User login
E-mailing patients
I’ve never lived in a world without e-mail. No, I’m not one of those millennial kids; e-mail has been around for a long time. Sending messages between computers dates to the 1960s, but most people consider 1971 to be the birth of e-mail. That’s when Ray Tomlinson added the @ symbol to separate users’ names from their e-mail addresses.
Today, e-mail is ubiquitous. You can e-mail your mother, your colleagues, or your cable company. You can even e-mail the president of the United States. Other than the pope and most physicians, there aren’t many people you cannot e-mail. (Although, interestingly, you can reach His Holiness on Twitter @Pontifex.)
We physicians have historically had a few good reasons to avoid e-mailing patients, but many of those objections are unwarranted. As part the meaningful use EHR incentive program from the Centers for Medicare & Medicaid Services, secure messaging will now be required to be eligible for rewards. Although many physicians cite security as a concern, most electronic medical record systems now have patient portals that allow for secure, safe messaging. Encroachment into private time, however, is still a concern for many physicians.
At Kaiser Permanente (KP), we’ve been using secure e-mails with our patients for more than 5 years. When we started, I had some of the same concerns as most doctors: When am I going to have time to do this? What types of questions will patients send? As it turns out, the system has been wildly popular for patients. In 2013 alone, we replied to more than 14 million patient messages. We encourage our patients to use e-mail to stay connected with us, because it leads to improved patient experiences and improved outcomes.
Managing e-mail in-boxes is difficult work, and we KP physicians constantly try to find ways to be more efficient. E-mail does sometimes encroach on my personal time, but I’ve discovered that’s okay. As it turns out, e-mail encroaches on my entrepreneurial brother’s personal time, my financial planner’s personal time, and my plumber’s personal time. Being always connected is a modern luxury and a curse. It’s also part of being a professional.
Here are some steps I’ve taken to manage my patient e-mails. First, I always remember that this electronic message is connected to a real person with real worry. Second, I remember how appreciative patients are to get a message from their doctor. E-mail a patient after 8 p.m., and they will never forget you. Third, clearly delineate time to take care of business. It never feels burdensome in part because I am in control. I choose to e-mail patients not because I have to but because I’m that doctor and it makes me feel good.
This weekend, for example, I did patient messages in a Jackson Hole, Wyo., coffee shop while on vacation. Just as I opened my computer, I noticed a young guy in a fleece jacket next to me checking his e-mail while his wife and two kids enjoyed muffins and hot cocoa. While I was waiting for my wife, Susan, to order our lattes, I overheard him make a call to his office: “Yes, I’m out, but why don’t you e-mail me that and I’ll get right back to you.”
I’m right with you, buddy, I think. I use my token and the wifi there in Wyoming to access my patient e-mails. There are only five. The messages are like most I receive: “I have a new spot,” or “The cream you gave me isn’t working,” or “My acne is better, so should I reduce the spironolactone?” I hammer replies out in 10 minutes.
My wife returns with lattes and opens the local paper while I review 14 biopsy results from 2 days ago. For most of them, I use a template and the secure e-mail to send patients their results. I then send a few notes to some patients, advising them to follow up with me for excisional surgeries.
The work I was doing was not additive; the questions my patients sent would have had to be addressed at some time. In fact, if they had called, then they would have left a message with a nurse who would have sent a message to me, which I would have had to reply to, and then send the message back to the nurse who would have to reply to the patient.
Despite our love/hate relationship with it, e-mail has been one of the great innovations of the 20th century, and it is the primary form of communication in the business world. According to one study, more than 100 billion business e-mails were sent and received every day in 2013. Yet, fewer than one-third of physicians use e-mail to communicate with their patients.Personally, I have found patients to be generally understanding, courteous, and appreciative of e-mail. Of course, there are a few who don’t follow good etiquette. (One of my primary care colleagues relates a story of a patient who e-mailed her every time she had a bowel movement. Gastroenteritis can significantly add to e-mail burden, apparently.)
There’s no doubt that e-mail will soon become the primary way to communicate with patients. Based on our experience at KP, this will ultimately be to the benefit of both doctors and patients. A June 2014 survey by Catalyst Healthcare Research showed that 93% of patients preferred to see a physician who offers e-mail communication with his or her patients. More than one-quarter of those respondents said they’d be willing to pay a $25 charge for such communication. It’s not surprising; as with all businesses, not just medicine, that patients want more channels of communication, not fewer. Fortunately for them, many of today’s medical residents are being trained to use electronic communication with patients. For instance, a 2013 study published in the Postgraduate Medical Journal found that 57% of residents used e-mail to communicate with patients.
My wife finished reading the Jackson Hole Daily newspaper and outlined our hike to Taggart Lake. And I finished answering my messages. The guy sitting next to me is still tapping away at his keyboard. I make eye contact and say, “Almost done?” “Yup,” he replies, “Better for me to just knock it out now, because I’ll just have to deal with it on Monday.” I agree.
Susan and I pack up and head for the trail, which is thankfully connection free. Let’s just hope we don’t run into any bears.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.
I’ve never lived in a world without e-mail. No, I’m not one of those millennial kids; e-mail has been around for a long time. Sending messages between computers dates to the 1960s, but most people consider 1971 to be the birth of e-mail. That’s when Ray Tomlinson added the @ symbol to separate users’ names from their e-mail addresses.
Today, e-mail is ubiquitous. You can e-mail your mother, your colleagues, or your cable company. You can even e-mail the president of the United States. Other than the pope and most physicians, there aren’t many people you cannot e-mail. (Although, interestingly, you can reach His Holiness on Twitter @Pontifex.)
We physicians have historically had a few good reasons to avoid e-mailing patients, but many of those objections are unwarranted. As part the meaningful use EHR incentive program from the Centers for Medicare & Medicaid Services, secure messaging will now be required to be eligible for rewards. Although many physicians cite security as a concern, most electronic medical record systems now have patient portals that allow for secure, safe messaging. Encroachment into private time, however, is still a concern for many physicians.
At Kaiser Permanente (KP), we’ve been using secure e-mails with our patients for more than 5 years. When we started, I had some of the same concerns as most doctors: When am I going to have time to do this? What types of questions will patients send? As it turns out, the system has been wildly popular for patients. In 2013 alone, we replied to more than 14 million patient messages. We encourage our patients to use e-mail to stay connected with us, because it leads to improved patient experiences and improved outcomes.
Managing e-mail in-boxes is difficult work, and we KP physicians constantly try to find ways to be more efficient. E-mail does sometimes encroach on my personal time, but I’ve discovered that’s okay. As it turns out, e-mail encroaches on my entrepreneurial brother’s personal time, my financial planner’s personal time, and my plumber’s personal time. Being always connected is a modern luxury and a curse. It’s also part of being a professional.
Here are some steps I’ve taken to manage my patient e-mails. First, I always remember that this electronic message is connected to a real person with real worry. Second, I remember how appreciative patients are to get a message from their doctor. E-mail a patient after 8 p.m., and they will never forget you. Third, clearly delineate time to take care of business. It never feels burdensome in part because I am in control. I choose to e-mail patients not because I have to but because I’m that doctor and it makes me feel good.
This weekend, for example, I did patient messages in a Jackson Hole, Wyo., coffee shop while on vacation. Just as I opened my computer, I noticed a young guy in a fleece jacket next to me checking his e-mail while his wife and two kids enjoyed muffins and hot cocoa. While I was waiting for my wife, Susan, to order our lattes, I overheard him make a call to his office: “Yes, I’m out, but why don’t you e-mail me that and I’ll get right back to you.”
I’m right with you, buddy, I think. I use my token and the wifi there in Wyoming to access my patient e-mails. There are only five. The messages are like most I receive: “I have a new spot,” or “The cream you gave me isn’t working,” or “My acne is better, so should I reduce the spironolactone?” I hammer replies out in 10 minutes.
My wife returns with lattes and opens the local paper while I review 14 biopsy results from 2 days ago. For most of them, I use a template and the secure e-mail to send patients their results. I then send a few notes to some patients, advising them to follow up with me for excisional surgeries.
The work I was doing was not additive; the questions my patients sent would have had to be addressed at some time. In fact, if they had called, then they would have left a message with a nurse who would have sent a message to me, which I would have had to reply to, and then send the message back to the nurse who would have to reply to the patient.
Despite our love/hate relationship with it, e-mail has been one of the great innovations of the 20th century, and it is the primary form of communication in the business world. According to one study, more than 100 billion business e-mails were sent and received every day in 2013. Yet, fewer than one-third of physicians use e-mail to communicate with their patients.Personally, I have found patients to be generally understanding, courteous, and appreciative of e-mail. Of course, there are a few who don’t follow good etiquette. (One of my primary care colleagues relates a story of a patient who e-mailed her every time she had a bowel movement. Gastroenteritis can significantly add to e-mail burden, apparently.)
There’s no doubt that e-mail will soon become the primary way to communicate with patients. Based on our experience at KP, this will ultimately be to the benefit of both doctors and patients. A June 2014 survey by Catalyst Healthcare Research showed that 93% of patients preferred to see a physician who offers e-mail communication with his or her patients. More than one-quarter of those respondents said they’d be willing to pay a $25 charge for such communication. It’s not surprising; as with all businesses, not just medicine, that patients want more channels of communication, not fewer. Fortunately for them, many of today’s medical residents are being trained to use electronic communication with patients. For instance, a 2013 study published in the Postgraduate Medical Journal found that 57% of residents used e-mail to communicate with patients.
My wife finished reading the Jackson Hole Daily newspaper and outlined our hike to Taggart Lake. And I finished answering my messages. The guy sitting next to me is still tapping away at his keyboard. I make eye contact and say, “Almost done?” “Yup,” he replies, “Better for me to just knock it out now, because I’ll just have to deal with it on Monday.” I agree.
Susan and I pack up and head for the trail, which is thankfully connection free. Let’s just hope we don’t run into any bears.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.
I’ve never lived in a world without e-mail. No, I’m not one of those millennial kids; e-mail has been around for a long time. Sending messages between computers dates to the 1960s, but most people consider 1971 to be the birth of e-mail. That’s when Ray Tomlinson added the @ symbol to separate users’ names from their e-mail addresses.
Today, e-mail is ubiquitous. You can e-mail your mother, your colleagues, or your cable company. You can even e-mail the president of the United States. Other than the pope and most physicians, there aren’t many people you cannot e-mail. (Although, interestingly, you can reach His Holiness on Twitter @Pontifex.)
We physicians have historically had a few good reasons to avoid e-mailing patients, but many of those objections are unwarranted. As part the meaningful use EHR incentive program from the Centers for Medicare & Medicaid Services, secure messaging will now be required to be eligible for rewards. Although many physicians cite security as a concern, most electronic medical record systems now have patient portals that allow for secure, safe messaging. Encroachment into private time, however, is still a concern for many physicians.
At Kaiser Permanente (KP), we’ve been using secure e-mails with our patients for more than 5 years. When we started, I had some of the same concerns as most doctors: When am I going to have time to do this? What types of questions will patients send? As it turns out, the system has been wildly popular for patients. In 2013 alone, we replied to more than 14 million patient messages. We encourage our patients to use e-mail to stay connected with us, because it leads to improved patient experiences and improved outcomes.
Managing e-mail in-boxes is difficult work, and we KP physicians constantly try to find ways to be more efficient. E-mail does sometimes encroach on my personal time, but I’ve discovered that’s okay. As it turns out, e-mail encroaches on my entrepreneurial brother’s personal time, my financial planner’s personal time, and my plumber’s personal time. Being always connected is a modern luxury and a curse. It’s also part of being a professional.
Here are some steps I’ve taken to manage my patient e-mails. First, I always remember that this electronic message is connected to a real person with real worry. Second, I remember how appreciative patients are to get a message from their doctor. E-mail a patient after 8 p.m., and they will never forget you. Third, clearly delineate time to take care of business. It never feels burdensome in part because I am in control. I choose to e-mail patients not because I have to but because I’m that doctor and it makes me feel good.
This weekend, for example, I did patient messages in a Jackson Hole, Wyo., coffee shop while on vacation. Just as I opened my computer, I noticed a young guy in a fleece jacket next to me checking his e-mail while his wife and two kids enjoyed muffins and hot cocoa. While I was waiting for my wife, Susan, to order our lattes, I overheard him make a call to his office: “Yes, I’m out, but why don’t you e-mail me that and I’ll get right back to you.”
I’m right with you, buddy, I think. I use my token and the wifi there in Wyoming to access my patient e-mails. There are only five. The messages are like most I receive: “I have a new spot,” or “The cream you gave me isn’t working,” or “My acne is better, so should I reduce the spironolactone?” I hammer replies out in 10 minutes.
My wife returns with lattes and opens the local paper while I review 14 biopsy results from 2 days ago. For most of them, I use a template and the secure e-mail to send patients their results. I then send a few notes to some patients, advising them to follow up with me for excisional surgeries.
The work I was doing was not additive; the questions my patients sent would have had to be addressed at some time. In fact, if they had called, then they would have left a message with a nurse who would have sent a message to me, which I would have had to reply to, and then send the message back to the nurse who would have to reply to the patient.
Despite our love/hate relationship with it, e-mail has been one of the great innovations of the 20th century, and it is the primary form of communication in the business world. According to one study, more than 100 billion business e-mails were sent and received every day in 2013. Yet, fewer than one-third of physicians use e-mail to communicate with their patients.Personally, I have found patients to be generally understanding, courteous, and appreciative of e-mail. Of course, there are a few who don’t follow good etiquette. (One of my primary care colleagues relates a story of a patient who e-mailed her every time she had a bowel movement. Gastroenteritis can significantly add to e-mail burden, apparently.)
There’s no doubt that e-mail will soon become the primary way to communicate with patients. Based on our experience at KP, this will ultimately be to the benefit of both doctors and patients. A June 2014 survey by Catalyst Healthcare Research showed that 93% of patients preferred to see a physician who offers e-mail communication with his or her patients. More than one-quarter of those respondents said they’d be willing to pay a $25 charge for such communication. It’s not surprising; as with all businesses, not just medicine, that patients want more channels of communication, not fewer. Fortunately for them, many of today’s medical residents are being trained to use electronic communication with patients. For instance, a 2013 study published in the Postgraduate Medical Journal found that 57% of residents used e-mail to communicate with patients.
My wife finished reading the Jackson Hole Daily newspaper and outlined our hike to Taggart Lake. And I finished answering my messages. The guy sitting next to me is still tapping away at his keyboard. I make eye contact and say, “Almost done?” “Yup,” he replies, “Better for me to just knock it out now, because I’ll just have to deal with it on Monday.” I agree.
Susan and I pack up and head for the trail, which is thankfully connection free. Let’s just hope we don’t run into any bears.
Dr. Benabio is a partner physician in the department of dermatology of the Southern California Permanente Group in San Diego, and volunteer clinical assistant professor at the University of California, San Diego. Dr. Benabio is @dermdoc on Twitter.

Sedative-hypnotics for sleepless geriatric patients
Mr. R, 75, is having difficulty sleeping. When he goes to bed, he lies there for what seems like forever, unable to fall asleep. He feels “so tired” and ends up taking naps during the day, but he cannot break this cycle. He has tried using over-the-counter products with little relief.
Mr. R’s primary care physician prescribes zaleplon, 10 mg/d, and asks him to call the clinic in 2 weeks to discuss his progress. He takes zaleplon as directed for several nights and begins to feel “sluggish” during the day, both mentally and physically, despite reporting an increase in the overall amount of sleep at night.
Sedative-hypnotic drugs are among the most commonly used medications in the United States. Use of these drugs, as well as anxiolytics, has increased from 2.8% between 1988 and 1994 to 4.7% between 2007 and 2010, according to the Department of Health and Human Services.1 In 2011, drugs categorized as sedative-hypnotics or antipsychotics were involved in 6.1% of all human exposures identified in the American Association of Poison Control Centers’ National Poison Data System.2 Therefore, an understanding of clinical and pharmacological variables related to safe and effective use is important for clinicians prescribing and monitoring therapy with these agents.
Neuropsychiatric disorders are prevalent among geriatric patients and are associated with age-related physiologic changes in the CNS.3 Such changes involve:
• neuroanatomy (brain atrophy, decreased neuronal density, increased plaque formation)
• neurotransmitters (reduced cholinergic transmission, decreased synthesis of dopamine and catecholamines), and
• neurophysiology (reduced cerebral blood flow).
These physiologic processes manifest as alterations in mental status, reflexes, sensation, gait, balance, and sleep. Examples of sleep changes among geriatric patients include decreased sleep efficiency, more frequent awakenings, and more variable sleep duration.3,4 Sleep disorders also may be related to mental disorders and other medical conditions.5 For example, the prevalence of sleep-related respiratory disorders, such as obstructive sleep apnea and central sleep apnea, increases with age.6
Sleep disorders are common among geriatric patients. In a large epidemiologic study of sleep complaints in patients age ≥65, more than one-half of patients had at least 1 sleep complaint (ie, difficulty falling asleep, trouble waking up, early awakening, need for naps, and feeling ill-rested).7 As many as 34% of patients reported symptoms of insomnia. In an analysis of National Ambulatory Medical Survey Data over 6 years, 24.8% to 27.9% of sleep-related medical office visits were attributed to patients age ≥65.8
Pharmacology in aging
Prescribing sedative-hypnotic drugs is not routinely recommended for older patients with a sleep disorder. Geriatric patients, compared with younger patients, are at higher risk of iatrogenic complications because of polypharmacy, comorbidities, relative renal and hepatic insufficiency, and other physiologic changes leading to alterations in drug exposure and metabolism (Table 1).9-12
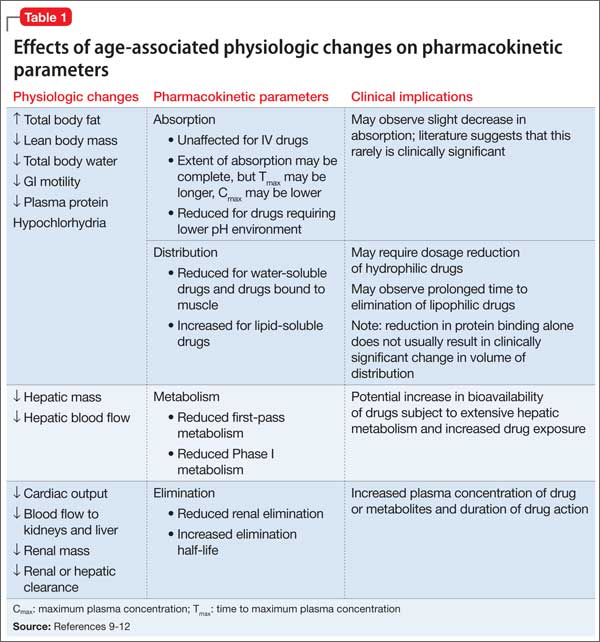
Aging is associated with changes in body composition, including an increase in total body fat and decrease in lean body mass and total body water. These changes, as well as a prolonged GI transit time, decrease in active gut transporters, decreased blood perfusion, and decrease in plasma proteins such as albumin (because of reduced liver function or malnutrition), may lead to alteration in drug absorption patterns and may increase the volume of distribution for lipophilic drugs. Additionally, the elimination half-life of some drugs may increase with age because of larger volumes of distribution and reduction in hepatic or renal clearance.
The clinical significance of these changes is not well established. Although the process of drug absorption can change with age, the amount of drug absorbed might not be significantly affected. An increase in the volume of distribution and reduction in drug metabolism and clearance might lead to increasing amounts of circulating drug and duration of drug exposure, putting geriatric patients at an increased risk for adverse effects and drug toxicity.9
Among these mechanisms, Dolder et al11 hypothesized that drug metabolism catalyzed by cytochrome P450 (CYP) enzymes and renal excretion may be of greatest concern. Although in vitro studies suggest that concentration of CYP enzymes does not decline with age, in vivo studies have demonstrated reduced CYP activity in geriatric patients.11,12 Theoretically, a reduction in CYP activity would increase the bioavailability of drugs, especially those that are subject to extensive first-pass (ie, hepatic) metabolism, and may lead to a reduction in systemic clearance.
Independent of metabolic changes, geriatric patients are at risk of reduced renal clearance because of age-related changes in glomerular filtration rate. Pharmacodynamic changes might be observed in older patients and could be a concern even in the setting of unaltered pharmacokinetic factors.9 These changes usually require administering smaller drug dosages.
Sedative-hypnotic medications
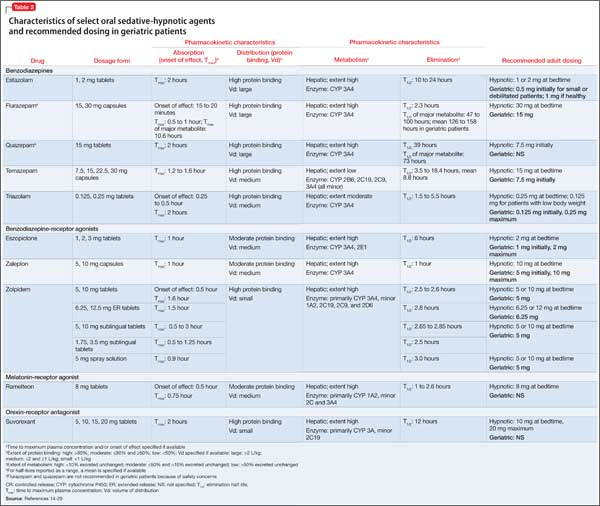
Sedative-hypnotic agents include several barbiturates, benzodiazepines (BZDs), non-BZD benzodiazepine-receptor agonists (BzRAs), a melatonin-receptor agonist (ie, ramelteon), and an orexin-receptor antagonist (ie, suvorexant).13,14Table 214-29 summarizes selected sedative-hypnotic drugs. Additional drug classes used to treat insomnia include:
• sedating antidepressants (trazodone, amitriptyline, doxepin, mirtazapine)
• antiepileptic drugs (gabapentin, tiagabine)
• atypical antipsychotics (quetiapine, olanzapine).
FDA-approved agents for treating insomnia include amobarbital, butabarbital, pentobarbital, phenobarbital, secobarbital, chloral hydrate, diphenhydramine, doxylamine, doxepin, estazolam, flurazepam, lorazepam, quazepam, temazepam, triazolam, eszopiclone, zaleplon, zolpidem, ramelteon, and suvorexant. Not all of these drugs are recommended for use in geriatric patients. Barbiturates, for example, should be avoided.30
Pharmacokinetic characteristics vary among drugs and drug classes. Choice of pharmacotherapy should account for patient and drug characteristics and the specific sleep complaint. Sleep disorders may be variously characterized as difficulty with sleep initiation, duration, consolidation, or quality.13 Therefore, onset and duration of effect are important drug-related considerations. Sedative-hypnotic drugs with a short time-to-onset may be ideal for patients with sleep-onset insomnia.
The drugs’ duration of effect (eg, presence of active metabolites, long elimination half-life) also must be reviewed. A long elimination half-life may lead to increased drug exposure and unwanted side effects such as residual daytime drowsiness. Despite this, sedative-hypnotic drugs with a longer duration of effect (eg, intermediate- or long-acting drugs) may be best for patients with insomnia defined by difficulty maintaining sleep.
Benzodiazepines vary in their time to onset of effect, rate of elimination, and metabolism.15-21 BZDs that are FDA- approved for use as sedative-hypnotics are listed in Table 2.14-29 These BZDs have different onsets of effect as evidenced by time to achieve maximum plasma concentration (Tmax), ranging from 0.5 hours (flurazepam) to 2 hours (estazolam, quazepam, triazolam). The elimination half-life varies widely among these medications, from 1.5 hours (triazolam) to >100 hours (flurazepam). Flurazepam’s long half-life is attributable to its active major metabolite. Although most BZDs are metabolized hepatically, temazepam is subject to minimal hepatic metabolism.
Benzodiazepine-receptor agonists. There is substantial variation in the pharmacokinetic characteristics of BzRAs.15,16,22-28 There also are differences among the zolpidem dosage forms; sublingual formulations have the shortest onset of effect. Eszopiclone and zaleplon have low protein binding compared with zolpidem. Elimination half-lives vary among drugs with the shortest attributed to zaleplon (1 hour) and longest to eszopiclone (6 hours). All BzRAs are subject to extensive hepatic metabolism.
Ramelteon. Singular in its class, ramelteon is a treatment option for insomnia.29 This drug has a short onset of effect, moderate protein binding, and extensive hepatic metabolism. Ramelteon is primarily excreted in the urine as its metabolites, and the drug half-life is relatively short.
Suvorexant is the latest addition to the sedative-hypnotic armamentarium, approved by the FDA in August 2014 for difficulty with sleep onset and/or sleep maintenance.14 As an orexin-receptor antagonist, suvorexant represents a novel pharmacologic class. Suvorexant exhibits moderately rapid absorption with time to peak concentration ranging from 30 minutes to 6 hours in fasting conditions; absorption is delayed when taken with or soon after a meal. The drug is highly protein bound and extensively metabolized, primarily through CYP3A. The manufacturer recommends dose reduction (5 mg at bedtime) in patients taking moderate CYP3A inhibitors and avoiding suvorexant in patients taking strong CYP3A inhibitors. Suvorexant is primarily excreted through feces and the mean half-life is relatively long.
Considering these characteristics and age-related physiologic changes, the practitioner should be concerned about drugs that undergo extensive hepatic metabolism. Age-related reductions in CYP activity may lead to an increase in drug bioavailability and a decrease in the systemic clearance,11 which might be associated with an increase in elimination half-life and duration of action. Dosage adjustments are recommended for several BZDs (lower initial and maximum dosages for most agents) and BzRAs.17-28 No dosage adjustments for ramelteon or suvorexant in geriatric patients have been specified14,29; the manufacturers for both products assert that no differences in safety and efficacy have been observed between older and younger adult patients.
Alternative and complementary medications
Several non-prescription products, including over-the-counter drugs (eg, diphenhy-dramine, doxylamine) and herbal therapies (eg, melatonin, valerian), are used for their sedative-hypnotic properties. There is a lack of evidence supporting using diphenhydra-mine in patients with chronic insomnia, and tolerance to its hypnotic effect has been reported with repeated use.31 Concerns about anticholinergic toxicity and CNS depression limit its use in geriatric patients. Among herbal therapies, melatonin may have the strongest evidence for its ability to alleviate sleep disorders in geriatric patients32; however, meta-analyses have demonstrated small effects of melatonin on sleep latency and minimal differences in wake time after sleep onset and total sleep time.13
Clinical practice guidelines
Non-pharmacotherapeutic interventions, such as behavioral (eg, sleep hygiene measures) and psychological therapy, are recommended for initial management of sleep disorders in geriatric patients.13,33 In conjunction, the American Medical Directors Association (AMDA) recommends address ing underlying causes and exacerbating factors (eg, medical condition or medication).33 The AMDA recommends avoiding long-term pharmacotherapy and advises caution with BZD-hypnotic drugs, tricyclic antidepressants, and antihistamines. The American Academy of Sleep Medicine (AASM) recommends an initial treatment period of 2 to 4 weeks, followed by re-evaluation of continued need for treatment.13 The AASM recommends short- or intermediate-acting BzRAs or ramelteon for initial pharmacologic management of primary insomnias and insomnias comorbid with other conditions. The AASM also recommends specific dosages of BzRAs and BZDs for geriatric patients, which coincide with manufacturer-recommended dosages (Table 2).14-29
Barbiturates, chloral hydrate, and non-barbiturate, non-BZD drugs such as meprobamate are not recommended because of potential significant adverse effects and tolerance/dependence, and low therapeutic index. The AASM advises caution when using prescription drugs off-label for insomnia (eg, antidepressants, antiepileptics, antipsychotics) and recommends avoiding them, if possible, because of limited evidence supporting their use.13
Safety concerns
Two commonly used references contain recommendations for sedative-hypnotic medication use in geriatric patients.30,34 According to Gallagher et al’s34 Screening Tool of Older Person’s Prescriptions (STOPP), long-term (>1 month) use of long-acting BZDs (eg, flurazepam, diazepam) and prolonged use (>1 week) of first-generation antihistamines (eg, diphenhydramine, doxylamine) should be avoided in patients age ≥65 because of the risk of sedation, confusion, and anticholinergic side effects. STOPP recognizes that any use of BZDs, neuroleptics, or first-generation antihistamines may contribute to postural imbalance; therefore these agents are not recommended in older patients at risk for falls.
In the 2012 American Geriatrics Society (AGS) Beers Criteria, the AGS recommends avoiding barbiturates in older adults because of the high rate of physical dependence, tolerance to sleep effects, and overdose risk at low dosages.30 The AGS also recommends avoiding BZDs, stating that older adults have increased sensitivity to these agents and are at an increased risk of cognitive impairment, delirium, falls, fractures, and motor vehicle accidents when taking these drugs. Non-BZD BzRAs also should not be prescribed to patients with a history of falls or fractures, unless safer alternatives are not available.
The FDA has issued several advisory reports regarding sedative-hypnotic drugs. In 2007, all manufacturers of sedative-hypnotic drugs were required to modify their product labeling to include stronger language about potential risks.35 Among these changes, warnings for anaphylaxis and complex sleep-related behaviors were added. Also, the FDA requested that manufacturers of sedative-hypnotic drugs develop and provide patient medication guides, advising consumers on the potential risks and precautions associated with these drugs. More recently, the FDA announced changes to dosing recommendations for zolpidem-containing products because of the risk of impaired mental alertness36; manufacturers were required to lower the recommended dosages for each product.
Manufacturers of FDA-approved sedative-hypnotic drugs urge caution when prescribing these medications for geriatric patients, citing the potential for increased sensitivity, manifesting as marked excitement, depression, or confusion (eg, barbiturates), and greater risk for dosage-related adverse effects (eg, oversedation, dizziness, confusion, impaired psychomotor performance, ataxia).17-29
Use in clinical practice
Several variables should be considered when evaluating appropriateness of pharmacotherapy, including characteristics of the drug and the patient. Geriatric patients may be prone to comorbidities resulting from age-related physiologic changes. These diseases may be confounding (ie, contributing to sleep disorders); examples include medical illnesses, such as hyperthyroidism and arthritis, and psychiatric illnesses, such as depression and anxiety.37 Other conditions, such as renal and hepatic dysfunction, may lead to alteration in drug exposure. These conditions should be assessed through routine renal function tests (eg, serum creatinine and glomerular filtration rate) and liver function tests (eg, serum albumin and liver transaminases).
Multiple comorbidities suggest a higher likelihood of polypharmacy, leading to other drug-related issues (eg, drug-drug interactions). Although these issues may guide therapy by restricting medication options, their potential contribution to the underlying sleep complaints should be considered.37 Several drugs commonly used by geriatric patients may affect wakefulness (eg, analgesics, antidepressants, and antihypertensives [sedating], and thyroid hormones, corticosteroids, and CNS stimulants [alerting]).
CASE CONTINUED
In Mr. R’s case, zaleplon was initiated at 10 mg/d. Because of his age and the nature of his sleep disorder, the choice of sedative-hypnotic was suitable; however, the prescribed dosage was inappropriate. The sluggishness Mr. R experienced likely was a manifestation of increased exposure to the drug. According to manufacturer and AASM recommendations, a more appropriate dosage is 5 mg/d.13,23 Mr. R’s medical history and current medications, and his hepatic and renal function, should be assessed. If Mr. R continues to have issues with sleep initiation, zaleplon, 5 mg at bedtime, should be considered.
Related Resources
• Institute for Safe Medication Practices. www.ismp.org.
• MedWatch: The FDA Safety Information and Adverse Event Reporting Program. www.fda.gov/Safety/MedWatch/default.htm.
Drug Brand Names
Amitriptyline • Elavil Mirtazapine • Remeron
Amobarbital • Amytal Olanzapine • Zyprexa
Butabarbital • Butisol Pentobarbital • Nembutal
Chloral hydrate • Somnote Phenobarbital • Luminal
Diazepam • Valium Quazepam • Doral
Diphenhydramine • Benadryl, others Quetiapine • Seroquel
Doxepin • Silenor Ramelteon • Rozerem
Doxylamine • Unisom, others Secobarbital • Seconal
Estazolam • ProSom Suvorexant • Belsomra
Eszopiclone • Lunesta Temazepam • Restoril
Flurazepam • Dalmane Tiagabine • Gabitril
Gabapentin • Neurontin, Trazodone • Desyrel
Gralise, Horizant Zaleplon • Sonata
Lorazepam • Ativan Zolpidem • Ambien, Edluar,
Meprobamate • Equanil Intermezzo, Zolpimist
Acknowledgement
Vicki L. Ellingrod, PharmD, FCCP, is the series editor of Savvy Psychopharmacology.
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. National Center for Health Statistics. Health, United States, 2012, with special feature on emergency care. http://www. cdc.gov/nchs/data/hus/hus12.pdf. Published May 2013. Accessed August 22, 2014.
2. Bronstein AC, Spyker DA, Cantilena LR Jr, et al. 2011 Annual report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 29th annual report. Clin Toxicol (Phila). 2012;50(10): 911-1164.
3. Inouye SK. Neuropsychiatric aspects of aging. In: Goldman L, Schafer AI, eds. Goldman’s cecil medicine. 24th ed. Philadelphia, PA: Elsevier Saunders; 2011:114-116.
4. Diagnostic and statistical manual of mental disorders, 4th ed. Washington, DC: American Psychiatric Association; 1994.
5. American Psychiatric Association. Highlights of changes from DSM-IV-TR to DSM-5. http://www.psychiatry. org/File%20Library/Practice/DSM/DSM-5/Changes-from-DSM-IV-TR--to-DSM-5.pdf. 2013. Accessed August 22, 2014.
6. Edwards BA, O’Driscoll DM, Ali A, et al. Aging and sleep: physiology and pathophysiology. Semin Respir Crit Care Med. 2010;31(5):618-633.
7. Foley DJ, Monjan AA, Brown SL, et al. Sleep complaints among elderly persons: an epidemiologic study of three communities. Sleep. 1995;18(6):425-432.
8. Morlock RJ, Tan M, Mitchell DY. Patient characteristics and patterns of drug use for sleep complaints in the United States: analysis of National Ambulatory Medical Survey Data, 1997-2002. Clin Ther. 2006;28(7):1044-1053.
9. Diasio RB. Principles of drug therapy. In: Goldman L, Schafer AI, eds. Goldman’s Cecil medicine. 24th ed. Philadelphia, PA: Elsevier Saunders; 2011:124-132.
10. Hilmer SN, Ford GA. General principles of pharmacology. In: Halter JB, Ouslander JG, Tinetti ME, et al, eds. Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill; 2009:103-122.
11. Dolder C, Nelson M, McKinsey J. Use of non-benzodiazepine hypnotics in the elderly: are all agents the same? CNS Drugs. 2007;21(5):389-405.
12. Klotz U. Pharmacokinetics and drug metabolism in the elderly. Drug Metab Rev. 2009;41(2):67-76.
13. Schutte-Rodin S, Broch L, Buysse D, et al. Clinical guideline for the evaluation and management of chronic insomnia in adults. J Clin Sleep Med. 2008;4(5):487-504.
14. Belsomra [package insert]. Whitehouse Station, NJ: Merck & Co., Inc.; 2014.
15. Micromedex Healthcare Series. Greenwood Village, CO: Thomson Healthcare. http://micromedex.com. Accessed August 22, 2014.
16. Lexicomp. St. Louis, MO: Wolters Kluwer Health. http:// www.lexi.com. Accessed August 22, 2014.
17. Estazolam [package insert]. Corona, CA: Watson Pharma, Inc; 2008.
18. Flurazepam [package insert]. Eatontown, NJ: West-Ward Pharmaceutical Corp; 2010.
19. Doral [package insert]. Las Vegas, NV: Nuro Pharma, Inc; 2013.
20. Restoril [package insert]. Hazelwood, MO: Mallinckrodt Inc; 2010.
21. Halcion [package insert]. New York, NY: Pharmacia & Upjohn Co; 2013.
22. Lunesta [package insert]. Marlborough, MA: Sunovion Pharmaceuticals Inc; 2012.
23. Sonata [package insert]. New York, NY: Pfizer Inc; 2013.
24. Ambien [package insert]. Bridgewater, NJ: Sanofi-Aventis; 2013.
25. Ambien CR [package insert]. Bridgewater, NJ: Sanofi- Aventis; 2013.
26. Edluar [package insert]. Somerset, NJ: Meda Pharmaceuticals Inc; 2009.
27. Intermezzo [package insert]. Point Richmond, CA: Transcept Pharmaceuticals, Inc; 2011.
28. Zolpimist [package insert]. Richmond, VA: ECR Pharmaceuticals; 2013.
29. Rozerem [package insert]. Deerfield, IL: Takeda Pharmaceuticals America, Inc; 2010.
30. The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60(4):616-631.
31. Kirkwood CK, Melton ST. Insomnia, drowsiness, and fatigue. In: Krinsky DL, Berardi RR, Ferreri SP, et al, eds. Handbook of nonprescription drugs: an interactive approach to self-care. 17th ed. Washington, DC: American Pharmacists Association; 2012:867-884.
32. Insomnia. In: Natural Standard. Somerville, MA: Natural Standard. https://naturalmedicines.therapeuticresearch. com/databases/medical-conditions/i/insomnia.aspx. Accessed August 22, 2014.
33. American Medical Directors Association. Clinical practice guideline: sleep disorders. Columbia, MD: American Medical Directors Association; 2006.
34. Gallagher P, Ryan C, Byrne S, et al. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther. 2008;46(2):72-83.
35. Food and Drug Administration. FDA requests label change for all sleep disorder drug products. http://www.fda. gov/newsevents/newsroom/pressannouncements/2007/ ucm108868.htm. Published March 14, 2007. Accessed August 22, 2014.
36. Food and Drug Administration. FDA drug safety communication: risk of next-morning impairment after use of insomnia drugs; FDA requires lower recommended doses for certain drugs containing zolpidem (Ambien, Ambien CR, Edluar, and Zolpimist). http://www.fda.gov/drugs/ drugsafety/ucm334033.htm. Published January 10, 2013. Accessed August 22, 2014.
37. Cohen-Zion M, Ancoli-Israel S. Sleep disorders. In: Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill; 2009:671-682.
Mr. R, 75, is having difficulty sleeping. When he goes to bed, he lies there for what seems like forever, unable to fall asleep. He feels “so tired” and ends up taking naps during the day, but he cannot break this cycle. He has tried using over-the-counter products with little relief.
Mr. R’s primary care physician prescribes zaleplon, 10 mg/d, and asks him to call the clinic in 2 weeks to discuss his progress. He takes zaleplon as directed for several nights and begins to feel “sluggish” during the day, both mentally and physically, despite reporting an increase in the overall amount of sleep at night.
Sedative-hypnotic drugs are among the most commonly used medications in the United States. Use of these drugs, as well as anxiolytics, has increased from 2.8% between 1988 and 1994 to 4.7% between 2007 and 2010, according to the Department of Health and Human Services.1 In 2011, drugs categorized as sedative-hypnotics or antipsychotics were involved in 6.1% of all human exposures identified in the American Association of Poison Control Centers’ National Poison Data System.2 Therefore, an understanding of clinical and pharmacological variables related to safe and effective use is important for clinicians prescribing and monitoring therapy with these agents.
Neuropsychiatric disorders are prevalent among geriatric patients and are associated with age-related physiologic changes in the CNS.3 Such changes involve:
• neuroanatomy (brain atrophy, decreased neuronal density, increased plaque formation)
• neurotransmitters (reduced cholinergic transmission, decreased synthesis of dopamine and catecholamines), and
• neurophysiology (reduced cerebral blood flow).
These physiologic processes manifest as alterations in mental status, reflexes, sensation, gait, balance, and sleep. Examples of sleep changes among geriatric patients include decreased sleep efficiency, more frequent awakenings, and more variable sleep duration.3,4 Sleep disorders also may be related to mental disorders and other medical conditions.5 For example, the prevalence of sleep-related respiratory disorders, such as obstructive sleep apnea and central sleep apnea, increases with age.6
Sleep disorders are common among geriatric patients. In a large epidemiologic study of sleep complaints in patients age ≥65, more than one-half of patients had at least 1 sleep complaint (ie, difficulty falling asleep, trouble waking up, early awakening, need for naps, and feeling ill-rested).7 As many as 34% of patients reported symptoms of insomnia. In an analysis of National Ambulatory Medical Survey Data over 6 years, 24.8% to 27.9% of sleep-related medical office visits were attributed to patients age ≥65.8
Pharmacology in aging
Prescribing sedative-hypnotic drugs is not routinely recommended for older patients with a sleep disorder. Geriatric patients, compared with younger patients, are at higher risk of iatrogenic complications because of polypharmacy, comorbidities, relative renal and hepatic insufficiency, and other physiologic changes leading to alterations in drug exposure and metabolism (Table 1).9-12
Aging is associated with changes in body composition, including an increase in total body fat and decrease in lean body mass and total body water. These changes, as well as a prolonged GI transit time, decrease in active gut transporters, decreased blood perfusion, and decrease in plasma proteins such as albumin (because of reduced liver function or malnutrition), may lead to alteration in drug absorption patterns and may increase the volume of distribution for lipophilic drugs. Additionally, the elimination half-life of some drugs may increase with age because of larger volumes of distribution and reduction in hepatic or renal clearance.
The clinical significance of these changes is not well established. Although the process of drug absorption can change with age, the amount of drug absorbed might not be significantly affected. An increase in the volume of distribution and reduction in drug metabolism and clearance might lead to increasing amounts of circulating drug and duration of drug exposure, putting geriatric patients at an increased risk for adverse effects and drug toxicity.9
Among these mechanisms, Dolder et al11 hypothesized that drug metabolism catalyzed by cytochrome P450 (CYP) enzymes and renal excretion may be of greatest concern. Although in vitro studies suggest that concentration of CYP enzymes does not decline with age, in vivo studies have demonstrated reduced CYP activity in geriatric patients.11,12 Theoretically, a reduction in CYP activity would increase the bioavailability of drugs, especially those that are subject to extensive first-pass (ie, hepatic) metabolism, and may lead to a reduction in systemic clearance.
Independent of metabolic changes, geriatric patients are at risk of reduced renal clearance because of age-related changes in glomerular filtration rate. Pharmacodynamic changes might be observed in older patients and could be a concern even in the setting of unaltered pharmacokinetic factors.9 These changes usually require administering smaller drug dosages.
Sedative-hypnotic medications
Sedative-hypnotic agents include several barbiturates, benzodiazepines (BZDs), non-BZD benzodiazepine-receptor agonists (BzRAs), a melatonin-receptor agonist (ie, ramelteon), and an orexin-receptor antagonist (ie, suvorexant).13,14Table 214-29 summarizes selected sedative-hypnotic drugs. Additional drug classes used to treat insomnia include:
• sedating antidepressants (trazodone, amitriptyline, doxepin, mirtazapine)
• antiepileptic drugs (gabapentin, tiagabine)
• atypical antipsychotics (quetiapine, olanzapine).
FDA-approved agents for treating insomnia include amobarbital, butabarbital, pentobarbital, phenobarbital, secobarbital, chloral hydrate, diphenhydramine, doxylamine, doxepin, estazolam, flurazepam, lorazepam, quazepam, temazepam, triazolam, eszopiclone, zaleplon, zolpidem, ramelteon, and suvorexant. Not all of these drugs are recommended for use in geriatric patients. Barbiturates, for example, should be avoided.30
Pharmacokinetic characteristics vary among drugs and drug classes. Choice of pharmacotherapy should account for patient and drug characteristics and the specific sleep complaint. Sleep disorders may be variously characterized as difficulty with sleep initiation, duration, consolidation, or quality.13 Therefore, onset and duration of effect are important drug-related considerations. Sedative-hypnotic drugs with a short time-to-onset may be ideal for patients with sleep-onset insomnia.
The drugs’ duration of effect (eg, presence of active metabolites, long elimination half-life) also must be reviewed. A long elimination half-life may lead to increased drug exposure and unwanted side effects such as residual daytime drowsiness. Despite this, sedative-hypnotic drugs with a longer duration of effect (eg, intermediate- or long-acting drugs) may be best for patients with insomnia defined by difficulty maintaining sleep.
Benzodiazepines vary in their time to onset of effect, rate of elimination, and metabolism.15-21 BZDs that are FDA- approved for use as sedative-hypnotics are listed in Table 2.14-29 These BZDs have different onsets of effect as evidenced by time to achieve maximum plasma concentration (Tmax), ranging from 0.5 hours (flurazepam) to 2 hours (estazolam, quazepam, triazolam). The elimination half-life varies widely among these medications, from 1.5 hours (triazolam) to >100 hours (flurazepam). Flurazepam’s long half-life is attributable to its active major metabolite. Although most BZDs are metabolized hepatically, temazepam is subject to minimal hepatic metabolism.
Benzodiazepine-receptor agonists. There is substantial variation in the pharmacokinetic characteristics of BzRAs.15,16,22-28 There also are differences among the zolpidem dosage forms; sublingual formulations have the shortest onset of effect. Eszopiclone and zaleplon have low protein binding compared with zolpidem. Elimination half-lives vary among drugs with the shortest attributed to zaleplon (1 hour) and longest to eszopiclone (6 hours). All BzRAs are subject to extensive hepatic metabolism.
Ramelteon. Singular in its class, ramelteon is a treatment option for insomnia.29 This drug has a short onset of effect, moderate protein binding, and extensive hepatic metabolism. Ramelteon is primarily excreted in the urine as its metabolites, and the drug half-life is relatively short.
Suvorexant is the latest addition to the sedative-hypnotic armamentarium, approved by the FDA in August 2014 for difficulty with sleep onset and/or sleep maintenance.14 As an orexin-receptor antagonist, suvorexant represents a novel pharmacologic class. Suvorexant exhibits moderately rapid absorption with time to peak concentration ranging from 30 minutes to 6 hours in fasting conditions; absorption is delayed when taken with or soon after a meal. The drug is highly protein bound and extensively metabolized, primarily through CYP3A. The manufacturer recommends dose reduction (5 mg at bedtime) in patients taking moderate CYP3A inhibitors and avoiding suvorexant in patients taking strong CYP3A inhibitors. Suvorexant is primarily excreted through feces and the mean half-life is relatively long.
Considering these characteristics and age-related physiologic changes, the practitioner should be concerned about drugs that undergo extensive hepatic metabolism. Age-related reductions in CYP activity may lead to an increase in drug bioavailability and a decrease in the systemic clearance,11 which might be associated with an increase in elimination half-life and duration of action. Dosage adjustments are recommended for several BZDs (lower initial and maximum dosages for most agents) and BzRAs.17-28 No dosage adjustments for ramelteon or suvorexant in geriatric patients have been specified14,29; the manufacturers for both products assert that no differences in safety and efficacy have been observed between older and younger adult patients.
Alternative and complementary medications
Several non-prescription products, including over-the-counter drugs (eg, diphenhy-dramine, doxylamine) and herbal therapies (eg, melatonin, valerian), are used for their sedative-hypnotic properties. There is a lack of evidence supporting using diphenhydra-mine in patients with chronic insomnia, and tolerance to its hypnotic effect has been reported with repeated use.31 Concerns about anticholinergic toxicity and CNS depression limit its use in geriatric patients. Among herbal therapies, melatonin may have the strongest evidence for its ability to alleviate sleep disorders in geriatric patients32; however, meta-analyses have demonstrated small effects of melatonin on sleep latency and minimal differences in wake time after sleep onset and total sleep time.13
Clinical practice guidelines
Non-pharmacotherapeutic interventions, such as behavioral (eg, sleep hygiene measures) and psychological therapy, are recommended for initial management of sleep disorders in geriatric patients.13,33 In conjunction, the American Medical Directors Association (AMDA) recommends address ing underlying causes and exacerbating factors (eg, medical condition or medication).33 The AMDA recommends avoiding long-term pharmacotherapy and advises caution with BZD-hypnotic drugs, tricyclic antidepressants, and antihistamines. The American Academy of Sleep Medicine (AASM) recommends an initial treatment period of 2 to 4 weeks, followed by re-evaluation of continued need for treatment.13 The AASM recommends short- or intermediate-acting BzRAs or ramelteon for initial pharmacologic management of primary insomnias and insomnias comorbid with other conditions. The AASM also recommends specific dosages of BzRAs and BZDs for geriatric patients, which coincide with manufacturer-recommended dosages (Table 2).14-29
Barbiturates, chloral hydrate, and non-barbiturate, non-BZD drugs such as meprobamate are not recommended because of potential significant adverse effects and tolerance/dependence, and low therapeutic index. The AASM advises caution when using prescription drugs off-label for insomnia (eg, antidepressants, antiepileptics, antipsychotics) and recommends avoiding them, if possible, because of limited evidence supporting their use.13
Safety concerns
Two commonly used references contain recommendations for sedative-hypnotic medication use in geriatric patients.30,34 According to Gallagher et al’s34 Screening Tool of Older Person’s Prescriptions (STOPP), long-term (>1 month) use of long-acting BZDs (eg, flurazepam, diazepam) and prolonged use (>1 week) of first-generation antihistamines (eg, diphenhydramine, doxylamine) should be avoided in patients age ≥65 because of the risk of sedation, confusion, and anticholinergic side effects. STOPP recognizes that any use of BZDs, neuroleptics, or first-generation antihistamines may contribute to postural imbalance; therefore these agents are not recommended in older patients at risk for falls.
In the 2012 American Geriatrics Society (AGS) Beers Criteria, the AGS recommends avoiding barbiturates in older adults because of the high rate of physical dependence, tolerance to sleep effects, and overdose risk at low dosages.30 The AGS also recommends avoiding BZDs, stating that older adults have increased sensitivity to these agents and are at an increased risk of cognitive impairment, delirium, falls, fractures, and motor vehicle accidents when taking these drugs. Non-BZD BzRAs also should not be prescribed to patients with a history of falls or fractures, unless safer alternatives are not available.
The FDA has issued several advisory reports regarding sedative-hypnotic drugs. In 2007, all manufacturers of sedative-hypnotic drugs were required to modify their product labeling to include stronger language about potential risks.35 Among these changes, warnings for anaphylaxis and complex sleep-related behaviors were added. Also, the FDA requested that manufacturers of sedative-hypnotic drugs develop and provide patient medication guides, advising consumers on the potential risks and precautions associated with these drugs. More recently, the FDA announced changes to dosing recommendations for zolpidem-containing products because of the risk of impaired mental alertness36; manufacturers were required to lower the recommended dosages for each product.
Manufacturers of FDA-approved sedative-hypnotic drugs urge caution when prescribing these medications for geriatric patients, citing the potential for increased sensitivity, manifesting as marked excitement, depression, or confusion (eg, barbiturates), and greater risk for dosage-related adverse effects (eg, oversedation, dizziness, confusion, impaired psychomotor performance, ataxia).17-29
Use in clinical practice
Several variables should be considered when evaluating appropriateness of pharmacotherapy, including characteristics of the drug and the patient. Geriatric patients may be prone to comorbidities resulting from age-related physiologic changes. These diseases may be confounding (ie, contributing to sleep disorders); examples include medical illnesses, such as hyperthyroidism and arthritis, and psychiatric illnesses, such as depression and anxiety.37 Other conditions, such as renal and hepatic dysfunction, may lead to alteration in drug exposure. These conditions should be assessed through routine renal function tests (eg, serum creatinine and glomerular filtration rate) and liver function tests (eg, serum albumin and liver transaminases).
Multiple comorbidities suggest a higher likelihood of polypharmacy, leading to other drug-related issues (eg, drug-drug interactions). Although these issues may guide therapy by restricting medication options, their potential contribution to the underlying sleep complaints should be considered.37 Several drugs commonly used by geriatric patients may affect wakefulness (eg, analgesics, antidepressants, and antihypertensives [sedating], and thyroid hormones, corticosteroids, and CNS stimulants [alerting]).
CASE CONTINUED
In Mr. R’s case, zaleplon was initiated at 10 mg/d. Because of his age and the nature of his sleep disorder, the choice of sedative-hypnotic was suitable; however, the prescribed dosage was inappropriate. The sluggishness Mr. R experienced likely was a manifestation of increased exposure to the drug. According to manufacturer and AASM recommendations, a more appropriate dosage is 5 mg/d.13,23 Mr. R’s medical history and current medications, and his hepatic and renal function, should be assessed. If Mr. R continues to have issues with sleep initiation, zaleplon, 5 mg at bedtime, should be considered.
Related Resources
• Institute for Safe Medication Practices. www.ismp.org.
• MedWatch: The FDA Safety Information and Adverse Event Reporting Program. www.fda.gov/Safety/MedWatch/default.htm.
Drug Brand Names
Amitriptyline • Elavil Mirtazapine • Remeron
Amobarbital • Amytal Olanzapine • Zyprexa
Butabarbital • Butisol Pentobarbital • Nembutal
Chloral hydrate • Somnote Phenobarbital • Luminal
Diazepam • Valium Quazepam • Doral
Diphenhydramine • Benadryl, others Quetiapine • Seroquel
Doxepin • Silenor Ramelteon • Rozerem
Doxylamine • Unisom, others Secobarbital • Seconal
Estazolam • ProSom Suvorexant • Belsomra
Eszopiclone • Lunesta Temazepam • Restoril
Flurazepam • Dalmane Tiagabine • Gabitril
Gabapentin • Neurontin, Trazodone • Desyrel
Gralise, Horizant Zaleplon • Sonata
Lorazepam • Ativan Zolpidem • Ambien, Edluar,
Meprobamate • Equanil Intermezzo, Zolpimist
Acknowledgement
Vicki L. Ellingrod, PharmD, FCCP, is the series editor of Savvy Psychopharmacology.
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Mr. R, 75, is having difficulty sleeping. When he goes to bed, he lies there for what seems like forever, unable to fall asleep. He feels “so tired” and ends up taking naps during the day, but he cannot break this cycle. He has tried using over-the-counter products with little relief.
Mr. R’s primary care physician prescribes zaleplon, 10 mg/d, and asks him to call the clinic in 2 weeks to discuss his progress. He takes zaleplon as directed for several nights and begins to feel “sluggish” during the day, both mentally and physically, despite reporting an increase in the overall amount of sleep at night.
Sedative-hypnotic drugs are among the most commonly used medications in the United States. Use of these drugs, as well as anxiolytics, has increased from 2.8% between 1988 and 1994 to 4.7% between 2007 and 2010, according to the Department of Health and Human Services.1 In 2011, drugs categorized as sedative-hypnotics or antipsychotics were involved in 6.1% of all human exposures identified in the American Association of Poison Control Centers’ National Poison Data System.2 Therefore, an understanding of clinical and pharmacological variables related to safe and effective use is important for clinicians prescribing and monitoring therapy with these agents.
Neuropsychiatric disorders are prevalent among geriatric patients and are associated with age-related physiologic changes in the CNS.3 Such changes involve:
• neuroanatomy (brain atrophy, decreased neuronal density, increased plaque formation)
• neurotransmitters (reduced cholinergic transmission, decreased synthesis of dopamine and catecholamines), and
• neurophysiology (reduced cerebral blood flow).
These physiologic processes manifest as alterations in mental status, reflexes, sensation, gait, balance, and sleep. Examples of sleep changes among geriatric patients include decreased sleep efficiency, more frequent awakenings, and more variable sleep duration.3,4 Sleep disorders also may be related to mental disorders and other medical conditions.5 For example, the prevalence of sleep-related respiratory disorders, such as obstructive sleep apnea and central sleep apnea, increases with age.6
Sleep disorders are common among geriatric patients. In a large epidemiologic study of sleep complaints in patients age ≥65, more than one-half of patients had at least 1 sleep complaint (ie, difficulty falling asleep, trouble waking up, early awakening, need for naps, and feeling ill-rested).7 As many as 34% of patients reported symptoms of insomnia. In an analysis of National Ambulatory Medical Survey Data over 6 years, 24.8% to 27.9% of sleep-related medical office visits were attributed to patients age ≥65.8
Pharmacology in aging
Prescribing sedative-hypnotic drugs is not routinely recommended for older patients with a sleep disorder. Geriatric patients, compared with younger patients, are at higher risk of iatrogenic complications because of polypharmacy, comorbidities, relative renal and hepatic insufficiency, and other physiologic changes leading to alterations in drug exposure and metabolism (Table 1).9-12
Aging is associated with changes in body composition, including an increase in total body fat and decrease in lean body mass and total body water. These changes, as well as a prolonged GI transit time, decrease in active gut transporters, decreased blood perfusion, and decrease in plasma proteins such as albumin (because of reduced liver function or malnutrition), may lead to alteration in drug absorption patterns and may increase the volume of distribution for lipophilic drugs. Additionally, the elimination half-life of some drugs may increase with age because of larger volumes of distribution and reduction in hepatic or renal clearance.
The clinical significance of these changes is not well established. Although the process of drug absorption can change with age, the amount of drug absorbed might not be significantly affected. An increase in the volume of distribution and reduction in drug metabolism and clearance might lead to increasing amounts of circulating drug and duration of drug exposure, putting geriatric patients at an increased risk for adverse effects and drug toxicity.9
Among these mechanisms, Dolder et al11 hypothesized that drug metabolism catalyzed by cytochrome P450 (CYP) enzymes and renal excretion may be of greatest concern. Although in vitro studies suggest that concentration of CYP enzymes does not decline with age, in vivo studies have demonstrated reduced CYP activity in geriatric patients.11,12 Theoretically, a reduction in CYP activity would increase the bioavailability of drugs, especially those that are subject to extensive first-pass (ie, hepatic) metabolism, and may lead to a reduction in systemic clearance.
Independent of metabolic changes, geriatric patients are at risk of reduced renal clearance because of age-related changes in glomerular filtration rate. Pharmacodynamic changes might be observed in older patients and could be a concern even in the setting of unaltered pharmacokinetic factors.9 These changes usually require administering smaller drug dosages.
Sedative-hypnotic medications
Sedative-hypnotic agents include several barbiturates, benzodiazepines (BZDs), non-BZD benzodiazepine-receptor agonists (BzRAs), a melatonin-receptor agonist (ie, ramelteon), and an orexin-receptor antagonist (ie, suvorexant).13,14Table 214-29 summarizes selected sedative-hypnotic drugs. Additional drug classes used to treat insomnia include:
• sedating antidepressants (trazodone, amitriptyline, doxepin, mirtazapine)
• antiepileptic drugs (gabapentin, tiagabine)
• atypical antipsychotics (quetiapine, olanzapine).
FDA-approved agents for treating insomnia include amobarbital, butabarbital, pentobarbital, phenobarbital, secobarbital, chloral hydrate, diphenhydramine, doxylamine, doxepin, estazolam, flurazepam, lorazepam, quazepam, temazepam, triazolam, eszopiclone, zaleplon, zolpidem, ramelteon, and suvorexant. Not all of these drugs are recommended for use in geriatric patients. Barbiturates, for example, should be avoided.30
Pharmacokinetic characteristics vary among drugs and drug classes. Choice of pharmacotherapy should account for patient and drug characteristics and the specific sleep complaint. Sleep disorders may be variously characterized as difficulty with sleep initiation, duration, consolidation, or quality.13 Therefore, onset and duration of effect are important drug-related considerations. Sedative-hypnotic drugs with a short time-to-onset may be ideal for patients with sleep-onset insomnia.
The drugs’ duration of effect (eg, presence of active metabolites, long elimination half-life) also must be reviewed. A long elimination half-life may lead to increased drug exposure and unwanted side effects such as residual daytime drowsiness. Despite this, sedative-hypnotic drugs with a longer duration of effect (eg, intermediate- or long-acting drugs) may be best for patients with insomnia defined by difficulty maintaining sleep.
Benzodiazepines vary in their time to onset of effect, rate of elimination, and metabolism.15-21 BZDs that are FDA- approved for use as sedative-hypnotics are listed in Table 2.14-29 These BZDs have different onsets of effect as evidenced by time to achieve maximum plasma concentration (Tmax), ranging from 0.5 hours (flurazepam) to 2 hours (estazolam, quazepam, triazolam). The elimination half-life varies widely among these medications, from 1.5 hours (triazolam) to >100 hours (flurazepam). Flurazepam’s long half-life is attributable to its active major metabolite. Although most BZDs are metabolized hepatically, temazepam is subject to minimal hepatic metabolism.
Benzodiazepine-receptor agonists. There is substantial variation in the pharmacokinetic characteristics of BzRAs.15,16,22-28 There also are differences among the zolpidem dosage forms; sublingual formulations have the shortest onset of effect. Eszopiclone and zaleplon have low protein binding compared with zolpidem. Elimination half-lives vary among drugs with the shortest attributed to zaleplon (1 hour) and longest to eszopiclone (6 hours). All BzRAs are subject to extensive hepatic metabolism.
Ramelteon. Singular in its class, ramelteon is a treatment option for insomnia.29 This drug has a short onset of effect, moderate protein binding, and extensive hepatic metabolism. Ramelteon is primarily excreted in the urine as its metabolites, and the drug half-life is relatively short.
Suvorexant is the latest addition to the sedative-hypnotic armamentarium, approved by the FDA in August 2014 for difficulty with sleep onset and/or sleep maintenance.14 As an orexin-receptor antagonist, suvorexant represents a novel pharmacologic class. Suvorexant exhibits moderately rapid absorption with time to peak concentration ranging from 30 minutes to 6 hours in fasting conditions; absorption is delayed when taken with or soon after a meal. The drug is highly protein bound and extensively metabolized, primarily through CYP3A. The manufacturer recommends dose reduction (5 mg at bedtime) in patients taking moderate CYP3A inhibitors and avoiding suvorexant in patients taking strong CYP3A inhibitors. Suvorexant is primarily excreted through feces and the mean half-life is relatively long.
Considering these characteristics and age-related physiologic changes, the practitioner should be concerned about drugs that undergo extensive hepatic metabolism. Age-related reductions in CYP activity may lead to an increase in drug bioavailability and a decrease in the systemic clearance,11 which might be associated with an increase in elimination half-life and duration of action. Dosage adjustments are recommended for several BZDs (lower initial and maximum dosages for most agents) and BzRAs.17-28 No dosage adjustments for ramelteon or suvorexant in geriatric patients have been specified14,29; the manufacturers for both products assert that no differences in safety and efficacy have been observed between older and younger adult patients.
Alternative and complementary medications
Several non-prescription products, including over-the-counter drugs (eg, diphenhy-dramine, doxylamine) and herbal therapies (eg, melatonin, valerian), are used for their sedative-hypnotic properties. There is a lack of evidence supporting using diphenhydra-mine in patients with chronic insomnia, and tolerance to its hypnotic effect has been reported with repeated use.31 Concerns about anticholinergic toxicity and CNS depression limit its use in geriatric patients. Among herbal therapies, melatonin may have the strongest evidence for its ability to alleviate sleep disorders in geriatric patients32; however, meta-analyses have demonstrated small effects of melatonin on sleep latency and minimal differences in wake time after sleep onset and total sleep time.13
Clinical practice guidelines
Non-pharmacotherapeutic interventions, such as behavioral (eg, sleep hygiene measures) and psychological therapy, are recommended for initial management of sleep disorders in geriatric patients.13,33 In conjunction, the American Medical Directors Association (AMDA) recommends address ing underlying causes and exacerbating factors (eg, medical condition or medication).33 The AMDA recommends avoiding long-term pharmacotherapy and advises caution with BZD-hypnotic drugs, tricyclic antidepressants, and antihistamines. The American Academy of Sleep Medicine (AASM) recommends an initial treatment period of 2 to 4 weeks, followed by re-evaluation of continued need for treatment.13 The AASM recommends short- or intermediate-acting BzRAs or ramelteon for initial pharmacologic management of primary insomnias and insomnias comorbid with other conditions. The AASM also recommends specific dosages of BzRAs and BZDs for geriatric patients, which coincide with manufacturer-recommended dosages (Table 2).14-29
Barbiturates, chloral hydrate, and non-barbiturate, non-BZD drugs such as meprobamate are not recommended because of potential significant adverse effects and tolerance/dependence, and low therapeutic index. The AASM advises caution when using prescription drugs off-label for insomnia (eg, antidepressants, antiepileptics, antipsychotics) and recommends avoiding them, if possible, because of limited evidence supporting their use.13
Safety concerns
Two commonly used references contain recommendations for sedative-hypnotic medication use in geriatric patients.30,34 According to Gallagher et al’s34 Screening Tool of Older Person’s Prescriptions (STOPP), long-term (>1 month) use of long-acting BZDs (eg, flurazepam, diazepam) and prolonged use (>1 week) of first-generation antihistamines (eg, diphenhydramine, doxylamine) should be avoided in patients age ≥65 because of the risk of sedation, confusion, and anticholinergic side effects. STOPP recognizes that any use of BZDs, neuroleptics, or first-generation antihistamines may contribute to postural imbalance; therefore these agents are not recommended in older patients at risk for falls.
In the 2012 American Geriatrics Society (AGS) Beers Criteria, the AGS recommends avoiding barbiturates in older adults because of the high rate of physical dependence, tolerance to sleep effects, and overdose risk at low dosages.30 The AGS also recommends avoiding BZDs, stating that older adults have increased sensitivity to these agents and are at an increased risk of cognitive impairment, delirium, falls, fractures, and motor vehicle accidents when taking these drugs. Non-BZD BzRAs also should not be prescribed to patients with a history of falls or fractures, unless safer alternatives are not available.
The FDA has issued several advisory reports regarding sedative-hypnotic drugs. In 2007, all manufacturers of sedative-hypnotic drugs were required to modify their product labeling to include stronger language about potential risks.35 Among these changes, warnings for anaphylaxis and complex sleep-related behaviors were added. Also, the FDA requested that manufacturers of sedative-hypnotic drugs develop and provide patient medication guides, advising consumers on the potential risks and precautions associated with these drugs. More recently, the FDA announced changes to dosing recommendations for zolpidem-containing products because of the risk of impaired mental alertness36; manufacturers were required to lower the recommended dosages for each product.
Manufacturers of FDA-approved sedative-hypnotic drugs urge caution when prescribing these medications for geriatric patients, citing the potential for increased sensitivity, manifesting as marked excitement, depression, or confusion (eg, barbiturates), and greater risk for dosage-related adverse effects (eg, oversedation, dizziness, confusion, impaired psychomotor performance, ataxia).17-29
Use in clinical practice
Several variables should be considered when evaluating appropriateness of pharmacotherapy, including characteristics of the drug and the patient. Geriatric patients may be prone to comorbidities resulting from age-related physiologic changes. These diseases may be confounding (ie, contributing to sleep disorders); examples include medical illnesses, such as hyperthyroidism and arthritis, and psychiatric illnesses, such as depression and anxiety.37 Other conditions, such as renal and hepatic dysfunction, may lead to alteration in drug exposure. These conditions should be assessed through routine renal function tests (eg, serum creatinine and glomerular filtration rate) and liver function tests (eg, serum albumin and liver transaminases).
Multiple comorbidities suggest a higher likelihood of polypharmacy, leading to other drug-related issues (eg, drug-drug interactions). Although these issues may guide therapy by restricting medication options, their potential contribution to the underlying sleep complaints should be considered.37 Several drugs commonly used by geriatric patients may affect wakefulness (eg, analgesics, antidepressants, and antihypertensives [sedating], and thyroid hormones, corticosteroids, and CNS stimulants [alerting]).
CASE CONTINUED
In Mr. R’s case, zaleplon was initiated at 10 mg/d. Because of his age and the nature of his sleep disorder, the choice of sedative-hypnotic was suitable; however, the prescribed dosage was inappropriate. The sluggishness Mr. R experienced likely was a manifestation of increased exposure to the drug. According to manufacturer and AASM recommendations, a more appropriate dosage is 5 mg/d.13,23 Mr. R’s medical history and current medications, and his hepatic and renal function, should be assessed. If Mr. R continues to have issues with sleep initiation, zaleplon, 5 mg at bedtime, should be considered.
Related Resources
• Institute for Safe Medication Practices. www.ismp.org.
• MedWatch: The FDA Safety Information and Adverse Event Reporting Program. www.fda.gov/Safety/MedWatch/default.htm.
Drug Brand Names
Amitriptyline • Elavil Mirtazapine • Remeron
Amobarbital • Amytal Olanzapine • Zyprexa
Butabarbital • Butisol Pentobarbital • Nembutal
Chloral hydrate • Somnote Phenobarbital • Luminal
Diazepam • Valium Quazepam • Doral
Diphenhydramine • Benadryl, others Quetiapine • Seroquel
Doxepin • Silenor Ramelteon • Rozerem
Doxylamine • Unisom, others Secobarbital • Seconal
Estazolam • ProSom Suvorexant • Belsomra
Eszopiclone • Lunesta Temazepam • Restoril
Flurazepam • Dalmane Tiagabine • Gabitril
Gabapentin • Neurontin, Trazodone • Desyrel
Gralise, Horizant Zaleplon • Sonata
Lorazepam • Ativan Zolpidem • Ambien, Edluar,
Meprobamate • Equanil Intermezzo, Zolpimist
Acknowledgement
Vicki L. Ellingrod, PharmD, FCCP, is the series editor of Savvy Psychopharmacology.
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. National Center for Health Statistics. Health, United States, 2012, with special feature on emergency care. http://www. cdc.gov/nchs/data/hus/hus12.pdf. Published May 2013. Accessed August 22, 2014.
2. Bronstein AC, Spyker DA, Cantilena LR Jr, et al. 2011 Annual report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 29th annual report. Clin Toxicol (Phila). 2012;50(10): 911-1164.
3. Inouye SK. Neuropsychiatric aspects of aging. In: Goldman L, Schafer AI, eds. Goldman’s cecil medicine. 24th ed. Philadelphia, PA: Elsevier Saunders; 2011:114-116.
4. Diagnostic and statistical manual of mental disorders, 4th ed. Washington, DC: American Psychiatric Association; 1994.
5. American Psychiatric Association. Highlights of changes from DSM-IV-TR to DSM-5. http://www.psychiatry. org/File%20Library/Practice/DSM/DSM-5/Changes-from-DSM-IV-TR--to-DSM-5.pdf. 2013. Accessed August 22, 2014.
6. Edwards BA, O’Driscoll DM, Ali A, et al. Aging and sleep: physiology and pathophysiology. Semin Respir Crit Care Med. 2010;31(5):618-633.
7. Foley DJ, Monjan AA, Brown SL, et al. Sleep complaints among elderly persons: an epidemiologic study of three communities. Sleep. 1995;18(6):425-432.
8. Morlock RJ, Tan M, Mitchell DY. Patient characteristics and patterns of drug use for sleep complaints in the United States: analysis of National Ambulatory Medical Survey Data, 1997-2002. Clin Ther. 2006;28(7):1044-1053.
9. Diasio RB. Principles of drug therapy. In: Goldman L, Schafer AI, eds. Goldman’s Cecil medicine. 24th ed. Philadelphia, PA: Elsevier Saunders; 2011:124-132.
10. Hilmer SN, Ford GA. General principles of pharmacology. In: Halter JB, Ouslander JG, Tinetti ME, et al, eds. Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill; 2009:103-122.
11. Dolder C, Nelson M, McKinsey J. Use of non-benzodiazepine hypnotics in the elderly: are all agents the same? CNS Drugs. 2007;21(5):389-405.
12. Klotz U. Pharmacokinetics and drug metabolism in the elderly. Drug Metab Rev. 2009;41(2):67-76.
13. Schutte-Rodin S, Broch L, Buysse D, et al. Clinical guideline for the evaluation and management of chronic insomnia in adults. J Clin Sleep Med. 2008;4(5):487-504.
14. Belsomra [package insert]. Whitehouse Station, NJ: Merck & Co., Inc.; 2014.
15. Micromedex Healthcare Series. Greenwood Village, CO: Thomson Healthcare. http://micromedex.com. Accessed August 22, 2014.
16. Lexicomp. St. Louis, MO: Wolters Kluwer Health. http:// www.lexi.com. Accessed August 22, 2014.
17. Estazolam [package insert]. Corona, CA: Watson Pharma, Inc; 2008.
18. Flurazepam [package insert]. Eatontown, NJ: West-Ward Pharmaceutical Corp; 2010.
19. Doral [package insert]. Las Vegas, NV: Nuro Pharma, Inc; 2013.
20. Restoril [package insert]. Hazelwood, MO: Mallinckrodt Inc; 2010.
21. Halcion [package insert]. New York, NY: Pharmacia & Upjohn Co; 2013.
22. Lunesta [package insert]. Marlborough, MA: Sunovion Pharmaceuticals Inc; 2012.
23. Sonata [package insert]. New York, NY: Pfizer Inc; 2013.
24. Ambien [package insert]. Bridgewater, NJ: Sanofi-Aventis; 2013.
25. Ambien CR [package insert]. Bridgewater, NJ: Sanofi- Aventis; 2013.
26. Edluar [package insert]. Somerset, NJ: Meda Pharmaceuticals Inc; 2009.
27. Intermezzo [package insert]. Point Richmond, CA: Transcept Pharmaceuticals, Inc; 2011.
28. Zolpimist [package insert]. Richmond, VA: ECR Pharmaceuticals; 2013.
29. Rozerem [package insert]. Deerfield, IL: Takeda Pharmaceuticals America, Inc; 2010.
30. The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60(4):616-631.
31. Kirkwood CK, Melton ST. Insomnia, drowsiness, and fatigue. In: Krinsky DL, Berardi RR, Ferreri SP, et al, eds. Handbook of nonprescription drugs: an interactive approach to self-care. 17th ed. Washington, DC: American Pharmacists Association; 2012:867-884.
32. Insomnia. In: Natural Standard. Somerville, MA: Natural Standard. https://naturalmedicines.therapeuticresearch. com/databases/medical-conditions/i/insomnia.aspx. Accessed August 22, 2014.
33. American Medical Directors Association. Clinical practice guideline: sleep disorders. Columbia, MD: American Medical Directors Association; 2006.
34. Gallagher P, Ryan C, Byrne S, et al. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther. 2008;46(2):72-83.
35. Food and Drug Administration. FDA requests label change for all sleep disorder drug products. http://www.fda. gov/newsevents/newsroom/pressannouncements/2007/ ucm108868.htm. Published March 14, 2007. Accessed August 22, 2014.
36. Food and Drug Administration. FDA drug safety communication: risk of next-morning impairment after use of insomnia drugs; FDA requires lower recommended doses for certain drugs containing zolpidem (Ambien, Ambien CR, Edluar, and Zolpimist). http://www.fda.gov/drugs/ drugsafety/ucm334033.htm. Published January 10, 2013. Accessed August 22, 2014.
37. Cohen-Zion M, Ancoli-Israel S. Sleep disorders. In: Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill; 2009:671-682.
1. National Center for Health Statistics. Health, United States, 2012, with special feature on emergency care. http://www. cdc.gov/nchs/data/hus/hus12.pdf. Published May 2013. Accessed August 22, 2014.
2. Bronstein AC, Spyker DA, Cantilena LR Jr, et al. 2011 Annual report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 29th annual report. Clin Toxicol (Phila). 2012;50(10): 911-1164.
3. Inouye SK. Neuropsychiatric aspects of aging. In: Goldman L, Schafer AI, eds. Goldman’s cecil medicine. 24th ed. Philadelphia, PA: Elsevier Saunders; 2011:114-116.
4. Diagnostic and statistical manual of mental disorders, 4th ed. Washington, DC: American Psychiatric Association; 1994.
5. American Psychiatric Association. Highlights of changes from DSM-IV-TR to DSM-5. http://www.psychiatry. org/File%20Library/Practice/DSM/DSM-5/Changes-from-DSM-IV-TR--to-DSM-5.pdf. 2013. Accessed August 22, 2014.
6. Edwards BA, O’Driscoll DM, Ali A, et al. Aging and sleep: physiology and pathophysiology. Semin Respir Crit Care Med. 2010;31(5):618-633.
7. Foley DJ, Monjan AA, Brown SL, et al. Sleep complaints among elderly persons: an epidemiologic study of three communities. Sleep. 1995;18(6):425-432.
8. Morlock RJ, Tan M, Mitchell DY. Patient characteristics and patterns of drug use for sleep complaints in the United States: analysis of National Ambulatory Medical Survey Data, 1997-2002. Clin Ther. 2006;28(7):1044-1053.
9. Diasio RB. Principles of drug therapy. In: Goldman L, Schafer AI, eds. Goldman’s Cecil medicine. 24th ed. Philadelphia, PA: Elsevier Saunders; 2011:124-132.
10. Hilmer SN, Ford GA. General principles of pharmacology. In: Halter JB, Ouslander JG, Tinetti ME, et al, eds. Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill; 2009:103-122.
11. Dolder C, Nelson M, McKinsey J. Use of non-benzodiazepine hypnotics in the elderly: are all agents the same? CNS Drugs. 2007;21(5):389-405.
12. Klotz U. Pharmacokinetics and drug metabolism in the elderly. Drug Metab Rev. 2009;41(2):67-76.
13. Schutte-Rodin S, Broch L, Buysse D, et al. Clinical guideline for the evaluation and management of chronic insomnia in adults. J Clin Sleep Med. 2008;4(5):487-504.
14. Belsomra [package insert]. Whitehouse Station, NJ: Merck & Co., Inc.; 2014.
15. Micromedex Healthcare Series. Greenwood Village, CO: Thomson Healthcare. http://micromedex.com. Accessed August 22, 2014.
16. Lexicomp. St. Louis, MO: Wolters Kluwer Health. http:// www.lexi.com. Accessed August 22, 2014.
17. Estazolam [package insert]. Corona, CA: Watson Pharma, Inc; 2008.
18. Flurazepam [package insert]. Eatontown, NJ: West-Ward Pharmaceutical Corp; 2010.
19. Doral [package insert]. Las Vegas, NV: Nuro Pharma, Inc; 2013.
20. Restoril [package insert]. Hazelwood, MO: Mallinckrodt Inc; 2010.
21. Halcion [package insert]. New York, NY: Pharmacia & Upjohn Co; 2013.
22. Lunesta [package insert]. Marlborough, MA: Sunovion Pharmaceuticals Inc; 2012.
23. Sonata [package insert]. New York, NY: Pfizer Inc; 2013.
24. Ambien [package insert]. Bridgewater, NJ: Sanofi-Aventis; 2013.
25. Ambien CR [package insert]. Bridgewater, NJ: Sanofi- Aventis; 2013.
26. Edluar [package insert]. Somerset, NJ: Meda Pharmaceuticals Inc; 2009.
27. Intermezzo [package insert]. Point Richmond, CA: Transcept Pharmaceuticals, Inc; 2011.
28. Zolpimist [package insert]. Richmond, VA: ECR Pharmaceuticals; 2013.
29. Rozerem [package insert]. Deerfield, IL: Takeda Pharmaceuticals America, Inc; 2010.
30. The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60(4):616-631.
31. Kirkwood CK, Melton ST. Insomnia, drowsiness, and fatigue. In: Krinsky DL, Berardi RR, Ferreri SP, et al, eds. Handbook of nonprescription drugs: an interactive approach to self-care. 17th ed. Washington, DC: American Pharmacists Association; 2012:867-884.
32. Insomnia. In: Natural Standard. Somerville, MA: Natural Standard. https://naturalmedicines.therapeuticresearch. com/databases/medical-conditions/i/insomnia.aspx. Accessed August 22, 2014.
33. American Medical Directors Association. Clinical practice guideline: sleep disorders. Columbia, MD: American Medical Directors Association; 2006.
34. Gallagher P, Ryan C, Byrne S, et al. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther. 2008;46(2):72-83.
35. Food and Drug Administration. FDA requests label change for all sleep disorder drug products. http://www.fda. gov/newsevents/newsroom/pressannouncements/2007/ ucm108868.htm. Published March 14, 2007. Accessed August 22, 2014.
36. Food and Drug Administration. FDA drug safety communication: risk of next-morning impairment after use of insomnia drugs; FDA requires lower recommended doses for certain drugs containing zolpidem (Ambien, Ambien CR, Edluar, and Zolpimist). http://www.fda.gov/drugs/ drugsafety/ucm334033.htm. Published January 10, 2013. Accessed August 22, 2014.
37. Cohen-Zion M, Ancoli-Israel S. Sleep disorders. In: Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill; 2009:671-682.
Managing Your Practice: What is your practice worth?
At least once during your career, you probably will have to put a value on your practice. The need arises more often than you might think – if you sell it, of course (more on that next month); but also for estate planning, preparation of financial statements, or divorce negotiations; or when an associate joins or leaves your office; or if you have occasion to combine or partner your practice with one or more others, as I will discuss in detail in a future issue.
As you might guess, a medical practice is trickier to value than an ordinary business, and usually requires the services of an experienced professional appraiser. Entire books have been written about the process, so I can’t hope to cover it completely in a few hundred words, but three basic yardsticks are essential for a practice appraisal:
Tangible assets: equipment, cash, accounts receivable, and other property owned by the practice.
Liabilities: accounts payable, outstanding loans, and anything else owed to others.
Intangible assets: sometimes called “good will” – the reputation of the physicians, the location and name recognition of the practice, the loyalty and volume of patients, and other, well, intangibles.
Armed with those numbers, an appraiser can then determine the “equity,” or book value, of the practice.
Valuing tangible assets is comparatively straightforward, but there are several ways to do it, and when reviewing a practice appraisal you should ask which of them was used. Depreciated value is the book value of equipment and supplies as determined by their purchase price, less the amount their value has decreased since purchase. Remaining useful life value estimates how long the equipment can be expected to last. Market (or replacement) value is the amount it would cost on the open market to replace all equipment and supplies.
Intangible assets are more difficult to value. Many components are analyzed, including location, interior and exterior decor, accessibility to patients, age and functional status of equipment, systems in place to promote efficiency, reasons patients come back (if they do), and the overall reputation of the practice in the community. Other important factors include the “payer mix” (what percentage pays cash, how many third-party contracts are in place and how well they pay, etc.), the extent and strength of the referral base, and the presence of clinical studies or other supplemental income streams.
It is also important to determine to what extent intangible assets are transferrable. For example, unique skills with a laser, neurotoxins, or filler substances (or extraordinary personal charisma) may increase your practice’s value to you, but they are worthless to the next owner, and he or she will be unwilling to pay for them unless your services become part of the deal.
Once again, there are many ways to estimate intangible asset value, and once again you should ask which were used. Cash flow analysis works on the assumption that cash flow is a measure of intangible value. Capitalization of earnings puts a value, or capitalization, on the practice’s income streams using a variety of assumptions. Guideline comparison uses various databases to compare your practice with other, similar ones that have changed hands in the past.
Two newer techniques, which some consider to provide a better estimate of intangible assets, are the replacement method, which estimates the costs of starting the practice over again in the current market; and the excess earnings method, which measures how far above average your practice’s earnings are (and thus its overall value).
Asset-based valuation is the most popular, but by no means the only, method available. Income-based valuation looks at the source and strength of a practice’s income stream as a creator of value, as well as whether or not the income stream under a different owner would mirror its present one. This in turn becomes the basis for an understanding of the fair market value of both tangible and intangible assets. Market valuation combines the asset-based and income-based approaches, along with an analysis of sales and mergers of comparable practices in the community, to determine the value of a practice in its local market.
Whatever methods are used, it is important that the appraisal be done by an experienced financial consultant, that all techniques used in the valuation be divulged and explained, and that documentation is supplied to support the conclusions reached. This is especially important if the appraisal will be relied upon in the sale or merger of the practice. I’ll talk about sales and mergers over the next several columns.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Skin & Allergy News.
At least once during your career, you probably will have to put a value on your practice. The need arises more often than you might think – if you sell it, of course (more on that next month); but also for estate planning, preparation of financial statements, or divorce negotiations; or when an associate joins or leaves your office; or if you have occasion to combine or partner your practice with one or more others, as I will discuss in detail in a future issue.
As you might guess, a medical practice is trickier to value than an ordinary business, and usually requires the services of an experienced professional appraiser. Entire books have been written about the process, so I can’t hope to cover it completely in a few hundred words, but three basic yardsticks are essential for a practice appraisal:
Tangible assets: equipment, cash, accounts receivable, and other property owned by the practice.
Liabilities: accounts payable, outstanding loans, and anything else owed to others.
Intangible assets: sometimes called “good will” – the reputation of the physicians, the location and name recognition of the practice, the loyalty and volume of patients, and other, well, intangibles.
Armed with those numbers, an appraiser can then determine the “equity,” or book value, of the practice.
Valuing tangible assets is comparatively straightforward, but there are several ways to do it, and when reviewing a practice appraisal you should ask which of them was used. Depreciated value is the book value of equipment and supplies as determined by their purchase price, less the amount their value has decreased since purchase. Remaining useful life value estimates how long the equipment can be expected to last. Market (or replacement) value is the amount it would cost on the open market to replace all equipment and supplies.
Intangible assets are more difficult to value. Many components are analyzed, including location, interior and exterior decor, accessibility to patients, age and functional status of equipment, systems in place to promote efficiency, reasons patients come back (if they do), and the overall reputation of the practice in the community. Other important factors include the “payer mix” (what percentage pays cash, how many third-party contracts are in place and how well they pay, etc.), the extent and strength of the referral base, and the presence of clinical studies or other supplemental income streams.
It is also important to determine to what extent intangible assets are transferrable. For example, unique skills with a laser, neurotoxins, or filler substances (or extraordinary personal charisma) may increase your practice’s value to you, but they are worthless to the next owner, and he or she will be unwilling to pay for them unless your services become part of the deal.
Once again, there are many ways to estimate intangible asset value, and once again you should ask which were used. Cash flow analysis works on the assumption that cash flow is a measure of intangible value. Capitalization of earnings puts a value, or capitalization, on the practice’s income streams using a variety of assumptions. Guideline comparison uses various databases to compare your practice with other, similar ones that have changed hands in the past.
Two newer techniques, which some consider to provide a better estimate of intangible assets, are the replacement method, which estimates the costs of starting the practice over again in the current market; and the excess earnings method, which measures how far above average your practice’s earnings are (and thus its overall value).
Asset-based valuation is the most popular, but by no means the only, method available. Income-based valuation looks at the source and strength of a practice’s income stream as a creator of value, as well as whether or not the income stream under a different owner would mirror its present one. This in turn becomes the basis for an understanding of the fair market value of both tangible and intangible assets. Market valuation combines the asset-based and income-based approaches, along with an analysis of sales and mergers of comparable practices in the community, to determine the value of a practice in its local market.
Whatever methods are used, it is important that the appraisal be done by an experienced financial consultant, that all techniques used in the valuation be divulged and explained, and that documentation is supplied to support the conclusions reached. This is especially important if the appraisal will be relied upon in the sale or merger of the practice. I’ll talk about sales and mergers over the next several columns.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Skin & Allergy News.
At least once during your career, you probably will have to put a value on your practice. The need arises more often than you might think – if you sell it, of course (more on that next month); but also for estate planning, preparation of financial statements, or divorce negotiations; or when an associate joins or leaves your office; or if you have occasion to combine or partner your practice with one or more others, as I will discuss in detail in a future issue.
As you might guess, a medical practice is trickier to value than an ordinary business, and usually requires the services of an experienced professional appraiser. Entire books have been written about the process, so I can’t hope to cover it completely in a few hundred words, but three basic yardsticks are essential for a practice appraisal:
Tangible assets: equipment, cash, accounts receivable, and other property owned by the practice.
Liabilities: accounts payable, outstanding loans, and anything else owed to others.
Intangible assets: sometimes called “good will” – the reputation of the physicians, the location and name recognition of the practice, the loyalty and volume of patients, and other, well, intangibles.
Armed with those numbers, an appraiser can then determine the “equity,” or book value, of the practice.
Valuing tangible assets is comparatively straightforward, but there are several ways to do it, and when reviewing a practice appraisal you should ask which of them was used. Depreciated value is the book value of equipment and supplies as determined by their purchase price, less the amount their value has decreased since purchase. Remaining useful life value estimates how long the equipment can be expected to last. Market (or replacement) value is the amount it would cost on the open market to replace all equipment and supplies.
Intangible assets are more difficult to value. Many components are analyzed, including location, interior and exterior decor, accessibility to patients, age and functional status of equipment, systems in place to promote efficiency, reasons patients come back (if they do), and the overall reputation of the practice in the community. Other important factors include the “payer mix” (what percentage pays cash, how many third-party contracts are in place and how well they pay, etc.), the extent and strength of the referral base, and the presence of clinical studies or other supplemental income streams.
It is also important to determine to what extent intangible assets are transferrable. For example, unique skills with a laser, neurotoxins, or filler substances (or extraordinary personal charisma) may increase your practice’s value to you, but they are worthless to the next owner, and he or she will be unwilling to pay for them unless your services become part of the deal.
Once again, there are many ways to estimate intangible asset value, and once again you should ask which were used. Cash flow analysis works on the assumption that cash flow is a measure of intangible value. Capitalization of earnings puts a value, or capitalization, on the practice’s income streams using a variety of assumptions. Guideline comparison uses various databases to compare your practice with other, similar ones that have changed hands in the past.
Two newer techniques, which some consider to provide a better estimate of intangible assets, are the replacement method, which estimates the costs of starting the practice over again in the current market; and the excess earnings method, which measures how far above average your practice’s earnings are (and thus its overall value).
Asset-based valuation is the most popular, but by no means the only, method available. Income-based valuation looks at the source and strength of a practice’s income stream as a creator of value, as well as whether or not the income stream under a different owner would mirror its present one. This in turn becomes the basis for an understanding of the fair market value of both tangible and intangible assets. Market valuation combines the asset-based and income-based approaches, along with an analysis of sales and mergers of comparable practices in the community, to determine the value of a practice in its local market.
Whatever methods are used, it is important that the appraisal be done by an experienced financial consultant, that all techniques used in the valuation be divulged and explained, and that documentation is supplied to support the conclusions reached. This is especially important if the appraisal will be relied upon in the sale or merger of the practice. I’ll talk about sales and mergers over the next several columns.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Skin & Allergy News.

A new form to fill out
I got my Medicare card 2 years ago (guess how old I am?). At this year’s physical exam (my first exam under new rules that let Medicare pay for routine annual physicals), the clerk asked me to fill out the “Health-Risk Assessment” form my PCP would need for billing.
This form had two pages. Page 1 listed 26 questions, each to be answered by checking off one of the following six choices: Never, Sometimes, Seldom, Often, Always, and Not Applicable.

Right away you see a problem. If this were an SAT test, say, where I actually cared whether or not I passed, I would summon a proctor and demand to know the difference between “Sometimes” and “Seldom,” or whether “Always” includes when I’m asleep, intoxicated, or filling out forms.
I will not burden you with all 26 questions. Instead, I’ll present several (these are the actual questions, folks, word for word), along with the answers I would have given had I not been hamstrung by the Six Categories. Each question is headed, “In the past 4 weeks.”
Q: How much have you felt little interest or pleasure?
A: I have very much felt little interest, and very little felt much interest. On the other hand, I have much interest in the little pleasure I have felt, and much pleasure in the little interest I have had.
Q: Has your physical and emotional health limited your social activities with family, friends, neighbors or groups?
A: No, but lack of money has.
Q: Have you needed help preparing your own meals?
A: Yes, ever since I got married, but that was more than 4 weeks ago. I can still make omelets, though.
Q: Are you having difficulties driving your car?
A: Do you know Boston drivers?
Q: Have you needed help managing your finances?
A: Not since 2008, and then it was my broker who needed the help.
Q: Have you needed help with household chores?
A: Never do ‘em.
Q: Do you have concerns about your memory?
A: What?
Q: DO YOU HAVE CONCERNS ABOUT YOUR MEMORY?
A: Not so much about what I can’t remember, mostly about what I can.
Q: Do any of your friends/family have concerns about your memory?
A: No, other than whether I’ll remember them in my will.
Q: Have you had sexual problems?
A: Too much. Too little. I forget. But that’s just the last 4 weeks. Six weeks ago was amazing.
Q: Have problems using a telephone?
A: Damn right. Cellular connectivity around here stinks.
Q: Do you exercise for about 20 minutes, 3 or more days a week?
A: I always exercise sometimes. I sometimes exercise always. Could you repeat the question?
Q: Does your home have throw rugs?
A: It has rugs, but nobody throws them.
Q: Does your home have poor lighting?
A: Ever since they outlawed incandescents. When I flip the switch, they’re fully lit by the time I finish breakfast, but by then it’s time to turn them off and go to work.
Q: During the past 4 weeks, how have things been going for you?
A: The Red Sox are doing lousy. Did you have to ask?
The form ends with thanks for taking the time to fill out the form and concludes with this cheery note: “Your responses will help you receive the best health and health care possible.”
When my physical was done, my doctor found the form in my paper pile. “I see you filled it out,” she said.
“By the way,” I asked her. ‘”What do you do with these forms?”
“Absolutely nothing,” she said.
“You don’t have to submit them for tabulation or something?”
“No,” she said.
If you’re not on Medicare yet, this is what you have to look forward to. Always.
Sometimes.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Skin & Allergy News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years.
I got my Medicare card 2 years ago (guess how old I am?). At this year’s physical exam (my first exam under new rules that let Medicare pay for routine annual physicals), the clerk asked me to fill out the “Health-Risk Assessment” form my PCP would need for billing.
This form had two pages. Page 1 listed 26 questions, each to be answered by checking off one of the following six choices: Never, Sometimes, Seldom, Often, Always, and Not Applicable.
Right away you see a problem. If this were an SAT test, say, where I actually cared whether or not I passed, I would summon a proctor and demand to know the difference between “Sometimes” and “Seldom,” or whether “Always” includes when I’m asleep, intoxicated, or filling out forms.
I will not burden you with all 26 questions. Instead, I’ll present several (these are the actual questions, folks, word for word), along with the answers I would have given had I not been hamstrung by the Six Categories. Each question is headed, “In the past 4 weeks.”
Q: How much have you felt little interest or pleasure?
A: I have very much felt little interest, and very little felt much interest. On the other hand, I have much interest in the little pleasure I have felt, and much pleasure in the little interest I have had.
Q: Has your physical and emotional health limited your social activities with family, friends, neighbors or groups?
A: No, but lack of money has.
Q: Have you needed help preparing your own meals?
A: Yes, ever since I got married, but that was more than 4 weeks ago. I can still make omelets, though.
Q: Are you having difficulties driving your car?
A: Do you know Boston drivers?
Q: Have you needed help managing your finances?
A: Not since 2008, and then it was my broker who needed the help.
Q: Have you needed help with household chores?
A: Never do ‘em.
Q: Do you have concerns about your memory?
A: What?
Q: DO YOU HAVE CONCERNS ABOUT YOUR MEMORY?
A: Not so much about what I can’t remember, mostly about what I can.
Q: Do any of your friends/family have concerns about your memory?
A: No, other than whether I’ll remember them in my will.
Q: Have you had sexual problems?
A: Too much. Too little. I forget. But that’s just the last 4 weeks. Six weeks ago was amazing.
Q: Have problems using a telephone?
A: Damn right. Cellular connectivity around here stinks.
Q: Do you exercise for about 20 minutes, 3 or more days a week?
A: I always exercise sometimes. I sometimes exercise always. Could you repeat the question?
Q: Does your home have throw rugs?
A: It has rugs, but nobody throws them.
Q: Does your home have poor lighting?
A: Ever since they outlawed incandescents. When I flip the switch, they’re fully lit by the time I finish breakfast, but by then it’s time to turn them off and go to work.
Q: During the past 4 weeks, how have things been going for you?
A: The Red Sox are doing lousy. Did you have to ask?
The form ends with thanks for taking the time to fill out the form and concludes with this cheery note: “Your responses will help you receive the best health and health care possible.”
When my physical was done, my doctor found the form in my paper pile. “I see you filled it out,” she said.
“By the way,” I asked her. ‘”What do you do with these forms?”
“Absolutely nothing,” she said.
“You don’t have to submit them for tabulation or something?”
“No,” she said.
If you’re not on Medicare yet, this is what you have to look forward to. Always.
Sometimes.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Skin & Allergy News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years.
I got my Medicare card 2 years ago (guess how old I am?). At this year’s physical exam (my first exam under new rules that let Medicare pay for routine annual physicals), the clerk asked me to fill out the “Health-Risk Assessment” form my PCP would need for billing.
This form had two pages. Page 1 listed 26 questions, each to be answered by checking off one of the following six choices: Never, Sometimes, Seldom, Often, Always, and Not Applicable.
Right away you see a problem. If this were an SAT test, say, where I actually cared whether or not I passed, I would summon a proctor and demand to know the difference between “Sometimes” and “Seldom,” or whether “Always” includes when I’m asleep, intoxicated, or filling out forms.
I will not burden you with all 26 questions. Instead, I’ll present several (these are the actual questions, folks, word for word), along with the answers I would have given had I not been hamstrung by the Six Categories. Each question is headed, “In the past 4 weeks.”
Q: How much have you felt little interest or pleasure?
A: I have very much felt little interest, and very little felt much interest. On the other hand, I have much interest in the little pleasure I have felt, and much pleasure in the little interest I have had.
Q: Has your physical and emotional health limited your social activities with family, friends, neighbors or groups?
A: No, but lack of money has.
Q: Have you needed help preparing your own meals?
A: Yes, ever since I got married, but that was more than 4 weeks ago. I can still make omelets, though.
Q: Are you having difficulties driving your car?
A: Do you know Boston drivers?
Q: Have you needed help managing your finances?
A: Not since 2008, and then it was my broker who needed the help.
Q: Have you needed help with household chores?
A: Never do ‘em.
Q: Do you have concerns about your memory?
A: What?
Q: DO YOU HAVE CONCERNS ABOUT YOUR MEMORY?
A: Not so much about what I can’t remember, mostly about what I can.
Q: Do any of your friends/family have concerns about your memory?
A: No, other than whether I’ll remember them in my will.
Q: Have you had sexual problems?
A: Too much. Too little. I forget. But that’s just the last 4 weeks. Six weeks ago was amazing.
Q: Have problems using a telephone?
A: Damn right. Cellular connectivity around here stinks.
Q: Do you exercise for about 20 minutes, 3 or more days a week?
A: I always exercise sometimes. I sometimes exercise always. Could you repeat the question?
Q: Does your home have throw rugs?
A: It has rugs, but nobody throws them.
Q: Does your home have poor lighting?
A: Ever since they outlawed incandescents. When I flip the switch, they’re fully lit by the time I finish breakfast, but by then it’s time to turn them off and go to work.
Q: During the past 4 weeks, how have things been going for you?
A: The Red Sox are doing lousy. Did you have to ask?
The form ends with thanks for taking the time to fill out the form and concludes with this cheery note: “Your responses will help you receive the best health and health care possible.”
When my physical was done, my doctor found the form in my paper pile. “I see you filled it out,” she said.
“By the way,” I asked her. ‘”What do you do with these forms?”
“Absolutely nothing,” she said.
“You don’t have to submit them for tabulation or something?”
“No,” she said.
If you’re not on Medicare yet, this is what you have to look forward to. Always.
Sometimes.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Skin & Allergy News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years.

Most VTE therapies produce comparable results, analysis suggests

Credit: CDC
A newly published meta-analysis suggests most anticoagulant therapies produce similar results in patients with venous thromboembolism (VTE).
Using data from 45 randomized trials, investigators compared 8 anticoagulation options and found that most were associated with similar rates of VTE recurrence and bleeding.
They did find that unfractionated heparin (UFH) plus a vitamin K antagonist (VKA) conferred the greatest risk of VTE recurrence.
And rivaroxaban and apixaban were associated with the lowest rates of bleeding.
Two treatments—apixaban and low-molecular-weight heparin (LMWH) plus edoxaban—had the highest probability of being the best therapy. And apixaban had the greatest probability of being the least harmful therapy.
Lana A. Castellucci, MD, of the Ottawa Hospital Research Institute in Ontario, Canada, and her colleagues reported these results in JAMA.
The team conducted this meta-analysis to compare the efficacy and safety of 8 anticoagulation options: rivaroxaban, apixaban, LMWH, LMWH plus dabigatran, LMWH plus edoxaban, LMWH plus a VKA, UFH plus a VKA, and fondaparinux plus a VKA.
A search of the medical literature revealed 45 randomized trials comparing treatment options for VTE. They included a total of 44,989 patients.
VTE recurrence
The investigators first compared the risk of VTE recurrence with LMWH-VKA to all other treatment strategies. They found that 6 of the other options were associated with a lower rate of VTE recurrence than LMWH-VKA.
The only exception was UFH-VKA. During 3 months of treatment, 1.84% of patients who received UFH-VKA had a VTE recurrence, compared to 1.30% of patients treated with LMWH-VKA.
When the investigators used UFH-VKA as the comparator, they found that LMWH-VKA and LMWH alone were the only treatments associated with a reduction in recurrent VTE.
Stepwise comparisons of the remaining treatment strategies did not reveal significant differences in VTE recurrence.
However, the investigators found that LMWH-edoxaban and apixaban had the greatest probability of being the best therapy—at 33.1% and 31.6%, respectively.
Bleeding risk
Compared with LMWH-VKA, rivaroxaban and apixaban were associated with the lowest bleeding risk. The incidence of major bleeding during 3 months of anticoagulation was 0.49% for rivaroxaban, 0.28% for apixaban, and 0.89% for LMWH-VKA.
For all other treatments, the risk of bleeding did not differ significantly from the risk associated with LMWH-VKA.
Additional pairwise comparisons showed that rivaroxaban, apixaban, or both were associated with the lowest bleeding rates compared with UFH-VKA, fondaparinux-VKA, LMWH-dabigatran, and LMWH-edoxaban.
Apixaban was associated with the greatest probability of being the least harmful therapy (88.9%).
Considering these results together, Dr Castellucci and her colleagues concluded that most of the VTE treatments studied elicited comparable safety and efficacy outcomes.
However, UFH-VKA may be the least effective strategy for managing VTE, and rivaroxaban and apixaban may be associated with the lowest risk of bleeding. ![]()
Credit: CDC
A newly published meta-analysis suggests most anticoagulant therapies produce similar results in patients with venous thromboembolism (VTE).
Using data from 45 randomized trials, investigators compared 8 anticoagulation options and found that most were associated with similar rates of VTE recurrence and bleeding.
They did find that unfractionated heparin (UFH) plus a vitamin K antagonist (VKA) conferred the greatest risk of VTE recurrence.
And rivaroxaban and apixaban were associated with the lowest rates of bleeding.
Two treatments—apixaban and low-molecular-weight heparin (LMWH) plus edoxaban—had the highest probability of being the best therapy. And apixaban had the greatest probability of being the least harmful therapy.
Lana A. Castellucci, MD, of the Ottawa Hospital Research Institute in Ontario, Canada, and her colleagues reported these results in JAMA.
The team conducted this meta-analysis to compare the efficacy and safety of 8 anticoagulation options: rivaroxaban, apixaban, LMWH, LMWH plus dabigatran, LMWH plus edoxaban, LMWH plus a VKA, UFH plus a VKA, and fondaparinux plus a VKA.
A search of the medical literature revealed 45 randomized trials comparing treatment options for VTE. They included a total of 44,989 patients.
VTE recurrence
The investigators first compared the risk of VTE recurrence with LMWH-VKA to all other treatment strategies. They found that 6 of the other options were associated with a lower rate of VTE recurrence than LMWH-VKA.
The only exception was UFH-VKA. During 3 months of treatment, 1.84% of patients who received UFH-VKA had a VTE recurrence, compared to 1.30% of patients treated with LMWH-VKA.
When the investigators used UFH-VKA as the comparator, they found that LMWH-VKA and LMWH alone were the only treatments associated with a reduction in recurrent VTE.
Stepwise comparisons of the remaining treatment strategies did not reveal significant differences in VTE recurrence.
However, the investigators found that LMWH-edoxaban and apixaban had the greatest probability of being the best therapy—at 33.1% and 31.6%, respectively.
Bleeding risk
Compared with LMWH-VKA, rivaroxaban and apixaban were associated with the lowest bleeding risk. The incidence of major bleeding during 3 months of anticoagulation was 0.49% for rivaroxaban, 0.28% for apixaban, and 0.89% for LMWH-VKA.
For all other treatments, the risk of bleeding did not differ significantly from the risk associated with LMWH-VKA.
Additional pairwise comparisons showed that rivaroxaban, apixaban, or both were associated with the lowest bleeding rates compared with UFH-VKA, fondaparinux-VKA, LMWH-dabigatran, and LMWH-edoxaban.
Apixaban was associated with the greatest probability of being the least harmful therapy (88.9%).
Considering these results together, Dr Castellucci and her colleagues concluded that most of the VTE treatments studied elicited comparable safety and efficacy outcomes.
However, UFH-VKA may be the least effective strategy for managing VTE, and rivaroxaban and apixaban may be associated with the lowest risk of bleeding. ![]()
Credit: CDC
A newly published meta-analysis suggests most anticoagulant therapies produce similar results in patients with venous thromboembolism (VTE).
Using data from 45 randomized trials, investigators compared 8 anticoagulation options and found that most were associated with similar rates of VTE recurrence and bleeding.
They did find that unfractionated heparin (UFH) plus a vitamin K antagonist (VKA) conferred the greatest risk of VTE recurrence.
And rivaroxaban and apixaban were associated with the lowest rates of bleeding.
Two treatments—apixaban and low-molecular-weight heparin (LMWH) plus edoxaban—had the highest probability of being the best therapy. And apixaban had the greatest probability of being the least harmful therapy.
Lana A. Castellucci, MD, of the Ottawa Hospital Research Institute in Ontario, Canada, and her colleagues reported these results in JAMA.
The team conducted this meta-analysis to compare the efficacy and safety of 8 anticoagulation options: rivaroxaban, apixaban, LMWH, LMWH plus dabigatran, LMWH plus edoxaban, LMWH plus a VKA, UFH plus a VKA, and fondaparinux plus a VKA.
A search of the medical literature revealed 45 randomized trials comparing treatment options for VTE. They included a total of 44,989 patients.
VTE recurrence
The investigators first compared the risk of VTE recurrence with LMWH-VKA to all other treatment strategies. They found that 6 of the other options were associated with a lower rate of VTE recurrence than LMWH-VKA.
The only exception was UFH-VKA. During 3 months of treatment, 1.84% of patients who received UFH-VKA had a VTE recurrence, compared to 1.30% of patients treated with LMWH-VKA.
When the investigators used UFH-VKA as the comparator, they found that LMWH-VKA and LMWH alone were the only treatments associated with a reduction in recurrent VTE.
Stepwise comparisons of the remaining treatment strategies did not reveal significant differences in VTE recurrence.
However, the investigators found that LMWH-edoxaban and apixaban had the greatest probability of being the best therapy—at 33.1% and 31.6%, respectively.
Bleeding risk
Compared with LMWH-VKA, rivaroxaban and apixaban were associated with the lowest bleeding risk. The incidence of major bleeding during 3 months of anticoagulation was 0.49% for rivaroxaban, 0.28% for apixaban, and 0.89% for LMWH-VKA.
For all other treatments, the risk of bleeding did not differ significantly from the risk associated with LMWH-VKA.
Additional pairwise comparisons showed that rivaroxaban, apixaban, or both were associated with the lowest bleeding rates compared with UFH-VKA, fondaparinux-VKA, LMWH-dabigatran, and LMWH-edoxaban.
Apixaban was associated with the greatest probability of being the least harmful therapy (88.9%).
Considering these results together, Dr Castellucci and her colleagues concluded that most of the VTE treatments studied elicited comparable safety and efficacy outcomes.
However, UFH-VKA may be the least effective strategy for managing VTE, and rivaroxaban and apixaban may be associated with the lowest risk of bleeding. ![]()
FDA approves treatment for kids with hemophilia B

The US Food and Drug Administration (FDA) has approved a recombinant factor IX product (Rixubis) for use in children with hemophilia B.
Rixubis is indicated for routine prophylactic treatment, control and prevention of bleeding episodes, and perioperative management in these patients.
Rixubis was the first recombinant factor IX product to gain FDA approval for routine prophylaxis and control of bleeding episodes in adults with hemophilia B.
The latest FDA approval is based on results of a trial investigating the efficacy and safety of Rixubis in 23 previously treated male patients younger than 12 years of age who had severe or moderately severe hemophilia B.
The patients received a twice-weekly Rixubis prophylaxis regimen (mean dose 56 IU/kg) for a mean treatment duration of 6 months and a mean of 54 exposure days.
The median annualized bleeding rate was 2.0 (0.0 for spontaneous bleeds and joint bleeds). Nine patients (39.1%) experienced no bleeds, and 23 bleeding episodes (88.5%) were treated with 1 to 2 infusions.
There were no reports of inhibitor development, severe allergic reactions, thrombotic events, or treatment-related adverse events.
These data were presented at the 2013 ASH Annual Meeting (abstract 1118).
Common adverse reactions observed in more than 1% of subjects in clinical studies of Rixubis were dysgeusia, pain in an extremity, and a positive test for furin antibody. Rixubis may pose a risk of hypersensitivity reactions, inhibitor development, nephrotic syndrome, and thromboembolic complications.
Rixubis is contraindicated in patients who have known hypersensitivity to the product or its excipients (including hamster protein), patients with disseminated intravascular coagulation, and those with signs of fibrinolysis.
For more details on Rixubis, see the full prescribing information. Rixubis is under development by Baxter International Inc. ![]()
The US Food and Drug Administration (FDA) has approved a recombinant factor IX product (Rixubis) for use in children with hemophilia B.
Rixubis is indicated for routine prophylactic treatment, control and prevention of bleeding episodes, and perioperative management in these patients.
Rixubis was the first recombinant factor IX product to gain FDA approval for routine prophylaxis and control of bleeding episodes in adults with hemophilia B.
The latest FDA approval is based on results of a trial investigating the efficacy and safety of Rixubis in 23 previously treated male patients younger than 12 years of age who had severe or moderately severe hemophilia B.
The patients received a twice-weekly Rixubis prophylaxis regimen (mean dose 56 IU/kg) for a mean treatment duration of 6 months and a mean of 54 exposure days.
The median annualized bleeding rate was 2.0 (0.0 for spontaneous bleeds and joint bleeds). Nine patients (39.1%) experienced no bleeds, and 23 bleeding episodes (88.5%) were treated with 1 to 2 infusions.
There were no reports of inhibitor development, severe allergic reactions, thrombotic events, or treatment-related adverse events.
These data were presented at the 2013 ASH Annual Meeting (abstract 1118).
Common adverse reactions observed in more than 1% of subjects in clinical studies of Rixubis were dysgeusia, pain in an extremity, and a positive test for furin antibody. Rixubis may pose a risk of hypersensitivity reactions, inhibitor development, nephrotic syndrome, and thromboembolic complications.
Rixubis is contraindicated in patients who have known hypersensitivity to the product or its excipients (including hamster protein), patients with disseminated intravascular coagulation, and those with signs of fibrinolysis.
For more details on Rixubis, see the full prescribing information. Rixubis is under development by Baxter International Inc. ![]()
The US Food and Drug Administration (FDA) has approved a recombinant factor IX product (Rixubis) for use in children with hemophilia B.
Rixubis is indicated for routine prophylactic treatment, control and prevention of bleeding episodes, and perioperative management in these patients.
Rixubis was the first recombinant factor IX product to gain FDA approval for routine prophylaxis and control of bleeding episodes in adults with hemophilia B.
The latest FDA approval is based on results of a trial investigating the efficacy and safety of Rixubis in 23 previously treated male patients younger than 12 years of age who had severe or moderately severe hemophilia B.
The patients received a twice-weekly Rixubis prophylaxis regimen (mean dose 56 IU/kg) for a mean treatment duration of 6 months and a mean of 54 exposure days.
The median annualized bleeding rate was 2.0 (0.0 for spontaneous bleeds and joint bleeds). Nine patients (39.1%) experienced no bleeds, and 23 bleeding episodes (88.5%) were treated with 1 to 2 infusions.
There were no reports of inhibitor development, severe allergic reactions, thrombotic events, or treatment-related adverse events.
These data were presented at the 2013 ASH Annual Meeting (abstract 1118).
Common adverse reactions observed in more than 1% of subjects in clinical studies of Rixubis were dysgeusia, pain in an extremity, and a positive test for furin antibody. Rixubis may pose a risk of hypersensitivity reactions, inhibitor development, nephrotic syndrome, and thromboembolic complications.
Rixubis is contraindicated in patients who have known hypersensitivity to the product or its excipients (including hamster protein), patients with disseminated intravascular coagulation, and those with signs of fibrinolysis.
For more details on Rixubis, see the full prescribing information. Rixubis is under development by Baxter International Inc. ![]()
Protein discovery points the way to sepsis treatment

Credit: Eric Smith
A protein that helps the innate immune system target bacteria and viruses can fight sepsis by interacting with histones, according to research
published in Science Signaling.
The pattern recognition protein pentraxin 3 (PTX3) is known to activate the body’s immune system in response to sepsis conditions.
But researchers thought the protein might have an additional role in sepsis pathogenesis, in the form of host protection against extracellular histones.
They knew that, during sepsis, histones escape from dead cells and kill nearby healthy cells, causing inflammation.
And the team’s experiments showed that PTX3 forms strong bonds with histones and disrupts their cellular toxicity, specifically by bundling the histones into aggregates that no longer kill healthy cells.
“We observed extraordinarily rapid and tight interaction with histone, which we recognized as coaggregation after a variety of experiments,” said study author Takao Hamakubo, MD, PhD, of the University of Tokyo in Japan.
The researchers also found that mice pretreated with PTX3 and infused with histones showed reduced inflammation.
So the team decided to investigate the effects of PTX3 in 2 mouse models of sepsis. In both models, the protein substantially reduced mortality.
PTX3 worked even when administered hours after a sepsis-inducing procedure called cecal ligation and puncture, in which fecal material is released into the abdomen to generate a strong immune response.
The researchers said these results suggest the host-protective effects of PTX3 in sepsis are a result of its coaggregation with histones rather than its ability to mediate pattern recognition. And this effect provides a potential basis for treating sepsis by protecting cells from the toxic effects of extracellular histones.
“To our knowledge, this is the first report of coaggregation between different proteins that is protective to the host,” Dr Hamakubo said. “We expect our findings lead to a novel understanding of protein interaction and that they will benefit people who are suffering from severe illness.” ![]()
Credit: Eric Smith
A protein that helps the innate immune system target bacteria and viruses can fight sepsis by interacting with histones, according to research
published in Science Signaling.
The pattern recognition protein pentraxin 3 (PTX3) is known to activate the body’s immune system in response to sepsis conditions.
But researchers thought the protein might have an additional role in sepsis pathogenesis, in the form of host protection against extracellular histones.
They knew that, during sepsis, histones escape from dead cells and kill nearby healthy cells, causing inflammation.
And the team’s experiments showed that PTX3 forms strong bonds with histones and disrupts their cellular toxicity, specifically by bundling the histones into aggregates that no longer kill healthy cells.
“We observed extraordinarily rapid and tight interaction with histone, which we recognized as coaggregation after a variety of experiments,” said study author Takao Hamakubo, MD, PhD, of the University of Tokyo in Japan.
The researchers also found that mice pretreated with PTX3 and infused with histones showed reduced inflammation.
So the team decided to investigate the effects of PTX3 in 2 mouse models of sepsis. In both models, the protein substantially reduced mortality.
PTX3 worked even when administered hours after a sepsis-inducing procedure called cecal ligation and puncture, in which fecal material is released into the abdomen to generate a strong immune response.
The researchers said these results suggest the host-protective effects of PTX3 in sepsis are a result of its coaggregation with histones rather than its ability to mediate pattern recognition. And this effect provides a potential basis for treating sepsis by protecting cells from the toxic effects of extracellular histones.
“To our knowledge, this is the first report of coaggregation between different proteins that is protective to the host,” Dr Hamakubo said. “We expect our findings lead to a novel understanding of protein interaction and that they will benefit people who are suffering from severe illness.” ![]()
Credit: Eric Smith
A protein that helps the innate immune system target bacteria and viruses can fight sepsis by interacting with histones, according to research
published in Science Signaling.
The pattern recognition protein pentraxin 3 (PTX3) is known to activate the body’s immune system in response to sepsis conditions.
But researchers thought the protein might have an additional role in sepsis pathogenesis, in the form of host protection against extracellular histones.
They knew that, during sepsis, histones escape from dead cells and kill nearby healthy cells, causing inflammation.
And the team’s experiments showed that PTX3 forms strong bonds with histones and disrupts their cellular toxicity, specifically by bundling the histones into aggregates that no longer kill healthy cells.
“We observed extraordinarily rapid and tight interaction with histone, which we recognized as coaggregation after a variety of experiments,” said study author Takao Hamakubo, MD, PhD, of the University of Tokyo in Japan.
The researchers also found that mice pretreated with PTX3 and infused with histones showed reduced inflammation.
So the team decided to investigate the effects of PTX3 in 2 mouse models of sepsis. In both models, the protein substantially reduced mortality.
PTX3 worked even when administered hours after a sepsis-inducing procedure called cecal ligation and puncture, in which fecal material is released into the abdomen to generate a strong immune response.
The researchers said these results suggest the host-protective effects of PTX3 in sepsis are a result of its coaggregation with histones rather than its ability to mediate pattern recognition. And this effect provides a potential basis for treating sepsis by protecting cells from the toxic effects of extracellular histones.
“To our knowledge, this is the first report of coaggregation between different proteins that is protective to the host,” Dr Hamakubo said. “We expect our findings lead to a novel understanding of protein interaction and that they will benefit people who are suffering from severe illness.” ![]()
New assay could prove useful in HSCT
![]()
Credit: Chad McNeeley
Researchers say they’ve developed an assay that allows for ultrasensitive DNA detection.
This haplotype-based assay could be used to detect relapse in patients who have undergone hematopoietic stem cell transplant (HSCT).
In fact, the researchers believe it would enable relapse detection earlier than existing microsatellite-based assays.
The new assay could also be used to detect microchimerism in solid organ transplants, in forensics, and for patient identification.
James Eshleman, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues described this assay in The Journal of Molecular Diagnostics.
The team noted that most bone marrow engraftment testing currently uses microsatellites or short tandem repeats that are resolved by capillary electrophoresis.
“Repeat testing will only detect DNA that makes up at least 1% of a DNA sample, so it’s not great for situations in which results depend on small amounts of material within a larger sample,” Dr Eshleman said.
In these situations, evaluating single-nucleotide polymorphisms (SNPs) might seem like a better choice, but this method has a high error rate. Dr Eshleman and his colleagues found they could circumvent this problem by analyzing blocks of closely spaced SNPs, or haplotypes.
To test their method, the researchers chose the HLA-A locus. They aligned common HLA-A alleles and identified a region containing 18 closely spaced SNPs. The team then tested a series of primers surrounding this region and selected the best pair on the basis of amplification efficiency and specificity.
They found it easy to differentiate some combinations of HLA-A alleles but not others. For instance, they discovered that 11 SNPs differentiate allele A*01 from A*02. But A*02 and HLA-A* 68:01:01:01 have a single SNP difference.
To test the possible cross talk between molecules that vary by 11 SNPs, the researchers sequenced 2 samples—one homozygous for A*01 and another homozygous for A*02—and analyzed each for the other allele. They found that, when there are enough discriminating SNPs between 2 individuals’ alleles, the haplotype assay is highly specific.
To evaluate the assay’s accuracy and limit of detection, the researchers generated various dilutions of 2 cell lines with known HLA-A genotypes. They made dilutions with cell mixes varying from 1 in 1 million (0.0001%) to 1 in 100 (1%), using 10 million cells for each dilution.
The team isolated DNA and performed PCR using 600 ng of DNA. And they sequenced each sample at least twice.
The assay proved highly precise at the 0.1% cell mix but less precise at the 0.01% cell mix.
“[Nevertheless,] we could detect cells when they made up just 0.01% of the mixture, which is a big improvement over the current method, which can only detect DNA that makes up 1% to 5% of a sample,” Dr Eshleman said.
The researchers also used their assay to test samples from 18 HSCT patients whose donor-patient HLA genotypes varied by at least 4 SNPs. All but 1 sample tested positive for some level of patient DNA, and the positives ranged from 0.001% to 1.47% patient DNA.
Finally, the team analyzed the human genome using the 1000 Genomes database and identified many additional loci that could be used with their assay. ![]()
![]()
Credit: Chad McNeeley
Researchers say they’ve developed an assay that allows for ultrasensitive DNA detection.
This haplotype-based assay could be used to detect relapse in patients who have undergone hematopoietic stem cell transplant (HSCT).
In fact, the researchers believe it would enable relapse detection earlier than existing microsatellite-based assays.
The new assay could also be used to detect microchimerism in solid organ transplants, in forensics, and for patient identification.
James Eshleman, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues described this assay in The Journal of Molecular Diagnostics.
The team noted that most bone marrow engraftment testing currently uses microsatellites or short tandem repeats that are resolved by capillary electrophoresis.
“Repeat testing will only detect DNA that makes up at least 1% of a DNA sample, so it’s not great for situations in which results depend on small amounts of material within a larger sample,” Dr Eshleman said.
In these situations, evaluating single-nucleotide polymorphisms (SNPs) might seem like a better choice, but this method has a high error rate. Dr Eshleman and his colleagues found they could circumvent this problem by analyzing blocks of closely spaced SNPs, or haplotypes.
To test their method, the researchers chose the HLA-A locus. They aligned common HLA-A alleles and identified a region containing 18 closely spaced SNPs. The team then tested a series of primers surrounding this region and selected the best pair on the basis of amplification efficiency and specificity.
They found it easy to differentiate some combinations of HLA-A alleles but not others. For instance, they discovered that 11 SNPs differentiate allele A*01 from A*02. But A*02 and HLA-A* 68:01:01:01 have a single SNP difference.
To test the possible cross talk between molecules that vary by 11 SNPs, the researchers sequenced 2 samples—one homozygous for A*01 and another homozygous for A*02—and analyzed each for the other allele. They found that, when there are enough discriminating SNPs between 2 individuals’ alleles, the haplotype assay is highly specific.
To evaluate the assay’s accuracy and limit of detection, the researchers generated various dilutions of 2 cell lines with known HLA-A genotypes. They made dilutions with cell mixes varying from 1 in 1 million (0.0001%) to 1 in 100 (1%), using 10 million cells for each dilution.
The team isolated DNA and performed PCR using 600 ng of DNA. And they sequenced each sample at least twice.
The assay proved highly precise at the 0.1% cell mix but less precise at the 0.01% cell mix.
“[Nevertheless,] we could detect cells when they made up just 0.01% of the mixture, which is a big improvement over the current method, which can only detect DNA that makes up 1% to 5% of a sample,” Dr Eshleman said.
The researchers also used their assay to test samples from 18 HSCT patients whose donor-patient HLA genotypes varied by at least 4 SNPs. All but 1 sample tested positive for some level of patient DNA, and the positives ranged from 0.001% to 1.47% patient DNA.
Finally, the team analyzed the human genome using the 1000 Genomes database and identified many additional loci that could be used with their assay. ![]()
![]()
Credit: Chad McNeeley
Researchers say they’ve developed an assay that allows for ultrasensitive DNA detection.
This haplotype-based assay could be used to detect relapse in patients who have undergone hematopoietic stem cell transplant (HSCT).
In fact, the researchers believe it would enable relapse detection earlier than existing microsatellite-based assays.
The new assay could also be used to detect microchimerism in solid organ transplants, in forensics, and for patient identification.
James Eshleman, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland, and his colleagues described this assay in The Journal of Molecular Diagnostics.
The team noted that most bone marrow engraftment testing currently uses microsatellites or short tandem repeats that are resolved by capillary electrophoresis.
“Repeat testing will only detect DNA that makes up at least 1% of a DNA sample, so it’s not great for situations in which results depend on small amounts of material within a larger sample,” Dr Eshleman said.
In these situations, evaluating single-nucleotide polymorphisms (SNPs) might seem like a better choice, but this method has a high error rate. Dr Eshleman and his colleagues found they could circumvent this problem by analyzing blocks of closely spaced SNPs, or haplotypes.
To test their method, the researchers chose the HLA-A locus. They aligned common HLA-A alleles and identified a region containing 18 closely spaced SNPs. The team then tested a series of primers surrounding this region and selected the best pair on the basis of amplification efficiency and specificity.
They found it easy to differentiate some combinations of HLA-A alleles but not others. For instance, they discovered that 11 SNPs differentiate allele A*01 from A*02. But A*02 and HLA-A* 68:01:01:01 have a single SNP difference.
To test the possible cross talk between molecules that vary by 11 SNPs, the researchers sequenced 2 samples—one homozygous for A*01 and another homozygous for A*02—and analyzed each for the other allele. They found that, when there are enough discriminating SNPs between 2 individuals’ alleles, the haplotype assay is highly specific.
To evaluate the assay’s accuracy and limit of detection, the researchers generated various dilutions of 2 cell lines with known HLA-A genotypes. They made dilutions with cell mixes varying from 1 in 1 million (0.0001%) to 1 in 100 (1%), using 10 million cells for each dilution.
The team isolated DNA and performed PCR using 600 ng of DNA. And they sequenced each sample at least twice.
The assay proved highly precise at the 0.1% cell mix but less precise at the 0.01% cell mix.
“[Nevertheless,] we could detect cells when they made up just 0.01% of the mixture, which is a big improvement over the current method, which can only detect DNA that makes up 1% to 5% of a sample,” Dr Eshleman said.
The researchers also used their assay to test samples from 18 HSCT patients whose donor-patient HLA genotypes varied by at least 4 SNPs. All but 1 sample tested positive for some level of patient DNA, and the positives ranged from 0.001% to 1.47% patient DNA.
Finally, the team analyzed the human genome using the 1000 Genomes database and identified many additional loci that could be used with their assay. ![]()
Most acute VTE therapies yield similar outcomes
For patients with acute venous thromboembolism, both clinical and safety outcomes were similar among seven of eight possible treatment strategies assessed in a network meta-analysis published online Sept. 16 in JAMA.
Clinicians have several treatment options but little guidance for choosing among them when managing acute VTE. Many strategies have shown promising results when assessed in single studies, but there have been few direct comparison studies. So investigators performed a network meta-analysis of 45 articles involving 44,989 patients, which enabled them to compare the safety and efficacy of eight possible approaches. The sample sizes of these studies ranged from 60 to 8,240 participants, with a median of 298. The median follow-up period was 3 months, with a range of 3-8 months.
The currently accepted standard treatment for acute VTE is the use of parenteral low-molecular-weight heparin (LMWH) for a minimum of 5 days, followed by transition to a vitamin K antagonist. This approach was compared against parenteral unfractionated heparin followed by a vitamin K antagonist; parenteral fondaparinux followed by a vitamin K antagonist; parenteral LMWH combined with dabigatran; parenteral LMWH combined with edoxaban; oral rivaroxaban; oral apixaban; and parenteral LMWH alone, said Dr. Lana A. Castellucci of the Ottawa Hospital Research Institute, University of Ottawa, and her associates.
Compared with standard parenteral LMWH plus a vitamin K antagonist, six of these approaches yielded comparable reductions in recurrent VTE and induced comparable rates of major bleeding, the investigators said (JAMA 2014 September 16 [doi:10.1001/jama.2014.10538]).
The only strategy that was less effective at reducing the rate of recurrent VTE was parenteral unfractionated heparin plus a vitamin K antagonist. However, “there are clinical circumstances that necessitate the use of unfractionated heparin, including for patients with severe renal insufficiency and those with massive or submassive pulmonary embolism who are potential candidates for thrombolysis or thrombectomy,” Dr. Castellucci and her associates noted.
Oral rivaroxaban and oral apixaban appeared to be associated with the lowest risk of major bleeding. “Future direct comparison trials, patient-level network meta-analyses, or high-quality nonrandomized studies are required to confirm our findings,” they added.
This study was supported by the Heart and Stroke Foundation of Canada, the University of Ottawa, the Canadian Institutes of Health Research, the Canadian Network and Centre for Trials Internationally, and the Heart and Stroke Foundation of Ontario. Dr. Castellucci reported no financial conflicts of interest; some of her associates reported ties to Bayer, Biomerieux, Boehringer Ingelheim, Bristol-Myers Squibb, Leo Pharma, Pfizer, and Sanofi.
*Correction, 9/17/2014: An earlier version of this article misstated the Key Clinical Point in the Vitals section.
For patients with acute venous thromboembolism, both clinical and safety outcomes were similar among seven of eight possible treatment strategies assessed in a network meta-analysis published online Sept. 16 in JAMA.
Clinicians have several treatment options but little guidance for choosing among them when managing acute VTE. Many strategies have shown promising results when assessed in single studies, but there have been few direct comparison studies. So investigators performed a network meta-analysis of 45 articles involving 44,989 patients, which enabled them to compare the safety and efficacy of eight possible approaches. The sample sizes of these studies ranged from 60 to 8,240 participants, with a median of 298. The median follow-up period was 3 months, with a range of 3-8 months.
The currently accepted standard treatment for acute VTE is the use of parenteral low-molecular-weight heparin (LMWH) for a minimum of 5 days, followed by transition to a vitamin K antagonist. This approach was compared against parenteral unfractionated heparin followed by a vitamin K antagonist; parenteral fondaparinux followed by a vitamin K antagonist; parenteral LMWH combined with dabigatran; parenteral LMWH combined with edoxaban; oral rivaroxaban; oral apixaban; and parenteral LMWH alone, said Dr. Lana A. Castellucci of the Ottawa Hospital Research Institute, University of Ottawa, and her associates.
Compared with standard parenteral LMWH plus a vitamin K antagonist, six of these approaches yielded comparable reductions in recurrent VTE and induced comparable rates of major bleeding, the investigators said (JAMA 2014 September 16 [doi:10.1001/jama.2014.10538]).
The only strategy that was less effective at reducing the rate of recurrent VTE was parenteral unfractionated heparin plus a vitamin K antagonist. However, “there are clinical circumstances that necessitate the use of unfractionated heparin, including for patients with severe renal insufficiency and those with massive or submassive pulmonary embolism who are potential candidates for thrombolysis or thrombectomy,” Dr. Castellucci and her associates noted.
Oral rivaroxaban and oral apixaban appeared to be associated with the lowest risk of major bleeding. “Future direct comparison trials, patient-level network meta-analyses, or high-quality nonrandomized studies are required to confirm our findings,” they added.
This study was supported by the Heart and Stroke Foundation of Canada, the University of Ottawa, the Canadian Institutes of Health Research, the Canadian Network and Centre for Trials Internationally, and the Heart and Stroke Foundation of Ontario. Dr. Castellucci reported no financial conflicts of interest; some of her associates reported ties to Bayer, Biomerieux, Boehringer Ingelheim, Bristol-Myers Squibb, Leo Pharma, Pfizer, and Sanofi.
*Correction, 9/17/2014: An earlier version of this article misstated the Key Clinical Point in the Vitals section.
For patients with acute venous thromboembolism, both clinical and safety outcomes were similar among seven of eight possible treatment strategies assessed in a network meta-analysis published online Sept. 16 in JAMA.
Clinicians have several treatment options but little guidance for choosing among them when managing acute VTE. Many strategies have shown promising results when assessed in single studies, but there have been few direct comparison studies. So investigators performed a network meta-analysis of 45 articles involving 44,989 patients, which enabled them to compare the safety and efficacy of eight possible approaches. The sample sizes of these studies ranged from 60 to 8,240 participants, with a median of 298. The median follow-up period was 3 months, with a range of 3-8 months.
The currently accepted standard treatment for acute VTE is the use of parenteral low-molecular-weight heparin (LMWH) for a minimum of 5 days, followed by transition to a vitamin K antagonist. This approach was compared against parenteral unfractionated heparin followed by a vitamin K antagonist; parenteral fondaparinux followed by a vitamin K antagonist; parenteral LMWH combined with dabigatran; parenteral LMWH combined with edoxaban; oral rivaroxaban; oral apixaban; and parenteral LMWH alone, said Dr. Lana A. Castellucci of the Ottawa Hospital Research Institute, University of Ottawa, and her associates.
Compared with standard parenteral LMWH plus a vitamin K antagonist, six of these approaches yielded comparable reductions in recurrent VTE and induced comparable rates of major bleeding, the investigators said (JAMA 2014 September 16 [doi:10.1001/jama.2014.10538]).
The only strategy that was less effective at reducing the rate of recurrent VTE was parenteral unfractionated heparin plus a vitamin K antagonist. However, “there are clinical circumstances that necessitate the use of unfractionated heparin, including for patients with severe renal insufficiency and those with massive or submassive pulmonary embolism who are potential candidates for thrombolysis or thrombectomy,” Dr. Castellucci and her associates noted.
Oral rivaroxaban and oral apixaban appeared to be associated with the lowest risk of major bleeding. “Future direct comparison trials, patient-level network meta-analyses, or high-quality nonrandomized studies are required to confirm our findings,” they added.
This study was supported by the Heart and Stroke Foundation of Canada, the University of Ottawa, the Canadian Institutes of Health Research, the Canadian Network and Centre for Trials Internationally, and the Heart and Stroke Foundation of Ontario. Dr. Castellucci reported no financial conflicts of interest; some of her associates reported ties to Bayer, Biomerieux, Boehringer Ingelheim, Bristol-Myers Squibb, Leo Pharma, Pfizer, and Sanofi.
*Correction, 9/17/2014: An earlier version of this article misstated the Key Clinical Point in the Vitals section.
FROM JAMA
Key clinical point: Seven of the eight available VTE therapies are equally safe and effective.*
Major finding: Compared with standard parenteral LMWH plus a vitamin K antagonist, six treatment approaches yielded comparable reductions in recurrent VTE and induced comparable rates of major bleeding; the only approach that was less effective at reducing the rate of recurrent VTE was parenteral unfractionated heparin plus a vitamin K antagonist.
Data source: A network meta-analysis of 45 articles on studies involving 44,989 patients with acute VTE who were treated using any of eight strategies and followed for a median of 3 months.
Disclosures: This study was supported by the Heart and Stroke Foundation of Canada, the University of Ottawa, the Canadian Institutes of Health Research, the Canadian Network and Centre for Trials Internationally, and the Heart and Stroke Foundation of Ontario. Dr. Castellucci reported no financial conflicts of interest; some of her associates reported ties to Bayer, Biomerieux, Boehringer Ingelheim, Bristol-Myers Squibb, Leo Pharma, Pfizer, and Sanofi.
Probiotics for IBS
Irritable bowel syndrome affects up to 15% of the U.S. adult population, which may be an underestimate. When patients are managing themselves well, their clinical course can be routine. When their self-management is poor, IBS can make life exceedingly challenging for both patients and their clinicians. Many of us may be stepping up our game in patients with known IBS experiencing symptoms, first by recommending a diet low in FODMAPs (fermentable oligo-, di-, and monosaccharides and polyols), which have been shown to reduce IBS symptoms.
My experience is that patients who have been struggling for years with IBS have a high degree of health literacy. And they are usually receptive to trying new things that might make their lives better. The exceptions are the occasional patients who are convinced that they do not have IBS and that their clinicians are just too poorly informed to figure out what the real cause is.
Anything else we can recommend?
Jun Sik Yoon and colleagues have published a clinical trial evaluating the effectiveness of multispecies probiotics on IBS symptoms and changes in the gut microbiota. In this randomized, placebo-controlled trial, 49 subjects (25 probiotics, 24 placebo) with clinically-diagnosed IBS received tablets twice a day for 4 weeks. The primary outcome was the proportion of individuals whose IBS symptoms were substantially relieved at 4 weeks.
Probiotics were associated with a significantly higher proportion of patients with reductions in IBS symptoms (68% vs. 37.5%; P < .05). Probiotics also improved abdominal pain/discomfort and bloating. Fecal analysis revealed increases in the microbiota obtained with the probiotics (J. Gastroenterol. Hepatol. 2014;29:52-9).
So probiotics may help our patients with IBS if a low FODMAP diet does not. But what probiotic (i.e., containing which species) should we select? Species may have different effects on gut motility. Importantly, taking probiotics with certain species does not mean that those species will set up permanent residence in the colon. In the current study, only three of the six species contained in the probiotics were still in the stool after 4 weeks. The author concluded that the alleviation in bowel symptoms was attributable to Bifidobacterium lactis, Lactobacillus rhamnosus, and Streptococcus thermophiles. So let’s tell patients to look for probiotics with these species.
Probiotics are generally safe with the only possible contraindication being their use in patients with a severely immunocompromised state, but this is debatable. But now we have another evidence-based tool for our patients struggling with symptom recrudescence.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.
Irritable bowel syndrome affects up to 15% of the U.S. adult population, which may be an underestimate. When patients are managing themselves well, their clinical course can be routine. When their self-management is poor, IBS can make life exceedingly challenging for both patients and their clinicians. Many of us may be stepping up our game in patients with known IBS experiencing symptoms, first by recommending a diet low in FODMAPs (fermentable oligo-, di-, and monosaccharides and polyols), which have been shown to reduce IBS symptoms.
My experience is that patients who have been struggling for years with IBS have a high degree of health literacy. And they are usually receptive to trying new things that might make their lives better. The exceptions are the occasional patients who are convinced that they do not have IBS and that their clinicians are just too poorly informed to figure out what the real cause is.
Anything else we can recommend?
Jun Sik Yoon and colleagues have published a clinical trial evaluating the effectiveness of multispecies probiotics on IBS symptoms and changes in the gut microbiota. In this randomized, placebo-controlled trial, 49 subjects (25 probiotics, 24 placebo) with clinically-diagnosed IBS received tablets twice a day for 4 weeks. The primary outcome was the proportion of individuals whose IBS symptoms were substantially relieved at 4 weeks.
Probiotics were associated with a significantly higher proportion of patients with reductions in IBS symptoms (68% vs. 37.5%; P < .05). Probiotics also improved abdominal pain/discomfort and bloating. Fecal analysis revealed increases in the microbiota obtained with the probiotics (J. Gastroenterol. Hepatol. 2014;29:52-9).
So probiotics may help our patients with IBS if a low FODMAP diet does not. But what probiotic (i.e., containing which species) should we select? Species may have different effects on gut motility. Importantly, taking probiotics with certain species does not mean that those species will set up permanent residence in the colon. In the current study, only three of the six species contained in the probiotics were still in the stool after 4 weeks. The author concluded that the alleviation in bowel symptoms was attributable to Bifidobacterium lactis, Lactobacillus rhamnosus, and Streptococcus thermophiles. So let’s tell patients to look for probiotics with these species.
Probiotics are generally safe with the only possible contraindication being their use in patients with a severely immunocompromised state, but this is debatable. But now we have another evidence-based tool for our patients struggling with symptom recrudescence.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.
Irritable bowel syndrome affects up to 15% of the U.S. adult population, which may be an underestimate. When patients are managing themselves well, their clinical course can be routine. When their self-management is poor, IBS can make life exceedingly challenging for both patients and their clinicians. Many of us may be stepping up our game in patients with known IBS experiencing symptoms, first by recommending a diet low in FODMAPs (fermentable oligo-, di-, and monosaccharides and polyols), which have been shown to reduce IBS symptoms.
My experience is that patients who have been struggling for years with IBS have a high degree of health literacy. And they are usually receptive to trying new things that might make their lives better. The exceptions are the occasional patients who are convinced that they do not have IBS and that their clinicians are just too poorly informed to figure out what the real cause is.
Anything else we can recommend?
Jun Sik Yoon and colleagues have published a clinical trial evaluating the effectiveness of multispecies probiotics on IBS symptoms and changes in the gut microbiota. In this randomized, placebo-controlled trial, 49 subjects (25 probiotics, 24 placebo) with clinically-diagnosed IBS received tablets twice a day for 4 weeks. The primary outcome was the proportion of individuals whose IBS symptoms were substantially relieved at 4 weeks.
Probiotics were associated with a significantly higher proportion of patients with reductions in IBS symptoms (68% vs. 37.5%; P < .05). Probiotics also improved abdominal pain/discomfort and bloating. Fecal analysis revealed increases in the microbiota obtained with the probiotics (J. Gastroenterol. Hepatol. 2014;29:52-9).
So probiotics may help our patients with IBS if a low FODMAP diet does not. But what probiotic (i.e., containing which species) should we select? Species may have different effects on gut motility. Importantly, taking probiotics with certain species does not mean that those species will set up permanent residence in the colon. In the current study, only three of the six species contained in the probiotics were still in the stool after 4 weeks. The author concluded that the alleviation in bowel symptoms was attributable to Bifidobacterium lactis, Lactobacillus rhamnosus, and Streptococcus thermophiles. So let’s tell patients to look for probiotics with these species.
Probiotics are generally safe with the only possible contraindication being their use in patients with a severely immunocompromised state, but this is debatable. But now we have another evidence-based tool for our patients struggling with symptom recrudescence.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician.
