User login
SNOWMASS, COLO. – The risk of irreversible hydroxychloroquine toxic retinopathy is much greater than previously appreciated, Dr. James T. Rosenbaum cautioned at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“I remember when I was a fellow a paper was published saying Plaquenil [hydroxychloroquine] is safer than aspirin, it lowers lipids, and everyone should be taking it,” recalled Dr. Rosenbaum, professor of inflammatory diseases and chief of the division of arthritis and rheumatic diseases at Oregon Health and Science University, and chief of ophthalmology at the Devers Eye Institute in Portland, Ore.
He doesn’t feel that way anymore.
Dr. Rosenbaum highlighted a major recent study from Kaiser Permanente of Northern California which underscored the retinal hazards of long-term hydroxychloroquine. The retrospective, case-control study included 2,361 Kaiser Permanente patients who used the drug continuously for at least 5 years.
Evaluation by visual field testing and/or spectral domain optical coherence tomography (OCT) showed the overall prevalence of retinal thinning and photoreceptor damage or visual field loss was 7.5%. The risk climbed with greater daily dosage and duration of therapy, reaching a prevalence of nearly 20% after 20 years on hydroxychloroquine (JAMA Ophthalmol. 2014;132:1453-60).
“This really shakes my belief,” Dr. Rosenbaum confessed. “I really thought that anyone could take hydroxychloroquine with great impunity, but it turns out we really have to be careful with the dosage and the duration of therapy. I think we probably should routinely be reducing the dosage after 5 years of use, and in females who are under 5’6” we might need to be adjusting the dosage.
“Look, I think hydroxychloroquine is the greatest drug. I think everyone with rheumatoid arthritis and lupus should be on hydroxychloroquine. But I do think that after 5 years you want to monitor, and you should start thinking about having the patient take the drug 12 times per week instead of 14 times per week,” he added.
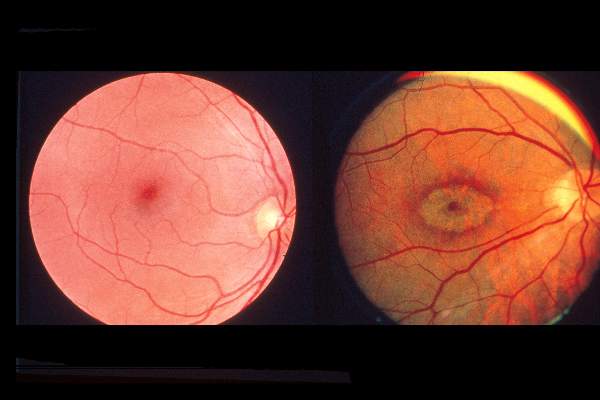
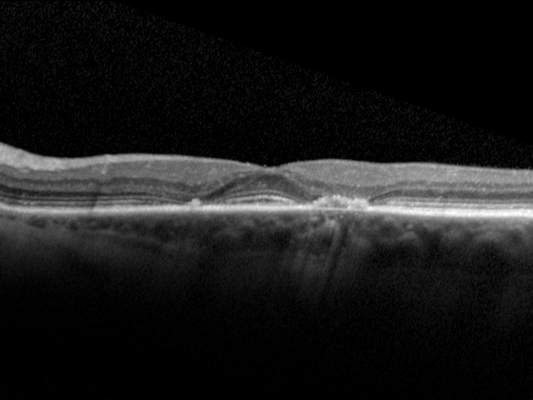
Dr. Rosenbaum called OCT “an absolutely invaluable diagnostic technique.” It provides objective findings enabling physicians to catch hydroxychloroquine retinopathy early, well before development of the classic hydroxychloroquine-induced severe bullseye maculopathy.
With no risk to the patient, the OCT laser reflects off the eye, permitting close inspection of the nine layers of the retina. Toxicity due to hydroxychloroquine or other antimalarials is manifest in what ophthalmologists call the flying saucer sign or sombrero sign because of its distinctive appearance, the result of fovial thinning and loss of the inner segment/outer segment junction.
Dr. Rosenbaum credited Dr. Michael F. Marmor, professor of ophthalmology at Stanford (Calif.) University, as the driving force behind the new appreciation of the full scope of hydroxychloroquine toxic retinopathy. Dr. Marmor was coauthor of the recent Kaiser Permanente study and has also collaborated with rheumatologist Dr. Fred Wolfe of the National Databank for Rheumatic Diseases in a large study (Arthritis Care Res. 2010;62:775-84). In addition, Dr. Marmor chaired the American Academy of Ophthalmology committee that drew up revised guidelines for screening for hydroxychloroquine retinopathy (Ophthalmology 2011;118:415-22).
Those guidelines call for screening when a patient first goes on hydroxychloroquine and then not again until the 5-year mark, since toxicity is rare within the first 5 years of treatment. After 5 years of use, annual screening is recommended. The screening should include a visual field exam as well as one of the advanced objective technologies: spectral domain OCT, autofluorescence, or multifocal electroretinography. Use of the outmoded Amsler grid is discouraged.
Dr. Rosenbaum advised his colleagues to send their patients to a practitioner who utilizes spectral domain OCT.
“Multifocal ERG is painful, time consuming, and you wouldn’t want to undergo it. Autofluorescence is equally as good as OCT but not as many centers do it; optometrists now often have OCT in their office,” he observed.
The Kaiser Permanente study identified several key risk factors for hydroxychloroquine retinopathy. The investigators were unable to identify a safe dosage of hydroxychloroquine, but they noted that for daily consumption of 4.0-5.0 mg/kg of real body weight, the prevalence was low – less than 2% – for the first 10 years of use. However, the prevalence climbed sharply thereafter. The researchers determined that real body weight predicted risk better than did ideal weight and should be used by clinicians in their dosing calculations. Patients on more than 5.0 mg/kg of real body weight daily had a 5.7-fold greater prevalence of hydroxychloroquine retinopathy.
Chronic kidney disease, defined as an estimated glomerular filtration rate below 60 mL/min, was associated with a twofold increased risk. Concurrent use of tamoxifen – a drug that appears to be toxic to the retina in its own right – was associated with a 4.6-fold increased risk of hydroxychloroquine retinopathy.
Audience members at the symposium asked how worried they and their patients really need to be, and just how often these subtle early abnormalities translate to functional visual impairment.
“When you can see the structural damage and see the damage functionally on the field exam, and you know that it’s going to increase over time, I think you need an awfully good lawyer to continue with the use of therapy,” Dr. Rosenbaum replied. “This is early change, and many patients may not even be aware of it. But I would much rather find it early than persist with treatment. And I’m thankful that now we have a mechanism to prevent it from progressing.”
Does the retinopathy reverse upon drug discontinuation? “Maybe a smidgen, but it’s neurologic damage. I think for the most part, if you catch it early and it stabilizes, that’s the best we can do,” according to Dr. Rosenbaum.
And remember: Eighty percent of people who have taken hydroxychloroquine for 20 years do not have retinal toxicity, he added.
Dr. Rosenbaum reported receiving consulting fees from a dozen pharmaceutical companies and research grants from AbbVie, Eyegate, Genentech, and pSivida.
SNOWMASS, COLO. – The risk of irreversible hydroxychloroquine toxic retinopathy is much greater than previously appreciated, Dr. James T. Rosenbaum cautioned at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“I remember when I was a fellow a paper was published saying Plaquenil [hydroxychloroquine] is safer than aspirin, it lowers lipids, and everyone should be taking it,” recalled Dr. Rosenbaum, professor of inflammatory diseases and chief of the division of arthritis and rheumatic diseases at Oregon Health and Science University, and chief of ophthalmology at the Devers Eye Institute in Portland, Ore.
He doesn’t feel that way anymore.
Dr. Rosenbaum highlighted a major recent study from Kaiser Permanente of Northern California which underscored the retinal hazards of long-term hydroxychloroquine. The retrospective, case-control study included 2,361 Kaiser Permanente patients who used the drug continuously for at least 5 years.
Evaluation by visual field testing and/or spectral domain optical coherence tomography (OCT) showed the overall prevalence of retinal thinning and photoreceptor damage or visual field loss was 7.5%. The risk climbed with greater daily dosage and duration of therapy, reaching a prevalence of nearly 20% after 20 years on hydroxychloroquine (JAMA Ophthalmol. 2014;132:1453-60).
“This really shakes my belief,” Dr. Rosenbaum confessed. “I really thought that anyone could take hydroxychloroquine with great impunity, but it turns out we really have to be careful with the dosage and the duration of therapy. I think we probably should routinely be reducing the dosage after 5 years of use, and in females who are under 5’6” we might need to be adjusting the dosage.
“Look, I think hydroxychloroquine is the greatest drug. I think everyone with rheumatoid arthritis and lupus should be on hydroxychloroquine. But I do think that after 5 years you want to monitor, and you should start thinking about having the patient take the drug 12 times per week instead of 14 times per week,” he added.
Dr. Rosenbaum called OCT “an absolutely invaluable diagnostic technique.” It provides objective findings enabling physicians to catch hydroxychloroquine retinopathy early, well before development of the classic hydroxychloroquine-induced severe bullseye maculopathy.
With no risk to the patient, the OCT laser reflects off the eye, permitting close inspection of the nine layers of the retina. Toxicity due to hydroxychloroquine or other antimalarials is manifest in what ophthalmologists call the flying saucer sign or sombrero sign because of its distinctive appearance, the result of fovial thinning and loss of the inner segment/outer segment junction.
Dr. Rosenbaum credited Dr. Michael F. Marmor, professor of ophthalmology at Stanford (Calif.) University, as the driving force behind the new appreciation of the full scope of hydroxychloroquine toxic retinopathy. Dr. Marmor was coauthor of the recent Kaiser Permanente study and has also collaborated with rheumatologist Dr. Fred Wolfe of the National Databank for Rheumatic Diseases in a large study (Arthritis Care Res. 2010;62:775-84). In addition, Dr. Marmor chaired the American Academy of Ophthalmology committee that drew up revised guidelines for screening for hydroxychloroquine retinopathy (Ophthalmology 2011;118:415-22).
Those guidelines call for screening when a patient first goes on hydroxychloroquine and then not again until the 5-year mark, since toxicity is rare within the first 5 years of treatment. After 5 years of use, annual screening is recommended. The screening should include a visual field exam as well as one of the advanced objective technologies: spectral domain OCT, autofluorescence, or multifocal electroretinography. Use of the outmoded Amsler grid is discouraged.
Dr. Rosenbaum advised his colleagues to send their patients to a practitioner who utilizes spectral domain OCT.
“Multifocal ERG is painful, time consuming, and you wouldn’t want to undergo it. Autofluorescence is equally as good as OCT but not as many centers do it; optometrists now often have OCT in their office,” he observed.
The Kaiser Permanente study identified several key risk factors for hydroxychloroquine retinopathy. The investigators were unable to identify a safe dosage of hydroxychloroquine, but they noted that for daily consumption of 4.0-5.0 mg/kg of real body weight, the prevalence was low – less than 2% – for the first 10 years of use. However, the prevalence climbed sharply thereafter. The researchers determined that real body weight predicted risk better than did ideal weight and should be used by clinicians in their dosing calculations. Patients on more than 5.0 mg/kg of real body weight daily had a 5.7-fold greater prevalence of hydroxychloroquine retinopathy.
Chronic kidney disease, defined as an estimated glomerular filtration rate below 60 mL/min, was associated with a twofold increased risk. Concurrent use of tamoxifen – a drug that appears to be toxic to the retina in its own right – was associated with a 4.6-fold increased risk of hydroxychloroquine retinopathy.
Audience members at the symposium asked how worried they and their patients really need to be, and just how often these subtle early abnormalities translate to functional visual impairment.
“When you can see the structural damage and see the damage functionally on the field exam, and you know that it’s going to increase over time, I think you need an awfully good lawyer to continue with the use of therapy,” Dr. Rosenbaum replied. “This is early change, and many patients may not even be aware of it. But I would much rather find it early than persist with treatment. And I’m thankful that now we have a mechanism to prevent it from progressing.”
Does the retinopathy reverse upon drug discontinuation? “Maybe a smidgen, but it’s neurologic damage. I think for the most part, if you catch it early and it stabilizes, that’s the best we can do,” according to Dr. Rosenbaum.
And remember: Eighty percent of people who have taken hydroxychloroquine for 20 years do not have retinal toxicity, he added.
Dr. Rosenbaum reported receiving consulting fees from a dozen pharmaceutical companies and research grants from AbbVie, Eyegate, Genentech, and pSivida.
SNOWMASS, COLO. – The risk of irreversible hydroxychloroquine toxic retinopathy is much greater than previously appreciated, Dr. James T. Rosenbaum cautioned at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“I remember when I was a fellow a paper was published saying Plaquenil [hydroxychloroquine] is safer than aspirin, it lowers lipids, and everyone should be taking it,” recalled Dr. Rosenbaum, professor of inflammatory diseases and chief of the division of arthritis and rheumatic diseases at Oregon Health and Science University, and chief of ophthalmology at the Devers Eye Institute in Portland, Ore.
He doesn’t feel that way anymore.
Dr. Rosenbaum highlighted a major recent study from Kaiser Permanente of Northern California which underscored the retinal hazards of long-term hydroxychloroquine. The retrospective, case-control study included 2,361 Kaiser Permanente patients who used the drug continuously for at least 5 years.
Evaluation by visual field testing and/or spectral domain optical coherence tomography (OCT) showed the overall prevalence of retinal thinning and photoreceptor damage or visual field loss was 7.5%. The risk climbed with greater daily dosage and duration of therapy, reaching a prevalence of nearly 20% after 20 years on hydroxychloroquine (JAMA Ophthalmol. 2014;132:1453-60).
“This really shakes my belief,” Dr. Rosenbaum confessed. “I really thought that anyone could take hydroxychloroquine with great impunity, but it turns out we really have to be careful with the dosage and the duration of therapy. I think we probably should routinely be reducing the dosage after 5 years of use, and in females who are under 5’6” we might need to be adjusting the dosage.
“Look, I think hydroxychloroquine is the greatest drug. I think everyone with rheumatoid arthritis and lupus should be on hydroxychloroquine. But I do think that after 5 years you want to monitor, and you should start thinking about having the patient take the drug 12 times per week instead of 14 times per week,” he added.
Dr. Rosenbaum called OCT “an absolutely invaluable diagnostic technique.” It provides objective findings enabling physicians to catch hydroxychloroquine retinopathy early, well before development of the classic hydroxychloroquine-induced severe bullseye maculopathy.
With no risk to the patient, the OCT laser reflects off the eye, permitting close inspection of the nine layers of the retina. Toxicity due to hydroxychloroquine or other antimalarials is manifest in what ophthalmologists call the flying saucer sign or sombrero sign because of its distinctive appearance, the result of fovial thinning and loss of the inner segment/outer segment junction.
Dr. Rosenbaum credited Dr. Michael F. Marmor, professor of ophthalmology at Stanford (Calif.) University, as the driving force behind the new appreciation of the full scope of hydroxychloroquine toxic retinopathy. Dr. Marmor was coauthor of the recent Kaiser Permanente study and has also collaborated with rheumatologist Dr. Fred Wolfe of the National Databank for Rheumatic Diseases in a large study (Arthritis Care Res. 2010;62:775-84). In addition, Dr. Marmor chaired the American Academy of Ophthalmology committee that drew up revised guidelines for screening for hydroxychloroquine retinopathy (Ophthalmology 2011;118:415-22).
Those guidelines call for screening when a patient first goes on hydroxychloroquine and then not again until the 5-year mark, since toxicity is rare within the first 5 years of treatment. After 5 years of use, annual screening is recommended. The screening should include a visual field exam as well as one of the advanced objective technologies: spectral domain OCT, autofluorescence, or multifocal electroretinography. Use of the outmoded Amsler grid is discouraged.
Dr. Rosenbaum advised his colleagues to send their patients to a practitioner who utilizes spectral domain OCT.
“Multifocal ERG is painful, time consuming, and you wouldn’t want to undergo it. Autofluorescence is equally as good as OCT but not as many centers do it; optometrists now often have OCT in their office,” he observed.
The Kaiser Permanente study identified several key risk factors for hydroxychloroquine retinopathy. The investigators were unable to identify a safe dosage of hydroxychloroquine, but they noted that for daily consumption of 4.0-5.0 mg/kg of real body weight, the prevalence was low – less than 2% – for the first 10 years of use. However, the prevalence climbed sharply thereafter. The researchers determined that real body weight predicted risk better than did ideal weight and should be used by clinicians in their dosing calculations. Patients on more than 5.0 mg/kg of real body weight daily had a 5.7-fold greater prevalence of hydroxychloroquine retinopathy.
Chronic kidney disease, defined as an estimated glomerular filtration rate below 60 mL/min, was associated with a twofold increased risk. Concurrent use of tamoxifen – a drug that appears to be toxic to the retina in its own right – was associated with a 4.6-fold increased risk of hydroxychloroquine retinopathy.
Audience members at the symposium asked how worried they and their patients really need to be, and just how often these subtle early abnormalities translate to functional visual impairment.
“When you can see the structural damage and see the damage functionally on the field exam, and you know that it’s going to increase over time, I think you need an awfully good lawyer to continue with the use of therapy,” Dr. Rosenbaum replied. “This is early change, and many patients may not even be aware of it. But I would much rather find it early than persist with treatment. And I’m thankful that now we have a mechanism to prevent it from progressing.”
Does the retinopathy reverse upon drug discontinuation? “Maybe a smidgen, but it’s neurologic damage. I think for the most part, if you catch it early and it stabilizes, that’s the best we can do,” according to Dr. Rosenbaum.
And remember: Eighty percent of people who have taken hydroxychloroquine for 20 years do not have retinal toxicity, he added.
Dr. Rosenbaum reported receiving consulting fees from a dozen pharmaceutical companies and research grants from AbbVie, Eyegate, Genentech, and pSivida.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM