A 20-year-old woman with no significant medical history presented to the ED with a several-month history of worsening abdominal pain. She reported that although she previously had been evaluated at multiple EDs, no cause of her abdominal pain had been identified. The patient further noted that the pain had significantly increased the day of this presentation.
Figure 1
Physical examination revealed guarding and rebound tenderness in the midabdomen. Computed tomography (CT) studies of the abdomen and pelvis were performed; representative scout and axial images of the upper abdomen are shown above (Figures 1 and 2).
Figure 2
What is the suspected diagnosis?
Answer
The scout image of the abdomen revealed a distended stomach (white arrows, Figure 3), which displaced multiple loops of small bowel into the lower abdomen. The axial image through the upper abdomen showed air and solid material within the distended stomach (white arrows, Figure 4). Multiple foci of extraluminal (free) air were seen anteriorly (white asterisks, Figure 4). A coronal reformat of the CT better demonstrated the distended stomach filled with debris (white arrows, Figure 5), extraluminal air (white asterisk, Figure 5), and pneumatosis (air within the walls of multiple small bowel loops; red arrows, Figure 5).
These findings indicated a bowel obstruction and perforation due to the presence of a gastric bezoar. Upon further questioning, the patient admitted to a stress-related habit of eating her own hair (trichophagia) over the past 3 to 4 months.
Figure 3
Bezoars
Gastric bezoars are aggregates of nondigestible material that collect within the gastrointestinal system, usually fruit/vegetable matter (phytobezoars) or hair (trichobezoars). Phytobezoars are most common in patients with a history of reduced gastric motility and/or prior gastric surgery. Trichobezoars, similar to the one seen in this case, typically occur in young women and/or patients with psychiatric illness.1
Gastric bezoars are typically located in the gastric body but may extend into the small bowel and cause bowel obstruction. Trichobezoars that extend into the small bowel are referred to as “Rapunzel syndrome” (based on the fairy tale of the princess with long hair).
Figure 4
Clinical Presentation
Patients with gastric bezoars often present to the ED with nonspecific complaints of abdominal pain, including early satiety, weight loss, signs of anemia, abdominal pain, bloating, and symptoms of small bowel obstruction (SBO).2 Obtaining a thorough history is important to identify trichophagia, as only a small percentage of patients have evidence of alopecia on examination.
Figure 5
Workup
The workup for patients with gastric bezoars typically involves multiple imaging modalities. While abdominal radiography may demonstrate distention of the stomach, these findings are often nonspecific, and the characteristic feature of a mass with a diffusely mottled appearance is visualized in less than 20% of cases.
Computed tomography is the test of choice for detecting a bezoar, with a reported sensitivity of 97%.3 This modality is also useful for assessing the size of a bezoar and evaluating for complications such as SBO, perforation (free-air), or pneumatosis—all of which were revealed on this patient’s CT studies.
Treatment
The treatment for patients with large or obstructing gastric bezoars is surgical resection; both open and laparoscopic techniques have been described in the literature.2,4 The patient in this case was admitted to the hospital, where she underwent surgical removal of the bezoar. She was discharged home on hospital day 6 with outpatient psychiatric follow-up.
References
1. Guniganti P, Bradenham CH, Raptis C, Menias CO, Mellnick VM. Radiographics. 2015;35(7):1909-1921. doi:10.1148/rg.2015150062. 2. Fallon SC, Slater BJ, Larimer EL, Brandt ML, Lopez ME. The surgical management of Rapunzel syndrome: a case series and literature review. J Pediatr Surg. 2013;48(4):830-834. doi:10.1016/j.jpedsurg.2012.07.046. 3. Ripollés T, García-Aguayo J, Martínez MJ, Gil P. Gastrointestinal Bezoars: Sonographic and CT Characteristics. AJR Am J Roentgenol. 2001;177(1):65-69. doi:10.2214/ajr.177.1.1770065. 4. Flaherty DC, Aguilar F, Pradhan B, Grewal H. Rapunzel syndrome due to ingested hair extensions: Surgical and psychiatric considerations. Int J Surg Case Rep. 2015;17:155-157. doi:10.1016/j.ijscr.2015.11.009.
An otherwise healthy 20-year-old woman presented for evaluation of severe chronic abdominal pain.
An otherwise healthy 20-year-old woman presented for evaluation of severe chronic abdominal pain.
A 20-year-old woman with no significant medical history presented to the ED with a several-month history of worsening abdominal pain. She reported that although she previously had been evaluated at multiple EDs, no cause of her abdominal pain had been identified. The patient further noted that the pain had significantly increased the day of this presentation.
Figure 1
Physical examination revealed guarding and rebound tenderness in the midabdomen. Computed tomography (CT) studies of the abdomen and pelvis were performed; representative scout and axial images of the upper abdomen are shown above (Figures 1 and 2).
Figure 2
What is the suspected diagnosis?
Answer
The scout image of the abdomen revealed a distended stomach (white arrows, Figure 3), which displaced multiple loops of small bowel into the lower abdomen. The axial image through the upper abdomen showed air and solid material within the distended stomach (white arrows, Figure 4). Multiple foci of extraluminal (free) air were seen anteriorly (white asterisks, Figure 4). A coronal reformat of the CT better demonstrated the distended stomach filled with debris (white arrows, Figure 5), extraluminal air (white asterisk, Figure 5), and pneumatosis (air within the walls of multiple small bowel loops; red arrows, Figure 5).
These findings indicated a bowel obstruction and perforation due to the presence of a gastric bezoar. Upon further questioning, the patient admitted to a stress-related habit of eating her own hair (trichophagia) over the past 3 to 4 months.
Figure 3
Bezoars
Gastric bezoars are aggregates of nondigestible material that collect within the gastrointestinal system, usually fruit/vegetable matter (phytobezoars) or hair (trichobezoars). Phytobezoars are most common in patients with a history of reduced gastric motility and/or prior gastric surgery. Trichobezoars, similar to the one seen in this case, typically occur in young women and/or patients with psychiatric illness.1
Gastric bezoars are typically located in the gastric body but may extend into the small bowel and cause bowel obstruction. Trichobezoars that extend into the small bowel are referred to as “Rapunzel syndrome” (based on the fairy tale of the princess with long hair).
Figure 4
Clinical Presentation
Patients with gastric bezoars often present to the ED with nonspecific complaints of abdominal pain, including early satiety, weight loss, signs of anemia, abdominal pain, bloating, and symptoms of small bowel obstruction (SBO).2 Obtaining a thorough history is important to identify trichophagia, as only a small percentage of patients have evidence of alopecia on examination.
Figure 5
Workup
The workup for patients with gastric bezoars typically involves multiple imaging modalities. While abdominal radiography may demonstrate distention of the stomach, these findings are often nonspecific, and the characteristic feature of a mass with a diffusely mottled appearance is visualized in less than 20% of cases.
Computed tomography is the test of choice for detecting a bezoar, with a reported sensitivity of 97%.3 This modality is also useful for assessing the size of a bezoar and evaluating for complications such as SBO, perforation (free-air), or pneumatosis—all of which were revealed on this patient’s CT studies.
Treatment
The treatment for patients with large or obstructing gastric bezoars is surgical resection; both open and laparoscopic techniques have been described in the literature.2,4 The patient in this case was admitted to the hospital, where she underwent surgical removal of the bezoar. She was discharged home on hospital day 6 with outpatient psychiatric follow-up.
A 20-year-old woman with no significant medical history presented to the ED with a several-month history of worsening abdominal pain. She reported that although she previously had been evaluated at multiple EDs, no cause of her abdominal pain had been identified. The patient further noted that the pain had significantly increased the day of this presentation.
Figure 1
Physical examination revealed guarding and rebound tenderness in the midabdomen. Computed tomography (CT) studies of the abdomen and pelvis were performed; representative scout and axial images of the upper abdomen are shown above (Figures 1 and 2).
Figure 2
What is the suspected diagnosis?
Answer
The scout image of the abdomen revealed a distended stomach (white arrows, Figure 3), which displaced multiple loops of small bowel into the lower abdomen. The axial image through the upper abdomen showed air and solid material within the distended stomach (white arrows, Figure 4). Multiple foci of extraluminal (free) air were seen anteriorly (white asterisks, Figure 4). A coronal reformat of the CT better demonstrated the distended stomach filled with debris (white arrows, Figure 5), extraluminal air (white asterisk, Figure 5), and pneumatosis (air within the walls of multiple small bowel loops; red arrows, Figure 5).
These findings indicated a bowel obstruction and perforation due to the presence of a gastric bezoar. Upon further questioning, the patient admitted to a stress-related habit of eating her own hair (trichophagia) over the past 3 to 4 months.
Figure 3
Bezoars
Gastric bezoars are aggregates of nondigestible material that collect within the gastrointestinal system, usually fruit/vegetable matter (phytobezoars) or hair (trichobezoars). Phytobezoars are most common in patients with a history of reduced gastric motility and/or prior gastric surgery. Trichobezoars, similar to the one seen in this case, typically occur in young women and/or patients with psychiatric illness.1
Gastric bezoars are typically located in the gastric body but may extend into the small bowel and cause bowel obstruction. Trichobezoars that extend into the small bowel are referred to as “Rapunzel syndrome” (based on the fairy tale of the princess with long hair).
Figure 4
Clinical Presentation
Patients with gastric bezoars often present to the ED with nonspecific complaints of abdominal pain, including early satiety, weight loss, signs of anemia, abdominal pain, bloating, and symptoms of small bowel obstruction (SBO).2 Obtaining a thorough history is important to identify trichophagia, as only a small percentage of patients have evidence of alopecia on examination.
Figure 5
Workup
The workup for patients with gastric bezoars typically involves multiple imaging modalities. While abdominal radiography may demonstrate distention of the stomach, these findings are often nonspecific, and the characteristic feature of a mass with a diffusely mottled appearance is visualized in less than 20% of cases.
Computed tomography is the test of choice for detecting a bezoar, with a reported sensitivity of 97%.3 This modality is also useful for assessing the size of a bezoar and evaluating for complications such as SBO, perforation (free-air), or pneumatosis—all of which were revealed on this patient’s CT studies.
Treatment
The treatment for patients with large or obstructing gastric bezoars is surgical resection; both open and laparoscopic techniques have been described in the literature.2,4 The patient in this case was admitted to the hospital, where she underwent surgical removal of the bezoar. She was discharged home on hospital day 6 with outpatient psychiatric follow-up.
References
1. Guniganti P, Bradenham CH, Raptis C, Menias CO, Mellnick VM. Radiographics. 2015;35(7):1909-1921. doi:10.1148/rg.2015150062. 2. Fallon SC, Slater BJ, Larimer EL, Brandt ML, Lopez ME. The surgical management of Rapunzel syndrome: a case series and literature review. J Pediatr Surg. 2013;48(4):830-834. doi:10.1016/j.jpedsurg.2012.07.046. 3. Ripollés T, García-Aguayo J, Martínez MJ, Gil P. Gastrointestinal Bezoars: Sonographic and CT Characteristics. AJR Am J Roentgenol. 2001;177(1):65-69. doi:10.2214/ajr.177.1.1770065. 4. Flaherty DC, Aguilar F, Pradhan B, Grewal H. Rapunzel syndrome due to ingested hair extensions: Surgical and psychiatric considerations. Int J Surg Case Rep. 2015;17:155-157. doi:10.1016/j.ijscr.2015.11.009.
References
1. Guniganti P, Bradenham CH, Raptis C, Menias CO, Mellnick VM. Radiographics. 2015;35(7):1909-1921. doi:10.1148/rg.2015150062. 2. Fallon SC, Slater BJ, Larimer EL, Brandt ML, Lopez ME. The surgical management of Rapunzel syndrome: a case series and literature review. J Pediatr Surg. 2013;48(4):830-834. doi:10.1016/j.jpedsurg.2012.07.046. 3. Ripollés T, García-Aguayo J, Martínez MJ, Gil P. Gastrointestinal Bezoars: Sonographic and CT Characteristics. AJR Am J Roentgenol. 2001;177(1):65-69. doi:10.2214/ajr.177.1.1770065. 4. Flaherty DC, Aguilar F, Pradhan B, Grewal H. Rapunzel syndrome due to ingested hair extensions: Surgical and psychiatric considerations. Int J Surg Case Rep. 2015;17:155-157. doi:10.1016/j.ijscr.2015.11.009.
First EDition: Novel Blood Collection System May Reduce Contamination Rates, more
BY JEFF BAUER
Use of a blood collection system that diverts and sequesters the initial 1.5 to 2 mL of blood was associated with a significant decrease in blood culture contamination compared to standard practice, according to an open-label trial conducted at a single ED. The results were published online in the journal Clinical Infectious Diseases.
An estimated 0.6% to 6% of blood cultures are contaminated. Some blood cultures may become contaminated by skin fragments colonized with bacteria that are dislodged during venipuncture. Such false-positive results lead to increased costs and harm associated with unnecessary additional testing and treatment.
Researchers at the University of Nebraska Medical Center evaluated a novel sterile blood collection system, the SteriPath initial specimen diversion device (ISDD), to determine if it could reduce contamination rates by diverting and excluding the initial portion of collected blood. Investigators evaluated 1,808 blood cultures from 904 adult ED patients at an urban 689-bed university hospital. The patients’ mean age was 59 years, and 55% were male. For each patient, the first 20-mL blood sample was obtained using a standard procedure in which blood was drawn into a syringe and then injected into blood culture vials. A second 20-mL sample was obtained using the ISDD; the initial 1.5 to 2 mL of blood was diverted into a holding chamber, and the rest of the sample was directed into the blood culture vials. A culture was determined to be contaminated if one or more of several skin-residing organisms, including coagulase-negative staphylococci, Propionibacterium species, Micrococcus species, viridans group streptococci, Corynebacterium species, or Bacillus species, was recovered from only one of the paired cultures.
Compared to standard practice, use of the ISDD was associated with a significant reduction in blood culture contamination. Overall, two of the 904 samples (0.22%) collected with the ISDD were contaminated, compared to 16 of the 904 samples (1.78%) collected via standard practice (P = .001). Sensitivity was not affected by use of the ISDD; true septicemia was observed in 65 of 904 samples (7.2%) collected via ISDD and 69 of 904 samples (7.6%) collected via standard procedure (P = .41).
Rupp ME, Cavalieri RJ, Marolf C, Lyden E. Reduction in blood culture contamination through use of initial specimen diversion device. Clin Infect Dis. 2017 Apr 3. [Epub ahead of print]. doi:10.1093/cid/cix304.
FDA: Fluoroquinolone Use Not Linked to Retinal Detachment, Aortic Problems
LUCAS FRANKI
FRONTLINE MEDICAL NEWS
The Food and Drug Administration (FDA) has found no evidence of a link between fluoroquinolone antibiotic use and retinal detachment or aortic aneurysm and dissection, according to a new Drug Safety Communication update on potential serious, disabling adverse effects of oral and injectable fluoroquinolones.
Fluoroquinolones are used to treat acute bacterial sinusitis, acute bacterial exacerbation of chronic bronchitis, and uncomplicated urinary tract infections.
In a Safety Communication published May 12, 2016, the FDA noted that serious adverse effects were possible from fluoroquinolone usage and that fluoroquinolones should be prescribed only when no other treatment options are possible. Serious adverse effects associated with fluoroquinolone use include hallucination, depression, suicidal thoughts, tendinitis and tendon rupture, a pins-and-needles feeling in the arms and legs, joint pain and swelling, skin rash, and severe diarrhea.
After reviewing patient cases and study findings, the FDA said the evidence did not support an association between fluoroquinolone use and potential retinal or aortic dangers, according to its May 10, 2017, Drug Safety Communication update.
“We will continue to assess safety issues with fluoroquinolones, and will update the public if additional actions are needed,” the FDA said in a statement.
US Food and Drug Administration. FDA Drug Safety Communication: FDA updates warnings for oral and injectable fluoroquinolone antibiotics due to disabling side effects. May 10, 2017. https://www.fda.gov/Drugs/DrugSafety/ucm511530.htm. Accessed May 25, 2017.
Intravenous tPA Increases Risk of Mortality in Children With Acute Ischemic Stroke
SHARON WORCESTER
FRONTLINE MEDICAL NEWS
Intravenous thrombolysis with tissue plasminogen activator (tPA) is associated with adverse outcomes, including an increased risk of death, in children with acute ischemic stroke, based on a review of cases from the 2006-2010 Nationwide Inpatient Survey.
Of 20,587 patients ages 0 to 17 years who were included in the survey, 198 received an intervention, including tPA in 169 patients, intra-arterial thrombectomy (IAT) in five patients, and both tPA and IAT in 24 patients. The overall mortality rate was 7.8%, but in those who received tPA, it was 13.8%, compared with 7.7% in those who did not, Kathryn Ess, MD, of Rush University Medical Center, Chicago, reported at the annual meeting of the American Academy of Neurology. No deaths occurred in those who underwent only IAT, said Dr Ess.
Other outcomes were also worse for those who received tPA. For example, untreated patients were more likely to be discharged home than were tPA-treated patients (67.8% vs 47.5%), and intracerebral hemorrhage was more common in treated vs untreated patients (10.1% vs 3.8%). Costs for treated patients averaged $200,346 vs $123,015 for untreated patients.
Children included in the review had a mean age of 6 years, 43.9% were girls, and 47.7% were white. Treated patients were older (10 years vs 5.9 years), and comorbidities included Moyamoya disease in 12.4% of patients, cardiac valvular disease in 6.6%, and sickle cell disease in 6.5%. Those who received tPA had a higher prevalence of procoagulable conditions (15.2% vs 2%). Of note, the higher prevalence of intracerebral hemorrhage in treated patients was not explained by Moyamoya or sickle cell disease, as patients with those comorbidities were less likely than those without those conditions to receive treatment, Dr Ess said.
Though limited by the retrospective study design, small numbers of treated patients, a lack of data on stroke severity or functional outcomes, and the inclusion of data from years before newer thrombectomy devices became available, the findings highlight concerns about the safety and efficacy of tPA in children with ischemic stroke, she said, noting that few studies have looked at the utility of tPA with or without IAT in the pediatric population.
“Studies of the efficacy of ischemic stroke treatment in adults can’t necessarily be extrapolated to children,” she said, adding that this is especially true given the difference in etiologies of pediatric acute ischemic stroke.
Indeed, the findings underscore “the age-old adage that children are not just little adults,” said Andrew Southerland, MD, of the University of Virginia, Charlottesville, who was the discussant for the session. “We need prospective clinical trials in children,” he said.
HCV Seroconversion Rate 0.1% After Occupational Exposure
BIANCA NOGRADY
FRONTLINE MEDICAL NEWS
An analysis of 13 years of accidental occupational exposures to hepatitis C virus (HCV)-contaminated fluids or instruments has revealed a seroconversion rate of just 0.1%, significantly lower than that previously reported in the literature. This finding is from a longitudinal analysis of data from a prospectively maintained database of 1,361 occupational injuries involving HCV-positive source that occurred between 2002 and 2015 conducted by Francesco M. Egro, MD, and his colleagues from the University of Pittsburgh Medical Center. Results were published online in the American Journal of Infection Control.
The two incidents of seroconversion occurred in patients who were exposed to blood from an HCV-positive patient via percutaneous injuries to the thumb from a hollow-bore needle, representing an overall seroconversion rate of 0.1%. In both cases, the source patients whose blood was involved were not coinfected with hepatitis B virus or human immunodeficiency virus.
Researchers also conducted a review of literature on needlestick injuries and occupational exposure to HCV-infected blood and fluids; from this review, they calculated an overall seroconversion rate average of 0.7%, with an average rate of 0.8% for percutaneous exposures. The review did not include mucomembranous exposure, as there were not enough data.
In this study, 65% of exposures were caused by percutaneous injuries and 34% were caused by mucocutaneous injuries; the cause of the remaining 1% was uncertain.
The hand was the most common site of injury (63%), followed by the face and neck (28%), and the arm, foot, leg, or trunk (4%). There was no record of the anatomical location of the injury in 5% of cases.
In nearly three-quarters of cases, blood was the source of exposure, while blood-containing saliva accounted for 3% of cases. The remaining 24% of cases were linked to other fluids, such as peritoneal fluid, tracheal secretions, amniotic fluid, bloody irrigation fluid, and blood-containing feces.
“The risk of transmission after exposure to HCV-positive patients’ fluids or tissues other than blood is expected to be low, but has not been formally quantified,” the authors wrote. “Although there have been reports of HCV seroconversion after human bites and after punching a HCV-positive individual in the teeth, percutaneous exposures to the blood of a HCV-positive source remain the most common cause of occupational HCV transmission.”
While the rate of seroconversion was low, the authors encouraged prompt reporting, testing, and follow-up of exposed individuals.
Egro FM, Nwaiwu CA, Smith S, Harper JD, Spiess AM. Seroconversion rates among health care workers exposed to hepatitis C virus-contaminated body fluids: The University of Pittsburgh 13-year experience. Am J Infect Control. 2017 Apr 24. [Epub ahead of print]. doi:10.1016/j.ajic.2017.03.011.
Use of a blood collection system that diverts and sequesters the initial 1.5 to 2 mL of blood was associated with a significant decrease in blood culture contamination compared to standard practice, according to an open-label trial conducted at a single ED. The results were published online in the journal Clinical Infectious Diseases.
An estimated 0.6% to 6% of blood cultures are contaminated. Some blood cultures may become contaminated by skin fragments colonized with bacteria that are dislodged during venipuncture. Such false-positive results lead to increased costs and harm associated with unnecessary additional testing and treatment.
Researchers at the University of Nebraska Medical Center evaluated a novel sterile blood collection system, the SteriPath initial specimen diversion device (ISDD), to determine if it could reduce contamination rates by diverting and excluding the initial portion of collected blood. Investigators evaluated 1,808 blood cultures from 904 adult ED patients at an urban 689-bed university hospital. The patients’ mean age was 59 years, and 55% were male. For each patient, the first 20-mL blood sample was obtained using a standard procedure in which blood was drawn into a syringe and then injected into blood culture vials. A second 20-mL sample was obtained using the ISDD; the initial 1.5 to 2 mL of blood was diverted into a holding chamber, and the rest of the sample was directed into the blood culture vials. A culture was determined to be contaminated if one or more of several skin-residing organisms, including coagulase-negative staphylococci, Propionibacterium species, Micrococcus species, viridans group streptococci, Corynebacterium species, or Bacillus species, was recovered from only one of the paired cultures.
Compared to standard practice, use of the ISDD was associated with a significant reduction in blood culture contamination. Overall, two of the 904 samples (0.22%) collected with the ISDD were contaminated, compared to 16 of the 904 samples (1.78%) collected via standard practice (P = .001). Sensitivity was not affected by use of the ISDD; true septicemia was observed in 65 of 904 samples (7.2%) collected via ISDD and 69 of 904 samples (7.6%) collected via standard procedure (P = .41).
Rupp ME, Cavalieri RJ, Marolf C, Lyden E. Reduction in blood culture contamination through use of initial specimen diversion device. Clin Infect Dis. 2017 Apr 3. [Epub ahead of print]. doi:10.1093/cid/cix304.
FDA: Fluoroquinolone Use Not Linked to Retinal Detachment, Aortic Problems
LUCAS FRANKI
FRONTLINE MEDICAL NEWS
The Food and Drug Administration (FDA) has found no evidence of a link between fluoroquinolone antibiotic use and retinal detachment or aortic aneurysm and dissection, according to a new Drug Safety Communication update on potential serious, disabling adverse effects of oral and injectable fluoroquinolones.
Fluoroquinolones are used to treat acute bacterial sinusitis, acute bacterial exacerbation of chronic bronchitis, and uncomplicated urinary tract infections.
In a Safety Communication published May 12, 2016, the FDA noted that serious adverse effects were possible from fluoroquinolone usage and that fluoroquinolones should be prescribed only when no other treatment options are possible. Serious adverse effects associated with fluoroquinolone use include hallucination, depression, suicidal thoughts, tendinitis and tendon rupture, a pins-and-needles feeling in the arms and legs, joint pain and swelling, skin rash, and severe diarrhea.
After reviewing patient cases and study findings, the FDA said the evidence did not support an association between fluoroquinolone use and potential retinal or aortic dangers, according to its May 10, 2017, Drug Safety Communication update.
“We will continue to assess safety issues with fluoroquinolones, and will update the public if additional actions are needed,” the FDA said in a statement.
US Food and Drug Administration. FDA Drug Safety Communication: FDA updates warnings for oral and injectable fluoroquinolone antibiotics due to disabling side effects. May 10, 2017. https://www.fda.gov/Drugs/DrugSafety/ucm511530.htm. Accessed May 25, 2017.
Intravenous tPA Increases Risk of Mortality in Children With Acute Ischemic Stroke
SHARON WORCESTER
FRONTLINE MEDICAL NEWS
Intravenous thrombolysis with tissue plasminogen activator (tPA) is associated with adverse outcomes, including an increased risk of death, in children with acute ischemic stroke, based on a review of cases from the 2006-2010 Nationwide Inpatient Survey.
Of 20,587 patients ages 0 to 17 years who were included in the survey, 198 received an intervention, including tPA in 169 patients, intra-arterial thrombectomy (IAT) in five patients, and both tPA and IAT in 24 patients. The overall mortality rate was 7.8%, but in those who received tPA, it was 13.8%, compared with 7.7% in those who did not, Kathryn Ess, MD, of Rush University Medical Center, Chicago, reported at the annual meeting of the American Academy of Neurology. No deaths occurred in those who underwent only IAT, said Dr Ess.
Other outcomes were also worse for those who received tPA. For example, untreated patients were more likely to be discharged home than were tPA-treated patients (67.8% vs 47.5%), and intracerebral hemorrhage was more common in treated vs untreated patients (10.1% vs 3.8%). Costs for treated patients averaged $200,346 vs $123,015 for untreated patients.
Children included in the review had a mean age of 6 years, 43.9% were girls, and 47.7% were white. Treated patients were older (10 years vs 5.9 years), and comorbidities included Moyamoya disease in 12.4% of patients, cardiac valvular disease in 6.6%, and sickle cell disease in 6.5%. Those who received tPA had a higher prevalence of procoagulable conditions (15.2% vs 2%). Of note, the higher prevalence of intracerebral hemorrhage in treated patients was not explained by Moyamoya or sickle cell disease, as patients with those comorbidities were less likely than those without those conditions to receive treatment, Dr Ess said.
Though limited by the retrospective study design, small numbers of treated patients, a lack of data on stroke severity or functional outcomes, and the inclusion of data from years before newer thrombectomy devices became available, the findings highlight concerns about the safety and efficacy of tPA in children with ischemic stroke, she said, noting that few studies have looked at the utility of tPA with or without IAT in the pediatric population.
“Studies of the efficacy of ischemic stroke treatment in adults can’t necessarily be extrapolated to children,” she said, adding that this is especially true given the difference in etiologies of pediatric acute ischemic stroke.
Indeed, the findings underscore “the age-old adage that children are not just little adults,” said Andrew Southerland, MD, of the University of Virginia, Charlottesville, who was the discussant for the session. “We need prospective clinical trials in children,” he said.
HCV Seroconversion Rate 0.1% After Occupational Exposure
BIANCA NOGRADY
FRONTLINE MEDICAL NEWS
An analysis of 13 years of accidental occupational exposures to hepatitis C virus (HCV)-contaminated fluids or instruments has revealed a seroconversion rate of just 0.1%, significantly lower than that previously reported in the literature. This finding is from a longitudinal analysis of data from a prospectively maintained database of 1,361 occupational injuries involving HCV-positive source that occurred between 2002 and 2015 conducted by Francesco M. Egro, MD, and his colleagues from the University of Pittsburgh Medical Center. Results were published online in the American Journal of Infection Control.
The two incidents of seroconversion occurred in patients who were exposed to blood from an HCV-positive patient via percutaneous injuries to the thumb from a hollow-bore needle, representing an overall seroconversion rate of 0.1%. In both cases, the source patients whose blood was involved were not coinfected with hepatitis B virus or human immunodeficiency virus.
Researchers also conducted a review of literature on needlestick injuries and occupational exposure to HCV-infected blood and fluids; from this review, they calculated an overall seroconversion rate average of 0.7%, with an average rate of 0.8% for percutaneous exposures. The review did not include mucomembranous exposure, as there were not enough data.
In this study, 65% of exposures were caused by percutaneous injuries and 34% were caused by mucocutaneous injuries; the cause of the remaining 1% was uncertain.
The hand was the most common site of injury (63%), followed by the face and neck (28%), and the arm, foot, leg, or trunk (4%). There was no record of the anatomical location of the injury in 5% of cases.
In nearly three-quarters of cases, blood was the source of exposure, while blood-containing saliva accounted for 3% of cases. The remaining 24% of cases were linked to other fluids, such as peritoneal fluid, tracheal secretions, amniotic fluid, bloody irrigation fluid, and blood-containing feces.
“The risk of transmission after exposure to HCV-positive patients’ fluids or tissues other than blood is expected to be low, but has not been formally quantified,” the authors wrote. “Although there have been reports of HCV seroconversion after human bites and after punching a HCV-positive individual in the teeth, percutaneous exposures to the blood of a HCV-positive source remain the most common cause of occupational HCV transmission.”
While the rate of seroconversion was low, the authors encouraged prompt reporting, testing, and follow-up of exposed individuals.
Egro FM, Nwaiwu CA, Smith S, Harper JD, Spiess AM. Seroconversion rates among health care workers exposed to hepatitis C virus-contaminated body fluids: The University of Pittsburgh 13-year experience. Am J Infect Control. 2017 Apr 24. [Epub ahead of print]. doi:10.1016/j.ajic.2017.03.011.
BY JEFF BAUER
Use of a blood collection system that diverts and sequesters the initial 1.5 to 2 mL of blood was associated with a significant decrease in blood culture contamination compared to standard practice, according to an open-label trial conducted at a single ED. The results were published online in the journal Clinical Infectious Diseases.
An estimated 0.6% to 6% of blood cultures are contaminated. Some blood cultures may become contaminated by skin fragments colonized with bacteria that are dislodged during venipuncture. Such false-positive results lead to increased costs and harm associated with unnecessary additional testing and treatment.
Researchers at the University of Nebraska Medical Center evaluated a novel sterile blood collection system, the SteriPath initial specimen diversion device (ISDD), to determine if it could reduce contamination rates by diverting and excluding the initial portion of collected blood. Investigators evaluated 1,808 blood cultures from 904 adult ED patients at an urban 689-bed university hospital. The patients’ mean age was 59 years, and 55% were male. For each patient, the first 20-mL blood sample was obtained using a standard procedure in which blood was drawn into a syringe and then injected into blood culture vials. A second 20-mL sample was obtained using the ISDD; the initial 1.5 to 2 mL of blood was diverted into a holding chamber, and the rest of the sample was directed into the blood culture vials. A culture was determined to be contaminated if one or more of several skin-residing organisms, including coagulase-negative staphylococci, Propionibacterium species, Micrococcus species, viridans group streptococci, Corynebacterium species, or Bacillus species, was recovered from only one of the paired cultures.
Compared to standard practice, use of the ISDD was associated with a significant reduction in blood culture contamination. Overall, two of the 904 samples (0.22%) collected with the ISDD were contaminated, compared to 16 of the 904 samples (1.78%) collected via standard practice (P = .001). Sensitivity was not affected by use of the ISDD; true septicemia was observed in 65 of 904 samples (7.2%) collected via ISDD and 69 of 904 samples (7.6%) collected via standard procedure (P = .41).
Rupp ME, Cavalieri RJ, Marolf C, Lyden E. Reduction in blood culture contamination through use of initial specimen diversion device. Clin Infect Dis. 2017 Apr 3. [Epub ahead of print]. doi:10.1093/cid/cix304.
FDA: Fluoroquinolone Use Not Linked to Retinal Detachment, Aortic Problems
LUCAS FRANKI
FRONTLINE MEDICAL NEWS
The Food and Drug Administration (FDA) has found no evidence of a link between fluoroquinolone antibiotic use and retinal detachment or aortic aneurysm and dissection, according to a new Drug Safety Communication update on potential serious, disabling adverse effects of oral and injectable fluoroquinolones.
Fluoroquinolones are used to treat acute bacterial sinusitis, acute bacterial exacerbation of chronic bronchitis, and uncomplicated urinary tract infections.
In a Safety Communication published May 12, 2016, the FDA noted that serious adverse effects were possible from fluoroquinolone usage and that fluoroquinolones should be prescribed only when no other treatment options are possible. Serious adverse effects associated with fluoroquinolone use include hallucination, depression, suicidal thoughts, tendinitis and tendon rupture, a pins-and-needles feeling in the arms and legs, joint pain and swelling, skin rash, and severe diarrhea.
After reviewing patient cases and study findings, the FDA said the evidence did not support an association between fluoroquinolone use and potential retinal or aortic dangers, according to its May 10, 2017, Drug Safety Communication update.
“We will continue to assess safety issues with fluoroquinolones, and will update the public if additional actions are needed,” the FDA said in a statement.
US Food and Drug Administration. FDA Drug Safety Communication: FDA updates warnings for oral and injectable fluoroquinolone antibiotics due to disabling side effects. May 10, 2017. https://www.fda.gov/Drugs/DrugSafety/ucm511530.htm. Accessed May 25, 2017.
Intravenous tPA Increases Risk of Mortality in Children With Acute Ischemic Stroke
SHARON WORCESTER
FRONTLINE MEDICAL NEWS
Intravenous thrombolysis with tissue plasminogen activator (tPA) is associated with adverse outcomes, including an increased risk of death, in children with acute ischemic stroke, based on a review of cases from the 2006-2010 Nationwide Inpatient Survey.
Of 20,587 patients ages 0 to 17 years who were included in the survey, 198 received an intervention, including tPA in 169 patients, intra-arterial thrombectomy (IAT) in five patients, and both tPA and IAT in 24 patients. The overall mortality rate was 7.8%, but in those who received tPA, it was 13.8%, compared with 7.7% in those who did not, Kathryn Ess, MD, of Rush University Medical Center, Chicago, reported at the annual meeting of the American Academy of Neurology. No deaths occurred in those who underwent only IAT, said Dr Ess.
Other outcomes were also worse for those who received tPA. For example, untreated patients were more likely to be discharged home than were tPA-treated patients (67.8% vs 47.5%), and intracerebral hemorrhage was more common in treated vs untreated patients (10.1% vs 3.8%). Costs for treated patients averaged $200,346 vs $123,015 for untreated patients.
Children included in the review had a mean age of 6 years, 43.9% were girls, and 47.7% were white. Treated patients were older (10 years vs 5.9 years), and comorbidities included Moyamoya disease in 12.4% of patients, cardiac valvular disease in 6.6%, and sickle cell disease in 6.5%. Those who received tPA had a higher prevalence of procoagulable conditions (15.2% vs 2%). Of note, the higher prevalence of intracerebral hemorrhage in treated patients was not explained by Moyamoya or sickle cell disease, as patients with those comorbidities were less likely than those without those conditions to receive treatment, Dr Ess said.
Though limited by the retrospective study design, small numbers of treated patients, a lack of data on stroke severity or functional outcomes, and the inclusion of data from years before newer thrombectomy devices became available, the findings highlight concerns about the safety and efficacy of tPA in children with ischemic stroke, she said, noting that few studies have looked at the utility of tPA with or without IAT in the pediatric population.
“Studies of the efficacy of ischemic stroke treatment in adults can’t necessarily be extrapolated to children,” she said, adding that this is especially true given the difference in etiologies of pediatric acute ischemic stroke.
Indeed, the findings underscore “the age-old adage that children are not just little adults,” said Andrew Southerland, MD, of the University of Virginia, Charlottesville, who was the discussant for the session. “We need prospective clinical trials in children,” he said.
HCV Seroconversion Rate 0.1% After Occupational Exposure
BIANCA NOGRADY
FRONTLINE MEDICAL NEWS
An analysis of 13 years of accidental occupational exposures to hepatitis C virus (HCV)-contaminated fluids or instruments has revealed a seroconversion rate of just 0.1%, significantly lower than that previously reported in the literature. This finding is from a longitudinal analysis of data from a prospectively maintained database of 1,361 occupational injuries involving HCV-positive source that occurred between 2002 and 2015 conducted by Francesco M. Egro, MD, and his colleagues from the University of Pittsburgh Medical Center. Results were published online in the American Journal of Infection Control.
The two incidents of seroconversion occurred in patients who were exposed to blood from an HCV-positive patient via percutaneous injuries to the thumb from a hollow-bore needle, representing an overall seroconversion rate of 0.1%. In both cases, the source patients whose blood was involved were not coinfected with hepatitis B virus or human immunodeficiency virus.
Researchers also conducted a review of literature on needlestick injuries and occupational exposure to HCV-infected blood and fluids; from this review, they calculated an overall seroconversion rate average of 0.7%, with an average rate of 0.8% for percutaneous exposures. The review did not include mucomembranous exposure, as there were not enough data.
In this study, 65% of exposures were caused by percutaneous injuries and 34% were caused by mucocutaneous injuries; the cause of the remaining 1% was uncertain.
The hand was the most common site of injury (63%), followed by the face and neck (28%), and the arm, foot, leg, or trunk (4%). There was no record of the anatomical location of the injury in 5% of cases.
In nearly three-quarters of cases, blood was the source of exposure, while blood-containing saliva accounted for 3% of cases. The remaining 24% of cases were linked to other fluids, such as peritoneal fluid, tracheal secretions, amniotic fluid, bloody irrigation fluid, and blood-containing feces.
“The risk of transmission after exposure to HCV-positive patients’ fluids or tissues other than blood is expected to be low, but has not been formally quantified,” the authors wrote. “Although there have been reports of HCV seroconversion after human bites and after punching a HCV-positive individual in the teeth, percutaneous exposures to the blood of a HCV-positive source remain the most common cause of occupational HCV transmission.”
While the rate of seroconversion was low, the authors encouraged prompt reporting, testing, and follow-up of exposed individuals.
Egro FM, Nwaiwu CA, Smith S, Harper JD, Spiess AM. Seroconversion rates among health care workers exposed to hepatitis C virus-contaminated body fluids: The University of Pittsburgh 13-year experience. Am J Infect Control. 2017 Apr 24. [Epub ahead of print]. doi:10.1016/j.ajic.2017.03.011.
Dr. Lipetskaia is Assistant Professor, Department of Obstetrics and Gynecology, University of Rochester School of Medicine and Dentistry, Rochester, New York.
Dr. Doyle is Assistant Professor, Department of Obstetrics and Gynecology, University of Rochester School of Medicine and Dentistry, Rochester, New York.
Dr. Wood is Research Associate Professor, Departments of Obstetrics and Gynecology, Urology, and Neuroscience, University of Rochester School of Medicine and Dentistry, Rochester, New York.
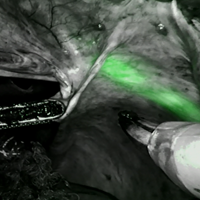
Dr. Lipetskaia reports no financial relationships relevant to this video. Dr. Doyle reports that she receives grant or research support from the University of Rochester and has other financial relationships with ENDOGLOW, LLC. Dr. Wood reports that he receives grant or research support from IMAGEN, Inc, and the University of Rochester, and is a consultant to ENDOGLOW, LLC, and IMAGEN, Inc.
Dr. Lipetskaia is Assistant Professor, Department of Obstetrics and Gynecology, University of Rochester School of Medicine and Dentistry, Rochester, New York.
Dr. Doyle is Assistant Professor, Department of Obstetrics and Gynecology, University of Rochester School of Medicine and Dentistry, Rochester, New York.
Dr. Wood is Research Associate Professor, Departments of Obstetrics and Gynecology, Urology, and Neuroscience, University of Rochester School of Medicine and Dentistry, Rochester, New York.
Dr. Lipetskaia reports no financial relationships relevant to this video. Dr. Doyle reports that she receives grant or research support from the University of Rochester and has other financial relationships with ENDOGLOW, LLC. Dr. Wood reports that he receives grant or research support from IMAGEN, Inc, and the University of Rochester, and is a consultant to ENDOGLOW, LLC, and IMAGEN, Inc.
Author and Disclosure Information
Dr. Lipetskaia is Assistant Professor, Department of Obstetrics and Gynecology, University of Rochester School of Medicine and Dentistry, Rochester, New York.
Dr. Doyle is Assistant Professor, Department of Obstetrics and Gynecology, University of Rochester School of Medicine and Dentistry, Rochester, New York.
Dr. Wood is Research Associate Professor, Departments of Obstetrics and Gynecology, Urology, and Neuroscience, University of Rochester School of Medicine and Dentistry, Rochester, New York.
Dr. Lipetskaia reports no financial relationships relevant to this video. Dr. Doyle reports that she receives grant or research support from the University of Rochester and has other financial relationships with ENDOGLOW, LLC. Dr. Wood reports that he receives grant or research support from IMAGEN, Inc, and the University of Rochester, and is a consultant to ENDOGLOW, LLC, and IMAGEN, Inc.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Visit the Society of Gynecologic Surgeons online: sgsonline.org
SAN DIEGO – Psychiatrists may encounter refugee patients from war-torn countries in virtually every part of the United States with complex mental health needs, including high rates of posttraumatic stress disorder, chronic pain, and somatic symptoms, according to two presenters at the annual meeting of the American Psychiatric Association.
Over the past decade, refugees from Middle Eastern counties – particularly Iraq, Syria, and Afghanistan – have increased fourfold as a percentage of all refugees in the United States, while those from Sub-Saharan Africa continue to make up a large share. Despite heated political wrangling, the U.S. Department of State recently increased limits on the number of refugees that can be accepted. California, Texas, New York, Michigan, Ohio, and Washington are the states resettling the most new arrivals.
Refugees with trauma exposure have high rates of posttraumatic stress disorder, chronic pain, and somatic symptoms. In addition, recent research suggests, these refugees may have poorly understood stressors related to migration and adjustment that also may be significant contributors to mental illness risk. Despite this, refugees generally have less access to mental health care than does the general population.
The presenters shared their perspectives on refugee mental health with findings that could inform the timing and nature of interventions in these potentially vulnerable populations.
Cynthia L. Arfken, PhD, of Wayne State University in Detroit, presented results from an ongoing cohort study of Syrian families presenting to a primary care clinic as part of their State Department–mandated health check upon resettlement. Arash Javanbakht, MD, also of the university, led the research.
The investigators recruited families at a primary care clinic in southeastern Michigan, where refugees receive health assessments within the first month of arrival in the United States.
The researchers consecutively enrolled and evaluated 297 individuals, including 59 children aged 6 and older (mean age, 11.3) from Syria. These families represented 95% of refugees seen at the clinic during the study period, from June to December 2016.
The researchers also collected hair and saliva samples from consenting families for a separate study looking at biomarkers and mental health outcomes.
Adults were screened for PTSD using the PTSD checklist for adults, and children for anxiety using the Screen for Child Anxiety Related Emotional Disorders, or SCARED, measure. Psychiatric nurses and bilingual health care workers helped the team obtain consent and conduct assessments.
The researchers found that 61% of the children had a probable anxiety diagnosis, and nearly 85% had probable separation anxiety. Higher child anxiety scores were associated with higher PTSD scores in mothers (P = .05).
Dr. Arfken said in an interview that she and her team were “shocked” at the high prevalence of probable anxiety disorders in the cohort, in part because they’d conducted an earlier study enrolling adult Iraqi refugees and “found hardly any psychiatric symptoms at all.”
The high levels of anxiety seen among the Syrian refugees may be related to the severity of the ongoing conflict, Dr. Arfken said. The children’s results were sufficiently jarring to the team that “we changed our whole plan,” she said, “to concentrate on following up both the children who showed distress and those who did not.” They also attempted some nonmedical interventions, such as dance and mindfulness groups.
Also at the conference, Christopher Morrow, MD, of the University of Maryland in Baltimore, presented findings from a case study that illuminates some of the potential mental health risks for resettled refugees.
Dr. Morrow described a 31-year-old man from Afghanistan who had worked for the U.S. Special Forces in Afghanistan as a translator and subsequently entered the United States as a refugee. About a year later he was admitted to an inpatient psychiatric unit after a violent suicide attempt and was treated for depression.
The researchers noted that the patient had no previous history of depression or other mental illness prior to arriving in the United States. “His symptoms developed over the course of the first year of resettlement,” Dr. Morrow said in an interview.
This patient, Dr. Morrow said, was single and was not religious, leaving him not inclined to join a mosque or other Islamic community group. He was placed in an unskilled work assignment, despite his well-developed skills as a translator. Over the course of a year, he became increasingly isolated and “decompensated to the point where there was a really violent suicide attempt.
“We think that some kind of programmed follow-up – be it a community resource or through primary care – could have helped stabilize him before he got to a point of real hopelessness,” Dr. Morrow said.
Dr. Morrow and his colleagues proposed two interventions as adjustments to current health policy for refugees: adding universal mental health screening to each refugee’s health check in the first month after arrival, and scheduling follow-up later in the resettlement process.
“If there is active follow-up, a way that you could check in with these individuals as they’re acclimating, that’s probably the point where you could intervene best,” he said.
Dr. Morrow and Dr. Arfken disclosed no conflicts of interest related to their research.
SAN DIEGO – Psychiatrists may encounter refugee patients from war-torn countries in virtually every part of the United States with complex mental health needs, including high rates of posttraumatic stress disorder, chronic pain, and somatic symptoms, according to two presenters at the annual meeting of the American Psychiatric Association.
Over the past decade, refugees from Middle Eastern counties – particularly Iraq, Syria, and Afghanistan – have increased fourfold as a percentage of all refugees in the United States, while those from Sub-Saharan Africa continue to make up a large share. Despite heated political wrangling, the U.S. Department of State recently increased limits on the number of refugees that can be accepted. California, Texas, New York, Michigan, Ohio, and Washington are the states resettling the most new arrivals.
Refugees with trauma exposure have high rates of posttraumatic stress disorder, chronic pain, and somatic symptoms. In addition, recent research suggests, these refugees may have poorly understood stressors related to migration and adjustment that also may be significant contributors to mental illness risk. Despite this, refugees generally have less access to mental health care than does the general population.
The presenters shared their perspectives on refugee mental health with findings that could inform the timing and nature of interventions in these potentially vulnerable populations.
Cynthia L. Arfken, PhD, of Wayne State University in Detroit, presented results from an ongoing cohort study of Syrian families presenting to a primary care clinic as part of their State Department–mandated health check upon resettlement. Arash Javanbakht, MD, also of the university, led the research.
The investigators recruited families at a primary care clinic in southeastern Michigan, where refugees receive health assessments within the first month of arrival in the United States.
The researchers consecutively enrolled and evaluated 297 individuals, including 59 children aged 6 and older (mean age, 11.3) from Syria. These families represented 95% of refugees seen at the clinic during the study period, from June to December 2016.
The researchers also collected hair and saliva samples from consenting families for a separate study looking at biomarkers and mental health outcomes.
Adults were screened for PTSD using the PTSD checklist for adults, and children for anxiety using the Screen for Child Anxiety Related Emotional Disorders, or SCARED, measure. Psychiatric nurses and bilingual health care workers helped the team obtain consent and conduct assessments.
The researchers found that 61% of the children had a probable anxiety diagnosis, and nearly 85% had probable separation anxiety. Higher child anxiety scores were associated with higher PTSD scores in mothers (P = .05).
Dr. Arfken said in an interview that she and her team were “shocked” at the high prevalence of probable anxiety disorders in the cohort, in part because they’d conducted an earlier study enrolling adult Iraqi refugees and “found hardly any psychiatric symptoms at all.”
The high levels of anxiety seen among the Syrian refugees may be related to the severity of the ongoing conflict, Dr. Arfken said. The children’s results were sufficiently jarring to the team that “we changed our whole plan,” she said, “to concentrate on following up both the children who showed distress and those who did not.” They also attempted some nonmedical interventions, such as dance and mindfulness groups.
Also at the conference, Christopher Morrow, MD, of the University of Maryland in Baltimore, presented findings from a case study that illuminates some of the potential mental health risks for resettled refugees.
Dr. Morrow described a 31-year-old man from Afghanistan who had worked for the U.S. Special Forces in Afghanistan as a translator and subsequently entered the United States as a refugee. About a year later he was admitted to an inpatient psychiatric unit after a violent suicide attempt and was treated for depression.
The researchers noted that the patient had no previous history of depression or other mental illness prior to arriving in the United States. “His symptoms developed over the course of the first year of resettlement,” Dr. Morrow said in an interview.
This patient, Dr. Morrow said, was single and was not religious, leaving him not inclined to join a mosque or other Islamic community group. He was placed in an unskilled work assignment, despite his well-developed skills as a translator. Over the course of a year, he became increasingly isolated and “decompensated to the point where there was a really violent suicide attempt.
“We think that some kind of programmed follow-up – be it a community resource or through primary care – could have helped stabilize him before he got to a point of real hopelessness,” Dr. Morrow said.
Dr. Morrow and his colleagues proposed two interventions as adjustments to current health policy for refugees: adding universal mental health screening to each refugee’s health check in the first month after arrival, and scheduling follow-up later in the resettlement process.
“If there is active follow-up, a way that you could check in with these individuals as they’re acclimating, that’s probably the point where you could intervene best,” he said.
Dr. Morrow and Dr. Arfken disclosed no conflicts of interest related to their research.
SAN DIEGO – Psychiatrists may encounter refugee patients from war-torn countries in virtually every part of the United States with complex mental health needs, including high rates of posttraumatic stress disorder, chronic pain, and somatic symptoms, according to two presenters at the annual meeting of the American Psychiatric Association.
Over the past decade, refugees from Middle Eastern counties – particularly Iraq, Syria, and Afghanistan – have increased fourfold as a percentage of all refugees in the United States, while those from Sub-Saharan Africa continue to make up a large share. Despite heated political wrangling, the U.S. Department of State recently increased limits on the number of refugees that can be accepted. California, Texas, New York, Michigan, Ohio, and Washington are the states resettling the most new arrivals.
Refugees with trauma exposure have high rates of posttraumatic stress disorder, chronic pain, and somatic symptoms. In addition, recent research suggests, these refugees may have poorly understood stressors related to migration and adjustment that also may be significant contributors to mental illness risk. Despite this, refugees generally have less access to mental health care than does the general population.
The presenters shared their perspectives on refugee mental health with findings that could inform the timing and nature of interventions in these potentially vulnerable populations.
Cynthia L. Arfken, PhD, of Wayne State University in Detroit, presented results from an ongoing cohort study of Syrian families presenting to a primary care clinic as part of their State Department–mandated health check upon resettlement. Arash Javanbakht, MD, also of the university, led the research.
The investigators recruited families at a primary care clinic in southeastern Michigan, where refugees receive health assessments within the first month of arrival in the United States.
The researchers consecutively enrolled and evaluated 297 individuals, including 59 children aged 6 and older (mean age, 11.3) from Syria. These families represented 95% of refugees seen at the clinic during the study period, from June to December 2016.
The researchers also collected hair and saliva samples from consenting families for a separate study looking at biomarkers and mental health outcomes.
Adults were screened for PTSD using the PTSD checklist for adults, and children for anxiety using the Screen for Child Anxiety Related Emotional Disorders, or SCARED, measure. Psychiatric nurses and bilingual health care workers helped the team obtain consent and conduct assessments.
The researchers found that 61% of the children had a probable anxiety diagnosis, and nearly 85% had probable separation anxiety. Higher child anxiety scores were associated with higher PTSD scores in mothers (P = .05).
Dr. Arfken said in an interview that she and her team were “shocked” at the high prevalence of probable anxiety disorders in the cohort, in part because they’d conducted an earlier study enrolling adult Iraqi refugees and “found hardly any psychiatric symptoms at all.”
The high levels of anxiety seen among the Syrian refugees may be related to the severity of the ongoing conflict, Dr. Arfken said. The children’s results were sufficiently jarring to the team that “we changed our whole plan,” she said, “to concentrate on following up both the children who showed distress and those who did not.” They also attempted some nonmedical interventions, such as dance and mindfulness groups.
Also at the conference, Christopher Morrow, MD, of the University of Maryland in Baltimore, presented findings from a case study that illuminates some of the potential mental health risks for resettled refugees.
Dr. Morrow described a 31-year-old man from Afghanistan who had worked for the U.S. Special Forces in Afghanistan as a translator and subsequently entered the United States as a refugee. About a year later he was admitted to an inpatient psychiatric unit after a violent suicide attempt and was treated for depression.
The researchers noted that the patient had no previous history of depression or other mental illness prior to arriving in the United States. “His symptoms developed over the course of the first year of resettlement,” Dr. Morrow said in an interview.
This patient, Dr. Morrow said, was single and was not religious, leaving him not inclined to join a mosque or other Islamic community group. He was placed in an unskilled work assignment, despite his well-developed skills as a translator. Over the course of a year, he became increasingly isolated and “decompensated to the point where there was a really violent suicide attempt.
“We think that some kind of programmed follow-up – be it a community resource or through primary care – could have helped stabilize him before he got to a point of real hopelessness,” Dr. Morrow said.
Dr. Morrow and his colleagues proposed two interventions as adjustments to current health policy for refugees: adding universal mental health screening to each refugee’s health check in the first month after arrival, and scheduling follow-up later in the resettlement process.
“If there is active follow-up, a way that you could check in with these individuals as they’re acclimating, that’s probably the point where you could intervene best,” he said.
Dr. Morrow and Dr. Arfken disclosed no conflicts of interest related to their research.
Children often present for evaluation of a melanocytic lesion that is new, evolving, or worrisome to parents and caregivers.
“In the pediatric health care system, malignant melanoma is considered an especially heinous crime. In San Diego, dedicated pediatric providers who identify this disease are members of an elite squad known as the mole patrol unit.” Dr. Sheila Fallon Friedlander opened her presentation on pediatric moles with this tongue-in-cheek statement, adapted from the popular TV show “Law and Order SVU,” at a pediatric dermatology meeting sponsored by Rady Children’s Hospital–San Diego and University of California, San Diego.
Dr. Sheila Fallon FriedlanderChildhood and adolescent melanoma is rare, but the incidence in the United States has been steadily increasing over the past 35 years. A multicenter, retrospective review conducted by Wong et al., using the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) database between 1973 and 2009, detected 1,317 cases of melanoma for an incidence rate of 6 (95% confidence interval, 5.7-6.3), and revealed an average increase in adolescent melanoma of 2% per year. The greatest incidence occurred in girls aged 15-19 years, and individuals living in geographic locations with low ultraviolet-B exposure, intermittently exposed to intense UV rays (Pediatrics. 2013 May;131[5]:846-54).
Only 104 cases were diagnosed in children aged less than 10 years, and the melanoma incidence in this age group was relatively unchanging from 1973 to 2009. Dr. Friedlander further emphasized, “Pediatric melanoma is extremely uncommon in patients less than 10 years of age, but more likely to be atypical.”
She continued by describing a group of surgical oncologists at MD Anderson Cancer Center in Houston, who conducted a retrospective review of children with cutaneous melanoma between 1988 and 2007 included in the SEER database, to determine the influence of age on disease presentation. Preadolescents younger than age 10 years were more ethnically diverse (nonwhite), more frequently presented with nontruncal primary melanocytic lesions, and increasingly were diagnosed with advanced disease, compared with their adolescent counterparts (J Pediatr Surg. 2013 Nov;48[11]:2207-13).
The National Cancer Institute
Cordoro et al. conducted a similar large retrospective cohort study of children given the diagnosis of melanoma from 1984 to 2009 at the University of California, San Francisco (J Am Acad Dermatol. 2013 Jun;68[6] 913-25). Discovering that 60% of 70 children did not present with classic ABCDE findings (asymmetry, border, color, diameter, evolving), this group suggested additional ABCD detection criteria (amelanosis, bleeding, bumps, color uniformity, variable diameter, and de novo development) to facilitate earlier diagnosis and treatment of pediatric melanoma.
Congenital melanocytic nevi (CMN) may have increased risk for malignant potential, and can be challenging for pediatric providers to manage. Among all CMN, the increase in melanoma risk is estimated as less than 1%. The risk for malignant melanoma is further increased in individuals with large or giant CMN (greater than 20 cm diameter adult size), with an absolute risk of approximately 2%-5%. The number of satellite nevi also is considered in risk stratification. The presence of greater than 20 satellite nevi is associated with a greater than fivefold risk of neurocutaneous melanosis. There is no documented association between an increased quantity of satellite nevi and malignant melanoma.
“One particularly challenging pigmented lesion identified among pediatric patients is a Spitz nevus,” according to Dr. Friedlander. This lesion presents with greater cytologic atypia than other benign congenital and acquired nevi, and often clinically mimics malignant melanoma if identified in adults. There also exists a subset of atypical Spitz nevi, consisting of lesions with greater cytologic atypia than benign Spitz nevi. A retrospective review at Massachusetts General Hospital, Boston, of 157 cases of Spitz-type melanocytic lesions identified between 1987 and 2002 revealed increased melanoma risk, minimal mortality, and moderate risk of regional lymph node metastasis (Arch Dermatol. 2011;147[10]:1173-9).
“Classic pediatric Spitz nevi with typical clinical features and history may be managed conservatively with clinical monitoring alone, but those with concerning features such as bleeding, asymmetry, or ulceration should be excised with clear margins,” Dr. Friedlander emphasized. She discouraged sentinel lymph node biopsy, however, given the positive outcomes of 24 patients at Boston Children’s Hospital with atypical Spitz nevi treated with excision alone, published by Cerrato et al. (Pediatr Dermatol. 2011 Dec 30;29[4]:448-53).
“In light of the rising incidence of pediatric melanoma, we need to identify high-risk patients, educate about mole surveillance, and encourage sun protection,” Dr. Friedlander stressed. Children with phenotype of Fitzpatrick I (fair skin, blonde or red hair, and blue eye color) are at highest risk, as are those with a high density of freckles who burn easily and tan poorly. Further risk factors highlighted include excessive sun exposure, indoor tanning, use of phototoxic medications, immunosuppression, and genetics. The first and best line of defense against harmful ultraviolet radiation is covering up (clothing with a tight weave, wet suits, and hats).
The American Academy of Pediatrics encourages staying in the shade when possible, and limiting sun exposure during the peak sun intensity hours, between 10 a.m. and 4 p.m. When physical protection is not possible, the American Academy of Dermatology endorses the application of water resistant, broad spectrum SPF of greater than 30 at least every 2 hours.
Children often present for evaluation of a melanocytic lesion that is new, evolving, or worrisome to parents and caregivers.
“In the pediatric health care system, malignant melanoma is considered an especially heinous crime. In San Diego, dedicated pediatric providers who identify this disease are members of an elite squad known as the mole patrol unit.” Dr. Sheila Fallon Friedlander opened her presentation on pediatric moles with this tongue-in-cheek statement, adapted from the popular TV show “Law and Order SVU,” at a pediatric dermatology meeting sponsored by Rady Children’s Hospital–San Diego and University of California, San Diego.
Dr. Sheila Fallon FriedlanderChildhood and adolescent melanoma is rare, but the incidence in the United States has been steadily increasing over the past 35 years. A multicenter, retrospective review conducted by Wong et al., using the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) database between 1973 and 2009, detected 1,317 cases of melanoma for an incidence rate of 6 (95% confidence interval, 5.7-6.3), and revealed an average increase in adolescent melanoma of 2% per year. The greatest incidence occurred in girls aged 15-19 years, and individuals living in geographic locations with low ultraviolet-B exposure, intermittently exposed to intense UV rays (Pediatrics. 2013 May;131[5]:846-54).
Only 104 cases were diagnosed in children aged less than 10 years, and the melanoma incidence in this age group was relatively unchanging from 1973 to 2009. Dr. Friedlander further emphasized, “Pediatric melanoma is extremely uncommon in patients less than 10 years of age, but more likely to be atypical.”
She continued by describing a group of surgical oncologists at MD Anderson Cancer Center in Houston, who conducted a retrospective review of children with cutaneous melanoma between 1988 and 2007 included in the SEER database, to determine the influence of age on disease presentation. Preadolescents younger than age 10 years were more ethnically diverse (nonwhite), more frequently presented with nontruncal primary melanocytic lesions, and increasingly were diagnosed with advanced disease, compared with their adolescent counterparts (J Pediatr Surg. 2013 Nov;48[11]:2207-13).
The National Cancer Institute
Cordoro et al. conducted a similar large retrospective cohort study of children given the diagnosis of melanoma from 1984 to 2009 at the University of California, San Francisco (J Am Acad Dermatol. 2013 Jun;68[6] 913-25). Discovering that 60% of 70 children did not present with classic ABCDE findings (asymmetry, border, color, diameter, evolving), this group suggested additional ABCD detection criteria (amelanosis, bleeding, bumps, color uniformity, variable diameter, and de novo development) to facilitate earlier diagnosis and treatment of pediatric melanoma.
Congenital melanocytic nevi (CMN) may have increased risk for malignant potential, and can be challenging for pediatric providers to manage. Among all CMN, the increase in melanoma risk is estimated as less than 1%. The risk for malignant melanoma is further increased in individuals with large or giant CMN (greater than 20 cm diameter adult size), with an absolute risk of approximately 2%-5%. The number of satellite nevi also is considered in risk stratification. The presence of greater than 20 satellite nevi is associated with a greater than fivefold risk of neurocutaneous melanosis. There is no documented association between an increased quantity of satellite nevi and malignant melanoma.
“One particularly challenging pigmented lesion identified among pediatric patients is a Spitz nevus,” according to Dr. Friedlander. This lesion presents with greater cytologic atypia than other benign congenital and acquired nevi, and often clinically mimics malignant melanoma if identified in adults. There also exists a subset of atypical Spitz nevi, consisting of lesions with greater cytologic atypia than benign Spitz nevi. A retrospective review at Massachusetts General Hospital, Boston, of 157 cases of Spitz-type melanocytic lesions identified between 1987 and 2002 revealed increased melanoma risk, minimal mortality, and moderate risk of regional lymph node metastasis (Arch Dermatol. 2011;147[10]:1173-9).
“Classic pediatric Spitz nevi with typical clinical features and history may be managed conservatively with clinical monitoring alone, but those with concerning features such as bleeding, asymmetry, or ulceration should be excised with clear margins,” Dr. Friedlander emphasized. She discouraged sentinel lymph node biopsy, however, given the positive outcomes of 24 patients at Boston Children’s Hospital with atypical Spitz nevi treated with excision alone, published by Cerrato et al. (Pediatr Dermatol. 2011 Dec 30;29[4]:448-53).
“In light of the rising incidence of pediatric melanoma, we need to identify high-risk patients, educate about mole surveillance, and encourage sun protection,” Dr. Friedlander stressed. Children with phenotype of Fitzpatrick I (fair skin, blonde or red hair, and blue eye color) are at highest risk, as are those with a high density of freckles who burn easily and tan poorly. Further risk factors highlighted include excessive sun exposure, indoor tanning, use of phototoxic medications, immunosuppression, and genetics. The first and best line of defense against harmful ultraviolet radiation is covering up (clothing with a tight weave, wet suits, and hats).
The American Academy of Pediatrics encourages staying in the shade when possible, and limiting sun exposure during the peak sun intensity hours, between 10 a.m. and 4 p.m. When physical protection is not possible, the American Academy of Dermatology endorses the application of water resistant, broad spectrum SPF of greater than 30 at least every 2 hours.
Children often present for evaluation of a melanocytic lesion that is new, evolving, or worrisome to parents and caregivers.
“In the pediatric health care system, malignant melanoma is considered an especially heinous crime. In San Diego, dedicated pediatric providers who identify this disease are members of an elite squad known as the mole patrol unit.” Dr. Sheila Fallon Friedlander opened her presentation on pediatric moles with this tongue-in-cheek statement, adapted from the popular TV show “Law and Order SVU,” at a pediatric dermatology meeting sponsored by Rady Children’s Hospital–San Diego and University of California, San Diego.
Dr. Sheila Fallon FriedlanderChildhood and adolescent melanoma is rare, but the incidence in the United States has been steadily increasing over the past 35 years. A multicenter, retrospective review conducted by Wong et al., using the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) database between 1973 and 2009, detected 1,317 cases of melanoma for an incidence rate of 6 (95% confidence interval, 5.7-6.3), and revealed an average increase in adolescent melanoma of 2% per year. The greatest incidence occurred in girls aged 15-19 years, and individuals living in geographic locations with low ultraviolet-B exposure, intermittently exposed to intense UV rays (Pediatrics. 2013 May;131[5]:846-54).
Only 104 cases were diagnosed in children aged less than 10 years, and the melanoma incidence in this age group was relatively unchanging from 1973 to 2009. Dr. Friedlander further emphasized, “Pediatric melanoma is extremely uncommon in patients less than 10 years of age, but more likely to be atypical.”
She continued by describing a group of surgical oncologists at MD Anderson Cancer Center in Houston, who conducted a retrospective review of children with cutaneous melanoma between 1988 and 2007 included in the SEER database, to determine the influence of age on disease presentation. Preadolescents younger than age 10 years were more ethnically diverse (nonwhite), more frequently presented with nontruncal primary melanocytic lesions, and increasingly were diagnosed with advanced disease, compared with their adolescent counterparts (J Pediatr Surg. 2013 Nov;48[11]:2207-13).
The National Cancer Institute
Cordoro et al. conducted a similar large retrospective cohort study of children given the diagnosis of melanoma from 1984 to 2009 at the University of California, San Francisco (J Am Acad Dermatol. 2013 Jun;68[6] 913-25). Discovering that 60% of 70 children did not present with classic ABCDE findings (asymmetry, border, color, diameter, evolving), this group suggested additional ABCD detection criteria (amelanosis, bleeding, bumps, color uniformity, variable diameter, and de novo development) to facilitate earlier diagnosis and treatment of pediatric melanoma.
Congenital melanocytic nevi (CMN) may have increased risk for malignant potential, and can be challenging for pediatric providers to manage. Among all CMN, the increase in melanoma risk is estimated as less than 1%. The risk for malignant melanoma is further increased in individuals with large or giant CMN (greater than 20 cm diameter adult size), with an absolute risk of approximately 2%-5%. The number of satellite nevi also is considered in risk stratification. The presence of greater than 20 satellite nevi is associated with a greater than fivefold risk of neurocutaneous melanosis. There is no documented association between an increased quantity of satellite nevi and malignant melanoma.
“One particularly challenging pigmented lesion identified among pediatric patients is a Spitz nevus,” according to Dr. Friedlander. This lesion presents with greater cytologic atypia than other benign congenital and acquired nevi, and often clinically mimics malignant melanoma if identified in adults. There also exists a subset of atypical Spitz nevi, consisting of lesions with greater cytologic atypia than benign Spitz nevi. A retrospective review at Massachusetts General Hospital, Boston, of 157 cases of Spitz-type melanocytic lesions identified between 1987 and 2002 revealed increased melanoma risk, minimal mortality, and moderate risk of regional lymph node metastasis (Arch Dermatol. 2011;147[10]:1173-9).
“Classic pediatric Spitz nevi with typical clinical features and history may be managed conservatively with clinical monitoring alone, but those with concerning features such as bleeding, asymmetry, or ulceration should be excised with clear margins,” Dr. Friedlander emphasized. She discouraged sentinel lymph node biopsy, however, given the positive outcomes of 24 patients at Boston Children’s Hospital with atypical Spitz nevi treated with excision alone, published by Cerrato et al. (Pediatr Dermatol. 2011 Dec 30;29[4]:448-53).
“In light of the rising incidence of pediatric melanoma, we need to identify high-risk patients, educate about mole surveillance, and encourage sun protection,” Dr. Friedlander stressed. Children with phenotype of Fitzpatrick I (fair skin, blonde or red hair, and blue eye color) are at highest risk, as are those with a high density of freckles who burn easily and tan poorly. Further risk factors highlighted include excessive sun exposure, indoor tanning, use of phototoxic medications, immunosuppression, and genetics. The first and best line of defense against harmful ultraviolet radiation is covering up (clothing with a tight weave, wet suits, and hats).
The American Academy of Pediatrics encourages staying in the shade when possible, and limiting sun exposure during the peak sun intensity hours, between 10 a.m. and 4 p.m. When physical protection is not possible, the American Academy of Dermatology endorses the application of water resistant, broad spectrum SPF of greater than 30 at least every 2 hours.
In the absence of a typical presentation, combining direct microscopy plus nail clipping histopathology – two diagnostic tests with different sensitivities and specificities – raises the likelihood of correctly diagnosing onychomycosis, according to a report published in Mycoses.
It is often difficult to diagnose nail diseases based solely on clinical features, and laboratory techniques for diagnosing onychomycoses in particular “remain a challenge,” said Fernanda G. Lavorato, MD, of Universidade do Estado do Rio de Janeiro, and her associates.
Isolating filamentous fungi in cultures is considered the preferred method for diagnosing the disorder, but this method lacks sensitivity and is not always accessible, since some dermatologic centers don’t have a mycology laboratory with personnel trained in sample collection and fungal processing.
copyright Manuel-F-O/Thinkstock
The investigators assessed the performance of cultures and two inexpensive and readily available techniques, direct microscopy and nail clipping for histopathological examination, at identifying toenail onychomycoses caused by dermatophyte and nondermatophyte molds. Their study sample comprised 212 adults who presented for diagnosis and treatment of toenail lesions to a single center during a 2-year period. Each patient had at least one lesion 2 mm wide and 3-5 mm long on the affected toenail.
The mean patient age was 58.8 years (range, 27-86 years). Most study participants (77.8%) had more than 1 affected nail. Many (29.7%) also had symptoms or signs of cutaneous lesions on the palm, sole, or interdigital region.
Direct microscopy was the most sensitive diagnostic test, correctly identifying 100% of the 122 cases of onychomycosis. In contrast, cultures identified only 34.4% of cases. This low sensitivity for culture testing was expected, and was “likely due to the rapid growth of fungi and bacteria comprising the local microbiota, which often prevents the growth of pathogenic fungi, particularly of slow-growing dermatophytes,” Dr. Lavorato and her associates said (Mycoses. 2017 May 15. doi:10.1111/myc.12633).
Histopathology of nail clippings was the most specific diagnostic test, correctly identifying 77% of cases. “Nail clipping histopathologic analysis complements the [microscopic] examination, particularly in cases of strong clinical suspicion but repeatedly negative mycological tests,” the investigators noted.
Direct microscopy showed greater accuracy with nondermatophytes, while nail clipping showed greater accuracy for dermatophytes, they added.
In this study, Trichophyton rubrum and T. mentagrophytes were the most frequently isolated dermatophytes, found in 70% and 23% of cases, respectively. Neoscytalidium dimidatum and Fusarium species were the most frequently isolated nondermatophytes, found in 44% and 28% of cases, respectively. In addition, Candida yeasts were isolated in samples from 14% of patients, and bacterial colonies were isolated in 70%.
The Mycology Laboratory at Pedro Ernesto University Hospital supported the study. Dr. Lavorato and her associates reported having no relevant financial disclosures.
In the absence of a typical presentation, combining direct microscopy plus nail clipping histopathology – two diagnostic tests with different sensitivities and specificities – raises the likelihood of correctly diagnosing onychomycosis, according to a report published in Mycoses.
It is often difficult to diagnose nail diseases based solely on clinical features, and laboratory techniques for diagnosing onychomycoses in particular “remain a challenge,” said Fernanda G. Lavorato, MD, of Universidade do Estado do Rio de Janeiro, and her associates.
Isolating filamentous fungi in cultures is considered the preferred method for diagnosing the disorder, but this method lacks sensitivity and is not always accessible, since some dermatologic centers don’t have a mycology laboratory with personnel trained in sample collection and fungal processing.
copyright Manuel-F-O/Thinkstock
The investigators assessed the performance of cultures and two inexpensive and readily available techniques, direct microscopy and nail clipping for histopathological examination, at identifying toenail onychomycoses caused by dermatophyte and nondermatophyte molds. Their study sample comprised 212 adults who presented for diagnosis and treatment of toenail lesions to a single center during a 2-year period. Each patient had at least one lesion 2 mm wide and 3-5 mm long on the affected toenail.
The mean patient age was 58.8 years (range, 27-86 years). Most study participants (77.8%) had more than 1 affected nail. Many (29.7%) also had symptoms or signs of cutaneous lesions on the palm, sole, or interdigital region.
Direct microscopy was the most sensitive diagnostic test, correctly identifying 100% of the 122 cases of onychomycosis. In contrast, cultures identified only 34.4% of cases. This low sensitivity for culture testing was expected, and was “likely due to the rapid growth of fungi and bacteria comprising the local microbiota, which often prevents the growth of pathogenic fungi, particularly of slow-growing dermatophytes,” Dr. Lavorato and her associates said (Mycoses. 2017 May 15. doi:10.1111/myc.12633).
Histopathology of nail clippings was the most specific diagnostic test, correctly identifying 77% of cases. “Nail clipping histopathologic analysis complements the [microscopic] examination, particularly in cases of strong clinical suspicion but repeatedly negative mycological tests,” the investigators noted.
Direct microscopy showed greater accuracy with nondermatophytes, while nail clipping showed greater accuracy for dermatophytes, they added.
In this study, Trichophyton rubrum and T. mentagrophytes were the most frequently isolated dermatophytes, found in 70% and 23% of cases, respectively. Neoscytalidium dimidatum and Fusarium species were the most frequently isolated nondermatophytes, found in 44% and 28% of cases, respectively. In addition, Candida yeasts were isolated in samples from 14% of patients, and bacterial colonies were isolated in 70%.
The Mycology Laboratory at Pedro Ernesto University Hospital supported the study. Dr. Lavorato and her associates reported having no relevant financial disclosures.
In the absence of a typical presentation, combining direct microscopy plus nail clipping histopathology – two diagnostic tests with different sensitivities and specificities – raises the likelihood of correctly diagnosing onychomycosis, according to a report published in Mycoses.
It is often difficult to diagnose nail diseases based solely on clinical features, and laboratory techniques for diagnosing onychomycoses in particular “remain a challenge,” said Fernanda G. Lavorato, MD, of Universidade do Estado do Rio de Janeiro, and her associates.
Isolating filamentous fungi in cultures is considered the preferred method for diagnosing the disorder, but this method lacks sensitivity and is not always accessible, since some dermatologic centers don’t have a mycology laboratory with personnel trained in sample collection and fungal processing.
copyright Manuel-F-O/Thinkstock
The investigators assessed the performance of cultures and two inexpensive and readily available techniques, direct microscopy and nail clipping for histopathological examination, at identifying toenail onychomycoses caused by dermatophyte and nondermatophyte molds. Their study sample comprised 212 adults who presented for diagnosis and treatment of toenail lesions to a single center during a 2-year period. Each patient had at least one lesion 2 mm wide and 3-5 mm long on the affected toenail.
The mean patient age was 58.8 years (range, 27-86 years). Most study participants (77.8%) had more than 1 affected nail. Many (29.7%) also had symptoms or signs of cutaneous lesions on the palm, sole, or interdigital region.
Direct microscopy was the most sensitive diagnostic test, correctly identifying 100% of the 122 cases of onychomycosis. In contrast, cultures identified only 34.4% of cases. This low sensitivity for culture testing was expected, and was “likely due to the rapid growth of fungi and bacteria comprising the local microbiota, which often prevents the growth of pathogenic fungi, particularly of slow-growing dermatophytes,” Dr. Lavorato and her associates said (Mycoses. 2017 May 15. doi:10.1111/myc.12633).
Histopathology of nail clippings was the most specific diagnostic test, correctly identifying 77% of cases. “Nail clipping histopathologic analysis complements the [microscopic] examination, particularly in cases of strong clinical suspicion but repeatedly negative mycological tests,” the investigators noted.
Direct microscopy showed greater accuracy with nondermatophytes, while nail clipping showed greater accuracy for dermatophytes, they added.
In this study, Trichophyton rubrum and T. mentagrophytes were the most frequently isolated dermatophytes, found in 70% and 23% of cases, respectively. Neoscytalidium dimidatum and Fusarium species were the most frequently isolated nondermatophytes, found in 44% and 28% of cases, respectively. In addition, Candida yeasts were isolated in samples from 14% of patients, and bacterial colonies were isolated in 70%.
The Mycology Laboratory at Pedro Ernesto University Hospital supported the study. Dr. Lavorato and her associates reported having no relevant financial disclosures.
Key clinical point: In the absence of a typical clinical presentation, combining direct microscopy plus nail clipping histopathology – two diagnostic tests with different sensitivities and specificities – raises the likelihood of correctly diagnosing onychomycosis.
Major finding: Direct microscopy was the most sensitive diagnostic test, correctly identifying 100% of the 122 cases of onychomycosis, while histopathology of nail clippings was the most specific diagnostic test, correctly identifying 77% of cases.
Data source: A single-center prospective cross-sectional study involving 212 adults suspected of having onychomycosis during a 2-year period.
Disclosures: The Mycology Laboratory at Pedro Ernesto University Hospital supported the study. Dr. Lavorato and her associates reported having no relevant financial disclosures.
For the May-June issue of the Journal of Community and Supportive Oncology, the Editor in Chief, Dr David Henry, discusses an editorial by Kevin Knopf, a JCSO editor, about drawing on modern portfolio theory to improve cancer care. Side effects come under scrutiny this issue, with a How We Do It article on prehabilitation for lymphedema in head and neck cancer patients, a Review article that examines pancreatitis associated with newer classes of antineoplastic therapies, and a research article that looks at prescriber adherence to antiemetic guidelines with trifluridine-tipiracil. In other research articles, investigators report on physician attitudes and prevalence of molecular testing in lung cancer; a comprehensive assessment of cancer survivors’ concerns to inform program development; and perceived financial hardship among patients with advanced cancer. Two Case Reports address the treatment of Kaposi sarcoma in patients with AIDS, and a third describes a rare case of hypoglycemia induced by a classic gastrointestinal stromal tumor. Finally, Dr Henry summarizes an in-depth interview on cardiotoxicity, which he did with his colleague, Dr Joseph Carver.
For the May-June issue of the Journal of Community and Supportive Oncology, the Editor in Chief, Dr David Henry, discusses an editorial by Kevin Knopf, a JCSO editor, about drawing on modern portfolio theory to improve cancer care. Side effects come under scrutiny this issue, with a How We Do It article on prehabilitation for lymphedema in head and neck cancer patients, a Review article that examines pancreatitis associated with newer classes of antineoplastic therapies, and a research article that looks at prescriber adherence to antiemetic guidelines with trifluridine-tipiracil. In other research articles, investigators report on physician attitudes and prevalence of molecular testing in lung cancer; a comprehensive assessment of cancer survivors’ concerns to inform program development; and perceived financial hardship among patients with advanced cancer. Two Case Reports address the treatment of Kaposi sarcoma in patients with AIDS, and a third describes a rare case of hypoglycemia induced by a classic gastrointestinal stromal tumor. Finally, Dr Henry summarizes an in-depth interview on cardiotoxicity, which he did with his colleague, Dr Joseph Carver.
Listen to the podcast below.
For the May-June issue of the Journal of Community and Supportive Oncology, the Editor in Chief, Dr David Henry, discusses an editorial by Kevin Knopf, a JCSO editor, about drawing on modern portfolio theory to improve cancer care. Side effects come under scrutiny this issue, with a How We Do It article on prehabilitation for lymphedema in head and neck cancer patients, a Review article that examines pancreatitis associated with newer classes of antineoplastic therapies, and a research article that looks at prescriber adherence to antiemetic guidelines with trifluridine-tipiracil. In other research articles, investigators report on physician attitudes and prevalence of molecular testing in lung cancer; a comprehensive assessment of cancer survivors’ concerns to inform program development; and perceived financial hardship among patients with advanced cancer. Two Case Reports address the treatment of Kaposi sarcoma in patients with AIDS, and a third describes a rare case of hypoglycemia induced by a classic gastrointestinal stromal tumor. Finally, Dr Henry summarizes an in-depth interview on cardiotoxicity, which he did with his colleague, Dr Joseph Carver.
NEW ORLEANS – Risk tolerance to current disease modifying therapies by patients with multiple sclerosis varies widely, results from a large national survey demonstrated.
“We have therapies available with a wide range of risks,” study author Sneha Natarajan, PhD, said in an interview at the annual meeting of the Consortium of Multiple Sclerosis Centers. “Some of the risks are relatively minor like injection site reactions or flu-like symptoms and some are as bad as PML [progressive multifocal leukoencephalopathy], which can be fatal. We don’t know what kind of risks people tolerate.”
Doug Brunk/Frontline Medical News
Dr. Sneha Natarajan
To find out, she and her associates conducted a survey of participants of North American Research Committee on Multiple Sclerosis and visitors to the National Multiple Sclerosis Society website who reported having MS. The benefit of a hypothetical oral disease modifying therapy (DMT) was set at 50% reduction in clinical relapses and 30% reduction in disability progression. The researchers chose six different risk scenarios to evaluate tolerance to six risks: risk of infection, skin rash, kidney injury, thyroid injury, liver injury, and risk of PML. Starting from a risk tolerance of 1:1,000, the risk was adjusted to identify the highest risk tolerated, ranging from “would take regardless of the risk of death” to “no acceptable risk.”
Dr. Natarajan, research coordinator at the Mellen Center for Multiple Sclerosis at the Cleveland Clinic, reported results from 3,371 survey respondents. Their mean age was 55 years, 93% were white, 61% had the relapsing-remitting form of MS, and 53% were currently taking a DMT. Overall, respondents reported the highest risk tolerance for infection or thyroid risks (1:1,000 for both) and lowest risk tolerance for PML and kidney injury risks (1:1,000,000 for both). Males reported a higher risk tolerance to all six risks (P less than .0001 for all). Females reported a risk tolerance to skin rash that was similar to kidney injury and PML.
“There is a pattern to the risks that our patients accept,” Dr. Natarajan said. “I don’t think a doctor would not recommend a therapy benefit because of a skin rash [risk], but he may need to address the concerns of the patient upfront and have a talk with the patient.”
The researchers also found that current DMT users expressed increased risk tolerance for all outcomes, compared with those not using any DMT (P less than .001). Higher risk tolerance was also expressed by respondents who were older, more disabled, and by those taking infusion therapies.
The National Multiple Sclerosis Society funded the study. Dr. Natarajan reported having no financial disclosures.
NEW ORLEANS – Risk tolerance to current disease modifying therapies by patients with multiple sclerosis varies widely, results from a large national survey demonstrated.
“We have therapies available with a wide range of risks,” study author Sneha Natarajan, PhD, said in an interview at the annual meeting of the Consortium of Multiple Sclerosis Centers. “Some of the risks are relatively minor like injection site reactions or flu-like symptoms and some are as bad as PML [progressive multifocal leukoencephalopathy], which can be fatal. We don’t know what kind of risks people tolerate.”
Doug Brunk/Frontline Medical News
Dr. Sneha Natarajan
To find out, she and her associates conducted a survey of participants of North American Research Committee on Multiple Sclerosis and visitors to the National Multiple Sclerosis Society website who reported having MS. The benefit of a hypothetical oral disease modifying therapy (DMT) was set at 50% reduction in clinical relapses and 30% reduction in disability progression. The researchers chose six different risk scenarios to evaluate tolerance to six risks: risk of infection, skin rash, kidney injury, thyroid injury, liver injury, and risk of PML. Starting from a risk tolerance of 1:1,000, the risk was adjusted to identify the highest risk tolerated, ranging from “would take regardless of the risk of death” to “no acceptable risk.”
Dr. Natarajan, research coordinator at the Mellen Center for Multiple Sclerosis at the Cleveland Clinic, reported results from 3,371 survey respondents. Their mean age was 55 years, 93% were white, 61% had the relapsing-remitting form of MS, and 53% were currently taking a DMT. Overall, respondents reported the highest risk tolerance for infection or thyroid risks (1:1,000 for both) and lowest risk tolerance for PML and kidney injury risks (1:1,000,000 for both). Males reported a higher risk tolerance to all six risks (P less than .0001 for all). Females reported a risk tolerance to skin rash that was similar to kidney injury and PML.
“There is a pattern to the risks that our patients accept,” Dr. Natarajan said. “I don’t think a doctor would not recommend a therapy benefit because of a skin rash [risk], but he may need to address the concerns of the patient upfront and have a talk with the patient.”
The researchers also found that current DMT users expressed increased risk tolerance for all outcomes, compared with those not using any DMT (P less than .001). Higher risk tolerance was also expressed by respondents who were older, more disabled, and by those taking infusion therapies.
The National Multiple Sclerosis Society funded the study. Dr. Natarajan reported having no financial disclosures.
NEW ORLEANS – Risk tolerance to current disease modifying therapies by patients with multiple sclerosis varies widely, results from a large national survey demonstrated.
“We have therapies available with a wide range of risks,” study author Sneha Natarajan, PhD, said in an interview at the annual meeting of the Consortium of Multiple Sclerosis Centers. “Some of the risks are relatively minor like injection site reactions or flu-like symptoms and some are as bad as PML [progressive multifocal leukoencephalopathy], which can be fatal. We don’t know what kind of risks people tolerate.”
Doug Brunk/Frontline Medical News
Dr. Sneha Natarajan
To find out, she and her associates conducted a survey of participants of North American Research Committee on Multiple Sclerosis and visitors to the National Multiple Sclerosis Society website who reported having MS. The benefit of a hypothetical oral disease modifying therapy (DMT) was set at 50% reduction in clinical relapses and 30% reduction in disability progression. The researchers chose six different risk scenarios to evaluate tolerance to six risks: risk of infection, skin rash, kidney injury, thyroid injury, liver injury, and risk of PML. Starting from a risk tolerance of 1:1,000, the risk was adjusted to identify the highest risk tolerated, ranging from “would take regardless of the risk of death” to “no acceptable risk.”
Dr. Natarajan, research coordinator at the Mellen Center for Multiple Sclerosis at the Cleveland Clinic, reported results from 3,371 survey respondents. Their mean age was 55 years, 93% were white, 61% had the relapsing-remitting form of MS, and 53% were currently taking a DMT. Overall, respondents reported the highest risk tolerance for infection or thyroid risks (1:1,000 for both) and lowest risk tolerance for PML and kidney injury risks (1:1,000,000 for both). Males reported a higher risk tolerance to all six risks (P less than .0001 for all). Females reported a risk tolerance to skin rash that was similar to kidney injury and PML.
“There is a pattern to the risks that our patients accept,” Dr. Natarajan said. “I don’t think a doctor would not recommend a therapy benefit because of a skin rash [risk], but he may need to address the concerns of the patient upfront and have a talk with the patient.”
The researchers also found that current DMT users expressed increased risk tolerance for all outcomes, compared with those not using any DMT (P less than .001). Higher risk tolerance was also expressed by respondents who were older, more disabled, and by those taking infusion therapies.
The National Multiple Sclerosis Society funded the study. Dr. Natarajan reported having no financial disclosures.
Key clinical point: People with MS report different levels of tolerance to various risks associated with DMTs.
Major finding: Survey respondents reported the highest risk tolerance for infection or thyroid risks (1:1,000 for both) and lowest risk tolerance for PML and kidney injury risks (1:1,000,000 for both).
Data source: A survey of 3,371 people who reported having MS.
Disclosures: The National Multiple Sclerosis Society funded the study. Dr. Natarajan reported having no financial disclosures.
Clinical Question: Do family reports of adverse events improve incident detection, compared with clinician reports and hospital incident reports?
Background: Hospital incident reports, which are voluntary and suffer from underreporting, capture only a fraction of errors and adverse events (defined as errors resulting in harm). Systematic, prospective surveillance by researchers is the gold standard but is time consuming and expensive. The authors hypothesized that family reports would improve error and adverse event detection.
Study Design: Prospective cohort study.
Setting: Four U.S. pediatric hospitals.
Synopsis: The authors developed a Family Safety Interview, administered weekly and on discharge, and compared reporting of errors and adverse events to clinician reports, hospital incident reports, and systematic review of records by researchers. Of 989 hospitalized pediatric patients, 746 parents/caregivers completed interviews between December 2014 and July 2015. From all sources, the authors found a total of 179 errors and 113 adverse events. Families reported a total of 39 of these 179 errors (including 19 unique errors not reported elsewhere) and 33 of 113 adverse events (8 unique).
Overall, error rates with family-reported errors were 15.5% higher (95% confidence interval, 9.0%-22.3%) than without. Adverse event rates with family reporting were 9.8% higher (95% CI, 3.1%-16.9%) than without. Family-reported error rates were 5 times higher (95% CI, 1.9-13.0) than hospital incident report rates.
The study showed that family-reported error and adverse event rates were significantly higher than voluntary, clinician-only hospital incident report rates. The study was limited to pediatric hospitals on general pediatric and subspecialty services, though findings potentially may be applicable more broadly (for example, adult and surgical services).
Bottom Line: Using a structured interview, families report significantly higher rates of errors and adverse events, compared with other sources.
Reference: Khan A, Coffey M, Litterer KP, et al. Families as partners in hospital error and adverse event surveillance. JAMA Pediatrics. Published online Feb 27, 2017. doi: 10.1001/jamapediatrics.2016.4812.
Clinical Question: Do family reports of adverse events improve incident detection, compared with clinician reports and hospital incident reports?
Background: Hospital incident reports, which are voluntary and suffer from underreporting, capture only a fraction of errors and adverse events (defined as errors resulting in harm). Systematic, prospective surveillance by researchers is the gold standard but is time consuming and expensive. The authors hypothesized that family reports would improve error and adverse event detection.
Study Design: Prospective cohort study.
Setting: Four U.S. pediatric hospitals.
Synopsis: The authors developed a Family Safety Interview, administered weekly and on discharge, and compared reporting of errors and adverse events to clinician reports, hospital incident reports, and systematic review of records by researchers. Of 989 hospitalized pediatric patients, 746 parents/caregivers completed interviews between December 2014 and July 2015. From all sources, the authors found a total of 179 errors and 113 adverse events. Families reported a total of 39 of these 179 errors (including 19 unique errors not reported elsewhere) and 33 of 113 adverse events (8 unique).
Overall, error rates with family-reported errors were 15.5% higher (95% confidence interval, 9.0%-22.3%) than without. Adverse event rates with family reporting were 9.8% higher (95% CI, 3.1%-16.9%) than without. Family-reported error rates were 5 times higher (95% CI, 1.9-13.0) than hospital incident report rates.
The study showed that family-reported error and adverse event rates were significantly higher than voluntary, clinician-only hospital incident report rates. The study was limited to pediatric hospitals on general pediatric and subspecialty services, though findings potentially may be applicable more broadly (for example, adult and surgical services).
Bottom Line: Using a structured interview, families report significantly higher rates of errors and adverse events, compared with other sources.
Reference: Khan A, Coffey M, Litterer KP, et al. Families as partners in hospital error and adverse event surveillance. JAMA Pediatrics. Published online Feb 27, 2017. doi: 10.1001/jamapediatrics.2016.4812.
Clinical Question: Do family reports of adverse events improve incident detection, compared with clinician reports and hospital incident reports?
Background: Hospital incident reports, which are voluntary and suffer from underreporting, capture only a fraction of errors and adverse events (defined as errors resulting in harm). Systematic, prospective surveillance by researchers is the gold standard but is time consuming and expensive. The authors hypothesized that family reports would improve error and adverse event detection.
Study Design: Prospective cohort study.
Setting: Four U.S. pediatric hospitals.
Synopsis: The authors developed a Family Safety Interview, administered weekly and on discharge, and compared reporting of errors and adverse events to clinician reports, hospital incident reports, and systematic review of records by researchers. Of 989 hospitalized pediatric patients, 746 parents/caregivers completed interviews between December 2014 and July 2015. From all sources, the authors found a total of 179 errors and 113 adverse events. Families reported a total of 39 of these 179 errors (including 19 unique errors not reported elsewhere) and 33 of 113 adverse events (8 unique).
Overall, error rates with family-reported errors were 15.5% higher (95% confidence interval, 9.0%-22.3%) than without. Adverse event rates with family reporting were 9.8% higher (95% CI, 3.1%-16.9%) than without. Family-reported error rates were 5 times higher (95% CI, 1.9-13.0) than hospital incident report rates.
The study showed that family-reported error and adverse event rates were significantly higher than voluntary, clinician-only hospital incident report rates. The study was limited to pediatric hospitals on general pediatric and subspecialty services, though findings potentially may be applicable more broadly (for example, adult and surgical services).
Bottom Line: Using a structured interview, families report significantly higher rates of errors and adverse events, compared with other sources.
Reference: Khan A, Coffey M, Litterer KP, et al. Families as partners in hospital error and adverse event surveillance. JAMA Pediatrics. Published online Feb 27, 2017. doi: 10.1001/jamapediatrics.2016.4812.
SCOTTSDALE, ARIZ. – Linda L.M. Worley, MD, was stunned when a meeting she’d requested with her supervisor to address a shortage of beds turned into a rebuke.
“You’re on the tenure track, Linda. If you want to keep your job 6 years from now, you’d best pick up the pace. You need to see 20 private patients a week, and get moving on your research and publications,” Dr. Worley remembers the supervisor saying. At the time, she was a 32-year-old mother of two, wife, academic faculty physician, and sole attending running a general hospital consultation liaison psychiatry department and the college of medicine student mental health service. She also worked as the 24/7 on-call psychiatrist for a week at a time, said Dr. Worley, now a staff psychiatrist in the Fayetteville, Ark., Veterans Health Care System of the Ozarks and chief mental health officer for South Central VA Health Care Network.
Dr. Linda Worley
Dr. Worley’s immediate response was to go home and “collapse into anguished sobs,” she said in an interview. Her ultimate response, however, was to change tack, as a sailor does to make the most of how the wind is blowing. “When I told my husband I couldn’t manage and felt as though I was capsizing, he told me to ‘reef in my sails,’ ” she said, describing the technique sailors use to reduce their exposure to dangerously strong winds. “That was the day my Smooth Sailing Life nautical metaphor first crystallized.”
Over the decades of an academic medical career complete with tenure, and dozens of published articles and book chapters, Dr. Worley has developed a system for achieving success while avoiding burnout, based on nautical references. In a session cofacilitated by Cynthia M. Stonnington, MD, chair of psychiatry and psychology at the Mayo Clinic’s campus in Scottsdale, Ariz., Dr. Worley presented her tips for self-care at the annual meeting of the American College of Psychiatrists.
“I use the nautical framework as a bio-psycho-social-spiritual model,” Dr. Worley said in an interview. “I teach it to medical students; I teach it to residents; I teach it to distressed physicians. I even teach it to patients when I am explaining a framework for a necessary treatment approach. With sailing, you have to stay in balance. That’s the same with taking good care of ourselves so we are less likely to get sick physically and mentally,” said Dr. Worley, who commutes to Nashville, Tenn., several times a year as part of her appointment as an adjunct professor of medicine at Vanderbilt University.
Her “Smooth Sailing Life” seminars have evolved over the past 20 years and are rooted in her training in psychosomatic medicine, which she said emphasizes the complexity of the entire person. “It’s about the biology and about the emotions, and the bridge between them,” according to Dr. Worley, who has a website, SmoothSailingLife.com, and is working on a book aimed at helping to meet what she said has been a steadily growing thirst for her approach to developing resilience.
“I am not studying anyone, but I am helping people to self-diagnose. I teach people how to avoid having to see a psychiatrist or a mental health provider but also to feel good about reaching out for help when necessary,” she said. “Life is far too short to suffer needlessly.”
In the interview, Dr. Worley said she adapts her presentations to the venue and the time allowed. Key aspects of her system include:
• Care for your yacht, which is the body, including the brain. “You only get one, and if you’re going to have a chance of winning the regatta, you have to take care of it. This means getting good sleep, nutrition, exercise, preventive care, rest, and rejuvenation, including vacation,” Dr. Worley said.
• Chart your course; have a navigational plan that includes your life goals and aspirations. Identify and rely upon “landmarks,” such as being a good spouse, mother, physician, or friend for the most authentic definition of personal success. “These are like buoys that keep us sailing in the right direction,” she said.
• Reef in your sails, meaning mind the “winds that come at us from every side,” she said. This includes triaging tasks and not letting perfectionism get in the way. “Perfectionists take too long to tack; they don’t know when it’s time to turn in the other direction,” she said. “If you want to finish the race, you have to do the best you can in the time you have.” This was the lesson Dr. Worley said she learned that day when she was a young physician feeling overwhelmed.
• Empty your bilge, the nautical term for removing waste water from within the hull. Dr. Worley uses this as a metaphor for identifying and expressing negative emotions of fear, anxiety, sadness, and frustration. “These vital emotions are giving us important messages. It is important to recognize that they are present. Name and accept them, and understand what they are trying to tell us. Is it a symptom of an underlying illness that needs treatment? A conflict in a relationship? A need not being met? Are you living your deepest values? Express the emotions and sort through the best response,” she said. “It’s all part of emotional intelligence.”
• Keep an even keel, which is Dr. Worley’s way of stating the importance of being connected to love and to living your deepest values. “The keel is your character, your connection to meaning, a spiritual connection. In medicine, we shy away from that. I have only lately ventured into talking about this,” she said, noting that this connection can come in numerous ways, such as meditation, and being in nature or with animals. “It’s very personal. It’s hard to quantify, but I have witnessed it and its healing power within the therapeutic alliance.”
In break-out sessions during her well-attended talk at the meeting, Dr. Worley listened as psychiatrists of all levels of experience and responsibility, ranging from medical directors to those in private community practice, shared the kinds of concerns she said she often encounters in her role as a core faculty member of the Program for Distressed Physicians at the Vanderbilt Center for Professional Health.
“Changes in medicine have been so frustrating; physicians are at their wits’ end. We don’t recruit people into medicine because they have a skill set for expressing their emotions, or taking care of themselves, or dealing with conflict,” she said. “That’s okay. They can learn it.”
SCOTTSDALE, ARIZ. – Linda L.M. Worley, MD, was stunned when a meeting she’d requested with her supervisor to address a shortage of beds turned into a rebuke.
“You’re on the tenure track, Linda. If you want to keep your job 6 years from now, you’d best pick up the pace. You need to see 20 private patients a week, and get moving on your research and publications,” Dr. Worley remembers the supervisor saying. At the time, she was a 32-year-old mother of two, wife, academic faculty physician, and sole attending running a general hospital consultation liaison psychiatry department and the college of medicine student mental health service. She also worked as the 24/7 on-call psychiatrist for a week at a time, said Dr. Worley, now a staff psychiatrist in the Fayetteville, Ark., Veterans Health Care System of the Ozarks and chief mental health officer for South Central VA Health Care Network.
Dr. Linda Worley
Dr. Worley’s immediate response was to go home and “collapse into anguished sobs,” she said in an interview. Her ultimate response, however, was to change tack, as a sailor does to make the most of how the wind is blowing. “When I told my husband I couldn’t manage and felt as though I was capsizing, he told me to ‘reef in my sails,’ ” she said, describing the technique sailors use to reduce their exposure to dangerously strong winds. “That was the day my Smooth Sailing Life nautical metaphor first crystallized.”
Over the decades of an academic medical career complete with tenure, and dozens of published articles and book chapters, Dr. Worley has developed a system for achieving success while avoiding burnout, based on nautical references. In a session cofacilitated by Cynthia M. Stonnington, MD, chair of psychiatry and psychology at the Mayo Clinic’s campus in Scottsdale, Ariz., Dr. Worley presented her tips for self-care at the annual meeting of the American College of Psychiatrists.
“I use the nautical framework as a bio-psycho-social-spiritual model,” Dr. Worley said in an interview. “I teach it to medical students; I teach it to residents; I teach it to distressed physicians. I even teach it to patients when I am explaining a framework for a necessary treatment approach. With sailing, you have to stay in balance. That’s the same with taking good care of ourselves so we are less likely to get sick physically and mentally,” said Dr. Worley, who commutes to Nashville, Tenn., several times a year as part of her appointment as an adjunct professor of medicine at Vanderbilt University.
Her “Smooth Sailing Life” seminars have evolved over the past 20 years and are rooted in her training in psychosomatic medicine, which she said emphasizes the complexity of the entire person. “It’s about the biology and about the emotions, and the bridge between them,” according to Dr. Worley, who has a website, SmoothSailingLife.com, and is working on a book aimed at helping to meet what she said has been a steadily growing thirst for her approach to developing resilience.
“I am not studying anyone, but I am helping people to self-diagnose. I teach people how to avoid having to see a psychiatrist or a mental health provider but also to feel good about reaching out for help when necessary,” she said. “Life is far too short to suffer needlessly.”
In the interview, Dr. Worley said she adapts her presentations to the venue and the time allowed. Key aspects of her system include:
• Care for your yacht, which is the body, including the brain. “You only get one, and if you’re going to have a chance of winning the regatta, you have to take care of it. This means getting good sleep, nutrition, exercise, preventive care, rest, and rejuvenation, including vacation,” Dr. Worley said.
• Chart your course; have a navigational plan that includes your life goals and aspirations. Identify and rely upon “landmarks,” such as being a good spouse, mother, physician, or friend for the most authentic definition of personal success. “These are like buoys that keep us sailing in the right direction,” she said.
• Reef in your sails, meaning mind the “winds that come at us from every side,” she said. This includes triaging tasks and not letting perfectionism get in the way. “Perfectionists take too long to tack; they don’t know when it’s time to turn in the other direction,” she said. “If you want to finish the race, you have to do the best you can in the time you have.” This was the lesson Dr. Worley said she learned that day when she was a young physician feeling overwhelmed.
• Empty your bilge, the nautical term for removing waste water from within the hull. Dr. Worley uses this as a metaphor for identifying and expressing negative emotions of fear, anxiety, sadness, and frustration. “These vital emotions are giving us important messages. It is important to recognize that they are present. Name and accept them, and understand what they are trying to tell us. Is it a symptom of an underlying illness that needs treatment? A conflict in a relationship? A need not being met? Are you living your deepest values? Express the emotions and sort through the best response,” she said. “It’s all part of emotional intelligence.”
• Keep an even keel, which is Dr. Worley’s way of stating the importance of being connected to love and to living your deepest values. “The keel is your character, your connection to meaning, a spiritual connection. In medicine, we shy away from that. I have only lately ventured into talking about this,” she said, noting that this connection can come in numerous ways, such as meditation, and being in nature or with animals. “It’s very personal. It’s hard to quantify, but I have witnessed it and its healing power within the therapeutic alliance.”
In break-out sessions during her well-attended talk at the meeting, Dr. Worley listened as psychiatrists of all levels of experience and responsibility, ranging from medical directors to those in private community practice, shared the kinds of concerns she said she often encounters in her role as a core faculty member of the Program for Distressed Physicians at the Vanderbilt Center for Professional Health.
“Changes in medicine have been so frustrating; physicians are at their wits’ end. We don’t recruit people into medicine because they have a skill set for expressing their emotions, or taking care of themselves, or dealing with conflict,” she said. “That’s okay. They can learn it.”
SCOTTSDALE, ARIZ. – Linda L.M. Worley, MD, was stunned when a meeting she’d requested with her supervisor to address a shortage of beds turned into a rebuke.
“You’re on the tenure track, Linda. If you want to keep your job 6 years from now, you’d best pick up the pace. You need to see 20 private patients a week, and get moving on your research and publications,” Dr. Worley remembers the supervisor saying. At the time, she was a 32-year-old mother of two, wife, academic faculty physician, and sole attending running a general hospital consultation liaison psychiatry department and the college of medicine student mental health service. She also worked as the 24/7 on-call psychiatrist for a week at a time, said Dr. Worley, now a staff psychiatrist in the Fayetteville, Ark., Veterans Health Care System of the Ozarks and chief mental health officer for South Central VA Health Care Network.
Dr. Linda Worley
Dr. Worley’s immediate response was to go home and “collapse into anguished sobs,” she said in an interview. Her ultimate response, however, was to change tack, as a sailor does to make the most of how the wind is blowing. “When I told my husband I couldn’t manage and felt as though I was capsizing, he told me to ‘reef in my sails,’ ” she said, describing the technique sailors use to reduce their exposure to dangerously strong winds. “That was the day my Smooth Sailing Life nautical metaphor first crystallized.”
Over the decades of an academic medical career complete with tenure, and dozens of published articles and book chapters, Dr. Worley has developed a system for achieving success while avoiding burnout, based on nautical references. In a session cofacilitated by Cynthia M. Stonnington, MD, chair of psychiatry and psychology at the Mayo Clinic’s campus in Scottsdale, Ariz., Dr. Worley presented her tips for self-care at the annual meeting of the American College of Psychiatrists.
“I use the nautical framework as a bio-psycho-social-spiritual model,” Dr. Worley said in an interview. “I teach it to medical students; I teach it to residents; I teach it to distressed physicians. I even teach it to patients when I am explaining a framework for a necessary treatment approach. With sailing, you have to stay in balance. That’s the same with taking good care of ourselves so we are less likely to get sick physically and mentally,” said Dr. Worley, who commutes to Nashville, Tenn., several times a year as part of her appointment as an adjunct professor of medicine at Vanderbilt University.
Her “Smooth Sailing Life” seminars have evolved over the past 20 years and are rooted in her training in psychosomatic medicine, which she said emphasizes the complexity of the entire person. “It’s about the biology and about the emotions, and the bridge between them,” according to Dr. Worley, who has a website, SmoothSailingLife.com, and is working on a book aimed at helping to meet what she said has been a steadily growing thirst for her approach to developing resilience.
“I am not studying anyone, but I am helping people to self-diagnose. I teach people how to avoid having to see a psychiatrist or a mental health provider but also to feel good about reaching out for help when necessary,” she said. “Life is far too short to suffer needlessly.”
In the interview, Dr. Worley said she adapts her presentations to the venue and the time allowed. Key aspects of her system include:
• Care for your yacht, which is the body, including the brain. “You only get one, and if you’re going to have a chance of winning the regatta, you have to take care of it. This means getting good sleep, nutrition, exercise, preventive care, rest, and rejuvenation, including vacation,” Dr. Worley said.
• Chart your course; have a navigational plan that includes your life goals and aspirations. Identify and rely upon “landmarks,” such as being a good spouse, mother, physician, or friend for the most authentic definition of personal success. “These are like buoys that keep us sailing in the right direction,” she said.
• Reef in your sails, meaning mind the “winds that come at us from every side,” she said. This includes triaging tasks and not letting perfectionism get in the way. “Perfectionists take too long to tack; they don’t know when it’s time to turn in the other direction,” she said. “If you want to finish the race, you have to do the best you can in the time you have.” This was the lesson Dr. Worley said she learned that day when she was a young physician feeling overwhelmed.
• Empty your bilge, the nautical term for removing waste water from within the hull. Dr. Worley uses this as a metaphor for identifying and expressing negative emotions of fear, anxiety, sadness, and frustration. “These vital emotions are giving us important messages. It is important to recognize that they are present. Name and accept them, and understand what they are trying to tell us. Is it a symptom of an underlying illness that needs treatment? A conflict in a relationship? A need not being met? Are you living your deepest values? Express the emotions and sort through the best response,” she said. “It’s all part of emotional intelligence.”
• Keep an even keel, which is Dr. Worley’s way of stating the importance of being connected to love and to living your deepest values. “The keel is your character, your connection to meaning, a spiritual connection. In medicine, we shy away from that. I have only lately ventured into talking about this,” she said, noting that this connection can come in numerous ways, such as meditation, and being in nature or with animals. “It’s very personal. It’s hard to quantify, but I have witnessed it and its healing power within the therapeutic alliance.”
In break-out sessions during her well-attended talk at the meeting, Dr. Worley listened as psychiatrists of all levels of experience and responsibility, ranging from medical directors to those in private community practice, shared the kinds of concerns she said she often encounters in her role as a core faculty member of the Program for Distressed Physicians at the Vanderbilt Center for Professional Health.
“Changes in medicine have been so frustrating; physicians are at their wits’ end. We don’t recruit people into medicine because they have a skill set for expressing their emotions, or taking care of themselves, or dealing with conflict,” she said. “That’s okay. They can learn it.”