User login
Quality of Life in Aging Multiple Sclerosis Patients
Study Overview
Objective. To evaluate the association between clinical and demographic factors and health-related quality of life (HRQOL) among older people with multiple sclerosis (MS).
Design. Cross-sectional survey-based study.
Setting and participants. Patients with MS aged 60 years or older were recruited from 4 MS centers in Long Island, NY. Patients with severe cognitive impairment as determined by the health care practitioner were excluded. Participants were asked to complete 3 surveys at 3 different time-points. In the first survey, participants completed the Morisky Medication Adherence Scale and the Patient Multiple Sclerosis Neuropsychological Screening Questionnaire (P-MSNQ). The second survey was the Multiple Sclerosis Quality of Life-54 (MSQOL-54), and the third survey included the Beck Depression Inventory-II (BDI-II) and a disability status self-assessment scale. Cognitive function was measured at the time of recruitment using the Symbol Digit Modalities Test (SDMT).
Analysis. The Andersen Healthcare Utilization model was used to structure the multivariate regression analysis. This model identifies multiple domains affecting quality of life, and the variables from the surveys were categorized according to domain: predisposing characteristics (demographic variables), enabling resources (caregiver support and living situation), needs (eg, health-related measures), and health behaviors (medication use, adherence).
Main results. A total of 211 completed the first survey, 188 the second, and 179 the third. 80% were female and 95% were white. Average age was 65.5 (SD 5.6) years. 56% of respondents’ self-reported scores on the SDMT classified them as cognitively impaired. Risk of neuropsychological impairment, depression, and disability status were significantly associated with a decreased mental and physical HRQOL. Significantly, there was a strong association between predisposing characteristics and QOL. Being widowed and remaining employed were the strongest predictors of better physical QOL and having an education level of high school or less was a predictor of lower mental HRQOL.
Conclusion. Clinicians should measure HRQOL in older MS patients regularly and assess for depression and cognitive impairment.
Commentary
Quality of life is an important marker of MS patients’ well-being as they cope with this chronic illness [1]. The progression of the disease and its symptomatology often negatively affect HRQOL. However, multiple psychosocial factors, such as coping, mood, self-efficacy, and perceived support, affect QOL of patients with MS more than biological variables such as weakness or burden of radiologic disease [2]. For example, many self-report HRQOL indices are strongly predicted by measures of depression [3]. In addition, many studies have found a positive association between physical disability and reduced QOL [4,5]. Further, while perceived HRQOL may be a meaningful outcome in itself, it may also be a predictor for outcomes such as disability-related changes [6].
MS leads to disability and loss of function in all age-groups, but only a few studies have focused on HRQOL among elderly patients with MS. As patients with MS age, they may develop comorbidities such as hypertension and diabetes that may affect HRQOL. However, in a previous study comparing QOL between older and younger patients with MS, elderly and younger patients with MS had similar QOL even though the elderly patients had more physical limitations [7].
The strength of the current study was using the Andersen Healthcare Utilization regression model in the analysis, since it factors in multiple influences on health status. The striking evidence that employment and being widowed were linked to better physical QOL suggest that older MS patients may have better adaptation and adjustment to their illness. Researchers have shown that the widowed elderly often take on more responsibilities and tasks when they lose their partner, which leads to increased self-esteem and QOL [8]. Another advantage of the study was the fact that the investigators evaluated the different exposure variables and their associations with mental and physical QOL while identifying multiple confounding variables. Additionally, the use of 2 cognitive assessment tools provided a stronger assessment of patients’ cognitive function.
The main weakness of the study was using a cross-sectional study design with convenience sampling. The convenience sample was based on voluntary participation, which may result in self-selection bias. In addition, the self-report design is subject to the usual limitations of self-reporting for data collection: participants may exaggerate symptoms in order to make their situation seem worse or may under-report the severity or frequency of symptoms in order to minimize their problems. While the overall sample size was 211, not all respondents completed all the surveys, and response rates varied by questions. Thus, missing data may have affected results, but which data are missing is not discernable from the paper. That patients were from a single geographic area and had relatively high education levels (44% with college or above) are among the factors that limit the generalizability of the study. Another limitation is the use of the Beck Depression Inventory, which was not specifically designed for use in the elderly. In addition, the results of this study might have been affected by unmeasured confounding variables, for example daily physical activity, which can be a factor that modifies between depression, cognition, and QOL.
Applications for Clinical Practice
This study reinforces the importance of monitoring older MS patients for factors that may influence their HRQOL. The presence of depression, disability, and cognitive impairment should be assessed for regularly. Clinicians should encourage and empower elderly patients to continue with activities, including employment, that promote their mental and physical well-being and help maintain their independence. Assessing patients with geriatric-specific tools may provide more reliable and accurate assessment data that better accounts for aging dynamics. In addition, comobidities must be managed appropriately.
—Aliza Bitton Ben-Zacharia, DNP, ANP, and Allison Squires, PhD, RN, New York University College of Nursing
1. Opara JA, Jaracz K, Brola W. Quality of life in multiple sclerosis. J Med Life 2010;3:352–8.
2. Mitchell AJ, Benito-León J, González JM, Rivera-Navarro J. Quality of life and its assessment in multiple sclerosis: integrating physical and psychological components of wellbeing. Lancet Neurol 2005;4:556–66.
3. Benedict RH, Wahlig E, Bakshi R, et al. Predicting quality of life in multiple sclerosis: accounting for physical disability, fatigue, cognition, mood disorder, personality, and behavior change. J Neurol Sci 2005;231:29–34.
4. Göksel Karatepe A, Kaya T, Günaydn R, et al. Quality of life in patients with multiple sclerosis: the impact of depression, fatigue, and disability. Int J Rehabil Res 2011;34:290–8.
5. Nortvedt MW, Riise T, Myhr KM, Nyland HI. Quality of life in multiple sclerosis: measuring the disease effects more broadly. Neurology 1999;53:1098–103.
6. Visschedijk MA, Uitdehaag BM, Klein M, et al. Value of health-related quality of life to predict disability course in multiple sclerosis. Neurology 2004;63:2046–50.
7. Ploughman M, Austin MW, Murdoch M, et al. Factors influencing healthy aging with multiple sclerosis: a qualitative study. Disabil Rehabil 2012;34:26–33.
8. Minden SL, Frankel D, Hadden LS, et al. Disability in elderly people with multiple sclerosis: An analysis of baseline data from the Sonya Slifka Longitudinal Multiple Sclerosis Study. NeuroRehabilitation. 2004;19:55–67.
Study Overview
Objective. To evaluate the association between clinical and demographic factors and health-related quality of life (HRQOL) among older people with multiple sclerosis (MS).
Design. Cross-sectional survey-based study.
Setting and participants. Patients with MS aged 60 years or older were recruited from 4 MS centers in Long Island, NY. Patients with severe cognitive impairment as determined by the health care practitioner were excluded. Participants were asked to complete 3 surveys at 3 different time-points. In the first survey, participants completed the Morisky Medication Adherence Scale and the Patient Multiple Sclerosis Neuropsychological Screening Questionnaire (P-MSNQ). The second survey was the Multiple Sclerosis Quality of Life-54 (MSQOL-54), and the third survey included the Beck Depression Inventory-II (BDI-II) and a disability status self-assessment scale. Cognitive function was measured at the time of recruitment using the Symbol Digit Modalities Test (SDMT).
Analysis. The Andersen Healthcare Utilization model was used to structure the multivariate regression analysis. This model identifies multiple domains affecting quality of life, and the variables from the surveys were categorized according to domain: predisposing characteristics (demographic variables), enabling resources (caregiver support and living situation), needs (eg, health-related measures), and health behaviors (medication use, adherence).
Main results. A total of 211 completed the first survey, 188 the second, and 179 the third. 80% were female and 95% were white. Average age was 65.5 (SD 5.6) years. 56% of respondents’ self-reported scores on the SDMT classified them as cognitively impaired. Risk of neuropsychological impairment, depression, and disability status were significantly associated with a decreased mental and physical HRQOL. Significantly, there was a strong association between predisposing characteristics and QOL. Being widowed and remaining employed were the strongest predictors of better physical QOL and having an education level of high school or less was a predictor of lower mental HRQOL.
Conclusion. Clinicians should measure HRQOL in older MS patients regularly and assess for depression and cognitive impairment.
Commentary
Quality of life is an important marker of MS patients’ well-being as they cope with this chronic illness [1]. The progression of the disease and its symptomatology often negatively affect HRQOL. However, multiple psychosocial factors, such as coping, mood, self-efficacy, and perceived support, affect QOL of patients with MS more than biological variables such as weakness or burden of radiologic disease [2]. For example, many self-report HRQOL indices are strongly predicted by measures of depression [3]. In addition, many studies have found a positive association between physical disability and reduced QOL [4,5]. Further, while perceived HRQOL may be a meaningful outcome in itself, it may also be a predictor for outcomes such as disability-related changes [6].
MS leads to disability and loss of function in all age-groups, but only a few studies have focused on HRQOL among elderly patients with MS. As patients with MS age, they may develop comorbidities such as hypertension and diabetes that may affect HRQOL. However, in a previous study comparing QOL between older and younger patients with MS, elderly and younger patients with MS had similar QOL even though the elderly patients had more physical limitations [7].
The strength of the current study was using the Andersen Healthcare Utilization regression model in the analysis, since it factors in multiple influences on health status. The striking evidence that employment and being widowed were linked to better physical QOL suggest that older MS patients may have better adaptation and adjustment to their illness. Researchers have shown that the widowed elderly often take on more responsibilities and tasks when they lose their partner, which leads to increased self-esteem and QOL [8]. Another advantage of the study was the fact that the investigators evaluated the different exposure variables and their associations with mental and physical QOL while identifying multiple confounding variables. Additionally, the use of 2 cognitive assessment tools provided a stronger assessment of patients’ cognitive function.
The main weakness of the study was using a cross-sectional study design with convenience sampling. The convenience sample was based on voluntary participation, which may result in self-selection bias. In addition, the self-report design is subject to the usual limitations of self-reporting for data collection: participants may exaggerate symptoms in order to make their situation seem worse or may under-report the severity or frequency of symptoms in order to minimize their problems. While the overall sample size was 211, not all respondents completed all the surveys, and response rates varied by questions. Thus, missing data may have affected results, but which data are missing is not discernable from the paper. That patients were from a single geographic area and had relatively high education levels (44% with college or above) are among the factors that limit the generalizability of the study. Another limitation is the use of the Beck Depression Inventory, which was not specifically designed for use in the elderly. In addition, the results of this study might have been affected by unmeasured confounding variables, for example daily physical activity, which can be a factor that modifies between depression, cognition, and QOL.
Applications for Clinical Practice
This study reinforces the importance of monitoring older MS patients for factors that may influence their HRQOL. The presence of depression, disability, and cognitive impairment should be assessed for regularly. Clinicians should encourage and empower elderly patients to continue with activities, including employment, that promote their mental and physical well-being and help maintain their independence. Assessing patients with geriatric-specific tools may provide more reliable and accurate assessment data that better accounts for aging dynamics. In addition, comobidities must be managed appropriately.
—Aliza Bitton Ben-Zacharia, DNP, ANP, and Allison Squires, PhD, RN, New York University College of Nursing
Study Overview
Objective. To evaluate the association between clinical and demographic factors and health-related quality of life (HRQOL) among older people with multiple sclerosis (MS).
Design. Cross-sectional survey-based study.
Setting and participants. Patients with MS aged 60 years or older were recruited from 4 MS centers in Long Island, NY. Patients with severe cognitive impairment as determined by the health care practitioner were excluded. Participants were asked to complete 3 surveys at 3 different time-points. In the first survey, participants completed the Morisky Medication Adherence Scale and the Patient Multiple Sclerosis Neuropsychological Screening Questionnaire (P-MSNQ). The second survey was the Multiple Sclerosis Quality of Life-54 (MSQOL-54), and the third survey included the Beck Depression Inventory-II (BDI-II) and a disability status self-assessment scale. Cognitive function was measured at the time of recruitment using the Symbol Digit Modalities Test (SDMT).
Analysis. The Andersen Healthcare Utilization model was used to structure the multivariate regression analysis. This model identifies multiple domains affecting quality of life, and the variables from the surveys were categorized according to domain: predisposing characteristics (demographic variables), enabling resources (caregiver support and living situation), needs (eg, health-related measures), and health behaviors (medication use, adherence).
Main results. A total of 211 completed the first survey, 188 the second, and 179 the third. 80% were female and 95% were white. Average age was 65.5 (SD 5.6) years. 56% of respondents’ self-reported scores on the SDMT classified them as cognitively impaired. Risk of neuropsychological impairment, depression, and disability status were significantly associated with a decreased mental and physical HRQOL. Significantly, there was a strong association between predisposing characteristics and QOL. Being widowed and remaining employed were the strongest predictors of better physical QOL and having an education level of high school or less was a predictor of lower mental HRQOL.
Conclusion. Clinicians should measure HRQOL in older MS patients regularly and assess for depression and cognitive impairment.
Commentary
Quality of life is an important marker of MS patients’ well-being as they cope with this chronic illness [1]. The progression of the disease and its symptomatology often negatively affect HRQOL. However, multiple psychosocial factors, such as coping, mood, self-efficacy, and perceived support, affect QOL of patients with MS more than biological variables such as weakness or burden of radiologic disease [2]. For example, many self-report HRQOL indices are strongly predicted by measures of depression [3]. In addition, many studies have found a positive association between physical disability and reduced QOL [4,5]. Further, while perceived HRQOL may be a meaningful outcome in itself, it may also be a predictor for outcomes such as disability-related changes [6].
MS leads to disability and loss of function in all age-groups, but only a few studies have focused on HRQOL among elderly patients with MS. As patients with MS age, they may develop comorbidities such as hypertension and diabetes that may affect HRQOL. However, in a previous study comparing QOL between older and younger patients with MS, elderly and younger patients with MS had similar QOL even though the elderly patients had more physical limitations [7].
The strength of the current study was using the Andersen Healthcare Utilization regression model in the analysis, since it factors in multiple influences on health status. The striking evidence that employment and being widowed were linked to better physical QOL suggest that older MS patients may have better adaptation and adjustment to their illness. Researchers have shown that the widowed elderly often take on more responsibilities and tasks when they lose their partner, which leads to increased self-esteem and QOL [8]. Another advantage of the study was the fact that the investigators evaluated the different exposure variables and their associations with mental and physical QOL while identifying multiple confounding variables. Additionally, the use of 2 cognitive assessment tools provided a stronger assessment of patients’ cognitive function.
The main weakness of the study was using a cross-sectional study design with convenience sampling. The convenience sample was based on voluntary participation, which may result in self-selection bias. In addition, the self-report design is subject to the usual limitations of self-reporting for data collection: participants may exaggerate symptoms in order to make their situation seem worse or may under-report the severity or frequency of symptoms in order to minimize their problems. While the overall sample size was 211, not all respondents completed all the surveys, and response rates varied by questions. Thus, missing data may have affected results, but which data are missing is not discernable from the paper. That patients were from a single geographic area and had relatively high education levels (44% with college or above) are among the factors that limit the generalizability of the study. Another limitation is the use of the Beck Depression Inventory, which was not specifically designed for use in the elderly. In addition, the results of this study might have been affected by unmeasured confounding variables, for example daily physical activity, which can be a factor that modifies between depression, cognition, and QOL.
Applications for Clinical Practice
This study reinforces the importance of monitoring older MS patients for factors that may influence their HRQOL. The presence of depression, disability, and cognitive impairment should be assessed for regularly. Clinicians should encourage and empower elderly patients to continue with activities, including employment, that promote their mental and physical well-being and help maintain their independence. Assessing patients with geriatric-specific tools may provide more reliable and accurate assessment data that better accounts for aging dynamics. In addition, comobidities must be managed appropriately.
—Aliza Bitton Ben-Zacharia, DNP, ANP, and Allison Squires, PhD, RN, New York University College of Nursing
1. Opara JA, Jaracz K, Brola W. Quality of life in multiple sclerosis. J Med Life 2010;3:352–8.
2. Mitchell AJ, Benito-León J, González JM, Rivera-Navarro J. Quality of life and its assessment in multiple sclerosis: integrating physical and psychological components of wellbeing. Lancet Neurol 2005;4:556–66.
3. Benedict RH, Wahlig E, Bakshi R, et al. Predicting quality of life in multiple sclerosis: accounting for physical disability, fatigue, cognition, mood disorder, personality, and behavior change. J Neurol Sci 2005;231:29–34.
4. Göksel Karatepe A, Kaya T, Günaydn R, et al. Quality of life in patients with multiple sclerosis: the impact of depression, fatigue, and disability. Int J Rehabil Res 2011;34:290–8.
5. Nortvedt MW, Riise T, Myhr KM, Nyland HI. Quality of life in multiple sclerosis: measuring the disease effects more broadly. Neurology 1999;53:1098–103.
6. Visschedijk MA, Uitdehaag BM, Klein M, et al. Value of health-related quality of life to predict disability course in multiple sclerosis. Neurology 2004;63:2046–50.
7. Ploughman M, Austin MW, Murdoch M, et al. Factors influencing healthy aging with multiple sclerosis: a qualitative study. Disabil Rehabil 2012;34:26–33.
8. Minden SL, Frankel D, Hadden LS, et al. Disability in elderly people with multiple sclerosis: An analysis of baseline data from the Sonya Slifka Longitudinal Multiple Sclerosis Study. NeuroRehabilitation. 2004;19:55–67.
1. Opara JA, Jaracz K, Brola W. Quality of life in multiple sclerosis. J Med Life 2010;3:352–8.
2. Mitchell AJ, Benito-León J, González JM, Rivera-Navarro J. Quality of life and its assessment in multiple sclerosis: integrating physical and psychological components of wellbeing. Lancet Neurol 2005;4:556–66.
3. Benedict RH, Wahlig E, Bakshi R, et al. Predicting quality of life in multiple sclerosis: accounting for physical disability, fatigue, cognition, mood disorder, personality, and behavior change. J Neurol Sci 2005;231:29–34.
4. Göksel Karatepe A, Kaya T, Günaydn R, et al. Quality of life in patients with multiple sclerosis: the impact of depression, fatigue, and disability. Int J Rehabil Res 2011;34:290–8.
5. Nortvedt MW, Riise T, Myhr KM, Nyland HI. Quality of life in multiple sclerosis: measuring the disease effects more broadly. Neurology 1999;53:1098–103.
6. Visschedijk MA, Uitdehaag BM, Klein M, et al. Value of health-related quality of life to predict disability course in multiple sclerosis. Neurology 2004;63:2046–50.
7. Ploughman M, Austin MW, Murdoch M, et al. Factors influencing healthy aging with multiple sclerosis: a qualitative study. Disabil Rehabil 2012;34:26–33.
8. Minden SL, Frankel D, Hadden LS, et al. Disability in elderly people with multiple sclerosis: An analysis of baseline data from the Sonya Slifka Longitudinal Multiple Sclerosis Study. NeuroRehabilitation. 2004;19:55–67.
Self-Monitoring and Self-Titration of Antihypertensive Medications Result in Better Systolic Blood Pressure Control
Study Overview
Objective. To examine the effect of self-monitoring of blood pressure and self-titration of antihypertensive medications among hypertensive patients with cardiovascular disease, diabetes, or chronic kidney disease.
Design. Unblinded randomized controlled trial.
Setting and participants. The study was conducted in central and east England. Patients with poorly controlled blood pressure with a last recorded systolic blood pressure of at least 145 mm Hg at 59 UK primary care practices were invited to participate. Patients had to be at least 35 years old and have at least 1 of the following comorbidities: transient ischemic attack or stroke, stage 3 chronic kidney disease, or history of coronary artery bypass graft surgery, myocardial infarction, or angina. Patients were excluded if they could not self-monitor blood pressure, had dementia or failed a cognitive screen using the short-orientation memory concentration test, had postural hypotension, took more than 3 antihypertensive medications, had an acute cardiovascular event within the previous 3 months, were receiving care from a specialist for their hypertension, were pregnant, or had a terminal disease. Participants were randomized to the self-management intervention or usual care.
Intervention. Patients in the self-management group were asked to monitor their blood pressure using an automated blood pressure monitor and to titrate their blood pressure medications using an individualized 3-step plan devised by the patient with their family physician. They were trained to do these tasks in 2- or 3-hour sessions. Patients were instructed to take their blood pressure twice each morning for the first week of each month; if 4 or more blood pressure readings during the measurement week for 2 consecutive months were higher than the target blood pressure, patients were to follow their individualized plan to change their medications. The target blood pressure was 120/75 mm Hg, following British guidelines for patients with stroke, diabetes, chronic kidney disease, or coronary heart disease. If patients exhausted all 3 steps for medication titration, they were to return to their family physician for additional instructions. Patients in the usual care group had a routine blood pressure check and medication review appointment with their family physician, which was followed by follow-up care at the discretion of the family physician for blood pressure measurement, blood pressure targets, or adjustment of medication.
Main outcome measure. The primary outcome was systolic blood pressure at 12 months. The difference in outcomes between the intervention and usual care groups was examined while accounting for baseline blood pressure and other clinical factors. 6 blood pressures were taken at 1-minute intervals after an initial 5 minutes of rest. Blood pressure was taken by an electronic automated blood pressure machine. The mean of the second and third readings were used as primary outcome. Outcome assessor was not blinded to group assignment. The primary analysis included all cases with complete data, and a sensitivity analysis with multiple imputations was also performed. Preplanned subgroup analyses included older vs. younger age-groups, men vs. women, and other risk groups.
Main results. Among 10,764 patients assessed for eligibility, 3353 were excluded as they were considered by their family physician to be housebound, have a terminal illness, or not be a suitable candidate. Among the 7411 invited to participate, 4207 did not respond to the invitation and 2003 declined participation (with a third who did not want to alter their own medications, and a third who did not want to measure their own blood pressure). Among the 1201 who attended the baseline clinic, 138 withdrew their consent and 508 were deemed ineligible. A total of 555 were randomized, and 220 in the intervention group and 230 in the control group completed the study and provided outcome data (81%). Patients in the self-management group had a 9.2 mm Hg–lower systolic blood pressure at 12 months (95% CI, 5.7–12.7) compared with the usual care group. The self-management group also had a larger increase in the intake of antihypertensive drugs compared with controls, with an increase in both doses and number of medications. Although adverse symptoms were common in both groups, there were no significant differences in adverse symptoms between groups.
Conclusions. Self-management of hypertension among patients with stroke, cardiovascular disease, and other high-risk conditions is safe and effective in achieving better blood pressure control.
Commentary
Hypertension is a major public health problem. Significant resources have been devoted to advance hypertension management through research, practice improvements, and guideline developments; however, blood pressure control among those with hypertension in the United States remains suboptimal—with only about half achieving adequate control [1].
Advances in technology have made home blood pressure monitoring possible. It offers several advantages to traditional office-based blood pressure management [2], and several studies have shown home blood pressure telemonitoring and team care can achieve better outcomes than office-based management [3]. A significant contribution of the current study is that it demonstrated that the self-management approach is both safe and effective even in high-risk patients, who are perhaps the most likely to have adverse events from treatment but also the most likely to derive benefit from adequate treatment of hypertension.
Although the self-management approach has promise, it also has potential drawbacks. Specifically, as demonstrated by the low enrollment rate in this study, this intervention may not be suitable for all patients. About two-thirds of those who responded to the initial enrollment attempt ultimately declined participation because they did not want to modify their own medications or did not want to perform the tasks of home blood pressure monitoring. This perhaps is a realistic assessment of who may ultimately benefit from this approach—patients who wish to have an active role in managing their medical problems and have the ability to do so. For the clinician, it is important to identify patients who are able to manage the complex task of adjusting their medication regimen; otherwise, the potential for harm may be magnified.
Engaging patients in the management of their chronic disease is a growing trend in chronic disease management. Bringing management of hypertension to patients’ homes, as the accompanying editorial in the issue pointed out, reflects patient-centeredness at its best and represents an important step toward the adaptation of treatment for patients who want to actively take part in their own care [2].
Applications for Clinical Practice
Self-management of blood pressure in patients at high risk of cardiovascular disease appears feasible. As the editorialists note, this study is an important step toward adaptation of treatment for patients who want to actively take part in their own risk-factor control [2]. More research is needed to study the effects of self-titration on long-term outcomes and to identify the appropriate protocols that can be applied by clinicians in the community, both for patient selection and education and medication adjustment.
—William Hung, MD, MPH
1. Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988-2008. JAMA 2010;303:2043–50.
2. Nilsson PM, Nystrom FH. Self-titration of antihypertensive therapy in high-risk patients. Bringing it home. JAMA 2014;312:795–6.
3. Margolis KL, Asche SE, Bergdall AR, et al. Effect of home blood pressure telemonitoring and pharmacist management on blood pressure control. a cluster randomized clinical trial. JAMA 2013;310:46–56.
Study Overview
Objective. To examine the effect of self-monitoring of blood pressure and self-titration of antihypertensive medications among hypertensive patients with cardiovascular disease, diabetes, or chronic kidney disease.
Design. Unblinded randomized controlled trial.
Setting and participants. The study was conducted in central and east England. Patients with poorly controlled blood pressure with a last recorded systolic blood pressure of at least 145 mm Hg at 59 UK primary care practices were invited to participate. Patients had to be at least 35 years old and have at least 1 of the following comorbidities: transient ischemic attack or stroke, stage 3 chronic kidney disease, or history of coronary artery bypass graft surgery, myocardial infarction, or angina. Patients were excluded if they could not self-monitor blood pressure, had dementia or failed a cognitive screen using the short-orientation memory concentration test, had postural hypotension, took more than 3 antihypertensive medications, had an acute cardiovascular event within the previous 3 months, were receiving care from a specialist for their hypertension, were pregnant, or had a terminal disease. Participants were randomized to the self-management intervention or usual care.
Intervention. Patients in the self-management group were asked to monitor their blood pressure using an automated blood pressure monitor and to titrate their blood pressure medications using an individualized 3-step plan devised by the patient with their family physician. They were trained to do these tasks in 2- or 3-hour sessions. Patients were instructed to take their blood pressure twice each morning for the first week of each month; if 4 or more blood pressure readings during the measurement week for 2 consecutive months were higher than the target blood pressure, patients were to follow their individualized plan to change their medications. The target blood pressure was 120/75 mm Hg, following British guidelines for patients with stroke, diabetes, chronic kidney disease, or coronary heart disease. If patients exhausted all 3 steps for medication titration, they were to return to their family physician for additional instructions. Patients in the usual care group had a routine blood pressure check and medication review appointment with their family physician, which was followed by follow-up care at the discretion of the family physician for blood pressure measurement, blood pressure targets, or adjustment of medication.
Main outcome measure. The primary outcome was systolic blood pressure at 12 months. The difference in outcomes between the intervention and usual care groups was examined while accounting for baseline blood pressure and other clinical factors. 6 blood pressures were taken at 1-minute intervals after an initial 5 minutes of rest. Blood pressure was taken by an electronic automated blood pressure machine. The mean of the second and third readings were used as primary outcome. Outcome assessor was not blinded to group assignment. The primary analysis included all cases with complete data, and a sensitivity analysis with multiple imputations was also performed. Preplanned subgroup analyses included older vs. younger age-groups, men vs. women, and other risk groups.
Main results. Among 10,764 patients assessed for eligibility, 3353 were excluded as they were considered by their family physician to be housebound, have a terminal illness, or not be a suitable candidate. Among the 7411 invited to participate, 4207 did not respond to the invitation and 2003 declined participation (with a third who did not want to alter their own medications, and a third who did not want to measure their own blood pressure). Among the 1201 who attended the baseline clinic, 138 withdrew their consent and 508 were deemed ineligible. A total of 555 were randomized, and 220 in the intervention group and 230 in the control group completed the study and provided outcome data (81%). Patients in the self-management group had a 9.2 mm Hg–lower systolic blood pressure at 12 months (95% CI, 5.7–12.7) compared with the usual care group. The self-management group also had a larger increase in the intake of antihypertensive drugs compared with controls, with an increase in both doses and number of medications. Although adverse symptoms were common in both groups, there were no significant differences in adverse symptoms between groups.
Conclusions. Self-management of hypertension among patients with stroke, cardiovascular disease, and other high-risk conditions is safe and effective in achieving better blood pressure control.
Commentary
Hypertension is a major public health problem. Significant resources have been devoted to advance hypertension management through research, practice improvements, and guideline developments; however, blood pressure control among those with hypertension in the United States remains suboptimal—with only about half achieving adequate control [1].
Advances in technology have made home blood pressure monitoring possible. It offers several advantages to traditional office-based blood pressure management [2], and several studies have shown home blood pressure telemonitoring and team care can achieve better outcomes than office-based management [3]. A significant contribution of the current study is that it demonstrated that the self-management approach is both safe and effective even in high-risk patients, who are perhaps the most likely to have adverse events from treatment but also the most likely to derive benefit from adequate treatment of hypertension.
Although the self-management approach has promise, it also has potential drawbacks. Specifically, as demonstrated by the low enrollment rate in this study, this intervention may not be suitable for all patients. About two-thirds of those who responded to the initial enrollment attempt ultimately declined participation because they did not want to modify their own medications or did not want to perform the tasks of home blood pressure monitoring. This perhaps is a realistic assessment of who may ultimately benefit from this approach—patients who wish to have an active role in managing their medical problems and have the ability to do so. For the clinician, it is important to identify patients who are able to manage the complex task of adjusting their medication regimen; otherwise, the potential for harm may be magnified.
Engaging patients in the management of their chronic disease is a growing trend in chronic disease management. Bringing management of hypertension to patients’ homes, as the accompanying editorial in the issue pointed out, reflects patient-centeredness at its best and represents an important step toward the adaptation of treatment for patients who want to actively take part in their own care [2].
Applications for Clinical Practice
Self-management of blood pressure in patients at high risk of cardiovascular disease appears feasible. As the editorialists note, this study is an important step toward adaptation of treatment for patients who want to actively take part in their own risk-factor control [2]. More research is needed to study the effects of self-titration on long-term outcomes and to identify the appropriate protocols that can be applied by clinicians in the community, both for patient selection and education and medication adjustment.
—William Hung, MD, MPH
Study Overview
Objective. To examine the effect of self-monitoring of blood pressure and self-titration of antihypertensive medications among hypertensive patients with cardiovascular disease, diabetes, or chronic kidney disease.
Design. Unblinded randomized controlled trial.
Setting and participants. The study was conducted in central and east England. Patients with poorly controlled blood pressure with a last recorded systolic blood pressure of at least 145 mm Hg at 59 UK primary care practices were invited to participate. Patients had to be at least 35 years old and have at least 1 of the following comorbidities: transient ischemic attack or stroke, stage 3 chronic kidney disease, or history of coronary artery bypass graft surgery, myocardial infarction, or angina. Patients were excluded if they could not self-monitor blood pressure, had dementia or failed a cognitive screen using the short-orientation memory concentration test, had postural hypotension, took more than 3 antihypertensive medications, had an acute cardiovascular event within the previous 3 months, were receiving care from a specialist for their hypertension, were pregnant, or had a terminal disease. Participants were randomized to the self-management intervention or usual care.
Intervention. Patients in the self-management group were asked to monitor their blood pressure using an automated blood pressure monitor and to titrate their blood pressure medications using an individualized 3-step plan devised by the patient with their family physician. They were trained to do these tasks in 2- or 3-hour sessions. Patients were instructed to take their blood pressure twice each morning for the first week of each month; if 4 or more blood pressure readings during the measurement week for 2 consecutive months were higher than the target blood pressure, patients were to follow their individualized plan to change their medications. The target blood pressure was 120/75 mm Hg, following British guidelines for patients with stroke, diabetes, chronic kidney disease, or coronary heart disease. If patients exhausted all 3 steps for medication titration, they were to return to their family physician for additional instructions. Patients in the usual care group had a routine blood pressure check and medication review appointment with their family physician, which was followed by follow-up care at the discretion of the family physician for blood pressure measurement, blood pressure targets, or adjustment of medication.
Main outcome measure. The primary outcome was systolic blood pressure at 12 months. The difference in outcomes between the intervention and usual care groups was examined while accounting for baseline blood pressure and other clinical factors. 6 blood pressures were taken at 1-minute intervals after an initial 5 minutes of rest. Blood pressure was taken by an electronic automated blood pressure machine. The mean of the second and third readings were used as primary outcome. Outcome assessor was not blinded to group assignment. The primary analysis included all cases with complete data, and a sensitivity analysis with multiple imputations was also performed. Preplanned subgroup analyses included older vs. younger age-groups, men vs. women, and other risk groups.
Main results. Among 10,764 patients assessed for eligibility, 3353 were excluded as they were considered by their family physician to be housebound, have a terminal illness, or not be a suitable candidate. Among the 7411 invited to participate, 4207 did not respond to the invitation and 2003 declined participation (with a third who did not want to alter their own medications, and a third who did not want to measure their own blood pressure). Among the 1201 who attended the baseline clinic, 138 withdrew their consent and 508 were deemed ineligible. A total of 555 were randomized, and 220 in the intervention group and 230 in the control group completed the study and provided outcome data (81%). Patients in the self-management group had a 9.2 mm Hg–lower systolic blood pressure at 12 months (95% CI, 5.7–12.7) compared with the usual care group. The self-management group also had a larger increase in the intake of antihypertensive drugs compared with controls, with an increase in both doses and number of medications. Although adverse symptoms were common in both groups, there were no significant differences in adverse symptoms between groups.
Conclusions. Self-management of hypertension among patients with stroke, cardiovascular disease, and other high-risk conditions is safe and effective in achieving better blood pressure control.
Commentary
Hypertension is a major public health problem. Significant resources have been devoted to advance hypertension management through research, practice improvements, and guideline developments; however, blood pressure control among those with hypertension in the United States remains suboptimal—with only about half achieving adequate control [1].
Advances in technology have made home blood pressure monitoring possible. It offers several advantages to traditional office-based blood pressure management [2], and several studies have shown home blood pressure telemonitoring and team care can achieve better outcomes than office-based management [3]. A significant contribution of the current study is that it demonstrated that the self-management approach is both safe and effective even in high-risk patients, who are perhaps the most likely to have adverse events from treatment but also the most likely to derive benefit from adequate treatment of hypertension.
Although the self-management approach has promise, it also has potential drawbacks. Specifically, as demonstrated by the low enrollment rate in this study, this intervention may not be suitable for all patients. About two-thirds of those who responded to the initial enrollment attempt ultimately declined participation because they did not want to modify their own medications or did not want to perform the tasks of home blood pressure monitoring. This perhaps is a realistic assessment of who may ultimately benefit from this approach—patients who wish to have an active role in managing their medical problems and have the ability to do so. For the clinician, it is important to identify patients who are able to manage the complex task of adjusting their medication regimen; otherwise, the potential for harm may be magnified.
Engaging patients in the management of their chronic disease is a growing trend in chronic disease management. Bringing management of hypertension to patients’ homes, as the accompanying editorial in the issue pointed out, reflects patient-centeredness at its best and represents an important step toward the adaptation of treatment for patients who want to actively take part in their own care [2].
Applications for Clinical Practice
Self-management of blood pressure in patients at high risk of cardiovascular disease appears feasible. As the editorialists note, this study is an important step toward adaptation of treatment for patients who want to actively take part in their own risk-factor control [2]. More research is needed to study the effects of self-titration on long-term outcomes and to identify the appropriate protocols that can be applied by clinicians in the community, both for patient selection and education and medication adjustment.
—William Hung, MD, MPH
1. Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988-2008. JAMA 2010;303:2043–50.
2. Nilsson PM, Nystrom FH. Self-titration of antihypertensive therapy in high-risk patients. Bringing it home. JAMA 2014;312:795–6.
3. Margolis KL, Asche SE, Bergdall AR, et al. Effect of home blood pressure telemonitoring and pharmacist management on blood pressure control. a cluster randomized clinical trial. JAMA 2013;310:46–56.
1. Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988-2008. JAMA 2010;303:2043–50.
2. Nilsson PM, Nystrom FH. Self-titration of antihypertensive therapy in high-risk patients. Bringing it home. JAMA 2014;312:795–6.
3. Margolis KL, Asche SE, Bergdall AR, et al. Effect of home blood pressure telemonitoring and pharmacist management on blood pressure control. a cluster randomized clinical trial. JAMA 2013;310:46–56.
CBT-i Coach

The VA National Center for PTSD, Stanford School of Medicine, and the DoD National Center for Telehealth and Technology collaborated to bring users the CBT-i (cognitive behavioral therapy for insomnia) Coach mobile app. Cognitive behavioral therapy is a nonmedication treatment that is based on scientific knowledge. The goals of CBT-i are “to help you fall asleep, stay asleep, and improve your daytime functioning as a result of better sleep at night.”
The CBT-i Coach is designed for patients engaged in CBT-i or who have experienced symptoms of insomnia and want to improve their sleep habits. Although the app is intended to augment face-to-face care with a health care professional, there are plenty of applications for users who are not enrolled in CBT-i and are not satisfied with the amount or quality of sleep they are getting.
SLEEP 101
Without knowing what or why sleep may need to be improved, it can be difficult to know what adjustments to make. To overcome a possible learning curve, users can navigate from the Learn option in the app menu to a section called “Sleep 101.” Here, the app lays out the fundamentals of sleep and why we need it, the stages of sleep and related brain-wave activity patterns, and what regulates our sleep and wakefulness.

The CBT-i approach is explained by its 2 parts: cognitive and behavioral aspects. The cognitive elements focus on “thoughts, feelings, and expectations about sleep and insomnia that may stand in the way of good sleep.” Behavioral aspects help people “adopt personal sleep habits that, based on the science of sleep, will help them sleep better.”
Important tips are provided in the “What is CBT-i,” section, including how dangerous it is to keep weapons within easy access of where an individual is sleeping and the important distinction between feeling sleepy and feeling tired. The app notes that sleepy refers to an actual need for sleep, whereas tired can mean that the person simply has low energy. Understanding this distinction, among many others, can aid us in determining when our bodies need sleep and how to enhance the process of falling asleep.
Also within the Learn menu is a section called “Habits and Sleep.” Here, users can scroll through a list of habits that may cause sleep issues and explore what they can do to make improvements. This list includes habits that might keep a person awake (exercise, worrying in bed, watching the clock, and napping), substances we might ingest that disrupt sleep (eating, caffeine, alcohol, and nicotine), and what can be done to improve sleep (winding down, limiting the bedroom to 2 activities, and getting comfortable).
TOOLS
“Create New Sleep Habits” is the first section within the Tools menu. Here, the app notes, “Incorporating new habits into your nighttime routine can help sleep come more easily.” Lists for middle of the night activities when you can’t sleep, setting up a proper sleep environment, and activities to keep you awake until your prescribed bedtime are all intended to lead to improved quality of sleep.

Another tool focuses on preventing insomnia, offering a self-administered quiz to determine personal areas that may need improvement. As the user grows more comfortable with the CBT-i Coach and uses it over a period of time, sleeping difficulties may still naturally return. The app reinforces “this is normal” and provides the quiz as a way for users to keep tabs on themselves and their habits to determine why their sleeping difficulties may have returned.
The app also includes a glossary to explain any language used in the app that the user doesn’t understand.
MY SLEEP
Tracking sleep patterns with the Sleep Diary can be useful for self-assessment and can provide a vital snapshot for the health care professional who is treating a patient for insomnia. All fields must be filled in, including how many times the user woke up in the middle of the night and how long it took him or her to fall asleep. If the app notices any inconsistencies the diary will prompt the user to correct any inaccurately entered field(s) before the entry can be saved. An optional push notification reminder to update the sleep diary is available, and the user can set this for any time of day.
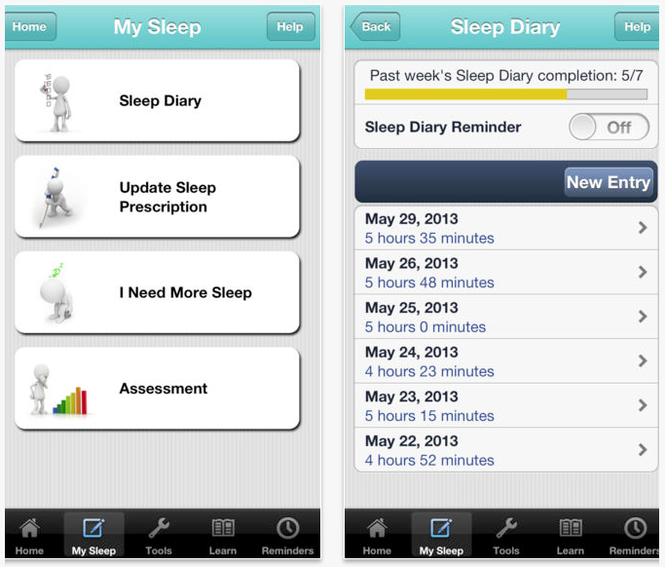
Other optional reminders may be found in the primary app menu at the bottom of the screen, and the user may select from any of the following: Sleep Diary Entry, Wind Down Time, Prescribed Bed Time, Prescribed Wake Time, Update Sleep Prescription, Take Assessment, Stop Caffeine, and Worry Time.
FINAL THOUGHTS
There is enough information in this app to keep a person busy for hours. But once it becomes part of a daily routine, users will find that with a bit of guidance, exercises, and personal modifications, a good night’s sleep, or at least one that’s improved, may be within reach.
For someone who is experiencing difficulties sleeping, it is critical to work with a health care professional who can determine and help treat any underlying causes of the insomnia.
The VA National Center for PTSD, Stanford School of Medicine, and the DoD National Center for Telehealth and Technology collaborated to bring users the CBT-i (cognitive behavioral therapy for insomnia) Coach mobile app. Cognitive behavioral therapy is a nonmedication treatment that is based on scientific knowledge. The goals of CBT-i are “to help you fall asleep, stay asleep, and improve your daytime functioning as a result of better sleep at night.”
The CBT-i Coach is designed for patients engaged in CBT-i or who have experienced symptoms of insomnia and want to improve their sleep habits. Although the app is intended to augment face-to-face care with a health care professional, there are plenty of applications for users who are not enrolled in CBT-i and are not satisfied with the amount or quality of sleep they are getting.
SLEEP 101
Without knowing what or why sleep may need to be improved, it can be difficult to know what adjustments to make. To overcome a possible learning curve, users can navigate from the Learn option in the app menu to a section called “Sleep 101.” Here, the app lays out the fundamentals of sleep and why we need it, the stages of sleep and related brain-wave activity patterns, and what regulates our sleep and wakefulness.
The CBT-i approach is explained by its 2 parts: cognitive and behavioral aspects. The cognitive elements focus on “thoughts, feelings, and expectations about sleep and insomnia that may stand in the way of good sleep.” Behavioral aspects help people “adopt personal sleep habits that, based on the science of sleep, will help them sleep better.”
Important tips are provided in the “What is CBT-i,” section, including how dangerous it is to keep weapons within easy access of where an individual is sleeping and the important distinction between feeling sleepy and feeling tired. The app notes that sleepy refers to an actual need for sleep, whereas tired can mean that the person simply has low energy. Understanding this distinction, among many others, can aid us in determining when our bodies need sleep and how to enhance the process of falling asleep.
Also within the Learn menu is a section called “Habits and Sleep.” Here, users can scroll through a list of habits that may cause sleep issues and explore what they can do to make improvements. This list includes habits that might keep a person awake (exercise, worrying in bed, watching the clock, and napping), substances we might ingest that disrupt sleep (eating, caffeine, alcohol, and nicotine), and what can be done to improve sleep (winding down, limiting the bedroom to 2 activities, and getting comfortable).
TOOLS
“Create New Sleep Habits” is the first section within the Tools menu. Here, the app notes, “Incorporating new habits into your nighttime routine can help sleep come more easily.” Lists for middle of the night activities when you can’t sleep, setting up a proper sleep environment, and activities to keep you awake until your prescribed bedtime are all intended to lead to improved quality of sleep.
Another tool focuses on preventing insomnia, offering a self-administered quiz to determine personal areas that may need improvement. As the user grows more comfortable with the CBT-i Coach and uses it over a period of time, sleeping difficulties may still naturally return. The app reinforces “this is normal” and provides the quiz as a way for users to keep tabs on themselves and their habits to determine why their sleeping difficulties may have returned.
The app also includes a glossary to explain any language used in the app that the user doesn’t understand.
MY SLEEP
Tracking sleep patterns with the Sleep Diary can be useful for self-assessment and can provide a vital snapshot for the health care professional who is treating a patient for insomnia. All fields must be filled in, including how many times the user woke up in the middle of the night and how long it took him or her to fall asleep. If the app notices any inconsistencies the diary will prompt the user to correct any inaccurately entered field(s) before the entry can be saved. An optional push notification reminder to update the sleep diary is available, and the user can set this for any time of day.
Other optional reminders may be found in the primary app menu at the bottom of the screen, and the user may select from any of the following: Sleep Diary Entry, Wind Down Time, Prescribed Bed Time, Prescribed Wake Time, Update Sleep Prescription, Take Assessment, Stop Caffeine, and Worry Time.
FINAL THOUGHTS
There is enough information in this app to keep a person busy for hours. But once it becomes part of a daily routine, users will find that with a bit of guidance, exercises, and personal modifications, a good night’s sleep, or at least one that’s improved, may be within reach.
For someone who is experiencing difficulties sleeping, it is critical to work with a health care professional who can determine and help treat any underlying causes of the insomnia.
The VA National Center for PTSD, Stanford School of Medicine, and the DoD National Center for Telehealth and Technology collaborated to bring users the CBT-i (cognitive behavioral therapy for insomnia) Coach mobile app. Cognitive behavioral therapy is a nonmedication treatment that is based on scientific knowledge. The goals of CBT-i are “to help you fall asleep, stay asleep, and improve your daytime functioning as a result of better sleep at night.”
The CBT-i Coach is designed for patients engaged in CBT-i or who have experienced symptoms of insomnia and want to improve their sleep habits. Although the app is intended to augment face-to-face care with a health care professional, there are plenty of applications for users who are not enrolled in CBT-i and are not satisfied with the amount or quality of sleep they are getting.
SLEEP 101
Without knowing what or why sleep may need to be improved, it can be difficult to know what adjustments to make. To overcome a possible learning curve, users can navigate from the Learn option in the app menu to a section called “Sleep 101.” Here, the app lays out the fundamentals of sleep and why we need it, the stages of sleep and related brain-wave activity patterns, and what regulates our sleep and wakefulness.
The CBT-i approach is explained by its 2 parts: cognitive and behavioral aspects. The cognitive elements focus on “thoughts, feelings, and expectations about sleep and insomnia that may stand in the way of good sleep.” Behavioral aspects help people “adopt personal sleep habits that, based on the science of sleep, will help them sleep better.”
Important tips are provided in the “What is CBT-i,” section, including how dangerous it is to keep weapons within easy access of where an individual is sleeping and the important distinction between feeling sleepy and feeling tired. The app notes that sleepy refers to an actual need for sleep, whereas tired can mean that the person simply has low energy. Understanding this distinction, among many others, can aid us in determining when our bodies need sleep and how to enhance the process of falling asleep.
Also within the Learn menu is a section called “Habits and Sleep.” Here, users can scroll through a list of habits that may cause sleep issues and explore what they can do to make improvements. This list includes habits that might keep a person awake (exercise, worrying in bed, watching the clock, and napping), substances we might ingest that disrupt sleep (eating, caffeine, alcohol, and nicotine), and what can be done to improve sleep (winding down, limiting the bedroom to 2 activities, and getting comfortable).
TOOLS
“Create New Sleep Habits” is the first section within the Tools menu. Here, the app notes, “Incorporating new habits into your nighttime routine can help sleep come more easily.” Lists for middle of the night activities when you can’t sleep, setting up a proper sleep environment, and activities to keep you awake until your prescribed bedtime are all intended to lead to improved quality of sleep.
Another tool focuses on preventing insomnia, offering a self-administered quiz to determine personal areas that may need improvement. As the user grows more comfortable with the CBT-i Coach and uses it over a period of time, sleeping difficulties may still naturally return. The app reinforces “this is normal” and provides the quiz as a way for users to keep tabs on themselves and their habits to determine why their sleeping difficulties may have returned.
The app also includes a glossary to explain any language used in the app that the user doesn’t understand.
MY SLEEP
Tracking sleep patterns with the Sleep Diary can be useful for self-assessment and can provide a vital snapshot for the health care professional who is treating a patient for insomnia. All fields must be filled in, including how many times the user woke up in the middle of the night and how long it took him or her to fall asleep. If the app notices any inconsistencies the diary will prompt the user to correct any inaccurately entered field(s) before the entry can be saved. An optional push notification reminder to update the sleep diary is available, and the user can set this for any time of day.
Other optional reminders may be found in the primary app menu at the bottom of the screen, and the user may select from any of the following: Sleep Diary Entry, Wind Down Time, Prescribed Bed Time, Prescribed Wake Time, Update Sleep Prescription, Take Assessment, Stop Caffeine, and Worry Time.
FINAL THOUGHTS
There is enough information in this app to keep a person busy for hours. But once it becomes part of a daily routine, users will find that with a bit of guidance, exercises, and personal modifications, a good night’s sleep, or at least one that’s improved, may be within reach.
For someone who is experiencing difficulties sleeping, it is critical to work with a health care professional who can determine and help treat any underlying causes of the insomnia.
ETBs prove effective against lymphoma and myeloma

Credit: Rhoda Baer
PHILADELPHIA—A pair of engineered toxin bodies (ETBs) can successfully treat Burkitt lymphoma and multiple myeloma, according to preclinical research presented at the AACR conference Hematologic Malignancies: Translating Discoveries to Novel Therapies.
The ETBs, known as MT-4007 and MT-4007-D, work by targeting CD38.
They greatly reduced tumor burden and improved survival in mouse models. And they were well-tolerated, even at the highest doses administered.
“In this study, we found that the growth of human cancer cells in mice was substantially decreased, or the cells were even eliminated, following treatment with our investigational CD38-targeted therapy,” said Erin K. Willert, PhD, of Molecular Templates Inc., in Georgetown, Texas.
Dr Willert and her colleagues explained that ETBs are derived from the ribosome-inactivating alpha subunit of Shiga-like toxin 1 (SLT-1A). They have been engineered to contain a target binding domain fused to a modified SLT-1A protein, which allows for delivery to a cell surface target—in this case, CD38.
Upon binding to a CD38-expressing cell, the ETB enters the cell, routes to the cytosol, halts protein synthesis, and kills the cell.
The researchers first tested MT-4007 and MT-4007-D in a range of human cell lines. The agents exhibited cytotoxicity in CD38+ Burkitt lymphoma and multiple myeloma cell lines (H929, Daudi, ST486, and Raji). But neither agent proved cytotoxic in CD38- cell lines (U266, SKBR3, and HCC1954).
The team then moved on to test MT-4007 in a mouse model of Burkitt lymphoma. Following injection with Daudi-Luc cells, mice received no treatment or MT-4007 at 0.05 mg/kg, 0.5 mg/kg, or 2 mg/kg on days 3, 5, 8, 10, and 12.
Treated mice exhibited significantly reduced tumor burden compared to controls. The mean tumor burden for mice that received MT-4007 at 0.05 mg/kg was 29% of the control tumor burden (P<0.0001). It was 0.4% for mice that received 0.50 mg/kg (P<0.0001) and 0.02% for mice that received 2 mg/kg (P<0.0001).
In a model of multiple myeloma, MT-4007-D provided a dose-dependent delay in tumor growth. After receiving injections of H929 cells, mice received no treatment or MT-4007-D at 0.5 mg/kg, 2 mg/kg, or 3 mg/kg on days 1, 3, 5, 8, 10, and 12.
The researchers assessed efficacy by measuring the time to endpoint, which was a tumor volume of 2000 mm3. The median time to endpoint was 22.3 days in controls, 21.2 days in the 0.5 mg/kg arm (not significant), 24.5 days in the 2 mg/kg arm (P=0.004), and 26.2 days in the 3 mg/kg arm (P=0.04).
The team assessed safety using body weight. They found that all treated groups of mice maintained a stable weight, suggesting MT-4007-D is well-tolerated.
The researchers also noted that, in a previous dose-finding study, the maximum-tolerated dose of MT-4007 was not reached at the highest dose administered to mice (2 mg/kg), which suggests MT-4007 is well tolerated as well.
Finally, Dr Willert and her colleagues found that MT-4007 extends survival in models of Burkitt lymphoma. The team euthanized mice if they had a greater than 20% loss in body weight or symptoms such as hind limb paralysis.
In the control group, all 10 mice died, and the median survival was 34 days. In the 0.5 mg/kg treatment group, 5 mice died, and the median survival was 59.5 days (P=0.0002).
One mouse died in the 0.5 mg/kg group (P<0.0001), and none of the mice died in the 2 mg/kg group (P<0.0001). The median survival was undefined for both groups.
Dr Willert said these results suggest the ETBs should be moved forward to clinical trials in CD38+ B-cell malignancies such as multiple myeloma. And because the ETBs work differently from other treatments, they might prove effective in relapsed or refractory patients.
However, more preclinical research is needed before the ETBs can be tested in patients. MT-4007-D is under investigation in preclinical studies now.
This research was funded by Molecular Templates Inc., makers of MT-4007 and MT-4007-D. ![]()
Credit: Rhoda Baer
PHILADELPHIA—A pair of engineered toxin bodies (ETBs) can successfully treat Burkitt lymphoma and multiple myeloma, according to preclinical research presented at the AACR conference Hematologic Malignancies: Translating Discoveries to Novel Therapies.
The ETBs, known as MT-4007 and MT-4007-D, work by targeting CD38.
They greatly reduced tumor burden and improved survival in mouse models. And they were well-tolerated, even at the highest doses administered.
“In this study, we found that the growth of human cancer cells in mice was substantially decreased, or the cells were even eliminated, following treatment with our investigational CD38-targeted therapy,” said Erin K. Willert, PhD, of Molecular Templates Inc., in Georgetown, Texas.
Dr Willert and her colleagues explained that ETBs are derived from the ribosome-inactivating alpha subunit of Shiga-like toxin 1 (SLT-1A). They have been engineered to contain a target binding domain fused to a modified SLT-1A protein, which allows for delivery to a cell surface target—in this case, CD38.
Upon binding to a CD38-expressing cell, the ETB enters the cell, routes to the cytosol, halts protein synthesis, and kills the cell.
The researchers first tested MT-4007 and MT-4007-D in a range of human cell lines. The agents exhibited cytotoxicity in CD38+ Burkitt lymphoma and multiple myeloma cell lines (H929, Daudi, ST486, and Raji). But neither agent proved cytotoxic in CD38- cell lines (U266, SKBR3, and HCC1954).
The team then moved on to test MT-4007 in a mouse model of Burkitt lymphoma. Following injection with Daudi-Luc cells, mice received no treatment or MT-4007 at 0.05 mg/kg, 0.5 mg/kg, or 2 mg/kg on days 3, 5, 8, 10, and 12.
Treated mice exhibited significantly reduced tumor burden compared to controls. The mean tumor burden for mice that received MT-4007 at 0.05 mg/kg was 29% of the control tumor burden (P<0.0001). It was 0.4% for mice that received 0.50 mg/kg (P<0.0001) and 0.02% for mice that received 2 mg/kg (P<0.0001).
In a model of multiple myeloma, MT-4007-D provided a dose-dependent delay in tumor growth. After receiving injections of H929 cells, mice received no treatment or MT-4007-D at 0.5 mg/kg, 2 mg/kg, or 3 mg/kg on days 1, 3, 5, 8, 10, and 12.
The researchers assessed efficacy by measuring the time to endpoint, which was a tumor volume of 2000 mm3. The median time to endpoint was 22.3 days in controls, 21.2 days in the 0.5 mg/kg arm (not significant), 24.5 days in the 2 mg/kg arm (P=0.004), and 26.2 days in the 3 mg/kg arm (P=0.04).
The team assessed safety using body weight. They found that all treated groups of mice maintained a stable weight, suggesting MT-4007-D is well-tolerated.
The researchers also noted that, in a previous dose-finding study, the maximum-tolerated dose of MT-4007 was not reached at the highest dose administered to mice (2 mg/kg), which suggests MT-4007 is well tolerated as well.
Finally, Dr Willert and her colleagues found that MT-4007 extends survival in models of Burkitt lymphoma. The team euthanized mice if they had a greater than 20% loss in body weight or symptoms such as hind limb paralysis.
In the control group, all 10 mice died, and the median survival was 34 days. In the 0.5 mg/kg treatment group, 5 mice died, and the median survival was 59.5 days (P=0.0002).
One mouse died in the 0.5 mg/kg group (P<0.0001), and none of the mice died in the 2 mg/kg group (P<0.0001). The median survival was undefined for both groups.
Dr Willert said these results suggest the ETBs should be moved forward to clinical trials in CD38+ B-cell malignancies such as multiple myeloma. And because the ETBs work differently from other treatments, they might prove effective in relapsed or refractory patients.
However, more preclinical research is needed before the ETBs can be tested in patients. MT-4007-D is under investigation in preclinical studies now.
This research was funded by Molecular Templates Inc., makers of MT-4007 and MT-4007-D. ![]()
Credit: Rhoda Baer
PHILADELPHIA—A pair of engineered toxin bodies (ETBs) can successfully treat Burkitt lymphoma and multiple myeloma, according to preclinical research presented at the AACR conference Hematologic Malignancies: Translating Discoveries to Novel Therapies.
The ETBs, known as MT-4007 and MT-4007-D, work by targeting CD38.
They greatly reduced tumor burden and improved survival in mouse models. And they were well-tolerated, even at the highest doses administered.
“In this study, we found that the growth of human cancer cells in mice was substantially decreased, or the cells were even eliminated, following treatment with our investigational CD38-targeted therapy,” said Erin K. Willert, PhD, of Molecular Templates Inc., in Georgetown, Texas.
Dr Willert and her colleagues explained that ETBs are derived from the ribosome-inactivating alpha subunit of Shiga-like toxin 1 (SLT-1A). They have been engineered to contain a target binding domain fused to a modified SLT-1A protein, which allows for delivery to a cell surface target—in this case, CD38.
Upon binding to a CD38-expressing cell, the ETB enters the cell, routes to the cytosol, halts protein synthesis, and kills the cell.
The researchers first tested MT-4007 and MT-4007-D in a range of human cell lines. The agents exhibited cytotoxicity in CD38+ Burkitt lymphoma and multiple myeloma cell lines (H929, Daudi, ST486, and Raji). But neither agent proved cytotoxic in CD38- cell lines (U266, SKBR3, and HCC1954).
The team then moved on to test MT-4007 in a mouse model of Burkitt lymphoma. Following injection with Daudi-Luc cells, mice received no treatment or MT-4007 at 0.05 mg/kg, 0.5 mg/kg, or 2 mg/kg on days 3, 5, 8, 10, and 12.
Treated mice exhibited significantly reduced tumor burden compared to controls. The mean tumor burden for mice that received MT-4007 at 0.05 mg/kg was 29% of the control tumor burden (P<0.0001). It was 0.4% for mice that received 0.50 mg/kg (P<0.0001) and 0.02% for mice that received 2 mg/kg (P<0.0001).
In a model of multiple myeloma, MT-4007-D provided a dose-dependent delay in tumor growth. After receiving injections of H929 cells, mice received no treatment or MT-4007-D at 0.5 mg/kg, 2 mg/kg, or 3 mg/kg on days 1, 3, 5, 8, 10, and 12.
The researchers assessed efficacy by measuring the time to endpoint, which was a tumor volume of 2000 mm3. The median time to endpoint was 22.3 days in controls, 21.2 days in the 0.5 mg/kg arm (not significant), 24.5 days in the 2 mg/kg arm (P=0.004), and 26.2 days in the 3 mg/kg arm (P=0.04).
The team assessed safety using body weight. They found that all treated groups of mice maintained a stable weight, suggesting MT-4007-D is well-tolerated.
The researchers also noted that, in a previous dose-finding study, the maximum-tolerated dose of MT-4007 was not reached at the highest dose administered to mice (2 mg/kg), which suggests MT-4007 is well tolerated as well.
Finally, Dr Willert and her colleagues found that MT-4007 extends survival in models of Burkitt lymphoma. The team euthanized mice if they had a greater than 20% loss in body weight or symptoms such as hind limb paralysis.
In the control group, all 10 mice died, and the median survival was 34 days. In the 0.5 mg/kg treatment group, 5 mice died, and the median survival was 59.5 days (P=0.0002).
One mouse died in the 0.5 mg/kg group (P<0.0001), and none of the mice died in the 2 mg/kg group (P<0.0001). The median survival was undefined for both groups.
Dr Willert said these results suggest the ETBs should be moved forward to clinical trials in CD38+ B-cell malignancies such as multiple myeloma. And because the ETBs work differently from other treatments, they might prove effective in relapsed or refractory patients.
However, more preclinical research is needed before the ETBs can be tested in patients. MT-4007-D is under investigation in preclinical studies now.
This research was funded by Molecular Templates Inc., makers of MT-4007 and MT-4007-D. ![]()
Platelets respond to their surroundings, study shows

Credit: Andre E.X. Brown
Platelets can sense and respond to their surroundings, according to research published in PNAS.
Researchers reported that platelets can detect mechanical aspects of their environment and transduce those cues into biological signals.
Experiments showed that platelets could sense the stiffness of a fibrin/fibrinogen substrate, and increasing stiffness was associated with increased platelet adhesion, spreading, and activation.
“Platelets are smarter than we give them credit for, in that they are able to sense the physical characteristics of their environment and respond in a graduated way,” said study author Wilbur Lam, MD, PhD, of the Emory University School of Medicine in Atlanta, Georgia.
He and his colleagues were able to separate physical and biochemical effects on platelet behavior by forming polymer gels with different degrees of stiffness and then overlaying each with the same coating of fibrinogen.
With stiffer gels, the researchers observed an increase in platelet adhesion, spreading, and activation. This behavior was most pronounced when the concentration of fibrinogen was relatively low.
“This variability helps to explain platelet behavior in the 3D context of a clot in the body, which can be quite heterogenous in makeup,” Dr Lam said.
The researchers were also able to dissect platelet biochemistry by allowing the platelets to adhere and then spread on the various gels under the influence of drugs that interfere with different biochemical steps.
The team found that integrins, which engage the fibrinogen, and the protein Rac1 are involved in the initial mechanical sensing during adhesion. Myosin and actin, components of the cytoskeleton, are responsible for platelet spreading.
“We found that the initial adhesion and later spreading are separable, because different biochemical pathways are involved in each step,” Dr Lam said. “Our data show that mechanosensing can occur and plays important roles even when the cellular structural building blocks are fairly basic, even when the nucleus is absent.”
The researchers believe these findings could influence the design of medical devices, as modifying the stiffness of materials used in these devices might reduce the formation of blood clots. The results could also guide the refinement of anticoagulant therapy. ![]()
Credit: Andre E.X. Brown
Platelets can sense and respond to their surroundings, according to research published in PNAS.
Researchers reported that platelets can detect mechanical aspects of their environment and transduce those cues into biological signals.
Experiments showed that platelets could sense the stiffness of a fibrin/fibrinogen substrate, and increasing stiffness was associated with increased platelet adhesion, spreading, and activation.
“Platelets are smarter than we give them credit for, in that they are able to sense the physical characteristics of their environment and respond in a graduated way,” said study author Wilbur Lam, MD, PhD, of the Emory University School of Medicine in Atlanta, Georgia.
He and his colleagues were able to separate physical and biochemical effects on platelet behavior by forming polymer gels with different degrees of stiffness and then overlaying each with the same coating of fibrinogen.
With stiffer gels, the researchers observed an increase in platelet adhesion, spreading, and activation. This behavior was most pronounced when the concentration of fibrinogen was relatively low.
“This variability helps to explain platelet behavior in the 3D context of a clot in the body, which can be quite heterogenous in makeup,” Dr Lam said.
The researchers were also able to dissect platelet biochemistry by allowing the platelets to adhere and then spread on the various gels under the influence of drugs that interfere with different biochemical steps.
The team found that integrins, which engage the fibrinogen, and the protein Rac1 are involved in the initial mechanical sensing during adhesion. Myosin and actin, components of the cytoskeleton, are responsible for platelet spreading.
“We found that the initial adhesion and later spreading are separable, because different biochemical pathways are involved in each step,” Dr Lam said. “Our data show that mechanosensing can occur and plays important roles even when the cellular structural building blocks are fairly basic, even when the nucleus is absent.”
The researchers believe these findings could influence the design of medical devices, as modifying the stiffness of materials used in these devices might reduce the formation of blood clots. The results could also guide the refinement of anticoagulant therapy. ![]()
Credit: Andre E.X. Brown
Platelets can sense and respond to their surroundings, according to research published in PNAS.
Researchers reported that platelets can detect mechanical aspects of their environment and transduce those cues into biological signals.
Experiments showed that platelets could sense the stiffness of a fibrin/fibrinogen substrate, and increasing stiffness was associated with increased platelet adhesion, spreading, and activation.
“Platelets are smarter than we give them credit for, in that they are able to sense the physical characteristics of their environment and respond in a graduated way,” said study author Wilbur Lam, MD, PhD, of the Emory University School of Medicine in Atlanta, Georgia.
He and his colleagues were able to separate physical and biochemical effects on platelet behavior by forming polymer gels with different degrees of stiffness and then overlaying each with the same coating of fibrinogen.
With stiffer gels, the researchers observed an increase in platelet adhesion, spreading, and activation. This behavior was most pronounced when the concentration of fibrinogen was relatively low.
“This variability helps to explain platelet behavior in the 3D context of a clot in the body, which can be quite heterogenous in makeup,” Dr Lam said.
The researchers were also able to dissect platelet biochemistry by allowing the platelets to adhere and then spread on the various gels under the influence of drugs that interfere with different biochemical steps.
The team found that integrins, which engage the fibrinogen, and the protein Rac1 are involved in the initial mechanical sensing during adhesion. Myosin and actin, components of the cytoskeleton, are responsible for platelet spreading.
“We found that the initial adhesion and later spreading are separable, because different biochemical pathways are involved in each step,” Dr Lam said. “Our data show that mechanosensing can occur and plays important roles even when the cellular structural building blocks are fairly basic, even when the nucleus is absent.”
The researchers believe these findings could influence the design of medical devices, as modifying the stiffness of materials used in these devices might reduce the formation of blood clots. The results could also guide the refinement of anticoagulant therapy. ![]()
Team tracks cell therapy using MRI

Scientists say they have devised a way to track the movements, destination, and persistence of a broad range of cellular therapies, without resorting to invasive procedures.
In Magnetic Resonance in Medicine, the researchers described the first human tests using a perfluorocarbon (PFC) tracer in combination with non-invasive magnetic resonance imaging (MRI) to track therapeutic immune cells injected into patients with colorectal cancer.
“Initially, we see this technique used for clinical trials that involve tests of new cell therapies,” said study author Eric T. Ahrens, PhD, of the University of California, San Diego.
“Clinical development of cell therapies can be accelerated by providing feedback regarding cell motility, optimal delivery routes, individual therapeutic doses, and engraftment success.”
Currently, there is no accepted way to image cells in the human body that covers a broad range of cell types and diseases. Earlier techniques have used metal ion-based vascular MRI contrast agents and radioisotopes.
The former have proven difficult to differentiate in vivo. The latter raise concerns about radiation toxicity and do not provide the anatomical detail available with MRIs.
“This is the first human PFC cell tracking agent, which is a new way to do MRI cell tracking,” Dr Ahrens said. “It’s the first example of a clinical MRI agent designed specifically for cell tracking.”
He and his colleagues used a PFC tracer agent and an MRI technique that directly detects fluorine atoms in labeled cells. Fluorine atoms naturally occur in extremely low concentrations in the body, making it easier to observe cells labeled with fluorine using MRI.
In this case, the modified and labeled dendritic cells were first prepared from white blood cells extracted from the patient. The cells were then injected into patients with stage 4 metastatic colorectal cancer to stimulate an anticancer T-cell immune response.
The researchers did not assess the efficacy of the cell therapy, only their ability to detect the labeled cells and monitor what happened to them. Dr Ahrens said the technique worked as expected, with the surprising finding that only half of the delivered cell vaccine remained at the inoculation site after 24 hours.
“The imaging agent technology has been shown to be able to tag any cell type that is of interest,” Dr Ahrens said. “It is a platform imaging technology for a wide range of diseases and applications.”
“Non-invasive cell tracking may help lower regulatory barriers,” he added. “For example, new stem cell therapies can be slow to obtain regulatory approvals, in part, because it is difficult, if not impossible, with current approaches to verify survival and location of transplanted cells.”
“And cell therapy trials generally have a high cost per patient. Tools that allow the investigator to gain a ‘richer’ data set from individual patients mean it may be possible to reduce patient numbers enrolled in a trial, thus reducing total trial cost.” ![]()
Scientists say they have devised a way to track the movements, destination, and persistence of a broad range of cellular therapies, without resorting to invasive procedures.
In Magnetic Resonance in Medicine, the researchers described the first human tests using a perfluorocarbon (PFC) tracer in combination with non-invasive magnetic resonance imaging (MRI) to track therapeutic immune cells injected into patients with colorectal cancer.
“Initially, we see this technique used for clinical trials that involve tests of new cell therapies,” said study author Eric T. Ahrens, PhD, of the University of California, San Diego.
“Clinical development of cell therapies can be accelerated by providing feedback regarding cell motility, optimal delivery routes, individual therapeutic doses, and engraftment success.”
Currently, there is no accepted way to image cells in the human body that covers a broad range of cell types and diseases. Earlier techniques have used metal ion-based vascular MRI contrast agents and radioisotopes.
The former have proven difficult to differentiate in vivo. The latter raise concerns about radiation toxicity and do not provide the anatomical detail available with MRIs.
“This is the first human PFC cell tracking agent, which is a new way to do MRI cell tracking,” Dr Ahrens said. “It’s the first example of a clinical MRI agent designed specifically for cell tracking.”
He and his colleagues used a PFC tracer agent and an MRI technique that directly detects fluorine atoms in labeled cells. Fluorine atoms naturally occur in extremely low concentrations in the body, making it easier to observe cells labeled with fluorine using MRI.
In this case, the modified and labeled dendritic cells were first prepared from white blood cells extracted from the patient. The cells were then injected into patients with stage 4 metastatic colorectal cancer to stimulate an anticancer T-cell immune response.
The researchers did not assess the efficacy of the cell therapy, only their ability to detect the labeled cells and monitor what happened to them. Dr Ahrens said the technique worked as expected, with the surprising finding that only half of the delivered cell vaccine remained at the inoculation site after 24 hours.
“The imaging agent technology has been shown to be able to tag any cell type that is of interest,” Dr Ahrens said. “It is a platform imaging technology for a wide range of diseases and applications.”
“Non-invasive cell tracking may help lower regulatory barriers,” he added. “For example, new stem cell therapies can be slow to obtain regulatory approvals, in part, because it is difficult, if not impossible, with current approaches to verify survival and location of transplanted cells.”
“And cell therapy trials generally have a high cost per patient. Tools that allow the investigator to gain a ‘richer’ data set from individual patients mean it may be possible to reduce patient numbers enrolled in a trial, thus reducing total trial cost.” ![]()
Scientists say they have devised a way to track the movements, destination, and persistence of a broad range of cellular therapies, without resorting to invasive procedures.
In Magnetic Resonance in Medicine, the researchers described the first human tests using a perfluorocarbon (PFC) tracer in combination with non-invasive magnetic resonance imaging (MRI) to track therapeutic immune cells injected into patients with colorectal cancer.
“Initially, we see this technique used for clinical trials that involve tests of new cell therapies,” said study author Eric T. Ahrens, PhD, of the University of California, San Diego.
“Clinical development of cell therapies can be accelerated by providing feedback regarding cell motility, optimal delivery routes, individual therapeutic doses, and engraftment success.”
Currently, there is no accepted way to image cells in the human body that covers a broad range of cell types and diseases. Earlier techniques have used metal ion-based vascular MRI contrast agents and radioisotopes.
The former have proven difficult to differentiate in vivo. The latter raise concerns about radiation toxicity and do not provide the anatomical detail available with MRIs.
“This is the first human PFC cell tracking agent, which is a new way to do MRI cell tracking,” Dr Ahrens said. “It’s the first example of a clinical MRI agent designed specifically for cell tracking.”
He and his colleagues used a PFC tracer agent and an MRI technique that directly detects fluorine atoms in labeled cells. Fluorine atoms naturally occur in extremely low concentrations in the body, making it easier to observe cells labeled with fluorine using MRI.
In this case, the modified and labeled dendritic cells were first prepared from white blood cells extracted from the patient. The cells were then injected into patients with stage 4 metastatic colorectal cancer to stimulate an anticancer T-cell immune response.
The researchers did not assess the efficacy of the cell therapy, only their ability to detect the labeled cells and monitor what happened to them. Dr Ahrens said the technique worked as expected, with the surprising finding that only half of the delivered cell vaccine remained at the inoculation site after 24 hours.
“The imaging agent technology has been shown to be able to tag any cell type that is of interest,” Dr Ahrens said. “It is a platform imaging technology for a wide range of diseases and applications.”
“Non-invasive cell tracking may help lower regulatory barriers,” he added. “For example, new stem cell therapies can be slow to obtain regulatory approvals, in part, because it is difficult, if not impossible, with current approaches to verify survival and location of transplanted cells.”
“And cell therapy trials generally have a high cost per patient. Tools that allow the investigator to gain a ‘richer’ data set from individual patients mean it may be possible to reduce patient numbers enrolled in a trial, thus reducing total trial cost.” ![]()
Drugs demonstrate inconsistent synergy in CLL, MCL

PHILADELPHIA—The Bcl-2 inhibitor ABT-199 and the Bruton tyrosine kinase inhibitor ibrutinib can have a synergistic effect against mantle cell lymphoma (MCL) and chronic lymphocytic leukemia (CLL), preclinical data suggest.
In one set of experiments with MCL and CLL samples, the drugs induced apoptosis at a much higher rate when used together than when used alone.
However, in other experiments with CLL samples, ABT-199 and ibrutinib did not consistently display synergistic cytoxicity.
The researchers said this indicates substantial patient heterogeneity in response to the combination that may be due to variations in the genetic landscape.
Michael J. Weber, PhD, of the University of Virginia School of Medicine in Charlottesville, and his colleagues presented this research at the AACR conference Hematologic Malignancies: Translating Discoveries to Novel Therapies.
“We took an empirical but systematic approach to identify combinations of drugs that might improve the ability of ibrutinib to kill cancer cells,” Dr Weber said. “The combination of ibrutinib and ABT-199 was, by far, the most effective in our assays, and we are in the very earliest stages of planning a clinical trial to test this combination in the clinic.”
In previous studies, Dr Weber and his colleagues found that ibrutinib synergized with both ABT-199 and the proteasome inhibitor carfilzomib to kill MCL cell lines. In this study, the team assessed the effects of exposure to these 2 combinations on samples from patients with MCL or CLL.
The researchers found that apoptosis occurred in 23% of cells exposed to ABT-199 and ibrutinib in combination, compared to 3.8% of cells exposed to ibrutinib and 3% exposed to ABT-199.
The combination of ibrutinib and carfilzomib also increased apoptosis in MCL and CLL cells compared to either agent alone, though to a lesser degree than the ABT-199 combination. Apoptosis occurred in 5.5% of cells exposed to ibrutinib and carfilzomib, 3.8% exposed to ibrutinib, and 1.7% exposed to carfilzomib.
The researchers observed minimal apoptosis in normal T cells, both with the single agents and the combinations.
Further analysis showed that ibrutinib and ABT-199 worked synergistically to cause apoptosis in leukemic cells from 5 of 9 patients with CLL.
According to Dr Weber, the variable response to this combination points to the importance of understanding how these combinations work, so we can match the treatments with the most appropriate patients.
“Ibrutinib and ABT-199 target different pathways involved in promoting cancer cell survival and growth,” Dr Weber said.
“This is very intriguing because, in most instances where cancer cells are resistant to a particular molecularly targeted drug, we find that cancer cells adapt and find new ways to reactivate the pathway being targeted by the drug and that combinations of drugs targeting this pathway in different ways can improve outcomes. Here, we found that targeting a pathway outside the primary pathway was effective.”
This study was funded by the University of Virginia Cancer Center. Dr Weber declared no conflicts of interest. ![]()
PHILADELPHIA—The Bcl-2 inhibitor ABT-199 and the Bruton tyrosine kinase inhibitor ibrutinib can have a synergistic effect against mantle cell lymphoma (MCL) and chronic lymphocytic leukemia (CLL), preclinical data suggest.
In one set of experiments with MCL and CLL samples, the drugs induced apoptosis at a much higher rate when used together than when used alone.
However, in other experiments with CLL samples, ABT-199 and ibrutinib did not consistently display synergistic cytoxicity.
The researchers said this indicates substantial patient heterogeneity in response to the combination that may be due to variations in the genetic landscape.
Michael J. Weber, PhD, of the University of Virginia School of Medicine in Charlottesville, and his colleagues presented this research at the AACR conference Hematologic Malignancies: Translating Discoveries to Novel Therapies.
“We took an empirical but systematic approach to identify combinations of drugs that might improve the ability of ibrutinib to kill cancer cells,” Dr Weber said. “The combination of ibrutinib and ABT-199 was, by far, the most effective in our assays, and we are in the very earliest stages of planning a clinical trial to test this combination in the clinic.”
In previous studies, Dr Weber and his colleagues found that ibrutinib synergized with both ABT-199 and the proteasome inhibitor carfilzomib to kill MCL cell lines. In this study, the team assessed the effects of exposure to these 2 combinations on samples from patients with MCL or CLL.
The researchers found that apoptosis occurred in 23% of cells exposed to ABT-199 and ibrutinib in combination, compared to 3.8% of cells exposed to ibrutinib and 3% exposed to ABT-199.
The combination of ibrutinib and carfilzomib also increased apoptosis in MCL and CLL cells compared to either agent alone, though to a lesser degree than the ABT-199 combination. Apoptosis occurred in 5.5% of cells exposed to ibrutinib and carfilzomib, 3.8% exposed to ibrutinib, and 1.7% exposed to carfilzomib.
The researchers observed minimal apoptosis in normal T cells, both with the single agents and the combinations.
Further analysis showed that ibrutinib and ABT-199 worked synergistically to cause apoptosis in leukemic cells from 5 of 9 patients with CLL.
According to Dr Weber, the variable response to this combination points to the importance of understanding how these combinations work, so we can match the treatments with the most appropriate patients.
“Ibrutinib and ABT-199 target different pathways involved in promoting cancer cell survival and growth,” Dr Weber said.
“This is very intriguing because, in most instances where cancer cells are resistant to a particular molecularly targeted drug, we find that cancer cells adapt and find new ways to reactivate the pathway being targeted by the drug and that combinations of drugs targeting this pathway in different ways can improve outcomes. Here, we found that targeting a pathway outside the primary pathway was effective.”
This study was funded by the University of Virginia Cancer Center. Dr Weber declared no conflicts of interest. ![]()
PHILADELPHIA—The Bcl-2 inhibitor ABT-199 and the Bruton tyrosine kinase inhibitor ibrutinib can have a synergistic effect against mantle cell lymphoma (MCL) and chronic lymphocytic leukemia (CLL), preclinical data suggest.
In one set of experiments with MCL and CLL samples, the drugs induced apoptosis at a much higher rate when used together than when used alone.
However, in other experiments with CLL samples, ABT-199 and ibrutinib did not consistently display synergistic cytoxicity.
The researchers said this indicates substantial patient heterogeneity in response to the combination that may be due to variations in the genetic landscape.
Michael J. Weber, PhD, of the University of Virginia School of Medicine in Charlottesville, and his colleagues presented this research at the AACR conference Hematologic Malignancies: Translating Discoveries to Novel Therapies.
“We took an empirical but systematic approach to identify combinations of drugs that might improve the ability of ibrutinib to kill cancer cells,” Dr Weber said. “The combination of ibrutinib and ABT-199 was, by far, the most effective in our assays, and we are in the very earliest stages of planning a clinical trial to test this combination in the clinic.”
In previous studies, Dr Weber and his colleagues found that ibrutinib synergized with both ABT-199 and the proteasome inhibitor carfilzomib to kill MCL cell lines. In this study, the team assessed the effects of exposure to these 2 combinations on samples from patients with MCL or CLL.
The researchers found that apoptosis occurred in 23% of cells exposed to ABT-199 and ibrutinib in combination, compared to 3.8% of cells exposed to ibrutinib and 3% exposed to ABT-199.
The combination of ibrutinib and carfilzomib also increased apoptosis in MCL and CLL cells compared to either agent alone, though to a lesser degree than the ABT-199 combination. Apoptosis occurred in 5.5% of cells exposed to ibrutinib and carfilzomib, 3.8% exposed to ibrutinib, and 1.7% exposed to carfilzomib.
The researchers observed minimal apoptosis in normal T cells, both with the single agents and the combinations.
Further analysis showed that ibrutinib and ABT-199 worked synergistically to cause apoptosis in leukemic cells from 5 of 9 patients with CLL.
According to Dr Weber, the variable response to this combination points to the importance of understanding how these combinations work, so we can match the treatments with the most appropriate patients.
“Ibrutinib and ABT-199 target different pathways involved in promoting cancer cell survival and growth,” Dr Weber said.
“This is very intriguing because, in most instances where cancer cells are resistant to a particular molecularly targeted drug, we find that cancer cells adapt and find new ways to reactivate the pathway being targeted by the drug and that combinations of drugs targeting this pathway in different ways can improve outcomes. Here, we found that targeting a pathway outside the primary pathway was effective.”
This study was funded by the University of Virginia Cancer Center. Dr Weber declared no conflicts of interest. ![]()
Closing large dermal defects much like a Victorian corset
EDINBURGH – Barbed absorbable sutures are a useful new tool to facilitate dermal closure of facial and nonfacial defects following tumor resection.
“These are not the bad old sutures that you might of heard about before, that were nonabsorbable sutures and attempted for use in cosmetic procedures,” Dr. John Strasswimmer said at the 15th World Congress on Cancers of the Skin.
Last year, Dr. Strasswimmer, medical director of melanoma and cutaneous oncology at the Lynn Cancer Institute in Boca Raton, Fla., reported his initial experience using a procedure he calls “Corseta” to close a large Mohs defect on the trunk of an 83-year-old man (JAMA Dermatol. 2013;149:853-4).

The procedure employs a barbed, bioabsorbable suture (Ethicon’s Stratafix and Covidien’s V-Loc) that is run in a continuous vertical looping manner in the subcutaneous layer, with minimal to no undermining of the wound. Undermining is typically used in cutaneous surgery to relieve tension or provide structure around anatomical landmarks, but it can increase the risk of bleeding, swelling, and patient discomfort, he said.
Instead, the first suture pass is placed in the deepest portion of the subcutaneous tissue and brought out within the more superficial subcutaneous layer. Each bite of the barbed suture extends peripherally at least 2.0 cm from the edge of the wound, so the point of tension is lateral to the wound margins. At every two passes, tension is placed evenly across the sutures to close the deepest layer of tissue and to engage the barbs, much like closing of a Victorian corset, Dr. Strasswimmer said.
The second arm of the suture is passed in a similar manner in the subcutaneous plane, superficial to the first pass.
“This is a lacing, not a suturing technique,” he said. “You get tissue approximation, but more importantly, because we’re bringing in all that deep tissue, you automatically get beautiful wound-edge eversion and very nice cosmetic results.”
Because the sutures have barbs cut into them, however, a 0-0 weight polydioxane or other absorbable material suture can have a breaking strength of a #2-0 suture. “You have to look very carefully at the manufacturer’s sizing and strength requirements,” Dr. Strasswimmer cautioned.
Since their initial case report, Dr. Strasswimmer and his colleagues have expanded use of the Corseta technique to more than 600 facial and nonfacial reconstructions. The Corseta procedure is not as helpful for curved topography such as the central face or scalp, he said in an interview. Still, of the 600 or so cases, none required conversion to another closure technique.
“The traditional closure technique would not have worked in those challenging cases,” Dr. Strasswimmer said. “In the most difficult situations, such as older patients with severely atrophic skin, even the best suturing won’t work. In that case, the Corseta at least produces a partial closure, thereby reducing the wound and accelerating healing.” The Corseta procedure is often coupled with tumescent anesthesia to decrease the risk of bleeding, particularly in patients on anticoagulation, he noted.
The conference was sponsored by the Skin Cancer Foundation.
EDINBURGH – Barbed absorbable sutures are a useful new tool to facilitate dermal closure of facial and nonfacial defects following tumor resection.
“These are not the bad old sutures that you might of heard about before, that were nonabsorbable sutures and attempted for use in cosmetic procedures,” Dr. John Strasswimmer said at the 15th World Congress on Cancers of the Skin.
Last year, Dr. Strasswimmer, medical director of melanoma and cutaneous oncology at the Lynn Cancer Institute in Boca Raton, Fla., reported his initial experience using a procedure he calls “Corseta” to close a large Mohs defect on the trunk of an 83-year-old man (JAMA Dermatol. 2013;149:853-4).
The procedure employs a barbed, bioabsorbable suture (Ethicon’s Stratafix and Covidien’s V-Loc) that is run in a continuous vertical looping manner in the subcutaneous layer, with minimal to no undermining of the wound. Undermining is typically used in cutaneous surgery to relieve tension or provide structure around anatomical landmarks, but it can increase the risk of bleeding, swelling, and patient discomfort, he said.
Instead, the first suture pass is placed in the deepest portion of the subcutaneous tissue and brought out within the more superficial subcutaneous layer. Each bite of the barbed suture extends peripherally at least 2.0 cm from the edge of the wound, so the point of tension is lateral to the wound margins. At every two passes, tension is placed evenly across the sutures to close the deepest layer of tissue and to engage the barbs, much like closing of a Victorian corset, Dr. Strasswimmer said.
The second arm of the suture is passed in a similar manner in the subcutaneous plane, superficial to the first pass.
“This is a lacing, not a suturing technique,” he said. “You get tissue approximation, but more importantly, because we’re bringing in all that deep tissue, you automatically get beautiful wound-edge eversion and very nice cosmetic results.”
Because the sutures have barbs cut into them, however, a 0-0 weight polydioxane or other absorbable material suture can have a breaking strength of a #2-0 suture. “You have to look very carefully at the manufacturer’s sizing and strength requirements,” Dr. Strasswimmer cautioned.
Since their initial case report, Dr. Strasswimmer and his colleagues have expanded use of the Corseta technique to more than 600 facial and nonfacial reconstructions. The Corseta procedure is not as helpful for curved topography such as the central face or scalp, he said in an interview. Still, of the 600 or so cases, none required conversion to another closure technique.
“The traditional closure technique would not have worked in those challenging cases,” Dr. Strasswimmer said. “In the most difficult situations, such as older patients with severely atrophic skin, even the best suturing won’t work. In that case, the Corseta at least produces a partial closure, thereby reducing the wound and accelerating healing.” The Corseta procedure is often coupled with tumescent anesthesia to decrease the risk of bleeding, particularly in patients on anticoagulation, he noted.
The conference was sponsored by the Skin Cancer Foundation.
EDINBURGH – Barbed absorbable sutures are a useful new tool to facilitate dermal closure of facial and nonfacial defects following tumor resection.
“These are not the bad old sutures that you might of heard about before, that were nonabsorbable sutures and attempted for use in cosmetic procedures,” Dr. John Strasswimmer said at the 15th World Congress on Cancers of the Skin.
Last year, Dr. Strasswimmer, medical director of melanoma and cutaneous oncology at the Lynn Cancer Institute in Boca Raton, Fla., reported his initial experience using a procedure he calls “Corseta” to close a large Mohs defect on the trunk of an 83-year-old man (JAMA Dermatol. 2013;149:853-4).
The procedure employs a barbed, bioabsorbable suture (Ethicon’s Stratafix and Covidien’s V-Loc) that is run in a continuous vertical looping manner in the subcutaneous layer, with minimal to no undermining of the wound. Undermining is typically used in cutaneous surgery to relieve tension or provide structure around anatomical landmarks, but it can increase the risk of bleeding, swelling, and patient discomfort, he said.
Instead, the first suture pass is placed in the deepest portion of the subcutaneous tissue and brought out within the more superficial subcutaneous layer. Each bite of the barbed suture extends peripherally at least 2.0 cm from the edge of the wound, so the point of tension is lateral to the wound margins. At every two passes, tension is placed evenly across the sutures to close the deepest layer of tissue and to engage the barbs, much like closing of a Victorian corset, Dr. Strasswimmer said.
The second arm of the suture is passed in a similar manner in the subcutaneous plane, superficial to the first pass.
“This is a lacing, not a suturing technique,” he said. “You get tissue approximation, but more importantly, because we’re bringing in all that deep tissue, you automatically get beautiful wound-edge eversion and very nice cosmetic results.”
Because the sutures have barbs cut into them, however, a 0-0 weight polydioxane or other absorbable material suture can have a breaking strength of a #2-0 suture. “You have to look very carefully at the manufacturer’s sizing and strength requirements,” Dr. Strasswimmer cautioned.
Since their initial case report, Dr. Strasswimmer and his colleagues have expanded use of the Corseta technique to more than 600 facial and nonfacial reconstructions. The Corseta procedure is not as helpful for curved topography such as the central face or scalp, he said in an interview. Still, of the 600 or so cases, none required conversion to another closure technique.
“The traditional closure technique would not have worked in those challenging cases,” Dr. Strasswimmer said. “In the most difficult situations, such as older patients with severely atrophic skin, even the best suturing won’t work. In that case, the Corseta at least produces a partial closure, thereby reducing the wound and accelerating healing.” The Corseta procedure is often coupled with tumescent anesthesia to decrease the risk of bleeding, particularly in patients on anticoagulation, he noted.
The conference was sponsored by the Skin Cancer Foundation.
EXPERT ANALYSIS FROM WCCS 2014

Durable responses in metastatic melanoma, improved PFS in advanced colorectal cancer
High rate of durable responses to pembrolizumab in metastatic melanoma
Maintenance improves PFS in patients with metastatic colorectal cancer
Key clinical point Patients with metastatic colorectal cancer who have at least stable disease after induction chemotherapy may benefit from maintenance therapy with capecitabine and bevacizumab, though further studies on quality of life are needed. Major finding The median time to second progression (PFS2) for patients with metastatic colorectal cancer following induction and re-treatment was a median of 8.5 months for observation, compared with 11.7 months for maintenance with capecitabine and bevacizumab. Data source Randomized controlled trial of 588 patients from 64 hospitals in the Netherlands.
Click on the PDF icon at the top of this introduction to read the full article.
High rate of durable responses to pembrolizumab in metastatic melanoma
Maintenance improves PFS in patients with metastatic colorectal cancer
Key clinical point Patients with metastatic colorectal cancer who have at least stable disease after induction chemotherapy may benefit from maintenance therapy with capecitabine and bevacizumab, though further studies on quality of life are needed. Major finding The median time to second progression (PFS2) for patients with metastatic colorectal cancer following induction and re-treatment was a median of 8.5 months for observation, compared with 11.7 months for maintenance with capecitabine and bevacizumab. Data source Randomized controlled trial of 588 patients from 64 hospitals in the Netherlands.
Click on the PDF icon at the top of this introduction to read the full article.
High rate of durable responses to pembrolizumab in metastatic melanoma
Maintenance improves PFS in patients with metastatic colorectal cancer
Key clinical point Patients with metastatic colorectal cancer who have at least stable disease after induction chemotherapy may benefit from maintenance therapy with capecitabine and bevacizumab, though further studies on quality of life are needed. Major finding The median time to second progression (PFS2) for patients with metastatic colorectal cancer following induction and re-treatment was a median of 8.5 months for observation, compared with 11.7 months for maintenance with capecitabine and bevacizumab. Data source Randomized controlled trial of 588 patients from 64 hospitals in the Netherlands.
Click on the PDF icon at the top of this introduction to read the full article.
Total laparoscopic versus laparoscopic supracervical hysterectomy
It gives me great pleasure to introduce this month’s surgical video. The following feature presentation was produced by my third-year fellow, Mireille Truong, MD, and my third-year resident, Sarah Horvath, MD. The focus of this surgical video is to compare and contrast total laparoscopic hysterectomy (TLH) with laparoscopic supracervical hysterectomy (LSH). The indication for the TLH case was refractory dysmenorrhea and for the LSH case was as part of a concomitant sacrocervicopexy. The particular methods for specimen removal demonstrated include through the colpotomy for TLH and cold knife manual morcellation within a bag using an Alexis retractor for LSH.
The objectives of this surgical video are to:
- Highlight the clinical advantages and disadvantages between cervical removal or retention at the time of a minimally invasive laparoscopic hysterectomy
- Demonstrate the surgical nuances between TLH and LSH
- Provide a potential resource for patient counseling as well as medical student and resident education.
I encourage you to share this video as an educational resource with your colleagues, residents, students, and patients alike.

I hope to see you at the AAGL Global Congress on Minimally Invasive Gynecology in Vancouver, November 17–21, 2014. Visit www.aagl.org/globalcongress for more information.
— Dr. Arnold Advincula, AAGL 2014 Scientific Program Chair
Share your thoughts on this video! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
It gives me great pleasure to introduce this month’s surgical video. The following feature presentation was produced by my third-year fellow, Mireille Truong, MD, and my third-year resident, Sarah Horvath, MD. The focus of this surgical video is to compare and contrast total laparoscopic hysterectomy (TLH) with laparoscopic supracervical hysterectomy (LSH). The indication for the TLH case was refractory dysmenorrhea and for the LSH case was as part of a concomitant sacrocervicopexy. The particular methods for specimen removal demonstrated include through the colpotomy for TLH and cold knife manual morcellation within a bag using an Alexis retractor for LSH.
The objectives of this surgical video are to:
- Highlight the clinical advantages and disadvantages between cervical removal or retention at the time of a minimally invasive laparoscopic hysterectomy
- Demonstrate the surgical nuances between TLH and LSH
- Provide a potential resource for patient counseling as well as medical student and resident education.
I encourage you to share this video as an educational resource with your colleagues, residents, students, and patients alike.
I hope to see you at the AAGL Global Congress on Minimally Invasive Gynecology in Vancouver, November 17–21, 2014. Visit www.aagl.org/globalcongress for more information.
— Dr. Arnold Advincula, AAGL 2014 Scientific Program Chair
Share your thoughts on this video! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
It gives me great pleasure to introduce this month’s surgical video. The following feature presentation was produced by my third-year fellow, Mireille Truong, MD, and my third-year resident, Sarah Horvath, MD. The focus of this surgical video is to compare and contrast total laparoscopic hysterectomy (TLH) with laparoscopic supracervical hysterectomy (LSH). The indication for the TLH case was refractory dysmenorrhea and for the LSH case was as part of a concomitant sacrocervicopexy. The particular methods for specimen removal demonstrated include through the colpotomy for TLH and cold knife manual morcellation within a bag using an Alexis retractor for LSH.
The objectives of this surgical video are to:
- Highlight the clinical advantages and disadvantages between cervical removal or retention at the time of a minimally invasive laparoscopic hysterectomy
- Demonstrate the surgical nuances between TLH and LSH
- Provide a potential resource for patient counseling as well as medical student and resident education.
I encourage you to share this video as an educational resource with your colleagues, residents, students, and patients alike.
I hope to see you at the AAGL Global Congress on Minimally Invasive Gynecology in Vancouver, November 17–21, 2014. Visit www.aagl.org/globalcongress for more information.
— Dr. Arnold Advincula, AAGL 2014 Scientific Program Chair
Share your thoughts on this video! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.