under anesthesia.
My personal practice is to initiate a statin prior to high-risk surgery or in patients with multiple cardiac risk factors if the risk-factor profile presents a clear indication for long-term statin use. If no risk factors are present, I am more reluctant to initiate a statin because of a lack of supportive data.
Beware the rebound effect with statin withdrawal
Statin withdrawal for several days following surgery is a common practice, since statins are given orally and their pleiotropic effects are underappreciated.
A withdrawal effect leading to abrogation of clinical benefit has been observed with perioperative use of short-acting statins, whose anti-inflammatory properties do not effectively extend to the postoperative period. Acute withdrawal has been associated with an increase in markers of inflammation and oxidative stress, and an increase in cardiac events has been observed with acute withdrawal of statins during periods of instability when compared with continuation of statin therapy.11
For these reasons, a long-acting statin is preferred preoperatively in patients whose oral intake will be compromised for several days after surgery (eg, in gastric surgery). The optimal statin for preventing the withdrawal effect is unknown. We chose extended-release fluvastatin in DECREASE III because its biological effect appears to last at least 4 days12 even though analysis of serum levels of the drug indicates a shorter half-life.
ANOTHER POTENTIAL BENEFIT: ENHANCED RECOVERY OF KIDNEY FUNCTION
Postoperative renal dysfunction is an ominous sign
Renal ischemic reperfusion injury is inevitable after vascular surgery that requires aortic cross-clamping. This is significant, as renal dysfunction after surgery is an ominous long-term sign that indicates abundant atherosclerosis. Complete recovery after acute kidney injury portends an improved long-term outcome, whereas patients with persistent renal dysfunction after vascular surgery have poor long-term outcomes.
A benefit from statins?
Statins may offer an effective means of preventing or shortening the course of acute kidney injury after surgery. Statins have been reported to lengthen survival of chronic kidney disease patients with sepsis or infectious complications and to improve the course of acute kidney injury in aging rats.13–15 These findings prompted my colleagues and I to conduct a retrospective study to evaluate whether statins may ameliorate reperfusion injury in the kidney after aortic cross-clamping.16
Promising findings from an observational review
We reviewed the records of all patients who had undergone vascular surgery at Erasmus Medical Center from January 1995 to June 2006 to examine the relation between preoperative statin use and renal function after suprarenal aortic cross-clamping.16 Of the 1,944 patients who met inclusion criteria, 515 (26.5%) were statin users. Postoperative kidney injury was defined as more than a 10% reduction in creatinine clearance on postoperative day 1 or 2 compared with baseline. Recovery of kidney function was defined as a creatinine clearance of greater than 90% of the baseline value by postoperative day 3.
The clinical characteristics of the populations with and without kidney injury after aortic cross-clamping were similar, including baseline creatinine clearance and serum creatinine.
Acute kidney injury within 2 days of surgery occurred in 664 patients (34%), of which 313 (47%) had complete recovery of kidney function at postoperative day 3. Although the incidence of postoperative kidney injury was similar among statin users and nonusers, statin use was associated with an increased chance of complete recovery of kidney function at day 3 (odds ratio = 2.0; 95% CI, 1.0–3.8).
All-cause mortality was assessed during a mean follow-up of 6.24 years. Statin use was associated with improved long-term survival, regardless of any change in kidney function (hazard ratio for death = 0.60; 95% CI, 0.48–0.75). Among the four broad patient groups, survival was highest among statin users with no postoperative kidney injury, followed by statin users who had kidney injury, then by nonusers of statins with no kidney injury, and finally by nonusers of statins who had kidney injury.
We concluded that perioperative statin use was associated with clinically significant recovery from acute kidney injury after high-risk vascular surgery and, more importantly, with improved long-term survival regardless of the presence of kidney injury. These promising findings require confirmation in prospective trials.
SUMMARY
Vascular surgery carries a high risk of perioperative mortality. Perioperative use of extended-release fluvastatin is associated with a reduced incidence of myocardial ischemia and the composite of MI and cardiovascular death at 30 days following surgery. These beneficial clinical outcomes are achieved without an increase in the incidence of side effects, including liver dysfunction and myopathy. Preoperative initiation of a long-acting statin is a reasonable strategy for reducing the risks associated with vascular surgery, and offers a bridge to postoperative statin continuation to blunt the inflammatory stress of surgery. Ischemic reperfusion injury is a major cause of renal dysfunction following vascular surgery. Statin therapy appears to help restore kidney function after aortic cross-clamping in patients undergoing high-risk vascular surgery.
DISCUSSION
Question from the audience: The majority of patients randomized in DECREASE III had relatively normal cholesterol levels. Do you believe those patients are biologically different from patients with physiologic vascular disease and elevated cholesterol levels?
Dr. Poldermans: We enrolled patients with various baseline cholesterol levels, and we found that these levels were not related to postoperative outcome. It would be a good idea to examine inflammation status just prior to surgery in patients with lower cholesterol levels to see if they have different outcomes from those with high cholesterol.
Question from the audience: If a patient is already on a short-acting statin and we know that he or she won’t be able to take a statin postoperatively, should we change to a long-acting statin just prior to surgery?
Dr. Poldermans: To be honest, this is a financial issue. If you have the opportunity, the best course would be to prescribe a statin with a prolonged half-life or an extended-release formulation. Of course, it’s not always possible to prescribe one particular statin. You have to negotiate what is feasible and hope to initiate the statin as early as possible to reduce risk.
Question from the audience: In studies conducted outside the perioperative setting, such as PROVE IT (Pravastatin or Atorvastatin Evaluation and Infection Therapy) and a substudy of REVERSAL (Reversing Atherosclerosis with Aggressive Lipid Lowering), it took about 30 days after statin initiation for hsCRP levels to minimize, and at least that long for halting of plaque progression to be detected by intravascular ultrasonography. Given that, does it make sense to delay nonurgent surgery in a patient in whom you’re worried about a postoperative MI?
Dr. Poldermans: Rat studies show improved blood flow and reduced thrombosis within hours of statin initiation. In the perioperative setting, therefore, initiating a statin within 30 days may be appropriate, but nobody knows the exact timing for optimal effect. Since there are no data to answer this question, I would not postpone surgery for this reason.
- Cohen MC, Aretz TH. Histological analysis of coronary artery lesions in fatal postoperative myocardial infarction. Cardiovasc Pathol 1999; 8:133–139.
- Dawood MM, Gutpa DK, Southern J, et al. Pathology of fatal perioperative myocardial infarction: implications regarding pathophysiology and prevention. Int J Cardiol 1996; 57:37–44.
- Ridker PM, Cannon CP, Morrow D, et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med 2005; 352:20–28.
- Poldermans D, Bax J, Boersma E, et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. European Society of Cardiology Web site. http://www.escardio.org/guidelines-surveys/esc-guidelines/GuidelinesDocuments/guidelines-perioperative-cardiac-care-FT.pdf. Posted September 1, 2009. Accessed September 3, 2009.
- Durazzo AE, Machado FS, Ikeoka DT, et al. Reduction in cardiovascular events after vascular surgery with atorvastatin: a randomized trial. J Vasc Surg 2004; 39:967–976.
- Lindenauer PK, Pekow P, Wang K, Gutierrez B, Benjamin EM. Lipid-lowering therapy and in-hospital mortality following major noncardiac surgery. JAMA 2004; 291:2092–2099.
- Kertai MD, Boersma E, Westerhout CM, et al. A combination of statins and beta-blockers is independently associated with a reduction in the incidence of perioperative mortality and nonfatal myocardial infarction in patients undergoing abdominal aortic aneurysm surgery. Eur J Vasc Endovasc Surg 2004; 28:343–352.
- O’Neil-Callahan K, Katsimaglis G, Tepper MR, et al. Statins decrease perioperative cardiac complications in patients undergoing noncardiac vascular surgery: the Statins for Risk Reduction in Surgery (StaRRS). J Am Coll Cardiol 2005; 45:336–342.
- Poldermans D, Bax JJ, Kertai MD, et al. Statins are associated with a reduced incidence of perioperative mortality in patients undergoing major noncardiac vascular surgery. Circulation 2003; 107:1848–1851.
- Schouten O, Boersma E, Hoeks SE, et al, for the Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. Fluvastatin and perioperative events in patients undergoing vascular surgery. N Engl J Med 2009; 361:980–989.
- Heeschen C, Hamm CW, Laufs U, Snapinn S, Bohm M, White HD. Withdrawal of statins increases event rates in patients with acute coronary syndromes. Circulation 2002; 105:1446–1452.
- Schouten O, Hoeks SE, Welten GM, et al. Effect of statin withdrawal on frequency of cardiac events after vascular surgery. Am J Cardiol 2007; 100:316–320.
- Gupta R, Plantinga LC, Fink NE, et al. Statin use and hospitalization for sepsis in patients with chronic kidney disease. JAMA 2007; 297:1455–1464.
- Yasuda H, Yuen PS, Hu X, et al. Simvastatin improves sepsis-induced mortality and acute kidney injury via renal vascular effects. Kidney Int 2006; 69:1535–1542.
- Sabbatini M, Pisani A, Uccello F, et al. Atorvastatin improves the course of ischemic acute renal failure in aging rats. J Am Soc Nephrol 2004; 15:901–909.
- Welten GMJM, Chonchol M, Schouten O, et al. Statin use is associated with early recovery of kidney injury after vascular surgery and improved long-term outcome. Nephrol Dial Transplant 2008; 23:3867–3873.
Current uncertainty over the best approach for preventing fatal perioperative myocardial infarction (MI) lies in our inability, despite sophisticated testing methods, to detect unstable coronary plaque prior to surgery. Unstable plaque can be present in patients with coronary lumina that appear normal on coronary angiography. Therefore, reliance on medical therapy to blunt inflammation is currently the best practice for minimizing the risk that unstable plaque poses.
Perioperative use of statins is a cornerstone of such therapy. This article briefly reviews the rationale for perioperative statin use in the setting of noncardiac surgery, presents the latest evidence on the clinical effects of perioperative statin use, and considers the potential role for statins in promoting recovery from acute kidney injury after vascular surgery.
FATAL MI: ORIGINS AND APPROACHES TO RISK REDUCTION
Fatal perioperative MI has two potential origins.1,2 One is a culprit coronary plaque that fissures and ruptures, causing a cascade of thrombogenic events (hemorrhage and thrombosis) inside the vessel wall, culminating in an MI. Less often, fatal perioperative MI results from long-lasting myocardial ischemia (a demand/supply mismatch of oxygen), typically as a consequence of a fixed coronary stenosis.
In nearly half of patients with fatal MI, coronary inflammation is a key contributor. In the perioperative setting, surgical stress induces the release of inflammatory cytokines that disrupt smooth muscle cells in the endothelium and contribute to disruption of a nonobstructing coronary plaque, predisposing to acute thrombus formation.
Risk reduction depends on pathophysiology
Strategies for minimizing the risk of perioperative MI depend on the pathophysiology involved. In the case of oxygen demand/supply mismatch as a result of flow-limiting stenosis, a beta-blocker and coronary revascularization, if possible, may be useful.
In the more common case of unstable plaque, a multifactorial strategy appears optimal, involving the following:
- Statin therapy to reduce coronary inflammation
- Aspirin to blunt the prothrombotic milieu postoperatively
- Chronic low-dose beta-blockade to decrease myocardial oxygen demand or inhibit plaque rupture.
A particular role for statins
Ridker et al found that patients with an acute coronary syndrome who experience a decline in high-sensitivity C-reactive protein (hsCRP) level after treatment with a statin have improved clinical outcomes compared with those whose hsCRP level remains high, regardless of their resultant low-density lipoprotein (LDL) cholesterol level.3
Among surgical patients, those most at risk for poor cardiovascular outcomes are those who undergo vascular surgery. In Europe, the cardiovascular death rate in such patients is approximately 2%.4
Retrospective cohort data and data from randomized clinical trials have demonstrated reductions in perioperative cardiac complications with statin use in patients undergoing various types of noncardiac vascular surgery.5–9 In light of these data, my colleagues and I recently undertook a prospective study to examine the effect of perioperative statin use on cardiovascular complications in patients undergoing vascular surgery.10 Key details and findings are surveyed in the following section.
DECREASE III: PROSPECTIVE EVIDENCE FOR ISCHEMIC BENEFIT FROM PERIOPERATIVE STATINS
The Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echo III (DECREASE III) was conducted at a single center (Erasmus Medical Center, Rotterdam, the Netherlands) in a randomized, double-blind, placebo-controlled manner.10
Patients and study design
The study population included 497 statin-naïve patients who were scheduled for one of four noncardiac vascular surgical procedures (repair or revascularization for abdominal aortic aneurysm, abdominal aortic stenosis, lower limb arterial stenosis, or carotid artery stenosis). Patients with unstable coronary artery disease or left main disease were excluded.
Patients were randomized to placebo or extended-release fluvastatin (80 mg/day) starting on the day of randomization, which was a median of 37 days before surgery. Treatment was continued until 30 days after surgery.
Extended-release fluvastatin was chosen because its long half-life permits a bridge to the early postoperative period, during which oral medications are not permitted in patients undergoing high-risk vascular surgery.
The primary end point was the occurrence of myocardial ischemia as assessed by three methods:
- Holter monitoring during the first 72 postoperative hours
- Measurement of troponin T on days 1, 3, 7, and 30
- Additional electrocardiographic recordings on days 7 and 30.
The secondary end point was a composite of cardiovascular death and nonfatal MI during the first 30 postoperative days.
Baseline characteristics were similar between the two randomized groups, with a median age approaching 66 years. About three-fourths of the patients were male, one-fourth had a history of MI, one-fourth had angina pectoris, one-fifth had diabetes mellitus, and nearly 30% had a history of cerebrovascular accident or transient ischemic attack.
All patients were being treated with a beta-blocker, about 60% with antiplatelet therapy, more than one-fourth with anticoagulant therapy, nearly half with either an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, and more than one-fourth with diuretics. There were no significant differences between the groups in the proportion of patients on each of these therapies.
Results: Reductions in inflammatory markers
Baseline levels of hsCRP and interleukin-6 (IL-6) were comparable between the groups. In patients randomized to placebo, the hsCRP level increased by 3%, from a median of 5.80 mg/L at randomization to 6.00 mg/L immediately prior to surgery. In contrast, the hsCRP level in patients randomized to extended-release fluvastatin decreased by 21%, from a median of 5.93 mg/L to 4.66 mg/L. The between-group difference in the change in hsCRP level was statistically significant (P < .001). There was also a significantly greater reduction from baseline in median level of IL-6 among fluvastatin recipients compared with placebo recipients (–33% vs –4%; P < .001).
The specificity of hsCRP for cardiac inflammation is not yet known, but measures of hsCRP and IL-6 can provide a fingerprint of inflammatory activity prior to surgery. Other inflammatory and noninflammatory markers are being investigated to better identify (prior to surgery) those high-risk patients most likely to benefit from perioperative statin use.
Results: Favorable effect on clinical end points
The incidence of the primary end point—myocardial ischemia 30 days after surgery—was significantly lower in the patients randomized to extended-release fluvastatin compared with placebo (10.9% vs 18.9%; P = .016), as was the incidence of the secondary end point of cardiovascular death or nonfatal MI (4.8% vs 10.1%; P = .039).
Safety: No effects on liver function or evidence of increased myopathy
We concluded that initiation of therapy with a long-acting statin should be considered in statin-naïve patients undergoing vascular surgery.
PERIOPERATIVE STATIN USE: PRACTICAL CONSIDERATIONS
Inflammation, not cholesterol, should be the target
The optimal statin choice and the target level of LDL cholesterol immediately prior to surgery remain controversial. It may be that the more potent statins induce more side effects during surgery, but any such claim is speculative since no comparative studies exist. Regardless, the purpose of perioperative statin use should be reduction of the inflammatory stress response to surgery, with the long-term goal being achievement of recommended target lipid levels.
In particular, patients with peripheral arterial disease should have a statin initiated prior to high-risk vascular surgery (if they are not already receiving one), to increase the odds of recovering renal function after surgery (see section below) and to improve long-term outcomes.
Who are the best candidates?
Patients with multiple cardiac risk factors represent an especially high-risk group that benefits the most from statin therapy prior to vascular surgery, as they are likely to have more extensive disease and more extensive inflammation in the coronary artery tree.
Given the low incidence of side effects associated with statins, initiating a statin in patients with multiple cardiac risk factors who are undergoing intermediate-risk surgery may seem appropriate, but no data from large randomized trials are available to support this practice. Caution is in order when extrapolating data from studies conducted in the high-risk vascular surgery context to other surgical settings, since statins may pose hidden side effects such as liver dysfunction and myopathy, which may be missed in patients under anesthesia.
My personal practice is to initiate a statin prior to high-risk surgery or in patients with multiple cardiac risk factors if the risk-factor profile presents a clear indication for long-term statin use. If no risk factors are present, I am more reluctant to initiate a statin because of a lack of supportive data.
Beware the rebound effect with statin withdrawal
Statin withdrawal for several days following surgery is a common practice, since statins are given orally and their pleiotropic effects are underappreciated.
A withdrawal effect leading to abrogation of clinical benefit has been observed with perioperative use of short-acting statins, whose anti-inflammatory properties do not effectively extend to the postoperative period. Acute withdrawal has been associated with an increase in markers of inflammation and oxidative stress, and an increase in cardiac events has been observed with acute withdrawal of statins during periods of instability when compared with continuation of statin therapy.11
For these reasons, a long-acting statin is preferred preoperatively in patients whose oral intake will be compromised for several days after surgery (eg, in gastric surgery). The optimal statin for preventing the withdrawal effect is unknown. We chose extended-release fluvastatin in DECREASE III because its biological effect appears to last at least 4 days12 even though analysis of serum levels of the drug indicates a shorter half-life.
ANOTHER POTENTIAL BENEFIT: ENHANCED RECOVERY OF KIDNEY FUNCTION
Postoperative renal dysfunction is an ominous sign
Renal ischemic reperfusion injury is inevitable after vascular surgery that requires aortic cross-clamping. This is significant, as renal dysfunction after surgery is an ominous long-term sign that indicates abundant atherosclerosis. Complete recovery after acute kidney injury portends an improved long-term outcome, whereas patients with persistent renal dysfunction after vascular surgery have poor long-term outcomes.
A benefit from statins?
Statins may offer an effective means of preventing or shortening the course of acute kidney injury after surgery. Statins have been reported to lengthen survival of chronic kidney disease patients with sepsis or infectious complications and to improve the course of acute kidney injury in aging rats.13–15 These findings prompted my colleagues and I to conduct a retrospective study to evaluate whether statins may ameliorate reperfusion injury in the kidney after aortic cross-clamping.16
Promising findings from an observational review
We reviewed the records of all patients who had undergone vascular surgery at Erasmus Medical Center from January 1995 to June 2006 to examine the relation between preoperative statin use and renal function after suprarenal aortic cross-clamping.16 Of the 1,944 patients who met inclusion criteria, 515 (26.5%) were statin users. Postoperative kidney injury was defined as more than a 10% reduction in creatinine clearance on postoperative day 1 or 2 compared with baseline. Recovery of kidney function was defined as a creatinine clearance of greater than 90% of the baseline value by postoperative day 3.
The clinical characteristics of the populations with and without kidney injury after aortic cross-clamping were similar, including baseline creatinine clearance and serum creatinine.
Acute kidney injury within 2 days of surgery occurred in 664 patients (34%), of which 313 (47%) had complete recovery of kidney function at postoperative day 3. Although the incidence of postoperative kidney injury was similar among statin users and nonusers, statin use was associated with an increased chance of complete recovery of kidney function at day 3 (odds ratio = 2.0; 95% CI, 1.0–3.8).
All-cause mortality was assessed during a mean follow-up of 6.24 years. Statin use was associated with improved long-term survival, regardless of any change in kidney function (hazard ratio for death = 0.60; 95% CI, 0.48–0.75). Among the four broad patient groups, survival was highest among statin users with no postoperative kidney injury, followed by statin users who had kidney injury, then by nonusers of statins with no kidney injury, and finally by nonusers of statins who had kidney injury.
We concluded that perioperative statin use was associated with clinically significant recovery from acute kidney injury after high-risk vascular surgery and, more importantly, with improved long-term survival regardless of the presence of kidney injury. These promising findings require confirmation in prospective trials.
SUMMARY
Vascular surgery carries a high risk of perioperative mortality. Perioperative use of extended-release fluvastatin is associated with a reduced incidence of myocardial ischemia and the composite of MI and cardiovascular death at 30 days following surgery. These beneficial clinical outcomes are achieved without an increase in the incidence of side effects, including liver dysfunction and myopathy. Preoperative initiation of a long-acting statin is a reasonable strategy for reducing the risks associated with vascular surgery, and offers a bridge to postoperative statin continuation to blunt the inflammatory stress of surgery. Ischemic reperfusion injury is a major cause of renal dysfunction following vascular surgery. Statin therapy appears to help restore kidney function after aortic cross-clamping in patients undergoing high-risk vascular surgery.
DISCUSSION
Question from the audience: The majority of patients randomized in DECREASE III had relatively normal cholesterol levels. Do you believe those patients are biologically different from patients with physiologic vascular disease and elevated cholesterol levels?
Dr. Poldermans: We enrolled patients with various baseline cholesterol levels, and we found that these levels were not related to postoperative outcome. It would be a good idea to examine inflammation status just prior to surgery in patients with lower cholesterol levels to see if they have different outcomes from those with high cholesterol.
Question from the audience: If a patient is already on a short-acting statin and we know that he or she won’t be able to take a statin postoperatively, should we change to a long-acting statin just prior to surgery?
Dr. Poldermans: To be honest, this is a financial issue. If you have the opportunity, the best course would be to prescribe a statin with a prolonged half-life or an extended-release formulation. Of course, it’s not always possible to prescribe one particular statin. You have to negotiate what is feasible and hope to initiate the statin as early as possible to reduce risk.
Question from the audience: In studies conducted outside the perioperative setting, such as PROVE IT (Pravastatin or Atorvastatin Evaluation and Infection Therapy) and a substudy of REVERSAL (Reversing Atherosclerosis with Aggressive Lipid Lowering), it took about 30 days after statin initiation for hsCRP levels to minimize, and at least that long for halting of plaque progression to be detected by intravascular ultrasonography. Given that, does it make sense to delay nonurgent surgery in a patient in whom you’re worried about a postoperative MI?
Dr. Poldermans: Rat studies show improved blood flow and reduced thrombosis within hours of statin initiation. In the perioperative setting, therefore, initiating a statin within 30 days may be appropriate, but nobody knows the exact timing for optimal effect. Since there are no data to answer this question, I would not postpone surgery for this reason.
Current uncertainty over the best approach for preventing fatal perioperative myocardial infarction (MI) lies in our inability, despite sophisticated testing methods, to detect unstable coronary plaque prior to surgery. Unstable plaque can be present in patients with coronary lumina that appear normal on coronary angiography. Therefore, reliance on medical therapy to blunt inflammation is currently the best practice for minimizing the risk that unstable plaque poses.
Perioperative use of statins is a cornerstone of such therapy. This article briefly reviews the rationale for perioperative statin use in the setting of noncardiac surgery, presents the latest evidence on the clinical effects of perioperative statin use, and considers the potential role for statins in promoting recovery from acute kidney injury after vascular surgery.
FATAL MI: ORIGINS AND APPROACHES TO RISK REDUCTION
Fatal perioperative MI has two potential origins.1,2 One is a culprit coronary plaque that fissures and ruptures, causing a cascade of thrombogenic events (hemorrhage and thrombosis) inside the vessel wall, culminating in an MI. Less often, fatal perioperative MI results from long-lasting myocardial ischemia (a demand/supply mismatch of oxygen), typically as a consequence of a fixed coronary stenosis.
In nearly half of patients with fatal MI, coronary inflammation is a key contributor. In the perioperative setting, surgical stress induces the release of inflammatory cytokines that disrupt smooth muscle cells in the endothelium and contribute to disruption of a nonobstructing coronary plaque, predisposing to acute thrombus formation.
Risk reduction depends on pathophysiology
Strategies for minimizing the risk of perioperative MI depend on the pathophysiology involved. In the case of oxygen demand/supply mismatch as a result of flow-limiting stenosis, a beta-blocker and coronary revascularization, if possible, may be useful.
In the more common case of unstable plaque, a multifactorial strategy appears optimal, involving the following:
- Statin therapy to reduce coronary inflammation
- Aspirin to blunt the prothrombotic milieu postoperatively
- Chronic low-dose beta-blockade to decrease myocardial oxygen demand or inhibit plaque rupture.
A particular role for statins
Ridker et al found that patients with an acute coronary syndrome who experience a decline in high-sensitivity C-reactive protein (hsCRP) level after treatment with a statin have improved clinical outcomes compared with those whose hsCRP level remains high, regardless of their resultant low-density lipoprotein (LDL) cholesterol level.3
Among surgical patients, those most at risk for poor cardiovascular outcomes are those who undergo vascular surgery. In Europe, the cardiovascular death rate in such patients is approximately 2%.4
Retrospective cohort data and data from randomized clinical trials have demonstrated reductions in perioperative cardiac complications with statin use in patients undergoing various types of noncardiac vascular surgery.5–9 In light of these data, my colleagues and I recently undertook a prospective study to examine the effect of perioperative statin use on cardiovascular complications in patients undergoing vascular surgery.10 Key details and findings are surveyed in the following section.
DECREASE III: PROSPECTIVE EVIDENCE FOR ISCHEMIC BENEFIT FROM PERIOPERATIVE STATINS
The Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echo III (DECREASE III) was conducted at a single center (Erasmus Medical Center, Rotterdam, the Netherlands) in a randomized, double-blind, placebo-controlled manner.10
Patients and study design
The study population included 497 statin-naïve patients who were scheduled for one of four noncardiac vascular surgical procedures (repair or revascularization for abdominal aortic aneurysm, abdominal aortic stenosis, lower limb arterial stenosis, or carotid artery stenosis). Patients with unstable coronary artery disease or left main disease were excluded.
Patients were randomized to placebo or extended-release fluvastatin (80 mg/day) starting on the day of randomization, which was a median of 37 days before surgery. Treatment was continued until 30 days after surgery.
Extended-release fluvastatin was chosen because its long half-life permits a bridge to the early postoperative period, during which oral medications are not permitted in patients undergoing high-risk vascular surgery.
The primary end point was the occurrence of myocardial ischemia as assessed by three methods:
- Holter monitoring during the first 72 postoperative hours
- Measurement of troponin T on days 1, 3, 7, and 30
- Additional electrocardiographic recordings on days 7 and 30.
The secondary end point was a composite of cardiovascular death and nonfatal MI during the first 30 postoperative days.
Baseline characteristics were similar between the two randomized groups, with a median age approaching 66 years. About three-fourths of the patients were male, one-fourth had a history of MI, one-fourth had angina pectoris, one-fifth had diabetes mellitus, and nearly 30% had a history of cerebrovascular accident or transient ischemic attack.
All patients were being treated with a beta-blocker, about 60% with antiplatelet therapy, more than one-fourth with anticoagulant therapy, nearly half with either an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, and more than one-fourth with diuretics. There were no significant differences between the groups in the proportion of patients on each of these therapies.
Results: Reductions in inflammatory markers
Baseline levels of hsCRP and interleukin-6 (IL-6) were comparable between the groups. In patients randomized to placebo, the hsCRP level increased by 3%, from a median of 5.80 mg/L at randomization to 6.00 mg/L immediately prior to surgery. In contrast, the hsCRP level in patients randomized to extended-release fluvastatin decreased by 21%, from a median of 5.93 mg/L to 4.66 mg/L. The between-group difference in the change in hsCRP level was statistically significant (P < .001). There was also a significantly greater reduction from baseline in median level of IL-6 among fluvastatin recipients compared with placebo recipients (–33% vs –4%; P < .001).
The specificity of hsCRP for cardiac inflammation is not yet known, but measures of hsCRP and IL-6 can provide a fingerprint of inflammatory activity prior to surgery. Other inflammatory and noninflammatory markers are being investigated to better identify (prior to surgery) those high-risk patients most likely to benefit from perioperative statin use.
Results: Favorable effect on clinical end points
The incidence of the primary end point—myocardial ischemia 30 days after surgery—was significantly lower in the patients randomized to extended-release fluvastatin compared with placebo (10.9% vs 18.9%; P = .016), as was the incidence of the secondary end point of cardiovascular death or nonfatal MI (4.8% vs 10.1%; P = .039).
Safety: No effects on liver function or evidence of increased myopathy
We concluded that initiation of therapy with a long-acting statin should be considered in statin-naïve patients undergoing vascular surgery.
PERIOPERATIVE STATIN USE: PRACTICAL CONSIDERATIONS
Inflammation, not cholesterol, should be the target
The optimal statin choice and the target level of LDL cholesterol immediately prior to surgery remain controversial. It may be that the more potent statins induce more side effects during surgery, but any such claim is speculative since no comparative studies exist. Regardless, the purpose of perioperative statin use should be reduction of the inflammatory stress response to surgery, with the long-term goal being achievement of recommended target lipid levels.
In particular, patients with peripheral arterial disease should have a statin initiated prior to high-risk vascular surgery (if they are not already receiving one), to increase the odds of recovering renal function after surgery (see section below) and to improve long-term outcomes.
Who are the best candidates?
Patients with multiple cardiac risk factors represent an especially high-risk group that benefits the most from statin therapy prior to vascular surgery, as they are likely to have more extensive disease and more extensive inflammation in the coronary artery tree.
Given the low incidence of side effects associated with statins, initiating a statin in patients with multiple cardiac risk factors who are undergoing intermediate-risk surgery may seem appropriate, but no data from large randomized trials are available to support this practice. Caution is in order when extrapolating data from studies conducted in the high-risk vascular surgery context to other surgical settings, since statins may pose hidden side effects such as liver dysfunction and myopathy, which may be missed in patients under anesthesia.
My personal practice is to initiate a statin prior to high-risk surgery or in patients with multiple cardiac risk factors if the risk-factor profile presents a clear indication for long-term statin use. If no risk factors are present, I am more reluctant to initiate a statin because of a lack of supportive data.
Beware the rebound effect with statin withdrawal
Statin withdrawal for several days following surgery is a common practice, since statins are given orally and their pleiotropic effects are underappreciated.
A withdrawal effect leading to abrogation of clinical benefit has been observed with perioperative use of short-acting statins, whose anti-inflammatory properties do not effectively extend to the postoperative period. Acute withdrawal has been associated with an increase in markers of inflammation and oxidative stress, and an increase in cardiac events has been observed with acute withdrawal of statins during periods of instability when compared with continuation of statin therapy.11
For these reasons, a long-acting statin is preferred preoperatively in patients whose oral intake will be compromised for several days after surgery (eg, in gastric surgery). The optimal statin for preventing the withdrawal effect is unknown. We chose extended-release fluvastatin in DECREASE III because its biological effect appears to last at least 4 days12 even though analysis of serum levels of the drug indicates a shorter half-life.
ANOTHER POTENTIAL BENEFIT: ENHANCED RECOVERY OF KIDNEY FUNCTION
Postoperative renal dysfunction is an ominous sign
Renal ischemic reperfusion injury is inevitable after vascular surgery that requires aortic cross-clamping. This is significant, as renal dysfunction after surgery is an ominous long-term sign that indicates abundant atherosclerosis. Complete recovery after acute kidney injury portends an improved long-term outcome, whereas patients with persistent renal dysfunction after vascular surgery have poor long-term outcomes.
A benefit from statins?
Statins may offer an effective means of preventing or shortening the course of acute kidney injury after surgery. Statins have been reported to lengthen survival of chronic kidney disease patients with sepsis or infectious complications and to improve the course of acute kidney injury in aging rats.13–15 These findings prompted my colleagues and I to conduct a retrospective study to evaluate whether statins may ameliorate reperfusion injury in the kidney after aortic cross-clamping.16
Promising findings from an observational review
We reviewed the records of all patients who had undergone vascular surgery at Erasmus Medical Center from January 1995 to June 2006 to examine the relation between preoperative statin use and renal function after suprarenal aortic cross-clamping.16 Of the 1,944 patients who met inclusion criteria, 515 (26.5%) were statin users. Postoperative kidney injury was defined as more than a 10% reduction in creatinine clearance on postoperative day 1 or 2 compared with baseline. Recovery of kidney function was defined as a creatinine clearance of greater than 90% of the baseline value by postoperative day 3.
The clinical characteristics of the populations with and without kidney injury after aortic cross-clamping were similar, including baseline creatinine clearance and serum creatinine.
Acute kidney injury within 2 days of surgery occurred in 664 patients (34%), of which 313 (47%) had complete recovery of kidney function at postoperative day 3. Although the incidence of postoperative kidney injury was similar among statin users and nonusers, statin use was associated with an increased chance of complete recovery of kidney function at day 3 (odds ratio = 2.0; 95% CI, 1.0–3.8).
All-cause mortality was assessed during a mean follow-up of 6.24 years. Statin use was associated with improved long-term survival, regardless of any change in kidney function (hazard ratio for death = 0.60; 95% CI, 0.48–0.75). Among the four broad patient groups, survival was highest among statin users with no postoperative kidney injury, followed by statin users who had kidney injury, then by nonusers of statins with no kidney injury, and finally by nonusers of statins who had kidney injury.
We concluded that perioperative statin use was associated with clinically significant recovery from acute kidney injury after high-risk vascular surgery and, more importantly, with improved long-term survival regardless of the presence of kidney injury. These promising findings require confirmation in prospective trials.
SUMMARY
Vascular surgery carries a high risk of perioperative mortality. Perioperative use of extended-release fluvastatin is associated with a reduced incidence of myocardial ischemia and the composite of MI and cardiovascular death at 30 days following surgery. These beneficial clinical outcomes are achieved without an increase in the incidence of side effects, including liver dysfunction and myopathy. Preoperative initiation of a long-acting statin is a reasonable strategy for reducing the risks associated with vascular surgery, and offers a bridge to postoperative statin continuation to blunt the inflammatory stress of surgery. Ischemic reperfusion injury is a major cause of renal dysfunction following vascular surgery. Statin therapy appears to help restore kidney function after aortic cross-clamping in patients undergoing high-risk vascular surgery.
DISCUSSION
Question from the audience: The majority of patients randomized in DECREASE III had relatively normal cholesterol levels. Do you believe those patients are biologically different from patients with physiologic vascular disease and elevated cholesterol levels?
Dr. Poldermans: We enrolled patients with various baseline cholesterol levels, and we found that these levels were not related to postoperative outcome. It would be a good idea to examine inflammation status just prior to surgery in patients with lower cholesterol levels to see if they have different outcomes from those with high cholesterol.
Question from the audience: If a patient is already on a short-acting statin and we know that he or she won’t be able to take a statin postoperatively, should we change to a long-acting statin just prior to surgery?
Dr. Poldermans: To be honest, this is a financial issue. If you have the opportunity, the best course would be to prescribe a statin with a prolonged half-life or an extended-release formulation. Of course, it’s not always possible to prescribe one particular statin. You have to negotiate what is feasible and hope to initiate the statin as early as possible to reduce risk.
Question from the audience: In studies conducted outside the perioperative setting, such as PROVE IT (Pravastatin or Atorvastatin Evaluation and Infection Therapy) and a substudy of REVERSAL (Reversing Atherosclerosis with Aggressive Lipid Lowering), it took about 30 days after statin initiation for hsCRP levels to minimize, and at least that long for halting of plaque progression to be detected by intravascular ultrasonography. Given that, does it make sense to delay nonurgent surgery in a patient in whom you’re worried about a postoperative MI?
Dr. Poldermans: Rat studies show improved blood flow and reduced thrombosis within hours of statin initiation. In the perioperative setting, therefore, initiating a statin within 30 days may be appropriate, but nobody knows the exact timing for optimal effect. Since there are no data to answer this question, I would not postpone surgery for this reason.
- Cohen MC, Aretz TH. Histological analysis of coronary artery lesions in fatal postoperative myocardial infarction. Cardiovasc Pathol 1999; 8:133–139.
- Dawood MM, Gutpa DK, Southern J, et al. Pathology of fatal perioperative myocardial infarction: implications regarding pathophysiology and prevention. Int J Cardiol 1996; 57:37–44.
- Ridker PM, Cannon CP, Morrow D, et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med 2005; 352:20–28.
- Poldermans D, Bax J, Boersma E, et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. European Society of Cardiology Web site. http://www.escardio.org/guidelines-surveys/esc-guidelines/GuidelinesDocuments/guidelines-perioperative-cardiac-care-FT.pdf. Posted September 1, 2009. Accessed September 3, 2009.
- Durazzo AE, Machado FS, Ikeoka DT, et al. Reduction in cardiovascular events after vascular surgery with atorvastatin: a randomized trial. J Vasc Surg 2004; 39:967–976.
- Lindenauer PK, Pekow P, Wang K, Gutierrez B, Benjamin EM. Lipid-lowering therapy and in-hospital mortality following major noncardiac surgery. JAMA 2004; 291:2092–2099.
- Kertai MD, Boersma E, Westerhout CM, et al. A combination of statins and beta-blockers is independently associated with a reduction in the incidence of perioperative mortality and nonfatal myocardial infarction in patients undergoing abdominal aortic aneurysm surgery. Eur J Vasc Endovasc Surg 2004; 28:343–352.
- O’Neil-Callahan K, Katsimaglis G, Tepper MR, et al. Statins decrease perioperative cardiac complications in patients undergoing noncardiac vascular surgery: the Statins for Risk Reduction in Surgery (StaRRS). J Am Coll Cardiol 2005; 45:336–342.
- Poldermans D, Bax JJ, Kertai MD, et al. Statins are associated with a reduced incidence of perioperative mortality in patients undergoing major noncardiac vascular surgery. Circulation 2003; 107:1848–1851.
- Schouten O, Boersma E, Hoeks SE, et al, for the Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. Fluvastatin and perioperative events in patients undergoing vascular surgery. N Engl J Med 2009; 361:980–989.
- Heeschen C, Hamm CW, Laufs U, Snapinn S, Bohm M, White HD. Withdrawal of statins increases event rates in patients with acute coronary syndromes. Circulation 2002; 105:1446–1452.
- Schouten O, Hoeks SE, Welten GM, et al. Effect of statin withdrawal on frequency of cardiac events after vascular surgery. Am J Cardiol 2007; 100:316–320.
- Gupta R, Plantinga LC, Fink NE, et al. Statin use and hospitalization for sepsis in patients with chronic kidney disease. JAMA 2007; 297:1455–1464.
- Yasuda H, Yuen PS, Hu X, et al. Simvastatin improves sepsis-induced mortality and acute kidney injury via renal vascular effects. Kidney Int 2006; 69:1535–1542.
- Sabbatini M, Pisani A, Uccello F, et al. Atorvastatin improves the course of ischemic acute renal failure in aging rats. J Am Soc Nephrol 2004; 15:901–909.
- Welten GMJM, Chonchol M, Schouten O, et al. Statin use is associated with early recovery of kidney injury after vascular surgery and improved long-term outcome. Nephrol Dial Transplant 2008; 23:3867–3873.
- Cohen MC, Aretz TH. Histological analysis of coronary artery lesions in fatal postoperative myocardial infarction. Cardiovasc Pathol 1999; 8:133–139.
- Dawood MM, Gutpa DK, Southern J, et al. Pathology of fatal perioperative myocardial infarction: implications regarding pathophysiology and prevention. Int J Cardiol 1996; 57:37–44.
- Ridker PM, Cannon CP, Morrow D, et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med 2005; 352:20–28.
- Poldermans D, Bax J, Boersma E, et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. European Society of Cardiology Web site. http://www.escardio.org/guidelines-surveys/esc-guidelines/GuidelinesDocuments/guidelines-perioperative-cardiac-care-FT.pdf. Posted September 1, 2009. Accessed September 3, 2009.
- Durazzo AE, Machado FS, Ikeoka DT, et al. Reduction in cardiovascular events after vascular surgery with atorvastatin: a randomized trial. J Vasc Surg 2004; 39:967–976.
- Lindenauer PK, Pekow P, Wang K, Gutierrez B, Benjamin EM. Lipid-lowering therapy and in-hospital mortality following major noncardiac surgery. JAMA 2004; 291:2092–2099.
- Kertai MD, Boersma E, Westerhout CM, et al. A combination of statins and beta-blockers is independently associated with a reduction in the incidence of perioperative mortality and nonfatal myocardial infarction in patients undergoing abdominal aortic aneurysm surgery. Eur J Vasc Endovasc Surg 2004; 28:343–352.
- O’Neil-Callahan K, Katsimaglis G, Tepper MR, et al. Statins decrease perioperative cardiac complications in patients undergoing noncardiac vascular surgery: the Statins for Risk Reduction in Surgery (StaRRS). J Am Coll Cardiol 2005; 45:336–342.
- Poldermans D, Bax JJ, Kertai MD, et al. Statins are associated with a reduced incidence of perioperative mortality in patients undergoing major noncardiac vascular surgery. Circulation 2003; 107:1848–1851.
- Schouten O, Boersma E, Hoeks SE, et al, for the Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. Fluvastatin and perioperative events in patients undergoing vascular surgery. N Engl J Med 2009; 361:980–989.
- Heeschen C, Hamm CW, Laufs U, Snapinn S, Bohm M, White HD. Withdrawal of statins increases event rates in patients with acute coronary syndromes. Circulation 2002; 105:1446–1452.
- Schouten O, Hoeks SE, Welten GM, et al. Effect of statin withdrawal on frequency of cardiac events after vascular surgery. Am J Cardiol 2007; 100:316–320.
- Gupta R, Plantinga LC, Fink NE, et al. Statin use and hospitalization for sepsis in patients with chronic kidney disease. JAMA 2007; 297:1455–1464.
- Yasuda H, Yuen PS, Hu X, et al. Simvastatin improves sepsis-induced mortality and acute kidney injury via renal vascular effects. Kidney Int 2006; 69:1535–1542.
- Sabbatini M, Pisani A, Uccello F, et al. Atorvastatin improves the course of ischemic acute renal failure in aging rats. J Am Soc Nephrol 2004; 15:901–909.
- Welten GMJM, Chonchol M, Schouten O, et al. Statin use is associated with early recovery of kidney injury after vascular surgery and improved long-term outcome. Nephrol Dial Transplant 2008; 23:3867–3873.
KEY POINTS
- The inflammatory and oxidative stress induced by vascular surgery can be blunted by statin therapy.
- Statin therapy started preoperatively can reduce the incidence of myocardial ischemia and the level of inflammatory markers in patients undergoing high-risk vascular surgery.
- The purpose of perioperative statin use should be reduction of the inflammatory stress response to surgery, with the long-term goal being achievement of target lipid levels.
- A long-acting statin is preferred preoperatively to best extend the anti-inflammatory effects into the postoperative period. Statin therapy should be continued postoperatively, if possible, to avoid deleterious acute withdrawal effects.
The experts debate: Perioperative beta-blockade for noncardiac surgery—proven safe or not?
NOTE: The individual co-authors in this debate-based article are responsible only for those views within their respective bylined subsections and those views ascribed to them in the rebuttals and discussion at the end.
Perioperative beta-blockade improves outcomes
By Don Poldermans, MD, PhD
It is my contention that perioperative beta-blockade improves mortality and cardiac outcomes in select high- and intermediate-risk patients undergoing noncardiac surgery. Patients on chronic beta-blocker therapy should have it continued perioperatively. For patients not already on beta-blockade who are at cardiac risk, initiation of low-dose beta-blocker therapy should be considered prior to surgery; such therapy should be started approximately 1 month before surgery, with dose titration to achieve hemodynamic stability. Reports of increased stroke rates with perioperative beta-blockade appear to be due to inappropriate acute administration of high-dose beta-blocker therapy.
THE PHYSIOLOGIC RATIONALE FOR PERIOPERATIVE BETA-BLOCKADE
Perioperative myocardial infarction (MI) can occur by one of two mechanisms, both of which can be attenuated by beta-blockade:
- The stress induced by surgery can cause an asymptomatic coronary plaque to become unstable and rupture, resulting in complete occlusion of a portion of the coronary tree. This type of perioperative MI occurs typically in patients with multiple risk factors for MI absent a critical coronary stenosis. The perioperative risk associated with unstable plaque can be reduced pharmacologically with aspirin, statins, and chronic beta-blocker therapy.
- Alternately, a fixed coronary stenosis can predispose to a mismatch of oxygen demand and supply, leading to myocardial ischemia and infarction. The patient with a fixed coronary lesion typically presents with stable angina pectoris, and the at-risk stenosis is identified through a stress echocardiogram or nuclear scan. The risk conferred by flow-limiting stable plaque can be reduced by coronary revascularization and a short course of beta-blocker therapy prior to surgery.
INITIAL SUPPORTIVE DATA
Mangano and colleagues were the first to evaluate perioperative beta-blockade in a randomized, controlled fashion.1,2 In their study of 200 surgical patients with or at risk for coronary artery disease, oral atenolol administered perioperatively was associated with a 50% reduction (compared with placebo) in the incidence of postoperative myocardial ischemia as measured by three-lead Holter monitoring.2 During 2 years of follow-up, mortality was significantly lower in the atenolol group (10%) than in the placebo group (21%) (P = .019).1
In the Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography (DECREASE I), my research group randomized 112 high-risk patients (as identified by dobutamine echocardiography) to standard perioperative care alone or standard perioperative care plus bisoprolol starting 30 days prior to major vascular surgery.3 The dosage of bisoprolol was titrated to achieve a target heart rate of 60 to 70 beats per minute. Thirty days after surgery, the incidence of the primary end point—a composite of death from cardiac causes or nonfatal MI—was reduced from 34% in the standard-care group to 3.4% in the bisoprolol group (P < .001). Thus, in this unblinded study in a population with proven coronary artery disease, beta-blockade clearly improved outcomes.
Additional studies of perioperative beta-blocker use have produced a wide range of outcomes, with most favoring beta-blockade, albeit usually not to a statistically significant degree.4–13 Notably, only some of these trials were randomized, they used various beta-blocker regimens at various doses, they were conducted in patients with varying degrees of cardiac risk, and many had small sample sizes.
What emerged from these trials was the idea that perioperative beta-blockade in patients with coronary artery disease produces an effect similar to that of long-term beta-blockade in reducing the risk of cardiovascular events in post-MI patients and in those with coronary artery disease and heart failure.
THE POISE STUDY AND ITS IMPLICATIONS
Results of the Perioperative Ischemic Evaluation (POISE) were published in 2008, in which 8,351 noncardiac surgery patients with or at risk of atherosclerotic disease were randomized to placebo or extended-release metoprolol succinate started 2 to 4 hours preoperatively and continued for 30 days.14 Metoprolol was associated with a clear reduction in the primary end point, a composite of cardiovascular death, nonfatal MI, or nonfatal cardiac arrest (5.8% vs 6.9% with placebo; hazard ratio [HR] = 0.84 [95% CI, 0.70–0.99]; P = .0399), but this effect was offset by significant increases in total mortality and stroke incidence in the metoprolol group. Mortality was 3.1% with metoprolol versus 2.3% with placebo (HR = 1.33 [95% CI, 1.03–1.74]; P = .0317), and stroke incidence was 1.0% with metoprolol versus 0.5% with placebo (HR = 2.17 [95% CI, 1.26–3.74]; P = .0053). Cerebral infarction, not bleeding, explained most of the excess mortality with metoprolol.
Of the 60 strokes in POISE, 49 were ischemic in origin, 3 were hemorrhagic, and 8 were of uncertain etiology. Preoperative predictors of stroke were the use of clopidogrel and a history of stroke or transient ischemic attack. Postoperative predictors of stroke included intraoperative bleeding and intraoperative hypotension. These predictors suggest a diseased cerebrovascular tree or unstable hemodynamics during the intraoperative period in the patients who suffered a stroke.
Does dosing explain the rise in mortality and strokes?
Could the fatal outcomes associated with the beta-blocker in POISE be attributed to the dosage of metoprolol? In the study, 100 mg of metoprolol was started immediately prior to surgery, and an additional 100 mg could be given, depending on the hemodynamic response. Maintenance therapy (200 mg/day) was started on the same day, making it possible that a patient could have received as much as 400 mg of metoprolol the day of surgery. The starting dose of metoprolol used in POISE was two to eight times the commonly prescribed dose.
The initial 100-mg dose of metoprolol used in POISE has a similar beta1-receptor blockade potency compared with the 5-mg dose of bisoprolol used in DECREASE I.3 However, in DECREASE I, bisoprolol was initiated 30 days prior to surgery and was titrated, if necessary, according to heart rate. The maintenance dose of bisoprolol was half of the maintenance dose used in POISE. In the later DECREASE trials, the starting dose of bisoprolol was only 2.5 mg. Therefore, there was a huge difference in beta-blocker dosing between POISE and DECREASE.
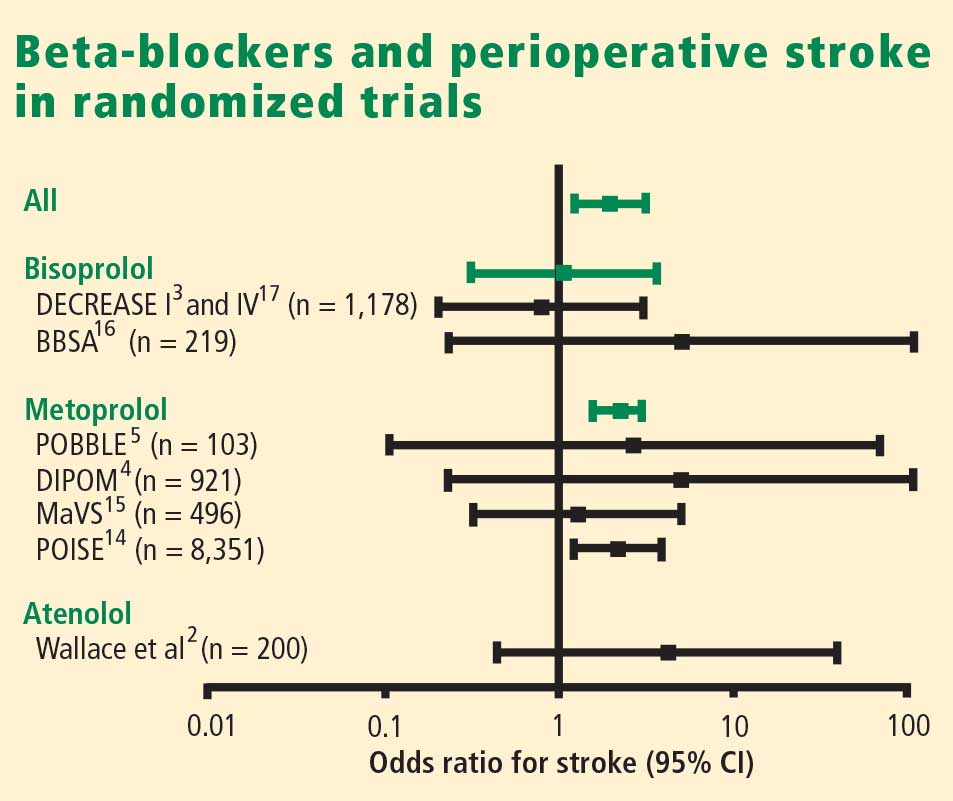
What about timing of beta-blocker initiation?
The POISE findings may also be explained in part by the timing of beta-blocker initiation. Whereas bisoprolol was carefully titrated for 30 days before surgery in DECREASE, metoprolol was initiated just before surgery in POISE, and the maximum recommended dose may have been prescribed during the first 24 hours, although subsequent dosing was 200 mg daily, which is 50% of the maximum daily therapeutic dose. This extremely narrow time window for titration may be important, since the beneficial effects of beta-blockade on coronary plaque stability are likely to take weeks to develop.
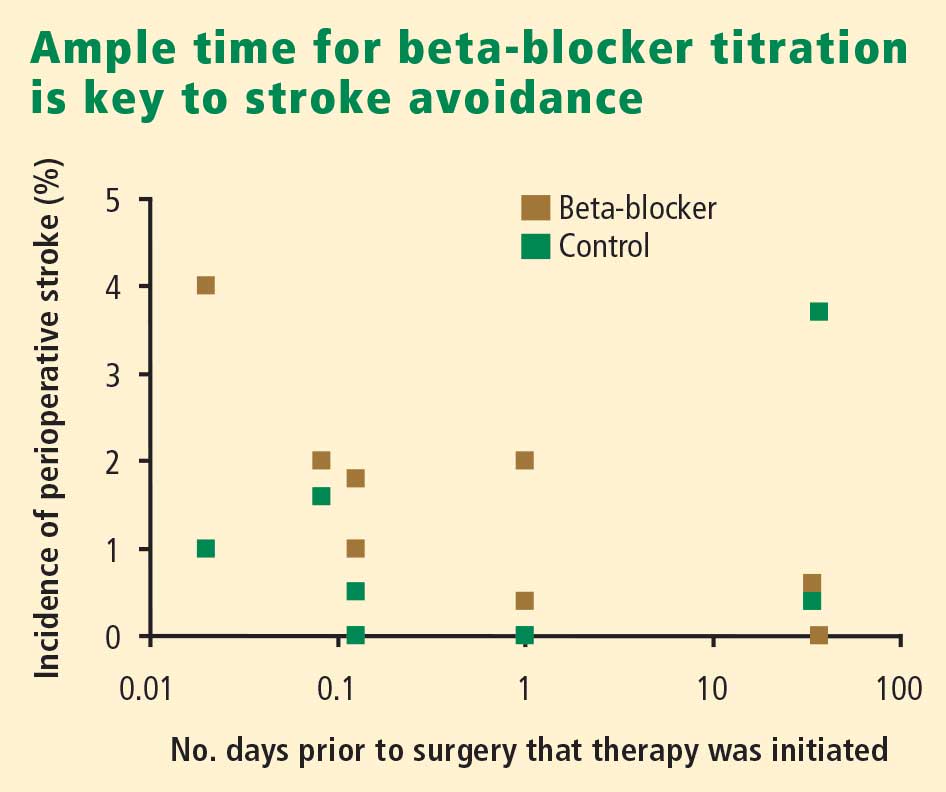
Reassurance from a large case-control study
My colleagues and I conducted a case-control study from among more than 75,000 patients who underwent noncardiac, nonvascular surgery at our institution, Erasmus Medical Center, from 1991 to 2001.18 The cases were the 989 patients who died in the hospital postoperatively; the controls were 1,879 survivors matched with the cases for age, sex, the year the surgery was performed, and the type of surgery. The incidence of perioperative stroke was 0.5%, which is comparable to the rate found in the literature. Risk factors predictive of stroke were the presence of diabetes, cerebrovascular disease, peripheral arterial disease, atrial fibrillation, coronary artery disease, and hypertension. Notably, no relationship was found between chronic beta-blocker use and stroke.
WHAT ABOUT PATIENTS AT INTERMEDIATE RISK?
Because the effect of perioperative beta-blockade has traditionally been ill defined in surgical patients at intermediate risk of cardiovascular events, the DECREASE study group recently completed a study (DECREASE IV) to assess perioperative bisoprolol in terms of cardiac morbidity and mortality in intermediate-risk patients undergoing elective noncardiovascular surgery.17 Enrollees had a score of 1 to 2 on the Revised Cardiac Risk Index of Lee et al,19 which corresponds to an estimated risk of between 1% and 6% for a perioperative cardiovascular event.17
DECREASE IV also aimed to assess the effect of perioperative fluvastatin, so a 2 x 2 factorial design was used in which the study’s 1,066 patients were randomized to receive bisoprolol, fluvastatin, combination treatment, or combination placebo control. Bisoprolol was initiated up to 30 days prior to surgery, and the 2.5-mg daily starting dosage was titrated according to the patient’s heart rate to achieve a target rate of 50 to 70 beats per minute. Fluvastatin was also started up to 30 days prior to surgery. Patients who received bisoprolol (with or without fluvastatin) had a significant reduction in the 30-day incidence of cardiac death and nonfatal MI compared with those who did not receive bisoprolol (2.1% vs 6.0%; HR = 0.34 [95% CI, 0.17–0.67]; P = .002). Fluvastatin was associated with a favorable trend on this end point, but statistical significance was not achieved (P = .17).17
There was no difference among treatment groups in the incidence of stroke (4 strokes in the 533 patients who received bisoprolol vs 3 strokes in the 533 patients who did not),17 which further suggests that the increased stroke rate seen with beta-blockade in POISE may have been due to dosage, timing of initiation, or both.
CONCLUSIONS
Dose-related hypotension may explain POISE findings
Our understanding of postoperative stroke is incomplete, but it appears that dosing of a beta-blocker can be a contributor, especially with respect to the potential side effect of hypotension during surgery. Keep in mind that the average age of patients in POISE was approximately 70 years and that patients were naïve to beta-blockers. Some may have had asymptomatic left ventricular dysfunction, and we know that starting a beta-blocker at a high dose in such patients may lead to hypotension. At my institution we routinely perform echocardiographic screening of all patients scheduled for surgery, and we have found that more than half of the patients with heart failure have it uncovered only through this screening.
It is not the medicine alone that can cause perioperative hypotension; other factors may induce hypotension, requiring beta-blocker titration and careful monitoring of hemodynamics during surgery.
Advice: Start early and titrate dose; continue chronic beta-blockade
My advice is as follows:
- If a patient is on chronic beta-blocker therapy, do not stop it perioperatively. We have seen devastating outcomes in the Netherlands when patients had their beta-blockers stopped immediately before surgery. Consider adjusting the dose, but do not stop it entirely. If a beta-blocker is on board and the patient develops hypotension or bradycardia during surgery, treat the symptoms and check for sepsis.
- In a patient not on a beta-blocker, consider adding one if the patient is at intermediate or high risk of a cardiac event, but start at a low dosage (ie, 2.5 mg/day for bisoprolol and 25 mg/day for metoprolol). Treatment ideally should be started 30 days preoperatively; in the Netherlands, we have the chance to start well in advance of surgery so we can titrate the dose according to hemodynamics.
- If a beta-blocker is not started because of insufficient time for titration, do not add one to treat tachycardia that develops during surgery, since tachycardia may represent a response to normal defense mechanisms.
Safety of perioperative beta-blocker use has not been adequately demonstrated
By P.J. Devereaux, MD, PhD
I contend that perioperative beta-blockade is a practice not grounded in evidence-based medicine, and its overall safety has increasingly come into question as more data from large, high-quality trials have emerged. I will begin with a historical overview of perioperative beta-blocker use, review the results of the POISE trial (for which I was the co-principal investigator), explore the major questions raised by this trial, and conclude with some take-away messages.
THE HISTORY OF PERIOPERATIVE BETA-BLOCKADE
In the 1970s, physicians were encouraged to hold beta-blockers prior to surgery out of concern that these medications may inhibit the required cardiovascular response when patients developed hypotension, and could thereby lead to serious adverse consequences.
In the 1980s, new research associated tachycardia with perioperative cardiovascular events, leading to proposals to implement perioperative beta-blocker use.
In the 1990s, two randomized trials with a total sample size of 312 patients1,3 suggested that perioperative beta-blockers had a large treatment effect in preventing major cardiovascular events and death. These small trials had several methodological limitations:
- One trial3 was unblinded in a setting in which the vast majority of MIs are clinically silent.
- One trial3 was stopped early—after randomizing only 112 patients—for unexpected large treatment effects.
- One of the studies1 failed to follow intention-to-treat principle.
Nevertheless, guidelines developed at the time by the American College of Cardiology and the American Heart Association (ACC/AHA) recommended the use of perioperative beta-blockers on the basis of the physiological rationale and these two small clinical trials. That recommendation was retained in the latest (2007) update of the ACC/AHA perioperative guidelines.20
In 2006, two clinical trials with a total sample size of 1,417 were completed,4,15 surpassing the total size of previous trials by more than fourfold. These two more recent trials did not suffer from the methodological limitations of earlier trials. These trials showed no benefit of perioperative beta-blocker use; in fact, there was a trend toward worse outcomes in the beta-blocker recipients.4,15 Despite these new data, guidelines committees continued to recommend perioperative beta-blockade.20
THE POISE TRIAL
Study design
This was the context into which the POISE results were released in 2008. POISE was a randomized, controlled, blinded trial of patients 45 years or older scheduled for noncardiac surgery who had, or were at high risk of, atherosclerotic disease.14 The intervention consisted of metoprolol succinate (metoprolol controlled release [CR]) or placebo started 2 to 4 hours preoperatively (if heart rate was ≥ 50 beats per minute and systolic blood pressure [SBP] was ≥ 100 mm Hg) and continued for 30 days. The target dosage of metoprolol was 200 mg once daily. No patients received the recommended maximum dosage of 400 mg over 24 hours. The main outcome measure was a 30-day composite of cardiovascular death, nonfatal MI, or nonfatal cardiac arrest.
We randomized 9,298 patients in a 1:1 ratio to metoprolol or placebo. We encountered data fraud at a number of centers that prompted exclusion of data from 474 patients allocated to metoprolol and 473 allocated to placebo. Therefore, the total number of patients available for the intention-to-treat analysis was 8,351, from 190 centers in 23 countries.
Results
The risk of the primary composite outcome was reduced by 16% (relative reduction) in recipients of metoprolol CR compared with placebo recipients (P = .0399). Significantly fewer nonfatal MIs occurred in the metoprolol CR group than in the placebo group (152 [3.6%] vs 215 [5.1%]; P = .0008), leaving little doubt that perioperative beta-blockade prevents MI.
In contrast, total mortality was increased in the beta-blocker group, with 129 deaths among those assigned to metoprolol CR and 97 among those assigned to placebo (P = .0317), and the incidence of stroke was also significantly greater in the metoprolol CR group (1.0% vs. 0.5%; P = .0053).
Consistency with findings from other trials
The POISE data are consistent with those from a 2008 meta-analysis of high-quality randomized controlled trials in noncardiac surgery patients, which showed a significantly greater risk of death among patients assigned to a beta-blocker than among controls who were not (160 deaths [2.8%] vs 127 deaths [2.3%]; odds ratio [OR] = 1.27 [95% CI, 1.01–1.61]).21 This meta-analysis also found a significantly greater risk of nonfatal stroke in beta-blocker recipients compared with controls (38 [0.7%] vs 17 [0.3%]; OR = 2.16 [95% CI, 1.27–3.68]).
I also contend that the DECREASE IV trial supports the POISE findings in that although few strokes were encountered in DECREASE IV, the trend was in the direction of harm in the beta-blocker group, which had 4 strokes among 533 patients versus 3 strokes among 533 patients not receiving the beta-blocker.17
Predictive role of hypotension
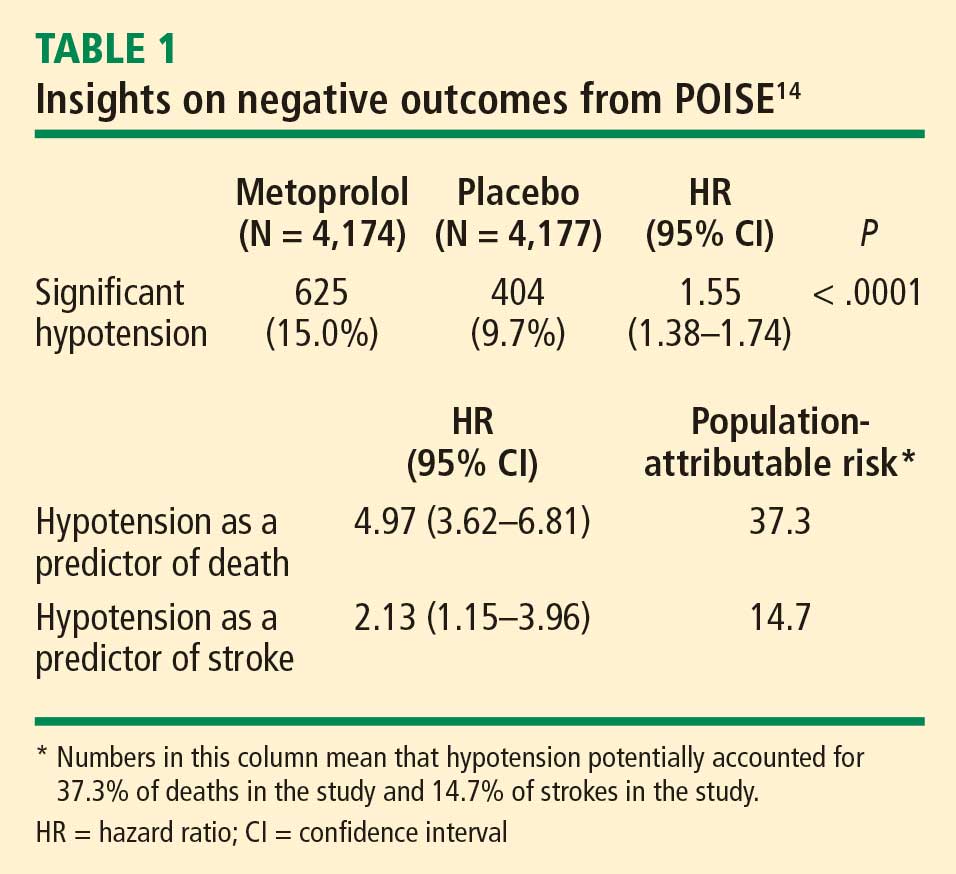
The link between hypotension and death in POISE is consistent with findings from the largest beta-blocker trial undertaken, COMMIT (Clopidogrel and Metoprolol in Myocardial Infarction Trial), in which 45,852 patients with acute MI were randomized to metoprolol or placebo.22 In COMMIT, metoprolol had no effect on 30-day all-cause mortality but significantly reduced the risk of arrhythmic death, a benefit that was countered by a significantly increased risk of death from shock with a beta-blocker in acute MI. Clinically significant hypotension is much more common in the perioperative setting than in acute MI, which may explain the excess number of deaths observed with metoprolol in POISE as opposed to metoprolol’s neutral effect on mortality in COMMIT.
ANSWERING THE CRITICS
Several criticisms have been raised about POISE, as detailed below.
Beta-blocker dose
Some contend that a lower dose of beta-blocker would provide benefit and minimize risk, but this assertion must be supported by evidence from a large clinical trial. The targeted dosage of metoprolol in POISE represents 50% of the maximum daily therapeutic dose. Further, the protocol called for decreasing the dosage to 100 mg/day if SBP dropped to less than 100 mm Hg or if heart rate fell to less than 45 beats per minute.
The two small trials on which guideline recommendations for perioperative beta-blockade are primarily based1,3 had a sample size that was 4% of that in POISE, which calls into question the reliability of their results. The study by Mangano et al used atenolol at a target dosage that was 50% of the maximum daily therapeutic dose,1 the same as with metoprolol in POISE. DECREASE initiated bisoprolol at 25% of the maximum daily therapeutic dose, and allowed for titration to 50% of the maximum daily therapeutic dose.3
As the second largest study of perioperative beta-blockade, the Diabetic Postoperative Mortality and Morbidity (DIPOM) trial enrolled 921 patients who were assigned to placebo or controlled-release metoprolol with a target dosage that was 25% of the maximum daily therapeutic dose.4 The 30-day outcomes from DIPOM showed a trend toward an excess of death and stroke despite using only one-half the dosage in POISE and the same dosage as in DECREASE.
Timing of beta-blocker initiation
Another contention is that earlier beta-blocker initiation would be better. The issue with timing of initiation is not benefit, as POISE showed that starting a beta-blocker hours before surgery results in a reduction in the risk of MI. The issue is whether giving a beta-blocker earlier makes administering the drug safer. Nearly 10% of placebo recipients in POISE developed clinically significant hypotension, which suggests that the titrated dosage of a beta-blocker that appears effective preoperatively is unlikely to inform a safe dose after surgery, when hypotension is common.
The practicality of titrating the dose of beta-blocker prior to surgery also comes into play. Most patients referred to my institution for surgery are seen 1 to 2 weeks in advance, at the earliest. Real-world practice at present simply does not afford us the luxury of seeing patients three to four times before surgery in order to titrate the beta-blocker dose.
POISE did not address chronic beta-blocker therapy
It is important to remember that POISE excluded patients on chronic beta-blocker therapy and thus did not attempt to address the perioperative management of such patients who undergo noncardiac surgery. My suspicion is that perioperative continuation of beta-blockade in these patients is the best course of action, but this too has not been studied robustly, so we need a large controlled trial to confirm that this practice is indeed safe.
CONCLUSIONS
The POISE results suggest that for every 1,000 patients treated, perioperative metoprolol would:
- Prevent 15 MIs, 3 cardiac revascularizations, and 7 new cases of atrial fibrillation
- Result in 8 excess deaths, 5 strokes, 53 cases of clinically significant hypotension, and 42 cases of clinically significant bradycardia.
The central take-away message is that patients are unlikely to want a perioperative beta-blocker if they are unwilling to accept a probable increase in mortality or if they place three times more value on avoiding a perioperative stroke than on avoiding an MI.
It has been 10 years since the recommendation to use perioperatove beta-blockers was incorporated into perioperative practice guidelines. Assuming only 10% of physicians acted on this recommendation, 100 million patients have received a perioperative beta-blocker over this time as a result. If the POISE results are applicable, a full 800,000 of these patients died and another 500,000 suffered perioperative strokes as a result of being given a beta-blocker. This issue is not to be taken lightly, given the evidence to suggest harm.
Though it is possible that an alternative beta-blocker regimen to the one used in POISE may provide benefit without substantial harm, the data suggest this is not probable. The POISE data highlight the risk of making assumptions, as well as the importance of and need for large, high-quality randomized trials in the perioperative setting.
It is time for perioperative medicine to enter the age of evidence-based practice and embrace one of its central tenets: only large trials are reliable when it comes to therapeutic questions.
Rebuttals and discussion
POLDERMANS REBUTTAL: MORE TRANSPARENCY NEEDED IN POISE DOSING DATA
Dr. Poldermans: The initial paper describing the POISE trial design did indeed indicate that it was possible for a patient to receive 400 mg of metoprolol on the first day of treatment. We need to see the actual doses of metoprolol given to all patients in POISE who had a perioperative stroke. If you show me these data, the issue will be much easier to discuss.
Our data from randomized trials are consistent in showing that a titrated dosing regimen using bisoprolol reduces the incidence of postoperative cardiac events with no increase in the number of strokes.
My take-home message is that if you want to use beta-blockers, use them sensibly, use them carefully, and act during surgery. If many of your patients are developing hypotension, then you are doing something wrong.
DEVEREAUX REBUTTAL: A SHIFT IN THINKING IS REQUIRED
Dr. Devereaux: The data from POISE are fully available, and I take issue with Dr. Poldermans’ contention that a patient could have received as much as 400 mg of metoprolol CR on the day of surgery; this was not an option according to protocol. I believe his statement is misleading in the same way that it is misleading to indicate that in the DECREASE trial patients may have received 20 mg of bisoprolol within 24 hours of surgery. It is possible that a patient in DECREASE could have gone to surgery at 2:00 pm and may have taken his or her bisoprolol at 10:00 am that morning. The following morning (in the hospital), it is possible that the patient would have received his or her bisoprolol 10 mg at 7:00 or 8:00 am (ie, 20 mg within 24 hours of surgery). Although this is possible and something similar could have happened within POISE, it does not reflect a patient receiving an effective dose of metoprolol CR 400 mg or bisoprolol 20 mg over a 24-hour period.
I worry about the distortion of reality in perioperative medicine that leads so many of us to believe that randomization is magical despite small sample sizes. Small randomized trials are at profound risk of imbalance between the randomized groups, whether we see it or not, and the results are therefore simply not reliable.
Unless we shift our thinking, we make ourselves susceptible to overconfidence in the benefits of a certain intervention before the data from large clinical trials become available. In the meantime, as we have seen from POISE, an intervention may have negative consequences that are not apparent from small clinical trials.
The reality of excess stroke with perioperative beta-blockers is consistent across all the trials. It does not mean that we cannot find another way to give beta-blockers safely, but if we want to establish safety, we need a large trial that unequivocally demonstrates safety, as opposed to simply using observational data, retrospective cohorts, or comparisons between two nonrandomized trials. Until we have large data sets, it is very difficult to say that we can give beta-blockers safely.
DISCUSSION WITH THE AUDIENCE
Moderator*: Dr. Devereaux, was the hypotension in POISE related to the long-acting beta-blocker itself or to the large dose of if that was used? Similarly, were the strokes a result of the drug itself or of the hypotension?
Dr. Devereaux: I must take issue with your premise that the dose of metoprolol used in POISE was “large.” As I noted, Mangano’s study used its beta-blocker (atenolol) at 50% of its maximum daily therapeutic dose,1 the same proportion used in POISE, and Dr. Poldermans’ own DECREASE trial allowed titration of bisoprolol up to 50% of the maximum daily therapeutic dose.3 The DIPOM trial used half the dose of metoprolol that we used, yet it too yielded a trend toward more death and stroke in the beta-blocker group.4 So it’s not that the dose we used was at some excessive level. At the same time, that does not mean that a smaller dose may not have achieved a similarly significant benefit in cardiac outcomes.
We can’t explain most of the strokes. Because most strokes were ischemic, I suspect that the explanation may lie in the threshold used to define clinically significant hypotension. We used an SBP cutoff of less than 90 mm Hg, but we did not classify large drops in SBP, such as from 180 to 95 mm Hg, as clinically significant hypotension. The high incidence of clinically significant hypotension in the placebo group—about 10%—suggests that hypotension was likely the driving factor for stroke. The beta-blocker exacerbated the hypotension, but its more important effect may have been that it made it harder for the body to overcome the hypotension. That is the exact same signal observed in the COMMIT trial in the setting of acute MI.22
Dr. Poldermans: I’d like to see the intraoperative blood pressure data for the 60 patients who suffered strokes in POISE. We could then find out exactly when the hypotension occurred, what kind of hypotension it was, what the patient’s initial blood pressure reading was, and so on. If we had access to this information, we could determine which occurred first—the hypotension or the stroke.
Dr. Devereaux: Although trials can indicate a signal, they can’t explain with certainty the pathway through which the outcome occurred. For example, we know that beta-blockers prevent MI, but we don’t know how. What’s most impressive about the stroke issue is the consistency across all the perioperative beta-blocker trials: every one shows a direction of excess stroke with beta-blockers.
Question from the audience: The patient groups studied in DECREASE and POISE were different. DECREASE studied a very high-risk vascular surgery group with known coronary artery disease on the basis of echocardiography. POISE included patients undergoing emergency surgery and patients with sepsis. Can you describe the outcomes in POISE solely among the patients who underwent elective vascular surgery, similar to the patients studied in DECREASE?
Dr. Devereaux: In terms of the benefit to bisoprolol in very high-risk patients in DECREASE, remember that it was a study of 112 patients. That’s far too small a trial to establish safety or efficacy. The benefit of perioperative beta-blockade in preventing MI is unequivocal because it’s consistent across all trials. But the real issue is, was it safe?
Interestingly, in POISE, the groups at highest risk looked like they benefited the least, not the most. The notion of targeting high-risk people is not supported by POISE; if anything, the POISE results went in the direction of harm with beta-blockade in high-risk patients. That being said, the P value for interaction is not statistically significant, but it’s heading in the direction of harm. So I wouldn’t take comfort in believing that if we simply target high-risk patients, beta-blockers become safe.
Question from the audience: I believe that the seven or eight studies that showed higher stroke rates with beta-blockers all gave beta-blockade within 24 hours of surgery. Only in DECREASE was it given days and weeks in advance of surgery. Can you comment?
Dr. Poldermans: There’s clearly a relation between the time of beta-blocker initiation and the incidence of stroke. If you look at the randomized trials, you see an increased incidence of stroke in patients in whom beta-blockers are started just prior to surgery but not in patients who are on chronic beta-blockers. In our case-control study,18 we screened more than 185,000 patients for stroke and could not detect an increased incidence of stroke in those on chronic beta-blocker therapy. So stroke indeed has something to do with starting beta-blockers just before surgery.
Dr. Devereaux: In DECREASE IV, bisoprolol was started up to 1 month before surgery, yet there were 4 strokes in the bisoprolol group versus 3 in the control group.17
Dr. Poldermans: Yes, but that difference is not statistically meaningful.
Comment from the audience: I’m uncomfortable with the way Dr. Devereaux stresses the importance of significant findings from large randomized trials but then quibbles about a stroke rate of 4 versus 3, which is not statistically significant. Keep it scientific: either there is or there isn’t a P value that achieves significance.
Though I congratulate you on a great trial, any resident in my program would be fired for pursuing your strategy of perioperative care in POISE, which included using an SBP of 100 mm Hg as the threshold for stopping the beta-blocker regardless of preoperative blood pressure. An SBP of 100 mm Hg is not the definition of hypotension. Most anesthesiologists and perioperative physicians peg the beta-blockade to a reasonable level based on the preoperative blood pressure. They titrate in fluids and titrate in the beta-blocker. Certainly the timing is an issue—we don’t recommend giving it right before the operation.
Dr. Devereaux: I referred to the stroke rates in DECREASE IV because Dr. Poldermans has claimed that the excess in strokes has occurred in all trials but his, yet DECREASE IV was one of his trials and also one in which bisoprolol was started early. I’m not claiming statistical significance between the 3 versus 4 strokes in DECREASE IV, but the stroke trend is in the same direction as in the other trials, so it tells us nothing with regard to safety. My point is, has anyone proven safety? As much as we’d like to imagine that beta-blockers are safe perioperatively—and maybe they are—it has not been proven. The largest trials at present are consistent with a signal toward harm.
It’s easy to criticize the methodology after a trial is done. A number of us came together and thought we had a reasonable protocol for POISE. We found a reduction in the incidence of MI but more strokes and higher mortality with perioperative metoprolol. Does this mean there is not a safe way to give a beta-blocker and derive the benefit? Of course not. But at the moment the evidence does not support a way to give a beta-blocker safely. Do we need to find a way to give it safely? Of course we do.
For example, the design of POISE II is factorial, looking at aspirin versus placebo as well as clonidine versus placebo. There are a number of factors about clonidine that suggest we might be able to achieve the benefits we saw in POISE and avoid the risk, but until we do a large trial, we’re not going to know.
Comment from the audience: It’s important that we clearly understand the conclusion from POISE. It’s not that the administration of beta-blockers is not safe. It’s that the administration of a beta-blocker, as your methodology applied it, was not totally safe. Those are two very different conclusions.
Dr. Devereaux: I would say the conclusion is that the way that beta-blockers are being given has not been proven to be safe. The result is consistent. It’s even consistent with DECREASE IV.
Moderator: I believe in large clinical trials, but they must apply to real-life practice. POISE did not address the practices of many people in this room, particularly regarding the doses of metoprolol used. So it is hard for us to apply the findings in clinical practice. Those of you who design large trials need to think through your trial design very thoroughly, considering the millions of dollars that go into these trials. It’s not fair to clinicians to do a study that may have little clinical relevance.
Dr. Devereaux: Investigators from 190 centers in 23 countries were involved in POISE, and all of them thought we had a reasonable approach and methodology. That doesn’t mean it was perfect, yet the criticisms we are hearing now did not surface while the trial was ongoing.
Comment from the audience: My hospital in Australia contributed to the POISE study. When it started 6 or 7 years ago, the cardiologists were using beta-blockers liberally and haphazardly. It was a huge challenge to convince them that conducting the trial was justifiable—that the case for perioperative beta-blockers had not been absolutely and overwhelmingly proved. They wanted to put beta-blockers in the water supply at the doses we’re talking about.
It would be interesting to do separate analyses of the data from the various countries involved in POISE. In Australia, the percentage of the population on chronic beta-blockers—who therefore would have been ineligible for the trial—is now quite high. Most patients who need to be on beta-blockers long term are on them, whereas that was not the case 15 years ago. The population is changing even while we’re doing the trials. Australian cardiologists are no longer putting every patient on perioperative beta-blockers; they’re thinking about it first.
Dr. Devereaux: A compelling feature of POISE as an international trial is its consistency of outcomes across the planet. No matter where we looked, the outcomes were consistent: in Asia, Europe, North America, and Australia.
Moderator: Would each of you summarize your take-home message for clinicians?
Dr. Devereaux: I urge clinicians to actually read the trials themselves rather than just relying on the advice of guideline writers. It’s important not to allow ourselves to become entrenched in a practice without evidence, just because we’ve done it for so long. If you told your patients the number of MIs prevented and the potential number of excess strokes and deaths, I suspect the average patient would conclude it’s not a great trade-off.
Remember that two-thirds of MIs in the perioperative setting are clinically silent. That doesn’t mean they’re not important, but the strokes, in contrast, are profoundly devastating. One-third of patients with stroke in POISE were dead within 30 days, and of those who survived, 60% were incapacitated, needing help with everyday activities.
I encourage clinicians to read the POISE manuscript with a fresh perspective, regardless of how you’ve practiced until now. Then ask yourself whether you really are comfortable with the safety of perioperative beta-blockers at this time. Of course, that doesn’t mean the evidence won’t change in the future.
Dr. Poldermans: The main imperative is to improve postoperative care. We strongly believe that perioperative beta-blockers work in the general population. If you have a patient who needs to be on a beta-blocker after surgery, why not start it preoperatively? I believe that dosing and timing of initiation are important. If you have the opportunity to start the beta-blocker prior to surgery, do so at a reasonable dose and start early. Patients in whom beta-blockers are started immediately prior to surgery may be worse off, with a higher incidence of stroke.
*Amir K. Jaffer, MD, University of Miami Miller School of Medicine, served as moderator of the debate and the discussion period.
- Mangano DT, Layug EL, Wallace A, Tateo I. Effect of atenolol on mortality and cardiovascular morbidity after noncardiac surgery: Multicenter Study of Perioperative Ischemia Research Group. N Engl J Med 1996; 335:1713–1720.
- Wallace A, Layug B, Tateo I, et al. Prophylactic atenolol reduces postoperative myocardial ischemia: McSPI Research Group. Anesthesiology 1998; 88:7–17.
- Poldermans D, Boersma E, Bax JJ, et al. The effect of bisoprolol on perioperative mortality and myocardial infarction in high-risk patients undergoing vascular surgery: Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. N Engl J Med 1999; 341:1789–1794.
- Juul AB, Wetterslev J, Gluud C, et al. Effect of perioperative b-blockade in patients with diabetes undergoing major non-cardiac surgery: randomised placebo controlled, blinded multicentre trial. BMJ 2006; 332:1482.
- Brady AR, Gibbs JS, Greenhalgh RM, et al. Perioperative beta-blockade (POBBLE) for patients undergoing infrarenal vascular surgery: results of a randomized double-blind controlled trial. J Vasc Surg 2005; 41:602–609.
- Cucchiara RF, Benefiel DJ, Matteo RS, DeWood M, Albin MS. Evaluation of esmolol in controlling increases in heart rate and blood pressure during endotracheal intubation in patients undergoing carotid endarterectomy. Anesthesiology 1986; 65:528–531.
- Magnusson J, Thulin T, Werner O, Järhult J, Thomson D. Haemodynamic effects of pretreatment with metoprolol in hypertensive patients undergoing surgery. Br J Anaesth 1986; 58:251–260.
- Stone JG, Foëx P, Sear JW, et al. Myocardial ischemia in untreated hypertensive patients: effect of a single small oral dose of a beta-adrenergic blocking agent. Anesthesiology 1988; 68:495–500.
- Jakobsen CJ, Bille S, Ahlburg P, et al. Perioperative metoprolol reduces the frequency of atrial fibrillation after thoracotomy for lung resection. J Cardiothorac Vasc Anesth 1997; 11:746–751.
- Bayliff CD, Massel DR, Inculet RI, et al. Propranolol for the prevention of postoperative arrhythmias in general thoracic surgery. Ann Thorac Surg 1999; 67:182–186.
- Raby KE, Brull SJ, Timimi F, et al. The effect of heart rate control on myocardial ischemia among high-risk patients after vascular surgery. Anesth Analg 1999; 88:477–482.
- Zaugg M, Tagliente T, Lucchinetti E, et al. Beneficial effects from beta-adrenergic blockade in elderly patients undergoing noncardiac surgery. Anesthesiology 1999; 91:1674–1686.
- Urban MK, Markowitz SM, Gordon MA, et al. Postoperative prophylactic administration of beta-adrenergic blockers in patients at risk for myocardial ischemia. Anesth Analg 2000; 90:1257–1261.
- POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet 2008; 371:1839–1847.
- Yang H, Raymer K, Butler R, et al. The effects of perioperative beta-blockade: results of the Metoprolol after Vascular Surgery (MaVS) study, a randomized controlled trial. Am Heart J 2006; 152:983–990.
- Zaugg M, Bestman L, Wacker J, et al. Adrenergic receptor genotype but not perioperative bisoprolol therapy may determine cardiovascular outcome in at-risk patients undergoing surgery with spinal block: the Swiss Beta Blocker in Spinal Anesthesia (BBSA) study. Anesthesiology 2007; 107:33–44.
- Dunkelgrun M, Boersma E, Schouten O, et al. Bisoprolol and fluvastatin for reduction of perioperative cardiac mortality and myocardial infarction in intermediate-risk patients undergoing noncardiac surgery. A randomized controlled trial (DECREASE-IV). Ann Surg 2009; 249:921–926.
- Noordzij PG, Poldermans D, Schouten O, et al. Beta-blockers and statins are individually associated with reduced mortality in patients undergoing noncardiac, nonvascular surgery. Coron Artery Dis 2007; 18:67–72.
- Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999; 100:1043–1049.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2007; 50:1707–1732.
- Bangalore S, Wetterslev J, Pranesh S, et al. Perioperative beta blockers in patients having non-cardiac surgery: a meta-analysis. Lancet 2008; 372:1962–1976.
- COMMIT (Clopidogrel and Metoprolol in Myocardial Infarction Trial) collaborative group. Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet 2005; 366:1622–1632.
NOTE: The individual co-authors in this debate-based article are responsible only for those views within their respective bylined subsections and those views ascribed to them in the rebuttals and discussion at the end.
Perioperative beta-blockade improves outcomes
By Don Poldermans, MD, PhD
It is my contention that perioperative beta-blockade improves mortality and cardiac outcomes in select high- and intermediate-risk patients undergoing noncardiac surgery. Patients on chronic beta-blocker therapy should have it continued perioperatively. For patients not already on beta-blockade who are at cardiac risk, initiation of low-dose beta-blocker therapy should be considered prior to surgery; such therapy should be started approximately 1 month before surgery, with dose titration to achieve hemodynamic stability. Reports of increased stroke rates with perioperative beta-blockade appear to be due to inappropriate acute administration of high-dose beta-blocker therapy.
THE PHYSIOLOGIC RATIONALE FOR PERIOPERATIVE BETA-BLOCKADE
Perioperative myocardial infarction (MI) can occur by one of two mechanisms, both of which can be attenuated by beta-blockade:
- The stress induced by surgery can cause an asymptomatic coronary plaque to become unstable and rupture, resulting in complete occlusion of a portion of the coronary tree. This type of perioperative MI occurs typically in patients with multiple risk factors for MI absent a critical coronary stenosis. The perioperative risk associated with unstable plaque can be reduced pharmacologically with aspirin, statins, and chronic beta-blocker therapy.
- Alternately, a fixed coronary stenosis can predispose to a mismatch of oxygen demand and supply, leading to myocardial ischemia and infarction. The patient with a fixed coronary lesion typically presents with stable angina pectoris, and the at-risk stenosis is identified through a stress echocardiogram or nuclear scan. The risk conferred by flow-limiting stable plaque can be reduced by coronary revascularization and a short course of beta-blocker therapy prior to surgery.
INITIAL SUPPORTIVE DATA
Mangano and colleagues were the first to evaluate perioperative beta-blockade in a randomized, controlled fashion.1,2 In their study of 200 surgical patients with or at risk for coronary artery disease, oral atenolol administered perioperatively was associated with a 50% reduction (compared with placebo) in the incidence of postoperative myocardial ischemia as measured by three-lead Holter monitoring.2 During 2 years of follow-up, mortality was significantly lower in the atenolol group (10%) than in the placebo group (21%) (P = .019).1
In the Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography (DECREASE I), my research group randomized 112 high-risk patients (as identified by dobutamine echocardiography) to standard perioperative care alone or standard perioperative care plus bisoprolol starting 30 days prior to major vascular surgery.3 The dosage of bisoprolol was titrated to achieve a target heart rate of 60 to 70 beats per minute. Thirty days after surgery, the incidence of the primary end point—a composite of death from cardiac causes or nonfatal MI—was reduced from 34% in the standard-care group to 3.4% in the bisoprolol group (P < .001). Thus, in this unblinded study in a population with proven coronary artery disease, beta-blockade clearly improved outcomes.
Additional studies of perioperative beta-blocker use have produced a wide range of outcomes, with most favoring beta-blockade, albeit usually not to a statistically significant degree.4–13 Notably, only some of these trials were randomized, they used various beta-blocker regimens at various doses, they were conducted in patients with varying degrees of cardiac risk, and many had small sample sizes.
What emerged from these trials was the idea that perioperative beta-blockade in patients with coronary artery disease produces an effect similar to that of long-term beta-blockade in reducing the risk of cardiovascular events in post-MI patients and in those with coronary artery disease and heart failure.
THE POISE STUDY AND ITS IMPLICATIONS
Results of the Perioperative Ischemic Evaluation (POISE) were published in 2008, in which 8,351 noncardiac surgery patients with or at risk of atherosclerotic disease were randomized to placebo or extended-release metoprolol succinate started 2 to 4 hours preoperatively and continued for 30 days.14 Metoprolol was associated with a clear reduction in the primary end point, a composite of cardiovascular death, nonfatal MI, or nonfatal cardiac arrest (5.8% vs 6.9% with placebo; hazard ratio [HR] = 0.84 [95% CI, 0.70–0.99]; P = .0399), but this effect was offset by significant increases in total mortality and stroke incidence in the metoprolol group. Mortality was 3.1% with metoprolol versus 2.3% with placebo (HR = 1.33 [95% CI, 1.03–1.74]; P = .0317), and stroke incidence was 1.0% with metoprolol versus 0.5% with placebo (HR = 2.17 [95% CI, 1.26–3.74]; P = .0053). Cerebral infarction, not bleeding, explained most of the excess mortality with metoprolol.
Of the 60 strokes in POISE, 49 were ischemic in origin, 3 were hemorrhagic, and 8 were of uncertain etiology. Preoperative predictors of stroke were the use of clopidogrel and a history of stroke or transient ischemic attack. Postoperative predictors of stroke included intraoperative bleeding and intraoperative hypotension. These predictors suggest a diseased cerebrovascular tree or unstable hemodynamics during the intraoperative period in the patients who suffered a stroke.
Does dosing explain the rise in mortality and strokes?
Could the fatal outcomes associated with the beta-blocker in POISE be attributed to the dosage of metoprolol? In the study, 100 mg of metoprolol was started immediately prior to surgery, and an additional 100 mg could be given, depending on the hemodynamic response. Maintenance therapy (200 mg/day) was started on the same day, making it possible that a patient could have received as much as 400 mg of metoprolol the day of surgery. The starting dose of metoprolol used in POISE was two to eight times the commonly prescribed dose.
The initial 100-mg dose of metoprolol used in POISE has a similar beta1-receptor blockade potency compared with the 5-mg dose of bisoprolol used in DECREASE I.3 However, in DECREASE I, bisoprolol was initiated 30 days prior to surgery and was titrated, if necessary, according to heart rate. The maintenance dose of bisoprolol was half of the maintenance dose used in POISE. In the later DECREASE trials, the starting dose of bisoprolol was only 2.5 mg. Therefore, there was a huge difference in beta-blocker dosing between POISE and DECREASE.
What about timing of beta-blocker initiation?
The POISE findings may also be explained in part by the timing of beta-blocker initiation. Whereas bisoprolol was carefully titrated for 30 days before surgery in DECREASE, metoprolol was initiated just before surgery in POISE, and the maximum recommended dose may have been prescribed during the first 24 hours, although subsequent dosing was 200 mg daily, which is 50% of the maximum daily therapeutic dose. This extremely narrow time window for titration may be important, since the beneficial effects of beta-blockade on coronary plaque stability are likely to take weeks to develop.
Reassurance from a large case-control study
My colleagues and I conducted a case-control study from among more than 75,000 patients who underwent noncardiac, nonvascular surgery at our institution, Erasmus Medical Center, from 1991 to 2001.18 The cases were the 989 patients who died in the hospital postoperatively; the controls were 1,879 survivors matched with the cases for age, sex, the year the surgery was performed, and the type of surgery. The incidence of perioperative stroke was 0.5%, which is comparable to the rate found in the literature. Risk factors predictive of stroke were the presence of diabetes, cerebrovascular disease, peripheral arterial disease, atrial fibrillation, coronary artery disease, and hypertension. Notably, no relationship was found between chronic beta-blocker use and stroke.
WHAT ABOUT PATIENTS AT INTERMEDIATE RISK?
Because the effect of perioperative beta-blockade has traditionally been ill defined in surgical patients at intermediate risk of cardiovascular events, the DECREASE study group recently completed a study (DECREASE IV) to assess perioperative bisoprolol in terms of cardiac morbidity and mortality in intermediate-risk patients undergoing elective noncardiovascular surgery.17 Enrollees had a score of 1 to 2 on the Revised Cardiac Risk Index of Lee et al,19 which corresponds to an estimated risk of between 1% and 6% for a perioperative cardiovascular event.17
DECREASE IV also aimed to assess the effect of perioperative fluvastatin, so a 2 x 2 factorial design was used in which the study’s 1,066 patients were randomized to receive bisoprolol, fluvastatin, combination treatment, or combination placebo control. Bisoprolol was initiated up to 30 days prior to surgery, and the 2.5-mg daily starting dosage was titrated according to the patient’s heart rate to achieve a target rate of 50 to 70 beats per minute. Fluvastatin was also started up to 30 days prior to surgery. Patients who received bisoprolol (with or without fluvastatin) had a significant reduction in the 30-day incidence of cardiac death and nonfatal MI compared with those who did not receive bisoprolol (2.1% vs 6.0%; HR = 0.34 [95% CI, 0.17–0.67]; P = .002). Fluvastatin was associated with a favorable trend on this end point, but statistical significance was not achieved (P = .17).17
There was no difference among treatment groups in the incidence of stroke (4 strokes in the 533 patients who received bisoprolol vs 3 strokes in the 533 patients who did not),17 which further suggests that the increased stroke rate seen with beta-blockade in POISE may have been due to dosage, timing of initiation, or both.
CONCLUSIONS
Dose-related hypotension may explain POISE findings
Our understanding of postoperative stroke is incomplete, but it appears that dosing of a beta-blocker can be a contributor, especially with respect to the potential side effect of hypotension during surgery. Keep in mind that the average age of patients in POISE was approximately 70 years and that patients were naïve to beta-blockers. Some may have had asymptomatic left ventricular dysfunction, and we know that starting a beta-blocker at a high dose in such patients may lead to hypotension. At my institution we routinely perform echocardiographic screening of all patients scheduled for surgery, and we have found that more than half of the patients with heart failure have it uncovered only through this screening.
It is not the medicine alone that can cause perioperative hypotension; other factors may induce hypotension, requiring beta-blocker titration and careful monitoring of hemodynamics during surgery.
Advice: Start early and titrate dose; continue chronic beta-blockade
My advice is as follows:
- If a patient is on chronic beta-blocker therapy, do not stop it perioperatively. We have seen devastating outcomes in the Netherlands when patients had their beta-blockers stopped immediately before surgery. Consider adjusting the dose, but do not stop it entirely. If a beta-blocker is on board and the patient develops hypotension or bradycardia during surgery, treat the symptoms and check for sepsis.
- In a patient not on a beta-blocker, consider adding one if the patient is at intermediate or high risk of a cardiac event, but start at a low dosage (ie, 2.5 mg/day for bisoprolol and 25 mg/day for metoprolol). Treatment ideally should be started 30 days preoperatively; in the Netherlands, we have the chance to start well in advance of surgery so we can titrate the dose according to hemodynamics.
- If a beta-blocker is not started because of insufficient time for titration, do not add one to treat tachycardia that develops during surgery, since tachycardia may represent a response to normal defense mechanisms.
Safety of perioperative beta-blocker use has not been adequately demonstrated
By P.J. Devereaux, MD, PhD
I contend that perioperative beta-blockade is a practice not grounded in evidence-based medicine, and its overall safety has increasingly come into question as more data from large, high-quality trials have emerged. I will begin with a historical overview of perioperative beta-blocker use, review the results of the POISE trial (for which I was the co-principal investigator), explore the major questions raised by this trial, and conclude with some take-away messages.
THE HISTORY OF PERIOPERATIVE BETA-BLOCKADE
In the 1970s, physicians were encouraged to hold beta-blockers prior to surgery out of concern that these medications may inhibit the required cardiovascular response when patients developed hypotension, and could thereby lead to serious adverse consequences.
In the 1980s, new research associated tachycardia with perioperative cardiovascular events, leading to proposals to implement perioperative beta-blocker use.
In the 1990s, two randomized trials with a total sample size of 312 patients1,3 suggested that perioperative beta-blockers had a large treatment effect in preventing major cardiovascular events and death. These small trials had several methodological limitations:
- One trial3 was unblinded in a setting in which the vast majority of MIs are clinically silent.
- One trial3 was stopped early—after randomizing only 112 patients—for unexpected large treatment effects.
- One of the studies1 failed to follow intention-to-treat principle.
Nevertheless, guidelines developed at the time by the American College of Cardiology and the American Heart Association (ACC/AHA) recommended the use of perioperative beta-blockers on the basis of the physiological rationale and these two small clinical trials. That recommendation was retained in the latest (2007) update of the ACC/AHA perioperative guidelines.20
In 2006, two clinical trials with a total sample size of 1,417 were completed,4,15 surpassing the total size of previous trials by more than fourfold. These two more recent trials did not suffer from the methodological limitations of earlier trials. These trials showed no benefit of perioperative beta-blocker use; in fact, there was a trend toward worse outcomes in the beta-blocker recipients.4,15 Despite these new data, guidelines committees continued to recommend perioperative beta-blockade.20
THE POISE TRIAL
Study design
This was the context into which the POISE results were released in 2008. POISE was a randomized, controlled, blinded trial of patients 45 years or older scheduled for noncardiac surgery who had, or were at high risk of, atherosclerotic disease.14 The intervention consisted of metoprolol succinate (metoprolol controlled release [CR]) or placebo started 2 to 4 hours preoperatively (if heart rate was ≥ 50 beats per minute and systolic blood pressure [SBP] was ≥ 100 mm Hg) and continued for 30 days. The target dosage of metoprolol was 200 mg once daily. No patients received the recommended maximum dosage of 400 mg over 24 hours. The main outcome measure was a 30-day composite of cardiovascular death, nonfatal MI, or nonfatal cardiac arrest.
We randomized 9,298 patients in a 1:1 ratio to metoprolol or placebo. We encountered data fraud at a number of centers that prompted exclusion of data from 474 patients allocated to metoprolol and 473 allocated to placebo. Therefore, the total number of patients available for the intention-to-treat analysis was 8,351, from 190 centers in 23 countries.
Results
The risk of the primary composite outcome was reduced by 16% (relative reduction) in recipients of metoprolol CR compared with placebo recipients (P = .0399). Significantly fewer nonfatal MIs occurred in the metoprolol CR group than in the placebo group (152 [3.6%] vs 215 [5.1%]; P = .0008), leaving little doubt that perioperative beta-blockade prevents MI.
In contrast, total mortality was increased in the beta-blocker group, with 129 deaths among those assigned to metoprolol CR and 97 among those assigned to placebo (P = .0317), and the incidence of stroke was also significantly greater in the metoprolol CR group (1.0% vs. 0.5%; P = .0053).
Consistency with findings from other trials
The POISE data are consistent with those from a 2008 meta-analysis of high-quality randomized controlled trials in noncardiac surgery patients, which showed a significantly greater risk of death among patients assigned to a beta-blocker than among controls who were not (160 deaths [2.8%] vs 127 deaths [2.3%]; odds ratio [OR] = 1.27 [95% CI, 1.01–1.61]).21 This meta-analysis also found a significantly greater risk of nonfatal stroke in beta-blocker recipients compared with controls (38 [0.7%] vs 17 [0.3%]; OR = 2.16 [95% CI, 1.27–3.68]).
I also contend that the DECREASE IV trial supports the POISE findings in that although few strokes were encountered in DECREASE IV, the trend was in the direction of harm in the beta-blocker group, which had 4 strokes among 533 patients versus 3 strokes among 533 patients not receiving the beta-blocker.17
Predictive role of hypotension
The link between hypotension and death in POISE is consistent with findings from the largest beta-blocker trial undertaken, COMMIT (Clopidogrel and Metoprolol in Myocardial Infarction Trial), in which 45,852 patients with acute MI were randomized to metoprolol or placebo.22 In COMMIT, metoprolol had no effect on 30-day all-cause mortality but significantly reduced the risk of arrhythmic death, a benefit that was countered by a significantly increased risk of death from shock with a beta-blocker in acute MI. Clinically significant hypotension is much more common in the perioperative setting than in acute MI, which may explain the excess number of deaths observed with metoprolol in POISE as opposed to metoprolol’s neutral effect on mortality in COMMIT.
ANSWERING THE CRITICS
Several criticisms have been raised about POISE, as detailed below.
Beta-blocker dose
Some contend that a lower dose of beta-blocker would provide benefit and minimize risk, but this assertion must be supported by evidence from a large clinical trial. The targeted dosage of metoprolol in POISE represents 50% of the maximum daily therapeutic dose. Further, the protocol called for decreasing the dosage to 100 mg/day if SBP dropped to less than 100 mm Hg or if heart rate fell to less than 45 beats per minute.
The two small trials on which guideline recommendations for perioperative beta-blockade are primarily based1,3 had a sample size that was 4% of that in POISE, which calls into question the reliability of their results. The study by Mangano et al used atenolol at a target dosage that was 50% of the maximum daily therapeutic dose,1 the same as with metoprolol in POISE. DECREASE initiated bisoprolol at 25% of the maximum daily therapeutic dose, and allowed for titration to 50% of the maximum daily therapeutic dose.3
As the second largest study of perioperative beta-blockade, the Diabetic Postoperative Mortality and Morbidity (DIPOM) trial enrolled 921 patients who were assigned to placebo or controlled-release metoprolol with a target dosage that was 25% of the maximum daily therapeutic dose.4 The 30-day outcomes from DIPOM showed a trend toward an excess of death and stroke despite using only one-half the dosage in POISE and the same dosage as in DECREASE.
Timing of beta-blocker initiation
Another contention is that earlier beta-blocker initiation would be better. The issue with timing of initiation is not benefit, as POISE showed that starting a beta-blocker hours before surgery results in a reduction in the risk of MI. The issue is whether giving a beta-blocker earlier makes administering the drug safer. Nearly 10% of placebo recipients in POISE developed clinically significant hypotension, which suggests that the titrated dosage of a beta-blocker that appears effective preoperatively is unlikely to inform a safe dose after surgery, when hypotension is common.
The practicality of titrating the dose of beta-blocker prior to surgery also comes into play. Most patients referred to my institution for surgery are seen 1 to 2 weeks in advance, at the earliest. Real-world practice at present simply does not afford us the luxury of seeing patients three to four times before surgery in order to titrate the beta-blocker dose.
POISE did not address chronic beta-blocker therapy
It is important to remember that POISE excluded patients on chronic beta-blocker therapy and thus did not attempt to address the perioperative management of such patients who undergo noncardiac surgery. My suspicion is that perioperative continuation of beta-blockade in these patients is the best course of action, but this too has not been studied robustly, so we need a large controlled trial to confirm that this practice is indeed safe.
CONCLUSIONS
The POISE results suggest that for every 1,000 patients treated, perioperative metoprolol would:
- Prevent 15 MIs, 3 cardiac revascularizations, and 7 new cases of atrial fibrillation
- Result in 8 excess deaths, 5 strokes, 53 cases of clinically significant hypotension, and 42 cases of clinically significant bradycardia.
The central take-away message is that patients are unlikely to want a perioperative beta-blocker if they are unwilling to accept a probable increase in mortality or if they place three times more value on avoiding a perioperative stroke than on avoiding an MI.
It has been 10 years since the recommendation to use perioperatove beta-blockers was incorporated into perioperative practice guidelines. Assuming only 10% of physicians acted on this recommendation, 100 million patients have received a perioperative beta-blocker over this time as a result. If the POISE results are applicable, a full 800,000 of these patients died and another 500,000 suffered perioperative strokes as a result of being given a beta-blocker. This issue is not to be taken lightly, given the evidence to suggest harm.
Though it is possible that an alternative beta-blocker regimen to the one used in POISE may provide benefit without substantial harm, the data suggest this is not probable. The POISE data highlight the risk of making assumptions, as well as the importance of and need for large, high-quality randomized trials in the perioperative setting.
It is time for perioperative medicine to enter the age of evidence-based practice and embrace one of its central tenets: only large trials are reliable when it comes to therapeutic questions.
Rebuttals and discussion
POLDERMANS REBUTTAL: MORE TRANSPARENCY NEEDED IN POISE DOSING DATA
Dr. Poldermans: The initial paper describing the POISE trial design did indeed indicate that it was possible for a patient to receive 400 mg of metoprolol on the first day of treatment. We need to see the actual doses of metoprolol given to all patients in POISE who had a perioperative stroke. If you show me these data, the issue will be much easier to discuss.
Our data from randomized trials are consistent in showing that a titrated dosing regimen using bisoprolol reduces the incidence of postoperative cardiac events with no increase in the number of strokes.
My take-home message is that if you want to use beta-blockers, use them sensibly, use them carefully, and act during surgery. If many of your patients are developing hypotension, then you are doing something wrong.
DEVEREAUX REBUTTAL: A SHIFT IN THINKING IS REQUIRED
Dr. Devereaux: The data from POISE are fully available, and I take issue with Dr. Poldermans’ contention that a patient could have received as much as 400 mg of metoprolol CR on the day of surgery; this was not an option according to protocol. I believe his statement is misleading in the same way that it is misleading to indicate that in the DECREASE trial patients may have received 20 mg of bisoprolol within 24 hours of surgery. It is possible that a patient in DECREASE could have gone to surgery at 2:00 pm and may have taken his or her bisoprolol at 10:00 am that morning. The following morning (in the hospital), it is possible that the patient would have received his or her bisoprolol 10 mg at 7:00 or 8:00 am (ie, 20 mg within 24 hours of surgery). Although this is possible and something similar could have happened within POISE, it does not reflect a patient receiving an effective dose of metoprolol CR 400 mg or bisoprolol 20 mg over a 24-hour period.
I worry about the distortion of reality in perioperative medicine that leads so many of us to believe that randomization is magical despite small sample sizes. Small randomized trials are at profound risk of imbalance between the randomized groups, whether we see it or not, and the results are therefore simply not reliable.
Unless we shift our thinking, we make ourselves susceptible to overconfidence in the benefits of a certain intervention before the data from large clinical trials become available. In the meantime, as we have seen from POISE, an intervention may have negative consequences that are not apparent from small clinical trials.
The reality of excess stroke with perioperative beta-blockers is consistent across all the trials. It does not mean that we cannot find another way to give beta-blockers safely, but if we want to establish safety, we need a large trial that unequivocally demonstrates safety, as opposed to simply using observational data, retrospective cohorts, or comparisons between two nonrandomized trials. Until we have large data sets, it is very difficult to say that we can give beta-blockers safely.
DISCUSSION WITH THE AUDIENCE
Moderator*: Dr. Devereaux, was the hypotension in POISE related to the long-acting beta-blocker itself or to the large dose of if that was used? Similarly, were the strokes a result of the drug itself or of the hypotension?
Dr. Devereaux: I must take issue with your premise that the dose of metoprolol used in POISE was “large.” As I noted, Mangano’s study used its beta-blocker (atenolol) at 50% of its maximum daily therapeutic dose,1 the same proportion used in POISE, and Dr. Poldermans’ own DECREASE trial allowed titration of bisoprolol up to 50% of the maximum daily therapeutic dose.3 The DIPOM trial used half the dose of metoprolol that we used, yet it too yielded a trend toward more death and stroke in the beta-blocker group.4 So it’s not that the dose we used was at some excessive level. At the same time, that does not mean that a smaller dose may not have achieved a similarly significant benefit in cardiac outcomes.
We can’t explain most of the strokes. Because most strokes were ischemic, I suspect that the explanation may lie in the threshold used to define clinically significant hypotension. We used an SBP cutoff of less than 90 mm Hg, but we did not classify large drops in SBP, such as from 180 to 95 mm Hg, as clinically significant hypotension. The high incidence of clinically significant hypotension in the placebo group—about 10%—suggests that hypotension was likely the driving factor for stroke. The beta-blocker exacerbated the hypotension, but its more important effect may have been that it made it harder for the body to overcome the hypotension. That is the exact same signal observed in the COMMIT trial in the setting of acute MI.22
Dr. Poldermans: I’d like to see the intraoperative blood pressure data for the 60 patients who suffered strokes in POISE. We could then find out exactly when the hypotension occurred, what kind of hypotension it was, what the patient’s initial blood pressure reading was, and so on. If we had access to this information, we could determine which occurred first—the hypotension or the stroke.
Dr. Devereaux: Although trials can indicate a signal, they can’t explain with certainty the pathway through which the outcome occurred. For example, we know that beta-blockers prevent MI, but we don’t know how. What’s most impressive about the stroke issue is the consistency across all the perioperative beta-blocker trials: every one shows a direction of excess stroke with beta-blockers.
Question from the audience: The patient groups studied in DECREASE and POISE were different. DECREASE studied a very high-risk vascular surgery group with known coronary artery disease on the basis of echocardiography. POISE included patients undergoing emergency surgery and patients with sepsis. Can you describe the outcomes in POISE solely among the patients who underwent elective vascular surgery, similar to the patients studied in DECREASE?
Dr. Devereaux: In terms of the benefit to bisoprolol in very high-risk patients in DECREASE, remember that it was a study of 112 patients. That’s far too small a trial to establish safety or efficacy. The benefit of perioperative beta-blockade in preventing MI is unequivocal because it’s consistent across all trials. But the real issue is, was it safe?
Interestingly, in POISE, the groups at highest risk looked like they benefited the least, not the most. The notion of targeting high-risk people is not supported by POISE; if anything, the POISE results went in the direction of harm with beta-blockade in high-risk patients. That being said, the P value for interaction is not statistically significant, but it’s heading in the direction of harm. So I wouldn’t take comfort in believing that if we simply target high-risk patients, beta-blockers become safe.
Question from the audience: I believe that the seven or eight studies that showed higher stroke rates with beta-blockers all gave beta-blockade within 24 hours of surgery. Only in DECREASE was it given days and weeks in advance of surgery. Can you comment?
Dr. Poldermans: There’s clearly a relation between the time of beta-blocker initiation and the incidence of stroke. If you look at the randomized trials, you see an increased incidence of stroke in patients in whom beta-blockers are started just prior to surgery but not in patients who are on chronic beta-blockers. In our case-control study,18 we screened more than 185,000 patients for stroke and could not detect an increased incidence of stroke in those on chronic beta-blocker therapy. So stroke indeed has something to do with starting beta-blockers just before surgery.
Dr. Devereaux: In DECREASE IV, bisoprolol was started up to 1 month before surgery, yet there were 4 strokes in the bisoprolol group versus 3 in the control group.17
Dr. Poldermans: Yes, but that difference is not statistically meaningful.
Comment from the audience: I’m uncomfortable with the way Dr. Devereaux stresses the importance of significant findings from large randomized trials but then quibbles about a stroke rate of 4 versus 3, which is not statistically significant. Keep it scientific: either there is or there isn’t a P value that achieves significance.
Though I congratulate you on a great trial, any resident in my program would be fired for pursuing your strategy of perioperative care in POISE, which included using an SBP of 100 mm Hg as the threshold for stopping the beta-blocker regardless of preoperative blood pressure. An SBP of 100 mm Hg is not the definition of hypotension. Most anesthesiologists and perioperative physicians peg the beta-blockade to a reasonable level based on the preoperative blood pressure. They titrate in fluids and titrate in the beta-blocker. Certainly the timing is an issue—we don’t recommend giving it right before the operation.
Dr. Devereaux: I referred to the stroke rates in DECREASE IV because Dr. Poldermans has claimed that the excess in strokes has occurred in all trials but his, yet DECREASE IV was one of his trials and also one in which bisoprolol was started early. I’m not claiming statistical significance between the 3 versus 4 strokes in DECREASE IV, but the stroke trend is in the same direction as in the other trials, so it tells us nothing with regard to safety. My point is, has anyone proven safety? As much as we’d like to imagine that beta-blockers are safe perioperatively—and maybe they are—it has not been proven. The largest trials at present are consistent with a signal toward harm.
It’s easy to criticize the methodology after a trial is done. A number of us came together and thought we had a reasonable protocol for POISE. We found a reduction in the incidence of MI but more strokes and higher mortality with perioperative metoprolol. Does this mean there is not a safe way to give a beta-blocker and derive the benefit? Of course not. But at the moment the evidence does not support a way to give a beta-blocker safely. Do we need to find a way to give it safely? Of course we do.
For example, the design of POISE II is factorial, looking at aspirin versus placebo as well as clonidine versus placebo. There are a number of factors about clonidine that suggest we might be able to achieve the benefits we saw in POISE and avoid the risk, but until we do a large trial, we’re not going to know.
Comment from the audience: It’s important that we clearly understand the conclusion from POISE. It’s not that the administration of beta-blockers is not safe. It’s that the administration of a beta-blocker, as your methodology applied it, was not totally safe. Those are two very different conclusions.
Dr. Devereaux: I would say the conclusion is that the way that beta-blockers are being given has not been proven to be safe. The result is consistent. It’s even consistent with DECREASE IV.
Moderator: I believe in large clinical trials, but they must apply to real-life practice. POISE did not address the practices of many people in this room, particularly regarding the doses of metoprolol used. So it is hard for us to apply the findings in clinical practice. Those of you who design large trials need to think through your trial design very thoroughly, considering the millions of dollars that go into these trials. It’s not fair to clinicians to do a study that may have little clinical relevance.
Dr. Devereaux: Investigators from 190 centers in 23 countries were involved in POISE, and all of them thought we had a reasonable approach and methodology. That doesn’t mean it was perfect, yet the criticisms we are hearing now did not surface while the trial was ongoing.
Comment from the audience: My hospital in Australia contributed to the POISE study. When it started 6 or 7 years ago, the cardiologists were using beta-blockers liberally and haphazardly. It was a huge challenge to convince them that conducting the trial was justifiable—that the case for perioperative beta-blockers had not been absolutely and overwhelmingly proved. They wanted to put beta-blockers in the water supply at the doses we’re talking about.
It would be interesting to do separate analyses of the data from the various countries involved in POISE. In Australia, the percentage of the population on chronic beta-blockers—who therefore would have been ineligible for the trial—is now quite high. Most patients who need to be on beta-blockers long term are on them, whereas that was not the case 15 years ago. The population is changing even while we’re doing the trials. Australian cardiologists are no longer putting every patient on perioperative beta-blockers; they’re thinking about it first.
Dr. Devereaux: A compelling feature of POISE as an international trial is its consistency of outcomes across the planet. No matter where we looked, the outcomes were consistent: in Asia, Europe, North America, and Australia.
Moderator: Would each of you summarize your take-home message for clinicians?
Dr. Devereaux: I urge clinicians to actually read the trials themselves rather than just relying on the advice of guideline writers. It’s important not to allow ourselves to become entrenched in a practice without evidence, just because we’ve done it for so long. If you told your patients the number of MIs prevented and the potential number of excess strokes and deaths, I suspect the average patient would conclude it’s not a great trade-off.
Remember that two-thirds of MIs in the perioperative setting are clinically silent. That doesn’t mean they’re not important, but the strokes, in contrast, are profoundly devastating. One-third of patients with stroke in POISE were dead within 30 days, and of those who survived, 60% were incapacitated, needing help with everyday activities.
I encourage clinicians to read the POISE manuscript with a fresh perspective, regardless of how you’ve practiced until now. Then ask yourself whether you really are comfortable with the safety of perioperative beta-blockers at this time. Of course, that doesn’t mean the evidence won’t change in the future.
Dr. Poldermans: The main imperative is to improve postoperative care. We strongly believe that perioperative beta-blockers work in the general population. If you have a patient who needs to be on a beta-blocker after surgery, why not start it preoperatively? I believe that dosing and timing of initiation are important. If you have the opportunity to start the beta-blocker prior to surgery, do so at a reasonable dose and start early. Patients in whom beta-blockers are started immediately prior to surgery may be worse off, with a higher incidence of stroke.
*Amir K. Jaffer, MD, University of Miami Miller School of Medicine, served as moderator of the debate and the discussion period.
NOTE: The individual co-authors in this debate-based article are responsible only for those views within their respective bylined subsections and those views ascribed to them in the rebuttals and discussion at the end.
Perioperative beta-blockade improves outcomes
By Don Poldermans, MD, PhD
It is my contention that perioperative beta-blockade improves mortality and cardiac outcomes in select high- and intermediate-risk patients undergoing noncardiac surgery. Patients on chronic beta-blocker therapy should have it continued perioperatively. For patients not already on beta-blockade who are at cardiac risk, initiation of low-dose beta-blocker therapy should be considered prior to surgery; such therapy should be started approximately 1 month before surgery, with dose titration to achieve hemodynamic stability. Reports of increased stroke rates with perioperative beta-blockade appear to be due to inappropriate acute administration of high-dose beta-blocker therapy.
THE PHYSIOLOGIC RATIONALE FOR PERIOPERATIVE BETA-BLOCKADE
Perioperative myocardial infarction (MI) can occur by one of two mechanisms, both of which can be attenuated by beta-blockade:
- The stress induced by surgery can cause an asymptomatic coronary plaque to become unstable and rupture, resulting in complete occlusion of a portion of the coronary tree. This type of perioperative MI occurs typically in patients with multiple risk factors for MI absent a critical coronary stenosis. The perioperative risk associated with unstable plaque can be reduced pharmacologically with aspirin, statins, and chronic beta-blocker therapy.
- Alternately, a fixed coronary stenosis can predispose to a mismatch of oxygen demand and supply, leading to myocardial ischemia and infarction. The patient with a fixed coronary lesion typically presents with stable angina pectoris, and the at-risk stenosis is identified through a stress echocardiogram or nuclear scan. The risk conferred by flow-limiting stable plaque can be reduced by coronary revascularization and a short course of beta-blocker therapy prior to surgery.
INITIAL SUPPORTIVE DATA
Mangano and colleagues were the first to evaluate perioperative beta-blockade in a randomized, controlled fashion.1,2 In their study of 200 surgical patients with or at risk for coronary artery disease, oral atenolol administered perioperatively was associated with a 50% reduction (compared with placebo) in the incidence of postoperative myocardial ischemia as measured by three-lead Holter monitoring.2 During 2 years of follow-up, mortality was significantly lower in the atenolol group (10%) than in the placebo group (21%) (P = .019).1
In the Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography (DECREASE I), my research group randomized 112 high-risk patients (as identified by dobutamine echocardiography) to standard perioperative care alone or standard perioperative care plus bisoprolol starting 30 days prior to major vascular surgery.3 The dosage of bisoprolol was titrated to achieve a target heart rate of 60 to 70 beats per minute. Thirty days after surgery, the incidence of the primary end point—a composite of death from cardiac causes or nonfatal MI—was reduced from 34% in the standard-care group to 3.4% in the bisoprolol group (P < .001). Thus, in this unblinded study in a population with proven coronary artery disease, beta-blockade clearly improved outcomes.
Additional studies of perioperative beta-blocker use have produced a wide range of outcomes, with most favoring beta-blockade, albeit usually not to a statistically significant degree.4–13 Notably, only some of these trials were randomized, they used various beta-blocker regimens at various doses, they were conducted in patients with varying degrees of cardiac risk, and many had small sample sizes.
What emerged from these trials was the idea that perioperative beta-blockade in patients with coronary artery disease produces an effect similar to that of long-term beta-blockade in reducing the risk of cardiovascular events in post-MI patients and in those with coronary artery disease and heart failure.
THE POISE STUDY AND ITS IMPLICATIONS
Results of the Perioperative Ischemic Evaluation (POISE) were published in 2008, in which 8,351 noncardiac surgery patients with or at risk of atherosclerotic disease were randomized to placebo or extended-release metoprolol succinate started 2 to 4 hours preoperatively and continued for 30 days.14 Metoprolol was associated with a clear reduction in the primary end point, a composite of cardiovascular death, nonfatal MI, or nonfatal cardiac arrest (5.8% vs 6.9% with placebo; hazard ratio [HR] = 0.84 [95% CI, 0.70–0.99]; P = .0399), but this effect was offset by significant increases in total mortality and stroke incidence in the metoprolol group. Mortality was 3.1% with metoprolol versus 2.3% with placebo (HR = 1.33 [95% CI, 1.03–1.74]; P = .0317), and stroke incidence was 1.0% with metoprolol versus 0.5% with placebo (HR = 2.17 [95% CI, 1.26–3.74]; P = .0053). Cerebral infarction, not bleeding, explained most of the excess mortality with metoprolol.
Of the 60 strokes in POISE, 49 were ischemic in origin, 3 were hemorrhagic, and 8 were of uncertain etiology. Preoperative predictors of stroke were the use of clopidogrel and a history of stroke or transient ischemic attack. Postoperative predictors of stroke included intraoperative bleeding and intraoperative hypotension. These predictors suggest a diseased cerebrovascular tree or unstable hemodynamics during the intraoperative period in the patients who suffered a stroke.
Does dosing explain the rise in mortality and strokes?
Could the fatal outcomes associated with the beta-blocker in POISE be attributed to the dosage of metoprolol? In the study, 100 mg of metoprolol was started immediately prior to surgery, and an additional 100 mg could be given, depending on the hemodynamic response. Maintenance therapy (200 mg/day) was started on the same day, making it possible that a patient could have received as much as 400 mg of metoprolol the day of surgery. The starting dose of metoprolol used in POISE was two to eight times the commonly prescribed dose.
The initial 100-mg dose of metoprolol used in POISE has a similar beta1-receptor blockade potency compared with the 5-mg dose of bisoprolol used in DECREASE I.3 However, in DECREASE I, bisoprolol was initiated 30 days prior to surgery and was titrated, if necessary, according to heart rate. The maintenance dose of bisoprolol was half of the maintenance dose used in POISE. In the later DECREASE trials, the starting dose of bisoprolol was only 2.5 mg. Therefore, there was a huge difference in beta-blocker dosing between POISE and DECREASE.
What about timing of beta-blocker initiation?
The POISE findings may also be explained in part by the timing of beta-blocker initiation. Whereas bisoprolol was carefully titrated for 30 days before surgery in DECREASE, metoprolol was initiated just before surgery in POISE, and the maximum recommended dose may have been prescribed during the first 24 hours, although subsequent dosing was 200 mg daily, which is 50% of the maximum daily therapeutic dose. This extremely narrow time window for titration may be important, since the beneficial effects of beta-blockade on coronary plaque stability are likely to take weeks to develop.
Reassurance from a large case-control study
My colleagues and I conducted a case-control study from among more than 75,000 patients who underwent noncardiac, nonvascular surgery at our institution, Erasmus Medical Center, from 1991 to 2001.18 The cases were the 989 patients who died in the hospital postoperatively; the controls were 1,879 survivors matched with the cases for age, sex, the year the surgery was performed, and the type of surgery. The incidence of perioperative stroke was 0.5%, which is comparable to the rate found in the literature. Risk factors predictive of stroke were the presence of diabetes, cerebrovascular disease, peripheral arterial disease, atrial fibrillation, coronary artery disease, and hypertension. Notably, no relationship was found between chronic beta-blocker use and stroke.
WHAT ABOUT PATIENTS AT INTERMEDIATE RISK?
Because the effect of perioperative beta-blockade has traditionally been ill defined in surgical patients at intermediate risk of cardiovascular events, the DECREASE study group recently completed a study (DECREASE IV) to assess perioperative bisoprolol in terms of cardiac morbidity and mortality in intermediate-risk patients undergoing elective noncardiovascular surgery.17 Enrollees had a score of 1 to 2 on the Revised Cardiac Risk Index of Lee et al,19 which corresponds to an estimated risk of between 1% and 6% for a perioperative cardiovascular event.17
DECREASE IV also aimed to assess the effect of perioperative fluvastatin, so a 2 x 2 factorial design was used in which the study’s 1,066 patients were randomized to receive bisoprolol, fluvastatin, combination treatment, or combination placebo control. Bisoprolol was initiated up to 30 days prior to surgery, and the 2.5-mg daily starting dosage was titrated according to the patient’s heart rate to achieve a target rate of 50 to 70 beats per minute. Fluvastatin was also started up to 30 days prior to surgery. Patients who received bisoprolol (with or without fluvastatin) had a significant reduction in the 30-day incidence of cardiac death and nonfatal MI compared with those who did not receive bisoprolol (2.1% vs 6.0%; HR = 0.34 [95% CI, 0.17–0.67]; P = .002). Fluvastatin was associated with a favorable trend on this end point, but statistical significance was not achieved (P = .17).17
There was no difference among treatment groups in the incidence of stroke (4 strokes in the 533 patients who received bisoprolol vs 3 strokes in the 533 patients who did not),17 which further suggests that the increased stroke rate seen with beta-blockade in POISE may have been due to dosage, timing of initiation, or both.
CONCLUSIONS
Dose-related hypotension may explain POISE findings
Our understanding of postoperative stroke is incomplete, but it appears that dosing of a beta-blocker can be a contributor, especially with respect to the potential side effect of hypotension during surgery. Keep in mind that the average age of patients in POISE was approximately 70 years and that patients were naïve to beta-blockers. Some may have had asymptomatic left ventricular dysfunction, and we know that starting a beta-blocker at a high dose in such patients may lead to hypotension. At my institution we routinely perform echocardiographic screening of all patients scheduled for surgery, and we have found that more than half of the patients with heart failure have it uncovered only through this screening.
It is not the medicine alone that can cause perioperative hypotension; other factors may induce hypotension, requiring beta-blocker titration and careful monitoring of hemodynamics during surgery.
Advice: Start early and titrate dose; continue chronic beta-blockade
My advice is as follows:
- If a patient is on chronic beta-blocker therapy, do not stop it perioperatively. We have seen devastating outcomes in the Netherlands when patients had their beta-blockers stopped immediately before surgery. Consider adjusting the dose, but do not stop it entirely. If a beta-blocker is on board and the patient develops hypotension or bradycardia during surgery, treat the symptoms and check for sepsis.
- In a patient not on a beta-blocker, consider adding one if the patient is at intermediate or high risk of a cardiac event, but start at a low dosage (ie, 2.5 mg/day for bisoprolol and 25 mg/day for metoprolol). Treatment ideally should be started 30 days preoperatively; in the Netherlands, we have the chance to start well in advance of surgery so we can titrate the dose according to hemodynamics.
- If a beta-blocker is not started because of insufficient time for titration, do not add one to treat tachycardia that develops during surgery, since tachycardia may represent a response to normal defense mechanisms.
Safety of perioperative beta-blocker use has not been adequately demonstrated
By P.J. Devereaux, MD, PhD
I contend that perioperative beta-blockade is a practice not grounded in evidence-based medicine, and its overall safety has increasingly come into question as more data from large, high-quality trials have emerged. I will begin with a historical overview of perioperative beta-blocker use, review the results of the POISE trial (for which I was the co-principal investigator), explore the major questions raised by this trial, and conclude with some take-away messages.
THE HISTORY OF PERIOPERATIVE BETA-BLOCKADE
In the 1970s, physicians were encouraged to hold beta-blockers prior to surgery out of concern that these medications may inhibit the required cardiovascular response when patients developed hypotension, and could thereby lead to serious adverse consequences.
In the 1980s, new research associated tachycardia with perioperative cardiovascular events, leading to proposals to implement perioperative beta-blocker use.
In the 1990s, two randomized trials with a total sample size of 312 patients1,3 suggested that perioperative beta-blockers had a large treatment effect in preventing major cardiovascular events and death. These small trials had several methodological limitations:
- One trial3 was unblinded in a setting in which the vast majority of MIs are clinically silent.
- One trial3 was stopped early—after randomizing only 112 patients—for unexpected large treatment effects.
- One of the studies1 failed to follow intention-to-treat principle.
Nevertheless, guidelines developed at the time by the American College of Cardiology and the American Heart Association (ACC/AHA) recommended the use of perioperative beta-blockers on the basis of the physiological rationale and these two small clinical trials. That recommendation was retained in the latest (2007) update of the ACC/AHA perioperative guidelines.20
In 2006, two clinical trials with a total sample size of 1,417 were completed,4,15 surpassing the total size of previous trials by more than fourfold. These two more recent trials did not suffer from the methodological limitations of earlier trials. These trials showed no benefit of perioperative beta-blocker use; in fact, there was a trend toward worse outcomes in the beta-blocker recipients.4,15 Despite these new data, guidelines committees continued to recommend perioperative beta-blockade.20
THE POISE TRIAL
Study design
This was the context into which the POISE results were released in 2008. POISE was a randomized, controlled, blinded trial of patients 45 years or older scheduled for noncardiac surgery who had, or were at high risk of, atherosclerotic disease.14 The intervention consisted of metoprolol succinate (metoprolol controlled release [CR]) or placebo started 2 to 4 hours preoperatively (if heart rate was ≥ 50 beats per minute and systolic blood pressure [SBP] was ≥ 100 mm Hg) and continued for 30 days. The target dosage of metoprolol was 200 mg once daily. No patients received the recommended maximum dosage of 400 mg over 24 hours. The main outcome measure was a 30-day composite of cardiovascular death, nonfatal MI, or nonfatal cardiac arrest.
We randomized 9,298 patients in a 1:1 ratio to metoprolol or placebo. We encountered data fraud at a number of centers that prompted exclusion of data from 474 patients allocated to metoprolol and 473 allocated to placebo. Therefore, the total number of patients available for the intention-to-treat analysis was 8,351, from 190 centers in 23 countries.
Results
The risk of the primary composite outcome was reduced by 16% (relative reduction) in recipients of metoprolol CR compared with placebo recipients (P = .0399). Significantly fewer nonfatal MIs occurred in the metoprolol CR group than in the placebo group (152 [3.6%] vs 215 [5.1%]; P = .0008), leaving little doubt that perioperative beta-blockade prevents MI.
In contrast, total mortality was increased in the beta-blocker group, with 129 deaths among those assigned to metoprolol CR and 97 among those assigned to placebo (P = .0317), and the incidence of stroke was also significantly greater in the metoprolol CR group (1.0% vs. 0.5%; P = .0053).
Consistency with findings from other trials
The POISE data are consistent with those from a 2008 meta-analysis of high-quality randomized controlled trials in noncardiac surgery patients, which showed a significantly greater risk of death among patients assigned to a beta-blocker than among controls who were not (160 deaths [2.8%] vs 127 deaths [2.3%]; odds ratio [OR] = 1.27 [95% CI, 1.01–1.61]).21 This meta-analysis also found a significantly greater risk of nonfatal stroke in beta-blocker recipients compared with controls (38 [0.7%] vs 17 [0.3%]; OR = 2.16 [95% CI, 1.27–3.68]).
I also contend that the DECREASE IV trial supports the POISE findings in that although few strokes were encountered in DECREASE IV, the trend was in the direction of harm in the beta-blocker group, which had 4 strokes among 533 patients versus 3 strokes among 533 patients not receiving the beta-blocker.17
Predictive role of hypotension
The link between hypotension and death in POISE is consistent with findings from the largest beta-blocker trial undertaken, COMMIT (Clopidogrel and Metoprolol in Myocardial Infarction Trial), in which 45,852 patients with acute MI were randomized to metoprolol or placebo.22 In COMMIT, metoprolol had no effect on 30-day all-cause mortality but significantly reduced the risk of arrhythmic death, a benefit that was countered by a significantly increased risk of death from shock with a beta-blocker in acute MI. Clinically significant hypotension is much more common in the perioperative setting than in acute MI, which may explain the excess number of deaths observed with metoprolol in POISE as opposed to metoprolol’s neutral effect on mortality in COMMIT.
ANSWERING THE CRITICS
Several criticisms have been raised about POISE, as detailed below.
Beta-blocker dose
Some contend that a lower dose of beta-blocker would provide benefit and minimize risk, but this assertion must be supported by evidence from a large clinical trial. The targeted dosage of metoprolol in POISE represents 50% of the maximum daily therapeutic dose. Further, the protocol called for decreasing the dosage to 100 mg/day if SBP dropped to less than 100 mm Hg or if heart rate fell to less than 45 beats per minute.
The two small trials on which guideline recommendations for perioperative beta-blockade are primarily based1,3 had a sample size that was 4% of that in POISE, which calls into question the reliability of their results. The study by Mangano et al used atenolol at a target dosage that was 50% of the maximum daily therapeutic dose,1 the same as with metoprolol in POISE. DECREASE initiated bisoprolol at 25% of the maximum daily therapeutic dose, and allowed for titration to 50% of the maximum daily therapeutic dose.3
As the second largest study of perioperative beta-blockade, the Diabetic Postoperative Mortality and Morbidity (DIPOM) trial enrolled 921 patients who were assigned to placebo or controlled-release metoprolol with a target dosage that was 25% of the maximum daily therapeutic dose.4 The 30-day outcomes from DIPOM showed a trend toward an excess of death and stroke despite using only one-half the dosage in POISE and the same dosage as in DECREASE.
Timing of beta-blocker initiation
Another contention is that earlier beta-blocker initiation would be better. The issue with timing of initiation is not benefit, as POISE showed that starting a beta-blocker hours before surgery results in a reduction in the risk of MI. The issue is whether giving a beta-blocker earlier makes administering the drug safer. Nearly 10% of placebo recipients in POISE developed clinically significant hypotension, which suggests that the titrated dosage of a beta-blocker that appears effective preoperatively is unlikely to inform a safe dose after surgery, when hypotension is common.
The practicality of titrating the dose of beta-blocker prior to surgery also comes into play. Most patients referred to my institution for surgery are seen 1 to 2 weeks in advance, at the earliest. Real-world practice at present simply does not afford us the luxury of seeing patients three to four times before surgery in order to titrate the beta-blocker dose.
POISE did not address chronic beta-blocker therapy
It is important to remember that POISE excluded patients on chronic beta-blocker therapy and thus did not attempt to address the perioperative management of such patients who undergo noncardiac surgery. My suspicion is that perioperative continuation of beta-blockade in these patients is the best course of action, but this too has not been studied robustly, so we need a large controlled trial to confirm that this practice is indeed safe.
CONCLUSIONS
The POISE results suggest that for every 1,000 patients treated, perioperative metoprolol would:
- Prevent 15 MIs, 3 cardiac revascularizations, and 7 new cases of atrial fibrillation
- Result in 8 excess deaths, 5 strokes, 53 cases of clinically significant hypotension, and 42 cases of clinically significant bradycardia.
The central take-away message is that patients are unlikely to want a perioperative beta-blocker if they are unwilling to accept a probable increase in mortality or if they place three times more value on avoiding a perioperative stroke than on avoiding an MI.
It has been 10 years since the recommendation to use perioperatove beta-blockers was incorporated into perioperative practice guidelines. Assuming only 10% of physicians acted on this recommendation, 100 million patients have received a perioperative beta-blocker over this time as a result. If the POISE results are applicable, a full 800,000 of these patients died and another 500,000 suffered perioperative strokes as a result of being given a beta-blocker. This issue is not to be taken lightly, given the evidence to suggest harm.
Though it is possible that an alternative beta-blocker regimen to the one used in POISE may provide benefit without substantial harm, the data suggest this is not probable. The POISE data highlight the risk of making assumptions, as well as the importance of and need for large, high-quality randomized trials in the perioperative setting.
It is time for perioperative medicine to enter the age of evidence-based practice and embrace one of its central tenets: only large trials are reliable when it comes to therapeutic questions.
Rebuttals and discussion
POLDERMANS REBUTTAL: MORE TRANSPARENCY NEEDED IN POISE DOSING DATA
Dr. Poldermans: The initial paper describing the POISE trial design did indeed indicate that it was possible for a patient to receive 400 mg of metoprolol on the first day of treatment. We need to see the actual doses of metoprolol given to all patients in POISE who had a perioperative stroke. If you show me these data, the issue will be much easier to discuss.
Our data from randomized trials are consistent in showing that a titrated dosing regimen using bisoprolol reduces the incidence of postoperative cardiac events with no increase in the number of strokes.
My take-home message is that if you want to use beta-blockers, use them sensibly, use them carefully, and act during surgery. If many of your patients are developing hypotension, then you are doing something wrong.
DEVEREAUX REBUTTAL: A SHIFT IN THINKING IS REQUIRED
Dr. Devereaux: The data from POISE are fully available, and I take issue with Dr. Poldermans’ contention that a patient could have received as much as 400 mg of metoprolol CR on the day of surgery; this was not an option according to protocol. I believe his statement is misleading in the same way that it is misleading to indicate that in the DECREASE trial patients may have received 20 mg of bisoprolol within 24 hours of surgery. It is possible that a patient in DECREASE could have gone to surgery at 2:00 pm and may have taken his or her bisoprolol at 10:00 am that morning. The following morning (in the hospital), it is possible that the patient would have received his or her bisoprolol 10 mg at 7:00 or 8:00 am (ie, 20 mg within 24 hours of surgery). Although this is possible and something similar could have happened within POISE, it does not reflect a patient receiving an effective dose of metoprolol CR 400 mg or bisoprolol 20 mg over a 24-hour period.
I worry about the distortion of reality in perioperative medicine that leads so many of us to believe that randomization is magical despite small sample sizes. Small randomized trials are at profound risk of imbalance between the randomized groups, whether we see it or not, and the results are therefore simply not reliable.
Unless we shift our thinking, we make ourselves susceptible to overconfidence in the benefits of a certain intervention before the data from large clinical trials become available. In the meantime, as we have seen from POISE, an intervention may have negative consequences that are not apparent from small clinical trials.
The reality of excess stroke with perioperative beta-blockers is consistent across all the trials. It does not mean that we cannot find another way to give beta-blockers safely, but if we want to establish safety, we need a large trial that unequivocally demonstrates safety, as opposed to simply using observational data, retrospective cohorts, or comparisons between two nonrandomized trials. Until we have large data sets, it is very difficult to say that we can give beta-blockers safely.
DISCUSSION WITH THE AUDIENCE
Moderator*: Dr. Devereaux, was the hypotension in POISE related to the long-acting beta-blocker itself or to the large dose of if that was used? Similarly, were the strokes a result of the drug itself or of the hypotension?
Dr. Devereaux: I must take issue with your premise that the dose of metoprolol used in POISE was “large.” As I noted, Mangano’s study used its beta-blocker (atenolol) at 50% of its maximum daily therapeutic dose,1 the same proportion used in POISE, and Dr. Poldermans’ own DECREASE trial allowed titration of bisoprolol up to 50% of the maximum daily therapeutic dose.3 The DIPOM trial used half the dose of metoprolol that we used, yet it too yielded a trend toward more death and stroke in the beta-blocker group.4 So it’s not that the dose we used was at some excessive level. At the same time, that does not mean that a smaller dose may not have achieved a similarly significant benefit in cardiac outcomes.
We can’t explain most of the strokes. Because most strokes were ischemic, I suspect that the explanation may lie in the threshold used to define clinically significant hypotension. We used an SBP cutoff of less than 90 mm Hg, but we did not classify large drops in SBP, such as from 180 to 95 mm Hg, as clinically significant hypotension. The high incidence of clinically significant hypotension in the placebo group—about 10%—suggests that hypotension was likely the driving factor for stroke. The beta-blocker exacerbated the hypotension, but its more important effect may have been that it made it harder for the body to overcome the hypotension. That is the exact same signal observed in the COMMIT trial in the setting of acute MI.22
Dr. Poldermans: I’d like to see the intraoperative blood pressure data for the 60 patients who suffered strokes in POISE. We could then find out exactly when the hypotension occurred, what kind of hypotension it was, what the patient’s initial blood pressure reading was, and so on. If we had access to this information, we could determine which occurred first—the hypotension or the stroke.
Dr. Devereaux: Although trials can indicate a signal, they can’t explain with certainty the pathway through which the outcome occurred. For example, we know that beta-blockers prevent MI, but we don’t know how. What’s most impressive about the stroke issue is the consistency across all the perioperative beta-blocker trials: every one shows a direction of excess stroke with beta-blockers.
Question from the audience: The patient groups studied in DECREASE and POISE were different. DECREASE studied a very high-risk vascular surgery group with known coronary artery disease on the basis of echocardiography. POISE included patients undergoing emergency surgery and patients with sepsis. Can you describe the outcomes in POISE solely among the patients who underwent elective vascular surgery, similar to the patients studied in DECREASE?
Dr. Devereaux: In terms of the benefit to bisoprolol in very high-risk patients in DECREASE, remember that it was a study of 112 patients. That’s far too small a trial to establish safety or efficacy. The benefit of perioperative beta-blockade in preventing MI is unequivocal because it’s consistent across all trials. But the real issue is, was it safe?
Interestingly, in POISE, the groups at highest risk looked like they benefited the least, not the most. The notion of targeting high-risk people is not supported by POISE; if anything, the POISE results went in the direction of harm with beta-blockade in high-risk patients. That being said, the P value for interaction is not statistically significant, but it’s heading in the direction of harm. So I wouldn’t take comfort in believing that if we simply target high-risk patients, beta-blockers become safe.
Question from the audience: I believe that the seven or eight studies that showed higher stroke rates with beta-blockers all gave beta-blockade within 24 hours of surgery. Only in DECREASE was it given days and weeks in advance of surgery. Can you comment?
Dr. Poldermans: There’s clearly a relation between the time of beta-blocker initiation and the incidence of stroke. If you look at the randomized trials, you see an increased incidence of stroke in patients in whom beta-blockers are started just prior to surgery but not in patients who are on chronic beta-blockers. In our case-control study,18 we screened more than 185,000 patients for stroke and could not detect an increased incidence of stroke in those on chronic beta-blocker therapy. So stroke indeed has something to do with starting beta-blockers just before surgery.
Dr. Devereaux: In DECREASE IV, bisoprolol was started up to 1 month before surgery, yet there were 4 strokes in the bisoprolol group versus 3 in the control group.17
Dr. Poldermans: Yes, but that difference is not statistically meaningful.
Comment from the audience: I’m uncomfortable with the way Dr. Devereaux stresses the importance of significant findings from large randomized trials but then quibbles about a stroke rate of 4 versus 3, which is not statistically significant. Keep it scientific: either there is or there isn’t a P value that achieves significance.
Though I congratulate you on a great trial, any resident in my program would be fired for pursuing your strategy of perioperative care in POISE, which included using an SBP of 100 mm Hg as the threshold for stopping the beta-blocker regardless of preoperative blood pressure. An SBP of 100 mm Hg is not the definition of hypotension. Most anesthesiologists and perioperative physicians peg the beta-blockade to a reasonable level based on the preoperative blood pressure. They titrate in fluids and titrate in the beta-blocker. Certainly the timing is an issue—we don’t recommend giving it right before the operation.
Dr. Devereaux: I referred to the stroke rates in DECREASE IV because Dr. Poldermans has claimed that the excess in strokes has occurred in all trials but his, yet DECREASE IV was one of his trials and also one in which bisoprolol was started early. I’m not claiming statistical significance between the 3 versus 4 strokes in DECREASE IV, but the stroke trend is in the same direction as in the other trials, so it tells us nothing with regard to safety. My point is, has anyone proven safety? As much as we’d like to imagine that beta-blockers are safe perioperatively—and maybe they are—it has not been proven. The largest trials at present are consistent with a signal toward harm.
It’s easy to criticize the methodology after a trial is done. A number of us came together and thought we had a reasonable protocol for POISE. We found a reduction in the incidence of MI but more strokes and higher mortality with perioperative metoprolol. Does this mean there is not a safe way to give a beta-blocker and derive the benefit? Of course not. But at the moment the evidence does not support a way to give a beta-blocker safely. Do we need to find a way to give it safely? Of course we do.
For example, the design of POISE II is factorial, looking at aspirin versus placebo as well as clonidine versus placebo. There are a number of factors about clonidine that suggest we might be able to achieve the benefits we saw in POISE and avoid the risk, but until we do a large trial, we’re not going to know.
Comment from the audience: It’s important that we clearly understand the conclusion from POISE. It’s not that the administration of beta-blockers is not safe. It’s that the administration of a beta-blocker, as your methodology applied it, was not totally safe. Those are two very different conclusions.
Dr. Devereaux: I would say the conclusion is that the way that beta-blockers are being given has not been proven to be safe. The result is consistent. It’s even consistent with DECREASE IV.
Moderator: I believe in large clinical trials, but they must apply to real-life practice. POISE did not address the practices of many people in this room, particularly regarding the doses of metoprolol used. So it is hard for us to apply the findings in clinical practice. Those of you who design large trials need to think through your trial design very thoroughly, considering the millions of dollars that go into these trials. It’s not fair to clinicians to do a study that may have little clinical relevance.
Dr. Devereaux: Investigators from 190 centers in 23 countries were involved in POISE, and all of them thought we had a reasonable approach and methodology. That doesn’t mean it was perfect, yet the criticisms we are hearing now did not surface while the trial was ongoing.
Comment from the audience: My hospital in Australia contributed to the POISE study. When it started 6 or 7 years ago, the cardiologists were using beta-blockers liberally and haphazardly. It was a huge challenge to convince them that conducting the trial was justifiable—that the case for perioperative beta-blockers had not been absolutely and overwhelmingly proved. They wanted to put beta-blockers in the water supply at the doses we’re talking about.
It would be interesting to do separate analyses of the data from the various countries involved in POISE. In Australia, the percentage of the population on chronic beta-blockers—who therefore would have been ineligible for the trial—is now quite high. Most patients who need to be on beta-blockers long term are on them, whereas that was not the case 15 years ago. The population is changing even while we’re doing the trials. Australian cardiologists are no longer putting every patient on perioperative beta-blockers; they’re thinking about it first.
Dr. Devereaux: A compelling feature of POISE as an international trial is its consistency of outcomes across the planet. No matter where we looked, the outcomes were consistent: in Asia, Europe, North America, and Australia.
Moderator: Would each of you summarize your take-home message for clinicians?
Dr. Devereaux: I urge clinicians to actually read the trials themselves rather than just relying on the advice of guideline writers. It’s important not to allow ourselves to become entrenched in a practice without evidence, just because we’ve done it for so long. If you told your patients the number of MIs prevented and the potential number of excess strokes and deaths, I suspect the average patient would conclude it’s not a great trade-off.
Remember that two-thirds of MIs in the perioperative setting are clinically silent. That doesn’t mean they’re not important, but the strokes, in contrast, are profoundly devastating. One-third of patients with stroke in POISE were dead within 30 days, and of those who survived, 60% were incapacitated, needing help with everyday activities.
I encourage clinicians to read the POISE manuscript with a fresh perspective, regardless of how you’ve practiced until now. Then ask yourself whether you really are comfortable with the safety of perioperative beta-blockers at this time. Of course, that doesn’t mean the evidence won’t change in the future.
Dr. Poldermans: The main imperative is to improve postoperative care. We strongly believe that perioperative beta-blockers work in the general population. If you have a patient who needs to be on a beta-blocker after surgery, why not start it preoperatively? I believe that dosing and timing of initiation are important. If you have the opportunity to start the beta-blocker prior to surgery, do so at a reasonable dose and start early. Patients in whom beta-blockers are started immediately prior to surgery may be worse off, with a higher incidence of stroke.
*Amir K. Jaffer, MD, University of Miami Miller School of Medicine, served as moderator of the debate and the discussion period.
- Mangano DT, Layug EL, Wallace A, Tateo I. Effect of atenolol on mortality and cardiovascular morbidity after noncardiac surgery: Multicenter Study of Perioperative Ischemia Research Group. N Engl J Med 1996; 335:1713–1720.
- Wallace A, Layug B, Tateo I, et al. Prophylactic atenolol reduces postoperative myocardial ischemia: McSPI Research Group. Anesthesiology 1998; 88:7–17.
- Poldermans D, Boersma E, Bax JJ, et al. The effect of bisoprolol on perioperative mortality and myocardial infarction in high-risk patients undergoing vascular surgery: Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. N Engl J Med 1999; 341:1789–1794.
- Juul AB, Wetterslev J, Gluud C, et al. Effect of perioperative b-blockade in patients with diabetes undergoing major non-cardiac surgery: randomised placebo controlled, blinded multicentre trial. BMJ 2006; 332:1482.
- Brady AR, Gibbs JS, Greenhalgh RM, et al. Perioperative beta-blockade (POBBLE) for patients undergoing infrarenal vascular surgery: results of a randomized double-blind controlled trial. J Vasc Surg 2005; 41:602–609.
- Cucchiara RF, Benefiel DJ, Matteo RS, DeWood M, Albin MS. Evaluation of esmolol in controlling increases in heart rate and blood pressure during endotracheal intubation in patients undergoing carotid endarterectomy. Anesthesiology 1986; 65:528–531.
- Magnusson J, Thulin T, Werner O, Järhult J, Thomson D. Haemodynamic effects of pretreatment with metoprolol in hypertensive patients undergoing surgery. Br J Anaesth 1986; 58:251–260.
- Stone JG, Foëx P, Sear JW, et al. Myocardial ischemia in untreated hypertensive patients: effect of a single small oral dose of a beta-adrenergic blocking agent. Anesthesiology 1988; 68:495–500.
- Jakobsen CJ, Bille S, Ahlburg P, et al. Perioperative metoprolol reduces the frequency of atrial fibrillation after thoracotomy for lung resection. J Cardiothorac Vasc Anesth 1997; 11:746–751.
- Bayliff CD, Massel DR, Inculet RI, et al. Propranolol for the prevention of postoperative arrhythmias in general thoracic surgery. Ann Thorac Surg 1999; 67:182–186.
- Raby KE, Brull SJ, Timimi F, et al. The effect of heart rate control on myocardial ischemia among high-risk patients after vascular surgery. Anesth Analg 1999; 88:477–482.
- Zaugg M, Tagliente T, Lucchinetti E, et al. Beneficial effects from beta-adrenergic blockade in elderly patients undergoing noncardiac surgery. Anesthesiology 1999; 91:1674–1686.
- Urban MK, Markowitz SM, Gordon MA, et al. Postoperative prophylactic administration of beta-adrenergic blockers in patients at risk for myocardial ischemia. Anesth Analg 2000; 90:1257–1261.
- POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet 2008; 371:1839–1847.
- Yang H, Raymer K, Butler R, et al. The effects of perioperative beta-blockade: results of the Metoprolol after Vascular Surgery (MaVS) study, a randomized controlled trial. Am Heart J 2006; 152:983–990.
- Zaugg M, Bestman L, Wacker J, et al. Adrenergic receptor genotype but not perioperative bisoprolol therapy may determine cardiovascular outcome in at-risk patients undergoing surgery with spinal block: the Swiss Beta Blocker in Spinal Anesthesia (BBSA) study. Anesthesiology 2007; 107:33–44.
- Dunkelgrun M, Boersma E, Schouten O, et al. Bisoprolol and fluvastatin for reduction of perioperative cardiac mortality and myocardial infarction in intermediate-risk patients undergoing noncardiac surgery. A randomized controlled trial (DECREASE-IV). Ann Surg 2009; 249:921–926.
- Noordzij PG, Poldermans D, Schouten O, et al. Beta-blockers and statins are individually associated with reduced mortality in patients undergoing noncardiac, nonvascular surgery. Coron Artery Dis 2007; 18:67–72.
- Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999; 100:1043–1049.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2007; 50:1707–1732.
- Bangalore S, Wetterslev J, Pranesh S, et al. Perioperative beta blockers in patients having non-cardiac surgery: a meta-analysis. Lancet 2008; 372:1962–1976.
- COMMIT (Clopidogrel and Metoprolol in Myocardial Infarction Trial) collaborative group. Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet 2005; 366:1622–1632.
- Mangano DT, Layug EL, Wallace A, Tateo I. Effect of atenolol on mortality and cardiovascular morbidity after noncardiac surgery: Multicenter Study of Perioperative Ischemia Research Group. N Engl J Med 1996; 335:1713–1720.
- Wallace A, Layug B, Tateo I, et al. Prophylactic atenolol reduces postoperative myocardial ischemia: McSPI Research Group. Anesthesiology 1998; 88:7–17.
- Poldermans D, Boersma E, Bax JJ, et al. The effect of bisoprolol on perioperative mortality and myocardial infarction in high-risk patients undergoing vascular surgery: Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. N Engl J Med 1999; 341:1789–1794.
- Juul AB, Wetterslev J, Gluud C, et al. Effect of perioperative b-blockade in patients with diabetes undergoing major non-cardiac surgery: randomised placebo controlled, blinded multicentre trial. BMJ 2006; 332:1482.
- Brady AR, Gibbs JS, Greenhalgh RM, et al. Perioperative beta-blockade (POBBLE) for patients undergoing infrarenal vascular surgery: results of a randomized double-blind controlled trial. J Vasc Surg 2005; 41:602–609.
- Cucchiara RF, Benefiel DJ, Matteo RS, DeWood M, Albin MS. Evaluation of esmolol in controlling increases in heart rate and blood pressure during endotracheal intubation in patients undergoing carotid endarterectomy. Anesthesiology 1986; 65:528–531.
- Magnusson J, Thulin T, Werner O, Järhult J, Thomson D. Haemodynamic effects of pretreatment with metoprolol in hypertensive patients undergoing surgery. Br J Anaesth 1986; 58:251–260.
- Stone JG, Foëx P, Sear JW, et al. Myocardial ischemia in untreated hypertensive patients: effect of a single small oral dose of a beta-adrenergic blocking agent. Anesthesiology 1988; 68:495–500.
- Jakobsen CJ, Bille S, Ahlburg P, et al. Perioperative metoprolol reduces the frequency of atrial fibrillation after thoracotomy for lung resection. J Cardiothorac Vasc Anesth 1997; 11:746–751.
- Bayliff CD, Massel DR, Inculet RI, et al. Propranolol for the prevention of postoperative arrhythmias in general thoracic surgery. Ann Thorac Surg 1999; 67:182–186.
- Raby KE, Brull SJ, Timimi F, et al. The effect of heart rate control on myocardial ischemia among high-risk patients after vascular surgery. Anesth Analg 1999; 88:477–482.
- Zaugg M, Tagliente T, Lucchinetti E, et al. Beneficial effects from beta-adrenergic blockade in elderly patients undergoing noncardiac surgery. Anesthesiology 1999; 91:1674–1686.
- Urban MK, Markowitz SM, Gordon MA, et al. Postoperative prophylactic administration of beta-adrenergic blockers in patients at risk for myocardial ischemia. Anesth Analg 2000; 90:1257–1261.
- POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet 2008; 371:1839–1847.
- Yang H, Raymer K, Butler R, et al. The effects of perioperative beta-blockade: results of the Metoprolol after Vascular Surgery (MaVS) study, a randomized controlled trial. Am Heart J 2006; 152:983–990.
- Zaugg M, Bestman L, Wacker J, et al. Adrenergic receptor genotype but not perioperative bisoprolol therapy may determine cardiovascular outcome in at-risk patients undergoing surgery with spinal block: the Swiss Beta Blocker in Spinal Anesthesia (BBSA) study. Anesthesiology 2007; 107:33–44.
- Dunkelgrun M, Boersma E, Schouten O, et al. Bisoprolol and fluvastatin for reduction of perioperative cardiac mortality and myocardial infarction in intermediate-risk patients undergoing noncardiac surgery. A randomized controlled trial (DECREASE-IV). Ann Surg 2009; 249:921–926.
- Noordzij PG, Poldermans D, Schouten O, et al. Beta-blockers and statins are individually associated with reduced mortality in patients undergoing noncardiac, nonvascular surgery. Coron Artery Dis 2007; 18:67–72.
- Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999; 100:1043–1049.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2007; 50:1707–1732.
- Bangalore S, Wetterslev J, Pranesh S, et al. Perioperative beta blockers in patients having non-cardiac surgery: a meta-analysis. Lancet 2008; 372:1962–1976.
- COMMIT (Clopidogrel and Metoprolol in Myocardial Infarction Trial) collaborative group. Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet 2005; 366:1622–1632.
Perioperative considerations for patients with liver disease
Assessing patients with liver disease for surgery is one of the most common reasons for hepatology consultation in the hospital. This review focuses on practical aspects of evaluating patients with known or suspected liver disease and provides guidance for determining whether it is safe to proceed with surgery in such patients. I begin with a case study to introduce some common clinical challenges and then revisit the case—with relevant teaching points—at the end.
CASE: A MIDDLE-AGED MAN WITH LIVER DISEASE SCHEDULED FOR CARDIAC SURGERY
A 57-year-old man with a history of liver disease is referred for preoperative assessment. It is 6:30 pm, and the patient has just arrived in the hospital; he is scheduled for coronary artery bypass graft surgery (CABG) early tomorrow morning for ischemic heart disease. Ten years ago, he was diagnosed with hepatitis C virus infection; 2 years later, he had a cholecystectomy. He has a remote history of intravenous drug use.
The sub-intern asks for an assessment of operative risk as well as advice on the type of anesthesia to be used.
HEPATIC EFFECTS OF ANESTHESIA
Anesthesiologists are keenly aware of the hepatic effects of anesthesia and that they must carefully choose anesthetics for patients with liver disease. There are a number of at least theoretical concerns about using particular anesthetics:
- Inhaled anesthetics, such as isoflurane, cause systemic vasodilation and depress cardiac output. These effects are of concern since many patients with advanced liver disease already have a hyperdynamic circulation because of peripheral vasodilation.
- Spinal or epidural anesthetics may reduce mean arterial pressure, which is of concern for similar reasons.
- Nitrous oxide has less of a depressive effect unless the patient has concomitant hypercapnia.
Another consideration is the hepatic metabolism of anesthetic agents. Use of halothane, which is 20% metabolized by the liver, is now uncommon, particularly if there is any concern about liver disease. In contrast, enflurane is only 4% metabolized by the liver. Numerous other anesthetics—including isoflurane, desflurane, and sevoflurane—have only minimal hepatic metabolism (< 0.2%), which makes them, along with nitrous oxide, the best anesthetic choices for patients with liver disease.
ASSESSING OPERATIVE RISK
The more important issue in the consultation for our patient is the degree of operative risk associated with his underlying liver disease. A number of factors are pertinent, including the etiology and severity of the liver disease and the type of surgery planned.
Acute liver disease has higher operative risk
Literature dating back 40 years has associated acute viral and alcoholic hepatitis with poor outcomes in surgical patients. Major elective surgery for a patient with suspected acute hepatitis A, for example, should be deferred until the patient has recovered, barring some compelling reason for greater urgency, such as a perforated viscus.
In chronic liver disease, hepatocellular function predicts outcome
When a patient with liver disease is evaluated for surgery, evidence should be sought to determine whether an index complication has already occurred. Because the patient in our case study had a cholecystectomy several years before, I would also ask, “What did the surgeon say your liver looked like? Did you have any bleeding problems afterwards? Did you develop ascites?”
It is also important to determine whether portal hypertension is present. For a patient with liver disease, otherwise unexplained thrombocytopenia is a useful indicator of portal hypertension.
Systems for scoring liver disease severity
Even a surgical patient with well-compensated liver disease is at risk for developing complications postoperatively, particularly if abdominal surgery is planned. Risk should be assessed in all patients with liver disease using either the Child-Pugh scoring system or the Model for End-Stage Liver Disease (MELD) scoring system.
The Child-Pugh score, which assigns 1 to 3 points according to the presence/absence and levels of each of five simple factors (bilirubin, albumin, prothrombin time/international normalized ratio [INR], ascites, and encephalopathy stage), has been used for decades to assess the severity of liver disease. Patients with Child-Pugh class A disease (score of 5–6) have well-compensated cirrhosis and good synthetic function, and therefore have essentially no restrictions for undergoing surgery. For patients in Child-Pugh class B (score of 7–9), the risk of perioperative complications and mortality is higher and any major hepatic surgery (such as hepatic resection) should be avoided. Patients with class C cirrhosis (score of 10–15) are not candidates for any major elective surgery and should be considered for liver transplantation referral.
The MELD scoring system was developed more recently and is used to prioritize eligibility for liver transplantation. Calculated using a mathematical formula that incorporates three objective patient variables—
creatinine, bilirubin, and INR—the MELD score correlates very well with prognosis. The score can be calculated by an online MELD calculator such as the one at www.unos.org/resources.2 A patient with a high MELD score is unlikely to survive for more than a few months without liver transplantation; a patient with a low MELD score is likely to survive for at least 12 months. Calculating the MELD score is now one of the first assessments in any patient suspected of having cirrhosis.
Risk factors for complications and death
In a retrospective study to identify factors associated with complications and mortality in surgical patients with cirrhosis, Ziser et al reviewed the records of 733 patients with cirrhosis who underwent surgical procedures (except liver transplantation) at the Mayo Clinic over an 11-year period (1980–1991).3 The mortality rate within 30 days of surgery was 11.6%. Long-term follow-up showed that most deaths occurred within the first few months after surgery, when many patients succumbed to pneumonia or renal insufficiency.
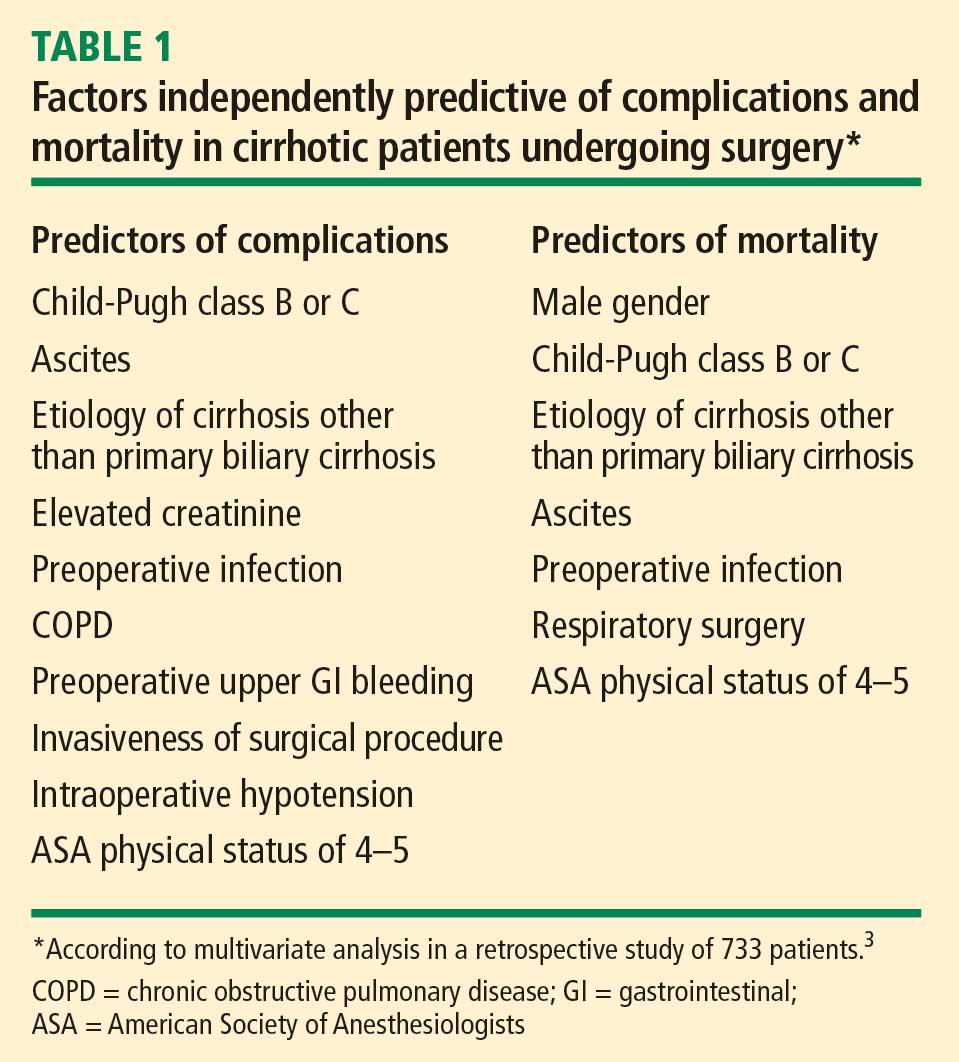
Risk factors have strong cumulative power
The study by Ziser et al also underscored the cumulative effect of risk factors, as the probability of developing a perioperative complication increased dramatically with the number of risk factors (as identified by multiavariate analysis) that a patient had, as follows3:
- 9.3% risk of complications with 1 risk factor
- 14.5% risk with 2 factors
- 33.5% risk with 3 factors
- 63.0% risk with 4 or 5 factors
- 73.3% risk with 6 factors
- 100% risk with 7 or 8 factors.
Postoperative complications: Beware hepatorenal syndrome
The most common postoperative complications in the study by Ziser et al were pneumonia, other infections, ventilation dependency, and ascites.3
Possibly the most ominous perioperative complication in a patient with liver disease is the onset of renal insufficiency, which may be precipitated by a number of factors, including nephrotoxic drugs and intraoperative hypotension. Renal insufficiency is usually a predictor of markedly reduced survival and a sign that hepatorenal syndrome may have developed.
Hepatorenal syndrome, which occurred in 3.3% of patients in the analysis by Ziser et al,3 is the presence of renal failure in a patient with cirrhosis. It is characterized by advanced liver failure and severe sinusoidal portal hypertension. The renal failure is said to be “functional” because significant histological changes are absent on kidney biopsy. Marked arteriolar vasodilation occurs in the extrarenal circulation with renal vasoconstriction leading to reduced glomerular filtration.
IMPORTANCE OF SURGICAL PROCEDURE TYPE
In addition to the patient-specific risk factors discussed above, certain surgical procedures deserve special consideration in patients with liver disease.
Cholecystectomy: Open vs closed
Patients with liver disease have the same indication for cholecystectomy as anyone else does: symptomatic gallstone disease. Patients with cirrhosis who are found to have incidental gallstones on ultrasonography should not undergo cholecystectomy unless the gallstones are symptomatic, as liver function may deteriorate after surgery.
For a patient with liver disease undergoing cholecystectomy, a common concern is whether an open or closed procedure should be done. Conventional wisdom had been that a patient with underlying liver disease (particularly cirrhosis) should have an open procedure so that the surgeon could more easily control bleeding, but that notion has changed in recent years with evidence supporting the safety of a laparoscopic approach in patients with liver disease.
One study supporting this new strategy is a retrospective review of 50 patients who had undergone cholecystectomy for symptomatic gallstone disease at the Mayo Clinic between 1990 and 1997.4 The procedure was open in half of the patients and laparoscopic in the other half. All patients had Child-Pugh class A or B cirrhosis. The indications for surgery were acute cholecystitis, biliary colic, or pancreatitis, and the number of patients with each of these indications was comparable between the open-surgery and laparoscopy groups. Three patients who initially underwent laparoscopy were converted to open cholecystectomy: two for bleeding and one for poor access. The study found that laparoscopic cholecystectomy was associated with statistically significant reductions in operating room time, blood loss, and length of hospital stay. No deaths occurred in either group. The authors concluded that laparoscopic cholecystectomy is safe in patients with cirrhosis and offers several advantages over an open surgical approach.
In light of these findings and other recent evidence, laparoscopic cholecystectomy should be recommended for patients with liver disease unless they have ascites or other evidence of overt hepatic decompensation, in which case cholecystectomy itself is contraindicated.
Cardiac surgery with bypass poses extra risk
Patients with liver disease undergoing open heart surgery with cardiopulmonary bypass are at especially high risk because of the effect on hepatic hemodynamics. This risk was demonstrated in a retrospective review of all patients with cirrhosis who underwent cardiac surgery with cardiopulmonary bypass at the Cleveland Clinic from 1992 to 2002.5 Of the 44 patients identified, 12 (27%) developed hepatic decompensation and 7 (16%) died. Hepatic decompensation was a major factor in all the deaths.
The MELD and Child-Pugh scores correlated well with one another in this study and were highly associated with hepatic decompensation and death. The best cutoff values for predicting mortality and hepatic decompensation were found to be a score greater than 7 in the Child-Pugh system and a score greater than 13 in the MELD system. (For context, receipt of a donor liver via a transplant list in the United States requires a MELD score of at least 15.) The study confirmed that the Child-Pugh score, which is easy to determine at the bedside, remains a reliable predictor of poor outcomes.5
CASE REVISITED: POSTOPERATIVE LIVER FUNCTION DECLINE―HOW SERIOUS IS IT?
Our patient undergoes the CABG procedure, and 3 days later you are asked to see him. According to the sub-intern, although the surgery was successful, the patient is now “in liver failure.” After hearing this news, the family is anxious to discuss liver transplantation.
On examination, the patient is alert and extubated, so he is clearly not encephalopathic. His wound is clean and shows no sign of infection. He appears to be mildly icteric, and he may have some ascites, based on mild flank dullness.
His laboratory test results are as follows:
- Bilirubin, 3.1 mg/dL (normal range, 0.3–1.2)
- INR, 1.2 (0.9–1.2)
- Alanine aminotransferase (ALT), 300 U/L (10–40)
- Creatinine, 0.9 mg/dL (0.6–1.2).
Although the bilirubin and ALT are elevated, it is notable that the creatinine is normal. This pattern is not uncommon after elective surgery in a patient with underlying cirrhosis. Renal dysfunction is the biggest concern in the perioperative management of a patient with liver disease, as it is an indicator that the patient may develop overt hepatic decompensation. Likely reasons for the patient’s ALT elevation are the effects of cardiopulmonary bypass and possible intraoperative hypotension.
The family needs to be told that the patient is not in liver failure and that it is best to wait with the expectation that he will do fine unless other complications supervene.
You advise cautious diuresis, and the ALT falls over the next few days. The bilirubin declines to 2.0 mg/dL. At this point, you advise discharge planning.
One need not wait for the bilirubin to return to normal: after an acute hepatic insult such as ischemic hepatitis or intraoperative hypotension, bilirubin is the last indicator to improve. Bilirubin is in part albumin-bound, and the half-life of albumin is 18 days, so a patient can remain icteric for some time after the rest of the liver function tests have returned to normal.
DISCUSSION
Question from the audience: What are your recommendations regarding platelet transfusion if the platelet count is less than 50,000 in a patient with liver disease?
Dr. Martin: For patients with thrombocytopenia, it is prudent to get the platelet count above 60,000 before any procedure. We will not even do a blind liver biopsy in a patient with a platelet count of less than 60,000.
Question from the audience: A study from the Annals of Surgery concludes that patients with liver disease do poorly with a hemoglobin of less than 10 g/dL. Would you transfuse aggressively before surgery?
Dr. Martin: For a patient with anemia, I don’t like to use aggressive transfusion if cirrhosis is present because the portal pressure may go up and increase the risk of variceal hemorrhage. If there is adequate time for a work-up, one can screen for varices by endoscopy. If there is evidence of overt hepatic decompensation and portal hypertension (esophageal varices, a palpable spleen, and thrombocytopenia), I wouldn’t try to get the hemoglobin much above 10 g/dL.
Question from the audience: How would you modify prophylaxis for deep vein thrombosis following hip or knee replacement surgery in patients with liver disease?
Dr. Martin: I would base it on the INR. Patients who are already mildly coagulopathic tend to be very sensitive to warfarin in the long term. For immediate perioperative prophylaxis, I would not administer anything if the patient had a platelet count below 60,000; otherwise I would probably proceed as usual.
Question from the audience: You said that we shouldn’t operate on patients with acute hepatitis, but we frequently encounter patients with drug-induced hepatitis, such as from anticholesterol drugs. These patients’ ALT and aspartate aminotransferase (AST) levels can remain elevated for 2 or 3 months. How long should we delay surgery? For example, is it dangerous to proceed with a mastectomy a month after discontinuing the drug if the liver enzymes are still around 100 U/L?
Dr. Martin: It’s worth noting that much of the literature on surgery in patients with acute viral hepatitis is 30 or 40 years old. If such a patient had a compelling reason to have surgery, you might wait until the liver enzymes were trending downward and you were confident that the patient was recovering.
Question from the audience: How do you manage patients who have varices or have had variceal bleeding in the past? Many of them are on beta-blockers, such as propranolol, which can cause hypotension intraoperatively.
Dr. Martin: The standard of care is to prescribe beta-blockers for a patient with large varices, or to ablate the varices by endoscopy, which is my practice. In general, I would discontinue propranolol on the morning of surgery. If possible, however, I would have the patient undergo endoscopy before surgery to assess the likelihood of short-term variceal bleeding. If the varices look to be at low risk of bleeding, the beta-blocker can safely be stopped. If they look to be at high risk of bleeding, the surgery should be delayed for a few weeks, if possible, so that the varices can be ablated, which usually takes two or three sessions.
Question from the audience: I deal with many referrals, and I struggle with how aggressive a work-up I should do for patients undergoing elective surgery when a new abnormality is found in one of their liver function tests.
Dr. Martin: I would try to establish whether the abnormality is a chronic problem. Has the patient been told about an abnormal liver test in the past? Ask if the patient has been a blood donor, as measurement of ALT and some hepatitis serologies would have been required. Also ask if he or she has ever taken out a big life insurance policy, which also would have required liver function testing. If the abnormality is chronic, you may proceed with surgery if the bilirubin and INR are normal. In the absence of chronicity, surgery should be delayed for further work-up only in patients with indicators of significant liver disease—either markedly abnormal liver tests, thrombocytopenia, or coagulopathy.
Follow-up question: But patients rarely know whether they’ve had elevated liver enzymes in the past. You said not to worry about enzyme abnormalities unless they are markedly elevated, but how high is that?
Dr. Martin: AST and ALT are indicators of liver injury rather than of synthetic function. The true liver function tests are really albumin, bilirubin, and prothrombin time. Paradoxically, one of the best liver function tests is the platelet count. For me, a red flag for a patient with newly recognized liver disease is any degree of thrombocytopenia or coagulopathy or an elevation of bilirubin above the upper limit of normal. A patient with a platelet count of 90,000 and an INR above 1.2 has significant underlying liver disease, and I would be very concerned. Unless it’s a dire emergency, such a patient would need further evaluation before proceeding with surgery. In contrast, a patient with an ALT of 89, an AST of 65, and normal prothrombin time and platelet count should be safe to proceed to surgery. But such a patient needs an evaluation for liver disease afterward.
Question from the audience: My institution performs many liver resections for metastases or primary liver cancers. Our liver surgeons routinely discontinue statins 2 to 3 weeks before liver surgery, but it has been said at this summit that is not necessary. What’s your opinion?
Dr. Martin: I think that statins get a very bad rap in terms of hepatotoxity. Most patients with metabolic syndrome have hyperlipidemia, which can cause fatty liver disease and hepatic dysfunction. Statins help bring the lipid levels down. Hepatologists do not regard statins as major culprits in causing liver problems. I don’t believe there’s any particular indication to stop them before a patient undergoes hepatic surgery.
Question from the audience: I assess patients 1 or 2 weeks before surgery. For a patient with coagulopathy whom you suspect has underlying liver disease, is there any value in trying to treat the coagulopathy with vitamin K?
Dr. Martin: It can be worthwhile to try 10 mg subcutaneously for 3 days to see whether the situation improves, but if the patient has severe parenchymal liver disease, the vitamin K won’t help much.
- Ginés P, Quintero E, Arroyo V, et al. Compensated cirrhosis: natural history and prognostic factors. Hepatology 1987; 7:122–128.
- MELD/PELD calculator. United Network for Organ Sharing Web site. http://www.unos.org/resources/MeldPeldCalculator.asp?index=98. Accessed May 8, 2009.
- Ziser A, Plevak DJ, Wiesner RH, Rakela J, Offord KP, Brown DL. Morbidity and mortality in cirrhotic patients undergoing anesthesia and surgery. Anesthesiology 1999; 90:42–53.
- Poggio JL, Rowland CM, Gores GJ, et al. A comparison of laparoscopic and open cholecystectomy in patients with compensated cirrhosis and symptomatic gallstone disease. Surgery 2000; 127:405–411.
- Suman A, Barnes DS, Zein NN, et al. Predicting outcome after cardiac surgery in patients with cirrhosis: a comparison of Child-Pugh and MELD scores. Clin Gastroenterol Hepatol 2004; 2:719–723.
Assessing patients with liver disease for surgery is one of the most common reasons for hepatology consultation in the hospital. This review focuses on practical aspects of evaluating patients with known or suspected liver disease and provides guidance for determining whether it is safe to proceed with surgery in such patients. I begin with a case study to introduce some common clinical challenges and then revisit the case—with relevant teaching points—at the end.
CASE: A MIDDLE-AGED MAN WITH LIVER DISEASE SCHEDULED FOR CARDIAC SURGERY
A 57-year-old man with a history of liver disease is referred for preoperative assessment. It is 6:30 pm, and the patient has just arrived in the hospital; he is scheduled for coronary artery bypass graft surgery (CABG) early tomorrow morning for ischemic heart disease. Ten years ago, he was diagnosed with hepatitis C virus infection; 2 years later, he had a cholecystectomy. He has a remote history of intravenous drug use.
The sub-intern asks for an assessment of operative risk as well as advice on the type of anesthesia to be used.
HEPATIC EFFECTS OF ANESTHESIA
Anesthesiologists are keenly aware of the hepatic effects of anesthesia and that they must carefully choose anesthetics for patients with liver disease. There are a number of at least theoretical concerns about using particular anesthetics:
- Inhaled anesthetics, such as isoflurane, cause systemic vasodilation and depress cardiac output. These effects are of concern since many patients with advanced liver disease already have a hyperdynamic circulation because of peripheral vasodilation.
- Spinal or epidural anesthetics may reduce mean arterial pressure, which is of concern for similar reasons.
- Nitrous oxide has less of a depressive effect unless the patient has concomitant hypercapnia.
Another consideration is the hepatic metabolism of anesthetic agents. Use of halothane, which is 20% metabolized by the liver, is now uncommon, particularly if there is any concern about liver disease. In contrast, enflurane is only 4% metabolized by the liver. Numerous other anesthetics—including isoflurane, desflurane, and sevoflurane—have only minimal hepatic metabolism (< 0.2%), which makes them, along with nitrous oxide, the best anesthetic choices for patients with liver disease.
ASSESSING OPERATIVE RISK
The more important issue in the consultation for our patient is the degree of operative risk associated with his underlying liver disease. A number of factors are pertinent, including the etiology and severity of the liver disease and the type of surgery planned.
Acute liver disease has higher operative risk
Literature dating back 40 years has associated acute viral and alcoholic hepatitis with poor outcomes in surgical patients. Major elective surgery for a patient with suspected acute hepatitis A, for example, should be deferred until the patient has recovered, barring some compelling reason for greater urgency, such as a perforated viscus.
In chronic liver disease, hepatocellular function predicts outcome
When a patient with liver disease is evaluated for surgery, evidence should be sought to determine whether an index complication has already occurred. Because the patient in our case study had a cholecystectomy several years before, I would also ask, “What did the surgeon say your liver looked like? Did you have any bleeding problems afterwards? Did you develop ascites?”
It is also important to determine whether portal hypertension is present. For a patient with liver disease, otherwise unexplained thrombocytopenia is a useful indicator of portal hypertension.
Systems for scoring liver disease severity
Even a surgical patient with well-compensated liver disease is at risk for developing complications postoperatively, particularly if abdominal surgery is planned. Risk should be assessed in all patients with liver disease using either the Child-Pugh scoring system or the Model for End-Stage Liver Disease (MELD) scoring system.
The Child-Pugh score, which assigns 1 to 3 points according to the presence/absence and levels of each of five simple factors (bilirubin, albumin, prothrombin time/international normalized ratio [INR], ascites, and encephalopathy stage), has been used for decades to assess the severity of liver disease. Patients with Child-Pugh class A disease (score of 5–6) have well-compensated cirrhosis and good synthetic function, and therefore have essentially no restrictions for undergoing surgery. For patients in Child-Pugh class B (score of 7–9), the risk of perioperative complications and mortality is higher and any major hepatic surgery (such as hepatic resection) should be avoided. Patients with class C cirrhosis (score of 10–15) are not candidates for any major elective surgery and should be considered for liver transplantation referral.
The MELD scoring system was developed more recently and is used to prioritize eligibility for liver transplantation. Calculated using a mathematical formula that incorporates three objective patient variables—
creatinine, bilirubin, and INR—the MELD score correlates very well with prognosis. The score can be calculated by an online MELD calculator such as the one at www.unos.org/resources.2 A patient with a high MELD score is unlikely to survive for more than a few months without liver transplantation; a patient with a low MELD score is likely to survive for at least 12 months. Calculating the MELD score is now one of the first assessments in any patient suspected of having cirrhosis.
Risk factors for complications and death
In a retrospective study to identify factors associated with complications and mortality in surgical patients with cirrhosis, Ziser et al reviewed the records of 733 patients with cirrhosis who underwent surgical procedures (except liver transplantation) at the Mayo Clinic over an 11-year period (1980–1991).3 The mortality rate within 30 days of surgery was 11.6%. Long-term follow-up showed that most deaths occurred within the first few months after surgery, when many patients succumbed to pneumonia or renal insufficiency.
Risk factors have strong cumulative power
The study by Ziser et al also underscored the cumulative effect of risk factors, as the probability of developing a perioperative complication increased dramatically with the number of risk factors (as identified by multiavariate analysis) that a patient had, as follows3:
- 9.3% risk of complications with 1 risk factor
- 14.5% risk with 2 factors
- 33.5% risk with 3 factors
- 63.0% risk with 4 or 5 factors
- 73.3% risk with 6 factors
- 100% risk with 7 or 8 factors.
Postoperative complications: Beware hepatorenal syndrome
The most common postoperative complications in the study by Ziser et al were pneumonia, other infections, ventilation dependency, and ascites.3
Possibly the most ominous perioperative complication in a patient with liver disease is the onset of renal insufficiency, which may be precipitated by a number of factors, including nephrotoxic drugs and intraoperative hypotension. Renal insufficiency is usually a predictor of markedly reduced survival and a sign that hepatorenal syndrome may have developed.
Hepatorenal syndrome, which occurred in 3.3% of patients in the analysis by Ziser et al,3 is the presence of renal failure in a patient with cirrhosis. It is characterized by advanced liver failure and severe sinusoidal portal hypertension. The renal failure is said to be “functional” because significant histological changes are absent on kidney biopsy. Marked arteriolar vasodilation occurs in the extrarenal circulation with renal vasoconstriction leading to reduced glomerular filtration.
IMPORTANCE OF SURGICAL PROCEDURE TYPE
In addition to the patient-specific risk factors discussed above, certain surgical procedures deserve special consideration in patients with liver disease.
Cholecystectomy: Open vs closed
Patients with liver disease have the same indication for cholecystectomy as anyone else does: symptomatic gallstone disease. Patients with cirrhosis who are found to have incidental gallstones on ultrasonography should not undergo cholecystectomy unless the gallstones are symptomatic, as liver function may deteriorate after surgery.
For a patient with liver disease undergoing cholecystectomy, a common concern is whether an open or closed procedure should be done. Conventional wisdom had been that a patient with underlying liver disease (particularly cirrhosis) should have an open procedure so that the surgeon could more easily control bleeding, but that notion has changed in recent years with evidence supporting the safety of a laparoscopic approach in patients with liver disease.
One study supporting this new strategy is a retrospective review of 50 patients who had undergone cholecystectomy for symptomatic gallstone disease at the Mayo Clinic between 1990 and 1997.4 The procedure was open in half of the patients and laparoscopic in the other half. All patients had Child-Pugh class A or B cirrhosis. The indications for surgery were acute cholecystitis, biliary colic, or pancreatitis, and the number of patients with each of these indications was comparable between the open-surgery and laparoscopy groups. Three patients who initially underwent laparoscopy were converted to open cholecystectomy: two for bleeding and one for poor access. The study found that laparoscopic cholecystectomy was associated with statistically significant reductions in operating room time, blood loss, and length of hospital stay. No deaths occurred in either group. The authors concluded that laparoscopic cholecystectomy is safe in patients with cirrhosis and offers several advantages over an open surgical approach.
In light of these findings and other recent evidence, laparoscopic cholecystectomy should be recommended for patients with liver disease unless they have ascites or other evidence of overt hepatic decompensation, in which case cholecystectomy itself is contraindicated.
Cardiac surgery with bypass poses extra risk
Patients with liver disease undergoing open heart surgery with cardiopulmonary bypass are at especially high risk because of the effect on hepatic hemodynamics. This risk was demonstrated in a retrospective review of all patients with cirrhosis who underwent cardiac surgery with cardiopulmonary bypass at the Cleveland Clinic from 1992 to 2002.5 Of the 44 patients identified, 12 (27%) developed hepatic decompensation and 7 (16%) died. Hepatic decompensation was a major factor in all the deaths.
The MELD and Child-Pugh scores correlated well with one another in this study and were highly associated with hepatic decompensation and death. The best cutoff values for predicting mortality and hepatic decompensation were found to be a score greater than 7 in the Child-Pugh system and a score greater than 13 in the MELD system. (For context, receipt of a donor liver via a transplant list in the United States requires a MELD score of at least 15.) The study confirmed that the Child-Pugh score, which is easy to determine at the bedside, remains a reliable predictor of poor outcomes.5
CASE REVISITED: POSTOPERATIVE LIVER FUNCTION DECLINE―HOW SERIOUS IS IT?
Our patient undergoes the CABG procedure, and 3 days later you are asked to see him. According to the sub-intern, although the surgery was successful, the patient is now “in liver failure.” After hearing this news, the family is anxious to discuss liver transplantation.
On examination, the patient is alert and extubated, so he is clearly not encephalopathic. His wound is clean and shows no sign of infection. He appears to be mildly icteric, and he may have some ascites, based on mild flank dullness.
His laboratory test results are as follows:
- Bilirubin, 3.1 mg/dL (normal range, 0.3–1.2)
- INR, 1.2 (0.9–1.2)
- Alanine aminotransferase (ALT), 300 U/L (10–40)
- Creatinine, 0.9 mg/dL (0.6–1.2).
Although the bilirubin and ALT are elevated, it is notable that the creatinine is normal. This pattern is not uncommon after elective surgery in a patient with underlying cirrhosis. Renal dysfunction is the biggest concern in the perioperative management of a patient with liver disease, as it is an indicator that the patient may develop overt hepatic decompensation. Likely reasons for the patient’s ALT elevation are the effects of cardiopulmonary bypass and possible intraoperative hypotension.
The family needs to be told that the patient is not in liver failure and that it is best to wait with the expectation that he will do fine unless other complications supervene.
You advise cautious diuresis, and the ALT falls over the next few days. The bilirubin declines to 2.0 mg/dL. At this point, you advise discharge planning.
One need not wait for the bilirubin to return to normal: after an acute hepatic insult such as ischemic hepatitis or intraoperative hypotension, bilirubin is the last indicator to improve. Bilirubin is in part albumin-bound, and the half-life of albumin is 18 days, so a patient can remain icteric for some time after the rest of the liver function tests have returned to normal.
DISCUSSION
Question from the audience: What are your recommendations regarding platelet transfusion if the platelet count is less than 50,000 in a patient with liver disease?
Dr. Martin: For patients with thrombocytopenia, it is prudent to get the platelet count above 60,000 before any procedure. We will not even do a blind liver biopsy in a patient with a platelet count of less than 60,000.
Question from the audience: A study from the Annals of Surgery concludes that patients with liver disease do poorly with a hemoglobin of less than 10 g/dL. Would you transfuse aggressively before surgery?
Dr. Martin: For a patient with anemia, I don’t like to use aggressive transfusion if cirrhosis is present because the portal pressure may go up and increase the risk of variceal hemorrhage. If there is adequate time for a work-up, one can screen for varices by endoscopy. If there is evidence of overt hepatic decompensation and portal hypertension (esophageal varices, a palpable spleen, and thrombocytopenia), I wouldn’t try to get the hemoglobin much above 10 g/dL.
Question from the audience: How would you modify prophylaxis for deep vein thrombosis following hip or knee replacement surgery in patients with liver disease?
Dr. Martin: I would base it on the INR. Patients who are already mildly coagulopathic tend to be very sensitive to warfarin in the long term. For immediate perioperative prophylaxis, I would not administer anything if the patient had a platelet count below 60,000; otherwise I would probably proceed as usual.
Question from the audience: You said that we shouldn’t operate on patients with acute hepatitis, but we frequently encounter patients with drug-induced hepatitis, such as from anticholesterol drugs. These patients’ ALT and aspartate aminotransferase (AST) levels can remain elevated for 2 or 3 months. How long should we delay surgery? For example, is it dangerous to proceed with a mastectomy a month after discontinuing the drug if the liver enzymes are still around 100 U/L?
Dr. Martin: It’s worth noting that much of the literature on surgery in patients with acute viral hepatitis is 30 or 40 years old. If such a patient had a compelling reason to have surgery, you might wait until the liver enzymes were trending downward and you were confident that the patient was recovering.
Question from the audience: How do you manage patients who have varices or have had variceal bleeding in the past? Many of them are on beta-blockers, such as propranolol, which can cause hypotension intraoperatively.
Dr. Martin: The standard of care is to prescribe beta-blockers for a patient with large varices, or to ablate the varices by endoscopy, which is my practice. In general, I would discontinue propranolol on the morning of surgery. If possible, however, I would have the patient undergo endoscopy before surgery to assess the likelihood of short-term variceal bleeding. If the varices look to be at low risk of bleeding, the beta-blocker can safely be stopped. If they look to be at high risk of bleeding, the surgery should be delayed for a few weeks, if possible, so that the varices can be ablated, which usually takes two or three sessions.
Question from the audience: I deal with many referrals, and I struggle with how aggressive a work-up I should do for patients undergoing elective surgery when a new abnormality is found in one of their liver function tests.
Dr. Martin: I would try to establish whether the abnormality is a chronic problem. Has the patient been told about an abnormal liver test in the past? Ask if the patient has been a blood donor, as measurement of ALT and some hepatitis serologies would have been required. Also ask if he or she has ever taken out a big life insurance policy, which also would have required liver function testing. If the abnormality is chronic, you may proceed with surgery if the bilirubin and INR are normal. In the absence of chronicity, surgery should be delayed for further work-up only in patients with indicators of significant liver disease—either markedly abnormal liver tests, thrombocytopenia, or coagulopathy.
Follow-up question: But patients rarely know whether they’ve had elevated liver enzymes in the past. You said not to worry about enzyme abnormalities unless they are markedly elevated, but how high is that?
Dr. Martin: AST and ALT are indicators of liver injury rather than of synthetic function. The true liver function tests are really albumin, bilirubin, and prothrombin time. Paradoxically, one of the best liver function tests is the platelet count. For me, a red flag for a patient with newly recognized liver disease is any degree of thrombocytopenia or coagulopathy or an elevation of bilirubin above the upper limit of normal. A patient with a platelet count of 90,000 and an INR above 1.2 has significant underlying liver disease, and I would be very concerned. Unless it’s a dire emergency, such a patient would need further evaluation before proceeding with surgery. In contrast, a patient with an ALT of 89, an AST of 65, and normal prothrombin time and platelet count should be safe to proceed to surgery. But such a patient needs an evaluation for liver disease afterward.
Question from the audience: My institution performs many liver resections for metastases or primary liver cancers. Our liver surgeons routinely discontinue statins 2 to 3 weeks before liver surgery, but it has been said at this summit that is not necessary. What’s your opinion?
Dr. Martin: I think that statins get a very bad rap in terms of hepatotoxity. Most patients with metabolic syndrome have hyperlipidemia, which can cause fatty liver disease and hepatic dysfunction. Statins help bring the lipid levels down. Hepatologists do not regard statins as major culprits in causing liver problems. I don’t believe there’s any particular indication to stop them before a patient undergoes hepatic surgery.
Question from the audience: I assess patients 1 or 2 weeks before surgery. For a patient with coagulopathy whom you suspect has underlying liver disease, is there any value in trying to treat the coagulopathy with vitamin K?
Dr. Martin: It can be worthwhile to try 10 mg subcutaneously for 3 days to see whether the situation improves, but if the patient has severe parenchymal liver disease, the vitamin K won’t help much.
Assessing patients with liver disease for surgery is one of the most common reasons for hepatology consultation in the hospital. This review focuses on practical aspects of evaluating patients with known or suspected liver disease and provides guidance for determining whether it is safe to proceed with surgery in such patients. I begin with a case study to introduce some common clinical challenges and then revisit the case—with relevant teaching points—at the end.
CASE: A MIDDLE-AGED MAN WITH LIVER DISEASE SCHEDULED FOR CARDIAC SURGERY
A 57-year-old man with a history of liver disease is referred for preoperative assessment. It is 6:30 pm, and the patient has just arrived in the hospital; he is scheduled for coronary artery bypass graft surgery (CABG) early tomorrow morning for ischemic heart disease. Ten years ago, he was diagnosed with hepatitis C virus infection; 2 years later, he had a cholecystectomy. He has a remote history of intravenous drug use.
The sub-intern asks for an assessment of operative risk as well as advice on the type of anesthesia to be used.
HEPATIC EFFECTS OF ANESTHESIA
Anesthesiologists are keenly aware of the hepatic effects of anesthesia and that they must carefully choose anesthetics for patients with liver disease. There are a number of at least theoretical concerns about using particular anesthetics:
- Inhaled anesthetics, such as isoflurane, cause systemic vasodilation and depress cardiac output. These effects are of concern since many patients with advanced liver disease already have a hyperdynamic circulation because of peripheral vasodilation.
- Spinal or epidural anesthetics may reduce mean arterial pressure, which is of concern for similar reasons.
- Nitrous oxide has less of a depressive effect unless the patient has concomitant hypercapnia.
Another consideration is the hepatic metabolism of anesthetic agents. Use of halothane, which is 20% metabolized by the liver, is now uncommon, particularly if there is any concern about liver disease. In contrast, enflurane is only 4% metabolized by the liver. Numerous other anesthetics—including isoflurane, desflurane, and sevoflurane—have only minimal hepatic metabolism (< 0.2%), which makes them, along with nitrous oxide, the best anesthetic choices for patients with liver disease.
ASSESSING OPERATIVE RISK
The more important issue in the consultation for our patient is the degree of operative risk associated with his underlying liver disease. A number of factors are pertinent, including the etiology and severity of the liver disease and the type of surgery planned.
Acute liver disease has higher operative risk
Literature dating back 40 years has associated acute viral and alcoholic hepatitis with poor outcomes in surgical patients. Major elective surgery for a patient with suspected acute hepatitis A, for example, should be deferred until the patient has recovered, barring some compelling reason for greater urgency, such as a perforated viscus.
In chronic liver disease, hepatocellular function predicts outcome
When a patient with liver disease is evaluated for surgery, evidence should be sought to determine whether an index complication has already occurred. Because the patient in our case study had a cholecystectomy several years before, I would also ask, “What did the surgeon say your liver looked like? Did you have any bleeding problems afterwards? Did you develop ascites?”
It is also important to determine whether portal hypertension is present. For a patient with liver disease, otherwise unexplained thrombocytopenia is a useful indicator of portal hypertension.
Systems for scoring liver disease severity
Even a surgical patient with well-compensated liver disease is at risk for developing complications postoperatively, particularly if abdominal surgery is planned. Risk should be assessed in all patients with liver disease using either the Child-Pugh scoring system or the Model for End-Stage Liver Disease (MELD) scoring system.
The Child-Pugh score, which assigns 1 to 3 points according to the presence/absence and levels of each of five simple factors (bilirubin, albumin, prothrombin time/international normalized ratio [INR], ascites, and encephalopathy stage), has been used for decades to assess the severity of liver disease. Patients with Child-Pugh class A disease (score of 5–6) have well-compensated cirrhosis and good synthetic function, and therefore have essentially no restrictions for undergoing surgery. For patients in Child-Pugh class B (score of 7–9), the risk of perioperative complications and mortality is higher and any major hepatic surgery (such as hepatic resection) should be avoided. Patients with class C cirrhosis (score of 10–15) are not candidates for any major elective surgery and should be considered for liver transplantation referral.
The MELD scoring system was developed more recently and is used to prioritize eligibility for liver transplantation. Calculated using a mathematical formula that incorporates three objective patient variables—
creatinine, bilirubin, and INR—the MELD score correlates very well with prognosis. The score can be calculated by an online MELD calculator such as the one at www.unos.org/resources.2 A patient with a high MELD score is unlikely to survive for more than a few months without liver transplantation; a patient with a low MELD score is likely to survive for at least 12 months. Calculating the MELD score is now one of the first assessments in any patient suspected of having cirrhosis.
Risk factors for complications and death
In a retrospective study to identify factors associated with complications and mortality in surgical patients with cirrhosis, Ziser et al reviewed the records of 733 patients with cirrhosis who underwent surgical procedures (except liver transplantation) at the Mayo Clinic over an 11-year period (1980–1991).3 The mortality rate within 30 days of surgery was 11.6%. Long-term follow-up showed that most deaths occurred within the first few months after surgery, when many patients succumbed to pneumonia or renal insufficiency.
Risk factors have strong cumulative power
The study by Ziser et al also underscored the cumulative effect of risk factors, as the probability of developing a perioperative complication increased dramatically with the number of risk factors (as identified by multiavariate analysis) that a patient had, as follows3:
- 9.3% risk of complications with 1 risk factor
- 14.5% risk with 2 factors
- 33.5% risk with 3 factors
- 63.0% risk with 4 or 5 factors
- 73.3% risk with 6 factors
- 100% risk with 7 or 8 factors.
Postoperative complications: Beware hepatorenal syndrome
The most common postoperative complications in the study by Ziser et al were pneumonia, other infections, ventilation dependency, and ascites.3
Possibly the most ominous perioperative complication in a patient with liver disease is the onset of renal insufficiency, which may be precipitated by a number of factors, including nephrotoxic drugs and intraoperative hypotension. Renal insufficiency is usually a predictor of markedly reduced survival and a sign that hepatorenal syndrome may have developed.
Hepatorenal syndrome, which occurred in 3.3% of patients in the analysis by Ziser et al,3 is the presence of renal failure in a patient with cirrhosis. It is characterized by advanced liver failure and severe sinusoidal portal hypertension. The renal failure is said to be “functional” because significant histological changes are absent on kidney biopsy. Marked arteriolar vasodilation occurs in the extrarenal circulation with renal vasoconstriction leading to reduced glomerular filtration.
IMPORTANCE OF SURGICAL PROCEDURE TYPE
In addition to the patient-specific risk factors discussed above, certain surgical procedures deserve special consideration in patients with liver disease.
Cholecystectomy: Open vs closed
Patients with liver disease have the same indication for cholecystectomy as anyone else does: symptomatic gallstone disease. Patients with cirrhosis who are found to have incidental gallstones on ultrasonography should not undergo cholecystectomy unless the gallstones are symptomatic, as liver function may deteriorate after surgery.
For a patient with liver disease undergoing cholecystectomy, a common concern is whether an open or closed procedure should be done. Conventional wisdom had been that a patient with underlying liver disease (particularly cirrhosis) should have an open procedure so that the surgeon could more easily control bleeding, but that notion has changed in recent years with evidence supporting the safety of a laparoscopic approach in patients with liver disease.
One study supporting this new strategy is a retrospective review of 50 patients who had undergone cholecystectomy for symptomatic gallstone disease at the Mayo Clinic between 1990 and 1997.4 The procedure was open in half of the patients and laparoscopic in the other half. All patients had Child-Pugh class A or B cirrhosis. The indications for surgery were acute cholecystitis, biliary colic, or pancreatitis, and the number of patients with each of these indications was comparable between the open-surgery and laparoscopy groups. Three patients who initially underwent laparoscopy were converted to open cholecystectomy: two for bleeding and one for poor access. The study found that laparoscopic cholecystectomy was associated with statistically significant reductions in operating room time, blood loss, and length of hospital stay. No deaths occurred in either group. The authors concluded that laparoscopic cholecystectomy is safe in patients with cirrhosis and offers several advantages over an open surgical approach.
In light of these findings and other recent evidence, laparoscopic cholecystectomy should be recommended for patients with liver disease unless they have ascites or other evidence of overt hepatic decompensation, in which case cholecystectomy itself is contraindicated.
Cardiac surgery with bypass poses extra risk
Patients with liver disease undergoing open heart surgery with cardiopulmonary bypass are at especially high risk because of the effect on hepatic hemodynamics. This risk was demonstrated in a retrospective review of all patients with cirrhosis who underwent cardiac surgery with cardiopulmonary bypass at the Cleveland Clinic from 1992 to 2002.5 Of the 44 patients identified, 12 (27%) developed hepatic decompensation and 7 (16%) died. Hepatic decompensation was a major factor in all the deaths.
The MELD and Child-Pugh scores correlated well with one another in this study and were highly associated with hepatic decompensation and death. The best cutoff values for predicting mortality and hepatic decompensation were found to be a score greater than 7 in the Child-Pugh system and a score greater than 13 in the MELD system. (For context, receipt of a donor liver via a transplant list in the United States requires a MELD score of at least 15.) The study confirmed that the Child-Pugh score, which is easy to determine at the bedside, remains a reliable predictor of poor outcomes.5
CASE REVISITED: POSTOPERATIVE LIVER FUNCTION DECLINE―HOW SERIOUS IS IT?
Our patient undergoes the CABG procedure, and 3 days later you are asked to see him. According to the sub-intern, although the surgery was successful, the patient is now “in liver failure.” After hearing this news, the family is anxious to discuss liver transplantation.
On examination, the patient is alert and extubated, so he is clearly not encephalopathic. His wound is clean and shows no sign of infection. He appears to be mildly icteric, and he may have some ascites, based on mild flank dullness.
His laboratory test results are as follows:
- Bilirubin, 3.1 mg/dL (normal range, 0.3–1.2)
- INR, 1.2 (0.9–1.2)
- Alanine aminotransferase (ALT), 300 U/L (10–40)
- Creatinine, 0.9 mg/dL (0.6–1.2).
Although the bilirubin and ALT are elevated, it is notable that the creatinine is normal. This pattern is not uncommon after elective surgery in a patient with underlying cirrhosis. Renal dysfunction is the biggest concern in the perioperative management of a patient with liver disease, as it is an indicator that the patient may develop overt hepatic decompensation. Likely reasons for the patient’s ALT elevation are the effects of cardiopulmonary bypass and possible intraoperative hypotension.
The family needs to be told that the patient is not in liver failure and that it is best to wait with the expectation that he will do fine unless other complications supervene.
You advise cautious diuresis, and the ALT falls over the next few days. The bilirubin declines to 2.0 mg/dL. At this point, you advise discharge planning.
One need not wait for the bilirubin to return to normal: after an acute hepatic insult such as ischemic hepatitis or intraoperative hypotension, bilirubin is the last indicator to improve. Bilirubin is in part albumin-bound, and the half-life of albumin is 18 days, so a patient can remain icteric for some time after the rest of the liver function tests have returned to normal.
DISCUSSION
Question from the audience: What are your recommendations regarding platelet transfusion if the platelet count is less than 50,000 in a patient with liver disease?
Dr. Martin: For patients with thrombocytopenia, it is prudent to get the platelet count above 60,000 before any procedure. We will not even do a blind liver biopsy in a patient with a platelet count of less than 60,000.
Question from the audience: A study from the Annals of Surgery concludes that patients with liver disease do poorly with a hemoglobin of less than 10 g/dL. Would you transfuse aggressively before surgery?
Dr. Martin: For a patient with anemia, I don’t like to use aggressive transfusion if cirrhosis is present because the portal pressure may go up and increase the risk of variceal hemorrhage. If there is adequate time for a work-up, one can screen for varices by endoscopy. If there is evidence of overt hepatic decompensation and portal hypertension (esophageal varices, a palpable spleen, and thrombocytopenia), I wouldn’t try to get the hemoglobin much above 10 g/dL.
Question from the audience: How would you modify prophylaxis for deep vein thrombosis following hip or knee replacement surgery in patients with liver disease?
Dr. Martin: I would base it on the INR. Patients who are already mildly coagulopathic tend to be very sensitive to warfarin in the long term. For immediate perioperative prophylaxis, I would not administer anything if the patient had a platelet count below 60,000; otherwise I would probably proceed as usual.
Question from the audience: You said that we shouldn’t operate on patients with acute hepatitis, but we frequently encounter patients with drug-induced hepatitis, such as from anticholesterol drugs. These patients’ ALT and aspartate aminotransferase (AST) levels can remain elevated for 2 or 3 months. How long should we delay surgery? For example, is it dangerous to proceed with a mastectomy a month after discontinuing the drug if the liver enzymes are still around 100 U/L?
Dr. Martin: It’s worth noting that much of the literature on surgery in patients with acute viral hepatitis is 30 or 40 years old. If such a patient had a compelling reason to have surgery, you might wait until the liver enzymes were trending downward and you were confident that the patient was recovering.
Question from the audience: How do you manage patients who have varices or have had variceal bleeding in the past? Many of them are on beta-blockers, such as propranolol, which can cause hypotension intraoperatively.
Dr. Martin: The standard of care is to prescribe beta-blockers for a patient with large varices, or to ablate the varices by endoscopy, which is my practice. In general, I would discontinue propranolol on the morning of surgery. If possible, however, I would have the patient undergo endoscopy before surgery to assess the likelihood of short-term variceal bleeding. If the varices look to be at low risk of bleeding, the beta-blocker can safely be stopped. If they look to be at high risk of bleeding, the surgery should be delayed for a few weeks, if possible, so that the varices can be ablated, which usually takes two or three sessions.
Question from the audience: I deal with many referrals, and I struggle with how aggressive a work-up I should do for patients undergoing elective surgery when a new abnormality is found in one of their liver function tests.
Dr. Martin: I would try to establish whether the abnormality is a chronic problem. Has the patient been told about an abnormal liver test in the past? Ask if the patient has been a blood donor, as measurement of ALT and some hepatitis serologies would have been required. Also ask if he or she has ever taken out a big life insurance policy, which also would have required liver function testing. If the abnormality is chronic, you may proceed with surgery if the bilirubin and INR are normal. In the absence of chronicity, surgery should be delayed for further work-up only in patients with indicators of significant liver disease—either markedly abnormal liver tests, thrombocytopenia, or coagulopathy.
Follow-up question: But patients rarely know whether they’ve had elevated liver enzymes in the past. You said not to worry about enzyme abnormalities unless they are markedly elevated, but how high is that?
Dr. Martin: AST and ALT are indicators of liver injury rather than of synthetic function. The true liver function tests are really albumin, bilirubin, and prothrombin time. Paradoxically, one of the best liver function tests is the platelet count. For me, a red flag for a patient with newly recognized liver disease is any degree of thrombocytopenia or coagulopathy or an elevation of bilirubin above the upper limit of normal. A patient with a platelet count of 90,000 and an INR above 1.2 has significant underlying liver disease, and I would be very concerned. Unless it’s a dire emergency, such a patient would need further evaluation before proceeding with surgery. In contrast, a patient with an ALT of 89, an AST of 65, and normal prothrombin time and platelet count should be safe to proceed to surgery. But such a patient needs an evaluation for liver disease afterward.
Question from the audience: My institution performs many liver resections for metastases or primary liver cancers. Our liver surgeons routinely discontinue statins 2 to 3 weeks before liver surgery, but it has been said at this summit that is not necessary. What’s your opinion?
Dr. Martin: I think that statins get a very bad rap in terms of hepatotoxity. Most patients with metabolic syndrome have hyperlipidemia, which can cause fatty liver disease and hepatic dysfunction. Statins help bring the lipid levels down. Hepatologists do not regard statins as major culprits in causing liver problems. I don’t believe there’s any particular indication to stop them before a patient undergoes hepatic surgery.
Question from the audience: I assess patients 1 or 2 weeks before surgery. For a patient with coagulopathy whom you suspect has underlying liver disease, is there any value in trying to treat the coagulopathy with vitamin K?
Dr. Martin: It can be worthwhile to try 10 mg subcutaneously for 3 days to see whether the situation improves, but if the patient has severe parenchymal liver disease, the vitamin K won’t help much.
- Ginés P, Quintero E, Arroyo V, et al. Compensated cirrhosis: natural history and prognostic factors. Hepatology 1987; 7:122–128.
- MELD/PELD calculator. United Network for Organ Sharing Web site. http://www.unos.org/resources/MeldPeldCalculator.asp?index=98. Accessed May 8, 2009.
- Ziser A, Plevak DJ, Wiesner RH, Rakela J, Offord KP, Brown DL. Morbidity and mortality in cirrhotic patients undergoing anesthesia and surgery. Anesthesiology 1999; 90:42–53.
- Poggio JL, Rowland CM, Gores GJ, et al. A comparison of laparoscopic and open cholecystectomy in patients with compensated cirrhosis and symptomatic gallstone disease. Surgery 2000; 127:405–411.
- Suman A, Barnes DS, Zein NN, et al. Predicting outcome after cardiac surgery in patients with cirrhosis: a comparison of Child-Pugh and MELD scores. Clin Gastroenterol Hepatol 2004; 2:719–723.
- Ginés P, Quintero E, Arroyo V, et al. Compensated cirrhosis: natural history and prognostic factors. Hepatology 1987; 7:122–128.
- MELD/PELD calculator. United Network for Organ Sharing Web site. http://www.unos.org/resources/MeldPeldCalculator.asp?index=98. Accessed May 8, 2009.
- Ziser A, Plevak DJ, Wiesner RH, Rakela J, Offord KP, Brown DL. Morbidity and mortality in cirrhotic patients undergoing anesthesia and surgery. Anesthesiology 1999; 90:42–53.
- Poggio JL, Rowland CM, Gores GJ, et al. A comparison of laparoscopic and open cholecystectomy in patients with compensated cirrhosis and symptomatic gallstone disease. Surgery 2000; 127:405–411.
- Suman A, Barnes DS, Zein NN, et al. Predicting outcome after cardiac surgery in patients with cirrhosis: a comparison of Child-Pugh and MELD scores. Clin Gastroenterol Hepatol 2004; 2:719–723.
KEY POINTS
- Patients with acute hepatitis should delay elective surgery until after their hepatitis resolves.
- Patients with chronic liver disease who have developed any index complication—variceal hemorrhage, ascites, hepatic encephalopathy, or jaundice—are at increased risk for postoperative complications and death.
- The Child-Pugh and MELD scores appear to be comparably effective in predicting surgical outcomes in patients with liver disease.
- Cardiac surgery with cardiopulmonary bypass and abdominal surgery are particularly high-risk procedures in patients with liver disease.
- If cholecystectomy is indicated in a patient with compensated liver disease, laparoscopy should be the initial approach, with conversion to an open procedure only if necessary.