User login
Pediatric psoriasis carries sharply increased risk of selected autoimmune comorbidities
GENEVA – Pediatric psoriasis is associated with sharply increased risks of selected autoimmune diseases, according to a cross-sectional study encompassing every child and adolescent in Denmark.
"Even though the absolute risk of many of these conditions remains rare in childhood, clinicians should keep these associations in mind because they can greatly add to the total disease burden. In particular, we advise focusing on extracutaneous symptoms when treating psoriasis in children,” Christoffer Blegvad, MD, said at the annual congress of the European Academy of Dermatology and Venereology.

He presented a cross-sectional study in which Denmark’s vaunted system of comprehensive national registries was harnessed to obtain health information on all individuals under age 18 years living in Denmark as of the end of 2012. The study population comprised 1,925 children and adolescents with dermatologist-diagnosed psoriasis, including those with psoriasis mild enough to be managed with topical therapies, and 1,194,712 youths without psoriasis.
In a first-pass unadjusted analysis, the psoriasis patients were at significantly increased risk for all nine of the autoimmune diseases examined. When the investigators adjusted for age, sex, and an individual’s health care utilization as reflected in his or her number of dermatology visits, the children and adolescents with psoriasis remained at tenfold increased risk for comorbid psoriatic arthritis, 6.6-fold risk for rheumatoid arthritis, 4.8-fold risk for vitiligo, and smaller yet significantly increased risks for several other autoimmune diseases, compared with individuals without psoriasis.
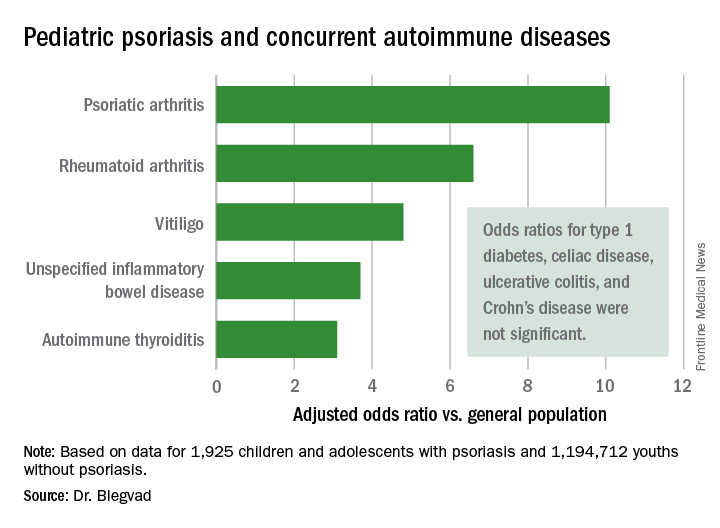
Indeed, while the presence of pediatric psoriasis was associated with an adjusted 4.4-fold increased risk of having at least one autoimmune disease, psoriasis patients with one of the selected autoimmune diseases were at 7.3-fold greater risk of having two or more autoimmune diseases, compared with individuals with one autoimmune disease who didn’t have psoriasis.
This is the first study to show such a clustering effect in either pediatric or adult psoriasis patients. The finding highlights the complex genetic underpinnings of psoriasis, which has previously been shown to share genetic susceptibility loci with inflammatory bowel disease and various other autoimmune diseases, Dr. Blegvad noted.
A small caveat: The psoriatic arthritis category also included individuals with juvenile idiopathic arthritis and juvenile psoriatic arthritis, because the clinical signs and symptoms of the three disorders often are difficult to distinguish in young patients.
Dr. Blegvad reported having no financial conflicts regarding the study, funded by Herlev and Gentofte Hospital and the LEO Foundation.
GENEVA – Pediatric psoriasis is associated with sharply increased risks of selected autoimmune diseases, according to a cross-sectional study encompassing every child and adolescent in Denmark.
"Even though the absolute risk of many of these conditions remains rare in childhood, clinicians should keep these associations in mind because they can greatly add to the total disease burden. In particular, we advise focusing on extracutaneous symptoms when treating psoriasis in children,” Christoffer Blegvad, MD, said at the annual congress of the European Academy of Dermatology and Venereology.
He presented a cross-sectional study in which Denmark’s vaunted system of comprehensive national registries was harnessed to obtain health information on all individuals under age 18 years living in Denmark as of the end of 2012. The study population comprised 1,925 children and adolescents with dermatologist-diagnosed psoriasis, including those with psoriasis mild enough to be managed with topical therapies, and 1,194,712 youths without psoriasis.
In a first-pass unadjusted analysis, the psoriasis patients were at significantly increased risk for all nine of the autoimmune diseases examined. When the investigators adjusted for age, sex, and an individual’s health care utilization as reflected in his or her number of dermatology visits, the children and adolescents with psoriasis remained at tenfold increased risk for comorbid psoriatic arthritis, 6.6-fold risk for rheumatoid arthritis, 4.8-fold risk for vitiligo, and smaller yet significantly increased risks for several other autoimmune diseases, compared with individuals without psoriasis.
Indeed, while the presence of pediatric psoriasis was associated with an adjusted 4.4-fold increased risk of having at least one autoimmune disease, psoriasis patients with one of the selected autoimmune diseases were at 7.3-fold greater risk of having two or more autoimmune diseases, compared with individuals with one autoimmune disease who didn’t have psoriasis.
This is the first study to show such a clustering effect in either pediatric or adult psoriasis patients. The finding highlights the complex genetic underpinnings of psoriasis, which has previously been shown to share genetic susceptibility loci with inflammatory bowel disease and various other autoimmune diseases, Dr. Blegvad noted.
A small caveat: The psoriatic arthritis category also included individuals with juvenile idiopathic arthritis and juvenile psoriatic arthritis, because the clinical signs and symptoms of the three disorders often are difficult to distinguish in young patients.
Dr. Blegvad reported having no financial conflicts regarding the study, funded by Herlev and Gentofte Hospital and the LEO Foundation.
GENEVA – Pediatric psoriasis is associated with sharply increased risks of selected autoimmune diseases, according to a cross-sectional study encompassing every child and adolescent in Denmark.
"Even though the absolute risk of many of these conditions remains rare in childhood, clinicians should keep these associations in mind because they can greatly add to the total disease burden. In particular, we advise focusing on extracutaneous symptoms when treating psoriasis in children,” Christoffer Blegvad, MD, said at the annual congress of the European Academy of Dermatology and Venereology.
He presented a cross-sectional study in which Denmark’s vaunted system of comprehensive national registries was harnessed to obtain health information on all individuals under age 18 years living in Denmark as of the end of 2012. The study population comprised 1,925 children and adolescents with dermatologist-diagnosed psoriasis, including those with psoriasis mild enough to be managed with topical therapies, and 1,194,712 youths without psoriasis.
In a first-pass unadjusted analysis, the psoriasis patients were at significantly increased risk for all nine of the autoimmune diseases examined. When the investigators adjusted for age, sex, and an individual’s health care utilization as reflected in his or her number of dermatology visits, the children and adolescents with psoriasis remained at tenfold increased risk for comorbid psoriatic arthritis, 6.6-fold risk for rheumatoid arthritis, 4.8-fold risk for vitiligo, and smaller yet significantly increased risks for several other autoimmune diseases, compared with individuals without psoriasis.
Indeed, while the presence of pediatric psoriasis was associated with an adjusted 4.4-fold increased risk of having at least one autoimmune disease, psoriasis patients with one of the selected autoimmune diseases were at 7.3-fold greater risk of having two or more autoimmune diseases, compared with individuals with one autoimmune disease who didn’t have psoriasis.
This is the first study to show such a clustering effect in either pediatric or adult psoriasis patients. The finding highlights the complex genetic underpinnings of psoriasis, which has previously been shown to share genetic susceptibility loci with inflammatory bowel disease and various other autoimmune diseases, Dr. Blegvad noted.
A small caveat: The psoriatic arthritis category also included individuals with juvenile idiopathic arthritis and juvenile psoriatic arthritis, because the clinical signs and symptoms of the three disorders often are difficult to distinguish in young patients.
Dr. Blegvad reported having no financial conflicts regarding the study, funded by Herlev and Gentofte Hospital and the LEO Foundation.
AT THE EADV CONGRESS
Key clinical point:
Major finding: Pediatric psoriasis patients were at an adjusted 6.6-fold increased risk of comorbid rheumatoid arthritis, 4.8-fold risk of vitiligo, and significantly increased risks of several other autoimmune diseases, compared with matched youths without psoriasis.
Data source: A cross-sectional study of all children and adolescents living in Denmark at the end of 2012.
Disclosures: The presenter reported having no financial conflicts regarding the study, funded by Herlev and Gentofte Hospital and the LEO Foundation.
Are those hemorrhoids? Get to know the anorectal imitators
ESTES PARK, COLO. – As a colorectal surgeon, Michelle Cowan, MD, sees a steady parade of primary care referrals for surgical evaluation of hemorrhoids.
The thing is, most of the time, the referred patients don’t have hemorrhoids. They have one of the other common anorectal disorders, including anal fissure, anoperineal abscess, fistula-in-ano, or an anorectal sexually transmitted infection, according to Dr. Cowan.

The diagnostic challenge stems from the fact that most common anorectal diseases – whether benign or malignant – present with the same constellation of symptoms: pain, bleeding, itching or burning, swelling, and leakage.
The quality and intensity of the pain “down under” provides a useful clue in differentiating the disorders.
“Hemorrhoids rarely cause legit pain,” said Dr. Cowan, who practices at the University of Colorado at Denver, Aurora. “Excruciating pain, where the patient will only sit on one side, that’s typically an abscess, a fissure, or an STI.”
The exceptions in the hemorrhoid realm are external thrombosed hemorrhoids, which are exceedingly painful but also readily identifiable, and incarcerated hemorrhoids, which are quite rare.
The pain associated with an anal fissure is distinct from that of an abscess or thrombosed hemorrhoid – it’s a throbbing pain lasting minutes to hours per episode.
“These are the people who won’t sit down in your office,” Dr. Cowan said.
Anal fissure is a common condition in young and middle-aged adults, and especially in peripartum women. The pathophysiology involves microtrauma, typically either because of passing rock-hard stools, diarrhea, or the rigors of childbirth, any of which can cause a break in the anal mucosa. That break causes the internal sphincter muscle to go into spasm, temporarily choking off the blood supply to the area of the fissure. Those wounds won’t heal on their own. Close to 90% of the fissures are located in the posterior midline; if the fissure is ectopic, it’s time to consider Crohn’s disease, HIV infection, tuberculosis, cancer, and other possibilities.
The patient with an anoperineal abscess presents with extreme pain, a sensation of fullness in the anus and rectum, erythema, fullness of the perineum, drainage, and sometimes fever.
“This is legit pain, like with a fissure or thrombosed hemorrhoids,” she explained. “Patients with any of these conditions can tell you exactly when they went from feeling normal to when the pain started.”
The abscess is caused by an infected anal gland. The location is most commonly perianal or ischioanal. If that’s not the suppuration site, the abscess is intersphincteric or supralevator, in which case a confirmatory CT scan is called for before proceeding with treatment.
Regardless of the suspected cause of a patient’s anorectal symptoms, any GI bleeding needs to be taken seriously. Young adults are the only segment of the population in whom the incidence of colorectal cancer is going up. In response, the American Society for Gastrointestinal Endoscopy and other groups now recommend colonoscopy for all patients older than age 40 years with GI bleeding, even if their family histories for colorectal cancer are negative and they lack other high-risk factors. For those younger than age 40 years, flexible sigmoidoscopy is recommended, even if it’s obvious that the patient has external thrombosed hemorrhoids that are bleeding.
“I tell people that I will not do hemorrhoid surgery until they have the scope,” Dr. Cowan said.
Office-based treatment of common anorectal disorders
Nonoperative treatment of anal fissures and internal hemorrhoids is all about encouraging patient adherence.
“Patient expectations are often overlooked,” according to the surgeon. “It’s rare that these patients actually need to go to surgery, but they oftentimes don’t do what we tell them to do, which is why they end up in my office.”
With anal fissure, the goal is to relax the spastic sphincter muscle, allowing the fissure to heal. That can be accomplished medically or surgically.
Medically, treatment consists of increased water intake, incorporation of more fiber in the diet, undertaking warm sitz baths a couple times a day, and application of a pea-sized amount of topical 2% diltiazem three times daily on the outside of the anus for 6-8 weeks.
“Compliance is huge. This whole thing is about consistency. Oftentimes, the reason treatment fails is people can’t do this. They feel good after about a week, so they stop before the fissure is completely healed,” she said.
The topical diltiazem must be prepared at a compounding pharmacy. It’s usually covered by insurance. Even if it’s not, an 8-week prescription costs only about $25. The drug is effective in up to 95% of patients who follow the instructions.
Topical 0.2% nitroglycerin, an alternative treatment, is less attractive because 30% of patients experience often-disabling headaches as a side effect. Topical diltiazem has a much better side effect profile, Dr. Cowan noted. If a patient shows a partial response to 6-8 weeks of topical diltiazem, it’s worth prescribing a second round. If the fissure still hasn’t healed after that, it’s time for referral to a surgeon. The options are onabotulinumtoxinA (Botox) and lateral internal sphincterotomy.
Botox is effective in 60%-80% of patients, she explained, providing temporary benefit lasting up to 3 months with a much lower risk of incontinence than with lateral internal sphincterotomy. Open and closed sphincterotomy techniques yield a similar success rate, with healing in 93% of cases.
For internal hemorrhoids, stool softeners, 25-30 g of fiber supplements per day, warm sitz baths, avoiding straining during defecation, and not loitering on the toilet are key elements in achieving symptomatic control nonoperatively.
Patients who don’t have a bathtub in which to take sitz baths can accomplish the same thing using an easily removable, commercially available device that fits over a toilet bowl.
Disposable baby wipes for adults have become the No. 1 cause of anal itching and are to be shunned by patients with internal hemorrhoids or other anorectal disorders.
“Patients often engage in excessive wiping because of the poor consistency of their bowel movements,” Dr. Cowan explained. “If they’re pasty and not coming out in one fell swoop, it leads to residue that patients appropriately feel they need to wipe multiple times to keep clean. The majority of these dipe wipes for adults are alcohol based, and even though on your exam you may see nothing, the dipe wipes cause microexcoriations of the skin. The patient itches and doesn’t know why.”
Primary care physicians can readily learn to do mucosal banding for grade II and III prolapsing hemorrhoids in the office, she noted. However, banding should never be attempted on external thrombosed hemorrhoids, though.
Surgical excisional hemorrhoidectomy is a lasting solution for such hemorrhoids, but patients need to understand that even though it’s only a 10- to 15-minute procedure performed in an outpatient setting, it’s excruciatingly painful for a week – and that’s not the end of the story.
“I tell patients to take a week off work,” the surgeon said. “And don’t sit on a donut; it pulls on the suture line. Pillows are okay. But it takes 6-8 weeks to heal, so even though they’re only in excruciating pain for about a week, they have to poop past the suture line, so they’ve got to avoid rock-hard stools.”
With an anoperineal abscess, first-line treatment is incision of the abscess as close as possible to the anus, followed by placement of a drain to be left in place for 7-10 days. Prophylactic antibiotics are reserved for immunosuppressed patients.
Patients need to understand up front that, 30%-50% of the time, a fistula can develop after drainage of an abscess. Indeed, abscessed anoperineal fistula is one of the most common conditions Dr. Cowan sees in the emergency department and clinic. The telltale symptoms are recurrent abscess and/or persistent drainage. Those patients need referral to a colorectal surgeon.
“Fistula-in-ano is a frustrating disease for the patient and the surgeon. As surgeons, we like to fix – and there’s really no good option,” according to Dr. Cowan.
Among the surgical treatment options are debridement followed by fibrin glue injection, an anal fistula plug, an endorectal flap closure, and ligation of the intersphincteric fistula tract, or LIFT, procedure.
Dr. Cowan reported serving as a consultant to Applied Medical.
ESTES PARK, COLO. – As a colorectal surgeon, Michelle Cowan, MD, sees a steady parade of primary care referrals for surgical evaluation of hemorrhoids.
The thing is, most of the time, the referred patients don’t have hemorrhoids. They have one of the other common anorectal disorders, including anal fissure, anoperineal abscess, fistula-in-ano, or an anorectal sexually transmitted infection, according to Dr. Cowan.
The diagnostic challenge stems from the fact that most common anorectal diseases – whether benign or malignant – present with the same constellation of symptoms: pain, bleeding, itching or burning, swelling, and leakage.
The quality and intensity of the pain “down under” provides a useful clue in differentiating the disorders.
“Hemorrhoids rarely cause legit pain,” said Dr. Cowan, who practices at the University of Colorado at Denver, Aurora. “Excruciating pain, where the patient will only sit on one side, that’s typically an abscess, a fissure, or an STI.”
The exceptions in the hemorrhoid realm are external thrombosed hemorrhoids, which are exceedingly painful but also readily identifiable, and incarcerated hemorrhoids, which are quite rare.
The pain associated with an anal fissure is distinct from that of an abscess or thrombosed hemorrhoid – it’s a throbbing pain lasting minutes to hours per episode.
“These are the people who won’t sit down in your office,” Dr. Cowan said.
Anal fissure is a common condition in young and middle-aged adults, and especially in peripartum women. The pathophysiology involves microtrauma, typically either because of passing rock-hard stools, diarrhea, or the rigors of childbirth, any of which can cause a break in the anal mucosa. That break causes the internal sphincter muscle to go into spasm, temporarily choking off the blood supply to the area of the fissure. Those wounds won’t heal on their own. Close to 90% of the fissures are located in the posterior midline; if the fissure is ectopic, it’s time to consider Crohn’s disease, HIV infection, tuberculosis, cancer, and other possibilities.
The patient with an anoperineal abscess presents with extreme pain, a sensation of fullness in the anus and rectum, erythema, fullness of the perineum, drainage, and sometimes fever.
“This is legit pain, like with a fissure or thrombosed hemorrhoids,” she explained. “Patients with any of these conditions can tell you exactly when they went from feeling normal to when the pain started.”
The abscess is caused by an infected anal gland. The location is most commonly perianal or ischioanal. If that’s not the suppuration site, the abscess is intersphincteric or supralevator, in which case a confirmatory CT scan is called for before proceeding with treatment.
Regardless of the suspected cause of a patient’s anorectal symptoms, any GI bleeding needs to be taken seriously. Young adults are the only segment of the population in whom the incidence of colorectal cancer is going up. In response, the American Society for Gastrointestinal Endoscopy and other groups now recommend colonoscopy for all patients older than age 40 years with GI bleeding, even if their family histories for colorectal cancer are negative and they lack other high-risk factors. For those younger than age 40 years, flexible sigmoidoscopy is recommended, even if it’s obvious that the patient has external thrombosed hemorrhoids that are bleeding.
“I tell people that I will not do hemorrhoid surgery until they have the scope,” Dr. Cowan said.
Office-based treatment of common anorectal disorders
Nonoperative treatment of anal fissures and internal hemorrhoids is all about encouraging patient adherence.
“Patient expectations are often overlooked,” according to the surgeon. “It’s rare that these patients actually need to go to surgery, but they oftentimes don’t do what we tell them to do, which is why they end up in my office.”
With anal fissure, the goal is to relax the spastic sphincter muscle, allowing the fissure to heal. That can be accomplished medically or surgically.
Medically, treatment consists of increased water intake, incorporation of more fiber in the diet, undertaking warm sitz baths a couple times a day, and application of a pea-sized amount of topical 2% diltiazem three times daily on the outside of the anus for 6-8 weeks.
“Compliance is huge. This whole thing is about consistency. Oftentimes, the reason treatment fails is people can’t do this. They feel good after about a week, so they stop before the fissure is completely healed,” she said.
The topical diltiazem must be prepared at a compounding pharmacy. It’s usually covered by insurance. Even if it’s not, an 8-week prescription costs only about $25. The drug is effective in up to 95% of patients who follow the instructions.
Topical 0.2% nitroglycerin, an alternative treatment, is less attractive because 30% of patients experience often-disabling headaches as a side effect. Topical diltiazem has a much better side effect profile, Dr. Cowan noted. If a patient shows a partial response to 6-8 weeks of topical diltiazem, it’s worth prescribing a second round. If the fissure still hasn’t healed after that, it’s time for referral to a surgeon. The options are onabotulinumtoxinA (Botox) and lateral internal sphincterotomy.
Botox is effective in 60%-80% of patients, she explained, providing temporary benefit lasting up to 3 months with a much lower risk of incontinence than with lateral internal sphincterotomy. Open and closed sphincterotomy techniques yield a similar success rate, with healing in 93% of cases.
For internal hemorrhoids, stool softeners, 25-30 g of fiber supplements per day, warm sitz baths, avoiding straining during defecation, and not loitering on the toilet are key elements in achieving symptomatic control nonoperatively.
Patients who don’t have a bathtub in which to take sitz baths can accomplish the same thing using an easily removable, commercially available device that fits over a toilet bowl.
Disposable baby wipes for adults have become the No. 1 cause of anal itching and are to be shunned by patients with internal hemorrhoids or other anorectal disorders.
“Patients often engage in excessive wiping because of the poor consistency of their bowel movements,” Dr. Cowan explained. “If they’re pasty and not coming out in one fell swoop, it leads to residue that patients appropriately feel they need to wipe multiple times to keep clean. The majority of these dipe wipes for adults are alcohol based, and even though on your exam you may see nothing, the dipe wipes cause microexcoriations of the skin. The patient itches and doesn’t know why.”
Primary care physicians can readily learn to do mucosal banding for grade II and III prolapsing hemorrhoids in the office, she noted. However, banding should never be attempted on external thrombosed hemorrhoids, though.
Surgical excisional hemorrhoidectomy is a lasting solution for such hemorrhoids, but patients need to understand that even though it’s only a 10- to 15-minute procedure performed in an outpatient setting, it’s excruciatingly painful for a week – and that’s not the end of the story.
“I tell patients to take a week off work,” the surgeon said. “And don’t sit on a donut; it pulls on the suture line. Pillows are okay. But it takes 6-8 weeks to heal, so even though they’re only in excruciating pain for about a week, they have to poop past the suture line, so they’ve got to avoid rock-hard stools.”
With an anoperineal abscess, first-line treatment is incision of the abscess as close as possible to the anus, followed by placement of a drain to be left in place for 7-10 days. Prophylactic antibiotics are reserved for immunosuppressed patients.
Patients need to understand up front that, 30%-50% of the time, a fistula can develop after drainage of an abscess. Indeed, abscessed anoperineal fistula is one of the most common conditions Dr. Cowan sees in the emergency department and clinic. The telltale symptoms are recurrent abscess and/or persistent drainage. Those patients need referral to a colorectal surgeon.
“Fistula-in-ano is a frustrating disease for the patient and the surgeon. As surgeons, we like to fix – and there’s really no good option,” according to Dr. Cowan.
Among the surgical treatment options are debridement followed by fibrin glue injection, an anal fistula plug, an endorectal flap closure, and ligation of the intersphincteric fistula tract, or LIFT, procedure.
Dr. Cowan reported serving as a consultant to Applied Medical.
ESTES PARK, COLO. – As a colorectal surgeon, Michelle Cowan, MD, sees a steady parade of primary care referrals for surgical evaluation of hemorrhoids.
The thing is, most of the time, the referred patients don’t have hemorrhoids. They have one of the other common anorectal disorders, including anal fissure, anoperineal abscess, fistula-in-ano, or an anorectal sexually transmitted infection, according to Dr. Cowan.
The diagnostic challenge stems from the fact that most common anorectal diseases – whether benign or malignant – present with the same constellation of symptoms: pain, bleeding, itching or burning, swelling, and leakage.
The quality and intensity of the pain “down under” provides a useful clue in differentiating the disorders.
“Hemorrhoids rarely cause legit pain,” said Dr. Cowan, who practices at the University of Colorado at Denver, Aurora. “Excruciating pain, where the patient will only sit on one side, that’s typically an abscess, a fissure, or an STI.”
The exceptions in the hemorrhoid realm are external thrombosed hemorrhoids, which are exceedingly painful but also readily identifiable, and incarcerated hemorrhoids, which are quite rare.
The pain associated with an anal fissure is distinct from that of an abscess or thrombosed hemorrhoid – it’s a throbbing pain lasting minutes to hours per episode.
“These are the people who won’t sit down in your office,” Dr. Cowan said.
Anal fissure is a common condition in young and middle-aged adults, and especially in peripartum women. The pathophysiology involves microtrauma, typically either because of passing rock-hard stools, diarrhea, or the rigors of childbirth, any of which can cause a break in the anal mucosa. That break causes the internal sphincter muscle to go into spasm, temporarily choking off the blood supply to the area of the fissure. Those wounds won’t heal on their own. Close to 90% of the fissures are located in the posterior midline; if the fissure is ectopic, it’s time to consider Crohn’s disease, HIV infection, tuberculosis, cancer, and other possibilities.
The patient with an anoperineal abscess presents with extreme pain, a sensation of fullness in the anus and rectum, erythema, fullness of the perineum, drainage, and sometimes fever.
“This is legit pain, like with a fissure or thrombosed hemorrhoids,” she explained. “Patients with any of these conditions can tell you exactly when they went from feeling normal to when the pain started.”
The abscess is caused by an infected anal gland. The location is most commonly perianal or ischioanal. If that’s not the suppuration site, the abscess is intersphincteric or supralevator, in which case a confirmatory CT scan is called for before proceeding with treatment.
Regardless of the suspected cause of a patient’s anorectal symptoms, any GI bleeding needs to be taken seriously. Young adults are the only segment of the population in whom the incidence of colorectal cancer is going up. In response, the American Society for Gastrointestinal Endoscopy and other groups now recommend colonoscopy for all patients older than age 40 years with GI bleeding, even if their family histories for colorectal cancer are negative and they lack other high-risk factors. For those younger than age 40 years, flexible sigmoidoscopy is recommended, even if it’s obvious that the patient has external thrombosed hemorrhoids that are bleeding.
“I tell people that I will not do hemorrhoid surgery until they have the scope,” Dr. Cowan said.
Office-based treatment of common anorectal disorders
Nonoperative treatment of anal fissures and internal hemorrhoids is all about encouraging patient adherence.
“Patient expectations are often overlooked,” according to the surgeon. “It’s rare that these patients actually need to go to surgery, but they oftentimes don’t do what we tell them to do, which is why they end up in my office.”
With anal fissure, the goal is to relax the spastic sphincter muscle, allowing the fissure to heal. That can be accomplished medically or surgically.
Medically, treatment consists of increased water intake, incorporation of more fiber in the diet, undertaking warm sitz baths a couple times a day, and application of a pea-sized amount of topical 2% diltiazem three times daily on the outside of the anus for 6-8 weeks.
“Compliance is huge. This whole thing is about consistency. Oftentimes, the reason treatment fails is people can’t do this. They feel good after about a week, so they stop before the fissure is completely healed,” she said.
The topical diltiazem must be prepared at a compounding pharmacy. It’s usually covered by insurance. Even if it’s not, an 8-week prescription costs only about $25. The drug is effective in up to 95% of patients who follow the instructions.
Topical 0.2% nitroglycerin, an alternative treatment, is less attractive because 30% of patients experience often-disabling headaches as a side effect. Topical diltiazem has a much better side effect profile, Dr. Cowan noted. If a patient shows a partial response to 6-8 weeks of topical diltiazem, it’s worth prescribing a second round. If the fissure still hasn’t healed after that, it’s time for referral to a surgeon. The options are onabotulinumtoxinA (Botox) and lateral internal sphincterotomy.
Botox is effective in 60%-80% of patients, she explained, providing temporary benefit lasting up to 3 months with a much lower risk of incontinence than with lateral internal sphincterotomy. Open and closed sphincterotomy techniques yield a similar success rate, with healing in 93% of cases.
For internal hemorrhoids, stool softeners, 25-30 g of fiber supplements per day, warm sitz baths, avoiding straining during defecation, and not loitering on the toilet are key elements in achieving symptomatic control nonoperatively.
Patients who don’t have a bathtub in which to take sitz baths can accomplish the same thing using an easily removable, commercially available device that fits over a toilet bowl.
Disposable baby wipes for adults have become the No. 1 cause of anal itching and are to be shunned by patients with internal hemorrhoids or other anorectal disorders.
“Patients often engage in excessive wiping because of the poor consistency of their bowel movements,” Dr. Cowan explained. “If they’re pasty and not coming out in one fell swoop, it leads to residue that patients appropriately feel they need to wipe multiple times to keep clean. The majority of these dipe wipes for adults are alcohol based, and even though on your exam you may see nothing, the dipe wipes cause microexcoriations of the skin. The patient itches and doesn’t know why.”
Primary care physicians can readily learn to do mucosal banding for grade II and III prolapsing hemorrhoids in the office, she noted. However, banding should never be attempted on external thrombosed hemorrhoids, though.
Surgical excisional hemorrhoidectomy is a lasting solution for such hemorrhoids, but patients need to understand that even though it’s only a 10- to 15-minute procedure performed in an outpatient setting, it’s excruciatingly painful for a week – and that’s not the end of the story.
“I tell patients to take a week off work,” the surgeon said. “And don’t sit on a donut; it pulls on the suture line. Pillows are okay. But it takes 6-8 weeks to heal, so even though they’re only in excruciating pain for about a week, they have to poop past the suture line, so they’ve got to avoid rock-hard stools.”
With an anoperineal abscess, first-line treatment is incision of the abscess as close as possible to the anus, followed by placement of a drain to be left in place for 7-10 days. Prophylactic antibiotics are reserved for immunosuppressed patients.
Patients need to understand up front that, 30%-50% of the time, a fistula can develop after drainage of an abscess. Indeed, abscessed anoperineal fistula is one of the most common conditions Dr. Cowan sees in the emergency department and clinic. The telltale symptoms are recurrent abscess and/or persistent drainage. Those patients need referral to a colorectal surgeon.
“Fistula-in-ano is a frustrating disease for the patient and the surgeon. As surgeons, we like to fix – and there’s really no good option,” according to Dr. Cowan.
Among the surgical treatment options are debridement followed by fibrin glue injection, an anal fistula plug, an endorectal flap closure, and ligation of the intersphincteric fistula tract, or LIFT, procedure.
Dr. Cowan reported serving as a consultant to Applied Medical.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM
Genital psoriasis is the worst: Patients sound off
GENEVA – The great majority of patients with genital psoriasis say their symptoms in the genital area are worse than elsewhere on the body, Kim A. Meeuwis, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
She presented a qualitative study in which 20 patients with longstanding genital psoriasis sounded off, sharing their perspectives on the disease in one-on-one, semistructured, face-to-face interviews.

Genital psoriasis is common. Epidemiologic studies show 30%-60% of psoriasis patients experience genital involvement at some point in the course of their disease. Yet patients seldom discuss their genital psoriasis with their physicians, and the patient perspective on how the experience of genital psoriasis differs from that of having psoriasis at other locations has been addressed only sparsely in the literature. This lack of attention was the impetus for the current study, she explained.
The 20 participants in the study had an average 18-year history of plaque psoriasis, with an average 7.5-year history of genital involvement. The genital psoriasis was rated moderate or severe in 70% of subjects at the time of the study.
The most commonly reported symptoms of genital psoriasis were itch and discomfort, each of which was cited by all study participants. This was followed by erythema, cited by 95%; stinging and burning, also cited by 95%; pain, cited by 85%; scaling, by 75%; and cracking, by 30%.
Of the patients in the study, 85% reported that their pain and/or discomfort were worse in the genital area than at other sites, and 10% said they were highly self-conscious about their genital psoriasis because others had misidentified them as having a sexually transmitted infection.
Since this was a qualitative study, Dr. Meeuwis provided representative quotes from several patients, including one who asserted, “I really only have discomfort on my psoriasis on the rest of my body ... in my genitals is the only place that actually has pain, or the itching is ... really, really bad.”
Dr. Meeuwis said the study results hold an important lesson for physicians who treat psoriasis: “Due to differences in patient experiences between genital and nongenital skin, it’s really important to make time for the specific evaluation of genital involvement in taking care of patients with psoriasis – and to be sure to ask about it.”
Dr. Meeuwis reported serving as a consultant to Eli Lilly, which sponsored the study, as well as being on an advisory board to Beiersdorf.
GENEVA – The great majority of patients with genital psoriasis say their symptoms in the genital area are worse than elsewhere on the body, Kim A. Meeuwis, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
She presented a qualitative study in which 20 patients with longstanding genital psoriasis sounded off, sharing their perspectives on the disease in one-on-one, semistructured, face-to-face interviews.
Genital psoriasis is common. Epidemiologic studies show 30%-60% of psoriasis patients experience genital involvement at some point in the course of their disease. Yet patients seldom discuss their genital psoriasis with their physicians, and the patient perspective on how the experience of genital psoriasis differs from that of having psoriasis at other locations has been addressed only sparsely in the literature. This lack of attention was the impetus for the current study, she explained.
The 20 participants in the study had an average 18-year history of plaque psoriasis, with an average 7.5-year history of genital involvement. The genital psoriasis was rated moderate or severe in 70% of subjects at the time of the study.
The most commonly reported symptoms of genital psoriasis were itch and discomfort, each of which was cited by all study participants. This was followed by erythema, cited by 95%; stinging and burning, also cited by 95%; pain, cited by 85%; scaling, by 75%; and cracking, by 30%.
Of the patients in the study, 85% reported that their pain and/or discomfort were worse in the genital area than at other sites, and 10% said they were highly self-conscious about their genital psoriasis because others had misidentified them as having a sexually transmitted infection.
Since this was a qualitative study, Dr. Meeuwis provided representative quotes from several patients, including one who asserted, “I really only have discomfort on my psoriasis on the rest of my body ... in my genitals is the only place that actually has pain, or the itching is ... really, really bad.”
Dr. Meeuwis said the study results hold an important lesson for physicians who treat psoriasis: “Due to differences in patient experiences between genital and nongenital skin, it’s really important to make time for the specific evaluation of genital involvement in taking care of patients with psoriasis – and to be sure to ask about it.”
Dr. Meeuwis reported serving as a consultant to Eli Lilly, which sponsored the study, as well as being on an advisory board to Beiersdorf.
GENEVA – The great majority of patients with genital psoriasis say their symptoms in the genital area are worse than elsewhere on the body, Kim A. Meeuwis, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
She presented a qualitative study in which 20 patients with longstanding genital psoriasis sounded off, sharing their perspectives on the disease in one-on-one, semistructured, face-to-face interviews.
Genital psoriasis is common. Epidemiologic studies show 30%-60% of psoriasis patients experience genital involvement at some point in the course of their disease. Yet patients seldom discuss their genital psoriasis with their physicians, and the patient perspective on how the experience of genital psoriasis differs from that of having psoriasis at other locations has been addressed only sparsely in the literature. This lack of attention was the impetus for the current study, she explained.
The 20 participants in the study had an average 18-year history of plaque psoriasis, with an average 7.5-year history of genital involvement. The genital psoriasis was rated moderate or severe in 70% of subjects at the time of the study.
The most commonly reported symptoms of genital psoriasis were itch and discomfort, each of which was cited by all study participants. This was followed by erythema, cited by 95%; stinging and burning, also cited by 95%; pain, cited by 85%; scaling, by 75%; and cracking, by 30%.
Of the patients in the study, 85% reported that their pain and/or discomfort were worse in the genital area than at other sites, and 10% said they were highly self-conscious about their genital psoriasis because others had misidentified them as having a sexually transmitted infection.
Since this was a qualitative study, Dr. Meeuwis provided representative quotes from several patients, including one who asserted, “I really only have discomfort on my psoriasis on the rest of my body ... in my genitals is the only place that actually has pain, or the itching is ... really, really bad.”
Dr. Meeuwis said the study results hold an important lesson for physicians who treat psoriasis: “Due to differences in patient experiences between genital and nongenital skin, it’s really important to make time for the specific evaluation of genital involvement in taking care of patients with psoriasis – and to be sure to ask about it.”
Dr. Meeuwis reported serving as a consultant to Eli Lilly, which sponsored the study, as well as being on an advisory board to Beiersdorf.
AT THE EADV CONGRESS
Key clinical point:
Major finding: Of the participants in a study of genital psoriasis, 100% reported that a hallmark of their genital disease was itching and discomfort.
Data source: A qualitative study that involved one-on-one interviews with 20 patients with genital psoriasis, who shared their experiences as to how genital involvement differs from their psoriasis elsewhere.
Disclosures: The study was sponsored by Eli Lilly. The presenter reported serving as a consultant to the company.
Ixekizumab has profound impact on genital psoriasis
GENEVA – The interleukin-17A inhibitor ixekizumab provided rapid clearance of genital psoriasis in a phase 3b clinical trial, with significant improvement seen as early as week 1, Caitriona Ryan, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The highly targeted monoclonal antibody also improved the intense itching that’s a particularly prominent feature of genital psoriasis.

“Genital psoriasis is a hidden part of psoriasis. Unfortunately, as dermatologists we do a bad job of evaluating our patients for it. They are ashamed and embarrassed to bring up the topic with their dermatologists. Hopefully, this study will create some awareness around the topic,” she said.
This was the first-ever randomized trial to evaluate the effect of a biologic agent specifically on genital psoriasis. It was also the first study of a biologic in psoriasis patients with less than 10% body surface area involved.
“That’s a very important thing,” according to the dermatologist. “There are lots of patients with genital psoriasis who have less than 10% body surface area involved and therefore don’t qualify for biologic therapy, even though their genital psoriasis can be incredibly debilitating.”
The 12-week, multicenter, double-blind trial included 149 patients with a baseline static Physician’s Global Assessment of Genitalia (sPGA-G) score of at least 3 on a 0-5 scale. All participants had failed to respond to at least one topical therapy for their genital psoriasis, such as a corticosteroid, a calcineurin inhibitor, or a vitamin D analog. The subjects averaged a 16-year history of psoriasis and a 9-year history of genital psoriasis. Thirty-eight percent of participants had an involved body surface area of at least 1% but less than 10%.
Patients were randomized to ixekizumab (Taltz) given in the usual way – a subcutaneous loading dose of 160 mg, followed by repeat 80-mg injections every 2 weeks – or placebo.
The primary study endpoint was achievement of an sPGA-G score of 0 or 1, meaning clear or almost clear, as assessed by blinded investigators. At the 12-week mark, the rate was 73% in the ixekizumab group and 8% in controls. The sPGA-G score already differed significantly between the two study arms at the first assessment, after 1 week. The treatment success rate was closely similar in patients with or without at least 10% total body surface area involved.
A key secondary endpoint concerned sexual health. Among patients who at baseline indicated that in the past week, their genital psoriasis “sometimes,” “often,” or “always” limited the frequency of their sexual activity, at week 12, 78% of those in the ixekizumab group answered the same question on the Sexual Frequency Questionnaire “never” or “rarely,” compared with 21% of controls.
“This is huge. It’s such an important part of our patients’ lives, and there was a big difference by week 1,” Dr. Ryan noted.
On another secondary endpoint, 60% of the ixekizumab group reported at least a 3-point improvement in the 0-10 Genital Itch Numeric Rating Scale at week 12, compared with 8% of controls, with a statistically significant difference apparent at week 2.
“Itch is the most frequently reported symptom in our patients with genital psoriasis, and it seems to be much more impactful than itch from psoriasis elsewhere,” Dr. Ryan commented.
The side effect profile of ixekizumab was the same as has been seen in larger, longer-term studies. There were no serious ixekizumab-related adverse events, and no cases of candidiasis.
The study was sponsored by Eli Lilly. Dr. Ryan reported serving as an advisory board member to and/or receiving honoraria from that company and more than half a dozen other pharmaceutical companies.
GENEVA – The interleukin-17A inhibitor ixekizumab provided rapid clearance of genital psoriasis in a phase 3b clinical trial, with significant improvement seen as early as week 1, Caitriona Ryan, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The highly targeted monoclonal antibody also improved the intense itching that’s a particularly prominent feature of genital psoriasis.
“Genital psoriasis is a hidden part of psoriasis. Unfortunately, as dermatologists we do a bad job of evaluating our patients for it. They are ashamed and embarrassed to bring up the topic with their dermatologists. Hopefully, this study will create some awareness around the topic,” she said.
This was the first-ever randomized trial to evaluate the effect of a biologic agent specifically on genital psoriasis. It was also the first study of a biologic in psoriasis patients with less than 10% body surface area involved.
“That’s a very important thing,” according to the dermatologist. “There are lots of patients with genital psoriasis who have less than 10% body surface area involved and therefore don’t qualify for biologic therapy, even though their genital psoriasis can be incredibly debilitating.”
The 12-week, multicenter, double-blind trial included 149 patients with a baseline static Physician’s Global Assessment of Genitalia (sPGA-G) score of at least 3 on a 0-5 scale. All participants had failed to respond to at least one topical therapy for their genital psoriasis, such as a corticosteroid, a calcineurin inhibitor, or a vitamin D analog. The subjects averaged a 16-year history of psoriasis and a 9-year history of genital psoriasis. Thirty-eight percent of participants had an involved body surface area of at least 1% but less than 10%.
Patients were randomized to ixekizumab (Taltz) given in the usual way – a subcutaneous loading dose of 160 mg, followed by repeat 80-mg injections every 2 weeks – or placebo.
The primary study endpoint was achievement of an sPGA-G score of 0 or 1, meaning clear or almost clear, as assessed by blinded investigators. At the 12-week mark, the rate was 73% in the ixekizumab group and 8% in controls. The sPGA-G score already differed significantly between the two study arms at the first assessment, after 1 week. The treatment success rate was closely similar in patients with or without at least 10% total body surface area involved.
A key secondary endpoint concerned sexual health. Among patients who at baseline indicated that in the past week, their genital psoriasis “sometimes,” “often,” or “always” limited the frequency of their sexual activity, at week 12, 78% of those in the ixekizumab group answered the same question on the Sexual Frequency Questionnaire “never” or “rarely,” compared with 21% of controls.
“This is huge. It’s such an important part of our patients’ lives, and there was a big difference by week 1,” Dr. Ryan noted.
On another secondary endpoint, 60% of the ixekizumab group reported at least a 3-point improvement in the 0-10 Genital Itch Numeric Rating Scale at week 12, compared with 8% of controls, with a statistically significant difference apparent at week 2.
“Itch is the most frequently reported symptom in our patients with genital psoriasis, and it seems to be much more impactful than itch from psoriasis elsewhere,” Dr. Ryan commented.
The side effect profile of ixekizumab was the same as has been seen in larger, longer-term studies. There were no serious ixekizumab-related adverse events, and no cases of candidiasis.
The study was sponsored by Eli Lilly. Dr. Ryan reported serving as an advisory board member to and/or receiving honoraria from that company and more than half a dozen other pharmaceutical companies.
GENEVA – The interleukin-17A inhibitor ixekizumab provided rapid clearance of genital psoriasis in a phase 3b clinical trial, with significant improvement seen as early as week 1, Caitriona Ryan, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The highly targeted monoclonal antibody also improved the intense itching that’s a particularly prominent feature of genital psoriasis.
“Genital psoriasis is a hidden part of psoriasis. Unfortunately, as dermatologists we do a bad job of evaluating our patients for it. They are ashamed and embarrassed to bring up the topic with their dermatologists. Hopefully, this study will create some awareness around the topic,” she said.
This was the first-ever randomized trial to evaluate the effect of a biologic agent specifically on genital psoriasis. It was also the first study of a biologic in psoriasis patients with less than 10% body surface area involved.
“That’s a very important thing,” according to the dermatologist. “There are lots of patients with genital psoriasis who have less than 10% body surface area involved and therefore don’t qualify for biologic therapy, even though their genital psoriasis can be incredibly debilitating.”
The 12-week, multicenter, double-blind trial included 149 patients with a baseline static Physician’s Global Assessment of Genitalia (sPGA-G) score of at least 3 on a 0-5 scale. All participants had failed to respond to at least one topical therapy for their genital psoriasis, such as a corticosteroid, a calcineurin inhibitor, or a vitamin D analog. The subjects averaged a 16-year history of psoriasis and a 9-year history of genital psoriasis. Thirty-eight percent of participants had an involved body surface area of at least 1% but less than 10%.
Patients were randomized to ixekizumab (Taltz) given in the usual way – a subcutaneous loading dose of 160 mg, followed by repeat 80-mg injections every 2 weeks – or placebo.
The primary study endpoint was achievement of an sPGA-G score of 0 or 1, meaning clear or almost clear, as assessed by blinded investigators. At the 12-week mark, the rate was 73% in the ixekizumab group and 8% in controls. The sPGA-G score already differed significantly between the two study arms at the first assessment, after 1 week. The treatment success rate was closely similar in patients with or without at least 10% total body surface area involved.
A key secondary endpoint concerned sexual health. Among patients who at baseline indicated that in the past week, their genital psoriasis “sometimes,” “often,” or “always” limited the frequency of their sexual activity, at week 12, 78% of those in the ixekizumab group answered the same question on the Sexual Frequency Questionnaire “never” or “rarely,” compared with 21% of controls.
“This is huge. It’s such an important part of our patients’ lives, and there was a big difference by week 1,” Dr. Ryan noted.
On another secondary endpoint, 60% of the ixekizumab group reported at least a 3-point improvement in the 0-10 Genital Itch Numeric Rating Scale at week 12, compared with 8% of controls, with a statistically significant difference apparent at week 2.
“Itch is the most frequently reported symptom in our patients with genital psoriasis, and it seems to be much more impactful than itch from psoriasis elsewhere,” Dr. Ryan commented.
The side effect profile of ixekizumab was the same as has been seen in larger, longer-term studies. There were no serious ixekizumab-related adverse events, and no cases of candidiasis.
The study was sponsored by Eli Lilly. Dr. Ryan reported serving as an advisory board member to and/or receiving honoraria from that company and more than half a dozen other pharmaceutical companies.
AT THE EADV CONGRESS
Key clinical point: First-ever trial of a biologic agent in genital psoriasis shows heartening results.
Major finding: 73% of patients with moderate to severe genital psoriasis were clear or almost clear of their genital disease after 12 weeks of ixekizumab, vs. 8% of controls.
Data source: This was a randomized, double-blind, placebo-controlled, multicenter, 12-week clinical trial in 149 patients with moderate to severe genital psoriasis.
Disclosures: The study was sponsored by Eli Lilly. The presenter reported serving as an advisory board member to and/or receiving honoraria from that company and more than half a dozen other pharmaceutical companies.
Physical inactivity in youth is an independent risk factor for schizophrenia
PARIS – Low physical activity in childhood and adolescence was independently associated with later development of schizophrenia and other nonaffective psychotic disorders in the large, prospective, population-based Cardiovascular Risk in Young Finns cohort study, Jarmo Hietala, MD, PhD, reported at the annual congress of the European College of Neuropsychopharmacology.
The key question now: Is this risk factor remediable? That is, will a pediatric exercise intervention that results in improved physical fitness also reduce the risk of later nonaffective psychosis? Given that there are really no downsides to physical activity, the Finnish data make a strong case for including exercise and physical activity interventions in investigational psychosis prevention programs targeting high-risk youth, according to Dr. Hietala, professor of psychiatry at the University of Turku (Finland).

Dr. Hietala and his coinvestigators tapped into comprehensive national registries in order to identify all study participants with a psychiatric diagnosis of sufficient severity to have resulted in hospitalization up to 2012. Forty-one patients were hospitalized for schizophrenia spectrum disorders, 47 for other forms of nonaffective psychosis, 43 for personality disorders, 111 for affective disorders, and 49 with alcohol and other substance use disorders.
In a multivariate analysis adjusted for sex, age, body mass index, birth weight, non-preterm birth, and maternal mental disorders, each 1-point decrement in the pediatric physical activity index was associated with a 26% increase in the risk of developing any nonaffective psychosis and, more specifically, a 43% increased risk of schizophrenia.
Moreover, nonparticipation in organized sports competitions was independently associated with a 2.58-fold increased risk of any nonaffective psychosis and a 4.88-fold increased risk of schizophrenia. And social isolation as reflected in spending less time in common activities with friends during leisure time was associated with a 71% increased risk of nonaffective psychosis and a 76% increased risk of schizophrenia.
Of note, schizophrenia was the only psychiatric disorder associated with low physical activity in childhood and adolescence. Sedentary youths were not at increased risk of later hospitalization for affective disorders or other forms of mental illness.
“Our results have relevance for preemptive psychiatry and provide rationale for including exercise in early interventions for psychosis,” the psychiatrist said.
Current programs aimed at preventing schizophrenia in youth at high risk because of family history typically emphasize avoidance of street drugs, the importance of seeking out constructive social interactions, stress reduction techniques, and cognitive-behavioral therapy aimed at promoting a positive world view.
Formal evaluation of physical activity as part of a preventive approach has a sound theoretic basis, according to Dr. Hietala. He cited an influential essay called “Rethinking Schizophrenia” by the then-director of the National Institute of Mental Health, Thomas R. Insel, MD. In that article, Dr. Insel highlights the past half-century of largely unsatisfactory results with pharmacotherapy and goes on to make the case for considering schizophrenia as a neurodevelopmental disorder in which, he argues, “psychosis is a late, potentially preventable stage of the illness” (Nature. 2010 Nov 11;468[7321]:187-93).
This view of schizophrenia as a neurodevelopmental disorder has quickly come to dominate thinking within the field. Dr. Hietala noted that the schizophrenia spectrum chapter in the DSM-5 includes a greater focus on abnormal behavior and catatonia as a core domain alongside classic features, such as delusions, hallucinations, negative symptoms, and disorganized speech.
“My view of schizophrenia is that the psychotic symptoms are a secondary phenomenon, a complication of the disease that has been going on for a while. It’s a pity that we focus so much on the psychotic symptoms rather than the cognitive or negative or affective symptoms,” he said.
The hope is that a long-term physical activity intervention in at-risk youth will stimulate neurodevelopmental catch-up, thereby thwarting their predisposition to schizophrenia.
“Human development is not a linear process; it happens in spurts of rapid growth followed by consolidation periods,” Dr. Hietala said.
However, even if it turns out that an early physical activity intervention does not reduce the risk of developing schizophrenia, it might favorably alter its course in important ways, according to Dr. Hietala.
Individuals with schizophrenia are known to be at increased risk for metabolic syndrome and premature death tied to cardiovascular disease. A recent meta-analysis of 16 prospective cohort studies totaling more than 1 million men and women found that mortality during follow-up was 59% greater in those who sat for more than 8 hours per day and were in the lowest quartile of physical activity, compared with those sitting for less than 4 hours per day who were in the top quartile of physical activity, at more than 35.5 metabolic equivalent hours per week.
But there was no increased risk of mortality among those who sat for more than 8 hours per day and were also in the highest quartile of physical activity. The implication is that high levels of moderate-intensity physical activity eliminates the increased risk of death associated with high sitting time (Lancet. 2016 Sep 24;388[10051]:1302-10). That’s a finding that could be applicable to patients with schizophrenia.
Dr. Hietala reported having no financial conflicts regarding the Cardiovascular Risk in Young Finns study, which is supported by the Academy of Finland, the Social Insurance Institution of Finland, and grants from nonprofit foundations.
PARIS – Low physical activity in childhood and adolescence was independently associated with later development of schizophrenia and other nonaffective psychotic disorders in the large, prospective, population-based Cardiovascular Risk in Young Finns cohort study, Jarmo Hietala, MD, PhD, reported at the annual congress of the European College of Neuropsychopharmacology.
The key question now: Is this risk factor remediable? That is, will a pediatric exercise intervention that results in improved physical fitness also reduce the risk of later nonaffective psychosis? Given that there are really no downsides to physical activity, the Finnish data make a strong case for including exercise and physical activity interventions in investigational psychosis prevention programs targeting high-risk youth, according to Dr. Hietala, professor of psychiatry at the University of Turku (Finland).
Dr. Hietala and his coinvestigators tapped into comprehensive national registries in order to identify all study participants with a psychiatric diagnosis of sufficient severity to have resulted in hospitalization up to 2012. Forty-one patients were hospitalized for schizophrenia spectrum disorders, 47 for other forms of nonaffective psychosis, 43 for personality disorders, 111 for affective disorders, and 49 with alcohol and other substance use disorders.
In a multivariate analysis adjusted for sex, age, body mass index, birth weight, non-preterm birth, and maternal mental disorders, each 1-point decrement in the pediatric physical activity index was associated with a 26% increase in the risk of developing any nonaffective psychosis and, more specifically, a 43% increased risk of schizophrenia.
Moreover, nonparticipation in organized sports competitions was independently associated with a 2.58-fold increased risk of any nonaffective psychosis and a 4.88-fold increased risk of schizophrenia. And social isolation as reflected in spending less time in common activities with friends during leisure time was associated with a 71% increased risk of nonaffective psychosis and a 76% increased risk of schizophrenia.
Of note, schizophrenia was the only psychiatric disorder associated with low physical activity in childhood and adolescence. Sedentary youths were not at increased risk of later hospitalization for affective disorders or other forms of mental illness.
“Our results have relevance for preemptive psychiatry and provide rationale for including exercise in early interventions for psychosis,” the psychiatrist said.
Current programs aimed at preventing schizophrenia in youth at high risk because of family history typically emphasize avoidance of street drugs, the importance of seeking out constructive social interactions, stress reduction techniques, and cognitive-behavioral therapy aimed at promoting a positive world view.
Formal evaluation of physical activity as part of a preventive approach has a sound theoretic basis, according to Dr. Hietala. He cited an influential essay called “Rethinking Schizophrenia” by the then-director of the National Institute of Mental Health, Thomas R. Insel, MD. In that article, Dr. Insel highlights the past half-century of largely unsatisfactory results with pharmacotherapy and goes on to make the case for considering schizophrenia as a neurodevelopmental disorder in which, he argues, “psychosis is a late, potentially preventable stage of the illness” (Nature. 2010 Nov 11;468[7321]:187-93).
This view of schizophrenia as a neurodevelopmental disorder has quickly come to dominate thinking within the field. Dr. Hietala noted that the schizophrenia spectrum chapter in the DSM-5 includes a greater focus on abnormal behavior and catatonia as a core domain alongside classic features, such as delusions, hallucinations, negative symptoms, and disorganized speech.
“My view of schizophrenia is that the psychotic symptoms are a secondary phenomenon, a complication of the disease that has been going on for a while. It’s a pity that we focus so much on the psychotic symptoms rather than the cognitive or negative or affective symptoms,” he said.
The hope is that a long-term physical activity intervention in at-risk youth will stimulate neurodevelopmental catch-up, thereby thwarting their predisposition to schizophrenia.
“Human development is not a linear process; it happens in spurts of rapid growth followed by consolidation periods,” Dr. Hietala said.
However, even if it turns out that an early physical activity intervention does not reduce the risk of developing schizophrenia, it might favorably alter its course in important ways, according to Dr. Hietala.
Individuals with schizophrenia are known to be at increased risk for metabolic syndrome and premature death tied to cardiovascular disease. A recent meta-analysis of 16 prospective cohort studies totaling more than 1 million men and women found that mortality during follow-up was 59% greater in those who sat for more than 8 hours per day and were in the lowest quartile of physical activity, compared with those sitting for less than 4 hours per day who were in the top quartile of physical activity, at more than 35.5 metabolic equivalent hours per week.
But there was no increased risk of mortality among those who sat for more than 8 hours per day and were also in the highest quartile of physical activity. The implication is that high levels of moderate-intensity physical activity eliminates the increased risk of death associated with high sitting time (Lancet. 2016 Sep 24;388[10051]:1302-10). That’s a finding that could be applicable to patients with schizophrenia.
Dr. Hietala reported having no financial conflicts regarding the Cardiovascular Risk in Young Finns study, which is supported by the Academy of Finland, the Social Insurance Institution of Finland, and grants from nonprofit foundations.
PARIS – Low physical activity in childhood and adolescence was independently associated with later development of schizophrenia and other nonaffective psychotic disorders in the large, prospective, population-based Cardiovascular Risk in Young Finns cohort study, Jarmo Hietala, MD, PhD, reported at the annual congress of the European College of Neuropsychopharmacology.
The key question now: Is this risk factor remediable? That is, will a pediatric exercise intervention that results in improved physical fitness also reduce the risk of later nonaffective psychosis? Given that there are really no downsides to physical activity, the Finnish data make a strong case for including exercise and physical activity interventions in investigational psychosis prevention programs targeting high-risk youth, according to Dr. Hietala, professor of psychiatry at the University of Turku (Finland).
Dr. Hietala and his coinvestigators tapped into comprehensive national registries in order to identify all study participants with a psychiatric diagnosis of sufficient severity to have resulted in hospitalization up to 2012. Forty-one patients were hospitalized for schizophrenia spectrum disorders, 47 for other forms of nonaffective psychosis, 43 for personality disorders, 111 for affective disorders, and 49 with alcohol and other substance use disorders.
In a multivariate analysis adjusted for sex, age, body mass index, birth weight, non-preterm birth, and maternal mental disorders, each 1-point decrement in the pediatric physical activity index was associated with a 26% increase in the risk of developing any nonaffective psychosis and, more specifically, a 43% increased risk of schizophrenia.
Moreover, nonparticipation in organized sports competitions was independently associated with a 2.58-fold increased risk of any nonaffective psychosis and a 4.88-fold increased risk of schizophrenia. And social isolation as reflected in spending less time in common activities with friends during leisure time was associated with a 71% increased risk of nonaffective psychosis and a 76% increased risk of schizophrenia.
Of note, schizophrenia was the only psychiatric disorder associated with low physical activity in childhood and adolescence. Sedentary youths were not at increased risk of later hospitalization for affective disorders or other forms of mental illness.
“Our results have relevance for preemptive psychiatry and provide rationale for including exercise in early interventions for psychosis,” the psychiatrist said.
Current programs aimed at preventing schizophrenia in youth at high risk because of family history typically emphasize avoidance of street drugs, the importance of seeking out constructive social interactions, stress reduction techniques, and cognitive-behavioral therapy aimed at promoting a positive world view.
Formal evaluation of physical activity as part of a preventive approach has a sound theoretic basis, according to Dr. Hietala. He cited an influential essay called “Rethinking Schizophrenia” by the then-director of the National Institute of Mental Health, Thomas R. Insel, MD. In that article, Dr. Insel highlights the past half-century of largely unsatisfactory results with pharmacotherapy and goes on to make the case for considering schizophrenia as a neurodevelopmental disorder in which, he argues, “psychosis is a late, potentially preventable stage of the illness” (Nature. 2010 Nov 11;468[7321]:187-93).
This view of schizophrenia as a neurodevelopmental disorder has quickly come to dominate thinking within the field. Dr. Hietala noted that the schizophrenia spectrum chapter in the DSM-5 includes a greater focus on abnormal behavior and catatonia as a core domain alongside classic features, such as delusions, hallucinations, negative symptoms, and disorganized speech.
“My view of schizophrenia is that the psychotic symptoms are a secondary phenomenon, a complication of the disease that has been going on for a while. It’s a pity that we focus so much on the psychotic symptoms rather than the cognitive or negative or affective symptoms,” he said.
The hope is that a long-term physical activity intervention in at-risk youth will stimulate neurodevelopmental catch-up, thereby thwarting their predisposition to schizophrenia.
“Human development is not a linear process; it happens in spurts of rapid growth followed by consolidation periods,” Dr. Hietala said.
However, even if it turns out that an early physical activity intervention does not reduce the risk of developing schizophrenia, it might favorably alter its course in important ways, according to Dr. Hietala.
Individuals with schizophrenia are known to be at increased risk for metabolic syndrome and premature death tied to cardiovascular disease. A recent meta-analysis of 16 prospective cohort studies totaling more than 1 million men and women found that mortality during follow-up was 59% greater in those who sat for more than 8 hours per day and were in the lowest quartile of physical activity, compared with those sitting for less than 4 hours per day who were in the top quartile of physical activity, at more than 35.5 metabolic equivalent hours per week.
But there was no increased risk of mortality among those who sat for more than 8 hours per day and were also in the highest quartile of physical activity. The implication is that high levels of moderate-intensity physical activity eliminates the increased risk of death associated with high sitting time (Lancet. 2016 Sep 24;388[10051]:1302-10). That’s a finding that could be applicable to patients with schizophrenia.
Dr. Hietala reported having no financial conflicts regarding the Cardiovascular Risk in Young Finns study, which is supported by the Academy of Finland, the Social Insurance Institution of Finland, and grants from nonprofit foundations.
AT THE ECNP CONGRESS
Key clinical point:
Major finding: Each 1-point decrement on a physical activity score recorded during childhood and adolescence was independently associated with a 43% increased risk of later development of schizophrenia.
Data source: The Cardiovascular Risk in Young Finns study is an ongoing prospective, population-based study of nearly 3,600 Finns who were aged 3-18 years old when the study began in 1980.
Disclosures: The presenter reported having no financial conflicts regarding the study, which is supported by the Academy of Finland, the Social Insurance Institution of Finland, and grants from nonprofit foundations.
Hyperlipidemia diagnosis protects against breast cancer
BARCELONA – Women diagnosed with hyperlipidemia had a strikingly reduced risk of subsequently developing breast cancer in a big-data, case-control study, Paul R. Carter, MD, reported at the annual congress of the European Society of Cardiology.
Moreover, those baseline hyperlipidemic women who later got breast cancer had a 40% lower risk of all-cause mortality than did matched nonhyperlipidemic controls diagnosed with the malignancy during follow-up, according to Dr. Carter, a cardiology fellow at Cambridge (England) University.
The inference isn’t that hyperlipidemia somehow protects against the most common type of cancer in women. Indeed, preclinical evidence indicates high cholesterol drives several key steps in carcinogenesis. Rather, the strong implication is that the explanation for the observed preventive effect lies in the pleotropic effects of the statin therapy routinely prescribed in accordance with guidelines once women received the diagnosis of hyperlipidemia, he continued.
“The results of this study provide the strongest justification to date for a clinical trial evaluating the protective effect of statins in patients with breast cancer, and this is what we intend to do,” according to Dr. Carter.
He presented a retrospective longitudinal study of the Algorithm for Comorbidities, Associations, Length of Stay and Mortality database, comprising more than 1.2 million patients admitted for various reasons to selected hospitals in northern England during 2000-2014. This big-data study entailed recruitment of 16,043 women aged 40 years and older who were diagnosed with hyperlipidemia during their hospital stay along with an equal number of age-matched women with normal lipid levels. None of the participants had a breast cancer diagnosis at baseline.

The all-cause mortality rate in baseline hyperlipidemic women who later developed breast cancer was 27.4%, significantly lower than the 37.4% rate in normolipidemic women with breast cancer. This translated into an adjusted 40% relative risk reduction.
All-cause mortality occurred during follow-up in 13.7% of breast cancer–free women with baseline hyperlipidemia, compared with 23.6% of nonhyperlipidemic controls without breast cancer.
In an analysis adjusted for age, ethnicity, and the top-10 causes of death in the U.K., women with baseline hyperlipidemia were 40% less likely to die during follow-up than were women without high cholesterol.
Dr. Carter reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
BARCELONA – Women diagnosed with hyperlipidemia had a strikingly reduced risk of subsequently developing breast cancer in a big-data, case-control study, Paul R. Carter, MD, reported at the annual congress of the European Society of Cardiology.
Moreover, those baseline hyperlipidemic women who later got breast cancer had a 40% lower risk of all-cause mortality than did matched nonhyperlipidemic controls diagnosed with the malignancy during follow-up, according to Dr. Carter, a cardiology fellow at Cambridge (England) University.
The inference isn’t that hyperlipidemia somehow protects against the most common type of cancer in women. Indeed, preclinical evidence indicates high cholesterol drives several key steps in carcinogenesis. Rather, the strong implication is that the explanation for the observed preventive effect lies in the pleotropic effects of the statin therapy routinely prescribed in accordance with guidelines once women received the diagnosis of hyperlipidemia, he continued.
“The results of this study provide the strongest justification to date for a clinical trial evaluating the protective effect of statins in patients with breast cancer, and this is what we intend to do,” according to Dr. Carter.
He presented a retrospective longitudinal study of the Algorithm for Comorbidities, Associations, Length of Stay and Mortality database, comprising more than 1.2 million patients admitted for various reasons to selected hospitals in northern England during 2000-2014. This big-data study entailed recruitment of 16,043 women aged 40 years and older who were diagnosed with hyperlipidemia during their hospital stay along with an equal number of age-matched women with normal lipid levels. None of the participants had a breast cancer diagnosis at baseline.
The all-cause mortality rate in baseline hyperlipidemic women who later developed breast cancer was 27.4%, significantly lower than the 37.4% rate in normolipidemic women with breast cancer. This translated into an adjusted 40% relative risk reduction.
All-cause mortality occurred during follow-up in 13.7% of breast cancer–free women with baseline hyperlipidemia, compared with 23.6% of nonhyperlipidemic controls without breast cancer.
In an analysis adjusted for age, ethnicity, and the top-10 causes of death in the U.K., women with baseline hyperlipidemia were 40% less likely to die during follow-up than were women without high cholesterol.
Dr. Carter reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
BARCELONA – Women diagnosed with hyperlipidemia had a strikingly reduced risk of subsequently developing breast cancer in a big-data, case-control study, Paul R. Carter, MD, reported at the annual congress of the European Society of Cardiology.
Moreover, those baseline hyperlipidemic women who later got breast cancer had a 40% lower risk of all-cause mortality than did matched nonhyperlipidemic controls diagnosed with the malignancy during follow-up, according to Dr. Carter, a cardiology fellow at Cambridge (England) University.
The inference isn’t that hyperlipidemia somehow protects against the most common type of cancer in women. Indeed, preclinical evidence indicates high cholesterol drives several key steps in carcinogenesis. Rather, the strong implication is that the explanation for the observed preventive effect lies in the pleotropic effects of the statin therapy routinely prescribed in accordance with guidelines once women received the diagnosis of hyperlipidemia, he continued.
“The results of this study provide the strongest justification to date for a clinical trial evaluating the protective effect of statins in patients with breast cancer, and this is what we intend to do,” according to Dr. Carter.
He presented a retrospective longitudinal study of the Algorithm for Comorbidities, Associations, Length of Stay and Mortality database, comprising more than 1.2 million patients admitted for various reasons to selected hospitals in northern England during 2000-2014. This big-data study entailed recruitment of 16,043 women aged 40 years and older who were diagnosed with hyperlipidemia during their hospital stay along with an equal number of age-matched women with normal lipid levels. None of the participants had a breast cancer diagnosis at baseline.
The all-cause mortality rate in baseline hyperlipidemic women who later developed breast cancer was 27.4%, significantly lower than the 37.4% rate in normolipidemic women with breast cancer. This translated into an adjusted 40% relative risk reduction.
All-cause mortality occurred during follow-up in 13.7% of breast cancer–free women with baseline hyperlipidemia, compared with 23.6% of nonhyperlipidemic controls without breast cancer.
In an analysis adjusted for age, ethnicity, and the top-10 causes of death in the U.K., women with baseline hyperlipidemia were 40% less likely to die during follow-up than were women without high cholesterol.
Dr. Carter reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
AT THE ESC CONGRESS 2017
Key clinical point:
Major finding: The risk of subsequent development of breast cancer was one-third lower in women diagnosed with hyperlipidemia than in controls with normal lipid levels.
Data source: A retrospective longitudinal case-control study of 16,043 U.K. women aged 40 years or older when diagnosed with hyperlipidemia and an equal number of age-matched women with normal lipids.
Disclosures: The presenter reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.

Avoid sildenafil for pulmonary hypertension after corrected valvular disease
BARCELONA – Off-label use of the phosphodiesterase-5 inhibitor sildenafil to treat residual pulmonary hypertension after successful correction of valvular heart disease is not merely ineffective, it’s counterproductive, according to the results of the randomized, placebo-controlled SIOVAC study.
“We believe based upon our results that off-label use of sildenafil in patients with left heart disease-pulmonary hypertension due to valvular disease should be discouraged,” Javier Bermejo, MD, declared at the annual congress of the European Society of Cardiology.

Sildenafil is approved with a solid, evidence-based indication for treating some other types of pulmonary hypertension. Many cardiologists also prescribe the drug off label for residual pulmonary hypertension in patients with corrected valve disease, hoping that it will be of benefit, since there is currently no approved treatment for this common and serious condition associated with increased mortality. But because the anecdotal literature on sildenafil for this specific type of pulmonary hypertension is mixed, Dr. Bermejo and his coinvestigators in the Spanish Network Center for Cardiovascular Research decided to conduct a multicenter randomized trial.
SIOVAC (Sildenafil for Improving Clinical Outcomes After Valvular Correction) comprised 200 patients with residual pulmonary hypertension after corrected valvular heart disease at 17 Spanish general hospitals. The patients were randomized to receive sildenafil at 40 mg t.i.d. or placebo for 6 months in this double-blind trial.
The primary endpoint was a standardized composite clinical score widely used in heart failure trials. It consists of all-cause mortality, hospital admission for heart failure, worsening exercise tolerance, and deterioration in a global self-assessment rating.
The shocker for the investigators – who had expected a positive study – was that 33% of patients in the sildenafil group worsened significantly on the composite clinical score at 6 months, compared with 14% of placebo-treated controls, said Dr. Bermejo, a cardiologist at Gregorio Marañón University Hospital in Madrid.
Moreover, only 27% of the sildenafil group improved, compared with 44% of controls. About one-third of patients in both groups remained unchanged over the course of the 6-month trial.
Dr. Bermejo noted that valvular disease is considered the next cardiac epidemic because of its strong association with advancing age and the rapid aging of the population worldwide. Pulmonary hypertension occurs is virtually all patients with severe mitral disease and in up to two-thirds of those with asymptomatic aortic stenosis. Regression of the pulmonary hypertension is often incomplete after successful surgical or transcatheter correction of the valvular lesion.
Discussant Irene M. Lang, MD, called SIOVAC “a very clear study.” It convincingly establishes that sildenafil – a vasodilator – is ineffective for the treatment of what the current ESC/European Respiratory Society guidelines on pulmonary hypertension call isolated post-capillary pulmonary hypertension, a condition defined hemodynamically by a diastolic pulmonary vascular pressure gradient of less than 7 mm Hg and/or a pulmonary vascular resistance below 3 Wood units (Eur Heart J. 2016 Jan 1;37[1]:67-119.)
The SIOVAC findings underscore the strong IIIC recommendation in the European guidelines that the use of approved therapies for pulmonary arterial hypertension is not recommended in patients with left heart disease-pulmonary hypertension, added Dr. Lang, a coauthor of the guidelines and professor of vascular biology at the Medical University of Vienna.
The Spanish government funded SIOVAC. Dr. Bermejo reported having no financial conflicts of interest.
BARCELONA – Off-label use of the phosphodiesterase-5 inhibitor sildenafil to treat residual pulmonary hypertension after successful correction of valvular heart disease is not merely ineffective, it’s counterproductive, according to the results of the randomized, placebo-controlled SIOVAC study.
“We believe based upon our results that off-label use of sildenafil in patients with left heart disease-pulmonary hypertension due to valvular disease should be discouraged,” Javier Bermejo, MD, declared at the annual congress of the European Society of Cardiology.
Sildenafil is approved with a solid, evidence-based indication for treating some other types of pulmonary hypertension. Many cardiologists also prescribe the drug off label for residual pulmonary hypertension in patients with corrected valve disease, hoping that it will be of benefit, since there is currently no approved treatment for this common and serious condition associated with increased mortality. But because the anecdotal literature on sildenafil for this specific type of pulmonary hypertension is mixed, Dr. Bermejo and his coinvestigators in the Spanish Network Center for Cardiovascular Research decided to conduct a multicenter randomized trial.
SIOVAC (Sildenafil for Improving Clinical Outcomes After Valvular Correction) comprised 200 patients with residual pulmonary hypertension after corrected valvular heart disease at 17 Spanish general hospitals. The patients were randomized to receive sildenafil at 40 mg t.i.d. or placebo for 6 months in this double-blind trial.
The primary endpoint was a standardized composite clinical score widely used in heart failure trials. It consists of all-cause mortality, hospital admission for heart failure, worsening exercise tolerance, and deterioration in a global self-assessment rating.
The shocker for the investigators – who had expected a positive study – was that 33% of patients in the sildenafil group worsened significantly on the composite clinical score at 6 months, compared with 14% of placebo-treated controls, said Dr. Bermejo, a cardiologist at Gregorio Marañón University Hospital in Madrid.
Moreover, only 27% of the sildenafil group improved, compared with 44% of controls. About one-third of patients in both groups remained unchanged over the course of the 6-month trial.
Dr. Bermejo noted that valvular disease is considered the next cardiac epidemic because of its strong association with advancing age and the rapid aging of the population worldwide. Pulmonary hypertension occurs is virtually all patients with severe mitral disease and in up to two-thirds of those with asymptomatic aortic stenosis. Regression of the pulmonary hypertension is often incomplete after successful surgical or transcatheter correction of the valvular lesion.
Discussant Irene M. Lang, MD, called SIOVAC “a very clear study.” It convincingly establishes that sildenafil – a vasodilator – is ineffective for the treatment of what the current ESC/European Respiratory Society guidelines on pulmonary hypertension call isolated post-capillary pulmonary hypertension, a condition defined hemodynamically by a diastolic pulmonary vascular pressure gradient of less than 7 mm Hg and/or a pulmonary vascular resistance below 3 Wood units (Eur Heart J. 2016 Jan 1;37[1]:67-119.)
The SIOVAC findings underscore the strong IIIC recommendation in the European guidelines that the use of approved therapies for pulmonary arterial hypertension is not recommended in patients with left heart disease-pulmonary hypertension, added Dr. Lang, a coauthor of the guidelines and professor of vascular biology at the Medical University of Vienna.
The Spanish government funded SIOVAC. Dr. Bermejo reported having no financial conflicts of interest.
BARCELONA – Off-label use of the phosphodiesterase-5 inhibitor sildenafil to treat residual pulmonary hypertension after successful correction of valvular heart disease is not merely ineffective, it’s counterproductive, according to the results of the randomized, placebo-controlled SIOVAC study.
“We believe based upon our results that off-label use of sildenafil in patients with left heart disease-pulmonary hypertension due to valvular disease should be discouraged,” Javier Bermejo, MD, declared at the annual congress of the European Society of Cardiology.
Sildenafil is approved with a solid, evidence-based indication for treating some other types of pulmonary hypertension. Many cardiologists also prescribe the drug off label for residual pulmonary hypertension in patients with corrected valve disease, hoping that it will be of benefit, since there is currently no approved treatment for this common and serious condition associated with increased mortality. But because the anecdotal literature on sildenafil for this specific type of pulmonary hypertension is mixed, Dr. Bermejo and his coinvestigators in the Spanish Network Center for Cardiovascular Research decided to conduct a multicenter randomized trial.
SIOVAC (Sildenafil for Improving Clinical Outcomes After Valvular Correction) comprised 200 patients with residual pulmonary hypertension after corrected valvular heart disease at 17 Spanish general hospitals. The patients were randomized to receive sildenafil at 40 mg t.i.d. or placebo for 6 months in this double-blind trial.
The primary endpoint was a standardized composite clinical score widely used in heart failure trials. It consists of all-cause mortality, hospital admission for heart failure, worsening exercise tolerance, and deterioration in a global self-assessment rating.
The shocker for the investigators – who had expected a positive study – was that 33% of patients in the sildenafil group worsened significantly on the composite clinical score at 6 months, compared with 14% of placebo-treated controls, said Dr. Bermejo, a cardiologist at Gregorio Marañón University Hospital in Madrid.
Moreover, only 27% of the sildenafil group improved, compared with 44% of controls. About one-third of patients in both groups remained unchanged over the course of the 6-month trial.
Dr. Bermejo noted that valvular disease is considered the next cardiac epidemic because of its strong association with advancing age and the rapid aging of the population worldwide. Pulmonary hypertension occurs is virtually all patients with severe mitral disease and in up to two-thirds of those with asymptomatic aortic stenosis. Regression of the pulmonary hypertension is often incomplete after successful surgical or transcatheter correction of the valvular lesion.
Discussant Irene M. Lang, MD, called SIOVAC “a very clear study.” It convincingly establishes that sildenafil – a vasodilator – is ineffective for the treatment of what the current ESC/European Respiratory Society guidelines on pulmonary hypertension call isolated post-capillary pulmonary hypertension, a condition defined hemodynamically by a diastolic pulmonary vascular pressure gradient of less than 7 mm Hg and/or a pulmonary vascular resistance below 3 Wood units (Eur Heart J. 2016 Jan 1;37[1]:67-119.)
The SIOVAC findings underscore the strong IIIC recommendation in the European guidelines that the use of approved therapies for pulmonary arterial hypertension is not recommended in patients with left heart disease-pulmonary hypertension, added Dr. Lang, a coauthor of the guidelines and professor of vascular biology at the Medical University of Vienna.
The Spanish government funded SIOVAC. Dr. Bermejo reported having no financial conflicts of interest.
AT THE ESC CONGRESS 2017
Key clinical point:
Major finding: One-third of patients with residual pulmonary hypertension after successful correction of valvular heart disease experienced significant clinical worsening during 6 months of sildenafil therapy, compared with 14% on placebo.
Data source: SIOVAC, a 6-month, double-blind, placebo-controlled study of 200 patients with residual pulmonary hypertension after correction for valvular heart disease.
Disclosures: The Spanish government funded SIOVAC. The presenter reported having no financial conflicts of interest.
HOPE-3 wades into fray regarding optimal blood pressure targets
BARCELONA – How low to go in treating hypertension is a topic of considerable recent controversy. Now the HOPE-3 trial investigators have weighed in, reporting that optimal outcomes in their landmark randomized trial were seen with an achieved, on-treatment systolic blood pressure of 130-140 mm Hg and a diastolic blood pressure of 75-80 mm Hg, Eva M. Lonn, MD, reported at the annual congress of the European Society of Cardiology.
Those results stand in glaring contrast to the findings of the much-discussed SPRINT trial, in which hypertensive patients fared best with an on-treatment SBP driven below 120 mm Hg (N Engl J Med. 2015 Nov 26; 373:2103-16).

“Please note that lower blood pressures, both systolic and diastolic, weren’t associated with lower risk, whereas higher blood pressures considerably increased the risk for major vascular events,” she added.
HOPE-3 (the Third Heart Outcomes Prevention Evaluation) included 12,705 patients in 21 countries who did not have cardiovascular disease and were at intermediate risk, with an average age of 65 years at enrollment and a Framinhgam Risk Score of about 10%. They were randomized double-blind in a 2x2 factorial design to rosuvastatin at 10 mg per day or placebo and/or candesartan at 16 mg plus hydrochlorothiazide at 12.5 mg per day or placebo and prospectively followed for a median of 5.6 years.
The primary outcomes of HOPE-3 have been published (N Engl J Med. 2016 May 26;374[21]:2009-20 and 2021-31). This was a practice-changing trial that opened the door to broader use of statin therapy for primary prevention.
At the ESC congress in Barcelona, Dr. Lonn presented a secondary post-hoc analysis that focused on the impact of antihypertensive therapy in HOPE-3. The results shed new light on the optimal blood pressure levels for triggering initation of antihypertensive therapy, as well as defining the achieved blood pressures that resulted in the greatest reductions in major vascular events.
As this was essentially an all-comers trial of intermediate-risk patients, participants presented with a range of blood pressures at baseline. But more than 4,700 subjects had a baseline SBP of 140-159.9 mm Hg, and 833 had an SBP of 160 mm Hg or more.
The candesartan/hydrochlorothiazide regimen resulted in what Dr. Lonn termed a “moderate” net placebo-subtracted blood pressure reduction of 6/3 mm Hg. The higher the baseline blood pressure, the bigger the reduction.
In the one-third of subjects with a baseline SBP greater than 143.5 mm Hg, antihypertensive therapy resulted in a significant 27% reduction in the composite endpoint of cardiovascular death, MI, or stroke compared with placebo. Those with a baseline SBP of 150 mm Hg or more showed even greater benefit from antihypertensive therapy, with a composite event rate of 4.8% compared with 7.2% for placebo, representing a 34% relative risk reduction in which the event curves began separating at about 2 years.
In contrast, antihypertensive therapy brought no significant reduction in events in patients in the lower two tertiles of baseline SBP. And there was no association at all between baseline DBP and major cardiovascular events across the range of DBP values evaluated in HOPE-3.
But wait: Things get more interesting, according to the cardiac electrophysiologist.
“I find the association between mean in-trial blood pressure as recorded in many measurements and vascular outcomes to be the most interesting analysis. This may be a better look at the association between blood pressure and outcomes than a measurement obtained just once or twice at baseline,” she explained.
Of note, among the 6,356 subjects on candesartan/hydrochlorothiazide, those with a mean on-treatment SBP of 160 mm Hg or more had a 2.61% per year rate of the composite of cardiovascular death, MI, stroke, rescue from cardiac arrest, heart failure, or revascularization. This was more than three-fold higher than the 0.75% per year rate in patients with an on-treatment SBP of 120-139.9 mm Hg. The composite event rate was also significantly higher in those with a mean on-treatment SBP of 140-159.9 mm Hg, at 1.4% per year. The event rate in patients with an on-treatment SBP below 120 mm Hg was identical to that of patients with a value of 120-139.9 mm Hg.
Only among patients with an on-treatment DBP of 90 mm Hg or more was the composite event rate significantly greater than in those with a DBP of 70-79.9 mm Hg, who had the lowest event rate by a margin of 1.89% versus 0.75% per year.
An Australian cardiologist in the audience who has been involved in revamping hypertension treatment guidelines Down Under expressed frustration. He only recently succeeded in wrangling his fellow panelists into incorporating the SPRINT results into the draft guidelines; now HOPE-3 is sending a very different message. What gives? Could the disparate findings simply be due to play of chance? he asked.
Highly unlikely, Dr. Lonn replied.
“There were substantial differences between our trials,” she explained. “First of all, the SPRINT population was at substantially higher risk. They either had to have established cardiovascular disease – we eliminated those people – or significant renal disease – we eliminated those people, too – or age greater than 75, or a Framingham Risk Score above 15%.”
Also, the SPRINT protocol controversially called for unattended blood pressure measurement.
“This is a very pure way ot eliminating white coat hypertension, but it is different from other studies, so it is very difficult to compare SPRINT to older studies or to HOPE-3. Some other investigators have suggested that the difference between attended and unattended blood pressure is close to 10 mm Hg. So our SBP of 130 mm Hg, which had the best outcomes in HOPE-3, may be the same as about 120 mm Hg in SPRINT,” according to Dr. Lonn.
HOPE-3 was funded by the Canadian Institutes of Health Research and AstraZeneca. Dr. Lonn reported serving as a consultant to and receiving research grants from AstraZeneca, Amgen, Bayer, and Novartis.
BARCELONA – How low to go in treating hypertension is a topic of considerable recent controversy. Now the HOPE-3 trial investigators have weighed in, reporting that optimal outcomes in their landmark randomized trial were seen with an achieved, on-treatment systolic blood pressure of 130-140 mm Hg and a diastolic blood pressure of 75-80 mm Hg, Eva M. Lonn, MD, reported at the annual congress of the European Society of Cardiology.
Those results stand in glaring contrast to the findings of the much-discussed SPRINT trial, in which hypertensive patients fared best with an on-treatment SBP driven below 120 mm Hg (N Engl J Med. 2015 Nov 26; 373:2103-16).
“Please note that lower blood pressures, both systolic and diastolic, weren’t associated with lower risk, whereas higher blood pressures considerably increased the risk for major vascular events,” she added.
HOPE-3 (the Third Heart Outcomes Prevention Evaluation) included 12,705 patients in 21 countries who did not have cardiovascular disease and were at intermediate risk, with an average age of 65 years at enrollment and a Framinhgam Risk Score of about 10%. They were randomized double-blind in a 2x2 factorial design to rosuvastatin at 10 mg per day or placebo and/or candesartan at 16 mg plus hydrochlorothiazide at 12.5 mg per day or placebo and prospectively followed for a median of 5.6 years.
The primary outcomes of HOPE-3 have been published (N Engl J Med. 2016 May 26;374[21]:2009-20 and 2021-31). This was a practice-changing trial that opened the door to broader use of statin therapy for primary prevention.
At the ESC congress in Barcelona, Dr. Lonn presented a secondary post-hoc analysis that focused on the impact of antihypertensive therapy in HOPE-3. The results shed new light on the optimal blood pressure levels for triggering initation of antihypertensive therapy, as well as defining the achieved blood pressures that resulted in the greatest reductions in major vascular events.
As this was essentially an all-comers trial of intermediate-risk patients, participants presented with a range of blood pressures at baseline. But more than 4,700 subjects had a baseline SBP of 140-159.9 mm Hg, and 833 had an SBP of 160 mm Hg or more.
The candesartan/hydrochlorothiazide regimen resulted in what Dr. Lonn termed a “moderate” net placebo-subtracted blood pressure reduction of 6/3 mm Hg. The higher the baseline blood pressure, the bigger the reduction.
In the one-third of subjects with a baseline SBP greater than 143.5 mm Hg, antihypertensive therapy resulted in a significant 27% reduction in the composite endpoint of cardiovascular death, MI, or stroke compared with placebo. Those with a baseline SBP of 150 mm Hg or more showed even greater benefit from antihypertensive therapy, with a composite event rate of 4.8% compared with 7.2% for placebo, representing a 34% relative risk reduction in which the event curves began separating at about 2 years.
In contrast, antihypertensive therapy brought no significant reduction in events in patients in the lower two tertiles of baseline SBP. And there was no association at all between baseline DBP and major cardiovascular events across the range of DBP values evaluated in HOPE-3.
But wait: Things get more interesting, according to the cardiac electrophysiologist.
“I find the association between mean in-trial blood pressure as recorded in many measurements and vascular outcomes to be the most interesting analysis. This may be a better look at the association between blood pressure and outcomes than a measurement obtained just once or twice at baseline,” she explained.
Of note, among the 6,356 subjects on candesartan/hydrochlorothiazide, those with a mean on-treatment SBP of 160 mm Hg or more had a 2.61% per year rate of the composite of cardiovascular death, MI, stroke, rescue from cardiac arrest, heart failure, or revascularization. This was more than three-fold higher than the 0.75% per year rate in patients with an on-treatment SBP of 120-139.9 mm Hg. The composite event rate was also significantly higher in those with a mean on-treatment SBP of 140-159.9 mm Hg, at 1.4% per year. The event rate in patients with an on-treatment SBP below 120 mm Hg was identical to that of patients with a value of 120-139.9 mm Hg.
Only among patients with an on-treatment DBP of 90 mm Hg or more was the composite event rate significantly greater than in those with a DBP of 70-79.9 mm Hg, who had the lowest event rate by a margin of 1.89% versus 0.75% per year.
An Australian cardiologist in the audience who has been involved in revamping hypertension treatment guidelines Down Under expressed frustration. He only recently succeeded in wrangling his fellow panelists into incorporating the SPRINT results into the draft guidelines; now HOPE-3 is sending a very different message. What gives? Could the disparate findings simply be due to play of chance? he asked.
Highly unlikely, Dr. Lonn replied.
“There were substantial differences between our trials,” she explained. “First of all, the SPRINT population was at substantially higher risk. They either had to have established cardiovascular disease – we eliminated those people – or significant renal disease – we eliminated those people, too – or age greater than 75, or a Framingham Risk Score above 15%.”
Also, the SPRINT protocol controversially called for unattended blood pressure measurement.
“This is a very pure way ot eliminating white coat hypertension, but it is different from other studies, so it is very difficult to compare SPRINT to older studies or to HOPE-3. Some other investigators have suggested that the difference between attended and unattended blood pressure is close to 10 mm Hg. So our SBP of 130 mm Hg, which had the best outcomes in HOPE-3, may be the same as about 120 mm Hg in SPRINT,” according to Dr. Lonn.
HOPE-3 was funded by the Canadian Institutes of Health Research and AstraZeneca. Dr. Lonn reported serving as a consultant to and receiving research grants from AstraZeneca, Amgen, Bayer, and Novartis.
BARCELONA – How low to go in treating hypertension is a topic of considerable recent controversy. Now the HOPE-3 trial investigators have weighed in, reporting that optimal outcomes in their landmark randomized trial were seen with an achieved, on-treatment systolic blood pressure of 130-140 mm Hg and a diastolic blood pressure of 75-80 mm Hg, Eva M. Lonn, MD, reported at the annual congress of the European Society of Cardiology.
Those results stand in glaring contrast to the findings of the much-discussed SPRINT trial, in which hypertensive patients fared best with an on-treatment SBP driven below 120 mm Hg (N Engl J Med. 2015 Nov 26; 373:2103-16).
“Please note that lower blood pressures, both systolic and diastolic, weren’t associated with lower risk, whereas higher blood pressures considerably increased the risk for major vascular events,” she added.
HOPE-3 (the Third Heart Outcomes Prevention Evaluation) included 12,705 patients in 21 countries who did not have cardiovascular disease and were at intermediate risk, with an average age of 65 years at enrollment and a Framinhgam Risk Score of about 10%. They were randomized double-blind in a 2x2 factorial design to rosuvastatin at 10 mg per day or placebo and/or candesartan at 16 mg plus hydrochlorothiazide at 12.5 mg per day or placebo and prospectively followed for a median of 5.6 years.
The primary outcomes of HOPE-3 have been published (N Engl J Med. 2016 May 26;374[21]:2009-20 and 2021-31). This was a practice-changing trial that opened the door to broader use of statin therapy for primary prevention.
At the ESC congress in Barcelona, Dr. Lonn presented a secondary post-hoc analysis that focused on the impact of antihypertensive therapy in HOPE-3. The results shed new light on the optimal blood pressure levels for triggering initation of antihypertensive therapy, as well as defining the achieved blood pressures that resulted in the greatest reductions in major vascular events.
As this was essentially an all-comers trial of intermediate-risk patients, participants presented with a range of blood pressures at baseline. But more than 4,700 subjects had a baseline SBP of 140-159.9 mm Hg, and 833 had an SBP of 160 mm Hg or more.
The candesartan/hydrochlorothiazide regimen resulted in what Dr. Lonn termed a “moderate” net placebo-subtracted blood pressure reduction of 6/3 mm Hg. The higher the baseline blood pressure, the bigger the reduction.
In the one-third of subjects with a baseline SBP greater than 143.5 mm Hg, antihypertensive therapy resulted in a significant 27% reduction in the composite endpoint of cardiovascular death, MI, or stroke compared with placebo. Those with a baseline SBP of 150 mm Hg or more showed even greater benefit from antihypertensive therapy, with a composite event rate of 4.8% compared with 7.2% for placebo, representing a 34% relative risk reduction in which the event curves began separating at about 2 years.
In contrast, antihypertensive therapy brought no significant reduction in events in patients in the lower two tertiles of baseline SBP. And there was no association at all between baseline DBP and major cardiovascular events across the range of DBP values evaluated in HOPE-3.
But wait: Things get more interesting, according to the cardiac electrophysiologist.
“I find the association between mean in-trial blood pressure as recorded in many measurements and vascular outcomes to be the most interesting analysis. This may be a better look at the association between blood pressure and outcomes than a measurement obtained just once or twice at baseline,” she explained.
Of note, among the 6,356 subjects on candesartan/hydrochlorothiazide, those with a mean on-treatment SBP of 160 mm Hg or more had a 2.61% per year rate of the composite of cardiovascular death, MI, stroke, rescue from cardiac arrest, heart failure, or revascularization. This was more than three-fold higher than the 0.75% per year rate in patients with an on-treatment SBP of 120-139.9 mm Hg. The composite event rate was also significantly higher in those with a mean on-treatment SBP of 140-159.9 mm Hg, at 1.4% per year. The event rate in patients with an on-treatment SBP below 120 mm Hg was identical to that of patients with a value of 120-139.9 mm Hg.
Only among patients with an on-treatment DBP of 90 mm Hg or more was the composite event rate significantly greater than in those with a DBP of 70-79.9 mm Hg, who had the lowest event rate by a margin of 1.89% versus 0.75% per year.
An Australian cardiologist in the audience who has been involved in revamping hypertension treatment guidelines Down Under expressed frustration. He only recently succeeded in wrangling his fellow panelists into incorporating the SPRINT results into the draft guidelines; now HOPE-3 is sending a very different message. What gives? Could the disparate findings simply be due to play of chance? he asked.
Highly unlikely, Dr. Lonn replied.
“There were substantial differences between our trials,” she explained. “First of all, the SPRINT population was at substantially higher risk. They either had to have established cardiovascular disease – we eliminated those people – or significant renal disease – we eliminated those people, too – or age greater than 75, or a Framingham Risk Score above 15%.”
Also, the SPRINT protocol controversially called for unattended blood pressure measurement.
“This is a very pure way ot eliminating white coat hypertension, but it is different from other studies, so it is very difficult to compare SPRINT to older studies or to HOPE-3. Some other investigators have suggested that the difference between attended and unattended blood pressure is close to 10 mm Hg. So our SBP of 130 mm Hg, which had the best outcomes in HOPE-3, may be the same as about 120 mm Hg in SPRINT,” according to Dr. Lonn.
HOPE-3 was funded by the Canadian Institutes of Health Research and AstraZeneca. Dr. Lonn reported serving as a consultant to and receiving research grants from AstraZeneca, Amgen, Bayer, and Novartis.
AT THE ESC CONGRESS 2017
Key clinical point:
Major finding: The on-treatment systolic blood pressure target associated with the greatest reduction in vascular events in the HOPE-3 trial was 130-140 mm Hg.
Data source: The HOPE-3 trial was a randomized, double-blind, placebo-controlled study of 12,705 intermediate-cardiovascular-risk patients in 21 countries who were prospectively followed for a median 5.6 years.
Disclosures: HOPE-3 was funded by the Canadian Institutes of Health Research and AstraZeneca. The presenter reported serving as a consultant to and receiving research grants from AstraZeneca, Amgen, Bayer, and Novartis.
Obesity paradox slings its weight around in atrial fibrillation
BARCELONA – The obesity paradox is alive and well in the rapidly growing population with atrial fibrillation, Samuel Z. Goldhaber, MD, reported at the annual congress of the European Society of Cardiology.
In an analysis of 22,541 participants in the international registry known as GARFIELD-AF (Global Anticoagulation Registry in the Field-Atrial Fibrillation) – the largest ongoing prospective AF registry in the world – all-cause mortality during the first 2 years after diagnosis of the arrhythmia paradoxically decreased as body mass index increased all the way up to a ceiling of 40 kg/m2, according to Dr. Goldhaber, professor of medicine at Harvard Medical School and section head of vascular medicine and director of the thrombosis research group at Brigham and Women’s Hospital, Boston.
“It’s pretty impressive. This degree of mortality reduction with overweight and obesity is of about the same magnitude you might get with thrombolytic therapy for an acute MI, or with beta blocker therapy or statins post-MI,” the cardiologist said in an interview.
This newly described obesity paradox in AF is all the more baffling in light of the heavy cardiovascular risk factor burden that accompanied increased BMI. For example, the prevalence of type 2 diabetes rose from 14.1% among normal-weight individuals with AF, to 19.7% in the overweight, 27.5% in the obese, 34.6% in those with a BMI of 35 to less than 40 kg/m2, and 41.6% in patients with a BMI of 40 kg/m2 or more.
“It’s perplexing,” Dr. Goldhaber confessed. “I think there’s some hidden message here that we haven’t decoded yet.”
Patients with AF who were at the low extreme of the BMI spectrum -- the 3.3% who were underweight, with a BMI below 20 kg/m2 – fared particularly poorly. Their 2-year all-cause mortality rate of 8.71 per 100 person-years was by far the highest of any BMI class in the study. But that’s relatively straightforward to understand, as it’s likely that many underweight patients with AF were frail and/or had cancer. Indeed, only 49% of deaths in the underweight group were due to cardiovascular disease, in contrast to 64% of deaths in persons whose BMI was 40 kg/m2 or more.
Interestingly, only 5%-6% of all deaths in GARFIELD-AF were due to stroke; deaths from heart failure were far more common.
Overall, 71% of patients who presented with newly diagnosed AF in GARFIELD-AF were overweight or obese. The only contributory factor to the obesity paradox that Dr. Goldhaber could spot was that the heavier patients were younger at diagnosis of AF. But this age disparity seems unlikely to overcome their massive burden of multiple other cardiovascular risk factors. So he solicited theories from his audience. One physician argued that morbidly obese individuals are sedentary, so they don’t leave the house as much as leaner AF patients.
“You stay at home because you cannot move. You don’t get into fatal car accidents. You don’t get into conflicts and get murdered,” the physician postulated.
Dr. Goldhaber wasn’t convinced.
“When I go out to bars or dancing, I look around at people, and I estimate that a lot of them have a BMI of 35,” he commented.
Another proposed theory was that overweight and obese AF patients exercise less, so they inhale less of the airborne toxic fine particulates present in the urban environment. The adverse health impact of air pollution is a particularly hot topic of late among European cardiologists, but the notion that obese AF patients fare better because they don’t exercise runs contrary to a wealth of data supporting the health benefits of working out.
The GARFIELD-AF registry is funded by Bayer AG. Dr. Goldhaber reported receiving research grants and/or serving as a consultant to Bayer and numerous other entities, including the National Heart, Lung and Blood Institute.
BARCELONA – The obesity paradox is alive and well in the rapidly growing population with atrial fibrillation, Samuel Z. Goldhaber, MD, reported at the annual congress of the European Society of Cardiology.
In an analysis of 22,541 participants in the international registry known as GARFIELD-AF (Global Anticoagulation Registry in the Field-Atrial Fibrillation) – the largest ongoing prospective AF registry in the world – all-cause mortality during the first 2 years after diagnosis of the arrhythmia paradoxically decreased as body mass index increased all the way up to a ceiling of 40 kg/m2, according to Dr. Goldhaber, professor of medicine at Harvard Medical School and section head of vascular medicine and director of the thrombosis research group at Brigham and Women’s Hospital, Boston.
“It’s pretty impressive. This degree of mortality reduction with overweight and obesity is of about the same magnitude you might get with thrombolytic therapy for an acute MI, or with beta blocker therapy or statins post-MI,” the cardiologist said in an interview.
This newly described obesity paradox in AF is all the more baffling in light of the heavy cardiovascular risk factor burden that accompanied increased BMI. For example, the prevalence of type 2 diabetes rose from 14.1% among normal-weight individuals with AF, to 19.7% in the overweight, 27.5% in the obese, 34.6% in those with a BMI of 35 to less than 40 kg/m2, and 41.6% in patients with a BMI of 40 kg/m2 or more.
“It’s perplexing,” Dr. Goldhaber confessed. “I think there’s some hidden message here that we haven’t decoded yet.”
Patients with AF who were at the low extreme of the BMI spectrum -- the 3.3% who were underweight, with a BMI below 20 kg/m2 – fared particularly poorly. Their 2-year all-cause mortality rate of 8.71 per 100 person-years was by far the highest of any BMI class in the study. But that’s relatively straightforward to understand, as it’s likely that many underweight patients with AF were frail and/or had cancer. Indeed, only 49% of deaths in the underweight group were due to cardiovascular disease, in contrast to 64% of deaths in persons whose BMI was 40 kg/m2 or more.
Interestingly, only 5%-6% of all deaths in GARFIELD-AF were due to stroke; deaths from heart failure were far more common.
Overall, 71% of patients who presented with newly diagnosed AF in GARFIELD-AF were overweight or obese. The only contributory factor to the obesity paradox that Dr. Goldhaber could spot was that the heavier patients were younger at diagnosis of AF. But this age disparity seems unlikely to overcome their massive burden of multiple other cardiovascular risk factors. So he solicited theories from his audience. One physician argued that morbidly obese individuals are sedentary, so they don’t leave the house as much as leaner AF patients.
“You stay at home because you cannot move. You don’t get into fatal car accidents. You don’t get into conflicts and get murdered,” the physician postulated.
Dr. Goldhaber wasn’t convinced.
“When I go out to bars or dancing, I look around at people, and I estimate that a lot of them have a BMI of 35,” he commented.
Another proposed theory was that overweight and obese AF patients exercise less, so they inhale less of the airborne toxic fine particulates present in the urban environment. The adverse health impact of air pollution is a particularly hot topic of late among European cardiologists, but the notion that obese AF patients fare better because they don’t exercise runs contrary to a wealth of data supporting the health benefits of working out.
The GARFIELD-AF registry is funded by Bayer AG. Dr. Goldhaber reported receiving research grants and/or serving as a consultant to Bayer and numerous other entities, including the National Heart, Lung and Blood Institute.
BARCELONA – The obesity paradox is alive and well in the rapidly growing population with atrial fibrillation, Samuel Z. Goldhaber, MD, reported at the annual congress of the European Society of Cardiology.
In an analysis of 22,541 participants in the international registry known as GARFIELD-AF (Global Anticoagulation Registry in the Field-Atrial Fibrillation) – the largest ongoing prospective AF registry in the world – all-cause mortality during the first 2 years after diagnosis of the arrhythmia paradoxically decreased as body mass index increased all the way up to a ceiling of 40 kg/m2, according to Dr. Goldhaber, professor of medicine at Harvard Medical School and section head of vascular medicine and director of the thrombosis research group at Brigham and Women’s Hospital, Boston.
“It’s pretty impressive. This degree of mortality reduction with overweight and obesity is of about the same magnitude you might get with thrombolytic therapy for an acute MI, or with beta blocker therapy or statins post-MI,” the cardiologist said in an interview.
This newly described obesity paradox in AF is all the more baffling in light of the heavy cardiovascular risk factor burden that accompanied increased BMI. For example, the prevalence of type 2 diabetes rose from 14.1% among normal-weight individuals with AF, to 19.7% in the overweight, 27.5% in the obese, 34.6% in those with a BMI of 35 to less than 40 kg/m2, and 41.6% in patients with a BMI of 40 kg/m2 or more.
“It’s perplexing,” Dr. Goldhaber confessed. “I think there’s some hidden message here that we haven’t decoded yet.”
Patients with AF who were at the low extreme of the BMI spectrum -- the 3.3% who were underweight, with a BMI below 20 kg/m2 – fared particularly poorly. Their 2-year all-cause mortality rate of 8.71 per 100 person-years was by far the highest of any BMI class in the study. But that’s relatively straightforward to understand, as it’s likely that many underweight patients with AF were frail and/or had cancer. Indeed, only 49% of deaths in the underweight group were due to cardiovascular disease, in contrast to 64% of deaths in persons whose BMI was 40 kg/m2 or more.
Interestingly, only 5%-6% of all deaths in GARFIELD-AF were due to stroke; deaths from heart failure were far more common.
Overall, 71% of patients who presented with newly diagnosed AF in GARFIELD-AF were overweight or obese. The only contributory factor to the obesity paradox that Dr. Goldhaber could spot was that the heavier patients were younger at diagnosis of AF. But this age disparity seems unlikely to overcome their massive burden of multiple other cardiovascular risk factors. So he solicited theories from his audience. One physician argued that morbidly obese individuals are sedentary, so they don’t leave the house as much as leaner AF patients.
“You stay at home because you cannot move. You don’t get into fatal car accidents. You don’t get into conflicts and get murdered,” the physician postulated.
Dr. Goldhaber wasn’t convinced.
“When I go out to bars or dancing, I look around at people, and I estimate that a lot of them have a BMI of 35,” he commented.
Another proposed theory was that overweight and obese AF patients exercise less, so they inhale less of the airborne toxic fine particulates present in the urban environment. The adverse health impact of air pollution is a particularly hot topic of late among European cardiologists, but the notion that obese AF patients fare better because they don’t exercise runs contrary to a wealth of data supporting the health benefits of working out.
The GARFIELD-AF registry is funded by Bayer AG. Dr. Goldhaber reported receiving research grants and/or serving as a consultant to Bayer and numerous other entities, including the National Heart, Lung and Blood Institute.
AT THE ESC CONGRESS 2017
Key clinical point:
Major finding: Two-year all-cause mortality following diagnosis of atrial fibrillation fell substantially in stepwise fashion with increasing body mass index, for reasons unknown.
Data source: GARFIELD-AF is an ongoing enormous international prospective registry of patients newly diagnosed with atrial fibrillation.
Disclosures: The GARFIELD-AF registry is funded by Bayer AG. The presenter reported receiving research grants and/or consultant fees from that company and numerous others.
Surgical left atrial appendage closure slashes stroke risk
BARCELONA – Routine surgical closure of the left atrial appendage during open heart surgery provides long-term protection against cerebral ischemic events, according to the findings of the first-ever randomized controlled trial to address the issue.
“I think we can say, based on our study, that it would be advisable to routinely add surgical closure of the left atrial appendage to planned open heart surgery,” Jesper Park-Hansen, MD, said at the annual congress of the European Society of Cardiology.

In light of the demonstrated success of percutaneous closure of the LAA using the Watchman and other devices for stroke prevention in patients with atrial fibrillation, Dr. Park-Hansen and his coinvestigators at the University of Copenhagen organized LAACS (the Left Atrial Appendage Closure Study). The goal was to generate solid, randomized trial evidence as to whether preemptive routine surgical closure of the LAA at the time of cardiac surgery is of benefit. Some cardiac surgeons already do this routinely; many others don’t because of the lack of Level 1 supporting evidence.
LAACS included 141 patients randomized to surgical LAA closure or not at the point of first-time open heart surgery. The study population included patients with and without a history of atrial fibrillation. LAA closure was accomplished via a purse string closure with a silk string around the neck of the appendage backed up by an additional single running suture. Transesophageal echocardiography performed in 10 patients a mean of 520 days post closure showed no signs of leakage or incomplete closure.
The primary composite outcome was comprised of clinical stroke or transient ischemic attack diagnosed by a neurologist, or a silent cerebral infarct detected on MRI performed 2-4 weeks post discharge and again at least 6 months later. At a mean follow-up of 3.7 years and a maximum of 6 years, this outcome had occurred in 6.3% of the LAAC group, significantly lower than the 18.3% rate in controls. All but one patient with a cerebral ischemic event in the control group had atrial fibrillation. The risk of an event was unrelated to whether or not a patient had a history of atrial fibrillation prior to surgery or to CHA2DS2-VASc score.
Dr. Park-Hansen emphasized that he and his coinvestigators don’t consider LAACS to be the final word on routine prophylactic appendage closure.
“This is the first randomized study. We are eager to move on to another randomized study on a larger scale. That is the next step for us,” he said.
“The challenge now – and what we will be discussing with our surgeons – is to agree on a feasible safe and effective means of left atrial appendage closure. My personal opinion is the Lariat suture delivery device or some other easily reproducible method of closure could be a good way to go,” Dr. Park-Hansen added.
The research group’s cardiac surgeons already have ruled out excision and stapling because of concerns about bleeding risk and the additional cost imposed by stapling.
Discussant Volkmar Falk, MD, commented that LAACS was too small, probably severely underpowered, should have included a preoperative MRI so investigators could reliably capture perioperative silent cerebral infarcts, and the double suture purse string is “probably not the best method” to occlude the LAA.
“LAACS addresses an important question, but alas, it does not provide the answer,” declared Dr. Falk, professor and director of the department of cardiothoracic and vascular surgery at Charité Medical University in Berlin.
Dr. Park-Hansen and Dr. Falk reported having no financial conflicts of interest.
BARCELONA – Routine surgical closure of the left atrial appendage during open heart surgery provides long-term protection against cerebral ischemic events, according to the findings of the first-ever randomized controlled trial to address the issue.
“I think we can say, based on our study, that it would be advisable to routinely add surgical closure of the left atrial appendage to planned open heart surgery,” Jesper Park-Hansen, MD, said at the annual congress of the European Society of Cardiology.
In light of the demonstrated success of percutaneous closure of the LAA using the Watchman and other devices for stroke prevention in patients with atrial fibrillation, Dr. Park-Hansen and his coinvestigators at the University of Copenhagen organized LAACS (the Left Atrial Appendage Closure Study). The goal was to generate solid, randomized trial evidence as to whether preemptive routine surgical closure of the LAA at the time of cardiac surgery is of benefit. Some cardiac surgeons already do this routinely; many others don’t because of the lack of Level 1 supporting evidence.
LAACS included 141 patients randomized to surgical LAA closure or not at the point of first-time open heart surgery. The study population included patients with and without a history of atrial fibrillation. LAA closure was accomplished via a purse string closure with a silk string around the neck of the appendage backed up by an additional single running suture. Transesophageal echocardiography performed in 10 patients a mean of 520 days post closure showed no signs of leakage or incomplete closure.
The primary composite outcome was comprised of clinical stroke or transient ischemic attack diagnosed by a neurologist, or a silent cerebral infarct detected on MRI performed 2-4 weeks post discharge and again at least 6 months later. At a mean follow-up of 3.7 years and a maximum of 6 years, this outcome had occurred in 6.3% of the LAAC group, significantly lower than the 18.3% rate in controls. All but one patient with a cerebral ischemic event in the control group had atrial fibrillation. The risk of an event was unrelated to whether or not a patient had a history of atrial fibrillation prior to surgery or to CHA2DS2-VASc score.
Dr. Park-Hansen emphasized that he and his coinvestigators don’t consider LAACS to be the final word on routine prophylactic appendage closure.
“This is the first randomized study. We are eager to move on to another randomized study on a larger scale. That is the next step for us,” he said.
“The challenge now – and what we will be discussing with our surgeons – is to agree on a feasible safe and effective means of left atrial appendage closure. My personal opinion is the Lariat suture delivery device or some other easily reproducible method of closure could be a good way to go,” Dr. Park-Hansen added.
The research group’s cardiac surgeons already have ruled out excision and stapling because of concerns about bleeding risk and the additional cost imposed by stapling.
Discussant Volkmar Falk, MD, commented that LAACS was too small, probably severely underpowered, should have included a preoperative MRI so investigators could reliably capture perioperative silent cerebral infarcts, and the double suture purse string is “probably not the best method” to occlude the LAA.
“LAACS addresses an important question, but alas, it does not provide the answer,” declared Dr. Falk, professor and director of the department of cardiothoracic and vascular surgery at Charité Medical University in Berlin.
Dr. Park-Hansen and Dr. Falk reported having no financial conflicts of interest.
BARCELONA – Routine surgical closure of the left atrial appendage during open heart surgery provides long-term protection against cerebral ischemic events, according to the findings of the first-ever randomized controlled trial to address the issue.
“I think we can say, based on our study, that it would be advisable to routinely add surgical closure of the left atrial appendage to planned open heart surgery,” Jesper Park-Hansen, MD, said at the annual congress of the European Society of Cardiology.
In light of the demonstrated success of percutaneous closure of the LAA using the Watchman and other devices for stroke prevention in patients with atrial fibrillation, Dr. Park-Hansen and his coinvestigators at the University of Copenhagen organized LAACS (the Left Atrial Appendage Closure Study). The goal was to generate solid, randomized trial evidence as to whether preemptive routine surgical closure of the LAA at the time of cardiac surgery is of benefit. Some cardiac surgeons already do this routinely; many others don’t because of the lack of Level 1 supporting evidence.
LAACS included 141 patients randomized to surgical LAA closure or not at the point of first-time open heart surgery. The study population included patients with and without a history of atrial fibrillation. LAA closure was accomplished via a purse string closure with a silk string around the neck of the appendage backed up by an additional single running suture. Transesophageal echocardiography performed in 10 patients a mean of 520 days post closure showed no signs of leakage or incomplete closure.
The primary composite outcome was comprised of clinical stroke or transient ischemic attack diagnosed by a neurologist, or a silent cerebral infarct detected on MRI performed 2-4 weeks post discharge and again at least 6 months later. At a mean follow-up of 3.7 years and a maximum of 6 years, this outcome had occurred in 6.3% of the LAAC group, significantly lower than the 18.3% rate in controls. All but one patient with a cerebral ischemic event in the control group had atrial fibrillation. The risk of an event was unrelated to whether or not a patient had a history of atrial fibrillation prior to surgery or to CHA2DS2-VASc score.
Dr. Park-Hansen emphasized that he and his coinvestigators don’t consider LAACS to be the final word on routine prophylactic appendage closure.
“This is the first randomized study. We are eager to move on to another randomized study on a larger scale. That is the next step for us,” he said.
“The challenge now – and what we will be discussing with our surgeons – is to agree on a feasible safe and effective means of left atrial appendage closure. My personal opinion is the Lariat suture delivery device or some other easily reproducible method of closure could be a good way to go,” Dr. Park-Hansen added.
The research group’s cardiac surgeons already have ruled out excision and stapling because of concerns about bleeding risk and the additional cost imposed by stapling.
Discussant Volkmar Falk, MD, commented that LAACS was too small, probably severely underpowered, should have included a preoperative MRI so investigators could reliably capture perioperative silent cerebral infarcts, and the double suture purse string is “probably not the best method” to occlude the LAA.
“LAACS addresses an important question, but alas, it does not provide the answer,” declared Dr. Falk, professor and director of the department of cardiothoracic and vascular surgery at Charité Medical University in Berlin.
Dr. Park-Hansen and Dr. Falk reported having no financial conflicts of interest.
AT THE ESC CONGRESS 2017
Key clinical point:
Major finding: The composite rate of clinical stroke, TIA, or silent cerebral infarct in the years following open heart surgery was threefold higher in patients randomized to no prophylactic surgical closure of the left atrial appendage, compared with patients who got appendage closure during their surgery.
Data source: A randomized trial in which 141 patients undergoing first-time open heart surgery were assigned to prophylactic surgical closure of the left atrial appendage or not.
Disclosures: The study was conducted free of commercial support. The presenter reported having no financial conflicts of interest.