User login
PARIS – The obesity paradox appears to apply to patients undergoing transcatheter aortic valve replacement (TAVR) but doesn’t extend to those with surgical aortic valve replacement (SAVR), Dr. Marco Spaziano reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
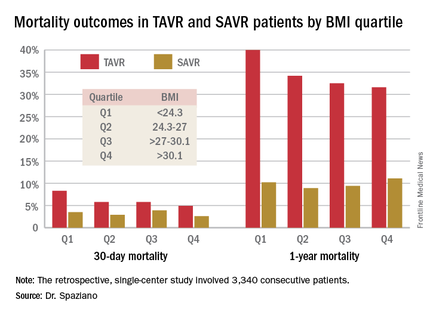
He presented a retrospective single-center study of 3,340 consecutive patients who underwent either TAVR or SAVR, with all valve replacement procedures being performed by the same surgeons. Investigators divided the patients – 1,301 with TAVR, 2,039 SAVR – into quartiles on the basis of body mass index.

Rates of 30-day and 1-year mortality, major vascular complications, and major bleeding events were consistently lowest in TAVR patients in the top body mass index (BMI) quartile, defined as greater than 30.1 kg/m2, and highest in those in the bottom quartile, reserved for patients with a BMI below 24.3 kg/m2.
It’s worth noting that with a mean BMI of 21.8 kg/m2 in the bottom BMI quartile, most patients in that group were actually normal weight, not underweight, observed Dr. Spaziano of the Paris South Cardiovascular Institute in Massy, France.
Among the TAVR group, there were no significant differences between the BMI quartiles in TAVR devices, size, or procedural approach.
The TAVR patients’ BMI quartile had no impact on other outcomes, including rates of stroke, MI, permanent pacemaker implantation, acute kidney injury, or aortic regurgitation.
While being overweight or obese was protective in TAVR patients, BMI quartiles had no relationship with outcomes in the SAVR cohort. The SAVR patients were on average about 10 years younger than the TAVR group, and their logistic EuroSCORE – a tool for estimating mortality risk after cardiac surgery – was much lower as well.
The obesity paradox remains an ongoing puzzle and source of intrigue for physicians in many different specialties. The paradox is this: Obesity is well established as a major risk factor for the development of cardiovascular diseases and diabetes, yet a higher BMI seems to be associated with lower mortality and better procedural outcomes for patients once they actually have a number of chronic diseases, including coronary artery disease, heart failure, peripheral arterial disease, hypertension, stroke, chronic obstructive pulmonary disease, renal disease, and acute venous thromboembolism.
The TAVR obesity paradox findings really got under the skin of at least one audience member.
“What’s the message?” he asked. “We’re telling people to lose weight, eat healthy, run thousands of miles and so forth, but then we’re supposed to tell patients undergoing a high-risk procedure that if you’re overweight you somehow survive better, live longer, feel better?”
Dr. Spaziano said the independent predictors of mortality in the lowest-BMI quartile of TAVR patients were a high serum creatinine, chronic obstructive pulmonary disease, and low BMI. Therein lies a likely explanation for the obesity paradox, at least in this particular study: The TAVR patients were generally sicker than the SAVR patients, which is why they weren’t undergoing surgery, and the lowest-BMI TAVR group was frailer than the others. Also, perhaps the heaviest patients benefited from having more energy reserves to draw upon.
He reported having no financial conflicts regarding this study, conducted free of commercial support.
PARIS – The obesity paradox appears to apply to patients undergoing transcatheter aortic valve replacement (TAVR) but doesn’t extend to those with surgical aortic valve replacement (SAVR), Dr. Marco Spaziano reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
He presented a retrospective single-center study of 3,340 consecutive patients who underwent either TAVR or SAVR, with all valve replacement procedures being performed by the same surgeons. Investigators divided the patients – 1,301 with TAVR, 2,039 SAVR – into quartiles on the basis of body mass index.
Rates of 30-day and 1-year mortality, major vascular complications, and major bleeding events were consistently lowest in TAVR patients in the top body mass index (BMI) quartile, defined as greater than 30.1 kg/m2, and highest in those in the bottom quartile, reserved for patients with a BMI below 24.3 kg/m2.
It’s worth noting that with a mean BMI of 21.8 kg/m2 in the bottom BMI quartile, most patients in that group were actually normal weight, not underweight, observed Dr. Spaziano of the Paris South Cardiovascular Institute in Massy, France.
Among the TAVR group, there were no significant differences between the BMI quartiles in TAVR devices, size, or procedural approach.
The TAVR patients’ BMI quartile had no impact on other outcomes, including rates of stroke, MI, permanent pacemaker implantation, acute kidney injury, or aortic regurgitation.
While being overweight or obese was protective in TAVR patients, BMI quartiles had no relationship with outcomes in the SAVR cohort. The SAVR patients were on average about 10 years younger than the TAVR group, and their logistic EuroSCORE – a tool for estimating mortality risk after cardiac surgery – was much lower as well.
The obesity paradox remains an ongoing puzzle and source of intrigue for physicians in many different specialties. The paradox is this: Obesity is well established as a major risk factor for the development of cardiovascular diseases and diabetes, yet a higher BMI seems to be associated with lower mortality and better procedural outcomes for patients once they actually have a number of chronic diseases, including coronary artery disease, heart failure, peripheral arterial disease, hypertension, stroke, chronic obstructive pulmonary disease, renal disease, and acute venous thromboembolism.
The TAVR obesity paradox findings really got under the skin of at least one audience member.
“What’s the message?” he asked. “We’re telling people to lose weight, eat healthy, run thousands of miles and so forth, but then we’re supposed to tell patients undergoing a high-risk procedure that if you’re overweight you somehow survive better, live longer, feel better?”
Dr. Spaziano said the independent predictors of mortality in the lowest-BMI quartile of TAVR patients were a high serum creatinine, chronic obstructive pulmonary disease, and low BMI. Therein lies a likely explanation for the obesity paradox, at least in this particular study: The TAVR patients were generally sicker than the SAVR patients, which is why they weren’t undergoing surgery, and the lowest-BMI TAVR group was frailer than the others. Also, perhaps the heaviest patients benefited from having more energy reserves to draw upon.
He reported having no financial conflicts regarding this study, conducted free of commercial support.
PARIS – The obesity paradox appears to apply to patients undergoing transcatheter aortic valve replacement (TAVR) but doesn’t extend to those with surgical aortic valve replacement (SAVR), Dr. Marco Spaziano reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
He presented a retrospective single-center study of 3,340 consecutive patients who underwent either TAVR or SAVR, with all valve replacement procedures being performed by the same surgeons. Investigators divided the patients – 1,301 with TAVR, 2,039 SAVR – into quartiles on the basis of body mass index.
Rates of 30-day and 1-year mortality, major vascular complications, and major bleeding events were consistently lowest in TAVR patients in the top body mass index (BMI) quartile, defined as greater than 30.1 kg/m2, and highest in those in the bottom quartile, reserved for patients with a BMI below 24.3 kg/m2.
It’s worth noting that with a mean BMI of 21.8 kg/m2 in the bottom BMI quartile, most patients in that group were actually normal weight, not underweight, observed Dr. Spaziano of the Paris South Cardiovascular Institute in Massy, France.
Among the TAVR group, there were no significant differences between the BMI quartiles in TAVR devices, size, or procedural approach.
The TAVR patients’ BMI quartile had no impact on other outcomes, including rates of stroke, MI, permanent pacemaker implantation, acute kidney injury, or aortic regurgitation.
While being overweight or obese was protective in TAVR patients, BMI quartiles had no relationship with outcomes in the SAVR cohort. The SAVR patients were on average about 10 years younger than the TAVR group, and their logistic EuroSCORE – a tool for estimating mortality risk after cardiac surgery – was much lower as well.
The obesity paradox remains an ongoing puzzle and source of intrigue for physicians in many different specialties. The paradox is this: Obesity is well established as a major risk factor for the development of cardiovascular diseases and diabetes, yet a higher BMI seems to be associated with lower mortality and better procedural outcomes for patients once they actually have a number of chronic diseases, including coronary artery disease, heart failure, peripheral arterial disease, hypertension, stroke, chronic obstructive pulmonary disease, renal disease, and acute venous thromboembolism.
The TAVR obesity paradox findings really got under the skin of at least one audience member.
“What’s the message?” he asked. “We’re telling people to lose weight, eat healthy, run thousands of miles and so forth, but then we’re supposed to tell patients undergoing a high-risk procedure that if you’re overweight you somehow survive better, live longer, feel better?”
Dr. Spaziano said the independent predictors of mortality in the lowest-BMI quartile of TAVR patients were a high serum creatinine, chronic obstructive pulmonary disease, and low BMI. Therein lies a likely explanation for the obesity paradox, at least in this particular study: The TAVR patients were generally sicker than the SAVR patients, which is why they weren’t undergoing surgery, and the lowest-BMI TAVR group was frailer than the others. Also, perhaps the heaviest patients benefited from having more energy reserves to draw upon.
He reported having no financial conflicts regarding this study, conducted free of commercial support.
AT EUROPCR 2016
Key clinical point: Being overweight or obese may have a protective effect in patients undergoing transcatheter aortic valve replacement, but not in those who have surgical replacement.
Major finding: Thirty-day mortality was 4.9% in TAVR patients in the top BMI quartile and climbed stepwise with lowering BMIs.
Data source: A single-center retrospective study of 3,340 consecutive patients who underwent TAVR or SAVR.
Disclosures: The presenter reported having no financial conflicts regarding this study, conducted free of commercial support.
