User login
Integrating behavioral health and primary care
This is the fourth in a series of articles from the National Center for Excellence in Primary Care Research (NCEPCR) in the Agency for Healthcare Research and Quality (AHRQ). This series introduces sets of tools and resources designed to help your practice.
Many patients with anxiety, depression, behavioral problems, substance abuse, and other mental and behavioral health conditions turn to their primary care providers as their first, and often only, source of mental health care. Unfortunately, this care may not be as effective as patients and primary care personnel would hope or expect it to be. Problems exist with missed or inaccurate diagnoses, referrals and coordination of care, and other failures in detection and treatment (NIMH Integrated Care Web site, accessed Oct. 1, 2017).

Through the Academy’s web portal interested clinicians, health care administrators, quality improvement specialists, and others can access a wide range of resources related to behavioral health integration. A hallmark of the site is the Integration Playbook, developed as a guide to integrating behavioral health in primary care and other ambulatory care settings. The Playbook assists the growing number of primary care practices and health systems that are beginning to design and implement integrated behavioral health services. The Playbook’s implementation framework is designed to be meaningful at any level of integration development.

One challenge in implementing primary care and behavioral health integration is connecting the community engaged in integrated health care. Often behavioral health and primary care providers operate within the same building or organization but are not be aware of each other’s presence. One goal of the Academy is to unite these disparate efforts and direct providers towards one another in an attempt to facilitate collaboration. In the same vein, the Academy aims to offer resources to patients and the community on integration, including the identification of integrated practices they can access.
In addition, in order to measure quality of care in this new approach to health care delivery, the Academy created the Atlas of Integrated Behavioral Health Care Quality Measures. Intended for practices and teams that wish to understand whether they are providing high-quality integrated behavioral health care or are preparing to implement integrated care, the Atlas aims to support the field of integrated behavioral health care measurement by 1) presenting a framework for understanding measurement of integrated care; 2) providing a list of existing measures relevant to integrated behavioral health care; and 3) organizing the measures by the framework and by user goals to facilitate selection of measures.
Links from the NCEPCR site:
Tools and Resources for Research, Quality Improvement, and Practice
https://www.ahrq.gov/ncepcr/research-qi-practice/practice-transformation-qi.html
Academy Web Portal: https://www.integrationacademy.ahrq.gov
The Integration Playbook: https://integrationacademy.ahrq.gov/playbook/about-playbook
Lexicon: https://integrationacademy.ahrq.gov/lexicon
Atlas of Integrated Behavioral Health Care Quality Measures: https://integrationacademy.ahrq.gov/resources/ibhc-measures-atlas
These and other tools can be found at the NCEPCR Web site: https://www.ahrq.gov/ncepcr.
Dr. Genevro is a health scientist at AHRQ. Dr. Ganiats is director, National Center for Excellence in Primary Care Research, AHRQ.
This is the fourth in a series of articles from the National Center for Excellence in Primary Care Research (NCEPCR) in the Agency for Healthcare Research and Quality (AHRQ). This series introduces sets of tools and resources designed to help your practice.
Many patients with anxiety, depression, behavioral problems, substance abuse, and other mental and behavioral health conditions turn to their primary care providers as their first, and often only, source of mental health care. Unfortunately, this care may not be as effective as patients and primary care personnel would hope or expect it to be. Problems exist with missed or inaccurate diagnoses, referrals and coordination of care, and other failures in detection and treatment (NIMH Integrated Care Web site, accessed Oct. 1, 2017).
Through the Academy’s web portal interested clinicians, health care administrators, quality improvement specialists, and others can access a wide range of resources related to behavioral health integration. A hallmark of the site is the Integration Playbook, developed as a guide to integrating behavioral health in primary care and other ambulatory care settings. The Playbook assists the growing number of primary care practices and health systems that are beginning to design and implement integrated behavioral health services. The Playbook’s implementation framework is designed to be meaningful at any level of integration development.
One challenge in implementing primary care and behavioral health integration is connecting the community engaged in integrated health care. Often behavioral health and primary care providers operate within the same building or organization but are not be aware of each other’s presence. One goal of the Academy is to unite these disparate efforts and direct providers towards one another in an attempt to facilitate collaboration. In the same vein, the Academy aims to offer resources to patients and the community on integration, including the identification of integrated practices they can access.
In addition, in order to measure quality of care in this new approach to health care delivery, the Academy created the Atlas of Integrated Behavioral Health Care Quality Measures. Intended for practices and teams that wish to understand whether they are providing high-quality integrated behavioral health care or are preparing to implement integrated care, the Atlas aims to support the field of integrated behavioral health care measurement by 1) presenting a framework for understanding measurement of integrated care; 2) providing a list of existing measures relevant to integrated behavioral health care; and 3) organizing the measures by the framework and by user goals to facilitate selection of measures.
Links from the NCEPCR site:
Tools and Resources for Research, Quality Improvement, and Practice
https://www.ahrq.gov/ncepcr/research-qi-practice/practice-transformation-qi.html
Academy Web Portal: https://www.integrationacademy.ahrq.gov
The Integration Playbook: https://integrationacademy.ahrq.gov/playbook/about-playbook
Lexicon: https://integrationacademy.ahrq.gov/lexicon
Atlas of Integrated Behavioral Health Care Quality Measures: https://integrationacademy.ahrq.gov/resources/ibhc-measures-atlas
These and other tools can be found at the NCEPCR Web site: https://www.ahrq.gov/ncepcr.
Dr. Genevro is a health scientist at AHRQ. Dr. Ganiats is director, National Center for Excellence in Primary Care Research, AHRQ.
This is the fourth in a series of articles from the National Center for Excellence in Primary Care Research (NCEPCR) in the Agency for Healthcare Research and Quality (AHRQ). This series introduces sets of tools and resources designed to help your practice.
Many patients with anxiety, depression, behavioral problems, substance abuse, and other mental and behavioral health conditions turn to their primary care providers as their first, and often only, source of mental health care. Unfortunately, this care may not be as effective as patients and primary care personnel would hope or expect it to be. Problems exist with missed or inaccurate diagnoses, referrals and coordination of care, and other failures in detection and treatment (NIMH Integrated Care Web site, accessed Oct. 1, 2017).
Through the Academy’s web portal interested clinicians, health care administrators, quality improvement specialists, and others can access a wide range of resources related to behavioral health integration. A hallmark of the site is the Integration Playbook, developed as a guide to integrating behavioral health in primary care and other ambulatory care settings. The Playbook assists the growing number of primary care practices and health systems that are beginning to design and implement integrated behavioral health services. The Playbook’s implementation framework is designed to be meaningful at any level of integration development.
One challenge in implementing primary care and behavioral health integration is connecting the community engaged in integrated health care. Often behavioral health and primary care providers operate within the same building or organization but are not be aware of each other’s presence. One goal of the Academy is to unite these disparate efforts and direct providers towards one another in an attempt to facilitate collaboration. In the same vein, the Academy aims to offer resources to patients and the community on integration, including the identification of integrated practices they can access.
In addition, in order to measure quality of care in this new approach to health care delivery, the Academy created the Atlas of Integrated Behavioral Health Care Quality Measures. Intended for practices and teams that wish to understand whether they are providing high-quality integrated behavioral health care or are preparing to implement integrated care, the Atlas aims to support the field of integrated behavioral health care measurement by 1) presenting a framework for understanding measurement of integrated care; 2) providing a list of existing measures relevant to integrated behavioral health care; and 3) organizing the measures by the framework and by user goals to facilitate selection of measures.
Links from the NCEPCR site:
Tools and Resources for Research, Quality Improvement, and Practice
https://www.ahrq.gov/ncepcr/research-qi-practice/practice-transformation-qi.html
Academy Web Portal: https://www.integrationacademy.ahrq.gov
The Integration Playbook: https://integrationacademy.ahrq.gov/playbook/about-playbook
Lexicon: https://integrationacademy.ahrq.gov/lexicon
Atlas of Integrated Behavioral Health Care Quality Measures: https://integrationacademy.ahrq.gov/resources/ibhc-measures-atlas
These and other tools can be found at the NCEPCR Web site: https://www.ahrq.gov/ncepcr.
Dr. Genevro is a health scientist at AHRQ. Dr. Ganiats is director, National Center for Excellence in Primary Care Research, AHRQ.
ADHD and the role of wellness
ADHD is a very common disorder with several medication treatment options. There also are wellness and parenting strategies that can address aspects of the challenges of ADHD that are not perfectly covered by medication, such as excess symptoms, times of day that are not covered, or oppositional behavior that often develops secondarily.
Case summary
James is a 6-year-old boy who has been an active, high-energy child since preschool. He has had difficulty with wiggling around in kindergarten and preschool, talking excessively, and being unable to follow directions and pay attention. He is impulsive, disruptive, and frequently doesn’t listen to what his parents tell him to do. Parents and teachers rank him in the clinical range for hyperactivity, impulsivity, and attention problems on standardized rating scales.
Discussion
When we first discuss a new diagnosis with a family, we have the opportunity to shape the family’s expectations about that diagnosis and how it should be addressed. When I discuss ADHD with a new family, I want them to understand the symptoms of inattention, hyperactivity, and impulsiveness, and that these symptoms are not the child’s fault, but rather related to the way his brain is connected. At the same time, I also emphasize that these connections are not entirely fixed, that they mature over time, and that they are affected by experiences in life. In particular, I stress that positive experiences and wellness activities can influence the brain in a positive way. While, of course, I discuss the range of medications that can address these issues, I also deal with wellness in the treatment plan.

Exercise
Studies in humans and animals have provided background evidence that exercise increases the release of neurotransmitters such as dopamine and norepinephrine that are important in the pathophysiology of ADHD. Cerillo-Urbina et al. did a meta-analysis in 2015 of randomized controlled trials and found medium to large effect sizes for a variety of physical activity programs with respect to attention, hyperactivity, and impulsivity, although the study quality was generally low.1 Clearly we need additional more rigorous studies, but given the positive direction of outcomes, the lack of side effects, and the many other positive effects of exercise, it does not seem too soon to add exercise as a prescription for our patients with ADHD. I review this evidence with families, ask them about physical activity they like, and ask if they are willing to work toward an hour of exercise a day.
Sleep
Many children with ADHD have problems with sleep even before they start on stimulant medications, which can further affect sleep. Addressing sleep early on can improve ADHD symptoms, as well as help parents change or avoid patterns like having children fall asleep to the sound of a television. Brief sleep hygiene and cognitive-behavioral therapy interventions over three visits were demonstrated in a randomized controlled trial by Hisock et al. to improve ADHD symptoms and behavioral function.2 These psychosocial interventions clearly are the first line in addressing sleep problems in ADHD, and can benefit even sleep problems connected to medication.
Parent training

Treatment plan
1. Have the child exercise 1 hour every day. Have fun!
2. Establish a nightly bedtime routine, with a bath at 7:30 p.m., brushing of teeth, a story, and lights out at 8 with no TV in the room.
3. Check out the CHADD website for Parent to Parent.
4. Start a trial of stimulant medication.
5. Return in 2 weeks to monitor these interventions, adjust goals, and adjust medications.
When to refer
Many parents will be able to put such a plan in motion with your support and that of other parents. If they are struggling, therapists, psychologists, and psychiatrists trained in motivational and behavioral methods can provide more individualized parent training. Also consider whether the parents themselves may have ADHD and could use referral and treatment.
Dr. Hall is assistant professor of psychiatry and pediatrics at the University of Vermont, Burlington. She said she had no relevant financial disclosures.
References
1. Child Care Health Dev. 2015 Nov;41(6):779-88.
2. BMJ. 2015. doi: 10.1136/bmj.h68.
ADHD is a very common disorder with several medication treatment options. There also are wellness and parenting strategies that can address aspects of the challenges of ADHD that are not perfectly covered by medication, such as excess symptoms, times of day that are not covered, or oppositional behavior that often develops secondarily.
Case summary
James is a 6-year-old boy who has been an active, high-energy child since preschool. He has had difficulty with wiggling around in kindergarten and preschool, talking excessively, and being unable to follow directions and pay attention. He is impulsive, disruptive, and frequently doesn’t listen to what his parents tell him to do. Parents and teachers rank him in the clinical range for hyperactivity, impulsivity, and attention problems on standardized rating scales.
Discussion
When we first discuss a new diagnosis with a family, we have the opportunity to shape the family’s expectations about that diagnosis and how it should be addressed. When I discuss ADHD with a new family, I want them to understand the symptoms of inattention, hyperactivity, and impulsiveness, and that these symptoms are not the child’s fault, but rather related to the way his brain is connected. At the same time, I also emphasize that these connections are not entirely fixed, that they mature over time, and that they are affected by experiences in life. In particular, I stress that positive experiences and wellness activities can influence the brain in a positive way. While, of course, I discuss the range of medications that can address these issues, I also deal with wellness in the treatment plan.
Exercise
Studies in humans and animals have provided background evidence that exercise increases the release of neurotransmitters such as dopamine and norepinephrine that are important in the pathophysiology of ADHD. Cerillo-Urbina et al. did a meta-analysis in 2015 of randomized controlled trials and found medium to large effect sizes for a variety of physical activity programs with respect to attention, hyperactivity, and impulsivity, although the study quality was generally low.1 Clearly we need additional more rigorous studies, but given the positive direction of outcomes, the lack of side effects, and the many other positive effects of exercise, it does not seem too soon to add exercise as a prescription for our patients with ADHD. I review this evidence with families, ask them about physical activity they like, and ask if they are willing to work toward an hour of exercise a day.
Sleep
Many children with ADHD have problems with sleep even before they start on stimulant medications, which can further affect sleep. Addressing sleep early on can improve ADHD symptoms, as well as help parents change or avoid patterns like having children fall asleep to the sound of a television. Brief sleep hygiene and cognitive-behavioral therapy interventions over three visits were demonstrated in a randomized controlled trial by Hisock et al. to improve ADHD symptoms and behavioral function.2 These psychosocial interventions clearly are the first line in addressing sleep problems in ADHD, and can benefit even sleep problems connected to medication.
Parent training
Treatment plan
1. Have the child exercise 1 hour every day. Have fun!
2. Establish a nightly bedtime routine, with a bath at 7:30 p.m., brushing of teeth, a story, and lights out at 8 with no TV in the room.
3. Check out the CHADD website for Parent to Parent.
4. Start a trial of stimulant medication.
5. Return in 2 weeks to monitor these interventions, adjust goals, and adjust medications.
When to refer
Many parents will be able to put such a plan in motion with your support and that of other parents. If they are struggling, therapists, psychologists, and psychiatrists trained in motivational and behavioral methods can provide more individualized parent training. Also consider whether the parents themselves may have ADHD and could use referral and treatment.
Dr. Hall is assistant professor of psychiatry and pediatrics at the University of Vermont, Burlington. She said she had no relevant financial disclosures.
References
1. Child Care Health Dev. 2015 Nov;41(6):779-88.
2. BMJ. 2015. doi: 10.1136/bmj.h68.
ADHD is a very common disorder with several medication treatment options. There also are wellness and parenting strategies that can address aspects of the challenges of ADHD that are not perfectly covered by medication, such as excess symptoms, times of day that are not covered, or oppositional behavior that often develops secondarily.
Case summary
James is a 6-year-old boy who has been an active, high-energy child since preschool. He has had difficulty with wiggling around in kindergarten and preschool, talking excessively, and being unable to follow directions and pay attention. He is impulsive, disruptive, and frequently doesn’t listen to what his parents tell him to do. Parents and teachers rank him in the clinical range for hyperactivity, impulsivity, and attention problems on standardized rating scales.
Discussion
When we first discuss a new diagnosis with a family, we have the opportunity to shape the family’s expectations about that diagnosis and how it should be addressed. When I discuss ADHD with a new family, I want them to understand the symptoms of inattention, hyperactivity, and impulsiveness, and that these symptoms are not the child’s fault, but rather related to the way his brain is connected. At the same time, I also emphasize that these connections are not entirely fixed, that they mature over time, and that they are affected by experiences in life. In particular, I stress that positive experiences and wellness activities can influence the brain in a positive way. While, of course, I discuss the range of medications that can address these issues, I also deal with wellness in the treatment plan.
Exercise
Studies in humans and animals have provided background evidence that exercise increases the release of neurotransmitters such as dopamine and norepinephrine that are important in the pathophysiology of ADHD. Cerillo-Urbina et al. did a meta-analysis in 2015 of randomized controlled trials and found medium to large effect sizes for a variety of physical activity programs with respect to attention, hyperactivity, and impulsivity, although the study quality was generally low.1 Clearly we need additional more rigorous studies, but given the positive direction of outcomes, the lack of side effects, and the many other positive effects of exercise, it does not seem too soon to add exercise as a prescription for our patients with ADHD. I review this evidence with families, ask them about physical activity they like, and ask if they are willing to work toward an hour of exercise a day.
Sleep
Many children with ADHD have problems with sleep even before they start on stimulant medications, which can further affect sleep. Addressing sleep early on can improve ADHD symptoms, as well as help parents change or avoid patterns like having children fall asleep to the sound of a television. Brief sleep hygiene and cognitive-behavioral therapy interventions over three visits were demonstrated in a randomized controlled trial by Hisock et al. to improve ADHD symptoms and behavioral function.2 These psychosocial interventions clearly are the first line in addressing sleep problems in ADHD, and can benefit even sleep problems connected to medication.
Parent training
Treatment plan
1. Have the child exercise 1 hour every day. Have fun!
2. Establish a nightly bedtime routine, with a bath at 7:30 p.m., brushing of teeth, a story, and lights out at 8 with no TV in the room.
3. Check out the CHADD website for Parent to Parent.
4. Start a trial of stimulant medication.
5. Return in 2 weeks to monitor these interventions, adjust goals, and adjust medications.
When to refer
Many parents will be able to put such a plan in motion with your support and that of other parents. If they are struggling, therapists, psychologists, and psychiatrists trained in motivational and behavioral methods can provide more individualized parent training. Also consider whether the parents themselves may have ADHD and could use referral and treatment.
Dr. Hall is assistant professor of psychiatry and pediatrics at the University of Vermont, Burlington. She said she had no relevant financial disclosures.
References
1. Child Care Health Dev. 2015 Nov;41(6):779-88.
2. BMJ. 2015. doi: 10.1136/bmj.h68.
Ending hazing as a rite of manhood on college campuses
Is hazing a necessary rite of passage in Greek life, or a terrible tradition that needs to end once and for all?
There can be no justification for hazing, especially after the recent tragic deaths of fraternity pledges at Florida State University, Texas State University, and Louisiana State University. The horror of hazing has been brought home by the refiling of charges against several Penn State fraternity members in the torturous death last February of Timothy Piazza, which was recorded on videotape. In response to recent deaths and injuries, some colleges have suspended Greek life activities on campus. Unfortunately, hazing deaths are not new to college campuses but have a been a problem for several years, with 40 deaths in the last decade. The majority of these deaths involved the forced consumption of large amounts of alcohol, but some have involved beatings and other forms of abuse.
What exactly is hazing? According to the organization StopHazing (stophazing.org), it is “any activity expected of someone joining or participating in a group that humiliates, degrades, abuses, or endangers them regardless of a person’s willingness to participate.” Activities may involve alcohol consumption, humiliation, sleep deprivation, physical abuse, and sexual abuse. Hazing is not just a problem of fraternities; half of college students joining clubs, teams, and other organizations experience hazing. In fact, half of young adults have been hazed by the time they graduate from high school.
Given its inherent dangers, we have to wonder, why does hazing continue? The National Public Radio show 1A offered one answer to this troubling question on its Nov. 15 show, “How to Stop Hazing.” Two panel members, a filmmaker and a professor, discussed their own hazing experiences in college fraternities that included being forced to drink too much alcohol, eating noxious products, and being subjected to violence. One of the panel members talked about hazing other people. Both men admitted that the hazing process made them feel closer to their fraternity brothers: They formed lifelong bonds and also became stronger in facing adversity. In many ways, hazing was a masculine rite of passage. Neither panel member condoned the behaviors they were subjected to or participated in, and in fact suggested that college men should find new ways to bond and have a sense of belonging.
Even though the panelists were not promoting hazing, I was struck by their almost fond recollection of these experiences. I, in contrast, have no fond memory of an incident that I would consider medical hazing. During my internship when working on an internal medicine unit, I was ordered back to work after 2 days at home with the flu, although I was still febrile and coughing up a storm. That week, I was punished with an extra night of on-call duty. This incident did not leave me embracing the camaraderie and hardiness of my medical colleagues. It left me more determined than ever to treat peers and trainees with care and compassion, and never to abuse my power.

In our own practices as psychiatrists, we can play a role in helping our young adult male patients avoid hazing experiences, which have the potential to lead to depression, anxiety, posttraumatic stress disorder, and suicidal behaviors. We can work with our male patients to develop a sense of belonging and an understanding of who they are as men, without putting their lives or others’ lives at risk. In my work as a college counseling center psychiatrist for over 2 decades, I have often addressed the issues of masculinity, friendship, and peer pressure with my male patients. For those of you who work with young adult men, particularly in the college population, here are some tips:
1. Talk with your male patients about healthy versus harmful relationships. No relationship should involve the intentional infliction of physical or emotional pain. Men will acknowledge that a man hitting a girlfriend is abusive. They need to understand that male fraternity brothers hitting each other or forcing someone to drink a large volume of alcohol is equally abusive. Encourage your patients to know their limits and set boundaries if they are asked to do something dangerous to themselves or others.
2. Role play with your patients how to say no to their peers. I did that with a patient who was drinking too much in general with his fraternity brothers. He was afraid they would reject him if he drank less. He was pleasantly surprised when they did not pressure him to drink more, but instead encouraged him to do what is healthy for him.
3. Encourage your patients to have strong social connections on campus. Well-run fraternities can provide these friendship without inflicting pain. Intramural sports, singing groups, bands, and volunteer organizations all provide great ways to connect and also have a sense of accomplishment. Social connections improve grades, physical health, and emotional health.
4. Encourage your male patients to accept who they are, without embracing one stereotype of what it means to be a man. Social media often promotes unattainable physical images, and some male patients will take supplements or even steroids to build up muscle mass. Promote a healthy lifestyle without extremes in exercise and diet. Explore with your patient what it means to be a man in the 21st century, at a time when typical gender roles are being challenged.
5. Listen for cues about your patients’ relationship with their fathers, which have a large impact on how they view masculinity. Many of the male patients I see discuss how they are trying to be more in touch with and expressive about their feelings, after watching their fathers hold in their emotions or use alcohol to numb emotional pain. Some patients have been able to model and encourage a greater openness with their fathers, while others have been met with silence. As a patient is creating his own life story, his father’s history is always in the background.
Should all fraternities be shut down to end the hazing problem? I don’t believe this is the answer. Each campus has a different fraternity culture, and fraternities on many campuses can be a positive force. I have heard young men describe how fraternities encouraged them academically, discouraged excessive drinking, and promoted ethical behavior. But given that abuses have been prevalent on certain campuses, it is incumbent upon universities to enforce safe behaviors. Fraternity brothers who hurt others should be prosecuted, not protected.
The hazing on campuses needs to stop, and we as psychiatrists should talk about this important issue with our patients and sometimes their parents. We can educate our patients about this insidious form of physical and emotional abuse; we can encourage them not to be bystanders when this happens; and we can promote a culture of respect on our campuses.
Hazing is not just a campus but a national cultural problem, as we are finding from the avalanche of news reports about sexual harassment and assault in the political and entertainment worlds. Victims are exposed to abuses and then deterred from reporting them as a condition of staying in and advancing in the professions they love. Hazing is an abuse of power that we as psychiatrists must continue to fight. We should teach our young adult men the mantra that is now being used by some fraternities, “Real men don’t haze.”
Dr. Morris is an associate professor of psychiatry and associate program director for student health psychiatry at the University of Florida, Gainesville. She is the author of The Campus Cure: A Parent’s Guide to Mental Health and Wellness for College Students, which will be published by Rowman & Littlefield of Lanham, Md., in January 2018.
Is hazing a necessary rite of passage in Greek life, or a terrible tradition that needs to end once and for all?
There can be no justification for hazing, especially after the recent tragic deaths of fraternity pledges at Florida State University, Texas State University, and Louisiana State University. The horror of hazing has been brought home by the refiling of charges against several Penn State fraternity members in the torturous death last February of Timothy Piazza, which was recorded on videotape. In response to recent deaths and injuries, some colleges have suspended Greek life activities on campus. Unfortunately, hazing deaths are not new to college campuses but have a been a problem for several years, with 40 deaths in the last decade. The majority of these deaths involved the forced consumption of large amounts of alcohol, but some have involved beatings and other forms of abuse.
What exactly is hazing? According to the organization StopHazing (stophazing.org), it is “any activity expected of someone joining or participating in a group that humiliates, degrades, abuses, or endangers them regardless of a person’s willingness to participate.” Activities may involve alcohol consumption, humiliation, sleep deprivation, physical abuse, and sexual abuse. Hazing is not just a problem of fraternities; half of college students joining clubs, teams, and other organizations experience hazing. In fact, half of young adults have been hazed by the time they graduate from high school.
Given its inherent dangers, we have to wonder, why does hazing continue? The National Public Radio show 1A offered one answer to this troubling question on its Nov. 15 show, “How to Stop Hazing.” Two panel members, a filmmaker and a professor, discussed their own hazing experiences in college fraternities that included being forced to drink too much alcohol, eating noxious products, and being subjected to violence. One of the panel members talked about hazing other people. Both men admitted that the hazing process made them feel closer to their fraternity brothers: They formed lifelong bonds and also became stronger in facing adversity. In many ways, hazing was a masculine rite of passage. Neither panel member condoned the behaviors they were subjected to or participated in, and in fact suggested that college men should find new ways to bond and have a sense of belonging.
Even though the panelists were not promoting hazing, I was struck by their almost fond recollection of these experiences. I, in contrast, have no fond memory of an incident that I would consider medical hazing. During my internship when working on an internal medicine unit, I was ordered back to work after 2 days at home with the flu, although I was still febrile and coughing up a storm. That week, I was punished with an extra night of on-call duty. This incident did not leave me embracing the camaraderie and hardiness of my medical colleagues. It left me more determined than ever to treat peers and trainees with care and compassion, and never to abuse my power.
In our own practices as psychiatrists, we can play a role in helping our young adult male patients avoid hazing experiences, which have the potential to lead to depression, anxiety, posttraumatic stress disorder, and suicidal behaviors. We can work with our male patients to develop a sense of belonging and an understanding of who they are as men, without putting their lives or others’ lives at risk. In my work as a college counseling center psychiatrist for over 2 decades, I have often addressed the issues of masculinity, friendship, and peer pressure with my male patients. For those of you who work with young adult men, particularly in the college population, here are some tips:
1. Talk with your male patients about healthy versus harmful relationships. No relationship should involve the intentional infliction of physical or emotional pain. Men will acknowledge that a man hitting a girlfriend is abusive. They need to understand that male fraternity brothers hitting each other or forcing someone to drink a large volume of alcohol is equally abusive. Encourage your patients to know their limits and set boundaries if they are asked to do something dangerous to themselves or others.
2. Role play with your patients how to say no to their peers. I did that with a patient who was drinking too much in general with his fraternity brothers. He was afraid they would reject him if he drank less. He was pleasantly surprised when they did not pressure him to drink more, but instead encouraged him to do what is healthy for him.
3. Encourage your patients to have strong social connections on campus. Well-run fraternities can provide these friendship without inflicting pain. Intramural sports, singing groups, bands, and volunteer organizations all provide great ways to connect and also have a sense of accomplishment. Social connections improve grades, physical health, and emotional health.
4. Encourage your male patients to accept who they are, without embracing one stereotype of what it means to be a man. Social media often promotes unattainable physical images, and some male patients will take supplements or even steroids to build up muscle mass. Promote a healthy lifestyle without extremes in exercise and diet. Explore with your patient what it means to be a man in the 21st century, at a time when typical gender roles are being challenged.
5. Listen for cues about your patients’ relationship with their fathers, which have a large impact on how they view masculinity. Many of the male patients I see discuss how they are trying to be more in touch with and expressive about their feelings, after watching their fathers hold in their emotions or use alcohol to numb emotional pain. Some patients have been able to model and encourage a greater openness with their fathers, while others have been met with silence. As a patient is creating his own life story, his father’s history is always in the background.
Should all fraternities be shut down to end the hazing problem? I don’t believe this is the answer. Each campus has a different fraternity culture, and fraternities on many campuses can be a positive force. I have heard young men describe how fraternities encouraged them academically, discouraged excessive drinking, and promoted ethical behavior. But given that abuses have been prevalent on certain campuses, it is incumbent upon universities to enforce safe behaviors. Fraternity brothers who hurt others should be prosecuted, not protected.
The hazing on campuses needs to stop, and we as psychiatrists should talk about this important issue with our patients and sometimes their parents. We can educate our patients about this insidious form of physical and emotional abuse; we can encourage them not to be bystanders when this happens; and we can promote a culture of respect on our campuses.
Hazing is not just a campus but a national cultural problem, as we are finding from the avalanche of news reports about sexual harassment and assault in the political and entertainment worlds. Victims are exposed to abuses and then deterred from reporting them as a condition of staying in and advancing in the professions they love. Hazing is an abuse of power that we as psychiatrists must continue to fight. We should teach our young adult men the mantra that is now being used by some fraternities, “Real men don’t haze.”
Dr. Morris is an associate professor of psychiatry and associate program director for student health psychiatry at the University of Florida, Gainesville. She is the author of The Campus Cure: A Parent’s Guide to Mental Health and Wellness for College Students, which will be published by Rowman & Littlefield of Lanham, Md., in January 2018.
Is hazing a necessary rite of passage in Greek life, or a terrible tradition that needs to end once and for all?
There can be no justification for hazing, especially after the recent tragic deaths of fraternity pledges at Florida State University, Texas State University, and Louisiana State University. The horror of hazing has been brought home by the refiling of charges against several Penn State fraternity members in the torturous death last February of Timothy Piazza, which was recorded on videotape. In response to recent deaths and injuries, some colleges have suspended Greek life activities on campus. Unfortunately, hazing deaths are not new to college campuses but have a been a problem for several years, with 40 deaths in the last decade. The majority of these deaths involved the forced consumption of large amounts of alcohol, but some have involved beatings and other forms of abuse.
What exactly is hazing? According to the organization StopHazing (stophazing.org), it is “any activity expected of someone joining or participating in a group that humiliates, degrades, abuses, or endangers them regardless of a person’s willingness to participate.” Activities may involve alcohol consumption, humiliation, sleep deprivation, physical abuse, and sexual abuse. Hazing is not just a problem of fraternities; half of college students joining clubs, teams, and other organizations experience hazing. In fact, half of young adults have been hazed by the time they graduate from high school.
Given its inherent dangers, we have to wonder, why does hazing continue? The National Public Radio show 1A offered one answer to this troubling question on its Nov. 15 show, “How to Stop Hazing.” Two panel members, a filmmaker and a professor, discussed their own hazing experiences in college fraternities that included being forced to drink too much alcohol, eating noxious products, and being subjected to violence. One of the panel members talked about hazing other people. Both men admitted that the hazing process made them feel closer to their fraternity brothers: They formed lifelong bonds and also became stronger in facing adversity. In many ways, hazing was a masculine rite of passage. Neither panel member condoned the behaviors they were subjected to or participated in, and in fact suggested that college men should find new ways to bond and have a sense of belonging.
Even though the panelists were not promoting hazing, I was struck by their almost fond recollection of these experiences. I, in contrast, have no fond memory of an incident that I would consider medical hazing. During my internship when working on an internal medicine unit, I was ordered back to work after 2 days at home with the flu, although I was still febrile and coughing up a storm. That week, I was punished with an extra night of on-call duty. This incident did not leave me embracing the camaraderie and hardiness of my medical colleagues. It left me more determined than ever to treat peers and trainees with care and compassion, and never to abuse my power.
In our own practices as psychiatrists, we can play a role in helping our young adult male patients avoid hazing experiences, which have the potential to lead to depression, anxiety, posttraumatic stress disorder, and suicidal behaviors. We can work with our male patients to develop a sense of belonging and an understanding of who they are as men, without putting their lives or others’ lives at risk. In my work as a college counseling center psychiatrist for over 2 decades, I have often addressed the issues of masculinity, friendship, and peer pressure with my male patients. For those of you who work with young adult men, particularly in the college population, here are some tips:
1. Talk with your male patients about healthy versus harmful relationships. No relationship should involve the intentional infliction of physical or emotional pain. Men will acknowledge that a man hitting a girlfriend is abusive. They need to understand that male fraternity brothers hitting each other or forcing someone to drink a large volume of alcohol is equally abusive. Encourage your patients to know their limits and set boundaries if they are asked to do something dangerous to themselves or others.
2. Role play with your patients how to say no to their peers. I did that with a patient who was drinking too much in general with his fraternity brothers. He was afraid they would reject him if he drank less. He was pleasantly surprised when they did not pressure him to drink more, but instead encouraged him to do what is healthy for him.
3. Encourage your patients to have strong social connections on campus. Well-run fraternities can provide these friendship without inflicting pain. Intramural sports, singing groups, bands, and volunteer organizations all provide great ways to connect and also have a sense of accomplishment. Social connections improve grades, physical health, and emotional health.
4. Encourage your male patients to accept who they are, without embracing one stereotype of what it means to be a man. Social media often promotes unattainable physical images, and some male patients will take supplements or even steroids to build up muscle mass. Promote a healthy lifestyle without extremes in exercise and diet. Explore with your patient what it means to be a man in the 21st century, at a time when typical gender roles are being challenged.
5. Listen for cues about your patients’ relationship with their fathers, which have a large impact on how they view masculinity. Many of the male patients I see discuss how they are trying to be more in touch with and expressive about their feelings, after watching their fathers hold in their emotions or use alcohol to numb emotional pain. Some patients have been able to model and encourage a greater openness with their fathers, while others have been met with silence. As a patient is creating his own life story, his father’s history is always in the background.
Should all fraternities be shut down to end the hazing problem? I don’t believe this is the answer. Each campus has a different fraternity culture, and fraternities on many campuses can be a positive force. I have heard young men describe how fraternities encouraged them academically, discouraged excessive drinking, and promoted ethical behavior. But given that abuses have been prevalent on certain campuses, it is incumbent upon universities to enforce safe behaviors. Fraternity brothers who hurt others should be prosecuted, not protected.
The hazing on campuses needs to stop, and we as psychiatrists should talk about this important issue with our patients and sometimes their parents. We can educate our patients about this insidious form of physical and emotional abuse; we can encourage them not to be bystanders when this happens; and we can promote a culture of respect on our campuses.
Hazing is not just a campus but a national cultural problem, as we are finding from the avalanche of news reports about sexual harassment and assault in the political and entertainment worlds. Victims are exposed to abuses and then deterred from reporting them as a condition of staying in and advancing in the professions they love. Hazing is an abuse of power that we as psychiatrists must continue to fight. We should teach our young adult men the mantra that is now being used by some fraternities, “Real men don’t haze.”
Dr. Morris is an associate professor of psychiatry and associate program director for student health psychiatry at the University of Florida, Gainesville. She is the author of The Campus Cure: A Parent’s Guide to Mental Health and Wellness for College Students, which will be published by Rowman & Littlefield of Lanham, Md., in January 2018.
Educational innovation
My son’s in medical school,” Fred told me. “First year.”
“Which school?”
Fred named a newly-chartered one.
“Really innovative curriculum,” he said.
“He got into a different school, too,” he said, “but he didn’t like how that school had canceled all lectures. Students just watch the lecture videos on their devices, so they scratched all the live ones.”
“Now that they don’t need lecturers, did they cut tuition?” I asked.
We both chuckled.

I was exposed to educational innovation on Day One of medical school, in the fall of 1968. (Go ahead, do the math.) The Dean addressed our entering class. “We’ve abolished tests,” he said. “We cut preclinical study from 2 years to 18 months, followed by one comprehensive exam.
"We want to get you into the clinic right away," he said, "because you chose to be doctors to help people. Even during the preclinical period, you’ll be getting not just dry frontal teaching but exposure to actual patients.”
We guessed that sounded good, especially the part about no tests. Less day-to-day studying. A lot less.
We still had lectures, of course, on biochemistry, anatomy, and so forth (they ran out of time and did all four extremities in 1 hour), but we felt little need to pay close attention. After all, any details we’d have to memorize would be diluted over three semesters, and 18 months was so far away.
As to the lectures themselves, I’ve never been diagnosed with actual narcolepsy, but when they turned out the lights and started showing slides, I fell fast asleep. Always have.
Most of us passed the comprehensive exam and moved on to the clinic. (We didn’t get into med school without knowing how to take tests, did we?)
The basic science faculty hated this educational innovation and recognized – correctly – that without tests we would take their classes less seriously. A couple of years later, the students themselves demanded that the tests be reinstated; lack of regular, numerical feedback made them anxious. So it was back to exams every 2 weeks. Poor devils.
Fast forward 40 years. Over lunch at a friend’s house, I recently met a young woman in her second year at a medical school in Chicago. “The school has an exciting, innovative curriculum,” she told me.
“No kidding,” I said. “What’s that?”
“They want to get us into the clinic as soon as possible,” she replied. “So they cut preclinical years to 18 months. And no regular tests. Just a comprehensive exam at the end. Much less day-to-day pressure.”
“Very innovative,” I observed.
***
Once in practice, I joined the clinical faculty of a local medical school. For 35 years, I hosted senior medical students for a month-long elective. During that time, I tried to pass on some of the things that weren’t on the standard academic curriculum. For instance, that patients have their own ideas about what is wrong with them, how it got that way, and what to do about it. That medical advice is less an order than a negotiation. Students seemed to find such notions – and their daily illustrations in the office – of some interest.
I put these and related deep thoughts between the covers of a book and sent a copy to the medical school registrar, from whom I had heard little over the years unless my student evaluations were 2 days late. My cover letter suggested that the school’s educators might be curious about what I’d been teaching their charges for 35 years.

The registrar replied by e-mail. “Thank you for your book,” she wrote. “I showed it to our dean of education, who told me that we would definitely not be changing our curriculum on the basis of your book. You might contact the medical librarian to see if they want to display it.”
I didn’t recall thinking, much less saying, that my ruminations ought to overturn the medical curriculum. I just thought they might be of some passing interest, coming as they did from an outside perspective.
Not so much, it turns out.
There are, in any event, so many exciting vistas of educational innovation to develop: genomics, precision medicine, and folding doctors into health care teams, and replacing clinical judgment with algorithms. The next generation of physicians, innovatively educated, will surpass all predecessors, just as we did.
Anyhow, they'll be bound to know more about the origins and insertions of the leg muscles. They could hardly know any less.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@frontlinemedcom.com.
My son’s in medical school,” Fred told me. “First year.”
“Which school?”
Fred named a newly-chartered one.
“Really innovative curriculum,” he said.
“He got into a different school, too,” he said, “but he didn’t like how that school had canceled all lectures. Students just watch the lecture videos on their devices, so they scratched all the live ones.”
“Now that they don’t need lecturers, did they cut tuition?” I asked.
We both chuckled.
I was exposed to educational innovation on Day One of medical school, in the fall of 1968. (Go ahead, do the math.) The Dean addressed our entering class. “We’ve abolished tests,” he said. “We cut preclinical study from 2 years to 18 months, followed by one comprehensive exam.
"We want to get you into the clinic right away," he said, "because you chose to be doctors to help people. Even during the preclinical period, you’ll be getting not just dry frontal teaching but exposure to actual patients.”
We guessed that sounded good, especially the part about no tests. Less day-to-day studying. A lot less.
We still had lectures, of course, on biochemistry, anatomy, and so forth (they ran out of time and did all four extremities in 1 hour), but we felt little need to pay close attention. After all, any details we’d have to memorize would be diluted over three semesters, and 18 months was so far away.
As to the lectures themselves, I’ve never been diagnosed with actual narcolepsy, but when they turned out the lights and started showing slides, I fell fast asleep. Always have.
Most of us passed the comprehensive exam and moved on to the clinic. (We didn’t get into med school without knowing how to take tests, did we?)
The basic science faculty hated this educational innovation and recognized – correctly – that without tests we would take their classes less seriously. A couple of years later, the students themselves demanded that the tests be reinstated; lack of regular, numerical feedback made them anxious. So it was back to exams every 2 weeks. Poor devils.
Fast forward 40 years. Over lunch at a friend’s house, I recently met a young woman in her second year at a medical school in Chicago. “The school has an exciting, innovative curriculum,” she told me.
“No kidding,” I said. “What’s that?”
“They want to get us into the clinic as soon as possible,” she replied. “So they cut preclinical years to 18 months. And no regular tests. Just a comprehensive exam at the end. Much less day-to-day pressure.”
“Very innovative,” I observed.
***
Once in practice, I joined the clinical faculty of a local medical school. For 35 years, I hosted senior medical students for a month-long elective. During that time, I tried to pass on some of the things that weren’t on the standard academic curriculum. For instance, that patients have their own ideas about what is wrong with them, how it got that way, and what to do about it. That medical advice is less an order than a negotiation. Students seemed to find such notions – and their daily illustrations in the office – of some interest.
I put these and related deep thoughts between the covers of a book and sent a copy to the medical school registrar, from whom I had heard little over the years unless my student evaluations were 2 days late. My cover letter suggested that the school’s educators might be curious about what I’d been teaching their charges for 35 years.
The registrar replied by e-mail. “Thank you for your book,” she wrote. “I showed it to our dean of education, who told me that we would definitely not be changing our curriculum on the basis of your book. You might contact the medical librarian to see if they want to display it.”
I didn’t recall thinking, much less saying, that my ruminations ought to overturn the medical curriculum. I just thought they might be of some passing interest, coming as they did from an outside perspective.
Not so much, it turns out.
There are, in any event, so many exciting vistas of educational innovation to develop: genomics, precision medicine, and folding doctors into health care teams, and replacing clinical judgment with algorithms. The next generation of physicians, innovatively educated, will surpass all predecessors, just as we did.
Anyhow, they'll be bound to know more about the origins and insertions of the leg muscles. They could hardly know any less.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@frontlinemedcom.com.
My son’s in medical school,” Fred told me. “First year.”
“Which school?”
Fred named a newly-chartered one.
“Really innovative curriculum,” he said.
“He got into a different school, too,” he said, “but he didn’t like how that school had canceled all lectures. Students just watch the lecture videos on their devices, so they scratched all the live ones.”
“Now that they don’t need lecturers, did they cut tuition?” I asked.
We both chuckled.
I was exposed to educational innovation on Day One of medical school, in the fall of 1968. (Go ahead, do the math.) The Dean addressed our entering class. “We’ve abolished tests,” he said. “We cut preclinical study from 2 years to 18 months, followed by one comprehensive exam.
"We want to get you into the clinic right away," he said, "because you chose to be doctors to help people. Even during the preclinical period, you’ll be getting not just dry frontal teaching but exposure to actual patients.”
We guessed that sounded good, especially the part about no tests. Less day-to-day studying. A lot less.
We still had lectures, of course, on biochemistry, anatomy, and so forth (they ran out of time and did all four extremities in 1 hour), but we felt little need to pay close attention. After all, any details we’d have to memorize would be diluted over three semesters, and 18 months was so far away.
As to the lectures themselves, I’ve never been diagnosed with actual narcolepsy, but when they turned out the lights and started showing slides, I fell fast asleep. Always have.
Most of us passed the comprehensive exam and moved on to the clinic. (We didn’t get into med school without knowing how to take tests, did we?)
The basic science faculty hated this educational innovation and recognized – correctly – that without tests we would take their classes less seriously. A couple of years later, the students themselves demanded that the tests be reinstated; lack of regular, numerical feedback made them anxious. So it was back to exams every 2 weeks. Poor devils.
Fast forward 40 years. Over lunch at a friend’s house, I recently met a young woman in her second year at a medical school in Chicago. “The school has an exciting, innovative curriculum,” she told me.
“No kidding,” I said. “What’s that?”
“They want to get us into the clinic as soon as possible,” she replied. “So they cut preclinical years to 18 months. And no regular tests. Just a comprehensive exam at the end. Much less day-to-day pressure.”
“Very innovative,” I observed.
***
Once in practice, I joined the clinical faculty of a local medical school. For 35 years, I hosted senior medical students for a month-long elective. During that time, I tried to pass on some of the things that weren’t on the standard academic curriculum. For instance, that patients have their own ideas about what is wrong with them, how it got that way, and what to do about it. That medical advice is less an order than a negotiation. Students seemed to find such notions – and their daily illustrations in the office – of some interest.
I put these and related deep thoughts between the covers of a book and sent a copy to the medical school registrar, from whom I had heard little over the years unless my student evaluations were 2 days late. My cover letter suggested that the school’s educators might be curious about what I’d been teaching their charges for 35 years.
The registrar replied by e-mail. “Thank you for your book,” she wrote. “I showed it to our dean of education, who told me that we would definitely not be changing our curriculum on the basis of your book. You might contact the medical librarian to see if they want to display it.”
I didn’t recall thinking, much less saying, that my ruminations ought to overturn the medical curriculum. I just thought they might be of some passing interest, coming as they did from an outside perspective.
Not so much, it turns out.
There are, in any event, so many exciting vistas of educational innovation to develop: genomics, precision medicine, and folding doctors into health care teams, and replacing clinical judgment with algorithms. The next generation of physicians, innovatively educated, will surpass all predecessors, just as we did.
Anyhow, they'll be bound to know more about the origins and insertions of the leg muscles. They could hardly know any less.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@frontlinemedcom.com.
A program to increase flu vaccine compliance
. It won’t hurt your bottom line either and actually will help it. A flu shot program potentially can be run by a licensed practical nurse, registered nurse, physician’s assistant, or pediatric nurse practitioner, depending on your state’s law regarding vaccine administration by other than a physician, thus freeing up the physician to see well-child and sick-call patients.
It’s easy to set up a flu shot program and run it. Start preparing in June, preceding the upcoming flu season. Designate several Saturdays and or Sundays in September, October, November, December, and January as flu shot Saturdays and/or Sundays. And if Columbus day falls on a weekday, consider adding Columbus Day to your program dates as the kids often are off from school that day (check the local school calendar).
Next, prepare a postcard to be mailed to all patients on the lists your EMR produced for you. Keep the postcard simple. Announce the program, and state the dates the flu shot program is running. Ask parents to call to make an appointment for a flu vaccine only by appointment “with the program.” In addition to mailing a postcard, announce the flu shot program by sending out automated telephone calls and emails to all three lists the EMR has produced for you. The postcard mailing is your first contact, essentially announcing the program with dates and times. An automated phone call may be used to announce a specific date for which you are “now booking.” A good option when using automated phone calls is to allow the caller to press “zero” to be connected to the office to schedule a “flu shot only” appointment! Finally, emails announcing the dates of the program simply will reinforce information about the program.

Mr. Berman has been providing practice management services to physicians and other medical providers since 1983. He is the CEO of a pediatrics practice with locations in Staten Island and Brooklyn, N.Y. He holds a faculty appointment at State University of New York, Brooklyn, as a lecturer for the department of family medicine’s residency training program. He has no disclosures to report. Email him at pdnews@frontlinemedcom.com.
. It won’t hurt your bottom line either and actually will help it. A flu shot program potentially can be run by a licensed practical nurse, registered nurse, physician’s assistant, or pediatric nurse practitioner, depending on your state’s law regarding vaccine administration by other than a physician, thus freeing up the physician to see well-child and sick-call patients.
It’s easy to set up a flu shot program and run it. Start preparing in June, preceding the upcoming flu season. Designate several Saturdays and or Sundays in September, October, November, December, and January as flu shot Saturdays and/or Sundays. And if Columbus day falls on a weekday, consider adding Columbus Day to your program dates as the kids often are off from school that day (check the local school calendar).
Next, prepare a postcard to be mailed to all patients on the lists your EMR produced for you. Keep the postcard simple. Announce the program, and state the dates the flu shot program is running. Ask parents to call to make an appointment for a flu vaccine only by appointment “with the program.” In addition to mailing a postcard, announce the flu shot program by sending out automated telephone calls and emails to all three lists the EMR has produced for you. The postcard mailing is your first contact, essentially announcing the program with dates and times. An automated phone call may be used to announce a specific date for which you are “now booking.” A good option when using automated phone calls is to allow the caller to press “zero” to be connected to the office to schedule a “flu shot only” appointment! Finally, emails announcing the dates of the program simply will reinforce information about the program.
Mr. Berman has been providing practice management services to physicians and other medical providers since 1983. He is the CEO of a pediatrics practice with locations in Staten Island and Brooklyn, N.Y. He holds a faculty appointment at State University of New York, Brooklyn, as a lecturer for the department of family medicine’s residency training program. He has no disclosures to report. Email him at pdnews@frontlinemedcom.com.
. It won’t hurt your bottom line either and actually will help it. A flu shot program potentially can be run by a licensed practical nurse, registered nurse, physician’s assistant, or pediatric nurse practitioner, depending on your state’s law regarding vaccine administration by other than a physician, thus freeing up the physician to see well-child and sick-call patients.
It’s easy to set up a flu shot program and run it. Start preparing in June, preceding the upcoming flu season. Designate several Saturdays and or Sundays in September, October, November, December, and January as flu shot Saturdays and/or Sundays. And if Columbus day falls on a weekday, consider adding Columbus Day to your program dates as the kids often are off from school that day (check the local school calendar).
Next, prepare a postcard to be mailed to all patients on the lists your EMR produced for you. Keep the postcard simple. Announce the program, and state the dates the flu shot program is running. Ask parents to call to make an appointment for a flu vaccine only by appointment “with the program.” In addition to mailing a postcard, announce the flu shot program by sending out automated telephone calls and emails to all three lists the EMR has produced for you. The postcard mailing is your first contact, essentially announcing the program with dates and times. An automated phone call may be used to announce a specific date for which you are “now booking.” A good option when using automated phone calls is to allow the caller to press “zero” to be connected to the office to schedule a “flu shot only” appointment! Finally, emails announcing the dates of the program simply will reinforce information about the program.
Mr. Berman has been providing practice management services to physicians and other medical providers since 1983. He is the CEO of a pediatrics practice with locations in Staten Island and Brooklyn, N.Y. He holds a faculty appointment at State University of New York, Brooklyn, as a lecturer for the department of family medicine’s residency training program. He has no disclosures to report. Email him at pdnews@frontlinemedcom.com.
New opportunities for gastroenterology leadership in the evolving payment reform landscape
This year’s Congressional debate over repealing or reforming key provisions of the Affordable Care Act was contentious in large part because of the high and rising costs of health care. Though a new health care reform bill is now unlikely, it remains critical to continue the discussion on how to deliver and pay for care in a way that addresses these high costs and makes coverage more affordable through more efficient and high-quality approaches.1

Illustrating the bipartisan nature of payment reforms, the Medicare Access and CHIP Reauthorization Act (MACRA) passed with more than 90% support in both the House and Senate in 2015. MACRA provides a 5% bonus payment for physicians who receive a significant part of their Medicare payments in an advanced APM, which involves some downside financial risk. In addition, any physician who participates significantly in a broader range of Medicare APMs, including many without downside risk, receives an exception from the reporting requirements for the new Merit-Based Incentive Payment System (MIPS) and would report on APM performance measures instead.
However, the details of payment reform are challenging and will benefit from engagement and leadership by physicians – including in gastroenterology. A new survey shows that the Department of Health and Human Services has achieved its goal of having 30% of health care payments tied to APMs by the end of 2016.3 It hopes to have 50% by the end of 2018.

Physician-Focused Payment Model Technical Advisory Committee’s role in recommending new payment models
The paucity of APMs was one reason the MACRA law established the Physician-Focused Payment Model Technical Advisory Committee (PTAC). Organizations can submit proposals for new Medicare payment models to PTAC, which then are reviewed according to 10 established criteria. The criteria place particular emphasis on the scope of the APM, the APM’s ability to increase quality while maintaining or decreasing costs, and whether the payment methodology improves on current policy. PTAC then makes recommendations to CMS for full implementation of a proposal, limited testing (a pilot program), or no implementation.

The fate of the two GI APMs offers broad insight on the path forward for new specialized-care models. Although PTAC focuses on physician payment, its criteria and critiques emphasize that the primary focus of any APM should be on the full spectrum of patient care. Project Sonar likely received a positive recommendation because it focused on shifting payment to improving chronic care and avoiding complications. Although the colonoscopy proposal was withdrawn, we can gain a sense of PTAC’s concerns through the preliminary review.5 The review argues the proposal did not sufficiently address how it would lead to a more efficient, better integrated, and higher quality screening that improves patient health. More specifically, the review criticized the proposal for focusing primarily on a site-of-service shift and offering fewer details on how the APM would reduce overutilization.
Overall, PTAC’s deliberations at both its April and September meetings suggest that it will deeply scrutinize models focusing only on a single procedure or specialty, or ones that it believes do not sufficiently coordinate with primary care or other specialties, because it does not believe that such models have a sufficiently comprehensive patient focus. These PTAC reviews also suggest that the Committee will recommend programs with ideas they find viable, even if committee members have expressed concerns about certain aspects. Indeed, despite preliminary recommendations against 6 initial proposals, the full Committee has approved 3 of them for limited testing. The Committee was receptive to the argument that without testing APMs in the real world, even if those programs have limitations, the field cannot move forward.

Implications for gastrointestinal practice and planning
Despite the many challenges in payment model development, the broader march toward APMs will continue, driven by increasing pressures to provide access to quality care while controlling costs. Further developments in several areas bear watching because they could accelerate opportunities for gastroenterologists.
Most notable is the considerable payment model innovation underway in private health insurance plans and state Medicaid plans, models that could develop into PTAC submissions. Project Sonar was first implemented in collaboration with a private payer in Illinois. Similarly, the inflammatory bowel disease specialty medical home was developed at the University of Pittsburgh. Both successfully have achieved the Triple Aim, improving patient experience and population health while decreasing medical costs.6 The private sector can serve as a testing ground for new APMs and the new administration’s desire to support innovative private sector models of care reform makes CMS likely to take further steps to support these approaches.
Second, working with both private and public payers, gastroenterologists could expand the concept of a specialty medical home or a primary-specialty coordinated medical home by incorporating more aspects of GI care. Chronic liver disease, chronic pancreatitis, and irritable bowel syndrome all could benefit from these approaches.7 Medical home models generally include a shift from fee-for-service payments by providing per-patient payments (potentially risk-adjusted) to the coordinating physician for a period of time. That per-member per-month payment may enable additional patient-centric services such as extending access to care, regular patient outreach to monitor changes in health status, and partnering with primary care and other providers to help patients access treatment for comorbid conditions.
Third, as evidenced by the PTAC critique on the Comprehensive Colonoscopy APM, a revised approach is needed for bundled episode payment reforms to better support endoscopists focused on performing high-quality procedures. Given their procedural focus, these physicians will need to show the value of endoscopic services in well-coordinated patient care. Site-of-service shifts are helpful where appropriate, but bundle proposals also must consider coordination with primary care providers on appropriate referrals, encouragement of non-endoscopic approaches, preparation technique to minimize the number of procedures that have to be repeated, and reducing anesthesia care for low-risk patients. These considerations generally suggest a broader episode payment model related to the goals of the procedure, rather than endoscopy-based bundles alone.
For example, a bundled payment for colorectal cancer screening, covering a full episode of treatment beyond a single colonoscopy, would make it easier for gastroenterologists to work more effectively with primary care providers to reduce gaps in colorectal cancer screening rates at the lowest possible overall cost. This bundle could be implemented by a specialized GI practice in conjunction with a primary care medical home or an ACO. If such a broad bundle is too much of a practice shift, an endoscopy-based episode payment could include performance measures and limited additional payments related to these same patient-focused objectives.
The kinds of reforms described earlier could work well with both primary care–focused and ACO models. However, there are technical challenges in dealing with overlapping payment reforms, and gastroenterologists should look for further guidance from CMS on how bundled episode payments and other specialized-care payment reforms will interact with APMs for primary care, such as ACOs and the Project Sonar model recommended by PTAC.8
Despite the broader shift toward APMs, it remains likely that many gastroenterologists will participate in the fee-for-service–based MIPS program in the near term. These physicians still will face fundamental pressures to deliver better value. Here, there may be opportunities to improve coordination in the MIPS program through additional care coordination payments for chronic disease, complementing the chronic care management payments that primary care physicians receive. Such payments would encourage further development and testing of more meaningful and outcome-oriented performance measures related to GI care.
Finally, GI care would benefit from better evidence for all GI-related payment reforms. Many of these reforms will be implemented outside of Medicare, but do not have results reported in a manner that make it easy to assess their impact and potential for broader implementation. Building an evidence base is feasible without imposing large costs or additional burdens on practices, especially when evaluations are implemented along with payment reforms, and offers the best way for organizations to learn and improve based on what works and what does not.9
Conclusions
Though the health care debate has ended in Congress for now, the march toward payment reform will continue. To accelerate progress, continued leadership from gastroenterologists is needed, especially in finding solutions that move beyond traditional GI practice. Collaborative incremental models that advance population health and are feasible to implement will provide the best opportunity for practice reform. Effective partnerships with primary care are particularly important to help avoid traditional gatekeeper approaches, and move toward a patient-centric model of shared accountability in which specialists function as a key partner in a medical neighborhood.10 Gastroenterologists can shape these steps, not only through PTAC and Medicare APMs, but through the other steps described earlier, and have a unique role in developing new models that leverage their specialty expertise. However, these models cannot be developed in isolation, and increased collaboration with primary care and other medical and nonmedical specialists will be critical. Physicians should start identifying opportunities to improve their practices and build these relationships now. These investments will allow them to thrive as new payment models come online.
References
1. Dzau V.J., McClellan M.B., McGinnis J.M. Vital directions for health and health care: priorities from a National Academy of Medicine initiative. JAMA 2017;317:1461-70.
2. Alternative Payment Model Framework Progress Tracking Work Group. Alternative payment model (APM) framework. Health
Care Payment Learning and Action Network. Available from: https://hcp-lan.org/workproducts/apm-whitepaper.pdf. Accessed: January 12, 2016.
3. Health Care Payment Learning and Action Network. APM Measurement: Progress of Alternative Payment Models. Available from: http://hcp-lan.org/workproducts/measurement_discussion%20article_2017.pdf Accessed November 2, 2017.
4. McClellan M., McStay F., Saunders R. The roadmap to physician payment reform: what it will take for all clinicians to succeed
under MACRA. Health Affairs Blog. Available from: http://healthaffairs.org/blog/2016/08/30/the-roadmap-to-physicianpayment-reform-what-it-will-take-for-all-clinicians-to-succeedunder-macra/. Accessed: August 30, 2016.
5. Medows R., Casale P., Berenson R. Preliminary review team report to the physician-focused Payment Model Technical Advisory Committee (PTAC). Physician-Focused Payment Model Technical Advisory Committee. Available from: https://aspe.hhs.gov/system/files/pdf/255906/DHNPRTReport.pdf. Accessed: March 22, 2017.
6. Regueiro M., Click B., Holder D., et al. Constructing an inflammatory bowel disease patient–centered medical home. Clin Gastroenterol Hepatol. 2017;15:1148-53.
7. Meier S.K., Shah N.D., Talwalkar J.A., et al. Adapting the patient-centered specialty practice model for populations with cirrhosis. Clin Gastroenterol Hepatol. 2016;14:492-6.
8. Pham H., Chernew M., Shrank W., et al. Market momentum, spillover effects, and evidence-based decision making on payment reform. Health Affairs Blog. Available from: http:// healthaffairs.org/blog/2017/05/24/market-momentum-spillovereffects-and-evidence-based-decision-making-on-paymentreform/. Accessed: May 24, 2017.
9. McClellan M., Richards R., Japinga M. Evidence on payment reform: where are the gaps? Health Affairs Blog. Available from: http://healthaffairs.org/blog/2017/04/25/evidence-onpayment-reform-where-are-the-gaps/. Accessed: April 25, 2017.
10. Huang X., Rosenthal M.B. Transforming specialty practice – the patient-centered medical neighborhood. N Engl J Med 2014;370:1376-9.
Mr. Japinga, Dr. Saunders, and Dr. McClellan are at the Duke-Margolis Center for Health Policy, Washington; Dr. Gellad is in the division of gastroenterology at the Duke University School of Medicine and at the Durham VA Medical Center, Durham, N.C. Dr. Gellad was supported by a Career Development Award from Veterans Affairs Health Services Research (CDA 14-158). The authors had no conflicts of interest.
This year’s Congressional debate over repealing or reforming key provisions of the Affordable Care Act was contentious in large part because of the high and rising costs of health care. Though a new health care reform bill is now unlikely, it remains critical to continue the discussion on how to deliver and pay for care in a way that addresses these high costs and makes coverage more affordable through more efficient and high-quality approaches.1
Illustrating the bipartisan nature of payment reforms, the Medicare Access and CHIP Reauthorization Act (MACRA) passed with more than 90% support in both the House and Senate in 2015. MACRA provides a 5% bonus payment for physicians who receive a significant part of their Medicare payments in an advanced APM, which involves some downside financial risk. In addition, any physician who participates significantly in a broader range of Medicare APMs, including many without downside risk, receives an exception from the reporting requirements for the new Merit-Based Incentive Payment System (MIPS) and would report on APM performance measures instead.
However, the details of payment reform are challenging and will benefit from engagement and leadership by physicians – including in gastroenterology. A new survey shows that the Department of Health and Human Services has achieved its goal of having 30% of health care payments tied to APMs by the end of 2016.3 It hopes to have 50% by the end of 2018.
Physician-Focused Payment Model Technical Advisory Committee’s role in recommending new payment models
The paucity of APMs was one reason the MACRA law established the Physician-Focused Payment Model Technical Advisory Committee (PTAC). Organizations can submit proposals for new Medicare payment models to PTAC, which then are reviewed according to 10 established criteria. The criteria place particular emphasis on the scope of the APM, the APM’s ability to increase quality while maintaining or decreasing costs, and whether the payment methodology improves on current policy. PTAC then makes recommendations to CMS for full implementation of a proposal, limited testing (a pilot program), or no implementation.
The fate of the two GI APMs offers broad insight on the path forward for new specialized-care models. Although PTAC focuses on physician payment, its criteria and critiques emphasize that the primary focus of any APM should be on the full spectrum of patient care. Project Sonar likely received a positive recommendation because it focused on shifting payment to improving chronic care and avoiding complications. Although the colonoscopy proposal was withdrawn, we can gain a sense of PTAC’s concerns through the preliminary review.5 The review argues the proposal did not sufficiently address how it would lead to a more efficient, better integrated, and higher quality screening that improves patient health. More specifically, the review criticized the proposal for focusing primarily on a site-of-service shift and offering fewer details on how the APM would reduce overutilization.
Overall, PTAC’s deliberations at both its April and September meetings suggest that it will deeply scrutinize models focusing only on a single procedure or specialty, or ones that it believes do not sufficiently coordinate with primary care or other specialties, because it does not believe that such models have a sufficiently comprehensive patient focus. These PTAC reviews also suggest that the Committee will recommend programs with ideas they find viable, even if committee members have expressed concerns about certain aspects. Indeed, despite preliminary recommendations against 6 initial proposals, the full Committee has approved 3 of them for limited testing. The Committee was receptive to the argument that without testing APMs in the real world, even if those programs have limitations, the field cannot move forward.
Implications for gastrointestinal practice and planning
Despite the many challenges in payment model development, the broader march toward APMs will continue, driven by increasing pressures to provide access to quality care while controlling costs. Further developments in several areas bear watching because they could accelerate opportunities for gastroenterologists.
Most notable is the considerable payment model innovation underway in private health insurance plans and state Medicaid plans, models that could develop into PTAC submissions. Project Sonar was first implemented in collaboration with a private payer in Illinois. Similarly, the inflammatory bowel disease specialty medical home was developed at the University of Pittsburgh. Both successfully have achieved the Triple Aim, improving patient experience and population health while decreasing medical costs.6 The private sector can serve as a testing ground for new APMs and the new administration’s desire to support innovative private sector models of care reform makes CMS likely to take further steps to support these approaches.
Second, working with both private and public payers, gastroenterologists could expand the concept of a specialty medical home or a primary-specialty coordinated medical home by incorporating more aspects of GI care. Chronic liver disease, chronic pancreatitis, and irritable bowel syndrome all could benefit from these approaches.7 Medical home models generally include a shift from fee-for-service payments by providing per-patient payments (potentially risk-adjusted) to the coordinating physician for a period of time. That per-member per-month payment may enable additional patient-centric services such as extending access to care, regular patient outreach to monitor changes in health status, and partnering with primary care and other providers to help patients access treatment for comorbid conditions.
Third, as evidenced by the PTAC critique on the Comprehensive Colonoscopy APM, a revised approach is needed for bundled episode payment reforms to better support endoscopists focused on performing high-quality procedures. Given their procedural focus, these physicians will need to show the value of endoscopic services in well-coordinated patient care. Site-of-service shifts are helpful where appropriate, but bundle proposals also must consider coordination with primary care providers on appropriate referrals, encouragement of non-endoscopic approaches, preparation technique to minimize the number of procedures that have to be repeated, and reducing anesthesia care for low-risk patients. These considerations generally suggest a broader episode payment model related to the goals of the procedure, rather than endoscopy-based bundles alone.
For example, a bundled payment for colorectal cancer screening, covering a full episode of treatment beyond a single colonoscopy, would make it easier for gastroenterologists to work more effectively with primary care providers to reduce gaps in colorectal cancer screening rates at the lowest possible overall cost. This bundle could be implemented by a specialized GI practice in conjunction with a primary care medical home or an ACO. If such a broad bundle is too much of a practice shift, an endoscopy-based episode payment could include performance measures and limited additional payments related to these same patient-focused objectives.
The kinds of reforms described earlier could work well with both primary care–focused and ACO models. However, there are technical challenges in dealing with overlapping payment reforms, and gastroenterologists should look for further guidance from CMS on how bundled episode payments and other specialized-care payment reforms will interact with APMs for primary care, such as ACOs and the Project Sonar model recommended by PTAC.8
Despite the broader shift toward APMs, it remains likely that many gastroenterologists will participate in the fee-for-service–based MIPS program in the near term. These physicians still will face fundamental pressures to deliver better value. Here, there may be opportunities to improve coordination in the MIPS program through additional care coordination payments for chronic disease, complementing the chronic care management payments that primary care physicians receive. Such payments would encourage further development and testing of more meaningful and outcome-oriented performance measures related to GI care.
Finally, GI care would benefit from better evidence for all GI-related payment reforms. Many of these reforms will be implemented outside of Medicare, but do not have results reported in a manner that make it easy to assess their impact and potential for broader implementation. Building an evidence base is feasible without imposing large costs or additional burdens on practices, especially when evaluations are implemented along with payment reforms, and offers the best way for organizations to learn and improve based on what works and what does not.9
Conclusions
Though the health care debate has ended in Congress for now, the march toward payment reform will continue. To accelerate progress, continued leadership from gastroenterologists is needed, especially in finding solutions that move beyond traditional GI practice. Collaborative incremental models that advance population health and are feasible to implement will provide the best opportunity for practice reform. Effective partnerships with primary care are particularly important to help avoid traditional gatekeeper approaches, and move toward a patient-centric model of shared accountability in which specialists function as a key partner in a medical neighborhood.10 Gastroenterologists can shape these steps, not only through PTAC and Medicare APMs, but through the other steps described earlier, and have a unique role in developing new models that leverage their specialty expertise. However, these models cannot be developed in isolation, and increased collaboration with primary care and other medical and nonmedical specialists will be critical. Physicians should start identifying opportunities to improve their practices and build these relationships now. These investments will allow them to thrive as new payment models come online.
References
1. Dzau V.J., McClellan M.B., McGinnis J.M. Vital directions for health and health care: priorities from a National Academy of Medicine initiative. JAMA 2017;317:1461-70.
2. Alternative Payment Model Framework Progress Tracking Work Group. Alternative payment model (APM) framework. Health
Care Payment Learning and Action Network. Available from: https://hcp-lan.org/workproducts/apm-whitepaper.pdf. Accessed: January 12, 2016.
3. Health Care Payment Learning and Action Network. APM Measurement: Progress of Alternative Payment Models. Available from: http://hcp-lan.org/workproducts/measurement_discussion%20article_2017.pdf Accessed November 2, 2017.
4. McClellan M., McStay F., Saunders R. The roadmap to physician payment reform: what it will take for all clinicians to succeed
under MACRA. Health Affairs Blog. Available from: http://healthaffairs.org/blog/2016/08/30/the-roadmap-to-physicianpayment-reform-what-it-will-take-for-all-clinicians-to-succeedunder-macra/. Accessed: August 30, 2016.
5. Medows R., Casale P., Berenson R. Preliminary review team report to the physician-focused Payment Model Technical Advisory Committee (PTAC). Physician-Focused Payment Model Technical Advisory Committee. Available from: https://aspe.hhs.gov/system/files/pdf/255906/DHNPRTReport.pdf. Accessed: March 22, 2017.
6. Regueiro M., Click B., Holder D., et al. Constructing an inflammatory bowel disease patient–centered medical home. Clin Gastroenterol Hepatol. 2017;15:1148-53.
7. Meier S.K., Shah N.D., Talwalkar J.A., et al. Adapting the patient-centered specialty practice model for populations with cirrhosis. Clin Gastroenterol Hepatol. 2016;14:492-6.
8. Pham H., Chernew M., Shrank W., et al. Market momentum, spillover effects, and evidence-based decision making on payment reform. Health Affairs Blog. Available from: http:// healthaffairs.org/blog/2017/05/24/market-momentum-spillovereffects-and-evidence-based-decision-making-on-paymentreform/. Accessed: May 24, 2017.
9. McClellan M., Richards R., Japinga M. Evidence on payment reform: where are the gaps? Health Affairs Blog. Available from: http://healthaffairs.org/blog/2017/04/25/evidence-onpayment-reform-where-are-the-gaps/. Accessed: April 25, 2017.
10. Huang X., Rosenthal M.B. Transforming specialty practice – the patient-centered medical neighborhood. N Engl J Med 2014;370:1376-9.
Mr. Japinga, Dr. Saunders, and Dr. McClellan are at the Duke-Margolis Center for Health Policy, Washington; Dr. Gellad is in the division of gastroenterology at the Duke University School of Medicine and at the Durham VA Medical Center, Durham, N.C. Dr. Gellad was supported by a Career Development Award from Veterans Affairs Health Services Research (CDA 14-158). The authors had no conflicts of interest.
This year’s Congressional debate over repealing or reforming key provisions of the Affordable Care Act was contentious in large part because of the high and rising costs of health care. Though a new health care reform bill is now unlikely, it remains critical to continue the discussion on how to deliver and pay for care in a way that addresses these high costs and makes coverage more affordable through more efficient and high-quality approaches.1
Illustrating the bipartisan nature of payment reforms, the Medicare Access and CHIP Reauthorization Act (MACRA) passed with more than 90% support in both the House and Senate in 2015. MACRA provides a 5% bonus payment for physicians who receive a significant part of their Medicare payments in an advanced APM, which involves some downside financial risk. In addition, any physician who participates significantly in a broader range of Medicare APMs, including many without downside risk, receives an exception from the reporting requirements for the new Merit-Based Incentive Payment System (MIPS) and would report on APM performance measures instead.
However, the details of payment reform are challenging and will benefit from engagement and leadership by physicians – including in gastroenterology. A new survey shows that the Department of Health and Human Services has achieved its goal of having 30% of health care payments tied to APMs by the end of 2016.3 It hopes to have 50% by the end of 2018.
Physician-Focused Payment Model Technical Advisory Committee’s role in recommending new payment models
The paucity of APMs was one reason the MACRA law established the Physician-Focused Payment Model Technical Advisory Committee (PTAC). Organizations can submit proposals for new Medicare payment models to PTAC, which then are reviewed according to 10 established criteria. The criteria place particular emphasis on the scope of the APM, the APM’s ability to increase quality while maintaining or decreasing costs, and whether the payment methodology improves on current policy. PTAC then makes recommendations to CMS for full implementation of a proposal, limited testing (a pilot program), or no implementation.
The fate of the two GI APMs offers broad insight on the path forward for new specialized-care models. Although PTAC focuses on physician payment, its criteria and critiques emphasize that the primary focus of any APM should be on the full spectrum of patient care. Project Sonar likely received a positive recommendation because it focused on shifting payment to improving chronic care and avoiding complications. Although the colonoscopy proposal was withdrawn, we can gain a sense of PTAC’s concerns through the preliminary review.5 The review argues the proposal did not sufficiently address how it would lead to a more efficient, better integrated, and higher quality screening that improves patient health. More specifically, the review criticized the proposal for focusing primarily on a site-of-service shift and offering fewer details on how the APM would reduce overutilization.
Overall, PTAC’s deliberations at both its April and September meetings suggest that it will deeply scrutinize models focusing only on a single procedure or specialty, or ones that it believes do not sufficiently coordinate with primary care or other specialties, because it does not believe that such models have a sufficiently comprehensive patient focus. These PTAC reviews also suggest that the Committee will recommend programs with ideas they find viable, even if committee members have expressed concerns about certain aspects. Indeed, despite preliminary recommendations against 6 initial proposals, the full Committee has approved 3 of them for limited testing. The Committee was receptive to the argument that without testing APMs in the real world, even if those programs have limitations, the field cannot move forward.
Implications for gastrointestinal practice and planning
Despite the many challenges in payment model development, the broader march toward APMs will continue, driven by increasing pressures to provide access to quality care while controlling costs. Further developments in several areas bear watching because they could accelerate opportunities for gastroenterologists.
Most notable is the considerable payment model innovation underway in private health insurance plans and state Medicaid plans, models that could develop into PTAC submissions. Project Sonar was first implemented in collaboration with a private payer in Illinois. Similarly, the inflammatory bowel disease specialty medical home was developed at the University of Pittsburgh. Both successfully have achieved the Triple Aim, improving patient experience and population health while decreasing medical costs.6 The private sector can serve as a testing ground for new APMs and the new administration’s desire to support innovative private sector models of care reform makes CMS likely to take further steps to support these approaches.
Second, working with both private and public payers, gastroenterologists could expand the concept of a specialty medical home or a primary-specialty coordinated medical home by incorporating more aspects of GI care. Chronic liver disease, chronic pancreatitis, and irritable bowel syndrome all could benefit from these approaches.7 Medical home models generally include a shift from fee-for-service payments by providing per-patient payments (potentially risk-adjusted) to the coordinating physician for a period of time. That per-member per-month payment may enable additional patient-centric services such as extending access to care, regular patient outreach to monitor changes in health status, and partnering with primary care and other providers to help patients access treatment for comorbid conditions.
Third, as evidenced by the PTAC critique on the Comprehensive Colonoscopy APM, a revised approach is needed for bundled episode payment reforms to better support endoscopists focused on performing high-quality procedures. Given their procedural focus, these physicians will need to show the value of endoscopic services in well-coordinated patient care. Site-of-service shifts are helpful where appropriate, but bundle proposals also must consider coordination with primary care providers on appropriate referrals, encouragement of non-endoscopic approaches, preparation technique to minimize the number of procedures that have to be repeated, and reducing anesthesia care for low-risk patients. These considerations generally suggest a broader episode payment model related to the goals of the procedure, rather than endoscopy-based bundles alone.
For example, a bundled payment for colorectal cancer screening, covering a full episode of treatment beyond a single colonoscopy, would make it easier for gastroenterologists to work more effectively with primary care providers to reduce gaps in colorectal cancer screening rates at the lowest possible overall cost. This bundle could be implemented by a specialized GI practice in conjunction with a primary care medical home or an ACO. If such a broad bundle is too much of a practice shift, an endoscopy-based episode payment could include performance measures and limited additional payments related to these same patient-focused objectives.
The kinds of reforms described earlier could work well with both primary care–focused and ACO models. However, there are technical challenges in dealing with overlapping payment reforms, and gastroenterologists should look for further guidance from CMS on how bundled episode payments and other specialized-care payment reforms will interact with APMs for primary care, such as ACOs and the Project Sonar model recommended by PTAC.8
Despite the broader shift toward APMs, it remains likely that many gastroenterologists will participate in the fee-for-service–based MIPS program in the near term. These physicians still will face fundamental pressures to deliver better value. Here, there may be opportunities to improve coordination in the MIPS program through additional care coordination payments for chronic disease, complementing the chronic care management payments that primary care physicians receive. Such payments would encourage further development and testing of more meaningful and outcome-oriented performance measures related to GI care.
Finally, GI care would benefit from better evidence for all GI-related payment reforms. Many of these reforms will be implemented outside of Medicare, but do not have results reported in a manner that make it easy to assess their impact and potential for broader implementation. Building an evidence base is feasible without imposing large costs or additional burdens on practices, especially when evaluations are implemented along with payment reforms, and offers the best way for organizations to learn and improve based on what works and what does not.9
Conclusions
Though the health care debate has ended in Congress for now, the march toward payment reform will continue. To accelerate progress, continued leadership from gastroenterologists is needed, especially in finding solutions that move beyond traditional GI practice. Collaborative incremental models that advance population health and are feasible to implement will provide the best opportunity for practice reform. Effective partnerships with primary care are particularly important to help avoid traditional gatekeeper approaches, and move toward a patient-centric model of shared accountability in which specialists function as a key partner in a medical neighborhood.10 Gastroenterologists can shape these steps, not only through PTAC and Medicare APMs, but through the other steps described earlier, and have a unique role in developing new models that leverage their specialty expertise. However, these models cannot be developed in isolation, and increased collaboration with primary care and other medical and nonmedical specialists will be critical. Physicians should start identifying opportunities to improve their practices and build these relationships now. These investments will allow them to thrive as new payment models come online.
References
1. Dzau V.J., McClellan M.B., McGinnis J.M. Vital directions for health and health care: priorities from a National Academy of Medicine initiative. JAMA 2017;317:1461-70.
2. Alternative Payment Model Framework Progress Tracking Work Group. Alternative payment model (APM) framework. Health
Care Payment Learning and Action Network. Available from: https://hcp-lan.org/workproducts/apm-whitepaper.pdf. Accessed: January 12, 2016.
3. Health Care Payment Learning and Action Network. APM Measurement: Progress of Alternative Payment Models. Available from: http://hcp-lan.org/workproducts/measurement_discussion%20article_2017.pdf Accessed November 2, 2017.
4. McClellan M., McStay F., Saunders R. The roadmap to physician payment reform: what it will take for all clinicians to succeed
under MACRA. Health Affairs Blog. Available from: http://healthaffairs.org/blog/2016/08/30/the-roadmap-to-physicianpayment-reform-what-it-will-take-for-all-clinicians-to-succeedunder-macra/. Accessed: August 30, 2016.
5. Medows R., Casale P., Berenson R. Preliminary review team report to the physician-focused Payment Model Technical Advisory Committee (PTAC). Physician-Focused Payment Model Technical Advisory Committee. Available from: https://aspe.hhs.gov/system/files/pdf/255906/DHNPRTReport.pdf. Accessed: March 22, 2017.
6. Regueiro M., Click B., Holder D., et al. Constructing an inflammatory bowel disease patient–centered medical home. Clin Gastroenterol Hepatol. 2017;15:1148-53.
7. Meier S.K., Shah N.D., Talwalkar J.A., et al. Adapting the patient-centered specialty practice model for populations with cirrhosis. Clin Gastroenterol Hepatol. 2016;14:492-6.
8. Pham H., Chernew M., Shrank W., et al. Market momentum, spillover effects, and evidence-based decision making on payment reform. Health Affairs Blog. Available from: http:// healthaffairs.org/blog/2017/05/24/market-momentum-spillovereffects-and-evidence-based-decision-making-on-paymentreform/. Accessed: May 24, 2017.
9. McClellan M., Richards R., Japinga M. Evidence on payment reform: where are the gaps? Health Affairs Blog. Available from: http://healthaffairs.org/blog/2017/04/25/evidence-onpayment-reform-where-are-the-gaps/. Accessed: April 25, 2017.
10. Huang X., Rosenthal M.B. Transforming specialty practice – the patient-centered medical neighborhood. N Engl J Med 2014;370:1376-9.
Mr. Japinga, Dr. Saunders, and Dr. McClellan are at the Duke-Margolis Center for Health Policy, Washington; Dr. Gellad is in the division of gastroenterology at the Duke University School of Medicine and at the Durham VA Medical Center, Durham, N.C. Dr. Gellad was supported by a Career Development Award from Veterans Affairs Health Services Research (CDA 14-158). The authors had no conflicts of interest.
Systems biology – A primer
Systems biology is relatively new. It is an interdisciplinary field that focuses on complex interactions within biological systems using a holistic approach in the pursuit of scientific discovery.
The systems biology approach seeks to integrate biological knowledge to understand how cells and molecules interact with one another. A key component is computational and mathematical modeling. The ever-increasing amount of biological data, and the judgment that this data cannot be understood by simply drawing lines between interacting cells and molecules, explains the demand for a systematic approach.
Prominent examples for biological systems are the immune system and the nervous system, which already have the word ”system” included. Although the idea of system-level understanding is not new, the growing interest in applying the systems approach has been driven by breakthrough advances in molecular biology and bioinformatics.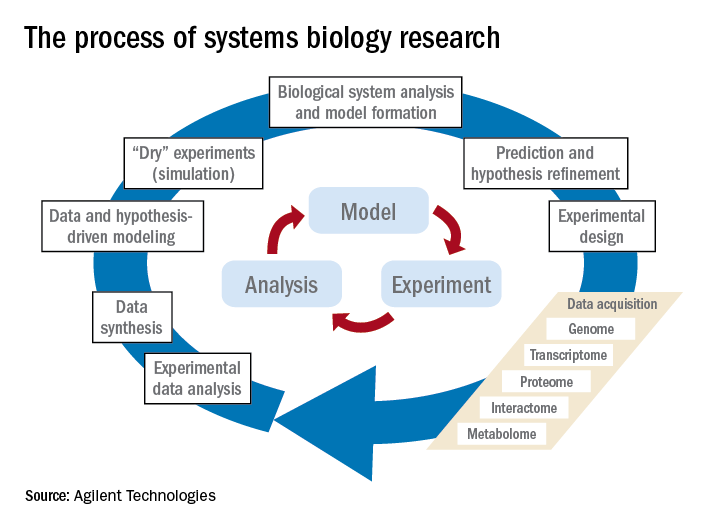
Over the past 10 years, our group has identified highly significant differences in immune functioning between the 10% of children who frequently develop acute otitis media (i.e., those who are “otitis prone”) and the children who develop AOM infrequently (60% of children) or not at all (30% of children). We also have identified a cohort of about 10% of children who fail to respond to infant vaccinations (low vaccine responders), compared with children who respond with protective immunity and establishment of immune memory. The differences in children who are prone to AOM vs. those who are not and in low vaccine responders vs. normal vaccine responders include differences in cytokine molecules in blood (providing biosignatures), reduced antibodies, immune memory, and aberrant intercellular signaling networks after otopathogen exposure (AOM prone vs. non–AOM prone) and routine pediatric vaccination (low vs. normal vaccine responders).

Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute at Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. He has no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.
Systems biology is relatively new. It is an interdisciplinary field that focuses on complex interactions within biological systems using a holistic approach in the pursuit of scientific discovery.
The systems biology approach seeks to integrate biological knowledge to understand how cells and molecules interact with one another. A key component is computational and mathematical modeling. The ever-increasing amount of biological data, and the judgment that this data cannot be understood by simply drawing lines between interacting cells and molecules, explains the demand for a systematic approach.
Prominent examples for biological systems are the immune system and the nervous system, which already have the word ”system” included. Although the idea of system-level understanding is not new, the growing interest in applying the systems approach has been driven by breakthrough advances in molecular biology and bioinformatics.
Over the past 10 years, our group has identified highly significant differences in immune functioning between the 10% of children who frequently develop acute otitis media (i.e., those who are “otitis prone”) and the children who develop AOM infrequently (60% of children) or not at all (30% of children). We also have identified a cohort of about 10% of children who fail to respond to infant vaccinations (low vaccine responders), compared with children who respond with protective immunity and establishment of immune memory. The differences in children who are prone to AOM vs. those who are not and in low vaccine responders vs. normal vaccine responders include differences in cytokine molecules in blood (providing biosignatures), reduced antibodies, immune memory, and aberrant intercellular signaling networks after otopathogen exposure (AOM prone vs. non–AOM prone) and routine pediatric vaccination (low vs. normal vaccine responders).
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute at Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. He has no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.
Systems biology is relatively new. It is an interdisciplinary field that focuses on complex interactions within biological systems using a holistic approach in the pursuit of scientific discovery.
The systems biology approach seeks to integrate biological knowledge to understand how cells and molecules interact with one another. A key component is computational and mathematical modeling. The ever-increasing amount of biological data, and the judgment that this data cannot be understood by simply drawing lines between interacting cells and molecules, explains the demand for a systematic approach.
Prominent examples for biological systems are the immune system and the nervous system, which already have the word ”system” included. Although the idea of system-level understanding is not new, the growing interest in applying the systems approach has been driven by breakthrough advances in molecular biology and bioinformatics.
Over the past 10 years, our group has identified highly significant differences in immune functioning between the 10% of children who frequently develop acute otitis media (i.e., those who are “otitis prone”) and the children who develop AOM infrequently (60% of children) or not at all (30% of children). We also have identified a cohort of about 10% of children who fail to respond to infant vaccinations (low vaccine responders), compared with children who respond with protective immunity and establishment of immune memory. The differences in children who are prone to AOM vs. those who are not and in low vaccine responders vs. normal vaccine responders include differences in cytokine molecules in blood (providing biosignatures), reduced antibodies, immune memory, and aberrant intercellular signaling networks after otopathogen exposure (AOM prone vs. non–AOM prone) and routine pediatric vaccination (low vs. normal vaccine responders).
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute at Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. He has no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.
Well, I figured it out ... I owe my soul to the company store
Going to sell you your practice?
You know I am certain that we physicians are never going to be paid much more than we get paid right now. Now we may get occasional 0.5% increases from Medicare, but after no pay increase for 15 years and with the new unachievable payments for quality, I am not optimistic. So, I have been talking to corporate physician buyout companies, specifically amalgamators of dermatologists. I mean, in the words of the “Fat Man” in “The House of God,” who wants to pass up a “fortuna”?
In June 2017, as far as I can tell, there were 17 corporate dermatology groups out there employing about 1,200 “providers” which includes extenders, and there are several “models” of assimilation.
There are extremes on either end. The least invasive is the group that buys you for a dollar, hopefully has better insurance contracts, and charges you a percentage for billing and management of your practice. If you want, you can buy yourself back for a dollar. In this setting, you just have to keep a close eye on how expenses are calculated. And there is no guarantee that this group won’t sell out to venture capital in the future, so you have to be prepared to reassume control of your practice if you don’t want to be acquired along with the group.
Another category is what I call the bottom feeders, who set up multiple dermatology shopfronts manned by nurse practitioners and physician assistants, who are loosely supervised by a physician, often remotely, who may not even be a dermatologist. The only requirement is that they have a medical license in that state. This group will come to town and bid for all the dermatology work from managed care companies. Typically, they are happy to settle for 85% of Medicare payments.
The more common model is based on acquiring practices, then selling them to other venture capital groups for a return to other venture capital groups. Venture capital groups are behind all the corporate practice acquisitions except for one, which funds out of a personal fortune. They all view medicine, particularly dermatology, as a fragmented industry that they can consolidate for a profit.
The basic plan of these groups is to pay you five to eight times EBITDA (earnings before interest, taxes, depreciation, and amortization) up front, which works out to be about 2 or 3 years net profits. Usually, they want you to take at least 40% of your “buyout” as company stock, which they promise may appreciate greatly, but has no liquidity until they sell to another venture capital group and maybe not even then. The cash you receive can mostly be treated as capital gains if you negotiate it correctly, which will be taxed at 23.8% (the 20% tax rate plus the Affordable Care Act 3.8% supplemental tax, instead of 39.6%, the top current federal bracket.
Generally, their expectations are that you will get 40% of the practice income as salary, overhead will be 40%, and their profit is 20%. So their buyout is really a loan from them, which will be paid off in 5 years. Admittedly, the buyout will be taxed less than your current income, with a possible equity kicker when they flip the practice, which they hope to do three or four times! Also, be aware, the physicians who got in early and represent them get a piece of what you would have been paid (usually $50,000-$100,000 in stock) for recruiting you. There is a reason they are working the company booth at meetings! It’s “Amway for Dermatologists.”
The company then owns your practice, you are an employee, and you owe them at least 5 years of service. They put you on a salary, which is less than you made previously – and interestingly, the difference again usually pays their original investment off in 5 years, usually with some interest. If you are a younger physician who owns the practice, with a longer practice future, you should receive a higher percentage of your former income. If the company can “boost” your practice income, you could make as much as or more than you did before, but most of these outfits do not have better insurance contracts. Their “boost” is based on hiring more physician assistants or nurse practitioners, and having you supervise them.
Once you sell and are owned by the company, they strongly suggest (but do not require, which is illegal) that you send your dermatopathology to your fellow employee, in another state, whom you have never met and probably never will. They will also suggest you send your Mohs cases to a fellow employee you’ve never heard of, who comes to town a couple of days a month to perform the surgeries. They take over your human resources, including your policies and payroll, which may be good if you have overpaid cranky employees you just can’t bear to fire because they have been with you so long. They will standardize everyone’s pay and benefits. They take over your billing, and may be able to get you more reasonable health insurance, and will have a standardized benefit plan. If you need to buy anything for the practice, you will fill out a requisition form. Major capital purchases must be approved in advance.
Your contract will specify that you have to work, on average, at least as many days per year as you have the last 3 years. If you leave early, you will have to pay the money you received, plus penalties. In addition, you may have a 2-year, 20-mile noncompete agreement clause (although this is negotiable) around all sites they operate, anywhere in the United States. If you die, they have an insurance policy on you.
Young employed doctors don’t get the “buy out” or the equity, although they can “buy in” later. They become cogs in the wheel.
The groups then try to roll up as many practices as possible so they can resell the amalgamation to a larger private equity fund eventually for 10-15 times EBITDA if the group is large enough. Maybe so, maybe not, but I have a strong feeling this is not going to end well. These equity funds work with borrowed money, and want double their investment and profit in 5 years or less.

The biggest losers, however, are the patients. They become a commodity, to be pushed through the office, and will not enjoy the benefits of the best consultants, but instead will have to select from the employees of the company store.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at dermnews@frontlinemedcom.com.
Going to sell you your practice?
You know I am certain that we physicians are never going to be paid much more than we get paid right now. Now we may get occasional 0.5% increases from Medicare, but after no pay increase for 15 years and with the new unachievable payments for quality, I am not optimistic. So, I have been talking to corporate physician buyout companies, specifically amalgamators of dermatologists. I mean, in the words of the “Fat Man” in “The House of God,” who wants to pass up a “fortuna”?
In June 2017, as far as I can tell, there were 17 corporate dermatology groups out there employing about 1,200 “providers” which includes extenders, and there are several “models” of assimilation.
There are extremes on either end. The least invasive is the group that buys you for a dollar, hopefully has better insurance contracts, and charges you a percentage for billing and management of your practice. If you want, you can buy yourself back for a dollar. In this setting, you just have to keep a close eye on how expenses are calculated. And there is no guarantee that this group won’t sell out to venture capital in the future, so you have to be prepared to reassume control of your practice if you don’t want to be acquired along with the group.
Another category is what I call the bottom feeders, who set up multiple dermatology shopfronts manned by nurse practitioners and physician assistants, who are loosely supervised by a physician, often remotely, who may not even be a dermatologist. The only requirement is that they have a medical license in that state. This group will come to town and bid for all the dermatology work from managed care companies. Typically, they are happy to settle for 85% of Medicare payments.
The more common model is based on acquiring practices, then selling them to other venture capital groups for a return to other venture capital groups. Venture capital groups are behind all the corporate practice acquisitions except for one, which funds out of a personal fortune. They all view medicine, particularly dermatology, as a fragmented industry that they can consolidate for a profit.
The basic plan of these groups is to pay you five to eight times EBITDA (earnings before interest, taxes, depreciation, and amortization) up front, which works out to be about 2 or 3 years net profits. Usually, they want you to take at least 40% of your “buyout” as company stock, which they promise may appreciate greatly, but has no liquidity until they sell to another venture capital group and maybe not even then. The cash you receive can mostly be treated as capital gains if you negotiate it correctly, which will be taxed at 23.8% (the 20% tax rate plus the Affordable Care Act 3.8% supplemental tax, instead of 39.6%, the top current federal bracket.
Generally, their expectations are that you will get 40% of the practice income as salary, overhead will be 40%, and their profit is 20%. So their buyout is really a loan from them, which will be paid off in 5 years. Admittedly, the buyout will be taxed less than your current income, with a possible equity kicker when they flip the practice, which they hope to do three or four times! Also, be aware, the physicians who got in early and represent them get a piece of what you would have been paid (usually $50,000-$100,000 in stock) for recruiting you. There is a reason they are working the company booth at meetings! It’s “Amway for Dermatologists.”
The company then owns your practice, you are an employee, and you owe them at least 5 years of service. They put you on a salary, which is less than you made previously – and interestingly, the difference again usually pays their original investment off in 5 years, usually with some interest. If you are a younger physician who owns the practice, with a longer practice future, you should receive a higher percentage of your former income. If the company can “boost” your practice income, you could make as much as or more than you did before, but most of these outfits do not have better insurance contracts. Their “boost” is based on hiring more physician assistants or nurse practitioners, and having you supervise them.
Once you sell and are owned by the company, they strongly suggest (but do not require, which is illegal) that you send your dermatopathology to your fellow employee, in another state, whom you have never met and probably never will. They will also suggest you send your Mohs cases to a fellow employee you’ve never heard of, who comes to town a couple of days a month to perform the surgeries. They take over your human resources, including your policies and payroll, which may be good if you have overpaid cranky employees you just can’t bear to fire because they have been with you so long. They will standardize everyone’s pay and benefits. They take over your billing, and may be able to get you more reasonable health insurance, and will have a standardized benefit plan. If you need to buy anything for the practice, you will fill out a requisition form. Major capital purchases must be approved in advance.
Your contract will specify that you have to work, on average, at least as many days per year as you have the last 3 years. If you leave early, you will have to pay the money you received, plus penalties. In addition, you may have a 2-year, 20-mile noncompete agreement clause (although this is negotiable) around all sites they operate, anywhere in the United States. If you die, they have an insurance policy on you.
Young employed doctors don’t get the “buy out” or the equity, although they can “buy in” later. They become cogs in the wheel.
The groups then try to roll up as many practices as possible so they can resell the amalgamation to a larger private equity fund eventually for 10-15 times EBITDA if the group is large enough. Maybe so, maybe not, but I have a strong feeling this is not going to end well. These equity funds work with borrowed money, and want double their investment and profit in 5 years or less.
The biggest losers, however, are the patients. They become a commodity, to be pushed through the office, and will not enjoy the benefits of the best consultants, but instead will have to select from the employees of the company store.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at dermnews@frontlinemedcom.com.
Going to sell you your practice?
You know I am certain that we physicians are never going to be paid much more than we get paid right now. Now we may get occasional 0.5% increases from Medicare, but after no pay increase for 15 years and with the new unachievable payments for quality, I am not optimistic. So, I have been talking to corporate physician buyout companies, specifically amalgamators of dermatologists. I mean, in the words of the “Fat Man” in “The House of God,” who wants to pass up a “fortuna”?
In June 2017, as far as I can tell, there were 17 corporate dermatology groups out there employing about 1,200 “providers” which includes extenders, and there are several “models” of assimilation.
There are extremes on either end. The least invasive is the group that buys you for a dollar, hopefully has better insurance contracts, and charges you a percentage for billing and management of your practice. If you want, you can buy yourself back for a dollar. In this setting, you just have to keep a close eye on how expenses are calculated. And there is no guarantee that this group won’t sell out to venture capital in the future, so you have to be prepared to reassume control of your practice if you don’t want to be acquired along with the group.
Another category is what I call the bottom feeders, who set up multiple dermatology shopfronts manned by nurse practitioners and physician assistants, who are loosely supervised by a physician, often remotely, who may not even be a dermatologist. The only requirement is that they have a medical license in that state. This group will come to town and bid for all the dermatology work from managed care companies. Typically, they are happy to settle for 85% of Medicare payments.
The more common model is based on acquiring practices, then selling them to other venture capital groups for a return to other venture capital groups. Venture capital groups are behind all the corporate practice acquisitions except for one, which funds out of a personal fortune. They all view medicine, particularly dermatology, as a fragmented industry that they can consolidate for a profit.
The basic plan of these groups is to pay you five to eight times EBITDA (earnings before interest, taxes, depreciation, and amortization) up front, which works out to be about 2 or 3 years net profits. Usually, they want you to take at least 40% of your “buyout” as company stock, which they promise may appreciate greatly, but has no liquidity until they sell to another venture capital group and maybe not even then. The cash you receive can mostly be treated as capital gains if you negotiate it correctly, which will be taxed at 23.8% (the 20% tax rate plus the Affordable Care Act 3.8% supplemental tax, instead of 39.6%, the top current federal bracket.
Generally, their expectations are that you will get 40% of the practice income as salary, overhead will be 40%, and their profit is 20%. So their buyout is really a loan from them, which will be paid off in 5 years. Admittedly, the buyout will be taxed less than your current income, with a possible equity kicker when they flip the practice, which they hope to do three or four times! Also, be aware, the physicians who got in early and represent them get a piece of what you would have been paid (usually $50,000-$100,000 in stock) for recruiting you. There is a reason they are working the company booth at meetings! It’s “Amway for Dermatologists.”
The company then owns your practice, you are an employee, and you owe them at least 5 years of service. They put you on a salary, which is less than you made previously – and interestingly, the difference again usually pays their original investment off in 5 years, usually with some interest. If you are a younger physician who owns the practice, with a longer practice future, you should receive a higher percentage of your former income. If the company can “boost” your practice income, you could make as much as or more than you did before, but most of these outfits do not have better insurance contracts. Their “boost” is based on hiring more physician assistants or nurse practitioners, and having you supervise them.
Once you sell and are owned by the company, they strongly suggest (but do not require, which is illegal) that you send your dermatopathology to your fellow employee, in another state, whom you have never met and probably never will. They will also suggest you send your Mohs cases to a fellow employee you’ve never heard of, who comes to town a couple of days a month to perform the surgeries. They take over your human resources, including your policies and payroll, which may be good if you have overpaid cranky employees you just can’t bear to fire because they have been with you so long. They will standardize everyone’s pay and benefits. They take over your billing, and may be able to get you more reasonable health insurance, and will have a standardized benefit plan. If you need to buy anything for the practice, you will fill out a requisition form. Major capital purchases must be approved in advance.
Your contract will specify that you have to work, on average, at least as many days per year as you have the last 3 years. If you leave early, you will have to pay the money you received, plus penalties. In addition, you may have a 2-year, 20-mile noncompete agreement clause (although this is negotiable) around all sites they operate, anywhere in the United States. If you die, they have an insurance policy on you.
Young employed doctors don’t get the “buy out” or the equity, although they can “buy in” later. They become cogs in the wheel.
The groups then try to roll up as many practices as possible so they can resell the amalgamation to a larger private equity fund eventually for 10-15 times EBITDA if the group is large enough. Maybe so, maybe not, but I have a strong feeling this is not going to end well. These equity funds work with borrowed money, and want double their investment and profit in 5 years or less.
The biggest losers, however, are the patients. They become a commodity, to be pushed through the office, and will not enjoy the benefits of the best consultants, but instead will have to select from the employees of the company store.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at dermnews@frontlinemedcom.com.

Health care panhandlers: A symptom of our system’s baked-in pressures?
A few nights a week after work I have to stop by the store for this or that.
In the last 1-2 months there’s always been a couple at the parking lot exit, both in wheelchairs, with a big sign asking for money to help one of them beat cancer. They even have the amount listed.
But, by the same token, they could be quite legitimate. The American health care system is full of cracks that seriously ill people can slip through. One recent survey found that about 30% of Americans had trouble paying their medical bills.
It’s easy to look at people like this and think, “I’ll never let that happen to me.” We assume they must be smokers, or irresponsible spenders, or some other reason that makes us feel we won’t stumble into the same pitfalls. That’s reassuring, and sometimes true, but not always. And probably more often than we want to realize.
The world is full of people and families devastated by bad luck. Through no fault of their own, they develop a terrible medical condition or suffer grievous injuries, and suddenly, decent, hard-working, previously healthy people are facing foreclosure and financial ruin. It could, quite literally, be any of us.
Case in point: My family has good insurance and has averaged $10,000 in out-of-pocket medical expenses per year for the last several years. That’s for routine stuff: meeting deductibles, copays on medications, tests, and doctor visits, a few ER trips, etc. The only real “surprise” in there was when my wife broke her leg and needed surgery.

If the panhandlers really did have legitimate medical issues, I might be willing to help out. I give to charity. My grandmother and parents stressed that value to me, and I try to teach it to my kids. But, sadly, we live in a world full of con artists who try to make money by taking advantage of caring peoples’ feelings. Look at all the scams that immediately cropped up following the recent hurricane and wildfire disasters. Without knowing the truth, I’d rather give to an organization like the Salvation Army or Red Cross, hoping they have more experience than I do in sorting out who’s really in need.
As a doctor, I also try to justify it by thinking about how much care I do for “free.” This includes uninsured hospital patients we all see on call, knowing we’ll end up writing their bill off as a loss, and bounced checks for copays and deductible portions that we know we’ll never see.
But, no matter how I try to rationalize it, it still bothers me when I see them sitting there as I leave the store. I don’t know if they’re legitimate. But if they are, they aren’t alone, and there’s something seriously wrong with our health care system.
[polldaddy:9876776]
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
A few nights a week after work I have to stop by the store for this or that.
In the last 1-2 months there’s always been a couple at the parking lot exit, both in wheelchairs, with a big sign asking for money to help one of them beat cancer. They even have the amount listed.
But, by the same token, they could be quite legitimate. The American health care system is full of cracks that seriously ill people can slip through. One recent survey found that about 30% of Americans had trouble paying their medical bills.
It’s easy to look at people like this and think, “I’ll never let that happen to me.” We assume they must be smokers, or irresponsible spenders, or some other reason that makes us feel we won’t stumble into the same pitfalls. That’s reassuring, and sometimes true, but not always. And probably more often than we want to realize.
The world is full of people and families devastated by bad luck. Through no fault of their own, they develop a terrible medical condition or suffer grievous injuries, and suddenly, decent, hard-working, previously healthy people are facing foreclosure and financial ruin. It could, quite literally, be any of us.
Case in point: My family has good insurance and has averaged $10,000 in out-of-pocket medical expenses per year for the last several years. That’s for routine stuff: meeting deductibles, copays on medications, tests, and doctor visits, a few ER trips, etc. The only real “surprise” in there was when my wife broke her leg and needed surgery.
If the panhandlers really did have legitimate medical issues, I might be willing to help out. I give to charity. My grandmother and parents stressed that value to me, and I try to teach it to my kids. But, sadly, we live in a world full of con artists who try to make money by taking advantage of caring peoples’ feelings. Look at all the scams that immediately cropped up following the recent hurricane and wildfire disasters. Without knowing the truth, I’d rather give to an organization like the Salvation Army or Red Cross, hoping they have more experience than I do in sorting out who’s really in need.
As a doctor, I also try to justify it by thinking about how much care I do for “free.” This includes uninsured hospital patients we all see on call, knowing we’ll end up writing their bill off as a loss, and bounced checks for copays and deductible portions that we know we’ll never see.
But, no matter how I try to rationalize it, it still bothers me when I see them sitting there as I leave the store. I don’t know if they’re legitimate. But if they are, they aren’t alone, and there’s something seriously wrong with our health care system.
[polldaddy:9876776]
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
A few nights a week after work I have to stop by the store for this or that.
In the last 1-2 months there’s always been a couple at the parking lot exit, both in wheelchairs, with a big sign asking for money to help one of them beat cancer. They even have the amount listed.
But, by the same token, they could be quite legitimate. The American health care system is full of cracks that seriously ill people can slip through. One recent survey found that about 30% of Americans had trouble paying their medical bills.
It’s easy to look at people like this and think, “I’ll never let that happen to me.” We assume they must be smokers, or irresponsible spenders, or some other reason that makes us feel we won’t stumble into the same pitfalls. That’s reassuring, and sometimes true, but not always. And probably more often than we want to realize.
The world is full of people and families devastated by bad luck. Through no fault of their own, they develop a terrible medical condition or suffer grievous injuries, and suddenly, decent, hard-working, previously healthy people are facing foreclosure and financial ruin. It could, quite literally, be any of us.
Case in point: My family has good insurance and has averaged $10,000 in out-of-pocket medical expenses per year for the last several years. That’s for routine stuff: meeting deductibles, copays on medications, tests, and doctor visits, a few ER trips, etc. The only real “surprise” in there was when my wife broke her leg and needed surgery.
If the panhandlers really did have legitimate medical issues, I might be willing to help out. I give to charity. My grandmother and parents stressed that value to me, and I try to teach it to my kids. But, sadly, we live in a world full of con artists who try to make money by taking advantage of caring peoples’ feelings. Look at all the scams that immediately cropped up following the recent hurricane and wildfire disasters. Without knowing the truth, I’d rather give to an organization like the Salvation Army or Red Cross, hoping they have more experience than I do in sorting out who’s really in need.
As a doctor, I also try to justify it by thinking about how much care I do for “free.” This includes uninsured hospital patients we all see on call, knowing we’ll end up writing their bill off as a loss, and bounced checks for copays and deductible portions that we know we’ll never see.
But, no matter how I try to rationalize it, it still bothers me when I see them sitting there as I leave the store. I don’t know if they’re legitimate. But if they are, they aren’t alone, and there’s something seriously wrong with our health care system.
[polldaddy:9876776]
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Your online reputation
Have you ever run across an unfair or even malicious comment about you or your practice on one of those “doctor-rating” web sites? Some curmudgeon, angry about something totally irrelevant to your clinical skills, decided to publicly trash you; and the site, of course, made no effort to authenticate the writer or fact-check the complaint.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management; but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.

Leave design and SEO to the pros, but don’t delegate the content itself; as captain of the ship you are responsible for all the facts and opinions on your site. And remember that, once it’s online, it’s online forever; consider the ramifications of anything you post on any site – yours or others – before hitting the “send” button. “The most damaging item about you,” one consultant told me, “could well be something you posted yourself.” Just ask any of several prominent politicians who have famously sabotaged their own careers online.
That said, don’t be shy about creating content. Patients appreciate factual information, but they value your opinions too. Add a blog to your web site and write about subjects – medical and otherwise – that interest you. If you have expertise in a particular field, be sure to write about that.
Incidentally, if the URL for your web site is not your own name, you should register your name as a separate domain name – even if you never use it – to be sure that a trickster or troll, or someone with the same name but a bad reputation, doesn’t get it.
A web site is a powerful resource, but not the only one. Take advantage of Google’s free profiling tool at https://profiles.google.com/me, where you can create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. Your Google profile will, of course, be at or near the top of any Google search.
Wikipedia articles also go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is done and updated regularly. Remember that Wikipedia’s conflict of interest rules forbid adding or editing content about yourself, so someone with a theoretically “neutral point of view” will have to do it for you.
Other useful resources are the social networking sites. Whatever your opinion of online networks, the reality is that personal pages on Facebook, LinkedIn, and Twitter rank very high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a “professional” network.) Make your (noncontroversial) opinions known on these portals. Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – also need to be mentioned prominently.
Set up an RSS news feed for yourself (directions to follow in the next two columns), so you’ll know immediately if your name pops up in news or gossip sites, or on blogs. If something untrue is posted about you, take action. Reputable news sites and blogs have their own reputations to protect and can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely or corrected within the original article. An erratum on the last page of the next edition will be ignored and will leave the false information online, intact.
Doctor-rating sites typically refuse to remove unfair comments unless they are blatantly libelous or a case of mistaken identity; but there is nothing wrong with encouraging happy patients to post favorable reviews on those sites. Sauce for the goose, and all that.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.
Have you ever run across an unfair or even malicious comment about you or your practice on one of those “doctor-rating” web sites? Some curmudgeon, angry about something totally irrelevant to your clinical skills, decided to publicly trash you; and the site, of course, made no effort to authenticate the writer or fact-check the complaint.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management; but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.
Leave design and SEO to the pros, but don’t delegate the content itself; as captain of the ship you are responsible for all the facts and opinions on your site. And remember that, once it’s online, it’s online forever; consider the ramifications of anything you post on any site – yours or others – before hitting the “send” button. “The most damaging item about you,” one consultant told me, “could well be something you posted yourself.” Just ask any of several prominent politicians who have famously sabotaged their own careers online.
That said, don’t be shy about creating content. Patients appreciate factual information, but they value your opinions too. Add a blog to your web site and write about subjects – medical and otherwise – that interest you. If you have expertise in a particular field, be sure to write about that.
Incidentally, if the URL for your web site is not your own name, you should register your name as a separate domain name – even if you never use it – to be sure that a trickster or troll, or someone with the same name but a bad reputation, doesn’t get it.
A web site is a powerful resource, but not the only one. Take advantage of Google’s free profiling tool at https://profiles.google.com/me, where you can create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. Your Google profile will, of course, be at or near the top of any Google search.
Wikipedia articles also go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is done and updated regularly. Remember that Wikipedia’s conflict of interest rules forbid adding or editing content about yourself, so someone with a theoretically “neutral point of view” will have to do it for you.
Other useful resources are the social networking sites. Whatever your opinion of online networks, the reality is that personal pages on Facebook, LinkedIn, and Twitter rank very high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a “professional” network.) Make your (noncontroversial) opinions known on these portals. Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – also need to be mentioned prominently.
Set up an RSS news feed for yourself (directions to follow in the next two columns), so you’ll know immediately if your name pops up in news or gossip sites, or on blogs. If something untrue is posted about you, take action. Reputable news sites and blogs have their own reputations to protect and can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely or corrected within the original article. An erratum on the last page of the next edition will be ignored and will leave the false information online, intact.
Doctor-rating sites typically refuse to remove unfair comments unless they are blatantly libelous or a case of mistaken identity; but there is nothing wrong with encouraging happy patients to post favorable reviews on those sites. Sauce for the goose, and all that.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.
Have you ever run across an unfair or even malicious comment about you or your practice on one of those “doctor-rating” web sites? Some curmudgeon, angry about something totally irrelevant to your clinical skills, decided to publicly trash you; and the site, of course, made no effort to authenticate the writer or fact-check the complaint.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management; but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.
Leave design and SEO to the pros, but don’t delegate the content itself; as captain of the ship you are responsible for all the facts and opinions on your site. And remember that, once it’s online, it’s online forever; consider the ramifications of anything you post on any site – yours or others – before hitting the “send” button. “The most damaging item about you,” one consultant told me, “could well be something you posted yourself.” Just ask any of several prominent politicians who have famously sabotaged their own careers online.
That said, don’t be shy about creating content. Patients appreciate factual information, but they value your opinions too. Add a blog to your web site and write about subjects – medical and otherwise – that interest you. If you have expertise in a particular field, be sure to write about that.
Incidentally, if the URL for your web site is not your own name, you should register your name as a separate domain name – even if you never use it – to be sure that a trickster or troll, or someone with the same name but a bad reputation, doesn’t get it.
A web site is a powerful resource, but not the only one. Take advantage of Google’s free profiling tool at https://profiles.google.com/me, where you can create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. Your Google profile will, of course, be at or near the top of any Google search.
Wikipedia articles also go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is done and updated regularly. Remember that Wikipedia’s conflict of interest rules forbid adding or editing content about yourself, so someone with a theoretically “neutral point of view” will have to do it for you.
Other useful resources are the social networking sites. Whatever your opinion of online networks, the reality is that personal pages on Facebook, LinkedIn, and Twitter rank very high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a “professional” network.) Make your (noncontroversial) opinions known on these portals. Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – also need to be mentioned prominently.
Set up an RSS news feed for yourself (directions to follow in the next two columns), so you’ll know immediately if your name pops up in news or gossip sites, or on blogs. If something untrue is posted about you, take action. Reputable news sites and blogs have their own reputations to protect and can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely or corrected within the original article. An erratum on the last page of the next edition will be ignored and will leave the false information online, intact.
Doctor-rating sites typically refuse to remove unfair comments unless they are blatantly libelous or a case of mistaken identity; but there is nothing wrong with encouraging happy patients to post favorable reviews on those sites. Sauce for the goose, and all that.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@frontlinemedcom.com.
