User login
Physician reimbursement 2021: Who are the big winners?
Amid all the chaos and problems caused by COVID-19, one might hope that physicians would get a break on their complicated payment-reporting programs.
But that’s not the case: The government recently released the 2021 proposed rule for the Quality Payment Program (QPP), often referred to by its most popular participation track, the Merit-Based Incentive Payment System (MIPS). The program, which launched in 2017, gets annual updates, and this year is no different.
Some good news has made primary care and some other physicians happy.
The government’s proposal includes significant changes to reimbursement for all physicians.
Specialties that rely heavily on office-based E/M services are delighted at this change. Those include internists, family physicians, neurologists, pulmonologists, dermatologists, and all other specialties that rely heavily on office encounters.
According to the estimates from the Centers for Medicare & Medicaid Services (CMS), endocrinologists and rheumatologists are the big winners, at 17% and 16% projected increases, respectively. The government has been pushing to make this shift in reimbursement from surgeries and procedures to office visits for years. Although some physicians may celebrate the change, others will not.
The reimbursement plan for professional services depends on budget neutrality, meaning that the budget increases need to be counterbalanced by budget declines. Specialties that rely heavily on procedures and surgeries will suffer losses. These corresponding reductions felt by proceduralists and surgeons will counterbalance the good fortune of physicians who rely on office visits for the bulk of their revenue. Radiologists, for example, are projected by CMS to experience a 11% downturn, and cardiac surgeons face a 9% decline.
These consequences are significant. The 2021 shift may be the single biggest transfer of reimbursement in the history of the scale, which was adopted in the early 1990s.
If the change affected only Medicare reimbursement, perhaps it would be less significant. Because the majority of private payers use the government’s scale – the resource-based relative value scale – the impact will reverberate across physicians’ bottom lines. Given the state of many physicians’ finances, driven by the pandemic, this may send some affected physicians into a downward spiral.
The boost to E/M reimbursement – which represents approximately 20% of the overall Medicare payout to physicians each year – puts downward pressure on the professional services conversion factor as well.
For 2021, it is proposed to be $32.2605, representing a decrease of $3.83 from the 2020 conversion factor of $36.0896. The resultant conversion factor – which serves as a multiplier applied to the relative value unit to come up with the payment – effectively reduces payments to physicians across the board by 10.6%. Thus, even those who enjoy the benefits of the new E/M increases will see the potential reimbursement high point cut down.
Before launching into the changes in store for 2021, it’s good to determine whether you are an eligible clinician: You need to have more than $90,000 in Medicare Part B charges per year, see more than 200 Medicare Part B patients per year, and provide 200 or more covered professional services to Part B patients.
The program is voluntary, but there are steep penalties for eligible clinicians who don’t participate. For the 2021 reporting year, a 9% penalty will be imposed on Medicare reimbursement in 2023 in the event of participation failure. You can verify your participation status here; you’ll need your National Provider Identifier to run the search, but it takes only seconds to determine your eligibility.
A 9% penalty is a pretty big hit to your income. With 9% at stake, eligible clinicians need to actively engage in the program. Although there have been changes, the basic four-category system remains the same for the MIPS track, as follows: quality, cost, improvement activities, and promoting interoperability.
The four category weights, used to evaluate performance, are changing in 2021. Cost category weight goes up by 5 percentage points, to be 20% of the clinician’s score, and the quality category goes down by 5 percentage points to contribute 40% to the weight. Promoting interoperability remains 25% of the score, with improvement activities constituting the final 15%.
Other key changes include the following:
- The CMS’s Web interface for submission for quality measures will be shuttered in 2021. Users of this submission method will have to find and use another way to report their quality measures.
- Quality measures will be scored against pre-COVID benchmarks in lieu of comparisons with the 2020 reporting year; 206 quality measures are proposed for 2021, compared with the current list of 219.
- Telehealth will be incorporated in the cost category by updates to the measure specifications for the episode-based and total per capita cost measures.
- A new health information exchange measure is added to the promoting interoperability category, and “incorporating” replaces “reconciling” in the reporting requirement “Support Electronic Referral Loops by Receiving and Incorporating Health Information.”
To avoid the 9% penalty, eligible clinicians must earn 50 points in 2021, up from 45 in the current year. Achieving “exceptional performance” remains at 85 points. This elevated level of engagement allows access to a pot of money Congress set aside for high performers.
Many physicians feel that too much work is required to earn the “paltry” bonuses; even a perfect score of 100 has only resulted in bonuses of 1.88% and 1.68%, respectively, in the past 2 years. That includes the $500 million allocation that Congress set aside; this extra funding to reward exceptional performance is only available for the first 6 years of the law. Although the 2019 scores have been released to participants, CMS has not yet announced the overall national average, but it’s expected to be minimal.
The combination of meager payouts and a diminishing funding mechanism has physicians questioning participation altogether. My recent conversations with physicians who qualify for the program revealed their intention to participate, but only at a level to achieve the minimum threshold of 45 points this year and 50 in 2021. With so little upside, it’s impossible to make a business case to aim for the stars.
Perhaps the biggest change in 2021, however, is that the program is not making the previously planned switch to MIPS Value Pathways (MVPs). MVPs were designed to align the four performance categories around a specialty, medical condition, or patient population.
CMS introduced MVPs by giving an example of diabetes: “Endocrinologist reports same ‘foundation’ of PI [promoting interoperability] and population health measures as all other clinicians but now has a MIPS Value Pathway with measures and activities that focus on diabetes prevention and treatment.” CMS had expected MVPs to launch in 2021 for all program participants; because of the pandemic, CMS announced an extension for at least 1 year. This comes as a relief to physicians who are just trying to keep the lights on given the financial pressures brought on by the pandemic.
MVPs, however, will be incorporated into the MIPS Alternative Payment Model (APM) participation segment. This will affect many physicians because this is the path that accountable care organizations (ACOs) have taken. If you are part of an ACO and you report through it, you’ll see some more changes than your colleagues in 2021.
The good news is that ACOs that participate in MIPS and the Medicare Shared Savings Program will have to report only once to satisfy the requirements for both programs. The construct for this new APM-based program is called the “APM Performance Pathway.” This pathway incorporates six population health–based measures that cross-cut specialties.
CMS is also proposing that telemedicine reimbursement will become permanent. As of now, telemedicine services will only be paid when a public health emergency has been declared. This ability to reimburse physicians for telemedicine would end when the current public health emergency is over. CMS is proposing to extend reimbursement beyond the pandemic, which will benefit all physicians who perform these remote encounters.
The CMS proposal would also make some other requirements easier to achieve. The use of codes 99495 and 99496 – the transitional care management codes – is expanding by reducing several key accompanying-services restrictions. Before the public health emergency, there were constraints related to scope of practice; the proposal would extend the ability of advanced practice providers to order diagnostic tests, even after the public health emergency ends.
Furthermore, the proposal reduces restrictions related to billing for remote physiologic monitoring services and outlines the possibility of a new, higher-paying virtual visit code.
Although the Quality Payment Program will undergo some changes, they are minor. Be aware of the requirement to hit the 50-point mark to avoid the steep penalties, however. Perhaps greater benefit will be achieved through the government’s continued push to refine the reimbursement system. As a result of budget neutrality, however, these changes will boost some physicians while resulting in losses for others.
The government’s proposed changes are not final, and there is a period during which they are accepting comments on the proposal; the final rule will be announced in November.
If you want to wash your hands of this now, apply for the 2020 performance year hardship for the Quality Payment Program. The application is now open and available through December 31, 2020; completing it will release you of any program requirements in 2020 (and avoid that hefty 9% penalty on your 2022 reimbursement).
This way, you won’t have to concern yourself with any of these rules until next year; the government’s extension of this “get out of jail free” card is a welcome relief for physicians who are frustrated by the regulatory burdens despite the pressure exerted by COVID. Spending 15 minutes to complete this form is well worth your time and may eliminate much of your worry.
A version of this article originally appeared on Medscape.com.
Amid all the chaos and problems caused by COVID-19, one might hope that physicians would get a break on their complicated payment-reporting programs.
But that’s not the case: The government recently released the 2021 proposed rule for the Quality Payment Program (QPP), often referred to by its most popular participation track, the Merit-Based Incentive Payment System (MIPS). The program, which launched in 2017, gets annual updates, and this year is no different.
Some good news has made primary care and some other physicians happy.
The government’s proposal includes significant changes to reimbursement for all physicians.
Specialties that rely heavily on office-based E/M services are delighted at this change. Those include internists, family physicians, neurologists, pulmonologists, dermatologists, and all other specialties that rely heavily on office encounters.
According to the estimates from the Centers for Medicare & Medicaid Services (CMS), endocrinologists and rheumatologists are the big winners, at 17% and 16% projected increases, respectively. The government has been pushing to make this shift in reimbursement from surgeries and procedures to office visits for years. Although some physicians may celebrate the change, others will not.
The reimbursement plan for professional services depends on budget neutrality, meaning that the budget increases need to be counterbalanced by budget declines. Specialties that rely heavily on procedures and surgeries will suffer losses. These corresponding reductions felt by proceduralists and surgeons will counterbalance the good fortune of physicians who rely on office visits for the bulk of their revenue. Radiologists, for example, are projected by CMS to experience a 11% downturn, and cardiac surgeons face a 9% decline.
These consequences are significant. The 2021 shift may be the single biggest transfer of reimbursement in the history of the scale, which was adopted in the early 1990s.
If the change affected only Medicare reimbursement, perhaps it would be less significant. Because the majority of private payers use the government’s scale – the resource-based relative value scale – the impact will reverberate across physicians’ bottom lines. Given the state of many physicians’ finances, driven by the pandemic, this may send some affected physicians into a downward spiral.
The boost to E/M reimbursement – which represents approximately 20% of the overall Medicare payout to physicians each year – puts downward pressure on the professional services conversion factor as well.
For 2021, it is proposed to be $32.2605, representing a decrease of $3.83 from the 2020 conversion factor of $36.0896. The resultant conversion factor – which serves as a multiplier applied to the relative value unit to come up with the payment – effectively reduces payments to physicians across the board by 10.6%. Thus, even those who enjoy the benefits of the new E/M increases will see the potential reimbursement high point cut down.
Before launching into the changes in store for 2021, it’s good to determine whether you are an eligible clinician: You need to have more than $90,000 in Medicare Part B charges per year, see more than 200 Medicare Part B patients per year, and provide 200 or more covered professional services to Part B patients.
The program is voluntary, but there are steep penalties for eligible clinicians who don’t participate. For the 2021 reporting year, a 9% penalty will be imposed on Medicare reimbursement in 2023 in the event of participation failure. You can verify your participation status here; you’ll need your National Provider Identifier to run the search, but it takes only seconds to determine your eligibility.
A 9% penalty is a pretty big hit to your income. With 9% at stake, eligible clinicians need to actively engage in the program. Although there have been changes, the basic four-category system remains the same for the MIPS track, as follows: quality, cost, improvement activities, and promoting interoperability.
The four category weights, used to evaluate performance, are changing in 2021. Cost category weight goes up by 5 percentage points, to be 20% of the clinician’s score, and the quality category goes down by 5 percentage points to contribute 40% to the weight. Promoting interoperability remains 25% of the score, with improvement activities constituting the final 15%.
Other key changes include the following:
- The CMS’s Web interface for submission for quality measures will be shuttered in 2021. Users of this submission method will have to find and use another way to report their quality measures.
- Quality measures will be scored against pre-COVID benchmarks in lieu of comparisons with the 2020 reporting year; 206 quality measures are proposed for 2021, compared with the current list of 219.
- Telehealth will be incorporated in the cost category by updates to the measure specifications for the episode-based and total per capita cost measures.
- A new health information exchange measure is added to the promoting interoperability category, and “incorporating” replaces “reconciling” in the reporting requirement “Support Electronic Referral Loops by Receiving and Incorporating Health Information.”
To avoid the 9% penalty, eligible clinicians must earn 50 points in 2021, up from 45 in the current year. Achieving “exceptional performance” remains at 85 points. This elevated level of engagement allows access to a pot of money Congress set aside for high performers.
Many physicians feel that too much work is required to earn the “paltry” bonuses; even a perfect score of 100 has only resulted in bonuses of 1.88% and 1.68%, respectively, in the past 2 years. That includes the $500 million allocation that Congress set aside; this extra funding to reward exceptional performance is only available for the first 6 years of the law. Although the 2019 scores have been released to participants, CMS has not yet announced the overall national average, but it’s expected to be minimal.
The combination of meager payouts and a diminishing funding mechanism has physicians questioning participation altogether. My recent conversations with physicians who qualify for the program revealed their intention to participate, but only at a level to achieve the minimum threshold of 45 points this year and 50 in 2021. With so little upside, it’s impossible to make a business case to aim for the stars.
Perhaps the biggest change in 2021, however, is that the program is not making the previously planned switch to MIPS Value Pathways (MVPs). MVPs were designed to align the four performance categories around a specialty, medical condition, or patient population.
CMS introduced MVPs by giving an example of diabetes: “Endocrinologist reports same ‘foundation’ of PI [promoting interoperability] and population health measures as all other clinicians but now has a MIPS Value Pathway with measures and activities that focus on diabetes prevention and treatment.” CMS had expected MVPs to launch in 2021 for all program participants; because of the pandemic, CMS announced an extension for at least 1 year. This comes as a relief to physicians who are just trying to keep the lights on given the financial pressures brought on by the pandemic.
MVPs, however, will be incorporated into the MIPS Alternative Payment Model (APM) participation segment. This will affect many physicians because this is the path that accountable care organizations (ACOs) have taken. If you are part of an ACO and you report through it, you’ll see some more changes than your colleagues in 2021.
The good news is that ACOs that participate in MIPS and the Medicare Shared Savings Program will have to report only once to satisfy the requirements for both programs. The construct for this new APM-based program is called the “APM Performance Pathway.” This pathway incorporates six population health–based measures that cross-cut specialties.
CMS is also proposing that telemedicine reimbursement will become permanent. As of now, telemedicine services will only be paid when a public health emergency has been declared. This ability to reimburse physicians for telemedicine would end when the current public health emergency is over. CMS is proposing to extend reimbursement beyond the pandemic, which will benefit all physicians who perform these remote encounters.
The CMS proposal would also make some other requirements easier to achieve. The use of codes 99495 and 99496 – the transitional care management codes – is expanding by reducing several key accompanying-services restrictions. Before the public health emergency, there were constraints related to scope of practice; the proposal would extend the ability of advanced practice providers to order diagnostic tests, even after the public health emergency ends.
Furthermore, the proposal reduces restrictions related to billing for remote physiologic monitoring services and outlines the possibility of a new, higher-paying virtual visit code.
Although the Quality Payment Program will undergo some changes, they are minor. Be aware of the requirement to hit the 50-point mark to avoid the steep penalties, however. Perhaps greater benefit will be achieved through the government’s continued push to refine the reimbursement system. As a result of budget neutrality, however, these changes will boost some physicians while resulting in losses for others.
The government’s proposed changes are not final, and there is a period during which they are accepting comments on the proposal; the final rule will be announced in November.
If you want to wash your hands of this now, apply for the 2020 performance year hardship for the Quality Payment Program. The application is now open and available through December 31, 2020; completing it will release you of any program requirements in 2020 (and avoid that hefty 9% penalty on your 2022 reimbursement).
This way, you won’t have to concern yourself with any of these rules until next year; the government’s extension of this “get out of jail free” card is a welcome relief for physicians who are frustrated by the regulatory burdens despite the pressure exerted by COVID. Spending 15 minutes to complete this form is well worth your time and may eliminate much of your worry.
A version of this article originally appeared on Medscape.com.
Amid all the chaos and problems caused by COVID-19, one might hope that physicians would get a break on their complicated payment-reporting programs.
But that’s not the case: The government recently released the 2021 proposed rule for the Quality Payment Program (QPP), often referred to by its most popular participation track, the Merit-Based Incentive Payment System (MIPS). The program, which launched in 2017, gets annual updates, and this year is no different.
Some good news has made primary care and some other physicians happy.
The government’s proposal includes significant changes to reimbursement for all physicians.
Specialties that rely heavily on office-based E/M services are delighted at this change. Those include internists, family physicians, neurologists, pulmonologists, dermatologists, and all other specialties that rely heavily on office encounters.
According to the estimates from the Centers for Medicare & Medicaid Services (CMS), endocrinologists and rheumatologists are the big winners, at 17% and 16% projected increases, respectively. The government has been pushing to make this shift in reimbursement from surgeries and procedures to office visits for years. Although some physicians may celebrate the change, others will not.
The reimbursement plan for professional services depends on budget neutrality, meaning that the budget increases need to be counterbalanced by budget declines. Specialties that rely heavily on procedures and surgeries will suffer losses. These corresponding reductions felt by proceduralists and surgeons will counterbalance the good fortune of physicians who rely on office visits for the bulk of their revenue. Radiologists, for example, are projected by CMS to experience a 11% downturn, and cardiac surgeons face a 9% decline.
These consequences are significant. The 2021 shift may be the single biggest transfer of reimbursement in the history of the scale, which was adopted in the early 1990s.
If the change affected only Medicare reimbursement, perhaps it would be less significant. Because the majority of private payers use the government’s scale – the resource-based relative value scale – the impact will reverberate across physicians’ bottom lines. Given the state of many physicians’ finances, driven by the pandemic, this may send some affected physicians into a downward spiral.
The boost to E/M reimbursement – which represents approximately 20% of the overall Medicare payout to physicians each year – puts downward pressure on the professional services conversion factor as well.
For 2021, it is proposed to be $32.2605, representing a decrease of $3.83 from the 2020 conversion factor of $36.0896. The resultant conversion factor – which serves as a multiplier applied to the relative value unit to come up with the payment – effectively reduces payments to physicians across the board by 10.6%. Thus, even those who enjoy the benefits of the new E/M increases will see the potential reimbursement high point cut down.
Before launching into the changes in store for 2021, it’s good to determine whether you are an eligible clinician: You need to have more than $90,000 in Medicare Part B charges per year, see more than 200 Medicare Part B patients per year, and provide 200 or more covered professional services to Part B patients.
The program is voluntary, but there are steep penalties for eligible clinicians who don’t participate. For the 2021 reporting year, a 9% penalty will be imposed on Medicare reimbursement in 2023 in the event of participation failure. You can verify your participation status here; you’ll need your National Provider Identifier to run the search, but it takes only seconds to determine your eligibility.
A 9% penalty is a pretty big hit to your income. With 9% at stake, eligible clinicians need to actively engage in the program. Although there have been changes, the basic four-category system remains the same for the MIPS track, as follows: quality, cost, improvement activities, and promoting interoperability.
The four category weights, used to evaluate performance, are changing in 2021. Cost category weight goes up by 5 percentage points, to be 20% of the clinician’s score, and the quality category goes down by 5 percentage points to contribute 40% to the weight. Promoting interoperability remains 25% of the score, with improvement activities constituting the final 15%.
Other key changes include the following:
- The CMS’s Web interface for submission for quality measures will be shuttered in 2021. Users of this submission method will have to find and use another way to report their quality measures.
- Quality measures will be scored against pre-COVID benchmarks in lieu of comparisons with the 2020 reporting year; 206 quality measures are proposed for 2021, compared with the current list of 219.
- Telehealth will be incorporated in the cost category by updates to the measure specifications for the episode-based and total per capita cost measures.
- A new health information exchange measure is added to the promoting interoperability category, and “incorporating” replaces “reconciling” in the reporting requirement “Support Electronic Referral Loops by Receiving and Incorporating Health Information.”
To avoid the 9% penalty, eligible clinicians must earn 50 points in 2021, up from 45 in the current year. Achieving “exceptional performance” remains at 85 points. This elevated level of engagement allows access to a pot of money Congress set aside for high performers.
Many physicians feel that too much work is required to earn the “paltry” bonuses; even a perfect score of 100 has only resulted in bonuses of 1.88% and 1.68%, respectively, in the past 2 years. That includes the $500 million allocation that Congress set aside; this extra funding to reward exceptional performance is only available for the first 6 years of the law. Although the 2019 scores have been released to participants, CMS has not yet announced the overall national average, but it’s expected to be minimal.
The combination of meager payouts and a diminishing funding mechanism has physicians questioning participation altogether. My recent conversations with physicians who qualify for the program revealed their intention to participate, but only at a level to achieve the minimum threshold of 45 points this year and 50 in 2021. With so little upside, it’s impossible to make a business case to aim for the stars.
Perhaps the biggest change in 2021, however, is that the program is not making the previously planned switch to MIPS Value Pathways (MVPs). MVPs were designed to align the four performance categories around a specialty, medical condition, or patient population.
CMS introduced MVPs by giving an example of diabetes: “Endocrinologist reports same ‘foundation’ of PI [promoting interoperability] and population health measures as all other clinicians but now has a MIPS Value Pathway with measures and activities that focus on diabetes prevention and treatment.” CMS had expected MVPs to launch in 2021 for all program participants; because of the pandemic, CMS announced an extension for at least 1 year. This comes as a relief to physicians who are just trying to keep the lights on given the financial pressures brought on by the pandemic.
MVPs, however, will be incorporated into the MIPS Alternative Payment Model (APM) participation segment. This will affect many physicians because this is the path that accountable care organizations (ACOs) have taken. If you are part of an ACO and you report through it, you’ll see some more changes than your colleagues in 2021.
The good news is that ACOs that participate in MIPS and the Medicare Shared Savings Program will have to report only once to satisfy the requirements for both programs. The construct for this new APM-based program is called the “APM Performance Pathway.” This pathway incorporates six population health–based measures that cross-cut specialties.
CMS is also proposing that telemedicine reimbursement will become permanent. As of now, telemedicine services will only be paid when a public health emergency has been declared. This ability to reimburse physicians for telemedicine would end when the current public health emergency is over. CMS is proposing to extend reimbursement beyond the pandemic, which will benefit all physicians who perform these remote encounters.
The CMS proposal would also make some other requirements easier to achieve. The use of codes 99495 and 99496 – the transitional care management codes – is expanding by reducing several key accompanying-services restrictions. Before the public health emergency, there were constraints related to scope of practice; the proposal would extend the ability of advanced practice providers to order diagnostic tests, even after the public health emergency ends.
Furthermore, the proposal reduces restrictions related to billing for remote physiologic monitoring services and outlines the possibility of a new, higher-paying virtual visit code.
Although the Quality Payment Program will undergo some changes, they are minor. Be aware of the requirement to hit the 50-point mark to avoid the steep penalties, however. Perhaps greater benefit will be achieved through the government’s continued push to refine the reimbursement system. As a result of budget neutrality, however, these changes will boost some physicians while resulting in losses for others.
The government’s proposed changes are not final, and there is a period during which they are accepting comments on the proposal; the final rule will be announced in November.
If you want to wash your hands of this now, apply for the 2020 performance year hardship for the Quality Payment Program. The application is now open and available through December 31, 2020; completing it will release you of any program requirements in 2020 (and avoid that hefty 9% penalty on your 2022 reimbursement).
This way, you won’t have to concern yourself with any of these rules until next year; the government’s extension of this “get out of jail free” card is a welcome relief for physicians who are frustrated by the regulatory burdens despite the pressure exerted by COVID. Spending 15 minutes to complete this form is well worth your time and may eliminate much of your worry.
A version of this article originally appeared on Medscape.com.
Too many patient call messages
In a recent study published in the Journal of the American Medical Informatics Association that used EHR logs, researchers found that “Clinicians with the highest volume of patient call messages have almost 4 times the odds of burnout compared with clinicians with the fewest.” And they discovered that “No other workload measures were significantly associated with burnout.” Like the majority of papers I skim through, it states the obvious. Doesn’t it makes sense that the busiest of providers should be more vulnerable to stress related symptoms? But is that really true for every provider? Being “busy” doesn’t guarantee that you are productive nor does it mean that the stuff you are doing while you are busy is fulfilling or rewarding either emotionally or financially. Certainly, slogging through a long list of patient call messages at the end of the day does qualify as being busy, but it is more likely to generate anger and frustration than it is fulfillment.

Just because you have a large practice, does that mean that you will necessarily have more messages to review and calls to return than a provider with a smaller practice. Maybe you manage your practice and your time so well that you actually have fewer messages and calls to return and, therefore, are less vulnerable to burnout.
There are three general strategies that you might be employing that result in fewer messages and calls that require your response. It may be that you have developed a handbook of frequently asked questions and trained your staff to use it as a reference in a way that reduces the number of messages that filter to you. Creating this triage book and finding the right personnel took time, but it didn’t necessarily mean that you had to hire staff with extensive training, which can be expensive. In-house training of raw talent that has demonstrated common sense and good communication skills can be cost effective and rewarding. You probably already have discovered that continued attention to quality control is an important part of this strategy. Included in your handbook you may have included a clearcut triage system for the questions that the staff can’t answer. Is it a question you must answer (a) as soon as you finish with this patient, (b) before lunch, or (c) at the end of the day? (Category (c) is of course strongly discouraged).
The second general group of strategies you may be using to keep your calls and messages to a minimum is anticipatory guidance. As you wrap up each visit, are you anticipating what calls it might generate? This of course depends on the nature of the problem and the personality of the patient. From your experience you can probably predict most of the questions that are likely going to crop up after the patient arrives home. Preemptively answering these before patients leave and providing a personalized handout that you discuss with them may easily be saving you two or three calls a day. Because you can’t anticipate every question, you have found that promising a follow-up call in a day or 2 encourages the patients to hold their questions and wait for you or your assistant to call.

Finally, you may have discovered long ago that in many cases it is easier and more efficient to see the patient rather than having your staff spend half their time building and maintaining a communication wall around you. This is particularly true if, during the initial contact with your office, the patients have made it clear that they would like to be seen. This strategy is based on commons sense, but for many physicians and their office staff it may require a dramatic shift in attitude. You may have needed to become more comfortable squeezing in short visits at which the goal is to simply begin the dual processes of anxiety relief and diagnosis. In the beginning, you may have had to frequently remind your staff that their primary goal is patient satisfaction and not protecting you from seeing “too many” patients. Ironically, by being over protective, they may have been contributing to burnout when simply cutting to the chase and having the patient come in to be seen would have generated fewer stress-producing calls and messages.
Enabling a system that generates an excess of patient messages is looking for trouble.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
In a recent study published in the Journal of the American Medical Informatics Association that used EHR logs, researchers found that “Clinicians with the highest volume of patient call messages have almost 4 times the odds of burnout compared with clinicians with the fewest.” And they discovered that “No other workload measures were significantly associated with burnout.” Like the majority of papers I skim through, it states the obvious. Doesn’t it makes sense that the busiest of providers should be more vulnerable to stress related symptoms? But is that really true for every provider? Being “busy” doesn’t guarantee that you are productive nor does it mean that the stuff you are doing while you are busy is fulfilling or rewarding either emotionally or financially. Certainly, slogging through a long list of patient call messages at the end of the day does qualify as being busy, but it is more likely to generate anger and frustration than it is fulfillment.
Just because you have a large practice, does that mean that you will necessarily have more messages to review and calls to return than a provider with a smaller practice. Maybe you manage your practice and your time so well that you actually have fewer messages and calls to return and, therefore, are less vulnerable to burnout.
There are three general strategies that you might be employing that result in fewer messages and calls that require your response. It may be that you have developed a handbook of frequently asked questions and trained your staff to use it as a reference in a way that reduces the number of messages that filter to you. Creating this triage book and finding the right personnel took time, but it didn’t necessarily mean that you had to hire staff with extensive training, which can be expensive. In-house training of raw talent that has demonstrated common sense and good communication skills can be cost effective and rewarding. You probably already have discovered that continued attention to quality control is an important part of this strategy. Included in your handbook you may have included a clearcut triage system for the questions that the staff can’t answer. Is it a question you must answer (a) as soon as you finish with this patient, (b) before lunch, or (c) at the end of the day? (Category (c) is of course strongly discouraged).
The second general group of strategies you may be using to keep your calls and messages to a minimum is anticipatory guidance. As you wrap up each visit, are you anticipating what calls it might generate? This of course depends on the nature of the problem and the personality of the patient. From your experience you can probably predict most of the questions that are likely going to crop up after the patient arrives home. Preemptively answering these before patients leave and providing a personalized handout that you discuss with them may easily be saving you two or three calls a day. Because you can’t anticipate every question, you have found that promising a follow-up call in a day or 2 encourages the patients to hold their questions and wait for you or your assistant to call.
Finally, you may have discovered long ago that in many cases it is easier and more efficient to see the patient rather than having your staff spend half their time building and maintaining a communication wall around you. This is particularly true if, during the initial contact with your office, the patients have made it clear that they would like to be seen. This strategy is based on commons sense, but for many physicians and their office staff it may require a dramatic shift in attitude. You may have needed to become more comfortable squeezing in short visits at which the goal is to simply begin the dual processes of anxiety relief and diagnosis. In the beginning, you may have had to frequently remind your staff that their primary goal is patient satisfaction and not protecting you from seeing “too many” patients. Ironically, by being over protective, they may have been contributing to burnout when simply cutting to the chase and having the patient come in to be seen would have generated fewer stress-producing calls and messages.
Enabling a system that generates an excess of patient messages is looking for trouble.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
In a recent study published in the Journal of the American Medical Informatics Association that used EHR logs, researchers found that “Clinicians with the highest volume of patient call messages have almost 4 times the odds of burnout compared with clinicians with the fewest.” And they discovered that “No other workload measures were significantly associated with burnout.” Like the majority of papers I skim through, it states the obvious. Doesn’t it makes sense that the busiest of providers should be more vulnerable to stress related symptoms? But is that really true for every provider? Being “busy” doesn’t guarantee that you are productive nor does it mean that the stuff you are doing while you are busy is fulfilling or rewarding either emotionally or financially. Certainly, slogging through a long list of patient call messages at the end of the day does qualify as being busy, but it is more likely to generate anger and frustration than it is fulfillment.
Just because you have a large practice, does that mean that you will necessarily have more messages to review and calls to return than a provider with a smaller practice. Maybe you manage your practice and your time so well that you actually have fewer messages and calls to return and, therefore, are less vulnerable to burnout.
There are three general strategies that you might be employing that result in fewer messages and calls that require your response. It may be that you have developed a handbook of frequently asked questions and trained your staff to use it as a reference in a way that reduces the number of messages that filter to you. Creating this triage book and finding the right personnel took time, but it didn’t necessarily mean that you had to hire staff with extensive training, which can be expensive. In-house training of raw talent that has demonstrated common sense and good communication skills can be cost effective and rewarding. You probably already have discovered that continued attention to quality control is an important part of this strategy. Included in your handbook you may have included a clearcut triage system for the questions that the staff can’t answer. Is it a question you must answer (a) as soon as you finish with this patient, (b) before lunch, or (c) at the end of the day? (Category (c) is of course strongly discouraged).
The second general group of strategies you may be using to keep your calls and messages to a minimum is anticipatory guidance. As you wrap up each visit, are you anticipating what calls it might generate? This of course depends on the nature of the problem and the personality of the patient. From your experience you can probably predict most of the questions that are likely going to crop up after the patient arrives home. Preemptively answering these before patients leave and providing a personalized handout that you discuss with them may easily be saving you two or three calls a day. Because you can’t anticipate every question, you have found that promising a follow-up call in a day or 2 encourages the patients to hold their questions and wait for you or your assistant to call.
Finally, you may have discovered long ago that in many cases it is easier and more efficient to see the patient rather than having your staff spend half their time building and maintaining a communication wall around you. This is particularly true if, during the initial contact with your office, the patients have made it clear that they would like to be seen. This strategy is based on commons sense, but for many physicians and their office staff it may require a dramatic shift in attitude. You may have needed to become more comfortable squeezing in short visits at which the goal is to simply begin the dual processes of anxiety relief and diagnosis. In the beginning, you may have had to frequently remind your staff that their primary goal is patient satisfaction and not protecting you from seeing “too many” patients. Ironically, by being over protective, they may have been contributing to burnout when simply cutting to the chase and having the patient come in to be seen would have generated fewer stress-producing calls and messages.
Enabling a system that generates an excess of patient messages is looking for trouble.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Election gift for Florida? Trump poised to approve drug imports from Canada
Over the objections of drugmakers, the Trump administration is expected within weeks to finalize its plan that would allow states to import some prescription medicines from Canada.
Six states – Colorado, Florida, Maine, New Hampshire, New Mexico, and Vermont – have passed laws allowing them to seek federal approval to buy drugs from Canada to give their residents access to lower-cost medicines.
But industry observers say the drug importation proposal under review by the administration is squarely aimed at Florida – the most populous swing state in the November election. Trump’s support of the idea initially came at the urging of Florida Gov. Ron DeSantis, a close Republican ally.
The DeSantis administration is so confident Trump will move ahead with allowing drug importation that it put out a request June 30 for private companies to bid on a three-year, $30 million contract to run the program. It hopes to award the contract in December.
Industry experts say Florida is likely to be the first state to win federal approval for a drug importation plan – something that could occur before the November election.
“Approving Florida would feel like the politically astute thing to do,” said Mara Baer, a health consultant who has worked with Colorado on its importation proposal.
Ben England, CEO of FDAImports, a consulting firm in Glen Burnie, Maryland, said the OMB typically has 60 days to review final rules, although he expects this one could be completed before Nov. 3 and predicted there’s a small chance it could get finalized and Florida’s request approved by then. “It’s an election year, so I do see the current administration trying to use this as a talking point to say ‘Look what we’ve accomplished,’” he said.
Florida also makes sense because of the large number of retirees, who face high costs for medicines despite Medicare drug coverage.
The DeSantis administration did not respond to requests for comment.
Trump boasted about his importation plan during an October speech in The Villages, a large retirement community about 60 miles northwest of Orlando. “We will soon allow the safe and legal importation of prescription drugs from other countries, including the country of Canada, where, believe it or not, they pay much less money for the exact same drug,” Trump said, with DeSantis in attendance. “Stand up, Ron. Boy, he wants this so badly.”
The Food and Drug Administration released a detailed proposal last December and sought comments. A final plan was delivered Sept. 10 to the Office of Management and Budget for review, signaling it could be unveiled within weeks.
The proposal would regulate how states set up their own programs for importing drugs from Canada.
Prices are cheaper because Canada limits how much drugmakers can charge for medicines. The United States lets free markets dictate drug prices.
The pharmaceutical industry signaled it will likely sue the Trump administration if it goes forward with its importation plans, saying the plan violates several federal laws and the U.S. Constitution.
But the most stinging rebuke of the Trump importation plan came from the Canadian government, which said the proposal would make it harder for Canadian citizens to get drugs, putting their health at risk.
“Canada will employ all necessary measures to safeguard access for Canadians to needed drugs,” the Canadian government wrote in a letter to the FDA about the draft proposal. “The Canadian drug market and manufacturing capacity are too small to meet the demand of both Canadian and American consumers for prescription drugs.”
Without buy-in from Canada, any plan to import medicines is unlikely to succeed, officials said.
Ena Backus, director of Health Care Reform in Vermont, who has worked on setting up an importation program there, said states will need help from Canada. “Our state importation program relies on a willing partner in Canada,” she said.
For decades, Americans have been buying drugs from Canada for personal use — either by driving over the border, ordering medication on the Internet, or using storefronts that connect them to foreign pharmacies. Though illegal, the FDA has generally permitted purchases for individual use.
About 4 million Americans import lower-cost medicines for personal use each year, and about 20 million say they or someone in their household have done so because the prices are much lower in other countries, according to surveys.
The practice has been popular in Florida. More than a dozen storefronts across the state help consumers connect to pharmacies in Canada and other countries. Several cities, state and school districts in Florida help employees get drugs from Canada.
The administration’s proposal builds on a 2000 law that opened the door to allowing drug importation from Canada. But that provision could take effect only if the Health and Human Services secretary certified importation as safe, something that Democratic and Republican administrations have refused to do.
The drug industry for years has said allowing drugs to be imported from Canada would disrupt the nation’s supply chain and make it easier for unsafe or counterfeit medications to enter the market.
Trump, who made lowering prescription drug prices a signature promise in his 2016 campaign, has been eager to fulfill his pledge. In July 2019, at Trump’s direction, HHS Secretary Alex Azar said the federal government was “open for business” on drug importation, a year after calling drug importation a “gimmick.”
The administration envisions a system in which a Canadian-licensed wholesaler buys directly from a manufacturer for drugs approved for sale in Canada and exports the drugs to a U.S. wholesaler/importer under contract to a state.
Florida’s legislation – approved in 2019 – would set up two importation programs. The first would focus on getting drugs for state programs such as Medicaid, the Department of Corrections and county health departments. State officials said they expect the programs would save the state about $150 million annually.
The second program would be geared to the broader state population.
In response to the draft rule, the states seeking to start a drug importation program suggested changes to the administration’s proposal.
“Should the final rule not address these areas of concern, Colorado will struggle to find appropriate partners and realize significant savings for consumers,” Kim Bimestefer, executive director of the Colorado Department of Health Care Policy & Financing, told the FDA in March.
Among the state’s concerns is that it would be limited to using only one Canadian wholesaler, and without competition the state fears prices might not be as low as officials hoped. Bimestefer also noted that under the draft rule, the federal government would approve the importation program for only two years and states need a longer time frame to get buy-in from wholesalers and other partners.
Colorado officials estimate importing drugs from Canada could cut prices by 54% for cancer drugs and 75% for cardiac medicines. The state also noted the diabetes drug Jardiance costs $400 a month in the United States and sells for $85 in Canada.
Several states worry some of the most expensive drugs – including injectable and biologic medicines – were exempt from the federal rule. Those drug classes are not allowed to be imported under the 2000 law.
However, in an executive order in July, Trump said he would allow insulin to be imported if Azar determined it is required for emergency medical care. An HHS spokesman would not say whether Azar has done that.
Jane Horvath, a health policy consultant in College Park, Md., said the administration faces several challenges getting an importation program up and running, including possible opposition from the pharmaceutical industry and limits on classes of drugs that can be sold over the border.
“Despite the barriers, the programs are still quite worthwhile to pursue,” she said.
Maine’s top health official said the administration should work with the Canadian government to address Canada’s concerns. HHS officials refused to say whether such discussions have started.
Officials in Vermont, where the program would also include consumers covered by private insurance, remain hopeful.
“Given that we want to reduce the burden of health care costs on residents in our state, then it is important to pursue this option if there is a clear pathway forward,” Backus said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente. This story also ran on Miami Herald.
Over the objections of drugmakers, the Trump administration is expected within weeks to finalize its plan that would allow states to import some prescription medicines from Canada.
Six states – Colorado, Florida, Maine, New Hampshire, New Mexico, and Vermont – have passed laws allowing them to seek federal approval to buy drugs from Canada to give their residents access to lower-cost medicines.
But industry observers say the drug importation proposal under review by the administration is squarely aimed at Florida – the most populous swing state in the November election. Trump’s support of the idea initially came at the urging of Florida Gov. Ron DeSantis, a close Republican ally.
The DeSantis administration is so confident Trump will move ahead with allowing drug importation that it put out a request June 30 for private companies to bid on a three-year, $30 million contract to run the program. It hopes to award the contract in December.
Industry experts say Florida is likely to be the first state to win federal approval for a drug importation plan – something that could occur before the November election.
“Approving Florida would feel like the politically astute thing to do,” said Mara Baer, a health consultant who has worked with Colorado on its importation proposal.
Ben England, CEO of FDAImports, a consulting firm in Glen Burnie, Maryland, said the OMB typically has 60 days to review final rules, although he expects this one could be completed before Nov. 3 and predicted there’s a small chance it could get finalized and Florida’s request approved by then. “It’s an election year, so I do see the current administration trying to use this as a talking point to say ‘Look what we’ve accomplished,’” he said.
Florida also makes sense because of the large number of retirees, who face high costs for medicines despite Medicare drug coverage.
The DeSantis administration did not respond to requests for comment.
Trump boasted about his importation plan during an October speech in The Villages, a large retirement community about 60 miles northwest of Orlando. “We will soon allow the safe and legal importation of prescription drugs from other countries, including the country of Canada, where, believe it or not, they pay much less money for the exact same drug,” Trump said, with DeSantis in attendance. “Stand up, Ron. Boy, he wants this so badly.”
The Food and Drug Administration released a detailed proposal last December and sought comments. A final plan was delivered Sept. 10 to the Office of Management and Budget for review, signaling it could be unveiled within weeks.
The proposal would regulate how states set up their own programs for importing drugs from Canada.
Prices are cheaper because Canada limits how much drugmakers can charge for medicines. The United States lets free markets dictate drug prices.
The pharmaceutical industry signaled it will likely sue the Trump administration if it goes forward with its importation plans, saying the plan violates several federal laws and the U.S. Constitution.
But the most stinging rebuke of the Trump importation plan came from the Canadian government, which said the proposal would make it harder for Canadian citizens to get drugs, putting their health at risk.
“Canada will employ all necessary measures to safeguard access for Canadians to needed drugs,” the Canadian government wrote in a letter to the FDA about the draft proposal. “The Canadian drug market and manufacturing capacity are too small to meet the demand of both Canadian and American consumers for prescription drugs.”
Without buy-in from Canada, any plan to import medicines is unlikely to succeed, officials said.
Ena Backus, director of Health Care Reform in Vermont, who has worked on setting up an importation program there, said states will need help from Canada. “Our state importation program relies on a willing partner in Canada,” she said.
For decades, Americans have been buying drugs from Canada for personal use — either by driving over the border, ordering medication on the Internet, or using storefronts that connect them to foreign pharmacies. Though illegal, the FDA has generally permitted purchases for individual use.
About 4 million Americans import lower-cost medicines for personal use each year, and about 20 million say they or someone in their household have done so because the prices are much lower in other countries, according to surveys.
The practice has been popular in Florida. More than a dozen storefronts across the state help consumers connect to pharmacies in Canada and other countries. Several cities, state and school districts in Florida help employees get drugs from Canada.
The administration’s proposal builds on a 2000 law that opened the door to allowing drug importation from Canada. But that provision could take effect only if the Health and Human Services secretary certified importation as safe, something that Democratic and Republican administrations have refused to do.
The drug industry for years has said allowing drugs to be imported from Canada would disrupt the nation’s supply chain and make it easier for unsafe or counterfeit medications to enter the market.
Trump, who made lowering prescription drug prices a signature promise in his 2016 campaign, has been eager to fulfill his pledge. In July 2019, at Trump’s direction, HHS Secretary Alex Azar said the federal government was “open for business” on drug importation, a year after calling drug importation a “gimmick.”
The administration envisions a system in which a Canadian-licensed wholesaler buys directly from a manufacturer for drugs approved for sale in Canada and exports the drugs to a U.S. wholesaler/importer under contract to a state.
Florida’s legislation – approved in 2019 – would set up two importation programs. The first would focus on getting drugs for state programs such as Medicaid, the Department of Corrections and county health departments. State officials said they expect the programs would save the state about $150 million annually.
The second program would be geared to the broader state population.
In response to the draft rule, the states seeking to start a drug importation program suggested changes to the administration’s proposal.
“Should the final rule not address these areas of concern, Colorado will struggle to find appropriate partners and realize significant savings for consumers,” Kim Bimestefer, executive director of the Colorado Department of Health Care Policy & Financing, told the FDA in March.
Among the state’s concerns is that it would be limited to using only one Canadian wholesaler, and without competition the state fears prices might not be as low as officials hoped. Bimestefer also noted that under the draft rule, the federal government would approve the importation program for only two years and states need a longer time frame to get buy-in from wholesalers and other partners.
Colorado officials estimate importing drugs from Canada could cut prices by 54% for cancer drugs and 75% for cardiac medicines. The state also noted the diabetes drug Jardiance costs $400 a month in the United States and sells for $85 in Canada.
Several states worry some of the most expensive drugs – including injectable and biologic medicines – were exempt from the federal rule. Those drug classes are not allowed to be imported under the 2000 law.
However, in an executive order in July, Trump said he would allow insulin to be imported if Azar determined it is required for emergency medical care. An HHS spokesman would not say whether Azar has done that.
Jane Horvath, a health policy consultant in College Park, Md., said the administration faces several challenges getting an importation program up and running, including possible opposition from the pharmaceutical industry and limits on classes of drugs that can be sold over the border.
“Despite the barriers, the programs are still quite worthwhile to pursue,” she said.
Maine’s top health official said the administration should work with the Canadian government to address Canada’s concerns. HHS officials refused to say whether such discussions have started.
Officials in Vermont, where the program would also include consumers covered by private insurance, remain hopeful.
“Given that we want to reduce the burden of health care costs on residents in our state, then it is important to pursue this option if there is a clear pathway forward,” Backus said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente. This story also ran on Miami Herald.
Over the objections of drugmakers, the Trump administration is expected within weeks to finalize its plan that would allow states to import some prescription medicines from Canada.
Six states – Colorado, Florida, Maine, New Hampshire, New Mexico, and Vermont – have passed laws allowing them to seek federal approval to buy drugs from Canada to give their residents access to lower-cost medicines.
But industry observers say the drug importation proposal under review by the administration is squarely aimed at Florida – the most populous swing state in the November election. Trump’s support of the idea initially came at the urging of Florida Gov. Ron DeSantis, a close Republican ally.
The DeSantis administration is so confident Trump will move ahead with allowing drug importation that it put out a request June 30 for private companies to bid on a three-year, $30 million contract to run the program. It hopes to award the contract in December.
Industry experts say Florida is likely to be the first state to win federal approval for a drug importation plan – something that could occur before the November election.
“Approving Florida would feel like the politically astute thing to do,” said Mara Baer, a health consultant who has worked with Colorado on its importation proposal.
Ben England, CEO of FDAImports, a consulting firm in Glen Burnie, Maryland, said the OMB typically has 60 days to review final rules, although he expects this one could be completed before Nov. 3 and predicted there’s a small chance it could get finalized and Florida’s request approved by then. “It’s an election year, so I do see the current administration trying to use this as a talking point to say ‘Look what we’ve accomplished,’” he said.
Florida also makes sense because of the large number of retirees, who face high costs for medicines despite Medicare drug coverage.
The DeSantis administration did not respond to requests for comment.
Trump boasted about his importation plan during an October speech in The Villages, a large retirement community about 60 miles northwest of Orlando. “We will soon allow the safe and legal importation of prescription drugs from other countries, including the country of Canada, where, believe it or not, they pay much less money for the exact same drug,” Trump said, with DeSantis in attendance. “Stand up, Ron. Boy, he wants this so badly.”
The Food and Drug Administration released a detailed proposal last December and sought comments. A final plan was delivered Sept. 10 to the Office of Management and Budget for review, signaling it could be unveiled within weeks.
The proposal would regulate how states set up their own programs for importing drugs from Canada.
Prices are cheaper because Canada limits how much drugmakers can charge for medicines. The United States lets free markets dictate drug prices.
The pharmaceutical industry signaled it will likely sue the Trump administration if it goes forward with its importation plans, saying the plan violates several federal laws and the U.S. Constitution.
But the most stinging rebuke of the Trump importation plan came from the Canadian government, which said the proposal would make it harder for Canadian citizens to get drugs, putting their health at risk.
“Canada will employ all necessary measures to safeguard access for Canadians to needed drugs,” the Canadian government wrote in a letter to the FDA about the draft proposal. “The Canadian drug market and manufacturing capacity are too small to meet the demand of both Canadian and American consumers for prescription drugs.”
Without buy-in from Canada, any plan to import medicines is unlikely to succeed, officials said.
Ena Backus, director of Health Care Reform in Vermont, who has worked on setting up an importation program there, said states will need help from Canada. “Our state importation program relies on a willing partner in Canada,” she said.
For decades, Americans have been buying drugs from Canada for personal use — either by driving over the border, ordering medication on the Internet, or using storefronts that connect them to foreign pharmacies. Though illegal, the FDA has generally permitted purchases for individual use.
About 4 million Americans import lower-cost medicines for personal use each year, and about 20 million say they or someone in their household have done so because the prices are much lower in other countries, according to surveys.
The practice has been popular in Florida. More than a dozen storefronts across the state help consumers connect to pharmacies in Canada and other countries. Several cities, state and school districts in Florida help employees get drugs from Canada.
The administration’s proposal builds on a 2000 law that opened the door to allowing drug importation from Canada. But that provision could take effect only if the Health and Human Services secretary certified importation as safe, something that Democratic and Republican administrations have refused to do.
The drug industry for years has said allowing drugs to be imported from Canada would disrupt the nation’s supply chain and make it easier for unsafe or counterfeit medications to enter the market.
Trump, who made lowering prescription drug prices a signature promise in his 2016 campaign, has been eager to fulfill his pledge. In July 2019, at Trump’s direction, HHS Secretary Alex Azar said the federal government was “open for business” on drug importation, a year after calling drug importation a “gimmick.”
The administration envisions a system in which a Canadian-licensed wholesaler buys directly from a manufacturer for drugs approved for sale in Canada and exports the drugs to a U.S. wholesaler/importer under contract to a state.
Florida’s legislation – approved in 2019 – would set up two importation programs. The first would focus on getting drugs for state programs such as Medicaid, the Department of Corrections and county health departments. State officials said they expect the programs would save the state about $150 million annually.
The second program would be geared to the broader state population.
In response to the draft rule, the states seeking to start a drug importation program suggested changes to the administration’s proposal.
“Should the final rule not address these areas of concern, Colorado will struggle to find appropriate partners and realize significant savings for consumers,” Kim Bimestefer, executive director of the Colorado Department of Health Care Policy & Financing, told the FDA in March.
Among the state’s concerns is that it would be limited to using only one Canadian wholesaler, and without competition the state fears prices might not be as low as officials hoped. Bimestefer also noted that under the draft rule, the federal government would approve the importation program for only two years and states need a longer time frame to get buy-in from wholesalers and other partners.
Colorado officials estimate importing drugs from Canada could cut prices by 54% for cancer drugs and 75% for cardiac medicines. The state also noted the diabetes drug Jardiance costs $400 a month in the United States and sells for $85 in Canada.
Several states worry some of the most expensive drugs – including injectable and biologic medicines – were exempt from the federal rule. Those drug classes are not allowed to be imported under the 2000 law.
However, in an executive order in July, Trump said he would allow insulin to be imported if Azar determined it is required for emergency medical care. An HHS spokesman would not say whether Azar has done that.
Jane Horvath, a health policy consultant in College Park, Md., said the administration faces several challenges getting an importation program up and running, including possible opposition from the pharmaceutical industry and limits on classes of drugs that can be sold over the border.
“Despite the barriers, the programs are still quite worthwhile to pursue,” she said.
Maine’s top health official said the administration should work with the Canadian government to address Canada’s concerns. HHS officials refused to say whether such discussions have started.
Officials in Vermont, where the program would also include consumers covered by private insurance, remain hopeful.
“Given that we want to reduce the burden of health care costs on residents in our state, then it is important to pursue this option if there is a clear pathway forward,” Backus said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente. This story also ran on Miami Herald.
Many Americans still concerned about access to health care
according to the results of a survey conducted Aug. 7-26.
Nationally, 23.8% of respondents said that they were very concerned about being able to receive care during the pandemic, and another 27.4% said that they were somewhat concerned. Just under a quarter, 24.3%, said they were not very concerned, while 20.4% were not at all concerned, the COVID-19 Consortium for Understanding the Public’s Policy Preferences Across States reported after surveying 21,196 adults.
At the state level, Mississippi had the most adults (35.5%) who were very concerned about their access to care, followed by Texas (32.7%) and Nevada (32.4%). The residents of Montana were least likely (10.5%) to be very concerned, with Vermont next at 11.6% and Wyoming slightly higher at 13.8%. Montana also had the highest proportion of adults, 30.2%, who were not at all concerned, the consortium’s data show.
When asked about getting the coronavirus themselves, 67.8% of U.S. adults came down on the concerned side (33.3% somewhat and 34.5% very concerned) versus 30.8% who were not concerned (18.6% were not very concerned; 12.2% were not concerned at all.). Respondents’ concern was higher for their family members’ risk of getting coronavirus: 30.2% were somewhat concerned and 47.6% were very concerned, the consortium said.
Among many other topics, respondents were asked how closely they had followed recommended health guidelines in the last week, with the two extremes shown here:
- Avoiding contact with other people: 49.3% very closely, 4.8% not at all closely.
- Frequently washing hands: 74.7% very, 1.6% not at all.
- Disinfecting often-touched surfaces: 54.4% very, 4.3% not at all.
- Wearing a face mask in public: 75.7% very, 3.5% not at all.
The consortium is a joint project of the Network Science Institute of Northeastern University; the Shorenstein Center on Media, Politics, and Public Policy of Harvard University; Harvard Medical School; the School of Communication and Information at Rutgers University; and the department of political science at Northwestern University. The project is supported by grants from the National Science Foundation.
according to the results of a survey conducted Aug. 7-26.
Nationally, 23.8% of respondents said that they were very concerned about being able to receive care during the pandemic, and another 27.4% said that they were somewhat concerned. Just under a quarter, 24.3%, said they were not very concerned, while 20.4% were not at all concerned, the COVID-19 Consortium for Understanding the Public’s Policy Preferences Across States reported after surveying 21,196 adults.
At the state level, Mississippi had the most adults (35.5%) who were very concerned about their access to care, followed by Texas (32.7%) and Nevada (32.4%). The residents of Montana were least likely (10.5%) to be very concerned, with Vermont next at 11.6% and Wyoming slightly higher at 13.8%. Montana also had the highest proportion of adults, 30.2%, who were not at all concerned, the consortium’s data show.
When asked about getting the coronavirus themselves, 67.8% of U.S. adults came down on the concerned side (33.3% somewhat and 34.5% very concerned) versus 30.8% who were not concerned (18.6% were not very concerned; 12.2% were not concerned at all.). Respondents’ concern was higher for their family members’ risk of getting coronavirus: 30.2% were somewhat concerned and 47.6% were very concerned, the consortium said.
Among many other topics, respondents were asked how closely they had followed recommended health guidelines in the last week, with the two extremes shown here:
- Avoiding contact with other people: 49.3% very closely, 4.8% not at all closely.
- Frequently washing hands: 74.7% very, 1.6% not at all.
- Disinfecting often-touched surfaces: 54.4% very, 4.3% not at all.
- Wearing a face mask in public: 75.7% very, 3.5% not at all.
The consortium is a joint project of the Network Science Institute of Northeastern University; the Shorenstein Center on Media, Politics, and Public Policy of Harvard University; Harvard Medical School; the School of Communication and Information at Rutgers University; and the department of political science at Northwestern University. The project is supported by grants from the National Science Foundation.
according to the results of a survey conducted Aug. 7-26.
Nationally, 23.8% of respondents said that they were very concerned about being able to receive care during the pandemic, and another 27.4% said that they were somewhat concerned. Just under a quarter, 24.3%, said they were not very concerned, while 20.4% were not at all concerned, the COVID-19 Consortium for Understanding the Public’s Policy Preferences Across States reported after surveying 21,196 adults.
At the state level, Mississippi had the most adults (35.5%) who were very concerned about their access to care, followed by Texas (32.7%) and Nevada (32.4%). The residents of Montana were least likely (10.5%) to be very concerned, with Vermont next at 11.6% and Wyoming slightly higher at 13.8%. Montana also had the highest proportion of adults, 30.2%, who were not at all concerned, the consortium’s data show.
When asked about getting the coronavirus themselves, 67.8% of U.S. adults came down on the concerned side (33.3% somewhat and 34.5% very concerned) versus 30.8% who were not concerned (18.6% were not very concerned; 12.2% were not concerned at all.). Respondents’ concern was higher for their family members’ risk of getting coronavirus: 30.2% were somewhat concerned and 47.6% were very concerned, the consortium said.
Among many other topics, respondents were asked how closely they had followed recommended health guidelines in the last week, with the two extremes shown here:
- Avoiding contact with other people: 49.3% very closely, 4.8% not at all closely.
- Frequently washing hands: 74.7% very, 1.6% not at all.
- Disinfecting often-touched surfaces: 54.4% very, 4.3% not at all.
- Wearing a face mask in public: 75.7% very, 3.5% not at all.
The consortium is a joint project of the Network Science Institute of Northeastern University; the Shorenstein Center on Media, Politics, and Public Policy of Harvard University; Harvard Medical School; the School of Communication and Information at Rutgers University; and the department of political science at Northwestern University. The project is supported by grants from the National Science Foundation.
Even in a virtual environment, the Society of Gynecologic Surgeons delivers without a “glitch”
Earlier this year, I was honored to serve as the Scientific Program Chair for the 46th Annual Scientific Meeting of the Society of Gynecologic Surgeons (SGS). This year’s meeting was the first ever (and hopefully last) “virtual” scientific meeting, which consisted of a hybrid of prerecorded and live presentations. Although faculty and attendees were not able to be together physically, the essence of the lively SGS meetings came through loud and clear. We still had “discussants” comment on the oral presentations and ask questions of the presenters. These questions and answers were all done live—without a glitch! Many thanks to all who made this meeting possible.
In addition to the outstanding abstract and video presentations, there were 4 superb postgraduate courses:
- Mikio Nihira, MD, chaired “Enhanced recovery after surgery: Overcoming barriers to implementation.”
- Charles Hanes, MD, headed up “It’s all about the apex: The key to successful POP surgery.”
- Cara King, DO, MS, led “Total laparoscopic hysterectomy: Pushing the envelope.”
- Vincent Lucente, MD, chaired “Transvaginal reconstructive pelvic surgery using graft augmentation post-FDA.”
Many special thanks to Dr. Lucente who transformed his course into a wonderful article for this special section of
One of our exceptional keynote speakers was Marc Beer (a serial entrepreneur and cofounder, chairman, and CEO of Renovia, Inc.), whose talk was entitled “A primer on medical device innovation—How to avoid common pitfalls while realizing your vision.” Mr. Beer has turned this topic into a unique article for this special section (see next month’s issue for Part 2).
Our TeLinde Lecture, entitled “Artificial intelligence in surgery,” was delivered by the dynamic Vicente Gracias, MD, professor of surgery at Robert Wood Johnson University Hospital, New Brunswick, New Jersey. We also held 2 live panel discussions that were very popular. The first, “Work-life balance and gynecologic surgery,” featured various perspectives from Drs. Kristie Green, Sally Huber, Catherine Matthews, and Charles Rardin. The second panel discussion, entitled “Understanding, managing, and benefiting from your e-presence,” by experts Heather Schueppert; Chief Marketing Officer at Unified Physician Management, Brad Bowman, MD; and Peter Lotze, MD. Both of these panel discussions are included in this special section as well.
I hope you enjoy the content of this special section of
Earlier this year, I was honored to serve as the Scientific Program Chair for the 46th Annual Scientific Meeting of the Society of Gynecologic Surgeons (SGS). This year’s meeting was the first ever (and hopefully last) “virtual” scientific meeting, which consisted of a hybrid of prerecorded and live presentations. Although faculty and attendees were not able to be together physically, the essence of the lively SGS meetings came through loud and clear. We still had “discussants” comment on the oral presentations and ask questions of the presenters. These questions and answers were all done live—without a glitch! Many thanks to all who made this meeting possible.
In addition to the outstanding abstract and video presentations, there were 4 superb postgraduate courses:
- Mikio Nihira, MD, chaired “Enhanced recovery after surgery: Overcoming barriers to implementation.”
- Charles Hanes, MD, headed up “It’s all about the apex: The key to successful POP surgery.”
- Cara King, DO, MS, led “Total laparoscopic hysterectomy: Pushing the envelope.”
- Vincent Lucente, MD, chaired “Transvaginal reconstructive pelvic surgery using graft augmentation post-FDA.”
Many special thanks to Dr. Lucente who transformed his course into a wonderful article for this special section of
One of our exceptional keynote speakers was Marc Beer (a serial entrepreneur and cofounder, chairman, and CEO of Renovia, Inc.), whose talk was entitled “A primer on medical device innovation—How to avoid common pitfalls while realizing your vision.” Mr. Beer has turned this topic into a unique article for this special section (see next month’s issue for Part 2).
Our TeLinde Lecture, entitled “Artificial intelligence in surgery,” was delivered by the dynamic Vicente Gracias, MD, professor of surgery at Robert Wood Johnson University Hospital, New Brunswick, New Jersey. We also held 2 live panel discussions that were very popular. The first, “Work-life balance and gynecologic surgery,” featured various perspectives from Drs. Kristie Green, Sally Huber, Catherine Matthews, and Charles Rardin. The second panel discussion, entitled “Understanding, managing, and benefiting from your e-presence,” by experts Heather Schueppert; Chief Marketing Officer at Unified Physician Management, Brad Bowman, MD; and Peter Lotze, MD. Both of these panel discussions are included in this special section as well.
I hope you enjoy the content of this special section of
Earlier this year, I was honored to serve as the Scientific Program Chair for the 46th Annual Scientific Meeting of the Society of Gynecologic Surgeons (SGS). This year’s meeting was the first ever (and hopefully last) “virtual” scientific meeting, which consisted of a hybrid of prerecorded and live presentations. Although faculty and attendees were not able to be together physically, the essence of the lively SGS meetings came through loud and clear. We still had “discussants” comment on the oral presentations and ask questions of the presenters. These questions and answers were all done live—without a glitch! Many thanks to all who made this meeting possible.
In addition to the outstanding abstract and video presentations, there were 4 superb postgraduate courses:
- Mikio Nihira, MD, chaired “Enhanced recovery after surgery: Overcoming barriers to implementation.”
- Charles Hanes, MD, headed up “It’s all about the apex: The key to successful POP surgery.”
- Cara King, DO, MS, led “Total laparoscopic hysterectomy: Pushing the envelope.”
- Vincent Lucente, MD, chaired “Transvaginal reconstructive pelvic surgery using graft augmentation post-FDA.”
Many special thanks to Dr. Lucente who transformed his course into a wonderful article for this special section of
One of our exceptional keynote speakers was Marc Beer (a serial entrepreneur and cofounder, chairman, and CEO of Renovia, Inc.), whose talk was entitled “A primer on medical device innovation—How to avoid common pitfalls while realizing your vision.” Mr. Beer has turned this topic into a unique article for this special section (see next month’s issue for Part 2).
Our TeLinde Lecture, entitled “Artificial intelligence in surgery,” was delivered by the dynamic Vicente Gracias, MD, professor of surgery at Robert Wood Johnson University Hospital, New Brunswick, New Jersey. We also held 2 live panel discussions that were very popular. The first, “Work-life balance and gynecologic surgery,” featured various perspectives from Drs. Kristie Green, Sally Huber, Catherine Matthews, and Charles Rardin. The second panel discussion, entitled “Understanding, managing, and benefiting from your e-presence,” by experts Heather Schueppert; Chief Marketing Officer at Unified Physician Management, Brad Bowman, MD; and Peter Lotze, MD. Both of these panel discussions are included in this special section as well.
I hope you enjoy the content of this special section of
Exorcising your ghosts
The COVID-19 pandemic has affected private medical practices on so many levels, not least of which is the loss of employees to illness, fear of illness, early retirement, and other reasons.
![]()
If you’re not hip to the slang, “ghosting” is the situation in which an employee disappears without any warning, notice, or explanation. It usually occurs after a candidate accepts a job offer, and you schedule their first day of work. That day dawns, but the new hire never arrives. Less commonly, an employee who has been with you for some time simply stops showing up and cannot be contacted.
Many employers think of ghosting as a relatively new phenomenon, and blame it on the irresponsibility of younger age groups – millennials, in particular. In fact, it has been an issue for many years across all age groups, and employers often share more of the responsibility than they think.
While total prevention is impossible, there are steps you can take as an employer to minimize ghosting in your practice.
- Your hiring process needs to be efficient. If you wait too long to schedule an interview with a promising candidate or to offer them the job, another job offer could lure them away. At the very least, a lengthy process or a lack of transparency may make the applicant apprehensive about accepting a job with you, particularly if other employers are pursuing them.
- Keep applicants in the loop. Follow up with every candidate; let them know where they are in your hiring process. Applicants who have no clue whether they have a shot at the job are going to start looking elsewhere. And make sure they know the job description and starting salary from the outset.
- Talk to new hires before their first day. Contact them personally to see if they have any questions or concerns, and let them know that you’re looking forward to their arrival.
- Once they start, make them feel welcome. An employee’s first few days on the job set the tone for the rest of the employment relationship. During this time, clearly communicate what the employee can expect from you and what you expect from them. Take time to discuss key issues, such as work schedules, timekeeping practices, how performance is measured, and dress codes. Introduce them to coworkers, and get them started shadowing more experienced staff members.
- Take a hard look at your supervision and your supervisors. Business people like to say that employees don’t quit their job, they quit their boss. If an employee quits – with or without notice – it may very well be because of a poor working relationship with you or the supervisor. To be effective, you and your supervisors need to be diligent in setting goals, managing performance, and applying workplace rules and policies. Numerous third-party companies provide training and guidance in these areas when needed.
- Recognize and reward. As I’ve written many times, positive feedback is a simple, low-cost way to improve employee retention. It demonstrates that you value an employee’s contributions and sets an excellent example for other employees. Effective recognition can come from anyone – including patients – and should be given openly. (Another old adage: “Praise publicly, criticize privately.”) It never hurts to catch an employee doing something right and acknowledge it.
- Don’t jump to conclusions. If a new hire or employee is absent without notice, don’t just assume you’ve been ghosted. There may be extenuating circumstances, such as an emergency or illness. In some states, an employee’s absence is protected under a law where the employee may not be required to provide advance notice, and taking adverse action could violate these laws. Establish procedures for attempting to contact absent employees, and make sure you’re complying with all applicable leave laws before taking any action.

If an employee does abandon their job, think before you act. Comply with all applicable laws. Act consistently with how you’ve handled similar situations in the past. Your attorney should be involved, especially if the decision involves termination. Notify the employee in writing. As with all employment decisions, keep adequate documentation in case the decision is ever challenged, or you need it to support future disciplinary decisions.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no disclosures related to this column. Write to him at dermnews@mdedge.com.
The COVID-19 pandemic has affected private medical practices on so many levels, not least of which is the loss of employees to illness, fear of illness, early retirement, and other reasons.
![]()
If you’re not hip to the slang, “ghosting” is the situation in which an employee disappears without any warning, notice, or explanation. It usually occurs after a candidate accepts a job offer, and you schedule their first day of work. That day dawns, but the new hire never arrives. Less commonly, an employee who has been with you for some time simply stops showing up and cannot be contacted.
Many employers think of ghosting as a relatively new phenomenon, and blame it on the irresponsibility of younger age groups – millennials, in particular. In fact, it has been an issue for many years across all age groups, and employers often share more of the responsibility than they think.
While total prevention is impossible, there are steps you can take as an employer to minimize ghosting in your practice.
- Your hiring process needs to be efficient. If you wait too long to schedule an interview with a promising candidate or to offer them the job, another job offer could lure them away. At the very least, a lengthy process or a lack of transparency may make the applicant apprehensive about accepting a job with you, particularly if other employers are pursuing them.
- Keep applicants in the loop. Follow up with every candidate; let them know where they are in your hiring process. Applicants who have no clue whether they have a shot at the job are going to start looking elsewhere. And make sure they know the job description and starting salary from the outset.
- Talk to new hires before their first day. Contact them personally to see if they have any questions or concerns, and let them know that you’re looking forward to their arrival.
- Once they start, make them feel welcome. An employee’s first few days on the job set the tone for the rest of the employment relationship. During this time, clearly communicate what the employee can expect from you and what you expect from them. Take time to discuss key issues, such as work schedules, timekeeping practices, how performance is measured, and dress codes. Introduce them to coworkers, and get them started shadowing more experienced staff members.
- Take a hard look at your supervision and your supervisors. Business people like to say that employees don’t quit their job, they quit their boss. If an employee quits – with or without notice – it may very well be because of a poor working relationship with you or the supervisor. To be effective, you and your supervisors need to be diligent in setting goals, managing performance, and applying workplace rules and policies. Numerous third-party companies provide training and guidance in these areas when needed.
- Recognize and reward. As I’ve written many times, positive feedback is a simple, low-cost way to improve employee retention. It demonstrates that you value an employee’s contributions and sets an excellent example for other employees. Effective recognition can come from anyone – including patients – and should be given openly. (Another old adage: “Praise publicly, criticize privately.”) It never hurts to catch an employee doing something right and acknowledge it.
- Don’t jump to conclusions. If a new hire or employee is absent without notice, don’t just assume you’ve been ghosted. There may be extenuating circumstances, such as an emergency or illness. In some states, an employee’s absence is protected under a law where the employee may not be required to provide advance notice, and taking adverse action could violate these laws. Establish procedures for attempting to contact absent employees, and make sure you’re complying with all applicable leave laws before taking any action.
If an employee does abandon their job, think before you act. Comply with all applicable laws. Act consistently with how you’ve handled similar situations in the past. Your attorney should be involved, especially if the decision involves termination. Notify the employee in writing. As with all employment decisions, keep adequate documentation in case the decision is ever challenged, or you need it to support future disciplinary decisions.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no disclosures related to this column. Write to him at dermnews@mdedge.com.
The COVID-19 pandemic has affected private medical practices on so many levels, not least of which is the loss of employees to illness, fear of illness, early retirement, and other reasons.
![]()
If you’re not hip to the slang, “ghosting” is the situation in which an employee disappears without any warning, notice, or explanation. It usually occurs after a candidate accepts a job offer, and you schedule their first day of work. That day dawns, but the new hire never arrives. Less commonly, an employee who has been with you for some time simply stops showing up and cannot be contacted.
Many employers think of ghosting as a relatively new phenomenon, and blame it on the irresponsibility of younger age groups – millennials, in particular. In fact, it has been an issue for many years across all age groups, and employers often share more of the responsibility than they think.
While total prevention is impossible, there are steps you can take as an employer to minimize ghosting in your practice.
- Your hiring process needs to be efficient. If you wait too long to schedule an interview with a promising candidate or to offer them the job, another job offer could lure them away. At the very least, a lengthy process or a lack of transparency may make the applicant apprehensive about accepting a job with you, particularly if other employers are pursuing them.
- Keep applicants in the loop. Follow up with every candidate; let them know where they are in your hiring process. Applicants who have no clue whether they have a shot at the job are going to start looking elsewhere. And make sure they know the job description and starting salary from the outset.
- Talk to new hires before their first day. Contact them personally to see if they have any questions or concerns, and let them know that you’re looking forward to their arrival.
- Once they start, make them feel welcome. An employee’s first few days on the job set the tone for the rest of the employment relationship. During this time, clearly communicate what the employee can expect from you and what you expect from them. Take time to discuss key issues, such as work schedules, timekeeping practices, how performance is measured, and dress codes. Introduce them to coworkers, and get them started shadowing more experienced staff members.
- Take a hard look at your supervision and your supervisors. Business people like to say that employees don’t quit their job, they quit their boss. If an employee quits – with or without notice – it may very well be because of a poor working relationship with you or the supervisor. To be effective, you and your supervisors need to be diligent in setting goals, managing performance, and applying workplace rules and policies. Numerous third-party companies provide training and guidance in these areas when needed.
- Recognize and reward. As I’ve written many times, positive feedback is a simple, low-cost way to improve employee retention. It demonstrates that you value an employee’s contributions and sets an excellent example for other employees. Effective recognition can come from anyone – including patients – and should be given openly. (Another old adage: “Praise publicly, criticize privately.”) It never hurts to catch an employee doing something right and acknowledge it.
- Don’t jump to conclusions. If a new hire or employee is absent without notice, don’t just assume you’ve been ghosted. There may be extenuating circumstances, such as an emergency or illness. In some states, an employee’s absence is protected under a law where the employee may not be required to provide advance notice, and taking adverse action could violate these laws. Establish procedures for attempting to contact absent employees, and make sure you’re complying with all applicable leave laws before taking any action.
If an employee does abandon their job, think before you act. Comply with all applicable laws. Act consistently with how you’ve handled similar situations in the past. Your attorney should be involved, especially if the decision involves termination. Notify the employee in writing. As with all employment decisions, keep adequate documentation in case the decision is ever challenged, or you need it to support future disciplinary decisions.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. He has no disclosures related to this column. Write to him at dermnews@mdedge.com.

Studying in Dermatology Residency
Dermatology residency can feel like drinking from a firehose, in which one is bombarded with so much information that it is impossible to retain any content. This article provides an overview of available resources and a guide on how to tailor studying throughout one’s training.
Prior to Residency
There are several resources that provide an introduction to dermatology and are appropriate for all medical students, regardless of intended specialty. The American Academy of Dermatology offers a free basic dermatology curriculum (https://www.aad.org/member/education/residents/bdc), with a choice of a 2- or 4-week course consisting of modules such as skin examination, basic science of the skin, dermatologic therapies, and specific dermatologic conditions. VisualDx offers LearnDerm (https://www.visualdx.com/learnderm/), which includes a 5-part tutorial and quiz focused on the skin examination, morphology, and lesion distribution. Lookingbill and Marks’ Principles of Dermatology1 is a book at an appropriate level for a medical student to learn about the fundamentals of dermatology. These resources may be helpful for residents to review immediately before starting dermatology residency (toward the end of intern year for most).
First Year
During the beginning of dermatology residency (postgraduate year [PGY] 2 for most), the fire hose of information feels most daunting. During this time, studying should focus on engendering a broad overview of dermatology. Most residencies maintain a textbook reading schedule, which provides a framework from which residents may structure their studying. Selection of a textbook tends to be program dependent. Even if the details of reading the textbook do not stick when reading it the first time, benefits include becoming familiar with what information one is expected to learn as a dermatologist and developing a strong foundation upon which one may continue to build. Based on my informal discussions with current residents, some reported that reading the textbook did not work well for them, citing too much minutiae in the textbooks and/or a preference for a more active learning approach. These residents instead focused on reading a review book for a broad overview, accompanied by a textbook or VisualDx when a more detailed reference is necessary. Table 1 provides a list of textbooks and mobile applications (apps) that residents may find helpful.
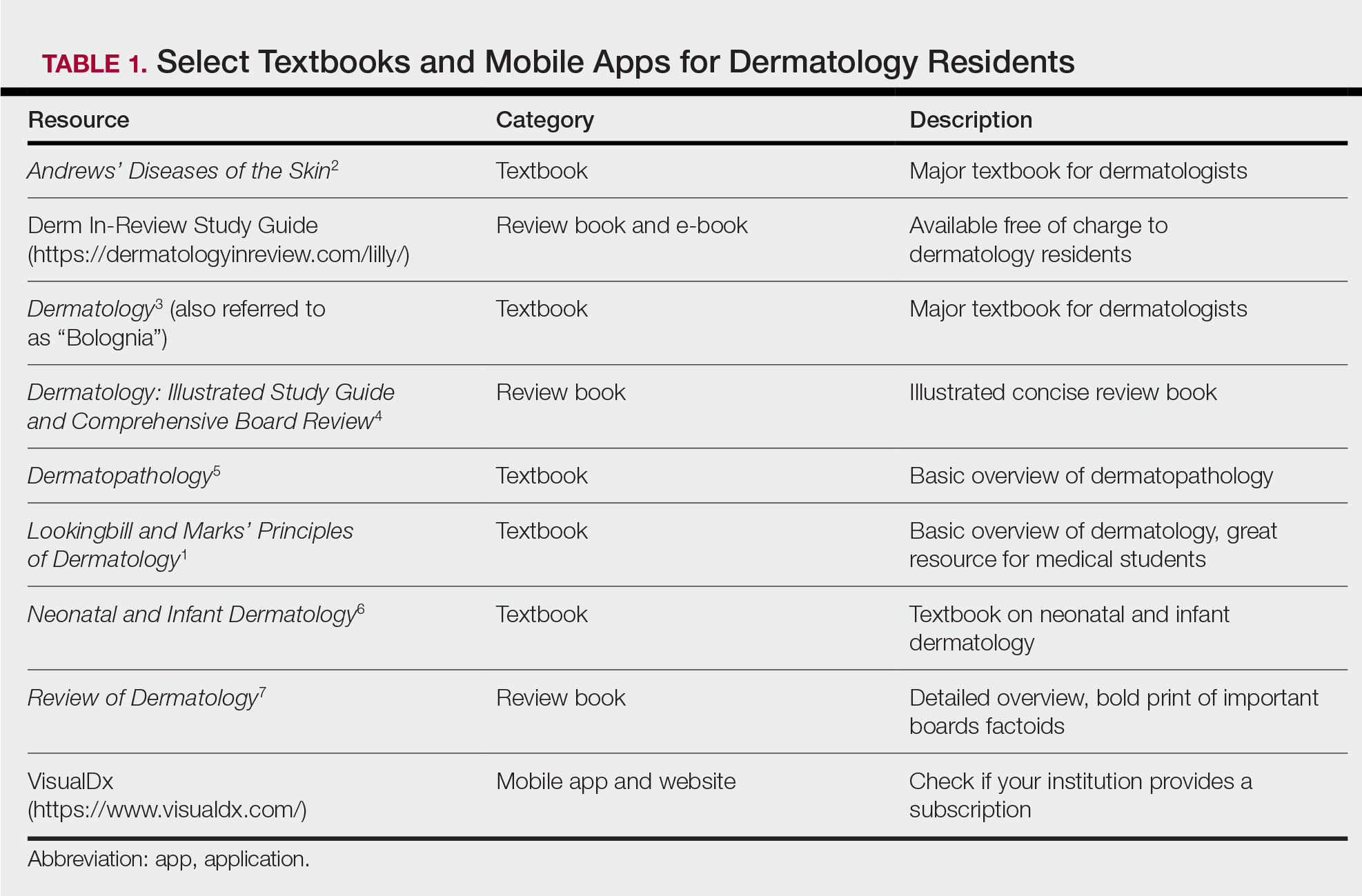
First-year residents may begin their efforts in synthesizing this new knowledge base toward the end of the year in preparation for the BASIC examination. The American Board of Dermatology provides a content outline as well as sample questions on their website (https://www.abderm.org/residents-and-fellows/exam-of-the-future-information-center.aspx#content), which may be used to guide more focused studying efforts during the weeks leading up to the examination.
Second Year
For second-year residents (PGY-3 for most) studying should focus on deepening and consolidating the broad foundation that was established during their first year. For many, this pursuit involves rereading the textbook chapters alongside more active learning measures, such as taking notes and quizzing oneself using flashcard apps and question banks (Table 2). Others may benefit from listening to podcasts (Table 3) or other sources utilizing audiovisual content, including attending conferences and other lectures virtually, which is becoming increasingly available in the setting of the coronavirus disease 2019 pandemic (Table 4). Because there are so many resources available to support these efforts, residents should be encouraged to try out a variety to determine what works best.
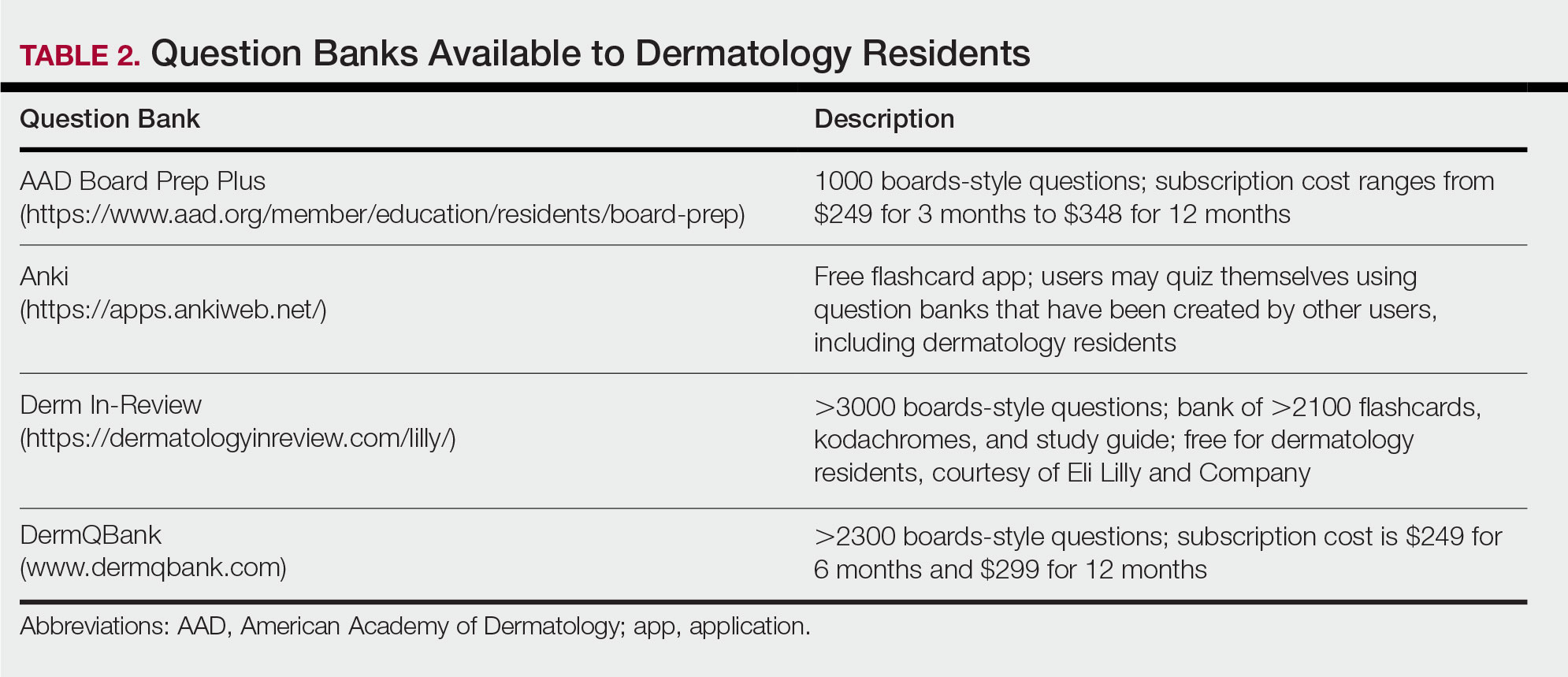
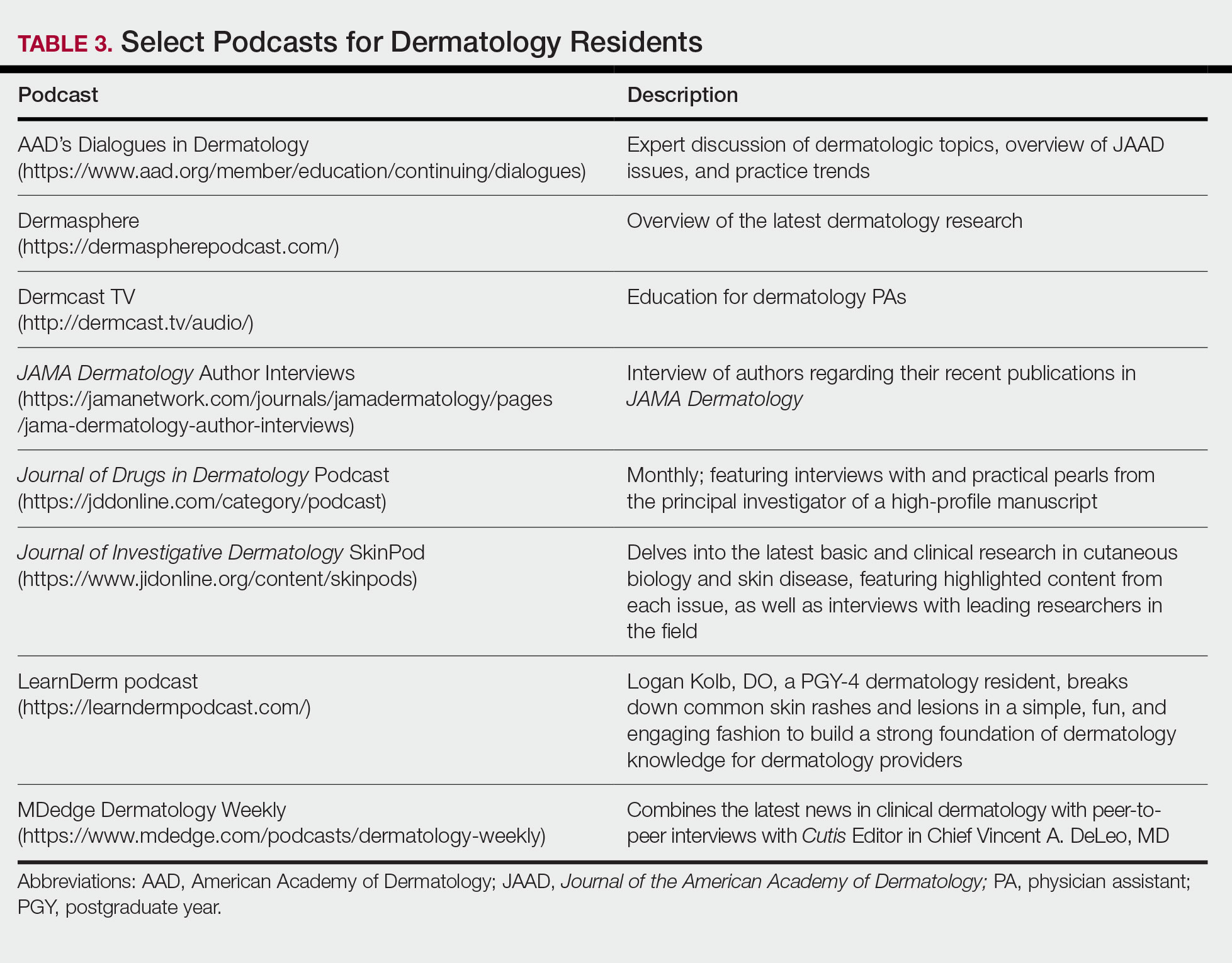
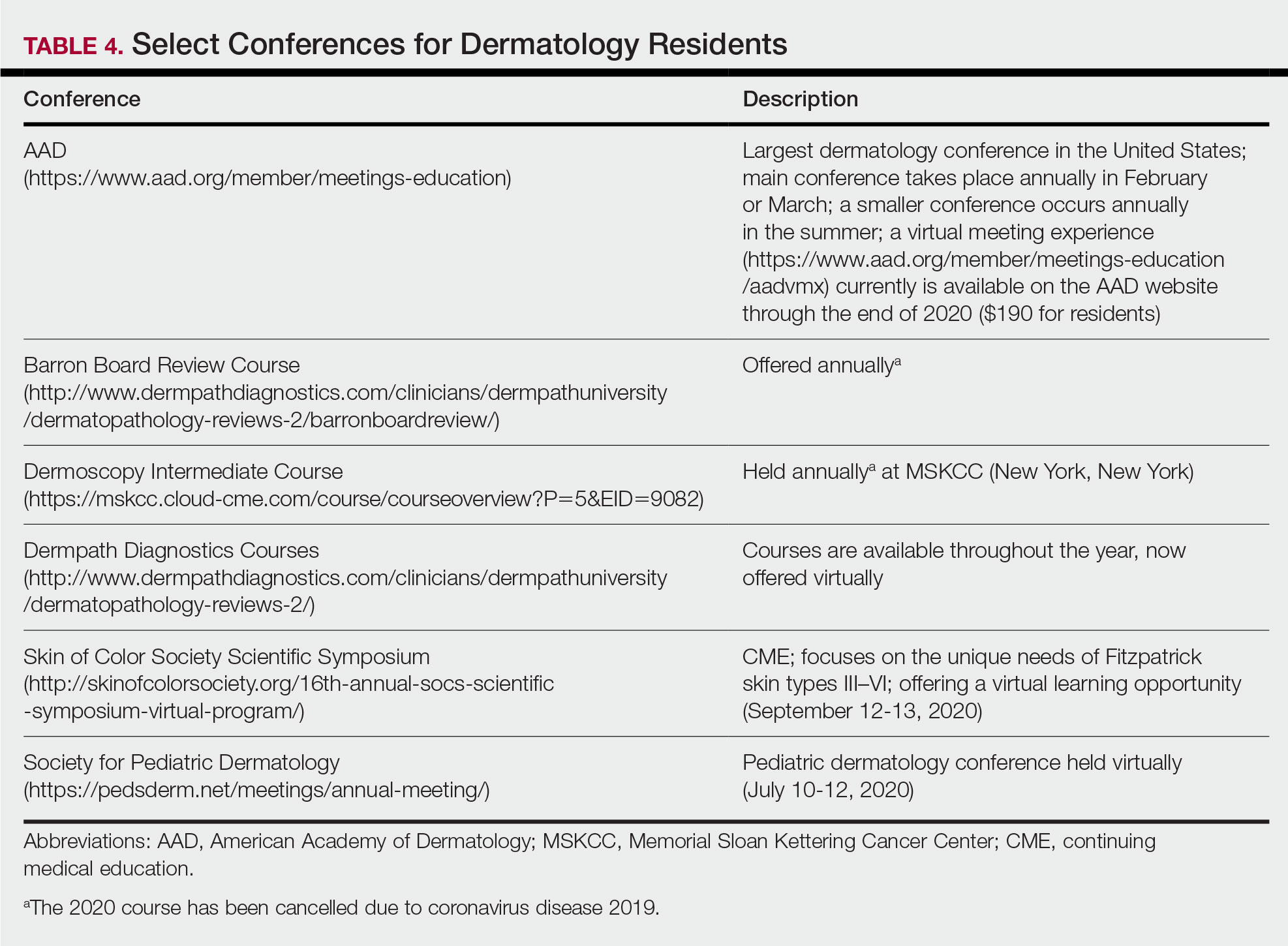
Toward the end of second year, studying may be tailored to preparing for the CORE examinations using the resources of one’s choice. Based on my discussions with current residents, a combination of reading review books, reviewing one’s personal notes, and quizzing through question banks and/or flashcard apps could be used.
In addition to maintaining a consistent and organized study schedule, second-year residents should continue to read in depth on topics related to patients for whom they are caring and stay on top of the dermatology literature. Table 5 provides a list of medical journals that dermatology residents should aim to read. The Journal of the American Academy of Dermatology’s continuing medical education series (https://www.jaad.org/content/collection-cme) may be particularly helpful to residents. In this series, experts review a variety of dermatologic topics in depth paired with quiz questions.
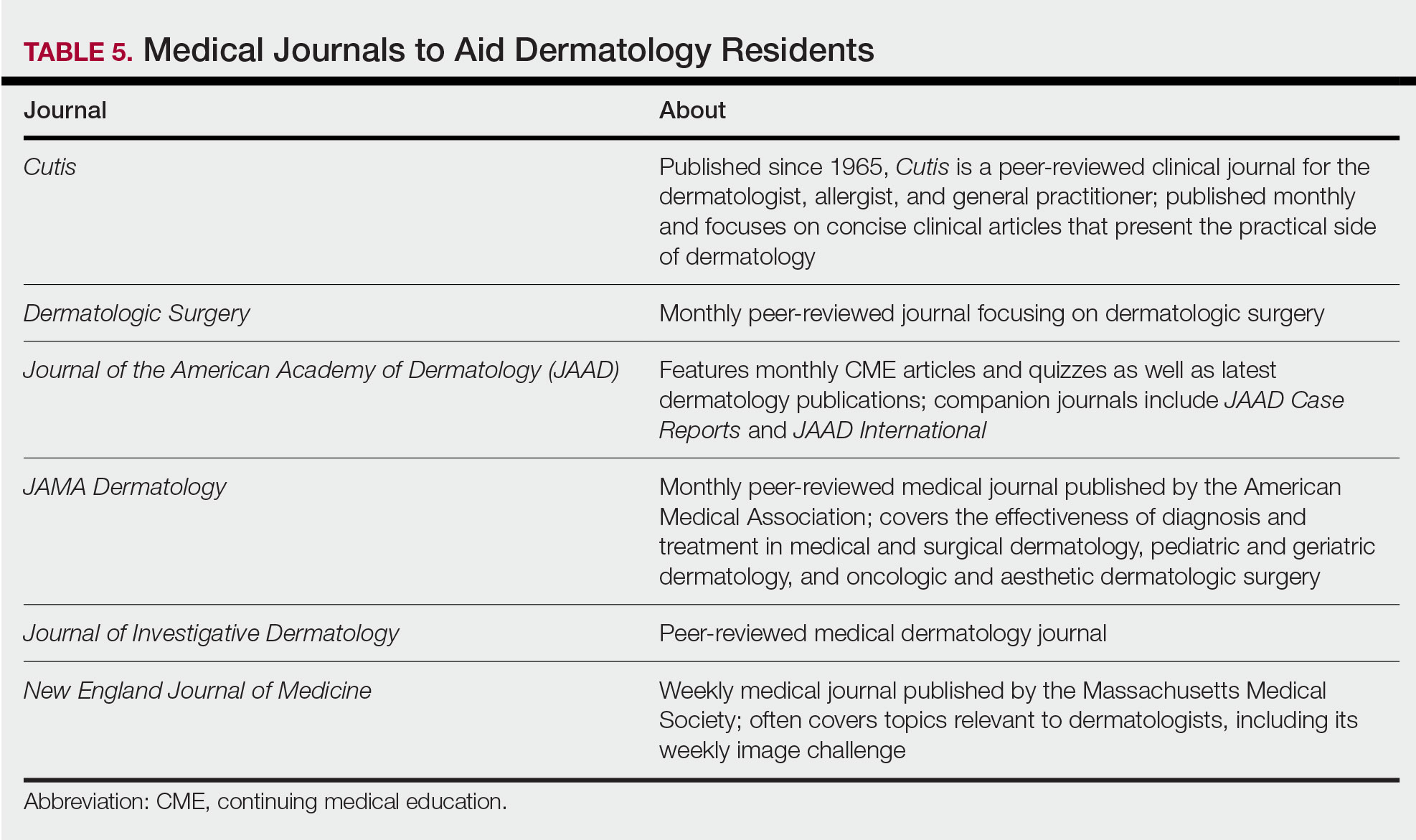
Third Year
As a third-year resident (PGY-4 for most), studying should focus on deepening one’s knowledge base and beginning preparation for the boards examination. At this point, residents should stick to a limited selection of resources (ie, 1 textbook, 1 review book, 1 question bank) for in-depth study. More time should be spent on active learning, such as note-taking and question banks. Boards review courses historically have been available to dermatology residents, namely the Barron Board Review course and a plenary session at the American Academy of Dermatology Annual Conference (Table 4).
Consistent Habits
Studying strategies can and should differ throughout dermatology residency, though consistency is necessary throughout. It is helpful to plan study schedules in advance—yearly, monthly, weekly—and aim to stick to them as much as possible. Finding what works for each individual may take trial and error. For some, it may mean waking up early to study before work, whereas others may do better in the evenings. It also is helpful to utilize a combination of longer blocks of studying (ie, weekend days), with consistent shorter blocks of time during the week. Many residents also learn to take advantage of time spent commuting by listening to podcasts in the car or reading while on public transportation.
Final Thoughts
There are many resources available to support residents in their learning such as textbooks, journals, podcasts, flashcards, question banks, and more. The path to mastery will be individualized for each resident, likely using a unique combination of resources. The beginning of residency is a good time to explore a variety of resources to see what works best, whereas at the end studying becomes more targeted.
- Marks Jr JG, Miller JJ. Lookingbill and Marks’ Principles of Dermatology. 6th ed. China: Elsevier; 2019.
- James WD, Elston DM, Treat JR. Andrews’ Diseases of the Skin. 13th ed. China: Elsevier; 2019.
- Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 4th ed. China: Elsevier; 2018.
- Jain S. Dermatology: Illustrated Study Guide and Comprehensive Board Review. New York, NY: Springer; 2012.
- Elston DM, Ferringer T, Ko C, et al. Dermatopathology. 2nd ed. China: Elsevier Saunders; 2014.
- Eichenfield LF, Frieden IJ, eds. Neonatal and Infant Dermatology. London, England: Saunders; 2015.
- Alikhan A, Hocker TLH, eds. Review of Dermatology. China: Elsevier; 2017.
Dermatology residency can feel like drinking from a firehose, in which one is bombarded with so much information that it is impossible to retain any content. This article provides an overview of available resources and a guide on how to tailor studying throughout one’s training.
Prior to Residency
There are several resources that provide an introduction to dermatology and are appropriate for all medical students, regardless of intended specialty. The American Academy of Dermatology offers a free basic dermatology curriculum (https://www.aad.org/member/education/residents/bdc), with a choice of a 2- or 4-week course consisting of modules such as skin examination, basic science of the skin, dermatologic therapies, and specific dermatologic conditions. VisualDx offers LearnDerm (https://www.visualdx.com/learnderm/), which includes a 5-part tutorial and quiz focused on the skin examination, morphology, and lesion distribution. Lookingbill and Marks’ Principles of Dermatology1 is a book at an appropriate level for a medical student to learn about the fundamentals of dermatology. These resources may be helpful for residents to review immediately before starting dermatology residency (toward the end of intern year for most).
First Year
During the beginning of dermatology residency (postgraduate year [PGY] 2 for most), the fire hose of information feels most daunting. During this time, studying should focus on engendering a broad overview of dermatology. Most residencies maintain a textbook reading schedule, which provides a framework from which residents may structure their studying. Selection of a textbook tends to be program dependent. Even if the details of reading the textbook do not stick when reading it the first time, benefits include becoming familiar with what information one is expected to learn as a dermatologist and developing a strong foundation upon which one may continue to build. Based on my informal discussions with current residents, some reported that reading the textbook did not work well for them, citing too much minutiae in the textbooks and/or a preference for a more active learning approach. These residents instead focused on reading a review book for a broad overview, accompanied by a textbook or VisualDx when a more detailed reference is necessary. Table 1 provides a list of textbooks and mobile applications (apps) that residents may find helpful.
First-year residents may begin their efforts in synthesizing this new knowledge base toward the end of the year in preparation for the BASIC examination. The American Board of Dermatology provides a content outline as well as sample questions on their website (https://www.abderm.org/residents-and-fellows/exam-of-the-future-information-center.aspx#content), which may be used to guide more focused studying efforts during the weeks leading up to the examination.
Second Year
For second-year residents (PGY-3 for most) studying should focus on deepening and consolidating the broad foundation that was established during their first year. For many, this pursuit involves rereading the textbook chapters alongside more active learning measures, such as taking notes and quizzing oneself using flashcard apps and question banks (Table 2). Others may benefit from listening to podcasts (Table 3) or other sources utilizing audiovisual content, including attending conferences and other lectures virtually, which is becoming increasingly available in the setting of the coronavirus disease 2019 pandemic (Table 4). Because there are so many resources available to support these efforts, residents should be encouraged to try out a variety to determine what works best.
Toward the end of second year, studying may be tailored to preparing for the CORE examinations using the resources of one’s choice. Based on my discussions with current residents, a combination of reading review books, reviewing one’s personal notes, and quizzing through question banks and/or flashcard apps could be used.
In addition to maintaining a consistent and organized study schedule, second-year residents should continue to read in depth on topics related to patients for whom they are caring and stay on top of the dermatology literature. Table 5 provides a list of medical journals that dermatology residents should aim to read. The Journal of the American Academy of Dermatology’s continuing medical education series (https://www.jaad.org/content/collection-cme) may be particularly helpful to residents. In this series, experts review a variety of dermatologic topics in depth paired with quiz questions.
Third Year
As a third-year resident (PGY-4 for most), studying should focus on deepening one’s knowledge base and beginning preparation for the boards examination. At this point, residents should stick to a limited selection of resources (ie, 1 textbook, 1 review book, 1 question bank) for in-depth study. More time should be spent on active learning, such as note-taking and question banks. Boards review courses historically have been available to dermatology residents, namely the Barron Board Review course and a plenary session at the American Academy of Dermatology Annual Conference (Table 4).
Consistent Habits
Studying strategies can and should differ throughout dermatology residency, though consistency is necessary throughout. It is helpful to plan study schedules in advance—yearly, monthly, weekly—and aim to stick to them as much as possible. Finding what works for each individual may take trial and error. For some, it may mean waking up early to study before work, whereas others may do better in the evenings. It also is helpful to utilize a combination of longer blocks of studying (ie, weekend days), with consistent shorter blocks of time during the week. Many residents also learn to take advantage of time spent commuting by listening to podcasts in the car or reading while on public transportation.
Final Thoughts
There are many resources available to support residents in their learning such as textbooks, journals, podcasts, flashcards, question banks, and more. The path to mastery will be individualized for each resident, likely using a unique combination of resources. The beginning of residency is a good time to explore a variety of resources to see what works best, whereas at the end studying becomes more targeted.
Dermatology residency can feel like drinking from a firehose, in which one is bombarded with so much information that it is impossible to retain any content. This article provides an overview of available resources and a guide on how to tailor studying throughout one’s training.
Prior to Residency
There are several resources that provide an introduction to dermatology and are appropriate for all medical students, regardless of intended specialty. The American Academy of Dermatology offers a free basic dermatology curriculum (https://www.aad.org/member/education/residents/bdc), with a choice of a 2- or 4-week course consisting of modules such as skin examination, basic science of the skin, dermatologic therapies, and specific dermatologic conditions. VisualDx offers LearnDerm (https://www.visualdx.com/learnderm/), which includes a 5-part tutorial and quiz focused on the skin examination, morphology, and lesion distribution. Lookingbill and Marks’ Principles of Dermatology1 is a book at an appropriate level for a medical student to learn about the fundamentals of dermatology. These resources may be helpful for residents to review immediately before starting dermatology residency (toward the end of intern year for most).
First Year
During the beginning of dermatology residency (postgraduate year [PGY] 2 for most), the fire hose of information feels most daunting. During this time, studying should focus on engendering a broad overview of dermatology. Most residencies maintain a textbook reading schedule, which provides a framework from which residents may structure their studying. Selection of a textbook tends to be program dependent. Even if the details of reading the textbook do not stick when reading it the first time, benefits include becoming familiar with what information one is expected to learn as a dermatologist and developing a strong foundation upon which one may continue to build. Based on my informal discussions with current residents, some reported that reading the textbook did not work well for them, citing too much minutiae in the textbooks and/or a preference for a more active learning approach. These residents instead focused on reading a review book for a broad overview, accompanied by a textbook or VisualDx when a more detailed reference is necessary. Table 1 provides a list of textbooks and mobile applications (apps) that residents may find helpful.
First-year residents may begin their efforts in synthesizing this new knowledge base toward the end of the year in preparation for the BASIC examination. The American Board of Dermatology provides a content outline as well as sample questions on their website (https://www.abderm.org/residents-and-fellows/exam-of-the-future-information-center.aspx#content), which may be used to guide more focused studying efforts during the weeks leading up to the examination.
Second Year
For second-year residents (PGY-3 for most) studying should focus on deepening and consolidating the broad foundation that was established during their first year. For many, this pursuit involves rereading the textbook chapters alongside more active learning measures, such as taking notes and quizzing oneself using flashcard apps and question banks (Table 2). Others may benefit from listening to podcasts (Table 3) or other sources utilizing audiovisual content, including attending conferences and other lectures virtually, which is becoming increasingly available in the setting of the coronavirus disease 2019 pandemic (Table 4). Because there are so many resources available to support these efforts, residents should be encouraged to try out a variety to determine what works best.
Toward the end of second year, studying may be tailored to preparing for the CORE examinations using the resources of one’s choice. Based on my discussions with current residents, a combination of reading review books, reviewing one’s personal notes, and quizzing through question banks and/or flashcard apps could be used.
In addition to maintaining a consistent and organized study schedule, second-year residents should continue to read in depth on topics related to patients for whom they are caring and stay on top of the dermatology literature. Table 5 provides a list of medical journals that dermatology residents should aim to read. The Journal of the American Academy of Dermatology’s continuing medical education series (https://www.jaad.org/content/collection-cme) may be particularly helpful to residents. In this series, experts review a variety of dermatologic topics in depth paired with quiz questions.
Third Year
As a third-year resident (PGY-4 for most), studying should focus on deepening one’s knowledge base and beginning preparation for the boards examination. At this point, residents should stick to a limited selection of resources (ie, 1 textbook, 1 review book, 1 question bank) for in-depth study. More time should be spent on active learning, such as note-taking and question banks. Boards review courses historically have been available to dermatology residents, namely the Barron Board Review course and a plenary session at the American Academy of Dermatology Annual Conference (Table 4).
Consistent Habits
Studying strategies can and should differ throughout dermatology residency, though consistency is necessary throughout. It is helpful to plan study schedules in advance—yearly, monthly, weekly—and aim to stick to them as much as possible. Finding what works for each individual may take trial and error. For some, it may mean waking up early to study before work, whereas others may do better in the evenings. It also is helpful to utilize a combination of longer blocks of studying (ie, weekend days), with consistent shorter blocks of time during the week. Many residents also learn to take advantage of time spent commuting by listening to podcasts in the car or reading while on public transportation.
Final Thoughts
There are many resources available to support residents in their learning such as textbooks, journals, podcasts, flashcards, question banks, and more. The path to mastery will be individualized for each resident, likely using a unique combination of resources. The beginning of residency is a good time to explore a variety of resources to see what works best, whereas at the end studying becomes more targeted.
- Marks Jr JG, Miller JJ. Lookingbill and Marks’ Principles of Dermatology. 6th ed. China: Elsevier; 2019.
- James WD, Elston DM, Treat JR. Andrews’ Diseases of the Skin. 13th ed. China: Elsevier; 2019.
- Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 4th ed. China: Elsevier; 2018.
- Jain S. Dermatology: Illustrated Study Guide and Comprehensive Board Review. New York, NY: Springer; 2012.
- Elston DM, Ferringer T, Ko C, et al. Dermatopathology. 2nd ed. China: Elsevier Saunders; 2014.
- Eichenfield LF, Frieden IJ, eds. Neonatal and Infant Dermatology. London, England: Saunders; 2015.
- Alikhan A, Hocker TLH, eds. Review of Dermatology. China: Elsevier; 2017.
- Marks Jr JG, Miller JJ. Lookingbill and Marks’ Principles of Dermatology. 6th ed. China: Elsevier; 2019.
- James WD, Elston DM, Treat JR. Andrews’ Diseases of the Skin. 13th ed. China: Elsevier; 2019.
- Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 4th ed. China: Elsevier; 2018.
- Jain S. Dermatology: Illustrated Study Guide and Comprehensive Board Review. New York, NY: Springer; 2012.
- Elston DM, Ferringer T, Ko C, et al. Dermatopathology. 2nd ed. China: Elsevier Saunders; 2014.
- Eichenfield LF, Frieden IJ, eds. Neonatal and Infant Dermatology. London, England: Saunders; 2015.
- Alikhan A, Hocker TLH, eds. Review of Dermatology. China: Elsevier; 2017.
Resident Pearls
- Independent study is a large component of dermatology residency.
- Consistent habits and a tailored approach will support optimal learning for each dermatology resident.
- The beginning of residency is a good time to explore a variety of resources to see what works best. Toward the end of residency, as studying becomes more targeted, residents may benefit from sticking to the resources with which they are most comfortable.

Physician income drops, burnout spikes globally in pandemic
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
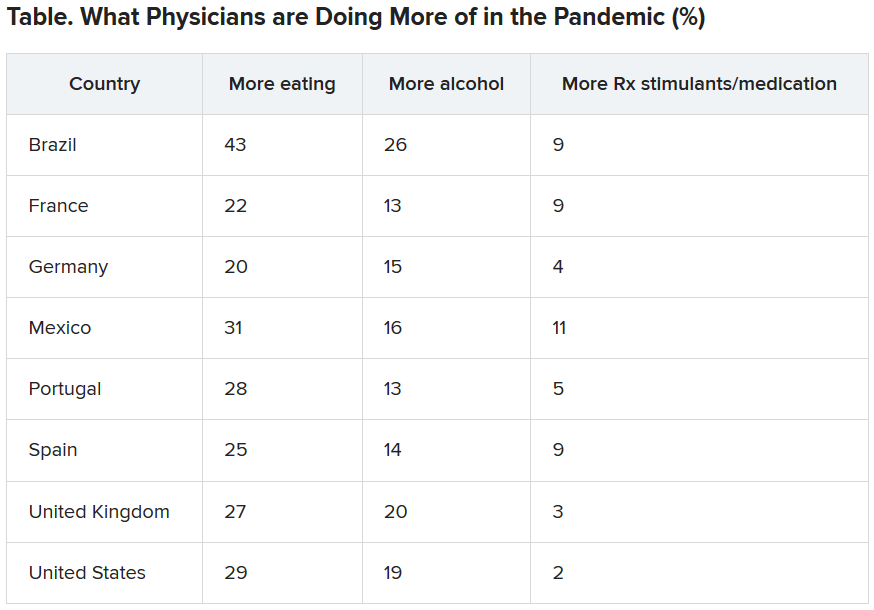
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
The march of immunotherapy continues at ESMO 2020
The use of immunotherapy for upper gastrointestinal tumors and renal cancer, ALK- and EGFR-targeted agents in non–small cell lung cancer (NSCLC), and the next step in personalized prostate cancer management will all be subjects of headlining presentations at the ESMO Virtual Congress 2020.
The conference will, like so many other major events, be held online this year because of the COVID-19 pandemic.
John B. Haanen, PhD, ESMO 2020 scientific chair, who is from the Netherlands Cancer Institute, Amsterdam, the Netherlands, told Medscape Medical News that, because the congress is being held online this year, fewer abstracts were submitted; nevertheless, “We were very happy to see ... that the quality was very good.”
The number of submissions was not the only problem the organizing committee had to face in transforming the ESMO Congress into a virtual meeting.
They were unable to fit the scientific and educational programs together and so have had to split them over two consecutive weekends. Moreover, many of the sessions were highly interactive and needed to be either adapted or omitted.
“So the program is somewhat different,” Haanen said. He noted that “the presentations were also made shorter, especially on the educational sessions, because...we can’t expect people to sit behind screens for hours listening to long presentations.”
He added: “That was out of the question.”
Haanen is nevertheless hopeful that the virtual meeting will be “very exciting.”
Solange Peters, MD, PhD, ESMO president, who is also affiliated with the Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland, said in a press conference that it was a “sacrifice” to move ESMO 2020 online and that “there were very sad moments” when deciding on the content.
However, there were some benefits from the change.
She said that all of the ESMO meetings this year have seen “huge” increases in the number of attendees and the geographical span or reach of each of the conferences.
“So suddenly you also realize that, what is one of the missions of ESMO being to convey education globally ... was probably better reached, better achieved with the virtual format,” she commented.
Presidential symposia
Turning to the program, Haanen first picked out the third presidential symposium, which will be held on Monday, September 21. This will focus entirely on upper gastrointestinal tumors in both the adjuvant and metastatic setting.
He said that in recent years, “very little progress has been made” in this area, with treatment mostly consisting of chemotherapy and chemoradiotherapy.
However, this year’s presentations will explore the addition of immunotherapy either to chemotherapy or as an adjuvant treatment following completion of standard-of-care treatment for local disease.
Haanen said that the results will be “very interesting ... and may change current practice,” something that “is very important for both doctors and their patients.”
On Saturday, September 19, the first presidential symposium will include two presentations on lung cancer that Haanen said will offer some “exciting new [results] that I am sure will change clinical practice.”
One will be on the CROWN phase 3 trial comparing lorlatinib and crizotinib in the first-line treatment of patients with advanced ALK-positive NSCLC.
The other will present results on central nervous system disease recurrence from the ADAURA phase 3 trial of osimertinib adjuvant therapy in patients with resected EGFR-mutated NSCLC.
The same session will also see new data in advanced renal cell carcinoma from CheckMate 9ER, in which the c-Met and VEGFR2 inhibitor cabozantinib (Cabometyx) was combined with nivolumab (Opdivo) and compared to sunitinib (Sutent) in untreated patients.
“Last year, there were already some exciting results of the combination of axitinib [Inlyta], either with pembrolizumab [Keytruda] or with avelumab [Bavencio]...in the first-line setting in metastatic clear cell renal cell cancer,” Hannen said.
“Clearly there was a survival advantage over the standard of care, sunitinib,” he added.
This year, not only will efficacy data from CheckMate 9ER be presented but also quality-of-life results.
“That’s very important, because what everybody is afraid of is that, by adding drugs, you always get more impact on the quality of life, but you will see that the quality-of-life results are very exciting,” he said.
The second presidential symposium will feature studies on prostate cancer, notably the phase 3 IPATential150 trial of abiraterone (Zytiga) plus either ipatasertib or placebo in metastatic castration-resistant prostate cancer.
Ipatasertib targets Akt, and Haanen said that “by adding it to, let’s say, standard-of-care treatment ... the question of course of will be, Does that have a better outcome?”
He believes the results will be a “very nice illustration” that prostate cancer management is heading in the direction of personalized treatment.
Alongside the presidential symposia, there will be a number of proffered paper sessions on the latest results in all aspects of oncology, including results from the ASCENT trial in triple-negative breast cancer, as well as a dedicated COVID-19 track.
Haanen said that the ESMO Virtual Congress 2020, coming after the AACR and ASCO annual meetings, has the “advantage” of being able to present the latest outcomes of patients treated with chemotherapy and immunotherapy against the backdrop of the pandemic.
This will include a study from the ESMO Resilience Task Force on the impact of COVID-19 on oncology professionals both in terms of their personal distress and burnout and their job performance.
“I think that is very important,” Haanen said, “especially because the whole thing with COVID-19 is not yet over, and everybody is preparing for a second wave in the fall and winter.
“It may help us give us clues on how we can protect ourselves or each other to prevent burnout or other problems that we as healthcare caregivers face in this difficult period.”
Next year
For next year, Peters remains hopeful that the ESMO 2021 meeting will take place as planned in Paris.
She anticipates that, indeed, ESMO meetings will be able to take place from spring next year.
This will depend on a vaccine for COVID-19 becoming widely available, although oncologists in some countries may still not be able to travel.
This means “starting probably with hybrid formats, with some of the faculty being on site and some not, [and] the same thing for the attendees,” Peters said.
She suggested that, for ESMO Congress 2021 to work as an on-site meeting, it will require at least half or two-thirds of the originally anticipated number of attendees.
“I hope that Paris next year will happen,” Peters said, adding that it “will probably happen with less attendees – that’s fine, but [still] with a large number of faculty and attendees.”
The commentators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The use of immunotherapy for upper gastrointestinal tumors and renal cancer, ALK- and EGFR-targeted agents in non–small cell lung cancer (NSCLC), and the next step in personalized prostate cancer management will all be subjects of headlining presentations at the ESMO Virtual Congress 2020.
The conference will, like so many other major events, be held online this year because of the COVID-19 pandemic.
John B. Haanen, PhD, ESMO 2020 scientific chair, who is from the Netherlands Cancer Institute, Amsterdam, the Netherlands, told Medscape Medical News that, because the congress is being held online this year, fewer abstracts were submitted; nevertheless, “We were very happy to see ... that the quality was very good.”
The number of submissions was not the only problem the organizing committee had to face in transforming the ESMO Congress into a virtual meeting.
They were unable to fit the scientific and educational programs together and so have had to split them over two consecutive weekends. Moreover, many of the sessions were highly interactive and needed to be either adapted or omitted.
“So the program is somewhat different,” Haanen said. He noted that “the presentations were also made shorter, especially on the educational sessions, because...we can’t expect people to sit behind screens for hours listening to long presentations.”
He added: “That was out of the question.”
Haanen is nevertheless hopeful that the virtual meeting will be “very exciting.”
Solange Peters, MD, PhD, ESMO president, who is also affiliated with the Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland, said in a press conference that it was a “sacrifice” to move ESMO 2020 online and that “there were very sad moments” when deciding on the content.
However, there were some benefits from the change.
She said that all of the ESMO meetings this year have seen “huge” increases in the number of attendees and the geographical span or reach of each of the conferences.
“So suddenly you also realize that, what is one of the missions of ESMO being to convey education globally ... was probably better reached, better achieved with the virtual format,” she commented.
Presidential symposia
Turning to the program, Haanen first picked out the third presidential symposium, which will be held on Monday, September 21. This will focus entirely on upper gastrointestinal tumors in both the adjuvant and metastatic setting.
He said that in recent years, “very little progress has been made” in this area, with treatment mostly consisting of chemotherapy and chemoradiotherapy.
However, this year’s presentations will explore the addition of immunotherapy either to chemotherapy or as an adjuvant treatment following completion of standard-of-care treatment for local disease.
Haanen said that the results will be “very interesting ... and may change current practice,” something that “is very important for both doctors and their patients.”
On Saturday, September 19, the first presidential symposium will include two presentations on lung cancer that Haanen said will offer some “exciting new [results] that I am sure will change clinical practice.”
One will be on the CROWN phase 3 trial comparing lorlatinib and crizotinib in the first-line treatment of patients with advanced ALK-positive NSCLC.
The other will present results on central nervous system disease recurrence from the ADAURA phase 3 trial of osimertinib adjuvant therapy in patients with resected EGFR-mutated NSCLC.
The same session will also see new data in advanced renal cell carcinoma from CheckMate 9ER, in which the c-Met and VEGFR2 inhibitor cabozantinib (Cabometyx) was combined with nivolumab (Opdivo) and compared to sunitinib (Sutent) in untreated patients.
“Last year, there were already some exciting results of the combination of axitinib [Inlyta], either with pembrolizumab [Keytruda] or with avelumab [Bavencio]...in the first-line setting in metastatic clear cell renal cell cancer,” Hannen said.
“Clearly there was a survival advantage over the standard of care, sunitinib,” he added.
This year, not only will efficacy data from CheckMate 9ER be presented but also quality-of-life results.
“That’s very important, because what everybody is afraid of is that, by adding drugs, you always get more impact on the quality of life, but you will see that the quality-of-life results are very exciting,” he said.
The second presidential symposium will feature studies on prostate cancer, notably the phase 3 IPATential150 trial of abiraterone (Zytiga) plus either ipatasertib or placebo in metastatic castration-resistant prostate cancer.
Ipatasertib targets Akt, and Haanen said that “by adding it to, let’s say, standard-of-care treatment ... the question of course of will be, Does that have a better outcome?”
He believes the results will be a “very nice illustration” that prostate cancer management is heading in the direction of personalized treatment.
Alongside the presidential symposia, there will be a number of proffered paper sessions on the latest results in all aspects of oncology, including results from the ASCENT trial in triple-negative breast cancer, as well as a dedicated COVID-19 track.
Haanen said that the ESMO Virtual Congress 2020, coming after the AACR and ASCO annual meetings, has the “advantage” of being able to present the latest outcomes of patients treated with chemotherapy and immunotherapy against the backdrop of the pandemic.
This will include a study from the ESMO Resilience Task Force on the impact of COVID-19 on oncology professionals both in terms of their personal distress and burnout and their job performance.
“I think that is very important,” Haanen said, “especially because the whole thing with COVID-19 is not yet over, and everybody is preparing for a second wave in the fall and winter.
“It may help us give us clues on how we can protect ourselves or each other to prevent burnout or other problems that we as healthcare caregivers face in this difficult period.”
Next year
For next year, Peters remains hopeful that the ESMO 2021 meeting will take place as planned in Paris.
She anticipates that, indeed, ESMO meetings will be able to take place from spring next year.
This will depend on a vaccine for COVID-19 becoming widely available, although oncologists in some countries may still not be able to travel.
This means “starting probably with hybrid formats, with some of the faculty being on site and some not, [and] the same thing for the attendees,” Peters said.
She suggested that, for ESMO Congress 2021 to work as an on-site meeting, it will require at least half or two-thirds of the originally anticipated number of attendees.
“I hope that Paris next year will happen,” Peters said, adding that it “will probably happen with less attendees – that’s fine, but [still] with a large number of faculty and attendees.”
The commentators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The use of immunotherapy for upper gastrointestinal tumors and renal cancer, ALK- and EGFR-targeted agents in non–small cell lung cancer (NSCLC), and the next step in personalized prostate cancer management will all be subjects of headlining presentations at the ESMO Virtual Congress 2020.
The conference will, like so many other major events, be held online this year because of the COVID-19 pandemic.
John B. Haanen, PhD, ESMO 2020 scientific chair, who is from the Netherlands Cancer Institute, Amsterdam, the Netherlands, told Medscape Medical News that, because the congress is being held online this year, fewer abstracts were submitted; nevertheless, “We were very happy to see ... that the quality was very good.”
The number of submissions was not the only problem the organizing committee had to face in transforming the ESMO Congress into a virtual meeting.
They were unable to fit the scientific and educational programs together and so have had to split them over two consecutive weekends. Moreover, many of the sessions were highly interactive and needed to be either adapted or omitted.
“So the program is somewhat different,” Haanen said. He noted that “the presentations were also made shorter, especially on the educational sessions, because...we can’t expect people to sit behind screens for hours listening to long presentations.”
He added: “That was out of the question.”
Haanen is nevertheless hopeful that the virtual meeting will be “very exciting.”
Solange Peters, MD, PhD, ESMO president, who is also affiliated with the Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland, said in a press conference that it was a “sacrifice” to move ESMO 2020 online and that “there were very sad moments” when deciding on the content.
However, there were some benefits from the change.
She said that all of the ESMO meetings this year have seen “huge” increases in the number of attendees and the geographical span or reach of each of the conferences.
“So suddenly you also realize that, what is one of the missions of ESMO being to convey education globally ... was probably better reached, better achieved with the virtual format,” she commented.
Presidential symposia
Turning to the program, Haanen first picked out the third presidential symposium, which will be held on Monday, September 21. This will focus entirely on upper gastrointestinal tumors in both the adjuvant and metastatic setting.
He said that in recent years, “very little progress has been made” in this area, with treatment mostly consisting of chemotherapy and chemoradiotherapy.
However, this year’s presentations will explore the addition of immunotherapy either to chemotherapy or as an adjuvant treatment following completion of standard-of-care treatment for local disease.
Haanen said that the results will be “very interesting ... and may change current practice,” something that “is very important for both doctors and their patients.”
On Saturday, September 19, the first presidential symposium will include two presentations on lung cancer that Haanen said will offer some “exciting new [results] that I am sure will change clinical practice.”
One will be on the CROWN phase 3 trial comparing lorlatinib and crizotinib in the first-line treatment of patients with advanced ALK-positive NSCLC.
The other will present results on central nervous system disease recurrence from the ADAURA phase 3 trial of osimertinib adjuvant therapy in patients with resected EGFR-mutated NSCLC.
The same session will also see new data in advanced renal cell carcinoma from CheckMate 9ER, in which the c-Met and VEGFR2 inhibitor cabozantinib (Cabometyx) was combined with nivolumab (Opdivo) and compared to sunitinib (Sutent) in untreated patients.
“Last year, there were already some exciting results of the combination of axitinib [Inlyta], either with pembrolizumab [Keytruda] or with avelumab [Bavencio]...in the first-line setting in metastatic clear cell renal cell cancer,” Hannen said.
“Clearly there was a survival advantage over the standard of care, sunitinib,” he added.
This year, not only will efficacy data from CheckMate 9ER be presented but also quality-of-life results.
“That’s very important, because what everybody is afraid of is that, by adding drugs, you always get more impact on the quality of life, but you will see that the quality-of-life results are very exciting,” he said.
The second presidential symposium will feature studies on prostate cancer, notably the phase 3 IPATential150 trial of abiraterone (Zytiga) plus either ipatasertib or placebo in metastatic castration-resistant prostate cancer.
Ipatasertib targets Akt, and Haanen said that “by adding it to, let’s say, standard-of-care treatment ... the question of course of will be, Does that have a better outcome?”
He believes the results will be a “very nice illustration” that prostate cancer management is heading in the direction of personalized treatment.
Alongside the presidential symposia, there will be a number of proffered paper sessions on the latest results in all aspects of oncology, including results from the ASCENT trial in triple-negative breast cancer, as well as a dedicated COVID-19 track.
Haanen said that the ESMO Virtual Congress 2020, coming after the AACR and ASCO annual meetings, has the “advantage” of being able to present the latest outcomes of patients treated with chemotherapy and immunotherapy against the backdrop of the pandemic.
This will include a study from the ESMO Resilience Task Force on the impact of COVID-19 on oncology professionals both in terms of their personal distress and burnout and their job performance.
“I think that is very important,” Haanen said, “especially because the whole thing with COVID-19 is not yet over, and everybody is preparing for a second wave in the fall and winter.
“It may help us give us clues on how we can protect ourselves or each other to prevent burnout or other problems that we as healthcare caregivers face in this difficult period.”
Next year
For next year, Peters remains hopeful that the ESMO 2021 meeting will take place as planned in Paris.
She anticipates that, indeed, ESMO meetings will be able to take place from spring next year.
This will depend on a vaccine for COVID-19 becoming widely available, although oncologists in some countries may still not be able to travel.
This means “starting probably with hybrid formats, with some of the faculty being on site and some not, [and] the same thing for the attendees,” Peters said.
She suggested that, for ESMO Congress 2021 to work as an on-site meeting, it will require at least half or two-thirds of the originally anticipated number of attendees.
“I hope that Paris next year will happen,” Peters said, adding that it “will probably happen with less attendees – that’s fine, but [still] with a large number of faculty and attendees.”
The commentators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
FROM ESMO 2020
New billing code for added COVID practice expense
The American Medical Association on Sept. 8 announced that a new code, 99072, is intended to cover additional supplies, materials, and clinical staff time over and above those usually included in an office visit when performed during a declared public health emergency, as defined by law, attributable to respiratory-transmitted infectious disease, the AMA said in a release.
Fifty national medical specialty societies and other organizations worked with the AMA’s Specialty Society RVS Update Committee over the summer to collect data on the costs of maintaining safe medical offices during the public health emergency. It has submitted recommendations to the Centers for Medicare & Medicaid Services seeking to persuade the federal agencies to recognize the new 99072 payment code.
The intention is to recognize the extra expenses involved in steps now routinely taken to reduce the risk for COVID transmission from office visits, Current Procedural Terminology Editorial Panel Chair Mark S. Synovec, MD, said in an interview. Some practices have adapted by having staff screen patients before they enter offices and making arrangements to keep patients at a safe distance from others during their visits, he said.
“Everyone’s life has significantly changed because of COVID and the health care system has dramatically changed,” Dr. Synovec said. “It was pretty clear that the status quo was not going to work.”
Physician practices will welcome this change, said Veronica Bradley, CPC, a senior industry adviser to the Medical Group Management Association. An office visit that in the past may have involved only basic infection control measures, such as donning a pair of gloves, now may involve clinicians taking the time to put on more extensive protective gear, she said.
“Now they are taking a heck of a lot more precautions, and there’s more time and more supplies being consumed,” Ms. Bradley said in an interview.
Code looks ahead to future use
The AMA explained how this new code differs from CPT code 99070, which is typically reported for supplies and materials that may be used or provided to patients during an office visit.
The new 99072 code applies only during declared public health emergencies and applies only to additional items required to support “a safe in-person provision” of evaluation, treatment, and procedures, the AMA said.
“These items contrast with those typically reported with code 99070, which focuses on additional supplies provided over and above those usually included with a specific service, such as drugs, intravenous catheters, or trays,” the AMA said.
The CPT panel sought to structure the new code for covering COVID practice expenses so that it could not be abused, and also looked ahead to the future, Dr. Synovec said.
“It’s a code that you would put on during a public health emergency as defined by law that would be related to a respiratory-transmitted infectious disease. Obviously we meant it for SARS-CoV-2,” he said. “Hopefully we can go another 100 years before we have another pandemic, but we also wanted to prepare something where if we have another airborne respiratory virus that requires additional practice expenses as seen this time, it would be available for use.”
The AMA also announced a second addition, CPT code 86413, that anticipates greater use of quantitative measurements of SARS-CoV-2 antibodies, as opposed to a qualitative assessment (positive/negative) provided by laboratory tests reported by other CPT codes.
More information is available on the AMA website.
A version of this article originally appeared on Medscape.com.
The American Medical Association on Sept. 8 announced that a new code, 99072, is intended to cover additional supplies, materials, and clinical staff time over and above those usually included in an office visit when performed during a declared public health emergency, as defined by law, attributable to respiratory-transmitted infectious disease, the AMA said in a release.
Fifty national medical specialty societies and other organizations worked with the AMA’s Specialty Society RVS Update Committee over the summer to collect data on the costs of maintaining safe medical offices during the public health emergency. It has submitted recommendations to the Centers for Medicare & Medicaid Services seeking to persuade the federal agencies to recognize the new 99072 payment code.
The intention is to recognize the extra expenses involved in steps now routinely taken to reduce the risk for COVID transmission from office visits, Current Procedural Terminology Editorial Panel Chair Mark S. Synovec, MD, said in an interview. Some practices have adapted by having staff screen patients before they enter offices and making arrangements to keep patients at a safe distance from others during their visits, he said.
“Everyone’s life has significantly changed because of COVID and the health care system has dramatically changed,” Dr. Synovec said. “It was pretty clear that the status quo was not going to work.”
Physician practices will welcome this change, said Veronica Bradley, CPC, a senior industry adviser to the Medical Group Management Association. An office visit that in the past may have involved only basic infection control measures, such as donning a pair of gloves, now may involve clinicians taking the time to put on more extensive protective gear, she said.
“Now they are taking a heck of a lot more precautions, and there’s more time and more supplies being consumed,” Ms. Bradley said in an interview.
Code looks ahead to future use
The AMA explained how this new code differs from CPT code 99070, which is typically reported for supplies and materials that may be used or provided to patients during an office visit.
The new 99072 code applies only during declared public health emergencies and applies only to additional items required to support “a safe in-person provision” of evaluation, treatment, and procedures, the AMA said.
“These items contrast with those typically reported with code 99070, which focuses on additional supplies provided over and above those usually included with a specific service, such as drugs, intravenous catheters, or trays,” the AMA said.
The CPT panel sought to structure the new code for covering COVID practice expenses so that it could not be abused, and also looked ahead to the future, Dr. Synovec said.
“It’s a code that you would put on during a public health emergency as defined by law that would be related to a respiratory-transmitted infectious disease. Obviously we meant it for SARS-CoV-2,” he said. “Hopefully we can go another 100 years before we have another pandemic, but we also wanted to prepare something where if we have another airborne respiratory virus that requires additional practice expenses as seen this time, it would be available for use.”
The AMA also announced a second addition, CPT code 86413, that anticipates greater use of quantitative measurements of SARS-CoV-2 antibodies, as opposed to a qualitative assessment (positive/negative) provided by laboratory tests reported by other CPT codes.
More information is available on the AMA website.
A version of this article originally appeared on Medscape.com.
The American Medical Association on Sept. 8 announced that a new code, 99072, is intended to cover additional supplies, materials, and clinical staff time over and above those usually included in an office visit when performed during a declared public health emergency, as defined by law, attributable to respiratory-transmitted infectious disease, the AMA said in a release.
Fifty national medical specialty societies and other organizations worked with the AMA’s Specialty Society RVS Update Committee over the summer to collect data on the costs of maintaining safe medical offices during the public health emergency. It has submitted recommendations to the Centers for Medicare & Medicaid Services seeking to persuade the federal agencies to recognize the new 99072 payment code.
The intention is to recognize the extra expenses involved in steps now routinely taken to reduce the risk for COVID transmission from office visits, Current Procedural Terminology Editorial Panel Chair Mark S. Synovec, MD, said in an interview. Some practices have adapted by having staff screen patients before they enter offices and making arrangements to keep patients at a safe distance from others during their visits, he said.
“Everyone’s life has significantly changed because of COVID and the health care system has dramatically changed,” Dr. Synovec said. “It was pretty clear that the status quo was not going to work.”
Physician practices will welcome this change, said Veronica Bradley, CPC, a senior industry adviser to the Medical Group Management Association. An office visit that in the past may have involved only basic infection control measures, such as donning a pair of gloves, now may involve clinicians taking the time to put on more extensive protective gear, she said.
“Now they are taking a heck of a lot more precautions, and there’s more time and more supplies being consumed,” Ms. Bradley said in an interview.
Code looks ahead to future use
The AMA explained how this new code differs from CPT code 99070, which is typically reported for supplies and materials that may be used or provided to patients during an office visit.
The new 99072 code applies only during declared public health emergencies and applies only to additional items required to support “a safe in-person provision” of evaluation, treatment, and procedures, the AMA said.
“These items contrast with those typically reported with code 99070, which focuses on additional supplies provided over and above those usually included with a specific service, such as drugs, intravenous catheters, or trays,” the AMA said.
The CPT panel sought to structure the new code for covering COVID practice expenses so that it could not be abused, and also looked ahead to the future, Dr. Synovec said.
“It’s a code that you would put on during a public health emergency as defined by law that would be related to a respiratory-transmitted infectious disease. Obviously we meant it for SARS-CoV-2,” he said. “Hopefully we can go another 100 years before we have another pandemic, but we also wanted to prepare something where if we have another airborne respiratory virus that requires additional practice expenses as seen this time, it would be available for use.”
The AMA also announced a second addition, CPT code 86413, that anticipates greater use of quantitative measurements of SARS-CoV-2 antibodies, as opposed to a qualitative assessment (positive/negative) provided by laboratory tests reported by other CPT codes.
More information is available on the AMA website.
A version of this article originally appeared on Medscape.com.