User login
Increasing number of children being poisoned by liquid nicotine
Doctors say a 2016 law aimed at lowering the risk contained a big flaw, NBC News reported. The Child Nicotine Poisoning Prevention Act required child-resistant packaging on vaping liquid – but not on the vaping devices themselves.
Contact with the vaping liquid, or liquid nicotine, can cause children to get dizzy, pass out, and suffer drops in blood pressure. A few drops of the liquid can be fatal for a toddler.
Last year, 6,731 cases of vaping-related nicotine exposure were reported, according to Poison Help. “As of June 30, 2023, poison centers have managed 3,863 exposure cases about e-cigarette devices and liquid nicotine,” the organization said.
“Poison centers began receiving calls about e-cigarettes and liquid nicotine products in 2011, which coincides with the initial period where these products reached the U.S. market,” according to Poison Help.
“These products often contain a greater concentration of nicotine, a stimulant, than other nicotine/tobacco products on the market. Some children and toddlers who come in contact with e-cigarette devices or liquid nicotine have become very ill; some even requiring emergency department visits with nausea and vomiting being the most significant symptoms.”
Toxicologist Ryan Marino, MD, told NBC that refillable vapes are designed to hold liquid nicotine in a central reservoir, making them dangerous to children.
“Even vapes that appear more child-resistant – because their nicotine is sealed inside a removable cartridge – present a risk, because the cartridges can be pried open,” NBC said. “And some disposable e-cigarettes, now the top-selling type on the market, allow users to take thousands of ‘puffs’ and contain as much nicotine as multiple packs of cigarettes.”
A spokesperson for the vaping industry said all e-liquid bottles made in this country conform to U.S. law.
“Not only are the caps child-resistant, but the flow of liquid is restricted so that only small amounts can be dispensed,” said April Meyers of the Smoke-Free Alternatives Trade Association, which represents the vaping industry.
A version of this article first appeared on WebMD.com.
Doctors say a 2016 law aimed at lowering the risk contained a big flaw, NBC News reported. The Child Nicotine Poisoning Prevention Act required child-resistant packaging on vaping liquid – but not on the vaping devices themselves.
Contact with the vaping liquid, or liquid nicotine, can cause children to get dizzy, pass out, and suffer drops in blood pressure. A few drops of the liquid can be fatal for a toddler.
Last year, 6,731 cases of vaping-related nicotine exposure were reported, according to Poison Help. “As of June 30, 2023, poison centers have managed 3,863 exposure cases about e-cigarette devices and liquid nicotine,” the organization said.
“Poison centers began receiving calls about e-cigarettes and liquid nicotine products in 2011, which coincides with the initial period where these products reached the U.S. market,” according to Poison Help.
“These products often contain a greater concentration of nicotine, a stimulant, than other nicotine/tobacco products on the market. Some children and toddlers who come in contact with e-cigarette devices or liquid nicotine have become very ill; some even requiring emergency department visits with nausea and vomiting being the most significant symptoms.”
Toxicologist Ryan Marino, MD, told NBC that refillable vapes are designed to hold liquid nicotine in a central reservoir, making them dangerous to children.
“Even vapes that appear more child-resistant – because their nicotine is sealed inside a removable cartridge – present a risk, because the cartridges can be pried open,” NBC said. “And some disposable e-cigarettes, now the top-selling type on the market, allow users to take thousands of ‘puffs’ and contain as much nicotine as multiple packs of cigarettes.”
A spokesperson for the vaping industry said all e-liquid bottles made in this country conform to U.S. law.
“Not only are the caps child-resistant, but the flow of liquid is restricted so that only small amounts can be dispensed,” said April Meyers of the Smoke-Free Alternatives Trade Association, which represents the vaping industry.
A version of this article first appeared on WebMD.com.
Doctors say a 2016 law aimed at lowering the risk contained a big flaw, NBC News reported. The Child Nicotine Poisoning Prevention Act required child-resistant packaging on vaping liquid – but not on the vaping devices themselves.
Contact with the vaping liquid, or liquid nicotine, can cause children to get dizzy, pass out, and suffer drops in blood pressure. A few drops of the liquid can be fatal for a toddler.
Last year, 6,731 cases of vaping-related nicotine exposure were reported, according to Poison Help. “As of June 30, 2023, poison centers have managed 3,863 exposure cases about e-cigarette devices and liquid nicotine,” the organization said.
“Poison centers began receiving calls about e-cigarettes and liquid nicotine products in 2011, which coincides with the initial period where these products reached the U.S. market,” according to Poison Help.
“These products often contain a greater concentration of nicotine, a stimulant, than other nicotine/tobacco products on the market. Some children and toddlers who come in contact with e-cigarette devices or liquid nicotine have become very ill; some even requiring emergency department visits with nausea and vomiting being the most significant symptoms.”
Toxicologist Ryan Marino, MD, told NBC that refillable vapes are designed to hold liquid nicotine in a central reservoir, making them dangerous to children.
“Even vapes that appear more child-resistant – because their nicotine is sealed inside a removable cartridge – present a risk, because the cartridges can be pried open,” NBC said. “And some disposable e-cigarettes, now the top-selling type on the market, allow users to take thousands of ‘puffs’ and contain as much nicotine as multiple packs of cigarettes.”
A spokesperson for the vaping industry said all e-liquid bottles made in this country conform to U.S. law.
“Not only are the caps child-resistant, but the flow of liquid is restricted so that only small amounts can be dispensed,” said April Meyers of the Smoke-Free Alternatives Trade Association, which represents the vaping industry.
A version of this article first appeared on WebMD.com.
Sulfonylureas as street drugs: Hidden hypoglycemia cause
SEATTLE – .
“Physicians should be aware of this possibility and consider intentional or unintentional sulfonylurea abuse, with or without other drugs,” Amanda McKenna, MD, a first-year endocrinology fellow at the Mayo Clinic, Jacksonville, Fla., and colleagues say in a poster presented at the annual scientific & clinical congress of the American Association of Clinical Endocrinology.
The new case, seen in Florida, involves a 33-year-old man with a history of narcotic dependence and anxiety but not diabetes. At the time of presentation, the patient was unconscious and diaphoretic. The patient’s blood glucose level was 18 mg/dL. He had purchased two unmarked, light blue pills on the street which he thought were Valiums but turned out to be glyburide.
Sulfonylureas have no potential for abuse, but they physically resemble Valiums and are easier for illicit drug dealers to obtain because they’re not a controlled substance, and they can be sold for considerably more money, Dr. McKenna said in an interview.
“He thought he was getting Valium, but what he really purchased was glyburide. ... When he took it, he developed sweating and weakness. He probably thought he was having a bad trip, but it was really low blood sugar,” she said.
Similar cases go back nearly two decades
Similar cases have been reported as far back as 2004 in different parts of the United States. A 2004 article reports five cases in which people in San Francisco were “admitted to the hospital for hypoglycemia as a result of a drug purchased on the streets as a presumed benzodiazepine.”
Two more cases of “glyburide poisoning by ingestion of ‘street Valium,’ ” also from San Francisco, were reported in 2012. And in another case presented at the 2022 Endocrine Society meeting, sulfonylurea had been cut with cocaine, presumably to increase the volume.
The lead author of the 2012 article, Craig Smollin, MD, medical director of the California Poison Control System, San Francisco Division, and professor of emergency medicine at the University of California, San Francisco, told this news organization that his team has seen “a handful of cases over the years” but that “it is hard to say how common it is because hypoglycemia is common in this patient population for a variety of reasons.”
Persistent hypoglycemia led to the source
In the current case, paramedics treated the patient with D50W, and his blood glucose level increased from 18 mg/dL to 109 mg/dL. He regained consciousness but then developed recurrent hypoglycemia, and his blood glucose level dropped back to 15 mg/dL in the ED. Urine toxicology results were positive for benzodiazepines, cannabis, and cocaine.
Laboratory results showed elevations in levels of insulin (47.4 mIU/mL), C-peptide (5.4 ng/mL), and glucose (44 mg/dL). He was again treated with D50W, and his blood glucose level returned to normal over 20 hours. Once alert and oriented, he reported no personal or family history of diabetes. A 72-hour fast showed no evidence of insulinoma. A sulfonylurea screen was positive for glyburide. He was discharged home in stable condition. How many more cases have been missed?
Dr. McKenna pointed out that a typical urine toxicology screen for drugs wouldn’t detect a sulfonylurea. “The screen for hypoglycemic agents is a blood test, not a urine screen, so it’s completely different in the workup, and you really have to be thinking about that. It typically takes a while to come back,” she said.
She added that if the hypoglycemia resolves and testing isn’t conducted, the cause of the low blood sugar level might be missed. “If the hypoglycemia doesn’t persist, the [ED] physician wouldn’t consult endocrine. ... Is this happening more than we think?”
Ocreotide: A ‘unique antidote’
In their article, Dr. Smollin and colleagues describe the use of ocreotide, a long-acting somatostatin agonist that reverses the insulin-releasing effect of sulfonylureas on pancreatic beta cells, resulting in diminished insulin secretion. Unlike glucose supplementation, ocreotide doesn’t stimulate additional insulin release. It is of longer duration than glucagon, the authors say.
“The management of sulfonylurea overdose includes administration of glucose but also may include the use of octreotide, a unique antidote for sulfonylurea induced hypoglycemia,” Dr. Smollin said.
However, he also cautioned, “there is a broad differential diagnosis for hypoglycemia, and clinicians must consider many alternative diagnoses.”
Dr. McKenna and Dr. Smollin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SEATTLE – .
“Physicians should be aware of this possibility and consider intentional or unintentional sulfonylurea abuse, with or without other drugs,” Amanda McKenna, MD, a first-year endocrinology fellow at the Mayo Clinic, Jacksonville, Fla., and colleagues say in a poster presented at the annual scientific & clinical congress of the American Association of Clinical Endocrinology.
The new case, seen in Florida, involves a 33-year-old man with a history of narcotic dependence and anxiety but not diabetes. At the time of presentation, the patient was unconscious and diaphoretic. The patient’s blood glucose level was 18 mg/dL. He had purchased two unmarked, light blue pills on the street which he thought were Valiums but turned out to be glyburide.
Sulfonylureas have no potential for abuse, but they physically resemble Valiums and are easier for illicit drug dealers to obtain because they’re not a controlled substance, and they can be sold for considerably more money, Dr. McKenna said in an interview.
“He thought he was getting Valium, but what he really purchased was glyburide. ... When he took it, he developed sweating and weakness. He probably thought he was having a bad trip, but it was really low blood sugar,” she said.
Similar cases go back nearly two decades
Similar cases have been reported as far back as 2004 in different parts of the United States. A 2004 article reports five cases in which people in San Francisco were “admitted to the hospital for hypoglycemia as a result of a drug purchased on the streets as a presumed benzodiazepine.”
Two more cases of “glyburide poisoning by ingestion of ‘street Valium,’ ” also from San Francisco, were reported in 2012. And in another case presented at the 2022 Endocrine Society meeting, sulfonylurea had been cut with cocaine, presumably to increase the volume.
The lead author of the 2012 article, Craig Smollin, MD, medical director of the California Poison Control System, San Francisco Division, and professor of emergency medicine at the University of California, San Francisco, told this news organization that his team has seen “a handful of cases over the years” but that “it is hard to say how common it is because hypoglycemia is common in this patient population for a variety of reasons.”
Persistent hypoglycemia led to the source
In the current case, paramedics treated the patient with D50W, and his blood glucose level increased from 18 mg/dL to 109 mg/dL. He regained consciousness but then developed recurrent hypoglycemia, and his blood glucose level dropped back to 15 mg/dL in the ED. Urine toxicology results were positive for benzodiazepines, cannabis, and cocaine.
Laboratory results showed elevations in levels of insulin (47.4 mIU/mL), C-peptide (5.4 ng/mL), and glucose (44 mg/dL). He was again treated with D50W, and his blood glucose level returned to normal over 20 hours. Once alert and oriented, he reported no personal or family history of diabetes. A 72-hour fast showed no evidence of insulinoma. A sulfonylurea screen was positive for glyburide. He was discharged home in stable condition. How many more cases have been missed?
Dr. McKenna pointed out that a typical urine toxicology screen for drugs wouldn’t detect a sulfonylurea. “The screen for hypoglycemic agents is a blood test, not a urine screen, so it’s completely different in the workup, and you really have to be thinking about that. It typically takes a while to come back,” she said.
She added that if the hypoglycemia resolves and testing isn’t conducted, the cause of the low blood sugar level might be missed. “If the hypoglycemia doesn’t persist, the [ED] physician wouldn’t consult endocrine. ... Is this happening more than we think?”
Ocreotide: A ‘unique antidote’
In their article, Dr. Smollin and colleagues describe the use of ocreotide, a long-acting somatostatin agonist that reverses the insulin-releasing effect of sulfonylureas on pancreatic beta cells, resulting in diminished insulin secretion. Unlike glucose supplementation, ocreotide doesn’t stimulate additional insulin release. It is of longer duration than glucagon, the authors say.
“The management of sulfonylurea overdose includes administration of glucose but also may include the use of octreotide, a unique antidote for sulfonylurea induced hypoglycemia,” Dr. Smollin said.
However, he also cautioned, “there is a broad differential diagnosis for hypoglycemia, and clinicians must consider many alternative diagnoses.”
Dr. McKenna and Dr. Smollin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SEATTLE – .
“Physicians should be aware of this possibility and consider intentional or unintentional sulfonylurea abuse, with or without other drugs,” Amanda McKenna, MD, a first-year endocrinology fellow at the Mayo Clinic, Jacksonville, Fla., and colleagues say in a poster presented at the annual scientific & clinical congress of the American Association of Clinical Endocrinology.
The new case, seen in Florida, involves a 33-year-old man with a history of narcotic dependence and anxiety but not diabetes. At the time of presentation, the patient was unconscious and diaphoretic. The patient’s blood glucose level was 18 mg/dL. He had purchased two unmarked, light blue pills on the street which he thought were Valiums but turned out to be glyburide.
Sulfonylureas have no potential for abuse, but they physically resemble Valiums and are easier for illicit drug dealers to obtain because they’re not a controlled substance, and they can be sold for considerably more money, Dr. McKenna said in an interview.
“He thought he was getting Valium, but what he really purchased was glyburide. ... When he took it, he developed sweating and weakness. He probably thought he was having a bad trip, but it was really low blood sugar,” she said.
Similar cases go back nearly two decades
Similar cases have been reported as far back as 2004 in different parts of the United States. A 2004 article reports five cases in which people in San Francisco were “admitted to the hospital for hypoglycemia as a result of a drug purchased on the streets as a presumed benzodiazepine.”
Two more cases of “glyburide poisoning by ingestion of ‘street Valium,’ ” also from San Francisco, were reported in 2012. And in another case presented at the 2022 Endocrine Society meeting, sulfonylurea had been cut with cocaine, presumably to increase the volume.
The lead author of the 2012 article, Craig Smollin, MD, medical director of the California Poison Control System, San Francisco Division, and professor of emergency medicine at the University of California, San Francisco, told this news organization that his team has seen “a handful of cases over the years” but that “it is hard to say how common it is because hypoglycemia is common in this patient population for a variety of reasons.”
Persistent hypoglycemia led to the source
In the current case, paramedics treated the patient with D50W, and his blood glucose level increased from 18 mg/dL to 109 mg/dL. He regained consciousness but then developed recurrent hypoglycemia, and his blood glucose level dropped back to 15 mg/dL in the ED. Urine toxicology results were positive for benzodiazepines, cannabis, and cocaine.
Laboratory results showed elevations in levels of insulin (47.4 mIU/mL), C-peptide (5.4 ng/mL), and glucose (44 mg/dL). He was again treated with D50W, and his blood glucose level returned to normal over 20 hours. Once alert and oriented, he reported no personal or family history of diabetes. A 72-hour fast showed no evidence of insulinoma. A sulfonylurea screen was positive for glyburide. He was discharged home in stable condition. How many more cases have been missed?
Dr. McKenna pointed out that a typical urine toxicology screen for drugs wouldn’t detect a sulfonylurea. “The screen for hypoglycemic agents is a blood test, not a urine screen, so it’s completely different in the workup, and you really have to be thinking about that. It typically takes a while to come back,” she said.
She added that if the hypoglycemia resolves and testing isn’t conducted, the cause of the low blood sugar level might be missed. “If the hypoglycemia doesn’t persist, the [ED] physician wouldn’t consult endocrine. ... Is this happening more than we think?”
Ocreotide: A ‘unique antidote’
In their article, Dr. Smollin and colleagues describe the use of ocreotide, a long-acting somatostatin agonist that reverses the insulin-releasing effect of sulfonylureas on pancreatic beta cells, resulting in diminished insulin secretion. Unlike glucose supplementation, ocreotide doesn’t stimulate additional insulin release. It is of longer duration than glucagon, the authors say.
“The management of sulfonylurea overdose includes administration of glucose but also may include the use of octreotide, a unique antidote for sulfonylurea induced hypoglycemia,” Dr. Smollin said.
However, he also cautioned, “there is a broad differential diagnosis for hypoglycemia, and clinicians must consider many alternative diagnoses.”
Dr. McKenna and Dr. Smollin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT AACE 2023
‘Shocking’ data on what’s really in melatonin gummies
New data may explain the recent massive jump in pediatric hospitalizations.
Thenvestigators found that consuming some products as directed could expose consumers, including children, to doses that are 40-130 times greater than what’s recommended.
“The results were quite shocking,” lead researcher Pieter Cohen, MD, with Harvard Medical School, Boston, and Cambridge Health Alliance, Somerville, Mass., said in an interview.
“Melatonin gummies contained up to 347% more melatonin than what was listed on the label, and some products also contained cannabidiol; in one brand of melatonin gummies, there was zero melatonin, just CBD,” Dr. Cohen said.
The study was published online in JAMA.
530% jump in pediatric hospitalizations
Melatonin products are not approved by the Food and Drug Administration but are sold over the counter or online.
Previous research from JAMA has shown the use of melatonin has increased over the past 2 decades among people of all ages.
With increased use has come a spike in reports of melatonin overdose, calls to poison control centers, and related ED visits for children.
Federal data show the number of U.S. children who unintentionally ingested melatonin supplements jumped 530% from 2012 to 2021. More than 4,000 of the reported ingestions led to a hospital stay; 287 children required intensive care, and two children died.
It was unclear why melatonin supplements were causing these harms, which led Dr. Cohen’s team to analyze 25 unique brands of “melatonin” gummies purchased online.
One product didn’t contain any melatonin but did contain 31.3 mg of CBD.
In the remaining products, the quantity of melatonin ranged from 1.3 mg to 13.1 mg per serving. The actual quantity of melatonin ranged from 74% to 347% of the labeled quantity, the researchers found.
They note that for a young adult who takes as little as 0.1-0.3 mg of melatonin, plasma concentrations can increase into the normal night-time range.
Of the 25 products (88%) analyzed, 22 were inaccurately labeled, and only 3 (12%) contained a quantity of melatonin that was within 10% (plus or minus) of the declared quantity.
Five products listed CBD as an ingredient. The listed quantity ranged from 10.6 mg to 31.3 mg per serving, although the actual quantity of CBD ranged from 104% to 118% of the labeled quantity.
Inquire about use in kids
A limitation of the study is that only one sample of each brand was analyzed, and only gummies were analyzed. It is not known whether the results are generalizable to melatonin products sold as tablets and capsules in the United States or whether the quantity of melatonin within an individual brand may vary from batch to batch.
A recent study from Canada showed similar results. In an analysis of 16 Canadian melatonin brands, the actual dose of melatonin ranged from 17% to 478% of the declared quantity.
It’s estimated that more than 1% of all U.S. children use melatonin supplements, most commonly for sleep, stress, and relaxation.
“Given new research as to the excessive quantities of melatonin in gummies, caution should be used if considering their use,” said Dr. Cohen.
“It’s important to inquire about melatonin use when caring for children, particularly when parents express concerns about their child’s sleep,” he added.
The American Academy of Sleep Medicine recently issued a health advisory encouraging parents to talk to a health care professional before giving melatonin or any supplement to children.
Children don’t need melatonin
Commenting on the study, Michael Breus, PhD, clinical psychologist and founder of TheSleepDoctor.com, agreed that analyzing only one sample of each brand is a key limitation “because supplements are made in batches, and gummies in particular are difficult to distribute the active ingredient evenly.
“But even with that being said, 88% of them were labeled incorrectly, so even if there were a few single-sample issues, I kind of doubt its all of them,” Dr. Breus said.
“Kids as a general rule do not need melatonin. Their brains make almost four times the necessary amount already. If you start giving kids pills to help them sleep, then they start to have a pill problem, causing another issue,” Dr. Breus added.
“Most children’s falling asleep and staying sleep issues can be treated with behavioral measures like cognitive-behavioral therapy for insomnia,” he said.
The study had no specific funding. Dr. Cohen has received research support from Consumers Union and PEW Charitable Trusts and royalties from UptoDate. Dr. Breus disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New data may explain the recent massive jump in pediatric hospitalizations.
Thenvestigators found that consuming some products as directed could expose consumers, including children, to doses that are 40-130 times greater than what’s recommended.
“The results were quite shocking,” lead researcher Pieter Cohen, MD, with Harvard Medical School, Boston, and Cambridge Health Alliance, Somerville, Mass., said in an interview.
“Melatonin gummies contained up to 347% more melatonin than what was listed on the label, and some products also contained cannabidiol; in one brand of melatonin gummies, there was zero melatonin, just CBD,” Dr. Cohen said.
The study was published online in JAMA.
530% jump in pediatric hospitalizations
Melatonin products are not approved by the Food and Drug Administration but are sold over the counter or online.
Previous research from JAMA has shown the use of melatonin has increased over the past 2 decades among people of all ages.
With increased use has come a spike in reports of melatonin overdose, calls to poison control centers, and related ED visits for children.
Federal data show the number of U.S. children who unintentionally ingested melatonin supplements jumped 530% from 2012 to 2021. More than 4,000 of the reported ingestions led to a hospital stay; 287 children required intensive care, and two children died.
It was unclear why melatonin supplements were causing these harms, which led Dr. Cohen’s team to analyze 25 unique brands of “melatonin” gummies purchased online.
One product didn’t contain any melatonin but did contain 31.3 mg of CBD.
In the remaining products, the quantity of melatonin ranged from 1.3 mg to 13.1 mg per serving. The actual quantity of melatonin ranged from 74% to 347% of the labeled quantity, the researchers found.
They note that for a young adult who takes as little as 0.1-0.3 mg of melatonin, plasma concentrations can increase into the normal night-time range.
Of the 25 products (88%) analyzed, 22 were inaccurately labeled, and only 3 (12%) contained a quantity of melatonin that was within 10% (plus or minus) of the declared quantity.
Five products listed CBD as an ingredient. The listed quantity ranged from 10.6 mg to 31.3 mg per serving, although the actual quantity of CBD ranged from 104% to 118% of the labeled quantity.
Inquire about use in kids
A limitation of the study is that only one sample of each brand was analyzed, and only gummies were analyzed. It is not known whether the results are generalizable to melatonin products sold as tablets and capsules in the United States or whether the quantity of melatonin within an individual brand may vary from batch to batch.
A recent study from Canada showed similar results. In an analysis of 16 Canadian melatonin brands, the actual dose of melatonin ranged from 17% to 478% of the declared quantity.
It’s estimated that more than 1% of all U.S. children use melatonin supplements, most commonly for sleep, stress, and relaxation.
“Given new research as to the excessive quantities of melatonin in gummies, caution should be used if considering their use,” said Dr. Cohen.
“It’s important to inquire about melatonin use when caring for children, particularly when parents express concerns about their child’s sleep,” he added.
The American Academy of Sleep Medicine recently issued a health advisory encouraging parents to talk to a health care professional before giving melatonin or any supplement to children.
Children don’t need melatonin
Commenting on the study, Michael Breus, PhD, clinical psychologist and founder of TheSleepDoctor.com, agreed that analyzing only one sample of each brand is a key limitation “because supplements are made in batches, and gummies in particular are difficult to distribute the active ingredient evenly.
“But even with that being said, 88% of them were labeled incorrectly, so even if there were a few single-sample issues, I kind of doubt its all of them,” Dr. Breus said.
“Kids as a general rule do not need melatonin. Their brains make almost four times the necessary amount already. If you start giving kids pills to help them sleep, then they start to have a pill problem, causing another issue,” Dr. Breus added.
“Most children’s falling asleep and staying sleep issues can be treated with behavioral measures like cognitive-behavioral therapy for insomnia,” he said.
The study had no specific funding. Dr. Cohen has received research support from Consumers Union and PEW Charitable Trusts and royalties from UptoDate. Dr. Breus disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New data may explain the recent massive jump in pediatric hospitalizations.
Thenvestigators found that consuming some products as directed could expose consumers, including children, to doses that are 40-130 times greater than what’s recommended.
“The results were quite shocking,” lead researcher Pieter Cohen, MD, with Harvard Medical School, Boston, and Cambridge Health Alliance, Somerville, Mass., said in an interview.
“Melatonin gummies contained up to 347% more melatonin than what was listed on the label, and some products also contained cannabidiol; in one brand of melatonin gummies, there was zero melatonin, just CBD,” Dr. Cohen said.
The study was published online in JAMA.
530% jump in pediatric hospitalizations
Melatonin products are not approved by the Food and Drug Administration but are sold over the counter or online.
Previous research from JAMA has shown the use of melatonin has increased over the past 2 decades among people of all ages.
With increased use has come a spike in reports of melatonin overdose, calls to poison control centers, and related ED visits for children.
Federal data show the number of U.S. children who unintentionally ingested melatonin supplements jumped 530% from 2012 to 2021. More than 4,000 of the reported ingestions led to a hospital stay; 287 children required intensive care, and two children died.
It was unclear why melatonin supplements were causing these harms, which led Dr. Cohen’s team to analyze 25 unique brands of “melatonin” gummies purchased online.
One product didn’t contain any melatonin but did contain 31.3 mg of CBD.
In the remaining products, the quantity of melatonin ranged from 1.3 mg to 13.1 mg per serving. The actual quantity of melatonin ranged from 74% to 347% of the labeled quantity, the researchers found.
They note that for a young adult who takes as little as 0.1-0.3 mg of melatonin, plasma concentrations can increase into the normal night-time range.
Of the 25 products (88%) analyzed, 22 were inaccurately labeled, and only 3 (12%) contained a quantity of melatonin that was within 10% (plus or minus) of the declared quantity.
Five products listed CBD as an ingredient. The listed quantity ranged from 10.6 mg to 31.3 mg per serving, although the actual quantity of CBD ranged from 104% to 118% of the labeled quantity.
Inquire about use in kids
A limitation of the study is that only one sample of each brand was analyzed, and only gummies were analyzed. It is not known whether the results are generalizable to melatonin products sold as tablets and capsules in the United States or whether the quantity of melatonin within an individual brand may vary from batch to batch.
A recent study from Canada showed similar results. In an analysis of 16 Canadian melatonin brands, the actual dose of melatonin ranged from 17% to 478% of the declared quantity.
It’s estimated that more than 1% of all U.S. children use melatonin supplements, most commonly for sleep, stress, and relaxation.
“Given new research as to the excessive quantities of melatonin in gummies, caution should be used if considering their use,” said Dr. Cohen.
“It’s important to inquire about melatonin use when caring for children, particularly when parents express concerns about their child’s sleep,” he added.
The American Academy of Sleep Medicine recently issued a health advisory encouraging parents to talk to a health care professional before giving melatonin or any supplement to children.
Children don’t need melatonin
Commenting on the study, Michael Breus, PhD, clinical psychologist and founder of TheSleepDoctor.com, agreed that analyzing only one sample of each brand is a key limitation “because supplements are made in batches, and gummies in particular are difficult to distribute the active ingredient evenly.
“But even with that being said, 88% of them were labeled incorrectly, so even if there were a few single-sample issues, I kind of doubt its all of them,” Dr. Breus said.
“Kids as a general rule do not need melatonin. Their brains make almost four times the necessary amount already. If you start giving kids pills to help them sleep, then they start to have a pill problem, causing another issue,” Dr. Breus added.
“Most children’s falling asleep and staying sleep issues can be treated with behavioral measures like cognitive-behavioral therapy for insomnia,” he said.
The study had no specific funding. Dr. Cohen has received research support from Consumers Union and PEW Charitable Trusts and royalties from UptoDate. Dr. Breus disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA
How safe is the blackout rage gallon drinking trend?
This discussion was recorded on April 6, 2023. This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining us today is Dr. Lewis Nelson, professor and chair of emergency medicine at Rutgers New Jersey Medical School and a certified medical toxicologist.
Today, we will be discussing an important and disturbing Gen Z trend circulating on social media, known as blackout rage gallon, or BORG.
Welcome, Lewis.
Lewis S. Nelson, MD: Thanks for having me.
Dr. Glatter: Thanks so much for joining us. This trend that’s been circulating on social media is really disturbing. It has elements that focus on binge drinking: Talking about taking a jug; emptying half of it out; and putting one fifth of vodka and some electrolytes, caffeine, or other things too is just incredibly disturbing. Teens and parents are looking at this. I’ll let you jump into the discussion.
Dr. Nelson: You’re totally right, it is disturbing. Binge drinking is a huge problem in this country in general. It’s a particular problem with young people – teenagers and young adults. I don’t think people appreciate the dangers associated with binge drinking, such as the amount of alcohol they consume and some of the unintended consequences of doing that.
To frame things quickly, we think there are probably around six people a day in the United States who die of alcohol poisoning. Alcohol poisoning basically is binge drinking to such an extent that you die of the alcohol itself. You’re not dying of a car crash or doing something that injures you. You’re dying of the alcohol. You’re drinking so much that your breathing slows, it stops, you have heart rhythm disturbances, and so on. It totals about 2,200 people a year in the United States.
Dr. Glatter: That’s alarming. For this trend, their argument is that half of the gallon is water. Therefore, I’m fine. I can drink it over 8-12 hours and it’s not an issue. How would you respond to that?
Dr. Nelson: Well, alcohol is alcohol. It’s all about how much you take in over what time period. I guess, in concept, it could be safer if you do it right. That’s not the way it’s been, so to speak, marketed on the various social media platforms. It’s meant to be a way to protect yourself from having your drink spiked or eating or ingesting contaminants from other people’s mouths when you share glasses or dip cups into communal pots like jungle juice or something.
Clearly, if you’re going to drink a large amount of alcohol over a short or long period of time, you do run the risk of having significant consequences, including bad decision-making if you’re just a little drunk all the way down to that of the complications you described about alcohol poisoning.
Dr. Glatter: There has been a comment made that this could be a form of harm reduction. The point of harm reduction is that we run trials, we validate it, and we test it. This, certainly in my mind, is no form of true harm reduction. I think you would agree.
Dr. Nelson: Many things that are marketed as harm reduction aren’t. There could be some aspects of this that could be considered harm reduction. You may believe – and there’s no reason not to – that protecting your drink is a good idea. If you’re at a bar and you leave your glass open and somebody put something in it, you can be drugged. Drug-facilitated sexual assault, for example, is a big issue. That means you have to leave your glass unattended. If you tend to your glass, it’s probably fine. One of the ways of harm reduction they mention is that by having a cap and having this bottle with you at all times, that can’t happen.
Now, in fairness, by far the drug most commonly associated with sexual assault is alcohol. It’s not gamma-hydroxybutyrate or ketamine. It’s not the other things that people are concerned about. Those happen, but those are small problems in the big picture. It’s drinking too much.
A form of harm reduction that you can comment on perhaps is that you make this drink concoction yourself, so you know what is in there. You can take that bottle, pour out half the water, and fill up the other half with water and nobody’s going to know. More likely, the way they say you should do it is you take your gallon jug, you pour it out, and you fill it up with one fifth of vodka.
One fifth of vodka is the same amount of volume as a bottle of wine. At 750 mL, that’s a huge amount of alcohol. If you measure the number of shots in that bottle, it’s about 17 shots. Even if you drink that over 6 hours, that’s still several shots an hour. That’s a large amount of alcohol. You might do two or three shots once and then not drink for a few hours. To sit and drink two or three shots an hour for 6 hours, that’s just an exceptional amount of alcohol.
They flavorize it and add caffeine, which only adds to the risk. It doesn’t make it in any way safer. With the volume, 1 gal of water or equivalent over a short period of time in and of itself could be a problem. There’s a large amount of mismessaging here. Whether something’s harm reduction, it could flip around to be easily construed or understood as being harmful.
Not to mention, the idea that when you make something safer, one of the unintended consequences of harm reduction is what we call risk compensation. This is best probably described as what’s called the Peltzman effect. The way that we think about airbags and seatbelts is that they’re going to reduce car crash deaths; and they do, but people drive faster and more recklessly because they know they’re safe.
This is a well-described problem in epidemiology: You expect a certain amount of harm reduction through some implemented process, but you don’t meet that because people take increased risks.
Dr. Glatter: Right. The idea of not developing a hangover is common among many teens and 20-somethings, thinking that because there’s hydration there, because half of it is water, it’s just not going to happen. There’s your “harm reduction,” but your judgment’s impaired. It’s day drinking at its best, all day long. Then someone has the idea to get behind the wheel. These are the disastrous consequences that we all fear.
Dr. Nelson: There is a great example, perhaps of an unintended consequence of harm reduction. By putting caffeine in it, depending on how much caffeine you put in, some of these mixtures can have up to 1,000 mg of caffeine. Remember, a cup of coffee is about 1-200 mg, so you’re talking about several cups of coffee. The idea is that you will not be able to sense, as you normally do, how drunk you are. You’re not going to be a sleepy drunk, you’re going to be an awake drunk.
The idea that you’re going to have to drive so you’re going to drink a strong cup of black coffee before you go driving, you’re not going to drive any better. I can assure you that. You’re going to be more awake, perhaps, and not fall asleep at the wheel, but you’re still going to have psychomotor impairment. Your judgment is going to be impaired. There’s nothing good that comes with adding caffeine except that you’re going to be awake.
From a hangover perspective, there are many things that we’ve guessed at or suggested as either prevention or cures for hangovers. I don’t doubt that you’re going to have some volume depletion if you drink a large amount of alcohol. Alcohol’s a diuretic, so you’re going to lose more volume than you bring in.
Hydrating is probably always a good idea, but there is hydrating and then there’s overhydrating. We don’t need volumes like that. If you drink a cup or two of water, you’re probably fine. You don’t need to drink half a gallon of water. That can lead to problems like delusional hyponatremia, and so forth. There’s not any clear benefit to doing it.
If you want to prevent a hangover, one of the ways you might do it is by using vodka. There are nice data that show that clear alcohols typically, particularly vodka, don’t have many of the congeners that make the specific forms of alcohol what they are. Bourbon smells and tastes like bourbon because of these little molecules, these alkalis and ketones and amino acids and things that make it taste and smell the way it does. That’s true for all the other alcohols.
Vodka has the least amount of that. Even wine and beer have those in them, but vodka is basically alcohol mixed with water. It’s probably the least hangover-prone of all the alcohols; but still, if you drink a lot of vodka, you’re going to have a hangover. It’s just a dose-response curve to how much alcohol you drink, to how drunk you get, and to how much of a hangover you’re going to have.
Dr. Glatter: The hangover is really what it’s about because people want to be functional the next day. There are many companies out there that market hangover remedies, but people are using this as the hangover remedy in a way that’s socially accepted. That’s a good point you make.
The question is how do we get the message out to parents and teens? What’s the best way you feel to really sound the alarm here?
Dr. Nelson: These are challenging issues. We face this all the time with all the sorts of social media in particular. Most parents are not as savvy on social media as their kids are. You have to know what your children are doing. You should know what they’re listening to and watching. You do have to pay attention to the media directed at parents that will inform you a little bit about what your kids are doing. You have to talk with your kids and make sure they understand what it is that they’re doing.
We do this with our kids for some things. Hopefully, we talk about drinking, smoking, sex, and other things with our children (like driving if they get to that stage) and make sure they understand what the risks are and how to mitigate those risks. Being an attentive parent is part of it.
Sometimes you need outside messengers to do it. We’d like to believe that these social media companies are able to police themselves – at least they pay lip service to the fact they do. They have warnings that they’ll take things down that aren’t socially appropriate. Whether they do or not, I don’t know, because you keep seeing things about BORG on these media sites. If they are doing it, they’re not doing it efficiently or quickly enough.
Dr. Glatter: There has to be some censorship. These are young persons who are impressionable, who have developing brains, who are looking at this, thinking that if it’s out there on social media, such as TikTok or Instagram, then it’s okay to do so. That message has to be driven home.
Dr. Nelson: That’s a great point, and it’s tough. We know there’s been debate over the liability of social media or what they post, and whether or not they should be held liable like a more conventional media company or not. That’s politics and philosophy, and we’re probably not going to solve it here.
All these things wind up going viral and there’s probably got to be some filter on things that go viral. Maybe they need to have a bit more attentiveness to that when those things start happening. Now, clearly not every one of these is viral. When you think about some of the challenges we’ve seen in the past, such as the Tide Pod challenge and cinnamon challenge, some of these things could be quickly figured out to be dangerous.
I remember that the ice bucket challenge for amyotrophic lateral sclerosis was pretty benign. You pour a bucket of water over your head, and people aren’t really getting hurt. That’s fun and good, and let people go out and do that. That could pass through the filter. When you start to see people drinking excessive amounts of alcohol, it doesn’t take an emergency physician to know that’s not a good thing. Any parent should know that if my kid drinks half a bottle or a bottle of vodka over a short period of time, that just can’t be okay.
Dr. Glatter: It’s a public health issue. That’s what we need to elevate it to because ultimately that’s what it impacts: welfare and safety.
Speaking of buckets, there’s a new bucket challenge, wherein unsuspecting people have a bucket put on their head, can’t breathe, and then pass out. There’s been a number of these reported and actually filmed on social media. Here’s another example of dangerous types of behavior that essentially are a form of assault. Unsuspecting people suffer injuries from young children and teens trying to play pranks.
Again, had there not been this medium, we wouldn’t necessarily see the extent of the injuries. I guess going forward, the next step would be to send a message to colleges that there should be some form of warning if this trend is seen, at least from a public health standpoint.
Dr. Nelson: Education is a necessary thing to do, but it’s almost never the real solution to a problem. We can educate people as best we can that they need to do things right. At some point, we’re going to need to regulate it or manage it somehow.
Whether it’s through a carrot or a stick approach, or whether you want to give people kudos for doing the right thing or punish them for doing something wrong, that’s a tough decision to make and one that is going to be made by a parent or guardian, a school official, or law enforcement. Somehow, we have to figure out how to make this happen.
There’s not going to be a single size that fits all for this. At some level, we have to do something to educate and regulate. The balance between those two things is going to be political and philosophical in nature.
Dr. Glatter: Right, and the element of peer pressure and conformity in this is really part of the element. If we try to remove that aspect of it, then often these trends would go away. That aspect of conformity and peer pressure is instrumental in fueling these trends. Maybe we can make a full gallon of water be the trend without any alcohol in there.
Dr. Nelson: We say water is only water, but as a medical toxicologist, I can tell you that one of the foundations in medical toxicology is that everything is toxic. It’s just the dose that determines the toxicity. Oxygen is toxic, water is toxic. Everything’s toxic if you take enough of it.
We know that whether it’s psychogenic or intentional, polydipsia by drinking excessive amounts of water, especially without electrolytes, is one of the reasons they say you should add electrolytes. That’s all relative as well, because depending on the electrolyte and how much you put in and things like that, that could also become dangerous. Drinking excessive amounts of water like they’re suggesting, which sounds like a good thing to prevent hangover and so on, can in and of itself be a problem too.
Dr. Glatter: Right, and we know that there’s no magic bullet for a hangover. Obviously, abstinence is the only thing that truly works.
Dr. Nelson: Or moderation.
Dr. Glatter: Until research proves further.
Thank you so much. You’ve made some really important points. Thank you for talking about the BORG phenomenon, how it relates to society in general, and what we can do to try to change people’s perception of alcohol and the bigger picture of binge drinking. I really appreciate it.
Dr. Nelson: Thanks, Rob, for having me. It’s an important topic and hopefully we can get a handle on this. I appreciate your time.
Dr. Glatter is an attending physician at Lenox Hill Hospital in New York City and assistant professor of emergency medicine at Hofstra University, Hempstead, N.Y. Dr. Nelson is professor and chair of the department of emergency medicine and chief of the division of medical toxicology at Rutgers New Jersey Medical School, Newark. He is a member of the board of directors of the American Board of Emergency Medicine, the Accreditation Council for Continuing Medical Education, and Association of Academic Chairs in Emergency Medicine and is past-president of the American College of Medical Toxicology. Dr. Glatter and Dr. Nelson disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
This discussion was recorded on April 6, 2023. This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining us today is Dr. Lewis Nelson, professor and chair of emergency medicine at Rutgers New Jersey Medical School and a certified medical toxicologist.
Today, we will be discussing an important and disturbing Gen Z trend circulating on social media, known as blackout rage gallon, or BORG.
Welcome, Lewis.
Lewis S. Nelson, MD: Thanks for having me.
Dr. Glatter: Thanks so much for joining us. This trend that’s been circulating on social media is really disturbing. It has elements that focus on binge drinking: Talking about taking a jug; emptying half of it out; and putting one fifth of vodka and some electrolytes, caffeine, or other things too is just incredibly disturbing. Teens and parents are looking at this. I’ll let you jump into the discussion.
Dr. Nelson: You’re totally right, it is disturbing. Binge drinking is a huge problem in this country in general. It’s a particular problem with young people – teenagers and young adults. I don’t think people appreciate the dangers associated with binge drinking, such as the amount of alcohol they consume and some of the unintended consequences of doing that.
To frame things quickly, we think there are probably around six people a day in the United States who die of alcohol poisoning. Alcohol poisoning basically is binge drinking to such an extent that you die of the alcohol itself. You’re not dying of a car crash or doing something that injures you. You’re dying of the alcohol. You’re drinking so much that your breathing slows, it stops, you have heart rhythm disturbances, and so on. It totals about 2,200 people a year in the United States.
Dr. Glatter: That’s alarming. For this trend, their argument is that half of the gallon is water. Therefore, I’m fine. I can drink it over 8-12 hours and it’s not an issue. How would you respond to that?
Dr. Nelson: Well, alcohol is alcohol. It’s all about how much you take in over what time period. I guess, in concept, it could be safer if you do it right. That’s not the way it’s been, so to speak, marketed on the various social media platforms. It’s meant to be a way to protect yourself from having your drink spiked or eating or ingesting contaminants from other people’s mouths when you share glasses or dip cups into communal pots like jungle juice or something.
Clearly, if you’re going to drink a large amount of alcohol over a short or long period of time, you do run the risk of having significant consequences, including bad decision-making if you’re just a little drunk all the way down to that of the complications you described about alcohol poisoning.
Dr. Glatter: There has been a comment made that this could be a form of harm reduction. The point of harm reduction is that we run trials, we validate it, and we test it. This, certainly in my mind, is no form of true harm reduction. I think you would agree.
Dr. Nelson: Many things that are marketed as harm reduction aren’t. There could be some aspects of this that could be considered harm reduction. You may believe – and there’s no reason not to – that protecting your drink is a good idea. If you’re at a bar and you leave your glass open and somebody put something in it, you can be drugged. Drug-facilitated sexual assault, for example, is a big issue. That means you have to leave your glass unattended. If you tend to your glass, it’s probably fine. One of the ways of harm reduction they mention is that by having a cap and having this bottle with you at all times, that can’t happen.
Now, in fairness, by far the drug most commonly associated with sexual assault is alcohol. It’s not gamma-hydroxybutyrate or ketamine. It’s not the other things that people are concerned about. Those happen, but those are small problems in the big picture. It’s drinking too much.
A form of harm reduction that you can comment on perhaps is that you make this drink concoction yourself, so you know what is in there. You can take that bottle, pour out half the water, and fill up the other half with water and nobody’s going to know. More likely, the way they say you should do it is you take your gallon jug, you pour it out, and you fill it up with one fifth of vodka.
One fifth of vodka is the same amount of volume as a bottle of wine. At 750 mL, that’s a huge amount of alcohol. If you measure the number of shots in that bottle, it’s about 17 shots. Even if you drink that over 6 hours, that’s still several shots an hour. That’s a large amount of alcohol. You might do two or three shots once and then not drink for a few hours. To sit and drink two or three shots an hour for 6 hours, that’s just an exceptional amount of alcohol.
They flavorize it and add caffeine, which only adds to the risk. It doesn’t make it in any way safer. With the volume, 1 gal of water or equivalent over a short period of time in and of itself could be a problem. There’s a large amount of mismessaging here. Whether something’s harm reduction, it could flip around to be easily construed or understood as being harmful.
Not to mention, the idea that when you make something safer, one of the unintended consequences of harm reduction is what we call risk compensation. This is best probably described as what’s called the Peltzman effect. The way that we think about airbags and seatbelts is that they’re going to reduce car crash deaths; and they do, but people drive faster and more recklessly because they know they’re safe.
This is a well-described problem in epidemiology: You expect a certain amount of harm reduction through some implemented process, but you don’t meet that because people take increased risks.
Dr. Glatter: Right. The idea of not developing a hangover is common among many teens and 20-somethings, thinking that because there’s hydration there, because half of it is water, it’s just not going to happen. There’s your “harm reduction,” but your judgment’s impaired. It’s day drinking at its best, all day long. Then someone has the idea to get behind the wheel. These are the disastrous consequences that we all fear.
Dr. Nelson: There is a great example, perhaps of an unintended consequence of harm reduction. By putting caffeine in it, depending on how much caffeine you put in, some of these mixtures can have up to 1,000 mg of caffeine. Remember, a cup of coffee is about 1-200 mg, so you’re talking about several cups of coffee. The idea is that you will not be able to sense, as you normally do, how drunk you are. You’re not going to be a sleepy drunk, you’re going to be an awake drunk.
The idea that you’re going to have to drive so you’re going to drink a strong cup of black coffee before you go driving, you’re not going to drive any better. I can assure you that. You’re going to be more awake, perhaps, and not fall asleep at the wheel, but you’re still going to have psychomotor impairment. Your judgment is going to be impaired. There’s nothing good that comes with adding caffeine except that you’re going to be awake.
From a hangover perspective, there are many things that we’ve guessed at or suggested as either prevention or cures for hangovers. I don’t doubt that you’re going to have some volume depletion if you drink a large amount of alcohol. Alcohol’s a diuretic, so you’re going to lose more volume than you bring in.
Hydrating is probably always a good idea, but there is hydrating and then there’s overhydrating. We don’t need volumes like that. If you drink a cup or two of water, you’re probably fine. You don’t need to drink half a gallon of water. That can lead to problems like delusional hyponatremia, and so forth. There’s not any clear benefit to doing it.
If you want to prevent a hangover, one of the ways you might do it is by using vodka. There are nice data that show that clear alcohols typically, particularly vodka, don’t have many of the congeners that make the specific forms of alcohol what they are. Bourbon smells and tastes like bourbon because of these little molecules, these alkalis and ketones and amino acids and things that make it taste and smell the way it does. That’s true for all the other alcohols.
Vodka has the least amount of that. Even wine and beer have those in them, but vodka is basically alcohol mixed with water. It’s probably the least hangover-prone of all the alcohols; but still, if you drink a lot of vodka, you’re going to have a hangover. It’s just a dose-response curve to how much alcohol you drink, to how drunk you get, and to how much of a hangover you’re going to have.
Dr. Glatter: The hangover is really what it’s about because people want to be functional the next day. There are many companies out there that market hangover remedies, but people are using this as the hangover remedy in a way that’s socially accepted. That’s a good point you make.
The question is how do we get the message out to parents and teens? What’s the best way you feel to really sound the alarm here?
Dr. Nelson: These are challenging issues. We face this all the time with all the sorts of social media in particular. Most parents are not as savvy on social media as their kids are. You have to know what your children are doing. You should know what they’re listening to and watching. You do have to pay attention to the media directed at parents that will inform you a little bit about what your kids are doing. You have to talk with your kids and make sure they understand what it is that they’re doing.
We do this with our kids for some things. Hopefully, we talk about drinking, smoking, sex, and other things with our children (like driving if they get to that stage) and make sure they understand what the risks are and how to mitigate those risks. Being an attentive parent is part of it.
Sometimes you need outside messengers to do it. We’d like to believe that these social media companies are able to police themselves – at least they pay lip service to the fact they do. They have warnings that they’ll take things down that aren’t socially appropriate. Whether they do or not, I don’t know, because you keep seeing things about BORG on these media sites. If they are doing it, they’re not doing it efficiently or quickly enough.
Dr. Glatter: There has to be some censorship. These are young persons who are impressionable, who have developing brains, who are looking at this, thinking that if it’s out there on social media, such as TikTok or Instagram, then it’s okay to do so. That message has to be driven home.
Dr. Nelson: That’s a great point, and it’s tough. We know there’s been debate over the liability of social media or what they post, and whether or not they should be held liable like a more conventional media company or not. That’s politics and philosophy, and we’re probably not going to solve it here.
All these things wind up going viral and there’s probably got to be some filter on things that go viral. Maybe they need to have a bit more attentiveness to that when those things start happening. Now, clearly not every one of these is viral. When you think about some of the challenges we’ve seen in the past, such as the Tide Pod challenge and cinnamon challenge, some of these things could be quickly figured out to be dangerous.
I remember that the ice bucket challenge for amyotrophic lateral sclerosis was pretty benign. You pour a bucket of water over your head, and people aren’t really getting hurt. That’s fun and good, and let people go out and do that. That could pass through the filter. When you start to see people drinking excessive amounts of alcohol, it doesn’t take an emergency physician to know that’s not a good thing. Any parent should know that if my kid drinks half a bottle or a bottle of vodka over a short period of time, that just can’t be okay.
Dr. Glatter: It’s a public health issue. That’s what we need to elevate it to because ultimately that’s what it impacts: welfare and safety.
Speaking of buckets, there’s a new bucket challenge, wherein unsuspecting people have a bucket put on their head, can’t breathe, and then pass out. There’s been a number of these reported and actually filmed on social media. Here’s another example of dangerous types of behavior that essentially are a form of assault. Unsuspecting people suffer injuries from young children and teens trying to play pranks.
Again, had there not been this medium, we wouldn’t necessarily see the extent of the injuries. I guess going forward, the next step would be to send a message to colleges that there should be some form of warning if this trend is seen, at least from a public health standpoint.
Dr. Nelson: Education is a necessary thing to do, but it’s almost never the real solution to a problem. We can educate people as best we can that they need to do things right. At some point, we’re going to need to regulate it or manage it somehow.
Whether it’s through a carrot or a stick approach, or whether you want to give people kudos for doing the right thing or punish them for doing something wrong, that’s a tough decision to make and one that is going to be made by a parent or guardian, a school official, or law enforcement. Somehow, we have to figure out how to make this happen.
There’s not going to be a single size that fits all for this. At some level, we have to do something to educate and regulate. The balance between those two things is going to be political and philosophical in nature.
Dr. Glatter: Right, and the element of peer pressure and conformity in this is really part of the element. If we try to remove that aspect of it, then often these trends would go away. That aspect of conformity and peer pressure is instrumental in fueling these trends. Maybe we can make a full gallon of water be the trend without any alcohol in there.
Dr. Nelson: We say water is only water, but as a medical toxicologist, I can tell you that one of the foundations in medical toxicology is that everything is toxic. It’s just the dose that determines the toxicity. Oxygen is toxic, water is toxic. Everything’s toxic if you take enough of it.
We know that whether it’s psychogenic or intentional, polydipsia by drinking excessive amounts of water, especially without electrolytes, is one of the reasons they say you should add electrolytes. That’s all relative as well, because depending on the electrolyte and how much you put in and things like that, that could also become dangerous. Drinking excessive amounts of water like they’re suggesting, which sounds like a good thing to prevent hangover and so on, can in and of itself be a problem too.
Dr. Glatter: Right, and we know that there’s no magic bullet for a hangover. Obviously, abstinence is the only thing that truly works.
Dr. Nelson: Or moderation.
Dr. Glatter: Until research proves further.
Thank you so much. You’ve made some really important points. Thank you for talking about the BORG phenomenon, how it relates to society in general, and what we can do to try to change people’s perception of alcohol and the bigger picture of binge drinking. I really appreciate it.
Dr. Nelson: Thanks, Rob, for having me. It’s an important topic and hopefully we can get a handle on this. I appreciate your time.
Dr. Glatter is an attending physician at Lenox Hill Hospital in New York City and assistant professor of emergency medicine at Hofstra University, Hempstead, N.Y. Dr. Nelson is professor and chair of the department of emergency medicine and chief of the division of medical toxicology at Rutgers New Jersey Medical School, Newark. He is a member of the board of directors of the American Board of Emergency Medicine, the Accreditation Council for Continuing Medical Education, and Association of Academic Chairs in Emergency Medicine and is past-president of the American College of Medical Toxicology. Dr. Glatter and Dr. Nelson disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
This discussion was recorded on April 6, 2023. This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining us today is Dr. Lewis Nelson, professor and chair of emergency medicine at Rutgers New Jersey Medical School and a certified medical toxicologist.
Today, we will be discussing an important and disturbing Gen Z trend circulating on social media, known as blackout rage gallon, or BORG.
Welcome, Lewis.
Lewis S. Nelson, MD: Thanks for having me.
Dr. Glatter: Thanks so much for joining us. This trend that’s been circulating on social media is really disturbing. It has elements that focus on binge drinking: Talking about taking a jug; emptying half of it out; and putting one fifth of vodka and some electrolytes, caffeine, or other things too is just incredibly disturbing. Teens and parents are looking at this. I’ll let you jump into the discussion.
Dr. Nelson: You’re totally right, it is disturbing. Binge drinking is a huge problem in this country in general. It’s a particular problem with young people – teenagers and young adults. I don’t think people appreciate the dangers associated with binge drinking, such as the amount of alcohol they consume and some of the unintended consequences of doing that.
To frame things quickly, we think there are probably around six people a day in the United States who die of alcohol poisoning. Alcohol poisoning basically is binge drinking to such an extent that you die of the alcohol itself. You’re not dying of a car crash or doing something that injures you. You’re dying of the alcohol. You’re drinking so much that your breathing slows, it stops, you have heart rhythm disturbances, and so on. It totals about 2,200 people a year in the United States.
Dr. Glatter: That’s alarming. For this trend, their argument is that half of the gallon is water. Therefore, I’m fine. I can drink it over 8-12 hours and it’s not an issue. How would you respond to that?
Dr. Nelson: Well, alcohol is alcohol. It’s all about how much you take in over what time period. I guess, in concept, it could be safer if you do it right. That’s not the way it’s been, so to speak, marketed on the various social media platforms. It’s meant to be a way to protect yourself from having your drink spiked or eating or ingesting contaminants from other people’s mouths when you share glasses or dip cups into communal pots like jungle juice or something.
Clearly, if you’re going to drink a large amount of alcohol over a short or long period of time, you do run the risk of having significant consequences, including bad decision-making if you’re just a little drunk all the way down to that of the complications you described about alcohol poisoning.
Dr. Glatter: There has been a comment made that this could be a form of harm reduction. The point of harm reduction is that we run trials, we validate it, and we test it. This, certainly in my mind, is no form of true harm reduction. I think you would agree.
Dr. Nelson: Many things that are marketed as harm reduction aren’t. There could be some aspects of this that could be considered harm reduction. You may believe – and there’s no reason not to – that protecting your drink is a good idea. If you’re at a bar and you leave your glass open and somebody put something in it, you can be drugged. Drug-facilitated sexual assault, for example, is a big issue. That means you have to leave your glass unattended. If you tend to your glass, it’s probably fine. One of the ways of harm reduction they mention is that by having a cap and having this bottle with you at all times, that can’t happen.
Now, in fairness, by far the drug most commonly associated with sexual assault is alcohol. It’s not gamma-hydroxybutyrate or ketamine. It’s not the other things that people are concerned about. Those happen, but those are small problems in the big picture. It’s drinking too much.
A form of harm reduction that you can comment on perhaps is that you make this drink concoction yourself, so you know what is in there. You can take that bottle, pour out half the water, and fill up the other half with water and nobody’s going to know. More likely, the way they say you should do it is you take your gallon jug, you pour it out, and you fill it up with one fifth of vodka.
One fifth of vodka is the same amount of volume as a bottle of wine. At 750 mL, that’s a huge amount of alcohol. If you measure the number of shots in that bottle, it’s about 17 shots. Even if you drink that over 6 hours, that’s still several shots an hour. That’s a large amount of alcohol. You might do two or three shots once and then not drink for a few hours. To sit and drink two or three shots an hour for 6 hours, that’s just an exceptional amount of alcohol.
They flavorize it and add caffeine, which only adds to the risk. It doesn’t make it in any way safer. With the volume, 1 gal of water or equivalent over a short period of time in and of itself could be a problem. There’s a large amount of mismessaging here. Whether something’s harm reduction, it could flip around to be easily construed or understood as being harmful.
Not to mention, the idea that when you make something safer, one of the unintended consequences of harm reduction is what we call risk compensation. This is best probably described as what’s called the Peltzman effect. The way that we think about airbags and seatbelts is that they’re going to reduce car crash deaths; and they do, but people drive faster and more recklessly because they know they’re safe.
This is a well-described problem in epidemiology: You expect a certain amount of harm reduction through some implemented process, but you don’t meet that because people take increased risks.
Dr. Glatter: Right. The idea of not developing a hangover is common among many teens and 20-somethings, thinking that because there’s hydration there, because half of it is water, it’s just not going to happen. There’s your “harm reduction,” but your judgment’s impaired. It’s day drinking at its best, all day long. Then someone has the idea to get behind the wheel. These are the disastrous consequences that we all fear.
Dr. Nelson: There is a great example, perhaps of an unintended consequence of harm reduction. By putting caffeine in it, depending on how much caffeine you put in, some of these mixtures can have up to 1,000 mg of caffeine. Remember, a cup of coffee is about 1-200 mg, so you’re talking about several cups of coffee. The idea is that you will not be able to sense, as you normally do, how drunk you are. You’re not going to be a sleepy drunk, you’re going to be an awake drunk.
The idea that you’re going to have to drive so you’re going to drink a strong cup of black coffee before you go driving, you’re not going to drive any better. I can assure you that. You’re going to be more awake, perhaps, and not fall asleep at the wheel, but you’re still going to have psychomotor impairment. Your judgment is going to be impaired. There’s nothing good that comes with adding caffeine except that you’re going to be awake.
From a hangover perspective, there are many things that we’ve guessed at or suggested as either prevention or cures for hangovers. I don’t doubt that you’re going to have some volume depletion if you drink a large amount of alcohol. Alcohol’s a diuretic, so you’re going to lose more volume than you bring in.
Hydrating is probably always a good idea, but there is hydrating and then there’s overhydrating. We don’t need volumes like that. If you drink a cup or two of water, you’re probably fine. You don’t need to drink half a gallon of water. That can lead to problems like delusional hyponatremia, and so forth. There’s not any clear benefit to doing it.
If you want to prevent a hangover, one of the ways you might do it is by using vodka. There are nice data that show that clear alcohols typically, particularly vodka, don’t have many of the congeners that make the specific forms of alcohol what they are. Bourbon smells and tastes like bourbon because of these little molecules, these alkalis and ketones and amino acids and things that make it taste and smell the way it does. That’s true for all the other alcohols.
Vodka has the least amount of that. Even wine and beer have those in them, but vodka is basically alcohol mixed with water. It’s probably the least hangover-prone of all the alcohols; but still, if you drink a lot of vodka, you’re going to have a hangover. It’s just a dose-response curve to how much alcohol you drink, to how drunk you get, and to how much of a hangover you’re going to have.
Dr. Glatter: The hangover is really what it’s about because people want to be functional the next day. There are many companies out there that market hangover remedies, but people are using this as the hangover remedy in a way that’s socially accepted. That’s a good point you make.
The question is how do we get the message out to parents and teens? What’s the best way you feel to really sound the alarm here?
Dr. Nelson: These are challenging issues. We face this all the time with all the sorts of social media in particular. Most parents are not as savvy on social media as their kids are. You have to know what your children are doing. You should know what they’re listening to and watching. You do have to pay attention to the media directed at parents that will inform you a little bit about what your kids are doing. You have to talk with your kids and make sure they understand what it is that they’re doing.
We do this with our kids for some things. Hopefully, we talk about drinking, smoking, sex, and other things with our children (like driving if they get to that stage) and make sure they understand what the risks are and how to mitigate those risks. Being an attentive parent is part of it.
Sometimes you need outside messengers to do it. We’d like to believe that these social media companies are able to police themselves – at least they pay lip service to the fact they do. They have warnings that they’ll take things down that aren’t socially appropriate. Whether they do or not, I don’t know, because you keep seeing things about BORG on these media sites. If they are doing it, they’re not doing it efficiently or quickly enough.
Dr. Glatter: There has to be some censorship. These are young persons who are impressionable, who have developing brains, who are looking at this, thinking that if it’s out there on social media, such as TikTok or Instagram, then it’s okay to do so. That message has to be driven home.
Dr. Nelson: That’s a great point, and it’s tough. We know there’s been debate over the liability of social media or what they post, and whether or not they should be held liable like a more conventional media company or not. That’s politics and philosophy, and we’re probably not going to solve it here.
All these things wind up going viral and there’s probably got to be some filter on things that go viral. Maybe they need to have a bit more attentiveness to that when those things start happening. Now, clearly not every one of these is viral. When you think about some of the challenges we’ve seen in the past, such as the Tide Pod challenge and cinnamon challenge, some of these things could be quickly figured out to be dangerous.
I remember that the ice bucket challenge for amyotrophic lateral sclerosis was pretty benign. You pour a bucket of water over your head, and people aren’t really getting hurt. That’s fun and good, and let people go out and do that. That could pass through the filter. When you start to see people drinking excessive amounts of alcohol, it doesn’t take an emergency physician to know that’s not a good thing. Any parent should know that if my kid drinks half a bottle or a bottle of vodka over a short period of time, that just can’t be okay.
Dr. Glatter: It’s a public health issue. That’s what we need to elevate it to because ultimately that’s what it impacts: welfare and safety.
Speaking of buckets, there’s a new bucket challenge, wherein unsuspecting people have a bucket put on their head, can’t breathe, and then pass out. There’s been a number of these reported and actually filmed on social media. Here’s another example of dangerous types of behavior that essentially are a form of assault. Unsuspecting people suffer injuries from young children and teens trying to play pranks.
Again, had there not been this medium, we wouldn’t necessarily see the extent of the injuries. I guess going forward, the next step would be to send a message to colleges that there should be some form of warning if this trend is seen, at least from a public health standpoint.
Dr. Nelson: Education is a necessary thing to do, but it’s almost never the real solution to a problem. We can educate people as best we can that they need to do things right. At some point, we’re going to need to regulate it or manage it somehow.
Whether it’s through a carrot or a stick approach, or whether you want to give people kudos for doing the right thing or punish them for doing something wrong, that’s a tough decision to make and one that is going to be made by a parent or guardian, a school official, or law enforcement. Somehow, we have to figure out how to make this happen.
There’s not going to be a single size that fits all for this. At some level, we have to do something to educate and regulate. The balance between those two things is going to be political and philosophical in nature.
Dr. Glatter: Right, and the element of peer pressure and conformity in this is really part of the element. If we try to remove that aspect of it, then often these trends would go away. That aspect of conformity and peer pressure is instrumental in fueling these trends. Maybe we can make a full gallon of water be the trend without any alcohol in there.
Dr. Nelson: We say water is only water, but as a medical toxicologist, I can tell you that one of the foundations in medical toxicology is that everything is toxic. It’s just the dose that determines the toxicity. Oxygen is toxic, water is toxic. Everything’s toxic if you take enough of it.
We know that whether it’s psychogenic or intentional, polydipsia by drinking excessive amounts of water, especially without electrolytes, is one of the reasons they say you should add electrolytes. That’s all relative as well, because depending on the electrolyte and how much you put in and things like that, that could also become dangerous. Drinking excessive amounts of water like they’re suggesting, which sounds like a good thing to prevent hangover and so on, can in and of itself be a problem too.
Dr. Glatter: Right, and we know that there’s no magic bullet for a hangover. Obviously, abstinence is the only thing that truly works.
Dr. Nelson: Or moderation.
Dr. Glatter: Until research proves further.
Thank you so much. You’ve made some really important points. Thank you for talking about the BORG phenomenon, how it relates to society in general, and what we can do to try to change people’s perception of alcohol and the bigger picture of binge drinking. I really appreciate it.
Dr. Nelson: Thanks, Rob, for having me. It’s an important topic and hopefully we can get a handle on this. I appreciate your time.
Dr. Glatter is an attending physician at Lenox Hill Hospital in New York City and assistant professor of emergency medicine at Hofstra University, Hempstead, N.Y. Dr. Nelson is professor and chair of the department of emergency medicine and chief of the division of medical toxicology at Rutgers New Jersey Medical School, Newark. He is a member of the board of directors of the American Board of Emergency Medicine, the Accreditation Council for Continuing Medical Education, and Association of Academic Chairs in Emergency Medicine and is past-president of the American College of Medical Toxicology. Dr. Glatter and Dr. Nelson disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Tranq-contaminated fentanyl now in 48 states, DEA warns
The DEA warning comes on the heels of a Food and Drug Administration announcement that it would begin more closely monitoring imports of the raw materials and bulk shipments of xylazine, also known as “tranq” and “zombie drug.”
Xylazine was first approved by the FDA in 1972 as a sedative and analgesic for use only in animals, but is increasingly being detected in illicit street drugs, and is often mixed with fentanyl, cocaine, and methamphetamine.
The FDA warned in November that naloxone (Narcan) would not reverse xylazine-related overdoses because the tranquilizer is not an opioid. It does suppress respiration and repeated exposures may lead to dependence and withdrawal, said the agency. Users are also experiencing severe necrosis at injection sites.
“Xylazine is making the deadliest drug threat our country has ever faced, fentanyl, even deadlier,” said DEA Administrator Anne Milgram in a statement. “The DEA Laboratory System is reporting that in 2022 approximately 23% of fentanyl powder and 7% of fentanyl pills seized by the DEA contained xylazine.”
Xylazine use has spread quickly, from its start in the Philadelphia area to the Northeast, the South, and most recently the West.
Citing data from the Centers for Disease Control and Prevention, the DEA said that 66% of the 107,735 overdose deaths for the year ending August 2022 involved synthetic opioids such as fentanyl. The DEA said that the Sinaloa Cartel and Jalisco Cartel in Mexico, using chemicals sourced from China, are primarily responsible for trafficking fentanyl in the United States.
A version of this article originally appeared on Medscape.com.
The DEA warning comes on the heels of a Food and Drug Administration announcement that it would begin more closely monitoring imports of the raw materials and bulk shipments of xylazine, also known as “tranq” and “zombie drug.”
Xylazine was first approved by the FDA in 1972 as a sedative and analgesic for use only in animals, but is increasingly being detected in illicit street drugs, and is often mixed with fentanyl, cocaine, and methamphetamine.
The FDA warned in November that naloxone (Narcan) would not reverse xylazine-related overdoses because the tranquilizer is not an opioid. It does suppress respiration and repeated exposures may lead to dependence and withdrawal, said the agency. Users are also experiencing severe necrosis at injection sites.
“Xylazine is making the deadliest drug threat our country has ever faced, fentanyl, even deadlier,” said DEA Administrator Anne Milgram in a statement. “The DEA Laboratory System is reporting that in 2022 approximately 23% of fentanyl powder and 7% of fentanyl pills seized by the DEA contained xylazine.”
Xylazine use has spread quickly, from its start in the Philadelphia area to the Northeast, the South, and most recently the West.
Citing data from the Centers for Disease Control and Prevention, the DEA said that 66% of the 107,735 overdose deaths for the year ending August 2022 involved synthetic opioids such as fentanyl. The DEA said that the Sinaloa Cartel and Jalisco Cartel in Mexico, using chemicals sourced from China, are primarily responsible for trafficking fentanyl in the United States.
A version of this article originally appeared on Medscape.com.
The DEA warning comes on the heels of a Food and Drug Administration announcement that it would begin more closely monitoring imports of the raw materials and bulk shipments of xylazine, also known as “tranq” and “zombie drug.”
Xylazine was first approved by the FDA in 1972 as a sedative and analgesic for use only in animals, but is increasingly being detected in illicit street drugs, and is often mixed with fentanyl, cocaine, and methamphetamine.
The FDA warned in November that naloxone (Narcan) would not reverse xylazine-related overdoses because the tranquilizer is not an opioid. It does suppress respiration and repeated exposures may lead to dependence and withdrawal, said the agency. Users are also experiencing severe necrosis at injection sites.
“Xylazine is making the deadliest drug threat our country has ever faced, fentanyl, even deadlier,” said DEA Administrator Anne Milgram in a statement. “The DEA Laboratory System is reporting that in 2022 approximately 23% of fentanyl powder and 7% of fentanyl pills seized by the DEA contained xylazine.”
Xylazine use has spread quickly, from its start in the Philadelphia area to the Northeast, the South, and most recently the West.
Citing data from the Centers for Disease Control and Prevention, the DEA said that 66% of the 107,735 overdose deaths for the year ending August 2022 involved synthetic opioids such as fentanyl. The DEA said that the Sinaloa Cartel and Jalisco Cartel in Mexico, using chemicals sourced from China, are primarily responsible for trafficking fentanyl in the United States.
A version of this article originally appeared on Medscape.com.
Opioid overdose is an important cause of postpartum death
(OUD), according to research published in Obstetrics and Gynecology.
Opioid overdose deaths account for up to 10% of pregnancy-associated deaths in the United States, and 75% of the deliveries of women with OUD are covered by Medicaid, according to lead author Elizabeth Suarez, PhD, MPH, with the division of pharmacoepidemiology and pharmacoeconomics at Brigham and Women’s Hospital and Harvard Medical School in Boston, and colleagues.
Nearly 5 million deliveries studied
Researchers studied claims data from Medicaid and the National Death Index database in the United States from 2006 to 2013 for 4,972,061 deliveries. They also identified a subgroup of women with a documented history of OUD in the 3 months before delivery.
They found the incidence of postpartum opioid overdose deaths was 5.4 per 100,000 deliveries (95% confidence interval, 4.5-6.4) among all in the study and 118 per 100,000 (95% CI, 84-163) among individuals with OUD.
Incidence of all-cause postpartum death was six times higher in women with OUD than in all the women studied. Common causes of death of those with OUD were other drug- and alcohol-related deaths (47/100,000); suicide (26/100,000); and other injuries, including accidents and falls (33/100,000).
Risk factors strongly linked with postpartum opioid overdose death included mental health and other substance use disorders.
Medication significantly lowers death risk
The authors also documented the benefit of buprenorphine or methadone for OUD.
For women with OUD who used medication to treat OUD post partum, odds of opioid overdose death were 60% lower (odds ratio, 0.4; 95% CI 0.1-0.9).
As important as use of medication, Marcela Smid, MD, MS, writes in an accompanying editorial, is noting that 80% of the women in this study who died of opioid overdoses had contact with a health care provider before death.
“Both of these results indicate that we have the means and opportunity to prevent these deaths,” writes Dr. Smid, with the division of maternal fetal medicine, University of Utah Health in Salt Lake City.
Dismal numbers on ob.gyns. trained to prescribe medications
She points out some barriers, however. Most clinicians, she notes, lack time and training to prescribe buprenorphine, and in 2019, fewer than 2% of ob.gyns. who accept Medicaid were able to prescribe it.
Her charge to ob.gyns.: “We need to help identify individuals who are at high risk of OUD or opioid overdose by screening.” A validated screening tool should be used at prenatal and postpartum appointments.
On a bigger scale, she urges Medicaid to be expanded for a full year post partum through the American Rescue Act’s State Plan Amendment, something only 28 states and Washington, D.C., have done so far.
Dr. Smid points out some good news, however: President Joe Biden signed the Consolidated Appropriations Act 2023, which eliminated the “X” waiver.
Now all clinicians who have a Drug Enforcement Administration registration that includes Schedule III authority can prescribe buprenorphine for OUD if applicable state law allows it.
But that calls for medical schools and residency programs to prioritize addiction medicine as a core competency, Dr. Smid says.
Getting naloxone to patients, families
One of the potential interventions the study authors suggest is providing naloxone prescriptions and training to pregnant and postpartum women who have a substance use history and to their partners and significant others.
However, Mishka Terplan, MD, MPH, told this publication, “It’s one thing to write a prescription; it’s another thing for the person to actually get the medication.” He is medical director of the Friends Research Institute in Baltimore, an ob.gyn. who specializes in addiction medicine.
“What can we do?” We can think about how to get naloxone into people’s hands at discharge from the hospital after they give birth, instead of prescribing. That would mean that health systems need to prioritize this, he said. “We give people discharge medications all the time.”
Still, naloxone can’t be seen as the answer, he said.
He compares it to defibrillators in public places, which are for rescues, not reversing a population problem.
“Some people think that naloxone reversals are doing something about OUD. It’s doing about as much about OUD as defibrillators do for cardiovascular disease,” he said.
The best help, he says, will be continuation of treatment.
“Addiction is a chronic condition,” he says, “but often we only provide episodic care. We see that particularly in pregnancy. Once the pregnancy is finished, there’s not categorical continuation of insurance.”
Even if you do have insurance, it’s hard to find a clinic that’s family friendly, he notes. “You might not feel comfortable taking your newborn and standing in line in the morning to get your daily methodone dose. We have to make those environments more welcoming.”
Problem probably understated
He also says that though the study was well done given the data available, he’s frustrated that researchers still have to depend on billing data and can’t capture factors such as child care availability, living wages, and continuation of health insurance. Additionally, not everyone is coded correctly for OUD.
“It’s all Medicaid, so it’s only people who continued with care,” he pointed out. That means these numbers may actually underrepresent the problem.
Still, he says it’s important to realize the magnitude of deaths this study does highlight in this population.
In people with OUD in the postpartum period, the deaths are more than 1 in 1,000.
“That should be alarming,” Dr. Terplan said. “That’s a very big number from a public health perspective.”
Coauthor Kathryn J. Gray received payment from Aetion Inc., Roche, and BillionToOne. Funds were paid to the University of Utah for Dr. Smid from Alydia Inc. for being the site principal investigator for a study of the JADA device, and from Gilead for Dr. Smid’s study of hepatitis C in pregnancy; she was also a consultant for Organon and Rhia Ventures. Dr. Terplan reports no relevant financial relationships.
(OUD), according to research published in Obstetrics and Gynecology.
Opioid overdose deaths account for up to 10% of pregnancy-associated deaths in the United States, and 75% of the deliveries of women with OUD are covered by Medicaid, according to lead author Elizabeth Suarez, PhD, MPH, with the division of pharmacoepidemiology and pharmacoeconomics at Brigham and Women’s Hospital and Harvard Medical School in Boston, and colleagues.
Nearly 5 million deliveries studied
Researchers studied claims data from Medicaid and the National Death Index database in the United States from 2006 to 2013 for 4,972,061 deliveries. They also identified a subgroup of women with a documented history of OUD in the 3 months before delivery.
They found the incidence of postpartum opioid overdose deaths was 5.4 per 100,000 deliveries (95% confidence interval, 4.5-6.4) among all in the study and 118 per 100,000 (95% CI, 84-163) among individuals with OUD.
Incidence of all-cause postpartum death was six times higher in women with OUD than in all the women studied. Common causes of death of those with OUD were other drug- and alcohol-related deaths (47/100,000); suicide (26/100,000); and other injuries, including accidents and falls (33/100,000).
Risk factors strongly linked with postpartum opioid overdose death included mental health and other substance use disorders.
Medication significantly lowers death risk
The authors also documented the benefit of buprenorphine or methadone for OUD.
For women with OUD who used medication to treat OUD post partum, odds of opioid overdose death were 60% lower (odds ratio, 0.4; 95% CI 0.1-0.9).
As important as use of medication, Marcela Smid, MD, MS, writes in an accompanying editorial, is noting that 80% of the women in this study who died of opioid overdoses had contact with a health care provider before death.
“Both of these results indicate that we have the means and opportunity to prevent these deaths,” writes Dr. Smid, with the division of maternal fetal medicine, University of Utah Health in Salt Lake City.
Dismal numbers on ob.gyns. trained to prescribe medications
She points out some barriers, however. Most clinicians, she notes, lack time and training to prescribe buprenorphine, and in 2019, fewer than 2% of ob.gyns. who accept Medicaid were able to prescribe it.
Her charge to ob.gyns.: “We need to help identify individuals who are at high risk of OUD or opioid overdose by screening.” A validated screening tool should be used at prenatal and postpartum appointments.
On a bigger scale, she urges Medicaid to be expanded for a full year post partum through the American Rescue Act’s State Plan Amendment, something only 28 states and Washington, D.C., have done so far.
Dr. Smid points out some good news, however: President Joe Biden signed the Consolidated Appropriations Act 2023, which eliminated the “X” waiver.
Now all clinicians who have a Drug Enforcement Administration registration that includes Schedule III authority can prescribe buprenorphine for OUD if applicable state law allows it.
But that calls for medical schools and residency programs to prioritize addiction medicine as a core competency, Dr. Smid says.
Getting naloxone to patients, families
One of the potential interventions the study authors suggest is providing naloxone prescriptions and training to pregnant and postpartum women who have a substance use history and to their partners and significant others.
However, Mishka Terplan, MD, MPH, told this publication, “It’s one thing to write a prescription; it’s another thing for the person to actually get the medication.” He is medical director of the Friends Research Institute in Baltimore, an ob.gyn. who specializes in addiction medicine.
“What can we do?” We can think about how to get naloxone into people’s hands at discharge from the hospital after they give birth, instead of prescribing. That would mean that health systems need to prioritize this, he said. “We give people discharge medications all the time.”
Still, naloxone can’t be seen as the answer, he said.
He compares it to defibrillators in public places, which are for rescues, not reversing a population problem.
“Some people think that naloxone reversals are doing something about OUD. It’s doing about as much about OUD as defibrillators do for cardiovascular disease,” he said.
The best help, he says, will be continuation of treatment.
“Addiction is a chronic condition,” he says, “but often we only provide episodic care. We see that particularly in pregnancy. Once the pregnancy is finished, there’s not categorical continuation of insurance.”
Even if you do have insurance, it’s hard to find a clinic that’s family friendly, he notes. “You might not feel comfortable taking your newborn and standing in line in the morning to get your daily methodone dose. We have to make those environments more welcoming.”
Problem probably understated
He also says that though the study was well done given the data available, he’s frustrated that researchers still have to depend on billing data and can’t capture factors such as child care availability, living wages, and continuation of health insurance. Additionally, not everyone is coded correctly for OUD.
“It’s all Medicaid, so it’s only people who continued with care,” he pointed out. That means these numbers may actually underrepresent the problem.
Still, he says it’s important to realize the magnitude of deaths this study does highlight in this population.
In people with OUD in the postpartum period, the deaths are more than 1 in 1,000.
“That should be alarming,” Dr. Terplan said. “That’s a very big number from a public health perspective.”
Coauthor Kathryn J. Gray received payment from Aetion Inc., Roche, and BillionToOne. Funds were paid to the University of Utah for Dr. Smid from Alydia Inc. for being the site principal investigator for a study of the JADA device, and from Gilead for Dr. Smid’s study of hepatitis C in pregnancy; she was also a consultant for Organon and Rhia Ventures. Dr. Terplan reports no relevant financial relationships.
(OUD), according to research published in Obstetrics and Gynecology.
Opioid overdose deaths account for up to 10% of pregnancy-associated deaths in the United States, and 75% of the deliveries of women with OUD are covered by Medicaid, according to lead author Elizabeth Suarez, PhD, MPH, with the division of pharmacoepidemiology and pharmacoeconomics at Brigham and Women’s Hospital and Harvard Medical School in Boston, and colleagues.
Nearly 5 million deliveries studied
Researchers studied claims data from Medicaid and the National Death Index database in the United States from 2006 to 2013 for 4,972,061 deliveries. They also identified a subgroup of women with a documented history of OUD in the 3 months before delivery.
They found the incidence of postpartum opioid overdose deaths was 5.4 per 100,000 deliveries (95% confidence interval, 4.5-6.4) among all in the study and 118 per 100,000 (95% CI, 84-163) among individuals with OUD.
Incidence of all-cause postpartum death was six times higher in women with OUD than in all the women studied. Common causes of death of those with OUD were other drug- and alcohol-related deaths (47/100,000); suicide (26/100,000); and other injuries, including accidents and falls (33/100,000).
Risk factors strongly linked with postpartum opioid overdose death included mental health and other substance use disorders.
Medication significantly lowers death risk
The authors also documented the benefit of buprenorphine or methadone for OUD.
For women with OUD who used medication to treat OUD post partum, odds of opioid overdose death were 60% lower (odds ratio, 0.4; 95% CI 0.1-0.9).
As important as use of medication, Marcela Smid, MD, MS, writes in an accompanying editorial, is noting that 80% of the women in this study who died of opioid overdoses had contact with a health care provider before death.
“Both of these results indicate that we have the means and opportunity to prevent these deaths,” writes Dr. Smid, with the division of maternal fetal medicine, University of Utah Health in Salt Lake City.
Dismal numbers on ob.gyns. trained to prescribe medications
She points out some barriers, however. Most clinicians, she notes, lack time and training to prescribe buprenorphine, and in 2019, fewer than 2% of ob.gyns. who accept Medicaid were able to prescribe it.
Her charge to ob.gyns.: “We need to help identify individuals who are at high risk of OUD or opioid overdose by screening.” A validated screening tool should be used at prenatal and postpartum appointments.
On a bigger scale, she urges Medicaid to be expanded for a full year post partum through the American Rescue Act’s State Plan Amendment, something only 28 states and Washington, D.C., have done so far.
Dr. Smid points out some good news, however: President Joe Biden signed the Consolidated Appropriations Act 2023, which eliminated the “X” waiver.
Now all clinicians who have a Drug Enforcement Administration registration that includes Schedule III authority can prescribe buprenorphine for OUD if applicable state law allows it.
But that calls for medical schools and residency programs to prioritize addiction medicine as a core competency, Dr. Smid says.
Getting naloxone to patients, families
One of the potential interventions the study authors suggest is providing naloxone prescriptions and training to pregnant and postpartum women who have a substance use history and to their partners and significant others.
However, Mishka Terplan, MD, MPH, told this publication, “It’s one thing to write a prescription; it’s another thing for the person to actually get the medication.” He is medical director of the Friends Research Institute in Baltimore, an ob.gyn. who specializes in addiction medicine.
“What can we do?” We can think about how to get naloxone into people’s hands at discharge from the hospital after they give birth, instead of prescribing. That would mean that health systems need to prioritize this, he said. “We give people discharge medications all the time.”
Still, naloxone can’t be seen as the answer, he said.
He compares it to defibrillators in public places, which are for rescues, not reversing a population problem.
“Some people think that naloxone reversals are doing something about OUD. It’s doing about as much about OUD as defibrillators do for cardiovascular disease,” he said.
The best help, he says, will be continuation of treatment.
“Addiction is a chronic condition,” he says, “but often we only provide episodic care. We see that particularly in pregnancy. Once the pregnancy is finished, there’s not categorical continuation of insurance.”
Even if you do have insurance, it’s hard to find a clinic that’s family friendly, he notes. “You might not feel comfortable taking your newborn and standing in line in the morning to get your daily methodone dose. We have to make those environments more welcoming.”
Problem probably understated
He also says that though the study was well done given the data available, he’s frustrated that researchers still have to depend on billing data and can’t capture factors such as child care availability, living wages, and continuation of health insurance. Additionally, not everyone is coded correctly for OUD.
“It’s all Medicaid, so it’s only people who continued with care,” he pointed out. That means these numbers may actually underrepresent the problem.
Still, he says it’s important to realize the magnitude of deaths this study does highlight in this population.
In people with OUD in the postpartum period, the deaths are more than 1 in 1,000.
“That should be alarming,” Dr. Terplan said. “That’s a very big number from a public health perspective.”
Coauthor Kathryn J. Gray received payment from Aetion Inc., Roche, and BillionToOne. Funds were paid to the University of Utah for Dr. Smid from Alydia Inc. for being the site principal investigator for a study of the JADA device, and from Gilead for Dr. Smid’s study of hepatitis C in pregnancy; she was also a consultant for Organon and Rhia Ventures. Dr. Terplan reports no relevant financial relationships.
FROM OBSTETRICS AND GYNECOLOGY
FDA moves to stop the spread of illicit ‘tranq’ in the U.S.
The agency issued an import alert, which gives it the power to detain raw ingredients or bulk finished product if the shipments are suspected to be in violation of the law. Xylazine was first approved by the FDA in 1972 as a sedative and analgesic for use only in animals.
It is increasingly being detected and is usually mixed with fentanyl, cocaine, methamphetamine, and other illicit drugs. A January 2023 study by Nashville-based testing company Aegis Sciences found xylazine in 413 of about 60,000 urine samples and in 25 of 39 states that submitted tests. The vast majority of xylazine-positive samples also tested positive for fentanyl.
The FDA said it would continue to ensure the availability of xylazine for veterinary use, and the American Veterinary Medicine Association said in a statement that it “supports such efforts to combat illicit drug use.”
FDA Commissioner Robert M. Califf, MD, said in a statement that the agency “remains concerned about the increasing prevalence of xylazine mixed with illicit drugs, and this action is one part of broader efforts the agency is undertaking to address this issue.”

In November, the agency warned health care providers that because xylazine is not an opioid, the overdose reversal agent naloxone would not be effective. Xylazine acts as a central alpha-2-adrenergic receptor agonist in the brainstem, causing a rapid decrease in the release of norepinephrine and dopamine in the central nervous system. Its use can lead to central nervous system and respiratory depression, said the FDA.
Clinicians have scrambled to treat severe necrotic skin ulcerations that develop at injection sites.
Xylazine is relatively cheap and easy to access, said the Drug Enforcement Administration and Department of Justice in a November joint report. The drug is “readily available for purchase on other Internet sites in liquid and powder form, often with no association to the veterinary profession nor requirements to prove legitimate need,” said the Justice Department. A buyer can purchase xylazine powder online from Chinese suppliers for $6-$20 per kilogram, according to the report.
In 2021, xylazine-positive overdoses were highest in the South, which experienced a 1,127% increase from 2020, the Justice Department reported. The same year, there were 1,281 overdoses involving the substance in the Northeast and 351 in the Midwest.
There were just 34 overdoses involving xylazine in the West in 2021, but its use appears to be growing. The San Francisco Department of Public Health said it had detected low levels of xylazine in four people who died of overdoses in December and January.
“Identifying xylazine in San Francisco is concerning,” said the department in a statement, adding that it had not yet seen evidence of skin wounds in injection drug users in the city.
In late February, the Los Angeles County Department of Public Health issued a warning to first responders and health care professionals that xylazine had been detected in the area’s illicit drug supply.
The department said it will “work closely with other partners to understand the extent of the possible xylazine contamination in the illicit drug supply to increase awareness and education to the public.”
The FDA commissioner said the agency will coordinate with public health officials to more closely track xylazine.
“We will continue to use all tools at our disposal and partner with the Drug Enforcement Administration and other federal, state, local agencies, and stakeholders as appropriate to stem these illicit activities and protect public health,” said Dr. Califf.
A version of this article first appeared on Medscape.com.
The agency issued an import alert, which gives it the power to detain raw ingredients or bulk finished product if the shipments are suspected to be in violation of the law. Xylazine was first approved by the FDA in 1972 as a sedative and analgesic for use only in animals.
It is increasingly being detected and is usually mixed with fentanyl, cocaine, methamphetamine, and other illicit drugs. A January 2023 study by Nashville-based testing company Aegis Sciences found xylazine in 413 of about 60,000 urine samples and in 25 of 39 states that submitted tests. The vast majority of xylazine-positive samples also tested positive for fentanyl.
The FDA said it would continue to ensure the availability of xylazine for veterinary use, and the American Veterinary Medicine Association said in a statement that it “supports such efforts to combat illicit drug use.”
FDA Commissioner Robert M. Califf, MD, said in a statement that the agency “remains concerned about the increasing prevalence of xylazine mixed with illicit drugs, and this action is one part of broader efforts the agency is undertaking to address this issue.”
In November, the agency warned health care providers that because xylazine is not an opioid, the overdose reversal agent naloxone would not be effective. Xylazine acts as a central alpha-2-adrenergic receptor agonist in the brainstem, causing a rapid decrease in the release of norepinephrine and dopamine in the central nervous system. Its use can lead to central nervous system and respiratory depression, said the FDA.
Clinicians have scrambled to treat severe necrotic skin ulcerations that develop at injection sites.
Xylazine is relatively cheap and easy to access, said the Drug Enforcement Administration and Department of Justice in a November joint report. The drug is “readily available for purchase on other Internet sites in liquid and powder form, often with no association to the veterinary profession nor requirements to prove legitimate need,” said the Justice Department. A buyer can purchase xylazine powder online from Chinese suppliers for $6-$20 per kilogram, according to the report.
In 2021, xylazine-positive overdoses were highest in the South, which experienced a 1,127% increase from 2020, the Justice Department reported. The same year, there were 1,281 overdoses involving the substance in the Northeast and 351 in the Midwest.
There were just 34 overdoses involving xylazine in the West in 2021, but its use appears to be growing. The San Francisco Department of Public Health said it had detected low levels of xylazine in four people who died of overdoses in December and January.
“Identifying xylazine in San Francisco is concerning,” said the department in a statement, adding that it had not yet seen evidence of skin wounds in injection drug users in the city.
In late February, the Los Angeles County Department of Public Health issued a warning to first responders and health care professionals that xylazine had been detected in the area’s illicit drug supply.
The department said it will “work closely with other partners to understand the extent of the possible xylazine contamination in the illicit drug supply to increase awareness and education to the public.”
The FDA commissioner said the agency will coordinate with public health officials to more closely track xylazine.
“We will continue to use all tools at our disposal and partner with the Drug Enforcement Administration and other federal, state, local agencies, and stakeholders as appropriate to stem these illicit activities and protect public health,” said Dr. Califf.
A version of this article first appeared on Medscape.com.
The agency issued an import alert, which gives it the power to detain raw ingredients or bulk finished product if the shipments are suspected to be in violation of the law. Xylazine was first approved by the FDA in 1972 as a sedative and analgesic for use only in animals.
It is increasingly being detected and is usually mixed with fentanyl, cocaine, methamphetamine, and other illicit drugs. A January 2023 study by Nashville-based testing company Aegis Sciences found xylazine in 413 of about 60,000 urine samples and in 25 of 39 states that submitted tests. The vast majority of xylazine-positive samples also tested positive for fentanyl.
The FDA said it would continue to ensure the availability of xylazine for veterinary use, and the American Veterinary Medicine Association said in a statement that it “supports such efforts to combat illicit drug use.”
FDA Commissioner Robert M. Califf, MD, said in a statement that the agency “remains concerned about the increasing prevalence of xylazine mixed with illicit drugs, and this action is one part of broader efforts the agency is undertaking to address this issue.”
In November, the agency warned health care providers that because xylazine is not an opioid, the overdose reversal agent naloxone would not be effective. Xylazine acts as a central alpha-2-adrenergic receptor agonist in the brainstem, causing a rapid decrease in the release of norepinephrine and dopamine in the central nervous system. Its use can lead to central nervous system and respiratory depression, said the FDA.
Clinicians have scrambled to treat severe necrotic skin ulcerations that develop at injection sites.
Xylazine is relatively cheap and easy to access, said the Drug Enforcement Administration and Department of Justice in a November joint report. The drug is “readily available for purchase on other Internet sites in liquid and powder form, often with no association to the veterinary profession nor requirements to prove legitimate need,” said the Justice Department. A buyer can purchase xylazine powder online from Chinese suppliers for $6-$20 per kilogram, according to the report.
In 2021, xylazine-positive overdoses were highest in the South, which experienced a 1,127% increase from 2020, the Justice Department reported. The same year, there were 1,281 overdoses involving the substance in the Northeast and 351 in the Midwest.
There were just 34 overdoses involving xylazine in the West in 2021, but its use appears to be growing. The San Francisco Department of Public Health said it had detected low levels of xylazine in four people who died of overdoses in December and January.
“Identifying xylazine in San Francisco is concerning,” said the department in a statement, adding that it had not yet seen evidence of skin wounds in injection drug users in the city.
In late February, the Los Angeles County Department of Public Health issued a warning to first responders and health care professionals that xylazine had been detected in the area’s illicit drug supply.
The department said it will “work closely with other partners to understand the extent of the possible xylazine contamination in the illicit drug supply to increase awareness and education to the public.”
The FDA commissioner said the agency will coordinate with public health officials to more closely track xylazine.
“We will continue to use all tools at our disposal and partner with the Drug Enforcement Administration and other federal, state, local agencies, and stakeholders as appropriate to stem these illicit activities and protect public health,” said Dr. Califf.
A version of this article first appeared on Medscape.com.
Buprenorphine proves effective for fentanyl users in the ED
based on data from nearly 900 individuals.
California EDs include a facilitation program known as CA Bridge for the treatment of opioid use disorder. Guidelines for CA Bridge call for high-dose buprenorphine to treat patients in drug withdrawal, with doses starting at 8-16 mg, Hannah Snyder, MD, of the University of California, San Francisco, and colleagues wrote.
“Buprenorphine has been repeatedly shown to save lives and prevent overdoses,” Dr. Snyder said in an interview. “We know that emergency department–initiated buprenorphine is an essential tool for increasing access. In the era of fentanyl, both patients and providers have expressed concerns that buprenorphine may not work as well as it did when patients were more likely to be using heroin or opioid pills.
“This retrospective cohort study provides additional information about emergency department buprenorphine as fentanyl becomes increasingly prevalent.”
In a research letter published in JAMA Network Open, the investigators reviewed data from the electronic health records of 896 patients who presented with opioid use disorder (OUD) at 16 CA Bridge EDs between Jan. 1, 2020, and April 30, 2020. All patients with OUD were included regardless of chief concern, current treatment, treatment desires, or withdrawal. A total of 87 individuals reported fentanyl use; if no fentanyl use was reported, the patient was classified as not using fentanyl. The median age of the patients was 35 years, two thirds were male, approximately 46% were White and non-Hispanic, and 30% had unstable housing.
The primary outcome was follow-up engagement at 7-14 days and 25-37 days.
A total of 492 patients received buprenorphine, including 44 fentanyl users, and 439 initiated high doses of 8-32 mg. At a 30-day follow-up, eight patients had precipitated withdrawal, including two cases in fentanyl users; none of these cases required hospital admission.
The follow-up engagement was similar for both groups, with adjusted odds ratios of 0.60 for administered buprenorphine at the initial ED encounter, 1.09 for 7-day follow-up, and 1.33 for 30-day follow-up.
The findings were limited by the retrospective design and use of clinical documentation, which likely resulted in underreporting of fentanyl use and follow-up, the researchers noted. However, the results supported the effectiveness of buprenorphine for ED patients in withdrawal with a history of fentanyl exposure.
“We were pleased to see that precipitated withdrawal was relatively uncommon in this study, and that patients who did and did not use fentanyl followed up at similar rates,” said Dr. Snyder. “This aligns with our clinical experience and prior research showing that emergency department buprenorphine starts continue to be an essential tool.”
The message for clinicians: “If a patient presents to the emergency department in objective opioid withdrawal and desires buprenorphine, they should be offered treatment in that moment,” Dr. Snyder said. “Treatment protocols used by hospitals in this study are available online. Emergency departments can offer compassionate and evidence-based treatment initiation 24 hours a day, 7 days a week, 365 days a year.”
More data needed on dosing strategies
“We need additional research to determine best practices for patients who use fentanyl and want to start buprenorphine, but are not yet in withdrawal,” Dr. Snyder said. “Doses of buprenorphine like those in this study are only appropriate for patients who are in withdrawal with objective signs, so some patients may struggle to wait long enough after their last use to go into sufficient withdrawal.”
Precipitated withdrawal does occur in some cases, said Dr. Snyder. “If it does, the emergency department is a very good place to manage it. We need additional research to determine best practices in management to make patients as comfortable as possible, including additional high-dose buprenorphine as well as additional adjunctive agents.”
Findings support buprenorphine
“The classic approach to buprenorphine initiation, which emerged from psychiatry outpatient office visits, is to start with very small doses of buprenorphine [2-4 mg] and titrate up slowly,” Reuben J. Strayer, MD, said in an interview.
“This dose range turns out to be the ‘sour spot’ most likely to cause the most important complication around buprenorphine initiation–precipitated withdrawal,” said Dr. Strayer, the director of addiction medicine in the emergency medicine department at Maimonides Medical Center, New York.
“One of the current focus areas of OUD treatment research is determining how to initiate buprenorphine without entailing a period of spontaneous withdrawal and without causing precipitated withdrawal,” Strayer explained. “The two primary strategies are low-dose buprenorphine initiation [LDBI, less than 2 mg, sometimes called microdosing] and high-dose [HDBI, ≥ 16 mg] buprenorphine initiation. HDBI is attractive because the primary treatment of buprenorphine-precipitated withdrawal is more buprenorphine.
“Additionally, using a high dose up front immediately transitions the patient to therapeutic blood levels, which protects the patient from withdrawal, cravings, and overdose from dangerous opioids (heroin, fentanyl, oxycodone).”
However, “the contamination and now replacement of heroin with fentanyl in the street drug supply has challenged buprenorphine initiation, because fentanyl, when used chronically, accumulates in the body and leaks into the bloodstream slowly over time, preventing the opioid washout that is required to eliminate the risk of precipitated withdrawal when buprenorphine is administered,” said Dr. Strayer.
The current study demonstrates that patients who are initiated with a first dose of 8-16 mg buprenorphine are unlikely to experience precipitated withdrawal and are successfully transitioned to buprenorphine maintenance and clinic follow-up, Dr. Snyder said, but he was surprised by the low rate of precipitated withdrawal in the current study, “which is discordant with what is being anecdotally reported across the country.”
However, the take-home message for clinicians is the support for the initiation of buprenorphine in emergency department settings at a starting dose of 8-16 mg, regardless of reported fentanyl use, he said. “Given the huge impact buprenorphine therapy has on OUD-related mortality, clinicians should make every effort to initiate buprenorphine for OUD patients at every opportunity, and precipitated withdrawal is very unlikely in appropriately selected patients.
“Many clinicians remain reluctant to initiate buprenorphine in ED settings for unfamiliarity with the drug, fear of precipitated withdrawal, or concerns around the certainty of outpatient follow-up,” Dr. Snyder said. “Education, encouragement, systems programming, such as including decision support within the electronic health record, and role-modeling from local champions will promote wider adoption of this lifesaving practice.”
Looking ahead, “more research, including prospective research, is needed to refine best practices around buprenorphine administration,” said Dr. Snyder. Questions to address include which patients are most at risk for precipitated withdrawal and whether there are alternatives to standard initiation dosing that are sufficiently unlikely to cause precipitated withdrawal. “Possibly effective alternatives include buprenorphine initiation by administration of long-acting injectable depot buprenorphine, which accumulates slowly, potentially avoiding precipitated withdrawal, as well as a slow intravenous buprenorphine infusion such as 9 mg given over 12 hours.”
The study received no outside funding. Dr. Snyder disclosed grants from the Substance Abuse and Mental Health Services Administration and the California Department of Health Care Services during the study. Dr. Strayer reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
based on data from nearly 900 individuals.
California EDs include a facilitation program known as CA Bridge for the treatment of opioid use disorder. Guidelines for CA Bridge call for high-dose buprenorphine to treat patients in drug withdrawal, with doses starting at 8-16 mg, Hannah Snyder, MD, of the University of California, San Francisco, and colleagues wrote.
“Buprenorphine has been repeatedly shown to save lives and prevent overdoses,” Dr. Snyder said in an interview. “We know that emergency department–initiated buprenorphine is an essential tool for increasing access. In the era of fentanyl, both patients and providers have expressed concerns that buprenorphine may not work as well as it did when patients were more likely to be using heroin or opioid pills.
“This retrospective cohort study provides additional information about emergency department buprenorphine as fentanyl becomes increasingly prevalent.”
In a research letter published in JAMA Network Open, the investigators reviewed data from the electronic health records of 896 patients who presented with opioid use disorder (OUD) at 16 CA Bridge EDs between Jan. 1, 2020, and April 30, 2020. All patients with OUD were included regardless of chief concern, current treatment, treatment desires, or withdrawal. A total of 87 individuals reported fentanyl use; if no fentanyl use was reported, the patient was classified as not using fentanyl. The median age of the patients was 35 years, two thirds were male, approximately 46% were White and non-Hispanic, and 30% had unstable housing.
The primary outcome was follow-up engagement at 7-14 days and 25-37 days.
A total of 492 patients received buprenorphine, including 44 fentanyl users, and 439 initiated high doses of 8-32 mg. At a 30-day follow-up, eight patients had precipitated withdrawal, including two cases in fentanyl users; none of these cases required hospital admission.
The follow-up engagement was similar for both groups, with adjusted odds ratios of 0.60 for administered buprenorphine at the initial ED encounter, 1.09 for 7-day follow-up, and 1.33 for 30-day follow-up.
The findings were limited by the retrospective design and use of clinical documentation, which likely resulted in underreporting of fentanyl use and follow-up, the researchers noted. However, the results supported the effectiveness of buprenorphine for ED patients in withdrawal with a history of fentanyl exposure.
“We were pleased to see that precipitated withdrawal was relatively uncommon in this study, and that patients who did and did not use fentanyl followed up at similar rates,” said Dr. Snyder. “This aligns with our clinical experience and prior research showing that emergency department buprenorphine starts continue to be an essential tool.”
The message for clinicians: “If a patient presents to the emergency department in objective opioid withdrawal and desires buprenorphine, they should be offered treatment in that moment,” Dr. Snyder said. “Treatment protocols used by hospitals in this study are available online. Emergency departments can offer compassionate and evidence-based treatment initiation 24 hours a day, 7 days a week, 365 days a year.”
More data needed on dosing strategies
“We need additional research to determine best practices for patients who use fentanyl and want to start buprenorphine, but are not yet in withdrawal,” Dr. Snyder said. “Doses of buprenorphine like those in this study are only appropriate for patients who are in withdrawal with objective signs, so some patients may struggle to wait long enough after their last use to go into sufficient withdrawal.”
Precipitated withdrawal does occur in some cases, said Dr. Snyder. “If it does, the emergency department is a very good place to manage it. We need additional research to determine best practices in management to make patients as comfortable as possible, including additional high-dose buprenorphine as well as additional adjunctive agents.”
Findings support buprenorphine
“The classic approach to buprenorphine initiation, which emerged from psychiatry outpatient office visits, is to start with very small doses of buprenorphine [2-4 mg] and titrate up slowly,” Reuben J. Strayer, MD, said in an interview.
“This dose range turns out to be the ‘sour spot’ most likely to cause the most important complication around buprenorphine initiation–precipitated withdrawal,” said Dr. Strayer, the director of addiction medicine in the emergency medicine department at Maimonides Medical Center, New York.
“One of the current focus areas of OUD treatment research is determining how to initiate buprenorphine without entailing a period of spontaneous withdrawal and without causing precipitated withdrawal,” Strayer explained. “The two primary strategies are low-dose buprenorphine initiation [LDBI, less than 2 mg, sometimes called microdosing] and high-dose [HDBI, ≥ 16 mg] buprenorphine initiation. HDBI is attractive because the primary treatment of buprenorphine-precipitated withdrawal is more buprenorphine.
“Additionally, using a high dose up front immediately transitions the patient to therapeutic blood levels, which protects the patient from withdrawal, cravings, and overdose from dangerous opioids (heroin, fentanyl, oxycodone).”
However, “the contamination and now replacement of heroin with fentanyl in the street drug supply has challenged buprenorphine initiation, because fentanyl, when used chronically, accumulates in the body and leaks into the bloodstream slowly over time, preventing the opioid washout that is required to eliminate the risk of precipitated withdrawal when buprenorphine is administered,” said Dr. Strayer.
The current study demonstrates that patients who are initiated with a first dose of 8-16 mg buprenorphine are unlikely to experience precipitated withdrawal and are successfully transitioned to buprenorphine maintenance and clinic follow-up, Dr. Snyder said, but he was surprised by the low rate of precipitated withdrawal in the current study, “which is discordant with what is being anecdotally reported across the country.”
However, the take-home message for clinicians is the support for the initiation of buprenorphine in emergency department settings at a starting dose of 8-16 mg, regardless of reported fentanyl use, he said. “Given the huge impact buprenorphine therapy has on OUD-related mortality, clinicians should make every effort to initiate buprenorphine for OUD patients at every opportunity, and precipitated withdrawal is very unlikely in appropriately selected patients.
“Many clinicians remain reluctant to initiate buprenorphine in ED settings for unfamiliarity with the drug, fear of precipitated withdrawal, or concerns around the certainty of outpatient follow-up,” Dr. Snyder said. “Education, encouragement, systems programming, such as including decision support within the electronic health record, and role-modeling from local champions will promote wider adoption of this lifesaving practice.”
Looking ahead, “more research, including prospective research, is needed to refine best practices around buprenorphine administration,” said Dr. Snyder. Questions to address include which patients are most at risk for precipitated withdrawal and whether there are alternatives to standard initiation dosing that are sufficiently unlikely to cause precipitated withdrawal. “Possibly effective alternatives include buprenorphine initiation by administration of long-acting injectable depot buprenorphine, which accumulates slowly, potentially avoiding precipitated withdrawal, as well as a slow intravenous buprenorphine infusion such as 9 mg given over 12 hours.”
The study received no outside funding. Dr. Snyder disclosed grants from the Substance Abuse and Mental Health Services Administration and the California Department of Health Care Services during the study. Dr. Strayer reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
based on data from nearly 900 individuals.
California EDs include a facilitation program known as CA Bridge for the treatment of opioid use disorder. Guidelines for CA Bridge call for high-dose buprenorphine to treat patients in drug withdrawal, with doses starting at 8-16 mg, Hannah Snyder, MD, of the University of California, San Francisco, and colleagues wrote.
“Buprenorphine has been repeatedly shown to save lives and prevent overdoses,” Dr. Snyder said in an interview. “We know that emergency department–initiated buprenorphine is an essential tool for increasing access. In the era of fentanyl, both patients and providers have expressed concerns that buprenorphine may not work as well as it did when patients were more likely to be using heroin or opioid pills.
“This retrospective cohort study provides additional information about emergency department buprenorphine as fentanyl becomes increasingly prevalent.”
In a research letter published in JAMA Network Open, the investigators reviewed data from the electronic health records of 896 patients who presented with opioid use disorder (OUD) at 16 CA Bridge EDs between Jan. 1, 2020, and April 30, 2020. All patients with OUD were included regardless of chief concern, current treatment, treatment desires, or withdrawal. A total of 87 individuals reported fentanyl use; if no fentanyl use was reported, the patient was classified as not using fentanyl. The median age of the patients was 35 years, two thirds were male, approximately 46% were White and non-Hispanic, and 30% had unstable housing.
The primary outcome was follow-up engagement at 7-14 days and 25-37 days.
A total of 492 patients received buprenorphine, including 44 fentanyl users, and 439 initiated high doses of 8-32 mg. At a 30-day follow-up, eight patients had precipitated withdrawal, including two cases in fentanyl users; none of these cases required hospital admission.
The follow-up engagement was similar for both groups, with adjusted odds ratios of 0.60 for administered buprenorphine at the initial ED encounter, 1.09 for 7-day follow-up, and 1.33 for 30-day follow-up.
The findings were limited by the retrospective design and use of clinical documentation, which likely resulted in underreporting of fentanyl use and follow-up, the researchers noted. However, the results supported the effectiveness of buprenorphine for ED patients in withdrawal with a history of fentanyl exposure.
“We were pleased to see that precipitated withdrawal was relatively uncommon in this study, and that patients who did and did not use fentanyl followed up at similar rates,” said Dr. Snyder. “This aligns with our clinical experience and prior research showing that emergency department buprenorphine starts continue to be an essential tool.”
The message for clinicians: “If a patient presents to the emergency department in objective opioid withdrawal and desires buprenorphine, they should be offered treatment in that moment,” Dr. Snyder said. “Treatment protocols used by hospitals in this study are available online. Emergency departments can offer compassionate and evidence-based treatment initiation 24 hours a day, 7 days a week, 365 days a year.”
More data needed on dosing strategies
“We need additional research to determine best practices for patients who use fentanyl and want to start buprenorphine, but are not yet in withdrawal,” Dr. Snyder said. “Doses of buprenorphine like those in this study are only appropriate for patients who are in withdrawal with objective signs, so some patients may struggle to wait long enough after their last use to go into sufficient withdrawal.”
Precipitated withdrawal does occur in some cases, said Dr. Snyder. “If it does, the emergency department is a very good place to manage it. We need additional research to determine best practices in management to make patients as comfortable as possible, including additional high-dose buprenorphine as well as additional adjunctive agents.”
Findings support buprenorphine
“The classic approach to buprenorphine initiation, which emerged from psychiatry outpatient office visits, is to start with very small doses of buprenorphine [2-4 mg] and titrate up slowly,” Reuben J. Strayer, MD, said in an interview.
“This dose range turns out to be the ‘sour spot’ most likely to cause the most important complication around buprenorphine initiation–precipitated withdrawal,” said Dr. Strayer, the director of addiction medicine in the emergency medicine department at Maimonides Medical Center, New York.
“One of the current focus areas of OUD treatment research is determining how to initiate buprenorphine without entailing a period of spontaneous withdrawal and without causing precipitated withdrawal,” Strayer explained. “The two primary strategies are low-dose buprenorphine initiation [LDBI, less than 2 mg, sometimes called microdosing] and high-dose [HDBI, ≥ 16 mg] buprenorphine initiation. HDBI is attractive because the primary treatment of buprenorphine-precipitated withdrawal is more buprenorphine.
“Additionally, using a high dose up front immediately transitions the patient to therapeutic blood levels, which protects the patient from withdrawal, cravings, and overdose from dangerous opioids (heroin, fentanyl, oxycodone).”
However, “the contamination and now replacement of heroin with fentanyl in the street drug supply has challenged buprenorphine initiation, because fentanyl, when used chronically, accumulates in the body and leaks into the bloodstream slowly over time, preventing the opioid washout that is required to eliminate the risk of precipitated withdrawal when buprenorphine is administered,” said Dr. Strayer.
The current study demonstrates that patients who are initiated with a first dose of 8-16 mg buprenorphine are unlikely to experience precipitated withdrawal and are successfully transitioned to buprenorphine maintenance and clinic follow-up, Dr. Snyder said, but he was surprised by the low rate of precipitated withdrawal in the current study, “which is discordant with what is being anecdotally reported across the country.”
However, the take-home message for clinicians is the support for the initiation of buprenorphine in emergency department settings at a starting dose of 8-16 mg, regardless of reported fentanyl use, he said. “Given the huge impact buprenorphine therapy has on OUD-related mortality, clinicians should make every effort to initiate buprenorphine for OUD patients at every opportunity, and precipitated withdrawal is very unlikely in appropriately selected patients.
“Many clinicians remain reluctant to initiate buprenorphine in ED settings for unfamiliarity with the drug, fear of precipitated withdrawal, or concerns around the certainty of outpatient follow-up,” Dr. Snyder said. “Education, encouragement, systems programming, such as including decision support within the electronic health record, and role-modeling from local champions will promote wider adoption of this lifesaving practice.”
Looking ahead, “more research, including prospective research, is needed to refine best practices around buprenorphine administration,” said Dr. Snyder. Questions to address include which patients are most at risk for precipitated withdrawal and whether there are alternatives to standard initiation dosing that are sufficiently unlikely to cause precipitated withdrawal. “Possibly effective alternatives include buprenorphine initiation by administration of long-acting injectable depot buprenorphine, which accumulates slowly, potentially avoiding precipitated withdrawal, as well as a slow intravenous buprenorphine infusion such as 9 mg given over 12 hours.”
The study received no outside funding. Dr. Snyder disclosed grants from the Substance Abuse and Mental Health Services Administration and the California Department of Health Care Services during the study. Dr. Strayer reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM JAMA NETWORK OPEN
No spike in overdose deaths from relaxed buprenorphine regulations
Researchers say the data add weight to the argument for permanently adopting the pandemic-era prescribing regulations for buprenorphine, a treatment for opioid use disorder.
“We saw no evidence that increased availability of buprenorphine through the loosening of rules around prescribing and dispensing of buprenorphine during the pandemic increased overdose deaths,” investigator Wilson Compton, MD, deputy director of the National Institute on Drug Abuse, told this news organization.
“This is reassuring that, even when we opened up the doors to easier access to buprenorphine, we didn’t see that most serious consequence,” Dr. Compton said.
The findings were published online in JAMA Network Open .
Cause and effect
Federal agencies relaxed prescribing regulations for buprenorphine in March 2020 to make it easier for clinicians to prescribe the drug via telemedicine and for patients to take the medication at home.
The number of buprenorphine prescriptions has increased since that change, with more than 1 million people receiving the medication in 2021 from retail pharmacies in the United States.
However, questions remained about whether increased access would lead to an increase in buprenorphine-involved overdose.
Researchers with NIDA and the Centers for Disease Control and Prevention analyzed data from the State Unintentional Drug Overdose Reporting System, a CDC database that combines medical examiner and coroner reports and postmortem toxicology testing.
The study included information about overdose deaths from July 2019 to June 2021 in 46 states and the District of Columbia.
Between July 2019 and June 2021, there were 1,955 buprenorphine-involved overdose deaths, which accounted for 2.2% of all drug overdose deaths and 2.6% of opioid-involved overdose deaths.
However, researchers went beyond overall numbers and evaluated details from coroner’s and medical examiner reports, something they had not done before.
“For the first time we looked at the characteristics of decedents from buprenorphine because this has not been studied in this type of detail with a near-national sample,” Dr. Compton said.
“That allowed us to look at patterns of use of other substances as well as the circumstances that are recorded at the death scene that are in the data set,” he added.
Important insights
Reports from nearly all buprenorphine-involved deaths included the presence of at least one other drug, compared with opioid overdose deaths that typically involved only one drug.
“This is consistent with the pharmacology of buprenorphine being a partial agonist, so it may not be as fatal all by itself as some of the other opioids,” Dr. Compton said.
Deaths involving buprenorphine were less likely to include illicitly manufactured fentanyls, and other prescription medications were more often found on the scene, such as antidepressants.
Compared with opioid decedents, buprenorphine decedents were more likely to be women, age 35-44, White, and receiving treatment for mental health conditions, including for substance use disorder (SUD).
These kinds of characteristics provide important insights about potential ways to improve safety and clinical outcomes, Dr. Compton noted.
“When we see things like a little higher rate of SUD treatment and this evidence of other prescription drugs on the scene, and some higher rates of antidepressants in these decedents than I might have expected, I’m very curious about their use of other medical services outside of substance use treatment, because that might be a place where some interventions could be implemented,” he said.
A similar study showed pandemic-era policy changes that allowed methadone to be taken at home was followed by a decrease in methadone-related overdose deaths.
The new findings are consistent with those results, Dr. Compton said.
‘Chipping away’ at stigma
Commenting on the study, O. Trent Hall, DO, assistant professor of addiction medicine, Department of Psychiatry and Behavioral Health, Ohio State University Wexner Medical Center, Columbus, said that, although he welcomed the findings, they aren’t unexpected.
“Buprenorphine is well established as a safe and effective medication for opioid use disorder and as a physician who routinely cares for patients in the hospital after opioid overdose, I am not at all surprised by these results,” said Dr. Hall, who was not involved with the research.
“When my patients leave the hospital with a buprenorphine prescription, they are much less likely to return with another overdose or serious opioid-related medical problem,” he added.
U.S. drug overdose deaths topped 100,000 for the first time in 2021, and most were opioid-related. Although the latest data from the CDC shows drug overdose deaths have been declining slowly since early 2022, the numbers remain high.
Buprenorphine is one of only two drugs known to reduce the risk of opioid overdose. While prescriptions have increased since 2020, the medication remains underutilized, despite its known effectiveness in treating opioid use disorder.
Dr. Hall noted that research such as the new study could help increase buprenorphine’s use.
“Studies like this one chip away at the stigma that has been misapplied to buprenorphine,” he said. “I hope this article will encourage more providers to offer buprenorphine to patients with opioid use disorder.”
The study was funded internally by NIDA and the CDC. Dr. Compton reported owning stock in General Electric, 3M, and Pfizer outside the submitted work. Dr. Hall has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers say the data add weight to the argument for permanently adopting the pandemic-era prescribing regulations for buprenorphine, a treatment for opioid use disorder.
“We saw no evidence that increased availability of buprenorphine through the loosening of rules around prescribing and dispensing of buprenorphine during the pandemic increased overdose deaths,” investigator Wilson Compton, MD, deputy director of the National Institute on Drug Abuse, told this news organization.
“This is reassuring that, even when we opened up the doors to easier access to buprenorphine, we didn’t see that most serious consequence,” Dr. Compton said.
The findings were published online in JAMA Network Open .
Cause and effect
Federal agencies relaxed prescribing regulations for buprenorphine in March 2020 to make it easier for clinicians to prescribe the drug via telemedicine and for patients to take the medication at home.
The number of buprenorphine prescriptions has increased since that change, with more than 1 million people receiving the medication in 2021 from retail pharmacies in the United States.
However, questions remained about whether increased access would lead to an increase in buprenorphine-involved overdose.
Researchers with NIDA and the Centers for Disease Control and Prevention analyzed data from the State Unintentional Drug Overdose Reporting System, a CDC database that combines medical examiner and coroner reports and postmortem toxicology testing.
The study included information about overdose deaths from July 2019 to June 2021 in 46 states and the District of Columbia.
Between July 2019 and June 2021, there were 1,955 buprenorphine-involved overdose deaths, which accounted for 2.2% of all drug overdose deaths and 2.6% of opioid-involved overdose deaths.
However, researchers went beyond overall numbers and evaluated details from coroner’s and medical examiner reports, something they had not done before.
“For the first time we looked at the characteristics of decedents from buprenorphine because this has not been studied in this type of detail with a near-national sample,” Dr. Compton said.
“That allowed us to look at patterns of use of other substances as well as the circumstances that are recorded at the death scene that are in the data set,” he added.
Important insights
Reports from nearly all buprenorphine-involved deaths included the presence of at least one other drug, compared with opioid overdose deaths that typically involved only one drug.
“This is consistent with the pharmacology of buprenorphine being a partial agonist, so it may not be as fatal all by itself as some of the other opioids,” Dr. Compton said.
Deaths involving buprenorphine were less likely to include illicitly manufactured fentanyls, and other prescription medications were more often found on the scene, such as antidepressants.
Compared with opioid decedents, buprenorphine decedents were more likely to be women, age 35-44, White, and receiving treatment for mental health conditions, including for substance use disorder (SUD).
These kinds of characteristics provide important insights about potential ways to improve safety and clinical outcomes, Dr. Compton noted.
“When we see things like a little higher rate of SUD treatment and this evidence of other prescription drugs on the scene, and some higher rates of antidepressants in these decedents than I might have expected, I’m very curious about their use of other medical services outside of substance use treatment, because that might be a place where some interventions could be implemented,” he said.
A similar study showed pandemic-era policy changes that allowed methadone to be taken at home was followed by a decrease in methadone-related overdose deaths.
The new findings are consistent with those results, Dr. Compton said.
‘Chipping away’ at stigma
Commenting on the study, O. Trent Hall, DO, assistant professor of addiction medicine, Department of Psychiatry and Behavioral Health, Ohio State University Wexner Medical Center, Columbus, said that, although he welcomed the findings, they aren’t unexpected.
“Buprenorphine is well established as a safe and effective medication for opioid use disorder and as a physician who routinely cares for patients in the hospital after opioid overdose, I am not at all surprised by these results,” said Dr. Hall, who was not involved with the research.
“When my patients leave the hospital with a buprenorphine prescription, they are much less likely to return with another overdose or serious opioid-related medical problem,” he added.
U.S. drug overdose deaths topped 100,000 for the first time in 2021, and most were opioid-related. Although the latest data from the CDC shows drug overdose deaths have been declining slowly since early 2022, the numbers remain high.
Buprenorphine is one of only two drugs known to reduce the risk of opioid overdose. While prescriptions have increased since 2020, the medication remains underutilized, despite its known effectiveness in treating opioid use disorder.
Dr. Hall noted that research such as the new study could help increase buprenorphine’s use.
“Studies like this one chip away at the stigma that has been misapplied to buprenorphine,” he said. “I hope this article will encourage more providers to offer buprenorphine to patients with opioid use disorder.”
The study was funded internally by NIDA and the CDC. Dr. Compton reported owning stock in General Electric, 3M, and Pfizer outside the submitted work. Dr. Hall has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers say the data add weight to the argument for permanently adopting the pandemic-era prescribing regulations for buprenorphine, a treatment for opioid use disorder.
“We saw no evidence that increased availability of buprenorphine through the loosening of rules around prescribing and dispensing of buprenorphine during the pandemic increased overdose deaths,” investigator Wilson Compton, MD, deputy director of the National Institute on Drug Abuse, told this news organization.
“This is reassuring that, even when we opened up the doors to easier access to buprenorphine, we didn’t see that most serious consequence,” Dr. Compton said.
The findings were published online in JAMA Network Open .
Cause and effect
Federal agencies relaxed prescribing regulations for buprenorphine in March 2020 to make it easier for clinicians to prescribe the drug via telemedicine and for patients to take the medication at home.
The number of buprenorphine prescriptions has increased since that change, with more than 1 million people receiving the medication in 2021 from retail pharmacies in the United States.
However, questions remained about whether increased access would lead to an increase in buprenorphine-involved overdose.
Researchers with NIDA and the Centers for Disease Control and Prevention analyzed data from the State Unintentional Drug Overdose Reporting System, a CDC database that combines medical examiner and coroner reports and postmortem toxicology testing.
The study included information about overdose deaths from July 2019 to June 2021 in 46 states and the District of Columbia.
Between July 2019 and June 2021, there were 1,955 buprenorphine-involved overdose deaths, which accounted for 2.2% of all drug overdose deaths and 2.6% of opioid-involved overdose deaths.
However, researchers went beyond overall numbers and evaluated details from coroner’s and medical examiner reports, something they had not done before.
“For the first time we looked at the characteristics of decedents from buprenorphine because this has not been studied in this type of detail with a near-national sample,” Dr. Compton said.
“That allowed us to look at patterns of use of other substances as well as the circumstances that are recorded at the death scene that are in the data set,” he added.
Important insights
Reports from nearly all buprenorphine-involved deaths included the presence of at least one other drug, compared with opioid overdose deaths that typically involved only one drug.
“This is consistent with the pharmacology of buprenorphine being a partial agonist, so it may not be as fatal all by itself as some of the other opioids,” Dr. Compton said.
Deaths involving buprenorphine were less likely to include illicitly manufactured fentanyls, and other prescription medications were more often found on the scene, such as antidepressants.
Compared with opioid decedents, buprenorphine decedents were more likely to be women, age 35-44, White, and receiving treatment for mental health conditions, including for substance use disorder (SUD).
These kinds of characteristics provide important insights about potential ways to improve safety and clinical outcomes, Dr. Compton noted.
“When we see things like a little higher rate of SUD treatment and this evidence of other prescription drugs on the scene, and some higher rates of antidepressants in these decedents than I might have expected, I’m very curious about their use of other medical services outside of substance use treatment, because that might be a place where some interventions could be implemented,” he said.
A similar study showed pandemic-era policy changes that allowed methadone to be taken at home was followed by a decrease in methadone-related overdose deaths.
The new findings are consistent with those results, Dr. Compton said.
‘Chipping away’ at stigma
Commenting on the study, O. Trent Hall, DO, assistant professor of addiction medicine, Department of Psychiatry and Behavioral Health, Ohio State University Wexner Medical Center, Columbus, said that, although he welcomed the findings, they aren’t unexpected.
“Buprenorphine is well established as a safe and effective medication for opioid use disorder and as a physician who routinely cares for patients in the hospital after opioid overdose, I am not at all surprised by these results,” said Dr. Hall, who was not involved with the research.
“When my patients leave the hospital with a buprenorphine prescription, they are much less likely to return with another overdose or serious opioid-related medical problem,” he added.
U.S. drug overdose deaths topped 100,000 for the first time in 2021, and most were opioid-related. Although the latest data from the CDC shows drug overdose deaths have been declining slowly since early 2022, the numbers remain high.
Buprenorphine is one of only two drugs known to reduce the risk of opioid overdose. While prescriptions have increased since 2020, the medication remains underutilized, despite its known effectiveness in treating opioid use disorder.
Dr. Hall noted that research such as the new study could help increase buprenorphine’s use.
“Studies like this one chip away at the stigma that has been misapplied to buprenorphine,” he said. “I hope this article will encourage more providers to offer buprenorphine to patients with opioid use disorder.”
The study was funded internally by NIDA and the CDC. Dr. Compton reported owning stock in General Electric, 3M, and Pfizer outside the submitted work. Dr. Hall has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Massive rise in drug overdose deaths driven by opioids
The 376% represents the change in age-adjusted overdose deaths per 100,000 population, which went from 6.9 in 2001 to 32.4 in 2021, as the total number of deaths rose from 19,394 to 106,699 (450%) over that time period, the NCHS said in a recent data brief. That total made 2021 the first year ever with more than 100,000 overdose deaths.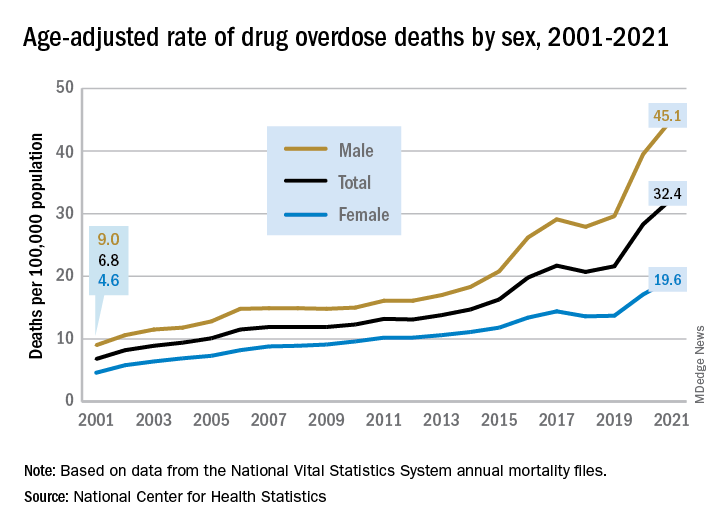
Since the age-adjusted rate stood at 21.6 per 100,000 in 2019, that means 42% of the total increase over 20 years actually occurred in 2020 and 2021. The number of deaths increased by about 36,000 over those 2 years, accounting for 41% of the total annual increase from 2001 to 2021, based on data from the National Vital Statistics System mortality files.
The overdose death rate was significantly higher for males than females for all of the years from 2001 to 2021, with males seeing an increase from 9.0 to 45.1 per 100,000 and females going from 4.6 to 19.6 deaths per 100,000. In the single year from 2020 to 2021, the age-adjusted rate was up by 14% for males and 15% for females, the mortality-file data show.
Analysis by age showed an even larger effect in some groups from 2020 to 2021. Drug overdose deaths jumped 28% among adults aged 65 years and older, more than any other group, and by 21% in those aged 55-64 years, according to the NCHS.
The only age group for which deaths didn’t increase significantly from 2020 to 2021 was 15- to 24-year-olds, whose rate rose by just 3%. The age group with the highest rate in both 2020 and 2021, however, was the 35- to 44-year-olds: 53.9 and 62.0 overdose deaths per 100,000, respectively, for an increase of 15%, the NCHS said in the report.
The drugs now involved in overdose deaths are most often opioids, a change from 2001. That year, opioids were involved in 49% of all overdose deaths, but by 2021 that share had increased to 75%. The trend for opioid-related deaths almost matches that of overall deaths over the 20-year span, and the significantly increasing trend that began for all overdose deaths in 2013 closely follows that of synthetic opioids such as fentanyl and tramadol, the report shows.
Overdose deaths involving cocaine and psychostimulants such as methamphetamine, amphetamine, and methylphenidate also show similar increases. The cocaine-related death rate rose 22% from 2020 to 2021 and is up by 421% since 2012, while the corresponding increases for psychostimulant deaths were 33% and 2,400%, the NCHS said.
The 376% represents the change in age-adjusted overdose deaths per 100,000 population, which went from 6.9 in 2001 to 32.4 in 2021, as the total number of deaths rose from 19,394 to 106,699 (450%) over that time period, the NCHS said in a recent data brief. That total made 2021 the first year ever with more than 100,000 overdose deaths.
Since the age-adjusted rate stood at 21.6 per 100,000 in 2019, that means 42% of the total increase over 20 years actually occurred in 2020 and 2021. The number of deaths increased by about 36,000 over those 2 years, accounting for 41% of the total annual increase from 2001 to 2021, based on data from the National Vital Statistics System mortality files.
The overdose death rate was significantly higher for males than females for all of the years from 2001 to 2021, with males seeing an increase from 9.0 to 45.1 per 100,000 and females going from 4.6 to 19.6 deaths per 100,000. In the single year from 2020 to 2021, the age-adjusted rate was up by 14% for males and 15% for females, the mortality-file data show.
Analysis by age showed an even larger effect in some groups from 2020 to 2021. Drug overdose deaths jumped 28% among adults aged 65 years and older, more than any other group, and by 21% in those aged 55-64 years, according to the NCHS.
The only age group for which deaths didn’t increase significantly from 2020 to 2021 was 15- to 24-year-olds, whose rate rose by just 3%. The age group with the highest rate in both 2020 and 2021, however, was the 35- to 44-year-olds: 53.9 and 62.0 overdose deaths per 100,000, respectively, for an increase of 15%, the NCHS said in the report.
The drugs now involved in overdose deaths are most often opioids, a change from 2001. That year, opioids were involved in 49% of all overdose deaths, but by 2021 that share had increased to 75%. The trend for opioid-related deaths almost matches that of overall deaths over the 20-year span, and the significantly increasing trend that began for all overdose deaths in 2013 closely follows that of synthetic opioids such as fentanyl and tramadol, the report shows.
Overdose deaths involving cocaine and psychostimulants such as methamphetamine, amphetamine, and methylphenidate also show similar increases. The cocaine-related death rate rose 22% from 2020 to 2021 and is up by 421% since 2012, while the corresponding increases for psychostimulant deaths were 33% and 2,400%, the NCHS said.
The 376% represents the change in age-adjusted overdose deaths per 100,000 population, which went from 6.9 in 2001 to 32.4 in 2021, as the total number of deaths rose from 19,394 to 106,699 (450%) over that time period, the NCHS said in a recent data brief. That total made 2021 the first year ever with more than 100,000 overdose deaths.
Since the age-adjusted rate stood at 21.6 per 100,000 in 2019, that means 42% of the total increase over 20 years actually occurred in 2020 and 2021. The number of deaths increased by about 36,000 over those 2 years, accounting for 41% of the total annual increase from 2001 to 2021, based on data from the National Vital Statistics System mortality files.
The overdose death rate was significantly higher for males than females for all of the years from 2001 to 2021, with males seeing an increase from 9.0 to 45.1 per 100,000 and females going from 4.6 to 19.6 deaths per 100,000. In the single year from 2020 to 2021, the age-adjusted rate was up by 14% for males and 15% for females, the mortality-file data show.
Analysis by age showed an even larger effect in some groups from 2020 to 2021. Drug overdose deaths jumped 28% among adults aged 65 years and older, more than any other group, and by 21% in those aged 55-64 years, according to the NCHS.
The only age group for which deaths didn’t increase significantly from 2020 to 2021 was 15- to 24-year-olds, whose rate rose by just 3%. The age group with the highest rate in both 2020 and 2021, however, was the 35- to 44-year-olds: 53.9 and 62.0 overdose deaths per 100,000, respectively, for an increase of 15%, the NCHS said in the report.
The drugs now involved in overdose deaths are most often opioids, a change from 2001. That year, opioids were involved in 49% of all overdose deaths, but by 2021 that share had increased to 75%. The trend for opioid-related deaths almost matches that of overall deaths over the 20-year span, and the significantly increasing trend that began for all overdose deaths in 2013 closely follows that of synthetic opioids such as fentanyl and tramadol, the report shows.
Overdose deaths involving cocaine and psychostimulants such as methamphetamine, amphetamine, and methylphenidate also show similar increases. The cocaine-related death rate rose 22% from 2020 to 2021 and is up by 421% since 2012, while the corresponding increases for psychostimulant deaths were 33% and 2,400%, the NCHS said.