User login
Ro-CHOP: Toxicity increases with efficacy
SAN FRANCISCO—Adding romidepsin to CHOP can enhance the regimen’s efficacy against peripheral T-cell lymphoma (PTCL), but the combination can also induce severe toxicity, results of a phase 1b/2 study have shown.
In patients with previously untreated PTCL, romidepsin plus CHOP elicited an overall response rate of about 69%.
But all patients experienced adverse events, a median of 49 per patient. In addition, rates of hematologic toxicities were high, and 3 patients experienced acute cardiac toxicity.
Bertrand Coiffier, MD, PhD, of CHU Lyon Sud in Pierre Benite, France, presented these findings at the 7th Annual T-cell Lymphoma Forum. Dr Coiffier and other researchers involved in this study receive funds from Celgene, the company developing romidepsin.
“CHOP is widely accepted,” Dr Coiffier noted. “It’s the most-used regimen for peripheral T-cell lymphoma, but it’s not the best one, and we certainly have regimens that do produce more [complete responses] and longer responses.”
He said researchers decided to test romidepsin in combination with CHOP because studies have suggested that romidepsin has very good efficacy in relapsed/refractory peripheral T-cell lymphoma, and the toxicities associated with romidepsin and CHOP alone have been managable.
So the researchers tested the combination in 37 patients with untreated PTCL, most of whom were male (n=20). The median age was 57, and 37.8% were older than 60. About 95% of patients had stage III/IV disease, and about 89% had an ECOG performance status less than 2.
Most patients had angioimmunoblastic T-cell lymphoma (n=17), followed by PTCL not otherwise specified (n=13), ALK- anaplastic large-cell lymphoma (n=3), enteropathy-associated T-cell lymphoma (n=1), hepatosplenic T-cell lymphoma (n=1), primary cutaneous CD4+ small/medium T-cell lymphoma (n=1), and “other” (n=1).
Early DLTs
The researchers used a standard “3+3” dose-escalation scheme, starting with a romidepsin dose of 10 mg/m2 given on days 1 and 8.
In the first 2 cycles, there were 3 dose-limiting toxicities (DLTs)—1 case of grade 3 syncope, 1 case of grade 3 general status alteration, and 1 case of grade 3 hematologic toxicity (neutropenia and thrombocytopenia) lasting longer than 7 days.
“So we looked at the definition of the criteria for DLT, and we thought that, this time, they were too severe,” Dr Coiffier said. “After a lot of discussion between all the investigators, we decided to modify the criteria for DLT regarding neutropenia or thrombocytopenia and to allow a little more toxicity before saying it’s a DLT.”
A DLT was initially defined as grade 3/4 non-hematologic toxicity, grade 3 hematologic toxicity lasting more than 7 days, or grade 4 hematologic toxicity lasting more than 3 days. The researchers modified the criteria so that hematologic toxicities would not be considered DLTs if they lasted less than 10 days for grade 3 or less than 7 days for grade 4.
When the team decreased the romidepsin dose to 8 mg/m2, they did not observe any DLTs according to the new criteria. The same was true when they raised the dose back up to 10 mg/m2.
There were, however, DLTs when the dose was increased to 12 mg/m2. In cohort 5, there was a case of grade 3 cardiac failure, and in cohort 6, there were 2 cases of grade 3 nausea.
Nevertheless, 12 mg/m2 became the phase 2 dose. In all, 25 patients received romidepsin at that dose.
Safety data
Twenty-six of 37 patients completed the 8 planned cycles of treatment. Five patients discontinued treatment due to progression and 6 due to toxicity (5 due to thrombocytopenia).
“One hundred percent of patients experienced at least one adverse event, but most of them were grade 1 or 2 [84%] and occurred during the first 2 cycles [38%],” Dr Coiffier said. “There were no deaths related to adverse events.”
Severe toxicities occurred during the expansion phase. There was a case of severe peripheral sensory neuropathy that led to treatment discontinuation, and there were 3 cases of acute cardiac toxicity. They all occurred after the first cycle, and none were fatal.
The rate of hematologic toxicity was high. Neutropenia occurred in all patients, thrombocytopenia in 94%, and anemia in 89%.
Grade 3/4 adverse events included neutropenia (85%), thrombocytopenia (35%), febrile neutropenia (19%), general status deterioration (13%), nausea/vomiting (10%), anemia (8%), hypophosphatemia (8%), fatigue (5%), mucositis (5%), decreased appetite (5%), hypocalcemia (3%), hyponatremia (3%), hypokalemia (3%), hypomagnesemia (3%), dysgeusia (3%), and peripheral sensory neuropathy (3%).
Response, survival, and next steps
About 51% of patients (18/35) achieved a complete response, and 17% (n=6) had a partial response. Twenty-six percent of patients (n=9) progressed.
The median follow-up was 30 months. The estimated 1-year progression-free survival was 57%, and the estimated 1-year overall survival was 82%.
“The [overall survival] curve is certainly much better than you would expect with just standard CHOP,” Dr Coiffier noted.
He added that this research has progressed to a phase 3 study comparing romidepsin and CHOP in combination to CHOP alone. There are 7 countries participating (France, Belgium, South Korea, Spain, Italy, Germany, and Portugal), and 100 patients have been enrolled thus far. ![]()
SAN FRANCISCO—Adding romidepsin to CHOP can enhance the regimen’s efficacy against peripheral T-cell lymphoma (PTCL), but the combination can also induce severe toxicity, results of a phase 1b/2 study have shown.
In patients with previously untreated PTCL, romidepsin plus CHOP elicited an overall response rate of about 69%.
But all patients experienced adverse events, a median of 49 per patient. In addition, rates of hematologic toxicities were high, and 3 patients experienced acute cardiac toxicity.
Bertrand Coiffier, MD, PhD, of CHU Lyon Sud in Pierre Benite, France, presented these findings at the 7th Annual T-cell Lymphoma Forum. Dr Coiffier and other researchers involved in this study receive funds from Celgene, the company developing romidepsin.
“CHOP is widely accepted,” Dr Coiffier noted. “It’s the most-used regimen for peripheral T-cell lymphoma, but it’s not the best one, and we certainly have regimens that do produce more [complete responses] and longer responses.”
He said researchers decided to test romidepsin in combination with CHOP because studies have suggested that romidepsin has very good efficacy in relapsed/refractory peripheral T-cell lymphoma, and the toxicities associated with romidepsin and CHOP alone have been managable.
So the researchers tested the combination in 37 patients with untreated PTCL, most of whom were male (n=20). The median age was 57, and 37.8% were older than 60. About 95% of patients had stage III/IV disease, and about 89% had an ECOG performance status less than 2.
Most patients had angioimmunoblastic T-cell lymphoma (n=17), followed by PTCL not otherwise specified (n=13), ALK- anaplastic large-cell lymphoma (n=3), enteropathy-associated T-cell lymphoma (n=1), hepatosplenic T-cell lymphoma (n=1), primary cutaneous CD4+ small/medium T-cell lymphoma (n=1), and “other” (n=1).
Early DLTs
The researchers used a standard “3+3” dose-escalation scheme, starting with a romidepsin dose of 10 mg/m2 given on days 1 and 8.
In the first 2 cycles, there were 3 dose-limiting toxicities (DLTs)—1 case of grade 3 syncope, 1 case of grade 3 general status alteration, and 1 case of grade 3 hematologic toxicity (neutropenia and thrombocytopenia) lasting longer than 7 days.
“So we looked at the definition of the criteria for DLT, and we thought that, this time, they were too severe,” Dr Coiffier said. “After a lot of discussion between all the investigators, we decided to modify the criteria for DLT regarding neutropenia or thrombocytopenia and to allow a little more toxicity before saying it’s a DLT.”
A DLT was initially defined as grade 3/4 non-hematologic toxicity, grade 3 hematologic toxicity lasting more than 7 days, or grade 4 hematologic toxicity lasting more than 3 days. The researchers modified the criteria so that hematologic toxicities would not be considered DLTs if they lasted less than 10 days for grade 3 or less than 7 days for grade 4.
When the team decreased the romidepsin dose to 8 mg/m2, they did not observe any DLTs according to the new criteria. The same was true when they raised the dose back up to 10 mg/m2.
There were, however, DLTs when the dose was increased to 12 mg/m2. In cohort 5, there was a case of grade 3 cardiac failure, and in cohort 6, there were 2 cases of grade 3 nausea.
Nevertheless, 12 mg/m2 became the phase 2 dose. In all, 25 patients received romidepsin at that dose.
Safety data
Twenty-six of 37 patients completed the 8 planned cycles of treatment. Five patients discontinued treatment due to progression and 6 due to toxicity (5 due to thrombocytopenia).
“One hundred percent of patients experienced at least one adverse event, but most of them were grade 1 or 2 [84%] and occurred during the first 2 cycles [38%],” Dr Coiffier said. “There were no deaths related to adverse events.”
Severe toxicities occurred during the expansion phase. There was a case of severe peripheral sensory neuropathy that led to treatment discontinuation, and there were 3 cases of acute cardiac toxicity. They all occurred after the first cycle, and none were fatal.
The rate of hematologic toxicity was high. Neutropenia occurred in all patients, thrombocytopenia in 94%, and anemia in 89%.
Grade 3/4 adverse events included neutropenia (85%), thrombocytopenia (35%), febrile neutropenia (19%), general status deterioration (13%), nausea/vomiting (10%), anemia (8%), hypophosphatemia (8%), fatigue (5%), mucositis (5%), decreased appetite (5%), hypocalcemia (3%), hyponatremia (3%), hypokalemia (3%), hypomagnesemia (3%), dysgeusia (3%), and peripheral sensory neuropathy (3%).
Response, survival, and next steps
About 51% of patients (18/35) achieved a complete response, and 17% (n=6) had a partial response. Twenty-six percent of patients (n=9) progressed.
The median follow-up was 30 months. The estimated 1-year progression-free survival was 57%, and the estimated 1-year overall survival was 82%.
“The [overall survival] curve is certainly much better than you would expect with just standard CHOP,” Dr Coiffier noted.
He added that this research has progressed to a phase 3 study comparing romidepsin and CHOP in combination to CHOP alone. There are 7 countries participating (France, Belgium, South Korea, Spain, Italy, Germany, and Portugal), and 100 patients have been enrolled thus far. ![]()
SAN FRANCISCO—Adding romidepsin to CHOP can enhance the regimen’s efficacy against peripheral T-cell lymphoma (PTCL), but the combination can also induce severe toxicity, results of a phase 1b/2 study have shown.
In patients with previously untreated PTCL, romidepsin plus CHOP elicited an overall response rate of about 69%.
But all patients experienced adverse events, a median of 49 per patient. In addition, rates of hematologic toxicities were high, and 3 patients experienced acute cardiac toxicity.
Bertrand Coiffier, MD, PhD, of CHU Lyon Sud in Pierre Benite, France, presented these findings at the 7th Annual T-cell Lymphoma Forum. Dr Coiffier and other researchers involved in this study receive funds from Celgene, the company developing romidepsin.
“CHOP is widely accepted,” Dr Coiffier noted. “It’s the most-used regimen for peripheral T-cell lymphoma, but it’s not the best one, and we certainly have regimens that do produce more [complete responses] and longer responses.”
He said researchers decided to test romidepsin in combination with CHOP because studies have suggested that romidepsin has very good efficacy in relapsed/refractory peripheral T-cell lymphoma, and the toxicities associated with romidepsin and CHOP alone have been managable.
So the researchers tested the combination in 37 patients with untreated PTCL, most of whom were male (n=20). The median age was 57, and 37.8% were older than 60. About 95% of patients had stage III/IV disease, and about 89% had an ECOG performance status less than 2.
Most patients had angioimmunoblastic T-cell lymphoma (n=17), followed by PTCL not otherwise specified (n=13), ALK- anaplastic large-cell lymphoma (n=3), enteropathy-associated T-cell lymphoma (n=1), hepatosplenic T-cell lymphoma (n=1), primary cutaneous CD4+ small/medium T-cell lymphoma (n=1), and “other” (n=1).
Early DLTs
The researchers used a standard “3+3” dose-escalation scheme, starting with a romidepsin dose of 10 mg/m2 given on days 1 and 8.
In the first 2 cycles, there were 3 dose-limiting toxicities (DLTs)—1 case of grade 3 syncope, 1 case of grade 3 general status alteration, and 1 case of grade 3 hematologic toxicity (neutropenia and thrombocytopenia) lasting longer than 7 days.
“So we looked at the definition of the criteria for DLT, and we thought that, this time, they were too severe,” Dr Coiffier said. “After a lot of discussion between all the investigators, we decided to modify the criteria for DLT regarding neutropenia or thrombocytopenia and to allow a little more toxicity before saying it’s a DLT.”
A DLT was initially defined as grade 3/4 non-hematologic toxicity, grade 3 hematologic toxicity lasting more than 7 days, or grade 4 hematologic toxicity lasting more than 3 days. The researchers modified the criteria so that hematologic toxicities would not be considered DLTs if they lasted less than 10 days for grade 3 or less than 7 days for grade 4.
When the team decreased the romidepsin dose to 8 mg/m2, they did not observe any DLTs according to the new criteria. The same was true when they raised the dose back up to 10 mg/m2.
There were, however, DLTs when the dose was increased to 12 mg/m2. In cohort 5, there was a case of grade 3 cardiac failure, and in cohort 6, there were 2 cases of grade 3 nausea.
Nevertheless, 12 mg/m2 became the phase 2 dose. In all, 25 patients received romidepsin at that dose.
Safety data
Twenty-six of 37 patients completed the 8 planned cycles of treatment. Five patients discontinued treatment due to progression and 6 due to toxicity (5 due to thrombocytopenia).
“One hundred percent of patients experienced at least one adverse event, but most of them were grade 1 or 2 [84%] and occurred during the first 2 cycles [38%],” Dr Coiffier said. “There were no deaths related to adverse events.”
Severe toxicities occurred during the expansion phase. There was a case of severe peripheral sensory neuropathy that led to treatment discontinuation, and there were 3 cases of acute cardiac toxicity. They all occurred after the first cycle, and none were fatal.
The rate of hematologic toxicity was high. Neutropenia occurred in all patients, thrombocytopenia in 94%, and anemia in 89%.
Grade 3/4 adverse events included neutropenia (85%), thrombocytopenia (35%), febrile neutropenia (19%), general status deterioration (13%), nausea/vomiting (10%), anemia (8%), hypophosphatemia (8%), fatigue (5%), mucositis (5%), decreased appetite (5%), hypocalcemia (3%), hyponatremia (3%), hypokalemia (3%), hypomagnesemia (3%), dysgeusia (3%), and peripheral sensory neuropathy (3%).
Response, survival, and next steps
About 51% of patients (18/35) achieved a complete response, and 17% (n=6) had a partial response. Twenty-six percent of patients (n=9) progressed.
The median follow-up was 30 months. The estimated 1-year progression-free survival was 57%, and the estimated 1-year overall survival was 82%.
“The [overall survival] curve is certainly much better than you would expect with just standard CHOP,” Dr Coiffier noted.
He added that this research has progressed to a phase 3 study comparing romidepsin and CHOP in combination to CHOP alone. There are 7 countries participating (France, Belgium, South Korea, Spain, Italy, Germany, and Portugal), and 100 patients have been enrolled thus far. ![]()
Anticoagulant now available in US pharmacies

Photo by Rhoda Baer
The oral factor Xa inhibitor edoxaban (Savaysa) is now available in US pharmacies, according to Daiichi Sankyo Company, Limited, the company developing the drug.
Savaysa is approved by the US Food and Drug Administration to reduce the risk of stroke and systemic embolism (SE) in patients with non-valvular atrial fibrillation (NVAF), as well as for the treatment of deep vein thrombosis and pulmonary embolism following 5 to 10 days of initial therapy with a parenteral anticoagulant.
According to Savaysa’s label, it should not be used in NVAF patients with creatinine clearance levels greater than 95 mL/min because, in that population, there is an increased risk of ischemic stroke with the drug compared to warfarin.
Daiichi Sankyo has developed resources for physicians and patients to help ensure patients can begin and/or remain on Savaysa per physician instructions.
The Savaysa Savings Plus program will include a reimbursement hotline to assist patients and prescribers who request help understanding a patient’s available coverage. Eligible patients who are prescribed Savaysa can enroll in a copay savings program and pay $4 per month through the Savaysa Savings Card.
Vouchers will also be available to provide patients and doctors with a way to try Savaysa at no cost to see if it is right for the patient.
In addition, the Savaysa Patient Assistance Program will offer assistance to qualified individuals, providing free product to eligible patients who are prescribed Savaysa, are uninsured, and are unable to identify alternative payment sources.
The approval of Savaysa in the US is based on data from the ENGAGE AF-TIMI 48 trial and the Hokusai-VTE trial. ![]()
Photo by Rhoda Baer
The oral factor Xa inhibitor edoxaban (Savaysa) is now available in US pharmacies, according to Daiichi Sankyo Company, Limited, the company developing the drug.
Savaysa is approved by the US Food and Drug Administration to reduce the risk of stroke and systemic embolism (SE) in patients with non-valvular atrial fibrillation (NVAF), as well as for the treatment of deep vein thrombosis and pulmonary embolism following 5 to 10 days of initial therapy with a parenteral anticoagulant.
According to Savaysa’s label, it should not be used in NVAF patients with creatinine clearance levels greater than 95 mL/min because, in that population, there is an increased risk of ischemic stroke with the drug compared to warfarin.
Daiichi Sankyo has developed resources for physicians and patients to help ensure patients can begin and/or remain on Savaysa per physician instructions.
The Savaysa Savings Plus program will include a reimbursement hotline to assist patients and prescribers who request help understanding a patient’s available coverage. Eligible patients who are prescribed Savaysa can enroll in a copay savings program and pay $4 per month through the Savaysa Savings Card.
Vouchers will also be available to provide patients and doctors with a way to try Savaysa at no cost to see if it is right for the patient.
In addition, the Savaysa Patient Assistance Program will offer assistance to qualified individuals, providing free product to eligible patients who are prescribed Savaysa, are uninsured, and are unable to identify alternative payment sources.
The approval of Savaysa in the US is based on data from the ENGAGE AF-TIMI 48 trial and the Hokusai-VTE trial. ![]()
Photo by Rhoda Baer
The oral factor Xa inhibitor edoxaban (Savaysa) is now available in US pharmacies, according to Daiichi Sankyo Company, Limited, the company developing the drug.
Savaysa is approved by the US Food and Drug Administration to reduce the risk of stroke and systemic embolism (SE) in patients with non-valvular atrial fibrillation (NVAF), as well as for the treatment of deep vein thrombosis and pulmonary embolism following 5 to 10 days of initial therapy with a parenteral anticoagulant.
According to Savaysa’s label, it should not be used in NVAF patients with creatinine clearance levels greater than 95 mL/min because, in that population, there is an increased risk of ischemic stroke with the drug compared to warfarin.
Daiichi Sankyo has developed resources for physicians and patients to help ensure patients can begin and/or remain on Savaysa per physician instructions.
The Savaysa Savings Plus program will include a reimbursement hotline to assist patients and prescribers who request help understanding a patient’s available coverage. Eligible patients who are prescribed Savaysa can enroll in a copay savings program and pay $4 per month through the Savaysa Savings Card.
Vouchers will also be available to provide patients and doctors with a way to try Savaysa at no cost to see if it is right for the patient.
In addition, the Savaysa Patient Assistance Program will offer assistance to qualified individuals, providing free product to eligible patients who are prescribed Savaysa, are uninsured, and are unable to identify alternative payment sources.
The approval of Savaysa in the US is based on data from the ENGAGE AF-TIMI 48 trial and the Hokusai-VTE trial. ![]()
FDA clears new blood-draw device

Photo courtesy of
Velano Vascular
The US Food and Drug Administration (FDA) has cleared for marketing a device that reduces the need for venipunctures for in-hospital blood draws.
Velano Vascular’s blood-draw device resembles a common syringe.
It allows peripheral intravenous catheters to be repurposed to draw blood from patients, thereby reducing the need for additional needle sticks among patients receiving medications and hydration via intravenous delivery.
The single-use device will soon be used for clinical evaluation in select hospitals, including the University of Pennsylvania in Philadelphia and University Hospitals Case Medical Center of Cleveland in Ohio.
“A fundamental benefit of this technology is reducing the ‘pin cushion effect,’ in which hospitalized patients are ‘stuck’ several times daily to obtain blood tests,” said Eric M. Stone, co-founder and chief executive officer of Velano Vascular, the company developing the blood-draw device.
“Oftentimes, the draw procedure is plagued by multiple failed attempts. The FDA’s clearance of this novel technology validates the existing clinical need and will allow us to expedite our efforts to bring this innovation to patients, healthcare providers, and hospitals around the world.”
According to research conducted by Velano Vascular, 1 of every 3 hospital patients is stuck 2 or more times daily for blood draws, with a significant subset of these patients receiving 3 or more blood draws, along with numerous needle sticks.
Twenty-eight percent of adult venipunctures and 44% of pediatric venipunctures require more than one stick to successfully draw blood.
“Traditional blood draws are one of the most common and most problematic healthcare procedures,” said Karen Daley, PhD, RN, past president of the American Nurses Association and a healthcare worker safety advocate.
“It is an antiquated technology that creates pain and anxiety for many patients, a significant safety risk for healthcare professionals, and a real inefficiency in our healthcare system. Velano Vascular has developed a common-sense solution to this pervasive, long-standing problem.” ![]()
Photo courtesy of
Velano Vascular
The US Food and Drug Administration (FDA) has cleared for marketing a device that reduces the need for venipunctures for in-hospital blood draws.
Velano Vascular’s blood-draw device resembles a common syringe.
It allows peripheral intravenous catheters to be repurposed to draw blood from patients, thereby reducing the need for additional needle sticks among patients receiving medications and hydration via intravenous delivery.
The single-use device will soon be used for clinical evaluation in select hospitals, including the University of Pennsylvania in Philadelphia and University Hospitals Case Medical Center of Cleveland in Ohio.
“A fundamental benefit of this technology is reducing the ‘pin cushion effect,’ in which hospitalized patients are ‘stuck’ several times daily to obtain blood tests,” said Eric M. Stone, co-founder and chief executive officer of Velano Vascular, the company developing the blood-draw device.
“Oftentimes, the draw procedure is plagued by multiple failed attempts. The FDA’s clearance of this novel technology validates the existing clinical need and will allow us to expedite our efforts to bring this innovation to patients, healthcare providers, and hospitals around the world.”
According to research conducted by Velano Vascular, 1 of every 3 hospital patients is stuck 2 or more times daily for blood draws, with a significant subset of these patients receiving 3 or more blood draws, along with numerous needle sticks.
Twenty-eight percent of adult venipunctures and 44% of pediatric venipunctures require more than one stick to successfully draw blood.
“Traditional blood draws are one of the most common and most problematic healthcare procedures,” said Karen Daley, PhD, RN, past president of the American Nurses Association and a healthcare worker safety advocate.
“It is an antiquated technology that creates pain and anxiety for many patients, a significant safety risk for healthcare professionals, and a real inefficiency in our healthcare system. Velano Vascular has developed a common-sense solution to this pervasive, long-standing problem.” ![]()
Photo courtesy of
Velano Vascular
The US Food and Drug Administration (FDA) has cleared for marketing a device that reduces the need for venipunctures for in-hospital blood draws.
Velano Vascular’s blood-draw device resembles a common syringe.
It allows peripheral intravenous catheters to be repurposed to draw blood from patients, thereby reducing the need for additional needle sticks among patients receiving medications and hydration via intravenous delivery.
The single-use device will soon be used for clinical evaluation in select hospitals, including the University of Pennsylvania in Philadelphia and University Hospitals Case Medical Center of Cleveland in Ohio.
“A fundamental benefit of this technology is reducing the ‘pin cushion effect,’ in which hospitalized patients are ‘stuck’ several times daily to obtain blood tests,” said Eric M. Stone, co-founder and chief executive officer of Velano Vascular, the company developing the blood-draw device.
“Oftentimes, the draw procedure is plagued by multiple failed attempts. The FDA’s clearance of this novel technology validates the existing clinical need and will allow us to expedite our efforts to bring this innovation to patients, healthcare providers, and hospitals around the world.”
According to research conducted by Velano Vascular, 1 of every 3 hospital patients is stuck 2 or more times daily for blood draws, with a significant subset of these patients receiving 3 or more blood draws, along with numerous needle sticks.
Twenty-eight percent of adult venipunctures and 44% of pediatric venipunctures require more than one stick to successfully draw blood.
“Traditional blood draws are one of the most common and most problematic healthcare procedures,” said Karen Daley, PhD, RN, past president of the American Nurses Association and a healthcare worker safety advocate.
“It is an antiquated technology that creates pain and anxiety for many patients, a significant safety risk for healthcare professionals, and a real inefficiency in our healthcare system. Velano Vascular has developed a common-sense solution to this pervasive, long-standing problem.” ![]()
More donated hearts rejected, even as wait list grows
Only about one in three available hearts was accepted for transplant in the United States in 2010, down from 44% 2 decades ago, researchers reported online Feb. 9 in the American Journal of Transplantation.
The decline stems in part from transplant centers rejecting “marginal” donor hearts, belying a growing need for heart transplants, longer waiting times, and multiple campaigns to expand the use of organs donated for transplantation, said Dr. Kiran Khush of Stanford (Calif.) University and her associates.

The researchers analyzed data on 82,053 potential donor hearts from the Organ Procurement and Transplantation Network. In 1995, 44% of available hearts were accepted for transplant, compared with only 29% in 2006 and 32% in 2010, they found. Meanwhile, rejection rates for donor hearts rose from 37% in 1995 to 52% in 2010, they reported (Am. J. Transplant. 2015 Feb. 10 [doi:10.1111/ajt.13055]).
Several factors might explain the trends, the investigators said. Potential heart donors tended to be older and more often had hypertension and diabetes by the final years of the study period, and transplant centers were less likely to accept hearts from such individuals. Also, mechanical circulatory devices were more commonly used, and centers might hesitate to transplant “marginal” hearts into “stable” recipients of such devices, Dr. Khush and her associates said. Furthermore, government scrutiny of post-transplant outcomes might make centers more conservative when evaluating potential donors, they added.
The study also uncovered regional variations in acceptance rates for donor hearts, with the lowest – about 25%-28% – found primarily in the southeastern United States. “Unfortunately, there are no standard guidelines for donor heart evaluation and acceptance, resulting in considerable inconsistencies in the types of donor hearts that are accepted by different transplant centers, and likely resulting in nonrecovery of potentially useful organs,” the investigators said. The findings “lend support to research and policy efforts aimed at establishing evidence-based criteria for donor heart evaluation and acceptance,” they added.
The work was supported by the National Heart, Lung, and Blood Institute; the National Institute of Diabetes and Digestive and Kidney Diseases; and the Health Resources and Services Administration. The authors reported having no conflicts of interest.
Only about one in three available hearts was accepted for transplant in the United States in 2010, down from 44% 2 decades ago, researchers reported online Feb. 9 in the American Journal of Transplantation.
The decline stems in part from transplant centers rejecting “marginal” donor hearts, belying a growing need for heart transplants, longer waiting times, and multiple campaigns to expand the use of organs donated for transplantation, said Dr. Kiran Khush of Stanford (Calif.) University and her associates.
The researchers analyzed data on 82,053 potential donor hearts from the Organ Procurement and Transplantation Network. In 1995, 44% of available hearts were accepted for transplant, compared with only 29% in 2006 and 32% in 2010, they found. Meanwhile, rejection rates for donor hearts rose from 37% in 1995 to 52% in 2010, they reported (Am. J. Transplant. 2015 Feb. 10 [doi:10.1111/ajt.13055]).
Several factors might explain the trends, the investigators said. Potential heart donors tended to be older and more often had hypertension and diabetes by the final years of the study period, and transplant centers were less likely to accept hearts from such individuals. Also, mechanical circulatory devices were more commonly used, and centers might hesitate to transplant “marginal” hearts into “stable” recipients of such devices, Dr. Khush and her associates said. Furthermore, government scrutiny of post-transplant outcomes might make centers more conservative when evaluating potential donors, they added.
The study also uncovered regional variations in acceptance rates for donor hearts, with the lowest – about 25%-28% – found primarily in the southeastern United States. “Unfortunately, there are no standard guidelines for donor heart evaluation and acceptance, resulting in considerable inconsistencies in the types of donor hearts that are accepted by different transplant centers, and likely resulting in nonrecovery of potentially useful organs,” the investigators said. The findings “lend support to research and policy efforts aimed at establishing evidence-based criteria for donor heart evaluation and acceptance,” they added.
The work was supported by the National Heart, Lung, and Blood Institute; the National Institute of Diabetes and Digestive and Kidney Diseases; and the Health Resources and Services Administration. The authors reported having no conflicts of interest.
Only about one in three available hearts was accepted for transplant in the United States in 2010, down from 44% 2 decades ago, researchers reported online Feb. 9 in the American Journal of Transplantation.
The decline stems in part from transplant centers rejecting “marginal” donor hearts, belying a growing need for heart transplants, longer waiting times, and multiple campaigns to expand the use of organs donated for transplantation, said Dr. Kiran Khush of Stanford (Calif.) University and her associates.
The researchers analyzed data on 82,053 potential donor hearts from the Organ Procurement and Transplantation Network. In 1995, 44% of available hearts were accepted for transplant, compared with only 29% in 2006 and 32% in 2010, they found. Meanwhile, rejection rates for donor hearts rose from 37% in 1995 to 52% in 2010, they reported (Am. J. Transplant. 2015 Feb. 10 [doi:10.1111/ajt.13055]).
Several factors might explain the trends, the investigators said. Potential heart donors tended to be older and more often had hypertension and diabetes by the final years of the study period, and transplant centers were less likely to accept hearts from such individuals. Also, mechanical circulatory devices were more commonly used, and centers might hesitate to transplant “marginal” hearts into “stable” recipients of such devices, Dr. Khush and her associates said. Furthermore, government scrutiny of post-transplant outcomes might make centers more conservative when evaluating potential donors, they added.
The study also uncovered regional variations in acceptance rates for donor hearts, with the lowest – about 25%-28% – found primarily in the southeastern United States. “Unfortunately, there are no standard guidelines for donor heart evaluation and acceptance, resulting in considerable inconsistencies in the types of donor hearts that are accepted by different transplant centers, and likely resulting in nonrecovery of potentially useful organs,” the investigators said. The findings “lend support to research and policy efforts aimed at establishing evidence-based criteria for donor heart evaluation and acceptance,” they added.
The work was supported by the National Heart, Lung, and Blood Institute; the National Institute of Diabetes and Digestive and Kidney Diseases; and the Health Resources and Services Administration. The authors reported having no conflicts of interest.
FROM THE AMERICAN JOURNAL OF TRANSPLANTATION
Key clinical point: Acceptance rates of hearts donated for transplantation have declined substantially in the United States.
Major finding: Only 32% of donated hearts were accepted for transplant in 2010, compared with 44% in 1995.
Data source: Analysis of 82,053 potential donor hearts from the Organ Procurement and Transplantation Network.
Disclosures: The study was supported by the National Heart, Lung, and Blood Institute; the National Institute of Diabetes and Digestive and Kidney Diseases; and the Health Resources and Services Administration. The authors reported having no conflicts of interest.

Overall survival plateaus at 3 years for ipilimumab-treated melanoma patients
Among patients with advanced melanoma who were treated with ipilimumab, about 20%-26% survived to 3 years, and these patients are likely to have a good long-term outcome, according to a pooled analysis of survival data published online Feb. 9 in the Journal of Clinical Oncology.
Investigators pooled data from ten prospective (including two phase III trials) and two retrospective studies with a total of 1,257 previously treated and 604 treatment-naive patients. At least 3 years after receiving ipilimumab, 254 patients were still alive, with a median follow up for this subset of 69 months. Around year 3, the Kaplan-Meier overall survival (OS) curve began to plateau and extended to 9.9 years for the longest survival follow-up.
“These results suggest that the majority of patients who reached this milestone time point had a low risk of death thereafter,” wrote Dr. Dirk Schadendorf and his associates (J. Clin. Oncol. 2015 Feb. 9 [doi:10.1200/JCO.2014.56.2736]).
Compared with patients who were previously treated, treatment-naive patients had a higher median overall survival (13.5 months [95% confidence interval, 11.9-15.4] vs. 10.7 months [9.6-11.4]) and higher 3-year-survival rates (26% [21%-30%] vs. 20% [18%-23%]). No definitive conclusion could be drawn from this observation, however, since nonrandomized subsets were used for this analysis. Subset analysis by dose showed similar median OS and 3-year survival rates for ipilimumab 3 mg/kg, 10 mg/kg, and other dosing regimens.
The researchers expanded the study to include overall survival (OS) data from 2,985 patients enrolled in a U.S. multicenter, open-label, expanded-access treatment protocol (EAP). This group included patients with poorer prognostic factors, some of whom were ineligible for clinical trials. The expanded group showed a lower median OS of 9.5 months and 3 year–survival rate of 21%, with the familiar OS curve plateau around 3 years that extended up to 10 years in some patients.
While this analysis only examined overall survival rates, individual ipilimumab studies that tracked patient responses to the drug have shown that some proportion of long-term survivors did not achieve a response. Identifying the specific disease characteristics of the long-term survivors will require further study.
“Considering the historic median OS of approximately 8-10 months and a 5-year survival rate of approximately 10% in advanced melanoma, the results presented herein are encouraging for patients diagnosed with this aggressive disease,” the authors wrote.
Dr. Schadendorf and his associates demonstrate a plateau in the survival curve of ipilimumab-treated patients beginning at about 3 years and representing about 21% of the treatment group. The curve suggests that those who survive to 3 years are highly likely to have a good long-term outcome, which provides a strong motivating factor in the decision to consider ipilimumab treatment. While pooled data adds information far beyond individual trials, a major drawback lies in the loss of control data necessary to isolate the added benefit of the study drug.
An indirect comparison using historic control series, in this case a large cohort documented in the American Joint Committee on Cancer (AJCC) Melanoma Staging Database, can substitute for missing control data in the pooled analysis. Reviewing data for stage IIIc and IV patients, the overall survival Kaplan-Meier curves in this population also show a plateau, but much later than that reported for ipilimumab, at beyond 8 years.
The AJCC melanoma classification gives survival rates at 3, 5, and 10 years of 19%, 13%, and 9%, respectively. Comparison with ipilimumab data suggests that survival at 3 years is similar, but thereafter improves with ipilimumab by 10% over other treatments that were available at the time. This difference is similar to the percentage of patients who achieved objective responses with ipilimumab. Although assessing response rate and progression-free survival in patients treated with ipilimumab presents challenges, the long-term benefits of ipilimumab could be better ascertained if information on the number of patients in the 21% plateau who were disease free or stably maintaining response had been collected.
Evaluation of long-term benefits of ipilimumab should consider toxicities and costs, as it is one of the most costly systemic therapies used for cancer treatment. The phase III trial using the drug at 3 mg/kg demonstrated that the large majority of patients had no serious adverse effects. If older patients and those with advanced disease are candidates, then the 10%-15% of grade 3 or 4 adverse events may translate to hospitalization and added expense, putting health regulatory systems in the position to deny widespread use of the agent despite proven benefit.
As the first agent to benefit overall survival of patients with advanced melanoma, ipilimumab may pave the way to broader improvements in a larger proportion of patients by combining with targeted therapies, such as BRAF and MEK inhibitors, and other new immunotherapies, such as anti-PD-1 antibodies.
Dr. Antoni Ribas is an oncologist with the Jonsson Comprehensive Cancer Center, Los Angles, and Dr. Keith T. Flaherty is an oncologist with Massachusetts General Hospital Cancer Center, Boston. These remarks were part of an editorial accompanying the report (J. Clin. Oncol. 2015 Feb. 9 [doi:10.1200/JCO.2014.56.2736]). Dr. Ribas has an advisory role with Merck, Amgen, Novartis, GlaxoSmithKline, and Genentech/Roche. Dr. Flaherty has an advisory role with GlaxoSmithKline, Genentech/Roche, Novartis, and Merck.
Dr. Schadendorf and his associates demonstrate a plateau in the survival curve of ipilimumab-treated patients beginning at about 3 years and representing about 21% of the treatment group. The curve suggests that those who survive to 3 years are highly likely to have a good long-term outcome, which provides a strong motivating factor in the decision to consider ipilimumab treatment. While pooled data adds information far beyond individual trials, a major drawback lies in the loss of control data necessary to isolate the added benefit of the study drug.
An indirect comparison using historic control series, in this case a large cohort documented in the American Joint Committee on Cancer (AJCC) Melanoma Staging Database, can substitute for missing control data in the pooled analysis. Reviewing data for stage IIIc and IV patients, the overall survival Kaplan-Meier curves in this population also show a plateau, but much later than that reported for ipilimumab, at beyond 8 years.
The AJCC melanoma classification gives survival rates at 3, 5, and 10 years of 19%, 13%, and 9%, respectively. Comparison with ipilimumab data suggests that survival at 3 years is similar, but thereafter improves with ipilimumab by 10% over other treatments that were available at the time. This difference is similar to the percentage of patients who achieved objective responses with ipilimumab. Although assessing response rate and progression-free survival in patients treated with ipilimumab presents challenges, the long-term benefits of ipilimumab could be better ascertained if information on the number of patients in the 21% plateau who were disease free or stably maintaining response had been collected.
Evaluation of long-term benefits of ipilimumab should consider toxicities and costs, as it is one of the most costly systemic therapies used for cancer treatment. The phase III trial using the drug at 3 mg/kg demonstrated that the large majority of patients had no serious adverse effects. If older patients and those with advanced disease are candidates, then the 10%-15% of grade 3 or 4 adverse events may translate to hospitalization and added expense, putting health regulatory systems in the position to deny widespread use of the agent despite proven benefit.
As the first agent to benefit overall survival of patients with advanced melanoma, ipilimumab may pave the way to broader improvements in a larger proportion of patients by combining with targeted therapies, such as BRAF and MEK inhibitors, and other new immunotherapies, such as anti-PD-1 antibodies.
Dr. Antoni Ribas is an oncologist with the Jonsson Comprehensive Cancer Center, Los Angles, and Dr. Keith T. Flaherty is an oncologist with Massachusetts General Hospital Cancer Center, Boston. These remarks were part of an editorial accompanying the report (J. Clin. Oncol. 2015 Feb. 9 [doi:10.1200/JCO.2014.56.2736]). Dr. Ribas has an advisory role with Merck, Amgen, Novartis, GlaxoSmithKline, and Genentech/Roche. Dr. Flaherty has an advisory role with GlaxoSmithKline, Genentech/Roche, Novartis, and Merck.
Dr. Schadendorf and his associates demonstrate a plateau in the survival curve of ipilimumab-treated patients beginning at about 3 years and representing about 21% of the treatment group. The curve suggests that those who survive to 3 years are highly likely to have a good long-term outcome, which provides a strong motivating factor in the decision to consider ipilimumab treatment. While pooled data adds information far beyond individual trials, a major drawback lies in the loss of control data necessary to isolate the added benefit of the study drug.
An indirect comparison using historic control series, in this case a large cohort documented in the American Joint Committee on Cancer (AJCC) Melanoma Staging Database, can substitute for missing control data in the pooled analysis. Reviewing data for stage IIIc and IV patients, the overall survival Kaplan-Meier curves in this population also show a plateau, but much later than that reported for ipilimumab, at beyond 8 years.
The AJCC melanoma classification gives survival rates at 3, 5, and 10 years of 19%, 13%, and 9%, respectively. Comparison with ipilimumab data suggests that survival at 3 years is similar, but thereafter improves with ipilimumab by 10% over other treatments that were available at the time. This difference is similar to the percentage of patients who achieved objective responses with ipilimumab. Although assessing response rate and progression-free survival in patients treated with ipilimumab presents challenges, the long-term benefits of ipilimumab could be better ascertained if information on the number of patients in the 21% plateau who were disease free or stably maintaining response had been collected.
Evaluation of long-term benefits of ipilimumab should consider toxicities and costs, as it is one of the most costly systemic therapies used for cancer treatment. The phase III trial using the drug at 3 mg/kg demonstrated that the large majority of patients had no serious adverse effects. If older patients and those with advanced disease are candidates, then the 10%-15% of grade 3 or 4 adverse events may translate to hospitalization and added expense, putting health regulatory systems in the position to deny widespread use of the agent despite proven benefit.
As the first agent to benefit overall survival of patients with advanced melanoma, ipilimumab may pave the way to broader improvements in a larger proportion of patients by combining with targeted therapies, such as BRAF and MEK inhibitors, and other new immunotherapies, such as anti-PD-1 antibodies.
Dr. Antoni Ribas is an oncologist with the Jonsson Comprehensive Cancer Center, Los Angles, and Dr. Keith T. Flaherty is an oncologist with Massachusetts General Hospital Cancer Center, Boston. These remarks were part of an editorial accompanying the report (J. Clin. Oncol. 2015 Feb. 9 [doi:10.1200/JCO.2014.56.2736]). Dr. Ribas has an advisory role with Merck, Amgen, Novartis, GlaxoSmithKline, and Genentech/Roche. Dr. Flaherty has an advisory role with GlaxoSmithKline, Genentech/Roche, Novartis, and Merck.
Among patients with advanced melanoma who were treated with ipilimumab, about 20%-26% survived to 3 years, and these patients are likely to have a good long-term outcome, according to a pooled analysis of survival data published online Feb. 9 in the Journal of Clinical Oncology.
Investigators pooled data from ten prospective (including two phase III trials) and two retrospective studies with a total of 1,257 previously treated and 604 treatment-naive patients. At least 3 years after receiving ipilimumab, 254 patients were still alive, with a median follow up for this subset of 69 months. Around year 3, the Kaplan-Meier overall survival (OS) curve began to plateau and extended to 9.9 years for the longest survival follow-up.
“These results suggest that the majority of patients who reached this milestone time point had a low risk of death thereafter,” wrote Dr. Dirk Schadendorf and his associates (J. Clin. Oncol. 2015 Feb. 9 [doi:10.1200/JCO.2014.56.2736]).
Compared with patients who were previously treated, treatment-naive patients had a higher median overall survival (13.5 months [95% confidence interval, 11.9-15.4] vs. 10.7 months [9.6-11.4]) and higher 3-year-survival rates (26% [21%-30%] vs. 20% [18%-23%]). No definitive conclusion could be drawn from this observation, however, since nonrandomized subsets were used for this analysis. Subset analysis by dose showed similar median OS and 3-year survival rates for ipilimumab 3 mg/kg, 10 mg/kg, and other dosing regimens.
The researchers expanded the study to include overall survival (OS) data from 2,985 patients enrolled in a U.S. multicenter, open-label, expanded-access treatment protocol (EAP). This group included patients with poorer prognostic factors, some of whom were ineligible for clinical trials. The expanded group showed a lower median OS of 9.5 months and 3 year–survival rate of 21%, with the familiar OS curve plateau around 3 years that extended up to 10 years in some patients.
While this analysis only examined overall survival rates, individual ipilimumab studies that tracked patient responses to the drug have shown that some proportion of long-term survivors did not achieve a response. Identifying the specific disease characteristics of the long-term survivors will require further study.
“Considering the historic median OS of approximately 8-10 months and a 5-year survival rate of approximately 10% in advanced melanoma, the results presented herein are encouraging for patients diagnosed with this aggressive disease,” the authors wrote.
Among patients with advanced melanoma who were treated with ipilimumab, about 20%-26% survived to 3 years, and these patients are likely to have a good long-term outcome, according to a pooled analysis of survival data published online Feb. 9 in the Journal of Clinical Oncology.
Investigators pooled data from ten prospective (including two phase III trials) and two retrospective studies with a total of 1,257 previously treated and 604 treatment-naive patients. At least 3 years after receiving ipilimumab, 254 patients were still alive, with a median follow up for this subset of 69 months. Around year 3, the Kaplan-Meier overall survival (OS) curve began to plateau and extended to 9.9 years for the longest survival follow-up.
“These results suggest that the majority of patients who reached this milestone time point had a low risk of death thereafter,” wrote Dr. Dirk Schadendorf and his associates (J. Clin. Oncol. 2015 Feb. 9 [doi:10.1200/JCO.2014.56.2736]).
Compared with patients who were previously treated, treatment-naive patients had a higher median overall survival (13.5 months [95% confidence interval, 11.9-15.4] vs. 10.7 months [9.6-11.4]) and higher 3-year-survival rates (26% [21%-30%] vs. 20% [18%-23%]). No definitive conclusion could be drawn from this observation, however, since nonrandomized subsets were used for this analysis. Subset analysis by dose showed similar median OS and 3-year survival rates for ipilimumab 3 mg/kg, 10 mg/kg, and other dosing regimens.
The researchers expanded the study to include overall survival (OS) data from 2,985 patients enrolled in a U.S. multicenter, open-label, expanded-access treatment protocol (EAP). This group included patients with poorer prognostic factors, some of whom were ineligible for clinical trials. The expanded group showed a lower median OS of 9.5 months and 3 year–survival rate of 21%, with the familiar OS curve plateau around 3 years that extended up to 10 years in some patients.
While this analysis only examined overall survival rates, individual ipilimumab studies that tracked patient responses to the drug have shown that some proportion of long-term survivors did not achieve a response. Identifying the specific disease characteristics of the long-term survivors will require further study.
“Considering the historic median OS of approximately 8-10 months and a 5-year survival rate of approximately 10% in advanced melanoma, the results presented herein are encouraging for patients diagnosed with this aggressive disease,” the authors wrote.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Ipilimumab-treated advanced melanoma patients alive at 3 years tend to have good long-term outcomes.
Major finding: Around year 3, the Kaplan-Meier OS curve began to plateau and extended to 9.9 years for the longest survival follow-up.
Data source: Pooled overall survival data from 12 studies including 1,861 ipilimumab-treated patients with advanced melanoma.
Disclosures: Dr. Schadendorf disclosed that he is a consultant for Bristol-Myers Squibb. Bristol-Myers Squibb sponsored this study.
ASCO endorses ACS guidelines for prostate cancer survivor care
The American Society of Clinical Oncology has endorsed the American Cancer Society Prostate Cancer Survivorship Care Guidelines, a 39-point list with recommendations on continuing care for prostate care survivors, but with a number of qualifying statements and modifications.
The guidelines, developed by a workgroup of 16 multidisciplinary experts specializing in the care of prostate cancer patients and the long-term effects of their treatments, are intended as points of reference for primary care providers, medical oncologists, urologists, and other health care providers.
Areas covered in the guidelines include health promotion, surveillance for recurrence, screening and early detection of second primary cancers, assessment and management of physical and psychosocial long-term and late effects, and care coordination and practice implications.Read the full list of recommendations here: (doi: 10.1200/JCO.2014.60.2557).
The American Society of Clinical Oncology has endorsed the American Cancer Society Prostate Cancer Survivorship Care Guidelines, a 39-point list with recommendations on continuing care for prostate care survivors, but with a number of qualifying statements and modifications.
The guidelines, developed by a workgroup of 16 multidisciplinary experts specializing in the care of prostate cancer patients and the long-term effects of their treatments, are intended as points of reference for primary care providers, medical oncologists, urologists, and other health care providers.
Areas covered in the guidelines include health promotion, surveillance for recurrence, screening and early detection of second primary cancers, assessment and management of physical and psychosocial long-term and late effects, and care coordination and practice implications.Read the full list of recommendations here: (doi: 10.1200/JCO.2014.60.2557).
The American Society of Clinical Oncology has endorsed the American Cancer Society Prostate Cancer Survivorship Care Guidelines, a 39-point list with recommendations on continuing care for prostate care survivors, but with a number of qualifying statements and modifications.
The guidelines, developed by a workgroup of 16 multidisciplinary experts specializing in the care of prostate cancer patients and the long-term effects of their treatments, are intended as points of reference for primary care providers, medical oncologists, urologists, and other health care providers.
Areas covered in the guidelines include health promotion, surveillance for recurrence, screening and early detection of second primary cancers, assessment and management of physical and psychosocial long-term and late effects, and care coordination and practice implications.Read the full list of recommendations here: (doi: 10.1200/JCO.2014.60.2557).
Psychopharmacology in primary care faces challenges
NEW YORK – Incorporating psychiatric assessment and treatment into a busy primary care practice is not easy, but it is doable.
“Every time I start a patient on a [psychiatric] medication I have a moment of trepidation, even though I have now done this for about 4 years,” Dr. Diane E. Bloomfield said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry. “It still does not come easily to me,” said Dr. Bloomfield, a general-practice pediatrician at the family care center of Montefiore Medical Center in New York.

Inclusion of mental health as part of routine pediatric practice is a new concept. “Until recently, we pediatricians did not think of mental health as part of daily practice,” she said.
Dr. Bloomfield cited three factors that pose the greatest challenges to integrating psychiatry into her practice: time constraints, reimbursement, and knowledge gaps.
Reimbursement limitations contribute to the time issue. Most of Dr. Bloomfield’s patients are covered by Medicaid, which allows for a 15-minute session with each patient and family. That’s barely enough time to assess a child’s social and emotional development, in addition to all the other bases she must cover during an appointment, but she tries to carve out time for more challenging cases by scheduling them near the end of her day.
Dr. Bloomfield said that she routinely administers the Pediatric Symptom Checklist to all her patients who are 4-18 years old. She recommended that pediatricians take advantage of all the screening tools that the American Academy of Pediatrics (AAP) includes with its practice guidelines, along with the other mental health resources on the AAP website. Using improved coding on her billings also allowed her to arrange reimbursement for more of the time she spends on mental health conditions.
Reducing the knowledge gap can be more complicated. Many pediatricians, Dr. Bloomfield included, did not prescribe methylphenidate or selective serotonin reuptake inhibitors (SSRIs) during training. The boxed warning that the Food and Drug Administration put on antidepressants starting in 2004 has been another factor dampening drug psychotherapy by pediatricians, dissuading them from treating depression, she said.
Some of these dilemmas decreased when the AAP released in 2010 two algorithms that provided a framework for identifying and managing mental health and substance abuse concerns in primary care (Pediatrics 2010;125:S109-25). Neither algorithm, however, dealt with psychopharmacology.
Survey results have shown that many pediatricians become more willing to prescribe SSRIs if they can consult with a psychiatrist about the diagnosis and treatment. Pediatricians are generally more comfortable prescribing stimulants for attention-deficit/hyperactivity disorder (ADHD). “We see a lot of kids with ADHD, so we think we need to do something for them. In addition, medications for ADHD either work or don’t work, but they don’t cause suicidality,” Dr. Bloomfield said.
An AAP working group that included Dr. Bloomfield recently introduced a pilot program for a revised residency curriculum that includes a mental health module as well as a second module that focuses on anxiety diagnosis and management. In addition, certain states, including Massachusetts and New York, have introduced postresidency education programs that deal with child and adolescent psychiatry, including drug treatment.
Dr. Bloomfield said that she had taken training courses in the New York program. “It gave me the tools for evaluating patients and it taught me how to start medications in a safe way.” The midcareer training she received through New York’s Child and Adolescent Psychiatry for Primary Care program “made me much more confident that I could address my patients’ psychosocial needs.” Today, Dr. Bloomfield said she tries to manage children and adolescents with mild depression herself and not refer them to a specialist.
“Pediatricians are quite willing” to include psychiatric interventions in their practice, but we need support from psychiatrists to receive the necessary education and adequate reimbursement,” Dr. Bloomfield said.
On Twitter @mitchelzoler
NEW YORK – Incorporating psychiatric assessment and treatment into a busy primary care practice is not easy, but it is doable.
“Every time I start a patient on a [psychiatric] medication I have a moment of trepidation, even though I have now done this for about 4 years,” Dr. Diane E. Bloomfield said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry. “It still does not come easily to me,” said Dr. Bloomfield, a general-practice pediatrician at the family care center of Montefiore Medical Center in New York.
Inclusion of mental health as part of routine pediatric practice is a new concept. “Until recently, we pediatricians did not think of mental health as part of daily practice,” she said.
Dr. Bloomfield cited three factors that pose the greatest challenges to integrating psychiatry into her practice: time constraints, reimbursement, and knowledge gaps.
Reimbursement limitations contribute to the time issue. Most of Dr. Bloomfield’s patients are covered by Medicaid, which allows for a 15-minute session with each patient and family. That’s barely enough time to assess a child’s social and emotional development, in addition to all the other bases she must cover during an appointment, but she tries to carve out time for more challenging cases by scheduling them near the end of her day.
Dr. Bloomfield said that she routinely administers the Pediatric Symptom Checklist to all her patients who are 4-18 years old. She recommended that pediatricians take advantage of all the screening tools that the American Academy of Pediatrics (AAP) includes with its practice guidelines, along with the other mental health resources on the AAP website. Using improved coding on her billings also allowed her to arrange reimbursement for more of the time she spends on mental health conditions.
Reducing the knowledge gap can be more complicated. Many pediatricians, Dr. Bloomfield included, did not prescribe methylphenidate or selective serotonin reuptake inhibitors (SSRIs) during training. The boxed warning that the Food and Drug Administration put on antidepressants starting in 2004 has been another factor dampening drug psychotherapy by pediatricians, dissuading them from treating depression, she said.
Some of these dilemmas decreased when the AAP released in 2010 two algorithms that provided a framework for identifying and managing mental health and substance abuse concerns in primary care (Pediatrics 2010;125:S109-25). Neither algorithm, however, dealt with psychopharmacology.
Survey results have shown that many pediatricians become more willing to prescribe SSRIs if they can consult with a psychiatrist about the diagnosis and treatment. Pediatricians are generally more comfortable prescribing stimulants for attention-deficit/hyperactivity disorder (ADHD). “We see a lot of kids with ADHD, so we think we need to do something for them. In addition, medications for ADHD either work or don’t work, but they don’t cause suicidality,” Dr. Bloomfield said.
An AAP working group that included Dr. Bloomfield recently introduced a pilot program for a revised residency curriculum that includes a mental health module as well as a second module that focuses on anxiety diagnosis and management. In addition, certain states, including Massachusetts and New York, have introduced postresidency education programs that deal with child and adolescent psychiatry, including drug treatment.
Dr. Bloomfield said that she had taken training courses in the New York program. “It gave me the tools for evaluating patients and it taught me how to start medications in a safe way.” The midcareer training she received through New York’s Child and Adolescent Psychiatry for Primary Care program “made me much more confident that I could address my patients’ psychosocial needs.” Today, Dr. Bloomfield said she tries to manage children and adolescents with mild depression herself and not refer them to a specialist.
“Pediatricians are quite willing” to include psychiatric interventions in their practice, but we need support from psychiatrists to receive the necessary education and adequate reimbursement,” Dr. Bloomfield said.
On Twitter @mitchelzoler
NEW YORK – Incorporating psychiatric assessment and treatment into a busy primary care practice is not easy, but it is doable.
“Every time I start a patient on a [psychiatric] medication I have a moment of trepidation, even though I have now done this for about 4 years,” Dr. Diane E. Bloomfield said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry. “It still does not come easily to me,” said Dr. Bloomfield, a general-practice pediatrician at the family care center of Montefiore Medical Center in New York.
Inclusion of mental health as part of routine pediatric practice is a new concept. “Until recently, we pediatricians did not think of mental health as part of daily practice,” she said.
Dr. Bloomfield cited three factors that pose the greatest challenges to integrating psychiatry into her practice: time constraints, reimbursement, and knowledge gaps.
Reimbursement limitations contribute to the time issue. Most of Dr. Bloomfield’s patients are covered by Medicaid, which allows for a 15-minute session with each patient and family. That’s barely enough time to assess a child’s social and emotional development, in addition to all the other bases she must cover during an appointment, but she tries to carve out time for more challenging cases by scheduling them near the end of her day.
Dr. Bloomfield said that she routinely administers the Pediatric Symptom Checklist to all her patients who are 4-18 years old. She recommended that pediatricians take advantage of all the screening tools that the American Academy of Pediatrics (AAP) includes with its practice guidelines, along with the other mental health resources on the AAP website. Using improved coding on her billings also allowed her to arrange reimbursement for more of the time she spends on mental health conditions.
Reducing the knowledge gap can be more complicated. Many pediatricians, Dr. Bloomfield included, did not prescribe methylphenidate or selective serotonin reuptake inhibitors (SSRIs) during training. The boxed warning that the Food and Drug Administration put on antidepressants starting in 2004 has been another factor dampening drug psychotherapy by pediatricians, dissuading them from treating depression, she said.
Some of these dilemmas decreased when the AAP released in 2010 two algorithms that provided a framework for identifying and managing mental health and substance abuse concerns in primary care (Pediatrics 2010;125:S109-25). Neither algorithm, however, dealt with psychopharmacology.
Survey results have shown that many pediatricians become more willing to prescribe SSRIs if they can consult with a psychiatrist about the diagnosis and treatment. Pediatricians are generally more comfortable prescribing stimulants for attention-deficit/hyperactivity disorder (ADHD). “We see a lot of kids with ADHD, so we think we need to do something for them. In addition, medications for ADHD either work or don’t work, but they don’t cause suicidality,” Dr. Bloomfield said.
An AAP working group that included Dr. Bloomfield recently introduced a pilot program for a revised residency curriculum that includes a mental health module as well as a second module that focuses on anxiety diagnosis and management. In addition, certain states, including Massachusetts and New York, have introduced postresidency education programs that deal with child and adolescent psychiatry, including drug treatment.
Dr. Bloomfield said that she had taken training courses in the New York program. “It gave me the tools for evaluating patients and it taught me how to start medications in a safe way.” The midcareer training she received through New York’s Child and Adolescent Psychiatry for Primary Care program “made me much more confident that I could address my patients’ psychosocial needs.” Today, Dr. Bloomfield said she tries to manage children and adolescents with mild depression herself and not refer them to a specialist.
“Pediatricians are quite willing” to include psychiatric interventions in their practice, but we need support from psychiatrists to receive the necessary education and adequate reimbursement,” Dr. Bloomfield said.
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE

NASH on the rise as a cause of liver transplants
Since 2004, there’s been almost a tripling of the number of nonalcoholic steatohepatitis patients waiting for liver transplants; the condition is now the second leading reason to be put on the waiting list in the United States, according to a study published in the March issue of Gastroenterology.*
Even so and for reasons that are not fully clear, adults with nonalcoholic steatohepatitis (NASH) are less likely to survive for 90 days on the wait list than are patients with alcoholic liver disease (ALD), and less likely to get a new liver within 90 days than are patients with ALD, hepatitis C virus (HCV), or a blend of both. For now, HCV remains the No. 1 reason for liver transplants in the United States (Gastroenterology 2014 Nov. 24 [doi: 10.1053/j.gastro.2014.11.039]).
“Our study provides valuable information about the changing epidemiology of chronic liver disease among wait-listed patients, and adds greatly to our understanding of the epidemiology of NASH in the United States,” the researchers wrote. The rapid rise in the prevalence of NASH is “a direct consequence of the worldwide obesity epidemic” as well as greater awareness of the condition. An expected decline in HCV-related cirrhosis due to effective antiviral therapy “will further contribute to the changing epidemiology of patients awaiting liver transplants in the United States,” said the authors, led by Dr. Robert Wong of the division of gastroenterology and hepatology at Highland Hospital, Oakland, Calif.
“Given the expected continued rise in the number of NASH patients awaiting liver transplant, additional research is needed to improve wait-list survival and ... outcomes among this cohort. In addition, the projection that overall donor availability will significantly diminish in the next 15-20 years emphasizes the need for additional research to improve liver transplant opportunities for NASH patients, including the option of living donor[s],” they said.
The researchers analyzed data from the United Network for Organ Sharing and Organ Procurement and Transplantation Network registry.
From 2004 to 2013, new wait-list registrants with NASH increased by 170% from 804 to 2,174; those with ALD increased by 45% from 1,400 to 2,024; and those with HCV increased by 14% from 2,887 to 3,291. Registrants with both HCV and ALD decreased by 9% from 880 to 803. NASH became the second-leading disease among liver transplant wait-list registrants in 2013.
Patients with ALD had a significantly higher Model for End-Stage Liver Disease (MELD) score at the time of registration than did others. However, after adjustment for MELD and other variables, patients with ALD were less likely to die within 90 days than were NASH patients (OR 0.77; 95% CI 0.67–0.89; P < .001). No difference was seen in wait-list mortality between NASH and HCV and HCV/ALD patients.
Compared with NASH, patients with HCV (OR 1.45; 95% CI 1.35–1.55; P < .001), ALD (OR 1.15; 95% CI: 1.06–1.24; P < .001), and HCV/ALD (OR 1.29; 95% CI 1.18–1.42; P < .001) were all significantly more likely to receive a liver after 3 months on the wait list.
A “potential explanation for these observations might be etiology-specific differences in disease progression, such that more aggressive etiologies (e.g., HCV or HCV/ALD) can have a more rapid rise in MELD score, receive liver transplant, and have lower wait-list mortality, and etiologies with less rapid progression (e.g., NASH) can have slower rise in MELD score over time, lower rates of LT, but no significant increase in wait-list mortality,” the investigators said.
Overall 1-year wait-list survival among NASH patients decreased from 42.8% in 2004-2008 to 25.6% in 2009-2013, and overall 1-year probability of receiving liver transplant among NASH patients also decreased from 42.1% in 2004-2008 to 39.6% in 2009-2013. The trends were similar for other etiologies, perhaps in part because there are more people waiting for a liver.
The authors said they have no financial conflicts to disclose.
*A change was made to the text on 3/12/2015.
Since 2004, there’s been almost a tripling of the number of nonalcoholic steatohepatitis patients waiting for liver transplants; the condition is now the second leading reason to be put on the waiting list in the United States, according to a study published in the March issue of Gastroenterology.*
Even so and for reasons that are not fully clear, adults with nonalcoholic steatohepatitis (NASH) are less likely to survive for 90 days on the wait list than are patients with alcoholic liver disease (ALD), and less likely to get a new liver within 90 days than are patients with ALD, hepatitis C virus (HCV), or a blend of both. For now, HCV remains the No. 1 reason for liver transplants in the United States (Gastroenterology 2014 Nov. 24 [doi: 10.1053/j.gastro.2014.11.039]).
“Our study provides valuable information about the changing epidemiology of chronic liver disease among wait-listed patients, and adds greatly to our understanding of the epidemiology of NASH in the United States,” the researchers wrote. The rapid rise in the prevalence of NASH is “a direct consequence of the worldwide obesity epidemic” as well as greater awareness of the condition. An expected decline in HCV-related cirrhosis due to effective antiviral therapy “will further contribute to the changing epidemiology of patients awaiting liver transplants in the United States,” said the authors, led by Dr. Robert Wong of the division of gastroenterology and hepatology at Highland Hospital, Oakland, Calif.
“Given the expected continued rise in the number of NASH patients awaiting liver transplant, additional research is needed to improve wait-list survival and ... outcomes among this cohort. In addition, the projection that overall donor availability will significantly diminish in the next 15-20 years emphasizes the need for additional research to improve liver transplant opportunities for NASH patients, including the option of living donor[s],” they said.
The researchers analyzed data from the United Network for Organ Sharing and Organ Procurement and Transplantation Network registry.
From 2004 to 2013, new wait-list registrants with NASH increased by 170% from 804 to 2,174; those with ALD increased by 45% from 1,400 to 2,024; and those with HCV increased by 14% from 2,887 to 3,291. Registrants with both HCV and ALD decreased by 9% from 880 to 803. NASH became the second-leading disease among liver transplant wait-list registrants in 2013.
Patients with ALD had a significantly higher Model for End-Stage Liver Disease (MELD) score at the time of registration than did others. However, after adjustment for MELD and other variables, patients with ALD were less likely to die within 90 days than were NASH patients (OR 0.77; 95% CI 0.67–0.89; P < .001). No difference was seen in wait-list mortality between NASH and HCV and HCV/ALD patients.
Compared with NASH, patients with HCV (OR 1.45; 95% CI 1.35–1.55; P < .001), ALD (OR 1.15; 95% CI: 1.06–1.24; P < .001), and HCV/ALD (OR 1.29; 95% CI 1.18–1.42; P < .001) were all significantly more likely to receive a liver after 3 months on the wait list.
A “potential explanation for these observations might be etiology-specific differences in disease progression, such that more aggressive etiologies (e.g., HCV or HCV/ALD) can have a more rapid rise in MELD score, receive liver transplant, and have lower wait-list mortality, and etiologies with less rapid progression (e.g., NASH) can have slower rise in MELD score over time, lower rates of LT, but no significant increase in wait-list mortality,” the investigators said.
Overall 1-year wait-list survival among NASH patients decreased from 42.8% in 2004-2008 to 25.6% in 2009-2013, and overall 1-year probability of receiving liver transplant among NASH patients also decreased from 42.1% in 2004-2008 to 39.6% in 2009-2013. The trends were similar for other etiologies, perhaps in part because there are more people waiting for a liver.
The authors said they have no financial conflicts to disclose.
*A change was made to the text on 3/12/2015.
Since 2004, there’s been almost a tripling of the number of nonalcoholic steatohepatitis patients waiting for liver transplants; the condition is now the second leading reason to be put on the waiting list in the United States, according to a study published in the March issue of Gastroenterology.*
Even so and for reasons that are not fully clear, adults with nonalcoholic steatohepatitis (NASH) are less likely to survive for 90 days on the wait list than are patients with alcoholic liver disease (ALD), and less likely to get a new liver within 90 days than are patients with ALD, hepatitis C virus (HCV), or a blend of both. For now, HCV remains the No. 1 reason for liver transplants in the United States (Gastroenterology 2014 Nov. 24 [doi: 10.1053/j.gastro.2014.11.039]).
“Our study provides valuable information about the changing epidemiology of chronic liver disease among wait-listed patients, and adds greatly to our understanding of the epidemiology of NASH in the United States,” the researchers wrote. The rapid rise in the prevalence of NASH is “a direct consequence of the worldwide obesity epidemic” as well as greater awareness of the condition. An expected decline in HCV-related cirrhosis due to effective antiviral therapy “will further contribute to the changing epidemiology of patients awaiting liver transplants in the United States,” said the authors, led by Dr. Robert Wong of the division of gastroenterology and hepatology at Highland Hospital, Oakland, Calif.
“Given the expected continued rise in the number of NASH patients awaiting liver transplant, additional research is needed to improve wait-list survival and ... outcomes among this cohort. In addition, the projection that overall donor availability will significantly diminish in the next 15-20 years emphasizes the need for additional research to improve liver transplant opportunities for NASH patients, including the option of living donor[s],” they said.
The researchers analyzed data from the United Network for Organ Sharing and Organ Procurement and Transplantation Network registry.
From 2004 to 2013, new wait-list registrants with NASH increased by 170% from 804 to 2,174; those with ALD increased by 45% from 1,400 to 2,024; and those with HCV increased by 14% from 2,887 to 3,291. Registrants with both HCV and ALD decreased by 9% from 880 to 803. NASH became the second-leading disease among liver transplant wait-list registrants in 2013.
Patients with ALD had a significantly higher Model for End-Stage Liver Disease (MELD) score at the time of registration than did others. However, after adjustment for MELD and other variables, patients with ALD were less likely to die within 90 days than were NASH patients (OR 0.77; 95% CI 0.67–0.89; P < .001). No difference was seen in wait-list mortality between NASH and HCV and HCV/ALD patients.
Compared with NASH, patients with HCV (OR 1.45; 95% CI 1.35–1.55; P < .001), ALD (OR 1.15; 95% CI: 1.06–1.24; P < .001), and HCV/ALD (OR 1.29; 95% CI 1.18–1.42; P < .001) were all significantly more likely to receive a liver after 3 months on the wait list.
A “potential explanation for these observations might be etiology-specific differences in disease progression, such that more aggressive etiologies (e.g., HCV or HCV/ALD) can have a more rapid rise in MELD score, receive liver transplant, and have lower wait-list mortality, and etiologies with less rapid progression (e.g., NASH) can have slower rise in MELD score over time, lower rates of LT, but no significant increase in wait-list mortality,” the investigators said.
Overall 1-year wait-list survival among NASH patients decreased from 42.8% in 2004-2008 to 25.6% in 2009-2013, and overall 1-year probability of receiving liver transplant among NASH patients also decreased from 42.1% in 2004-2008 to 39.6% in 2009-2013. The trends were similar for other etiologies, perhaps in part because there are more people waiting for a liver.
The authors said they have no financial conflicts to disclose.
*A change was made to the text on 3/12/2015.
FROM GASTROENTEROLOGY
Key clinical point: As the epidemiology of liver transplantation changes in the United States, more needs to be done to ensure good outcomes in NASH patients.
Major finding: From 2004 to 2013, new wait-list registrants with NASH increased by 170% from 804 to 2,174.
Data source: The United Network for Organ Sharing and Organ Procurement and Transplantation Network registry.
Disclosures: The authors said they have no relevant disclosures.
LISTEN NOW: SHM Launches a Patient Experience Committee
{kind=link}
Advance Care Planning Among Patients with Heart Failure: A Review of Challenges and Approaches to Better Communication
From the Rand Corporation and UCLA Fielding School of Public Health, Santa Monica, CA (Dr. Ahluwalia) and University of Southern California, Leonard Davis School of Gerontology, Los Angeles, CA (Dr. Enguidanos).
Abstract
- Objective: To review the relevance of advance care planning to heart failure management, describe key advance care planning challenges, and provide clinicians with actionable guidance for engaging in advance care planning conversations.
- Methods: Review of the literature.
- Results: Although most patients with heart failure prefer to receive thorough and honest information about their health condition and prognosis, the unpredictability of the heart failure trajectory coupled with physician barriers including discomfort with emotionally-laden topics and difficulty identifying the “right” time to engage in advance care planning, and systems barriers such as inadequate clinic time and limited reimbursement, impede timely engagement in advance care planning discussions. Approaches to effective advance care planning communication include using open-ended questions to stimulate patient engagement, evaluating how much information the patient wants to ensure patient-centeredness, and using empathic language to demonstrate support and understanding. While successful models of advance care planning communication have been identified, replication is limited due to the resource intense nature of these approaches.
- Conclusion: Challenges to advance care planning discussions among patients with heart failure may be mitigated through the establishment of communication quality standards as well as guidelines promoting early and ongoing advance care planning discussions, as well as reimbursement for outpatient discussions.
Heart failure, a leading cause of death, disability, and health care costs in the United States, is an incurable and life-limiting illness that is becoming increasingly prevalent due to an aging population and improved life expectancy. Approximately 5.3 million Americans are currently living with heart failure [1], with more than 550,000 new cases diagnosed each year [2]. Heart failure disproportionately affects older adults; about 80% of all cases occur in persons aged 65 years or older [3], and heart failure is the leading cause of hospital admissions among older adults [4]. The burden and impact of heart failure peaks near the end of life; 80% of Medicare beneficiaries with heart failure are hospitalized in the last 6 months of life [5].
The Trajectory of Heart Failure
Patients with heart failure experience a highly variable, nonlinear clinical trajectory marked by progressive deterioration and frequent exacerbations requiring hospitalization [6]. Their prognosis, though uncertain, is poor, with reported 1-year mortality rates following a hospitalization between 30% and 50% and 5-year mortality as high as 75% [7–11], a survival rate worse than that of some cancers [12]. Patients with heart failure caused by ischemic heart disease are at high risk for sudden cardiac death, particularly at earlier stages of the disease, which can confound the ability to appropriately plan for the future [13]. Those who survive to more advanced stages of heart failure face worsening quality of life [14–16], driven by a high prevalence of fatigue, breathlessness, pain, and depression [17–24]. Indeed, patients with heart failure have a similar symptom burden to patients with advanced cancer [25]. Older adults with heart failure also have a high comorbidity burden that further complicates both symptomology and disease trajectory with implications for decision-making about life-prolonging heart failure therapies [26,27].
Advance Care Planning in Heart Failure
The unpredictable nature of heart failure makes it difficult for patients and families to plan and prepare for their future, yet it is this very uncertainty that makes advance care planning (ACP) so critical for heart failure patients. Clear and honest patient-clinician communication about ACP, including an exploration of patient values and goals for care in the context of prognostic information, is essential to patient-centered treatment decision-making [28]. This is particularly relevant in heart failure, where a range of high-intensity, invasive, and costly interventions are increasingly being applied (eg, ventricular assist devices) without equivalent attention to quality of life and patients’ long-term goals for care.
Patients with heart failure and their families face multiple complex treatment decisions along the trajectory of their illness, such as discontinuation of beta blockers among patients with refractory fluid overload or angiotensin-converting enzyme inhibitors in end-stage patients with symptomatic hypotension [29,30]. In end-stage heart failure patients, deactivation of an implantable cardiac defibrillator might be considered to avoid the pain and distress associated with repeated shocks. In contrast, other interventions such as cardiac resynchronization therapy and continuous inotropic infusion have quality of life benefits; continuation of these therapies may be appropriate even when discontinuing other interventions. Such decisions should be guided by a thorough understanding of the patient’s expressed preferences and values, ideally assessed early in the trajectory of the disease and continuously re-evaluated as the diseases progresses.
The American Heart Association supports early and regular patient-provider ACP discussions to guide heart failure patients’ future decision-making [31], and recommends that such discussions be initiated in the outpatient setting, prior to and in anticipation of clinical decline. ACP communication plays a critical role in enhancing patients’ understanding of their diagnosis, treatment, prognosis, and choices in end-of-life care [31]. ACP communication also helps the clinician to better understand the context within which patients and their caregivers might make health care decisions, including their values and preferences for care. Patient-provider discussions about ACP focused on understanding patient values and initiated early in the trajectory of serious illness can support future in-the-moment decision-making, and is likely more effective than asking patients to make specific treatment decisions in advance [32]. A growing body of rigorous research has shown that ACP communication is associated with greater preference-concordant care and congruence in patient-surrogate understanding of patient preferences, lower costs, and less aggressive care at the end of life [33–37].
Patient Preferences for ACP Communication
Most patients with heart failure and their caregivers want honest disclosure regarding prognosis and to receive information about the expected trajectory of their disease [38–41] as early as possible [38] to help them plan and prepare for their future. Patients and their caregivers prefer to have these conversations with their physician [38] or other provider most familiar with the patient and family [39]. Patients also express a preference for support with dealing with the uncertainty inherent to heart failure [39]. Although most patients and caregivers desire to receive clear and honest communication about their disease, it is important to note that patients may vary in the extent of information they prefer to receive about their heart failure, with some individuals preferring not to talk about the end of life and future care needs at all [39,42–44].
Challenges to ACP Communication in Heart Failure
Despite patient and caregiver preferences for ACP communication with their providers, evidence suggests such communication occurs infrequently [40,45] and that heart failure patients may lack important information about their prognosis and treatment options [40,44,46,47]. For example, patients may not recognize the terminal nature of heart failure, and may be unaware of the range of treatment options, including hospice, available to them. Evidence also demonstrates that ACP is infrequently discussed with their health care providers [40], resulting in these conversations being avoided or deferred until an emergent clinical situation [44,48] when hasty questions about treatment choices may yield uncertain and conflicting answers not representative of a patient’s underlying values.
The infrequent, late, and often lack of discussions about ACP are driven by several challenges. First, the uncertain trajectory of heart failure makes communication regarding “what to expect” difficult. Prognostication is an immense challenge in heart failure [40,49–52], making it harder to talk about end-of-life issues and hindering the ability of patients, caregivers and health care providers to plan and prepare for the future. It is often difficult for clinicians, who face the challenge of instilling hope in the face of truthful disclosure [53], to identify the “right time” to initiate such discussions.
Second, a lack of time, particularly during outpatient visits, impedes physician ability to have considered discussions about future care needs and preferences [32,54]. The U.S. health care system currently lacks financial reimbursement for these discussions, which poses a significant barrier to the integration of ACP conversations into routine clinical practice. Moreover, these conversations are lengthy and iterative [53]. ACP discussions that are focused on facilitating patient-centered decision-making ideally begin with a discussion of expected prognosis, followed by an exploration of patient preferences and values for health care, and then a review of treatment options to be considered in the context of those preferences. Often additional time is needed for completing advance directive documents or for charting key outcomes from these discussions. Clinicians today are frequently overloaded with addressing multiple medical issues during outpatient visits that leave little time for non-medical tasks such as ACP discussions. The lack of financial incentives to support in-depth discussions is a critical challenge in improving ACP.
Third, a lack of training in specialized communication skills, particularly focused on empathic and emotionally sensitive disclosure, may further hinder physicians from initiating frank discussions with their patients. ACP conversations are highly sensitive and fraught with emotional complexity, and clinicians understandably experience discomfort with breaking bad news [49,51,55] or with broader issues of decline and death [51,56,57]. Physicians tend to be most comfortable addressing cognitive aspects of communication; addressing the emotional needs of patients is harder. Medical school training teaches detachment in physician practice, perhaps as a way of coping with the sadness they regularly confront and in maintaining their ability to provide clinical care. In fact, physicians describe their most difficult encounters as those with the most negative expressed emotions and miss opportunities to respond with empathy [58–60], a critical skill in effective patient-physician communication that is associated with improved patient satisfaction [61,62]. While patients value good communication skills in their health care encounters, many providers feel they lack the necessary skills to lead effective ACP discussions [49,63].
Finally, information gaps with regards to heart failure contribute to delayed or absent conversations about planning for future care. Many heart failure patients have a limited understanding of their disease [32,40,44,55], particularly an inaccurate perception that heart failure is not a terminal and life-limiting illness [42,49,64]. Compounding this is the fact that even some health care providers are reluctant to acknowledge the terminal nature of heart failure [50,56]. Without frank acknowledgement of the terminal nature of heart failure, the initiation of discussions regarding end-of-life care will remain difficult if not impossible.
Approaches to ACP in Heart Failure
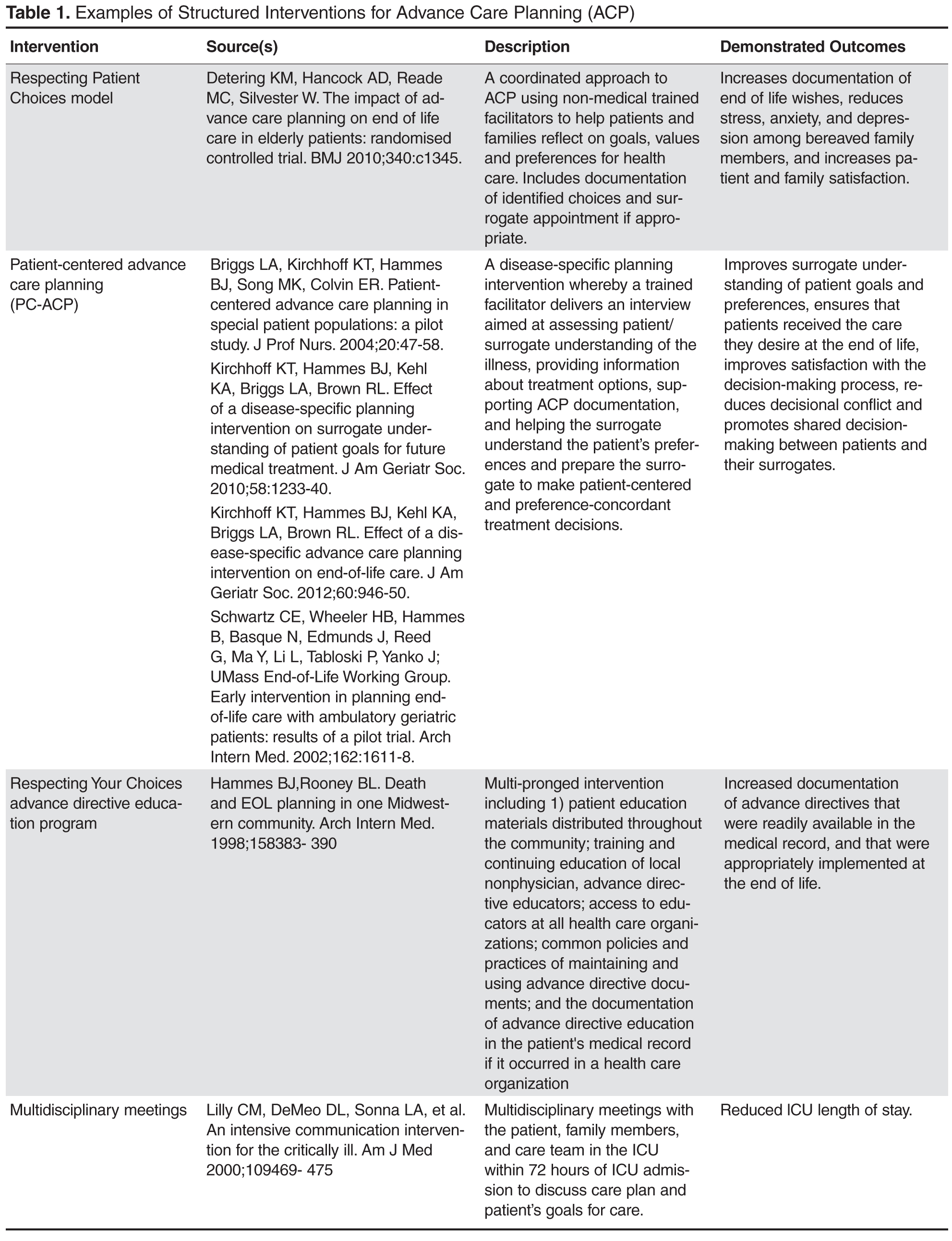
When Is the Right Time?
Given the complexity and unpredictable trajectory of heart failure, indicators of disease progression, including changes in health status and health service use, may serve as useful signals to help clinicians identify the appropriate time to initiate care planning discussions. Repeated hospital admissions for heart failure are strongly associated with increased mortality. In a sample of community heart failure patients [8], median survival after the first, second, and third hospitalization was 2.4, 1.4, and 1.0 years, respectively. In light of this, a patient with 1 or more hospitalizations in a 12-month period may be an appropriate candidate for an ACP conversation. Similarly, comorbidity in patients with heart failure may signal the relevance and need for discussions about future care. In a sample of Medicare beneficiaries with advanced heart failure, an increasing burden of comorbidity was associated with significantly higher mortality, as were certain conditions (COPD, CKD, dementia, depression) and combinations of conditions (eg, CKD and dementia) [26]. Davidson and colleagues [68] suggest a list of clinical indicators signaling the need for an ACP conversation, including any of the following:
- > 1 episodes of exacerbation of heart failure leading to hospital admission
- New York Heart Association Class IV heart failure
- Decline in function and mobility
- Unexplained weight loss
- Resting pulse rate greater than 100 beats/minute
- Raised serum creatinine (> 150 µmol/L)
- Low serum sodium (< 135 mmol/L)
- Low serum albumen (< 33 g/L)
- High dose of loop diuretic (eg, furosemide ≥ 160 mg daily)
Given the considerable complexity and multisystem nature of heart failure, none of these indicators alone can signal certainty about disease progression and consequent outcomes; however, they can serve as a useful heuristic for helping clinicians identify appropriate times to raise the topic of ACP with their patients.
What Do I Say? Structuring the Conversation
Heart failure patients and their caregivers may vary in their preferences for hearing information about their disease; therefore, it is critical to open any conversation about planning for future in the context of their illness by asking what and how much information is desired. This includes evaluating how involved in decision-making the patient wants to be. Previously suggested language includes [69,70]:
- Would you like to consider all the options, or my opinion about the options that fit best with what I know about you?
- Some people like to know everything about their disease and be involved in all decision making. Others do not want all the news and would rather the doctor talk to __________. Which kind of person are you? How involved do you want to be in these decisions?
- Would you like me to tell you the full details of your condition?
- If you prefer not to hear the details, is there someone in your family who you trust to receive this information?
After establishing the patient’s preferences for hearing different types of information and level of involvement in decision-making about their care, the ask-tell-ask model [69,71] provides a useful approach to communicating with patients and their families. The conversation generally begins by asking patients what he or she understands about their illness (eg, “What do you understand about your heart failure?”; “I want to make sure we’re on the same page; what have other doctors told you?”). Building on what the patient already knows, the clinician can then disclose new information, correct misunderstandings, or confirm impressions and expectations the patient might have. In this way, information is tailored to the patient’s understanding and aimed at addressing potential knowledge gaps, all within the context of their preferences. Finally, the clinician asks the patient to describe their new understanding and whether or not they have questions or concerns (eg, “To make sure I did a good job of explaining to you, can you tell me what you now know about your condition from our conversation?”; “I know I’ve covered a lot and I want to make sure I was clear. When you get home, how are you going to explain what I’ve told you to your spouse?”). This approach encourages communication and exchange between patient and physician. Additionally, expressions of concern promote relationship building and bonding between physician and patient.
Keeping the Conversation Going
ACP communication can cover a wide range of topics beyond disease and prognostic disclosure by the provider to the patient. A critical aspect of ACP conversations is an exploration of the patient’s values and preferences, which can be used to help contextualize treatment choices and subsequently guide in-the-moment decision-making [72]. Using open-ended questions throughout the conversation gives the patient an opportunity to reflect on and communicate their wishes and values and allows them to engage in the conversation on their own terms. Examples of discussion-stimulating questions include [69,73]:
- What concerns you most about your illness?
- How is treatment going for you (your family)?
- As you think about your illness, what is the best and worst that might happen?
- What are your greatest hopes about your health?
- What has been most difficult about this illness for you?
- Looking back at your life, what has been important to you?
- At this point, what is most important for you to do?
Language
Central to this process is the use of empathic language to demonstrate support and understanding. An expression of empathy is also an appropriate way to acknowledge and share difficult emotions when it becomes hard to know where to take the conversation next. Quill and colleagues [74] suggest the following empathic responses to patients’ emotional expressions:
- I wish for that too
- It's unfortunate that things aren't different
- I am so sorry that this happened to you
- I understand how much you want that
- It must be very hard to accept the seriousness of this illness
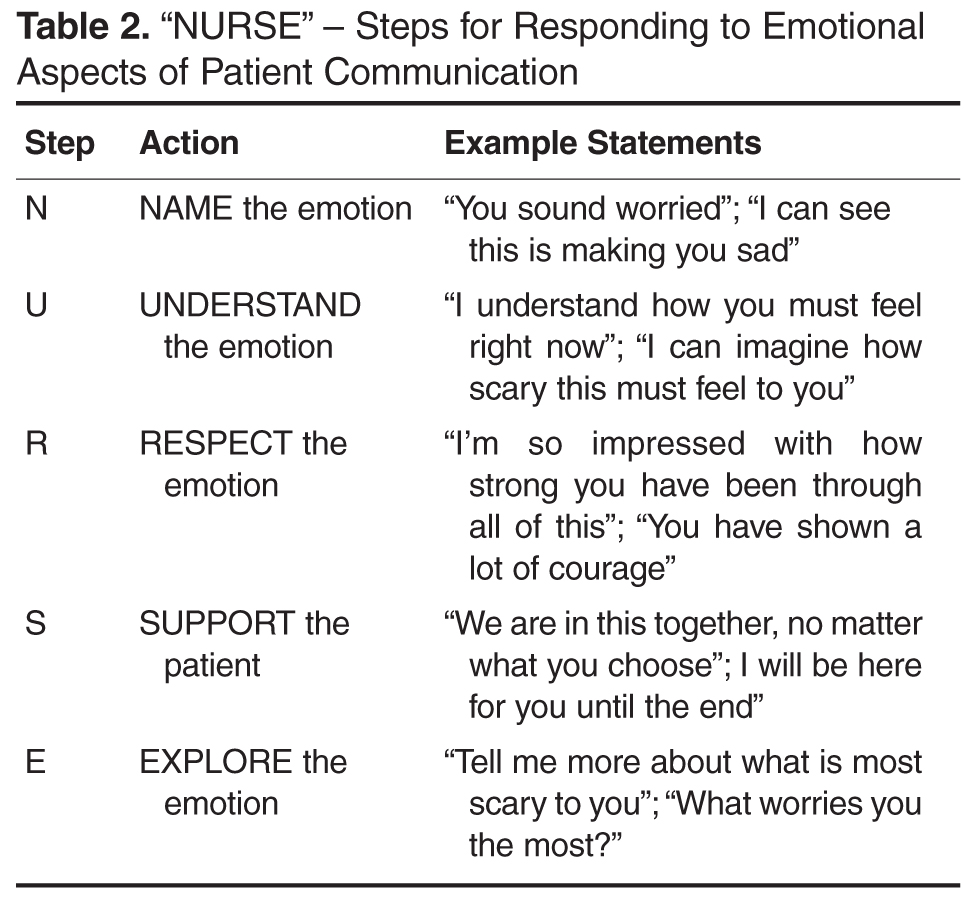
Relatedly, the use of medical jargon in ACP conversations can increase the distance between patients and their providers, and may hinder patient understanding. Physicians may use technical language out of habit, or as an unconscious way to emotionally separate themselves from the task of delivering bad news. However, clear communication using layperson terms is the most effective approach to providing information necessary to patient-centered decision making. Explaining medical procedures in simple terms can improve understanding and help to build trust with the physician (eg, “We will perform an angioplasty – a procedure where a special tube with a balloon on the end of it is inserted into your artery to stretch it open. This will improve blood flow and relieve some of the symptoms you are currently experiencing”.)
Cultural Issues in Communication
There are various cultural issues to consider and address when conducting ACP discussions with heart failure patients and their families. Heart failure disproportionately affects certain racial and ethnic groups (eg, African Americans) [77–79], and effective management of heart failure depends on the provision of culturally sensitive information and facilitation of culturally informed self-care behaviors. There is evidence of cultural variation in preferences for information and role in decision-making. For example, most white and African-American patients prefer to be fully informed of their condition [80], whereas other cultures may focus on protecting the patient from difficult information in order to maintain hope [80–86]. Moreover, even in cultures where nondisclosure is preferred, patients may want to be told the truth in an indirect, euphemistic, or even nonverbal manner [80,87–89]. These complexities underscore the importance of taking a patient-centered approach to ACP communication, respecting individuality and autonomy while ultimately facilitating decision-making [90,91].
Are There Effective Training Programs for ACP Communication?
Effective communication skills are a critical component of ACP conversations between clinicians and their patients; however, most clinicians do not receive formal training in ACP communication and believe it to be a difficult task [92]. Strong evidence of the effectiveness of communication skills training has yet to be established, largely due to variation in the approach to training and the specification of relevant outcomes. For example, a systematic review of communication skills training courses found that some courses are effective at improving different types of communication skills related to providing support and gathering information, but these courses lacked effectiveness in improving patient satisfaction or provider burnout and distress [93]. Similarly, a range of approaches to teaching clinicians effective ACP communication skills early in their medical training have been identified [94], but considerable variation in quality preclude any conclusions from being drawn about their effectiveness.
Despite these challenges, there are some studies of communication skills training courses that have demonstrated the ability to increase providers’ use of empathic and facilitative communication (eg, use of open-ended questions) [58,95], and to increase self-efficacy and confidence among providers [96]. One particular teaching model that is increasingly used in cancer care is Oncotalk (http://depts.washington.edu/oncotalk/). Oncotalk has been shown to significantly increase clinical skills in giving bad news and facilitating the transition to palliative care. Building on this success, the program has expanded to training courses focused on the intensive care setting (http://depts.washington.edu/icutalk/) and geriatrics care [97–99]. It is important to note, however, that the considerable time and resource-intensive nature of communication training programs limits widespread implementation of any one approach into routine medical education. More attention to the type and structure of communication skills training programs are needed as well as scalable approaches to assist clinicians in developing effective ACP communication skills.
Policy Implications of ACP and Future Directions
There is growing recognition of the need to improve ACP among patients with seriously illness, including heart failure. In a recent Institute of Medicine (IOM) report, Dying in America [100], the need for clinician-patient communication about ACP was identified as a primary area of improvement. Recommendations include the establishment of communication quality standards as well as guidelines promoting early and ongoing ACP discussions. This is supported by recommendations from medical professional societies for an iterative model of ACP that follows the course of a serious illness [2,101]. At early stages of the illness, ACP might be focused on helping patients clarify their broad health care values and raise awareness of their disease and expected prognosis. As the condition progresses, ACP discussion might focus on exploring disease-specific treatment options within the context of previously expressed preferences, as well as identifying changes in patients’ values over time, particularly as they gain experience with their illness and health status changes [102]. In late stages of the disease, ACP might focus on documenting specific treatment choices (eg, DNR orders) and on exploring options such as palliative care, while also ensuring that patients and caregivers are appropriately prepared for imminent decline and death.
The IOM report also calls for payment reforms to include reimbursement for outpatient ACP discussions [100]. There is burgeoning national support for developing reimbursement models for ACP discussions. The American Medical Association has recently released current procedural terminology (CPT) codes for ACP services, a first step toward urging Medicare to consider reimbursement for ACP discussions with physicians.
Finally, the IOM report calls for improved education and training in ACP communication across all disciplines and specialties providing care to patients with serious illness. These recommendations bring national attention to the current limitations surrounding ACP discussions for those with serious illness, including heart failure. Further research is needed to identify methods and care models to address the gap in communication skills, processes, and policies.
Corresponding author: Sangeeta C. Ahluwalia, Rand Corporation, 1776 Main St., Santa Monica, CA, 90401, sahluwal@rand.org.
Financial disclosures: None.
Author contributions: conception and design, SCA, SE; analysis and interpretation of data, SCA, SE; drafting of article, SCA, SE; critical revision of the article, SCA, SE.
1. American Heart Association. Heart disease and stroke statistics—2008 update. [Internet]. Available at www.americanheart.org/downloadable/heart/1200078608862HS_Stats%202008.final.pdf.
2. Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult—summary article. Circulation 2005;112:1825–52.
3. Masoudi FA, Havranek EP, Krumholz HM. The burden of chronic congestive heart failure in older persons: magnitude and implications for policy and research. Heart Fail Rev 2002;7:9–16.
4. McMurray JJ PM. Heart failure. Lancet 2005;365:1877–89.
5. Unroe KT, Greiner MA, Hernandez AF, et al. Resource use in the last 6 months of life among medicare beneficiaries with heart failure, 2000-2007. Arch Intern Med 2011;171:196–203.
6. Lunney JR, Lynn J, Foley DJ, et al. Patterns of functional decline at the end of life. JAMA 2003;289:2387–92.
7. Ko D, Alter D, Austin P, et al. Life expectancy after an index hospitalization for patients with heart failure: A population-based study. Am Heart J 2008;155:324–31.
8. Setoguchi S, Stevenson LW, Schneeweiss S. Repeated hospitalizations predict mortality in the community population with heart failure. Am Heart J 2007;154:260–6.
9. Jong P, Vowinskel E, Liu PP, et al. Prognosis and determinants for survival in patients newly hospitalized for heart failure. Arch Intern Med 2002;162:1689-94.
10. Thom T, Haase N, Rodamond W, et al. Heart disease and stroke statistics- 2006 update. Circulation 2006;113:e85-e151.
11. Shahar E, Lee S, Kim J, et al. Hospitalized heart failure: Rates and long-term mortality. J Card Fail 2004;10:374–9.
12. Kirkpatrick JN, Guger CJ, Arnsdorf MF, et al. Advance directives in the cardiac care unit. Am Heart J 2007;154:477–81.
13. Orn S, Dickstein K. How do heart failure patients die? Eur Heart J. 2002;4(suppl D).
14. Juenger J, Schellberg D, Kraemer S, et al. Health related quality of life in patients with congestive heart failure: comparison with other chronic disease and relation to functional variables. Heart 2002;87:235–41.
15. Steptoe A, Mohabir A, Mahon NG, et al. Health related quality of life and psychological wellbeing in patients with dilated cardiomyopathy. Heart 2000;83:645–50.
16. Johansson P, Agnebrink M, Dahlstrom U, et al. Measurement of health-related quality of life in chronic heart failure, form a nursing perspective--a review of the literature. Eur J Cardiovasc Nurs 2004;3:7–20.
17. Levenson J, McCarthy E, Lynn J, et al. The last six months of life for patients with congestive heart failure. J Am Geriatr Soc 2000;48(Suppl 5):S101–S109.
18. Sullivan M, Levy W, Russo J, Spertus J. Depression and health status in patients with advanced heart failure: a prospective study in tertiary care. J Card Fail 2004;10:390–6.
19. Bekelman DB, Havranek EP, Becker DM, et al. Symptoms, depression, and quality of life in patients with heart failure. J Card Fail 2007;13:643–8.
20. Godfrey CM, Harrison MB, Friedberg E, et al. The symptom of pain in individuals recently hospitalized for heart failure. J Cardiovasc Nurs 2007;22:368–74.
21. McCarthy M, Lay M, Addington-Hall J. Dying from heart disease. J R Coll Physicians Lond 1996;30:325–8.
22. Norgren L SS. Symptoms experienced in the last six months of life in patients with end-stage heart failure. Eur J Cardiovasc Nurs 2003;2:213–7.
23. Zambroski CH, Moser DK, Bhat G, et al. Impact of symptom prevalence and symptom burden on quality of life in patients with heart failure. Eur J Cardiovasc Nurs 2005;4:198–206.
24. Walke LM, Byers AL, Tinetti ME, et al. Range and severity of symptoms over time among older adults wih chronic obstructive pulmonary disease and heart failure. Arch Intern Med 2007;167:2503–8.
25. Bekelman DB, Rumsfeld JS, Havranek EP, et al. Symptom burden, depression, and spiritual well-being: a comparison of heart failure and advanced cancer patients. J Gen Intern Med 2009;24:592–8.
26. Ahluwalia SC, Gross CP, Chaudhry SI, et al. Impact of comorbidity on mortality among older persons with advanced heart failure. J Gen Intern Med 2012;27:513–9.
27. Ahluwalia SC, Gross CP, Chaudhry SI, et al. Change in comorbidity prevalence with advancing age among persons with heart failure. J Gen Intern Med 2011;26:1145–51.
28. Corrigan JM, Donaldson MS, Kohn LT, et al. A new health system for the 21st century. crossing the quality chasm. Washington, DC: Institute of Medicine, National Academy of Sciences, National Academies Press; 2001.
29. Kirchhoff KT, Hammes BJ, Kehl KA, et al. Effect of a disease-specific advance care planning intervention on end-of-life care. J Am Geriatr Soc 2012;60:946–50.
30. Kirchhoff KT, Hammes BJ, Kehl KA, et al. Effect of a disease-specific planning intervention on surrogate understanding of patient goals for future medical treatment. J Am Geriatr Soc 2010;58:1233–40.
31. Janssen DJ, Engelberg RA, Wouters EF, Curtis JR. Advance care planning for patients with COPD: past, present and future. Patient Educ Couns 2012;86:19–24.
32. Aldred H, Gott M, Gariballa S. Advanced heart failure: Impact on older patients and informal carers. J Adv Nurs 2005;49:116–24.
33. Zhang B, Wright AA, Huskamp HA, et al. Health care costs in the last week of life: Associations with end-of-life conversations. Arch Intern Med 2009;169:480–8.
34. Wright AA, Zhang B, Ray A, et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 2008;300:1665–73.
35. Mack JW, Smith TJ. Reasons why physicians do not have discussions about poor prognosis, why it matters, and what can be improved. J Clin Oncol 2012;30:2715–7.
36. Detering KM, Hancock AD, Reade MC, Silvester W. The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ 2010;340:c1345.
37. Schwartz CE, Wheeler HB, Hammes B, et al. Early intervention in planning end-of-life care with ambulatory geriatric patients: results of a pilot trial. Arch Intern Med 2002;162:1611–8.
38. Caldwell PH, Arthur HM, Demers C. Preferences of patients with heart failure for prognosis communication. Can J Cardiol 2007;23:791–6.
39. Bekelman DB, Nowels Ct, Retrum JH, et al. Giving voice to patients’ and family caregivers’ needs in chronic heart failure: implications for palliative care programs. J Palliat Med 2011;14:1317–24.
40. Harding R, Selman L, Beynon T, et al. Meeting the communication and information needs of chronic heart failure patients. J Pain Symptom Manage 2008;36:149–56.
41. Strachan PH, Ross H, Dodek PM, et al. Mind the gap: opportunities for improving end-of-life care for patients with advanced heart failure. Can J Cardiol 2009;25:635–40.
42. Ågård A, Hermerén G, Herlitz J. When is a patient with heart failure adequately informed? A study of patients’ knowledge of and attitudes toward medical information. Heart Lung 2004;33:219–26.
43. Gott M, Small N, Barnes S, et al. Older people’s views of a good death in heart failure: implications for palliative care provision. Soc Sci Med 2008;67:1113–21.
44. Murray SA, Boyd K, Kendall M, et al. Dying of lung cancer or cardiac failure: prospective qualitative interview study of patients and their carers in the community. BMJ 2002;325:929.
45. Ahluwalia SC, Levin JR, Lorenz KA, et al. Missed opportunities for advance care planning communication during outpatient clinic visits. J Gen Intern Med 2012;27:445–51.
46. Rodriguez KL, Appelt CJ, Switzer GE, et al. “They diagnosed bad heart”: a qualitative exploration of patients’ knowledge about and experiences with heart failure. Heart Lung. 2008;37:257–65.
47. Remme WJ,McMurray JJ, Rauch B, et al. Public awareness of heart failure in Europe: first results from SHAPE. Eur Heart J 2005;22:2413e21.
48. Golin CE, Wenger NS, Liu H, et al. A prospective study of patient-physician communication about resuscitation. J Am Geriatr Soc 2000;48(5 Suppl):S52–60.
49. Selman L, Harding R, Beynon T, et al. Improving end of life care for patients with chronic heart failure: ‘let’s hope it’ll get better when I know in my heart of hearts it won’t’. Heart 2007;93:963–7.
50. Barnes S, Gott M, Payne S, et al. Communication in heart failure: Perspectives from older people and primary care professionals. Health Soc Care Comm 2006;14:482–90.
51. Brännström M, Ekman I, Norberg A, et al. Living with severe chronic heart failure in palliative advanced home care. Eur J Cardiovasc Nurs 2006;5:295–302.
52. Barclay S, Momen N, Case-Upton S, et al. End-of-life care conversations with heart failure patients: a systematic literature review and narrative synthesis. Br J Gen Pract 2011;61:e49–62.
53. Whitney SN, McCullough LB, Fruge E, et al. Beyond breaking bad news: the roles of hope and hopefulness. Cancer 2008;113:442–5.
54. Tung EE, North F. Advance care planning in the primary care setting: a comparison of attending staff and resident barriers. Am J Hosp Palliat Care 2009;26:456–63.
55. Boyd K, Murray S, Kendall M, et al. Living with advanced heart failure: A prospective, community based study of patients and their carers. Eur J Heart Fail 2004;6:585–91.
56. Borbasi S, Wotton K, Redden M, et al. Letting go: A qualitative study of acute care and community nurses’ perceptions of a ‘good’ versus a ‘bad’ death. Austr Crit Care 2005 2005;18:104–13.
57. Hanratty B, Hibbert D, Mair F, et al. Doctors’ perceptions of palliative care for heart failure: Focus group study. BMJ 2002;325:581–5.
58. Fallowfield L, Jenkins V, Farewell V, et al. Efficacy of a communication skills training model for oncologists: a randomized controlled trial. Lancet 2002;359:650–6.
59. Platt F, Keller V. Empathic communication: a teachable and learnable skill. J Gen Intern Med 1994;9:222–6.
60. Morse D, Edwardsen E, Gordon H. Missed opportunities for interval empathy in lung cancer communication. Arch Intern Med 2008;22;168:1853–8.
61. Epstein R, Hadee T, Carroll J, et al. “Could this be something serious?” reassurance, uncertainty, and empathy in response to patients’ expressions of worry. J Gen Intern Med 2007;22:1731–9.
62. Stewart M. What is a successful doctor-patient interview? A study of interactions and outcomes. Soc Sci Med 1984;19:
167–75.
63. Wotton K, Borbasi S, Redden M. When all else has failed. Nurses’ perception of factors influencing palliative care for patients with end-stage heart failure. J Cardiovasc Nurs 2005;20:18–25.
64. Willems DL, Hak A, Visser F, Van der Wal G. Thoughts of patients with advanced heart failure on dying. Palliat Med 2004;18:564–72.
65. Briggs L, Kirchhoff K, Hammes B, et al. Patient-centered advance care planning in special patient populations: a pilot study. J Prof Nurs 2004;20:47–58.
66. Hammes B, Rooney B. Death and EOL planning in one midwestern community. Arch Intern Med 1998;158:390.
67. Lilly C, DeMeo D, Sonna L, et al. An intensive communication intervention for the critically ill. Am J Med 2000;109:469–75.
68. Davidson P, Macdonald P, Newton P, et al. End stage heart failure patients: Palliative care in general practice. Aust Fam Physician 2010;39:920.
69. Goodlin S, Quill T, Arnold R. Communication and decision-making about prognosis in heart failure care. J Card Fail 2008;14:106–13.
70. Analysis of U.S. hospital palliative care programs 2010 snapshot. Center to Advance Palliative Care (CAPC). Accessed 24 Nov 2014 at www.capc.org/news-and-events/releases/analysis-of-us-hospital-palliative-care-programs-2010-snapshot.pdf.
71. Back AL, Arnold RM, Baile WF, et al. Approaching difficult communication tasks in oncology. CA Cancer J Clin 2005;55:164–77.
72. Sudore RL, Fried TR, Redefining the “planning” in advance care planning: preparing for end-of-life decision making. Ann Intern Med 2010;153:256–61.
73. Lo B, Quill T, Tulsky J. Discussing palliative care with patients. Ann Intern Med 1999;130:744–9.
74. Quill T, Arnold R, Platt F. I wish things were different: Expressing wishes in response to loss, futility, and unrealistic hopes. Ann Intern Med 2001;135:551–5.
75. Pollak K, Arnold R, Jeffreys A, et al. Oncologist communication about emotion during visits with patients with advanced cancer. J Clin Oncol 2007;25:5748–52.
76. Back AL, Anderson WG, Bunch L, et al. Communication about cancer near the end of life. Cancer 2008;113(S7):1897–910.
77. Dries D, Exner D, Gersh B, et al. Racial differences in the outcome of left ventricular dysfunction. N Engl J Med 1999;340:609–16.
78. Alexander M, Grumbach K, Selby J, et al. Hospitalization for congestive heart failure. Explaining racial differences. JAMA 1995;274:1037–42.
79. Afzal A, Ananthasubramaniam K, Sharma N, et al. Racial differences in patients with heart failure. Clin Cardiol 1999;22:791–4.
80. Blackhall L, Murphy S, Frank G, et al. Ethnicity and attitudes toward patient autonomy. JAMA 1995;274:820–5.
81. Huang X, Butow P, Meiser B, et al. Attitudes and information needs of chinese migrant cancer patients and their relatives. Aust N Z J Med 1999;29:207–13.
82. Tan T, Teo F, Wong K, et al. Cancer: to tell or not to tell? Singapore Med J 1993;34:202–3.
83. Gorgaki S, Kalaidopoulou O, Liarmakopoulos I, et al. Nurses’ attitudes toward truthful communication with patients with cancer. A Greek study. Cancer Nurs 2002;25:436–41.
84. Harris J, Shao J, Sugarman J. Disclosure of cancer diagnosis and prognosis in northern Tanzania. Soc Sci Med 2003;56:905–13.
85. Goldstein D, Thewes B, Butow P. Communicating in a multicultural society. II: Greek community attitudes towards cancer in Australia. Intern Med J 2002;32:289–96.
86. Beyene Y. Medical disclosure and refugees. Telling bad news to Ethiopian patients. West J Med 1992;157:328–32.
87. Matsumura S, Bito S, Liu H, et al. Acculturation of attitudes toward end-of-life care: A cross-cultural survey of Japanese Americans and Japanese. J Gen Intern Med 2002;17:531–9.
88. Yick AG, Gupta R. Chinese cultural dimensions of death, dying, and bereavement: Focus group findings. J Cult Divers 2002 Summer;9:32–42.
89. Frank G, Blackhall L, Murphy S, et al. Ambiguity and hope: Disclosure preferences of less acculturated elderly Mexican Americans concerning terminal cancer—A case story. Camb Q Healthc Ethics 2002;11:117–26.
90. Hern HJ, Koenig B, Moore L, et al. The difference that culture can make in end-of-life decisionmaking. Camb Q Healthc Ethics 1998;7:27–48.
91. Kagawa-Singer M, Kassim-Lakha S. A strategy to reduce cross-cultural miscommunication and increase the likelihood of improving health outcomes. Acad Med 2003;78:577–87.
92. Barnett MM, Fisher JD, Cooke H, et al. Breaking bad news: consultants’ experience, previous education, and views on educational format and timing. Med Educ 2007;41:947–56.
93. Moore P, Rivera Mercado S, Grez Artigues M, Lawrie T. Communication skills training for healthcare professionals working with people who have cancer. Cochrane Database Syst Rev 2013;3CD003751.
94. Alelwani S, Ahmed Y. Medical training for communication of bad news: A literature review. J Educ Health Promot 2014;3
95. Delvaux N, Razavi D, Marchal S, et al. Effects of a 105 hour psychological training program on attitudes, communication skills and occupational stress in oncology: a randomised study. Br J Cancer 2004;90:106–14.
96. Baile WF, Lenzi R, Kudelka AP, et al. Improving physician-patient communication in cancer care: Outcome of a workshop for oncologists. J Cancer Educ 1997;12:166–73.
97. Back AL, Arnold RM, Baile WF, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Intern Med 2007;167:453–60.
98. Gelfman LP, Lindenberger E, Fernandez H, et al. The effectiveness of the Geritalk communication skills course: a real-time assessment of skill acquisition and deliberate practice. J Pain Sympt Manage 2014;48:738–44.
99. Kelley AS, Back AL, Arnold RM, et al. Geritalk: communication skills training for geriatric and palliative medicine fellows. J Am Geriatr Soc 2012;60:332–7.
100. Institute of Medicine. Dying in America: Improving quality and honoring individual preferences near the end of life. Washington, DC: National Academies Press; 2014.
101. Allen LA, Stevenson LW, Grady KL, et al. Decision making in advanced heart failure: a scientific statement From the American Heart Association. Circulation 2012;125:1928–52.
102. Ditto PH, Jacobson JA, Smucker WD, et al. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment preferences. Med Decis Making 2006;26:313–22.
From the Rand Corporation and UCLA Fielding School of Public Health, Santa Monica, CA (Dr. Ahluwalia) and University of Southern California, Leonard Davis School of Gerontology, Los Angeles, CA (Dr. Enguidanos).
Abstract
- Objective: To review the relevance of advance care planning to heart failure management, describe key advance care planning challenges, and provide clinicians with actionable guidance for engaging in advance care planning conversations.
- Methods: Review of the literature.
- Results: Although most patients with heart failure prefer to receive thorough and honest information about their health condition and prognosis, the unpredictability of the heart failure trajectory coupled with physician barriers including discomfort with emotionally-laden topics and difficulty identifying the “right” time to engage in advance care planning, and systems barriers such as inadequate clinic time and limited reimbursement, impede timely engagement in advance care planning discussions. Approaches to effective advance care planning communication include using open-ended questions to stimulate patient engagement, evaluating how much information the patient wants to ensure patient-centeredness, and using empathic language to demonstrate support and understanding. While successful models of advance care planning communication have been identified, replication is limited due to the resource intense nature of these approaches.
- Conclusion: Challenges to advance care planning discussions among patients with heart failure may be mitigated through the establishment of communication quality standards as well as guidelines promoting early and ongoing advance care planning discussions, as well as reimbursement for outpatient discussions.
Heart failure, a leading cause of death, disability, and health care costs in the United States, is an incurable and life-limiting illness that is becoming increasingly prevalent due to an aging population and improved life expectancy. Approximately 5.3 million Americans are currently living with heart failure [1], with more than 550,000 new cases diagnosed each year [2]. Heart failure disproportionately affects older adults; about 80% of all cases occur in persons aged 65 years or older [3], and heart failure is the leading cause of hospital admissions among older adults [4]. The burden and impact of heart failure peaks near the end of life; 80% of Medicare beneficiaries with heart failure are hospitalized in the last 6 months of life [5].
The Trajectory of Heart Failure
Patients with heart failure experience a highly variable, nonlinear clinical trajectory marked by progressive deterioration and frequent exacerbations requiring hospitalization [6]. Their prognosis, though uncertain, is poor, with reported 1-year mortality rates following a hospitalization between 30% and 50% and 5-year mortality as high as 75% [7–11], a survival rate worse than that of some cancers [12]. Patients with heart failure caused by ischemic heart disease are at high risk for sudden cardiac death, particularly at earlier stages of the disease, which can confound the ability to appropriately plan for the future [13]. Those who survive to more advanced stages of heart failure face worsening quality of life [14–16], driven by a high prevalence of fatigue, breathlessness, pain, and depression [17–24]. Indeed, patients with heart failure have a similar symptom burden to patients with advanced cancer [25]. Older adults with heart failure also have a high comorbidity burden that further complicates both symptomology and disease trajectory with implications for decision-making about life-prolonging heart failure therapies [26,27].
Advance Care Planning in Heart Failure
The unpredictable nature of heart failure makes it difficult for patients and families to plan and prepare for their future, yet it is this very uncertainty that makes advance care planning (ACP) so critical for heart failure patients. Clear and honest patient-clinician communication about ACP, including an exploration of patient values and goals for care in the context of prognostic information, is essential to patient-centered treatment decision-making [28]. This is particularly relevant in heart failure, where a range of high-intensity, invasive, and costly interventions are increasingly being applied (eg, ventricular assist devices) without equivalent attention to quality of life and patients’ long-term goals for care.
Patients with heart failure and their families face multiple complex treatment decisions along the trajectory of their illness, such as discontinuation of beta blockers among patients with refractory fluid overload or angiotensin-converting enzyme inhibitors in end-stage patients with symptomatic hypotension [29,30]. In end-stage heart failure patients, deactivation of an implantable cardiac defibrillator might be considered to avoid the pain and distress associated with repeated shocks. In contrast, other interventions such as cardiac resynchronization therapy and continuous inotropic infusion have quality of life benefits; continuation of these therapies may be appropriate even when discontinuing other interventions. Such decisions should be guided by a thorough understanding of the patient’s expressed preferences and values, ideally assessed early in the trajectory of the disease and continuously re-evaluated as the diseases progresses.
The American Heart Association supports early and regular patient-provider ACP discussions to guide heart failure patients’ future decision-making [31], and recommends that such discussions be initiated in the outpatient setting, prior to and in anticipation of clinical decline. ACP communication plays a critical role in enhancing patients’ understanding of their diagnosis, treatment, prognosis, and choices in end-of-life care [31]. ACP communication also helps the clinician to better understand the context within which patients and their caregivers might make health care decisions, including their values and preferences for care. Patient-provider discussions about ACP focused on understanding patient values and initiated early in the trajectory of serious illness can support future in-the-moment decision-making, and is likely more effective than asking patients to make specific treatment decisions in advance [32]. A growing body of rigorous research has shown that ACP communication is associated with greater preference-concordant care and congruence in patient-surrogate understanding of patient preferences, lower costs, and less aggressive care at the end of life [33–37].
Patient Preferences for ACP Communication
Most patients with heart failure and their caregivers want honest disclosure regarding prognosis and to receive information about the expected trajectory of their disease [38–41] as early as possible [38] to help them plan and prepare for their future. Patients and their caregivers prefer to have these conversations with their physician [38] or other provider most familiar with the patient and family [39]. Patients also express a preference for support with dealing with the uncertainty inherent to heart failure [39]. Although most patients and caregivers desire to receive clear and honest communication about their disease, it is important to note that patients may vary in the extent of information they prefer to receive about their heart failure, with some individuals preferring not to talk about the end of life and future care needs at all [39,42–44].
Challenges to ACP Communication in Heart Failure
Despite patient and caregiver preferences for ACP communication with their providers, evidence suggests such communication occurs infrequently [40,45] and that heart failure patients may lack important information about their prognosis and treatment options [40,44,46,47]. For example, patients may not recognize the terminal nature of heart failure, and may be unaware of the range of treatment options, including hospice, available to them. Evidence also demonstrates that ACP is infrequently discussed with their health care providers [40], resulting in these conversations being avoided or deferred until an emergent clinical situation [44,48] when hasty questions about treatment choices may yield uncertain and conflicting answers not representative of a patient’s underlying values.
The infrequent, late, and often lack of discussions about ACP are driven by several challenges. First, the uncertain trajectory of heart failure makes communication regarding “what to expect” difficult. Prognostication is an immense challenge in heart failure [40,49–52], making it harder to talk about end-of-life issues and hindering the ability of patients, caregivers and health care providers to plan and prepare for the future. It is often difficult for clinicians, who face the challenge of instilling hope in the face of truthful disclosure [53], to identify the “right time” to initiate such discussions.
Second, a lack of time, particularly during outpatient visits, impedes physician ability to have considered discussions about future care needs and preferences [32,54]. The U.S. health care system currently lacks financial reimbursement for these discussions, which poses a significant barrier to the integration of ACP conversations into routine clinical practice. Moreover, these conversations are lengthy and iterative [53]. ACP discussions that are focused on facilitating patient-centered decision-making ideally begin with a discussion of expected prognosis, followed by an exploration of patient preferences and values for health care, and then a review of treatment options to be considered in the context of those preferences. Often additional time is needed for completing advance directive documents or for charting key outcomes from these discussions. Clinicians today are frequently overloaded with addressing multiple medical issues during outpatient visits that leave little time for non-medical tasks such as ACP discussions. The lack of financial incentives to support in-depth discussions is a critical challenge in improving ACP.
Third, a lack of training in specialized communication skills, particularly focused on empathic and emotionally sensitive disclosure, may further hinder physicians from initiating frank discussions with their patients. ACP conversations are highly sensitive and fraught with emotional complexity, and clinicians understandably experience discomfort with breaking bad news [49,51,55] or with broader issues of decline and death [51,56,57]. Physicians tend to be most comfortable addressing cognitive aspects of communication; addressing the emotional needs of patients is harder. Medical school training teaches detachment in physician practice, perhaps as a way of coping with the sadness they regularly confront and in maintaining their ability to provide clinical care. In fact, physicians describe their most difficult encounters as those with the most negative expressed emotions and miss opportunities to respond with empathy [58–60], a critical skill in effective patient-physician communication that is associated with improved patient satisfaction [61,62]. While patients value good communication skills in their health care encounters, many providers feel they lack the necessary skills to lead effective ACP discussions [49,63].
Finally, information gaps with regards to heart failure contribute to delayed or absent conversations about planning for future care. Many heart failure patients have a limited understanding of their disease [32,40,44,55], particularly an inaccurate perception that heart failure is not a terminal and life-limiting illness [42,49,64]. Compounding this is the fact that even some health care providers are reluctant to acknowledge the terminal nature of heart failure [50,56]. Without frank acknowledgement of the terminal nature of heart failure, the initiation of discussions regarding end-of-life care will remain difficult if not impossible.
Approaches to ACP in Heart Failure
When Is the Right Time?
Given the complexity and unpredictable trajectory of heart failure, indicators of disease progression, including changes in health status and health service use, may serve as useful signals to help clinicians identify the appropriate time to initiate care planning discussions. Repeated hospital admissions for heart failure are strongly associated with increased mortality. In a sample of community heart failure patients [8], median survival after the first, second, and third hospitalization was 2.4, 1.4, and 1.0 years, respectively. In light of this, a patient with 1 or more hospitalizations in a 12-month period may be an appropriate candidate for an ACP conversation. Similarly, comorbidity in patients with heart failure may signal the relevance and need for discussions about future care. In a sample of Medicare beneficiaries with advanced heart failure, an increasing burden of comorbidity was associated with significantly higher mortality, as were certain conditions (COPD, CKD, dementia, depression) and combinations of conditions (eg, CKD and dementia) [26]. Davidson and colleagues [68] suggest a list of clinical indicators signaling the need for an ACP conversation, including any of the following:
- > 1 episodes of exacerbation of heart failure leading to hospital admission
- New York Heart Association Class IV heart failure
- Decline in function and mobility
- Unexplained weight loss
- Resting pulse rate greater than 100 beats/minute
- Raised serum creatinine (> 150 µmol/L)
- Low serum sodium (< 135 mmol/L)
- Low serum albumen (< 33 g/L)
- High dose of loop diuretic (eg, furosemide ≥ 160 mg daily)
Given the considerable complexity and multisystem nature of heart failure, none of these indicators alone can signal certainty about disease progression and consequent outcomes; however, they can serve as a useful heuristic for helping clinicians identify appropriate times to raise the topic of ACP with their patients.
What Do I Say? Structuring the Conversation
Heart failure patients and their caregivers may vary in their preferences for hearing information about their disease; therefore, it is critical to open any conversation about planning for future in the context of their illness by asking what and how much information is desired. This includes evaluating how involved in decision-making the patient wants to be. Previously suggested language includes [69,70]:
- Would you like to consider all the options, or my opinion about the options that fit best with what I know about you?
- Some people like to know everything about their disease and be involved in all decision making. Others do not want all the news and would rather the doctor talk to __________. Which kind of person are you? How involved do you want to be in these decisions?
- Would you like me to tell you the full details of your condition?
- If you prefer not to hear the details, is there someone in your family who you trust to receive this information?
After establishing the patient’s preferences for hearing different types of information and level of involvement in decision-making about their care, the ask-tell-ask model [69,71] provides a useful approach to communicating with patients and their families. The conversation generally begins by asking patients what he or she understands about their illness (eg, “What do you understand about your heart failure?”; “I want to make sure we’re on the same page; what have other doctors told you?”). Building on what the patient already knows, the clinician can then disclose new information, correct misunderstandings, or confirm impressions and expectations the patient might have. In this way, information is tailored to the patient’s understanding and aimed at addressing potential knowledge gaps, all within the context of their preferences. Finally, the clinician asks the patient to describe their new understanding and whether or not they have questions or concerns (eg, “To make sure I did a good job of explaining to you, can you tell me what you now know about your condition from our conversation?”; “I know I’ve covered a lot and I want to make sure I was clear. When you get home, how are you going to explain what I’ve told you to your spouse?”). This approach encourages communication and exchange between patient and physician. Additionally, expressions of concern promote relationship building and bonding between physician and patient.
Keeping the Conversation Going
ACP communication can cover a wide range of topics beyond disease and prognostic disclosure by the provider to the patient. A critical aspect of ACP conversations is an exploration of the patient’s values and preferences, which can be used to help contextualize treatment choices and subsequently guide in-the-moment decision-making [72]. Using open-ended questions throughout the conversation gives the patient an opportunity to reflect on and communicate their wishes and values and allows them to engage in the conversation on their own terms. Examples of discussion-stimulating questions include [69,73]:
- What concerns you most about your illness?
- How is treatment going for you (your family)?
- As you think about your illness, what is the best and worst that might happen?
- What are your greatest hopes about your health?
- What has been most difficult about this illness for you?
- Looking back at your life, what has been important to you?
- At this point, what is most important for you to do?
Language
Central to this process is the use of empathic language to demonstrate support and understanding. An expression of empathy is also an appropriate way to acknowledge and share difficult emotions when it becomes hard to know where to take the conversation next. Quill and colleagues [74] suggest the following empathic responses to patients’ emotional expressions:
- I wish for that too
- It's unfortunate that things aren't different
- I am so sorry that this happened to you
- I understand how much you want that
- It must be very hard to accept the seriousness of this illness
Relatedly, the use of medical jargon in ACP conversations can increase the distance between patients and their providers, and may hinder patient understanding. Physicians may use technical language out of habit, or as an unconscious way to emotionally separate themselves from the task of delivering bad news. However, clear communication using layperson terms is the most effective approach to providing information necessary to patient-centered decision making. Explaining medical procedures in simple terms can improve understanding and help to build trust with the physician (eg, “We will perform an angioplasty – a procedure where a special tube with a balloon on the end of it is inserted into your artery to stretch it open. This will improve blood flow and relieve some of the symptoms you are currently experiencing”.)
Cultural Issues in Communication
There are various cultural issues to consider and address when conducting ACP discussions with heart failure patients and their families. Heart failure disproportionately affects certain racial and ethnic groups (eg, African Americans) [77–79], and effective management of heart failure depends on the provision of culturally sensitive information and facilitation of culturally informed self-care behaviors. There is evidence of cultural variation in preferences for information and role in decision-making. For example, most white and African-American patients prefer to be fully informed of their condition [80], whereas other cultures may focus on protecting the patient from difficult information in order to maintain hope [80–86]. Moreover, even in cultures where nondisclosure is preferred, patients may want to be told the truth in an indirect, euphemistic, or even nonverbal manner [80,87–89]. These complexities underscore the importance of taking a patient-centered approach to ACP communication, respecting individuality and autonomy while ultimately facilitating decision-making [90,91].
Are There Effective Training Programs for ACP Communication?
Effective communication skills are a critical component of ACP conversations between clinicians and their patients; however, most clinicians do not receive formal training in ACP communication and believe it to be a difficult task [92]. Strong evidence of the effectiveness of communication skills training has yet to be established, largely due to variation in the approach to training and the specification of relevant outcomes. For example, a systematic review of communication skills training courses found that some courses are effective at improving different types of communication skills related to providing support and gathering information, but these courses lacked effectiveness in improving patient satisfaction or provider burnout and distress [93]. Similarly, a range of approaches to teaching clinicians effective ACP communication skills early in their medical training have been identified [94], but considerable variation in quality preclude any conclusions from being drawn about their effectiveness.
Despite these challenges, there are some studies of communication skills training courses that have demonstrated the ability to increase providers’ use of empathic and facilitative communication (eg, use of open-ended questions) [58,95], and to increase self-efficacy and confidence among providers [96]. One particular teaching model that is increasingly used in cancer care is Oncotalk (http://depts.washington.edu/oncotalk/). Oncotalk has been shown to significantly increase clinical skills in giving bad news and facilitating the transition to palliative care. Building on this success, the program has expanded to training courses focused on the intensive care setting (http://depts.washington.edu/icutalk/) and geriatrics care [97–99]. It is important to note, however, that the considerable time and resource-intensive nature of communication training programs limits widespread implementation of any one approach into routine medical education. More attention to the type and structure of communication skills training programs are needed as well as scalable approaches to assist clinicians in developing effective ACP communication skills.
Policy Implications of ACP and Future Directions
There is growing recognition of the need to improve ACP among patients with seriously illness, including heart failure. In a recent Institute of Medicine (IOM) report, Dying in America [100], the need for clinician-patient communication about ACP was identified as a primary area of improvement. Recommendations include the establishment of communication quality standards as well as guidelines promoting early and ongoing ACP discussions. This is supported by recommendations from medical professional societies for an iterative model of ACP that follows the course of a serious illness [2,101]. At early stages of the illness, ACP might be focused on helping patients clarify their broad health care values and raise awareness of their disease and expected prognosis. As the condition progresses, ACP discussion might focus on exploring disease-specific treatment options within the context of previously expressed preferences, as well as identifying changes in patients’ values over time, particularly as they gain experience with their illness and health status changes [102]. In late stages of the disease, ACP might focus on documenting specific treatment choices (eg, DNR orders) and on exploring options such as palliative care, while also ensuring that patients and caregivers are appropriately prepared for imminent decline and death.
The IOM report also calls for payment reforms to include reimbursement for outpatient ACP discussions [100]. There is burgeoning national support for developing reimbursement models for ACP discussions. The American Medical Association has recently released current procedural terminology (CPT) codes for ACP services, a first step toward urging Medicare to consider reimbursement for ACP discussions with physicians.
Finally, the IOM report calls for improved education and training in ACP communication across all disciplines and specialties providing care to patients with serious illness. These recommendations bring national attention to the current limitations surrounding ACP discussions for those with serious illness, including heart failure. Further research is needed to identify methods and care models to address the gap in communication skills, processes, and policies.
Corresponding author: Sangeeta C. Ahluwalia, Rand Corporation, 1776 Main St., Santa Monica, CA, 90401, sahluwal@rand.org.
Financial disclosures: None.
Author contributions: conception and design, SCA, SE; analysis and interpretation of data, SCA, SE; drafting of article, SCA, SE; critical revision of the article, SCA, SE.
From the Rand Corporation and UCLA Fielding School of Public Health, Santa Monica, CA (Dr. Ahluwalia) and University of Southern California, Leonard Davis School of Gerontology, Los Angeles, CA (Dr. Enguidanos).
Abstract
- Objective: To review the relevance of advance care planning to heart failure management, describe key advance care planning challenges, and provide clinicians with actionable guidance for engaging in advance care planning conversations.
- Methods: Review of the literature.
- Results: Although most patients with heart failure prefer to receive thorough and honest information about their health condition and prognosis, the unpredictability of the heart failure trajectory coupled with physician barriers including discomfort with emotionally-laden topics and difficulty identifying the “right” time to engage in advance care planning, and systems barriers such as inadequate clinic time and limited reimbursement, impede timely engagement in advance care planning discussions. Approaches to effective advance care planning communication include using open-ended questions to stimulate patient engagement, evaluating how much information the patient wants to ensure patient-centeredness, and using empathic language to demonstrate support and understanding. While successful models of advance care planning communication have been identified, replication is limited due to the resource intense nature of these approaches.
- Conclusion: Challenges to advance care planning discussions among patients with heart failure may be mitigated through the establishment of communication quality standards as well as guidelines promoting early and ongoing advance care planning discussions, as well as reimbursement for outpatient discussions.
Heart failure, a leading cause of death, disability, and health care costs in the United States, is an incurable and life-limiting illness that is becoming increasingly prevalent due to an aging population and improved life expectancy. Approximately 5.3 million Americans are currently living with heart failure [1], with more than 550,000 new cases diagnosed each year [2]. Heart failure disproportionately affects older adults; about 80% of all cases occur in persons aged 65 years or older [3], and heart failure is the leading cause of hospital admissions among older adults [4]. The burden and impact of heart failure peaks near the end of life; 80% of Medicare beneficiaries with heart failure are hospitalized in the last 6 months of life [5].
The Trajectory of Heart Failure
Patients with heart failure experience a highly variable, nonlinear clinical trajectory marked by progressive deterioration and frequent exacerbations requiring hospitalization [6]. Their prognosis, though uncertain, is poor, with reported 1-year mortality rates following a hospitalization between 30% and 50% and 5-year mortality as high as 75% [7–11], a survival rate worse than that of some cancers [12]. Patients with heart failure caused by ischemic heart disease are at high risk for sudden cardiac death, particularly at earlier stages of the disease, which can confound the ability to appropriately plan for the future [13]. Those who survive to more advanced stages of heart failure face worsening quality of life [14–16], driven by a high prevalence of fatigue, breathlessness, pain, and depression [17–24]. Indeed, patients with heart failure have a similar symptom burden to patients with advanced cancer [25]. Older adults with heart failure also have a high comorbidity burden that further complicates both symptomology and disease trajectory with implications for decision-making about life-prolonging heart failure therapies [26,27].
Advance Care Planning in Heart Failure
The unpredictable nature of heart failure makes it difficult for patients and families to plan and prepare for their future, yet it is this very uncertainty that makes advance care planning (ACP) so critical for heart failure patients. Clear and honest patient-clinician communication about ACP, including an exploration of patient values and goals for care in the context of prognostic information, is essential to patient-centered treatment decision-making [28]. This is particularly relevant in heart failure, where a range of high-intensity, invasive, and costly interventions are increasingly being applied (eg, ventricular assist devices) without equivalent attention to quality of life and patients’ long-term goals for care.
Patients with heart failure and their families face multiple complex treatment decisions along the trajectory of their illness, such as discontinuation of beta blockers among patients with refractory fluid overload or angiotensin-converting enzyme inhibitors in end-stage patients with symptomatic hypotension [29,30]. In end-stage heart failure patients, deactivation of an implantable cardiac defibrillator might be considered to avoid the pain and distress associated with repeated shocks. In contrast, other interventions such as cardiac resynchronization therapy and continuous inotropic infusion have quality of life benefits; continuation of these therapies may be appropriate even when discontinuing other interventions. Such decisions should be guided by a thorough understanding of the patient’s expressed preferences and values, ideally assessed early in the trajectory of the disease and continuously re-evaluated as the diseases progresses.
The American Heart Association supports early and regular patient-provider ACP discussions to guide heart failure patients’ future decision-making [31], and recommends that such discussions be initiated in the outpatient setting, prior to and in anticipation of clinical decline. ACP communication plays a critical role in enhancing patients’ understanding of their diagnosis, treatment, prognosis, and choices in end-of-life care [31]. ACP communication also helps the clinician to better understand the context within which patients and their caregivers might make health care decisions, including their values and preferences for care. Patient-provider discussions about ACP focused on understanding patient values and initiated early in the trajectory of serious illness can support future in-the-moment decision-making, and is likely more effective than asking patients to make specific treatment decisions in advance [32]. A growing body of rigorous research has shown that ACP communication is associated with greater preference-concordant care and congruence in patient-surrogate understanding of patient preferences, lower costs, and less aggressive care at the end of life [33–37].
Patient Preferences for ACP Communication
Most patients with heart failure and their caregivers want honest disclosure regarding prognosis and to receive information about the expected trajectory of their disease [38–41] as early as possible [38] to help them plan and prepare for their future. Patients and their caregivers prefer to have these conversations with their physician [38] or other provider most familiar with the patient and family [39]. Patients also express a preference for support with dealing with the uncertainty inherent to heart failure [39]. Although most patients and caregivers desire to receive clear and honest communication about their disease, it is important to note that patients may vary in the extent of information they prefer to receive about their heart failure, with some individuals preferring not to talk about the end of life and future care needs at all [39,42–44].
Challenges to ACP Communication in Heart Failure
Despite patient and caregiver preferences for ACP communication with their providers, evidence suggests such communication occurs infrequently [40,45] and that heart failure patients may lack important information about their prognosis and treatment options [40,44,46,47]. For example, patients may not recognize the terminal nature of heart failure, and may be unaware of the range of treatment options, including hospice, available to them. Evidence also demonstrates that ACP is infrequently discussed with their health care providers [40], resulting in these conversations being avoided or deferred until an emergent clinical situation [44,48] when hasty questions about treatment choices may yield uncertain and conflicting answers not representative of a patient’s underlying values.
The infrequent, late, and often lack of discussions about ACP are driven by several challenges. First, the uncertain trajectory of heart failure makes communication regarding “what to expect” difficult. Prognostication is an immense challenge in heart failure [40,49–52], making it harder to talk about end-of-life issues and hindering the ability of patients, caregivers and health care providers to plan and prepare for the future. It is often difficult for clinicians, who face the challenge of instilling hope in the face of truthful disclosure [53], to identify the “right time” to initiate such discussions.
Second, a lack of time, particularly during outpatient visits, impedes physician ability to have considered discussions about future care needs and preferences [32,54]. The U.S. health care system currently lacks financial reimbursement for these discussions, which poses a significant barrier to the integration of ACP conversations into routine clinical practice. Moreover, these conversations are lengthy and iterative [53]. ACP discussions that are focused on facilitating patient-centered decision-making ideally begin with a discussion of expected prognosis, followed by an exploration of patient preferences and values for health care, and then a review of treatment options to be considered in the context of those preferences. Often additional time is needed for completing advance directive documents or for charting key outcomes from these discussions. Clinicians today are frequently overloaded with addressing multiple medical issues during outpatient visits that leave little time for non-medical tasks such as ACP discussions. The lack of financial incentives to support in-depth discussions is a critical challenge in improving ACP.
Third, a lack of training in specialized communication skills, particularly focused on empathic and emotionally sensitive disclosure, may further hinder physicians from initiating frank discussions with their patients. ACP conversations are highly sensitive and fraught with emotional complexity, and clinicians understandably experience discomfort with breaking bad news [49,51,55] or with broader issues of decline and death [51,56,57]. Physicians tend to be most comfortable addressing cognitive aspects of communication; addressing the emotional needs of patients is harder. Medical school training teaches detachment in physician practice, perhaps as a way of coping with the sadness they regularly confront and in maintaining their ability to provide clinical care. In fact, physicians describe their most difficult encounters as those with the most negative expressed emotions and miss opportunities to respond with empathy [58–60], a critical skill in effective patient-physician communication that is associated with improved patient satisfaction [61,62]. While patients value good communication skills in their health care encounters, many providers feel they lack the necessary skills to lead effective ACP discussions [49,63].
Finally, information gaps with regards to heart failure contribute to delayed or absent conversations about planning for future care. Many heart failure patients have a limited understanding of their disease [32,40,44,55], particularly an inaccurate perception that heart failure is not a terminal and life-limiting illness [42,49,64]. Compounding this is the fact that even some health care providers are reluctant to acknowledge the terminal nature of heart failure [50,56]. Without frank acknowledgement of the terminal nature of heart failure, the initiation of discussions regarding end-of-life care will remain difficult if not impossible.
Approaches to ACP in Heart Failure
When Is the Right Time?
Given the complexity and unpredictable trajectory of heart failure, indicators of disease progression, including changes in health status and health service use, may serve as useful signals to help clinicians identify the appropriate time to initiate care planning discussions. Repeated hospital admissions for heart failure are strongly associated with increased mortality. In a sample of community heart failure patients [8], median survival after the first, second, and third hospitalization was 2.4, 1.4, and 1.0 years, respectively. In light of this, a patient with 1 or more hospitalizations in a 12-month period may be an appropriate candidate for an ACP conversation. Similarly, comorbidity in patients with heart failure may signal the relevance and need for discussions about future care. In a sample of Medicare beneficiaries with advanced heart failure, an increasing burden of comorbidity was associated with significantly higher mortality, as were certain conditions (COPD, CKD, dementia, depression) and combinations of conditions (eg, CKD and dementia) [26]. Davidson and colleagues [68] suggest a list of clinical indicators signaling the need for an ACP conversation, including any of the following:
- > 1 episodes of exacerbation of heart failure leading to hospital admission
- New York Heart Association Class IV heart failure
- Decline in function and mobility
- Unexplained weight loss
- Resting pulse rate greater than 100 beats/minute
- Raised serum creatinine (> 150 µmol/L)
- Low serum sodium (< 135 mmol/L)
- Low serum albumen (< 33 g/L)
- High dose of loop diuretic (eg, furosemide ≥ 160 mg daily)
Given the considerable complexity and multisystem nature of heart failure, none of these indicators alone can signal certainty about disease progression and consequent outcomes; however, they can serve as a useful heuristic for helping clinicians identify appropriate times to raise the topic of ACP with their patients.
What Do I Say? Structuring the Conversation
Heart failure patients and their caregivers may vary in their preferences for hearing information about their disease; therefore, it is critical to open any conversation about planning for future in the context of their illness by asking what and how much information is desired. This includes evaluating how involved in decision-making the patient wants to be. Previously suggested language includes [69,70]:
- Would you like to consider all the options, or my opinion about the options that fit best with what I know about you?
- Some people like to know everything about their disease and be involved in all decision making. Others do not want all the news and would rather the doctor talk to __________. Which kind of person are you? How involved do you want to be in these decisions?
- Would you like me to tell you the full details of your condition?
- If you prefer not to hear the details, is there someone in your family who you trust to receive this information?
After establishing the patient’s preferences for hearing different types of information and level of involvement in decision-making about their care, the ask-tell-ask model [69,71] provides a useful approach to communicating with patients and their families. The conversation generally begins by asking patients what he or she understands about their illness (eg, “What do you understand about your heart failure?”; “I want to make sure we’re on the same page; what have other doctors told you?”). Building on what the patient already knows, the clinician can then disclose new information, correct misunderstandings, or confirm impressions and expectations the patient might have. In this way, information is tailored to the patient’s understanding and aimed at addressing potential knowledge gaps, all within the context of their preferences. Finally, the clinician asks the patient to describe their new understanding and whether or not they have questions or concerns (eg, “To make sure I did a good job of explaining to you, can you tell me what you now know about your condition from our conversation?”; “I know I’ve covered a lot and I want to make sure I was clear. When you get home, how are you going to explain what I’ve told you to your spouse?”). This approach encourages communication and exchange between patient and physician. Additionally, expressions of concern promote relationship building and bonding between physician and patient.
Keeping the Conversation Going
ACP communication can cover a wide range of topics beyond disease and prognostic disclosure by the provider to the patient. A critical aspect of ACP conversations is an exploration of the patient’s values and preferences, which can be used to help contextualize treatment choices and subsequently guide in-the-moment decision-making [72]. Using open-ended questions throughout the conversation gives the patient an opportunity to reflect on and communicate their wishes and values and allows them to engage in the conversation on their own terms. Examples of discussion-stimulating questions include [69,73]:
- What concerns you most about your illness?
- How is treatment going for you (your family)?
- As you think about your illness, what is the best and worst that might happen?
- What are your greatest hopes about your health?
- What has been most difficult about this illness for you?
- Looking back at your life, what has been important to you?
- At this point, what is most important for you to do?
Language
Central to this process is the use of empathic language to demonstrate support and understanding. An expression of empathy is also an appropriate way to acknowledge and share difficult emotions when it becomes hard to know where to take the conversation next. Quill and colleagues [74] suggest the following empathic responses to patients’ emotional expressions:
- I wish for that too
- It's unfortunate that things aren't different
- I am so sorry that this happened to you
- I understand how much you want that
- It must be very hard to accept the seriousness of this illness
Relatedly, the use of medical jargon in ACP conversations can increase the distance between patients and their providers, and may hinder patient understanding. Physicians may use technical language out of habit, or as an unconscious way to emotionally separate themselves from the task of delivering bad news. However, clear communication using layperson terms is the most effective approach to providing information necessary to patient-centered decision making. Explaining medical procedures in simple terms can improve understanding and help to build trust with the physician (eg, “We will perform an angioplasty – a procedure where a special tube with a balloon on the end of it is inserted into your artery to stretch it open. This will improve blood flow and relieve some of the symptoms you are currently experiencing”.)
Cultural Issues in Communication
There are various cultural issues to consider and address when conducting ACP discussions with heart failure patients and their families. Heart failure disproportionately affects certain racial and ethnic groups (eg, African Americans) [77–79], and effective management of heart failure depends on the provision of culturally sensitive information and facilitation of culturally informed self-care behaviors. There is evidence of cultural variation in preferences for information and role in decision-making. For example, most white and African-American patients prefer to be fully informed of their condition [80], whereas other cultures may focus on protecting the patient from difficult information in order to maintain hope [80–86]. Moreover, even in cultures where nondisclosure is preferred, patients may want to be told the truth in an indirect, euphemistic, or even nonverbal manner [80,87–89]. These complexities underscore the importance of taking a patient-centered approach to ACP communication, respecting individuality and autonomy while ultimately facilitating decision-making [90,91].
Are There Effective Training Programs for ACP Communication?
Effective communication skills are a critical component of ACP conversations between clinicians and their patients; however, most clinicians do not receive formal training in ACP communication and believe it to be a difficult task [92]. Strong evidence of the effectiveness of communication skills training has yet to be established, largely due to variation in the approach to training and the specification of relevant outcomes. For example, a systematic review of communication skills training courses found that some courses are effective at improving different types of communication skills related to providing support and gathering information, but these courses lacked effectiveness in improving patient satisfaction or provider burnout and distress [93]. Similarly, a range of approaches to teaching clinicians effective ACP communication skills early in their medical training have been identified [94], but considerable variation in quality preclude any conclusions from being drawn about their effectiveness.
Despite these challenges, there are some studies of communication skills training courses that have demonstrated the ability to increase providers’ use of empathic and facilitative communication (eg, use of open-ended questions) [58,95], and to increase self-efficacy and confidence among providers [96]. One particular teaching model that is increasingly used in cancer care is Oncotalk (http://depts.washington.edu/oncotalk/). Oncotalk has been shown to significantly increase clinical skills in giving bad news and facilitating the transition to palliative care. Building on this success, the program has expanded to training courses focused on the intensive care setting (http://depts.washington.edu/icutalk/) and geriatrics care [97–99]. It is important to note, however, that the considerable time and resource-intensive nature of communication training programs limits widespread implementation of any one approach into routine medical education. More attention to the type and structure of communication skills training programs are needed as well as scalable approaches to assist clinicians in developing effective ACP communication skills.
Policy Implications of ACP and Future Directions
There is growing recognition of the need to improve ACP among patients with seriously illness, including heart failure. In a recent Institute of Medicine (IOM) report, Dying in America [100], the need for clinician-patient communication about ACP was identified as a primary area of improvement. Recommendations include the establishment of communication quality standards as well as guidelines promoting early and ongoing ACP discussions. This is supported by recommendations from medical professional societies for an iterative model of ACP that follows the course of a serious illness [2,101]. At early stages of the illness, ACP might be focused on helping patients clarify their broad health care values and raise awareness of their disease and expected prognosis. As the condition progresses, ACP discussion might focus on exploring disease-specific treatment options within the context of previously expressed preferences, as well as identifying changes in patients’ values over time, particularly as they gain experience with their illness and health status changes [102]. In late stages of the disease, ACP might focus on documenting specific treatment choices (eg, DNR orders) and on exploring options such as palliative care, while also ensuring that patients and caregivers are appropriately prepared for imminent decline and death.
The IOM report also calls for payment reforms to include reimbursement for outpatient ACP discussions [100]. There is burgeoning national support for developing reimbursement models for ACP discussions. The American Medical Association has recently released current procedural terminology (CPT) codes for ACP services, a first step toward urging Medicare to consider reimbursement for ACP discussions with physicians.
Finally, the IOM report calls for improved education and training in ACP communication across all disciplines and specialties providing care to patients with serious illness. These recommendations bring national attention to the current limitations surrounding ACP discussions for those with serious illness, including heart failure. Further research is needed to identify methods and care models to address the gap in communication skills, processes, and policies.
Corresponding author: Sangeeta C. Ahluwalia, Rand Corporation, 1776 Main St., Santa Monica, CA, 90401, sahluwal@rand.org.
Financial disclosures: None.
Author contributions: conception and design, SCA, SE; analysis and interpretation of data, SCA, SE; drafting of article, SCA, SE; critical revision of the article, SCA, SE.
1. American Heart Association. Heart disease and stroke statistics—2008 update. [Internet]. Available at www.americanheart.org/downloadable/heart/1200078608862HS_Stats%202008.final.pdf.
2. Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult—summary article. Circulation 2005;112:1825–52.
3. Masoudi FA, Havranek EP, Krumholz HM. The burden of chronic congestive heart failure in older persons: magnitude and implications for policy and research. Heart Fail Rev 2002;7:9–16.
4. McMurray JJ PM. Heart failure. Lancet 2005;365:1877–89.
5. Unroe KT, Greiner MA, Hernandez AF, et al. Resource use in the last 6 months of life among medicare beneficiaries with heart failure, 2000-2007. Arch Intern Med 2011;171:196–203.
6. Lunney JR, Lynn J, Foley DJ, et al. Patterns of functional decline at the end of life. JAMA 2003;289:2387–92.
7. Ko D, Alter D, Austin P, et al. Life expectancy after an index hospitalization for patients with heart failure: A population-based study. Am Heart J 2008;155:324–31.
8. Setoguchi S, Stevenson LW, Schneeweiss S. Repeated hospitalizations predict mortality in the community population with heart failure. Am Heart J 2007;154:260–6.
9. Jong P, Vowinskel E, Liu PP, et al. Prognosis and determinants for survival in patients newly hospitalized for heart failure. Arch Intern Med 2002;162:1689-94.
10. Thom T, Haase N, Rodamond W, et al. Heart disease and stroke statistics- 2006 update. Circulation 2006;113:e85-e151.
11. Shahar E, Lee S, Kim J, et al. Hospitalized heart failure: Rates and long-term mortality. J Card Fail 2004;10:374–9.
12. Kirkpatrick JN, Guger CJ, Arnsdorf MF, et al. Advance directives in the cardiac care unit. Am Heart J 2007;154:477–81.
13. Orn S, Dickstein K. How do heart failure patients die? Eur Heart J. 2002;4(suppl D).
14. Juenger J, Schellberg D, Kraemer S, et al. Health related quality of life in patients with congestive heart failure: comparison with other chronic disease and relation to functional variables. Heart 2002;87:235–41.
15. Steptoe A, Mohabir A, Mahon NG, et al. Health related quality of life and psychological wellbeing in patients with dilated cardiomyopathy. Heart 2000;83:645–50.
16. Johansson P, Agnebrink M, Dahlstrom U, et al. Measurement of health-related quality of life in chronic heart failure, form a nursing perspective--a review of the literature. Eur J Cardiovasc Nurs 2004;3:7–20.
17. Levenson J, McCarthy E, Lynn J, et al. The last six months of life for patients with congestive heart failure. J Am Geriatr Soc 2000;48(Suppl 5):S101–S109.
18. Sullivan M, Levy W, Russo J, Spertus J. Depression and health status in patients with advanced heart failure: a prospective study in tertiary care. J Card Fail 2004;10:390–6.
19. Bekelman DB, Havranek EP, Becker DM, et al. Symptoms, depression, and quality of life in patients with heart failure. J Card Fail 2007;13:643–8.
20. Godfrey CM, Harrison MB, Friedberg E, et al. The symptom of pain in individuals recently hospitalized for heart failure. J Cardiovasc Nurs 2007;22:368–74.
21. McCarthy M, Lay M, Addington-Hall J. Dying from heart disease. J R Coll Physicians Lond 1996;30:325–8.
22. Norgren L SS. Symptoms experienced in the last six months of life in patients with end-stage heart failure. Eur J Cardiovasc Nurs 2003;2:213–7.
23. Zambroski CH, Moser DK, Bhat G, et al. Impact of symptom prevalence and symptom burden on quality of life in patients with heart failure. Eur J Cardiovasc Nurs 2005;4:198–206.
24. Walke LM, Byers AL, Tinetti ME, et al. Range and severity of symptoms over time among older adults wih chronic obstructive pulmonary disease and heart failure. Arch Intern Med 2007;167:2503–8.
25. Bekelman DB, Rumsfeld JS, Havranek EP, et al. Symptom burden, depression, and spiritual well-being: a comparison of heart failure and advanced cancer patients. J Gen Intern Med 2009;24:592–8.
26. Ahluwalia SC, Gross CP, Chaudhry SI, et al. Impact of comorbidity on mortality among older persons with advanced heart failure. J Gen Intern Med 2012;27:513–9.
27. Ahluwalia SC, Gross CP, Chaudhry SI, et al. Change in comorbidity prevalence with advancing age among persons with heart failure. J Gen Intern Med 2011;26:1145–51.
28. Corrigan JM, Donaldson MS, Kohn LT, et al. A new health system for the 21st century. crossing the quality chasm. Washington, DC: Institute of Medicine, National Academy of Sciences, National Academies Press; 2001.
29. Kirchhoff KT, Hammes BJ, Kehl KA, et al. Effect of a disease-specific advance care planning intervention on end-of-life care. J Am Geriatr Soc 2012;60:946–50.
30. Kirchhoff KT, Hammes BJ, Kehl KA, et al. Effect of a disease-specific planning intervention on surrogate understanding of patient goals for future medical treatment. J Am Geriatr Soc 2010;58:1233–40.
31. Janssen DJ, Engelberg RA, Wouters EF, Curtis JR. Advance care planning for patients with COPD: past, present and future. Patient Educ Couns 2012;86:19–24.
32. Aldred H, Gott M, Gariballa S. Advanced heart failure: Impact on older patients and informal carers. J Adv Nurs 2005;49:116–24.
33. Zhang B, Wright AA, Huskamp HA, et al. Health care costs in the last week of life: Associations with end-of-life conversations. Arch Intern Med 2009;169:480–8.
34. Wright AA, Zhang B, Ray A, et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 2008;300:1665–73.
35. Mack JW, Smith TJ. Reasons why physicians do not have discussions about poor prognosis, why it matters, and what can be improved. J Clin Oncol 2012;30:2715–7.
36. Detering KM, Hancock AD, Reade MC, Silvester W. The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ 2010;340:c1345.
37. Schwartz CE, Wheeler HB, Hammes B, et al. Early intervention in planning end-of-life care with ambulatory geriatric patients: results of a pilot trial. Arch Intern Med 2002;162:1611–8.
38. Caldwell PH, Arthur HM, Demers C. Preferences of patients with heart failure for prognosis communication. Can J Cardiol 2007;23:791–6.
39. Bekelman DB, Nowels Ct, Retrum JH, et al. Giving voice to patients’ and family caregivers’ needs in chronic heart failure: implications for palliative care programs. J Palliat Med 2011;14:1317–24.
40. Harding R, Selman L, Beynon T, et al. Meeting the communication and information needs of chronic heart failure patients. J Pain Symptom Manage 2008;36:149–56.
41. Strachan PH, Ross H, Dodek PM, et al. Mind the gap: opportunities for improving end-of-life care for patients with advanced heart failure. Can J Cardiol 2009;25:635–40.
42. Ågård A, Hermerén G, Herlitz J. When is a patient with heart failure adequately informed? A study of patients’ knowledge of and attitudes toward medical information. Heart Lung 2004;33:219–26.
43. Gott M, Small N, Barnes S, et al. Older people’s views of a good death in heart failure: implications for palliative care provision. Soc Sci Med 2008;67:1113–21.
44. Murray SA, Boyd K, Kendall M, et al. Dying of lung cancer or cardiac failure: prospective qualitative interview study of patients and their carers in the community. BMJ 2002;325:929.
45. Ahluwalia SC, Levin JR, Lorenz KA, et al. Missed opportunities for advance care planning communication during outpatient clinic visits. J Gen Intern Med 2012;27:445–51.
46. Rodriguez KL, Appelt CJ, Switzer GE, et al. “They diagnosed bad heart”: a qualitative exploration of patients’ knowledge about and experiences with heart failure. Heart Lung. 2008;37:257–65.
47. Remme WJ,McMurray JJ, Rauch B, et al. Public awareness of heart failure in Europe: first results from SHAPE. Eur Heart J 2005;22:2413e21.
48. Golin CE, Wenger NS, Liu H, et al. A prospective study of patient-physician communication about resuscitation. J Am Geriatr Soc 2000;48(5 Suppl):S52–60.
49. Selman L, Harding R, Beynon T, et al. Improving end of life care for patients with chronic heart failure: ‘let’s hope it’ll get better when I know in my heart of hearts it won’t’. Heart 2007;93:963–7.
50. Barnes S, Gott M, Payne S, et al. Communication in heart failure: Perspectives from older people and primary care professionals. Health Soc Care Comm 2006;14:482–90.
51. Brännström M, Ekman I, Norberg A, et al. Living with severe chronic heart failure in palliative advanced home care. Eur J Cardiovasc Nurs 2006;5:295–302.
52. Barclay S, Momen N, Case-Upton S, et al. End-of-life care conversations with heart failure patients: a systematic literature review and narrative synthesis. Br J Gen Pract 2011;61:e49–62.
53. Whitney SN, McCullough LB, Fruge E, et al. Beyond breaking bad news: the roles of hope and hopefulness. Cancer 2008;113:442–5.
54. Tung EE, North F. Advance care planning in the primary care setting: a comparison of attending staff and resident barriers. Am J Hosp Palliat Care 2009;26:456–63.
55. Boyd K, Murray S, Kendall M, et al. Living with advanced heart failure: A prospective, community based study of patients and their carers. Eur J Heart Fail 2004;6:585–91.
56. Borbasi S, Wotton K, Redden M, et al. Letting go: A qualitative study of acute care and community nurses’ perceptions of a ‘good’ versus a ‘bad’ death. Austr Crit Care 2005 2005;18:104–13.
57. Hanratty B, Hibbert D, Mair F, et al. Doctors’ perceptions of palliative care for heart failure: Focus group study. BMJ 2002;325:581–5.
58. Fallowfield L, Jenkins V, Farewell V, et al. Efficacy of a communication skills training model for oncologists: a randomized controlled trial. Lancet 2002;359:650–6.
59. Platt F, Keller V. Empathic communication: a teachable and learnable skill. J Gen Intern Med 1994;9:222–6.
60. Morse D, Edwardsen E, Gordon H. Missed opportunities for interval empathy in lung cancer communication. Arch Intern Med 2008;22;168:1853–8.
61. Epstein R, Hadee T, Carroll J, et al. “Could this be something serious?” reassurance, uncertainty, and empathy in response to patients’ expressions of worry. J Gen Intern Med 2007;22:1731–9.
62. Stewart M. What is a successful doctor-patient interview? A study of interactions and outcomes. Soc Sci Med 1984;19:
167–75.
63. Wotton K, Borbasi S, Redden M. When all else has failed. Nurses’ perception of factors influencing palliative care for patients with end-stage heart failure. J Cardiovasc Nurs 2005;20:18–25.
64. Willems DL, Hak A, Visser F, Van der Wal G. Thoughts of patients with advanced heart failure on dying. Palliat Med 2004;18:564–72.
65. Briggs L, Kirchhoff K, Hammes B, et al. Patient-centered advance care planning in special patient populations: a pilot study. J Prof Nurs 2004;20:47–58.
66. Hammes B, Rooney B. Death and EOL planning in one midwestern community. Arch Intern Med 1998;158:390.
67. Lilly C, DeMeo D, Sonna L, et al. An intensive communication intervention for the critically ill. Am J Med 2000;109:469–75.
68. Davidson P, Macdonald P, Newton P, et al. End stage heart failure patients: Palliative care in general practice. Aust Fam Physician 2010;39:920.
69. Goodlin S, Quill T, Arnold R. Communication and decision-making about prognosis in heart failure care. J Card Fail 2008;14:106–13.
70. Analysis of U.S. hospital palliative care programs 2010 snapshot. Center to Advance Palliative Care (CAPC). Accessed 24 Nov 2014 at www.capc.org/news-and-events/releases/analysis-of-us-hospital-palliative-care-programs-2010-snapshot.pdf.
71. Back AL, Arnold RM, Baile WF, et al. Approaching difficult communication tasks in oncology. CA Cancer J Clin 2005;55:164–77.
72. Sudore RL, Fried TR, Redefining the “planning” in advance care planning: preparing for end-of-life decision making. Ann Intern Med 2010;153:256–61.
73. Lo B, Quill T, Tulsky J. Discussing palliative care with patients. Ann Intern Med 1999;130:744–9.
74. Quill T, Arnold R, Platt F. I wish things were different: Expressing wishes in response to loss, futility, and unrealistic hopes. Ann Intern Med 2001;135:551–5.
75. Pollak K, Arnold R, Jeffreys A, et al. Oncologist communication about emotion during visits with patients with advanced cancer. J Clin Oncol 2007;25:5748–52.
76. Back AL, Anderson WG, Bunch L, et al. Communication about cancer near the end of life. Cancer 2008;113(S7):1897–910.
77. Dries D, Exner D, Gersh B, et al. Racial differences in the outcome of left ventricular dysfunction. N Engl J Med 1999;340:609–16.
78. Alexander M, Grumbach K, Selby J, et al. Hospitalization for congestive heart failure. Explaining racial differences. JAMA 1995;274:1037–42.
79. Afzal A, Ananthasubramaniam K, Sharma N, et al. Racial differences in patients with heart failure. Clin Cardiol 1999;22:791–4.
80. Blackhall L, Murphy S, Frank G, et al. Ethnicity and attitudes toward patient autonomy. JAMA 1995;274:820–5.
81. Huang X, Butow P, Meiser B, et al. Attitudes and information needs of chinese migrant cancer patients and their relatives. Aust N Z J Med 1999;29:207–13.
82. Tan T, Teo F, Wong K, et al. Cancer: to tell or not to tell? Singapore Med J 1993;34:202–3.
83. Gorgaki S, Kalaidopoulou O, Liarmakopoulos I, et al. Nurses’ attitudes toward truthful communication with patients with cancer. A Greek study. Cancer Nurs 2002;25:436–41.
84. Harris J, Shao J, Sugarman J. Disclosure of cancer diagnosis and prognosis in northern Tanzania. Soc Sci Med 2003;56:905–13.
85. Goldstein D, Thewes B, Butow P. Communicating in a multicultural society. II: Greek community attitudes towards cancer in Australia. Intern Med J 2002;32:289–96.
86. Beyene Y. Medical disclosure and refugees. Telling bad news to Ethiopian patients. West J Med 1992;157:328–32.
87. Matsumura S, Bito S, Liu H, et al. Acculturation of attitudes toward end-of-life care: A cross-cultural survey of Japanese Americans and Japanese. J Gen Intern Med 2002;17:531–9.
88. Yick AG, Gupta R. Chinese cultural dimensions of death, dying, and bereavement: Focus group findings. J Cult Divers 2002 Summer;9:32–42.
89. Frank G, Blackhall L, Murphy S, et al. Ambiguity and hope: Disclosure preferences of less acculturated elderly Mexican Americans concerning terminal cancer—A case story. Camb Q Healthc Ethics 2002;11:117–26.
90. Hern HJ, Koenig B, Moore L, et al. The difference that culture can make in end-of-life decisionmaking. Camb Q Healthc Ethics 1998;7:27–48.
91. Kagawa-Singer M, Kassim-Lakha S. A strategy to reduce cross-cultural miscommunication and increase the likelihood of improving health outcomes. Acad Med 2003;78:577–87.
92. Barnett MM, Fisher JD, Cooke H, et al. Breaking bad news: consultants’ experience, previous education, and views on educational format and timing. Med Educ 2007;41:947–56.
93. Moore P, Rivera Mercado S, Grez Artigues M, Lawrie T. Communication skills training for healthcare professionals working with people who have cancer. Cochrane Database Syst Rev 2013;3CD003751.
94. Alelwani S, Ahmed Y. Medical training for communication of bad news: A literature review. J Educ Health Promot 2014;3
95. Delvaux N, Razavi D, Marchal S, et al. Effects of a 105 hour psychological training program on attitudes, communication skills and occupational stress in oncology: a randomised study. Br J Cancer 2004;90:106–14.
96. Baile WF, Lenzi R, Kudelka AP, et al. Improving physician-patient communication in cancer care: Outcome of a workshop for oncologists. J Cancer Educ 1997;12:166–73.
97. Back AL, Arnold RM, Baile WF, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Intern Med 2007;167:453–60.
98. Gelfman LP, Lindenberger E, Fernandez H, et al. The effectiveness of the Geritalk communication skills course: a real-time assessment of skill acquisition and deliberate practice. J Pain Sympt Manage 2014;48:738–44.
99. Kelley AS, Back AL, Arnold RM, et al. Geritalk: communication skills training for geriatric and palliative medicine fellows. J Am Geriatr Soc 2012;60:332–7.
100. Institute of Medicine. Dying in America: Improving quality and honoring individual preferences near the end of life. Washington, DC: National Academies Press; 2014.
101. Allen LA, Stevenson LW, Grady KL, et al. Decision making in advanced heart failure: a scientific statement From the American Heart Association. Circulation 2012;125:1928–52.
102. Ditto PH, Jacobson JA, Smucker WD, et al. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment preferences. Med Decis Making 2006;26:313–22.
1. American Heart Association. Heart disease and stroke statistics—2008 update. [Internet]. Available at www.americanheart.org/downloadable/heart/1200078608862HS_Stats%202008.final.pdf.
2. Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult—summary article. Circulation 2005;112:1825–52.
3. Masoudi FA, Havranek EP, Krumholz HM. The burden of chronic congestive heart failure in older persons: magnitude and implications for policy and research. Heart Fail Rev 2002;7:9–16.
4. McMurray JJ PM. Heart failure. Lancet 2005;365:1877–89.
5. Unroe KT, Greiner MA, Hernandez AF, et al. Resource use in the last 6 months of life among medicare beneficiaries with heart failure, 2000-2007. Arch Intern Med 2011;171:196–203.
6. Lunney JR, Lynn J, Foley DJ, et al. Patterns of functional decline at the end of life. JAMA 2003;289:2387–92.
7. Ko D, Alter D, Austin P, et al. Life expectancy after an index hospitalization for patients with heart failure: A population-based study. Am Heart J 2008;155:324–31.
8. Setoguchi S, Stevenson LW, Schneeweiss S. Repeated hospitalizations predict mortality in the community population with heart failure. Am Heart J 2007;154:260–6.
9. Jong P, Vowinskel E, Liu PP, et al. Prognosis and determinants for survival in patients newly hospitalized for heart failure. Arch Intern Med 2002;162:1689-94.
10. Thom T, Haase N, Rodamond W, et al. Heart disease and stroke statistics- 2006 update. Circulation 2006;113:e85-e151.
11. Shahar E, Lee S, Kim J, et al. Hospitalized heart failure: Rates and long-term mortality. J Card Fail 2004;10:374–9.
12. Kirkpatrick JN, Guger CJ, Arnsdorf MF, et al. Advance directives in the cardiac care unit. Am Heart J 2007;154:477–81.
13. Orn S, Dickstein K. How do heart failure patients die? Eur Heart J. 2002;4(suppl D).
14. Juenger J, Schellberg D, Kraemer S, et al. Health related quality of life in patients with congestive heart failure: comparison with other chronic disease and relation to functional variables. Heart 2002;87:235–41.
15. Steptoe A, Mohabir A, Mahon NG, et al. Health related quality of life and psychological wellbeing in patients with dilated cardiomyopathy. Heart 2000;83:645–50.
16. Johansson P, Agnebrink M, Dahlstrom U, et al. Measurement of health-related quality of life in chronic heart failure, form a nursing perspective--a review of the literature. Eur J Cardiovasc Nurs 2004;3:7–20.
17. Levenson J, McCarthy E, Lynn J, et al. The last six months of life for patients with congestive heart failure. J Am Geriatr Soc 2000;48(Suppl 5):S101–S109.
18. Sullivan M, Levy W, Russo J, Spertus J. Depression and health status in patients with advanced heart failure: a prospective study in tertiary care. J Card Fail 2004;10:390–6.
19. Bekelman DB, Havranek EP, Becker DM, et al. Symptoms, depression, and quality of life in patients with heart failure. J Card Fail 2007;13:643–8.
20. Godfrey CM, Harrison MB, Friedberg E, et al. The symptom of pain in individuals recently hospitalized for heart failure. J Cardiovasc Nurs 2007;22:368–74.
21. McCarthy M, Lay M, Addington-Hall J. Dying from heart disease. J R Coll Physicians Lond 1996;30:325–8.
22. Norgren L SS. Symptoms experienced in the last six months of life in patients with end-stage heart failure. Eur J Cardiovasc Nurs 2003;2:213–7.
23. Zambroski CH, Moser DK, Bhat G, et al. Impact of symptom prevalence and symptom burden on quality of life in patients with heart failure. Eur J Cardiovasc Nurs 2005;4:198–206.
24. Walke LM, Byers AL, Tinetti ME, et al. Range and severity of symptoms over time among older adults wih chronic obstructive pulmonary disease and heart failure. Arch Intern Med 2007;167:2503–8.
25. Bekelman DB, Rumsfeld JS, Havranek EP, et al. Symptom burden, depression, and spiritual well-being: a comparison of heart failure and advanced cancer patients. J Gen Intern Med 2009;24:592–8.
26. Ahluwalia SC, Gross CP, Chaudhry SI, et al. Impact of comorbidity on mortality among older persons with advanced heart failure. J Gen Intern Med 2012;27:513–9.
27. Ahluwalia SC, Gross CP, Chaudhry SI, et al. Change in comorbidity prevalence with advancing age among persons with heart failure. J Gen Intern Med 2011;26:1145–51.
28. Corrigan JM, Donaldson MS, Kohn LT, et al. A new health system for the 21st century. crossing the quality chasm. Washington, DC: Institute of Medicine, National Academy of Sciences, National Academies Press; 2001.
29. Kirchhoff KT, Hammes BJ, Kehl KA, et al. Effect of a disease-specific advance care planning intervention on end-of-life care. J Am Geriatr Soc 2012;60:946–50.
30. Kirchhoff KT, Hammes BJ, Kehl KA, et al. Effect of a disease-specific planning intervention on surrogate understanding of patient goals for future medical treatment. J Am Geriatr Soc 2010;58:1233–40.
31. Janssen DJ, Engelberg RA, Wouters EF, Curtis JR. Advance care planning for patients with COPD: past, present and future. Patient Educ Couns 2012;86:19–24.
32. Aldred H, Gott M, Gariballa S. Advanced heart failure: Impact on older patients and informal carers. J Adv Nurs 2005;49:116–24.
33. Zhang B, Wright AA, Huskamp HA, et al. Health care costs in the last week of life: Associations with end-of-life conversations. Arch Intern Med 2009;169:480–8.
34. Wright AA, Zhang B, Ray A, et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 2008;300:1665–73.
35. Mack JW, Smith TJ. Reasons why physicians do not have discussions about poor prognosis, why it matters, and what can be improved. J Clin Oncol 2012;30:2715–7.
36. Detering KM, Hancock AD, Reade MC, Silvester W. The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ 2010;340:c1345.
37. Schwartz CE, Wheeler HB, Hammes B, et al. Early intervention in planning end-of-life care with ambulatory geriatric patients: results of a pilot trial. Arch Intern Med 2002;162:1611–8.
38. Caldwell PH, Arthur HM, Demers C. Preferences of patients with heart failure for prognosis communication. Can J Cardiol 2007;23:791–6.
39. Bekelman DB, Nowels Ct, Retrum JH, et al. Giving voice to patients’ and family caregivers’ needs in chronic heart failure: implications for palliative care programs. J Palliat Med 2011;14:1317–24.
40. Harding R, Selman L, Beynon T, et al. Meeting the communication and information needs of chronic heart failure patients. J Pain Symptom Manage 2008;36:149–56.
41. Strachan PH, Ross H, Dodek PM, et al. Mind the gap: opportunities for improving end-of-life care for patients with advanced heart failure. Can J Cardiol 2009;25:635–40.
42. Ågård A, Hermerén G, Herlitz J. When is a patient with heart failure adequately informed? A study of patients’ knowledge of and attitudes toward medical information. Heart Lung 2004;33:219–26.
43. Gott M, Small N, Barnes S, et al. Older people’s views of a good death in heart failure: implications for palliative care provision. Soc Sci Med 2008;67:1113–21.
44. Murray SA, Boyd K, Kendall M, et al. Dying of lung cancer or cardiac failure: prospective qualitative interview study of patients and their carers in the community. BMJ 2002;325:929.
45. Ahluwalia SC, Levin JR, Lorenz KA, et al. Missed opportunities for advance care planning communication during outpatient clinic visits. J Gen Intern Med 2012;27:445–51.
46. Rodriguez KL, Appelt CJ, Switzer GE, et al. “They diagnosed bad heart”: a qualitative exploration of patients’ knowledge about and experiences with heart failure. Heart Lung. 2008;37:257–65.
47. Remme WJ,McMurray JJ, Rauch B, et al. Public awareness of heart failure in Europe: first results from SHAPE. Eur Heart J 2005;22:2413e21.
48. Golin CE, Wenger NS, Liu H, et al. A prospective study of patient-physician communication about resuscitation. J Am Geriatr Soc 2000;48(5 Suppl):S52–60.
49. Selman L, Harding R, Beynon T, et al. Improving end of life care for patients with chronic heart failure: ‘let’s hope it’ll get better when I know in my heart of hearts it won’t’. Heart 2007;93:963–7.
50. Barnes S, Gott M, Payne S, et al. Communication in heart failure: Perspectives from older people and primary care professionals. Health Soc Care Comm 2006;14:482–90.
51. Brännström M, Ekman I, Norberg A, et al. Living with severe chronic heart failure in palliative advanced home care. Eur J Cardiovasc Nurs 2006;5:295–302.
52. Barclay S, Momen N, Case-Upton S, et al. End-of-life care conversations with heart failure patients: a systematic literature review and narrative synthesis. Br J Gen Pract 2011;61:e49–62.
53. Whitney SN, McCullough LB, Fruge E, et al. Beyond breaking bad news: the roles of hope and hopefulness. Cancer 2008;113:442–5.
54. Tung EE, North F. Advance care planning in the primary care setting: a comparison of attending staff and resident barriers. Am J Hosp Palliat Care 2009;26:456–63.
55. Boyd K, Murray S, Kendall M, et al. Living with advanced heart failure: A prospective, community based study of patients and their carers. Eur J Heart Fail 2004;6:585–91.
56. Borbasi S, Wotton K, Redden M, et al. Letting go: A qualitative study of acute care and community nurses’ perceptions of a ‘good’ versus a ‘bad’ death. Austr Crit Care 2005 2005;18:104–13.
57. Hanratty B, Hibbert D, Mair F, et al. Doctors’ perceptions of palliative care for heart failure: Focus group study. BMJ 2002;325:581–5.
58. Fallowfield L, Jenkins V, Farewell V, et al. Efficacy of a communication skills training model for oncologists: a randomized controlled trial. Lancet 2002;359:650–6.
59. Platt F, Keller V. Empathic communication: a teachable and learnable skill. J Gen Intern Med 1994;9:222–6.
60. Morse D, Edwardsen E, Gordon H. Missed opportunities for interval empathy in lung cancer communication. Arch Intern Med 2008;22;168:1853–8.
61. Epstein R, Hadee T, Carroll J, et al. “Could this be something serious?” reassurance, uncertainty, and empathy in response to patients’ expressions of worry. J Gen Intern Med 2007;22:1731–9.
62. Stewart M. What is a successful doctor-patient interview? A study of interactions and outcomes. Soc Sci Med 1984;19:
167–75.
63. Wotton K, Borbasi S, Redden M. When all else has failed. Nurses’ perception of factors influencing palliative care for patients with end-stage heart failure. J Cardiovasc Nurs 2005;20:18–25.
64. Willems DL, Hak A, Visser F, Van der Wal G. Thoughts of patients with advanced heart failure on dying. Palliat Med 2004;18:564–72.
65. Briggs L, Kirchhoff K, Hammes B, et al. Patient-centered advance care planning in special patient populations: a pilot study. J Prof Nurs 2004;20:47–58.
66. Hammes B, Rooney B. Death and EOL planning in one midwestern community. Arch Intern Med 1998;158:390.
67. Lilly C, DeMeo D, Sonna L, et al. An intensive communication intervention for the critically ill. Am J Med 2000;109:469–75.
68. Davidson P, Macdonald P, Newton P, et al. End stage heart failure patients: Palliative care in general practice. Aust Fam Physician 2010;39:920.
69. Goodlin S, Quill T, Arnold R. Communication and decision-making about prognosis in heart failure care. J Card Fail 2008;14:106–13.
70. Analysis of U.S. hospital palliative care programs 2010 snapshot. Center to Advance Palliative Care (CAPC). Accessed 24 Nov 2014 at www.capc.org/news-and-events/releases/analysis-of-us-hospital-palliative-care-programs-2010-snapshot.pdf.
71. Back AL, Arnold RM, Baile WF, et al. Approaching difficult communication tasks in oncology. CA Cancer J Clin 2005;55:164–77.
72. Sudore RL, Fried TR, Redefining the “planning” in advance care planning: preparing for end-of-life decision making. Ann Intern Med 2010;153:256–61.
73. Lo B, Quill T, Tulsky J. Discussing palliative care with patients. Ann Intern Med 1999;130:744–9.
74. Quill T, Arnold R, Platt F. I wish things were different: Expressing wishes in response to loss, futility, and unrealistic hopes. Ann Intern Med 2001;135:551–5.
75. Pollak K, Arnold R, Jeffreys A, et al. Oncologist communication about emotion during visits with patients with advanced cancer. J Clin Oncol 2007;25:5748–52.
76. Back AL, Anderson WG, Bunch L, et al. Communication about cancer near the end of life. Cancer 2008;113(S7):1897–910.
77. Dries D, Exner D, Gersh B, et al. Racial differences in the outcome of left ventricular dysfunction. N Engl J Med 1999;340:609–16.
78. Alexander M, Grumbach K, Selby J, et al. Hospitalization for congestive heart failure. Explaining racial differences. JAMA 1995;274:1037–42.
79. Afzal A, Ananthasubramaniam K, Sharma N, et al. Racial differences in patients with heart failure. Clin Cardiol 1999;22:791–4.
80. Blackhall L, Murphy S, Frank G, et al. Ethnicity and attitudes toward patient autonomy. JAMA 1995;274:820–5.
81. Huang X, Butow P, Meiser B, et al. Attitudes and information needs of chinese migrant cancer patients and their relatives. Aust N Z J Med 1999;29:207–13.
82. Tan T, Teo F, Wong K, et al. Cancer: to tell or not to tell? Singapore Med J 1993;34:202–3.
83. Gorgaki S, Kalaidopoulou O, Liarmakopoulos I, et al. Nurses’ attitudes toward truthful communication with patients with cancer. A Greek study. Cancer Nurs 2002;25:436–41.
84. Harris J, Shao J, Sugarman J. Disclosure of cancer diagnosis and prognosis in northern Tanzania. Soc Sci Med 2003;56:905–13.
85. Goldstein D, Thewes B, Butow P. Communicating in a multicultural society. II: Greek community attitudes towards cancer in Australia. Intern Med J 2002;32:289–96.
86. Beyene Y. Medical disclosure and refugees. Telling bad news to Ethiopian patients. West J Med 1992;157:328–32.
87. Matsumura S, Bito S, Liu H, et al. Acculturation of attitudes toward end-of-life care: A cross-cultural survey of Japanese Americans and Japanese. J Gen Intern Med 2002;17:531–9.
88. Yick AG, Gupta R. Chinese cultural dimensions of death, dying, and bereavement: Focus group findings. J Cult Divers 2002 Summer;9:32–42.
89. Frank G, Blackhall L, Murphy S, et al. Ambiguity and hope: Disclosure preferences of less acculturated elderly Mexican Americans concerning terminal cancer—A case story. Camb Q Healthc Ethics 2002;11:117–26.
90. Hern HJ, Koenig B, Moore L, et al. The difference that culture can make in end-of-life decisionmaking. Camb Q Healthc Ethics 1998;7:27–48.
91. Kagawa-Singer M, Kassim-Lakha S. A strategy to reduce cross-cultural miscommunication and increase the likelihood of improving health outcomes. Acad Med 2003;78:577–87.
92. Barnett MM, Fisher JD, Cooke H, et al. Breaking bad news: consultants’ experience, previous education, and views on educational format and timing. Med Educ 2007;41:947–56.
93. Moore P, Rivera Mercado S, Grez Artigues M, Lawrie T. Communication skills training for healthcare professionals working with people who have cancer. Cochrane Database Syst Rev 2013;3CD003751.
94. Alelwani S, Ahmed Y. Medical training for communication of bad news: A literature review. J Educ Health Promot 2014;3
95. Delvaux N, Razavi D, Marchal S, et al. Effects of a 105 hour psychological training program on attitudes, communication skills and occupational stress in oncology: a randomised study. Br J Cancer 2004;90:106–14.
96. Baile WF, Lenzi R, Kudelka AP, et al. Improving physician-patient communication in cancer care: Outcome of a workshop for oncologists. J Cancer Educ 1997;12:166–73.
97. Back AL, Arnold RM, Baile WF, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Intern Med 2007;167:453–60.
98. Gelfman LP, Lindenberger E, Fernandez H, et al. The effectiveness of the Geritalk communication skills course: a real-time assessment of skill acquisition and deliberate practice. J Pain Sympt Manage 2014;48:738–44.
99. Kelley AS, Back AL, Arnold RM, et al. Geritalk: communication skills training for geriatric and palliative medicine fellows. J Am Geriatr Soc 2012;60:332–7.
100. Institute of Medicine. Dying in America: Improving quality and honoring individual preferences near the end of life. Washington, DC: National Academies Press; 2014.
101. Allen LA, Stevenson LW, Grady KL, et al. Decision making in advanced heart failure: a scientific statement From the American Heart Association. Circulation 2012;125:1928–52.
102. Ditto PH, Jacobson JA, Smucker WD, et al. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment preferences. Med Decis Making 2006;26:313–22.