User login
USPSTF backs away from cotesting in cervical cancer screening
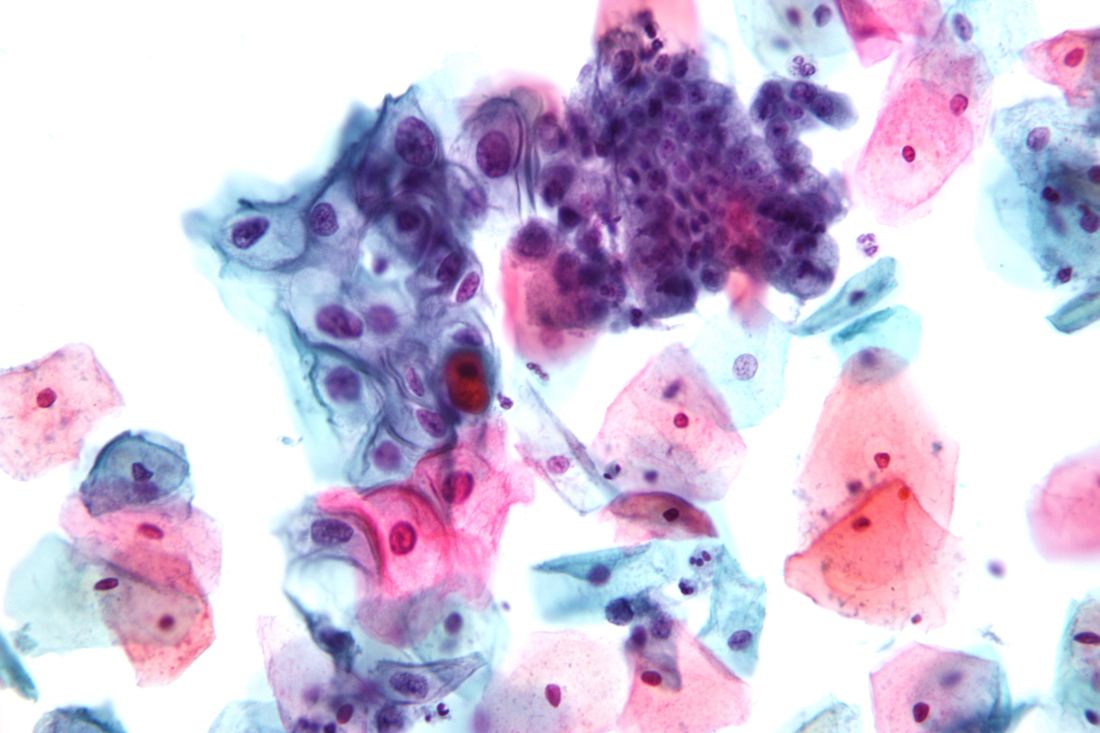
Women aged 30-65 years should be offered a choice between two cervical cancer screening methods, according to draft recommendations from the U.S. Preventive Services Task Force. The recommendations were released on Sept. 12.
The Task Force continues to recommend that women in their 20s be screened every 3 years via cervical cytology, but in a change from the 2012 recommendations, the researchers now advise clinicians to offer women aged 30-65 years a choice of either cytology every 3 years or the high-risk human papillomavirus (hrHPV) test every 5 years as a method of screening for cervical cancer. Cotesting is no longer recommended.
Offering women aged 30-65 years a screening choice received an A recommendation. The draft retains the previous Task Force position and D recommendation against cervical cancer screening for certain groups, including women younger than 21 years, women aged 65 and older with a history of screening and a low risk of cervical cancer, and women who have had a hysterectomy.
The USPSTF based the draft recommendations in part on a review of four randomized, controlled trials of cotesting hrHPV and cytology that included more than 130,000 women.
“Modeling found that cotesting does not offer any benefit in terms of cancer reduction or life-years gained over hrHPV testing alone but increases the number of tests and procedures per each cancer case averted,” the Task Force members noted in the draft recommendation statement. “Therefore, the USPSTF concluded that there is convincing evidence that screening with either cytology alone or hrHPV testing alone provides substantial benefit and is preferable to cotesting” in otherwise healthy women aged 30-65 years.
The American College of Obstetricians and Gynecologists currently recommends cotesting with cytology and HPV testing every 5 years or cytology alone every 3 years in women aged 30-65 years (Obstet Gynecol. 2016;128[4]:e111-30).
The USPSTF draft recommendations do not apply to women at increased risk for cervical cancer, including those with compromised immune systems or those who have cervical intraepithelial neoplasia grade 2 or 3.
The draft recommendations are available online for public comment from Sept. 12 through Oct. 9, 2017, at the USPSTF website, www.uspreventiveservicestaskforce.org.
Women aged 30-65 years should be offered a choice between two cervical cancer screening methods, according to draft recommendations from the U.S. Preventive Services Task Force. The recommendations were released on Sept. 12.
The Task Force continues to recommend that women in their 20s be screened every 3 years via cervical cytology, but in a change from the 2012 recommendations, the researchers now advise clinicians to offer women aged 30-65 years a choice of either cytology every 3 years or the high-risk human papillomavirus (hrHPV) test every 5 years as a method of screening for cervical cancer. Cotesting is no longer recommended.
Offering women aged 30-65 years a screening choice received an A recommendation. The draft retains the previous Task Force position and D recommendation against cervical cancer screening for certain groups, including women younger than 21 years, women aged 65 and older with a history of screening and a low risk of cervical cancer, and women who have had a hysterectomy.
The USPSTF based the draft recommendations in part on a review of four randomized, controlled trials of cotesting hrHPV and cytology that included more than 130,000 women.
“Modeling found that cotesting does not offer any benefit in terms of cancer reduction or life-years gained over hrHPV testing alone but increases the number of tests and procedures per each cancer case averted,” the Task Force members noted in the draft recommendation statement. “Therefore, the USPSTF concluded that there is convincing evidence that screening with either cytology alone or hrHPV testing alone provides substantial benefit and is preferable to cotesting” in otherwise healthy women aged 30-65 years.
The American College of Obstetricians and Gynecologists currently recommends cotesting with cytology and HPV testing every 5 years or cytology alone every 3 years in women aged 30-65 years (Obstet Gynecol. 2016;128[4]:e111-30).
The USPSTF draft recommendations do not apply to women at increased risk for cervical cancer, including those with compromised immune systems or those who have cervical intraepithelial neoplasia grade 2 or 3.
The draft recommendations are available online for public comment from Sept. 12 through Oct. 9, 2017, at the USPSTF website, www.uspreventiveservicestaskforce.org.
Women aged 30-65 years should be offered a choice between two cervical cancer screening methods, according to draft recommendations from the U.S. Preventive Services Task Force. The recommendations were released on Sept. 12.
The Task Force continues to recommend that women in their 20s be screened every 3 years via cervical cytology, but in a change from the 2012 recommendations, the researchers now advise clinicians to offer women aged 30-65 years a choice of either cytology every 3 years or the high-risk human papillomavirus (hrHPV) test every 5 years as a method of screening for cervical cancer. Cotesting is no longer recommended.
Offering women aged 30-65 years a screening choice received an A recommendation. The draft retains the previous Task Force position and D recommendation against cervical cancer screening for certain groups, including women younger than 21 years, women aged 65 and older with a history of screening and a low risk of cervical cancer, and women who have had a hysterectomy.
The USPSTF based the draft recommendations in part on a review of four randomized, controlled trials of cotesting hrHPV and cytology that included more than 130,000 women.
“Modeling found that cotesting does not offer any benefit in terms of cancer reduction or life-years gained over hrHPV testing alone but increases the number of tests and procedures per each cancer case averted,” the Task Force members noted in the draft recommendation statement. “Therefore, the USPSTF concluded that there is convincing evidence that screening with either cytology alone or hrHPV testing alone provides substantial benefit and is preferable to cotesting” in otherwise healthy women aged 30-65 years.
The American College of Obstetricians and Gynecologists currently recommends cotesting with cytology and HPV testing every 5 years or cytology alone every 3 years in women aged 30-65 years (Obstet Gynecol. 2016;128[4]:e111-30).
The USPSTF draft recommendations do not apply to women at increased risk for cervical cancer, including those with compromised immune systems or those who have cervical intraepithelial neoplasia grade 2 or 3.
The draft recommendations are available online for public comment from Sept. 12 through Oct. 9, 2017, at the USPSTF website, www.uspreventiveservicestaskforce.org.
Check children’s eyes early for best corrections
or its risk factors with the goal of improving visual acuity, publishing its final recommendation statement and evidence summary online Sept. 5 in JAMA.
A review of the latest evidence supports a B recommendation for vision screening at least once in children aged 3-5 years, but the evidence is insufficient to determine the balance of risks and benefits for vision screening in children younger than 3 years (meriting an I statement from the USPSTF). The recommendation updates the 2011 USPSTF recommendation, which also recommended vision screening for children aged 3-5 years with a B recommendation.
“The prevalence of amblyopia, strabismus, and anisometropia ranges from 1% to 6% among children younger than 6 years in the United States,” which can lead to permanent vision loss if left untreated, chair and corresponding author David C. Grossman, MD, of Kaiser Permanente Washington Health Research Institute, Seattle, and colleagues noted in the recommendation statement (JAMA. 2017;318:836-44).
The USPSTF found “inadequate evidence that treatment reduced the incidence of long-term amblyopia or improved school performance, functioning, or quality of life.” However, the USPSTF concluded that the harms of screening and treating preschool children for amblyopia and its risk factors were small, and that treatment improved visual acuity, “which is likely to result in permanent improvements throughout life.”
The benefits of early treatment were characterized as moderate because of the risk of permanent, uncorrectable vision loss associated with untreated amblyopia, “and the benefits of screening and treatment can be experienced over a child’s lifetime,” the researchers said.
The evidence report accompanying the recommendations contained data from 40 studies with 34,709 participants, and addressed issues including the benefits of screening, accuracy of vision screening tests, and the potential harms and benefits of treatments including eye patches and glasses (JAMA. 2017;318:845-58).
“Studies directly evaluating the effectiveness of screening were limited and do not establish whether vision screening in preschool children is better than no screening,” Daniel E. Jonas, MD, of RTI International–University of North Carolina at Chapel Hill Evidence-based Practice Center and his colleagues wrote in the evidence report.
Therefore, the Task Force called for additional research while recommending at least one screening.
The study was funded by the Agency for Healthcare Research and Quality. The researchers had no financial conflicts to disclose.
Read the complete recommendations online at http://www.uspreventiveservicestaskforce.org.
or its risk factors with the goal of improving visual acuity, publishing its final recommendation statement and evidence summary online Sept. 5 in JAMA.
A review of the latest evidence supports a B recommendation for vision screening at least once in children aged 3-5 years, but the evidence is insufficient to determine the balance of risks and benefits for vision screening in children younger than 3 years (meriting an I statement from the USPSTF). The recommendation updates the 2011 USPSTF recommendation, which also recommended vision screening for children aged 3-5 years with a B recommendation.
“The prevalence of amblyopia, strabismus, and anisometropia ranges from 1% to 6% among children younger than 6 years in the United States,” which can lead to permanent vision loss if left untreated, chair and corresponding author David C. Grossman, MD, of Kaiser Permanente Washington Health Research Institute, Seattle, and colleagues noted in the recommendation statement (JAMA. 2017;318:836-44).
The USPSTF found “inadequate evidence that treatment reduced the incidence of long-term amblyopia or improved school performance, functioning, or quality of life.” However, the USPSTF concluded that the harms of screening and treating preschool children for amblyopia and its risk factors were small, and that treatment improved visual acuity, “which is likely to result in permanent improvements throughout life.”
The benefits of early treatment were characterized as moderate because of the risk of permanent, uncorrectable vision loss associated with untreated amblyopia, “and the benefits of screening and treatment can be experienced over a child’s lifetime,” the researchers said.
The evidence report accompanying the recommendations contained data from 40 studies with 34,709 participants, and addressed issues including the benefits of screening, accuracy of vision screening tests, and the potential harms and benefits of treatments including eye patches and glasses (JAMA. 2017;318:845-58).
“Studies directly evaluating the effectiveness of screening were limited and do not establish whether vision screening in preschool children is better than no screening,” Daniel E. Jonas, MD, of RTI International–University of North Carolina at Chapel Hill Evidence-based Practice Center and his colleagues wrote in the evidence report.
Therefore, the Task Force called for additional research while recommending at least one screening.
The study was funded by the Agency for Healthcare Research and Quality. The researchers had no financial conflicts to disclose.
Read the complete recommendations online at http://www.uspreventiveservicestaskforce.org.
or its risk factors with the goal of improving visual acuity, publishing its final recommendation statement and evidence summary online Sept. 5 in JAMA.
A review of the latest evidence supports a B recommendation for vision screening at least once in children aged 3-5 years, but the evidence is insufficient to determine the balance of risks and benefits for vision screening in children younger than 3 years (meriting an I statement from the USPSTF). The recommendation updates the 2011 USPSTF recommendation, which also recommended vision screening for children aged 3-5 years with a B recommendation.
“The prevalence of amblyopia, strabismus, and anisometropia ranges from 1% to 6% among children younger than 6 years in the United States,” which can lead to permanent vision loss if left untreated, chair and corresponding author David C. Grossman, MD, of Kaiser Permanente Washington Health Research Institute, Seattle, and colleagues noted in the recommendation statement (JAMA. 2017;318:836-44).
The USPSTF found “inadequate evidence that treatment reduced the incidence of long-term amblyopia or improved school performance, functioning, or quality of life.” However, the USPSTF concluded that the harms of screening and treating preschool children for amblyopia and its risk factors were small, and that treatment improved visual acuity, “which is likely to result in permanent improvements throughout life.”
The benefits of early treatment were characterized as moderate because of the risk of permanent, uncorrectable vision loss associated with untreated amblyopia, “and the benefits of screening and treatment can be experienced over a child’s lifetime,” the researchers said.
The evidence report accompanying the recommendations contained data from 40 studies with 34,709 participants, and addressed issues including the benefits of screening, accuracy of vision screening tests, and the potential harms and benefits of treatments including eye patches and glasses (JAMA. 2017;318:845-58).
“Studies directly evaluating the effectiveness of screening were limited and do not establish whether vision screening in preschool children is better than no screening,” Daniel E. Jonas, MD, of RTI International–University of North Carolina at Chapel Hill Evidence-based Practice Center and his colleagues wrote in the evidence report.
Therefore, the Task Force called for additional research while recommending at least one screening.
The study was funded by the Agency for Healthcare Research and Quality. The researchers had no financial conflicts to disclose.
Read the complete recommendations online at http://www.uspreventiveservicestaskforce.org.
FROM JAMA
Intraoperative ketamine makes no dent in postop delirium or pain
Postoperative delirium remains a problem without an effective solution, wrote Michael S. Avidan, MBBCh, FCASA, of Washington University, Saint Louis, and his colleagues (Lancet 2017;390[10091]:267-75).
Recent guidelines published by the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council include ketamine as a recommended component of multimodal pain therapy for several commonly performed surgeries. “Before recommending widespread administration of an intraoperative bolus of subanaesthetic ketamine, demonstrating that ketamine decreases either delirium or pain, or both, without incurring adverse effects in a large, pragmatic trial was warranted,” the researchers said.
In the PODCAST (Prevention of Delirium and Complications Associated With Surgical Treatments) trial, the researchers randomized 672 patients over the age of 60 undergoing major open surgery under general anesthesia (such as open cardiac or noncardiac surgery, urological surgery, gynecologic surgery, or intra-abdominal surgery) to 0.5 mg/kg ketamine (227), 1.0 mg/kg ketamine (223), or placebo (222). The ketamine or placebo was given after anesthesia and before surgical incision.
Overall, no difference in the incidence of delirium occurred between patients in the combined ketamine groups (19.5%) and the placebo group (19.8%), and there was no significant difference in delirium across all three treatment groups.
No differences in pain based on visual analog scale scores were observed across the three groups, and overall adverse event rates were similar as well: approximately 40.8% in the 1.0-mg ketamine group, 39.6% in the 0.5-mg ketamine group, and 36.9% in the placebo group.
The study findings were limited by several factors, including a study population potentially too small to show an effect of ketamine on delirium, and a lack of data on other variables that might contribute to delirium and pain, the researchers noted. However, the results suggest that “despite present evidence and guidelines, the administration of a subanaesthetic ketamine dose during surgery is not useful for preventing postoperative delirium (primary outcome) or reducing postoperative pain and minimising opioid consumption (related secondary outcomes),” and appears to increase postoperative hallucinations and nightmares to an extent that might be prohibitive, they said.
The National Institutes of Health and Cancer Center Support funded the study. The researchers had no financial conflicts to disclose.
Postoperative delirium remains a problem without an effective solution, wrote Michael S. Avidan, MBBCh, FCASA, of Washington University, Saint Louis, and his colleagues (Lancet 2017;390[10091]:267-75).
Recent guidelines published by the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council include ketamine as a recommended component of multimodal pain therapy for several commonly performed surgeries. “Before recommending widespread administration of an intraoperative bolus of subanaesthetic ketamine, demonstrating that ketamine decreases either delirium or pain, or both, without incurring adverse effects in a large, pragmatic trial was warranted,” the researchers said.
In the PODCAST (Prevention of Delirium and Complications Associated With Surgical Treatments) trial, the researchers randomized 672 patients over the age of 60 undergoing major open surgery under general anesthesia (such as open cardiac or noncardiac surgery, urological surgery, gynecologic surgery, or intra-abdominal surgery) to 0.5 mg/kg ketamine (227), 1.0 mg/kg ketamine (223), or placebo (222). The ketamine or placebo was given after anesthesia and before surgical incision.
Overall, no difference in the incidence of delirium occurred between patients in the combined ketamine groups (19.5%) and the placebo group (19.8%), and there was no significant difference in delirium across all three treatment groups.
No differences in pain based on visual analog scale scores were observed across the three groups, and overall adverse event rates were similar as well: approximately 40.8% in the 1.0-mg ketamine group, 39.6% in the 0.5-mg ketamine group, and 36.9% in the placebo group.
The study findings were limited by several factors, including a study population potentially too small to show an effect of ketamine on delirium, and a lack of data on other variables that might contribute to delirium and pain, the researchers noted. However, the results suggest that “despite present evidence and guidelines, the administration of a subanaesthetic ketamine dose during surgery is not useful for preventing postoperative delirium (primary outcome) or reducing postoperative pain and minimising opioid consumption (related secondary outcomes),” and appears to increase postoperative hallucinations and nightmares to an extent that might be prohibitive, they said.
The National Institutes of Health and Cancer Center Support funded the study. The researchers had no financial conflicts to disclose.
Postoperative delirium remains a problem without an effective solution, wrote Michael S. Avidan, MBBCh, FCASA, of Washington University, Saint Louis, and his colleagues (Lancet 2017;390[10091]:267-75).
Recent guidelines published by the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council include ketamine as a recommended component of multimodal pain therapy for several commonly performed surgeries. “Before recommending widespread administration of an intraoperative bolus of subanaesthetic ketamine, demonstrating that ketamine decreases either delirium or pain, or both, without incurring adverse effects in a large, pragmatic trial was warranted,” the researchers said.
In the PODCAST (Prevention of Delirium and Complications Associated With Surgical Treatments) trial, the researchers randomized 672 patients over the age of 60 undergoing major open surgery under general anesthesia (such as open cardiac or noncardiac surgery, urological surgery, gynecologic surgery, or intra-abdominal surgery) to 0.5 mg/kg ketamine (227), 1.0 mg/kg ketamine (223), or placebo (222). The ketamine or placebo was given after anesthesia and before surgical incision.
Overall, no difference in the incidence of delirium occurred between patients in the combined ketamine groups (19.5%) and the placebo group (19.8%), and there was no significant difference in delirium across all three treatment groups.
No differences in pain based on visual analog scale scores were observed across the three groups, and overall adverse event rates were similar as well: approximately 40.8% in the 1.0-mg ketamine group, 39.6% in the 0.5-mg ketamine group, and 36.9% in the placebo group.
The study findings were limited by several factors, including a study population potentially too small to show an effect of ketamine on delirium, and a lack of data on other variables that might contribute to delirium and pain, the researchers noted. However, the results suggest that “despite present evidence and guidelines, the administration of a subanaesthetic ketamine dose during surgery is not useful for preventing postoperative delirium (primary outcome) or reducing postoperative pain and minimising opioid consumption (related secondary outcomes),” and appears to increase postoperative hallucinations and nightmares to an extent that might be prohibitive, they said.
The National Institutes of Health and Cancer Center Support funded the study. The researchers had no financial conflicts to disclose.
FROM THE LANCET
Key clinical point: Ketamine failed to reduce postoperative delirium in older adults.
Major finding: No difference was observed in the incidence of postoperative delirium between patients given ketamine before surgical incision and patients on placebo.
Data source: The Prevention of Delirium and Complications Associated With Surgical Treatments study, a randomized, multicenter trial of 672 adults older than 60 years.
Disclosures: The National Institutes of Health and Cancer Center Support funded the study. The researchers had no financial conflicts to disclose.
BMI z scores fall short for tracking severe obesity
, based on data from nearly 7,000 children in the Bogalusa Heart Study.
The current parameters used in the Centers for Disease Control and Prevention growth charts for children with high body mass index (BMI) “can result in estimates that differ substantially from those that are observed and constrains the maximum BMI z that is attainable at a given sex and age,” wrote David S. Freedman, PhD, of the Centers for Disease Control and Prevention in Atlanta, and Gerald S. Berenson, MD, of Louisiana State University Health Sciences Center, New Orleans, (Pediatrics. 2017;140:e20171072).
The BMI adjusted z score (BMIaz) or the BMI expressed as a percentage of the 95th percentile (%BMIp95) “will provide more accurate information on body size over time among children with very high BMIs,” they said.
In children with severe obesity, BMI z was a weaker measure (r = 0.46) than were measures of %BMIp95 (r = 0.61) or BMIaz scores with no upper boundary (r = 0.65).
BMI z scores were weakest when applied to children younger than 10 years, with correlations of r = 0.36 for BMI z vs. correlations of 0.60 and 0.57 for BMIaz and %BMIp95, respectively.
The results were limited by several factors including the age of the data (40 years ago, when the prevalence of severe obesity was lower, 2% compared with approximately 6% now) and long intervals between exams in some cases (5 years or more), the researchers noted. However, the results suggest that BMI z values “can differ substantially from empirical estimates, have an effective upper limit, and are strongly influenced by sex and age,” they said. As an alternative, the researchers recommended that “very high BMIs should be should expressed as z scores on the basis of linear extrapolations of a fixed SD or as percentage of the CDC 95th percentile,” or using multilevel models that adjust for age and sex.
The researchers had no financial conflicts to disclose. The National Institute on Aging, the National Heart, Lung, and Blood Institute, and the National Institutes of Health funded the study.
The use of BMI z scores to assess and track severe obesity in children should be abandoned.
In the study by Freedman et al., BMI z scores, which are extrapolations of BMI measurements, did not correlate well with other measures of adiposity. Their use to assess severe obesity is problematic because large changes in weight and BMI are linked to small changes in BMI z or BMI percentiles.

William H. Dietz, MD, PhD, is at the Sumner M. Redstone Global Center for Prevention and Wellness, Milken Institute School of Public Health at George Washington University in Washington. He had no relevant financial disclosures, but disclosed that he serves on the scientific advisory board for Weight Watchers and is on the board of directors for the Partnership for a Healthier America. He discussed the article by Freedman et al. in an editorial (Pediatrics. 2017;140:e20172148).
The use of BMI z scores to assess and track severe obesity in children should be abandoned.
In the study by Freedman et al., BMI z scores, which are extrapolations of BMI measurements, did not correlate well with other measures of adiposity. Their use to assess severe obesity is problematic because large changes in weight and BMI are linked to small changes in BMI z or BMI percentiles.
William H. Dietz, MD, PhD, is at the Sumner M. Redstone Global Center for Prevention and Wellness, Milken Institute School of Public Health at George Washington University in Washington. He had no relevant financial disclosures, but disclosed that he serves on the scientific advisory board for Weight Watchers and is on the board of directors for the Partnership for a Healthier America. He discussed the article by Freedman et al. in an editorial (Pediatrics. 2017;140:e20172148).
The use of BMI z scores to assess and track severe obesity in children should be abandoned.
In the study by Freedman et al., BMI z scores, which are extrapolations of BMI measurements, did not correlate well with other measures of adiposity. Their use to assess severe obesity is problematic because large changes in weight and BMI are linked to small changes in BMI z or BMI percentiles.
William H. Dietz, MD, PhD, is at the Sumner M. Redstone Global Center for Prevention and Wellness, Milken Institute School of Public Health at George Washington University in Washington. He had no relevant financial disclosures, but disclosed that he serves on the scientific advisory board for Weight Watchers and is on the board of directors for the Partnership for a Healthier America. He discussed the article by Freedman et al. in an editorial (Pediatrics. 2017;140:e20172148).
, based on data from nearly 7,000 children in the Bogalusa Heart Study.
The current parameters used in the Centers for Disease Control and Prevention growth charts for children with high body mass index (BMI) “can result in estimates that differ substantially from those that are observed and constrains the maximum BMI z that is attainable at a given sex and age,” wrote David S. Freedman, PhD, of the Centers for Disease Control and Prevention in Atlanta, and Gerald S. Berenson, MD, of Louisiana State University Health Sciences Center, New Orleans, (Pediatrics. 2017;140:e20171072).
The BMI adjusted z score (BMIaz) or the BMI expressed as a percentage of the 95th percentile (%BMIp95) “will provide more accurate information on body size over time among children with very high BMIs,” they said.
In children with severe obesity, BMI z was a weaker measure (r = 0.46) than were measures of %BMIp95 (r = 0.61) or BMIaz scores with no upper boundary (r = 0.65).
BMI z scores were weakest when applied to children younger than 10 years, with correlations of r = 0.36 for BMI z vs. correlations of 0.60 and 0.57 for BMIaz and %BMIp95, respectively.
The results were limited by several factors including the age of the data (40 years ago, when the prevalence of severe obesity was lower, 2% compared with approximately 6% now) and long intervals between exams in some cases (5 years or more), the researchers noted. However, the results suggest that BMI z values “can differ substantially from empirical estimates, have an effective upper limit, and are strongly influenced by sex and age,” they said. As an alternative, the researchers recommended that “very high BMIs should be should expressed as z scores on the basis of linear extrapolations of a fixed SD or as percentage of the CDC 95th percentile,” or using multilevel models that adjust for age and sex.
The researchers had no financial conflicts to disclose. The National Institute on Aging, the National Heart, Lung, and Blood Institute, and the National Institutes of Health funded the study.
, based on data from nearly 7,000 children in the Bogalusa Heart Study.
The current parameters used in the Centers for Disease Control and Prevention growth charts for children with high body mass index (BMI) “can result in estimates that differ substantially from those that are observed and constrains the maximum BMI z that is attainable at a given sex and age,” wrote David S. Freedman, PhD, of the Centers for Disease Control and Prevention in Atlanta, and Gerald S. Berenson, MD, of Louisiana State University Health Sciences Center, New Orleans, (Pediatrics. 2017;140:e20171072).
The BMI adjusted z score (BMIaz) or the BMI expressed as a percentage of the 95th percentile (%BMIp95) “will provide more accurate information on body size over time among children with very high BMIs,” they said.
In children with severe obesity, BMI z was a weaker measure (r = 0.46) than were measures of %BMIp95 (r = 0.61) or BMIaz scores with no upper boundary (r = 0.65).
BMI z scores were weakest when applied to children younger than 10 years, with correlations of r = 0.36 for BMI z vs. correlations of 0.60 and 0.57 for BMIaz and %BMIp95, respectively.
The results were limited by several factors including the age of the data (40 years ago, when the prevalence of severe obesity was lower, 2% compared with approximately 6% now) and long intervals between exams in some cases (5 years or more), the researchers noted. However, the results suggest that BMI z values “can differ substantially from empirical estimates, have an effective upper limit, and are strongly influenced by sex and age,” they said. As an alternative, the researchers recommended that “very high BMIs should be should expressed as z scores on the basis of linear extrapolations of a fixed SD or as percentage of the CDC 95th percentile,” or using multilevel models that adjust for age and sex.
The researchers had no financial conflicts to disclose. The National Institute on Aging, the National Heart, Lung, and Blood Institute, and the National Institutes of Health funded the study.
FROM PEDIATRICS
Key clinical point: BMI z scores are weak trackers of severe obesity in children.
Major finding: Correlations were weaker for BMI z scores (r = 0.46) than for metrics of BMI using the 95th percentile or z scores with no upper bound (r = approximately 0.6) over 2.8 years.
Data source: The study is based on longitudinal data from 6,994 children participating in the Bogalusa Heart study, including 247 children with severe obesity.
Disclosures: The researchers had no relevant financial conflicts to disclose. The National Institute on Aging, the National Heart, Lung, and Blood Institute, and the National Institutes of Health funded the study.
Brain scan study suggests serotonin drives early cognitive decline
Serotonin levels may play an early role in cognitive decline, according to imaging data from a group of study participants with mild cognitive impairment.
Previous studies have shown a link between a loss of serotonin neurons as part of normal aging and as part of the development of Alzheimer’s disease, wrote Gwenn S. Smith, PhD, of Johns Hopkins University in Baltimore, and her colleagues. However, “it is not known whether serotonin degeneration occurs in the preclinical stages or later in the course of AD,” the researchers said. The researchers used MRI and PET imaging to measure serotonin transporters (SERT) in the brains of 28 adults with mild cognitive impairment (MCI) and 28 healthy controls.
Overall, MCI participants showed significantly lower SERT, compared with the healthy controls; the loss of SERT in the MCI group ranged from 10% to 38%. No significant regions of higher SERT were noted in the MCI group, compared with the controls, and no significant differences were noted in gray matter volume.
The participants were recruited from the community or from the Johns Hopkins University Alzheimer’s Disease Research Center. All of the subjects underwent several evaluations, including the Clinical Dementia Rating Scale and the Mini-Mental State Examination, and mild cognitive impairment was defined as a cognitive decline mainly in the ability to remember sequences or organization, as well as having lower scores on tests such as the California Verbal Learning Test (Neurobiol Dis. 2017 Sep;105:33-41). The average age of the participants was 66 years, and about 45% were women.
The study results were limited by several factors, including lack of arterial blood for quantification purposes and the absence of partial-volume correction in assessing the brain images, reported Dr. Smith, a professor of psychiatry and behavioral sciences at the university, and her colleagues.
However, the findings suggest that “the loss of SERT in MCI may have a substantial impact on brain function and behavior given the widespread distribution of SERT in the brain and the evidence that serotonin modulates other neurotransmitters (glutamate, norepinephrine, dopamine, and acetylcholine) implicated in AD and potentially MCI,” they emphasized.
Based on the findings, next steps for research could include targeting receptors that detect serotonin on message-receiving cells. “The substantially lower SERT in MCI observed in the present study suggests that the serotonin system may represent an important target for prevention and treatment,” the researchers noted.
Dr. Smith has received research funding from the National Institutes of Health and Functional Neuromodulation. This study was supported by the NIH.
Serotonin levels may play an early role in cognitive decline, according to imaging data from a group of study participants with mild cognitive impairment.
Previous studies have shown a link between a loss of serotonin neurons as part of normal aging and as part of the development of Alzheimer’s disease, wrote Gwenn S. Smith, PhD, of Johns Hopkins University in Baltimore, and her colleagues. However, “it is not known whether serotonin degeneration occurs in the preclinical stages or later in the course of AD,” the researchers said. The researchers used MRI and PET imaging to measure serotonin transporters (SERT) in the brains of 28 adults with mild cognitive impairment (MCI) and 28 healthy controls.
Overall, MCI participants showed significantly lower SERT, compared with the healthy controls; the loss of SERT in the MCI group ranged from 10% to 38%. No significant regions of higher SERT were noted in the MCI group, compared with the controls, and no significant differences were noted in gray matter volume.
The participants were recruited from the community or from the Johns Hopkins University Alzheimer’s Disease Research Center. All of the subjects underwent several evaluations, including the Clinical Dementia Rating Scale and the Mini-Mental State Examination, and mild cognitive impairment was defined as a cognitive decline mainly in the ability to remember sequences or organization, as well as having lower scores on tests such as the California Verbal Learning Test (Neurobiol Dis. 2017 Sep;105:33-41). The average age of the participants was 66 years, and about 45% were women.
The study results were limited by several factors, including lack of arterial blood for quantification purposes and the absence of partial-volume correction in assessing the brain images, reported Dr. Smith, a professor of psychiatry and behavioral sciences at the university, and her colleagues.
However, the findings suggest that “the loss of SERT in MCI may have a substantial impact on brain function and behavior given the widespread distribution of SERT in the brain and the evidence that serotonin modulates other neurotransmitters (glutamate, norepinephrine, dopamine, and acetylcholine) implicated in AD and potentially MCI,” they emphasized.
Based on the findings, next steps for research could include targeting receptors that detect serotonin on message-receiving cells. “The substantially lower SERT in MCI observed in the present study suggests that the serotonin system may represent an important target for prevention and treatment,” the researchers noted.
Dr. Smith has received research funding from the National Institutes of Health and Functional Neuromodulation. This study was supported by the NIH.
Serotonin levels may play an early role in cognitive decline, according to imaging data from a group of study participants with mild cognitive impairment.
Previous studies have shown a link between a loss of serotonin neurons as part of normal aging and as part of the development of Alzheimer’s disease, wrote Gwenn S. Smith, PhD, of Johns Hopkins University in Baltimore, and her colleagues. However, “it is not known whether serotonin degeneration occurs in the preclinical stages or later in the course of AD,” the researchers said. The researchers used MRI and PET imaging to measure serotonin transporters (SERT) in the brains of 28 adults with mild cognitive impairment (MCI) and 28 healthy controls.
Overall, MCI participants showed significantly lower SERT, compared with the healthy controls; the loss of SERT in the MCI group ranged from 10% to 38%. No significant regions of higher SERT were noted in the MCI group, compared with the controls, and no significant differences were noted in gray matter volume.
The participants were recruited from the community or from the Johns Hopkins University Alzheimer’s Disease Research Center. All of the subjects underwent several evaluations, including the Clinical Dementia Rating Scale and the Mini-Mental State Examination, and mild cognitive impairment was defined as a cognitive decline mainly in the ability to remember sequences or organization, as well as having lower scores on tests such as the California Verbal Learning Test (Neurobiol Dis. 2017 Sep;105:33-41). The average age of the participants was 66 years, and about 45% were women.
The study results were limited by several factors, including lack of arterial blood for quantification purposes and the absence of partial-volume correction in assessing the brain images, reported Dr. Smith, a professor of psychiatry and behavioral sciences at the university, and her colleagues.
However, the findings suggest that “the loss of SERT in MCI may have a substantial impact on brain function and behavior given the widespread distribution of SERT in the brain and the evidence that serotonin modulates other neurotransmitters (glutamate, norepinephrine, dopamine, and acetylcholine) implicated in AD and potentially MCI,” they emphasized.
Based on the findings, next steps for research could include targeting receptors that detect serotonin on message-receiving cells. “The substantially lower SERT in MCI observed in the present study suggests that the serotonin system may represent an important target for prevention and treatment,” the researchers noted.
Dr. Smith has received research funding from the National Institutes of Health and Functional Neuromodulation. This study was supported by the NIH.
FROM NEUROBIOLOGY OF DISEASE
Key clinical point: Levels of serotonin transporters were significantly lower in the cortical, striatal, thalamic, and limbic regions of the brain of adults with mild cognitive impairment, compared with healthy controls.
Major finding: The decrease in serotonin transporters (SERT) ranged from 10% to 38% in MCI adults, compared with healthy controls.
Data source: The data come from a comparison study of 28 adults with MCI and 28 healthy controls.
Disclosures: Dr. Smith has received research funding from the National Institutes of Health and Functional Neuromodulation. The study was supported by the NIH.
Cannabis shows inconsistent benefits for pain, PTSD
Chronic pain and posttraumatic stress disorder are among the top reasons given by patients seeking medical marijuana in states where it is legal, but there is little scientific evidence to support its value for treating either condition, based on the results of a pair of systemic evidence reviews conducted by the U.S. Department of Veterans Affairs.
The findings were published online Aug. 14 in the Annals of Internal Medicine.

In the PTSD study, Maya E. O’Neil, PhD, of the VA Portland (Ore.) Health Care System, and colleagues found no significant evidence to support the effectiveness of cannabis for relieving symptoms (Ann Intern Med. 2017 Aug 14. doi: 10.7326/M17-0477). The researchers reviewed data from two systematic reviews and three primary studies.
One of the larger studies (included in one of the systematic reviews) included 47,000 veterans in VA intensive PTSD programs during 1992-2011. In fact, after controlling for demographic factors and other confounding variables, individuals who continued to use cannabis or started using cannabis showed worse PTSD symptoms than did nonusers after 4 months.
“Findings from [randomized, controlled trials] are needed to help determine whether and to what extent cannabis may improve PTSD symptoms, and further studies also are needed to clarify harms in patients with PTSD,” the researchers noted.
In the review of chronic pain literature, Shannon M. Nugent, PhD, also of the VA Portland (Ore.) Health Care System, and her colleagues examined 27 trials, 11 reviews, and 32 primary studies (Ann Intern Med. 2017 Aug 14. doi: 10.7326/M17-0155).
“Across nine studies, intervention patients were more likely to report at least 30% improvement in pain,” the investigators said. But this finding was specific to tetrahydrocannabinol (THC), the researchers said, and evidence of the ability of cannabis to relieve other types of pain, such as cancer pain and multiple sclerosis pain, was insufficient.
In addition, the researchers found a low strength of evidence association between cannabis use and the development of psychotic symptoms, and a moderate strength of evidence association between cannabis use and impaired cognitive function in the general population. “However, our confidence in the findings is limited by inconsistent findings among included studies, inadequate assessment of exposure, and inadequate adjustment for confounding among the studies” they said.
Although no significant differences were noted in rates of adverse events between cannabis users and nonusers, some data suggested users had an increased risk for short-term adverse events that ranged from dizziness to paranoia and suicide attempts.
Other potential harms associated with cannabis use included decreased lung function, increased risk of complications from infectious diseases, cannabis hyperemesis syndrome, and increased risk of violent behavior.
“Even though we did not find strong, consistent evidence of benefit, clinicians will still need to engage in evidence-based discussions with patients managing chronic pain who are using or requesting to use cannabis,” the researchers wrote.
The researchers had no financial conflicts to disclose. The study was commissioned by the Veterans Health Administration.
“The systematic reviews highlight an alarming lack of high-quality data from which to draw firm conclusions about the efficacy of cannabis for these conditions, for which cannabis is both sanctioned and commonly used,” wrote Sachin Patel, MD, PhD, in an accompanying editorial (Ann Intern Med. 2017 Aug 14. doi: 10.7326/M17-1713).
“Even if future studies reveal a clear lack of substantial benefit of cannabis for pain or PTSD, legislation is unlikely to remove these conditions from the lists of indications for medical cannabis,” he cautioned. “It will be up to front-line practicing physicians to learn about the harms and benefits of cannabis, educate their patients on these topics, and make evidence-based recommendations about using cannabis and related products for various health conditions.
“In parallel, the research community must pursue high-quality studies and disseminate the results to clinicians and the public. In this context, these reviews are must-reads for all physicians, especially those practicing in states where medical cannabis is legal,” Dr. Patel added.
Dr. Patel is affiliated with Vanderbilt Psychiatric Hospital in Nashville, Tenn. He had no relevant financial conflicts to disclose, but reported receiving grants from Lundbeck.
“The systematic reviews highlight an alarming lack of high-quality data from which to draw firm conclusions about the efficacy of cannabis for these conditions, for which cannabis is both sanctioned and commonly used,” wrote Sachin Patel, MD, PhD, in an accompanying editorial (Ann Intern Med. 2017 Aug 14. doi: 10.7326/M17-1713).
“Even if future studies reveal a clear lack of substantial benefit of cannabis for pain or PTSD, legislation is unlikely to remove these conditions from the lists of indications for medical cannabis,” he cautioned. “It will be up to front-line practicing physicians to learn about the harms and benefits of cannabis, educate their patients on these topics, and make evidence-based recommendations about using cannabis and related products for various health conditions.
“In parallel, the research community must pursue high-quality studies and disseminate the results to clinicians and the public. In this context, these reviews are must-reads for all physicians, especially those practicing in states where medical cannabis is legal,” Dr. Patel added.
Dr. Patel is affiliated with Vanderbilt Psychiatric Hospital in Nashville, Tenn. He had no relevant financial conflicts to disclose, but reported receiving grants from Lundbeck.
“The systematic reviews highlight an alarming lack of high-quality data from which to draw firm conclusions about the efficacy of cannabis for these conditions, for which cannabis is both sanctioned and commonly used,” wrote Sachin Patel, MD, PhD, in an accompanying editorial (Ann Intern Med. 2017 Aug 14. doi: 10.7326/M17-1713).
“Even if future studies reveal a clear lack of substantial benefit of cannabis for pain or PTSD, legislation is unlikely to remove these conditions from the lists of indications for medical cannabis,” he cautioned. “It will be up to front-line practicing physicians to learn about the harms and benefits of cannabis, educate their patients on these topics, and make evidence-based recommendations about using cannabis and related products for various health conditions.
“In parallel, the research community must pursue high-quality studies and disseminate the results to clinicians and the public. In this context, these reviews are must-reads for all physicians, especially those practicing in states where medical cannabis is legal,” Dr. Patel added.
Dr. Patel is affiliated with Vanderbilt Psychiatric Hospital in Nashville, Tenn. He had no relevant financial conflicts to disclose, but reported receiving grants from Lundbeck.
Chronic pain and posttraumatic stress disorder are among the top reasons given by patients seeking medical marijuana in states where it is legal, but there is little scientific evidence to support its value for treating either condition, based on the results of a pair of systemic evidence reviews conducted by the U.S. Department of Veterans Affairs.
The findings were published online Aug. 14 in the Annals of Internal Medicine.
In the PTSD study, Maya E. O’Neil, PhD, of the VA Portland (Ore.) Health Care System, and colleagues found no significant evidence to support the effectiveness of cannabis for relieving symptoms (Ann Intern Med. 2017 Aug 14. doi: 10.7326/M17-0477). The researchers reviewed data from two systematic reviews and three primary studies.
One of the larger studies (included in one of the systematic reviews) included 47,000 veterans in VA intensive PTSD programs during 1992-2011. In fact, after controlling for demographic factors and other confounding variables, individuals who continued to use cannabis or started using cannabis showed worse PTSD symptoms than did nonusers after 4 months.
“Findings from [randomized, controlled trials] are needed to help determine whether and to what extent cannabis may improve PTSD symptoms, and further studies also are needed to clarify harms in patients with PTSD,” the researchers noted.
In the review of chronic pain literature, Shannon M. Nugent, PhD, also of the VA Portland (Ore.) Health Care System, and her colleagues examined 27 trials, 11 reviews, and 32 primary studies (Ann Intern Med. 2017 Aug 14. doi: 10.7326/M17-0155).
“Across nine studies, intervention patients were more likely to report at least 30% improvement in pain,” the investigators said. But this finding was specific to tetrahydrocannabinol (THC), the researchers said, and evidence of the ability of cannabis to relieve other types of pain, such as cancer pain and multiple sclerosis pain, was insufficient.
In addition, the researchers found a low strength of evidence association between cannabis use and the development of psychotic symptoms, and a moderate strength of evidence association between cannabis use and impaired cognitive function in the general population. “However, our confidence in the findings is limited by inconsistent findings among included studies, inadequate assessment of exposure, and inadequate adjustment for confounding among the studies” they said.
Although no significant differences were noted in rates of adverse events between cannabis users and nonusers, some data suggested users had an increased risk for short-term adverse events that ranged from dizziness to paranoia and suicide attempts.
Other potential harms associated with cannabis use included decreased lung function, increased risk of complications from infectious diseases, cannabis hyperemesis syndrome, and increased risk of violent behavior.
“Even though we did not find strong, consistent evidence of benefit, clinicians will still need to engage in evidence-based discussions with patients managing chronic pain who are using or requesting to use cannabis,” the researchers wrote.
The researchers had no financial conflicts to disclose. The study was commissioned by the Veterans Health Administration.
Chronic pain and posttraumatic stress disorder are among the top reasons given by patients seeking medical marijuana in states where it is legal, but there is little scientific evidence to support its value for treating either condition, based on the results of a pair of systemic evidence reviews conducted by the U.S. Department of Veterans Affairs.
The findings were published online Aug. 14 in the Annals of Internal Medicine.
In the PTSD study, Maya E. O’Neil, PhD, of the VA Portland (Ore.) Health Care System, and colleagues found no significant evidence to support the effectiveness of cannabis for relieving symptoms (Ann Intern Med. 2017 Aug 14. doi: 10.7326/M17-0477). The researchers reviewed data from two systematic reviews and three primary studies.
One of the larger studies (included in one of the systematic reviews) included 47,000 veterans in VA intensive PTSD programs during 1992-2011. In fact, after controlling for demographic factors and other confounding variables, individuals who continued to use cannabis or started using cannabis showed worse PTSD symptoms than did nonusers after 4 months.
“Findings from [randomized, controlled trials] are needed to help determine whether and to what extent cannabis may improve PTSD symptoms, and further studies also are needed to clarify harms in patients with PTSD,” the researchers noted.
In the review of chronic pain literature, Shannon M. Nugent, PhD, also of the VA Portland (Ore.) Health Care System, and her colleagues examined 27 trials, 11 reviews, and 32 primary studies (Ann Intern Med. 2017 Aug 14. doi: 10.7326/M17-0155).
“Across nine studies, intervention patients were more likely to report at least 30% improvement in pain,” the investigators said. But this finding was specific to tetrahydrocannabinol (THC), the researchers said, and evidence of the ability of cannabis to relieve other types of pain, such as cancer pain and multiple sclerosis pain, was insufficient.
In addition, the researchers found a low strength of evidence association between cannabis use and the development of psychotic symptoms, and a moderate strength of evidence association between cannabis use and impaired cognitive function in the general population. “However, our confidence in the findings is limited by inconsistent findings among included studies, inadequate assessment of exposure, and inadequate adjustment for confounding among the studies” they said.
Although no significant differences were noted in rates of adverse events between cannabis users and nonusers, some data suggested users had an increased risk for short-term adverse events that ranged from dizziness to paranoia and suicide attempts.
Other potential harms associated with cannabis use included decreased lung function, increased risk of complications from infectious diseases, cannabis hyperemesis syndrome, and increased risk of violent behavior.
“Even though we did not find strong, consistent evidence of benefit, clinicians will still need to engage in evidence-based discussions with patients managing chronic pain who are using or requesting to use cannabis,” the researchers wrote.
The researchers had no financial conflicts to disclose. The study was commissioned by the Veterans Health Administration.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point:
Major finding: One study of cannabis use for neuropathic pain showed an approximately 30% improvement in pain, but researchers found no significant impact on relieving other types of chronic pain or PTSD symptoms.
Data source: The data come from a chronic pain review that included 27 trials, 11 systematic reviews, and 32 primary studies; and a PTSD review that included 2 systematic reviews and 3 primary studies.
Disclosures: The researchers had no financial conflicts to disclose. The study was commissioned by the Veterans Health Administration.
Marijuana use triples risk of death from hypertension
The risk of death from hypertension is three times greater in adults who use marijuana, compared with nonusers, based on data from a retrospective study of 1,213 adults.
Changes in the legalization of marijuana may promote increased recreational use, but data on the long-term effects of marijuana use on cardiovascular and cerebrovascular mortality are limited, wrote Barbara A. Yankey, PhD, of Georgia State University, Atlanta, and her colleagues.

Data on 686 users and 527 nonusers were combined with the 2011 mortality data from the National Center for Health Statistics (Eur J Prev Cardiol. 2017 Aug 9; doi: 10.1177/2047487317723212).
Overall, marijuana users had a 3.42 times greater risk of death from hypertension than did nonusers (95% confidence interval, 1.20-9.79), and the risk increased by 1.04 for each year of use (95% CI, 1.00-1.07). The average duration of marijuana use was 11.5 years. At the time of study entry, the average age of the participants was 38 years, and the average body mass index was 29 kg/m2; 23% of marijuana users and 21% of nonusers had a prior diagnosis of hypertension.
Of the study participants, 20% used marijuana and smoked cigarettes, 16% used marijuana and were past smokers, 5% were past smokers, and 4% only smoked cigarettes. “In our study, increase in risk for hypertension, [heart disease], or cerebrovascular disease mortality associated with cigarette use was not significant,” the researchers wrote. They attributed this factor to the small sample size and noted that the dangers of cigarette smoking to the cardiovascular system are well established.
The study findings were limited by the relatively small sample size and potentially inaccurate data on the duration of marijuana use, the researchers said.
However, the results suggest that “cardiovascular risk associated with marijuana use may be greater than the cardiovascular risk already established for cigarette smoking,” and longitudinal studies are warranted, they concluded.
The researchers had no financial conflicts to disclose.
The risk of death from hypertension is three times greater in adults who use marijuana, compared with nonusers, based on data from a retrospective study of 1,213 adults.
Changes in the legalization of marijuana may promote increased recreational use, but data on the long-term effects of marijuana use on cardiovascular and cerebrovascular mortality are limited, wrote Barbara A. Yankey, PhD, of Georgia State University, Atlanta, and her colleagues.
Data on 686 users and 527 nonusers were combined with the 2011 mortality data from the National Center for Health Statistics (Eur J Prev Cardiol. 2017 Aug 9; doi: 10.1177/2047487317723212).
Overall, marijuana users had a 3.42 times greater risk of death from hypertension than did nonusers (95% confidence interval, 1.20-9.79), and the risk increased by 1.04 for each year of use (95% CI, 1.00-1.07). The average duration of marijuana use was 11.5 years. At the time of study entry, the average age of the participants was 38 years, and the average body mass index was 29 kg/m2; 23% of marijuana users and 21% of nonusers had a prior diagnosis of hypertension.
Of the study participants, 20% used marijuana and smoked cigarettes, 16% used marijuana and were past smokers, 5% were past smokers, and 4% only smoked cigarettes. “In our study, increase in risk for hypertension, [heart disease], or cerebrovascular disease mortality associated with cigarette use was not significant,” the researchers wrote. They attributed this factor to the small sample size and noted that the dangers of cigarette smoking to the cardiovascular system are well established.
The study findings were limited by the relatively small sample size and potentially inaccurate data on the duration of marijuana use, the researchers said.
However, the results suggest that “cardiovascular risk associated with marijuana use may be greater than the cardiovascular risk already established for cigarette smoking,” and longitudinal studies are warranted, they concluded.
The researchers had no financial conflicts to disclose.
The risk of death from hypertension is three times greater in adults who use marijuana, compared with nonusers, based on data from a retrospective study of 1,213 adults.
Changes in the legalization of marijuana may promote increased recreational use, but data on the long-term effects of marijuana use on cardiovascular and cerebrovascular mortality are limited, wrote Barbara A. Yankey, PhD, of Georgia State University, Atlanta, and her colleagues.
Data on 686 users and 527 nonusers were combined with the 2011 mortality data from the National Center for Health Statistics (Eur J Prev Cardiol. 2017 Aug 9; doi: 10.1177/2047487317723212).
Overall, marijuana users had a 3.42 times greater risk of death from hypertension than did nonusers (95% confidence interval, 1.20-9.79), and the risk increased by 1.04 for each year of use (95% CI, 1.00-1.07). The average duration of marijuana use was 11.5 years. At the time of study entry, the average age of the participants was 38 years, and the average body mass index was 29 kg/m2; 23% of marijuana users and 21% of nonusers had a prior diagnosis of hypertension.
Of the study participants, 20% used marijuana and smoked cigarettes, 16% used marijuana and were past smokers, 5% were past smokers, and 4% only smoked cigarettes. “In our study, increase in risk for hypertension, [heart disease], or cerebrovascular disease mortality associated with cigarette use was not significant,” the researchers wrote. They attributed this factor to the small sample size and noted that the dangers of cigarette smoking to the cardiovascular system are well established.
The study findings were limited by the relatively small sample size and potentially inaccurate data on the duration of marijuana use, the researchers said.
However, the results suggest that “cardiovascular risk associated with marijuana use may be greater than the cardiovascular risk already established for cigarette smoking,” and longitudinal studies are warranted, they concluded.
The researchers had no financial conflicts to disclose.
FROM THE EUROPEAN JOURNAL OF PREVENTIVE CARDIOLOGY
Key clinical point: A history of marijuana use significantly increases the risk of death from hypertension.
Major finding: Marijuana users had a 3.42 times higher risk of death from hypertension and a 1.04 times increased risk of death for each year of use.
Data source: A retrospective study of 1,213 adults aged 20 years and older using data from National Health and Nutrition Examination Survey and the National Center for Health Statistics.
Disclosures: The researchers had no financial conflicts to disclose.
Childhood poverty sets stage for adult heart disease
Children from the poorest families show signs of thicker carotid artery walls that may raise their risk for heart attack and stroke as adults, according to data from a longitudinal study of more than 1,000 families in Australia.
“Understanding when associations between SEP [socioeconomic position] and CVD [cardiovascular disease] first appear may help address the increasing social gradients in CVD outcomes and risk factors,” wrote Richard S. Liu, MD, of the Murdoch Children’s Research Institute, Parkville, Australia, and colleagues.
The researchers reviewed data from 1,477 families in Australia. Socioeconomic position of the children’s families was measured biennially at age 0-1 year and onward, and the researchers used imaging to measure the right carotid arteries of children between age 11 and 12 years. Overall, children in the lowest socioeconomic quartile at age 11-12 years were 46% more likely than those in the highest quartile to have thicker carotid arteries (defined as greater than the 75th percentile).
“In univariable analyses, each quartile increment higher of family SEP was associated with a 3.7-micrometer thicker carotid intima-media thickness [IMT],” and the association remained significant in a multivariate analysis controlling for cardiovascular risk factors including secondhand smoke, body weight, and blood pressure, the researchers wrote.
The socioeconomic status of the family had a greater impact than that of the neighborhood, they noted.
In addition, low socioeconomic status of a child’s family at age 2-3 years was associated with thickness in carotid artery measurements at age 11-12 years.
The study findings were limited by several factors, including a lack of data on the clinical consequences of increased carotid thickness in children, as well as the need for investigation of other signs of subclinical atherosclerosis, the researchers said. However, “consistent evidence showed an association between SEP from early life and midchildhood carotid IMT,” and additional research is needed to explore the impact of household factors on childhood health, they emphasized.
The findings were published online Aug. 9 in the Journal of the American Heart Association (J Am Heart Assoc. 2017;6:e0059255).
The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
Children from the poorest families show signs of thicker carotid artery walls that may raise their risk for heart attack and stroke as adults, according to data from a longitudinal study of more than 1,000 families in Australia.
“Understanding when associations between SEP [socioeconomic position] and CVD [cardiovascular disease] first appear may help address the increasing social gradients in CVD outcomes and risk factors,” wrote Richard S. Liu, MD, of the Murdoch Children’s Research Institute, Parkville, Australia, and colleagues.
The researchers reviewed data from 1,477 families in Australia. Socioeconomic position of the children’s families was measured biennially at age 0-1 year and onward, and the researchers used imaging to measure the right carotid arteries of children between age 11 and 12 years. Overall, children in the lowest socioeconomic quartile at age 11-12 years were 46% more likely than those in the highest quartile to have thicker carotid arteries (defined as greater than the 75th percentile).
“In univariable analyses, each quartile increment higher of family SEP was associated with a 3.7-micrometer thicker carotid intima-media thickness [IMT],” and the association remained significant in a multivariate analysis controlling for cardiovascular risk factors including secondhand smoke, body weight, and blood pressure, the researchers wrote.
The socioeconomic status of the family had a greater impact than that of the neighborhood, they noted.
In addition, low socioeconomic status of a child’s family at age 2-3 years was associated with thickness in carotid artery measurements at age 11-12 years.
The study findings were limited by several factors, including a lack of data on the clinical consequences of increased carotid thickness in children, as well as the need for investigation of other signs of subclinical atherosclerosis, the researchers said. However, “consistent evidence showed an association between SEP from early life and midchildhood carotid IMT,” and additional research is needed to explore the impact of household factors on childhood health, they emphasized.
The findings were published online Aug. 9 in the Journal of the American Heart Association (J Am Heart Assoc. 2017;6:e0059255).
The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
Children from the poorest families show signs of thicker carotid artery walls that may raise their risk for heart attack and stroke as adults, according to data from a longitudinal study of more than 1,000 families in Australia.
“Understanding when associations between SEP [socioeconomic position] and CVD [cardiovascular disease] first appear may help address the increasing social gradients in CVD outcomes and risk factors,” wrote Richard S. Liu, MD, of the Murdoch Children’s Research Institute, Parkville, Australia, and colleagues.
The researchers reviewed data from 1,477 families in Australia. Socioeconomic position of the children’s families was measured biennially at age 0-1 year and onward, and the researchers used imaging to measure the right carotid arteries of children between age 11 and 12 years. Overall, children in the lowest socioeconomic quartile at age 11-12 years were 46% more likely than those in the highest quartile to have thicker carotid arteries (defined as greater than the 75th percentile).
“In univariable analyses, each quartile increment higher of family SEP was associated with a 3.7-micrometer thicker carotid intima-media thickness [IMT],” and the association remained significant in a multivariate analysis controlling for cardiovascular risk factors including secondhand smoke, body weight, and blood pressure, the researchers wrote.
The socioeconomic status of the family had a greater impact than that of the neighborhood, they noted.
In addition, low socioeconomic status of a child’s family at age 2-3 years was associated with thickness in carotid artery measurements at age 11-12 years.
The study findings were limited by several factors, including a lack of data on the clinical consequences of increased carotid thickness in children, as well as the need for investigation of other signs of subclinical atherosclerosis, the researchers said. However, “consistent evidence showed an association between SEP from early life and midchildhood carotid IMT,” and additional research is needed to explore the impact of household factors on childhood health, they emphasized.
The findings were published online Aug. 9 in the Journal of the American Heart Association (J Am Heart Assoc. 2017;6:e0059255).
The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF THE AMERICAN HEART ASSOCIATION
Key clinical point: Low socioeconomic status of families was significantly linked with thicker carotid arteries in children at age 11-12 years, which could increase the risk of stroke in adulthood.
Major finding: Children in the lowest socioeconomic group at age 11-12 years were 46% more likely to have carotid intima-media thickness at a level above the 75th percentile.
Data source: A longitudinal study of children from 1,477 families in Australia.
Disclosures: The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
Botox smooths prep for hernia surgery
Injections of onabotulinumtoxinA prior to hernia surgery relaxed the abdominal muscles and increased abdominal wall length by an average of 8 cm, based on data from an observational study of 56 patients. The findings were published online in Surgical Endoscopy.
Although laparoscopic ventral hernia repair has a lower recurrence rate than open repair, expanding the abdominal wall remains a challenge, wrote Omar Rodriguez-Acevedo, MD, of the Hernia Institute Australia, Edgecliff, New South Wales, Australia, and colleagues (Surg Endosc. 2017 Jul 21. doi: 10.1007/s00464-017-5750-3).

Nearly three-fourths of the patients (73%) had at least one previous repair. The patients underwent injections of either 200 units or 300 units of BTA between 7 and 14 days before surgery. The average age of the patients was 60 years, and the average body mass index was 40 kg/m2. A subset of 18 patients with larger defects underwent preoperative progressive pneumoperitoneum (PPP) in addition to receiving BTA injections.
Overall, BTA injections significantly increased lateral abdominal length in all subgroups. On average, the length increase per side was 4.4 cm in the 300-unit group, 3.6 cm in the 200-unit group, 4.2 cm in the BtA-only group, and 3.7 cm in the BTA-plus-PPP group. In a pooled analysis, the average gain in length was 4.0 per side.
No significant difference in abdominal wall lengthening was observed between the 200-unit and 300-unit patients or between the BTA-plus-PPP and BTA-only patients.
Overall, the injections were well tolerated, and no complications required intervention, the researchers said. The most common side effects included superficial bruising at the injection site, bloating sensations, weak coughing, and back pain.
The findings were limited by the small study population and by the short follow-up period, and additional long-term follow-up is needed to identify delayed hernia recurrence, the researchers noted. However, the results suggest that “the flaccid paralysis delivered by BTA resulted in the relaxation, elongation, and thinning of the chronically contracted abdominal lateral wall musculature,” which “consequently facilitates laparoscopic repair and primary closure of large defects under minimal tension,” they said.
The researchers had no financial conflicts to disclose.
Injections of onabotulinumtoxinA prior to hernia surgery relaxed the abdominal muscles and increased abdominal wall length by an average of 8 cm, based on data from an observational study of 56 patients. The findings were published online in Surgical Endoscopy.
Although laparoscopic ventral hernia repair has a lower recurrence rate than open repair, expanding the abdominal wall remains a challenge, wrote Omar Rodriguez-Acevedo, MD, of the Hernia Institute Australia, Edgecliff, New South Wales, Australia, and colleagues (Surg Endosc. 2017 Jul 21. doi: 10.1007/s00464-017-5750-3).
Nearly three-fourths of the patients (73%) had at least one previous repair. The patients underwent injections of either 200 units or 300 units of BTA between 7 and 14 days before surgery. The average age of the patients was 60 years, and the average body mass index was 40 kg/m2. A subset of 18 patients with larger defects underwent preoperative progressive pneumoperitoneum (PPP) in addition to receiving BTA injections.
Overall, BTA injections significantly increased lateral abdominal length in all subgroups. On average, the length increase per side was 4.4 cm in the 300-unit group, 3.6 cm in the 200-unit group, 4.2 cm in the BtA-only group, and 3.7 cm in the BTA-plus-PPP group. In a pooled analysis, the average gain in length was 4.0 per side.
No significant difference in abdominal wall lengthening was observed between the 200-unit and 300-unit patients or between the BTA-plus-PPP and BTA-only patients.
Overall, the injections were well tolerated, and no complications required intervention, the researchers said. The most common side effects included superficial bruising at the injection site, bloating sensations, weak coughing, and back pain.
The findings were limited by the small study population and by the short follow-up period, and additional long-term follow-up is needed to identify delayed hernia recurrence, the researchers noted. However, the results suggest that “the flaccid paralysis delivered by BTA resulted in the relaxation, elongation, and thinning of the chronically contracted abdominal lateral wall musculature,” which “consequently facilitates laparoscopic repair and primary closure of large defects under minimal tension,” they said.
The researchers had no financial conflicts to disclose.
Injections of onabotulinumtoxinA prior to hernia surgery relaxed the abdominal muscles and increased abdominal wall length by an average of 8 cm, based on data from an observational study of 56 patients. The findings were published online in Surgical Endoscopy.
Although laparoscopic ventral hernia repair has a lower recurrence rate than open repair, expanding the abdominal wall remains a challenge, wrote Omar Rodriguez-Acevedo, MD, of the Hernia Institute Australia, Edgecliff, New South Wales, Australia, and colleagues (Surg Endosc. 2017 Jul 21. doi: 10.1007/s00464-017-5750-3).
Nearly three-fourths of the patients (73%) had at least one previous repair. The patients underwent injections of either 200 units or 300 units of BTA between 7 and 14 days before surgery. The average age of the patients was 60 years, and the average body mass index was 40 kg/m2. A subset of 18 patients with larger defects underwent preoperative progressive pneumoperitoneum (PPP) in addition to receiving BTA injections.
Overall, BTA injections significantly increased lateral abdominal length in all subgroups. On average, the length increase per side was 4.4 cm in the 300-unit group, 3.6 cm in the 200-unit group, 4.2 cm in the BtA-only group, and 3.7 cm in the BTA-plus-PPP group. In a pooled analysis, the average gain in length was 4.0 per side.
No significant difference in abdominal wall lengthening was observed between the 200-unit and 300-unit patients or between the BTA-plus-PPP and BTA-only patients.
Overall, the injections were well tolerated, and no complications required intervention, the researchers said. The most common side effects included superficial bruising at the injection site, bloating sensations, weak coughing, and back pain.
The findings were limited by the small study population and by the short follow-up period, and additional long-term follow-up is needed to identify delayed hernia recurrence, the researchers noted. However, the results suggest that “the flaccid paralysis delivered by BTA resulted in the relaxation, elongation, and thinning of the chronically contracted abdominal lateral wall musculature,” which “consequently facilitates laparoscopic repair and primary closure of large defects under minimal tension,” they said.
The researchers had no financial conflicts to disclose.
FROM SURGICAL ENDOSCOPY
Key clinical point: Injection with botulinum toxin A prior to hernia repair serves as an effective surgical preparation by temporarily paralyzing the lateral abdominal wall muscles.
Major finding: A comparison of pre- and post-onabotulinumtoxinA images of the abdominal wall showed an unstretched average increase in length of 8.0 cm.
Data source: A prospective, observational study of 56 adults who underwent elective ventral hernia repairs at a single center.
Disclosures: The researchers had no financial conflicts to disclose.
Hormonal IUD is most cost-effective menorrhagia management
Quality of life was higher, and costs were lower, with the levonorgestrel-releasing intrauterine system for treatment of heavy menstrual bleeding than with three other common treatments, according to data from a model and a hypothetical population of 100,000 premenopausal women. The findings were published online in the American Journal of Obstetrics and Gynecology.

“As health systems and policies continue to emphasize value-based treatment decisions, it is important to give physicians and patients the tools to understand the health and economic trade-offs associated with each of these options,” Jennifer C. Spencer of the University of North Carolina, Chapel Hill, and her colleagues wrote (Am J Obstet Gynecol. 2017 Jul 25. doi: 10.1016/j.ajog.2017.07.024).
Overall, LNG-IUS was superior to hysterectomy and both types of endometrial ablation in terms of cost and quality of life, although quality of life scores were similar across all four treatments.
LNG-IUS was cost effective, compared with hysterectomy, in 90% of scenarios. Both types of ablation were similarly more cost effective, compared with hysterectomy; resectoscopic endometrial ablation was more cost effective in 44% of scenarios, nonresectoscopic endometrial ablation was more cost effective in 53% of scenarios.
“The 5-year cost of women undergoing LNG-IUS was $4,500, about half the cost of endometrial ablation ($9,500) and about one-third the cost of hysterectomy ($13,500),” the researchers noted.
“Our analysis finds strong evidence in favor of LNG-IUS as a cost-saving, dominant alternative to hysterectomy for women with heavy menstrual bleeding,” they wrote.
If LNG-IUS is not an option, the model shows that hysterectomy resulted in better quality of life in the majority of simulations but is cost effective in just over half of the simulations, compared with either resectoscopic or nonresectoscopic ablation.
“The comparative cost effectiveness of endometrial ablation and hysterectomy highlights important trade-offs for patients and providers to consider when selecting between treatment options, such as the need for future procedures or the potential for rare, but serious, complications,” the researchers wrote.
No other studies on this topic have been conducted in the United States, but the findings are consistent with results from studies conducted outside the United States, the researchers wrote.
The study was limited by the short follow-up period and the inability to extend the model to women with large fibroids, polyps, or other uterine pathologies.
Two of the authors reported receiving grant funding from Pfizer for an unrelated study. Other authors reported serving as consultants for Teleflex Medical, Applied Medical, and Olympus.
Quality of life was higher, and costs were lower, with the levonorgestrel-releasing intrauterine system for treatment of heavy menstrual bleeding than with three other common treatments, according to data from a model and a hypothetical population of 100,000 premenopausal women. The findings were published online in the American Journal of Obstetrics and Gynecology.
“As health systems and policies continue to emphasize value-based treatment decisions, it is important to give physicians and patients the tools to understand the health and economic trade-offs associated with each of these options,” Jennifer C. Spencer of the University of North Carolina, Chapel Hill, and her colleagues wrote (Am J Obstet Gynecol. 2017 Jul 25. doi: 10.1016/j.ajog.2017.07.024).
Overall, LNG-IUS was superior to hysterectomy and both types of endometrial ablation in terms of cost and quality of life, although quality of life scores were similar across all four treatments.
LNG-IUS was cost effective, compared with hysterectomy, in 90% of scenarios. Both types of ablation were similarly more cost effective, compared with hysterectomy; resectoscopic endometrial ablation was more cost effective in 44% of scenarios, nonresectoscopic endometrial ablation was more cost effective in 53% of scenarios.
“The 5-year cost of women undergoing LNG-IUS was $4,500, about half the cost of endometrial ablation ($9,500) and about one-third the cost of hysterectomy ($13,500),” the researchers noted.
“Our analysis finds strong evidence in favor of LNG-IUS as a cost-saving, dominant alternative to hysterectomy for women with heavy menstrual bleeding,” they wrote.
If LNG-IUS is not an option, the model shows that hysterectomy resulted in better quality of life in the majority of simulations but is cost effective in just over half of the simulations, compared with either resectoscopic or nonresectoscopic ablation.
“The comparative cost effectiveness of endometrial ablation and hysterectomy highlights important trade-offs for patients and providers to consider when selecting between treatment options, such as the need for future procedures or the potential for rare, but serious, complications,” the researchers wrote.
No other studies on this topic have been conducted in the United States, but the findings are consistent with results from studies conducted outside the United States, the researchers wrote.
The study was limited by the short follow-up period and the inability to extend the model to women with large fibroids, polyps, or other uterine pathologies.
Two of the authors reported receiving grant funding from Pfizer for an unrelated study. Other authors reported serving as consultants for Teleflex Medical, Applied Medical, and Olympus.
Quality of life was higher, and costs were lower, with the levonorgestrel-releasing intrauterine system for treatment of heavy menstrual bleeding than with three other common treatments, according to data from a model and a hypothetical population of 100,000 premenopausal women. The findings were published online in the American Journal of Obstetrics and Gynecology.
“As health systems and policies continue to emphasize value-based treatment decisions, it is important to give physicians and patients the tools to understand the health and economic trade-offs associated with each of these options,” Jennifer C. Spencer of the University of North Carolina, Chapel Hill, and her colleagues wrote (Am J Obstet Gynecol. 2017 Jul 25. doi: 10.1016/j.ajog.2017.07.024).
Overall, LNG-IUS was superior to hysterectomy and both types of endometrial ablation in terms of cost and quality of life, although quality of life scores were similar across all four treatments.
LNG-IUS was cost effective, compared with hysterectomy, in 90% of scenarios. Both types of ablation were similarly more cost effective, compared with hysterectomy; resectoscopic endometrial ablation was more cost effective in 44% of scenarios, nonresectoscopic endometrial ablation was more cost effective in 53% of scenarios.
“The 5-year cost of women undergoing LNG-IUS was $4,500, about half the cost of endometrial ablation ($9,500) and about one-third the cost of hysterectomy ($13,500),” the researchers noted.
“Our analysis finds strong evidence in favor of LNG-IUS as a cost-saving, dominant alternative to hysterectomy for women with heavy menstrual bleeding,” they wrote.
If LNG-IUS is not an option, the model shows that hysterectomy resulted in better quality of life in the majority of simulations but is cost effective in just over half of the simulations, compared with either resectoscopic or nonresectoscopic ablation.
“The comparative cost effectiveness of endometrial ablation and hysterectomy highlights important trade-offs for patients and providers to consider when selecting between treatment options, such as the need for future procedures or the potential for rare, but serious, complications,” the researchers wrote.
No other studies on this topic have been conducted in the United States, but the findings are consistent with results from studies conducted outside the United States, the researchers wrote.
The study was limited by the short follow-up period and the inability to extend the model to women with large fibroids, polyps, or other uterine pathologies.
Two of the authors reported receiving grant funding from Pfizer for an unrelated study. Other authors reported serving as consultants for Teleflex Medical, Applied Medical, and Olympus.
FROM AMERICAN JOURNAL OF OBSTETRICS AND GYNECOLOGY
Key clinical point:
Major finding: LNG-IUS is the most cost-effective option in 90% of scenarios, compared with hysterectomy.
Data source: The data come from a model created using a literature review of four treatment options: resectoscopic ablation, nonresectoscopic ablation, hysterectomy, and LNG-IUS. It included a hypothetical cohort of 100,000 premenopausal women.
Disclosures: Two of the authors reported receiving grant funding from Pfizer for an unrelated study. Other authors reported serving as consultants for Teleflex Medical, Applied Medical, and Olympus.