User login
Cutaneous Presentation of T-Cell Prolymphocytic Leukemia
Cutaneous Mastocytosis: A Case of Bullous Urticaria Pigmentosa

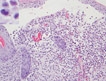
Langerhans Cell Histiocytosis
Postcoital vomiting after taking sildenafil?
When you think of sildenafil citrate for the treatment of erectile dysfunction (ED), what adverse effects come to mind? Chances are you think of some of the most common adverse reactions, such as headache (16%), flushing (10%), and dyspepsia (7%), with the latter more common (17%) at higher doses.1 Or perhaps you think of diarrhea (3%) or maybe even dizziness (2%). But chances are, you don’t think of vomiting, which is reported to occur in <2% of patients.1 In fact, an OVID search for the terms PDE5 inhibitors and vomiting revealed no reports of postcoital emesis. In the case we report here, however, postcoital vomiting secondary to sildenafil use did occur.
Our patient, a 43-year-old African-American man with a 23-year history of diabetes and hypertension, sought help for ED. His medications included insulin 70/30 and irbesartan/hydrochlorothiazide (Avalide) 150/12.5 mg daily, due to a history of ACE inhibitor-induced cough. He denied the use of tobacco and recreational drugs but admitted to consuming 6 to 10 beers on Friday nights. He followed no special diet or exercise regimen. A review of systems was negative except for the ED, presumed to be organic as the physical exam was unrevealing.
The patient was not using nitrates and had no known contraindications for sildenafil, and therapy was initiated at 50 mg as needed prior to sexual activity. On follow-up, he reported an acceptable erectile response but noted the onset of postcoital emesis. He denied associated nausea, but reported that on multiple occasions, emesis occurred soon after ejaculation, typically occurring about 90 minutes after ingestion of sildenafil.
The adverse effect profile of sildenafil may be divided into vasodilator effects and enzymatic inhibitor effects.2 It is postulated that an emetic response may be associated with PDE4 inhibitors secondary to release of mediators 5-HT, substance P, and noradrenaline analogous to presynaptic α2-adrenoreceptor inhibition.3
A study by Robichaud et al showed that administration of PDE4 inhibitors reduced the duration of anesthesia induced by a combination of xylazine and ketamine—a correlate of emesis in nonvomiting species (rodents).3 But it is not known if inhibition of PDE4 promotes emesis in humans or if a similar effect occurs with PDE5 inhibitors like sildenafil.3,4 Mild cross-reactivity of sildenafil with PDE6 (present in the retina) explains the visual disturbances associated with the drug (changes in color perception, blurry vision, and light sensitivity)5 and lends further credibility to possible cross-reactivity between PDE4 and PDE5.
Emesis in the absence of nausea or other gastrointestinal (GI) symptoms supports a drug-related effect, rather than a complication associated with type 2 diabetes or binge drinking. The patient denied symptoms of fullness, upper abdominal pain, or reduced hunger, all of which correlate better with delayed gastric emptying associated with diabetic gastroparesis than nausea or vomiting.5
The patient’s weekly consumption of beer meets the criteria for binge drinking defined by the National Institute of Alcohol Abuse and Alcoholism;6 however, emesis associated with ingestion of sildenafil occurred independent of alcohol ingestion, according to our patient.
The patient was advised to try sildenafil both with and without food to determine if either scenario would ameliorate symptoms of vomiting, and to reduce the dosage to 25 mg. Since he now has another health care team, we do not know whether he tried again with sildenafil or another PDE5 inhibitor.
Another case in the literature struck us as remarkably similar. A case report published in 2002 described a 79-year-old man who experienced vestibular symptoms 2 hours after taking sildenafil for the first time, including horizontal nystagmus with rotator components and vomiting.2 The similar time frame as our patient’s complaints also indicates a drug-related phenomenon. The observation of vomiting appears to be unique in the literature and supports its inclusion in published reports that include the long list of sildenafil’s potential adverse effects.
Michelle Lamb, PharmD
Nancy Brahm, PharmD
Mark D. Fox, MD
Tulsa, Okla
1. Viagra (sildenafil citrate) tablets [package insert]. New York NY: Pfizer; 2010. Available at: http://media.pfizer.com/files/products/uspi_viagra.pdf. Accessed January 23, 2013.
2. Hamzavi J, Schmetterer L, Formanek M. Vestibular symptoms as a complication of sildenafil: a case report. Wein Klin Wochenschr. 2002;114:54-55.
3. Robichaud A, Stamatiou PB, Jin S-LC, et al. Deletion of phosphodiesterase 4D in mice shortens α2-adrenoreceptor-mediated anesthesia, a behavioral correlate of emesis. J Clin Invest. 2002;110:1045-1052.
4. Giembycz MA. 4D or not 4D - the emetogenic basis of PDE4 inhibitors uncovered? Trends Pharmacol Sci. 2002;23:548.-
5. Camilleri M, Bharucha AE, Farrugia G. Epidemiology mechanisms, and management of diabetic gastroparesis. Clin Gastroenterol Hepatol. 2011;9:5-12.
6. National Institute of Alcohol Abuse and Alcoholism. NIAAA council approves definition of binge drinking. NIAAA Newsletter. 2004;3:3.-
When you think of sildenafil citrate for the treatment of erectile dysfunction (ED), what adverse effects come to mind? Chances are you think of some of the most common adverse reactions, such as headache (16%), flushing (10%), and dyspepsia (7%), with the latter more common (17%) at higher doses.1 Or perhaps you think of diarrhea (3%) or maybe even dizziness (2%). But chances are, you don’t think of vomiting, which is reported to occur in <2% of patients.1 In fact, an OVID search for the terms PDE5 inhibitors and vomiting revealed no reports of postcoital emesis. In the case we report here, however, postcoital vomiting secondary to sildenafil use did occur.
Our patient, a 43-year-old African-American man with a 23-year history of diabetes and hypertension, sought help for ED. His medications included insulin 70/30 and irbesartan/hydrochlorothiazide (Avalide) 150/12.5 mg daily, due to a history of ACE inhibitor-induced cough. He denied the use of tobacco and recreational drugs but admitted to consuming 6 to 10 beers on Friday nights. He followed no special diet or exercise regimen. A review of systems was negative except for the ED, presumed to be organic as the physical exam was unrevealing.
The patient was not using nitrates and had no known contraindications for sildenafil, and therapy was initiated at 50 mg as needed prior to sexual activity. On follow-up, he reported an acceptable erectile response but noted the onset of postcoital emesis. He denied associated nausea, but reported that on multiple occasions, emesis occurred soon after ejaculation, typically occurring about 90 minutes after ingestion of sildenafil.
The adverse effect profile of sildenafil may be divided into vasodilator effects and enzymatic inhibitor effects.2 It is postulated that an emetic response may be associated with PDE4 inhibitors secondary to release of mediators 5-HT, substance P, and noradrenaline analogous to presynaptic α2-adrenoreceptor inhibition.3
A study by Robichaud et al showed that administration of PDE4 inhibitors reduced the duration of anesthesia induced by a combination of xylazine and ketamine—a correlate of emesis in nonvomiting species (rodents).3 But it is not known if inhibition of PDE4 promotes emesis in humans or if a similar effect occurs with PDE5 inhibitors like sildenafil.3,4 Mild cross-reactivity of sildenafil with PDE6 (present in the retina) explains the visual disturbances associated with the drug (changes in color perception, blurry vision, and light sensitivity)5 and lends further credibility to possible cross-reactivity between PDE4 and PDE5.
Emesis in the absence of nausea or other gastrointestinal (GI) symptoms supports a drug-related effect, rather than a complication associated with type 2 diabetes or binge drinking. The patient denied symptoms of fullness, upper abdominal pain, or reduced hunger, all of which correlate better with delayed gastric emptying associated with diabetic gastroparesis than nausea or vomiting.5
The patient’s weekly consumption of beer meets the criteria for binge drinking defined by the National Institute of Alcohol Abuse and Alcoholism;6 however, emesis associated with ingestion of sildenafil occurred independent of alcohol ingestion, according to our patient.
The patient was advised to try sildenafil both with and without food to determine if either scenario would ameliorate symptoms of vomiting, and to reduce the dosage to 25 mg. Since he now has another health care team, we do not know whether he tried again with sildenafil or another PDE5 inhibitor.
Another case in the literature struck us as remarkably similar. A case report published in 2002 described a 79-year-old man who experienced vestibular symptoms 2 hours after taking sildenafil for the first time, including horizontal nystagmus with rotator components and vomiting.2 The similar time frame as our patient’s complaints also indicates a drug-related phenomenon. The observation of vomiting appears to be unique in the literature and supports its inclusion in published reports that include the long list of sildenafil’s potential adverse effects.
Michelle Lamb, PharmD
Nancy Brahm, PharmD
Mark D. Fox, MD
Tulsa, Okla
When you think of sildenafil citrate for the treatment of erectile dysfunction (ED), what adverse effects come to mind? Chances are you think of some of the most common adverse reactions, such as headache (16%), flushing (10%), and dyspepsia (7%), with the latter more common (17%) at higher doses.1 Or perhaps you think of diarrhea (3%) or maybe even dizziness (2%). But chances are, you don’t think of vomiting, which is reported to occur in <2% of patients.1 In fact, an OVID search for the terms PDE5 inhibitors and vomiting revealed no reports of postcoital emesis. In the case we report here, however, postcoital vomiting secondary to sildenafil use did occur.
Our patient, a 43-year-old African-American man with a 23-year history of diabetes and hypertension, sought help for ED. His medications included insulin 70/30 and irbesartan/hydrochlorothiazide (Avalide) 150/12.5 mg daily, due to a history of ACE inhibitor-induced cough. He denied the use of tobacco and recreational drugs but admitted to consuming 6 to 10 beers on Friday nights. He followed no special diet or exercise regimen. A review of systems was negative except for the ED, presumed to be organic as the physical exam was unrevealing.
The patient was not using nitrates and had no known contraindications for sildenafil, and therapy was initiated at 50 mg as needed prior to sexual activity. On follow-up, he reported an acceptable erectile response but noted the onset of postcoital emesis. He denied associated nausea, but reported that on multiple occasions, emesis occurred soon after ejaculation, typically occurring about 90 minutes after ingestion of sildenafil.
The adverse effect profile of sildenafil may be divided into vasodilator effects and enzymatic inhibitor effects.2 It is postulated that an emetic response may be associated with PDE4 inhibitors secondary to release of mediators 5-HT, substance P, and noradrenaline analogous to presynaptic α2-adrenoreceptor inhibition.3
A study by Robichaud et al showed that administration of PDE4 inhibitors reduced the duration of anesthesia induced by a combination of xylazine and ketamine—a correlate of emesis in nonvomiting species (rodents).3 But it is not known if inhibition of PDE4 promotes emesis in humans or if a similar effect occurs with PDE5 inhibitors like sildenafil.3,4 Mild cross-reactivity of sildenafil with PDE6 (present in the retina) explains the visual disturbances associated with the drug (changes in color perception, blurry vision, and light sensitivity)5 and lends further credibility to possible cross-reactivity between PDE4 and PDE5.
Emesis in the absence of nausea or other gastrointestinal (GI) symptoms supports a drug-related effect, rather than a complication associated with type 2 diabetes or binge drinking. The patient denied symptoms of fullness, upper abdominal pain, or reduced hunger, all of which correlate better with delayed gastric emptying associated with diabetic gastroparesis than nausea or vomiting.5
The patient’s weekly consumption of beer meets the criteria for binge drinking defined by the National Institute of Alcohol Abuse and Alcoholism;6 however, emesis associated with ingestion of sildenafil occurred independent of alcohol ingestion, according to our patient.
The patient was advised to try sildenafil both with and without food to determine if either scenario would ameliorate symptoms of vomiting, and to reduce the dosage to 25 mg. Since he now has another health care team, we do not know whether he tried again with sildenafil or another PDE5 inhibitor.
Another case in the literature struck us as remarkably similar. A case report published in 2002 described a 79-year-old man who experienced vestibular symptoms 2 hours after taking sildenafil for the first time, including horizontal nystagmus with rotator components and vomiting.2 The similar time frame as our patient’s complaints also indicates a drug-related phenomenon. The observation of vomiting appears to be unique in the literature and supports its inclusion in published reports that include the long list of sildenafil’s potential adverse effects.
Michelle Lamb, PharmD
Nancy Brahm, PharmD
Mark D. Fox, MD
Tulsa, Okla
1. Viagra (sildenafil citrate) tablets [package insert]. New York NY: Pfizer; 2010. Available at: http://media.pfizer.com/files/products/uspi_viagra.pdf. Accessed January 23, 2013.
2. Hamzavi J, Schmetterer L, Formanek M. Vestibular symptoms as a complication of sildenafil: a case report. Wein Klin Wochenschr. 2002;114:54-55.
3. Robichaud A, Stamatiou PB, Jin S-LC, et al. Deletion of phosphodiesterase 4D in mice shortens α2-adrenoreceptor-mediated anesthesia, a behavioral correlate of emesis. J Clin Invest. 2002;110:1045-1052.
4. Giembycz MA. 4D or not 4D - the emetogenic basis of PDE4 inhibitors uncovered? Trends Pharmacol Sci. 2002;23:548.-
5. Camilleri M, Bharucha AE, Farrugia G. Epidemiology mechanisms, and management of diabetic gastroparesis. Clin Gastroenterol Hepatol. 2011;9:5-12.
6. National Institute of Alcohol Abuse and Alcoholism. NIAAA council approves definition of binge drinking. NIAAA Newsletter. 2004;3:3.-
1. Viagra (sildenafil citrate) tablets [package insert]. New York NY: Pfizer; 2010. Available at: http://media.pfizer.com/files/products/uspi_viagra.pdf. Accessed January 23, 2013.
2. Hamzavi J, Schmetterer L, Formanek M. Vestibular symptoms as a complication of sildenafil: a case report. Wein Klin Wochenschr. 2002;114:54-55.
3. Robichaud A, Stamatiou PB, Jin S-LC, et al. Deletion of phosphodiesterase 4D in mice shortens α2-adrenoreceptor-mediated anesthesia, a behavioral correlate of emesis. J Clin Invest. 2002;110:1045-1052.
4. Giembycz MA. 4D or not 4D - the emetogenic basis of PDE4 inhibitors uncovered? Trends Pharmacol Sci. 2002;23:548.-
5. Camilleri M, Bharucha AE, Farrugia G. Epidemiology mechanisms, and management of diabetic gastroparesis. Clin Gastroenterol Hepatol. 2011;9:5-12.
6. National Institute of Alcohol Abuse and Alcoholism. NIAAA council approves definition of binge drinking. NIAAA Newsletter. 2004;3:3.-
Bipolar disorder or something else?
CASE: Unclear diagnosis
Police find Ms. S, age 31, extremely intoxicated and drinking alcohol in her car in a city park parking lot. In the emergency room, she becomes increasingly somnolent and clinicians intubate her trachea to protect her airway. Lab testing shows she has elevated acetaminophen and lithium serum levels, and she is transferred to our hospital for further management after being started on N-acetylcysteine to treat acetaminophen toxicity. Her “ex-fiancé,” the father of her 2 children, saw her earlier the day of the episode and says she was distraught, intoxicated, and had several empty pill bottles in her purse.
In our hospital, Ms. S’ lithium level increases from 2.3 mEq/L to a peak of 5.32 mEq/L, and she undergoes hemodialysis. On hospital day 2, her serum lithium level is trending downward. After Ms. S is able to breathe spontaneously, her trachea is extubated and her hemodialysis line is removed. A psychiatric consultation is obtained, but she is unable to provide a coherent history and the treating clinicians believe she has delirium caused by multiple factors.
On hospital day 3, Ms. S’ delirium clears enough for her to engage in an interview, and she is transferred to our inpatient psychiatry ward for further monitoring and stabilization.
She reports that she was diagnosed with bipolar disorder (BD) at age 12, when she faced multiple psychosocial stressors, including physical abuse by her mother’s boyfriend. She took several psychotropics—although she cannot remember which ones—until age 14, when she stopped all medications until the year before her current hospitalization. Although throughout adolescence and adulthood Ms. S experienced chronic irritability, anxiety, impulsive behavior, poor self-esteem, abusive relationships, self-cutting, and depressed mood, she maintains that she felt worse when she was taking psychotropics and doubts the BD diagnosis. She attributes her longstanding mood issues to low self-worth, a “codependent nature,” and a tendency to gravitate toward abusive relationships. Although she admits to experimenting with several illicit drugs during adolescence, she denies more recent substance use and states she drinks alcohol only once every few months.
The authors’ observations
BD is underdiagnosed in several patient populations, such as individuals previously diagnosed with MDD.1-3 Misdiagnosis can have severe implications, including delay in receiving treatment with effective medications (eg, mood stabilizers) or use of agents that can induce mania or rapid-cycling, such as antidepressants. Perhaps in response to this concern, in recent years clinicians increasingly have diagnosed BD in adolescents and adults. An analysis of a national database of physician practices found a 40-fold increase in office visits for BD among youth and a near doubling among adults from 1994 to 2003.4
Although underdiagnosis of BD remains important, some researchers have suggested that overdiagnosis may be more prevalent and equally harmful. In a study of 180 patients being treated for depression in a family care clinic, there was a 21.6% initial underdiagnosis rate among those eventually found to have BD.1 However, among 43 patients with a prior BD diagnosis, the diagnosis was not confirmed in 33%.1 In a study of 700 psychiatric outpatients in Rhode Island, only 43% of 145 patients who reported a prior BD diagnosis had that diagnosis confirmed.5 Three times as many patients were overdiagnosed with BD as underdiagnosed.
Are there characteristics common to individuals incorrectly diagnosed with BD? In a study that compared patients who had been mistakenly diagnosed with BD with those who had not been diagnosed with BD, the overdiagnosis group was significantly more likely to be diagnosed with a personality disorder, in particular borderline or antisocial personality disorder.6 Only lifetime and current BPD, current posttraumatic stress disorder (PTSD), and lifetime impulse control disorders were independently associated with BD overdiagnosis. The odds ratio for overdiagnosis of BD in patients found to have BPD was 3.7.
EVALUATION: Rethink the diagnosis
In the last few months, Ms. S had complained to her primary care provider (PCP) of worsening anxiety and depressed mood. She was the victim of ongoing physical and emotional abuse by her ex-fiancé and was concerned that she may lose custody of her 2 sons. Approximately 8 months before admission, Ms. S’ PCP prescribed lithium, 450 mg, 3 times a day, for “mood stabilization” and depression because she’d already been diagnosed with BD. This was the first mood stabilizer she’d taken since she was 14. She also was taking unknown doses of hydrocodone/acetaminophen, cyclobenzaprine, and tramadol for pain and temazepam for insomnia. Ms. S continued to suffer from labile and depressed mood, and fought with her ex-fiancé and legal authorities to maintain custody of her 2 children until she was found in the park.
Throughout her hospitalization she denies that she attempted suicide that day, and maintains that this incident was caused by unintentional mismanagement of her medications. Although she continues to have a sense of low self-worth, she denies feeling depressed; in contrast, she says she feels like she has a “new lease on life.” During several interviews she cannot provide a history of any prolonged (ie, several days) episodes of elevated mood, increased goal-directed behavior, decreased need for sleep, tangential thought, pressured speech, or other symptoms that suggest hypomania or mania. She does not endorse prolonged periods of neurovegetative symptoms that would indicate a major depressive episode.
We feel that Ms. S’ symptoms of affective dysregulation, impulsivity, and interpersonal dysfunction are consistent with BPD, and we determine that she meets 6 of the 9 DSM-IV-TR diagnostic features of BPD (≥5 are required for a BPD diagnosis) (Table 1).7 Ms. S describes efforts to avoid abandonment, unstable and intense interpersonal relationships, marked and persistent unstable self-image, recurrent suicidal and self-mutilating behavior, affective instability, and chronic feelings of emptiness. She is discharged to follow up with a psychotherapist and family practitioner. She is not continued on any psychotropic medications.
The authors’ observations
Although it can be difficult to accurately diagnose psychiatric illness during a brief inpatient hospitalization, several clinicians who cared for Ms. S felt that her presentation was more consistent with BPD than BD. Her case is an example of the potential harm of incorrectly diagnosing personality-disordered patients with BD. Ms. S is impulsive and used lithium—a medication that is the standard of care for BD—in an overdose, which lead to a costly and dangerous hospitalization marked by a difficult tracheal intubation and hemodialysis.
Table 1
DSM-IV-TR diagnostic criteria for borderline personality disorder
| A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity, as indicated by ≥5 of the following: |
|
| Source: Reference 7 |
Distinguishing BD and BPD
There is considerable overlap in symptoms of BD and BPD. Although the episodic nature of BD is well differentiated from the more chronic course of BPD, many hypomania and mania symptoms are similar to those of BPD (Table 2).7 For example, patients with BD or BPD may exhibit impulsive behavior and labile moods. Substance use, risky and self-destructive behaviors, and inflammatory interpersonal relationships can occur in both disorders. Some researchers have suggested that pathophysiologically, BPD may fall on a spectrum of bipolar illness, and have proposed a clinical entity they call bipolar type IV or ultra-rapid cycling BD.2,8,9 There may be more co-occurrence of BD with BPD than would be expected by chance10; 1 review of BPD studies found the rate of comorbid BD ranged from 5.6% to 19%.11 However, because of differences in several factors—including phenomenology, family prevalence, longitudinal course, and medication response—some researchers have concluded that evidence does not support categorizing BPD as part of a bipolar spectrum.10-14 Nonetheless, BPD and other personality disorders often co-occur with axis I disorders, including MDD, BD, or PTSD.
Some research has suggested that the increasing availability and marketing campaigns of medications to treat BD may promote diagnosis of the disorder.15 Zimmerman15 hypothesizes that physicians may be more likely to diagnose a condition that responds to medication (ie, BD) than one that is less responsive (ie, BPD). Financial compensation for treating axis I disorders is significantly better than for treating personality disorders.16 The inpatient setting confers barriers to accurately diagnosing personality disorders, including limits on the amount of time that clinicians can spend with patients or ability to communicate with sources of collateral information. A patient’s observed personality and behaviors while hospitalized may not accurately reflect his or her personality and behaviors in that patient’s “natural” environment.
Several diagnostic strategies can help distinguish BPD from BD. For BD to be the primary diagnosis, a patient must have had a hypomanic or manic episode. Sustained episodes of elation or extreme irritability without evident stressors suggest BD rather than BPD.10 According to Gunderson et al,10 “repeated angry outbursts, suicide attempts, or acts of deliberate self harm that are reactive to interpersonal stress and reflect extreme rejection sensitivity are axiomatic of borderline personality disorder.” In a review of clinical practice, Gunderson17 found that hypersensitivity to rejection and fearful preoccupation with expected abandonment are the most distinctive characteristics of BPD patients. He suggested that clinicians can establish the diagnosis by asking patients directly if they believe the criteria for BPD characterize them, which also can help a patient to accept the diagnosis.
Finally, during a short hospitalization, it can be helpful to obtain collateral information from the patient’s friends and family or further characterize the time course of symptoms and diagnostic features in the patient’s natural environment. Clinicians who are reluctant to diagnose BPD in an inpatient setting could suggest the presence of borderline traits or discuss the possibility of the BPD diagnosis in documentation (eg, in the assessment or formulation). Doing so would avoid a premature BPD diagnosis and allow outpatient providers to confirm or rule out personality disorder diagnoses over time. It is important to screen patients with BPD for co-occurring axis I disorders, including BD, MDD, PTSD, and substance abuse.
A false-positive BD diagnosis in patients with BPD has serious treatment implications. Antipsychotics, antidepressants, and anticonvulsants have been used to target BPD symptoms such as affective dysregulation, impulsivity, and cognitive/perceptual abnormalities, but no medications are FDA-approved for treating BPD. American Psychiatric Association guidelines recommend symptom-based pharmacologic strategies for BPD,18 although some researchers believe that these recommendations are out-of-date and not evidence-based.17,19 Some evidence suggests pharmacotherapy can have modest short-term benefits on specific BPD symptoms, but no data suggest that medication can reduce the severity of BPD or lead to remission.19-23 Just 1 randomized controlled trial (N = 17) has examined lithium for BPD and found no effect on mood.11,24
Misdiagnosis of BD in the context of BPD may create unrealistic expectations regarding the potential efficacy of medications for relieving symptoms. Patients may be diverted from potentially helpful psychotherapeutic treatments—such as DBT or mentalization therapy—which evidence suggests can effectively reduce symptoms, the need for additional treatments, and self-harm or suicidal behaviors.10,17,19 Evidence from long-term longitudinal studies suggests that psychosocial or psychotherapeutic treatment may protect against suicide in BPD patients.25
Table 2
DSM-IV-TR diagnostic criteria for a manic episode
|
The DSM-IV-TR diagnostic criteria for a hypomanic episode are similar to criteria for a manic episode, except:
|
| Source: Reference 7 |
Related Resources
- National Education Alliance Borderline Personality Disorder. www.borderlinepersonalitydisorder.com.
- Hoffman PD, Steiner-Grossman P. Borderline personality disorder: meeting the challenges to successful treatment. Philadelphia, PA: Haworth Press; 2008.
Drug Brand Names
- Cyclobenzaprine • Flexeril
- Hydrocodone/acetaminophen • Lorcet, Vicodin, others
- Lithium • Eskalith, Lithobid
- Temazepam • Restoril
- Tramadol • Ultram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Hirschfeld RM, Cass AR, Holt DC, et al. Screening for bipolar disorder in patients treated for depression in a family medicine clinic. J Am Board Fam Pract. 2005;18(4):233-239.
2. Ghaemi SN, Ko JY, Goodwin FK. “Cade’s disease” and beyond: Misdiagnosis antidepressant use, and a proposed definition for bipolar spectrum disorder. Can J Psychiatry. 2002;47(2):125-134.
3. Bowden CL. Strategies to reduce misdiagnosis of bipolar depression. Psychiatr Serv. 2001;52(1):51-55.
4. Moreno C, Laje G, Blanco C, et al. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Arch Gen Psychiatry. 2007;64(9):1032-1039.
5. Zimmerman M, Ruggero CJ, Chelminski I, et al. Is bipolar disorder overdiagnosed? J Clin Psychiatry. 2008;69(6):935-940.
6. Zimmerman M, Ruggero CJ, Chelminski I, et al. Psychiatric diagnoses in patients previously overdiagnosed with bipolar disorder. J Clin Psychiatry. 2010;71(1):26-31.
7. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
8. Akiskal HS. The bipolar spectrum-the shaping of a new paradigm in psychiatry. Curr Psychiatry Rep. 2002;4(1):1-3.
9. Akiskal HS, Pinto O. The evolving bipolar spectrum. Prototypes I II, III, and IV. Psychiatr Clin North Am. 1999;22(3):517-534, vii.
10. Gunderson JG, Weinberg I, Daversa MT, et al. Descriptive and longitudinal observations on the relationship of borderline personality disorder and bipolar disorder. Am J Psychiatry. 2006;163(7):1173-1178.
11. Paris J, Gunderson J, Weinberg I. The interface between borderline personality disorder and bipolar spectrum disorders. Compr Psychiatry. 2007;48(2):145-154.
12. Paris J. Why psychiatrists are reluctant to diagnose: borderline personality disorder. Psychiatry (Edgmont). 2007;4(1):35-39.
13. Paris J. Borderline or bipolar? Distinguishing borderline personality disorder from bipolar spectrum disorders. Harv Rev Psychiatry. 2004;12(3):140-145.
14. Ruggero CJ, Zimmerman M, Chelminski I, et al. Borderline personality disorder and the misdiagnosis of bipolar disorder. J Psychiatr Res. 2010;44(6):405-408.
15. Zimmerman M. Problems diagnosing bipolar disorder in clinical practice. Expert Rev Neurother. 2010;10(7):1019-1021.
16. Stone MH. Relationship of borderline personality disorder and bipolar disorder. Am J Psychiatry. 2006;163(7):1126-1128.
17. Gunderson JG. Clinical practice. Borderline personality disorder. N Engl J Med. 2011;364(21):2037-2042.
18. American Psychiatric Association. Practice guideline for the treatment of patients with borderline personality disorder. Washington D.C.: American Psychiatric Association; 2001.
19. Paris J. The treatment of borderline personality disorder: implications of research on diagnosis etiology, and outcome. Annu Rev Clin Psychol. 2009;5:277-290.
20. Stoffers J, Völlm BA, Rücker G, et al. Pharmacological interventions for borderline personality disorder. Cochrane Database Syst Rev. 2010;(6):CD005653.-
21. Ripoll LH, Triebwasser J, Siever LJ. Evidence-based pharmacotherapy for personality disorders. Int J Neuropsychopharmacol. 2011;14(9):1257-1288.
22. Mercer D, Douglass AB, Links PS. Meta-analyses of mood stabilizers antidepressants and antipsychotics in the treatment of borderline personality disorder: effectiveness for depression and anger symptoms. J Pers Disord. 2009;23(2):156-174.
23. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. Br J Psychiatry. 2010;196(1):4-12.
24. Links PS, Steiner M, Boiago I, et al. Lithium therapy for borderline patients: preliminary findings. J Pers Disord. 1990;4(2):173-181.
25. Goodman M, Roiff T, Oakes AH, et al. Suicidal risk and management in borderline personality disorder. Curr Psychiatry Rep. 2012;14(1):79-85.
CASE: Unclear diagnosis
Police find Ms. S, age 31, extremely intoxicated and drinking alcohol in her car in a city park parking lot. In the emergency room, she becomes increasingly somnolent and clinicians intubate her trachea to protect her airway. Lab testing shows she has elevated acetaminophen and lithium serum levels, and she is transferred to our hospital for further management after being started on N-acetylcysteine to treat acetaminophen toxicity. Her “ex-fiancé,” the father of her 2 children, saw her earlier the day of the episode and says she was distraught, intoxicated, and had several empty pill bottles in her purse.
In our hospital, Ms. S’ lithium level increases from 2.3 mEq/L to a peak of 5.32 mEq/L, and she undergoes hemodialysis. On hospital day 2, her serum lithium level is trending downward. After Ms. S is able to breathe spontaneously, her trachea is extubated and her hemodialysis line is removed. A psychiatric consultation is obtained, but she is unable to provide a coherent history and the treating clinicians believe she has delirium caused by multiple factors.
On hospital day 3, Ms. S’ delirium clears enough for her to engage in an interview, and she is transferred to our inpatient psychiatry ward for further monitoring and stabilization.
She reports that she was diagnosed with bipolar disorder (BD) at age 12, when she faced multiple psychosocial stressors, including physical abuse by her mother’s boyfriend. She took several psychotropics—although she cannot remember which ones—until age 14, when she stopped all medications until the year before her current hospitalization. Although throughout adolescence and adulthood Ms. S experienced chronic irritability, anxiety, impulsive behavior, poor self-esteem, abusive relationships, self-cutting, and depressed mood, she maintains that she felt worse when she was taking psychotropics and doubts the BD diagnosis. She attributes her longstanding mood issues to low self-worth, a “codependent nature,” and a tendency to gravitate toward abusive relationships. Although she admits to experimenting with several illicit drugs during adolescence, she denies more recent substance use and states she drinks alcohol only once every few months.
The authors’ observations
BD is underdiagnosed in several patient populations, such as individuals previously diagnosed with MDD.1-3 Misdiagnosis can have severe implications, including delay in receiving treatment with effective medications (eg, mood stabilizers) or use of agents that can induce mania or rapid-cycling, such as antidepressants. Perhaps in response to this concern, in recent years clinicians increasingly have diagnosed BD in adolescents and adults. An analysis of a national database of physician practices found a 40-fold increase in office visits for BD among youth and a near doubling among adults from 1994 to 2003.4
Although underdiagnosis of BD remains important, some researchers have suggested that overdiagnosis may be more prevalent and equally harmful. In a study of 180 patients being treated for depression in a family care clinic, there was a 21.6% initial underdiagnosis rate among those eventually found to have BD.1 However, among 43 patients with a prior BD diagnosis, the diagnosis was not confirmed in 33%.1 In a study of 700 psychiatric outpatients in Rhode Island, only 43% of 145 patients who reported a prior BD diagnosis had that diagnosis confirmed.5 Three times as many patients were overdiagnosed with BD as underdiagnosed.
Are there characteristics common to individuals incorrectly diagnosed with BD? In a study that compared patients who had been mistakenly diagnosed with BD with those who had not been diagnosed with BD, the overdiagnosis group was significantly more likely to be diagnosed with a personality disorder, in particular borderline or antisocial personality disorder.6 Only lifetime and current BPD, current posttraumatic stress disorder (PTSD), and lifetime impulse control disorders were independently associated with BD overdiagnosis. The odds ratio for overdiagnosis of BD in patients found to have BPD was 3.7.
EVALUATION: Rethink the diagnosis
In the last few months, Ms. S had complained to her primary care provider (PCP) of worsening anxiety and depressed mood. She was the victim of ongoing physical and emotional abuse by her ex-fiancé and was concerned that she may lose custody of her 2 sons. Approximately 8 months before admission, Ms. S’ PCP prescribed lithium, 450 mg, 3 times a day, for “mood stabilization” and depression because she’d already been diagnosed with BD. This was the first mood stabilizer she’d taken since she was 14. She also was taking unknown doses of hydrocodone/acetaminophen, cyclobenzaprine, and tramadol for pain and temazepam for insomnia. Ms. S continued to suffer from labile and depressed mood, and fought with her ex-fiancé and legal authorities to maintain custody of her 2 children until she was found in the park.
Throughout her hospitalization she denies that she attempted suicide that day, and maintains that this incident was caused by unintentional mismanagement of her medications. Although she continues to have a sense of low self-worth, she denies feeling depressed; in contrast, she says she feels like she has a “new lease on life.” During several interviews she cannot provide a history of any prolonged (ie, several days) episodes of elevated mood, increased goal-directed behavior, decreased need for sleep, tangential thought, pressured speech, or other symptoms that suggest hypomania or mania. She does not endorse prolonged periods of neurovegetative symptoms that would indicate a major depressive episode.
We feel that Ms. S’ symptoms of affective dysregulation, impulsivity, and interpersonal dysfunction are consistent with BPD, and we determine that she meets 6 of the 9 DSM-IV-TR diagnostic features of BPD (≥5 are required for a BPD diagnosis) (Table 1).7 Ms. S describes efforts to avoid abandonment, unstable and intense interpersonal relationships, marked and persistent unstable self-image, recurrent suicidal and self-mutilating behavior, affective instability, and chronic feelings of emptiness. She is discharged to follow up with a psychotherapist and family practitioner. She is not continued on any psychotropic medications.
The authors’ observations
Although it can be difficult to accurately diagnose psychiatric illness during a brief inpatient hospitalization, several clinicians who cared for Ms. S felt that her presentation was more consistent with BPD than BD. Her case is an example of the potential harm of incorrectly diagnosing personality-disordered patients with BD. Ms. S is impulsive and used lithium—a medication that is the standard of care for BD—in an overdose, which lead to a costly and dangerous hospitalization marked by a difficult tracheal intubation and hemodialysis.
Table 1
DSM-IV-TR diagnostic criteria for borderline personality disorder
| A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity, as indicated by ≥5 of the following: |
|
| Source: Reference 7 |
Distinguishing BD and BPD
There is considerable overlap in symptoms of BD and BPD. Although the episodic nature of BD is well differentiated from the more chronic course of BPD, many hypomania and mania symptoms are similar to those of BPD (Table 2).7 For example, patients with BD or BPD may exhibit impulsive behavior and labile moods. Substance use, risky and self-destructive behaviors, and inflammatory interpersonal relationships can occur in both disorders. Some researchers have suggested that pathophysiologically, BPD may fall on a spectrum of bipolar illness, and have proposed a clinical entity they call bipolar type IV or ultra-rapid cycling BD.2,8,9 There may be more co-occurrence of BD with BPD than would be expected by chance10; 1 review of BPD studies found the rate of comorbid BD ranged from 5.6% to 19%.11 However, because of differences in several factors—including phenomenology, family prevalence, longitudinal course, and medication response—some researchers have concluded that evidence does not support categorizing BPD as part of a bipolar spectrum.10-14 Nonetheless, BPD and other personality disorders often co-occur with axis I disorders, including MDD, BD, or PTSD.
Some research has suggested that the increasing availability and marketing campaigns of medications to treat BD may promote diagnosis of the disorder.15 Zimmerman15 hypothesizes that physicians may be more likely to diagnose a condition that responds to medication (ie, BD) than one that is less responsive (ie, BPD). Financial compensation for treating axis I disorders is significantly better than for treating personality disorders.16 The inpatient setting confers barriers to accurately diagnosing personality disorders, including limits on the amount of time that clinicians can spend with patients or ability to communicate with sources of collateral information. A patient’s observed personality and behaviors while hospitalized may not accurately reflect his or her personality and behaviors in that patient’s “natural” environment.
Several diagnostic strategies can help distinguish BPD from BD. For BD to be the primary diagnosis, a patient must have had a hypomanic or manic episode. Sustained episodes of elation or extreme irritability without evident stressors suggest BD rather than BPD.10 According to Gunderson et al,10 “repeated angry outbursts, suicide attempts, or acts of deliberate self harm that are reactive to interpersonal stress and reflect extreme rejection sensitivity are axiomatic of borderline personality disorder.” In a review of clinical practice, Gunderson17 found that hypersensitivity to rejection and fearful preoccupation with expected abandonment are the most distinctive characteristics of BPD patients. He suggested that clinicians can establish the diagnosis by asking patients directly if they believe the criteria for BPD characterize them, which also can help a patient to accept the diagnosis.
Finally, during a short hospitalization, it can be helpful to obtain collateral information from the patient’s friends and family or further characterize the time course of symptoms and diagnostic features in the patient’s natural environment. Clinicians who are reluctant to diagnose BPD in an inpatient setting could suggest the presence of borderline traits or discuss the possibility of the BPD diagnosis in documentation (eg, in the assessment or formulation). Doing so would avoid a premature BPD diagnosis and allow outpatient providers to confirm or rule out personality disorder diagnoses over time. It is important to screen patients with BPD for co-occurring axis I disorders, including BD, MDD, PTSD, and substance abuse.
A false-positive BD diagnosis in patients with BPD has serious treatment implications. Antipsychotics, antidepressants, and anticonvulsants have been used to target BPD symptoms such as affective dysregulation, impulsivity, and cognitive/perceptual abnormalities, but no medications are FDA-approved for treating BPD. American Psychiatric Association guidelines recommend symptom-based pharmacologic strategies for BPD,18 although some researchers believe that these recommendations are out-of-date and not evidence-based.17,19 Some evidence suggests pharmacotherapy can have modest short-term benefits on specific BPD symptoms, but no data suggest that medication can reduce the severity of BPD or lead to remission.19-23 Just 1 randomized controlled trial (N = 17) has examined lithium for BPD and found no effect on mood.11,24
Misdiagnosis of BD in the context of BPD may create unrealistic expectations regarding the potential efficacy of medications for relieving symptoms. Patients may be diverted from potentially helpful psychotherapeutic treatments—such as DBT or mentalization therapy—which evidence suggests can effectively reduce symptoms, the need for additional treatments, and self-harm or suicidal behaviors.10,17,19 Evidence from long-term longitudinal studies suggests that psychosocial or psychotherapeutic treatment may protect against suicide in BPD patients.25
Table 2
DSM-IV-TR diagnostic criteria for a manic episode
|
The DSM-IV-TR diagnostic criteria for a hypomanic episode are similar to criteria for a manic episode, except:
|
| Source: Reference 7 |
Related Resources
- National Education Alliance Borderline Personality Disorder. www.borderlinepersonalitydisorder.com.
- Hoffman PD, Steiner-Grossman P. Borderline personality disorder: meeting the challenges to successful treatment. Philadelphia, PA: Haworth Press; 2008.
Drug Brand Names
- Cyclobenzaprine • Flexeril
- Hydrocodone/acetaminophen • Lorcet, Vicodin, others
- Lithium • Eskalith, Lithobid
- Temazepam • Restoril
- Tramadol • Ultram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Unclear diagnosis
Police find Ms. S, age 31, extremely intoxicated and drinking alcohol in her car in a city park parking lot. In the emergency room, she becomes increasingly somnolent and clinicians intubate her trachea to protect her airway. Lab testing shows she has elevated acetaminophen and lithium serum levels, and she is transferred to our hospital for further management after being started on N-acetylcysteine to treat acetaminophen toxicity. Her “ex-fiancé,” the father of her 2 children, saw her earlier the day of the episode and says she was distraught, intoxicated, and had several empty pill bottles in her purse.
In our hospital, Ms. S’ lithium level increases from 2.3 mEq/L to a peak of 5.32 mEq/L, and she undergoes hemodialysis. On hospital day 2, her serum lithium level is trending downward. After Ms. S is able to breathe spontaneously, her trachea is extubated and her hemodialysis line is removed. A psychiatric consultation is obtained, but she is unable to provide a coherent history and the treating clinicians believe she has delirium caused by multiple factors.
On hospital day 3, Ms. S’ delirium clears enough for her to engage in an interview, and she is transferred to our inpatient psychiatry ward for further monitoring and stabilization.
She reports that she was diagnosed with bipolar disorder (BD) at age 12, when she faced multiple psychosocial stressors, including physical abuse by her mother’s boyfriend. She took several psychotropics—although she cannot remember which ones—until age 14, when she stopped all medications until the year before her current hospitalization. Although throughout adolescence and adulthood Ms. S experienced chronic irritability, anxiety, impulsive behavior, poor self-esteem, abusive relationships, self-cutting, and depressed mood, she maintains that she felt worse when she was taking psychotropics and doubts the BD diagnosis. She attributes her longstanding mood issues to low self-worth, a “codependent nature,” and a tendency to gravitate toward abusive relationships. Although she admits to experimenting with several illicit drugs during adolescence, she denies more recent substance use and states she drinks alcohol only once every few months.
The authors’ observations
BD is underdiagnosed in several patient populations, such as individuals previously diagnosed with MDD.1-3 Misdiagnosis can have severe implications, including delay in receiving treatment with effective medications (eg, mood stabilizers) or use of agents that can induce mania or rapid-cycling, such as antidepressants. Perhaps in response to this concern, in recent years clinicians increasingly have diagnosed BD in adolescents and adults. An analysis of a national database of physician practices found a 40-fold increase in office visits for BD among youth and a near doubling among adults from 1994 to 2003.4
Although underdiagnosis of BD remains important, some researchers have suggested that overdiagnosis may be more prevalent and equally harmful. In a study of 180 patients being treated for depression in a family care clinic, there was a 21.6% initial underdiagnosis rate among those eventually found to have BD.1 However, among 43 patients with a prior BD diagnosis, the diagnosis was not confirmed in 33%.1 In a study of 700 psychiatric outpatients in Rhode Island, only 43% of 145 patients who reported a prior BD diagnosis had that diagnosis confirmed.5 Three times as many patients were overdiagnosed with BD as underdiagnosed.
Are there characteristics common to individuals incorrectly diagnosed with BD? In a study that compared patients who had been mistakenly diagnosed with BD with those who had not been diagnosed with BD, the overdiagnosis group was significantly more likely to be diagnosed with a personality disorder, in particular borderline or antisocial personality disorder.6 Only lifetime and current BPD, current posttraumatic stress disorder (PTSD), and lifetime impulse control disorders were independently associated with BD overdiagnosis. The odds ratio for overdiagnosis of BD in patients found to have BPD was 3.7.
EVALUATION: Rethink the diagnosis
In the last few months, Ms. S had complained to her primary care provider (PCP) of worsening anxiety and depressed mood. She was the victim of ongoing physical and emotional abuse by her ex-fiancé and was concerned that she may lose custody of her 2 sons. Approximately 8 months before admission, Ms. S’ PCP prescribed lithium, 450 mg, 3 times a day, for “mood stabilization” and depression because she’d already been diagnosed with BD. This was the first mood stabilizer she’d taken since she was 14. She also was taking unknown doses of hydrocodone/acetaminophen, cyclobenzaprine, and tramadol for pain and temazepam for insomnia. Ms. S continued to suffer from labile and depressed mood, and fought with her ex-fiancé and legal authorities to maintain custody of her 2 children until she was found in the park.
Throughout her hospitalization she denies that she attempted suicide that day, and maintains that this incident was caused by unintentional mismanagement of her medications. Although she continues to have a sense of low self-worth, she denies feeling depressed; in contrast, she says she feels like she has a “new lease on life.” During several interviews she cannot provide a history of any prolonged (ie, several days) episodes of elevated mood, increased goal-directed behavior, decreased need for sleep, tangential thought, pressured speech, or other symptoms that suggest hypomania or mania. She does not endorse prolonged periods of neurovegetative symptoms that would indicate a major depressive episode.
We feel that Ms. S’ symptoms of affective dysregulation, impulsivity, and interpersonal dysfunction are consistent with BPD, and we determine that she meets 6 of the 9 DSM-IV-TR diagnostic features of BPD (≥5 are required for a BPD diagnosis) (Table 1).7 Ms. S describes efforts to avoid abandonment, unstable and intense interpersonal relationships, marked and persistent unstable self-image, recurrent suicidal and self-mutilating behavior, affective instability, and chronic feelings of emptiness. She is discharged to follow up with a psychotherapist and family practitioner. She is not continued on any psychotropic medications.
The authors’ observations
Although it can be difficult to accurately diagnose psychiatric illness during a brief inpatient hospitalization, several clinicians who cared for Ms. S felt that her presentation was more consistent with BPD than BD. Her case is an example of the potential harm of incorrectly diagnosing personality-disordered patients with BD. Ms. S is impulsive and used lithium—a medication that is the standard of care for BD—in an overdose, which lead to a costly and dangerous hospitalization marked by a difficult tracheal intubation and hemodialysis.
Table 1
DSM-IV-TR diagnostic criteria for borderline personality disorder
| A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity, as indicated by ≥5 of the following: |
|
| Source: Reference 7 |
Distinguishing BD and BPD
There is considerable overlap in symptoms of BD and BPD. Although the episodic nature of BD is well differentiated from the more chronic course of BPD, many hypomania and mania symptoms are similar to those of BPD (Table 2).7 For example, patients with BD or BPD may exhibit impulsive behavior and labile moods. Substance use, risky and self-destructive behaviors, and inflammatory interpersonal relationships can occur in both disorders. Some researchers have suggested that pathophysiologically, BPD may fall on a spectrum of bipolar illness, and have proposed a clinical entity they call bipolar type IV or ultra-rapid cycling BD.2,8,9 There may be more co-occurrence of BD with BPD than would be expected by chance10; 1 review of BPD studies found the rate of comorbid BD ranged from 5.6% to 19%.11 However, because of differences in several factors—including phenomenology, family prevalence, longitudinal course, and medication response—some researchers have concluded that evidence does not support categorizing BPD as part of a bipolar spectrum.10-14 Nonetheless, BPD and other personality disorders often co-occur with axis I disorders, including MDD, BD, or PTSD.
Some research has suggested that the increasing availability and marketing campaigns of medications to treat BD may promote diagnosis of the disorder.15 Zimmerman15 hypothesizes that physicians may be more likely to diagnose a condition that responds to medication (ie, BD) than one that is less responsive (ie, BPD). Financial compensation for treating axis I disorders is significantly better than for treating personality disorders.16 The inpatient setting confers barriers to accurately diagnosing personality disorders, including limits on the amount of time that clinicians can spend with patients or ability to communicate with sources of collateral information. A patient’s observed personality and behaviors while hospitalized may not accurately reflect his or her personality and behaviors in that patient’s “natural” environment.
Several diagnostic strategies can help distinguish BPD from BD. For BD to be the primary diagnosis, a patient must have had a hypomanic or manic episode. Sustained episodes of elation or extreme irritability without evident stressors suggest BD rather than BPD.10 According to Gunderson et al,10 “repeated angry outbursts, suicide attempts, or acts of deliberate self harm that are reactive to interpersonal stress and reflect extreme rejection sensitivity are axiomatic of borderline personality disorder.” In a review of clinical practice, Gunderson17 found that hypersensitivity to rejection and fearful preoccupation with expected abandonment are the most distinctive characteristics of BPD patients. He suggested that clinicians can establish the diagnosis by asking patients directly if they believe the criteria for BPD characterize them, which also can help a patient to accept the diagnosis.
Finally, during a short hospitalization, it can be helpful to obtain collateral information from the patient’s friends and family or further characterize the time course of symptoms and diagnostic features in the patient’s natural environment. Clinicians who are reluctant to diagnose BPD in an inpatient setting could suggest the presence of borderline traits or discuss the possibility of the BPD diagnosis in documentation (eg, in the assessment or formulation). Doing so would avoid a premature BPD diagnosis and allow outpatient providers to confirm or rule out personality disorder diagnoses over time. It is important to screen patients with BPD for co-occurring axis I disorders, including BD, MDD, PTSD, and substance abuse.
A false-positive BD diagnosis in patients with BPD has serious treatment implications. Antipsychotics, antidepressants, and anticonvulsants have been used to target BPD symptoms such as affective dysregulation, impulsivity, and cognitive/perceptual abnormalities, but no medications are FDA-approved for treating BPD. American Psychiatric Association guidelines recommend symptom-based pharmacologic strategies for BPD,18 although some researchers believe that these recommendations are out-of-date and not evidence-based.17,19 Some evidence suggests pharmacotherapy can have modest short-term benefits on specific BPD symptoms, but no data suggest that medication can reduce the severity of BPD or lead to remission.19-23 Just 1 randomized controlled trial (N = 17) has examined lithium for BPD and found no effect on mood.11,24
Misdiagnosis of BD in the context of BPD may create unrealistic expectations regarding the potential efficacy of medications for relieving symptoms. Patients may be diverted from potentially helpful psychotherapeutic treatments—such as DBT or mentalization therapy—which evidence suggests can effectively reduce symptoms, the need for additional treatments, and self-harm or suicidal behaviors.10,17,19 Evidence from long-term longitudinal studies suggests that psychosocial or psychotherapeutic treatment may protect against suicide in BPD patients.25
Table 2
DSM-IV-TR diagnostic criteria for a manic episode
|
The DSM-IV-TR diagnostic criteria for a hypomanic episode are similar to criteria for a manic episode, except:
|
| Source: Reference 7 |
Related Resources
- National Education Alliance Borderline Personality Disorder. www.borderlinepersonalitydisorder.com.
- Hoffman PD, Steiner-Grossman P. Borderline personality disorder: meeting the challenges to successful treatment. Philadelphia, PA: Haworth Press; 2008.
Drug Brand Names
- Cyclobenzaprine • Flexeril
- Hydrocodone/acetaminophen • Lorcet, Vicodin, others
- Lithium • Eskalith, Lithobid
- Temazepam • Restoril
- Tramadol • Ultram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Hirschfeld RM, Cass AR, Holt DC, et al. Screening for bipolar disorder in patients treated for depression in a family medicine clinic. J Am Board Fam Pract. 2005;18(4):233-239.
2. Ghaemi SN, Ko JY, Goodwin FK. “Cade’s disease” and beyond: Misdiagnosis antidepressant use, and a proposed definition for bipolar spectrum disorder. Can J Psychiatry. 2002;47(2):125-134.
3. Bowden CL. Strategies to reduce misdiagnosis of bipolar depression. Psychiatr Serv. 2001;52(1):51-55.
4. Moreno C, Laje G, Blanco C, et al. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Arch Gen Psychiatry. 2007;64(9):1032-1039.
5. Zimmerman M, Ruggero CJ, Chelminski I, et al. Is bipolar disorder overdiagnosed? J Clin Psychiatry. 2008;69(6):935-940.
6. Zimmerman M, Ruggero CJ, Chelminski I, et al. Psychiatric diagnoses in patients previously overdiagnosed with bipolar disorder. J Clin Psychiatry. 2010;71(1):26-31.
7. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
8. Akiskal HS. The bipolar spectrum-the shaping of a new paradigm in psychiatry. Curr Psychiatry Rep. 2002;4(1):1-3.
9. Akiskal HS, Pinto O. The evolving bipolar spectrum. Prototypes I II, III, and IV. Psychiatr Clin North Am. 1999;22(3):517-534, vii.
10. Gunderson JG, Weinberg I, Daversa MT, et al. Descriptive and longitudinal observations on the relationship of borderline personality disorder and bipolar disorder. Am J Psychiatry. 2006;163(7):1173-1178.
11. Paris J, Gunderson J, Weinberg I. The interface between borderline personality disorder and bipolar spectrum disorders. Compr Psychiatry. 2007;48(2):145-154.
12. Paris J. Why psychiatrists are reluctant to diagnose: borderline personality disorder. Psychiatry (Edgmont). 2007;4(1):35-39.
13. Paris J. Borderline or bipolar? Distinguishing borderline personality disorder from bipolar spectrum disorders. Harv Rev Psychiatry. 2004;12(3):140-145.
14. Ruggero CJ, Zimmerman M, Chelminski I, et al. Borderline personality disorder and the misdiagnosis of bipolar disorder. J Psychiatr Res. 2010;44(6):405-408.
15. Zimmerman M. Problems diagnosing bipolar disorder in clinical practice. Expert Rev Neurother. 2010;10(7):1019-1021.
16. Stone MH. Relationship of borderline personality disorder and bipolar disorder. Am J Psychiatry. 2006;163(7):1126-1128.
17. Gunderson JG. Clinical practice. Borderline personality disorder. N Engl J Med. 2011;364(21):2037-2042.
18. American Psychiatric Association. Practice guideline for the treatment of patients with borderline personality disorder. Washington D.C.: American Psychiatric Association; 2001.
19. Paris J. The treatment of borderline personality disorder: implications of research on diagnosis etiology, and outcome. Annu Rev Clin Psychol. 2009;5:277-290.
20. Stoffers J, Völlm BA, Rücker G, et al. Pharmacological interventions for borderline personality disorder. Cochrane Database Syst Rev. 2010;(6):CD005653.-
21. Ripoll LH, Triebwasser J, Siever LJ. Evidence-based pharmacotherapy for personality disorders. Int J Neuropsychopharmacol. 2011;14(9):1257-1288.
22. Mercer D, Douglass AB, Links PS. Meta-analyses of mood stabilizers antidepressants and antipsychotics in the treatment of borderline personality disorder: effectiveness for depression and anger symptoms. J Pers Disord. 2009;23(2):156-174.
23. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. Br J Psychiatry. 2010;196(1):4-12.
24. Links PS, Steiner M, Boiago I, et al. Lithium therapy for borderline patients: preliminary findings. J Pers Disord. 1990;4(2):173-181.
25. Goodman M, Roiff T, Oakes AH, et al. Suicidal risk and management in borderline personality disorder. Curr Psychiatry Rep. 2012;14(1):79-85.
1. Hirschfeld RM, Cass AR, Holt DC, et al. Screening for bipolar disorder in patients treated for depression in a family medicine clinic. J Am Board Fam Pract. 2005;18(4):233-239.
2. Ghaemi SN, Ko JY, Goodwin FK. “Cade’s disease” and beyond: Misdiagnosis antidepressant use, and a proposed definition for bipolar spectrum disorder. Can J Psychiatry. 2002;47(2):125-134.
3. Bowden CL. Strategies to reduce misdiagnosis of bipolar depression. Psychiatr Serv. 2001;52(1):51-55.
4. Moreno C, Laje G, Blanco C, et al. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Arch Gen Psychiatry. 2007;64(9):1032-1039.
5. Zimmerman M, Ruggero CJ, Chelminski I, et al. Is bipolar disorder overdiagnosed? J Clin Psychiatry. 2008;69(6):935-940.
6. Zimmerman M, Ruggero CJ, Chelminski I, et al. Psychiatric diagnoses in patients previously overdiagnosed with bipolar disorder. J Clin Psychiatry. 2010;71(1):26-31.
7. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
8. Akiskal HS. The bipolar spectrum-the shaping of a new paradigm in psychiatry. Curr Psychiatry Rep. 2002;4(1):1-3.
9. Akiskal HS, Pinto O. The evolving bipolar spectrum. Prototypes I II, III, and IV. Psychiatr Clin North Am. 1999;22(3):517-534, vii.
10. Gunderson JG, Weinberg I, Daversa MT, et al. Descriptive and longitudinal observations on the relationship of borderline personality disorder and bipolar disorder. Am J Psychiatry. 2006;163(7):1173-1178.
11. Paris J, Gunderson J, Weinberg I. The interface between borderline personality disorder and bipolar spectrum disorders. Compr Psychiatry. 2007;48(2):145-154.
12. Paris J. Why psychiatrists are reluctant to diagnose: borderline personality disorder. Psychiatry (Edgmont). 2007;4(1):35-39.
13. Paris J. Borderline or bipolar? Distinguishing borderline personality disorder from bipolar spectrum disorders. Harv Rev Psychiatry. 2004;12(3):140-145.
14. Ruggero CJ, Zimmerman M, Chelminski I, et al. Borderline personality disorder and the misdiagnosis of bipolar disorder. J Psychiatr Res. 2010;44(6):405-408.
15. Zimmerman M. Problems diagnosing bipolar disorder in clinical practice. Expert Rev Neurother. 2010;10(7):1019-1021.
16. Stone MH. Relationship of borderline personality disorder and bipolar disorder. Am J Psychiatry. 2006;163(7):1126-1128.
17. Gunderson JG. Clinical practice. Borderline personality disorder. N Engl J Med. 2011;364(21):2037-2042.
18. American Psychiatric Association. Practice guideline for the treatment of patients with borderline personality disorder. Washington D.C.: American Psychiatric Association; 2001.
19. Paris J. The treatment of borderline personality disorder: implications of research on diagnosis etiology, and outcome. Annu Rev Clin Psychol. 2009;5:277-290.
20. Stoffers J, Völlm BA, Rücker G, et al. Pharmacological interventions for borderline personality disorder. Cochrane Database Syst Rev. 2010;(6):CD005653.-
21. Ripoll LH, Triebwasser J, Siever LJ. Evidence-based pharmacotherapy for personality disorders. Int J Neuropsychopharmacol. 2011;14(9):1257-1288.
22. Mercer D, Douglass AB, Links PS. Meta-analyses of mood stabilizers antidepressants and antipsychotics in the treatment of borderline personality disorder: effectiveness for depression and anger symptoms. J Pers Disord. 2009;23(2):156-174.
23. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. Br J Psychiatry. 2010;196(1):4-12.
24. Links PS, Steiner M, Boiago I, et al. Lithium therapy for borderline patients: preliminary findings. J Pers Disord. 1990;4(2):173-181.
25. Goodman M, Roiff T, Oakes AH, et al. Suicidal risk and management in borderline personality disorder. Curr Psychiatry Rep. 2012;14(1):79-85.
Have you tried these innovative alternatives to antibiotics for UTI prevention?
The authors report no financial relationships relevant to this article.
CASE: Recurrent UTI and antibiotic resistance
A 53-year-old postmenopausal woman with a history of culture-proven recurrent Escherichia coli urinary tract infections (UTIs) presents to the clinic with symptoms of UTI. She was previously treated with a postcoital regimen of trimethoprim/sulfamethoxazole, based on sensitivities identified by culture. A past work-up of her upper and lower urinary tract was negative. You send a catheterized specimen for culture; again, E. coli is identified as the pathogen but proves resistant to her current antibiotic regimen.
What treatment alternatives, aside from antibiotics, are available for this patient—and how might they affect resistance?
Increased antibiotic usage has led to greater bacterial resistance, which is perpetuated by clonal spread. Resistant strains of E. coli have been found in household members, suggesting host-host transmission as a mechanism for dissemination. Alternative treatments that reduce the use of antibiotics may minimize bacterial resistance and increase the efficacy of treatment. In the TABLE , we summarize alternative approaches to the treatment of recurrent UTI. We also describe a strategy to alleviate symptoms.
Alternatives to antibiotics in the treatment and prevention of recurrent UTI
| Category | Type | Examples and doses, if recommended |
|---|---|---|
| Vaginal estrogen | Conjugated estrogen cream Estradiol
| Premarin cream, 0.5–2 g vaginally twice weekly
|
| Nutritive agents | Cranberry juice Cranberry tablets Cystopurin Lactobacilli Blueberry products | Not recommended 1 tablet (300 to 400 mg, depending on manufacturer) twice daily Not recommended Vivag, EcoVag, 1 capsule daily by vagina for 5 days, then once weekly for 10 weeks Not recommended |
| Anti-infective drugs | Methenamine hippurate Methenamine mandelate Methylene blue | Urex or Hiprex, 1 g orally twice daily Mandelamine, 1 g orally 4 times daily Future therapy |
| Urinary acidifiers | Vitamin C/ascorbic acid | 1–3 g orally 3–4 times daily |
| Herbal remedies | Uva ursi Forskolin | Not recommended for long-term use Not recommended |
| Behavioral changes | Adequate hydration Postcoital voiding |
Vaginal estrogen is the only proven alternative to antibiotics for postmenopausal women
A lack of estrogen is a risk factor for UTI and is associated with atrophic mucosa, leading to decreased colonization with lactobacilli, increased vaginal pH, and E. coli colonization.
A randomized, double-blind, placebo-controlled trial of intravaginal estriol cream versus placebo in 93 postmenopausal women found a significant decrease in the rate of UTI among women who used the cream.1 After 8 months of follow-up, the incidence of UTI was 0.5 vs 5.9 episodes per patient-year (P <.001). Interestingly, all pretreatment cultures were negative for lactobacilli. One month after treatment, 61% of women in the estriol group were culture-positive for lactobacilli, compared with 0% of the placebo group.1
A 2008 Cochrane review of nine studies concluded that vaginal estrogen reduces the number of UTIs in postmenopausal women, with variation based on the type of estrogen and duration of use.2
Adverse effects are mild
Twenty-eight percent of the estriol group in the randomized trial described above withdrew from treatment, with 20% citing local side effects, including vaginal irritation, burning, or itching—all of which were mild and self-limited.1 Other possible adverse effects include breast tenderness, vaginal bleeding or spotting, and discharge.2
Clinical recommendations
Given the efficacy of this therapy, we recommend topical estrogen for postmenopausal patients with recurrent UTIs.
Cranberry juice may reduce UTI, but many patients withdraw
from treatment
Cranberries belong to the Vaccinium species, which contains all flavonoids, including anthocyanins and proanthocyanidins. It was previously thought that the acidification of urine produced an antibacterial effect, but several trials have documented no change in urine levels of hippuric acid when cranberry products are given, with no acidification of the urine.3 Current theory suggests that cranberries prevent bacteria from adhering to the uroepithelial cells of the walls of the bladder, by blocking expression of E. coli’s adhesion molecule, P. fimbriae, so that bacteria are unable to penetrate the mucosal surface.4,5 The major benefit of cranberry products over antibiotic prophylaxis is that they do not have the potential for resistance.4
A 2008 Cochrane review concluded that cranberry juice may reduce symptomatic UTIs, particularly among young, sexually active women—but there is a high rate of withdrawal from treatment.6 The optimal method of administration and dose remain unclear. In contrast, two recent randomized, controlled trials—published after the Cochrane review—found no difference in the rate of recurrent UTI in premenopausal women.7,8 Adverse effects in these two trials included constipation, heartburn, loose stools, vaginal itching and dryness, and migraines. Of note, there was no statistical difference in side effects between the cranberry and placebo groups.7
Vaccinium tablets may be protective in older women
Cranberry extracts of 500 mg to 1,000 mg daily have been compared with antimicrobial prophylaxis in two randomized, double-blind, controlled trials. The trials demonstrated mixed benefits. Trimethoprim/sulfamethoxazole was associated with a lower rate of UTI in younger women, compared with cranberry extracts alone (P=.02), while cranberry extracts were slightly more effective than trimethoprim alone in older women.9,10 Cranberry tablets were not associated with bacterial resistance, were cheaper, and were viewed as a more natural option. The interventions were equally well tolerated.
Overall efficacy of cranberry tablets is unclear. Side effects, albeit mild, included gastrointestinal disturbances, vaginal complaints, and rash or urticaria. There was no significant difference in the rate of adverse effects between antimicrobial treatment and cranberry tablets.9
Cystopurin has not been studied
Cystopurin is an over-the-counter (OTC) tablet containing cranberry extract and potassium citrate that is taken three times daily (3 g/dose) for 2 days. Interestingly, although a proposed mechanism for the efficacy of vitamin C and cranberry juice has been a reduction of pH, potassium citrate is an alkalizing agent that is reported to relieve burning and reduce urinary urgency and frequency. No studies have assessed this medication in the treatment of a UTI or its symptoms.
Clinical recommendations
The evidence is mixed on the use of cranberry products to reduce recurrent UTI. However, given the limited side effects associated with these products, we offer cranberry tablets to patients who have recurrent UTIs who are interested in a more natural alternative.
We generally do not recommend cranberry juice because the added fluid volume tends to exacerbate frequency and urgency symptoms.

Lactobacilli suppositories may benefit
postmenopausal women
Lactobacilli are fastidious gram-positive rods and are usually the dominant component of the vaginal flora.11 They prevent colonization and infection by more virulent bacteria by competing for adhesion receptors and nutrients as well as producing antimicrobial substances such as hydrogen peroxide and lactic acid. A decrease in lactobacilli leaves the urinary tract susceptible to infectious organisms that may colonize the vaginal mucosa and increase the risk of recurrent UTI.12-14
A 2008 review of randomized, controlled trials of oral lactobacilli and UTI was inconclusive, due to inconsistent dosing strategies and small sample sizes.15 A 2011 randomized, double-blind, placebo-controlled phase 2 trial of Lactin-V, a lactobacilli vaginal suppository, found that it reduced the rate of recurrent UTI. Lactin-V contains a hydrogen-peroxide–producing Lactobacillus crispatus developed as a probiotic that was determined to be safe and tolerable as a vaginal suppository in a phase 1 trial.16 The phase 2 trial enrolled 100 young premenopausal women with a history of recurrent UTI who took either Lactin-V or placebo daily for 5 days, then weekly for 10 weeks. Women in the Lactin-V group who had high levels of L. crispatus colonization experienced a significant reduction in the rate of UTI (15% vs 27% in the placebo group), but the effect did not reach statistical significance.14
Little difference in adverse effects
Adverse effects were reported among 56% of patients who received Lactin-V versus 50% of those given placebo. The most common of these were vaginal discharge, itching, and moderate abdominal discomfort.14 Although lactobacillus can potentially promote UTI, this phenomenon is rare.11
Regrettably, Lactin-V is not currently available in the United States. However, there are other lactobacilli vaginal suppositories on the market ( TABLE ). Given the low risk associated with their use, they should be considered as an alternative for patients who cannot or will not use estrogen.
Clinical recommendations
Probiotics such as lactobacilli are categorized as “dietary supplements”; as such, they are not regulated by the US Food and Drug Administration. We recommend the use of lactobacilli suppositories in postmenopausal women who have a contraindication to (or prefer to avoid) vaginal estrogen.
Skip blueberry products for now
Like cranberries, blueberries belong to the Vaccinium species and are thought to interfere with bacterial adhesion to the walls of the bladder. One in vitro trial suggests that blueberries also have antiproliferation effects, although no clinical studies have been performed to date to further investigate safety or efficacy.4 Consequently, we do not recommend use of these products.
Methenamine salts may benefit some populations
These anti-infective agents, including methenamine hippurate and methenamine mandelate, often are used to prevent UTI. They are found in combination OTC medications, such as Prosed DS and Urelle. Methenamine salts are bacteriostatic to all urinary tract pathogens due to their production of formaldehyde.3,16
Although methenamine produces varying concentrations of formaldehyde, depending on the acidity of the urine, there is no evidence that acidified urine enhances methenamine’s effects.16
Advantages of methenamine include the fact that it produces no changes in gut flora, poses no risk for antimicrobial resistance, and has low toxicity. It also is low in cost.17
Methenamine is contraindicated in patients with renal insufficiency or severe hepatic disease.
Adverse reactions are generally mild and include gastrointestinal disturbances, skin rashes, dysuria, and microscopic hematuria.16
Methenamine hippurate
A 2007 Cochrane review, deemed up to date in 2010, analyzed 13 randomized, controlled trials involving 2,032 participants. Subgroup analyses suggested that methenamine hippurate may be of some benefit to patients without renal tract abnormalities; these patients experienced significantly reduced symptoms after short-term treatment of 1 week or less.
Patients with spinal injury do not appear to benefit from treatment, according to a randomized, double-blind, placebo-controlled trial by Lee and colleagues.18
Methenamine mandelate
This agent is commonly used to prevent recurrent UTI, although there is a paucity of randomized, controlled trials to support its use. One such trial in patients with neurogenic bladder found that methenamine mandelate with acidification was superior to placebo (P <.02) for preventing UTI.19 Beyond this population, however, it’s difficult to assess methenamine’s efficacy in the prevention of recurrent UTI.
Methylene blue may be useful in the elderly
Methylene blue is a light-activated compound described as “photodynamic antimicrobial chemotherapy” (PACT). Once illuminated, it becomes a bactericide, causing excitation of electrons followed by one of two reactions:
- reduction oxidation
- formation of a labile singlet oxygen and then oxidation.
This makes resistance unlikely.
In an in vitro study, methylene blue was as effective as levofloxacin against Pseudomonas aeruginosa, Klebsiella pneumonia, Proteus mirabilis, Enterococcus, and Staphylococcus aureus when illuminated.
Potential benefits of this mode of treatment include local exposure and no drug interactions.
We suggest that methylene blue be placed and illuminated with a special catheter that would target UTI in the elderly population, among whom 52% of UTIs are associated with use of catheters.20 In vivo effects, adverse effects, and cost are not known, which limits current applicability of this compound.
Vitamin C may reduce UTI in pregnancy
The proposed mechanism for the efficacy of vitamin C for the treatment of UTI is the acidification of urine, which is believed to reduce the proliferation of bacteria. However, several studies have shown that vitamin C, at various doses, does not reliably reduce urine pH.15,21,22 Nonetheless, ascorbic acid was tested for its effect on UTI prevention during pregnancy.
In a single-blind trial, 110 pregnant women were divided into two groups (55 in each group):
- One group received ferrous sulfate (200 mg), folic acid (5 mg), and vitamin C (100 mg) daily for 3 months
- The other received ferrous sulfate (200 mg) and folic acid (5 mg) daily for 3 months.
Urine was cultured monthly. The incidence of UTI was significantly lower in the group receiving vitamin C (12.7%), compared with the control group (29.1%) (P=.03; odds ratio [OR], 0.35).23
Uva ursi may have a prophylactic effect
Uva ursi (UVA-E) is one of the most commonly used herbal supplements for treatment of UTI. The crude extract from Bearberry or Arctostaphylos uva-ursi has been shown to act as an antimicrobial by decreasing bacterial adherence.24 In addition, investigators have found the extract to have diuretic and anti-inflammatory properties.25,26 However, few studies have explored its efficacy. One randomized, controlled trial that included 57 women (30 allocated to UVA-E and 27 to placebo) found a statistically significant reduction in the rate of recurrence at 1 year among women taking UVA-E, compared with those who did not.27
Note that the women in this trial were given UVA-E for 1 month only. Long-term use of this herb has not been studied and may cause liver damage.
In a mouse model, forskolin reduced urinary-tract E. coli
This herb is derived from Indian coleus (Coleus forskohlii), a member of the mint family. It has been used primarily for its antiasthmatic, spasmolytic, and antihypertensive effects. It is believed to activate adenylate cyclase, increasing intracellular cyclic AMP (cAMP) concentrations and activating a number of key enzymatic pathways.28
The findings of a recent observational study have spurred the use of forskolin in the treatment of recurrent UTI.29 In the study, conducted on mice, when forskolin was injected into the bladder, intracellular E. coli decreased.
It is theorized that the incorporation of bacteria into intracellular vesicles of the bladder prevents exposure to antibiotics. When combined with an antibiotic, forskolin may increase bacterial elimination and thus lower the risk of recurrent infection. However, no randomized trials have evaluated the efficacy of this treatment.
Patients who are already taking antihypertensive medications should be cautious when using this herb, as it may lead to a drop in blood pressure.
Behavior changes are risk-free
One of the natural mechanisms that promotes bacterial elimination and prevents bacterial growth is urination. A recent review article on the subject found several contradictory studies on the effect of fluid intake on the risk of UTI.30 Although there is no definitive evidence that susceptibility to UTI is linked to fluid intake, adequate hydration may reduce the risk of recurrent infection.
Similarly, voiding shortly after sexual intercourse may prevent UTI. One case-control study found a modest protective effect in patients who voided after intercourse.31
Clinical recommendations
Given the low risk of these measures, it seems reasonable to recommend postcoital voiding and increased fluid intake to prevent recurrent UTI.
A focus on symptoms
Phenazopyridine, the chemical found in numerous OTC medications, such as Pyridium, AZO, and Uristat, was discovered by Swiss chemist Bernhard Joos in the 1950s. Its mechanism of action is still unclear, but approximately 65% of the oral dose is excreted by the kidneys, where it has a direct topical analgesic effect.32,33
Clinical recommendations
Patients should be warned that phenazopyridine will lead to orange urine discoloration.
The medication is generally well tolerated but should be used with caution in patients with acute renal failure, hemolytic anemia, or methemoglobinemia, as it may exacerbate these conditions.
Last words
Recurrent UTIs are common and impose a significant financial burden on our healthcare system. Although there are several antibiotic treatment options and dosing regimens available, increasing antibiotic resistance has made management of recurrent UTIs more difficult. Effective alternative treatments that reduce the reliance on antibiotics may minimize bacterial resistance and decrease the financial burden of this common condition.
CASE: Resolved
To reduce vaginal E. coli, the patient is started on vaginal estrogen cream. She is also advised to purchase cranberry tablets to help prevent future infections. Last, she is counseled about behavioral changes she can make and prescribed a short course of antibiotics to treat her culture-proven infection.
We want to hear from you! Tell us what you think.
URINARY PROBLEMS?
CLICK HERE to access 9 articles about treating urinary incontinence and urinary tract infections, published in OBG MANAGEMENTin 2012.
1. Raz R, Stamm W. A controlled trial of intravaginal estriol in postmenopausal women with recurrent urinary tract infections. N Engl J Med. 1993;329(11):753-756.
2. Perrotta C, Aznar M, Mejia R, Albert X, Ng CW. Oestrogens for preventing recurrent urinary tract infection in postmenopausal women. Cochrane Database Syst Rev. 2008;2:CD005131.-
3. Mayrer AR, Andriole VT. Urinary tract antiseptics. Med Clin North Am. 1982;66(1):199-208.
4. Jepson RG, Craig JC. A systematic review of the evidence for cranberries and blueberries in UTI prevention. Mol Nutr Food Res. 2007;51(6):738-745.
5. Salvatore S, Salvatore S, Cattoni E, et al. Urinary tract infections in women. Eur J Obstet Gynecol Reprod Biol. 2011;156(2):131-136.
6. Jepson RG, Craig JC. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev. 2008;1:CD001321.-
7. Stapleton AE, Dziura J, Hooton TM, et al. Recurrent urinary tract infection and urinary Escherichia coli in women ingesting cranberry juice daily: a randomized controlled trial. Mayo Clin Proc. 2012;87(2):143-150.
8. Barbosa-Cesnik C, Brown MB, Buxton M, Zhang L, DeBusscher J, Foxman B. Cranberry juice fails to prevent recurrent urinary tract infection: results from a randomized placebo-controlled trial. Clin Infect Dis. 2011;52(1):23-30.
9. Beerepoot MAJ, Reit G, Nys S, et al. Cranberries vs antibiotics to prevent urinary tract infections. Arch Intern Med. 2011;171(14):1270-1278.
10. McMurdo MET, Argo I, Phillips G, Daly F, Davey P. Cranberry or trimethoprim for the prevention of recurrent urinary tract infections? A randomized controlled trial in older women. J Antimicrob Chemother. 2009;63(2):389-395.
11. Barrons R, Tassone D. Use of Lactobacillus probiotics for bacterial genitourinary infections in women: a review. Clinical Therapeutics. 2008;30(3):453-468.
12. Miller JL, Krieger JN. Urinary tract infections: cranberry juice underwear, and probiotics in the 21st century. Urol Clin N Am. 2002;29(3):695-699.
13. Osset J, Bartolome R, Garcia E, et al. Assessment of the capacity of Lactobacillus to inhibit the growth of uropathogens and block their adhesion to vaginal epithelial cells. J Infect Dis. 2001;183(3):485-491.
14. Stapleton AE, Au-Yeung M, Hooton TM, et al. Randomized, placebo-controlled phase 2 trial of Lactobacillus crispatus probiotic given intravaginally for prevention of recurrent urinary tract infection. Clin Infect Dis. 2011;52(10):1212-1217.
15. Castello T, Girona L, Gomez MR, Mena Mur A, Garcia L. The possible value of ascorbic acid as a prophylactic agent for urinary tract infection. Spinal Cord. 1996;34(10):592-593.
16. Gleckman R, Alvarez S, Joubert DW, Matthews SJ. Drug therapy reviews: methenamine mandelate and methenamine hippurate. Am J Hosp Pharm. 1979;36(11):1509-1512.
17. Vainrub B, Musher DM. Lack of effect of methenamine in suppression of or prophylaxis against, chronic urinary tract infection. Antimicrob Agents Chemother. 1977;12(5):625-629.
18. Lee BB, Simpson JM, Craig JC, Bhuta T. Methenamine hippurate for preventing urinary tract infections. Cochrane Database Syst Rev. 2007;4:CD003265.-
19. Kevorkian CG, Merritt JL, Ilstrup DM. Methenamine mandelate with acidification: an effective urinary antiseptic in patients with neurogenic bladder. Mayo Clin Proc. 1984;59(8):523-529.
20. Wainwright M, Stanforth A, Jones R, Loughran C, Meegan K. Photoantimicrobials as a potential local approach to geriatric UTIs. Lett Appl Microbiol. 2010;50(5):486-492.
21. Bannwart C, Hagmaier V, Straumann E, Hofer H, Buillemier JP, Trutishauser G. Modification of urinary pH through ascorbic acid. Helv Chir Acta. 1981;48(3-4):425-428.
22. Hetey SK, Kleinberg ML, Parker WD, Johnson EW. Effect of ascorbic acid on urine pH in patients with injured spinal cords. Am J Hosp Pharm. 1980;37(2):235-237.
23. Ochoa-Brust GJ, Fernandez AR, Villanueva-Ruiz GJ, et al. Daily intake of 100 mg ascorbic acid as urinary tract infection prophylactic agent during pregnancy. Acta Obstet Gynecol Scand. 2007;86(7):783-787.
24. Turi M, Turi E, Kotjalg S, Mikelsaar M. Influence of aqueous extracts of medicinal plants on surface hydrophobicity of Escherichia coli strains of different origin. APMIS. 1997;105(12):956-962.
25. Beaux D, Fleurentin J, Mortier F. Effect of extracts of Orthosiphon stamineus Benth Hieracium pilosellaL., Sambucus nigra L. and Arctostaphylos uva-ursi (L.) Spreng. in rats. Phytother Res. 1999;13(3):222-225.
26. Kubo M, Ito M, Nakata H, Matsuda H. Pharmacological studies on leaf of Arctostaphylos uva-ursi (L.) Spreng. I. Combined effect of 50% methanolic extract from Arctostaphylos uva-ursi (L.) Spreng. (bearberry leaf) and prednisolone on immuno-inflammation [article in Japanese]. Yakugaku Zasshi. 1990;110(1):59-67.
27. Larsson B, Jonasson A, Fianu S. Prophylactic effect of UVA-E in women with recurrent cystitis: a preliminary report. Curr Ther Res. 1993;53(4):441-443.
28. Christenson JT, Thulesius D, Nazzal MM. The effect of forskolin on blood flow platelet metabolism, aggregation and ATP release. Vasa. 1995;24(1):56-61.
29. Bishop BL, Duncan MJ, Song J, Li G, Zaas D, Abraham SN. Cyclic AMP-regulated exocytosis of Escherichia coli from infected bladder epithelial cells. Nat Med. 2007;13(5):625-630.
30. Beetz R. Mild dehydration: a risk factor of urinary tract infection? Eur J Clin Nutr. 2003;57(Suppl 2):S52-58.
31. Foxman B, Chi JW. Health behavior and urinary tract infection in college-aged women. J Clin Epidemiol. 1990;43(4):329-337.
32. Thomas BH, Whitehouse LW, Solomonraj G, Paul CJ. Excretion of phenazopyridine and its metabolites in the urine of humans rats, mice, and guinea pigs. J Pharm Sci. 1990;79(4):321-325.
33. Aizawa N, Wyndaele JJ. Effects of phenazopyridine on rat bladder primary afferent activity and comparison with lidocaine and acetaminophen. Neurourol Urodyn. 2010;29(8):1445-1550.
Patrick A. Nosti, MD
Dr. Nosti is a Fellow in Female Pelvic Medicine and Reconstructive Surgery at Washington Hospital Center and Georgetown University Medical Center in Washington, DC.
Kate C. Arnold
Ms. Arnold is a medical student at Georgetown University School of Medicine in Washington, DC.
Cheryl B. Iglesia, MD
Dr. Iglesia is Director of the Section of Female Pelvic Medicine and Reconstructive Surgery at Washington Hospital Center. She is also Associate Professor, Departments of Obstetrics and Gynecology and Urology, at Georgetown University School of Medicine in Washington, DC. She serves on the OBG Management Board of Editors.
Patrick A. Nosti, MD
Dr. Nosti is a Fellow in Female Pelvic Medicine and Reconstructive Surgery at Washington Hospital Center and Georgetown University Medical Center in Washington, DC.
Kate C. Arnold
Ms. Arnold is a medical student at Georgetown University School of Medicine in Washington, DC.
Cheryl B. Iglesia, MD
Dr. Iglesia is Director of the Section of Female Pelvic Medicine and Reconstructive Surgery at Washington Hospital Center. She is also Associate Professor, Departments of Obstetrics and Gynecology and Urology, at Georgetown University School of Medicine in Washington, DC. She serves on the OBG Management Board of Editors.
Patrick A. Nosti, MD
Dr. Nosti is a Fellow in Female Pelvic Medicine and Reconstructive Surgery at Washington Hospital Center and Georgetown University Medical Center in Washington, DC.
Kate C. Arnold
Ms. Arnold is a medical student at Georgetown University School of Medicine in Washington, DC.
Cheryl B. Iglesia, MD
Dr. Iglesia is Director of the Section of Female Pelvic Medicine and Reconstructive Surgery at Washington Hospital Center. She is also Associate Professor, Departments of Obstetrics and Gynecology and Urology, at Georgetown University School of Medicine in Washington, DC. She serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this article.
CASE: Recurrent UTI and antibiotic resistance
A 53-year-old postmenopausal woman with a history of culture-proven recurrent Escherichia coli urinary tract infections (UTIs) presents to the clinic with symptoms of UTI. She was previously treated with a postcoital regimen of trimethoprim/sulfamethoxazole, based on sensitivities identified by culture. A past work-up of her upper and lower urinary tract was negative. You send a catheterized specimen for culture; again, E. coli is identified as the pathogen but proves resistant to her current antibiotic regimen.
What treatment alternatives, aside from antibiotics, are available for this patient—and how might they affect resistance?
Increased antibiotic usage has led to greater bacterial resistance, which is perpetuated by clonal spread. Resistant strains of E. coli have been found in household members, suggesting host-host transmission as a mechanism for dissemination. Alternative treatments that reduce the use of antibiotics may minimize bacterial resistance and increase the efficacy of treatment. In the TABLE , we summarize alternative approaches to the treatment of recurrent UTI. We also describe a strategy to alleviate symptoms.
Alternatives to antibiotics in the treatment and prevention of recurrent UTI
| Category | Type | Examples and doses, if recommended |
|---|---|---|
| Vaginal estrogen | Conjugated estrogen cream Estradiol
| Premarin cream, 0.5–2 g vaginally twice weekly
|
| Nutritive agents | Cranberry juice Cranberry tablets Cystopurin Lactobacilli Blueberry products | Not recommended 1 tablet (300 to 400 mg, depending on manufacturer) twice daily Not recommended Vivag, EcoVag, 1 capsule daily by vagina for 5 days, then once weekly for 10 weeks Not recommended |
| Anti-infective drugs | Methenamine hippurate Methenamine mandelate Methylene blue | Urex or Hiprex, 1 g orally twice daily Mandelamine, 1 g orally 4 times daily Future therapy |
| Urinary acidifiers | Vitamin C/ascorbic acid | 1–3 g orally 3–4 times daily |
| Herbal remedies | Uva ursi Forskolin | Not recommended for long-term use Not recommended |
| Behavioral changes | Adequate hydration Postcoital voiding |
Vaginal estrogen is the only proven alternative to antibiotics for postmenopausal women
A lack of estrogen is a risk factor for UTI and is associated with atrophic mucosa, leading to decreased colonization with lactobacilli, increased vaginal pH, and E. coli colonization.
A randomized, double-blind, placebo-controlled trial of intravaginal estriol cream versus placebo in 93 postmenopausal women found a significant decrease in the rate of UTI among women who used the cream.1 After 8 months of follow-up, the incidence of UTI was 0.5 vs 5.9 episodes per patient-year (P <.001). Interestingly, all pretreatment cultures were negative for lactobacilli. One month after treatment, 61% of women in the estriol group were culture-positive for lactobacilli, compared with 0% of the placebo group.1
A 2008 Cochrane review of nine studies concluded that vaginal estrogen reduces the number of UTIs in postmenopausal women, with variation based on the type of estrogen and duration of use.2
Adverse effects are mild
Twenty-eight percent of the estriol group in the randomized trial described above withdrew from treatment, with 20% citing local side effects, including vaginal irritation, burning, or itching—all of which were mild and self-limited.1 Other possible adverse effects include breast tenderness, vaginal bleeding or spotting, and discharge.2
Clinical recommendations
Given the efficacy of this therapy, we recommend topical estrogen for postmenopausal patients with recurrent UTIs.
Cranberry juice may reduce UTI, but many patients withdraw
from treatment
Cranberries belong to the Vaccinium species, which contains all flavonoids, including anthocyanins and proanthocyanidins. It was previously thought that the acidification of urine produced an antibacterial effect, but several trials have documented no change in urine levels of hippuric acid when cranberry products are given, with no acidification of the urine.3 Current theory suggests that cranberries prevent bacteria from adhering to the uroepithelial cells of the walls of the bladder, by blocking expression of E. coli’s adhesion molecule, P. fimbriae, so that bacteria are unable to penetrate the mucosal surface.4,5 The major benefit of cranberry products over antibiotic prophylaxis is that they do not have the potential for resistance.4
A 2008 Cochrane review concluded that cranberry juice may reduce symptomatic UTIs, particularly among young, sexually active women—but there is a high rate of withdrawal from treatment.6 The optimal method of administration and dose remain unclear. In contrast, two recent randomized, controlled trials—published after the Cochrane review—found no difference in the rate of recurrent UTI in premenopausal women.7,8 Adverse effects in these two trials included constipation, heartburn, loose stools, vaginal itching and dryness, and migraines. Of note, there was no statistical difference in side effects between the cranberry and placebo groups.7
Vaccinium tablets may be protective in older women
Cranberry extracts of 500 mg to 1,000 mg daily have been compared with antimicrobial prophylaxis in two randomized, double-blind, controlled trials. The trials demonstrated mixed benefits. Trimethoprim/sulfamethoxazole was associated with a lower rate of UTI in younger women, compared with cranberry extracts alone (P=.02), while cranberry extracts were slightly more effective than trimethoprim alone in older women.9,10 Cranberry tablets were not associated with bacterial resistance, were cheaper, and were viewed as a more natural option. The interventions were equally well tolerated.
Overall efficacy of cranberry tablets is unclear. Side effects, albeit mild, included gastrointestinal disturbances, vaginal complaints, and rash or urticaria. There was no significant difference in the rate of adverse effects between antimicrobial treatment and cranberry tablets.9
Cystopurin has not been studied
Cystopurin is an over-the-counter (OTC) tablet containing cranberry extract and potassium citrate that is taken three times daily (3 g/dose) for 2 days. Interestingly, although a proposed mechanism for the efficacy of vitamin C and cranberry juice has been a reduction of pH, potassium citrate is an alkalizing agent that is reported to relieve burning and reduce urinary urgency and frequency. No studies have assessed this medication in the treatment of a UTI or its symptoms.
Clinical recommendations
The evidence is mixed on the use of cranberry products to reduce recurrent UTI. However, given the limited side effects associated with these products, we offer cranberry tablets to patients who have recurrent UTIs who are interested in a more natural alternative.
We generally do not recommend cranberry juice because the added fluid volume tends to exacerbate frequency and urgency symptoms.
Lactobacilli suppositories may benefit
postmenopausal women
Lactobacilli are fastidious gram-positive rods and are usually the dominant component of the vaginal flora.11 They prevent colonization and infection by more virulent bacteria by competing for adhesion receptors and nutrients as well as producing antimicrobial substances such as hydrogen peroxide and lactic acid. A decrease in lactobacilli leaves the urinary tract susceptible to infectious organisms that may colonize the vaginal mucosa and increase the risk of recurrent UTI.12-14
A 2008 review of randomized, controlled trials of oral lactobacilli and UTI was inconclusive, due to inconsistent dosing strategies and small sample sizes.15 A 2011 randomized, double-blind, placebo-controlled phase 2 trial of Lactin-V, a lactobacilli vaginal suppository, found that it reduced the rate of recurrent UTI. Lactin-V contains a hydrogen-peroxide–producing Lactobacillus crispatus developed as a probiotic that was determined to be safe and tolerable as a vaginal suppository in a phase 1 trial.16 The phase 2 trial enrolled 100 young premenopausal women with a history of recurrent UTI who took either Lactin-V or placebo daily for 5 days, then weekly for 10 weeks. Women in the Lactin-V group who had high levels of L. crispatus colonization experienced a significant reduction in the rate of UTI (15% vs 27% in the placebo group), but the effect did not reach statistical significance.14
Little difference in adverse effects
Adverse effects were reported among 56% of patients who received Lactin-V versus 50% of those given placebo. The most common of these were vaginal discharge, itching, and moderate abdominal discomfort.14 Although lactobacillus can potentially promote UTI, this phenomenon is rare.11
Regrettably, Lactin-V is not currently available in the United States. However, there are other lactobacilli vaginal suppositories on the market ( TABLE ). Given the low risk associated with their use, they should be considered as an alternative for patients who cannot or will not use estrogen.
Clinical recommendations
Probiotics such as lactobacilli are categorized as “dietary supplements”; as such, they are not regulated by the US Food and Drug Administration. We recommend the use of lactobacilli suppositories in postmenopausal women who have a contraindication to (or prefer to avoid) vaginal estrogen.
Skip blueberry products for now
Like cranberries, blueberries belong to the Vaccinium species and are thought to interfere with bacterial adhesion to the walls of the bladder. One in vitro trial suggests that blueberries also have antiproliferation effects, although no clinical studies have been performed to date to further investigate safety or efficacy.4 Consequently, we do not recommend use of these products.
Methenamine salts may benefit some populations
These anti-infective agents, including methenamine hippurate and methenamine mandelate, often are used to prevent UTI. They are found in combination OTC medications, such as Prosed DS and Urelle. Methenamine salts are bacteriostatic to all urinary tract pathogens due to their production of formaldehyde.3,16
Although methenamine produces varying concentrations of formaldehyde, depending on the acidity of the urine, there is no evidence that acidified urine enhances methenamine’s effects.16
Advantages of methenamine include the fact that it produces no changes in gut flora, poses no risk for antimicrobial resistance, and has low toxicity. It also is low in cost.17
Methenamine is contraindicated in patients with renal insufficiency or severe hepatic disease.
Adverse reactions are generally mild and include gastrointestinal disturbances, skin rashes, dysuria, and microscopic hematuria.16
Methenamine hippurate
A 2007 Cochrane review, deemed up to date in 2010, analyzed 13 randomized, controlled trials involving 2,032 participants. Subgroup analyses suggested that methenamine hippurate may be of some benefit to patients without renal tract abnormalities; these patients experienced significantly reduced symptoms after short-term treatment of 1 week or less.
Patients with spinal injury do not appear to benefit from treatment, according to a randomized, double-blind, placebo-controlled trial by Lee and colleagues.18
Methenamine mandelate
This agent is commonly used to prevent recurrent UTI, although there is a paucity of randomized, controlled trials to support its use. One such trial in patients with neurogenic bladder found that methenamine mandelate with acidification was superior to placebo (P <.02) for preventing UTI.19 Beyond this population, however, it’s difficult to assess methenamine’s efficacy in the prevention of recurrent UTI.
Methylene blue may be useful in the elderly
Methylene blue is a light-activated compound described as “photodynamic antimicrobial chemotherapy” (PACT). Once illuminated, it becomes a bactericide, causing excitation of electrons followed by one of two reactions:
- reduction oxidation
- formation of a labile singlet oxygen and then oxidation.
This makes resistance unlikely.
In an in vitro study, methylene blue was as effective as levofloxacin against Pseudomonas aeruginosa, Klebsiella pneumonia, Proteus mirabilis, Enterococcus, and Staphylococcus aureus when illuminated.
Potential benefits of this mode of treatment include local exposure and no drug interactions.
We suggest that methylene blue be placed and illuminated with a special catheter that would target UTI in the elderly population, among whom 52% of UTIs are associated with use of catheters.20 In vivo effects, adverse effects, and cost are not known, which limits current applicability of this compound.
Vitamin C may reduce UTI in pregnancy
The proposed mechanism for the efficacy of vitamin C for the treatment of UTI is the acidification of urine, which is believed to reduce the proliferation of bacteria. However, several studies have shown that vitamin C, at various doses, does not reliably reduce urine pH.15,21,22 Nonetheless, ascorbic acid was tested for its effect on UTI prevention during pregnancy.
In a single-blind trial, 110 pregnant women were divided into two groups (55 in each group):
- One group received ferrous sulfate (200 mg), folic acid (5 mg), and vitamin C (100 mg) daily for 3 months
- The other received ferrous sulfate (200 mg) and folic acid (5 mg) daily for 3 months.
Urine was cultured monthly. The incidence of UTI was significantly lower in the group receiving vitamin C (12.7%), compared with the control group (29.1%) (P=.03; odds ratio [OR], 0.35).23
Uva ursi may have a prophylactic effect
Uva ursi (UVA-E) is one of the most commonly used herbal supplements for treatment of UTI. The crude extract from Bearberry or Arctostaphylos uva-ursi has been shown to act as an antimicrobial by decreasing bacterial adherence.24 In addition, investigators have found the extract to have diuretic and anti-inflammatory properties.25,26 However, few studies have explored its efficacy. One randomized, controlled trial that included 57 women (30 allocated to UVA-E and 27 to placebo) found a statistically significant reduction in the rate of recurrence at 1 year among women taking UVA-E, compared with those who did not.27
Note that the women in this trial were given UVA-E for 1 month only. Long-term use of this herb has not been studied and may cause liver damage.
In a mouse model, forskolin reduced urinary-tract E. coli
This herb is derived from Indian coleus (Coleus forskohlii), a member of the mint family. It has been used primarily for its antiasthmatic, spasmolytic, and antihypertensive effects. It is believed to activate adenylate cyclase, increasing intracellular cyclic AMP (cAMP) concentrations and activating a number of key enzymatic pathways.28
The findings of a recent observational study have spurred the use of forskolin in the treatment of recurrent UTI.29 In the study, conducted on mice, when forskolin was injected into the bladder, intracellular E. coli decreased.
It is theorized that the incorporation of bacteria into intracellular vesicles of the bladder prevents exposure to antibiotics. When combined with an antibiotic, forskolin may increase bacterial elimination and thus lower the risk of recurrent infection. However, no randomized trials have evaluated the efficacy of this treatment.
Patients who are already taking antihypertensive medications should be cautious when using this herb, as it may lead to a drop in blood pressure.
Behavior changes are risk-free
One of the natural mechanisms that promotes bacterial elimination and prevents bacterial growth is urination. A recent review article on the subject found several contradictory studies on the effect of fluid intake on the risk of UTI.30 Although there is no definitive evidence that susceptibility to UTI is linked to fluid intake, adequate hydration may reduce the risk of recurrent infection.
Similarly, voiding shortly after sexual intercourse may prevent UTI. One case-control study found a modest protective effect in patients who voided after intercourse.31
Clinical recommendations
Given the low risk of these measures, it seems reasonable to recommend postcoital voiding and increased fluid intake to prevent recurrent UTI.
A focus on symptoms
Phenazopyridine, the chemical found in numerous OTC medications, such as Pyridium, AZO, and Uristat, was discovered by Swiss chemist Bernhard Joos in the 1950s. Its mechanism of action is still unclear, but approximately 65% of the oral dose is excreted by the kidneys, where it has a direct topical analgesic effect.32,33
Clinical recommendations
Patients should be warned that phenazopyridine will lead to orange urine discoloration.
The medication is generally well tolerated but should be used with caution in patients with acute renal failure, hemolytic anemia, or methemoglobinemia, as it may exacerbate these conditions.
Last words
Recurrent UTIs are common and impose a significant financial burden on our healthcare system. Although there are several antibiotic treatment options and dosing regimens available, increasing antibiotic resistance has made management of recurrent UTIs more difficult. Effective alternative treatments that reduce the reliance on antibiotics may minimize bacterial resistance and decrease the financial burden of this common condition.
CASE: Resolved
To reduce vaginal E. coli, the patient is started on vaginal estrogen cream. She is also advised to purchase cranberry tablets to help prevent future infections. Last, she is counseled about behavioral changes she can make and prescribed a short course of antibiotics to treat her culture-proven infection.
We want to hear from you! Tell us what you think.
URINARY PROBLEMS?
CLICK HERE to access 9 articles about treating urinary incontinence and urinary tract infections, published in OBG MANAGEMENTin 2012.
The authors report no financial relationships relevant to this article.
CASE: Recurrent UTI and antibiotic resistance
A 53-year-old postmenopausal woman with a history of culture-proven recurrent Escherichia coli urinary tract infections (UTIs) presents to the clinic with symptoms of UTI. She was previously treated with a postcoital regimen of trimethoprim/sulfamethoxazole, based on sensitivities identified by culture. A past work-up of her upper and lower urinary tract was negative. You send a catheterized specimen for culture; again, E. coli is identified as the pathogen but proves resistant to her current antibiotic regimen.
What treatment alternatives, aside from antibiotics, are available for this patient—and how might they affect resistance?
Increased antibiotic usage has led to greater bacterial resistance, which is perpetuated by clonal spread. Resistant strains of E. coli have been found in household members, suggesting host-host transmission as a mechanism for dissemination. Alternative treatments that reduce the use of antibiotics may minimize bacterial resistance and increase the efficacy of treatment. In the TABLE , we summarize alternative approaches to the treatment of recurrent UTI. We also describe a strategy to alleviate symptoms.
Alternatives to antibiotics in the treatment and prevention of recurrent UTI
| Category | Type | Examples and doses, if recommended |
|---|---|---|
| Vaginal estrogen | Conjugated estrogen cream Estradiol
| Premarin cream, 0.5–2 g vaginally twice weekly
|
| Nutritive agents | Cranberry juice Cranberry tablets Cystopurin Lactobacilli Blueberry products | Not recommended 1 tablet (300 to 400 mg, depending on manufacturer) twice daily Not recommended Vivag, EcoVag, 1 capsule daily by vagina for 5 days, then once weekly for 10 weeks Not recommended |
| Anti-infective drugs | Methenamine hippurate Methenamine mandelate Methylene blue | Urex or Hiprex, 1 g orally twice daily Mandelamine, 1 g orally 4 times daily Future therapy |
| Urinary acidifiers | Vitamin C/ascorbic acid | 1–3 g orally 3–4 times daily |
| Herbal remedies | Uva ursi Forskolin | Not recommended for long-term use Not recommended |
| Behavioral changes | Adequate hydration Postcoital voiding |
Vaginal estrogen is the only proven alternative to antibiotics for postmenopausal women
A lack of estrogen is a risk factor for UTI and is associated with atrophic mucosa, leading to decreased colonization with lactobacilli, increased vaginal pH, and E. coli colonization.
A randomized, double-blind, placebo-controlled trial of intravaginal estriol cream versus placebo in 93 postmenopausal women found a significant decrease in the rate of UTI among women who used the cream.1 After 8 months of follow-up, the incidence of UTI was 0.5 vs 5.9 episodes per patient-year (P <.001). Interestingly, all pretreatment cultures were negative for lactobacilli. One month after treatment, 61% of women in the estriol group were culture-positive for lactobacilli, compared with 0% of the placebo group.1
A 2008 Cochrane review of nine studies concluded that vaginal estrogen reduces the number of UTIs in postmenopausal women, with variation based on the type of estrogen and duration of use.2
Adverse effects are mild
Twenty-eight percent of the estriol group in the randomized trial described above withdrew from treatment, with 20% citing local side effects, including vaginal irritation, burning, or itching—all of which were mild and self-limited.1 Other possible adverse effects include breast tenderness, vaginal bleeding or spotting, and discharge.2
Clinical recommendations
Given the efficacy of this therapy, we recommend topical estrogen for postmenopausal patients with recurrent UTIs.
Cranberry juice may reduce UTI, but many patients withdraw
from treatment
Cranberries belong to the Vaccinium species, which contains all flavonoids, including anthocyanins and proanthocyanidins. It was previously thought that the acidification of urine produced an antibacterial effect, but several trials have documented no change in urine levels of hippuric acid when cranberry products are given, with no acidification of the urine.3 Current theory suggests that cranberries prevent bacteria from adhering to the uroepithelial cells of the walls of the bladder, by blocking expression of E. coli’s adhesion molecule, P. fimbriae, so that bacteria are unable to penetrate the mucosal surface.4,5 The major benefit of cranberry products over antibiotic prophylaxis is that they do not have the potential for resistance.4
A 2008 Cochrane review concluded that cranberry juice may reduce symptomatic UTIs, particularly among young, sexually active women—but there is a high rate of withdrawal from treatment.6 The optimal method of administration and dose remain unclear. In contrast, two recent randomized, controlled trials—published after the Cochrane review—found no difference in the rate of recurrent UTI in premenopausal women.7,8 Adverse effects in these two trials included constipation, heartburn, loose stools, vaginal itching and dryness, and migraines. Of note, there was no statistical difference in side effects between the cranberry and placebo groups.7
Vaccinium tablets may be protective in older women
Cranberry extracts of 500 mg to 1,000 mg daily have been compared with antimicrobial prophylaxis in two randomized, double-blind, controlled trials. The trials demonstrated mixed benefits. Trimethoprim/sulfamethoxazole was associated with a lower rate of UTI in younger women, compared with cranberry extracts alone (P=.02), while cranberry extracts were slightly more effective than trimethoprim alone in older women.9,10 Cranberry tablets were not associated with bacterial resistance, were cheaper, and were viewed as a more natural option. The interventions were equally well tolerated.
Overall efficacy of cranberry tablets is unclear. Side effects, albeit mild, included gastrointestinal disturbances, vaginal complaints, and rash or urticaria. There was no significant difference in the rate of adverse effects between antimicrobial treatment and cranberry tablets.9
Cystopurin has not been studied
Cystopurin is an over-the-counter (OTC) tablet containing cranberry extract and potassium citrate that is taken three times daily (3 g/dose) for 2 days. Interestingly, although a proposed mechanism for the efficacy of vitamin C and cranberry juice has been a reduction of pH, potassium citrate is an alkalizing agent that is reported to relieve burning and reduce urinary urgency and frequency. No studies have assessed this medication in the treatment of a UTI or its symptoms.
Clinical recommendations
The evidence is mixed on the use of cranberry products to reduce recurrent UTI. However, given the limited side effects associated with these products, we offer cranberry tablets to patients who have recurrent UTIs who are interested in a more natural alternative.
We generally do not recommend cranberry juice because the added fluid volume tends to exacerbate frequency and urgency symptoms.
Lactobacilli suppositories may benefit
postmenopausal women
Lactobacilli are fastidious gram-positive rods and are usually the dominant component of the vaginal flora.11 They prevent colonization and infection by more virulent bacteria by competing for adhesion receptors and nutrients as well as producing antimicrobial substances such as hydrogen peroxide and lactic acid. A decrease in lactobacilli leaves the urinary tract susceptible to infectious organisms that may colonize the vaginal mucosa and increase the risk of recurrent UTI.12-14
A 2008 review of randomized, controlled trials of oral lactobacilli and UTI was inconclusive, due to inconsistent dosing strategies and small sample sizes.15 A 2011 randomized, double-blind, placebo-controlled phase 2 trial of Lactin-V, a lactobacilli vaginal suppository, found that it reduced the rate of recurrent UTI. Lactin-V contains a hydrogen-peroxide–producing Lactobacillus crispatus developed as a probiotic that was determined to be safe and tolerable as a vaginal suppository in a phase 1 trial.16 The phase 2 trial enrolled 100 young premenopausal women with a history of recurrent UTI who took either Lactin-V or placebo daily for 5 days, then weekly for 10 weeks. Women in the Lactin-V group who had high levels of L. crispatus colonization experienced a significant reduction in the rate of UTI (15% vs 27% in the placebo group), but the effect did not reach statistical significance.14
Little difference in adverse effects
Adverse effects were reported among 56% of patients who received Lactin-V versus 50% of those given placebo. The most common of these were vaginal discharge, itching, and moderate abdominal discomfort.14 Although lactobacillus can potentially promote UTI, this phenomenon is rare.11
Regrettably, Lactin-V is not currently available in the United States. However, there are other lactobacilli vaginal suppositories on the market ( TABLE ). Given the low risk associated with their use, they should be considered as an alternative for patients who cannot or will not use estrogen.
Clinical recommendations
Probiotics such as lactobacilli are categorized as “dietary supplements”; as such, they are not regulated by the US Food and Drug Administration. We recommend the use of lactobacilli suppositories in postmenopausal women who have a contraindication to (or prefer to avoid) vaginal estrogen.
Skip blueberry products for now
Like cranberries, blueberries belong to the Vaccinium species and are thought to interfere with bacterial adhesion to the walls of the bladder. One in vitro trial suggests that blueberries also have antiproliferation effects, although no clinical studies have been performed to date to further investigate safety or efficacy.4 Consequently, we do not recommend use of these products.
Methenamine salts may benefit some populations
These anti-infective agents, including methenamine hippurate and methenamine mandelate, often are used to prevent UTI. They are found in combination OTC medications, such as Prosed DS and Urelle. Methenamine salts are bacteriostatic to all urinary tract pathogens due to their production of formaldehyde.3,16
Although methenamine produces varying concentrations of formaldehyde, depending on the acidity of the urine, there is no evidence that acidified urine enhances methenamine’s effects.16
Advantages of methenamine include the fact that it produces no changes in gut flora, poses no risk for antimicrobial resistance, and has low toxicity. It also is low in cost.17
Methenamine is contraindicated in patients with renal insufficiency or severe hepatic disease.
Adverse reactions are generally mild and include gastrointestinal disturbances, skin rashes, dysuria, and microscopic hematuria.16
Methenamine hippurate
A 2007 Cochrane review, deemed up to date in 2010, analyzed 13 randomized, controlled trials involving 2,032 participants. Subgroup analyses suggested that methenamine hippurate may be of some benefit to patients without renal tract abnormalities; these patients experienced significantly reduced symptoms after short-term treatment of 1 week or less.
Patients with spinal injury do not appear to benefit from treatment, according to a randomized, double-blind, placebo-controlled trial by Lee and colleagues.18
Methenamine mandelate
This agent is commonly used to prevent recurrent UTI, although there is a paucity of randomized, controlled trials to support its use. One such trial in patients with neurogenic bladder found that methenamine mandelate with acidification was superior to placebo (P <.02) for preventing UTI.19 Beyond this population, however, it’s difficult to assess methenamine’s efficacy in the prevention of recurrent UTI.
Methylene blue may be useful in the elderly
Methylene blue is a light-activated compound described as “photodynamic antimicrobial chemotherapy” (PACT). Once illuminated, it becomes a bactericide, causing excitation of electrons followed by one of two reactions:
- reduction oxidation
- formation of a labile singlet oxygen and then oxidation.
This makes resistance unlikely.
In an in vitro study, methylene blue was as effective as levofloxacin against Pseudomonas aeruginosa, Klebsiella pneumonia, Proteus mirabilis, Enterococcus, and Staphylococcus aureus when illuminated.
Potential benefits of this mode of treatment include local exposure and no drug interactions.
We suggest that methylene blue be placed and illuminated with a special catheter that would target UTI in the elderly population, among whom 52% of UTIs are associated with use of catheters.20 In vivo effects, adverse effects, and cost are not known, which limits current applicability of this compound.
Vitamin C may reduce UTI in pregnancy
The proposed mechanism for the efficacy of vitamin C for the treatment of UTI is the acidification of urine, which is believed to reduce the proliferation of bacteria. However, several studies have shown that vitamin C, at various doses, does not reliably reduce urine pH.15,21,22 Nonetheless, ascorbic acid was tested for its effect on UTI prevention during pregnancy.
In a single-blind trial, 110 pregnant women were divided into two groups (55 in each group):
- One group received ferrous sulfate (200 mg), folic acid (5 mg), and vitamin C (100 mg) daily for 3 months
- The other received ferrous sulfate (200 mg) and folic acid (5 mg) daily for 3 months.
Urine was cultured monthly. The incidence of UTI was significantly lower in the group receiving vitamin C (12.7%), compared with the control group (29.1%) (P=.03; odds ratio [OR], 0.35).23
Uva ursi may have a prophylactic effect
Uva ursi (UVA-E) is one of the most commonly used herbal supplements for treatment of UTI. The crude extract from Bearberry or Arctostaphylos uva-ursi has been shown to act as an antimicrobial by decreasing bacterial adherence.24 In addition, investigators have found the extract to have diuretic and anti-inflammatory properties.25,26 However, few studies have explored its efficacy. One randomized, controlled trial that included 57 women (30 allocated to UVA-E and 27 to placebo) found a statistically significant reduction in the rate of recurrence at 1 year among women taking UVA-E, compared with those who did not.27
Note that the women in this trial were given UVA-E for 1 month only. Long-term use of this herb has not been studied and may cause liver damage.
In a mouse model, forskolin reduced urinary-tract E. coli
This herb is derived from Indian coleus (Coleus forskohlii), a member of the mint family. It has been used primarily for its antiasthmatic, spasmolytic, and antihypertensive effects. It is believed to activate adenylate cyclase, increasing intracellular cyclic AMP (cAMP) concentrations and activating a number of key enzymatic pathways.28
The findings of a recent observational study have spurred the use of forskolin in the treatment of recurrent UTI.29 In the study, conducted on mice, when forskolin was injected into the bladder, intracellular E. coli decreased.
It is theorized that the incorporation of bacteria into intracellular vesicles of the bladder prevents exposure to antibiotics. When combined with an antibiotic, forskolin may increase bacterial elimination and thus lower the risk of recurrent infection. However, no randomized trials have evaluated the efficacy of this treatment.
Patients who are already taking antihypertensive medications should be cautious when using this herb, as it may lead to a drop in blood pressure.
Behavior changes are risk-free
One of the natural mechanisms that promotes bacterial elimination and prevents bacterial growth is urination. A recent review article on the subject found several contradictory studies on the effect of fluid intake on the risk of UTI.30 Although there is no definitive evidence that susceptibility to UTI is linked to fluid intake, adequate hydration may reduce the risk of recurrent infection.
Similarly, voiding shortly after sexual intercourse may prevent UTI. One case-control study found a modest protective effect in patients who voided after intercourse.31
Clinical recommendations
Given the low risk of these measures, it seems reasonable to recommend postcoital voiding and increased fluid intake to prevent recurrent UTI.
A focus on symptoms
Phenazopyridine, the chemical found in numerous OTC medications, such as Pyridium, AZO, and Uristat, was discovered by Swiss chemist Bernhard Joos in the 1950s. Its mechanism of action is still unclear, but approximately 65% of the oral dose is excreted by the kidneys, where it has a direct topical analgesic effect.32,33
Clinical recommendations
Patients should be warned that phenazopyridine will lead to orange urine discoloration.
The medication is generally well tolerated but should be used with caution in patients with acute renal failure, hemolytic anemia, or methemoglobinemia, as it may exacerbate these conditions.
Last words
Recurrent UTIs are common and impose a significant financial burden on our healthcare system. Although there are several antibiotic treatment options and dosing regimens available, increasing antibiotic resistance has made management of recurrent UTIs more difficult. Effective alternative treatments that reduce the reliance on antibiotics may minimize bacterial resistance and decrease the financial burden of this common condition.
CASE: Resolved
To reduce vaginal E. coli, the patient is started on vaginal estrogen cream. She is also advised to purchase cranberry tablets to help prevent future infections. Last, she is counseled about behavioral changes she can make and prescribed a short course of antibiotics to treat her culture-proven infection.
We want to hear from you! Tell us what you think.
URINARY PROBLEMS?
CLICK HERE to access 9 articles about treating urinary incontinence and urinary tract infections, published in OBG MANAGEMENTin 2012.
1. Raz R, Stamm W. A controlled trial of intravaginal estriol in postmenopausal women with recurrent urinary tract infections. N Engl J Med. 1993;329(11):753-756.
2. Perrotta C, Aznar M, Mejia R, Albert X, Ng CW. Oestrogens for preventing recurrent urinary tract infection in postmenopausal women. Cochrane Database Syst Rev. 2008;2:CD005131.-
3. Mayrer AR, Andriole VT. Urinary tract antiseptics. Med Clin North Am. 1982;66(1):199-208.
4. Jepson RG, Craig JC. A systematic review of the evidence for cranberries and blueberries in UTI prevention. Mol Nutr Food Res. 2007;51(6):738-745.
5. Salvatore S, Salvatore S, Cattoni E, et al. Urinary tract infections in women. Eur J Obstet Gynecol Reprod Biol. 2011;156(2):131-136.
6. Jepson RG, Craig JC. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev. 2008;1:CD001321.-
7. Stapleton AE, Dziura J, Hooton TM, et al. Recurrent urinary tract infection and urinary Escherichia coli in women ingesting cranberry juice daily: a randomized controlled trial. Mayo Clin Proc. 2012;87(2):143-150.
8. Barbosa-Cesnik C, Brown MB, Buxton M, Zhang L, DeBusscher J, Foxman B. Cranberry juice fails to prevent recurrent urinary tract infection: results from a randomized placebo-controlled trial. Clin Infect Dis. 2011;52(1):23-30.
9. Beerepoot MAJ, Reit G, Nys S, et al. Cranberries vs antibiotics to prevent urinary tract infections. Arch Intern Med. 2011;171(14):1270-1278.
10. McMurdo MET, Argo I, Phillips G, Daly F, Davey P. Cranberry or trimethoprim for the prevention of recurrent urinary tract infections? A randomized controlled trial in older women. J Antimicrob Chemother. 2009;63(2):389-395.
11. Barrons R, Tassone D. Use of Lactobacillus probiotics for bacterial genitourinary infections in women: a review. Clinical Therapeutics. 2008;30(3):453-468.
12. Miller JL, Krieger JN. Urinary tract infections: cranberry juice underwear, and probiotics in the 21st century. Urol Clin N Am. 2002;29(3):695-699.
13. Osset J, Bartolome R, Garcia E, et al. Assessment of the capacity of Lactobacillus to inhibit the growth of uropathogens and block their adhesion to vaginal epithelial cells. J Infect Dis. 2001;183(3):485-491.
14. Stapleton AE, Au-Yeung M, Hooton TM, et al. Randomized, placebo-controlled phase 2 trial of Lactobacillus crispatus probiotic given intravaginally for prevention of recurrent urinary tract infection. Clin Infect Dis. 2011;52(10):1212-1217.
15. Castello T, Girona L, Gomez MR, Mena Mur A, Garcia L. The possible value of ascorbic acid as a prophylactic agent for urinary tract infection. Spinal Cord. 1996;34(10):592-593.
16. Gleckman R, Alvarez S, Joubert DW, Matthews SJ. Drug therapy reviews: methenamine mandelate and methenamine hippurate. Am J Hosp Pharm. 1979;36(11):1509-1512.
17. Vainrub B, Musher DM. Lack of effect of methenamine in suppression of or prophylaxis against, chronic urinary tract infection. Antimicrob Agents Chemother. 1977;12(5):625-629.
18. Lee BB, Simpson JM, Craig JC, Bhuta T. Methenamine hippurate for preventing urinary tract infections. Cochrane Database Syst Rev. 2007;4:CD003265.-
19. Kevorkian CG, Merritt JL, Ilstrup DM. Methenamine mandelate with acidification: an effective urinary antiseptic in patients with neurogenic bladder. Mayo Clin Proc. 1984;59(8):523-529.
20. Wainwright M, Stanforth A, Jones R, Loughran C, Meegan K. Photoantimicrobials as a potential local approach to geriatric UTIs. Lett Appl Microbiol. 2010;50(5):486-492.
21. Bannwart C, Hagmaier V, Straumann E, Hofer H, Buillemier JP, Trutishauser G. Modification of urinary pH through ascorbic acid. Helv Chir Acta. 1981;48(3-4):425-428.
22. Hetey SK, Kleinberg ML, Parker WD, Johnson EW. Effect of ascorbic acid on urine pH in patients with injured spinal cords. Am J Hosp Pharm. 1980;37(2):235-237.
23. Ochoa-Brust GJ, Fernandez AR, Villanueva-Ruiz GJ, et al. Daily intake of 100 mg ascorbic acid as urinary tract infection prophylactic agent during pregnancy. Acta Obstet Gynecol Scand. 2007;86(7):783-787.
24. Turi M, Turi E, Kotjalg S, Mikelsaar M. Influence of aqueous extracts of medicinal plants on surface hydrophobicity of Escherichia coli strains of different origin. APMIS. 1997;105(12):956-962.
25. Beaux D, Fleurentin J, Mortier F. Effect of extracts of Orthosiphon stamineus Benth Hieracium pilosellaL., Sambucus nigra L. and Arctostaphylos uva-ursi (L.) Spreng. in rats. Phytother Res. 1999;13(3):222-225.
26. Kubo M, Ito M, Nakata H, Matsuda H. Pharmacological studies on leaf of Arctostaphylos uva-ursi (L.) Spreng. I. Combined effect of 50% methanolic extract from Arctostaphylos uva-ursi (L.) Spreng. (bearberry leaf) and prednisolone on immuno-inflammation [article in Japanese]. Yakugaku Zasshi. 1990;110(1):59-67.
27. Larsson B, Jonasson A, Fianu S. Prophylactic effect of UVA-E in women with recurrent cystitis: a preliminary report. Curr Ther Res. 1993;53(4):441-443.
28. Christenson JT, Thulesius D, Nazzal MM. The effect of forskolin on blood flow platelet metabolism, aggregation and ATP release. Vasa. 1995;24(1):56-61.
29. Bishop BL, Duncan MJ, Song J, Li G, Zaas D, Abraham SN. Cyclic AMP-regulated exocytosis of Escherichia coli from infected bladder epithelial cells. Nat Med. 2007;13(5):625-630.
30. Beetz R. Mild dehydration: a risk factor of urinary tract infection? Eur J Clin Nutr. 2003;57(Suppl 2):S52-58.
31. Foxman B, Chi JW. Health behavior and urinary tract infection in college-aged women. J Clin Epidemiol. 1990;43(4):329-337.
32. Thomas BH, Whitehouse LW, Solomonraj G, Paul CJ. Excretion of phenazopyridine and its metabolites in the urine of humans rats, mice, and guinea pigs. J Pharm Sci. 1990;79(4):321-325.
33. Aizawa N, Wyndaele JJ. Effects of phenazopyridine on rat bladder primary afferent activity and comparison with lidocaine and acetaminophen. Neurourol Urodyn. 2010;29(8):1445-1550.
1. Raz R, Stamm W. A controlled trial of intravaginal estriol in postmenopausal women with recurrent urinary tract infections. N Engl J Med. 1993;329(11):753-756.
2. Perrotta C, Aznar M, Mejia R, Albert X, Ng CW. Oestrogens for preventing recurrent urinary tract infection in postmenopausal women. Cochrane Database Syst Rev. 2008;2:CD005131.-
3. Mayrer AR, Andriole VT. Urinary tract antiseptics. Med Clin North Am. 1982;66(1):199-208.
4. Jepson RG, Craig JC. A systematic review of the evidence for cranberries and blueberries in UTI prevention. Mol Nutr Food Res. 2007;51(6):738-745.
5. Salvatore S, Salvatore S, Cattoni E, et al. Urinary tract infections in women. Eur J Obstet Gynecol Reprod Biol. 2011;156(2):131-136.
6. Jepson RG, Craig JC. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev. 2008;1:CD001321.-
7. Stapleton AE, Dziura J, Hooton TM, et al. Recurrent urinary tract infection and urinary Escherichia coli in women ingesting cranberry juice daily: a randomized controlled trial. Mayo Clin Proc. 2012;87(2):143-150.
8. Barbosa-Cesnik C, Brown MB, Buxton M, Zhang L, DeBusscher J, Foxman B. Cranberry juice fails to prevent recurrent urinary tract infection: results from a randomized placebo-controlled trial. Clin Infect Dis. 2011;52(1):23-30.
9. Beerepoot MAJ, Reit G, Nys S, et al. Cranberries vs antibiotics to prevent urinary tract infections. Arch Intern Med. 2011;171(14):1270-1278.
10. McMurdo MET, Argo I, Phillips G, Daly F, Davey P. Cranberry or trimethoprim for the prevention of recurrent urinary tract infections? A randomized controlled trial in older women. J Antimicrob Chemother. 2009;63(2):389-395.
11. Barrons R, Tassone D. Use of Lactobacillus probiotics for bacterial genitourinary infections in women: a review. Clinical Therapeutics. 2008;30(3):453-468.
12. Miller JL, Krieger JN. Urinary tract infections: cranberry juice underwear, and probiotics in the 21st century. Urol Clin N Am. 2002;29(3):695-699.
13. Osset J, Bartolome R, Garcia E, et al. Assessment of the capacity of Lactobacillus to inhibit the growth of uropathogens and block their adhesion to vaginal epithelial cells. J Infect Dis. 2001;183(3):485-491.
14. Stapleton AE, Au-Yeung M, Hooton TM, et al. Randomized, placebo-controlled phase 2 trial of Lactobacillus crispatus probiotic given intravaginally for prevention of recurrent urinary tract infection. Clin Infect Dis. 2011;52(10):1212-1217.
15. Castello T, Girona L, Gomez MR, Mena Mur A, Garcia L. The possible value of ascorbic acid as a prophylactic agent for urinary tract infection. Spinal Cord. 1996;34(10):592-593.
16. Gleckman R, Alvarez S, Joubert DW, Matthews SJ. Drug therapy reviews: methenamine mandelate and methenamine hippurate. Am J Hosp Pharm. 1979;36(11):1509-1512.
17. Vainrub B, Musher DM. Lack of effect of methenamine in suppression of or prophylaxis against, chronic urinary tract infection. Antimicrob Agents Chemother. 1977;12(5):625-629.
18. Lee BB, Simpson JM, Craig JC, Bhuta T. Methenamine hippurate for preventing urinary tract infections. Cochrane Database Syst Rev. 2007;4:CD003265.-
19. Kevorkian CG, Merritt JL, Ilstrup DM. Methenamine mandelate with acidification: an effective urinary antiseptic in patients with neurogenic bladder. Mayo Clin Proc. 1984;59(8):523-529.
20. Wainwright M, Stanforth A, Jones R, Loughran C, Meegan K. Photoantimicrobials as a potential local approach to geriatric UTIs. Lett Appl Microbiol. 2010;50(5):486-492.
21. Bannwart C, Hagmaier V, Straumann E, Hofer H, Buillemier JP, Trutishauser G. Modification of urinary pH through ascorbic acid. Helv Chir Acta. 1981;48(3-4):425-428.
22. Hetey SK, Kleinberg ML, Parker WD, Johnson EW. Effect of ascorbic acid on urine pH in patients with injured spinal cords. Am J Hosp Pharm. 1980;37(2):235-237.
23. Ochoa-Brust GJ, Fernandez AR, Villanueva-Ruiz GJ, et al. Daily intake of 100 mg ascorbic acid as urinary tract infection prophylactic agent during pregnancy. Acta Obstet Gynecol Scand. 2007;86(7):783-787.
24. Turi M, Turi E, Kotjalg S, Mikelsaar M. Influence of aqueous extracts of medicinal plants on surface hydrophobicity of Escherichia coli strains of different origin. APMIS. 1997;105(12):956-962.
25. Beaux D, Fleurentin J, Mortier F. Effect of extracts of Orthosiphon stamineus Benth Hieracium pilosellaL., Sambucus nigra L. and Arctostaphylos uva-ursi (L.) Spreng. in rats. Phytother Res. 1999;13(3):222-225.
26. Kubo M, Ito M, Nakata H, Matsuda H. Pharmacological studies on leaf of Arctostaphylos uva-ursi (L.) Spreng. I. Combined effect of 50% methanolic extract from Arctostaphylos uva-ursi (L.) Spreng. (bearberry leaf) and prednisolone on immuno-inflammation [article in Japanese]. Yakugaku Zasshi. 1990;110(1):59-67.
27. Larsson B, Jonasson A, Fianu S. Prophylactic effect of UVA-E in women with recurrent cystitis: a preliminary report. Curr Ther Res. 1993;53(4):441-443.
28. Christenson JT, Thulesius D, Nazzal MM. The effect of forskolin on blood flow platelet metabolism, aggregation and ATP release. Vasa. 1995;24(1):56-61.
29. Bishop BL, Duncan MJ, Song J, Li G, Zaas D, Abraham SN. Cyclic AMP-regulated exocytosis of Escherichia coli from infected bladder epithelial cells. Nat Med. 2007;13(5):625-630.
30. Beetz R. Mild dehydration: a risk factor of urinary tract infection? Eur J Clin Nutr. 2003;57(Suppl 2):S52-58.
31. Foxman B, Chi JW. Health behavior and urinary tract infection in college-aged women. J Clin Epidemiol. 1990;43(4):329-337.
32. Thomas BH, Whitehouse LW, Solomonraj G, Paul CJ. Excretion of phenazopyridine and its metabolites in the urine of humans rats, mice, and guinea pigs. J Pharm Sci. 1990;79(4):321-325.
33. Aizawa N, Wyndaele JJ. Effects of phenazopyridine on rat bladder primary afferent activity and comparison with lidocaine and acetaminophen. Neurourol Urodyn. 2010;29(8):1445-1550.
How reliable is self-testing for gonorrhea and chlamydia among men who have sex with men?
Background Recent studies have demonstrated a high prevalence of pharyngeal (P) and rectal (R) Neisseria gonorrhoeae (GC) and Chlamydia trachomatis (CT) infections among men who have sex with men (MSM). Guidelines by the Centers for Disease Control and Prevention recommend testing at least annually. But surveys of medical providers suggest that adherence to these guidelines is minimal as a result of limited time and staff. Because of these concerns, we evaluated the feasibility and accuracy of patient self-testing.
Methods Three-hundred seventy-four patients at a Washington, DC clinic who identified themselves as MSM and requested testing for sexually transmitted infections (STIs) participated in the study. Patients performed self-screening using the Gen-Probe APTIMA Combo 2 (AC2) kit after viewing written and pictorial instructions. Trained providers also screened patients. We randomized the order in which patients or providers performed testing.
Results Among those receiving specific tests, 8% of patients tested positive for R-GC, 9.3% for P-GC, 12.7% for R-CT, and 1.3% for P-CT. We performed McNemar tests, stratified by infection type and anatomic site to evaluate concordance. Self-administered testing was significantly better at identifying P-GC (discordant: 3%) and R-GC (discordant: 2.9%) (P≤.01), and had results similar to provider- administered testing for P-CT (discordant: 0.5%) and R-CT (discordant: 1.1%) detection.
Conclusions The equivalent or better detection rates for rectal and oral gonorrhea and chlamydia among patients suggest that patients are capable of performing their own screening for STIs, which may increase infection detection and treatment.
The prevalence of Neisseria gonorrhoeae (GC) and Chlamydia trachomatis (CT) infections among men who have sex with men (MSM) are common but unfortunately difficult to identify as a result of their anatomic location and lack of symptoms. In recent studies, 3.7% to 14.9% of MSM tested positive for GC, and 1.7% to 10.7% tested positive for CT on a first screening.1-4 Even more striking, however, was that many of these infections were extragenital and asymptomatic, with rectal GC infections 5 times more common than urethral in one study,3 and more than 80% of rectal GC and CT infections reportedly asymptomatic in another.2
Given the prevalence of undetected infection, the Centers for Disease Control and Prevention (CDC) recommends screening all sexually active MSM at least yearly for rectal GC and CT and pharyngeal GC infections in addition to urethral infections.5 However, research suggests that relatively few physicians follow these recommendations. In a survey of 3509 physicians, less than 14% reported screening their male patients for gonorrhea and chlamydia.6 In another survey, approximately one-third of providers reported not having enough staff to talk with patients about sexually transmitted infections (STIs) and testing, not having enough time in patient visits, and having difficulty keeping up with guidelines for caring for high-risk patients, including MSM.7
These studies raise concern that GC and CT infections will go undiagnosed; failure to detect these infections in MSM is particularly dangerous, given the STIs’ relationship to human immunodeficiency virus (HIV) transmission.8 Urethral GC infections have been shown to increase shedding of HIV in semen,9 and a recent study of MSM also demonstrated that having had multiple rectal GC or CT infections within a 2-year period made HIV seroconversion more likely.10
Due to the importance of identifying GC and CT infections and providers’ concerns about lack of time to do so, studies have explored the possibility of patient-administered testing, which has numerous potential benefits. It decreases the time that a health care provider has to spend on STI testing, and it could lead to screening of larger numbers of patients. It may also enable providers to reach patient populations that are often not appropriately screened, including MSM, prison inmates, homeless patients, drug users, adolescents, and patients in rural or disadvantaged areas.11-19
Comparisons of patient- and clinician-collected samples have yielded encouraging results about the ability of MSM to perform self-administered testing. There was 98% concordance between patient and provider results for rectal GC/CT swabs in one study.20 And another study found that self-collected rectal swabs had equivalent or better sensitivity and specificity for GC/CT detection than provider-collected swabs.21
Only one study has explored both pharyngeal and rectal self-testing of MSM patients, and it found that patient and provider results were concordant for 91.6% of rectal specimens and 93.6% of pharyngeal specimens. Most discordant cases involved patient-identified positives where the provider test was negative. The study authors considered these likely false positives; most occurred in patients who were positive for GC at another site, making cross-contamination probable.22 It is important to investigate further, however, because it is also possible that patients were identifying cases that providers missed.
The aim of our study, therefore, was to explore the ability of MSM patients to perform both pharyngeal and rectal testing for gonorrhea and chlamydia by evaluating the concordance of patient- and provider- administered testing results. We designed the study so that both patients and trained providers performed testing using Gen-Probe’s APTIMA Combo 2 (AC2) kits at pharyngeal, rectal, or both sites, depending on the patient’s recent sexual practices. As discussed, prior studies suggested that concordance would be good for rectal swab specimens. But only one study had examined pharyngeal swab concordance in addition to rectal, and it led to concerns about patient-generated false positives. We wanted our study to evaluate whether patient-administered testing produced accurate results for both pharyngeal and rectal specimens, and whether patient testing behaviors led to cross-contamination and subsequent false-positives when performing both tests.
METHODS
Patient recruitment and eligibility
We recruited patients from STI testing clinics and from primary and HIV care clinics at the Whitman-Walker Clinic in Washington, DC from September 15, 2009 to April 19, 2011. Eligible participants were men who’d had sex with men in the last 6 months and who wanted testing for gonorrhea and chlamydia. The presence of symptoms, reports of condom use during sex, and HIV status did not affect eligibility.
Interested patients signed a consent form and completed a behavioral questionnaire, which included questions about demographics and sexual behavior. A patient’s responses to this questionnaire determined whether he was eligible to participate and the type of testing needed. For example, if a patient had had only oral or anal sex but not both, we limited testing to either pharyngeal or rectal swabbing.
Testing procedures
We randomized patients to either perform self-testing first or to have provider-administered testing first. When patients were ready to self-administer the swabs, we gave them placards that explained how to properly collect samples23 and Gen-Probe AC2 testing kits (Hologic Gen-Probe, San Diego, Calif) for each test they needed to perform. The provider remained in the room while the patient performed the testing to ensure that the patient made an attempt at screening and to identify any common problems with the instructions. If the provider observed problems with how the patient performed the screening, he or she recorded that on a spreadsheet after the patient left.
The 4 providers who performed testing (a nursing student, a medical student, and 2 clinical research assistants) had all been previously trained in STI testing techniques by clinic MDs. When these providers performed testing, they swabbed the patient twice at each site. One of these swabs was stored for research testing, and the other went immediately to the clinic laboratory for testing so that the patient could receive the standard of care antibiotic treatment if the test was positive. The designated research samples were tested in a Gen-Probe laboratory in California.
Statistical methods
Based on a previous study by Lampinen et al that examined concordance between patient- and provider-obtained rectal swabs, we planned on a total sample of 360 patients to achieve 80% power in detecting a difference in positive tests of 5% between patients and clinicians at a one-sided 5% significance level.24 This plan assumed that the percentage of discordant pairs would be 15%, where one pair consists of one test result each from a clinician and a patient at the same site. We performed sample-size calculations in nQuery Advisor version 6.0 (Statistical Solutions, Saugus, Mass). Ultimately, we enrolled 374 men in the study. We tested 5 patients twice, but only their first screening was included in the primary analyses.
We entered demographic and behavioral data from the patient questionnaires into an online database. We also generated descriptive statistics for demographics and baseline characteristics from the questionnaires.
We performed an exact McNemar’s test for each anatomic site and STI to evaluate whether there were significant differences between patient- and provider-performed swabs. We also calculated Kappa coefficients for each site and STI as a measure of concordance. We regarded as positive any test results that were equivocal, because in clinical practice a provider would likely provide treatment. However, we also performed McNemar testing and Kappa calculations with these results excluded and classified as negative to ensure that no significant differences resulted. We evaluated statistical significance at the 0.05 level (2-sided), and performed all analyses in SAS software version 9.2 (SAS Institute, Cary, NC).
RESULTS
The patients who enrolled in the study represented a wide range of ages and ethnic backgrounds, with a median age of 33 years and with Caucasian patients accounting for 54.8%. Patients who had had sex with only men in the past year accounted for 89.8% of the sample, while 8.6% had both male and female partners (the final 1.6% had either no sex partners or missing data). The average number of male partners in the last 2 months was 2. As for sexual practice, 86.9% had insertive oral intercourse in the past year, 70.8% had insertive anal intercourse, 87.2% had receptive oral intercourse, and 67.9% had receptive anal intercourse (TABLE 1).
Considering only provider-identified positives, 5.1% of the patients tested positive for rectal gonorrhea, 11.6% for rectal chlamydia, 6.3% for pharyngeal gonorrhea, and 0.8% for pharyngeal chlamydia (TABLE 2). Considering both provider- and patient-identified positives, 8.0% of patients tested positive for rectal gonorrhea, 9.3% for pharyngeal gonorrhea, 12.7% for rectal chlamydia, and 1.3% for pharyngeal chlamydia. Five equivocal results were identified—2 for a patient rectal gonorrhea test, one for a patient pharyngeal gonorrhea test, one for a provider pharyngeal gonorrhea test, and one for a provider rectal chlamydia test.
In only one case did a provider identify a positive result when the patient’s result was negative. In 23 cases, however, the patient identified a positive result when the provider’s result was negative. Patients identified significantly more positives for rectal and pharyngeal gonorrhea than providers, but there were no significant differences in patient and provider results for the chlamydia tests.
Even with these 24 discordant results, there was ≥75% concordance between patient and provider results on all tests, with very strong concordance (95%) for rectal chlamydia results (TABLE 2). When we re-ran the McNemar tests and the Kappa coefficients with equivocal results considered missing and negative, there were no statistically significant differences when compared with the calculations done with equivocal results considered positive.
Some difficulties observed with self-testing. Observing providers noted anecdotally that there were minor difficulties with the self-administered testing instructions. Three patients spilled the preservative liquid in which swabs are placed, 5 patients used the incorrect swab to perform testing, and 2 other patients had samples that were noted as compromised by the provider. None of these documented problems involved the 24 discordant cases.
TABLE 1
Characteristics of men participating in the study
| Demographic | N=374 |
|---|---|
| Age, y | |
| Median | 33 |
| Range | 18-70 |
| n (%) | |
| Race/ethnicity | |
| White/non-Hispanic | 205 (54.8) |
| Black/non-Hispanic | 85 (22.7) |
| Latino/Hispanic | 40 (10.7) |
| Asian | 13 (3.5) |
| Mixed | 8 (2.1) |
| Other | 19 (5.1) |
| Missing data | 4 (1.1) |
| Modes of GC/CT testing | |
| Rectal and pharyngeal | 272 (72.7) |
| Rectal only | 5 (1.3) |
| Pharyngeal only | 97 (25.9) |
| Sexual partner(s) in the last 12 months | |
| Men | 336 (89.8) |
| Men and women | 32 (8.6) |
| None | 1 (0.3) |
| Missing data | 5 (1.3) |
| Number of male sexual partners in the past 30 days | |
| 0-1 | 178 (47.6) |
| 2-3 | 130 (34.8) |
| 4 or more | 64 (17.1) |
| Missing data | 2 (0.5) |
| Number of male sexual partners in the past 60 days | |
| 0-1 | 104 (27.8) |
| 2-3 | 135 (36.1) |
| 4 or more | 133 (35.6) |
| Missing data | 2 (0.5) |
| Practiced insertive oral intercourse in past 12 months | |
| Yes | 325 (86.9) |
| No | 20 (5.4) |
| Missing data | 29 (7.7) |
| Practiced insertive anal intercourse in past 12 months | |
| Yes | 265 (70.8) |
| No | 78 (20.9) |
| Missing data | 31 (8.3) |
| Practiced receptive oral intercourse in past 12 months | |
| Yes | 326 (87.2) |
| No | 20 (5.3) |
| Missing data | 28 (7.5) |
| Practiced receptive anal intercourse in past 12 months | |
| Yes | 254 (67.9) |
| No | 90 (24.1) |
| Missing data | 30 (8.0) |
| CT, Chlamydia trachomatis; GC, Neisseria gonorrhoeae. | |
TABLE 2
Comparison of provider and patient testing results for GC/CT by anatomic site reveals ≥75% concordance on all tests
| Patient test result | Total tests, N | Provider positive test result, n (%) | Provider negative test result, n (%) | P value | Kappa coefficient |
|---|---|---|---|---|---|
| Rectal GC Patient positive test result Patient negative test result | 276 | 14 (5.1) 0 | 8 (2.9)* 254 (92) | <.01 | 0.76 |
| Pharyngeal GC Patient positive test result Patient negative test result | 367 | 23 (6.3) 1 (0.3)* | 10 (2.7)* 333 (90.7) | .01 | 0.79 |
| Rectal CT Patient positive test result Patient negative test result | 276 | 32 (11.6) 0 | 3 (1.1)* 241 (87.3) | .25 | 0.95 |
| Pharyngeal CT Patient positive test result Patient negative test result | 367 | 3 (0.8) 0 | 2 (0.5)* 362 (98.7) | .50 | 0.75 |
| CT, Chlamydia trachomatis; GC, Neisseria gonorrhoeae. *Discordant patient-provider test results. | |||||
DISCUSSION
The prevalence of gonorrhea and chlamydia in this study population was similar to what has been observed in previous studies of MSM,1-4 which confirms the need for improved detection of infections. Self- administered testing is one possible means of increasing the number of patients who are screened and treated, as the results of this study suggest it is equally or more accurate than provider-administered testing at detecting cases of gonorrhea and chlamydia.
Patient and provider results were equivalent for chlamydia detection, and patients appeared to identify more cases of gonorrhea, although interpretation of the significance of this finding is difficult given the relatively small number of cases. However, it is likely that the 23 cases in which patients identified positives that providers did not were true positives, given the sensitivity (84%-100%) and specificity (≥99.4%) of the AC2 test for detecting GC and CT.25
Assuming that our population has a similar prevalence of these STIs as prior studies, we would expect positive predictive values of approximately 100% for rectal GC, 95% for pharyngeal GC, 86.4% for rectal CT, and 71.4% for pharyngeal CT.26
Possible explanations for patients achieving better results than providers in some cases. The most likely explanation for better patient performance on some of the tests is that patients swabbed more meticulously and contacted more surface area.
This was also seen in a study that compared the ability of patients and physicians to identify human papillomavirus infection in swabs taken from areas where skin scraping had been performed. Patients were found to collect an appropriate sample significantly more often, which was thought to be due to physician hesitation to thoroughly scrape the patient’s skin.27 In our study, patients were anecdotally observed to be less likely to gag on a self-administered throat swab and to have less visible tensing of the rectal sphincter on self-administered rectal swab, which could have contributed to improved results.
Potential changes to the patient instructions before clinical implementation. These results suggest that self-administered testing could be substituted for clinician-administered testing, potentially improving detection. But widespread implementation would require a few modifications to the testing instructions based on the trained providers’ observations. Although the evidence is anecdotal, providers noted that several patients had difficulty with the instructions. For example, the placard said to use only the swab with the “blue shaft,” but 5 patients got confused and used the white swab either in addition to or instead of the blue swab. (The additional white swab was intended for use in making wet preps, when women are tested.) Many more patients ultimately used the correct swab, but appeared confused by the presence of the additional swab in the kit.
The confusion in these situations might have been avoided if the instructions had told men to throw one swab away and to use only the “blue swab” or the swab with the “blue handle” to avoid potential confusion over the word “shaft.” Another helpful modification to the instructions would be to alert men to the presence of the preservative liquid in the tubes. Several patients laid the tube horizontally with the cap off and spilled much of the liquid. It was still possible to test these samples, and there were no discrepancies between patient and provider results involving them. But ensuring standardization of the test tube contents should still be a priority in editing the instructions.
Incorporating self-testing into clinical practice. While the results of this study suggest that self-testing could be used with a few modifications to the instructions, how best to incorporate self-testing into the clinical setting still needs to be addressed. It might be possible for patients to simply perform testing after a physical exam; for patients to come in when it is convenient for them and leave a sample in the lab; or even for patients to perform testing at home and bring the swabs back to their clinic at a later time.
We obtained the results in this study when patients performed testing in a clinic with a trained provider in the room. One concern in implementing widespread self-testing would be that a provider’s presence in our study might have made patients more likely to spend the time needed to read instructions thoroughly and to put effort into performing the test correctly. However, it is also possible that knowing a provider will be duplicating the testing could lead to decreased patient effort. It may be that having responsibility for one’s own test results is what ensures adequate performance.
Further studies could explore the impact of a provider in the room, but studies have already examined testing done in private and yielded similar results for concordance, which suggests that any impact of the provider’s presence was relatively minimal. A 2009-2010 study at a London clinic, for example, allowed patients to perform testing privately following instructions from a nurse and identified a 9.8% prevalence of rectal CT infection and a 4.2% prevalence of rectal GC infection. These results are similar to those seen in our study and therefore suggest that patients were appropriately identifying infections without observation.28
Another study published in 2012 demonstrated that GC/CT testing swabs sent through the mail without any accompanying transport medium yielded results equivalent to those for swabs shipped in the liquid medium. This approach would make testing at home significantly easier, as patients would not have to be concerned about appropriate storage of their samples before returning them to a clinic.29
Applicability to female patients. Implementation of self-administered testing should be considered for female patients. In fact, most prior studies on the feasibility of self-testing have focused on women, as detection of their chlamydia and gonorrhea infections is equally critical. CDC guidelines stress the importance of yearly chlamydia screening for all women <25 years and for women >25 years who are at high risk (ie, multiple partners); and yearly gonorrhea screening for women at high risk, given the risk of medical complications including pelvic inflammatory disease and infertility if infections are missed.5
Researchers have found that after women participate in self-testing, they report that they would get STI testing more regularly if they could perform it themselves.19,30 Additionally, in studies similar to ours, women performing testing for gonorrhea and chlamydia using self-collected vaginal swabs have achieved similar sensitivity and specificity results to provider-performed testing.12,15,31
Study limitations. This was a self- selected MSM sample seeking STI testing from an urban community health center. Thus, one might assume that the detection of pharyngeal and rectal gonorrhea and chlamydia infections was higher in this sample compared with the general MSM population. That seems unlikely, however, given the similarity (noted earlier) between our findings and data reported in previous studies.1-4 Additionally, the presence of a provider in the room may have influenced patient performance, as we discussed earlier.
It therefore appears that self-administered testing could have universal applicability. Once optimal ways to incorporate self-testing for both men and women are identified, providers should be able to comply with the CDC testing guidelines without an increase in time or staff needed, thereby leading to increased detection and treatment of STIs and benefits for both patients and providers.
CORRESPONDENCE
Michael W. Plankey, PhD, Georgetown University Medical Center, Department of Medicine, Division of Infectious Diseases, 2115 Wisconsin Avenue, NW, Suite 130, Washington, DC 20007; mwp23@georgetown.edu
1. Baker J, Plankey M, Josayma Y, et al. The prevalence of rectal, urethral, and pharyngeal Neisseria gonorrhoeae and Chlamydia trachomatis among asymptomatic men who have sex with men in a prospective cohort in Washington, D.C. AIDS Patient Care STDs. 2009;23:585-588.
2. Kent CK, Chaw JK, Wong W, et al. Prevalence of rectal, urethral, and pharyngeal chlamydia and gonorrhea detected in 2 clinical settings among men who have sex with men: San Francisco, California, 2003. Clin Infect Dis. 2005;41:67-74.
3. Mimiaga MJ, Helms DJ, Reisner SL, et al. Gonococcal, chlamydia, and syphilis infection positivity among MSM attending a large primary care clinic, Boston, 2003 to 2004. Sex Transm Dis. 2009;36:507-511.
4. Park J, Marcus JL, Pandori M, et al. Sentinel surveillance for pharyngeal chlamydia and gonorrhea among men who have sex with men—San Francisco, 2010. Sex Transm Dis. 2012;39:482-484.
5. Workowski KA, Berman S. Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
6. St Lawrence JS, Montano DE, Kasprzyk D, et al. STD screening, testing, case reporting, and clinical and partner notification practices: a national survey of US physicians. Am J Public Health. 2002;92:1784-1788.
7. Mark H, Irwin K, Sternberg M, et al. Providers’ perceived barriers to sexually transmitted disease care in 2 large health maintenance organizations. Sex Transm Dis. 2008;35:184-189.
8. Xu F, Sternberg MR, Markowitz LE. Men who have sex with men in the United States: demographic and behavioral characteristics and prevalence of HIV and HSV-2 infection: results from National Health and Nutrition Examination Survey 2001-2006. Sex Transm Dis. 2010;37:399-405.
9. Cohen MS, Hoffman IF, Royce RA, et al. Reduction of concentration of HIV-1 in semen after treatment of urethritis: implications for prevention of sexual transmission of HIV-1. AIDSCAP Malawi Research Group. Lancet. 1997;349:1868-1873.
10. Bernstein KT, Marcus JL, Nieri G, et al. Rectal gonorrhea and chlamydia reinfection is associated with increased risk of HIV seroconversion. J Acquir Immune Defic Syndr. 2010;53:537-543.
11. Bradshaw CS, Pierce LI, Tabrizi SN, et al. Screening injecting drug users for sexually transmitted infections and blood borne viruses using street outreach and self collected sampling. Sex Transm Infect. 2005;81:53-58.
12. Fang J, Husman C, DeSilva L, et al. Evaluation of self-collected vaginal swab, first void urine, and endocervical swab specimens for the detection of Chlamydia trachomatis and Neisseria gonorrhoeae in adolescent females. J Pediatr Adolesc Gynecol. 2008;21:355-360.
13. Gaydos CA. Nucleic acid amplification tests for gonorrhea and chlamydia: practice and applications. Infect Dis Clin North Am. 2005;19:367-386 ix.
14. Hobbs MM, van der Pol B, Totten P, et al. From the NIH: proceedings of a workshop on the importance of self-obtained vaginal specimens for detection of sexually transmitted infections. Sex Transm Dis. 2008;35:8-13.
15. Knox J, Tabrizi SN, Miller P, et al. Evaluation of self-collected samples in contrast to practitioner-collected samples for detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis by polymerase chain reaction among women living in remote areas. Sex Transm Dis. 2002;29:647-654.
16. Lippman SA, Jones HE, Luppi CG, et al. Home-based self-sampling and self-testing for sexually transmitted infections: acceptable and feasible alternatives to provider-based screening in low-income women in Sao Paulo, Brazil. Sex Transm Dis. 2007;34:421-428.
17. Newman SB, Nelson MB, Gaydos CA, et al. Female prisoners’ p of collection methods for testing for Chlamydia trachomatis and Neisseria gonorrhoeae infection. Sex Transm Dis. 2003;30:306-309.
18. Richardson E, Sellors JW, Mackinnon S, et al. Prevalence of Chlamydia trachomatis infections and specimen collection preference among women, using self-collected vaginal swabs in community settings. Sex Transm Dis. 2003;30:880-885.
19. Wiesenfeld HC, Lowry DL, Heine RP, et al. Self-collection of vaginal swabs for the detection of Chlamydia, gonorrhea, and trichomoniasis: opportunity to encourage sexually transmitted disease testing among adolescents. Sex Transm Dis. 2001;28:321-325.
20. van der Helm JJ, Hoebe CJ, van Rooijen MS, et al. High performance and acceptability of self-collected rectal swabs for diagnosis of Chlamydia trachomatis and Neisseria gonorrhoeae in men who have sex with men and women. Sex Transm Dis. 2009;36:493-497.
21. Moncada J, Schachter J, Liska S, et al. Evaluation of self-collected glans and rectal swabs from men who have sex with men for detection of Chlamydia trachomatis and Neisseria gonorrhoeae by use of nucleic acid amplification tests. J Clin Microbiol. 2009;47:1657-1662.
22. Alexander S, Ison C, Parry J, et al. Self-taken pharyngeal and rectal swabs are appropriate for the detection of Chlamydia trachomatis and Neisseria gonorrhoeae in asymptomatic men who have sex with men. Sex Transm Infect. 2008;84:488-492.
23. San Francisco City Clinic. Patient instructions for self-collected specimens: pharyngeal and rectal. Available at: http://www.sfcityclinic.org/providers. Accessed December 15 2011.
24. Lampinen TM, Latulippe L, van Niekerk D, et al. Illustrated instructions for self-collection of anorectal swab specimens and their adequacy for cytological examination. Sex Transm Dis. 2006;33:386-388.
25. Schachter J, Moncada J, Liska S, et al. Nucleic acid amplification tests in the diagnosis of chlamydial and gonococcal infections of the oropharynx and rectum in men who have sex with men. Sex Transm Dis. 2008;35:637-642.
26. Ota KV, Tamari IE, Smieja M, et al. Detection of Neisseria gonorrhoeae and Chlamydia trachomatis in pharyngeal and rectal specimens using the BD Probetec ET system, the Gen-Probe Aptima Combo 2 assay and culture. Sex Transm Infect. 2009;85:182-186.
27. Hernandez BY, McDuffie K, Goodman MT, et al. Comparison of physician- and self-collected genital specimens for detection of human papillomavirus in men. J Clin Microbiol. 2006;44:513-517.
28. Soni S, White JA. Self-screening for Neisseria gonorrhoeae and Chlamydia trachomatis in the human immunodeficiency virus clinic—high yields and high acceptability. Sex Transm Dis. 2011;38:1107-1109.
29. Gaydos CA, Farshy C, Barnes M, et al. Can mailed swab samples be dry-shipped for the detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis by nucleic acid amplification tests? Diagn Microbiol Infect Dis. 2012;73:16-20.
30. Chernesky MA, Hook EW, 3rd, Martin DH, et al. Women find it easy and prefer to collect their own vaginal swabs to diagnose Chlamydia trachomatis or Neisseria gonorrhoeae infections. Sex Transm Dis. 2005;32:729-733.
31. Polaneczky M, Quigley C, Pollock L, et al. Use of self-collected vaginal specimens for detection of Chlamydia trachomatis infection. Obstet Gynecol. 1998;91:375-378.
Background Recent studies have demonstrated a high prevalence of pharyngeal (P) and rectal (R) Neisseria gonorrhoeae (GC) and Chlamydia trachomatis (CT) infections among men who have sex with men (MSM). Guidelines by the Centers for Disease Control and Prevention recommend testing at least annually. But surveys of medical providers suggest that adherence to these guidelines is minimal as a result of limited time and staff. Because of these concerns, we evaluated the feasibility and accuracy of patient self-testing.
Methods Three-hundred seventy-four patients at a Washington, DC clinic who identified themselves as MSM and requested testing for sexually transmitted infections (STIs) participated in the study. Patients performed self-screening using the Gen-Probe APTIMA Combo 2 (AC2) kit after viewing written and pictorial instructions. Trained providers also screened patients. We randomized the order in which patients or providers performed testing.
Results Among those receiving specific tests, 8% of patients tested positive for R-GC, 9.3% for P-GC, 12.7% for R-CT, and 1.3% for P-CT. We performed McNemar tests, stratified by infection type and anatomic site to evaluate concordance. Self-administered testing was significantly better at identifying P-GC (discordant: 3%) and R-GC (discordant: 2.9%) (P≤.01), and had results similar to provider- administered testing for P-CT (discordant: 0.5%) and R-CT (discordant: 1.1%) detection.
Conclusions The equivalent or better detection rates for rectal and oral gonorrhea and chlamydia among patients suggest that patients are capable of performing their own screening for STIs, which may increase infection detection and treatment.
The prevalence of Neisseria gonorrhoeae (GC) and Chlamydia trachomatis (CT) infections among men who have sex with men (MSM) are common but unfortunately difficult to identify as a result of their anatomic location and lack of symptoms. In recent studies, 3.7% to 14.9% of MSM tested positive for GC, and 1.7% to 10.7% tested positive for CT on a first screening.1-4 Even more striking, however, was that many of these infections were extragenital and asymptomatic, with rectal GC infections 5 times more common than urethral in one study,3 and more than 80% of rectal GC and CT infections reportedly asymptomatic in another.2
Given the prevalence of undetected infection, the Centers for Disease Control and Prevention (CDC) recommends screening all sexually active MSM at least yearly for rectal GC and CT and pharyngeal GC infections in addition to urethral infections.5 However, research suggests that relatively few physicians follow these recommendations. In a survey of 3509 physicians, less than 14% reported screening their male patients for gonorrhea and chlamydia.6 In another survey, approximately one-third of providers reported not having enough staff to talk with patients about sexually transmitted infections (STIs) and testing, not having enough time in patient visits, and having difficulty keeping up with guidelines for caring for high-risk patients, including MSM.7
These studies raise concern that GC and CT infections will go undiagnosed; failure to detect these infections in MSM is particularly dangerous, given the STIs’ relationship to human immunodeficiency virus (HIV) transmission.8 Urethral GC infections have been shown to increase shedding of HIV in semen,9 and a recent study of MSM also demonstrated that having had multiple rectal GC or CT infections within a 2-year period made HIV seroconversion more likely.10
Due to the importance of identifying GC and CT infections and providers’ concerns about lack of time to do so, studies have explored the possibility of patient-administered testing, which has numerous potential benefits. It decreases the time that a health care provider has to spend on STI testing, and it could lead to screening of larger numbers of patients. It may also enable providers to reach patient populations that are often not appropriately screened, including MSM, prison inmates, homeless patients, drug users, adolescents, and patients in rural or disadvantaged areas.11-19
Comparisons of patient- and clinician-collected samples have yielded encouraging results about the ability of MSM to perform self-administered testing. There was 98% concordance between patient and provider results for rectal GC/CT swabs in one study.20 And another study found that self-collected rectal swabs had equivalent or better sensitivity and specificity for GC/CT detection than provider-collected swabs.21
Only one study has explored both pharyngeal and rectal self-testing of MSM patients, and it found that patient and provider results were concordant for 91.6% of rectal specimens and 93.6% of pharyngeal specimens. Most discordant cases involved patient-identified positives where the provider test was negative. The study authors considered these likely false positives; most occurred in patients who were positive for GC at another site, making cross-contamination probable.22 It is important to investigate further, however, because it is also possible that patients were identifying cases that providers missed.
The aim of our study, therefore, was to explore the ability of MSM patients to perform both pharyngeal and rectal testing for gonorrhea and chlamydia by evaluating the concordance of patient- and provider- administered testing results. We designed the study so that both patients and trained providers performed testing using Gen-Probe’s APTIMA Combo 2 (AC2) kits at pharyngeal, rectal, or both sites, depending on the patient’s recent sexual practices. As discussed, prior studies suggested that concordance would be good for rectal swab specimens. But only one study had examined pharyngeal swab concordance in addition to rectal, and it led to concerns about patient-generated false positives. We wanted our study to evaluate whether patient-administered testing produced accurate results for both pharyngeal and rectal specimens, and whether patient testing behaviors led to cross-contamination and subsequent false-positives when performing both tests.
METHODS
Patient recruitment and eligibility
We recruited patients from STI testing clinics and from primary and HIV care clinics at the Whitman-Walker Clinic in Washington, DC from September 15, 2009 to April 19, 2011. Eligible participants were men who’d had sex with men in the last 6 months and who wanted testing for gonorrhea and chlamydia. The presence of symptoms, reports of condom use during sex, and HIV status did not affect eligibility.
Interested patients signed a consent form and completed a behavioral questionnaire, which included questions about demographics and sexual behavior. A patient’s responses to this questionnaire determined whether he was eligible to participate and the type of testing needed. For example, if a patient had had only oral or anal sex but not both, we limited testing to either pharyngeal or rectal swabbing.
Testing procedures
We randomized patients to either perform self-testing first or to have provider-administered testing first. When patients were ready to self-administer the swabs, we gave them placards that explained how to properly collect samples23 and Gen-Probe AC2 testing kits (Hologic Gen-Probe, San Diego, Calif) for each test they needed to perform. The provider remained in the room while the patient performed the testing to ensure that the patient made an attempt at screening and to identify any common problems with the instructions. If the provider observed problems with how the patient performed the screening, he or she recorded that on a spreadsheet after the patient left.
The 4 providers who performed testing (a nursing student, a medical student, and 2 clinical research assistants) had all been previously trained in STI testing techniques by clinic MDs. When these providers performed testing, they swabbed the patient twice at each site. One of these swabs was stored for research testing, and the other went immediately to the clinic laboratory for testing so that the patient could receive the standard of care antibiotic treatment if the test was positive. The designated research samples were tested in a Gen-Probe laboratory in California.
Statistical methods
Based on a previous study by Lampinen et al that examined concordance between patient- and provider-obtained rectal swabs, we planned on a total sample of 360 patients to achieve 80% power in detecting a difference in positive tests of 5% between patients and clinicians at a one-sided 5% significance level.24 This plan assumed that the percentage of discordant pairs would be 15%, where one pair consists of one test result each from a clinician and a patient at the same site. We performed sample-size calculations in nQuery Advisor version 6.0 (Statistical Solutions, Saugus, Mass). Ultimately, we enrolled 374 men in the study. We tested 5 patients twice, but only their first screening was included in the primary analyses.
We entered demographic and behavioral data from the patient questionnaires into an online database. We also generated descriptive statistics for demographics and baseline characteristics from the questionnaires.
We performed an exact McNemar’s test for each anatomic site and STI to evaluate whether there were significant differences between patient- and provider-performed swabs. We also calculated Kappa coefficients for each site and STI as a measure of concordance. We regarded as positive any test results that were equivocal, because in clinical practice a provider would likely provide treatment. However, we also performed McNemar testing and Kappa calculations with these results excluded and classified as negative to ensure that no significant differences resulted. We evaluated statistical significance at the 0.05 level (2-sided), and performed all analyses in SAS software version 9.2 (SAS Institute, Cary, NC).
RESULTS
The patients who enrolled in the study represented a wide range of ages and ethnic backgrounds, with a median age of 33 years and with Caucasian patients accounting for 54.8%. Patients who had had sex with only men in the past year accounted for 89.8% of the sample, while 8.6% had both male and female partners (the final 1.6% had either no sex partners or missing data). The average number of male partners in the last 2 months was 2. As for sexual practice, 86.9% had insertive oral intercourse in the past year, 70.8% had insertive anal intercourse, 87.2% had receptive oral intercourse, and 67.9% had receptive anal intercourse (TABLE 1).
Considering only provider-identified positives, 5.1% of the patients tested positive for rectal gonorrhea, 11.6% for rectal chlamydia, 6.3% for pharyngeal gonorrhea, and 0.8% for pharyngeal chlamydia (TABLE 2). Considering both provider- and patient-identified positives, 8.0% of patients tested positive for rectal gonorrhea, 9.3% for pharyngeal gonorrhea, 12.7% for rectal chlamydia, and 1.3% for pharyngeal chlamydia. Five equivocal results were identified—2 for a patient rectal gonorrhea test, one for a patient pharyngeal gonorrhea test, one for a provider pharyngeal gonorrhea test, and one for a provider rectal chlamydia test.
In only one case did a provider identify a positive result when the patient’s result was negative. In 23 cases, however, the patient identified a positive result when the provider’s result was negative. Patients identified significantly more positives for rectal and pharyngeal gonorrhea than providers, but there were no significant differences in patient and provider results for the chlamydia tests.
Even with these 24 discordant results, there was ≥75% concordance between patient and provider results on all tests, with very strong concordance (95%) for rectal chlamydia results (TABLE 2). When we re-ran the McNemar tests and the Kappa coefficients with equivocal results considered missing and negative, there were no statistically significant differences when compared with the calculations done with equivocal results considered positive.
Some difficulties observed with self-testing. Observing providers noted anecdotally that there were minor difficulties with the self-administered testing instructions. Three patients spilled the preservative liquid in which swabs are placed, 5 patients used the incorrect swab to perform testing, and 2 other patients had samples that were noted as compromised by the provider. None of these documented problems involved the 24 discordant cases.
TABLE 1
Characteristics of men participating in the study
| Demographic | N=374 |
|---|---|
| Age, y | |
| Median | 33 |
| Range | 18-70 |
| n (%) | |
| Race/ethnicity | |
| White/non-Hispanic | 205 (54.8) |
| Black/non-Hispanic | 85 (22.7) |
| Latino/Hispanic | 40 (10.7) |
| Asian | 13 (3.5) |
| Mixed | 8 (2.1) |
| Other | 19 (5.1) |
| Missing data | 4 (1.1) |
| Modes of GC/CT testing | |
| Rectal and pharyngeal | 272 (72.7) |
| Rectal only | 5 (1.3) |
| Pharyngeal only | 97 (25.9) |
| Sexual partner(s) in the last 12 months | |
| Men | 336 (89.8) |
| Men and women | 32 (8.6) |
| None | 1 (0.3) |
| Missing data | 5 (1.3) |
| Number of male sexual partners in the past 30 days | |
| 0-1 | 178 (47.6) |
| 2-3 | 130 (34.8) |
| 4 or more | 64 (17.1) |
| Missing data | 2 (0.5) |
| Number of male sexual partners in the past 60 days | |
| 0-1 | 104 (27.8) |
| 2-3 | 135 (36.1) |
| 4 or more | 133 (35.6) |
| Missing data | 2 (0.5) |
| Practiced insertive oral intercourse in past 12 months | |
| Yes | 325 (86.9) |
| No | 20 (5.4) |
| Missing data | 29 (7.7) |
| Practiced insertive anal intercourse in past 12 months | |
| Yes | 265 (70.8) |
| No | 78 (20.9) |
| Missing data | 31 (8.3) |
| Practiced receptive oral intercourse in past 12 months | |
| Yes | 326 (87.2) |
| No | 20 (5.3) |
| Missing data | 28 (7.5) |
| Practiced receptive anal intercourse in past 12 months | |
| Yes | 254 (67.9) |
| No | 90 (24.1) |
| Missing data | 30 (8.0) |
| CT, Chlamydia trachomatis; GC, Neisseria gonorrhoeae. | |
TABLE 2
Comparison of provider and patient testing results for GC/CT by anatomic site reveals ≥75% concordance on all tests
| Patient test result | Total tests, N | Provider positive test result, n (%) | Provider negative test result, n (%) | P value | Kappa coefficient |
|---|---|---|---|---|---|
| Rectal GC Patient positive test result Patient negative test result | 276 | 14 (5.1) 0 | 8 (2.9)* 254 (92) | <.01 | 0.76 |
| Pharyngeal GC Patient positive test result Patient negative test result | 367 | 23 (6.3) 1 (0.3)* | 10 (2.7)* 333 (90.7) | .01 | 0.79 |
| Rectal CT Patient positive test result Patient negative test result | 276 | 32 (11.6) 0 | 3 (1.1)* 241 (87.3) | .25 | 0.95 |
| Pharyngeal CT Patient positive test result Patient negative test result | 367 | 3 (0.8) 0 | 2 (0.5)* 362 (98.7) | .50 | 0.75 |
| CT, Chlamydia trachomatis; GC, Neisseria gonorrhoeae. *Discordant patient-provider test results. | |||||
DISCUSSION
The prevalence of gonorrhea and chlamydia in this study population was similar to what has been observed in previous studies of MSM,1-4 which confirms the need for improved detection of infections. Self- administered testing is one possible means of increasing the number of patients who are screened and treated, as the results of this study suggest it is equally or more accurate than provider-administered testing at detecting cases of gonorrhea and chlamydia.
Patient and provider results were equivalent for chlamydia detection, and patients appeared to identify more cases of gonorrhea, although interpretation of the significance of this finding is difficult given the relatively small number of cases. However, it is likely that the 23 cases in which patients identified positives that providers did not were true positives, given the sensitivity (84%-100%) and specificity (≥99.4%) of the AC2 test for detecting GC and CT.25
Assuming that our population has a similar prevalence of these STIs as prior studies, we would expect positive predictive values of approximately 100% for rectal GC, 95% for pharyngeal GC, 86.4% for rectal CT, and 71.4% for pharyngeal CT.26
Possible explanations for patients achieving better results than providers in some cases. The most likely explanation for better patient performance on some of the tests is that patients swabbed more meticulously and contacted more surface area.
This was also seen in a study that compared the ability of patients and physicians to identify human papillomavirus infection in swabs taken from areas where skin scraping had been performed. Patients were found to collect an appropriate sample significantly more often, which was thought to be due to physician hesitation to thoroughly scrape the patient’s skin.27 In our study, patients were anecdotally observed to be less likely to gag on a self-administered throat swab and to have less visible tensing of the rectal sphincter on self-administered rectal swab, which could have contributed to improved results.
Potential changes to the patient instructions before clinical implementation. These results suggest that self-administered testing could be substituted for clinician-administered testing, potentially improving detection. But widespread implementation would require a few modifications to the testing instructions based on the trained providers’ observations. Although the evidence is anecdotal, providers noted that several patients had difficulty with the instructions. For example, the placard said to use only the swab with the “blue shaft,” but 5 patients got confused and used the white swab either in addition to or instead of the blue swab. (The additional white swab was intended for use in making wet preps, when women are tested.) Many more patients ultimately used the correct swab, but appeared confused by the presence of the additional swab in the kit.
The confusion in these situations might have been avoided if the instructions had told men to throw one swab away and to use only the “blue swab” or the swab with the “blue handle” to avoid potential confusion over the word “shaft.” Another helpful modification to the instructions would be to alert men to the presence of the preservative liquid in the tubes. Several patients laid the tube horizontally with the cap off and spilled much of the liquid. It was still possible to test these samples, and there were no discrepancies between patient and provider results involving them. But ensuring standardization of the test tube contents should still be a priority in editing the instructions.
Incorporating self-testing into clinical practice. While the results of this study suggest that self-testing could be used with a few modifications to the instructions, how best to incorporate self-testing into the clinical setting still needs to be addressed. It might be possible for patients to simply perform testing after a physical exam; for patients to come in when it is convenient for them and leave a sample in the lab; or even for patients to perform testing at home and bring the swabs back to their clinic at a later time.
We obtained the results in this study when patients performed testing in a clinic with a trained provider in the room. One concern in implementing widespread self-testing would be that a provider’s presence in our study might have made patients more likely to spend the time needed to read instructions thoroughly and to put effort into performing the test correctly. However, it is also possible that knowing a provider will be duplicating the testing could lead to decreased patient effort. It may be that having responsibility for one’s own test results is what ensures adequate performance.
Further studies could explore the impact of a provider in the room, but studies have already examined testing done in private and yielded similar results for concordance, which suggests that any impact of the provider’s presence was relatively minimal. A 2009-2010 study at a London clinic, for example, allowed patients to perform testing privately following instructions from a nurse and identified a 9.8% prevalence of rectal CT infection and a 4.2% prevalence of rectal GC infection. These results are similar to those seen in our study and therefore suggest that patients were appropriately identifying infections without observation.28
Another study published in 2012 demonstrated that GC/CT testing swabs sent through the mail without any accompanying transport medium yielded results equivalent to those for swabs shipped in the liquid medium. This approach would make testing at home significantly easier, as patients would not have to be concerned about appropriate storage of their samples before returning them to a clinic.29
Applicability to female patients. Implementation of self-administered testing should be considered for female patients. In fact, most prior studies on the feasibility of self-testing have focused on women, as detection of their chlamydia and gonorrhea infections is equally critical. CDC guidelines stress the importance of yearly chlamydia screening for all women <25 years and for women >25 years who are at high risk (ie, multiple partners); and yearly gonorrhea screening for women at high risk, given the risk of medical complications including pelvic inflammatory disease and infertility if infections are missed.5
Researchers have found that after women participate in self-testing, they report that they would get STI testing more regularly if they could perform it themselves.19,30 Additionally, in studies similar to ours, women performing testing for gonorrhea and chlamydia using self-collected vaginal swabs have achieved similar sensitivity and specificity results to provider-performed testing.12,15,31
Study limitations. This was a self- selected MSM sample seeking STI testing from an urban community health center. Thus, one might assume that the detection of pharyngeal and rectal gonorrhea and chlamydia infections was higher in this sample compared with the general MSM population. That seems unlikely, however, given the similarity (noted earlier) between our findings and data reported in previous studies.1-4 Additionally, the presence of a provider in the room may have influenced patient performance, as we discussed earlier.
It therefore appears that self-administered testing could have universal applicability. Once optimal ways to incorporate self-testing for both men and women are identified, providers should be able to comply with the CDC testing guidelines without an increase in time or staff needed, thereby leading to increased detection and treatment of STIs and benefits for both patients and providers.
CORRESPONDENCE
Michael W. Plankey, PhD, Georgetown University Medical Center, Department of Medicine, Division of Infectious Diseases, 2115 Wisconsin Avenue, NW, Suite 130, Washington, DC 20007; mwp23@georgetown.edu
Background Recent studies have demonstrated a high prevalence of pharyngeal (P) and rectal (R) Neisseria gonorrhoeae (GC) and Chlamydia trachomatis (CT) infections among men who have sex with men (MSM). Guidelines by the Centers for Disease Control and Prevention recommend testing at least annually. But surveys of medical providers suggest that adherence to these guidelines is minimal as a result of limited time and staff. Because of these concerns, we evaluated the feasibility and accuracy of patient self-testing.
Methods Three-hundred seventy-four patients at a Washington, DC clinic who identified themselves as MSM and requested testing for sexually transmitted infections (STIs) participated in the study. Patients performed self-screening using the Gen-Probe APTIMA Combo 2 (AC2) kit after viewing written and pictorial instructions. Trained providers also screened patients. We randomized the order in which patients or providers performed testing.
Results Among those receiving specific tests, 8% of patients tested positive for R-GC, 9.3% for P-GC, 12.7% for R-CT, and 1.3% for P-CT. We performed McNemar tests, stratified by infection type and anatomic site to evaluate concordance. Self-administered testing was significantly better at identifying P-GC (discordant: 3%) and R-GC (discordant: 2.9%) (P≤.01), and had results similar to provider- administered testing for P-CT (discordant: 0.5%) and R-CT (discordant: 1.1%) detection.
Conclusions The equivalent or better detection rates for rectal and oral gonorrhea and chlamydia among patients suggest that patients are capable of performing their own screening for STIs, which may increase infection detection and treatment.
The prevalence of Neisseria gonorrhoeae (GC) and Chlamydia trachomatis (CT) infections among men who have sex with men (MSM) are common but unfortunately difficult to identify as a result of their anatomic location and lack of symptoms. In recent studies, 3.7% to 14.9% of MSM tested positive for GC, and 1.7% to 10.7% tested positive for CT on a first screening.1-4 Even more striking, however, was that many of these infections were extragenital and asymptomatic, with rectal GC infections 5 times more common than urethral in one study,3 and more than 80% of rectal GC and CT infections reportedly asymptomatic in another.2
Given the prevalence of undetected infection, the Centers for Disease Control and Prevention (CDC) recommends screening all sexually active MSM at least yearly for rectal GC and CT and pharyngeal GC infections in addition to urethral infections.5 However, research suggests that relatively few physicians follow these recommendations. In a survey of 3509 physicians, less than 14% reported screening their male patients for gonorrhea and chlamydia.6 In another survey, approximately one-third of providers reported not having enough staff to talk with patients about sexually transmitted infections (STIs) and testing, not having enough time in patient visits, and having difficulty keeping up with guidelines for caring for high-risk patients, including MSM.7
These studies raise concern that GC and CT infections will go undiagnosed; failure to detect these infections in MSM is particularly dangerous, given the STIs’ relationship to human immunodeficiency virus (HIV) transmission.8 Urethral GC infections have been shown to increase shedding of HIV in semen,9 and a recent study of MSM also demonstrated that having had multiple rectal GC or CT infections within a 2-year period made HIV seroconversion more likely.10
Due to the importance of identifying GC and CT infections and providers’ concerns about lack of time to do so, studies have explored the possibility of patient-administered testing, which has numerous potential benefits. It decreases the time that a health care provider has to spend on STI testing, and it could lead to screening of larger numbers of patients. It may also enable providers to reach patient populations that are often not appropriately screened, including MSM, prison inmates, homeless patients, drug users, adolescents, and patients in rural or disadvantaged areas.11-19
Comparisons of patient- and clinician-collected samples have yielded encouraging results about the ability of MSM to perform self-administered testing. There was 98% concordance between patient and provider results for rectal GC/CT swabs in one study.20 And another study found that self-collected rectal swabs had equivalent or better sensitivity and specificity for GC/CT detection than provider-collected swabs.21
Only one study has explored both pharyngeal and rectal self-testing of MSM patients, and it found that patient and provider results were concordant for 91.6% of rectal specimens and 93.6% of pharyngeal specimens. Most discordant cases involved patient-identified positives where the provider test was negative. The study authors considered these likely false positives; most occurred in patients who were positive for GC at another site, making cross-contamination probable.22 It is important to investigate further, however, because it is also possible that patients were identifying cases that providers missed.
The aim of our study, therefore, was to explore the ability of MSM patients to perform both pharyngeal and rectal testing for gonorrhea and chlamydia by evaluating the concordance of patient- and provider- administered testing results. We designed the study so that both patients and trained providers performed testing using Gen-Probe’s APTIMA Combo 2 (AC2) kits at pharyngeal, rectal, or both sites, depending on the patient’s recent sexual practices. As discussed, prior studies suggested that concordance would be good for rectal swab specimens. But only one study had examined pharyngeal swab concordance in addition to rectal, and it led to concerns about patient-generated false positives. We wanted our study to evaluate whether patient-administered testing produced accurate results for both pharyngeal and rectal specimens, and whether patient testing behaviors led to cross-contamination and subsequent false-positives when performing both tests.
METHODS
Patient recruitment and eligibility
We recruited patients from STI testing clinics and from primary and HIV care clinics at the Whitman-Walker Clinic in Washington, DC from September 15, 2009 to April 19, 2011. Eligible participants were men who’d had sex with men in the last 6 months and who wanted testing for gonorrhea and chlamydia. The presence of symptoms, reports of condom use during sex, and HIV status did not affect eligibility.
Interested patients signed a consent form and completed a behavioral questionnaire, which included questions about demographics and sexual behavior. A patient’s responses to this questionnaire determined whether he was eligible to participate and the type of testing needed. For example, if a patient had had only oral or anal sex but not both, we limited testing to either pharyngeal or rectal swabbing.
Testing procedures
We randomized patients to either perform self-testing first or to have provider-administered testing first. When patients were ready to self-administer the swabs, we gave them placards that explained how to properly collect samples23 and Gen-Probe AC2 testing kits (Hologic Gen-Probe, San Diego, Calif) for each test they needed to perform. The provider remained in the room while the patient performed the testing to ensure that the patient made an attempt at screening and to identify any common problems with the instructions. If the provider observed problems with how the patient performed the screening, he or she recorded that on a spreadsheet after the patient left.
The 4 providers who performed testing (a nursing student, a medical student, and 2 clinical research assistants) had all been previously trained in STI testing techniques by clinic MDs. When these providers performed testing, they swabbed the patient twice at each site. One of these swabs was stored for research testing, and the other went immediately to the clinic laboratory for testing so that the patient could receive the standard of care antibiotic treatment if the test was positive. The designated research samples were tested in a Gen-Probe laboratory in California.
Statistical methods
Based on a previous study by Lampinen et al that examined concordance between patient- and provider-obtained rectal swabs, we planned on a total sample of 360 patients to achieve 80% power in detecting a difference in positive tests of 5% between patients and clinicians at a one-sided 5% significance level.24 This plan assumed that the percentage of discordant pairs would be 15%, where one pair consists of one test result each from a clinician and a patient at the same site. We performed sample-size calculations in nQuery Advisor version 6.0 (Statistical Solutions, Saugus, Mass). Ultimately, we enrolled 374 men in the study. We tested 5 patients twice, but only their first screening was included in the primary analyses.
We entered demographic and behavioral data from the patient questionnaires into an online database. We also generated descriptive statistics for demographics and baseline characteristics from the questionnaires.
We performed an exact McNemar’s test for each anatomic site and STI to evaluate whether there were significant differences between patient- and provider-performed swabs. We also calculated Kappa coefficients for each site and STI as a measure of concordance. We regarded as positive any test results that were equivocal, because in clinical practice a provider would likely provide treatment. However, we also performed McNemar testing and Kappa calculations with these results excluded and classified as negative to ensure that no significant differences resulted. We evaluated statistical significance at the 0.05 level (2-sided), and performed all analyses in SAS software version 9.2 (SAS Institute, Cary, NC).
RESULTS
The patients who enrolled in the study represented a wide range of ages and ethnic backgrounds, with a median age of 33 years and with Caucasian patients accounting for 54.8%. Patients who had had sex with only men in the past year accounted for 89.8% of the sample, while 8.6% had both male and female partners (the final 1.6% had either no sex partners or missing data). The average number of male partners in the last 2 months was 2. As for sexual practice, 86.9% had insertive oral intercourse in the past year, 70.8% had insertive anal intercourse, 87.2% had receptive oral intercourse, and 67.9% had receptive anal intercourse (TABLE 1).
Considering only provider-identified positives, 5.1% of the patients tested positive for rectal gonorrhea, 11.6% for rectal chlamydia, 6.3% for pharyngeal gonorrhea, and 0.8% for pharyngeal chlamydia (TABLE 2). Considering both provider- and patient-identified positives, 8.0% of patients tested positive for rectal gonorrhea, 9.3% for pharyngeal gonorrhea, 12.7% for rectal chlamydia, and 1.3% for pharyngeal chlamydia. Five equivocal results were identified—2 for a patient rectal gonorrhea test, one for a patient pharyngeal gonorrhea test, one for a provider pharyngeal gonorrhea test, and one for a provider rectal chlamydia test.
In only one case did a provider identify a positive result when the patient’s result was negative. In 23 cases, however, the patient identified a positive result when the provider’s result was negative. Patients identified significantly more positives for rectal and pharyngeal gonorrhea than providers, but there were no significant differences in patient and provider results for the chlamydia tests.
Even with these 24 discordant results, there was ≥75% concordance between patient and provider results on all tests, with very strong concordance (95%) for rectal chlamydia results (TABLE 2). When we re-ran the McNemar tests and the Kappa coefficients with equivocal results considered missing and negative, there were no statistically significant differences when compared with the calculations done with equivocal results considered positive.
Some difficulties observed with self-testing. Observing providers noted anecdotally that there were minor difficulties with the self-administered testing instructions. Three patients spilled the preservative liquid in which swabs are placed, 5 patients used the incorrect swab to perform testing, and 2 other patients had samples that were noted as compromised by the provider. None of these documented problems involved the 24 discordant cases.
TABLE 1
Characteristics of men participating in the study
| Demographic | N=374 |
|---|---|
| Age, y | |
| Median | 33 |
| Range | 18-70 |
| n (%) | |
| Race/ethnicity | |
| White/non-Hispanic | 205 (54.8) |
| Black/non-Hispanic | 85 (22.7) |
| Latino/Hispanic | 40 (10.7) |
| Asian | 13 (3.5) |
| Mixed | 8 (2.1) |
| Other | 19 (5.1) |
| Missing data | 4 (1.1) |
| Modes of GC/CT testing | |
| Rectal and pharyngeal | 272 (72.7) |
| Rectal only | 5 (1.3) |
| Pharyngeal only | 97 (25.9) |
| Sexual partner(s) in the last 12 months | |
| Men | 336 (89.8) |
| Men and women | 32 (8.6) |
| None | 1 (0.3) |
| Missing data | 5 (1.3) |
| Number of male sexual partners in the past 30 days | |
| 0-1 | 178 (47.6) |
| 2-3 | 130 (34.8) |
| 4 or more | 64 (17.1) |
| Missing data | 2 (0.5) |
| Number of male sexual partners in the past 60 days | |
| 0-1 | 104 (27.8) |
| 2-3 | 135 (36.1) |
| 4 or more | 133 (35.6) |
| Missing data | 2 (0.5) |
| Practiced insertive oral intercourse in past 12 months | |
| Yes | 325 (86.9) |
| No | 20 (5.4) |
| Missing data | 29 (7.7) |
| Practiced insertive anal intercourse in past 12 months | |
| Yes | 265 (70.8) |
| No | 78 (20.9) |
| Missing data | 31 (8.3) |
| Practiced receptive oral intercourse in past 12 months | |
| Yes | 326 (87.2) |
| No | 20 (5.3) |
| Missing data | 28 (7.5) |
| Practiced receptive anal intercourse in past 12 months | |
| Yes | 254 (67.9) |
| No | 90 (24.1) |
| Missing data | 30 (8.0) |
| CT, Chlamydia trachomatis; GC, Neisseria gonorrhoeae. | |
TABLE 2
Comparison of provider and patient testing results for GC/CT by anatomic site reveals ≥75% concordance on all tests
| Patient test result | Total tests, N | Provider positive test result, n (%) | Provider negative test result, n (%) | P value | Kappa coefficient |
|---|---|---|---|---|---|
| Rectal GC Patient positive test result Patient negative test result | 276 | 14 (5.1) 0 | 8 (2.9)* 254 (92) | <.01 | 0.76 |
| Pharyngeal GC Patient positive test result Patient negative test result | 367 | 23 (6.3) 1 (0.3)* | 10 (2.7)* 333 (90.7) | .01 | 0.79 |
| Rectal CT Patient positive test result Patient negative test result | 276 | 32 (11.6) 0 | 3 (1.1)* 241 (87.3) | .25 | 0.95 |
| Pharyngeal CT Patient positive test result Patient negative test result | 367 | 3 (0.8) 0 | 2 (0.5)* 362 (98.7) | .50 | 0.75 |
| CT, Chlamydia trachomatis; GC, Neisseria gonorrhoeae. *Discordant patient-provider test results. | |||||
DISCUSSION
The prevalence of gonorrhea and chlamydia in this study population was similar to what has been observed in previous studies of MSM,1-4 which confirms the need for improved detection of infections. Self- administered testing is one possible means of increasing the number of patients who are screened and treated, as the results of this study suggest it is equally or more accurate than provider-administered testing at detecting cases of gonorrhea and chlamydia.
Patient and provider results were equivalent for chlamydia detection, and patients appeared to identify more cases of gonorrhea, although interpretation of the significance of this finding is difficult given the relatively small number of cases. However, it is likely that the 23 cases in which patients identified positives that providers did not were true positives, given the sensitivity (84%-100%) and specificity (≥99.4%) of the AC2 test for detecting GC and CT.25
Assuming that our population has a similar prevalence of these STIs as prior studies, we would expect positive predictive values of approximately 100% for rectal GC, 95% for pharyngeal GC, 86.4% for rectal CT, and 71.4% for pharyngeal CT.26
Possible explanations for patients achieving better results than providers in some cases. The most likely explanation for better patient performance on some of the tests is that patients swabbed more meticulously and contacted more surface area.
This was also seen in a study that compared the ability of patients and physicians to identify human papillomavirus infection in swabs taken from areas where skin scraping had been performed. Patients were found to collect an appropriate sample significantly more often, which was thought to be due to physician hesitation to thoroughly scrape the patient’s skin.27 In our study, patients were anecdotally observed to be less likely to gag on a self-administered throat swab and to have less visible tensing of the rectal sphincter on self-administered rectal swab, which could have contributed to improved results.
Potential changes to the patient instructions before clinical implementation. These results suggest that self-administered testing could be substituted for clinician-administered testing, potentially improving detection. But widespread implementation would require a few modifications to the testing instructions based on the trained providers’ observations. Although the evidence is anecdotal, providers noted that several patients had difficulty with the instructions. For example, the placard said to use only the swab with the “blue shaft,” but 5 patients got confused and used the white swab either in addition to or instead of the blue swab. (The additional white swab was intended for use in making wet preps, when women are tested.) Many more patients ultimately used the correct swab, but appeared confused by the presence of the additional swab in the kit.
The confusion in these situations might have been avoided if the instructions had told men to throw one swab away and to use only the “blue swab” or the swab with the “blue handle” to avoid potential confusion over the word “shaft.” Another helpful modification to the instructions would be to alert men to the presence of the preservative liquid in the tubes. Several patients laid the tube horizontally with the cap off and spilled much of the liquid. It was still possible to test these samples, and there were no discrepancies between patient and provider results involving them. But ensuring standardization of the test tube contents should still be a priority in editing the instructions.
Incorporating self-testing into clinical practice. While the results of this study suggest that self-testing could be used with a few modifications to the instructions, how best to incorporate self-testing into the clinical setting still needs to be addressed. It might be possible for patients to simply perform testing after a physical exam; for patients to come in when it is convenient for them and leave a sample in the lab; or even for patients to perform testing at home and bring the swabs back to their clinic at a later time.
We obtained the results in this study when patients performed testing in a clinic with a trained provider in the room. One concern in implementing widespread self-testing would be that a provider’s presence in our study might have made patients more likely to spend the time needed to read instructions thoroughly and to put effort into performing the test correctly. However, it is also possible that knowing a provider will be duplicating the testing could lead to decreased patient effort. It may be that having responsibility for one’s own test results is what ensures adequate performance.
Further studies could explore the impact of a provider in the room, but studies have already examined testing done in private and yielded similar results for concordance, which suggests that any impact of the provider’s presence was relatively minimal. A 2009-2010 study at a London clinic, for example, allowed patients to perform testing privately following instructions from a nurse and identified a 9.8% prevalence of rectal CT infection and a 4.2% prevalence of rectal GC infection. These results are similar to those seen in our study and therefore suggest that patients were appropriately identifying infections without observation.28
Another study published in 2012 demonstrated that GC/CT testing swabs sent through the mail without any accompanying transport medium yielded results equivalent to those for swabs shipped in the liquid medium. This approach would make testing at home significantly easier, as patients would not have to be concerned about appropriate storage of their samples before returning them to a clinic.29
Applicability to female patients. Implementation of self-administered testing should be considered for female patients. In fact, most prior studies on the feasibility of self-testing have focused on women, as detection of their chlamydia and gonorrhea infections is equally critical. CDC guidelines stress the importance of yearly chlamydia screening for all women <25 years and for women >25 years who are at high risk (ie, multiple partners); and yearly gonorrhea screening for women at high risk, given the risk of medical complications including pelvic inflammatory disease and infertility if infections are missed.5
Researchers have found that after women participate in self-testing, they report that they would get STI testing more regularly if they could perform it themselves.19,30 Additionally, in studies similar to ours, women performing testing for gonorrhea and chlamydia using self-collected vaginal swabs have achieved similar sensitivity and specificity results to provider-performed testing.12,15,31
Study limitations. This was a self- selected MSM sample seeking STI testing from an urban community health center. Thus, one might assume that the detection of pharyngeal and rectal gonorrhea and chlamydia infections was higher in this sample compared with the general MSM population. That seems unlikely, however, given the similarity (noted earlier) between our findings and data reported in previous studies.1-4 Additionally, the presence of a provider in the room may have influenced patient performance, as we discussed earlier.
It therefore appears that self-administered testing could have universal applicability. Once optimal ways to incorporate self-testing for both men and women are identified, providers should be able to comply with the CDC testing guidelines without an increase in time or staff needed, thereby leading to increased detection and treatment of STIs and benefits for both patients and providers.
CORRESPONDENCE
Michael W. Plankey, PhD, Georgetown University Medical Center, Department of Medicine, Division of Infectious Diseases, 2115 Wisconsin Avenue, NW, Suite 130, Washington, DC 20007; mwp23@georgetown.edu
1. Baker J, Plankey M, Josayma Y, et al. The prevalence of rectal, urethral, and pharyngeal Neisseria gonorrhoeae and Chlamydia trachomatis among asymptomatic men who have sex with men in a prospective cohort in Washington, D.C. AIDS Patient Care STDs. 2009;23:585-588.
2. Kent CK, Chaw JK, Wong W, et al. Prevalence of rectal, urethral, and pharyngeal chlamydia and gonorrhea detected in 2 clinical settings among men who have sex with men: San Francisco, California, 2003. Clin Infect Dis. 2005;41:67-74.
3. Mimiaga MJ, Helms DJ, Reisner SL, et al. Gonococcal, chlamydia, and syphilis infection positivity among MSM attending a large primary care clinic, Boston, 2003 to 2004. Sex Transm Dis. 2009;36:507-511.
4. Park J, Marcus JL, Pandori M, et al. Sentinel surveillance for pharyngeal chlamydia and gonorrhea among men who have sex with men—San Francisco, 2010. Sex Transm Dis. 2012;39:482-484.
5. Workowski KA, Berman S. Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
6. St Lawrence JS, Montano DE, Kasprzyk D, et al. STD screening, testing, case reporting, and clinical and partner notification practices: a national survey of US physicians. Am J Public Health. 2002;92:1784-1788.
7. Mark H, Irwin K, Sternberg M, et al. Providers’ perceived barriers to sexually transmitted disease care in 2 large health maintenance organizations. Sex Transm Dis. 2008;35:184-189.
8. Xu F, Sternberg MR, Markowitz LE. Men who have sex with men in the United States: demographic and behavioral characteristics and prevalence of HIV and HSV-2 infection: results from National Health and Nutrition Examination Survey 2001-2006. Sex Transm Dis. 2010;37:399-405.
9. Cohen MS, Hoffman IF, Royce RA, et al. Reduction of concentration of HIV-1 in semen after treatment of urethritis: implications for prevention of sexual transmission of HIV-1. AIDSCAP Malawi Research Group. Lancet. 1997;349:1868-1873.
10. Bernstein KT, Marcus JL, Nieri G, et al. Rectal gonorrhea and chlamydia reinfection is associated with increased risk of HIV seroconversion. J Acquir Immune Defic Syndr. 2010;53:537-543.
11. Bradshaw CS, Pierce LI, Tabrizi SN, et al. Screening injecting drug users for sexually transmitted infections and blood borne viruses using street outreach and self collected sampling. Sex Transm Infect. 2005;81:53-58.
12. Fang J, Husman C, DeSilva L, et al. Evaluation of self-collected vaginal swab, first void urine, and endocervical swab specimens for the detection of Chlamydia trachomatis and Neisseria gonorrhoeae in adolescent females. J Pediatr Adolesc Gynecol. 2008;21:355-360.
13. Gaydos CA. Nucleic acid amplification tests for gonorrhea and chlamydia: practice and applications. Infect Dis Clin North Am. 2005;19:367-386 ix.
14. Hobbs MM, van der Pol B, Totten P, et al. From the NIH: proceedings of a workshop on the importance of self-obtained vaginal specimens for detection of sexually transmitted infections. Sex Transm Dis. 2008;35:8-13.
15. Knox J, Tabrizi SN, Miller P, et al. Evaluation of self-collected samples in contrast to practitioner-collected samples for detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis by polymerase chain reaction among women living in remote areas. Sex Transm Dis. 2002;29:647-654.
16. Lippman SA, Jones HE, Luppi CG, et al. Home-based self-sampling and self-testing for sexually transmitted infections: acceptable and feasible alternatives to provider-based screening in low-income women in Sao Paulo, Brazil. Sex Transm Dis. 2007;34:421-428.
17. Newman SB, Nelson MB, Gaydos CA, et al. Female prisoners’ p of collection methods for testing for Chlamydia trachomatis and Neisseria gonorrhoeae infection. Sex Transm Dis. 2003;30:306-309.
18. Richardson E, Sellors JW, Mackinnon S, et al. Prevalence of Chlamydia trachomatis infections and specimen collection preference among women, using self-collected vaginal swabs in community settings. Sex Transm Dis. 2003;30:880-885.
19. Wiesenfeld HC, Lowry DL, Heine RP, et al. Self-collection of vaginal swabs for the detection of Chlamydia, gonorrhea, and trichomoniasis: opportunity to encourage sexually transmitted disease testing among adolescents. Sex Transm Dis. 2001;28:321-325.
20. van der Helm JJ, Hoebe CJ, van Rooijen MS, et al. High performance and acceptability of self-collected rectal swabs for diagnosis of Chlamydia trachomatis and Neisseria gonorrhoeae in men who have sex with men and women. Sex Transm Dis. 2009;36:493-497.
21. Moncada J, Schachter J, Liska S, et al. Evaluation of self-collected glans and rectal swabs from men who have sex with men for detection of Chlamydia trachomatis and Neisseria gonorrhoeae by use of nucleic acid amplification tests. J Clin Microbiol. 2009;47:1657-1662.
22. Alexander S, Ison C, Parry J, et al. Self-taken pharyngeal and rectal swabs are appropriate for the detection of Chlamydia trachomatis and Neisseria gonorrhoeae in asymptomatic men who have sex with men. Sex Transm Infect. 2008;84:488-492.
23. San Francisco City Clinic. Patient instructions for self-collected specimens: pharyngeal and rectal. Available at: http://www.sfcityclinic.org/providers. Accessed December 15 2011.
24. Lampinen TM, Latulippe L, van Niekerk D, et al. Illustrated instructions for self-collection of anorectal swab specimens and their adequacy for cytological examination. Sex Transm Dis. 2006;33:386-388.
25. Schachter J, Moncada J, Liska S, et al. Nucleic acid amplification tests in the diagnosis of chlamydial and gonococcal infections of the oropharynx and rectum in men who have sex with men. Sex Transm Dis. 2008;35:637-642.
26. Ota KV, Tamari IE, Smieja M, et al. Detection of Neisseria gonorrhoeae and Chlamydia trachomatis in pharyngeal and rectal specimens using the BD Probetec ET system, the Gen-Probe Aptima Combo 2 assay and culture. Sex Transm Infect. 2009;85:182-186.
27. Hernandez BY, McDuffie K, Goodman MT, et al. Comparison of physician- and self-collected genital specimens for detection of human papillomavirus in men. J Clin Microbiol. 2006;44:513-517.
28. Soni S, White JA. Self-screening for Neisseria gonorrhoeae and Chlamydia trachomatis in the human immunodeficiency virus clinic—high yields and high acceptability. Sex Transm Dis. 2011;38:1107-1109.
29. Gaydos CA, Farshy C, Barnes M, et al. Can mailed swab samples be dry-shipped for the detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis by nucleic acid amplification tests? Diagn Microbiol Infect Dis. 2012;73:16-20.
30. Chernesky MA, Hook EW, 3rd, Martin DH, et al. Women find it easy and prefer to collect their own vaginal swabs to diagnose Chlamydia trachomatis or Neisseria gonorrhoeae infections. Sex Transm Dis. 2005;32:729-733.
31. Polaneczky M, Quigley C, Pollock L, et al. Use of self-collected vaginal specimens for detection of Chlamydia trachomatis infection. Obstet Gynecol. 1998;91:375-378.
1. Baker J, Plankey M, Josayma Y, et al. The prevalence of rectal, urethral, and pharyngeal Neisseria gonorrhoeae and Chlamydia trachomatis among asymptomatic men who have sex with men in a prospective cohort in Washington, D.C. AIDS Patient Care STDs. 2009;23:585-588.
2. Kent CK, Chaw JK, Wong W, et al. Prevalence of rectal, urethral, and pharyngeal chlamydia and gonorrhea detected in 2 clinical settings among men who have sex with men: San Francisco, California, 2003. Clin Infect Dis. 2005;41:67-74.
3. Mimiaga MJ, Helms DJ, Reisner SL, et al. Gonococcal, chlamydia, and syphilis infection positivity among MSM attending a large primary care clinic, Boston, 2003 to 2004. Sex Transm Dis. 2009;36:507-511.
4. Park J, Marcus JL, Pandori M, et al. Sentinel surveillance for pharyngeal chlamydia and gonorrhea among men who have sex with men—San Francisco, 2010. Sex Transm Dis. 2012;39:482-484.
5. Workowski KA, Berman S. Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines 2010. MMWR Recomm Rep. 2010;59(RR-12):1-110.
6. St Lawrence JS, Montano DE, Kasprzyk D, et al. STD screening, testing, case reporting, and clinical and partner notification practices: a national survey of US physicians. Am J Public Health. 2002;92:1784-1788.
7. Mark H, Irwin K, Sternberg M, et al. Providers’ perceived barriers to sexually transmitted disease care in 2 large health maintenance organizations. Sex Transm Dis. 2008;35:184-189.
8. Xu F, Sternberg MR, Markowitz LE. Men who have sex with men in the United States: demographic and behavioral characteristics and prevalence of HIV and HSV-2 infection: results from National Health and Nutrition Examination Survey 2001-2006. Sex Transm Dis. 2010;37:399-405.
9. Cohen MS, Hoffman IF, Royce RA, et al. Reduction of concentration of HIV-1 in semen after treatment of urethritis: implications for prevention of sexual transmission of HIV-1. AIDSCAP Malawi Research Group. Lancet. 1997;349:1868-1873.
10. Bernstein KT, Marcus JL, Nieri G, et al. Rectal gonorrhea and chlamydia reinfection is associated with increased risk of HIV seroconversion. J Acquir Immune Defic Syndr. 2010;53:537-543.
11. Bradshaw CS, Pierce LI, Tabrizi SN, et al. Screening injecting drug users for sexually transmitted infections and blood borne viruses using street outreach and self collected sampling. Sex Transm Infect. 2005;81:53-58.
12. Fang J, Husman C, DeSilva L, et al. Evaluation of self-collected vaginal swab, first void urine, and endocervical swab specimens for the detection of Chlamydia trachomatis and Neisseria gonorrhoeae in adolescent females. J Pediatr Adolesc Gynecol. 2008;21:355-360.
13. Gaydos CA. Nucleic acid amplification tests for gonorrhea and chlamydia: practice and applications. Infect Dis Clin North Am. 2005;19:367-386 ix.
14. Hobbs MM, van der Pol B, Totten P, et al. From the NIH: proceedings of a workshop on the importance of self-obtained vaginal specimens for detection of sexually transmitted infections. Sex Transm Dis. 2008;35:8-13.
15. Knox J, Tabrizi SN, Miller P, et al. Evaluation of self-collected samples in contrast to practitioner-collected samples for detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis by polymerase chain reaction among women living in remote areas. Sex Transm Dis. 2002;29:647-654.
16. Lippman SA, Jones HE, Luppi CG, et al. Home-based self-sampling and self-testing for sexually transmitted infections: acceptable and feasible alternatives to provider-based screening in low-income women in Sao Paulo, Brazil. Sex Transm Dis. 2007;34:421-428.
17. Newman SB, Nelson MB, Gaydos CA, et al. Female prisoners’ p of collection methods for testing for Chlamydia trachomatis and Neisseria gonorrhoeae infection. Sex Transm Dis. 2003;30:306-309.
18. Richardson E, Sellors JW, Mackinnon S, et al. Prevalence of Chlamydia trachomatis infections and specimen collection preference among women, using self-collected vaginal swabs in community settings. Sex Transm Dis. 2003;30:880-885.
19. Wiesenfeld HC, Lowry DL, Heine RP, et al. Self-collection of vaginal swabs for the detection of Chlamydia, gonorrhea, and trichomoniasis: opportunity to encourage sexually transmitted disease testing among adolescents. Sex Transm Dis. 2001;28:321-325.
20. van der Helm JJ, Hoebe CJ, van Rooijen MS, et al. High performance and acceptability of self-collected rectal swabs for diagnosis of Chlamydia trachomatis and Neisseria gonorrhoeae in men who have sex with men and women. Sex Transm Dis. 2009;36:493-497.
21. Moncada J, Schachter J, Liska S, et al. Evaluation of self-collected glans and rectal swabs from men who have sex with men for detection of Chlamydia trachomatis and Neisseria gonorrhoeae by use of nucleic acid amplification tests. J Clin Microbiol. 2009;47:1657-1662.
22. Alexander S, Ison C, Parry J, et al. Self-taken pharyngeal and rectal swabs are appropriate for the detection of Chlamydia trachomatis and Neisseria gonorrhoeae in asymptomatic men who have sex with men. Sex Transm Infect. 2008;84:488-492.
23. San Francisco City Clinic. Patient instructions for self-collected specimens: pharyngeal and rectal. Available at: http://www.sfcityclinic.org/providers. Accessed December 15 2011.
24. Lampinen TM, Latulippe L, van Niekerk D, et al. Illustrated instructions for self-collection of anorectal swab specimens and their adequacy for cytological examination. Sex Transm Dis. 2006;33:386-388.
25. Schachter J, Moncada J, Liska S, et al. Nucleic acid amplification tests in the diagnosis of chlamydial and gonococcal infections of the oropharynx and rectum in men who have sex with men. Sex Transm Dis. 2008;35:637-642.
26. Ota KV, Tamari IE, Smieja M, et al. Detection of Neisseria gonorrhoeae and Chlamydia trachomatis in pharyngeal and rectal specimens using the BD Probetec ET system, the Gen-Probe Aptima Combo 2 assay and culture. Sex Transm Infect. 2009;85:182-186.
27. Hernandez BY, McDuffie K, Goodman MT, et al. Comparison of physician- and self-collected genital specimens for detection of human papillomavirus in men. J Clin Microbiol. 2006;44:513-517.
28. Soni S, White JA. Self-screening for Neisseria gonorrhoeae and Chlamydia trachomatis in the human immunodeficiency virus clinic—high yields and high acceptability. Sex Transm Dis. 2011;38:1107-1109.
29. Gaydos CA, Farshy C, Barnes M, et al. Can mailed swab samples be dry-shipped for the detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis by nucleic acid amplification tests? Diagn Microbiol Infect Dis. 2012;73:16-20.
30. Chernesky MA, Hook EW, 3rd, Martin DH, et al. Women find it easy and prefer to collect their own vaginal swabs to diagnose Chlamydia trachomatis or Neisseria gonorrhoeae infections. Sex Transm Dis. 2005;32:729-733.
31. Polaneczky M, Quigley C, Pollock L, et al. Use of self-collected vaginal specimens for detection of Chlamydia trachomatis infection. Obstet Gynecol. 1998;91:375-378.
Top gynecologic surgeons gather for 2012 PAGS
Mark Walters, MD
![]()
Susan B. Levy, MD
![]()
![]()
Tomasso Falcone, MD
![]()
Amy Garcia, MD
More than 300 physicians attended the 15th annual Pelvic Anatomy and Gynecologic Surgery (PAGS) symposium December 13–15, 2012, in Las Vegas. One likely reason was an abundance of offerings, including:
- a laparoscopist’s view of pelvic and abdominal anatomy
- case-based discussion of the evaluation of female pelvic floor disorders
- a surgical video fest with expert discussion and audience participation
- an in-depth look at fibroid management
- a focus on hysterectomy, from the vaginal approach to single-port laparoscopy and robotics
- a panel discussion of pelvic pain and its management
- tips on avoiding and managing laparoscopic and other complications
- a breakout session on endometriosis surgery
- the latest on evaluation and management of fetal incontinence.
Here are a few additional highlights of the 2012 program:
Surgery for stress incontinence: Which sling is for which patient?
When it comes to slings, one size does not fit all. That point was emphasized by Mark Walters, MD, in a comprehensive session that described the surgical techniques behind various bladder-neck and midurethral sling procedures, as well as the associated cure rates, complications, and pros and cons. To watch a 7-minute video in which Dr. Walters elaborates on patient-selection criteria, CLICK HERE .
Surgical approach to prolapse—what I do and why I do it

“That’s something you have to come to grips with in your own practice—what’s best in your hands?” he said.
While showing videos of actual surgeries, he described specific techniques, pearls, and pitfalls, and emphasized the importance of cystoscopy to rule out bladder injury.
Keynote address: The economics of surgical gynecology

She also described the current payment environment, explained why the current trend in health-care spending is unsustainable, and stressed the need to find areas in surgical gynecologic practice that may benefit from improvements in health-care delivery. CLICK HERE for Dr. Levy’s overview of the issues on video.
After Dr. Levy’s keynote address on the economics of surgical gynecology, OBG Management gathered the opinions of four participants: Gary Bostrom, MD, of California; Richard Robinson, MD, of Georgia; Timothy Hall, MD, of North Carolina; and Todd Slater, MD, of Ohio. To hear their points of view, CLICK HERE .
Myomectomy: Open to robotic approaches
“Myomectomy is not a dying art by any stretch,” said PAGS Co-Chair Tommaso Falcone, MD, in opening this session. “In fact, it’s expected to increase,” he added, as more women seek to preserve their uterus.
He then proceeded to describe management approaches (including watchful waiting), indications for myomectomy, and surgical options, including data on both perioperative and reproductive outcomes.
CLICK HERE for a video summary of Dr. Falcone’s talk.
Laparoscopic supracervical hysterectomy
As more women seek to preserve their cervix at the time of hysterectomy, the supracervical approach is becoming increasingly common. Amy Garcia, MD, described the indications, technique, benefits, and risks associated with this procedure. CLICK HERE to hear Dr. Garcia highlight the key points of her talk.
Join me in Las Vegas for FUUS 2013!

“This is a unique meeting,” says Dr. Karram, “as it addresses both urologic and gynecologic issues related to female pelvic medicine and reconstructive surgery.” It’s also timely—with the first board exam for the subspecialty of female pelvic medicine and reconstructive surgery being held in June 2013. Prepare yourself to meet the demand for physicians who have the expertise to evaluate pelvic floor disorders.
“The meeting is attended by 50% gynecologists and 50% urologists, has many breakout sessions, and covers a variety of topics—everything from vaginal surgery for prolapse, voiding dysfunction, and types of reconstructive procedures with laparoscopic and robotic approaches,” says Dr. Karram, who is excited for this year’s special symposium by Karl J. Kreder, Jr, MD, on April 20 that addresses pelvic pain syndromes. For a complete agenda and registration details, visit www.fuus-cme.org.
Mark Walters, MD
![]()
Susan B. Levy, MD
![]()
![]()
Tomasso Falcone, MD
![]()
Amy Garcia, MD
More than 300 physicians attended the 15th annual Pelvic Anatomy and Gynecologic Surgery (PAGS) symposium December 13–15, 2012, in Las Vegas. One likely reason was an abundance of offerings, including:
- a laparoscopist’s view of pelvic and abdominal anatomy
- case-based discussion of the evaluation of female pelvic floor disorders
- a surgical video fest with expert discussion and audience participation
- an in-depth look at fibroid management
- a focus on hysterectomy, from the vaginal approach to single-port laparoscopy and robotics
- a panel discussion of pelvic pain and its management
- tips on avoiding and managing laparoscopic and other complications
- a breakout session on endometriosis surgery
- the latest on evaluation and management of fetal incontinence.
Here are a few additional highlights of the 2012 program:
Surgery for stress incontinence: Which sling is for which patient?
When it comes to slings, one size does not fit all. That point was emphasized by Mark Walters, MD, in a comprehensive session that described the surgical techniques behind various bladder-neck and midurethral sling procedures, as well as the associated cure rates, complications, and pros and cons. To watch a 7-minute video in which Dr. Walters elaborates on patient-selection criteria, CLICK HERE .
Surgical approach to prolapse—what I do and why I do it
“That’s something you have to come to grips with in your own practice—what’s best in your hands?” he said.
While showing videos of actual surgeries, he described specific techniques, pearls, and pitfalls, and emphasized the importance of cystoscopy to rule out bladder injury.
Keynote address: The economics of surgical gynecology
She also described the current payment environment, explained why the current trend in health-care spending is unsustainable, and stressed the need to find areas in surgical gynecologic practice that may benefit from improvements in health-care delivery. CLICK HERE for Dr. Levy’s overview of the issues on video.
After Dr. Levy’s keynote address on the economics of surgical gynecology, OBG Management gathered the opinions of four participants: Gary Bostrom, MD, of California; Richard Robinson, MD, of Georgia; Timothy Hall, MD, of North Carolina; and Todd Slater, MD, of Ohio. To hear their points of view, CLICK HERE .
Myomectomy: Open to robotic approaches
“Myomectomy is not a dying art by any stretch,” said PAGS Co-Chair Tommaso Falcone, MD, in opening this session. “In fact, it’s expected to increase,” he added, as more women seek to preserve their uterus.
He then proceeded to describe management approaches (including watchful waiting), indications for myomectomy, and surgical options, including data on both perioperative and reproductive outcomes.
CLICK HERE for a video summary of Dr. Falcone’s talk.
Laparoscopic supracervical hysterectomy
As more women seek to preserve their cervix at the time of hysterectomy, the supracervical approach is becoming increasingly common. Amy Garcia, MD, described the indications, technique, benefits, and risks associated with this procedure. CLICK HERE to hear Dr. Garcia highlight the key points of her talk.
Join me in Las Vegas for FUUS 2013!
“This is a unique meeting,” says Dr. Karram, “as it addresses both urologic and gynecologic issues related to female pelvic medicine and reconstructive surgery.” It’s also timely—with the first board exam for the subspecialty of female pelvic medicine and reconstructive surgery being held in June 2013. Prepare yourself to meet the demand for physicians who have the expertise to evaluate pelvic floor disorders.
“The meeting is attended by 50% gynecologists and 50% urologists, has many breakout sessions, and covers a variety of topics—everything from vaginal surgery for prolapse, voiding dysfunction, and types of reconstructive procedures with laparoscopic and robotic approaches,” says Dr. Karram, who is excited for this year’s special symposium by Karl J. Kreder, Jr, MD, on April 20 that addresses pelvic pain syndromes. For a complete agenda and registration details, visit www.fuus-cme.org.
Mark Walters, MD
![]()
Susan B. Levy, MD
![]()
![]()
Tomasso Falcone, MD
![]()
Amy Garcia, MD
More than 300 physicians attended the 15th annual Pelvic Anatomy and Gynecologic Surgery (PAGS) symposium December 13–15, 2012, in Las Vegas. One likely reason was an abundance of offerings, including:
- a laparoscopist’s view of pelvic and abdominal anatomy
- case-based discussion of the evaluation of female pelvic floor disorders
- a surgical video fest with expert discussion and audience participation
- an in-depth look at fibroid management
- a focus on hysterectomy, from the vaginal approach to single-port laparoscopy and robotics
- a panel discussion of pelvic pain and its management
- tips on avoiding and managing laparoscopic and other complications
- a breakout session on endometriosis surgery
- the latest on evaluation and management of fetal incontinence.
Here are a few additional highlights of the 2012 program:
Surgery for stress incontinence: Which sling is for which patient?
When it comes to slings, one size does not fit all. That point was emphasized by Mark Walters, MD, in a comprehensive session that described the surgical techniques behind various bladder-neck and midurethral sling procedures, as well as the associated cure rates, complications, and pros and cons. To watch a 7-minute video in which Dr. Walters elaborates on patient-selection criteria, CLICK HERE .
Surgical approach to prolapse—what I do and why I do it
“That’s something you have to come to grips with in your own practice—what’s best in your hands?” he said.
While showing videos of actual surgeries, he described specific techniques, pearls, and pitfalls, and emphasized the importance of cystoscopy to rule out bladder injury.
Keynote address: The economics of surgical gynecology
She also described the current payment environment, explained why the current trend in health-care spending is unsustainable, and stressed the need to find areas in surgical gynecologic practice that may benefit from improvements in health-care delivery. CLICK HERE for Dr. Levy’s overview of the issues on video.
After Dr. Levy’s keynote address on the economics of surgical gynecology, OBG Management gathered the opinions of four participants: Gary Bostrom, MD, of California; Richard Robinson, MD, of Georgia; Timothy Hall, MD, of North Carolina; and Todd Slater, MD, of Ohio. To hear their points of view, CLICK HERE .
Myomectomy: Open to robotic approaches
“Myomectomy is not a dying art by any stretch,” said PAGS Co-Chair Tommaso Falcone, MD, in opening this session. “In fact, it’s expected to increase,” he added, as more women seek to preserve their uterus.
He then proceeded to describe management approaches (including watchful waiting), indications for myomectomy, and surgical options, including data on both perioperative and reproductive outcomes.
CLICK HERE for a video summary of Dr. Falcone’s talk.
Laparoscopic supracervical hysterectomy
As more women seek to preserve their cervix at the time of hysterectomy, the supracervical approach is becoming increasingly common. Amy Garcia, MD, described the indications, technique, benefits, and risks associated with this procedure. CLICK HERE to hear Dr. Garcia highlight the key points of her talk.
Join me in Las Vegas for FUUS 2013!
“This is a unique meeting,” says Dr. Karram, “as it addresses both urologic and gynecologic issues related to female pelvic medicine and reconstructive surgery.” It’s also timely—with the first board exam for the subspecialty of female pelvic medicine and reconstructive surgery being held in June 2013. Prepare yourself to meet the demand for physicians who have the expertise to evaluate pelvic floor disorders.
“The meeting is attended by 50% gynecologists and 50% urologists, has many breakout sessions, and covers a variety of topics—everything from vaginal surgery for prolapse, voiding dysfunction, and types of reconstructive procedures with laparoscopic and robotic approaches,” says Dr. Karram, who is excited for this year’s special symposium by Karl J. Kreder, Jr, MD, on April 20 that addresses pelvic pain syndromes. For a complete agenda and registration details, visit www.fuus-cme.org.
Failure to diagnose preeclampsia … and more

A MOTHER CALLED HER OBGYN at 34 weeks’ gestation with complaints of a headache, swelling, and weight gain. The ObGyn prescribed Tylenol. The next morning, the mother was found unconscious on her kitchen floor. She was taken to the emergency department (ED), where she underwent a cesarean delivery and brain surgery. The child, born prematurely, suffered a stroke that resulted in brain damage and cerebral palsy (CP).
PARENTS’ CLAIM The ObGyn should have immediately evaluated the mother when she called with a headache. Failure to recognize eclampsia led to severe hypertension.
PHYSICIAN’S DEFENSE When the mother called the ObGyn, she reported a headache and diarrhea, and asked if it was all right to take Tylenol. The ObGyn claimed she asked the mother several questions and the mother’s answers included that the headache was not severe and that she’d had it for a few hours. The mother denied blurred vision, abdominal or uterine pain, and reported that she was not vomiting. The ObGyn believed that the mother had a virus and recommended Tylenol. The fetus’ stroke had occurred the day prior to the mother’s eclamptic episode.
VERDICT At first, a Pennsylvania defense verdict was returned. After an appeal, the second trial resulted in a $3.75 million verdict.
Spontaneous home birth goes badly awry
A WOMAN SPONTANEOUSLY DELIVERED her fourth baby at home. An ambulance transported the mother and child to the ED. Upon arrival, the child had depressed breathing. The pediatrician ordered a chest x-ray, which indicated a collapsed lung. A chest tube was inserted. The infant was monitored for the next 2 hours, when transfer to another hospital was arranged because her condition worsened. She sustained brain damage from the respiratory problems and died 2 days after birth.
PARENTS’ CLAIM The pediatrician failed to establish an airway and place a central line.
PHYSICIAN’S DEFENSE The newborn’s breathing difficulties were due to aspiration of meconium. The fetus suffered an in-utero hypoxic event due to a small placenta.
VERDICT A Kentucky defense verdict was returned.
NICU team not called early enough
AN INFANT’S HEART RATE was 100 bpm at birth. She was blue and not breathing, and suffered seizures in the first 24 hours of life. She was found to have brain damage, CP, and spastic quadriplegia. She requires a feeding tube and is unable to speak or walk.
PARENTS’ CLAIM The nurse should have called the NICU team before the baby’s birth because fetal distress was evident. The team arrived and began resuscitation 5 minutes after birth. The delay allowed for a lack of oxygen, which caused brain damage.
DEFENDANTS’ DEFENSE A placental infection caused the baby’s distress.
VERDICT A $8,583,000 Ohio verdict was returned against the hospital.
Woman not told cancer had spread to nodes
A 56-YEAR-OLD WOMAN underwent right breast mastectomy. The surgeon did not remove any lymph nodes despite radiologic evidence of possible nodal involvement. After the mastectomy, the surgeon advised the patient to see an oncologist.
The patient could not get an appointment with the oncologist for 6 months. During that visit, the oncologist told her that cancer had invaded lymph nodes that had not been removed. The cancer metastasized to a lung. Despite surgery, she was told that recurrence was inevitable.
PATIENT’S CLAIM Metastasis could have been avoided if the lymph nodes had been removed at mastectomy. The surgeon had not told her about lymph node involvement, which contributed to the delay in seeing the oncologist.
PHYSICIAN’S DEFENSE Removal of the lymph nodes was not necessary—immediate chemotherapy could have effectively addressed the cancer. The patient was told of the lymph node involvement and clearly advised that prompt chemotherapy was necessary.
VERDICT A $500,000 New York verdict was returned for past pain and suffering. Defense posttrial motions were denied. The judge granted the patient’s motion for future pain and suffering and awarded $500,000.

A WOMAN WENT TO THE HOSPITAL FOR THE BIRTH of her eighth child. She had received no prenatal care, although she had a history of preeclampsia. Upon arrival at the ED, she had decreased blood pressure. Two on-call ObGyns delivered the baby. Shoulder dystocia was encountered, and after several unsuccessful attempts were made to dislodge the shoulder, a rescue cesarean delivery was performed. The child has a brachial plexus injury.
PARENTS’ CLAIM The ObGyns failed to perform a cesarean delivery in a timely manner, and used excessive force in attempting to free the baby’s shoulder.
PHYSICIAN’S DEFENSE All appropriate measures were taken in an effort to facilitate a prompt and injury-free delivery.
VERDICT A $1,250,000 Ohio verdict was returned.
Failure to detect fetal growth restriction
A CHILD WAS DELIVERED BY AN OBGYN and a neonatologist. The child has CP with developmental delays and spastic quadriplegia. She requires constant care.
PARENTS’ CLAIM The child’s CP was caused by an hypoxic event that occurred 3 hours before delivery. The fetus was extremely small, which increased the susceptibility to hypoxic events. The ObGyn was negligent in failing to diagnose fetal growth restriction caused by placental insufficiency. The fetal monitor showed an abnormal heart rate during that 3-hour span. Fetal distress should have prompted action by the ObGyn; a cesarean delivery could have avoided the injury.
DEFENDANTS’ DEFENSE Prenatal tests, including ultrasonography, indicated that the fetus had grown appropriately. Fetal heart-rate monitors did not reveal problematic heart function. The child’s CP was due to chronic hypoxia that could not have been detected or prevented.
VERDICT A $6.5 million New York settlement was reached.
Emergency cesarean after fetal distress
AFTER A NORMAL PREGNANCY, an emergency cesarean delivery was performed when the fetal monitor indicated fetal distress. The child suffered hypoxic ischemic encephalopathy resulting in permanent neurologic deficits.
PARENTS’ CLAIM The nurse failed to timely alert the physician of decelerations shown on the fetal heart-rate monitor. A cesarean should have been performed earlier.
DEFENDANT’S DEFENSE The cesarean was performed when fetal distress was evident.
VERDICT A Massachusetts defense verdict was returned.
Pelvic abscess after hysterectomy
A WOMAN UNDERWENT a total vaginal hysterectomy without prophylactic antibiotics. Six days after discharge, she went to the ED with fever, chills, abdominal pain, and diarrhea. She was given antibiotics and admitted after a CT scan and physical examination suggested an infection. At discharge 6 days later, antibiotics were not prescribed because she had been afebrile for over 48 hours. She continued to have abdominal distention, and returned to the hospital the next day with an ultrasound taken elsewhere that revealed a 9-cm pelvic abscess. She underwent bilateral salpingo-oophorectomy and was discharged after 4 days, this time with antibiotics. She continued to have diarrhea, severe abdominal pain, and weight loss for a year.
PATIENT’S CLAIM Prophylactic antibiotics should have been prescribed prior to surgery, and continued when she left the hospital the first time.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A confidential Utah settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska ( www.verdictslaska.com ). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
A MOTHER CALLED HER OBGYN at 34 weeks’ gestation with complaints of a headache, swelling, and weight gain. The ObGyn prescribed Tylenol. The next morning, the mother was found unconscious on her kitchen floor. She was taken to the emergency department (ED), where she underwent a cesarean delivery and brain surgery. The child, born prematurely, suffered a stroke that resulted in brain damage and cerebral palsy (CP).
PARENTS’ CLAIM The ObGyn should have immediately evaluated the mother when she called with a headache. Failure to recognize eclampsia led to severe hypertension.
PHYSICIAN’S DEFENSE When the mother called the ObGyn, she reported a headache and diarrhea, and asked if it was all right to take Tylenol. The ObGyn claimed she asked the mother several questions and the mother’s answers included that the headache was not severe and that she’d had it for a few hours. The mother denied blurred vision, abdominal or uterine pain, and reported that she was not vomiting. The ObGyn believed that the mother had a virus and recommended Tylenol. The fetus’ stroke had occurred the day prior to the mother’s eclamptic episode.
VERDICT At first, a Pennsylvania defense verdict was returned. After an appeal, the second trial resulted in a $3.75 million verdict.
Spontaneous home birth goes badly awry
A WOMAN SPONTANEOUSLY DELIVERED her fourth baby at home. An ambulance transported the mother and child to the ED. Upon arrival, the child had depressed breathing. The pediatrician ordered a chest x-ray, which indicated a collapsed lung. A chest tube was inserted. The infant was monitored for the next 2 hours, when transfer to another hospital was arranged because her condition worsened. She sustained brain damage from the respiratory problems and died 2 days after birth.
PARENTS’ CLAIM The pediatrician failed to establish an airway and place a central line.
PHYSICIAN’S DEFENSE The newborn’s breathing difficulties were due to aspiration of meconium. The fetus suffered an in-utero hypoxic event due to a small placenta.
VERDICT A Kentucky defense verdict was returned.
NICU team not called early enough
AN INFANT’S HEART RATE was 100 bpm at birth. She was blue and not breathing, and suffered seizures in the first 24 hours of life. She was found to have brain damage, CP, and spastic quadriplegia. She requires a feeding tube and is unable to speak or walk.
PARENTS’ CLAIM The nurse should have called the NICU team before the baby’s birth because fetal distress was evident. The team arrived and began resuscitation 5 minutes after birth. The delay allowed for a lack of oxygen, which caused brain damage.
DEFENDANTS’ DEFENSE A placental infection caused the baby’s distress.
VERDICT A $8,583,000 Ohio verdict was returned against the hospital.
Woman not told cancer had spread to nodes
A 56-YEAR-OLD WOMAN underwent right breast mastectomy. The surgeon did not remove any lymph nodes despite radiologic evidence of possible nodal involvement. After the mastectomy, the surgeon advised the patient to see an oncologist.
The patient could not get an appointment with the oncologist for 6 months. During that visit, the oncologist told her that cancer had invaded lymph nodes that had not been removed. The cancer metastasized to a lung. Despite surgery, she was told that recurrence was inevitable.
PATIENT’S CLAIM Metastasis could have been avoided if the lymph nodes had been removed at mastectomy. The surgeon had not told her about lymph node involvement, which contributed to the delay in seeing the oncologist.
PHYSICIAN’S DEFENSE Removal of the lymph nodes was not necessary—immediate chemotherapy could have effectively addressed the cancer. The patient was told of the lymph node involvement and clearly advised that prompt chemotherapy was necessary.
VERDICT A $500,000 New York verdict was returned for past pain and suffering. Defense posttrial motions were denied. The judge granted the patient’s motion for future pain and suffering and awarded $500,000.
A WOMAN WENT TO THE HOSPITAL FOR THE BIRTH of her eighth child. She had received no prenatal care, although she had a history of preeclampsia. Upon arrival at the ED, she had decreased blood pressure. Two on-call ObGyns delivered the baby. Shoulder dystocia was encountered, and after several unsuccessful attempts were made to dislodge the shoulder, a rescue cesarean delivery was performed. The child has a brachial plexus injury.
PARENTS’ CLAIM The ObGyns failed to perform a cesarean delivery in a timely manner, and used excessive force in attempting to free the baby’s shoulder.
PHYSICIAN’S DEFENSE All appropriate measures were taken in an effort to facilitate a prompt and injury-free delivery.
VERDICT A $1,250,000 Ohio verdict was returned.
Failure to detect fetal growth restriction
A CHILD WAS DELIVERED BY AN OBGYN and a neonatologist. The child has CP with developmental delays and spastic quadriplegia. She requires constant care.
PARENTS’ CLAIM The child’s CP was caused by an hypoxic event that occurred 3 hours before delivery. The fetus was extremely small, which increased the susceptibility to hypoxic events. The ObGyn was negligent in failing to diagnose fetal growth restriction caused by placental insufficiency. The fetal monitor showed an abnormal heart rate during that 3-hour span. Fetal distress should have prompted action by the ObGyn; a cesarean delivery could have avoided the injury.
DEFENDANTS’ DEFENSE Prenatal tests, including ultrasonography, indicated that the fetus had grown appropriately. Fetal heart-rate monitors did not reveal problematic heart function. The child’s CP was due to chronic hypoxia that could not have been detected or prevented.
VERDICT A $6.5 million New York settlement was reached.
Emergency cesarean after fetal distress
AFTER A NORMAL PREGNANCY, an emergency cesarean delivery was performed when the fetal monitor indicated fetal distress. The child suffered hypoxic ischemic encephalopathy resulting in permanent neurologic deficits.
PARENTS’ CLAIM The nurse failed to timely alert the physician of decelerations shown on the fetal heart-rate monitor. A cesarean should have been performed earlier.
DEFENDANT’S DEFENSE The cesarean was performed when fetal distress was evident.
VERDICT A Massachusetts defense verdict was returned.
Pelvic abscess after hysterectomy
A WOMAN UNDERWENT a total vaginal hysterectomy without prophylactic antibiotics. Six days after discharge, she went to the ED with fever, chills, abdominal pain, and diarrhea. She was given antibiotics and admitted after a CT scan and physical examination suggested an infection. At discharge 6 days later, antibiotics were not prescribed because she had been afebrile for over 48 hours. She continued to have abdominal distention, and returned to the hospital the next day with an ultrasound taken elsewhere that revealed a 9-cm pelvic abscess. She underwent bilateral salpingo-oophorectomy and was discharged after 4 days, this time with antibiotics. She continued to have diarrhea, severe abdominal pain, and weight loss for a year.
PATIENT’S CLAIM Prophylactic antibiotics should have been prescribed prior to surgery, and continued when she left the hospital the first time.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A confidential Utah settlement was reached.
A MOTHER CALLED HER OBGYN at 34 weeks’ gestation with complaints of a headache, swelling, and weight gain. The ObGyn prescribed Tylenol. The next morning, the mother was found unconscious on her kitchen floor. She was taken to the emergency department (ED), where she underwent a cesarean delivery and brain surgery. The child, born prematurely, suffered a stroke that resulted in brain damage and cerebral palsy (CP).
PARENTS’ CLAIM The ObGyn should have immediately evaluated the mother when she called with a headache. Failure to recognize eclampsia led to severe hypertension.
PHYSICIAN’S DEFENSE When the mother called the ObGyn, she reported a headache and diarrhea, and asked if it was all right to take Tylenol. The ObGyn claimed she asked the mother several questions and the mother’s answers included that the headache was not severe and that she’d had it for a few hours. The mother denied blurred vision, abdominal or uterine pain, and reported that she was not vomiting. The ObGyn believed that the mother had a virus and recommended Tylenol. The fetus’ stroke had occurred the day prior to the mother’s eclamptic episode.
VERDICT At first, a Pennsylvania defense verdict was returned. After an appeal, the second trial resulted in a $3.75 million verdict.
Spontaneous home birth goes badly awry
A WOMAN SPONTANEOUSLY DELIVERED her fourth baby at home. An ambulance transported the mother and child to the ED. Upon arrival, the child had depressed breathing. The pediatrician ordered a chest x-ray, which indicated a collapsed lung. A chest tube was inserted. The infant was monitored for the next 2 hours, when transfer to another hospital was arranged because her condition worsened. She sustained brain damage from the respiratory problems and died 2 days after birth.
PARENTS’ CLAIM The pediatrician failed to establish an airway and place a central line.
PHYSICIAN’S DEFENSE The newborn’s breathing difficulties were due to aspiration of meconium. The fetus suffered an in-utero hypoxic event due to a small placenta.
VERDICT A Kentucky defense verdict was returned.
NICU team not called early enough
AN INFANT’S HEART RATE was 100 bpm at birth. She was blue and not breathing, and suffered seizures in the first 24 hours of life. She was found to have brain damage, CP, and spastic quadriplegia. She requires a feeding tube and is unable to speak or walk.
PARENTS’ CLAIM The nurse should have called the NICU team before the baby’s birth because fetal distress was evident. The team arrived and began resuscitation 5 minutes after birth. The delay allowed for a lack of oxygen, which caused brain damage.
DEFENDANTS’ DEFENSE A placental infection caused the baby’s distress.
VERDICT A $8,583,000 Ohio verdict was returned against the hospital.
Woman not told cancer had spread to nodes
A 56-YEAR-OLD WOMAN underwent right breast mastectomy. The surgeon did not remove any lymph nodes despite radiologic evidence of possible nodal involvement. After the mastectomy, the surgeon advised the patient to see an oncologist.
The patient could not get an appointment with the oncologist for 6 months. During that visit, the oncologist told her that cancer had invaded lymph nodes that had not been removed. The cancer metastasized to a lung. Despite surgery, she was told that recurrence was inevitable.
PATIENT’S CLAIM Metastasis could have been avoided if the lymph nodes had been removed at mastectomy. The surgeon had not told her about lymph node involvement, which contributed to the delay in seeing the oncologist.
PHYSICIAN’S DEFENSE Removal of the lymph nodes was not necessary—immediate chemotherapy could have effectively addressed the cancer. The patient was told of the lymph node involvement and clearly advised that prompt chemotherapy was necessary.
VERDICT A $500,000 New York verdict was returned for past pain and suffering. Defense posttrial motions were denied. The judge granted the patient’s motion for future pain and suffering and awarded $500,000.
A WOMAN WENT TO THE HOSPITAL FOR THE BIRTH of her eighth child. She had received no prenatal care, although she had a history of preeclampsia. Upon arrival at the ED, she had decreased blood pressure. Two on-call ObGyns delivered the baby. Shoulder dystocia was encountered, and after several unsuccessful attempts were made to dislodge the shoulder, a rescue cesarean delivery was performed. The child has a brachial plexus injury.
PARENTS’ CLAIM The ObGyns failed to perform a cesarean delivery in a timely manner, and used excessive force in attempting to free the baby’s shoulder.
PHYSICIAN’S DEFENSE All appropriate measures were taken in an effort to facilitate a prompt and injury-free delivery.
VERDICT A $1,250,000 Ohio verdict was returned.
Failure to detect fetal growth restriction
A CHILD WAS DELIVERED BY AN OBGYN and a neonatologist. The child has CP with developmental delays and spastic quadriplegia. She requires constant care.
PARENTS’ CLAIM The child’s CP was caused by an hypoxic event that occurred 3 hours before delivery. The fetus was extremely small, which increased the susceptibility to hypoxic events. The ObGyn was negligent in failing to diagnose fetal growth restriction caused by placental insufficiency. The fetal monitor showed an abnormal heart rate during that 3-hour span. Fetal distress should have prompted action by the ObGyn; a cesarean delivery could have avoided the injury.
DEFENDANTS’ DEFENSE Prenatal tests, including ultrasonography, indicated that the fetus had grown appropriately. Fetal heart-rate monitors did not reveal problematic heart function. The child’s CP was due to chronic hypoxia that could not have been detected or prevented.
VERDICT A $6.5 million New York settlement was reached.
Emergency cesarean after fetal distress
AFTER A NORMAL PREGNANCY, an emergency cesarean delivery was performed when the fetal monitor indicated fetal distress. The child suffered hypoxic ischemic encephalopathy resulting in permanent neurologic deficits.
PARENTS’ CLAIM The nurse failed to timely alert the physician of decelerations shown on the fetal heart-rate monitor. A cesarean should have been performed earlier.
DEFENDANT’S DEFENSE The cesarean was performed when fetal distress was evident.
VERDICT A Massachusetts defense verdict was returned.
Pelvic abscess after hysterectomy
A WOMAN UNDERWENT a total vaginal hysterectomy without prophylactic antibiotics. Six days after discharge, she went to the ED with fever, chills, abdominal pain, and diarrhea. She was given antibiotics and admitted after a CT scan and physical examination suggested an infection. At discharge 6 days later, antibiotics were not prescribed because she had been afebrile for over 48 hours. She continued to have abdominal distention, and returned to the hospital the next day with an ultrasound taken elsewhere that revealed a 9-cm pelvic abscess. She underwent bilateral salpingo-oophorectomy and was discharged after 4 days, this time with antibiotics. She continued to have diarrhea, severe abdominal pain, and weight loss for a year.
PATIENT’S CLAIM Prophylactic antibiotics should have been prescribed prior to surgery, and continued when she left the hospital the first time.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A confidential Utah settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska ( www.verdictslaska.com ). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska ( www.verdictslaska.com ). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Delayed MI diagnosis ends in disability, huge ($126M) verdict … more
Delayed heart attack diagnosis ends in disability and a huge verdict
DESPITE FEELING ILL ON AWAKENING, a 50-year-old woman went to work, where she suffered crushing chest pain radiating down her left arm and up to her jaw. Her coworker (and husband at the time) recognized the symptoms of a heart attack and drove her to the emergency department (ED).
An electrocardiogram (EKG) performed more than 4 hours later was read as not indicating a heart attack. The patient was given pain medication and an antianxiety drug because she had a history of anxiety. She spent the night at the hospital, lying on a gurney in a hallway at times.
In the morning, her husband called his own cardiologist, whose office was across the street from the hospital. The cardiologist came to the ED and immediately arranged to have the patient transferred by ambulance to the intensive care unit at another hospital.
Upon arrival, the patient was immediately sent to the hospital’s cardiac catheterization lab, where a heart attack was diagnosed. She underwent immediate surgery, during which she suffered dissection of an artery. Because of damage to her heart, she couldn’t return to work.
PLAINTIFF’S CLAIM The patient lost 70% of her heart’s pumping capacity and would require a heart transplant eventually. A cardiologist should have evaluated the patient immediately upon her arrival at the first hospital; the EKG done at that hospital was misread. On the catheterization film taken before surgery at the second hospital, the front portion of the patient’s heart was motionless.
THE DEFENSE The dissection during surgery caused the patient’s injuries.
VERDICT $126.6 million New York verdict.
COMMENT I do some malpractice case review and have seen 2 cases just like this one. If it sounds like a horse (myocardial infarction), it is a horse until proven otherwise. I’ve heard of men in their 40s seeking urgent care, being diagnosed with dyspepsia, and dying within 2 days.
Inadequate INR monitoring implicated in woman's death
A 59-YEAR-OLD WOMAN was diagnosed with atrial fibrillation and heart failure by a cardiologist and put on warfarin, which the cardiologist discontinued after a few days. Warfarin was resumed when the patient underwent surgery to place a mechanical heart valve.
The patient’s international normalized ratio (INR) was tested daily while she was in the hospital, and warfarin was stopped several times. She was discharged with a prescription for 2 mg warfarin because her INR was 2.2, below the therapeutic range.
At a follow-up visit, the cardiologist checked the INR, which was 3.1. He saw the patient in the office again 8 days later, and 6 days after that a call was made to him, but no further blood tests were performed.
Eight days after the call, the patient was found unresponsive, with indications of gastrointestinal (GI) bleeding, and taken to the emergency department. Her INR level was at least 24.4, the highest the equipment could measure. In addition to GI bleeding, she had bleeding in her lungs. She died the next day.
PLAINTIFF’S CLAIM The defendants didn’t monitor INR properly; the doctor knew the importance of monitoring INR while the patient was taking warfarin.
THE DEFENSE The INR level was normal at the posthospital visit. That measurement, along with the monitoring done while the patient was hospitalized, was appropriate monitoring. The patient died of sepsis, not exsanguination.
VERDICT $386,648 net California verdict.
COMMENT This could have happened to any of us. If you monitor warfarin in your practice, make sure the follow-up system is water tight. Use a registry and double checking system. Be sure you know who is responsible during care transitions.
Delayed heart attack diagnosis ends in disability and a huge verdict
DESPITE FEELING ILL ON AWAKENING, a 50-year-old woman went to work, where she suffered crushing chest pain radiating down her left arm and up to her jaw. Her coworker (and husband at the time) recognized the symptoms of a heart attack and drove her to the emergency department (ED).
An electrocardiogram (EKG) performed more than 4 hours later was read as not indicating a heart attack. The patient was given pain medication and an antianxiety drug because she had a history of anxiety. She spent the night at the hospital, lying on a gurney in a hallway at times.
In the morning, her husband called his own cardiologist, whose office was across the street from the hospital. The cardiologist came to the ED and immediately arranged to have the patient transferred by ambulance to the intensive care unit at another hospital.
Upon arrival, the patient was immediately sent to the hospital’s cardiac catheterization lab, where a heart attack was diagnosed. She underwent immediate surgery, during which she suffered dissection of an artery. Because of damage to her heart, she couldn’t return to work.
PLAINTIFF’S CLAIM The patient lost 70% of her heart’s pumping capacity and would require a heart transplant eventually. A cardiologist should have evaluated the patient immediately upon her arrival at the first hospital; the EKG done at that hospital was misread. On the catheterization film taken before surgery at the second hospital, the front portion of the patient’s heart was motionless.
THE DEFENSE The dissection during surgery caused the patient’s injuries.
VERDICT $126.6 million New York verdict.
COMMENT I do some malpractice case review and have seen 2 cases just like this one. If it sounds like a horse (myocardial infarction), it is a horse until proven otherwise. I’ve heard of men in their 40s seeking urgent care, being diagnosed with dyspepsia, and dying within 2 days.
Inadequate INR monitoring implicated in woman's death
A 59-YEAR-OLD WOMAN was diagnosed with atrial fibrillation and heart failure by a cardiologist and put on warfarin, which the cardiologist discontinued after a few days. Warfarin was resumed when the patient underwent surgery to place a mechanical heart valve.
The patient’s international normalized ratio (INR) was tested daily while she was in the hospital, and warfarin was stopped several times. She was discharged with a prescription for 2 mg warfarin because her INR was 2.2, below the therapeutic range.
At a follow-up visit, the cardiologist checked the INR, which was 3.1. He saw the patient in the office again 8 days later, and 6 days after that a call was made to him, but no further blood tests were performed.
Eight days after the call, the patient was found unresponsive, with indications of gastrointestinal (GI) bleeding, and taken to the emergency department. Her INR level was at least 24.4, the highest the equipment could measure. In addition to GI bleeding, she had bleeding in her lungs. She died the next day.
PLAINTIFF’S CLAIM The defendants didn’t monitor INR properly; the doctor knew the importance of monitoring INR while the patient was taking warfarin.
THE DEFENSE The INR level was normal at the posthospital visit. That measurement, along with the monitoring done while the patient was hospitalized, was appropriate monitoring. The patient died of sepsis, not exsanguination.
VERDICT $386,648 net California verdict.
COMMENT This could have happened to any of us. If you monitor warfarin in your practice, make sure the follow-up system is water tight. Use a registry and double checking system. Be sure you know who is responsible during care transitions.
Delayed heart attack diagnosis ends in disability and a huge verdict
DESPITE FEELING ILL ON AWAKENING, a 50-year-old woman went to work, where she suffered crushing chest pain radiating down her left arm and up to her jaw. Her coworker (and husband at the time) recognized the symptoms of a heart attack and drove her to the emergency department (ED).
An electrocardiogram (EKG) performed more than 4 hours later was read as not indicating a heart attack. The patient was given pain medication and an antianxiety drug because she had a history of anxiety. She spent the night at the hospital, lying on a gurney in a hallway at times.
In the morning, her husband called his own cardiologist, whose office was across the street from the hospital. The cardiologist came to the ED and immediately arranged to have the patient transferred by ambulance to the intensive care unit at another hospital.
Upon arrival, the patient was immediately sent to the hospital’s cardiac catheterization lab, where a heart attack was diagnosed. She underwent immediate surgery, during which she suffered dissection of an artery. Because of damage to her heart, she couldn’t return to work.
PLAINTIFF’S CLAIM The patient lost 70% of her heart’s pumping capacity and would require a heart transplant eventually. A cardiologist should have evaluated the patient immediately upon her arrival at the first hospital; the EKG done at that hospital was misread. On the catheterization film taken before surgery at the second hospital, the front portion of the patient’s heart was motionless.
THE DEFENSE The dissection during surgery caused the patient’s injuries.
VERDICT $126.6 million New York verdict.
COMMENT I do some malpractice case review and have seen 2 cases just like this one. If it sounds like a horse (myocardial infarction), it is a horse until proven otherwise. I’ve heard of men in their 40s seeking urgent care, being diagnosed with dyspepsia, and dying within 2 days.
Inadequate INR monitoring implicated in woman's death
A 59-YEAR-OLD WOMAN was diagnosed with atrial fibrillation and heart failure by a cardiologist and put on warfarin, which the cardiologist discontinued after a few days. Warfarin was resumed when the patient underwent surgery to place a mechanical heart valve.
The patient’s international normalized ratio (INR) was tested daily while she was in the hospital, and warfarin was stopped several times. She was discharged with a prescription for 2 mg warfarin because her INR was 2.2, below the therapeutic range.
At a follow-up visit, the cardiologist checked the INR, which was 3.1. He saw the patient in the office again 8 days later, and 6 days after that a call was made to him, but no further blood tests were performed.
Eight days after the call, the patient was found unresponsive, with indications of gastrointestinal (GI) bleeding, and taken to the emergency department. Her INR level was at least 24.4, the highest the equipment could measure. In addition to GI bleeding, she had bleeding in her lungs. She died the next day.
PLAINTIFF’S CLAIM The defendants didn’t monitor INR properly; the doctor knew the importance of monitoring INR while the patient was taking warfarin.
THE DEFENSE The INR level was normal at the posthospital visit. That measurement, along with the monitoring done while the patient was hospitalized, was appropriate monitoring. The patient died of sepsis, not exsanguination.
VERDICT $386,648 net California verdict.
COMMENT This could have happened to any of us. If you monitor warfarin in your practice, make sure the follow-up system is water tight. Use a registry and double checking system. Be sure you know who is responsible during care transitions.