User login
Neurology Reviews covers innovative and emerging news in neurology and neuroscience every month, with a focus on practical approaches to treating Parkinson's disease, epilepsy, headache, stroke, multiple sclerosis, Alzheimer's disease, and other neurologic disorders.
PML
Progressive multifocal leukoencephalopathy
Rituxan
The leading independent newspaper covering neurology news and commentary.
Percentage of doctors who are Black barely changed in 120 years
according to a new study.
In 1900, 1.3% of physicians were Black. In 1940, 2.8% of physicians were Black, and by 2018 – when almost 13% of the population was Black – 5.4% of doctors were Black, reports Dan Ly, MD, PhD, MPP, an assistant professor of medicine at the University of California, Los Angeles, in a study published online April 19, 2021, in the Journal of General Internal Medicine.
The proportion of male Black physicians was 2.7% in 1940 and 2.6% in 2018.
Dr. Ly also found a significant wage gap. The median income earned by White doctors was $50,000 more than the median income of Black physicians in 2018. Dr. Ly based his findings on the U.S. Census Decennial Census long form, accessed via IPUMS, a free database funded by the National Institutes of Health and other organizations.
“If we care about the health of the population, particularly the health of Black patients, we should care about how small the proportion of our physicians who are Black is and the extremely slow progress we have made as a medical system in increasing that proportion,” Dr. Ly said in an interview.
Dr. Ly said he took on this research in part because previous studies have shown that Black patients are more likely to seek preventive care from Black doctors. Thus, increasing the numbers of Black physicians could narrow gaps in life expectancy between Whites and Blacks.
He also wanted to see whether progress had been made as a result of various medical organizations and the Association of American Medical Colleges undertaking initiatives to increase workforce diversity. There has been “very, very little” progress, he said.
Norma Poll-Hunter, PhD, the AAMC’s senior director of workforce diversity, said Dr. Ly’s report “was not surprising at all.”
The AAMC reported in 2014 that the number of Black men who apply to and matriculate into medical schools has been declining since 1978. That year, there were 1,410 Black male applicants and 542 Black enrollees. In 2014, there were 1,337 applicants and 515 enrollees.
Since 2014, Black male enrollment has increased slightly, rising from 2.4% in the 2014-2015 school year to 2.9% in the 2019-2020 year, the AAMC reported last year.
In addition, among other historically underrepresented minorities, “we really have seen very small progress” despite the increase in the number of medical schools, Dr. Poll-Hunter said in an interview.
The AAMC and the National Medical Association consider the lack of Black male applicants and matriculants to be a national crisis. The two groups started an alliance in 2020 aimed at finding ways to amplify and support Black men’s interest in medicine and the biomedical sciences and to “develop systems-based solutions to address exclusionary practices that create barriers for Black men and prevent them from having equitable opportunities to successfully enroll in medical school.”
Solutions include requiring medical school admissions committees and application screeners to undergo implicit bias awareness and mitigation training, adopting holistic admissions reviews, and incentivizing institutions of higher learning to partner with Black communities in urban and rural school systems to establish K-12 health sciences academies, said NMA President Leon McDougle, MD, MPH.
“There are the systems factors, and racism is a big one that we have to tackle,” said Dr. Poll-Hunter.
Diversity isn’t just about numbers, said Dr. McDougle, a professor of family medicine and associate dean for diversity and inclusion at Ohio State University, Columbus. “We know that medical school graduates who are African American or Black, Hispanic or Latinx, or American Indian or Alaskan Native are more likely to serve those communities as practicing physicians.
“The COVID-19 pandemic highlighted the urgent need for more African American or Black, Hispanic or Latinx, or American Indian or Alaskan Native physicians,” he said. “Inadequate access to culturally competent care has exacerbated existing health disparities, resulting in death and hospitalization rates up to three to four times the rates of European American or White people.”
Dr. Poll-Hunter also said that studies have shown that diversity in the classroom creates a more enriched learning environment and increases civic mindedness and cognitive complexity, “as well as helps us understand people who are different than ourselves.”
The diversity goal “is not about quotas, it’s about excellence,” she said. “We know that there’s talent that exists, and we want to make sure that everyone has an opportunity to be successful.”
Dr. Ly has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new study.
In 1900, 1.3% of physicians were Black. In 1940, 2.8% of physicians were Black, and by 2018 – when almost 13% of the population was Black – 5.4% of doctors were Black, reports Dan Ly, MD, PhD, MPP, an assistant professor of medicine at the University of California, Los Angeles, in a study published online April 19, 2021, in the Journal of General Internal Medicine.
The proportion of male Black physicians was 2.7% in 1940 and 2.6% in 2018.
Dr. Ly also found a significant wage gap. The median income earned by White doctors was $50,000 more than the median income of Black physicians in 2018. Dr. Ly based his findings on the U.S. Census Decennial Census long form, accessed via IPUMS, a free database funded by the National Institutes of Health and other organizations.
“If we care about the health of the population, particularly the health of Black patients, we should care about how small the proportion of our physicians who are Black is and the extremely slow progress we have made as a medical system in increasing that proportion,” Dr. Ly said in an interview.
Dr. Ly said he took on this research in part because previous studies have shown that Black patients are more likely to seek preventive care from Black doctors. Thus, increasing the numbers of Black physicians could narrow gaps in life expectancy between Whites and Blacks.
He also wanted to see whether progress had been made as a result of various medical organizations and the Association of American Medical Colleges undertaking initiatives to increase workforce diversity. There has been “very, very little” progress, he said.
Norma Poll-Hunter, PhD, the AAMC’s senior director of workforce diversity, said Dr. Ly’s report “was not surprising at all.”
The AAMC reported in 2014 that the number of Black men who apply to and matriculate into medical schools has been declining since 1978. That year, there were 1,410 Black male applicants and 542 Black enrollees. In 2014, there were 1,337 applicants and 515 enrollees.
Since 2014, Black male enrollment has increased slightly, rising from 2.4% in the 2014-2015 school year to 2.9% in the 2019-2020 year, the AAMC reported last year.
In addition, among other historically underrepresented minorities, “we really have seen very small progress” despite the increase in the number of medical schools, Dr. Poll-Hunter said in an interview.
The AAMC and the National Medical Association consider the lack of Black male applicants and matriculants to be a national crisis. The two groups started an alliance in 2020 aimed at finding ways to amplify and support Black men’s interest in medicine and the biomedical sciences and to “develop systems-based solutions to address exclusionary practices that create barriers for Black men and prevent them from having equitable opportunities to successfully enroll in medical school.”
Solutions include requiring medical school admissions committees and application screeners to undergo implicit bias awareness and mitigation training, adopting holistic admissions reviews, and incentivizing institutions of higher learning to partner with Black communities in urban and rural school systems to establish K-12 health sciences academies, said NMA President Leon McDougle, MD, MPH.
“There are the systems factors, and racism is a big one that we have to tackle,” said Dr. Poll-Hunter.
Diversity isn’t just about numbers, said Dr. McDougle, a professor of family medicine and associate dean for diversity and inclusion at Ohio State University, Columbus. “We know that medical school graduates who are African American or Black, Hispanic or Latinx, or American Indian or Alaskan Native are more likely to serve those communities as practicing physicians.
“The COVID-19 pandemic highlighted the urgent need for more African American or Black, Hispanic or Latinx, or American Indian or Alaskan Native physicians,” he said. “Inadequate access to culturally competent care has exacerbated existing health disparities, resulting in death and hospitalization rates up to three to four times the rates of European American or White people.”
Dr. Poll-Hunter also said that studies have shown that diversity in the classroom creates a more enriched learning environment and increases civic mindedness and cognitive complexity, “as well as helps us understand people who are different than ourselves.”
The diversity goal “is not about quotas, it’s about excellence,” she said. “We know that there’s talent that exists, and we want to make sure that everyone has an opportunity to be successful.”
Dr. Ly has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new study.
In 1900, 1.3% of physicians were Black. In 1940, 2.8% of physicians were Black, and by 2018 – when almost 13% of the population was Black – 5.4% of doctors were Black, reports Dan Ly, MD, PhD, MPP, an assistant professor of medicine at the University of California, Los Angeles, in a study published online April 19, 2021, in the Journal of General Internal Medicine.
The proportion of male Black physicians was 2.7% in 1940 and 2.6% in 2018.
Dr. Ly also found a significant wage gap. The median income earned by White doctors was $50,000 more than the median income of Black physicians in 2018. Dr. Ly based his findings on the U.S. Census Decennial Census long form, accessed via IPUMS, a free database funded by the National Institutes of Health and other organizations.
“If we care about the health of the population, particularly the health of Black patients, we should care about how small the proportion of our physicians who are Black is and the extremely slow progress we have made as a medical system in increasing that proportion,” Dr. Ly said in an interview.
Dr. Ly said he took on this research in part because previous studies have shown that Black patients are more likely to seek preventive care from Black doctors. Thus, increasing the numbers of Black physicians could narrow gaps in life expectancy between Whites and Blacks.
He also wanted to see whether progress had been made as a result of various medical organizations and the Association of American Medical Colleges undertaking initiatives to increase workforce diversity. There has been “very, very little” progress, he said.
Norma Poll-Hunter, PhD, the AAMC’s senior director of workforce diversity, said Dr. Ly’s report “was not surprising at all.”
The AAMC reported in 2014 that the number of Black men who apply to and matriculate into medical schools has been declining since 1978. That year, there were 1,410 Black male applicants and 542 Black enrollees. In 2014, there were 1,337 applicants and 515 enrollees.
Since 2014, Black male enrollment has increased slightly, rising from 2.4% in the 2014-2015 school year to 2.9% in the 2019-2020 year, the AAMC reported last year.
In addition, among other historically underrepresented minorities, “we really have seen very small progress” despite the increase in the number of medical schools, Dr. Poll-Hunter said in an interview.
The AAMC and the National Medical Association consider the lack of Black male applicants and matriculants to be a national crisis. The two groups started an alliance in 2020 aimed at finding ways to amplify and support Black men’s interest in medicine and the biomedical sciences and to “develop systems-based solutions to address exclusionary practices that create barriers for Black men and prevent them from having equitable opportunities to successfully enroll in medical school.”
Solutions include requiring medical school admissions committees and application screeners to undergo implicit bias awareness and mitigation training, adopting holistic admissions reviews, and incentivizing institutions of higher learning to partner with Black communities in urban and rural school systems to establish K-12 health sciences academies, said NMA President Leon McDougle, MD, MPH.
“There are the systems factors, and racism is a big one that we have to tackle,” said Dr. Poll-Hunter.
Diversity isn’t just about numbers, said Dr. McDougle, a professor of family medicine and associate dean for diversity and inclusion at Ohio State University, Columbus. “We know that medical school graduates who are African American or Black, Hispanic or Latinx, or American Indian or Alaskan Native are more likely to serve those communities as practicing physicians.
“The COVID-19 pandemic highlighted the urgent need for more African American or Black, Hispanic or Latinx, or American Indian or Alaskan Native physicians,” he said. “Inadequate access to culturally competent care has exacerbated existing health disparities, resulting in death and hospitalization rates up to three to four times the rates of European American or White people.”
Dr. Poll-Hunter also said that studies have shown that diversity in the classroom creates a more enriched learning environment and increases civic mindedness and cognitive complexity, “as well as helps us understand people who are different than ourselves.”
The diversity goal “is not about quotas, it’s about excellence,” she said. “We know that there’s talent that exists, and we want to make sure that everyone has an opportunity to be successful.”
Dr. Ly has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID-19 infection conveys imperfect immunity in young adults
Do your patients think that getting COVID-19 is fully protective against subsequent reinfection? Tell it to the Marines.
A study of U.S. Marine recruits on their way to boot camp at Parris Island, S.C., showed that those who were seropositive at baseline, indicating prior exposure to SARS-CoV-2, remained at some risk for reinfection. They had about one-fifth the risk of subsequent infection, compared with seronegative recruits during basic training, but reinfections did occur.
The study, by Stuart C. Sealfon, MD, of Icahn School of Medicine at Mount Sinai in New York, and colleagues, was published in The Lancet Respiratory Medicine.
“Although antibodies induced by initial infection are largely protective, they do not guarantee effective SARS-CoV-2 neutralization activity or immunity against subsequent infection,” they wrote.
An infectious disease specialist who was not involved in the study said that the findings provide further evidence about the level of immunity acquired after an infection.
“It’s quite clear that reinfections do occur, they are of public health importance, and they’re something we need to be mindful of in terms of advising patients about whether a prior infection protects them from reinfection,” Mark Siedner, MD, MPH, a clinician and researcher in the division of infectious diseases at Massachusetts General Hospital, Boston, said in an interview.
The study results reinforce that “not all antibodies are the same,” said Sachin Gupta, MD, an attending physician in pulmonary and critical care medicine at Alameda Health System in Oakland, Calif. “We’re seeing still that 10% of folks who have antibodies can get infected again,” he said in an interview.

CHARM initiative
Dr. Sealfon and colleagues presented an analysis of data from the ironically named CHARM (COVID-19 Health Action Response for Marines) prospective study.
CHARM included U.S. Marine recruits, most of them male, aged 18-20 years, who were instructed to follow a 2-week unsupervised quarantine at home, after which they reported to a Marine-supervised facility for an additional 2-week quarantine.
At baseline, participants were tested for SARS-CoV-2 immunoglobulin G (IgG) seropositivity, defined as a dilution of 1:150 or more on receptor-binding domain and full-length spike protein enzyme-linked immunosorbent assay (ELISA).
The recruits filled out questionnaires asking them to report any of 14 specific COVID-19–related symptoms or any other unspecified symptom, as well as demographic information, risk factors, and a brief medical history.
Investigators tested recruits for SARS-CoV-2 infection by polymerase chain reaction (PCR) assay at weeks 0, 1, and 2 of quarantine, and any who had positive PCR results during quarantine were excluded.
Participants who had three negative swab PCR results during quarantine and a baseline serology test at the beginning of the supervised quarantine period – either seronegative or seropositive – then went on to enjoy their basic training at the Marine Corps Recruit Depot, Parris Island, S.C.
The participants were followed prospectively with PCR tests at weeks 2, 4, and 6 in both the seropositive and seronegative groups, and sera were obtained at the same time.
Holes in immunologic armor
Full data were available for a total of 189 participants who were seropositive and 2,247 who were seronegative at enrollment.
In all, 19 of 189 seropositive recruits (10%) had at least one PCR test positive for SARS-CoV-2 infection during the 6-week follow-up period. This translated into an incidence of 1.1 cases per person-year.
Of the 2,247 participants seronegative at baseline, 1,079 tested positive (6.2 cases per person-year; incidence rate ratio 0.18).
It appeared that antibodies provided some protection for seropositive recruits, as evidenced by a higher likelihood of infection among those with lower baseline full-length spike protein IgG titers than in those with higher baseline titers (hazard ratio 0.4, P < .001).
Among the seropositive participants who did acquire a second SARS-CoV-2 infection, viral loads in mid-turbinate nasal swabs were about 10-fold lower than in seronegative recruits who acquired infections during follow-up.
“This finding suggests that some reinfected individuals could have a similar capacity to transmit infection as those who are infected for the first time. The rate at which reinfection occurs after vaccines and natural immunity is important for estimating the proportion of the population that needs to be vaccinated to suppress the pandemic,” the investigators wrote.
Baseline neutralizing antibody titers were detected in 45 of the first 54 seropositive recruits who remained PCR negative throughout follow-up, but also in 6 of 19 seropositive participants who became infected during the 6 weeks of observation.
Lessons
Both Dr. Siedner and Dr. Gupta agreed with the authors that the risks for reinfection that were observed in young, physically fit people may differ for other populations, such as women (only 10% of seropositive recruits and 8% of seronegative recruits were female), older patients, or those who are immunocompromised.
Given that the adjusted odds ratio for reinfection in this study was nearly identical to that of a recent British study comparing infection rates between seropositive and seronegative health care workers, the risk of reinfection for other young adults and for the general population may be similar, Dr. Sealfon and colleagues wrote.
Adding to the challenge of reaching herd immunity is the observation that some patients who have recovered from COVID-19 are skeptical about the need for further protection.
“There are patients who feel like vaccination is of low benefit to them, and I think these are the same people who would be hesitant to get the vaccine anyway,” Dr. Gupta said.
Although no vaccine is perfect – the vaccine failure rate from the mRNA-based vaccines from Moderna and Pfizer/Biontech is about 5% – the protections they afford are unmistakable, Dr. Siedner said.
“I think it’s important to make the distinction that most postvaccination infections by and large have been very mild,” he said. “In people with normal immune systems, we have not seen an onslaught of postvaccination infections requiring hospitalization. Even if people do get infected after vaccination, the vaccines protect people from severe infection, and that’s what we want them to do.”
The investigators stated, “Young adults, of whom a high proportion are asymptomatically infected and become seropositive in the absence of known infection, can be an important source of transmission to more vulnerable populations. Evaluating the protection against subsequent SARS-CoV-2 infection conferred by seropositivity in young adults is important for determining the need for vaccinating previously infected individuals in this age group.”
The study was funded by the Defense Health Agency and Defense Advanced Research Projects Agency. Dr. Sealfon, Dr. Siedner, and Dr. Gupta have no conflicts of interest to report. Dr. Gupta is a member of the editorial advisory board for this publication.
Do your patients think that getting COVID-19 is fully protective against subsequent reinfection? Tell it to the Marines.
A study of U.S. Marine recruits on their way to boot camp at Parris Island, S.C., showed that those who were seropositive at baseline, indicating prior exposure to SARS-CoV-2, remained at some risk for reinfection. They had about one-fifth the risk of subsequent infection, compared with seronegative recruits during basic training, but reinfections did occur.
The study, by Stuart C. Sealfon, MD, of Icahn School of Medicine at Mount Sinai in New York, and colleagues, was published in The Lancet Respiratory Medicine.
“Although antibodies induced by initial infection are largely protective, they do not guarantee effective SARS-CoV-2 neutralization activity or immunity against subsequent infection,” they wrote.
An infectious disease specialist who was not involved in the study said that the findings provide further evidence about the level of immunity acquired after an infection.
“It’s quite clear that reinfections do occur, they are of public health importance, and they’re something we need to be mindful of in terms of advising patients about whether a prior infection protects them from reinfection,” Mark Siedner, MD, MPH, a clinician and researcher in the division of infectious diseases at Massachusetts General Hospital, Boston, said in an interview.
The study results reinforce that “not all antibodies are the same,” said Sachin Gupta, MD, an attending physician in pulmonary and critical care medicine at Alameda Health System in Oakland, Calif. “We’re seeing still that 10% of folks who have antibodies can get infected again,” he said in an interview.
CHARM initiative
Dr. Sealfon and colleagues presented an analysis of data from the ironically named CHARM (COVID-19 Health Action Response for Marines) prospective study.
CHARM included U.S. Marine recruits, most of them male, aged 18-20 years, who were instructed to follow a 2-week unsupervised quarantine at home, after which they reported to a Marine-supervised facility for an additional 2-week quarantine.
At baseline, participants were tested for SARS-CoV-2 immunoglobulin G (IgG) seropositivity, defined as a dilution of 1:150 or more on receptor-binding domain and full-length spike protein enzyme-linked immunosorbent assay (ELISA).
The recruits filled out questionnaires asking them to report any of 14 specific COVID-19–related symptoms or any other unspecified symptom, as well as demographic information, risk factors, and a brief medical history.
Investigators tested recruits for SARS-CoV-2 infection by polymerase chain reaction (PCR) assay at weeks 0, 1, and 2 of quarantine, and any who had positive PCR results during quarantine were excluded.
Participants who had three negative swab PCR results during quarantine and a baseline serology test at the beginning of the supervised quarantine period – either seronegative or seropositive – then went on to enjoy their basic training at the Marine Corps Recruit Depot, Parris Island, S.C.
The participants were followed prospectively with PCR tests at weeks 2, 4, and 6 in both the seropositive and seronegative groups, and sera were obtained at the same time.
Holes in immunologic armor
Full data were available for a total of 189 participants who were seropositive and 2,247 who were seronegative at enrollment.
In all, 19 of 189 seropositive recruits (10%) had at least one PCR test positive for SARS-CoV-2 infection during the 6-week follow-up period. This translated into an incidence of 1.1 cases per person-year.
Of the 2,247 participants seronegative at baseline, 1,079 tested positive (6.2 cases per person-year; incidence rate ratio 0.18).
It appeared that antibodies provided some protection for seropositive recruits, as evidenced by a higher likelihood of infection among those with lower baseline full-length spike protein IgG titers than in those with higher baseline titers (hazard ratio 0.4, P < .001).
Among the seropositive participants who did acquire a second SARS-CoV-2 infection, viral loads in mid-turbinate nasal swabs were about 10-fold lower than in seronegative recruits who acquired infections during follow-up.
“This finding suggests that some reinfected individuals could have a similar capacity to transmit infection as those who are infected for the first time. The rate at which reinfection occurs after vaccines and natural immunity is important for estimating the proportion of the population that needs to be vaccinated to suppress the pandemic,” the investigators wrote.
Baseline neutralizing antibody titers were detected in 45 of the first 54 seropositive recruits who remained PCR negative throughout follow-up, but also in 6 of 19 seropositive participants who became infected during the 6 weeks of observation.
Lessons
Both Dr. Siedner and Dr. Gupta agreed with the authors that the risks for reinfection that were observed in young, physically fit people may differ for other populations, such as women (only 10% of seropositive recruits and 8% of seronegative recruits were female), older patients, or those who are immunocompromised.
Given that the adjusted odds ratio for reinfection in this study was nearly identical to that of a recent British study comparing infection rates between seropositive and seronegative health care workers, the risk of reinfection for other young adults and for the general population may be similar, Dr. Sealfon and colleagues wrote.
Adding to the challenge of reaching herd immunity is the observation that some patients who have recovered from COVID-19 are skeptical about the need for further protection.
“There are patients who feel like vaccination is of low benefit to them, and I think these are the same people who would be hesitant to get the vaccine anyway,” Dr. Gupta said.
Although no vaccine is perfect – the vaccine failure rate from the mRNA-based vaccines from Moderna and Pfizer/Biontech is about 5% – the protections they afford are unmistakable, Dr. Siedner said.
“I think it’s important to make the distinction that most postvaccination infections by and large have been very mild,” he said. “In people with normal immune systems, we have not seen an onslaught of postvaccination infections requiring hospitalization. Even if people do get infected after vaccination, the vaccines protect people from severe infection, and that’s what we want them to do.”
The investigators stated, “Young adults, of whom a high proportion are asymptomatically infected and become seropositive in the absence of known infection, can be an important source of transmission to more vulnerable populations. Evaluating the protection against subsequent SARS-CoV-2 infection conferred by seropositivity in young adults is important for determining the need for vaccinating previously infected individuals in this age group.”
The study was funded by the Defense Health Agency and Defense Advanced Research Projects Agency. Dr. Sealfon, Dr. Siedner, and Dr. Gupta have no conflicts of interest to report. Dr. Gupta is a member of the editorial advisory board for this publication.
Do your patients think that getting COVID-19 is fully protective against subsequent reinfection? Tell it to the Marines.
A study of U.S. Marine recruits on their way to boot camp at Parris Island, S.C., showed that those who were seropositive at baseline, indicating prior exposure to SARS-CoV-2, remained at some risk for reinfection. They had about one-fifth the risk of subsequent infection, compared with seronegative recruits during basic training, but reinfections did occur.
The study, by Stuart C. Sealfon, MD, of Icahn School of Medicine at Mount Sinai in New York, and colleagues, was published in The Lancet Respiratory Medicine.
“Although antibodies induced by initial infection are largely protective, they do not guarantee effective SARS-CoV-2 neutralization activity or immunity against subsequent infection,” they wrote.
An infectious disease specialist who was not involved in the study said that the findings provide further evidence about the level of immunity acquired after an infection.
“It’s quite clear that reinfections do occur, they are of public health importance, and they’re something we need to be mindful of in terms of advising patients about whether a prior infection protects them from reinfection,” Mark Siedner, MD, MPH, a clinician and researcher in the division of infectious diseases at Massachusetts General Hospital, Boston, said in an interview.
The study results reinforce that “not all antibodies are the same,” said Sachin Gupta, MD, an attending physician in pulmonary and critical care medicine at Alameda Health System in Oakland, Calif. “We’re seeing still that 10% of folks who have antibodies can get infected again,” he said in an interview.
CHARM initiative
Dr. Sealfon and colleagues presented an analysis of data from the ironically named CHARM (COVID-19 Health Action Response for Marines) prospective study.
CHARM included U.S. Marine recruits, most of them male, aged 18-20 years, who were instructed to follow a 2-week unsupervised quarantine at home, after which they reported to a Marine-supervised facility for an additional 2-week quarantine.
At baseline, participants were tested for SARS-CoV-2 immunoglobulin G (IgG) seropositivity, defined as a dilution of 1:150 or more on receptor-binding domain and full-length spike protein enzyme-linked immunosorbent assay (ELISA).
The recruits filled out questionnaires asking them to report any of 14 specific COVID-19–related symptoms or any other unspecified symptom, as well as demographic information, risk factors, and a brief medical history.
Investigators tested recruits for SARS-CoV-2 infection by polymerase chain reaction (PCR) assay at weeks 0, 1, and 2 of quarantine, and any who had positive PCR results during quarantine were excluded.
Participants who had three negative swab PCR results during quarantine and a baseline serology test at the beginning of the supervised quarantine period – either seronegative or seropositive – then went on to enjoy their basic training at the Marine Corps Recruit Depot, Parris Island, S.C.
The participants were followed prospectively with PCR tests at weeks 2, 4, and 6 in both the seropositive and seronegative groups, and sera were obtained at the same time.
Holes in immunologic armor
Full data were available for a total of 189 participants who were seropositive and 2,247 who were seronegative at enrollment.
In all, 19 of 189 seropositive recruits (10%) had at least one PCR test positive for SARS-CoV-2 infection during the 6-week follow-up period. This translated into an incidence of 1.1 cases per person-year.
Of the 2,247 participants seronegative at baseline, 1,079 tested positive (6.2 cases per person-year; incidence rate ratio 0.18).
It appeared that antibodies provided some protection for seropositive recruits, as evidenced by a higher likelihood of infection among those with lower baseline full-length spike protein IgG titers than in those with higher baseline titers (hazard ratio 0.4, P < .001).
Among the seropositive participants who did acquire a second SARS-CoV-2 infection, viral loads in mid-turbinate nasal swabs were about 10-fold lower than in seronegative recruits who acquired infections during follow-up.
“This finding suggests that some reinfected individuals could have a similar capacity to transmit infection as those who are infected for the first time. The rate at which reinfection occurs after vaccines and natural immunity is important for estimating the proportion of the population that needs to be vaccinated to suppress the pandemic,” the investigators wrote.
Baseline neutralizing antibody titers were detected in 45 of the first 54 seropositive recruits who remained PCR negative throughout follow-up, but also in 6 of 19 seropositive participants who became infected during the 6 weeks of observation.
Lessons
Both Dr. Siedner and Dr. Gupta agreed with the authors that the risks for reinfection that were observed in young, physically fit people may differ for other populations, such as women (only 10% of seropositive recruits and 8% of seronegative recruits were female), older patients, or those who are immunocompromised.
Given that the adjusted odds ratio for reinfection in this study was nearly identical to that of a recent British study comparing infection rates between seropositive and seronegative health care workers, the risk of reinfection for other young adults and for the general population may be similar, Dr. Sealfon and colleagues wrote.
Adding to the challenge of reaching herd immunity is the observation that some patients who have recovered from COVID-19 are skeptical about the need for further protection.
“There are patients who feel like vaccination is of low benefit to them, and I think these are the same people who would be hesitant to get the vaccine anyway,” Dr. Gupta said.
Although no vaccine is perfect – the vaccine failure rate from the mRNA-based vaccines from Moderna and Pfizer/Biontech is about 5% – the protections they afford are unmistakable, Dr. Siedner said.
“I think it’s important to make the distinction that most postvaccination infections by and large have been very mild,” he said. “In people with normal immune systems, we have not seen an onslaught of postvaccination infections requiring hospitalization. Even if people do get infected after vaccination, the vaccines protect people from severe infection, and that’s what we want them to do.”
The investigators stated, “Young adults, of whom a high proportion are asymptomatically infected and become seropositive in the absence of known infection, can be an important source of transmission to more vulnerable populations. Evaluating the protection against subsequent SARS-CoV-2 infection conferred by seropositivity in young adults is important for determining the need for vaccinating previously infected individuals in this age group.”
The study was funded by the Defense Health Agency and Defense Advanced Research Projects Agency. Dr. Sealfon, Dr. Siedner, and Dr. Gupta have no conflicts of interest to report. Dr. Gupta is a member of the editorial advisory board for this publication.
FROM THE LANCET RESPIRATORY MEDICINE
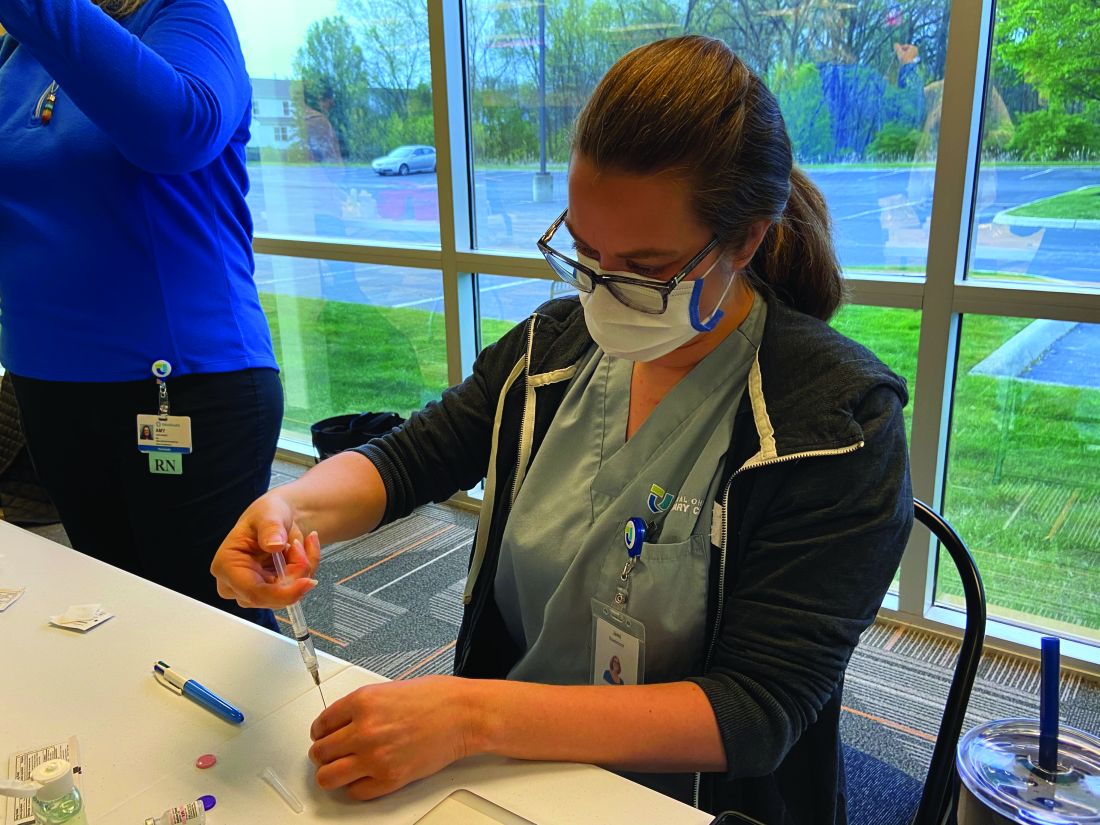
Vaccinating homebound patients is an uphill battle

There are about 2 million to 4 million homebound patients in the United States, according to a webinar from The Trust for America’s Health, which was broadcast in March. But many of these individuals have not been vaccinated yet because of logistical challenges.
Some homebound COVID-19 immunization programs are administering Moderna and Pfizer vaccines to their patients, but many state, city, and local programs administered the Johnson & Johnson vaccine after it was cleared for use by the Food and Drug Administration in February 2021. The efficacy of the one-shot vaccine, as well as it being easier to store and ship than the Moderna and Pfizer vaccines, makes getting it to homebound patients less challenging.
“With Pfizer and Moderna, transportation is a challenge because the temperature demands and the fragility of [messenger] RNA–based vaccines,” Brent Feorene, executive director of the American Academy of Home Care Medicine, said in an interview. That’s why [the Johnson & Johnson] vaccine held such promise – it’s less fragile, [can be stored in] higher temperatures, and was a one shot.”
Other hurdles to getting homebound patients vaccinated had already been in place prior to the 10-day-pause on using the J&J vaccine that occurred for federal agencies to consider possible serious side effects linked to it.
Many roadblocks to vaccination
Although many homebound patients can’t readily go out into the community and be exposed to the COVID-19 virus themselves, they are dependent on caregivers and family members who do go out into the community.
“Their friends, family, neighbors, home health aides, and other kinds of health care workers come into the home,” said Shawn Amer, clinical program director at Central Ohio Primary Care in Columbus.
Nurses from Ms. Amer’s practice vaccinated approximately ten homebound patients with the J&J vaccine through a pilot program in March. Then on April 24, nurses from Central Ohio Primary Care vaccinated just under 40 homebound patients and about a handful of their caregivers who were not able to get their vaccines elsewhere, according to Ms. Amer. This time they used the Pfizer vaccine and will be returning to these patients’ homes on May 15 to administer the second dose.
“Any time you are getting in the car and adding miles, it adds complexity,” Ms. Amer said.
“We called patients 24 to 36 hours before coming to their homes to make sure they were ready, but we learned that just because the healthcare power of attorney agrees to a patient getting vaccinated does not mean that patient will be willing to get the vaccine when the nurse shows up," she noted.
Ms. Amer elaborated that three patients with dementia refused the vaccine when nurses arrived at their home on April 24.
“We had to pivot and find other people,” Ms. Amer. Her practice ended up having to waste one shot.
Expenses are greater
The higher costs of getting homebound patients vaccinated is an additional hurdle to getting these vulnerable individuals protected by COVID-19 shots.
Vaccinating patients in their homes “doesn’t require a lot of technology, but it does require a lot of time” and the staffing expense becomes part of the challenge, Ms. Amer noted.
For each of the two days that Central Ohio Primary Care provides the Pfizer vaccine to homebound patients, the practice needs to pay seven nurses to administer the vaccine, Ms. Amer explained.
There have also been reports of organizations that administer the vaccines – which are free for patients because the federal government is paying for them – not being paid enough by Medicare to cover staff time and efforts to vaccinate patients in their homes, Kaiser Health News reported. According to the Centers for Medicare & Medicaid Services, they pay $40 for the administration of a single-dose COVID-19 vaccine and, for COVID-19 vaccines requiring multiple doses, Medicare pays approximately $40 for each dose in the series. These rates were implemented after March 15. Before that date, the rates were even lower, with the Medicare reimbursement rates for initial doses of COVID-19 vaccines being $16.94 and final doses being $28.39.
William Dombi, president of the National Association for Home Care & Hospice, told Kaiser Health News that the actual cost of these homebound visits are closer to $150 or $160.
“The reimbursement for the injection is pretty minimal,” Mr. Feorene said. “So unless you’re a larger organization and able to have staff to deploy some of your smaller practices, just couldn’t afford to do it.”
Many homebound patients have also been unable to get the lifesaving shots because of logistical roadblocks and many practices not being able to do home visits.
“I think that initially when the [Centers for Disease Control and Prevention] came out with vaccine guidance for medical providers, they offered no guidance for in-home medical providers and we had to go back and ask for that, which they did produce,” Mr. Feorene said. “And we’re grateful for that. But I think just this general understanding that there is a population of folks that are [limited to their home], that they do receive medical care and other care in the home, and that we have to remember that the medical providers who provide care in the home are also primary care providers.”
Furthermore, trying to navigate or find programs delivering vaccines to the homebound can be difficult depending on where a patient lives.
While some programs have been launched on the country or city level – the New York Fire Department launched a pilot program to bring the Johnson & Johnson vaccine to homebound seniors – other programs have been spearheaded by hospital networks like Northwell and Mount Sinai. However, many of these hospital networks only reach out to people who already have a relationship with the hospital.
Ms Amer said identifying homebound patients and reaching out to them can be tough and can contribute to the logistics and time involved in setting patients up for the vaccine.
“Reaching some of these patients is difficult,” Ms. Amer noted. “Sometimes the best way to reach them or get a hold of them is through their caregiver. And so do you have the right phone number? Do you have the right name?”
Overcoming the challenges
With the absence of a national plan targeting homebound patients, many local initiatives were launched to help these individuals get vaccinated. Local fire department paramedics have gone door to door to administer the COVID-19 vaccine in cities like Chicago, New York, and Miami. The suspension of the Johnson & Johnson vaccine resulted in the suspension of in-home vaccinations for some people in New York City. However, the program resumed after the FDA and CDC lifted the pause on April 24.

Health systems like Mount Sinai vaccinated approximately 530 people through the Mount Sinai Visiting Doctors Program, including patients and their caregivers, according to Peter Gliatto, MD, associate director of the Mount Sinai Visiting Doctors Program.
“In different cities, townships, and jurisdictions, different health departments and different provider groups are approaching [the distribution of the COVID-19 vaccine] slightly differently,” Ms. Amer said. So a lot of the decisions surrounding the distribution of shots are local or dependent on local resourcing.
People who live in rural areas present a unique challenge, but Mr. Feorene said reaching out to local emergency medical services or the local health departments can provide some insight on what their town is doing to vaccinate homebound patients.
“I think understanding what a [public health department] is doing would be the very first place to start,” Mr. Feorene said in an interview.
If a patient is bedridden and is mobile enough to sit in a car, Mr. Feorene also recommends finding out if there are vaccine fairs “within a reasonable driving distance.”
Ms. Amer said continuing this mission of getting homebound patients vaccinated is necessary for public health.
“Even if it’s going to take longer to vaccinate these homebound patients, we still have to make an effort. So much of the country’s vaccine efforts have been focused on getting as many shots in as many arms as quickly as possible. And that is definitely super important,” she said.
Ms. Amer is working with her practice’s primary care physicians to try to identify all of those patients who are functionally debilitated or unable to leave their home to get vaccinated and that Central Ohio Primary Care will vaccinate more homebound patients, she added.
The experts interviewed in this article have no conflicts.
Katie Lennon contributed to this report.
This article was updated 4/29/21.
There are about 2 million to 4 million homebound patients in the United States, according to a webinar from The Trust for America’s Health, which was broadcast in March. But many of these individuals have not been vaccinated yet because of logistical challenges.
Some homebound COVID-19 immunization programs are administering Moderna and Pfizer vaccines to their patients, but many state, city, and local programs administered the Johnson & Johnson vaccine after it was cleared for use by the Food and Drug Administration in February 2021. The efficacy of the one-shot vaccine, as well as it being easier to store and ship than the Moderna and Pfizer vaccines, makes getting it to homebound patients less challenging.
“With Pfizer and Moderna, transportation is a challenge because the temperature demands and the fragility of [messenger] RNA–based vaccines,” Brent Feorene, executive director of the American Academy of Home Care Medicine, said in an interview. That’s why [the Johnson & Johnson] vaccine held such promise – it’s less fragile, [can be stored in] higher temperatures, and was a one shot.”
Other hurdles to getting homebound patients vaccinated had already been in place prior to the 10-day-pause on using the J&J vaccine that occurred for federal agencies to consider possible serious side effects linked to it.
Many roadblocks to vaccination
Although many homebound patients can’t readily go out into the community and be exposed to the COVID-19 virus themselves, they are dependent on caregivers and family members who do go out into the community.
“Their friends, family, neighbors, home health aides, and other kinds of health care workers come into the home,” said Shawn Amer, clinical program director at Central Ohio Primary Care in Columbus.
Nurses from Ms. Amer’s practice vaccinated approximately ten homebound patients with the J&J vaccine through a pilot program in March. Then on April 24, nurses from Central Ohio Primary Care vaccinated just under 40 homebound patients and about a handful of their caregivers who were not able to get their vaccines elsewhere, according to Ms. Amer. This time they used the Pfizer vaccine and will be returning to these patients’ homes on May 15 to administer the second dose.
“Any time you are getting in the car and adding miles, it adds complexity,” Ms. Amer said.
“We called patients 24 to 36 hours before coming to their homes to make sure they were ready, but we learned that just because the healthcare power of attorney agrees to a patient getting vaccinated does not mean that patient will be willing to get the vaccine when the nurse shows up," she noted.
Ms. Amer elaborated that three patients with dementia refused the vaccine when nurses arrived at their home on April 24.
“We had to pivot and find other people,” Ms. Amer. Her practice ended up having to waste one shot.
Expenses are greater
The higher costs of getting homebound patients vaccinated is an additional hurdle to getting these vulnerable individuals protected by COVID-19 shots.
Vaccinating patients in their homes “doesn’t require a lot of technology, but it does require a lot of time” and the staffing expense becomes part of the challenge, Ms. Amer noted.
For each of the two days that Central Ohio Primary Care provides the Pfizer vaccine to homebound patients, the practice needs to pay seven nurses to administer the vaccine, Ms. Amer explained.
There have also been reports of organizations that administer the vaccines – which are free for patients because the federal government is paying for them – not being paid enough by Medicare to cover staff time and efforts to vaccinate patients in their homes, Kaiser Health News reported. According to the Centers for Medicare & Medicaid Services, they pay $40 for the administration of a single-dose COVID-19 vaccine and, for COVID-19 vaccines requiring multiple doses, Medicare pays approximately $40 for each dose in the series. These rates were implemented after March 15. Before that date, the rates were even lower, with the Medicare reimbursement rates for initial doses of COVID-19 vaccines being $16.94 and final doses being $28.39.
William Dombi, president of the National Association for Home Care & Hospice, told Kaiser Health News that the actual cost of these homebound visits are closer to $150 or $160.
“The reimbursement for the injection is pretty minimal,” Mr. Feorene said. “So unless you’re a larger organization and able to have staff to deploy some of your smaller practices, just couldn’t afford to do it.”
Many homebound patients have also been unable to get the lifesaving shots because of logistical roadblocks and many practices not being able to do home visits.
“I think that initially when the [Centers for Disease Control and Prevention] came out with vaccine guidance for medical providers, they offered no guidance for in-home medical providers and we had to go back and ask for that, which they did produce,” Mr. Feorene said. “And we’re grateful for that. But I think just this general understanding that there is a population of folks that are [limited to their home], that they do receive medical care and other care in the home, and that we have to remember that the medical providers who provide care in the home are also primary care providers.”
Furthermore, trying to navigate or find programs delivering vaccines to the homebound can be difficult depending on where a patient lives.
While some programs have been launched on the country or city level – the New York Fire Department launched a pilot program to bring the Johnson & Johnson vaccine to homebound seniors – other programs have been spearheaded by hospital networks like Northwell and Mount Sinai. However, many of these hospital networks only reach out to people who already have a relationship with the hospital.
Ms Amer said identifying homebound patients and reaching out to them can be tough and can contribute to the logistics and time involved in setting patients up for the vaccine.
“Reaching some of these patients is difficult,” Ms. Amer noted. “Sometimes the best way to reach them or get a hold of them is through their caregiver. And so do you have the right phone number? Do you have the right name?”
Overcoming the challenges
With the absence of a national plan targeting homebound patients, many local initiatives were launched to help these individuals get vaccinated. Local fire department paramedics have gone door to door to administer the COVID-19 vaccine in cities like Chicago, New York, and Miami. The suspension of the Johnson & Johnson vaccine resulted in the suspension of in-home vaccinations for some people in New York City. However, the program resumed after the FDA and CDC lifted the pause on April 24.
Health systems like Mount Sinai vaccinated approximately 530 people through the Mount Sinai Visiting Doctors Program, including patients and their caregivers, according to Peter Gliatto, MD, associate director of the Mount Sinai Visiting Doctors Program.
“In different cities, townships, and jurisdictions, different health departments and different provider groups are approaching [the distribution of the COVID-19 vaccine] slightly differently,” Ms. Amer said. So a lot of the decisions surrounding the distribution of shots are local or dependent on local resourcing.
People who live in rural areas present a unique challenge, but Mr. Feorene said reaching out to local emergency medical services or the local health departments can provide some insight on what their town is doing to vaccinate homebound patients.
“I think understanding what a [public health department] is doing would be the very first place to start,” Mr. Feorene said in an interview.
If a patient is bedridden and is mobile enough to sit in a car, Mr. Feorene also recommends finding out if there are vaccine fairs “within a reasonable driving distance.”
Ms. Amer said continuing this mission of getting homebound patients vaccinated is necessary for public health.
“Even if it’s going to take longer to vaccinate these homebound patients, we still have to make an effort. So much of the country’s vaccine efforts have been focused on getting as many shots in as many arms as quickly as possible. And that is definitely super important,” she said.
Ms. Amer is working with her practice’s primary care physicians to try to identify all of those patients who are functionally debilitated or unable to leave their home to get vaccinated and that Central Ohio Primary Care will vaccinate more homebound patients, she added.
The experts interviewed in this article have no conflicts.
Katie Lennon contributed to this report.
This article was updated 4/29/21.
There are about 2 million to 4 million homebound patients in the United States, according to a webinar from The Trust for America’s Health, which was broadcast in March. But many of these individuals have not been vaccinated yet because of logistical challenges.
Some homebound COVID-19 immunization programs are administering Moderna and Pfizer vaccines to their patients, but many state, city, and local programs administered the Johnson & Johnson vaccine after it was cleared for use by the Food and Drug Administration in February 2021. The efficacy of the one-shot vaccine, as well as it being easier to store and ship than the Moderna and Pfizer vaccines, makes getting it to homebound patients less challenging.
“With Pfizer and Moderna, transportation is a challenge because the temperature demands and the fragility of [messenger] RNA–based vaccines,” Brent Feorene, executive director of the American Academy of Home Care Medicine, said in an interview. That’s why [the Johnson & Johnson] vaccine held such promise – it’s less fragile, [can be stored in] higher temperatures, and was a one shot.”
Other hurdles to getting homebound patients vaccinated had already been in place prior to the 10-day-pause on using the J&J vaccine that occurred for federal agencies to consider possible serious side effects linked to it.
Many roadblocks to vaccination
Although many homebound patients can’t readily go out into the community and be exposed to the COVID-19 virus themselves, they are dependent on caregivers and family members who do go out into the community.
“Their friends, family, neighbors, home health aides, and other kinds of health care workers come into the home,” said Shawn Amer, clinical program director at Central Ohio Primary Care in Columbus.
Nurses from Ms. Amer’s practice vaccinated approximately ten homebound patients with the J&J vaccine through a pilot program in March. Then on April 24, nurses from Central Ohio Primary Care vaccinated just under 40 homebound patients and about a handful of their caregivers who were not able to get their vaccines elsewhere, according to Ms. Amer. This time they used the Pfizer vaccine and will be returning to these patients’ homes on May 15 to administer the second dose.
“Any time you are getting in the car and adding miles, it adds complexity,” Ms. Amer said.
“We called patients 24 to 36 hours before coming to their homes to make sure they were ready, but we learned that just because the healthcare power of attorney agrees to a patient getting vaccinated does not mean that patient will be willing to get the vaccine when the nurse shows up," she noted.
Ms. Amer elaborated that three patients with dementia refused the vaccine when nurses arrived at their home on April 24.
“We had to pivot and find other people,” Ms. Amer. Her practice ended up having to waste one shot.
Expenses are greater
The higher costs of getting homebound patients vaccinated is an additional hurdle to getting these vulnerable individuals protected by COVID-19 shots.
Vaccinating patients in their homes “doesn’t require a lot of technology, but it does require a lot of time” and the staffing expense becomes part of the challenge, Ms. Amer noted.
For each of the two days that Central Ohio Primary Care provides the Pfizer vaccine to homebound patients, the practice needs to pay seven nurses to administer the vaccine, Ms. Amer explained.
There have also been reports of organizations that administer the vaccines – which are free for patients because the federal government is paying for them – not being paid enough by Medicare to cover staff time and efforts to vaccinate patients in their homes, Kaiser Health News reported. According to the Centers for Medicare & Medicaid Services, they pay $40 for the administration of a single-dose COVID-19 vaccine and, for COVID-19 vaccines requiring multiple doses, Medicare pays approximately $40 for each dose in the series. These rates were implemented after March 15. Before that date, the rates were even lower, with the Medicare reimbursement rates for initial doses of COVID-19 vaccines being $16.94 and final doses being $28.39.
William Dombi, president of the National Association for Home Care & Hospice, told Kaiser Health News that the actual cost of these homebound visits are closer to $150 or $160.
“The reimbursement for the injection is pretty minimal,” Mr. Feorene said. “So unless you’re a larger organization and able to have staff to deploy some of your smaller practices, just couldn’t afford to do it.”
Many homebound patients have also been unable to get the lifesaving shots because of logistical roadblocks and many practices not being able to do home visits.
“I think that initially when the [Centers for Disease Control and Prevention] came out with vaccine guidance for medical providers, they offered no guidance for in-home medical providers and we had to go back and ask for that, which they did produce,” Mr. Feorene said. “And we’re grateful for that. But I think just this general understanding that there is a population of folks that are [limited to their home], that they do receive medical care and other care in the home, and that we have to remember that the medical providers who provide care in the home are also primary care providers.”
Furthermore, trying to navigate or find programs delivering vaccines to the homebound can be difficult depending on where a patient lives.
While some programs have been launched on the country or city level – the New York Fire Department launched a pilot program to bring the Johnson & Johnson vaccine to homebound seniors – other programs have been spearheaded by hospital networks like Northwell and Mount Sinai. However, many of these hospital networks only reach out to people who already have a relationship with the hospital.
Ms Amer said identifying homebound patients and reaching out to them can be tough and can contribute to the logistics and time involved in setting patients up for the vaccine.
“Reaching some of these patients is difficult,” Ms. Amer noted. “Sometimes the best way to reach them or get a hold of them is through their caregiver. And so do you have the right phone number? Do you have the right name?”
Overcoming the challenges
With the absence of a national plan targeting homebound patients, many local initiatives were launched to help these individuals get vaccinated. Local fire department paramedics have gone door to door to administer the COVID-19 vaccine in cities like Chicago, New York, and Miami. The suspension of the Johnson & Johnson vaccine resulted in the suspension of in-home vaccinations for some people in New York City. However, the program resumed after the FDA and CDC lifted the pause on April 24.
Health systems like Mount Sinai vaccinated approximately 530 people through the Mount Sinai Visiting Doctors Program, including patients and their caregivers, according to Peter Gliatto, MD, associate director of the Mount Sinai Visiting Doctors Program.
“In different cities, townships, and jurisdictions, different health departments and different provider groups are approaching [the distribution of the COVID-19 vaccine] slightly differently,” Ms. Amer said. So a lot of the decisions surrounding the distribution of shots are local or dependent on local resourcing.
People who live in rural areas present a unique challenge, but Mr. Feorene said reaching out to local emergency medical services or the local health departments can provide some insight on what their town is doing to vaccinate homebound patients.
“I think understanding what a [public health department] is doing would be the very first place to start,” Mr. Feorene said in an interview.
If a patient is bedridden and is mobile enough to sit in a car, Mr. Feorene also recommends finding out if there are vaccine fairs “within a reasonable driving distance.”
Ms. Amer said continuing this mission of getting homebound patients vaccinated is necessary for public health.
“Even if it’s going to take longer to vaccinate these homebound patients, we still have to make an effort. So much of the country’s vaccine efforts have been focused on getting as many shots in as many arms as quickly as possible. And that is definitely super important,” she said.
Ms. Amer is working with her practice’s primary care physicians to try to identify all of those patients who are functionally debilitated or unable to leave their home to get vaccinated and that Central Ohio Primary Care will vaccinate more homebound patients, she added.
The experts interviewed in this article have no conflicts.
Katie Lennon contributed to this report.
This article was updated 4/29/21.
Cannabis for migraine strongly linked to rebound headache
, preliminary research suggests, although the direction of the relationship is unclear. Researchers at Stanford (Calif.) University found a significant increase in the likelihood of medication overuse headache (rebound headache) in chronic migraine patients who use cannabis.

“This study shows that there is some kind of association between cannabis use and medication overuse headache in people with chronic migraine,” said lead investigator Niushen Zhang, MD, a clinical assistant professor at Stanford.
“But it is unclear at this time whether patients are using cannabis to treat medication overuse headache or if cannabis is contributing to the development medication overuse headache, or both,” she said.
The findings were presented at the American Academy of Neurology’s 2021 annual meeting.
Sixfold increase
“Medication overuse occurs in about 1% to 3% of the general population. It affects nearly one-third of the patients (mostly patients with chronic migraine) seen at tertiary care centers such as the Stanford Headache Center,” Dr. Zhang said.
From clinical observations, patients with chronic migraine and medication overuse headache appear to be concomitantly using cannabis products, yet there is currently very little research on this topic, she added.
To investigate, the researchers reviewed the records of 368 adults who experienced chronic migraine (15 or more migraine days per month) for at least 1 year. Of the 368 patients, 150 were using cannabis, and 218 were not. In addition, 212 had medication overuse headache, and 156 did not.
Results showed that patients who used cannabis were nearly six times more likely to have medication overuse headache than those who did not use cannabis (odds ratio, 5.99; 95% confidence interval, 3.45-10.43; P < .0001).
There were significant bidirectional relationships between current cannabis use, opioid use, and medication overuse headache.
Jury out on cannabis for migraine
Commenting on the findings, Teshamae Monteith, MD, of the University of Miami, noted, “With increased legalization, greater access, and less stigmatization, there are more individuals using cannabis for migraine, but there is no solid evidence to suggest that cannabis is effective for acute or preventive treatment of migraine.”
The study is “interesting,” Dr. Monteith said, but, owing to methodologic limitations, it is not clear that cannabis contributes to medication overuse headache. “Patients with medication overuse headaches may have more comorbidities, such as anxiety, depression, and sleep disorders, that are driving the cannabis use. The patients on cannabis also had higher rates of opiate use, which itself is a stronger contributor to medication overuse headache and may indicate the presence of other pain disorders,” Dr. Monteith said.
“It is not clear if these patients were appropriately treated with migraine prevention; patients that use cannabis sometimes report that they prefer to avoid pharmaceutical treatments, such as antidepressants, etc., used for migraine,” Dr. Monteith noted.
She said that at this point, she would advise clinicians to ask about cannabis use “and let patients know that we do not know enough about the long-term effects of cannabis on the migraine brain.”
Most importantly, Dr. Monteith said, she would “encourage clinicians to be sensitive to the high prevalence of migraine, chronic migraine, and medication overuse. If we can treat more effectively and prevent migraine progression, which includes addressing comorbidities, there would be a lot less medication overuse headache.”
Also weighing in on the study, Jessica Ailani, MD, director, Medstar Georgetown Headache Center, Washington, D.C., noted that there is no conclusive evidence that cannabis is an effective acute or preventive treatment for migraine. “There is a suggestion that cannabis can help treat a migraine attack, but there is uncertainty about concentration of cannabidiol (CBD) to tetrahydrocannabinol (THC) needed to achieve pain freedom,” Dr. Ailani said.
“There has also been some concern about interactions between CBD and other medications used to treat migraine and that CBD can cause a condition known as reversible cerebral vasoconstrictive syndrome. These are reasons to be cautious with CBD,” Dr. Ailani added.
“At this time there is limited advice we can give our patients except that more studies need to be done. If cannabis is used, it should be reported, and medications that may interact with cannabis should be avoided. A headache calendar should be kept to ensure frequency of migraine and headache attacks do not go up,” said Dr. Ailani.
The study had no specific funding. Dr. Zhang, Dr. Monteith, and Dr. Ailani have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, preliminary research suggests, although the direction of the relationship is unclear. Researchers at Stanford (Calif.) University found a significant increase in the likelihood of medication overuse headache (rebound headache) in chronic migraine patients who use cannabis.
“This study shows that there is some kind of association between cannabis use and medication overuse headache in people with chronic migraine,” said lead investigator Niushen Zhang, MD, a clinical assistant professor at Stanford.
“But it is unclear at this time whether patients are using cannabis to treat medication overuse headache or if cannabis is contributing to the development medication overuse headache, or both,” she said.
The findings were presented at the American Academy of Neurology’s 2021 annual meeting.
Sixfold increase
“Medication overuse occurs in about 1% to 3% of the general population. It affects nearly one-third of the patients (mostly patients with chronic migraine) seen at tertiary care centers such as the Stanford Headache Center,” Dr. Zhang said.
From clinical observations, patients with chronic migraine and medication overuse headache appear to be concomitantly using cannabis products, yet there is currently very little research on this topic, she added.
To investigate, the researchers reviewed the records of 368 adults who experienced chronic migraine (15 or more migraine days per month) for at least 1 year. Of the 368 patients, 150 were using cannabis, and 218 were not. In addition, 212 had medication overuse headache, and 156 did not.
Results showed that patients who used cannabis were nearly six times more likely to have medication overuse headache than those who did not use cannabis (odds ratio, 5.99; 95% confidence interval, 3.45-10.43; P < .0001).
There were significant bidirectional relationships between current cannabis use, opioid use, and medication overuse headache.
Jury out on cannabis for migraine
Commenting on the findings, Teshamae Monteith, MD, of the University of Miami, noted, “With increased legalization, greater access, and less stigmatization, there are more individuals using cannabis for migraine, but there is no solid evidence to suggest that cannabis is effective for acute or preventive treatment of migraine.”
The study is “interesting,” Dr. Monteith said, but, owing to methodologic limitations, it is not clear that cannabis contributes to medication overuse headache. “Patients with medication overuse headaches may have more comorbidities, such as anxiety, depression, and sleep disorders, that are driving the cannabis use. The patients on cannabis also had higher rates of opiate use, which itself is a stronger contributor to medication overuse headache and may indicate the presence of other pain disorders,” Dr. Monteith said.
“It is not clear if these patients were appropriately treated with migraine prevention; patients that use cannabis sometimes report that they prefer to avoid pharmaceutical treatments, such as antidepressants, etc., used for migraine,” Dr. Monteith noted.
She said that at this point, she would advise clinicians to ask about cannabis use “and let patients know that we do not know enough about the long-term effects of cannabis on the migraine brain.”
Most importantly, Dr. Monteith said, she would “encourage clinicians to be sensitive to the high prevalence of migraine, chronic migraine, and medication overuse. If we can treat more effectively and prevent migraine progression, which includes addressing comorbidities, there would be a lot less medication overuse headache.”
Also weighing in on the study, Jessica Ailani, MD, director, Medstar Georgetown Headache Center, Washington, D.C., noted that there is no conclusive evidence that cannabis is an effective acute or preventive treatment for migraine. “There is a suggestion that cannabis can help treat a migraine attack, but there is uncertainty about concentration of cannabidiol (CBD) to tetrahydrocannabinol (THC) needed to achieve pain freedom,” Dr. Ailani said.
“There has also been some concern about interactions between CBD and other medications used to treat migraine and that CBD can cause a condition known as reversible cerebral vasoconstrictive syndrome. These are reasons to be cautious with CBD,” Dr. Ailani added.
“At this time there is limited advice we can give our patients except that more studies need to be done. If cannabis is used, it should be reported, and medications that may interact with cannabis should be avoided. A headache calendar should be kept to ensure frequency of migraine and headache attacks do not go up,” said Dr. Ailani.
The study had no specific funding. Dr. Zhang, Dr. Monteith, and Dr. Ailani have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, preliminary research suggests, although the direction of the relationship is unclear. Researchers at Stanford (Calif.) University found a significant increase in the likelihood of medication overuse headache (rebound headache) in chronic migraine patients who use cannabis.
“This study shows that there is some kind of association between cannabis use and medication overuse headache in people with chronic migraine,” said lead investigator Niushen Zhang, MD, a clinical assistant professor at Stanford.
“But it is unclear at this time whether patients are using cannabis to treat medication overuse headache or if cannabis is contributing to the development medication overuse headache, or both,” she said.
The findings were presented at the American Academy of Neurology’s 2021 annual meeting.
Sixfold increase
“Medication overuse occurs in about 1% to 3% of the general population. It affects nearly one-third of the patients (mostly patients with chronic migraine) seen at tertiary care centers such as the Stanford Headache Center,” Dr. Zhang said.
From clinical observations, patients with chronic migraine and medication overuse headache appear to be concomitantly using cannabis products, yet there is currently very little research on this topic, she added.
To investigate, the researchers reviewed the records of 368 adults who experienced chronic migraine (15 or more migraine days per month) for at least 1 year. Of the 368 patients, 150 were using cannabis, and 218 were not. In addition, 212 had medication overuse headache, and 156 did not.
Results showed that patients who used cannabis were nearly six times more likely to have medication overuse headache than those who did not use cannabis (odds ratio, 5.99; 95% confidence interval, 3.45-10.43; P < .0001).
There were significant bidirectional relationships between current cannabis use, opioid use, and medication overuse headache.
Jury out on cannabis for migraine
Commenting on the findings, Teshamae Monteith, MD, of the University of Miami, noted, “With increased legalization, greater access, and less stigmatization, there are more individuals using cannabis for migraine, but there is no solid evidence to suggest that cannabis is effective for acute or preventive treatment of migraine.”
The study is “interesting,” Dr. Monteith said, but, owing to methodologic limitations, it is not clear that cannabis contributes to medication overuse headache. “Patients with medication overuse headaches may have more comorbidities, such as anxiety, depression, and sleep disorders, that are driving the cannabis use. The patients on cannabis also had higher rates of opiate use, which itself is a stronger contributor to medication overuse headache and may indicate the presence of other pain disorders,” Dr. Monteith said.
“It is not clear if these patients were appropriately treated with migraine prevention; patients that use cannabis sometimes report that they prefer to avoid pharmaceutical treatments, such as antidepressants, etc., used for migraine,” Dr. Monteith noted.
She said that at this point, she would advise clinicians to ask about cannabis use “and let patients know that we do not know enough about the long-term effects of cannabis on the migraine brain.”
Most importantly, Dr. Monteith said, she would “encourage clinicians to be sensitive to the high prevalence of migraine, chronic migraine, and medication overuse. If we can treat more effectively and prevent migraine progression, which includes addressing comorbidities, there would be a lot less medication overuse headache.”
Also weighing in on the study, Jessica Ailani, MD, director, Medstar Georgetown Headache Center, Washington, D.C., noted that there is no conclusive evidence that cannabis is an effective acute or preventive treatment for migraine. “There is a suggestion that cannabis can help treat a migraine attack, but there is uncertainty about concentration of cannabidiol (CBD) to tetrahydrocannabinol (THC) needed to achieve pain freedom,” Dr. Ailani said.
“There has also been some concern about interactions between CBD and other medications used to treat migraine and that CBD can cause a condition known as reversible cerebral vasoconstrictive syndrome. These are reasons to be cautious with CBD,” Dr. Ailani added.
“At this time there is limited advice we can give our patients except that more studies need to be done. If cannabis is used, it should be reported, and medications that may interact with cannabis should be avoided. A headache calendar should be kept to ensure frequency of migraine and headache attacks do not go up,” said Dr. Ailani.
The study had no specific funding. Dr. Zhang, Dr. Monteith, and Dr. Ailani have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
From AAN 2021
Nondopamine antipsychotic shows clinical signal in Parkinson’s disease psychosis
according to results of a proof-of-principle study presented at the 2021 annual meeting of the American Academy of Neurology.

In presenting study results, Stuart H. Isaacson, MD, of the Parkinson’s Disease and Movement Disorders Center in Boca Raton, Fla., noted the one potential advantage of SEP-363856 is that it does not require blood monitoring, unlike clozapine, often used as an alternative to pimavanserin, the only Food and Drug Administration–approved treatment for Parkinson’s disease psychosis.* Quetiapine has also been used off label for Parkinson’s disease psychosis, but Dr. Isaacson said this lacks the evidence supporting the other two options and has side effects including sedation and orthostatic hypotension.
“Other non–FDA-approved treatment options are limited due to their lack of efficacy, safety concerns, and exacerbation of motor symptoms,” he said.
The study involved 38 patients, 24 of whom received SEP-363856 and the rest placebo, and evaluated total scores for the novel Scale for the Assessment of Positive Symptoms for Parkinson’s Disease Psychosis (SAPS-PD) after 6 weeks of treatment. The treatment group was given one of three doses: 25 mg (n = 11), 50 mg (n = 9), and 75 mg (n = 10).
Dr. Isaacson described SEP-363856 as a novel molecule that has agonist activity at TARR1, which regulates dopamine, norepinephrine, and serotonin, as well as serotonin receptor 5-HT1A, but has no activity at the dopamine receptor D2.
“There did appear to be improvement with this medication in patients’ psychosis symptoms, using the SAPS-PD subscale to identify the frequency and severity of hallucinations and delusions, but there was also improvement in the placebo group in this small study,” Dr. Isaacson said. “That did not demonstrate significance.” The improvement was maintained through the study period.
But the gap between the treatment and placebo groups widened as the degree of response increased. The rates were identical for the 30% or above response and the 50% or above response subgroups: 27.3% and 37.5% for placebo and treatment groups, respectively. However, 25% of patients taking SEP-363856 had a 100% response in terms of SAPS-PD score versus 0% in the placebo group, Dr. Isaacson said.
The study also found Mini-Mental State Examination (MMSE) scores improved more in the treatment group, with the gap wider in those with baseline MMSE scores below 24 versus scores above 24: –5.2 (standard deviation, 2.81) versus –2.1 (SD, 3.00; P = .460).
“The scope of daytime and nighttime sleep both showed improvement, with the score for daytime sleep being significant,” Dr. Isaacson said of the treatment group. “Importantly, UPDRS [Unified Parkinson’s Disease Rating Scale] Part III motor scores showed no difference from placebo. Indeed, there was a trend toward improvement, but this again was not significant.” That’s noteworthy, he said, because other antipsychotics, with the exception of clozapine – which requires blood monitoring – are contraindicated in PDP because of their effect on motor function.
During question-and-answer, Dr. Isaacson noted that the complete response rate of 25% with SEP-363856 compared favorably with the 14% complete response rate reported with pimavanserin in the pivotal trial.
“Hopefully greater-powered studies will be performed to further identify and determine the safety and efficacy and tolerably of SEP-363856 in Parkinson’s psychosis, aiming to minimize the placebo effect and to try to hopefully identify its efficacy in relationship to other treatments,” Dr. Isaacson said.
“Right now with only one approved treatment, one that has efficacy but requires blood monitoring, and another treatment that may be fraught sometimes with sleepiness and other side effects, we need other alternatives for our patients as many of them resort to lowering and lowering their dopaminergic therapies with the consequence [of] worsening motor activity,” Dr. Isaacson said.

“This study further supports the concept that Parkinson’s disease psychosis involves much more than simply dopamine,” said Daniel E. Kremens, MD, codirector of the Parkinson’s disease and movement disorders division at Thomas Jefferson University, Philadelphia. “Targeting nondopaminergic targets allows us to treat the psychosis without worsening motor symptoms. By targeting TAAR-1 along with 5HT1A, SEP-363856 is a novel compound that appears to be well tolerated and may treat PDP without worsening motor symptoms,”
Sunovion Pharmaceuticals provided funding for the study. Dr. Isaacson has no financial relationships to disclose. Three study coauthors are employees of Sunovion. Dr. Kremens reported serving as a consultant to Sunovion.
*Correction, 5/17/21: An earlier version of this article misstated the blood monitoring requirements for pimavanserin.
according to results of a proof-of-principle study presented at the 2021 annual meeting of the American Academy of Neurology.
In presenting study results, Stuart H. Isaacson, MD, of the Parkinson’s Disease and Movement Disorders Center in Boca Raton, Fla., noted the one potential advantage of SEP-363856 is that it does not require blood monitoring, unlike clozapine, often used as an alternative to pimavanserin, the only Food and Drug Administration–approved treatment for Parkinson’s disease psychosis.* Quetiapine has also been used off label for Parkinson’s disease psychosis, but Dr. Isaacson said this lacks the evidence supporting the other two options and has side effects including sedation and orthostatic hypotension.
“Other non–FDA-approved treatment options are limited due to their lack of efficacy, safety concerns, and exacerbation of motor symptoms,” he said.
The study involved 38 patients, 24 of whom received SEP-363856 and the rest placebo, and evaluated total scores for the novel Scale for the Assessment of Positive Symptoms for Parkinson’s Disease Psychosis (SAPS-PD) after 6 weeks of treatment. The treatment group was given one of three doses: 25 mg (n = 11), 50 mg (n = 9), and 75 mg (n = 10).
Dr. Isaacson described SEP-363856 as a novel molecule that has agonist activity at TARR1, which regulates dopamine, norepinephrine, and serotonin, as well as serotonin receptor 5-HT1A, but has no activity at the dopamine receptor D2.
“There did appear to be improvement with this medication in patients’ psychosis symptoms, using the SAPS-PD subscale to identify the frequency and severity of hallucinations and delusions, but there was also improvement in the placebo group in this small study,” Dr. Isaacson said. “That did not demonstrate significance.” The improvement was maintained through the study period.
But the gap between the treatment and placebo groups widened as the degree of response increased. The rates were identical for the 30% or above response and the 50% or above response subgroups: 27.3% and 37.5% for placebo and treatment groups, respectively. However, 25% of patients taking SEP-363856 had a 100% response in terms of SAPS-PD score versus 0% in the placebo group, Dr. Isaacson said.
The study also found Mini-Mental State Examination (MMSE) scores improved more in the treatment group, with the gap wider in those with baseline MMSE scores below 24 versus scores above 24: –5.2 (standard deviation, 2.81) versus –2.1 (SD, 3.00; P = .460).
“The scope of daytime and nighttime sleep both showed improvement, with the score for daytime sleep being significant,” Dr. Isaacson said of the treatment group. “Importantly, UPDRS [Unified Parkinson’s Disease Rating Scale] Part III motor scores showed no difference from placebo. Indeed, there was a trend toward improvement, but this again was not significant.” That’s noteworthy, he said, because other antipsychotics, with the exception of clozapine – which requires blood monitoring – are contraindicated in PDP because of their effect on motor function.
During question-and-answer, Dr. Isaacson noted that the complete response rate of 25% with SEP-363856 compared favorably with the 14% complete response rate reported with pimavanserin in the pivotal trial.
“Hopefully greater-powered studies will be performed to further identify and determine the safety and efficacy and tolerably of SEP-363856 in Parkinson’s psychosis, aiming to minimize the placebo effect and to try to hopefully identify its efficacy in relationship to other treatments,” Dr. Isaacson said.
“Right now with only one approved treatment, one that has efficacy but requires blood monitoring, and another treatment that may be fraught sometimes with sleepiness and other side effects, we need other alternatives for our patients as many of them resort to lowering and lowering their dopaminergic therapies with the consequence [of] worsening motor activity,” Dr. Isaacson said.
“This study further supports the concept that Parkinson’s disease psychosis involves much more than simply dopamine,” said Daniel E. Kremens, MD, codirector of the Parkinson’s disease and movement disorders division at Thomas Jefferson University, Philadelphia. “Targeting nondopaminergic targets allows us to treat the psychosis without worsening motor symptoms. By targeting TAAR-1 along with 5HT1A, SEP-363856 is a novel compound that appears to be well tolerated and may treat PDP without worsening motor symptoms,”
Sunovion Pharmaceuticals provided funding for the study. Dr. Isaacson has no financial relationships to disclose. Three study coauthors are employees of Sunovion. Dr. Kremens reported serving as a consultant to Sunovion.
*Correction, 5/17/21: An earlier version of this article misstated the blood monitoring requirements for pimavanserin.
according to results of a proof-of-principle study presented at the 2021 annual meeting of the American Academy of Neurology.
In presenting study results, Stuart H. Isaacson, MD, of the Parkinson’s Disease and Movement Disorders Center in Boca Raton, Fla., noted the one potential advantage of SEP-363856 is that it does not require blood monitoring, unlike clozapine, often used as an alternative to pimavanserin, the only Food and Drug Administration–approved treatment for Parkinson’s disease psychosis.* Quetiapine has also been used off label for Parkinson’s disease psychosis, but Dr. Isaacson said this lacks the evidence supporting the other two options and has side effects including sedation and orthostatic hypotension.
“Other non–FDA-approved treatment options are limited due to their lack of efficacy, safety concerns, and exacerbation of motor symptoms,” he said.
The study involved 38 patients, 24 of whom received SEP-363856 and the rest placebo, and evaluated total scores for the novel Scale for the Assessment of Positive Symptoms for Parkinson’s Disease Psychosis (SAPS-PD) after 6 weeks of treatment. The treatment group was given one of three doses: 25 mg (n = 11), 50 mg (n = 9), and 75 mg (n = 10).
Dr. Isaacson described SEP-363856 as a novel molecule that has agonist activity at TARR1, which regulates dopamine, norepinephrine, and serotonin, as well as serotonin receptor 5-HT1A, but has no activity at the dopamine receptor D2.
“There did appear to be improvement with this medication in patients’ psychosis symptoms, using the SAPS-PD subscale to identify the frequency and severity of hallucinations and delusions, but there was also improvement in the placebo group in this small study,” Dr. Isaacson said. “That did not demonstrate significance.” The improvement was maintained through the study period.
But the gap between the treatment and placebo groups widened as the degree of response increased. The rates were identical for the 30% or above response and the 50% or above response subgroups: 27.3% and 37.5% for placebo and treatment groups, respectively. However, 25% of patients taking SEP-363856 had a 100% response in terms of SAPS-PD score versus 0% in the placebo group, Dr. Isaacson said.
The study also found Mini-Mental State Examination (MMSE) scores improved more in the treatment group, with the gap wider in those with baseline MMSE scores below 24 versus scores above 24: –5.2 (standard deviation, 2.81) versus –2.1 (SD, 3.00; P = .460).
“The scope of daytime and nighttime sleep both showed improvement, with the score for daytime sleep being significant,” Dr. Isaacson said of the treatment group. “Importantly, UPDRS [Unified Parkinson’s Disease Rating Scale] Part III motor scores showed no difference from placebo. Indeed, there was a trend toward improvement, but this again was not significant.” That’s noteworthy, he said, because other antipsychotics, with the exception of clozapine – which requires blood monitoring – are contraindicated in PDP because of their effect on motor function.
During question-and-answer, Dr. Isaacson noted that the complete response rate of 25% with SEP-363856 compared favorably with the 14% complete response rate reported with pimavanserin in the pivotal trial.
“Hopefully greater-powered studies will be performed to further identify and determine the safety and efficacy and tolerably of SEP-363856 in Parkinson’s psychosis, aiming to minimize the placebo effect and to try to hopefully identify its efficacy in relationship to other treatments,” Dr. Isaacson said.
“Right now with only one approved treatment, one that has efficacy but requires blood monitoring, and another treatment that may be fraught sometimes with sleepiness and other side effects, we need other alternatives for our patients as many of them resort to lowering and lowering their dopaminergic therapies with the consequence [of] worsening motor activity,” Dr. Isaacson said.
“This study further supports the concept that Parkinson’s disease psychosis involves much more than simply dopamine,” said Daniel E. Kremens, MD, codirector of the Parkinson’s disease and movement disorders division at Thomas Jefferson University, Philadelphia. “Targeting nondopaminergic targets allows us to treat the psychosis without worsening motor symptoms. By targeting TAAR-1 along with 5HT1A, SEP-363856 is a novel compound that appears to be well tolerated and may treat PDP without worsening motor symptoms,”
Sunovion Pharmaceuticals provided funding for the study. Dr. Isaacson has no financial relationships to disclose. Three study coauthors are employees of Sunovion. Dr. Kremens reported serving as a consultant to Sunovion.
*Correction, 5/17/21: An earlier version of this article misstated the blood monitoring requirements for pimavanserin.
FROM AAN 2021
Gene therapy shows promise for Sanfilippo syndrome
. Most of the benefit from the treatment came in patients who began treatment at younger age, but comparisons to natural history controls showed profound improvement among many recipients, some of whom attained normal developmental trajectories.
The study was presented at the American Academy of Neurology’s 2021 annual meeting by Kevin Flanigan, MD, an attending neurologist at Nationwide Children’s Hospital in Columbus, Ohio. He highlighted the improved developmental outcomes. “There’s been nothing shown to change the cognitive pathway of the disease. This is the first time it’s been seen as a treatment effect,” Dr. Flanigan said during a follow-up Q&A session.
The therapy was delivered using an adeno-associated virus-9 (AAV-9) vector, which led one questioner to ask about potential safety concerns, since AAV-associated risks date back to the death of Jesse Gelsinger in 1999. “There is concern about AAV therapies related to immune responses to potentially complement-mediated activation and thrombocytopenic syndrome, which has led to clinical holds on some other AAV-9 products related to muscular dystrophies. We’ve not seen signals of anything reminiscent of that, and we’re at AAV-9 dosages that are quite similar to what’s been used elsewhere in the field,” said Dr. Flanigan.
The results have him optimistic about the therapy. “I do think if it continues to be increasing divergent from the natural history, it will be questionable as to whether a subsequent trial will be necessary for this. That’s a decision for the [Food and Drug Administration] and the company to decide. Each observation point that goes by, each patient treated, and each time we get more data, I get more and more confident. It’s really gratifying to watch,” said Dr. Flanigan.
The study confirms the potential of gene replacement therapy autosomal recessive conditions, according to Nicholas Johnson, MD, associate professor of neurology at Virginia Commonwealth University, Richmond, as well as a fellow of the American Academy of Neurology. “Where the genetic problem is loss of gene function, the ability to replace that gene using a viral approach is going to be transformative across the board for many of these different conditions, including Sanfilippo syndrome,” said Dr. Johnson, who attended the session but was not involved in the research.
Toxicity could remain an issue, even in the absence of AAV-based safety concerns. “The rate limiting step in terms of gene replacement therapy development likely relates to the ability to provide those therapies to larger adults, because many approaches are weight based and it’s unclear what the upper limit of toxicity would be for adults,” said Dr. Johnson.
Transpher A study results
Dr. Flanigan presented results from Transpher A, a phase 1/2 clinical trial that has enrolled 20 patients to date in three cohorts: Cohort 1, with 3 patients, received 5 x 1,012 vg/kg, and had a mean follow-up of 58 months; cohort 2, with 3 patients, received 1 x 1,013 vg/kg, and had a mean follow-up of 49 months; and cohort 3, with 14 patients, received 3 x 1,013 vg/kg, with a mean follow-up of 24 months. Included patients ranged from birth to age 2, or older than age 2 with a development quotient of 60 or higher on the Bayley Scale.
Dr. Flanigan showed a plot of developmental progress compared with natural history controls, which showed that patients treated before age 2 or with a developmental quotient of 60 or higher had improved outcomes compared to other patients in the high dose cohort. They continued to show normal developmental progression at 30-36 months post treatment, at a time when the natural history data suggested they would suffer cognitive decline. Two years after administration, this group had cerebral spinal fluid levels of heparan sulfate that fell below the lower limit of detection. Patients in the high-dose cohort had normalized CSF levels of GM2 and GM3 gangliosides, and there were reductions in plasma heparan sulfate and urinary glycosaminoglycans. There was also a sustained decrease in liver volume.
The highest dose group was originally given to older patients, and most were similar to the natural history cohort, though some did stabilize. “More compellingly, patients (in the high-dose group) who were treated younger actually showed continued increase in development. One individual follows the normal development quotient line, and we would say that these are really quite distinct from what we typically see in patients,” said Dr. Flanigan.
The treatment was well tolerated. There were no deaths or treatment-related serious adverse events, and no clinically-significant adverse events within the first 5 years of follow-up.
The study was funded by Abeona Therapeutics. Dr. Flanigan has been on advisory boards for Apic Bio and 4D Molecular Therapeutics, consulted for Encoded Therapeutics, and has received royalties from Audentes Therapeutics. Dr. Flanigan has received funding from and been a consultant for Avidity.
. Most of the benefit from the treatment came in patients who began treatment at younger age, but comparisons to natural history controls showed profound improvement among many recipients, some of whom attained normal developmental trajectories.
The study was presented at the American Academy of Neurology’s 2021 annual meeting by Kevin Flanigan, MD, an attending neurologist at Nationwide Children’s Hospital in Columbus, Ohio. He highlighted the improved developmental outcomes. “There’s been nothing shown to change the cognitive pathway of the disease. This is the first time it’s been seen as a treatment effect,” Dr. Flanigan said during a follow-up Q&A session.
The therapy was delivered using an adeno-associated virus-9 (AAV-9) vector, which led one questioner to ask about potential safety concerns, since AAV-associated risks date back to the death of Jesse Gelsinger in 1999. “There is concern about AAV therapies related to immune responses to potentially complement-mediated activation and thrombocytopenic syndrome, which has led to clinical holds on some other AAV-9 products related to muscular dystrophies. We’ve not seen signals of anything reminiscent of that, and we’re at AAV-9 dosages that are quite similar to what’s been used elsewhere in the field,” said Dr. Flanigan.
The results have him optimistic about the therapy. “I do think if it continues to be increasing divergent from the natural history, it will be questionable as to whether a subsequent trial will be necessary for this. That’s a decision for the [Food and Drug Administration] and the company to decide. Each observation point that goes by, each patient treated, and each time we get more data, I get more and more confident. It’s really gratifying to watch,” said Dr. Flanigan.
The study confirms the potential of gene replacement therapy autosomal recessive conditions, according to Nicholas Johnson, MD, associate professor of neurology at Virginia Commonwealth University, Richmond, as well as a fellow of the American Academy of Neurology. “Where the genetic problem is loss of gene function, the ability to replace that gene using a viral approach is going to be transformative across the board for many of these different conditions, including Sanfilippo syndrome,” said Dr. Johnson, who attended the session but was not involved in the research.
Toxicity could remain an issue, even in the absence of AAV-based safety concerns. “The rate limiting step in terms of gene replacement therapy development likely relates to the ability to provide those therapies to larger adults, because many approaches are weight based and it’s unclear what the upper limit of toxicity would be for adults,” said Dr. Johnson.
Transpher A study results
Dr. Flanigan presented results from Transpher A, a phase 1/2 clinical trial that has enrolled 20 patients to date in three cohorts: Cohort 1, with 3 patients, received 5 x 1,012 vg/kg, and had a mean follow-up of 58 months; cohort 2, with 3 patients, received 1 x 1,013 vg/kg, and had a mean follow-up of 49 months; and cohort 3, with 14 patients, received 3 x 1,013 vg/kg, with a mean follow-up of 24 months. Included patients ranged from birth to age 2, or older than age 2 with a development quotient of 60 or higher on the Bayley Scale.
Dr. Flanigan showed a plot of developmental progress compared with natural history controls, which showed that patients treated before age 2 or with a developmental quotient of 60 or higher had improved outcomes compared to other patients in the high dose cohort. They continued to show normal developmental progression at 30-36 months post treatment, at a time when the natural history data suggested they would suffer cognitive decline. Two years after administration, this group had cerebral spinal fluid levels of heparan sulfate that fell below the lower limit of detection. Patients in the high-dose cohort had normalized CSF levels of GM2 and GM3 gangliosides, and there were reductions in plasma heparan sulfate and urinary glycosaminoglycans. There was also a sustained decrease in liver volume.
The highest dose group was originally given to older patients, and most were similar to the natural history cohort, though some did stabilize. “More compellingly, patients (in the high-dose group) who were treated younger actually showed continued increase in development. One individual follows the normal development quotient line, and we would say that these are really quite distinct from what we typically see in patients,” said Dr. Flanigan.
The treatment was well tolerated. There were no deaths or treatment-related serious adverse events, and no clinically-significant adverse events within the first 5 years of follow-up.
The study was funded by Abeona Therapeutics. Dr. Flanigan has been on advisory boards for Apic Bio and 4D Molecular Therapeutics, consulted for Encoded Therapeutics, and has received royalties from Audentes Therapeutics. Dr. Flanigan has received funding from and been a consultant for Avidity.
. Most of the benefit from the treatment came in patients who began treatment at younger age, but comparisons to natural history controls showed profound improvement among many recipients, some of whom attained normal developmental trajectories.
The study was presented at the American Academy of Neurology’s 2021 annual meeting by Kevin Flanigan, MD, an attending neurologist at Nationwide Children’s Hospital in Columbus, Ohio. He highlighted the improved developmental outcomes. “There’s been nothing shown to change the cognitive pathway of the disease. This is the first time it’s been seen as a treatment effect,” Dr. Flanigan said during a follow-up Q&A session.
The therapy was delivered using an adeno-associated virus-9 (AAV-9) vector, which led one questioner to ask about potential safety concerns, since AAV-associated risks date back to the death of Jesse Gelsinger in 1999. “There is concern about AAV therapies related to immune responses to potentially complement-mediated activation and thrombocytopenic syndrome, which has led to clinical holds on some other AAV-9 products related to muscular dystrophies. We’ve not seen signals of anything reminiscent of that, and we’re at AAV-9 dosages that are quite similar to what’s been used elsewhere in the field,” said Dr. Flanigan.
The results have him optimistic about the therapy. “I do think if it continues to be increasing divergent from the natural history, it will be questionable as to whether a subsequent trial will be necessary for this. That’s a decision for the [Food and Drug Administration] and the company to decide. Each observation point that goes by, each patient treated, and each time we get more data, I get more and more confident. It’s really gratifying to watch,” said Dr. Flanigan.
The study confirms the potential of gene replacement therapy autosomal recessive conditions, according to Nicholas Johnson, MD, associate professor of neurology at Virginia Commonwealth University, Richmond, as well as a fellow of the American Academy of Neurology. “Where the genetic problem is loss of gene function, the ability to replace that gene using a viral approach is going to be transformative across the board for many of these different conditions, including Sanfilippo syndrome,” said Dr. Johnson, who attended the session but was not involved in the research.
Toxicity could remain an issue, even in the absence of AAV-based safety concerns. “The rate limiting step in terms of gene replacement therapy development likely relates to the ability to provide those therapies to larger adults, because many approaches are weight based and it’s unclear what the upper limit of toxicity would be for adults,” said Dr. Johnson.
Transpher A study results
Dr. Flanigan presented results from Transpher A, a phase 1/2 clinical trial that has enrolled 20 patients to date in three cohorts: Cohort 1, with 3 patients, received 5 x 1,012 vg/kg, and had a mean follow-up of 58 months; cohort 2, with 3 patients, received 1 x 1,013 vg/kg, and had a mean follow-up of 49 months; and cohort 3, with 14 patients, received 3 x 1,013 vg/kg, with a mean follow-up of 24 months. Included patients ranged from birth to age 2, or older than age 2 with a development quotient of 60 or higher on the Bayley Scale.
Dr. Flanigan showed a plot of developmental progress compared with natural history controls, which showed that patients treated before age 2 or with a developmental quotient of 60 or higher had improved outcomes compared to other patients in the high dose cohort. They continued to show normal developmental progression at 30-36 months post treatment, at a time when the natural history data suggested they would suffer cognitive decline. Two years after administration, this group had cerebral spinal fluid levels of heparan sulfate that fell below the lower limit of detection. Patients in the high-dose cohort had normalized CSF levels of GM2 and GM3 gangliosides, and there were reductions in plasma heparan sulfate and urinary glycosaminoglycans. There was also a sustained decrease in liver volume.
The highest dose group was originally given to older patients, and most were similar to the natural history cohort, though some did stabilize. “More compellingly, patients (in the high-dose group) who were treated younger actually showed continued increase in development. One individual follows the normal development quotient line, and we would say that these are really quite distinct from what we typically see in patients,” said Dr. Flanigan.
The treatment was well tolerated. There were no deaths or treatment-related serious adverse events, and no clinically-significant adverse events within the first 5 years of follow-up.
The study was funded by Abeona Therapeutics. Dr. Flanigan has been on advisory boards for Apic Bio and 4D Molecular Therapeutics, consulted for Encoded Therapeutics, and has received royalties from Audentes Therapeutics. Dr. Flanigan has received funding from and been a consultant for Avidity.
FROM AAN 2021
Investigative gepant liver profile comparable with standard of care
according to results of a multicenter, open-label trial presented at the 2021 annual meeting of the American Academy of Neurology.

The trial included 739 patients, 543 of whom were randomized to daily oral atogepant with the remainder assigned to the existing standard of care oral migraine prevention medication, said Messoud Ashina, MD, PhD, of the Danish Headache Center at the University of Copenhagen. Initially, 67% (n = 364) of the atogepant patients reported treatment-emergent adverse events (TEAEs). However, he noted, the rate of TEAEs related to treatment was actually 18% (n = 98), and the rate of serious AEs was 4.4% (n = 24); 31 patients (5.7%) discontinued therapy because of TEAEs.
Those rates compared favorably with the standard of care group, Dr. Ashina said. In that group, the rate of TEAEs was 78.6% (154/196), and the rate of treatment-related TEAEs was 36.2% (n = 71).
In the atogepant group, the most common TEAEs were upper respiratory tract infection (10.3%, n = 56), constipation (7.2%, n = 39) and nausea (6.3%, n = 34). “With constipation in particular most cases were mild to moderate,” Dr. Ashina said. “Only one case was considered severe and it resolved before the end of the trial.” One patient discontinued treatment because of constipation.
Most significantly, said Dr. Ashina, “No hepatic safety issues were identified.” In the atogepant group, 2.4% of patients (n = 13) had ALT/AST levels at three times the upper limit of normal versus 3.2% (n = 6) in the standard of care group.
During question-and-answer, Dr. Ashina was pressed on the rate or urinary tract infections in the atogepant patients – 5.2% (n = 28), a measure not reported in the standard of care group – but he said there was no indication the UTIs resulted from atogepant itself. “I assume if there was some problems with urinary tract infections because of the kidneys then you would expect to see the lab data showing that,” he added in an interview. “There were no differences in lab abnormalities between the two groups.”
While Dr. Ashina said “I don’t think it’s something of concern” with regard to the UTI risk, he added: “It doesn’t mean that we don’t have to be careful. As physicians, we have to exhibit pharmacovigilance all the time, especially with the new drugs coming out over the next 5 years. But don’t panic.”
Stephen D. Silberstein, MD, director of the headache center at Thomas Jefferson University, Philadelphia, agreed that the hepatic values reported in the open-label trial are important. “What’s really nice about this study is the fact that we now know that this particular gepant when given on a regular basis for 1 year has no problem with liver or kidney function,” he said in an interview.
Dr. Ashina said once-daily oral atogepant could potentially be a desirable alternative migraine preventive treatment to monoclonal antibodies and their quarterly injections and a second-line therapy when other treatments don’t work. However, Dr. Silverstein noted that patients typically aren’t as compliant with self-administered oral medications as they are with periodic injections.
Allergan/AbbVie sponsored the trial. Dr. Ashina reported financial relationships with Allergan/AbbVie, Amgen, Eli Lilly, Lundbeck, Novartis, and Teva. Dr. Silberstein is a trial investigator.
according to results of a multicenter, open-label trial presented at the 2021 annual meeting of the American Academy of Neurology.
The trial included 739 patients, 543 of whom were randomized to daily oral atogepant with the remainder assigned to the existing standard of care oral migraine prevention medication, said Messoud Ashina, MD, PhD, of the Danish Headache Center at the University of Copenhagen. Initially, 67% (n = 364) of the atogepant patients reported treatment-emergent adverse events (TEAEs). However, he noted, the rate of TEAEs related to treatment was actually 18% (n = 98), and the rate of serious AEs was 4.4% (n = 24); 31 patients (5.7%) discontinued therapy because of TEAEs.
Those rates compared favorably with the standard of care group, Dr. Ashina said. In that group, the rate of TEAEs was 78.6% (154/196), and the rate of treatment-related TEAEs was 36.2% (n = 71).
In the atogepant group, the most common TEAEs were upper respiratory tract infection (10.3%, n = 56), constipation (7.2%, n = 39) and nausea (6.3%, n = 34). “With constipation in particular most cases were mild to moderate,” Dr. Ashina said. “Only one case was considered severe and it resolved before the end of the trial.” One patient discontinued treatment because of constipation.
Most significantly, said Dr. Ashina, “No hepatic safety issues were identified.” In the atogepant group, 2.4% of patients (n = 13) had ALT/AST levels at three times the upper limit of normal versus 3.2% (n = 6) in the standard of care group.
During question-and-answer, Dr. Ashina was pressed on the rate or urinary tract infections in the atogepant patients – 5.2% (n = 28), a measure not reported in the standard of care group – but he said there was no indication the UTIs resulted from atogepant itself. “I assume if there was some problems with urinary tract infections because of the kidneys then you would expect to see the lab data showing that,” he added in an interview. “There were no differences in lab abnormalities between the two groups.”
While Dr. Ashina said “I don’t think it’s something of concern” with regard to the UTI risk, he added: “It doesn’t mean that we don’t have to be careful. As physicians, we have to exhibit pharmacovigilance all the time, especially with the new drugs coming out over the next 5 years. But don’t panic.”
Stephen D. Silberstein, MD, director of the headache center at Thomas Jefferson University, Philadelphia, agreed that the hepatic values reported in the open-label trial are important. “What’s really nice about this study is the fact that we now know that this particular gepant when given on a regular basis for 1 year has no problem with liver or kidney function,” he said in an interview.
Dr. Ashina said once-daily oral atogepant could potentially be a desirable alternative migraine preventive treatment to monoclonal antibodies and their quarterly injections and a second-line therapy when other treatments don’t work. However, Dr. Silverstein noted that patients typically aren’t as compliant with self-administered oral medications as they are with periodic injections.
Allergan/AbbVie sponsored the trial. Dr. Ashina reported financial relationships with Allergan/AbbVie, Amgen, Eli Lilly, Lundbeck, Novartis, and Teva. Dr. Silberstein is a trial investigator.
according to results of a multicenter, open-label trial presented at the 2021 annual meeting of the American Academy of Neurology.
The trial included 739 patients, 543 of whom were randomized to daily oral atogepant with the remainder assigned to the existing standard of care oral migraine prevention medication, said Messoud Ashina, MD, PhD, of the Danish Headache Center at the University of Copenhagen. Initially, 67% (n = 364) of the atogepant patients reported treatment-emergent adverse events (TEAEs). However, he noted, the rate of TEAEs related to treatment was actually 18% (n = 98), and the rate of serious AEs was 4.4% (n = 24); 31 patients (5.7%) discontinued therapy because of TEAEs.
Those rates compared favorably with the standard of care group, Dr. Ashina said. In that group, the rate of TEAEs was 78.6% (154/196), and the rate of treatment-related TEAEs was 36.2% (n = 71).
In the atogepant group, the most common TEAEs were upper respiratory tract infection (10.3%, n = 56), constipation (7.2%, n = 39) and nausea (6.3%, n = 34). “With constipation in particular most cases were mild to moderate,” Dr. Ashina said. “Only one case was considered severe and it resolved before the end of the trial.” One patient discontinued treatment because of constipation.
Most significantly, said Dr. Ashina, “No hepatic safety issues were identified.” In the atogepant group, 2.4% of patients (n = 13) had ALT/AST levels at three times the upper limit of normal versus 3.2% (n = 6) in the standard of care group.
During question-and-answer, Dr. Ashina was pressed on the rate or urinary tract infections in the atogepant patients – 5.2% (n = 28), a measure not reported in the standard of care group – but he said there was no indication the UTIs resulted from atogepant itself. “I assume if there was some problems with urinary tract infections because of the kidneys then you would expect to see the lab data showing that,” he added in an interview. “There were no differences in lab abnormalities between the two groups.”
While Dr. Ashina said “I don’t think it’s something of concern” with regard to the UTI risk, he added: “It doesn’t mean that we don’t have to be careful. As physicians, we have to exhibit pharmacovigilance all the time, especially with the new drugs coming out over the next 5 years. But don’t panic.”
Stephen D. Silberstein, MD, director of the headache center at Thomas Jefferson University, Philadelphia, agreed that the hepatic values reported in the open-label trial are important. “What’s really nice about this study is the fact that we now know that this particular gepant when given on a regular basis for 1 year has no problem with liver or kidney function,” he said in an interview.
Dr. Ashina said once-daily oral atogepant could potentially be a desirable alternative migraine preventive treatment to monoclonal antibodies and their quarterly injections and a second-line therapy when other treatments don’t work. However, Dr. Silverstein noted that patients typically aren’t as compliant with self-administered oral medications as they are with periodic injections.
Allergan/AbbVie sponsored the trial. Dr. Ashina reported financial relationships with Allergan/AbbVie, Amgen, Eli Lilly, Lundbeck, Novartis, and Teva. Dr. Silberstein is a trial investigator.
FROM AAN 2021
The neurology of long-haul COVID-19
Long-haul neurologic symptoms of COVID-19 seem to be distinct from neurologic conditions found in acute disease. Much work remains to be done to understand the biological mechanisms behind these problems, but inflammation and autoimmune responses may play a role in some cases.

Those were some of the takeaways from a talk by Serena Spudich, MD, who presented her research at the 2021 annual meeting of the American Academy of Neurology. Dr. Spudich is the division chief of neurologic infections and global neurology and codirector of the Center for Neuroepidemiology and Clinical Neurological Research at Yale University, New Haven, Conn.
Examining the nervous system’s involvement in COVID-19
Even early on in the pandemic, it became clear that there were lingering complaints of neuromuscular problems, cognitive dysfunction, and mood and psychiatric issues. Breathing and heart rate problems also can arise. “There seems to be a preponderance of syndromes that reflect involvement of the nervous system,” said Dr. Spudich.
To try to understand the etiology of these persistent problems, Dr. Spudich said it’s important to examine the nervous system’s involvement in acute COVID-19. She has been involved in these efforts since early in the pandemic, when she ran an inpatient consult service at Yale dedicated to neurologic effects of acute COVID-19. She witnessed complications including stroke, encephalopathy, and seizures, among others.
Stroke during acute COVID-19 seemed to be associated with inflammation and endothelial activation or endotheliopathy. SARS-CoV-2 has been undetectable in the cerebrospinal fluid (CSF) of patients with acute COVID-19 and neurologic symptoms, but inflammatory cytokines can be present along with increased frequency of B cells. Anti–SARS-CoV-2 antibodies have also been found in CSF, some of which were auto reactive to brain tissue. The immune response was altered, compared with healthy controls, and in the CNS, compared with in the blood, “raising the question of whether inflammation and autoimmunity may be underlying causes of these syndromes,” said Dr. Spudich.
She also pointed to an MRI study of autopsied brain tissue of patients with COVID-19 and neurologic complications, which showed indications of both hemorrhagic and ischemic microvascular injury. “It’s just a reminder that, during acute COVID-19, there may be inflammation in the brain, there may be autoimmune reactions, and there may be vascular changes that underlie some of the neurologic syndromes that are seen,” said Dr. Spudich.
A panoply of different syndromes
In October, Yale set up a post-COVID neurologic clinic that brought together pulmonary, cardiology, and psychiatric specialists, many of whom saw the same patients, about 60% of whom had cognitive impairment, more than 40% had neuromuscular problems, and over 30% headache. “There’s not a single entity of a post-COVID neurologic syndrome. There’s a panoply of different syndromes that may have similar or distinct etiologies,” said Dr. Spudich.
Most patients were in their 30s, 40s, or 50s. That doesn’t necessarily mean this is the most common age range for these issues, though. There could be some bias if these individuals are seeking specialty care because they expected to recover from COVID-19 quickly. But it could be that there is something biologically unique among this age group that predisposes them to complications. Regardless, two out of three patients were never hospitalized, “suggesting that even mild COVID-19 can lead to some long-term sequelae,” said Dr. Spudich.
One potential explanation for long-term neurologic syndromes is that they are an extension of the inflammation, autoimmunity, and immune perturbation occurring during acute disease. One study looked at 18 cancer patients who had neurologic complications with COVID-19. Two months after onset, they had elevated markers of neuroinflammation and neuronal injury in the cerebral spinal fluid compared to cancer patients with no history of COVID-19.
Looking for biologic markers
An Italian study looked at patients who were evaluated during acute hospitalization and again 3 months later, and found that some markers of inflation in the blood were associated with later cognitive impairment. The patients were more severely ill, so it’s not clear what the findings mean for patients who present with neurologic symptoms after milder illness.
A PET scan study of 35 patients with persistent neurologic symptoms found patterns of reduced fluorodeoxyglucose uptake in some regions of the brain that are believed to be associated with some symptoms. Lower values were associated with greater severity for symptoms like memory dysfunction, and anosmia. “Why there might be hypometabolism in these regions I think needs to be assessed and used as a biomarker to associate hypometabolism with other kinds of processes in blood and spinal fluid,” said Dr. Spudich.
Along with colleagues at Yale, Dr. Spudich is conducting the MIND study, which is using PET and MRI imaging along with blood and CSF biomarkers to track the progress of patients after COVID-19. There are few results to discuss since only 20 patients have been recruited so far, except that brain imaging and blood values are generally normal despite neurologic complaints. Most were not hospitalized for COVID-19. Dr. Spudich highlighted one man in his 30s who developed new-onset psychosis, despite no previous history. Although clinical tests were all negative, a novel autoantibody detection method revealed a previously unknown autoreactive antibody in his spinal fluid. “This may suggest that there is autoantibody production in some individuals with post–COVID-19 psychosis, and potentially other syndromes,” said Dr. Spudich.
The research task ahead
The case illustrates the task ahead for neurology. “There’s a real research mandate to understand the biological substrates of these diverse disorders, not only to address the emergent public health concern and reduce the stigma in our patients, but to develop targeted therapeutic interventions,” said Dr. Spudich.

Anna Cervantes-Arslanian, MD, an associate professor of neurology at Boston University who also treats and studies patients with post-COVID neurologic symptoms, agreed with that assessment. “It’s not like every patient that has muscle aches and fatigue also has brain fog. It’s really hard to parse them out into specific phenotypes that are pretty classic. Some people will have all of those things, some will have very few of them,” said Dr. Cervantes-Arslanian. “We need to be able to identify them sand see if there is clustering of symptoms so we can better look into what the biological underpinnings are. That’s the first step to thinking about a therapeutic target.”
Dr. Spudich and Dr. Cervantes-Arslanian had no relevant financial disclosures.
Long-haul neurologic symptoms of COVID-19 seem to be distinct from neurologic conditions found in acute disease. Much work remains to be done to understand the biological mechanisms behind these problems, but inflammation and autoimmune responses may play a role in some cases.
Those were some of the takeaways from a talk by Serena Spudich, MD, who presented her research at the 2021 annual meeting of the American Academy of Neurology. Dr. Spudich is the division chief of neurologic infections and global neurology and codirector of the Center for Neuroepidemiology and Clinical Neurological Research at Yale University, New Haven, Conn.
Examining the nervous system’s involvement in COVID-19
Even early on in the pandemic, it became clear that there were lingering complaints of neuromuscular problems, cognitive dysfunction, and mood and psychiatric issues. Breathing and heart rate problems also can arise. “There seems to be a preponderance of syndromes that reflect involvement of the nervous system,” said Dr. Spudich.
To try to understand the etiology of these persistent problems, Dr. Spudich said it’s important to examine the nervous system’s involvement in acute COVID-19. She has been involved in these efforts since early in the pandemic, when she ran an inpatient consult service at Yale dedicated to neurologic effects of acute COVID-19. She witnessed complications including stroke, encephalopathy, and seizures, among others.
Stroke during acute COVID-19 seemed to be associated with inflammation and endothelial activation or endotheliopathy. SARS-CoV-2 has been undetectable in the cerebrospinal fluid (CSF) of patients with acute COVID-19 and neurologic symptoms, but inflammatory cytokines can be present along with increased frequency of B cells. Anti–SARS-CoV-2 antibodies have also been found in CSF, some of which were auto reactive to brain tissue. The immune response was altered, compared with healthy controls, and in the CNS, compared with in the blood, “raising the question of whether inflammation and autoimmunity may be underlying causes of these syndromes,” said Dr. Spudich.
She also pointed to an MRI study of autopsied brain tissue of patients with COVID-19 and neurologic complications, which showed indications of both hemorrhagic and ischemic microvascular injury. “It’s just a reminder that, during acute COVID-19, there may be inflammation in the brain, there may be autoimmune reactions, and there may be vascular changes that underlie some of the neurologic syndromes that are seen,” said Dr. Spudich.
A panoply of different syndromes
In October, Yale set up a post-COVID neurologic clinic that brought together pulmonary, cardiology, and psychiatric specialists, many of whom saw the same patients, about 60% of whom had cognitive impairment, more than 40% had neuromuscular problems, and over 30% headache. “There’s not a single entity of a post-COVID neurologic syndrome. There’s a panoply of different syndromes that may have similar or distinct etiologies,” said Dr. Spudich.
Most patients were in their 30s, 40s, or 50s. That doesn’t necessarily mean this is the most common age range for these issues, though. There could be some bias if these individuals are seeking specialty care because they expected to recover from COVID-19 quickly. But it could be that there is something biologically unique among this age group that predisposes them to complications. Regardless, two out of three patients were never hospitalized, “suggesting that even mild COVID-19 can lead to some long-term sequelae,” said Dr. Spudich.
One potential explanation for long-term neurologic syndromes is that they are an extension of the inflammation, autoimmunity, and immune perturbation occurring during acute disease. One study looked at 18 cancer patients who had neurologic complications with COVID-19. Two months after onset, they had elevated markers of neuroinflammation and neuronal injury in the cerebral spinal fluid compared to cancer patients with no history of COVID-19.
Looking for biologic markers
An Italian study looked at patients who were evaluated during acute hospitalization and again 3 months later, and found that some markers of inflation in the blood were associated with later cognitive impairment. The patients were more severely ill, so it’s not clear what the findings mean for patients who present with neurologic symptoms after milder illness.
A PET scan study of 35 patients with persistent neurologic symptoms found patterns of reduced fluorodeoxyglucose uptake in some regions of the brain that are believed to be associated with some symptoms. Lower values were associated with greater severity for symptoms like memory dysfunction, and anosmia. “Why there might be hypometabolism in these regions I think needs to be assessed and used as a biomarker to associate hypometabolism with other kinds of processes in blood and spinal fluid,” said Dr. Spudich.
Along with colleagues at Yale, Dr. Spudich is conducting the MIND study, which is using PET and MRI imaging along with blood and CSF biomarkers to track the progress of patients after COVID-19. There are few results to discuss since only 20 patients have been recruited so far, except that brain imaging and blood values are generally normal despite neurologic complaints. Most were not hospitalized for COVID-19. Dr. Spudich highlighted one man in his 30s who developed new-onset psychosis, despite no previous history. Although clinical tests were all negative, a novel autoantibody detection method revealed a previously unknown autoreactive antibody in his spinal fluid. “This may suggest that there is autoantibody production in some individuals with post–COVID-19 psychosis, and potentially other syndromes,” said Dr. Spudich.
The research task ahead
The case illustrates the task ahead for neurology. “There’s a real research mandate to understand the biological substrates of these diverse disorders, not only to address the emergent public health concern and reduce the stigma in our patients, but to develop targeted therapeutic interventions,” said Dr. Spudich.
Anna Cervantes-Arslanian, MD, an associate professor of neurology at Boston University who also treats and studies patients with post-COVID neurologic symptoms, agreed with that assessment. “It’s not like every patient that has muscle aches and fatigue also has brain fog. It’s really hard to parse them out into specific phenotypes that are pretty classic. Some people will have all of those things, some will have very few of them,” said Dr. Cervantes-Arslanian. “We need to be able to identify them sand see if there is clustering of symptoms so we can better look into what the biological underpinnings are. That’s the first step to thinking about a therapeutic target.”
Dr. Spudich and Dr. Cervantes-Arslanian had no relevant financial disclosures.
Long-haul neurologic symptoms of COVID-19 seem to be distinct from neurologic conditions found in acute disease. Much work remains to be done to understand the biological mechanisms behind these problems, but inflammation and autoimmune responses may play a role in some cases.
Those were some of the takeaways from a talk by Serena Spudich, MD, who presented her research at the 2021 annual meeting of the American Academy of Neurology. Dr. Spudich is the division chief of neurologic infections and global neurology and codirector of the Center for Neuroepidemiology and Clinical Neurological Research at Yale University, New Haven, Conn.
Examining the nervous system’s involvement in COVID-19
Even early on in the pandemic, it became clear that there were lingering complaints of neuromuscular problems, cognitive dysfunction, and mood and psychiatric issues. Breathing and heart rate problems also can arise. “There seems to be a preponderance of syndromes that reflect involvement of the nervous system,” said Dr. Spudich.
To try to understand the etiology of these persistent problems, Dr. Spudich said it’s important to examine the nervous system’s involvement in acute COVID-19. She has been involved in these efforts since early in the pandemic, when she ran an inpatient consult service at Yale dedicated to neurologic effects of acute COVID-19. She witnessed complications including stroke, encephalopathy, and seizures, among others.
Stroke during acute COVID-19 seemed to be associated with inflammation and endothelial activation or endotheliopathy. SARS-CoV-2 has been undetectable in the cerebrospinal fluid (CSF) of patients with acute COVID-19 and neurologic symptoms, but inflammatory cytokines can be present along with increased frequency of B cells. Anti–SARS-CoV-2 antibodies have also been found in CSF, some of which were auto reactive to brain tissue. The immune response was altered, compared with healthy controls, and in the CNS, compared with in the blood, “raising the question of whether inflammation and autoimmunity may be underlying causes of these syndromes,” said Dr. Spudich.
She also pointed to an MRI study of autopsied brain tissue of patients with COVID-19 and neurologic complications, which showed indications of both hemorrhagic and ischemic microvascular injury. “It’s just a reminder that, during acute COVID-19, there may be inflammation in the brain, there may be autoimmune reactions, and there may be vascular changes that underlie some of the neurologic syndromes that are seen,” said Dr. Spudich.
A panoply of different syndromes
In October, Yale set up a post-COVID neurologic clinic that brought together pulmonary, cardiology, and psychiatric specialists, many of whom saw the same patients, about 60% of whom had cognitive impairment, more than 40% had neuromuscular problems, and over 30% headache. “There’s not a single entity of a post-COVID neurologic syndrome. There’s a panoply of different syndromes that may have similar or distinct etiologies,” said Dr. Spudich.
Most patients were in their 30s, 40s, or 50s. That doesn’t necessarily mean this is the most common age range for these issues, though. There could be some bias if these individuals are seeking specialty care because they expected to recover from COVID-19 quickly. But it could be that there is something biologically unique among this age group that predisposes them to complications. Regardless, two out of three patients were never hospitalized, “suggesting that even mild COVID-19 can lead to some long-term sequelae,” said Dr. Spudich.
One potential explanation for long-term neurologic syndromes is that they are an extension of the inflammation, autoimmunity, and immune perturbation occurring during acute disease. One study looked at 18 cancer patients who had neurologic complications with COVID-19. Two months after onset, they had elevated markers of neuroinflammation and neuronal injury in the cerebral spinal fluid compared to cancer patients with no history of COVID-19.
Looking for biologic markers
An Italian study looked at patients who were evaluated during acute hospitalization and again 3 months later, and found that some markers of inflation in the blood were associated with later cognitive impairment. The patients were more severely ill, so it’s not clear what the findings mean for patients who present with neurologic symptoms after milder illness.
A PET scan study of 35 patients with persistent neurologic symptoms found patterns of reduced fluorodeoxyglucose uptake in some regions of the brain that are believed to be associated with some symptoms. Lower values were associated with greater severity for symptoms like memory dysfunction, and anosmia. “Why there might be hypometabolism in these regions I think needs to be assessed and used as a biomarker to associate hypometabolism with other kinds of processes in blood and spinal fluid,” said Dr. Spudich.
Along with colleagues at Yale, Dr. Spudich is conducting the MIND study, which is using PET and MRI imaging along with blood and CSF biomarkers to track the progress of patients after COVID-19. There are few results to discuss since only 20 patients have been recruited so far, except that brain imaging and blood values are generally normal despite neurologic complaints. Most were not hospitalized for COVID-19. Dr. Spudich highlighted one man in his 30s who developed new-onset psychosis, despite no previous history. Although clinical tests were all negative, a novel autoantibody detection method revealed a previously unknown autoreactive antibody in his spinal fluid. “This may suggest that there is autoantibody production in some individuals with post–COVID-19 psychosis, and potentially other syndromes,” said Dr. Spudich.
The research task ahead
The case illustrates the task ahead for neurology. “There’s a real research mandate to understand the biological substrates of these diverse disorders, not only to address the emergent public health concern and reduce the stigma in our patients, but to develop targeted therapeutic interventions,” said Dr. Spudich.
Anna Cervantes-Arslanian, MD, an associate professor of neurology at Boston University who also treats and studies patients with post-COVID neurologic symptoms, agreed with that assessment. “It’s not like every patient that has muscle aches and fatigue also has brain fog. It’s really hard to parse them out into specific phenotypes that are pretty classic. Some people will have all of those things, some will have very few of them,” said Dr. Cervantes-Arslanian. “We need to be able to identify them sand see if there is clustering of symptoms so we can better look into what the biological underpinnings are. That’s the first step to thinking about a therapeutic target.”
Dr. Spudich and Dr. Cervantes-Arslanian had no relevant financial disclosures.
FROM AAN 2021
Most patients with chronic inflammatory diseases have sufficient response to COVID-19 vaccination
Glucocorticoids and B-cell–depleting therapies are trouble spots
Although most patients with chronic inflammatory diseases mounted immune responses after two doses of mRNA-based COVID-19 vaccines, glucocorticoids and B-cell–depleting therapies markedly reduced the response, according to a recently published preprint of a new study.

The study, published on MedRxiv and not yet peer reviewed, involved a prospective look at 133 patients with chronic inflammatory disease (CID) and 53 patients with healthy immune systems at Washington University, St. Louis, and the University of California, San Francisco. It is regarded as the largest and most detailed study yet in how vaccines perform in people with immune-mediated inflammatory disease. The patients were enrolled between December 2020 and March 2021, and the most common diseases were inflammatory bowel disease (32%), rheumatoid arthritis (29%), spondyloarthritis (15%), and systemic lupus erythematosus (11%).
A ‘modest’ reduction in antibody response
Senior author Alfred Kim, MD, PhD, of the department of medicine at Washington University, said the overall results so far are encouraging.
“Most patients with an autoimmune disease that are on immunosuppression can mount antibody responses,” he said. “We’re seeing the majority of our subjects respond.”

The immune-healthy controls and most of the patients with CID had a robust immune response against the spike protein, although the CID group had a mean reduction in antibody titers that was three times lower than the controls (P = .0092). The CID group similarly had a 2.7-fold reduction in preventing neutralization, or halting the virus’ ability to infect (P < .0001), researchers reported.
This reduction in response is “modest,” he said.
“Is the level of reduction going to be detrimental for protection? Time will tell,” he said, adding that researchers anticipate that it won’t have a critical effect on protection because responses tended to be within the range of the immunocompetent controls, who themselves had wildly varied antibody titers across a 20-fold range. “ ‘Optimal’ isn’t necessarily the same as ‘sufficient.’ ”
Type of medication has big impact on antibody titers
But there was a wide variety of effects on the immune response depending on the medication. Glucorticoids resulted in a response that was 10 times lower than the immune-healthy controls, as well as fewer circulating plasmablasts after vaccination. Researchers found that 98% of controls were seropositive for antibody, compared with 92% of those with CID who were not taking prednisone, and 65% of CID patients on prednisone (P = .0006 and .0115, respectively). Prevention of neutralization of the virus was similarly reduced in those groups, compared with the controls. Dr. Kim noted this was a small sample size, with about 15 patients. These effects were seen regardless of the dose.
“We would’ve anticipated this would have been dose dependent, so this was a little bit surprising,” Dr. Kim said.
B-cell–depleting therapies, such as rituximab (Rituxan) and ocrelizumab (Ocrevus), reduced antibody titers by 36 times, compared with controls (P < .0001), with a similar reduction in preventing infection (P = .0066), the researchers found. The reduction in antibody titers was the most pronounced among those who had received B-cell–depleting therapies within the previous 6 months. Dr. Kim noted this was a small sample size, with about 10 patients.
CID study subjects taking an antimetabolite, including methotrexate, had an average of a two- to threefold reduction in antibody titers and in neutralization (P = .0006). This reduction was greatest with methotrexate, researchers found (P = .0027).
JAK inhibitors also significantly reduced antibody titers (P = .0066), but the reduction in neutralization of the virus was not significant. In addition, researchers found a reduction in antibody titers, the prevention of viral infection, and circulating plasmablasts among those on tumor necrosis factor (TNF) inhibitors, compared with controls, but these were insignificant statistically except for virus neutralization.
Dr. Kim said he hopes the glucocorticoid data spur physicians to try harder to wean patients off the drugs, when possible, in keeping with recommendations already in place.
“The general culture in rheumatology has been very lax about the need to reduce glucocorticoids,” he said. “This reinvigorates that call.” Questions about possible drug holidays from glucocorticoids remain, regarding how long a holiday would be needed, he said. He noted that many patients on glucocorticoids nonetheless mounted responses.
Those on B-cell–depleting therapies present a “much more difficult” question, he said. Some patients possibly could wait a bit longer than their normal, every-6-month schedule, but it’s an individual decision, he said. Since a booster of influenza vaccine has been found to enhance the response even within the 6-month window among ocrelizumab patients, a booster of COVID-19 vaccine might also help, although this remains to be studied.
The study group has already increased its sample size and is looking at adverse reactions and long-term immune responses, Dr. Kim said.
Encouraging, rather than discouraging, results
Leonard Calabrese, DO, professor of medicine at the Cleveland Clinic in Ohio, said the findings shouldn’t discourage clinicians from encouraging vaccination.

“There’s still a preponderance of people who will develop a robust antibody vaccine response,” he said.
He cautioned that the findings look only at antibodies to the spike protein and at plasmablasts. The reduction in these titers is “of concern,” he said, but “we don’t really know with certainty what are the effects of these drugs, and these data are on the overall biologic protective effect of the vaccine. There’s much more to a vaccine response than anti–spike protein and plasmablasts,” including cell-mediated immune response.
For an individual patient, the findings “mean a lot,” he said.
“I think that people who are on significant prednisone and B-cell–depleting agents, I think you have to share with them that there’s a reasonable chance that you’re not going to be making a response similar to healthy people,” he said. “Thus, even with your vaccine, we’re not going to cut you loose to do things that are violating social distancing and group settings. … Should you be hugging your grandchildren if you’re a rituximab vaccine recipient? I think I would wait until we have a little bit more data.”
Kevin Winthrop, MD, MPH, professor of ophthalmology at Oregon Health & Science University, Portland, where he studies vaccinations in the immunocompromised, said that glucocorticoids tend to have little effect on vaccinations generally at low doses.

When effects are seen they can be difficult to interpret, he said.
“It’s hard to extricate that from the effect of the underlying disease,” he said. The drug can be a proxy for worse disease control.
Although it’s a small study, it’s reassuring that overall the responses were similar to healthy controls.
For B-cell–depleting therapies, his usual guidance is to not give vaccine until a patient is at least 3 months out from their last dose, and not to restart until at least 2 weeks after vaccination.
“It’s not surprising that some of these DMARDs [disease-modifying antirheumatic drugs] do negatively affect vaccine response, particularly B-cell–depletion therapy. We need to do some studies to find a way to overcome that, or optimize delivery of the vaccine.”
Dr. Kim reported participating in consulting, advisory board, or speaker’s bureau for Alexion, Aurinia, Annexon Biosciences, Exagen Diagnostics, and GlaxoSmithKline, and receiving funding under a sponsored research agreement unrelated to the data in the paper from GlaxoSmithKline. Dr. Winthrop reported receiving consulting fees from Pfizer, AbbVie, UCB, Eli Lilly, Galapagos, GlaxoSmithKline, Roche, Gilead, Bristol-Myers Squibb, Regeneron, Sanofi, AstraZeneca, Novartis, and research grants from Bristol-Myers Squibb and Pfizer. Dr. Calabrese reported no relevant disclosures.
Glucocorticoids and B-cell–depleting therapies are trouble spots
Glucocorticoids and B-cell–depleting therapies are trouble spots
Although most patients with chronic inflammatory diseases mounted immune responses after two doses of mRNA-based COVID-19 vaccines, glucocorticoids and B-cell–depleting therapies markedly reduced the response, according to a recently published preprint of a new study.
The study, published on MedRxiv and not yet peer reviewed, involved a prospective look at 133 patients with chronic inflammatory disease (CID) and 53 patients with healthy immune systems at Washington University, St. Louis, and the University of California, San Francisco. It is regarded as the largest and most detailed study yet in how vaccines perform in people with immune-mediated inflammatory disease. The patients were enrolled between December 2020 and March 2021, and the most common diseases were inflammatory bowel disease (32%), rheumatoid arthritis (29%), spondyloarthritis (15%), and systemic lupus erythematosus (11%).
A ‘modest’ reduction in antibody response
Senior author Alfred Kim, MD, PhD, of the department of medicine at Washington University, said the overall results so far are encouraging.
“Most patients with an autoimmune disease that are on immunosuppression can mount antibody responses,” he said. “We’re seeing the majority of our subjects respond.”
The immune-healthy controls and most of the patients with CID had a robust immune response against the spike protein, although the CID group had a mean reduction in antibody titers that was three times lower than the controls (P = .0092). The CID group similarly had a 2.7-fold reduction in preventing neutralization, or halting the virus’ ability to infect (P < .0001), researchers reported.
This reduction in response is “modest,” he said.
“Is the level of reduction going to be detrimental for protection? Time will tell,” he said, adding that researchers anticipate that it won’t have a critical effect on protection because responses tended to be within the range of the immunocompetent controls, who themselves had wildly varied antibody titers across a 20-fold range. “ ‘Optimal’ isn’t necessarily the same as ‘sufficient.’ ”
Type of medication has big impact on antibody titers
But there was a wide variety of effects on the immune response depending on the medication. Glucorticoids resulted in a response that was 10 times lower than the immune-healthy controls, as well as fewer circulating plasmablasts after vaccination. Researchers found that 98% of controls were seropositive for antibody, compared with 92% of those with CID who were not taking prednisone, and 65% of CID patients on prednisone (P = .0006 and .0115, respectively). Prevention of neutralization of the virus was similarly reduced in those groups, compared with the controls. Dr. Kim noted this was a small sample size, with about 15 patients. These effects were seen regardless of the dose.
“We would’ve anticipated this would have been dose dependent, so this was a little bit surprising,” Dr. Kim said.
B-cell–depleting therapies, such as rituximab (Rituxan) and ocrelizumab (Ocrevus), reduced antibody titers by 36 times, compared with controls (P < .0001), with a similar reduction in preventing infection (P = .0066), the researchers found. The reduction in antibody titers was the most pronounced among those who had received B-cell–depleting therapies within the previous 6 months. Dr. Kim noted this was a small sample size, with about 10 patients.
CID study subjects taking an antimetabolite, including methotrexate, had an average of a two- to threefold reduction in antibody titers and in neutralization (P = .0006). This reduction was greatest with methotrexate, researchers found (P = .0027).
JAK inhibitors also significantly reduced antibody titers (P = .0066), but the reduction in neutralization of the virus was not significant. In addition, researchers found a reduction in antibody titers, the prevention of viral infection, and circulating plasmablasts among those on tumor necrosis factor (TNF) inhibitors, compared with controls, but these were insignificant statistically except for virus neutralization.
Dr. Kim said he hopes the glucocorticoid data spur physicians to try harder to wean patients off the drugs, when possible, in keeping with recommendations already in place.
“The general culture in rheumatology has been very lax about the need to reduce glucocorticoids,” he said. “This reinvigorates that call.” Questions about possible drug holidays from glucocorticoids remain, regarding how long a holiday would be needed, he said. He noted that many patients on glucocorticoids nonetheless mounted responses.
Those on B-cell–depleting therapies present a “much more difficult” question, he said. Some patients possibly could wait a bit longer than their normal, every-6-month schedule, but it’s an individual decision, he said. Since a booster of influenza vaccine has been found to enhance the response even within the 6-month window among ocrelizumab patients, a booster of COVID-19 vaccine might also help, although this remains to be studied.
The study group has already increased its sample size and is looking at adverse reactions and long-term immune responses, Dr. Kim said.
Encouraging, rather than discouraging, results
Leonard Calabrese, DO, professor of medicine at the Cleveland Clinic in Ohio, said the findings shouldn’t discourage clinicians from encouraging vaccination.
“There’s still a preponderance of people who will develop a robust antibody vaccine response,” he said.
He cautioned that the findings look only at antibodies to the spike protein and at plasmablasts. The reduction in these titers is “of concern,” he said, but “we don’t really know with certainty what are the effects of these drugs, and these data are on the overall biologic protective effect of the vaccine. There’s much more to a vaccine response than anti–spike protein and plasmablasts,” including cell-mediated immune response.
For an individual patient, the findings “mean a lot,” he said.
“I think that people who are on significant prednisone and B-cell–depleting agents, I think you have to share with them that there’s a reasonable chance that you’re not going to be making a response similar to healthy people,” he said. “Thus, even with your vaccine, we’re not going to cut you loose to do things that are violating social distancing and group settings. … Should you be hugging your grandchildren if you’re a rituximab vaccine recipient? I think I would wait until we have a little bit more data.”
Kevin Winthrop, MD, MPH, professor of ophthalmology at Oregon Health & Science University, Portland, where he studies vaccinations in the immunocompromised, said that glucocorticoids tend to have little effect on vaccinations generally at low doses.
When effects are seen they can be difficult to interpret, he said.
“It’s hard to extricate that from the effect of the underlying disease,” he said. The drug can be a proxy for worse disease control.
Although it’s a small study, it’s reassuring that overall the responses were similar to healthy controls.
For B-cell–depleting therapies, his usual guidance is to not give vaccine until a patient is at least 3 months out from their last dose, and not to restart until at least 2 weeks after vaccination.
“It’s not surprising that some of these DMARDs [disease-modifying antirheumatic drugs] do negatively affect vaccine response, particularly B-cell–depletion therapy. We need to do some studies to find a way to overcome that, or optimize delivery of the vaccine.”
Dr. Kim reported participating in consulting, advisory board, or speaker’s bureau for Alexion, Aurinia, Annexon Biosciences, Exagen Diagnostics, and GlaxoSmithKline, and receiving funding under a sponsored research agreement unrelated to the data in the paper from GlaxoSmithKline. Dr. Winthrop reported receiving consulting fees from Pfizer, AbbVie, UCB, Eli Lilly, Galapagos, GlaxoSmithKline, Roche, Gilead, Bristol-Myers Squibb, Regeneron, Sanofi, AstraZeneca, Novartis, and research grants from Bristol-Myers Squibb and Pfizer. Dr. Calabrese reported no relevant disclosures.
Although most patients with chronic inflammatory diseases mounted immune responses after two doses of mRNA-based COVID-19 vaccines, glucocorticoids and B-cell–depleting therapies markedly reduced the response, according to a recently published preprint of a new study.
The study, published on MedRxiv and not yet peer reviewed, involved a prospective look at 133 patients with chronic inflammatory disease (CID) and 53 patients with healthy immune systems at Washington University, St. Louis, and the University of California, San Francisco. It is regarded as the largest and most detailed study yet in how vaccines perform in people with immune-mediated inflammatory disease. The patients were enrolled between December 2020 and March 2021, and the most common diseases were inflammatory bowel disease (32%), rheumatoid arthritis (29%), spondyloarthritis (15%), and systemic lupus erythematosus (11%).
A ‘modest’ reduction in antibody response
Senior author Alfred Kim, MD, PhD, of the department of medicine at Washington University, said the overall results so far are encouraging.
“Most patients with an autoimmune disease that are on immunosuppression can mount antibody responses,” he said. “We’re seeing the majority of our subjects respond.”
The immune-healthy controls and most of the patients with CID had a robust immune response against the spike protein, although the CID group had a mean reduction in antibody titers that was three times lower than the controls (P = .0092). The CID group similarly had a 2.7-fold reduction in preventing neutralization, or halting the virus’ ability to infect (P < .0001), researchers reported.
This reduction in response is “modest,” he said.
“Is the level of reduction going to be detrimental for protection? Time will tell,” he said, adding that researchers anticipate that it won’t have a critical effect on protection because responses tended to be within the range of the immunocompetent controls, who themselves had wildly varied antibody titers across a 20-fold range. “ ‘Optimal’ isn’t necessarily the same as ‘sufficient.’ ”
Type of medication has big impact on antibody titers
But there was a wide variety of effects on the immune response depending on the medication. Glucorticoids resulted in a response that was 10 times lower than the immune-healthy controls, as well as fewer circulating plasmablasts after vaccination. Researchers found that 98% of controls were seropositive for antibody, compared with 92% of those with CID who were not taking prednisone, and 65% of CID patients on prednisone (P = .0006 and .0115, respectively). Prevention of neutralization of the virus was similarly reduced in those groups, compared with the controls. Dr. Kim noted this was a small sample size, with about 15 patients. These effects were seen regardless of the dose.
“We would’ve anticipated this would have been dose dependent, so this was a little bit surprising,” Dr. Kim said.
B-cell–depleting therapies, such as rituximab (Rituxan) and ocrelizumab (Ocrevus), reduced antibody titers by 36 times, compared with controls (P < .0001), with a similar reduction in preventing infection (P = .0066), the researchers found. The reduction in antibody titers was the most pronounced among those who had received B-cell–depleting therapies within the previous 6 months. Dr. Kim noted this was a small sample size, with about 10 patients.
CID study subjects taking an antimetabolite, including methotrexate, had an average of a two- to threefold reduction in antibody titers and in neutralization (P = .0006). This reduction was greatest with methotrexate, researchers found (P = .0027).
JAK inhibitors also significantly reduced antibody titers (P = .0066), but the reduction in neutralization of the virus was not significant. In addition, researchers found a reduction in antibody titers, the prevention of viral infection, and circulating plasmablasts among those on tumor necrosis factor (TNF) inhibitors, compared with controls, but these were insignificant statistically except for virus neutralization.
Dr. Kim said he hopes the glucocorticoid data spur physicians to try harder to wean patients off the drugs, when possible, in keeping with recommendations already in place.
“The general culture in rheumatology has been very lax about the need to reduce glucocorticoids,” he said. “This reinvigorates that call.” Questions about possible drug holidays from glucocorticoids remain, regarding how long a holiday would be needed, he said. He noted that many patients on glucocorticoids nonetheless mounted responses.
Those on B-cell–depleting therapies present a “much more difficult” question, he said. Some patients possibly could wait a bit longer than their normal, every-6-month schedule, but it’s an individual decision, he said. Since a booster of influenza vaccine has been found to enhance the response even within the 6-month window among ocrelizumab patients, a booster of COVID-19 vaccine might also help, although this remains to be studied.
The study group has already increased its sample size and is looking at adverse reactions and long-term immune responses, Dr. Kim said.
Encouraging, rather than discouraging, results
Leonard Calabrese, DO, professor of medicine at the Cleveland Clinic in Ohio, said the findings shouldn’t discourage clinicians from encouraging vaccination.
“There’s still a preponderance of people who will develop a robust antibody vaccine response,” he said.
He cautioned that the findings look only at antibodies to the spike protein and at plasmablasts. The reduction in these titers is “of concern,” he said, but “we don’t really know with certainty what are the effects of these drugs, and these data are on the overall biologic protective effect of the vaccine. There’s much more to a vaccine response than anti–spike protein and plasmablasts,” including cell-mediated immune response.
For an individual patient, the findings “mean a lot,” he said.
“I think that people who are on significant prednisone and B-cell–depleting agents, I think you have to share with them that there’s a reasonable chance that you’re not going to be making a response similar to healthy people,” he said. “Thus, even with your vaccine, we’re not going to cut you loose to do things that are violating social distancing and group settings. … Should you be hugging your grandchildren if you’re a rituximab vaccine recipient? I think I would wait until we have a little bit more data.”
Kevin Winthrop, MD, MPH, professor of ophthalmology at Oregon Health & Science University, Portland, where he studies vaccinations in the immunocompromised, said that glucocorticoids tend to have little effect on vaccinations generally at low doses.
When effects are seen they can be difficult to interpret, he said.
“It’s hard to extricate that from the effect of the underlying disease,” he said. The drug can be a proxy for worse disease control.
Although it’s a small study, it’s reassuring that overall the responses were similar to healthy controls.
For B-cell–depleting therapies, his usual guidance is to not give vaccine until a patient is at least 3 months out from their last dose, and not to restart until at least 2 weeks after vaccination.
“It’s not surprising that some of these DMARDs [disease-modifying antirheumatic drugs] do negatively affect vaccine response, particularly B-cell–depletion therapy. We need to do some studies to find a way to overcome that, or optimize delivery of the vaccine.”
Dr. Kim reported participating in consulting, advisory board, or speaker’s bureau for Alexion, Aurinia, Annexon Biosciences, Exagen Diagnostics, and GlaxoSmithKline, and receiving funding under a sponsored research agreement unrelated to the data in the paper from GlaxoSmithKline. Dr. Winthrop reported receiving consulting fees from Pfizer, AbbVie, UCB, Eli Lilly, Galapagos, GlaxoSmithKline, Roche, Gilead, Bristol-Myers Squibb, Regeneron, Sanofi, AstraZeneca, Novartis, and research grants from Bristol-Myers Squibb and Pfizer. Dr. Calabrese reported no relevant disclosures.
FROM MEDRXIV
Stroke is ‘not a common complication’ in COVID-19
One study showed a stroke rate of 2.2% among patients with COVID-19 admitted to intensive care in 52 different countries. Another found a stroke rate of 1.48% in patients hospitalized with COVID-19 from 70 different countries. These researchers also found a reduction in stroke presentations and stroke care during the pandemic.
Both studies will be presented at the American Academy of Neurology’s 2021 annual meeting.
“Stroke has been a known serious complication of COVID-19, with some studies reporting a higher-than-expected occurrence, especially in young people,” said coauthor of the intensive care study, Jonathon Fanning, MBBS, PhD, University of Queensland, Brisbane, Australia.
“However, among the sickest of COVID patients – those admitted to an ICU – our research found that stroke was not a common complication and that ischemic stroke did not increase the risk of death,” he added.
Hemorrhagic stroke more common?
In this study, researchers analyzed a database of 2,699 patients who were admitted to the intensive care unit with COVID-19 in 52 countries and found that 59 of these patients (2.2%) subsequently sustained a stroke.
Most of the strokes identified in this cohort were hemorrhagic (46%), with 32% being ischemic and 22% unspecified. Hemorrhagic stroke was associated with a fivefold increased risk for death compared with patients who did not have a stroke. Of those with a hemorrhagic stroke, 72% died, but only 15% died of the stroke. Rather, multiorgan failure was the leading cause of death.
There was no association between ischemic stroke and mortality.
“There is scarce research on new-onset stroke complicating ICU admissions, and many of the limitations of assessing stroke in ICU populations confound the true values and result in variability in reported incidence anywhere from a 1%-4% incidence,” Dr. Fanning said.
He noted that a large Korean study had shown a 1.2% rate of stroke in patients without COVID admitted to non-neurologic ICUs. “In light of this, I think this 2% is higher than we would expect in a general ICU population, but in the context of earlier reports of COVID-19–associated risk for stroke, this figure is actually somewhat reassuring,” Dr. Fanning said.
Asked how this study compared with the large American Heart Association study recently reported that showed an overall rate of ischemic stroke of 0.75%, Dr. Fanning said the two studies reported on different populations, which makes them difficult to compare.
“Our study specifically reports on new-onset stroke complicating ICU admission,” he noted. “The AHA study is a large study of all patients admitted to hospital, but both studies identified less than previous estimates of COVID-related stroke.”
Largest sample to date
The other study, which includes 119,967 COVID-19 hospitalizations and represents the largest sample reporting the concomitant diagnoses of stroke and SARS-CoV-2 infection to date, was presented at the AAN meeting by Thanh N. Nguyen, MD, a professor at Boston University.
This study has also been published online in Neurology, with first author Raul G. Nogueira, MD, Emory University, Atlanta.
In this international observational, retrospective study across 6 continents, 70 countries, and 457 stroke centers, there was a 1.48% stroke rate across 119,967 COVID-19 hospitalizations. SARS-CoV-2 infection was noted in 3.3% (1,722) of all stroke admissions, which numbered 52,026.
The researchers identified stroke diagnoses by the International Classification of Diseases, 10th revision, codes and/or classifications in stroke center databases, and rates of stroke hospitalizations and numbers of patients receiving thrombolysis were compared between the first 4 months of the pandemic (March to June 2020) compared with two control 4-month periods.
Global decline in stroke care during pandemic
Results showed a global decline in the number of stroke patients admitted to the hospital as well as acute stroke treatments, such as thrombolysis, during the first wave of the COVID-19 pandemic. The researchers found that there were 91,373 stroke admissions in the 4 months immediately before the pandemic, compared with 80,894 admissions during the first 4 pandemic months, representing an 11.5% decline.
They also report that 13,334 stroke patients received intravenous thrombolysis in the 4 months preceding the pandemic, compared with 11,570 during the first 4 pandemic months, representing a 13.2% drop.
Interhospital transfers after thrombolysis for a higher level of stroke care decreased from 1,337 before the pandemic to 1,178 during the pandemic, a reduction of 11.9%.
There were greater declines in primary compared with comprehensive stroke centers for stroke hospitalizations (change, –17.3% vs. –10.3%) and for the number of patients receiving thrombolysis (change, –15.5% vs. –12.6%).
The volume of stroke hospitalizations increased by 9.5% in the two later pandemic months (May, June) versus the two earlier months (March, April), with greater recovery in hospitals with lower COVID-19 hospitalization volume, high-volume stroke centers, and comprehensive stroke centers.
Dr. Nguyen suggested that reasons for the reductions in these stroke numbers at the beginning of the pandemic could include a reduction in stroke risk due to a reduction of exposure to other viral infections or patients not presenting to the hospital for fear of contracting the coronavirus.
The higher recovery of stroke volume in high-volume stroke centers and comprehensive stroke centers may represent patients with higher needs – those having more severe strokes – seeking care more frequently than those with milder symptoms, she noted.
“Preserving access to stroke care and emergency stroke care amidst a pandemic is as important as educating patients on the importance of presenting to the hospital in the event of stroke-like symptoms,” Dr. Nguyen concluded.
“We continue to advocate that if a patient has stroke-like symptoms, such as loss of speech, strength, vision, or balance, it is important for the patient to seek medical care as an emergency, as there are treatments that can improve a patient’s ability to recover from disabling stroke in earlier rather than later time windows,” she added.
In the publication, the authors wrote, “Our results concur with other recent reports on the collateral effects of the COVID-19 pandemic on stroke systems of care,” but added that “this is among the first descriptions of the change at a global level, including primary and comprehensive stroke centers.”
They said that hospital access related to high COVID-19 burden was unlikely a factor because the decline was seen in centers with a few or no patients with COVID-19. They suggested that patient fear of contracting coronavirus may have played a role, along with a decrease in presentation of transient ischemic attacks, mild strokes, or moderate strokes, and physical distancing measures may have prevented the timely witnessing of a stroke.
A version of this article first appeared on Medscape.com.
One study showed a stroke rate of 2.2% among patients with COVID-19 admitted to intensive care in 52 different countries. Another found a stroke rate of 1.48% in patients hospitalized with COVID-19 from 70 different countries. These researchers also found a reduction in stroke presentations and stroke care during the pandemic.
Both studies will be presented at the American Academy of Neurology’s 2021 annual meeting.
“Stroke has been a known serious complication of COVID-19, with some studies reporting a higher-than-expected occurrence, especially in young people,” said coauthor of the intensive care study, Jonathon Fanning, MBBS, PhD, University of Queensland, Brisbane, Australia.
“However, among the sickest of COVID patients – those admitted to an ICU – our research found that stroke was not a common complication and that ischemic stroke did not increase the risk of death,” he added.
Hemorrhagic stroke more common?
In this study, researchers analyzed a database of 2,699 patients who were admitted to the intensive care unit with COVID-19 in 52 countries and found that 59 of these patients (2.2%) subsequently sustained a stroke.
Most of the strokes identified in this cohort were hemorrhagic (46%), with 32% being ischemic and 22% unspecified. Hemorrhagic stroke was associated with a fivefold increased risk for death compared with patients who did not have a stroke. Of those with a hemorrhagic stroke, 72% died, but only 15% died of the stroke. Rather, multiorgan failure was the leading cause of death.
There was no association between ischemic stroke and mortality.
“There is scarce research on new-onset stroke complicating ICU admissions, and many of the limitations of assessing stroke in ICU populations confound the true values and result in variability in reported incidence anywhere from a 1%-4% incidence,” Dr. Fanning said.
He noted that a large Korean study had shown a 1.2% rate of stroke in patients without COVID admitted to non-neurologic ICUs. “In light of this, I think this 2% is higher than we would expect in a general ICU population, but in the context of earlier reports of COVID-19–associated risk for stroke, this figure is actually somewhat reassuring,” Dr. Fanning said.
Asked how this study compared with the large American Heart Association study recently reported that showed an overall rate of ischemic stroke of 0.75%, Dr. Fanning said the two studies reported on different populations, which makes them difficult to compare.
“Our study specifically reports on new-onset stroke complicating ICU admission,” he noted. “The AHA study is a large study of all patients admitted to hospital, but both studies identified less than previous estimates of COVID-related stroke.”
Largest sample to date
The other study, which includes 119,967 COVID-19 hospitalizations and represents the largest sample reporting the concomitant diagnoses of stroke and SARS-CoV-2 infection to date, was presented at the AAN meeting by Thanh N. Nguyen, MD, a professor at Boston University.
This study has also been published online in Neurology, with first author Raul G. Nogueira, MD, Emory University, Atlanta.
In this international observational, retrospective study across 6 continents, 70 countries, and 457 stroke centers, there was a 1.48% stroke rate across 119,967 COVID-19 hospitalizations. SARS-CoV-2 infection was noted in 3.3% (1,722) of all stroke admissions, which numbered 52,026.
The researchers identified stroke diagnoses by the International Classification of Diseases, 10th revision, codes and/or classifications in stroke center databases, and rates of stroke hospitalizations and numbers of patients receiving thrombolysis were compared between the first 4 months of the pandemic (March to June 2020) compared with two control 4-month periods.
Global decline in stroke care during pandemic
Results showed a global decline in the number of stroke patients admitted to the hospital as well as acute stroke treatments, such as thrombolysis, during the first wave of the COVID-19 pandemic. The researchers found that there were 91,373 stroke admissions in the 4 months immediately before the pandemic, compared with 80,894 admissions during the first 4 pandemic months, representing an 11.5% decline.
They also report that 13,334 stroke patients received intravenous thrombolysis in the 4 months preceding the pandemic, compared with 11,570 during the first 4 pandemic months, representing a 13.2% drop.
Interhospital transfers after thrombolysis for a higher level of stroke care decreased from 1,337 before the pandemic to 1,178 during the pandemic, a reduction of 11.9%.
There were greater declines in primary compared with comprehensive stroke centers for stroke hospitalizations (change, –17.3% vs. –10.3%) and for the number of patients receiving thrombolysis (change, –15.5% vs. –12.6%).
The volume of stroke hospitalizations increased by 9.5% in the two later pandemic months (May, June) versus the two earlier months (March, April), with greater recovery in hospitals with lower COVID-19 hospitalization volume, high-volume stroke centers, and comprehensive stroke centers.
Dr. Nguyen suggested that reasons for the reductions in these stroke numbers at the beginning of the pandemic could include a reduction in stroke risk due to a reduction of exposure to other viral infections or patients not presenting to the hospital for fear of contracting the coronavirus.
The higher recovery of stroke volume in high-volume stroke centers and comprehensive stroke centers may represent patients with higher needs – those having more severe strokes – seeking care more frequently than those with milder symptoms, she noted.
“Preserving access to stroke care and emergency stroke care amidst a pandemic is as important as educating patients on the importance of presenting to the hospital in the event of stroke-like symptoms,” Dr. Nguyen concluded.
“We continue to advocate that if a patient has stroke-like symptoms, such as loss of speech, strength, vision, or balance, it is important for the patient to seek medical care as an emergency, as there are treatments that can improve a patient’s ability to recover from disabling stroke in earlier rather than later time windows,” she added.
In the publication, the authors wrote, “Our results concur with other recent reports on the collateral effects of the COVID-19 pandemic on stroke systems of care,” but added that “this is among the first descriptions of the change at a global level, including primary and comprehensive stroke centers.”
They said that hospital access related to high COVID-19 burden was unlikely a factor because the decline was seen in centers with a few or no patients with COVID-19. They suggested that patient fear of contracting coronavirus may have played a role, along with a decrease in presentation of transient ischemic attacks, mild strokes, or moderate strokes, and physical distancing measures may have prevented the timely witnessing of a stroke.
A version of this article first appeared on Medscape.com.
One study showed a stroke rate of 2.2% among patients with COVID-19 admitted to intensive care in 52 different countries. Another found a stroke rate of 1.48% in patients hospitalized with COVID-19 from 70 different countries. These researchers also found a reduction in stroke presentations and stroke care during the pandemic.
Both studies will be presented at the American Academy of Neurology’s 2021 annual meeting.
“Stroke has been a known serious complication of COVID-19, with some studies reporting a higher-than-expected occurrence, especially in young people,” said coauthor of the intensive care study, Jonathon Fanning, MBBS, PhD, University of Queensland, Brisbane, Australia.
“However, among the sickest of COVID patients – those admitted to an ICU – our research found that stroke was not a common complication and that ischemic stroke did not increase the risk of death,” he added.
Hemorrhagic stroke more common?
In this study, researchers analyzed a database of 2,699 patients who were admitted to the intensive care unit with COVID-19 in 52 countries and found that 59 of these patients (2.2%) subsequently sustained a stroke.
Most of the strokes identified in this cohort were hemorrhagic (46%), with 32% being ischemic and 22% unspecified. Hemorrhagic stroke was associated with a fivefold increased risk for death compared with patients who did not have a stroke. Of those with a hemorrhagic stroke, 72% died, but only 15% died of the stroke. Rather, multiorgan failure was the leading cause of death.
There was no association between ischemic stroke and mortality.
“There is scarce research on new-onset stroke complicating ICU admissions, and many of the limitations of assessing stroke in ICU populations confound the true values and result in variability in reported incidence anywhere from a 1%-4% incidence,” Dr. Fanning said.
He noted that a large Korean study had shown a 1.2% rate of stroke in patients without COVID admitted to non-neurologic ICUs. “In light of this, I think this 2% is higher than we would expect in a general ICU population, but in the context of earlier reports of COVID-19–associated risk for stroke, this figure is actually somewhat reassuring,” Dr. Fanning said.
Asked how this study compared with the large American Heart Association study recently reported that showed an overall rate of ischemic stroke of 0.75%, Dr. Fanning said the two studies reported on different populations, which makes them difficult to compare.
“Our study specifically reports on new-onset stroke complicating ICU admission,” he noted. “The AHA study is a large study of all patients admitted to hospital, but both studies identified less than previous estimates of COVID-related stroke.”
Largest sample to date
The other study, which includes 119,967 COVID-19 hospitalizations and represents the largest sample reporting the concomitant diagnoses of stroke and SARS-CoV-2 infection to date, was presented at the AAN meeting by Thanh N. Nguyen, MD, a professor at Boston University.
This study has also been published online in Neurology, with first author Raul G. Nogueira, MD, Emory University, Atlanta.
In this international observational, retrospective study across 6 continents, 70 countries, and 457 stroke centers, there was a 1.48% stroke rate across 119,967 COVID-19 hospitalizations. SARS-CoV-2 infection was noted in 3.3% (1,722) of all stroke admissions, which numbered 52,026.
The researchers identified stroke diagnoses by the International Classification of Diseases, 10th revision, codes and/or classifications in stroke center databases, and rates of stroke hospitalizations and numbers of patients receiving thrombolysis were compared between the first 4 months of the pandemic (March to June 2020) compared with two control 4-month periods.
Global decline in stroke care during pandemic
Results showed a global decline in the number of stroke patients admitted to the hospital as well as acute stroke treatments, such as thrombolysis, during the first wave of the COVID-19 pandemic. The researchers found that there were 91,373 stroke admissions in the 4 months immediately before the pandemic, compared with 80,894 admissions during the first 4 pandemic months, representing an 11.5% decline.
They also report that 13,334 stroke patients received intravenous thrombolysis in the 4 months preceding the pandemic, compared with 11,570 during the first 4 pandemic months, representing a 13.2% drop.
Interhospital transfers after thrombolysis for a higher level of stroke care decreased from 1,337 before the pandemic to 1,178 during the pandemic, a reduction of 11.9%.
There were greater declines in primary compared with comprehensive stroke centers for stroke hospitalizations (change, –17.3% vs. –10.3%) and for the number of patients receiving thrombolysis (change, –15.5% vs. –12.6%).
The volume of stroke hospitalizations increased by 9.5% in the two later pandemic months (May, June) versus the two earlier months (March, April), with greater recovery in hospitals with lower COVID-19 hospitalization volume, high-volume stroke centers, and comprehensive stroke centers.
Dr. Nguyen suggested that reasons for the reductions in these stroke numbers at the beginning of the pandemic could include a reduction in stroke risk due to a reduction of exposure to other viral infections or patients not presenting to the hospital for fear of contracting the coronavirus.
The higher recovery of stroke volume in high-volume stroke centers and comprehensive stroke centers may represent patients with higher needs – those having more severe strokes – seeking care more frequently than those with milder symptoms, she noted.
“Preserving access to stroke care and emergency stroke care amidst a pandemic is as important as educating patients on the importance of presenting to the hospital in the event of stroke-like symptoms,” Dr. Nguyen concluded.
“We continue to advocate that if a patient has stroke-like symptoms, such as loss of speech, strength, vision, or balance, it is important for the patient to seek medical care as an emergency, as there are treatments that can improve a patient’s ability to recover from disabling stroke in earlier rather than later time windows,” she added.
In the publication, the authors wrote, “Our results concur with other recent reports on the collateral effects of the COVID-19 pandemic on stroke systems of care,” but added that “this is among the first descriptions of the change at a global level, including primary and comprehensive stroke centers.”
They said that hospital access related to high COVID-19 burden was unlikely a factor because the decline was seen in centers with a few or no patients with COVID-19. They suggested that patient fear of contracting coronavirus may have played a role, along with a decrease in presentation of transient ischemic attacks, mild strokes, or moderate strokes, and physical distancing measures may have prevented the timely witnessing of a stroke.
A version of this article first appeared on Medscape.com.
From AAN 2021