User login
Alarming increase in esophageal cancer in middle-aged adults
An alarming increase in both esophageal cancer (EC) and the primary precursor lesion for esophageal adenocarcinoma known as Barrett’s esophagus (BE) has been observed among middle-aged adults over the past 5 years, and it’s not because of better or more frequent screening, warn the authors of a new study from Florida.
“We found that the [prevalence of] esophageal cancer and Barrett’s esophagus may have in fact plateaued in the elderly, but there is a concerning increase in their prevalence in middle-aged adults despite the fact that there has been no increase in the use of endoscopy in this population,” Bashar Qumseya, MD, MPH, associate professor of medicine and chief of endoscopy, University of Florida, Gainesville, told a press briefing.
“This should be of great concern to physicians and to patients, and it is our suggestion that maybe we should consider screening middle-aged patients or even those at younger ages for both conditions,” he added.
The study was highlighted during a press briefing in advance of the annual Digestive Disease Week® (DDW).
Research network
The analysis was carried out using electronic health records from the OneFlorida Clinical Data Research Network, a database that covers over 40% of residents living in Florida. The researchers identified patients who had been diagnosed with EC or BE between 2012 and 2019. “The primary outcome of interest was the adjusted prevalence of EC and BE in the population,” they stated.
The cohort was categorized by age: those aged 18-44 years (young); those aged 45-64 years (middle-aged), and those older than 65 (elderly). The number of patients included in the database varied by year and ranged from 4,238,884 to 5,411,838 patients per year, the investigators noted. Interestingly, in the most recent year, 2019, more women, at over 57%, were diagnosed with EC than were men.
Over the study interval, the prevalence of EC remained stable among the elderly but nearly doubled among middle-aged patients, from a rate of 49 per 100,000 in 2012 to a rate of 94 per 100,000 in 2019.
Similarly, there was a 50% increase in BE over the same study interval, from 304 per 100,000 in 2012 to 466 per 100,000 in 2019, again in the middle-aged group. The increase in the prevalence of BE was highest in those aged 51-60 years, followed by those aged 61-70 years and then by those aged 41-50.
Data from the same cohort also indicated that the great majority of patients with multiple risk factors for EC or BE – obesity, diet, and gastroesophageal reflux disease – had never undergone endoscopy, “so we can definitely do better,” Dr. Qumseya said. One simple way to “do better” is to offer patients an endoscopy when they undergo their first colonoscopy at the recommended age of 45 years.
“I am not in a position to make the guidelines,”Dr. Qumseya commented. “But we do [already] have guidelines that suggest that patients with multiple risk factors [for EC and BE] be screened, and since we know from our data that this is not happening, I believe that if a patient has multiple risk factors, they should have at least one screening endoscopy at the time of colonoscopy. Otherwise, we are missing a good opportunity to do so, and personally, I think this is something that we should be considering.”
A version of this article first appeared on Medscape.com.
An alarming increase in both esophageal cancer (EC) and the primary precursor lesion for esophageal adenocarcinoma known as Barrett’s esophagus (BE) has been observed among middle-aged adults over the past 5 years, and it’s not because of better or more frequent screening, warn the authors of a new study from Florida.
“We found that the [prevalence of] esophageal cancer and Barrett’s esophagus may have in fact plateaued in the elderly, but there is a concerning increase in their prevalence in middle-aged adults despite the fact that there has been no increase in the use of endoscopy in this population,” Bashar Qumseya, MD, MPH, associate professor of medicine and chief of endoscopy, University of Florida, Gainesville, told a press briefing.
“This should be of great concern to physicians and to patients, and it is our suggestion that maybe we should consider screening middle-aged patients or even those at younger ages for both conditions,” he added.
The study was highlighted during a press briefing in advance of the annual Digestive Disease Week® (DDW).
Research network
The analysis was carried out using electronic health records from the OneFlorida Clinical Data Research Network, a database that covers over 40% of residents living in Florida. The researchers identified patients who had been diagnosed with EC or BE between 2012 and 2019. “The primary outcome of interest was the adjusted prevalence of EC and BE in the population,” they stated.
The cohort was categorized by age: those aged 18-44 years (young); those aged 45-64 years (middle-aged), and those older than 65 (elderly). The number of patients included in the database varied by year and ranged from 4,238,884 to 5,411,838 patients per year, the investigators noted. Interestingly, in the most recent year, 2019, more women, at over 57%, were diagnosed with EC than were men.
Over the study interval, the prevalence of EC remained stable among the elderly but nearly doubled among middle-aged patients, from a rate of 49 per 100,000 in 2012 to a rate of 94 per 100,000 in 2019.
Similarly, there was a 50% increase in BE over the same study interval, from 304 per 100,000 in 2012 to 466 per 100,000 in 2019, again in the middle-aged group. The increase in the prevalence of BE was highest in those aged 51-60 years, followed by those aged 61-70 years and then by those aged 41-50.
Data from the same cohort also indicated that the great majority of patients with multiple risk factors for EC or BE – obesity, diet, and gastroesophageal reflux disease – had never undergone endoscopy, “so we can definitely do better,” Dr. Qumseya said. One simple way to “do better” is to offer patients an endoscopy when they undergo their first colonoscopy at the recommended age of 45 years.
“I am not in a position to make the guidelines,”Dr. Qumseya commented. “But we do [already] have guidelines that suggest that patients with multiple risk factors [for EC and BE] be screened, and since we know from our data that this is not happening, I believe that if a patient has multiple risk factors, they should have at least one screening endoscopy at the time of colonoscopy. Otherwise, we are missing a good opportunity to do so, and personally, I think this is something that we should be considering.”
A version of this article first appeared on Medscape.com.
An alarming increase in both esophageal cancer (EC) and the primary precursor lesion for esophageal adenocarcinoma known as Barrett’s esophagus (BE) has been observed among middle-aged adults over the past 5 years, and it’s not because of better or more frequent screening, warn the authors of a new study from Florida.
“We found that the [prevalence of] esophageal cancer and Barrett’s esophagus may have in fact plateaued in the elderly, but there is a concerning increase in their prevalence in middle-aged adults despite the fact that there has been no increase in the use of endoscopy in this population,” Bashar Qumseya, MD, MPH, associate professor of medicine and chief of endoscopy, University of Florida, Gainesville, told a press briefing.
“This should be of great concern to physicians and to patients, and it is our suggestion that maybe we should consider screening middle-aged patients or even those at younger ages for both conditions,” he added.
The study was highlighted during a press briefing in advance of the annual Digestive Disease Week® (DDW).
Research network
The analysis was carried out using electronic health records from the OneFlorida Clinical Data Research Network, a database that covers over 40% of residents living in Florida. The researchers identified patients who had been diagnosed with EC or BE between 2012 and 2019. “The primary outcome of interest was the adjusted prevalence of EC and BE in the population,” they stated.
The cohort was categorized by age: those aged 18-44 years (young); those aged 45-64 years (middle-aged), and those older than 65 (elderly). The number of patients included in the database varied by year and ranged from 4,238,884 to 5,411,838 patients per year, the investigators noted. Interestingly, in the most recent year, 2019, more women, at over 57%, were diagnosed with EC than were men.
Over the study interval, the prevalence of EC remained stable among the elderly but nearly doubled among middle-aged patients, from a rate of 49 per 100,000 in 2012 to a rate of 94 per 100,000 in 2019.
Similarly, there was a 50% increase in BE over the same study interval, from 304 per 100,000 in 2012 to 466 per 100,000 in 2019, again in the middle-aged group. The increase in the prevalence of BE was highest in those aged 51-60 years, followed by those aged 61-70 years and then by those aged 41-50.
Data from the same cohort also indicated that the great majority of patients with multiple risk factors for EC or BE – obesity, diet, and gastroesophageal reflux disease – had never undergone endoscopy, “so we can definitely do better,” Dr. Qumseya said. One simple way to “do better” is to offer patients an endoscopy when they undergo their first colonoscopy at the recommended age of 45 years.
“I am not in a position to make the guidelines,”Dr. Qumseya commented. “But we do [already] have guidelines that suggest that patients with multiple risk factors [for EC and BE] be screened, and since we know from our data that this is not happening, I believe that if a patient has multiple risk factors, they should have at least one screening endoscopy at the time of colonoscopy. Otherwise, we are missing a good opportunity to do so, and personally, I think this is something that we should be considering.”
A version of this article first appeared on Medscape.com.
New insight into how brain stimulation eases major depression
For the first time, researchers understand what happens to the brain when patients with treatment-resistant depression receive repetitive transcranial magnetic stimulation (rTMS).
Using functional magnetic resonance imaging (fMRI), they showed that rTMS induces widespread alterations in functional connectivity in brain regions involved in emotion and motor control.
“‘How does rTMS work?’ is one of the most frequent questions I get in clinic. Providing an accurate explanation and narrative to patients is critical,” senior investigator Fidel Vila-Rodriguez, MD, PhD, director of the Non-Invasive Neurostimulation Therapies Laboratory, University of British Columbia, Vancouver, told this news organization.

“Our findings suggest that rTMS might rely on the brain’s capacity for change (neuroplasticity) to exert its effects and that rTMS effects on the brain are widespread beyond the focal area stimulated (functional network effects),” Dr. Vila-Rodriguez added.
The study was published online in the American Journal of Psychiatry.
Mechanistic insights
Although rTMS has proven efficacy for treatment-resistant depression, the mechanisms behind how it affects the brain are not well understood.
In the current study, researchers used fMRI to assess changes in functional connectivity induced by a single rTMS session in 26 women and 12 men with treatment-resistant depression.
They found that – from managing emotional responses to memory and motor control.
Following a 4-week course of rTMS, these connectivity changes predicted about 30% of the variance of improvement in scores on the Montgomery-Åsberg Depression Rating Scale after rTMS treatment.
The most robust predictive associations involved connections between prefrontal regions and motor, parietal, and insular cortices and between bilateral regions of the thalamus.
“By demonstrating this principle and identifying regions of the brain that are activated by rTMS, we can now try to understand whether this pattern can be used as a biomarker,” Dr. Vila-Rodriguez said in a news release.
“This work provides a mechanistic explanation of what rTMS does to treat depression and supports the notion that for rTMS to treat depressive symptoms a distributed change in brain activity (network or circuit base) is necessary,” he told this news organization.
With funding from the Canadian Institutes of Health Research (CIHR), the team will next see if they can use fMRI to guide rTMS at the individual level, with the ultimate goal of “personalizing” rTMS using individualized functional targets, Dr. Vila-Rodriguez said.
New generation of tms researchers
Reached for comment, Jonathan Downar, MD, PhD, department of psychiatry, University of Toronto, noted that TMS can be “very effective” for treatment-resistant depression, and it has a “very clean side effect profile compared to medications.”
What the field is trying to figure out now is “who it works for and how we can predict more effectively who’s going to benefit from it,” Dr. Downar said in an interview.
He noted that the study’s investigators are part of a “new generation of TMS researchers who are bringing new ideas into the fold and figuring out how to use brain imaging to personalize the treatment.” This study represents “a step” in that direction.
“A challenge for the field is that it’s often pretty easy to demonstrate a change at the group level, but the question is whether we can use that at the individual level. That’s a higher bar to meet, and we’re still not there yet,” Dr. Downar added.
Support for the study was provided by Brain Canada, the Michael Smith Foundation for Health Research and the Vancouver Coastal Health Research Institute. Dr. Vila-Rodriguez has received research support from CIHR, Brain Canada, the Michael Smith Foundation for Health Research, the Vancouver Coastal Health Research Institute, and the Weston Brain Institute for investigator-initiated research and philanthropic support from the Seedlings Foundation; he received in-kind equipment support from MagVenture for this investigator-initiated trial; and he has received honoraria for participation on an advisory board for Janssen. Dr. Downar has served as an adviser for BrainCheck, NeuroStim TMS, and Salience Neuro Health; received research grant from CIHR, National Institute for Mental Health, Brain Canada, Canadian Biomarker Integration Network in Depression, Ontario Brain Institute, Klarman Family Foundation, Arrell Family Foundation and the Edgestone Foundation; received travel stipends from Lundbeck and ANT Neuro; and received in-kind equipment support for investigator-initiated trials from MagVenture.
A version of this article first appeared on Medscape.com.
For the first time, researchers understand what happens to the brain when patients with treatment-resistant depression receive repetitive transcranial magnetic stimulation (rTMS).
Using functional magnetic resonance imaging (fMRI), they showed that rTMS induces widespread alterations in functional connectivity in brain regions involved in emotion and motor control.
“‘How does rTMS work?’ is one of the most frequent questions I get in clinic. Providing an accurate explanation and narrative to patients is critical,” senior investigator Fidel Vila-Rodriguez, MD, PhD, director of the Non-Invasive Neurostimulation Therapies Laboratory, University of British Columbia, Vancouver, told this news organization.
“Our findings suggest that rTMS might rely on the brain’s capacity for change (neuroplasticity) to exert its effects and that rTMS effects on the brain are widespread beyond the focal area stimulated (functional network effects),” Dr. Vila-Rodriguez added.
The study was published online in the American Journal of Psychiatry.
Mechanistic insights
Although rTMS has proven efficacy for treatment-resistant depression, the mechanisms behind how it affects the brain are not well understood.
In the current study, researchers used fMRI to assess changes in functional connectivity induced by a single rTMS session in 26 women and 12 men with treatment-resistant depression.
They found that – from managing emotional responses to memory and motor control.
Following a 4-week course of rTMS, these connectivity changes predicted about 30% of the variance of improvement in scores on the Montgomery-Åsberg Depression Rating Scale after rTMS treatment.
The most robust predictive associations involved connections between prefrontal regions and motor, parietal, and insular cortices and between bilateral regions of the thalamus.
“By demonstrating this principle and identifying regions of the brain that are activated by rTMS, we can now try to understand whether this pattern can be used as a biomarker,” Dr. Vila-Rodriguez said in a news release.
“This work provides a mechanistic explanation of what rTMS does to treat depression and supports the notion that for rTMS to treat depressive symptoms a distributed change in brain activity (network or circuit base) is necessary,” he told this news organization.
With funding from the Canadian Institutes of Health Research (CIHR), the team will next see if they can use fMRI to guide rTMS at the individual level, with the ultimate goal of “personalizing” rTMS using individualized functional targets, Dr. Vila-Rodriguez said.
New generation of tms researchers
Reached for comment, Jonathan Downar, MD, PhD, department of psychiatry, University of Toronto, noted that TMS can be “very effective” for treatment-resistant depression, and it has a “very clean side effect profile compared to medications.”
What the field is trying to figure out now is “who it works for and how we can predict more effectively who’s going to benefit from it,” Dr. Downar said in an interview.
He noted that the study’s investigators are part of a “new generation of TMS researchers who are bringing new ideas into the fold and figuring out how to use brain imaging to personalize the treatment.” This study represents “a step” in that direction.
“A challenge for the field is that it’s often pretty easy to demonstrate a change at the group level, but the question is whether we can use that at the individual level. That’s a higher bar to meet, and we’re still not there yet,” Dr. Downar added.
Support for the study was provided by Brain Canada, the Michael Smith Foundation for Health Research and the Vancouver Coastal Health Research Institute. Dr. Vila-Rodriguez has received research support from CIHR, Brain Canada, the Michael Smith Foundation for Health Research, the Vancouver Coastal Health Research Institute, and the Weston Brain Institute for investigator-initiated research and philanthropic support from the Seedlings Foundation; he received in-kind equipment support from MagVenture for this investigator-initiated trial; and he has received honoraria for participation on an advisory board for Janssen. Dr. Downar has served as an adviser for BrainCheck, NeuroStim TMS, and Salience Neuro Health; received research grant from CIHR, National Institute for Mental Health, Brain Canada, Canadian Biomarker Integration Network in Depression, Ontario Brain Institute, Klarman Family Foundation, Arrell Family Foundation and the Edgestone Foundation; received travel stipends from Lundbeck and ANT Neuro; and received in-kind equipment support for investigator-initiated trials from MagVenture.
A version of this article first appeared on Medscape.com.
For the first time, researchers understand what happens to the brain when patients with treatment-resistant depression receive repetitive transcranial magnetic stimulation (rTMS).
Using functional magnetic resonance imaging (fMRI), they showed that rTMS induces widespread alterations in functional connectivity in brain regions involved in emotion and motor control.
“‘How does rTMS work?’ is one of the most frequent questions I get in clinic. Providing an accurate explanation and narrative to patients is critical,” senior investigator Fidel Vila-Rodriguez, MD, PhD, director of the Non-Invasive Neurostimulation Therapies Laboratory, University of British Columbia, Vancouver, told this news organization.
“Our findings suggest that rTMS might rely on the brain’s capacity for change (neuroplasticity) to exert its effects and that rTMS effects on the brain are widespread beyond the focal area stimulated (functional network effects),” Dr. Vila-Rodriguez added.
The study was published online in the American Journal of Psychiatry.
Mechanistic insights
Although rTMS has proven efficacy for treatment-resistant depression, the mechanisms behind how it affects the brain are not well understood.
In the current study, researchers used fMRI to assess changes in functional connectivity induced by a single rTMS session in 26 women and 12 men with treatment-resistant depression.
They found that – from managing emotional responses to memory and motor control.
Following a 4-week course of rTMS, these connectivity changes predicted about 30% of the variance of improvement in scores on the Montgomery-Åsberg Depression Rating Scale after rTMS treatment.
The most robust predictive associations involved connections between prefrontal regions and motor, parietal, and insular cortices and between bilateral regions of the thalamus.
“By demonstrating this principle and identifying regions of the brain that are activated by rTMS, we can now try to understand whether this pattern can be used as a biomarker,” Dr. Vila-Rodriguez said in a news release.
“This work provides a mechanistic explanation of what rTMS does to treat depression and supports the notion that for rTMS to treat depressive symptoms a distributed change in brain activity (network or circuit base) is necessary,” he told this news organization.
With funding from the Canadian Institutes of Health Research (CIHR), the team will next see if they can use fMRI to guide rTMS at the individual level, with the ultimate goal of “personalizing” rTMS using individualized functional targets, Dr. Vila-Rodriguez said.
New generation of tms researchers
Reached for comment, Jonathan Downar, MD, PhD, department of psychiatry, University of Toronto, noted that TMS can be “very effective” for treatment-resistant depression, and it has a “very clean side effect profile compared to medications.”
What the field is trying to figure out now is “who it works for and how we can predict more effectively who’s going to benefit from it,” Dr. Downar said in an interview.
He noted that the study’s investigators are part of a “new generation of TMS researchers who are bringing new ideas into the fold and figuring out how to use brain imaging to personalize the treatment.” This study represents “a step” in that direction.
“A challenge for the field is that it’s often pretty easy to demonstrate a change at the group level, but the question is whether we can use that at the individual level. That’s a higher bar to meet, and we’re still not there yet,” Dr. Downar added.
Support for the study was provided by Brain Canada, the Michael Smith Foundation for Health Research and the Vancouver Coastal Health Research Institute. Dr. Vila-Rodriguez has received research support from CIHR, Brain Canada, the Michael Smith Foundation for Health Research, the Vancouver Coastal Health Research Institute, and the Weston Brain Institute for investigator-initiated research and philanthropic support from the Seedlings Foundation; he received in-kind equipment support from MagVenture for this investigator-initiated trial; and he has received honoraria for participation on an advisory board for Janssen. Dr. Downar has served as an adviser for BrainCheck, NeuroStim TMS, and Salience Neuro Health; received research grant from CIHR, National Institute for Mental Health, Brain Canada, Canadian Biomarker Integration Network in Depression, Ontario Brain Institute, Klarman Family Foundation, Arrell Family Foundation and the Edgestone Foundation; received travel stipends from Lundbeck and ANT Neuro; and received in-kind equipment support for investigator-initiated trials from MagVenture.
A version of this article first appeared on Medscape.com.
Type 2 Diabetes: Pathophysiology
SAFE-PAD shows long-term safety of paclitaxel devices
Patients who have paclitaxel-coated stents and balloons have survival and outcomes comparable to those who have a bare-metal stent or percutaneous transluminal angioplasty, according to updated results from a large study of almost 170,000 Medicare beneficiaries.
The SAFE-PAD study analyzed Medicare claims data of 168,533 patients, including 70,584 who were treated with drug-coated devices (DCD), from April 2015 through 2018.

Notably, Eric A. Secemsky, MD, MSc, said in an interview, that included more than 32,000 patients with more than 5 years of follow-up. He presented the results at the Society for Cardiovascular Angiography & Interventions annual scientific sessions.
“What we’re seeing now with this study is that paclitaxel-coated devices [PCDs] have the same long-term survival compared to those treated with non–drug-coated devices (NDCDs),” said Dr. Secemsky, director of vascular intervention at Beth Israel Deaconess Medical Center in Boston. “I think this is another important piece and some of the longest-term data in this size population to demonstrate the long-term safety of PCD, and hopefully it will help us get back to normal practice that has been halted now for over 3 years.”
That was a reference to the 2018 meta-analysis by Konstantinos Katsanos, MD, PhD, of Patras University in Greece, and colleagues, which showed an increased risk of death after PCD placements. That study threw a wet blanket of sorts on PCD use, Dr. Secemsky said.
The median follow-up for SAFE-PAD (formally called the Safety Assessment of Femoropopliteal Endovascular treatment with Paclitaxel-coated Devices) was 3.5 years, with the longest follow-up, 6.3 years. The weighted cumulative incidence of mortality at 6.3 years was 63.6% with NDCDs and 62.5% with DCDs (hazard ratio, 0.98; 95% confidence interval, 0.96-0.99; P < .0001). A subgroup analysis found no link between DCDs and increased death in low-risk patients, low-comorbid patients, inpatient or outpatient treatment, patients without critical limb ischemia, or patients treated with stents or balloon angioplasty alone.
“This report and the length of follow-up is one more piece that has continued to demonstrate safety with PCDs,” Dr. Secemsky said. He added that these results fall in line with smaller studies that failed to show a link between DCDs and long-term mortality, notably the SWEDEPAD randomized study of 2,289 patients evaluated through 4 years, and a subanalysis of 4,000 patients in VOYAGER-PAD through 42 months of follow-up.
“So we’ve really shown through these data sets and others that we can’t replicate any harms that we’ve seen in that Katsanos meta-analysis, and it suggests that there was some bias in that meta-analysis.”
Strengths of the study are its size and the way it followed the patients longitudinally, Sahil A. Parikh, MD, director of endovascular services at Columbia University Vagelos College of Physicians and Surgeons in New York, said in an interview.
With regard to its limitations, Dr. Parikh said, “On the other hand, it’s a claims database which doesn’t have the granularity about the patients’ specific procedural factors,” he said. “There are gaps that might further inform the value of lack thereof of the drug-coated device, but certainly at the topline, which is the hard endpoint of mortality, you can read quite a lot and you can assume that with such large numbers, the signal-to-noise ratio would be sufficiently sensitive that you get a real signal.”
With these updated SAFE-PAD results along with other studies, Dr. Parikh said, “If one weighs the risk benefit of cardiac lesion revascularization regarding requiring a repeat procedure vs. the risk of mortality from paclitaxel, if there is such a thing, I think most physicians have come back and the pendulum has swung back considering it reasonable to use paclitaxel products.”
That’s a message that will resonate with patients reluctant to return to the hospital since the COVID-19 outbreak, he said. “If you can tell them we can avoid a repeat trip to the hospital, they’re all for it,” Dr. Parikh said.
The study results were published simultaneously with Dr. Secemsky’s presentation. Funding for SAFE-PAD came from a multi-industry consortium consisting of BD, Boston Scientific, Cook Medical, Medtronic and Philips, which wasn’t involved in the study design or analysis.
Dr. Secemsky disclosed relationships with Abbott, BD, Bayer, Boston Scientific, Cook Medical, CSI, Endovascular Engineering, Inari, Janssen, Medtronic, Philips, and Venture Med. Dr. Parikh disclosed relationships with TriReme Medical, Boston Scientific, Heartflow, Cordis, Janssen, Terumo, Canon, Shockwave, Abiomed, Abbott, Cardiovascular Systems, Inari and Surmodics.
Patients who have paclitaxel-coated stents and balloons have survival and outcomes comparable to those who have a bare-metal stent or percutaneous transluminal angioplasty, according to updated results from a large study of almost 170,000 Medicare beneficiaries.
The SAFE-PAD study analyzed Medicare claims data of 168,533 patients, including 70,584 who were treated with drug-coated devices (DCD), from April 2015 through 2018.
Notably, Eric A. Secemsky, MD, MSc, said in an interview, that included more than 32,000 patients with more than 5 years of follow-up. He presented the results at the Society for Cardiovascular Angiography & Interventions annual scientific sessions.
“What we’re seeing now with this study is that paclitaxel-coated devices [PCDs] have the same long-term survival compared to those treated with non–drug-coated devices (NDCDs),” said Dr. Secemsky, director of vascular intervention at Beth Israel Deaconess Medical Center in Boston. “I think this is another important piece and some of the longest-term data in this size population to demonstrate the long-term safety of PCD, and hopefully it will help us get back to normal practice that has been halted now for over 3 years.”
That was a reference to the 2018 meta-analysis by Konstantinos Katsanos, MD, PhD, of Patras University in Greece, and colleagues, which showed an increased risk of death after PCD placements. That study threw a wet blanket of sorts on PCD use, Dr. Secemsky said.
The median follow-up for SAFE-PAD (formally called the Safety Assessment of Femoropopliteal Endovascular treatment with Paclitaxel-coated Devices) was 3.5 years, with the longest follow-up, 6.3 years. The weighted cumulative incidence of mortality at 6.3 years was 63.6% with NDCDs and 62.5% with DCDs (hazard ratio, 0.98; 95% confidence interval, 0.96-0.99; P < .0001). A subgroup analysis found no link between DCDs and increased death in low-risk patients, low-comorbid patients, inpatient or outpatient treatment, patients without critical limb ischemia, or patients treated with stents or balloon angioplasty alone.
“This report and the length of follow-up is one more piece that has continued to demonstrate safety with PCDs,” Dr. Secemsky said. He added that these results fall in line with smaller studies that failed to show a link between DCDs and long-term mortality, notably the SWEDEPAD randomized study of 2,289 patients evaluated through 4 years, and a subanalysis of 4,000 patients in VOYAGER-PAD through 42 months of follow-up.
“So we’ve really shown through these data sets and others that we can’t replicate any harms that we’ve seen in that Katsanos meta-analysis, and it suggests that there was some bias in that meta-analysis.”
Strengths of the study are its size and the way it followed the patients longitudinally, Sahil A. Parikh, MD, director of endovascular services at Columbia University Vagelos College of Physicians and Surgeons in New York, said in an interview.
With regard to its limitations, Dr. Parikh said, “On the other hand, it’s a claims database which doesn’t have the granularity about the patients’ specific procedural factors,” he said. “There are gaps that might further inform the value of lack thereof of the drug-coated device, but certainly at the topline, which is the hard endpoint of mortality, you can read quite a lot and you can assume that with such large numbers, the signal-to-noise ratio would be sufficiently sensitive that you get a real signal.”
With these updated SAFE-PAD results along with other studies, Dr. Parikh said, “If one weighs the risk benefit of cardiac lesion revascularization regarding requiring a repeat procedure vs. the risk of mortality from paclitaxel, if there is such a thing, I think most physicians have come back and the pendulum has swung back considering it reasonable to use paclitaxel products.”
That’s a message that will resonate with patients reluctant to return to the hospital since the COVID-19 outbreak, he said. “If you can tell them we can avoid a repeat trip to the hospital, they’re all for it,” Dr. Parikh said.
The study results were published simultaneously with Dr. Secemsky’s presentation. Funding for SAFE-PAD came from a multi-industry consortium consisting of BD, Boston Scientific, Cook Medical, Medtronic and Philips, which wasn’t involved in the study design or analysis.
Dr. Secemsky disclosed relationships with Abbott, BD, Bayer, Boston Scientific, Cook Medical, CSI, Endovascular Engineering, Inari, Janssen, Medtronic, Philips, and Venture Med. Dr. Parikh disclosed relationships with TriReme Medical, Boston Scientific, Heartflow, Cordis, Janssen, Terumo, Canon, Shockwave, Abiomed, Abbott, Cardiovascular Systems, Inari and Surmodics.
Patients who have paclitaxel-coated stents and balloons have survival and outcomes comparable to those who have a bare-metal stent or percutaneous transluminal angioplasty, according to updated results from a large study of almost 170,000 Medicare beneficiaries.
The SAFE-PAD study analyzed Medicare claims data of 168,533 patients, including 70,584 who were treated with drug-coated devices (DCD), from April 2015 through 2018.
Notably, Eric A. Secemsky, MD, MSc, said in an interview, that included more than 32,000 patients with more than 5 years of follow-up. He presented the results at the Society for Cardiovascular Angiography & Interventions annual scientific sessions.
“What we’re seeing now with this study is that paclitaxel-coated devices [PCDs] have the same long-term survival compared to those treated with non–drug-coated devices (NDCDs),” said Dr. Secemsky, director of vascular intervention at Beth Israel Deaconess Medical Center in Boston. “I think this is another important piece and some of the longest-term data in this size population to demonstrate the long-term safety of PCD, and hopefully it will help us get back to normal practice that has been halted now for over 3 years.”
That was a reference to the 2018 meta-analysis by Konstantinos Katsanos, MD, PhD, of Patras University in Greece, and colleagues, which showed an increased risk of death after PCD placements. That study threw a wet blanket of sorts on PCD use, Dr. Secemsky said.
The median follow-up for SAFE-PAD (formally called the Safety Assessment of Femoropopliteal Endovascular treatment with Paclitaxel-coated Devices) was 3.5 years, with the longest follow-up, 6.3 years. The weighted cumulative incidence of mortality at 6.3 years was 63.6% with NDCDs and 62.5% with DCDs (hazard ratio, 0.98; 95% confidence interval, 0.96-0.99; P < .0001). A subgroup analysis found no link between DCDs and increased death in low-risk patients, low-comorbid patients, inpatient or outpatient treatment, patients without critical limb ischemia, or patients treated with stents or balloon angioplasty alone.
“This report and the length of follow-up is one more piece that has continued to demonstrate safety with PCDs,” Dr. Secemsky said. He added that these results fall in line with smaller studies that failed to show a link between DCDs and long-term mortality, notably the SWEDEPAD randomized study of 2,289 patients evaluated through 4 years, and a subanalysis of 4,000 patients in VOYAGER-PAD through 42 months of follow-up.
“So we’ve really shown through these data sets and others that we can’t replicate any harms that we’ve seen in that Katsanos meta-analysis, and it suggests that there was some bias in that meta-analysis.”
Strengths of the study are its size and the way it followed the patients longitudinally, Sahil A. Parikh, MD, director of endovascular services at Columbia University Vagelos College of Physicians and Surgeons in New York, said in an interview.
With regard to its limitations, Dr. Parikh said, “On the other hand, it’s a claims database which doesn’t have the granularity about the patients’ specific procedural factors,” he said. “There are gaps that might further inform the value of lack thereof of the drug-coated device, but certainly at the topline, which is the hard endpoint of mortality, you can read quite a lot and you can assume that with such large numbers, the signal-to-noise ratio would be sufficiently sensitive that you get a real signal.”
With these updated SAFE-PAD results along with other studies, Dr. Parikh said, “If one weighs the risk benefit of cardiac lesion revascularization regarding requiring a repeat procedure vs. the risk of mortality from paclitaxel, if there is such a thing, I think most physicians have come back and the pendulum has swung back considering it reasonable to use paclitaxel products.”
That’s a message that will resonate with patients reluctant to return to the hospital since the COVID-19 outbreak, he said. “If you can tell them we can avoid a repeat trip to the hospital, they’re all for it,” Dr. Parikh said.
The study results were published simultaneously with Dr. Secemsky’s presentation. Funding for SAFE-PAD came from a multi-industry consortium consisting of BD, Boston Scientific, Cook Medical, Medtronic and Philips, which wasn’t involved in the study design or analysis.
Dr. Secemsky disclosed relationships with Abbott, BD, Bayer, Boston Scientific, Cook Medical, CSI, Endovascular Engineering, Inari, Janssen, Medtronic, Philips, and Venture Med. Dr. Parikh disclosed relationships with TriReme Medical, Boston Scientific, Heartflow, Cordis, Janssen, Terumo, Canon, Shockwave, Abiomed, Abbott, Cardiovascular Systems, Inari and Surmodics.
FROM SCAI 2022
A psychiatric patient confesses to murder: Now what?
NEW ORLEANS – The patient, a 60-year-old woman who’d just tried to kill herself by overdosing on gabapentin, felt the need to make a confession. As she told a resident psychiatrist late one night at a Philadelphia crisis response center, she’d just murdered two people and buried them in her backyard. More details kept coming, including who was dead and where their bodies were.
It didn’t take long for the attending physician’s phone to ring as the resident sought guidance. This wasn’t a typical “duty to warn” case since there was no one to warn of a threat of violence. But then what kind of case was it? As Meghan Musselman, MD, and colleagues noted in a report presented at the annual meeting of the American Psychiatric Association, the law and medical ethics didn’t present a clear-cut solution to whether the patient’s claim should be reported to the authorities.

“This was much more of a gray zone case than we typically see,” said Dr. Musselman, of the department of psychiatry at Temple University in Philadelphia, in an interview. “If someone is threatening to harm someone, most states have statutes about what to do in that situation. The same doesn’t really exist for when the crime has already happened.”
Even so, might the existing “duty to warn/protect” laws be helpful as a guide to what to do? Maybe, but it’s complicated. The laws, which address the waiving of therapist-patient confidentiality when violence is threatened, are widely variable. Some don’t specifically cover psychiatrists, according to the National Conference of State Legislatures. Some simply allow – but don’t require – certain mental-health professionals to take action regarding threats of violence without getting in trouble themselves.
There are no duty to warn/protect laws in Nevada, North Dakota, North Carolina, and Maine. Pennsylvania requires “mental-health professionals” to act when there’s a “clear and immediate danger to others or to society.”
In an interview, Columbia University, New York, psychiatrist and medical law/ethics specialist Paul S. Appelbaum, MD, said that “with the exception of situations like child abuse or elder abuse, for which psychiatrists are mandatory reporters, psychiatrists generally have the same responsibilities for reporting crimes as other citizens.”

He added that there is a crime in English common law known as “misprision” that refers to failing to report a felony. “A few states still have misprision statutes, but courts have tended to interpret them to require an affirmative act to conceal a crime, not just failure to report,” he said. “Unless the patient’s confession indicates a continuing threat to other people – e.g., a serial rapist or murderer – there is probably no obligation to report a previous crime.”
In this case, Dr. Musselman said, the physicians thought they might be able to waive confidentiality because it was possible that the alleged murder victims were still alive and in need of help.
However, the patient ultimately took the decision out of the hands of the psychiatrists and agreed to confess to the police. There’s a happy ending: The patient later recanted the story, Dr. Musselman said, and there was no follow-up by the authorities.
What should psychiatrists do in a similar situation? Besides the law, Dr. Musselman said, it’s important to consider medical ethics, confidentiality, and the greater good. “Doctors may have to ask themselves: Would I rather be sued because I’m breaking confidentiality or potentially play a part in someone’s suffering?”
She recommended reaching out to attorneys for legal guidance. “There’s a saying in forensic psychiatry by [Harvard University psychiatrist] Thomas Gutheil: Never worry alone.”
Dr. Applebaum agreed, and added: “Psychiatrists should consider the credibility of the patient’s confession: Could it represent a delusion? Is it being proffered as a way of manipulating the therapist? What is the extent to which, if valid, it indicates an ongoing threat to others? Is the patient is willing to contact the police and admit to the crime or authorize the psychiatrist to do so? Only in the case of a credible confession, an ongoing threat, and a patient unwilling to contact the police themselves should the psychiatrist seriously consider breaching confidentiality to report.”
No study funding or disclosures were reported.
NEW ORLEANS – The patient, a 60-year-old woman who’d just tried to kill herself by overdosing on gabapentin, felt the need to make a confession. As she told a resident psychiatrist late one night at a Philadelphia crisis response center, she’d just murdered two people and buried them in her backyard. More details kept coming, including who was dead and where their bodies were.
It didn’t take long for the attending physician’s phone to ring as the resident sought guidance. This wasn’t a typical “duty to warn” case since there was no one to warn of a threat of violence. But then what kind of case was it? As Meghan Musselman, MD, and colleagues noted in a report presented at the annual meeting of the American Psychiatric Association, the law and medical ethics didn’t present a clear-cut solution to whether the patient’s claim should be reported to the authorities.
“This was much more of a gray zone case than we typically see,” said Dr. Musselman, of the department of psychiatry at Temple University in Philadelphia, in an interview. “If someone is threatening to harm someone, most states have statutes about what to do in that situation. The same doesn’t really exist for when the crime has already happened.”
Even so, might the existing “duty to warn/protect” laws be helpful as a guide to what to do? Maybe, but it’s complicated. The laws, which address the waiving of therapist-patient confidentiality when violence is threatened, are widely variable. Some don’t specifically cover psychiatrists, according to the National Conference of State Legislatures. Some simply allow – but don’t require – certain mental-health professionals to take action regarding threats of violence without getting in trouble themselves.
There are no duty to warn/protect laws in Nevada, North Dakota, North Carolina, and Maine. Pennsylvania requires “mental-health professionals” to act when there’s a “clear and immediate danger to others or to society.”
In an interview, Columbia University, New York, psychiatrist and medical law/ethics specialist Paul S. Appelbaum, MD, said that “with the exception of situations like child abuse or elder abuse, for which psychiatrists are mandatory reporters, psychiatrists generally have the same responsibilities for reporting crimes as other citizens.”
He added that there is a crime in English common law known as “misprision” that refers to failing to report a felony. “A few states still have misprision statutes, but courts have tended to interpret them to require an affirmative act to conceal a crime, not just failure to report,” he said. “Unless the patient’s confession indicates a continuing threat to other people – e.g., a serial rapist or murderer – there is probably no obligation to report a previous crime.”
In this case, Dr. Musselman said, the physicians thought they might be able to waive confidentiality because it was possible that the alleged murder victims were still alive and in need of help.
However, the patient ultimately took the decision out of the hands of the psychiatrists and agreed to confess to the police. There’s a happy ending: The patient later recanted the story, Dr. Musselman said, and there was no follow-up by the authorities.
What should psychiatrists do in a similar situation? Besides the law, Dr. Musselman said, it’s important to consider medical ethics, confidentiality, and the greater good. “Doctors may have to ask themselves: Would I rather be sued because I’m breaking confidentiality or potentially play a part in someone’s suffering?”
She recommended reaching out to attorneys for legal guidance. “There’s a saying in forensic psychiatry by [Harvard University psychiatrist] Thomas Gutheil: Never worry alone.”
Dr. Applebaum agreed, and added: “Psychiatrists should consider the credibility of the patient’s confession: Could it represent a delusion? Is it being proffered as a way of manipulating the therapist? What is the extent to which, if valid, it indicates an ongoing threat to others? Is the patient is willing to contact the police and admit to the crime or authorize the psychiatrist to do so? Only in the case of a credible confession, an ongoing threat, and a patient unwilling to contact the police themselves should the psychiatrist seriously consider breaching confidentiality to report.”
No study funding or disclosures were reported.
NEW ORLEANS – The patient, a 60-year-old woman who’d just tried to kill herself by overdosing on gabapentin, felt the need to make a confession. As she told a resident psychiatrist late one night at a Philadelphia crisis response center, she’d just murdered two people and buried them in her backyard. More details kept coming, including who was dead and where their bodies were.
It didn’t take long for the attending physician’s phone to ring as the resident sought guidance. This wasn’t a typical “duty to warn” case since there was no one to warn of a threat of violence. But then what kind of case was it? As Meghan Musselman, MD, and colleagues noted in a report presented at the annual meeting of the American Psychiatric Association, the law and medical ethics didn’t present a clear-cut solution to whether the patient’s claim should be reported to the authorities.
“This was much more of a gray zone case than we typically see,” said Dr. Musselman, of the department of psychiatry at Temple University in Philadelphia, in an interview. “If someone is threatening to harm someone, most states have statutes about what to do in that situation. The same doesn’t really exist for when the crime has already happened.”
Even so, might the existing “duty to warn/protect” laws be helpful as a guide to what to do? Maybe, but it’s complicated. The laws, which address the waiving of therapist-patient confidentiality when violence is threatened, are widely variable. Some don’t specifically cover psychiatrists, according to the National Conference of State Legislatures. Some simply allow – but don’t require – certain mental-health professionals to take action regarding threats of violence without getting in trouble themselves.
There are no duty to warn/protect laws in Nevada, North Dakota, North Carolina, and Maine. Pennsylvania requires “mental-health professionals” to act when there’s a “clear and immediate danger to others or to society.”
In an interview, Columbia University, New York, psychiatrist and medical law/ethics specialist Paul S. Appelbaum, MD, said that “with the exception of situations like child abuse or elder abuse, for which psychiatrists are mandatory reporters, psychiatrists generally have the same responsibilities for reporting crimes as other citizens.”
He added that there is a crime in English common law known as “misprision” that refers to failing to report a felony. “A few states still have misprision statutes, but courts have tended to interpret them to require an affirmative act to conceal a crime, not just failure to report,” he said. “Unless the patient’s confession indicates a continuing threat to other people – e.g., a serial rapist or murderer – there is probably no obligation to report a previous crime.”
In this case, Dr. Musselman said, the physicians thought they might be able to waive confidentiality because it was possible that the alleged murder victims were still alive and in need of help.
However, the patient ultimately took the decision out of the hands of the psychiatrists and agreed to confess to the police. There’s a happy ending: The patient later recanted the story, Dr. Musselman said, and there was no follow-up by the authorities.
What should psychiatrists do in a similar situation? Besides the law, Dr. Musselman said, it’s important to consider medical ethics, confidentiality, and the greater good. “Doctors may have to ask themselves: Would I rather be sued because I’m breaking confidentiality or potentially play a part in someone’s suffering?”
She recommended reaching out to attorneys for legal guidance. “There’s a saying in forensic psychiatry by [Harvard University psychiatrist] Thomas Gutheil: Never worry alone.”
Dr. Applebaum agreed, and added: “Psychiatrists should consider the credibility of the patient’s confession: Could it represent a delusion? Is it being proffered as a way of manipulating the therapist? What is the extent to which, if valid, it indicates an ongoing threat to others? Is the patient is willing to contact the police and admit to the crime or authorize the psychiatrist to do so? Only in the case of a credible confession, an ongoing threat, and a patient unwilling to contact the police themselves should the psychiatrist seriously consider breaching confidentiality to report.”
No study funding or disclosures were reported.
AT APA 2022
Fever after a tropical trip: A guide to differential diagnosis
After 2 years of a pandemic in which traveling was barely possible, tropical diseases are becoming important once more. At a 2022 conference for internal medicine specialists, tropical medicine specialist Fritz Holst, MD, of the Center for Tropical and Travel Medicine in Marburg, Germany, explained what questions you should be asking travelers with a fever at your practice and how to proceed with a suspected case.
The following article is based on the lecture: “Differential Diagnosis of Fever After a Trip to the Tropics,” which Dr. Holst gave at the 128th conference of the German Society of Internal Medicine.
A meta-analysis of studies concerning the topic, “returnee travelers from the tropics with fever,” was published in 2020. According to the analysis, purely tropical infections make up a third (33%) of fever diagnoses worldwide following an exotic trip. Malaria accounts for a fifth (22%), 5% are dengue fever, and 2.2% are typhoid (enteric fever).
In 26% of the returnee travelers investigated, nontropical infections were the cause of the fever. Acute gastroenteritis was responsible for 14%, and respiratory infections were responsible for 13%. In 18% of the cases, the cause of the fever remained unclear.
In Germany, the number of malaria cases has increased, said Dr. Holst. In Hessen, for example, there was recently a malaria fatality. “What we should do has been forgotten again,” he warned. More attention should also be paid once more to prophylaxis.
How to proceed
Dr. Holst described the following steps for treating recently returned travelers who are sick:
- Severely ill or not: If there are signs of a severe disease, such as dyspnea, signs of bleeding, hypotension, or central nervous system symptoms, the patient should be referred to a clinic. A diagnosis should be made within 1 day and treatment should be started.
- Transmissible or dangerous disease: This question should be quickly clarified to protect health care personnel, especially those treating patients. By using a thorough medical history (discussed below), a range of diseases may be clarified.
- Disease outbreak in destination country: Find out about possible disease outbreaks in the country that the traveler visited.
- Malaria? Immediate diagnostics: Malaria should always be excluded in patients at the practice on the same day by using a thick blood smear, even if no fever is present. If this is not possible because of time constraints, the affected person should be transferred directly to the clinic.
- Fever independent of the travel? Exclude other causes of the fever (for example, endocarditis).
- Involve tropical medicine specialists in a timely manner.
Nine mandatory questions
Dr. Holst also listed nine questions that clinicians should ask this patient population.
Where were you exactly?
Depending on the regional prevalence of tropical diseases, certain pathogens can be excluded quickly. Approximately 35% of travelers returning from Africa have malaria, whereas typhoid is much rarer. In contrast, typhoid and dengue fever are much more widespread in Southeast Asia. In Latin America, this is the case for both dengue fever and leptospirosis.
When did you travel?
By using the incubation time of the pathogen in question, as well as the time of return journey, you can determine which diseases are possible and which are not. In one patient who visited the practice 4 weeks after his return, dengue or typhoid were excluded.
Where did you stay overnight?
Whether in an unhygienic bed or under the stars, the question regarding how and where travelers stayed overnight provides important evidence of the following nocturnal vectors:
- Sandflies: Leishmaniasis
- Kissing bugs: Chagas disease
- Fleas: Spotted fever, bubonic plague
- Mosquitoes: Malaria, dengue, filariasis
What did you eat?
Many infections can be attributed to careless eating. For example, when eating fish, crabs, crawfish, or frogs, especially if raw, liver fluke, lung fluke, or ciguatera should be considered. Mussel toxins have been found on the coast of Kenya and even in the south of France. In North African countries, you should be cautious when eating nonpasteurized milk products (for example, camel milk). They can transmit the pathogens for brucellosis and tuberculosis. In beef or pork that has not been cooked thoroughly, there is the risk of trichinosis or of a tapeworm. Even vegetarians need to be careful. Infections with the common liver fluke are possible after eating watercress.
What have you been doing?
You can only get some diseases through certain activities, said Dr. Holst. If long-distance travelers tell you about the following excursions, prick up your ears:
- Freshwater contact: Schistosomiasis, leptospirosis
- Caving: Histoplasmosis, rabies
- Excavations: Anthrax, coccidioidomycosis
- Camel tour: MERS coronavirus (Do not mount a sniffling camel!)
- Walking around barefoot: Strongyloides, hookworm
Was there contact with animals?
Because of the risk of rabies following contact with cats or biting apes, Dr. Holst advised long-distance travelers to get vaccinated.
Were there new sexual partners?
In the event of new sexual contacts, tests for hepatitis A, B, C, and HIV should be performed.
Are you undergoing medical treatment?
The patient may already be under medical supervision because of having a disease.
What prophylactic measures did you take before traveling?
To progress in the differential diagnosis, questions should also be asked regarding prophylactic measures. Vaccination against hepatitis A provides very efficient infection protection, whereas vaccines against typhoid offer a much lower level of protection.
Diagnostic tests
As long as there are no abnormalities, such as meningism or heart murmurs, further diagnostics include routine infectiologic laboratory investigations (C-reactive protein, blood count, etc), blood culture (aerobic, anaerobic), a urine dipstick test, and rapid tests for malaria and dengue.
To exclude malaria, a thick blood smear should always be performed on the same day, said Dr. Holst. “The rapid test is occasionally negative. But you often only detect tertian malaria in the thick blood smear. And you have to repeat the diagnostics the following day.” For this, it is important to know that a single test result does not exclude malaria right away. In contrast, detecting malaria antibodies is obsolete. Depending on the result, further tests include serologies, antigen investigations, and polymerase chain reaction.
Treat early
A complete set of results is not always available promptly. Experts recommend that, “if you already have a hunch, then start the therapy, even without a definite diagnosis.” This applies in particular for the suspected diagnoses in the following table.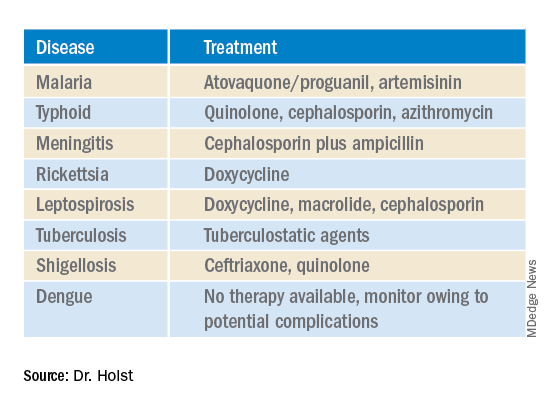
This article was translated from Coliquio. A version of this article appeared on Medscape.com.
After 2 years of a pandemic in which traveling was barely possible, tropical diseases are becoming important once more. At a 2022 conference for internal medicine specialists, tropical medicine specialist Fritz Holst, MD, of the Center for Tropical and Travel Medicine in Marburg, Germany, explained what questions you should be asking travelers with a fever at your practice and how to proceed with a suspected case.
The following article is based on the lecture: “Differential Diagnosis of Fever After a Trip to the Tropics,” which Dr. Holst gave at the 128th conference of the German Society of Internal Medicine.
A meta-analysis of studies concerning the topic, “returnee travelers from the tropics with fever,” was published in 2020. According to the analysis, purely tropical infections make up a third (33%) of fever diagnoses worldwide following an exotic trip. Malaria accounts for a fifth (22%), 5% are dengue fever, and 2.2% are typhoid (enteric fever).
In 26% of the returnee travelers investigated, nontropical infections were the cause of the fever. Acute gastroenteritis was responsible for 14%, and respiratory infections were responsible for 13%. In 18% of the cases, the cause of the fever remained unclear.
In Germany, the number of malaria cases has increased, said Dr. Holst. In Hessen, for example, there was recently a malaria fatality. “What we should do has been forgotten again,” he warned. More attention should also be paid once more to prophylaxis.
How to proceed
Dr. Holst described the following steps for treating recently returned travelers who are sick:
- Severely ill or not: If there are signs of a severe disease, such as dyspnea, signs of bleeding, hypotension, or central nervous system symptoms, the patient should be referred to a clinic. A diagnosis should be made within 1 day and treatment should be started.
- Transmissible or dangerous disease: This question should be quickly clarified to protect health care personnel, especially those treating patients. By using a thorough medical history (discussed below), a range of diseases may be clarified.
- Disease outbreak in destination country: Find out about possible disease outbreaks in the country that the traveler visited.
- Malaria? Immediate diagnostics: Malaria should always be excluded in patients at the practice on the same day by using a thick blood smear, even if no fever is present. If this is not possible because of time constraints, the affected person should be transferred directly to the clinic.
- Fever independent of the travel? Exclude other causes of the fever (for example, endocarditis).
- Involve tropical medicine specialists in a timely manner.
Nine mandatory questions
Dr. Holst also listed nine questions that clinicians should ask this patient population.
Where were you exactly?
Depending on the regional prevalence of tropical diseases, certain pathogens can be excluded quickly. Approximately 35% of travelers returning from Africa have malaria, whereas typhoid is much rarer. In contrast, typhoid and dengue fever are much more widespread in Southeast Asia. In Latin America, this is the case for both dengue fever and leptospirosis.
When did you travel?
By using the incubation time of the pathogen in question, as well as the time of return journey, you can determine which diseases are possible and which are not. In one patient who visited the practice 4 weeks after his return, dengue or typhoid were excluded.
Where did you stay overnight?
Whether in an unhygienic bed or under the stars, the question regarding how and where travelers stayed overnight provides important evidence of the following nocturnal vectors:
- Sandflies: Leishmaniasis
- Kissing bugs: Chagas disease
- Fleas: Spotted fever, bubonic plague
- Mosquitoes: Malaria, dengue, filariasis
What did you eat?
Many infections can be attributed to careless eating. For example, when eating fish, crabs, crawfish, or frogs, especially if raw, liver fluke, lung fluke, or ciguatera should be considered. Mussel toxins have been found on the coast of Kenya and even in the south of France. In North African countries, you should be cautious when eating nonpasteurized milk products (for example, camel milk). They can transmit the pathogens for brucellosis and tuberculosis. In beef or pork that has not been cooked thoroughly, there is the risk of trichinosis or of a tapeworm. Even vegetarians need to be careful. Infections with the common liver fluke are possible after eating watercress.
What have you been doing?
You can only get some diseases through certain activities, said Dr. Holst. If long-distance travelers tell you about the following excursions, prick up your ears:
- Freshwater contact: Schistosomiasis, leptospirosis
- Caving: Histoplasmosis, rabies
- Excavations: Anthrax, coccidioidomycosis
- Camel tour: MERS coronavirus (Do not mount a sniffling camel!)
- Walking around barefoot: Strongyloides, hookworm
Was there contact with animals?
Because of the risk of rabies following contact with cats or biting apes, Dr. Holst advised long-distance travelers to get vaccinated.
Were there new sexual partners?
In the event of new sexual contacts, tests for hepatitis A, B, C, and HIV should be performed.
Are you undergoing medical treatment?
The patient may already be under medical supervision because of having a disease.
What prophylactic measures did you take before traveling?
To progress in the differential diagnosis, questions should also be asked regarding prophylactic measures. Vaccination against hepatitis A provides very efficient infection protection, whereas vaccines against typhoid offer a much lower level of protection.
Diagnostic tests
As long as there are no abnormalities, such as meningism or heart murmurs, further diagnostics include routine infectiologic laboratory investigations (C-reactive protein, blood count, etc), blood culture (aerobic, anaerobic), a urine dipstick test, and rapid tests for malaria and dengue.
To exclude malaria, a thick blood smear should always be performed on the same day, said Dr. Holst. “The rapid test is occasionally negative. But you often only detect tertian malaria in the thick blood smear. And you have to repeat the diagnostics the following day.” For this, it is important to know that a single test result does not exclude malaria right away. In contrast, detecting malaria antibodies is obsolete. Depending on the result, further tests include serologies, antigen investigations, and polymerase chain reaction.
Treat early
A complete set of results is not always available promptly. Experts recommend that, “if you already have a hunch, then start the therapy, even without a definite diagnosis.” This applies in particular for the suspected diagnoses in the following table.
This article was translated from Coliquio. A version of this article appeared on Medscape.com.
After 2 years of a pandemic in which traveling was barely possible, tropical diseases are becoming important once more. At a 2022 conference for internal medicine specialists, tropical medicine specialist Fritz Holst, MD, of the Center for Tropical and Travel Medicine in Marburg, Germany, explained what questions you should be asking travelers with a fever at your practice and how to proceed with a suspected case.
The following article is based on the lecture: “Differential Diagnosis of Fever After a Trip to the Tropics,” which Dr. Holst gave at the 128th conference of the German Society of Internal Medicine.
A meta-analysis of studies concerning the topic, “returnee travelers from the tropics with fever,” was published in 2020. According to the analysis, purely tropical infections make up a third (33%) of fever diagnoses worldwide following an exotic trip. Malaria accounts for a fifth (22%), 5% are dengue fever, and 2.2% are typhoid (enteric fever).
In 26% of the returnee travelers investigated, nontropical infections were the cause of the fever. Acute gastroenteritis was responsible for 14%, and respiratory infections were responsible for 13%. In 18% of the cases, the cause of the fever remained unclear.
In Germany, the number of malaria cases has increased, said Dr. Holst. In Hessen, for example, there was recently a malaria fatality. “What we should do has been forgotten again,” he warned. More attention should also be paid once more to prophylaxis.
How to proceed
Dr. Holst described the following steps for treating recently returned travelers who are sick:
- Severely ill or not: If there are signs of a severe disease, such as dyspnea, signs of bleeding, hypotension, or central nervous system symptoms, the patient should be referred to a clinic. A diagnosis should be made within 1 day and treatment should be started.
- Transmissible or dangerous disease: This question should be quickly clarified to protect health care personnel, especially those treating patients. By using a thorough medical history (discussed below), a range of diseases may be clarified.
- Disease outbreak in destination country: Find out about possible disease outbreaks in the country that the traveler visited.
- Malaria? Immediate diagnostics: Malaria should always be excluded in patients at the practice on the same day by using a thick blood smear, even if no fever is present. If this is not possible because of time constraints, the affected person should be transferred directly to the clinic.
- Fever independent of the travel? Exclude other causes of the fever (for example, endocarditis).
- Involve tropical medicine specialists in a timely manner.
Nine mandatory questions
Dr. Holst also listed nine questions that clinicians should ask this patient population.
Where were you exactly?
Depending on the regional prevalence of tropical diseases, certain pathogens can be excluded quickly. Approximately 35% of travelers returning from Africa have malaria, whereas typhoid is much rarer. In contrast, typhoid and dengue fever are much more widespread in Southeast Asia. In Latin America, this is the case for both dengue fever and leptospirosis.
When did you travel?
By using the incubation time of the pathogen in question, as well as the time of return journey, you can determine which diseases are possible and which are not. In one patient who visited the practice 4 weeks after his return, dengue or typhoid were excluded.
Where did you stay overnight?
Whether in an unhygienic bed or under the stars, the question regarding how and where travelers stayed overnight provides important evidence of the following nocturnal vectors:
- Sandflies: Leishmaniasis
- Kissing bugs: Chagas disease
- Fleas: Spotted fever, bubonic plague
- Mosquitoes: Malaria, dengue, filariasis
What did you eat?
Many infections can be attributed to careless eating. For example, when eating fish, crabs, crawfish, or frogs, especially if raw, liver fluke, lung fluke, or ciguatera should be considered. Mussel toxins have been found on the coast of Kenya and even in the south of France. In North African countries, you should be cautious when eating nonpasteurized milk products (for example, camel milk). They can transmit the pathogens for brucellosis and tuberculosis. In beef or pork that has not been cooked thoroughly, there is the risk of trichinosis or of a tapeworm. Even vegetarians need to be careful. Infections with the common liver fluke are possible after eating watercress.
What have you been doing?
You can only get some diseases through certain activities, said Dr. Holst. If long-distance travelers tell you about the following excursions, prick up your ears:
- Freshwater contact: Schistosomiasis, leptospirosis
- Caving: Histoplasmosis, rabies
- Excavations: Anthrax, coccidioidomycosis
- Camel tour: MERS coronavirus (Do not mount a sniffling camel!)
- Walking around barefoot: Strongyloides, hookworm
Was there contact with animals?
Because of the risk of rabies following contact with cats or biting apes, Dr. Holst advised long-distance travelers to get vaccinated.
Were there new sexual partners?
In the event of new sexual contacts, tests for hepatitis A, B, C, and HIV should be performed.
Are you undergoing medical treatment?
The patient may already be under medical supervision because of having a disease.
What prophylactic measures did you take before traveling?
To progress in the differential diagnosis, questions should also be asked regarding prophylactic measures. Vaccination against hepatitis A provides very efficient infection protection, whereas vaccines against typhoid offer a much lower level of protection.
Diagnostic tests
As long as there are no abnormalities, such as meningism or heart murmurs, further diagnostics include routine infectiologic laboratory investigations (C-reactive protein, blood count, etc), blood culture (aerobic, anaerobic), a urine dipstick test, and rapid tests for malaria and dengue.
To exclude malaria, a thick blood smear should always be performed on the same day, said Dr. Holst. “The rapid test is occasionally negative. But you often only detect tertian malaria in the thick blood smear. And you have to repeat the diagnostics the following day.” For this, it is important to know that a single test result does not exclude malaria right away. In contrast, detecting malaria antibodies is obsolete. Depending on the result, further tests include serologies, antigen investigations, and polymerase chain reaction.
Treat early
A complete set of results is not always available promptly. Experts recommend that, “if you already have a hunch, then start the therapy, even without a definite diagnosis.” This applies in particular for the suspected diagnoses in the following table.
This article was translated from Coliquio. A version of this article appeared on Medscape.com.
Doxycycline bests azithromycin for anorectal chlamydia in women
NEW YORK (Reuters) – A one-week course of doxycycline was superior to a single dose of azithromycin in women with concurrent vaginal and anorectal chlamydia infection in an unblinded randomized controlled trial, mirroring previous results in men.
Researchers suggest that doxycycline should be the first-line therapy for chlamydia infection in women.
“It is clear we must consider that any woman with a urogenital infection must have an effective treatment for the anal infection, since nearly 80% of women have an anal infection concomitant with the vaginal infection,” Dr. Bertille de Barbeyrac of the University of Bordeaux, France, told Reuters Health by email.
However, she noted that “even [though] the study shows that doxycycline is more effective than azithromycin on anal infection, other studies are needed to prove that residual anal infection after treatment with azithromycin can be a source of vaginal contamination and therefore justify changing practices and eliminating azithromycin as a treatment for lower urogenital chlamydial infection in women.”
“There are other reasons [to make] this change,” she added, “such as the acquisition of macrolide resistance by M. genitalium following heavy use of azithromycin.”
As reported in The Lancet Infectious Diseases, Dr. Barbeyrac and colleagues randomly assigned 460 women (median age, 21) to either doxycycline or azithromycin in a multicenter, open-label superiority trial.
Participants received either azithromycin (a single 1-g dose, with or without food) or doxycycline (100 mg in the morning and evening at mealtimes for 7 days – that is, 100 mg of doxycycline twice daily).
The primary outcome was that the microbiological anorectal cure rate, defined as a C. trachomatis-negative nucleic acid amplification test (NAAT), resulted in anorectal specimens six weeks after treatment initiation among women who had a baseline positive result (about half the women in each treatment group).
Ninety-four percent of the doxycycline group versus 85% of the azithromycin group had an anorectal cure (adjusted odds ratio with imputation of missing values, 0.43).
Adverse events possibly related to treatment occurred in 11% of the doxycycline group versus 13% of the azithromycin group. Gastrointestinal disorders were most frequent, occurring in 8% of the doxycycline and 11% of the azithromycin groups.
Summing up, the authors write, “The microbiological anorectal cure rate was significantly lower among women who received a single dose of azithromycin than among those who received a 1-week course of doxycycline. This finding suggests that doxycycline should be the first-line therapy for C trachomatis infection in women.”
Dr. Meleen Chuang, medical director of women’s health at the Family Health Centers at NYU Langone, Brooklyn, commented in an email to Reuters Health that after reviewing this study “as well as CDC and WHO recommendations updated as of 2022, health care providers should be treating C. trachomatis infections with doxycycline 100 mg twice a day for seven days as first-line therapy rather than azithromycin, [given] concerns of increasing macrolide drug resistance against Mycoplasma genitalium and Neisseria gonorrhea.”
“Our clinicians also see the growing uptick of syphilis, gonorrhea, and chlamydia infections in our population, similarly to the rest of the United States since 2020,” she noted. “With the increase in STD infection ... treatment with doxycycline therapy with an important caveat to the patient to complete the one-week treatment regimen is extremely important.”
Dr. Latasha Murphy of the Gynecologic Care Institute at Mercy, Baltimore, also commented in an email to Reuters Health. She noted, “this study does not mirror my clinical experience. More patients have side effects from doxycycline than azithromycin in my experience. Also, anorectal screening is not routine in STD screening.”
“If any major changes to clinical care are made,” she said, “it may be for more consistent screening for anorectal disease. This may ultimately lead to doxycycline being the first line-treatment. More research is needed before making any definitive changes.”
Reuters Health Information © 2022
NEW YORK (Reuters) – A one-week course of doxycycline was superior to a single dose of azithromycin in women with concurrent vaginal and anorectal chlamydia infection in an unblinded randomized controlled trial, mirroring previous results in men.
Researchers suggest that doxycycline should be the first-line therapy for chlamydia infection in women.
“It is clear we must consider that any woman with a urogenital infection must have an effective treatment for the anal infection, since nearly 80% of women have an anal infection concomitant with the vaginal infection,” Dr. Bertille de Barbeyrac of the University of Bordeaux, France, told Reuters Health by email.
However, she noted that “even [though] the study shows that doxycycline is more effective than azithromycin on anal infection, other studies are needed to prove that residual anal infection after treatment with azithromycin can be a source of vaginal contamination and therefore justify changing practices and eliminating azithromycin as a treatment for lower urogenital chlamydial infection in women.”
“There are other reasons [to make] this change,” she added, “such as the acquisition of macrolide resistance by M. genitalium following heavy use of azithromycin.”
As reported in The Lancet Infectious Diseases, Dr. Barbeyrac and colleagues randomly assigned 460 women (median age, 21) to either doxycycline or azithromycin in a multicenter, open-label superiority trial.
Participants received either azithromycin (a single 1-g dose, with or without food) or doxycycline (100 mg in the morning and evening at mealtimes for 7 days – that is, 100 mg of doxycycline twice daily).
The primary outcome was that the microbiological anorectal cure rate, defined as a C. trachomatis-negative nucleic acid amplification test (NAAT), resulted in anorectal specimens six weeks after treatment initiation among women who had a baseline positive result (about half the women in each treatment group).
Ninety-four percent of the doxycycline group versus 85% of the azithromycin group had an anorectal cure (adjusted odds ratio with imputation of missing values, 0.43).
Adverse events possibly related to treatment occurred in 11% of the doxycycline group versus 13% of the azithromycin group. Gastrointestinal disorders were most frequent, occurring in 8% of the doxycycline and 11% of the azithromycin groups.
Summing up, the authors write, “The microbiological anorectal cure rate was significantly lower among women who received a single dose of azithromycin than among those who received a 1-week course of doxycycline. This finding suggests that doxycycline should be the first-line therapy for C trachomatis infection in women.”
Dr. Meleen Chuang, medical director of women’s health at the Family Health Centers at NYU Langone, Brooklyn, commented in an email to Reuters Health that after reviewing this study “as well as CDC and WHO recommendations updated as of 2022, health care providers should be treating C. trachomatis infections with doxycycline 100 mg twice a day for seven days as first-line therapy rather than azithromycin, [given] concerns of increasing macrolide drug resistance against Mycoplasma genitalium and Neisseria gonorrhea.”
“Our clinicians also see the growing uptick of syphilis, gonorrhea, and chlamydia infections in our population, similarly to the rest of the United States since 2020,” she noted. “With the increase in STD infection ... treatment with doxycycline therapy with an important caveat to the patient to complete the one-week treatment regimen is extremely important.”
Dr. Latasha Murphy of the Gynecologic Care Institute at Mercy, Baltimore, also commented in an email to Reuters Health. She noted, “this study does not mirror my clinical experience. More patients have side effects from doxycycline than azithromycin in my experience. Also, anorectal screening is not routine in STD screening.”
“If any major changes to clinical care are made,” she said, “it may be for more consistent screening for anorectal disease. This may ultimately lead to doxycycline being the first line-treatment. More research is needed before making any definitive changes.”
Reuters Health Information © 2022
NEW YORK (Reuters) – A one-week course of doxycycline was superior to a single dose of azithromycin in women with concurrent vaginal and anorectal chlamydia infection in an unblinded randomized controlled trial, mirroring previous results in men.
Researchers suggest that doxycycline should be the first-line therapy for chlamydia infection in women.
“It is clear we must consider that any woman with a urogenital infection must have an effective treatment for the anal infection, since nearly 80% of women have an anal infection concomitant with the vaginal infection,” Dr. Bertille de Barbeyrac of the University of Bordeaux, France, told Reuters Health by email.
However, she noted that “even [though] the study shows that doxycycline is more effective than azithromycin on anal infection, other studies are needed to prove that residual anal infection after treatment with azithromycin can be a source of vaginal contamination and therefore justify changing practices and eliminating azithromycin as a treatment for lower urogenital chlamydial infection in women.”
“There are other reasons [to make] this change,” she added, “such as the acquisition of macrolide resistance by M. genitalium following heavy use of azithromycin.”
As reported in The Lancet Infectious Diseases, Dr. Barbeyrac and colleagues randomly assigned 460 women (median age, 21) to either doxycycline or azithromycin in a multicenter, open-label superiority trial.
Participants received either azithromycin (a single 1-g dose, with or without food) or doxycycline (100 mg in the morning and evening at mealtimes for 7 days – that is, 100 mg of doxycycline twice daily).
The primary outcome was that the microbiological anorectal cure rate, defined as a C. trachomatis-negative nucleic acid amplification test (NAAT), resulted in anorectal specimens six weeks after treatment initiation among women who had a baseline positive result (about half the women in each treatment group).
Ninety-four percent of the doxycycline group versus 85% of the azithromycin group had an anorectal cure (adjusted odds ratio with imputation of missing values, 0.43).
Adverse events possibly related to treatment occurred in 11% of the doxycycline group versus 13% of the azithromycin group. Gastrointestinal disorders were most frequent, occurring in 8% of the doxycycline and 11% of the azithromycin groups.
Summing up, the authors write, “The microbiological anorectal cure rate was significantly lower among women who received a single dose of azithromycin than among those who received a 1-week course of doxycycline. This finding suggests that doxycycline should be the first-line therapy for C trachomatis infection in women.”
Dr. Meleen Chuang, medical director of women’s health at the Family Health Centers at NYU Langone, Brooklyn, commented in an email to Reuters Health that after reviewing this study “as well as CDC and WHO recommendations updated as of 2022, health care providers should be treating C. trachomatis infections with doxycycline 100 mg twice a day for seven days as first-line therapy rather than azithromycin, [given] concerns of increasing macrolide drug resistance against Mycoplasma genitalium and Neisseria gonorrhea.”
“Our clinicians also see the growing uptick of syphilis, gonorrhea, and chlamydia infections in our population, similarly to the rest of the United States since 2020,” she noted. “With the increase in STD infection ... treatment with doxycycline therapy with an important caveat to the patient to complete the one-week treatment regimen is extremely important.”
Dr. Latasha Murphy of the Gynecologic Care Institute at Mercy, Baltimore, also commented in an email to Reuters Health. She noted, “this study does not mirror my clinical experience. More patients have side effects from doxycycline than azithromycin in my experience. Also, anorectal screening is not routine in STD screening.”
“If any major changes to clinical care are made,” she said, “it may be for more consistent screening for anorectal disease. This may ultimately lead to doxycycline being the first line-treatment. More research is needed before making any definitive changes.”
Reuters Health Information © 2022
CRC screening: Blood test accuracy compared to colonoscopy
The first prospective study to evaluate the accuracy of a blood test for people being screened for colorectal cancer (CRC) revealed a high sensitivity and specificity.
At 90% specificity, the blood assay (Guardant Health) was 100% sensitive for detecting CRC. At 95% specificity, sensitivity was 88%.
The blood assay detects circulating tumor DNA from cancer in the bloodstream, which is then analyzed for multiple factors, including cancer genetics and methylation.
Lead author Paloma Peinado, MD, a medical oncologist at HM Hospitales, Madrid, and colleagues, called the results similar to those seen with noninvasive, stool-based testing, noting that the “sensitivity and specificity of the blood-based test reached clinically significant thresholds.”
“The reported performance, combined with a more acceptable mode of testing, suggests that this blood-based test may be a viable CRC screening option,” they added.
The study was presented at Digestive Disease Week® (DDW) 2022, held virtually and in San Diego.
Dr. Peinado and colleagues studied 557 people who agreed to have blood drawn at the time of their colonoscopy. They enrolled participants at four hospitals in Spain.
One-third of participants (33%) who sought CRC screening were at average risk. Of the remainder, 49% were symptomatic, 11% had a positive family history of CRC, 6% had a positive stool-based test result, and 1% presented for colonoscopy for other reasons.
The prospective observational study included people age 45-84 years. The median age of participants was 55 years, and just over half (52%) were women.
The prevalence rate of colorectal adenocarcinoma was 2.6%. Eight patients had stage I cancer, three had stage II cancer, two had stage III cancer, and two had stage IV cancer.
The study was designed to follow patients for 1 year after screening. To date, 14% of participants have reached this point.
Not a general population screening study
“We definitely we need more studies like this,” said Barbara H. Jung, MD, chair of the department of medicine at the University of Washington, Seattle, when asked to comment on the study.
“We need to find other ways to detect colorectal cancer early, to enhance the screening, and to broaden it to a larger population who may not be amenable to the other techniques.”
Dr. Jung added a caveat that the study population included people at a higher risk for CRC. Therefore, she said, it was a screening study but not a general population, average-risk screening study.
However, she said, “that does not mean that this could not be optimized in the future.”
Ideally, we need tests for every application, including people who are asymptomatic, Dr. Jung said.
Dr. Peinado reports no relevant financial relationships. Some of the study authors are employees of Guardant Health. Dr. Jung reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The first prospective study to evaluate the accuracy of a blood test for people being screened for colorectal cancer (CRC) revealed a high sensitivity and specificity.
At 90% specificity, the blood assay (Guardant Health) was 100% sensitive for detecting CRC. At 95% specificity, sensitivity was 88%.
The blood assay detects circulating tumor DNA from cancer in the bloodstream, which is then analyzed for multiple factors, including cancer genetics and methylation.
Lead author Paloma Peinado, MD, a medical oncologist at HM Hospitales, Madrid, and colleagues, called the results similar to those seen with noninvasive, stool-based testing, noting that the “sensitivity and specificity of the blood-based test reached clinically significant thresholds.”
“The reported performance, combined with a more acceptable mode of testing, suggests that this blood-based test may be a viable CRC screening option,” they added.
The study was presented at Digestive Disease Week® (DDW) 2022, held virtually and in San Diego.
Dr. Peinado and colleagues studied 557 people who agreed to have blood drawn at the time of their colonoscopy. They enrolled participants at four hospitals in Spain.
One-third of participants (33%) who sought CRC screening were at average risk. Of the remainder, 49% were symptomatic, 11% had a positive family history of CRC, 6% had a positive stool-based test result, and 1% presented for colonoscopy for other reasons.
The prospective observational study included people age 45-84 years. The median age of participants was 55 years, and just over half (52%) were women.
The prevalence rate of colorectal adenocarcinoma was 2.6%. Eight patients had stage I cancer, three had stage II cancer, two had stage III cancer, and two had stage IV cancer.
The study was designed to follow patients for 1 year after screening. To date, 14% of participants have reached this point.
Not a general population screening study
“We definitely we need more studies like this,” said Barbara H. Jung, MD, chair of the department of medicine at the University of Washington, Seattle, when asked to comment on the study.
“We need to find other ways to detect colorectal cancer early, to enhance the screening, and to broaden it to a larger population who may not be amenable to the other techniques.”
Dr. Jung added a caveat that the study population included people at a higher risk for CRC. Therefore, she said, it was a screening study but not a general population, average-risk screening study.
However, she said, “that does not mean that this could not be optimized in the future.”
Ideally, we need tests for every application, including people who are asymptomatic, Dr. Jung said.
Dr. Peinado reports no relevant financial relationships. Some of the study authors are employees of Guardant Health. Dr. Jung reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The first prospective study to evaluate the accuracy of a blood test for people being screened for colorectal cancer (CRC) revealed a high sensitivity and specificity.
At 90% specificity, the blood assay (Guardant Health) was 100% sensitive for detecting CRC. At 95% specificity, sensitivity was 88%.
The blood assay detects circulating tumor DNA from cancer in the bloodstream, which is then analyzed for multiple factors, including cancer genetics and methylation.
Lead author Paloma Peinado, MD, a medical oncologist at HM Hospitales, Madrid, and colleagues, called the results similar to those seen with noninvasive, stool-based testing, noting that the “sensitivity and specificity of the blood-based test reached clinically significant thresholds.”
“The reported performance, combined with a more acceptable mode of testing, suggests that this blood-based test may be a viable CRC screening option,” they added.
The study was presented at Digestive Disease Week® (DDW) 2022, held virtually and in San Diego.
Dr. Peinado and colleagues studied 557 people who agreed to have blood drawn at the time of their colonoscopy. They enrolled participants at four hospitals in Spain.
One-third of participants (33%) who sought CRC screening were at average risk. Of the remainder, 49% were symptomatic, 11% had a positive family history of CRC, 6% had a positive stool-based test result, and 1% presented for colonoscopy for other reasons.
The prospective observational study included people age 45-84 years. The median age of participants was 55 years, and just over half (52%) were women.
The prevalence rate of colorectal adenocarcinoma was 2.6%. Eight patients had stage I cancer, three had stage II cancer, two had stage III cancer, and two had stage IV cancer.
The study was designed to follow patients for 1 year after screening. To date, 14% of participants have reached this point.
Not a general population screening study
“We definitely we need more studies like this,” said Barbara H. Jung, MD, chair of the department of medicine at the University of Washington, Seattle, when asked to comment on the study.
“We need to find other ways to detect colorectal cancer early, to enhance the screening, and to broaden it to a larger population who may not be amenable to the other techniques.”
Dr. Jung added a caveat that the study population included people at a higher risk for CRC. Therefore, she said, it was a screening study but not a general population, average-risk screening study.
However, she said, “that does not mean that this could not be optimized in the future.”
Ideally, we need tests for every application, including people who are asymptomatic, Dr. Jung said.
Dr. Peinado reports no relevant financial relationships. Some of the study authors are employees of Guardant Health. Dr. Jung reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Roe v. Wade’s pending fall raises privacy concerns
If Roe v. Wade is overturned, can criminal prosecutors or tech companies use smartphone data against someone?
Now that the future of U.S. abortion laws hangs in the balance, many women are questioning the degree of caution needed to keep their cyber activity confidential – especially period and fertility tracking apps, smartphone location data, and social media interactions.
Cybersecurity and legal experts say the answer largely boils down to one major issue: The right to privacy.
“There’s this notion of the expectation of privacy,” said Brad Malin, PhD, professor of biomedical informatics, biostatistics, and computer science at Vanderbilt University in Nashville, Tenn.
Dr. Malin said it’s directly related to bodily privacy that a person expects they have control of as part of their own environment.
According to Dr. Malin, this is “why this whole notion of Roe v. Wade at the present moment is really relevant. The right to privacy is mentioned about a dozen times within the law for the case.
“This is why we don’t know what’s going to happen with Roe v. Wade, but it worries a lot of privacy professionals,” he said. “It leads down this slippery slope of if you don’t even have control over your own body, then with electronic communications … we might as well not even start.”
Legal protections
The Fourth Amendment of the U.S. Constitution protects people against unreasonable searches and seizures.
To acquire cyber data that could be used as evidence in courts in states where abortion is deemed a crime, prosecutors would still have to go through standard criminal procedures, said Anthony Michael Kreis, JD, a constitutional law professor at Georgia State University, Atlanta.
But the data they do get could still be used in court against someone who is suspected of having had an abortion or who “miscarried under circumstances law enforcement officers found suspicious,” Mr. Kreis said.
And there’s another possibility, he noted: States holding women who end their pregnancies criminally or civilly responsible for “leaving their jurisdiction to obtain an abortion out-of-state.”
“That legal mechanism may abridge the constitutional right to travel, but it is not out of the realm of possibilities in a post-Roe America,” said Mr. Kreis.
But while many anti-abortion groups have said that criminalizing abortion or limiting access to contraception is not the end goal, “history is not promising here,” said Ellen Wright Clayton, MD, JD, professor of pediatrics and professor of law at Vanderbilt University.
She referred to a recent proposal from lawmakers in Louisiana to classify abortion as homicide.
The bill didn’t get far in the House of Representatives, but the concern is warranted, said Dr. Clayton.
Period and fertility tracking apps
Health information privacy laws, like the Health Insurance Portability and Accountability Act (HIPAA), do not protect information on period and fertility tracking apps.
Right now, there are no signs that people plan to use period and fertility tracking data to advance a prochoice agenda, according to Adam Levin, JD, a cybersecurity expert and founder of CyberScout, a global identity and data protection company.
Still, a cycle tracking app “created by a company owned by an antiabortion activist” is totally feasible, said Mr. Levin.
If you want to ensure your data is safe from such meddling, you may want to delete your app, he said, noting that using the notepad feature on your smartphone could be a safer alternative, as could using old-fashioned pen and paper.
You don’t have to stop with period and fertility tracking apps, either.
For any apps you share personal information with, set privacy settings “as tightly as possible” – and reconsider using apps if these options are unavailable, Mr. Levin advised.
“Make sure that company is not engaging in social or political activism that does not align with your politics.”
New York State Attorney General Letitia James recently spoke on the topic, noting on May 13 that “people use fertility tracking apps and location services every day, but if they’re not careful their personal information can end up in the wrong hands.
“With abortion rights in jeopardy, it’s more important than ever that everyone take their digital privacy seriously,” she said. “I urge everyone, especially those visiting abortion clinics or seeking abortion care, to follow the tips offered by my office and be more careful of the apps and websites they use.”
The New York State Attorney General’s Office recommends women use encrypted messaging when communicating about personal health information or behaviors, and to be careful about what they share on social media posts. The office also suggests turning off location and personalized advertising options on their smartphones.
Cellphone location data
Dr. Malin said there are several ways that location services could be used to track where a woman uses her smartphone. An app could track locations if someone grants permission through the app end user agreement, for example.
A second but less likely scenario would be the service provider tracking the pings coming off cellphone towers to find a smartphone.
So what recourse does a woman have if tracked by a third-party app?
“It’s a really tricky situation there because it depends on if the individual was put expressly in harm’s way,” Dr. Malin said. What’s more, tracking someone out in public is not prohibited in general.
“There’s a big difference between documenting what an individual does within a Planned Parenthood clinic versus what they do outside of it,” he said.
Dr. Malin said it’s better that regulations protect all smartphone users rather than requiring each person to remember to turn off the location tracker and then turn it back on again. Also, it should be more of an opt-in situation – where app developers must ask permission to track app usage or location services – versus making each woman opt out.
Think before you share
Vindictive or untrustworthy partners and family members of women in abusive relationships could also be a cause of concern, said Mr. Kreis.
“Individuals within a woman’s closest circles could hold abortions over their head or threaten reporting them for reproductive health care or miscarriages,” he said.
It’s not uncommon for women to experience domestic violence after having an abortion, particularly if their partners were unaware they had the procedure, according to Dr. Clayton.
She said women should also be mindful of what they share on social media.
Dr. Clayton gave the example of a woman seeking advice on where to get a safe abortion or how to order certain medications.
“If someone goes online to look for that, that’s potentially dangerous.”
A version of this article first appeared on WebMD.com.
If Roe v. Wade is overturned, can criminal prosecutors or tech companies use smartphone data against someone?
Now that the future of U.S. abortion laws hangs in the balance, many women are questioning the degree of caution needed to keep their cyber activity confidential – especially period and fertility tracking apps, smartphone location data, and social media interactions.
Cybersecurity and legal experts say the answer largely boils down to one major issue: The right to privacy.
“There’s this notion of the expectation of privacy,” said Brad Malin, PhD, professor of biomedical informatics, biostatistics, and computer science at Vanderbilt University in Nashville, Tenn.
Dr. Malin said it’s directly related to bodily privacy that a person expects they have control of as part of their own environment.
According to Dr. Malin, this is “why this whole notion of Roe v. Wade at the present moment is really relevant. The right to privacy is mentioned about a dozen times within the law for the case.
“This is why we don’t know what’s going to happen with Roe v. Wade, but it worries a lot of privacy professionals,” he said. “It leads down this slippery slope of if you don’t even have control over your own body, then with electronic communications … we might as well not even start.”
Legal protections
The Fourth Amendment of the U.S. Constitution protects people against unreasonable searches and seizures.
To acquire cyber data that could be used as evidence in courts in states where abortion is deemed a crime, prosecutors would still have to go through standard criminal procedures, said Anthony Michael Kreis, JD, a constitutional law professor at Georgia State University, Atlanta.
But the data they do get could still be used in court against someone who is suspected of having had an abortion or who “miscarried under circumstances law enforcement officers found suspicious,” Mr. Kreis said.
And there’s another possibility, he noted: States holding women who end their pregnancies criminally or civilly responsible for “leaving their jurisdiction to obtain an abortion out-of-state.”
“That legal mechanism may abridge the constitutional right to travel, but it is not out of the realm of possibilities in a post-Roe America,” said Mr. Kreis.
But while many anti-abortion groups have said that criminalizing abortion or limiting access to contraception is not the end goal, “history is not promising here,” said Ellen Wright Clayton, MD, JD, professor of pediatrics and professor of law at Vanderbilt University.
She referred to a recent proposal from lawmakers in Louisiana to classify abortion as homicide.
The bill didn’t get far in the House of Representatives, but the concern is warranted, said Dr. Clayton.
Period and fertility tracking apps
Health information privacy laws, like the Health Insurance Portability and Accountability Act (HIPAA), do not protect information on period and fertility tracking apps.
Right now, there are no signs that people plan to use period and fertility tracking data to advance a prochoice agenda, according to Adam Levin, JD, a cybersecurity expert and founder of CyberScout, a global identity and data protection company.
Still, a cycle tracking app “created by a company owned by an antiabortion activist” is totally feasible, said Mr. Levin.
If you want to ensure your data is safe from such meddling, you may want to delete your app, he said, noting that using the notepad feature on your smartphone could be a safer alternative, as could using old-fashioned pen and paper.
You don’t have to stop with period and fertility tracking apps, either.
For any apps you share personal information with, set privacy settings “as tightly as possible” – and reconsider using apps if these options are unavailable, Mr. Levin advised.
“Make sure that company is not engaging in social or political activism that does not align with your politics.”
New York State Attorney General Letitia James recently spoke on the topic, noting on May 13 that “people use fertility tracking apps and location services every day, but if they’re not careful their personal information can end up in the wrong hands.
“With abortion rights in jeopardy, it’s more important than ever that everyone take their digital privacy seriously,” she said. “I urge everyone, especially those visiting abortion clinics or seeking abortion care, to follow the tips offered by my office and be more careful of the apps and websites they use.”
The New York State Attorney General’s Office recommends women use encrypted messaging when communicating about personal health information or behaviors, and to be careful about what they share on social media posts. The office also suggests turning off location and personalized advertising options on their smartphones.
Cellphone location data
Dr. Malin said there are several ways that location services could be used to track where a woman uses her smartphone. An app could track locations if someone grants permission through the app end user agreement, for example.
A second but less likely scenario would be the service provider tracking the pings coming off cellphone towers to find a smartphone.
So what recourse does a woman have if tracked by a third-party app?
“It’s a really tricky situation there because it depends on if the individual was put expressly in harm’s way,” Dr. Malin said. What’s more, tracking someone out in public is not prohibited in general.
“There’s a big difference between documenting what an individual does within a Planned Parenthood clinic versus what they do outside of it,” he said.
Dr. Malin said it’s better that regulations protect all smartphone users rather than requiring each person to remember to turn off the location tracker and then turn it back on again. Also, it should be more of an opt-in situation – where app developers must ask permission to track app usage or location services – versus making each woman opt out.
Think before you share
Vindictive or untrustworthy partners and family members of women in abusive relationships could also be a cause of concern, said Mr. Kreis.
“Individuals within a woman’s closest circles could hold abortions over their head or threaten reporting them for reproductive health care or miscarriages,” he said.
It’s not uncommon for women to experience domestic violence after having an abortion, particularly if their partners were unaware they had the procedure, according to Dr. Clayton.
She said women should also be mindful of what they share on social media.
Dr. Clayton gave the example of a woman seeking advice on where to get a safe abortion or how to order certain medications.
“If someone goes online to look for that, that’s potentially dangerous.”
A version of this article first appeared on WebMD.com.
If Roe v. Wade is overturned, can criminal prosecutors or tech companies use smartphone data against someone?
Now that the future of U.S. abortion laws hangs in the balance, many women are questioning the degree of caution needed to keep their cyber activity confidential – especially period and fertility tracking apps, smartphone location data, and social media interactions.
Cybersecurity and legal experts say the answer largely boils down to one major issue: The right to privacy.
“There’s this notion of the expectation of privacy,” said Brad Malin, PhD, professor of biomedical informatics, biostatistics, and computer science at Vanderbilt University in Nashville, Tenn.
Dr. Malin said it’s directly related to bodily privacy that a person expects they have control of as part of their own environment.
According to Dr. Malin, this is “why this whole notion of Roe v. Wade at the present moment is really relevant. The right to privacy is mentioned about a dozen times within the law for the case.
“This is why we don’t know what’s going to happen with Roe v. Wade, but it worries a lot of privacy professionals,” he said. “It leads down this slippery slope of if you don’t even have control over your own body, then with electronic communications … we might as well not even start.”
Legal protections
The Fourth Amendment of the U.S. Constitution protects people against unreasonable searches and seizures.
To acquire cyber data that could be used as evidence in courts in states where abortion is deemed a crime, prosecutors would still have to go through standard criminal procedures, said Anthony Michael Kreis, JD, a constitutional law professor at Georgia State University, Atlanta.
But the data they do get could still be used in court against someone who is suspected of having had an abortion or who “miscarried under circumstances law enforcement officers found suspicious,” Mr. Kreis said.
And there’s another possibility, he noted: States holding women who end their pregnancies criminally or civilly responsible for “leaving their jurisdiction to obtain an abortion out-of-state.”
“That legal mechanism may abridge the constitutional right to travel, but it is not out of the realm of possibilities in a post-Roe America,” said Mr. Kreis.
But while many anti-abortion groups have said that criminalizing abortion or limiting access to contraception is not the end goal, “history is not promising here,” said Ellen Wright Clayton, MD, JD, professor of pediatrics and professor of law at Vanderbilt University.
She referred to a recent proposal from lawmakers in Louisiana to classify abortion as homicide.
The bill didn’t get far in the House of Representatives, but the concern is warranted, said Dr. Clayton.
Period and fertility tracking apps
Health information privacy laws, like the Health Insurance Portability and Accountability Act (HIPAA), do not protect information on period and fertility tracking apps.
Right now, there are no signs that people plan to use period and fertility tracking data to advance a prochoice agenda, according to Adam Levin, JD, a cybersecurity expert and founder of CyberScout, a global identity and data protection company.
Still, a cycle tracking app “created by a company owned by an antiabortion activist” is totally feasible, said Mr. Levin.
If you want to ensure your data is safe from such meddling, you may want to delete your app, he said, noting that using the notepad feature on your smartphone could be a safer alternative, as could using old-fashioned pen and paper.
You don’t have to stop with period and fertility tracking apps, either.
For any apps you share personal information with, set privacy settings “as tightly as possible” – and reconsider using apps if these options are unavailable, Mr. Levin advised.
“Make sure that company is not engaging in social or political activism that does not align with your politics.”
New York State Attorney General Letitia James recently spoke on the topic, noting on May 13 that “people use fertility tracking apps and location services every day, but if they’re not careful their personal information can end up in the wrong hands.
“With abortion rights in jeopardy, it’s more important than ever that everyone take their digital privacy seriously,” she said. “I urge everyone, especially those visiting abortion clinics or seeking abortion care, to follow the tips offered by my office and be more careful of the apps and websites they use.”
The New York State Attorney General’s Office recommends women use encrypted messaging when communicating about personal health information or behaviors, and to be careful about what they share on social media posts. The office also suggests turning off location and personalized advertising options on their smartphones.
Cellphone location data
Dr. Malin said there are several ways that location services could be used to track where a woman uses her smartphone. An app could track locations if someone grants permission through the app end user agreement, for example.
A second but less likely scenario would be the service provider tracking the pings coming off cellphone towers to find a smartphone.
So what recourse does a woman have if tracked by a third-party app?
“It’s a really tricky situation there because it depends on if the individual was put expressly in harm’s way,” Dr. Malin said. What’s more, tracking someone out in public is not prohibited in general.
“There’s a big difference between documenting what an individual does within a Planned Parenthood clinic versus what they do outside of it,” he said.
Dr. Malin said it’s better that regulations protect all smartphone users rather than requiring each person to remember to turn off the location tracker and then turn it back on again. Also, it should be more of an opt-in situation – where app developers must ask permission to track app usage or location services – versus making each woman opt out.
Think before you share
Vindictive or untrustworthy partners and family members of women in abusive relationships could also be a cause of concern, said Mr. Kreis.
“Individuals within a woman’s closest circles could hold abortions over their head or threaten reporting them for reproductive health care or miscarriages,” he said.
It’s not uncommon for women to experience domestic violence after having an abortion, particularly if their partners were unaware they had the procedure, according to Dr. Clayton.
She said women should also be mindful of what they share on social media.
Dr. Clayton gave the example of a woman seeking advice on where to get a safe abortion or how to order certain medications.
“If someone goes online to look for that, that’s potentially dangerous.”
A version of this article first appeared on WebMD.com.
How to manage drug interactions with Paxlovid for COVID-19
Misinformation about nirmatrelvir/ritonavir (Paxlovid, Pfizer) for treating mild to moderate COVID-19 in patients at high risk for severe disease is feeding misunderstanding among prescribers and patients, two experts from the Infectious Diseases Society of America (IDSA) have said.
They briefed reporters on potential drug interactions and uncommon cases of a “rebound” effect with the drug, which was granted emergency use authorization by the Food and Drug Administration last December for patients at least 12 years old.
The drug combination works “like a pair of scissors chopping up proteins that are made as the virus replicates inside of cells. Inhibiting that enzyme leads to the cessation of replication,” said Jason C. Gallagher, PharmD, of Temple University School of Pharmacy, Philadelphia.
That’s important because other treatments that target the spike protein, such as monoclonal antibodies, can lose their efficacy as the virus changes. He said that while that’s not impossible for Paxlovid, “we have not seen variants emerging that are resistant to it.”
Potential drug interactions
IDSA recently published updated guidance on potential interactions between Paxlovid and the top 100 drugs, and important considerations for prescribing.
“There is a concern that people have not been prescribing it because of fear of these interactions,” Dr. Gallagher said, explaining that, while in some cases those fears may be valid, in many instances the interaction is manageable.
One example is in two popular statins for heart disease, lovastatin and simvastatin.
“That’s an interaction that can be managed by holding [those drugs] for the 5 days that someone receives Paxlovid,” he said.
Misinformation also is circulating about distribution status of Paxlovid, Dr. Gallagher said.
“We’re in a very different state from that standpoint than we were a month or 2 months ago,” he said, adding that it is widely available in not all but a large number of pharmacies throughout the United States.
He emphasized the importance of drug reconciliation, as many patients will go to a different pharmacy for Paxlovid than they might for their usual prescriptions, so without a full accounting of prescriptions and supplements potential interactions may be missed.
Important interactions to watch
Melanie Thompson, MD, cochair of the HIVMA/IDSA HIV Primary Care Guidance Panel, highlighted some classes of drugs to watch, among them the antiarrhythmics, most of which are contraindicated with Paxlovid.
There are also important interactions with a number of cancer drugs, and consults with oncologists will be critical, she said.
“Likewise, people who have had transplants are likely to be on drugs that have significant ritonavir interactions,” Dr. Thompson said.
People on ergot drugs for migraine cannot take Paxlovid, she said, and “people who take colchicine for gout have to be very careful.”
She said it’s better not to use colchicine while taking Paxlovid, as it is contraindicated, “but it can be managed in certain circumstances with substantial dose reduction.”
A number of mental health drugs can be managed with Paxlovid, Dr. Thompson said. For the antipsychotic drug quetiapine, (Seroquel), a “substantial decrease in dose is required.”
Viagra for ED can be managed
Use of Viagra depends on why it’s being used, Dr. Thompson said. If it’s used for pulmonary hypertension, it is used at a very high dose and that is contraindicated. But if used for erectile dysfunction, the dose needs to be managed when people are on Paxlovid.
She said prescribers must know the kidney function of patients.
“There is a dose reduction that is required if people have impaired kidney function but below a certain level of function, which is 30 mL/min, it’s not recommended to give Paxlovid.”
Dr. Thompson highlighted two other websites for thorough, printable information on drug-drug interactions with Paxlovid: the University of Liverpool’s drug interaction checker and a printable handout from the University of Waterloo in Ontario, Canada.
“We need a 24/7 clinician hotline for Paxlovid to really make it accessible,” she said.
No data yet on ‘rebound’ effect
As to a few recent reports of a “rebound” effect, of people developing COVID-19 symptoms after completing a course of Paxlovid, there are not enough data yet to determine a clear pattern or cause.
“All we have are anecdotal data,” Dr. Thompson said. Current questions for study include whether the 5-day course is not long enough, she said, and whether people more at risk should be given a second course of Paxlovid if they do rebound.
Dr. Gallagher said it’s important to remember that the therapy goal of the drug is to prevent hospitalizations and deaths, and while any rebound is problematic, “it’s possible the use of the medication has already saved a life.”
Dr. Gallagher and Dr. Thompson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Misinformation about nirmatrelvir/ritonavir (Paxlovid, Pfizer) for treating mild to moderate COVID-19 in patients at high risk for severe disease is feeding misunderstanding among prescribers and patients, two experts from the Infectious Diseases Society of America (IDSA) have said.
They briefed reporters on potential drug interactions and uncommon cases of a “rebound” effect with the drug, which was granted emergency use authorization by the Food and Drug Administration last December for patients at least 12 years old.
The drug combination works “like a pair of scissors chopping up proteins that are made as the virus replicates inside of cells. Inhibiting that enzyme leads to the cessation of replication,” said Jason C. Gallagher, PharmD, of Temple University School of Pharmacy, Philadelphia.
That’s important because other treatments that target the spike protein, such as monoclonal antibodies, can lose their efficacy as the virus changes. He said that while that’s not impossible for Paxlovid, “we have not seen variants emerging that are resistant to it.”
Potential drug interactions
IDSA recently published updated guidance on potential interactions between Paxlovid and the top 100 drugs, and important considerations for prescribing.
“There is a concern that people have not been prescribing it because of fear of these interactions,” Dr. Gallagher said, explaining that, while in some cases those fears may be valid, in many instances the interaction is manageable.
One example is in two popular statins for heart disease, lovastatin and simvastatin.
“That’s an interaction that can be managed by holding [those drugs] for the 5 days that someone receives Paxlovid,” he said.
Misinformation also is circulating about distribution status of Paxlovid, Dr. Gallagher said.
“We’re in a very different state from that standpoint than we were a month or 2 months ago,” he said, adding that it is widely available in not all but a large number of pharmacies throughout the United States.
He emphasized the importance of drug reconciliation, as many patients will go to a different pharmacy for Paxlovid than they might for their usual prescriptions, so without a full accounting of prescriptions and supplements potential interactions may be missed.
Important interactions to watch
Melanie Thompson, MD, cochair of the HIVMA/IDSA HIV Primary Care Guidance Panel, highlighted some classes of drugs to watch, among them the antiarrhythmics, most of which are contraindicated with Paxlovid.
There are also important interactions with a number of cancer drugs, and consults with oncologists will be critical, she said.
“Likewise, people who have had transplants are likely to be on drugs that have significant ritonavir interactions,” Dr. Thompson said.
People on ergot drugs for migraine cannot take Paxlovid, she said, and “people who take colchicine for gout have to be very careful.”
She said it’s better not to use colchicine while taking Paxlovid, as it is contraindicated, “but it can be managed in certain circumstances with substantial dose reduction.”
A number of mental health drugs can be managed with Paxlovid, Dr. Thompson said. For the antipsychotic drug quetiapine, (Seroquel), a “substantial decrease in dose is required.”
Viagra for ED can be managed
Use of Viagra depends on why it’s being used, Dr. Thompson said. If it’s used for pulmonary hypertension, it is used at a very high dose and that is contraindicated. But if used for erectile dysfunction, the dose needs to be managed when people are on Paxlovid.
She said prescribers must know the kidney function of patients.
“There is a dose reduction that is required if people have impaired kidney function but below a certain level of function, which is 30 mL/min, it’s not recommended to give Paxlovid.”
Dr. Thompson highlighted two other websites for thorough, printable information on drug-drug interactions with Paxlovid: the University of Liverpool’s drug interaction checker and a printable handout from the University of Waterloo in Ontario, Canada.
“We need a 24/7 clinician hotline for Paxlovid to really make it accessible,” she said.
No data yet on ‘rebound’ effect
As to a few recent reports of a “rebound” effect, of people developing COVID-19 symptoms after completing a course of Paxlovid, there are not enough data yet to determine a clear pattern or cause.
“All we have are anecdotal data,” Dr. Thompson said. Current questions for study include whether the 5-day course is not long enough, she said, and whether people more at risk should be given a second course of Paxlovid if they do rebound.
Dr. Gallagher said it’s important to remember that the therapy goal of the drug is to prevent hospitalizations and deaths, and while any rebound is problematic, “it’s possible the use of the medication has already saved a life.”
Dr. Gallagher and Dr. Thompson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Misinformation about nirmatrelvir/ritonavir (Paxlovid, Pfizer) for treating mild to moderate COVID-19 in patients at high risk for severe disease is feeding misunderstanding among prescribers and patients, two experts from the Infectious Diseases Society of America (IDSA) have said.
They briefed reporters on potential drug interactions and uncommon cases of a “rebound” effect with the drug, which was granted emergency use authorization by the Food and Drug Administration last December for patients at least 12 years old.
The drug combination works “like a pair of scissors chopping up proteins that are made as the virus replicates inside of cells. Inhibiting that enzyme leads to the cessation of replication,” said Jason C. Gallagher, PharmD, of Temple University School of Pharmacy, Philadelphia.
That’s important because other treatments that target the spike protein, such as monoclonal antibodies, can lose their efficacy as the virus changes. He said that while that’s not impossible for Paxlovid, “we have not seen variants emerging that are resistant to it.”
Potential drug interactions
IDSA recently published updated guidance on potential interactions between Paxlovid and the top 100 drugs, and important considerations for prescribing.
“There is a concern that people have not been prescribing it because of fear of these interactions,” Dr. Gallagher said, explaining that, while in some cases those fears may be valid, in many instances the interaction is manageable.
One example is in two popular statins for heart disease, lovastatin and simvastatin.
“That’s an interaction that can be managed by holding [those drugs] for the 5 days that someone receives Paxlovid,” he said.
Misinformation also is circulating about distribution status of Paxlovid, Dr. Gallagher said.
“We’re in a very different state from that standpoint than we were a month or 2 months ago,” he said, adding that it is widely available in not all but a large number of pharmacies throughout the United States.
He emphasized the importance of drug reconciliation, as many patients will go to a different pharmacy for Paxlovid than they might for their usual prescriptions, so without a full accounting of prescriptions and supplements potential interactions may be missed.
Important interactions to watch
Melanie Thompson, MD, cochair of the HIVMA/IDSA HIV Primary Care Guidance Panel, highlighted some classes of drugs to watch, among them the antiarrhythmics, most of which are contraindicated with Paxlovid.
There are also important interactions with a number of cancer drugs, and consults with oncologists will be critical, she said.
“Likewise, people who have had transplants are likely to be on drugs that have significant ritonavir interactions,” Dr. Thompson said.
People on ergot drugs for migraine cannot take Paxlovid, she said, and “people who take colchicine for gout have to be very careful.”
She said it’s better not to use colchicine while taking Paxlovid, as it is contraindicated, “but it can be managed in certain circumstances with substantial dose reduction.”
A number of mental health drugs can be managed with Paxlovid, Dr. Thompson said. For the antipsychotic drug quetiapine, (Seroquel), a “substantial decrease in dose is required.”
Viagra for ED can be managed
Use of Viagra depends on why it’s being used, Dr. Thompson said. If it’s used for pulmonary hypertension, it is used at a very high dose and that is contraindicated. But if used for erectile dysfunction, the dose needs to be managed when people are on Paxlovid.
She said prescribers must know the kidney function of patients.
“There is a dose reduction that is required if people have impaired kidney function but below a certain level of function, which is 30 mL/min, it’s not recommended to give Paxlovid.”
Dr. Thompson highlighted two other websites for thorough, printable information on drug-drug interactions with Paxlovid: the University of Liverpool’s drug interaction checker and a printable handout from the University of Waterloo in Ontario, Canada.
“We need a 24/7 clinician hotline for Paxlovid to really make it accessible,” she said.
No data yet on ‘rebound’ effect
As to a few recent reports of a “rebound” effect, of people developing COVID-19 symptoms after completing a course of Paxlovid, there are not enough data yet to determine a clear pattern or cause.
“All we have are anecdotal data,” Dr. Thompson said. Current questions for study include whether the 5-day course is not long enough, she said, and whether people more at risk should be given a second course of Paxlovid if they do rebound.
Dr. Gallagher said it’s important to remember that the therapy goal of the drug is to prevent hospitalizations and deaths, and while any rebound is problematic, “it’s possible the use of the medication has already saved a life.”
Dr. Gallagher and Dr. Thompson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.