User login
Diet’s link to RA risk centers on alcohol, fish, sugar consumption
SNOWMASS, COLO. – Moderate alcohol intake and fish consumption are the two dietary factors supported by the strongest epidemiologic evidence for a protective effect against development of rheumatoid arthritis, while sugar-sweetened sodas are associated with increased risk of the disease.
“Sugar-sweetened soft drinks are now the primary source of sugar in the American diet. This consumption has increased astronomically over the past 30 years,” Dr. Karen H. Costenbader observed at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.

Obesity, one consequence of America’s love affair with sugar, is a moderately potent independent risk factor for RA, according to several studies, including one carried out by Dr. Costenbader and her colleagues at Brigham and Women’s Hospital and Harvard University, Boston.
They followed nearly 220,000 women enrolled in the Nurses Health Study (NHS) and NHS II prospective cohort studies. During 4.7 million person-years of follow-up, women who were diagnosed with RA before age 55 were 45% more likely to be overweight and 65% more likely to be obese than were women without RA at that age. The association was stronger for seropositive than seronegative RA. Moreover, in an analysis that considered cumulative years of obesity as something akin to pack-years of smoking, the investigators found strong evidence of a dose effect, such that 10 cumulative years of being obese was associated with a 37% increased risk of RA by age 55 (Ann. Rheum. Dis. 2014;73:1914-22).
These findings were consistent with the results of a retrospective, population-based study of Olmsted County, Minn., residents conducted by investigators at the Mayo Clinic. They found that a history of obesity was associated with a 24% increased likelihood of developing RA. The investigators calculated that obesity could account for 52% of the sharp increase in the incidence of RA seen in the county, as elsewhere, between 1985 and 2007 (Arthritis Care Res. 2013;65:71-7).
The mechanism by which obesity may boost the development of RA is unknown. Speculation has focused on inflammation as the likely mediator. Visceral fat secretes proinflammatory cytokines, with resultant elevations in C-reactive protein, TNF-alpha, and other biomarkers of systemic inflammation, Dr. Costenbader said.
The importance of eating fish as a protector against developing RA is also supported by multiple epidemiologic studies. Investigators at the Karolinska Institute in Stockholm demonstrated in a study of 1,889 Swedish RA patients and 2,145 controls that eating oily fish on as few as 1-3 occasions per month was associated with a 20% reduction in the odds of developing RA (Epidemiology 2009;20:896-901).
The Swedish findings were confirmed in a recent, not-yet-published analysis of women enrolled in the Nurses’ Health Study and NHS II. Dr. Costenbader and coworkers showed that eating fish at least once per month was associated with a 28% reduction in RA risk, compared with never-eaters of fish.
The evidence for a preventive effect of eating fish and a contributory role of obesity in the development of RA is sufficiently strong that these two behavioral factors have been incorporated in the Personalized Risk Estimator for Rheumatoid Arthritis (PRE-RA) Family Study. This is an ongoing National Institutes of Health–funded, prospective, randomized, controlled trial being conducted by Dr. Costenbader and others at Brigham and Women’s Hospital.
The PRE-RA Family Study is designed to compare the willingness to change RA-associated behaviors among first-degree relatives of RA patients after exposure to an online personalized risk-estimation tool and education program. The four behavioral factors included in the risk estimator – and targeted for change in the online risk education program – are cigarette smoking, excess body weight, low fish intake, and poor oral health.
Dr. Costenbader said “the sweet spot” for alcohol consumption in terms of reducing RA risk was 5.0-9.9 g/day – equivalent to one-half to one drink – in an analysis of incident RA cases she and her coinvestigators performed in the NHS and NHS II cohorts (Arthritis Rheumatol. 2014;66:1998-2005).
In the sugar-sweetened soda study, she and her coworkers found that nurses who drank more than one serving per day had a 63% greater risk of developing seropositive RA compared with those who consumed less than one per month. Restricting the analysis to women with onset of RA after age 55, the association grew markedly stronger, with one or more soft drinks per day linked to a 2.64-fold increased risk (Am. J. Clin. Nutr. 2014;100:959-67).
Lots of other dietary factors, including coffee, tea, red meat, protein, vitamins and antioxidant-rich foods, and the Mediterranean diet pattern, have been looked at by various investigators. None have panned out.
Dr. Costenbader’s research is supported by the NIH and the Arthritis Foundation. She reported having no financial conflicts.
SNOWMASS, COLO. – Moderate alcohol intake and fish consumption are the two dietary factors supported by the strongest epidemiologic evidence for a protective effect against development of rheumatoid arthritis, while sugar-sweetened sodas are associated with increased risk of the disease.
“Sugar-sweetened soft drinks are now the primary source of sugar in the American diet. This consumption has increased astronomically over the past 30 years,” Dr. Karen H. Costenbader observed at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Obesity, one consequence of America’s love affair with sugar, is a moderately potent independent risk factor for RA, according to several studies, including one carried out by Dr. Costenbader and her colleagues at Brigham and Women’s Hospital and Harvard University, Boston.
They followed nearly 220,000 women enrolled in the Nurses Health Study (NHS) and NHS II prospective cohort studies. During 4.7 million person-years of follow-up, women who were diagnosed with RA before age 55 were 45% more likely to be overweight and 65% more likely to be obese than were women without RA at that age. The association was stronger for seropositive than seronegative RA. Moreover, in an analysis that considered cumulative years of obesity as something akin to pack-years of smoking, the investigators found strong evidence of a dose effect, such that 10 cumulative years of being obese was associated with a 37% increased risk of RA by age 55 (Ann. Rheum. Dis. 2014;73:1914-22).
These findings were consistent with the results of a retrospective, population-based study of Olmsted County, Minn., residents conducted by investigators at the Mayo Clinic. They found that a history of obesity was associated with a 24% increased likelihood of developing RA. The investigators calculated that obesity could account for 52% of the sharp increase in the incidence of RA seen in the county, as elsewhere, between 1985 and 2007 (Arthritis Care Res. 2013;65:71-7).
The mechanism by which obesity may boost the development of RA is unknown. Speculation has focused on inflammation as the likely mediator. Visceral fat secretes proinflammatory cytokines, with resultant elevations in C-reactive protein, TNF-alpha, and other biomarkers of systemic inflammation, Dr. Costenbader said.
The importance of eating fish as a protector against developing RA is also supported by multiple epidemiologic studies. Investigators at the Karolinska Institute in Stockholm demonstrated in a study of 1,889 Swedish RA patients and 2,145 controls that eating oily fish on as few as 1-3 occasions per month was associated with a 20% reduction in the odds of developing RA (Epidemiology 2009;20:896-901).
The Swedish findings were confirmed in a recent, not-yet-published analysis of women enrolled in the Nurses’ Health Study and NHS II. Dr. Costenbader and coworkers showed that eating fish at least once per month was associated with a 28% reduction in RA risk, compared with never-eaters of fish.
The evidence for a preventive effect of eating fish and a contributory role of obesity in the development of RA is sufficiently strong that these two behavioral factors have been incorporated in the Personalized Risk Estimator for Rheumatoid Arthritis (PRE-RA) Family Study. This is an ongoing National Institutes of Health–funded, prospective, randomized, controlled trial being conducted by Dr. Costenbader and others at Brigham and Women’s Hospital.
The PRE-RA Family Study is designed to compare the willingness to change RA-associated behaviors among first-degree relatives of RA patients after exposure to an online personalized risk-estimation tool and education program. The four behavioral factors included in the risk estimator – and targeted for change in the online risk education program – are cigarette smoking, excess body weight, low fish intake, and poor oral health.
Dr. Costenbader said “the sweet spot” for alcohol consumption in terms of reducing RA risk was 5.0-9.9 g/day – equivalent to one-half to one drink – in an analysis of incident RA cases she and her coinvestigators performed in the NHS and NHS II cohorts (Arthritis Rheumatol. 2014;66:1998-2005).
In the sugar-sweetened soda study, she and her coworkers found that nurses who drank more than one serving per day had a 63% greater risk of developing seropositive RA compared with those who consumed less than one per month. Restricting the analysis to women with onset of RA after age 55, the association grew markedly stronger, with one or more soft drinks per day linked to a 2.64-fold increased risk (Am. J. Clin. Nutr. 2014;100:959-67).
Lots of other dietary factors, including coffee, tea, red meat, protein, vitamins and antioxidant-rich foods, and the Mediterranean diet pattern, have been looked at by various investigators. None have panned out.
Dr. Costenbader’s research is supported by the NIH and the Arthritis Foundation. She reported having no financial conflicts.
SNOWMASS, COLO. – Moderate alcohol intake and fish consumption are the two dietary factors supported by the strongest epidemiologic evidence for a protective effect against development of rheumatoid arthritis, while sugar-sweetened sodas are associated with increased risk of the disease.
“Sugar-sweetened soft drinks are now the primary source of sugar in the American diet. This consumption has increased astronomically over the past 30 years,” Dr. Karen H. Costenbader observed at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Obesity, one consequence of America’s love affair with sugar, is a moderately potent independent risk factor for RA, according to several studies, including one carried out by Dr. Costenbader and her colleagues at Brigham and Women’s Hospital and Harvard University, Boston.
They followed nearly 220,000 women enrolled in the Nurses Health Study (NHS) and NHS II prospective cohort studies. During 4.7 million person-years of follow-up, women who were diagnosed with RA before age 55 were 45% more likely to be overweight and 65% more likely to be obese than were women without RA at that age. The association was stronger for seropositive than seronegative RA. Moreover, in an analysis that considered cumulative years of obesity as something akin to pack-years of smoking, the investigators found strong evidence of a dose effect, such that 10 cumulative years of being obese was associated with a 37% increased risk of RA by age 55 (Ann. Rheum. Dis. 2014;73:1914-22).
These findings were consistent with the results of a retrospective, population-based study of Olmsted County, Minn., residents conducted by investigators at the Mayo Clinic. They found that a history of obesity was associated with a 24% increased likelihood of developing RA. The investigators calculated that obesity could account for 52% of the sharp increase in the incidence of RA seen in the county, as elsewhere, between 1985 and 2007 (Arthritis Care Res. 2013;65:71-7).
The mechanism by which obesity may boost the development of RA is unknown. Speculation has focused on inflammation as the likely mediator. Visceral fat secretes proinflammatory cytokines, with resultant elevations in C-reactive protein, TNF-alpha, and other biomarkers of systemic inflammation, Dr. Costenbader said.
The importance of eating fish as a protector against developing RA is also supported by multiple epidemiologic studies. Investigators at the Karolinska Institute in Stockholm demonstrated in a study of 1,889 Swedish RA patients and 2,145 controls that eating oily fish on as few as 1-3 occasions per month was associated with a 20% reduction in the odds of developing RA (Epidemiology 2009;20:896-901).
The Swedish findings were confirmed in a recent, not-yet-published analysis of women enrolled in the Nurses’ Health Study and NHS II. Dr. Costenbader and coworkers showed that eating fish at least once per month was associated with a 28% reduction in RA risk, compared with never-eaters of fish.
The evidence for a preventive effect of eating fish and a contributory role of obesity in the development of RA is sufficiently strong that these two behavioral factors have been incorporated in the Personalized Risk Estimator for Rheumatoid Arthritis (PRE-RA) Family Study. This is an ongoing National Institutes of Health–funded, prospective, randomized, controlled trial being conducted by Dr. Costenbader and others at Brigham and Women’s Hospital.
The PRE-RA Family Study is designed to compare the willingness to change RA-associated behaviors among first-degree relatives of RA patients after exposure to an online personalized risk-estimation tool and education program. The four behavioral factors included in the risk estimator – and targeted for change in the online risk education program – are cigarette smoking, excess body weight, low fish intake, and poor oral health.
Dr. Costenbader said “the sweet spot” for alcohol consumption in terms of reducing RA risk was 5.0-9.9 g/day – equivalent to one-half to one drink – in an analysis of incident RA cases she and her coinvestigators performed in the NHS and NHS II cohorts (Arthritis Rheumatol. 2014;66:1998-2005).
In the sugar-sweetened soda study, she and her coworkers found that nurses who drank more than one serving per day had a 63% greater risk of developing seropositive RA compared with those who consumed less than one per month. Restricting the analysis to women with onset of RA after age 55, the association grew markedly stronger, with one or more soft drinks per day linked to a 2.64-fold increased risk (Am. J. Clin. Nutr. 2014;100:959-67).
Lots of other dietary factors, including coffee, tea, red meat, protein, vitamins and antioxidant-rich foods, and the Mediterranean diet pattern, have been looked at by various investigators. None have panned out.
Dr. Costenbader’s research is supported by the NIH and the Arthritis Foundation. She reported having no financial conflicts.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM

Microbiome research is decades away from benefiting human health
MAUI, HAWAII – Don’t look for findings about the human microbiome to have any imminent impact on health, said rheumatologist Peter Lipsky.
The human microbiome “is the most exciting area in science at the moment, but also the most hyped. There’s a tendency in this field driven both by scientists and the NIH [National Institutes of Health], as well as by commercial interests, to explain every [condition as it relates to] the microbiome,” he said at the 2015 Rheumatology Winter Clinical Symposium.
Most of our understanding about the microbiome comes from “very reductionist experiments” in genetically altered mice, often raised in germ-free environments “where you can control everything.” The findings have no clear use in human medicine, and have not led to any breakthroughs. To date, there have been only a few microbiome studies in people, and they’ve been solely descriptive, said Dr. Lipsky, former chief of the autoimmunity branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
Microbiome research examines how normal human bacteria might have something to do with illness. The field has much in common with human genome mapping in the mid-1990s; it is in the data-gathering phase with little evidence of benefit.
It will take decades to fully figure out how vast and ever-changing communities of bacteria interact with each other and the human body, and how to selectively manipulate them to improve human health. Humans carry about 3 pounds of bacteria on and in their bodies, with bacterial cells outnumbering human cells by about 10:1. Those 3 pounds are composed of thousands of bacterial species, and new species are being discovered almost daily, thanks to advances in molecular technology.
“It’s impossible with the technology that we have now to integrate the actions of all these organisms,” said Dr. Lipsky of Charlottesville, Va.
Even so, the Internet is awash in ads for prebiotics, probiotics, and other products to balance the human microbiome. There are companies that take stool samples to diagnose and correct microbiome imbalances.
“Does this make any sense today? No,” Dr. Lipsky said. “You are never going to be able to stop patients from taking risks, but there is a certain amount of caution that needs to be exerted here. What you can tell patients is that this is an exciting area, but it’s in its early stage. There is really no scientific basis for any of these products. Most of them probably don’t do any harm, but I don’t know that for certain. The same organism that might protect against colon cancer could facilitate rheumatoid arthritis or periodontal disease,” he said.
Dr. Lipsky supported his thesis with a review of the latest human findings. One study found an aberration in oral microbiota in new-onset rheumatoid arthritis (RA). A stool sample study correlated an overabundance of gut Prevotella copri with RA. Another found changes in gut bacteria in psoriasis and psoriatic arthritis that seem similar to those seen in inflammatory bowel disease. It’s unknown if the disease caused the imbalance or visa versa.
Another small study found a drop in gut Firmicutes families in lupus (mBio 2014;5:e01548-14). “How and why this microbial community influences [lupus] remains to be elucidated,” the authors noted.
Dr. Lipsky is an adviser for Janssen and a consultant for Pfizer.
MAUI, HAWAII – Don’t look for findings about the human microbiome to have any imminent impact on health, said rheumatologist Peter Lipsky.
The human microbiome “is the most exciting area in science at the moment, but also the most hyped. There’s a tendency in this field driven both by scientists and the NIH [National Institutes of Health], as well as by commercial interests, to explain every [condition as it relates to] the microbiome,” he said at the 2015 Rheumatology Winter Clinical Symposium.
Most of our understanding about the microbiome comes from “very reductionist experiments” in genetically altered mice, often raised in germ-free environments “where you can control everything.” The findings have no clear use in human medicine, and have not led to any breakthroughs. To date, there have been only a few microbiome studies in people, and they’ve been solely descriptive, said Dr. Lipsky, former chief of the autoimmunity branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
Microbiome research examines how normal human bacteria might have something to do with illness. The field has much in common with human genome mapping in the mid-1990s; it is in the data-gathering phase with little evidence of benefit.
It will take decades to fully figure out how vast and ever-changing communities of bacteria interact with each other and the human body, and how to selectively manipulate them to improve human health. Humans carry about 3 pounds of bacteria on and in their bodies, with bacterial cells outnumbering human cells by about 10:1. Those 3 pounds are composed of thousands of bacterial species, and new species are being discovered almost daily, thanks to advances in molecular technology.
“It’s impossible with the technology that we have now to integrate the actions of all these organisms,” said Dr. Lipsky of Charlottesville, Va.
Even so, the Internet is awash in ads for prebiotics, probiotics, and other products to balance the human microbiome. There are companies that take stool samples to diagnose and correct microbiome imbalances.
“Does this make any sense today? No,” Dr. Lipsky said. “You are never going to be able to stop patients from taking risks, but there is a certain amount of caution that needs to be exerted here. What you can tell patients is that this is an exciting area, but it’s in its early stage. There is really no scientific basis for any of these products. Most of them probably don’t do any harm, but I don’t know that for certain. The same organism that might protect against colon cancer could facilitate rheumatoid arthritis or periodontal disease,” he said.
Dr. Lipsky supported his thesis with a review of the latest human findings. One study found an aberration in oral microbiota in new-onset rheumatoid arthritis (RA). A stool sample study correlated an overabundance of gut Prevotella copri with RA. Another found changes in gut bacteria in psoriasis and psoriatic arthritis that seem similar to those seen in inflammatory bowel disease. It’s unknown if the disease caused the imbalance or visa versa.
Another small study found a drop in gut Firmicutes families in lupus (mBio 2014;5:e01548-14). “How and why this microbial community influences [lupus] remains to be elucidated,” the authors noted.
Dr. Lipsky is an adviser for Janssen and a consultant for Pfizer.
MAUI, HAWAII – Don’t look for findings about the human microbiome to have any imminent impact on health, said rheumatologist Peter Lipsky.
The human microbiome “is the most exciting area in science at the moment, but also the most hyped. There’s a tendency in this field driven both by scientists and the NIH [National Institutes of Health], as well as by commercial interests, to explain every [condition as it relates to] the microbiome,” he said at the 2015 Rheumatology Winter Clinical Symposium.
Most of our understanding about the microbiome comes from “very reductionist experiments” in genetically altered mice, often raised in germ-free environments “where you can control everything.” The findings have no clear use in human medicine, and have not led to any breakthroughs. To date, there have been only a few microbiome studies in people, and they’ve been solely descriptive, said Dr. Lipsky, former chief of the autoimmunity branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
Microbiome research examines how normal human bacteria might have something to do with illness. The field has much in common with human genome mapping in the mid-1990s; it is in the data-gathering phase with little evidence of benefit.
It will take decades to fully figure out how vast and ever-changing communities of bacteria interact with each other and the human body, and how to selectively manipulate them to improve human health. Humans carry about 3 pounds of bacteria on and in their bodies, with bacterial cells outnumbering human cells by about 10:1. Those 3 pounds are composed of thousands of bacterial species, and new species are being discovered almost daily, thanks to advances in molecular technology.
“It’s impossible with the technology that we have now to integrate the actions of all these organisms,” said Dr. Lipsky of Charlottesville, Va.
Even so, the Internet is awash in ads for prebiotics, probiotics, and other products to balance the human microbiome. There are companies that take stool samples to diagnose and correct microbiome imbalances.
“Does this make any sense today? No,” Dr. Lipsky said. “You are never going to be able to stop patients from taking risks, but there is a certain amount of caution that needs to be exerted here. What you can tell patients is that this is an exciting area, but it’s in its early stage. There is really no scientific basis for any of these products. Most of them probably don’t do any harm, but I don’t know that for certain. The same organism that might protect against colon cancer could facilitate rheumatoid arthritis or periodontal disease,” he said.
Dr. Lipsky supported his thesis with a review of the latest human findings. One study found an aberration in oral microbiota in new-onset rheumatoid arthritis (RA). A stool sample study correlated an overabundance of gut Prevotella copri with RA. Another found changes in gut bacteria in psoriasis and psoriatic arthritis that seem similar to those seen in inflammatory bowel disease. It’s unknown if the disease caused the imbalance or visa versa.
Another small study found a drop in gut Firmicutes families in lupus (mBio 2014;5:e01548-14). “How and why this microbial community influences [lupus] remains to be elucidated,” the authors noted.
Dr. Lipsky is an adviser for Janssen and a consultant for Pfizer.
EXPERT ANALYSIS FROM RWCS 2015

Infliximab most common cause of drug-induced liver injury
Infliximab caused liver injury in 8.3% of treated patients in a prospective study, exceeding rates for other tumor necrosis factor-alpha antagonists, investigators reported online in Clinical Gastroenterology and Hepatology.
The findings show that “liver injury associated with the use of TNF-alpha antagonists is more common than previously reported, occurring in 1 in 120 of those exposed to infliximab,” said Dr. Einar S. Björnsson at the University of Iceland in Reykjavik and his associates. Furthermore, neither anti-TNF treatment dose nor baseline antinuclear acid antibody (ANA) status predicted which patients would develop drug-induced liver injury (DILI), the researchers said.
Since emerging in the 1990s, anti-TNF agents have dramatically altered the treatment landscape for autoimmune diseases such as rheumatoid arthritis, psoriasis, and inflammatory bowel disease. Although they are known to cause liver damage in some patients, data on the topic mainly come from single case reports, the researchers said (Clin. Gastroenterol. Hepatol. 2014 [doi: http://dx.doi.org/10.1016/j.cgh.2014.07.062]) To better understand the association, the researchers prospectively studied patients who received anti-TNF agents between 2009 and 2013 at the University Hospital in Iceland. They defined liver injury as aspartate aminotransferase or alanine aminotransferase (ALT) levels that were at least triple the normal upper limit, or alkaline phosphatase levels of at least double the upper limit.
A total of 1,776 patients were treated with anti-TNF agents during the 5-year study period, the researchers reported. In all, 11 developed drug-induced liver injury (DILI), of which nine cases were caused by infliximab, they said. Liver injury developed in 8.3% of patients treated with infliximab, compared with only 3.7% of those who received adalimumab and 2.3% of those given etanercept, they added. In a past analysis, the researchers calculated that one in every 148 patients would develop DILI during 2 years of treatment with infliximab (Gastroenterology 2014;144:1419-25). Patients who developed DILI on one anti-TNF agent were able to switch therapies without DILI recurring, the investigators said. Seven patients were switched from infliximab to adalimumab, etanercept, or both, and one was switched to infliximab after developing DILI on adalimumab, they added.
The researchers also compared the 11 cases to 22 randomized controls matched by age, sex, underlying condition, and treatment. Notably, among the 11 patients diagnosed with DILI, just 1 (9%) was receiving methotrexate at the time of diagnosis, compared with 59% of the controls (P = .009), they reported. “The reason for this is not clear,” they added. “Methotrexate has been shown to lead to a decrease in circulating autoantibodies in cutaneous lupus erythematosus, but the influence of methotrexate could not be confirmed during infliximab treatment.”
Five of the 11 patients with DILI had liver biopsies, of which three showed severe acute hepatitis, two indicated mild unspecified chronic hepatitis, and one showed pure canalicular cholestasis, the researchers reported. About half the patients needed steroids acutely, but “the vast majority” did not need long-term steroid treatment, they said. Exactly how anti-TNF agents cause liver injury remains unclear, they added. Future studies might evaluate whether these drugs trigger CD4 T cells to react against liver cells, as is the case in classic autoimmune hepatitis, they said.
The researchers reported no funding sources and declared having no conflicts of interest.
Infliximab caused liver injury in 8.3% of treated patients in a prospective study, exceeding rates for other tumor necrosis factor-alpha antagonists, investigators reported online in Clinical Gastroenterology and Hepatology.
The findings show that “liver injury associated with the use of TNF-alpha antagonists is more common than previously reported, occurring in 1 in 120 of those exposed to infliximab,” said Dr. Einar S. Björnsson at the University of Iceland in Reykjavik and his associates. Furthermore, neither anti-TNF treatment dose nor baseline antinuclear acid antibody (ANA) status predicted which patients would develop drug-induced liver injury (DILI), the researchers said.
Since emerging in the 1990s, anti-TNF agents have dramatically altered the treatment landscape for autoimmune diseases such as rheumatoid arthritis, psoriasis, and inflammatory bowel disease. Although they are known to cause liver damage in some patients, data on the topic mainly come from single case reports, the researchers said (Clin. Gastroenterol. Hepatol. 2014 [doi: http://dx.doi.org/10.1016/j.cgh.2014.07.062]) To better understand the association, the researchers prospectively studied patients who received anti-TNF agents between 2009 and 2013 at the University Hospital in Iceland. They defined liver injury as aspartate aminotransferase or alanine aminotransferase (ALT) levels that were at least triple the normal upper limit, or alkaline phosphatase levels of at least double the upper limit.
A total of 1,776 patients were treated with anti-TNF agents during the 5-year study period, the researchers reported. In all, 11 developed drug-induced liver injury (DILI), of which nine cases were caused by infliximab, they said. Liver injury developed in 8.3% of patients treated with infliximab, compared with only 3.7% of those who received adalimumab and 2.3% of those given etanercept, they added. In a past analysis, the researchers calculated that one in every 148 patients would develop DILI during 2 years of treatment with infliximab (Gastroenterology 2014;144:1419-25). Patients who developed DILI on one anti-TNF agent were able to switch therapies without DILI recurring, the investigators said. Seven patients were switched from infliximab to adalimumab, etanercept, or both, and one was switched to infliximab after developing DILI on adalimumab, they added.
The researchers also compared the 11 cases to 22 randomized controls matched by age, sex, underlying condition, and treatment. Notably, among the 11 patients diagnosed with DILI, just 1 (9%) was receiving methotrexate at the time of diagnosis, compared with 59% of the controls (P = .009), they reported. “The reason for this is not clear,” they added. “Methotrexate has been shown to lead to a decrease in circulating autoantibodies in cutaneous lupus erythematosus, but the influence of methotrexate could not be confirmed during infliximab treatment.”
Five of the 11 patients with DILI had liver biopsies, of which three showed severe acute hepatitis, two indicated mild unspecified chronic hepatitis, and one showed pure canalicular cholestasis, the researchers reported. About half the patients needed steroids acutely, but “the vast majority” did not need long-term steroid treatment, they said. Exactly how anti-TNF agents cause liver injury remains unclear, they added. Future studies might evaluate whether these drugs trigger CD4 T cells to react against liver cells, as is the case in classic autoimmune hepatitis, they said.
The researchers reported no funding sources and declared having no conflicts of interest.
Infliximab caused liver injury in 8.3% of treated patients in a prospective study, exceeding rates for other tumor necrosis factor-alpha antagonists, investigators reported online in Clinical Gastroenterology and Hepatology.
The findings show that “liver injury associated with the use of TNF-alpha antagonists is more common than previously reported, occurring in 1 in 120 of those exposed to infliximab,” said Dr. Einar S. Björnsson at the University of Iceland in Reykjavik and his associates. Furthermore, neither anti-TNF treatment dose nor baseline antinuclear acid antibody (ANA) status predicted which patients would develop drug-induced liver injury (DILI), the researchers said.
Since emerging in the 1990s, anti-TNF agents have dramatically altered the treatment landscape for autoimmune diseases such as rheumatoid arthritis, psoriasis, and inflammatory bowel disease. Although they are known to cause liver damage in some patients, data on the topic mainly come from single case reports, the researchers said (Clin. Gastroenterol. Hepatol. 2014 [doi: http://dx.doi.org/10.1016/j.cgh.2014.07.062]) To better understand the association, the researchers prospectively studied patients who received anti-TNF agents between 2009 and 2013 at the University Hospital in Iceland. They defined liver injury as aspartate aminotransferase or alanine aminotransferase (ALT) levels that were at least triple the normal upper limit, or alkaline phosphatase levels of at least double the upper limit.
A total of 1,776 patients were treated with anti-TNF agents during the 5-year study period, the researchers reported. In all, 11 developed drug-induced liver injury (DILI), of which nine cases were caused by infliximab, they said. Liver injury developed in 8.3% of patients treated with infliximab, compared with only 3.7% of those who received adalimumab and 2.3% of those given etanercept, they added. In a past analysis, the researchers calculated that one in every 148 patients would develop DILI during 2 years of treatment with infliximab (Gastroenterology 2014;144:1419-25). Patients who developed DILI on one anti-TNF agent were able to switch therapies without DILI recurring, the investigators said. Seven patients were switched from infliximab to adalimumab, etanercept, or both, and one was switched to infliximab after developing DILI on adalimumab, they added.
The researchers also compared the 11 cases to 22 randomized controls matched by age, sex, underlying condition, and treatment. Notably, among the 11 patients diagnosed with DILI, just 1 (9%) was receiving methotrexate at the time of diagnosis, compared with 59% of the controls (P = .009), they reported. “The reason for this is not clear,” they added. “Methotrexate has been shown to lead to a decrease in circulating autoantibodies in cutaneous lupus erythematosus, but the influence of methotrexate could not be confirmed during infliximab treatment.”
Five of the 11 patients with DILI had liver biopsies, of which three showed severe acute hepatitis, two indicated mild unspecified chronic hepatitis, and one showed pure canalicular cholestasis, the researchers reported. About half the patients needed steroids acutely, but “the vast majority” did not need long-term steroid treatment, they said. Exactly how anti-TNF agents cause liver injury remains unclear, they added. Future studies might evaluate whether these drugs trigger CD4 T cells to react against liver cells, as is the case in classic autoimmune hepatitis, they said.
The researchers reported no funding sources and declared having no conflicts of interest.
Key clinical point: Infliximab was the most common anti–tumor necrosis factor-alpha agent linked to liver injury.
Major finding: Rates of drug-induced liver injury were highest among patients treated with infliximab (8.3%), compared with 3.7% for adalimumab and 2.3% for etanercept.
Data source: Prospective study of 11 cases of drug-induced liver injury and 22 controls.
Disclosures: The researchers declared no funding sources or conflicts of interest.
VIDEO: True remission necessary before tapering or discontinuing RA drugs
MAUI, HAWAII– Discontinuing medications when rheumatoid arthritis patients are doing well is a hot topic in rheumatology lately, but it’s tricky.
The idea is to give patients a break from the costs and side effects of steroids, methotrexate, and biologics. Whether or not doing so is a good idea has a lot to do with how you define remission, and the odds of recapturing patients if they flare.
Advice from Dr. Roy Fleischmann, a clinical professor of rheumatology at the University of Texas Southwestern Medical Center in Dallas, might help. At the 2015 Rheumatology Winter Clinical Symposium, he shared his know-how about tapering and discontinuing treatments, culled from his professional experience and the literature on the subject in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MAUI, HAWAII– Discontinuing medications when rheumatoid arthritis patients are doing well is a hot topic in rheumatology lately, but it’s tricky.
The idea is to give patients a break from the costs and side effects of steroids, methotrexate, and biologics. Whether or not doing so is a good idea has a lot to do with how you define remission, and the odds of recapturing patients if they flare.
Advice from Dr. Roy Fleischmann, a clinical professor of rheumatology at the University of Texas Southwestern Medical Center in Dallas, might help. At the 2015 Rheumatology Winter Clinical Symposium, he shared his know-how about tapering and discontinuing treatments, culled from his professional experience and the literature on the subject in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MAUI, HAWAII– Discontinuing medications when rheumatoid arthritis patients are doing well is a hot topic in rheumatology lately, but it’s tricky.
The idea is to give patients a break from the costs and side effects of steroids, methotrexate, and biologics. Whether or not doing so is a good idea has a lot to do with how you define remission, and the odds of recapturing patients if they flare.
Advice from Dr. Roy Fleischmann, a clinical professor of rheumatology at the University of Texas Southwestern Medical Center in Dallas, might help. At the 2015 Rheumatology Winter Clinical Symposium, he shared his know-how about tapering and discontinuing treatments, culled from his professional experience and the literature on the subject in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT RWCS 2015

What’s new with methotrexate for rheumatoid arthritis
SNOWMASS, COLO. – Can an old rheumatoid arthritis drug – like an old dog – learn new tricks?
When that drug is methotrexate, the answer is definitely yes, according to Dr. Michael E. Weinblatt, professor of medicine at Harvard Medical School, Boston.
Clinically important advances and refinements continue to be made in the use of this venerable drug, a treatment mainstay for RA since the mid-1980s.
“I had the pleasure of participating in a symposium on methotrexate organized by Dr. Joel Kremer at last year’s annual ACR meeting in Boston. This is the second one we’ve done, and I must tell you, the number of people in attendance was extraordinary. We probably filled one of the largest conference rooms for the second time in 2 years. And the questions went on forever. So even though methotrexate is an old drug, there still remains great interest in it,” he observed at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Here’s what’s new:
Subcutaneous methotrexate for RA is finally legit.
Multiple studies over the past 15 years have established that at methotrexate doses above 15-20 mg/week, subcutaneous therapy achieves superior efficacy, compared with oral therapy. For this reason, rheumatologists have long used once-weekly subcutaneous injections of methotrexate in RA patients with an inadequate clinical response to oral therapy. However, as payers have often informed them, this has been off-label usage. Not any longer. Rheumatoid arthritis is now an FDA-approved indication for subcutaneous methotrexate. Moreover, two easy-to-use, single-dose, once-weekly, autoinjector formulations are now on the market, known as Otrexup and Rasuvo.
In a randomized, crossover study of various doses of oral methotrexate versus Otrexup in 49 RA patients, the systemic bioavailability of oral methotrexate plateaued at doses of 15 mg/week or above. In contrast, the systemic exposure of subcutaneous methotrexate continued to increase linearly out to 25 mg/week, the highest dose studied. And this greater bioavailability wasn’t associated with an increase in adverse events (Ann. Rheum. Dis. 2014;73:1549-51).
Split-dose oral therapy improves bioavailability.
When methotrexate was first prescribed for RA in the mid-1980s, it was given in a pulsed-dose regimen: 8 a.m., 8 p.m., and again at 8 a.m. the next morning. Three doses over a 24-hour period, once weekly.
“Over time, most of us shifted to a once-a-week regimen for convenience, ease-of-administration, and because of some concerns about liver exposure. We’ve come to appreciate, however, that if you dose-escalate methotrexate, a significant percentage of patients do not absorb the drug at doses above 15-20 mg once weekly. But pharmacokinetic studies have demonstrated you get higher drug concentrations with a split dose,” according to the rheumatologist.
For example, a crossover study involving 10 patients on stable doses of oral methotrexate at 25-35 mg/week showed that splitting a dose into two halves given 8 hours apart resulted in 28% greater bioavailability, compared with the standard single dose. Indeed, the bioavailability with the oral split dose was comparable to that achieved with subcutaneous administration (J. Rheumatol. 2006;33:481-5).
“Many of us are now splitting the dose of methotrexate at doses above 17.5-20 mg/week. I would like to caution, however, that this does not mean you should give the drug on Mondays and Thursdays. This was studied 40 years ago at the [National Institutes of Health]. It caused more acute toxicity, including bone marrow suppression, and more chronic toxicity, such as liver disease. So the drug should only be administered over one 24-hour period per week,” Dr. Weinblatt advised.
Methotrexate: the next statin?
Four cohort studies over the past 10 years have reported that methotrexate appears to reduce cardiovascular mortality in RA patients. Registry data are also supportive. The evidence is sufficiently strong that a definitive randomized clinical trial is now well underway. This major study, known as the Cardiovascular Inflammation Reduction Trial (CIRT), is funded by the National Heart, Lung, and Blood Institute and led by renowned cardiologist Dr. Paul Ridker, the Eugene Braunwald Professor of Medicine at Harvard Medical School. It will enroll 7,000 subjects – none with RA – at roughly 350 U.S. and Canadian sites.
Participants are high–cardiovascular risk patients with a history of acute MI within the previous 5 years plus type 2 diabetes or metabolic syndrome. They are being randomized to guideline-directed medical care plus either oral methotrexate at 10-20 mg/week or placebo for 2-4 years. The primary endpoint is cardiovascular death, nonfatal MI, or stroke.
The proposed mechanism of benefit is methotrexate’s anti-inflammatory effect. If the results of CIRT are positive, this low-cost generic drug with a thoroughly understood safety profile could transform preventive cardiology; lowering systemic inflammation would potentially join LDL lowering via statins as a cornerstone of disease prevention.
“This is one of the most exciting areas involving methotrexate,” commented Dr. Weinblatt, a participating investigator in CIRT.
Methotrexate boosts efficacy of selected biologics.
Concomitant methotrexate is known to increase the clinical efficacy of anti–tumor necrosis factor biologics and rituximab. Studies in patients on infliximab or adalimumab have shown that background methotrexate raises serum concentrations of the biologics by 20%-25%, which is presumably the explanation for the increased efficacy. Whether methotrexate enhances or attenuates the efficacy of the oral small-molecule JAK inhibitors is now under study.
One intriguing cohort study has shown that methotrexate reduces the immunogenicity of adalimumab in dose-dependent fashion; the higher the dose of methotrexate, the less ability patients had to develop blocking antibodies against adalimumab (Ann. Rheum. Dis. 2012;71:1914-5).
More recently, the randomized, double-blind CONCERTO trial conducted in 395 methotrexate- and biologic-naive RA patients extended this work. Participants were randomized to open-label adalimumab plus weekly blinded methotrexate at 2.5, 5, 10, or 20 mg. Clinical outcomes at 26 weeks as reflected in 28-joint count disease activity score and other measures were significantly better in patients on 10 or 20 mg/week of methotrexate. Serum adalimumab levels were higher in patients on those doses of methotrexate than in those on 2.5 or 5 mg/week as well (Ann. Rheum. Dis. 2014 Feb. 18 [doi:10.1136/annrheumdis-2013-204769]).
There’s an important lesson here for patient management: “If you’re going to dose-reduce your methotrexate in patients with low disease activity or in remission, there is a threshold at which you should probably stop reducing the methotrexate, at least when your patient is on this biologic,” according to Dr. Weinblatt.
In contrast, no methotrexate dose-threshold effect occurs with etanercept, he added.
Methotrexate and the liver.
A national observational cohort study of 659 military veterans over age 65 when they started methotrexate for RA or other rheumatic diseases found a 6% incidence of moderately elevated liver enzymes during a mean follow-up period of 7 months. The investigators identified a series of independent risk factors for liver function test abnormalities. Obesity was associated with a 1.9-fold increased risk, a serum total cholesterol greater than 240 mg/dL conferred a 5.8-fold elevated risk, abnormal liver function tests premethotrexate was associated with a 3.2-fold increased risk, and lack of folic acid supplementation brought a 2.2-fold increase in risk (Arthritis Care Res. 2014;66:1159-66).
“This study confirms what a lot of us have been worried about,” Dr. Weinblatt commented. That is, the risk of methotrexate-related liver toxicity is particularly high in older patients with characteristics consistent with the metabolic syndrome, a condition that has reached epidemic proportions.
A strong take-home message from this study, he added, is that patients should not start on methotrexate if they have abnormal liver function tests. That guidance was included in the original guidelines for methotrexate in RA published back in the mid-1990s.
“I think rheumatologists have kind of lost sight of that. You probably should find out why those tests are elevated. In many cases you’ll find it may be related to NASH [nonalcoholic steatohepatitis],” he said. “I actually think obesity is one of the greatest risk factors for methotrexate toxicity.”
Dr. Weinblatt reported receiving consulting fees or other remuneration from more than two dozen pharmaceutical companies.
SNOWMASS, COLO. – Can an old rheumatoid arthritis drug – like an old dog – learn new tricks?
When that drug is methotrexate, the answer is definitely yes, according to Dr. Michael E. Weinblatt, professor of medicine at Harvard Medical School, Boston.
Clinically important advances and refinements continue to be made in the use of this venerable drug, a treatment mainstay for RA since the mid-1980s.
“I had the pleasure of participating in a symposium on methotrexate organized by Dr. Joel Kremer at last year’s annual ACR meeting in Boston. This is the second one we’ve done, and I must tell you, the number of people in attendance was extraordinary. We probably filled one of the largest conference rooms for the second time in 2 years. And the questions went on forever. So even though methotrexate is an old drug, there still remains great interest in it,” he observed at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Here’s what’s new:
Subcutaneous methotrexate for RA is finally legit.
Multiple studies over the past 15 years have established that at methotrexate doses above 15-20 mg/week, subcutaneous therapy achieves superior efficacy, compared with oral therapy. For this reason, rheumatologists have long used once-weekly subcutaneous injections of methotrexate in RA patients with an inadequate clinical response to oral therapy. However, as payers have often informed them, this has been off-label usage. Not any longer. Rheumatoid arthritis is now an FDA-approved indication for subcutaneous methotrexate. Moreover, two easy-to-use, single-dose, once-weekly, autoinjector formulations are now on the market, known as Otrexup and Rasuvo.
In a randomized, crossover study of various doses of oral methotrexate versus Otrexup in 49 RA patients, the systemic bioavailability of oral methotrexate plateaued at doses of 15 mg/week or above. In contrast, the systemic exposure of subcutaneous methotrexate continued to increase linearly out to 25 mg/week, the highest dose studied. And this greater bioavailability wasn’t associated with an increase in adverse events (Ann. Rheum. Dis. 2014;73:1549-51).
Split-dose oral therapy improves bioavailability.
When methotrexate was first prescribed for RA in the mid-1980s, it was given in a pulsed-dose regimen: 8 a.m., 8 p.m., and again at 8 a.m. the next morning. Three doses over a 24-hour period, once weekly.
“Over time, most of us shifted to a once-a-week regimen for convenience, ease-of-administration, and because of some concerns about liver exposure. We’ve come to appreciate, however, that if you dose-escalate methotrexate, a significant percentage of patients do not absorb the drug at doses above 15-20 mg once weekly. But pharmacokinetic studies have demonstrated you get higher drug concentrations with a split dose,” according to the rheumatologist.
For example, a crossover study involving 10 patients on stable doses of oral methotrexate at 25-35 mg/week showed that splitting a dose into two halves given 8 hours apart resulted in 28% greater bioavailability, compared with the standard single dose. Indeed, the bioavailability with the oral split dose was comparable to that achieved with subcutaneous administration (J. Rheumatol. 2006;33:481-5).
“Many of us are now splitting the dose of methotrexate at doses above 17.5-20 mg/week. I would like to caution, however, that this does not mean you should give the drug on Mondays and Thursdays. This was studied 40 years ago at the [National Institutes of Health]. It caused more acute toxicity, including bone marrow suppression, and more chronic toxicity, such as liver disease. So the drug should only be administered over one 24-hour period per week,” Dr. Weinblatt advised.
Methotrexate: the next statin?
Four cohort studies over the past 10 years have reported that methotrexate appears to reduce cardiovascular mortality in RA patients. Registry data are also supportive. The evidence is sufficiently strong that a definitive randomized clinical trial is now well underway. This major study, known as the Cardiovascular Inflammation Reduction Trial (CIRT), is funded by the National Heart, Lung, and Blood Institute and led by renowned cardiologist Dr. Paul Ridker, the Eugene Braunwald Professor of Medicine at Harvard Medical School. It will enroll 7,000 subjects – none with RA – at roughly 350 U.S. and Canadian sites.
Participants are high–cardiovascular risk patients with a history of acute MI within the previous 5 years plus type 2 diabetes or metabolic syndrome. They are being randomized to guideline-directed medical care plus either oral methotrexate at 10-20 mg/week or placebo for 2-4 years. The primary endpoint is cardiovascular death, nonfatal MI, or stroke.
The proposed mechanism of benefit is methotrexate’s anti-inflammatory effect. If the results of CIRT are positive, this low-cost generic drug with a thoroughly understood safety profile could transform preventive cardiology; lowering systemic inflammation would potentially join LDL lowering via statins as a cornerstone of disease prevention.
“This is one of the most exciting areas involving methotrexate,” commented Dr. Weinblatt, a participating investigator in CIRT.
Methotrexate boosts efficacy of selected biologics.
Concomitant methotrexate is known to increase the clinical efficacy of anti–tumor necrosis factor biologics and rituximab. Studies in patients on infliximab or adalimumab have shown that background methotrexate raises serum concentrations of the biologics by 20%-25%, which is presumably the explanation for the increased efficacy. Whether methotrexate enhances or attenuates the efficacy of the oral small-molecule JAK inhibitors is now under study.
One intriguing cohort study has shown that methotrexate reduces the immunogenicity of adalimumab in dose-dependent fashion; the higher the dose of methotrexate, the less ability patients had to develop blocking antibodies against adalimumab (Ann. Rheum. Dis. 2012;71:1914-5).
More recently, the randomized, double-blind CONCERTO trial conducted in 395 methotrexate- and biologic-naive RA patients extended this work. Participants were randomized to open-label adalimumab plus weekly blinded methotrexate at 2.5, 5, 10, or 20 mg. Clinical outcomes at 26 weeks as reflected in 28-joint count disease activity score and other measures were significantly better in patients on 10 or 20 mg/week of methotrexate. Serum adalimumab levels were higher in patients on those doses of methotrexate than in those on 2.5 or 5 mg/week as well (Ann. Rheum. Dis. 2014 Feb. 18 [doi:10.1136/annrheumdis-2013-204769]).
There’s an important lesson here for patient management: “If you’re going to dose-reduce your methotrexate in patients with low disease activity or in remission, there is a threshold at which you should probably stop reducing the methotrexate, at least when your patient is on this biologic,” according to Dr. Weinblatt.
In contrast, no methotrexate dose-threshold effect occurs with etanercept, he added.
Methotrexate and the liver.
A national observational cohort study of 659 military veterans over age 65 when they started methotrexate for RA or other rheumatic diseases found a 6% incidence of moderately elevated liver enzymes during a mean follow-up period of 7 months. The investigators identified a series of independent risk factors for liver function test abnormalities. Obesity was associated with a 1.9-fold increased risk, a serum total cholesterol greater than 240 mg/dL conferred a 5.8-fold elevated risk, abnormal liver function tests premethotrexate was associated with a 3.2-fold increased risk, and lack of folic acid supplementation brought a 2.2-fold increase in risk (Arthritis Care Res. 2014;66:1159-66).
“This study confirms what a lot of us have been worried about,” Dr. Weinblatt commented. That is, the risk of methotrexate-related liver toxicity is particularly high in older patients with characteristics consistent with the metabolic syndrome, a condition that has reached epidemic proportions.
A strong take-home message from this study, he added, is that patients should not start on methotrexate if they have abnormal liver function tests. That guidance was included in the original guidelines for methotrexate in RA published back in the mid-1990s.
“I think rheumatologists have kind of lost sight of that. You probably should find out why those tests are elevated. In many cases you’ll find it may be related to NASH [nonalcoholic steatohepatitis],” he said. “I actually think obesity is one of the greatest risk factors for methotrexate toxicity.”
Dr. Weinblatt reported receiving consulting fees or other remuneration from more than two dozen pharmaceutical companies.
SNOWMASS, COLO. – Can an old rheumatoid arthritis drug – like an old dog – learn new tricks?
When that drug is methotrexate, the answer is definitely yes, according to Dr. Michael E. Weinblatt, professor of medicine at Harvard Medical School, Boston.
Clinically important advances and refinements continue to be made in the use of this venerable drug, a treatment mainstay for RA since the mid-1980s.
“I had the pleasure of participating in a symposium on methotrexate organized by Dr. Joel Kremer at last year’s annual ACR meeting in Boston. This is the second one we’ve done, and I must tell you, the number of people in attendance was extraordinary. We probably filled one of the largest conference rooms for the second time in 2 years. And the questions went on forever. So even though methotrexate is an old drug, there still remains great interest in it,” he observed at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Here’s what’s new:
Subcutaneous methotrexate for RA is finally legit.
Multiple studies over the past 15 years have established that at methotrexate doses above 15-20 mg/week, subcutaneous therapy achieves superior efficacy, compared with oral therapy. For this reason, rheumatologists have long used once-weekly subcutaneous injections of methotrexate in RA patients with an inadequate clinical response to oral therapy. However, as payers have often informed them, this has been off-label usage. Not any longer. Rheumatoid arthritis is now an FDA-approved indication for subcutaneous methotrexate. Moreover, two easy-to-use, single-dose, once-weekly, autoinjector formulations are now on the market, known as Otrexup and Rasuvo.
In a randomized, crossover study of various doses of oral methotrexate versus Otrexup in 49 RA patients, the systemic bioavailability of oral methotrexate plateaued at doses of 15 mg/week or above. In contrast, the systemic exposure of subcutaneous methotrexate continued to increase linearly out to 25 mg/week, the highest dose studied. And this greater bioavailability wasn’t associated with an increase in adverse events (Ann. Rheum. Dis. 2014;73:1549-51).
Split-dose oral therapy improves bioavailability.
When methotrexate was first prescribed for RA in the mid-1980s, it was given in a pulsed-dose regimen: 8 a.m., 8 p.m., and again at 8 a.m. the next morning. Three doses over a 24-hour period, once weekly.
“Over time, most of us shifted to a once-a-week regimen for convenience, ease-of-administration, and because of some concerns about liver exposure. We’ve come to appreciate, however, that if you dose-escalate methotrexate, a significant percentage of patients do not absorb the drug at doses above 15-20 mg once weekly. But pharmacokinetic studies have demonstrated you get higher drug concentrations with a split dose,” according to the rheumatologist.
For example, a crossover study involving 10 patients on stable doses of oral methotrexate at 25-35 mg/week showed that splitting a dose into two halves given 8 hours apart resulted in 28% greater bioavailability, compared with the standard single dose. Indeed, the bioavailability with the oral split dose was comparable to that achieved with subcutaneous administration (J. Rheumatol. 2006;33:481-5).
“Many of us are now splitting the dose of methotrexate at doses above 17.5-20 mg/week. I would like to caution, however, that this does not mean you should give the drug on Mondays and Thursdays. This was studied 40 years ago at the [National Institutes of Health]. It caused more acute toxicity, including bone marrow suppression, and more chronic toxicity, such as liver disease. So the drug should only be administered over one 24-hour period per week,” Dr. Weinblatt advised.
Methotrexate: the next statin?
Four cohort studies over the past 10 years have reported that methotrexate appears to reduce cardiovascular mortality in RA patients. Registry data are also supportive. The evidence is sufficiently strong that a definitive randomized clinical trial is now well underway. This major study, known as the Cardiovascular Inflammation Reduction Trial (CIRT), is funded by the National Heart, Lung, and Blood Institute and led by renowned cardiologist Dr. Paul Ridker, the Eugene Braunwald Professor of Medicine at Harvard Medical School. It will enroll 7,000 subjects – none with RA – at roughly 350 U.S. and Canadian sites.
Participants are high–cardiovascular risk patients with a history of acute MI within the previous 5 years plus type 2 diabetes or metabolic syndrome. They are being randomized to guideline-directed medical care plus either oral methotrexate at 10-20 mg/week or placebo for 2-4 years. The primary endpoint is cardiovascular death, nonfatal MI, or stroke.
The proposed mechanism of benefit is methotrexate’s anti-inflammatory effect. If the results of CIRT are positive, this low-cost generic drug with a thoroughly understood safety profile could transform preventive cardiology; lowering systemic inflammation would potentially join LDL lowering via statins as a cornerstone of disease prevention.
“This is one of the most exciting areas involving methotrexate,” commented Dr. Weinblatt, a participating investigator in CIRT.
Methotrexate boosts efficacy of selected biologics.
Concomitant methotrexate is known to increase the clinical efficacy of anti–tumor necrosis factor biologics and rituximab. Studies in patients on infliximab or adalimumab have shown that background methotrexate raises serum concentrations of the biologics by 20%-25%, which is presumably the explanation for the increased efficacy. Whether methotrexate enhances or attenuates the efficacy of the oral small-molecule JAK inhibitors is now under study.
One intriguing cohort study has shown that methotrexate reduces the immunogenicity of adalimumab in dose-dependent fashion; the higher the dose of methotrexate, the less ability patients had to develop blocking antibodies against adalimumab (Ann. Rheum. Dis. 2012;71:1914-5).
More recently, the randomized, double-blind CONCERTO trial conducted in 395 methotrexate- and biologic-naive RA patients extended this work. Participants were randomized to open-label adalimumab plus weekly blinded methotrexate at 2.5, 5, 10, or 20 mg. Clinical outcomes at 26 weeks as reflected in 28-joint count disease activity score and other measures were significantly better in patients on 10 or 20 mg/week of methotrexate. Serum adalimumab levels were higher in patients on those doses of methotrexate than in those on 2.5 or 5 mg/week as well (Ann. Rheum. Dis. 2014 Feb. 18 [doi:10.1136/annrheumdis-2013-204769]).
There’s an important lesson here for patient management: “If you’re going to dose-reduce your methotrexate in patients with low disease activity or in remission, there is a threshold at which you should probably stop reducing the methotrexate, at least when your patient is on this biologic,” according to Dr. Weinblatt.
In contrast, no methotrexate dose-threshold effect occurs with etanercept, he added.
Methotrexate and the liver.
A national observational cohort study of 659 military veterans over age 65 when they started methotrexate for RA or other rheumatic diseases found a 6% incidence of moderately elevated liver enzymes during a mean follow-up period of 7 months. The investigators identified a series of independent risk factors for liver function test abnormalities. Obesity was associated with a 1.9-fold increased risk, a serum total cholesterol greater than 240 mg/dL conferred a 5.8-fold elevated risk, abnormal liver function tests premethotrexate was associated with a 3.2-fold increased risk, and lack of folic acid supplementation brought a 2.2-fold increase in risk (Arthritis Care Res. 2014;66:1159-66).
“This study confirms what a lot of us have been worried about,” Dr. Weinblatt commented. That is, the risk of methotrexate-related liver toxicity is particularly high in older patients with characteristics consistent with the metabolic syndrome, a condition that has reached epidemic proportions.
A strong take-home message from this study, he added, is that patients should not start on methotrexate if they have abnormal liver function tests. That guidance was included in the original guidelines for methotrexate in RA published back in the mid-1990s.
“I think rheumatologists have kind of lost sight of that. You probably should find out why those tests are elevated. In many cases you’ll find it may be related to NASH [nonalcoholic steatohepatitis],” he said. “I actually think obesity is one of the greatest risk factors for methotrexate toxicity.”
Dr. Weinblatt reported receiving consulting fees or other remuneration from more than two dozen pharmaceutical companies.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM

Rituximab for RA: Think like a European
SNOWMASS, COLO. – When it comes to prescribing rituximab in patients with rheumatoid arthritis, maybe it’s time to think like a European.
In response to a persuasive French study, rheumatologists across Europe have embraced a lower-dose rituximab regimen: Patients who achieve a moderate or good EULAR response to the standard initial induction dosing of two 1,000-mg doses given intravenously 2 weeks apart receive thereafter a single 1,000-mg dose every 6 months rather than the licensed maintenance dosing of two 1,000-mg IV injections every 6 months.
“They showed that one dose every 6 months is as good as two doses every 6 months. This is a strategy that our European colleagues have actively adopted. It’s a cost-effective strategy, and I think it’s actually an appropriate strategy to use and one we’re using routinely now in our rheumatoid patients after we’ve induced a response with the initial induction dosing,” Dr. Michael E. Weinblatt, professor of medicine at Harvard Medical School, Boston, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
The French study was an open-label, prospective, multicenter, noninferiority study involving 225 rheumatoid arthritis patients with an inadequate response to anti–tumor necrosis factor (anti-TNF) agents and a 6-month moderate or good EULAR response to rituximab (Rituxan) induction therapy coupled with methotrexate. They were randomized to rituximab retreatment at 6-month intervals at either a single 1,000-mg dose or the two 1,000-mg doses as described in the product labeling. At 104 weeks, disease activity as measured by the mean disease activity in 28 joints plus C-reactive protein level area under the curve was similar in the two treatment arms. So was the safety profile (Ann. Rheum. Dis. 2014;73:1508-14).
Dr. Weinblatt also provided an update on rituximab and infections. Two studies presented at last fall’s annual meeting of the American College of Rheumatology in Boston shed new light on this perennially hot topic.
In one, Dr. Kenneth G. Saag of the University of Alabama, Birmingham, and coinvestigators provided an update from the ongoing prospective, observational SUNSTONE cohort study, whose goal is to evaluate in a real-world setting the safety of rituximab in rheumatoid arthritis patients refractory to anti-TNF therapies. At a mean 4-year duration of follow-up in 938 patients who received a mean of four courses of rituximab, 17% of patients had experienced significant infections as defined either by the Food and Drug Administration serious adverse event criteria or need for intravenous antibiotics. The key finding from this intermediate analysis: The serious infection incidence rate did not increase with time and multiple courses of rituximab.
That’s reassuring, Dr. Weinblatt observed, and so is the finding that, in the 338 SUNSTONE participants who switched from rituximab to another biologic agent, there wasn’t any associated increased risk of serious infection.
All of the biologics carry an increased risk of infection. The one rituximab-associated infection that gives rheumatologists particular pause – and that has blunted the use of the anti-B-cell agent in the United States – is progressive multifocal leukoencephalopathy (PML). Indeed, rituximab is the only biologic agent or small molecule prescribed by rheumatologists that carries a warning label about PML, and the only one whose use is restricted to patients who’ve failed a first biologic.
“That means you have to – and should – discuss this with your patients,” Dr. Weinblatt noted.
At last November’s annual ACR meeting, Dr. Leonard H. Calabrese of the Cleveland Clinic and Dr. Eamonn Molloy of St. Vincent University Hospital, Dublin, provided an analysis of data released in response to their Freedom of Information Act request that the FDA provide information on all cases of PML recorded in the agency’s Adverse Event Reporting System through August 2012. In Dr. Weinblatt’s view, these data are reassuring.
“The rates are actually quite low. It’s a rare event. It’s clearly associated with rituximab, though,” he said.
Indeed, 30 confirmed cases of PML have been associated with biologic therapies for autoimmune rheumatic diseases, including 11 in patients with RA, 11 with systemic lupus erythematosus, and 5 with dermato/polymyositis. The median age was 53 years, and 25 of the 30 patients were women. Twenty-six cases occurred in patients who had most recently been on rituximab, the other four in patients who were on anti-TNF therapies at the time. Abatacept, belimumab, tocilizumab, and anakinra were not linked to PML.
PML developed after a median of two courses of rituximab. The median time interval was 15 months from the first rituximab infusion and 5 months from the last, but many confounders were present, making it difficult to draw definitive conclusions about causality. For example, four patients with PML had been on concomitant rituximab and cyclophosphamide, and another five had received cyclophosphamide prior to going on rituximab. Eighteen of 26 rituximab-treated patients were on one or more additional immunosuppressive agents at the time they were diagnosed with PML. Two patients had previously received cancer chemotherapy. Another five had significant lymphopenia.
Dr. Weinblatt reported receiving consulting fees or other remuneration from more than two dozen pharmaceutical companies, including Genentech, which markets rituximab.
SNOWMASS, COLO. – When it comes to prescribing rituximab in patients with rheumatoid arthritis, maybe it’s time to think like a European.
In response to a persuasive French study, rheumatologists across Europe have embraced a lower-dose rituximab regimen: Patients who achieve a moderate or good EULAR response to the standard initial induction dosing of two 1,000-mg doses given intravenously 2 weeks apart receive thereafter a single 1,000-mg dose every 6 months rather than the licensed maintenance dosing of two 1,000-mg IV injections every 6 months.
“They showed that one dose every 6 months is as good as two doses every 6 months. This is a strategy that our European colleagues have actively adopted. It’s a cost-effective strategy, and I think it’s actually an appropriate strategy to use and one we’re using routinely now in our rheumatoid patients after we’ve induced a response with the initial induction dosing,” Dr. Michael E. Weinblatt, professor of medicine at Harvard Medical School, Boston, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
The French study was an open-label, prospective, multicenter, noninferiority study involving 225 rheumatoid arthritis patients with an inadequate response to anti–tumor necrosis factor (anti-TNF) agents and a 6-month moderate or good EULAR response to rituximab (Rituxan) induction therapy coupled with methotrexate. They were randomized to rituximab retreatment at 6-month intervals at either a single 1,000-mg dose or the two 1,000-mg doses as described in the product labeling. At 104 weeks, disease activity as measured by the mean disease activity in 28 joints plus C-reactive protein level area under the curve was similar in the two treatment arms. So was the safety profile (Ann. Rheum. Dis. 2014;73:1508-14).
Dr. Weinblatt also provided an update on rituximab and infections. Two studies presented at last fall’s annual meeting of the American College of Rheumatology in Boston shed new light on this perennially hot topic.
In one, Dr. Kenneth G. Saag of the University of Alabama, Birmingham, and coinvestigators provided an update from the ongoing prospective, observational SUNSTONE cohort study, whose goal is to evaluate in a real-world setting the safety of rituximab in rheumatoid arthritis patients refractory to anti-TNF therapies. At a mean 4-year duration of follow-up in 938 patients who received a mean of four courses of rituximab, 17% of patients had experienced significant infections as defined either by the Food and Drug Administration serious adverse event criteria or need for intravenous antibiotics. The key finding from this intermediate analysis: The serious infection incidence rate did not increase with time and multiple courses of rituximab.
That’s reassuring, Dr. Weinblatt observed, and so is the finding that, in the 338 SUNSTONE participants who switched from rituximab to another biologic agent, there wasn’t any associated increased risk of serious infection.
All of the biologics carry an increased risk of infection. The one rituximab-associated infection that gives rheumatologists particular pause – and that has blunted the use of the anti-B-cell agent in the United States – is progressive multifocal leukoencephalopathy (PML). Indeed, rituximab is the only biologic agent or small molecule prescribed by rheumatologists that carries a warning label about PML, and the only one whose use is restricted to patients who’ve failed a first biologic.
“That means you have to – and should – discuss this with your patients,” Dr. Weinblatt noted.
At last November’s annual ACR meeting, Dr. Leonard H. Calabrese of the Cleveland Clinic and Dr. Eamonn Molloy of St. Vincent University Hospital, Dublin, provided an analysis of data released in response to their Freedom of Information Act request that the FDA provide information on all cases of PML recorded in the agency’s Adverse Event Reporting System through August 2012. In Dr. Weinblatt’s view, these data are reassuring.
“The rates are actually quite low. It’s a rare event. It’s clearly associated with rituximab, though,” he said.
Indeed, 30 confirmed cases of PML have been associated with biologic therapies for autoimmune rheumatic diseases, including 11 in patients with RA, 11 with systemic lupus erythematosus, and 5 with dermato/polymyositis. The median age was 53 years, and 25 of the 30 patients were women. Twenty-six cases occurred in patients who had most recently been on rituximab, the other four in patients who were on anti-TNF therapies at the time. Abatacept, belimumab, tocilizumab, and anakinra were not linked to PML.
PML developed after a median of two courses of rituximab. The median time interval was 15 months from the first rituximab infusion and 5 months from the last, but many confounders were present, making it difficult to draw definitive conclusions about causality. For example, four patients with PML had been on concomitant rituximab and cyclophosphamide, and another five had received cyclophosphamide prior to going on rituximab. Eighteen of 26 rituximab-treated patients were on one or more additional immunosuppressive agents at the time they were diagnosed with PML. Two patients had previously received cancer chemotherapy. Another five had significant lymphopenia.
Dr. Weinblatt reported receiving consulting fees or other remuneration from more than two dozen pharmaceutical companies, including Genentech, which markets rituximab.
SNOWMASS, COLO. – When it comes to prescribing rituximab in patients with rheumatoid arthritis, maybe it’s time to think like a European.
In response to a persuasive French study, rheumatologists across Europe have embraced a lower-dose rituximab regimen: Patients who achieve a moderate or good EULAR response to the standard initial induction dosing of two 1,000-mg doses given intravenously 2 weeks apart receive thereafter a single 1,000-mg dose every 6 months rather than the licensed maintenance dosing of two 1,000-mg IV injections every 6 months.
“They showed that one dose every 6 months is as good as two doses every 6 months. This is a strategy that our European colleagues have actively adopted. It’s a cost-effective strategy, and I think it’s actually an appropriate strategy to use and one we’re using routinely now in our rheumatoid patients after we’ve induced a response with the initial induction dosing,” Dr. Michael E. Weinblatt, professor of medicine at Harvard Medical School, Boston, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
The French study was an open-label, prospective, multicenter, noninferiority study involving 225 rheumatoid arthritis patients with an inadequate response to anti–tumor necrosis factor (anti-TNF) agents and a 6-month moderate or good EULAR response to rituximab (Rituxan) induction therapy coupled with methotrexate. They were randomized to rituximab retreatment at 6-month intervals at either a single 1,000-mg dose or the two 1,000-mg doses as described in the product labeling. At 104 weeks, disease activity as measured by the mean disease activity in 28 joints plus C-reactive protein level area under the curve was similar in the two treatment arms. So was the safety profile (Ann. Rheum. Dis. 2014;73:1508-14).
Dr. Weinblatt also provided an update on rituximab and infections. Two studies presented at last fall’s annual meeting of the American College of Rheumatology in Boston shed new light on this perennially hot topic.
In one, Dr. Kenneth G. Saag of the University of Alabama, Birmingham, and coinvestigators provided an update from the ongoing prospective, observational SUNSTONE cohort study, whose goal is to evaluate in a real-world setting the safety of rituximab in rheumatoid arthritis patients refractory to anti-TNF therapies. At a mean 4-year duration of follow-up in 938 patients who received a mean of four courses of rituximab, 17% of patients had experienced significant infections as defined either by the Food and Drug Administration serious adverse event criteria or need for intravenous antibiotics. The key finding from this intermediate analysis: The serious infection incidence rate did not increase with time and multiple courses of rituximab.
That’s reassuring, Dr. Weinblatt observed, and so is the finding that, in the 338 SUNSTONE participants who switched from rituximab to another biologic agent, there wasn’t any associated increased risk of serious infection.
All of the biologics carry an increased risk of infection. The one rituximab-associated infection that gives rheumatologists particular pause – and that has blunted the use of the anti-B-cell agent in the United States – is progressive multifocal leukoencephalopathy (PML). Indeed, rituximab is the only biologic agent or small molecule prescribed by rheumatologists that carries a warning label about PML, and the only one whose use is restricted to patients who’ve failed a first biologic.
“That means you have to – and should – discuss this with your patients,” Dr. Weinblatt noted.
At last November’s annual ACR meeting, Dr. Leonard H. Calabrese of the Cleveland Clinic and Dr. Eamonn Molloy of St. Vincent University Hospital, Dublin, provided an analysis of data released in response to their Freedom of Information Act request that the FDA provide information on all cases of PML recorded in the agency’s Adverse Event Reporting System through August 2012. In Dr. Weinblatt’s view, these data are reassuring.
“The rates are actually quite low. It’s a rare event. It’s clearly associated with rituximab, though,” he said.
Indeed, 30 confirmed cases of PML have been associated with biologic therapies for autoimmune rheumatic diseases, including 11 in patients with RA, 11 with systemic lupus erythematosus, and 5 with dermato/polymyositis. The median age was 53 years, and 25 of the 30 patients were women. Twenty-six cases occurred in patients who had most recently been on rituximab, the other four in patients who were on anti-TNF therapies at the time. Abatacept, belimumab, tocilizumab, and anakinra were not linked to PML.
PML developed after a median of two courses of rituximab. The median time interval was 15 months from the first rituximab infusion and 5 months from the last, but many confounders were present, making it difficult to draw definitive conclusions about causality. For example, four patients with PML had been on concomitant rituximab and cyclophosphamide, and another five had received cyclophosphamide prior to going on rituximab. Eighteen of 26 rituximab-treated patients were on one or more additional immunosuppressive agents at the time they were diagnosed with PML. Two patients had previously received cancer chemotherapy. Another five had significant lymphopenia.
Dr. Weinblatt reported receiving consulting fees or other remuneration from more than two dozen pharmaceutical companies, including Genentech, which markets rituximab.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM
VIDEO: As biosimilars arrive in U.S., treatment questions arise
MAUI, HAWAII – There’s been fairly brisk uptake of biosimilar infliximab in Europe, both for new patients and as a possible switch from Remicade.
That biosimilar infliximab, Remsima, was submitted for U.S. approval in 2014, and a Food and Drug Administration advisory panel recently recommended approval of a biosimilar for filgrastim (Neupogen).
The agents are in the vanguard of what is sure to be an expanding market in the United States as biologics come off patent. Additional infliximab replacements are in the works, as well as biosimilars for etanercept, adalimumab, rituximab, and others.
For rheumatologists, that could mean less expensive treatments for patients, but it’s also likely to make treatment more complicated. Given the complexity of the molecules, the differences between biosimilars and familiar brands could be a bit more marked than those between small-molecule generics and their branded counterparts.
In a video interview at the 2015 Rheumatology Winter Clinical Symposium, Dr. Arthur F. Kavanaugh, a rheumatology professor at the University of California, San Diego, outlined the latest developments and shared his thoughts on the rapidly evolving field.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MAUI, HAWAII – There’s been fairly brisk uptake of biosimilar infliximab in Europe, both for new patients and as a possible switch from Remicade.
That biosimilar infliximab, Remsima, was submitted for U.S. approval in 2014, and a Food and Drug Administration advisory panel recently recommended approval of a biosimilar for filgrastim (Neupogen).
The agents are in the vanguard of what is sure to be an expanding market in the United States as biologics come off patent. Additional infliximab replacements are in the works, as well as biosimilars for etanercept, adalimumab, rituximab, and others.
For rheumatologists, that could mean less expensive treatments for patients, but it’s also likely to make treatment more complicated. Given the complexity of the molecules, the differences between biosimilars and familiar brands could be a bit more marked than those between small-molecule generics and their branded counterparts.
In a video interview at the 2015 Rheumatology Winter Clinical Symposium, Dr. Arthur F. Kavanaugh, a rheumatology professor at the University of California, San Diego, outlined the latest developments and shared his thoughts on the rapidly evolving field.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MAUI, HAWAII – There’s been fairly brisk uptake of biosimilar infliximab in Europe, both for new patients and as a possible switch from Remicade.
That biosimilar infliximab, Remsima, was submitted for U.S. approval in 2014, and a Food and Drug Administration advisory panel recently recommended approval of a biosimilar for filgrastim (Neupogen).
The agents are in the vanguard of what is sure to be an expanding market in the United States as biologics come off patent. Additional infliximab replacements are in the works, as well as biosimilars for etanercept, adalimumab, rituximab, and others.
For rheumatologists, that could mean less expensive treatments for patients, but it’s also likely to make treatment more complicated. Given the complexity of the molecules, the differences between biosimilars and familiar brands could be a bit more marked than those between small-molecule generics and their branded counterparts.
In a video interview at the 2015 Rheumatology Winter Clinical Symposium, Dr. Arthur F. Kavanaugh, a rheumatology professor at the University of California, San Diego, outlined the latest developments and shared his thoughts on the rapidly evolving field.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT RWCS 2015

New concerns rise over iatrogenic hydroxychloroquine retinopathy
SNOWMASS, COLO. – The risk of irreversible hydroxychloroquine toxic retinopathy is much greater than previously appreciated, Dr. James T. Rosenbaum cautioned at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“I remember when I was a fellow a paper was published saying Plaquenil [hydroxychloroquine] is safer than aspirin, it lowers lipids, and everyone should be taking it,” recalled Dr. Rosenbaum, professor of inflammatory diseases and chief of the division of arthritis and rheumatic diseases at Oregon Health and Science University, and chief of ophthalmology at the Devers Eye Institute in Portland, Ore.
He doesn’t feel that way anymore.
Dr. Rosenbaum highlighted a major recent study from Kaiser Permanente of Northern California which underscored the retinal hazards of long-term hydroxychloroquine. The retrospective, case-control study included 2,361 Kaiser Permanente patients who used the drug continuously for at least 5 years.
Evaluation by visual field testing and/or spectral domain optical coherence tomography (OCT) showed the overall prevalence of retinal thinning and photoreceptor damage or visual field loss was 7.5%. The risk climbed with greater daily dosage and duration of therapy, reaching a prevalence of nearly 20% after 20 years on hydroxychloroquine (JAMA Ophthalmol. 2014;132:1453-60).
“This really shakes my belief,” Dr. Rosenbaum confessed. “I really thought that anyone could take hydroxychloroquine with great impunity, but it turns out we really have to be careful with the dosage and the duration of therapy. I think we probably should routinely be reducing the dosage after 5 years of use, and in females who are under 5’6” we might need to be adjusting the dosage.
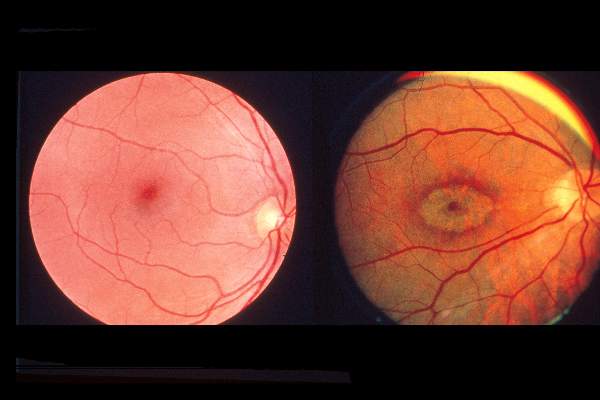
“Look, I think hydroxychloroquine is the greatest drug. I think everyone with rheumatoid arthritis and lupus should be on hydroxychloroquine. But I do think that after 5 years you want to monitor, and you should start thinking about having the patient take the drug 12 times per week instead of 14 times per week,” he added.
Dr. Rosenbaum called OCT “an absolutely invaluable diagnostic technique.” It provides objective findings enabling physicians to catch hydroxychloroquine retinopathy early, well before development of the classic hydroxychloroquine-induced severe bullseye maculopathy.
With no risk to the patient, the OCT laser reflects off the eye, permitting close inspection of the nine layers of the retina. Toxicity due to hydroxychloroquine or other antimalarials is manifest in what ophthalmologists call the flying saucer sign or sombrero sign because of its distinctive appearance, the result of fovial thinning and loss of the inner segment/outer segment junction.
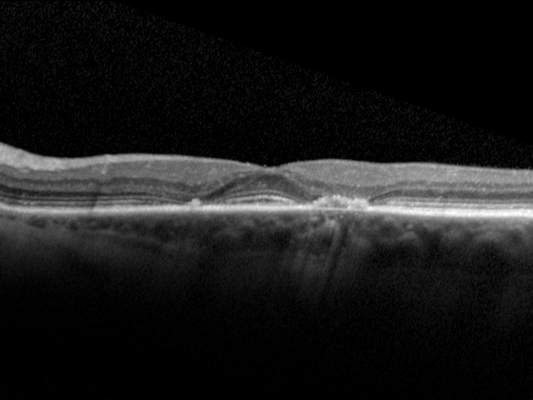
Dr. Rosenbaum credited Dr. Michael F. Marmor, professor of ophthalmology at Stanford (Calif.) University, as the driving force behind the new appreciation of the full scope of hydroxychloroquine toxic retinopathy. Dr. Marmor was coauthor of the recent Kaiser Permanente study and has also collaborated with rheumatologist Dr. Fred Wolfe of the National Databank for Rheumatic Diseases in a large study (Arthritis Care Res. 2010;62:775-84). In addition, Dr. Marmor chaired the American Academy of Ophthalmology committee that drew up revised guidelines for screening for hydroxychloroquine retinopathy (Ophthalmology 2011;118:415-22).
Those guidelines call for screening when a patient first goes on hydroxychloroquine and then not again until the 5-year mark, since toxicity is rare within the first 5 years of treatment. After 5 years of use, annual screening is recommended. The screening should include a visual field exam as well as one of the advanced objective technologies: spectral domain OCT, autofluorescence, or multifocal electroretinography. Use of the outmoded Amsler grid is discouraged.
Dr. Rosenbaum advised his colleagues to send their patients to a practitioner who utilizes spectral domain OCT.
“Multifocal ERG is painful, time consuming, and you wouldn’t want to undergo it. Autofluorescence is equally as good as OCT but not as many centers do it; optometrists now often have OCT in their office,” he observed.
The Kaiser Permanente study identified several key risk factors for hydroxychloroquine retinopathy. The investigators were unable to identify a safe dosage of hydroxychloroquine, but they noted that for daily consumption of 4.0-5.0 mg/kg of real body weight, the prevalence was low – less than 2% – for the first 10 years of use. However, the prevalence climbed sharply thereafter. The researchers determined that real body weight predicted risk better than did ideal weight and should be used by clinicians in their dosing calculations. Patients on more than 5.0 mg/kg of real body weight daily had a 5.7-fold greater prevalence of hydroxychloroquine retinopathy.
Chronic kidney disease, defined as an estimated glomerular filtration rate below 60 mL/min, was associated with a twofold increased risk. Concurrent use of tamoxifen – a drug that appears to be toxic to the retina in its own right – was associated with a 4.6-fold increased risk of hydroxychloroquine retinopathy.
Audience members at the symposium asked how worried they and their patients really need to be, and just how often these subtle early abnormalities translate to functional visual impairment.
“When you can see the structural damage and see the damage functionally on the field exam, and you know that it’s going to increase over time, I think you need an awfully good lawyer to continue with the use of therapy,” Dr. Rosenbaum replied. “This is early change, and many patients may not even be aware of it. But I would much rather find it early than persist with treatment. And I’m thankful that now we have a mechanism to prevent it from progressing.”
Does the retinopathy reverse upon drug discontinuation? “Maybe a smidgen, but it’s neurologic damage. I think for the most part, if you catch it early and it stabilizes, that’s the best we can do,” according to Dr. Rosenbaum.
And remember: Eighty percent of people who have taken hydroxychloroquine for 20 years do not have retinal toxicity, he added.
Dr. Rosenbaum reported receiving consulting fees from a dozen pharmaceutical companies and research grants from AbbVie, Eyegate, Genentech, and pSivida.
SNOWMASS, COLO. – The risk of irreversible hydroxychloroquine toxic retinopathy is much greater than previously appreciated, Dr. James T. Rosenbaum cautioned at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“I remember when I was a fellow a paper was published saying Plaquenil [hydroxychloroquine] is safer than aspirin, it lowers lipids, and everyone should be taking it,” recalled Dr. Rosenbaum, professor of inflammatory diseases and chief of the division of arthritis and rheumatic diseases at Oregon Health and Science University, and chief of ophthalmology at the Devers Eye Institute in Portland, Ore.
He doesn’t feel that way anymore.
Dr. Rosenbaum highlighted a major recent study from Kaiser Permanente of Northern California which underscored the retinal hazards of long-term hydroxychloroquine. The retrospective, case-control study included 2,361 Kaiser Permanente patients who used the drug continuously for at least 5 years.
Evaluation by visual field testing and/or spectral domain optical coherence tomography (OCT) showed the overall prevalence of retinal thinning and photoreceptor damage or visual field loss was 7.5%. The risk climbed with greater daily dosage and duration of therapy, reaching a prevalence of nearly 20% after 20 years on hydroxychloroquine (JAMA Ophthalmol. 2014;132:1453-60).
“This really shakes my belief,” Dr. Rosenbaum confessed. “I really thought that anyone could take hydroxychloroquine with great impunity, but it turns out we really have to be careful with the dosage and the duration of therapy. I think we probably should routinely be reducing the dosage after 5 years of use, and in females who are under 5’6” we might need to be adjusting the dosage.
“Look, I think hydroxychloroquine is the greatest drug. I think everyone with rheumatoid arthritis and lupus should be on hydroxychloroquine. But I do think that after 5 years you want to monitor, and you should start thinking about having the patient take the drug 12 times per week instead of 14 times per week,” he added.
Dr. Rosenbaum called OCT “an absolutely invaluable diagnostic technique.” It provides objective findings enabling physicians to catch hydroxychloroquine retinopathy early, well before development of the classic hydroxychloroquine-induced severe bullseye maculopathy.
With no risk to the patient, the OCT laser reflects off the eye, permitting close inspection of the nine layers of the retina. Toxicity due to hydroxychloroquine or other antimalarials is manifest in what ophthalmologists call the flying saucer sign or sombrero sign because of its distinctive appearance, the result of fovial thinning and loss of the inner segment/outer segment junction.
Dr. Rosenbaum credited Dr. Michael F. Marmor, professor of ophthalmology at Stanford (Calif.) University, as the driving force behind the new appreciation of the full scope of hydroxychloroquine toxic retinopathy. Dr. Marmor was coauthor of the recent Kaiser Permanente study and has also collaborated with rheumatologist Dr. Fred Wolfe of the National Databank for Rheumatic Diseases in a large study (Arthritis Care Res. 2010;62:775-84). In addition, Dr. Marmor chaired the American Academy of Ophthalmology committee that drew up revised guidelines for screening for hydroxychloroquine retinopathy (Ophthalmology 2011;118:415-22).
Those guidelines call for screening when a patient first goes on hydroxychloroquine and then not again until the 5-year mark, since toxicity is rare within the first 5 years of treatment. After 5 years of use, annual screening is recommended. The screening should include a visual field exam as well as one of the advanced objective technologies: spectral domain OCT, autofluorescence, or multifocal electroretinography. Use of the outmoded Amsler grid is discouraged.
Dr. Rosenbaum advised his colleagues to send their patients to a practitioner who utilizes spectral domain OCT.
“Multifocal ERG is painful, time consuming, and you wouldn’t want to undergo it. Autofluorescence is equally as good as OCT but not as many centers do it; optometrists now often have OCT in their office,” he observed.
The Kaiser Permanente study identified several key risk factors for hydroxychloroquine retinopathy. The investigators were unable to identify a safe dosage of hydroxychloroquine, but they noted that for daily consumption of 4.0-5.0 mg/kg of real body weight, the prevalence was low – less than 2% – for the first 10 years of use. However, the prevalence climbed sharply thereafter. The researchers determined that real body weight predicted risk better than did ideal weight and should be used by clinicians in their dosing calculations. Patients on more than 5.0 mg/kg of real body weight daily had a 5.7-fold greater prevalence of hydroxychloroquine retinopathy.
Chronic kidney disease, defined as an estimated glomerular filtration rate below 60 mL/min, was associated with a twofold increased risk. Concurrent use of tamoxifen – a drug that appears to be toxic to the retina in its own right – was associated with a 4.6-fold increased risk of hydroxychloroquine retinopathy.
Audience members at the symposium asked how worried they and their patients really need to be, and just how often these subtle early abnormalities translate to functional visual impairment.
“When you can see the structural damage and see the damage functionally on the field exam, and you know that it’s going to increase over time, I think you need an awfully good lawyer to continue with the use of therapy,” Dr. Rosenbaum replied. “This is early change, and many patients may not even be aware of it. But I would much rather find it early than persist with treatment. And I’m thankful that now we have a mechanism to prevent it from progressing.”
Does the retinopathy reverse upon drug discontinuation? “Maybe a smidgen, but it’s neurologic damage. I think for the most part, if you catch it early and it stabilizes, that’s the best we can do,” according to Dr. Rosenbaum.
And remember: Eighty percent of people who have taken hydroxychloroquine for 20 years do not have retinal toxicity, he added.
Dr. Rosenbaum reported receiving consulting fees from a dozen pharmaceutical companies and research grants from AbbVie, Eyegate, Genentech, and pSivida.
SNOWMASS, COLO. – The risk of irreversible hydroxychloroquine toxic retinopathy is much greater than previously appreciated, Dr. James T. Rosenbaum cautioned at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“I remember when I was a fellow a paper was published saying Plaquenil [hydroxychloroquine] is safer than aspirin, it lowers lipids, and everyone should be taking it,” recalled Dr. Rosenbaum, professor of inflammatory diseases and chief of the division of arthritis and rheumatic diseases at Oregon Health and Science University, and chief of ophthalmology at the Devers Eye Institute in Portland, Ore.
He doesn’t feel that way anymore.
Dr. Rosenbaum highlighted a major recent study from Kaiser Permanente of Northern California which underscored the retinal hazards of long-term hydroxychloroquine. The retrospective, case-control study included 2,361 Kaiser Permanente patients who used the drug continuously for at least 5 years.
Evaluation by visual field testing and/or spectral domain optical coherence tomography (OCT) showed the overall prevalence of retinal thinning and photoreceptor damage or visual field loss was 7.5%. The risk climbed with greater daily dosage and duration of therapy, reaching a prevalence of nearly 20% after 20 years on hydroxychloroquine (JAMA Ophthalmol. 2014;132:1453-60).
“This really shakes my belief,” Dr. Rosenbaum confessed. “I really thought that anyone could take hydroxychloroquine with great impunity, but it turns out we really have to be careful with the dosage and the duration of therapy. I think we probably should routinely be reducing the dosage after 5 years of use, and in females who are under 5’6” we might need to be adjusting the dosage.
“Look, I think hydroxychloroquine is the greatest drug. I think everyone with rheumatoid arthritis and lupus should be on hydroxychloroquine. But I do think that after 5 years you want to monitor, and you should start thinking about having the patient take the drug 12 times per week instead of 14 times per week,” he added.
Dr. Rosenbaum called OCT “an absolutely invaluable diagnostic technique.” It provides objective findings enabling physicians to catch hydroxychloroquine retinopathy early, well before development of the classic hydroxychloroquine-induced severe bullseye maculopathy.
With no risk to the patient, the OCT laser reflects off the eye, permitting close inspection of the nine layers of the retina. Toxicity due to hydroxychloroquine or other antimalarials is manifest in what ophthalmologists call the flying saucer sign or sombrero sign because of its distinctive appearance, the result of fovial thinning and loss of the inner segment/outer segment junction.
Dr. Rosenbaum credited Dr. Michael F. Marmor, professor of ophthalmology at Stanford (Calif.) University, as the driving force behind the new appreciation of the full scope of hydroxychloroquine toxic retinopathy. Dr. Marmor was coauthor of the recent Kaiser Permanente study and has also collaborated with rheumatologist Dr. Fred Wolfe of the National Databank for Rheumatic Diseases in a large study (Arthritis Care Res. 2010;62:775-84). In addition, Dr. Marmor chaired the American Academy of Ophthalmology committee that drew up revised guidelines for screening for hydroxychloroquine retinopathy (Ophthalmology 2011;118:415-22).
Those guidelines call for screening when a patient first goes on hydroxychloroquine and then not again until the 5-year mark, since toxicity is rare within the first 5 years of treatment. After 5 years of use, annual screening is recommended. The screening should include a visual field exam as well as one of the advanced objective technologies: spectral domain OCT, autofluorescence, or multifocal electroretinography. Use of the outmoded Amsler grid is discouraged.
Dr. Rosenbaum advised his colleagues to send their patients to a practitioner who utilizes spectral domain OCT.
“Multifocal ERG is painful, time consuming, and you wouldn’t want to undergo it. Autofluorescence is equally as good as OCT but not as many centers do it; optometrists now often have OCT in their office,” he observed.
The Kaiser Permanente study identified several key risk factors for hydroxychloroquine retinopathy. The investigators were unable to identify a safe dosage of hydroxychloroquine, but they noted that for daily consumption of 4.0-5.0 mg/kg of real body weight, the prevalence was low – less than 2% – for the first 10 years of use. However, the prevalence climbed sharply thereafter. The researchers determined that real body weight predicted risk better than did ideal weight and should be used by clinicians in their dosing calculations. Patients on more than 5.0 mg/kg of real body weight daily had a 5.7-fold greater prevalence of hydroxychloroquine retinopathy.
Chronic kidney disease, defined as an estimated glomerular filtration rate below 60 mL/min, was associated with a twofold increased risk. Concurrent use of tamoxifen – a drug that appears to be toxic to the retina in its own right – was associated with a 4.6-fold increased risk of hydroxychloroquine retinopathy.
Audience members at the symposium asked how worried they and their patients really need to be, and just how often these subtle early abnormalities translate to functional visual impairment.
“When you can see the structural damage and see the damage functionally on the field exam, and you know that it’s going to increase over time, I think you need an awfully good lawyer to continue with the use of therapy,” Dr. Rosenbaum replied. “This is early change, and many patients may not even be aware of it. But I would much rather find it early than persist with treatment. And I’m thankful that now we have a mechanism to prevent it from progressing.”
Does the retinopathy reverse upon drug discontinuation? “Maybe a smidgen, but it’s neurologic damage. I think for the most part, if you catch it early and it stabilizes, that’s the best we can do,” according to Dr. Rosenbaum.
And remember: Eighty percent of people who have taken hydroxychloroquine for 20 years do not have retinal toxicity, he added.
Dr. Rosenbaum reported receiving consulting fees from a dozen pharmaceutical companies and research grants from AbbVie, Eyegate, Genentech, and pSivida.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM
Acute RA flares increase risk of cardiovascular disease
Exposure to acute flares of rheumatoid arthritis significantly increases the risk of cardiovascular diseases, according to findings from a population-based cohort study conducted by Dr. Elena Myasoedova and her associates.
Each exposure to a rheumatoid arthritis (RA) flare lasting 6 weeks increased the risk of cardiovascular disease (CVD) by about 7% in the study of 525 patients aged 30 years or older who were identified during 1988-2007 as meeting 1987 American College of Rheumatology criteria for RA. CVD risk for RA patients in remission was similar to a random sample of patients without RA with similar age and sex. Patients who had increased cumulative moving averages in daily calculations of two methods for estimating RA severity, the RA medical Records-Based Index of Severity (RARBIS) and Claims-Based Index of RA Severity (CIRAS), had significantly higher risk of CVD (hazard ratios, 1.16 and 1.38, respectively). For each year spent in the highest CIRAS tertile, CVD risk rose by 18% when compared with time in the lowest tertile, the investigators found.
“These findings imply important cardiovascular benefits associated with improved flare management and tight inflammation control in RA,” the researchers concluded.
Read the full study published Jan. 30 in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-206411).
Exposure to acute flares of rheumatoid arthritis significantly increases the risk of cardiovascular diseases, according to findings from a population-based cohort study conducted by Dr. Elena Myasoedova and her associates.
Each exposure to a rheumatoid arthritis (RA) flare lasting 6 weeks increased the risk of cardiovascular disease (CVD) by about 7% in the study of 525 patients aged 30 years or older who were identified during 1988-2007 as meeting 1987 American College of Rheumatology criteria for RA. CVD risk for RA patients in remission was similar to a random sample of patients without RA with similar age and sex. Patients who had increased cumulative moving averages in daily calculations of two methods for estimating RA severity, the RA medical Records-Based Index of Severity (RARBIS) and Claims-Based Index of RA Severity (CIRAS), had significantly higher risk of CVD (hazard ratios, 1.16 and 1.38, respectively). For each year spent in the highest CIRAS tertile, CVD risk rose by 18% when compared with time in the lowest tertile, the investigators found.
“These findings imply important cardiovascular benefits associated with improved flare management and tight inflammation control in RA,” the researchers concluded.
Read the full study published Jan. 30 in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-206411).
Exposure to acute flares of rheumatoid arthritis significantly increases the risk of cardiovascular diseases, according to findings from a population-based cohort study conducted by Dr. Elena Myasoedova and her associates.
Each exposure to a rheumatoid arthritis (RA) flare lasting 6 weeks increased the risk of cardiovascular disease (CVD) by about 7% in the study of 525 patients aged 30 years or older who were identified during 1988-2007 as meeting 1987 American College of Rheumatology criteria for RA. CVD risk for RA patients in remission was similar to a random sample of patients without RA with similar age and sex. Patients who had increased cumulative moving averages in daily calculations of two methods for estimating RA severity, the RA medical Records-Based Index of Severity (RARBIS) and Claims-Based Index of RA Severity (CIRAS), had significantly higher risk of CVD (hazard ratios, 1.16 and 1.38, respectively). For each year spent in the highest CIRAS tertile, CVD risk rose by 18% when compared with time in the lowest tertile, the investigators found.
“These findings imply important cardiovascular benefits associated with improved flare management and tight inflammation control in RA,” the researchers concluded.
Read the full study published Jan. 30 in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-206411).
RA risk lowered by recent gastrointestinal and urogenital infections
People with gastrointestinal or urogenital infections in the 2 years prior to answering a questionnaire had significantly lower odds of having rheumatoid arthritis in a Swedish population-based case-control study, Dr. Maria E. C. Sandberg and her associates reported.
Gastroenteritis, urinary tract infections, and genital infections were significantly associated with a lower likelihood of having rheumatoid arthritis. Prostatitis, a much less common disease, had a protective effect at a similar magnitude, but a smaller sample size meant the association was not statistically significant. No association was found for sinusitis, tonsillitis, and pneumonia.
The sites of infections that conferred a decreased risk in the study were primarily infected with gram-negative bacteria, while the sites in which infections did not confer a decreased risk were primarily infected with gram-positive bacteria, the researchers noted.
The investigators noted that the findings “could be particularly interesting in light of emerging data implicating that the microbiome in the gut may play a role in RA pathogenesis since mucosal sites are exposed to a high load of bacterial antigens and may thus represent the site of initiation or modification of inflammation in RA.”
Read the full article published online Feb. 4 in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-206493).
People with gastrointestinal or urogenital infections in the 2 years prior to answering a questionnaire had significantly lower odds of having rheumatoid arthritis in a Swedish population-based case-control study, Dr. Maria E. C. Sandberg and her associates reported.
Gastroenteritis, urinary tract infections, and genital infections were significantly associated with a lower likelihood of having rheumatoid arthritis. Prostatitis, a much less common disease, had a protective effect at a similar magnitude, but a smaller sample size meant the association was not statistically significant. No association was found for sinusitis, tonsillitis, and pneumonia.
The sites of infections that conferred a decreased risk in the study were primarily infected with gram-negative bacteria, while the sites in which infections did not confer a decreased risk were primarily infected with gram-positive bacteria, the researchers noted.
The investigators noted that the findings “could be particularly interesting in light of emerging data implicating that the microbiome in the gut may play a role in RA pathogenesis since mucosal sites are exposed to a high load of bacterial antigens and may thus represent the site of initiation or modification of inflammation in RA.”
Read the full article published online Feb. 4 in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-206493).
People with gastrointestinal or urogenital infections in the 2 years prior to answering a questionnaire had significantly lower odds of having rheumatoid arthritis in a Swedish population-based case-control study, Dr. Maria E. C. Sandberg and her associates reported.
Gastroenteritis, urinary tract infections, and genital infections were significantly associated with a lower likelihood of having rheumatoid arthritis. Prostatitis, a much less common disease, had a protective effect at a similar magnitude, but a smaller sample size meant the association was not statistically significant. No association was found for sinusitis, tonsillitis, and pneumonia.
The sites of infections that conferred a decreased risk in the study were primarily infected with gram-negative bacteria, while the sites in which infections did not confer a decreased risk were primarily infected with gram-positive bacteria, the researchers noted.
The investigators noted that the findings “could be particularly interesting in light of emerging data implicating that the microbiome in the gut may play a role in RA pathogenesis since mucosal sites are exposed to a high load of bacterial antigens and may thus represent the site of initiation or modification of inflammation in RA.”
Read the full article published online Feb. 4 in Annals of the Rheumatic Diseases (doi:10.1136/annrheumdis-2014-206493).