User login
Genetic risk factor found for RA-associated interstitial lung disease
CHICAGO – Rheumatoid arthritis–associated interstitial lung disease and idiopathic pulmonary fibrosis without RA share a common genetic underpinning whose hallmark is a gain-of-function MUC5B gene promoter variant that cranks up mucin production in the lungs, Pierre-Antoine Juge, MD, reported at the annual meeting of the American College of Rheumatology.

He presented a seven-country genetic case-control study of 620 patients with RA-associated interstitial lung disease (RA-ILD), 614 with RA but no ILD, and 5,448 unaffected controls. The key finding was that the MUC5B promoter variant rs35705950, already known to be the strongest genetic risk factor for idiopathic pulmonary fibrosis (IPF), also contributes substantially to the risk of RA-ILD.
Indeed, the presence of the MUC5B promoter variant in patients with RA proved to be associated with substantially higher risk of RA-ILD than the previously recognized risk factors for RA-ILD, including cigarette smoking and the human leukocyte antigen locus for RA, according to Dr. Juge, a rheumatologist at Bichat Hospital–Claude Bernard and Paris Diderot University.
MUC5B encodes for mucin production in the lungs. The increased risk of RA-ILD conferred by the presence of the MUC5B promoter variant was confined to the 41% of RA-ILD patients with a pattern of usual interstitial pneumonia (UIP) or possible UIP on high-resolution CT. The presence of the MUC5B promoter variant in RA patients was independently associated with an adjusted 6.1-fold increased risk of ILD with a UIP pattern on imaging – marked by honeycombing, reticular abnormalities, and subpleural involvement – compared with RA patients who didn’t possess the gain-of-function MUC5B variant. The risk of other types of RA-ILD wasn’t affected by the presence or absence of the MUC5B variant.
The MUC5B promoter variant was not a risk factor for development of RA.
These findings have potentially important implications for clinical practice, given that clinically significant ILD is present in about 10% of all RA patients and occult ILD is detectable using high-resolution CT in up to half of individuals with RA, Dr. Juge observed. Detection of the MUC5B promoter variant could be used to screen patients with RA for preclinical ILD. Also, there is now a sound rationale to study drugs known to be effective for IPF as potential treatments for RA-ILD, he said.
Dr. Juge reported having no financial conflicts regarding the study, which was sponsored by the National Institutes of Health, the U.S. Department of Defense, the French Rheumatology Society, the Japanese Society for the Promotion of Science, Fondation Arthritis, and the Nina Ireland Program for Lung Health.
In conjunction with his presentation in Chicago, the study was published online in the New England Journal of Medicine (doi: 10.1056/NEJMoa1801562).
SOURCE: Juge P-A et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 1819.
CHICAGO – Rheumatoid arthritis–associated interstitial lung disease and idiopathic pulmonary fibrosis without RA share a common genetic underpinning whose hallmark is a gain-of-function MUC5B gene promoter variant that cranks up mucin production in the lungs, Pierre-Antoine Juge, MD, reported at the annual meeting of the American College of Rheumatology.
He presented a seven-country genetic case-control study of 620 patients with RA-associated interstitial lung disease (RA-ILD), 614 with RA but no ILD, and 5,448 unaffected controls. The key finding was that the MUC5B promoter variant rs35705950, already known to be the strongest genetic risk factor for idiopathic pulmonary fibrosis (IPF), also contributes substantially to the risk of RA-ILD.
Indeed, the presence of the MUC5B promoter variant in patients with RA proved to be associated with substantially higher risk of RA-ILD than the previously recognized risk factors for RA-ILD, including cigarette smoking and the human leukocyte antigen locus for RA, according to Dr. Juge, a rheumatologist at Bichat Hospital–Claude Bernard and Paris Diderot University.
MUC5B encodes for mucin production in the lungs. The increased risk of RA-ILD conferred by the presence of the MUC5B promoter variant was confined to the 41% of RA-ILD patients with a pattern of usual interstitial pneumonia (UIP) or possible UIP on high-resolution CT. The presence of the MUC5B promoter variant in RA patients was independently associated with an adjusted 6.1-fold increased risk of ILD with a UIP pattern on imaging – marked by honeycombing, reticular abnormalities, and subpleural involvement – compared with RA patients who didn’t possess the gain-of-function MUC5B variant. The risk of other types of RA-ILD wasn’t affected by the presence or absence of the MUC5B variant.
The MUC5B promoter variant was not a risk factor for development of RA.
These findings have potentially important implications for clinical practice, given that clinically significant ILD is present in about 10% of all RA patients and occult ILD is detectable using high-resolution CT in up to half of individuals with RA, Dr. Juge observed. Detection of the MUC5B promoter variant could be used to screen patients with RA for preclinical ILD. Also, there is now a sound rationale to study drugs known to be effective for IPF as potential treatments for RA-ILD, he said.
Dr. Juge reported having no financial conflicts regarding the study, which was sponsored by the National Institutes of Health, the U.S. Department of Defense, the French Rheumatology Society, the Japanese Society for the Promotion of Science, Fondation Arthritis, and the Nina Ireland Program for Lung Health.
In conjunction with his presentation in Chicago, the study was published online in the New England Journal of Medicine (doi: 10.1056/NEJMoa1801562).
SOURCE: Juge P-A et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 1819.
CHICAGO – Rheumatoid arthritis–associated interstitial lung disease and idiopathic pulmonary fibrosis without RA share a common genetic underpinning whose hallmark is a gain-of-function MUC5B gene promoter variant that cranks up mucin production in the lungs, Pierre-Antoine Juge, MD, reported at the annual meeting of the American College of Rheumatology.
He presented a seven-country genetic case-control study of 620 patients with RA-associated interstitial lung disease (RA-ILD), 614 with RA but no ILD, and 5,448 unaffected controls. The key finding was that the MUC5B promoter variant rs35705950, already known to be the strongest genetic risk factor for idiopathic pulmonary fibrosis (IPF), also contributes substantially to the risk of RA-ILD.
Indeed, the presence of the MUC5B promoter variant in patients with RA proved to be associated with substantially higher risk of RA-ILD than the previously recognized risk factors for RA-ILD, including cigarette smoking and the human leukocyte antigen locus for RA, according to Dr. Juge, a rheumatologist at Bichat Hospital–Claude Bernard and Paris Diderot University.
MUC5B encodes for mucin production in the lungs. The increased risk of RA-ILD conferred by the presence of the MUC5B promoter variant was confined to the 41% of RA-ILD patients with a pattern of usual interstitial pneumonia (UIP) or possible UIP on high-resolution CT. The presence of the MUC5B promoter variant in RA patients was independently associated with an adjusted 6.1-fold increased risk of ILD with a UIP pattern on imaging – marked by honeycombing, reticular abnormalities, and subpleural involvement – compared with RA patients who didn’t possess the gain-of-function MUC5B variant. The risk of other types of RA-ILD wasn’t affected by the presence or absence of the MUC5B variant.
The MUC5B promoter variant was not a risk factor for development of RA.
These findings have potentially important implications for clinical practice, given that clinically significant ILD is present in about 10% of all RA patients and occult ILD is detectable using high-resolution CT in up to half of individuals with RA, Dr. Juge observed. Detection of the MUC5B promoter variant could be used to screen patients with RA for preclinical ILD. Also, there is now a sound rationale to study drugs known to be effective for IPF as potential treatments for RA-ILD, he said.
Dr. Juge reported having no financial conflicts regarding the study, which was sponsored by the National Institutes of Health, the U.S. Department of Defense, the French Rheumatology Society, the Japanese Society for the Promotion of Science, Fondation Arthritis, and the Nina Ireland Program for Lung Health.
In conjunction with his presentation in Chicago, the study was published online in the New England Journal of Medicine (doi: 10.1056/NEJMoa1801562).
SOURCE: Juge P-A et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 1819.
REPORTING FROM THE ACR ANNUAL MEETING
Palindromic rheumatism has a distinct imaging phenotype
Palindromic rheumatism, while often challenging to distinguish from persistent arthritis, has a distinct imaging pattern characterized by extracapsular inflammation, often with no synovitis, results of a recent prospective study show.
Finding the phenotype on ultrasound evaluation may help to separate cases of inflammatory arthritis, which may need early disease-modifying treatment, from palindromic rheumatism, which can be managed conservatively, the study authors reported in Annals of the Rheumatic Diseases.
“These findings may refine diagnosis and improve management of this important condition,” wrote Kulveer Mankia, MD, of the Leeds (England) Institute of Rheumatic and Musculoskeletal Medicine, and his coauthors.
High-resolution imaging studies in palindromic rheumatism have been sparse, in part because of the sporadic nature of flares in these patients, according to Dr. Mankia and his colleagues.
Their report included 79 patients with palindromic rheumatism recruited from two U.K. rheumatology clinics and a national primary care program and compared them with other populations.
The patients underwent ultrasound evaluation by experienced rheumatologists and sonographers, as well as MRI on the most symptomatic region during flares. Those results were compared with clinical and ultrasound assessments in a cohort of patients with new-onset RA, and a second cohort of anticyclic citrullinated peptide (CCP)–positive at-risk individuals.
The investigators were able to assess 31 of the palindromic rheumatism patients during a flare episode. Extracapsular inflammation was frequently found during these episodes, with one or more instances of periarticular inflammation, peritendinous edema, or subcutaneous edema occurring in 19 (61%) of 31 patients.
However, tenosynovitis was detected in just seven of those patients (23%), while peritendinous edema was seen in three (10%).
By contrast, ultrasound abnormalities were infrequent in 27 nonflare evaluations taken in those 31 patients. For example, just four scans (15%) showed extracapsular inflammation.
Overall, extracapsular inflammation was found in 65% of palindromic rheumatism patients, compared with just 29% of new-onset RA cases (P less than .023).
Of particular note, extracapsular inflammation without synovitis was specific for palindromic rheumatism, occurring in 42%, compared with only 4% of RA cases (P = .003) and 6% of anti–CCP-positive at-risk patients (P = .0012).
A total of 13 of the 79 palindromic rheumatism patients (16%) went on to develop persistent inflammatory arthritis over a median follow-up of 42-49 days. Of the 31 patients evaluated during flare, 7 (23%) developed persistent inflammatory arthritis over the follow-up period. Those seven patients all met American College of Rheumatology/European League Against Rheumatism (EULAR) 2010 classification criteria for RA.
The MRI studies concurred with the ultrasound findings and identified some additional abnormalities, the investigators reported.
Altogether, these imaging findings are important to note because of the “variable” progression seen in palindromic rheumatism, Dr. Mankia and his colleagues wrote.
While anti-CCP antibody positivity confers high risk of progression in palindromic rheumatism, presence of this marker does not always mean the patient will develop persistent arthritis on follow-up, they added. In fact, this study showed that, among 47 anti–CCP-positive palindromic rheumatism patients, 35 (74%) did not develop persistent inflammatory arthritis in follow-up.
“In clinical practice, these patients may be inappropriately treated [e.g., with methotrexate] as they often meet ACR/EULAR criteria for rheumatoid arthritis,” the investigators wrote in their report.
Funding for the study came from the National Institute for Health Research Leeds Clinical Research Facility with additional support from an Arthritis Research U.K. grant. The authors reported no competing interests related to their study.
SOURCE: Mankia K et al. Ann Rheum Dis. 2018 Oct 8. doi: 10.1136/annrheumdis-2018-214175.
Palindromic rheumatism, while often challenging to distinguish from persistent arthritis, has a distinct imaging pattern characterized by extracapsular inflammation, often with no synovitis, results of a recent prospective study show.
Finding the phenotype on ultrasound evaluation may help to separate cases of inflammatory arthritis, which may need early disease-modifying treatment, from palindromic rheumatism, which can be managed conservatively, the study authors reported in Annals of the Rheumatic Diseases.
“These findings may refine diagnosis and improve management of this important condition,” wrote Kulveer Mankia, MD, of the Leeds (England) Institute of Rheumatic and Musculoskeletal Medicine, and his coauthors.
High-resolution imaging studies in palindromic rheumatism have been sparse, in part because of the sporadic nature of flares in these patients, according to Dr. Mankia and his colleagues.
Their report included 79 patients with palindromic rheumatism recruited from two U.K. rheumatology clinics and a national primary care program and compared them with other populations.
The patients underwent ultrasound evaluation by experienced rheumatologists and sonographers, as well as MRI on the most symptomatic region during flares. Those results were compared with clinical and ultrasound assessments in a cohort of patients with new-onset RA, and a second cohort of anticyclic citrullinated peptide (CCP)–positive at-risk individuals.
The investigators were able to assess 31 of the palindromic rheumatism patients during a flare episode. Extracapsular inflammation was frequently found during these episodes, with one or more instances of periarticular inflammation, peritendinous edema, or subcutaneous edema occurring in 19 (61%) of 31 patients.
However, tenosynovitis was detected in just seven of those patients (23%), while peritendinous edema was seen in three (10%).
By contrast, ultrasound abnormalities were infrequent in 27 nonflare evaluations taken in those 31 patients. For example, just four scans (15%) showed extracapsular inflammation.
Overall, extracapsular inflammation was found in 65% of palindromic rheumatism patients, compared with just 29% of new-onset RA cases (P less than .023).
Of particular note, extracapsular inflammation without synovitis was specific for palindromic rheumatism, occurring in 42%, compared with only 4% of RA cases (P = .003) and 6% of anti–CCP-positive at-risk patients (P = .0012).
A total of 13 of the 79 palindromic rheumatism patients (16%) went on to develop persistent inflammatory arthritis over a median follow-up of 42-49 days. Of the 31 patients evaluated during flare, 7 (23%) developed persistent inflammatory arthritis over the follow-up period. Those seven patients all met American College of Rheumatology/European League Against Rheumatism (EULAR) 2010 classification criteria for RA.
The MRI studies concurred with the ultrasound findings and identified some additional abnormalities, the investigators reported.
Altogether, these imaging findings are important to note because of the “variable” progression seen in palindromic rheumatism, Dr. Mankia and his colleagues wrote.
While anti-CCP antibody positivity confers high risk of progression in palindromic rheumatism, presence of this marker does not always mean the patient will develop persistent arthritis on follow-up, they added. In fact, this study showed that, among 47 anti–CCP-positive palindromic rheumatism patients, 35 (74%) did not develop persistent inflammatory arthritis in follow-up.
“In clinical practice, these patients may be inappropriately treated [e.g., with methotrexate] as they often meet ACR/EULAR criteria for rheumatoid arthritis,” the investigators wrote in their report.
Funding for the study came from the National Institute for Health Research Leeds Clinical Research Facility with additional support from an Arthritis Research U.K. grant. The authors reported no competing interests related to their study.
SOURCE: Mankia K et al. Ann Rheum Dis. 2018 Oct 8. doi: 10.1136/annrheumdis-2018-214175.
Palindromic rheumatism, while often challenging to distinguish from persistent arthritis, has a distinct imaging pattern characterized by extracapsular inflammation, often with no synovitis, results of a recent prospective study show.
Finding the phenotype on ultrasound evaluation may help to separate cases of inflammatory arthritis, which may need early disease-modifying treatment, from palindromic rheumatism, which can be managed conservatively, the study authors reported in Annals of the Rheumatic Diseases.
“These findings may refine diagnosis and improve management of this important condition,” wrote Kulveer Mankia, MD, of the Leeds (England) Institute of Rheumatic and Musculoskeletal Medicine, and his coauthors.
High-resolution imaging studies in palindromic rheumatism have been sparse, in part because of the sporadic nature of flares in these patients, according to Dr. Mankia and his colleagues.
Their report included 79 patients with palindromic rheumatism recruited from two U.K. rheumatology clinics and a national primary care program and compared them with other populations.
The patients underwent ultrasound evaluation by experienced rheumatologists and sonographers, as well as MRI on the most symptomatic region during flares. Those results were compared with clinical and ultrasound assessments in a cohort of patients with new-onset RA, and a second cohort of anticyclic citrullinated peptide (CCP)–positive at-risk individuals.
The investigators were able to assess 31 of the palindromic rheumatism patients during a flare episode. Extracapsular inflammation was frequently found during these episodes, with one or more instances of periarticular inflammation, peritendinous edema, or subcutaneous edema occurring in 19 (61%) of 31 patients.
However, tenosynovitis was detected in just seven of those patients (23%), while peritendinous edema was seen in three (10%).
By contrast, ultrasound abnormalities were infrequent in 27 nonflare evaluations taken in those 31 patients. For example, just four scans (15%) showed extracapsular inflammation.
Overall, extracapsular inflammation was found in 65% of palindromic rheumatism patients, compared with just 29% of new-onset RA cases (P less than .023).
Of particular note, extracapsular inflammation without synovitis was specific for palindromic rheumatism, occurring in 42%, compared with only 4% of RA cases (P = .003) and 6% of anti–CCP-positive at-risk patients (P = .0012).
A total of 13 of the 79 palindromic rheumatism patients (16%) went on to develop persistent inflammatory arthritis over a median follow-up of 42-49 days. Of the 31 patients evaluated during flare, 7 (23%) developed persistent inflammatory arthritis over the follow-up period. Those seven patients all met American College of Rheumatology/European League Against Rheumatism (EULAR) 2010 classification criteria for RA.
The MRI studies concurred with the ultrasound findings and identified some additional abnormalities, the investigators reported.
Altogether, these imaging findings are important to note because of the “variable” progression seen in palindromic rheumatism, Dr. Mankia and his colleagues wrote.
While anti-CCP antibody positivity confers high risk of progression in palindromic rheumatism, presence of this marker does not always mean the patient will develop persistent arthritis on follow-up, they added. In fact, this study showed that, among 47 anti–CCP-positive palindromic rheumatism patients, 35 (74%) did not develop persistent inflammatory arthritis in follow-up.
“In clinical practice, these patients may be inappropriately treated [e.g., with methotrexate] as they often meet ACR/EULAR criteria for rheumatoid arthritis,” the investigators wrote in their report.
Funding for the study came from the National Institute for Health Research Leeds Clinical Research Facility with additional support from an Arthritis Research U.K. grant. The authors reported no competing interests related to their study.
SOURCE: Mankia K et al. Ann Rheum Dis. 2018 Oct 8. doi: 10.1136/annrheumdis-2018-214175.
FROM ANNALS OF THE RHEUMATIC DISEASES
Key clinical point: The
Major finding: Extracapsular inflammation without synovitis occurred in 42% of palindromic rheumatism patients, versus 4% of RA cases (P = .003) and 6% of anticyclic citrullinated peptide–positive at-risk patients (P = .0012).
Study details: A prospective study of 79 patients with palindromic rheumatism, including comparisons with new-onset RA and anticyclic citrullinated peptide–positive at-risk patient cohorts.
Disclosures: Funding for the study came from the National Institute for Health Research Leeds Clinical Research Facility and Arthritis Research U.K. The study authors reported no competing interests.
Source: Mankia K et al. Ann Rheum Dis. 2018 Oct 8. doi: 10.1136/annrheumdis-2018-214175.
High-dose flu vaccine in RA patients beats standard dose
CHICAGO – The administration of high-dose vs. standard-dose influenza vaccine provided substantially better immune responses in seropositive rheumatoid arthritis patients in a randomized, active-controlled trial.
High-dose trivalent influenza vaccine is known to improve immune responses in the elderly, but the current findings, which were presented at the annual meeting of the American College of Rheumatology, are the first to document a successful intervention to enhance vaccine responses in immunocompromised patients, according to Inés Colmegna, MD, of McGill University, Montreal.
Dr. Colmegna and her colleagues assessed antibody responses to either standard-dose (15 mcg of hemagglutinin per strain) quadrivalent inactivated influenza vaccine (SD-QIV) or high-dose (60 mcg of hemagglutinin per strain) trivalent inactivated influenza vaccine (HD-TIV) in 140 and 139 patients, respectively.
Seroprotection rates prior to vaccination were comparable in the two groups, but the high-dose recipients had consistently higher overall responses to vaccination.
Seroconversion rates were 22.3% vs. 8.6% (odds ratio, 2.93) for the H3N2 strain (A/HongKong/4801/2014), and 44.6% vs. 28.6% (OR, 1.93) for the B Victoria Lin strain (B/Brisbane/60/2008). For the H1N1 strain A/California/7/2009 in 2016-2017 and closely related A/Michigan/45/2015 in 2017-2018, the seroconversion rates were 51.1% vs. 30.0% (OR, 2.91) and 46.4% vs. 24.6% (OR, 2.79), respectively. Seroprotection rates for the H3N2 strain were 48.5% vs. 30.9%, and for the B Victoria Lin strain, 60.0% vs. 50.7%. The seroprotection rates for the H1N1 strains together were and 80.4% vs. 73.5%, Dr. Colmegna said.
Seroconversion was defined as at least a fourfold serum hemagglutination inhibition (HI) antibody increase from prevaccination level (day 0), and seroprotection was defined as percent with HI titers of 1:40 or greater at postvaccination day 28.
After the researchers controlled for age, vaccine type, treatment type in the 3 months prior to vaccination and during the study period, Charlson comorbidity index, and RA duration, the only significant predictors of vaccine seroresponse were vaccine dose and age.
The findings are notable because RA patients have a nearly threefold increase in the risk of contracting influenza infection or related illness, compared with age-matched healthy controls, because of “inherent immune dysfunction associated with RA, comorbidities, the age of our patients, and immunosuppressive therapy,” Dr. Colmegna said.
For this reason, RA patients are a priority group for annual vaccination. However, while vaccination remains the most effective method for preventing influenza and its associated complications, vaccine-induced antibody responses and protection in RA are suboptimal, she explained, noting that this puts them at increased risk for severe influenza.
“There is a high priority to develop new approaches to try to decrease this risk,” she said.
It was unknown whether HD-TIV – the only currently available high-dose influenza vaccine – would safely enhance antibody production in RA as it does in the elderly, so she and her colleagues recruited patients from a tertiary care center during the 2016-2017 and 2017-2018 Northern Hemisphere influenza seasons for this study.
The mean age of the patients was 61 years, and 80% were women. All were on stable treatment with either disease-modifying antirheumatic drugs (DMARDs) or biologics for at least 3 months prior to vaccination; treatment types included DMARDs in 138 patients (49.5%), anticytokine therapy in 92 patients (33%), and anti-B-cell therapy and small molecules in 49 patients (17.6%). An analysis by treatment type showed a possible reduction in the rate of seroconversion in patients who received anti-B-cell therapy and small molecules, but the number of patients in the group was too small to make definitive conclusions, Dr. Colmegna said.
Treatment in all groups was safe, with no differences in adverse events between those receiving high- or standard-dose vaccine, and none of the adverse events were related to treatment.
Further, the high-dose vaccine was not associated with an increase in disease activity.
“We believe that these results will likely change clinical practice,” she concluded.
Dr. Colmegna reported having no disclosures.
SOURCE: Colmegna I et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 837.
CHICAGO – The administration of high-dose vs. standard-dose influenza vaccine provided substantially better immune responses in seropositive rheumatoid arthritis patients in a randomized, active-controlled trial.
High-dose trivalent influenza vaccine is known to improve immune responses in the elderly, but the current findings, which were presented at the annual meeting of the American College of Rheumatology, are the first to document a successful intervention to enhance vaccine responses in immunocompromised patients, according to Inés Colmegna, MD, of McGill University, Montreal.
Dr. Colmegna and her colleagues assessed antibody responses to either standard-dose (15 mcg of hemagglutinin per strain) quadrivalent inactivated influenza vaccine (SD-QIV) or high-dose (60 mcg of hemagglutinin per strain) trivalent inactivated influenza vaccine (HD-TIV) in 140 and 139 patients, respectively.
Seroprotection rates prior to vaccination were comparable in the two groups, but the high-dose recipients had consistently higher overall responses to vaccination.
Seroconversion rates were 22.3% vs. 8.6% (odds ratio, 2.93) for the H3N2 strain (A/HongKong/4801/2014), and 44.6% vs. 28.6% (OR, 1.93) for the B Victoria Lin strain (B/Brisbane/60/2008). For the H1N1 strain A/California/7/2009 in 2016-2017 and closely related A/Michigan/45/2015 in 2017-2018, the seroconversion rates were 51.1% vs. 30.0% (OR, 2.91) and 46.4% vs. 24.6% (OR, 2.79), respectively. Seroprotection rates for the H3N2 strain were 48.5% vs. 30.9%, and for the B Victoria Lin strain, 60.0% vs. 50.7%. The seroprotection rates for the H1N1 strains together were and 80.4% vs. 73.5%, Dr. Colmegna said.
Seroconversion was defined as at least a fourfold serum hemagglutination inhibition (HI) antibody increase from prevaccination level (day 0), and seroprotection was defined as percent with HI titers of 1:40 or greater at postvaccination day 28.
After the researchers controlled for age, vaccine type, treatment type in the 3 months prior to vaccination and during the study period, Charlson comorbidity index, and RA duration, the only significant predictors of vaccine seroresponse were vaccine dose and age.
The findings are notable because RA patients have a nearly threefold increase in the risk of contracting influenza infection or related illness, compared with age-matched healthy controls, because of “inherent immune dysfunction associated with RA, comorbidities, the age of our patients, and immunosuppressive therapy,” Dr. Colmegna said.
For this reason, RA patients are a priority group for annual vaccination. However, while vaccination remains the most effective method for preventing influenza and its associated complications, vaccine-induced antibody responses and protection in RA are suboptimal, she explained, noting that this puts them at increased risk for severe influenza.
“There is a high priority to develop new approaches to try to decrease this risk,” she said.
It was unknown whether HD-TIV – the only currently available high-dose influenza vaccine – would safely enhance antibody production in RA as it does in the elderly, so she and her colleagues recruited patients from a tertiary care center during the 2016-2017 and 2017-2018 Northern Hemisphere influenza seasons for this study.
The mean age of the patients was 61 years, and 80% were women. All were on stable treatment with either disease-modifying antirheumatic drugs (DMARDs) or biologics for at least 3 months prior to vaccination; treatment types included DMARDs in 138 patients (49.5%), anticytokine therapy in 92 patients (33%), and anti-B-cell therapy and small molecules in 49 patients (17.6%). An analysis by treatment type showed a possible reduction in the rate of seroconversion in patients who received anti-B-cell therapy and small molecules, but the number of patients in the group was too small to make definitive conclusions, Dr. Colmegna said.
Treatment in all groups was safe, with no differences in adverse events between those receiving high- or standard-dose vaccine, and none of the adverse events were related to treatment.
Further, the high-dose vaccine was not associated with an increase in disease activity.
“We believe that these results will likely change clinical practice,” she concluded.
Dr. Colmegna reported having no disclosures.
SOURCE: Colmegna I et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 837.
CHICAGO – The administration of high-dose vs. standard-dose influenza vaccine provided substantially better immune responses in seropositive rheumatoid arthritis patients in a randomized, active-controlled trial.
High-dose trivalent influenza vaccine is known to improve immune responses in the elderly, but the current findings, which were presented at the annual meeting of the American College of Rheumatology, are the first to document a successful intervention to enhance vaccine responses in immunocompromised patients, according to Inés Colmegna, MD, of McGill University, Montreal.
Dr. Colmegna and her colleagues assessed antibody responses to either standard-dose (15 mcg of hemagglutinin per strain) quadrivalent inactivated influenza vaccine (SD-QIV) or high-dose (60 mcg of hemagglutinin per strain) trivalent inactivated influenza vaccine (HD-TIV) in 140 and 139 patients, respectively.
Seroprotection rates prior to vaccination were comparable in the two groups, but the high-dose recipients had consistently higher overall responses to vaccination.
Seroconversion rates were 22.3% vs. 8.6% (odds ratio, 2.93) for the H3N2 strain (A/HongKong/4801/2014), and 44.6% vs. 28.6% (OR, 1.93) for the B Victoria Lin strain (B/Brisbane/60/2008). For the H1N1 strain A/California/7/2009 in 2016-2017 and closely related A/Michigan/45/2015 in 2017-2018, the seroconversion rates were 51.1% vs. 30.0% (OR, 2.91) and 46.4% vs. 24.6% (OR, 2.79), respectively. Seroprotection rates for the H3N2 strain were 48.5% vs. 30.9%, and for the B Victoria Lin strain, 60.0% vs. 50.7%. The seroprotection rates for the H1N1 strains together were and 80.4% vs. 73.5%, Dr. Colmegna said.
Seroconversion was defined as at least a fourfold serum hemagglutination inhibition (HI) antibody increase from prevaccination level (day 0), and seroprotection was defined as percent with HI titers of 1:40 or greater at postvaccination day 28.
After the researchers controlled for age, vaccine type, treatment type in the 3 months prior to vaccination and during the study period, Charlson comorbidity index, and RA duration, the only significant predictors of vaccine seroresponse were vaccine dose and age.
The findings are notable because RA patients have a nearly threefold increase in the risk of contracting influenza infection or related illness, compared with age-matched healthy controls, because of “inherent immune dysfunction associated with RA, comorbidities, the age of our patients, and immunosuppressive therapy,” Dr. Colmegna said.
For this reason, RA patients are a priority group for annual vaccination. However, while vaccination remains the most effective method for preventing influenza and its associated complications, vaccine-induced antibody responses and protection in RA are suboptimal, she explained, noting that this puts them at increased risk for severe influenza.
“There is a high priority to develop new approaches to try to decrease this risk,” she said.
It was unknown whether HD-TIV – the only currently available high-dose influenza vaccine – would safely enhance antibody production in RA as it does in the elderly, so she and her colleagues recruited patients from a tertiary care center during the 2016-2017 and 2017-2018 Northern Hemisphere influenza seasons for this study.
The mean age of the patients was 61 years, and 80% were women. All were on stable treatment with either disease-modifying antirheumatic drugs (DMARDs) or biologics for at least 3 months prior to vaccination; treatment types included DMARDs in 138 patients (49.5%), anticytokine therapy in 92 patients (33%), and anti-B-cell therapy and small molecules in 49 patients (17.6%). An analysis by treatment type showed a possible reduction in the rate of seroconversion in patients who received anti-B-cell therapy and small molecules, but the number of patients in the group was too small to make definitive conclusions, Dr. Colmegna said.
Treatment in all groups was safe, with no differences in adverse events between those receiving high- or standard-dose vaccine, and none of the adverse events were related to treatment.
Further, the high-dose vaccine was not associated with an increase in disease activity.
“We believe that these results will likely change clinical practice,” she concluded.
Dr. Colmegna reported having no disclosures.
SOURCE: Colmegna I et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 837.
REPORTING FROM THE ACR ANNUAL MEETING
Key clinical point: High- vs. standard-dose flu vaccine improves immune responses in RA patients.
Major finding: High-dose trivalent inactivated influenza vaccine was associated with greater odds of H3N2, B Victoria Lin, and H1N1 seroconversion.
Study details: A randomized, active-controlled trial of 279 RA patients
Disclosures: Dr. Colmegna reported having no disclosures.
Source: Colmegna I et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 837.

Multiple interventions boost RA treat-to-target success
CHICAGO – A novel disease-management approach that paired routine monitoring of the clinical status of patients with RA and training for their rheumatologists on how to refine their treat-to-target practices led to a modest but meaningful boost in the achievement of treat-to-target goals in a single-center study with 2,549 patients.
After 1 year, patients assigned to the intervention program had a 12% improvement in their treat-to-target implementation score, compared with patients who received standard care, an increase that was “clinically meaningful,” Cianna L. Leatherwood, MD, said while presenting a poster at the annual meeting of the American College of Rheumatology.
This increased score represented improvements in its four components: measuring disease activity, using a disease activity score in treatment decision making, documenting evidence for creating a treatment goal, and making shared decisions, Dr. Leatherwood explained in a video interview. Some of Dr. Leatherwood’s collaborators in this study from Brigham and Women’s Hospital in Boston developed and first introduced the treat-to-target implementation score a few years ago (Arthritis Rheum. 2017 July;69[7]:1374-80).
The major interventions used in this program included having patients complete the Routine Assessment of Patient Index Data 3 index (Rheum Dis Clin North Am. 2009 Nov;35[4]:773-8) at every clinic encounter, focus-group discussions with panels of patients both prior to and during the year-long program, and monthly “learning collaborative sessions” for the nine rheumatologists in the intervention arm to discuss and develop treat-to-target practices, said Dr. Leatherwood, a rheumatologist at Kaiser Permanente in Oakland, Calif. The physicians in the intervention group also received frequent email reminders about adopting a treat-to-target approach. The control arm of the study included 11 rheumatologists who did not participate in these sessions or receive the reminders.
Dr. Leatherwood expressed confidence that other health systems could now adapt and use the treatment model she and her associates developed and tested after tailoring it to better match their local conditions.
The study received partial funding from Pfizer. Dr. Leatherwood had no disclosures to report.
SOURCE: Leatherwood CL et al. ACR Annual Meeting, Abstract 326.
CHICAGO – A novel disease-management approach that paired routine monitoring of the clinical status of patients with RA and training for their rheumatologists on how to refine their treat-to-target practices led to a modest but meaningful boost in the achievement of treat-to-target goals in a single-center study with 2,549 patients.
After 1 year, patients assigned to the intervention program had a 12% improvement in their treat-to-target implementation score, compared with patients who received standard care, an increase that was “clinically meaningful,” Cianna L. Leatherwood, MD, said while presenting a poster at the annual meeting of the American College of Rheumatology.
This increased score represented improvements in its four components: measuring disease activity, using a disease activity score in treatment decision making, documenting evidence for creating a treatment goal, and making shared decisions, Dr. Leatherwood explained in a video interview. Some of Dr. Leatherwood’s collaborators in this study from Brigham and Women’s Hospital in Boston developed and first introduced the treat-to-target implementation score a few years ago (Arthritis Rheum. 2017 July;69[7]:1374-80).
The major interventions used in this program included having patients complete the Routine Assessment of Patient Index Data 3 index (Rheum Dis Clin North Am. 2009 Nov;35[4]:773-8) at every clinic encounter, focus-group discussions with panels of patients both prior to and during the year-long program, and monthly “learning collaborative sessions” for the nine rheumatologists in the intervention arm to discuss and develop treat-to-target practices, said Dr. Leatherwood, a rheumatologist at Kaiser Permanente in Oakland, Calif. The physicians in the intervention group also received frequent email reminders about adopting a treat-to-target approach. The control arm of the study included 11 rheumatologists who did not participate in these sessions or receive the reminders.
Dr. Leatherwood expressed confidence that other health systems could now adapt and use the treatment model she and her associates developed and tested after tailoring it to better match their local conditions.
The study received partial funding from Pfizer. Dr. Leatherwood had no disclosures to report.
SOURCE: Leatherwood CL et al. ACR Annual Meeting, Abstract 326.
CHICAGO – A novel disease-management approach that paired routine monitoring of the clinical status of patients with RA and training for their rheumatologists on how to refine their treat-to-target practices led to a modest but meaningful boost in the achievement of treat-to-target goals in a single-center study with 2,549 patients.
After 1 year, patients assigned to the intervention program had a 12% improvement in their treat-to-target implementation score, compared with patients who received standard care, an increase that was “clinically meaningful,” Cianna L. Leatherwood, MD, said while presenting a poster at the annual meeting of the American College of Rheumatology.
This increased score represented improvements in its four components: measuring disease activity, using a disease activity score in treatment decision making, documenting evidence for creating a treatment goal, and making shared decisions, Dr. Leatherwood explained in a video interview. Some of Dr. Leatherwood’s collaborators in this study from Brigham and Women’s Hospital in Boston developed and first introduced the treat-to-target implementation score a few years ago (Arthritis Rheum. 2017 July;69[7]:1374-80).
The major interventions used in this program included having patients complete the Routine Assessment of Patient Index Data 3 index (Rheum Dis Clin North Am. 2009 Nov;35[4]:773-8) at every clinic encounter, focus-group discussions with panels of patients both prior to and during the year-long program, and monthly “learning collaborative sessions” for the nine rheumatologists in the intervention arm to discuss and develop treat-to-target practices, said Dr. Leatherwood, a rheumatologist at Kaiser Permanente in Oakland, Calif. The physicians in the intervention group also received frequent email reminders about adopting a treat-to-target approach. The control arm of the study included 11 rheumatologists who did not participate in these sessions or receive the reminders.
Dr. Leatherwood expressed confidence that other health systems could now adapt and use the treatment model she and her associates developed and tested after tailoring it to better match their local conditions.
The study received partial funding from Pfizer. Dr. Leatherwood had no disclosures to report.
SOURCE: Leatherwood CL et al. ACR Annual Meeting, Abstract 326.
REPORTING FROM THE ACR ANNUAL MEETING
Key clinical point:
Major finding: After 1 year, the treat-to-target implementation score in the intervention patients was 12% higher than among the control patients.
Study details: A single-center, controlled study with 2,549 RA patients and 22 rheumatologists.
Disclosures: The study received partial funding from Pfizer. Dr. Leatherwood had no disclosures to report.
Source: Leatherwood CL et al. ACR Annual Meeting, Abstract 326.

Novel blood test brings RA prevention closer to reality
CHICAGO – A positive B cell clonality test in a peripheral blood sample predicts imminent onset of rheumatoid arthritis with a high degree of accuracy in at-risk individuals, Niek de Vries, MD, PhD, reported at the annual meeting of the American College of Rheumatology.

This finding, now confirmed twice over in separate validation studies, opens the door to trials of pharmacologic treatment aimed at preventing rheumatoid arthritis (RA).
“In my view, a positive test might be an indication for preventive treatment and retesting at 1 year to evaluate the treatment effect,” said Dr. de Vries, professor of rheumatology at the University of Amsterdam.
Many patients with RA experience a pre-RA phase marked by joint pain, the presence of RA-specific autoantibodies, IgM rheumatoid factor, and/or anticitrullinated protein antibodies, but no synovial inflammation. The challenge in attempting to develop RA preventive strategies targeting this population is that only about 28% of them go on to develop RA within 3 years. Exposing the entire preclinical-phase population to powerful antirheumatic drugs to try to prevent RA in the minority who are actually headed for overt disease is not an attractive strategy.
That’s why Dr. de Vries and his coinvestigators developed a method of B cell receptor (BCR) analysis using PCR and next-generation sequencing techniques. They determined that when a clone comprised more than 0.5% of the total B cell receptor population, it can be considered an expanded or dominant clone. They then demonstrated that when a patient in the pre-RA phase has five or more dominant clones in a peripheral blood sample, that can be considered a positive BCR test. In two published studies, they showed that a positive BCR test in the pre-RA stage accurately predicts onset of overt RA within the next several years (Ann Rheum Dis. 2017 Nov;76[11]:1924-30 and Ann Rheum Dis. 2018;77:151). They have also shown that at the time of RA onset, the BCR clones disappear from peripheral blood and reappear in the synovium.
At the ACR annual meeting, Dr. de Vries presented the results of a new BCR test validation study, this one involving 129 pre–RA-phase Dutch patients. The purpose of this study was to learn whether the BCR test is more predictive than clinical predictors such as the Risk Rule Model, and also to determine whether a higher number of dominant clones predicts RA onset even more accurately than the five-or-more clone threshold the investigators had been using. The answer to both questions proved to be yes.
Thirty-five percent of the 129 pre-RA subjects had a positive BCR test as defined by the presence of five or more expanded clones. A total of 75% of them went on to develop RA within the next 3 years. None of the BCR test-negative patients did. That result translated to a test sensitivity of 100%, a specificity of 87%, a positive predictive value of 71%, and a negative predictive value of 100%. A positive BCR blood test was associated with a 120-fold increased risk of an RA diagnosis within 3 years.
The investigators also compared outcomes in the 17% of study participants with a high degree of BCR test positivity, defined as the presence of nine or more expanded clones, versus the 18% of subjects whose positive BCR test had five to eight clones. Overall, 91% with a highly positive BCR test featuring nine or more clones developed RA within 3 years, compared with 55% of those with five to eight clones.
These findings permit categorization of pre-RA patients into three groups. Those with a negative BCR test can be reassured that their 3-year risk of developing RA is similar to the background risk in the general population. Those with a mid-range positive BCR test – that is, five to eight dominant clones – should probably be retested periodically, although the optimum interval is still under study. And patients with a highly positive BCR test might be candidates for preventive therapy.
Before RA-preventive therapy during the high-risk pre-RA phase can be introduced into routine clinical practice, however, several issues need to be resolved, Dr. de Vries continued. Although a single dose of rituximab (Rituxan) showed efficacy in a proof-of-concept study, that was off-label therapy. There is as yet no approved agent for prevention of RA in high-risk patients. Also, the risk/benefit ratio of preventive therapy will need to be determined. And rheumatologists will have to figure out how to identify these high-risk pre-RA individuals early, when preventive therapy is likely to most effective.
Several audience members observed that the Dutch investigators’ BCR test using PCR and next-generation sequencing is technically complex. They asked if the BCR results might correlate with any far more readily available serologic tests. The answer is no, according to Dr. de Vries.
“I think it’s very important to realize that what we test is the migration of B cells or plasmablast-like cells through the blood at the moment that we’re testing. This is completely different from a serological assessment of antibody production by plasma cells which are present in the bone marrow, which changes very little despite effective treatment. In contrast, if we test B cell migration while a patient gets corticosteroids we see an immediate disappearance of all these cells. So it’s a different parameter,” the rheumatologist explained.
The Dutch Arthritis Association funded the study. Dr. de Vries noted that he is a coinventor of the BCR test, the intellectual property rights for which belong to the University of Amsterdam. He receives research funding from Pfizer, Roche, Janssen, and GlaxoSmithKline.
SOURCE: de Vries N et al. Arthritis Rheumatol. 2018;70(Suppl 10). Abstract 835.
CHICAGO – A positive B cell clonality test in a peripheral blood sample predicts imminent onset of rheumatoid arthritis with a high degree of accuracy in at-risk individuals, Niek de Vries, MD, PhD, reported at the annual meeting of the American College of Rheumatology.
This finding, now confirmed twice over in separate validation studies, opens the door to trials of pharmacologic treatment aimed at preventing rheumatoid arthritis (RA).
“In my view, a positive test might be an indication for preventive treatment and retesting at 1 year to evaluate the treatment effect,” said Dr. de Vries, professor of rheumatology at the University of Amsterdam.
Many patients with RA experience a pre-RA phase marked by joint pain, the presence of RA-specific autoantibodies, IgM rheumatoid factor, and/or anticitrullinated protein antibodies, but no synovial inflammation. The challenge in attempting to develop RA preventive strategies targeting this population is that only about 28% of them go on to develop RA within 3 years. Exposing the entire preclinical-phase population to powerful antirheumatic drugs to try to prevent RA in the minority who are actually headed for overt disease is not an attractive strategy.
That’s why Dr. de Vries and his coinvestigators developed a method of B cell receptor (BCR) analysis using PCR and next-generation sequencing techniques. They determined that when a clone comprised more than 0.5% of the total B cell receptor population, it can be considered an expanded or dominant clone. They then demonstrated that when a patient in the pre-RA phase has five or more dominant clones in a peripheral blood sample, that can be considered a positive BCR test. In two published studies, they showed that a positive BCR test in the pre-RA stage accurately predicts onset of overt RA within the next several years (Ann Rheum Dis. 2017 Nov;76[11]:1924-30 and Ann Rheum Dis. 2018;77:151). They have also shown that at the time of RA onset, the BCR clones disappear from peripheral blood and reappear in the synovium.
At the ACR annual meeting, Dr. de Vries presented the results of a new BCR test validation study, this one involving 129 pre–RA-phase Dutch patients. The purpose of this study was to learn whether the BCR test is more predictive than clinical predictors such as the Risk Rule Model, and also to determine whether a higher number of dominant clones predicts RA onset even more accurately than the five-or-more clone threshold the investigators had been using. The answer to both questions proved to be yes.
Thirty-five percent of the 129 pre-RA subjects had a positive BCR test as defined by the presence of five or more expanded clones. A total of 75% of them went on to develop RA within the next 3 years. None of the BCR test-negative patients did. That result translated to a test sensitivity of 100%, a specificity of 87%, a positive predictive value of 71%, and a negative predictive value of 100%. A positive BCR blood test was associated with a 120-fold increased risk of an RA diagnosis within 3 years.
The investigators also compared outcomes in the 17% of study participants with a high degree of BCR test positivity, defined as the presence of nine or more expanded clones, versus the 18% of subjects whose positive BCR test had five to eight clones. Overall, 91% with a highly positive BCR test featuring nine or more clones developed RA within 3 years, compared with 55% of those with five to eight clones.
These findings permit categorization of pre-RA patients into three groups. Those with a negative BCR test can be reassured that their 3-year risk of developing RA is similar to the background risk in the general population. Those with a mid-range positive BCR test – that is, five to eight dominant clones – should probably be retested periodically, although the optimum interval is still under study. And patients with a highly positive BCR test might be candidates for preventive therapy.
Before RA-preventive therapy during the high-risk pre-RA phase can be introduced into routine clinical practice, however, several issues need to be resolved, Dr. de Vries continued. Although a single dose of rituximab (Rituxan) showed efficacy in a proof-of-concept study, that was off-label therapy. There is as yet no approved agent for prevention of RA in high-risk patients. Also, the risk/benefit ratio of preventive therapy will need to be determined. And rheumatologists will have to figure out how to identify these high-risk pre-RA individuals early, when preventive therapy is likely to most effective.
Several audience members observed that the Dutch investigators’ BCR test using PCR and next-generation sequencing is technically complex. They asked if the BCR results might correlate with any far more readily available serologic tests. The answer is no, according to Dr. de Vries.
“I think it’s very important to realize that what we test is the migration of B cells or plasmablast-like cells through the blood at the moment that we’re testing. This is completely different from a serological assessment of antibody production by plasma cells which are present in the bone marrow, which changes very little despite effective treatment. In contrast, if we test B cell migration while a patient gets corticosteroids we see an immediate disappearance of all these cells. So it’s a different parameter,” the rheumatologist explained.
The Dutch Arthritis Association funded the study. Dr. de Vries noted that he is a coinventor of the BCR test, the intellectual property rights for which belong to the University of Amsterdam. He receives research funding from Pfizer, Roche, Janssen, and GlaxoSmithKline.
SOURCE: de Vries N et al. Arthritis Rheumatol. 2018;70(Suppl 10). Abstract 835.
CHICAGO – A positive B cell clonality test in a peripheral blood sample predicts imminent onset of rheumatoid arthritis with a high degree of accuracy in at-risk individuals, Niek de Vries, MD, PhD, reported at the annual meeting of the American College of Rheumatology.
This finding, now confirmed twice over in separate validation studies, opens the door to trials of pharmacologic treatment aimed at preventing rheumatoid arthritis (RA).
“In my view, a positive test might be an indication for preventive treatment and retesting at 1 year to evaluate the treatment effect,” said Dr. de Vries, professor of rheumatology at the University of Amsterdam.
Many patients with RA experience a pre-RA phase marked by joint pain, the presence of RA-specific autoantibodies, IgM rheumatoid factor, and/or anticitrullinated protein antibodies, but no synovial inflammation. The challenge in attempting to develop RA preventive strategies targeting this population is that only about 28% of them go on to develop RA within 3 years. Exposing the entire preclinical-phase population to powerful antirheumatic drugs to try to prevent RA in the minority who are actually headed for overt disease is not an attractive strategy.
That’s why Dr. de Vries and his coinvestigators developed a method of B cell receptor (BCR) analysis using PCR and next-generation sequencing techniques. They determined that when a clone comprised more than 0.5% of the total B cell receptor population, it can be considered an expanded or dominant clone. They then demonstrated that when a patient in the pre-RA phase has five or more dominant clones in a peripheral blood sample, that can be considered a positive BCR test. In two published studies, they showed that a positive BCR test in the pre-RA stage accurately predicts onset of overt RA within the next several years (Ann Rheum Dis. 2017 Nov;76[11]:1924-30 and Ann Rheum Dis. 2018;77:151). They have also shown that at the time of RA onset, the BCR clones disappear from peripheral blood and reappear in the synovium.
At the ACR annual meeting, Dr. de Vries presented the results of a new BCR test validation study, this one involving 129 pre–RA-phase Dutch patients. The purpose of this study was to learn whether the BCR test is more predictive than clinical predictors such as the Risk Rule Model, and also to determine whether a higher number of dominant clones predicts RA onset even more accurately than the five-or-more clone threshold the investigators had been using. The answer to both questions proved to be yes.
Thirty-five percent of the 129 pre-RA subjects had a positive BCR test as defined by the presence of five or more expanded clones. A total of 75% of them went on to develop RA within the next 3 years. None of the BCR test-negative patients did. That result translated to a test sensitivity of 100%, a specificity of 87%, a positive predictive value of 71%, and a negative predictive value of 100%. A positive BCR blood test was associated with a 120-fold increased risk of an RA diagnosis within 3 years.
The investigators also compared outcomes in the 17% of study participants with a high degree of BCR test positivity, defined as the presence of nine or more expanded clones, versus the 18% of subjects whose positive BCR test had five to eight clones. Overall, 91% with a highly positive BCR test featuring nine or more clones developed RA within 3 years, compared with 55% of those with five to eight clones.
These findings permit categorization of pre-RA patients into three groups. Those with a negative BCR test can be reassured that their 3-year risk of developing RA is similar to the background risk in the general population. Those with a mid-range positive BCR test – that is, five to eight dominant clones – should probably be retested periodically, although the optimum interval is still under study. And patients with a highly positive BCR test might be candidates for preventive therapy.
Before RA-preventive therapy during the high-risk pre-RA phase can be introduced into routine clinical practice, however, several issues need to be resolved, Dr. de Vries continued. Although a single dose of rituximab (Rituxan) showed efficacy in a proof-of-concept study, that was off-label therapy. There is as yet no approved agent for prevention of RA in high-risk patients. Also, the risk/benefit ratio of preventive therapy will need to be determined. And rheumatologists will have to figure out how to identify these high-risk pre-RA individuals early, when preventive therapy is likely to most effective.
Several audience members observed that the Dutch investigators’ BCR test using PCR and next-generation sequencing is technically complex. They asked if the BCR results might correlate with any far more readily available serologic tests. The answer is no, according to Dr. de Vries.
“I think it’s very important to realize that what we test is the migration of B cells or plasmablast-like cells through the blood at the moment that we’re testing. This is completely different from a serological assessment of antibody production by plasma cells which are present in the bone marrow, which changes very little despite effective treatment. In contrast, if we test B cell migration while a patient gets corticosteroids we see an immediate disappearance of all these cells. So it’s a different parameter,” the rheumatologist explained.
The Dutch Arthritis Association funded the study. Dr. de Vries noted that he is a coinventor of the BCR test, the intellectual property rights for which belong to the University of Amsterdam. He receives research funding from Pfizer, Roche, Janssen, and GlaxoSmithKline.
SOURCE: de Vries N et al. Arthritis Rheumatol. 2018;70(Suppl 10). Abstract 835.
REPORTING FROM THE ACR ANNUAL MEETING
Key clinical point: A peripheral blood sample showing a high level of expanded B cell receptor clones accurately predicts looming onset of rheumatoid arthritis.
Major finding: Ninety-one percent of patients with a highly positive B cell receptor clonality blood test developed rheumatoid arthritis within the next 3 years.
Study details: This study included 129 patients deemed at high risk for developing rheumatoid arthritis who were followed for 3 years.
Disclosures: The Dutch Arthritis Association funded the study. The presenter noted that he is a coinventor of the B cell receptor blood test, the intellectual property rights for which belong to the University of Amsterdam.
Source: De Vries N et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 835.
Clinically meaningful change determined for RAPID-3 in active RA
An improvement of nearly 4 points on a 30-point, patient-scored disease severity index appears to be clinically meaningful for adults with active RA, according to a recent clinical trial analysis.

A 3.8-point decrease represented the minimal clinically important improvement in the Routine Assessment of Patient Index Data 3 (RAPID-3) index, investigators reported in The Journal of Rheumatology.
“Clinicians may feel comfortable documenting and monitoring patient status, recognizing an improvement of 3.8 units in patients with active RA to be meaningful in routine patient care,” Michael M. Ward, MD, PhD, of the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), and his coinvestigators wrote.
The RAPID-3 index consists of three patient self-report measures out of the seven-item RA Core Data Set: physical function, pain, and patient’s global assessment. The index was initially designed to be feasible in routine care, such that a patient could fill it out in the waiting area, Dr. Ward and his colleagues noted in their report.
Previous investigations have shown that RAPID-3 is highly correlated with the 28-joint count Disease Activity Score (DAS28) and the Clinical Disease Activity Index, and in one study, it was more likely than erythrocyte sedimentation rate (ESR) to identify incomplete responses to methotrexate.
However, prior to the present study, there were no reported estimates of the minimal clinically important improvement for the RAPID-3 index.
Knowing whether or not a decrease in RAPID-3 is clinically meaningful to patients would help clinicians interpret those changes in response to treatment, Dr. Ward and his coauthors wrote.
In the current study, RAPID-3 was calculated before and after escalation of treatment in a prospective study involving 250 adults with active RA, including 195 women (78%). The mean age of the patients was 51 years, and the median duration of RA was more than 6 years.
At the patients’ baseline visit and evaluation, rheumatologists prescribed prednisone, a new disease-modifying treatment, a new biologic, or increased the dose of a current treatment. The follow-up visit occurred at 4 months for most patients, though follow-up was at 1 month for prednisone-treated patients because of an expected rapid response.
At baseline, the mean RAPID-3 score was 16.3, which improved to 11.1 at the follow-up visit, for a mean change of –5.2 points, according to the investigators. The standardized response mean was –0.79 (95% confidence interval, –0.71 to –0.88), which investigators said demonstrated good sensitivity to change.
They found that the minimal clinically important improvement was –3.8 in a statistical analysis that optimized sensitivity and specificity, and –3.5 and –4.1 by alternate statistical criteria.
However, Dr. Ward and his coauthors cautioned that these estimates should be applied only to patient groups that have high levels of RA activity, similar to this study, in which patients had a baseline mean DAS28-ESR of 6.16 and a mean Simplified Disease Activity Index of 38.6.
Patients with low RA activity are closer to an acceptable symptom state, making the minimal clinically important improvement less relevant. “The margin for symptom improvement becomes smaller and ultimately indiscernible as the level of activity decreases,” they explained in their report.
The study was supported in part through the NIAMS Intramural Research Program and a grant from the U.S. Public Health Service. No conflicts of interest were reported.
SOURCE: Ward MM et al. J Rheumatol. 2018 Oct 15. doi: 10.3899/jrheum.180153.
An improvement of nearly 4 points on a 30-point, patient-scored disease severity index appears to be clinically meaningful for adults with active RA, according to a recent clinical trial analysis.
A 3.8-point decrease represented the minimal clinically important improvement in the Routine Assessment of Patient Index Data 3 (RAPID-3) index, investigators reported in The Journal of Rheumatology.
“Clinicians may feel comfortable documenting and monitoring patient status, recognizing an improvement of 3.8 units in patients with active RA to be meaningful in routine patient care,” Michael M. Ward, MD, PhD, of the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), and his coinvestigators wrote.
The RAPID-3 index consists of three patient self-report measures out of the seven-item RA Core Data Set: physical function, pain, and patient’s global assessment. The index was initially designed to be feasible in routine care, such that a patient could fill it out in the waiting area, Dr. Ward and his colleagues noted in their report.
Previous investigations have shown that RAPID-3 is highly correlated with the 28-joint count Disease Activity Score (DAS28) and the Clinical Disease Activity Index, and in one study, it was more likely than erythrocyte sedimentation rate (ESR) to identify incomplete responses to methotrexate.
However, prior to the present study, there were no reported estimates of the minimal clinically important improvement for the RAPID-3 index.
Knowing whether or not a decrease in RAPID-3 is clinically meaningful to patients would help clinicians interpret those changes in response to treatment, Dr. Ward and his coauthors wrote.
In the current study, RAPID-3 was calculated before and after escalation of treatment in a prospective study involving 250 adults with active RA, including 195 women (78%). The mean age of the patients was 51 years, and the median duration of RA was more than 6 years.
At the patients’ baseline visit and evaluation, rheumatologists prescribed prednisone, a new disease-modifying treatment, a new biologic, or increased the dose of a current treatment. The follow-up visit occurred at 4 months for most patients, though follow-up was at 1 month for prednisone-treated patients because of an expected rapid response.
At baseline, the mean RAPID-3 score was 16.3, which improved to 11.1 at the follow-up visit, for a mean change of –5.2 points, according to the investigators. The standardized response mean was –0.79 (95% confidence interval, –0.71 to –0.88), which investigators said demonstrated good sensitivity to change.
They found that the minimal clinically important improvement was –3.8 in a statistical analysis that optimized sensitivity and specificity, and –3.5 and –4.1 by alternate statistical criteria.
However, Dr. Ward and his coauthors cautioned that these estimates should be applied only to patient groups that have high levels of RA activity, similar to this study, in which patients had a baseline mean DAS28-ESR of 6.16 and a mean Simplified Disease Activity Index of 38.6.
Patients with low RA activity are closer to an acceptable symptom state, making the minimal clinically important improvement less relevant. “The margin for symptom improvement becomes smaller and ultimately indiscernible as the level of activity decreases,” they explained in their report.
The study was supported in part through the NIAMS Intramural Research Program and a grant from the U.S. Public Health Service. No conflicts of interest were reported.
SOURCE: Ward MM et al. J Rheumatol. 2018 Oct 15. doi: 10.3899/jrheum.180153.
An improvement of nearly 4 points on a 30-point, patient-scored disease severity index appears to be clinically meaningful for adults with active RA, according to a recent clinical trial analysis.
A 3.8-point decrease represented the minimal clinically important improvement in the Routine Assessment of Patient Index Data 3 (RAPID-3) index, investigators reported in The Journal of Rheumatology.
“Clinicians may feel comfortable documenting and monitoring patient status, recognizing an improvement of 3.8 units in patients with active RA to be meaningful in routine patient care,” Michael M. Ward, MD, PhD, of the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), and his coinvestigators wrote.
The RAPID-3 index consists of three patient self-report measures out of the seven-item RA Core Data Set: physical function, pain, and patient’s global assessment. The index was initially designed to be feasible in routine care, such that a patient could fill it out in the waiting area, Dr. Ward and his colleagues noted in their report.
Previous investigations have shown that RAPID-3 is highly correlated with the 28-joint count Disease Activity Score (DAS28) and the Clinical Disease Activity Index, and in one study, it was more likely than erythrocyte sedimentation rate (ESR) to identify incomplete responses to methotrexate.
However, prior to the present study, there were no reported estimates of the minimal clinically important improvement for the RAPID-3 index.
Knowing whether or not a decrease in RAPID-3 is clinically meaningful to patients would help clinicians interpret those changes in response to treatment, Dr. Ward and his coauthors wrote.
In the current study, RAPID-3 was calculated before and after escalation of treatment in a prospective study involving 250 adults with active RA, including 195 women (78%). The mean age of the patients was 51 years, and the median duration of RA was more than 6 years.
At the patients’ baseline visit and evaluation, rheumatologists prescribed prednisone, a new disease-modifying treatment, a new biologic, or increased the dose of a current treatment. The follow-up visit occurred at 4 months for most patients, though follow-up was at 1 month for prednisone-treated patients because of an expected rapid response.
At baseline, the mean RAPID-3 score was 16.3, which improved to 11.1 at the follow-up visit, for a mean change of –5.2 points, according to the investigators. The standardized response mean was –0.79 (95% confidence interval, –0.71 to –0.88), which investigators said demonstrated good sensitivity to change.
They found that the minimal clinically important improvement was –3.8 in a statistical analysis that optimized sensitivity and specificity, and –3.5 and –4.1 by alternate statistical criteria.
However, Dr. Ward and his coauthors cautioned that these estimates should be applied only to patient groups that have high levels of RA activity, similar to this study, in which patients had a baseline mean DAS28-ESR of 6.16 and a mean Simplified Disease Activity Index of 38.6.
Patients with low RA activity are closer to an acceptable symptom state, making the minimal clinically important improvement less relevant. “The margin for symptom improvement becomes smaller and ultimately indiscernible as the level of activity decreases,” they explained in their report.
The study was supported in part through the NIAMS Intramural Research Program and a grant from the U.S. Public Health Service. No conflicts of interest were reported.
SOURCE: Ward MM et al. J Rheumatol. 2018 Oct 15. doi: 10.3899/jrheum.180153.
FROM THE JOURNAL OF RHEUMATOLOGY
Key clinical point:
Major finding: Minimal clinically important improvement was –3.8 in a statistical analysis that optimized sensitivity and specificity, and –3.5 and –4.1 by alternate statistical criteria.
Study details: A prospective study of patient-reported outcome measures in 250 adults with active RA.
Disclosures: The study was supported in part through the National Institute of Arthritis and Musculoskeletal and Skin Diseases Intramural Research Program and a grant from the U.S. Public Health Service. No conflicts of interest were reported.
Source: Ward MM et al. J Rheumatol. 2018 Oct 15. doi: 10.3899/jrheum.180153.
Glucocorticoids plus tofacitinib may boost herpes zoster risk
Concomitant use of glucocorticoids with tofacitinib in rheumatoid arthritis may double the risk of herpes zoster, but methotrexate does not appear to increase the risk, outcomes from a cohort study of 8,030 rheumatoid arthritis patients – including 222 cases of herpes zoster – suggest.

Using information from Medicare and MarketScan, researchers found that dual therapy with tofacitinib and glucocorticoids was associated with a 96% increase in the risk of herpes zoster, compared with monotherapy with the Janus kinase inhibitor tofacitinib (95% confidence interval, 33%-188%). The crude incidence rate in those taking concomitant tofacitinib and glucocorticoids was 6 cases per 100 patient-years, compared with an incidence rate of 3.4 cases per 100 patient-years with tofacitinib monotherapy.
However, the addition of methotrexate therapy to tofacitinib was not associated with an increased risk of herpes zoster, and the incidence rate in patients on this dual therapy was 3.7 cases per 100 patient-years, Jeffrey R. Curtis, MD, MS, MPH, of the University of Alabama at Birmingham and his coauthors reported in Arthritis Care & Research.
Women – who constituted 80% of the study population – showed a significantly increased risk of herpes zoster, as did older patients.
The study also found that individuals who had received the live herpes zoster vaccine showed a trend toward a decrease in risk.
“We saw a strong trend for decreased risk related to vaccination with the live agent (Zostavax); the concern with this form of vaccination is that any live vaccination is potentially dangerous in patients receiving potent immunosuppression,” Dr. Curtis and his associates wrote.
“The risks for disease flare, and potentially problematic tolerability related to a relatively high incidence of grade 3 (severe) systemic reactogenicity, may limit enthusiasm until specific data in an RA population is available,” they wrote. However, they noted that a randomized, controlled trial of the live virus vaccine was underway in patients with rheumatoid arthritis who were being treated with tumor necrosis factor inhibitors and suggested that vaccination should be considered in at-risk patients who didn’t have contraindications.
The authors noted that the effect of glucocorticoid exposure on herpes zoster risk in patients taking tofacitinib was similar to that seen in rheumatoid arthritis patients receiving conventional synthetic disease-modifying antirheumatic drugs or biologic therapies.
The study was partly funded by the Patient-Centered Outcomes Research Institute. Two authors declared research grants and other funding from the pharmaceutical industry, but no other conflicts of interest were declared.
SOURCE: Curtis J et al. Arthritis Care Res. 2018 Oct 8. doi: 10.1002/acr.23769.
Concomitant use of glucocorticoids with tofacitinib in rheumatoid arthritis may double the risk of herpes zoster, but methotrexate does not appear to increase the risk, outcomes from a cohort study of 8,030 rheumatoid arthritis patients – including 222 cases of herpes zoster – suggest.
Using information from Medicare and MarketScan, researchers found that dual therapy with tofacitinib and glucocorticoids was associated with a 96% increase in the risk of herpes zoster, compared with monotherapy with the Janus kinase inhibitor tofacitinib (95% confidence interval, 33%-188%). The crude incidence rate in those taking concomitant tofacitinib and glucocorticoids was 6 cases per 100 patient-years, compared with an incidence rate of 3.4 cases per 100 patient-years with tofacitinib monotherapy.
However, the addition of methotrexate therapy to tofacitinib was not associated with an increased risk of herpes zoster, and the incidence rate in patients on this dual therapy was 3.7 cases per 100 patient-years, Jeffrey R. Curtis, MD, MS, MPH, of the University of Alabama at Birmingham and his coauthors reported in Arthritis Care & Research.
Women – who constituted 80% of the study population – showed a significantly increased risk of herpes zoster, as did older patients.
The study also found that individuals who had received the live herpes zoster vaccine showed a trend toward a decrease in risk.
“We saw a strong trend for decreased risk related to vaccination with the live agent (Zostavax); the concern with this form of vaccination is that any live vaccination is potentially dangerous in patients receiving potent immunosuppression,” Dr. Curtis and his associates wrote.
“The risks for disease flare, and potentially problematic tolerability related to a relatively high incidence of grade 3 (severe) systemic reactogenicity, may limit enthusiasm until specific data in an RA population is available,” they wrote. However, they noted that a randomized, controlled trial of the live virus vaccine was underway in patients with rheumatoid arthritis who were being treated with tumor necrosis factor inhibitors and suggested that vaccination should be considered in at-risk patients who didn’t have contraindications.
The authors noted that the effect of glucocorticoid exposure on herpes zoster risk in patients taking tofacitinib was similar to that seen in rheumatoid arthritis patients receiving conventional synthetic disease-modifying antirheumatic drugs or biologic therapies.
The study was partly funded by the Patient-Centered Outcomes Research Institute. Two authors declared research grants and other funding from the pharmaceutical industry, but no other conflicts of interest were declared.
SOURCE: Curtis J et al. Arthritis Care Res. 2018 Oct 8. doi: 10.1002/acr.23769.
Concomitant use of glucocorticoids with tofacitinib in rheumatoid arthritis may double the risk of herpes zoster, but methotrexate does not appear to increase the risk, outcomes from a cohort study of 8,030 rheumatoid arthritis patients – including 222 cases of herpes zoster – suggest.
Using information from Medicare and MarketScan, researchers found that dual therapy with tofacitinib and glucocorticoids was associated with a 96% increase in the risk of herpes zoster, compared with monotherapy with the Janus kinase inhibitor tofacitinib (95% confidence interval, 33%-188%). The crude incidence rate in those taking concomitant tofacitinib and glucocorticoids was 6 cases per 100 patient-years, compared with an incidence rate of 3.4 cases per 100 patient-years with tofacitinib monotherapy.
However, the addition of methotrexate therapy to tofacitinib was not associated with an increased risk of herpes zoster, and the incidence rate in patients on this dual therapy was 3.7 cases per 100 patient-years, Jeffrey R. Curtis, MD, MS, MPH, of the University of Alabama at Birmingham and his coauthors reported in Arthritis Care & Research.
Women – who constituted 80% of the study population – showed a significantly increased risk of herpes zoster, as did older patients.
The study also found that individuals who had received the live herpes zoster vaccine showed a trend toward a decrease in risk.
“We saw a strong trend for decreased risk related to vaccination with the live agent (Zostavax); the concern with this form of vaccination is that any live vaccination is potentially dangerous in patients receiving potent immunosuppression,” Dr. Curtis and his associates wrote.
“The risks for disease flare, and potentially problematic tolerability related to a relatively high incidence of grade 3 (severe) systemic reactogenicity, may limit enthusiasm until specific data in an RA population is available,” they wrote. However, they noted that a randomized, controlled trial of the live virus vaccine was underway in patients with rheumatoid arthritis who were being treated with tumor necrosis factor inhibitors and suggested that vaccination should be considered in at-risk patients who didn’t have contraindications.
The authors noted that the effect of glucocorticoid exposure on herpes zoster risk in patients taking tofacitinib was similar to that seen in rheumatoid arthritis patients receiving conventional synthetic disease-modifying antirheumatic drugs or biologic therapies.
The study was partly funded by the Patient-Centered Outcomes Research Institute. Two authors declared research grants and other funding from the pharmaceutical industry, but no other conflicts of interest were declared.
SOURCE: Curtis J et al. Arthritis Care Res. 2018 Oct 8. doi: 10.1002/acr.23769.
FROM ARTHRITIS CARE & RESEARCH
Key clinical point: Patients treated with concomitant glucocorticoids and tofacitinib showed increased risk of herpes zoster.
Major finding: Concomitant use of glucocorticoids and tofacitinib is associated with nearly twofold increase in the risk of herpes zoster.
Study details: Cohort study using data from 8,030 rheumatoid arthritis patients.
Disclosures: The study was partly funded by the Patient-Centered Outcomes Research Institute. Two authors declared research grants and other funding from the pharmaceutical industry, but no other conflicts of interest were declared.
Source: Curtis J et al. Arthritis Care Res. 2018 Oct 8. doi: 10.1002/acr.23769.
Flu vaccination lags among patients with psoriasis
Psoriasis patients are more vulnerable to systemic infections, including influenza-related pneumonia, but a new study shows that they are less likely to receive the influenza vaccine than patients with RA.

Vaccination rates were higher in psoriasis patients aged over 50 years, those who were female, and those with other chronic medical conditions, however.
Megan H. Noe, MD, of the department of dermatology at the University of Pennsylvania, Philadelphia, and her coauthors referred to recent evidence suggesting that psoriasis involves systemic inflammation that increase the risk of comorbidities and that hospitalization rates for serious infections, including lower respiratory tract infections and pneumonia, are higher among adults with psoriasis than those who do not have psoriasis.
drawing from administrative and commercial claims data from OptumInsight Clinformatics Data Mart. They examined all adult patients with psoriasis, RA, or chronic hypertension who required oral antihypertensive medication. The study population included individuals tracked during the 2010-2011 flu season and 24 months prior (September 2008 to March 2011). This year was chosen because it was labeled as a “typical” season by the Centers for Disease Control and Prevention.
The primary outcome was a claim for an influenza vaccine, and covariates included age, length of residency, gender, and a clinical history of a range of conditions known to be associated with greater risk of influenza complications.
The population included 17,078 patients with psoriasis, 21,832 with RA, and 496,972 with chronic hypertension. After controlling for sex and age, the probability of getting a flu vaccine was similar between psoriasis and hypertension patients, but RA patients were more likely to be vaccinated than patients with psoriasis (odds ratio, 1.08; 95% confidence interval, 1.03-1.13). But the likelihood varied with age: 30-year-old patients with RA were more likely than a 30-year-old psoriasis patient to get a flu shot (OR, 1.30; 95% CI, 1.18-1.45), while a 70-year-old patient with RA was about as likely to get the flu vaccine as a 70-year-old patient with psoriasis.
Female psoriasis patients were more likely to get a flu shot than males (OR, 1.29; 95% CI, 1.20-1.38). Among the psoriasis patients, having some medical comorbidities were linked to a greater likelihood of being vaccinated, including asthma (OR, 1.58; 95% CI, 1.40-1.77), chronic liver disease (OR, 1.23; 95%, 1.03-1.47), diabetes (OR, 1.48; 95% CI, 1.36-1.63), HIV (OR, 3.68; 95% CI, 2.06-6.57), history of malignancy (OR, 1.21; 95% CI, 1.09-1.34), and psoriatic arthritis (OR, 1.40; 95% CI, 1.25-1.58).
There was no association between the use of an oral systemic therapy or biologic treatment and vaccination rates.
The authors suggested that psoriasis patients, especially younger ones, may not get adequate counseling on the value of the flu vaccine from their physicians. Studies have shown that, among the American public, health care providers are the most influential source of information about the flu vaccine. Among younger patients, the dermatologist may be a psoriasis patient’s primary health care provider, so it is important for dermatologists to counsel patients about the recommended vaccines, the authors wrote.
“Further research understanding why adults with psoriasis do not receive recommended vaccinations will help to create targeted interventions to improve vaccination rates and decrease hospitalizations in adults with psoriasis,” they concluded.
The study relied on administrative claims, so the results may not be generalizable to patients with insurance types other than those in the database or who are uninsured, the authors noted.
This study was funded by the National Psoriasis Foundation, the Dermatology Foundation, and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Noe and three other authors did not report any disclosures, the fifth author reported multiple disclosures related to various pharmaceutical companies.
SOURCE: Noe MH et al. J Invest Dermatol. 2018 Oct 10. doi: 10.1016/j.jid.2018.09.012.
Psoriasis patients are more vulnerable to systemic infections, including influenza-related pneumonia, but a new study shows that they are less likely to receive the influenza vaccine than patients with RA.
Vaccination rates were higher in psoriasis patients aged over 50 years, those who were female, and those with other chronic medical conditions, however.
Megan H. Noe, MD, of the department of dermatology at the University of Pennsylvania, Philadelphia, and her coauthors referred to recent evidence suggesting that psoriasis involves systemic inflammation that increase the risk of comorbidities and that hospitalization rates for serious infections, including lower respiratory tract infections and pneumonia, are higher among adults with psoriasis than those who do not have psoriasis.
drawing from administrative and commercial claims data from OptumInsight Clinformatics Data Mart. They examined all adult patients with psoriasis, RA, or chronic hypertension who required oral antihypertensive medication. The study population included individuals tracked during the 2010-2011 flu season and 24 months prior (September 2008 to March 2011). This year was chosen because it was labeled as a “typical” season by the Centers for Disease Control and Prevention.
The primary outcome was a claim for an influenza vaccine, and covariates included age, length of residency, gender, and a clinical history of a range of conditions known to be associated with greater risk of influenza complications.
The population included 17,078 patients with psoriasis, 21,832 with RA, and 496,972 with chronic hypertension. After controlling for sex and age, the probability of getting a flu vaccine was similar between psoriasis and hypertension patients, but RA patients were more likely to be vaccinated than patients with psoriasis (odds ratio, 1.08; 95% confidence interval, 1.03-1.13). But the likelihood varied with age: 30-year-old patients with RA were more likely than a 30-year-old psoriasis patient to get a flu shot (OR, 1.30; 95% CI, 1.18-1.45), while a 70-year-old patient with RA was about as likely to get the flu vaccine as a 70-year-old patient with psoriasis.
Female psoriasis patients were more likely to get a flu shot than males (OR, 1.29; 95% CI, 1.20-1.38). Among the psoriasis patients, having some medical comorbidities were linked to a greater likelihood of being vaccinated, including asthma (OR, 1.58; 95% CI, 1.40-1.77), chronic liver disease (OR, 1.23; 95%, 1.03-1.47), diabetes (OR, 1.48; 95% CI, 1.36-1.63), HIV (OR, 3.68; 95% CI, 2.06-6.57), history of malignancy (OR, 1.21; 95% CI, 1.09-1.34), and psoriatic arthritis (OR, 1.40; 95% CI, 1.25-1.58).
There was no association between the use of an oral systemic therapy or biologic treatment and vaccination rates.
The authors suggested that psoriasis patients, especially younger ones, may not get adequate counseling on the value of the flu vaccine from their physicians. Studies have shown that, among the American public, health care providers are the most influential source of information about the flu vaccine. Among younger patients, the dermatologist may be a psoriasis patient’s primary health care provider, so it is important for dermatologists to counsel patients about the recommended vaccines, the authors wrote.
“Further research understanding why adults with psoriasis do not receive recommended vaccinations will help to create targeted interventions to improve vaccination rates and decrease hospitalizations in adults with psoriasis,” they concluded.
The study relied on administrative claims, so the results may not be generalizable to patients with insurance types other than those in the database or who are uninsured, the authors noted.
This study was funded by the National Psoriasis Foundation, the Dermatology Foundation, and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Noe and three other authors did not report any disclosures, the fifth author reported multiple disclosures related to various pharmaceutical companies.
SOURCE: Noe MH et al. J Invest Dermatol. 2018 Oct 10. doi: 10.1016/j.jid.2018.09.012.
Psoriasis patients are more vulnerable to systemic infections, including influenza-related pneumonia, but a new study shows that they are less likely to receive the influenza vaccine than patients with RA.
Vaccination rates were higher in psoriasis patients aged over 50 years, those who were female, and those with other chronic medical conditions, however.
Megan H. Noe, MD, of the department of dermatology at the University of Pennsylvania, Philadelphia, and her coauthors referred to recent evidence suggesting that psoriasis involves systemic inflammation that increase the risk of comorbidities and that hospitalization rates for serious infections, including lower respiratory tract infections and pneumonia, are higher among adults with psoriasis than those who do not have psoriasis.
drawing from administrative and commercial claims data from OptumInsight Clinformatics Data Mart. They examined all adult patients with psoriasis, RA, or chronic hypertension who required oral antihypertensive medication. The study population included individuals tracked during the 2010-2011 flu season and 24 months prior (September 2008 to March 2011). This year was chosen because it was labeled as a “typical” season by the Centers for Disease Control and Prevention.
The primary outcome was a claim for an influenza vaccine, and covariates included age, length of residency, gender, and a clinical history of a range of conditions known to be associated with greater risk of influenza complications.
The population included 17,078 patients with psoriasis, 21,832 with RA, and 496,972 with chronic hypertension. After controlling for sex and age, the probability of getting a flu vaccine was similar between psoriasis and hypertension patients, but RA patients were more likely to be vaccinated than patients with psoriasis (odds ratio, 1.08; 95% confidence interval, 1.03-1.13). But the likelihood varied with age: 30-year-old patients with RA were more likely than a 30-year-old psoriasis patient to get a flu shot (OR, 1.30; 95% CI, 1.18-1.45), while a 70-year-old patient with RA was about as likely to get the flu vaccine as a 70-year-old patient with psoriasis.
Female psoriasis patients were more likely to get a flu shot than males (OR, 1.29; 95% CI, 1.20-1.38). Among the psoriasis patients, having some medical comorbidities were linked to a greater likelihood of being vaccinated, including asthma (OR, 1.58; 95% CI, 1.40-1.77), chronic liver disease (OR, 1.23; 95%, 1.03-1.47), diabetes (OR, 1.48; 95% CI, 1.36-1.63), HIV (OR, 3.68; 95% CI, 2.06-6.57), history of malignancy (OR, 1.21; 95% CI, 1.09-1.34), and psoriatic arthritis (OR, 1.40; 95% CI, 1.25-1.58).
There was no association between the use of an oral systemic therapy or biologic treatment and vaccination rates.
The authors suggested that psoriasis patients, especially younger ones, may not get adequate counseling on the value of the flu vaccine from their physicians. Studies have shown that, among the American public, health care providers are the most influential source of information about the flu vaccine. Among younger patients, the dermatologist may be a psoriasis patient’s primary health care provider, so it is important for dermatologists to counsel patients about the recommended vaccines, the authors wrote.
“Further research understanding why adults with psoriasis do not receive recommended vaccinations will help to create targeted interventions to improve vaccination rates and decrease hospitalizations in adults with psoriasis,” they concluded.
The study relied on administrative claims, so the results may not be generalizable to patients with insurance types other than those in the database or who are uninsured, the authors noted.
This study was funded by the National Psoriasis Foundation, the Dermatology Foundation, and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Noe and three other authors did not report any disclosures, the fifth author reported multiple disclosures related to various pharmaceutical companies.
SOURCE: Noe MH et al. J Invest Dermatol. 2018 Oct 10. doi: 10.1016/j.jid.2018.09.012.
FROM THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
Key clinical point: Despite vulnerability to complications, fewer psoriasis patients received the vaccine, compared with RA patients.
Major finding: Patients with RA were 8% more likely to receive a flu vaccine than patients with psoriasis.
Study details: A retrospective cohort study of 535,882 subjects with psoriasis, RA, or hypertension.
Disclosures: This study was funded by the National Psoriasis Foundation, the Dermatology Foundation, and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Four authors did not report any disclosures; the fifth author reported multiple disclosures related to various pharmaceutical companies.
Source: Noe MH et al. J Invest Dermatol. 2018 Oct 10. doi: 10.1016/j.jid.2018.09.012.
Inflammatory arthritis a common rheumatic adverse event with ICIs
Inflammatory arthritis (IA) is the most common rheumatic adverse event seen in people on immune checkpoint inhibitor (ICI) therapy and can largely be managed by rheumatologists without the need to halt cancer treatment, according to Michael D. Richter, MD, of the Mayo School of Graduate Medical Education, Rochester, Minn., and his colleagues.

The investigators’ observations of patients seen at the Mayo Clinic over a 7-year period suggested that “IA should not be seen as a contraindication to continuing or restarting ICIs, ” although continuing ICI therapy concurrently with high-dose steroids is “generally not recommended.” Previous estimates of rheumatic adverse events with ICIs had ranged from 1% to 10%, and management had largely been based on the experience of experts and findings from retrospective studies, they noted.
“This study aims to add granularity to the existing literature by describing the prevalence, clinical characteristics, and treatment outcomes of a large, single-institution cohort of patients with rheumatic immune-related adverse events,” Dr. Richter and his associates wrote in an article published in Arthritis & Rheumatology.
The analysis included 1,293 patients who had received treatment with any ICI at the Mayo Clinic between January 2011 and March 2018. Patients who had received treatment at other centers but were seen at the Mayo clinic for their rheumatic adverse event were also included.
Overall, 61 patients experienced a rheumatic immune-related adverse event (Rh-irAE) related to checkpoint inhibitor treatment; 43 were from the Mayo cohort and 18 were from other centers. The average age of the patients was 62.6 years, and almost half (49%) were female.
New-onset inflammatory arthritis was the most common Rh-irAE reported (n = 34), with the majority of patients presenting with polyarticular symptoms (n = 22; 65%).
Most of these patients were managed by a rheumatologist and were treated with systemic glucocorticoids (n = 26; 76%) for an average duration of 18 weeks. Five of the patients also required disease-modifying antirheumatic drugs and eight needed NSAIDS or intra-articular steroids.
The investigators noted that almost half of the patients (47%) experienced a complete resolution of symptoms during the study period, although few achieved this while they were still on the cancer treatment.
According to the investigators, the clinical characteristics of IA in their cohort support the existing literature: “Time of symptom onset is generally 4-8 weeks after starting ICI therapy. … The majority of patients require long courses of systemic glucocorticoids. And very few achieve complete symptom resolution while continuing ICI therapy,” they wrote.
The database analysis also revealed that a further 10 patients developed myopathy, with all patients presenting with myalgias and weaknesses. Five had bulbar myopathy, and four patients were diagnosed with concomitant myocarditis. All of these patients were treated with glucocorticoids for an average treatment duration of 15 weeks.
Complete resolution of the myopathy was observed in 70%, but two patients died from complications related to myocarditis and bulbar myopathy.
Other rheumatic events included four cases of vasculitis and four cases of polymyalgia rheumatica and six cases of diffuse systemic sclerosis or sicca syndromes.
“In lieu of controlled prospective studies, this cohort may serve as a guide for rheumatologists managing and counseling patients with Rh-IrAEs,” the investigators concluded.
“It remains unclear why some patients develop Rh-irAEs, and so far no genomic risk factors have been identified, though the varied clinical phenotypes of Rh-irAEs certainly suggest multiple underlying immunopathogenic mechanisms. Further prospective studies that distinguish between subsets of Rh-irAEs are necessary to better understand their pathophysiology and improve clinical care,” they added.
They noted that a limitation of the study was its reliance on retrospective data and clinician diagnoses.
None of the authors declared any financial or other conflicts of interest.
SOURCE: Richter MD et al. Arthritis Rheumatol. 2018 Oct 3. doi: 10.1002/art.40745.
Inflammatory arthritis (IA) is the most common rheumatic adverse event seen in people on immune checkpoint inhibitor (ICI) therapy and can largely be managed by rheumatologists without the need to halt cancer treatment, according to Michael D. Richter, MD, of the Mayo School of Graduate Medical Education, Rochester, Minn., and his colleagues.
The investigators’ observations of patients seen at the Mayo Clinic over a 7-year period suggested that “IA should not be seen as a contraindication to continuing or restarting ICIs, ” although continuing ICI therapy concurrently with high-dose steroids is “generally not recommended.” Previous estimates of rheumatic adverse events with ICIs had ranged from 1% to 10%, and management had largely been based on the experience of experts and findings from retrospective studies, they noted.
“This study aims to add granularity to the existing literature by describing the prevalence, clinical characteristics, and treatment outcomes of a large, single-institution cohort of patients with rheumatic immune-related adverse events,” Dr. Richter and his associates wrote in an article published in Arthritis & Rheumatology.
The analysis included 1,293 patients who had received treatment with any ICI at the Mayo Clinic between January 2011 and March 2018. Patients who had received treatment at other centers but were seen at the Mayo clinic for their rheumatic adverse event were also included.
Overall, 61 patients experienced a rheumatic immune-related adverse event (Rh-irAE) related to checkpoint inhibitor treatment; 43 were from the Mayo cohort and 18 were from other centers. The average age of the patients was 62.6 years, and almost half (49%) were female.
New-onset inflammatory arthritis was the most common Rh-irAE reported (n = 34), with the majority of patients presenting with polyarticular symptoms (n = 22; 65%).
Most of these patients were managed by a rheumatologist and were treated with systemic glucocorticoids (n = 26; 76%) for an average duration of 18 weeks. Five of the patients also required disease-modifying antirheumatic drugs and eight needed NSAIDS or intra-articular steroids.
The investigators noted that almost half of the patients (47%) experienced a complete resolution of symptoms during the study period, although few achieved this while they were still on the cancer treatment.
According to the investigators, the clinical characteristics of IA in their cohort support the existing literature: “Time of symptom onset is generally 4-8 weeks after starting ICI therapy. … The majority of patients require long courses of systemic glucocorticoids. And very few achieve complete symptom resolution while continuing ICI therapy,” they wrote.
The database analysis also revealed that a further 10 patients developed myopathy, with all patients presenting with myalgias and weaknesses. Five had bulbar myopathy, and four patients were diagnosed with concomitant myocarditis. All of these patients were treated with glucocorticoids for an average treatment duration of 15 weeks.
Complete resolution of the myopathy was observed in 70%, but two patients died from complications related to myocarditis and bulbar myopathy.
Other rheumatic events included four cases of vasculitis and four cases of polymyalgia rheumatica and six cases of diffuse systemic sclerosis or sicca syndromes.
“In lieu of controlled prospective studies, this cohort may serve as a guide for rheumatologists managing and counseling patients with Rh-IrAEs,” the investigators concluded.
“It remains unclear why some patients develop Rh-irAEs, and so far no genomic risk factors have been identified, though the varied clinical phenotypes of Rh-irAEs certainly suggest multiple underlying immunopathogenic mechanisms. Further prospective studies that distinguish between subsets of Rh-irAEs are necessary to better understand their pathophysiology and improve clinical care,” they added.
They noted that a limitation of the study was its reliance on retrospective data and clinician diagnoses.
None of the authors declared any financial or other conflicts of interest.
SOURCE: Richter MD et al. Arthritis Rheumatol. 2018 Oct 3. doi: 10.1002/art.40745.
Inflammatory arthritis (IA) is the most common rheumatic adverse event seen in people on immune checkpoint inhibitor (ICI) therapy and can largely be managed by rheumatologists without the need to halt cancer treatment, according to Michael D. Richter, MD, of the Mayo School of Graduate Medical Education, Rochester, Minn., and his colleagues.
The investigators’ observations of patients seen at the Mayo Clinic over a 7-year period suggested that “IA should not be seen as a contraindication to continuing or restarting ICIs, ” although continuing ICI therapy concurrently with high-dose steroids is “generally not recommended.” Previous estimates of rheumatic adverse events with ICIs had ranged from 1% to 10%, and management had largely been based on the experience of experts and findings from retrospective studies, they noted.
“This study aims to add granularity to the existing literature by describing the prevalence, clinical characteristics, and treatment outcomes of a large, single-institution cohort of patients with rheumatic immune-related adverse events,” Dr. Richter and his associates wrote in an article published in Arthritis & Rheumatology.
The analysis included 1,293 patients who had received treatment with any ICI at the Mayo Clinic between January 2011 and March 2018. Patients who had received treatment at other centers but were seen at the Mayo clinic for their rheumatic adverse event were also included.
Overall, 61 patients experienced a rheumatic immune-related adverse event (Rh-irAE) related to checkpoint inhibitor treatment; 43 were from the Mayo cohort and 18 were from other centers. The average age of the patients was 62.6 years, and almost half (49%) were female.
New-onset inflammatory arthritis was the most common Rh-irAE reported (n = 34), with the majority of patients presenting with polyarticular symptoms (n = 22; 65%).
Most of these patients were managed by a rheumatologist and were treated with systemic glucocorticoids (n = 26; 76%) for an average duration of 18 weeks. Five of the patients also required disease-modifying antirheumatic drugs and eight needed NSAIDS or intra-articular steroids.
The investigators noted that almost half of the patients (47%) experienced a complete resolution of symptoms during the study period, although few achieved this while they were still on the cancer treatment.
According to the investigators, the clinical characteristics of IA in their cohort support the existing literature: “Time of symptom onset is generally 4-8 weeks after starting ICI therapy. … The majority of patients require long courses of systemic glucocorticoids. And very few achieve complete symptom resolution while continuing ICI therapy,” they wrote.
The database analysis also revealed that a further 10 patients developed myopathy, with all patients presenting with myalgias and weaknesses. Five had bulbar myopathy, and four patients were diagnosed with concomitant myocarditis. All of these patients were treated with glucocorticoids for an average treatment duration of 15 weeks.
Complete resolution of the myopathy was observed in 70%, but two patients died from complications related to myocarditis and bulbar myopathy.
Other rheumatic events included four cases of vasculitis and four cases of polymyalgia rheumatica and six cases of diffuse systemic sclerosis or sicca syndromes.
“In lieu of controlled prospective studies, this cohort may serve as a guide for rheumatologists managing and counseling patients with Rh-IrAEs,” the investigators concluded.
“It remains unclear why some patients develop Rh-irAEs, and so far no genomic risk factors have been identified, though the varied clinical phenotypes of Rh-irAEs certainly suggest multiple underlying immunopathogenic mechanisms. Further prospective studies that distinguish between subsets of Rh-irAEs are necessary to better understand their pathophysiology and improve clinical care,” they added.
They noted that a limitation of the study was its reliance on retrospective data and clinician diagnoses.
None of the authors declared any financial or other conflicts of interest.
SOURCE: Richter MD et al. Arthritis Rheumatol. 2018 Oct 3. doi: 10.1002/art.40745.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point: Inflammatory arthritis (IA) is the most common form of rheumatic immune-related adverse event (Rh-irAE) related to ICI treatment. The majority of patients with an Rh-irAE (90% in the current cohort) remained on ICI treatment, which suggests that IA should not be seen as a contraindication to continuing or restarting ICI treatment.
Major finding: Among a cohort of 1,293 patients and 18 patients who received ICI therapy at other centers, 61 cases of Rh-irAE were identified. Over half (n = 34) of these patients presented with IA.
Study details: A retrospective analysis of a database of all patients who received any ICI at the Mayo Clinic between January 2011 and March 2018.
Disclosures: None of the authors declared any financial or other conflicts of interest.
Source: Richter MD et al. Arthritis Rheumatol. 2018 Oct 3. doi: 10.1002/art.40745.
Anxiety and depression widespread among arthritis patients
Adults with arthritis are almost twice as likely to have symptoms of anxiety than depression, but the depressed patients are more likely to receive treatment, according to the Centers for Disease Control and Prevention.
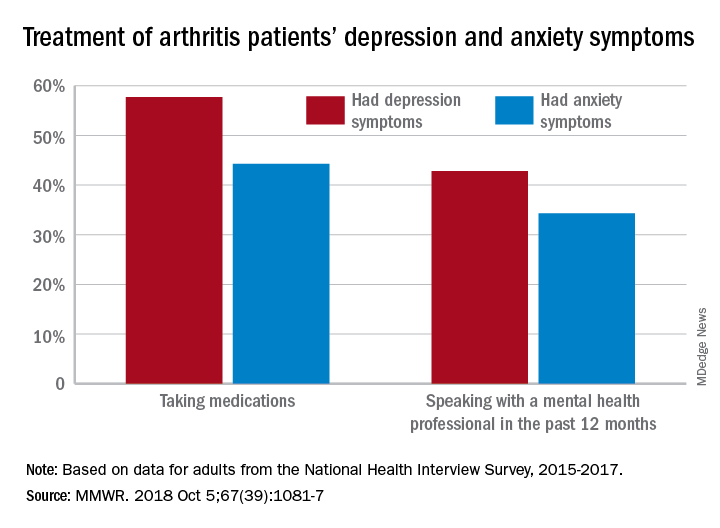
During 2015-2017, the prevalence of anxiety symptoms was 22.5% in adults with arthritis, compared with 12.1% for depression symptoms. Treatment of those symptoms, however, was another story: 57.7% of arthritis patients with depression symptoms were taking medications, versus 44.3% of those with anxiety symptoms, and 42.8% of those with symptoms of depression reported seeing a mental health professional the past 12 months, compared with 34.3% of adults with anxiety, Dana Guglielmo, MPH, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report.
Prevalences of anxiety and depression symptoms varied considerably by sociodemographic characteristic during 2015-2017. Anxiety and depression were both more common in those aged 18-44 years (28.3% and 13.7%, respectively) than in those aged over 65 (9.7% and 6.2%), and women with arthritis were more likely than were men to experience symptoms of anxiety (26.9% vs. 16%) and depression (14% vs. 9.2%), the investigators said, based on data from the National Health Interview Survey.
Among racial/ethnic groups, the prevalence of anxiety was highest for whites (23.9%) and lowest for Asians (10.6%), who also had lowest depression symptom prevalence at 3.3%, with American Indians/Alaska Natives highest at 15.4%. Adults categorized as other/multiple race, however, were highest in both cases at 32.3% for anxiety and 17.4% for depression, Ms. Guglielmo and her associates said.
The overall prevalence of anxiety and depression symptoms in patients with arthritis was much higher than in those without arthritis – 10.7% for anxiety and 4.7% for depression – which “suggests that all adults with arthritis would benefit from mental health screening,” they noted.
, and encouraging physical activity, which is an effective nonpharmacologic strategy that can help reduce the symptoms of anxiety and depression, improve arthritis symptoms, and promote better quality of life,” the investigators wrote.
SOURCE: Guglielmo D et al. MMWR. 2018 Oct 5;67(39):1081-7.
Adults with arthritis are almost twice as likely to have symptoms of anxiety than depression, but the depressed patients are more likely to receive treatment, according to the Centers for Disease Control and Prevention.
During 2015-2017, the prevalence of anxiety symptoms was 22.5% in adults with arthritis, compared with 12.1% for depression symptoms. Treatment of those symptoms, however, was another story: 57.7% of arthritis patients with depression symptoms were taking medications, versus 44.3% of those with anxiety symptoms, and 42.8% of those with symptoms of depression reported seeing a mental health professional the past 12 months, compared with 34.3% of adults with anxiety, Dana Guglielmo, MPH, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report.
Prevalences of anxiety and depression symptoms varied considerably by sociodemographic characteristic during 2015-2017. Anxiety and depression were both more common in those aged 18-44 years (28.3% and 13.7%, respectively) than in those aged over 65 (9.7% and 6.2%), and women with arthritis were more likely than were men to experience symptoms of anxiety (26.9% vs. 16%) and depression (14% vs. 9.2%), the investigators said, based on data from the National Health Interview Survey.
Among racial/ethnic groups, the prevalence of anxiety was highest for whites (23.9%) and lowest for Asians (10.6%), who also had lowest depression symptom prevalence at 3.3%, with American Indians/Alaska Natives highest at 15.4%. Adults categorized as other/multiple race, however, were highest in both cases at 32.3% for anxiety and 17.4% for depression, Ms. Guglielmo and her associates said.
The overall prevalence of anxiety and depression symptoms in patients with arthritis was much higher than in those without arthritis – 10.7% for anxiety and 4.7% for depression – which “suggests that all adults with arthritis would benefit from mental health screening,” they noted.
, and encouraging physical activity, which is an effective nonpharmacologic strategy that can help reduce the symptoms of anxiety and depression, improve arthritis symptoms, and promote better quality of life,” the investigators wrote.
SOURCE: Guglielmo D et al. MMWR. 2018 Oct 5;67(39):1081-7.
Adults with arthritis are almost twice as likely to have symptoms of anxiety than depression, but the depressed patients are more likely to receive treatment, according to the Centers for Disease Control and Prevention.
During 2015-2017, the prevalence of anxiety symptoms was 22.5% in adults with arthritis, compared with 12.1% for depression symptoms. Treatment of those symptoms, however, was another story: 57.7% of arthritis patients with depression symptoms were taking medications, versus 44.3% of those with anxiety symptoms, and 42.8% of those with symptoms of depression reported seeing a mental health professional the past 12 months, compared with 34.3% of adults with anxiety, Dana Guglielmo, MPH, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report.
Prevalences of anxiety and depression symptoms varied considerably by sociodemographic characteristic during 2015-2017. Anxiety and depression were both more common in those aged 18-44 years (28.3% and 13.7%, respectively) than in those aged over 65 (9.7% and 6.2%), and women with arthritis were more likely than were men to experience symptoms of anxiety (26.9% vs. 16%) and depression (14% vs. 9.2%), the investigators said, based on data from the National Health Interview Survey.
Among racial/ethnic groups, the prevalence of anxiety was highest for whites (23.9%) and lowest for Asians (10.6%), who also had lowest depression symptom prevalence at 3.3%, with American Indians/Alaska Natives highest at 15.4%. Adults categorized as other/multiple race, however, were highest in both cases at 32.3% for anxiety and 17.4% for depression, Ms. Guglielmo and her associates said.
The overall prevalence of anxiety and depression symptoms in patients with arthritis was much higher than in those without arthritis – 10.7% for anxiety and 4.7% for depression – which “suggests that all adults with arthritis would benefit from mental health screening,” they noted.
, and encouraging physical activity, which is an effective nonpharmacologic strategy that can help reduce the symptoms of anxiety and depression, improve arthritis symptoms, and promote better quality of life,” the investigators wrote.
SOURCE: Guglielmo D et al. MMWR. 2018 Oct 5;67(39):1081-7.
FROM MMWR