User login
Knee Surgery Not Necessary for Middle-Aged Patients with Mild Osteoarthritis
New meta-analysis evidence suggests that there is no benefit to having arthroscopic meniscal debridement for degenerative meniscal tears in comparison with nonoperative treatments or sham treatments in middle-aged patients with mild or no concomitant osteoarthritis. The findings were published August 25 online ahead of print in the Canadian Medical Association Journal.
“Doctors need to carefully weigh the costs and benefits when deciding who should undergo such surgery,” said Moin Khan, MD, lead author of the study and research fellow in orthopedic surgery in the Michael G. DeGroote School of Medicine at McMaster University in Hamilton, Ontario.

Dr. Khan and colleagues conducted a meta-analysis of 7 randomized controlled trials published between 1946 and January 20, 2014, on arthroscopic partial meniscectomy in patients with mild to no osteoarthritis compared with nonoperative treatments. Two reviewers independently screened all abstracts and titles for eligibility. In total, there were 811 knees in 805 patients with a mean age of 56 years. The pooled treatment effect of arthroscopic surgery did not show a significant or minimally important difference between treatment arms for long-term functional outcomes. Short-term functional outcomes between groups were significant but did not exceed the threshold for minimally important difference. Arthroscopic surgery did not result in a significant improvement in either short- or long-term pain scores.
“This study shows that surgery should not be the initial option for middle-age or older patients, as there is limited evidence supporting partial meniscectomy surgery for meniscus tears,” Dr. Khan said. “Other treatments should be used first.”
“Arthroscopic debridement or washout of knee osteoarthritis has come under lots of scrutiny based upon trials that suggest patients get no benefit from the procedure. We’re concerned that many surgeons worldwide may still be doing this procedure,” stated the researchers.
Suggested Reading
Khan M, Evaniew N, Bedi A, et al. Arthroscopic surgery for degenerative tears of the meniscus: a systematic review and meta-analysis. CMAJ. 2014 Aug 25. pii: cmaj.140433. [Epub ahead of print]
New meta-analysis evidence suggests that there is no benefit to having arthroscopic meniscal debridement for degenerative meniscal tears in comparison with nonoperative treatments or sham treatments in middle-aged patients with mild or no concomitant osteoarthritis. The findings were published August 25 online ahead of print in the Canadian Medical Association Journal.
“Doctors need to carefully weigh the costs and benefits when deciding who should undergo such surgery,” said Moin Khan, MD, lead author of the study and research fellow in orthopedic surgery in the Michael G. DeGroote School of Medicine at McMaster University in Hamilton, Ontario.
Dr. Khan and colleagues conducted a meta-analysis of 7 randomized controlled trials published between 1946 and January 20, 2014, on arthroscopic partial meniscectomy in patients with mild to no osteoarthritis compared with nonoperative treatments. Two reviewers independently screened all abstracts and titles for eligibility. In total, there were 811 knees in 805 patients with a mean age of 56 years. The pooled treatment effect of arthroscopic surgery did not show a significant or minimally important difference between treatment arms for long-term functional outcomes. Short-term functional outcomes between groups were significant but did not exceed the threshold for minimally important difference. Arthroscopic surgery did not result in a significant improvement in either short- or long-term pain scores.
“This study shows that surgery should not be the initial option for middle-age or older patients, as there is limited evidence supporting partial meniscectomy surgery for meniscus tears,” Dr. Khan said. “Other treatments should be used first.”
“Arthroscopic debridement or washout of knee osteoarthritis has come under lots of scrutiny based upon trials that suggest patients get no benefit from the procedure. We’re concerned that many surgeons worldwide may still be doing this procedure,” stated the researchers.
New meta-analysis evidence suggests that there is no benefit to having arthroscopic meniscal debridement for degenerative meniscal tears in comparison with nonoperative treatments or sham treatments in middle-aged patients with mild or no concomitant osteoarthritis. The findings were published August 25 online ahead of print in the Canadian Medical Association Journal.
“Doctors need to carefully weigh the costs and benefits when deciding who should undergo such surgery,” said Moin Khan, MD, lead author of the study and research fellow in orthopedic surgery in the Michael G. DeGroote School of Medicine at McMaster University in Hamilton, Ontario.
Dr. Khan and colleagues conducted a meta-analysis of 7 randomized controlled trials published between 1946 and January 20, 2014, on arthroscopic partial meniscectomy in patients with mild to no osteoarthritis compared with nonoperative treatments. Two reviewers independently screened all abstracts and titles for eligibility. In total, there were 811 knees in 805 patients with a mean age of 56 years. The pooled treatment effect of arthroscopic surgery did not show a significant or minimally important difference between treatment arms for long-term functional outcomes. Short-term functional outcomes between groups were significant but did not exceed the threshold for minimally important difference. Arthroscopic surgery did not result in a significant improvement in either short- or long-term pain scores.
“This study shows that surgery should not be the initial option for middle-age or older patients, as there is limited evidence supporting partial meniscectomy surgery for meniscus tears,” Dr. Khan said. “Other treatments should be used first.”
“Arthroscopic debridement or washout of knee osteoarthritis has come under lots of scrutiny based upon trials that suggest patients get no benefit from the procedure. We’re concerned that many surgeons worldwide may still be doing this procedure,” stated the researchers.
Suggested Reading
Khan M, Evaniew N, Bedi A, et al. Arthroscopic surgery for degenerative tears of the meniscus: a systematic review and meta-analysis. CMAJ. 2014 Aug 25. pii: cmaj.140433. [Epub ahead of print]
Suggested Reading
Khan M, Evaniew N, Bedi A, et al. Arthroscopic surgery for degenerative tears of the meniscus: a systematic review and meta-analysis. CMAJ. 2014 Aug 25. pii: cmaj.140433. [Epub ahead of print]

Baby Has Rash; Parents Feel Itchy
A 5-month-old baby is brought in by his parents for evaluation of a rash that manifested on his hands several weeks ago. It then spread to his arms and trunk and is now essentially everywhere except his face. Despite a number of treatment attempts, including use of oral antibiotics (cephalexin suspension 125/5 cc) and OTC topical steroid creams, the problem has persisted.
Prior to dermatology, they had consulted a pediatrician. He suggested the child might have scabies, for which he prescribed permethrin cream. The parents tried it, but it made little if any difference.
Neither the child nor his parents are atopic. However, both parents have recently started to feel itchy.

EXAMINATION
The child is afebrile and in no acute distress. Hundreds of tiny papules are scattered on his trunk, arms, and legs, with a particular concentration on his palms. Several of the papules, on closer examination, prove to be vesicles (ie, filled with clear fluid).
One of these lesions, on the child’s volar wrist, is scraped and the sample examined under the microscope. Magnification at 10x power reveals an adult scabies organism and a number of rugby ball–shaped eggs.
Both parents are also examined and found to have probable scabies as well. The mother’s lesions are concentrated around the anterior axillary areas and waistline. The father’s are on his volar wrists and penis.
What is the diagnosis?
DISCUSSION
This case nicely illustrates several issues revolving around the diagnosis of scabies. One might think this would be a simple matter: Diagnose, then treat. Alas, it is seldom so.
For one thing, the diagnosis of scabies needs to be confirmed, whenever possible, with microscopic findings of scabetic elements. Without this, patient and provider confidence are lacking—a situation that often leads to shotgun treatment.
In addition, had the diagnosis been confirmed prior to presentation to dermatology, the previously consulted providers might have considered treating the whole family and trying to identify the source of the infestation. Both of these are absolutely crucial to successful treatment.
Several factors make the diagnosis of scabies difficult in infants. Any part of an infant’s thin, soft, relatively hairless skin is fair game (whereas, in adults, scabies rarely affects skin above the neck). Furthermore, although infants with scabies undoubtedly itch—probably just as much as adults—they are totally inept excoriators and even worse historians. In contrast, adults with scabies will scratch continuously while in the exam room and complain bitterly 24/7.
Once the diagnosis is established, a crucial element of dealing effectively with scabies is education—in this case, of the parents. They must understand the nature of the problem in specific terms. For example, scabies cannot be caught from or given to nonhuman hosts (eg, animals). And while I advise affected families to clean areas such as beds, sofas, and bathrooms, I also emphasize that the organism does not reside in or multiply on inanimate objects. Despite my best efforts, though, some families become almost hysterical: steam-cleaning every surface, calling pest control, washing bedding and towels multiple times, and calling me three times a day.
Families must also understand that treatment of all household members must be coordinated and done twice, seven to 10 days apart, in order to kill freshly hatched organisms. This child was treated with permethrin 5% cream, applied to the entire body and left on overnight, then washed off the next morning (twice per the schedule outlined above). In addition to permethrin, the adults were treated with ivermectin (200 mcg/kg) on the same schedule. Even with these extensive measures, recurrence would not be surprising.
Most often, when treatment “fails,” it is because the diagnosis was not scabies in the first place. In confirmed cases, treatment will be unsuccessful if all family members are not adequately (and concurrently) treated. Another problem occurs when the actual source is outside the home (daycare, sleepovers, sexual partner) and remains unidentified—dooming the family to recurrence. (Institutional scabies—from nursing homes, group living, etc—can be far more difficult to deal with and is beyond the scope of this article.)
The differential for scabies includes—most significantly—atopic dermatitis, which it can closely resemble.
TAKE-HOME LEARNING POINTS
• Scabies can show up almost anywhere on an infant’s body, because the skin is so thin, hairless, and soft.
• If the baby has scabies, chances are the parents and siblings have it too.
• Someone brings scabies into the family, and unless the source is identified and treated, the problem will recur.
• Microscopic examination (KOH) for scabetic elements is a crucial component of diagnosis and treatment.
• Scabies sarcoptes var humani is species-specific and cannot be given to or caught from an animal.
• Permethrin cream 5% is considered safe for infants ages 2 months and older.
A 5-month-old baby is brought in by his parents for evaluation of a rash that manifested on his hands several weeks ago. It then spread to his arms and trunk and is now essentially everywhere except his face. Despite a number of treatment attempts, including use of oral antibiotics (cephalexin suspension 125/5 cc) and OTC topical steroid creams, the problem has persisted.
Prior to dermatology, they had consulted a pediatrician. He suggested the child might have scabies, for which he prescribed permethrin cream. The parents tried it, but it made little if any difference.
Neither the child nor his parents are atopic. However, both parents have recently started to feel itchy.
EXAMINATION
The child is afebrile and in no acute distress. Hundreds of tiny papules are scattered on his trunk, arms, and legs, with a particular concentration on his palms. Several of the papules, on closer examination, prove to be vesicles (ie, filled with clear fluid).
One of these lesions, on the child’s volar wrist, is scraped and the sample examined under the microscope. Magnification at 10x power reveals an adult scabies organism and a number of rugby ball–shaped eggs.
Both parents are also examined and found to have probable scabies as well. The mother’s lesions are concentrated around the anterior axillary areas and waistline. The father’s are on his volar wrists and penis.
What is the diagnosis?
DISCUSSION
This case nicely illustrates several issues revolving around the diagnosis of scabies. One might think this would be a simple matter: Diagnose, then treat. Alas, it is seldom so.
For one thing, the diagnosis of scabies needs to be confirmed, whenever possible, with microscopic findings of scabetic elements. Without this, patient and provider confidence are lacking—a situation that often leads to shotgun treatment.
In addition, had the diagnosis been confirmed prior to presentation to dermatology, the previously consulted providers might have considered treating the whole family and trying to identify the source of the infestation. Both of these are absolutely crucial to successful treatment.
Several factors make the diagnosis of scabies difficult in infants. Any part of an infant’s thin, soft, relatively hairless skin is fair game (whereas, in adults, scabies rarely affects skin above the neck). Furthermore, although infants with scabies undoubtedly itch—probably just as much as adults—they are totally inept excoriators and even worse historians. In contrast, adults with scabies will scratch continuously while in the exam room and complain bitterly 24/7.
Once the diagnosis is established, a crucial element of dealing effectively with scabies is education—in this case, of the parents. They must understand the nature of the problem in specific terms. For example, scabies cannot be caught from or given to nonhuman hosts (eg, animals). And while I advise affected families to clean areas such as beds, sofas, and bathrooms, I also emphasize that the organism does not reside in or multiply on inanimate objects. Despite my best efforts, though, some families become almost hysterical: steam-cleaning every surface, calling pest control, washing bedding and towels multiple times, and calling me three times a day.
Families must also understand that treatment of all household members must be coordinated and done twice, seven to 10 days apart, in order to kill freshly hatched organisms. This child was treated with permethrin 5% cream, applied to the entire body and left on overnight, then washed off the next morning (twice per the schedule outlined above). In addition to permethrin, the adults were treated with ivermectin (200 mcg/kg) on the same schedule. Even with these extensive measures, recurrence would not be surprising.
Most often, when treatment “fails,” it is because the diagnosis was not scabies in the first place. In confirmed cases, treatment will be unsuccessful if all family members are not adequately (and concurrently) treated. Another problem occurs when the actual source is outside the home (daycare, sleepovers, sexual partner) and remains unidentified—dooming the family to recurrence. (Institutional scabies—from nursing homes, group living, etc—can be far more difficult to deal with and is beyond the scope of this article.)
The differential for scabies includes—most significantly—atopic dermatitis, which it can closely resemble.
TAKE-HOME LEARNING POINTS
• Scabies can show up almost anywhere on an infant’s body, because the skin is so thin, hairless, and soft.
• If the baby has scabies, chances are the parents and siblings have it too.
• Someone brings scabies into the family, and unless the source is identified and treated, the problem will recur.
• Microscopic examination (KOH) for scabetic elements is a crucial component of diagnosis and treatment.
• Scabies sarcoptes var humani is species-specific and cannot be given to or caught from an animal.
• Permethrin cream 5% is considered safe for infants ages 2 months and older.
A 5-month-old baby is brought in by his parents for evaluation of a rash that manifested on his hands several weeks ago. It then spread to his arms and trunk and is now essentially everywhere except his face. Despite a number of treatment attempts, including use of oral antibiotics (cephalexin suspension 125/5 cc) and OTC topical steroid creams, the problem has persisted.
Prior to dermatology, they had consulted a pediatrician. He suggested the child might have scabies, for which he prescribed permethrin cream. The parents tried it, but it made little if any difference.
Neither the child nor his parents are atopic. However, both parents have recently started to feel itchy.
EXAMINATION
The child is afebrile and in no acute distress. Hundreds of tiny papules are scattered on his trunk, arms, and legs, with a particular concentration on his palms. Several of the papules, on closer examination, prove to be vesicles (ie, filled with clear fluid).
One of these lesions, on the child’s volar wrist, is scraped and the sample examined under the microscope. Magnification at 10x power reveals an adult scabies organism and a number of rugby ball–shaped eggs.
Both parents are also examined and found to have probable scabies as well. The mother’s lesions are concentrated around the anterior axillary areas and waistline. The father’s are on his volar wrists and penis.
What is the diagnosis?
DISCUSSION
This case nicely illustrates several issues revolving around the diagnosis of scabies. One might think this would be a simple matter: Diagnose, then treat. Alas, it is seldom so.
For one thing, the diagnosis of scabies needs to be confirmed, whenever possible, with microscopic findings of scabetic elements. Without this, patient and provider confidence are lacking—a situation that often leads to shotgun treatment.
In addition, had the diagnosis been confirmed prior to presentation to dermatology, the previously consulted providers might have considered treating the whole family and trying to identify the source of the infestation. Both of these are absolutely crucial to successful treatment.
Several factors make the diagnosis of scabies difficult in infants. Any part of an infant’s thin, soft, relatively hairless skin is fair game (whereas, in adults, scabies rarely affects skin above the neck). Furthermore, although infants with scabies undoubtedly itch—probably just as much as adults—they are totally inept excoriators and even worse historians. In contrast, adults with scabies will scratch continuously while in the exam room and complain bitterly 24/7.
Once the diagnosis is established, a crucial element of dealing effectively with scabies is education—in this case, of the parents. They must understand the nature of the problem in specific terms. For example, scabies cannot be caught from or given to nonhuman hosts (eg, animals). And while I advise affected families to clean areas such as beds, sofas, and bathrooms, I also emphasize that the organism does not reside in or multiply on inanimate objects. Despite my best efforts, though, some families become almost hysterical: steam-cleaning every surface, calling pest control, washing bedding and towels multiple times, and calling me three times a day.
Families must also understand that treatment of all household members must be coordinated and done twice, seven to 10 days apart, in order to kill freshly hatched organisms. This child was treated with permethrin 5% cream, applied to the entire body and left on overnight, then washed off the next morning (twice per the schedule outlined above). In addition to permethrin, the adults were treated with ivermectin (200 mcg/kg) on the same schedule. Even with these extensive measures, recurrence would not be surprising.
Most often, when treatment “fails,” it is because the diagnosis was not scabies in the first place. In confirmed cases, treatment will be unsuccessful if all family members are not adequately (and concurrently) treated. Another problem occurs when the actual source is outside the home (daycare, sleepovers, sexual partner) and remains unidentified—dooming the family to recurrence. (Institutional scabies—from nursing homes, group living, etc—can be far more difficult to deal with and is beyond the scope of this article.)
The differential for scabies includes—most significantly—atopic dermatitis, which it can closely resemble.
TAKE-HOME LEARNING POINTS
• Scabies can show up almost anywhere on an infant’s body, because the skin is so thin, hairless, and soft.
• If the baby has scabies, chances are the parents and siblings have it too.
• Someone brings scabies into the family, and unless the source is identified and treated, the problem will recur.
• Microscopic examination (KOH) for scabetic elements is a crucial component of diagnosis and treatment.
• Scabies sarcoptes var humani is species-specific and cannot be given to or caught from an animal.
• Permethrin cream 5% is considered safe for infants ages 2 months and older.

Care your way to LOS solutions
High-quality care, optimal length of stay (LOS), patient satisfaction, cost-effectiveness – all part of the hospitalists’ creed, our raison d’être. But with these exist national, as well as local imperatives, some of which carry penalties and/or rewards. Public and private organizations devote a huge amount of resources into setting higher and higher bars of excellence for physicians. Individual hospitals adapt and tweak the methods of other centers that have outstanding track records in hopes they, too, may enjoy similar success. Yet, at the end of the day, we are the foot soldiers.
Insurers should not mandate the care we provide. Government should not have to tell us what is acceptable practice and what is not. And hospital administrators – God bless them – should not have to stab blindly in the dark for solutions to the problems that plague their individual institutions. After all, we physicians are at the patients’ bedsides. We talk to them and their families, consult effective and efficient specialists, write orders to take care of them, and ultimately discharge them to their next phase in care.
There is a tremendous amount of low-hanging fruit we easily could seize upon to make our hospitals run more smoothly and make our patients much happier (though the processes and procedures that make one institution ineffective may not plague the next).

For instance, many hospitals have a peak time for admissions, as well as for discharges, and these two times frequently do not coincide. As a result, there may be a backlog of patients in the emergency department (ED) awaiting a clean bed. Invariably, meanwhile, there are patients pacing the halls anxiously waiting for the doctor to arrive to discharge them. But if that doctor is busy seeing a new or very sick patient, that discharge may just have to wait, sometimes for several hours. Here, I have learned to try to look for opportunities instead of focusing on obstacles.
If I anticipate that a patient will be discharged the following day, I try prepare the discharge summary and patient instruction sheet, and to write the prescriptions a day in advance (when time permits). That way, on the following day, instead of devoting 45 minutes to reviewing the records of a lengthy hospital stay, I can simply check on the patient to confirm that she has no new problems and that her examination is stable. Within seconds, I can type in a discharge order and move along to the next patient. Even in the midst of a very busy day, I can typically work in this type of visit fairly early.
On the other hand, if the same patient is likely to be discharged the day after I leave the service, the same preparation by me can save my partner a great deal of time the next day. If everything is already done except the official discharge order, she, too, can likely discharge the patient early in the day, instead of late in the evening after she learns the entire service. (Who likes going home in the dark anyway?)

The patient is happier. The administration is happier to have more beds freed up earlier. The little old lady in the ED with a comminuted hip fracture will get a nice warm bed quicker, and the rounder is less stressed. Everyone wins!
Listening to our patients’ desires, not just their needs can also go a long way in patient satisfaction.
I recently had a patient who was visiting from the other side of the country who, unfortunately, wound up in our ED for cellulitis. She was part of a historical group from California who had traveled to the Washington, D.C., area to attend a national function. The event was to culminate in a banquet that evening – a banquet that she was going to miss. When I saw her, she acknowledged she was getting better on the intravenous vancomycin that was started in the ED the night before, and though the line of demarcation drawn by my partner clearly showed her infection was improving, she still had mild-moderate cellulitis. Her history of methicillin-resistant Staphylococcus aureus (MRSA) made me uncomfortable discharging her on a regimen that would “probably” cover MRSA, and we all know that linezolid (Zyvox) can be incredibly expensive if not on a patient’s formulary. There we were at 5 p.m. on a Saturday. Who would be reachable for a prior authorization?
As I looked down at her sad face and saw the disappointment in her eyes, I had to do something! She was in the area for a great cause; the hospitalization was an unexpected nuisance that threatened to destroy her entire trip. The solution was simple. I called her pharmacist in California and found out that her copay for Zyvox was an affordable $30, so I could safely discharge her in time for her banquet. While that falls far short of an near-miracle that changed a life, my simple effort made a big difference for her.
The point is that when we focus on the patient’s entire needs – not just the disease that brought them to the hospital in the first place – we can create solutions to many of their problems. Sometimes it’s the finishing touches, not just the medical care, that patients remember most.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.
High-quality care, optimal length of stay (LOS), patient satisfaction, cost-effectiveness – all part of the hospitalists’ creed, our raison d’être. But with these exist national, as well as local imperatives, some of which carry penalties and/or rewards. Public and private organizations devote a huge amount of resources into setting higher and higher bars of excellence for physicians. Individual hospitals adapt and tweak the methods of other centers that have outstanding track records in hopes they, too, may enjoy similar success. Yet, at the end of the day, we are the foot soldiers.
Insurers should not mandate the care we provide. Government should not have to tell us what is acceptable practice and what is not. And hospital administrators – God bless them – should not have to stab blindly in the dark for solutions to the problems that plague their individual institutions. After all, we physicians are at the patients’ bedsides. We talk to them and their families, consult effective and efficient specialists, write orders to take care of them, and ultimately discharge them to their next phase in care.
There is a tremendous amount of low-hanging fruit we easily could seize upon to make our hospitals run more smoothly and make our patients much happier (though the processes and procedures that make one institution ineffective may not plague the next).
For instance, many hospitals have a peak time for admissions, as well as for discharges, and these two times frequently do not coincide. As a result, there may be a backlog of patients in the emergency department (ED) awaiting a clean bed. Invariably, meanwhile, there are patients pacing the halls anxiously waiting for the doctor to arrive to discharge them. But if that doctor is busy seeing a new or very sick patient, that discharge may just have to wait, sometimes for several hours. Here, I have learned to try to look for opportunities instead of focusing on obstacles.
If I anticipate that a patient will be discharged the following day, I try prepare the discharge summary and patient instruction sheet, and to write the prescriptions a day in advance (when time permits). That way, on the following day, instead of devoting 45 minutes to reviewing the records of a lengthy hospital stay, I can simply check on the patient to confirm that she has no new problems and that her examination is stable. Within seconds, I can type in a discharge order and move along to the next patient. Even in the midst of a very busy day, I can typically work in this type of visit fairly early.
On the other hand, if the same patient is likely to be discharged the day after I leave the service, the same preparation by me can save my partner a great deal of time the next day. If everything is already done except the official discharge order, she, too, can likely discharge the patient early in the day, instead of late in the evening after she learns the entire service. (Who likes going home in the dark anyway?)
The patient is happier. The administration is happier to have more beds freed up earlier. The little old lady in the ED with a comminuted hip fracture will get a nice warm bed quicker, and the rounder is less stressed. Everyone wins!
Listening to our patients’ desires, not just their needs can also go a long way in patient satisfaction.
I recently had a patient who was visiting from the other side of the country who, unfortunately, wound up in our ED for cellulitis. She was part of a historical group from California who had traveled to the Washington, D.C., area to attend a national function. The event was to culminate in a banquet that evening – a banquet that she was going to miss. When I saw her, she acknowledged she was getting better on the intravenous vancomycin that was started in the ED the night before, and though the line of demarcation drawn by my partner clearly showed her infection was improving, she still had mild-moderate cellulitis. Her history of methicillin-resistant Staphylococcus aureus (MRSA) made me uncomfortable discharging her on a regimen that would “probably” cover MRSA, and we all know that linezolid (Zyvox) can be incredibly expensive if not on a patient’s formulary. There we were at 5 p.m. on a Saturday. Who would be reachable for a prior authorization?
As I looked down at her sad face and saw the disappointment in her eyes, I had to do something! She was in the area for a great cause; the hospitalization was an unexpected nuisance that threatened to destroy her entire trip. The solution was simple. I called her pharmacist in California and found out that her copay for Zyvox was an affordable $30, so I could safely discharge her in time for her banquet. While that falls far short of an near-miracle that changed a life, my simple effort made a big difference for her.
The point is that when we focus on the patient’s entire needs – not just the disease that brought them to the hospital in the first place – we can create solutions to many of their problems. Sometimes it’s the finishing touches, not just the medical care, that patients remember most.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.
High-quality care, optimal length of stay (LOS), patient satisfaction, cost-effectiveness – all part of the hospitalists’ creed, our raison d’être. But with these exist national, as well as local imperatives, some of which carry penalties and/or rewards. Public and private organizations devote a huge amount of resources into setting higher and higher bars of excellence for physicians. Individual hospitals adapt and tweak the methods of other centers that have outstanding track records in hopes they, too, may enjoy similar success. Yet, at the end of the day, we are the foot soldiers.
Insurers should not mandate the care we provide. Government should not have to tell us what is acceptable practice and what is not. And hospital administrators – God bless them – should not have to stab blindly in the dark for solutions to the problems that plague their individual institutions. After all, we physicians are at the patients’ bedsides. We talk to them and their families, consult effective and efficient specialists, write orders to take care of them, and ultimately discharge them to their next phase in care.
There is a tremendous amount of low-hanging fruit we easily could seize upon to make our hospitals run more smoothly and make our patients much happier (though the processes and procedures that make one institution ineffective may not plague the next).
For instance, many hospitals have a peak time for admissions, as well as for discharges, and these two times frequently do not coincide. As a result, there may be a backlog of patients in the emergency department (ED) awaiting a clean bed. Invariably, meanwhile, there are patients pacing the halls anxiously waiting for the doctor to arrive to discharge them. But if that doctor is busy seeing a new or very sick patient, that discharge may just have to wait, sometimes for several hours. Here, I have learned to try to look for opportunities instead of focusing on obstacles.
If I anticipate that a patient will be discharged the following day, I try prepare the discharge summary and patient instruction sheet, and to write the prescriptions a day in advance (when time permits). That way, on the following day, instead of devoting 45 minutes to reviewing the records of a lengthy hospital stay, I can simply check on the patient to confirm that she has no new problems and that her examination is stable. Within seconds, I can type in a discharge order and move along to the next patient. Even in the midst of a very busy day, I can typically work in this type of visit fairly early.
On the other hand, if the same patient is likely to be discharged the day after I leave the service, the same preparation by me can save my partner a great deal of time the next day. If everything is already done except the official discharge order, she, too, can likely discharge the patient early in the day, instead of late in the evening after she learns the entire service. (Who likes going home in the dark anyway?)
The patient is happier. The administration is happier to have more beds freed up earlier. The little old lady in the ED with a comminuted hip fracture will get a nice warm bed quicker, and the rounder is less stressed. Everyone wins!
Listening to our patients’ desires, not just their needs can also go a long way in patient satisfaction.
I recently had a patient who was visiting from the other side of the country who, unfortunately, wound up in our ED for cellulitis. She was part of a historical group from California who had traveled to the Washington, D.C., area to attend a national function. The event was to culminate in a banquet that evening – a banquet that she was going to miss. When I saw her, she acknowledged she was getting better on the intravenous vancomycin that was started in the ED the night before, and though the line of demarcation drawn by my partner clearly showed her infection was improving, she still had mild-moderate cellulitis. Her history of methicillin-resistant Staphylococcus aureus (MRSA) made me uncomfortable discharging her on a regimen that would “probably” cover MRSA, and we all know that linezolid (Zyvox) can be incredibly expensive if not on a patient’s formulary. There we were at 5 p.m. on a Saturday. Who would be reachable for a prior authorization?
As I looked down at her sad face and saw the disappointment in her eyes, I had to do something! She was in the area for a great cause; the hospitalization was an unexpected nuisance that threatened to destroy her entire trip. The solution was simple. I called her pharmacist in California and found out that her copay for Zyvox was an affordable $30, so I could safely discharge her in time for her banquet. While that falls far short of an near-miracle that changed a life, my simple effort made a big difference for her.
The point is that when we focus on the patient’s entire needs – not just the disease that brought them to the hospital in the first place – we can create solutions to many of their problems. Sometimes it’s the finishing touches, not just the medical care, that patients remember most.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.

Study supports new gold standard for FL

PET-CT should be the new standard for response assessment in patients with follicular lymphoma (FL), according to researchers.
The group found evidence suggesting that PET-CT is more accurate than conventional CT in measuring treatment response and predicting survival in patients with FL.
“Our findings have important implications for patients with follicular lymphoma,” said study author Judith Trotman, MBChB, of the University of Sydney in Australia.
“Compared to conventional CT scanning, PET-CT is more accurate in mapping out the lymphoma and better identifies the majority of patients who have a prolonged remission after treatment.”
Dr Trotman and her colleagues reported these findings in The Lancet Haematology. The results will also be discussed at the International Workshop on PET in Lymphoma in Menton, France, which is taking place September 19-20.
By assessing imaging performed in 3 clinical trials, the researchers examined the link between PET-CT status and survival following first-line immunochemotherapy for advanced FL.
Independent, masked reviewers evaluated scans of 246 patients who underwent both PET-CT and traditional CT imaging within 3 months of their last dose of therapy. Patients were followed for a median of 54.8 months.
Seventeen percent of patients had a positive post-induction PET scan, according to a cutoff of 4 or higher on the 5PS.
When the researchers compared patients with a positive PET scan to those with a negative scan, the hazard ratio (HR) for progression-free survival (PFS) was 3.9 (P<0.0001). For overall survival, the HR was 6.7 (P=0.0002).
The 4-year PFS was 23.2% in patients with a positive PET scan and 63.4% in those who had a negative PET scan (P<0.0001). The 4-year overall survival was 87.2% and 97.1%, respectively (P<0.0001).
The researchers also discovered that conventional CT-based response—complete response or unconfirmed complete response compared to partial response—was weakly predictive of PFS. The HR was 1.7 (P=0.017).
“Our study shows that PET-CT is much better in evaluating treatment response and is an early predictor of survival,” Dr Trotman said. “This greater accuracy will assist physicians to more effectively monitor their patients.”
“We expect this research will result in PET-CT imaging replacing CT, becoming the new gold standard to evaluate patients with follicular lymphoma after treatment. Importantly, it will be a platform for future studies of response-adapted therapies aimed to improve the poor outcomes for those patients who remain PET-positive.”
This study may also pave the way for several new research opportunities, according to Bruce Cheson, MD, of Georgetown University in Washington DC, who wrote a comment article related to this study.
“One such possibility would be to assess if an early reaction to the PET scan result improves patient outcome,” he wrote. “Thus, patients with a positive PET scan after induction therapy could be randomly assigned to either deferred treatment until disease progression or immediate intervention.”
“A preferable alternative would be to introduce a unique agent at that time, such as the newly developed small molecules (eg, idelalisib, ibrutinib, or ABT-199) in a novel combination.” ![]()
PET-CT should be the new standard for response assessment in patients with follicular lymphoma (FL), according to researchers.
The group found evidence suggesting that PET-CT is more accurate than conventional CT in measuring treatment response and predicting survival in patients with FL.
“Our findings have important implications for patients with follicular lymphoma,” said study author Judith Trotman, MBChB, of the University of Sydney in Australia.
“Compared to conventional CT scanning, PET-CT is more accurate in mapping out the lymphoma and better identifies the majority of patients who have a prolonged remission after treatment.”
Dr Trotman and her colleagues reported these findings in The Lancet Haematology. The results will also be discussed at the International Workshop on PET in Lymphoma in Menton, France, which is taking place September 19-20.
By assessing imaging performed in 3 clinical trials, the researchers examined the link between PET-CT status and survival following first-line immunochemotherapy for advanced FL.
Independent, masked reviewers evaluated scans of 246 patients who underwent both PET-CT and traditional CT imaging within 3 months of their last dose of therapy. Patients were followed for a median of 54.8 months.
Seventeen percent of patients had a positive post-induction PET scan, according to a cutoff of 4 or higher on the 5PS.
When the researchers compared patients with a positive PET scan to those with a negative scan, the hazard ratio (HR) for progression-free survival (PFS) was 3.9 (P<0.0001). For overall survival, the HR was 6.7 (P=0.0002).
The 4-year PFS was 23.2% in patients with a positive PET scan and 63.4% in those who had a negative PET scan (P<0.0001). The 4-year overall survival was 87.2% and 97.1%, respectively (P<0.0001).
The researchers also discovered that conventional CT-based response—complete response or unconfirmed complete response compared to partial response—was weakly predictive of PFS. The HR was 1.7 (P=0.017).
“Our study shows that PET-CT is much better in evaluating treatment response and is an early predictor of survival,” Dr Trotman said. “This greater accuracy will assist physicians to more effectively monitor their patients.”
“We expect this research will result in PET-CT imaging replacing CT, becoming the new gold standard to evaluate patients with follicular lymphoma after treatment. Importantly, it will be a platform for future studies of response-adapted therapies aimed to improve the poor outcomes for those patients who remain PET-positive.”
This study may also pave the way for several new research opportunities, according to Bruce Cheson, MD, of Georgetown University in Washington DC, who wrote a comment article related to this study.
“One such possibility would be to assess if an early reaction to the PET scan result improves patient outcome,” he wrote. “Thus, patients with a positive PET scan after induction therapy could be randomly assigned to either deferred treatment until disease progression or immediate intervention.”
“A preferable alternative would be to introduce a unique agent at that time, such as the newly developed small molecules (eg, idelalisib, ibrutinib, or ABT-199) in a novel combination.” ![]()
PET-CT should be the new standard for response assessment in patients with follicular lymphoma (FL), according to researchers.
The group found evidence suggesting that PET-CT is more accurate than conventional CT in measuring treatment response and predicting survival in patients with FL.
“Our findings have important implications for patients with follicular lymphoma,” said study author Judith Trotman, MBChB, of the University of Sydney in Australia.
“Compared to conventional CT scanning, PET-CT is more accurate in mapping out the lymphoma and better identifies the majority of patients who have a prolonged remission after treatment.”
Dr Trotman and her colleagues reported these findings in The Lancet Haematology. The results will also be discussed at the International Workshop on PET in Lymphoma in Menton, France, which is taking place September 19-20.
By assessing imaging performed in 3 clinical trials, the researchers examined the link between PET-CT status and survival following first-line immunochemotherapy for advanced FL.
Independent, masked reviewers evaluated scans of 246 patients who underwent both PET-CT and traditional CT imaging within 3 months of their last dose of therapy. Patients were followed for a median of 54.8 months.
Seventeen percent of patients had a positive post-induction PET scan, according to a cutoff of 4 or higher on the 5PS.
When the researchers compared patients with a positive PET scan to those with a negative scan, the hazard ratio (HR) for progression-free survival (PFS) was 3.9 (P<0.0001). For overall survival, the HR was 6.7 (P=0.0002).
The 4-year PFS was 23.2% in patients with a positive PET scan and 63.4% in those who had a negative PET scan (P<0.0001). The 4-year overall survival was 87.2% and 97.1%, respectively (P<0.0001).
The researchers also discovered that conventional CT-based response—complete response or unconfirmed complete response compared to partial response—was weakly predictive of PFS. The HR was 1.7 (P=0.017).
“Our study shows that PET-CT is much better in evaluating treatment response and is an early predictor of survival,” Dr Trotman said. “This greater accuracy will assist physicians to more effectively monitor their patients.”
“We expect this research will result in PET-CT imaging replacing CT, becoming the new gold standard to evaluate patients with follicular lymphoma after treatment. Importantly, it will be a platform for future studies of response-adapted therapies aimed to improve the poor outcomes for those patients who remain PET-positive.”
This study may also pave the way for several new research opportunities, according to Bruce Cheson, MD, of Georgetown University in Washington DC, who wrote a comment article related to this study.
“One such possibility would be to assess if an early reaction to the PET scan result improves patient outcome,” he wrote. “Thus, patients with a positive PET scan after induction therapy could be randomly assigned to either deferred treatment until disease progression or immediate intervention.”
“A preferable alternative would be to introduce a unique agent at that time, such as the newly developed small molecules (eg, idelalisib, ibrutinib, or ABT-199) in a novel combination.” ![]()
Group investigates link between implants and ALCL

Credit: FDA
A newly published review provides insight into anaplastic large-cell lymphoma (ALCL) associated with breast implants.
Previous reports have demonstrated a link between breast implants and ALCL, but the reasons why implants may contribute to this type of lymphoma have remained unclear.
So Suzanne Turner, PhD, of the University of Cambridge in the UK, and her colleagues evaluated the 71 recorded cases of implant-associated ALCL (iALCL).
The researchers recounted their findings in Mutation Research/Reviews in Mutations Research.
The team calculated that the absolute risk of developing iALCL is low, ranging from 1:500,000 to 1:3,000,000 patients with breast implants per year.
Among the 71 cases of iALCL, the average patient was 50 years of age. The average time from breast augmentation/reconstruction to iALCL diagnosis was 10 years.
Most of the cases presented in the capsule surrounding the implant, as part of the periprosthetic fluid or the capsule itself.
The majority of cases were ALK-negative but had a good prognosis. Of the 49 cases where information on the patients’ progress was available, there were 5 deaths.
Some patients received chemotherapy and radiotherapy, but many achieved remission once the implant and surrounding tissue were removed. This suggests it is the body’s abnormal immune response to the implant that is causing iALCL, the researchers said.
There is some evidence to suggest that having any type of prosthetic implant can increase the risk of lymphoma. And some researchers have suggested that lifestyle differences between patients with and without breast implants may be at the root of iALCL.
But Dr Turner and her colleagues said the biological features of lymphomas in the presence of implants, such as the lack of ALK and the proximity to the implant, suggest a real link.
“It’s becoming clear that implant-related ALCL is a distinct clinical entity in itself,” Dr Turner said. “There are still unanswered questions, and only by getting to the bottom of this very rare disease will we be able to find alternative ways to treat it.” ![]()
Credit: FDA
A newly published review provides insight into anaplastic large-cell lymphoma (ALCL) associated with breast implants.
Previous reports have demonstrated a link between breast implants and ALCL, but the reasons why implants may contribute to this type of lymphoma have remained unclear.
So Suzanne Turner, PhD, of the University of Cambridge in the UK, and her colleagues evaluated the 71 recorded cases of implant-associated ALCL (iALCL).
The researchers recounted their findings in Mutation Research/Reviews in Mutations Research.
The team calculated that the absolute risk of developing iALCL is low, ranging from 1:500,000 to 1:3,000,000 patients with breast implants per year.
Among the 71 cases of iALCL, the average patient was 50 years of age. The average time from breast augmentation/reconstruction to iALCL diagnosis was 10 years.
Most of the cases presented in the capsule surrounding the implant, as part of the periprosthetic fluid or the capsule itself.
The majority of cases were ALK-negative but had a good prognosis. Of the 49 cases where information on the patients’ progress was available, there were 5 deaths.
Some patients received chemotherapy and radiotherapy, but many achieved remission once the implant and surrounding tissue were removed. This suggests it is the body’s abnormal immune response to the implant that is causing iALCL, the researchers said.
There is some evidence to suggest that having any type of prosthetic implant can increase the risk of lymphoma. And some researchers have suggested that lifestyle differences between patients with and without breast implants may be at the root of iALCL.
But Dr Turner and her colleagues said the biological features of lymphomas in the presence of implants, such as the lack of ALK and the proximity to the implant, suggest a real link.
“It’s becoming clear that implant-related ALCL is a distinct clinical entity in itself,” Dr Turner said. “There are still unanswered questions, and only by getting to the bottom of this very rare disease will we be able to find alternative ways to treat it.” ![]()
Credit: FDA
A newly published review provides insight into anaplastic large-cell lymphoma (ALCL) associated with breast implants.
Previous reports have demonstrated a link between breast implants and ALCL, but the reasons why implants may contribute to this type of lymphoma have remained unclear.
So Suzanne Turner, PhD, of the University of Cambridge in the UK, and her colleagues evaluated the 71 recorded cases of implant-associated ALCL (iALCL).
The researchers recounted their findings in Mutation Research/Reviews in Mutations Research.
The team calculated that the absolute risk of developing iALCL is low, ranging from 1:500,000 to 1:3,000,000 patients with breast implants per year.
Among the 71 cases of iALCL, the average patient was 50 years of age. The average time from breast augmentation/reconstruction to iALCL diagnosis was 10 years.
Most of the cases presented in the capsule surrounding the implant, as part of the periprosthetic fluid or the capsule itself.
The majority of cases were ALK-negative but had a good prognosis. Of the 49 cases where information on the patients’ progress was available, there were 5 deaths.
Some patients received chemotherapy and radiotherapy, but many achieved remission once the implant and surrounding tissue were removed. This suggests it is the body’s abnormal immune response to the implant that is causing iALCL, the researchers said.
There is some evidence to suggest that having any type of prosthetic implant can increase the risk of lymphoma. And some researchers have suggested that lifestyle differences between patients with and without breast implants may be at the root of iALCL.
But Dr Turner and her colleagues said the biological features of lymphomas in the presence of implants, such as the lack of ALK and the proximity to the implant, suggest a real link.
“It’s becoming clear that implant-related ALCL is a distinct clinical entity in itself,” Dr Turner said. “There are still unanswered questions, and only by getting to the bottom of this very rare disease will we be able to find alternative ways to treat it.” ![]()
Shorter duration of DAPT appears safe

Credit: Andre E.X. Brown
WASHINGTON, DC—New research indicates that patients may only need 6 months of dual antiplatelet therapy (DAPT) after receiving a second-generation drug-eluting stent.
Results of the SECURITY trial showed that patients had similar outcomes whether they received DAPT for 6 months or a full year.
The proportion of patients who met a composite endpoint of cardiac, thrombotic, and bleeding events was low among both treatment groups at the 12- and 24-month time points.
Antonio Colombo, MD, of San Raffaele Scientific Institute in Milan, Italy, and his colleagues reported these findings at TCT 2014 and in the Journal of the American College of Cardiology.
SECURITY was a randomized, multicenter study that aimed to address the need for prolonged use of DAPT following the implantation of a second-generation drug-eluting stent for patients without high-risk acute coronary syndromes.
Patients with a diagnosis of stable or unstable angina or documented silent ischemia undergoing revascularization with at least 1 second-generation drug-eluting stent were eligible for the study. The stents used were the Endeavor Resolute (Medtronic), Xience (Abbott), Promus (Boston Scientific), Nobori (Terumo Corporation), and the Biomatrix (Biosensors Europe SA).
Of 1399 patients, 682 were randomized to 6 months of DAPT, and 717 were randomized to 12 months of treatment. They received clopidogrel at 75 mg per day for at least 3 days before the procedure or a pre-procedural loading dose of a minimum of 300 mg of clopidogrel, if they were not on chronic clopidogrel therapy.
In the post-procedure period, patients received 75 mg of clopidogrel for 6 or 12 months, according to randomization. They also received aspirin indefinitely. And once the new antiplatelet compounds prasugrel and ticagrelor hit the market, they were allowed as treatment options in a protocol amendment.
At 12 months, the incidence of the primary endpoint—the composite of cardiac death, myocardial infarction (MI), stroke, definite or probable stent thrombosis, or BARC type 3 or 5 bleeding—was 4.5% in the 6-month DAPT group and 3.7% in the 12-month DAPT group (P=0.469).
After 24 months, the 6-month and 12-month groups still showed similar incidences of cardiac death (0.9% vs 0.8%, P=0.925), MI (3.1% vs 2.6%, P=0.636), stroke (0.9% vs 0.4%, P=0.636), stent thrombosis (0.4% vs 0.4%, P=0.951), and BARC 3 or 5 bleeding (0.7% vs 1.1%, P=0.496).
Rates of the secondary endpoint—a composite of cardiac death, spontaneous MI, stroke, definite or probable stent thrombosis, or BARC type 2, 3, or 5 bleeding at 12 and 24 months—were also similar among the 6-month and 12-month treatment groups.
At 12 months, the incidence of the secondary composite endpoint was 5.3% in the 6-month group and 4.0% in the 12-month group (P=0.273). In the year that followed, both groups had lower incidences of secondary composite endpoints—1.5% and 2.2%, respectively (P=0.289).
A multivariable analysis showed that an age of 75 years or older, the type of stent used, the mean number of stents implanted, the mean stent length, and the mean stent size were all significant independent predictors of the primary endpoint.
The SECURITY trial was funded by grants from Medtronic and Terumo, makers of 2 brands of drug-eluting stents used in the study. ![]()
Credit: Andre E.X. Brown
WASHINGTON, DC—New research indicates that patients may only need 6 months of dual antiplatelet therapy (DAPT) after receiving a second-generation drug-eluting stent.
Results of the SECURITY trial showed that patients had similar outcomes whether they received DAPT for 6 months or a full year.
The proportion of patients who met a composite endpoint of cardiac, thrombotic, and bleeding events was low among both treatment groups at the 12- and 24-month time points.
Antonio Colombo, MD, of San Raffaele Scientific Institute in Milan, Italy, and his colleagues reported these findings at TCT 2014 and in the Journal of the American College of Cardiology.
SECURITY was a randomized, multicenter study that aimed to address the need for prolonged use of DAPT following the implantation of a second-generation drug-eluting stent for patients without high-risk acute coronary syndromes.
Patients with a diagnosis of stable or unstable angina or documented silent ischemia undergoing revascularization with at least 1 second-generation drug-eluting stent were eligible for the study. The stents used were the Endeavor Resolute (Medtronic), Xience (Abbott), Promus (Boston Scientific), Nobori (Terumo Corporation), and the Biomatrix (Biosensors Europe SA).
Of 1399 patients, 682 were randomized to 6 months of DAPT, and 717 were randomized to 12 months of treatment. They received clopidogrel at 75 mg per day for at least 3 days before the procedure or a pre-procedural loading dose of a minimum of 300 mg of clopidogrel, if they were not on chronic clopidogrel therapy.
In the post-procedure period, patients received 75 mg of clopidogrel for 6 or 12 months, according to randomization. They also received aspirin indefinitely. And once the new antiplatelet compounds prasugrel and ticagrelor hit the market, they were allowed as treatment options in a protocol amendment.
At 12 months, the incidence of the primary endpoint—the composite of cardiac death, myocardial infarction (MI), stroke, definite or probable stent thrombosis, or BARC type 3 or 5 bleeding—was 4.5% in the 6-month DAPT group and 3.7% in the 12-month DAPT group (P=0.469).
After 24 months, the 6-month and 12-month groups still showed similar incidences of cardiac death (0.9% vs 0.8%, P=0.925), MI (3.1% vs 2.6%, P=0.636), stroke (0.9% vs 0.4%, P=0.636), stent thrombosis (0.4% vs 0.4%, P=0.951), and BARC 3 or 5 bleeding (0.7% vs 1.1%, P=0.496).
Rates of the secondary endpoint—a composite of cardiac death, spontaneous MI, stroke, definite or probable stent thrombosis, or BARC type 2, 3, or 5 bleeding at 12 and 24 months—were also similar among the 6-month and 12-month treatment groups.
At 12 months, the incidence of the secondary composite endpoint was 5.3% in the 6-month group and 4.0% in the 12-month group (P=0.273). In the year that followed, both groups had lower incidences of secondary composite endpoints—1.5% and 2.2%, respectively (P=0.289).
A multivariable analysis showed that an age of 75 years or older, the type of stent used, the mean number of stents implanted, the mean stent length, and the mean stent size were all significant independent predictors of the primary endpoint.
The SECURITY trial was funded by grants from Medtronic and Terumo, makers of 2 brands of drug-eluting stents used in the study. ![]()
Credit: Andre E.X. Brown
WASHINGTON, DC—New research indicates that patients may only need 6 months of dual antiplatelet therapy (DAPT) after receiving a second-generation drug-eluting stent.
Results of the SECURITY trial showed that patients had similar outcomes whether they received DAPT for 6 months or a full year.
The proportion of patients who met a composite endpoint of cardiac, thrombotic, and bleeding events was low among both treatment groups at the 12- and 24-month time points.
Antonio Colombo, MD, of San Raffaele Scientific Institute in Milan, Italy, and his colleagues reported these findings at TCT 2014 and in the Journal of the American College of Cardiology.
SECURITY was a randomized, multicenter study that aimed to address the need for prolonged use of DAPT following the implantation of a second-generation drug-eluting stent for patients without high-risk acute coronary syndromes.
Patients with a diagnosis of stable or unstable angina or documented silent ischemia undergoing revascularization with at least 1 second-generation drug-eluting stent were eligible for the study. The stents used were the Endeavor Resolute (Medtronic), Xience (Abbott), Promus (Boston Scientific), Nobori (Terumo Corporation), and the Biomatrix (Biosensors Europe SA).
Of 1399 patients, 682 were randomized to 6 months of DAPT, and 717 were randomized to 12 months of treatment. They received clopidogrel at 75 mg per day for at least 3 days before the procedure or a pre-procedural loading dose of a minimum of 300 mg of clopidogrel, if they were not on chronic clopidogrel therapy.
In the post-procedure period, patients received 75 mg of clopidogrel for 6 or 12 months, according to randomization. They also received aspirin indefinitely. And once the new antiplatelet compounds prasugrel and ticagrelor hit the market, they were allowed as treatment options in a protocol amendment.
At 12 months, the incidence of the primary endpoint—the composite of cardiac death, myocardial infarction (MI), stroke, definite or probable stent thrombosis, or BARC type 3 or 5 bleeding—was 4.5% in the 6-month DAPT group and 3.7% in the 12-month DAPT group (P=0.469).
After 24 months, the 6-month and 12-month groups still showed similar incidences of cardiac death (0.9% vs 0.8%, P=0.925), MI (3.1% vs 2.6%, P=0.636), stroke (0.9% vs 0.4%, P=0.636), stent thrombosis (0.4% vs 0.4%, P=0.951), and BARC 3 or 5 bleeding (0.7% vs 1.1%, P=0.496).
Rates of the secondary endpoint—a composite of cardiac death, spontaneous MI, stroke, definite or probable stent thrombosis, or BARC type 2, 3, or 5 bleeding at 12 and 24 months—were also similar among the 6-month and 12-month treatment groups.
At 12 months, the incidence of the secondary composite endpoint was 5.3% in the 6-month group and 4.0% in the 12-month group (P=0.273). In the year that followed, both groups had lower incidences of secondary composite endpoints—1.5% and 2.2%, respectively (P=0.289).
A multivariable analysis showed that an age of 75 years or older, the type of stent used, the mean number of stents implanted, the mean stent length, and the mean stent size were all significant independent predictors of the primary endpoint.
The SECURITY trial was funded by grants from Medtronic and Terumo, makers of 2 brands of drug-eluting stents used in the study. ![]()
Bivalirudin bests heparin in BRIGHT trial

Credit: Bill Branson
WASHINGTON, DC—The latest results from the BRIGHT trial suggest bivalirudin confers benefits over heparin monotherapy and heparin plus tirofiban for patients with acute myocardial infarction undergoing percutaneous coronary intervention.
Patients who received bivalirudin had a significantly lower incidence of net adverse clinical events (NACE), a composite of death from any cause, reinfarction, ischemia-driven target vessel revascularization, stroke, or any bleeding, both at 30 days and at 1 year.
Bivalirudin conferred a lower risk of bleeding at both time points as well.
However, there were no significant differences between the treatment arms with regard to stent thrombosis or major adverse cardiac and cerebral events (MACCE), a composite of death from any cause, reinfarction, ischemia-driven target vessel revascularization, or stroke.
Yaling Han, MD, of the General Hospital of Shenyang Military Region in China, presented these data at TCT 2014.
The BRIGHT trial included 2194 patients who had acute myocardial infarction and were eligible for emergency percutaneous coronary intervention. They were randomized to receive bivalirudin alone (n=735), heparin alone (n=729), or heparin plus tirofiban (n=730).
The primary endpoint was NACE at 30 days. Secondary endpoints were NACE at 1 year, any bleeding at 30 days and 1 year, and MACCE at 30 days and 1 year. Safety endpoints were thrombocytopenia at 30 days and stent thrombosis at 30 days and 1 year.
Bivalirudin was superior to both heparin monotherapy and heparin plus tirofiban in reducing the primary composite endpoint. At 30 days, NACE had occurred in 8.8%, 13.2%, and 17.0% of patients, respectively (P<0.001).
Bivalirudin was also superior with regard to bleeding at 30 days. Bleeding occurred in 4.1% of patients in the bivalirudin arm, 7.5% in the heparin arm, and 12.3% in the heparin-tirofiban arm (P<0.001).
However, there was no significant difference between the arms for the incidence of MACCE at 30 days—5.0%, 5.8%, and 4.9%, respectively (P=0.74). Likewise, there was no significant difference in the rate of stent thrombosis at 30 days—0.6%, 0.9%, and 0.7%, respectively (P=0.77).
There were differences between the arms in the 30-day thrombocytopenia rate, which was 0.1% in the bivalirudin arm, 0.7% in the heparin arm, and 1.1% in the heparin-tirofiban arm (P=0.04 for bivalirudin vs pooled heparin, P=0.12 for bivalirudin vs heparin, P=0.02 for bivalirudin vs heparin-tirofiban).
The differences between the treatment arms at 1 year were similar to those observed at the 30-day mark. Bivalirudin remained significantly superior when it came to NACE and bleeding, but there were no significant differences with regard to MACCE and stent thrombosis.
At 1-year, NACE had occurred in 12.8% of patients in the bivalirudin arm, 16.5% in the heparin arm, and 20.5% in the heparin-tirofiban arm (P<0.001). Bleeding had occurred in 6.3%, 9.9%, and 14.2% of patients, respectively (P<0.001).
The incidence of MACCE was 6.7% in the bivalirudin arm, 7.3% in the heparin arm, and 6.8%, in the heparin-tirofiban arm. And stent thrombosis had occurred in 1.2%, 1.9%, and 1.2% of patients, respectively.
This research was funded by Salubris Pharmaceutical Co. Ltd, makers of bivalirudin, and the National Key Science and Technology R&D project of the 12th Five-Year Plan. ![]()
Credit: Bill Branson
WASHINGTON, DC—The latest results from the BRIGHT trial suggest bivalirudin confers benefits over heparin monotherapy and heparin plus tirofiban for patients with acute myocardial infarction undergoing percutaneous coronary intervention.
Patients who received bivalirudin had a significantly lower incidence of net adverse clinical events (NACE), a composite of death from any cause, reinfarction, ischemia-driven target vessel revascularization, stroke, or any bleeding, both at 30 days and at 1 year.
Bivalirudin conferred a lower risk of bleeding at both time points as well.
However, there were no significant differences between the treatment arms with regard to stent thrombosis or major adverse cardiac and cerebral events (MACCE), a composite of death from any cause, reinfarction, ischemia-driven target vessel revascularization, or stroke.
Yaling Han, MD, of the General Hospital of Shenyang Military Region in China, presented these data at TCT 2014.
The BRIGHT trial included 2194 patients who had acute myocardial infarction and were eligible for emergency percutaneous coronary intervention. They were randomized to receive bivalirudin alone (n=735), heparin alone (n=729), or heparin plus tirofiban (n=730).
The primary endpoint was NACE at 30 days. Secondary endpoints were NACE at 1 year, any bleeding at 30 days and 1 year, and MACCE at 30 days and 1 year. Safety endpoints were thrombocytopenia at 30 days and stent thrombosis at 30 days and 1 year.
Bivalirudin was superior to both heparin monotherapy and heparin plus tirofiban in reducing the primary composite endpoint. At 30 days, NACE had occurred in 8.8%, 13.2%, and 17.0% of patients, respectively (P<0.001).
Bivalirudin was also superior with regard to bleeding at 30 days. Bleeding occurred in 4.1% of patients in the bivalirudin arm, 7.5% in the heparin arm, and 12.3% in the heparin-tirofiban arm (P<0.001).
However, there was no significant difference between the arms for the incidence of MACCE at 30 days—5.0%, 5.8%, and 4.9%, respectively (P=0.74). Likewise, there was no significant difference in the rate of stent thrombosis at 30 days—0.6%, 0.9%, and 0.7%, respectively (P=0.77).
There were differences between the arms in the 30-day thrombocytopenia rate, which was 0.1% in the bivalirudin arm, 0.7% in the heparin arm, and 1.1% in the heparin-tirofiban arm (P=0.04 for bivalirudin vs pooled heparin, P=0.12 for bivalirudin vs heparin, P=0.02 for bivalirudin vs heparin-tirofiban).
The differences between the treatment arms at 1 year were similar to those observed at the 30-day mark. Bivalirudin remained significantly superior when it came to NACE and bleeding, but there were no significant differences with regard to MACCE and stent thrombosis.
At 1-year, NACE had occurred in 12.8% of patients in the bivalirudin arm, 16.5% in the heparin arm, and 20.5% in the heparin-tirofiban arm (P<0.001). Bleeding had occurred in 6.3%, 9.9%, and 14.2% of patients, respectively (P<0.001).
The incidence of MACCE was 6.7% in the bivalirudin arm, 7.3% in the heparin arm, and 6.8%, in the heparin-tirofiban arm. And stent thrombosis had occurred in 1.2%, 1.9%, and 1.2% of patients, respectively.
This research was funded by Salubris Pharmaceutical Co. Ltd, makers of bivalirudin, and the National Key Science and Technology R&D project of the 12th Five-Year Plan. ![]()
Credit: Bill Branson
WASHINGTON, DC—The latest results from the BRIGHT trial suggest bivalirudin confers benefits over heparin monotherapy and heparin plus tirofiban for patients with acute myocardial infarction undergoing percutaneous coronary intervention.
Patients who received bivalirudin had a significantly lower incidence of net adverse clinical events (NACE), a composite of death from any cause, reinfarction, ischemia-driven target vessel revascularization, stroke, or any bleeding, both at 30 days and at 1 year.
Bivalirudin conferred a lower risk of bleeding at both time points as well.
However, there were no significant differences between the treatment arms with regard to stent thrombosis or major adverse cardiac and cerebral events (MACCE), a composite of death from any cause, reinfarction, ischemia-driven target vessel revascularization, or stroke.
Yaling Han, MD, of the General Hospital of Shenyang Military Region in China, presented these data at TCT 2014.
The BRIGHT trial included 2194 patients who had acute myocardial infarction and were eligible for emergency percutaneous coronary intervention. They were randomized to receive bivalirudin alone (n=735), heparin alone (n=729), or heparin plus tirofiban (n=730).
The primary endpoint was NACE at 30 days. Secondary endpoints were NACE at 1 year, any bleeding at 30 days and 1 year, and MACCE at 30 days and 1 year. Safety endpoints were thrombocytopenia at 30 days and stent thrombosis at 30 days and 1 year.
Bivalirudin was superior to both heparin monotherapy and heparin plus tirofiban in reducing the primary composite endpoint. At 30 days, NACE had occurred in 8.8%, 13.2%, and 17.0% of patients, respectively (P<0.001).
Bivalirudin was also superior with regard to bleeding at 30 days. Bleeding occurred in 4.1% of patients in the bivalirudin arm, 7.5% in the heparin arm, and 12.3% in the heparin-tirofiban arm (P<0.001).
However, there was no significant difference between the arms for the incidence of MACCE at 30 days—5.0%, 5.8%, and 4.9%, respectively (P=0.74). Likewise, there was no significant difference in the rate of stent thrombosis at 30 days—0.6%, 0.9%, and 0.7%, respectively (P=0.77).
There were differences between the arms in the 30-day thrombocytopenia rate, which was 0.1% in the bivalirudin arm, 0.7% in the heparin arm, and 1.1% in the heparin-tirofiban arm (P=0.04 for bivalirudin vs pooled heparin, P=0.12 for bivalirudin vs heparin, P=0.02 for bivalirudin vs heparin-tirofiban).
The differences between the treatment arms at 1 year were similar to those observed at the 30-day mark. Bivalirudin remained significantly superior when it came to NACE and bleeding, but there were no significant differences with regard to MACCE and stent thrombosis.
At 1-year, NACE had occurred in 12.8% of patients in the bivalirudin arm, 16.5% in the heparin arm, and 20.5% in the heparin-tirofiban arm (P<0.001). Bleeding had occurred in 6.3%, 9.9%, and 14.2% of patients, respectively (P<0.001).
The incidence of MACCE was 6.7% in the bivalirudin arm, 7.3% in the heparin arm, and 6.8%, in the heparin-tirofiban arm. And stent thrombosis had occurred in 1.2%, 1.9%, and 1.2% of patients, respectively.
This research was funded by Salubris Pharmaceutical Co. Ltd, makers of bivalirudin, and the National Key Science and Technology R&D project of the 12th Five-Year Plan. ![]()
Honey
Honeybees (Apis mellifera, A. cerana, A. dorsata, A. floria, A. andreniformis, A. koschevnikov, and A. laborisa) play a key role in propagating numerous plants, flower nectar, and flower pollen as well as in pollinating approximately one-third of common agricultural crops, including fruits, vegetables, nuts, and seeds (Time magazine; Proc. Biol. Sci. 2007;274[1608]:303-13). Indeed, the honeybee is the lone insect that produces food regularly consumed by human beings (Am. J. Ther. 2014;21:304-23). Honey, which contains more than 180 compounds, is produced by honeybees from flower nectar. This sweet food product is supersaturated in sugar, and also contains phenolic acids, flavonoids, ascorbic acid, alpha-tocopherol, carotenoids, the enzymes glucose oxidase and catalase, organic and amino acids, and proteins (J. Food Sci. 2008;73:R117-24). Honey has been used since ancient times in Ayurvedic medicine to treat diabetes and has long been used to treat infected wounds (Ayu 2012;33:178-82; Clin. Infect. Dis. 2009;49:1541-9). Currently, honey is used in Ayurvedic medicine to treat acne, and it is incorporated in various cosmetic formulations such as facial washes, skin moisturizers, and hair conditioners (Ayu 2012;33:178-82).
History
For at least 2,700 years, traditional medical practice has included the use of topically applied honey for various conditions, with many modern researchers retrospectively attributing this usage to the antibacterial activity of honey (Am. J. Ther. 2014;21:304-23; Clin. Infect. Dis. 2008;46:1677-82). Honey served as a potent anti-inflammatory and antibacterial agent in folk remedies in ancient Egypt, Greece, and Rome, with written references to the medical application of bee products dating back to ancientEgypt, India, and China (Am. J. Ther. 2014;21:304-23; Cancer Res. 1993;53:1255-61; Evid. Based Complement. Alternat. Med. 2013;2013:697390)). For more than 4,000 years, honey has been used in Ayurvedic medicine, and its use has been traced to the Xin dynasty in China (Am. J. Ther. 2014;21:304-23). The antibacterial characteristics of honey were first reported in 1892 (IUBMB Life 2012;64:48-55). Russia and Germany used honey for wound treatment through World War I. The traditional medical application of honey began to subside with the advent of antibiotics in the 1940s(Burns 2013; 39:1514-25; Int. J. Clin. Pract. 2007;61:1705-7).
Chemistry
Myriad biological functions are associated with honey (antibacterial, antioxidant, antitumor, anti-inflammatory, antibrowning, and antiviral) and ascribed mainly to its constituent phenolic compounds, such as flavonoids, including chrysin (J. Food Sci. 2008;73:R117-24). Indeed, medical grade honeys such as manuka honey (a monofloral honey derived from Leptospermum scoparium, a member of the Myrtaceae family, native to New Zealand) and Medihoney® (a standardized mix of Australian and New Zealand honeys) are rich in flavonoids (Int. J. Clin. Pract. 2007;61:1705-7;J. Int. Acad. Periodontol. 2004;6:63-7; Evid. Based Complement. Alternat. Med. 2009;6:165-73;J. Agric. Food Chem. 2012;60:7229-37). Honey has a pH ranging from 3.2 to 4.5 and an acidity level that stymies the growth of many microorganisms (Burns 2013;39:1514-25; J. Clin. Nurs. 2008;17:2604-23; Nurs. Times. 2006;102:40-2; Br. J. Community Nurs. 2004;Suppl:S21-7 ).
Antibacterial activity
In 2008, Kwakman et al. found that within 24 hours, 10%-40% (vol/vol) medical grade honey (Revamil) destroyed antibiotic-susceptible and antibiotic-resistant isolates of Staphylococcus aureus,S. epidermidis, Enterococcus faecium, Escherichia coli, Pseudomonas aeruginosa, Enterobacter cloacae, and Klebsiella oxytoca. After 2 days of honey application, they also observed a 100-fold decrease in forearm skin colonization in healthy volunteers, with the number of positive skin cultures declining by 76%. The researchers concluded that Revamil exhibits significant potential to prevent or treat infections, including those spawned by multidrug-resistant bacteria (Clin. Infect. Dis. 2008;46:1677-82). Honey has been demonstrated to be clinically effective in treating several kinds of wound infections, reducing skin colonization of multiple bacteria, including methicillin-resistant S. aureus (Clin. Infect. Dis. 2008;46:1677-82) and enhancing wound healing, without provoking adverse effects ( Clin. Infect. Dis. 2009;49:1541-9). Manuka honey and Medihoney are the main forms of medical grade honey used in clinical practice. Nonmedical grade honey may contain viable bacterial spores (including clostridia), and manifest less predictable antibacterial properties (Clin. Infect. Dis. 2009;49:1541-9).
Honey is used in over-the-counter products as a moisturizing agent and in hair-conditioning products based on its strong humectant properties. It is also used in home remedies to treat burns, wounds, eczema, and dermatitis, especially in Asia (Ayu 2012;33:178-8).
Seborrheic dermatitis/dandruff
In 2001, Al-Waili assessed the potential of topically applied crude honey (90% honey diluted in warm water) to treat chronic seborrheic dermatitis of the scalp, face, and chest in 30 patients (20 males and 10 females, aged 15-60 years). Over the initial 4 weeks of treatment, honey was gently rubbed onto lesions every other day for 2-3 minutes at a time, with the ointment left on for 3 hours before gentle warm-water rinsing. Then, in a 6-month prophylactic phase, the participants were divided into a once-weekly treatment group and a control group. Skin lesions healed completely within 2 weeks in the treatment group, after significant reductions in itching and scaling in just the first week. Subjective improvements in hair loss were also reported. Relapse was observed in 12 of the 15 subjects in the control group within 2-4 months of therapy cessation and none in the treatment group. The author concluded that weekly use of crude honey significantly improves seborrheic dermatitis symptoms and related hair loss (Eur. J. Med. Res. 2001;6:306-8).
Wound healing
In February 2013, Jull published a review of 25 randomized and quasirandomized trials evaluating honey in the treatment of acute or chronic wounds, finding that honey might delay healing in partial- and full-thickness burns, compared with early excision and grafting, but it does not significantly enhance healing of chronic venous leg ulcers. They suggested that while honey may prove to be more effective than some conventional dressings for such ulcers, evidence is currently insufficient to support this claim ( Cochrane Database Syst. Rev. 2013;2:CD005083). Later that year, Vandamme et al. identified 55 studies in a literature review suggesting that honey stimulates healing of burns, ulcers, and other wounds. They also found, despite some methodologic concerns, that honey exerts antibacterial activity in burn treatment and deodorizing, debridement, anti-inflammatory, and analgesic activity ( Burns 2013;39:1514-25).
Conclusion
Honey has a long history of traditional medicinal use and has been found to display significant biologic activity, including antibacterial, antioxidant, antitumor, anti-inflammatory, antibrowning, and antiviral. The antibacterial properties of honey are particularly compelling. While more research, in the form of randomized, controlled trials, is needed prior to incorporating bee products into the dermatologic armamentarium as first-line therapies, the potential of honey usage for skin care is promising.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in Miami Beach. She founded the cosmetic dermatology center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (McGraw-Hill, April 2002), and a book for consumers, “The Skin Type Solution” (Bantam, 2006). She has contributed to the Cosmeceutical Critique column in Skin & Allergy News since January 2001. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Galderma, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Stiefel, Topix Pharmaceuticals, and Unilever.
Honeybees (Apis mellifera, A. cerana, A. dorsata, A. floria, A. andreniformis, A. koschevnikov, and A. laborisa) play a key role in propagating numerous plants, flower nectar, and flower pollen as well as in pollinating approximately one-third of common agricultural crops, including fruits, vegetables, nuts, and seeds (Time magazine; Proc. Biol. Sci. 2007;274[1608]:303-13). Indeed, the honeybee is the lone insect that produces food regularly consumed by human beings (Am. J. Ther. 2014;21:304-23). Honey, which contains more than 180 compounds, is produced by honeybees from flower nectar. This sweet food product is supersaturated in sugar, and also contains phenolic acids, flavonoids, ascorbic acid, alpha-tocopherol, carotenoids, the enzymes glucose oxidase and catalase, organic and amino acids, and proteins (J. Food Sci. 2008;73:R117-24). Honey has been used since ancient times in Ayurvedic medicine to treat diabetes and has long been used to treat infected wounds (Ayu 2012;33:178-82; Clin. Infect. Dis. 2009;49:1541-9). Currently, honey is used in Ayurvedic medicine to treat acne, and it is incorporated in various cosmetic formulations such as facial washes, skin moisturizers, and hair conditioners (Ayu 2012;33:178-82).
History
For at least 2,700 years, traditional medical practice has included the use of topically applied honey for various conditions, with many modern researchers retrospectively attributing this usage to the antibacterial activity of honey (Am. J. Ther. 2014;21:304-23; Clin. Infect. Dis. 2008;46:1677-82). Honey served as a potent anti-inflammatory and antibacterial agent in folk remedies in ancient Egypt, Greece, and Rome, with written references to the medical application of bee products dating back to ancientEgypt, India, and China (Am. J. Ther. 2014;21:304-23; Cancer Res. 1993;53:1255-61; Evid. Based Complement. Alternat. Med. 2013;2013:697390)). For more than 4,000 years, honey has been used in Ayurvedic medicine, and its use has been traced to the Xin dynasty in China (Am. J. Ther. 2014;21:304-23). The antibacterial characteristics of honey were first reported in 1892 (IUBMB Life 2012;64:48-55). Russia and Germany used honey for wound treatment through World War I. The traditional medical application of honey began to subside with the advent of antibiotics in the 1940s(Burns 2013; 39:1514-25; Int. J. Clin. Pract. 2007;61:1705-7).
Chemistry
Myriad biological functions are associated with honey (antibacterial, antioxidant, antitumor, anti-inflammatory, antibrowning, and antiviral) and ascribed mainly to its constituent phenolic compounds, such as flavonoids, including chrysin (J. Food Sci. 2008;73:R117-24). Indeed, medical grade honeys such as manuka honey (a monofloral honey derived from Leptospermum scoparium, a member of the Myrtaceae family, native to New Zealand) and Medihoney® (a standardized mix of Australian and New Zealand honeys) are rich in flavonoids (Int. J. Clin. Pract. 2007;61:1705-7;J. Int. Acad. Periodontol. 2004;6:63-7; Evid. Based Complement. Alternat. Med. 2009;6:165-73;J. Agric. Food Chem. 2012;60:7229-37). Honey has a pH ranging from 3.2 to 4.5 and an acidity level that stymies the growth of many microorganisms (Burns 2013;39:1514-25; J. Clin. Nurs. 2008;17:2604-23; Nurs. Times. 2006;102:40-2; Br. J. Community Nurs. 2004;Suppl:S21-7 ).
Antibacterial activity
In 2008, Kwakman et al. found that within 24 hours, 10%-40% (vol/vol) medical grade honey (Revamil) destroyed antibiotic-susceptible and antibiotic-resistant isolates of Staphylococcus aureus,S. epidermidis, Enterococcus faecium, Escherichia coli, Pseudomonas aeruginosa, Enterobacter cloacae, and Klebsiella oxytoca. After 2 days of honey application, they also observed a 100-fold decrease in forearm skin colonization in healthy volunteers, with the number of positive skin cultures declining by 76%. The researchers concluded that Revamil exhibits significant potential to prevent or treat infections, including those spawned by multidrug-resistant bacteria (Clin. Infect. Dis. 2008;46:1677-82). Honey has been demonstrated to be clinically effective in treating several kinds of wound infections, reducing skin colonization of multiple bacteria, including methicillin-resistant S. aureus (Clin. Infect. Dis. 2008;46:1677-82) and enhancing wound healing, without provoking adverse effects ( Clin. Infect. Dis. 2009;49:1541-9). Manuka honey and Medihoney are the main forms of medical grade honey used in clinical practice. Nonmedical grade honey may contain viable bacterial spores (including clostridia), and manifest less predictable antibacterial properties (Clin. Infect. Dis. 2009;49:1541-9).
Honey is used in over-the-counter products as a moisturizing agent and in hair-conditioning products based on its strong humectant properties. It is also used in home remedies to treat burns, wounds, eczema, and dermatitis, especially in Asia (Ayu 2012;33:178-8).
Seborrheic dermatitis/dandruff
In 2001, Al-Waili assessed the potential of topically applied crude honey (90% honey diluted in warm water) to treat chronic seborrheic dermatitis of the scalp, face, and chest in 30 patients (20 males and 10 females, aged 15-60 years). Over the initial 4 weeks of treatment, honey was gently rubbed onto lesions every other day for 2-3 minutes at a time, with the ointment left on for 3 hours before gentle warm-water rinsing. Then, in a 6-month prophylactic phase, the participants were divided into a once-weekly treatment group and a control group. Skin lesions healed completely within 2 weeks in the treatment group, after significant reductions in itching and scaling in just the first week. Subjective improvements in hair loss were also reported. Relapse was observed in 12 of the 15 subjects in the control group within 2-4 months of therapy cessation and none in the treatment group. The author concluded that weekly use of crude honey significantly improves seborrheic dermatitis symptoms and related hair loss (Eur. J. Med. Res. 2001;6:306-8).
Wound healing
In February 2013, Jull published a review of 25 randomized and quasirandomized trials evaluating honey in the treatment of acute or chronic wounds, finding that honey might delay healing in partial- and full-thickness burns, compared with early excision and grafting, but it does not significantly enhance healing of chronic venous leg ulcers. They suggested that while honey may prove to be more effective than some conventional dressings for such ulcers, evidence is currently insufficient to support this claim ( Cochrane Database Syst. Rev. 2013;2:CD005083). Later that year, Vandamme et al. identified 55 studies in a literature review suggesting that honey stimulates healing of burns, ulcers, and other wounds. They also found, despite some methodologic concerns, that honey exerts antibacterial activity in burn treatment and deodorizing, debridement, anti-inflammatory, and analgesic activity ( Burns 2013;39:1514-25).
Conclusion
Honey has a long history of traditional medicinal use and has been found to display significant biologic activity, including antibacterial, antioxidant, antitumor, anti-inflammatory, antibrowning, and antiviral. The antibacterial properties of honey are particularly compelling. While more research, in the form of randomized, controlled trials, is needed prior to incorporating bee products into the dermatologic armamentarium as first-line therapies, the potential of honey usage for skin care is promising.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in Miami Beach. She founded the cosmetic dermatology center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (McGraw-Hill, April 2002), and a book for consumers, “The Skin Type Solution” (Bantam, 2006). She has contributed to the Cosmeceutical Critique column in Skin & Allergy News since January 2001. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Galderma, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Stiefel, Topix Pharmaceuticals, and Unilever.
Honeybees (Apis mellifera, A. cerana, A. dorsata, A. floria, A. andreniformis, A. koschevnikov, and A. laborisa) play a key role in propagating numerous plants, flower nectar, and flower pollen as well as in pollinating approximately one-third of common agricultural crops, including fruits, vegetables, nuts, and seeds (Time magazine; Proc. Biol. Sci. 2007;274[1608]:303-13). Indeed, the honeybee is the lone insect that produces food regularly consumed by human beings (Am. J. Ther. 2014;21:304-23). Honey, which contains more than 180 compounds, is produced by honeybees from flower nectar. This sweet food product is supersaturated in sugar, and also contains phenolic acids, flavonoids, ascorbic acid, alpha-tocopherol, carotenoids, the enzymes glucose oxidase and catalase, organic and amino acids, and proteins (J. Food Sci. 2008;73:R117-24). Honey has been used since ancient times in Ayurvedic medicine to treat diabetes and has long been used to treat infected wounds (Ayu 2012;33:178-82; Clin. Infect. Dis. 2009;49:1541-9). Currently, honey is used in Ayurvedic medicine to treat acne, and it is incorporated in various cosmetic formulations such as facial washes, skin moisturizers, and hair conditioners (Ayu 2012;33:178-82).
History
For at least 2,700 years, traditional medical practice has included the use of topically applied honey for various conditions, with many modern researchers retrospectively attributing this usage to the antibacterial activity of honey (Am. J. Ther. 2014;21:304-23; Clin. Infect. Dis. 2008;46:1677-82). Honey served as a potent anti-inflammatory and antibacterial agent in folk remedies in ancient Egypt, Greece, and Rome, with written references to the medical application of bee products dating back to ancientEgypt, India, and China (Am. J. Ther. 2014;21:304-23; Cancer Res. 1993;53:1255-61; Evid. Based Complement. Alternat. Med. 2013;2013:697390)). For more than 4,000 years, honey has been used in Ayurvedic medicine, and its use has been traced to the Xin dynasty in China (Am. J. Ther. 2014;21:304-23). The antibacterial characteristics of honey were first reported in 1892 (IUBMB Life 2012;64:48-55). Russia and Germany used honey for wound treatment through World War I. The traditional medical application of honey began to subside with the advent of antibiotics in the 1940s(Burns 2013; 39:1514-25; Int. J. Clin. Pract. 2007;61:1705-7).
Chemistry
Myriad biological functions are associated with honey (antibacterial, antioxidant, antitumor, anti-inflammatory, antibrowning, and antiviral) and ascribed mainly to its constituent phenolic compounds, such as flavonoids, including chrysin (J. Food Sci. 2008;73:R117-24). Indeed, medical grade honeys such as manuka honey (a monofloral honey derived from Leptospermum scoparium, a member of the Myrtaceae family, native to New Zealand) and Medihoney® (a standardized mix of Australian and New Zealand honeys) are rich in flavonoids (Int. J. Clin. Pract. 2007;61:1705-7;J. Int. Acad. Periodontol. 2004;6:63-7; Evid. Based Complement. Alternat. Med. 2009;6:165-73;J. Agric. Food Chem. 2012;60:7229-37). Honey has a pH ranging from 3.2 to 4.5 and an acidity level that stymies the growth of many microorganisms (Burns 2013;39:1514-25; J. Clin. Nurs. 2008;17:2604-23; Nurs. Times. 2006;102:40-2; Br. J. Community Nurs. 2004;Suppl:S21-7 ).
Antibacterial activity
In 2008, Kwakman et al. found that within 24 hours, 10%-40% (vol/vol) medical grade honey (Revamil) destroyed antibiotic-susceptible and antibiotic-resistant isolates of Staphylococcus aureus,S. epidermidis, Enterococcus faecium, Escherichia coli, Pseudomonas aeruginosa, Enterobacter cloacae, and Klebsiella oxytoca. After 2 days of honey application, they also observed a 100-fold decrease in forearm skin colonization in healthy volunteers, with the number of positive skin cultures declining by 76%. The researchers concluded that Revamil exhibits significant potential to prevent or treat infections, including those spawned by multidrug-resistant bacteria (Clin. Infect. Dis. 2008;46:1677-82). Honey has been demonstrated to be clinically effective in treating several kinds of wound infections, reducing skin colonization of multiple bacteria, including methicillin-resistant S. aureus (Clin. Infect. Dis. 2008;46:1677-82) and enhancing wound healing, without provoking adverse effects ( Clin. Infect. Dis. 2009;49:1541-9). Manuka honey and Medihoney are the main forms of medical grade honey used in clinical practice. Nonmedical grade honey may contain viable bacterial spores (including clostridia), and manifest less predictable antibacterial properties (Clin. Infect. Dis. 2009;49:1541-9).
Honey is used in over-the-counter products as a moisturizing agent and in hair-conditioning products based on its strong humectant properties. It is also used in home remedies to treat burns, wounds, eczema, and dermatitis, especially in Asia (Ayu 2012;33:178-8).
Seborrheic dermatitis/dandruff
In 2001, Al-Waili assessed the potential of topically applied crude honey (90% honey diluted in warm water) to treat chronic seborrheic dermatitis of the scalp, face, and chest in 30 patients (20 males and 10 females, aged 15-60 years). Over the initial 4 weeks of treatment, honey was gently rubbed onto lesions every other day for 2-3 minutes at a time, with the ointment left on for 3 hours before gentle warm-water rinsing. Then, in a 6-month prophylactic phase, the participants were divided into a once-weekly treatment group and a control group. Skin lesions healed completely within 2 weeks in the treatment group, after significant reductions in itching and scaling in just the first week. Subjective improvements in hair loss were also reported. Relapse was observed in 12 of the 15 subjects in the control group within 2-4 months of therapy cessation and none in the treatment group. The author concluded that weekly use of crude honey significantly improves seborrheic dermatitis symptoms and related hair loss (Eur. J. Med. Res. 2001;6:306-8).
Wound healing
In February 2013, Jull published a review of 25 randomized and quasirandomized trials evaluating honey in the treatment of acute or chronic wounds, finding that honey might delay healing in partial- and full-thickness burns, compared with early excision and grafting, but it does not significantly enhance healing of chronic venous leg ulcers. They suggested that while honey may prove to be more effective than some conventional dressings for such ulcers, evidence is currently insufficient to support this claim ( Cochrane Database Syst. Rev. 2013;2:CD005083). Later that year, Vandamme et al. identified 55 studies in a literature review suggesting that honey stimulates healing of burns, ulcers, and other wounds. They also found, despite some methodologic concerns, that honey exerts antibacterial activity in burn treatment and deodorizing, debridement, anti-inflammatory, and analgesic activity ( Burns 2013;39:1514-25).
Conclusion
Honey has a long history of traditional medicinal use and has been found to display significant biologic activity, including antibacterial, antioxidant, antitumor, anti-inflammatory, antibrowning, and antiviral. The antibacterial properties of honey are particularly compelling. While more research, in the form of randomized, controlled trials, is needed prior to incorporating bee products into the dermatologic armamentarium as first-line therapies, the potential of honey usage for skin care is promising.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in Miami Beach. She founded the cosmetic dermatology center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (McGraw-Hill, April 2002), and a book for consumers, “The Skin Type Solution” (Bantam, 2006). She has contributed to the Cosmeceutical Critique column in Skin & Allergy News since January 2001. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Galderma, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Stiefel, Topix Pharmaceuticals, and Unilever.

Depressed, suicidal, and brittle in her bones
CASE Broken down
Ms. E, age 20, is a college student who has had major depressive disorder for several years and a genetic bone disease (osteogenesis imperfecta, mixed type III and IV). She presents with depression, anxiety, and suicidal ideation. She reports recent worsening of her depressive symptoms, including anhedonia, excessive sleep, difficulty concentrating, and feeling overwhelmed, hopeless, and worthless. She also describes frequent thoughts of suicide with the plan of putting herself in oncoming traffic, although she has no history of suicide attempts.
Previously, her primary care physician prescribed lorazepam, 0.5 mg, as needed for anxiety, and sertraline, 100 mg/d, for depression and anxiety. She experienced only partial improvement in symptoms, however.
In addition to depressive symptoms, Ms. E describes manic symptoms lasting for as long as 3 to 5 days, including decreased need for sleep, increased energy, pressured speech, racing thoughts, distractibility, spending excessive money on cosmetics, and risking her safety—given her skeletal disorder— by participating in high-impact stage-combat classes. She denies auditory and visual hallucinations, homicidal ideation, and delusions.
The medical history is significant for osteogenesis imperfecta, which has caused 62 fractures and required 16 surgeries. Ms. E is a theater major who, despite her short stature and wheelchair use, reports enjoying her acting career and says she does not feel demoralized by her medical condition. She describes overcoming her physical disabilities with pride and confidence. However, her recent worsening mood symptoms have left her unable to concentrate and feeling overwhelmed with school.
Ms. E is voluntarily admitted to an inpatient psychiatric unit with a diagnosis of bipolar I disorder with rapid cycling, most recent episode mixed. Because of her bone fragility, the treatment team considers what would be an appropriate course of drug treatment to control bipolar symptoms while minimizing risk of bone loss.
Which medications are associated with decreased bone mineral density?
a) citalopram
b) haloperidol
c) carbamazepine
d) paliperidone
e) all of the above
The authors’ observations
Osteogenesis imperfecta is a genetic condition caused by mutations in genes implicated in collagen production. As a result, bones are brittle and prone to fracture. Different classes of psychotropics have been shown to increase risk of bone fractures through a variety of mechanisms. Clinicians often must choose appropriate pharmacotherapy for patients at high risk of fracture, including postmenopausal women, older patients, malnourished persons, and those with hormonal deficiencies leading to osteoporosis.
To assist our clinical decision-making, we reviewed the literature to establish appropriate management of a patient with increased bone fragility and new-onset bipolar disorder. We considered all classes of medications used to treat bipolar disorder, including antipsychotics, antidepressants, lithium, and anticonvulsants.
Antipsychotics
In population-based studies, prolactin-elevating antipsychotics have been associated with decreased bone mineral density and increased risk of fracture.1 Additional studies on geriatric and non-geriatric populations have supported these findings.2,3
The mechanism through which fracture risk is increased likely is related to antipsychotics’ effect on serum prolactin and cortisol levels. Antipsychotics act as antagonists on D2 receptors in the hypothalamic tubero-infundibular pathway, therefore preventing inhibition of prolactin. Long-term elevation in serum prolactin can cause loss of bone mineral density through secondary hypogonadism and direct effects on target tissues. Additional modifying factors include smoking and estrogen use.
The degree to which antipsychotics increase fracture risk might be related to the degree of serum prolactin elevation.4 Antipsychotics previously have been grouped by the degree of prolactin elevation, categorizing them as high, medium, and low or no potential to elevate serum prolactin.4 Based on this classification, typical antipsychotics, risperidone, and paliperidone have the highest potential to elevate prolactin. Accordingly, antipsychotics with the lowest fracture risk are those that have the lowest risk of serum prolactin elevation: ziprasidone, asenapine, quetiapine, and clozapine. Aripiprazole may lower prolactin in some patients. This is supported by studies noting reduced bone mineral density5,6 and increased risk of fracture1 with high-potential vs low- or no-potential antipsychotics. Because of these findings, it is crucial to consider the potential risk of prolactin elevation when treating patients at increased risk of fracture. Providers should consider low/no potential antipsychotic medications before considering those with medium or high potential (Table).
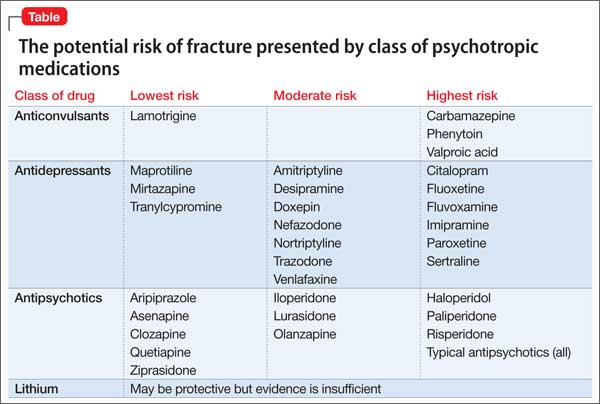
Antidepressants
In a meta-analysis, antidepressants were shown to increase fracture risk by 70% to 90%.2 However, the relative risk varies by antidepressant class. Several studies have shown that selective serotonin reuptake inhibitors (SSRIs) are associated with a higher risk of fracture compared with tricyclic antidepressants (TCAs).7 In addition, antidepressants with a high affinity for the serotonin transporter, including citalopram, fluoxetine, fluvoxamine, paroxetine, sertraline, and imipramine, have been associated with greater risk of osteoporotic fracture compared with those with low affinity.8
The mechanisms by which antidepressants increase fracture risk are complex, although the strongest evidence implicates a direct effect on bone metabolism via the 5-HTT receptor. This receptor, found on osteoblasts and osteoclasts, plays an important role in bone metabolism; it is through this receptor that SSRIs might inhibit osteoblasts and promote osteoclast activity, thereby disrupting bone microarchitecture. Additional studies are needed to further describe the mechanism of the association among antidepressants, bone mineral density, and fracture risk.
Fracture risk is associated with duration of use rather than dosage. Population-based studies show a higher fracture risk for new users of TCAs compared with continuous users, and the risk of fracture with SSRIs seems to increase slightly over time.9 No association has been identified between fracture risk and antidepressant dosage. According to the literature, drugs with low affinity for the serotonin transporter, such as maprotiline and mirtazapine, likely are the safest antidepressants for patients at increased risk of fracture. Options also include other TCAs and any antidepressant with low affinity for the serotonin receptor.7,8
Lithium
Studies on lithium and bone mineral density have shown mixed results. Older studies found that lithium had a negative or no effect on bone mineral density or the parathyroid hormone level.10 More recent investigations, however, suggest that the drug has a protective effect on bone mineral density, although this has not been replicated in all studies.
In a mouse model, lithium has been shown to enhance bone formation and improve bone mass, at least in part by activation of the Wnt signaling pathway through an inhibitory effect on glycogen synthase kinase-3β.11 In humans, lithium-treated adults had lower serum alkaline phosphate, osteocalcin, and C-telopeptide levels compared with controls, suggesting a state of decreased bone remodeling and increased turnover.12 There is a paucity of clinical data on the effect of lithium on fracture risk. Additional studies are necessary to elucidate lithium’s mechanism on bone mineral density and determine the magnitude of the clinical effect.
Anticonvulsants
The association among anticonvulsants, decreased bone mineral density, and increased risk of fracture is well-established in the literature.13 However, causality is difficult to determine, because many studies were of patients with a seizure disorder, who often have additional risk factors for fracture, including seizure-related trauma, drowsiness, and slowed reflexes.
Mechanisms through which anticonvulsants increase fracture risk include increased bone resorption, secondary hypoparathyroidism, and pseudohypoparathyroidism. Markers of bone resorption were elevated in patients receiving an antiepileptic.14 This effect might be enhanced by co-administration of cytochrome P450 (CYP450) enzyme-inducing anticonvulsants and CYP450 enzyme-inhibiting medications, such as valproate. Long-term treatment with valproate may produce reduction of bone mass and increased risk of fractures; however, other studies disagree with this finding.15
In addition to CYP450-inducing effects, phenytoin, carbamezapine, and phenobarbital can increase catabolism of vitamin D, which is associated with osteomalacia.14 This results in decreased intestinal absorption of calcium, hypocalcemia, and secondary hyperparathyroidism, which also increases fracture risk. Anticonvulsants also might increase resistance to pseudohypoparathyroidism and inhibit calcitonin secretion.
Lamotrigine has not been shown to interfere with bone accrual16 and may be a safer mood stabilizer for patients at high risk of fracture. For patients at increased risk of fracture, it is important to select an anticonvulsant wisely to minimize fracture risk.
How would you treat Ms. E during her hospitalization for bipolar disorder?
a) carbamazepine
b) lithium
c) risperidone
d) mirtazapine
TREATMENT Minimizing polypharmacy
Because many pharmacotherapeutic options for managing bipolar disorder can increase the risk of fracture, clinicians must be aware of the relative risk of each class of medication and each individual drug. We initiated lithium, 300 mg, 3 times a day, to stabilize Ms. E’s mood. Although clinical data are inconclusive regarding lithium’s effect on fracture risk, we felt that the benefit of acute mood stabilization outweighed the risk of decreased bone mineral index.
We selected aripiprazole, 10 mg/d, as an adjunctive treatment because of its minimal effect on serum prolactin levels.4 We considered prescribing an antidepressant but decided against it because we were concerned about manic switching.
Polypharmacy is another important consideration for Ms. E. Several studies have identified polypharmacy, particularly with antipsychotics, as an independent risk factor for fracture.3 Therefore, we sought to minimize the number of medications Ms. E receives. Although lithium monotherapy is an option, we thought that her mood symptoms were severe enough that the risk of inadequately treating her bipolar symptoms outweighed the additional risk of fracture from dual therapy with lithium and aripiprazole. Untreated or inadequately treated depression is associated with a higher fracture risk. Therefore, we avoided prescribing >2 medications to mitigate any excessive risk of fracture from polypharmacy.
Bottom Line
Different classes of medications—antipsychotics, anticonvulsants, antidepressants, and lithium—used for treating bipolar disorder have been shown to increase risk of bone fracture through a variety of mechanisms. Anticonvulsants and prolactin-elevating antipsychotics are associated with increased fracture risk; evidence on lithium is mixed. Fracture risk with antidepressants is associated with duration of use, rather than dosage.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Howard L, Kirkwood G, Leese M. Risk of hip fracture in patients with a history of schizophrenia. Br J Psychiatry. 2007;190:129-134.
2. Takkouche B, Montes-Martínez A, Gill SS, et al. Psychotropic medications and the risk of fracture: a meta-analysis. Drug Saf. 2007;30(2):171-184.
3. Sørensen HJ, Jensen SO, Nielsen J. Schizophrenia, antipsychotics and risk of hip fracture: a population-based analysis. Eur Neuropsychopharmacol. 2013;23(8):872-878.
4. Rahman T, Clevenger CV, Kaklamani V, et al. Antipsychotic treatment in breast cancer patients. Am J Psychiatry. 2014;171(6):616-621.
5. Bilici M, Cakirbay H, Guler M, et al. Classical and atypical neuroleptics, and bone mineral density, in patients with schizophrenia. Int J Neurosci. 2002;112(7):817-828.
6. Becker D, Liver O, Mester R, et al. Risperidone, but not olanzapine, decreases bone mineral density in female premenopausal schizophrenia patients. J Clin Psychiatry. 2003;64(7):761-766.
7. Bolton JM, Metge C, Lix L, et al. Fracture risk from psychotropic medications: a population-based analysis. J Clin Psychopharmacol. 2008;28(4):384-391.
8. Verdel BM, Souverein PC, Egberts TC, et al. Use of antidepressant drugs and risk of osteoporotic and non-osteoporotic fractures. Bone. 2010;47(3):604-609.
9. Diem SJ, Ruppert K, Cauley JA. Rates of bone loss among women initiating antidepressant medication use in midlife. J Clin Endocrinol Metab. 2013;(11):4355-4363.
10. Plenge P, Rafaelsen OJ. Lithium effects on calcium, magnesium and phosphate in man: effects on balance, bone mineral content, faecal and urinary excretion. Acta Psychiatr Scand. 1982;66(5):361-373.
11. Clément-Lacroix P, Ai M, Morvan F, et al. Lrp5-independent activation of Wnt signaling by lithium chloride increases bone formation and bone mass in mice. Proc Natl Acad Sci U S A. 2005;102(48):17406-17411.
12. Zamani A, Omrani GR, Nasab MM. Lithium’s effect on bone mineral density. Bone. 2009;44(2):331-334.
13. Swanton J, Simister R, Altmann D, et al. Bone mineral density in institutionalised patients with refractory epilepsy. Seizure. 2007;16(6):538-541.
14. Pack AM, Morrell MJ. Epilepsy and bone health in adults. Epilepsy Behav. 2004;5(suppl 2):S24-S29.
15. Pack AM. Bone disease in epilepsy. Curr Neurol Neurosci Rep. 2004;4(4):329-334.
16. Sheth RD, Hermann BP. Bone mineral density with lamotrigine monotherapy for epilepsy. Pediatr Neurol. 2007;37(4):250-254.
CASE Broken down
Ms. E, age 20, is a college student who has had major depressive disorder for several years and a genetic bone disease (osteogenesis imperfecta, mixed type III and IV). She presents with depression, anxiety, and suicidal ideation. She reports recent worsening of her depressive symptoms, including anhedonia, excessive sleep, difficulty concentrating, and feeling overwhelmed, hopeless, and worthless. She also describes frequent thoughts of suicide with the plan of putting herself in oncoming traffic, although she has no history of suicide attempts.
Previously, her primary care physician prescribed lorazepam, 0.5 mg, as needed for anxiety, and sertraline, 100 mg/d, for depression and anxiety. She experienced only partial improvement in symptoms, however.
In addition to depressive symptoms, Ms. E describes manic symptoms lasting for as long as 3 to 5 days, including decreased need for sleep, increased energy, pressured speech, racing thoughts, distractibility, spending excessive money on cosmetics, and risking her safety—given her skeletal disorder— by participating in high-impact stage-combat classes. She denies auditory and visual hallucinations, homicidal ideation, and delusions.
The medical history is significant for osteogenesis imperfecta, which has caused 62 fractures and required 16 surgeries. Ms. E is a theater major who, despite her short stature and wheelchair use, reports enjoying her acting career and says she does not feel demoralized by her medical condition. She describes overcoming her physical disabilities with pride and confidence. However, her recent worsening mood symptoms have left her unable to concentrate and feeling overwhelmed with school.
Ms. E is voluntarily admitted to an inpatient psychiatric unit with a diagnosis of bipolar I disorder with rapid cycling, most recent episode mixed. Because of her bone fragility, the treatment team considers what would be an appropriate course of drug treatment to control bipolar symptoms while minimizing risk of bone loss.
Which medications are associated with decreased bone mineral density?
a) citalopram
b) haloperidol
c) carbamazepine
d) paliperidone
e) all of the above
The authors’ observations
Osteogenesis imperfecta is a genetic condition caused by mutations in genes implicated in collagen production. As a result, bones are brittle and prone to fracture. Different classes of psychotropics have been shown to increase risk of bone fractures through a variety of mechanisms. Clinicians often must choose appropriate pharmacotherapy for patients at high risk of fracture, including postmenopausal women, older patients, malnourished persons, and those with hormonal deficiencies leading to osteoporosis.
To assist our clinical decision-making, we reviewed the literature to establish appropriate management of a patient with increased bone fragility and new-onset bipolar disorder. We considered all classes of medications used to treat bipolar disorder, including antipsychotics, antidepressants, lithium, and anticonvulsants.
Antipsychotics
In population-based studies, prolactin-elevating antipsychotics have been associated with decreased bone mineral density and increased risk of fracture.1 Additional studies on geriatric and non-geriatric populations have supported these findings.2,3
The mechanism through which fracture risk is increased likely is related to antipsychotics’ effect on serum prolactin and cortisol levels. Antipsychotics act as antagonists on D2 receptors in the hypothalamic tubero-infundibular pathway, therefore preventing inhibition of prolactin. Long-term elevation in serum prolactin can cause loss of bone mineral density through secondary hypogonadism and direct effects on target tissues. Additional modifying factors include smoking and estrogen use.
The degree to which antipsychotics increase fracture risk might be related to the degree of serum prolactin elevation.4 Antipsychotics previously have been grouped by the degree of prolactin elevation, categorizing them as high, medium, and low or no potential to elevate serum prolactin.4 Based on this classification, typical antipsychotics, risperidone, and paliperidone have the highest potential to elevate prolactin. Accordingly, antipsychotics with the lowest fracture risk are those that have the lowest risk of serum prolactin elevation: ziprasidone, asenapine, quetiapine, and clozapine. Aripiprazole may lower prolactin in some patients. This is supported by studies noting reduced bone mineral density5,6 and increased risk of fracture1 with high-potential vs low- or no-potential antipsychotics. Because of these findings, it is crucial to consider the potential risk of prolactin elevation when treating patients at increased risk of fracture. Providers should consider low/no potential antipsychotic medications before considering those with medium or high potential (Table).
Antidepressants
In a meta-analysis, antidepressants were shown to increase fracture risk by 70% to 90%.2 However, the relative risk varies by antidepressant class. Several studies have shown that selective serotonin reuptake inhibitors (SSRIs) are associated with a higher risk of fracture compared with tricyclic antidepressants (TCAs).7 In addition, antidepressants with a high affinity for the serotonin transporter, including citalopram, fluoxetine, fluvoxamine, paroxetine, sertraline, and imipramine, have been associated with greater risk of osteoporotic fracture compared with those with low affinity.8
The mechanisms by which antidepressants increase fracture risk are complex, although the strongest evidence implicates a direct effect on bone metabolism via the 5-HTT receptor. This receptor, found on osteoblasts and osteoclasts, plays an important role in bone metabolism; it is through this receptor that SSRIs might inhibit osteoblasts and promote osteoclast activity, thereby disrupting bone microarchitecture. Additional studies are needed to further describe the mechanism of the association among antidepressants, bone mineral density, and fracture risk.
Fracture risk is associated with duration of use rather than dosage. Population-based studies show a higher fracture risk for new users of TCAs compared with continuous users, and the risk of fracture with SSRIs seems to increase slightly over time.9 No association has been identified between fracture risk and antidepressant dosage. According to the literature, drugs with low affinity for the serotonin transporter, such as maprotiline and mirtazapine, likely are the safest antidepressants for patients at increased risk of fracture. Options also include other TCAs and any antidepressant with low affinity for the serotonin receptor.7,8
Lithium
Studies on lithium and bone mineral density have shown mixed results. Older studies found that lithium had a negative or no effect on bone mineral density or the parathyroid hormone level.10 More recent investigations, however, suggest that the drug has a protective effect on bone mineral density, although this has not been replicated in all studies.
In a mouse model, lithium has been shown to enhance bone formation and improve bone mass, at least in part by activation of the Wnt signaling pathway through an inhibitory effect on glycogen synthase kinase-3β.11 In humans, lithium-treated adults had lower serum alkaline phosphate, osteocalcin, and C-telopeptide levels compared with controls, suggesting a state of decreased bone remodeling and increased turnover.12 There is a paucity of clinical data on the effect of lithium on fracture risk. Additional studies are necessary to elucidate lithium’s mechanism on bone mineral density and determine the magnitude of the clinical effect.
Anticonvulsants
The association among anticonvulsants, decreased bone mineral density, and increased risk of fracture is well-established in the literature.13 However, causality is difficult to determine, because many studies were of patients with a seizure disorder, who often have additional risk factors for fracture, including seizure-related trauma, drowsiness, and slowed reflexes.
Mechanisms through which anticonvulsants increase fracture risk include increased bone resorption, secondary hypoparathyroidism, and pseudohypoparathyroidism. Markers of bone resorption were elevated in patients receiving an antiepileptic.14 This effect might be enhanced by co-administration of cytochrome P450 (CYP450) enzyme-inducing anticonvulsants and CYP450 enzyme-inhibiting medications, such as valproate. Long-term treatment with valproate may produce reduction of bone mass and increased risk of fractures; however, other studies disagree with this finding.15
In addition to CYP450-inducing effects, phenytoin, carbamezapine, and phenobarbital can increase catabolism of vitamin D, which is associated with osteomalacia.14 This results in decreased intestinal absorption of calcium, hypocalcemia, and secondary hyperparathyroidism, which also increases fracture risk. Anticonvulsants also might increase resistance to pseudohypoparathyroidism and inhibit calcitonin secretion.
Lamotrigine has not been shown to interfere with bone accrual16 and may be a safer mood stabilizer for patients at high risk of fracture. For patients at increased risk of fracture, it is important to select an anticonvulsant wisely to minimize fracture risk.
How would you treat Ms. E during her hospitalization for bipolar disorder?
a) carbamazepine
b) lithium
c) risperidone
d) mirtazapine
TREATMENT Minimizing polypharmacy
Because many pharmacotherapeutic options for managing bipolar disorder can increase the risk of fracture, clinicians must be aware of the relative risk of each class of medication and each individual drug. We initiated lithium, 300 mg, 3 times a day, to stabilize Ms. E’s mood. Although clinical data are inconclusive regarding lithium’s effect on fracture risk, we felt that the benefit of acute mood stabilization outweighed the risk of decreased bone mineral index.
We selected aripiprazole, 10 mg/d, as an adjunctive treatment because of its minimal effect on serum prolactin levels.4 We considered prescribing an antidepressant but decided against it because we were concerned about manic switching.
Polypharmacy is another important consideration for Ms. E. Several studies have identified polypharmacy, particularly with antipsychotics, as an independent risk factor for fracture.3 Therefore, we sought to minimize the number of medications Ms. E receives. Although lithium monotherapy is an option, we thought that her mood symptoms were severe enough that the risk of inadequately treating her bipolar symptoms outweighed the additional risk of fracture from dual therapy with lithium and aripiprazole. Untreated or inadequately treated depression is associated with a higher fracture risk. Therefore, we avoided prescribing >2 medications to mitigate any excessive risk of fracture from polypharmacy.
Bottom Line
Different classes of medications—antipsychotics, anticonvulsants, antidepressants, and lithium—used for treating bipolar disorder have been shown to increase risk of bone fracture through a variety of mechanisms. Anticonvulsants and prolactin-elevating antipsychotics are associated with increased fracture risk; evidence on lithium is mixed. Fracture risk with antidepressants is associated with duration of use, rather than dosage.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE Broken down
Ms. E, age 20, is a college student who has had major depressive disorder for several years and a genetic bone disease (osteogenesis imperfecta, mixed type III and IV). She presents with depression, anxiety, and suicidal ideation. She reports recent worsening of her depressive symptoms, including anhedonia, excessive sleep, difficulty concentrating, and feeling overwhelmed, hopeless, and worthless. She also describes frequent thoughts of suicide with the plan of putting herself in oncoming traffic, although she has no history of suicide attempts.
Previously, her primary care physician prescribed lorazepam, 0.5 mg, as needed for anxiety, and sertraline, 100 mg/d, for depression and anxiety. She experienced only partial improvement in symptoms, however.
In addition to depressive symptoms, Ms. E describes manic symptoms lasting for as long as 3 to 5 days, including decreased need for sleep, increased energy, pressured speech, racing thoughts, distractibility, spending excessive money on cosmetics, and risking her safety—given her skeletal disorder— by participating in high-impact stage-combat classes. She denies auditory and visual hallucinations, homicidal ideation, and delusions.
The medical history is significant for osteogenesis imperfecta, which has caused 62 fractures and required 16 surgeries. Ms. E is a theater major who, despite her short stature and wheelchair use, reports enjoying her acting career and says she does not feel demoralized by her medical condition. She describes overcoming her physical disabilities with pride and confidence. However, her recent worsening mood symptoms have left her unable to concentrate and feeling overwhelmed with school.
Ms. E is voluntarily admitted to an inpatient psychiatric unit with a diagnosis of bipolar I disorder with rapid cycling, most recent episode mixed. Because of her bone fragility, the treatment team considers what would be an appropriate course of drug treatment to control bipolar symptoms while minimizing risk of bone loss.
Which medications are associated with decreased bone mineral density?
a) citalopram
b) haloperidol
c) carbamazepine
d) paliperidone
e) all of the above
The authors’ observations
Osteogenesis imperfecta is a genetic condition caused by mutations in genes implicated in collagen production. As a result, bones are brittle and prone to fracture. Different classes of psychotropics have been shown to increase risk of bone fractures through a variety of mechanisms. Clinicians often must choose appropriate pharmacotherapy for patients at high risk of fracture, including postmenopausal women, older patients, malnourished persons, and those with hormonal deficiencies leading to osteoporosis.
To assist our clinical decision-making, we reviewed the literature to establish appropriate management of a patient with increased bone fragility and new-onset bipolar disorder. We considered all classes of medications used to treat bipolar disorder, including antipsychotics, antidepressants, lithium, and anticonvulsants.
Antipsychotics
In population-based studies, prolactin-elevating antipsychotics have been associated with decreased bone mineral density and increased risk of fracture.1 Additional studies on geriatric and non-geriatric populations have supported these findings.2,3
The mechanism through which fracture risk is increased likely is related to antipsychotics’ effect on serum prolactin and cortisol levels. Antipsychotics act as antagonists on D2 receptors in the hypothalamic tubero-infundibular pathway, therefore preventing inhibition of prolactin. Long-term elevation in serum prolactin can cause loss of bone mineral density through secondary hypogonadism and direct effects on target tissues. Additional modifying factors include smoking and estrogen use.
The degree to which antipsychotics increase fracture risk might be related to the degree of serum prolactin elevation.4 Antipsychotics previously have been grouped by the degree of prolactin elevation, categorizing them as high, medium, and low or no potential to elevate serum prolactin.4 Based on this classification, typical antipsychotics, risperidone, and paliperidone have the highest potential to elevate prolactin. Accordingly, antipsychotics with the lowest fracture risk are those that have the lowest risk of serum prolactin elevation: ziprasidone, asenapine, quetiapine, and clozapine. Aripiprazole may lower prolactin in some patients. This is supported by studies noting reduced bone mineral density5,6 and increased risk of fracture1 with high-potential vs low- or no-potential antipsychotics. Because of these findings, it is crucial to consider the potential risk of prolactin elevation when treating patients at increased risk of fracture. Providers should consider low/no potential antipsychotic medications before considering those with medium or high potential (Table).
Antidepressants
In a meta-analysis, antidepressants were shown to increase fracture risk by 70% to 90%.2 However, the relative risk varies by antidepressant class. Several studies have shown that selective serotonin reuptake inhibitors (SSRIs) are associated with a higher risk of fracture compared with tricyclic antidepressants (TCAs).7 In addition, antidepressants with a high affinity for the serotonin transporter, including citalopram, fluoxetine, fluvoxamine, paroxetine, sertraline, and imipramine, have been associated with greater risk of osteoporotic fracture compared with those with low affinity.8
The mechanisms by which antidepressants increase fracture risk are complex, although the strongest evidence implicates a direct effect on bone metabolism via the 5-HTT receptor. This receptor, found on osteoblasts and osteoclasts, plays an important role in bone metabolism; it is through this receptor that SSRIs might inhibit osteoblasts and promote osteoclast activity, thereby disrupting bone microarchitecture. Additional studies are needed to further describe the mechanism of the association among antidepressants, bone mineral density, and fracture risk.
Fracture risk is associated with duration of use rather than dosage. Population-based studies show a higher fracture risk for new users of TCAs compared with continuous users, and the risk of fracture with SSRIs seems to increase slightly over time.9 No association has been identified between fracture risk and antidepressant dosage. According to the literature, drugs with low affinity for the serotonin transporter, such as maprotiline and mirtazapine, likely are the safest antidepressants for patients at increased risk of fracture. Options also include other TCAs and any antidepressant with low affinity for the serotonin receptor.7,8
Lithium
Studies on lithium and bone mineral density have shown mixed results. Older studies found that lithium had a negative or no effect on bone mineral density or the parathyroid hormone level.10 More recent investigations, however, suggest that the drug has a protective effect on bone mineral density, although this has not been replicated in all studies.
In a mouse model, lithium has been shown to enhance bone formation and improve bone mass, at least in part by activation of the Wnt signaling pathway through an inhibitory effect on glycogen synthase kinase-3β.11 In humans, lithium-treated adults had lower serum alkaline phosphate, osteocalcin, and C-telopeptide levels compared with controls, suggesting a state of decreased bone remodeling and increased turnover.12 There is a paucity of clinical data on the effect of lithium on fracture risk. Additional studies are necessary to elucidate lithium’s mechanism on bone mineral density and determine the magnitude of the clinical effect.
Anticonvulsants
The association among anticonvulsants, decreased bone mineral density, and increased risk of fracture is well-established in the literature.13 However, causality is difficult to determine, because many studies were of patients with a seizure disorder, who often have additional risk factors for fracture, including seizure-related trauma, drowsiness, and slowed reflexes.
Mechanisms through which anticonvulsants increase fracture risk include increased bone resorption, secondary hypoparathyroidism, and pseudohypoparathyroidism. Markers of bone resorption were elevated in patients receiving an antiepileptic.14 This effect might be enhanced by co-administration of cytochrome P450 (CYP450) enzyme-inducing anticonvulsants and CYP450 enzyme-inhibiting medications, such as valproate. Long-term treatment with valproate may produce reduction of bone mass and increased risk of fractures; however, other studies disagree with this finding.15
In addition to CYP450-inducing effects, phenytoin, carbamezapine, and phenobarbital can increase catabolism of vitamin D, which is associated with osteomalacia.14 This results in decreased intestinal absorption of calcium, hypocalcemia, and secondary hyperparathyroidism, which also increases fracture risk. Anticonvulsants also might increase resistance to pseudohypoparathyroidism and inhibit calcitonin secretion.
Lamotrigine has not been shown to interfere with bone accrual16 and may be a safer mood stabilizer for patients at high risk of fracture. For patients at increased risk of fracture, it is important to select an anticonvulsant wisely to minimize fracture risk.
How would you treat Ms. E during her hospitalization for bipolar disorder?
a) carbamazepine
b) lithium
c) risperidone
d) mirtazapine
TREATMENT Minimizing polypharmacy
Because many pharmacotherapeutic options for managing bipolar disorder can increase the risk of fracture, clinicians must be aware of the relative risk of each class of medication and each individual drug. We initiated lithium, 300 mg, 3 times a day, to stabilize Ms. E’s mood. Although clinical data are inconclusive regarding lithium’s effect on fracture risk, we felt that the benefit of acute mood stabilization outweighed the risk of decreased bone mineral index.
We selected aripiprazole, 10 mg/d, as an adjunctive treatment because of its minimal effect on serum prolactin levels.4 We considered prescribing an antidepressant but decided against it because we were concerned about manic switching.
Polypharmacy is another important consideration for Ms. E. Several studies have identified polypharmacy, particularly with antipsychotics, as an independent risk factor for fracture.3 Therefore, we sought to minimize the number of medications Ms. E receives. Although lithium monotherapy is an option, we thought that her mood symptoms were severe enough that the risk of inadequately treating her bipolar symptoms outweighed the additional risk of fracture from dual therapy with lithium and aripiprazole. Untreated or inadequately treated depression is associated with a higher fracture risk. Therefore, we avoided prescribing >2 medications to mitigate any excessive risk of fracture from polypharmacy.
Bottom Line
Different classes of medications—antipsychotics, anticonvulsants, antidepressants, and lithium—used for treating bipolar disorder have been shown to increase risk of bone fracture through a variety of mechanisms. Anticonvulsants and prolactin-elevating antipsychotics are associated with increased fracture risk; evidence on lithium is mixed. Fracture risk with antidepressants is associated with duration of use, rather than dosage.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Howard L, Kirkwood G, Leese M. Risk of hip fracture in patients with a history of schizophrenia. Br J Psychiatry. 2007;190:129-134.
2. Takkouche B, Montes-Martínez A, Gill SS, et al. Psychotropic medications and the risk of fracture: a meta-analysis. Drug Saf. 2007;30(2):171-184.
3. Sørensen HJ, Jensen SO, Nielsen J. Schizophrenia, antipsychotics and risk of hip fracture: a population-based analysis. Eur Neuropsychopharmacol. 2013;23(8):872-878.
4. Rahman T, Clevenger CV, Kaklamani V, et al. Antipsychotic treatment in breast cancer patients. Am J Psychiatry. 2014;171(6):616-621.
5. Bilici M, Cakirbay H, Guler M, et al. Classical and atypical neuroleptics, and bone mineral density, in patients with schizophrenia. Int J Neurosci. 2002;112(7):817-828.
6. Becker D, Liver O, Mester R, et al. Risperidone, but not olanzapine, decreases bone mineral density in female premenopausal schizophrenia patients. J Clin Psychiatry. 2003;64(7):761-766.
7. Bolton JM, Metge C, Lix L, et al. Fracture risk from psychotropic medications: a population-based analysis. J Clin Psychopharmacol. 2008;28(4):384-391.
8. Verdel BM, Souverein PC, Egberts TC, et al. Use of antidepressant drugs and risk of osteoporotic and non-osteoporotic fractures. Bone. 2010;47(3):604-609.
9. Diem SJ, Ruppert K, Cauley JA. Rates of bone loss among women initiating antidepressant medication use in midlife. J Clin Endocrinol Metab. 2013;(11):4355-4363.
10. Plenge P, Rafaelsen OJ. Lithium effects on calcium, magnesium and phosphate in man: effects on balance, bone mineral content, faecal and urinary excretion. Acta Psychiatr Scand. 1982;66(5):361-373.
11. Clément-Lacroix P, Ai M, Morvan F, et al. Lrp5-independent activation of Wnt signaling by lithium chloride increases bone formation and bone mass in mice. Proc Natl Acad Sci U S A. 2005;102(48):17406-17411.
12. Zamani A, Omrani GR, Nasab MM. Lithium’s effect on bone mineral density. Bone. 2009;44(2):331-334.
13. Swanton J, Simister R, Altmann D, et al. Bone mineral density in institutionalised patients with refractory epilepsy. Seizure. 2007;16(6):538-541.
14. Pack AM, Morrell MJ. Epilepsy and bone health in adults. Epilepsy Behav. 2004;5(suppl 2):S24-S29.
15. Pack AM. Bone disease in epilepsy. Curr Neurol Neurosci Rep. 2004;4(4):329-334.
16. Sheth RD, Hermann BP. Bone mineral density with lamotrigine monotherapy for epilepsy. Pediatr Neurol. 2007;37(4):250-254.
1. Howard L, Kirkwood G, Leese M. Risk of hip fracture in patients with a history of schizophrenia. Br J Psychiatry. 2007;190:129-134.
2. Takkouche B, Montes-Martínez A, Gill SS, et al. Psychotropic medications and the risk of fracture: a meta-analysis. Drug Saf. 2007;30(2):171-184.
3. Sørensen HJ, Jensen SO, Nielsen J. Schizophrenia, antipsychotics and risk of hip fracture: a population-based analysis. Eur Neuropsychopharmacol. 2013;23(8):872-878.
4. Rahman T, Clevenger CV, Kaklamani V, et al. Antipsychotic treatment in breast cancer patients. Am J Psychiatry. 2014;171(6):616-621.
5. Bilici M, Cakirbay H, Guler M, et al. Classical and atypical neuroleptics, and bone mineral density, in patients with schizophrenia. Int J Neurosci. 2002;112(7):817-828.
6. Becker D, Liver O, Mester R, et al. Risperidone, but not olanzapine, decreases bone mineral density in female premenopausal schizophrenia patients. J Clin Psychiatry. 2003;64(7):761-766.
7. Bolton JM, Metge C, Lix L, et al. Fracture risk from psychotropic medications: a population-based analysis. J Clin Psychopharmacol. 2008;28(4):384-391.
8. Verdel BM, Souverein PC, Egberts TC, et al. Use of antidepressant drugs and risk of osteoporotic and non-osteoporotic fractures. Bone. 2010;47(3):604-609.
9. Diem SJ, Ruppert K, Cauley JA. Rates of bone loss among women initiating antidepressant medication use in midlife. J Clin Endocrinol Metab. 2013;(11):4355-4363.
10. Plenge P, Rafaelsen OJ. Lithium effects on calcium, magnesium and phosphate in man: effects on balance, bone mineral content, faecal and urinary excretion. Acta Psychiatr Scand. 1982;66(5):361-373.
11. Clément-Lacroix P, Ai M, Morvan F, et al. Lrp5-independent activation of Wnt signaling by lithium chloride increases bone formation and bone mass in mice. Proc Natl Acad Sci U S A. 2005;102(48):17406-17411.
12. Zamani A, Omrani GR, Nasab MM. Lithium’s effect on bone mineral density. Bone. 2009;44(2):331-334.
13. Swanton J, Simister R, Altmann D, et al. Bone mineral density in institutionalised patients with refractory epilepsy. Seizure. 2007;16(6):538-541.
14. Pack AM, Morrell MJ. Epilepsy and bone health in adults. Epilepsy Behav. 2004;5(suppl 2):S24-S29.
15. Pack AM. Bone disease in epilepsy. Curr Neurol Neurosci Rep. 2004;4(4):329-334.
16. Sheth RD, Hermann BP. Bone mineral density with lamotrigine monotherapy for epilepsy. Pediatr Neurol. 2007;37(4):250-254.
Man Awakens With "Fluttering" in His Chest
ANSWER
This ECG is consistent with coarse atrial fibrillation with a rapid ventricular response and a nonspecific T-wave abnormality. The patient’s presentation is strongly suggestive of lone atrial fibrillation: This was the first incidence, it occurred in the absence of an existing heart condition, and it presented with an abrupt onset of increased heart rate and dyspnea.
Lone atrial fibrillation most commonly occurs in men in their 40s and 50s. It is vagally mediated, occurring during sleep or relaxation and after food and/or alcohol consumption.
The patient was cardioverted to normal sinus rhythm in the ED without difficulty, and follow-up was arranged.
ANSWER
This ECG is consistent with coarse atrial fibrillation with a rapid ventricular response and a nonspecific T-wave abnormality. The patient’s presentation is strongly suggestive of lone atrial fibrillation: This was the first incidence, it occurred in the absence of an existing heart condition, and it presented with an abrupt onset of increased heart rate and dyspnea.
Lone atrial fibrillation most commonly occurs in men in their 40s and 50s. It is vagally mediated, occurring during sleep or relaxation and after food and/or alcohol consumption.
The patient was cardioverted to normal sinus rhythm in the ED without difficulty, and follow-up was arranged.
ANSWER
This ECG is consistent with coarse atrial fibrillation with a rapid ventricular response and a nonspecific T-wave abnormality. The patient’s presentation is strongly suggestive of lone atrial fibrillation: This was the first incidence, it occurred in the absence of an existing heart condition, and it presented with an abrupt onset of increased heart rate and dyspnea.
Lone atrial fibrillation most commonly occurs in men in their 40s and 50s. It is vagally mediated, occurring during sleep or relaxation and after food and/or alcohol consumption.
The patient was cardioverted to normal sinus rhythm in the ED without difficulty, and follow-up was arranged.
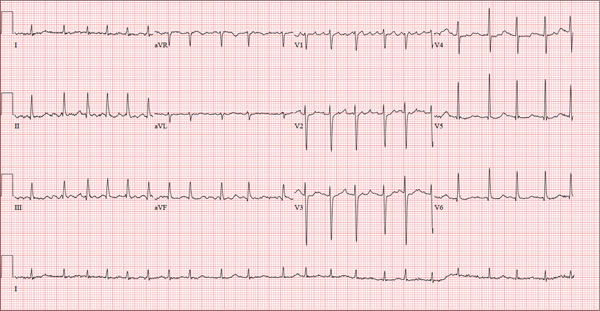
A 56-year-old man presents to the emergency department (ED) complaining of shortness of breath and a rapid heart rate. He went to bed at his regular time (10:30 pm) last night and woke up at 3:30 am with a fluttering sensation in his chest. He checked his pulse; it was 120 beats/min. Alarmed, he got out of bed and noted he was short of breath as he walked to the bathroom. He went back to bed, but after approximately 20 minutes without relief, he decided to call his son to take him to the ED. The time from onset of symptoms until arrival at the ED was two hours. During that time, his symptoms did not change. When you examine the patient, he states that he is typically in excellent health and has never experienced either shortness of breath or a rapid heart rate before. He denies a history of cardiac or pulmonary disease and has never had chest pain, syncope, or near-syncope. Medical history is unremarkable. Surgical history is remarkable for a tonsillectomy in childhood and an appendectomy for acute appendicitis at age 18. The patient has no known drug allergies and is taking ibuprofen for a recent ankle sprain but is on no other medications. He works as a certified public accountant and has a sedentary lifestyle. He drinks two to three glasses of wine each evening, does not smoke, and denies recreational or naturopathic medication use. He is a widower (his wife died of breast cancer at age 44) and has one son who lives in the same housing complex. The review of systems is remarkable for a recent left ankle sprain, which occurred when the patient slipped on the carpet at home. Vital signs include a blood pressure of 144/84 mm Hg; pulse, 130 beats/min; respiratory rate, 18 breaths/min-1; O2 saturation, 98%; and temperature, 98.9°F. His height is 5 ft 9 in and his weight, 223 lb. The physical exam reveals an obese white male in mild distress. The HEENT exam reveals corrective lenses and the absence of tonsils. The neck shows no evidence of thyromegaly or jugular venous distention. The lungs are clear in all fields. The cardiac rhythm is irregular with a rate of 130 beats/min. There are no murmurs or extra heart sounds audible. The abdomen is obese and nontender, with no palpable masses. An old surgical scar is evident in the right lower quadrant, consistent with his history of an appendectomy. The lower extremities show no evidence of peripheral edema. Mild discomfort is present with examination of the left ankle. Peripheral pulses are strong and equal, and the neurologic exam is intact. An ECG is obtained that reveals a ventricular rate of 131 beats/min; PR interval, not measured; QRS duration, 82 ms; QT/QTc interval, 374/552 ms; no P axis; R axis, 68°; and T axis, 36°. What is your interpretation of this ECG?