User login
Primary arrhythmia syndromes: Common cause of pediatric sudden cardiac death
CHICAGO – Just over one-half of all sudden deaths in a large pediatric case series were due to a primary arrhythmia syndrome, Dr. Grazia Delle Donne reported at the annual meeting of the American College of Cardiology.
She presented an analysis of all patients under the age of 18 years who were referred to London’s Royal Brompton Hospital for post mortem examination following presumed sudden cardiac death during 1991-2013. Royal Brompton is a national referral center for sudden cardiac death.
The review was undertaken because sudden cardiac death in the pediatric population occurs infrequently. Little is known about the prevalence of the various causes, noted Dr. Delle Donne of Royal Brompton.

Of the 398 subjects, 266 (67%) were female. The median age at death was 14 years. Twenty-two percent of the fatalities occurred during or immediately after exercise. Thirty-nine percent occurred while at rest.
Thirty-one percent of subjects had a family history of sudden cardiac death, another 14% had a family history of cardiomyopathy, and in 5% of cases there was a significant family history of arrhythmia.
Five percent of the children were known to have congenital heart disease. Eighteen percent of the children had a history of syncope.
Investigators determined that a primary arrhythmia syndrome such as long QT or Brugada syndrome was the cause of sudden death in 54% of cases. Death was attributed to cardiomyopathy in 15% cases, congenital heart disease in 8%, myocarditis in 6%, and coronary anomalies in 5%, with miscellaneous causes accounting for the remainder.
Dr. Delle Donne reported having no financial conflicts of interest regarding her presentation.
CHICAGO – Just over one-half of all sudden deaths in a large pediatric case series were due to a primary arrhythmia syndrome, Dr. Grazia Delle Donne reported at the annual meeting of the American College of Cardiology.
She presented an analysis of all patients under the age of 18 years who were referred to London’s Royal Brompton Hospital for post mortem examination following presumed sudden cardiac death during 1991-2013. Royal Brompton is a national referral center for sudden cardiac death.
The review was undertaken because sudden cardiac death in the pediatric population occurs infrequently. Little is known about the prevalence of the various causes, noted Dr. Delle Donne of Royal Brompton.
Of the 398 subjects, 266 (67%) were female. The median age at death was 14 years. Twenty-two percent of the fatalities occurred during or immediately after exercise. Thirty-nine percent occurred while at rest.
Thirty-one percent of subjects had a family history of sudden cardiac death, another 14% had a family history of cardiomyopathy, and in 5% of cases there was a significant family history of arrhythmia.
Five percent of the children were known to have congenital heart disease. Eighteen percent of the children had a history of syncope.
Investigators determined that a primary arrhythmia syndrome such as long QT or Brugada syndrome was the cause of sudden death in 54% of cases. Death was attributed to cardiomyopathy in 15% cases, congenital heart disease in 8%, myocarditis in 6%, and coronary anomalies in 5%, with miscellaneous causes accounting for the remainder.
Dr. Delle Donne reported having no financial conflicts of interest regarding her presentation.
CHICAGO – Just over one-half of all sudden deaths in a large pediatric case series were due to a primary arrhythmia syndrome, Dr. Grazia Delle Donne reported at the annual meeting of the American College of Cardiology.
She presented an analysis of all patients under the age of 18 years who were referred to London’s Royal Brompton Hospital for post mortem examination following presumed sudden cardiac death during 1991-2013. Royal Brompton is a national referral center for sudden cardiac death.
The review was undertaken because sudden cardiac death in the pediatric population occurs infrequently. Little is known about the prevalence of the various causes, noted Dr. Delle Donne of Royal Brompton.
Of the 398 subjects, 266 (67%) were female. The median age at death was 14 years. Twenty-two percent of the fatalities occurred during or immediately after exercise. Thirty-nine percent occurred while at rest.
Thirty-one percent of subjects had a family history of sudden cardiac death, another 14% had a family history of cardiomyopathy, and in 5% of cases there was a significant family history of arrhythmia.
Five percent of the children were known to have congenital heart disease. Eighteen percent of the children had a history of syncope.
Investigators determined that a primary arrhythmia syndrome such as long QT or Brugada syndrome was the cause of sudden death in 54% of cases. Death was attributed to cardiomyopathy in 15% cases, congenital heart disease in 8%, myocarditis in 6%, and coronary anomalies in 5%, with miscellaneous causes accounting for the remainder.
Dr. Delle Donne reported having no financial conflicts of interest regarding her presentation.
AT ACC 16
Key clinical point: Primary arrhythmia syndromes accounted for most cases of sudden cardiac death in a large pediatric case series.
Major finding: Family history of sudden cardiac death was present in 31% of 398 cases.
Data source: A retrospective review of all 398 cases of sudden cardiac death in childhood referred for post mortem examination at a British center during 1991-2013.
Disclosures: Dr. Delle Donne reported having no financial conflicts of interest.

Cardiovascular consequences of extreme prematurity persist into late adolescence
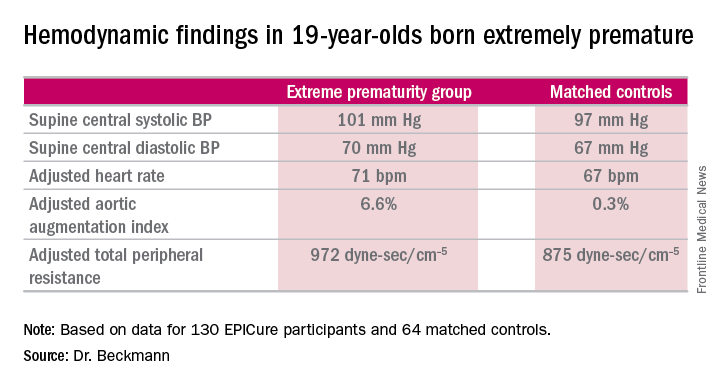
CHICAGO – The abnormal arterial hemodynamics identified in 11-year-olds with an extremely preterm birth persist at age 19, according to an update from the landmark longitudinal EPICure study.
“Given the implications of these significant findings, cardiovascular monitoring and risk prevention would be highly recommended for all individuals born extremely preterm,” Dr. Joanne Beckmann said in presenting the EPICure results on the long-term consequences of extreme prematurity at the annual meeting of the American College of Cardiology.
EPICure is a longitudinal study investigating health outcomes in a national cohort of babies born extremely preterm at 22-25 weeks’ gestation in the United Kingdom during 1995-1996. It is the longest such study conducted anywhere.
“Neonatal survival at the lowest gestations has improved significantly since the 1990s with the advancement in neonatal care treatments and the implementation of evidence-based practices. Therefore, long-term health outcomes following extremely preterm birth will have increasing relevance to adult physicians,” observed Dr. Beckmann of University College London.
She reported on the results of detailed cardiovascular assessments conducted in 130 extremely premature EPICure participants and 64 matched controls who made it to London for 2 days of health testing when they turned 19 years of age. The findings update the results of similar comprehensive examinations done at age 11 years.
The extremely premature birth (EP) subjects were shorter and weighed less than did the controls. The two groups had similar seated systolic and diastolic blood pressure, and cardiac index didn’t differ between the two groups. However, the EP group had significantly higher supine central systolic and diastolic blood pressure and a higher heart rate.
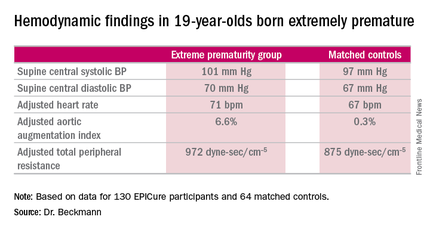
Moreover, the increases in aortic augmentation index – a composite of arterial stiffness and global wave reflections – and total peripheral resistance seen in the EP group at age 11 years persisted at the 19-year mark. It’s unclear whether the abnormal peripheral resistance in the EP group is structural or functional in nature. All hemodynamic differences between the two groups remained significant after adjustment for potential confounders.
Aortic pulse wave velocity was not significantly different between the two groups of 19-year-olds.
Data pertaining to other aspects of health in the 19-year-olds are now being analyzed. At the age-11 assessment, the EP group was found to have significantly impaired lung function (J Pediatr. 2012 Oct;161[4]:595-601.e2), high risk for neurodevelopmental disability (Pediatrics. 2009 Aug;124[2]:3249-57), a high rate of learning impairments, and an 18-fold increased risk of poor academic attainment compared to their matched peers (Arch Dis Child Fetal Neonatal Ed. 2009 Jul;94[4]:F283-9).
EPICure is funded by the Medical Research Council. Dr. Beckmann reported having no financial conflicts of interest.
CHICAGO – The abnormal arterial hemodynamics identified in 11-year-olds with an extremely preterm birth persist at age 19, according to an update from the landmark longitudinal EPICure study.
“Given the implications of these significant findings, cardiovascular monitoring and risk prevention would be highly recommended for all individuals born extremely preterm,” Dr. Joanne Beckmann said in presenting the EPICure results on the long-term consequences of extreme prematurity at the annual meeting of the American College of Cardiology.
EPICure is a longitudinal study investigating health outcomes in a national cohort of babies born extremely preterm at 22-25 weeks’ gestation in the United Kingdom during 1995-1996. It is the longest such study conducted anywhere.
“Neonatal survival at the lowest gestations has improved significantly since the 1990s with the advancement in neonatal care treatments and the implementation of evidence-based practices. Therefore, long-term health outcomes following extremely preterm birth will have increasing relevance to adult physicians,” observed Dr. Beckmann of University College London.
She reported on the results of detailed cardiovascular assessments conducted in 130 extremely premature EPICure participants and 64 matched controls who made it to London for 2 days of health testing when they turned 19 years of age. The findings update the results of similar comprehensive examinations done at age 11 years.
The extremely premature birth (EP) subjects were shorter and weighed less than did the controls. The two groups had similar seated systolic and diastolic blood pressure, and cardiac index didn’t differ between the two groups. However, the EP group had significantly higher supine central systolic and diastolic blood pressure and a higher heart rate.
Moreover, the increases in aortic augmentation index – a composite of arterial stiffness and global wave reflections – and total peripheral resistance seen in the EP group at age 11 years persisted at the 19-year mark. It’s unclear whether the abnormal peripheral resistance in the EP group is structural or functional in nature. All hemodynamic differences between the two groups remained significant after adjustment for potential confounders.
Aortic pulse wave velocity was not significantly different between the two groups of 19-year-olds.
Data pertaining to other aspects of health in the 19-year-olds are now being analyzed. At the age-11 assessment, the EP group was found to have significantly impaired lung function (J Pediatr. 2012 Oct;161[4]:595-601.e2), high risk for neurodevelopmental disability (Pediatrics. 2009 Aug;124[2]:3249-57), a high rate of learning impairments, and an 18-fold increased risk of poor academic attainment compared to their matched peers (Arch Dis Child Fetal Neonatal Ed. 2009 Jul;94[4]:F283-9).
EPICure is funded by the Medical Research Council. Dr. Beckmann reported having no financial conflicts of interest.
CHICAGO – The abnormal arterial hemodynamics identified in 11-year-olds with an extremely preterm birth persist at age 19, according to an update from the landmark longitudinal EPICure study.
“Given the implications of these significant findings, cardiovascular monitoring and risk prevention would be highly recommended for all individuals born extremely preterm,” Dr. Joanne Beckmann said in presenting the EPICure results on the long-term consequences of extreme prematurity at the annual meeting of the American College of Cardiology.
EPICure is a longitudinal study investigating health outcomes in a national cohort of babies born extremely preterm at 22-25 weeks’ gestation in the United Kingdom during 1995-1996. It is the longest such study conducted anywhere.
“Neonatal survival at the lowest gestations has improved significantly since the 1990s with the advancement in neonatal care treatments and the implementation of evidence-based practices. Therefore, long-term health outcomes following extremely preterm birth will have increasing relevance to adult physicians,” observed Dr. Beckmann of University College London.
She reported on the results of detailed cardiovascular assessments conducted in 130 extremely premature EPICure participants and 64 matched controls who made it to London for 2 days of health testing when they turned 19 years of age. The findings update the results of similar comprehensive examinations done at age 11 years.
The extremely premature birth (EP) subjects were shorter and weighed less than did the controls. The two groups had similar seated systolic and diastolic blood pressure, and cardiac index didn’t differ between the two groups. However, the EP group had significantly higher supine central systolic and diastolic blood pressure and a higher heart rate.
Moreover, the increases in aortic augmentation index – a composite of arterial stiffness and global wave reflections – and total peripheral resistance seen in the EP group at age 11 years persisted at the 19-year mark. It’s unclear whether the abnormal peripheral resistance in the EP group is structural or functional in nature. All hemodynamic differences between the two groups remained significant after adjustment for potential confounders.
Aortic pulse wave velocity was not significantly different between the two groups of 19-year-olds.
Data pertaining to other aspects of health in the 19-year-olds are now being analyzed. At the age-11 assessment, the EP group was found to have significantly impaired lung function (J Pediatr. 2012 Oct;161[4]:595-601.e2), high risk for neurodevelopmental disability (Pediatrics. 2009 Aug;124[2]:3249-57), a high rate of learning impairments, and an 18-fold increased risk of poor academic attainment compared to their matched peers (Arch Dis Child Fetal Neonatal Ed. 2009 Jul;94[4]:F283-9).
EPICure is funded by the Medical Research Council. Dr. Beckmann reported having no financial conflicts of interest.
AT ACC 16
Key clinical point: At age 19 years, persons born extremely premature still show significant abnormalities in arterial hemodynamics and peripheral resistance.
Major finding: The adjusted aortic augmentation index was 6.6% in 19-year-olds born at 22-25 weeks gestation compared with 0.3% in matched controls.
Data source: EPICure, a longitudinal study of health outcomes in a national cohort of babies born extremely preterm at 22-25 weeks gestation in the United Kingdom during 1995-1996.
Disclosures: EPICure is funded by the Medical Research Council. The presenter reported having no financial conflicts of interest.
Acute viral bronchiolitis hospital stay not shortened by hypertonic saline
The results of two previously published meta-analyses supporting a shortening of hospital length of stay following the use of hypertonic saline in infants with acute viral bronchiolitis are unreliable, according to a study published in JAMA Pediatrics.
Hypertonic saline should not be expected to shorten the length of hospital stay for those with acute viral bronchiolitis in typical hospital settings in the United States, Dr. Corinne G. Brooks of the Leadership in Preventive Medicine and Pediatrics Residencies at the Dartmouth-Hitchcock Medical Center in Lebanon, N.H., and her associates concluded.
The investigators reached this conclusion after reanalyzing data from the 18 randomized clinical trials using hypertonic saline in infants with bronchiolitis reporting hospital length of stay as an outcome measure in the two previously published meta-analyses, after finding no additional data sources through a literature search. The studies included 2,063 infants (63% male), with a mean age of 4.2 months and a mean length of stay of 3.6 days (JAMA Pediatr. 2016 Apr 18. doi: 10.1001/jamapediatrics.2016.0079).
Dr. Brooks explained the rationale behind the study by pointing out that the previously published analyses failed to address and account for the large amount of study heterogeneity in the assessed cohort of studies, necessitating a reanalysis of the full data set to investigate factors with the potential to introduce such heterogeneity.
The reanalysis produced two significant findings, which collectively accounted for all of the heterogeneity between the assessed studies. First, one of the study populations was determined to be a significant outlier with very different criteria for discharge and substantially longer expected hospital length of stay. Because the statistical significance of the weighted mean difference in hospital length of stay attributable to the use of hypertonic saline was sensitive to the removal of this study population, heterogeneity was found to resolve to moderate to acceptable levels. Second, an important baseline difference between the treatment arms in day of illness at study enrollment was found. Patients presenting later in their illness were more likely to be allocated to the hypertonic saline treatment arm in 6 of the 18 studies assessed, most of which were small positive studies. Therefore, this difference accounted for a systematic bias favoring treatment groups.
Based on their reanalysis of the available data, Dr. Brooks and her associates said that the appearance of a meaningful reduction in the length of hospital stay for infants with acute viral bronchiolitis was a direct result of the inappropriate combination of studies with clinically significant differences in outcome definitions, and the previously unnoticed systematic bias in treatment group allocation.
No external funding was provided. None of the authors reported any conflicts of interest.
When infants below 1 year of age experience viral bronchiolitis, usually from respiratory syncytial virus (RSV), they sometimes get admitted to hospital for supportive care. In hospital, the main goals are to reduce the work of breathing and tachypnea and increase oxygen saturation in the blood. In addition to supplemental oxygen, the use of hypertonic saline nebulizations has been proposed, studied, and endorsed by some investigators based on randomized trials.

|
Dr. Michael Pichichero |
In this paper from a group at Dartmouth Medical Center, we learn that a recent conclusion of benefit from hypertonic saline nebulizations on hospital length of stay likely was incorrect. The authors correctly point out that meta-analysis is a tricky business because it relies on a reasonable homogeneity among the populations included in the individual studies. If there is heterogeneity, this can complicate interpretation, although there are statistical maneuvers that can help determine if the heterogeneity that is inherent in meta-analyses has a major impact on conclusions, as appears to have occurred here.
When we must hospitalize an infant with bronchiolitis for hypoxemia, it creates a lot of stress for the family. As physicians, we seek to do anything that might help get the child home sooner – thus the 18 studies published on trying hypertonic saline, with varied results. I suspect that this paper from the Dartmouth group will not end the debate or deter future research into treatments that might help these babies.
Michael E. Pichichero, M.D., a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero commented in an interview. He said he had no relevant financial disclosures.
When infants below 1 year of age experience viral bronchiolitis, usually from respiratory syncytial virus (RSV), they sometimes get admitted to hospital for supportive care. In hospital, the main goals are to reduce the work of breathing and tachypnea and increase oxygen saturation in the blood. In addition to supplemental oxygen, the use of hypertonic saline nebulizations has been proposed, studied, and endorsed by some investigators based on randomized trials.
|
|
Dr. Michael Pichichero |
In this paper from a group at Dartmouth Medical Center, we learn that a recent conclusion of benefit from hypertonic saline nebulizations on hospital length of stay likely was incorrect. The authors correctly point out that meta-analysis is a tricky business because it relies on a reasonable homogeneity among the populations included in the individual studies. If there is heterogeneity, this can complicate interpretation, although there are statistical maneuvers that can help determine if the heterogeneity that is inherent in meta-analyses has a major impact on conclusions, as appears to have occurred here.
When we must hospitalize an infant with bronchiolitis for hypoxemia, it creates a lot of stress for the family. As physicians, we seek to do anything that might help get the child home sooner – thus the 18 studies published on trying hypertonic saline, with varied results. I suspect that this paper from the Dartmouth group will not end the debate or deter future research into treatments that might help these babies.
Michael E. Pichichero, M.D., a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero commented in an interview. He said he had no relevant financial disclosures.
When infants below 1 year of age experience viral bronchiolitis, usually from respiratory syncytial virus (RSV), they sometimes get admitted to hospital for supportive care. In hospital, the main goals are to reduce the work of breathing and tachypnea and increase oxygen saturation in the blood. In addition to supplemental oxygen, the use of hypertonic saline nebulizations has been proposed, studied, and endorsed by some investigators based on randomized trials.
|
|
Dr. Michael Pichichero |
In this paper from a group at Dartmouth Medical Center, we learn that a recent conclusion of benefit from hypertonic saline nebulizations on hospital length of stay likely was incorrect. The authors correctly point out that meta-analysis is a tricky business because it relies on a reasonable homogeneity among the populations included in the individual studies. If there is heterogeneity, this can complicate interpretation, although there are statistical maneuvers that can help determine if the heterogeneity that is inherent in meta-analyses has a major impact on conclusions, as appears to have occurred here.
When we must hospitalize an infant with bronchiolitis for hypoxemia, it creates a lot of stress for the family. As physicians, we seek to do anything that might help get the child home sooner – thus the 18 studies published on trying hypertonic saline, with varied results. I suspect that this paper from the Dartmouth group will not end the debate or deter future research into treatments that might help these babies.
Michael E. Pichichero, M.D., a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero commented in an interview. He said he had no relevant financial disclosures.
The results of two previously published meta-analyses supporting a shortening of hospital length of stay following the use of hypertonic saline in infants with acute viral bronchiolitis are unreliable, according to a study published in JAMA Pediatrics.
Hypertonic saline should not be expected to shorten the length of hospital stay for those with acute viral bronchiolitis in typical hospital settings in the United States, Dr. Corinne G. Brooks of the Leadership in Preventive Medicine and Pediatrics Residencies at the Dartmouth-Hitchcock Medical Center in Lebanon, N.H., and her associates concluded.
The investigators reached this conclusion after reanalyzing data from the 18 randomized clinical trials using hypertonic saline in infants with bronchiolitis reporting hospital length of stay as an outcome measure in the two previously published meta-analyses, after finding no additional data sources through a literature search. The studies included 2,063 infants (63% male), with a mean age of 4.2 months and a mean length of stay of 3.6 days (JAMA Pediatr. 2016 Apr 18. doi: 10.1001/jamapediatrics.2016.0079).
Dr. Brooks explained the rationale behind the study by pointing out that the previously published analyses failed to address and account for the large amount of study heterogeneity in the assessed cohort of studies, necessitating a reanalysis of the full data set to investigate factors with the potential to introduce such heterogeneity.
The reanalysis produced two significant findings, which collectively accounted for all of the heterogeneity between the assessed studies. First, one of the study populations was determined to be a significant outlier with very different criteria for discharge and substantially longer expected hospital length of stay. Because the statistical significance of the weighted mean difference in hospital length of stay attributable to the use of hypertonic saline was sensitive to the removal of this study population, heterogeneity was found to resolve to moderate to acceptable levels. Second, an important baseline difference between the treatment arms in day of illness at study enrollment was found. Patients presenting later in their illness were more likely to be allocated to the hypertonic saline treatment arm in 6 of the 18 studies assessed, most of which were small positive studies. Therefore, this difference accounted for a systematic bias favoring treatment groups.
Based on their reanalysis of the available data, Dr. Brooks and her associates said that the appearance of a meaningful reduction in the length of hospital stay for infants with acute viral bronchiolitis was a direct result of the inappropriate combination of studies with clinically significant differences in outcome definitions, and the previously unnoticed systematic bias in treatment group allocation.
No external funding was provided. None of the authors reported any conflicts of interest.
The results of two previously published meta-analyses supporting a shortening of hospital length of stay following the use of hypertonic saline in infants with acute viral bronchiolitis are unreliable, according to a study published in JAMA Pediatrics.
Hypertonic saline should not be expected to shorten the length of hospital stay for those with acute viral bronchiolitis in typical hospital settings in the United States, Dr. Corinne G. Brooks of the Leadership in Preventive Medicine and Pediatrics Residencies at the Dartmouth-Hitchcock Medical Center in Lebanon, N.H., and her associates concluded.
The investigators reached this conclusion after reanalyzing data from the 18 randomized clinical trials using hypertonic saline in infants with bronchiolitis reporting hospital length of stay as an outcome measure in the two previously published meta-analyses, after finding no additional data sources through a literature search. The studies included 2,063 infants (63% male), with a mean age of 4.2 months and a mean length of stay of 3.6 days (JAMA Pediatr. 2016 Apr 18. doi: 10.1001/jamapediatrics.2016.0079).
Dr. Brooks explained the rationale behind the study by pointing out that the previously published analyses failed to address and account for the large amount of study heterogeneity in the assessed cohort of studies, necessitating a reanalysis of the full data set to investigate factors with the potential to introduce such heterogeneity.
The reanalysis produced two significant findings, which collectively accounted for all of the heterogeneity between the assessed studies. First, one of the study populations was determined to be a significant outlier with very different criteria for discharge and substantially longer expected hospital length of stay. Because the statistical significance of the weighted mean difference in hospital length of stay attributable to the use of hypertonic saline was sensitive to the removal of this study population, heterogeneity was found to resolve to moderate to acceptable levels. Second, an important baseline difference between the treatment arms in day of illness at study enrollment was found. Patients presenting later in their illness were more likely to be allocated to the hypertonic saline treatment arm in 6 of the 18 studies assessed, most of which were small positive studies. Therefore, this difference accounted for a systematic bias favoring treatment groups.
Based on their reanalysis of the available data, Dr. Brooks and her associates said that the appearance of a meaningful reduction in the length of hospital stay for infants with acute viral bronchiolitis was a direct result of the inappropriate combination of studies with clinically significant differences in outcome definitions, and the previously unnoticed systematic bias in treatment group allocation.
No external funding was provided. None of the authors reported any conflicts of interest.
FROM JAMA PEDIATRICS
Key clinical point: Physicians should not expect hypertonic saline to shorten hospital length of stay for those with acute viral bronchiolitis.
Major finding: Removal of heterogeneity from recent meta-analyses refutes the utility of hypertonic saline in reducing hospital length of stay for acute viral bronchiolitis.
Data sources: Two previously published meta-analyses pertaining to the use of hypertonic saline and hospital length of stay for acute viral bronchiolitis in infants.
Disclosures: No external funding was provided. None of the authors reported any conflicts of interest.

CDC Reports Major Drop in Teen Birth Rates Among Minorities
Pregnancy rates among Hispanic and black teens are at an all-time low, reflecting overall declines in teen birth rates, new data show.
The Centers for Disease Control and Prevention reported on April 28 that the rate of Hispanic teens giving birth in the United States has dropped by more than half since 2006. During that same time period, there was a 44% drop in the birth rate for black teens.
Although these dramatic declines occurred against the backdrop of an overall decrease of about 40% in teen birth rates during the last decade, the CDC also reported that birth rates among Hispanics and black teens are still twice as high as they are for whites.
“The United States has made remarkable progress in reducing both teen pregnancy and racial and ethnic differences, but the reality is, too many American teens are still having babies,” Dr. Tom Frieden, CDC director, said in a statement. “By better understanding the many factors that contribute to teen pregnancy, we can better design, implement, evaluate, and improve prevention interventions and further reduce disparities.”
Overall, the birth rate among girls aged 15-19 years dropped from 41.1 to 24.2 per 1,000 from 2006 to 2014. The largest decline occurred in Hispanics, going from 77.4 to 38.0 per 1,000. The next biggest rate decline was in black teens, which fell from 61.9 to 34.9 per 1,000. The rate for white teens declined by 35%, falling from 26.7 to 17.3 per 1,000 (MMWR Morb Mortal Wkly Rep. 2016 Apr;65:409-14).
The CDC report indicated state- and community-level patterns, including that rates were notably higher among all races and ethnicities where unemployment is also high, but income and education levels are low. In some states with low overall birth rates, certain counties experienced higher rates. The highest rates nationwide tended to be in counties located in southern and southwestern states.
“These data underscore that the solution to our nation’s teen pregnancy problem is not going to be a one-size-fits-all – teen birth rates vary greatly across state lines and even within states,” Lisa Romero, Dr.P.H., a health scientist in the CDC’s Division of Reproductive Health, and the report’s lead author, said in a statement. “We can ensure the success of teen pregnancy prevention efforts by capitalizing on the expertise of our state and local public health colleagues. Together, we can work to implement proven prevention programs that take into account unique, local needs.”
The study is based on statistics for births to girls aged 15-19 years occurring between 2006 and 2014, taken from the National Vital Statistics System (NVSS). County-level NVSS data from 2013 and 2014 was also used, as were data from the American Community Survey between 2010 and 2014.
Pregnancy rates among Hispanic and black teens are at an all-time low, reflecting overall declines in teen birth rates, new data show.
The Centers for Disease Control and Prevention reported on April 28 that the rate of Hispanic teens giving birth in the United States has dropped by more than half since 2006. During that same time period, there was a 44% drop in the birth rate for black teens.
Although these dramatic declines occurred against the backdrop of an overall decrease of about 40% in teen birth rates during the last decade, the CDC also reported that birth rates among Hispanics and black teens are still twice as high as they are for whites.
“The United States has made remarkable progress in reducing both teen pregnancy and racial and ethnic differences, but the reality is, too many American teens are still having babies,” Dr. Tom Frieden, CDC director, said in a statement. “By better understanding the many factors that contribute to teen pregnancy, we can better design, implement, evaluate, and improve prevention interventions and further reduce disparities.”
Overall, the birth rate among girls aged 15-19 years dropped from 41.1 to 24.2 per 1,000 from 2006 to 2014. The largest decline occurred in Hispanics, going from 77.4 to 38.0 per 1,000. The next biggest rate decline was in black teens, which fell from 61.9 to 34.9 per 1,000. The rate for white teens declined by 35%, falling from 26.7 to 17.3 per 1,000 (MMWR Morb Mortal Wkly Rep. 2016 Apr;65:409-14).
The CDC report indicated state- and community-level patterns, including that rates were notably higher among all races and ethnicities where unemployment is also high, but income and education levels are low. In some states with low overall birth rates, certain counties experienced higher rates. The highest rates nationwide tended to be in counties located in southern and southwestern states.
“These data underscore that the solution to our nation’s teen pregnancy problem is not going to be a one-size-fits-all – teen birth rates vary greatly across state lines and even within states,” Lisa Romero, Dr.P.H., a health scientist in the CDC’s Division of Reproductive Health, and the report’s lead author, said in a statement. “We can ensure the success of teen pregnancy prevention efforts by capitalizing on the expertise of our state and local public health colleagues. Together, we can work to implement proven prevention programs that take into account unique, local needs.”
The study is based on statistics for births to girls aged 15-19 years occurring between 2006 and 2014, taken from the National Vital Statistics System (NVSS). County-level NVSS data from 2013 and 2014 was also used, as were data from the American Community Survey between 2010 and 2014.
Pregnancy rates among Hispanic and black teens are at an all-time low, reflecting overall declines in teen birth rates, new data show.
The Centers for Disease Control and Prevention reported on April 28 that the rate of Hispanic teens giving birth in the United States has dropped by more than half since 2006. During that same time period, there was a 44% drop in the birth rate for black teens.
Although these dramatic declines occurred against the backdrop of an overall decrease of about 40% in teen birth rates during the last decade, the CDC also reported that birth rates among Hispanics and black teens are still twice as high as they are for whites.
“The United States has made remarkable progress in reducing both teen pregnancy and racial and ethnic differences, but the reality is, too many American teens are still having babies,” Dr. Tom Frieden, CDC director, said in a statement. “By better understanding the many factors that contribute to teen pregnancy, we can better design, implement, evaluate, and improve prevention interventions and further reduce disparities.”
Overall, the birth rate among girls aged 15-19 years dropped from 41.1 to 24.2 per 1,000 from 2006 to 2014. The largest decline occurred in Hispanics, going from 77.4 to 38.0 per 1,000. The next biggest rate decline was in black teens, which fell from 61.9 to 34.9 per 1,000. The rate for white teens declined by 35%, falling from 26.7 to 17.3 per 1,000 (MMWR Morb Mortal Wkly Rep. 2016 Apr;65:409-14).
The CDC report indicated state- and community-level patterns, including that rates were notably higher among all races and ethnicities where unemployment is also high, but income and education levels are low. In some states with low overall birth rates, certain counties experienced higher rates. The highest rates nationwide tended to be in counties located in southern and southwestern states.
“These data underscore that the solution to our nation’s teen pregnancy problem is not going to be a one-size-fits-all – teen birth rates vary greatly across state lines and even within states,” Lisa Romero, Dr.P.H., a health scientist in the CDC’s Division of Reproductive Health, and the report’s lead author, said in a statement. “We can ensure the success of teen pregnancy prevention efforts by capitalizing on the expertise of our state and local public health colleagues. Together, we can work to implement proven prevention programs that take into account unique, local needs.”
The study is based on statistics for births to girls aged 15-19 years occurring between 2006 and 2014, taken from the National Vital Statistics System (NVSS). County-level NVSS data from 2013 and 2014 was also used, as were data from the American Community Survey between 2010 and 2014.
FROM MMWR
CDC reports major drop in teen birth rates among minorities
Pregnancy rates among Hispanic and black teens are at an all-time low, reflecting overall declines in teen birth rates, new data show.
The Centers for Disease Control and Prevention reported on April 28 that the rate of Hispanic teens giving birth in the United States has dropped by more than half since 2006. During that same time period, there was a 44% drop in the birth rate for black teens.
Although these dramatic declines occurred against the backdrop of an overall decrease of about 40% in teen birth rates during the last decade, the CDC also reported that birth rates among Hispanics and black teens are still twice as high as they are for whites.
“The United States has made remarkable progress in reducing both teen pregnancy and racial and ethnic differences, but the reality is, too many American teens are still having babies,” Dr. Tom Frieden, CDC director, said in a statement. “By better understanding the many factors that contribute to teen pregnancy, we can better design, implement, evaluate, and improve prevention interventions and further reduce disparities.”
Overall, the birth rate among girls aged 15-19 years dropped from 41.1 to 24.2 per 1,000 from 2006 to 2014. The largest decline occurred in Hispanics, going from 77.4 to 38.0 per 1,000. The next biggest rate decline was in black teens, which fell from 61.9 to 34.9 per 1,000. The rate for white teens declined by 35%, falling from 26.7 to 17.3 per 1,000 (MMWR Morb Mortal Wkly Rep. 2016 Apr;65:409-14).
The CDC report indicated state- and community-level patterns, including that rates were notably higher among all races and ethnicities where unemployment is also high, but income and education levels are low. In some states with low overall birth rates, certain counties experienced higher rates. The highest rates nationwide tended to be in counties located in southern and southwestern states.
“These data underscore that the solution to our nation’s teen pregnancy problem is not going to be a one-size-fits-all – teen birth rates vary greatly across state lines and even within states,” Lisa Romero, Dr.P.H., a health scientist in the CDC’s Division of Reproductive Health, and the report’s lead author, said in a statement. “We can ensure the success of teen pregnancy prevention efforts by capitalizing on the expertise of our state and local public health colleagues. Together, we can work to implement proven prevention programs that take into account unique, local needs.”
The study is based on statistics for births to girls aged 15-19 years occurring between 2006 and 2014, taken from the National Vital Statistics System (NVSS). County-level NVSS data from 2013 and 2014 was also used, as were data from the American Community Survey between 2010 and 2014.
On Twitter @whitneymcknight
Pregnancy rates among Hispanic and black teens are at an all-time low, reflecting overall declines in teen birth rates, new data show.
The Centers for Disease Control and Prevention reported on April 28 that the rate of Hispanic teens giving birth in the United States has dropped by more than half since 2006. During that same time period, there was a 44% drop in the birth rate for black teens.
Although these dramatic declines occurred against the backdrop of an overall decrease of about 40% in teen birth rates during the last decade, the CDC also reported that birth rates among Hispanics and black teens are still twice as high as they are for whites.
“The United States has made remarkable progress in reducing both teen pregnancy and racial and ethnic differences, but the reality is, too many American teens are still having babies,” Dr. Tom Frieden, CDC director, said in a statement. “By better understanding the many factors that contribute to teen pregnancy, we can better design, implement, evaluate, and improve prevention interventions and further reduce disparities.”
Overall, the birth rate among girls aged 15-19 years dropped from 41.1 to 24.2 per 1,000 from 2006 to 2014. The largest decline occurred in Hispanics, going from 77.4 to 38.0 per 1,000. The next biggest rate decline was in black teens, which fell from 61.9 to 34.9 per 1,000. The rate for white teens declined by 35%, falling from 26.7 to 17.3 per 1,000 (MMWR Morb Mortal Wkly Rep. 2016 Apr;65:409-14).
The CDC report indicated state- and community-level patterns, including that rates were notably higher among all races and ethnicities where unemployment is also high, but income and education levels are low. In some states with low overall birth rates, certain counties experienced higher rates. The highest rates nationwide tended to be in counties located in southern and southwestern states.
“These data underscore that the solution to our nation’s teen pregnancy problem is not going to be a one-size-fits-all – teen birth rates vary greatly across state lines and even within states,” Lisa Romero, Dr.P.H., a health scientist in the CDC’s Division of Reproductive Health, and the report’s lead author, said in a statement. “We can ensure the success of teen pregnancy prevention efforts by capitalizing on the expertise of our state and local public health colleagues. Together, we can work to implement proven prevention programs that take into account unique, local needs.”
The study is based on statistics for births to girls aged 15-19 years occurring between 2006 and 2014, taken from the National Vital Statistics System (NVSS). County-level NVSS data from 2013 and 2014 was also used, as were data from the American Community Survey between 2010 and 2014.
On Twitter @whitneymcknight
Pregnancy rates among Hispanic and black teens are at an all-time low, reflecting overall declines in teen birth rates, new data show.
The Centers for Disease Control and Prevention reported on April 28 that the rate of Hispanic teens giving birth in the United States has dropped by more than half since 2006. During that same time period, there was a 44% drop in the birth rate for black teens.
Although these dramatic declines occurred against the backdrop of an overall decrease of about 40% in teen birth rates during the last decade, the CDC also reported that birth rates among Hispanics and black teens are still twice as high as they are for whites.
“The United States has made remarkable progress in reducing both teen pregnancy and racial and ethnic differences, but the reality is, too many American teens are still having babies,” Dr. Tom Frieden, CDC director, said in a statement. “By better understanding the many factors that contribute to teen pregnancy, we can better design, implement, evaluate, and improve prevention interventions and further reduce disparities.”
Overall, the birth rate among girls aged 15-19 years dropped from 41.1 to 24.2 per 1,000 from 2006 to 2014. The largest decline occurred in Hispanics, going from 77.4 to 38.0 per 1,000. The next biggest rate decline was in black teens, which fell from 61.9 to 34.9 per 1,000. The rate for white teens declined by 35%, falling from 26.7 to 17.3 per 1,000 (MMWR Morb Mortal Wkly Rep. 2016 Apr;65:409-14).
The CDC report indicated state- and community-level patterns, including that rates were notably higher among all races and ethnicities where unemployment is also high, but income and education levels are low. In some states with low overall birth rates, certain counties experienced higher rates. The highest rates nationwide tended to be in counties located in southern and southwestern states.
“These data underscore that the solution to our nation’s teen pregnancy problem is not going to be a one-size-fits-all – teen birth rates vary greatly across state lines and even within states,” Lisa Romero, Dr.P.H., a health scientist in the CDC’s Division of Reproductive Health, and the report’s lead author, said in a statement. “We can ensure the success of teen pregnancy prevention efforts by capitalizing on the expertise of our state and local public health colleagues. Together, we can work to implement proven prevention programs that take into account unique, local needs.”
The study is based on statistics for births to girls aged 15-19 years occurring between 2006 and 2014, taken from the National Vital Statistics System (NVSS). County-level NVSS data from 2013 and 2014 was also used, as were data from the American Community Survey between 2010 and 2014.
On Twitter @whitneymcknight
FROM MMWR
Doppler Ultrasound Headset Performs Well at Spotting Sports-related Concussion
VANCOUVER – A new transcranial Doppler platform that analyzes subtle changes in the cerebral blood flow waveform performed well in detecting sports-related concussion in a cohort study of 238 Los Angeles high school athletes.
The investigational headset device was able to differentiate between those with and without a recent concussion 83% of the time, investigators reported at the annual meeting of the American Academy of Neurology. In contrast, traditional transcranial Doppler analysis detected a recent concussion only 50%-60% of the time.
“Over the last few years, there has been growing evidence that cerebral hemodynamics are altered following sports-related concussion,” senior author Robert Hamilton, Ph.D., cofounder and chief science officer of Neural Analytics in Los Angeles, commented in a session and interview.
Most studies in this area have used MRI or traditional transcranial Doppler analysis, he said. However, the former is costly, time consuming, and not portable, and the latter has not proven very accurate.
As traditional Doppler analysis disregards the majority of waveform data, Dr. Hamilton and his colleagues developed an advanced platform that uses machine learning to analyze the entire shape of the cerebral blood flow velocity waveform through quantitative cerebral hemodynamics.
They compared the advanced analysis with traditional analysis among 69 high school athletes in contact sports who had sustained a concussion an average of 6 days earlier and a control group of 169 unaffected age-matched high school athletes from contact and noncontact sports.
Both groups had bilateral monitoring of blood flow in the middle cerebral artery with transcranial Doppler while they followed a standard cerebrovascular reactivity protocol that included rest and breath holding.
Results showed that for differentiating between athletes who did and did not have concussion, the advanced analysis had an area under the receiver operating characteristic curve of 83%. (Sensitivity was 72%, specificity was 82%, and overall accuracy was 80%.)
In comparison, the area under the curve was substantially lower for the traditional analysis measures: It was 55% for mean velocity (100% sensitivity, 0% specificity, 76% accuracy), 52% for the pulsatility index (86% sensitivity, 23% specificity, 61% accuracy), and 60% for the cerebrovascular reactivity index (51% sensitivity, 68% specificity, 64% accuracy).
“Unfortunately, concussion diagnostics and management today are basically subjective,” Dr. Hamilton commented. The advanced analysis may therefore improve the situation by providing objective evidence of blood flow dysfunction after injury.
The new analysis platform “is easy to use and portable, and [testing] can be done very quickly, within 5 minutes,” he noted. “The nice thing is it can be done on the sideline, in the emergency room, or in a doctor’s office.”
The investigators will next use the advanced analysis to track recovery of blood flow regulation after sports-related concussion and will compare its performance with that of additional modalities, such as MRI, according to Dr. Hamilton. Furthermore, they are testing it in various other populations: adolescents, college athletes, and members of the military.
“Ultimately, blood flow dysfunction is also important in a wide variety of conditions, such as stroke and dementia,” he pointed out. “So those are conditions that we are looking at to study this year and moving forward in the future.”
The research was supported by the National Institutes of Health and the National Science Foundation.
VANCOUVER – A new transcranial Doppler platform that analyzes subtle changes in the cerebral blood flow waveform performed well in detecting sports-related concussion in a cohort study of 238 Los Angeles high school athletes.
The investigational headset device was able to differentiate between those with and without a recent concussion 83% of the time, investigators reported at the annual meeting of the American Academy of Neurology. In contrast, traditional transcranial Doppler analysis detected a recent concussion only 50%-60% of the time.
“Over the last few years, there has been growing evidence that cerebral hemodynamics are altered following sports-related concussion,” senior author Robert Hamilton, Ph.D., cofounder and chief science officer of Neural Analytics in Los Angeles, commented in a session and interview.
Most studies in this area have used MRI or traditional transcranial Doppler analysis, he said. However, the former is costly, time consuming, and not portable, and the latter has not proven very accurate.
As traditional Doppler analysis disregards the majority of waveform data, Dr. Hamilton and his colleagues developed an advanced platform that uses machine learning to analyze the entire shape of the cerebral blood flow velocity waveform through quantitative cerebral hemodynamics.
They compared the advanced analysis with traditional analysis among 69 high school athletes in contact sports who had sustained a concussion an average of 6 days earlier and a control group of 169 unaffected age-matched high school athletes from contact and noncontact sports.
Both groups had bilateral monitoring of blood flow in the middle cerebral artery with transcranial Doppler while they followed a standard cerebrovascular reactivity protocol that included rest and breath holding.
Results showed that for differentiating between athletes who did and did not have concussion, the advanced analysis had an area under the receiver operating characteristic curve of 83%. (Sensitivity was 72%, specificity was 82%, and overall accuracy was 80%.)
In comparison, the area under the curve was substantially lower for the traditional analysis measures: It was 55% for mean velocity (100% sensitivity, 0% specificity, 76% accuracy), 52% for the pulsatility index (86% sensitivity, 23% specificity, 61% accuracy), and 60% for the cerebrovascular reactivity index (51% sensitivity, 68% specificity, 64% accuracy).
“Unfortunately, concussion diagnostics and management today are basically subjective,” Dr. Hamilton commented. The advanced analysis may therefore improve the situation by providing objective evidence of blood flow dysfunction after injury.
The new analysis platform “is easy to use and portable, and [testing] can be done very quickly, within 5 minutes,” he noted. “The nice thing is it can be done on the sideline, in the emergency room, or in a doctor’s office.”
The investigators will next use the advanced analysis to track recovery of blood flow regulation after sports-related concussion and will compare its performance with that of additional modalities, such as MRI, according to Dr. Hamilton. Furthermore, they are testing it in various other populations: adolescents, college athletes, and members of the military.
“Ultimately, blood flow dysfunction is also important in a wide variety of conditions, such as stroke and dementia,” he pointed out. “So those are conditions that we are looking at to study this year and moving forward in the future.”
The research was supported by the National Institutes of Health and the National Science Foundation.
VANCOUVER – A new transcranial Doppler platform that analyzes subtle changes in the cerebral blood flow waveform performed well in detecting sports-related concussion in a cohort study of 238 Los Angeles high school athletes.
The investigational headset device was able to differentiate between those with and without a recent concussion 83% of the time, investigators reported at the annual meeting of the American Academy of Neurology. In contrast, traditional transcranial Doppler analysis detected a recent concussion only 50%-60% of the time.
“Over the last few years, there has been growing evidence that cerebral hemodynamics are altered following sports-related concussion,” senior author Robert Hamilton, Ph.D., cofounder and chief science officer of Neural Analytics in Los Angeles, commented in a session and interview.
Most studies in this area have used MRI or traditional transcranial Doppler analysis, he said. However, the former is costly, time consuming, and not portable, and the latter has not proven very accurate.
As traditional Doppler analysis disregards the majority of waveform data, Dr. Hamilton and his colleagues developed an advanced platform that uses machine learning to analyze the entire shape of the cerebral blood flow velocity waveform through quantitative cerebral hemodynamics.
They compared the advanced analysis with traditional analysis among 69 high school athletes in contact sports who had sustained a concussion an average of 6 days earlier and a control group of 169 unaffected age-matched high school athletes from contact and noncontact sports.
Both groups had bilateral monitoring of blood flow in the middle cerebral artery with transcranial Doppler while they followed a standard cerebrovascular reactivity protocol that included rest and breath holding.
Results showed that for differentiating between athletes who did and did not have concussion, the advanced analysis had an area under the receiver operating characteristic curve of 83%. (Sensitivity was 72%, specificity was 82%, and overall accuracy was 80%.)
In comparison, the area under the curve was substantially lower for the traditional analysis measures: It was 55% for mean velocity (100% sensitivity, 0% specificity, 76% accuracy), 52% for the pulsatility index (86% sensitivity, 23% specificity, 61% accuracy), and 60% for the cerebrovascular reactivity index (51% sensitivity, 68% specificity, 64% accuracy).
“Unfortunately, concussion diagnostics and management today are basically subjective,” Dr. Hamilton commented. The advanced analysis may therefore improve the situation by providing objective evidence of blood flow dysfunction after injury.
The new analysis platform “is easy to use and portable, and [testing] can be done very quickly, within 5 minutes,” he noted. “The nice thing is it can be done on the sideline, in the emergency room, or in a doctor’s office.”
The investigators will next use the advanced analysis to track recovery of blood flow regulation after sports-related concussion and will compare its performance with that of additional modalities, such as MRI, according to Dr. Hamilton. Furthermore, they are testing it in various other populations: adolescents, college athletes, and members of the military.
“Ultimately, blood flow dysfunction is also important in a wide variety of conditions, such as stroke and dementia,” he pointed out. “So those are conditions that we are looking at to study this year and moving forward in the future.”
The research was supported by the National Institutes of Health and the National Science Foundation.
AT THE AAN 2016 ANNUAL MEETING
Doppler ultrasound headset performs well at spotting sports-related concussion
VANCOUVER – A new transcranial Doppler platform that analyzes subtle changes in the cerebral blood flow waveform performed well in detecting sports-related concussion in a cohort study of 238 Los Angeles high school athletes.
The investigational headset device was able to differentiate between those with and without a recent concussion 83% of the time, investigators reported at the annual meeting of the American Academy of Neurology. In contrast, traditional transcranial Doppler analysis detected a recent concussion only 50%-60% of the time.
“Over the last few years, there has been growing evidence that cerebral hemodynamics are altered following sports-related concussion,” senior author Robert Hamilton, Ph.D., cofounder and chief science officer of Neural Analytics in Los Angeles, commented in a session and interview.
Most studies in this area have used MRI or traditional transcranial Doppler analysis, he said. However, the former is costly, time consuming, and not portable, and the latter has not proven very accurate.
As traditional Doppler analysis disregards the majority of waveform data, Dr. Hamilton and his colleagues developed an advanced platform that uses machine learning to analyze the entire shape of the cerebral blood flow velocity waveform through quantitative cerebral hemodynamics.
They compared the advanced analysis with traditional analysis among 69 high school athletes in contact sports who had sustained a concussion an average of 6 days earlier and a control group of 169 unaffected age-matched high school athletes from contact and noncontact sports.
Both groups had bilateral monitoring of blood flow in the middle cerebral artery with transcranial Doppler while they followed a standard cerebrovascular reactivity protocol that included rest and breath holding.
Results showed that for differentiating between athletes who did and did not have concussion, the advanced analysis had an area under the receiver operating characteristic curve of 83%. (Sensitivity was 72%, specificity was 82%, and overall accuracy was 80%.)
In comparison, the area under the curve was substantially lower for the traditional analysis measures: It was 55% for mean velocity (100% sensitivity, 0% specificity, 76% accuracy), 52% for the pulsatility index (86% sensitivity, 23% specificity, 61% accuracy), and 60% for the cerebrovascular reactivity index (51% sensitivity, 68% specificity, 64% accuracy).
“Unfortunately, concussion diagnostics and management today are basically subjective,” Dr. Hamilton commented. The advanced analysis may therefore improve the situation by providing objective evidence of blood flow dysfunction after injury.
The new analysis platform “is easy to use and portable, and [testing] can be done very quickly, within 5 minutes,” he noted. “The nice thing is it can be done on the sideline, in the emergency room, or in a doctor’s office.”
The investigators will next use the advanced analysis to track recovery of blood flow regulation after sports-related concussion and will compare its performance with that of additional modalities, such as MRI, according to Dr. Hamilton. Furthermore, they are testing it in various other populations: adolescents, college athletes, and members of the military.
“Ultimately, blood flow dysfunction is also important in a wide variety of conditions, such as stroke and dementia,” he pointed out. “So those are conditions that we are looking at to study this year and moving forward in the future.”
The research was supported by the National Institutes of Health and the National Science Foundation.
VANCOUVER – A new transcranial Doppler platform that analyzes subtle changes in the cerebral blood flow waveform performed well in detecting sports-related concussion in a cohort study of 238 Los Angeles high school athletes.
The investigational headset device was able to differentiate between those with and without a recent concussion 83% of the time, investigators reported at the annual meeting of the American Academy of Neurology. In contrast, traditional transcranial Doppler analysis detected a recent concussion only 50%-60% of the time.
“Over the last few years, there has been growing evidence that cerebral hemodynamics are altered following sports-related concussion,” senior author Robert Hamilton, Ph.D., cofounder and chief science officer of Neural Analytics in Los Angeles, commented in a session and interview.
Most studies in this area have used MRI or traditional transcranial Doppler analysis, he said. However, the former is costly, time consuming, and not portable, and the latter has not proven very accurate.
As traditional Doppler analysis disregards the majority of waveform data, Dr. Hamilton and his colleagues developed an advanced platform that uses machine learning to analyze the entire shape of the cerebral blood flow velocity waveform through quantitative cerebral hemodynamics.
They compared the advanced analysis with traditional analysis among 69 high school athletes in contact sports who had sustained a concussion an average of 6 days earlier and a control group of 169 unaffected age-matched high school athletes from contact and noncontact sports.
Both groups had bilateral monitoring of blood flow in the middle cerebral artery with transcranial Doppler while they followed a standard cerebrovascular reactivity protocol that included rest and breath holding.
Results showed that for differentiating between athletes who did and did not have concussion, the advanced analysis had an area under the receiver operating characteristic curve of 83%. (Sensitivity was 72%, specificity was 82%, and overall accuracy was 80%.)
In comparison, the area under the curve was substantially lower for the traditional analysis measures: It was 55% for mean velocity (100% sensitivity, 0% specificity, 76% accuracy), 52% for the pulsatility index (86% sensitivity, 23% specificity, 61% accuracy), and 60% for the cerebrovascular reactivity index (51% sensitivity, 68% specificity, 64% accuracy).
“Unfortunately, concussion diagnostics and management today are basically subjective,” Dr. Hamilton commented. The advanced analysis may therefore improve the situation by providing objective evidence of blood flow dysfunction after injury.
The new analysis platform “is easy to use and portable, and [testing] can be done very quickly, within 5 minutes,” he noted. “The nice thing is it can be done on the sideline, in the emergency room, or in a doctor’s office.”
The investigators will next use the advanced analysis to track recovery of blood flow regulation after sports-related concussion and will compare its performance with that of additional modalities, such as MRI, according to Dr. Hamilton. Furthermore, they are testing it in various other populations: adolescents, college athletes, and members of the military.
“Ultimately, blood flow dysfunction is also important in a wide variety of conditions, such as stroke and dementia,” he pointed out. “So those are conditions that we are looking at to study this year and moving forward in the future.”
The research was supported by the National Institutes of Health and the National Science Foundation.
VANCOUVER – A new transcranial Doppler platform that analyzes subtle changes in the cerebral blood flow waveform performed well in detecting sports-related concussion in a cohort study of 238 Los Angeles high school athletes.
The investigational headset device was able to differentiate between those with and without a recent concussion 83% of the time, investigators reported at the annual meeting of the American Academy of Neurology. In contrast, traditional transcranial Doppler analysis detected a recent concussion only 50%-60% of the time.
“Over the last few years, there has been growing evidence that cerebral hemodynamics are altered following sports-related concussion,” senior author Robert Hamilton, Ph.D., cofounder and chief science officer of Neural Analytics in Los Angeles, commented in a session and interview.
Most studies in this area have used MRI or traditional transcranial Doppler analysis, he said. However, the former is costly, time consuming, and not portable, and the latter has not proven very accurate.
As traditional Doppler analysis disregards the majority of waveform data, Dr. Hamilton and his colleagues developed an advanced platform that uses machine learning to analyze the entire shape of the cerebral blood flow velocity waveform through quantitative cerebral hemodynamics.
They compared the advanced analysis with traditional analysis among 69 high school athletes in contact sports who had sustained a concussion an average of 6 days earlier and a control group of 169 unaffected age-matched high school athletes from contact and noncontact sports.
Both groups had bilateral monitoring of blood flow in the middle cerebral artery with transcranial Doppler while they followed a standard cerebrovascular reactivity protocol that included rest and breath holding.
Results showed that for differentiating between athletes who did and did not have concussion, the advanced analysis had an area under the receiver operating characteristic curve of 83%. (Sensitivity was 72%, specificity was 82%, and overall accuracy was 80%.)
In comparison, the area under the curve was substantially lower for the traditional analysis measures: It was 55% for mean velocity (100% sensitivity, 0% specificity, 76% accuracy), 52% for the pulsatility index (86% sensitivity, 23% specificity, 61% accuracy), and 60% for the cerebrovascular reactivity index (51% sensitivity, 68% specificity, 64% accuracy).
“Unfortunately, concussion diagnostics and management today are basically subjective,” Dr. Hamilton commented. The advanced analysis may therefore improve the situation by providing objective evidence of blood flow dysfunction after injury.
The new analysis platform “is easy to use and portable, and [testing] can be done very quickly, within 5 minutes,” he noted. “The nice thing is it can be done on the sideline, in the emergency room, or in a doctor’s office.”
The investigators will next use the advanced analysis to track recovery of blood flow regulation after sports-related concussion and will compare its performance with that of additional modalities, such as MRI, according to Dr. Hamilton. Furthermore, they are testing it in various other populations: adolescents, college athletes, and members of the military.
“Ultimately, blood flow dysfunction is also important in a wide variety of conditions, such as stroke and dementia,” he pointed out. “So those are conditions that we are looking at to study this year and moving forward in the future.”
The research was supported by the National Institutes of Health and the National Science Foundation.
AT THE AAN 2016 ANNUAL MEETING
Key clinical point: Advanced transcranial Doppler analysis may improve identification of athletes with concussion at the point of care.
Major finding: For differentiating between athletes who did and did not have concussion, the advanced analysis had an area under the receiver operating characteristic curve of 83%.
Data source: A cohort study of 69 concussed and 169 nonconcussed high school athletes.
Disclosures: Dr. Hamilton disclosed that he is a cofounder and chief science officer of Neural Analytics. The study was supported by the National Institutes of Health and the National Science Foundation.
A Practical Overview of Pediatric Atopic Dermatitis, Part 2: Triggers and Grading
Atopic dermatitis (AD) may be triggered by viral infections, food allergens, weather, and other causes, and it may trigger an inflammatory progression known as the atopic march. This article reviews research on triggers of pediatric AD so that dermatologists may discuss trigger avoidance with patients and guardians. Other factors affecting AD development include genetics and hygiene. Grading of AD also is discussed.
The Atopic March
The persistence of AD in untreated skin can trigger an inflammatory progression called the atopic march in which food and environmental allergies as well as asthma may occur progressively due to ongoing inflammatory triggering.1 In a study of asthma and food allergy reporting and management in public schools in Chicago, Illinois, food allergies were seen in 9.3% of asthmatic students (n=18,000), and 40.1% of food allergic students (n=4000) had asthma.2 An observational study by Flohr et al3 in London, England, included 619 exclusively breastfed infants who were recruited at 3 months of age. The investigators determined that food sensitization was unrelated to the presence of filaggrin mutations, type of eczema (flexural vs nonflexural), and transepidermal water loss but was associated with AD severity as determined by SCORAD (SCORing Atopic Dermatitis), a composite score of AD that includes pruritus as a factor in severity. Other AD associations included 3 leading food allergens: eggs, milk, and peanuts. No association with cod, wheat, or sesame allergy was noted. The investigators concluded that AD and AD severity were the leading skin-related risk factors for food allergies and therefore food allergy development in breastfed infants was probably mediated by cutaneous antigen-presenting cells.3
The skin has been documented to react to contact with known food allergens4 and is known to be a route of allergic sensitization to allergens such as fragrance in patients with AD.5,6 Two phenotypes of eczema that have been associated with asthma development are severe AD disease and multiple environmental allergies, supporting the theory of the atopic march.7 There also is evidence that release of danger-associated proteins from an impaired barrier also may trigger asthma.8 An analysis of the 2007 National Survey of Children’s Health, a population-based study of91,642 children aged 0 to 17 years, showed that children with AD had a higher prevalence of comorbid asthma (25.1% vs 12.3%), hay fever (34.4% vs 14.3%), and food allergies (15.1% vs 3.6%) compared to children without AD.9 A recent article provided detailed information on how food and diet interplay with AD.10
Triggers of Disease Flares
Triggers are the leading source of AD flare initiation, and avoidance of triggers is an important mechanism by which patients can control disease activity. Despite the best skin care and trigger avoidance, disease flares occur, sometimes due to ongoing inflammation and other times due to inability to prevent flares such as heat and humidity. A survey of patients with AD in Spain identified the following triggers: cosmetic products, clothing, mites, detergents/soaps, and temperature changes.11 In childhood, wool also is a known trigger of AD.12 Viral infections including respiratory syncytial virus may trigger the first onset of AD.13 Patients with AD may become allergic to fragrance and metals causing disease exacerbation on exposure.14,15 Food allergens contribute to approximately 40% of cases of AD in infancy but are not the cause of AD. The best evidence for improvement of AD with food allergen avoidance exists for egg white allergy.16 Food avoidance programs should be developed in conjunction with an allergist, as it is no longer advised in many cases to completely withdraw foods; therefore, an allergist has to assess the level of allergic severity and the risk-benefit ratio of food avoidance or introduction.17 Emotional stressors, heat, and humidity, as well as indoor heating in the winter months, can cause AD flares.18
A study by Silverberg et al19 provided evidence of climate influences on the US prevalence of childhood eczema using a merged analysis of the 2007 National Survey of Children’s Health and the 2006-2007 National Climate Data Center and Weather Service. Results showed that eczema prevalence was significantly lower when associated with higher annual relative humidity (P=.01), UV index (P<.0001), and highest-quartile air temperature (P=.002).19 The Pediatric Eczema Elective Registry also showed that warm, humid, and high-sun-exposure climates are associated with poorly controlled eczema in affected patients.20 The association of eczema with latitude as well as its negative association with mean annual outdoor temperature has been described by Weiland et al21 in the ISAAC (International Study of Asthma and Allergies in Childhood) study. Long airplane flights in low humidity can trigger eczema in adults. Climate has been postulated to affect eczema through alterations in filaggrin and skin barrier function.22 Indoor temperature and humidity regulation may be used adjunctively for daily flare prevention.
Genetics and AD
Of 762 infants in a birth cohort with a parent with atopy in Cincinnati, Ohio, 39% developed eczema by the age of 3 years. Single nucleotide polymorphisms of IL-4Rα 175 V and CD14-159 C/T were linked to greater eczema risk at 2 to 3 years of age.23 Monozygotic twins have a concordance rate of 0.72 to 0.86 versus 0.21 to 0.23 in dizygotic twins, demonstrating a strong genetic component in the development of AD.24 Linkage to AD has been positively made to the epidermal differentiation complex on human chromosome 1q21, which contains the genes for filaggrin and other proteins such as loricrin. Other genes linked to AD include the serine protease inhibitor SPINK5 (serine peptidase inhibitor, Kazal type 5) implicated in Netherton syndrome (triad of ichthyosis linearis circumflexa, bamboo hair, and atopic disorders); RANTES (regulated on activation, normal T-expressed, and secreted), which has been associated with severity of AD; IL-4; and IL-13.5,25,26
The Hygiene Hypothesis
Atopic dermatitis is more common in wealthy developed countries, leading some to believe that hygiene and relative reduction in illness via vaccination have contributed to the rise of AD prevalence in developed nations.13,27 There currently is evidence demonstrating that wild-type varicella infection confers long-standing protection against AD and mediates reduced total IgE and peripheral blood lymphocytes.27
Grading of AD
Grading of AD is a subject of controversy, as there currently are no uniform grading scales.28 A recent outcomes group attempted to determine the best scale for disease monitoring. Schmitt et al29 presented the Harmonizing Outcome Measures for Eczema (HOME) roadmap, which was intended to determine a core outcome set for eczema; however, because these outcome measurements have not yet been standardized, only the eczema assessment and severity index (EASI) scoring system meets criteria for standardization. In clinical practice, physicians often assign mild, moderate, or severe labeling based on their general sense of the disease extent using an investigator global assessment score.28
The EASI score is a well-validated composite score of AD severity based on 4 body regions: (1) head and neck, (2) trunk (including genital area), (3) upper limbs, and (4) lower limbs (including buttocks). The total area of involvement in each region is graded on a scale of 0 to 6, and AD severity is graded as a composite of 4 parameters (ranked on a scale of 0–3), including redness (erythema, inflammation), thickness (induration, papulation, swelling [acute eczema]), scratching (excoriation), and lichenification (prurigo nodules [chronic eczema]). The surface area of each region relative to body size is used as a multiplying factor, resulting in the following severity strata: 0=clear; 0.1–1.0=almost clear; 1.1–7.0=mild; 7.1–21.0=moderate; 21.1–50.0=severe; 50.1–72.0=very severe (κ=0.75).30-32 The six area, six sign AD (SASSAD) score32,33 is a similar score without adjustment for body surface area by region.34
An older, now less frequently used eczema score is the SCORAD, which addressed surface area by rule of nines and severity of 6 features—redness, swelling, oozing/crusting, scratch marks, skin thickening (lichenification), dryness (assessed in an area with no inflammation)—by region on a scale of 0 to 3. A subjective symptom parameter for itching and sleeplessness helped highlight that these comorbidities are important in gauging disease activity and impact on a child’s life.35
Natural History of AD
The clinical dogma has been that AD would improve with age, with reduction at grade school entry and perhaps full disappearance in adulthood; however, 3 recent surveys have suggested otherwise. The ISAAC group has found prevalence of AD in wealthy developed countries among children aged 6 to 7 years to be at a consistent increase.36 A US-based survey from the National Health Interview Survey showed a 1-year prevalence of 10.2% of active AD in adults and 9.8% when occupational dermatitis was excluded.37 Halvorsen et al38 demonstrated that eczema prevalence is 9.7% in individuals aged 18 to 19 years.
A prospective trial of eighth graders followed from 1995 to 2010 demonstrated that AD persisted in 50% at school age. Persistent eczema into adulthood was associated with early-onset childhood allergic rhinitis and hand eczema.39 In a cohort of hand eczema patients (N=368), 28% had AD and 39% had an atopic illness.40 An association with allergic contact dermatitis and increased IgE to Malassezia furfur was further associated.41
Conclusion
The role of triggers and allergens in disease activity in AD is an important consideration in children with AD and requires ongoing consideration with age and varied exposures. Understanding the grading of AD is important in evaluating clinical trial data. The natural history of AD has changed, which is important for the practitioner to note when counseling patients and guardians.
- Li M. Current evidence of epidermal barrier dysfunction and thymic stromal lymphopoietin in the atopic march. Eur Respir Rev. 2014;23:292-298.
- Gupta RS, Rivkina V, DeSantiago-Cardenas L, et al. Asthma and food allergy management in Chicago public schools. Pediatrics. 2014;134:729-736.
- Flohr C, Perkin M, Logan K, et al. Atopic dermatitis and disease severity are the main risk factors for food sensitization in exclusively breastfed infants. J Invest Dermatol. 2014;134:345-350.
- Silverberg NB. Food, glorious food. Cutis. 2011;87:267-268.
- De Benedetto A, Kubo A, Beck LA. Skin barrier disruption: a requirement for allergen sensitization? J Invest Dermatol. 2012;132:949-963.
- Thyssen JP, McFadden JP, Kimber I. The multiple factors affecting the association between atopic dermatitis and contact sensitization. Allergy. 2014;69:28-36.
- Amat F, Saint-Pierre P, Bourrat E, et al. Early-onset atopic dermatitis in children: which are the phenotypes at risk of asthma? results from the ORCA Cohort. PLoS One. 2015;10:e0131369.
- Demehri S, Morimoto M, Holtzman MJ, et al. Skin-derived TSLP triggers progression from epidermal-barrier defects to asthma. PLoS Biol. 2009;7:e1000067.
- Silverberg JI, Simpson EL. Association between severe eczema in children and multiple comorbid conditions and increased healthcare utilization. Pediatr Allergy Immunol. 2013;24:476-486.
- Silverberg NB, Lee-Wong M, Yosipovitch G. Diet and atopic dermatitis. Cutis. 2016;97:227-232.
- Ortiz de Frutos FJ, Torrelo A, de Lucas R, et al. Patient perspectives on triggers, adherence to medical recommendations, and disease control in atopic dermatitis: the DATOP study. Actas Dermosifiliogr. 2014;105:487-496.
- Ricci G, Patrizi A, Bellini F, et al. Use of textiles in atopic dermatitis: care of atopic dermatitis. Curr Probl Dermatol. 2006;33:127-143.
- Welliver RC, Wong DT, Sun M, et al. The development of respiratory syncytial virus-specific IgE and the release of histamine in nasopharyngeal secretions after infection. N Engl J Med. 1981;305:841-846.
- Aquino M, Fonacier L. The role of contact dermatitis in patients with atopic dermatitis. J Allergy Clin Immunol Pract. 2014;2:382-387.
- Brod BA, Treat JR, Rothe MJ, et al. Allergic contact dermatitis: kids are not just little people. Clin Dermatol. 2015;33:605-612.
- Martorell A, Alonso E, Boné J, et al. Position document: IgE-mediated allergy to egg protein. Allergol Immunopathol (Madr). 2013;41:320-336.
- Sicherer SH. Early introduction of peanut to infants at high allergic risk can reduce peanut allergy at age 5 years [published online September 17, 2015]. Evid Based Med. 2015;20:204.
- Kiken DA, Silverberg NB. Atopic dermatitis in children, part 1: epidemiology, clinical features, and complications. Cutis. 2006;78:241-247.
- Silverberg JI, Hanifin J, Simpson EL. Climatic factors are associated with childhood eczema prevalence in the United States. J Invest Dermatol. 2013;133:1752-1759.
- Sargen MR, Hoffstad O, Margolis DJ. Warm, humid, and high sun exposure climates are associated with poorly controlled eczema: PEER (Pediatric Eczema Elective Registry) cohort, 2004-2012. J Invest Dermatol. 2014;134:51-57.
- Weiland SK, Hüsing A, Strachan DP, et al. Climate and the prevalence of symptoms of asthma, allergic rhinitis, and atopic eczema in children. Occup Environ Med. 2004;61:609-615.
- Langan SM, Irvine AD. Childhood eczema and the importance of the physical environment. J Invest Dermatol. 2013;133:1706-1709.
- Biagini Myers JM, Wang N, LeMasters GK, et al. Genetic and environmental risk factors for childhood eczema development and allergic sensitization in the CCAAPS cohort. J Invest Dermatol. 2010;130:430-437.
- Brown SJ, McLean WH. Eczema genetics: current state of knowledge and future goals. J Invest Dermatol. 2009;129:543-552.
- Hanifin JM. Evolving concepts of pathogenesis in atopic dermatitis and other eczemas. J Invest Dermatol. 2009;129:320-322.
- Paller AS. Latest approaches to treating atopic dermatitis. Chem Immunol Allergy. 2012;96:132-140.
- Silverberg JI, Norowitz KB, Kleiman E, et al. Association between varicella zoster virus infection and atopic dermatitis in early and late childhood: a case-control study. J Allergy Clin Immunol. 2010;126:300-305.
- Futamura M, Leshem YA, Thomas KS, et al. A systematic review of Investigator Global Assessment (IGA) in atopic dermatitis (AD) trials: many options, no standards. J Am Acad Dermatol. 2016;74:288-294.
- Schmitt J, Apfelbacher C, Spuls PI, et al. The Harmonizing Outcome Measures for Eczema (HOME) roadmap: a methodological framework to develop core sets of outcome measurements in dermatology. J Invest Dermatol. 2015;135:24-30.
- Hanifin JM, Thurston M, Omoto M, et al. The eczema area and severity index (EASI): assessment of reliability in atopic dermatitis. EASI Evaluator Group. Exp Dermatol. 2001;10:11-18.
- Leshem YA, Hajar T, Hanifin JM, et al. What the Eczema Area and Severity Index score tells us about the severity of atopic dermatitis: an interpretability study. Br J Dermatol. 2015;172:1353-1357.
- Barbier N, Paul C, Luger T, et al. Validation of the Eczema Area and Severity Index for atopic dermatitis in a cohort of 1550 patients from the pimecrolimus cream 1% randomized controlled clinical trials programme. Br J Dermatol. 2004;150:96-102.
- Berth-Jones J. Six area, six sign atopic dermatitis (SASSAD) severity score: a simple system for monitoring disease activity in atopic dermatitis. Br J Dermatol. 1996;135(suppl 48):25-30.
- Zhao CY, Tran AQ, Lazo-Dizon JP, et al. A pilot comparison study of four clinician-rated atopic dermatitis severity scales. Br J Dermatol. 2015;173:488-497.
- Kunz B, Oranje AP, Labrèze L, et al. Clinical validation and guidelines for the SCORAD index: consensus report of the European Task Force on Atopic Dermatitis. Dermatology. 1997;195:10-19.
- Williams H, Stewart A, von Mutius E, et al. Is eczema really on the increase worldwide? J Allergy Clin Immunol. 2008;121:947-954.
- Silverberg JI, Hanifin JM. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population-based study. J Allergy Clin Immunol. 2013;132:1132-1138.
- Halvorsen JA, Lien L, Dalgard F, et al. Suicidal ideation, mental health problems, and social function in adolescents with eczema: a population-based study. J Invest Dermatol. 2014;134:1847-1854.
- Mortz CG, Andersen KE, Dellgren C, et al. Atopic dermatitis from adolescence to adulthood in the TOACS cohort: prevalence, persistence, and comorbidities. Allergy. 2015;70:836-845.
- Rystedt I. Atopic background in patients with occupational hand eczema. Contact Dermatitis. 1985;12:247-254.
- Mortz CG, Andersen KE, Dellgren C, et al. Atopic dermatitis from adolescence to adulthood in the TOACS cohort: prevalence, persistence and comorbidities. Allergy. 2015;70:836-845.
Atopic dermatitis (AD) may be triggered by viral infections, food allergens, weather, and other causes, and it may trigger an inflammatory progression known as the atopic march. This article reviews research on triggers of pediatric AD so that dermatologists may discuss trigger avoidance with patients and guardians. Other factors affecting AD development include genetics and hygiene. Grading of AD also is discussed.
The Atopic March
The persistence of AD in untreated skin can trigger an inflammatory progression called the atopic march in which food and environmental allergies as well as asthma may occur progressively due to ongoing inflammatory triggering.1 In a study of asthma and food allergy reporting and management in public schools in Chicago, Illinois, food allergies were seen in 9.3% of asthmatic students (n=18,000), and 40.1% of food allergic students (n=4000) had asthma.2 An observational study by Flohr et al3 in London, England, included 619 exclusively breastfed infants who were recruited at 3 months of age. The investigators determined that food sensitization was unrelated to the presence of filaggrin mutations, type of eczema (flexural vs nonflexural), and transepidermal water loss but was associated with AD severity as determined by SCORAD (SCORing Atopic Dermatitis), a composite score of AD that includes pruritus as a factor in severity. Other AD associations included 3 leading food allergens: eggs, milk, and peanuts. No association with cod, wheat, or sesame allergy was noted. The investigators concluded that AD and AD severity were the leading skin-related risk factors for food allergies and therefore food allergy development in breastfed infants was probably mediated by cutaneous antigen-presenting cells.3
The skin has been documented to react to contact with known food allergens4 and is known to be a route of allergic sensitization to allergens such as fragrance in patients with AD.5,6 Two phenotypes of eczema that have been associated with asthma development are severe AD disease and multiple environmental allergies, supporting the theory of the atopic march.7 There also is evidence that release of danger-associated proteins from an impaired barrier also may trigger asthma.8 An analysis of the 2007 National Survey of Children’s Health, a population-based study of91,642 children aged 0 to 17 years, showed that children with AD had a higher prevalence of comorbid asthma (25.1% vs 12.3%), hay fever (34.4% vs 14.3%), and food allergies (15.1% vs 3.6%) compared to children without AD.9 A recent article provided detailed information on how food and diet interplay with AD.10
Triggers of Disease Flares
Triggers are the leading source of AD flare initiation, and avoidance of triggers is an important mechanism by which patients can control disease activity. Despite the best skin care and trigger avoidance, disease flares occur, sometimes due to ongoing inflammation and other times due to inability to prevent flares such as heat and humidity. A survey of patients with AD in Spain identified the following triggers: cosmetic products, clothing, mites, detergents/soaps, and temperature changes.11 In childhood, wool also is a known trigger of AD.12 Viral infections including respiratory syncytial virus may trigger the first onset of AD.13 Patients with AD may become allergic to fragrance and metals causing disease exacerbation on exposure.14,15 Food allergens contribute to approximately 40% of cases of AD in infancy but are not the cause of AD. The best evidence for improvement of AD with food allergen avoidance exists for egg white allergy.16 Food avoidance programs should be developed in conjunction with an allergist, as it is no longer advised in many cases to completely withdraw foods; therefore, an allergist has to assess the level of allergic severity and the risk-benefit ratio of food avoidance or introduction.17 Emotional stressors, heat, and humidity, as well as indoor heating in the winter months, can cause AD flares.18
A study by Silverberg et al19 provided evidence of climate influences on the US prevalence of childhood eczema using a merged analysis of the 2007 National Survey of Children’s Health and the 2006-2007 National Climate Data Center and Weather Service. Results showed that eczema prevalence was significantly lower when associated with higher annual relative humidity (P=.01), UV index (P<.0001), and highest-quartile air temperature (P=.002).19 The Pediatric Eczema Elective Registry also showed that warm, humid, and high-sun-exposure climates are associated with poorly controlled eczema in affected patients.20 The association of eczema with latitude as well as its negative association with mean annual outdoor temperature has been described by Weiland et al21 in the ISAAC (International Study of Asthma and Allergies in Childhood) study. Long airplane flights in low humidity can trigger eczema in adults. Climate has been postulated to affect eczema through alterations in filaggrin and skin barrier function.22 Indoor temperature and humidity regulation may be used adjunctively for daily flare prevention.
Genetics and AD
Of 762 infants in a birth cohort with a parent with atopy in Cincinnati, Ohio, 39% developed eczema by the age of 3 years. Single nucleotide polymorphisms of IL-4Rα 175 V and CD14-159 C/T were linked to greater eczema risk at 2 to 3 years of age.23 Monozygotic twins have a concordance rate of 0.72 to 0.86 versus 0.21 to 0.23 in dizygotic twins, demonstrating a strong genetic component in the development of AD.24 Linkage to AD has been positively made to the epidermal differentiation complex on human chromosome 1q21, which contains the genes for filaggrin and other proteins such as loricrin. Other genes linked to AD include the serine protease inhibitor SPINK5 (serine peptidase inhibitor, Kazal type 5) implicated in Netherton syndrome (triad of ichthyosis linearis circumflexa, bamboo hair, and atopic disorders); RANTES (regulated on activation, normal T-expressed, and secreted), which has been associated with severity of AD; IL-4; and IL-13.5,25,26
The Hygiene Hypothesis
Atopic dermatitis is more common in wealthy developed countries, leading some to believe that hygiene and relative reduction in illness via vaccination have contributed to the rise of AD prevalence in developed nations.13,27 There currently is evidence demonstrating that wild-type varicella infection confers long-standing protection against AD and mediates reduced total IgE and peripheral blood lymphocytes.27
Grading of AD
Grading of AD is a subject of controversy, as there currently are no uniform grading scales.28 A recent outcomes group attempted to determine the best scale for disease monitoring. Schmitt et al29 presented the Harmonizing Outcome Measures for Eczema (HOME) roadmap, which was intended to determine a core outcome set for eczema; however, because these outcome measurements have not yet been standardized, only the eczema assessment and severity index (EASI) scoring system meets criteria for standardization. In clinical practice, physicians often assign mild, moderate, or severe labeling based on their general sense of the disease extent using an investigator global assessment score.28
The EASI score is a well-validated composite score of AD severity based on 4 body regions: (1) head and neck, (2) trunk (including genital area), (3) upper limbs, and (4) lower limbs (including buttocks). The total area of involvement in each region is graded on a scale of 0 to 6, and AD severity is graded as a composite of 4 parameters (ranked on a scale of 0–3), including redness (erythema, inflammation), thickness (induration, papulation, swelling [acute eczema]), scratching (excoriation), and lichenification (prurigo nodules [chronic eczema]). The surface area of each region relative to body size is used as a multiplying factor, resulting in the following severity strata: 0=clear; 0.1–1.0=almost clear; 1.1–7.0=mild; 7.1–21.0=moderate; 21.1–50.0=severe; 50.1–72.0=very severe (κ=0.75).30-32 The six area, six sign AD (SASSAD) score32,33 is a similar score without adjustment for body surface area by region.34
An older, now less frequently used eczema score is the SCORAD, which addressed surface area by rule of nines and severity of 6 features—redness, swelling, oozing/crusting, scratch marks, skin thickening (lichenification), dryness (assessed in an area with no inflammation)—by region on a scale of 0 to 3. A subjective symptom parameter for itching and sleeplessness helped highlight that these comorbidities are important in gauging disease activity and impact on a child’s life.35
Natural History of AD
The clinical dogma has been that AD would improve with age, with reduction at grade school entry and perhaps full disappearance in adulthood; however, 3 recent surveys have suggested otherwise. The ISAAC group has found prevalence of AD in wealthy developed countries among children aged 6 to 7 years to be at a consistent increase.36 A US-based survey from the National Health Interview Survey showed a 1-year prevalence of 10.2% of active AD in adults and 9.8% when occupational dermatitis was excluded.37 Halvorsen et al38 demonstrated that eczema prevalence is 9.7% in individuals aged 18 to 19 years.
A prospective trial of eighth graders followed from 1995 to 2010 demonstrated that AD persisted in 50% at school age. Persistent eczema into adulthood was associated with early-onset childhood allergic rhinitis and hand eczema.39 In a cohort of hand eczema patients (N=368), 28% had AD and 39% had an atopic illness.40 An association with allergic contact dermatitis and increased IgE to Malassezia furfur was further associated.41
Conclusion
The role of triggers and allergens in disease activity in AD is an important consideration in children with AD and requires ongoing consideration with age and varied exposures. Understanding the grading of AD is important in evaluating clinical trial data. The natural history of AD has changed, which is important for the practitioner to note when counseling patients and guardians.
Atopic dermatitis (AD) may be triggered by viral infections, food allergens, weather, and other causes, and it may trigger an inflammatory progression known as the atopic march. This article reviews research on triggers of pediatric AD so that dermatologists may discuss trigger avoidance with patients and guardians. Other factors affecting AD development include genetics and hygiene. Grading of AD also is discussed.
The Atopic March
The persistence of AD in untreated skin can trigger an inflammatory progression called the atopic march in which food and environmental allergies as well as asthma may occur progressively due to ongoing inflammatory triggering.1 In a study of asthma and food allergy reporting and management in public schools in Chicago, Illinois, food allergies were seen in 9.3% of asthmatic students (n=18,000), and 40.1% of food allergic students (n=4000) had asthma.2 An observational study by Flohr et al3 in London, England, included 619 exclusively breastfed infants who were recruited at 3 months of age. The investigators determined that food sensitization was unrelated to the presence of filaggrin mutations, type of eczema (flexural vs nonflexural), and transepidermal water loss but was associated with AD severity as determined by SCORAD (SCORing Atopic Dermatitis), a composite score of AD that includes pruritus as a factor in severity. Other AD associations included 3 leading food allergens: eggs, milk, and peanuts. No association with cod, wheat, or sesame allergy was noted. The investigators concluded that AD and AD severity were the leading skin-related risk factors for food allergies and therefore food allergy development in breastfed infants was probably mediated by cutaneous antigen-presenting cells.3
The skin has been documented to react to contact with known food allergens4 and is known to be a route of allergic sensitization to allergens such as fragrance in patients with AD.5,6 Two phenotypes of eczema that have been associated with asthma development are severe AD disease and multiple environmental allergies, supporting the theory of the atopic march.7 There also is evidence that release of danger-associated proteins from an impaired barrier also may trigger asthma.8 An analysis of the 2007 National Survey of Children’s Health, a population-based study of91,642 children aged 0 to 17 years, showed that children with AD had a higher prevalence of comorbid asthma (25.1% vs 12.3%), hay fever (34.4% vs 14.3%), and food allergies (15.1% vs 3.6%) compared to children without AD.9 A recent article provided detailed information on how food and diet interplay with AD.10
Triggers of Disease Flares
Triggers are the leading source of AD flare initiation, and avoidance of triggers is an important mechanism by which patients can control disease activity. Despite the best skin care and trigger avoidance, disease flares occur, sometimes due to ongoing inflammation and other times due to inability to prevent flares such as heat and humidity. A survey of patients with AD in Spain identified the following triggers: cosmetic products, clothing, mites, detergents/soaps, and temperature changes.11 In childhood, wool also is a known trigger of AD.12 Viral infections including respiratory syncytial virus may trigger the first onset of AD.13 Patients with AD may become allergic to fragrance and metals causing disease exacerbation on exposure.14,15 Food allergens contribute to approximately 40% of cases of AD in infancy but are not the cause of AD. The best evidence for improvement of AD with food allergen avoidance exists for egg white allergy.16 Food avoidance programs should be developed in conjunction with an allergist, as it is no longer advised in many cases to completely withdraw foods; therefore, an allergist has to assess the level of allergic severity and the risk-benefit ratio of food avoidance or introduction.17 Emotional stressors, heat, and humidity, as well as indoor heating in the winter months, can cause AD flares.18
A study by Silverberg et al19 provided evidence of climate influences on the US prevalence of childhood eczema using a merged analysis of the 2007 National Survey of Children’s Health and the 2006-2007 National Climate Data Center and Weather Service. Results showed that eczema prevalence was significantly lower when associated with higher annual relative humidity (P=.01), UV index (P<.0001), and highest-quartile air temperature (P=.002).19 The Pediatric Eczema Elective Registry also showed that warm, humid, and high-sun-exposure climates are associated with poorly controlled eczema in affected patients.20 The association of eczema with latitude as well as its negative association with mean annual outdoor temperature has been described by Weiland et al21 in the ISAAC (International Study of Asthma and Allergies in Childhood) study. Long airplane flights in low humidity can trigger eczema in adults. Climate has been postulated to affect eczema through alterations in filaggrin and skin barrier function.22 Indoor temperature and humidity regulation may be used adjunctively for daily flare prevention.
Genetics and AD
Of 762 infants in a birth cohort with a parent with atopy in Cincinnati, Ohio, 39% developed eczema by the age of 3 years. Single nucleotide polymorphisms of IL-4Rα 175 V and CD14-159 C/T were linked to greater eczema risk at 2 to 3 years of age.23 Monozygotic twins have a concordance rate of 0.72 to 0.86 versus 0.21 to 0.23 in dizygotic twins, demonstrating a strong genetic component in the development of AD.24 Linkage to AD has been positively made to the epidermal differentiation complex on human chromosome 1q21, which contains the genes for filaggrin and other proteins such as loricrin. Other genes linked to AD include the serine protease inhibitor SPINK5 (serine peptidase inhibitor, Kazal type 5) implicated in Netherton syndrome (triad of ichthyosis linearis circumflexa, bamboo hair, and atopic disorders); RANTES (regulated on activation, normal T-expressed, and secreted), which has been associated with severity of AD; IL-4; and IL-13.5,25,26
The Hygiene Hypothesis
Atopic dermatitis is more common in wealthy developed countries, leading some to believe that hygiene and relative reduction in illness via vaccination have contributed to the rise of AD prevalence in developed nations.13,27 There currently is evidence demonstrating that wild-type varicella infection confers long-standing protection against AD and mediates reduced total IgE and peripheral blood lymphocytes.27
Grading of AD
Grading of AD is a subject of controversy, as there currently are no uniform grading scales.28 A recent outcomes group attempted to determine the best scale for disease monitoring. Schmitt et al29 presented the Harmonizing Outcome Measures for Eczema (HOME) roadmap, which was intended to determine a core outcome set for eczema; however, because these outcome measurements have not yet been standardized, only the eczema assessment and severity index (EASI) scoring system meets criteria for standardization. In clinical practice, physicians often assign mild, moderate, or severe labeling based on their general sense of the disease extent using an investigator global assessment score.28
The EASI score is a well-validated composite score of AD severity based on 4 body regions: (1) head and neck, (2) trunk (including genital area), (3) upper limbs, and (4) lower limbs (including buttocks). The total area of involvement in each region is graded on a scale of 0 to 6, and AD severity is graded as a composite of 4 parameters (ranked on a scale of 0–3), including redness (erythema, inflammation), thickness (induration, papulation, swelling [acute eczema]), scratching (excoriation), and lichenification (prurigo nodules [chronic eczema]). The surface area of each region relative to body size is used as a multiplying factor, resulting in the following severity strata: 0=clear; 0.1–1.0=almost clear; 1.1–7.0=mild; 7.1–21.0=moderate; 21.1–50.0=severe; 50.1–72.0=very severe (κ=0.75).30-32 The six area, six sign AD (SASSAD) score32,33 is a similar score without adjustment for body surface area by region.34
An older, now less frequently used eczema score is the SCORAD, which addressed surface area by rule of nines and severity of 6 features—redness, swelling, oozing/crusting, scratch marks, skin thickening (lichenification), dryness (assessed in an area with no inflammation)—by region on a scale of 0 to 3. A subjective symptom parameter for itching and sleeplessness helped highlight that these comorbidities are important in gauging disease activity and impact on a child’s life.35
Natural History of AD
The clinical dogma has been that AD would improve with age, with reduction at grade school entry and perhaps full disappearance in adulthood; however, 3 recent surveys have suggested otherwise. The ISAAC group has found prevalence of AD in wealthy developed countries among children aged 6 to 7 years to be at a consistent increase.36 A US-based survey from the National Health Interview Survey showed a 1-year prevalence of 10.2% of active AD in adults and 9.8% when occupational dermatitis was excluded.37 Halvorsen et al38 demonstrated that eczema prevalence is 9.7% in individuals aged 18 to 19 years.
A prospective trial of eighth graders followed from 1995 to 2010 demonstrated that AD persisted in 50% at school age. Persistent eczema into adulthood was associated with early-onset childhood allergic rhinitis and hand eczema.39 In a cohort of hand eczema patients (N=368), 28% had AD and 39% had an atopic illness.40 An association with allergic contact dermatitis and increased IgE to Malassezia furfur was further associated.41
Conclusion
The role of triggers and allergens in disease activity in AD is an important consideration in children with AD and requires ongoing consideration with age and varied exposures. Understanding the grading of AD is important in evaluating clinical trial data. The natural history of AD has changed, which is important for the practitioner to note when counseling patients and guardians.
- Li M. Current evidence of epidermal barrier dysfunction and thymic stromal lymphopoietin in the atopic march. Eur Respir Rev. 2014;23:292-298.
- Gupta RS, Rivkina V, DeSantiago-Cardenas L, et al. Asthma and food allergy management in Chicago public schools. Pediatrics. 2014;134:729-736.
- Flohr C, Perkin M, Logan K, et al. Atopic dermatitis and disease severity are the main risk factors for food sensitization in exclusively breastfed infants. J Invest Dermatol. 2014;134:345-350.
- Silverberg NB. Food, glorious food. Cutis. 2011;87:267-268.
- De Benedetto A, Kubo A, Beck LA. Skin barrier disruption: a requirement for allergen sensitization? J Invest Dermatol. 2012;132:949-963.
- Thyssen JP, McFadden JP, Kimber I. The multiple factors affecting the association between atopic dermatitis and contact sensitization. Allergy. 2014;69:28-36.
- Amat F, Saint-Pierre P, Bourrat E, et al. Early-onset atopic dermatitis in children: which are the phenotypes at risk of asthma? results from the ORCA Cohort. PLoS One. 2015;10:e0131369.
- Demehri S, Morimoto M, Holtzman MJ, et al. Skin-derived TSLP triggers progression from epidermal-barrier defects to asthma. PLoS Biol. 2009;7:e1000067.
- Silverberg JI, Simpson EL. Association between severe eczema in children and multiple comorbid conditions and increased healthcare utilization. Pediatr Allergy Immunol. 2013;24:476-486.
- Silverberg NB, Lee-Wong M, Yosipovitch G. Diet and atopic dermatitis. Cutis. 2016;97:227-232.
- Ortiz de Frutos FJ, Torrelo A, de Lucas R, et al. Patient perspectives on triggers, adherence to medical recommendations, and disease control in atopic dermatitis: the DATOP study. Actas Dermosifiliogr. 2014;105:487-496.
- Ricci G, Patrizi A, Bellini F, et al. Use of textiles in atopic dermatitis: care of atopic dermatitis. Curr Probl Dermatol. 2006;33:127-143.
- Welliver RC, Wong DT, Sun M, et al. The development of respiratory syncytial virus-specific IgE and the release of histamine in nasopharyngeal secretions after infection. N Engl J Med. 1981;305:841-846.
- Aquino M, Fonacier L. The role of contact dermatitis in patients with atopic dermatitis. J Allergy Clin Immunol Pract. 2014;2:382-387.
- Brod BA, Treat JR, Rothe MJ, et al. Allergic contact dermatitis: kids are not just little people. Clin Dermatol. 2015;33:605-612.
- Martorell A, Alonso E, Boné J, et al. Position document: IgE-mediated allergy to egg protein. Allergol Immunopathol (Madr). 2013;41:320-336.
- Sicherer SH. Early introduction of peanut to infants at high allergic risk can reduce peanut allergy at age 5 years [published online September 17, 2015]. Evid Based Med. 2015;20:204.
- Kiken DA, Silverberg NB. Atopic dermatitis in children, part 1: epidemiology, clinical features, and complications. Cutis. 2006;78:241-247.
- Silverberg JI, Hanifin J, Simpson EL. Climatic factors are associated with childhood eczema prevalence in the United States. J Invest Dermatol. 2013;133:1752-1759.
- Sargen MR, Hoffstad O, Margolis DJ. Warm, humid, and high sun exposure climates are associated with poorly controlled eczema: PEER (Pediatric Eczema Elective Registry) cohort, 2004-2012. J Invest Dermatol. 2014;134:51-57.
- Weiland SK, Hüsing A, Strachan DP, et al. Climate and the prevalence of symptoms of asthma, allergic rhinitis, and atopic eczema in children. Occup Environ Med. 2004;61:609-615.
- Langan SM, Irvine AD. Childhood eczema and the importance of the physical environment. J Invest Dermatol. 2013;133:1706-1709.
- Biagini Myers JM, Wang N, LeMasters GK, et al. Genetic and environmental risk factors for childhood eczema development and allergic sensitization in the CCAAPS cohort. J Invest Dermatol. 2010;130:430-437.
- Brown SJ, McLean WH. Eczema genetics: current state of knowledge and future goals. J Invest Dermatol. 2009;129:543-552.
- Hanifin JM. Evolving concepts of pathogenesis in atopic dermatitis and other eczemas. J Invest Dermatol. 2009;129:320-322.
- Paller AS. Latest approaches to treating atopic dermatitis. Chem Immunol Allergy. 2012;96:132-140.
- Silverberg JI, Norowitz KB, Kleiman E, et al. Association between varicella zoster virus infection and atopic dermatitis in early and late childhood: a case-control study. J Allergy Clin Immunol. 2010;126:300-305.
- Futamura M, Leshem YA, Thomas KS, et al. A systematic review of Investigator Global Assessment (IGA) in atopic dermatitis (AD) trials: many options, no standards. J Am Acad Dermatol. 2016;74:288-294.
- Schmitt J, Apfelbacher C, Spuls PI, et al. The Harmonizing Outcome Measures for Eczema (HOME) roadmap: a methodological framework to develop core sets of outcome measurements in dermatology. J Invest Dermatol. 2015;135:24-30.
- Hanifin JM, Thurston M, Omoto M, et al. The eczema area and severity index (EASI): assessment of reliability in atopic dermatitis. EASI Evaluator Group. Exp Dermatol. 2001;10:11-18.
- Leshem YA, Hajar T, Hanifin JM, et al. What the Eczema Area and Severity Index score tells us about the severity of atopic dermatitis: an interpretability study. Br J Dermatol. 2015;172:1353-1357.
- Barbier N, Paul C, Luger T, et al. Validation of the Eczema Area and Severity Index for atopic dermatitis in a cohort of 1550 patients from the pimecrolimus cream 1% randomized controlled clinical trials programme. Br J Dermatol. 2004;150:96-102.
- Berth-Jones J. Six area, six sign atopic dermatitis (SASSAD) severity score: a simple system for monitoring disease activity in atopic dermatitis. Br J Dermatol. 1996;135(suppl 48):25-30.
- Zhao CY, Tran AQ, Lazo-Dizon JP, et al. A pilot comparison study of four clinician-rated atopic dermatitis severity scales. Br J Dermatol. 2015;173:488-497.
- Kunz B, Oranje AP, Labrèze L, et al. Clinical validation and guidelines for the SCORAD index: consensus report of the European Task Force on Atopic Dermatitis. Dermatology. 1997;195:10-19.
- Williams H, Stewart A, von Mutius E, et al. Is eczema really on the increase worldwide? J Allergy Clin Immunol. 2008;121:947-954.
- Silverberg JI, Hanifin JM. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population-based study. J Allergy Clin Immunol. 2013;132:1132-1138.
- Halvorsen JA, Lien L, Dalgard F, et al. Suicidal ideation, mental health problems, and social function in adolescents with eczema: a population-based study. J Invest Dermatol. 2014;134:1847-1854.
- Mortz CG, Andersen KE, Dellgren C, et al. Atopic dermatitis from adolescence to adulthood in the TOACS cohort: prevalence, persistence, and comorbidities. Allergy. 2015;70:836-845.
- Rystedt I. Atopic background in patients with occupational hand eczema. Contact Dermatitis. 1985;12:247-254.
- Mortz CG, Andersen KE, Dellgren C, et al. Atopic dermatitis from adolescence to adulthood in the TOACS cohort: prevalence, persistence and comorbidities. Allergy. 2015;70:836-845.
- Li M. Current evidence of epidermal barrier dysfunction and thymic stromal lymphopoietin in the atopic march. Eur Respir Rev. 2014;23:292-298.
- Gupta RS, Rivkina V, DeSantiago-Cardenas L, et al. Asthma and food allergy management in Chicago public schools. Pediatrics. 2014;134:729-736.
- Flohr C, Perkin M, Logan K, et al. Atopic dermatitis and disease severity are the main risk factors for food sensitization in exclusively breastfed infants. J Invest Dermatol. 2014;134:345-350.
- Silverberg NB. Food, glorious food. Cutis. 2011;87:267-268.
- De Benedetto A, Kubo A, Beck LA. Skin barrier disruption: a requirement for allergen sensitization? J Invest Dermatol. 2012;132:949-963.
- Thyssen JP, McFadden JP, Kimber I. The multiple factors affecting the association between atopic dermatitis and contact sensitization. Allergy. 2014;69:28-36.
- Amat F, Saint-Pierre P, Bourrat E, et al. Early-onset atopic dermatitis in children: which are the phenotypes at risk of asthma? results from the ORCA Cohort. PLoS One. 2015;10:e0131369.
- Demehri S, Morimoto M, Holtzman MJ, et al. Skin-derived TSLP triggers progression from epidermal-barrier defects to asthma. PLoS Biol. 2009;7:e1000067.
- Silverberg JI, Simpson EL. Association between severe eczema in children and multiple comorbid conditions and increased healthcare utilization. Pediatr Allergy Immunol. 2013;24:476-486.
- Silverberg NB, Lee-Wong M, Yosipovitch G. Diet and atopic dermatitis. Cutis. 2016;97:227-232.
- Ortiz de Frutos FJ, Torrelo A, de Lucas R, et al. Patient perspectives on triggers, adherence to medical recommendations, and disease control in atopic dermatitis: the DATOP study. Actas Dermosifiliogr. 2014;105:487-496.
- Ricci G, Patrizi A, Bellini F, et al. Use of textiles in atopic dermatitis: care of atopic dermatitis. Curr Probl Dermatol. 2006;33:127-143.
- Welliver RC, Wong DT, Sun M, et al. The development of respiratory syncytial virus-specific IgE and the release of histamine in nasopharyngeal secretions after infection. N Engl J Med. 1981;305:841-846.
- Aquino M, Fonacier L. The role of contact dermatitis in patients with atopic dermatitis. J Allergy Clin Immunol Pract. 2014;2:382-387.
- Brod BA, Treat JR, Rothe MJ, et al. Allergic contact dermatitis: kids are not just little people. Clin Dermatol. 2015;33:605-612.
- Martorell A, Alonso E, Boné J, et al. Position document: IgE-mediated allergy to egg protein. Allergol Immunopathol (Madr). 2013;41:320-336.
- Sicherer SH. Early introduction of peanut to infants at high allergic risk can reduce peanut allergy at age 5 years [published online September 17, 2015]. Evid Based Med. 2015;20:204.
- Kiken DA, Silverberg NB. Atopic dermatitis in children, part 1: epidemiology, clinical features, and complications. Cutis. 2006;78:241-247.
- Silverberg JI, Hanifin J, Simpson EL. Climatic factors are associated with childhood eczema prevalence in the United States. J Invest Dermatol. 2013;133:1752-1759.
- Sargen MR, Hoffstad O, Margolis DJ. Warm, humid, and high sun exposure climates are associated with poorly controlled eczema: PEER (Pediatric Eczema Elective Registry) cohort, 2004-2012. J Invest Dermatol. 2014;134:51-57.
- Weiland SK, Hüsing A, Strachan DP, et al. Climate and the prevalence of symptoms of asthma, allergic rhinitis, and atopic eczema in children. Occup Environ Med. 2004;61:609-615.
- Langan SM, Irvine AD. Childhood eczema and the importance of the physical environment. J Invest Dermatol. 2013;133:1706-1709.
- Biagini Myers JM, Wang N, LeMasters GK, et al. Genetic and environmental risk factors for childhood eczema development and allergic sensitization in the CCAAPS cohort. J Invest Dermatol. 2010;130:430-437.
- Brown SJ, McLean WH. Eczema genetics: current state of knowledge and future goals. J Invest Dermatol. 2009;129:543-552.
- Hanifin JM. Evolving concepts of pathogenesis in atopic dermatitis and other eczemas. J Invest Dermatol. 2009;129:320-322.
- Paller AS. Latest approaches to treating atopic dermatitis. Chem Immunol Allergy. 2012;96:132-140.
- Silverberg JI, Norowitz KB, Kleiman E, et al. Association between varicella zoster virus infection and atopic dermatitis in early and late childhood: a case-control study. J Allergy Clin Immunol. 2010;126:300-305.
- Futamura M, Leshem YA, Thomas KS, et al. A systematic review of Investigator Global Assessment (IGA) in atopic dermatitis (AD) trials: many options, no standards. J Am Acad Dermatol. 2016;74:288-294.
- Schmitt J, Apfelbacher C, Spuls PI, et al. The Harmonizing Outcome Measures for Eczema (HOME) roadmap: a methodological framework to develop core sets of outcome measurements in dermatology. J Invest Dermatol. 2015;135:24-30.
- Hanifin JM, Thurston M, Omoto M, et al. The eczema area and severity index (EASI): assessment of reliability in atopic dermatitis. EASI Evaluator Group. Exp Dermatol. 2001;10:11-18.
- Leshem YA, Hajar T, Hanifin JM, et al. What the Eczema Area and Severity Index score tells us about the severity of atopic dermatitis: an interpretability study. Br J Dermatol. 2015;172:1353-1357.
- Barbier N, Paul C, Luger T, et al. Validation of the Eczema Area and Severity Index for atopic dermatitis in a cohort of 1550 patients from the pimecrolimus cream 1% randomized controlled clinical trials programme. Br J Dermatol. 2004;150:96-102.
- Berth-Jones J. Six area, six sign atopic dermatitis (SASSAD) severity score: a simple system for monitoring disease activity in atopic dermatitis. Br J Dermatol. 1996;135(suppl 48):25-30.
- Zhao CY, Tran AQ, Lazo-Dizon JP, et al. A pilot comparison study of four clinician-rated atopic dermatitis severity scales. Br J Dermatol. 2015;173:488-497.
- Kunz B, Oranje AP, Labrèze L, et al. Clinical validation and guidelines for the SCORAD index: consensus report of the European Task Force on Atopic Dermatitis. Dermatology. 1997;195:10-19.
- Williams H, Stewart A, von Mutius E, et al. Is eczema really on the increase worldwide? J Allergy Clin Immunol. 2008;121:947-954.
- Silverberg JI, Hanifin JM. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population-based study. J Allergy Clin Immunol. 2013;132:1132-1138.
- Halvorsen JA, Lien L, Dalgard F, et al. Suicidal ideation, mental health problems, and social function in adolescents with eczema: a population-based study. J Invest Dermatol. 2014;134:1847-1854.
- Mortz CG, Andersen KE, Dellgren C, et al. Atopic dermatitis from adolescence to adulthood in the TOACS cohort: prevalence, persistence, and comorbidities. Allergy. 2015;70:836-845.
- Rystedt I. Atopic background in patients with occupational hand eczema. Contact Dermatitis. 1985;12:247-254.
- Mortz CG, Andersen KE, Dellgren C, et al. Atopic dermatitis from adolescence to adulthood in the TOACS cohort: prevalence, persistence and comorbidities. Allergy. 2015;70:836-845.
Practice Points
- Atopic dermatitis (AD) can be triggered by viral infections, weather, and food allergens.
- The scoring of AD is largely used experimentally and includes the eczema assessment and severity index; the SCORAD (SCORing Atopic Dermatitis); and the six area, six sign AD (SASSAD) scores.
- There is a strong genetic contribution to the development of AD.
- Children with AD may have persistent disease into adulthood in half of cases.

Acute Bacterial Sinusitis in Children: Evaluation and Treatment
IN THIS ARTICLE
- Complications of acute bacterial sinusitis
- What are the medical options?
- AAP 2013 recommendations for initial antimicrobial treatment
Acute bacterial sinusitis (ABS) is a common diagnosis in pediatric patients. Of children who are evaluated for respiratory complaints, 6% to 7% meet clinical criteria for ABS.1 In addition to being a frequent complication of upper respiratory infection (URI), ABS in children has a significant financial impact. Direct health care expenditures attributed to sinusitis in children ages 12 or younger is $1.8 billion annually.2
Differentiating between viral URI and ABS is a diagnostic challenge for health care providers. In recent years, the American Academy of Pediatrics (AAP) and the Infectious Diseases Society of America (IDSA) have released clinical practice guidelines on the clinical diagnosis and management of ABS in children.3,4
URI AND ABS MANIFESTATIONS
URIs manifest with a predictable pattern of symptoms. Children may experience one to two days of fever, accompanied by constitutional symptoms, such as fatigue, headache, decreased appetite, and myalgia. Nasal discharge typically begins clear and becomes mucopurulent over the next few days; subsequently, it either resolves or becomes serous again at the end of the URI. Cough, hoarseness, malodorous breath, and pharyngitis may be present.3,5 Symptoms typically resolve over five to 10 days, with respiratory symptoms peaking at days 3 to 5. Importantly, in viral URIs, nasal congestion and cough improve toward the end of the illness.1,3
Persistent illness. Patients with ABS may experience persistent illness with nasal discharge (of any quality) and/or daytime cough that persists more than 10 days without improvement.3,4 These patients are differentiated from those with a viral URI by a lack of improvement in congestion and/or cough after 10 days of symptoms.3 While some children with viral illnesses may have persistant upper respiratory symptoms, these should be gradually resolving. Clinicians must take a thorough history to identify children who may have multiple consecutive URIs rather than one persistent illness that is not resolving.
Other diagnoses, such as allergic rhinitis, nasal foreign body, pertussis, influenza, and bacterial pharyngitis, must also be excluded. Children who present with persistent nasal congestion, with or without cough, after 10 days of illness without signs of improvement meet the criteria for ABS.3
Severe symptom onset. Children with ABS may experience severe onset of symptoms.3,4 These children have purulent nasal discharge for at least three consecutive days at onset of illness and concurrent fever (temperature, ≥ 102.2°F). In contrast, a viral URI typically presents with fever for less than 48 hours and clear nasal discharge that becomes purulent after the first few days of symptoms.
“Double sickening.” Finally, children with ABS may have a worsening course of symptoms or a “double sickening.”3,4 These patients experience typical URI symptoms that initially begin to improve, then worsen on day 6 or 7 of illness with increasing or new onset of considerable nasal drainage, daytime cough, or fever.
Continue for physical findings >>
PHYSICAL FINDINGS
Physical exam findings are not sufficient to distinguish between viral URI and ABS.1,3,5 Typical findings on examination may include nasal congestion, postnasal drip, erythematous turbinates, and/or injected posterior oropharynx. Malodorous breath may be present but is not diagnostic.3,5 The tympanic membranes should be examined for signs of concomitant acute otitis media (AOM) or otitis media with effusion. Swelling of the eyelids may be present. Facial pain may also be noted on physical exam.3
Clinicians should be mindful of the complications of sinusitis when performing the physical examination (see Table 1). The most common complications of ABS are orbital and may manifest with eyelid swelling, proptosis, or decreased extraocular movements. Patients with intracranial complications may present with headache, photophobia, seizure, meningeal signs, or focal neurologic signs.3
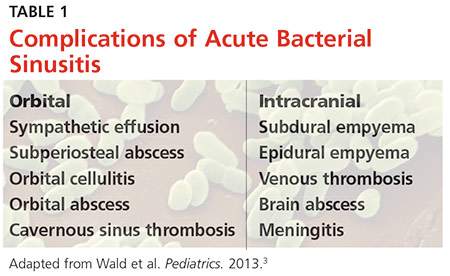
Continue to making the diagnosis >>
MAKING THE DIAGNOSIS
The diagnosis of ABS is a clinical one. Clinical guidelines from the AAP and IDSA for the diagnosis of ABS in children are very similar; both describe clinical presentations of persistent, severe, or worsening symptoms.3,4 This display of expert consensus allows clinicians to confidently distinguish between viral URIs and ABS by adhering to the strict diagnostic criteria already discussed.
Imaging
Radiographs and CT scans are not necessary to confirm the diagnosis of ABS. Imaging studies may reveal current or recent upper respiratory symptoms, including mucosal inflammation, opacities, and air-fluid levels6,7; however, no imaging study is available that can distinguish among mucosal inflammation and viral or bacterial infections. CT scans or MRI may be useful if clinicians suspect a complication of sinusitis.3,7
Microbiology
Historically, the microbiology of ABS has been determined by maxillary sinus aspiration. The most recent studies of this method, published in the 1980s, identified Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis as the most common bacterial pathogens.3,6,9 More recently, the microbiology of ABS has been linked with causative pathogens in AOM. The pathogenesis of ABS and AOM are similar, therefore allowing data from tympanocentesis in children with AOM to be used to determine the microbiology of children with ABS.10 Although S pneumoniae, H influenzae, and M catarrhalis remain common causative pathogens in ABS, the introduction of the 7- and 13-valent pneumococcal vaccines has altered the microbiology of AOM, and presumably ABS.11
Importantly, numbers of cases of AOM attributed to S pneumoniae have decreased while those attributed to H influenzae have increased.3,11 In addition, antimicrobial susceptibility of S pneumoniae and the prevalence of β-lactamase–positive H influenzae are important considerations when choosing appropriate antibiotics and can vary significantly by geographic region. Therefore, it is important that clinicians be aware of susceptibility patterns in the communities in which they practice.
Continue for the medical options >>
WHAT ARE THE MEDICAL OPTIONS?
Initial management of ABS in children is contingent on the symptom profile at presentation (persistent, worsening, or severe) and consideration of causative pathogens. While the consensus among experts is that children presenting with severe or worsening symptoms be treated initially with antibiotics,3,4 children who present with mild symptoms consistent with persistent illness may initially be treated with antibiotics or observed for an additional three days. This decision should be made thoughtfully and in collaboration with the patient’s parents or guardians. Any child with ABS who presents with persistent symptoms of illness and is managed initially by observation alone should be reassessed or treated with an antibiotic if symptoms worsen, if new symptoms appear, or if the child fails to improve within 72 hours.
Amoxicillin with or without clavulanate is the antibiotic of choice when ABS has been diagnosed and antibiotic treatment is indicated.1,3 AAP recommendations for antimicrobial treatment of ABS in children are stratified on the basis of age, severity of illness, day care attendance, and history of treatment with amoxicillin in the previous 30 days (see Table 2). Clinicians should rely on their knowledge of drug resistance in their community and judgment regarding severity of illness when choosing between amoxicillin and amoxicillin/clavulanate as initial treatment for ABS.3
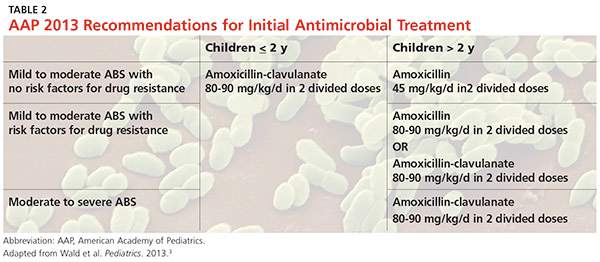
Recommendations for duration of antimicrobial treatment for ABS vary considerably. A reasonable suggestion is to continue to treat patients until they are symptom-free for seven days. For many patients, this will mean a 10-day treatment course, with flexibility to increase the duration as needed.3
Children with ABS should be reassessed if there are worsening signs or symptoms or lack of clinical improvement within 72 hours of initial management. Clinicians should evaluate whether the patient has been appropriately diagnosed and assessed for complications of ABS. If the diagnosis is confirmed and ABS complications are not suspected, the clinician may change antibiotics or initiate antibiotic therapy if the child was previously managed by observation only.3,4
A child who is vomiting or unable to tolerate PO medications may benefit from a single 50-gm/kg dose of ceftriaxone IV or IM with follow-up in 24 hours.3 Oral antibiotics may be started at the follow-up visit if the patient demonstrates clinical improvement.
When considering a change in antibiotic, the clinician should consider the possibility of drug resistance. If the child was initially treated with amoxicillin, high-dose amoxicillin/clavulanate may be prescribed. If high-dose amoxicillin/clavulanate was initially prescribed and the patient has not improved or is experiencing worsening symptoms, clindamycin with cefixime, linezolid with cefixime, or levofloxacin may be considered.3,4
Penicillin allergy
Patients with a history of a non–type 1 hypersensitivity reaction to amoxicillin may be treated with cefdinir, cefuroxime, cefpodoxime, or combination therapy with clindamycin plus a third-generation oral cephalosporin. Allergist referral for penicillin or cephalosporin skin testing may be considered before initiation of therapy.3,4,13
Adjuvant therapy
Decongestants, antihistamines, and nasal irrigation are frequently recommended in the management of ABS in children; however, the authors of a 2012 Cochrane review found no properly designed studies to evaluate the effectiveness of these treatments.13 Furthermore, there is insufficient evidence to clearly recommend the use of intranasal steroids as an adjuvant therapy in the treatment of ABS in children (although several randomized controlled studies demonstrate their effectiveness in adolescents and adults).3
Continue for the conclusion >>
CONCLUSION
ABS in children is diagnosed clinically by following a strict set of clinical criteria. Patients commonly present with one of three types of symptoms: persistent URI; severe purulent nasal discharge and fever for at least three consecutive days; or a double sickening. Physical examination findings vary and will not differentiate viral URI symptoms from a diagnosis of ABS. Imaging is not recommended for diagnosis but may be helpful if an orbital or intracranial complication of ABS is suspected.
S pneumoniae, H influenzae, and M catarrhalis continue to be the most common pathogens associated with ABS. However, since the introduction of the 7-valent pneumococcal vaccine, prevalence of H influenzae and β-lactamase–positive H influenzae has increased.
Treatment recommendations vary, based on suspected causative pathogens and presenting symptoms. Amoxicillin or amoxicillin-clavulanate is recommended as firstline antimicrobial treatment for ABS, with alternate antibiotic choices for patients with worsening symptoms or lack of improvement within 72 hours. An awareness of the community’s susceptibility patterns is essential for the clinician who cares for children at risk for ABS.
REFERENCES
1. Wald ER, Nash D, Eickhoff J. Effectiveness of amoxicillin/clavulanate potassium in the treatment of acute bacterial sinusitis in children. Pediatrics. 2009;124(1):9-15.
2. Ray NF, Baraniuk JN, Thamer M, et al. Healthcare expenditures for sinusitis in 1996: contributions of asthma, rhinitis, and other airway disorders. J Allergy Clin Immunol. 1999;103(3 pt 1):408-414.
3. Wald ER, Applegate KE, Bordley C, et al. Clinical practice guideline for the diagnosis and management of acute bacterial sinusitis in children aged 1 to 18 years. Pediatrics. 2013;132(1):e262-e280.
4. Chow AW, Benninger MS, Brook I, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54(8):1041-1045.
5. Shaikh N, Hoberman A, Kearney DH, et al. Signs and symptoms that differentiate acute sinusitis from viral upper respiratory tract infection. Pediatr Infect Dis J. 2013;32(10):1061-1065.
6. Kovatch AL, Wald ER, Ledesma-Medina J, et al. Maxillary sinus radiographs in children with nonrespiratory complaints. Pediatrics. 1984; 73(3):306-308.
7. Triulzi F, Zirpoli S. Imaging techniques in the diagnosis and management of rhinosinusitis in children. Pediatr Allergy Immunol. 2007;18(suppl 18):46-49.
8. Wald ER, Milmoe GJ, Bowen A, et al. Acute maxillary sinusitis in children. N Engl J Med. 1981;304(13):749-754.
9. Wald ER, Reilly JS, Casselbrant M, et al. Treatment of acute maxillary sinusitis in childhood: a comparative study of amoxicillin and cefaclor. J Pediatr. 1984;104(2):297-302.
10. Wald ER. Acute otitis media and acute bacterial sinusitis. Clin Infect Dis. 2011;52(suppl 4):S277-S283.
11. Casey JR, Adlowitz DG, Pichichero ME. New patterns in the otopathogens causing acute otitis media six to eight years after introduction of pneumococcal conjugate vaccine. Pediatr Infect Dis J. 2010;29(4):304-309.
12. Pichichero ME. A review of evidence supporting the American Academy of Pediatrics recommendation for prescribing cephalosporin antibiotics for penicillin-allergic patients. Pediatrics. 2004;115(4):1048-1057.
13. Shaikh N, Wald ER, Pi M. Decongestants, antihistamines and nasal irrigation for acute sinusitis in children. Cochrane Database Syst Rev. 2012;9:CD007909.
IN THIS ARTICLE
- Complications of acute bacterial sinusitis
- What are the medical options?
- AAP 2013 recommendations for initial antimicrobial treatment
Acute bacterial sinusitis (ABS) is a common diagnosis in pediatric patients. Of children who are evaluated for respiratory complaints, 6% to 7% meet clinical criteria for ABS.1 In addition to being a frequent complication of upper respiratory infection (URI), ABS in children has a significant financial impact. Direct health care expenditures attributed to sinusitis in children ages 12 or younger is $1.8 billion annually.2
Differentiating between viral URI and ABS is a diagnostic challenge for health care providers. In recent years, the American Academy of Pediatrics (AAP) and the Infectious Diseases Society of America (IDSA) have released clinical practice guidelines on the clinical diagnosis and management of ABS in children.3,4
URI AND ABS MANIFESTATIONS
URIs manifest with a predictable pattern of symptoms. Children may experience one to two days of fever, accompanied by constitutional symptoms, such as fatigue, headache, decreased appetite, and myalgia. Nasal discharge typically begins clear and becomes mucopurulent over the next few days; subsequently, it either resolves or becomes serous again at the end of the URI. Cough, hoarseness, malodorous breath, and pharyngitis may be present.3,5 Symptoms typically resolve over five to 10 days, with respiratory symptoms peaking at days 3 to 5. Importantly, in viral URIs, nasal congestion and cough improve toward the end of the illness.1,3
Persistent illness. Patients with ABS may experience persistent illness with nasal discharge (of any quality) and/or daytime cough that persists more than 10 days without improvement.3,4 These patients are differentiated from those with a viral URI by a lack of improvement in congestion and/or cough after 10 days of symptoms.3 While some children with viral illnesses may have persistant upper respiratory symptoms, these should be gradually resolving. Clinicians must take a thorough history to identify children who may have multiple consecutive URIs rather than one persistent illness that is not resolving.
Other diagnoses, such as allergic rhinitis, nasal foreign body, pertussis, influenza, and bacterial pharyngitis, must also be excluded. Children who present with persistent nasal congestion, with or without cough, after 10 days of illness without signs of improvement meet the criteria for ABS.3
Severe symptom onset. Children with ABS may experience severe onset of symptoms.3,4 These children have purulent nasal discharge for at least three consecutive days at onset of illness and concurrent fever (temperature, ≥ 102.2°F). In contrast, a viral URI typically presents with fever for less than 48 hours and clear nasal discharge that becomes purulent after the first few days of symptoms.
“Double sickening.” Finally, children with ABS may have a worsening course of symptoms or a “double sickening.”3,4 These patients experience typical URI symptoms that initially begin to improve, then worsen on day 6 or 7 of illness with increasing or new onset of considerable nasal drainage, daytime cough, or fever.
Continue for physical findings >>
PHYSICAL FINDINGS
Physical exam findings are not sufficient to distinguish between viral URI and ABS.1,3,5 Typical findings on examination may include nasal congestion, postnasal drip, erythematous turbinates, and/or injected posterior oropharynx. Malodorous breath may be present but is not diagnostic.3,5 The tympanic membranes should be examined for signs of concomitant acute otitis media (AOM) or otitis media with effusion. Swelling of the eyelids may be present. Facial pain may also be noted on physical exam.3
Clinicians should be mindful of the complications of sinusitis when performing the physical examination (see Table 1). The most common complications of ABS are orbital and may manifest with eyelid swelling, proptosis, or decreased extraocular movements. Patients with intracranial complications may present with headache, photophobia, seizure, meningeal signs, or focal neurologic signs.3
Continue to making the diagnosis >>
MAKING THE DIAGNOSIS
The diagnosis of ABS is a clinical one. Clinical guidelines from the AAP and IDSA for the diagnosis of ABS in children are very similar; both describe clinical presentations of persistent, severe, or worsening symptoms.3,4 This display of expert consensus allows clinicians to confidently distinguish between viral URIs and ABS by adhering to the strict diagnostic criteria already discussed.
Imaging
Radiographs and CT scans are not necessary to confirm the diagnosis of ABS. Imaging studies may reveal current or recent upper respiratory symptoms, including mucosal inflammation, opacities, and air-fluid levels6,7; however, no imaging study is available that can distinguish among mucosal inflammation and viral or bacterial infections. CT scans or MRI may be useful if clinicians suspect a complication of sinusitis.3,7
Microbiology
Historically, the microbiology of ABS has been determined by maxillary sinus aspiration. The most recent studies of this method, published in the 1980s, identified Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis as the most common bacterial pathogens.3,6,9 More recently, the microbiology of ABS has been linked with causative pathogens in AOM. The pathogenesis of ABS and AOM are similar, therefore allowing data from tympanocentesis in children with AOM to be used to determine the microbiology of children with ABS.10 Although S pneumoniae, H influenzae, and M catarrhalis remain common causative pathogens in ABS, the introduction of the 7- and 13-valent pneumococcal vaccines has altered the microbiology of AOM, and presumably ABS.11
Importantly, numbers of cases of AOM attributed to S pneumoniae have decreased while those attributed to H influenzae have increased.3,11 In addition, antimicrobial susceptibility of S pneumoniae and the prevalence of β-lactamase–positive H influenzae are important considerations when choosing appropriate antibiotics and can vary significantly by geographic region. Therefore, it is important that clinicians be aware of susceptibility patterns in the communities in which they practice.
Continue for the medical options >>
WHAT ARE THE MEDICAL OPTIONS?
Initial management of ABS in children is contingent on the symptom profile at presentation (persistent, worsening, or severe) and consideration of causative pathogens. While the consensus among experts is that children presenting with severe or worsening symptoms be treated initially with antibiotics,3,4 children who present with mild symptoms consistent with persistent illness may initially be treated with antibiotics or observed for an additional three days. This decision should be made thoughtfully and in collaboration with the patient’s parents or guardians. Any child with ABS who presents with persistent symptoms of illness and is managed initially by observation alone should be reassessed or treated with an antibiotic if symptoms worsen, if new symptoms appear, or if the child fails to improve within 72 hours.
Amoxicillin with or without clavulanate is the antibiotic of choice when ABS has been diagnosed and antibiotic treatment is indicated.1,3 AAP recommendations for antimicrobial treatment of ABS in children are stratified on the basis of age, severity of illness, day care attendance, and history of treatment with amoxicillin in the previous 30 days (see Table 2). Clinicians should rely on their knowledge of drug resistance in their community and judgment regarding severity of illness when choosing between amoxicillin and amoxicillin/clavulanate as initial treatment for ABS.3
Recommendations for duration of antimicrobial treatment for ABS vary considerably. A reasonable suggestion is to continue to treat patients until they are symptom-free for seven days. For many patients, this will mean a 10-day treatment course, with flexibility to increase the duration as needed.3
Children with ABS should be reassessed if there are worsening signs or symptoms or lack of clinical improvement within 72 hours of initial management. Clinicians should evaluate whether the patient has been appropriately diagnosed and assessed for complications of ABS. If the diagnosis is confirmed and ABS complications are not suspected, the clinician may change antibiotics or initiate antibiotic therapy if the child was previously managed by observation only.3,4
A child who is vomiting or unable to tolerate PO medications may benefit from a single 50-gm/kg dose of ceftriaxone IV or IM with follow-up in 24 hours.3 Oral antibiotics may be started at the follow-up visit if the patient demonstrates clinical improvement.
When considering a change in antibiotic, the clinician should consider the possibility of drug resistance. If the child was initially treated with amoxicillin, high-dose amoxicillin/clavulanate may be prescribed. If high-dose amoxicillin/clavulanate was initially prescribed and the patient has not improved or is experiencing worsening symptoms, clindamycin with cefixime, linezolid with cefixime, or levofloxacin may be considered.3,4
Penicillin allergy
Patients with a history of a non–type 1 hypersensitivity reaction to amoxicillin may be treated with cefdinir, cefuroxime, cefpodoxime, or combination therapy with clindamycin plus a third-generation oral cephalosporin. Allergist referral for penicillin or cephalosporin skin testing may be considered before initiation of therapy.3,4,13
Adjuvant therapy
Decongestants, antihistamines, and nasal irrigation are frequently recommended in the management of ABS in children; however, the authors of a 2012 Cochrane review found no properly designed studies to evaluate the effectiveness of these treatments.13 Furthermore, there is insufficient evidence to clearly recommend the use of intranasal steroids as an adjuvant therapy in the treatment of ABS in children (although several randomized controlled studies demonstrate their effectiveness in adolescents and adults).3
Continue for the conclusion >>
CONCLUSION
ABS in children is diagnosed clinically by following a strict set of clinical criteria. Patients commonly present with one of three types of symptoms: persistent URI; severe purulent nasal discharge and fever for at least three consecutive days; or a double sickening. Physical examination findings vary and will not differentiate viral URI symptoms from a diagnosis of ABS. Imaging is not recommended for diagnosis but may be helpful if an orbital or intracranial complication of ABS is suspected.
S pneumoniae, H influenzae, and M catarrhalis continue to be the most common pathogens associated with ABS. However, since the introduction of the 7-valent pneumococcal vaccine, prevalence of H influenzae and β-lactamase–positive H influenzae has increased.
Treatment recommendations vary, based on suspected causative pathogens and presenting symptoms. Amoxicillin or amoxicillin-clavulanate is recommended as firstline antimicrobial treatment for ABS, with alternate antibiotic choices for patients with worsening symptoms or lack of improvement within 72 hours. An awareness of the community’s susceptibility patterns is essential for the clinician who cares for children at risk for ABS.
REFERENCES
1. Wald ER, Nash D, Eickhoff J. Effectiveness of amoxicillin/clavulanate potassium in the treatment of acute bacterial sinusitis in children. Pediatrics. 2009;124(1):9-15.
2. Ray NF, Baraniuk JN, Thamer M, et al. Healthcare expenditures for sinusitis in 1996: contributions of asthma, rhinitis, and other airway disorders. J Allergy Clin Immunol. 1999;103(3 pt 1):408-414.
3. Wald ER, Applegate KE, Bordley C, et al. Clinical practice guideline for the diagnosis and management of acute bacterial sinusitis in children aged 1 to 18 years. Pediatrics. 2013;132(1):e262-e280.
4. Chow AW, Benninger MS, Brook I, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54(8):1041-1045.
5. Shaikh N, Hoberman A, Kearney DH, et al. Signs and symptoms that differentiate acute sinusitis from viral upper respiratory tract infection. Pediatr Infect Dis J. 2013;32(10):1061-1065.
6. Kovatch AL, Wald ER, Ledesma-Medina J, et al. Maxillary sinus radiographs in children with nonrespiratory complaints. Pediatrics. 1984; 73(3):306-308.
7. Triulzi F, Zirpoli S. Imaging techniques in the diagnosis and management of rhinosinusitis in children. Pediatr Allergy Immunol. 2007;18(suppl 18):46-49.
8. Wald ER, Milmoe GJ, Bowen A, et al. Acute maxillary sinusitis in children. N Engl J Med. 1981;304(13):749-754.
9. Wald ER, Reilly JS, Casselbrant M, et al. Treatment of acute maxillary sinusitis in childhood: a comparative study of amoxicillin and cefaclor. J Pediatr. 1984;104(2):297-302.
10. Wald ER. Acute otitis media and acute bacterial sinusitis. Clin Infect Dis. 2011;52(suppl 4):S277-S283.
11. Casey JR, Adlowitz DG, Pichichero ME. New patterns in the otopathogens causing acute otitis media six to eight years after introduction of pneumococcal conjugate vaccine. Pediatr Infect Dis J. 2010;29(4):304-309.
12. Pichichero ME. A review of evidence supporting the American Academy of Pediatrics recommendation for prescribing cephalosporin antibiotics for penicillin-allergic patients. Pediatrics. 2004;115(4):1048-1057.
13. Shaikh N, Wald ER, Pi M. Decongestants, antihistamines and nasal irrigation for acute sinusitis in children. Cochrane Database Syst Rev. 2012;9:CD007909.
IN THIS ARTICLE
- Complications of acute bacterial sinusitis
- What are the medical options?
- AAP 2013 recommendations for initial antimicrobial treatment
Acute bacterial sinusitis (ABS) is a common diagnosis in pediatric patients. Of children who are evaluated for respiratory complaints, 6% to 7% meet clinical criteria for ABS.1 In addition to being a frequent complication of upper respiratory infection (URI), ABS in children has a significant financial impact. Direct health care expenditures attributed to sinusitis in children ages 12 or younger is $1.8 billion annually.2
Differentiating between viral URI and ABS is a diagnostic challenge for health care providers. In recent years, the American Academy of Pediatrics (AAP) and the Infectious Diseases Society of America (IDSA) have released clinical practice guidelines on the clinical diagnosis and management of ABS in children.3,4
URI AND ABS MANIFESTATIONS
URIs manifest with a predictable pattern of symptoms. Children may experience one to two days of fever, accompanied by constitutional symptoms, such as fatigue, headache, decreased appetite, and myalgia. Nasal discharge typically begins clear and becomes mucopurulent over the next few days; subsequently, it either resolves or becomes serous again at the end of the URI. Cough, hoarseness, malodorous breath, and pharyngitis may be present.3,5 Symptoms typically resolve over five to 10 days, with respiratory symptoms peaking at days 3 to 5. Importantly, in viral URIs, nasal congestion and cough improve toward the end of the illness.1,3
Persistent illness. Patients with ABS may experience persistent illness with nasal discharge (of any quality) and/or daytime cough that persists more than 10 days without improvement.3,4 These patients are differentiated from those with a viral URI by a lack of improvement in congestion and/or cough after 10 days of symptoms.3 While some children with viral illnesses may have persistant upper respiratory symptoms, these should be gradually resolving. Clinicians must take a thorough history to identify children who may have multiple consecutive URIs rather than one persistent illness that is not resolving.
Other diagnoses, such as allergic rhinitis, nasal foreign body, pertussis, influenza, and bacterial pharyngitis, must also be excluded. Children who present with persistent nasal congestion, with or without cough, after 10 days of illness without signs of improvement meet the criteria for ABS.3
Severe symptom onset. Children with ABS may experience severe onset of symptoms.3,4 These children have purulent nasal discharge for at least three consecutive days at onset of illness and concurrent fever (temperature, ≥ 102.2°F). In contrast, a viral URI typically presents with fever for less than 48 hours and clear nasal discharge that becomes purulent after the first few days of symptoms.
“Double sickening.” Finally, children with ABS may have a worsening course of symptoms or a “double sickening.”3,4 These patients experience typical URI symptoms that initially begin to improve, then worsen on day 6 or 7 of illness with increasing or new onset of considerable nasal drainage, daytime cough, or fever.
Continue for physical findings >>
PHYSICAL FINDINGS
Physical exam findings are not sufficient to distinguish between viral URI and ABS.1,3,5 Typical findings on examination may include nasal congestion, postnasal drip, erythematous turbinates, and/or injected posterior oropharynx. Malodorous breath may be present but is not diagnostic.3,5 The tympanic membranes should be examined for signs of concomitant acute otitis media (AOM) or otitis media with effusion. Swelling of the eyelids may be present. Facial pain may also be noted on physical exam.3
Clinicians should be mindful of the complications of sinusitis when performing the physical examination (see Table 1). The most common complications of ABS are orbital and may manifest with eyelid swelling, proptosis, or decreased extraocular movements. Patients with intracranial complications may present with headache, photophobia, seizure, meningeal signs, or focal neurologic signs.3
Continue to making the diagnosis >>
MAKING THE DIAGNOSIS
The diagnosis of ABS is a clinical one. Clinical guidelines from the AAP and IDSA for the diagnosis of ABS in children are very similar; both describe clinical presentations of persistent, severe, or worsening symptoms.3,4 This display of expert consensus allows clinicians to confidently distinguish between viral URIs and ABS by adhering to the strict diagnostic criteria already discussed.
Imaging
Radiographs and CT scans are not necessary to confirm the diagnosis of ABS. Imaging studies may reveal current or recent upper respiratory symptoms, including mucosal inflammation, opacities, and air-fluid levels6,7; however, no imaging study is available that can distinguish among mucosal inflammation and viral or bacterial infections. CT scans or MRI may be useful if clinicians suspect a complication of sinusitis.3,7
Microbiology
Historically, the microbiology of ABS has been determined by maxillary sinus aspiration. The most recent studies of this method, published in the 1980s, identified Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis as the most common bacterial pathogens.3,6,9 More recently, the microbiology of ABS has been linked with causative pathogens in AOM. The pathogenesis of ABS and AOM are similar, therefore allowing data from tympanocentesis in children with AOM to be used to determine the microbiology of children with ABS.10 Although S pneumoniae, H influenzae, and M catarrhalis remain common causative pathogens in ABS, the introduction of the 7- and 13-valent pneumococcal vaccines has altered the microbiology of AOM, and presumably ABS.11
Importantly, numbers of cases of AOM attributed to S pneumoniae have decreased while those attributed to H influenzae have increased.3,11 In addition, antimicrobial susceptibility of S pneumoniae and the prevalence of β-lactamase–positive H influenzae are important considerations when choosing appropriate antibiotics and can vary significantly by geographic region. Therefore, it is important that clinicians be aware of susceptibility patterns in the communities in which they practice.
Continue for the medical options >>
WHAT ARE THE MEDICAL OPTIONS?
Initial management of ABS in children is contingent on the symptom profile at presentation (persistent, worsening, or severe) and consideration of causative pathogens. While the consensus among experts is that children presenting with severe or worsening symptoms be treated initially with antibiotics,3,4 children who present with mild symptoms consistent with persistent illness may initially be treated with antibiotics or observed for an additional three days. This decision should be made thoughtfully and in collaboration with the patient’s parents or guardians. Any child with ABS who presents with persistent symptoms of illness and is managed initially by observation alone should be reassessed or treated with an antibiotic if symptoms worsen, if new symptoms appear, or if the child fails to improve within 72 hours.
Amoxicillin with or without clavulanate is the antibiotic of choice when ABS has been diagnosed and antibiotic treatment is indicated.1,3 AAP recommendations for antimicrobial treatment of ABS in children are stratified on the basis of age, severity of illness, day care attendance, and history of treatment with amoxicillin in the previous 30 days (see Table 2). Clinicians should rely on their knowledge of drug resistance in their community and judgment regarding severity of illness when choosing between amoxicillin and amoxicillin/clavulanate as initial treatment for ABS.3
Recommendations for duration of antimicrobial treatment for ABS vary considerably. A reasonable suggestion is to continue to treat patients until they are symptom-free for seven days. For many patients, this will mean a 10-day treatment course, with flexibility to increase the duration as needed.3
Children with ABS should be reassessed if there are worsening signs or symptoms or lack of clinical improvement within 72 hours of initial management. Clinicians should evaluate whether the patient has been appropriately diagnosed and assessed for complications of ABS. If the diagnosis is confirmed and ABS complications are not suspected, the clinician may change antibiotics or initiate antibiotic therapy if the child was previously managed by observation only.3,4
A child who is vomiting or unable to tolerate PO medications may benefit from a single 50-gm/kg dose of ceftriaxone IV or IM with follow-up in 24 hours.3 Oral antibiotics may be started at the follow-up visit if the patient demonstrates clinical improvement.
When considering a change in antibiotic, the clinician should consider the possibility of drug resistance. If the child was initially treated with amoxicillin, high-dose amoxicillin/clavulanate may be prescribed. If high-dose amoxicillin/clavulanate was initially prescribed and the patient has not improved or is experiencing worsening symptoms, clindamycin with cefixime, linezolid with cefixime, or levofloxacin may be considered.3,4
Penicillin allergy
Patients with a history of a non–type 1 hypersensitivity reaction to amoxicillin may be treated with cefdinir, cefuroxime, cefpodoxime, or combination therapy with clindamycin plus a third-generation oral cephalosporin. Allergist referral for penicillin or cephalosporin skin testing may be considered before initiation of therapy.3,4,13
Adjuvant therapy
Decongestants, antihistamines, and nasal irrigation are frequently recommended in the management of ABS in children; however, the authors of a 2012 Cochrane review found no properly designed studies to evaluate the effectiveness of these treatments.13 Furthermore, there is insufficient evidence to clearly recommend the use of intranasal steroids as an adjuvant therapy in the treatment of ABS in children (although several randomized controlled studies demonstrate their effectiveness in adolescents and adults).3
Continue for the conclusion >>
CONCLUSION
ABS in children is diagnosed clinically by following a strict set of clinical criteria. Patients commonly present with one of three types of symptoms: persistent URI; severe purulent nasal discharge and fever for at least three consecutive days; or a double sickening. Physical examination findings vary and will not differentiate viral URI symptoms from a diagnosis of ABS. Imaging is not recommended for diagnosis but may be helpful if an orbital or intracranial complication of ABS is suspected.
S pneumoniae, H influenzae, and M catarrhalis continue to be the most common pathogens associated with ABS. However, since the introduction of the 7-valent pneumococcal vaccine, prevalence of H influenzae and β-lactamase–positive H influenzae has increased.
Treatment recommendations vary, based on suspected causative pathogens and presenting symptoms. Amoxicillin or amoxicillin-clavulanate is recommended as firstline antimicrobial treatment for ABS, with alternate antibiotic choices for patients with worsening symptoms or lack of improvement within 72 hours. An awareness of the community’s susceptibility patterns is essential for the clinician who cares for children at risk for ABS.
REFERENCES
1. Wald ER, Nash D, Eickhoff J. Effectiveness of amoxicillin/clavulanate potassium in the treatment of acute bacterial sinusitis in children. Pediatrics. 2009;124(1):9-15.
2. Ray NF, Baraniuk JN, Thamer M, et al. Healthcare expenditures for sinusitis in 1996: contributions of asthma, rhinitis, and other airway disorders. J Allergy Clin Immunol. 1999;103(3 pt 1):408-414.
3. Wald ER, Applegate KE, Bordley C, et al. Clinical practice guideline for the diagnosis and management of acute bacterial sinusitis in children aged 1 to 18 years. Pediatrics. 2013;132(1):e262-e280.
4. Chow AW, Benninger MS, Brook I, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54(8):1041-1045.
5. Shaikh N, Hoberman A, Kearney DH, et al. Signs and symptoms that differentiate acute sinusitis from viral upper respiratory tract infection. Pediatr Infect Dis J. 2013;32(10):1061-1065.
6. Kovatch AL, Wald ER, Ledesma-Medina J, et al. Maxillary sinus radiographs in children with nonrespiratory complaints. Pediatrics. 1984; 73(3):306-308.
7. Triulzi F, Zirpoli S. Imaging techniques in the diagnosis and management of rhinosinusitis in children. Pediatr Allergy Immunol. 2007;18(suppl 18):46-49.
8. Wald ER, Milmoe GJ, Bowen A, et al. Acute maxillary sinusitis in children. N Engl J Med. 1981;304(13):749-754.
9. Wald ER, Reilly JS, Casselbrant M, et al. Treatment of acute maxillary sinusitis in childhood: a comparative study of amoxicillin and cefaclor. J Pediatr. 1984;104(2):297-302.
10. Wald ER. Acute otitis media and acute bacterial sinusitis. Clin Infect Dis. 2011;52(suppl 4):S277-S283.
11. Casey JR, Adlowitz DG, Pichichero ME. New patterns in the otopathogens causing acute otitis media six to eight years after introduction of pneumococcal conjugate vaccine. Pediatr Infect Dis J. 2010;29(4):304-309.
12. Pichichero ME. A review of evidence supporting the American Academy of Pediatrics recommendation for prescribing cephalosporin antibiotics for penicillin-allergic patients. Pediatrics. 2004;115(4):1048-1057.
13. Shaikh N, Wald ER, Pi M. Decongestants, antihistamines and nasal irrigation for acute sinusitis in children. Cochrane Database Syst Rev. 2012;9:CD007909.
Bringing behavioral health services to pediatrics
Research shows that the foundation of lifelong health is established during a child’s earliest years, including the prenatal period, and is also determined by the health of the future mother before she becomes pregnant. Much like the foundation of a house, if a child’s early years are filled with nurturing experiences and limited exposure to toxic stress, a child is set to succeed and withstand future challenges. However, adverse childhood experiences and toxic stress can disproportionately derail a child’s developmental growth and can lead to negative impacts throughout the lifespan, including social, emotional, and cognitive impairment; adoption of health risk behaviors; disease, disability, and social problems; and potentially early death.
Furthermore, data from the National Comorbidity Survey–Replication Sample (NCS-R) found that the prevalence of various mental health disorders – including disorders related to mood, anxiety, impulse control, and substance abuse – increases with the cumulative number of adverse childhood experiences. Persons with four or more childhood adversities had an odds ratio of 7.3 for four disorder categories.

Combined with recent data from the World Health Organization suggesting that the global cost of untreated mental health disorders is approximately $1 trillion, there is a clear public health crisis on our doorstep. Seeing our vulnerable patient population in the Bronx, family after family struggling to cope, I asked myself – is the solution on our doorstep too?
The role of the pediatrician
During a child’s early years, a pediatrician’s role is to identify signs of early childhood adversity and toxic stress, and to provide targeted support for parents and caregivers (Pediatrics. 2012 Jan. doi: 10.1542/peds.2011-2662). Given this, child primary care providers face the following challenges:
• Is there an opportunity for us to identify children at risk of developing mental health problems within the primary care setting?
• If so, how early can we identify children who would benefit from specific preventive or therapeutic interventions to optimize their developmental and behavioral potential?
• What tools are available in primary care to accomplish this function, and how should we administer them?
Healthy Steps program evaluation
At Montefiore Medical Group, we have developed a program that helps pediatricians overcome these challenges. Based on the national Healthy Steps program, Montefiore offers integrated mental health services in pediatric primary care settings, and provides universal screening, assessment, and treatment of young children and their caregivers.
A quasiexperimental longitudinal study was conducted, involving follow-up of 124 children enrolled in Healthy Steps at their primary care pediatric setting and a comparison group from a clinic that did not receive this intervention. The aim of the study was to determine the relationship between maternal adverse childhood experiences (ACES) and child social-emotional development, as measured via the Ages and States Questionnaire: Social Emotional (ASQ:SE) at age 36 months.
Social-emotional development is thought to be critical in terms of a child’s ability to learn and get along with others. It is also a precursor to mental health. Our results showed that, without intervention, there was a dramatic link between maternal ACES score and at-risk social-emotional development for children at age 3 years. However, our Healthy Steps program appeared to moderate this otherwise powerful link, as children who received Healthy Steps, even if their mother had experienced abuse or neglect in her own childhood, had healthy social-emotional development at age 3 years.
As a result of the success of Healthy Steps at Montefiore, in 2014 we expanded our pediatric integrated behavioral health program to also include school age and adolescent patients. Today, we are serving approximately 90,000 pediatric patients at more than 21 sites in the Bronx and surrounding area. We provide universal behavioral health screening, including for autism and maternal depression, at well-child visits. We provide parental mental health services, within pediatrics, to parents of infants and toddlers struggling with perinatal mental health challenges, and we devote significant time to education of our primary care providers, to increase their confidence and competence regarding pediatric behavioral health.
Initial results for school age, adolescent program
Our early results regarding feasibility are promising. We found that more than 26% of children presenting to the primary care practices, well beyond national averages, were referred to our program during a 6-month study period. And while a referral unfortunately rarely leads to actual treatment in mental health, we found that more than half of referred patients attended at least one therapy session, and a warm hand-off (a unique feature of integrated care in which psychologists meet with a referred patient during the well-child visit in order to establish a level of trust between patient and provider) increased this to 63%.
Future steps
Our efforts suggest that integration of pediatric behavioral health specialists into primary care is feasible, efficacious, and beneficial to children and parents. We have had success at identifying children at risk for exposure to toxic stress early in their lifetimes and providing multigenerational treatment to these children to ensure healthy social-emotional development. We have shown that when we offer mental health treatment within primary care, even in an urban setting where stigma around mental illness runs high, we almost triple the national average of successful linkage to mental health services for school age and adolescent children. However, payment reform is needed to truly achieve population health. We must ensure preventive and multigenerational services are covered so that we may continue to treat children and families within the nonstigmatized and universally accessed setting of primary care.
Dr. Briggs is director of pediatric behavioral health services and Healthy Steps at Montefiore Medical Group and associate professor of clinical pediatrics at Albert Einstein College of Medicine, both in New York.
Research shows that the foundation of lifelong health is established during a child’s earliest years, including the prenatal period, and is also determined by the health of the future mother before she becomes pregnant. Much like the foundation of a house, if a child’s early years are filled with nurturing experiences and limited exposure to toxic stress, a child is set to succeed and withstand future challenges. However, adverse childhood experiences and toxic stress can disproportionately derail a child’s developmental growth and can lead to negative impacts throughout the lifespan, including social, emotional, and cognitive impairment; adoption of health risk behaviors; disease, disability, and social problems; and potentially early death.
Furthermore, data from the National Comorbidity Survey–Replication Sample (NCS-R) found that the prevalence of various mental health disorders – including disorders related to mood, anxiety, impulse control, and substance abuse – increases with the cumulative number of adverse childhood experiences. Persons with four or more childhood adversities had an odds ratio of 7.3 for four disorder categories.
Combined with recent data from the World Health Organization suggesting that the global cost of untreated mental health disorders is approximately $1 trillion, there is a clear public health crisis on our doorstep. Seeing our vulnerable patient population in the Bronx, family after family struggling to cope, I asked myself – is the solution on our doorstep too?
The role of the pediatrician
During a child’s early years, a pediatrician’s role is to identify signs of early childhood adversity and toxic stress, and to provide targeted support for parents and caregivers (Pediatrics. 2012 Jan. doi: 10.1542/peds.2011-2662). Given this, child primary care providers face the following challenges:
• Is there an opportunity for us to identify children at risk of developing mental health problems within the primary care setting?
• If so, how early can we identify children who would benefit from specific preventive or therapeutic interventions to optimize their developmental and behavioral potential?
• What tools are available in primary care to accomplish this function, and how should we administer them?
Healthy Steps program evaluation
At Montefiore Medical Group, we have developed a program that helps pediatricians overcome these challenges. Based on the national Healthy Steps program, Montefiore offers integrated mental health services in pediatric primary care settings, and provides universal screening, assessment, and treatment of young children and their caregivers.
A quasiexperimental longitudinal study was conducted, involving follow-up of 124 children enrolled in Healthy Steps at their primary care pediatric setting and a comparison group from a clinic that did not receive this intervention. The aim of the study was to determine the relationship between maternal adverse childhood experiences (ACES) and child social-emotional development, as measured via the Ages and States Questionnaire: Social Emotional (ASQ:SE) at age 36 months.
Social-emotional development is thought to be critical in terms of a child’s ability to learn and get along with others. It is also a precursor to mental health. Our results showed that, without intervention, there was a dramatic link between maternal ACES score and at-risk social-emotional development for children at age 3 years. However, our Healthy Steps program appeared to moderate this otherwise powerful link, as children who received Healthy Steps, even if their mother had experienced abuse or neglect in her own childhood, had healthy social-emotional development at age 3 years.
As a result of the success of Healthy Steps at Montefiore, in 2014 we expanded our pediatric integrated behavioral health program to also include school age and adolescent patients. Today, we are serving approximately 90,000 pediatric patients at more than 21 sites in the Bronx and surrounding area. We provide universal behavioral health screening, including for autism and maternal depression, at well-child visits. We provide parental mental health services, within pediatrics, to parents of infants and toddlers struggling with perinatal mental health challenges, and we devote significant time to education of our primary care providers, to increase their confidence and competence regarding pediatric behavioral health.
Initial results for school age, adolescent program
Our early results regarding feasibility are promising. We found that more than 26% of children presenting to the primary care practices, well beyond national averages, were referred to our program during a 6-month study period. And while a referral unfortunately rarely leads to actual treatment in mental health, we found that more than half of referred patients attended at least one therapy session, and a warm hand-off (a unique feature of integrated care in which psychologists meet with a referred patient during the well-child visit in order to establish a level of trust between patient and provider) increased this to 63%.
Future steps
Our efforts suggest that integration of pediatric behavioral health specialists into primary care is feasible, efficacious, and beneficial to children and parents. We have had success at identifying children at risk for exposure to toxic stress early in their lifetimes and providing multigenerational treatment to these children to ensure healthy social-emotional development. We have shown that when we offer mental health treatment within primary care, even in an urban setting where stigma around mental illness runs high, we almost triple the national average of successful linkage to mental health services for school age and adolescent children. However, payment reform is needed to truly achieve population health. We must ensure preventive and multigenerational services are covered so that we may continue to treat children and families within the nonstigmatized and universally accessed setting of primary care.
Dr. Briggs is director of pediatric behavioral health services and Healthy Steps at Montefiore Medical Group and associate professor of clinical pediatrics at Albert Einstein College of Medicine, both in New York.
Research shows that the foundation of lifelong health is established during a child’s earliest years, including the prenatal period, and is also determined by the health of the future mother before she becomes pregnant. Much like the foundation of a house, if a child’s early years are filled with nurturing experiences and limited exposure to toxic stress, a child is set to succeed and withstand future challenges. However, adverse childhood experiences and toxic stress can disproportionately derail a child’s developmental growth and can lead to negative impacts throughout the lifespan, including social, emotional, and cognitive impairment; adoption of health risk behaviors; disease, disability, and social problems; and potentially early death.
Furthermore, data from the National Comorbidity Survey–Replication Sample (NCS-R) found that the prevalence of various mental health disorders – including disorders related to mood, anxiety, impulse control, and substance abuse – increases with the cumulative number of adverse childhood experiences. Persons with four or more childhood adversities had an odds ratio of 7.3 for four disorder categories.
Combined with recent data from the World Health Organization suggesting that the global cost of untreated mental health disorders is approximately $1 trillion, there is a clear public health crisis on our doorstep. Seeing our vulnerable patient population in the Bronx, family after family struggling to cope, I asked myself – is the solution on our doorstep too?
The role of the pediatrician
During a child’s early years, a pediatrician’s role is to identify signs of early childhood adversity and toxic stress, and to provide targeted support for parents and caregivers (Pediatrics. 2012 Jan. doi: 10.1542/peds.2011-2662). Given this, child primary care providers face the following challenges:
• Is there an opportunity for us to identify children at risk of developing mental health problems within the primary care setting?
• If so, how early can we identify children who would benefit from specific preventive or therapeutic interventions to optimize their developmental and behavioral potential?
• What tools are available in primary care to accomplish this function, and how should we administer them?
Healthy Steps program evaluation
At Montefiore Medical Group, we have developed a program that helps pediatricians overcome these challenges. Based on the national Healthy Steps program, Montefiore offers integrated mental health services in pediatric primary care settings, and provides universal screening, assessment, and treatment of young children and their caregivers.
A quasiexperimental longitudinal study was conducted, involving follow-up of 124 children enrolled in Healthy Steps at their primary care pediatric setting and a comparison group from a clinic that did not receive this intervention. The aim of the study was to determine the relationship between maternal adverse childhood experiences (ACES) and child social-emotional development, as measured via the Ages and States Questionnaire: Social Emotional (ASQ:SE) at age 36 months.
Social-emotional development is thought to be critical in terms of a child’s ability to learn and get along with others. It is also a precursor to mental health. Our results showed that, without intervention, there was a dramatic link between maternal ACES score and at-risk social-emotional development for children at age 3 years. However, our Healthy Steps program appeared to moderate this otherwise powerful link, as children who received Healthy Steps, even if their mother had experienced abuse or neglect in her own childhood, had healthy social-emotional development at age 3 years.
As a result of the success of Healthy Steps at Montefiore, in 2014 we expanded our pediatric integrated behavioral health program to also include school age and adolescent patients. Today, we are serving approximately 90,000 pediatric patients at more than 21 sites in the Bronx and surrounding area. We provide universal behavioral health screening, including for autism and maternal depression, at well-child visits. We provide parental mental health services, within pediatrics, to parents of infants and toddlers struggling with perinatal mental health challenges, and we devote significant time to education of our primary care providers, to increase their confidence and competence regarding pediatric behavioral health.
Initial results for school age, adolescent program
Our early results regarding feasibility are promising. We found that more than 26% of children presenting to the primary care practices, well beyond national averages, were referred to our program during a 6-month study period. And while a referral unfortunately rarely leads to actual treatment in mental health, we found that more than half of referred patients attended at least one therapy session, and a warm hand-off (a unique feature of integrated care in which psychologists meet with a referred patient during the well-child visit in order to establish a level of trust between patient and provider) increased this to 63%.
Future steps
Our efforts suggest that integration of pediatric behavioral health specialists into primary care is feasible, efficacious, and beneficial to children and parents. We have had success at identifying children at risk for exposure to toxic stress early in their lifetimes and providing multigenerational treatment to these children to ensure healthy social-emotional development. We have shown that when we offer mental health treatment within primary care, even in an urban setting where stigma around mental illness runs high, we almost triple the national average of successful linkage to mental health services for school age and adolescent children. However, payment reform is needed to truly achieve population health. We must ensure preventive and multigenerational services are covered so that we may continue to treat children and families within the nonstigmatized and universally accessed setting of primary care.
Dr. Briggs is director of pediatric behavioral health services and Healthy Steps at Montefiore Medical Group and associate professor of clinical pediatrics at Albert Einstein College of Medicine, both in New York.
