User login
Real-world data are a wake-up call
In this edition of “Applying research to practice,” I highlight a study revealing real-world information about the clinical care of breast cancer patients with deleterious germline mutations.

While germline testing among breast cancer patients is becoming more commonplace, it isn’t clear how test results influence patient care. To gain some insight, Allison W. Kurian, MD, of Stanford (Calif.) University, and colleagues analyzed data on 20,568 women with stage 0-III breast cancer from the Surveillance, Epidemiology, and End Results (SEER) registries of Georgia and California (JAMA Oncol. 2020 Feb 6. doi: 10.1001/jamaoncol.2019.6400).
The researchers aimed to determine whether women with mutations in breast cancer–associated genes (BRCA1/2 or others) received guideline-concordant care to the same degree as women who lacked deleterious mutations. The authors evaluated guideline concordance with respect to three treatment modalities: surgery (bilateral vs. unilateral mastectomy in women who were eligible for unilateral surgery), radiotherapy after lumpectomy (for women aged less than 70 years with hormonally responsive, ErbB2-negative, stage I cancers), and chemotherapy (among women eligible for consideration of chemotherapy omission)
In alignment with guidelines, many clinicians correctly used genetic test results to guide surgical decisions. For example, 61.7% of women with BRCA mutations underwent bilateral mastectomy, compared with 24.3% who were mutation negative (odds ratio, 5.52). For other pathogenic variants (ATM, CDH1, CHEK2, NBN, NF1, PALB2, PTEN, and TP53), the rate of bilateral mastectomy was still elevated, albeit to a lesser degree (OR, 2.41).
In discord with guidelines, women with BRCA mutations were 78% less likely to receive radiotherapy after lumpectomy (OR, 0.22) and 76% more likely to receive chemotherapy for early-stage, hormone-positive disease (OR, 1.76), suggesting possible trends in under- and overtreatment, respectively. Chemotherapy utilization rates among mutation carriers and noncarriers became more similar after adjustment for clinical and demographic factors.
There are limits on the granularity of the SEER database, such that, if a patient had a mastectomy a year or more after lumpectomy in an effort to avoid radiotherapy, the database would not have reflected that. Clinical factors could have appropriately influenced chemotherapy receipt among patients with mutations, but those additional factors (including patient preference) would not be included in the SEER data.
The authors concluded that research should be conducted to confirm the results of this retrospective, population-based cohort analysis, in an effort to understand the decision-making process and consequences for long-term outcome.
How these findings should influence practice
With every new development, there are challenges – some expected, some unanticipated.
It is now feasible to obtain multigene panel testing reasonably inexpensively. There are concerns about undertesting of patients on the basis of family history alone. And some major professional organizations have endorsed routine gene panel testing for all breast cancer patients.
As a consequence of these factors, genetic test results are routinely available to clinicians who may lack formal training in clinical genetics. Whether these results influence the receipt of evidence-based clinical care is uncertain.
The information published by Dr. Kurian and colleagues is inherently limited by the methodology of a SEER database review. Among other limitations, as the authors comment:
- The genetic test results could have arrived after treatment decisions were made.
- Treatment delivered more than a year after diagnosis would not have been captured.
- There was selection of patients for genetic testing.
- There were few patients with particular germline mutations other than BRCA1/2 on whom to judge whether treatment was guideline concordant.
- The rationale for the treatment choices made by physicians and patients was not available.
- Impact of treatment choices on survival for carriers of deleterious mutations is uncertain.
Nonetheless, these data suggest a need to redouble efforts to educate patients, their family members, and health care professionals about evidence-based guidelines for care and the rationale for those recommendations.
Careful, prospective monitoring of any resultant differences in treatment outcome in patients treated with guideline-concordant and nonconcordant care is needed. When treatment choices appear to systematically deviate from published guidelines with no obvious rationale, it is a wake-up call for all of us.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers as well as expanding clinical trial access to medically underserved populations.
In this edition of “Applying research to practice,” I highlight a study revealing real-world information about the clinical care of breast cancer patients with deleterious germline mutations.
While germline testing among breast cancer patients is becoming more commonplace, it isn’t clear how test results influence patient care. To gain some insight, Allison W. Kurian, MD, of Stanford (Calif.) University, and colleagues analyzed data on 20,568 women with stage 0-III breast cancer from the Surveillance, Epidemiology, and End Results (SEER) registries of Georgia and California (JAMA Oncol. 2020 Feb 6. doi: 10.1001/jamaoncol.2019.6400).
The researchers aimed to determine whether women with mutations in breast cancer–associated genes (BRCA1/2 or others) received guideline-concordant care to the same degree as women who lacked deleterious mutations. The authors evaluated guideline concordance with respect to three treatment modalities: surgery (bilateral vs. unilateral mastectomy in women who were eligible for unilateral surgery), radiotherapy after lumpectomy (for women aged less than 70 years with hormonally responsive, ErbB2-negative, stage I cancers), and chemotherapy (among women eligible for consideration of chemotherapy omission)
In alignment with guidelines, many clinicians correctly used genetic test results to guide surgical decisions. For example, 61.7% of women with BRCA mutations underwent bilateral mastectomy, compared with 24.3% who were mutation negative (odds ratio, 5.52). For other pathogenic variants (ATM, CDH1, CHEK2, NBN, NF1, PALB2, PTEN, and TP53), the rate of bilateral mastectomy was still elevated, albeit to a lesser degree (OR, 2.41).
In discord with guidelines, women with BRCA mutations were 78% less likely to receive radiotherapy after lumpectomy (OR, 0.22) and 76% more likely to receive chemotherapy for early-stage, hormone-positive disease (OR, 1.76), suggesting possible trends in under- and overtreatment, respectively. Chemotherapy utilization rates among mutation carriers and noncarriers became more similar after adjustment for clinical and demographic factors.
There are limits on the granularity of the SEER database, such that, if a patient had a mastectomy a year or more after lumpectomy in an effort to avoid radiotherapy, the database would not have reflected that. Clinical factors could have appropriately influenced chemotherapy receipt among patients with mutations, but those additional factors (including patient preference) would not be included in the SEER data.
The authors concluded that research should be conducted to confirm the results of this retrospective, population-based cohort analysis, in an effort to understand the decision-making process and consequences for long-term outcome.
How these findings should influence practice
With every new development, there are challenges – some expected, some unanticipated.
It is now feasible to obtain multigene panel testing reasonably inexpensively. There are concerns about undertesting of patients on the basis of family history alone. And some major professional organizations have endorsed routine gene panel testing for all breast cancer patients.
As a consequence of these factors, genetic test results are routinely available to clinicians who may lack formal training in clinical genetics. Whether these results influence the receipt of evidence-based clinical care is uncertain.
The information published by Dr. Kurian and colleagues is inherently limited by the methodology of a SEER database review. Among other limitations, as the authors comment:
- The genetic test results could have arrived after treatment decisions were made.
- Treatment delivered more than a year after diagnosis would not have been captured.
- There was selection of patients for genetic testing.
- There were few patients with particular germline mutations other than BRCA1/2 on whom to judge whether treatment was guideline concordant.
- The rationale for the treatment choices made by physicians and patients was not available.
- Impact of treatment choices on survival for carriers of deleterious mutations is uncertain.
Nonetheless, these data suggest a need to redouble efforts to educate patients, their family members, and health care professionals about evidence-based guidelines for care and the rationale for those recommendations.
Careful, prospective monitoring of any resultant differences in treatment outcome in patients treated with guideline-concordant and nonconcordant care is needed. When treatment choices appear to systematically deviate from published guidelines with no obvious rationale, it is a wake-up call for all of us.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers as well as expanding clinical trial access to medically underserved populations.
In this edition of “Applying research to practice,” I highlight a study revealing real-world information about the clinical care of breast cancer patients with deleterious germline mutations.
While germline testing among breast cancer patients is becoming more commonplace, it isn’t clear how test results influence patient care. To gain some insight, Allison W. Kurian, MD, of Stanford (Calif.) University, and colleagues analyzed data on 20,568 women with stage 0-III breast cancer from the Surveillance, Epidemiology, and End Results (SEER) registries of Georgia and California (JAMA Oncol. 2020 Feb 6. doi: 10.1001/jamaoncol.2019.6400).
The researchers aimed to determine whether women with mutations in breast cancer–associated genes (BRCA1/2 or others) received guideline-concordant care to the same degree as women who lacked deleterious mutations. The authors evaluated guideline concordance with respect to three treatment modalities: surgery (bilateral vs. unilateral mastectomy in women who were eligible for unilateral surgery), radiotherapy after lumpectomy (for women aged less than 70 years with hormonally responsive, ErbB2-negative, stage I cancers), and chemotherapy (among women eligible for consideration of chemotherapy omission)
In alignment with guidelines, many clinicians correctly used genetic test results to guide surgical decisions. For example, 61.7% of women with BRCA mutations underwent bilateral mastectomy, compared with 24.3% who were mutation negative (odds ratio, 5.52). For other pathogenic variants (ATM, CDH1, CHEK2, NBN, NF1, PALB2, PTEN, and TP53), the rate of bilateral mastectomy was still elevated, albeit to a lesser degree (OR, 2.41).
In discord with guidelines, women with BRCA mutations were 78% less likely to receive radiotherapy after lumpectomy (OR, 0.22) and 76% more likely to receive chemotherapy for early-stage, hormone-positive disease (OR, 1.76), suggesting possible trends in under- and overtreatment, respectively. Chemotherapy utilization rates among mutation carriers and noncarriers became more similar after adjustment for clinical and demographic factors.
There are limits on the granularity of the SEER database, such that, if a patient had a mastectomy a year or more after lumpectomy in an effort to avoid radiotherapy, the database would not have reflected that. Clinical factors could have appropriately influenced chemotherapy receipt among patients with mutations, but those additional factors (including patient preference) would not be included in the SEER data.
The authors concluded that research should be conducted to confirm the results of this retrospective, population-based cohort analysis, in an effort to understand the decision-making process and consequences for long-term outcome.
How these findings should influence practice
With every new development, there are challenges – some expected, some unanticipated.
It is now feasible to obtain multigene panel testing reasonably inexpensively. There are concerns about undertesting of patients on the basis of family history alone. And some major professional organizations have endorsed routine gene panel testing for all breast cancer patients.
As a consequence of these factors, genetic test results are routinely available to clinicians who may lack formal training in clinical genetics. Whether these results influence the receipt of evidence-based clinical care is uncertain.
The information published by Dr. Kurian and colleagues is inherently limited by the methodology of a SEER database review. Among other limitations, as the authors comment:
- The genetic test results could have arrived after treatment decisions were made.
- Treatment delivered more than a year after diagnosis would not have been captured.
- There was selection of patients for genetic testing.
- There were few patients with particular germline mutations other than BRCA1/2 on whom to judge whether treatment was guideline concordant.
- The rationale for the treatment choices made by physicians and patients was not available.
- Impact of treatment choices on survival for carriers of deleterious mutations is uncertain.
Nonetheless, these data suggest a need to redouble efforts to educate patients, their family members, and health care professionals about evidence-based guidelines for care and the rationale for those recommendations.
Careful, prospective monitoring of any resultant differences in treatment outcome in patients treated with guideline-concordant and nonconcordant care is needed. When treatment choices appear to systematically deviate from published guidelines with no obvious rationale, it is a wake-up call for all of us.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers as well as expanding clinical trial access to medically underserved populations.
Hospital medicine physician leaders
The right skills and time to develop them
“When you get someone who knows what quality looks like and pair that with curiosity about new ways to think about leading, you end up with the people who are able to produce dramatic innovations in the field.”1
In medicine, a physician is trained to take charge in emergent situations and make potentially lifesaving efforts. However, when it comes to leading teams of individuals, not only must successful leaders have the right skills, they also need time to dedicate to the work of leadership.

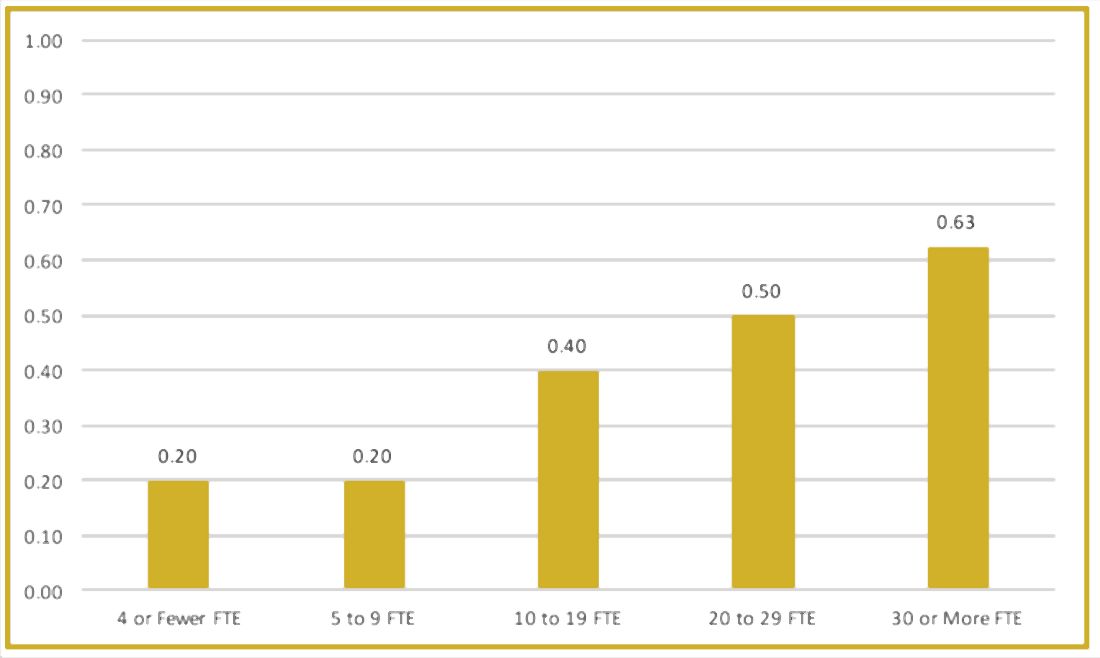
To better understand current approaches to dedicated hospital medicine group (HMG) leadership time, let’s examine the 2018 State of Hospital Medicine (SoHM) Report. The survey, upon which the Report was based, examined two aspects of leadership: 1) how much dedicated time a leader receives to manage the group; and 2) how the leader’s time is compensated. Looking closely at the data displayed in graphs from the SoHM Report (Figures 1, 2, and 3), we can see that dedicated administrative time is directly proportional to the size of the group.
In my current role as a regional medical director in the Dallas-Fort Worth market, I oversee some programs where the size is greater than 30 full-time equivalents (FTEs), and requires a full-time administrative physician leader to manage the group. Their daily administrative duties include, but are not limited to, addressing physician performance and behaviors, managing team performance metrics, dealing with consultants’ expectations, attending and leading various committee meetings at the hospital or the system level, attending and presenting performance reviews, leading and preparing for team meetings, as well as addressing and being innovative in leading new initiatives from the hospital partner system.
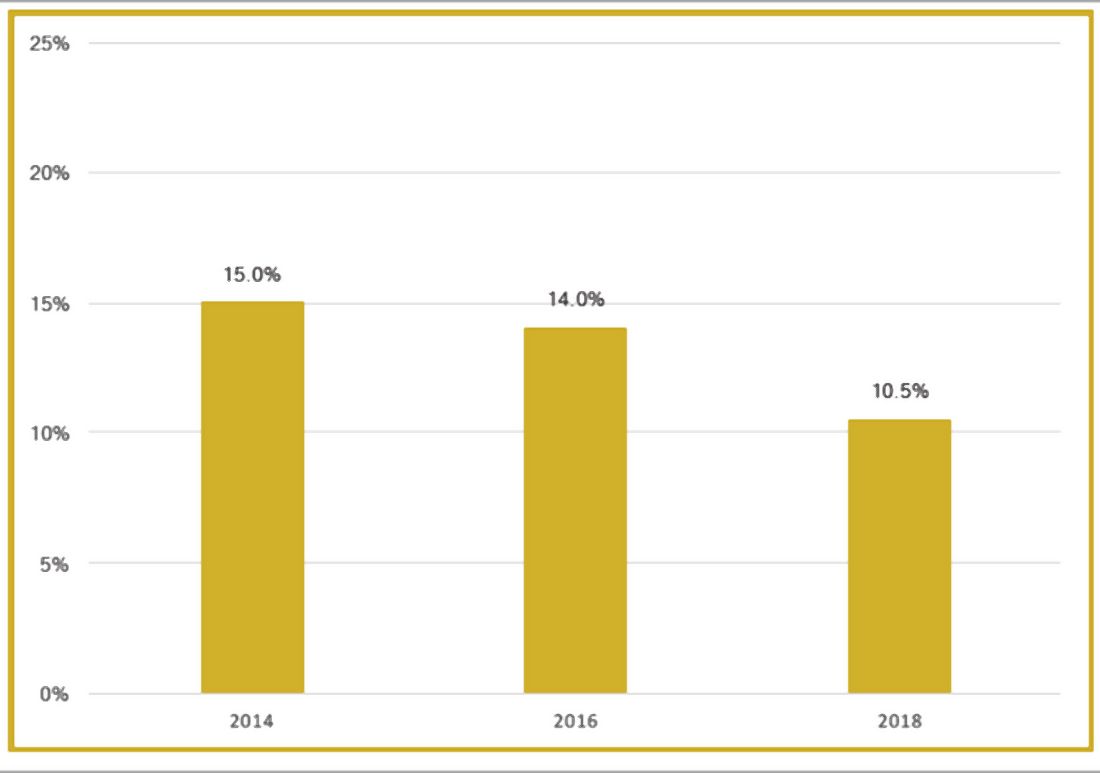
Although physician leaders are paid more for their work, the 2018 SoHM Report reveals a decline in the premium year over year. One of the reasons for the payment decline that I have encountered in various groups is that their incentives for leading the group are based on performance, as opposed to receiving a fixed stipend. Another reason is the presence of dedicated administrative support or the inclusion of a performance improvement staffer, such as an additional nurse or advanced practice provider, in the group.
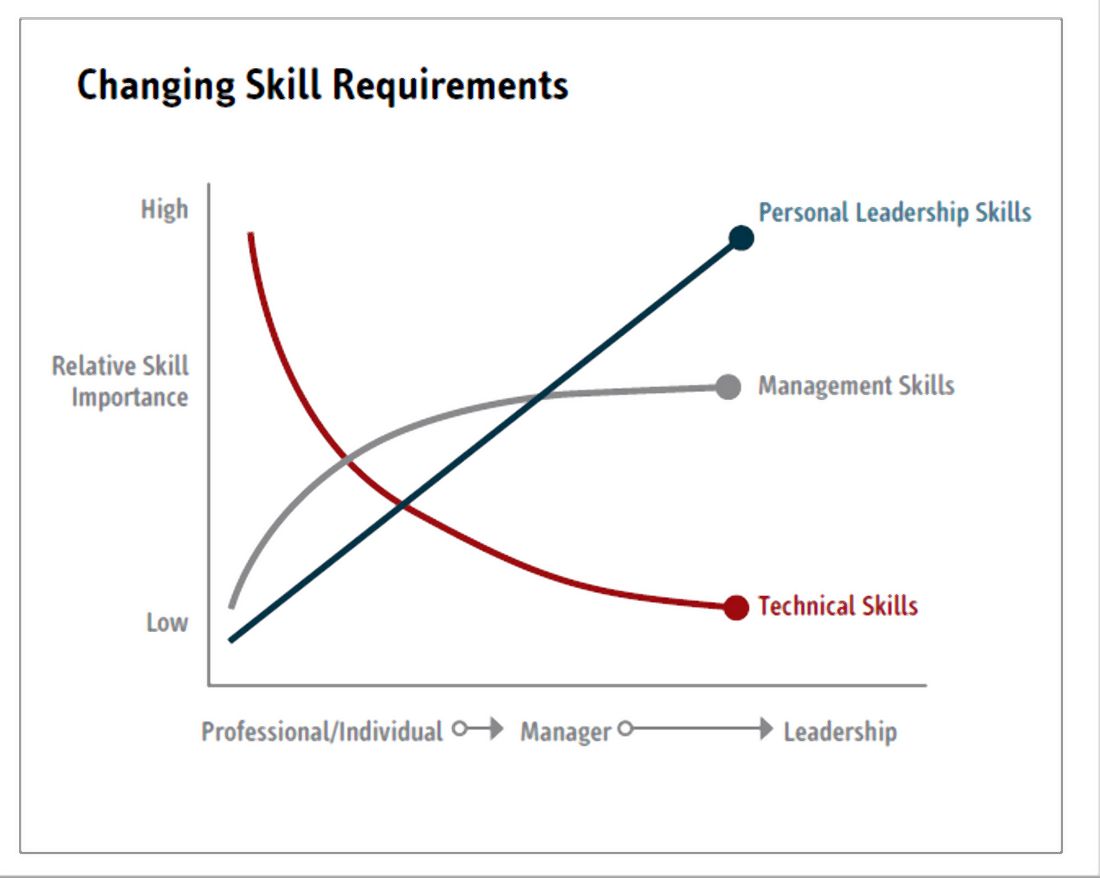
Evidence suggests that organizations and patients benefit when physicians take on leadership roles. Physician leaders play critical roles in providing high-quality patient care. How can the Society of Hospital Medicine help? Management degrees and leadership workshops have become a common pathway for many physicians, including myself. SHM provides one of the most thorough and relevant experiences through the SHM Leadership Academy. The focus of the Leadership Academy is on developing a broad set of additional leadership competencies across a spectrum of experience.5 As hospitalist physicians are often expected to fulfill a broader leadership void, we must pay attention to developing the leadership skills depicted in Figure 3. Hospital medicine is an ideal “proving ground” for future physician executives and leaders, as they often share the same characteristics required for success.
The leadership paths available in my organization, Sound Physicians, were recently highlighted in a New York Times article.3 Sound Physicians employs more than 3,000 physicians across the country, and has a pipeline for doctors to advance through structured rungs of leadership – emphasizing a different mix of clinical, strategic, and business skills at each stage, from individual practitioner to the C-suite. The training includes in-person and online courses, as well as an annual conference, to help doctors develop management and leadership competencies, and learn how to apply these skills within their organizations. Since introducing its leadership development program, the company reports less turnover, higher morale, and better growth. I personally have gone through the leadership training provided by Sound Physicians, and reflecting back, it has been a transformational experience for me. Leadership is a journey, not a destination, and as physicians we should strive to learn more from the health care leaders around us.
The administrative workload for hospital-based physician leaders will increase with the arrival of value-based programs and alternative payment models promoted by the Centers for Medicare and Medicaid Services. Lead hospitalist duties are not limited to daily operations, but can extend to leading the strategic vision of the hospital or health system. The 2020 SoHM Report will reflect these changes, as well as provide further information about how to manage and set expectations for physician leaders, based on group size and employment model.
Dr. Patel is a regional medical director with Sound Physicians. He manages more than 100 FTE hospitalists and advanced-practice providers (APPs) within multiple health systems and hospitals in the Texas market. He also serves as a member of the SHM Practice Analysis Committee and as a vice president of SHM North Texas Chapter.
References
1. Angood P and Birk S. The Value of Physician Leadership. Physician Exec. 2014 May-Jun;40(3):6-20.
2. Rice JA. Expanding the Need for Physician Leaders. Executive Insight, Advance Healthcare Network, Nov 16, 2011. Available at: http://healthcare-executive-insight.advanceweb.com/Features/Articles/Expanding-the-Need-for-Physician-Leaders.aspx.
3. Khullar D. Good leaders make good doctors. New York Times. 2019 Nov 21.
4. Beresford L. The State of Hospital Medicine in 2018. Hospitalist. 2019;23(1):1-11.
5. Harte B. Hospitalists can meet the demand for physician executives. Hospitalist. 2018 Nov 29.
The right skills and time to develop them
The right skills and time to develop them
“When you get someone who knows what quality looks like and pair that with curiosity about new ways to think about leading, you end up with the people who are able to produce dramatic innovations in the field.”1
In medicine, a physician is trained to take charge in emergent situations and make potentially lifesaving efforts. However, when it comes to leading teams of individuals, not only must successful leaders have the right skills, they also need time to dedicate to the work of leadership.
To better understand current approaches to dedicated hospital medicine group (HMG) leadership time, let’s examine the 2018 State of Hospital Medicine (SoHM) Report. The survey, upon which the Report was based, examined two aspects of leadership: 1) how much dedicated time a leader receives to manage the group; and 2) how the leader’s time is compensated. Looking closely at the data displayed in graphs from the SoHM Report (Figures 1, 2, and 3), we can see that dedicated administrative time is directly proportional to the size of the group.
In my current role as a regional medical director in the Dallas-Fort Worth market, I oversee some programs where the size is greater than 30 full-time equivalents (FTEs), and requires a full-time administrative physician leader to manage the group. Their daily administrative duties include, but are not limited to, addressing physician performance and behaviors, managing team performance metrics, dealing with consultants’ expectations, attending and leading various committee meetings at the hospital or the system level, attending and presenting performance reviews, leading and preparing for team meetings, as well as addressing and being innovative in leading new initiatives from the hospital partner system.
Although physician leaders are paid more for their work, the 2018 SoHM Report reveals a decline in the premium year over year. One of the reasons for the payment decline that I have encountered in various groups is that their incentives for leading the group are based on performance, as opposed to receiving a fixed stipend. Another reason is the presence of dedicated administrative support or the inclusion of a performance improvement staffer, such as an additional nurse or advanced practice provider, in the group.
Evidence suggests that organizations and patients benefit when physicians take on leadership roles. Physician leaders play critical roles in providing high-quality patient care. How can the Society of Hospital Medicine help? Management degrees and leadership workshops have become a common pathway for many physicians, including myself. SHM provides one of the most thorough and relevant experiences through the SHM Leadership Academy. The focus of the Leadership Academy is on developing a broad set of additional leadership competencies across a spectrum of experience.5 As hospitalist physicians are often expected to fulfill a broader leadership void, we must pay attention to developing the leadership skills depicted in Figure 3. Hospital medicine is an ideal “proving ground” for future physician executives and leaders, as they often share the same characteristics required for success.
The leadership paths available in my organization, Sound Physicians, were recently highlighted in a New York Times article.3 Sound Physicians employs more than 3,000 physicians across the country, and has a pipeline for doctors to advance through structured rungs of leadership – emphasizing a different mix of clinical, strategic, and business skills at each stage, from individual practitioner to the C-suite. The training includes in-person and online courses, as well as an annual conference, to help doctors develop management and leadership competencies, and learn how to apply these skills within their organizations. Since introducing its leadership development program, the company reports less turnover, higher morale, and better growth. I personally have gone through the leadership training provided by Sound Physicians, and reflecting back, it has been a transformational experience for me. Leadership is a journey, not a destination, and as physicians we should strive to learn more from the health care leaders around us.
The administrative workload for hospital-based physician leaders will increase with the arrival of value-based programs and alternative payment models promoted by the Centers for Medicare and Medicaid Services. Lead hospitalist duties are not limited to daily operations, but can extend to leading the strategic vision of the hospital or health system. The 2020 SoHM Report will reflect these changes, as well as provide further information about how to manage and set expectations for physician leaders, based on group size and employment model.
Dr. Patel is a regional medical director with Sound Physicians. He manages more than 100 FTE hospitalists and advanced-practice providers (APPs) within multiple health systems and hospitals in the Texas market. He also serves as a member of the SHM Practice Analysis Committee and as a vice president of SHM North Texas Chapter.
References
1. Angood P and Birk S. The Value of Physician Leadership. Physician Exec. 2014 May-Jun;40(3):6-20.
2. Rice JA. Expanding the Need for Physician Leaders. Executive Insight, Advance Healthcare Network, Nov 16, 2011. Available at: http://healthcare-executive-insight.advanceweb.com/Features/Articles/Expanding-the-Need-for-Physician-Leaders.aspx.
3. Khullar D. Good leaders make good doctors. New York Times. 2019 Nov 21.
4. Beresford L. The State of Hospital Medicine in 2018. Hospitalist. 2019;23(1):1-11.
5. Harte B. Hospitalists can meet the demand for physician executives. Hospitalist. 2018 Nov 29.
“When you get someone who knows what quality looks like and pair that with curiosity about new ways to think about leading, you end up with the people who are able to produce dramatic innovations in the field.”1
In medicine, a physician is trained to take charge in emergent situations and make potentially lifesaving efforts. However, when it comes to leading teams of individuals, not only must successful leaders have the right skills, they also need time to dedicate to the work of leadership.
To better understand current approaches to dedicated hospital medicine group (HMG) leadership time, let’s examine the 2018 State of Hospital Medicine (SoHM) Report. The survey, upon which the Report was based, examined two aspects of leadership: 1) how much dedicated time a leader receives to manage the group; and 2) how the leader’s time is compensated. Looking closely at the data displayed in graphs from the SoHM Report (Figures 1, 2, and 3), we can see that dedicated administrative time is directly proportional to the size of the group.
In my current role as a regional medical director in the Dallas-Fort Worth market, I oversee some programs where the size is greater than 30 full-time equivalents (FTEs), and requires a full-time administrative physician leader to manage the group. Their daily administrative duties include, but are not limited to, addressing physician performance and behaviors, managing team performance metrics, dealing with consultants’ expectations, attending and leading various committee meetings at the hospital or the system level, attending and presenting performance reviews, leading and preparing for team meetings, as well as addressing and being innovative in leading new initiatives from the hospital partner system.
Although physician leaders are paid more for their work, the 2018 SoHM Report reveals a decline in the premium year over year. One of the reasons for the payment decline that I have encountered in various groups is that their incentives for leading the group are based on performance, as opposed to receiving a fixed stipend. Another reason is the presence of dedicated administrative support or the inclusion of a performance improvement staffer, such as an additional nurse or advanced practice provider, in the group.
Evidence suggests that organizations and patients benefit when physicians take on leadership roles. Physician leaders play critical roles in providing high-quality patient care. How can the Society of Hospital Medicine help? Management degrees and leadership workshops have become a common pathway for many physicians, including myself. SHM provides one of the most thorough and relevant experiences through the SHM Leadership Academy. The focus of the Leadership Academy is on developing a broad set of additional leadership competencies across a spectrum of experience.5 As hospitalist physicians are often expected to fulfill a broader leadership void, we must pay attention to developing the leadership skills depicted in Figure 3. Hospital medicine is an ideal “proving ground” for future physician executives and leaders, as they often share the same characteristics required for success.
The leadership paths available in my organization, Sound Physicians, were recently highlighted in a New York Times article.3 Sound Physicians employs more than 3,000 physicians across the country, and has a pipeline for doctors to advance through structured rungs of leadership – emphasizing a different mix of clinical, strategic, and business skills at each stage, from individual practitioner to the C-suite. The training includes in-person and online courses, as well as an annual conference, to help doctors develop management and leadership competencies, and learn how to apply these skills within their organizations. Since introducing its leadership development program, the company reports less turnover, higher morale, and better growth. I personally have gone through the leadership training provided by Sound Physicians, and reflecting back, it has been a transformational experience for me. Leadership is a journey, not a destination, and as physicians we should strive to learn more from the health care leaders around us.
The administrative workload for hospital-based physician leaders will increase with the arrival of value-based programs and alternative payment models promoted by the Centers for Medicare and Medicaid Services. Lead hospitalist duties are not limited to daily operations, but can extend to leading the strategic vision of the hospital or health system. The 2020 SoHM Report will reflect these changes, as well as provide further information about how to manage and set expectations for physician leaders, based on group size and employment model.
Dr. Patel is a regional medical director with Sound Physicians. He manages more than 100 FTE hospitalists and advanced-practice providers (APPs) within multiple health systems and hospitals in the Texas market. He also serves as a member of the SHM Practice Analysis Committee and as a vice president of SHM North Texas Chapter.
References
1. Angood P and Birk S. The Value of Physician Leadership. Physician Exec. 2014 May-Jun;40(3):6-20.
2. Rice JA. Expanding the Need for Physician Leaders. Executive Insight, Advance Healthcare Network, Nov 16, 2011. Available at: http://healthcare-executive-insight.advanceweb.com/Features/Articles/Expanding-the-Need-for-Physician-Leaders.aspx.
3. Khullar D. Good leaders make good doctors. New York Times. 2019 Nov 21.
4. Beresford L. The State of Hospital Medicine in 2018. Hospitalist. 2019;23(1):1-11.
5. Harte B. Hospitalists can meet the demand for physician executives. Hospitalist. 2018 Nov 29.
Emeritus
“So what do you do all day?”
.

Asking what an emeritus does all day sounds fair, but the question is harder to answer than it sounds. Last year, I asked Dave, who was already retired. He took a day to think about it.
“Sometimes I sit on the back porch and watch the birds,” he said.
Dave has long been an avid bird-watcher. Along with golf and Facebook, watching birds is a pursuit that really engages many people, but I never understood it. I still don’t.
Over the years, I’ve met people whose experience of retirement has ranged from, “I’m so busy, I don’t know how I had time to work!” to, “I miss the gang and I’m bored,” to everything in between. Before I (semi-) retired, I made a plan to not make plans, at least at first: No new hobbies, cooking lessons, or anthropology courses. I figured I would figure it out.
So I am figuring it out. No rush. After a lifetime of rushing, not rushing is part of the point.
One hobby I cultivate is napping. I always get up early, no alarm needed. By late morning I am sometimes inclined to lie down for a bit. Taking a midmorning nap has always struck me as one of life’s great pleasures, though one I could rarely enjoy, unless you count dozing off standing up while a patient described an itch that started 17 years before, on a Thursday.
Now I can shut my eyes for half an hour and wake up refreshed, ready for the rest of the day.
During which I will do ...
An older friend of mine, now long gone, wrote a witty essay on being embarrassed to work at home. He refused to answer the phone during the day and hid from the postman. Contemplating retirement, I was afraid I would also feel that way, picturing myself a pitiful pensioner shuffling abroad at mid-day, looking for a park to poison pigeons in. That of course was before “working remotely” became a goal for cool young strivers. You see them around at all hours, with things sticking out of their ears, talking urgently to no one you can see.
Now I also walk the streets proudly at 11 a.m. or 2:45 p.m. I may get one of those earbuds that stick out at 45 degrees, so people can think my ear fungus has grown branches. Maybe they’ll imagine me a mastermind of an international CBD cartel. What they think doesn’t really matter.
One thing that I actually do all day is wonder why I spent so much of my career worrying about what other people think. Dr. Smith used to refer patients. No longer. Did I fail to meet her expectations? Mr. Trelawney came in weekly with itches and pains. No more. Did I roll my eyes too obviously?
Questions like these used to trouble me. Now I can’t recall why. Instead I worry about more important things, like who will play right field for the Red Sox this year.
Though I never signed up, I am an enrolled Baby Boomer, that navel-gazing cohort now passing from the scene while pretending it won’t. I never understood my generation when it was claiming to overturn the universe in the 1960s. Now its members write and read books with chirpy titles like “Amazing Aging!” as though – because we are so wonderfully special – age, infirmity, and decline will repeal themselves just for us.
Well, anyone can dream.
I go into the office a couple of half-days a week, when I’m in town. I like bantering with the gang and chatting with old patients. They wish me well and hope I’ll refer them to someone worthy when I hang them up for good, as many of their (and my) doctors already have.
Here is one thing I don’t do all day – manage human resource issues in the office. What’s to miss?
Now and then, with lessening frequency, I muse, “Well, if I do get bored, I can always spend more time in the office.”
Time for another nap.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semi-retired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@mdedge.com.
“So what do you do all day?”
.
Asking what an emeritus does all day sounds fair, but the question is harder to answer than it sounds. Last year, I asked Dave, who was already retired. He took a day to think about it.
“Sometimes I sit on the back porch and watch the birds,” he said.
Dave has long been an avid bird-watcher. Along with golf and Facebook, watching birds is a pursuit that really engages many people, but I never understood it. I still don’t.
Over the years, I’ve met people whose experience of retirement has ranged from, “I’m so busy, I don’t know how I had time to work!” to, “I miss the gang and I’m bored,” to everything in between. Before I (semi-) retired, I made a plan to not make plans, at least at first: No new hobbies, cooking lessons, or anthropology courses. I figured I would figure it out.
So I am figuring it out. No rush. After a lifetime of rushing, not rushing is part of the point.
One hobby I cultivate is napping. I always get up early, no alarm needed. By late morning I am sometimes inclined to lie down for a bit. Taking a midmorning nap has always struck me as one of life’s great pleasures, though one I could rarely enjoy, unless you count dozing off standing up while a patient described an itch that started 17 years before, on a Thursday.
Now I can shut my eyes for half an hour and wake up refreshed, ready for the rest of the day.
During which I will do ...
An older friend of mine, now long gone, wrote a witty essay on being embarrassed to work at home. He refused to answer the phone during the day and hid from the postman. Contemplating retirement, I was afraid I would also feel that way, picturing myself a pitiful pensioner shuffling abroad at mid-day, looking for a park to poison pigeons in. That of course was before “working remotely” became a goal for cool young strivers. You see them around at all hours, with things sticking out of their ears, talking urgently to no one you can see.
Now I also walk the streets proudly at 11 a.m. or 2:45 p.m. I may get one of those earbuds that stick out at 45 degrees, so people can think my ear fungus has grown branches. Maybe they’ll imagine me a mastermind of an international CBD cartel. What they think doesn’t really matter.
One thing that I actually do all day is wonder why I spent so much of my career worrying about what other people think. Dr. Smith used to refer patients. No longer. Did I fail to meet her expectations? Mr. Trelawney came in weekly with itches and pains. No more. Did I roll my eyes too obviously?
Questions like these used to trouble me. Now I can’t recall why. Instead I worry about more important things, like who will play right field for the Red Sox this year.
Though I never signed up, I am an enrolled Baby Boomer, that navel-gazing cohort now passing from the scene while pretending it won’t. I never understood my generation when it was claiming to overturn the universe in the 1960s. Now its members write and read books with chirpy titles like “Amazing Aging!” as though – because we are so wonderfully special – age, infirmity, and decline will repeal themselves just for us.
Well, anyone can dream.
I go into the office a couple of half-days a week, when I’m in town. I like bantering with the gang and chatting with old patients. They wish me well and hope I’ll refer them to someone worthy when I hang them up for good, as many of their (and my) doctors already have.
Here is one thing I don’t do all day – manage human resource issues in the office. What’s to miss?
Now and then, with lessening frequency, I muse, “Well, if I do get bored, I can always spend more time in the office.”
Time for another nap.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semi-retired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@mdedge.com.
“So what do you do all day?”
.
Asking what an emeritus does all day sounds fair, but the question is harder to answer than it sounds. Last year, I asked Dave, who was already retired. He took a day to think about it.
“Sometimes I sit on the back porch and watch the birds,” he said.
Dave has long been an avid bird-watcher. Along with golf and Facebook, watching birds is a pursuit that really engages many people, but I never understood it. I still don’t.
Over the years, I’ve met people whose experience of retirement has ranged from, “I’m so busy, I don’t know how I had time to work!” to, “I miss the gang and I’m bored,” to everything in between. Before I (semi-) retired, I made a plan to not make plans, at least at first: No new hobbies, cooking lessons, or anthropology courses. I figured I would figure it out.
So I am figuring it out. No rush. After a lifetime of rushing, not rushing is part of the point.
One hobby I cultivate is napping. I always get up early, no alarm needed. By late morning I am sometimes inclined to lie down for a bit. Taking a midmorning nap has always struck me as one of life’s great pleasures, though one I could rarely enjoy, unless you count dozing off standing up while a patient described an itch that started 17 years before, on a Thursday.
Now I can shut my eyes for half an hour and wake up refreshed, ready for the rest of the day.
During which I will do ...
An older friend of mine, now long gone, wrote a witty essay on being embarrassed to work at home. He refused to answer the phone during the day and hid from the postman. Contemplating retirement, I was afraid I would also feel that way, picturing myself a pitiful pensioner shuffling abroad at mid-day, looking for a park to poison pigeons in. That of course was before “working remotely” became a goal for cool young strivers. You see them around at all hours, with things sticking out of their ears, talking urgently to no one you can see.
Now I also walk the streets proudly at 11 a.m. or 2:45 p.m. I may get one of those earbuds that stick out at 45 degrees, so people can think my ear fungus has grown branches. Maybe they’ll imagine me a mastermind of an international CBD cartel. What they think doesn’t really matter.
One thing that I actually do all day is wonder why I spent so much of my career worrying about what other people think. Dr. Smith used to refer patients. No longer. Did I fail to meet her expectations? Mr. Trelawney came in weekly with itches and pains. No more. Did I roll my eyes too obviously?
Questions like these used to trouble me. Now I can’t recall why. Instead I worry about more important things, like who will play right field for the Red Sox this year.
Though I never signed up, I am an enrolled Baby Boomer, that navel-gazing cohort now passing from the scene while pretending it won’t. I never understood my generation when it was claiming to overturn the universe in the 1960s. Now its members write and read books with chirpy titles like “Amazing Aging!” as though – because we are so wonderfully special – age, infirmity, and decline will repeal themselves just for us.
Well, anyone can dream.
I go into the office a couple of half-days a week, when I’m in town. I like bantering with the gang and chatting with old patients. They wish me well and hope I’ll refer them to someone worthy when I hang them up for good, as many of their (and my) doctors already have.
Here is one thing I don’t do all day – manage human resource issues in the office. What’s to miss?
Now and then, with lessening frequency, I muse, “Well, if I do get bored, I can always spend more time in the office.”
Time for another nap.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semi-retired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@mdedge.com.
A 7-month-old male presents with perioral rash and fever
Patients with atopic dermatitis are at risk for developing the herpes simplex virus (HSV)–related skin complication “eczema herpeticum,” also known as Kaposi’s varicelliform eruption. Eczema herpeticum is characterized by cutaneous pain and vesicular skin lesions, most commonly secondary to infection with HSV-1. The condition may affect individuals with atopic dermatitis or other inflammatory skin disorders. Eczema herpeticum develops when the virus infects large areas of skin, rather than being confined to a small area as in the common cold sore. Eczema herpeticum often appears on the face and neck, although it can appear anywhere on the body. In some cases, the rash may be difficult to distinguish from a patient’s baseline eczema if the latter is poorly controlled. Skin symptoms of eczema herpeticum include clusters of small blisters that are itchy and painful; vesicles that appear red, purple, or black; purulent blisters; or crusting. Classically, the morphology of vesicles or crusted lesions shows a “cluster of grapes” appearance. Eczema herpeticum may present with a high fever, chills, and swollen lymph glands.

While a clinical diagnosis based on the history, physical findings, and morphologic appearance of the rash is reasonable, testing may confirm the diagnosis. The most sensitive and specific tests are polymerase chain reaction sequencing for HSV, direct fluorescent antibody stain, and/or viral culture, while Tzanck smear may show characteristic histologic changes. Treatment is with oral antiviral therapy and treatment of the eczema.
Hand, foot, and mouth disease (HFMD) is a common viral illness usually affecting infants and children. The infection often involves the hands, feet, mouth, and sometimes, the genitals and buttocks. The viral exanthem is most commonly caused by the coxsackievirus, of the enterovirus family. Coxsackievirus A16 and enterovirus A71 are the serotypes that are most commonly implicated as the causative agents. HFMD initially presents with a low-grade fever, reduced appetite, and general malaise. About 1-2 days later, the child may develop painful mouth sores with an exanthem that involves the dorsum of the hands, soles of the feet, buttocks, legs, and arms. The exanthem consists of vesicles surrounded by a thin halo of erythema, eventually rupturing and forming superficial ulcers with a gray-yellow base and erythematous rim. The exanthem is itchy, and can be macular, papular, or vesicular. The lesions are nonpruritic, and typically not painful. The diagnosis of HFMD usually is made clinically, although a physician can swab the mouth or get a stool sample for polymerase chain reaction, which will show the virus; treatment is supportive. In children with atopic dermatitis, lesions also can tend to concentrate in areas previously or currently affected by the dermatitis, similar to eczema herpeticum, and the terms eczema coxsackium or atypical HFMD are applicable. In young adults, the disease may present with erythematous papulovesicular lesions on the face, oral mucosa, extensor surfaces of the upper and lower extremities, and palms and soles; confluent, hemorrhagic, and crusted lesions also can be seen on the extremities. Systemic symptoms usually subside in a few days; the skin lesions resolve without scarring in days to weeks.

Secondary bacterial infection is not uncommon in eczema herpeticum patients, reflecting common Staphylococcus aureus infection in atopic dermatitis patients. Streptococcus also may be seen as a concurrent infection. Treatment of secondary bacterial infection may be considered based on clinic context and culture.
Impetiginized eczema also is in the differential diagnosis of eczema herpeticum. S. aureus and Streptococci are the most important causative organisms. Lesions can manifest as a single red papule or macule that quickly becomes vesicular or eroded. Subsequently, the content dries, forming honey-colored crusts. Impetigo may resolve spontaneously, although in the context of infected eczema both topical anti-inflammatory agents (e.g. topical corticosteroids) along with systemic antibiotics may be a reasonable treatment option. Although our patient had honey-colored crusting, the wound culture showed normal bacterial flora.

Primary varicella infection causes acute fever and rash, with an initial exanthem of disseminated pruritic erythematous macules that progress beyond the papular stage, forming clear, fluid-filled vesicles (like dewdrops on a rose petal). In children, the rash presents on the stomach, back, and face, and then spreads to other parts of the body. Blisters also can arise inside the mouth.
In this patient, perioral HSV PCR 1 was positive, and wound culture showed normal oral flora with no organisms or white blood cells seen. The patient responded well to oral acyclovir, and treatment of his underlying atopic dermatitis with low-potency topical corticosteroids.
Dr. Bhatti is a research fellow in pediatric dermatology at Rady Children’s Hospital and the University of California, San Diego. Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego. He is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego. Neither of the physicians had relevant financial disclosures. Email them at pdnews@mdedge.com.
Sources
Can Fam Physician. 2012 Dec;58(12):1358-61.
William L Weston, MD., William Howe, MD. UpToDate. Treatment of atopic dermatitis (eczema).
Christine Johnson, MD, Anna Wald, MD, MPH. UpToDate. Epidemiology, clinical manifestations, and diagnosis of herpes simplex virus type 1 infection.
Robert Sidbury, MD, MPH. UpToDate. Atypical exanthems in children.
National Eczema Association. Eczema herpeticum.
Centers for Disease Control and Prevention. Symptoms and diagnosis of hand, foot, and mouth disease (HFMD).
Patients with atopic dermatitis are at risk for developing the herpes simplex virus (HSV)–related skin complication “eczema herpeticum,” also known as Kaposi’s varicelliform eruption. Eczema herpeticum is characterized by cutaneous pain and vesicular skin lesions, most commonly secondary to infection with HSV-1. The condition may affect individuals with atopic dermatitis or other inflammatory skin disorders. Eczema herpeticum develops when the virus infects large areas of skin, rather than being confined to a small area as in the common cold sore. Eczema herpeticum often appears on the face and neck, although it can appear anywhere on the body. In some cases, the rash may be difficult to distinguish from a patient’s baseline eczema if the latter is poorly controlled. Skin symptoms of eczema herpeticum include clusters of small blisters that are itchy and painful; vesicles that appear red, purple, or black; purulent blisters; or crusting. Classically, the morphology of vesicles or crusted lesions shows a “cluster of grapes” appearance. Eczema herpeticum may present with a high fever, chills, and swollen lymph glands.
While a clinical diagnosis based on the history, physical findings, and morphologic appearance of the rash is reasonable, testing may confirm the diagnosis. The most sensitive and specific tests are polymerase chain reaction sequencing for HSV, direct fluorescent antibody stain, and/or viral culture, while Tzanck smear may show characteristic histologic changes. Treatment is with oral antiviral therapy and treatment of the eczema.
Hand, foot, and mouth disease (HFMD) is a common viral illness usually affecting infants and children. The infection often involves the hands, feet, mouth, and sometimes, the genitals and buttocks. The viral exanthem is most commonly caused by the coxsackievirus, of the enterovirus family. Coxsackievirus A16 and enterovirus A71 are the serotypes that are most commonly implicated as the causative agents. HFMD initially presents with a low-grade fever, reduced appetite, and general malaise. About 1-2 days later, the child may develop painful mouth sores with an exanthem that involves the dorsum of the hands, soles of the feet, buttocks, legs, and arms. The exanthem consists of vesicles surrounded by a thin halo of erythema, eventually rupturing and forming superficial ulcers with a gray-yellow base and erythematous rim. The exanthem is itchy, and can be macular, papular, or vesicular. The lesions are nonpruritic, and typically not painful. The diagnosis of HFMD usually is made clinically, although a physician can swab the mouth or get a stool sample for polymerase chain reaction, which will show the virus; treatment is supportive. In children with atopic dermatitis, lesions also can tend to concentrate in areas previously or currently affected by the dermatitis, similar to eczema herpeticum, and the terms eczema coxsackium or atypical HFMD are applicable. In young adults, the disease may present with erythematous papulovesicular lesions on the face, oral mucosa, extensor surfaces of the upper and lower extremities, and palms and soles; confluent, hemorrhagic, and crusted lesions also can be seen on the extremities. Systemic symptoms usually subside in a few days; the skin lesions resolve without scarring in days to weeks.
Secondary bacterial infection is not uncommon in eczema herpeticum patients, reflecting common Staphylococcus aureus infection in atopic dermatitis patients. Streptococcus also may be seen as a concurrent infection. Treatment of secondary bacterial infection may be considered based on clinic context and culture.
Impetiginized eczema also is in the differential diagnosis of eczema herpeticum. S. aureus and Streptococci are the most important causative organisms. Lesions can manifest as a single red papule or macule that quickly becomes vesicular or eroded. Subsequently, the content dries, forming honey-colored crusts. Impetigo may resolve spontaneously, although in the context of infected eczema both topical anti-inflammatory agents (e.g. topical corticosteroids) along with systemic antibiotics may be a reasonable treatment option. Although our patient had honey-colored crusting, the wound culture showed normal bacterial flora.
Primary varicella infection causes acute fever and rash, with an initial exanthem of disseminated pruritic erythematous macules that progress beyond the papular stage, forming clear, fluid-filled vesicles (like dewdrops on a rose petal). In children, the rash presents on the stomach, back, and face, and then spreads to other parts of the body. Blisters also can arise inside the mouth.
In this patient, perioral HSV PCR 1 was positive, and wound culture showed normal oral flora with no organisms or white blood cells seen. The patient responded well to oral acyclovir, and treatment of his underlying atopic dermatitis with low-potency topical corticosteroids.
Dr. Bhatti is a research fellow in pediatric dermatology at Rady Children’s Hospital and the University of California, San Diego. Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego. He is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego. Neither of the physicians had relevant financial disclosures. Email them at pdnews@mdedge.com.
Sources
Can Fam Physician. 2012 Dec;58(12):1358-61.
William L Weston, MD., William Howe, MD. UpToDate. Treatment of atopic dermatitis (eczema).
Christine Johnson, MD, Anna Wald, MD, MPH. UpToDate. Epidemiology, clinical manifestations, and diagnosis of herpes simplex virus type 1 infection.
Robert Sidbury, MD, MPH. UpToDate. Atypical exanthems in children.
National Eczema Association. Eczema herpeticum.
Centers for Disease Control and Prevention. Symptoms and diagnosis of hand, foot, and mouth disease (HFMD).
Patients with atopic dermatitis are at risk for developing the herpes simplex virus (HSV)–related skin complication “eczema herpeticum,” also known as Kaposi’s varicelliform eruption. Eczema herpeticum is characterized by cutaneous pain and vesicular skin lesions, most commonly secondary to infection with HSV-1. The condition may affect individuals with atopic dermatitis or other inflammatory skin disorders. Eczema herpeticum develops when the virus infects large areas of skin, rather than being confined to a small area as in the common cold sore. Eczema herpeticum often appears on the face and neck, although it can appear anywhere on the body. In some cases, the rash may be difficult to distinguish from a patient’s baseline eczema if the latter is poorly controlled. Skin symptoms of eczema herpeticum include clusters of small blisters that are itchy and painful; vesicles that appear red, purple, or black; purulent blisters; or crusting. Classically, the morphology of vesicles or crusted lesions shows a “cluster of grapes” appearance. Eczema herpeticum may present with a high fever, chills, and swollen lymph glands.
While a clinical diagnosis based on the history, physical findings, and morphologic appearance of the rash is reasonable, testing may confirm the diagnosis. The most sensitive and specific tests are polymerase chain reaction sequencing for HSV, direct fluorescent antibody stain, and/or viral culture, while Tzanck smear may show characteristic histologic changes. Treatment is with oral antiviral therapy and treatment of the eczema.
Hand, foot, and mouth disease (HFMD) is a common viral illness usually affecting infants and children. The infection often involves the hands, feet, mouth, and sometimes, the genitals and buttocks. The viral exanthem is most commonly caused by the coxsackievirus, of the enterovirus family. Coxsackievirus A16 and enterovirus A71 are the serotypes that are most commonly implicated as the causative agents. HFMD initially presents with a low-grade fever, reduced appetite, and general malaise. About 1-2 days later, the child may develop painful mouth sores with an exanthem that involves the dorsum of the hands, soles of the feet, buttocks, legs, and arms. The exanthem consists of vesicles surrounded by a thin halo of erythema, eventually rupturing and forming superficial ulcers with a gray-yellow base and erythematous rim. The exanthem is itchy, and can be macular, papular, or vesicular. The lesions are nonpruritic, and typically not painful. The diagnosis of HFMD usually is made clinically, although a physician can swab the mouth or get a stool sample for polymerase chain reaction, which will show the virus; treatment is supportive. In children with atopic dermatitis, lesions also can tend to concentrate in areas previously or currently affected by the dermatitis, similar to eczema herpeticum, and the terms eczema coxsackium or atypical HFMD are applicable. In young adults, the disease may present with erythematous papulovesicular lesions on the face, oral mucosa, extensor surfaces of the upper and lower extremities, and palms and soles; confluent, hemorrhagic, and crusted lesions also can be seen on the extremities. Systemic symptoms usually subside in a few days; the skin lesions resolve without scarring in days to weeks.
Secondary bacterial infection is not uncommon in eczema herpeticum patients, reflecting common Staphylococcus aureus infection in atopic dermatitis patients. Streptococcus also may be seen as a concurrent infection. Treatment of secondary bacterial infection may be considered based on clinic context and culture.
Impetiginized eczema also is in the differential diagnosis of eczema herpeticum. S. aureus and Streptococci are the most important causative organisms. Lesions can manifest as a single red papule or macule that quickly becomes vesicular or eroded. Subsequently, the content dries, forming honey-colored crusts. Impetigo may resolve spontaneously, although in the context of infected eczema both topical anti-inflammatory agents (e.g. topical corticosteroids) along with systemic antibiotics may be a reasonable treatment option. Although our patient had honey-colored crusting, the wound culture showed normal bacterial flora.
Primary varicella infection causes acute fever and rash, with an initial exanthem of disseminated pruritic erythematous macules that progress beyond the papular stage, forming clear, fluid-filled vesicles (like dewdrops on a rose petal). In children, the rash presents on the stomach, back, and face, and then spreads to other parts of the body. Blisters also can arise inside the mouth.
In this patient, perioral HSV PCR 1 was positive, and wound culture showed normal oral flora with no organisms or white blood cells seen. The patient responded well to oral acyclovir, and treatment of his underlying atopic dermatitis with low-potency topical corticosteroids.
Dr. Bhatti is a research fellow in pediatric dermatology at Rady Children’s Hospital and the University of California, San Diego. Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego. He is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego. Neither of the physicians had relevant financial disclosures. Email them at pdnews@mdedge.com.
Sources
Can Fam Physician. 2012 Dec;58(12):1358-61.
William L Weston, MD., William Howe, MD. UpToDate. Treatment of atopic dermatitis (eczema).
Christine Johnson, MD, Anna Wald, MD, MPH. UpToDate. Epidemiology, clinical manifestations, and diagnosis of herpes simplex virus type 1 infection.
Robert Sidbury, MD, MPH. UpToDate. Atypical exanthems in children.
National Eczema Association. Eczema herpeticum.
Centers for Disease Control and Prevention. Symptoms and diagnosis of hand, foot, and mouth disease (HFMD).

The pros and cons of pathology lab ownership: What early career GI doctors need to know
From colonoscopies to endoscopic ultrasound, gastroenterology is fundamentally a procedure-based specialty. Given that reality, making a decision to have as much control as possible over the entire process just makes sense for many GI practices.
Back in 2008, I was in charge of the process to develop a pathology lab at Arizona Digestive Health, a physician group with 26 locations throughout the state, as part of our decision to form a supergroup with eight ambulatory surgery centers. For us, having ambulatory surgery centers had been a game changer. We learned we could double our efficiency with procedures when we controlled the process from start to finish. We began to consider other processes – in this case pathology – that we could improve.
Prior to running our own pathology lab, doctors who read our slides were general pathologists who did not always understand the language of gastroenterology. We had results that came back by fax that were often cumbersome to read and did not always give us the information we needed in the way we needed it. Consistency was a problem. We knew we needed a change.
I cannot lie – setting up and running your own pathology lab is not always easy. But with the right factors in place, here are some benefits to consider when you are making a decision about joining a practice.
Quality, efficiency can lead to opportunity
Our lab has three GI fellowship–trained pathologists reading our slides. That means they are highly specialized and know exactly what we are looking for in a pathology report. We have a 24-hour turnaround for results. A courier service delivers biopsy specimens from our endoscopy centers to our path lab every day, and each morning our gastropathologists have a stack of pathology slides waiting for them. It’s added predictability and stability to the process, and we get the level of quality, specificity, and uniformity we need in a report.
The efficiencies are beneficial and it has given us more leverage in our negotiations with payers. We know what our costs are and have great quality metrics as well as read rates that we can provide. This signals to health plans that quality is a top priority for us.
We have also gained a reputational benefit with patients. Although much of the work is happening behind the scenes for our patients, they get results faster and a consistency with costs. It also allows us to easily access the slides of patients we have been seeing for years, giving us a richer data set and more confidence in our diagnosis.
Now that we have our own lab, we can look at our pathology data and conduct studies that will benefit all patients. For example, a few of our GI fellows were able to work with our pathologists to conduct a study on adenoma detection rates, exhausting a tissue block when no adenoma was found on initial review. We found a significant increase in adenoma detection using this method; we plan to publish results soon. The ability to conduct this kind of research is worth considering when early career gastroenterologists are selecting a practice to join.
And last but not least, having our own pathology lab acts as a unifying force for our group, which is spread out across 26 offices. When diagnoses are available and we get a call from our pathologist, we know to pick up the phone immediately.
What to consider before jumping in
Setting up our own pathology lab from the ground up was a learning process. We had enough patient volume for the move to make sense, so it is possible that smaller practices might not be able to make the investment if they have lower patient volume or cannot control their specimen flow. One option is to set up a technical lab and contract out for the slide reading. We felt it was important for our pathologists to also be our practice partners, and time has proven this to be a good decision for us.
We designed a lab with our work flow in mind, and it helped to have a pathologist on board from the beginning who knows gastroenterology. We even created our own lab information system with the help of a software engineer. It took a little bit over a year from conception to a functioning comprehensive lab.
Of course, there are regulatory factors to consider – the federal physician self-referral (Stark) law and the federal Anti-Markup Rule – come to mind. But we made sure to get a legal opinion that allows us to comply with the law. That’s something anyone who wants to make a move in this direction should do.
Looking back over the experience, I would not do anything differently. Yes, there are startup costs and a learning curve. But the quality we get from having our own pathology lab dedicated to GI and the efficiencies we have gained are well worth it.
Dr. Berggreen is the president of Arizona Digestive Health and chief strategy officer of the GI Alliance. He is also a board member of the Digestive Health Physicians Association. He received his doctorate at Louisiana State University, New Orleans. He is the former site director of the Good Samaritan GI Fellowship Program and named one of Phoenix Magazine’s “Top Docs.”
From colonoscopies to endoscopic ultrasound, gastroenterology is fundamentally a procedure-based specialty. Given that reality, making a decision to have as much control as possible over the entire process just makes sense for many GI practices.
Back in 2008, I was in charge of the process to develop a pathology lab at Arizona Digestive Health, a physician group with 26 locations throughout the state, as part of our decision to form a supergroup with eight ambulatory surgery centers. For us, having ambulatory surgery centers had been a game changer. We learned we could double our efficiency with procedures when we controlled the process from start to finish. We began to consider other processes – in this case pathology – that we could improve.
Prior to running our own pathology lab, doctors who read our slides were general pathologists who did not always understand the language of gastroenterology. We had results that came back by fax that were often cumbersome to read and did not always give us the information we needed in the way we needed it. Consistency was a problem. We knew we needed a change.
I cannot lie – setting up and running your own pathology lab is not always easy. But with the right factors in place, here are some benefits to consider when you are making a decision about joining a practice.
Quality, efficiency can lead to opportunity
Our lab has three GI fellowship–trained pathologists reading our slides. That means they are highly specialized and know exactly what we are looking for in a pathology report. We have a 24-hour turnaround for results. A courier service delivers biopsy specimens from our endoscopy centers to our path lab every day, and each morning our gastropathologists have a stack of pathology slides waiting for them. It’s added predictability and stability to the process, and we get the level of quality, specificity, and uniformity we need in a report.
The efficiencies are beneficial and it has given us more leverage in our negotiations with payers. We know what our costs are and have great quality metrics as well as read rates that we can provide. This signals to health plans that quality is a top priority for us.
We have also gained a reputational benefit with patients. Although much of the work is happening behind the scenes for our patients, they get results faster and a consistency with costs. It also allows us to easily access the slides of patients we have been seeing for years, giving us a richer data set and more confidence in our diagnosis.
Now that we have our own lab, we can look at our pathology data and conduct studies that will benefit all patients. For example, a few of our GI fellows were able to work with our pathologists to conduct a study on adenoma detection rates, exhausting a tissue block when no adenoma was found on initial review. We found a significant increase in adenoma detection using this method; we plan to publish results soon. The ability to conduct this kind of research is worth considering when early career gastroenterologists are selecting a practice to join.
And last but not least, having our own pathology lab acts as a unifying force for our group, which is spread out across 26 offices. When diagnoses are available and we get a call from our pathologist, we know to pick up the phone immediately.
What to consider before jumping in
Setting up our own pathology lab from the ground up was a learning process. We had enough patient volume for the move to make sense, so it is possible that smaller practices might not be able to make the investment if they have lower patient volume or cannot control their specimen flow. One option is to set up a technical lab and contract out for the slide reading. We felt it was important for our pathologists to also be our practice partners, and time has proven this to be a good decision for us.
We designed a lab with our work flow in mind, and it helped to have a pathologist on board from the beginning who knows gastroenterology. We even created our own lab information system with the help of a software engineer. It took a little bit over a year from conception to a functioning comprehensive lab.
Of course, there are regulatory factors to consider – the federal physician self-referral (Stark) law and the federal Anti-Markup Rule – come to mind. But we made sure to get a legal opinion that allows us to comply with the law. That’s something anyone who wants to make a move in this direction should do.
Looking back over the experience, I would not do anything differently. Yes, there are startup costs and a learning curve. But the quality we get from having our own pathology lab dedicated to GI and the efficiencies we have gained are well worth it.
Dr. Berggreen is the president of Arizona Digestive Health and chief strategy officer of the GI Alliance. He is also a board member of the Digestive Health Physicians Association. He received his doctorate at Louisiana State University, New Orleans. He is the former site director of the Good Samaritan GI Fellowship Program and named one of Phoenix Magazine’s “Top Docs.”
From colonoscopies to endoscopic ultrasound, gastroenterology is fundamentally a procedure-based specialty. Given that reality, making a decision to have as much control as possible over the entire process just makes sense for many GI practices.
Back in 2008, I was in charge of the process to develop a pathology lab at Arizona Digestive Health, a physician group with 26 locations throughout the state, as part of our decision to form a supergroup with eight ambulatory surgery centers. For us, having ambulatory surgery centers had been a game changer. We learned we could double our efficiency with procedures when we controlled the process from start to finish. We began to consider other processes – in this case pathology – that we could improve.
Prior to running our own pathology lab, doctors who read our slides were general pathologists who did not always understand the language of gastroenterology. We had results that came back by fax that were often cumbersome to read and did not always give us the information we needed in the way we needed it. Consistency was a problem. We knew we needed a change.
I cannot lie – setting up and running your own pathology lab is not always easy. But with the right factors in place, here are some benefits to consider when you are making a decision about joining a practice.
Quality, efficiency can lead to opportunity
Our lab has three GI fellowship–trained pathologists reading our slides. That means they are highly specialized and know exactly what we are looking for in a pathology report. We have a 24-hour turnaround for results. A courier service delivers biopsy specimens from our endoscopy centers to our path lab every day, and each morning our gastropathologists have a stack of pathology slides waiting for them. It’s added predictability and stability to the process, and we get the level of quality, specificity, and uniformity we need in a report.
The efficiencies are beneficial and it has given us more leverage in our negotiations with payers. We know what our costs are and have great quality metrics as well as read rates that we can provide. This signals to health plans that quality is a top priority for us.
We have also gained a reputational benefit with patients. Although much of the work is happening behind the scenes for our patients, they get results faster and a consistency with costs. It also allows us to easily access the slides of patients we have been seeing for years, giving us a richer data set and more confidence in our diagnosis.
Now that we have our own lab, we can look at our pathology data and conduct studies that will benefit all patients. For example, a few of our GI fellows were able to work with our pathologists to conduct a study on adenoma detection rates, exhausting a tissue block when no adenoma was found on initial review. We found a significant increase in adenoma detection using this method; we plan to publish results soon. The ability to conduct this kind of research is worth considering when early career gastroenterologists are selecting a practice to join.
And last but not least, having our own pathology lab acts as a unifying force for our group, which is spread out across 26 offices. When diagnoses are available and we get a call from our pathologist, we know to pick up the phone immediately.
What to consider before jumping in
Setting up our own pathology lab from the ground up was a learning process. We had enough patient volume for the move to make sense, so it is possible that smaller practices might not be able to make the investment if they have lower patient volume or cannot control their specimen flow. One option is to set up a technical lab and contract out for the slide reading. We felt it was important for our pathologists to also be our practice partners, and time has proven this to be a good decision for us.
We designed a lab with our work flow in mind, and it helped to have a pathologist on board from the beginning who knows gastroenterology. We even created our own lab information system with the help of a software engineer. It took a little bit over a year from conception to a functioning comprehensive lab.
Of course, there are regulatory factors to consider – the federal physician self-referral (Stark) law and the federal Anti-Markup Rule – come to mind. But we made sure to get a legal opinion that allows us to comply with the law. That’s something anyone who wants to make a move in this direction should do.
Looking back over the experience, I would not do anything differently. Yes, there are startup costs and a learning curve. But the quality we get from having our own pathology lab dedicated to GI and the efficiencies we have gained are well worth it.
Dr. Berggreen is the president of Arizona Digestive Health and chief strategy officer of the GI Alliance. He is also a board member of the Digestive Health Physicians Association. He received his doctorate at Louisiana State University, New Orleans. He is the former site director of the Good Samaritan GI Fellowship Program and named one of Phoenix Magazine’s “Top Docs.”
The role of medication in autism spectrum disorder
Efforts toward early identification and treatment are an important facet of the public health work in autism spectrum disorder (ASD).

The prevalence of ASD is rising. With the most recent estimate from the Centers from Disease Control and Prevention of 1 in 59* children aged 8 years,1 it is important for pediatric health care providers to have an understanding of current recommendations for treatment so they can counsel and guide affected families. ASD is a heterogeneous condition, so this article seeks to touch on broad principles, recognizing that clinicians must take into account the full clinical picture of each individual and family.
It is important to acknowledge that while there is no cure for ASD, there are treatment modalities that have an evidence base for addressing specific areas that may be impaired in children with autism. While it is beyond the scope of this article to review all of the potential areas of intervention in children with ASD, it is important to be keep in mind a few important principles.
1. The best evidenced treatment for addressing challenging and problematic behavior as well as improving a host of outcomes in children with ASD is itself behavioral in nature. These treatments are based on the principles of applied behavioral analysis,2 an educational and therapeutic approach which involves looking at antecedents and consequences of behaviors. This approach also looks to shape, motivate, and reinforce functional behaviors while discouraging harmful and disruptive ones.
2. Because communication often is impaired in children with ASD, providers always should investigate for possible medical causes of pain or discomfort that might explain sudden behavior change, as well as environmental changes that could be involved.
3. – because children with ASD often are particularly sensitive to medication side effects.
Irritability/aggression/extreme mood lability
There are only two medications with Food and Drug Administration labeling for an autism specific condition, and those are aripiprazole and risperidone, two second-generation antipsychotic agents approved for irritability associated with ASD on the basis of randomized controlled trials (RCTs) demonstrating their efficacy.3,4 Included under the umbrella of irritability are aggression, deliberate self-injurious behavior, extreme temper tantrums, and quick and extreme mood changes. For aripiprazole the approved ages are 6-17 years; a dosing range of 2-15 mg/day is recommended. For risperidone, the approved age range is 5-17 years; the recommended dosing range is 0.25-4 mg/day. Prior to starting either of these medications, a cardiac history should be obtained, and baseline laboratory values, particularly lipid levels and hemoglobin A1c (HbA1c) are recommended. All second-generation antipsychotics carry the risk of tardive dyskinesia (a movement disorder), as well as risk of weight gain and metabolic effects. Baseline weight prior to medication initiation with routine follow-up measurement is encouraged. In light of the burden of potential side effects, these medications tend to be reserved by clinicians for circumstances where there is a significant impact on functioning. Both medications are available in liquid form for children with difficulty swallowing pills.
ADHD
There are positive RCTs of methylphenidate in co-occurring ASD and ADHD,5 making it the preferred first line agent for treatment. Amphetamine salt based stimulant preparations do not have any RCTs in co-occurring ASD, but theoretically should be similarly effective. Again, the principle of starting low and going slow is applicable. Second line are the alpha 2 adrenergic agonists guanfacine and clonidine, both of whose long-acting formulations are approved for treatment of ADHD in children and adolescents without ASD, as well as atomoxetine, a selective norepinephrine reuptake inhibitor approved for ADHD. Guanfacine and atomoxetine have the stronger evidence base in the co-occurring condition. None of the second-line medications come in liquid preparation, although the immediate-release forms of guanfacine and clonidine both can be crushed and are used in clinical practice when the extended-release forms are not practicable.
Anxiety disorders and depression
Repetitive behaviors and insistence on sameness are broad headings that can be thought of as similar to obsessive compulsive disorder in children without ASD. However, controlled studies of SSRIs and clomipramine (a tricyclic antidepressant) have not shown a clear benefit in these behaviors in children with autism. There are no RCTs looking specifically at treatment of anxiety disorders in children with ASD, but expert consensus is that pharmacologic treatment is similar to that of children without ASD, with the SSRIs fluoxetine and sertraline the first-line agents due to the robust evidence for these two medications in treatment of anxiety disorders in children.6 Especially for kids with higher functioning ASD, cognitive behavioral therapy (CBT) should be considered and has some evidence for the co-occurring condition. Similarly, there are no RCTs for co-occurring depression in ASD, and clinical practice is to treat it as you would depression in the non-ASD population. Be aware that the studies of SSRIs in children with ASD reported higher than typical rates of behavioral activation on these medications, and again the principle of starting low and going slow is emphasized. Fluoxetine and sertraline both come in liquid form.
Insomnia
Insomnia is a common occurrence in children with ASD, and studies suggest melatonin can be effective, with immediate release clonidine a consideration with some limited evidence, if melatonin is not successful.

Finally I would be remiss in not mentioning that there is preliminary evidence from review7 and meta-analysis8 articles to suggest that regular exercise for individuals with ASD has a positive effect on multiple symptom domains, suggesting that this is an important additional treatment recommendation for children and families.
In conclusion, identification and treatment of ASD and co-occurring syndromes is often challenging, and while specialty referral often will be necessary, it is hoped that this overview provides a helpful frame of reference for primary care providers who encounter these conditions in clinical practice.
For further reading on this important subject, I recommend the American Academy of Child and Adolescent Psychiatry Practice Parameter for the Assessment and Treatment of Children and Adolescents with ASD and the Parents Medication Guide for Autism Spectrum Disorders.
Dr. Hoffnung is a pediatric psychiatrist at the University of Vermont Children’s Hospital and an assistant professor of psychiatry at the Robert Larner, M.D. College of Medicine at the University of Vermont, both in Burlington. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
References
1. MMWR Surveill Summ 2018;67(No. SS-6):1–23*
2. National Standards Project, Phase 2. National Autism Center 2015.
3. N Engl J Med. 2002 Aug 1;347(5):314-21.
4. J Am Acad Child Adolesc Psychiatry. 2009 Nov;48(11):1110-9.
5. Arch Gen Psychiatry. 2005 Nov;62(11):1266-74.
6. Pediatrics. 2016 Feb;137(Supplement 2):S115-S123.
7. Research in Autism Spectrum Disorders. 2010 Dec;4(4):565-76.
8. Research in Autism Spectrum Disorders. 2012;6(1):46-57.
*This article was updated 4/2/2020.
Efforts toward early identification and treatment are an important facet of the public health work in autism spectrum disorder (ASD).
The prevalence of ASD is rising. With the most recent estimate from the Centers from Disease Control and Prevention of 1 in 59* children aged 8 years,1 it is important for pediatric health care providers to have an understanding of current recommendations for treatment so they can counsel and guide affected families. ASD is a heterogeneous condition, so this article seeks to touch on broad principles, recognizing that clinicians must take into account the full clinical picture of each individual and family.
It is important to acknowledge that while there is no cure for ASD, there are treatment modalities that have an evidence base for addressing specific areas that may be impaired in children with autism. While it is beyond the scope of this article to review all of the potential areas of intervention in children with ASD, it is important to be keep in mind a few important principles.
1. The best evidenced treatment for addressing challenging and problematic behavior as well as improving a host of outcomes in children with ASD is itself behavioral in nature. These treatments are based on the principles of applied behavioral analysis,2 an educational and therapeutic approach which involves looking at antecedents and consequences of behaviors. This approach also looks to shape, motivate, and reinforce functional behaviors while discouraging harmful and disruptive ones.
2. Because communication often is impaired in children with ASD, providers always should investigate for possible medical causes of pain or discomfort that might explain sudden behavior change, as well as environmental changes that could be involved.
3. – because children with ASD often are particularly sensitive to medication side effects.
Irritability/aggression/extreme mood lability
There are only two medications with Food and Drug Administration labeling for an autism specific condition, and those are aripiprazole and risperidone, two second-generation antipsychotic agents approved for irritability associated with ASD on the basis of randomized controlled trials (RCTs) demonstrating their efficacy.3,4 Included under the umbrella of irritability are aggression, deliberate self-injurious behavior, extreme temper tantrums, and quick and extreme mood changes. For aripiprazole the approved ages are 6-17 years; a dosing range of 2-15 mg/day is recommended. For risperidone, the approved age range is 5-17 years; the recommended dosing range is 0.25-4 mg/day. Prior to starting either of these medications, a cardiac history should be obtained, and baseline laboratory values, particularly lipid levels and hemoglobin A1c (HbA1c) are recommended. All second-generation antipsychotics carry the risk of tardive dyskinesia (a movement disorder), as well as risk of weight gain and metabolic effects. Baseline weight prior to medication initiation with routine follow-up measurement is encouraged. In light of the burden of potential side effects, these medications tend to be reserved by clinicians for circumstances where there is a significant impact on functioning. Both medications are available in liquid form for children with difficulty swallowing pills.
ADHD
There are positive RCTs of methylphenidate in co-occurring ASD and ADHD,5 making it the preferred first line agent for treatment. Amphetamine salt based stimulant preparations do not have any RCTs in co-occurring ASD, but theoretically should be similarly effective. Again, the principle of starting low and going slow is applicable. Second line are the alpha 2 adrenergic agonists guanfacine and clonidine, both of whose long-acting formulations are approved for treatment of ADHD in children and adolescents without ASD, as well as atomoxetine, a selective norepinephrine reuptake inhibitor approved for ADHD. Guanfacine and atomoxetine have the stronger evidence base in the co-occurring condition. None of the second-line medications come in liquid preparation, although the immediate-release forms of guanfacine and clonidine both can be crushed and are used in clinical practice when the extended-release forms are not practicable.
Anxiety disorders and depression
Repetitive behaviors and insistence on sameness are broad headings that can be thought of as similar to obsessive compulsive disorder in children without ASD. However, controlled studies of SSRIs and clomipramine (a tricyclic antidepressant) have not shown a clear benefit in these behaviors in children with autism. There are no RCTs looking specifically at treatment of anxiety disorders in children with ASD, but expert consensus is that pharmacologic treatment is similar to that of children without ASD, with the SSRIs fluoxetine and sertraline the first-line agents due to the robust evidence for these two medications in treatment of anxiety disorders in children.6 Especially for kids with higher functioning ASD, cognitive behavioral therapy (CBT) should be considered and has some evidence for the co-occurring condition. Similarly, there are no RCTs for co-occurring depression in ASD, and clinical practice is to treat it as you would depression in the non-ASD population. Be aware that the studies of SSRIs in children with ASD reported higher than typical rates of behavioral activation on these medications, and again the principle of starting low and going slow is emphasized. Fluoxetine and sertraline both come in liquid form.
Insomnia
Insomnia is a common occurrence in children with ASD, and studies suggest melatonin can be effective, with immediate release clonidine a consideration with some limited evidence, if melatonin is not successful.
Finally I would be remiss in not mentioning that there is preliminary evidence from review7 and meta-analysis8 articles to suggest that regular exercise for individuals with ASD has a positive effect on multiple symptom domains, suggesting that this is an important additional treatment recommendation for children and families.
In conclusion, identification and treatment of ASD and co-occurring syndromes is often challenging, and while specialty referral often will be necessary, it is hoped that this overview provides a helpful frame of reference for primary care providers who encounter these conditions in clinical practice.
For further reading on this important subject, I recommend the American Academy of Child and Adolescent Psychiatry Practice Parameter for the Assessment and Treatment of Children and Adolescents with ASD and the Parents Medication Guide for Autism Spectrum Disorders.
Dr. Hoffnung is a pediatric psychiatrist at the University of Vermont Children’s Hospital and an assistant professor of psychiatry at the Robert Larner, M.D. College of Medicine at the University of Vermont, both in Burlington. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
References
1. MMWR Surveill Summ 2018;67(No. SS-6):1–23*
2. National Standards Project, Phase 2. National Autism Center 2015.
3. N Engl J Med. 2002 Aug 1;347(5):314-21.
4. J Am Acad Child Adolesc Psychiatry. 2009 Nov;48(11):1110-9.
5. Arch Gen Psychiatry. 2005 Nov;62(11):1266-74.
6. Pediatrics. 2016 Feb;137(Supplement 2):S115-S123.
7. Research in Autism Spectrum Disorders. 2010 Dec;4(4):565-76.
8. Research in Autism Spectrum Disorders. 2012;6(1):46-57.
*This article was updated 4/2/2020.
Efforts toward early identification and treatment are an important facet of the public health work in autism spectrum disorder (ASD).
The prevalence of ASD is rising. With the most recent estimate from the Centers from Disease Control and Prevention of 1 in 59* children aged 8 years,1 it is important for pediatric health care providers to have an understanding of current recommendations for treatment so they can counsel and guide affected families. ASD is a heterogeneous condition, so this article seeks to touch on broad principles, recognizing that clinicians must take into account the full clinical picture of each individual and family.
It is important to acknowledge that while there is no cure for ASD, there are treatment modalities that have an evidence base for addressing specific areas that may be impaired in children with autism. While it is beyond the scope of this article to review all of the potential areas of intervention in children with ASD, it is important to be keep in mind a few important principles.
1. The best evidenced treatment for addressing challenging and problematic behavior as well as improving a host of outcomes in children with ASD is itself behavioral in nature. These treatments are based on the principles of applied behavioral analysis,2 an educational and therapeutic approach which involves looking at antecedents and consequences of behaviors. This approach also looks to shape, motivate, and reinforce functional behaviors while discouraging harmful and disruptive ones.
2. Because communication often is impaired in children with ASD, providers always should investigate for possible medical causes of pain or discomfort that might explain sudden behavior change, as well as environmental changes that could be involved.
3. – because children with ASD often are particularly sensitive to medication side effects.
Irritability/aggression/extreme mood lability
There are only two medications with Food and Drug Administration labeling for an autism specific condition, and those are aripiprazole and risperidone, two second-generation antipsychotic agents approved for irritability associated with ASD on the basis of randomized controlled trials (RCTs) demonstrating their efficacy.3,4 Included under the umbrella of irritability are aggression, deliberate self-injurious behavior, extreme temper tantrums, and quick and extreme mood changes. For aripiprazole the approved ages are 6-17 years; a dosing range of 2-15 mg/day is recommended. For risperidone, the approved age range is 5-17 years; the recommended dosing range is 0.25-4 mg/day. Prior to starting either of these medications, a cardiac history should be obtained, and baseline laboratory values, particularly lipid levels and hemoglobin A1c (HbA1c) are recommended. All second-generation antipsychotics carry the risk of tardive dyskinesia (a movement disorder), as well as risk of weight gain and metabolic effects. Baseline weight prior to medication initiation with routine follow-up measurement is encouraged. In light of the burden of potential side effects, these medications tend to be reserved by clinicians for circumstances where there is a significant impact on functioning. Both medications are available in liquid form for children with difficulty swallowing pills.
ADHD
There are positive RCTs of methylphenidate in co-occurring ASD and ADHD,5 making it the preferred first line agent for treatment. Amphetamine salt based stimulant preparations do not have any RCTs in co-occurring ASD, but theoretically should be similarly effective. Again, the principle of starting low and going slow is applicable. Second line are the alpha 2 adrenergic agonists guanfacine and clonidine, both of whose long-acting formulations are approved for treatment of ADHD in children and adolescents without ASD, as well as atomoxetine, a selective norepinephrine reuptake inhibitor approved for ADHD. Guanfacine and atomoxetine have the stronger evidence base in the co-occurring condition. None of the second-line medications come in liquid preparation, although the immediate-release forms of guanfacine and clonidine both can be crushed and are used in clinical practice when the extended-release forms are not practicable.
Anxiety disorders and depression
Repetitive behaviors and insistence on sameness are broad headings that can be thought of as similar to obsessive compulsive disorder in children without ASD. However, controlled studies of SSRIs and clomipramine (a tricyclic antidepressant) have not shown a clear benefit in these behaviors in children with autism. There are no RCTs looking specifically at treatment of anxiety disorders in children with ASD, but expert consensus is that pharmacologic treatment is similar to that of children without ASD, with the SSRIs fluoxetine and sertraline the first-line agents due to the robust evidence for these two medications in treatment of anxiety disorders in children.6 Especially for kids with higher functioning ASD, cognitive behavioral therapy (CBT) should be considered and has some evidence for the co-occurring condition. Similarly, there are no RCTs for co-occurring depression in ASD, and clinical practice is to treat it as you would depression in the non-ASD population. Be aware that the studies of SSRIs in children with ASD reported higher than typical rates of behavioral activation on these medications, and again the principle of starting low and going slow is emphasized. Fluoxetine and sertraline both come in liquid form.
Insomnia
Insomnia is a common occurrence in children with ASD, and studies suggest melatonin can be effective, with immediate release clonidine a consideration with some limited evidence, if melatonin is not successful.
Finally I would be remiss in not mentioning that there is preliminary evidence from review7 and meta-analysis8 articles to suggest that regular exercise for individuals with ASD has a positive effect on multiple symptom domains, suggesting that this is an important additional treatment recommendation for children and families.
In conclusion, identification and treatment of ASD and co-occurring syndromes is often challenging, and while specialty referral often will be necessary, it is hoped that this overview provides a helpful frame of reference for primary care providers who encounter these conditions in clinical practice.
For further reading on this important subject, I recommend the American Academy of Child and Adolescent Psychiatry Practice Parameter for the Assessment and Treatment of Children and Adolescents with ASD and the Parents Medication Guide for Autism Spectrum Disorders.
Dr. Hoffnung is a pediatric psychiatrist at the University of Vermont Children’s Hospital and an assistant professor of psychiatry at the Robert Larner, M.D. College of Medicine at the University of Vermont, both in Burlington. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
References
1. MMWR Surveill Summ 2018;67(No. SS-6):1–23*
2. National Standards Project, Phase 2. National Autism Center 2015.
3. N Engl J Med. 2002 Aug 1;347(5):314-21.
4. J Am Acad Child Adolesc Psychiatry. 2009 Nov;48(11):1110-9.
5. Arch Gen Psychiatry. 2005 Nov;62(11):1266-74.
6. Pediatrics. 2016 Feb;137(Supplement 2):S115-S123.
7. Research in Autism Spectrum Disorders. 2010 Dec;4(4):565-76.
8. Research in Autism Spectrum Disorders. 2012;6(1):46-57.
*This article was updated 4/2/2020.
Medical identity theft
In his book, “Scam Me If You Can,” fraud expert Frank Abagnale relates the case of a 5-year-old boy whose pediatrician’s computer was hacked, compromising his name, birth date, Social Security number, insurance information, and medical records. The result was a bureaucratic nightmare that may well continue for the rest of that unfortunate young patient’s life. One can only speculate on the difficulties he might have as adult in obtaining a line of credit, or in proving his medical identity to physicians and hospitals.

– your Social Security number, bank account numbers, etc. – sells for about $25 on the black market; add health insurance and medical records, and the price can jump to $1,000 or more. That’s because there is a far greater potential yield from medical identity theft – and once your personal information and medical records are breached, they are in the Cloud for the rest of your life, available to anyone who wants to buy them. Older patients are particularly vulnerable: Medicare billing scams cost taxpayers more than $60 billion a year.
If your office’s computer system does not have effective fraud protection, you could be held liable for any fraud committed with information stolen from it – and if the information is resold years later and reused to commit more fraud, you’ll be liable for that, too. That’s why I strongly recommend that you invest in high-quality security technology and software, so that in the event of a breach, the security company will at least share in the fault and the liability. (As always, I have no financial interest in any product or industry mentioned in this column.)
Even with adequate protection, breaches can still occur, so all medical offices should have a breach response plan in place, covering how to halt security breaches, and how to handle any lost or stolen data. Your computer and security vendors can help with formulating such a plan. Patients affected by a breach need to be contacted as well, so they may put a freeze on accounts or send out fraud alerts.
Patients also need to be aware of the risks. If your EHR includes an online portal to communicate protected information to patients, it may be secure on your end, but patients are unlikely to have similar protection on their home computers. If you offer online patient portal services, you should make your patients aware of measures they can take to protect their data once it arrives on their computers or phones.
Patients should also be warned of the risks that come with sharing medical information with others. If they are asked to reveal medical data via phone or email, they need to ask who is requesting it, and why. Any unsolicited calls inquiring about their medical information, from someone who can’t or won’t confirm their identity, should be considered extremely suspicious.
We tell our patients to protect their insurance numbers as carefully as they guard their Social Security number and other valuable data, and to shred any medical paperwork they no longer need, including labels on prescription bottles. And if they see something on an Explanation of Benefits that doesn’t look right, they should question it immediately. We encourage them to take advantage of the free services at MyMedicare.gov, including Medicare Summary Notices provided every 3 months (if any services or medical supplies are received during that period), to make sure they’re being billed only for services they have received.

Your staff should be made aware of the potential for “friendly fraud,” which is defined as theft of identity and medical information by patients’ friends or family members. (According to some studies, as much as 50% of all medical identity theft may be committed this way.) Staffers should never divulge insurance numbers, diagnoses, lab reports, or any other privileged information to family or friends, whether by phone, fax, mail, or in person, without written permission from the patient. And when callers claiming to be patients request information about themselves, your employees should be alert for “red flags.” For example, legitimate patients won’t stumble over simple questions (such as “What is your birth date?”) or request test results or diagnoses that they should already know about.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
In his book, “Scam Me If You Can,” fraud expert Frank Abagnale relates the case of a 5-year-old boy whose pediatrician’s computer was hacked, compromising his name, birth date, Social Security number, insurance information, and medical records. The result was a bureaucratic nightmare that may well continue for the rest of that unfortunate young patient’s life. One can only speculate on the difficulties he might have as adult in obtaining a line of credit, or in proving his medical identity to physicians and hospitals.
– your Social Security number, bank account numbers, etc. – sells for about $25 on the black market; add health insurance and medical records, and the price can jump to $1,000 or more. That’s because there is a far greater potential yield from medical identity theft – and once your personal information and medical records are breached, they are in the Cloud for the rest of your life, available to anyone who wants to buy them. Older patients are particularly vulnerable: Medicare billing scams cost taxpayers more than $60 billion a year.
If your office’s computer system does not have effective fraud protection, you could be held liable for any fraud committed with information stolen from it – and if the information is resold years later and reused to commit more fraud, you’ll be liable for that, too. That’s why I strongly recommend that you invest in high-quality security technology and software, so that in the event of a breach, the security company will at least share in the fault and the liability. (As always, I have no financial interest in any product or industry mentioned in this column.)
Even with adequate protection, breaches can still occur, so all medical offices should have a breach response plan in place, covering how to halt security breaches, and how to handle any lost or stolen data. Your computer and security vendors can help with formulating such a plan. Patients affected by a breach need to be contacted as well, so they may put a freeze on accounts or send out fraud alerts.
Patients also need to be aware of the risks. If your EHR includes an online portal to communicate protected information to patients, it may be secure on your end, but patients are unlikely to have similar protection on their home computers. If you offer online patient portal services, you should make your patients aware of measures they can take to protect their data once it arrives on their computers or phones.
Patients should also be warned of the risks that come with sharing medical information with others. If they are asked to reveal medical data via phone or email, they need to ask who is requesting it, and why. Any unsolicited calls inquiring about their medical information, from someone who can’t or won’t confirm their identity, should be considered extremely suspicious.
We tell our patients to protect their insurance numbers as carefully as they guard their Social Security number and other valuable data, and to shred any medical paperwork they no longer need, including labels on prescription bottles. And if they see something on an Explanation of Benefits that doesn’t look right, they should question it immediately. We encourage them to take advantage of the free services at MyMedicare.gov, including Medicare Summary Notices provided every 3 months (if any services or medical supplies are received during that period), to make sure they’re being billed only for services they have received.
Your staff should be made aware of the potential for “friendly fraud,” which is defined as theft of identity and medical information by patients’ friends or family members. (According to some studies, as much as 50% of all medical identity theft may be committed this way.) Staffers should never divulge insurance numbers, diagnoses, lab reports, or any other privileged information to family or friends, whether by phone, fax, mail, or in person, without written permission from the patient. And when callers claiming to be patients request information about themselves, your employees should be alert for “red flags.” For example, legitimate patients won’t stumble over simple questions (such as “What is your birth date?”) or request test results or diagnoses that they should already know about.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
In his book, “Scam Me If You Can,” fraud expert Frank Abagnale relates the case of a 5-year-old boy whose pediatrician’s computer was hacked, compromising his name, birth date, Social Security number, insurance information, and medical records. The result was a bureaucratic nightmare that may well continue for the rest of that unfortunate young patient’s life. One can only speculate on the difficulties he might have as adult in obtaining a line of credit, or in proving his medical identity to physicians and hospitals.
– your Social Security number, bank account numbers, etc. – sells for about $25 on the black market; add health insurance and medical records, and the price can jump to $1,000 or more. That’s because there is a far greater potential yield from medical identity theft – and once your personal information and medical records are breached, they are in the Cloud for the rest of your life, available to anyone who wants to buy them. Older patients are particularly vulnerable: Medicare billing scams cost taxpayers more than $60 billion a year.
If your office’s computer system does not have effective fraud protection, you could be held liable for any fraud committed with information stolen from it – and if the information is resold years later and reused to commit more fraud, you’ll be liable for that, too. That’s why I strongly recommend that you invest in high-quality security technology and software, so that in the event of a breach, the security company will at least share in the fault and the liability. (As always, I have no financial interest in any product or industry mentioned in this column.)
Even with adequate protection, breaches can still occur, so all medical offices should have a breach response plan in place, covering how to halt security breaches, and how to handle any lost or stolen data. Your computer and security vendors can help with formulating such a plan. Patients affected by a breach need to be contacted as well, so they may put a freeze on accounts or send out fraud alerts.
Patients also need to be aware of the risks. If your EHR includes an online portal to communicate protected information to patients, it may be secure on your end, but patients are unlikely to have similar protection on their home computers. If you offer online patient portal services, you should make your patients aware of measures they can take to protect their data once it arrives on their computers or phones.
Patients should also be warned of the risks that come with sharing medical information with others. If they are asked to reveal medical data via phone or email, they need to ask who is requesting it, and why. Any unsolicited calls inquiring about their medical information, from someone who can’t or won’t confirm their identity, should be considered extremely suspicious.
We tell our patients to protect their insurance numbers as carefully as they guard their Social Security number and other valuable data, and to shred any medical paperwork they no longer need, including labels on prescription bottles. And if they see something on an Explanation of Benefits that doesn’t look right, they should question it immediately. We encourage them to take advantage of the free services at MyMedicare.gov, including Medicare Summary Notices provided every 3 months (if any services or medical supplies are received during that period), to make sure they’re being billed only for services they have received.
Your staff should be made aware of the potential for “friendly fraud,” which is defined as theft of identity and medical information by patients’ friends or family members. (According to some studies, as much as 50% of all medical identity theft may be committed this way.) Staffers should never divulge insurance numbers, diagnoses, lab reports, or any other privileged information to family or friends, whether by phone, fax, mail, or in person, without written permission from the patient. And when callers claiming to be patients request information about themselves, your employees should be alert for “red flags.” For example, legitimate patients won’t stumble over simple questions (such as “What is your birth date?”) or request test results or diagnoses that they should already know about.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
Does misplaced faith in modern medicine run at odds against healthier lifestyles?
Recently, a study in the Journal of the American Heart Association found that taking statins and blood pressure medications doesn’t lead to healthier lifestyles.

This should surprise no one practicing medicine today. With absolutely no scientific data to back up the next statement, I’m willing to bet a study on oral antiglycemics for type 2 diabetes would yield similar results.
The problem here is that these drugs don’t change human nature, and I’m not belittling their ability to reduce morbidity and mortality.
Developed nations nowadays live in a world of plenty. For most of us, there’s not only no shortage of food options, but the majority of what’s out there is the worst stuff for your health. Salty, dense calories, high-fat, sweetened – for most of us that’s a normal day of eating. It tastes good. Two million years of evolution have programmed us to eat similar stuff because in the wild it sustains survival.
In the city and suburbs, however, that’s not the case.
Food manufacturers make it and stores sell it because, quite bluntly, it makes money. The profit margin for unhealthy stuff is higher than that for fruits and vegetables. If you’re trying to run a successful business, which one would you choose to sell?
As long as people are going to eat unhealthy stuff, others will sell it to them. All the medical breakthroughs in the world won’t change that.
Same with exercise. Some people love to exercise. Some people catch the bug to do it consistently. But most try for a few weeks, usually in January-February, then give up because they don’t have time, or the will, or both.
Medical breakthroughs won’t fix that, either.
There’s also, I suspect, a component of misplaced faith in modern medicine. Like the mysterious “anti-calories” in a can of diet soda. You really do encounter people who think that drinking a diet soda and having a slice of chocolate cake will cancel each other out. Any doctor or nutritionist will scoff at this, but it’s amazing how many people think that doing one good thing (health wise) means you can equally do one bad thing at no penalty. Humans love magical thinking like that.

Unintentionally, the medications contribute to this belief. People figure if they’re lowering blood sugar or lipids, maybe they can eat more steak and ice cream. That’s an unintended consequence of modern medicine. It’s not even limited to nonmedical people. When Lipitor came to market in the late 1990s, one of my attendings called it “a license to eat.” Sadly, as the new study proves, he wasn’t that far from the truth.
People want an easy cure. A pill that makes it all better. That’s human nature. But the real problem, for all the great work we’ve done in medications, is that many patients don’t want to be an active participant in their own care. Exercising and maintaining a healthy diet are hard work, in spite of all the evidence showing their benefits (especially when combined with modern medicine, which is the whole idea in the first place). So it’s much easier for them to place all the responsibility on doctors and medications, and just take a simple pill to fix everything.
As this study shows, it doesn’t work that way.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, a study in the Journal of the American Heart Association found that taking statins and blood pressure medications doesn’t lead to healthier lifestyles.
This should surprise no one practicing medicine today. With absolutely no scientific data to back up the next statement, I’m willing to bet a study on oral antiglycemics for type 2 diabetes would yield similar results.
The problem here is that these drugs don’t change human nature, and I’m not belittling their ability to reduce morbidity and mortality.
Developed nations nowadays live in a world of plenty. For most of us, there’s not only no shortage of food options, but the majority of what’s out there is the worst stuff for your health. Salty, dense calories, high-fat, sweetened – for most of us that’s a normal day of eating. It tastes good. Two million years of evolution have programmed us to eat similar stuff because in the wild it sustains survival.
In the city and suburbs, however, that’s not the case.
Food manufacturers make it and stores sell it because, quite bluntly, it makes money. The profit margin for unhealthy stuff is higher than that for fruits and vegetables. If you’re trying to run a successful business, which one would you choose to sell?
As long as people are going to eat unhealthy stuff, others will sell it to them. All the medical breakthroughs in the world won’t change that.
Same with exercise. Some people love to exercise. Some people catch the bug to do it consistently. But most try for a few weeks, usually in January-February, then give up because they don’t have time, or the will, or both.
Medical breakthroughs won’t fix that, either.
There’s also, I suspect, a component of misplaced faith in modern medicine. Like the mysterious “anti-calories” in a can of diet soda. You really do encounter people who think that drinking a diet soda and having a slice of chocolate cake will cancel each other out. Any doctor or nutritionist will scoff at this, but it’s amazing how many people think that doing one good thing (health wise) means you can equally do one bad thing at no penalty. Humans love magical thinking like that.
Unintentionally, the medications contribute to this belief. People figure if they’re lowering blood sugar or lipids, maybe they can eat more steak and ice cream. That’s an unintended consequence of modern medicine. It’s not even limited to nonmedical people. When Lipitor came to market in the late 1990s, one of my attendings called it “a license to eat.” Sadly, as the new study proves, he wasn’t that far from the truth.
People want an easy cure. A pill that makes it all better. That’s human nature. But the real problem, for all the great work we’ve done in medications, is that many patients don’t want to be an active participant in their own care. Exercising and maintaining a healthy diet are hard work, in spite of all the evidence showing their benefits (especially when combined with modern medicine, which is the whole idea in the first place). So it’s much easier for them to place all the responsibility on doctors and medications, and just take a simple pill to fix everything.
As this study shows, it doesn’t work that way.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, a study in the Journal of the American Heart Association found that taking statins and blood pressure medications doesn’t lead to healthier lifestyles.
This should surprise no one practicing medicine today. With absolutely no scientific data to back up the next statement, I’m willing to bet a study on oral antiglycemics for type 2 diabetes would yield similar results.
The problem here is that these drugs don’t change human nature, and I’m not belittling their ability to reduce morbidity and mortality.
Developed nations nowadays live in a world of plenty. For most of us, there’s not only no shortage of food options, but the majority of what’s out there is the worst stuff for your health. Salty, dense calories, high-fat, sweetened – for most of us that’s a normal day of eating. It tastes good. Two million years of evolution have programmed us to eat similar stuff because in the wild it sustains survival.
In the city and suburbs, however, that’s not the case.
Food manufacturers make it and stores sell it because, quite bluntly, it makes money. The profit margin for unhealthy stuff is higher than that for fruits and vegetables. If you’re trying to run a successful business, which one would you choose to sell?
As long as people are going to eat unhealthy stuff, others will sell it to them. All the medical breakthroughs in the world won’t change that.
Same with exercise. Some people love to exercise. Some people catch the bug to do it consistently. But most try for a few weeks, usually in January-February, then give up because they don’t have time, or the will, or both.
Medical breakthroughs won’t fix that, either.
There’s also, I suspect, a component of misplaced faith in modern medicine. Like the mysterious “anti-calories” in a can of diet soda. You really do encounter people who think that drinking a diet soda and having a slice of chocolate cake will cancel each other out. Any doctor or nutritionist will scoff at this, but it’s amazing how many people think that doing one good thing (health wise) means you can equally do one bad thing at no penalty. Humans love magical thinking like that.
Unintentionally, the medications contribute to this belief. People figure if they’re lowering blood sugar or lipids, maybe they can eat more steak and ice cream. That’s an unintended consequence of modern medicine. It’s not even limited to nonmedical people. When Lipitor came to market in the late 1990s, one of my attendings called it “a license to eat.” Sadly, as the new study proves, he wasn’t that far from the truth.
People want an easy cure. A pill that makes it all better. That’s human nature. But the real problem, for all the great work we’ve done in medications, is that many patients don’t want to be an active participant in their own care. Exercising and maintaining a healthy diet are hard work, in spite of all the evidence showing their benefits (especially when combined with modern medicine, which is the whole idea in the first place). So it’s much easier for them to place all the responsibility on doctors and medications, and just take a simple pill to fix everything.
As this study shows, it doesn’t work that way.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
As physicians, accountability is part of our innate identity
Recently, Nicolas Badre, MD, challenged psychiatrists who care for patients involved in the legal system. He encouraged “a resurgence of personal accountability and responsibility.”
Using the chronically disenfranchised patients who are repetitiously shuttled between jails and mental hospitals as examples, he pointed out that we psychiatrists must “step up to the plate” and approach clinical problems with the attitude that “the buck stops with me.” As Dr. Badre pointed out, this is especially true when dealing with large, complex systems in which fragmented care exists without clear leadership. This, in turn, allows for a dissolution of accountability.
Accountability is a natural continuation of our training as physicians. We all remember the transition from medical student to intern, the steep learning curve as well as growth and maturation during this changeover. A dramatic transformation occurs over the course of 1 year, from medical students who tag along learning from patients to interns expected to be on their own for endless hours.
Over the course of those hours, we came to the understanding that people’s lives were in our hands. This causes a shift in our identity. This process continues throughout residency and onward in our careers. At some point, it becomes part of our innate identity as physicians or our professional sense of self – which is hard to describe to nonphysicians.
A profound example of a sense of accountability within the medical profession can be found in “How We Live,” a book by National Book Award winner Sherwin B. Nuland, MD. In the book, the late Dr. Nuland recounted how, as a 49-year-old seasoned surgeon working at Yale University, New Haven, Conn., and casually rounding on patients, he heard a frantic message: “Any general surgeon! Any general surgeon! Go immediately to the operating room – immediately – any general surgeon!”
The case involved a 42-year-old wife and mother who had been rushed to the ED after having been found in the community in a profound state of shock. In the ED, it was suspected that the patient was bleeding heavily from a ruptured tubal pregnancy. She was sped rapidly to the operating room with an undetectable blood pressure and a barely palpable pulse. The on-call ob.gyn. had been summoned from home, and he rushed to the operating room along with his department chairman.
Because the woman had lost much of her blood supply, there was no time for crossmatching. The anesthesiologist had placed large-bore intravenous lines and transfused her with O-negative blood (the universal donor blood type) to try maintain some level of blood pressure. Before she could be even fully anesthetized, the ob.gyn had made an incision in her lower abdomen. The bleeding he encountered was profound.
After a quick evaluation, the ob.gyn. realized that the blood was coming from above, not below, leading to the emergency page that Dr. Nuland heard. Dr. Nuland described bounding up the stairs three at a time. He recalled: “[A] very real apprehension had entered my mind. I might encounter a situation that was beyond me, something that I might make even worse, something that would cause me to regret for the rest of my life that I had answered the page’s insistent call instead of simply turning my back on its urgency and slinking off to my car before anyone noticed I was there.”
However, he could not see himself doing such a thing and he rushed up to the operating room because, “walking away from that kind of cry for help would have violated every precept taught me by my life and my training, and every bit of moral sense I had. … . I bear an obsessive preoccupation with accepting responsibility, amounting really to a compulsively neurotic sense of duty.”
And yet in the next few seconds, as he was running to the operating room, he wondered: “Am I about to botch something up? Will I, in one quick stroke of ineptness and fate, bring my career crashing down around my feet and with it my sense of what I am? Am I on my way to destroy an unknown patient and myself at the same time?”
In Dr. Nuland’s thoughts lie the conundrum of responsibility for physicians. Thankfully for Dr. Nuland, he was able to save the day and diagnose a rare case of rupture of an aneurysm of the splenic artery and keep the patient alive. This dramatic story involved a surgical colleague who had to make split-second decisions while a patient’s life hanged in the balance, but the same principles apply to us as psychiatrists.
I would note that, in the above example of the surgical patient, the “system” for saving the woman’s life was well organized and resourced to allow for a comprehensive and time-limited intervention into a life-threatening situation. There was an operating room staffed by various professionals who all had a defined role. It required the leader, Dr. Nuland, to step in, make the right diagnosis, and then issue commands to the identified professionals who all recognized his leadership and were skilled in carrying out their assigned duties. Dr. Nuland clearly was the leader once he took charge.
An outpatient psychiatrist facing a suicidal patient must deal with a different set of challenges, often involving various complex systems as well as multiple barriers. Clinical barriers include available interdisciplinary resources/personnel to assist not only with the critical encounter, but also with extended evaluation and treatment in a secure, well-resourced environment. Administrative barriers can include justifying the optimal treatment plan to payors. Our lethal patients often require both outpatient and inpatient services with sometimes-conflicting agendas. In a recent article, I pointed out some of the vexing problems that arise when communication and collaboration are poor between inpatient and outpatient psychiatrists. In such complex environments, it is less clear what is involved in the outpatient psychiatrist stepping up to the plate and asserting leadership.
An emotionally wrenching article about an emergency physician, Matthew E. Seaman, MD, who died by suicide, reminds us of the potential for suicide in a complicated patient (in this case, a medical colleague) involving complex systems. Plagued by a review of his care by the medical board (they had forced him to surrender his medical license and allowed the allegations to go public in lieu of further disciplinary proceedings), a subsequent lawsuit and an ultimate attempt by the plaintiff to obtain Dr. Seaman’s personal assets led to his worsening mental health. According to his wife, also a physician, he was getting “more depressed by the insults and assaults on his integrity and professionalism.”
Just before the investigation, he had received a 30-year pin from the American Board of Emergency Medicine for his “dedication to the specialty.” He fell into a deep depression from which he could not recover despite several psychiatric admissions and several medication trials. Along with his depression, he suffered from severe anxiety, a known risk factor for suicide. Dr. Seaman was feeling overwhelmed by the lengthy legal process targeting him as being negligent. He begged his attorney to settle the case, but his insurance carrier would not allow it. According to his wife: “All sense of human worth had been beaten out of him.”
Dr. Seaman had been known as resilient. He could handle complex ED situations, including simultaneously dealing with multiple traumas. He previously had been named in three malpractice lawsuits and had prevailed in each one. But his resilience had greatly diminished, and he became overwhelmed. He previously had, as a physician, been able to step up to the plate of accountability. But now, because of a confluence of depression and anxiety as well as the “insults and assaults on his integrity and professionalism,” he found life to be unbearable with the resulting tragic end.
So how would we as psychiatrists step up to the plate and be accountable when faced with a struggling fellow physician at risk for suicide such as Dr. Seaman?
Be aware of relevant risk factors
In addition to being aware of the usual risk factors for suicide, it would behoove us to also understand how physician suicides differ from suicides among nonphysicians.1 For example, physicians who have died by suicide were far more likely to have experienced job-related problems than nonphysicians, but less likely to have experienced the recent death of a loved one. Also noteworthy is that physicians who end their lives were more often married. In addition, Michael F. Myers, MD, a psychiatrist who has studied physician suicides, noted in the article about Dr. Seaman that struggling physicians are likely to suffer from shame and embarrassment.
Consider shame, burdensomeness, and secrecy
When suicide risk factors are taught to students and professionals, rarely is shame mentioned. Perhaps it is not a common risk factor in the general population, but shame and its cousin, disgrace, are known risk factors that likely apply more to people – such as physicians – who have built a reputation over their careers. One whole chapter is given to disgrace suicides in a book about suicide notes.2 A reputation often is one of the most important factors for professionals, which creates their sense of identity and, by extension, a sense of purpose in life.
When a doctor perceives that his or her reputation is being destroyed, it can produce a profound sense of shame, one of the most powerful of negative emotions.3 Another feature among completed suicides that applies more generally is perceived burdensomeness, according to Thomas E. Joiner Jr., PhD, one of the deep and innovative researchers in the field of suicidology.4 Once a doctor starts feeling that he has been a failure in his professional life and starts ruminating about it, the feelings of failure may generalize to other areas of his life, so that he starts feeling that he is a burden to his spouse. This, then, only increases his shame.
The issue of secrecy also is noteworthy. I was struck reading a book by Dr. Myers on physician suicide by the many spouses and family members who were caught completely unaware of problems when their spouse, a doctor, ended their lives by suicide.5 The doctors hid their problems well, perhaps not wanting to burden their family members. Also, if feelings of shame are an issue, then concealment tends to occur. This concealment of suicidality runs counter to the current narrative among some in the professional community that suicides are preventable (this despite the continuing increase in rates of suicide at the same time that there are increases in mental health services and suicide prevention programs).6
As pointed out in some of the letters quoted in Dr. Myers’s book, those who completed suicide are smart and know how to hide their symptoms well. Although Dr. Seaman’s wife, Linda Seaman, MD, was aware of her husband’s suicidality, when he eventually determined that he was going to end his life, he apparently did not reveal his more serious intention to her. Aside from spouses and family, determined suicide completers often hide their intentions from their clinicians.7
Attempt to obtain collateral information
By being aware of the usual and less-usual risk factors for suicide that our physician colleagues may present with as explained above, we can use strategies for mitigating risk. If secrecy because of shame and embarrassment prevents our physician patient from being fully candid, include the spouse or another significant family member in sessions. While the physician might hide his suicidal intent from both the clinician and spouse, it remains prudent to include the spouse in the treatment plan. Give the spouse a telephone number with which they can contact you if they notice any worrisome change in functioning or behavior. Collateral information often is helpful. (Example: Is the patient not eating, not sleeping, or giving away valued possessions?)
Assess for competency
In Dr. Seaman’s case, it was noted that, with a trial approaching, Dr. Seaman had written in a journal entry that he could not mentally endure a trial. “For me, the stress is overwhelming.” Such a patient, suffering from severe depression, often is unable to properly assist his attorney in his defense. The outpatient psychiatrist can notify the court or one of the attorneys that the competency of the physician patient is questionable (or express a definite opinion of incompetency), and offer the opinion that it would be best to postpone further legal action until the patient is in a more healthy state of mind.
Know when hospitalization is needed
Obviously, the process will go smoother if the admission is voluntary. If the patient physician resists and the psychiatrist believes that the risk for self-harm is too high for the physician patient to remain as an outpatient, try to get a spouse or family member to persuade him to be admitted. An involuntary admission opens up a whole new can of worms and may fracture the therapeutic alliance.
In the end, it might be better to take that risk rather than having a dead patient on your hands. If a hospitalization is necessary, contact the admitting psychiatrist and verbally express your concerns and the reasons why a hospitalization is needed. Ask the inpatient psychiatrist to contact you when a discharge is approaching so that you have an opportunity to ask relevant questions.
For example, during his second psychiatric admission, as the time for discharge was approaching, Dr. Seaman wrote: “I am not well enough for discharge. I am still mentally ill.” Ask the inpatient doctor whether the patient has gotten sufficiently better and he feels confident he can function as an outpatient. If there is a conflicting opinion about the readiness of the patient for discharge, notify the medical director of the service or an administrator about your concerns.
Ask for consultation
At any stage of the process consider getting consultation for a trusted colleague or senior clinician if you are failing to make progress. Sometimes it helps to get the perspective from a fresh pair of eyes or ears.
Get a reality check
Having recounted the inspiring story of Dr. Nuland’s magnificent efforts and joyous success in preserving a life that was on the verge of being lost in the battle against death at the last possible second, I would note the following: Surgeons will tell you that, despite their most heroic efforts and teamwork, there are times when luck runs out and the patient dies on the operating table. Also, small lapses, which all mortals are prone to despite their best efforts at conscientiousness, sometimes can lead to a bad outcome.
Similarly, in psychiatry, no matter how much effort we put into saving a life, sometimes it is all to no avail. Despite all we have learned about suicide and its risk factors, and no matter how much care we take to contain risk, our patients who are determined will find a way of ending their own lives. The vexing problem of suicide seems intractable. A suicide among our patients humbles us, but also hopefully inspires us to keep trying harder to step up to the plate of accountability.
In conclusion, for us physicians, accountability is not a facet, a trait, or even a pursuit, accountability is at the core of who are and how we define ourselves. Accountability is the reason we leap stairs three at time when we are urgently paged. Accountability is the reason malpractice lawsuits cut at the core of our self-image. Accountability allows us to always have hope for a positive outcome, despite overwhelming barriers, and gives our lives a sense of purpose.
For me, in preparing this article, accountability was reviewing and studying physician suicide and then applying best practices in risk assessment after reading the tragic story of Dr. Seaman. I hope I inspire you to do the same in the pursuit of helping our vulnerable patients.
Learning how to care for our complex patients is a never-ending journey.
References
1. Gold KJ. Gen Hosp Psychiatry. 2013 Jan;35(1):45-9.
2. Etkind M. ...Or Not to Be: A Collection of Suicide Notes. New York: Riverhead Books, 1997.
3. Lamia LC. Shame: A concealed, contagious, and dangerous emotion. Psychology Today. 2011 Apr 4.
4. Joiner TE. Why People Die by Suicide. Cambridge: Harvard University Press, 2005.
5. Myers MF. Why Physicians Die by Suicide. 2017.
6. National Institutes of Health. Suicide Prevention. https://www.nimh.nih.gov/health/topics/suicide-prevention/index.shtml.
7. Levy AG et al. JAMA Netw Open. 2019 Aug 14. doi: 10.1001/jamanetworkopen.2019.9277.
Dr. Kausch is a clinical and forensic psychiatrist who is on the faculty at Case Western Reserve University, Cleveland, as an assistant clinical professor. He spends most of his time seeing patients through the Akron General/Cleveland Clinic health system. He has published in the area of forensic psychiatry, addictions, pathological gambling, and suicide. He has recently taken an interest in conducting marital therapy and is now publishing in that area as well.
Recently, Nicolas Badre, MD, challenged psychiatrists who care for patients involved in the legal system. He encouraged “a resurgence of personal accountability and responsibility.”
Using the chronically disenfranchised patients who are repetitiously shuttled between jails and mental hospitals as examples, he pointed out that we psychiatrists must “step up to the plate” and approach clinical problems with the attitude that “the buck stops with me.” As Dr. Badre pointed out, this is especially true when dealing with large, complex systems in which fragmented care exists without clear leadership. This, in turn, allows for a dissolution of accountability.
Accountability is a natural continuation of our training as physicians. We all remember the transition from medical student to intern, the steep learning curve as well as growth and maturation during this changeover. A dramatic transformation occurs over the course of 1 year, from medical students who tag along learning from patients to interns expected to be on their own for endless hours.
Over the course of those hours, we came to the understanding that people’s lives were in our hands. This causes a shift in our identity. This process continues throughout residency and onward in our careers. At some point, it becomes part of our innate identity as physicians or our professional sense of self – which is hard to describe to nonphysicians.
A profound example of a sense of accountability within the medical profession can be found in “How We Live,” a book by National Book Award winner Sherwin B. Nuland, MD. In the book, the late Dr. Nuland recounted how, as a 49-year-old seasoned surgeon working at Yale University, New Haven, Conn., and casually rounding on patients, he heard a frantic message: “Any general surgeon! Any general surgeon! Go immediately to the operating room – immediately – any general surgeon!”
The case involved a 42-year-old wife and mother who had been rushed to the ED after having been found in the community in a profound state of shock. In the ED, it was suspected that the patient was bleeding heavily from a ruptured tubal pregnancy. She was sped rapidly to the operating room with an undetectable blood pressure and a barely palpable pulse. The on-call ob.gyn. had been summoned from home, and he rushed to the operating room along with his department chairman.
Because the woman had lost much of her blood supply, there was no time for crossmatching. The anesthesiologist had placed large-bore intravenous lines and transfused her with O-negative blood (the universal donor blood type) to try maintain some level of blood pressure. Before she could be even fully anesthetized, the ob.gyn had made an incision in her lower abdomen. The bleeding he encountered was profound.
After a quick evaluation, the ob.gyn. realized that the blood was coming from above, not below, leading to the emergency page that Dr. Nuland heard. Dr. Nuland described bounding up the stairs three at a time. He recalled: “[A] very real apprehension had entered my mind. I might encounter a situation that was beyond me, something that I might make even worse, something that would cause me to regret for the rest of my life that I had answered the page’s insistent call instead of simply turning my back on its urgency and slinking off to my car before anyone noticed I was there.”
However, he could not see himself doing such a thing and he rushed up to the operating room because, “walking away from that kind of cry for help would have violated every precept taught me by my life and my training, and every bit of moral sense I had. … . I bear an obsessive preoccupation with accepting responsibility, amounting really to a compulsively neurotic sense of duty.”
And yet in the next few seconds, as he was running to the operating room, he wondered: “Am I about to botch something up? Will I, in one quick stroke of ineptness and fate, bring my career crashing down around my feet and with it my sense of what I am? Am I on my way to destroy an unknown patient and myself at the same time?”
In Dr. Nuland’s thoughts lie the conundrum of responsibility for physicians. Thankfully for Dr. Nuland, he was able to save the day and diagnose a rare case of rupture of an aneurysm of the splenic artery and keep the patient alive. This dramatic story involved a surgical colleague who had to make split-second decisions while a patient’s life hanged in the balance, but the same principles apply to us as psychiatrists.
I would note that, in the above example of the surgical patient, the “system” for saving the woman’s life was well organized and resourced to allow for a comprehensive and time-limited intervention into a life-threatening situation. There was an operating room staffed by various professionals who all had a defined role. It required the leader, Dr. Nuland, to step in, make the right diagnosis, and then issue commands to the identified professionals who all recognized his leadership and were skilled in carrying out their assigned duties. Dr. Nuland clearly was the leader once he took charge.
An outpatient psychiatrist facing a suicidal patient must deal with a different set of challenges, often involving various complex systems as well as multiple barriers. Clinical barriers include available interdisciplinary resources/personnel to assist not only with the critical encounter, but also with extended evaluation and treatment in a secure, well-resourced environment. Administrative barriers can include justifying the optimal treatment plan to payors. Our lethal patients often require both outpatient and inpatient services with sometimes-conflicting agendas. In a recent article, I pointed out some of the vexing problems that arise when communication and collaboration are poor between inpatient and outpatient psychiatrists. In such complex environments, it is less clear what is involved in the outpatient psychiatrist stepping up to the plate and asserting leadership.
An emotionally wrenching article about an emergency physician, Matthew E. Seaman, MD, who died by suicide, reminds us of the potential for suicide in a complicated patient (in this case, a medical colleague) involving complex systems. Plagued by a review of his care by the medical board (they had forced him to surrender his medical license and allowed the allegations to go public in lieu of further disciplinary proceedings), a subsequent lawsuit and an ultimate attempt by the plaintiff to obtain Dr. Seaman’s personal assets led to his worsening mental health. According to his wife, also a physician, he was getting “more depressed by the insults and assaults on his integrity and professionalism.”
Just before the investigation, he had received a 30-year pin from the American Board of Emergency Medicine for his “dedication to the specialty.” He fell into a deep depression from which he could not recover despite several psychiatric admissions and several medication trials. Along with his depression, he suffered from severe anxiety, a known risk factor for suicide. Dr. Seaman was feeling overwhelmed by the lengthy legal process targeting him as being negligent. He begged his attorney to settle the case, but his insurance carrier would not allow it. According to his wife: “All sense of human worth had been beaten out of him.”
Dr. Seaman had been known as resilient. He could handle complex ED situations, including simultaneously dealing with multiple traumas. He previously had been named in three malpractice lawsuits and had prevailed in each one. But his resilience had greatly diminished, and he became overwhelmed. He previously had, as a physician, been able to step up to the plate of accountability. But now, because of a confluence of depression and anxiety as well as the “insults and assaults on his integrity and professionalism,” he found life to be unbearable with the resulting tragic end.
So how would we as psychiatrists step up to the plate and be accountable when faced with a struggling fellow physician at risk for suicide such as Dr. Seaman?
Be aware of relevant risk factors
In addition to being aware of the usual risk factors for suicide, it would behoove us to also understand how physician suicides differ from suicides among nonphysicians.1 For example, physicians who have died by suicide were far more likely to have experienced job-related problems than nonphysicians, but less likely to have experienced the recent death of a loved one. Also noteworthy is that physicians who end their lives were more often married. In addition, Michael F. Myers, MD, a psychiatrist who has studied physician suicides, noted in the article about Dr. Seaman that struggling physicians are likely to suffer from shame and embarrassment.
Consider shame, burdensomeness, and secrecy
When suicide risk factors are taught to students and professionals, rarely is shame mentioned. Perhaps it is not a common risk factor in the general population, but shame and its cousin, disgrace, are known risk factors that likely apply more to people – such as physicians – who have built a reputation over their careers. One whole chapter is given to disgrace suicides in a book about suicide notes.2 A reputation often is one of the most important factors for professionals, which creates their sense of identity and, by extension, a sense of purpose in life.
When a doctor perceives that his or her reputation is being destroyed, it can produce a profound sense of shame, one of the most powerful of negative emotions.3 Another feature among completed suicides that applies more generally is perceived burdensomeness, according to Thomas E. Joiner Jr., PhD, one of the deep and innovative researchers in the field of suicidology.4 Once a doctor starts feeling that he has been a failure in his professional life and starts ruminating about it, the feelings of failure may generalize to other areas of his life, so that he starts feeling that he is a burden to his spouse. This, then, only increases his shame.
The issue of secrecy also is noteworthy. I was struck reading a book by Dr. Myers on physician suicide by the many spouses and family members who were caught completely unaware of problems when their spouse, a doctor, ended their lives by suicide.5 The doctors hid their problems well, perhaps not wanting to burden their family members. Also, if feelings of shame are an issue, then concealment tends to occur. This concealment of suicidality runs counter to the current narrative among some in the professional community that suicides are preventable (this despite the continuing increase in rates of suicide at the same time that there are increases in mental health services and suicide prevention programs).6
As pointed out in some of the letters quoted in Dr. Myers’s book, those who completed suicide are smart and know how to hide their symptoms well. Although Dr. Seaman’s wife, Linda Seaman, MD, was aware of her husband’s suicidality, when he eventually determined that he was going to end his life, he apparently did not reveal his more serious intention to her. Aside from spouses and family, determined suicide completers often hide their intentions from their clinicians.7
Attempt to obtain collateral information
By being aware of the usual and less-usual risk factors for suicide that our physician colleagues may present with as explained above, we can use strategies for mitigating risk. If secrecy because of shame and embarrassment prevents our physician patient from being fully candid, include the spouse or another significant family member in sessions. While the physician might hide his suicidal intent from both the clinician and spouse, it remains prudent to include the spouse in the treatment plan. Give the spouse a telephone number with which they can contact you if they notice any worrisome change in functioning or behavior. Collateral information often is helpful. (Example: Is the patient not eating, not sleeping, or giving away valued possessions?)
Assess for competency
In Dr. Seaman’s case, it was noted that, with a trial approaching, Dr. Seaman had written in a journal entry that he could not mentally endure a trial. “For me, the stress is overwhelming.” Such a patient, suffering from severe depression, often is unable to properly assist his attorney in his defense. The outpatient psychiatrist can notify the court or one of the attorneys that the competency of the physician patient is questionable (or express a definite opinion of incompetency), and offer the opinion that it would be best to postpone further legal action until the patient is in a more healthy state of mind.
Know when hospitalization is needed
Obviously, the process will go smoother if the admission is voluntary. If the patient physician resists and the psychiatrist believes that the risk for self-harm is too high for the physician patient to remain as an outpatient, try to get a spouse or family member to persuade him to be admitted. An involuntary admission opens up a whole new can of worms and may fracture the therapeutic alliance.
In the end, it might be better to take that risk rather than having a dead patient on your hands. If a hospitalization is necessary, contact the admitting psychiatrist and verbally express your concerns and the reasons why a hospitalization is needed. Ask the inpatient psychiatrist to contact you when a discharge is approaching so that you have an opportunity to ask relevant questions.
For example, during his second psychiatric admission, as the time for discharge was approaching, Dr. Seaman wrote: “I am not well enough for discharge. I am still mentally ill.” Ask the inpatient doctor whether the patient has gotten sufficiently better and he feels confident he can function as an outpatient. If there is a conflicting opinion about the readiness of the patient for discharge, notify the medical director of the service or an administrator about your concerns.
Ask for consultation
At any stage of the process consider getting consultation for a trusted colleague or senior clinician if you are failing to make progress. Sometimes it helps to get the perspective from a fresh pair of eyes or ears.
Get a reality check
Having recounted the inspiring story of Dr. Nuland’s magnificent efforts and joyous success in preserving a life that was on the verge of being lost in the battle against death at the last possible second, I would note the following: Surgeons will tell you that, despite their most heroic efforts and teamwork, there are times when luck runs out and the patient dies on the operating table. Also, small lapses, which all mortals are prone to despite their best efforts at conscientiousness, sometimes can lead to a bad outcome.
Similarly, in psychiatry, no matter how much effort we put into saving a life, sometimes it is all to no avail. Despite all we have learned about suicide and its risk factors, and no matter how much care we take to contain risk, our patients who are determined will find a way of ending their own lives. The vexing problem of suicide seems intractable. A suicide among our patients humbles us, but also hopefully inspires us to keep trying harder to step up to the plate of accountability.
In conclusion, for us physicians, accountability is not a facet, a trait, or even a pursuit, accountability is at the core of who are and how we define ourselves. Accountability is the reason we leap stairs three at time when we are urgently paged. Accountability is the reason malpractice lawsuits cut at the core of our self-image. Accountability allows us to always have hope for a positive outcome, despite overwhelming barriers, and gives our lives a sense of purpose.
For me, in preparing this article, accountability was reviewing and studying physician suicide and then applying best practices in risk assessment after reading the tragic story of Dr. Seaman. I hope I inspire you to do the same in the pursuit of helping our vulnerable patients.
Learning how to care for our complex patients is a never-ending journey.
References
1. Gold KJ. Gen Hosp Psychiatry. 2013 Jan;35(1):45-9.
2. Etkind M. ...Or Not to Be: A Collection of Suicide Notes. New York: Riverhead Books, 1997.
3. Lamia LC. Shame: A concealed, contagious, and dangerous emotion. Psychology Today. 2011 Apr 4.
4. Joiner TE. Why People Die by Suicide. Cambridge: Harvard University Press, 2005.
5. Myers MF. Why Physicians Die by Suicide. 2017.
6. National Institutes of Health. Suicide Prevention. https://www.nimh.nih.gov/health/topics/suicide-prevention/index.shtml.
7. Levy AG et al. JAMA Netw Open. 2019 Aug 14. doi: 10.1001/jamanetworkopen.2019.9277.
Dr. Kausch is a clinical and forensic psychiatrist who is on the faculty at Case Western Reserve University, Cleveland, as an assistant clinical professor. He spends most of his time seeing patients through the Akron General/Cleveland Clinic health system. He has published in the area of forensic psychiatry, addictions, pathological gambling, and suicide. He has recently taken an interest in conducting marital therapy and is now publishing in that area as well.
Recently, Nicolas Badre, MD, challenged psychiatrists who care for patients involved in the legal system. He encouraged “a resurgence of personal accountability and responsibility.”
Using the chronically disenfranchised patients who are repetitiously shuttled between jails and mental hospitals as examples, he pointed out that we psychiatrists must “step up to the plate” and approach clinical problems with the attitude that “the buck stops with me.” As Dr. Badre pointed out, this is especially true when dealing with large, complex systems in which fragmented care exists without clear leadership. This, in turn, allows for a dissolution of accountability.
Accountability is a natural continuation of our training as physicians. We all remember the transition from medical student to intern, the steep learning curve as well as growth and maturation during this changeover. A dramatic transformation occurs over the course of 1 year, from medical students who tag along learning from patients to interns expected to be on their own for endless hours.
Over the course of those hours, we came to the understanding that people’s lives were in our hands. This causes a shift in our identity. This process continues throughout residency and onward in our careers. At some point, it becomes part of our innate identity as physicians or our professional sense of self – which is hard to describe to nonphysicians.
A profound example of a sense of accountability within the medical profession can be found in “How We Live,” a book by National Book Award winner Sherwin B. Nuland, MD. In the book, the late Dr. Nuland recounted how, as a 49-year-old seasoned surgeon working at Yale University, New Haven, Conn., and casually rounding on patients, he heard a frantic message: “Any general surgeon! Any general surgeon! Go immediately to the operating room – immediately – any general surgeon!”
The case involved a 42-year-old wife and mother who had been rushed to the ED after having been found in the community in a profound state of shock. In the ED, it was suspected that the patient was bleeding heavily from a ruptured tubal pregnancy. She was sped rapidly to the operating room with an undetectable blood pressure and a barely palpable pulse. The on-call ob.gyn. had been summoned from home, and he rushed to the operating room along with his department chairman.
Because the woman had lost much of her blood supply, there was no time for crossmatching. The anesthesiologist had placed large-bore intravenous lines and transfused her with O-negative blood (the universal donor blood type) to try maintain some level of blood pressure. Before she could be even fully anesthetized, the ob.gyn had made an incision in her lower abdomen. The bleeding he encountered was profound.
After a quick evaluation, the ob.gyn. realized that the blood was coming from above, not below, leading to the emergency page that Dr. Nuland heard. Dr. Nuland described bounding up the stairs three at a time. He recalled: “[A] very real apprehension had entered my mind. I might encounter a situation that was beyond me, something that I might make even worse, something that would cause me to regret for the rest of my life that I had answered the page’s insistent call instead of simply turning my back on its urgency and slinking off to my car before anyone noticed I was there.”
However, he could not see himself doing such a thing and he rushed up to the operating room because, “walking away from that kind of cry for help would have violated every precept taught me by my life and my training, and every bit of moral sense I had. … . I bear an obsessive preoccupation with accepting responsibility, amounting really to a compulsively neurotic sense of duty.”
And yet in the next few seconds, as he was running to the operating room, he wondered: “Am I about to botch something up? Will I, in one quick stroke of ineptness and fate, bring my career crashing down around my feet and with it my sense of what I am? Am I on my way to destroy an unknown patient and myself at the same time?”
In Dr. Nuland’s thoughts lie the conundrum of responsibility for physicians. Thankfully for Dr. Nuland, he was able to save the day and diagnose a rare case of rupture of an aneurysm of the splenic artery and keep the patient alive. This dramatic story involved a surgical colleague who had to make split-second decisions while a patient’s life hanged in the balance, but the same principles apply to us as psychiatrists.
I would note that, in the above example of the surgical patient, the “system” for saving the woman’s life was well organized and resourced to allow for a comprehensive and time-limited intervention into a life-threatening situation. There was an operating room staffed by various professionals who all had a defined role. It required the leader, Dr. Nuland, to step in, make the right diagnosis, and then issue commands to the identified professionals who all recognized his leadership and were skilled in carrying out their assigned duties. Dr. Nuland clearly was the leader once he took charge.
An outpatient psychiatrist facing a suicidal patient must deal with a different set of challenges, often involving various complex systems as well as multiple barriers. Clinical barriers include available interdisciplinary resources/personnel to assist not only with the critical encounter, but also with extended evaluation and treatment in a secure, well-resourced environment. Administrative barriers can include justifying the optimal treatment plan to payors. Our lethal patients often require both outpatient and inpatient services with sometimes-conflicting agendas. In a recent article, I pointed out some of the vexing problems that arise when communication and collaboration are poor between inpatient and outpatient psychiatrists. In such complex environments, it is less clear what is involved in the outpatient psychiatrist stepping up to the plate and asserting leadership.
An emotionally wrenching article about an emergency physician, Matthew E. Seaman, MD, who died by suicide, reminds us of the potential for suicide in a complicated patient (in this case, a medical colleague) involving complex systems. Plagued by a review of his care by the medical board (they had forced him to surrender his medical license and allowed the allegations to go public in lieu of further disciplinary proceedings), a subsequent lawsuit and an ultimate attempt by the plaintiff to obtain Dr. Seaman’s personal assets led to his worsening mental health. According to his wife, also a physician, he was getting “more depressed by the insults and assaults on his integrity and professionalism.”
Just before the investigation, he had received a 30-year pin from the American Board of Emergency Medicine for his “dedication to the specialty.” He fell into a deep depression from which he could not recover despite several psychiatric admissions and several medication trials. Along with his depression, he suffered from severe anxiety, a known risk factor for suicide. Dr. Seaman was feeling overwhelmed by the lengthy legal process targeting him as being negligent. He begged his attorney to settle the case, but his insurance carrier would not allow it. According to his wife: “All sense of human worth had been beaten out of him.”
Dr. Seaman had been known as resilient. He could handle complex ED situations, including simultaneously dealing with multiple traumas. He previously had been named in three malpractice lawsuits and had prevailed in each one. But his resilience had greatly diminished, and he became overwhelmed. He previously had, as a physician, been able to step up to the plate of accountability. But now, because of a confluence of depression and anxiety as well as the “insults and assaults on his integrity and professionalism,” he found life to be unbearable with the resulting tragic end.
So how would we as psychiatrists step up to the plate and be accountable when faced with a struggling fellow physician at risk for suicide such as Dr. Seaman?
Be aware of relevant risk factors
In addition to being aware of the usual risk factors for suicide, it would behoove us to also understand how physician suicides differ from suicides among nonphysicians.1 For example, physicians who have died by suicide were far more likely to have experienced job-related problems than nonphysicians, but less likely to have experienced the recent death of a loved one. Also noteworthy is that physicians who end their lives were more often married. In addition, Michael F. Myers, MD, a psychiatrist who has studied physician suicides, noted in the article about Dr. Seaman that struggling physicians are likely to suffer from shame and embarrassment.
Consider shame, burdensomeness, and secrecy
When suicide risk factors are taught to students and professionals, rarely is shame mentioned. Perhaps it is not a common risk factor in the general population, but shame and its cousin, disgrace, are known risk factors that likely apply more to people – such as physicians – who have built a reputation over their careers. One whole chapter is given to disgrace suicides in a book about suicide notes.2 A reputation often is one of the most important factors for professionals, which creates their sense of identity and, by extension, a sense of purpose in life.
When a doctor perceives that his or her reputation is being destroyed, it can produce a profound sense of shame, one of the most powerful of negative emotions.3 Another feature among completed suicides that applies more generally is perceived burdensomeness, according to Thomas E. Joiner Jr., PhD, one of the deep and innovative researchers in the field of suicidology.4 Once a doctor starts feeling that he has been a failure in his professional life and starts ruminating about it, the feelings of failure may generalize to other areas of his life, so that he starts feeling that he is a burden to his spouse. This, then, only increases his shame.
The issue of secrecy also is noteworthy. I was struck reading a book by Dr. Myers on physician suicide by the many spouses and family members who were caught completely unaware of problems when their spouse, a doctor, ended their lives by suicide.5 The doctors hid their problems well, perhaps not wanting to burden their family members. Also, if feelings of shame are an issue, then concealment tends to occur. This concealment of suicidality runs counter to the current narrative among some in the professional community that suicides are preventable (this despite the continuing increase in rates of suicide at the same time that there are increases in mental health services and suicide prevention programs).6
As pointed out in some of the letters quoted in Dr. Myers’s book, those who completed suicide are smart and know how to hide their symptoms well. Although Dr. Seaman’s wife, Linda Seaman, MD, was aware of her husband’s suicidality, when he eventually determined that he was going to end his life, he apparently did not reveal his more serious intention to her. Aside from spouses and family, determined suicide completers often hide their intentions from their clinicians.7
Attempt to obtain collateral information
By being aware of the usual and less-usual risk factors for suicide that our physician colleagues may present with as explained above, we can use strategies for mitigating risk. If secrecy because of shame and embarrassment prevents our physician patient from being fully candid, include the spouse or another significant family member in sessions. While the physician might hide his suicidal intent from both the clinician and spouse, it remains prudent to include the spouse in the treatment plan. Give the spouse a telephone number with which they can contact you if they notice any worrisome change in functioning or behavior. Collateral information often is helpful. (Example: Is the patient not eating, not sleeping, or giving away valued possessions?)
Assess for competency
In Dr. Seaman’s case, it was noted that, with a trial approaching, Dr. Seaman had written in a journal entry that he could not mentally endure a trial. “For me, the stress is overwhelming.” Such a patient, suffering from severe depression, often is unable to properly assist his attorney in his defense. The outpatient psychiatrist can notify the court or one of the attorneys that the competency of the physician patient is questionable (or express a definite opinion of incompetency), and offer the opinion that it would be best to postpone further legal action until the patient is in a more healthy state of mind.
Know when hospitalization is needed
Obviously, the process will go smoother if the admission is voluntary. If the patient physician resists and the psychiatrist believes that the risk for self-harm is too high for the physician patient to remain as an outpatient, try to get a spouse or family member to persuade him to be admitted. An involuntary admission opens up a whole new can of worms and may fracture the therapeutic alliance.
In the end, it might be better to take that risk rather than having a dead patient on your hands. If a hospitalization is necessary, contact the admitting psychiatrist and verbally express your concerns and the reasons why a hospitalization is needed. Ask the inpatient psychiatrist to contact you when a discharge is approaching so that you have an opportunity to ask relevant questions.
For example, during his second psychiatric admission, as the time for discharge was approaching, Dr. Seaman wrote: “I am not well enough for discharge. I am still mentally ill.” Ask the inpatient doctor whether the patient has gotten sufficiently better and he feels confident he can function as an outpatient. If there is a conflicting opinion about the readiness of the patient for discharge, notify the medical director of the service or an administrator about your concerns.
Ask for consultation
At any stage of the process consider getting consultation for a trusted colleague or senior clinician if you are failing to make progress. Sometimes it helps to get the perspective from a fresh pair of eyes or ears.
Get a reality check
Having recounted the inspiring story of Dr. Nuland’s magnificent efforts and joyous success in preserving a life that was on the verge of being lost in the battle against death at the last possible second, I would note the following: Surgeons will tell you that, despite their most heroic efforts and teamwork, there are times when luck runs out and the patient dies on the operating table. Also, small lapses, which all mortals are prone to despite their best efforts at conscientiousness, sometimes can lead to a bad outcome.
Similarly, in psychiatry, no matter how much effort we put into saving a life, sometimes it is all to no avail. Despite all we have learned about suicide and its risk factors, and no matter how much care we take to contain risk, our patients who are determined will find a way of ending their own lives. The vexing problem of suicide seems intractable. A suicide among our patients humbles us, but also hopefully inspires us to keep trying harder to step up to the plate of accountability.
In conclusion, for us physicians, accountability is not a facet, a trait, or even a pursuit, accountability is at the core of who are and how we define ourselves. Accountability is the reason we leap stairs three at time when we are urgently paged. Accountability is the reason malpractice lawsuits cut at the core of our self-image. Accountability allows us to always have hope for a positive outcome, despite overwhelming barriers, and gives our lives a sense of purpose.
For me, in preparing this article, accountability was reviewing and studying physician suicide and then applying best practices in risk assessment after reading the tragic story of Dr. Seaman. I hope I inspire you to do the same in the pursuit of helping our vulnerable patients.
Learning how to care for our complex patients is a never-ending journey.
References
1. Gold KJ. Gen Hosp Psychiatry. 2013 Jan;35(1):45-9.
2. Etkind M. ...Or Not to Be: A Collection of Suicide Notes. New York: Riverhead Books, 1997.
3. Lamia LC. Shame: A concealed, contagious, and dangerous emotion. Psychology Today. 2011 Apr 4.
4. Joiner TE. Why People Die by Suicide. Cambridge: Harvard University Press, 2005.
5. Myers MF. Why Physicians Die by Suicide. 2017.
6. National Institutes of Health. Suicide Prevention. https://www.nimh.nih.gov/health/topics/suicide-prevention/index.shtml.
7. Levy AG et al. JAMA Netw Open. 2019 Aug 14. doi: 10.1001/jamanetworkopen.2019.9277.
Dr. Kausch is a clinical and forensic psychiatrist who is on the faculty at Case Western Reserve University, Cleveland, as an assistant clinical professor. He spends most of his time seeing patients through the Akron General/Cleveland Clinic health system. He has published in the area of forensic psychiatry, addictions, pathological gambling, and suicide. He has recently taken an interest in conducting marital therapy and is now publishing in that area as well.
Under the influence
I don’t know how successful you have been at getting your adolescent patients to follow your suggestions, but I would guess that my batting average was in the low 100s. Even when I try stepping off my soapbox to involve the patient in a nonjudgmental dialogue, my successes pale in comparison to my failures.

Just looking at our national statistics for obesity, it’s pretty obvious that we are all doing a pretty rotten job of modifying our patients behaviors. You could point to a few encouraging numbers but they are few and far between. You could claim correctly that by the time a child reaches preschool, the die is already cast, throw up your arms, and not even raise the subject of diet with your overweight teenage patients.
A recent article in the journal Appetite hints at a group of strategies for molding patient behavior that so far have gotten very little attention from physicians (“Do perceived norms of social media users eating habits and preferences predict our own food consumption and BMI?” Appetite. 2020 Jan 18. doi: 10.1016/j.appet.2020.104611). Researchers at the department of psychology at Ashton University in Birmingham, England, surveyed more than 350 college-age students asking them about the dietary preference of their Facebook contacts and their own dietary habits. What the investigators found was that respondents who perceived their peers ate a healthy diet ate a healthier diet. Conversely, if the respondents thought their social media contacts ate junk food, they reported eating more of an unhealthy diet themselves.
In other words, it appears that, through social media, we have the potential to influence the eating habits of our patients’ peers. Before we get too excited, it should be pointed out that this study from England wasn’t of a long enough duration to demonstrate an effect on body mass index. And another study of 176 children recently published in Pediatrics found that while influencer marketing of unhealthy foods increased children’s immediate food intake, the equivalent marketing of healthy foods had no effect (“Social influencer marketing and children’s food intake: A randomized trial.” Pediatrics. 2019 Apr 1. doi: 10.1542/peds.2018-2554).
Not being terribly aware of the whos, whats, and wheres of influencers, I did a little bit of Internet searching at the Influencer Marketing hub and learned that influencers comes in all shapes and sizes, from “nanoinfluencers” who have acknowledged expertise and a very small Internet following numbering as few as a hundred to “megainfluencers” who have more than a million followers and might charge large entities a million dollars for a single post. The influencer’s content could appear as a blog, a YouTube video, a podcast, or simply a social media post.

The field of influencer marketing is new and growing exponentially. This initiative could come in the form of an office dedicated to Influencer Marketing created by the American Academy of Pediatrics. That group could search for megainfluencers who might be funded by the academy. But it also could develop a handbook for individual practitioners and groups to help them identify nano- and micro- (1,000-40,000 followers) influencers in their own practices.
You probably don’t ask your patients about their social media habits other than to caution them about time management. Maybe it’s time to dig a little deeper. You may find that you have a potent influencer hidden in your practice. She or he might just be willing to spread a good word or two for you.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
I don’t know how successful you have been at getting your adolescent patients to follow your suggestions, but I would guess that my batting average was in the low 100s. Even when I try stepping off my soapbox to involve the patient in a nonjudgmental dialogue, my successes pale in comparison to my failures.
Just looking at our national statistics for obesity, it’s pretty obvious that we are all doing a pretty rotten job of modifying our patients behaviors. You could point to a few encouraging numbers but they are few and far between. You could claim correctly that by the time a child reaches preschool, the die is already cast, throw up your arms, and not even raise the subject of diet with your overweight teenage patients.
A recent article in the journal Appetite hints at a group of strategies for molding patient behavior that so far have gotten very little attention from physicians (“Do perceived norms of social media users eating habits and preferences predict our own food consumption and BMI?” Appetite. 2020 Jan 18. doi: 10.1016/j.appet.2020.104611). Researchers at the department of psychology at Ashton University in Birmingham, England, surveyed more than 350 college-age students asking them about the dietary preference of their Facebook contacts and their own dietary habits. What the investigators found was that respondents who perceived their peers ate a healthy diet ate a healthier diet. Conversely, if the respondents thought their social media contacts ate junk food, they reported eating more of an unhealthy diet themselves.
In other words, it appears that, through social media, we have the potential to influence the eating habits of our patients’ peers. Before we get too excited, it should be pointed out that this study from England wasn’t of a long enough duration to demonstrate an effect on body mass index. And another study of 176 children recently published in Pediatrics found that while influencer marketing of unhealthy foods increased children’s immediate food intake, the equivalent marketing of healthy foods had no effect (“Social influencer marketing and children’s food intake: A randomized trial.” Pediatrics. 2019 Apr 1. doi: 10.1542/peds.2018-2554).
Not being terribly aware of the whos, whats, and wheres of influencers, I did a little bit of Internet searching at the Influencer Marketing hub and learned that influencers comes in all shapes and sizes, from “nanoinfluencers” who have acknowledged expertise and a very small Internet following numbering as few as a hundred to “megainfluencers” who have more than a million followers and might charge large entities a million dollars for a single post. The influencer’s content could appear as a blog, a YouTube video, a podcast, or simply a social media post.
The field of influencer marketing is new and growing exponentially. This initiative could come in the form of an office dedicated to Influencer Marketing created by the American Academy of Pediatrics. That group could search for megainfluencers who might be funded by the academy. But it also could develop a handbook for individual practitioners and groups to help them identify nano- and micro- (1,000-40,000 followers) influencers in their own practices.
You probably don’t ask your patients about their social media habits other than to caution them about time management. Maybe it’s time to dig a little deeper. You may find that you have a potent influencer hidden in your practice. She or he might just be willing to spread a good word or two for you.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
I don’t know how successful you have been at getting your adolescent patients to follow your suggestions, but I would guess that my batting average was in the low 100s. Even when I try stepping off my soapbox to involve the patient in a nonjudgmental dialogue, my successes pale in comparison to my failures.
Just looking at our national statistics for obesity, it’s pretty obvious that we are all doing a pretty rotten job of modifying our patients behaviors. You could point to a few encouraging numbers but they are few and far between. You could claim correctly that by the time a child reaches preschool, the die is already cast, throw up your arms, and not even raise the subject of diet with your overweight teenage patients.
A recent article in the journal Appetite hints at a group of strategies for molding patient behavior that so far have gotten very little attention from physicians (“Do perceived norms of social media users eating habits and preferences predict our own food consumption and BMI?” Appetite. 2020 Jan 18. doi: 10.1016/j.appet.2020.104611). Researchers at the department of psychology at Ashton University in Birmingham, England, surveyed more than 350 college-age students asking them about the dietary preference of their Facebook contacts and their own dietary habits. What the investigators found was that respondents who perceived their peers ate a healthy diet ate a healthier diet. Conversely, if the respondents thought their social media contacts ate junk food, they reported eating more of an unhealthy diet themselves.
In other words, it appears that, through social media, we have the potential to influence the eating habits of our patients’ peers. Before we get too excited, it should be pointed out that this study from England wasn’t of a long enough duration to demonstrate an effect on body mass index. And another study of 176 children recently published in Pediatrics found that while influencer marketing of unhealthy foods increased children’s immediate food intake, the equivalent marketing of healthy foods had no effect (“Social influencer marketing and children’s food intake: A randomized trial.” Pediatrics. 2019 Apr 1. doi: 10.1542/peds.2018-2554).
Not being terribly aware of the whos, whats, and wheres of influencers, I did a little bit of Internet searching at the Influencer Marketing hub and learned that influencers comes in all shapes and sizes, from “nanoinfluencers” who have acknowledged expertise and a very small Internet following numbering as few as a hundred to “megainfluencers” who have more than a million followers and might charge large entities a million dollars for a single post. The influencer’s content could appear as a blog, a YouTube video, a podcast, or simply a social media post.
The field of influencer marketing is new and growing exponentially. This initiative could come in the form of an office dedicated to Influencer Marketing created by the American Academy of Pediatrics. That group could search for megainfluencers who might be funded by the academy. But it also could develop a handbook for individual practitioners and groups to help them identify nano- and micro- (1,000-40,000 followers) influencers in their own practices.
You probably don’t ask your patients about their social media habits other than to caution them about time management. Maybe it’s time to dig a little deeper. You may find that you have a potent influencer hidden in your practice. She or he might just be willing to spread a good word or two for you.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.