User login
Give Her a Shoulder to Cry on

ANSWER
The radiograph demonstrates an acute horizontal fracture through the humeral neck. There is some slight lateral displacement of the fracture fragment.
The patient’s right arm was placed in a sling. Prompt orthopedic consultation was then obtained.
ANSWER
The radiograph demonstrates an acute horizontal fracture through the humeral neck. There is some slight lateral displacement of the fracture fragment.
The patient’s right arm was placed in a sling. Prompt orthopedic consultation was then obtained.
ANSWER
The radiograph demonstrates an acute horizontal fracture through the humeral neck. There is some slight lateral displacement of the fracture fragment.
The patient’s right arm was placed in a sling. Prompt orthopedic consultation was then obtained.

After a motor vehicle collision, a 70-year-old woman is brought to your emergency department by EMS personnel. She was a restrained driver in a vehicle crossing an intersection when she was broadsided by a tractor trailer traveling at high speed. Her airbags deployed, and she believes she briefly lost consciousness. Her biggest complaint is pain in her right shoulder.
Her medical history is significant for hypertension and hypothyroidism. On primary survey, you note an elderly woman who is in full cervical spine immobilization on a long backboard. Her Glasgow Coma Scale score is 15. She is in mild distress but has normal vital signs.
The patient has scattered abrasions and bruises on her body. Her right shoulder has mild to moderate tenderness to palpation and a decreased range of motion. Distally in that arm, she has good pulses and is neurovascularly intact.
You obtain a portable radiograph of the right shoulder (shown). What is your impression?

CardioMEMS cuts heart failure hospitalizations in post-approval study
NEW ORLEANS – Frequent, noninvasive measurement of pulmonary artery pressure in patients with advanced heart failure and an implanted CardioMEMS device that allows this measurement led to management that produced a substantial reduction in heart failure hospitalizations, compared with each patient’s history, in a real-world study.

The Food and Drug Administration–mandated CardioMEMS Post-Approval Study included 1,200 patients who received CardioMEMS implants after it received U.S. marketing approval. The study showed that when clinicians and patients used the device in routine practice, presumably as part of a structured management system designed to take advantage of the pulmonary artery (PA) pressures the device provides, the result safely produced a 58% cut in heart failure hospitalizations during the year following device placement when compared to each patient’s own hospitalization history during the year before they got the CardioMEMS device, David M. Shavelle, MD, said at the at the annual meeting of the American College of Cardiology. This statistically significant result for the study’s primary endpoint showed an absolute reduction in the average rate of heart failure hospitalizations from 1.24 per patient during the year before the CardioMEMS placement to 0.52 hospitalizations per patient during the 12 months after placement, an average reduction of 0.72 hospitalizations/patient, said Dr. Shavelle, an interventional cardiologist at the University of Southern California in Los Angeles.
Another notable finding was that this benefit from CardioMEMS placement and use occurred at roughly similar rates in patients with New York Heart Association class III heart failure regardless of whether they had a reduced ejection fraction (40% or less), a mid-range ejection fraction (41%-50%), or preserved ejection fraction (greater than 50%), making CardioMEMS use one of the few treatments to produce any proven benefit in patients with heart failure with preserved ejection fraction. In that subgroup, 30% of the 1,200 enrolled patients had an average cut of 0.68 hospitalizations in the year after CardioMEMS implantation, a 61% drop, relative to the year before they received the device.
The results also fulfilled the study’s two prespecified safety measures. Among the 1,214 patients in the study assessed for safety, which included the 1,200 patients who received the device and 4 patients in whom placement failed, 4 patients had a device or system related complication during the study, a 0.3% rate, compared with a prespecified objective performance criteria of less than 20%. Among the 1,200 patients with a functioning CardioMEMS sensor, one patient (0.1%) had a device failure, compared with the study’s objective performance criteria of less than 10%.
The performance of the CardioMEMS device and the benefit it provided to patients in the post-approval study closely tracked its performance during the published pivotal trial (Lancet. 2011 Feb 19;377[9766]:658-66). On the basis of the pivotal trial results, the FDA approved CardioMEMS for U.S. marketing in 2014. Since then, the company has reported that about 10,000 U.S. heart failure patients have received these devices, Dr. Shavelle said.
“The benefit was seen across the range of ejection fractions; that’s very important,” commented Gurusher Panjrath, MD, director of advanced heart failure at George Washington University in Washington and a designated discussant for Dr. Shavelle’s report. “The safety seemed very good, and the efficacy was consistent” with prior reports. “There also was high compliance. The key to success is the structure” of patient management, Dr. Pangroth said. “The data are limited by who is monitoring patients and their data and how much of that contact influences patient outcomes.”

That final comment by Dr. Panjrath highlighted the biggest caveat that heart failure clinicians have raised about judging the efficacy of CardioMEMS. To achieve clinical efficacy, the implanted device requires diligent, virtually daily interrogation and data transmission by the patient, assessment of a large amount of data for each patient by the patient’s clinical team, and responsiveness by the patient to medication adjustments directed by the clinical team to deal with episodes of rising PA pressure.
“The device itself has no benefit. It’s the actions prompted by the device that have benefit,” noted Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern University in Chicago and a second designated discussant for the report.

Dr. Shavelle agreed that for the CardioMEMS device to have an impact, one basic requirement is to identify patients who will cooperate with data collection and transmission and also with changes in their medications that are sent to them in response to PA pressure changes. This means selecting patients who appear to have problems with volume overload, including prior hospitalizations for decompensation, and patients who are comfortable interacting with their clinical-care providers. It also means excluding patients who are too sick to benefit from this intervention. He estimated that at his center more than 95% of class III heart failure patients who qualified for inclusion in the post-approval study by clinical criteria were also judged reasonable recipients of the device based on their willingness to cooperate with this system. He also estimated that at the University of Southern California the heart failure clinical team is now caring for about 150 patients with a CardioMEMS device implanted.
Another concern is teasing apart the specific benefit of collecting and using PA pressure data from the contact that the clinical team maintains with CardioMEMS patients.
“If nurses are contacting patients more often, is it the device or the communication? We need to look at that very carefully in a study that had no control group,” Dr. Yancy said in an interview. Contact with a nurse “is the best thing you can do for heart failure patients.”
Dr. Shavelle countered that several reports from past studies that assessed case management and regular monitoring of and contact with heart failure patients but without PA pressure data failed to showed any consistent benefit to patients.
“If you pick the right patients, CardioMEMS works. There is no question in my mind that the device works,” Dr. Shavelle said in an interview. “If you pick the wrong patient, who will not send the data or follow dose changes, then it won’t work.”
The study was sponsored by Abbott, the company that markets the CardioMEMS HF System. Dr. Shavelle has been a consultant to and speaker on behalf of Abbott Vascular and he has received research funding from Abbott Vascular, Abiomed, Biocardia, and V-Wave. Dr. Yancy had an unspecified financial relationship with Abbott Laboratories. Dr. Panjrath had no disclosures.
mzoler@mdedge.com
On Twitter @mitchelzoler
SOURCE: Shavelle DM et al. American College of Cardiology annual meeting, abstract 405-16.
NEW ORLEANS – Frequent, noninvasive measurement of pulmonary artery pressure in patients with advanced heart failure and an implanted CardioMEMS device that allows this measurement led to management that produced a substantial reduction in heart failure hospitalizations, compared with each patient’s history, in a real-world study.
The Food and Drug Administration–mandated CardioMEMS Post-Approval Study included 1,200 patients who received CardioMEMS implants after it received U.S. marketing approval. The study showed that when clinicians and patients used the device in routine practice, presumably as part of a structured management system designed to take advantage of the pulmonary artery (PA) pressures the device provides, the result safely produced a 58% cut in heart failure hospitalizations during the year following device placement when compared to each patient’s own hospitalization history during the year before they got the CardioMEMS device, David M. Shavelle, MD, said at the at the annual meeting of the American College of Cardiology. This statistically significant result for the study’s primary endpoint showed an absolute reduction in the average rate of heart failure hospitalizations from 1.24 per patient during the year before the CardioMEMS placement to 0.52 hospitalizations per patient during the 12 months after placement, an average reduction of 0.72 hospitalizations/patient, said Dr. Shavelle, an interventional cardiologist at the University of Southern California in Los Angeles.
Another notable finding was that this benefit from CardioMEMS placement and use occurred at roughly similar rates in patients with New York Heart Association class III heart failure regardless of whether they had a reduced ejection fraction (40% or less), a mid-range ejection fraction (41%-50%), or preserved ejection fraction (greater than 50%), making CardioMEMS use one of the few treatments to produce any proven benefit in patients with heart failure with preserved ejection fraction. In that subgroup, 30% of the 1,200 enrolled patients had an average cut of 0.68 hospitalizations in the year after CardioMEMS implantation, a 61% drop, relative to the year before they received the device.
The results also fulfilled the study’s two prespecified safety measures. Among the 1,214 patients in the study assessed for safety, which included the 1,200 patients who received the device and 4 patients in whom placement failed, 4 patients had a device or system related complication during the study, a 0.3% rate, compared with a prespecified objective performance criteria of less than 20%. Among the 1,200 patients with a functioning CardioMEMS sensor, one patient (0.1%) had a device failure, compared with the study’s objective performance criteria of less than 10%.
The performance of the CardioMEMS device and the benefit it provided to patients in the post-approval study closely tracked its performance during the published pivotal trial (Lancet. 2011 Feb 19;377[9766]:658-66). On the basis of the pivotal trial results, the FDA approved CardioMEMS for U.S. marketing in 2014. Since then, the company has reported that about 10,000 U.S. heart failure patients have received these devices, Dr. Shavelle said.
“The benefit was seen across the range of ejection fractions; that’s very important,” commented Gurusher Panjrath, MD, director of advanced heart failure at George Washington University in Washington and a designated discussant for Dr. Shavelle’s report. “The safety seemed very good, and the efficacy was consistent” with prior reports. “There also was high compliance. The key to success is the structure” of patient management, Dr. Pangroth said. “The data are limited by who is monitoring patients and their data and how much of that contact influences patient outcomes.”
That final comment by Dr. Panjrath highlighted the biggest caveat that heart failure clinicians have raised about judging the efficacy of CardioMEMS. To achieve clinical efficacy, the implanted device requires diligent, virtually daily interrogation and data transmission by the patient, assessment of a large amount of data for each patient by the patient’s clinical team, and responsiveness by the patient to medication adjustments directed by the clinical team to deal with episodes of rising PA pressure.
“The device itself has no benefit. It’s the actions prompted by the device that have benefit,” noted Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern University in Chicago and a second designated discussant for the report.
Dr. Shavelle agreed that for the CardioMEMS device to have an impact, one basic requirement is to identify patients who will cooperate with data collection and transmission and also with changes in their medications that are sent to them in response to PA pressure changes. This means selecting patients who appear to have problems with volume overload, including prior hospitalizations for decompensation, and patients who are comfortable interacting with their clinical-care providers. It also means excluding patients who are too sick to benefit from this intervention. He estimated that at his center more than 95% of class III heart failure patients who qualified for inclusion in the post-approval study by clinical criteria were also judged reasonable recipients of the device based on their willingness to cooperate with this system. He also estimated that at the University of Southern California the heart failure clinical team is now caring for about 150 patients with a CardioMEMS device implanted.
Another concern is teasing apart the specific benefit of collecting and using PA pressure data from the contact that the clinical team maintains with CardioMEMS patients.
“If nurses are contacting patients more often, is it the device or the communication? We need to look at that very carefully in a study that had no control group,” Dr. Yancy said in an interview. Contact with a nurse “is the best thing you can do for heart failure patients.”
Dr. Shavelle countered that several reports from past studies that assessed case management and regular monitoring of and contact with heart failure patients but without PA pressure data failed to showed any consistent benefit to patients.
“If you pick the right patients, CardioMEMS works. There is no question in my mind that the device works,” Dr. Shavelle said in an interview. “If you pick the wrong patient, who will not send the data or follow dose changes, then it won’t work.”
The study was sponsored by Abbott, the company that markets the CardioMEMS HF System. Dr. Shavelle has been a consultant to and speaker on behalf of Abbott Vascular and he has received research funding from Abbott Vascular, Abiomed, Biocardia, and V-Wave. Dr. Yancy had an unspecified financial relationship with Abbott Laboratories. Dr. Panjrath had no disclosures.
mzoler@mdedge.com
On Twitter @mitchelzoler
SOURCE: Shavelle DM et al. American College of Cardiology annual meeting, abstract 405-16.
NEW ORLEANS – Frequent, noninvasive measurement of pulmonary artery pressure in patients with advanced heart failure and an implanted CardioMEMS device that allows this measurement led to management that produced a substantial reduction in heart failure hospitalizations, compared with each patient’s history, in a real-world study.
The Food and Drug Administration–mandated CardioMEMS Post-Approval Study included 1,200 patients who received CardioMEMS implants after it received U.S. marketing approval. The study showed that when clinicians and patients used the device in routine practice, presumably as part of a structured management system designed to take advantage of the pulmonary artery (PA) pressures the device provides, the result safely produced a 58% cut in heart failure hospitalizations during the year following device placement when compared to each patient’s own hospitalization history during the year before they got the CardioMEMS device, David M. Shavelle, MD, said at the at the annual meeting of the American College of Cardiology. This statistically significant result for the study’s primary endpoint showed an absolute reduction in the average rate of heart failure hospitalizations from 1.24 per patient during the year before the CardioMEMS placement to 0.52 hospitalizations per patient during the 12 months after placement, an average reduction of 0.72 hospitalizations/patient, said Dr. Shavelle, an interventional cardiologist at the University of Southern California in Los Angeles.
Another notable finding was that this benefit from CardioMEMS placement and use occurred at roughly similar rates in patients with New York Heart Association class III heart failure regardless of whether they had a reduced ejection fraction (40% or less), a mid-range ejection fraction (41%-50%), or preserved ejection fraction (greater than 50%), making CardioMEMS use one of the few treatments to produce any proven benefit in patients with heart failure with preserved ejection fraction. In that subgroup, 30% of the 1,200 enrolled patients had an average cut of 0.68 hospitalizations in the year after CardioMEMS implantation, a 61% drop, relative to the year before they received the device.
The results also fulfilled the study’s two prespecified safety measures. Among the 1,214 patients in the study assessed for safety, which included the 1,200 patients who received the device and 4 patients in whom placement failed, 4 patients had a device or system related complication during the study, a 0.3% rate, compared with a prespecified objective performance criteria of less than 20%. Among the 1,200 patients with a functioning CardioMEMS sensor, one patient (0.1%) had a device failure, compared with the study’s objective performance criteria of less than 10%.
The performance of the CardioMEMS device and the benefit it provided to patients in the post-approval study closely tracked its performance during the published pivotal trial (Lancet. 2011 Feb 19;377[9766]:658-66). On the basis of the pivotal trial results, the FDA approved CardioMEMS for U.S. marketing in 2014. Since then, the company has reported that about 10,000 U.S. heart failure patients have received these devices, Dr. Shavelle said.
“The benefit was seen across the range of ejection fractions; that’s very important,” commented Gurusher Panjrath, MD, director of advanced heart failure at George Washington University in Washington and a designated discussant for Dr. Shavelle’s report. “The safety seemed very good, and the efficacy was consistent” with prior reports. “There also was high compliance. The key to success is the structure” of patient management, Dr. Pangroth said. “The data are limited by who is monitoring patients and their data and how much of that contact influences patient outcomes.”
That final comment by Dr. Panjrath highlighted the biggest caveat that heart failure clinicians have raised about judging the efficacy of CardioMEMS. To achieve clinical efficacy, the implanted device requires diligent, virtually daily interrogation and data transmission by the patient, assessment of a large amount of data for each patient by the patient’s clinical team, and responsiveness by the patient to medication adjustments directed by the clinical team to deal with episodes of rising PA pressure.
“The device itself has no benefit. It’s the actions prompted by the device that have benefit,” noted Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern University in Chicago and a second designated discussant for the report.
Dr. Shavelle agreed that for the CardioMEMS device to have an impact, one basic requirement is to identify patients who will cooperate with data collection and transmission and also with changes in their medications that are sent to them in response to PA pressure changes. This means selecting patients who appear to have problems with volume overload, including prior hospitalizations for decompensation, and patients who are comfortable interacting with their clinical-care providers. It also means excluding patients who are too sick to benefit from this intervention. He estimated that at his center more than 95% of class III heart failure patients who qualified for inclusion in the post-approval study by clinical criteria were also judged reasonable recipients of the device based on their willingness to cooperate with this system. He also estimated that at the University of Southern California the heart failure clinical team is now caring for about 150 patients with a CardioMEMS device implanted.
Another concern is teasing apart the specific benefit of collecting and using PA pressure data from the contact that the clinical team maintains with CardioMEMS patients.
“If nurses are contacting patients more often, is it the device or the communication? We need to look at that very carefully in a study that had no control group,” Dr. Yancy said in an interview. Contact with a nurse “is the best thing you can do for heart failure patients.”
Dr. Shavelle countered that several reports from past studies that assessed case management and regular monitoring of and contact with heart failure patients but without PA pressure data failed to showed any consistent benefit to patients.
“If you pick the right patients, CardioMEMS works. There is no question in my mind that the device works,” Dr. Shavelle said in an interview. “If you pick the wrong patient, who will not send the data or follow dose changes, then it won’t work.”
The study was sponsored by Abbott, the company that markets the CardioMEMS HF System. Dr. Shavelle has been a consultant to and speaker on behalf of Abbott Vascular and he has received research funding from Abbott Vascular, Abiomed, Biocardia, and V-Wave. Dr. Yancy had an unspecified financial relationship with Abbott Laboratories. Dr. Panjrath had no disclosures.
mzoler@mdedge.com
On Twitter @mitchelzoler
SOURCE: Shavelle DM et al. American College of Cardiology annual meeting, abstract 405-16.
REPORTING FROM ACC 2019
Ocrelizumab effective, safe in relapsing-remitting MS patients
PHILADELPHIA – Ocrelizumab is effective and safe in patients with relapsing-remitting multiple sclerosis who had inadequate responses to previous disease-modifying treatments, said an investigator reporting interim results of a recent nonrandomized study.
The findings of the 600+ patient CHORDS study suggest a positive risk-to-benefit ratio over nearly 1 year for this anti-CD20 monoclonal antibody, said Thomas P. Leist, MD, of Thomas Jefferson University, Philadelphia, at the annual meeting of the American Academy of Neurology (AAN).
“MRI activity has been significantly attenuated in these individuals, particularly, in the period from 24 to 48 weeks, and the overall safety that has been observed to date has been in line with what has been observed in clinical trials with this medication,” Dr. Leist said in a podium presentation.
While previous investigations demonstrated superiority to treatment with interferon in patients with relapsing multiple sclerosis, this phase IIIb study was needed to further clarify the effects of the treatment following suboptimal response to several disease modifying treatments, according to Dr. Leist and his co-investigators.
The intention-to-treat population of CHORDS consisted of 608 patients who received disease-modifying therapy for 6 or more months and discontinued it due to suboptimal response, which was defined as one or more clinically reported relapses, one or more T1 gadolinium-enhancing lesions, or two or more enlarging T2 lesions. They all received a 600 mg dose of ocrelizumab every 24 weeks for as many as 96 weeks.
With 48 weeks of follow-up, the majority of patients had no relapses, no enhancing T1 lesions, no new or enlarging T2 lesions, and no confirmed progression of disability. In all, 54.5% of the patients experienced none of those events, according to Dr. Leist.
The adjusted annualized relapse rate in this cohort was 0.065, he reported.
New MRI activity included 48 new T1 gadolinium-enhancing lesions in 1,174 MRI scans, for an adjusted rate of 0.023, he also reported, while there were 679 new or enlarging T2 lesions on 1,175 scans, for an adjusted rate of 0.581.
The safety in this population was comparable to the overall safety profile of ocrelizumab seen in other studies, according to Dr. Leist. A total of 25 patients, or 4.1%, experienced a serious adverse event, though none led to treatment withdrawal and only one led to a dose modification or interruption, the data show.
Dr. Leist reported disclosures related to Alkermes, Bayer, Biogen, EMD Serono, Genentech, Inc., Novartis, Sanofi Genzyme, Sun Pharma, and Teva Neuroscience.
SOURCE: Leist TP, et al. Presented at the 2019 American Academy of Neurology (AAN) Annual Meeting, May 4-10, 2019. Philadelphia. Presentation S56.007.
PHILADELPHIA – Ocrelizumab is effective and safe in patients with relapsing-remitting multiple sclerosis who had inadequate responses to previous disease-modifying treatments, said an investigator reporting interim results of a recent nonrandomized study.
The findings of the 600+ patient CHORDS study suggest a positive risk-to-benefit ratio over nearly 1 year for this anti-CD20 monoclonal antibody, said Thomas P. Leist, MD, of Thomas Jefferson University, Philadelphia, at the annual meeting of the American Academy of Neurology (AAN).
“MRI activity has been significantly attenuated in these individuals, particularly, in the period from 24 to 48 weeks, and the overall safety that has been observed to date has been in line with what has been observed in clinical trials with this medication,” Dr. Leist said in a podium presentation.
While previous investigations demonstrated superiority to treatment with interferon in patients with relapsing multiple sclerosis, this phase IIIb study was needed to further clarify the effects of the treatment following suboptimal response to several disease modifying treatments, according to Dr. Leist and his co-investigators.
The intention-to-treat population of CHORDS consisted of 608 patients who received disease-modifying therapy for 6 or more months and discontinued it due to suboptimal response, which was defined as one or more clinically reported relapses, one or more T1 gadolinium-enhancing lesions, or two or more enlarging T2 lesions. They all received a 600 mg dose of ocrelizumab every 24 weeks for as many as 96 weeks.
With 48 weeks of follow-up, the majority of patients had no relapses, no enhancing T1 lesions, no new or enlarging T2 lesions, and no confirmed progression of disability. In all, 54.5% of the patients experienced none of those events, according to Dr. Leist.
The adjusted annualized relapse rate in this cohort was 0.065, he reported.
New MRI activity included 48 new T1 gadolinium-enhancing lesions in 1,174 MRI scans, for an adjusted rate of 0.023, he also reported, while there were 679 new or enlarging T2 lesions on 1,175 scans, for an adjusted rate of 0.581.
The safety in this population was comparable to the overall safety profile of ocrelizumab seen in other studies, according to Dr. Leist. A total of 25 patients, or 4.1%, experienced a serious adverse event, though none led to treatment withdrawal and only one led to a dose modification or interruption, the data show.
Dr. Leist reported disclosures related to Alkermes, Bayer, Biogen, EMD Serono, Genentech, Inc., Novartis, Sanofi Genzyme, Sun Pharma, and Teva Neuroscience.
SOURCE: Leist TP, et al. Presented at the 2019 American Academy of Neurology (AAN) Annual Meeting, May 4-10, 2019. Philadelphia. Presentation S56.007.
PHILADELPHIA – Ocrelizumab is effective and safe in patients with relapsing-remitting multiple sclerosis who had inadequate responses to previous disease-modifying treatments, said an investigator reporting interim results of a recent nonrandomized study.
The findings of the 600+ patient CHORDS study suggest a positive risk-to-benefit ratio over nearly 1 year for this anti-CD20 monoclonal antibody, said Thomas P. Leist, MD, of Thomas Jefferson University, Philadelphia, at the annual meeting of the American Academy of Neurology (AAN).
“MRI activity has been significantly attenuated in these individuals, particularly, in the period from 24 to 48 weeks, and the overall safety that has been observed to date has been in line with what has been observed in clinical trials with this medication,” Dr. Leist said in a podium presentation.
While previous investigations demonstrated superiority to treatment with interferon in patients with relapsing multiple sclerosis, this phase IIIb study was needed to further clarify the effects of the treatment following suboptimal response to several disease modifying treatments, according to Dr. Leist and his co-investigators.
The intention-to-treat population of CHORDS consisted of 608 patients who received disease-modifying therapy for 6 or more months and discontinued it due to suboptimal response, which was defined as one or more clinically reported relapses, one or more T1 gadolinium-enhancing lesions, or two or more enlarging T2 lesions. They all received a 600 mg dose of ocrelizumab every 24 weeks for as many as 96 weeks.
With 48 weeks of follow-up, the majority of patients had no relapses, no enhancing T1 lesions, no new or enlarging T2 lesions, and no confirmed progression of disability. In all, 54.5% of the patients experienced none of those events, according to Dr. Leist.
The adjusted annualized relapse rate in this cohort was 0.065, he reported.
New MRI activity included 48 new T1 gadolinium-enhancing lesions in 1,174 MRI scans, for an adjusted rate of 0.023, he also reported, while there were 679 new or enlarging T2 lesions on 1,175 scans, for an adjusted rate of 0.581.
The safety in this population was comparable to the overall safety profile of ocrelizumab seen in other studies, according to Dr. Leist. A total of 25 patients, or 4.1%, experienced a serious adverse event, though none led to treatment withdrawal and only one led to a dose modification or interruption, the data show.
Dr. Leist reported disclosures related to Alkermes, Bayer, Biogen, EMD Serono, Genentech, Inc., Novartis, Sanofi Genzyme, Sun Pharma, and Teva Neuroscience.
SOURCE: Leist TP, et al. Presented at the 2019 American Academy of Neurology (AAN) Annual Meeting, May 4-10, 2019. Philadelphia. Presentation S56.007.
FROM AAN 2019
Gentamicin restores wound healing in hereditary epidermolysis bullosa
Rare progress seen in challenging disease
CHICAGO – Topical gentamicin counters the nonsense mutations that inhibit production of laminin 332 in infants with Herlitz junctional epidermolysis bullosa (H-JEB) to allow lesion healing, according to results of a small clinical study presented at the annual meeting of the Society for Investigative Dermatology.
“All of the children treated so far have responded,” reported Andrew Kwong, who will soon graduate from the Keck School of Medicine at the University of Southern California, Los Angeles.
H-JEB is an inherited blistering skin disease associated with nonsense mutations in the LAMA3, LAMB3, or LAMC2 genes that result in impaired production of functional laminin 332, an essential protein for epidermal-dermal adherence. At this time there are no effective therapies, and the disease is fatal.
The small clinical study was initiated after in vitro studies demonstrated that gentamicin restored functional laminin 332 in cultured keratinocytes from infants with H-JEB. The dose-dependent effect was credited to the ability of gentamicin to induce readthrough of premature stop codons that block production of laminin 332.
Data were presented on the first three infants with H-JEB treated with oral gentamicin. In each child, lesions were treated with topical 0.5% gentamicin twice daily for two weeks. Biopsies were taken prior to the initiation of treatment and at one and three months after treatment. The primary outcome was change in laminin 332, but clinical improvement was also monitored.
Although none of the infants had measurable laminin 332 prior to treatment, all lesions treated with topical gentamicin developed localized laminin 332 at the dermal-epidermal junction of the skin, Mr. Kwong reported. This expression, which was about 40% to 60% of that seen in normal skin, still persisted when evaluated three months after treatment.
The expression was associated with resolution of existing lesions and a reduced risk of developing new lesions, according to Mr. Kwong. In lesions that went untreated, there was no change.
Other molecular changes in the skin, such as increased expression and polarization of beta-4 integrin, were consistent with the ability of gentamicin to address the underlying pathophysiology of H-JEB. There were no adverse events observed.
By restoring functional laminin 332 in the skin, topical gentamicin appears to address the underlying cause of the bullae associated with H-JEB, but Mr. Kwong said that the next step is to determine whether intravenous gentamicin can address the systemic effects. If so, this treatment has the potential to improve survival. He reported that an infant with H-JEB was recently started on intravenous treatment, and initial results were encouraging.
Asked whether he would recommend topical gentamicin on the basis of these findings, Mr. Kwong cautioned that the case series remains very small, but he noted that the uniformity of the positive response is encouraging. He expects that off-label use of this novel and low-cost approach might be warranted in a population that has very limited therapeutic options.
SOURCE: Kwong A. SID 2019;S102, Abstract 594. Annual meeting of the Society for Investigative Dermatology.
Rare progress seen in challenging disease
Rare progress seen in challenging disease
CHICAGO – Topical gentamicin counters the nonsense mutations that inhibit production of laminin 332 in infants with Herlitz junctional epidermolysis bullosa (H-JEB) to allow lesion healing, according to results of a small clinical study presented at the annual meeting of the Society for Investigative Dermatology.
“All of the children treated so far have responded,” reported Andrew Kwong, who will soon graduate from the Keck School of Medicine at the University of Southern California, Los Angeles.
H-JEB is an inherited blistering skin disease associated with nonsense mutations in the LAMA3, LAMB3, or LAMC2 genes that result in impaired production of functional laminin 332, an essential protein for epidermal-dermal adherence. At this time there are no effective therapies, and the disease is fatal.
The small clinical study was initiated after in vitro studies demonstrated that gentamicin restored functional laminin 332 in cultured keratinocytes from infants with H-JEB. The dose-dependent effect was credited to the ability of gentamicin to induce readthrough of premature stop codons that block production of laminin 332.
Data were presented on the first three infants with H-JEB treated with oral gentamicin. In each child, lesions were treated with topical 0.5% gentamicin twice daily for two weeks. Biopsies were taken prior to the initiation of treatment and at one and three months after treatment. The primary outcome was change in laminin 332, but clinical improvement was also monitored.
Although none of the infants had measurable laminin 332 prior to treatment, all lesions treated with topical gentamicin developed localized laminin 332 at the dermal-epidermal junction of the skin, Mr. Kwong reported. This expression, which was about 40% to 60% of that seen in normal skin, still persisted when evaluated three months after treatment.
The expression was associated with resolution of existing lesions and a reduced risk of developing new lesions, according to Mr. Kwong. In lesions that went untreated, there was no change.
Other molecular changes in the skin, such as increased expression and polarization of beta-4 integrin, were consistent with the ability of gentamicin to address the underlying pathophysiology of H-JEB. There were no adverse events observed.
By restoring functional laminin 332 in the skin, topical gentamicin appears to address the underlying cause of the bullae associated with H-JEB, but Mr. Kwong said that the next step is to determine whether intravenous gentamicin can address the systemic effects. If so, this treatment has the potential to improve survival. He reported that an infant with H-JEB was recently started on intravenous treatment, and initial results were encouraging.
Asked whether he would recommend topical gentamicin on the basis of these findings, Mr. Kwong cautioned that the case series remains very small, but he noted that the uniformity of the positive response is encouraging. He expects that off-label use of this novel and low-cost approach might be warranted in a population that has very limited therapeutic options.
SOURCE: Kwong A. SID 2019;S102, Abstract 594. Annual meeting of the Society for Investigative Dermatology.
CHICAGO – Topical gentamicin counters the nonsense mutations that inhibit production of laminin 332 in infants with Herlitz junctional epidermolysis bullosa (H-JEB) to allow lesion healing, according to results of a small clinical study presented at the annual meeting of the Society for Investigative Dermatology.
“All of the children treated so far have responded,” reported Andrew Kwong, who will soon graduate from the Keck School of Medicine at the University of Southern California, Los Angeles.
H-JEB is an inherited blistering skin disease associated with nonsense mutations in the LAMA3, LAMB3, or LAMC2 genes that result in impaired production of functional laminin 332, an essential protein for epidermal-dermal adherence. At this time there are no effective therapies, and the disease is fatal.
The small clinical study was initiated after in vitro studies demonstrated that gentamicin restored functional laminin 332 in cultured keratinocytes from infants with H-JEB. The dose-dependent effect was credited to the ability of gentamicin to induce readthrough of premature stop codons that block production of laminin 332.
Data were presented on the first three infants with H-JEB treated with oral gentamicin. In each child, lesions were treated with topical 0.5% gentamicin twice daily for two weeks. Biopsies were taken prior to the initiation of treatment and at one and three months after treatment. The primary outcome was change in laminin 332, but clinical improvement was also monitored.
Although none of the infants had measurable laminin 332 prior to treatment, all lesions treated with topical gentamicin developed localized laminin 332 at the dermal-epidermal junction of the skin, Mr. Kwong reported. This expression, which was about 40% to 60% of that seen in normal skin, still persisted when evaluated three months after treatment.
The expression was associated with resolution of existing lesions and a reduced risk of developing new lesions, according to Mr. Kwong. In lesions that went untreated, there was no change.
Other molecular changes in the skin, such as increased expression and polarization of beta-4 integrin, were consistent with the ability of gentamicin to address the underlying pathophysiology of H-JEB. There were no adverse events observed.
By restoring functional laminin 332 in the skin, topical gentamicin appears to address the underlying cause of the bullae associated with H-JEB, but Mr. Kwong said that the next step is to determine whether intravenous gentamicin can address the systemic effects. If so, this treatment has the potential to improve survival. He reported that an infant with H-JEB was recently started on intravenous treatment, and initial results were encouraging.
Asked whether he would recommend topical gentamicin on the basis of these findings, Mr. Kwong cautioned that the case series remains very small, but he noted that the uniformity of the positive response is encouraging. He expects that off-label use of this novel and low-cost approach might be warranted in a population that has very limited therapeutic options.
SOURCE: Kwong A. SID 2019;S102, Abstract 594. Annual meeting of the Society for Investigative Dermatology.
REPORTING FROM SID 2019
Magnetic beads functionalized with VEGF could treat preeclampsia
A method of apheresis using vascular endothelial growth factor functionalized magnetic beads reduced levels of the soluble form of the vascular endothelial growth factor 1 in blood from women with preeclampsia, according to recent research published in the journal Hypertension.
The approach both reduces levels of the soluble form of the vascular endothelial growth factor 1 (sFlt-1) and releases placental growth factor (PlGF), which could help restore endothelial function in women with preeclampsia. The researchers said they chose sFlt-1 as a target because of “mounting evidence of its involvement in the pathogenesis of preeclampsia.” sFlt-1 has been suspected of inhibiting angiogenic signaling through “direct sequestration of angiogenic ligands” vascular endothelial growth factor (VEGF) and PlGF as well as “dominant-negative heterodimerization with surface VEGFRs.”
“During normal pregnancy, massive amounts of PlGF are produced by the placenta, reaching concentrations of free PlGF around 400 pg/mL, whereas during preeclampsia, free PlGF is extremely low due to the release of sFlt-1 into the maternal circulation,” the researchers said.
Using VEGF-functionalized magnetic beads, the researchers performed static and dynamic experiments using phosphate buffered saline (PBS), conditioned media, and plasma from women with preeclampsia. Under static conditions, there was a decrease of 33% for sFlt-1 and an increase of 27% for PlGF, while in dynamic conditions, there was a 40% decrease in sFlt-1 and a twofold increase in freed PlGF. When tested with plasma from women with preeclampsia, the ratio of sFlt-1/PlGF decreased by 63%, and VEGF release was associated with apheresis.
“This was a proof of concept study and our approach aims to restore physiologic levels of angiogenic factors,” Vassilis Tsatsaris, MD, PhD, of Cochin Hospital, Paris, said in a press release. “The reduction of sFlt-1 and the release of angiogenic factors is very significant and promising.”
Dr. Tsatsaris and his colleagues noted their next steps are to optimize the process of reducing sFlt-1 and examining how the approach works in an animal model.
“During normal pregnancy, circulating free VEGF levels are very low, almost undetectable with noncompetitive [enzyme-linked immunosorbent assay] ELISA. Whether these extremely low levels of VEGF have a physiological role during pregnancy is not known,” they wrote.
This study was funded by Agence Nationale pour la recherche, Institut Pierre Gilles de Gennes and the PremUP Foundation. One author reported receiving a grant from the Ecole Normale Supérieure and a second author reported receiving a grant from the Fondation pour la Recherche Médicale. The other authors report no relevant conflicts of interest.
SOURCE: Trapiella-Alfonso L et al. Hypertension. 2019. doi: 10.1161/HYPERTENSIONAHA.118.12380.
A method of apheresis using vascular endothelial growth factor functionalized magnetic beads reduced levels of the soluble form of the vascular endothelial growth factor 1 in blood from women with preeclampsia, according to recent research published in the journal Hypertension.
The approach both reduces levels of the soluble form of the vascular endothelial growth factor 1 (sFlt-1) and releases placental growth factor (PlGF), which could help restore endothelial function in women with preeclampsia. The researchers said they chose sFlt-1 as a target because of “mounting evidence of its involvement in the pathogenesis of preeclampsia.” sFlt-1 has been suspected of inhibiting angiogenic signaling through “direct sequestration of angiogenic ligands” vascular endothelial growth factor (VEGF) and PlGF as well as “dominant-negative heterodimerization with surface VEGFRs.”
“During normal pregnancy, massive amounts of PlGF are produced by the placenta, reaching concentrations of free PlGF around 400 pg/mL, whereas during preeclampsia, free PlGF is extremely low due to the release of sFlt-1 into the maternal circulation,” the researchers said.
Using VEGF-functionalized magnetic beads, the researchers performed static and dynamic experiments using phosphate buffered saline (PBS), conditioned media, and plasma from women with preeclampsia. Under static conditions, there was a decrease of 33% for sFlt-1 and an increase of 27% for PlGF, while in dynamic conditions, there was a 40% decrease in sFlt-1 and a twofold increase in freed PlGF. When tested with plasma from women with preeclampsia, the ratio of sFlt-1/PlGF decreased by 63%, and VEGF release was associated with apheresis.
“This was a proof of concept study and our approach aims to restore physiologic levels of angiogenic factors,” Vassilis Tsatsaris, MD, PhD, of Cochin Hospital, Paris, said in a press release. “The reduction of sFlt-1 and the release of angiogenic factors is very significant and promising.”
Dr. Tsatsaris and his colleagues noted their next steps are to optimize the process of reducing sFlt-1 and examining how the approach works in an animal model.
“During normal pregnancy, circulating free VEGF levels are very low, almost undetectable with noncompetitive [enzyme-linked immunosorbent assay] ELISA. Whether these extremely low levels of VEGF have a physiological role during pregnancy is not known,” they wrote.
This study was funded by Agence Nationale pour la recherche, Institut Pierre Gilles de Gennes and the PremUP Foundation. One author reported receiving a grant from the Ecole Normale Supérieure and a second author reported receiving a grant from the Fondation pour la Recherche Médicale. The other authors report no relevant conflicts of interest.
SOURCE: Trapiella-Alfonso L et al. Hypertension. 2019. doi: 10.1161/HYPERTENSIONAHA.118.12380.
A method of apheresis using vascular endothelial growth factor functionalized magnetic beads reduced levels of the soluble form of the vascular endothelial growth factor 1 in blood from women with preeclampsia, according to recent research published in the journal Hypertension.
The approach both reduces levels of the soluble form of the vascular endothelial growth factor 1 (sFlt-1) and releases placental growth factor (PlGF), which could help restore endothelial function in women with preeclampsia. The researchers said they chose sFlt-1 as a target because of “mounting evidence of its involvement in the pathogenesis of preeclampsia.” sFlt-1 has been suspected of inhibiting angiogenic signaling through “direct sequestration of angiogenic ligands” vascular endothelial growth factor (VEGF) and PlGF as well as “dominant-negative heterodimerization with surface VEGFRs.”
“During normal pregnancy, massive amounts of PlGF are produced by the placenta, reaching concentrations of free PlGF around 400 pg/mL, whereas during preeclampsia, free PlGF is extremely low due to the release of sFlt-1 into the maternal circulation,” the researchers said.
Using VEGF-functionalized magnetic beads, the researchers performed static and dynamic experiments using phosphate buffered saline (PBS), conditioned media, and plasma from women with preeclampsia. Under static conditions, there was a decrease of 33% for sFlt-1 and an increase of 27% for PlGF, while in dynamic conditions, there was a 40% decrease in sFlt-1 and a twofold increase in freed PlGF. When tested with plasma from women with preeclampsia, the ratio of sFlt-1/PlGF decreased by 63%, and VEGF release was associated with apheresis.
“This was a proof of concept study and our approach aims to restore physiologic levels of angiogenic factors,” Vassilis Tsatsaris, MD, PhD, of Cochin Hospital, Paris, said in a press release. “The reduction of sFlt-1 and the release of angiogenic factors is very significant and promising.”
Dr. Tsatsaris and his colleagues noted their next steps are to optimize the process of reducing sFlt-1 and examining how the approach works in an animal model.
“During normal pregnancy, circulating free VEGF levels are very low, almost undetectable with noncompetitive [enzyme-linked immunosorbent assay] ELISA. Whether these extremely low levels of VEGF have a physiological role during pregnancy is not known,” they wrote.
This study was funded by Agence Nationale pour la recherche, Institut Pierre Gilles de Gennes and the PremUP Foundation. One author reported receiving a grant from the Ecole Normale Supérieure and a second author reported receiving a grant from the Fondation pour la Recherche Médicale. The other authors report no relevant conflicts of interest.
SOURCE: Trapiella-Alfonso L et al. Hypertension. 2019. doi: 10.1161/HYPERTENSIONAHA.118.12380.
FROM HYPERTENSION
Key clinical point: Use of magnetic beads functionalized with vascular endothelial growth factor (VEGF) reduced the soluble form of endothelial growth factor 1 (sFlt-1) in the blood of women with preeclampsia.
Major finding: sFlt-1 was reduced by 40% under dynamic conditions, and there was a twofold increase in the amount of freed placental growth factor.
Study details: A proof-of-concept study using VEGF-functionalized magnetic beads and phosphate buffered saline (PBS), conditioned media, and plasma from women with preeclampsia.
Disclosures: This study was funded by Agence Nationale pour la recherche, Institut Pierre Gilles de Gennes, and the PremUP Foundation. One author reported receiving a grant from the Ecole Normale Supérieure and a second author reported receiving a grant from the Fondation pour la Recherche Médicale. The other authors reported no relevant conflicts of interest.
Source: Trapiella-Alfonso L et al. Hypertension. 2019. doi: 10.1161/HYPERTENSIONAHA.118.12380.
Post-treatment persistence of oral HPV in HNSCC predicts recurrence, death
Persistence of oral human papillomavirus (HPV) DNA after primary treatment of HPV-positive oral cavity or oropharyngeal head and neck squamous cell carcinoma (HNSCC) is a strong risk factor for poor outcomes, finds a prospective cohort study.

Investigators working under senior author Maura L. Gillison, MD, PhD, of the department of thoracic head and neck medical oncology at the University of Texas MD Anderson Cancer Center, Houston, collected serial oral rinses from 396 patients with HNSCC (217 with oropharyngeal cancer, 170 with oral cavity cancer, 9 with unknown primary cancer) treated at two institutions. Overall, 51% had HPV-positive tumors.
Patients with HPV-positive tumors were much more likely to have detectable oral HPV at diagnosis than their counterparts with HPV-negative tumors (84.2% vs 12.4%; P less than .001). Detection of oral HPV-16 DNA had good sensitivity (81%) and excellent specificity (100%) for HPV-16-positive tumors, Dr. Gillison and colleagues reported in JAMA Oncology.
Patients’ odds of having detectable tumor-type HPV fell during primary therapy (odds ratio per each postdiagnosis month, 0.41; P less than .001); in contrast, their odds of having of having detectable nontumor types did not. Current smokers were about half as likely to achieve clearing of tumor-type HPV DNA (hazard ratio, 0.49; P = .01).
Compared with counterparts who no longer had detectable tumor-type DNA after therapy, HPV-positive patients who did had dramatically poorer recurrence-free survival (55% vs. 88%; adjusted hazard ratio, 3.72; P less than .001) and overall survival (68% vs. 95%; adjusted hazard ratio, 6.61; P = .003).
In contrast, persistence of nontumor-type HPV DNA did not predict these outcomes among either patients with HPV-positive tumors or patients with HPV-negative tumors.
“Analysis of tumor type HPV DNA has considerable promise as a biomarker for treatment response and risk of progression,” Dr. Gillison and coinvestigators maintain.
“Our data suggest that a subset of patients with HPV-positive HNSCC at high-risk for locoregional recurrence can be identified by detection of persistent, oral HPV after treatment. However, the clinical utility may be constrained by a need to identify the tumor-type infection, a low-moderate positive predictive value for recurrence, and weak associations with risk of distant metastases,” they conclude. “Ongoing studies will evaluate whether multiplexed detection of plasma HPV DNA can improve these limitations.”
Dr. Gillison disclosed consulting for Roche Holding AG, Bristol-Myers Squibb, Merck & Co Inc., Celgene Corporation, Amgen, AstraZeneca, Rakuten Aspyrian Inc. (now known as Rakuten Medical), EMD Serono Inc., NewLink Genetics Corporation, and Genocea Biosciences. The study was supported by the Oral Cancer Foundation and The Ohio State University Comprehensive Cancer Center. Dr. Gillison is a Cancer Prevention and Research Institute of Texas Scholar.
SOURCE: Fakhry C et al. JAMA Oncol. 2019 May 2. doi: 10.1001/jamaoncol.2019.0439.
Persistence of oral human papillomavirus (HPV) DNA after primary treatment of HPV-positive oral cavity or oropharyngeal head and neck squamous cell carcinoma (HNSCC) is a strong risk factor for poor outcomes, finds a prospective cohort study.
Investigators working under senior author Maura L. Gillison, MD, PhD, of the department of thoracic head and neck medical oncology at the University of Texas MD Anderson Cancer Center, Houston, collected serial oral rinses from 396 patients with HNSCC (217 with oropharyngeal cancer, 170 with oral cavity cancer, 9 with unknown primary cancer) treated at two institutions. Overall, 51% had HPV-positive tumors.
Patients with HPV-positive tumors were much more likely to have detectable oral HPV at diagnosis than their counterparts with HPV-negative tumors (84.2% vs 12.4%; P less than .001). Detection of oral HPV-16 DNA had good sensitivity (81%) and excellent specificity (100%) for HPV-16-positive tumors, Dr. Gillison and colleagues reported in JAMA Oncology.
Patients’ odds of having detectable tumor-type HPV fell during primary therapy (odds ratio per each postdiagnosis month, 0.41; P less than .001); in contrast, their odds of having of having detectable nontumor types did not. Current smokers were about half as likely to achieve clearing of tumor-type HPV DNA (hazard ratio, 0.49; P = .01).
Compared with counterparts who no longer had detectable tumor-type DNA after therapy, HPV-positive patients who did had dramatically poorer recurrence-free survival (55% vs. 88%; adjusted hazard ratio, 3.72; P less than .001) and overall survival (68% vs. 95%; adjusted hazard ratio, 6.61; P = .003).
In contrast, persistence of nontumor-type HPV DNA did not predict these outcomes among either patients with HPV-positive tumors or patients with HPV-negative tumors.
“Analysis of tumor type HPV DNA has considerable promise as a biomarker for treatment response and risk of progression,” Dr. Gillison and coinvestigators maintain.
“Our data suggest that a subset of patients with HPV-positive HNSCC at high-risk for locoregional recurrence can be identified by detection of persistent, oral HPV after treatment. However, the clinical utility may be constrained by a need to identify the tumor-type infection, a low-moderate positive predictive value for recurrence, and weak associations with risk of distant metastases,” they conclude. “Ongoing studies will evaluate whether multiplexed detection of plasma HPV DNA can improve these limitations.”
Dr. Gillison disclosed consulting for Roche Holding AG, Bristol-Myers Squibb, Merck & Co Inc., Celgene Corporation, Amgen, AstraZeneca, Rakuten Aspyrian Inc. (now known as Rakuten Medical), EMD Serono Inc., NewLink Genetics Corporation, and Genocea Biosciences. The study was supported by the Oral Cancer Foundation and The Ohio State University Comprehensive Cancer Center. Dr. Gillison is a Cancer Prevention and Research Institute of Texas Scholar.
SOURCE: Fakhry C et al. JAMA Oncol. 2019 May 2. doi: 10.1001/jamaoncol.2019.0439.
Persistence of oral human papillomavirus (HPV) DNA after primary treatment of HPV-positive oral cavity or oropharyngeal head and neck squamous cell carcinoma (HNSCC) is a strong risk factor for poor outcomes, finds a prospective cohort study.
Investigators working under senior author Maura L. Gillison, MD, PhD, of the department of thoracic head and neck medical oncology at the University of Texas MD Anderson Cancer Center, Houston, collected serial oral rinses from 396 patients with HNSCC (217 with oropharyngeal cancer, 170 with oral cavity cancer, 9 with unknown primary cancer) treated at two institutions. Overall, 51% had HPV-positive tumors.
Patients with HPV-positive tumors were much more likely to have detectable oral HPV at diagnosis than their counterparts with HPV-negative tumors (84.2% vs 12.4%; P less than .001). Detection of oral HPV-16 DNA had good sensitivity (81%) and excellent specificity (100%) for HPV-16-positive tumors, Dr. Gillison and colleagues reported in JAMA Oncology.
Patients’ odds of having detectable tumor-type HPV fell during primary therapy (odds ratio per each postdiagnosis month, 0.41; P less than .001); in contrast, their odds of having of having detectable nontumor types did not. Current smokers were about half as likely to achieve clearing of tumor-type HPV DNA (hazard ratio, 0.49; P = .01).
Compared with counterparts who no longer had detectable tumor-type DNA after therapy, HPV-positive patients who did had dramatically poorer recurrence-free survival (55% vs. 88%; adjusted hazard ratio, 3.72; P less than .001) and overall survival (68% vs. 95%; adjusted hazard ratio, 6.61; P = .003).
In contrast, persistence of nontumor-type HPV DNA did not predict these outcomes among either patients with HPV-positive tumors or patients with HPV-negative tumors.
“Analysis of tumor type HPV DNA has considerable promise as a biomarker for treatment response and risk of progression,” Dr. Gillison and coinvestigators maintain.
“Our data suggest that a subset of patients with HPV-positive HNSCC at high-risk for locoregional recurrence can be identified by detection of persistent, oral HPV after treatment. However, the clinical utility may be constrained by a need to identify the tumor-type infection, a low-moderate positive predictive value for recurrence, and weak associations with risk of distant metastases,” they conclude. “Ongoing studies will evaluate whether multiplexed detection of plasma HPV DNA can improve these limitations.”
Dr. Gillison disclosed consulting for Roche Holding AG, Bristol-Myers Squibb, Merck & Co Inc., Celgene Corporation, Amgen, AstraZeneca, Rakuten Aspyrian Inc. (now known as Rakuten Medical), EMD Serono Inc., NewLink Genetics Corporation, and Genocea Biosciences. The study was supported by the Oral Cancer Foundation and The Ohio State University Comprehensive Cancer Center. Dr. Gillison is a Cancer Prevention and Research Institute of Texas Scholar.
SOURCE: Fakhry C et al. JAMA Oncol. 2019 May 2. doi: 10.1001/jamaoncol.2019.0439.
FROM JAMA ONCOLOGY
Key clinical point: Persistence of detectable tumor-type HPV DNA in oral rinses after primary treatment of HPV-positive HNSCC identifies patients at high risk for poor outcomes.
Major finding: HPV-positive patients with persistent oral tumor-type HPV DNA had sharply higher risks of 2-year recurrence-free survival events (hazard ratio, 3.72; P less than .001) and death (hazard ratio, 6.61; P = .003).
Study details: Prospective cohort study of 396 patients with newly diagnosed oral cavity or oropharyngeal HNSCC.
Disclosures: Dr. Gillison disclosed consulting for Roche Holding AG, Bristol-Myers Squibb, Merck & Co Inc., Celgene Corporation, Amgen, AstraZeneca, Rakuten Aspyrian Inc. (now known as Rakuten Medical), EMD Serono Inc., NewLink Genetics Corporation, and Genocea Biosciences. The study was supported by the Oral Cancer Foundation and The Ohio State University Comprehensive Cancer Center. Dr. Gillison is a Cancer Prevention and Research Institute of Texas Scholar.
Source: Gillison ML et al. JAMA Oncol. 2019 May 2. doi: 10.1001/jamaoncol.2019.0439.
FMT explored as a potential weight loss treatment
“Currently, fecal microbiota transplantation [FMT] can only be performed clinically in the US to treat recurrent Clostridium difficile infection,” lead study author Jessica R. Allegretti, MD, MPH, said during a media briefing in advance of the annual Digestive Disease Week.

“However, there is ongoing research to find out whether FMT works for other health conditions such as obesity, a condition which affects millions of people worldwide. [It’s] a condition that also increases the risk of developing many other illnesses, including diabetes, heart disease, and certain cancers. In my clinical practice, we regularly see patients who have not yet developed some of these other conditions related to obesity, but really do have difficulty losing weight. Through our research we wanted to focus on a population we call the medically uncompromised obese, and understand if FMT might be a viable treatment option for them,” she said.
Dr. Allegretti, director of the fecal microbiota transplant program at Brigham and Women’s Hospital, Boston, conducted a parallel study of 22 patients with a body mass index of 35 kg/m2 or higher who were metabolically healthy – defined as having no type 2 diabetes, nonalcoholic steatohepatitis (NASH), or metabolic syndrome. They randomized study participants 1:1 to receive 30 FMT capsules followed by two doses of 12 capsules over a 12-week period, or identical placebo capsules. A single healthy lean donor with a BMI of 17 kg/m2 was used.
The researchers assessed patients with a mixed meal tolerance test at baseline, week 6, and week 12 post-FMT, at which biomarkers GLP-1 and leptin were measured. Stool was collected at baseline and at one, four, six, eight, and 12 weeks post-FMT. The primary outcomes were safety and change in the area under the curve for GLP-1 at 12 weeks compared to baseline. Secondary endpoints include gut microbiome profiles and diversity as well as bile acid profiles at 12 weeks post FMT. Additional endpoints include a decrease in BMI and waist circumference at week 12. Standard stool microbiome and bile acid analysis was performed.
The mean age of the patients at baseline was 43 years, and their mean BMI was 41 kg/m2. Between baseline and week 12, the research observed no increase of GLP-1 in either group, while the change in leptin revealed an increase in the placebo group only (P less than .001). At week 12, no early changes in BMI were noted in either group (P = .51). No serious adverse events occurred in either arm.
Dr. Allegretti and her colleagues observed global signals of donor community engraftment following FMT, including an increase in alpha diversity and increased similarity to stool samples from the FMT donor – trends that were not observed in the placebo arm. In addition, bile acid analysis suggested a sustained decrease in taurocholic acid in the FMT arm, comparable with the donor – an effect that was not seen in the placebo arm. “We know that what leads to the germination of C. diff. spores is brought out by bile acids,” she said. “That’s one of the critical components of pathogenesis in that disease. My group has been able to show that after FMT, you regain bile acid homeostasis.”
Dr. Allegretti concluded her remarks by noting that the current study “adds an encouraging first step in trying to understand the role that the gut microbiome is playing in the pathogenesis of medically uncompromised obese patients. As a next step, we plan to seek more sensitive measures of GLP-1, as well as conduct additional research into varied doses of FMT capsules, as well as potentially investigating other microbial pathways to better understand the role the microbiome is playing in obesity.”
Somerville, Mass.–based Finch Therapeutics provided funding for the research. Dr. Allegretti reported having no financial disclosures.
SOURCE: Allegretti J et al. DDW 2019. Abstract 621.
“Currently, fecal microbiota transplantation [FMT] can only be performed clinically in the US to treat recurrent Clostridium difficile infection,” lead study author Jessica R. Allegretti, MD, MPH, said during a media briefing in advance of the annual Digestive Disease Week.
“However, there is ongoing research to find out whether FMT works for other health conditions such as obesity, a condition which affects millions of people worldwide. [It’s] a condition that also increases the risk of developing many other illnesses, including diabetes, heart disease, and certain cancers. In my clinical practice, we regularly see patients who have not yet developed some of these other conditions related to obesity, but really do have difficulty losing weight. Through our research we wanted to focus on a population we call the medically uncompromised obese, and understand if FMT might be a viable treatment option for them,” she said.
Dr. Allegretti, director of the fecal microbiota transplant program at Brigham and Women’s Hospital, Boston, conducted a parallel study of 22 patients with a body mass index of 35 kg/m2 or higher who were metabolically healthy – defined as having no type 2 diabetes, nonalcoholic steatohepatitis (NASH), or metabolic syndrome. They randomized study participants 1:1 to receive 30 FMT capsules followed by two doses of 12 capsules over a 12-week period, or identical placebo capsules. A single healthy lean donor with a BMI of 17 kg/m2 was used.
The researchers assessed patients with a mixed meal tolerance test at baseline, week 6, and week 12 post-FMT, at which biomarkers GLP-1 and leptin were measured. Stool was collected at baseline and at one, four, six, eight, and 12 weeks post-FMT. The primary outcomes were safety and change in the area under the curve for GLP-1 at 12 weeks compared to baseline. Secondary endpoints include gut microbiome profiles and diversity as well as bile acid profiles at 12 weeks post FMT. Additional endpoints include a decrease in BMI and waist circumference at week 12. Standard stool microbiome and bile acid analysis was performed.
The mean age of the patients at baseline was 43 years, and their mean BMI was 41 kg/m2. Between baseline and week 12, the research observed no increase of GLP-1 in either group, while the change in leptin revealed an increase in the placebo group only (P less than .001). At week 12, no early changes in BMI were noted in either group (P = .51). No serious adverse events occurred in either arm.
Dr. Allegretti and her colleagues observed global signals of donor community engraftment following FMT, including an increase in alpha diversity and increased similarity to stool samples from the FMT donor – trends that were not observed in the placebo arm. In addition, bile acid analysis suggested a sustained decrease in taurocholic acid in the FMT arm, comparable with the donor – an effect that was not seen in the placebo arm. “We know that what leads to the germination of C. diff. spores is brought out by bile acids,” she said. “That’s one of the critical components of pathogenesis in that disease. My group has been able to show that after FMT, you regain bile acid homeostasis.”
Dr. Allegretti concluded her remarks by noting that the current study “adds an encouraging first step in trying to understand the role that the gut microbiome is playing in the pathogenesis of medically uncompromised obese patients. As a next step, we plan to seek more sensitive measures of GLP-1, as well as conduct additional research into varied doses of FMT capsules, as well as potentially investigating other microbial pathways to better understand the role the microbiome is playing in obesity.”
Somerville, Mass.–based Finch Therapeutics provided funding for the research. Dr. Allegretti reported having no financial disclosures.
SOURCE: Allegretti J et al. DDW 2019. Abstract 621.
“Currently, fecal microbiota transplantation [FMT] can only be performed clinically in the US to treat recurrent Clostridium difficile infection,” lead study author Jessica R. Allegretti, MD, MPH, said during a media briefing in advance of the annual Digestive Disease Week.
“However, there is ongoing research to find out whether FMT works for other health conditions such as obesity, a condition which affects millions of people worldwide. [It’s] a condition that also increases the risk of developing many other illnesses, including diabetes, heart disease, and certain cancers. In my clinical practice, we regularly see patients who have not yet developed some of these other conditions related to obesity, but really do have difficulty losing weight. Through our research we wanted to focus on a population we call the medically uncompromised obese, and understand if FMT might be a viable treatment option for them,” she said.
Dr. Allegretti, director of the fecal microbiota transplant program at Brigham and Women’s Hospital, Boston, conducted a parallel study of 22 patients with a body mass index of 35 kg/m2 or higher who were metabolically healthy – defined as having no type 2 diabetes, nonalcoholic steatohepatitis (NASH), or metabolic syndrome. They randomized study participants 1:1 to receive 30 FMT capsules followed by two doses of 12 capsules over a 12-week period, or identical placebo capsules. A single healthy lean donor with a BMI of 17 kg/m2 was used.
The researchers assessed patients with a mixed meal tolerance test at baseline, week 6, and week 12 post-FMT, at which biomarkers GLP-1 and leptin were measured. Stool was collected at baseline and at one, four, six, eight, and 12 weeks post-FMT. The primary outcomes were safety and change in the area under the curve for GLP-1 at 12 weeks compared to baseline. Secondary endpoints include gut microbiome profiles and diversity as well as bile acid profiles at 12 weeks post FMT. Additional endpoints include a decrease in BMI and waist circumference at week 12. Standard stool microbiome and bile acid analysis was performed.
The mean age of the patients at baseline was 43 years, and their mean BMI was 41 kg/m2. Between baseline and week 12, the research observed no increase of GLP-1 in either group, while the change in leptin revealed an increase in the placebo group only (P less than .001). At week 12, no early changes in BMI were noted in either group (P = .51). No serious adverse events occurred in either arm.
Dr. Allegretti and her colleagues observed global signals of donor community engraftment following FMT, including an increase in alpha diversity and increased similarity to stool samples from the FMT donor – trends that were not observed in the placebo arm. In addition, bile acid analysis suggested a sustained decrease in taurocholic acid in the FMT arm, comparable with the donor – an effect that was not seen in the placebo arm. “We know that what leads to the germination of C. diff. spores is brought out by bile acids,” she said. “That’s one of the critical components of pathogenesis in that disease. My group has been able to show that after FMT, you regain bile acid homeostasis.”
Dr. Allegretti concluded her remarks by noting that the current study “adds an encouraging first step in trying to understand the role that the gut microbiome is playing in the pathogenesis of medically uncompromised obese patients. As a next step, we plan to seek more sensitive measures of GLP-1, as well as conduct additional research into varied doses of FMT capsules, as well as potentially investigating other microbial pathways to better understand the role the microbiome is playing in obesity.”
Somerville, Mass.–based Finch Therapeutics provided funding for the research. Dr. Allegretti reported having no financial disclosures.
SOURCE: Allegretti J et al. DDW 2019. Abstract 621.
REPORTING FROM DDW 2019
Key clinical point: Using capsules filled with fecal matter from a lean donor, researchers successfully changed some of the composition of the gut microbiota of patients with obesity.
Major finding: Following fecal microbiota transplantation, researchers detected a decrease in a specific bile acid and alterations in stool samples that showed increased similarity to those of the lean donor.
Study details: A randomized, placebo-controlled trial of 22 healthy obese patients.
Disclosures: Somerville, Mass.–based Finch Therapeutics provided funding for the research. Dr. Allegretti reported having no financial disclosures.
Source: Allegretti J et al. DDW 2019. Abstract 621.
Age may be a driver of therapeutic testosterone level in transgender men
LOS ANGELES – The dose of testosterone required to maintain a therapeutic level in transgender men is not correlated with body mass index but does decrease with age, results from a single-center study have shown.
“At this point, there are limited data regarding the dosing of testosterone in relation to age and BMI, which is what makes our work unique,” one of the study authors, Sushmitha Echt, MD, said in an interview following the annual scientific and clinical congress of the American Association of Clinical Endocrinologists.

“Although we have guidelines regarding initiating hormonal therapy for transgender patients, such as the Endocrine Society’s Clinical Practice Guidelines from 2017, we do not have much data regarding the optimal dosing of testosterone in transgender men. We hope that with more research, we will have more data to drive our treatment decisions for our transgender patients.”
Dr. Echt, an endocrinology fellow at North Shore University Hospital, Manhassett, NY, and her colleague, Aren Skolnick, DO, retrospectively evaluated 40 transgender men who were treated at the medical center between July 1, 2014 and July 1, 2018. They performed univariate and multivariate mixed-model analyses to determine the relationship between testosterone dose, age, and body mass index (BMI), and Cox regression analysis to determine the relationship between time to development of each physical attribute, testosterone dose, and route of administration.
The patients ranged in age from 18 to 54 years, and their mean baseline age was 25 years. At the time of their first visit, 32 of the patients were on intramuscular testosterone, four were on subcutaneous testosterone, and five were on the transdermal form.
By the end of the study, 28 patients remained on intramuscular testosterone, six were on the subcutaneous form, five were on the transdermal form, and one had transitioned to testosterone pellets. The majority of patients (37) became therapeutic during the course of the study, and the average therapeutic testosterone level was 551.7 ng/dL.
During an average follow-up time of one year, the researchers observed no correlation between testosterone dose and BMI. However, they found a negative correlation between testosterone dose and age, with or without adjustment for BMI (P = .016 and P = .020, respectively). Adjusted for BMI, the dose decreased by 2.0 mg for every one-year increase in age.
A subgroup analysis of the new patients again revealed a negative correlation between testosterone dose and age, with or without adjustment for BMI (P = .013 and P = .019, respectively). Adjusted for BMI, the dose decreased by 2.5 mg for every one-year increase in age.
Subgroup analysis of the patients already on testosterone therapy revealed no association between testosterone dose, age, and BMI. Among the new patients, no association was observed between time to development of each physical attribute and testosterone dose or route of administration. Among the new patients, 73% reported hair growth (mean time, 89 days), deepening of voice (51 days), and cessation of menses (136 days), and 59% reported clitoromegaly (51 days).
“The finding that surprised us the most is that the testosterone dose needed to maintain a therapeutic testosterone level in transgender men is not related to BMI,” Dr. Echt said. “Some medications are dosed based on body weight, and it was surprising to us that testosterone dosing was not related to weight in kilograms or BMI. Although the findings from our project suggest that the testosterone dose needed for hormonal therapy for transgender men may decrease with older age, further research and larger studies are needed in this field to help guide management of transgender patients.”
Dr. Echt acknowledged certain limitations of the study, including its small sample size. “At this point, our population of transgender patients has been increasing in our practice,” she said. “In the future, we would like to build upon our study by including more patients in our retrospective analysis and then stratify the results by mode of administration of testosterone.”
The researchers reported having no financial disclosures.
LOS ANGELES – The dose of testosterone required to maintain a therapeutic level in transgender men is not correlated with body mass index but does decrease with age, results from a single-center study have shown.
“At this point, there are limited data regarding the dosing of testosterone in relation to age and BMI, which is what makes our work unique,” one of the study authors, Sushmitha Echt, MD, said in an interview following the annual scientific and clinical congress of the American Association of Clinical Endocrinologists.
“Although we have guidelines regarding initiating hormonal therapy for transgender patients, such as the Endocrine Society’s Clinical Practice Guidelines from 2017, we do not have much data regarding the optimal dosing of testosterone in transgender men. We hope that with more research, we will have more data to drive our treatment decisions for our transgender patients.”
Dr. Echt, an endocrinology fellow at North Shore University Hospital, Manhassett, NY, and her colleague, Aren Skolnick, DO, retrospectively evaluated 40 transgender men who were treated at the medical center between July 1, 2014 and July 1, 2018. They performed univariate and multivariate mixed-model analyses to determine the relationship between testosterone dose, age, and body mass index (BMI), and Cox regression analysis to determine the relationship between time to development of each physical attribute, testosterone dose, and route of administration.
The patients ranged in age from 18 to 54 years, and their mean baseline age was 25 years. At the time of their first visit, 32 of the patients were on intramuscular testosterone, four were on subcutaneous testosterone, and five were on the transdermal form.
By the end of the study, 28 patients remained on intramuscular testosterone, six were on the subcutaneous form, five were on the transdermal form, and one had transitioned to testosterone pellets. The majority of patients (37) became therapeutic during the course of the study, and the average therapeutic testosterone level was 551.7 ng/dL.
During an average follow-up time of one year, the researchers observed no correlation between testosterone dose and BMI. However, they found a negative correlation between testosterone dose and age, with or without adjustment for BMI (P = .016 and P = .020, respectively). Adjusted for BMI, the dose decreased by 2.0 mg for every one-year increase in age.
A subgroup analysis of the new patients again revealed a negative correlation between testosterone dose and age, with or without adjustment for BMI (P = .013 and P = .019, respectively). Adjusted for BMI, the dose decreased by 2.5 mg for every one-year increase in age.
Subgroup analysis of the patients already on testosterone therapy revealed no association between testosterone dose, age, and BMI. Among the new patients, no association was observed between time to development of each physical attribute and testosterone dose or route of administration. Among the new patients, 73% reported hair growth (mean time, 89 days), deepening of voice (51 days), and cessation of menses (136 days), and 59% reported clitoromegaly (51 days).
“The finding that surprised us the most is that the testosterone dose needed to maintain a therapeutic testosterone level in transgender men is not related to BMI,” Dr. Echt said. “Some medications are dosed based on body weight, and it was surprising to us that testosterone dosing was not related to weight in kilograms or BMI. Although the findings from our project suggest that the testosterone dose needed for hormonal therapy for transgender men may decrease with older age, further research and larger studies are needed in this field to help guide management of transgender patients.”
Dr. Echt acknowledged certain limitations of the study, including its small sample size. “At this point, our population of transgender patients has been increasing in our practice,” she said. “In the future, we would like to build upon our study by including more patients in our retrospective analysis and then stratify the results by mode of administration of testosterone.”
The researchers reported having no financial disclosures.
LOS ANGELES – The dose of testosterone required to maintain a therapeutic level in transgender men is not correlated with body mass index but does decrease with age, results from a single-center study have shown.
“At this point, there are limited data regarding the dosing of testosterone in relation to age and BMI, which is what makes our work unique,” one of the study authors, Sushmitha Echt, MD, said in an interview following the annual scientific and clinical congress of the American Association of Clinical Endocrinologists.
“Although we have guidelines regarding initiating hormonal therapy for transgender patients, such as the Endocrine Society’s Clinical Practice Guidelines from 2017, we do not have much data regarding the optimal dosing of testosterone in transgender men. We hope that with more research, we will have more data to drive our treatment decisions for our transgender patients.”
Dr. Echt, an endocrinology fellow at North Shore University Hospital, Manhassett, NY, and her colleague, Aren Skolnick, DO, retrospectively evaluated 40 transgender men who were treated at the medical center between July 1, 2014 and July 1, 2018. They performed univariate and multivariate mixed-model analyses to determine the relationship between testosterone dose, age, and body mass index (BMI), and Cox regression analysis to determine the relationship between time to development of each physical attribute, testosterone dose, and route of administration.
The patients ranged in age from 18 to 54 years, and their mean baseline age was 25 years. At the time of their first visit, 32 of the patients were on intramuscular testosterone, four were on subcutaneous testosterone, and five were on the transdermal form.
By the end of the study, 28 patients remained on intramuscular testosterone, six were on the subcutaneous form, five were on the transdermal form, and one had transitioned to testosterone pellets. The majority of patients (37) became therapeutic during the course of the study, and the average therapeutic testosterone level was 551.7 ng/dL.
During an average follow-up time of one year, the researchers observed no correlation between testosterone dose and BMI. However, they found a negative correlation between testosterone dose and age, with or without adjustment for BMI (P = .016 and P = .020, respectively). Adjusted for BMI, the dose decreased by 2.0 mg for every one-year increase in age.
A subgroup analysis of the new patients again revealed a negative correlation between testosterone dose and age, with or without adjustment for BMI (P = .013 and P = .019, respectively). Adjusted for BMI, the dose decreased by 2.5 mg for every one-year increase in age.
Subgroup analysis of the patients already on testosterone therapy revealed no association between testosterone dose, age, and BMI. Among the new patients, no association was observed between time to development of each physical attribute and testosterone dose or route of administration. Among the new patients, 73% reported hair growth (mean time, 89 days), deepening of voice (51 days), and cessation of menses (136 days), and 59% reported clitoromegaly (51 days).
“The finding that surprised us the most is that the testosterone dose needed to maintain a therapeutic testosterone level in transgender men is not related to BMI,” Dr. Echt said. “Some medications are dosed based on body weight, and it was surprising to us that testosterone dosing was not related to weight in kilograms or BMI. Although the findings from our project suggest that the testosterone dose needed for hormonal therapy for transgender men may decrease with older age, further research and larger studies are needed in this field to help guide management of transgender patients.”
Dr. Echt acknowledged certain limitations of the study, including its small sample size. “At this point, our population of transgender patients has been increasing in our practice,” she said. “In the future, we would like to build upon our study by including more patients in our retrospective analysis and then stratify the results by mode of administration of testosterone.”
The researchers reported having no financial disclosures.
REPORTING FROM AACE 2019
Key clinical point:
Major finding: Adjusted for BMI, the dose of testosterone decreased by 2.0 mg for every one-year increase in age.
Study details: A retrospective analysis of 40 transgender men.
Disclosures: The researchers reported having no financial conflicts.
Green light therapy: A stop sign for pain?
MILWAUKEE – Exposure to green light therapy may significantly reduce pain in patients with chronic pain conditions, including migraine and fibromyalgia, an expert reported at the scientific meeting of the American Pain Society.
“There’s a subset of patients in every clinic whose pain doesn’t respond to medical therapies,” said Mohab M. Ibrahim, MD, PhD. “I always wonder what could be done with these patients.”
Dr. Ibrahim, who directs the chronic pain clinic at the University of Arizona, Tucson, walked attendees through an experimental process that began with an observation and has led to human clinical trials of green light therapy.
“Despite being a pharmacologist, I’m really interested in nonpharmacologic methods to manage pain,” he said.
Dr. Ibrahim said the idea for green light therapy came to him when he was speaking with his brother, who experiences migraines. His brother said his headaches were alleviated with time outside, in his back yard, or in one of the many parks in the city where he lives.
Knowing that spending time in nature had salutary effects in general, Dr. Ibrahim, an anesthesiologist and pain management specialist, wondered whether exposure to the sort of light found in nature, with blue skies and the green of a tree canopy, could help control pain.
To begin with, Dr. Ibrahim said, “the question was, do different colors have different behavior aspects on animals?”
Dr. Ibrahim and his collaborators exposed rats to light of various wavelengths across the color spectrum, as well as white and infrared light. They found that the rats who were exposed to blue and green light had a significantly longer latency period before withdrawing their hands and feet from a painfully hot stimulus, showing an antinociceptive effect with these wavelengths similar to that seen with analgesic medication.
“At that point, I decided to pursue green light and to forego blue, because blue can change the circadian rhythm,” said Dr. Ibrahim, adding, “Most pain patients have sleep disturbances to begin with, so to compound that issue is probably not a good idea.”
Dr. Ibrahim and his colleagues wanted to determine whether the analgesic effect had to do with rats seeing the green light or just being exposed to the light. Accordingly, the researchers fitted some rats with tiny, specially manufactured, completely opaque contact lenses. As a control, the researchers applied completely clear contact lenses to another group of rats. “I can’t tell you how many times we got bit, but by the end we got pretty good at it,” said Dr. Ibrahim.
Only the rats with clear lenses had prolonged latency in paw withdrawal to a noxious stimulus with green light exposure; for the rats with the blackout contact lenses, the effect was gone, “suggesting that the visual system is essential in mediating this effect,” noted Dr. Ibrahim.
This series of experiments also showed durable effects of green light exposure. In addition, the analgesic effect of green light did not wane over time, and higher “doses” were not required to achieve the same effect (as is the case with opioids, for example) (Pain. 2017 Feb;158[2]:347-60).
Clues to the mechanism of action came when Dr. Ibrahim and his colleagues administered naloxone to green light-exposed rats. “Naloxone reversed the effects of the green light, suggesting that the endogenous opioid system plays a role in this,” he said, adding that enkephalins were increased two- to threefold in the green light-exposed rats’ spinal cords, and astrocyte activation was reduced as well.
Similar experiments using a rat model of neuropathic pain showed a reversal of pain symptoms with green light exposure, offering promise that green light therapy could be effective in alleviating chronic as well as acute pain.
Moving to humans, Dr. Ibrahim enrolled a small group of individuals from his pain clinic who had refractory migraine into a study that exposed them either to white light or to green light. “These are patients who have failed everything…They have come to me, but I have nothing else to offer them,” he said.
The study had a crossover design. Participants in the small study had baseline pain scores of about 8/10, with no significant drop in pain with white light exposure. However, when the white light patients were crossed over to green light exposure, pain scores dropped to about 3/10. “That’s a greater than 50% reduction in the intensity of their migraine.”
Similar effects were seen in patients with fibromyalgia: “It was exactly the same story…When patients with white light exposure were crossed over [to green light], they had significant reductions in pain,” said Dr. Ibrahim.
“Their opioid use also decreased,” said Dr. Ibrahim. Medication use dropped in green light-exposed patients with migraine and fibromyalgia from an aggregate of about 280 morphine milligram equivalents (MME) to about 150 MME by the end of the study. The small size of the pilot study meant that those differences were not statistically significant.
“A multimodal approach to manage chronic pain patients is probably the best approach that we have so far,” said Dr. Ibrahim. An ongoing clinical trial randomizes patients with chronic pain to white light or green light therapy for two hours daily for 10 weeks, tracking pain scores, medication, and quality of life measures.
Future directions, said Dr. Ibrahim, include a study of the efficacy of green light therapy for patients with interstitial cystitis; another study will investigate green light for postoperative pain control. Sleep may also be improved by green light exposure, and Dr. Ibrahim and his colleagues plan to study this as well.
Dr. Ibrahim reported that his research was supported by the National Institutes of Health. He reported that he had no relevant conflicts of interest.
MILWAUKEE – Exposure to green light therapy may significantly reduce pain in patients with chronic pain conditions, including migraine and fibromyalgia, an expert reported at the scientific meeting of the American Pain Society.
“There’s a subset of patients in every clinic whose pain doesn’t respond to medical therapies,” said Mohab M. Ibrahim, MD, PhD. “I always wonder what could be done with these patients.”
Dr. Ibrahim, who directs the chronic pain clinic at the University of Arizona, Tucson, walked attendees through an experimental process that began with an observation and has led to human clinical trials of green light therapy.
“Despite being a pharmacologist, I’m really interested in nonpharmacologic methods to manage pain,” he said.
Dr. Ibrahim said the idea for green light therapy came to him when he was speaking with his brother, who experiences migraines. His brother said his headaches were alleviated with time outside, in his back yard, or in one of the many parks in the city where he lives.
Knowing that spending time in nature had salutary effects in general, Dr. Ibrahim, an anesthesiologist and pain management specialist, wondered whether exposure to the sort of light found in nature, with blue skies and the green of a tree canopy, could help control pain.
To begin with, Dr. Ibrahim said, “the question was, do different colors have different behavior aspects on animals?”
Dr. Ibrahim and his collaborators exposed rats to light of various wavelengths across the color spectrum, as well as white and infrared light. They found that the rats who were exposed to blue and green light had a significantly longer latency period before withdrawing their hands and feet from a painfully hot stimulus, showing an antinociceptive effect with these wavelengths similar to that seen with analgesic medication.
“At that point, I decided to pursue green light and to forego blue, because blue can change the circadian rhythm,” said Dr. Ibrahim, adding, “Most pain patients have sleep disturbances to begin with, so to compound that issue is probably not a good idea.”
Dr. Ibrahim and his colleagues wanted to determine whether the analgesic effect had to do with rats seeing the green light or just being exposed to the light. Accordingly, the researchers fitted some rats with tiny, specially manufactured, completely opaque contact lenses. As a control, the researchers applied completely clear contact lenses to another group of rats. “I can’t tell you how many times we got bit, but by the end we got pretty good at it,” said Dr. Ibrahim.
Only the rats with clear lenses had prolonged latency in paw withdrawal to a noxious stimulus with green light exposure; for the rats with the blackout contact lenses, the effect was gone, “suggesting that the visual system is essential in mediating this effect,” noted Dr. Ibrahim.
This series of experiments also showed durable effects of green light exposure. In addition, the analgesic effect of green light did not wane over time, and higher “doses” were not required to achieve the same effect (as is the case with opioids, for example) (Pain. 2017 Feb;158[2]:347-60).
Clues to the mechanism of action came when Dr. Ibrahim and his colleagues administered naloxone to green light-exposed rats. “Naloxone reversed the effects of the green light, suggesting that the endogenous opioid system plays a role in this,” he said, adding that enkephalins were increased two- to threefold in the green light-exposed rats’ spinal cords, and astrocyte activation was reduced as well.
Similar experiments using a rat model of neuropathic pain showed a reversal of pain symptoms with green light exposure, offering promise that green light therapy could be effective in alleviating chronic as well as acute pain.
Moving to humans, Dr. Ibrahim enrolled a small group of individuals from his pain clinic who had refractory migraine into a study that exposed them either to white light or to green light. “These are patients who have failed everything…They have come to me, but I have nothing else to offer them,” he said.
The study had a crossover design. Participants in the small study had baseline pain scores of about 8/10, with no significant drop in pain with white light exposure. However, when the white light patients were crossed over to green light exposure, pain scores dropped to about 3/10. “That’s a greater than 50% reduction in the intensity of their migraine.”
Similar effects were seen in patients with fibromyalgia: “It was exactly the same story…When patients with white light exposure were crossed over [to green light], they had significant reductions in pain,” said Dr. Ibrahim.
“Their opioid use also decreased,” said Dr. Ibrahim. Medication use dropped in green light-exposed patients with migraine and fibromyalgia from an aggregate of about 280 morphine milligram equivalents (MME) to about 150 MME by the end of the study. The small size of the pilot study meant that those differences were not statistically significant.
“A multimodal approach to manage chronic pain patients is probably the best approach that we have so far,” said Dr. Ibrahim. An ongoing clinical trial randomizes patients with chronic pain to white light or green light therapy for two hours daily for 10 weeks, tracking pain scores, medication, and quality of life measures.
Future directions, said Dr. Ibrahim, include a study of the efficacy of green light therapy for patients with interstitial cystitis; another study will investigate green light for postoperative pain control. Sleep may also be improved by green light exposure, and Dr. Ibrahim and his colleagues plan to study this as well.
Dr. Ibrahim reported that his research was supported by the National Institutes of Health. He reported that he had no relevant conflicts of interest.
MILWAUKEE – Exposure to green light therapy may significantly reduce pain in patients with chronic pain conditions, including migraine and fibromyalgia, an expert reported at the scientific meeting of the American Pain Society.
“There’s a subset of patients in every clinic whose pain doesn’t respond to medical therapies,” said Mohab M. Ibrahim, MD, PhD. “I always wonder what could be done with these patients.”
Dr. Ibrahim, who directs the chronic pain clinic at the University of Arizona, Tucson, walked attendees through an experimental process that began with an observation and has led to human clinical trials of green light therapy.
“Despite being a pharmacologist, I’m really interested in nonpharmacologic methods to manage pain,” he said.
Dr. Ibrahim said the idea for green light therapy came to him when he was speaking with his brother, who experiences migraines. His brother said his headaches were alleviated with time outside, in his back yard, or in one of the many parks in the city where he lives.
Knowing that spending time in nature had salutary effects in general, Dr. Ibrahim, an anesthesiologist and pain management specialist, wondered whether exposure to the sort of light found in nature, with blue skies and the green of a tree canopy, could help control pain.
To begin with, Dr. Ibrahim said, “the question was, do different colors have different behavior aspects on animals?”
Dr. Ibrahim and his collaborators exposed rats to light of various wavelengths across the color spectrum, as well as white and infrared light. They found that the rats who were exposed to blue and green light had a significantly longer latency period before withdrawing their hands and feet from a painfully hot stimulus, showing an antinociceptive effect with these wavelengths similar to that seen with analgesic medication.
“At that point, I decided to pursue green light and to forego blue, because blue can change the circadian rhythm,” said Dr. Ibrahim, adding, “Most pain patients have sleep disturbances to begin with, so to compound that issue is probably not a good idea.”
Dr. Ibrahim and his colleagues wanted to determine whether the analgesic effect had to do with rats seeing the green light or just being exposed to the light. Accordingly, the researchers fitted some rats with tiny, specially manufactured, completely opaque contact lenses. As a control, the researchers applied completely clear contact lenses to another group of rats. “I can’t tell you how many times we got bit, but by the end we got pretty good at it,” said Dr. Ibrahim.
Only the rats with clear lenses had prolonged latency in paw withdrawal to a noxious stimulus with green light exposure; for the rats with the blackout contact lenses, the effect was gone, “suggesting that the visual system is essential in mediating this effect,” noted Dr. Ibrahim.
This series of experiments also showed durable effects of green light exposure. In addition, the analgesic effect of green light did not wane over time, and higher “doses” were not required to achieve the same effect (as is the case with opioids, for example) (Pain. 2017 Feb;158[2]:347-60).
Clues to the mechanism of action came when Dr. Ibrahim and his colleagues administered naloxone to green light-exposed rats. “Naloxone reversed the effects of the green light, suggesting that the endogenous opioid system plays a role in this,” he said, adding that enkephalins were increased two- to threefold in the green light-exposed rats’ spinal cords, and astrocyte activation was reduced as well.
Similar experiments using a rat model of neuropathic pain showed a reversal of pain symptoms with green light exposure, offering promise that green light therapy could be effective in alleviating chronic as well as acute pain.
Moving to humans, Dr. Ibrahim enrolled a small group of individuals from his pain clinic who had refractory migraine into a study that exposed them either to white light or to green light. “These are patients who have failed everything…They have come to me, but I have nothing else to offer them,” he said.
The study had a crossover design. Participants in the small study had baseline pain scores of about 8/10, with no significant drop in pain with white light exposure. However, when the white light patients were crossed over to green light exposure, pain scores dropped to about 3/10. “That’s a greater than 50% reduction in the intensity of their migraine.”
Similar effects were seen in patients with fibromyalgia: “It was exactly the same story…When patients with white light exposure were crossed over [to green light], they had significant reductions in pain,” said Dr. Ibrahim.
“Their opioid use also decreased,” said Dr. Ibrahim. Medication use dropped in green light-exposed patients with migraine and fibromyalgia from an aggregate of about 280 morphine milligram equivalents (MME) to about 150 MME by the end of the study. The small size of the pilot study meant that those differences were not statistically significant.
“A multimodal approach to manage chronic pain patients is probably the best approach that we have so far,” said Dr. Ibrahim. An ongoing clinical trial randomizes patients with chronic pain to white light or green light therapy for two hours daily for 10 weeks, tracking pain scores, medication, and quality of life measures.
Future directions, said Dr. Ibrahim, include a study of the efficacy of green light therapy for patients with interstitial cystitis; another study will investigate green light for postoperative pain control. Sleep may also be improved by green light exposure, and Dr. Ibrahim and his colleagues plan to study this as well.
Dr. Ibrahim reported that his research was supported by the National Institutes of Health. He reported that he had no relevant conflicts of interest.
REPORTING FROM APS 2019
Subclinical hypothyroidism may be associated with increased cancer risks
LOS ANGELES – There is no consistent evidence to suggest that subclinical hypothyroidism is linked to an increased risk of incident breast, prostate, or colon cancer. The condition, however, may be linked to an increased risk of thyroid malignancy and to an increased risk of overall cancer mortality.
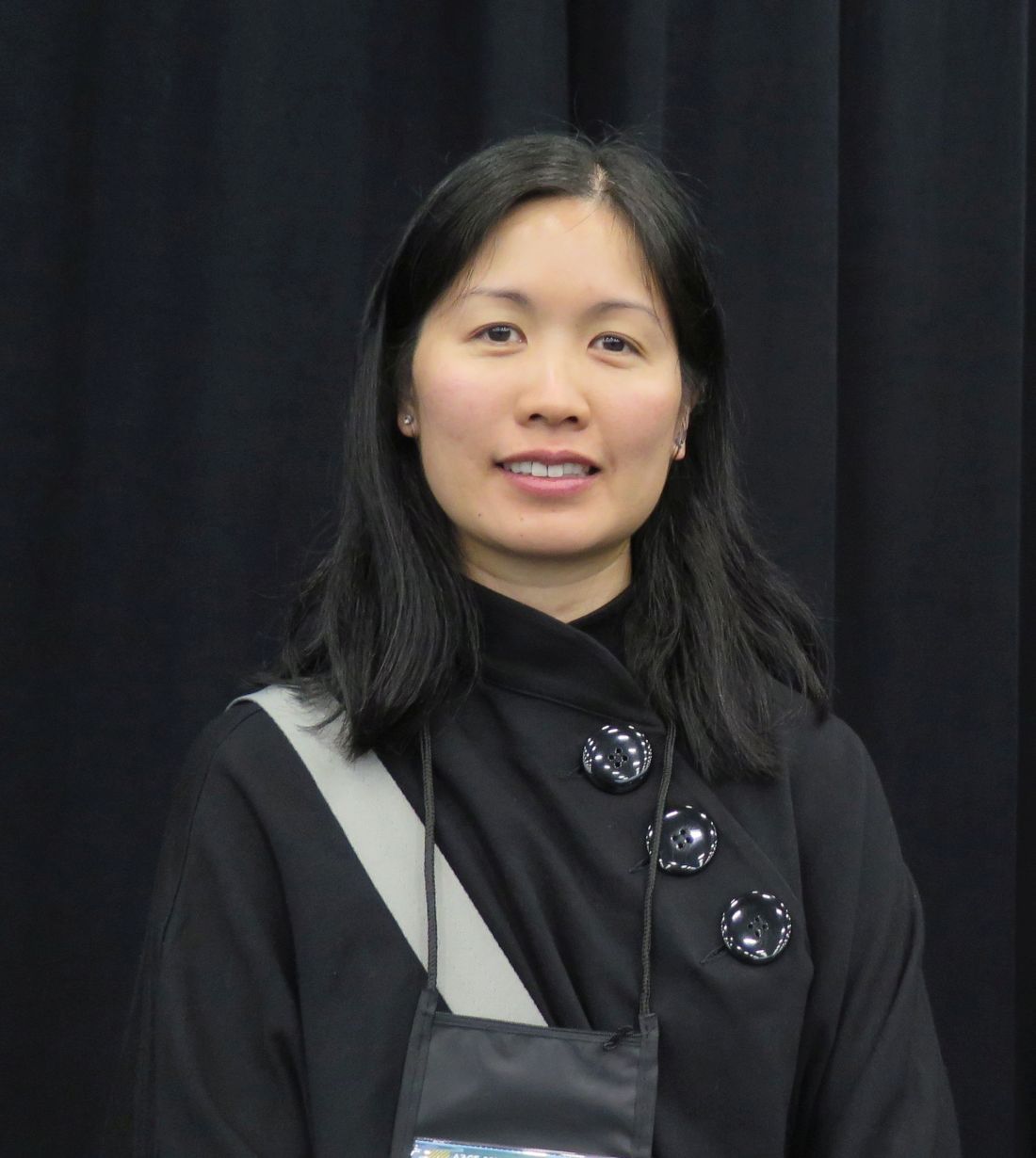
These findings come from the first systematic review to examine the effect of subclinical hypothyroidism on the risk of incident cancer and cancer mortality.
“Subclinical hypothyroidism is very prevalent,” lead study author Oriana Yu, MD, MSc, said in an interview at the annual scientific and clinical congress of the American Association of Clinical Endocrinologists. “It affects up to 10% of people, yet at this time we are uncertain as to whether or not [we should] treat them. Most studies have focused on cardiovascular outcomes, because we know that thyroid hormone is very important in lipid metabolism.”
Dr. Yu, an endocrinologist at McGill University, Montreal, and her colleagues searched the Ovid MEDLINE database for articles published from the date of its inception until Nov. 13, 2017, and combined words related to thyroid function and cancer in their search. They limited the analysis to randomized clinical trials and cohort and case-control studies in which the thyroid dysfunction chronologically preceded the cancer incidence or mortality by at least one year.
Of the 180 records screened, 51 full-text articles were assessed for eligibility. Of those, nine met the criteria for systematic review – seven related to cancer risk and two to cancer mortality. The studies were deemed to be of good to medium quality, but six of the nine were cohort studies, the rest case-control studies. “We had hoped to do a systematic review and meta-analysis, but there was high heterogeneity in the studies, especially in terms of different risk measures and outcomes reported,” Dr. Yu said. “As a result, we were not able to perform a meta-analysis.”
The researchers found that the studies had inconsistent findings when it came to the impact of subclinical hypothyroidism on the risk of breast, prostate, and colon cancer. For example, one prospective cohort study of 2,738 patients found no association between subclinical hypothyroidism and the risk of breast cancer (odds ratio, 1.9; 95% confidence interval, 0.8-4.9; Thyroid. 2005;15[11]:1253-9). Women with breast cancer, however, were more likely to have thyroid autoantibodies.
Meanwhile, a case-control study of 1,201 men found that those with elevated TSH levels had a decreased risk of prostate cancer (OR, 0.71; 95% CI, 0.47-1.06; PLoS One. 2012 Oct 30. doi: 10.1371/journal.pone.0047730). “That was a bit surprising to us,” Dr. Yu said. In addition, a nested case-control study of 103,044 patients found that subclinical hypothyroidism was linked to an increased risk for colon cancer (OR, 1.16; 95% CI, 1.08-1.24; J Natl Cancer Inst. 2015 Apr 8. doi: 10.1093/jnci/djv084).
Of the two studies that focused on cancer mortality, one retrospective cohort analysis of 4,735 patients showed that treatment of subclinical hypothyroidism was associated with a decreased risk of cancer mortality in those aged 40-70 years (hazard ratio, 0.59; 95% CI, 0.21-0.99; Arch Intern Med. 2012;172[10]:811-7). The other study, a retrospective cohort analysis of 115,746 patients, found that subclinical hypothyroidism was associated with an increased risk of cancer mortality (relative risk, 1.51; 95% CI, 1.06-2.15; PLoS One. 2015 Apr 1. doi: 10.1371/journal.pone.0122955).
“We need to interpret the cancer-related mortality findings with caution,” Dr. Yu said. “There’s concern about whether patients who are treated might be [generally] healthier or were less frail, compared with those who were not treated. Although these studies adjusted for a number of confounders, it may be difficult to measure and adjust for [those two] factors. That might explain the findings in the two studies on cancer-related mortality.”
Dr. Yu and two coauthors have received salary awards from the Fonds de recherche du Québec–Santé.
LOS ANGELES – There is no consistent evidence to suggest that subclinical hypothyroidism is linked to an increased risk of incident breast, prostate, or colon cancer. The condition, however, may be linked to an increased risk of thyroid malignancy and to an increased risk of overall cancer mortality.
These findings come from the first systematic review to examine the effect of subclinical hypothyroidism on the risk of incident cancer and cancer mortality.
“Subclinical hypothyroidism is very prevalent,” lead study author Oriana Yu, MD, MSc, said in an interview at the annual scientific and clinical congress of the American Association of Clinical Endocrinologists. “It affects up to 10% of people, yet at this time we are uncertain as to whether or not [we should] treat them. Most studies have focused on cardiovascular outcomes, because we know that thyroid hormone is very important in lipid metabolism.”
Dr. Yu, an endocrinologist at McGill University, Montreal, and her colleagues searched the Ovid MEDLINE database for articles published from the date of its inception until Nov. 13, 2017, and combined words related to thyroid function and cancer in their search. They limited the analysis to randomized clinical trials and cohort and case-control studies in which the thyroid dysfunction chronologically preceded the cancer incidence or mortality by at least one year.
Of the 180 records screened, 51 full-text articles were assessed for eligibility. Of those, nine met the criteria for systematic review – seven related to cancer risk and two to cancer mortality. The studies were deemed to be of good to medium quality, but six of the nine were cohort studies, the rest case-control studies. “We had hoped to do a systematic review and meta-analysis, but there was high heterogeneity in the studies, especially in terms of different risk measures and outcomes reported,” Dr. Yu said. “As a result, we were not able to perform a meta-analysis.”
The researchers found that the studies had inconsistent findings when it came to the impact of subclinical hypothyroidism on the risk of breast, prostate, and colon cancer. For example, one prospective cohort study of 2,738 patients found no association between subclinical hypothyroidism and the risk of breast cancer (odds ratio, 1.9; 95% confidence interval, 0.8-4.9; Thyroid. 2005;15[11]:1253-9). Women with breast cancer, however, were more likely to have thyroid autoantibodies.
Meanwhile, a case-control study of 1,201 men found that those with elevated TSH levels had a decreased risk of prostate cancer (OR, 0.71; 95% CI, 0.47-1.06; PLoS One. 2012 Oct 30. doi: 10.1371/journal.pone.0047730). “That was a bit surprising to us,” Dr. Yu said. In addition, a nested case-control study of 103,044 patients found that subclinical hypothyroidism was linked to an increased risk for colon cancer (OR, 1.16; 95% CI, 1.08-1.24; J Natl Cancer Inst. 2015 Apr 8. doi: 10.1093/jnci/djv084).
Of the two studies that focused on cancer mortality, one retrospective cohort analysis of 4,735 patients showed that treatment of subclinical hypothyroidism was associated with a decreased risk of cancer mortality in those aged 40-70 years (hazard ratio, 0.59; 95% CI, 0.21-0.99; Arch Intern Med. 2012;172[10]:811-7). The other study, a retrospective cohort analysis of 115,746 patients, found that subclinical hypothyroidism was associated with an increased risk of cancer mortality (relative risk, 1.51; 95% CI, 1.06-2.15; PLoS One. 2015 Apr 1. doi: 10.1371/journal.pone.0122955).
“We need to interpret the cancer-related mortality findings with caution,” Dr. Yu said. “There’s concern about whether patients who are treated might be [generally] healthier or were less frail, compared with those who were not treated. Although these studies adjusted for a number of confounders, it may be difficult to measure and adjust for [those two] factors. That might explain the findings in the two studies on cancer-related mortality.”
Dr. Yu and two coauthors have received salary awards from the Fonds de recherche du Québec–Santé.
LOS ANGELES – There is no consistent evidence to suggest that subclinical hypothyroidism is linked to an increased risk of incident breast, prostate, or colon cancer. The condition, however, may be linked to an increased risk of thyroid malignancy and to an increased risk of overall cancer mortality.
These findings come from the first systematic review to examine the effect of subclinical hypothyroidism on the risk of incident cancer and cancer mortality.
“Subclinical hypothyroidism is very prevalent,” lead study author Oriana Yu, MD, MSc, said in an interview at the annual scientific and clinical congress of the American Association of Clinical Endocrinologists. “It affects up to 10% of people, yet at this time we are uncertain as to whether or not [we should] treat them. Most studies have focused on cardiovascular outcomes, because we know that thyroid hormone is very important in lipid metabolism.”
Dr. Yu, an endocrinologist at McGill University, Montreal, and her colleagues searched the Ovid MEDLINE database for articles published from the date of its inception until Nov. 13, 2017, and combined words related to thyroid function and cancer in their search. They limited the analysis to randomized clinical trials and cohort and case-control studies in which the thyroid dysfunction chronologically preceded the cancer incidence or mortality by at least one year.
Of the 180 records screened, 51 full-text articles were assessed for eligibility. Of those, nine met the criteria for systematic review – seven related to cancer risk and two to cancer mortality. The studies were deemed to be of good to medium quality, but six of the nine were cohort studies, the rest case-control studies. “We had hoped to do a systematic review and meta-analysis, but there was high heterogeneity in the studies, especially in terms of different risk measures and outcomes reported,” Dr. Yu said. “As a result, we were not able to perform a meta-analysis.”
The researchers found that the studies had inconsistent findings when it came to the impact of subclinical hypothyroidism on the risk of breast, prostate, and colon cancer. For example, one prospective cohort study of 2,738 patients found no association between subclinical hypothyroidism and the risk of breast cancer (odds ratio, 1.9; 95% confidence interval, 0.8-4.9; Thyroid. 2005;15[11]:1253-9). Women with breast cancer, however, were more likely to have thyroid autoantibodies.
Meanwhile, a case-control study of 1,201 men found that those with elevated TSH levels had a decreased risk of prostate cancer (OR, 0.71; 95% CI, 0.47-1.06; PLoS One. 2012 Oct 30. doi: 10.1371/journal.pone.0047730). “That was a bit surprising to us,” Dr. Yu said. In addition, a nested case-control study of 103,044 patients found that subclinical hypothyroidism was linked to an increased risk for colon cancer (OR, 1.16; 95% CI, 1.08-1.24; J Natl Cancer Inst. 2015 Apr 8. doi: 10.1093/jnci/djv084).
Of the two studies that focused on cancer mortality, one retrospective cohort analysis of 4,735 patients showed that treatment of subclinical hypothyroidism was associated with a decreased risk of cancer mortality in those aged 40-70 years (hazard ratio, 0.59; 95% CI, 0.21-0.99; Arch Intern Med. 2012;172[10]:811-7). The other study, a retrospective cohort analysis of 115,746 patients, found that subclinical hypothyroidism was associated with an increased risk of cancer mortality (relative risk, 1.51; 95% CI, 1.06-2.15; PLoS One. 2015 Apr 1. doi: 10.1371/journal.pone.0122955).
“We need to interpret the cancer-related mortality findings with caution,” Dr. Yu said. “There’s concern about whether patients who are treated might be [generally] healthier or were less frail, compared with those who were not treated. Although these studies adjusted for a number of confounders, it may be difficult to measure and adjust for [those two] factors. That might explain the findings in the two studies on cancer-related mortality.”
Dr. Yu and two coauthors have received salary awards from the Fonds de recherche du Québec–Santé.
REPORTING FROM AACE 2019
Key clinical point: Further studies are needed to assess the association between untreated subclinical hypothyroidism and the risks of different types of cancer.
Major finding:
Study details: A systematic review of nine studies.
Disclosures: Dr. Yu and two coauthors have received salary awards from the Fonds de recherche du Québec–Santé.