User login
Mitchel is a reporter for MDedge based in the Philadelphia area. He started with the company in 1992, when it was International Medical News Group (IMNG), and has since covered a range of medical specialties. Mitchel trained as a virologist at Roswell Park Memorial Institute in Buffalo, and then worked briefly as a researcher at Boston Children's Hospital before pivoting to journalism as a AAAS Mass Media Fellow in 1980. His first reporting job was with Science Digest magazine, and from the mid-1980s to early-1990s he was a reporter with Medical World News. @mitchelzoler
Two approved antibiotics show new gonorrhea efficacy
VIENNA – Two combination regimens using antibiotics already approved for U.S. use eradicated urogenital gonorrhea infections with virtually 100% efficacy in a multicenter U.S. study with about 400 patients, providing solid evidence for the potential of both combinations as backup treatments for Neisseria gonorrhoeae at a time when resistance in the pathogen has whittled standard treatment options down to one primary drug, ceftriaxone.
"The emergence of cephalosporin resistance complicates empiric treatment" of gonorrhea infections, Dr. Robert D. Kirkcaldy said at the joint meeting of the International Society for Sexually Transmitted Diseases Research and the International Union Against Sexually Transmitted Infections.
The two new combinations he and his associates tested – gentamicin plus azithromycin (Zithromax) and gemifloxicin (Factive) plus azithromycin – "may be useful for patients unsuccessfully treated with ceftriaxone or patients with a cephalosporin allergy, but neither [of the two new combinations] is a magic bullet," said Dr. Kirkcaldy, a medical epidemiologist in the division of STD prevention at the Centers for Disease Control and Prevention. "The gastrointestinal side effects [seen with both new regimens] may limit their routine use."
Gastrointestinal adverse effects occurred in 47% of the patients who received gentamicin plus azithromycin and in 55% of those who got gemifloxacin plus azithromycin. But Dr. Kirkcaldy highlighted that all of these effects were mild to moderate, none was serious, and the vast majority of patients were able to hold the oral drugs they received for more than an hour; 3% of the gentamicin recipients and 8% of the gemifloxacin recipients vomited within an hour of receiving treatment and were excluded from the primary efficacy analysis as a result.
"These trial results are an exciting step in the right direction in the fight against drug-resistant gonorrhea, but patients need more oral options with fewer side effects," Dr. Gail Bolan, director of the CDC’s division of STD prevention, commented in a written statement.
Less than a year ago, in August 2012, a panel of CDC staffers and outside experts released updated recommendations for treating all types of uncomplicated gonococcal infections, including anorectal, pharyngeal, and urogenital infections. The CDC recommended a single intramuscular injection of ceftriaxone (Rocephin) along with a single oral dose of azithromycin or a 7-day course of doxycycline given b.i.d. (MMWR 2012;61:590-4).
This recommendation came about because of an increasing U.S. incidence of gonococcal infections by strains resistant to cefixime (Suprax), the prior mainstay of treatment. The need to move from cefixime to ceftriaxone also concerned the CDC. The agency projects that patients may soon also face ceftriaxone-resistant gonorrhea.
"Ceftriaxone became the one remaining first-line option. The antimicrobial pipeline is running dry, and N. gonorrhoeae continues to acquire resistance. We wanted to repurpose approved drugs that could be used for salvage treatment on cetriaxone failures and for patients allergic to cephalosporins," Dr. Kirkcaldy said.
The study enrolled patients aged 15-60 years who presented at any one of five participating U.S. medical centers with uncomplicated, untreated urogenital gonorrhea. The 401 patients who completed the study averaged about 28 years of age. About a third were men who have sex with men, slightly more than half were men who have sex with women, and about 10% were women. Just under 10% were HIV positive. Patients received either 240 mg gentamicin as an intramuscular injection at two separate sites (with the dosage adjusted downward for patients weighing 45 kg or less) or a single, 320-mg oral dose of gemifloxacin. All patients also received a 2-g oral dose of azithromycin.
Gentamicin, a drug primarily used for hospitalized patients with endocarditis, was chosen because of its known, modest (about 91.5%) efficacy for gonorrhea, low risk of toxicity with a single dose in otherwise healthy men and women, and its U.S. availability, Dr. Kirkcaldy said. Gemifloxacin was selected because it’s an oral drug approved for sale in the United States that’s been shown to be active in vitro against ciprofloxacin-resistant strains of N. gonorrhoeae. Azithromycin was added because of its known activity against gonorrhea, although with recent eradication rates of 97%-99%, it is now deemed too unreliable for monotherapy.
The study's primary efficacy endpoint was the percentage of patients who successfully received treatment and returned for a follow-up microbiologic test of eradication. This happened in all 202 patients treated with gentamicin plus azithromycin, and in 198 of the 199 (99.5%) treated with gemifloxacin plus azithromycin. A small percentage of the patients enrolled also had rectal or pharyngeal gonococcal infections in addition to their urogenital infection. Both treatments were 100% effective at eradicating infections at those sites, but the numbers were too small to conclusively prove efficacy for these sites, he said.
These new data will be considered as the CDC develops its next revision of the U.S. STD treatment guidelines, due out next year, Dr. Kirkcaldy said.
The study was sponsored by the National Institute of Allergy and Infectious Diseases. Dr. Kirkcaldy said he had no relevant financial disclosures.
On Twitter @mitchelzoler
VIENNA – Two combination regimens using antibiotics already approved for U.S. use eradicated urogenital gonorrhea infections with virtually 100% efficacy in a multicenter U.S. study with about 400 patients, providing solid evidence for the potential of both combinations as backup treatments for Neisseria gonorrhoeae at a time when resistance in the pathogen has whittled standard treatment options down to one primary drug, ceftriaxone.
"The emergence of cephalosporin resistance complicates empiric treatment" of gonorrhea infections, Dr. Robert D. Kirkcaldy said at the joint meeting of the International Society for Sexually Transmitted Diseases Research and the International Union Against Sexually Transmitted Infections.
The two new combinations he and his associates tested – gentamicin plus azithromycin (Zithromax) and gemifloxicin (Factive) plus azithromycin – "may be useful for patients unsuccessfully treated with ceftriaxone or patients with a cephalosporin allergy, but neither [of the two new combinations] is a magic bullet," said Dr. Kirkcaldy, a medical epidemiologist in the division of STD prevention at the Centers for Disease Control and Prevention. "The gastrointestinal side effects [seen with both new regimens] may limit their routine use."
Gastrointestinal adverse effects occurred in 47% of the patients who received gentamicin plus azithromycin and in 55% of those who got gemifloxacin plus azithromycin. But Dr. Kirkcaldy highlighted that all of these effects were mild to moderate, none was serious, and the vast majority of patients were able to hold the oral drugs they received for more than an hour; 3% of the gentamicin recipients and 8% of the gemifloxacin recipients vomited within an hour of receiving treatment and were excluded from the primary efficacy analysis as a result.
"These trial results are an exciting step in the right direction in the fight against drug-resistant gonorrhea, but patients need more oral options with fewer side effects," Dr. Gail Bolan, director of the CDC’s division of STD prevention, commented in a written statement.
Less than a year ago, in August 2012, a panel of CDC staffers and outside experts released updated recommendations for treating all types of uncomplicated gonococcal infections, including anorectal, pharyngeal, and urogenital infections. The CDC recommended a single intramuscular injection of ceftriaxone (Rocephin) along with a single oral dose of azithromycin or a 7-day course of doxycycline given b.i.d. (MMWR 2012;61:590-4).
This recommendation came about because of an increasing U.S. incidence of gonococcal infections by strains resistant to cefixime (Suprax), the prior mainstay of treatment. The need to move from cefixime to ceftriaxone also concerned the CDC. The agency projects that patients may soon also face ceftriaxone-resistant gonorrhea.
"Ceftriaxone became the one remaining first-line option. The antimicrobial pipeline is running dry, and N. gonorrhoeae continues to acquire resistance. We wanted to repurpose approved drugs that could be used for salvage treatment on cetriaxone failures and for patients allergic to cephalosporins," Dr. Kirkcaldy said.
The study enrolled patients aged 15-60 years who presented at any one of five participating U.S. medical centers with uncomplicated, untreated urogenital gonorrhea. The 401 patients who completed the study averaged about 28 years of age. About a third were men who have sex with men, slightly more than half were men who have sex with women, and about 10% were women. Just under 10% were HIV positive. Patients received either 240 mg gentamicin as an intramuscular injection at two separate sites (with the dosage adjusted downward for patients weighing 45 kg or less) or a single, 320-mg oral dose of gemifloxacin. All patients also received a 2-g oral dose of azithromycin.
Gentamicin, a drug primarily used for hospitalized patients with endocarditis, was chosen because of its known, modest (about 91.5%) efficacy for gonorrhea, low risk of toxicity with a single dose in otherwise healthy men and women, and its U.S. availability, Dr. Kirkcaldy said. Gemifloxacin was selected because it’s an oral drug approved for sale in the United States that’s been shown to be active in vitro against ciprofloxacin-resistant strains of N. gonorrhoeae. Azithromycin was added because of its known activity against gonorrhea, although with recent eradication rates of 97%-99%, it is now deemed too unreliable for monotherapy.
The study's primary efficacy endpoint was the percentage of patients who successfully received treatment and returned for a follow-up microbiologic test of eradication. This happened in all 202 patients treated with gentamicin plus azithromycin, and in 198 of the 199 (99.5%) treated with gemifloxacin plus azithromycin. A small percentage of the patients enrolled also had rectal or pharyngeal gonococcal infections in addition to their urogenital infection. Both treatments were 100% effective at eradicating infections at those sites, but the numbers were too small to conclusively prove efficacy for these sites, he said.
These new data will be considered as the CDC develops its next revision of the U.S. STD treatment guidelines, due out next year, Dr. Kirkcaldy said.
The study was sponsored by the National Institute of Allergy and Infectious Diseases. Dr. Kirkcaldy said he had no relevant financial disclosures.
On Twitter @mitchelzoler
VIENNA – Two combination regimens using antibiotics already approved for U.S. use eradicated urogenital gonorrhea infections with virtually 100% efficacy in a multicenter U.S. study with about 400 patients, providing solid evidence for the potential of both combinations as backup treatments for Neisseria gonorrhoeae at a time when resistance in the pathogen has whittled standard treatment options down to one primary drug, ceftriaxone.
"The emergence of cephalosporin resistance complicates empiric treatment" of gonorrhea infections, Dr. Robert D. Kirkcaldy said at the joint meeting of the International Society for Sexually Transmitted Diseases Research and the International Union Against Sexually Transmitted Infections.
The two new combinations he and his associates tested – gentamicin plus azithromycin (Zithromax) and gemifloxicin (Factive) plus azithromycin – "may be useful for patients unsuccessfully treated with ceftriaxone or patients with a cephalosporin allergy, but neither [of the two new combinations] is a magic bullet," said Dr. Kirkcaldy, a medical epidemiologist in the division of STD prevention at the Centers for Disease Control and Prevention. "The gastrointestinal side effects [seen with both new regimens] may limit their routine use."
Gastrointestinal adverse effects occurred in 47% of the patients who received gentamicin plus azithromycin and in 55% of those who got gemifloxacin plus azithromycin. But Dr. Kirkcaldy highlighted that all of these effects were mild to moderate, none was serious, and the vast majority of patients were able to hold the oral drugs they received for more than an hour; 3% of the gentamicin recipients and 8% of the gemifloxacin recipients vomited within an hour of receiving treatment and were excluded from the primary efficacy analysis as a result.
"These trial results are an exciting step in the right direction in the fight against drug-resistant gonorrhea, but patients need more oral options with fewer side effects," Dr. Gail Bolan, director of the CDC’s division of STD prevention, commented in a written statement.
Less than a year ago, in August 2012, a panel of CDC staffers and outside experts released updated recommendations for treating all types of uncomplicated gonococcal infections, including anorectal, pharyngeal, and urogenital infections. The CDC recommended a single intramuscular injection of ceftriaxone (Rocephin) along with a single oral dose of azithromycin or a 7-day course of doxycycline given b.i.d. (MMWR 2012;61:590-4).
This recommendation came about because of an increasing U.S. incidence of gonococcal infections by strains resistant to cefixime (Suprax), the prior mainstay of treatment. The need to move from cefixime to ceftriaxone also concerned the CDC. The agency projects that patients may soon also face ceftriaxone-resistant gonorrhea.
"Ceftriaxone became the one remaining first-line option. The antimicrobial pipeline is running dry, and N. gonorrhoeae continues to acquire resistance. We wanted to repurpose approved drugs that could be used for salvage treatment on cetriaxone failures and for patients allergic to cephalosporins," Dr. Kirkcaldy said.
The study enrolled patients aged 15-60 years who presented at any one of five participating U.S. medical centers with uncomplicated, untreated urogenital gonorrhea. The 401 patients who completed the study averaged about 28 years of age. About a third were men who have sex with men, slightly more than half were men who have sex with women, and about 10% were women. Just under 10% were HIV positive. Patients received either 240 mg gentamicin as an intramuscular injection at two separate sites (with the dosage adjusted downward for patients weighing 45 kg or less) or a single, 320-mg oral dose of gemifloxacin. All patients also received a 2-g oral dose of azithromycin.
Gentamicin, a drug primarily used for hospitalized patients with endocarditis, was chosen because of its known, modest (about 91.5%) efficacy for gonorrhea, low risk of toxicity with a single dose in otherwise healthy men and women, and its U.S. availability, Dr. Kirkcaldy said. Gemifloxacin was selected because it’s an oral drug approved for sale in the United States that’s been shown to be active in vitro against ciprofloxacin-resistant strains of N. gonorrhoeae. Azithromycin was added because of its known activity against gonorrhea, although with recent eradication rates of 97%-99%, it is now deemed too unreliable for monotherapy.
The study's primary efficacy endpoint was the percentage of patients who successfully received treatment and returned for a follow-up microbiologic test of eradication. This happened in all 202 patients treated with gentamicin plus azithromycin, and in 198 of the 199 (99.5%) treated with gemifloxacin plus azithromycin. A small percentage of the patients enrolled also had rectal or pharyngeal gonococcal infections in addition to their urogenital infection. Both treatments were 100% effective at eradicating infections at those sites, but the numbers were too small to conclusively prove efficacy for these sites, he said.
These new data will be considered as the CDC develops its next revision of the U.S. STD treatment guidelines, due out next year, Dr. Kirkcaldy said.
The study was sponsored by the National Institute of Allergy and Infectious Diseases. Dr. Kirkcaldy said he had no relevant financial disclosures.
On Twitter @mitchelzoler
AT THE STI & AIDS WORLD CONGRESS 2013

Two approved antibiotics show new gonorrhea efficacy
VIENNA – Two combination regimens using antibiotics already approved for U.S. use eradicated urogenital gonorrhea infections with virtually 100% efficacy in a multicenter U.S. study with about 400 patients, providing solid evidence for the potential of both combinations as backup treatments for Neisseria gonorrhoeae at a time when resistance in the pathogen has whittled standard treatment options down to one primary drug, ceftriaxone.
"The emergence of cephalosporin resistance complicates empiric treatment" of gonorrhea infections, Dr. Robert D. Kirkcaldy said at the joint meeting of the International Society for Sexually Transmitted Diseases Research and the International Union Against Sexually Transmitted Infections.

The two new combinations he and his associates tested – gentamicin plus azithromycin (Zithromax) and gemifloxicin (Factive) plus azithromycin – "may be useful for patients unsuccessfully treated with ceftriaxone or patients with a cephalosporin allergy, but neither [of the two new combinations] is a magic bullet," said Dr. Kirkcaldy, a medical epidemiologist in the division of STD prevention at the Centers for Disease Control and Prevention. "The gastrointestinal side effects [seen with both new regimens] may limit their routine use."
Gastrointestinal adverse effects occurred in 47% of the patients who received gentamicin plus azithromycin and in 55% of those who got gemifloxacin plus azithromycin. But Dr. Kirkcaldy highlighted that all of these effects were mild to moderate, none was serious, and the vast majority of patients were able to hold the oral drugs they received for more than an hour; 3% of the gentamicin recipients and 8% of the gemifloxacin recipients vomited within an hour of receiving treatment and were excluded from the primary efficacy analysis as a result.
"These trial results are an exciting step in the right direction in the fight against drug-resistant gonorrhea, but patients need more oral options with fewer side effects," Dr. Gail Bolan, director of the CDC’s division of STD prevention, commented in a written statement.
Less than a year ago, in August 2012, a panel of CDC staffers and outside experts released updated recommendations for treating all types of uncomplicated gonococcal infections, including anorectal, pharyngeal, and urogenital infections. The CDC recommended a single intramuscular injection of ceftriaxone (Rocephin) along with a single oral dose of azithromycin or a 7-day course of doxycycline given b.i.d. (MMWR 2012;61:590-4).
This recommendation came about because of an increasing U.S. incidence of gonococcal infections by strains resistant to cefixime (Suprax), the prior mainstay of treatment. The need to move from cefixime to ceftriaxone also concerned the CDC. The agency projects that patients may soon also face ceftriaxone-resistant gonorrhea.
"Ceftriaxone became the one remaining first-line option. The antimicrobial pipeline is running dry, and N. gonorrhoeae continues to acquire resistance. We wanted to repurpose approved drugs that could be used for salvage treatment on cetriaxone failures and for patients allergic to cephalosporins," Dr. Kirkcaldy said.
The study enrolled patients aged 15-60 years who presented at any one of five participating U.S. medical centers with uncomplicated, untreated urogenital gonorrhea. The 401 patients who completed the study averaged about 28 years of age. About a third were men who have sex with men, slightly more than half were men who have sex with women, and about 10% were women. Just under 10% were HIV positive. Patients received either 240 mg gentamicin as an intramuscular injection at two separate sites (with the dosage adjusted downward for patients weighing 45 kg or less) or a single, 320-mg oral dose of gemifloxacin. All patients also received a 2-g oral dose of azithromycin.
Gentamicin, a drug primarily used for hospitalized patients with endocarditis, was chosen because of its known, modest (about 91.5%) efficacy for gonorrhea, low risk of toxicity with a single dose in otherwise healthy men and women, and its U.S. availability, Dr. Kirkcaldy said. Gemifloxacin was selected because it’s an oral drug approved for sale in the United States that’s been shown to be active in vitro against ciprofloxacin-resistant strains of N. gonorrhoeae. Azithromycin was added because of its known activity against gonorrhea, although with recent eradication rates of 97%-99%, it is now deemed too unreliable for monotherapy.
The study's primary efficacy endpoint was the percentage of patients who successfully received treatment and returned for a follow-up microbiologic test of eradication. This happened in all 202 patients treated with gentamicin plus azithromycin, and in 198 of the 199 (99.5%) treated with gemifloxacin plus azithromycin. A small percentage of the patients enrolled also had rectal or pharyngeal gonococcal infections in addition to their urogenital infection. Both treatments were 100% effective at eradicating infections at those sites, but the numbers were too small to conclusively prove efficacy for these sites, he said.
These new data will be considered as the CDC develops its next revision of the U.S. STD treatment guidelines, due out next year, Dr. Kirkcaldy said.
The study was sponsored by the National Institute of Allergy and Infectious Diseases. Dr. Kirkcaldy said he had no relevant financial disclosures.
On Twitter @mitchelzoler
VIENNA – Two combination regimens using antibiotics already approved for U.S. use eradicated urogenital gonorrhea infections with virtually 100% efficacy in a multicenter U.S. study with about 400 patients, providing solid evidence for the potential of both combinations as backup treatments for Neisseria gonorrhoeae at a time when resistance in the pathogen has whittled standard treatment options down to one primary drug, ceftriaxone.
"The emergence of cephalosporin resistance complicates empiric treatment" of gonorrhea infections, Dr. Robert D. Kirkcaldy said at the joint meeting of the International Society for Sexually Transmitted Diseases Research and the International Union Against Sexually Transmitted Infections.
The two new combinations he and his associates tested – gentamicin plus azithromycin (Zithromax) and gemifloxicin (Factive) plus azithromycin – "may be useful for patients unsuccessfully treated with ceftriaxone or patients with a cephalosporin allergy, but neither [of the two new combinations] is a magic bullet," said Dr. Kirkcaldy, a medical epidemiologist in the division of STD prevention at the Centers for Disease Control and Prevention. "The gastrointestinal side effects [seen with both new regimens] may limit their routine use."
Gastrointestinal adverse effects occurred in 47% of the patients who received gentamicin plus azithromycin and in 55% of those who got gemifloxacin plus azithromycin. But Dr. Kirkcaldy highlighted that all of these effects were mild to moderate, none was serious, and the vast majority of patients were able to hold the oral drugs they received for more than an hour; 3% of the gentamicin recipients and 8% of the gemifloxacin recipients vomited within an hour of receiving treatment and were excluded from the primary efficacy analysis as a result.
"These trial results are an exciting step in the right direction in the fight against drug-resistant gonorrhea, but patients need more oral options with fewer side effects," Dr. Gail Bolan, director of the CDC’s division of STD prevention, commented in a written statement.
Less than a year ago, in August 2012, a panel of CDC staffers and outside experts released updated recommendations for treating all types of uncomplicated gonococcal infections, including anorectal, pharyngeal, and urogenital infections. The CDC recommended a single intramuscular injection of ceftriaxone (Rocephin) along with a single oral dose of azithromycin or a 7-day course of doxycycline given b.i.d. (MMWR 2012;61:590-4).
This recommendation came about because of an increasing U.S. incidence of gonococcal infections by strains resistant to cefixime (Suprax), the prior mainstay of treatment. The need to move from cefixime to ceftriaxone also concerned the CDC. The agency projects that patients may soon also face ceftriaxone-resistant gonorrhea.
"Ceftriaxone became the one remaining first-line option. The antimicrobial pipeline is running dry, and N. gonorrhoeae continues to acquire resistance. We wanted to repurpose approved drugs that could be used for salvage treatment on cetriaxone failures and for patients allergic to cephalosporins," Dr. Kirkcaldy said.
The study enrolled patients aged 15-60 years who presented at any one of five participating U.S. medical centers with uncomplicated, untreated urogenital gonorrhea. The 401 patients who completed the study averaged about 28 years of age. About a third were men who have sex with men, slightly more than half were men who have sex with women, and about 10% were women. Just under 10% were HIV positive. Patients received either 240 mg gentamicin as an intramuscular injection at two separate sites (with the dosage adjusted downward for patients weighing 45 kg or less) or a single, 320-mg oral dose of gemifloxacin. All patients also received a 2-g oral dose of azithromycin.
Gentamicin, a drug primarily used for hospitalized patients with endocarditis, was chosen because of its known, modest (about 91.5%) efficacy for gonorrhea, low risk of toxicity with a single dose in otherwise healthy men and women, and its U.S. availability, Dr. Kirkcaldy said. Gemifloxacin was selected because it’s an oral drug approved for sale in the United States that’s been shown to be active in vitro against ciprofloxacin-resistant strains of N. gonorrhoeae. Azithromycin was added because of its known activity against gonorrhea, although with recent eradication rates of 97%-99%, it is now deemed too unreliable for monotherapy.
The study's primary efficacy endpoint was the percentage of patients who successfully received treatment and returned for a follow-up microbiologic test of eradication. This happened in all 202 patients treated with gentamicin plus azithromycin, and in 198 of the 199 (99.5%) treated with gemifloxacin plus azithromycin. A small percentage of the patients enrolled also had rectal or pharyngeal gonococcal infections in addition to their urogenital infection. Both treatments were 100% effective at eradicating infections at those sites, but the numbers were too small to conclusively prove efficacy for these sites, he said.
These new data will be considered as the CDC develops its next revision of the U.S. STD treatment guidelines, due out next year, Dr. Kirkcaldy said.
The study was sponsored by the National Institute of Allergy and Infectious Diseases. Dr. Kirkcaldy said he had no relevant financial disclosures.
On Twitter @mitchelzoler
VIENNA – Two combination regimens using antibiotics already approved for U.S. use eradicated urogenital gonorrhea infections with virtually 100% efficacy in a multicenter U.S. study with about 400 patients, providing solid evidence for the potential of both combinations as backup treatments for Neisseria gonorrhoeae at a time when resistance in the pathogen has whittled standard treatment options down to one primary drug, ceftriaxone.
"The emergence of cephalosporin resistance complicates empiric treatment" of gonorrhea infections, Dr. Robert D. Kirkcaldy said at the joint meeting of the International Society for Sexually Transmitted Diseases Research and the International Union Against Sexually Transmitted Infections.
The two new combinations he and his associates tested – gentamicin plus azithromycin (Zithromax) and gemifloxicin (Factive) plus azithromycin – "may be useful for patients unsuccessfully treated with ceftriaxone or patients with a cephalosporin allergy, but neither [of the two new combinations] is a magic bullet," said Dr. Kirkcaldy, a medical epidemiologist in the division of STD prevention at the Centers for Disease Control and Prevention. "The gastrointestinal side effects [seen with both new regimens] may limit their routine use."
Gastrointestinal adverse effects occurred in 47% of the patients who received gentamicin plus azithromycin and in 55% of those who got gemifloxacin plus azithromycin. But Dr. Kirkcaldy highlighted that all of these effects were mild to moderate, none was serious, and the vast majority of patients were able to hold the oral drugs they received for more than an hour; 3% of the gentamicin recipients and 8% of the gemifloxacin recipients vomited within an hour of receiving treatment and were excluded from the primary efficacy analysis as a result.
"These trial results are an exciting step in the right direction in the fight against drug-resistant gonorrhea, but patients need more oral options with fewer side effects," Dr. Gail Bolan, director of the CDC’s division of STD prevention, commented in a written statement.
Less than a year ago, in August 2012, a panel of CDC staffers and outside experts released updated recommendations for treating all types of uncomplicated gonococcal infections, including anorectal, pharyngeal, and urogenital infections. The CDC recommended a single intramuscular injection of ceftriaxone (Rocephin) along with a single oral dose of azithromycin or a 7-day course of doxycycline given b.i.d. (MMWR 2012;61:590-4).
This recommendation came about because of an increasing U.S. incidence of gonococcal infections by strains resistant to cefixime (Suprax), the prior mainstay of treatment. The need to move from cefixime to ceftriaxone also concerned the CDC. The agency projects that patients may soon also face ceftriaxone-resistant gonorrhea.
"Ceftriaxone became the one remaining first-line option. The antimicrobial pipeline is running dry, and N. gonorrhoeae continues to acquire resistance. We wanted to repurpose approved drugs that could be used for salvage treatment on cetriaxone failures and for patients allergic to cephalosporins," Dr. Kirkcaldy said.
The study enrolled patients aged 15-60 years who presented at any one of five participating U.S. medical centers with uncomplicated, untreated urogenital gonorrhea. The 401 patients who completed the study averaged about 28 years of age. About a third were men who have sex with men, slightly more than half were men who have sex with women, and about 10% were women. Just under 10% were HIV positive. Patients received either 240 mg gentamicin as an intramuscular injection at two separate sites (with the dosage adjusted downward for patients weighing 45 kg or less) or a single, 320-mg oral dose of gemifloxacin. All patients also received a 2-g oral dose of azithromycin.
Gentamicin, a drug primarily used for hospitalized patients with endocarditis, was chosen because of its known, modest (about 91.5%) efficacy for gonorrhea, low risk of toxicity with a single dose in otherwise healthy men and women, and its U.S. availability, Dr. Kirkcaldy said. Gemifloxacin was selected because it’s an oral drug approved for sale in the United States that’s been shown to be active in vitro against ciprofloxacin-resistant strains of N. gonorrhoeae. Azithromycin was added because of its known activity against gonorrhea, although with recent eradication rates of 97%-99%, it is now deemed too unreliable for monotherapy.
The study's primary efficacy endpoint was the percentage of patients who successfully received treatment and returned for a follow-up microbiologic test of eradication. This happened in all 202 patients treated with gentamicin plus azithromycin, and in 198 of the 199 (99.5%) treated with gemifloxacin plus azithromycin. A small percentage of the patients enrolled also had rectal or pharyngeal gonococcal infections in addition to their urogenital infection. Both treatments were 100% effective at eradicating infections at those sites, but the numbers were too small to conclusively prove efficacy for these sites, he said.
These new data will be considered as the CDC develops its next revision of the U.S. STD treatment guidelines, due out next year, Dr. Kirkcaldy said.
The study was sponsored by the National Institute of Allergy and Infectious Diseases. Dr. Kirkcaldy said he had no relevant financial disclosures.
On Twitter @mitchelzoler
AT THE STI & AIDS WORLD CONGRESS 2013
Major finding: Gentamicin plus azithromycin was 100% effective and gemfloxacin plus azithromycin was 99.5% effective for eradication of urogenital gonorrhea.
Data source: An open-label study of two antibiotic regimens in 401 patients at five U.S. sites.
Disclosures: The study was sponsored by the National Institute of Allergy and Infectious Diseases. Dr. Kirkcaldy said he had no relevant financial disclosures.

Sickle cell disease linked to VTE risk
AMSTERDAM – Adult patients who become hospitalized and have sickle cell disease have about a sixfold increased risk of developing venous thromboembolism during the following weeks and months, compared with hospitalized patients without sickle cell disease, in a case-control study of more than 25,000 people admitted to or seen at California hospitals during 1990-2010.
Since 46% of the venous thromboembolism (VTE) episodes in patients with sickle cell disease happened within 30 days of a hospitalization or emergency department visit, the painful, inflammatory episodes that often drive patients with sickle cell disease to seek hospitalization may also provoke VTE said Dr. Ted Wun and his associates in a poster presented at a congress of the International Society on Thrombosis and Haemostasis. Relative immobilization during hospitalization may also play a role in triggering VTE in these patients, suggesting that "robust" thromboprophylaxis be applied to patients with sickle cell disease who enter a hospital, said Dr. Wun, professor of medicine and chief of hematology and oncology at the University of California, Davis, in Sacramento.
The analysis also showed the impact of VTE episodes. After 10 years of follow-up, cumulative mortality was just under 20% in patients with sickle cell disease who did not have a VTE, and more than 40% in patients who had a VTE, a statistically significant difference in an actuarial analysis.
The risk for VTE posed by sickle cell disease was even higher in the 42% of patients with severe sickle cell disease, defined as patients who had three or more hospitalizations or emergency department visits during the prior year. Patients in the severe subgroup had a 9.5-fold higher rate of VTE, compared with controls who had no sickle cell disease. Among the 58% of sickle cell patients without severe disease, the incidence of VTE was fourfold greater than among those without sickle cell disease.
Dr. Wun and his associates used data collected in the California Patient Discharge Dataset and in California’s Emergency Department Utilization database. They identified 4,280 patients 18-65 years old with sickle cell disease who were either hospitalized or seen at an emergency department during 1990-2010. They matched each of these sickle cell patients with five patients hospitalized or seen at emergency departments who did not have sickle cell disease. Matching included age, sex, race, ethnicity, and year of index event. The researchers could track each of the more than 25,000 total patients through subsequent hospitalizations and emergency-department visits by their unique identifier codes.
The patients with sickle cell disease averaged 28 years old, 91% were black, and during follow-up they had an 8% incidence of VTE.
The analysis also showed that comorbidities increased the risk for VTE, although not as strongly as sickle cell disease. For the entire group of more than 25,000 patients having three or more comorbidities linked with a threefold higher rate of VTEs, compared with those without any comorbidities. Among only patients with sickle cell disease, having three or more comorbidities boosted the VTE rate by a statistically-significant 67%, compared with sickle cell patients without any comorbidities. Female sex also significantly linked with a boosted VTE rate among patients with sickle cell disease. Women with sickle cell disease had 43% more VTE episodes than did men with sickle cell disease in the adjusted analysis.
Dr. Wun had no disclosures.
On Twitter @mitchelzoler
AMSTERDAM – Adult patients who become hospitalized and have sickle cell disease have about a sixfold increased risk of developing venous thromboembolism during the following weeks and months, compared with hospitalized patients without sickle cell disease, in a case-control study of more than 25,000 people admitted to or seen at California hospitals during 1990-2010.
Since 46% of the venous thromboembolism (VTE) episodes in patients with sickle cell disease happened within 30 days of a hospitalization or emergency department visit, the painful, inflammatory episodes that often drive patients with sickle cell disease to seek hospitalization may also provoke VTE said Dr. Ted Wun and his associates in a poster presented at a congress of the International Society on Thrombosis and Haemostasis. Relative immobilization during hospitalization may also play a role in triggering VTE in these patients, suggesting that "robust" thromboprophylaxis be applied to patients with sickle cell disease who enter a hospital, said Dr. Wun, professor of medicine and chief of hematology and oncology at the University of California, Davis, in Sacramento.
The analysis also showed the impact of VTE episodes. After 10 years of follow-up, cumulative mortality was just under 20% in patients with sickle cell disease who did not have a VTE, and more than 40% in patients who had a VTE, a statistically significant difference in an actuarial analysis.
The risk for VTE posed by sickle cell disease was even higher in the 42% of patients with severe sickle cell disease, defined as patients who had three or more hospitalizations or emergency department visits during the prior year. Patients in the severe subgroup had a 9.5-fold higher rate of VTE, compared with controls who had no sickle cell disease. Among the 58% of sickle cell patients without severe disease, the incidence of VTE was fourfold greater than among those without sickle cell disease.
Dr. Wun and his associates used data collected in the California Patient Discharge Dataset and in California’s Emergency Department Utilization database. They identified 4,280 patients 18-65 years old with sickle cell disease who were either hospitalized or seen at an emergency department during 1990-2010. They matched each of these sickle cell patients with five patients hospitalized or seen at emergency departments who did not have sickle cell disease. Matching included age, sex, race, ethnicity, and year of index event. The researchers could track each of the more than 25,000 total patients through subsequent hospitalizations and emergency-department visits by their unique identifier codes.
The patients with sickle cell disease averaged 28 years old, 91% were black, and during follow-up they had an 8% incidence of VTE.
The analysis also showed that comorbidities increased the risk for VTE, although not as strongly as sickle cell disease. For the entire group of more than 25,000 patients having three or more comorbidities linked with a threefold higher rate of VTEs, compared with those without any comorbidities. Among only patients with sickle cell disease, having three or more comorbidities boosted the VTE rate by a statistically-significant 67%, compared with sickle cell patients without any comorbidities. Female sex also significantly linked with a boosted VTE rate among patients with sickle cell disease. Women with sickle cell disease had 43% more VTE episodes than did men with sickle cell disease in the adjusted analysis.
Dr. Wun had no disclosures.
On Twitter @mitchelzoler
AMSTERDAM – Adult patients who become hospitalized and have sickle cell disease have about a sixfold increased risk of developing venous thromboembolism during the following weeks and months, compared with hospitalized patients without sickle cell disease, in a case-control study of more than 25,000 people admitted to or seen at California hospitals during 1990-2010.
Since 46% of the venous thromboembolism (VTE) episodes in patients with sickle cell disease happened within 30 days of a hospitalization or emergency department visit, the painful, inflammatory episodes that often drive patients with sickle cell disease to seek hospitalization may also provoke VTE said Dr. Ted Wun and his associates in a poster presented at a congress of the International Society on Thrombosis and Haemostasis. Relative immobilization during hospitalization may also play a role in triggering VTE in these patients, suggesting that "robust" thromboprophylaxis be applied to patients with sickle cell disease who enter a hospital, said Dr. Wun, professor of medicine and chief of hematology and oncology at the University of California, Davis, in Sacramento.
The analysis also showed the impact of VTE episodes. After 10 years of follow-up, cumulative mortality was just under 20% in patients with sickle cell disease who did not have a VTE, and more than 40% in patients who had a VTE, a statistically significant difference in an actuarial analysis.
The risk for VTE posed by sickle cell disease was even higher in the 42% of patients with severe sickle cell disease, defined as patients who had three or more hospitalizations or emergency department visits during the prior year. Patients in the severe subgroup had a 9.5-fold higher rate of VTE, compared with controls who had no sickle cell disease. Among the 58% of sickle cell patients without severe disease, the incidence of VTE was fourfold greater than among those without sickle cell disease.
Dr. Wun and his associates used data collected in the California Patient Discharge Dataset and in California’s Emergency Department Utilization database. They identified 4,280 patients 18-65 years old with sickle cell disease who were either hospitalized or seen at an emergency department during 1990-2010. They matched each of these sickle cell patients with five patients hospitalized or seen at emergency departments who did not have sickle cell disease. Matching included age, sex, race, ethnicity, and year of index event. The researchers could track each of the more than 25,000 total patients through subsequent hospitalizations and emergency-department visits by their unique identifier codes.
The patients with sickle cell disease averaged 28 years old, 91% were black, and during follow-up they had an 8% incidence of VTE.
The analysis also showed that comorbidities increased the risk for VTE, although not as strongly as sickle cell disease. For the entire group of more than 25,000 patients having three or more comorbidities linked with a threefold higher rate of VTEs, compared with those without any comorbidities. Among only patients with sickle cell disease, having three or more comorbidities boosted the VTE rate by a statistically-significant 67%, compared with sickle cell patients without any comorbidities. Female sex also significantly linked with a boosted VTE rate among patients with sickle cell disease. Women with sickle cell disease had 43% more VTE episodes than did men with sickle cell disease in the adjusted analysis.
Dr. Wun had no disclosures.
On Twitter @mitchelzoler
AT ISTH 2013
Ultrasound speeds new RA diagnoses
MADRID – Routine joint scans by ultrasound in patients with suspected rheumatoid arthritis led to faster diagnoses and quicker initiation of disease-modifying treatment in a multicenter-study of more than 250 patients.
But the results did not address whether this earlier diagnosis and treatment produced better outcomes. "While earlier diagnosis and treatment is known to lead to better outcomes, a large, prospective study is required to explore the long-term clinical impact and cost effectiveness of wider routine use of ultrasound by rheumatologists," Dr. Stephen Kelly said at the annual European Congress of Rheumatology.
Despite this current limitation of the available evidence, Dr. Kelly is convinced of the value of routine ultrasound examinations for joint assessment in patients with possible rheumatoid arthritis (RA). "You can see raging inflammation in joints that are not swollen or tender," he said in an interview. The discrepancy between clinical symptoms and the ultrasound appearance can be "surprising," said Dr. Kelly, a rheumatologist at Mile End Hospital in Barts Health NHS Trust in London.

The current study involved observation of patients referred by primary-care physicians to rheumatologists at four U.K. hospitals. Each of the four sites selected included some rheumatologists who routinely used ultrasound and others who did not. By the end of the study, 134 patients had been assessed with ultrasound joint examinations and 124 had been assessed without ultrasound. All patients were initially seen in the referral rheumatology clinics an average of 5 months after symptom onset. They had a mean age of about 53 years, and about 70% were women.
Among the 134 patients assessed initially with ultrasound, the average time to a formal RA diagnosis was 2.24 months, and the median time was 0.89 months. Among the patients not examined with ultrasound, a formal RA diagnosis was made at a mean of 2.76 months and a median of 2 months. These differences were statistically significant.
The investigators eventually diagnosed RA in 54 of the patients assessed with ultrasound and in 58 patients assessed without ultrasound. The median time to the start of treatment with a disease-modifying antirheumatic drug (DMARD) was 0.62 months among patients routinely examined with ultrasound and 1.41 months among those examined without ultrasound.
Put another way, among the patients eventually diagnosed with RA, 67% were diagnosed within a month of initial referral when their rheumatologists routinely used ultrasound, compared with 37% of the RA patients diagnosed within the first month when ultrasound wasn’t used. Initiation of DMARD treatment for the subgroup eventually diagnosed with RA happened in the first month for 63% of the patients routinely assessed by ultrasound, and in 32% of those worked-up without ultrasound.
In a further analysis, the rheumatologists who assessed 134 patients with ultrasound were asked whether their use of ultrasound made a difference. Fifty-three percent said that the first scan they obtained was instrumental in making their diagnosis, and 39% said that a subsequent ultrasound exam was critical in their diagnostic process.
The researchers also asked the rheumatologists who used ultrasound whether the ultrasound results played an important role in management decisions. Thirty-eight percent of the rheumatologists said that the first ultrasound scan they obtained played an important role in their management decisions, and 57% said that a subsequent ultrasound scan affected management.
The study was sponsored by AbbVie. Dr. Kelly said that he had no personal disclosures.
On Twitter @mitchelzoler
The main issue when imaging joints in patients with suspected rheumatoid arthritis (RA) or early disease is: What does imaging add to a standard clinical examination? Standard x-rays do not show many erosions in patients with early disease; ultrasound, as well as MRI, are much more sensitive. Both ultrasound and MRI can be very helpful for difficult-to-diagnose cases. In my experience, about 5%-10% of early-diagnosis cases benefit from using ultrasound or MRI imaging of joints.

|
|
Ultrasound is more widely used than MRI is and also costs less. You can examine multiple joints with ultrasound, you don’t need to inject contrast, and you can also use the ultrasound to guide injections. For all these reasons, ultrasound has rapidly become widely used to aid early diagnoses. But not every clinician has the expertise to perform ultrasound examinations, and it has not yet been definitively proven that using ultrasound routinely for diagnostically challenging cases is cost effective. I suspect it is cost effective to perform ultrasound examinations fairly broadly on patients suspected of having RA, compared with the financial and social costs of delayed RA diagnosis in which the patient goes untreated for an added period of time, but study results are still needed to prove this.
In June, I chaired a task force that issued the European League Against Rheumatism’s first recommendations on using joint imaging in the management of RA (Ann. Rheum. Dis. 2013;72:804-14). The 10 recommendations made by the task force include several that support and encourage the use of ultrasound or MRI for both the initial diagnosis of RA as well as subsequent management. However, because evidence is currently lacking to fully document the feasibility, cost, and training required to use methods like ultrasound in routine practice, our recommendations could not be unqualified. For example, our first recommendation says, "When there is diagnostic doubt, conventional radiography, ultrasound, or MRI can be used to improve the certainty of a diagnosis of RA above clinical criteria alone." The level of evidence for this recommendation is level III, which is not the highest level. In addition, note that the recommendation says "can be used" rather than mandating the use of ultrasound or another imaging method. In the same way, our third recommendation says, "Ultrasound and MRI are superior to clinical examination in the detection of joint inflammation; these techniques should be considered for more accurate assessment of inflammation." Again, the level of evidence, III, precluded us from saying anything more definitive than "should be considered."
The main issue when imaging joints in patients with suspected rheumatoid arthritis (RA) or early disease is: What does imaging add to a standard clinical examination? Standard x-rays do not show many erosions in patients with early disease; ultrasound, as well as MRI, are much more sensitive. Both ultrasound and MRI can be very helpful for difficult-to-diagnose cases. In my experience, about 5%-10% of early-diagnosis cases benefit from using ultrasound or MRI imaging of joints.
|
|
|
Ultrasound is more widely used than MRI is and also costs less. You can examine multiple joints with ultrasound, you don’t need to inject contrast, and you can also use the ultrasound to guide injections. For all these reasons, ultrasound has rapidly become widely used to aid early diagnoses. But not every clinician has the expertise to perform ultrasound examinations, and it has not yet been definitively proven that using ultrasound routinely for diagnostically challenging cases is cost effective. I suspect it is cost effective to perform ultrasound examinations fairly broadly on patients suspected of having RA, compared with the financial and social costs of delayed RA diagnosis in which the patient goes untreated for an added period of time, but study results are still needed to prove this.
In June, I chaired a task force that issued the European League Against Rheumatism’s first recommendations on using joint imaging in the management of RA (Ann. Rheum. Dis. 2013;72:804-14). The 10 recommendations made by the task force include several that support and encourage the use of ultrasound or MRI for both the initial diagnosis of RA as well as subsequent management. However, because evidence is currently lacking to fully document the feasibility, cost, and training required to use methods like ultrasound in routine practice, our recommendations could not be unqualified. For example, our first recommendation says, "When there is diagnostic doubt, conventional radiography, ultrasound, or MRI can be used to improve the certainty of a diagnosis of RA above clinical criteria alone." The level of evidence for this recommendation is level III, which is not the highest level. In addition, note that the recommendation says "can be used" rather than mandating the use of ultrasound or another imaging method. In the same way, our third recommendation says, "Ultrasound and MRI are superior to clinical examination in the detection of joint inflammation; these techniques should be considered for more accurate assessment of inflammation." Again, the level of evidence, III, precluded us from saying anything more definitive than "should be considered."
The main issue when imaging joints in patients with suspected rheumatoid arthritis (RA) or early disease is: What does imaging add to a standard clinical examination? Standard x-rays do not show many erosions in patients with early disease; ultrasound, as well as MRI, are much more sensitive. Both ultrasound and MRI can be very helpful for difficult-to-diagnose cases. In my experience, about 5%-10% of early-diagnosis cases benefit from using ultrasound or MRI imaging of joints.
|
|
|
Ultrasound is more widely used than MRI is and also costs less. You can examine multiple joints with ultrasound, you don’t need to inject contrast, and you can also use the ultrasound to guide injections. For all these reasons, ultrasound has rapidly become widely used to aid early diagnoses. But not every clinician has the expertise to perform ultrasound examinations, and it has not yet been definitively proven that using ultrasound routinely for diagnostically challenging cases is cost effective. I suspect it is cost effective to perform ultrasound examinations fairly broadly on patients suspected of having RA, compared with the financial and social costs of delayed RA diagnosis in which the patient goes untreated for an added period of time, but study results are still needed to prove this.
In June, I chaired a task force that issued the European League Against Rheumatism’s first recommendations on using joint imaging in the management of RA (Ann. Rheum. Dis. 2013;72:804-14). The 10 recommendations made by the task force include several that support and encourage the use of ultrasound or MRI for both the initial diagnosis of RA as well as subsequent management. However, because evidence is currently lacking to fully document the feasibility, cost, and training required to use methods like ultrasound in routine practice, our recommendations could not be unqualified. For example, our first recommendation says, "When there is diagnostic doubt, conventional radiography, ultrasound, or MRI can be used to improve the certainty of a diagnosis of RA above clinical criteria alone." The level of evidence for this recommendation is level III, which is not the highest level. In addition, note that the recommendation says "can be used" rather than mandating the use of ultrasound or another imaging method. In the same way, our third recommendation says, "Ultrasound and MRI are superior to clinical examination in the detection of joint inflammation; these techniques should be considered for more accurate assessment of inflammation." Again, the level of evidence, III, precluded us from saying anything more definitive than "should be considered."
MADRID – Routine joint scans by ultrasound in patients with suspected rheumatoid arthritis led to faster diagnoses and quicker initiation of disease-modifying treatment in a multicenter-study of more than 250 patients.
But the results did not address whether this earlier diagnosis and treatment produced better outcomes. "While earlier diagnosis and treatment is known to lead to better outcomes, a large, prospective study is required to explore the long-term clinical impact and cost effectiveness of wider routine use of ultrasound by rheumatologists," Dr. Stephen Kelly said at the annual European Congress of Rheumatology.
Despite this current limitation of the available evidence, Dr. Kelly is convinced of the value of routine ultrasound examinations for joint assessment in patients with possible rheumatoid arthritis (RA). "You can see raging inflammation in joints that are not swollen or tender," he said in an interview. The discrepancy between clinical symptoms and the ultrasound appearance can be "surprising," said Dr. Kelly, a rheumatologist at Mile End Hospital in Barts Health NHS Trust in London.
The current study involved observation of patients referred by primary-care physicians to rheumatologists at four U.K. hospitals. Each of the four sites selected included some rheumatologists who routinely used ultrasound and others who did not. By the end of the study, 134 patients had been assessed with ultrasound joint examinations and 124 had been assessed without ultrasound. All patients were initially seen in the referral rheumatology clinics an average of 5 months after symptom onset. They had a mean age of about 53 years, and about 70% were women.
Among the 134 patients assessed initially with ultrasound, the average time to a formal RA diagnosis was 2.24 months, and the median time was 0.89 months. Among the patients not examined with ultrasound, a formal RA diagnosis was made at a mean of 2.76 months and a median of 2 months. These differences were statistically significant.
The investigators eventually diagnosed RA in 54 of the patients assessed with ultrasound and in 58 patients assessed without ultrasound. The median time to the start of treatment with a disease-modifying antirheumatic drug (DMARD) was 0.62 months among patients routinely examined with ultrasound and 1.41 months among those examined without ultrasound.
Put another way, among the patients eventually diagnosed with RA, 67% were diagnosed within a month of initial referral when their rheumatologists routinely used ultrasound, compared with 37% of the RA patients diagnosed within the first month when ultrasound wasn’t used. Initiation of DMARD treatment for the subgroup eventually diagnosed with RA happened in the first month for 63% of the patients routinely assessed by ultrasound, and in 32% of those worked-up without ultrasound.
In a further analysis, the rheumatologists who assessed 134 patients with ultrasound were asked whether their use of ultrasound made a difference. Fifty-three percent said that the first scan they obtained was instrumental in making their diagnosis, and 39% said that a subsequent ultrasound exam was critical in their diagnostic process.
The researchers also asked the rheumatologists who used ultrasound whether the ultrasound results played an important role in management decisions. Thirty-eight percent of the rheumatologists said that the first ultrasound scan they obtained played an important role in their management decisions, and 57% said that a subsequent ultrasound scan affected management.
The study was sponsored by AbbVie. Dr. Kelly said that he had no personal disclosures.
On Twitter @mitchelzoler
MADRID – Routine joint scans by ultrasound in patients with suspected rheumatoid arthritis led to faster diagnoses and quicker initiation of disease-modifying treatment in a multicenter-study of more than 250 patients.
But the results did not address whether this earlier diagnosis and treatment produced better outcomes. "While earlier diagnosis and treatment is known to lead to better outcomes, a large, prospective study is required to explore the long-term clinical impact and cost effectiveness of wider routine use of ultrasound by rheumatologists," Dr. Stephen Kelly said at the annual European Congress of Rheumatology.
Despite this current limitation of the available evidence, Dr. Kelly is convinced of the value of routine ultrasound examinations for joint assessment in patients with possible rheumatoid arthritis (RA). "You can see raging inflammation in joints that are not swollen or tender," he said in an interview. The discrepancy between clinical symptoms and the ultrasound appearance can be "surprising," said Dr. Kelly, a rheumatologist at Mile End Hospital in Barts Health NHS Trust in London.
The current study involved observation of patients referred by primary-care physicians to rheumatologists at four U.K. hospitals. Each of the four sites selected included some rheumatologists who routinely used ultrasound and others who did not. By the end of the study, 134 patients had been assessed with ultrasound joint examinations and 124 had been assessed without ultrasound. All patients were initially seen in the referral rheumatology clinics an average of 5 months after symptom onset. They had a mean age of about 53 years, and about 70% were women.
Among the 134 patients assessed initially with ultrasound, the average time to a formal RA diagnosis was 2.24 months, and the median time was 0.89 months. Among the patients not examined with ultrasound, a formal RA diagnosis was made at a mean of 2.76 months and a median of 2 months. These differences were statistically significant.
The investigators eventually diagnosed RA in 54 of the patients assessed with ultrasound and in 58 patients assessed without ultrasound. The median time to the start of treatment with a disease-modifying antirheumatic drug (DMARD) was 0.62 months among patients routinely examined with ultrasound and 1.41 months among those examined without ultrasound.
Put another way, among the patients eventually diagnosed with RA, 67% were diagnosed within a month of initial referral when their rheumatologists routinely used ultrasound, compared with 37% of the RA patients diagnosed within the first month when ultrasound wasn’t used. Initiation of DMARD treatment for the subgroup eventually diagnosed with RA happened in the first month for 63% of the patients routinely assessed by ultrasound, and in 32% of those worked-up without ultrasound.
In a further analysis, the rheumatologists who assessed 134 patients with ultrasound were asked whether their use of ultrasound made a difference. Fifty-three percent said that the first scan they obtained was instrumental in making their diagnosis, and 39% said that a subsequent ultrasound exam was critical in their diagnostic process.
The researchers also asked the rheumatologists who used ultrasound whether the ultrasound results played an important role in management decisions. Thirty-eight percent of the rheumatologists said that the first ultrasound scan they obtained played an important role in their management decisions, and 57% said that a subsequent ultrasound scan affected management.
The study was sponsored by AbbVie. Dr. Kelly said that he had no personal disclosures.
On Twitter @mitchelzoler
AT THE EULAR CONGRESS 2013
Major finding: Rheumatoid arthritis diagnosis using ultrasound took a median of 0.89 months, compared with 2.00 months when ultrasound wasn’t used.
Data source: A prospective study of 258 patients with suspected rheumatoid arthritis who were examined at four U.K. centers.
Disclosures: The study was sponsored by AbbVie. Dr. Kelly said that he had no personal disclosures.
CDC moves to cast a wider Chlamydia screening net
VIENNA – Staffers at the Centers for Disease Control and Prevention are developing and will soon start prospectively testing a new approach of universal, opt-out chlamydial infection screening for girls and women aged 15-24 years. In making this change, CDC is recognizing that current U.S. recommendations for sexually active girls and women in this age group are producing woefully low screening rates of roughly 30%, according to CDC staffers.
CDC researchers developing this new approach to Chlamydia trachomatis screening performed a cost-effectiveness analysis of this screening paradigm and found it was "very cost effective," with an estimated incremental cost of $1,372 for each quality-adjusted life year gained. In contrast, the current risk-based approach to screening for chlamydial infections among women in this age range has a cost effectiveness of about $41,000 per quality-adjusted life year gained, Dr. Karen Hoover said at the joint meeting of the International Society for Sexually Transmitted Diseases Research and the International Union Against Sexually Transmitted Infections.

According to a preliminary economic analysis by Kwame Owusu-Edusei Jr., Ph.D., of the CDC’s Division of STD Prevention in Atlanta, universal, opt-out screening may prove to have the added benefit of boosting screening rates from the current level of 30% overall among sexually active girls and women aged 15-24 and as low as 11% in sexually-active 15-year-old girls to an overall rate of 52%. The CDC’s planned changes are expected to raise the participation level to at least 75% among the sexually-active subgroup (and an expected 5% participation rate among those who are not sexually active in this age group, who would be advised not to undergo screening).
The higher screening uptake rate should, within less than 5 years, cut the prevalence of chlamydial infection in these girls and women from the current levels of 3% to nearly 1%, and in the same time frame it should also drop infection rates among men from just over 2% to below 1%, said Dr. Hoover, an ob.gyn. and medical epidemiologist in the CDC’s Division of STD Prevention.
Another benefit would be removing the stigma that the current, risk-based system generates by making many girls and women feel that they have had "bad" sex or promiscuous sex because they are now at risk of harboring chlamydial infection and need screening, Dr. Hoover said. Universal screening with opt-out would "normalize" screening in the eyes of the target population.
Routine, annual screening of sexually-active U.S. girls and women aged 24 years and younger for chlamydial infection was first recommended by the U.S. Preventive Services Task Force for about a decade, and most recently in 2007 (Ann. Int. Med. 2007;147:128-34). The CDC also recommends this screening approach for girls and women aged 25 years and younger (MMWR 2010;59(RR12):1-110).
Although the new screening model is still in development, it would likely be patient centered and hinge on having the reception staffs at primary care physicians’ offices routinely ask girls and women in the target age group to supply a urine specimen or self-administered vaginal swab at the start of all visits to any primary care provider – gynecologists, pediatricians, family practice physicians, or internal medicine physicians – along with an information sheet or pamphlet. The process would resemble the way that pregnant U.S. women are routinely asked to supply a urine specimen at the start of all their antenatal office visits. "This is very simple for clinics to implement," Dr. Hoover said at the meeting.
Routine specimen collection from all girls and women in the target group would help remove the stigma from specimen collection, Dr. Hoover said in an interview. The information patients receive would encourage them to discuss screening with their physicians, when they could exercise their opt out.
Although this approach could result in a modest amount of overtesting, the huge cost-effectiveness advantage of universal opt-out screening compared with the current, risk-based approach leaves a lot of margin to accommodate some overtesting and still be cost effective.
The only other infectious disease currently screened in the United States by a universal, opt-out system in a target age group is HIV, she noted.
Dr. Hoover said that the CDC would like to pilot universal testing in several types of U.S. clinical practice. Testing of the screening model should start within a few years, she said.
"We need a paradigm shift; we need to do this differently. As long as we continue to rely on clinicians to change their behavior [and initiate more screening than they currently do] we will never get to where we want to be" with C. trachomatis screening, she said.
Dr. Hoover had no disclosures.
On Twitter @mitchelzoler
VIENNA – Staffers at the Centers for Disease Control and Prevention are developing and will soon start prospectively testing a new approach of universal, opt-out chlamydial infection screening for girls and women aged 15-24 years. In making this change, CDC is recognizing that current U.S. recommendations for sexually active girls and women in this age group are producing woefully low screening rates of roughly 30%, according to CDC staffers.
CDC researchers developing this new approach to Chlamydia trachomatis screening performed a cost-effectiveness analysis of this screening paradigm and found it was "very cost effective," with an estimated incremental cost of $1,372 for each quality-adjusted life year gained. In contrast, the current risk-based approach to screening for chlamydial infections among women in this age range has a cost effectiveness of about $41,000 per quality-adjusted life year gained, Dr. Karen Hoover said at the joint meeting of the International Society for Sexually Transmitted Diseases Research and the International Union Against Sexually Transmitted Infections.
According to a preliminary economic analysis by Kwame Owusu-Edusei Jr., Ph.D., of the CDC’s Division of STD Prevention in Atlanta, universal, opt-out screening may prove to have the added benefit of boosting screening rates from the current level of 30% overall among sexually active girls and women aged 15-24 and as low as 11% in sexually-active 15-year-old girls to an overall rate of 52%. The CDC’s planned changes are expected to raise the participation level to at least 75% among the sexually-active subgroup (and an expected 5% participation rate among those who are not sexually active in this age group, who would be advised not to undergo screening).
The higher screening uptake rate should, within less than 5 years, cut the prevalence of chlamydial infection in these girls and women from the current levels of 3% to nearly 1%, and in the same time frame it should also drop infection rates among men from just over 2% to below 1%, said Dr. Hoover, an ob.gyn. and medical epidemiologist in the CDC’s Division of STD Prevention.
Another benefit would be removing the stigma that the current, risk-based system generates by making many girls and women feel that they have had "bad" sex or promiscuous sex because they are now at risk of harboring chlamydial infection and need screening, Dr. Hoover said. Universal screening with opt-out would "normalize" screening in the eyes of the target population.
Routine, annual screening of sexually-active U.S. girls and women aged 24 years and younger for chlamydial infection was first recommended by the U.S. Preventive Services Task Force for about a decade, and most recently in 2007 (Ann. Int. Med. 2007;147:128-34). The CDC also recommends this screening approach for girls and women aged 25 years and younger (MMWR 2010;59(RR12):1-110).
Although the new screening model is still in development, it would likely be patient centered and hinge on having the reception staffs at primary care physicians’ offices routinely ask girls and women in the target age group to supply a urine specimen or self-administered vaginal swab at the start of all visits to any primary care provider – gynecologists, pediatricians, family practice physicians, or internal medicine physicians – along with an information sheet or pamphlet. The process would resemble the way that pregnant U.S. women are routinely asked to supply a urine specimen at the start of all their antenatal office visits. "This is very simple for clinics to implement," Dr. Hoover said at the meeting.
Routine specimen collection from all girls and women in the target group would help remove the stigma from specimen collection, Dr. Hoover said in an interview. The information patients receive would encourage them to discuss screening with their physicians, when they could exercise their opt out.
Although this approach could result in a modest amount of overtesting, the huge cost-effectiveness advantage of universal opt-out screening compared with the current, risk-based approach leaves a lot of margin to accommodate some overtesting and still be cost effective.
The only other infectious disease currently screened in the United States by a universal, opt-out system in a target age group is HIV, she noted.
Dr. Hoover said that the CDC would like to pilot universal testing in several types of U.S. clinical practice. Testing of the screening model should start within a few years, she said.
"We need a paradigm shift; we need to do this differently. As long as we continue to rely on clinicians to change their behavior [and initiate more screening than they currently do] we will never get to where we want to be" with C. trachomatis screening, she said.
Dr. Hoover had no disclosures.
On Twitter @mitchelzoler
VIENNA – Staffers at the Centers for Disease Control and Prevention are developing and will soon start prospectively testing a new approach of universal, opt-out chlamydial infection screening for girls and women aged 15-24 years. In making this change, CDC is recognizing that current U.S. recommendations for sexually active girls and women in this age group are producing woefully low screening rates of roughly 30%, according to CDC staffers.
CDC researchers developing this new approach to Chlamydia trachomatis screening performed a cost-effectiveness analysis of this screening paradigm and found it was "very cost effective," with an estimated incremental cost of $1,372 for each quality-adjusted life year gained. In contrast, the current risk-based approach to screening for chlamydial infections among women in this age range has a cost effectiveness of about $41,000 per quality-adjusted life year gained, Dr. Karen Hoover said at the joint meeting of the International Society for Sexually Transmitted Diseases Research and the International Union Against Sexually Transmitted Infections.
According to a preliminary economic analysis by Kwame Owusu-Edusei Jr., Ph.D., of the CDC’s Division of STD Prevention in Atlanta, universal, opt-out screening may prove to have the added benefit of boosting screening rates from the current level of 30% overall among sexually active girls and women aged 15-24 and as low as 11% in sexually-active 15-year-old girls to an overall rate of 52%. The CDC’s planned changes are expected to raise the participation level to at least 75% among the sexually-active subgroup (and an expected 5% participation rate among those who are not sexually active in this age group, who would be advised not to undergo screening).
The higher screening uptake rate should, within less than 5 years, cut the prevalence of chlamydial infection in these girls and women from the current levels of 3% to nearly 1%, and in the same time frame it should also drop infection rates among men from just over 2% to below 1%, said Dr. Hoover, an ob.gyn. and medical epidemiologist in the CDC’s Division of STD Prevention.
Another benefit would be removing the stigma that the current, risk-based system generates by making many girls and women feel that they have had "bad" sex or promiscuous sex because they are now at risk of harboring chlamydial infection and need screening, Dr. Hoover said. Universal screening with opt-out would "normalize" screening in the eyes of the target population.
Routine, annual screening of sexually-active U.S. girls and women aged 24 years and younger for chlamydial infection was first recommended by the U.S. Preventive Services Task Force for about a decade, and most recently in 2007 (Ann. Int. Med. 2007;147:128-34). The CDC also recommends this screening approach for girls and women aged 25 years and younger (MMWR 2010;59(RR12):1-110).
Although the new screening model is still in development, it would likely be patient centered and hinge on having the reception staffs at primary care physicians’ offices routinely ask girls and women in the target age group to supply a urine specimen or self-administered vaginal swab at the start of all visits to any primary care provider – gynecologists, pediatricians, family practice physicians, or internal medicine physicians – along with an information sheet or pamphlet. The process would resemble the way that pregnant U.S. women are routinely asked to supply a urine specimen at the start of all their antenatal office visits. "This is very simple for clinics to implement," Dr. Hoover said at the meeting.
Routine specimen collection from all girls and women in the target group would help remove the stigma from specimen collection, Dr. Hoover said in an interview. The information patients receive would encourage them to discuss screening with their physicians, when they could exercise their opt out.
Although this approach could result in a modest amount of overtesting, the huge cost-effectiveness advantage of universal opt-out screening compared with the current, risk-based approach leaves a lot of margin to accommodate some overtesting and still be cost effective.
The only other infectious disease currently screened in the United States by a universal, opt-out system in a target age group is HIV, she noted.
Dr. Hoover said that the CDC would like to pilot universal testing in several types of U.S. clinical practice. Testing of the screening model should start within a few years, she said.
"We need a paradigm shift; we need to do this differently. As long as we continue to rely on clinicians to change their behavior [and initiate more screening than they currently do] we will never get to where we want to be" with C. trachomatis screening, she said.
Dr. Hoover had no disclosures.
On Twitter @mitchelzoler
AT THE STI & AIDS WORLD CONGRESS 2013
Major finding: Universal, opt-out screening for chlamydial infection in U.S. women aged 15-24 years was projected to cost $1,372 per quality-adjusted life year.
Data source: A cost-effectiveness model developed by staffers at the Centers for Disease Control and Prevention.
Disclosures: Dr. Hoover had no disclosures.

Khorana score tracks risk of cancer death
AMSTERDAM – A score routinely used to quantify cancer patients’ risk for developing venous thromboembolism also can be used to gauge their risk of death, according to an analysis of data from more than 1,500 patients.
The new findings are only exploratory, but they suggest that the well-established risk calculator known as the Khorana score "may support clinical decision making not only for VTE prophylaxis but also for anticancer treatment strategies," Dr. Cihan Ay said at the Congress of the International Society on Thrombosis and Haemostasis.
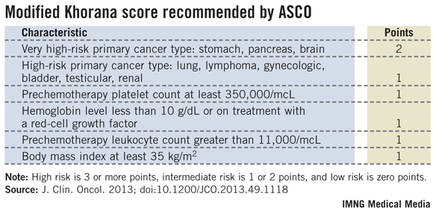
The link between higher Khorana scores and an increased rate of death over the following 2 years was independent of VTE occurrence, suggesting that the Khorana score identifies susceptibilities in addition to VTE than can cause death, said Dr. Ay, a hematologist-oncologist at the Medical University of Vienna.
Following the Khorana score’s introduction in 2008 by Dr. Alok Khorana and his associates (Blood 2008;111:4902-7) to assess a patient’s risk for VTE and need for anticoagulant prophylaxis, the score underwent several validations. Earlier this year, the score was adopted in a slightly modified form as part of the VTE management guidelines of the American Society of Clinical Oncology (J. Clin. Onc. 2013 [doi: 10.1200/JCO.2013.49.1118]).
The ASCO guidelines say that "the Panel recommends that patients with cancer be assessed for VTE risk at the time of chemotherapy initiation and periodically thereafter" using the slightly modified form of the Khorana score (see box). The 2013 formula from the ASCO Panel revised the original 2008 version of the Khorana score by adding primary brain tumors to the 2-point category and renal tumors to the 1-point category.

"The Khorana score is used to identify patients for primary thromboprophylaxis. My idea is to also use it to get information on general prognosis," Dr. Ay said in an interview. "There is often a discussion of the patient’s prognosis and how far to go with treatment, how intensive treatment should be. If patients have a poor prognosis, some treatments may not be worth trying."
Dr. Ay and his associates applied their own slight modification of the Khorana score to 1,544 patients with a variety of cancers enrolled in the Vienna Cancer and Thrombosis Study. The patients averaged 62 years old, about 45% were women, and they were followed for a mean of about 19 months, during which overall, all-cause mortality was 42%. The most common tumor type was lung cancer, in about 250 patients, followed by lymphoma, breast cancer, and brain tumors, which each affected more than 200 patients. The researchers modified the Khorana score by adding melanoma to the 1-point group of cancers and removing gynecologic, bladder, and testicular cancer from being assigned any points.
The analysis showed a strong link between patients’ Khorana scores at baseline, before treatment began, and their survival over the next 2 years of follow-up. The 466 patients (30%) with a score of 0 had a 27% mortality rate; the 489 patients (32%) with a score of 1 had a 38% mortality rate (adjusted hazard ratio, 61% compared with patients with a score of 0). The 405 patients (26%) with a score of 2 had a 51% mortality rate, a 2.8-fold increased mortality rate after adjustment, and the 184 patients (12%) with a score of 3 or more had a 63% mortality rate, a fourfold higher mortality rate after adjustment compared with patients with a score of 0. Between-group differences in mortality were all statistically significant. The hazard model adjusted for age, sex, and incident VTE.
Overall in the adjusted model, every 1-point increase in modified Khorana score linked with a statistically significant 56% increase in mortality, Dr. Ay said.
Dr. Ay said that he had no relevant disclosures.
On Twitter @mitchelzoler
AMSTERDAM – A score routinely used to quantify cancer patients’ risk for developing venous thromboembolism also can be used to gauge their risk of death, according to an analysis of data from more than 1,500 patients.
The new findings are only exploratory, but they suggest that the well-established risk calculator known as the Khorana score "may support clinical decision making not only for VTE prophylaxis but also for anticancer treatment strategies," Dr. Cihan Ay said at the Congress of the International Society on Thrombosis and Haemostasis.
The link between higher Khorana scores and an increased rate of death over the following 2 years was independent of VTE occurrence, suggesting that the Khorana score identifies susceptibilities in addition to VTE than can cause death, said Dr. Ay, a hematologist-oncologist at the Medical University of Vienna.
Following the Khorana score’s introduction in 2008 by Dr. Alok Khorana and his associates (Blood 2008;111:4902-7) to assess a patient’s risk for VTE and need for anticoagulant prophylaxis, the score underwent several validations. Earlier this year, the score was adopted in a slightly modified form as part of the VTE management guidelines of the American Society of Clinical Oncology (J. Clin. Onc. 2013 [doi: 10.1200/JCO.2013.49.1118]).
The ASCO guidelines say that "the Panel recommends that patients with cancer be assessed for VTE risk at the time of chemotherapy initiation and periodically thereafter" using the slightly modified form of the Khorana score (see box). The 2013 formula from the ASCO Panel revised the original 2008 version of the Khorana score by adding primary brain tumors to the 2-point category and renal tumors to the 1-point category.
"The Khorana score is used to identify patients for primary thromboprophylaxis. My idea is to also use it to get information on general prognosis," Dr. Ay said in an interview. "There is often a discussion of the patient’s prognosis and how far to go with treatment, how intensive treatment should be. If patients have a poor prognosis, some treatments may not be worth trying."
Dr. Ay and his associates applied their own slight modification of the Khorana score to 1,544 patients with a variety of cancers enrolled in the Vienna Cancer and Thrombosis Study. The patients averaged 62 years old, about 45% were women, and they were followed for a mean of about 19 months, during which overall, all-cause mortality was 42%. The most common tumor type was lung cancer, in about 250 patients, followed by lymphoma, breast cancer, and brain tumors, which each affected more than 200 patients. The researchers modified the Khorana score by adding melanoma to the 1-point group of cancers and removing gynecologic, bladder, and testicular cancer from being assigned any points.
The analysis showed a strong link between patients’ Khorana scores at baseline, before treatment began, and their survival over the next 2 years of follow-up. The 466 patients (30%) with a score of 0 had a 27% mortality rate; the 489 patients (32%) with a score of 1 had a 38% mortality rate (adjusted hazard ratio, 61% compared with patients with a score of 0). The 405 patients (26%) with a score of 2 had a 51% mortality rate, a 2.8-fold increased mortality rate after adjustment, and the 184 patients (12%) with a score of 3 or more had a 63% mortality rate, a fourfold higher mortality rate after adjustment compared with patients with a score of 0. Between-group differences in mortality were all statistically significant. The hazard model adjusted for age, sex, and incident VTE.
Overall in the adjusted model, every 1-point increase in modified Khorana score linked with a statistically significant 56% increase in mortality, Dr. Ay said.
Dr. Ay said that he had no relevant disclosures.
On Twitter @mitchelzoler
AMSTERDAM – A score routinely used to quantify cancer patients’ risk for developing venous thromboembolism also can be used to gauge their risk of death, according to an analysis of data from more than 1,500 patients.
The new findings are only exploratory, but they suggest that the well-established risk calculator known as the Khorana score "may support clinical decision making not only for VTE prophylaxis but also for anticancer treatment strategies," Dr. Cihan Ay said at the Congress of the International Society on Thrombosis and Haemostasis.
The link between higher Khorana scores and an increased rate of death over the following 2 years was independent of VTE occurrence, suggesting that the Khorana score identifies susceptibilities in addition to VTE than can cause death, said Dr. Ay, a hematologist-oncologist at the Medical University of Vienna.
Following the Khorana score’s introduction in 2008 by Dr. Alok Khorana and his associates (Blood 2008;111:4902-7) to assess a patient’s risk for VTE and need for anticoagulant prophylaxis, the score underwent several validations. Earlier this year, the score was adopted in a slightly modified form as part of the VTE management guidelines of the American Society of Clinical Oncology (J. Clin. Onc. 2013 [doi: 10.1200/JCO.2013.49.1118]).
The ASCO guidelines say that "the Panel recommends that patients with cancer be assessed for VTE risk at the time of chemotherapy initiation and periodically thereafter" using the slightly modified form of the Khorana score (see box). The 2013 formula from the ASCO Panel revised the original 2008 version of the Khorana score by adding primary brain tumors to the 2-point category and renal tumors to the 1-point category.
"The Khorana score is used to identify patients for primary thromboprophylaxis. My idea is to also use it to get information on general prognosis," Dr. Ay said in an interview. "There is often a discussion of the patient’s prognosis and how far to go with treatment, how intensive treatment should be. If patients have a poor prognosis, some treatments may not be worth trying."
Dr. Ay and his associates applied their own slight modification of the Khorana score to 1,544 patients with a variety of cancers enrolled in the Vienna Cancer and Thrombosis Study. The patients averaged 62 years old, about 45% were women, and they were followed for a mean of about 19 months, during which overall, all-cause mortality was 42%. The most common tumor type was lung cancer, in about 250 patients, followed by lymphoma, breast cancer, and brain tumors, which each affected more than 200 patients. The researchers modified the Khorana score by adding melanoma to the 1-point group of cancers and removing gynecologic, bladder, and testicular cancer from being assigned any points.
The analysis showed a strong link between patients’ Khorana scores at baseline, before treatment began, and their survival over the next 2 years of follow-up. The 466 patients (30%) with a score of 0 had a 27% mortality rate; the 489 patients (32%) with a score of 1 had a 38% mortality rate (adjusted hazard ratio, 61% compared with patients with a score of 0). The 405 patients (26%) with a score of 2 had a 51% mortality rate, a 2.8-fold increased mortality rate after adjustment, and the 184 patients (12%) with a score of 3 or more had a 63% mortality rate, a fourfold higher mortality rate after adjustment compared with patients with a score of 0. Between-group differences in mortality were all statistically significant. The hazard model adjusted for age, sex, and incident VTE.
Overall in the adjusted model, every 1-point increase in modified Khorana score linked with a statistically significant 56% increase in mortality, Dr. Ay said.
Dr. Ay said that he had no relevant disclosures.
On Twitter @mitchelzoler
AT THE 2013 ISTH CONGRESS
Major finding: In the adjusted model, every 1-point increase in modified Khorana score linked with a statistically significant 56% increase in mortality.
Data source: An analysis of 1,544 cancer patients followed prospectively at an Austrian center.
Disclosures: Dr. Ay said that he had no relevant disclosures.
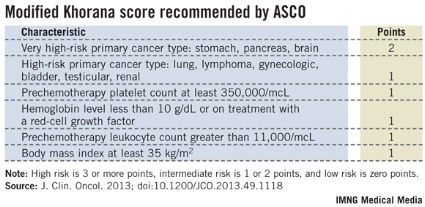
Expert panel sets broad SpA treat-to-target goals
MADRID – A panel of clinicians with expertise in the management of patients with spondyloarthritis took another step toward better defining this disease category and the goals of its treatment by producing the first "treat-to-target" recommendations for spondyloarthritis.
The new recommendations will "guide physicians, patients, and other stakeholders on how to optimize reduction of signs and symptoms and, ideally, outcomes, and will drive" the current research agenda, Dr. Josef S. Smolen said while presenting the panel’s recommendations at the annual European Congress of Rheumatology.

"Treat to target proposes a stepwise approach to achieving optimal outcomes based on available evidence and expert opinion. Treat to target has been successfully applied to management of diabetes, hypertension, hyperlipidemia, and rheumatoid arthritis," and the new task force set out to address whether it could be used when treating patients with spondyloarthritis (SpA), a question that required the expert task force to review the evidence for setting specific treatment goals for patients with SpA, said Dr. Smolen, professor of medicine at the Medical University of Vienna.
The task force eventually decided that the treat-to-target concept was applicable to SpA, but that the data available so far prevented the task force from setting specific treatment goals. While the recommendations underscore the importance of treating SpA patients with a goal of remission or inactive disease, and failing that, at least low disease activity, they fall short of giving clinicians guidance on how to best measure and define remission or low disease activity or how to achieve these goals.
For example, for axial SpA – the subtype that received the most specific recommendations – the panel advised clinicians to guide treatment decisions by using a "validated composite measure of disease activity" such as the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) plus acute phase reactants, or the Ankylosing Spondylitis Disease Activity Score (ASDAS) with or without functional measures such as the Bath Ankylosing Spondylitis Functional Index (BASFI). But the recommendations say nothing about what scores by these measures would define remission or low disease activity. The recommendations also talk about using other factors to further gauge axial SpA disease activity such as MRI analysis of inflammation and radiographic progression, but again Dr. Smolen provided no specific targets when using these measures.
For other, less well studied types of SpA, the new recommendations were even more nebulous. For psoriatic arthritis, the panel indicated that "validated measures of musculoskeletal disease activity" should be "performed and documented regularly" as should other factors such as spinal and extraarticular manifestations, imaging findings, and comorbidities, but the recommendations gave no specifics on what any of these measures might be or what level might equal remission or low disease. The same held true for peripheral SpA.
Other factors touched on by the new recommendations include the need for individualized and shared decision making between physicians and patients, the need for coordination of care among rheumatologists and other medical specialists who treat SpA patients (dermatologists, gastroenterologists, and ophthalmologists), and the need to take into account extraarticular manifestations of SpA diseases, comorbidities, and treatment risks along with the goal of low disease activity.
"I think it was important to document that there is a paucity of trials that have looked at strategies to treat" SpA. "For rheumatoid arthritis we have strategies, but not in spondyloarthritis, and I think it is important to say that," said Dr. Jürgen Braun, medical director of Rheumazentrum Ruhrgebiet in Herne, Germany.
SpA also lags behind rheumatoid arthritis by not having any treatments proven to slow radiographic progression. "Although we say that it is presumably important to treat inflammation [in patients with SpA], we are not sure," said Dr. Braun, who served as a member of the treat-to-target task force.
Even though the task force’s report highlights the absence of evidence for most facets of SpA management, "in the absence of evidence you need eminence, and that’s what was produced." Dr. Braun predicted that rheumatologists and other clinicians who care for patients with SpA would welcome these new recommendations despite their shortcomings. "What we say is what clinicians feel: If a patient’s CRP is elevated we must do something about it, but the evidence supporting this is limited. Presumably, it is important to treat inflammation, but we are not yet sure," he said in an interview.
"We don’t have trial results yet where you set up a quantifiable endpoint as your target, but that is coming," said Dr. Philip J. Mease, director of the rheumatology clinical research division at Swedish Medical Center in Seattle and a member of the task force. For example, the results from the Tight Control of Psoriatic Arthritis (TICOPA) trial "will tell us whether more aggressive treatment to a quantifiable target is appropriate and makes a difference. We anticipate that it will, but evidence is currently lacking." The primary endpoint of the TICOPA trial is change in the ACR20 response, but the trial includes several other clinical measures as secondary endpoints, including the Assessment in Ankylosing Spondylitis (ASAS), the BASDAI, and the psoriasis area severity index (PASI).
"The rheumatoid model is prompting us to develop quantifiable measures like the ASDAS and the new Psoriatic Arthritis Disease Activity Score (PASDAS) that we’ll start to see used. I just spoke with a colleague about the need to also develop a similar measure for peripheral SpA," Dr. Mease said in an interview.
The task force that developed the treat-to-target recommendations included 16 physicians and patients on its steering committee and 16 on an advisory committee. The majority came from various European locations, but about a quarter of the task force members were from the United States. To arrive at its recommendations, the task force used a comprehensive literature review that identified 22 published reports that addressed treatment targets for SpA (Ann. Rheum. Dis. 2013 June 10 [doi:10.1136/annrheumdis-2013-203860]). The treat-to-target recommendations were published online a few days before Dr. Smolen’s presentation at the meeting (Ann. Rheum. Dis. 2013 June 8 [doi:10.1136/annrheumdis-2013-203419]).
Dr. Smolen, Dr. Braun, and Dr. Mease said that they had no disclosures relevant to the topic.
On Twitter @mitchelzoler
MADRID – A panel of clinicians with expertise in the management of patients with spondyloarthritis took another step toward better defining this disease category and the goals of its treatment by producing the first "treat-to-target" recommendations for spondyloarthritis.
The new recommendations will "guide physicians, patients, and other stakeholders on how to optimize reduction of signs and symptoms and, ideally, outcomes, and will drive" the current research agenda, Dr. Josef S. Smolen said while presenting the panel’s recommendations at the annual European Congress of Rheumatology.
"Treat to target proposes a stepwise approach to achieving optimal outcomes based on available evidence and expert opinion. Treat to target has been successfully applied to management of diabetes, hypertension, hyperlipidemia, and rheumatoid arthritis," and the new task force set out to address whether it could be used when treating patients with spondyloarthritis (SpA), a question that required the expert task force to review the evidence for setting specific treatment goals for patients with SpA, said Dr. Smolen, professor of medicine at the Medical University of Vienna.
The task force eventually decided that the treat-to-target concept was applicable to SpA, but that the data available so far prevented the task force from setting specific treatment goals. While the recommendations underscore the importance of treating SpA patients with a goal of remission or inactive disease, and failing that, at least low disease activity, they fall short of giving clinicians guidance on how to best measure and define remission or low disease activity or how to achieve these goals.
For example, for axial SpA – the subtype that received the most specific recommendations – the panel advised clinicians to guide treatment decisions by using a "validated composite measure of disease activity" such as the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) plus acute phase reactants, or the Ankylosing Spondylitis Disease Activity Score (ASDAS) with or without functional measures such as the Bath Ankylosing Spondylitis Functional Index (BASFI). But the recommendations say nothing about what scores by these measures would define remission or low disease activity. The recommendations also talk about using other factors to further gauge axial SpA disease activity such as MRI analysis of inflammation and radiographic progression, but again Dr. Smolen provided no specific targets when using these measures.
For other, less well studied types of SpA, the new recommendations were even more nebulous. For psoriatic arthritis, the panel indicated that "validated measures of musculoskeletal disease activity" should be "performed and documented regularly" as should other factors such as spinal and extraarticular manifestations, imaging findings, and comorbidities, but the recommendations gave no specifics on what any of these measures might be or what level might equal remission or low disease. The same held true for peripheral SpA.
Other factors touched on by the new recommendations include the need for individualized and shared decision making between physicians and patients, the need for coordination of care among rheumatologists and other medical specialists who treat SpA patients (dermatologists, gastroenterologists, and ophthalmologists), and the need to take into account extraarticular manifestations of SpA diseases, comorbidities, and treatment risks along with the goal of low disease activity.
"I think it was important to document that there is a paucity of trials that have looked at strategies to treat" SpA. "For rheumatoid arthritis we have strategies, but not in spondyloarthritis, and I think it is important to say that," said Dr. Jürgen Braun, medical director of Rheumazentrum Ruhrgebiet in Herne, Germany.
SpA also lags behind rheumatoid arthritis by not having any treatments proven to slow radiographic progression. "Although we say that it is presumably important to treat inflammation [in patients with SpA], we are not sure," said Dr. Braun, who served as a member of the treat-to-target task force.
Even though the task force’s report highlights the absence of evidence for most facets of SpA management, "in the absence of evidence you need eminence, and that’s what was produced." Dr. Braun predicted that rheumatologists and other clinicians who care for patients with SpA would welcome these new recommendations despite their shortcomings. "What we say is what clinicians feel: If a patient’s CRP is elevated we must do something about it, but the evidence supporting this is limited. Presumably, it is important to treat inflammation, but we are not yet sure," he said in an interview.
"We don’t have trial results yet where you set up a quantifiable endpoint as your target, but that is coming," said Dr. Philip J. Mease, director of the rheumatology clinical research division at Swedish Medical Center in Seattle and a member of the task force. For example, the results from the Tight Control of Psoriatic Arthritis (TICOPA) trial "will tell us whether more aggressive treatment to a quantifiable target is appropriate and makes a difference. We anticipate that it will, but evidence is currently lacking." The primary endpoint of the TICOPA trial is change in the ACR20 response, but the trial includes several other clinical measures as secondary endpoints, including the Assessment in Ankylosing Spondylitis (ASAS), the BASDAI, and the psoriasis area severity index (PASI).
"The rheumatoid model is prompting us to develop quantifiable measures like the ASDAS and the new Psoriatic Arthritis Disease Activity Score (PASDAS) that we’ll start to see used. I just spoke with a colleague about the need to also develop a similar measure for peripheral SpA," Dr. Mease said in an interview.
The task force that developed the treat-to-target recommendations included 16 physicians and patients on its steering committee and 16 on an advisory committee. The majority came from various European locations, but about a quarter of the task force members were from the United States. To arrive at its recommendations, the task force used a comprehensive literature review that identified 22 published reports that addressed treatment targets for SpA (Ann. Rheum. Dis. 2013 June 10 [doi:10.1136/annrheumdis-2013-203860]). The treat-to-target recommendations were published online a few days before Dr. Smolen’s presentation at the meeting (Ann. Rheum. Dis. 2013 June 8 [doi:10.1136/annrheumdis-2013-203419]).
Dr. Smolen, Dr. Braun, and Dr. Mease said that they had no disclosures relevant to the topic.
On Twitter @mitchelzoler
MADRID – A panel of clinicians with expertise in the management of patients with spondyloarthritis took another step toward better defining this disease category and the goals of its treatment by producing the first "treat-to-target" recommendations for spondyloarthritis.
The new recommendations will "guide physicians, patients, and other stakeholders on how to optimize reduction of signs and symptoms and, ideally, outcomes, and will drive" the current research agenda, Dr. Josef S. Smolen said while presenting the panel’s recommendations at the annual European Congress of Rheumatology.
"Treat to target proposes a stepwise approach to achieving optimal outcomes based on available evidence and expert opinion. Treat to target has been successfully applied to management of diabetes, hypertension, hyperlipidemia, and rheumatoid arthritis," and the new task force set out to address whether it could be used when treating patients with spondyloarthritis (SpA), a question that required the expert task force to review the evidence for setting specific treatment goals for patients with SpA, said Dr. Smolen, professor of medicine at the Medical University of Vienna.
The task force eventually decided that the treat-to-target concept was applicable to SpA, but that the data available so far prevented the task force from setting specific treatment goals. While the recommendations underscore the importance of treating SpA patients with a goal of remission or inactive disease, and failing that, at least low disease activity, they fall short of giving clinicians guidance on how to best measure and define remission or low disease activity or how to achieve these goals.
For example, for axial SpA – the subtype that received the most specific recommendations – the panel advised clinicians to guide treatment decisions by using a "validated composite measure of disease activity" such as the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) plus acute phase reactants, or the Ankylosing Spondylitis Disease Activity Score (ASDAS) with or without functional measures such as the Bath Ankylosing Spondylitis Functional Index (BASFI). But the recommendations say nothing about what scores by these measures would define remission or low disease activity. The recommendations also talk about using other factors to further gauge axial SpA disease activity such as MRI analysis of inflammation and radiographic progression, but again Dr. Smolen provided no specific targets when using these measures.
For other, less well studied types of SpA, the new recommendations were even more nebulous. For psoriatic arthritis, the panel indicated that "validated measures of musculoskeletal disease activity" should be "performed and documented regularly" as should other factors such as spinal and extraarticular manifestations, imaging findings, and comorbidities, but the recommendations gave no specifics on what any of these measures might be or what level might equal remission or low disease. The same held true for peripheral SpA.
Other factors touched on by the new recommendations include the need for individualized and shared decision making between physicians and patients, the need for coordination of care among rheumatologists and other medical specialists who treat SpA patients (dermatologists, gastroenterologists, and ophthalmologists), and the need to take into account extraarticular manifestations of SpA diseases, comorbidities, and treatment risks along with the goal of low disease activity.
"I think it was important to document that there is a paucity of trials that have looked at strategies to treat" SpA. "For rheumatoid arthritis we have strategies, but not in spondyloarthritis, and I think it is important to say that," said Dr. Jürgen Braun, medical director of Rheumazentrum Ruhrgebiet in Herne, Germany.
SpA also lags behind rheumatoid arthritis by not having any treatments proven to slow radiographic progression. "Although we say that it is presumably important to treat inflammation [in patients with SpA], we are not sure," said Dr. Braun, who served as a member of the treat-to-target task force.
Even though the task force’s report highlights the absence of evidence for most facets of SpA management, "in the absence of evidence you need eminence, and that’s what was produced." Dr. Braun predicted that rheumatologists and other clinicians who care for patients with SpA would welcome these new recommendations despite their shortcomings. "What we say is what clinicians feel: If a patient’s CRP is elevated we must do something about it, but the evidence supporting this is limited. Presumably, it is important to treat inflammation, but we are not yet sure," he said in an interview.
"We don’t have trial results yet where you set up a quantifiable endpoint as your target, but that is coming," said Dr. Philip J. Mease, director of the rheumatology clinical research division at Swedish Medical Center in Seattle and a member of the task force. For example, the results from the Tight Control of Psoriatic Arthritis (TICOPA) trial "will tell us whether more aggressive treatment to a quantifiable target is appropriate and makes a difference. We anticipate that it will, but evidence is currently lacking." The primary endpoint of the TICOPA trial is change in the ACR20 response, but the trial includes several other clinical measures as secondary endpoints, including the Assessment in Ankylosing Spondylitis (ASAS), the BASDAI, and the psoriasis area severity index (PASI).
"The rheumatoid model is prompting us to develop quantifiable measures like the ASDAS and the new Psoriatic Arthritis Disease Activity Score (PASDAS) that we’ll start to see used. I just spoke with a colleague about the need to also develop a similar measure for peripheral SpA," Dr. Mease said in an interview.
The task force that developed the treat-to-target recommendations included 16 physicians and patients on its steering committee and 16 on an advisory committee. The majority came from various European locations, but about a quarter of the task force members were from the United States. To arrive at its recommendations, the task force used a comprehensive literature review that identified 22 published reports that addressed treatment targets for SpA (Ann. Rheum. Dis. 2013 June 10 [doi:10.1136/annrheumdis-2013-203860]). The treat-to-target recommendations were published online a few days before Dr. Smolen’s presentation at the meeting (Ann. Rheum. Dis. 2013 June 8 [doi:10.1136/annrheumdis-2013-203419]).
Dr. Smolen, Dr. Braun, and Dr. Mease said that they had no disclosures relevant to the topic.
On Twitter @mitchelzoler
AT THE EULAR CONGRESS 2013

VTE rate triples in pediatric cancer survivors
AMSTERDAM – Children, adolescents, and young adults who survived a diagnosis and treatment of cancer had a greater than threefold higher rate of acute venous thromboembolism during roughly 10 years of follow-up, compared with matched controls from the general population, in a study that included more than 30,000 Canadians.
The increased rate of VTE appeared to be linked to the chemotherapy and radiation treatments that patients received, because patients who were managed only by surgery had a substantially reduced rate of VTE during follow-up.

"Our working hypothesis is that VTE that develops during [initial] treatment of childhood cancers then places these patients at an increased risk" for a second VTE later in their life, Dr. Ketan P. Kulkarni said at the congress of the International Society on Thrombosis and Haemostasis.
If a first episode of VTE during or soon after the initial therapy that young cancer patients receive can be clearly established as a major risk factor for a subsequent episode of VTE, the next step would be to test whether improved prophylaxis during initial therapy can prevent a first episode and thereby also cut patients’ risk for a second VTE several months or years later. Clinicians who manage children, adolescents, and young adults with cancer need increased awareness that VTE "is a major problem" during both initial treatment and follow-up, Dr. Kulkarni said in an interview. "We think the VTEs during follow-up are recurrences of clots that first formed during treatment." He and his associates have begun to review the medical records of each survivor to better determine how many of the VTEs seen during follow-up were recurrences.
Another major finding from this analysis of people who survived at least 5 years following cancer diagnosis at age 0-24 years was that the entire range of cancers posed a VTE risk to patients, not just leukemia as some had previously though. The VTE rate during follow-up of the survivors was roughly the same regardless of whether patients had leukemia, lymphoma, carcinoma, or some other type of cancer.
"We have clearly dispelled the myth that it’s only leukemias. It’s all cancers," said Dr. Kulkarni, a pediatric hematologist-oncologist at the University of Alberta in Edmonton.
The researchers used provincial health insurance records from British Columbia during 1981-1999 to identify 2,857 patients who were aged 0-24 years at the time of their initial cancer diagnosis and then lived for at least another 5 years. The survivors averaged about 14 years old at the time of their initial cancer diagnosis. The investigators also assembled a control group matched by age and sex from the general British Columbia population, taking 10 controls for each case for a total of 28,570 controls.
During follow-up that ranged from 5 to 21 years and averaged nearly 10 years, they found that 43 survivors had an episode of VTE, a 1.5% incidence rate, compared with a 0.5% rate among the controls. In a multivariate analysis that controlled for sex, socioeconomic status, and region of residence, patients who were cancer survivors had a statistically significant, 3.4-fold increased rate of VTE compared with the controls, Dr. Kulkarni reported. Among the survivors the incidence of deep vein thrombosis was roughly 0.8%, the incidence of pulmonary embolism was roughly 0.5%, and VTE in other locations occurred in about 0.3% of the survivors (the total is 1.6% because of rounding). The incidence of VTEs was highest during the first 6 months following cancer diagnosis.
Cancer survivors who had been treated by surgery alone, without chemotherapy or radiation, had a statistically significant, 81% lower rate of developing a VTE compared with the patients treated by chemotherapy alone, radiation alone, or both.
"This supports the hypothesis that treatment by radiation or by chemotherapy increases the VTE risk," Dr. Kulkarni said.
The VTE rate was also substantially higher in survivors who had a relapse of their cancer during follow-up. Patients with relapses had a 2.5-fold higher rate of VTE compared with survivors who did not have a relapse.
Dr. Kulkarni said that he had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AMSTERDAM – Children, adolescents, and young adults who survived a diagnosis and treatment of cancer had a greater than threefold higher rate of acute venous thromboembolism during roughly 10 years of follow-up, compared with matched controls from the general population, in a study that included more than 30,000 Canadians.
The increased rate of VTE appeared to be linked to the chemotherapy and radiation treatments that patients received, because patients who were managed only by surgery had a substantially reduced rate of VTE during follow-up.
"Our working hypothesis is that VTE that develops during [initial] treatment of childhood cancers then places these patients at an increased risk" for a second VTE later in their life, Dr. Ketan P. Kulkarni said at the congress of the International Society on Thrombosis and Haemostasis.
If a first episode of VTE during or soon after the initial therapy that young cancer patients receive can be clearly established as a major risk factor for a subsequent episode of VTE, the next step would be to test whether improved prophylaxis during initial therapy can prevent a first episode and thereby also cut patients’ risk for a second VTE several months or years later. Clinicians who manage children, adolescents, and young adults with cancer need increased awareness that VTE "is a major problem" during both initial treatment and follow-up, Dr. Kulkarni said in an interview. "We think the VTEs during follow-up are recurrences of clots that first formed during treatment." He and his associates have begun to review the medical records of each survivor to better determine how many of the VTEs seen during follow-up were recurrences.
Another major finding from this analysis of people who survived at least 5 years following cancer diagnosis at age 0-24 years was that the entire range of cancers posed a VTE risk to patients, not just leukemia as some had previously though. The VTE rate during follow-up of the survivors was roughly the same regardless of whether patients had leukemia, lymphoma, carcinoma, or some other type of cancer.
"We have clearly dispelled the myth that it’s only leukemias. It’s all cancers," said Dr. Kulkarni, a pediatric hematologist-oncologist at the University of Alberta in Edmonton.
The researchers used provincial health insurance records from British Columbia during 1981-1999 to identify 2,857 patients who were aged 0-24 years at the time of their initial cancer diagnosis and then lived for at least another 5 years. The survivors averaged about 14 years old at the time of their initial cancer diagnosis. The investigators also assembled a control group matched by age and sex from the general British Columbia population, taking 10 controls for each case for a total of 28,570 controls.
During follow-up that ranged from 5 to 21 years and averaged nearly 10 years, they found that 43 survivors had an episode of VTE, a 1.5% incidence rate, compared with a 0.5% rate among the controls. In a multivariate analysis that controlled for sex, socioeconomic status, and region of residence, patients who were cancer survivors had a statistically significant, 3.4-fold increased rate of VTE compared with the controls, Dr. Kulkarni reported. Among the survivors the incidence of deep vein thrombosis was roughly 0.8%, the incidence of pulmonary embolism was roughly 0.5%, and VTE in other locations occurred in about 0.3% of the survivors (the total is 1.6% because of rounding). The incidence of VTEs was highest during the first 6 months following cancer diagnosis.
Cancer survivors who had been treated by surgery alone, without chemotherapy or radiation, had a statistically significant, 81% lower rate of developing a VTE compared with the patients treated by chemotherapy alone, radiation alone, or both.
"This supports the hypothesis that treatment by radiation or by chemotherapy increases the VTE risk," Dr. Kulkarni said.
The VTE rate was also substantially higher in survivors who had a relapse of their cancer during follow-up. Patients with relapses had a 2.5-fold higher rate of VTE compared with survivors who did not have a relapse.
Dr. Kulkarni said that he had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AMSTERDAM – Children, adolescents, and young adults who survived a diagnosis and treatment of cancer had a greater than threefold higher rate of acute venous thromboembolism during roughly 10 years of follow-up, compared with matched controls from the general population, in a study that included more than 30,000 Canadians.
The increased rate of VTE appeared to be linked to the chemotherapy and radiation treatments that patients received, because patients who were managed only by surgery had a substantially reduced rate of VTE during follow-up.
"Our working hypothesis is that VTE that develops during [initial] treatment of childhood cancers then places these patients at an increased risk" for a second VTE later in their life, Dr. Ketan P. Kulkarni said at the congress of the International Society on Thrombosis and Haemostasis.
If a first episode of VTE during or soon after the initial therapy that young cancer patients receive can be clearly established as a major risk factor for a subsequent episode of VTE, the next step would be to test whether improved prophylaxis during initial therapy can prevent a first episode and thereby also cut patients’ risk for a second VTE several months or years later. Clinicians who manage children, adolescents, and young adults with cancer need increased awareness that VTE "is a major problem" during both initial treatment and follow-up, Dr. Kulkarni said in an interview. "We think the VTEs during follow-up are recurrences of clots that first formed during treatment." He and his associates have begun to review the medical records of each survivor to better determine how many of the VTEs seen during follow-up were recurrences.
Another major finding from this analysis of people who survived at least 5 years following cancer diagnosis at age 0-24 years was that the entire range of cancers posed a VTE risk to patients, not just leukemia as some had previously though. The VTE rate during follow-up of the survivors was roughly the same regardless of whether patients had leukemia, lymphoma, carcinoma, or some other type of cancer.
"We have clearly dispelled the myth that it’s only leukemias. It’s all cancers," said Dr. Kulkarni, a pediatric hematologist-oncologist at the University of Alberta in Edmonton.
The researchers used provincial health insurance records from British Columbia during 1981-1999 to identify 2,857 patients who were aged 0-24 years at the time of their initial cancer diagnosis and then lived for at least another 5 years. The survivors averaged about 14 years old at the time of their initial cancer diagnosis. The investigators also assembled a control group matched by age and sex from the general British Columbia population, taking 10 controls for each case for a total of 28,570 controls.
During follow-up that ranged from 5 to 21 years and averaged nearly 10 years, they found that 43 survivors had an episode of VTE, a 1.5% incidence rate, compared with a 0.5% rate among the controls. In a multivariate analysis that controlled for sex, socioeconomic status, and region of residence, patients who were cancer survivors had a statistically significant, 3.4-fold increased rate of VTE compared with the controls, Dr. Kulkarni reported. Among the survivors the incidence of deep vein thrombosis was roughly 0.8%, the incidence of pulmonary embolism was roughly 0.5%, and VTE in other locations occurred in about 0.3% of the survivors (the total is 1.6% because of rounding). The incidence of VTEs was highest during the first 6 months following cancer diagnosis.
Cancer survivors who had been treated by surgery alone, without chemotherapy or radiation, had a statistically significant, 81% lower rate of developing a VTE compared with the patients treated by chemotherapy alone, radiation alone, or both.
"This supports the hypothesis that treatment by radiation or by chemotherapy increases the VTE risk," Dr. Kulkarni said.
The VTE rate was also substantially higher in survivors who had a relapse of their cancer during follow-up. Patients with relapses had a 2.5-fold higher rate of VTE compared with survivors who did not have a relapse.
Dr. Kulkarni said that he had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT THE 2013 ISTH CONGRESS
Major finding: Pediatric cancer survivors had a 3.4-fold increased rate of venous thromboembolism during follow-up, compared with controls.
Data source: Data came from a case-control study of 2,857 pediatric and young adult Canadian cancer survivors and 28,570 age-matched Canadian residents who did not have cancer, during an average follow-up of about 10 years.
Disclosures: Dr. Kulkarni said that he had no disclosures.

Bioresorbable coronary scaffolds quickly snag European role
PARIS – Bioresorbable coronary stents programmed to disappear look like they are here to stay.
Late last year, interventional cardiology began its slow but inexorable shift from metallic coronary stents to bioresorbable scaffolds that disappear from arteries within a couple of years, and in newer models, within several months.
The first bioresorbable coronary stent, called a bioresorbable vascular scaffold (BVS), came out for routine use in Europe last September under the brand name Absorb. While the U.S. pivotal trial for this BVS launched only in January, as early as last September interventionalists at a few European centers felt so convinced by the BVS concept that they designated it their "default" device for percutaneous coronary interventions (PCI). While early European results from more than 200 patients treated with default BVS were generally encouraging, although not without a problem, default BVS currently operates with enough exclusions and caveats to warrant a big asterisk.

A major lesson from "default" use of BVS is that they are clearly not for everyone right now. The largest default bioresorbable program reported so far includes 176 BVS placed by PCI in 174 patients during September 2012 through April 2013 at the Thoraxcenter in Rotterdam. Those 176 interventions were out of 1,018 procedures done in 958 patients during the same 8-month period. Despite having declared their default device, Thoraxcenter interventionalists decided that they needed something other than a BVS for more than 80% of their PCI patients, Dr. Robert-Jan van Geuns reported at the annual meeting of the European Association of Percutaneous Coronary Interventions.
The data so far are limited, "from small registries," not the sort of evidence that changes practice, admitted Dr. van Geuns, "but I think we are seeing where we are going" with BVS.
"With BVS, there is the hope for therapeutic benefit with possible vessel remodeling," said Dr. Stephan Windecker, professor and chief of cardiology at University Hospital in Bern, Switzerland. "I think it may have long-term benefits that we do not see" with conventional drug-eluting metallic stents. "There is strong evidence for a different way of vessel remodeling when the scaffold disappears," said Dr. Windecker, expressing the widely held but still clinically unproven view that treating patients with stents that disappear once they’ve done their job will be better for patients than are standard metal stents that stay in place forever.
Two Rotterdam BVS registries
Dr. van Geuns did not specify all the criteria his group applied for targeting BVS, aside from saying in an interview that they were younger patients with relatively few comorbidities and a life expectancy of at least 2 years so that they could potentially benefit from long-term advantages after a BVS disappears.

The Thoraxcenter’s 174 BVS-treated patients included 41 patients with a ST-elevation myocardial infarction who entered a separate review, two with prior coronary artery bypass surgery, and 131 who underwent PCI for other reasons who were the focus of Dr. van Geuns’ report. Procedural and clinical success occurred in 126 of the 131 patients (95%). The only complications during median follow-up of 137 days were two cases of stent thrombosis, one myocardial infarction in a nontarget vessel that occurred during the first 30 days after treatment, and one death. The operators generally found BVS to be deliverable, though with longer procedure times, more wires needed, and more predilatation of the PCI vessel, compared with what’s usual for placing metallic coronary stents.
The Polish ACS registry
Two other series reported at the meeting used BVS as the default device in patients with acute coronary syndrome (ACS). The POLAR ACS (Polish Absorb Registry for ACS) enrolled 88 ACS patients who received at least one BVS during November 2012-May 2013 when participating centers used BVS as their default devices for PCI. Treatment also included aspiration thrombectomy in 15 patients (17%), and predilatation of the infarct-related artery in 78 patients (89%).
The BVS intervention had 100% procedural success and produced robust, TIMI grade III flow in all of the treated patients, reported Dr. Dariusz Dudek, professor and head of interventional cardiology at Jagiellonian University in Krakow, Poland. The BVS was "easy to deliver," he said. But after predilatation and before BVS placement, one patient had no reflow and two had slow flow. Following completion of the procedure, one patient continued to have slow flow and four patients needed bail-out placement of another BVS. The only major adverse coronary event during hospitalization was need for PCI outside the target vessel.
"The data indicate at least similar safety and efficacy for BVS as for current drug-eluting stents," said Dr. Dudek, We can start replacing drug-eluting metal stents with BVS in many cases, especially for focal stenoses in younger patients."
But Dr. Chaim Lotan voiced concern about the incidence of low and slow blood flow during and after the ACS procedures. "Reduction of flow predicts mortality," he warned. "I think this is related to the aggressive vessel preparation," said Dr. Lotan, director of the heart institute at Hadassah Medical Center in Jerusalem.
Dr. Dudek acknowledged that the predilatation with a noncompliant balloon that BVS requires can trigger slow or no flow in the infarct vessel.
In response, Dr. Ron Waksman defended the BVS concept. "We see 4% restenosis after 3 years, and 6% after 4 years" with conventional drug-eluting metal stents. "These are unacceptable numbers. BVS is a new technology that guarantees that after 3 years there is no stent," said Dr. Waksman, associate director of cardiology at MedStar Washington Hospital Center.
The Czech STEMI registry
A third European registry of default BVS that began late last year focused on patients treated for ST-elevation MI at a participating center in the Czech Republic during December 2012-May 2013. Of the 87 patients who presented at participating centers with STEMI, 22 patients (25%) met prespecified criteria for undergoing BVS treatment, a BVS penetration level similar to the rate in the Thoraxcenter series. One eligibility criteria was life expectancy of at least 3 years. The 21-treated patients received 27 of 28 BVS successfully; one BVS could not be placed because of vessel tortuosity. Nineteen of the 21-BVS-treated patients achieved TIMI III grade coronary flow after PCI, with the other two patients reaching grade II flow, reported Dr. Petr Widimský, professor and head of the cardiocenter at Charles University in Prague. Common reasons why STEMI patients did not receive a BVS included no stent needed; a vessel too wide (more than 4.0 mm) to be treated by existing BVS sizes; or the presence of pulmonary edema or shock. During follow-up, one patient had a reinfarction caused by BVS thrombosis 3 days after stopping ticagrelor, but no patients had any episodes of clinical restenosis during follow-up of up to 5 months.
Based on the experience so far in three reported programs using BVS to treat patients with STEMI the key for successful use in these patients seems to be treating appropriately-sized coronary arteries because the possibility to post-dilate the BVS without breaking it is limited, said Dr. van Geuns.
Despite limited experience so far using BVS in routine practice, experts see the penetration the devices have made so far as a model for the future of interventional cardiology. During one panel discussion on BVS at the meeting, the widely shared consensus was that within a decade BVS numbers will surpass metallic stents for PCI and truly be the default device, with use in three-quarters or more of PCI patients.
A larger BVS registry
A larger record of BVS performance reported at the meeting came from a registry of 450 patients followed for 1 year after receiving one or two BVS at centers that participated in the ABSORB EXTEND trial. Average lesion length treated was just under 12 mm, and 93% of patients had a single lesion. During 12 months of follow-up, patients had one death, 13 myocardial infarctions, and eight instances of ischemia-driven target-vessel revascularization, for an overall major adverse event rate of 4.2%, reported Dr. Patrick W. Serruys, professor of interventional cardiology at the Thoraxcenter. Four cases of scaffold thrombosis (0.9%) occurred during 1 year follow-up.

Dr. Serruys showed how the BVS outcomes from the 450 patients in this registry compared with a historical series of patients who received the Xience V everolimus-eluting coronary stent in the SPIRIT II (Eurointervention 2007;3:315-20) and SPIRIT III (JAMA 2008:299:1903-13) trials. The 12-month major adverse cardiac events (MACE) rate of 4.2%, scaffold thrombosis rate of 0.9%, and the 2.9% MI rate seen with the Absorb BVS in the registry compared well with the 5.3% MACE rate, 0.7% definite stent thrombosis rate, and 2.3% MI rate seen with Xience V in the two older trials, Dr. Serruys noted. The BVS had no significant safety and efficacy differences, compared with historic results from a drug-eluting, metallic stent comparator, but with the added potential benefit of disappearing from the patient.
High expectations for BVS
"The noninferiority of BVS has been well established in patients with simple [coronary] disease, but in patients with diffuse disease, BVS may well be superior," said Dr. Ibrahim Al-Rashdan, director of the cardiac catheterization laboratory at in Kuwait Heart Center. "We can use BVS to avoid a metal jacket with diffuse disease. But lesion preparation and good vessel sizing is mandatory. And if the vessel is calcified you must use a rotablator; if you have any doubt, use a rotablator." Another limitation of BVS is that because they are made from polymers, they break when overexpanded, and the currently available models are bulkier than metallic stents and their bulkiness demands predilatation of the artery receiving a BVS. "There is consensus to use BVS for long lesions, and for patients with diabetes," said Dr. van Geuns.
But despite this support for BVS, their reception may be tepid so far at the grassroots’ level. "People are afraid of BVS because it’s a plastic stent," said Dr. Dudek. But while he conceded that BVS use requires precautions, "the technique is not so different from a regular DES [drug-eluting stent]," he said.

"The ideal lesions for BVS are soft, with no calcifications, and enough compliance of the vessel wall to accommodate the device so you don’t need to worry about full stent expansion. With BVS, there is hope to have therapeutic benefit with possible vessel remodeling." said Dr. Windecker. "There is strong evidence for a different way of vessel remodeling" with lesion regression. "This may also happen with metal stents, but with a metal stent, the remodeling won’t benefit the lumen because of the metallic wires. We have preliminary data from coronary imaging that the coronary seems to grow" around a BVS "in a way that does not compromise the lumen," Dr. Windecker said in an interview.
A focus for continued BVS development will be patients with diabetes because of the "clear limitation of drug-eluting stents" in these patients, he said. Future studies will also try to establish that BVS can prevent plaque rupture.
Dr. van Geuns said that he has been a consultant to and received honoraria from Stentys and Abbott Vascular. Dr. Windecker said that he has received grant support from Abbott, Biotronik, Boston Scientific, and several other companies. Dr. Dudek said that he has been a consultant to Biotronik, Abbott, Medtronic, and Boston Scientific. Dr. Lotan said that he has been a consultant to and stockholder in InspireMD and that he has received honoraria from Medtronic and other companies. Dr. Waksman said that he has been a consultant to Biotronik, Abbott Vascular, Boston Scientific, and Medtronic. Dr. Widimský said that he has been a consultant to Abbott Vascular, Boston Scientific, Medtronic, and several other companies. Dr. Serruys said that he had no disclosures. Dr. Al-Rashdan said that he had no disclosures.
On Twitter @mitchelzoler
PARIS – Bioresorbable coronary stents programmed to disappear look like they are here to stay.
Late last year, interventional cardiology began its slow but inexorable shift from metallic coronary stents to bioresorbable scaffolds that disappear from arteries within a couple of years, and in newer models, within several months.
The first bioresorbable coronary stent, called a bioresorbable vascular scaffold (BVS), came out for routine use in Europe last September under the brand name Absorb. While the U.S. pivotal trial for this BVS launched only in January, as early as last September interventionalists at a few European centers felt so convinced by the BVS concept that they designated it their "default" device for percutaneous coronary interventions (PCI). While early European results from more than 200 patients treated with default BVS were generally encouraging, although not without a problem, default BVS currently operates with enough exclusions and caveats to warrant a big asterisk.
A major lesson from "default" use of BVS is that they are clearly not for everyone right now. The largest default bioresorbable program reported so far includes 176 BVS placed by PCI in 174 patients during September 2012 through April 2013 at the Thoraxcenter in Rotterdam. Those 176 interventions were out of 1,018 procedures done in 958 patients during the same 8-month period. Despite having declared their default device, Thoraxcenter interventionalists decided that they needed something other than a BVS for more than 80% of their PCI patients, Dr. Robert-Jan van Geuns reported at the annual meeting of the European Association of Percutaneous Coronary Interventions.
The data so far are limited, "from small registries," not the sort of evidence that changes practice, admitted Dr. van Geuns, "but I think we are seeing where we are going" with BVS.
"With BVS, there is the hope for therapeutic benefit with possible vessel remodeling," said Dr. Stephan Windecker, professor and chief of cardiology at University Hospital in Bern, Switzerland. "I think it may have long-term benefits that we do not see" with conventional drug-eluting metallic stents. "There is strong evidence for a different way of vessel remodeling when the scaffold disappears," said Dr. Windecker, expressing the widely held but still clinically unproven view that treating patients with stents that disappear once they’ve done their job will be better for patients than are standard metal stents that stay in place forever.
Two Rotterdam BVS registries
Dr. van Geuns did not specify all the criteria his group applied for targeting BVS, aside from saying in an interview that they were younger patients with relatively few comorbidities and a life expectancy of at least 2 years so that they could potentially benefit from long-term advantages after a BVS disappears.
The Thoraxcenter’s 174 BVS-treated patients included 41 patients with a ST-elevation myocardial infarction who entered a separate review, two with prior coronary artery bypass surgery, and 131 who underwent PCI for other reasons who were the focus of Dr. van Geuns’ report. Procedural and clinical success occurred in 126 of the 131 patients (95%). The only complications during median follow-up of 137 days were two cases of stent thrombosis, one myocardial infarction in a nontarget vessel that occurred during the first 30 days after treatment, and one death. The operators generally found BVS to be deliverable, though with longer procedure times, more wires needed, and more predilatation of the PCI vessel, compared with what’s usual for placing metallic coronary stents.
The Polish ACS registry
Two other series reported at the meeting used BVS as the default device in patients with acute coronary syndrome (ACS). The POLAR ACS (Polish Absorb Registry for ACS) enrolled 88 ACS patients who received at least one BVS during November 2012-May 2013 when participating centers used BVS as their default devices for PCI. Treatment also included aspiration thrombectomy in 15 patients (17%), and predilatation of the infarct-related artery in 78 patients (89%).
The BVS intervention had 100% procedural success and produced robust, TIMI grade III flow in all of the treated patients, reported Dr. Dariusz Dudek, professor and head of interventional cardiology at Jagiellonian University in Krakow, Poland. The BVS was "easy to deliver," he said. But after predilatation and before BVS placement, one patient had no reflow and two had slow flow. Following completion of the procedure, one patient continued to have slow flow and four patients needed bail-out placement of another BVS. The only major adverse coronary event during hospitalization was need for PCI outside the target vessel.
"The data indicate at least similar safety and efficacy for BVS as for current drug-eluting stents," said Dr. Dudek, We can start replacing drug-eluting metal stents with BVS in many cases, especially for focal stenoses in younger patients."
But Dr. Chaim Lotan voiced concern about the incidence of low and slow blood flow during and after the ACS procedures. "Reduction of flow predicts mortality," he warned. "I think this is related to the aggressive vessel preparation," said Dr. Lotan, director of the heart institute at Hadassah Medical Center in Jerusalem.
Dr. Dudek acknowledged that the predilatation with a noncompliant balloon that BVS requires can trigger slow or no flow in the infarct vessel.
In response, Dr. Ron Waksman defended the BVS concept. "We see 4% restenosis after 3 years, and 6% after 4 years" with conventional drug-eluting metal stents. "These are unacceptable numbers. BVS is a new technology that guarantees that after 3 years there is no stent," said Dr. Waksman, associate director of cardiology at MedStar Washington Hospital Center.
The Czech STEMI registry
A third European registry of default BVS that began late last year focused on patients treated for ST-elevation MI at a participating center in the Czech Republic during December 2012-May 2013. Of the 87 patients who presented at participating centers with STEMI, 22 patients (25%) met prespecified criteria for undergoing BVS treatment, a BVS penetration level similar to the rate in the Thoraxcenter series. One eligibility criteria was life expectancy of at least 3 years. The 21-treated patients received 27 of 28 BVS successfully; one BVS could not be placed because of vessel tortuosity. Nineteen of the 21-BVS-treated patients achieved TIMI III grade coronary flow after PCI, with the other two patients reaching grade II flow, reported Dr. Petr Widimský, professor and head of the cardiocenter at Charles University in Prague. Common reasons why STEMI patients did not receive a BVS included no stent needed; a vessel too wide (more than 4.0 mm) to be treated by existing BVS sizes; or the presence of pulmonary edema or shock. During follow-up, one patient had a reinfarction caused by BVS thrombosis 3 days after stopping ticagrelor, but no patients had any episodes of clinical restenosis during follow-up of up to 5 months.
Based on the experience so far in three reported programs using BVS to treat patients with STEMI the key for successful use in these patients seems to be treating appropriately-sized coronary arteries because the possibility to post-dilate the BVS without breaking it is limited, said Dr. van Geuns.
Despite limited experience so far using BVS in routine practice, experts see the penetration the devices have made so far as a model for the future of interventional cardiology. During one panel discussion on BVS at the meeting, the widely shared consensus was that within a decade BVS numbers will surpass metallic stents for PCI and truly be the default device, with use in three-quarters or more of PCI patients.
A larger BVS registry
A larger record of BVS performance reported at the meeting came from a registry of 450 patients followed for 1 year after receiving one or two BVS at centers that participated in the ABSORB EXTEND trial. Average lesion length treated was just under 12 mm, and 93% of patients had a single lesion. During 12 months of follow-up, patients had one death, 13 myocardial infarctions, and eight instances of ischemia-driven target-vessel revascularization, for an overall major adverse event rate of 4.2%, reported Dr. Patrick W. Serruys, professor of interventional cardiology at the Thoraxcenter. Four cases of scaffold thrombosis (0.9%) occurred during 1 year follow-up.
Dr. Serruys showed how the BVS outcomes from the 450 patients in this registry compared with a historical series of patients who received the Xience V everolimus-eluting coronary stent in the SPIRIT II (Eurointervention 2007;3:315-20) and SPIRIT III (JAMA 2008:299:1903-13) trials. The 12-month major adverse cardiac events (MACE) rate of 4.2%, scaffold thrombosis rate of 0.9%, and the 2.9% MI rate seen with the Absorb BVS in the registry compared well with the 5.3% MACE rate, 0.7% definite stent thrombosis rate, and 2.3% MI rate seen with Xience V in the two older trials, Dr. Serruys noted. The BVS had no significant safety and efficacy differences, compared with historic results from a drug-eluting, metallic stent comparator, but with the added potential benefit of disappearing from the patient.
High expectations for BVS
"The noninferiority of BVS has been well established in patients with simple [coronary] disease, but in patients with diffuse disease, BVS may well be superior," said Dr. Ibrahim Al-Rashdan, director of the cardiac catheterization laboratory at in Kuwait Heart Center. "We can use BVS to avoid a metal jacket with diffuse disease. But lesion preparation and good vessel sizing is mandatory. And if the vessel is calcified you must use a rotablator; if you have any doubt, use a rotablator." Another limitation of BVS is that because they are made from polymers, they break when overexpanded, and the currently available models are bulkier than metallic stents and their bulkiness demands predilatation of the artery receiving a BVS. "There is consensus to use BVS for long lesions, and for patients with diabetes," said Dr. van Geuns.
But despite this support for BVS, their reception may be tepid so far at the grassroots’ level. "People are afraid of BVS because it’s a plastic stent," said Dr. Dudek. But while he conceded that BVS use requires precautions, "the technique is not so different from a regular DES [drug-eluting stent]," he said.
"The ideal lesions for BVS are soft, with no calcifications, and enough compliance of the vessel wall to accommodate the device so you don’t need to worry about full stent expansion. With BVS, there is hope to have therapeutic benefit with possible vessel remodeling." said Dr. Windecker. "There is strong evidence for a different way of vessel remodeling" with lesion regression. "This may also happen with metal stents, but with a metal stent, the remodeling won’t benefit the lumen because of the metallic wires. We have preliminary data from coronary imaging that the coronary seems to grow" around a BVS "in a way that does not compromise the lumen," Dr. Windecker said in an interview.
A focus for continued BVS development will be patients with diabetes because of the "clear limitation of drug-eluting stents" in these patients, he said. Future studies will also try to establish that BVS can prevent plaque rupture.
Dr. van Geuns said that he has been a consultant to and received honoraria from Stentys and Abbott Vascular. Dr. Windecker said that he has received grant support from Abbott, Biotronik, Boston Scientific, and several other companies. Dr. Dudek said that he has been a consultant to Biotronik, Abbott, Medtronic, and Boston Scientific. Dr. Lotan said that he has been a consultant to and stockholder in InspireMD and that he has received honoraria from Medtronic and other companies. Dr. Waksman said that he has been a consultant to Biotronik, Abbott Vascular, Boston Scientific, and Medtronic. Dr. Widimský said that he has been a consultant to Abbott Vascular, Boston Scientific, Medtronic, and several other companies. Dr. Serruys said that he had no disclosures. Dr. Al-Rashdan said that he had no disclosures.
On Twitter @mitchelzoler
PARIS – Bioresorbable coronary stents programmed to disappear look like they are here to stay.
Late last year, interventional cardiology began its slow but inexorable shift from metallic coronary stents to bioresorbable scaffolds that disappear from arteries within a couple of years, and in newer models, within several months.
The first bioresorbable coronary stent, called a bioresorbable vascular scaffold (BVS), came out for routine use in Europe last September under the brand name Absorb. While the U.S. pivotal trial for this BVS launched only in January, as early as last September interventionalists at a few European centers felt so convinced by the BVS concept that they designated it their "default" device for percutaneous coronary interventions (PCI). While early European results from more than 200 patients treated with default BVS were generally encouraging, although not without a problem, default BVS currently operates with enough exclusions and caveats to warrant a big asterisk.
A major lesson from "default" use of BVS is that they are clearly not for everyone right now. The largest default bioresorbable program reported so far includes 176 BVS placed by PCI in 174 patients during September 2012 through April 2013 at the Thoraxcenter in Rotterdam. Those 176 interventions were out of 1,018 procedures done in 958 patients during the same 8-month period. Despite having declared their default device, Thoraxcenter interventionalists decided that they needed something other than a BVS for more than 80% of their PCI patients, Dr. Robert-Jan van Geuns reported at the annual meeting of the European Association of Percutaneous Coronary Interventions.
The data so far are limited, "from small registries," not the sort of evidence that changes practice, admitted Dr. van Geuns, "but I think we are seeing where we are going" with BVS.
"With BVS, there is the hope for therapeutic benefit with possible vessel remodeling," said Dr. Stephan Windecker, professor and chief of cardiology at University Hospital in Bern, Switzerland. "I think it may have long-term benefits that we do not see" with conventional drug-eluting metallic stents. "There is strong evidence for a different way of vessel remodeling when the scaffold disappears," said Dr. Windecker, expressing the widely held but still clinically unproven view that treating patients with stents that disappear once they’ve done their job will be better for patients than are standard metal stents that stay in place forever.
Two Rotterdam BVS registries
Dr. van Geuns did not specify all the criteria his group applied for targeting BVS, aside from saying in an interview that they were younger patients with relatively few comorbidities and a life expectancy of at least 2 years so that they could potentially benefit from long-term advantages after a BVS disappears.
The Thoraxcenter’s 174 BVS-treated patients included 41 patients with a ST-elevation myocardial infarction who entered a separate review, two with prior coronary artery bypass surgery, and 131 who underwent PCI for other reasons who were the focus of Dr. van Geuns’ report. Procedural and clinical success occurred in 126 of the 131 patients (95%). The only complications during median follow-up of 137 days were two cases of stent thrombosis, one myocardial infarction in a nontarget vessel that occurred during the first 30 days after treatment, and one death. The operators generally found BVS to be deliverable, though with longer procedure times, more wires needed, and more predilatation of the PCI vessel, compared with what’s usual for placing metallic coronary stents.
The Polish ACS registry
Two other series reported at the meeting used BVS as the default device in patients with acute coronary syndrome (ACS). The POLAR ACS (Polish Absorb Registry for ACS) enrolled 88 ACS patients who received at least one BVS during November 2012-May 2013 when participating centers used BVS as their default devices for PCI. Treatment also included aspiration thrombectomy in 15 patients (17%), and predilatation of the infarct-related artery in 78 patients (89%).
The BVS intervention had 100% procedural success and produced robust, TIMI grade III flow in all of the treated patients, reported Dr. Dariusz Dudek, professor and head of interventional cardiology at Jagiellonian University in Krakow, Poland. The BVS was "easy to deliver," he said. But after predilatation and before BVS placement, one patient had no reflow and two had slow flow. Following completion of the procedure, one patient continued to have slow flow and four patients needed bail-out placement of another BVS. The only major adverse coronary event during hospitalization was need for PCI outside the target vessel.
"The data indicate at least similar safety and efficacy for BVS as for current drug-eluting stents," said Dr. Dudek, We can start replacing drug-eluting metal stents with BVS in many cases, especially for focal stenoses in younger patients."
But Dr. Chaim Lotan voiced concern about the incidence of low and slow blood flow during and after the ACS procedures. "Reduction of flow predicts mortality," he warned. "I think this is related to the aggressive vessel preparation," said Dr. Lotan, director of the heart institute at Hadassah Medical Center in Jerusalem.
Dr. Dudek acknowledged that the predilatation with a noncompliant balloon that BVS requires can trigger slow or no flow in the infarct vessel.
In response, Dr. Ron Waksman defended the BVS concept. "We see 4% restenosis after 3 years, and 6% after 4 years" with conventional drug-eluting metal stents. "These are unacceptable numbers. BVS is a new technology that guarantees that after 3 years there is no stent," said Dr. Waksman, associate director of cardiology at MedStar Washington Hospital Center.
The Czech STEMI registry
A third European registry of default BVS that began late last year focused on patients treated for ST-elevation MI at a participating center in the Czech Republic during December 2012-May 2013. Of the 87 patients who presented at participating centers with STEMI, 22 patients (25%) met prespecified criteria for undergoing BVS treatment, a BVS penetration level similar to the rate in the Thoraxcenter series. One eligibility criteria was life expectancy of at least 3 years. The 21-treated patients received 27 of 28 BVS successfully; one BVS could not be placed because of vessel tortuosity. Nineteen of the 21-BVS-treated patients achieved TIMI III grade coronary flow after PCI, with the other two patients reaching grade II flow, reported Dr. Petr Widimský, professor and head of the cardiocenter at Charles University in Prague. Common reasons why STEMI patients did not receive a BVS included no stent needed; a vessel too wide (more than 4.0 mm) to be treated by existing BVS sizes; or the presence of pulmonary edema or shock. During follow-up, one patient had a reinfarction caused by BVS thrombosis 3 days after stopping ticagrelor, but no patients had any episodes of clinical restenosis during follow-up of up to 5 months.
Based on the experience so far in three reported programs using BVS to treat patients with STEMI the key for successful use in these patients seems to be treating appropriately-sized coronary arteries because the possibility to post-dilate the BVS without breaking it is limited, said Dr. van Geuns.
Despite limited experience so far using BVS in routine practice, experts see the penetration the devices have made so far as a model for the future of interventional cardiology. During one panel discussion on BVS at the meeting, the widely shared consensus was that within a decade BVS numbers will surpass metallic stents for PCI and truly be the default device, with use in three-quarters or more of PCI patients.
A larger BVS registry
A larger record of BVS performance reported at the meeting came from a registry of 450 patients followed for 1 year after receiving one or two BVS at centers that participated in the ABSORB EXTEND trial. Average lesion length treated was just under 12 mm, and 93% of patients had a single lesion. During 12 months of follow-up, patients had one death, 13 myocardial infarctions, and eight instances of ischemia-driven target-vessel revascularization, for an overall major adverse event rate of 4.2%, reported Dr. Patrick W. Serruys, professor of interventional cardiology at the Thoraxcenter. Four cases of scaffold thrombosis (0.9%) occurred during 1 year follow-up.
Dr. Serruys showed how the BVS outcomes from the 450 patients in this registry compared with a historical series of patients who received the Xience V everolimus-eluting coronary stent in the SPIRIT II (Eurointervention 2007;3:315-20) and SPIRIT III (JAMA 2008:299:1903-13) trials. The 12-month major adverse cardiac events (MACE) rate of 4.2%, scaffold thrombosis rate of 0.9%, and the 2.9% MI rate seen with the Absorb BVS in the registry compared well with the 5.3% MACE rate, 0.7% definite stent thrombosis rate, and 2.3% MI rate seen with Xience V in the two older trials, Dr. Serruys noted. The BVS had no significant safety and efficacy differences, compared with historic results from a drug-eluting, metallic stent comparator, but with the added potential benefit of disappearing from the patient.
High expectations for BVS
"The noninferiority of BVS has been well established in patients with simple [coronary] disease, but in patients with diffuse disease, BVS may well be superior," said Dr. Ibrahim Al-Rashdan, director of the cardiac catheterization laboratory at in Kuwait Heart Center. "We can use BVS to avoid a metal jacket with diffuse disease. But lesion preparation and good vessel sizing is mandatory. And if the vessel is calcified you must use a rotablator; if you have any doubt, use a rotablator." Another limitation of BVS is that because they are made from polymers, they break when overexpanded, and the currently available models are bulkier than metallic stents and their bulkiness demands predilatation of the artery receiving a BVS. "There is consensus to use BVS for long lesions, and for patients with diabetes," said Dr. van Geuns.
But despite this support for BVS, their reception may be tepid so far at the grassroots’ level. "People are afraid of BVS because it’s a plastic stent," said Dr. Dudek. But while he conceded that BVS use requires precautions, "the technique is not so different from a regular DES [drug-eluting stent]," he said.
"The ideal lesions for BVS are soft, with no calcifications, and enough compliance of the vessel wall to accommodate the device so you don’t need to worry about full stent expansion. With BVS, there is hope to have therapeutic benefit with possible vessel remodeling." said Dr. Windecker. "There is strong evidence for a different way of vessel remodeling" with lesion regression. "This may also happen with metal stents, but with a metal stent, the remodeling won’t benefit the lumen because of the metallic wires. We have preliminary data from coronary imaging that the coronary seems to grow" around a BVS "in a way that does not compromise the lumen," Dr. Windecker said in an interview.
A focus for continued BVS development will be patients with diabetes because of the "clear limitation of drug-eluting stents" in these patients, he said. Future studies will also try to establish that BVS can prevent plaque rupture.
Dr. van Geuns said that he has been a consultant to and received honoraria from Stentys and Abbott Vascular. Dr. Windecker said that he has received grant support from Abbott, Biotronik, Boston Scientific, and several other companies. Dr. Dudek said that he has been a consultant to Biotronik, Abbott, Medtronic, and Boston Scientific. Dr. Lotan said that he has been a consultant to and stockholder in InspireMD and that he has received honoraria from Medtronic and other companies. Dr. Waksman said that he has been a consultant to Biotronik, Abbott Vascular, Boston Scientific, and Medtronic. Dr. Widimský said that he has been a consultant to Abbott Vascular, Boston Scientific, Medtronic, and several other companies. Dr. Serruys said that he had no disclosures. Dr. Al-Rashdan said that he had no disclosures.
On Twitter @mitchelzoler
EXPERT OPINION FROM EUROPCR 2013

DESolve Bioresorbable stent speeds coronary healing
PARIS – The monopoly Absorb has held in Europe since last September as the only bioresorbable vascular scaffold on the market is at an end.
In May, Elixir, a company that makes its own version of a different bioresorbable vascular scaffold (BVS), announced it received permission from the European Commission to market its DESolve BVS.
DESolve differs from Absorb by substantially disappearing within 6 months of placement with full resorption within a year, roughly twice the disappearing speed of Absorb, the first bioresorbable vascular scaffold on the European market.
This difference may have affected performance, said Dr. Alexandre Abizaid, who reported on a multicenter series of 126 patients who received DESolve BVS in a talk at the annual meeting of the European Association of Percutaneous Coronary Interventions.

"We got the same results after 6 months with this device as we see with Absorb after 2 or 3 years," said Dr. Abizaid, chief of coronary interventions at the Dante Pazzanese Cardiology Institute in São Paulo, Brazil."We saw the benefit from a BVS early on, with lumen enlargement and vessel enlargement.
"I would use this devise on the types of patients included in the study; younger patients with relatively short lesions, about 12 mm; patients who could benefit from vessel restoration; patients who might need coronary artery bypass surgery in the future; and patients with diabetes who seem to get the same results with this BVS as other patients. As we get more confident with the acute and long-term performance, we will expand the indications," Dr. Abizaid said.
Another feature of the DESolve BVS is that the 3.0-mm–diameter model can be balloon expanded to 4.8 mm before breaking, in contrast to the Absorb BVS, which can break when overexpansion surpasses 0.5 mm.
The results Dr. Abizaid reported on DESolve "led to the CE mark for the device. It will surely change our practice," commented Dr. Robert A. Byrne, an interventional cardiologist at the Heart Center in Munich. "When we have more bioresorbable scaffolds in the marketplace, we will see further development of this technology."
The DESolve Nx (notorolimus-eluting) pivotal trial included 126 patients at 13 centers in Brazil, New Zealand, and Europe. The study’s primary endpoint was the late lumen loss at 6 months, which averaged 0.21 mm, a rate that Dr. Byrne called "very good" compared with current standards.
Other measures reported by Dr. Abizaid further documented the extent of healing and vessel growth. "In the first 6 months, we usually see the lumen decrease due to scar tissue, but at 3-12 months we saw luminal enlargement that occurs as the scaffold degrades. There was a clear, statistically significant 17% increase in vessel area at 6 months, with a luminal increase of almost 10%, generally what we see after 3-4 years with Absorb," he said. In addition, imaging showed nearly 99% of all struts covered by tissue at 6 months. "The healing process is essentially complete" by then, he said.
Follow-up also showed low early recoil and no negative remodeling. In-segment binary restenosis occurred in one patient in whom the restenosis was within the scaffold, and in three patients where it occurred at the edge. During follow-up, clinically indicated revascularization was performed in two patients, a target vessel non–Q-wave myocardial infarction occurred in one patient, and cardiac death occurred in another.
"This device does its job to prevent negative remodeling in the first 4 months, and then it uncages the vessel, frees it to allow natural, positive remodeling. The potential advantages of the DESolve BVS are that degradation really happens within 1 year, and it gives you more freedom to postdilate if you need to. Having the device not fracture [during postdilation] is important," Dr. Abizaid said.
The DESolve Nx trial was sponsored by Elixir, which markets the stent. Dr. Abizaid said he has received research grants from Elixir, Abbott Vascular, Boston Scientific, and Medtronic. Dr. Byrne said his institution received research support from Biotronik.
On Twitter @mitchelzoler
PARIS – The monopoly Absorb has held in Europe since last September as the only bioresorbable vascular scaffold on the market is at an end.
In May, Elixir, a company that makes its own version of a different bioresorbable vascular scaffold (BVS), announced it received permission from the European Commission to market its DESolve BVS.
DESolve differs from Absorb by substantially disappearing within 6 months of placement with full resorption within a year, roughly twice the disappearing speed of Absorb, the first bioresorbable vascular scaffold on the European market.
This difference may have affected performance, said Dr. Alexandre Abizaid, who reported on a multicenter series of 126 patients who received DESolve BVS in a talk at the annual meeting of the European Association of Percutaneous Coronary Interventions.
"We got the same results after 6 months with this device as we see with Absorb after 2 or 3 years," said Dr. Abizaid, chief of coronary interventions at the Dante Pazzanese Cardiology Institute in São Paulo, Brazil."We saw the benefit from a BVS early on, with lumen enlargement and vessel enlargement.
"I would use this devise on the types of patients included in the study; younger patients with relatively short lesions, about 12 mm; patients who could benefit from vessel restoration; patients who might need coronary artery bypass surgery in the future; and patients with diabetes who seem to get the same results with this BVS as other patients. As we get more confident with the acute and long-term performance, we will expand the indications," Dr. Abizaid said.
Another feature of the DESolve BVS is that the 3.0-mm–diameter model can be balloon expanded to 4.8 mm before breaking, in contrast to the Absorb BVS, which can break when overexpansion surpasses 0.5 mm.
The results Dr. Abizaid reported on DESolve "led to the CE mark for the device. It will surely change our practice," commented Dr. Robert A. Byrne, an interventional cardiologist at the Heart Center in Munich. "When we have more bioresorbable scaffolds in the marketplace, we will see further development of this technology."
The DESolve Nx (notorolimus-eluting) pivotal trial included 126 patients at 13 centers in Brazil, New Zealand, and Europe. The study’s primary endpoint was the late lumen loss at 6 months, which averaged 0.21 mm, a rate that Dr. Byrne called "very good" compared with current standards.
Other measures reported by Dr. Abizaid further documented the extent of healing and vessel growth. "In the first 6 months, we usually see the lumen decrease due to scar tissue, but at 3-12 months we saw luminal enlargement that occurs as the scaffold degrades. There was a clear, statistically significant 17% increase in vessel area at 6 months, with a luminal increase of almost 10%, generally what we see after 3-4 years with Absorb," he said. In addition, imaging showed nearly 99% of all struts covered by tissue at 6 months. "The healing process is essentially complete" by then, he said.
Follow-up also showed low early recoil and no negative remodeling. In-segment binary restenosis occurred in one patient in whom the restenosis was within the scaffold, and in three patients where it occurred at the edge. During follow-up, clinically indicated revascularization was performed in two patients, a target vessel non–Q-wave myocardial infarction occurred in one patient, and cardiac death occurred in another.
"This device does its job to prevent negative remodeling in the first 4 months, and then it uncages the vessel, frees it to allow natural, positive remodeling. The potential advantages of the DESolve BVS are that degradation really happens within 1 year, and it gives you more freedom to postdilate if you need to. Having the device not fracture [during postdilation] is important," Dr. Abizaid said.
The DESolve Nx trial was sponsored by Elixir, which markets the stent. Dr. Abizaid said he has received research grants from Elixir, Abbott Vascular, Boston Scientific, and Medtronic. Dr. Byrne said his institution received research support from Biotronik.
On Twitter @mitchelzoler
PARIS – The monopoly Absorb has held in Europe since last September as the only bioresorbable vascular scaffold on the market is at an end.
In May, Elixir, a company that makes its own version of a different bioresorbable vascular scaffold (BVS), announced it received permission from the European Commission to market its DESolve BVS.
DESolve differs from Absorb by substantially disappearing within 6 months of placement with full resorption within a year, roughly twice the disappearing speed of Absorb, the first bioresorbable vascular scaffold on the European market.
This difference may have affected performance, said Dr. Alexandre Abizaid, who reported on a multicenter series of 126 patients who received DESolve BVS in a talk at the annual meeting of the European Association of Percutaneous Coronary Interventions.
"We got the same results after 6 months with this device as we see with Absorb after 2 or 3 years," said Dr. Abizaid, chief of coronary interventions at the Dante Pazzanese Cardiology Institute in São Paulo, Brazil."We saw the benefit from a BVS early on, with lumen enlargement and vessel enlargement.
"I would use this devise on the types of patients included in the study; younger patients with relatively short lesions, about 12 mm; patients who could benefit from vessel restoration; patients who might need coronary artery bypass surgery in the future; and patients with diabetes who seem to get the same results with this BVS as other patients. As we get more confident with the acute and long-term performance, we will expand the indications," Dr. Abizaid said.
Another feature of the DESolve BVS is that the 3.0-mm–diameter model can be balloon expanded to 4.8 mm before breaking, in contrast to the Absorb BVS, which can break when overexpansion surpasses 0.5 mm.
The results Dr. Abizaid reported on DESolve "led to the CE mark for the device. It will surely change our practice," commented Dr. Robert A. Byrne, an interventional cardiologist at the Heart Center in Munich. "When we have more bioresorbable scaffolds in the marketplace, we will see further development of this technology."
The DESolve Nx (notorolimus-eluting) pivotal trial included 126 patients at 13 centers in Brazil, New Zealand, and Europe. The study’s primary endpoint was the late lumen loss at 6 months, which averaged 0.21 mm, a rate that Dr. Byrne called "very good" compared with current standards.
Other measures reported by Dr. Abizaid further documented the extent of healing and vessel growth. "In the first 6 months, we usually see the lumen decrease due to scar tissue, but at 3-12 months we saw luminal enlargement that occurs as the scaffold degrades. There was a clear, statistically significant 17% increase in vessel area at 6 months, with a luminal increase of almost 10%, generally what we see after 3-4 years with Absorb," he said. In addition, imaging showed nearly 99% of all struts covered by tissue at 6 months. "The healing process is essentially complete" by then, he said.
Follow-up also showed low early recoil and no negative remodeling. In-segment binary restenosis occurred in one patient in whom the restenosis was within the scaffold, and in three patients where it occurred at the edge. During follow-up, clinically indicated revascularization was performed in two patients, a target vessel non–Q-wave myocardial infarction occurred in one patient, and cardiac death occurred in another.
"This device does its job to prevent negative remodeling in the first 4 months, and then it uncages the vessel, frees it to allow natural, positive remodeling. The potential advantages of the DESolve BVS are that degradation really happens within 1 year, and it gives you more freedom to postdilate if you need to. Having the device not fracture [during postdilation] is important," Dr. Abizaid said.
The DESolve Nx trial was sponsored by Elixir, which markets the stent. Dr. Abizaid said he has received research grants from Elixir, Abbott Vascular, Boston Scientific, and Medtronic. Dr. Byrne said his institution received research support from Biotronik.
On Twitter @mitchelzoler
AT EUROPCR 2013
Major finding: Patients averaged a 0.21-mm late lumen loss 6 months after receiving a DESolve bioresorbable vascular scaffold.
Data source: The DESolve Nx study in 126 patients with single lesions at 13 worldwide centers.
Disclosures: The DESolve Nx study was sponsored by Elixir, the company that markets the DESolve device. Dr. Abizaid said he has received research grants from Elixir, Abbott Vascular, Boston Scientific, and Medtronic. Dr. Byrne said his institution received research support from Biotronik.
