User login
Diagnosing Multiple Myeloma in Primary Care
IN THIS ARTICLE
- Presenting symptoms
- Diagnostic tests
- Differential diagnostic criteria
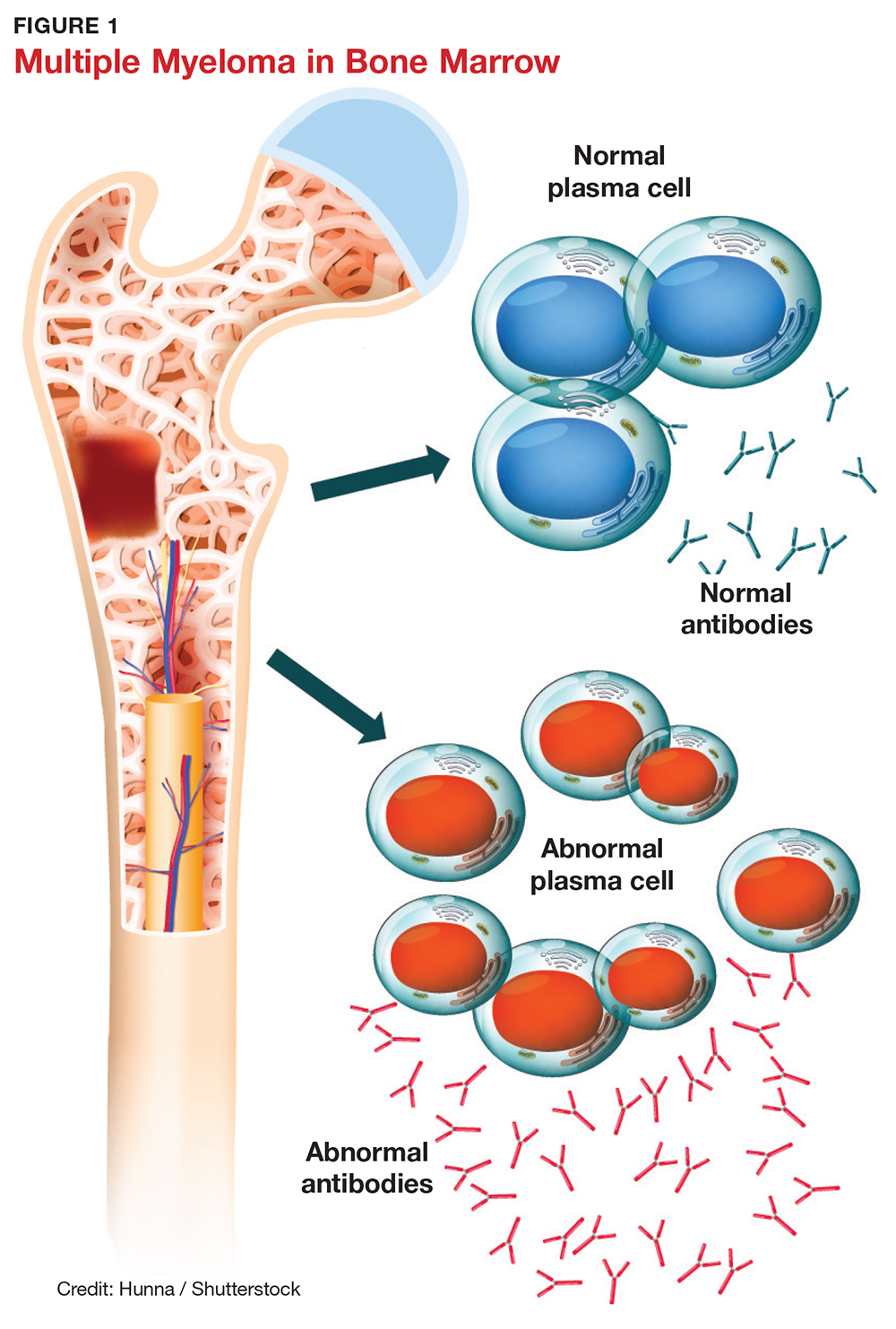
Multiple myeloma (MM) is a fatal, malignant neoplasm that originates in the plasma cells of bone marrow. A genetic mutation in the plasma cells creates myeloma cells, which replicate and produce monoclonal protein (M-protein). This accumulation of cells and abnormal protein can result in destruction and eventual marrow failure.1,2
MM’s insidious nature means it often goes undetected or misdiagnosed in its early stages; this delayed diagnosis can cause sequelae that limit quality of life. Furthermore, the five-year survival rate for myeloma varies by stage at which the disease is diagnosed: from 48% for distant (metastasized) myeloma to 71% for localized disease.3 It has also been noted that, in the past two decades, improvements in available treatment options and supportive care have contributed to a doubling of median survival time (from three years to six years).4 It is therefore paramount that providers be aware of MM and its signs to facilitate early diagnosis and treatment.
INCIDENCE AND EPIDEMIOLOGY
MM accounts for 1% of all cancers and about 10% of all hematologic malignancies.5 In 2017, the American Cancer Society estimated that more than 30,000 new cases of MM would be diagnosed in the United States.6 Additionally, MM was expected to cause more than 12,000 deaths last year.6
Median age at diagnosis is 69.3 In fact, 75% of men are older than 75 and 79% of women are older than 70 at diagnosis.1
Apart from age, other risk factors for MM have been identified but not fully explicated. For example, the disease is more common in men than in women (with men comprising two-thirds of new cases per year).3 MM is also two to three times more common in black than in white persons, making it the most common hematologic malignancy in this demographic group.3,7
The possibility of a genetic predisposition has also been studied. Several analyses have indicated an increased risk for MM in patients with a family history of the disease—as much as four times higher in those with an affected first-degree relative. This risk was further elevated in black compared with white patients (odds ratios, 17.4 and 1.5, respectively).7 However, many patients with MM have no relatives with this disorder.6,8
DISEASE PROGRESSION
Almost all patients who develop MM also experience an asymptomatic premalignant stage called monoclonal gammopathy of undetermined significance (MGUS). MGUS is present in 3% to 4% of the general population older than 50 and is often an incidental finding. This stage almost always precedes MM—but because it is asymptomatic, only 10% of individuals diagnosed with MM have a known history of MGUS.8
In some patients, an asymptomatic intermediate stage called smoldering multiple myeloma (SMM) can be identified. SMM progresses to MM at a rate of 10% per year for the first five years; the rate decreases to 3% per year over the following five years, and 1% per year after that.8
MM is not curable, but as noted, the survival rate is steadily increasing due to rapidly evolving treatment regimens. Discussion of treatment is outside the scope of this article, but early diagnosis can improve quality of life and clinical outcomes and prolong life expectancy.
SYMPTOMS
The initial symptoms of MM can be nonspecific and may lead the provider to suspect a host of other conditions.2,6 (Those for advanced disease are also vague but tend to be more pronounced.) These may include fatigue, weakness, easy bruising or bleeding, and bone pain. Other common clinical manifestations of MM are anemia, chronic infection, bone disease, and/or renal failure.1,4 Patients may also experience loss of appetite, nausea, vomiting, increased thirst, and increased urination.9
Recent studies have shown that patients with SMM and/or MGUS also exhibit early signs of bone disease and increased risk for fracture.10 Eighty percent of patients who progress to MM have evidence of pathologic bone fractures.10 It is also possible for bones in the spine to weaken and collapse, pressing on the spinal nerves. This is known as spinal cord compression, which can manifest with sudden, severe back pain or numbness and/or muscle weakness (most often in the legs).6
MM must be included in the differential diagnosis, particularly when symptoms do not point to one specific disease process. Without early diagnosis, disease progression can result in complications such as bone fracture and osteoporosis, reduced kidney function, peripheral neuropathy, chronic anemia, and ultimately, death.2,6 The presence of bone fractures increases mortality risk by 20%.10
DIAGNOSTIC WORKUP
Evidence of MM may be discovered during routine bloodwork and screening tests, while presenting symptoms or subtle changes in lab results can raise suspicion for the disease. Initial bloodwork abnormalities include anemia, elevated calcium levels, renal insufficiency, and/or elevated protein levels.8
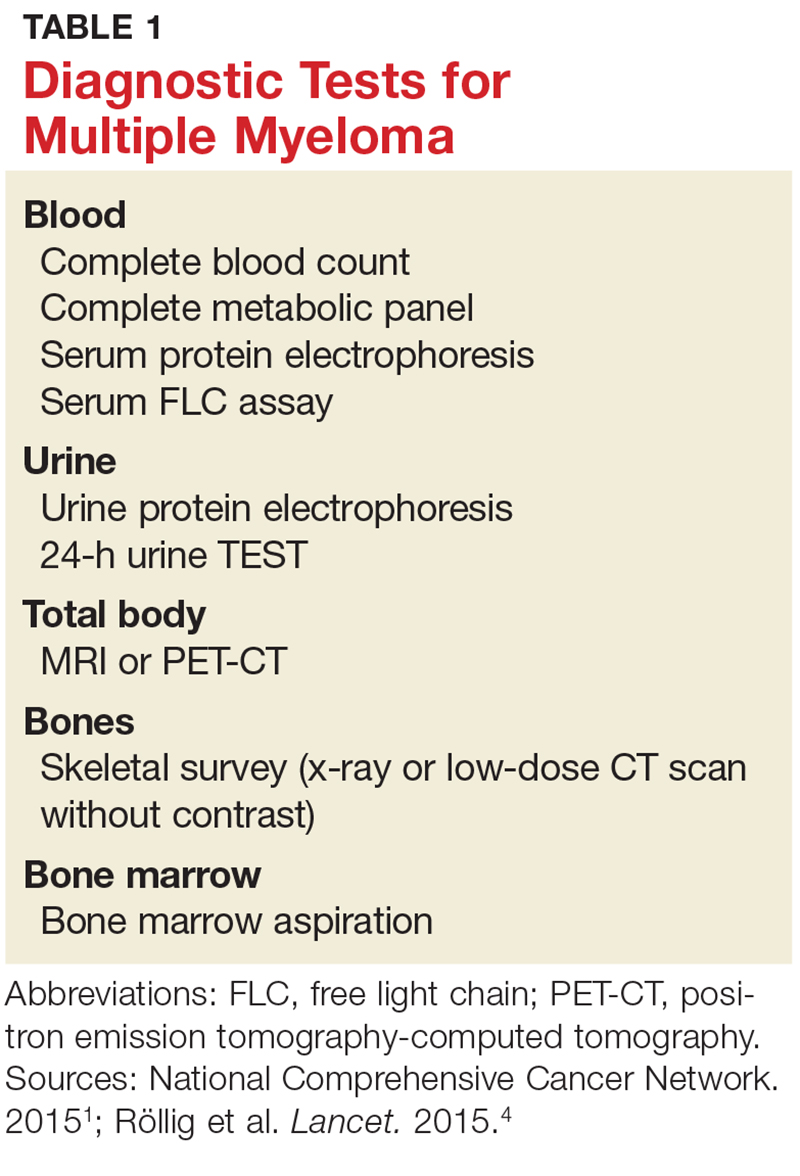
A combination of abnormalities in the complete blood count (CBC) and complete metabolic panel (CMP), along with symptoms, should alert the provider to the possibility of MM, prompting additional workup. Table 1 outlines suggested diagnostic tests; the possible findings are discussed below.
CBC. The CBC may reveal abnormalities including anemia (which occurs in 75% of patients with MM), thrombocytopenia, and leukopenia.1,8 These findings can contribute to fatigue, increased incidence of infection, and abnormal bruising of the skin.2,8
CMP. A CMP may show increases in serum calcium or protein. Hypercalcemia occurs in 15% of patients with MM, leading to symptoms such as loss of appetite, nausea, vomiting, increased urination, weakness, and confusion.8 An increase in protein may alter the albumin/globulin ratio, which should raise suspicion for MM. A decrease in albumin can signify disease severity. Also, the CMP may show worsening renal function and elevated serum creatinine, which occurs in 20% of patients with MM.8
Serum protein electrophoresis (SPEP). Suspicion of MM should prompt the clinician to evaluate proteins via SPEP. This test may be indicated for patients with anemia, hypercalcemia, bone pain, and unexplained neuropathy.9 The electrophoresis separates proteins based on their physical properties. This identifies the presence and amount of M-protein, which can determine the extent of the disease.1 M-protein is identified in approximately 82% of patients with MM using this test.8
Serum free light chain (FLC) assay. This diagnostic test can identify MM in individuals with high clinical suspicion for the disease but no discernible M-protein on SPEP; it increases sensitivity to 97%.8 The serum FLC assay evaluates for presence and ratio of free light chains—proteins produced by plasma cells. This test is also useful for monitoring treatment response and disease progression.1
Urine protein electrophoresis (UPEP). The UPEP separates proteins according to charge, which is helpful for classifying renal injury. Protein patterns are interpreted and may be reported as glomerular, tubular, or mixed. UPEP also tests for M-protein in the urine.1,11
24-hour urine. The 24-h urine test quantifies the amount and type of protein excreted in the urine and helps determine the extent of kidney disease.1
Skeletal survey. MM causes significant bone changes that can be identified with radiographic studies. The most common locations for fractures are the vertebral, pelvic, and clavicular areas.10 Currently, the skeletal survey is the gold standard for detecting fractures and osteolytic lesions associated with MM.10 Radiographic films ordered for other purposes may uncover abnormalities in bones.
Bone mineral density (BMD) test. Most often, BMD testing is used to evaluate treatment and progression of bone involvement. Because it can uncover osteopenia or osteoporosis, however, it can also be used to corroborate the diagnosis of MM.10
Once the presence of M-protein is identified, patients are referred for specialty care. At that time, further workup will include a bone marrow biopsy and imaging studies, such as additional radiographic films, CT scans (without contrast, as contrast dye can damage frail kidneys), and MRI.1,8 These diagnostic tests provide useful information for the classification of the disease and guide initiation of treatment.
CLASSIFICATION OF DISEASE
MM can be classified into three stages—MGUS, SMM, and MM—based on recommendations from the International Myeloma Working Group.12 Table 2 outlines the diagnostic criteria for each stage.
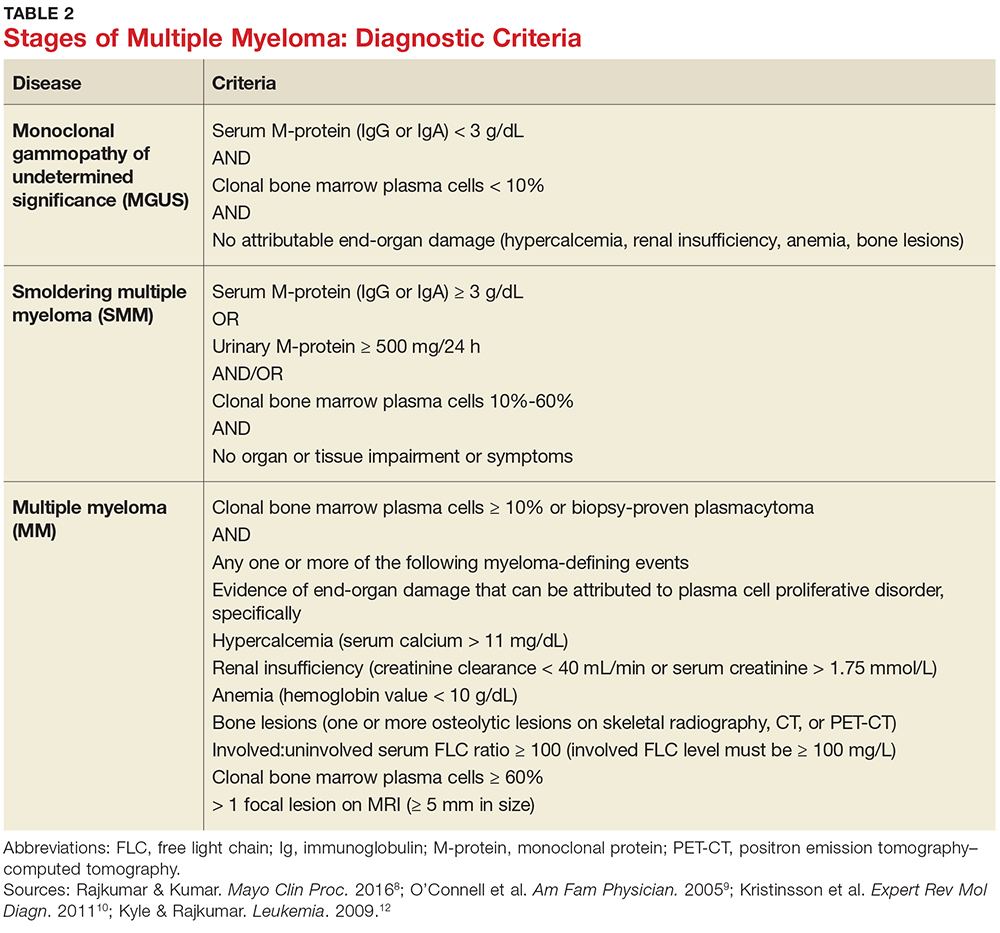
Individuals with MGUS and SMM are considered asymptomatic; guidelines do not recommend treatment for these patients. Those who are diagnosed with MM are referred to oncologists and treated based on current clinical practice guidelines.1
CONCLUSION
Multiple myeloma is a malignant neoplasm without a cure. Presenting symptoms may include anemia, bone pain, elevated creatinine or serum protein, fatigue, and hypercalcemia. Early diagnosis is key to early intervention and treatment, which can improve quality of life and clinical outcomes for those affected. Primary care providers play a major role in recognizing the subtle symptoms and ordering the appropriate diagnostic tests.
1. National Comprehensive Cancer Network. Multiple myeloma. NCCN clinical practice guidelines in oncology version 2.2015.
2. Rajkumar VS. Multiple myeloma symptoms, diagnosis, and staging. www.uptodate.com/contents/clinical-features-laboratory-manifestations-and-diagnosis-of-multiple-myeloma?source=machineLearning&search=multiple+myeloma&selectedTitle=1%7E150§ionRank=1&anchor=H25#H26. Accessed October 16, 2017.
3. National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer stat facts: myeloma. https://seer.cancer.gov/statfacts/html/mulmy.html. Accessed October 26, 2017.
4. Röllig C, Knop S, Bornhäuser M. Multiple myeloma. Lancet. 2015;385(9983):2197-2208.
5. Moreau P, San Miguel J, Sonneveld M, et al. Multiple myeloma: ESMO clinical practice guidelines. Ann Oncol. 2017;28(4):iv52-iv61.
6. American Cancer Society. Multiple myeloma. www.cancer.org/cancer/multiplemyeloma/detailedguide. Accessed October 16, 2017.
7. Koura DT, Langston AA. Inherited predisposition to multiple myeloma. Ther Adv Hematol. 2013;4(4):291-297.
8. Rajkumar SV, Kumar S. Multiple myeloma: diagnosis and treatment. Mayo Clin Proc. 2016;91:101-119.
9. O’Connell T, Horita TJ, Kasravi B. Understanding and interpreting serum electrophoresis. Am Fam Physician. 2005; 71(1):105-112.
10. Kristinsson SY, Minter AR, Korde N, et al. Bone disease in multiple myeloma and precursor disease; novel diagnostic approaches and implications on clinical management. Expert Rev Mol Diagn. 2011;11(6):593-603.
11. Jacobs D, DeMott W, Oxley D. Laboratory Test Handbook: Concise With Disease Index. Hudson, OH: Lexi-Comp; 2004.
12. Kyle RA, Rajkumar SV. Criteria for diagnosis, staging, risk stratification and response assessment of multiple myeloma. Leukemia. 2009;23(1):3-9.
IN THIS ARTICLE
- Presenting symptoms
- Diagnostic tests
- Differential diagnostic criteria
Multiple myeloma (MM) is a fatal, malignant neoplasm that originates in the plasma cells of bone marrow. A genetic mutation in the plasma cells creates myeloma cells, which replicate and produce monoclonal protein (M-protein). This accumulation of cells and abnormal protein can result in destruction and eventual marrow failure.1,2
MM’s insidious nature means it often goes undetected or misdiagnosed in its early stages; this delayed diagnosis can cause sequelae that limit quality of life. Furthermore, the five-year survival rate for myeloma varies by stage at which the disease is diagnosed: from 48% for distant (metastasized) myeloma to 71% for localized disease.3 It has also been noted that, in the past two decades, improvements in available treatment options and supportive care have contributed to a doubling of median survival time (from three years to six years).4 It is therefore paramount that providers be aware of MM and its signs to facilitate early diagnosis and treatment.
INCIDENCE AND EPIDEMIOLOGY
MM accounts for 1% of all cancers and about 10% of all hematologic malignancies.5 In 2017, the American Cancer Society estimated that more than 30,000 new cases of MM would be diagnosed in the United States.6 Additionally, MM was expected to cause more than 12,000 deaths last year.6
Median age at diagnosis is 69.3 In fact, 75% of men are older than 75 and 79% of women are older than 70 at diagnosis.1
Apart from age, other risk factors for MM have been identified but not fully explicated. For example, the disease is more common in men than in women (with men comprising two-thirds of new cases per year).3 MM is also two to three times more common in black than in white persons, making it the most common hematologic malignancy in this demographic group.3,7
The possibility of a genetic predisposition has also been studied. Several analyses have indicated an increased risk for MM in patients with a family history of the disease—as much as four times higher in those with an affected first-degree relative. This risk was further elevated in black compared with white patients (odds ratios, 17.4 and 1.5, respectively).7 However, many patients with MM have no relatives with this disorder.6,8
DISEASE PROGRESSION
Almost all patients who develop MM also experience an asymptomatic premalignant stage called monoclonal gammopathy of undetermined significance (MGUS). MGUS is present in 3% to 4% of the general population older than 50 and is often an incidental finding. This stage almost always precedes MM—but because it is asymptomatic, only 10% of individuals diagnosed with MM have a known history of MGUS.8
In some patients, an asymptomatic intermediate stage called smoldering multiple myeloma (SMM) can be identified. SMM progresses to MM at a rate of 10% per year for the first five years; the rate decreases to 3% per year over the following five years, and 1% per year after that.8
MM is not curable, but as noted, the survival rate is steadily increasing due to rapidly evolving treatment regimens. Discussion of treatment is outside the scope of this article, but early diagnosis can improve quality of life and clinical outcomes and prolong life expectancy.
SYMPTOMS
The initial symptoms of MM can be nonspecific and may lead the provider to suspect a host of other conditions.2,6 (Those for advanced disease are also vague but tend to be more pronounced.) These may include fatigue, weakness, easy bruising or bleeding, and bone pain. Other common clinical manifestations of MM are anemia, chronic infection, bone disease, and/or renal failure.1,4 Patients may also experience loss of appetite, nausea, vomiting, increased thirst, and increased urination.9
Recent studies have shown that patients with SMM and/or MGUS also exhibit early signs of bone disease and increased risk for fracture.10 Eighty percent of patients who progress to MM have evidence of pathologic bone fractures.10 It is also possible for bones in the spine to weaken and collapse, pressing on the spinal nerves. This is known as spinal cord compression, which can manifest with sudden, severe back pain or numbness and/or muscle weakness (most often in the legs).6
MM must be included in the differential diagnosis, particularly when symptoms do not point to one specific disease process. Without early diagnosis, disease progression can result in complications such as bone fracture and osteoporosis, reduced kidney function, peripheral neuropathy, chronic anemia, and ultimately, death.2,6 The presence of bone fractures increases mortality risk by 20%.10
DIAGNOSTIC WORKUP
Evidence of MM may be discovered during routine bloodwork and screening tests, while presenting symptoms or subtle changes in lab results can raise suspicion for the disease. Initial bloodwork abnormalities include anemia, elevated calcium levels, renal insufficiency, and/or elevated protein levels.8
A combination of abnormalities in the complete blood count (CBC) and complete metabolic panel (CMP), along with symptoms, should alert the provider to the possibility of MM, prompting additional workup. Table 1 outlines suggested diagnostic tests; the possible findings are discussed below.
CBC. The CBC may reveal abnormalities including anemia (which occurs in 75% of patients with MM), thrombocytopenia, and leukopenia.1,8 These findings can contribute to fatigue, increased incidence of infection, and abnormal bruising of the skin.2,8
CMP. A CMP may show increases in serum calcium or protein. Hypercalcemia occurs in 15% of patients with MM, leading to symptoms such as loss of appetite, nausea, vomiting, increased urination, weakness, and confusion.8 An increase in protein may alter the albumin/globulin ratio, which should raise suspicion for MM. A decrease in albumin can signify disease severity. Also, the CMP may show worsening renal function and elevated serum creatinine, which occurs in 20% of patients with MM.8
Serum protein electrophoresis (SPEP). Suspicion of MM should prompt the clinician to evaluate proteins via SPEP. This test may be indicated for patients with anemia, hypercalcemia, bone pain, and unexplained neuropathy.9 The electrophoresis separates proteins based on their physical properties. This identifies the presence and amount of M-protein, which can determine the extent of the disease.1 M-protein is identified in approximately 82% of patients with MM using this test.8
Serum free light chain (FLC) assay. This diagnostic test can identify MM in individuals with high clinical suspicion for the disease but no discernible M-protein on SPEP; it increases sensitivity to 97%.8 The serum FLC assay evaluates for presence and ratio of free light chains—proteins produced by plasma cells. This test is also useful for monitoring treatment response and disease progression.1
Urine protein electrophoresis (UPEP). The UPEP separates proteins according to charge, which is helpful for classifying renal injury. Protein patterns are interpreted and may be reported as glomerular, tubular, or mixed. UPEP also tests for M-protein in the urine.1,11
24-hour urine. The 24-h urine test quantifies the amount and type of protein excreted in the urine and helps determine the extent of kidney disease.1
Skeletal survey. MM causes significant bone changes that can be identified with radiographic studies. The most common locations for fractures are the vertebral, pelvic, and clavicular areas.10 Currently, the skeletal survey is the gold standard for detecting fractures and osteolytic lesions associated with MM.10 Radiographic films ordered for other purposes may uncover abnormalities in bones.
Bone mineral density (BMD) test. Most often, BMD testing is used to evaluate treatment and progression of bone involvement. Because it can uncover osteopenia or osteoporosis, however, it can also be used to corroborate the diagnosis of MM.10
Once the presence of M-protein is identified, patients are referred for specialty care. At that time, further workup will include a bone marrow biopsy and imaging studies, such as additional radiographic films, CT scans (without contrast, as contrast dye can damage frail kidneys), and MRI.1,8 These diagnostic tests provide useful information for the classification of the disease and guide initiation of treatment.
CLASSIFICATION OF DISEASE
MM can be classified into three stages—MGUS, SMM, and MM—based on recommendations from the International Myeloma Working Group.12 Table 2 outlines the diagnostic criteria for each stage.
Individuals with MGUS and SMM are considered asymptomatic; guidelines do not recommend treatment for these patients. Those who are diagnosed with MM are referred to oncologists and treated based on current clinical practice guidelines.1
CONCLUSION
Multiple myeloma is a malignant neoplasm without a cure. Presenting symptoms may include anemia, bone pain, elevated creatinine or serum protein, fatigue, and hypercalcemia. Early diagnosis is key to early intervention and treatment, which can improve quality of life and clinical outcomes for those affected. Primary care providers play a major role in recognizing the subtle symptoms and ordering the appropriate diagnostic tests.
IN THIS ARTICLE
- Presenting symptoms
- Diagnostic tests
- Differential diagnostic criteria
Multiple myeloma (MM) is a fatal, malignant neoplasm that originates in the plasma cells of bone marrow. A genetic mutation in the plasma cells creates myeloma cells, which replicate and produce monoclonal protein (M-protein). This accumulation of cells and abnormal protein can result in destruction and eventual marrow failure.1,2
MM’s insidious nature means it often goes undetected or misdiagnosed in its early stages; this delayed diagnosis can cause sequelae that limit quality of life. Furthermore, the five-year survival rate for myeloma varies by stage at which the disease is diagnosed: from 48% for distant (metastasized) myeloma to 71% for localized disease.3 It has also been noted that, in the past two decades, improvements in available treatment options and supportive care have contributed to a doubling of median survival time (from three years to six years).4 It is therefore paramount that providers be aware of MM and its signs to facilitate early diagnosis and treatment.
INCIDENCE AND EPIDEMIOLOGY
MM accounts for 1% of all cancers and about 10% of all hematologic malignancies.5 In 2017, the American Cancer Society estimated that more than 30,000 new cases of MM would be diagnosed in the United States.6 Additionally, MM was expected to cause more than 12,000 deaths last year.6
Median age at diagnosis is 69.3 In fact, 75% of men are older than 75 and 79% of women are older than 70 at diagnosis.1
Apart from age, other risk factors for MM have been identified but not fully explicated. For example, the disease is more common in men than in women (with men comprising two-thirds of new cases per year).3 MM is also two to three times more common in black than in white persons, making it the most common hematologic malignancy in this demographic group.3,7
The possibility of a genetic predisposition has also been studied. Several analyses have indicated an increased risk for MM in patients with a family history of the disease—as much as four times higher in those with an affected first-degree relative. This risk was further elevated in black compared with white patients (odds ratios, 17.4 and 1.5, respectively).7 However, many patients with MM have no relatives with this disorder.6,8
DISEASE PROGRESSION
Almost all patients who develop MM also experience an asymptomatic premalignant stage called monoclonal gammopathy of undetermined significance (MGUS). MGUS is present in 3% to 4% of the general population older than 50 and is often an incidental finding. This stage almost always precedes MM—but because it is asymptomatic, only 10% of individuals diagnosed with MM have a known history of MGUS.8
In some patients, an asymptomatic intermediate stage called smoldering multiple myeloma (SMM) can be identified. SMM progresses to MM at a rate of 10% per year for the first five years; the rate decreases to 3% per year over the following five years, and 1% per year after that.8
MM is not curable, but as noted, the survival rate is steadily increasing due to rapidly evolving treatment regimens. Discussion of treatment is outside the scope of this article, but early diagnosis can improve quality of life and clinical outcomes and prolong life expectancy.
SYMPTOMS
The initial symptoms of MM can be nonspecific and may lead the provider to suspect a host of other conditions.2,6 (Those for advanced disease are also vague but tend to be more pronounced.) These may include fatigue, weakness, easy bruising or bleeding, and bone pain. Other common clinical manifestations of MM are anemia, chronic infection, bone disease, and/or renal failure.1,4 Patients may also experience loss of appetite, nausea, vomiting, increased thirst, and increased urination.9
Recent studies have shown that patients with SMM and/or MGUS also exhibit early signs of bone disease and increased risk for fracture.10 Eighty percent of patients who progress to MM have evidence of pathologic bone fractures.10 It is also possible for bones in the spine to weaken and collapse, pressing on the spinal nerves. This is known as spinal cord compression, which can manifest with sudden, severe back pain or numbness and/or muscle weakness (most often in the legs).6
MM must be included in the differential diagnosis, particularly when symptoms do not point to one specific disease process. Without early diagnosis, disease progression can result in complications such as bone fracture and osteoporosis, reduced kidney function, peripheral neuropathy, chronic anemia, and ultimately, death.2,6 The presence of bone fractures increases mortality risk by 20%.10
DIAGNOSTIC WORKUP
Evidence of MM may be discovered during routine bloodwork and screening tests, while presenting symptoms or subtle changes in lab results can raise suspicion for the disease. Initial bloodwork abnormalities include anemia, elevated calcium levels, renal insufficiency, and/or elevated protein levels.8
A combination of abnormalities in the complete blood count (CBC) and complete metabolic panel (CMP), along with symptoms, should alert the provider to the possibility of MM, prompting additional workup. Table 1 outlines suggested diagnostic tests; the possible findings are discussed below.
CBC. The CBC may reveal abnormalities including anemia (which occurs in 75% of patients with MM), thrombocytopenia, and leukopenia.1,8 These findings can contribute to fatigue, increased incidence of infection, and abnormal bruising of the skin.2,8
CMP. A CMP may show increases in serum calcium or protein. Hypercalcemia occurs in 15% of patients with MM, leading to symptoms such as loss of appetite, nausea, vomiting, increased urination, weakness, and confusion.8 An increase in protein may alter the albumin/globulin ratio, which should raise suspicion for MM. A decrease in albumin can signify disease severity. Also, the CMP may show worsening renal function and elevated serum creatinine, which occurs in 20% of patients with MM.8
Serum protein electrophoresis (SPEP). Suspicion of MM should prompt the clinician to evaluate proteins via SPEP. This test may be indicated for patients with anemia, hypercalcemia, bone pain, and unexplained neuropathy.9 The electrophoresis separates proteins based on their physical properties. This identifies the presence and amount of M-protein, which can determine the extent of the disease.1 M-protein is identified in approximately 82% of patients with MM using this test.8
Serum free light chain (FLC) assay. This diagnostic test can identify MM in individuals with high clinical suspicion for the disease but no discernible M-protein on SPEP; it increases sensitivity to 97%.8 The serum FLC assay evaluates for presence and ratio of free light chains—proteins produced by plasma cells. This test is also useful for monitoring treatment response and disease progression.1
Urine protein electrophoresis (UPEP). The UPEP separates proteins according to charge, which is helpful for classifying renal injury. Protein patterns are interpreted and may be reported as glomerular, tubular, or mixed. UPEP also tests for M-protein in the urine.1,11
24-hour urine. The 24-h urine test quantifies the amount and type of protein excreted in the urine and helps determine the extent of kidney disease.1
Skeletal survey. MM causes significant bone changes that can be identified with radiographic studies. The most common locations for fractures are the vertebral, pelvic, and clavicular areas.10 Currently, the skeletal survey is the gold standard for detecting fractures and osteolytic lesions associated with MM.10 Radiographic films ordered for other purposes may uncover abnormalities in bones.
Bone mineral density (BMD) test. Most often, BMD testing is used to evaluate treatment and progression of bone involvement. Because it can uncover osteopenia or osteoporosis, however, it can also be used to corroborate the diagnosis of MM.10
Once the presence of M-protein is identified, patients are referred for specialty care. At that time, further workup will include a bone marrow biopsy and imaging studies, such as additional radiographic films, CT scans (without contrast, as contrast dye can damage frail kidneys), and MRI.1,8 These diagnostic tests provide useful information for the classification of the disease and guide initiation of treatment.
CLASSIFICATION OF DISEASE
MM can be classified into three stages—MGUS, SMM, and MM—based on recommendations from the International Myeloma Working Group.12 Table 2 outlines the diagnostic criteria for each stage.
Individuals with MGUS and SMM are considered asymptomatic; guidelines do not recommend treatment for these patients. Those who are diagnosed with MM are referred to oncologists and treated based on current clinical practice guidelines.1
CONCLUSION
Multiple myeloma is a malignant neoplasm without a cure. Presenting symptoms may include anemia, bone pain, elevated creatinine or serum protein, fatigue, and hypercalcemia. Early diagnosis is key to early intervention and treatment, which can improve quality of life and clinical outcomes for those affected. Primary care providers play a major role in recognizing the subtle symptoms and ordering the appropriate diagnostic tests.
1. National Comprehensive Cancer Network. Multiple myeloma. NCCN clinical practice guidelines in oncology version 2.2015.
2. Rajkumar VS. Multiple myeloma symptoms, diagnosis, and staging. www.uptodate.com/contents/clinical-features-laboratory-manifestations-and-diagnosis-of-multiple-myeloma?source=machineLearning&search=multiple+myeloma&selectedTitle=1%7E150§ionRank=1&anchor=H25#H26. Accessed October 16, 2017.
3. National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer stat facts: myeloma. https://seer.cancer.gov/statfacts/html/mulmy.html. Accessed October 26, 2017.
4. Röllig C, Knop S, Bornhäuser M. Multiple myeloma. Lancet. 2015;385(9983):2197-2208.
5. Moreau P, San Miguel J, Sonneveld M, et al. Multiple myeloma: ESMO clinical practice guidelines. Ann Oncol. 2017;28(4):iv52-iv61.
6. American Cancer Society. Multiple myeloma. www.cancer.org/cancer/multiplemyeloma/detailedguide. Accessed October 16, 2017.
7. Koura DT, Langston AA. Inherited predisposition to multiple myeloma. Ther Adv Hematol. 2013;4(4):291-297.
8. Rajkumar SV, Kumar S. Multiple myeloma: diagnosis and treatment. Mayo Clin Proc. 2016;91:101-119.
9. O’Connell T, Horita TJ, Kasravi B. Understanding and interpreting serum electrophoresis. Am Fam Physician. 2005; 71(1):105-112.
10. Kristinsson SY, Minter AR, Korde N, et al. Bone disease in multiple myeloma and precursor disease; novel diagnostic approaches and implications on clinical management. Expert Rev Mol Diagn. 2011;11(6):593-603.
11. Jacobs D, DeMott W, Oxley D. Laboratory Test Handbook: Concise With Disease Index. Hudson, OH: Lexi-Comp; 2004.
12. Kyle RA, Rajkumar SV. Criteria for diagnosis, staging, risk stratification and response assessment of multiple myeloma. Leukemia. 2009;23(1):3-9.
1. National Comprehensive Cancer Network. Multiple myeloma. NCCN clinical practice guidelines in oncology version 2.2015.
2. Rajkumar VS. Multiple myeloma symptoms, diagnosis, and staging. www.uptodate.com/contents/clinical-features-laboratory-manifestations-and-diagnosis-of-multiple-myeloma?source=machineLearning&search=multiple+myeloma&selectedTitle=1%7E150§ionRank=1&anchor=H25#H26. Accessed October 16, 2017.
3. National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer stat facts: myeloma. https://seer.cancer.gov/statfacts/html/mulmy.html. Accessed October 26, 2017.
4. Röllig C, Knop S, Bornhäuser M. Multiple myeloma. Lancet. 2015;385(9983):2197-2208.
5. Moreau P, San Miguel J, Sonneveld M, et al. Multiple myeloma: ESMO clinical practice guidelines. Ann Oncol. 2017;28(4):iv52-iv61.
6. American Cancer Society. Multiple myeloma. www.cancer.org/cancer/multiplemyeloma/detailedguide. Accessed October 16, 2017.
7. Koura DT, Langston AA. Inherited predisposition to multiple myeloma. Ther Adv Hematol. 2013;4(4):291-297.
8. Rajkumar SV, Kumar S. Multiple myeloma: diagnosis and treatment. Mayo Clin Proc. 2016;91:101-119.
9. O’Connell T, Horita TJ, Kasravi B. Understanding and interpreting serum electrophoresis. Am Fam Physician. 2005; 71(1):105-112.
10. Kristinsson SY, Minter AR, Korde N, et al. Bone disease in multiple myeloma and precursor disease; novel diagnostic approaches and implications on clinical management. Expert Rev Mol Diagn. 2011;11(6):593-603.
11. Jacobs D, DeMott W, Oxley D. Laboratory Test Handbook: Concise With Disease Index. Hudson, OH: Lexi-Comp; 2004.
12. Kyle RA, Rajkumar SV. Criteria for diagnosis, staging, risk stratification and response assessment of multiple myeloma. Leukemia. 2009;23(1):3-9.
Vascular Risk: What’s Really Important?
This video was filmed at Metabolic & Endocrine Disease Summit (MEDS). Click here to learn more.
This video was filmed at Metabolic & Endocrine Disease Summit (MEDS). Click here to learn more.
This video was filmed at Metabolic & Endocrine Disease Summit (MEDS). Click here to learn more.
Antiviral receives breakthrough designation for CMV

The US Food and Drug Administration (FDA) has granted breakthrough therapy designation to maribavir (SHP620) as a treatment for cytomegalovirus (CMV) infection and disease in transplant recipients who are resistant or refractory to prior therapy.
Maribavir, an antiviral therapy that belongs to a class of drugs called benzimidazole ribosides, is being evaluated in patients who have CMV infection after undergoing hematopoietic stem cell transplant or solid organ transplant.
The drug inhibits the CMV UL97 protein kinase and is thought to affect several critical processes in CMV replication, including viral DNA synthesis, viral gene expression, encapsidation, and egress of mature capsids from the nucleus.
The FDA granted maribavir breakthrough designation based on data from two phase 2 studies. For one of these studies (NCT00223925), data are not yet available.
The other study (NCT01611974) was presented at IDWeek 2016. This study included 120 patients ages 12 and older with CMV infection (≥1000 DNA copies/mL of blood plasma) that was resistant or refractory to (val)ganciclovir or foscarnet.
Forty-seven of the patients had received a hematopoietic stem cell transplant, and 73 had a solid organ transplant.
The patients were randomized to 1 of 3 twice-daily oral doses of maribavir—400 mg, 800 mg, or 1200 mg—for up to 24 weeks of treatment.
The study’s primary efficacy endpoint was the proportion of patients with confirmed undetectable plasma CMV DNA within 6 weeks of treatment. Sixty-seven percent (80/120) of patients met this endpoint. This included 70% (n=28) of patients in the 400 mg group, 63% (n=25) in the 800 mg group, and 67% (n=27) in the 1200 mg group.
CMV infection recurred in 30 patients, including 7 in the 400 mg group, 11 in the 800 mg group, and 12 in the 1200 mg group.
The incidence of treatment-emergent adverse events (AEs) was 78% (n=93) overall, 78% (n=31) in the 400 mg group, 80% (n=32) in the 800 mg group, and 75% (n=30) in the 1200 mg group.
Twenty-seven percent of patients died due to any AE, 1 of which (multi-organ failure) was considered possibly related to maribavir.
Forty-one patients (34%) discontinued treatment with maribavir due to an AE, including 17 patients who discontinued due to CMV infection.
Dysgeusia was the most common treatment-emergent AE and led to treatment discontinuation in 1 patient. Dysgeusia occurred in 65% (n=78) of all patients, including 60% (n=24) in the 400 mg group, 63% (n=25) in the 800 mg group, and 73% (n=29) in the 1200 mg group.
About breakthrough designation
The FDA’s breakthrough designation is intended to expedite the development and review of new treatments for serious or life-threatening conditions.
The designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need. ![]()
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation to maribavir (SHP620) as a treatment for cytomegalovirus (CMV) infection and disease in transplant recipients who are resistant or refractory to prior therapy.
Maribavir, an antiviral therapy that belongs to a class of drugs called benzimidazole ribosides, is being evaluated in patients who have CMV infection after undergoing hematopoietic stem cell transplant or solid organ transplant.
The drug inhibits the CMV UL97 protein kinase and is thought to affect several critical processes in CMV replication, including viral DNA synthesis, viral gene expression, encapsidation, and egress of mature capsids from the nucleus.
The FDA granted maribavir breakthrough designation based on data from two phase 2 studies. For one of these studies (NCT00223925), data are not yet available.
The other study (NCT01611974) was presented at IDWeek 2016. This study included 120 patients ages 12 and older with CMV infection (≥1000 DNA copies/mL of blood plasma) that was resistant or refractory to (val)ganciclovir or foscarnet.
Forty-seven of the patients had received a hematopoietic stem cell transplant, and 73 had a solid organ transplant.
The patients were randomized to 1 of 3 twice-daily oral doses of maribavir—400 mg, 800 mg, or 1200 mg—for up to 24 weeks of treatment.
The study’s primary efficacy endpoint was the proportion of patients with confirmed undetectable plasma CMV DNA within 6 weeks of treatment. Sixty-seven percent (80/120) of patients met this endpoint. This included 70% (n=28) of patients in the 400 mg group, 63% (n=25) in the 800 mg group, and 67% (n=27) in the 1200 mg group.
CMV infection recurred in 30 patients, including 7 in the 400 mg group, 11 in the 800 mg group, and 12 in the 1200 mg group.
The incidence of treatment-emergent adverse events (AEs) was 78% (n=93) overall, 78% (n=31) in the 400 mg group, 80% (n=32) in the 800 mg group, and 75% (n=30) in the 1200 mg group.
Twenty-seven percent of patients died due to any AE, 1 of which (multi-organ failure) was considered possibly related to maribavir.
Forty-one patients (34%) discontinued treatment with maribavir due to an AE, including 17 patients who discontinued due to CMV infection.
Dysgeusia was the most common treatment-emergent AE and led to treatment discontinuation in 1 patient. Dysgeusia occurred in 65% (n=78) of all patients, including 60% (n=24) in the 400 mg group, 63% (n=25) in the 800 mg group, and 73% (n=29) in the 1200 mg group.
About breakthrough designation
The FDA’s breakthrough designation is intended to expedite the development and review of new treatments for serious or life-threatening conditions.
The designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need. ![]()
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation to maribavir (SHP620) as a treatment for cytomegalovirus (CMV) infection and disease in transplant recipients who are resistant or refractory to prior therapy.
Maribavir, an antiviral therapy that belongs to a class of drugs called benzimidazole ribosides, is being evaluated in patients who have CMV infection after undergoing hematopoietic stem cell transplant or solid organ transplant.
The drug inhibits the CMV UL97 protein kinase and is thought to affect several critical processes in CMV replication, including viral DNA synthesis, viral gene expression, encapsidation, and egress of mature capsids from the nucleus.
The FDA granted maribavir breakthrough designation based on data from two phase 2 studies. For one of these studies (NCT00223925), data are not yet available.
The other study (NCT01611974) was presented at IDWeek 2016. This study included 120 patients ages 12 and older with CMV infection (≥1000 DNA copies/mL of blood plasma) that was resistant or refractory to (val)ganciclovir or foscarnet.
Forty-seven of the patients had received a hematopoietic stem cell transplant, and 73 had a solid organ transplant.
The patients were randomized to 1 of 3 twice-daily oral doses of maribavir—400 mg, 800 mg, or 1200 mg—for up to 24 weeks of treatment.
The study’s primary efficacy endpoint was the proportion of patients with confirmed undetectable plasma CMV DNA within 6 weeks of treatment. Sixty-seven percent (80/120) of patients met this endpoint. This included 70% (n=28) of patients in the 400 mg group, 63% (n=25) in the 800 mg group, and 67% (n=27) in the 1200 mg group.
CMV infection recurred in 30 patients, including 7 in the 400 mg group, 11 in the 800 mg group, and 12 in the 1200 mg group.
The incidence of treatment-emergent adverse events (AEs) was 78% (n=93) overall, 78% (n=31) in the 400 mg group, 80% (n=32) in the 800 mg group, and 75% (n=30) in the 1200 mg group.
Twenty-seven percent of patients died due to any AE, 1 of which (multi-organ failure) was considered possibly related to maribavir.
Forty-one patients (34%) discontinued treatment with maribavir due to an AE, including 17 patients who discontinued due to CMV infection.
Dysgeusia was the most common treatment-emergent AE and led to treatment discontinuation in 1 patient. Dysgeusia occurred in 65% (n=78) of all patients, including 60% (n=24) in the 400 mg group, 63% (n=25) in the 800 mg group, and 73% (n=29) in the 1200 mg group.
About breakthrough designation
The FDA’s breakthrough designation is intended to expedite the development and review of new treatments for serious or life-threatening conditions.
The designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need. ![]()
FDA approves denosumab for MM patients

The US Food and Drug Administration (FDA) has approved denosumab (XGEVA®) for use in patients with multiple myeloma (MM).
The drug was previously approved to prevent skeletal-related events in patients with bone metastases from solid tumors.
Now, denosumab is FDA-approved to prevent skeletal-related events in MM patients as well.
Denosumab is a fully human monoclonal antibody that binds to and neutralizes RANK ligand—a protein essential for the formation, function, and survival of osteoclasts—thereby inhibiting osteoclast-mediated bone destruction.
The FDA’s approval of denosumab in MM is based on data from the phase 3 '482 study, which were presented at the 2017 ASCO Annual Meeting last June.
In this trial, researchers compared denosumab to zoledronic acid for the prevention of skeletal-related events in 1718 adults with newly diagnosed MM and bone disease.
Patients were randomized to receive either subcutaneous denosumab at 120 mg and intravenous placebo every 4 weeks (n=859) or intravenous zoledronic acid at 4 mg (adjusted for renal function) and subcutaneous placebo every 4 weeks (n=859).
Denosumab proved non-inferior to zoledronic acid in delaying the time to first on-study skeletal-related event (pathologic fracture, radiation to bone, surgery to bone, or spinal cord compression). The hazard ratio (HR) was 0.98 (95% CI: 0.85, 1.14; P=0.01).
Denosumab was not superior to zoledronic acid in delaying the time to a first skeletal-related event or delaying the time to first-and-subsequent skeletal-related events.
Overall survival was comparable between the treatment arms. The HR was 0.90 (95% CI: 0.70, 1.16; P=0.41).
The median difference in progression-free survival favored denosumab by 10.7 months (HR=0.82, 95% CI: 0.68-0.99; descriptive P=0.036). The median progression-free survival was 46.1 months for denosumab and 35.4 months for zoledronic acid.
The most common adverse events in patients who received denosumab were diarrhea (34%), nausea (32%), anemia (22%), back pain (21%), thrombocytopenia (19%), peripheral edema (17%), hypocalcemia (16%), upper respiratory tract infection (15%), rash (14%) and headache (11%).
The most common adverse event resulting in discontinuation of denosumab was osteonecrosis of the jaw.
In the primary treatment phase of the study, osteonecrosis of the jaw was confirmed in 4.1% of patients in the denosumab arm (median exposure of 16 months; range, 1-50) and 2.8% of those in the zoledronic acid arm (median 15 months; range, 1-45 months). ![]()
The US Food and Drug Administration (FDA) has approved denosumab (XGEVA®) for use in patients with multiple myeloma (MM).
The drug was previously approved to prevent skeletal-related events in patients with bone metastases from solid tumors.
Now, denosumab is FDA-approved to prevent skeletal-related events in MM patients as well.
Denosumab is a fully human monoclonal antibody that binds to and neutralizes RANK ligand—a protein essential for the formation, function, and survival of osteoclasts—thereby inhibiting osteoclast-mediated bone destruction.
The FDA’s approval of denosumab in MM is based on data from the phase 3 '482 study, which were presented at the 2017 ASCO Annual Meeting last June.
In this trial, researchers compared denosumab to zoledronic acid for the prevention of skeletal-related events in 1718 adults with newly diagnosed MM and bone disease.
Patients were randomized to receive either subcutaneous denosumab at 120 mg and intravenous placebo every 4 weeks (n=859) or intravenous zoledronic acid at 4 mg (adjusted for renal function) and subcutaneous placebo every 4 weeks (n=859).
Denosumab proved non-inferior to zoledronic acid in delaying the time to first on-study skeletal-related event (pathologic fracture, radiation to bone, surgery to bone, or spinal cord compression). The hazard ratio (HR) was 0.98 (95% CI: 0.85, 1.14; P=0.01).
Denosumab was not superior to zoledronic acid in delaying the time to a first skeletal-related event or delaying the time to first-and-subsequent skeletal-related events.
Overall survival was comparable between the treatment arms. The HR was 0.90 (95% CI: 0.70, 1.16; P=0.41).
The median difference in progression-free survival favored denosumab by 10.7 months (HR=0.82, 95% CI: 0.68-0.99; descriptive P=0.036). The median progression-free survival was 46.1 months for denosumab and 35.4 months for zoledronic acid.
The most common adverse events in patients who received denosumab were diarrhea (34%), nausea (32%), anemia (22%), back pain (21%), thrombocytopenia (19%), peripheral edema (17%), hypocalcemia (16%), upper respiratory tract infection (15%), rash (14%) and headache (11%).
The most common adverse event resulting in discontinuation of denosumab was osteonecrosis of the jaw.
In the primary treatment phase of the study, osteonecrosis of the jaw was confirmed in 4.1% of patients in the denosumab arm (median exposure of 16 months; range, 1-50) and 2.8% of those in the zoledronic acid arm (median 15 months; range, 1-45 months). ![]()
The US Food and Drug Administration (FDA) has approved denosumab (XGEVA®) for use in patients with multiple myeloma (MM).
The drug was previously approved to prevent skeletal-related events in patients with bone metastases from solid tumors.
Now, denosumab is FDA-approved to prevent skeletal-related events in MM patients as well.
Denosumab is a fully human monoclonal antibody that binds to and neutralizes RANK ligand—a protein essential for the formation, function, and survival of osteoclasts—thereby inhibiting osteoclast-mediated bone destruction.
The FDA’s approval of denosumab in MM is based on data from the phase 3 '482 study, which were presented at the 2017 ASCO Annual Meeting last June.
In this trial, researchers compared denosumab to zoledronic acid for the prevention of skeletal-related events in 1718 adults with newly diagnosed MM and bone disease.
Patients were randomized to receive either subcutaneous denosumab at 120 mg and intravenous placebo every 4 weeks (n=859) or intravenous zoledronic acid at 4 mg (adjusted for renal function) and subcutaneous placebo every 4 weeks (n=859).
Denosumab proved non-inferior to zoledronic acid in delaying the time to first on-study skeletal-related event (pathologic fracture, radiation to bone, surgery to bone, or spinal cord compression). The hazard ratio (HR) was 0.98 (95% CI: 0.85, 1.14; P=0.01).
Denosumab was not superior to zoledronic acid in delaying the time to a first skeletal-related event or delaying the time to first-and-subsequent skeletal-related events.
Overall survival was comparable between the treatment arms. The HR was 0.90 (95% CI: 0.70, 1.16; P=0.41).
The median difference in progression-free survival favored denosumab by 10.7 months (HR=0.82, 95% CI: 0.68-0.99; descriptive P=0.036). The median progression-free survival was 46.1 months for denosumab and 35.4 months for zoledronic acid.
The most common adverse events in patients who received denosumab were diarrhea (34%), nausea (32%), anemia (22%), back pain (21%), thrombocytopenia (19%), peripheral edema (17%), hypocalcemia (16%), upper respiratory tract infection (15%), rash (14%) and headache (11%).
The most common adverse event resulting in discontinuation of denosumab was osteonecrosis of the jaw.
In the primary treatment phase of the study, osteonecrosis of the jaw was confirmed in 4.1% of patients in the denosumab arm (median exposure of 16 months; range, 1-50) and 2.8% of those in the zoledronic acid arm (median 15 months; range, 1-45 months). ![]()
Rituximab tackles relapse of severe, difficult-to-treat pemphigus
, based on data from a case series of 11 patients.
“We found that treatment with rituximab alone, even at a low dose, not only prevented relapse but also maintained complete remission with a better benefit-to-risk ratio than treatment with corticosteroids,” Julia Sanchez, MD, of Reims (France) University Hospital and her colleagues reported in a research letter in JAMA Dermatology.
The study population consisted of patients diagnosed with pemphigus at a single center from Jan. 1, 2014, to Dec. 31, 2014, and treated with at least one cycle of rituximab for corticosteroid dependence, corticosteroid resistance, or adverse events. All the patients were in remission at the time of the first maintenance dose of rituximab.
All patients received a 1-g rituximab infusion every 6 months for 24-67 months; some patients changed to a once-yearly dose after 18 months. Although 5 patients experienced grade 3 or 4 adverse events (1 patient had sepsis; 2, diabetes; 1, hypertension; and 2, endocrine disorders) between the initial therapy cycle and the first rituximab maintenance infusion, no adverse events were reported by any of the 11 patients during the maintenance therapy period.
All 11 patients remained in remission after their last follow-up visit (an average of 78 months after the first cycle), at which point 10 patients had discontinued the therapy.
“A progressive decrease in serum anti-desmoglein autoantibody levels to less than 14 U/mL occurred in all cases along with clinical complete remission even after maintenance therapy cessation,” Dr. Sanchez and her associates noted.
Future research should address questions including the optimal dose and dosing frequency of rituximab, as well as the cost-effectiveness of the treatment and criteria for treatment withdrawal, they said.
The researchers had no relevant financial conflicts disclosures.
SOURCE: JAMA Dermatol. 2017 Jan 3. doi: 10.1001/jamadermatol.2017.5176.
, based on data from a case series of 11 patients.
“We found that treatment with rituximab alone, even at a low dose, not only prevented relapse but also maintained complete remission with a better benefit-to-risk ratio than treatment with corticosteroids,” Julia Sanchez, MD, of Reims (France) University Hospital and her colleagues reported in a research letter in JAMA Dermatology.
The study population consisted of patients diagnosed with pemphigus at a single center from Jan. 1, 2014, to Dec. 31, 2014, and treated with at least one cycle of rituximab for corticosteroid dependence, corticosteroid resistance, or adverse events. All the patients were in remission at the time of the first maintenance dose of rituximab.
All patients received a 1-g rituximab infusion every 6 months for 24-67 months; some patients changed to a once-yearly dose after 18 months. Although 5 patients experienced grade 3 or 4 adverse events (1 patient had sepsis; 2, diabetes; 1, hypertension; and 2, endocrine disorders) between the initial therapy cycle and the first rituximab maintenance infusion, no adverse events were reported by any of the 11 patients during the maintenance therapy period.
All 11 patients remained in remission after their last follow-up visit (an average of 78 months after the first cycle), at which point 10 patients had discontinued the therapy.
“A progressive decrease in serum anti-desmoglein autoantibody levels to less than 14 U/mL occurred in all cases along with clinical complete remission even after maintenance therapy cessation,” Dr. Sanchez and her associates noted.
Future research should address questions including the optimal dose and dosing frequency of rituximab, as well as the cost-effectiveness of the treatment and criteria for treatment withdrawal, they said.
The researchers had no relevant financial conflicts disclosures.
SOURCE: JAMA Dermatol. 2017 Jan 3. doi: 10.1001/jamadermatol.2017.5176.
, based on data from a case series of 11 patients.
“We found that treatment with rituximab alone, even at a low dose, not only prevented relapse but also maintained complete remission with a better benefit-to-risk ratio than treatment with corticosteroids,” Julia Sanchez, MD, of Reims (France) University Hospital and her colleagues reported in a research letter in JAMA Dermatology.
The study population consisted of patients diagnosed with pemphigus at a single center from Jan. 1, 2014, to Dec. 31, 2014, and treated with at least one cycle of rituximab for corticosteroid dependence, corticosteroid resistance, or adverse events. All the patients were in remission at the time of the first maintenance dose of rituximab.
All patients received a 1-g rituximab infusion every 6 months for 24-67 months; some patients changed to a once-yearly dose after 18 months. Although 5 patients experienced grade 3 or 4 adverse events (1 patient had sepsis; 2, diabetes; 1, hypertension; and 2, endocrine disorders) between the initial therapy cycle and the first rituximab maintenance infusion, no adverse events were reported by any of the 11 patients during the maintenance therapy period.
All 11 patients remained in remission after their last follow-up visit (an average of 78 months after the first cycle), at which point 10 patients had discontinued the therapy.
“A progressive decrease in serum anti-desmoglein autoantibody levels to less than 14 U/mL occurred in all cases along with clinical complete remission even after maintenance therapy cessation,” Dr. Sanchez and her associates noted.
Future research should address questions including the optimal dose and dosing frequency of rituximab, as well as the cost-effectiveness of the treatment and criteria for treatment withdrawal, they said.
The researchers had no relevant financial conflicts disclosures.
SOURCE: JAMA Dermatol. 2017 Jan 3. doi: 10.1001/jamadermatol.2017.5176.
FROM JAMA DERMATOLOGY
Key clinical point: Treatment with rituximab prevented relapse and maintained remission in 11 patients with severe, difficult-to-treat pemphigus.
Major finding: All 11 patients treated with a 1-g dose of rituximab given every 6 months maintained remission at an average of 78 months after the first cycle.
Data source: The data come from a single-center, retrospective case series of 11 adults.
Disclosures: The researchers had no relevant financial disclosures.
Source: JAMA Dermatol. 2017 Jan 3. doi: 10.1001/jamadermatol.2017.5176.
FDA cites manufacturer of autologous stem cells for regulatory, manufacturing missteps
for manufacturing processes that may compromise its safety and for failing to toe the regulatory line in marketing.
American CryoStem received an FDA warning letter Jan. 3 demanding that the company comply with best-manufacturing processes and obtain an investigational new drug application if it wishes to continue marketing ATCELL for its currently advertised clinical indications and administration routes. These include intravenous, intrathecal, or aerosol inhalation of the product for anoxic brain injury, Parkinson’s disease, amyotrophic lateral sclerosis, stroke, and multiple sclerosis.
“Please be advised that, to lawfully market a drug that is a biological product, a valid biologics license must be in effect,” noted the letter. “Such licenses are issued only after a showing that the product is safe, pure, and potent. While in the development stage, such products may be distributed for clinical use in humans only if the sponsor has an investigational new drug application (IND) in effect as specified by FDA regulations. ATCELL is not the subject of an approved biologics license application nor is there an IND in effect. Based on this information, we have determined that your actions have violated the Food, Drug, and Cosmetic Act and the Public Health Service Act.”
FDA inspectors conducted a site inspection of American CryoStem in Eatontown, N.J., last summer, during which they “documented evidence of significant deviations from current good manufacturing practice.” The agency then provided the company a chance to respond to these issues. The new warning letter discussed each complaint, noting that some were inadequately addressed, and demanded that the company take action within 15 working days or face potential legal process, including seizure and/or injunction.
American CryoStem is one of the first companies to experience increased scrutiny under FDA’s new commitment to regulate the rapid growth and development of regenerative medicine products, which include novel cellular therapies, with the aim of ensuring their safety and effectiveness.
The new policy is designed to support the potential of cellular rejuvenation medicine, while protecting patients from “unscrupulous actors” who might endanger public health with untested products, according to FDA Commissioner Scott Gottlieb, MD. As enthusiasm for stem cell treatments surges, so are reports of adverse events. The New England Journal of Medicine recently reported on three patients with age-related macular degeneration who were blinded by intravitreal injection of autologous adipose-derived stem cells (N Engl J Med. 2017;376:1047-53).
Under the new policy, cell- and tissue-based products could be exempt from FDA premarket review only if they are removed from and implanted back into the same patient in their original form, or if the products are “minimally manipulated.” ATCELL fulfills neither qualification, the FDA warning letter said.
“You process adipose tissue ... to isolate cellular components of adipose tissue, commonly referred to as stromal vascular fraction [SVF]. Such processing is more than minimal manipulation because [it alters] the original relevant characteristics of the [tissue] relating to its utility for reconstruction, repair, or replacement. Then you process the SVF by expanding it in cell culture to manufacture ATCELL. Such expansion also is more than minimal manipulation because it alters the original relevant characteristics of the tissue.”
Furthermore, the letter noted, at least one of the components used in the clonal expansion process is investigational and not intended for human use. The manufacturer of that component, which was not named, “indicates the following: ‘Unless otherwise stated in our catalog or other company documentation accompanying the product(s), our products are intended for research use only and are not to be used for any other purpose, which includes but is not limited to, unauthorized commercial uses, in vitro diagnostic uses, ex vivo or in vivo therapeutic uses or any type of consumption or application to human and animals.”
The FDA also took exception with several equipment and lab safety issues. ATCELL was being created in areas that had no clean space designation – a serious concern, the letter said.
“American CryoStem’s unvalidated processes, inadequately controlled environment, lack of control of components used in production, and lack of sufficient and validated product testing ... pose a significant risk that ATCELL may be contaminated with microorganisms or have other serious product quality defects ... Because the product is administered to humans by various higher risk routes of administration, including intravenously, intrathecally, and by aerosol inhalation, if contaminated, its use could cause a range of adverse events, from infections to death.”
FDA also expressed concerns over a lack of consistent quality control testing of each batch and questioned whether the company’s method of shipping ATCELL to clinicians had been adequately validated.
Finally, the agency raised concerns that ATCELL, while it is labeled as being for research purposes only, may harm patients indirectly by preventing them from seeking timely treatment with proven therapies.
“ATCELL is intended to treat a variety of serious or life-threatening diseases or conditions, all of which are non-homologous uses,” the warning letter noted. “Such uses raise potential significant safety concerns because there is less basis on which to predict the product’s behavior in the recipient, and use of these unapproved products may cause users to delay or discontinue medical treatments that have been found safe and effective.”
SOURCE: FDA warning letter
for manufacturing processes that may compromise its safety and for failing to toe the regulatory line in marketing.
American CryoStem received an FDA warning letter Jan. 3 demanding that the company comply with best-manufacturing processes and obtain an investigational new drug application if it wishes to continue marketing ATCELL for its currently advertised clinical indications and administration routes. These include intravenous, intrathecal, or aerosol inhalation of the product for anoxic brain injury, Parkinson’s disease, amyotrophic lateral sclerosis, stroke, and multiple sclerosis.
“Please be advised that, to lawfully market a drug that is a biological product, a valid biologics license must be in effect,” noted the letter. “Such licenses are issued only after a showing that the product is safe, pure, and potent. While in the development stage, such products may be distributed for clinical use in humans only if the sponsor has an investigational new drug application (IND) in effect as specified by FDA regulations. ATCELL is not the subject of an approved biologics license application nor is there an IND in effect. Based on this information, we have determined that your actions have violated the Food, Drug, and Cosmetic Act and the Public Health Service Act.”
FDA inspectors conducted a site inspection of American CryoStem in Eatontown, N.J., last summer, during which they “documented evidence of significant deviations from current good manufacturing practice.” The agency then provided the company a chance to respond to these issues. The new warning letter discussed each complaint, noting that some were inadequately addressed, and demanded that the company take action within 15 working days or face potential legal process, including seizure and/or injunction.
American CryoStem is one of the first companies to experience increased scrutiny under FDA’s new commitment to regulate the rapid growth and development of regenerative medicine products, which include novel cellular therapies, with the aim of ensuring their safety and effectiveness.
The new policy is designed to support the potential of cellular rejuvenation medicine, while protecting patients from “unscrupulous actors” who might endanger public health with untested products, according to FDA Commissioner Scott Gottlieb, MD. As enthusiasm for stem cell treatments surges, so are reports of adverse events. The New England Journal of Medicine recently reported on three patients with age-related macular degeneration who were blinded by intravitreal injection of autologous adipose-derived stem cells (N Engl J Med. 2017;376:1047-53).
Under the new policy, cell- and tissue-based products could be exempt from FDA premarket review only if they are removed from and implanted back into the same patient in their original form, or if the products are “minimally manipulated.” ATCELL fulfills neither qualification, the FDA warning letter said.
“You process adipose tissue ... to isolate cellular components of adipose tissue, commonly referred to as stromal vascular fraction [SVF]. Such processing is more than minimal manipulation because [it alters] the original relevant characteristics of the [tissue] relating to its utility for reconstruction, repair, or replacement. Then you process the SVF by expanding it in cell culture to manufacture ATCELL. Such expansion also is more than minimal manipulation because it alters the original relevant characteristics of the tissue.”
Furthermore, the letter noted, at least one of the components used in the clonal expansion process is investigational and not intended for human use. The manufacturer of that component, which was not named, “indicates the following: ‘Unless otherwise stated in our catalog or other company documentation accompanying the product(s), our products are intended for research use only and are not to be used for any other purpose, which includes but is not limited to, unauthorized commercial uses, in vitro diagnostic uses, ex vivo or in vivo therapeutic uses or any type of consumption or application to human and animals.”
The FDA also took exception with several equipment and lab safety issues. ATCELL was being created in areas that had no clean space designation – a serious concern, the letter said.
“American CryoStem’s unvalidated processes, inadequately controlled environment, lack of control of components used in production, and lack of sufficient and validated product testing ... pose a significant risk that ATCELL may be contaminated with microorganisms or have other serious product quality defects ... Because the product is administered to humans by various higher risk routes of administration, including intravenously, intrathecally, and by aerosol inhalation, if contaminated, its use could cause a range of adverse events, from infections to death.”
FDA also expressed concerns over a lack of consistent quality control testing of each batch and questioned whether the company’s method of shipping ATCELL to clinicians had been adequately validated.
Finally, the agency raised concerns that ATCELL, while it is labeled as being for research purposes only, may harm patients indirectly by preventing them from seeking timely treatment with proven therapies.
“ATCELL is intended to treat a variety of serious or life-threatening diseases or conditions, all of which are non-homologous uses,” the warning letter noted. “Such uses raise potential significant safety concerns because there is less basis on which to predict the product’s behavior in the recipient, and use of these unapproved products may cause users to delay or discontinue medical treatments that have been found safe and effective.”
SOURCE: FDA warning letter
for manufacturing processes that may compromise its safety and for failing to toe the regulatory line in marketing.
American CryoStem received an FDA warning letter Jan. 3 demanding that the company comply with best-manufacturing processes and obtain an investigational new drug application if it wishes to continue marketing ATCELL for its currently advertised clinical indications and administration routes. These include intravenous, intrathecal, or aerosol inhalation of the product for anoxic brain injury, Parkinson’s disease, amyotrophic lateral sclerosis, stroke, and multiple sclerosis.
“Please be advised that, to lawfully market a drug that is a biological product, a valid biologics license must be in effect,” noted the letter. “Such licenses are issued only after a showing that the product is safe, pure, and potent. While in the development stage, such products may be distributed for clinical use in humans only if the sponsor has an investigational new drug application (IND) in effect as specified by FDA regulations. ATCELL is not the subject of an approved biologics license application nor is there an IND in effect. Based on this information, we have determined that your actions have violated the Food, Drug, and Cosmetic Act and the Public Health Service Act.”
FDA inspectors conducted a site inspection of American CryoStem in Eatontown, N.J., last summer, during which they “documented evidence of significant deviations from current good manufacturing practice.” The agency then provided the company a chance to respond to these issues. The new warning letter discussed each complaint, noting that some were inadequately addressed, and demanded that the company take action within 15 working days or face potential legal process, including seizure and/or injunction.
American CryoStem is one of the first companies to experience increased scrutiny under FDA’s new commitment to regulate the rapid growth and development of regenerative medicine products, which include novel cellular therapies, with the aim of ensuring their safety and effectiveness.
The new policy is designed to support the potential of cellular rejuvenation medicine, while protecting patients from “unscrupulous actors” who might endanger public health with untested products, according to FDA Commissioner Scott Gottlieb, MD. As enthusiasm for stem cell treatments surges, so are reports of adverse events. The New England Journal of Medicine recently reported on three patients with age-related macular degeneration who were blinded by intravitreal injection of autologous adipose-derived stem cells (N Engl J Med. 2017;376:1047-53).
Under the new policy, cell- and tissue-based products could be exempt from FDA premarket review only if they are removed from and implanted back into the same patient in their original form, or if the products are “minimally manipulated.” ATCELL fulfills neither qualification, the FDA warning letter said.
“You process adipose tissue ... to isolate cellular components of adipose tissue, commonly referred to as stromal vascular fraction [SVF]. Such processing is more than minimal manipulation because [it alters] the original relevant characteristics of the [tissue] relating to its utility for reconstruction, repair, or replacement. Then you process the SVF by expanding it in cell culture to manufacture ATCELL. Such expansion also is more than minimal manipulation because it alters the original relevant characteristics of the tissue.”
Furthermore, the letter noted, at least one of the components used in the clonal expansion process is investigational and not intended for human use. The manufacturer of that component, which was not named, “indicates the following: ‘Unless otherwise stated in our catalog or other company documentation accompanying the product(s), our products are intended for research use only and are not to be used for any other purpose, which includes but is not limited to, unauthorized commercial uses, in vitro diagnostic uses, ex vivo or in vivo therapeutic uses or any type of consumption or application to human and animals.”
The FDA also took exception with several equipment and lab safety issues. ATCELL was being created in areas that had no clean space designation – a serious concern, the letter said.
“American CryoStem’s unvalidated processes, inadequately controlled environment, lack of control of components used in production, and lack of sufficient and validated product testing ... pose a significant risk that ATCELL may be contaminated with microorganisms or have other serious product quality defects ... Because the product is administered to humans by various higher risk routes of administration, including intravenously, intrathecally, and by aerosol inhalation, if contaminated, its use could cause a range of adverse events, from infections to death.”
FDA also expressed concerns over a lack of consistent quality control testing of each batch and questioned whether the company’s method of shipping ATCELL to clinicians had been adequately validated.
Finally, the agency raised concerns that ATCELL, while it is labeled as being for research purposes only, may harm patients indirectly by preventing them from seeking timely treatment with proven therapies.
“ATCELL is intended to treat a variety of serious or life-threatening diseases or conditions, all of which are non-homologous uses,” the warning letter noted. “Such uses raise potential significant safety concerns because there is less basis on which to predict the product’s behavior in the recipient, and use of these unapproved products may cause users to delay or discontinue medical treatments that have been found safe and effective.”
SOURCE: FDA warning letter
Very preterm birth is linked to reduced risk of eczema
according to data from a meta-analysis of 18 studies.
Previous research suggests that low birth weight is protective against the development of atopic dermatitis, said Tingting Zhu, PhD, of West China Second University Hospital, Chengdu, and colleagues.
Preterm birth (before 37 completed weeks’ gestation) was divided into subgroups of extremely preterm (less than 28 weeks’ gestation), very preterm (28 weeks’ to less than 32 weeks’ gestation), and moderate/late preterm (32 weeks’ gestation to less than 37 weeks’ gestation).
In an analysis based on gestational age, children had a significantly reduced risk of eczema if they were very preterm (relative risk, 0.77; 95% confidence interval, 0.70-0.84, P less than .01; adjusted RR, 0.73; 95% CI, 0.64-0.82; P less than 0.01), compared with children born full term. The association between eczema and preterm birth was no longer significant among children born moderately preterm, Dr. Zhu and associates reported.
The reasons for the impact of very preterm birth on eczema are unclear, but maturation of the stratum corneum at 29-37 weeks’ gestational age could play a role, the researchers noted. Also, limited microflora in very preterm infants could affect acquiring immune tolerance and lead to reduced risk of eczema. The study was limited by several factors, including variations in gestational age and inconsistent assessments of eczema among the studies.
However, the large sample size lends strength to the results, and further studies are needed to explore how the environment, nutrition, immune system development, and skin barrier function impact the risk of eczema in very preterm infants, Dr. Zhu and associates said.
The researchers had no relevant financial disclosures. The researchers had no financial conflicts to disclose. The study was funded in part by the National Science Foundation of China, the Ministry of Health of China, and various other grants.
SOURCE: Zhu T et al. J Amer Dermatol. 2018. doi: 10.1016/j.jaad.2017.12.015.
according to data from a meta-analysis of 18 studies.
Previous research suggests that low birth weight is protective against the development of atopic dermatitis, said Tingting Zhu, PhD, of West China Second University Hospital, Chengdu, and colleagues.
Preterm birth (before 37 completed weeks’ gestation) was divided into subgroups of extremely preterm (less than 28 weeks’ gestation), very preterm (28 weeks’ to less than 32 weeks’ gestation), and moderate/late preterm (32 weeks’ gestation to less than 37 weeks’ gestation).
In an analysis based on gestational age, children had a significantly reduced risk of eczema if they were very preterm (relative risk, 0.77; 95% confidence interval, 0.70-0.84, P less than .01; adjusted RR, 0.73; 95% CI, 0.64-0.82; P less than 0.01), compared with children born full term. The association between eczema and preterm birth was no longer significant among children born moderately preterm, Dr. Zhu and associates reported.
The reasons for the impact of very preterm birth on eczema are unclear, but maturation of the stratum corneum at 29-37 weeks’ gestational age could play a role, the researchers noted. Also, limited microflora in very preterm infants could affect acquiring immune tolerance and lead to reduced risk of eczema. The study was limited by several factors, including variations in gestational age and inconsistent assessments of eczema among the studies.
However, the large sample size lends strength to the results, and further studies are needed to explore how the environment, nutrition, immune system development, and skin barrier function impact the risk of eczema in very preterm infants, Dr. Zhu and associates said.
The researchers had no relevant financial disclosures. The researchers had no financial conflicts to disclose. The study was funded in part by the National Science Foundation of China, the Ministry of Health of China, and various other grants.
SOURCE: Zhu T et al. J Amer Dermatol. 2018. doi: 10.1016/j.jaad.2017.12.015.
according to data from a meta-analysis of 18 studies.
Previous research suggests that low birth weight is protective against the development of atopic dermatitis, said Tingting Zhu, PhD, of West China Second University Hospital, Chengdu, and colleagues.
Preterm birth (before 37 completed weeks’ gestation) was divided into subgroups of extremely preterm (less than 28 weeks’ gestation), very preterm (28 weeks’ to less than 32 weeks’ gestation), and moderate/late preterm (32 weeks’ gestation to less than 37 weeks’ gestation).
In an analysis based on gestational age, children had a significantly reduced risk of eczema if they were very preterm (relative risk, 0.77; 95% confidence interval, 0.70-0.84, P less than .01; adjusted RR, 0.73; 95% CI, 0.64-0.82; P less than 0.01), compared with children born full term. The association between eczema and preterm birth was no longer significant among children born moderately preterm, Dr. Zhu and associates reported.
The reasons for the impact of very preterm birth on eczema are unclear, but maturation of the stratum corneum at 29-37 weeks’ gestational age could play a role, the researchers noted. Also, limited microflora in very preterm infants could affect acquiring immune tolerance and lead to reduced risk of eczema. The study was limited by several factors, including variations in gestational age and inconsistent assessments of eczema among the studies.
However, the large sample size lends strength to the results, and further studies are needed to explore how the environment, nutrition, immune system development, and skin barrier function impact the risk of eczema in very preterm infants, Dr. Zhu and associates said.
The researchers had no relevant financial disclosures. The researchers had no financial conflicts to disclose. The study was funded in part by the National Science Foundation of China, the Ministry of Health of China, and various other grants.
SOURCE: Zhu T et al. J Amer Dermatol. 2018. doi: 10.1016/j.jaad.2017.12.015.
FROM JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Key clinical point: Very preterm birth was associated with a significantly reduced risk of eczema, compared with full-term birth, but no difference in risk appeared between moderate preterm and full-term birth.
Major finding: Children had a significantly reduced risk of eczema if they were very preterm (RR, 0.77; 95% CI, 0.70-0.84; P less than .01; aRR 0.73, 95% CI, 0.64-0.82; P less than .01), compared with children born full term.
Data source: The data come from a meta-analysis of 18 studies.
Disclosures: The researchers had no financial conflicts to disclose. The study was funded in part by the National Science Foundation of China, the Ministry of Health of China, and various other grants.
Source: Zhu T et al. J Amer Dermatol. 2018. doi: 10.1016/j.jaad.2017.12.015.
The price of protection
It’s very likely that you have at least one or two female patients who play lacrosse. The sport has been reported to be the fastest-growing high school sport in the United States. (“Lacrosse is Actually America’s Fastest-Growing Sport,” by John Templon, BuzzFeed News, June 30, 2014). When I played in college, most of my teammates were products of prep schools in the Northeast or one of the few local hotbeds in Baltimore, Long Island, or the Finger Lakes Region of New York. But pickings were slim, and there was room for walk-ons like me looking to learn a new sport and stay in shape for football. Now hundreds of high schools in all parts of the country offer the sport for both boys and girls.

With growing awareness of the long-term effects of repeated head trauma, there has been a call from some parents and organizers of women’s lacrosse to require helmets on all players (“As Concussion Worries Rise, Girls’ Lacrosse Turns to Headgear,” by Bill Pennington, The New York Times, Nov 23, 2017). To those of us who have committed our professional lives to the health of children, the inclusion of helmets to the standard equipment for a female lacrosse player sounds like a good idea.
However, the proposed mandate has its critics, including several college coaches. Karen Corbett, women’s lacrosse coach at the University of Pennsylvania, has said that, players “will start to lead with their head because they feel protected, and that causes more injuries. We’ll become a more physical sport and a very different sport than we are today.”

Although I’m afraid that there are few data to support the validity of Dr. Hanley’s prediction, any observer of college hockey over the last 3 or 4 decades will tell you that he was unfortunately correct. There have been certainly fewer lacerations and eye injuries since face masks were introduced, but the game has become far more violent, and head, neck, and spine injuries have become more frequent. I think part of the problem is that game officials have been duped by the same false assumption as the players that more protection would make the game safer, and enforcement of the rules has not kept up with the technological changes.
There will always be injuries in any sport, but before we as physicians lend our support to a proposed change in protective equipment, we should step back and look at the broader picture. While the loss of an eye for an individual player is a tragedy, did we put several dozen more players at greater risk for spinal injury in college hockey with more protective gear? If adding headgear protects female lacrosse players from concussions, what might be the result if play becomes more physical? Protection can come with a price.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
It’s very likely that you have at least one or two female patients who play lacrosse. The sport has been reported to be the fastest-growing high school sport in the United States. (“Lacrosse is Actually America’s Fastest-Growing Sport,” by John Templon, BuzzFeed News, June 30, 2014). When I played in college, most of my teammates were products of prep schools in the Northeast or one of the few local hotbeds in Baltimore, Long Island, or the Finger Lakes Region of New York. But pickings were slim, and there was room for walk-ons like me looking to learn a new sport and stay in shape for football. Now hundreds of high schools in all parts of the country offer the sport for both boys and girls.
With growing awareness of the long-term effects of repeated head trauma, there has been a call from some parents and organizers of women’s lacrosse to require helmets on all players (“As Concussion Worries Rise, Girls’ Lacrosse Turns to Headgear,” by Bill Pennington, The New York Times, Nov 23, 2017). To those of us who have committed our professional lives to the health of children, the inclusion of helmets to the standard equipment for a female lacrosse player sounds like a good idea.
However, the proposed mandate has its critics, including several college coaches. Karen Corbett, women’s lacrosse coach at the University of Pennsylvania, has said that, players “will start to lead with their head because they feel protected, and that causes more injuries. We’ll become a more physical sport and a very different sport than we are today.”
Although I’m afraid that there are few data to support the validity of Dr. Hanley’s prediction, any observer of college hockey over the last 3 or 4 decades will tell you that he was unfortunately correct. There have been certainly fewer lacerations and eye injuries since face masks were introduced, but the game has become far more violent, and head, neck, and spine injuries have become more frequent. I think part of the problem is that game officials have been duped by the same false assumption as the players that more protection would make the game safer, and enforcement of the rules has not kept up with the technological changes.
There will always be injuries in any sport, but before we as physicians lend our support to a proposed change in protective equipment, we should step back and look at the broader picture. While the loss of an eye for an individual player is a tragedy, did we put several dozen more players at greater risk for spinal injury in college hockey with more protective gear? If adding headgear protects female lacrosse players from concussions, what might be the result if play becomes more physical? Protection can come with a price.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
It’s very likely that you have at least one or two female patients who play lacrosse. The sport has been reported to be the fastest-growing high school sport in the United States. (“Lacrosse is Actually America’s Fastest-Growing Sport,” by John Templon, BuzzFeed News, June 30, 2014). When I played in college, most of my teammates were products of prep schools in the Northeast or one of the few local hotbeds in Baltimore, Long Island, or the Finger Lakes Region of New York. But pickings were slim, and there was room for walk-ons like me looking to learn a new sport and stay in shape for football. Now hundreds of high schools in all parts of the country offer the sport for both boys and girls.
With growing awareness of the long-term effects of repeated head trauma, there has been a call from some parents and organizers of women’s lacrosse to require helmets on all players (“As Concussion Worries Rise, Girls’ Lacrosse Turns to Headgear,” by Bill Pennington, The New York Times, Nov 23, 2017). To those of us who have committed our professional lives to the health of children, the inclusion of helmets to the standard equipment for a female lacrosse player sounds like a good idea.
However, the proposed mandate has its critics, including several college coaches. Karen Corbett, women’s lacrosse coach at the University of Pennsylvania, has said that, players “will start to lead with their head because they feel protected, and that causes more injuries. We’ll become a more physical sport and a very different sport than we are today.”
Although I’m afraid that there are few data to support the validity of Dr. Hanley’s prediction, any observer of college hockey over the last 3 or 4 decades will tell you that he was unfortunately correct. There have been certainly fewer lacerations and eye injuries since face masks were introduced, but the game has become far more violent, and head, neck, and spine injuries have become more frequent. I think part of the problem is that game officials have been duped by the same false assumption as the players that more protection would make the game safer, and enforcement of the rules has not kept up with the technological changes.
There will always be injuries in any sport, but before we as physicians lend our support to a proposed change in protective equipment, we should step back and look at the broader picture. While the loss of an eye for an individual player is a tragedy, did we put several dozen more players at greater risk for spinal injury in college hockey with more protective gear? If adding headgear protects female lacrosse players from concussions, what might be the result if play becomes more physical? Protection can come with a price.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Early Hip Fracture Surgery Is Associated with Lower 30-Day Mortality
Study Overview
Objective. To determine the association between wait times for hip fracture surgery and outcomes after surgery and to identify the optimal time window for conducting hip fracture surgery.
Design. Observational cohort study.
Setting and participants. The study was conducted using population-based health administrative databases in Ontario, Canada. The databases collected information on health care services, physician and hospital information, and demographic characteristics in Ontario. The investigators used the databases to identify adults undergoing hip fracture surgery between April 2009 and March 2014. Excluded were adults who are non-Ontario residents, those with elective hospital admissions, those with prior hip fractures, and patients without hospital arrival time data. Other exclusion criteria include age younger than 45 years, those with delay in surgery longer than 10 days, surgery performed by a nonorthopedic surgeon, and those at hospitals with fewer than 5 hip fracture surgeries during the study period.
The primary independent variable was wait time for surgery, calculated from time from emergency department arrival until surgery and rounded in hours. Other covariates included in the analysis were patient characteristics including age, sex and comorbid conditions using the Deyo-Charlson comorbidity index, the Johns Hopkins Collapsed Aggregated Diagnosis Groups, and other validated algorithms. In addition, other conditions associated with hip fracture were included—osteomyelitis, bone cancer, other fractures, history of total hip arthroplasty, and multiple trauma. Additional covariates included median neighborhood household income quintile as a proxy for socioeconomic status, patient’s discharge disposition, and rural status. Characteristics of the procedure including procedure type, duration and timing (working vs. after hours) were assessed. Surgeon- and hospital-related factors included years since orthopedic certification as a proxy for surgeon experience and number of hip fracture procedures performed in the year preceding the event for surgeon and hospital. Other hospital characteristics included academic or community-based hospital, hospital size, and hospital’s capacity for performing nonelective surgery.
Main outcome measures. The main outcome measure was mortality within 30 days of being admitted for hip fracture surgery. Other secondary outcomes included mortality at 90 and 365 days after admission, medical complications within 30, 90, and 365 days, and a composite of mortality and any complications at these timeframes. Complications included myocardial infarction, deep vein thrombosis, pulmonary embolism and pneumonia. Statistical analysis include modeling for the probability of complications according to the time elapsed from emergency department arrival to surgery using risk adjusted spline analyses. The association between surgical wait time and mortality was graphically represented to visualize an inflection point when complications begin to rise. The area under the receiver operating characteristic curve was calculated at time thresholds around the area of inflection and the time producing the maximum area under the curve was selected as the threshold to classify patients
as receiving early or delayed surgery. Early and delayed patients were matched using propensity score with 1:1 matching without replacement. Outcomes were compared between early and delayed groups after matching and absolute risk differences were calculated using generalized estimating equations.
Main results. A total of 42,230 adults were included, with a mean age of 80.1 (SD 10.7) years; 70.5% were women. The average time from arrival to emergency room to surgery was 38.8 (SD 28.8) hours. The spline models identified an area of inflection at 24 hours when the risk of complications begins to rise. The investigators used 24 hours as a time point to classify patients into early or delayed surgery group. 33.6% of patients received early surgery and 66.4% had delayed surgery. Propensity score matching yielded a sample of 13,731 in each group. Patients with delayed surgery compared with early surgery had higher 30-day mortality (6.5% vs. 5.8%, absolute risk difference 0.79%), rate of pulmonary embolism (1.2% vs. 0.7%, absolute risk difference 0.51%), rate of myocardial infarction (1.2% vs. 0.8%, absolute risk difference 0.39%), and rate of pneumonia (4.6% vs. 3.7%, absolute risk difference 0.95%). For the composite outcome, 12.1% vs. 10.1% had mortality or complications in the delayed group and the early group respectively with an absolute difference of 2.16%. Outcomes at 90 days and 365 days were similar and remained significant. In subgroups of patients without comorbidity and those receiving surgery within 36 hours the results remained similar.
Conclusion. Early hip fracture surgery, defined as within 24 hours after arrival to emergency room, is associated with lower mortality and complications when compared to delayed surgery.
Commentary
Hip fracture affects predominantly older adults and leads to potential devastating consequences. Older adults who experience hip fracture have increased risk of functional decline, institutionalization, and death [1]. As hip fracture care often include surgical repair, many studies have examined the impact of timing of surgery on hip fracture outcomes, as the timing of surgery is a potentially modifiable factor that could impact patient outcomes [2]. Prior smaller cohort studies have demonstrated that delayed surgery may impact outcomes but the reasons for the delay, such as medical complexity, may also play a role in increasing the risk of adverse outcomes [3]. The current study adds to the previous literature by examining a large population-based cohort, thereby allowing for analysis that takes into account medical comorbidities using matching methods and sensitivity analyses that examined a sample without comorbidities. The study also employs a different approach to defining early vs. delayed surgery by using analytical methods to determine when risk of complications begins to rise. The results indicate that early surgery is associated with better outcomes at 30 days and beyond and that delaying surgery beyond 24 hours is associated with poorer patient outcomes.
Patients with hip fracture require care from multiple disciplines and care across multiple settings. These care components may also have an impact on patient outcomes, particularly outcomes at 90 and 365 days; some examples include anesthesia care during hip fracture surgery [4], pain control, early mobilization, and delirium prevention [1,5]. A limitation of utilizing administrative databases is that some of these potentially important factors that may affect outcome may not be included and thus cannot be controlled for. It is conceivable that early surgery may be associated with care characteristics that may also be favorable to outcomes. Another limitation is that it is still difficult to tease out the effect of medical complexity at the
time of hip fracture presentation, which may impact both timing of surgery and patient outcomes, despite sensitivity analyses that limit the sample to those who had surgery within 36 hours and also those without medical comorbidities according to the administrative data, and adjusting for antiplatelet or anticoagulant medications. It is also important to note that a randomized controlled trial may further elucidate the causal relationship between timing of surgery and patient outcomes. Despite the limitations of the study, the results make a strong case for limiting surgical wait time to within 24 hours from the time when the patient arrives in the emergency room.
Applications for Clinical Practice
Similar to how hospitals organize their care for patients with acute myocardial infarction for early reperfusion, and for patients with acute ischemic stroke with early thombolytic therapy, hip fracture care may need to be organized and coordinated in order to reduce surgical wait time to within 24 hours. Timely assessments by an orthopedic surgeon, anesthesiologist, and medical consultants to prepare patients for surgery and making available operating room and staff for hip fracture patients are necessary steps to reach the goal of reducing surgical wait time.
—William W. Hung, MD, MPH
1. Hung WW, Egol KA, Zuckerman JD, Siu AL. Hip fracture management: tailoring care for the older patient. JAMA 2012;307:2185–94.
2. Orosz GM, Magaziner J, Hannan EL, et al. Association of timing of surgery for hip fracture and patient outcomes. JAMA 2004;291:1738–43.
3. Vidán MT, Sánchez E, Gracia Y, et al. Causes and effects of surgical delay in patients with hip fracture: a cohort study. Ann Intern Med 2011;155:226–33.
4. Neuman MD, Silber JH, Elkassabany NM, et al. Comparative effectiveness of regional versus general anesthesia for hip fracture surgery in adults. Anesthesiology 2012;117: 72–92.
5. Grigoryan KV, Javedan H, Rudolph JL. Orthogeriatric care models and outcomes in hip fracture patients: a systematic review and meta-analysis. J Orthop Trauma 2014;28:e49–55.
Study Overview
Objective. To determine the association between wait times for hip fracture surgery and outcomes after surgery and to identify the optimal time window for conducting hip fracture surgery.
Design. Observational cohort study.
Setting and participants. The study was conducted using population-based health administrative databases in Ontario, Canada. The databases collected information on health care services, physician and hospital information, and demographic characteristics in Ontario. The investigators used the databases to identify adults undergoing hip fracture surgery between April 2009 and March 2014. Excluded were adults who are non-Ontario residents, those with elective hospital admissions, those with prior hip fractures, and patients without hospital arrival time data. Other exclusion criteria include age younger than 45 years, those with delay in surgery longer than 10 days, surgery performed by a nonorthopedic surgeon, and those at hospitals with fewer than 5 hip fracture surgeries during the study period.
The primary independent variable was wait time for surgery, calculated from time from emergency department arrival until surgery and rounded in hours. Other covariates included in the analysis were patient characteristics including age, sex and comorbid conditions using the Deyo-Charlson comorbidity index, the Johns Hopkins Collapsed Aggregated Diagnosis Groups, and other validated algorithms. In addition, other conditions associated with hip fracture were included—osteomyelitis, bone cancer, other fractures, history of total hip arthroplasty, and multiple trauma. Additional covariates included median neighborhood household income quintile as a proxy for socioeconomic status, patient’s discharge disposition, and rural status. Characteristics of the procedure including procedure type, duration and timing (working vs. after hours) were assessed. Surgeon- and hospital-related factors included years since orthopedic certification as a proxy for surgeon experience and number of hip fracture procedures performed in the year preceding the event for surgeon and hospital. Other hospital characteristics included academic or community-based hospital, hospital size, and hospital’s capacity for performing nonelective surgery.
Main outcome measures. The main outcome measure was mortality within 30 days of being admitted for hip fracture surgery. Other secondary outcomes included mortality at 90 and 365 days after admission, medical complications within 30, 90, and 365 days, and a composite of mortality and any complications at these timeframes. Complications included myocardial infarction, deep vein thrombosis, pulmonary embolism and pneumonia. Statistical analysis include modeling for the probability of complications according to the time elapsed from emergency department arrival to surgery using risk adjusted spline analyses. The association between surgical wait time and mortality was graphically represented to visualize an inflection point when complications begin to rise. The area under the receiver operating characteristic curve was calculated at time thresholds around the area of inflection and the time producing the maximum area under the curve was selected as the threshold to classify patients
as receiving early or delayed surgery. Early and delayed patients were matched using propensity score with 1:1 matching without replacement. Outcomes were compared between early and delayed groups after matching and absolute risk differences were calculated using generalized estimating equations.
Main results. A total of 42,230 adults were included, with a mean age of 80.1 (SD 10.7) years; 70.5% were women. The average time from arrival to emergency room to surgery was 38.8 (SD 28.8) hours. The spline models identified an area of inflection at 24 hours when the risk of complications begins to rise. The investigators used 24 hours as a time point to classify patients into early or delayed surgery group. 33.6% of patients received early surgery and 66.4% had delayed surgery. Propensity score matching yielded a sample of 13,731 in each group. Patients with delayed surgery compared with early surgery had higher 30-day mortality (6.5% vs. 5.8%, absolute risk difference 0.79%), rate of pulmonary embolism (1.2% vs. 0.7%, absolute risk difference 0.51%), rate of myocardial infarction (1.2% vs. 0.8%, absolute risk difference 0.39%), and rate of pneumonia (4.6% vs. 3.7%, absolute risk difference 0.95%). For the composite outcome, 12.1% vs. 10.1% had mortality or complications in the delayed group and the early group respectively with an absolute difference of 2.16%. Outcomes at 90 days and 365 days were similar and remained significant. In subgroups of patients without comorbidity and those receiving surgery within 36 hours the results remained similar.
Conclusion. Early hip fracture surgery, defined as within 24 hours after arrival to emergency room, is associated with lower mortality and complications when compared to delayed surgery.
Commentary
Hip fracture affects predominantly older adults and leads to potential devastating consequences. Older adults who experience hip fracture have increased risk of functional decline, institutionalization, and death [1]. As hip fracture care often include surgical repair, many studies have examined the impact of timing of surgery on hip fracture outcomes, as the timing of surgery is a potentially modifiable factor that could impact patient outcomes [2]. Prior smaller cohort studies have demonstrated that delayed surgery may impact outcomes but the reasons for the delay, such as medical complexity, may also play a role in increasing the risk of adverse outcomes [3]. The current study adds to the previous literature by examining a large population-based cohort, thereby allowing for analysis that takes into account medical comorbidities using matching methods and sensitivity analyses that examined a sample without comorbidities. The study also employs a different approach to defining early vs. delayed surgery by using analytical methods to determine when risk of complications begins to rise. The results indicate that early surgery is associated with better outcomes at 30 days and beyond and that delaying surgery beyond 24 hours is associated with poorer patient outcomes.
Patients with hip fracture require care from multiple disciplines and care across multiple settings. These care components may also have an impact on patient outcomes, particularly outcomes at 90 and 365 days; some examples include anesthesia care during hip fracture surgery [4], pain control, early mobilization, and delirium prevention [1,5]. A limitation of utilizing administrative databases is that some of these potentially important factors that may affect outcome may not be included and thus cannot be controlled for. It is conceivable that early surgery may be associated with care characteristics that may also be favorable to outcomes. Another limitation is that it is still difficult to tease out the effect of medical complexity at the
time of hip fracture presentation, which may impact both timing of surgery and patient outcomes, despite sensitivity analyses that limit the sample to those who had surgery within 36 hours and also those without medical comorbidities according to the administrative data, and adjusting for antiplatelet or anticoagulant medications. It is also important to note that a randomized controlled trial may further elucidate the causal relationship between timing of surgery and patient outcomes. Despite the limitations of the study, the results make a strong case for limiting surgical wait time to within 24 hours from the time when the patient arrives in the emergency room.
Applications for Clinical Practice
Similar to how hospitals organize their care for patients with acute myocardial infarction for early reperfusion, and for patients with acute ischemic stroke with early thombolytic therapy, hip fracture care may need to be organized and coordinated in order to reduce surgical wait time to within 24 hours. Timely assessments by an orthopedic surgeon, anesthesiologist, and medical consultants to prepare patients for surgery and making available operating room and staff for hip fracture patients are necessary steps to reach the goal of reducing surgical wait time.
—William W. Hung, MD, MPH
Study Overview
Objective. To determine the association between wait times for hip fracture surgery and outcomes after surgery and to identify the optimal time window for conducting hip fracture surgery.
Design. Observational cohort study.
Setting and participants. The study was conducted using population-based health administrative databases in Ontario, Canada. The databases collected information on health care services, physician and hospital information, and demographic characteristics in Ontario. The investigators used the databases to identify adults undergoing hip fracture surgery between April 2009 and March 2014. Excluded were adults who are non-Ontario residents, those with elective hospital admissions, those with prior hip fractures, and patients without hospital arrival time data. Other exclusion criteria include age younger than 45 years, those with delay in surgery longer than 10 days, surgery performed by a nonorthopedic surgeon, and those at hospitals with fewer than 5 hip fracture surgeries during the study period.
The primary independent variable was wait time for surgery, calculated from time from emergency department arrival until surgery and rounded in hours. Other covariates included in the analysis were patient characteristics including age, sex and comorbid conditions using the Deyo-Charlson comorbidity index, the Johns Hopkins Collapsed Aggregated Diagnosis Groups, and other validated algorithms. In addition, other conditions associated with hip fracture were included—osteomyelitis, bone cancer, other fractures, history of total hip arthroplasty, and multiple trauma. Additional covariates included median neighborhood household income quintile as a proxy for socioeconomic status, patient’s discharge disposition, and rural status. Characteristics of the procedure including procedure type, duration and timing (working vs. after hours) were assessed. Surgeon- and hospital-related factors included years since orthopedic certification as a proxy for surgeon experience and number of hip fracture procedures performed in the year preceding the event for surgeon and hospital. Other hospital characteristics included academic or community-based hospital, hospital size, and hospital’s capacity for performing nonelective surgery.
Main outcome measures. The main outcome measure was mortality within 30 days of being admitted for hip fracture surgery. Other secondary outcomes included mortality at 90 and 365 days after admission, medical complications within 30, 90, and 365 days, and a composite of mortality and any complications at these timeframes. Complications included myocardial infarction, deep vein thrombosis, pulmonary embolism and pneumonia. Statistical analysis include modeling for the probability of complications according to the time elapsed from emergency department arrival to surgery using risk adjusted spline analyses. The association between surgical wait time and mortality was graphically represented to visualize an inflection point when complications begin to rise. The area under the receiver operating characteristic curve was calculated at time thresholds around the area of inflection and the time producing the maximum area under the curve was selected as the threshold to classify patients
as receiving early or delayed surgery. Early and delayed patients were matched using propensity score with 1:1 matching without replacement. Outcomes were compared between early and delayed groups after matching and absolute risk differences were calculated using generalized estimating equations.
Main results. A total of 42,230 adults were included, with a mean age of 80.1 (SD 10.7) years; 70.5% were women. The average time from arrival to emergency room to surgery was 38.8 (SD 28.8) hours. The spline models identified an area of inflection at 24 hours when the risk of complications begins to rise. The investigators used 24 hours as a time point to classify patients into early or delayed surgery group. 33.6% of patients received early surgery and 66.4% had delayed surgery. Propensity score matching yielded a sample of 13,731 in each group. Patients with delayed surgery compared with early surgery had higher 30-day mortality (6.5% vs. 5.8%, absolute risk difference 0.79%), rate of pulmonary embolism (1.2% vs. 0.7%, absolute risk difference 0.51%), rate of myocardial infarction (1.2% vs. 0.8%, absolute risk difference 0.39%), and rate of pneumonia (4.6% vs. 3.7%, absolute risk difference 0.95%). For the composite outcome, 12.1% vs. 10.1% had mortality or complications in the delayed group and the early group respectively with an absolute difference of 2.16%. Outcomes at 90 days and 365 days were similar and remained significant. In subgroups of patients without comorbidity and those receiving surgery within 36 hours the results remained similar.
Conclusion. Early hip fracture surgery, defined as within 24 hours after arrival to emergency room, is associated with lower mortality and complications when compared to delayed surgery.
Commentary
Hip fracture affects predominantly older adults and leads to potential devastating consequences. Older adults who experience hip fracture have increased risk of functional decline, institutionalization, and death [1]. As hip fracture care often include surgical repair, many studies have examined the impact of timing of surgery on hip fracture outcomes, as the timing of surgery is a potentially modifiable factor that could impact patient outcomes [2]. Prior smaller cohort studies have demonstrated that delayed surgery may impact outcomes but the reasons for the delay, such as medical complexity, may also play a role in increasing the risk of adverse outcomes [3]. The current study adds to the previous literature by examining a large population-based cohort, thereby allowing for analysis that takes into account medical comorbidities using matching methods and sensitivity analyses that examined a sample without comorbidities. The study also employs a different approach to defining early vs. delayed surgery by using analytical methods to determine when risk of complications begins to rise. The results indicate that early surgery is associated with better outcomes at 30 days and beyond and that delaying surgery beyond 24 hours is associated with poorer patient outcomes.
Patients with hip fracture require care from multiple disciplines and care across multiple settings. These care components may also have an impact on patient outcomes, particularly outcomes at 90 and 365 days; some examples include anesthesia care during hip fracture surgery [4], pain control, early mobilization, and delirium prevention [1,5]. A limitation of utilizing administrative databases is that some of these potentially important factors that may affect outcome may not be included and thus cannot be controlled for. It is conceivable that early surgery may be associated with care characteristics that may also be favorable to outcomes. Another limitation is that it is still difficult to tease out the effect of medical complexity at the
time of hip fracture presentation, which may impact both timing of surgery and patient outcomes, despite sensitivity analyses that limit the sample to those who had surgery within 36 hours and also those without medical comorbidities according to the administrative data, and adjusting for antiplatelet or anticoagulant medications. It is also important to note that a randomized controlled trial may further elucidate the causal relationship between timing of surgery and patient outcomes. Despite the limitations of the study, the results make a strong case for limiting surgical wait time to within 24 hours from the time when the patient arrives in the emergency room.
Applications for Clinical Practice
Similar to how hospitals organize their care for patients with acute myocardial infarction for early reperfusion, and for patients with acute ischemic stroke with early thombolytic therapy, hip fracture care may need to be organized and coordinated in order to reduce surgical wait time to within 24 hours. Timely assessments by an orthopedic surgeon, anesthesiologist, and medical consultants to prepare patients for surgery and making available operating room and staff for hip fracture patients are necessary steps to reach the goal of reducing surgical wait time.
—William W. Hung, MD, MPH
1. Hung WW, Egol KA, Zuckerman JD, Siu AL. Hip fracture management: tailoring care for the older patient. JAMA 2012;307:2185–94.
2. Orosz GM, Magaziner J, Hannan EL, et al. Association of timing of surgery for hip fracture and patient outcomes. JAMA 2004;291:1738–43.
3. Vidán MT, Sánchez E, Gracia Y, et al. Causes and effects of surgical delay in patients with hip fracture: a cohort study. Ann Intern Med 2011;155:226–33.
4. Neuman MD, Silber JH, Elkassabany NM, et al. Comparative effectiveness of regional versus general anesthesia for hip fracture surgery in adults. Anesthesiology 2012;117: 72–92.
5. Grigoryan KV, Javedan H, Rudolph JL. Orthogeriatric care models and outcomes in hip fracture patients: a systematic review and meta-analysis. J Orthop Trauma 2014;28:e49–55.
1. Hung WW, Egol KA, Zuckerman JD, Siu AL. Hip fracture management: tailoring care for the older patient. JAMA 2012;307:2185–94.
2. Orosz GM, Magaziner J, Hannan EL, et al. Association of timing of surgery for hip fracture and patient outcomes. JAMA 2004;291:1738–43.
3. Vidán MT, Sánchez E, Gracia Y, et al. Causes and effects of surgical delay in patients with hip fracture: a cohort study. Ann Intern Med 2011;155:226–33.
4. Neuman MD, Silber JH, Elkassabany NM, et al. Comparative effectiveness of regional versus general anesthesia for hip fracture surgery in adults. Anesthesiology 2012;117: 72–92.
5. Grigoryan KV, Javedan H, Rudolph JL. Orthogeriatric care models and outcomes in hip fracture patients: a systematic review and meta-analysis. J Orthop Trauma 2014;28:e49–55.
Low caffeine in blood could be marker of early Parkinson’s
Low serum caffeine and caffeine metabolite levels after an overnight fast may be a sensitive way to detect the presence of Parkinson’s disease, according to the results of a new case-control study.
Levels of caffeine and its metabolites were also lower in Parkinson’s disease (PD) patients who had motor dysfunction, compared with those without motor dysfunction, but no differences in serum levels of caffeine metabolites could be detected between patients with mild to more severe stages of PD, reported Motoki Fujimaki, MD, of Juntendo University, Tokyo, and colleagues. The report was published online Jan. 3 in Neurology.
To test that idea, Dr. Fujimaki and associates recruited 31 healthy controls (18 women) and 108 patients with PD but no dementia (50 women). The control group’s mean caffeine intake of 115.81 mg/day (standard deviation, 69.22) was similar to PD patients’ intake of 107.50 mg/day (SD, 67.27).
Serum caffeine levels measured after an overnight fast showed that a cutoff of 33.04 pmol/10 mcL identified PD with an area under the curve (AUC) of 0.78 (sensitivity 76.9%, specificity 74.2%). Inclusion of the primary caffeine metabolites theophylline, theobromine, and paraxanthine improved the AUC to 0.87. When the researchers included all 11 measurable metabolites, the AUC jumped to 0.98.
Genetic analyses found no significant differences in the frequencies of caffeine metabolism–associated genetic variants between PD patients and controls.
The study was limited by the fact that it was conducted at a single university hospital, and the patient population did not include many severe cases. The algorithm should also be studied in other PD patient populations.
The study was funded by grants from several Japanese government agencies. Some of the authors have financial relationships with the pharmaceutical industry.
SOURCE: Fujimaki M et al. Neurology. 2018 Jan 3. doi: 10.1212/WNL.0000000000004888
A key question is what is causing the decrease in serum concentration found in patients with Parkinson’s disease? Nearly all of the patients were receiving treatment, which could have affected serum levels.
The researchers addressed this by looking for an association between serum caffeine metabolite levels and levodopa equivalent doses, and they found none.
Still, the validity of the study depends on whether caffeine metabolism may be affected by treatment. To demonstrate the utility of caffeine metabolites unequivocally, a future study will have to reproduce these results in patients with untreated PD or subjects at high risk of PD, such as those with prodromal signs of PD.
David G. Munoz, MD, is in the department of laboratory medicine and pathobiology at the University of Toronto. Shinsuke Fujioka, MD is in the department of neurology at Fukuoka (Japan) University. Dr. Munoz and Dr. Fujioka reported having no financial disclosures. Their comments are derived from an editorial accompanying the study by Dr. Fujimaki and colleagues (Neurology. 2018 Jan 3. doi: 10.1212/WNL.0000000000004898).
A key question is what is causing the decrease in serum concentration found in patients with Parkinson’s disease? Nearly all of the patients were receiving treatment, which could have affected serum levels.
The researchers addressed this by looking for an association between serum caffeine metabolite levels and levodopa equivalent doses, and they found none.
Still, the validity of the study depends on whether caffeine metabolism may be affected by treatment. To demonstrate the utility of caffeine metabolites unequivocally, a future study will have to reproduce these results in patients with untreated PD or subjects at high risk of PD, such as those with prodromal signs of PD.
David G. Munoz, MD, is in the department of laboratory medicine and pathobiology at the University of Toronto. Shinsuke Fujioka, MD is in the department of neurology at Fukuoka (Japan) University. Dr. Munoz and Dr. Fujioka reported having no financial disclosures. Their comments are derived from an editorial accompanying the study by Dr. Fujimaki and colleagues (Neurology. 2018 Jan 3. doi: 10.1212/WNL.0000000000004898).
A key question is what is causing the decrease in serum concentration found in patients with Parkinson’s disease? Nearly all of the patients were receiving treatment, which could have affected serum levels.
The researchers addressed this by looking for an association between serum caffeine metabolite levels and levodopa equivalent doses, and they found none.
Still, the validity of the study depends on whether caffeine metabolism may be affected by treatment. To demonstrate the utility of caffeine metabolites unequivocally, a future study will have to reproduce these results in patients with untreated PD or subjects at high risk of PD, such as those with prodromal signs of PD.
David G. Munoz, MD, is in the department of laboratory medicine and pathobiology at the University of Toronto. Shinsuke Fujioka, MD is in the department of neurology at Fukuoka (Japan) University. Dr. Munoz and Dr. Fujioka reported having no financial disclosures. Their comments are derived from an editorial accompanying the study by Dr. Fujimaki and colleagues (Neurology. 2018 Jan 3. doi: 10.1212/WNL.0000000000004898).
Low serum caffeine and caffeine metabolite levels after an overnight fast may be a sensitive way to detect the presence of Parkinson’s disease, according to the results of a new case-control study.
Levels of caffeine and its metabolites were also lower in Parkinson’s disease (PD) patients who had motor dysfunction, compared with those without motor dysfunction, but no differences in serum levels of caffeine metabolites could be detected between patients with mild to more severe stages of PD, reported Motoki Fujimaki, MD, of Juntendo University, Tokyo, and colleagues. The report was published online Jan. 3 in Neurology.
To test that idea, Dr. Fujimaki and associates recruited 31 healthy controls (18 women) and 108 patients with PD but no dementia (50 women). The control group’s mean caffeine intake of 115.81 mg/day (standard deviation, 69.22) was similar to PD patients’ intake of 107.50 mg/day (SD, 67.27).
Serum caffeine levels measured after an overnight fast showed that a cutoff of 33.04 pmol/10 mcL identified PD with an area under the curve (AUC) of 0.78 (sensitivity 76.9%, specificity 74.2%). Inclusion of the primary caffeine metabolites theophylline, theobromine, and paraxanthine improved the AUC to 0.87. When the researchers included all 11 measurable metabolites, the AUC jumped to 0.98.
Genetic analyses found no significant differences in the frequencies of caffeine metabolism–associated genetic variants between PD patients and controls.
The study was limited by the fact that it was conducted at a single university hospital, and the patient population did not include many severe cases. The algorithm should also be studied in other PD patient populations.
The study was funded by grants from several Japanese government agencies. Some of the authors have financial relationships with the pharmaceutical industry.
SOURCE: Fujimaki M et al. Neurology. 2018 Jan 3. doi: 10.1212/WNL.0000000000004888
Low serum caffeine and caffeine metabolite levels after an overnight fast may be a sensitive way to detect the presence of Parkinson’s disease, according to the results of a new case-control study.
Levels of caffeine and its metabolites were also lower in Parkinson’s disease (PD) patients who had motor dysfunction, compared with those without motor dysfunction, but no differences in serum levels of caffeine metabolites could be detected between patients with mild to more severe stages of PD, reported Motoki Fujimaki, MD, of Juntendo University, Tokyo, and colleagues. The report was published online Jan. 3 in Neurology.
To test that idea, Dr. Fujimaki and associates recruited 31 healthy controls (18 women) and 108 patients with PD but no dementia (50 women). The control group’s mean caffeine intake of 115.81 mg/day (standard deviation, 69.22) was similar to PD patients’ intake of 107.50 mg/day (SD, 67.27).
Serum caffeine levels measured after an overnight fast showed that a cutoff of 33.04 pmol/10 mcL identified PD with an area under the curve (AUC) of 0.78 (sensitivity 76.9%, specificity 74.2%). Inclusion of the primary caffeine metabolites theophylline, theobromine, and paraxanthine improved the AUC to 0.87. When the researchers included all 11 measurable metabolites, the AUC jumped to 0.98.
Genetic analyses found no significant differences in the frequencies of caffeine metabolism–associated genetic variants between PD patients and controls.
The study was limited by the fact that it was conducted at a single university hospital, and the patient population did not include many severe cases. The algorithm should also be studied in other PD patient populations.
The study was funded by grants from several Japanese government agencies. Some of the authors have financial relationships with the pharmaceutical industry.
SOURCE: Fujimaki M et al. Neurology. 2018 Jan 3. doi: 10.1212/WNL.0000000000004888
FROM NEUROLOGY
Key clinical point:
Major finding: Combining serum levels of caffeine and nine related metabolites identified individuals with PD with an AUC of 0.98.
Data source: Analysis of 108 Parkinson’s patients and 31 healthy controls.
Disclosures: The study was funded by grants from several Japanese government agencies. Some of the authors have financial relationships with the pharmaceutical industry.
Source: Fujimaki M et al., Neurology. 2018 Jan 3. doi: 10.1212/WNL.0000000000004888