User login
Uveitis in juvenile idiopathic arthritis may be preventable
MAUI, HAWAII – Uveitis is a common, highly destructive manifestation of juvenile idiopathic arthritis that is readily treatable when caught early, Dr. Anne M. Stevens said at the 2016 Rheumatology Winter Clinical Symposium.
Moreover, recent evidence from Germany suggests that uveitis may actually be preventable through early aggressive anti-inflammatory therapy, noted Dr. Stevens, a pediatric rheumatologist at Seattle Children’s Hospital and the University of Washington.

She cited a report from investigators participating in the National Pediatric Rheumatological Database in Germany. This large study included 3,512 juvenile idiopathic arthritis (JIA) patients with a mean age at arthritis onset of 7.8 years, a disease duration of less than 12 months at enrollment, and a mean follow-up of 3.6 years.
Uveitis occurred in 5.1% of patients within the first year after onset of JIA, and in another 7.1% following the first year. The key finding in the German study was that aggressive disease-modifying antirheumatic drug (DMARD) therapy during the year prior to uveitis significantly reduced the likelihood of developing this complication. Children on methotrexate during that time period were 37% less likely to develop uveitis than were those not on a DMARD. Moreover, patients placed on methotrexate within the first year after being diagnosed with JIA had a 71% relative risk reduction.
Patients on a tumor necrosis factor inhibitor during the year prior to uveitis had a 44% reduction in the risk of developing the eye complication. Most impressive of all, children on both methotrexate and a TNF inhibitor during the year prior to uveitis had a whopping 90% reduction in the risk of developing uveitis, compared with those not on a DMARD (Arthritis Care Res [Hoboken]. 2016 Jan;68[1]:46-54).
“I was fascinated by this study showing that treatment with two types of therapy may be preventive,” Dr. Stevens commented. “If this is substantiated in another large population-based cohort, it will be interesting to see if practice moves to treating the ANA [antinuclear antibody]–positive oligo JIA patients very early with TNF [tumor necrosis factor] inhibitors and methotrexate to prevent uveitis.”
The logic behind this aggressive preventive therapy lies in the fact that while uveitis occurs in about 20% of patients with oligoarticular JIA overall, roughly 90% of cases involve ANA-positive patients. For this reason, guidelines recommend slit lamp examinations every 3 months for a year in patients with young-onset, ANA-positive JIA.
“Imagine trying to do a slit lamp exam on a 2-year-old. It really helps to send these kids to a pediatric ophthalmologist who’s done a lot of them,” she advised.
The uveitis of JIA is typically anterior, asymptomatic, and low grade. It’s also a leading cause of blindness in childhood. Complications include band keratopathy, glaucomatous optic neuropathy, cataracts, and maculopathy.
“If we catch uveitis early, we can treat this disease really well now,” according to Dr. Stevens.
The initial therapy is short-term topical steroids. It’s important to keep in touch with the ophthalmologist regarding the slit lamp findings, however, because ophthalmologists generally tend to favor longer-term topical steroid therapy, while rheumatologists are appropriately primed to push on to more aggressive systemic therapy very quickly.
The first-line systemic agent for treatment of uveitis in patients with JIA is methotrexate at 1 mg/kg/week. If that doesn’t achieve satisfactory results, pediatric rheumatologists are quick to move on to second-line therapy with cyclosporine, azathioprine, or mycophenolate (CellCept).
“We move on fairly quickly if need be to TNF inhibitors, and we go with very high doses. The literature for infliximab [Remicade] is supportive of 20 mg/kg every 4 weeks. That’s what I use,” she continued.
High-dose adalimumab (Humira) is another option (J Rheumatol. 2013 Jan;40[1]:74-9). However, etanercept (Enbrel) is not effective for this condition. The use of abatacept (Orencia) or rituximab (Rituxan) in refractory patients is supported by favorable case reports.
Dr. Stevens reported having no financial interests relevant to her presentation.
MAUI, HAWAII – Uveitis is a common, highly destructive manifestation of juvenile idiopathic arthritis that is readily treatable when caught early, Dr. Anne M. Stevens said at the 2016 Rheumatology Winter Clinical Symposium.
Moreover, recent evidence from Germany suggests that uveitis may actually be preventable through early aggressive anti-inflammatory therapy, noted Dr. Stevens, a pediatric rheumatologist at Seattle Children’s Hospital and the University of Washington.
She cited a report from investigators participating in the National Pediatric Rheumatological Database in Germany. This large study included 3,512 juvenile idiopathic arthritis (JIA) patients with a mean age at arthritis onset of 7.8 years, a disease duration of less than 12 months at enrollment, and a mean follow-up of 3.6 years.
Uveitis occurred in 5.1% of patients within the first year after onset of JIA, and in another 7.1% following the first year. The key finding in the German study was that aggressive disease-modifying antirheumatic drug (DMARD) therapy during the year prior to uveitis significantly reduced the likelihood of developing this complication. Children on methotrexate during that time period were 37% less likely to develop uveitis than were those not on a DMARD. Moreover, patients placed on methotrexate within the first year after being diagnosed with JIA had a 71% relative risk reduction.
Patients on a tumor necrosis factor inhibitor during the year prior to uveitis had a 44% reduction in the risk of developing the eye complication. Most impressive of all, children on both methotrexate and a TNF inhibitor during the year prior to uveitis had a whopping 90% reduction in the risk of developing uveitis, compared with those not on a DMARD (Arthritis Care Res [Hoboken]. 2016 Jan;68[1]:46-54).
“I was fascinated by this study showing that treatment with two types of therapy may be preventive,” Dr. Stevens commented. “If this is substantiated in another large population-based cohort, it will be interesting to see if practice moves to treating the ANA [antinuclear antibody]–positive oligo JIA patients very early with TNF [tumor necrosis factor] inhibitors and methotrexate to prevent uveitis.”
The logic behind this aggressive preventive therapy lies in the fact that while uveitis occurs in about 20% of patients with oligoarticular JIA overall, roughly 90% of cases involve ANA-positive patients. For this reason, guidelines recommend slit lamp examinations every 3 months for a year in patients with young-onset, ANA-positive JIA.
“Imagine trying to do a slit lamp exam on a 2-year-old. It really helps to send these kids to a pediatric ophthalmologist who’s done a lot of them,” she advised.
The uveitis of JIA is typically anterior, asymptomatic, and low grade. It’s also a leading cause of blindness in childhood. Complications include band keratopathy, glaucomatous optic neuropathy, cataracts, and maculopathy.
“If we catch uveitis early, we can treat this disease really well now,” according to Dr. Stevens.
The initial therapy is short-term topical steroids. It’s important to keep in touch with the ophthalmologist regarding the slit lamp findings, however, because ophthalmologists generally tend to favor longer-term topical steroid therapy, while rheumatologists are appropriately primed to push on to more aggressive systemic therapy very quickly.
The first-line systemic agent for treatment of uveitis in patients with JIA is methotrexate at 1 mg/kg/week. If that doesn’t achieve satisfactory results, pediatric rheumatologists are quick to move on to second-line therapy with cyclosporine, azathioprine, or mycophenolate (CellCept).
“We move on fairly quickly if need be to TNF inhibitors, and we go with very high doses. The literature for infliximab [Remicade] is supportive of 20 mg/kg every 4 weeks. That’s what I use,” she continued.
High-dose adalimumab (Humira) is another option (J Rheumatol. 2013 Jan;40[1]:74-9). However, etanercept (Enbrel) is not effective for this condition. The use of abatacept (Orencia) or rituximab (Rituxan) in refractory patients is supported by favorable case reports.
Dr. Stevens reported having no financial interests relevant to her presentation.
MAUI, HAWAII – Uveitis is a common, highly destructive manifestation of juvenile idiopathic arthritis that is readily treatable when caught early, Dr. Anne M. Stevens said at the 2016 Rheumatology Winter Clinical Symposium.
Moreover, recent evidence from Germany suggests that uveitis may actually be preventable through early aggressive anti-inflammatory therapy, noted Dr. Stevens, a pediatric rheumatologist at Seattle Children’s Hospital and the University of Washington.
She cited a report from investigators participating in the National Pediatric Rheumatological Database in Germany. This large study included 3,512 juvenile idiopathic arthritis (JIA) patients with a mean age at arthritis onset of 7.8 years, a disease duration of less than 12 months at enrollment, and a mean follow-up of 3.6 years.
Uveitis occurred in 5.1% of patients within the first year after onset of JIA, and in another 7.1% following the first year. The key finding in the German study was that aggressive disease-modifying antirheumatic drug (DMARD) therapy during the year prior to uveitis significantly reduced the likelihood of developing this complication. Children on methotrexate during that time period were 37% less likely to develop uveitis than were those not on a DMARD. Moreover, patients placed on methotrexate within the first year after being diagnosed with JIA had a 71% relative risk reduction.
Patients on a tumor necrosis factor inhibitor during the year prior to uveitis had a 44% reduction in the risk of developing the eye complication. Most impressive of all, children on both methotrexate and a TNF inhibitor during the year prior to uveitis had a whopping 90% reduction in the risk of developing uveitis, compared with those not on a DMARD (Arthritis Care Res [Hoboken]. 2016 Jan;68[1]:46-54).
“I was fascinated by this study showing that treatment with two types of therapy may be preventive,” Dr. Stevens commented. “If this is substantiated in another large population-based cohort, it will be interesting to see if practice moves to treating the ANA [antinuclear antibody]–positive oligo JIA patients very early with TNF [tumor necrosis factor] inhibitors and methotrexate to prevent uveitis.”
The logic behind this aggressive preventive therapy lies in the fact that while uveitis occurs in about 20% of patients with oligoarticular JIA overall, roughly 90% of cases involve ANA-positive patients. For this reason, guidelines recommend slit lamp examinations every 3 months for a year in patients with young-onset, ANA-positive JIA.
“Imagine trying to do a slit lamp exam on a 2-year-old. It really helps to send these kids to a pediatric ophthalmologist who’s done a lot of them,” she advised.
The uveitis of JIA is typically anterior, asymptomatic, and low grade. It’s also a leading cause of blindness in childhood. Complications include band keratopathy, glaucomatous optic neuropathy, cataracts, and maculopathy.
“If we catch uveitis early, we can treat this disease really well now,” according to Dr. Stevens.
The initial therapy is short-term topical steroids. It’s important to keep in touch with the ophthalmologist regarding the slit lamp findings, however, because ophthalmologists generally tend to favor longer-term topical steroid therapy, while rheumatologists are appropriately primed to push on to more aggressive systemic therapy very quickly.
The first-line systemic agent for treatment of uveitis in patients with JIA is methotrexate at 1 mg/kg/week. If that doesn’t achieve satisfactory results, pediatric rheumatologists are quick to move on to second-line therapy with cyclosporine, azathioprine, or mycophenolate (CellCept).
“We move on fairly quickly if need be to TNF inhibitors, and we go with very high doses. The literature for infliximab [Remicade] is supportive of 20 mg/kg every 4 weeks. That’s what I use,” she continued.
High-dose adalimumab (Humira) is another option (J Rheumatol. 2013 Jan;40[1]:74-9). However, etanercept (Enbrel) is not effective for this condition. The use of abatacept (Orencia) or rituximab (Rituxan) in refractory patients is supported by favorable case reports.
Dr. Stevens reported having no financial interests relevant to her presentation.
EXPERT ANALYSIS FROM RWCS 2016

USPSTF draft recommendation nixes skin cancer screening
WAIKOLOA, HAWAII – In light of the U.S. Preventive Services Task Force’s recent rejection of population-based melanoma screening in a draft recommendation, the future of skin examination for early detection of melanoma most likely lies in the development of a targeted, risk-stratified screening approach, Dr. Michael A. Marchetti said at the Hawaii Dermatology Seminar.
The logical place to start would be in white men above age 50. They account for 50% of all melanoma deaths in the United States. Thus, this is a group where melanoma screening is most likely to bring significant demonstrable benefit with the least potential harm, according to Dr. Marchetti, a dermatologist at Memorial Sloan Kettering Cancer Center in New York.

In its December 2015 draft recommendation statement, the USPSTF declared “current evidence is insufficient to assess the balance of benefits and harms of visual skin cancer screening in adults.” The panel drew the same conclusion in its previous 2009 assessment, Dr. Marchetti noted at the seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
Panelists did not find persuasive the German SCREEN study (Skin Cancer Research to Provide Evidence for Effectiveness of Screening in Northern Germany), which initially generated enormous excitement among skin cancer experts worldwide. SCREEN investigators triumphantly reported a 48% drop in mortality from melanoma 5 years after the German state of Schleswig-Holstein instituted a population-based skin cancer screening program based upon total body skin examination by dermatologists and specially trained primary care physicians (J Am Acad Dermatol. 2012 Feb;66[2]:201-11).
However, the SCREEN study has since come under a variety of criticisms. The USPSTF took note, and in its December update declared the study had “important methodologic limitations” which “raise questions as to the plausibility of the observed effect.” In a best case scenario, according to the panelists, the benefit of the Schleswig-Holstein melanoma awareness campaign and free screening program worked out to at most one fewer melanoma death per 100,000 persons screened annually over a decade.
Dr. Marchetti noted that the German federal government found the SCREEN program initial results so impressive that a national program of free biannual skin cancer screening for all adults age 35 and older has been adopted. Disappointingly, however, investigators at the International Prevention Research Institute in Lyon, France, have reported that in the first 5 years of the national program, melanoma mortality rates not only didn’t decrease, they actually increased by 2.6% in men and 0.02% in women. Moreover, the same investigators determined that in the second 5-year period of screening in Schleswig-Holstein, melanoma mortality rates shot back up to levels seen before initiation of the screening program (BMJ Open. 2015 Sep 15;5[9]:e008158).
Dr. Marchetti said that based upon his reading of the USPSTF 2009 and December 2015 reports, he doesn’t think the panel takes issue with the concept that earlier detection of melanomas while they are thinner results in a much better prognosis. Their major concern is with the scarcity of data regarding the potential harms involved in population-based skin cancer screening, which include the cost and morbidity of the enormous number of skin biopsies which would result from such a screening program, with most of those biopsies coming back negative.
He added that he shares those reservations.
“I have a lot of concern about targeting low-risk populations for screening, particularly children and adolescents and dark-skinned individuals. I think in those circumstances we’re more likely to have greater harm,” the dermatologist said.
Indeed, he and his coinvestigators recently analyzed two large dermatopathology databases and concluded that during 2009-2013 in the United States, 1,035 biopsies of nevi were performed in patients age 19 years or younger in order to find one melanoma (JAMA Dermatol. 2015 Apr;151[4]:447-8).
Dr. Marchetti also recently published a viewpoint article in which he asserted that increased pressure to detect acral lentiginous melanoma in dark-skinned individuals could lead to significant harms with minimal return benefit (JAMA Dermatol. 2015 Oct;151[10]:1055-6).
The December 2015 update from USPSTF was the group’s draft document, with the final recommendations forthcoming this year. The public comment period has closed, and no major professional organization in the United States – not the American College of Physicians, the American Academy of Family Physicians, or even the American Academy of Dermatology – specifically recommends a clinical visual skin cancer screening examination.
In response to an audience question, session chair Dr. Ashfaq A. Marghoob commented that the USPSTF’s stance has big implications for physician reimbursement for skin cancer screening examinations in patients who have no symptoms or aren’t already under surveillance due to high risk of skin cancer.
“There is a code for screening, but by and large no insurance carrier will reimburse you if you use that code. In my experience, they’ll default to the U.S. Preventive Services Task Force that it’s a noncovered service. However, the minute you make your chief complaint ‘nevus,’ or ‘actinic keratosis,’ or ‘neoplasm undetermined’ and list skin cancer screening as a secondary service, then it’s covered,” said Dr. Marghoob, of Memorial Sloan Kettering Cancer Center, New York.
In addressing another audience question, he said he is not aware of any lawsuit ever having arisen directed at a physician who participated in “melanoma Monday” skin cancer screening using the American Academy of Dermatology forms with the examinee’s signature. Participating physicians are thoroughly protected.
Dr. Marchetti and Dr. Marghoob reported having no financial interests relevant to their presentations.
The SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – In light of the U.S. Preventive Services Task Force’s recent rejection of population-based melanoma screening in a draft recommendation, the future of skin examination for early detection of melanoma most likely lies in the development of a targeted, risk-stratified screening approach, Dr. Michael A. Marchetti said at the Hawaii Dermatology Seminar.
The logical place to start would be in white men above age 50. They account for 50% of all melanoma deaths in the United States. Thus, this is a group where melanoma screening is most likely to bring significant demonstrable benefit with the least potential harm, according to Dr. Marchetti, a dermatologist at Memorial Sloan Kettering Cancer Center in New York.
In its December 2015 draft recommendation statement, the USPSTF declared “current evidence is insufficient to assess the balance of benefits and harms of visual skin cancer screening in adults.” The panel drew the same conclusion in its previous 2009 assessment, Dr. Marchetti noted at the seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
Panelists did not find persuasive the German SCREEN study (Skin Cancer Research to Provide Evidence for Effectiveness of Screening in Northern Germany), which initially generated enormous excitement among skin cancer experts worldwide. SCREEN investigators triumphantly reported a 48% drop in mortality from melanoma 5 years after the German state of Schleswig-Holstein instituted a population-based skin cancer screening program based upon total body skin examination by dermatologists and specially trained primary care physicians (J Am Acad Dermatol. 2012 Feb;66[2]:201-11).
However, the SCREEN study has since come under a variety of criticisms. The USPSTF took note, and in its December update declared the study had “important methodologic limitations” which “raise questions as to the plausibility of the observed effect.” In a best case scenario, according to the panelists, the benefit of the Schleswig-Holstein melanoma awareness campaign and free screening program worked out to at most one fewer melanoma death per 100,000 persons screened annually over a decade.
Dr. Marchetti noted that the German federal government found the SCREEN program initial results so impressive that a national program of free biannual skin cancer screening for all adults age 35 and older has been adopted. Disappointingly, however, investigators at the International Prevention Research Institute in Lyon, France, have reported that in the first 5 years of the national program, melanoma mortality rates not only didn’t decrease, they actually increased by 2.6% in men and 0.02% in women. Moreover, the same investigators determined that in the second 5-year period of screening in Schleswig-Holstein, melanoma mortality rates shot back up to levels seen before initiation of the screening program (BMJ Open. 2015 Sep 15;5[9]:e008158).
Dr. Marchetti said that based upon his reading of the USPSTF 2009 and December 2015 reports, he doesn’t think the panel takes issue with the concept that earlier detection of melanomas while they are thinner results in a much better prognosis. Their major concern is with the scarcity of data regarding the potential harms involved in population-based skin cancer screening, which include the cost and morbidity of the enormous number of skin biopsies which would result from such a screening program, with most of those biopsies coming back negative.
He added that he shares those reservations.
“I have a lot of concern about targeting low-risk populations for screening, particularly children and adolescents and dark-skinned individuals. I think in those circumstances we’re more likely to have greater harm,” the dermatologist said.
Indeed, he and his coinvestigators recently analyzed two large dermatopathology databases and concluded that during 2009-2013 in the United States, 1,035 biopsies of nevi were performed in patients age 19 years or younger in order to find one melanoma (JAMA Dermatol. 2015 Apr;151[4]:447-8).
Dr. Marchetti also recently published a viewpoint article in which he asserted that increased pressure to detect acral lentiginous melanoma in dark-skinned individuals could lead to significant harms with minimal return benefit (JAMA Dermatol. 2015 Oct;151[10]:1055-6).
The December 2015 update from USPSTF was the group’s draft document, with the final recommendations forthcoming this year. The public comment period has closed, and no major professional organization in the United States – not the American College of Physicians, the American Academy of Family Physicians, or even the American Academy of Dermatology – specifically recommends a clinical visual skin cancer screening examination.
In response to an audience question, session chair Dr. Ashfaq A. Marghoob commented that the USPSTF’s stance has big implications for physician reimbursement for skin cancer screening examinations in patients who have no symptoms or aren’t already under surveillance due to high risk of skin cancer.
“There is a code for screening, but by and large no insurance carrier will reimburse you if you use that code. In my experience, they’ll default to the U.S. Preventive Services Task Force that it’s a noncovered service. However, the minute you make your chief complaint ‘nevus,’ or ‘actinic keratosis,’ or ‘neoplasm undetermined’ and list skin cancer screening as a secondary service, then it’s covered,” said Dr. Marghoob, of Memorial Sloan Kettering Cancer Center, New York.
In addressing another audience question, he said he is not aware of any lawsuit ever having arisen directed at a physician who participated in “melanoma Monday” skin cancer screening using the American Academy of Dermatology forms with the examinee’s signature. Participating physicians are thoroughly protected.
Dr. Marchetti and Dr. Marghoob reported having no financial interests relevant to their presentations.
The SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – In light of the U.S. Preventive Services Task Force’s recent rejection of population-based melanoma screening in a draft recommendation, the future of skin examination for early detection of melanoma most likely lies in the development of a targeted, risk-stratified screening approach, Dr. Michael A. Marchetti said at the Hawaii Dermatology Seminar.
The logical place to start would be in white men above age 50. They account for 50% of all melanoma deaths in the United States. Thus, this is a group where melanoma screening is most likely to bring significant demonstrable benefit with the least potential harm, according to Dr. Marchetti, a dermatologist at Memorial Sloan Kettering Cancer Center in New York.
In its December 2015 draft recommendation statement, the USPSTF declared “current evidence is insufficient to assess the balance of benefits and harms of visual skin cancer screening in adults.” The panel drew the same conclusion in its previous 2009 assessment, Dr. Marchetti noted at the seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
Panelists did not find persuasive the German SCREEN study (Skin Cancer Research to Provide Evidence for Effectiveness of Screening in Northern Germany), which initially generated enormous excitement among skin cancer experts worldwide. SCREEN investigators triumphantly reported a 48% drop in mortality from melanoma 5 years after the German state of Schleswig-Holstein instituted a population-based skin cancer screening program based upon total body skin examination by dermatologists and specially trained primary care physicians (J Am Acad Dermatol. 2012 Feb;66[2]:201-11).
However, the SCREEN study has since come under a variety of criticisms. The USPSTF took note, and in its December update declared the study had “important methodologic limitations” which “raise questions as to the plausibility of the observed effect.” In a best case scenario, according to the panelists, the benefit of the Schleswig-Holstein melanoma awareness campaign and free screening program worked out to at most one fewer melanoma death per 100,000 persons screened annually over a decade.
Dr. Marchetti noted that the German federal government found the SCREEN program initial results so impressive that a national program of free biannual skin cancer screening for all adults age 35 and older has been adopted. Disappointingly, however, investigators at the International Prevention Research Institute in Lyon, France, have reported that in the first 5 years of the national program, melanoma mortality rates not only didn’t decrease, they actually increased by 2.6% in men and 0.02% in women. Moreover, the same investigators determined that in the second 5-year period of screening in Schleswig-Holstein, melanoma mortality rates shot back up to levels seen before initiation of the screening program (BMJ Open. 2015 Sep 15;5[9]:e008158).
Dr. Marchetti said that based upon his reading of the USPSTF 2009 and December 2015 reports, he doesn’t think the panel takes issue with the concept that earlier detection of melanomas while they are thinner results in a much better prognosis. Their major concern is with the scarcity of data regarding the potential harms involved in population-based skin cancer screening, which include the cost and morbidity of the enormous number of skin biopsies which would result from such a screening program, with most of those biopsies coming back negative.
He added that he shares those reservations.
“I have a lot of concern about targeting low-risk populations for screening, particularly children and adolescents and dark-skinned individuals. I think in those circumstances we’re more likely to have greater harm,” the dermatologist said.
Indeed, he and his coinvestigators recently analyzed two large dermatopathology databases and concluded that during 2009-2013 in the United States, 1,035 biopsies of nevi were performed in patients age 19 years or younger in order to find one melanoma (JAMA Dermatol. 2015 Apr;151[4]:447-8).
Dr. Marchetti also recently published a viewpoint article in which he asserted that increased pressure to detect acral lentiginous melanoma in dark-skinned individuals could lead to significant harms with minimal return benefit (JAMA Dermatol. 2015 Oct;151[10]:1055-6).
The December 2015 update from USPSTF was the group’s draft document, with the final recommendations forthcoming this year. The public comment period has closed, and no major professional organization in the United States – not the American College of Physicians, the American Academy of Family Physicians, or even the American Academy of Dermatology – specifically recommends a clinical visual skin cancer screening examination.
In response to an audience question, session chair Dr. Ashfaq A. Marghoob commented that the USPSTF’s stance has big implications for physician reimbursement for skin cancer screening examinations in patients who have no symptoms or aren’t already under surveillance due to high risk of skin cancer.
“There is a code for screening, but by and large no insurance carrier will reimburse you if you use that code. In my experience, they’ll default to the U.S. Preventive Services Task Force that it’s a noncovered service. However, the minute you make your chief complaint ‘nevus,’ or ‘actinic keratosis,’ or ‘neoplasm undetermined’ and list skin cancer screening as a secondary service, then it’s covered,” said Dr. Marghoob, of Memorial Sloan Kettering Cancer Center, New York.
In addressing another audience question, he said he is not aware of any lawsuit ever having arisen directed at a physician who participated in “melanoma Monday” skin cancer screening using the American Academy of Dermatology forms with the examinee’s signature. Participating physicians are thoroughly protected.
Dr. Marchetti and Dr. Marghoob reported having no financial interests relevant to their presentations.
The SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM THE SDEF HAWAII DERMATOLOGY SEMINAR

Keep cancer prominent in differential diagnoses of pediatric rheumatic complaints
MAUI, HAWAII – The first thing nonpediatric rheumatologists need to understand about a child who presents with rheumatic complaints is the importance of ruling out malignancy, Dr. Anne M. Stevens stressed at the 2016 Rheumatology Winter Clinical Symposium.
“This is something I think we in pediatric rheumatology worry about a lot more than adult rheumatologists: malignancy and how to distinguish it from rheumatic diseases,” said Dr. Stevens, a pediatric rheumatologist at Seattle Children’s Hospital and the University of Washington.

And with there being only about 250 pediatric rheumatologists in the entire United States, and a handful of states having none at all, it’s important that physicians in other specialties be familiar with key differences between pediatric and adult rheumatic diseases, she added.
A diverse group of malignancies in children and teens can present with swollen joints or other rheumatic features. One of the biggest red flags suggestive of an underlying malignancy is disproportionate pain, especially nonarticular bone pain or tenderness or back pain as a major presenting feature.
The source of this bone or back pain may be a reactive arthritis in response to local bony changes caused by an osteosarcoma or neuroblastoma, or malignant effusions as a result of leukemia or lymphoma, Dr. Stevens explained.
Other atypical features that get her thinking about the possibility of underlying malignancy rather than juvenile idiopathic arthritis include weight loss, night sweats, fatigue, fever, and night pain. Overall, young patients with an undetected cancer just seem sicker than those with rheumatic disease, she continued.
In a classic retrospective study of 29 children and teens who initially presented to pediatric rheumatologists at the University of British Columbia and were ultimately found to have malignancy, the most common provisional rheumatologic diagnosis was juvenile rheumatoid arthritis in 12 of the 29. Five patients were thought by referring physicians to have a connective tissue disease, and three each were believed to have discitis or spondyloarthropathy. Other provisional diagnoses included systemic lupus erythematosus in two patients; Kawasaki disease in two; and Lyme disease, mixed connective tissue disease, and dermatomyositis in one each.
The final diagnoses included leukemia in 13 patients, neuroblastoma in 6, lymphoma in 3, Ewing sarcoma in 3, and single cases of ependymoma, thalamic glioma, epithelioma, and sarcoma (J Pediatr. 1999 Jan;134[1]:53-7).
Working backwards, the investigators developed a set of clinical clues helpful in detecting malignancy. Nonarticular bone pain was a prominent presenting complaint in 20 of the 29, bone tenderness in 8, and back pain in 9.
“Bone tenderness is not seen in juvenile idiopathic arthritis at all, and children under about age 10 just don’t get low back pain. That really alerts us to malignancy concern,” Dr. Stevens said.
Night sweats were present in four patients, severe constitutional symptoms in nine.
Two patients had true juvenile idiopathic arthritis, so that finding doesn’t rule out malignancy.
Surprisingly, the CBC was normal in three-quarters of patients. Antinuclear antibody testing is not helpful, as it can be strongly positive in the setting of pediatric malignancy, but lactate dehydrogenase and uric acid tests are important in making the differential diagnosis.
If there are any surprising findings raising concerns about possible malignancy, a bone marrow biopsy is essential.
“We have a lot of fights with our hematologists when we’re trying to get a bone marrow biopsy and they say, ‘No, the CBC is normal so you don’t need a bone marrow biopsy.’ But you have to get that bone marrow biopsy. A strategy that works is for us to say, ‘Could you please include a note in the chart that it’s okay for us to give steroids because you’re sure it’s not a lymphoma?’ Then we usually get it scheduled for the next day,” Dr. Stevens said.
She reported having no relevant financial disclosures.
MAUI, HAWAII – The first thing nonpediatric rheumatologists need to understand about a child who presents with rheumatic complaints is the importance of ruling out malignancy, Dr. Anne M. Stevens stressed at the 2016 Rheumatology Winter Clinical Symposium.
“This is something I think we in pediatric rheumatology worry about a lot more than adult rheumatologists: malignancy and how to distinguish it from rheumatic diseases,” said Dr. Stevens, a pediatric rheumatologist at Seattle Children’s Hospital and the University of Washington.
And with there being only about 250 pediatric rheumatologists in the entire United States, and a handful of states having none at all, it’s important that physicians in other specialties be familiar with key differences between pediatric and adult rheumatic diseases, she added.
A diverse group of malignancies in children and teens can present with swollen joints or other rheumatic features. One of the biggest red flags suggestive of an underlying malignancy is disproportionate pain, especially nonarticular bone pain or tenderness or back pain as a major presenting feature.
The source of this bone or back pain may be a reactive arthritis in response to local bony changes caused by an osteosarcoma or neuroblastoma, or malignant effusions as a result of leukemia or lymphoma, Dr. Stevens explained.
Other atypical features that get her thinking about the possibility of underlying malignancy rather than juvenile idiopathic arthritis include weight loss, night sweats, fatigue, fever, and night pain. Overall, young patients with an undetected cancer just seem sicker than those with rheumatic disease, she continued.
In a classic retrospective study of 29 children and teens who initially presented to pediatric rheumatologists at the University of British Columbia and were ultimately found to have malignancy, the most common provisional rheumatologic diagnosis was juvenile rheumatoid arthritis in 12 of the 29. Five patients were thought by referring physicians to have a connective tissue disease, and three each were believed to have discitis or spondyloarthropathy. Other provisional diagnoses included systemic lupus erythematosus in two patients; Kawasaki disease in two; and Lyme disease, mixed connective tissue disease, and dermatomyositis in one each.
The final diagnoses included leukemia in 13 patients, neuroblastoma in 6, lymphoma in 3, Ewing sarcoma in 3, and single cases of ependymoma, thalamic glioma, epithelioma, and sarcoma (J Pediatr. 1999 Jan;134[1]:53-7).
Working backwards, the investigators developed a set of clinical clues helpful in detecting malignancy. Nonarticular bone pain was a prominent presenting complaint in 20 of the 29, bone tenderness in 8, and back pain in 9.
“Bone tenderness is not seen in juvenile idiopathic arthritis at all, and children under about age 10 just don’t get low back pain. That really alerts us to malignancy concern,” Dr. Stevens said.
Night sweats were present in four patients, severe constitutional symptoms in nine.
Two patients had true juvenile idiopathic arthritis, so that finding doesn’t rule out malignancy.
Surprisingly, the CBC was normal in three-quarters of patients. Antinuclear antibody testing is not helpful, as it can be strongly positive in the setting of pediatric malignancy, but lactate dehydrogenase and uric acid tests are important in making the differential diagnosis.
If there are any surprising findings raising concerns about possible malignancy, a bone marrow biopsy is essential.
“We have a lot of fights with our hematologists when we’re trying to get a bone marrow biopsy and they say, ‘No, the CBC is normal so you don’t need a bone marrow biopsy.’ But you have to get that bone marrow biopsy. A strategy that works is for us to say, ‘Could you please include a note in the chart that it’s okay for us to give steroids because you’re sure it’s not a lymphoma?’ Then we usually get it scheduled for the next day,” Dr. Stevens said.
She reported having no relevant financial disclosures.
MAUI, HAWAII – The first thing nonpediatric rheumatologists need to understand about a child who presents with rheumatic complaints is the importance of ruling out malignancy, Dr. Anne M. Stevens stressed at the 2016 Rheumatology Winter Clinical Symposium.
“This is something I think we in pediatric rheumatology worry about a lot more than adult rheumatologists: malignancy and how to distinguish it from rheumatic diseases,” said Dr. Stevens, a pediatric rheumatologist at Seattle Children’s Hospital and the University of Washington.
And with there being only about 250 pediatric rheumatologists in the entire United States, and a handful of states having none at all, it’s important that physicians in other specialties be familiar with key differences between pediatric and adult rheumatic diseases, she added.
A diverse group of malignancies in children and teens can present with swollen joints or other rheumatic features. One of the biggest red flags suggestive of an underlying malignancy is disproportionate pain, especially nonarticular bone pain or tenderness or back pain as a major presenting feature.
The source of this bone or back pain may be a reactive arthritis in response to local bony changes caused by an osteosarcoma or neuroblastoma, or malignant effusions as a result of leukemia or lymphoma, Dr. Stevens explained.
Other atypical features that get her thinking about the possibility of underlying malignancy rather than juvenile idiopathic arthritis include weight loss, night sweats, fatigue, fever, and night pain. Overall, young patients with an undetected cancer just seem sicker than those with rheumatic disease, she continued.
In a classic retrospective study of 29 children and teens who initially presented to pediatric rheumatologists at the University of British Columbia and were ultimately found to have malignancy, the most common provisional rheumatologic diagnosis was juvenile rheumatoid arthritis in 12 of the 29. Five patients were thought by referring physicians to have a connective tissue disease, and three each were believed to have discitis or spondyloarthropathy. Other provisional diagnoses included systemic lupus erythematosus in two patients; Kawasaki disease in two; and Lyme disease, mixed connective tissue disease, and dermatomyositis in one each.
The final diagnoses included leukemia in 13 patients, neuroblastoma in 6, lymphoma in 3, Ewing sarcoma in 3, and single cases of ependymoma, thalamic glioma, epithelioma, and sarcoma (J Pediatr. 1999 Jan;134[1]:53-7).
Working backwards, the investigators developed a set of clinical clues helpful in detecting malignancy. Nonarticular bone pain was a prominent presenting complaint in 20 of the 29, bone tenderness in 8, and back pain in 9.
“Bone tenderness is not seen in juvenile idiopathic arthritis at all, and children under about age 10 just don’t get low back pain. That really alerts us to malignancy concern,” Dr. Stevens said.
Night sweats were present in four patients, severe constitutional symptoms in nine.
Two patients had true juvenile idiopathic arthritis, so that finding doesn’t rule out malignancy.
Surprisingly, the CBC was normal in three-quarters of patients. Antinuclear antibody testing is not helpful, as it can be strongly positive in the setting of pediatric malignancy, but lactate dehydrogenase and uric acid tests are important in making the differential diagnosis.
If there are any surprising findings raising concerns about possible malignancy, a bone marrow biopsy is essential.
“We have a lot of fights with our hematologists when we’re trying to get a bone marrow biopsy and they say, ‘No, the CBC is normal so you don’t need a bone marrow biopsy.’ But you have to get that bone marrow biopsy. A strategy that works is for us to say, ‘Could you please include a note in the chart that it’s okay for us to give steroids because you’re sure it’s not a lymphoma?’ Then we usually get it scheduled for the next day,” Dr. Stevens said.
She reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM RWCS 2016

Romosozumab, coming ACR guidelines mark recent high points in osteoporosis
MAUI, HAWAII – The investigational bone-building agent romosozumab provided the therapeutic highlight in the field of osteoporosis during the past year, Dr. Martin J. Bergman said at the 2016 Rheumatology Winter Clinical Symposium.
Romosozumab is a monoclonal antibody directed against sclerostin, a glycoprotein that prevents mesenchymal cells from becoming osteoblasts. By inhibiting sclerostin, romosozumab promotes osteoblast production. The result is increased bone mineral density and bone formation coupled with decreased bone resorption, providing physicians with a promising new avenue for rapidly building strong bone, explained Dr. Bergman of Drexel University in Philadelphia and chief of the section of rheumatology at Taylor Hospital in Ridley Park, Pa.
Romosozumab caught his eye in a 12-month randomized trial presented last fall at the annual meeting of the American College of Rheumatology. The 430 postmenopausal participants were assigned to blinded romosozumab at 210 mg delivered by subcutaneous injection once per month, blinded placebo, or open-label teriparatide (Forteo). The primary endpoint in this secondary analysis was change in bone strength as measured using the Food and Drug Administration–approved method of finite element analysis based upon quantitative CT imaging.
Romosozumab boosted bone strength at the spine by 27.3% at 12 months, compared with a 3.9% reduction from baseline with placebo and an 18.5% increase with teriparatide. At the hip, romosozumab delivered a 3.6% increase in bone strength versus no significant change from baseline in the other two study arms. Thus, romosozumab increased bone strength both in the cortical and trabecular compartments even more than did teriparatide, the most potent drug currently available for building bone mass.
“The numbers are very impressive,” Dr. Bergman observed. “Trabecular bone, cortical bone, whole bone – across the board, we haven’t seen similar numbers before. I think this is going to be a very exciting new approach to the treatment of osteoporosis. We need to keep an eye on this.”
Romosozumab, which is being codeveloped by Amgen and UCB, is now in phase III testing.
The other big news in osteoporosis is that later this year the ACR will undertake a revision of its 2010 guidelines for the prevention and treatment of glucocorticoid-induced osteoporosis (Arthritis Care Res [Hoboken]. 2010 Nov;62[11]:1515-26).
Among the actions that need to be taken are the incorporation of denosumab (Prolia) and ibandronate (Boniva) into the treatment recommendations, as well as clarification of the recommendation for supplemental calcium in light of recent evidence of an association between high serum calcium and increased cardiovascular risk. Most of the lifestyle modification recommendations in the current guidelines are supported by a weak level of evidence C, meaning “expert opinion,” and the hope is that the evidence has become stronger since 2010, he said.
Dr. Bergman reported having no financial conflicts regarding his presentation.
MAUI, HAWAII – The investigational bone-building agent romosozumab provided the therapeutic highlight in the field of osteoporosis during the past year, Dr. Martin J. Bergman said at the 2016 Rheumatology Winter Clinical Symposium.
Romosozumab is a monoclonal antibody directed against sclerostin, a glycoprotein that prevents mesenchymal cells from becoming osteoblasts. By inhibiting sclerostin, romosozumab promotes osteoblast production. The result is increased bone mineral density and bone formation coupled with decreased bone resorption, providing physicians with a promising new avenue for rapidly building strong bone, explained Dr. Bergman of Drexel University in Philadelphia and chief of the section of rheumatology at Taylor Hospital in Ridley Park, Pa.
Romosozumab caught his eye in a 12-month randomized trial presented last fall at the annual meeting of the American College of Rheumatology. The 430 postmenopausal participants were assigned to blinded romosozumab at 210 mg delivered by subcutaneous injection once per month, blinded placebo, or open-label teriparatide (Forteo). The primary endpoint in this secondary analysis was change in bone strength as measured using the Food and Drug Administration–approved method of finite element analysis based upon quantitative CT imaging.
Romosozumab boosted bone strength at the spine by 27.3% at 12 months, compared with a 3.9% reduction from baseline with placebo and an 18.5% increase with teriparatide. At the hip, romosozumab delivered a 3.6% increase in bone strength versus no significant change from baseline in the other two study arms. Thus, romosozumab increased bone strength both in the cortical and trabecular compartments even more than did teriparatide, the most potent drug currently available for building bone mass.
“The numbers are very impressive,” Dr. Bergman observed. “Trabecular bone, cortical bone, whole bone – across the board, we haven’t seen similar numbers before. I think this is going to be a very exciting new approach to the treatment of osteoporosis. We need to keep an eye on this.”
Romosozumab, which is being codeveloped by Amgen and UCB, is now in phase III testing.
The other big news in osteoporosis is that later this year the ACR will undertake a revision of its 2010 guidelines for the prevention and treatment of glucocorticoid-induced osteoporosis (Arthritis Care Res [Hoboken]. 2010 Nov;62[11]:1515-26).
Among the actions that need to be taken are the incorporation of denosumab (Prolia) and ibandronate (Boniva) into the treatment recommendations, as well as clarification of the recommendation for supplemental calcium in light of recent evidence of an association between high serum calcium and increased cardiovascular risk. Most of the lifestyle modification recommendations in the current guidelines are supported by a weak level of evidence C, meaning “expert opinion,” and the hope is that the evidence has become stronger since 2010, he said.
Dr. Bergman reported having no financial conflicts regarding his presentation.
MAUI, HAWAII – The investigational bone-building agent romosozumab provided the therapeutic highlight in the field of osteoporosis during the past year, Dr. Martin J. Bergman said at the 2016 Rheumatology Winter Clinical Symposium.
Romosozumab is a monoclonal antibody directed against sclerostin, a glycoprotein that prevents mesenchymal cells from becoming osteoblasts. By inhibiting sclerostin, romosozumab promotes osteoblast production. The result is increased bone mineral density and bone formation coupled with decreased bone resorption, providing physicians with a promising new avenue for rapidly building strong bone, explained Dr. Bergman of Drexel University in Philadelphia and chief of the section of rheumatology at Taylor Hospital in Ridley Park, Pa.
Romosozumab caught his eye in a 12-month randomized trial presented last fall at the annual meeting of the American College of Rheumatology. The 430 postmenopausal participants were assigned to blinded romosozumab at 210 mg delivered by subcutaneous injection once per month, blinded placebo, or open-label teriparatide (Forteo). The primary endpoint in this secondary analysis was change in bone strength as measured using the Food and Drug Administration–approved method of finite element analysis based upon quantitative CT imaging.
Romosozumab boosted bone strength at the spine by 27.3% at 12 months, compared with a 3.9% reduction from baseline with placebo and an 18.5% increase with teriparatide. At the hip, romosozumab delivered a 3.6% increase in bone strength versus no significant change from baseline in the other two study arms. Thus, romosozumab increased bone strength both in the cortical and trabecular compartments even more than did teriparatide, the most potent drug currently available for building bone mass.
“The numbers are very impressive,” Dr. Bergman observed. “Trabecular bone, cortical bone, whole bone – across the board, we haven’t seen similar numbers before. I think this is going to be a very exciting new approach to the treatment of osteoporosis. We need to keep an eye on this.”
Romosozumab, which is being codeveloped by Amgen and UCB, is now in phase III testing.
The other big news in osteoporosis is that later this year the ACR will undertake a revision of its 2010 guidelines for the prevention and treatment of glucocorticoid-induced osteoporosis (Arthritis Care Res [Hoboken]. 2010 Nov;62[11]:1515-26).
Among the actions that need to be taken are the incorporation of denosumab (Prolia) and ibandronate (Boniva) into the treatment recommendations, as well as clarification of the recommendation for supplemental calcium in light of recent evidence of an association between high serum calcium and increased cardiovascular risk. Most of the lifestyle modification recommendations in the current guidelines are supported by a weak level of evidence C, meaning “expert opinion,” and the hope is that the evidence has become stronger since 2010, he said.
Dr. Bergman reported having no financial conflicts regarding his presentation.
EXPERT ANALYSIS FROM RWCS 2016
NNTs show once-unimaginable psoriasis outcomes now readily attainable
WAIKOLOA, HAWAII – Scrutiny of the number needed to treat with various systemic drugs to achieve a Psoriasis Area and Severity Index–90 (PASI-90) response in psoriasis highlights the folly of current stepwise treatment strategies imposed upon dermatologists by many payers, Dr. Craig L. Leonardi asserted at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
“It’s time to rethink our goals,” declared Dr. Leonardi, a dermatologist at Saint Louis University and a noted clinical trialist.

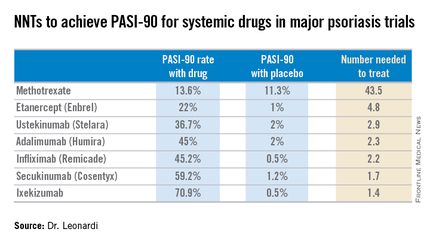
Most health plans insist that patients with moderate to severe psoriasis must have tried methotrexate and failed to achieve an adequate response before moving on to costlier biologic agents. But a PASI-90 response rate, indicative of 90% improvement in psoriasis area and severity, was achieved in only 13.6% of patients on methotrexate in the CHAMPION trial, compared with 59.2% and 70.9% of patients in phase III randomized trials of the interleukin-17 antagonists secukinumab (Cosentyx) and ixekizumab, respectively.
In other words, it is now routinely possible using highly effective medications to achieve a PASI-90 response in the majority of psoriasis patients, he noted.
Although statisticians say it isn’t appropriate to compare outcomes across clinical trials because study populations may differ, Dr. Leonardi decided it nevertheless would be illuminating to compare NNTs (the number of patients who needed to be treated with a medication instead of placebo to achieve one additional responder in a defined time period). In this analysis, he used data from phase III randomized, placebo-controlled clinical trials and Food and Drug Administration–regulated package inserts to calculate NNTs for systemic medications for psoriasis for the 10- to 16-week duration of phase III trials. The NNTs for a PASI-90 response ranged from a whopping 43.5 for methotrexate to 1.7 with secukinumab and 1.4 for ixekizumab.
“You can see immediately that methotrexate is outed as a weak and ineffective drug. And yet which drug are we usually asked to use first? Methotrexate. This is a structural problem that we have to solve in our specialty. We have to get with the insurance industry, we have to get with our guidelines of care and rewrite them. There is no reason that this drug should be placed in front of any of the other drugs, which are much more effective,” Dr. Leonardi said.
Viewing the data another way, the proportion of patients who achieved a PASI-75 response at the time of a major placebo-controlled clinical trial’s primary endpoint ranged from a low of 35.5% with methotrexate to 81.6% with secukinumab and 89.1% with ixekizumab. The NNTs to get a PASI-75 improvement with secukinumab and ixekizumab were, respectively, 1.3 and 1.2, compared to 6.0 for methotrexate.
“With an NNT of 1.2, if you treat 12 patients with ixekizumab, 10 of them are going to achieve PASI-75. This is a very different world than we had at the beginning of this adventure back in the early 2000s,” he observed.
In the modern era of highly effective biologic therapies for psoriasis, it makes sense to push as hard as possible in an effort to try to clear patients, according to Dr. Leonardi. That’s in part because the closer patients come to that once-nearly-unattainable goal, the better they actually feel, as underscored in the phase III results for ixekizumab.
In that study, the proportion of patients with a Dermatology Life Quality Index (DLQI) score of 0 or 1 at week 12 rose stepwise with the size of their PASI response. Among patients with a week-12 PASI response of 50 to less than 75, 18.8% had a DLQI of 0 or 1. For patients with a PASI-75 to less than PASI-90, it jumped to 52.3%. Among subjects with a PASI-90 to less than 100, 66.9% had a DLQI of 0 or 1. And among the 35.3% of ixekizumab-treated patients who had a PASI-100 response, the likelihood of a DLQI of 0 or 1 rose to 71.1%.
Noting that etanercept (Enbrel) is the only biologic on the market that achieves a PASI-75 response in less than half of treated patients, Dr. Leonardi said, “I’m over using etanercept as a first-line biologic. It’s the weakest biologic we can pick right now. I really like the highly efficacious drugs. I like adalimumab. I like the efficacy I see with ustekinumab. I like secukinumab. They are all preferred first-line drugs if I can get them, but it’s an insurance company world. I can’t tell you how many times I’ve heard, ‘Well, we’re not saying you can’t prescribe it, Dr. Leonardi, we’re just not going to pay for it.’ ”
Ixekizumab is under FDA review for psoriasis and a decision is expected within the first quarter of 2016, according to a spokesperson for Eli Lilly.
Dr. Leonardi is a recipient of research grants from well over a dozen pharmaceutical companies and is a consultant to and/or member of the speakers bureaus for AbbVie, Amgen, Boehringer Ingelheim, Celgene, Dermira, Janssen, Eli Lilly, Leo, Novartis, Pfizer, Sandoz, UCB, and Vitae.
SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – Scrutiny of the number needed to treat with various systemic drugs to achieve a Psoriasis Area and Severity Index–90 (PASI-90) response in psoriasis highlights the folly of current stepwise treatment strategies imposed upon dermatologists by many payers, Dr. Craig L. Leonardi asserted at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
“It’s time to rethink our goals,” declared Dr. Leonardi, a dermatologist at Saint Louis University and a noted clinical trialist.
Most health plans insist that patients with moderate to severe psoriasis must have tried methotrexate and failed to achieve an adequate response before moving on to costlier biologic agents. But a PASI-90 response rate, indicative of 90% improvement in psoriasis area and severity, was achieved in only 13.6% of patients on methotrexate in the CHAMPION trial, compared with 59.2% and 70.9% of patients in phase III randomized trials of the interleukin-17 antagonists secukinumab (Cosentyx) and ixekizumab, respectively.
In other words, it is now routinely possible using highly effective medications to achieve a PASI-90 response in the majority of psoriasis patients, he noted.
Although statisticians say it isn’t appropriate to compare outcomes across clinical trials because study populations may differ, Dr. Leonardi decided it nevertheless would be illuminating to compare NNTs (the number of patients who needed to be treated with a medication instead of placebo to achieve one additional responder in a defined time period). In this analysis, he used data from phase III randomized, placebo-controlled clinical trials and Food and Drug Administration–regulated package inserts to calculate NNTs for systemic medications for psoriasis for the 10- to 16-week duration of phase III trials. The NNTs for a PASI-90 response ranged from a whopping 43.5 for methotrexate to 1.7 with secukinumab and 1.4 for ixekizumab.
“You can see immediately that methotrexate is outed as a weak and ineffective drug. And yet which drug are we usually asked to use first? Methotrexate. This is a structural problem that we have to solve in our specialty. We have to get with the insurance industry, we have to get with our guidelines of care and rewrite them. There is no reason that this drug should be placed in front of any of the other drugs, which are much more effective,” Dr. Leonardi said.
Viewing the data another way, the proportion of patients who achieved a PASI-75 response at the time of a major placebo-controlled clinical trial’s primary endpoint ranged from a low of 35.5% with methotrexate to 81.6% with secukinumab and 89.1% with ixekizumab. The NNTs to get a PASI-75 improvement with secukinumab and ixekizumab were, respectively, 1.3 and 1.2, compared to 6.0 for methotrexate.
“With an NNT of 1.2, if you treat 12 patients with ixekizumab, 10 of them are going to achieve PASI-75. This is a very different world than we had at the beginning of this adventure back in the early 2000s,” he observed.
In the modern era of highly effective biologic therapies for psoriasis, it makes sense to push as hard as possible in an effort to try to clear patients, according to Dr. Leonardi. That’s in part because the closer patients come to that once-nearly-unattainable goal, the better they actually feel, as underscored in the phase III results for ixekizumab.
In that study, the proportion of patients with a Dermatology Life Quality Index (DLQI) score of 0 or 1 at week 12 rose stepwise with the size of their PASI response. Among patients with a week-12 PASI response of 50 to less than 75, 18.8% had a DLQI of 0 or 1. For patients with a PASI-75 to less than PASI-90, it jumped to 52.3%. Among subjects with a PASI-90 to less than 100, 66.9% had a DLQI of 0 or 1. And among the 35.3% of ixekizumab-treated patients who had a PASI-100 response, the likelihood of a DLQI of 0 or 1 rose to 71.1%.
Noting that etanercept (Enbrel) is the only biologic on the market that achieves a PASI-75 response in less than half of treated patients, Dr. Leonardi said, “I’m over using etanercept as a first-line biologic. It’s the weakest biologic we can pick right now. I really like the highly efficacious drugs. I like adalimumab. I like the efficacy I see with ustekinumab. I like secukinumab. They are all preferred first-line drugs if I can get them, but it’s an insurance company world. I can’t tell you how many times I’ve heard, ‘Well, we’re not saying you can’t prescribe it, Dr. Leonardi, we’re just not going to pay for it.’ ”
Ixekizumab is under FDA review for psoriasis and a decision is expected within the first quarter of 2016, according to a spokesperson for Eli Lilly.
Dr. Leonardi is a recipient of research grants from well over a dozen pharmaceutical companies and is a consultant to and/or member of the speakers bureaus for AbbVie, Amgen, Boehringer Ingelheim, Celgene, Dermira, Janssen, Eli Lilly, Leo, Novartis, Pfizer, Sandoz, UCB, and Vitae.
SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – Scrutiny of the number needed to treat with various systemic drugs to achieve a Psoriasis Area and Severity Index–90 (PASI-90) response in psoriasis highlights the folly of current stepwise treatment strategies imposed upon dermatologists by many payers, Dr. Craig L. Leonardi asserted at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
“It’s time to rethink our goals,” declared Dr. Leonardi, a dermatologist at Saint Louis University and a noted clinical trialist.
Most health plans insist that patients with moderate to severe psoriasis must have tried methotrexate and failed to achieve an adequate response before moving on to costlier biologic agents. But a PASI-90 response rate, indicative of 90% improvement in psoriasis area and severity, was achieved in only 13.6% of patients on methotrexate in the CHAMPION trial, compared with 59.2% and 70.9% of patients in phase III randomized trials of the interleukin-17 antagonists secukinumab (Cosentyx) and ixekizumab, respectively.
In other words, it is now routinely possible using highly effective medications to achieve a PASI-90 response in the majority of psoriasis patients, he noted.
Although statisticians say it isn’t appropriate to compare outcomes across clinical trials because study populations may differ, Dr. Leonardi decided it nevertheless would be illuminating to compare NNTs (the number of patients who needed to be treated with a medication instead of placebo to achieve one additional responder in a defined time period). In this analysis, he used data from phase III randomized, placebo-controlled clinical trials and Food and Drug Administration–regulated package inserts to calculate NNTs for systemic medications for psoriasis for the 10- to 16-week duration of phase III trials. The NNTs for a PASI-90 response ranged from a whopping 43.5 for methotrexate to 1.7 with secukinumab and 1.4 for ixekizumab.
“You can see immediately that methotrexate is outed as a weak and ineffective drug. And yet which drug are we usually asked to use first? Methotrexate. This is a structural problem that we have to solve in our specialty. We have to get with the insurance industry, we have to get with our guidelines of care and rewrite them. There is no reason that this drug should be placed in front of any of the other drugs, which are much more effective,” Dr. Leonardi said.
Viewing the data another way, the proportion of patients who achieved a PASI-75 response at the time of a major placebo-controlled clinical trial’s primary endpoint ranged from a low of 35.5% with methotrexate to 81.6% with secukinumab and 89.1% with ixekizumab. The NNTs to get a PASI-75 improvement with secukinumab and ixekizumab were, respectively, 1.3 and 1.2, compared to 6.0 for methotrexate.
“With an NNT of 1.2, if you treat 12 patients with ixekizumab, 10 of them are going to achieve PASI-75. This is a very different world than we had at the beginning of this adventure back in the early 2000s,” he observed.
In the modern era of highly effective biologic therapies for psoriasis, it makes sense to push as hard as possible in an effort to try to clear patients, according to Dr. Leonardi. That’s in part because the closer patients come to that once-nearly-unattainable goal, the better they actually feel, as underscored in the phase III results for ixekizumab.
In that study, the proportion of patients with a Dermatology Life Quality Index (DLQI) score of 0 or 1 at week 12 rose stepwise with the size of their PASI response. Among patients with a week-12 PASI response of 50 to less than 75, 18.8% had a DLQI of 0 or 1. For patients with a PASI-75 to less than PASI-90, it jumped to 52.3%. Among subjects with a PASI-90 to less than 100, 66.9% had a DLQI of 0 or 1. And among the 35.3% of ixekizumab-treated patients who had a PASI-100 response, the likelihood of a DLQI of 0 or 1 rose to 71.1%.
Noting that etanercept (Enbrel) is the only biologic on the market that achieves a PASI-75 response in less than half of treated patients, Dr. Leonardi said, “I’m over using etanercept as a first-line biologic. It’s the weakest biologic we can pick right now. I really like the highly efficacious drugs. I like adalimumab. I like the efficacy I see with ustekinumab. I like secukinumab. They are all preferred first-line drugs if I can get them, but it’s an insurance company world. I can’t tell you how many times I’ve heard, ‘Well, we’re not saying you can’t prescribe it, Dr. Leonardi, we’re just not going to pay for it.’ ”
Ixekizumab is under FDA review for psoriasis and a decision is expected within the first quarter of 2016, according to a spokesperson for Eli Lilly.
Dr. Leonardi is a recipient of research grants from well over a dozen pharmaceutical companies and is a consultant to and/or member of the speakers bureaus for AbbVie, Amgen, Boehringer Ingelheim, Celgene, Dermira, Janssen, Eli Lilly, Leo, Novartis, Pfizer, Sandoz, UCB, and Vitae.
SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR

Registry shows no increased cancer risk with biologics for psoriasis
WAIKOLOA, HAWAII – The latest update from the ongoing PSOLAR registry provides “very reassuring” evidence that the use of biologic agents to treat moderate to severe psoriasis doesn’t significantly increase malignancy risk other than for skin cancer, according to Dr. Kristina Callis Duffin.
Dr. Duffin of the department of dermatology at the University of Utah, Salt Lake City, cited a report presented by Dr. David Fiorentino, professor of dermatology at Stanford (Calif.) University, at the annual meeting of the European Academy of Dermatology and Venereology last October in Copenhagen. This update from the prospective international Psoriasis Longitudinal Assessment and Registry (PSOLAR) included 12,093 psoriasis patients deemed candidates for biologics, including 2,084 who did not go on a biologic agent while the rest did.

During 40,388 patient-years of prospective follow-up, or an average of 3.3 years, 455 patients were diagnosed with a malignancy other than skin cancer. The cumulative malignancy rate was 0.75 cases per 100 patient-years in patients on nonbiologic therapies, which was not significantly different from the rates of 0.51 per 100 patient-years in participants who started on ustekinumab (Stelara) at enrollment, 0.81 in patients on infliximab (Remicade), or 0.73 per 100 patient-years in those on other biologics, Dr. Duffin said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
“These are all very low rates,” commented Dr. Duffin.
The PSOLAR data are particularly valuable because the registry was set up specifically to prospectively examine the long-term safety and efficacy of biologic agents in psoriasis patients. In contrast, the landmark epidemiologic study led by Dr. Joel M. Gelfand of the University of Pennsylvania, Philadelphia, which concluded that mild psoriasis was associated with a 34% increased risk of lymphoma and that severe psoriasis carried a 59% greater risk than in nonpsoriatic controls (J Invest Dermatol. 2006 Oct;126[10]:2194-201), involved a retrospective analysis of the U.K. General Practice Research Database. And while that study had strength in numbers – it included more than 153,000 British psoriasis patients and nearly 800,000 controls – it wasn’t designed to look specifically at psoriasis patients.
It’s reassuring that the lymphoma rate of 0.47 cases per 100 patient-years in patients with severe psoriasis in the U.K. registry during the prebiologics era is virtually identical to the rates associated with biologic agents in PSOLAR to date, which ranged from 0.3 to 0.5 cases per 100 patient-years, Dr. Duffin said.
The PSOLAR findings are worth sharing with patients. As a result of direct-to-consumer advertising by pharmaceutical companies, psoriasis patients are typically quite concerned about the risk of cancer associated with biologic agents, she added.
“They hear the comment in the ad that serious infections and malignancies have been reported in patients on these drugs as ‘these drugs increase the risk of malignancy.’ So where I start this conversation is, ‘Actually, patients with psoriasis do have some increased risk of malignancy, but those malignancies are mostly nonmelanoma skin cancers and lymphoproliferative diseases,’” the dermatologist explained.
Much of this risk is probably related to the fact that patients with moderate to severe psoriasis often have an extensive history of exposure to immunosuppressive agents such as cyclosporine as well as UV light therapies, which increase the risk of skin cancer.
“You also have to consider the fact that psoriasis patients tend to have a lot of smoking behaviors and alcohol behaviors that increase cancer risk,” Dr. Duffin continued.
In shared decision making regarding the option of biologic therapy in psoriasis patients having a history of cancer or who develop cancer while on a biologic, she likes to pose a question: What scares you more: the risk of your cancer coming back or not being able to have a good quality of life?
“That gets them thinking,” she said.
She stressed that as part of discussions regarding the risk/benefit profile of biologic therapy in an individual with a history of cancer, or of continuing a biologic in someone diagnosed with a malignancy while on treatment, it’s important for the dermatologist to talk with the patient’s oncologist, who is best positioned to provide insight into the risk of cancer recurrence.
Dr. Duffin is a recipient of research grants from and a consultant to Janssen, which sponsors the PSOLAR registry, as well as to more than half a dozen other pharmaceutical companies. SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – The latest update from the ongoing PSOLAR registry provides “very reassuring” evidence that the use of biologic agents to treat moderate to severe psoriasis doesn’t significantly increase malignancy risk other than for skin cancer, according to Dr. Kristina Callis Duffin.
Dr. Duffin of the department of dermatology at the University of Utah, Salt Lake City, cited a report presented by Dr. David Fiorentino, professor of dermatology at Stanford (Calif.) University, at the annual meeting of the European Academy of Dermatology and Venereology last October in Copenhagen. This update from the prospective international Psoriasis Longitudinal Assessment and Registry (PSOLAR) included 12,093 psoriasis patients deemed candidates for biologics, including 2,084 who did not go on a biologic agent while the rest did.
During 40,388 patient-years of prospective follow-up, or an average of 3.3 years, 455 patients were diagnosed with a malignancy other than skin cancer. The cumulative malignancy rate was 0.75 cases per 100 patient-years in patients on nonbiologic therapies, which was not significantly different from the rates of 0.51 per 100 patient-years in participants who started on ustekinumab (Stelara) at enrollment, 0.81 in patients on infliximab (Remicade), or 0.73 per 100 patient-years in those on other biologics, Dr. Duffin said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
“These are all very low rates,” commented Dr. Duffin.
The PSOLAR data are particularly valuable because the registry was set up specifically to prospectively examine the long-term safety and efficacy of biologic agents in psoriasis patients. In contrast, the landmark epidemiologic study led by Dr. Joel M. Gelfand of the University of Pennsylvania, Philadelphia, which concluded that mild psoriasis was associated with a 34% increased risk of lymphoma and that severe psoriasis carried a 59% greater risk than in nonpsoriatic controls (J Invest Dermatol. 2006 Oct;126[10]:2194-201), involved a retrospective analysis of the U.K. General Practice Research Database. And while that study had strength in numbers – it included more than 153,000 British psoriasis patients and nearly 800,000 controls – it wasn’t designed to look specifically at psoriasis patients.
It’s reassuring that the lymphoma rate of 0.47 cases per 100 patient-years in patients with severe psoriasis in the U.K. registry during the prebiologics era is virtually identical to the rates associated with biologic agents in PSOLAR to date, which ranged from 0.3 to 0.5 cases per 100 patient-years, Dr. Duffin said.
The PSOLAR findings are worth sharing with patients. As a result of direct-to-consumer advertising by pharmaceutical companies, psoriasis patients are typically quite concerned about the risk of cancer associated with biologic agents, she added.
“They hear the comment in the ad that serious infections and malignancies have been reported in patients on these drugs as ‘these drugs increase the risk of malignancy.’ So where I start this conversation is, ‘Actually, patients with psoriasis do have some increased risk of malignancy, but those malignancies are mostly nonmelanoma skin cancers and lymphoproliferative diseases,’” the dermatologist explained.
Much of this risk is probably related to the fact that patients with moderate to severe psoriasis often have an extensive history of exposure to immunosuppressive agents such as cyclosporine as well as UV light therapies, which increase the risk of skin cancer.
“You also have to consider the fact that psoriasis patients tend to have a lot of smoking behaviors and alcohol behaviors that increase cancer risk,” Dr. Duffin continued.
In shared decision making regarding the option of biologic therapy in psoriasis patients having a history of cancer or who develop cancer while on a biologic, she likes to pose a question: What scares you more: the risk of your cancer coming back or not being able to have a good quality of life?
“That gets them thinking,” she said.
She stressed that as part of discussions regarding the risk/benefit profile of biologic therapy in an individual with a history of cancer, or of continuing a biologic in someone diagnosed with a malignancy while on treatment, it’s important for the dermatologist to talk with the patient’s oncologist, who is best positioned to provide insight into the risk of cancer recurrence.
Dr. Duffin is a recipient of research grants from and a consultant to Janssen, which sponsors the PSOLAR registry, as well as to more than half a dozen other pharmaceutical companies. SDEF and this news organization are owned by the same parent company.
WAIKOLOA, HAWAII – The latest update from the ongoing PSOLAR registry provides “very reassuring” evidence that the use of biologic agents to treat moderate to severe psoriasis doesn’t significantly increase malignancy risk other than for skin cancer, according to Dr. Kristina Callis Duffin.
Dr. Duffin of the department of dermatology at the University of Utah, Salt Lake City, cited a report presented by Dr. David Fiorentino, professor of dermatology at Stanford (Calif.) University, at the annual meeting of the European Academy of Dermatology and Venereology last October in Copenhagen. This update from the prospective international Psoriasis Longitudinal Assessment and Registry (PSOLAR) included 12,093 psoriasis patients deemed candidates for biologics, including 2,084 who did not go on a biologic agent while the rest did.
During 40,388 patient-years of prospective follow-up, or an average of 3.3 years, 455 patients were diagnosed with a malignancy other than skin cancer. The cumulative malignancy rate was 0.75 cases per 100 patient-years in patients on nonbiologic therapies, which was not significantly different from the rates of 0.51 per 100 patient-years in participants who started on ustekinumab (Stelara) at enrollment, 0.81 in patients on infliximab (Remicade), or 0.73 per 100 patient-years in those on other biologics, Dr. Duffin said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
“These are all very low rates,” commented Dr. Duffin.
The PSOLAR data are particularly valuable because the registry was set up specifically to prospectively examine the long-term safety and efficacy of biologic agents in psoriasis patients. In contrast, the landmark epidemiologic study led by Dr. Joel M. Gelfand of the University of Pennsylvania, Philadelphia, which concluded that mild psoriasis was associated with a 34% increased risk of lymphoma and that severe psoriasis carried a 59% greater risk than in nonpsoriatic controls (J Invest Dermatol. 2006 Oct;126[10]:2194-201), involved a retrospective analysis of the U.K. General Practice Research Database. And while that study had strength in numbers – it included more than 153,000 British psoriasis patients and nearly 800,000 controls – it wasn’t designed to look specifically at psoriasis patients.
It’s reassuring that the lymphoma rate of 0.47 cases per 100 patient-years in patients with severe psoriasis in the U.K. registry during the prebiologics era is virtually identical to the rates associated with biologic agents in PSOLAR to date, which ranged from 0.3 to 0.5 cases per 100 patient-years, Dr. Duffin said.
The PSOLAR findings are worth sharing with patients. As a result of direct-to-consumer advertising by pharmaceutical companies, psoriasis patients are typically quite concerned about the risk of cancer associated with biologic agents, she added.
“They hear the comment in the ad that serious infections and malignancies have been reported in patients on these drugs as ‘these drugs increase the risk of malignancy.’ So where I start this conversation is, ‘Actually, patients with psoriasis do have some increased risk of malignancy, but those malignancies are mostly nonmelanoma skin cancers and lymphoproliferative diseases,’” the dermatologist explained.
Much of this risk is probably related to the fact that patients with moderate to severe psoriasis often have an extensive history of exposure to immunosuppressive agents such as cyclosporine as well as UV light therapies, which increase the risk of skin cancer.
“You also have to consider the fact that psoriasis patients tend to have a lot of smoking behaviors and alcohol behaviors that increase cancer risk,” Dr. Duffin continued.
In shared decision making regarding the option of biologic therapy in psoriasis patients having a history of cancer or who develop cancer while on a biologic, she likes to pose a question: What scares you more: the risk of your cancer coming back or not being able to have a good quality of life?
“That gets them thinking,” she said.
She stressed that as part of discussions regarding the risk/benefit profile of biologic therapy in an individual with a history of cancer, or of continuing a biologic in someone diagnosed with a malignancy while on treatment, it’s important for the dermatologist to talk with the patient’s oncologist, who is best positioned to provide insight into the risk of cancer recurrence.
Dr. Duffin is a recipient of research grants from and a consultant to Janssen, which sponsors the PSOLAR registry, as well as to more than half a dozen other pharmaceutical companies. SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR

TAVR forges ahead in PARTNER III for low-risk patients
SNOWMASS, COLO. – The Food and Drug Administration has approved the first-ever U.S. randomized clinical trial of transcatheter aortic valve replacement versus open surgical replacement in low–surgical risk patients with symptomatic severe aortic stenosis.
The PARTNER III trial will enroll roughly 1,200 patients age 65 or older, all with a Society of Thoracic Surgeons risk score of less than 4%, at 50 sites beginning this spring, Dr. Vinod H. Thourani said at the Annual Cardiovascular Conference at Snowmass.

This is a noninferiority trial with a primary endpoint comprising a 1-year composite of death, stroke, or rehospitalization. The study is sponsored by Edwards Lifesciences, and patients randomized to transcatheter aortic valve replacement (TAVR) will receive the company’s low-profile Sapien 3 valve.
Coprincipal investigators are Dr. Michael J. Mack of the Baylor Health Care System in Plano, Tex., and Dr. Martin B. Leon of Columbia University, New York. Dr. Thourani is a member of the PARTNER III executive committee.
This is a study that could upend clinical practice, he observed.
“Are we going to have within the next 5 years 80%-90% of all patients who present with severe symptomatic aortic stenosis treated with transcatheter valves? We’re really at a major crossroads here, I believe,” said Dr. Thourani, professor of surgery and medicine and codirector of the structural heart and valve center at Emory University in Atlanta.
He ran down the numbers: Today, roughly 80% of all surgical aortic valve replacements (SAVR) in the United States are performed in low–surgical risk patients. These low-risk patients comprise roughly 65% of the total operable population with severe aortic stenosis. If PARTNER III and other data show that TAVR provides results comparable to SAVR in this group, Dr. Thourani predicted that it’s likely most low–surgical risk patients will opt for the less invasive approach. The appeal is no surgical incision, less pain, a shorter or no ICU stay, and faster return to normal activity.
Right now, U.S. and European guidelines state that TAVR is the preferred or alternative strategy to SAVR only in the relatively small group comprised of inoperable or high–surgical risk patients. In clinical practice, TAVR has already supplanted SAVR in the 10% of operable patients with high surgical risk. And TAVR is poised to do so in the roughly 25% of patients who fall into the intermediate–surgical risk category, according to the cardiothoracic surgeon.
He predicted that the 1-year outcomes of TAVR in more than 1,000 intermediate-risk participants in the PARTNER II trial will create a stir when presented this year, as a late-breaker at the annual meeting of the American College of Cardiology in Chicago. Although he stressed that he doesn’t know the results, the 30-day outcomes presented at last year’s Transcatheter Cardiovascular Therapeutics conference are extremely promising: a 1.1% all-cause mortality rate in patients with an average Society of Thoracic Surgeons risk score of 5.3%, for a stunning observed-to-expected ratio of just 0.21. Plus, a 1.0% rate of disabling stroke in this large multicenter randomized experience.
“That becomes really compelling data for us to think we’re ready now to go to the next step,” Dr. Thourani said. “My belief is at the rate we’re going, we’ll see most intermediate-risk patients going to TAVR.”
To date there has been only one randomized trial of TAVR versus SAVR in low–surgical risk patients: the Nordic Aortic Valve Intervention Trial (NOTION), which included 280 randomized patients with an average Society of Thoracic Surgeons risk score of 3%.
In the 2-year results presented by Dr. Lars Søndergaard of the University of Copenhagen at TCT 2015, all-cause mortality was 2.1% with TAVR and 3.7% with SAVR at 30 days, 4.9% with TAVR and 7.5% with SAVR at 12 months, and 8.0% versus 9.8% at 24 months. The 30-day rates of major bleeding, cardiogenic shock, atrial fibrillation, and acute kidney injury were all substantially lower in the TAVR group. All very impressive. However, Dr. Thourani found the TAVR patients’ pacemaker-requirement rate troubling. At 30 days post TAVR, 34% of patients had a pacemaker, compared with 1.6% of the SAVR group. By 24 months, 41% of the TAVR group had received a pacemaker, compared with just 4% of the SAVR group.
“What’s the acceptable pacemaker rate for someone utilizing TAVR – 5%, 10%, 40%? That’s something we as a community have to look at,” the surgeon observed. He noted that his purchase price for a TAVR valve is roughly $32,500, whereas a SAVR valve costs him $4,500. And at Emory, putting in a pacemaker costs an added $10,000-$15,000 for the device.
“If I’m putting a pacemaker in 40% of my TAVR patients at a cost of $40,000-$45,000 per patient for the valve and pacemaker, that becomes an issue,” Dr. Thourani said.
Other concerns surrounding TAVR, in addition to reimbursement, include the uncertain long-term impact of residual minimal paravalvular leak, which is common.
“We’re not done talking about paravalvular leak rates. As cardiologists you’re not okay with me giving your patient a minimal paravalvular leak post-SAVR. Are we going to change the bar a little bit for TAVR?” he mused.
Another issue is thrombosis of TAVR valve leaflets, Dr. Thourani continued. In a large patient series reported last year, this event occurred in 0.6% of patients, with an average of 181 days from TAVR to confirmatory abnormal imaging (Circ Cardiovasc Interv. 2015 Apr;8[4]. pii: e001779). Two clinical trials are gearing up to examine various anticoagulant strategies to address the problem.
Despite the various concerns, however, Dr. Thourani is extremely optimistic about TAVR’s future. It’s a booming field, with 396 U.S. TAVR centers as of 2015. The indications appear to be on the verge of expansion. Technical progress continues, with half a dozen TAVR valves in development in addition to the two now FDA approved.
“We have just scratched the surface of what we’re going to do in the management of severe aortic stenosis,” the surgeon promised.
The latest results of minimalist TAVR provide another reason for optimism regarding TAVR’s future.
Emory University surgeons and interventional cardiologists have been pacesetters in the minimalist TAVR approach. The key elements of minimalist TAVR are that the procedure is performed in the cardiac catheterization laboratory via transfemoral access, under conscious sedation, with transthoracic echocardiographic guidance, no Swan-Ganz catheter, and no ICU stay for most patients.
Dr. Thourani presented as-yet unpublished data on a recent series of 111 high–surgical risk patients who underwent minimalist TAVR with implantation of a Sapien 3 valve at Emory. Although their Society of Thoracic Surgeons risk score was 8%, there was zero 30-day mortality in this group. One patient had a major stroke, two had major vascular complications, and the 30-day readmission rate was just 3.8%.
“Can we get to these results universally? We think we can. This is the bar we need to start thinking about,” Dr. Thourani said.
Dr. Thourani reported serving as a consultant to Edwards Lifesciences and St. Jude Medical and receiving research grants from Abbott, Boston Scientific, Medtronic, and Sorin.
SNOWMASS, COLO. – The Food and Drug Administration has approved the first-ever U.S. randomized clinical trial of transcatheter aortic valve replacement versus open surgical replacement in low–surgical risk patients with symptomatic severe aortic stenosis.
The PARTNER III trial will enroll roughly 1,200 patients age 65 or older, all with a Society of Thoracic Surgeons risk score of less than 4%, at 50 sites beginning this spring, Dr. Vinod H. Thourani said at the Annual Cardiovascular Conference at Snowmass.
This is a noninferiority trial with a primary endpoint comprising a 1-year composite of death, stroke, or rehospitalization. The study is sponsored by Edwards Lifesciences, and patients randomized to transcatheter aortic valve replacement (TAVR) will receive the company’s low-profile Sapien 3 valve.
Coprincipal investigators are Dr. Michael J. Mack of the Baylor Health Care System in Plano, Tex., and Dr. Martin B. Leon of Columbia University, New York. Dr. Thourani is a member of the PARTNER III executive committee.
This is a study that could upend clinical practice, he observed.
“Are we going to have within the next 5 years 80%-90% of all patients who present with severe symptomatic aortic stenosis treated with transcatheter valves? We’re really at a major crossroads here, I believe,” said Dr. Thourani, professor of surgery and medicine and codirector of the structural heart and valve center at Emory University in Atlanta.
He ran down the numbers: Today, roughly 80% of all surgical aortic valve replacements (SAVR) in the United States are performed in low–surgical risk patients. These low-risk patients comprise roughly 65% of the total operable population with severe aortic stenosis. If PARTNER III and other data show that TAVR provides results comparable to SAVR in this group, Dr. Thourani predicted that it’s likely most low–surgical risk patients will opt for the less invasive approach. The appeal is no surgical incision, less pain, a shorter or no ICU stay, and faster return to normal activity.
Right now, U.S. and European guidelines state that TAVR is the preferred or alternative strategy to SAVR only in the relatively small group comprised of inoperable or high–surgical risk patients. In clinical practice, TAVR has already supplanted SAVR in the 10% of operable patients with high surgical risk. And TAVR is poised to do so in the roughly 25% of patients who fall into the intermediate–surgical risk category, according to the cardiothoracic surgeon.
He predicted that the 1-year outcomes of TAVR in more than 1,000 intermediate-risk participants in the PARTNER II trial will create a stir when presented this year, as a late-breaker at the annual meeting of the American College of Cardiology in Chicago. Although he stressed that he doesn’t know the results, the 30-day outcomes presented at last year’s Transcatheter Cardiovascular Therapeutics conference are extremely promising: a 1.1% all-cause mortality rate in patients with an average Society of Thoracic Surgeons risk score of 5.3%, for a stunning observed-to-expected ratio of just 0.21. Plus, a 1.0% rate of disabling stroke in this large multicenter randomized experience.
“That becomes really compelling data for us to think we’re ready now to go to the next step,” Dr. Thourani said. “My belief is at the rate we’re going, we’ll see most intermediate-risk patients going to TAVR.”
To date there has been only one randomized trial of TAVR versus SAVR in low–surgical risk patients: the Nordic Aortic Valve Intervention Trial (NOTION), which included 280 randomized patients with an average Society of Thoracic Surgeons risk score of 3%.
In the 2-year results presented by Dr. Lars Søndergaard of the University of Copenhagen at TCT 2015, all-cause mortality was 2.1% with TAVR and 3.7% with SAVR at 30 days, 4.9% with TAVR and 7.5% with SAVR at 12 months, and 8.0% versus 9.8% at 24 months. The 30-day rates of major bleeding, cardiogenic shock, atrial fibrillation, and acute kidney injury were all substantially lower in the TAVR group. All very impressive. However, Dr. Thourani found the TAVR patients’ pacemaker-requirement rate troubling. At 30 days post TAVR, 34% of patients had a pacemaker, compared with 1.6% of the SAVR group. By 24 months, 41% of the TAVR group had received a pacemaker, compared with just 4% of the SAVR group.
“What’s the acceptable pacemaker rate for someone utilizing TAVR – 5%, 10%, 40%? That’s something we as a community have to look at,” the surgeon observed. He noted that his purchase price for a TAVR valve is roughly $32,500, whereas a SAVR valve costs him $4,500. And at Emory, putting in a pacemaker costs an added $10,000-$15,000 for the device.
“If I’m putting a pacemaker in 40% of my TAVR patients at a cost of $40,000-$45,000 per patient for the valve and pacemaker, that becomes an issue,” Dr. Thourani said.
Other concerns surrounding TAVR, in addition to reimbursement, include the uncertain long-term impact of residual minimal paravalvular leak, which is common.
“We’re not done talking about paravalvular leak rates. As cardiologists you’re not okay with me giving your patient a minimal paravalvular leak post-SAVR. Are we going to change the bar a little bit for TAVR?” he mused.
Another issue is thrombosis of TAVR valve leaflets, Dr. Thourani continued. In a large patient series reported last year, this event occurred in 0.6% of patients, with an average of 181 days from TAVR to confirmatory abnormal imaging (Circ Cardiovasc Interv. 2015 Apr;8[4]. pii: e001779). Two clinical trials are gearing up to examine various anticoagulant strategies to address the problem.
Despite the various concerns, however, Dr. Thourani is extremely optimistic about TAVR’s future. It’s a booming field, with 396 U.S. TAVR centers as of 2015. The indications appear to be on the verge of expansion. Technical progress continues, with half a dozen TAVR valves in development in addition to the two now FDA approved.
“We have just scratched the surface of what we’re going to do in the management of severe aortic stenosis,” the surgeon promised.
The latest results of minimalist TAVR provide another reason for optimism regarding TAVR’s future.
Emory University surgeons and interventional cardiologists have been pacesetters in the minimalist TAVR approach. The key elements of minimalist TAVR are that the procedure is performed in the cardiac catheterization laboratory via transfemoral access, under conscious sedation, with transthoracic echocardiographic guidance, no Swan-Ganz catheter, and no ICU stay for most patients.
Dr. Thourani presented as-yet unpublished data on a recent series of 111 high–surgical risk patients who underwent minimalist TAVR with implantation of a Sapien 3 valve at Emory. Although their Society of Thoracic Surgeons risk score was 8%, there was zero 30-day mortality in this group. One patient had a major stroke, two had major vascular complications, and the 30-day readmission rate was just 3.8%.
“Can we get to these results universally? We think we can. This is the bar we need to start thinking about,” Dr. Thourani said.
Dr. Thourani reported serving as a consultant to Edwards Lifesciences and St. Jude Medical and receiving research grants from Abbott, Boston Scientific, Medtronic, and Sorin.
SNOWMASS, COLO. – The Food and Drug Administration has approved the first-ever U.S. randomized clinical trial of transcatheter aortic valve replacement versus open surgical replacement in low–surgical risk patients with symptomatic severe aortic stenosis.
The PARTNER III trial will enroll roughly 1,200 patients age 65 or older, all with a Society of Thoracic Surgeons risk score of less than 4%, at 50 sites beginning this spring, Dr. Vinod H. Thourani said at the Annual Cardiovascular Conference at Snowmass.
This is a noninferiority trial with a primary endpoint comprising a 1-year composite of death, stroke, or rehospitalization. The study is sponsored by Edwards Lifesciences, and patients randomized to transcatheter aortic valve replacement (TAVR) will receive the company’s low-profile Sapien 3 valve.
Coprincipal investigators are Dr. Michael J. Mack of the Baylor Health Care System in Plano, Tex., and Dr. Martin B. Leon of Columbia University, New York. Dr. Thourani is a member of the PARTNER III executive committee.
This is a study that could upend clinical practice, he observed.
“Are we going to have within the next 5 years 80%-90% of all patients who present with severe symptomatic aortic stenosis treated with transcatheter valves? We’re really at a major crossroads here, I believe,” said Dr. Thourani, professor of surgery and medicine and codirector of the structural heart and valve center at Emory University in Atlanta.
He ran down the numbers: Today, roughly 80% of all surgical aortic valve replacements (SAVR) in the United States are performed in low–surgical risk patients. These low-risk patients comprise roughly 65% of the total operable population with severe aortic stenosis. If PARTNER III and other data show that TAVR provides results comparable to SAVR in this group, Dr. Thourani predicted that it’s likely most low–surgical risk patients will opt for the less invasive approach. The appeal is no surgical incision, less pain, a shorter or no ICU stay, and faster return to normal activity.
Right now, U.S. and European guidelines state that TAVR is the preferred or alternative strategy to SAVR only in the relatively small group comprised of inoperable or high–surgical risk patients. In clinical practice, TAVR has already supplanted SAVR in the 10% of operable patients with high surgical risk. And TAVR is poised to do so in the roughly 25% of patients who fall into the intermediate–surgical risk category, according to the cardiothoracic surgeon.
He predicted that the 1-year outcomes of TAVR in more than 1,000 intermediate-risk participants in the PARTNER II trial will create a stir when presented this year, as a late-breaker at the annual meeting of the American College of Cardiology in Chicago. Although he stressed that he doesn’t know the results, the 30-day outcomes presented at last year’s Transcatheter Cardiovascular Therapeutics conference are extremely promising: a 1.1% all-cause mortality rate in patients with an average Society of Thoracic Surgeons risk score of 5.3%, for a stunning observed-to-expected ratio of just 0.21. Plus, a 1.0% rate of disabling stroke in this large multicenter randomized experience.
“That becomes really compelling data for us to think we’re ready now to go to the next step,” Dr. Thourani said. “My belief is at the rate we’re going, we’ll see most intermediate-risk patients going to TAVR.”
To date there has been only one randomized trial of TAVR versus SAVR in low–surgical risk patients: the Nordic Aortic Valve Intervention Trial (NOTION), which included 280 randomized patients with an average Society of Thoracic Surgeons risk score of 3%.
In the 2-year results presented by Dr. Lars Søndergaard of the University of Copenhagen at TCT 2015, all-cause mortality was 2.1% with TAVR and 3.7% with SAVR at 30 days, 4.9% with TAVR and 7.5% with SAVR at 12 months, and 8.0% versus 9.8% at 24 months. The 30-day rates of major bleeding, cardiogenic shock, atrial fibrillation, and acute kidney injury were all substantially lower in the TAVR group. All very impressive. However, Dr. Thourani found the TAVR patients’ pacemaker-requirement rate troubling. At 30 days post TAVR, 34% of patients had a pacemaker, compared with 1.6% of the SAVR group. By 24 months, 41% of the TAVR group had received a pacemaker, compared with just 4% of the SAVR group.
“What’s the acceptable pacemaker rate for someone utilizing TAVR – 5%, 10%, 40%? That’s something we as a community have to look at,” the surgeon observed. He noted that his purchase price for a TAVR valve is roughly $32,500, whereas a SAVR valve costs him $4,500. And at Emory, putting in a pacemaker costs an added $10,000-$15,000 for the device.
“If I’m putting a pacemaker in 40% of my TAVR patients at a cost of $40,000-$45,000 per patient for the valve and pacemaker, that becomes an issue,” Dr. Thourani said.
Other concerns surrounding TAVR, in addition to reimbursement, include the uncertain long-term impact of residual minimal paravalvular leak, which is common.
“We’re not done talking about paravalvular leak rates. As cardiologists you’re not okay with me giving your patient a minimal paravalvular leak post-SAVR. Are we going to change the bar a little bit for TAVR?” he mused.
Another issue is thrombosis of TAVR valve leaflets, Dr. Thourani continued. In a large patient series reported last year, this event occurred in 0.6% of patients, with an average of 181 days from TAVR to confirmatory abnormal imaging (Circ Cardiovasc Interv. 2015 Apr;8[4]. pii: e001779). Two clinical trials are gearing up to examine various anticoagulant strategies to address the problem.
Despite the various concerns, however, Dr. Thourani is extremely optimistic about TAVR’s future. It’s a booming field, with 396 U.S. TAVR centers as of 2015. The indications appear to be on the verge of expansion. Technical progress continues, with half a dozen TAVR valves in development in addition to the two now FDA approved.
“We have just scratched the surface of what we’re going to do in the management of severe aortic stenosis,” the surgeon promised.
The latest results of minimalist TAVR provide another reason for optimism regarding TAVR’s future.
Emory University surgeons and interventional cardiologists have been pacesetters in the minimalist TAVR approach. The key elements of minimalist TAVR are that the procedure is performed in the cardiac catheterization laboratory via transfemoral access, under conscious sedation, with transthoracic echocardiographic guidance, no Swan-Ganz catheter, and no ICU stay for most patients.
Dr. Thourani presented as-yet unpublished data on a recent series of 111 high–surgical risk patients who underwent minimalist TAVR with implantation of a Sapien 3 valve at Emory. Although their Society of Thoracic Surgeons risk score was 8%, there was zero 30-day mortality in this group. One patient had a major stroke, two had major vascular complications, and the 30-day readmission rate was just 3.8%.
“Can we get to these results universally? We think we can. This is the bar we need to start thinking about,” Dr. Thourani said.
Dr. Thourani reported serving as a consultant to Edwards Lifesciences and St. Jude Medical and receiving research grants from Abbott, Boston Scientific, Medtronic, and Sorin.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

Noninvasive Testing of Women with Suspected CAD Simplified
SNOWMASS, COLO. – Current American Heart Association consensus recommendations for noninvasive testing of women with suspected ischemic heart disease utilize a novel and simplified approach to pretest risk stratification.
The writing committee’s thinking was that a new risk assessment method specific to symptomatic women was needed. Conventional risk scores, such as the Framingham and American College of Cardiology/AHA atherosclerotic cardiovascular disease risk calculator, are weighted for risk evaluation in the general population of asymptomatic men and women, committee cochair Dr. Jennifer H. Mieres explained at the Annual Cardiovascular Conference at Snowmass.

The pretest risk assessment strategy for ischemic heart disease (IHD) described in the AHA consensus statement (Circulation. 2014 Jul 22;130[4]:350-79) is applicable only in women who present with chest pain symptoms or an ischemic equivalent such as excessive shortness of breath not attributable to underlying pulmonary disease. It’s designed to avoid overuse of costly noninvasive and invasive diagnostic testing, which has become common in concert with increasing physician awareness that the pattern of symptom presentation is broader in women than men with IHD.
Given the epidemiologic evidence that coronary heart disease tends to occur a decade later in women than men, the female-specific risk assessment method utilizes age as its starting point. In general, women who present with symptoms suggestive of IHD in their 50s are classified as low risk. Those in their 60s are deemed intermediate risk. And symptomatic women in their 70s are categorized as high risk. A patient gets bumped up one risk category if she has multiple cardiac risk factors or functional disability, according to Dr. Mieres, professor of cardiology and population health at Hofstra University in Hempstead, N.Y.
Functional disability is defined as inability to perform activities of daily living or as a limited exercise capacity estimated at less than 5 metabolic equivalents (METs) using the Duke Activities Status Index (DASI), a validated brief 12-item questionnaire suitable for patients to complete in the waiting room.
A symptomatic woman’s baseline fitness level is important for a couple of reasons. If she can’t perform basic activities of daily living or do more than 5 METs of exercise then the exercise treadmill test is not the initial diagnostic test of choice because she won’t be able to achieve maximum stress.
Plus, the landmark Women’s Ischemia Syndrome Evaluation (WISE) study showed that a symptomatic woman’s baseline fitness level is a powerful predictor of her prognosis: Participants who had an estimated exercise capacity of 4.7 METs or less based upon their DASI score had a 3.7-fold greater risk of death or nonfatal MI during follow-up did than those with a DASI score of 10 METs or more. Those with a DASI score of 4.8-7.4 METs were 2.1-fold more likely to experience death or MI, and women with an estimated exercise capacity of 7.5-9.9 METs based upon DASI were at 1.9-fold increased risk of death or MI, compared with those having a DASI score of at least 10 METs (J Am Coll Cardiol. 2006 Feb 7;47[3 Suppl]:S36-43).
In addition, the women’s IHD risk evaluation utilizes several high-risk equivalents which automatically move a symptomatic woman into the high-risk category regardless of her age. These are peripheral artery disease, longstanding poorly controlled diabetes, and a history of cerebrovascular accident, Dr. Mieres continued.
She stressed that most low-risk symptomatic women are not candidates for diagnostic testing. The exercise treadmill test is the first-line diagnostic test for women at intermediate risk for IHD who are functionally capable and have a normal resting ECG.
Stress imaging studies are reserved for intermediate- and high-risk women with resting ST-segment abnormalities, inability to exercise adequately, or an indeterminate exercise treadmill test.
Stress echocardiography gets a class I recommendation in these situations. So does stress myocardial perfusion imaging with SPECT or PET except in premenopausal women, where concerns about radiation exposure dictate that stress echo or stress cardiac magnetic resonance imaging is preferable.
Otherwise, stress cardiac magnetic resonance gets a class IIb – “may be reasonable” – recommendation as an initial imaging test in these situations.
Coronary artery calcium measurement via CT angiography gets a class IIb recommendation in intermediate-risk symptomatic women. This imaging method is unique in that it not only provides accurate information about the obstructive burden of CAD, but it measures the nonobstructive burden as well. That’s particularly important in women because they have a greater burden of nonobstructive CAD, defined as 1%-49% stenosis, than do men. Women with stress test abnormalities and nonobstructive CAD are no longer defined as having a false-positive test, as was traditionally the case; instead, their test is categorized as abnormal because the WISE study has shown they are at elevated IHD risk, Dr. Mieres said.
She reported having no financial conflicts regarding her presentation.
SNOWMASS, COLO. – Current American Heart Association consensus recommendations for noninvasive testing of women with suspected ischemic heart disease utilize a novel and simplified approach to pretest risk stratification.
The writing committee’s thinking was that a new risk assessment method specific to symptomatic women was needed. Conventional risk scores, such as the Framingham and American College of Cardiology/AHA atherosclerotic cardiovascular disease risk calculator, are weighted for risk evaluation in the general population of asymptomatic men and women, committee cochair Dr. Jennifer H. Mieres explained at the Annual Cardiovascular Conference at Snowmass.
The pretest risk assessment strategy for ischemic heart disease (IHD) described in the AHA consensus statement (Circulation. 2014 Jul 22;130[4]:350-79) is applicable only in women who present with chest pain symptoms or an ischemic equivalent such as excessive shortness of breath not attributable to underlying pulmonary disease. It’s designed to avoid overuse of costly noninvasive and invasive diagnostic testing, which has become common in concert with increasing physician awareness that the pattern of symptom presentation is broader in women than men with IHD.
Given the epidemiologic evidence that coronary heart disease tends to occur a decade later in women than men, the female-specific risk assessment method utilizes age as its starting point. In general, women who present with symptoms suggestive of IHD in their 50s are classified as low risk. Those in their 60s are deemed intermediate risk. And symptomatic women in their 70s are categorized as high risk. A patient gets bumped up one risk category if she has multiple cardiac risk factors or functional disability, according to Dr. Mieres, professor of cardiology and population health at Hofstra University in Hempstead, N.Y.
Functional disability is defined as inability to perform activities of daily living or as a limited exercise capacity estimated at less than 5 metabolic equivalents (METs) using the Duke Activities Status Index (DASI), a validated brief 12-item questionnaire suitable for patients to complete in the waiting room.
A symptomatic woman’s baseline fitness level is important for a couple of reasons. If she can’t perform basic activities of daily living or do more than 5 METs of exercise then the exercise treadmill test is not the initial diagnostic test of choice because she won’t be able to achieve maximum stress.
Plus, the landmark Women’s Ischemia Syndrome Evaluation (WISE) study showed that a symptomatic woman’s baseline fitness level is a powerful predictor of her prognosis: Participants who had an estimated exercise capacity of 4.7 METs or less based upon their DASI score had a 3.7-fold greater risk of death or nonfatal MI during follow-up did than those with a DASI score of 10 METs or more. Those with a DASI score of 4.8-7.4 METs were 2.1-fold more likely to experience death or MI, and women with an estimated exercise capacity of 7.5-9.9 METs based upon DASI were at 1.9-fold increased risk of death or MI, compared with those having a DASI score of at least 10 METs (J Am Coll Cardiol. 2006 Feb 7;47[3 Suppl]:S36-43).
In addition, the women’s IHD risk evaluation utilizes several high-risk equivalents which automatically move a symptomatic woman into the high-risk category regardless of her age. These are peripheral artery disease, longstanding poorly controlled diabetes, and a history of cerebrovascular accident, Dr. Mieres continued.
She stressed that most low-risk symptomatic women are not candidates for diagnostic testing. The exercise treadmill test is the first-line diagnostic test for women at intermediate risk for IHD who are functionally capable and have a normal resting ECG.
Stress imaging studies are reserved for intermediate- and high-risk women with resting ST-segment abnormalities, inability to exercise adequately, or an indeterminate exercise treadmill test.
Stress echocardiography gets a class I recommendation in these situations. So does stress myocardial perfusion imaging with SPECT or PET except in premenopausal women, where concerns about radiation exposure dictate that stress echo or stress cardiac magnetic resonance imaging is preferable.
Otherwise, stress cardiac magnetic resonance gets a class IIb – “may be reasonable” – recommendation as an initial imaging test in these situations.
Coronary artery calcium measurement via CT angiography gets a class IIb recommendation in intermediate-risk symptomatic women. This imaging method is unique in that it not only provides accurate information about the obstructive burden of CAD, but it measures the nonobstructive burden as well. That’s particularly important in women because they have a greater burden of nonobstructive CAD, defined as 1%-49% stenosis, than do men. Women with stress test abnormalities and nonobstructive CAD are no longer defined as having a false-positive test, as was traditionally the case; instead, their test is categorized as abnormal because the WISE study has shown they are at elevated IHD risk, Dr. Mieres said.
She reported having no financial conflicts regarding her presentation.
SNOWMASS, COLO. – Current American Heart Association consensus recommendations for noninvasive testing of women with suspected ischemic heart disease utilize a novel and simplified approach to pretest risk stratification.
The writing committee’s thinking was that a new risk assessment method specific to symptomatic women was needed. Conventional risk scores, such as the Framingham and American College of Cardiology/AHA atherosclerotic cardiovascular disease risk calculator, are weighted for risk evaluation in the general population of asymptomatic men and women, committee cochair Dr. Jennifer H. Mieres explained at the Annual Cardiovascular Conference at Snowmass.
The pretest risk assessment strategy for ischemic heart disease (IHD) described in the AHA consensus statement (Circulation. 2014 Jul 22;130[4]:350-79) is applicable only in women who present with chest pain symptoms or an ischemic equivalent such as excessive shortness of breath not attributable to underlying pulmonary disease. It’s designed to avoid overuse of costly noninvasive and invasive diagnostic testing, which has become common in concert with increasing physician awareness that the pattern of symptom presentation is broader in women than men with IHD.
Given the epidemiologic evidence that coronary heart disease tends to occur a decade later in women than men, the female-specific risk assessment method utilizes age as its starting point. In general, women who present with symptoms suggestive of IHD in their 50s are classified as low risk. Those in their 60s are deemed intermediate risk. And symptomatic women in their 70s are categorized as high risk. A patient gets bumped up one risk category if she has multiple cardiac risk factors or functional disability, according to Dr. Mieres, professor of cardiology and population health at Hofstra University in Hempstead, N.Y.
Functional disability is defined as inability to perform activities of daily living or as a limited exercise capacity estimated at less than 5 metabolic equivalents (METs) using the Duke Activities Status Index (DASI), a validated brief 12-item questionnaire suitable for patients to complete in the waiting room.
A symptomatic woman’s baseline fitness level is important for a couple of reasons. If she can’t perform basic activities of daily living or do more than 5 METs of exercise then the exercise treadmill test is not the initial diagnostic test of choice because she won’t be able to achieve maximum stress.
Plus, the landmark Women’s Ischemia Syndrome Evaluation (WISE) study showed that a symptomatic woman’s baseline fitness level is a powerful predictor of her prognosis: Participants who had an estimated exercise capacity of 4.7 METs or less based upon their DASI score had a 3.7-fold greater risk of death or nonfatal MI during follow-up did than those with a DASI score of 10 METs or more. Those with a DASI score of 4.8-7.4 METs were 2.1-fold more likely to experience death or MI, and women with an estimated exercise capacity of 7.5-9.9 METs based upon DASI were at 1.9-fold increased risk of death or MI, compared with those having a DASI score of at least 10 METs (J Am Coll Cardiol. 2006 Feb 7;47[3 Suppl]:S36-43).
In addition, the women’s IHD risk evaluation utilizes several high-risk equivalents which automatically move a symptomatic woman into the high-risk category regardless of her age. These are peripheral artery disease, longstanding poorly controlled diabetes, and a history of cerebrovascular accident, Dr. Mieres continued.
She stressed that most low-risk symptomatic women are not candidates for diagnostic testing. The exercise treadmill test is the first-line diagnostic test for women at intermediate risk for IHD who are functionally capable and have a normal resting ECG.
Stress imaging studies are reserved for intermediate- and high-risk women with resting ST-segment abnormalities, inability to exercise adequately, or an indeterminate exercise treadmill test.
Stress echocardiography gets a class I recommendation in these situations. So does stress myocardial perfusion imaging with SPECT or PET except in premenopausal women, where concerns about radiation exposure dictate that stress echo or stress cardiac magnetic resonance imaging is preferable.
Otherwise, stress cardiac magnetic resonance gets a class IIb – “may be reasonable” – recommendation as an initial imaging test in these situations.
Coronary artery calcium measurement via CT angiography gets a class IIb recommendation in intermediate-risk symptomatic women. This imaging method is unique in that it not only provides accurate information about the obstructive burden of CAD, but it measures the nonobstructive burden as well. That’s particularly important in women because they have a greater burden of nonobstructive CAD, defined as 1%-49% stenosis, than do men. Women with stress test abnormalities and nonobstructive CAD are no longer defined as having a false-positive test, as was traditionally the case; instead, their test is categorized as abnormal because the WISE study has shown they are at elevated IHD risk, Dr. Mieres said.
She reported having no financial conflicts regarding her presentation.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

Noninvasive testing of women with suspected CAD simplified
SNOWMASS, COLO. – Current American Heart Association consensus recommendations for noninvasive testing of women with suspected ischemic heart disease utilize a novel and simplified approach to pretest risk stratification.
The writing committee’s thinking was that a new risk assessment method specific to symptomatic women was needed. Conventional risk scores, such as the Framingham and American College of Cardiology/AHA atherosclerotic cardiovascular disease risk calculator, are weighted for risk evaluation in the general population of asymptomatic men and women, committee cochair Dr. Jennifer H. Mieres explained at the Annual Cardiovascular Conference at Snowmass.

The pretest risk assessment strategy for ischemic heart disease (IHD) described in the AHA consensus statement (Circulation. 2014 Jul 22;130[4]:350-79) is applicable only in women who present with chest pain symptoms or an ischemic equivalent such as excessive shortness of breath not attributable to underlying pulmonary disease. It’s designed to avoid overuse of costly noninvasive and invasive diagnostic testing, which has become common in concert with increasing physician awareness that the pattern of symptom presentation is broader in women than men with IHD.
Given the epidemiologic evidence that coronary heart disease tends to occur a decade later in women than men, the female-specific risk assessment method utilizes age as its starting point. In general, women who present with symptoms suggestive of IHD in their 50s are classified as low risk. Those in their 60s are deemed intermediate risk. And symptomatic women in their 70s are categorized as high risk. A patient gets bumped up one risk category if she has multiple cardiac risk factors or functional disability, according to Dr. Mieres, professor of cardiology and population health at Hofstra University in Hempstead, N.Y.
Functional disability is defined as inability to perform activities of daily living or as a limited exercise capacity estimated at less than 5 metabolic equivalents (METs) using the Duke Activities Status Index (DASI), a validated brief 12-item questionnaire suitable for patients to complete in the waiting room.
A symptomatic woman’s baseline fitness level is important for a couple of reasons. If she can’t perform basic activities of daily living or do more than 5 METs of exercise then the exercise treadmill test is not the initial diagnostic test of choice because she won’t be able to achieve maximum stress.
Plus, the landmark Women’s Ischemia Syndrome Evaluation (WISE) study showed that a symptomatic woman’s baseline fitness level is a powerful predictor of her prognosis: Participants who had an estimated exercise capacity of 4.7 METs or less based upon their DASI score had a 3.7-fold greater risk of death or nonfatal MI during follow-up did than those with a DASI score of 10 METs or more. Those with a DASI score of 4.8-7.4 METs were 2.1-fold more likely to experience death or MI, and women with an estimated exercise capacity of 7.5-9.9 METs based upon DASI were at 1.9-fold increased risk of death or MI, compared with those having a DASI score of at least 10 METs (J Am Coll Cardiol. 2006 Feb 7;47[3 Suppl]:S36-43).
In addition, the women’s IHD risk evaluation utilizes several high-risk equivalents which automatically move a symptomatic woman into the high-risk category regardless of her age. These are peripheral artery disease, longstanding poorly controlled diabetes, and a history of cerebrovascular accident, Dr. Mieres continued.
She stressed that most low-risk symptomatic women are not candidates for diagnostic testing. The exercise treadmill test is the first-line diagnostic test for women at intermediate risk for IHD who are functionally capable and have a normal resting ECG.
Stress imaging studies are reserved for intermediate- and high-risk women with resting ST-segment abnormalities, inability to exercise adequately, or an indeterminate exercise treadmill test.
Stress echocardiography gets a class I recommendation in these situations. So does stress myocardial perfusion imaging with SPECT or PET except in premenopausal women, where concerns about radiation exposure dictate that stress echo or stress cardiac magnetic resonance imaging is preferable.
Otherwise, stress cardiac magnetic resonance gets a class IIb – “may be reasonable” – recommendation as an initial imaging test in these situations.
Coronary artery calcium measurement via CT angiography gets a class IIb recommendation in intermediate-risk symptomatic women. This imaging method is unique in that it not only provides accurate information about the obstructive burden of CAD, but it measures the nonobstructive burden as well. That’s particularly important in women because they have a greater burden of nonobstructive CAD, defined as 1%-49% stenosis, than do men. Women with stress test abnormalities and nonobstructive CAD are no longer defined as having a false-positive test, as was traditionally the case; instead, their test is categorized as abnormal because the WISE study has shown they are at elevated IHD risk, Dr. Mieres said.
She reported having no financial conflicts regarding her presentation.
SNOWMASS, COLO. – Current American Heart Association consensus recommendations for noninvasive testing of women with suspected ischemic heart disease utilize a novel and simplified approach to pretest risk stratification.
The writing committee’s thinking was that a new risk assessment method specific to symptomatic women was needed. Conventional risk scores, such as the Framingham and American College of Cardiology/AHA atherosclerotic cardiovascular disease risk calculator, are weighted for risk evaluation in the general population of asymptomatic men and women, committee cochair Dr. Jennifer H. Mieres explained at the Annual Cardiovascular Conference at Snowmass.
The pretest risk assessment strategy for ischemic heart disease (IHD) described in the AHA consensus statement (Circulation. 2014 Jul 22;130[4]:350-79) is applicable only in women who present with chest pain symptoms or an ischemic equivalent such as excessive shortness of breath not attributable to underlying pulmonary disease. It’s designed to avoid overuse of costly noninvasive and invasive diagnostic testing, which has become common in concert with increasing physician awareness that the pattern of symptom presentation is broader in women than men with IHD.
Given the epidemiologic evidence that coronary heart disease tends to occur a decade later in women than men, the female-specific risk assessment method utilizes age as its starting point. In general, women who present with symptoms suggestive of IHD in their 50s are classified as low risk. Those in their 60s are deemed intermediate risk. And symptomatic women in their 70s are categorized as high risk. A patient gets bumped up one risk category if she has multiple cardiac risk factors or functional disability, according to Dr. Mieres, professor of cardiology and population health at Hofstra University in Hempstead, N.Y.
Functional disability is defined as inability to perform activities of daily living or as a limited exercise capacity estimated at less than 5 metabolic equivalents (METs) using the Duke Activities Status Index (DASI), a validated brief 12-item questionnaire suitable for patients to complete in the waiting room.
A symptomatic woman’s baseline fitness level is important for a couple of reasons. If she can’t perform basic activities of daily living or do more than 5 METs of exercise then the exercise treadmill test is not the initial diagnostic test of choice because she won’t be able to achieve maximum stress.
Plus, the landmark Women’s Ischemia Syndrome Evaluation (WISE) study showed that a symptomatic woman’s baseline fitness level is a powerful predictor of her prognosis: Participants who had an estimated exercise capacity of 4.7 METs or less based upon their DASI score had a 3.7-fold greater risk of death or nonfatal MI during follow-up did than those with a DASI score of 10 METs or more. Those with a DASI score of 4.8-7.4 METs were 2.1-fold more likely to experience death or MI, and women with an estimated exercise capacity of 7.5-9.9 METs based upon DASI were at 1.9-fold increased risk of death or MI, compared with those having a DASI score of at least 10 METs (J Am Coll Cardiol. 2006 Feb 7;47[3 Suppl]:S36-43).
In addition, the women’s IHD risk evaluation utilizes several high-risk equivalents which automatically move a symptomatic woman into the high-risk category regardless of her age. These are peripheral artery disease, longstanding poorly controlled diabetes, and a history of cerebrovascular accident, Dr. Mieres continued.
She stressed that most low-risk symptomatic women are not candidates for diagnostic testing. The exercise treadmill test is the first-line diagnostic test for women at intermediate risk for IHD who are functionally capable and have a normal resting ECG.
Stress imaging studies are reserved for intermediate- and high-risk women with resting ST-segment abnormalities, inability to exercise adequately, or an indeterminate exercise treadmill test.
Stress echocardiography gets a class I recommendation in these situations. So does stress myocardial perfusion imaging with SPECT or PET except in premenopausal women, where concerns about radiation exposure dictate that stress echo or stress cardiac magnetic resonance imaging is preferable.
Otherwise, stress cardiac magnetic resonance gets a class IIb – “may be reasonable” – recommendation as an initial imaging test in these situations.
Coronary artery calcium measurement via CT angiography gets a class IIb recommendation in intermediate-risk symptomatic women. This imaging method is unique in that it not only provides accurate information about the obstructive burden of CAD, but it measures the nonobstructive burden as well. That’s particularly important in women because they have a greater burden of nonobstructive CAD, defined as 1%-49% stenosis, than do men. Women with stress test abnormalities and nonobstructive CAD are no longer defined as having a false-positive test, as was traditionally the case; instead, their test is categorized as abnormal because the WISE study has shown they are at elevated IHD risk, Dr. Mieres said.
She reported having no financial conflicts regarding her presentation.
SNOWMASS, COLO. – Current American Heart Association consensus recommendations for noninvasive testing of women with suspected ischemic heart disease utilize a novel and simplified approach to pretest risk stratification.
The writing committee’s thinking was that a new risk assessment method specific to symptomatic women was needed. Conventional risk scores, such as the Framingham and American College of Cardiology/AHA atherosclerotic cardiovascular disease risk calculator, are weighted for risk evaluation in the general population of asymptomatic men and women, committee cochair Dr. Jennifer H. Mieres explained at the Annual Cardiovascular Conference at Snowmass.
The pretest risk assessment strategy for ischemic heart disease (IHD) described in the AHA consensus statement (Circulation. 2014 Jul 22;130[4]:350-79) is applicable only in women who present with chest pain symptoms or an ischemic equivalent such as excessive shortness of breath not attributable to underlying pulmonary disease. It’s designed to avoid overuse of costly noninvasive and invasive diagnostic testing, which has become common in concert with increasing physician awareness that the pattern of symptom presentation is broader in women than men with IHD.
Given the epidemiologic evidence that coronary heart disease tends to occur a decade later in women than men, the female-specific risk assessment method utilizes age as its starting point. In general, women who present with symptoms suggestive of IHD in their 50s are classified as low risk. Those in their 60s are deemed intermediate risk. And symptomatic women in their 70s are categorized as high risk. A patient gets bumped up one risk category if she has multiple cardiac risk factors or functional disability, according to Dr. Mieres, professor of cardiology and population health at Hofstra University in Hempstead, N.Y.
Functional disability is defined as inability to perform activities of daily living or as a limited exercise capacity estimated at less than 5 metabolic equivalents (METs) using the Duke Activities Status Index (DASI), a validated brief 12-item questionnaire suitable for patients to complete in the waiting room.
A symptomatic woman’s baseline fitness level is important for a couple of reasons. If she can’t perform basic activities of daily living or do more than 5 METs of exercise then the exercise treadmill test is not the initial diagnostic test of choice because she won’t be able to achieve maximum stress.
Plus, the landmark Women’s Ischemia Syndrome Evaluation (WISE) study showed that a symptomatic woman’s baseline fitness level is a powerful predictor of her prognosis: Participants who had an estimated exercise capacity of 4.7 METs or less based upon their DASI score had a 3.7-fold greater risk of death or nonfatal MI during follow-up did than those with a DASI score of 10 METs or more. Those with a DASI score of 4.8-7.4 METs were 2.1-fold more likely to experience death or MI, and women with an estimated exercise capacity of 7.5-9.9 METs based upon DASI were at 1.9-fold increased risk of death or MI, compared with those having a DASI score of at least 10 METs (J Am Coll Cardiol. 2006 Feb 7;47[3 Suppl]:S36-43).
In addition, the women’s IHD risk evaluation utilizes several high-risk equivalents which automatically move a symptomatic woman into the high-risk category regardless of her age. These are peripheral artery disease, longstanding poorly controlled diabetes, and a history of cerebrovascular accident, Dr. Mieres continued.
She stressed that most low-risk symptomatic women are not candidates for diagnostic testing. The exercise treadmill test is the first-line diagnostic test for women at intermediate risk for IHD who are functionally capable and have a normal resting ECG.
Stress imaging studies are reserved for intermediate- and high-risk women with resting ST-segment abnormalities, inability to exercise adequately, or an indeterminate exercise treadmill test.
Stress echocardiography gets a class I recommendation in these situations. So does stress myocardial perfusion imaging with SPECT or PET except in premenopausal women, where concerns about radiation exposure dictate that stress echo or stress cardiac magnetic resonance imaging is preferable.
Otherwise, stress cardiac magnetic resonance gets a class IIb – “may be reasonable” – recommendation as an initial imaging test in these situations.
Coronary artery calcium measurement via CT angiography gets a class IIb recommendation in intermediate-risk symptomatic women. This imaging method is unique in that it not only provides accurate information about the obstructive burden of CAD, but it measures the nonobstructive burden as well. That’s particularly important in women because they have a greater burden of nonobstructive CAD, defined as 1%-49% stenosis, than do men. Women with stress test abnormalities and nonobstructive CAD are no longer defined as having a false-positive test, as was traditionally the case; instead, their test is categorized as abnormal because the WISE study has shown they are at elevated IHD risk, Dr. Mieres said.
She reported having no financial conflicts regarding her presentation.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

Acute heart failure: What works, what doesn’t
SNOWMASS, COLO. – The primary treatment goal in patients hospitalized for acute decompensated heart failure is aggressive decongestion to get them feeling better and out of the hospital quicker – and the best way to achieve that is with high-dose loop diuretics administered intravenously at a dose equivalent to 2.5 times the previous oral dose, Dr. Akshay S. Desai said at the Annual Cardiovascular Conference at Snowmass.
This was the key lesson of the Diuretic Optimization Strategies Evaluation (DOSE) trial, a prospective double-blind randomized trial that provides physicians with the best available data on how to decongest patients with acute decompensated heart failure (ADHF), according to Dr. Desai, a coinvestigator. The study was conducted by the National Heart, Lung, and Blood Institute Heart Failure Clinical Research Network.

The DOSE trial showed that it really doesn’t matter whether the diuretic is administered intravenously by continuous infusion or a bolus every 12 hours. The important thing is the high-dose strategy. It proved to be safe and was associated with accelerated decongestion as manifest in greater relief of dyspnea, greater weight loss and fluid loss, and a larger reduction in serum brain natriuretic peptide at 72 hours than low-dose therapy equivalent to the patient’s previous oral dose (N Engl J Med. 2011 Mar 3;364[9]:797-805).
“The message for you in practice is that the route of diuretic administration is probably not important as long as you give an adequate dose. I would consider giving the higher dose of diuretic because it’s associated with more effective decongestion and perhaps shorter length of stay,” said Dr. Desai, director of heart failure disease management at Brigham and Women’s Hospital in Boston.
There is a trade-off in ADHF between effective decongestion and worsening renal function as reflected in increased serum creatinine levels. Transient worsening of renal function occurred more frequently with the high-dose strategy in the DOSE trial, but it had no impact on clinical outcomes at 60 days follow-up. This finding is consistent with the results of an important Italian study showing that worsening renal function alone isn’t independently associated with increased risk of death or ADHF readmission; the problems arise in patients with worsening renal function and persistent congestion (Circ Heart Fail. 2012 Jan;5[1]:54-62).
Worsening congestion drives most hospitalizations for heart failure. And patients who are still congested at discharge are at dramatically increased risk for death or readmission in the ensuing 6 months. Yet the limitations of current therapy mean that even in expert hands, a substantial proportion of patients are discharged with clinically significant congestion. For example, in a retrospective analysis of nearly 500 patients enrolled in ADHF studies conducted by physicians in the NHLBI Heart Failure Clinical Research Network, only 52% were discharged free of congestion (Circ Heart Fail. 2015 Jul;8[4]:741-8).
Beyond aggressive treatment with loop diuretics, what else is useful in achieving the goal of hospital discharge with normalized filling pressures? Not much, according to a considerable body of research on the topic.
“The data tell us more about what not to do than what to do,” according to Dr. Desai.
For example, even though aggressive salt and fluid restriction is often forced upon patients hospitalized for ADHF on the rationale that this strategy may make it easier for diuretics to work, it’s not an evidence-based practice. Indeed, in a randomized clinical trial with blinded outcome assessments, an in-hospital diet restricted to a maximum intake of 800 mg of sodium and 800 mL of fluid daily had no effect on weight loss or a clinical congestion score (JAMA Intern Med. 2013 June 24;173[12]:1058-64).
“What it did very effectively was make patients thirsty. There are probably some patients where restriction of sodium and fluid intake is important, but routine use of tight restrictions is probably more harmful than helpful,” he observed.
The list of failed once-promising alternatives to diuretics in the setting of ADHF is impressive. It includes milrinone, tolvaptan, nesiritide, levosimendan, tezosentan, low-dose dopamine, and ultrafiltration. All had a sound mechanistic basis for the belief that they might improve outcomes, but in clinical trials none of them did.
Although routine use of pulmonary artery catheters to guide decongestion therapy in ADHF isn’t warranted because it has not been shown to be better than clinical assessment, there are certain situations where it is extremely helpful. For example, in the patient who isn’t responding to adequate doses of loop diuretics, it becomes important to understand the hemodynamics, which may involve systemic vascular resistance or a cardiac output problem.
Other situations where it’s worthwhile to consider placement of a pulmonary artery catheter include the patient of uncertain fluid status where it’s not possible to confidently estimate cardiac output at the bedside or markedly worsening renal function with empiric therapy.
Dr. Desai reported receiving research funding from Novartis and St. Jude Medical and serving as a paid consultant to Merck, Relypsa, and St. Jude Medical.
SNOWMASS, COLO. – The primary treatment goal in patients hospitalized for acute decompensated heart failure is aggressive decongestion to get them feeling better and out of the hospital quicker – and the best way to achieve that is with high-dose loop diuretics administered intravenously at a dose equivalent to 2.5 times the previous oral dose, Dr. Akshay S. Desai said at the Annual Cardiovascular Conference at Snowmass.
This was the key lesson of the Diuretic Optimization Strategies Evaluation (DOSE) trial, a prospective double-blind randomized trial that provides physicians with the best available data on how to decongest patients with acute decompensated heart failure (ADHF), according to Dr. Desai, a coinvestigator. The study was conducted by the National Heart, Lung, and Blood Institute Heart Failure Clinical Research Network.
The DOSE trial showed that it really doesn’t matter whether the diuretic is administered intravenously by continuous infusion or a bolus every 12 hours. The important thing is the high-dose strategy. It proved to be safe and was associated with accelerated decongestion as manifest in greater relief of dyspnea, greater weight loss and fluid loss, and a larger reduction in serum brain natriuretic peptide at 72 hours than low-dose therapy equivalent to the patient’s previous oral dose (N Engl J Med. 2011 Mar 3;364[9]:797-805).
“The message for you in practice is that the route of diuretic administration is probably not important as long as you give an adequate dose. I would consider giving the higher dose of diuretic because it’s associated with more effective decongestion and perhaps shorter length of stay,” said Dr. Desai, director of heart failure disease management at Brigham and Women’s Hospital in Boston.
There is a trade-off in ADHF between effective decongestion and worsening renal function as reflected in increased serum creatinine levels. Transient worsening of renal function occurred more frequently with the high-dose strategy in the DOSE trial, but it had no impact on clinical outcomes at 60 days follow-up. This finding is consistent with the results of an important Italian study showing that worsening renal function alone isn’t independently associated with increased risk of death or ADHF readmission; the problems arise in patients with worsening renal function and persistent congestion (Circ Heart Fail. 2012 Jan;5[1]:54-62).
Worsening congestion drives most hospitalizations for heart failure. And patients who are still congested at discharge are at dramatically increased risk for death or readmission in the ensuing 6 months. Yet the limitations of current therapy mean that even in expert hands, a substantial proportion of patients are discharged with clinically significant congestion. For example, in a retrospective analysis of nearly 500 patients enrolled in ADHF studies conducted by physicians in the NHLBI Heart Failure Clinical Research Network, only 52% were discharged free of congestion (Circ Heart Fail. 2015 Jul;8[4]:741-8).
Beyond aggressive treatment with loop diuretics, what else is useful in achieving the goal of hospital discharge with normalized filling pressures? Not much, according to a considerable body of research on the topic.
“The data tell us more about what not to do than what to do,” according to Dr. Desai.
For example, even though aggressive salt and fluid restriction is often forced upon patients hospitalized for ADHF on the rationale that this strategy may make it easier for diuretics to work, it’s not an evidence-based practice. Indeed, in a randomized clinical trial with blinded outcome assessments, an in-hospital diet restricted to a maximum intake of 800 mg of sodium and 800 mL of fluid daily had no effect on weight loss or a clinical congestion score (JAMA Intern Med. 2013 June 24;173[12]:1058-64).
“What it did very effectively was make patients thirsty. There are probably some patients where restriction of sodium and fluid intake is important, but routine use of tight restrictions is probably more harmful than helpful,” he observed.
The list of failed once-promising alternatives to diuretics in the setting of ADHF is impressive. It includes milrinone, tolvaptan, nesiritide, levosimendan, tezosentan, low-dose dopamine, and ultrafiltration. All had a sound mechanistic basis for the belief that they might improve outcomes, but in clinical trials none of them did.
Although routine use of pulmonary artery catheters to guide decongestion therapy in ADHF isn’t warranted because it has not been shown to be better than clinical assessment, there are certain situations where it is extremely helpful. For example, in the patient who isn’t responding to adequate doses of loop diuretics, it becomes important to understand the hemodynamics, which may involve systemic vascular resistance or a cardiac output problem.
Other situations where it’s worthwhile to consider placement of a pulmonary artery catheter include the patient of uncertain fluid status where it’s not possible to confidently estimate cardiac output at the bedside or markedly worsening renal function with empiric therapy.
Dr. Desai reported receiving research funding from Novartis and St. Jude Medical and serving as a paid consultant to Merck, Relypsa, and St. Jude Medical.
SNOWMASS, COLO. – The primary treatment goal in patients hospitalized for acute decompensated heart failure is aggressive decongestion to get them feeling better and out of the hospital quicker – and the best way to achieve that is with high-dose loop diuretics administered intravenously at a dose equivalent to 2.5 times the previous oral dose, Dr. Akshay S. Desai said at the Annual Cardiovascular Conference at Snowmass.
This was the key lesson of the Diuretic Optimization Strategies Evaluation (DOSE) trial, a prospective double-blind randomized trial that provides physicians with the best available data on how to decongest patients with acute decompensated heart failure (ADHF), according to Dr. Desai, a coinvestigator. The study was conducted by the National Heart, Lung, and Blood Institute Heart Failure Clinical Research Network.
The DOSE trial showed that it really doesn’t matter whether the diuretic is administered intravenously by continuous infusion or a bolus every 12 hours. The important thing is the high-dose strategy. It proved to be safe and was associated with accelerated decongestion as manifest in greater relief of dyspnea, greater weight loss and fluid loss, and a larger reduction in serum brain natriuretic peptide at 72 hours than low-dose therapy equivalent to the patient’s previous oral dose (N Engl J Med. 2011 Mar 3;364[9]:797-805).
“The message for you in practice is that the route of diuretic administration is probably not important as long as you give an adequate dose. I would consider giving the higher dose of diuretic because it’s associated with more effective decongestion and perhaps shorter length of stay,” said Dr. Desai, director of heart failure disease management at Brigham and Women’s Hospital in Boston.
There is a trade-off in ADHF between effective decongestion and worsening renal function as reflected in increased serum creatinine levels. Transient worsening of renal function occurred more frequently with the high-dose strategy in the DOSE trial, but it had no impact on clinical outcomes at 60 days follow-up. This finding is consistent with the results of an important Italian study showing that worsening renal function alone isn’t independently associated with increased risk of death or ADHF readmission; the problems arise in patients with worsening renal function and persistent congestion (Circ Heart Fail. 2012 Jan;5[1]:54-62).
Worsening congestion drives most hospitalizations for heart failure. And patients who are still congested at discharge are at dramatically increased risk for death or readmission in the ensuing 6 months. Yet the limitations of current therapy mean that even in expert hands, a substantial proportion of patients are discharged with clinically significant congestion. For example, in a retrospective analysis of nearly 500 patients enrolled in ADHF studies conducted by physicians in the NHLBI Heart Failure Clinical Research Network, only 52% were discharged free of congestion (Circ Heart Fail. 2015 Jul;8[4]:741-8).
Beyond aggressive treatment with loop diuretics, what else is useful in achieving the goal of hospital discharge with normalized filling pressures? Not much, according to a considerable body of research on the topic.
“The data tell us more about what not to do than what to do,” according to Dr. Desai.
For example, even though aggressive salt and fluid restriction is often forced upon patients hospitalized for ADHF on the rationale that this strategy may make it easier for diuretics to work, it’s not an evidence-based practice. Indeed, in a randomized clinical trial with blinded outcome assessments, an in-hospital diet restricted to a maximum intake of 800 mg of sodium and 800 mL of fluid daily had no effect on weight loss or a clinical congestion score (JAMA Intern Med. 2013 June 24;173[12]:1058-64).
“What it did very effectively was make patients thirsty. There are probably some patients where restriction of sodium and fluid intake is important, but routine use of tight restrictions is probably more harmful than helpful,” he observed.
The list of failed once-promising alternatives to diuretics in the setting of ADHF is impressive. It includes milrinone, tolvaptan, nesiritide, levosimendan, tezosentan, low-dose dopamine, and ultrafiltration. All had a sound mechanistic basis for the belief that they might improve outcomes, but in clinical trials none of them did.
Although routine use of pulmonary artery catheters to guide decongestion therapy in ADHF isn’t warranted because it has not been shown to be better than clinical assessment, there are certain situations where it is extremely helpful. For example, in the patient who isn’t responding to adequate doses of loop diuretics, it becomes important to understand the hemodynamics, which may involve systemic vascular resistance or a cardiac output problem.
Other situations where it’s worthwhile to consider placement of a pulmonary artery catheter include the patient of uncertain fluid status where it’s not possible to confidently estimate cardiac output at the bedside or markedly worsening renal function with empiric therapy.
Dr. Desai reported receiving research funding from Novartis and St. Jude Medical and serving as a paid consultant to Merck, Relypsa, and St. Jude Medical.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
