User login
Benralizumab proves noninferior to mepolizumab for rare vasculitis, EGPA
SAN DIEGO – Treatment with benralizumab (Fasenra) achieved remission at 36 and 48 weeks at rates similar to those of mepolizumab (Nucala) in a head-to-head phase 3 trial of the two drugs for patients with a relapsing or refractory case of the rare vasculitis eosinophilic granulomatosis with polyangiitis (EGPA).
Benralizumab, a monoclonal antibody from AstraZeneca that binds to the alpha chain of the interleukin (IL)-5 receptor, is indicated as an add-on maintenance treatment for patients 12 years and older with severe eosinophilic asthma but is not currently approved for EGPA. Mepolizumab is a humanized monoclonal antibody targeting IL-5 and the only approved drug for EGPA.
Peter A. Merkel, MD, presented the trial, known as MANDARA, during a late-breaking poster session at the annual meeting of the American College of Rheumatology. A total of 140 patients with EGPA received either subcutaneous benralizumab 30 mg or mepolizumab 300 mg every 4 weeks for 52 weeks. The trial, which began recruitment in late 2019, was limited to patients at least 18 years of age with relapsing/refractory EGPA that required stable use of oral glucocorticoids (OGCs) and immunosuppressive therapy for at least 4 weeks prior to randomization, and the primary endpoint was the proportion of patients who achieved remission at weeks 36 and 48. Remission was defined as a Birmingham Vasculitis Activity Score (BVAS) of 0 plus an OGC dose of no more than 4 mg/day. Secondary endpoints included rates of accrued and maintained remission, OGC use, clinical benefit and complete response, blood eosinophil counts, total BVAS, and Vascular Damage Index scores. The mean age of the 140 patients was 52 years, and 60% were women.
Dr. Merkel and colleagues reported that the adjusted remission rate at both weeks 36 and 48 was 59.2% for those in the benralizumab arm and 56.5% for those in the mepolizumab arm (P = .7278). The percentage of patients who achieved a BVAS of 0 was similar between the two arms (83% in the benralizumab arm vs. 84.2% for those in the mepolizumab arm; P = .8502), as was the percentage of patients on an OGC dose of up to 4 mg/day (62.1% vs. 57.9%; P = .5942). At 48-52 weeks, 86.1% of patients in the benralizumab arm achieved up to a 50% reduction in OGC use, compared with 73.9% of those in the mepolizumab arm (P = .0611), and 41.4% of patients in the benralizumab arm achieved a 100% reduction in OGC use, compared with 25.8% of those in the mepolizumab arm (P = .0406).
In findings related to safety, the top three adverse events were COVID-19 (21.4% in the benralizumab arm vs. 27.1% in the mepolizumab arm, respectively), headache (17.1% vs. 15.7%), and arthralgia (17.1% vs. 11.4%).
“We were pleased with the findings because they met our expectations,” Dr. Merkel, chief of rheumatology and professor of medicine and epidemiology at the University of Pennsylvania, Philadelphia, said in an interview. “The hypothesis was that these two drugs would be equivalent and safe. The implication for patients is that they’ll have another treatment option for EGPA, which is an underrecognized disease with need for more effective treatments. I anticipate that the drug will be approved for use in EGPA, providing another option for treating this complicated multisystem eosinophilic-associated disease. Having more options for our biologic therapies is good.”
He characterized the retention of patients in MANDARA as “remarkable, despite the COVID-19 pandemic. Patients with rare diseases are quite dedicated to helping conduct research. They know that their disease is not common and that they could help others.”
The study was sponsored and funded by AstraZeneca. Dr. Merkel disclosed that he has received consulting fees and research support from many pharmaceutical companies, including AstraZeneca.
SAN DIEGO – Treatment with benralizumab (Fasenra) achieved remission at 36 and 48 weeks at rates similar to those of mepolizumab (Nucala) in a head-to-head phase 3 trial of the two drugs for patients with a relapsing or refractory case of the rare vasculitis eosinophilic granulomatosis with polyangiitis (EGPA).
Benralizumab, a monoclonal antibody from AstraZeneca that binds to the alpha chain of the interleukin (IL)-5 receptor, is indicated as an add-on maintenance treatment for patients 12 years and older with severe eosinophilic asthma but is not currently approved for EGPA. Mepolizumab is a humanized monoclonal antibody targeting IL-5 and the only approved drug for EGPA.
Peter A. Merkel, MD, presented the trial, known as MANDARA, during a late-breaking poster session at the annual meeting of the American College of Rheumatology. A total of 140 patients with EGPA received either subcutaneous benralizumab 30 mg or mepolizumab 300 mg every 4 weeks for 52 weeks. The trial, which began recruitment in late 2019, was limited to patients at least 18 years of age with relapsing/refractory EGPA that required stable use of oral glucocorticoids (OGCs) and immunosuppressive therapy for at least 4 weeks prior to randomization, and the primary endpoint was the proportion of patients who achieved remission at weeks 36 and 48. Remission was defined as a Birmingham Vasculitis Activity Score (BVAS) of 0 plus an OGC dose of no more than 4 mg/day. Secondary endpoints included rates of accrued and maintained remission, OGC use, clinical benefit and complete response, blood eosinophil counts, total BVAS, and Vascular Damage Index scores. The mean age of the 140 patients was 52 years, and 60% were women.
Dr. Merkel and colleagues reported that the adjusted remission rate at both weeks 36 and 48 was 59.2% for those in the benralizumab arm and 56.5% for those in the mepolizumab arm (P = .7278). The percentage of patients who achieved a BVAS of 0 was similar between the two arms (83% in the benralizumab arm vs. 84.2% for those in the mepolizumab arm; P = .8502), as was the percentage of patients on an OGC dose of up to 4 mg/day (62.1% vs. 57.9%; P = .5942). At 48-52 weeks, 86.1% of patients in the benralizumab arm achieved up to a 50% reduction in OGC use, compared with 73.9% of those in the mepolizumab arm (P = .0611), and 41.4% of patients in the benralizumab arm achieved a 100% reduction in OGC use, compared with 25.8% of those in the mepolizumab arm (P = .0406).
In findings related to safety, the top three adverse events were COVID-19 (21.4% in the benralizumab arm vs. 27.1% in the mepolizumab arm, respectively), headache (17.1% vs. 15.7%), and arthralgia (17.1% vs. 11.4%).
“We were pleased with the findings because they met our expectations,” Dr. Merkel, chief of rheumatology and professor of medicine and epidemiology at the University of Pennsylvania, Philadelphia, said in an interview. “The hypothesis was that these two drugs would be equivalent and safe. The implication for patients is that they’ll have another treatment option for EGPA, which is an underrecognized disease with need for more effective treatments. I anticipate that the drug will be approved for use in EGPA, providing another option for treating this complicated multisystem eosinophilic-associated disease. Having more options for our biologic therapies is good.”
He characterized the retention of patients in MANDARA as “remarkable, despite the COVID-19 pandemic. Patients with rare diseases are quite dedicated to helping conduct research. They know that their disease is not common and that they could help others.”
The study was sponsored and funded by AstraZeneca. Dr. Merkel disclosed that he has received consulting fees and research support from many pharmaceutical companies, including AstraZeneca.
SAN DIEGO – Treatment with benralizumab (Fasenra) achieved remission at 36 and 48 weeks at rates similar to those of mepolizumab (Nucala) in a head-to-head phase 3 trial of the two drugs for patients with a relapsing or refractory case of the rare vasculitis eosinophilic granulomatosis with polyangiitis (EGPA).
Benralizumab, a monoclonal antibody from AstraZeneca that binds to the alpha chain of the interleukin (IL)-5 receptor, is indicated as an add-on maintenance treatment for patients 12 years and older with severe eosinophilic asthma but is not currently approved for EGPA. Mepolizumab is a humanized monoclonal antibody targeting IL-5 and the only approved drug for EGPA.
Peter A. Merkel, MD, presented the trial, known as MANDARA, during a late-breaking poster session at the annual meeting of the American College of Rheumatology. A total of 140 patients with EGPA received either subcutaneous benralizumab 30 mg or mepolizumab 300 mg every 4 weeks for 52 weeks. The trial, which began recruitment in late 2019, was limited to patients at least 18 years of age with relapsing/refractory EGPA that required stable use of oral glucocorticoids (OGCs) and immunosuppressive therapy for at least 4 weeks prior to randomization, and the primary endpoint was the proportion of patients who achieved remission at weeks 36 and 48. Remission was defined as a Birmingham Vasculitis Activity Score (BVAS) of 0 plus an OGC dose of no more than 4 mg/day. Secondary endpoints included rates of accrued and maintained remission, OGC use, clinical benefit and complete response, blood eosinophil counts, total BVAS, and Vascular Damage Index scores. The mean age of the 140 patients was 52 years, and 60% were women.
Dr. Merkel and colleagues reported that the adjusted remission rate at both weeks 36 and 48 was 59.2% for those in the benralizumab arm and 56.5% for those in the mepolizumab arm (P = .7278). The percentage of patients who achieved a BVAS of 0 was similar between the two arms (83% in the benralizumab arm vs. 84.2% for those in the mepolizumab arm; P = .8502), as was the percentage of patients on an OGC dose of up to 4 mg/day (62.1% vs. 57.9%; P = .5942). At 48-52 weeks, 86.1% of patients in the benralizumab arm achieved up to a 50% reduction in OGC use, compared with 73.9% of those in the mepolizumab arm (P = .0611), and 41.4% of patients in the benralizumab arm achieved a 100% reduction in OGC use, compared with 25.8% of those in the mepolizumab arm (P = .0406).
In findings related to safety, the top three adverse events were COVID-19 (21.4% in the benralizumab arm vs. 27.1% in the mepolizumab arm, respectively), headache (17.1% vs. 15.7%), and arthralgia (17.1% vs. 11.4%).
“We were pleased with the findings because they met our expectations,” Dr. Merkel, chief of rheumatology and professor of medicine and epidemiology at the University of Pennsylvania, Philadelphia, said in an interview. “The hypothesis was that these two drugs would be equivalent and safe. The implication for patients is that they’ll have another treatment option for EGPA, which is an underrecognized disease with need for more effective treatments. I anticipate that the drug will be approved for use in EGPA, providing another option for treating this complicated multisystem eosinophilic-associated disease. Having more options for our biologic therapies is good.”
He characterized the retention of patients in MANDARA as “remarkable, despite the COVID-19 pandemic. Patients with rare diseases are quite dedicated to helping conduct research. They know that their disease is not common and that they could help others.”
The study was sponsored and funded by AstraZeneca. Dr. Merkel disclosed that he has received consulting fees and research support from many pharmaceutical companies, including AstraZeneca.
AT ACR 2023
Novel blood test can detect RA
SAN DIEGO – Researchers say they’ve developed a novel blood-based assay that can differentiate patients with seropositive or seronegative rheumatoid arthritis from healthy people and those with other inflammatory diseases or osteoarthritis.
While cautioning that the results need to be confirmed, University of Oxford (England) rheumatologist Peter Taylor, PhD, MA, told an audience at the annual meeting of the American College of Rheumatology that the test has an overall mean sensitivity of 90.8% (standard deviation, 0.94%; 95% confidence interval, 83.2%-95.4%) and mean specificity of 96.1% (SD, 0.64%; 95% CI, 92.7%-97.9%). The mean area under the curve (AUC) is 0.991 (SD, 0.001; 95% CI, 97.2%-99.6%).

“That is to say that it can correctly identify 96% of people without rheumatoid arthritis, and it can correctly identify over 90% of those who do have rheumatoid arthritis,” Dr. Taylor said. In the big picture, he said, “we’ve developed a blood-based assay that detects both organ-specific and systemic biological processes in patients with rheumatoid arthritis.”
Rheumatologist Kevin W. Byram, MD, of Vanderbilt University, Nashville, Tenn., who did not take part in the study but is familiar with its findings, noted in an interview that “there is a constant search for biomarkers to help aide in more accurate and faster diagnosis of all rheumatic conditions, including RA.”
He added that “a common clinical scenario for the rheumatologist is a patient presenting with painful and/or swollen joints and other features that might suggest a few different diagnoses. A diagnostic assay like this might help distinguish patients with RA from other inflammatory conditions or non-inflammatory conditions that might mimic RA.”
In his presentation, Dr. Taylor noted that “we haven’t yet integrated precision medicine into routine clinical practice in rheumatology.” While blood-based assays are prevalent in other types of clinical diagnostics, rheumatology relies on synovial biopsies that are “rarely used in routine clinical practice,” he said.
The new test is a “non-invasive DNA capture assay that can identify specific gene expression from synovium-specific signatures in blood plasma of patients with rheumatoid arthritis,” Dr. Taylor said. Specifically, it focuses on the “unique patterns and sizes of cell-free DNA,” he said. “Analysis of [long] fragments has the potential to give us a great deal of information about disease progression, potentially about customizing treatments and even evaluating the effectiveness of therapies.”
For the new study, researchers examined 229 samples from 191 patients, of whom 63.3% were White and 67.9% were female, with a median age of 56. A total of 89 patients with RA provided 89 samples and 102 without RA provided 140 samples, including 29 healthy controls (66 samples) and others with conditions such as psoriatic arthritis, ulcerative colitis, and osteoarthritis.
The machine learning model “identified 3,425 epigenetic features with statistically significant discrimination between the patients with and without rheumatoid arthritis,” Dr. Taylor said. These features were mapped to 929 genes which had some overlap with known blood pathway genes.
“Over and above that, there’s a whole set of these epigenetic features which represent novel pathways and potentially rich hunting ground for therapeutic targets and other translational investigation,” he said.
For seronegative cases, mean AUC was 0.971 (SD, 0.001; 95% CI, 93.8%-99.2%), sensitivity was 83.7% (SD, 2.03; 95% CI, 63.3%-91.8%) and specificity was 95.4% (SD, 0.69; 95% CI, 90.8%-97.5%).
Specificity for RA versus healthy controls was 100 (SD, 0; 95% CI, 94.4-100.0).
Dr. Byram described the study as small but intriguing. He cautioned that “there is always some likelihood that the actual components of the test are just recognizing some combination of things we are already testing in the clinic,” he said. Details about the patients in the study can offer insight into “whether the assay is actually just recognizing something about patients with RA that is truly different, or rather is it recognizing how a common factor among patients with RA is transcribed by the cell.”
Moving forward, “it is important to get a grasp of how these biomarkers might perform in various settings,” he said.
Dr. Taylor did not discuss the potential cost of the assay in his presentation. “Tests like these have to strike a real balance in being useful and cost-effective and, since they are still made by commercial companies with commercial interests, also make a margin for their owner,” Dr. Byram said. “Turnaround time is also an important factor to think about.”
Aqtual funded the study. Dr. Taylor reports consulting for AbbVie, Aqtual, Biogen, Fresenius Kabi, Galapagos, Gilead, GlaxoSmithKline, Janssen, Lilly, Nordic Pharma, Pfizer, Sanofi, and UCB and receiving grant support from Galapagos. The other study authors all have relationships with Aqtual, and some report various other disclosures. Dr. Byram has no disclosures.
SAN DIEGO – Researchers say they’ve developed a novel blood-based assay that can differentiate patients with seropositive or seronegative rheumatoid arthritis from healthy people and those with other inflammatory diseases or osteoarthritis.
While cautioning that the results need to be confirmed, University of Oxford (England) rheumatologist Peter Taylor, PhD, MA, told an audience at the annual meeting of the American College of Rheumatology that the test has an overall mean sensitivity of 90.8% (standard deviation, 0.94%; 95% confidence interval, 83.2%-95.4%) and mean specificity of 96.1% (SD, 0.64%; 95% CI, 92.7%-97.9%). The mean area under the curve (AUC) is 0.991 (SD, 0.001; 95% CI, 97.2%-99.6%).
“That is to say that it can correctly identify 96% of people without rheumatoid arthritis, and it can correctly identify over 90% of those who do have rheumatoid arthritis,” Dr. Taylor said. In the big picture, he said, “we’ve developed a blood-based assay that detects both organ-specific and systemic biological processes in patients with rheumatoid arthritis.”
Rheumatologist Kevin W. Byram, MD, of Vanderbilt University, Nashville, Tenn., who did not take part in the study but is familiar with its findings, noted in an interview that “there is a constant search for biomarkers to help aide in more accurate and faster diagnosis of all rheumatic conditions, including RA.”
He added that “a common clinical scenario for the rheumatologist is a patient presenting with painful and/or swollen joints and other features that might suggest a few different diagnoses. A diagnostic assay like this might help distinguish patients with RA from other inflammatory conditions or non-inflammatory conditions that might mimic RA.”
In his presentation, Dr. Taylor noted that “we haven’t yet integrated precision medicine into routine clinical practice in rheumatology.” While blood-based assays are prevalent in other types of clinical diagnostics, rheumatology relies on synovial biopsies that are “rarely used in routine clinical practice,” he said.
The new test is a “non-invasive DNA capture assay that can identify specific gene expression from synovium-specific signatures in blood plasma of patients with rheumatoid arthritis,” Dr. Taylor said. Specifically, it focuses on the “unique patterns and sizes of cell-free DNA,” he said. “Analysis of [long] fragments has the potential to give us a great deal of information about disease progression, potentially about customizing treatments and even evaluating the effectiveness of therapies.”
For the new study, researchers examined 229 samples from 191 patients, of whom 63.3% were White and 67.9% were female, with a median age of 56. A total of 89 patients with RA provided 89 samples and 102 without RA provided 140 samples, including 29 healthy controls (66 samples) and others with conditions such as psoriatic arthritis, ulcerative colitis, and osteoarthritis.
The machine learning model “identified 3,425 epigenetic features with statistically significant discrimination between the patients with and without rheumatoid arthritis,” Dr. Taylor said. These features were mapped to 929 genes which had some overlap with known blood pathway genes.
“Over and above that, there’s a whole set of these epigenetic features which represent novel pathways and potentially rich hunting ground for therapeutic targets and other translational investigation,” he said.
For seronegative cases, mean AUC was 0.971 (SD, 0.001; 95% CI, 93.8%-99.2%), sensitivity was 83.7% (SD, 2.03; 95% CI, 63.3%-91.8%) and specificity was 95.4% (SD, 0.69; 95% CI, 90.8%-97.5%).
Specificity for RA versus healthy controls was 100 (SD, 0; 95% CI, 94.4-100.0).
Dr. Byram described the study as small but intriguing. He cautioned that “there is always some likelihood that the actual components of the test are just recognizing some combination of things we are already testing in the clinic,” he said. Details about the patients in the study can offer insight into “whether the assay is actually just recognizing something about patients with RA that is truly different, or rather is it recognizing how a common factor among patients with RA is transcribed by the cell.”
Moving forward, “it is important to get a grasp of how these biomarkers might perform in various settings,” he said.
Dr. Taylor did not discuss the potential cost of the assay in his presentation. “Tests like these have to strike a real balance in being useful and cost-effective and, since they are still made by commercial companies with commercial interests, also make a margin for their owner,” Dr. Byram said. “Turnaround time is also an important factor to think about.”
Aqtual funded the study. Dr. Taylor reports consulting for AbbVie, Aqtual, Biogen, Fresenius Kabi, Galapagos, Gilead, GlaxoSmithKline, Janssen, Lilly, Nordic Pharma, Pfizer, Sanofi, and UCB and receiving grant support from Galapagos. The other study authors all have relationships with Aqtual, and some report various other disclosures. Dr. Byram has no disclosures.
SAN DIEGO – Researchers say they’ve developed a novel blood-based assay that can differentiate patients with seropositive or seronegative rheumatoid arthritis from healthy people and those with other inflammatory diseases or osteoarthritis.
While cautioning that the results need to be confirmed, University of Oxford (England) rheumatologist Peter Taylor, PhD, MA, told an audience at the annual meeting of the American College of Rheumatology that the test has an overall mean sensitivity of 90.8% (standard deviation, 0.94%; 95% confidence interval, 83.2%-95.4%) and mean specificity of 96.1% (SD, 0.64%; 95% CI, 92.7%-97.9%). The mean area under the curve (AUC) is 0.991 (SD, 0.001; 95% CI, 97.2%-99.6%).
“That is to say that it can correctly identify 96% of people without rheumatoid arthritis, and it can correctly identify over 90% of those who do have rheumatoid arthritis,” Dr. Taylor said. In the big picture, he said, “we’ve developed a blood-based assay that detects both organ-specific and systemic biological processes in patients with rheumatoid arthritis.”
Rheumatologist Kevin W. Byram, MD, of Vanderbilt University, Nashville, Tenn., who did not take part in the study but is familiar with its findings, noted in an interview that “there is a constant search for biomarkers to help aide in more accurate and faster diagnosis of all rheumatic conditions, including RA.”
He added that “a common clinical scenario for the rheumatologist is a patient presenting with painful and/or swollen joints and other features that might suggest a few different diagnoses. A diagnostic assay like this might help distinguish patients with RA from other inflammatory conditions or non-inflammatory conditions that might mimic RA.”
In his presentation, Dr. Taylor noted that “we haven’t yet integrated precision medicine into routine clinical practice in rheumatology.” While blood-based assays are prevalent in other types of clinical diagnostics, rheumatology relies on synovial biopsies that are “rarely used in routine clinical practice,” he said.
The new test is a “non-invasive DNA capture assay that can identify specific gene expression from synovium-specific signatures in blood plasma of patients with rheumatoid arthritis,” Dr. Taylor said. Specifically, it focuses on the “unique patterns and sizes of cell-free DNA,” he said. “Analysis of [long] fragments has the potential to give us a great deal of information about disease progression, potentially about customizing treatments and even evaluating the effectiveness of therapies.”
For the new study, researchers examined 229 samples from 191 patients, of whom 63.3% were White and 67.9% were female, with a median age of 56. A total of 89 patients with RA provided 89 samples and 102 without RA provided 140 samples, including 29 healthy controls (66 samples) and others with conditions such as psoriatic arthritis, ulcerative colitis, and osteoarthritis.
The machine learning model “identified 3,425 epigenetic features with statistically significant discrimination between the patients with and without rheumatoid arthritis,” Dr. Taylor said. These features were mapped to 929 genes which had some overlap with known blood pathway genes.
“Over and above that, there’s a whole set of these epigenetic features which represent novel pathways and potentially rich hunting ground for therapeutic targets and other translational investigation,” he said.
For seronegative cases, mean AUC was 0.971 (SD, 0.001; 95% CI, 93.8%-99.2%), sensitivity was 83.7% (SD, 2.03; 95% CI, 63.3%-91.8%) and specificity was 95.4% (SD, 0.69; 95% CI, 90.8%-97.5%).
Specificity for RA versus healthy controls was 100 (SD, 0; 95% CI, 94.4-100.0).
Dr. Byram described the study as small but intriguing. He cautioned that “there is always some likelihood that the actual components of the test are just recognizing some combination of things we are already testing in the clinic,” he said. Details about the patients in the study can offer insight into “whether the assay is actually just recognizing something about patients with RA that is truly different, or rather is it recognizing how a common factor among patients with RA is transcribed by the cell.”
Moving forward, “it is important to get a grasp of how these biomarkers might perform in various settings,” he said.
Dr. Taylor did not discuss the potential cost of the assay in his presentation. “Tests like these have to strike a real balance in being useful and cost-effective and, since they are still made by commercial companies with commercial interests, also make a margin for their owner,” Dr. Byram said. “Turnaround time is also an important factor to think about.”
Aqtual funded the study. Dr. Taylor reports consulting for AbbVie, Aqtual, Biogen, Fresenius Kabi, Galapagos, Gilead, GlaxoSmithKline, Janssen, Lilly, Nordic Pharma, Pfizer, Sanofi, and UCB and receiving grant support from Galapagos. The other study authors all have relationships with Aqtual, and some report various other disclosures. Dr. Byram has no disclosures.
AT ACR 2023
Split-dose methotrexate speeds RA response over single dose
SAN DIEGO – A split dose of methotrexate (MTX) given orally once per week showed significantly higher efficacy in patients with rheumatoid arthritis at 16 weeks, compared with a single MTX dose weekly, according to new research. By 24 weeks, efficacy measures were similar for both groups.
However, fewer patients in the split-dose group needed additional disease-modifying antirheumatic drugs (DMARDs) to control disease activity.
MTX is a highly utilized, inexpensive drug for RA, but only about 30% of patients can achieve low disease activity or remission on MTX monotherapy, said Varun Dhir, MD, MBBS, of the Postgraduate Institute of Medical Education and Research, Chandigarh, India. He co-authored and presented the research at the annual meeting of the American College of Rheumatology.
Part of the problem is that “oral methotrexate absorption from the gut reduces as the doses go up,” Dr. Dhir noted, because the transport mechanism gets saturated. MTX delivered subcutaneously is one way to improve efficacy, but patients can be needle-averse, and in some countries, like India, pre-filled syringes are not available, he said.
There is pharmacokinetic data dating back 20 years that suggest split-dose MTX could be more efficacious. “However, there are no randomized controlled trials to date, and the guidelines therefore are silent on this approach,” Dr. Dhir said.
To address this question, Dr. Dhir and colleagues recruited patients with RA from six centers across India. Patients were aged 18-60 years, seropositive (rheumatoid factor or anti-citrullinated protein antibodies), and had a disease duration of 5 years or fewer. Patients had active disease, defined as at least four tender joints and at least two swollen joints, and were not taking any DMARDs except for hydroxychloroquine and/or low-dose prednisolone.
A total of 253 patients were randomly assigned to a single 25-mg dose or a split-dose of MTX once weekly (10 mg in the morning and 15 mg in the evening on the same day). The primary outcome was a European Alliance of Associations for Rheumatology (EULAR) good response at 24 weeks. At the 16-week mark, if patients had not achieved low disease activity based on a 28-joint Disease Activity Score (DAS28) greater than 3.2, a blinded assessor could add either leflunomide or sulfasalazine to the continued MTX therapy.
At baseline, there was no difference between the groups’ DAS28, but after 16 weeks, DAS28 was significantly lower in the split-dose group, compared with the single-dose group (4.4 vs. 5.1; P < .001), and a higher percentage of patients in the split-dose group had a EULAR good response.
About three-quarters (76.6%) of patients in the split-dose group experienced an improvement of at least 20% in ACR response criteria (ACR20), compared with 52% in the single-dose group. The split-dose group also had higher proportion of patients achieving ACR50 and ACR70.
About one-third of the split-dose group (35%) added an additional DMARD at 16 weeks, compared with 54.5% of the single-dose group (P = .005).
After 24 weeks, DAS28 scores remained lower in the split-dose group (4.1 vs. 4.5; P = .03), but there were no other differences in treatment responses. Health Assessment Questionnaire scores were the same between both groups at 16 and 24 weeks.
The primary outcome was not met, although Dr. Dhir noted a flaw in the study design that could have affected the results. By allowing patients to add additional DMARDs at 16 weeks, “there were two factors which were affecting the primary outcome” at 24 weeks, he told this news organization. “I feel there was a robust result at least at 16 weeks.”
While there were no major adverse events, the split-dose group had higher rates of transaminitis (elevated liver enzymes) during the study, and low white blood cell count was higher in the single-dose group at 24 weeks. There was no difference in MTX intolerance between the two groups.
“It looks like [the split-dose group] gets out of the block faster. It’s a faster effect,” although the other group did catch up, Janet Pope, MD, MPH, of Western University, London, Ont., said in an interview. She was not involved with the research. Two positive results were the earlier ACR responses in the split-dose group as well as fewer patients in that same group needing to add another DMARD to therapy.
“In my opinion, if it’s equal cost, why not try it and see?” she said.
In a separate presentation referring to the abstract, Joan Bathon, MD, director of rheumatology at Columbia University, New York City, noted that these results align with ACR 2021 recommendations. Dr. Bathon was not involved with this study but was on the writing committee establishing those 2021 guidelines.
“The recommendation – with low certainty of evidence – was that for patients who are intolerant to MTX, that split-dose of oral MTX is worth trying before you switch to a different DMARD,” she said. “I think these data support that concept.”
Dr. Dhir and Dr. Bathon had no relevant financial relationships. Dr. Pope disclosed financial relationships with AbbVie/Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Fresenius Kabi, GlaxoSmithKline, Janssen, Mallinckrodt, Novartis, Organon, Pfizer, Sandoz, and Viatris.
A version of this article first appeared on Medscape.com.
SAN DIEGO – A split dose of methotrexate (MTX) given orally once per week showed significantly higher efficacy in patients with rheumatoid arthritis at 16 weeks, compared with a single MTX dose weekly, according to new research. By 24 weeks, efficacy measures were similar for both groups.
However, fewer patients in the split-dose group needed additional disease-modifying antirheumatic drugs (DMARDs) to control disease activity.
MTX is a highly utilized, inexpensive drug for RA, but only about 30% of patients can achieve low disease activity or remission on MTX monotherapy, said Varun Dhir, MD, MBBS, of the Postgraduate Institute of Medical Education and Research, Chandigarh, India. He co-authored and presented the research at the annual meeting of the American College of Rheumatology.
Part of the problem is that “oral methotrexate absorption from the gut reduces as the doses go up,” Dr. Dhir noted, because the transport mechanism gets saturated. MTX delivered subcutaneously is one way to improve efficacy, but patients can be needle-averse, and in some countries, like India, pre-filled syringes are not available, he said.
There is pharmacokinetic data dating back 20 years that suggest split-dose MTX could be more efficacious. “However, there are no randomized controlled trials to date, and the guidelines therefore are silent on this approach,” Dr. Dhir said.
To address this question, Dr. Dhir and colleagues recruited patients with RA from six centers across India. Patients were aged 18-60 years, seropositive (rheumatoid factor or anti-citrullinated protein antibodies), and had a disease duration of 5 years or fewer. Patients had active disease, defined as at least four tender joints and at least two swollen joints, and were not taking any DMARDs except for hydroxychloroquine and/or low-dose prednisolone.
A total of 253 patients were randomly assigned to a single 25-mg dose or a split-dose of MTX once weekly (10 mg in the morning and 15 mg in the evening on the same day). The primary outcome was a European Alliance of Associations for Rheumatology (EULAR) good response at 24 weeks. At the 16-week mark, if patients had not achieved low disease activity based on a 28-joint Disease Activity Score (DAS28) greater than 3.2, a blinded assessor could add either leflunomide or sulfasalazine to the continued MTX therapy.
At baseline, there was no difference between the groups’ DAS28, but after 16 weeks, DAS28 was significantly lower in the split-dose group, compared with the single-dose group (4.4 vs. 5.1; P < .001), and a higher percentage of patients in the split-dose group had a EULAR good response.
About three-quarters (76.6%) of patients in the split-dose group experienced an improvement of at least 20% in ACR response criteria (ACR20), compared with 52% in the single-dose group. The split-dose group also had higher proportion of patients achieving ACR50 and ACR70.
About one-third of the split-dose group (35%) added an additional DMARD at 16 weeks, compared with 54.5% of the single-dose group (P = .005).
After 24 weeks, DAS28 scores remained lower in the split-dose group (4.1 vs. 4.5; P = .03), but there were no other differences in treatment responses. Health Assessment Questionnaire scores were the same between both groups at 16 and 24 weeks.
The primary outcome was not met, although Dr. Dhir noted a flaw in the study design that could have affected the results. By allowing patients to add additional DMARDs at 16 weeks, “there were two factors which were affecting the primary outcome” at 24 weeks, he told this news organization. “I feel there was a robust result at least at 16 weeks.”
While there were no major adverse events, the split-dose group had higher rates of transaminitis (elevated liver enzymes) during the study, and low white blood cell count was higher in the single-dose group at 24 weeks. There was no difference in MTX intolerance between the two groups.
“It looks like [the split-dose group] gets out of the block faster. It’s a faster effect,” although the other group did catch up, Janet Pope, MD, MPH, of Western University, London, Ont., said in an interview. She was not involved with the research. Two positive results were the earlier ACR responses in the split-dose group as well as fewer patients in that same group needing to add another DMARD to therapy.
“In my opinion, if it’s equal cost, why not try it and see?” she said.
In a separate presentation referring to the abstract, Joan Bathon, MD, director of rheumatology at Columbia University, New York City, noted that these results align with ACR 2021 recommendations. Dr. Bathon was not involved with this study but was on the writing committee establishing those 2021 guidelines.
“The recommendation – with low certainty of evidence – was that for patients who are intolerant to MTX, that split-dose of oral MTX is worth trying before you switch to a different DMARD,” she said. “I think these data support that concept.”
Dr. Dhir and Dr. Bathon had no relevant financial relationships. Dr. Pope disclosed financial relationships with AbbVie/Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Fresenius Kabi, GlaxoSmithKline, Janssen, Mallinckrodt, Novartis, Organon, Pfizer, Sandoz, and Viatris.
A version of this article first appeared on Medscape.com.
SAN DIEGO – A split dose of methotrexate (MTX) given orally once per week showed significantly higher efficacy in patients with rheumatoid arthritis at 16 weeks, compared with a single MTX dose weekly, according to new research. By 24 weeks, efficacy measures were similar for both groups.
However, fewer patients in the split-dose group needed additional disease-modifying antirheumatic drugs (DMARDs) to control disease activity.
MTX is a highly utilized, inexpensive drug for RA, but only about 30% of patients can achieve low disease activity or remission on MTX monotherapy, said Varun Dhir, MD, MBBS, of the Postgraduate Institute of Medical Education and Research, Chandigarh, India. He co-authored and presented the research at the annual meeting of the American College of Rheumatology.
Part of the problem is that “oral methotrexate absorption from the gut reduces as the doses go up,” Dr. Dhir noted, because the transport mechanism gets saturated. MTX delivered subcutaneously is one way to improve efficacy, but patients can be needle-averse, and in some countries, like India, pre-filled syringes are not available, he said.
There is pharmacokinetic data dating back 20 years that suggest split-dose MTX could be more efficacious. “However, there are no randomized controlled trials to date, and the guidelines therefore are silent on this approach,” Dr. Dhir said.
To address this question, Dr. Dhir and colleagues recruited patients with RA from six centers across India. Patients were aged 18-60 years, seropositive (rheumatoid factor or anti-citrullinated protein antibodies), and had a disease duration of 5 years or fewer. Patients had active disease, defined as at least four tender joints and at least two swollen joints, and were not taking any DMARDs except for hydroxychloroquine and/or low-dose prednisolone.
A total of 253 patients were randomly assigned to a single 25-mg dose or a split-dose of MTX once weekly (10 mg in the morning and 15 mg in the evening on the same day). The primary outcome was a European Alliance of Associations for Rheumatology (EULAR) good response at 24 weeks. At the 16-week mark, if patients had not achieved low disease activity based on a 28-joint Disease Activity Score (DAS28) greater than 3.2, a blinded assessor could add either leflunomide or sulfasalazine to the continued MTX therapy.
At baseline, there was no difference between the groups’ DAS28, but after 16 weeks, DAS28 was significantly lower in the split-dose group, compared with the single-dose group (4.4 vs. 5.1; P < .001), and a higher percentage of patients in the split-dose group had a EULAR good response.
About three-quarters (76.6%) of patients in the split-dose group experienced an improvement of at least 20% in ACR response criteria (ACR20), compared with 52% in the single-dose group. The split-dose group also had higher proportion of patients achieving ACR50 and ACR70.
About one-third of the split-dose group (35%) added an additional DMARD at 16 weeks, compared with 54.5% of the single-dose group (P = .005).
After 24 weeks, DAS28 scores remained lower in the split-dose group (4.1 vs. 4.5; P = .03), but there were no other differences in treatment responses. Health Assessment Questionnaire scores were the same between both groups at 16 and 24 weeks.
The primary outcome was not met, although Dr. Dhir noted a flaw in the study design that could have affected the results. By allowing patients to add additional DMARDs at 16 weeks, “there were two factors which were affecting the primary outcome” at 24 weeks, he told this news organization. “I feel there was a robust result at least at 16 weeks.”
While there were no major adverse events, the split-dose group had higher rates of transaminitis (elevated liver enzymes) during the study, and low white blood cell count was higher in the single-dose group at 24 weeks. There was no difference in MTX intolerance between the two groups.
“It looks like [the split-dose group] gets out of the block faster. It’s a faster effect,” although the other group did catch up, Janet Pope, MD, MPH, of Western University, London, Ont., said in an interview. She was not involved with the research. Two positive results were the earlier ACR responses in the split-dose group as well as fewer patients in that same group needing to add another DMARD to therapy.
“In my opinion, if it’s equal cost, why not try it and see?” she said.
In a separate presentation referring to the abstract, Joan Bathon, MD, director of rheumatology at Columbia University, New York City, noted that these results align with ACR 2021 recommendations. Dr. Bathon was not involved with this study but was on the writing committee establishing those 2021 guidelines.
“The recommendation – with low certainty of evidence – was that for patients who are intolerant to MTX, that split-dose of oral MTX is worth trying before you switch to a different DMARD,” she said. “I think these data support that concept.”
Dr. Dhir and Dr. Bathon had no relevant financial relationships. Dr. Pope disclosed financial relationships with AbbVie/Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Fresenius Kabi, GlaxoSmithKline, Janssen, Mallinckrodt, Novartis, Organon, Pfizer, Sandoz, and Viatris.
A version of this article first appeared on Medscape.com.
AT ACR 2023

IV secukinumab, alternative to self-injections, reaches primary endpoints in PsA, axSpA
SAN DIEGO – Monthly use of intravenously administered secukinumab (Cosentyx) proved its efficacy over placebo in treating psoriatic arthritis (PsA) and axial spondyloarthritis (axSpA) in two industry-sponsored, randomized, double-blinded, phase 3 trials of the drug’s second and newly approved route of administration.
The studies of the human monoclonal antibody secukinumab, an interleukin-17 inhibitor, were presented at the annual meeting of the American College of Rheumatology. A subcutaneously injectable formulation of the drug is available, and the Food and Drug Administration approved the IV form for the conditions in October, although at a recommended lower monthly dose than the new trials examined.
In the PsA trial, 191 patients took IV secukinumab, and 190 took placebo. For the primary endpoint, the percentages who reached at least a 50% improvement in American College of Rheumatology response criteria (ACR 50) at 16 weeks were 31.4% and 6.3%, respectively (P < .0001).
In the axSpA trial, 264 patients took IV secukinumab, and 262 took placebo. The primary endpoint, at least a 40% improvement in Assessment of the Spondyloarthritis International Society response criteria (ASAS 40), was met at 16 weeks by 40.9% and 22.9%, respectively (P < .0001).
“Both studies appear to present clear efficacy of IV route administration of secukinumab with no clear increase in safety signals,” consultant rheumatologist Nicola Goodson, MBChB, PhD, of Aintree University Hospital in Liverpool, England, said in an interview.
“Offering IV administration as an option to patients is helpful,” added Dr. Goodson, who was not involved with the study but is familiar with its findings.
As Dr. Goodson explained, secukinumab “was the first IL [interleukin]-17 inhibitor used to treat spondyloarthropathies, and we have been using subcutaneous secukinumab to treat psoriasis, psoriatic arthritis, and axial spondyloarthritis/ankylosing spondylitis since 2016 in the U.K. Our experience with this medication has been good with similar efficacy to anti-TNF [tumor necrosis factor] therapy in axial spondyloarthritis. The medication is generally well-tolerated, and the subcutaneous pen injection device is easy for patients to use.”
However, IV treatment may speed up onset of action, she said, and it may be useful in situations when compliance is a challenge.
PsA trial details
In the PsA trial, known as INVIGORATE-2, researchers recruited patients who met the CASPAR criteria for active PsA with symptoms for ≥ 6 months, and had ≥ 3 tender joints out of 78 joints and ≥ 3 swollen joints out of 76.
Participants with a mean age of 48, including 55% females, were randomized 1:1 to receive placebo or secukinumab (6 mg/kg at baseline followed by 3 mg/kg every 4 weeks). Those in the placebo group were switched to the same monthly doses of secukinumab at 16 weeks.
“Patients who switched from the placebo had a similar increase of efficacy as the original treated group,” rheumatologist Alan J. Kivitz, MD, of the Altoona Center for Clinical Research, in Duncansville, Penn., said in his presentation at the meeting. Specifically, at 52 weeks, the groups had similar ACR 50 response rates: 58% with secukinumab and 64% with placebo-to-secukinumab.
The fact that patients in the original placebo group who received 3 mg IV doses without 6-mg loading doses achieved ACR response rates similar to those who took secukinumab during the whole trial “could suggest that the IV loading dose may not be required. This would need to be explored in a randomized head-to-head study, but it’s an interesting observation that may reduce costs and exposure to higher doses of medication at the start of treatment,” Dr. Goodson said.
Among the patients who received secukinumab at any point in the study, 63% had a treatment-emergent adverse event, including 5.9% with serious events. One death was reported in the placebo group before week 16. No other deaths were reported.
AxSpA trial details
In the axSpA trial, called INVIGORATE-1, researchers recruited people aged ≥18 years with a diagnosis of active radiographic axSpA according to modified New York criteria or nonradiographic axSpA according to ASAS criteria, and all had inflammatory back pain for ≥6 months with an onset before age 45. They were randomized at a 1:1 ratio to receive IV secukinumab (6 mg/kg loading dose, followed by 3 mg/kg every 4 weeks) or placebo for 16 weeks. At that point, the placebo group switched to the same monthly doses of IV secukinumab.
Participants had a mean age of about 39, and about one-third were female.
Following the statistical superiority in ASAS 40 response rates seen with IV secukinumab at week 16, patients who from there switched from placebo to IV secukinumab achieved comparable ASAS 40 response rates to those of patients originally randomized to secukinumab by week 24, reaching 66.8% for those on secukinumab the whole time and 74.9% for those who switched.
Secondary outcome measures were similar in both groups at week 52.
Among all patients who took secukinumab – the percentage with any adverse event was 63.2%, and 6% had a nonfatal adverse event deemed serious. There was one death during secukinumab treatment not suspected to be related to treatment.
In a presentation about the axSpA study findings, Atul Deodhar, MD, of Oregon Health & Science University, noted that “having an IV biologic available in the U.S. has some advantages. There are certain insurance providers such as Medicare where it is more economical for the patient to have an IV drug available.”
Dr. Deodhar also noted that in October the FDA approved a recommended lower dose for the IV treatment than in the study: 1.75 mg/kg instead of 3 mg/kg following the loading dose. That’s because the 3 mg/kg dose caused blood levels to be higher than those in the subcutaneous form, he said.
The FDA made the same dose recommendation for PsA.
Study limitations
Dr. Goodson, the U.K. consultant rheumatologist, noted a limitation of the trials: “It would have been interesting to compare IV to subcutaneous route secukinumab.” Still, the findings suggest that “the safety and efficacy of IV administration appears comparable,” she said.
“IV administration will have associated costs of attending hospital or infusion clinics,” she added, “and the cost of additional staff and administration need to be considered.”
Novartis, the maker of secukinumab, funded both studies. The PsA study authors report multiple relationships with industry, and some, such as Dr. Kivitz, have connections to Novartis. The axSpA study authors also report multiple relationships with industry, and some, such as Dr. Deodhar, have connections to Novartis. Some authors of both studies are Novartis employees. Dr. Goodson disclosed financial relationships with UCB and AbbVie.
SAN DIEGO – Monthly use of intravenously administered secukinumab (Cosentyx) proved its efficacy over placebo in treating psoriatic arthritis (PsA) and axial spondyloarthritis (axSpA) in two industry-sponsored, randomized, double-blinded, phase 3 trials of the drug’s second and newly approved route of administration.
The studies of the human monoclonal antibody secukinumab, an interleukin-17 inhibitor, were presented at the annual meeting of the American College of Rheumatology. A subcutaneously injectable formulation of the drug is available, and the Food and Drug Administration approved the IV form for the conditions in October, although at a recommended lower monthly dose than the new trials examined.
In the PsA trial, 191 patients took IV secukinumab, and 190 took placebo. For the primary endpoint, the percentages who reached at least a 50% improvement in American College of Rheumatology response criteria (ACR 50) at 16 weeks were 31.4% and 6.3%, respectively (P < .0001).
In the axSpA trial, 264 patients took IV secukinumab, and 262 took placebo. The primary endpoint, at least a 40% improvement in Assessment of the Spondyloarthritis International Society response criteria (ASAS 40), was met at 16 weeks by 40.9% and 22.9%, respectively (P < .0001).
“Both studies appear to present clear efficacy of IV route administration of secukinumab with no clear increase in safety signals,” consultant rheumatologist Nicola Goodson, MBChB, PhD, of Aintree University Hospital in Liverpool, England, said in an interview.
“Offering IV administration as an option to patients is helpful,” added Dr. Goodson, who was not involved with the study but is familiar with its findings.
As Dr. Goodson explained, secukinumab “was the first IL [interleukin]-17 inhibitor used to treat spondyloarthropathies, and we have been using subcutaneous secukinumab to treat psoriasis, psoriatic arthritis, and axial spondyloarthritis/ankylosing spondylitis since 2016 in the U.K. Our experience with this medication has been good with similar efficacy to anti-TNF [tumor necrosis factor] therapy in axial spondyloarthritis. The medication is generally well-tolerated, and the subcutaneous pen injection device is easy for patients to use.”
However, IV treatment may speed up onset of action, she said, and it may be useful in situations when compliance is a challenge.
PsA trial details
In the PsA trial, known as INVIGORATE-2, researchers recruited patients who met the CASPAR criteria for active PsA with symptoms for ≥ 6 months, and had ≥ 3 tender joints out of 78 joints and ≥ 3 swollen joints out of 76.
Participants with a mean age of 48, including 55% females, were randomized 1:1 to receive placebo or secukinumab (6 mg/kg at baseline followed by 3 mg/kg every 4 weeks). Those in the placebo group were switched to the same monthly doses of secukinumab at 16 weeks.
“Patients who switched from the placebo had a similar increase of efficacy as the original treated group,” rheumatologist Alan J. Kivitz, MD, of the Altoona Center for Clinical Research, in Duncansville, Penn., said in his presentation at the meeting. Specifically, at 52 weeks, the groups had similar ACR 50 response rates: 58% with secukinumab and 64% with placebo-to-secukinumab.
The fact that patients in the original placebo group who received 3 mg IV doses without 6-mg loading doses achieved ACR response rates similar to those who took secukinumab during the whole trial “could suggest that the IV loading dose may not be required. This would need to be explored in a randomized head-to-head study, but it’s an interesting observation that may reduce costs and exposure to higher doses of medication at the start of treatment,” Dr. Goodson said.
Among the patients who received secukinumab at any point in the study, 63% had a treatment-emergent adverse event, including 5.9% with serious events. One death was reported in the placebo group before week 16. No other deaths were reported.
AxSpA trial details
In the axSpA trial, called INVIGORATE-1, researchers recruited people aged ≥18 years with a diagnosis of active radiographic axSpA according to modified New York criteria or nonradiographic axSpA according to ASAS criteria, and all had inflammatory back pain for ≥6 months with an onset before age 45. They were randomized at a 1:1 ratio to receive IV secukinumab (6 mg/kg loading dose, followed by 3 mg/kg every 4 weeks) or placebo for 16 weeks. At that point, the placebo group switched to the same monthly doses of IV secukinumab.
Participants had a mean age of about 39, and about one-third were female.
Following the statistical superiority in ASAS 40 response rates seen with IV secukinumab at week 16, patients who from there switched from placebo to IV secukinumab achieved comparable ASAS 40 response rates to those of patients originally randomized to secukinumab by week 24, reaching 66.8% for those on secukinumab the whole time and 74.9% for those who switched.
Secondary outcome measures were similar in both groups at week 52.
Among all patients who took secukinumab – the percentage with any adverse event was 63.2%, and 6% had a nonfatal adverse event deemed serious. There was one death during secukinumab treatment not suspected to be related to treatment.
In a presentation about the axSpA study findings, Atul Deodhar, MD, of Oregon Health & Science University, noted that “having an IV biologic available in the U.S. has some advantages. There are certain insurance providers such as Medicare where it is more economical for the patient to have an IV drug available.”
Dr. Deodhar also noted that in October the FDA approved a recommended lower dose for the IV treatment than in the study: 1.75 mg/kg instead of 3 mg/kg following the loading dose. That’s because the 3 mg/kg dose caused blood levels to be higher than those in the subcutaneous form, he said.
The FDA made the same dose recommendation for PsA.
Study limitations
Dr. Goodson, the U.K. consultant rheumatologist, noted a limitation of the trials: “It would have been interesting to compare IV to subcutaneous route secukinumab.” Still, the findings suggest that “the safety and efficacy of IV administration appears comparable,” she said.
“IV administration will have associated costs of attending hospital or infusion clinics,” she added, “and the cost of additional staff and administration need to be considered.”
Novartis, the maker of secukinumab, funded both studies. The PsA study authors report multiple relationships with industry, and some, such as Dr. Kivitz, have connections to Novartis. The axSpA study authors also report multiple relationships with industry, and some, such as Dr. Deodhar, have connections to Novartis. Some authors of both studies are Novartis employees. Dr. Goodson disclosed financial relationships with UCB and AbbVie.
SAN DIEGO – Monthly use of intravenously administered secukinumab (Cosentyx) proved its efficacy over placebo in treating psoriatic arthritis (PsA) and axial spondyloarthritis (axSpA) in two industry-sponsored, randomized, double-blinded, phase 3 trials of the drug’s second and newly approved route of administration.
The studies of the human monoclonal antibody secukinumab, an interleukin-17 inhibitor, were presented at the annual meeting of the American College of Rheumatology. A subcutaneously injectable formulation of the drug is available, and the Food and Drug Administration approved the IV form for the conditions in October, although at a recommended lower monthly dose than the new trials examined.
In the PsA trial, 191 patients took IV secukinumab, and 190 took placebo. For the primary endpoint, the percentages who reached at least a 50% improvement in American College of Rheumatology response criteria (ACR 50) at 16 weeks were 31.4% and 6.3%, respectively (P < .0001).
In the axSpA trial, 264 patients took IV secukinumab, and 262 took placebo. The primary endpoint, at least a 40% improvement in Assessment of the Spondyloarthritis International Society response criteria (ASAS 40), was met at 16 weeks by 40.9% and 22.9%, respectively (P < .0001).
“Both studies appear to present clear efficacy of IV route administration of secukinumab with no clear increase in safety signals,” consultant rheumatologist Nicola Goodson, MBChB, PhD, of Aintree University Hospital in Liverpool, England, said in an interview.
“Offering IV administration as an option to patients is helpful,” added Dr. Goodson, who was not involved with the study but is familiar with its findings.
As Dr. Goodson explained, secukinumab “was the first IL [interleukin]-17 inhibitor used to treat spondyloarthropathies, and we have been using subcutaneous secukinumab to treat psoriasis, psoriatic arthritis, and axial spondyloarthritis/ankylosing spondylitis since 2016 in the U.K. Our experience with this medication has been good with similar efficacy to anti-TNF [tumor necrosis factor] therapy in axial spondyloarthritis. The medication is generally well-tolerated, and the subcutaneous pen injection device is easy for patients to use.”
However, IV treatment may speed up onset of action, she said, and it may be useful in situations when compliance is a challenge.
PsA trial details
In the PsA trial, known as INVIGORATE-2, researchers recruited patients who met the CASPAR criteria for active PsA with symptoms for ≥ 6 months, and had ≥ 3 tender joints out of 78 joints and ≥ 3 swollen joints out of 76.
Participants with a mean age of 48, including 55% females, were randomized 1:1 to receive placebo or secukinumab (6 mg/kg at baseline followed by 3 mg/kg every 4 weeks). Those in the placebo group were switched to the same monthly doses of secukinumab at 16 weeks.
“Patients who switched from the placebo had a similar increase of efficacy as the original treated group,” rheumatologist Alan J. Kivitz, MD, of the Altoona Center for Clinical Research, in Duncansville, Penn., said in his presentation at the meeting. Specifically, at 52 weeks, the groups had similar ACR 50 response rates: 58% with secukinumab and 64% with placebo-to-secukinumab.
The fact that patients in the original placebo group who received 3 mg IV doses without 6-mg loading doses achieved ACR response rates similar to those who took secukinumab during the whole trial “could suggest that the IV loading dose may not be required. This would need to be explored in a randomized head-to-head study, but it’s an interesting observation that may reduce costs and exposure to higher doses of medication at the start of treatment,” Dr. Goodson said.
Among the patients who received secukinumab at any point in the study, 63% had a treatment-emergent adverse event, including 5.9% with serious events. One death was reported in the placebo group before week 16. No other deaths were reported.
AxSpA trial details
In the axSpA trial, called INVIGORATE-1, researchers recruited people aged ≥18 years with a diagnosis of active radiographic axSpA according to modified New York criteria or nonradiographic axSpA according to ASAS criteria, and all had inflammatory back pain for ≥6 months with an onset before age 45. They were randomized at a 1:1 ratio to receive IV secukinumab (6 mg/kg loading dose, followed by 3 mg/kg every 4 weeks) or placebo for 16 weeks. At that point, the placebo group switched to the same monthly doses of IV secukinumab.
Participants had a mean age of about 39, and about one-third were female.
Following the statistical superiority in ASAS 40 response rates seen with IV secukinumab at week 16, patients who from there switched from placebo to IV secukinumab achieved comparable ASAS 40 response rates to those of patients originally randomized to secukinumab by week 24, reaching 66.8% for those on secukinumab the whole time and 74.9% for those who switched.
Secondary outcome measures were similar in both groups at week 52.
Among all patients who took secukinumab – the percentage with any adverse event was 63.2%, and 6% had a nonfatal adverse event deemed serious. There was one death during secukinumab treatment not suspected to be related to treatment.
In a presentation about the axSpA study findings, Atul Deodhar, MD, of Oregon Health & Science University, noted that “having an IV biologic available in the U.S. has some advantages. There are certain insurance providers such as Medicare where it is more economical for the patient to have an IV drug available.”
Dr. Deodhar also noted that in October the FDA approved a recommended lower dose for the IV treatment than in the study: 1.75 mg/kg instead of 3 mg/kg following the loading dose. That’s because the 3 mg/kg dose caused blood levels to be higher than those in the subcutaneous form, he said.
The FDA made the same dose recommendation for PsA.
Study limitations
Dr. Goodson, the U.K. consultant rheumatologist, noted a limitation of the trials: “It would have been interesting to compare IV to subcutaneous route secukinumab.” Still, the findings suggest that “the safety and efficacy of IV administration appears comparable,” she said.
“IV administration will have associated costs of attending hospital or infusion clinics,” she added, “and the cost of additional staff and administration need to be considered.”
Novartis, the maker of secukinumab, funded both studies. The PsA study authors report multiple relationships with industry, and some, such as Dr. Kivitz, have connections to Novartis. The axSpA study authors also report multiple relationships with industry, and some, such as Dr. Deodhar, have connections to Novartis. Some authors of both studies are Novartis employees. Dr. Goodson disclosed financial relationships with UCB and AbbVie.
AT ACR 2023
First referral guide issued for axial spondyloarthritis
SAN DIEGO – The Spondyloarthritis Research and Treatment Network (SPARTAN) has created the first referral recommendations for axial spondyloarthritis (axSpA).
The draft recommendations use a points scoring system, with the goal that at least one in three patients referred would be diagnosed with axSpA, an inflammatory arthritis that affects the central skeleton and shares a genetic overlap with skin psoriasis, inflammatory bowel disease, and inflammatory eye disease.

Patients with axSpA can wait 10 years after symptom onset to be diagnosed with the condition. There are currently no guidelines to advise clinicians on when to refer to a rheumatologist, and with the rheumatology workforce shortage, “it is impossible for rheumatologists to evaluate the 20% of adults in the U.S. who have chronic back pain,” said Maureen Dubreuil, MD, a rheumatologist at Boston University. She presented the work at the annual meeting of the American College of Rheumatology.
To address this issue, Dr. Dubreuil and colleagues conducted a literature review to determine how predictive different spondyloarthritis features were of eventual axSpA diagnosis. The interdisciplinary team identified 38 studies published before March 2022, and uncovered 28 individual potential features associated with axSpA, including pain sites, family history of axSpA and related conditions, blood markers of inflammation, genetic testing, and imaging findings.
Inflammatory back pain elements had the lower predictive values, with positive likelihood ratios (LR+) ranging from 1.15 to 2.32, while imaging findings were the most predictive (LR+s from 6.40 to 10.02).
Using a Delphi exercise and discrete choice experiments, members narrowed the checklist down to 10 features. These 10 features were assigned points, with a score of 3 points qualifying for a referral of adults 45 years or younger with chronic pain (3 or more months) in the back, hip, or buttock.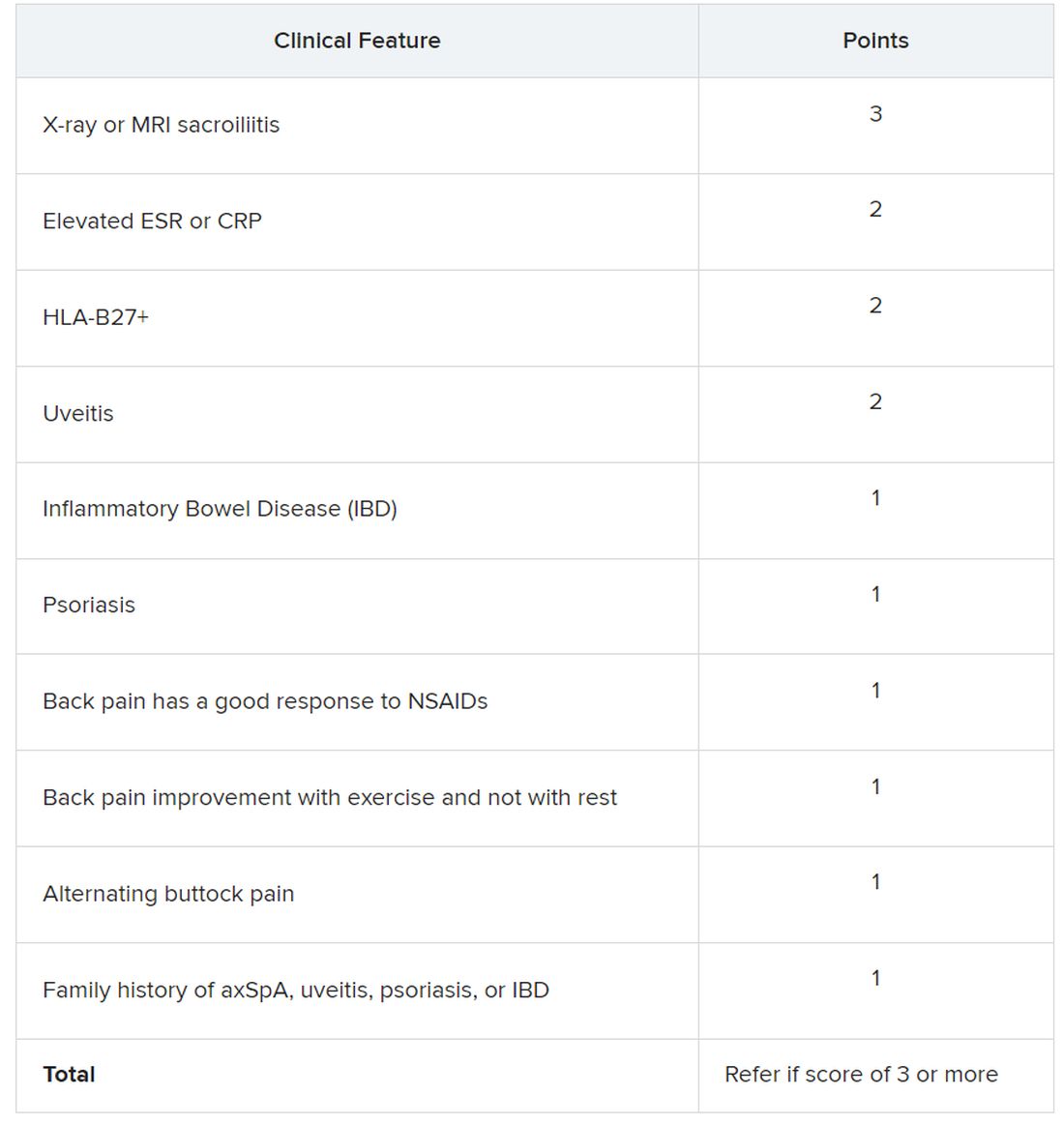
Sacroiliitis seen on imaging, either by x-ray or MRI, received the highest score of 3 points. Dr. Dubreuil emphasized that imaging was not required for a referral, but if a patient has received imaging “that shows sacroiliitis, that is sufficient for referral to a rheumatologist,” she said in her presentation.
Elevated erythrocyte sedimentation rate or C-reactive protein, HLA-B27 positivity, and uveitis score 2 points. Inflammatory bowel disease; psoriasis; back pain with good response to NSAIDs; back pain improvement with exercise and not with rest; alternating buttock pain; and family history of axial spondyloarthritis, uveitis, psoriasis, or IBD score 1 point.
Dr. Dubreuil and colleagues expect that these criteria for referral will result in about one in three referred adults aged 45 years or younger with chronic back pain being diagnosed with axSpA. They also say additional research is necessary to understand if these recommendations increase probability of axSpA diagnosis and reduce diagnostic delays.
“We’re now getting to the stage where we are creating this screening tool, but [testing the] performance of the screening tool is going to be the major next step,” said Mark Hwang, MD, of UTHealth Houston in an interview with this news organization. He is a member of SPARTAN but was not involved with authoring the recommendations. “Will the screening tool enhance the ability on the back end to identify axSpA? We don’t know yet.”
Jon Chan, MD, a rheumatologist at the University of British Columbia, Vancouver, agreed that these recommendations “are a good first step,” but that more awareness about axSpA from nonrheumatologists would also be helpful in identifying new axSpA patients. He is also a member of SPARTAN and comoderated with Dr. Hwang the session where the new recommendations were presented. “I think other diseases like rheumatoid arthritis or lupus have a lot more recognition in the nonrheumatology community,” he told this news organization.
Connecting with other health professionals who see a lot of patients with back pain – physiotherapists, chiropractors, and chronic pain physicians – could also be helpful, he added. “A lot of times, patients go straight to a physio and circumvent the doctor,” he said.
Dr. Chan reports success in educating other departments. “I put up a poster in the emergency department saying, ‘If you’re young with back pain and uveitis, you need to be seen by rheumatology,’ and we’ve identified a ton of axSpA patients that way,” he said. “Maybe their uveitis was very mild, but their back pain was quite severe, and no one really clued in.”
Dr. Dubreuil disclosed financial relationships with Amgen, Pfizer, and UCB Pharma. Her abstract coauthors disclosed financial relationships with multiple pharmaceutical companies. Dr. Hwang consults for UCB and has received research support from Janssen. Dr. Chan has relationships with AbbVie/Abbott, Eli Lilly, Janssen, Novartis, and UCB.
SAN DIEGO – The Spondyloarthritis Research and Treatment Network (SPARTAN) has created the first referral recommendations for axial spondyloarthritis (axSpA).
The draft recommendations use a points scoring system, with the goal that at least one in three patients referred would be diagnosed with axSpA, an inflammatory arthritis that affects the central skeleton and shares a genetic overlap with skin psoriasis, inflammatory bowel disease, and inflammatory eye disease.
Patients with axSpA can wait 10 years after symptom onset to be diagnosed with the condition. There are currently no guidelines to advise clinicians on when to refer to a rheumatologist, and with the rheumatology workforce shortage, “it is impossible for rheumatologists to evaluate the 20% of adults in the U.S. who have chronic back pain,” said Maureen Dubreuil, MD, a rheumatologist at Boston University. She presented the work at the annual meeting of the American College of Rheumatology.
To address this issue, Dr. Dubreuil and colleagues conducted a literature review to determine how predictive different spondyloarthritis features were of eventual axSpA diagnosis. The interdisciplinary team identified 38 studies published before March 2022, and uncovered 28 individual potential features associated with axSpA, including pain sites, family history of axSpA and related conditions, blood markers of inflammation, genetic testing, and imaging findings.
Inflammatory back pain elements had the lower predictive values, with positive likelihood ratios (LR+) ranging from 1.15 to 2.32, while imaging findings were the most predictive (LR+s from 6.40 to 10.02).
Using a Delphi exercise and discrete choice experiments, members narrowed the checklist down to 10 features. These 10 features were assigned points, with a score of 3 points qualifying for a referral of adults 45 years or younger with chronic pain (3 or more months) in the back, hip, or buttock.
Sacroiliitis seen on imaging, either by x-ray or MRI, received the highest score of 3 points. Dr. Dubreuil emphasized that imaging was not required for a referral, but if a patient has received imaging “that shows sacroiliitis, that is sufficient for referral to a rheumatologist,” she said in her presentation.
Elevated erythrocyte sedimentation rate or C-reactive protein, HLA-B27 positivity, and uveitis score 2 points. Inflammatory bowel disease; psoriasis; back pain with good response to NSAIDs; back pain improvement with exercise and not with rest; alternating buttock pain; and family history of axial spondyloarthritis, uveitis, psoriasis, or IBD score 1 point.
Dr. Dubreuil and colleagues expect that these criteria for referral will result in about one in three referred adults aged 45 years or younger with chronic back pain being diagnosed with axSpA. They also say additional research is necessary to understand if these recommendations increase probability of axSpA diagnosis and reduce diagnostic delays.
“We’re now getting to the stage where we are creating this screening tool, but [testing the] performance of the screening tool is going to be the major next step,” said Mark Hwang, MD, of UTHealth Houston in an interview with this news organization. He is a member of SPARTAN but was not involved with authoring the recommendations. “Will the screening tool enhance the ability on the back end to identify axSpA? We don’t know yet.”
Jon Chan, MD, a rheumatologist at the University of British Columbia, Vancouver, agreed that these recommendations “are a good first step,” but that more awareness about axSpA from nonrheumatologists would also be helpful in identifying new axSpA patients. He is also a member of SPARTAN and comoderated with Dr. Hwang the session where the new recommendations were presented. “I think other diseases like rheumatoid arthritis or lupus have a lot more recognition in the nonrheumatology community,” he told this news organization.
Connecting with other health professionals who see a lot of patients with back pain – physiotherapists, chiropractors, and chronic pain physicians – could also be helpful, he added. “A lot of times, patients go straight to a physio and circumvent the doctor,” he said.
Dr. Chan reports success in educating other departments. “I put up a poster in the emergency department saying, ‘If you’re young with back pain and uveitis, you need to be seen by rheumatology,’ and we’ve identified a ton of axSpA patients that way,” he said. “Maybe their uveitis was very mild, but their back pain was quite severe, and no one really clued in.”
Dr. Dubreuil disclosed financial relationships with Amgen, Pfizer, and UCB Pharma. Her abstract coauthors disclosed financial relationships with multiple pharmaceutical companies. Dr. Hwang consults for UCB and has received research support from Janssen. Dr. Chan has relationships with AbbVie/Abbott, Eli Lilly, Janssen, Novartis, and UCB.
SAN DIEGO – The Spondyloarthritis Research and Treatment Network (SPARTAN) has created the first referral recommendations for axial spondyloarthritis (axSpA).
The draft recommendations use a points scoring system, with the goal that at least one in three patients referred would be diagnosed with axSpA, an inflammatory arthritis that affects the central skeleton and shares a genetic overlap with skin psoriasis, inflammatory bowel disease, and inflammatory eye disease.
Patients with axSpA can wait 10 years after symptom onset to be diagnosed with the condition. There are currently no guidelines to advise clinicians on when to refer to a rheumatologist, and with the rheumatology workforce shortage, “it is impossible for rheumatologists to evaluate the 20% of adults in the U.S. who have chronic back pain,” said Maureen Dubreuil, MD, a rheumatologist at Boston University. She presented the work at the annual meeting of the American College of Rheumatology.
To address this issue, Dr. Dubreuil and colleagues conducted a literature review to determine how predictive different spondyloarthritis features were of eventual axSpA diagnosis. The interdisciplinary team identified 38 studies published before March 2022, and uncovered 28 individual potential features associated with axSpA, including pain sites, family history of axSpA and related conditions, blood markers of inflammation, genetic testing, and imaging findings.
Inflammatory back pain elements had the lower predictive values, with positive likelihood ratios (LR+) ranging from 1.15 to 2.32, while imaging findings were the most predictive (LR+s from 6.40 to 10.02).
Using a Delphi exercise and discrete choice experiments, members narrowed the checklist down to 10 features. These 10 features were assigned points, with a score of 3 points qualifying for a referral of adults 45 years or younger with chronic pain (3 or more months) in the back, hip, or buttock.
Sacroiliitis seen on imaging, either by x-ray or MRI, received the highest score of 3 points. Dr. Dubreuil emphasized that imaging was not required for a referral, but if a patient has received imaging “that shows sacroiliitis, that is sufficient for referral to a rheumatologist,” she said in her presentation.
Elevated erythrocyte sedimentation rate or C-reactive protein, HLA-B27 positivity, and uveitis score 2 points. Inflammatory bowel disease; psoriasis; back pain with good response to NSAIDs; back pain improvement with exercise and not with rest; alternating buttock pain; and family history of axial spondyloarthritis, uveitis, psoriasis, or IBD score 1 point.
Dr. Dubreuil and colleagues expect that these criteria for referral will result in about one in three referred adults aged 45 years or younger with chronic back pain being diagnosed with axSpA. They also say additional research is necessary to understand if these recommendations increase probability of axSpA diagnosis and reduce diagnostic delays.
“We’re now getting to the stage where we are creating this screening tool, but [testing the] performance of the screening tool is going to be the major next step,” said Mark Hwang, MD, of UTHealth Houston in an interview with this news organization. He is a member of SPARTAN but was not involved with authoring the recommendations. “Will the screening tool enhance the ability on the back end to identify axSpA? We don’t know yet.”
Jon Chan, MD, a rheumatologist at the University of British Columbia, Vancouver, agreed that these recommendations “are a good first step,” but that more awareness about axSpA from nonrheumatologists would also be helpful in identifying new axSpA patients. He is also a member of SPARTAN and comoderated with Dr. Hwang the session where the new recommendations were presented. “I think other diseases like rheumatoid arthritis or lupus have a lot more recognition in the nonrheumatology community,” he told this news organization.
Connecting with other health professionals who see a lot of patients with back pain – physiotherapists, chiropractors, and chronic pain physicians – could also be helpful, he added. “A lot of times, patients go straight to a physio and circumvent the doctor,” he said.
Dr. Chan reports success in educating other departments. “I put up a poster in the emergency department saying, ‘If you’re young with back pain and uveitis, you need to be seen by rheumatology,’ and we’ve identified a ton of axSpA patients that way,” he said. “Maybe their uveitis was very mild, but their back pain was quite severe, and no one really clued in.”
Dr. Dubreuil disclosed financial relationships with Amgen, Pfizer, and UCB Pharma. Her abstract coauthors disclosed financial relationships with multiple pharmaceutical companies. Dr. Hwang consults for UCB and has received research support from Janssen. Dr. Chan has relationships with AbbVie/Abbott, Eli Lilly, Janssen, Novartis, and UCB.
AT ACR 2023
Study takes fine-grained look at MACE risk with glucocorticoids in RA
SAN DIEGO – Even when taken at low doses and over short periods, glucocorticoids (GCs) were linked to a higher risk of major adverse cardiovascular events (MACE) over the long term in a Veterans Affairs population of older, mostly male patients with rheumatoid arthritis, a new retrospective cohort study has found.
The analysis of nearly 19,000 patients, presented by rheumatologist Beth Wallace, MD, MSc, at the annual meeting of the American College of Rheumatology, showed that the level of risk for MACE rose with the dose, duration, and recency of GC use, in which risk increased significantly at prednisone-equivalent doses as low as 5 mg/day, durations as short as 30 days, and with last use as long as 1 year before MACE.

“Up to half of RA patients in the United States use long-term glucocorticoids despite previous work suggesting they increase MACE in a dose-dependent way,” said Dr. Wallace, assistant professor of medicine at the University of Michigan, Ann Arbor, and a rheumatologist at the VA Ann Arbor Healthcare Center. “Our group previously presented work suggesting that less than 14 days of glucocorticoid use in a 6-month period is associated with a two-thirds increase in odds of MACE over the following 6 months, with 90 days of use associated with more than twofold increase.”
In recent years, researchers such as Dr. Wallace have focused attention on the risks of GCs in RA. The American College of Rheumatology and the European Alliance of Associations for Rheumatology emphasize avoiding long-term use of GCs in RA and keeping doses as small and over the shortest amount of time as possible.
When Dr. Wallace and colleagues looked at the clinical pattern of GC use for patients with RA during the past 2 years, those who took 5 mg, 7.5 mg, and 10 mg daily doses for 30 days and had stopped at least a year before had risk for MACE that rose significantly by 3%, 5%, and 7%, respectively, compared with those who didn’t take GCs in the past 2 years.
While those increases were small, risk for MACE rose even more for those who took the same daily doses for 90 days, increasing 10%, 15%, and 21%, respectively. Researchers linked current ongoing use of GCs for the past 90 days to a 13%, 19%, and 27% higher risk for MACE at those respective doses.
The findings “add to the literature suggesting that there is some risk even with low-dose steroids,” said Michael George, MD, assistant professor of rheumatology and epidemiology at the University of Pennsylvania, Philadelphia, who did not take part in the research but is familiar with the findings.

“We can see that even glucocorticoids taken several years ago may affect cardiovascular risk but that recent use has a bigger effect on risk,” Dr. George said in an interview. “This study also suggests that very low-dose use affects risk.”
For the new study, Dr. Wallace and colleagues examined a Veterans Affairs database and identified 18,882 patients with RA (mean age, 62.5 years; 84% male; 66% GC users) who met the criteria of being > 40 and < 90 years old. The subjects had an initial VA rheumatology visit during 2010-2018 and were excluded if they had a non-RA rheumatologic disorder, prior MACE, or heart failure. MACE was defined as MI, stroke/TIA, cardiac arrest, coronary revascularization, or death from CV cause.
A total of 16% of the cohort had the largest exposure to GCs, defined as use for 90 days or more; 23% had exposure of 14-89 days, and 14% had exposure of 1-13 days.
The median 5-year MACE risk at baseline was 5.3%, and 3,754 patients (19.9%) had high baseline MACE risk. Incident MACE occurred in 4.1% of patients, and the median time to MACE was 2.67 years (interquartile ratio, 1.26-4.45 years).
Covariates included factors such as age, race, sex, body mass index, smoking status, adjusted Elixhauser index, VA risk score for cardiovascular disease, cancer, hospitalization for infection, number of rheumatology clinic visits, and use of lipid-lowering drugs, opioids, methotrexate, biologics, and hydroxychloroquine.
Dr. Wallace noted limitations including the possibility of residual confounding and the influence of background cardiovascular risk. The study didn’t examine the clinical value of taking GCs or compare that to the potential risk. Nor did it examine cost or the risks and benefits of alternative therapeutic options.
A study released earlier this year suggested that patients taking daily prednisolone doses under 5 mg do not have a higher risk of MACE. Previous studies had reached conflicting results.
“Glucocorticoids can provide major benefits to patients, but these benefits must be balanced with the potential risks,” Dr. George said. At low doses, these risks may be small, but they are present. In many cases, escalating DMARD [disease-modifying antirheumatic drug] therapy may be safer than continuing glucocorticoids.”
He added that the risks of GCs may be especially high in older patients and in those who have cardiovascular risk factors: “Often biologics are avoided in these higher-risk patients. But in fact, in many cases biologics may be the safer choice.”
No study funding was reported. Dr. Wallace reported no relevant financial relationships, and some of the other authors reported various ties with industry. Dr. George reported research funding from GlaxoSmithKline and Janssen and consulting fees from AbbVie.
SAN DIEGO – Even when taken at low doses and over short periods, glucocorticoids (GCs) were linked to a higher risk of major adverse cardiovascular events (MACE) over the long term in a Veterans Affairs population of older, mostly male patients with rheumatoid arthritis, a new retrospective cohort study has found.
The analysis of nearly 19,000 patients, presented by rheumatologist Beth Wallace, MD, MSc, at the annual meeting of the American College of Rheumatology, showed that the level of risk for MACE rose with the dose, duration, and recency of GC use, in which risk increased significantly at prednisone-equivalent doses as low as 5 mg/day, durations as short as 30 days, and with last use as long as 1 year before MACE.
“Up to half of RA patients in the United States use long-term glucocorticoids despite previous work suggesting they increase MACE in a dose-dependent way,” said Dr. Wallace, assistant professor of medicine at the University of Michigan, Ann Arbor, and a rheumatologist at the VA Ann Arbor Healthcare Center. “Our group previously presented work suggesting that less than 14 days of glucocorticoid use in a 6-month period is associated with a two-thirds increase in odds of MACE over the following 6 months, with 90 days of use associated with more than twofold increase.”
In recent years, researchers such as Dr. Wallace have focused attention on the risks of GCs in RA. The American College of Rheumatology and the European Alliance of Associations for Rheumatology emphasize avoiding long-term use of GCs in RA and keeping doses as small and over the shortest amount of time as possible.
When Dr. Wallace and colleagues looked at the clinical pattern of GC use for patients with RA during the past 2 years, those who took 5 mg, 7.5 mg, and 10 mg daily doses for 30 days and had stopped at least a year before had risk for MACE that rose significantly by 3%, 5%, and 7%, respectively, compared with those who didn’t take GCs in the past 2 years.
While those increases were small, risk for MACE rose even more for those who took the same daily doses for 90 days, increasing 10%, 15%, and 21%, respectively. Researchers linked current ongoing use of GCs for the past 90 days to a 13%, 19%, and 27% higher risk for MACE at those respective doses.
The findings “add to the literature suggesting that there is some risk even with low-dose steroids,” said Michael George, MD, assistant professor of rheumatology and epidemiology at the University of Pennsylvania, Philadelphia, who did not take part in the research but is familiar with the findings.
“We can see that even glucocorticoids taken several years ago may affect cardiovascular risk but that recent use has a bigger effect on risk,” Dr. George said in an interview. “This study also suggests that very low-dose use affects risk.”
For the new study, Dr. Wallace and colleagues examined a Veterans Affairs database and identified 18,882 patients with RA (mean age, 62.5 years; 84% male; 66% GC users) who met the criteria of being > 40 and < 90 years old. The subjects had an initial VA rheumatology visit during 2010-2018 and were excluded if they had a non-RA rheumatologic disorder, prior MACE, or heart failure. MACE was defined as MI, stroke/TIA, cardiac arrest, coronary revascularization, or death from CV cause.
A total of 16% of the cohort had the largest exposure to GCs, defined as use for 90 days or more; 23% had exposure of 14-89 days, and 14% had exposure of 1-13 days.
The median 5-year MACE risk at baseline was 5.3%, and 3,754 patients (19.9%) had high baseline MACE risk. Incident MACE occurred in 4.1% of patients, and the median time to MACE was 2.67 years (interquartile ratio, 1.26-4.45 years).
Covariates included factors such as age, race, sex, body mass index, smoking status, adjusted Elixhauser index, VA risk score for cardiovascular disease, cancer, hospitalization for infection, number of rheumatology clinic visits, and use of lipid-lowering drugs, opioids, methotrexate, biologics, and hydroxychloroquine.
Dr. Wallace noted limitations including the possibility of residual confounding and the influence of background cardiovascular risk. The study didn’t examine the clinical value of taking GCs or compare that to the potential risk. Nor did it examine cost or the risks and benefits of alternative therapeutic options.
A study released earlier this year suggested that patients taking daily prednisolone doses under 5 mg do not have a higher risk of MACE. Previous studies had reached conflicting results.
“Glucocorticoids can provide major benefits to patients, but these benefits must be balanced with the potential risks,” Dr. George said. At low doses, these risks may be small, but they are present. In many cases, escalating DMARD [disease-modifying antirheumatic drug] therapy may be safer than continuing glucocorticoids.”
He added that the risks of GCs may be especially high in older patients and in those who have cardiovascular risk factors: “Often biologics are avoided in these higher-risk patients. But in fact, in many cases biologics may be the safer choice.”
No study funding was reported. Dr. Wallace reported no relevant financial relationships, and some of the other authors reported various ties with industry. Dr. George reported research funding from GlaxoSmithKline and Janssen and consulting fees from AbbVie.
SAN DIEGO – Even when taken at low doses and over short periods, glucocorticoids (GCs) were linked to a higher risk of major adverse cardiovascular events (MACE) over the long term in a Veterans Affairs population of older, mostly male patients with rheumatoid arthritis, a new retrospective cohort study has found.
The analysis of nearly 19,000 patients, presented by rheumatologist Beth Wallace, MD, MSc, at the annual meeting of the American College of Rheumatology, showed that the level of risk for MACE rose with the dose, duration, and recency of GC use, in which risk increased significantly at prednisone-equivalent doses as low as 5 mg/day, durations as short as 30 days, and with last use as long as 1 year before MACE.
“Up to half of RA patients in the United States use long-term glucocorticoids despite previous work suggesting they increase MACE in a dose-dependent way,” said Dr. Wallace, assistant professor of medicine at the University of Michigan, Ann Arbor, and a rheumatologist at the VA Ann Arbor Healthcare Center. “Our group previously presented work suggesting that less than 14 days of glucocorticoid use in a 6-month period is associated with a two-thirds increase in odds of MACE over the following 6 months, with 90 days of use associated with more than twofold increase.”
In recent years, researchers such as Dr. Wallace have focused attention on the risks of GCs in RA. The American College of Rheumatology and the European Alliance of Associations for Rheumatology emphasize avoiding long-term use of GCs in RA and keeping doses as small and over the shortest amount of time as possible.
When Dr. Wallace and colleagues looked at the clinical pattern of GC use for patients with RA during the past 2 years, those who took 5 mg, 7.5 mg, and 10 mg daily doses for 30 days and had stopped at least a year before had risk for MACE that rose significantly by 3%, 5%, and 7%, respectively, compared with those who didn’t take GCs in the past 2 years.
While those increases were small, risk for MACE rose even more for those who took the same daily doses for 90 days, increasing 10%, 15%, and 21%, respectively. Researchers linked current ongoing use of GCs for the past 90 days to a 13%, 19%, and 27% higher risk for MACE at those respective doses.
The findings “add to the literature suggesting that there is some risk even with low-dose steroids,” said Michael George, MD, assistant professor of rheumatology and epidemiology at the University of Pennsylvania, Philadelphia, who did not take part in the research but is familiar with the findings.
“We can see that even glucocorticoids taken several years ago may affect cardiovascular risk but that recent use has a bigger effect on risk,” Dr. George said in an interview. “This study also suggests that very low-dose use affects risk.”
For the new study, Dr. Wallace and colleagues examined a Veterans Affairs database and identified 18,882 patients with RA (mean age, 62.5 years; 84% male; 66% GC users) who met the criteria of being > 40 and < 90 years old. The subjects had an initial VA rheumatology visit during 2010-2018 and were excluded if they had a non-RA rheumatologic disorder, prior MACE, or heart failure. MACE was defined as MI, stroke/TIA, cardiac arrest, coronary revascularization, or death from CV cause.
A total of 16% of the cohort had the largest exposure to GCs, defined as use for 90 days or more; 23% had exposure of 14-89 days, and 14% had exposure of 1-13 days.
The median 5-year MACE risk at baseline was 5.3%, and 3,754 patients (19.9%) had high baseline MACE risk. Incident MACE occurred in 4.1% of patients, and the median time to MACE was 2.67 years (interquartile ratio, 1.26-4.45 years).
Covariates included factors such as age, race, sex, body mass index, smoking status, adjusted Elixhauser index, VA risk score for cardiovascular disease, cancer, hospitalization for infection, number of rheumatology clinic visits, and use of lipid-lowering drugs, opioids, methotrexate, biologics, and hydroxychloroquine.
Dr. Wallace noted limitations including the possibility of residual confounding and the influence of background cardiovascular risk. The study didn’t examine the clinical value of taking GCs or compare that to the potential risk. Nor did it examine cost or the risks and benefits of alternative therapeutic options.
A study released earlier this year suggested that patients taking daily prednisolone doses under 5 mg do not have a higher risk of MACE. Previous studies had reached conflicting results.
“Glucocorticoids can provide major benefits to patients, but these benefits must be balanced with the potential risks,” Dr. George said. At low doses, these risks may be small, but they are present. In many cases, escalating DMARD [disease-modifying antirheumatic drug] therapy may be safer than continuing glucocorticoids.”
He added that the risks of GCs may be especially high in older patients and in those who have cardiovascular risk factors: “Often biologics are avoided in these higher-risk patients. But in fact, in many cases biologics may be the safer choice.”
No study funding was reported. Dr. Wallace reported no relevant financial relationships, and some of the other authors reported various ties with industry. Dr. George reported research funding from GlaxoSmithKline and Janssen and consulting fees from AbbVie.
AT ACR 2023
AI tool perfect in study of inflammatory diseases
Artificial intelligence can distinguish overlapping inflammatory conditions with total accuracy, according to a new study presented at the annual meeting of the American College of Rheumatology.
Texas pediatricians faced a conundrum during the pandemic. Endemic typhus, a flea-borne tropical infection common to the region, is nearly indistinguishable from multisystem inflammatory syndrome in children (MIS-C), a rare condition set in motion by SARS-CoV-2 infection. Children with either ailment had seemingly identical symptoms: fever, rash, gastrointestinal issues, and in need of swift treatment. A diagnosis of endemic typhus can take 4-6 days to confirm.
Tiphanie Vogel, MD, PhD, a pediatric rheumatologist at Texas Children’s Hospital, Houston, and colleagues sought to create a tool to hasten diagnosis and, ideally, treatment. To do so, they incorporated machine learning and clinical factors available within the first 6 hours of the onset of symptoms.
The team analyzed 49 demographic, clinical, and laboratory measures from the medical records of 133 children with MIS-C and 87 with endemic typhus. Using deep learning, they narrowed the model to 30 essential features that became the backbone of AI-MET, a two-phase clinical-decision support system.
Phase 1 uses 17 clinical factors and can be performed on paper. If a patient’s score in phase 1 is not determinative, clinicians proceed to phase 2, which uses an additional 13 weighted factors and machine learning.
In testing, the two-part tool classified each of the 220 test patients perfectly. And it diagnosed a second group of 111 patients with MIS-C with 99% (110/111) accuracy.
Of note, “that first step classifies [a patient] correctly half of the time,” Dr. Vogel said, so the second, AI phase of the tool was necessary for only half of cases. Dr. Vogel said that’s a good sign; it means that the tool is useful in settings where AI may not always be feasible, like in a busy ED.
Melissa Mizesko, MD, a pediatric rheumatologist at Driscoll Children’s Hospital in Corpus Christi, Tex., said that the new tool could help clinicians streamline care. When cases of MIS-C peaked in Texas, clinicians often would start sick children on doxycycline and treat for MIS-C at the same time, then wait to see whether the antibiotic brought the fever down.
“This [new tool] is helpful if you live in a part of the country that has typhus,” said Jane Burns, MD, director of the Kawasaki Disease Research Center at the University of California, San Diego, who helped develop a similar AI-based tool to distinguish MIS-C from Kawasaki disease. But she encouraged the researchers to expand their testing to include other conditions. Although the AI model Dr. Vogel’s group developed can pinpoint MIS-C or endemic typhus, what if a child has neither condition? “It’s not often you’re dealing with a diagnosis between just two specific diseases,” Dr. Burns said.
Dr. Vogel is also interested in making AI-MET more efficient. “This go-round we prioritized perfect accuracy,” she said. But 30 clinical factors, with 17 of them recorded and calculated by hand, is a lot. “Could we still get this to be very accurate, maybe not perfect, with less inputs?”
In addition to refining AI-MET, which Texas Children’s eventually hopes to make available to other institutions, Dr. Vogel and associates are also considering other use cases for AI. Lupus is one option. “Maybe with machine learning we could identify clues at diagnosis that would help recommend targeted treatment,” she said
Dr. Vogel disclosed potential conflicts of interest with Moderna, Novartis, Pfizer, and SOBI. Dr. Burns and Dr. Mizesko disclosed no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
Artificial intelligence can distinguish overlapping inflammatory conditions with total accuracy, according to a new study presented at the annual meeting of the American College of Rheumatology.
Texas pediatricians faced a conundrum during the pandemic. Endemic typhus, a flea-borne tropical infection common to the region, is nearly indistinguishable from multisystem inflammatory syndrome in children (MIS-C), a rare condition set in motion by SARS-CoV-2 infection. Children with either ailment had seemingly identical symptoms: fever, rash, gastrointestinal issues, and in need of swift treatment. A diagnosis of endemic typhus can take 4-6 days to confirm.
Tiphanie Vogel, MD, PhD, a pediatric rheumatologist at Texas Children’s Hospital, Houston, and colleagues sought to create a tool to hasten diagnosis and, ideally, treatment. To do so, they incorporated machine learning and clinical factors available within the first 6 hours of the onset of symptoms.
The team analyzed 49 demographic, clinical, and laboratory measures from the medical records of 133 children with MIS-C and 87 with endemic typhus. Using deep learning, they narrowed the model to 30 essential features that became the backbone of AI-MET, a two-phase clinical-decision support system.
Phase 1 uses 17 clinical factors and can be performed on paper. If a patient’s score in phase 1 is not determinative, clinicians proceed to phase 2, which uses an additional 13 weighted factors and machine learning.
In testing, the two-part tool classified each of the 220 test patients perfectly. And it diagnosed a second group of 111 patients with MIS-C with 99% (110/111) accuracy.
Of note, “that first step classifies [a patient] correctly half of the time,” Dr. Vogel said, so the second, AI phase of the tool was necessary for only half of cases. Dr. Vogel said that’s a good sign; it means that the tool is useful in settings where AI may not always be feasible, like in a busy ED.
Melissa Mizesko, MD, a pediatric rheumatologist at Driscoll Children’s Hospital in Corpus Christi, Tex., said that the new tool could help clinicians streamline care. When cases of MIS-C peaked in Texas, clinicians often would start sick children on doxycycline and treat for MIS-C at the same time, then wait to see whether the antibiotic brought the fever down.
“This [new tool] is helpful if you live in a part of the country that has typhus,” said Jane Burns, MD, director of the Kawasaki Disease Research Center at the University of California, San Diego, who helped develop a similar AI-based tool to distinguish MIS-C from Kawasaki disease. But she encouraged the researchers to expand their testing to include other conditions. Although the AI model Dr. Vogel’s group developed can pinpoint MIS-C or endemic typhus, what if a child has neither condition? “It’s not often you’re dealing with a diagnosis between just two specific diseases,” Dr. Burns said.
Dr. Vogel is also interested in making AI-MET more efficient. “This go-round we prioritized perfect accuracy,” she said. But 30 clinical factors, with 17 of them recorded and calculated by hand, is a lot. “Could we still get this to be very accurate, maybe not perfect, with less inputs?”
In addition to refining AI-MET, which Texas Children’s eventually hopes to make available to other institutions, Dr. Vogel and associates are also considering other use cases for AI. Lupus is one option. “Maybe with machine learning we could identify clues at diagnosis that would help recommend targeted treatment,” she said
Dr. Vogel disclosed potential conflicts of interest with Moderna, Novartis, Pfizer, and SOBI. Dr. Burns and Dr. Mizesko disclosed no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
Artificial intelligence can distinguish overlapping inflammatory conditions with total accuracy, according to a new study presented at the annual meeting of the American College of Rheumatology.
Texas pediatricians faced a conundrum during the pandemic. Endemic typhus, a flea-borne tropical infection common to the region, is nearly indistinguishable from multisystem inflammatory syndrome in children (MIS-C), a rare condition set in motion by SARS-CoV-2 infection. Children with either ailment had seemingly identical symptoms: fever, rash, gastrointestinal issues, and in need of swift treatment. A diagnosis of endemic typhus can take 4-6 days to confirm.
Tiphanie Vogel, MD, PhD, a pediatric rheumatologist at Texas Children’s Hospital, Houston, and colleagues sought to create a tool to hasten diagnosis and, ideally, treatment. To do so, they incorporated machine learning and clinical factors available within the first 6 hours of the onset of symptoms.
The team analyzed 49 demographic, clinical, and laboratory measures from the medical records of 133 children with MIS-C and 87 with endemic typhus. Using deep learning, they narrowed the model to 30 essential features that became the backbone of AI-MET, a two-phase clinical-decision support system.
Phase 1 uses 17 clinical factors and can be performed on paper. If a patient’s score in phase 1 is not determinative, clinicians proceed to phase 2, which uses an additional 13 weighted factors and machine learning.
In testing, the two-part tool classified each of the 220 test patients perfectly. And it diagnosed a second group of 111 patients with MIS-C with 99% (110/111) accuracy.
Of note, “that first step classifies [a patient] correctly half of the time,” Dr. Vogel said, so the second, AI phase of the tool was necessary for only half of cases. Dr. Vogel said that’s a good sign; it means that the tool is useful in settings where AI may not always be feasible, like in a busy ED.
Melissa Mizesko, MD, a pediatric rheumatologist at Driscoll Children’s Hospital in Corpus Christi, Tex., said that the new tool could help clinicians streamline care. When cases of MIS-C peaked in Texas, clinicians often would start sick children on doxycycline and treat for MIS-C at the same time, then wait to see whether the antibiotic brought the fever down.
“This [new tool] is helpful if you live in a part of the country that has typhus,” said Jane Burns, MD, director of the Kawasaki Disease Research Center at the University of California, San Diego, who helped develop a similar AI-based tool to distinguish MIS-C from Kawasaki disease. But she encouraged the researchers to expand their testing to include other conditions. Although the AI model Dr. Vogel’s group developed can pinpoint MIS-C or endemic typhus, what if a child has neither condition? “It’s not often you’re dealing with a diagnosis between just two specific diseases,” Dr. Burns said.
Dr. Vogel is also interested in making AI-MET more efficient. “This go-round we prioritized perfect accuracy,” she said. But 30 clinical factors, with 17 of them recorded and calculated by hand, is a lot. “Could we still get this to be very accurate, maybe not perfect, with less inputs?”
In addition to refining AI-MET, which Texas Children’s eventually hopes to make available to other institutions, Dr. Vogel and associates are also considering other use cases for AI. Lupus is one option. “Maybe with machine learning we could identify clues at diagnosis that would help recommend targeted treatment,” she said
Dr. Vogel disclosed potential conflicts of interest with Moderna, Novartis, Pfizer, and SOBI. Dr. Burns and Dr. Mizesko disclosed no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
FROM ACR 2023
TNF inhibitors may be OK for treating RA-associated interstitial lung disease
SAN DIEGO – Patients with rheumatoid arthritis-associated interstitial lung disease (RA-ILD) who start a tumor necrosis factor inhibitor (TNFi) appear to have rates of survival and respiratory-related hospitalization similar to those initiating a non-TNFi biologic disease-modifying antirheumatic drug (bDMARD) or Janus kinase inhibitor (JAKi), results from a large pharmacoepidemiologic study show.
“These results challenge some of the findings in prior literature that perhaps TNFi should be avoided in RA-ILD,” lead study investigator Bryant R. England, MD, PhD, said in an interview. The findings were presented during a plenary session at the American College of Rheumatology annual meeting.

Dr. England, associate professor of rheumatology and immunology at the University of Nebraska Medical Center, Omaha, said that while RA-ILD carries a poor prognosis, a paucity of evidence exists on the effectiveness and safety of disease-modifying therapies in this population.
It’s a pleasant surprise “to see that the investigators were unable to demonstrate a significant difference in the risk of respiratory hospitalization or death between people with RA-ILD initiating non-TNFi/JAKi versus TNFi. Here is a unique situation where a so called ‘negative’ study contributes important information. This study provides needed safety data, as they were unable to show that TNFi results in worsening of severe RA-ILD outcomes,” Sindhu R. Johnson, MD, PhD, professor of medicine at the University of Toronto, said when asked for comment on the study.

“While this study does not address the use of these medications for the treatment of RA-ILD, these data suggest that TNFi may remain a treatment option for articular disease in people with RA-ILD,” said Dr. Johnson, who was not involved with the study.
For the study, Dr. England and colleagues drew from Veterans Health Administration data between 2006 and 2018 to identify patients with RA-ILD initiating TNFi or non-TNFi biologic/JAKi for the first time. Those who received ILD-focused therapies such as mycophenolate and antifibrotics were excluded from the analysis.
The researchers used validated administrative algorithms requiring multiple RA and ILD diagnostic codes to identify RA-ILD and used 1:1 propensity score matching to compare TNFi and non-TNFi biologic/JAKi factors such as health care use, comorbidities, and several RA-ILD factors, such as pretreatment forced vital capacity, obtained from electronic health records and administrative data. The primary outcome was a composite of time to respiratory-related hospitalization or death using Cox regression models.
Dr. England reported findings from 237 TNFi initiators and 237 non-TNFi/JAKi initiators. Their mean age was 68 years and 92% were male. After matching, the mean standardized differences of variables in the propensity score model improved, but a few variables remained slightly imbalanced, such as two markers of inflammation, inhaled corticosteroid use, and body mass index. The most frequently prescribed TNFi drugs were adalimumab (51%) and etanercept (37%), and the most frequently prescribed non-TNFi/JAKi drugs were rituximab (53%) and abatacept (28%).
The researchers observed no significant difference in the primary outcome between non-TNFi/JAKi and TNFi initiators (adjusted hazard ratio [aHR], 1.22; 95% confidence interval [CI], 0.92-1.60). They also observed no significant differences in respiratory hospitalization, all-cause mortality, or respiratory-related death at 1 and 3 years. In sensitivity analyses with modified cohort eligibility requirements, no significant differences in outcomes were observed between non-TNFi/JAKi and TNFi initiators.
During his presentation at the meeting, Dr. England posed the question: Are TNFi drugs safe to be used in RA-ILD?
“The answer is: It’s complex,” he said. “Our findings don’t suggest that we should be systematically avoiding TNFis with every single person with RA-ILD. But that’s different than whether there are specific subpopulations of RA-ILD for which the choice of these therapies may differ. Unfortunately, we could not address that in this study. We also could not address whether TNFis have efficacy at stopping, slowing, or reversing progression of the ILD itself. This calls for us as a field to gather together and pursue clinical trials to try to generate robust evidence that can guide these important clinical decisions that we’re making with our patients.”
He acknowledged certain limitations of the analysis, including its observational design. “So, despite best efforts to minimize bias with pharmacoepidemiologic designs and approaches, there could still be confounding and selection,” he said. “Additionally, RA-ILD is a heterogeneous disease characterized by different patterns and trajectories. While we did account for several RA- and ILD-related factors, we could not account for all heterogeneity in RA-ILD.”
When asked for comment on the study, session moderator Janet Pope, MD, MPH, professor of medicine in the division of rheumatology at the University of Western Ontario, London, said that the study findings surprised her.

“Sometimes RA patients on TNFis were thought to have more new or worsening ILD vs. [those on] non-TNFi bDMARDs, but most [data were] from older studies where TNFis were used as initial bDMARD in sicker patients,” she told this news organization. “So, data were confounded previously. Even in this study, there may have been channeling bias as it was not a randomized controlled trial. We need a definitive randomized controlled trial to answer this question of what the most optimal therapy for RA-ILD is.”
Dr. England reports receiving consulting fees and research support from Boehringer Ingelheim, and several coauthors reported financial relationships from various pharmaceutical companies and medical publishers. Dr. Johnson reports no relevant financial relationships. Dr. Pope reports being a consultant for several pharmaceutical companies. She has received grant/research support from AbbVie/Abbott and Eli Lilly and is an adviser for Boehringer Ingelheim.
A version of this article appeared on Medscape.com.
SAN DIEGO – Patients with rheumatoid arthritis-associated interstitial lung disease (RA-ILD) who start a tumor necrosis factor inhibitor (TNFi) appear to have rates of survival and respiratory-related hospitalization similar to those initiating a non-TNFi biologic disease-modifying antirheumatic drug (bDMARD) or Janus kinase inhibitor (JAKi), results from a large pharmacoepidemiologic study show.
“These results challenge some of the findings in prior literature that perhaps TNFi should be avoided in RA-ILD,” lead study investigator Bryant R. England, MD, PhD, said in an interview. The findings were presented during a plenary session at the American College of Rheumatology annual meeting.
Dr. England, associate professor of rheumatology and immunology at the University of Nebraska Medical Center, Omaha, said that while RA-ILD carries a poor prognosis, a paucity of evidence exists on the effectiveness and safety of disease-modifying therapies in this population.
It’s a pleasant surprise “to see that the investigators were unable to demonstrate a significant difference in the risk of respiratory hospitalization or death between people with RA-ILD initiating non-TNFi/JAKi versus TNFi. Here is a unique situation where a so called ‘negative’ study contributes important information. This study provides needed safety data, as they were unable to show that TNFi results in worsening of severe RA-ILD outcomes,” Sindhu R. Johnson, MD, PhD, professor of medicine at the University of Toronto, said when asked for comment on the study.
“While this study does not address the use of these medications for the treatment of RA-ILD, these data suggest that TNFi may remain a treatment option for articular disease in people with RA-ILD,” said Dr. Johnson, who was not involved with the study.
For the study, Dr. England and colleagues drew from Veterans Health Administration data between 2006 and 2018 to identify patients with RA-ILD initiating TNFi or non-TNFi biologic/JAKi for the first time. Those who received ILD-focused therapies such as mycophenolate and antifibrotics were excluded from the analysis.
The researchers used validated administrative algorithms requiring multiple RA and ILD diagnostic codes to identify RA-ILD and used 1:1 propensity score matching to compare TNFi and non-TNFi biologic/JAKi factors such as health care use, comorbidities, and several RA-ILD factors, such as pretreatment forced vital capacity, obtained from electronic health records and administrative data. The primary outcome was a composite of time to respiratory-related hospitalization or death using Cox regression models.
Dr. England reported findings from 237 TNFi initiators and 237 non-TNFi/JAKi initiators. Their mean age was 68 years and 92% were male. After matching, the mean standardized differences of variables in the propensity score model improved, but a few variables remained slightly imbalanced, such as two markers of inflammation, inhaled corticosteroid use, and body mass index. The most frequently prescribed TNFi drugs were adalimumab (51%) and etanercept (37%), and the most frequently prescribed non-TNFi/JAKi drugs were rituximab (53%) and abatacept (28%).
The researchers observed no significant difference in the primary outcome between non-TNFi/JAKi and TNFi initiators (adjusted hazard ratio [aHR], 1.22; 95% confidence interval [CI], 0.92-1.60). They also observed no significant differences in respiratory hospitalization, all-cause mortality, or respiratory-related death at 1 and 3 years. In sensitivity analyses with modified cohort eligibility requirements, no significant differences in outcomes were observed between non-TNFi/JAKi and TNFi initiators.
During his presentation at the meeting, Dr. England posed the question: Are TNFi drugs safe to be used in RA-ILD?
“The answer is: It’s complex,” he said. “Our findings don’t suggest that we should be systematically avoiding TNFis with every single person with RA-ILD. But that’s different than whether there are specific subpopulations of RA-ILD for which the choice of these therapies may differ. Unfortunately, we could not address that in this study. We also could not address whether TNFis have efficacy at stopping, slowing, or reversing progression of the ILD itself. This calls for us as a field to gather together and pursue clinical trials to try to generate robust evidence that can guide these important clinical decisions that we’re making with our patients.”
He acknowledged certain limitations of the analysis, including its observational design. “So, despite best efforts to minimize bias with pharmacoepidemiologic designs and approaches, there could still be confounding and selection,” he said. “Additionally, RA-ILD is a heterogeneous disease characterized by different patterns and trajectories. While we did account for several RA- and ILD-related factors, we could not account for all heterogeneity in RA-ILD.”
When asked for comment on the study, session moderator Janet Pope, MD, MPH, professor of medicine in the division of rheumatology at the University of Western Ontario, London, said that the study findings surprised her.
“Sometimes RA patients on TNFis were thought to have more new or worsening ILD vs. [those on] non-TNFi bDMARDs, but most [data were] from older studies where TNFis were used as initial bDMARD in sicker patients,” she told this news organization. “So, data were confounded previously. Even in this study, there may have been channeling bias as it was not a randomized controlled trial. We need a definitive randomized controlled trial to answer this question of what the most optimal therapy for RA-ILD is.”
Dr. England reports receiving consulting fees and research support from Boehringer Ingelheim, and several coauthors reported financial relationships from various pharmaceutical companies and medical publishers. Dr. Johnson reports no relevant financial relationships. Dr. Pope reports being a consultant for several pharmaceutical companies. She has received grant/research support from AbbVie/Abbott and Eli Lilly and is an adviser for Boehringer Ingelheim.
A version of this article appeared on Medscape.com.
SAN DIEGO – Patients with rheumatoid arthritis-associated interstitial lung disease (RA-ILD) who start a tumor necrosis factor inhibitor (TNFi) appear to have rates of survival and respiratory-related hospitalization similar to those initiating a non-TNFi biologic disease-modifying antirheumatic drug (bDMARD) or Janus kinase inhibitor (JAKi), results from a large pharmacoepidemiologic study show.
“These results challenge some of the findings in prior literature that perhaps TNFi should be avoided in RA-ILD,” lead study investigator Bryant R. England, MD, PhD, said in an interview. The findings were presented during a plenary session at the American College of Rheumatology annual meeting.
Dr. England, associate professor of rheumatology and immunology at the University of Nebraska Medical Center, Omaha, said that while RA-ILD carries a poor prognosis, a paucity of evidence exists on the effectiveness and safety of disease-modifying therapies in this population.
It’s a pleasant surprise “to see that the investigators were unable to demonstrate a significant difference in the risk of respiratory hospitalization or death between people with RA-ILD initiating non-TNFi/JAKi versus TNFi. Here is a unique situation where a so called ‘negative’ study contributes important information. This study provides needed safety data, as they were unable to show that TNFi results in worsening of severe RA-ILD outcomes,” Sindhu R. Johnson, MD, PhD, professor of medicine at the University of Toronto, said when asked for comment on the study.
“While this study does not address the use of these medications for the treatment of RA-ILD, these data suggest that TNFi may remain a treatment option for articular disease in people with RA-ILD,” said Dr. Johnson, who was not involved with the study.
For the study, Dr. England and colleagues drew from Veterans Health Administration data between 2006 and 2018 to identify patients with RA-ILD initiating TNFi or non-TNFi biologic/JAKi for the first time. Those who received ILD-focused therapies such as mycophenolate and antifibrotics were excluded from the analysis.
The researchers used validated administrative algorithms requiring multiple RA and ILD diagnostic codes to identify RA-ILD and used 1:1 propensity score matching to compare TNFi and non-TNFi biologic/JAKi factors such as health care use, comorbidities, and several RA-ILD factors, such as pretreatment forced vital capacity, obtained from electronic health records and administrative data. The primary outcome was a composite of time to respiratory-related hospitalization or death using Cox regression models.
Dr. England reported findings from 237 TNFi initiators and 237 non-TNFi/JAKi initiators. Their mean age was 68 years and 92% were male. After matching, the mean standardized differences of variables in the propensity score model improved, but a few variables remained slightly imbalanced, such as two markers of inflammation, inhaled corticosteroid use, and body mass index. The most frequently prescribed TNFi drugs were adalimumab (51%) and etanercept (37%), and the most frequently prescribed non-TNFi/JAKi drugs were rituximab (53%) and abatacept (28%).
The researchers observed no significant difference in the primary outcome between non-TNFi/JAKi and TNFi initiators (adjusted hazard ratio [aHR], 1.22; 95% confidence interval [CI], 0.92-1.60). They also observed no significant differences in respiratory hospitalization, all-cause mortality, or respiratory-related death at 1 and 3 years. In sensitivity analyses with modified cohort eligibility requirements, no significant differences in outcomes were observed between non-TNFi/JAKi and TNFi initiators.
During his presentation at the meeting, Dr. England posed the question: Are TNFi drugs safe to be used in RA-ILD?
“The answer is: It’s complex,” he said. “Our findings don’t suggest that we should be systematically avoiding TNFis with every single person with RA-ILD. But that’s different than whether there are specific subpopulations of RA-ILD for which the choice of these therapies may differ. Unfortunately, we could not address that in this study. We also could not address whether TNFis have efficacy at stopping, slowing, or reversing progression of the ILD itself. This calls for us as a field to gather together and pursue clinical trials to try to generate robust evidence that can guide these important clinical decisions that we’re making with our patients.”
He acknowledged certain limitations of the analysis, including its observational design. “So, despite best efforts to minimize bias with pharmacoepidemiologic designs and approaches, there could still be confounding and selection,” he said. “Additionally, RA-ILD is a heterogeneous disease characterized by different patterns and trajectories. While we did account for several RA- and ILD-related factors, we could not account for all heterogeneity in RA-ILD.”
When asked for comment on the study, session moderator Janet Pope, MD, MPH, professor of medicine in the division of rheumatology at the University of Western Ontario, London, said that the study findings surprised her.
“Sometimes RA patients on TNFis were thought to have more new or worsening ILD vs. [those on] non-TNFi bDMARDs, but most [data were] from older studies where TNFis were used as initial bDMARD in sicker patients,” she told this news organization. “So, data were confounded previously. Even in this study, there may have been channeling bias as it was not a randomized controlled trial. We need a definitive randomized controlled trial to answer this question of what the most optimal therapy for RA-ILD is.”
Dr. England reports receiving consulting fees and research support from Boehringer Ingelheim, and several coauthors reported financial relationships from various pharmaceutical companies and medical publishers. Dr. Johnson reports no relevant financial relationships. Dr. Pope reports being a consultant for several pharmaceutical companies. She has received grant/research support from AbbVie/Abbott and Eli Lilly and is an adviser for Boehringer Ingelheim.
A version of this article appeared on Medscape.com.
AT ACR 2023
Vasculitis confers higher risk for adverse pregnancy outcomes
SAN DIEGO – Pregnancy in patients with vasculitis had a higher risk for preterm delivery and preeclampsia/eclampsia – especially those with small-vessel vasculitis – compared with the general obstetric population, in a large analysis of administrative claims data presented at the American College of Rheumatology annual meeting.
“We suspect that there is a relationship between the increased risk of these serious hypertensive disorders and preterm delivery, given the higher risk of medically indicated preterm delivery,” one the of the study authors, Audra Horomanski, MD, said in an interview prior to her presentation in a plenary session at the meeting.
Limited data exist on the risks of pregnancy in patients with systemic vasculitis, according to Dr. Horomanski, a rheumatologist who directs the Stanford Vasculitis Clinic at Stanford (Calif.) University. “The majority of what we do know comes from relatively small cohort studies,” she said. “This is the first U.S., nationwide database study looking at the risk of preterm delivery and other adverse pregnancy outcomes.”

Drawing on administrative claims data from private health insurance providers, Dr. Horomanski and her colleagues identified all pregnancies regardless of outcome for patients with and without vasculitis from 2007 to 2021. They defined vasculitis as ≥ 2 ICD-coded outpatient visits or ≥ 1 ICD-coded inpatient visit occurring before the estimated last menstrual period (LMP), and they further categorized vasculitis by vessel size: large, medium, small, and variable, based on Chapel Hill Consensus Conference criteria. For a referent population, they included patients without vasculitis or other rheumatic disease, defined as no ICD-coded outpatient or inpatient visits for vasculitis, systemic lupus erythematosus, rheumatoid arthritis, systemic sclerosis, or juvenile idiopathic arthritis before LMP or during pregnancy. Next, the researchers described pregnancy outcomes in patients with vasculitis compared with the referent population, and explored pregnancy characteristics and complications in patients with vasculitis stratified by parity (nulliparous vs. multiparous).
Dr. Horomanski reported results from 665 pregnancies in 527 patients with vasculitis and 4,209,034 pregnancies in 2,932,379 patients from the referent population. Patients with vasculitis had higher rates of spontaneous abortion (21% vs. 19%), elective termination (6% vs. 5%), ectopic and molar pregnancy (4% vs. 3%), and preterm delivery (13% vs. 6%). Approximately 12% of pregnancies among patients with vasculitis were complicated by preeclampsia. Multiparous pregnancies had a slightly higher frequency of preterm delivery than did nulliparous pregnancies (14% vs. 13%) and were more often comorbid with gestational diabetes (11% vs. 6%) and prepregnancy hypertension (23% vs. 13%). Patients with small-vessel vasculitis had higher frequencies of spontaneous abortion, preterm delivery, and comorbidities among vasculitis subtypes.
“I was surprised that vasculitis patients were less likely to be diagnosed with gestational hypertension compared to the general population, but more likely to be diagnosed with preeclampsia/eclampsia,” Dr. Horomanski added. “It raises questions about whether vasculitis patients are more likely to be diagnosed with more serious hypertensive disorders of pregnancy due to their underlying systemic disease or due to the perceptions of the treating clinicians.”
She acknowledged certain limitations of the study, including the fact that it lacked information on race and ethnicity and was limited to privately insured individuals. This “suggests that we are likely missing patients with disabilities and those who are uninsured, both groups that may be at higher risk for adverse pregnancy outcomes,” she said. “We also have no information on disease activity or flare events which may contribute to these outcomes, particularly medically indicated preterm delivery. There is also a risk of misclassification due to the use of claims data and ICD coding. This misclassification may impact vasculitis diagnoses, parity, and early pregnancy losses.”
Despite the limitations, she said that the work “highlights the value of large database analysis as a complement to prior cohort studies to further clarify this complex picture. Overall, this information is valuable for the counseling of vasculitis patients considering pregnancy and for creating a plan to monitor for pregnancy complications.”
Lindsay S. Lally, MD, a rheumatologist with Hospital for Special Surgery in New York, who was asked to comment on the study, characterized the findings as “important in how many women with vasculitis and vasculitis pregnancies were identified. These data are a start at heightening our awareness about potential complications these women may experience during pregnancy. This study should help inform our family planning conversations with our vasculitis patients. Discussing potential reproductive risks, which are likely mediated by the disease itself, as well as the treatments that we prescribe, is important to help our vasculitis patients make informed decisions.”

Dr. Lally noted that an ongoing project through the Vasculitis Clinical Research Consortium includes a prospective registry of pregnant women with vasculitis, which asks pregnant patients to enter information throughout their pregnancy. “These studies will ultimately help optimize care of our vasculitis patients during pregnancy, ensuring the best outcomes for mother and baby,” she said.
Dr. Horomanski disclosed that she has received research support from Principia, BeiGene, Gilead, and the National Institutes of Health. Dr. Lally reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
SAN DIEGO – Pregnancy in patients with vasculitis had a higher risk for preterm delivery and preeclampsia/eclampsia – especially those with small-vessel vasculitis – compared with the general obstetric population, in a large analysis of administrative claims data presented at the American College of Rheumatology annual meeting.
“We suspect that there is a relationship between the increased risk of these serious hypertensive disorders and preterm delivery, given the higher risk of medically indicated preterm delivery,” one the of the study authors, Audra Horomanski, MD, said in an interview prior to her presentation in a plenary session at the meeting.
Limited data exist on the risks of pregnancy in patients with systemic vasculitis, according to Dr. Horomanski, a rheumatologist who directs the Stanford Vasculitis Clinic at Stanford (Calif.) University. “The majority of what we do know comes from relatively small cohort studies,” she said. “This is the first U.S., nationwide database study looking at the risk of preterm delivery and other adverse pregnancy outcomes.”
Drawing on administrative claims data from private health insurance providers, Dr. Horomanski and her colleagues identified all pregnancies regardless of outcome for patients with and without vasculitis from 2007 to 2021. They defined vasculitis as ≥ 2 ICD-coded outpatient visits or ≥ 1 ICD-coded inpatient visit occurring before the estimated last menstrual period (LMP), and they further categorized vasculitis by vessel size: large, medium, small, and variable, based on Chapel Hill Consensus Conference criteria. For a referent population, they included patients without vasculitis or other rheumatic disease, defined as no ICD-coded outpatient or inpatient visits for vasculitis, systemic lupus erythematosus, rheumatoid arthritis, systemic sclerosis, or juvenile idiopathic arthritis before LMP or during pregnancy. Next, the researchers described pregnancy outcomes in patients with vasculitis compared with the referent population, and explored pregnancy characteristics and complications in patients with vasculitis stratified by parity (nulliparous vs. multiparous).
Dr. Horomanski reported results from 665 pregnancies in 527 patients with vasculitis and 4,209,034 pregnancies in 2,932,379 patients from the referent population. Patients with vasculitis had higher rates of spontaneous abortion (21% vs. 19%), elective termination (6% vs. 5%), ectopic and molar pregnancy (4% vs. 3%), and preterm delivery (13% vs. 6%). Approximately 12% of pregnancies among patients with vasculitis were complicated by preeclampsia. Multiparous pregnancies had a slightly higher frequency of preterm delivery than did nulliparous pregnancies (14% vs. 13%) and were more often comorbid with gestational diabetes (11% vs. 6%) and prepregnancy hypertension (23% vs. 13%). Patients with small-vessel vasculitis had higher frequencies of spontaneous abortion, preterm delivery, and comorbidities among vasculitis subtypes.
“I was surprised that vasculitis patients were less likely to be diagnosed with gestational hypertension compared to the general population, but more likely to be diagnosed with preeclampsia/eclampsia,” Dr. Horomanski added. “It raises questions about whether vasculitis patients are more likely to be diagnosed with more serious hypertensive disorders of pregnancy due to their underlying systemic disease or due to the perceptions of the treating clinicians.”
She acknowledged certain limitations of the study, including the fact that it lacked information on race and ethnicity and was limited to privately insured individuals. This “suggests that we are likely missing patients with disabilities and those who are uninsured, both groups that may be at higher risk for adverse pregnancy outcomes,” she said. “We also have no information on disease activity or flare events which may contribute to these outcomes, particularly medically indicated preterm delivery. There is also a risk of misclassification due to the use of claims data and ICD coding. This misclassification may impact vasculitis diagnoses, parity, and early pregnancy losses.”
Despite the limitations, she said that the work “highlights the value of large database analysis as a complement to prior cohort studies to further clarify this complex picture. Overall, this information is valuable for the counseling of vasculitis patients considering pregnancy and for creating a plan to monitor for pregnancy complications.”
Lindsay S. Lally, MD, a rheumatologist with Hospital for Special Surgery in New York, who was asked to comment on the study, characterized the findings as “important in how many women with vasculitis and vasculitis pregnancies were identified. These data are a start at heightening our awareness about potential complications these women may experience during pregnancy. This study should help inform our family planning conversations with our vasculitis patients. Discussing potential reproductive risks, which are likely mediated by the disease itself, as well as the treatments that we prescribe, is important to help our vasculitis patients make informed decisions.”
Dr. Lally noted that an ongoing project through the Vasculitis Clinical Research Consortium includes a prospective registry of pregnant women with vasculitis, which asks pregnant patients to enter information throughout their pregnancy. “These studies will ultimately help optimize care of our vasculitis patients during pregnancy, ensuring the best outcomes for mother and baby,” she said.
Dr. Horomanski disclosed that she has received research support from Principia, BeiGene, Gilead, and the National Institutes of Health. Dr. Lally reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
SAN DIEGO – Pregnancy in patients with vasculitis had a higher risk for preterm delivery and preeclampsia/eclampsia – especially those with small-vessel vasculitis – compared with the general obstetric population, in a large analysis of administrative claims data presented at the American College of Rheumatology annual meeting.
“We suspect that there is a relationship between the increased risk of these serious hypertensive disorders and preterm delivery, given the higher risk of medically indicated preterm delivery,” one the of the study authors, Audra Horomanski, MD, said in an interview prior to her presentation in a plenary session at the meeting.
Limited data exist on the risks of pregnancy in patients with systemic vasculitis, according to Dr. Horomanski, a rheumatologist who directs the Stanford Vasculitis Clinic at Stanford (Calif.) University. “The majority of what we do know comes from relatively small cohort studies,” she said. “This is the first U.S., nationwide database study looking at the risk of preterm delivery and other adverse pregnancy outcomes.”
Drawing on administrative claims data from private health insurance providers, Dr. Horomanski and her colleagues identified all pregnancies regardless of outcome for patients with and without vasculitis from 2007 to 2021. They defined vasculitis as ≥ 2 ICD-coded outpatient visits or ≥ 1 ICD-coded inpatient visit occurring before the estimated last menstrual period (LMP), and they further categorized vasculitis by vessel size: large, medium, small, and variable, based on Chapel Hill Consensus Conference criteria. For a referent population, they included patients without vasculitis or other rheumatic disease, defined as no ICD-coded outpatient or inpatient visits for vasculitis, systemic lupus erythematosus, rheumatoid arthritis, systemic sclerosis, or juvenile idiopathic arthritis before LMP or during pregnancy. Next, the researchers described pregnancy outcomes in patients with vasculitis compared with the referent population, and explored pregnancy characteristics and complications in patients with vasculitis stratified by parity (nulliparous vs. multiparous).
Dr. Horomanski reported results from 665 pregnancies in 527 patients with vasculitis and 4,209,034 pregnancies in 2,932,379 patients from the referent population. Patients with vasculitis had higher rates of spontaneous abortion (21% vs. 19%), elective termination (6% vs. 5%), ectopic and molar pregnancy (4% vs. 3%), and preterm delivery (13% vs. 6%). Approximately 12% of pregnancies among patients with vasculitis were complicated by preeclampsia. Multiparous pregnancies had a slightly higher frequency of preterm delivery than did nulliparous pregnancies (14% vs. 13%) and were more often comorbid with gestational diabetes (11% vs. 6%) and prepregnancy hypertension (23% vs. 13%). Patients with small-vessel vasculitis had higher frequencies of spontaneous abortion, preterm delivery, and comorbidities among vasculitis subtypes.
“I was surprised that vasculitis patients were less likely to be diagnosed with gestational hypertension compared to the general population, but more likely to be diagnosed with preeclampsia/eclampsia,” Dr. Horomanski added. “It raises questions about whether vasculitis patients are more likely to be diagnosed with more serious hypertensive disorders of pregnancy due to their underlying systemic disease or due to the perceptions of the treating clinicians.”
She acknowledged certain limitations of the study, including the fact that it lacked information on race and ethnicity and was limited to privately insured individuals. This “suggests that we are likely missing patients with disabilities and those who are uninsured, both groups that may be at higher risk for adverse pregnancy outcomes,” she said. “We also have no information on disease activity or flare events which may contribute to these outcomes, particularly medically indicated preterm delivery. There is also a risk of misclassification due to the use of claims data and ICD coding. This misclassification may impact vasculitis diagnoses, parity, and early pregnancy losses.”
Despite the limitations, she said that the work “highlights the value of large database analysis as a complement to prior cohort studies to further clarify this complex picture. Overall, this information is valuable for the counseling of vasculitis patients considering pregnancy and for creating a plan to monitor for pregnancy complications.”
Lindsay S. Lally, MD, a rheumatologist with Hospital for Special Surgery in New York, who was asked to comment on the study, characterized the findings as “important in how many women with vasculitis and vasculitis pregnancies were identified. These data are a start at heightening our awareness about potential complications these women may experience during pregnancy. This study should help inform our family planning conversations with our vasculitis patients. Discussing potential reproductive risks, which are likely mediated by the disease itself, as well as the treatments that we prescribe, is important to help our vasculitis patients make informed decisions.”
Dr. Lally noted that an ongoing project through the Vasculitis Clinical Research Consortium includes a prospective registry of pregnant women with vasculitis, which asks pregnant patients to enter information throughout their pregnancy. “These studies will ultimately help optimize care of our vasculitis patients during pregnancy, ensuring the best outcomes for mother and baby,” she said.
Dr. Horomanski disclosed that she has received research support from Principia, BeiGene, Gilead, and the National Institutes of Health. Dr. Lally reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
AT ACR 2023
Apremilast beats placebo in early PsA affecting few joints
SAN DIEGO – Patients with early oligoarticular psoriatic arthritis (PsA) who took apremilast (Otezla) had more than double the response rate of placebo-treated patients by 16 weeks in a double-blind and randomized phase 4 study.
Oligoarticular PsA can significantly affect quality of life even though few joints are affected, and there’s a lack of relevant clinical data to guide treatment, said rheumatologist Philip J. Mease, MD, of the University of Washington and Swedish Medical Center, Seattle, who reported the results in a presentation at the annual meeting of the American College of Rheumatology.

The findings of the study, called FOREMOST, support the use of the drug in mild PsA, Alexis Ogdie, MD, director of the Penn Psoriatic Arthritis Clinic and the Penn Center for Clinical Epidemiology and Biostatistics at the University of Pennsylvania, Philadelphia, said in an interview. Dr. Ogdie, who was not involved with the research, noted that rheumatologists commonly prescribe apremilast for mild PsA, although previous research has focused on severe PsA cases.
By 16 weeks, 33.9% of 203 who received apremilast and 16% of 105 who received placebo (difference, 18.5%; 95% confidence interval, 8.9-28.1; P = .0008) met the trial’s primary outcome, a modified version of minimal disease activity score (MDA-Joints), which required attainment of 1 or fewer swollen and/or tender joints plus three of five additional criteria (psoriasis body surface area of 3% or less, a patient pain visual analog scale assessment of 15 mm or less out of 0-100 mm, a patient global assessment of 20 mm or less out of 0-100 mm, a Health Assessment Questionnaire-Disability Index score of 0.5 or less, and a Leeds Enthesitis Index score of 1 or less). The primary analysis was conducted only in joints affected at baseline.
The researchers recruited patients with 2-4 swollen and/or tender joints out of a total of 66-68 joints assessed; most patients (87%) randomized in the study had 4 or fewer active joints at baseline. The patients had a mean age of 50.9. The mean duration of PsA was 9.9 months, and 39.9% of patients were taking a conventional disease-modifying antirheumatic drug.
In a clinically important outcome, the percentage who had a patient-reported pain response improvement defined as “significant” reached 31.4% with placebo, compared with 48.8% for apremilast (difference, 17.7%; 95% CI, 6.0-29.4; P = .0044), and the percentage who reached a patient-reported pain response defined as “major” totaled 19.1% for placebo vs. 41.3% for apremilast (difference, 22.3%; 95% CI, 11.7-32.9; P = .002).

In an exploratory analysis of all joints, the percentages meeting MDA-Joints criteria for response were 7.9% with placebo and 21.3% with apremilast (difference, 13.6%; 95% CI, 5.9-21.4; P = .0028. Focusing on this exploratory analysis, Dr. Ogdie noted that examination of all joints is “more consistent” with the understanding of disease activity than only looking at the initial joints that had disease activity.
A post-hoc analysis among subjects with 2-4 affected joints found rates similar to the primary endpoint analysis: MDA-Joints response rates were reached by 34.4% of those who took apremilast and by 17.2% of those who took placebo.
When asked about the relatively low response rate for apremilast, Dr. Ogdie said the drug is “a really mild medication, which is why it belongs in the mild disease population. That’s balanced by the fact that it has a pretty good safety profile,” especially compared with the alternative of methotrexate, she said.
Almost all patients can tolerate apremilast, she said, although they may experience nausea or diarrhea. (The study found that adverse events were as expected for apremilast, and the drug was well tolerated.) Blood labs aren’t necessary, she added, as they are in patients taking methotrexate.
As for cost, apremilast is a highly expensive drug, especially when compared to methotrexate, which costs pennies per tablet at some pharmacies. Amgen, the manufacturer of apremilast, lists the price as $4,600 a month. Still, insurers generally cover apremilast, Dr. Ogdie said.
The study was sponsored by Amgen. Dr. Mease reported financial relationships with many pharmaceutical companies, including Amgen. Many other coauthors reported financial relationships with Amgen and other pharmaceutical companies or were employees of Amgen. Dr. Ogdie reported having multiple consulting relationships with pharmaceutical companies, including Amgen, and receiving grant funding from multiple companies as well as the National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Psoriasis Foundation, Rheumatology Research Foundation, and Forward Databank.
SAN DIEGO – Patients with early oligoarticular psoriatic arthritis (PsA) who took apremilast (Otezla) had more than double the response rate of placebo-treated patients by 16 weeks in a double-blind and randomized phase 4 study.
Oligoarticular PsA can significantly affect quality of life even though few joints are affected, and there’s a lack of relevant clinical data to guide treatment, said rheumatologist Philip J. Mease, MD, of the University of Washington and Swedish Medical Center, Seattle, who reported the results in a presentation at the annual meeting of the American College of Rheumatology.
The findings of the study, called FOREMOST, support the use of the drug in mild PsA, Alexis Ogdie, MD, director of the Penn Psoriatic Arthritis Clinic and the Penn Center for Clinical Epidemiology and Biostatistics at the University of Pennsylvania, Philadelphia, said in an interview. Dr. Ogdie, who was not involved with the research, noted that rheumatologists commonly prescribe apremilast for mild PsA, although previous research has focused on severe PsA cases.
By 16 weeks, 33.9% of 203 who received apremilast and 16% of 105 who received placebo (difference, 18.5%; 95% confidence interval, 8.9-28.1; P = .0008) met the trial’s primary outcome, a modified version of minimal disease activity score (MDA-Joints), which required attainment of 1 or fewer swollen and/or tender joints plus three of five additional criteria (psoriasis body surface area of 3% or less, a patient pain visual analog scale assessment of 15 mm or less out of 0-100 mm, a patient global assessment of 20 mm or less out of 0-100 mm, a Health Assessment Questionnaire-Disability Index score of 0.5 or less, and a Leeds Enthesitis Index score of 1 or less). The primary analysis was conducted only in joints affected at baseline.
The researchers recruited patients with 2-4 swollen and/or tender joints out of a total of 66-68 joints assessed; most patients (87%) randomized in the study had 4 or fewer active joints at baseline. The patients had a mean age of 50.9. The mean duration of PsA was 9.9 months, and 39.9% of patients were taking a conventional disease-modifying antirheumatic drug.
In a clinically important outcome, the percentage who had a patient-reported pain response improvement defined as “significant” reached 31.4% with placebo, compared with 48.8% for apremilast (difference, 17.7%; 95% CI, 6.0-29.4; P = .0044), and the percentage who reached a patient-reported pain response defined as “major” totaled 19.1% for placebo vs. 41.3% for apremilast (difference, 22.3%; 95% CI, 11.7-32.9; P = .002).
In an exploratory analysis of all joints, the percentages meeting MDA-Joints criteria for response were 7.9% with placebo and 21.3% with apremilast (difference, 13.6%; 95% CI, 5.9-21.4; P = .0028. Focusing on this exploratory analysis, Dr. Ogdie noted that examination of all joints is “more consistent” with the understanding of disease activity than only looking at the initial joints that had disease activity.
A post-hoc analysis among subjects with 2-4 affected joints found rates similar to the primary endpoint analysis: MDA-Joints response rates were reached by 34.4% of those who took apremilast and by 17.2% of those who took placebo.
When asked about the relatively low response rate for apremilast, Dr. Ogdie said the drug is “a really mild medication, which is why it belongs in the mild disease population. That’s balanced by the fact that it has a pretty good safety profile,” especially compared with the alternative of methotrexate, she said.
Almost all patients can tolerate apremilast, she said, although they may experience nausea or diarrhea. (The study found that adverse events were as expected for apremilast, and the drug was well tolerated.) Blood labs aren’t necessary, she added, as they are in patients taking methotrexate.
As for cost, apremilast is a highly expensive drug, especially when compared to methotrexate, which costs pennies per tablet at some pharmacies. Amgen, the manufacturer of apremilast, lists the price as $4,600 a month. Still, insurers generally cover apremilast, Dr. Ogdie said.
The study was sponsored by Amgen. Dr. Mease reported financial relationships with many pharmaceutical companies, including Amgen. Many other coauthors reported financial relationships with Amgen and other pharmaceutical companies or were employees of Amgen. Dr. Ogdie reported having multiple consulting relationships with pharmaceutical companies, including Amgen, and receiving grant funding from multiple companies as well as the National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Psoriasis Foundation, Rheumatology Research Foundation, and Forward Databank.
SAN DIEGO – Patients with early oligoarticular psoriatic arthritis (PsA) who took apremilast (Otezla) had more than double the response rate of placebo-treated patients by 16 weeks in a double-blind and randomized phase 4 study.
Oligoarticular PsA can significantly affect quality of life even though few joints are affected, and there’s a lack of relevant clinical data to guide treatment, said rheumatologist Philip J. Mease, MD, of the University of Washington and Swedish Medical Center, Seattle, who reported the results in a presentation at the annual meeting of the American College of Rheumatology.
The findings of the study, called FOREMOST, support the use of the drug in mild PsA, Alexis Ogdie, MD, director of the Penn Psoriatic Arthritis Clinic and the Penn Center for Clinical Epidemiology and Biostatistics at the University of Pennsylvania, Philadelphia, said in an interview. Dr. Ogdie, who was not involved with the research, noted that rheumatologists commonly prescribe apremilast for mild PsA, although previous research has focused on severe PsA cases.
By 16 weeks, 33.9% of 203 who received apremilast and 16% of 105 who received placebo (difference, 18.5%; 95% confidence interval, 8.9-28.1; P = .0008) met the trial’s primary outcome, a modified version of minimal disease activity score (MDA-Joints), which required attainment of 1 or fewer swollen and/or tender joints plus three of five additional criteria (psoriasis body surface area of 3% or less, a patient pain visual analog scale assessment of 15 mm or less out of 0-100 mm, a patient global assessment of 20 mm or less out of 0-100 mm, a Health Assessment Questionnaire-Disability Index score of 0.5 or less, and a Leeds Enthesitis Index score of 1 or less). The primary analysis was conducted only in joints affected at baseline.
The researchers recruited patients with 2-4 swollen and/or tender joints out of a total of 66-68 joints assessed; most patients (87%) randomized in the study had 4 or fewer active joints at baseline. The patients had a mean age of 50.9. The mean duration of PsA was 9.9 months, and 39.9% of patients were taking a conventional disease-modifying antirheumatic drug.
In a clinically important outcome, the percentage who had a patient-reported pain response improvement defined as “significant” reached 31.4% with placebo, compared with 48.8% for apremilast (difference, 17.7%; 95% CI, 6.0-29.4; P = .0044), and the percentage who reached a patient-reported pain response defined as “major” totaled 19.1% for placebo vs. 41.3% for apremilast (difference, 22.3%; 95% CI, 11.7-32.9; P = .002).
In an exploratory analysis of all joints, the percentages meeting MDA-Joints criteria for response were 7.9% with placebo and 21.3% with apremilast (difference, 13.6%; 95% CI, 5.9-21.4; P = .0028. Focusing on this exploratory analysis, Dr. Ogdie noted that examination of all joints is “more consistent” with the understanding of disease activity than only looking at the initial joints that had disease activity.
A post-hoc analysis among subjects with 2-4 affected joints found rates similar to the primary endpoint analysis: MDA-Joints response rates were reached by 34.4% of those who took apremilast and by 17.2% of those who took placebo.
When asked about the relatively low response rate for apremilast, Dr. Ogdie said the drug is “a really mild medication, which is why it belongs in the mild disease population. That’s balanced by the fact that it has a pretty good safety profile,” especially compared with the alternative of methotrexate, she said.
Almost all patients can tolerate apremilast, she said, although they may experience nausea or diarrhea. (The study found that adverse events were as expected for apremilast, and the drug was well tolerated.) Blood labs aren’t necessary, she added, as they are in patients taking methotrexate.
As for cost, apremilast is a highly expensive drug, especially when compared to methotrexate, which costs pennies per tablet at some pharmacies. Amgen, the manufacturer of apremilast, lists the price as $4,600 a month. Still, insurers generally cover apremilast, Dr. Ogdie said.
The study was sponsored by Amgen. Dr. Mease reported financial relationships with many pharmaceutical companies, including Amgen. Many other coauthors reported financial relationships with Amgen and other pharmaceutical companies or were employees of Amgen. Dr. Ogdie reported having multiple consulting relationships with pharmaceutical companies, including Amgen, and receiving grant funding from multiple companies as well as the National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Psoriasis Foundation, Rheumatology Research Foundation, and Forward Databank.
AT ACR 2023