User login
Adverse childhood experiences
Adverse childhood experiences (ACEs) are the traumatic experiences in a person’s life occurring before the age of 18 years that the person remembers as an adult and that have consequences on a diverse set of outcomes. ACEs include physical abuse, sexual abuse, emotional abuse, mental illness of a household member, problematic drinking or alcoholism of a household member, illegal street or prescription drug use by a household member, divorce or separation of a parent, domestic violence toward a parent, and incarceration of a household member. Each of these experiences before the age of 18 years increases the likelihood of not only adulthood depression, suicide, and substance use disorders, but also a range of nonpsychiatric outcomes such as heart disease and chronic lung disease.

Case summary
Ellie is a 16-year-old girl with a past history of ADHD and oppositionality who arrives on her own in a walk-in clinic to be seen for a sports physical. Ellie has been generally healthy and was previously on a stable medical regimen of methylphenidate but has not been taking it for about 1 year. The oppositionality that she previously experienced in her early school-age years has slowly decreased. She generally does well in school and is in several clubs. In the course of the history, Ellie reveals that her mother’s depression has been worse lately to the point where her mother has resumed her drinking and illegal opiate use. You discuss safety with Ellie, and she reveals that, while she has never been threatened or injured, there has been domestic violence in the home that Ellie felt responsible to try to stop by calling the police. This led to the one and only time that Ellie was physically struck. Her father is now incarcerated, and Ellie feels guilty. After a discussion with Ellie, you report this situation to social services, who already has the case on file. Ellie’s mental status exam, including a thorough examination of symptoms of mood disorders, anxiety, substance use, and PTSD, is within normal limits.
Case discussion
Ellie has suffered a set of ACEs. Specifically, her mother has a mental illness, has a drinking problem, and uses illegal drugs; Ellie has witnessed domestic violence toward her mother, has a family member who is incarcerated, and has suffered from physical abuse. This ACEs score of 6 puts her at markedly increased risk for multiple psychiatric and nonpsychiatric medical outcomes. Individuals with scores of 4 or above on the simple ACEs questionnaire have demonstrated a 4- to 12-fold increased health risks for alcoholism, drug abuse, depression, and suicide attempts. Further, studies have shown a twofold to fourfold increase in smoking, poor self-rated health, increased numbers of sexual partners and sexually transmitted disease, and 1.4- to 1.6-fold increase in physical inactivity and severe obesity (Am J Prev Med. 1998 May;14[4]:245-58). In Ellie’s case, her history of ADHD and family history of substance use puts her at even further increased risk for later substance use disorders.
While there is no pharmacotherapy or psychotherapy specific to the treatment of having suffered adversity, it is critical for the clinician to note her increased risk. Ellie would be an individual for whom health promotion and prevention would be critical. It is excellent that she is exercising and participating in sports, which appear to be protective. Careful counseling and follow-up with regard to her increased risk for psychiatric and nonpsychiatric disorders is paramount.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Email him at pdnews@frontlinemedcom.com.
Adverse childhood experiences (ACEs) are the traumatic experiences in a person’s life occurring before the age of 18 years that the person remembers as an adult and that have consequences on a diverse set of outcomes. ACEs include physical abuse, sexual abuse, emotional abuse, mental illness of a household member, problematic drinking or alcoholism of a household member, illegal street or prescription drug use by a household member, divorce or separation of a parent, domestic violence toward a parent, and incarceration of a household member. Each of these experiences before the age of 18 years increases the likelihood of not only adulthood depression, suicide, and substance use disorders, but also a range of nonpsychiatric outcomes such as heart disease and chronic lung disease.
Case summary
Ellie is a 16-year-old girl with a past history of ADHD and oppositionality who arrives on her own in a walk-in clinic to be seen for a sports physical. Ellie has been generally healthy and was previously on a stable medical regimen of methylphenidate but has not been taking it for about 1 year. The oppositionality that she previously experienced in her early school-age years has slowly decreased. She generally does well in school and is in several clubs. In the course of the history, Ellie reveals that her mother’s depression has been worse lately to the point where her mother has resumed her drinking and illegal opiate use. You discuss safety with Ellie, and she reveals that, while she has never been threatened or injured, there has been domestic violence in the home that Ellie felt responsible to try to stop by calling the police. This led to the one and only time that Ellie was physically struck. Her father is now incarcerated, and Ellie feels guilty. After a discussion with Ellie, you report this situation to social services, who already has the case on file. Ellie’s mental status exam, including a thorough examination of symptoms of mood disorders, anxiety, substance use, and PTSD, is within normal limits.
Case discussion
Ellie has suffered a set of ACEs. Specifically, her mother has a mental illness, has a drinking problem, and uses illegal drugs; Ellie has witnessed domestic violence toward her mother, has a family member who is incarcerated, and has suffered from physical abuse. This ACEs score of 6 puts her at markedly increased risk for multiple psychiatric and nonpsychiatric medical outcomes. Individuals with scores of 4 or above on the simple ACEs questionnaire have demonstrated a 4- to 12-fold increased health risks for alcoholism, drug abuse, depression, and suicide attempts. Further, studies have shown a twofold to fourfold increase in smoking, poor self-rated health, increased numbers of sexual partners and sexually transmitted disease, and 1.4- to 1.6-fold increase in physical inactivity and severe obesity (Am J Prev Med. 1998 May;14[4]:245-58). In Ellie’s case, her history of ADHD and family history of substance use puts her at even further increased risk for later substance use disorders.
While there is no pharmacotherapy or psychotherapy specific to the treatment of having suffered adversity, it is critical for the clinician to note her increased risk. Ellie would be an individual for whom health promotion and prevention would be critical. It is excellent that she is exercising and participating in sports, which appear to be protective. Careful counseling and follow-up with regard to her increased risk for psychiatric and nonpsychiatric disorders is paramount.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Email him at pdnews@frontlinemedcom.com.
Adverse childhood experiences (ACEs) are the traumatic experiences in a person’s life occurring before the age of 18 years that the person remembers as an adult and that have consequences on a diverse set of outcomes. ACEs include physical abuse, sexual abuse, emotional abuse, mental illness of a household member, problematic drinking or alcoholism of a household member, illegal street or prescription drug use by a household member, divorce or separation of a parent, domestic violence toward a parent, and incarceration of a household member. Each of these experiences before the age of 18 years increases the likelihood of not only adulthood depression, suicide, and substance use disorders, but also a range of nonpsychiatric outcomes such as heart disease and chronic lung disease.
Case summary
Ellie is a 16-year-old girl with a past history of ADHD and oppositionality who arrives on her own in a walk-in clinic to be seen for a sports physical. Ellie has been generally healthy and was previously on a stable medical regimen of methylphenidate but has not been taking it for about 1 year. The oppositionality that she previously experienced in her early school-age years has slowly decreased. She generally does well in school and is in several clubs. In the course of the history, Ellie reveals that her mother’s depression has been worse lately to the point where her mother has resumed her drinking and illegal opiate use. You discuss safety with Ellie, and she reveals that, while she has never been threatened or injured, there has been domestic violence in the home that Ellie felt responsible to try to stop by calling the police. This led to the one and only time that Ellie was physically struck. Her father is now incarcerated, and Ellie feels guilty. After a discussion with Ellie, you report this situation to social services, who already has the case on file. Ellie’s mental status exam, including a thorough examination of symptoms of mood disorders, anxiety, substance use, and PTSD, is within normal limits.
Case discussion
Ellie has suffered a set of ACEs. Specifically, her mother has a mental illness, has a drinking problem, and uses illegal drugs; Ellie has witnessed domestic violence toward her mother, has a family member who is incarcerated, and has suffered from physical abuse. This ACEs score of 6 puts her at markedly increased risk for multiple psychiatric and nonpsychiatric medical outcomes. Individuals with scores of 4 or above on the simple ACEs questionnaire have demonstrated a 4- to 12-fold increased health risks for alcoholism, drug abuse, depression, and suicide attempts. Further, studies have shown a twofold to fourfold increase in smoking, poor self-rated health, increased numbers of sexual partners and sexually transmitted disease, and 1.4- to 1.6-fold increase in physical inactivity and severe obesity (Am J Prev Med. 1998 May;14[4]:245-58). In Ellie’s case, her history of ADHD and family history of substance use puts her at even further increased risk for later substance use disorders.
While there is no pharmacotherapy or psychotherapy specific to the treatment of having suffered adversity, it is critical for the clinician to note her increased risk. Ellie would be an individual for whom health promotion and prevention would be critical. It is excellent that she is exercising and participating in sports, which appear to be protective. Careful counseling and follow-up with regard to her increased risk for psychiatric and nonpsychiatric disorders is paramount.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Email him at pdnews@frontlinemedcom.com.
Methotrexate prolonged efficacy of steroid injections in oligoarticular JIA
Oral methotrexate prolonged and slightly boosted the efficacy of intra-articular corticosteroid injections in children with oligoarticular juvenile idiopathic arthritis without causing serious adverse effects, based on the results of a first-in-kind multicenter, randomized, open-label trial.
“This combination could be considered as reference treatment in everyday clinical practice for pediatricians, particularly in children with higher erythrocyte sedimentation rate,” Angelo Ravelli, MD, of Istituto Giannini Gaslini, Genoa, Italy, and his associates wrote in The Lancet. The regimen also could take center stage in treat-to-target strategies for children with chronic arthritis, they said (Lancet. 2017 Feb 2. doi: 10.1016/S0140-6736[17]30065-X).
For the study, they randomly assigned 207 children and adolescents with oligoarticular juvenile idiopathic arthritis to receive intra-articular injections with triamcinolone hexacetonide or methylprednisolone acetate, either alone or with 15 mg/m2 oral methotrexate at a maximum dose of 20 mg. The primary endpoint was the proportion of patients with remission of all injected joints at 12 months.
Methotrexate missed this endpoint – 12-month remission rates were 34% in the injection-only group and 39% in the dual therapy group (P = .48). However, methotrexate seemed to prolong the time to arthritis flare. The median time to flare was 10.1 months (95% confidence interval, 7.6 to more than 16 months) when patients received injections plus methotrexate, and only 6 months (95% CI, 4.6-8.2 months) when they received injections only (hazard ratio, 0.67; 95% CI, 0.46-0.97; P = .03).
Consequently, the dual therapy group had a higher rate of remission at 6 months (67%; 95% CI, 56%-75%) than did the injection-only group (49%; 95% CI, 39%-58%). Cumulative remission rates at 12 months also were higher for dual therapy (46%), compared with injections only (35%).
Erythrocyte sedimentation rate predicted arthritis flare, but did not seem to affect the chances of methotrexate being effective, the researchers said. After controlling for erythrocyte sedimentation rate, methotrexate decreased the 12-month risk of flare by 47%, “although the statistical effect was marginal,” they noted (adjusted odds ratio, 0.53; 95% CI, 0.27-1.01; P = .05).
These findings support those of noncontrolled studies and can inform strategies for initial treatment of oligoarticular juvenile idiopathic arthritis because study participants had short disease durations, the researchers said. But they emphasized that the cohort excluded patients with monoarthritis of the knee, for whom they use only local injections, adding methotrexate if patients relapse soon after the knee is injected or if arthritis spreads to other joints within 6-12 months.
Rates of new-onset uveitis were less than 10% and did not significantly differ between arms. Methotrexate most frequently caused nausea, vomiting, or constipation, but eight patients developed elevated liver enzymes. One patient stopped methotrexate as a result, and five interrupted treatment or had dose reductions. Another patient stopped treatment because of gastrointestinal discomfort, but no there were no serious adverse effects of any type, the researchers said. They will follow the cohort for up to 2 years to evaluate longer-term safety, they added.
The Italian Agency of Drug Evaluation funded the study. Dr. Ravelli disclosed personal fees from AbbVie, Bristol-Myers Squibb, Novartis, Pfizer, Roche, and Johnson & Johnson. Several coinvestigators also disclosed ties to a number of pharmaceutical companies.
These outcomes [of adding methotrexate to intra-articular corticosteroids] seem of substantial benefit for the individual patient [with juvenile idiopathic arthritis]. However, we need to know more about the pathogenesis of this disease and to develop more robust and validated biomarkers to predict an individual’s disease course and response to therapy. Both oral and subcutaneous methotrexate are associated with nausea or intolerance symptoms in up to 40% of patients, which often causes noncompliance in children and adolescents. Therefore, knowledge of who will benefit most from early methotrexate therapy is important.

Nico M. Wulffraat, MD, is with the department of pediatric rheumatology at University Medical Center Utrecht (the Netherlands). He disclosed unrestricted grants from AbbVie, GlaxoSmithKline, Novartis, Pfizer, Roche, Sanofi, and Sobi. These comments are from his editorial accompanying Dr. Ravelli and his colleagues’ report (Lancet. 2017 Feb 2. doi: 10.1016/S0140-6736[17]30180-0).
These outcomes [of adding methotrexate to intra-articular corticosteroids] seem of substantial benefit for the individual patient [with juvenile idiopathic arthritis]. However, we need to know more about the pathogenesis of this disease and to develop more robust and validated biomarkers to predict an individual’s disease course and response to therapy. Both oral and subcutaneous methotrexate are associated with nausea or intolerance symptoms in up to 40% of patients, which often causes noncompliance in children and adolescents. Therefore, knowledge of who will benefit most from early methotrexate therapy is important.
Nico M. Wulffraat, MD, is with the department of pediatric rheumatology at University Medical Center Utrecht (the Netherlands). He disclosed unrestricted grants from AbbVie, GlaxoSmithKline, Novartis, Pfizer, Roche, Sanofi, and Sobi. These comments are from his editorial accompanying Dr. Ravelli and his colleagues’ report (Lancet. 2017 Feb 2. doi: 10.1016/S0140-6736[17]30180-0).
These outcomes [of adding methotrexate to intra-articular corticosteroids] seem of substantial benefit for the individual patient [with juvenile idiopathic arthritis]. However, we need to know more about the pathogenesis of this disease and to develop more robust and validated biomarkers to predict an individual’s disease course and response to therapy. Both oral and subcutaneous methotrexate are associated with nausea or intolerance symptoms in up to 40% of patients, which often causes noncompliance in children and adolescents. Therefore, knowledge of who will benefit most from early methotrexate therapy is important.
Nico M. Wulffraat, MD, is with the department of pediatric rheumatology at University Medical Center Utrecht (the Netherlands). He disclosed unrestricted grants from AbbVie, GlaxoSmithKline, Novartis, Pfizer, Roche, Sanofi, and Sobi. These comments are from his editorial accompanying Dr. Ravelli and his colleagues’ report (Lancet. 2017 Feb 2. doi: 10.1016/S0140-6736[17]30180-0).
Oral methotrexate prolonged and slightly boosted the efficacy of intra-articular corticosteroid injections in children with oligoarticular juvenile idiopathic arthritis without causing serious adverse effects, based on the results of a first-in-kind multicenter, randomized, open-label trial.
“This combination could be considered as reference treatment in everyday clinical practice for pediatricians, particularly in children with higher erythrocyte sedimentation rate,” Angelo Ravelli, MD, of Istituto Giannini Gaslini, Genoa, Italy, and his associates wrote in The Lancet. The regimen also could take center stage in treat-to-target strategies for children with chronic arthritis, they said (Lancet. 2017 Feb 2. doi: 10.1016/S0140-6736[17]30065-X).
For the study, they randomly assigned 207 children and adolescents with oligoarticular juvenile idiopathic arthritis to receive intra-articular injections with triamcinolone hexacetonide or methylprednisolone acetate, either alone or with 15 mg/m2 oral methotrexate at a maximum dose of 20 mg. The primary endpoint was the proportion of patients with remission of all injected joints at 12 months.
Methotrexate missed this endpoint – 12-month remission rates were 34% in the injection-only group and 39% in the dual therapy group (P = .48). However, methotrexate seemed to prolong the time to arthritis flare. The median time to flare was 10.1 months (95% confidence interval, 7.6 to more than 16 months) when patients received injections plus methotrexate, and only 6 months (95% CI, 4.6-8.2 months) when they received injections only (hazard ratio, 0.67; 95% CI, 0.46-0.97; P = .03).
Consequently, the dual therapy group had a higher rate of remission at 6 months (67%; 95% CI, 56%-75%) than did the injection-only group (49%; 95% CI, 39%-58%). Cumulative remission rates at 12 months also were higher for dual therapy (46%), compared with injections only (35%).
Erythrocyte sedimentation rate predicted arthritis flare, but did not seem to affect the chances of methotrexate being effective, the researchers said. After controlling for erythrocyte sedimentation rate, methotrexate decreased the 12-month risk of flare by 47%, “although the statistical effect was marginal,” they noted (adjusted odds ratio, 0.53; 95% CI, 0.27-1.01; P = .05).
These findings support those of noncontrolled studies and can inform strategies for initial treatment of oligoarticular juvenile idiopathic arthritis because study participants had short disease durations, the researchers said. But they emphasized that the cohort excluded patients with monoarthritis of the knee, for whom they use only local injections, adding methotrexate if patients relapse soon after the knee is injected or if arthritis spreads to other joints within 6-12 months.
Rates of new-onset uveitis were less than 10% and did not significantly differ between arms. Methotrexate most frequently caused nausea, vomiting, or constipation, but eight patients developed elevated liver enzymes. One patient stopped methotrexate as a result, and five interrupted treatment or had dose reductions. Another patient stopped treatment because of gastrointestinal discomfort, but no there were no serious adverse effects of any type, the researchers said. They will follow the cohort for up to 2 years to evaluate longer-term safety, they added.
The Italian Agency of Drug Evaluation funded the study. Dr. Ravelli disclosed personal fees from AbbVie, Bristol-Myers Squibb, Novartis, Pfizer, Roche, and Johnson & Johnson. Several coinvestigators also disclosed ties to a number of pharmaceutical companies.
Oral methotrexate prolonged and slightly boosted the efficacy of intra-articular corticosteroid injections in children with oligoarticular juvenile idiopathic arthritis without causing serious adverse effects, based on the results of a first-in-kind multicenter, randomized, open-label trial.
“This combination could be considered as reference treatment in everyday clinical practice for pediatricians, particularly in children with higher erythrocyte sedimentation rate,” Angelo Ravelli, MD, of Istituto Giannini Gaslini, Genoa, Italy, and his associates wrote in The Lancet. The regimen also could take center stage in treat-to-target strategies for children with chronic arthritis, they said (Lancet. 2017 Feb 2. doi: 10.1016/S0140-6736[17]30065-X).
For the study, they randomly assigned 207 children and adolescents with oligoarticular juvenile idiopathic arthritis to receive intra-articular injections with triamcinolone hexacetonide or methylprednisolone acetate, either alone or with 15 mg/m2 oral methotrexate at a maximum dose of 20 mg. The primary endpoint was the proportion of patients with remission of all injected joints at 12 months.
Methotrexate missed this endpoint – 12-month remission rates were 34% in the injection-only group and 39% in the dual therapy group (P = .48). However, methotrexate seemed to prolong the time to arthritis flare. The median time to flare was 10.1 months (95% confidence interval, 7.6 to more than 16 months) when patients received injections plus methotrexate, and only 6 months (95% CI, 4.6-8.2 months) when they received injections only (hazard ratio, 0.67; 95% CI, 0.46-0.97; P = .03).
Consequently, the dual therapy group had a higher rate of remission at 6 months (67%; 95% CI, 56%-75%) than did the injection-only group (49%; 95% CI, 39%-58%). Cumulative remission rates at 12 months also were higher for dual therapy (46%), compared with injections only (35%).
Erythrocyte sedimentation rate predicted arthritis flare, but did not seem to affect the chances of methotrexate being effective, the researchers said. After controlling for erythrocyte sedimentation rate, methotrexate decreased the 12-month risk of flare by 47%, “although the statistical effect was marginal,” they noted (adjusted odds ratio, 0.53; 95% CI, 0.27-1.01; P = .05).
These findings support those of noncontrolled studies and can inform strategies for initial treatment of oligoarticular juvenile idiopathic arthritis because study participants had short disease durations, the researchers said. But they emphasized that the cohort excluded patients with monoarthritis of the knee, for whom they use only local injections, adding methotrexate if patients relapse soon after the knee is injected or if arthritis spreads to other joints within 6-12 months.
Rates of new-onset uveitis were less than 10% and did not significantly differ between arms. Methotrexate most frequently caused nausea, vomiting, or constipation, but eight patients developed elevated liver enzymes. One patient stopped methotrexate as a result, and five interrupted treatment or had dose reductions. Another patient stopped treatment because of gastrointestinal discomfort, but no there were no serious adverse effects of any type, the researchers said. They will follow the cohort for up to 2 years to evaluate longer-term safety, they added.
The Italian Agency of Drug Evaluation funded the study. Dr. Ravelli disclosed personal fees from AbbVie, Bristol-Myers Squibb, Novartis, Pfizer, Roche, and Johnson & Johnson. Several coinvestigators also disclosed ties to a number of pharmaceutical companies.
FROM THE LANCET
Key clinical point:
Major finding: The primary endpoint, remission of arthritis in all injected joints at 12 months, occurred in 34% of patients who received intra-articular corticosteroids only and in 39% of those who also received oral methotrexate (P = .48). Median time to arthritis flare was 10.1 months with dual therapy and 6 months with injections only (HR, 0.67; P = .03).
Data source: A multicenter, open-label, randomized trial of 207 children younger than 18 years with oligoarticular juvenile idiopathic arthritis.
Disclosures: The Italian Agency of Drug Evaluation funded the study. Dr. Ravelli disclosed personal fees from AbbVie, Bristol-Myers Squibb, Novartis, Pfizer, Roche, and Johnson & Johnson. Several coinvestigators also disclosed ties to a number of pharmaceutical companies.
Mycobacterium tuberculosis: Overcoming one obstacle on the road to elimination
March 24 is World TB Day. It was on this date in 1882 that physician Robert Koch announced the discovery of Mycobacterium tuberculosis, the causative agent of tuberculosis. Worldwide, activities are planned to raise awareness of TB and to support initiatives for prevention, better control, and ultimately the elimination of this disease.
Globally in 2015, the World Health Organization estimated there were 10.4 million new cases of TB, including 1 million in children. Data from the United States reveal that after 20 years of annual decline, the incidence of TB has plateaued. In 2015, 9,563 cases of TB disease were reported, including 440 cases in children less than 15 years of age. While the overall incidence was 3 cases per 100,000, the incidence among foreign-born persons was 15.1 cases per 100,000. There were 3,201 cases (33.5%) among U.S.-born individuals. Foreign-born persons accounted for 66.2% of cases; however, the majority of those cases were diagnosed several years after their arrival in the United States. The top five countries of origin of these individuals were China, India, Mexico, the Philippines, and Vietnam. In contrast, only one-quarter of all pediatric cases occurred in foreign-born children. Four states (California, Florida, New York, and Texas) reported more than 500 cases each in 2015, as they have for the last 7 consecutive years. In 2015, these states accounted for slightly more than half (4,839) of all cases (MMWR 2016 Mar 25;65[11]:273-8).

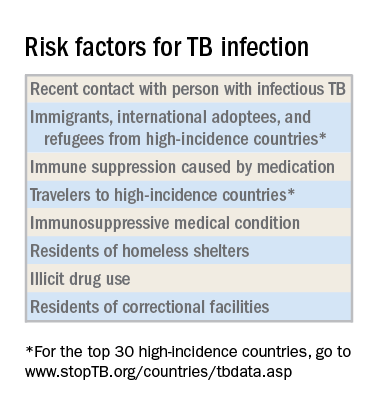
Why as pediatricians should we be concerned? TB in a child is a sentinel event and represents recent or ongoing transmission. Young children who are infected are more likely to progress to TB disease and develop severe manifestations such as miliary TB or meningitis. Children less than 4 years old and those with certain underlying disorders, including those with an immunodeficiency or who are receiving immunosuppressive agents, also are at greater risk for progression from infection to disease. Other predictors of disease progression include diagnosis of the infection within the past 2 years, use of chemotherapy and high-dose corticosteroids, as well as certain cancers, diabetes, and chronic renal failure.
Once infected, most children and adolescents remain asymptomatic. If disease occurs, symptoms develop 1-6 months after infection and include fever, cough, weight loss or failure to thrive, night sweats, and chills. Chest radiographic findings are nonspecific. Infiltrates and intrathoracic lymph node enlargement may or may not be present. However, our goal is to diagnose at-risk children with infection, treat them, and avoid their progression to TB disease.
Screening tests
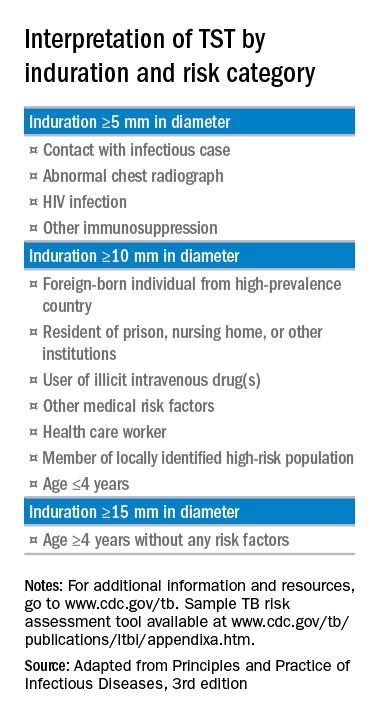
The interferon-gamma release assay is a blood test that has a greater specificity than TST and requires only one visit. A positive test is seen in both latent TB infection and TB disease. There is no cross-reaction with BCG. This is the ideal test for prior BCG recipients and others who are unlikely to return for TST readings and are at least 5 years of age.
A chest radiograph is required to differentiate latent TB infection from TB disease. Latent TB infection is diagnosed when there is an absence of parenchymal disease, opacification, or intrathoracic adenopathy.
Treatment of latent TB infection versus TB disease is beyond the scope of this article. Consultation with an infectious disease expert is recommended.
For additional information and resources, go to www.cdc.gov/tb, and for a sample TB risk assessment tool, go to www.cdc.gov/tb/publications/ltbi/appendixa.htm.
As we mark the passing of another World TB Day, we have one goal – to identify, screen, and treat children and adolescents at risk for latent TB infection and help eliminate future cases of TB disease.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
March 24 is World TB Day. It was on this date in 1882 that physician Robert Koch announced the discovery of Mycobacterium tuberculosis, the causative agent of tuberculosis. Worldwide, activities are planned to raise awareness of TB and to support initiatives for prevention, better control, and ultimately the elimination of this disease.
Globally in 2015, the World Health Organization estimated there were 10.4 million new cases of TB, including 1 million in children. Data from the United States reveal that after 20 years of annual decline, the incidence of TB has plateaued. In 2015, 9,563 cases of TB disease were reported, including 440 cases in children less than 15 years of age. While the overall incidence was 3 cases per 100,000, the incidence among foreign-born persons was 15.1 cases per 100,000. There were 3,201 cases (33.5%) among U.S.-born individuals. Foreign-born persons accounted for 66.2% of cases; however, the majority of those cases were diagnosed several years after their arrival in the United States. The top five countries of origin of these individuals were China, India, Mexico, the Philippines, and Vietnam. In contrast, only one-quarter of all pediatric cases occurred in foreign-born children. Four states (California, Florida, New York, and Texas) reported more than 500 cases each in 2015, as they have for the last 7 consecutive years. In 2015, these states accounted for slightly more than half (4,839) of all cases (MMWR 2016 Mar 25;65[11]:273-8).
Why as pediatricians should we be concerned? TB in a child is a sentinel event and represents recent or ongoing transmission. Young children who are infected are more likely to progress to TB disease and develop severe manifestations such as miliary TB or meningitis. Children less than 4 years old and those with certain underlying disorders, including those with an immunodeficiency or who are receiving immunosuppressive agents, also are at greater risk for progression from infection to disease. Other predictors of disease progression include diagnosis of the infection within the past 2 years, use of chemotherapy and high-dose corticosteroids, as well as certain cancers, diabetes, and chronic renal failure.
Once infected, most children and adolescents remain asymptomatic. If disease occurs, symptoms develop 1-6 months after infection and include fever, cough, weight loss or failure to thrive, night sweats, and chills. Chest radiographic findings are nonspecific. Infiltrates and intrathoracic lymph node enlargement may or may not be present. However, our goal is to diagnose at-risk children with infection, treat them, and avoid their progression to TB disease.
Screening tests
The interferon-gamma release assay is a blood test that has a greater specificity than TST and requires only one visit. A positive test is seen in both latent TB infection and TB disease. There is no cross-reaction with BCG. This is the ideal test for prior BCG recipients and others who are unlikely to return for TST readings and are at least 5 years of age.
A chest radiograph is required to differentiate latent TB infection from TB disease. Latent TB infection is diagnosed when there is an absence of parenchymal disease, opacification, or intrathoracic adenopathy.
Treatment of latent TB infection versus TB disease is beyond the scope of this article. Consultation with an infectious disease expert is recommended.
For additional information and resources, go to www.cdc.gov/tb, and for a sample TB risk assessment tool, go to www.cdc.gov/tb/publications/ltbi/appendixa.htm.
As we mark the passing of another World TB Day, we have one goal – to identify, screen, and treat children and adolescents at risk for latent TB infection and help eliminate future cases of TB disease.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
March 24 is World TB Day. It was on this date in 1882 that physician Robert Koch announced the discovery of Mycobacterium tuberculosis, the causative agent of tuberculosis. Worldwide, activities are planned to raise awareness of TB and to support initiatives for prevention, better control, and ultimately the elimination of this disease.
Globally in 2015, the World Health Organization estimated there were 10.4 million new cases of TB, including 1 million in children. Data from the United States reveal that after 20 years of annual decline, the incidence of TB has plateaued. In 2015, 9,563 cases of TB disease were reported, including 440 cases in children less than 15 years of age. While the overall incidence was 3 cases per 100,000, the incidence among foreign-born persons was 15.1 cases per 100,000. There were 3,201 cases (33.5%) among U.S.-born individuals. Foreign-born persons accounted for 66.2% of cases; however, the majority of those cases were diagnosed several years after their arrival in the United States. The top five countries of origin of these individuals were China, India, Mexico, the Philippines, and Vietnam. In contrast, only one-quarter of all pediatric cases occurred in foreign-born children. Four states (California, Florida, New York, and Texas) reported more than 500 cases each in 2015, as they have for the last 7 consecutive years. In 2015, these states accounted for slightly more than half (4,839) of all cases (MMWR 2016 Mar 25;65[11]:273-8).
Why as pediatricians should we be concerned? TB in a child is a sentinel event and represents recent or ongoing transmission. Young children who are infected are more likely to progress to TB disease and develop severe manifestations such as miliary TB or meningitis. Children less than 4 years old and those with certain underlying disorders, including those with an immunodeficiency or who are receiving immunosuppressive agents, also are at greater risk for progression from infection to disease. Other predictors of disease progression include diagnosis of the infection within the past 2 years, use of chemotherapy and high-dose corticosteroids, as well as certain cancers, diabetes, and chronic renal failure.
Once infected, most children and adolescents remain asymptomatic. If disease occurs, symptoms develop 1-6 months after infection and include fever, cough, weight loss or failure to thrive, night sweats, and chills. Chest radiographic findings are nonspecific. Infiltrates and intrathoracic lymph node enlargement may or may not be present. However, our goal is to diagnose at-risk children with infection, treat them, and avoid their progression to TB disease.
Screening tests
The interferon-gamma release assay is a blood test that has a greater specificity than TST and requires only one visit. A positive test is seen in both latent TB infection and TB disease. There is no cross-reaction with BCG. This is the ideal test for prior BCG recipients and others who are unlikely to return for TST readings and are at least 5 years of age.
A chest radiograph is required to differentiate latent TB infection from TB disease. Latent TB infection is diagnosed when there is an absence of parenchymal disease, opacification, or intrathoracic adenopathy.
Treatment of latent TB infection versus TB disease is beyond the scope of this article. Consultation with an infectious disease expert is recommended.
For additional information and resources, go to www.cdc.gov/tb, and for a sample TB risk assessment tool, go to www.cdc.gov/tb/publications/ltbi/appendixa.htm.
As we mark the passing of another World TB Day, we have one goal – to identify, screen, and treat children and adolescents at risk for latent TB infection and help eliminate future cases of TB disease.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
Pregnancy medical home reduces hospital visits, overall costs
LAS VEGAS – Women and their newborns who received care through a pregnancy medical home model used the emergency department less and had fewer inpatient stays, resulting in significant cost savings to a state health insurance plan.
In the single-center, retrospective cohort study, women who had at least one medical home visit had 897 emergency department visits per 1,000 member months, compared with 1,969/1,000 member months for patients who had no medical home visits (P less than .01). Newborns in the medical home group had fewer inpatient days per 1,000 member months as well, compared with non–medical home infants (698 vs. 1,799 days/member month, P less than .01). Inpatient stays for pregnant women receiving medical home care were also reduced (4,279 vs. 2,939 inpatient days, P less than .01).
The pregnancy medical home project was conducted jointly by the Texas Children’s Health Plan and Baylor College of Medicine. The care delivery model, offered from the Baylor Center for Children and Women, gave pregnant women enhanced access, used evidence-based protocols for treatment, and emphasized both quality care and the patient experience, said Dr. Suhag, professor of ob.gyn. at Baylor College of Medicine, Houston.
The pregnancy medical home includes extended hours, walk-in appointments, 24-hour nurse availability for triage, and a laborist model for hospital coverage.
From a payment perspective, the medical home is a fully capitated, full-risk model. “Our center is paid on a monthly basis to provide care to members of our panel,” Dr. Suhag said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
The primary outcomes measured by the study were the number of inpatient days and the rate of emergency department usage among pregnancy medical home participants, compared with nonparticipating pregnant women and newborns seen at the Center for Children and Women. Annualized cost savings for the pregnancy medical home model was a secondary outcome measure.
Over a 1-year period, the study examined claims data for pregnant women and newborns who were enrolled in the Texas Children’s Health Plan and were assigned to the pregnancy medical home panel. In total, 27,912 member months (including care for both women and newborns) were examined; of these, about 37% (10,402) were for women and newborns who had at least one medical home visit, and 63% (17,510) of the member months accrued to patients who had no medical home visits. Women and their infants were excluded from the cohort if they received care billed to another health plan.
Participation in the medical home group resulted in lower costs, with annualized estimated emergency department cost savings of $330,161 and $30,739 for pregnant women and newborns, respectively. The reduced number of inpatient days in the medical home group resulted in a total savings of $494,313 for pregnant women and $1,606,392 for newborns in this cohort.
The integrated care model, which used a care coordinator and provided care from multiple specialties at a single site, was likely the key to success, Dr. Suhag said. “With this access, 40% of our pregnant moms were able to access prenatal care in the first trimester, which likely improved outcomes and contributed to the cost savings,” she said.
The control group in the study was made up of individuals who had been randomized to the medical home, but who had chosen care from another provider instead. Because the researchers were relying on health claims data, they were not able to perform a detailed comparison between the two groups, leaving open the possibility that patient characteristics may have accounted for part of the differences in outcomes. Women “could self-select to receive care at the Center for Children and Women,” Dr. Suhag said in an interview. “It is possible that they are different than the women who did not choose care in our clinic.”
A strength of the study, Dr. Suhag said, is that it evaluated outcomes from the medical home model by comparing it to several other medical practices caring for a similar demographic in the same geographic area.
The study was conducted by the Texas Children’s Health Plan and Baylor College of Medicine. Dr. Suhag reported having no other outside sources of funding or conflicts of interest.
Dr. Suhag reported having no outside sources of funding beyond the study’s two sponsoring organizations and no conflicts of interest.
koakes@frontlinemedcom.com
On Twitter @karioakes
LAS VEGAS – Women and their newborns who received care through a pregnancy medical home model used the emergency department less and had fewer inpatient stays, resulting in significant cost savings to a state health insurance plan.
In the single-center, retrospective cohort study, women who had at least one medical home visit had 897 emergency department visits per 1,000 member months, compared with 1,969/1,000 member months for patients who had no medical home visits (P less than .01). Newborns in the medical home group had fewer inpatient days per 1,000 member months as well, compared with non–medical home infants (698 vs. 1,799 days/member month, P less than .01). Inpatient stays for pregnant women receiving medical home care were also reduced (4,279 vs. 2,939 inpatient days, P less than .01).
The pregnancy medical home project was conducted jointly by the Texas Children’s Health Plan and Baylor College of Medicine. The care delivery model, offered from the Baylor Center for Children and Women, gave pregnant women enhanced access, used evidence-based protocols for treatment, and emphasized both quality care and the patient experience, said Dr. Suhag, professor of ob.gyn. at Baylor College of Medicine, Houston.
The pregnancy medical home includes extended hours, walk-in appointments, 24-hour nurse availability for triage, and a laborist model for hospital coverage.
From a payment perspective, the medical home is a fully capitated, full-risk model. “Our center is paid on a monthly basis to provide care to members of our panel,” Dr. Suhag said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
The primary outcomes measured by the study were the number of inpatient days and the rate of emergency department usage among pregnancy medical home participants, compared with nonparticipating pregnant women and newborns seen at the Center for Children and Women. Annualized cost savings for the pregnancy medical home model was a secondary outcome measure.
Over a 1-year period, the study examined claims data for pregnant women and newborns who were enrolled in the Texas Children’s Health Plan and were assigned to the pregnancy medical home panel. In total, 27,912 member months (including care for both women and newborns) were examined; of these, about 37% (10,402) were for women and newborns who had at least one medical home visit, and 63% (17,510) of the member months accrued to patients who had no medical home visits. Women and their infants were excluded from the cohort if they received care billed to another health plan.
Participation in the medical home group resulted in lower costs, with annualized estimated emergency department cost savings of $330,161 and $30,739 for pregnant women and newborns, respectively. The reduced number of inpatient days in the medical home group resulted in a total savings of $494,313 for pregnant women and $1,606,392 for newborns in this cohort.
The integrated care model, which used a care coordinator and provided care from multiple specialties at a single site, was likely the key to success, Dr. Suhag said. “With this access, 40% of our pregnant moms were able to access prenatal care in the first trimester, which likely improved outcomes and contributed to the cost savings,” she said.
The control group in the study was made up of individuals who had been randomized to the medical home, but who had chosen care from another provider instead. Because the researchers were relying on health claims data, they were not able to perform a detailed comparison between the two groups, leaving open the possibility that patient characteristics may have accounted for part of the differences in outcomes. Women “could self-select to receive care at the Center for Children and Women,” Dr. Suhag said in an interview. “It is possible that they are different than the women who did not choose care in our clinic.”
A strength of the study, Dr. Suhag said, is that it evaluated outcomes from the medical home model by comparing it to several other medical practices caring for a similar demographic in the same geographic area.
The study was conducted by the Texas Children’s Health Plan and Baylor College of Medicine. Dr. Suhag reported having no other outside sources of funding or conflicts of interest.
Dr. Suhag reported having no outside sources of funding beyond the study’s two sponsoring organizations and no conflicts of interest.
koakes@frontlinemedcom.com
On Twitter @karioakes
LAS VEGAS – Women and their newborns who received care through a pregnancy medical home model used the emergency department less and had fewer inpatient stays, resulting in significant cost savings to a state health insurance plan.
In the single-center, retrospective cohort study, women who had at least one medical home visit had 897 emergency department visits per 1,000 member months, compared with 1,969/1,000 member months for patients who had no medical home visits (P less than .01). Newborns in the medical home group had fewer inpatient days per 1,000 member months as well, compared with non–medical home infants (698 vs. 1,799 days/member month, P less than .01). Inpatient stays for pregnant women receiving medical home care were also reduced (4,279 vs. 2,939 inpatient days, P less than .01).
The pregnancy medical home project was conducted jointly by the Texas Children’s Health Plan and Baylor College of Medicine. The care delivery model, offered from the Baylor Center for Children and Women, gave pregnant women enhanced access, used evidence-based protocols for treatment, and emphasized both quality care and the patient experience, said Dr. Suhag, professor of ob.gyn. at Baylor College of Medicine, Houston.
The pregnancy medical home includes extended hours, walk-in appointments, 24-hour nurse availability for triage, and a laborist model for hospital coverage.
From a payment perspective, the medical home is a fully capitated, full-risk model. “Our center is paid on a monthly basis to provide care to members of our panel,” Dr. Suhag said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
The primary outcomes measured by the study were the number of inpatient days and the rate of emergency department usage among pregnancy medical home participants, compared with nonparticipating pregnant women and newborns seen at the Center for Children and Women. Annualized cost savings for the pregnancy medical home model was a secondary outcome measure.
Over a 1-year period, the study examined claims data for pregnant women and newborns who were enrolled in the Texas Children’s Health Plan and were assigned to the pregnancy medical home panel. In total, 27,912 member months (including care for both women and newborns) were examined; of these, about 37% (10,402) were for women and newborns who had at least one medical home visit, and 63% (17,510) of the member months accrued to patients who had no medical home visits. Women and their infants were excluded from the cohort if they received care billed to another health plan.
Participation in the medical home group resulted in lower costs, with annualized estimated emergency department cost savings of $330,161 and $30,739 for pregnant women and newborns, respectively. The reduced number of inpatient days in the medical home group resulted in a total savings of $494,313 for pregnant women and $1,606,392 for newborns in this cohort.
The integrated care model, which used a care coordinator and provided care from multiple specialties at a single site, was likely the key to success, Dr. Suhag said. “With this access, 40% of our pregnant moms were able to access prenatal care in the first trimester, which likely improved outcomes and contributed to the cost savings,” she said.
The control group in the study was made up of individuals who had been randomized to the medical home, but who had chosen care from another provider instead. Because the researchers were relying on health claims data, they were not able to perform a detailed comparison between the two groups, leaving open the possibility that patient characteristics may have accounted for part of the differences in outcomes. Women “could self-select to receive care at the Center for Children and Women,” Dr. Suhag said in an interview. “It is possible that they are different than the women who did not choose care in our clinic.”
A strength of the study, Dr. Suhag said, is that it evaluated outcomes from the medical home model by comparing it to several other medical practices caring for a similar demographic in the same geographic area.
The study was conducted by the Texas Children’s Health Plan and Baylor College of Medicine. Dr. Suhag reported having no other outside sources of funding or conflicts of interest.
Dr. Suhag reported having no outside sources of funding beyond the study’s two sponsoring organizations and no conflicts of interest.
koakes@frontlinemedcom.com
On Twitter @karioakes
AT THE PREGNANCY MEETING
Key clinical point:
Major finding: Medical home patients had 897 emergency department visits, compared with 1,969 per 1,000 member months for non–medical home patients (P less than .01).
Data source: A retrospective cohort study of 27,912 patient member months comparing pregnancy medical home patients with non–medical home patients.
Disclosures: The study was conducted by the Texas Children’s Health Plan and Baylor College of Medicine. Dr. Suhag reported having no other outside sources of funding or conflicts of interest.
Pertussis susceptibility estimates call for public health push
, according to results of research by Lana Childs and Robert A. Bednarczyk, PhD.
There were 32,971 pertussis cases reported in 2014, a 15% increase over 2013; most cases occurred in children who were too young to be fully vaccinated and in preadolescents with waning immunity from their vaccines. In the United States, vaccine coverage during childhood tends to be high overall, but DTaP coverage (84% in 2014) “remains lower than coverage for other childhood vaccinations,” they noted.
“These findings emphasize the need for public health professionals to continue efforts to increase DTaP vaccine coverage in children and Tdap coverage in pregnant women, plan for potential outbreaks, and maintain immunity levels needed to prevent the spread of pertussis.” the investigators concluded.
Read more at (Ped Inf Dis J. 2017. doi: 10.1097/INF.0000000000001537).
, according to results of research by Lana Childs and Robert A. Bednarczyk, PhD.
There were 32,971 pertussis cases reported in 2014, a 15% increase over 2013; most cases occurred in children who were too young to be fully vaccinated and in preadolescents with waning immunity from their vaccines. In the United States, vaccine coverage during childhood tends to be high overall, but DTaP coverage (84% in 2014) “remains lower than coverage for other childhood vaccinations,” they noted.
“These findings emphasize the need for public health professionals to continue efforts to increase DTaP vaccine coverage in children and Tdap coverage in pregnant women, plan for potential outbreaks, and maintain immunity levels needed to prevent the spread of pertussis.” the investigators concluded.
Read more at (Ped Inf Dis J. 2017. doi: 10.1097/INF.0000000000001537).
, according to results of research by Lana Childs and Robert A. Bednarczyk, PhD.
There were 32,971 pertussis cases reported in 2014, a 15% increase over 2013; most cases occurred in children who were too young to be fully vaccinated and in preadolescents with waning immunity from their vaccines. In the United States, vaccine coverage during childhood tends to be high overall, but DTaP coverage (84% in 2014) “remains lower than coverage for other childhood vaccinations,” they noted.
“These findings emphasize the need for public health professionals to continue efforts to increase DTaP vaccine coverage in children and Tdap coverage in pregnant women, plan for potential outbreaks, and maintain immunity levels needed to prevent the spread of pertussis.” the investigators concluded.
Read more at (Ped Inf Dis J. 2017. doi: 10.1097/INF.0000000000001537).
FROM THE PEDIATRIC INFECTIOUS DISEASE JOURNAL
Twenty-five states at highest flu activity level
Flu activity in the United States continued to increase as half of the states reached the highest level of influenza-like illness (ILI) activity in the week ending Feb. 11, according to the Centers for Disease Control and Prevention.
For the week, the 25 states at level 10 on the CDC’s 1-10 scale of ILI activity were joined in the high range by Illinois and Kentucky at level 9 and Iowa at level 8, the CDC reported. The previous week, there were 23 states in the high range.
Of the nine flu-related pediatric deaths reported to the CDC during the latest week, eight occurred in earlier weeks. For the 2016-2017 season so far, 29 flu-related pediatric deaths have been reported, the CDC said.
Flu activity in the United States continued to increase as half of the states reached the highest level of influenza-like illness (ILI) activity in the week ending Feb. 11, according to the Centers for Disease Control and Prevention.
For the week, the 25 states at level 10 on the CDC’s 1-10 scale of ILI activity were joined in the high range by Illinois and Kentucky at level 9 and Iowa at level 8, the CDC reported. The previous week, there were 23 states in the high range.
Of the nine flu-related pediatric deaths reported to the CDC during the latest week, eight occurred in earlier weeks. For the 2016-2017 season so far, 29 flu-related pediatric deaths have been reported, the CDC said.
Flu activity in the United States continued to increase as half of the states reached the highest level of influenza-like illness (ILI) activity in the week ending Feb. 11, according to the Centers for Disease Control and Prevention.
For the week, the 25 states at level 10 on the CDC’s 1-10 scale of ILI activity were joined in the high range by Illinois and Kentucky at level 9 and Iowa at level 8, the CDC reported. The previous week, there were 23 states in the high range.
Of the nine flu-related pediatric deaths reported to the CDC during the latest week, eight occurred in earlier weeks. For the 2016-2017 season so far, 29 flu-related pediatric deaths have been reported, the CDC said.
Medication for life
Some areas of psychiatry would benefit from more controversy. One of them is the prescription of antidepressants to young people dealing with romantic disappointments.
I have seen many young men and women given an antidepressant for the very painful, but ordinary, romantic break-ups characteristic of this phase of life, who then become habituated to the drug. They take the medication indefinitely, their brains accommodate neurophysiologically to the presence of the chemical, and they become unable to discontinue it without intolerable withdrawal symptoms that look like an underlying illness. A parallel phenomenon occurs not infrequently with the use of amphetamines (and other stimulants) for attention-deficit hyperactivity disorder that is at times mistakenly diagnosed in this age group.

Antidepressants for early romantic disappointments
Mr. A, now in his 30s, became sullen and withdrawn at age 16 after a girl refused his romantic approaches. His well-intentioned parents took him to a psychiatrist, who, after a brief evaluation, prescribed fluoxetine. Mr. A is now well adjusted and happily married but unable to get off fluoxetine. Even when it is carefully tapered, 2 or 3 months after it is discontinued, he becomes anxious and depressed. This is an iatrogenic problem. It is not related to goings-on in his mind or his life; rather it is the result of his brain’s accommodation to a medication, producing a serious withdrawal syndrome.
His original psychiatrist made only a descriptive diagnosis. He did not inquire about what was going on in Mr. A’s mind and thus could not make a dynamic diagnosis (that is, a diagnosis of a patient’s central emotional conflicts, ability to function in relation to other people, strengths, and weaknesses). Mr. A, like many adolescents, had a lot of anxiety and guilt about sexual and romantic involvement, and potential success. He defended against his anxiety and guilt by assuring himself life would never work out for him. When the girl he admired rebuffed him, he immediately concluded this would perpetually be his fate, so the girl’s refusal was particularly painful. Mr. A feels that had this dynamic been discussed with him at the time, he may well not have needed medication at all.
Ms. B, like Mr. A, was prescribed antidepressants for depressive reactions to early romantic disappointments. Likewise, she self-punitively convinced herself, despite easily attracting men’s attentions, that these disappointments meant a lifetime alone. Ms. B has a family history of depression (although neither of her brothers struggles with it), and she felt that she needed the medications to help negotiate difficult periods. But should she have been on them for extended periods of time? Therapeutic attention to her emotional conflicts helped her to form lasting relationships, marry, and have children. Unable to get off the medications, she had to deal with the risks of their use during pregnancy, which she then subjected to the same sort of guilty self-accusations as she previously had used to limit her romantic prospects.
Ms. C came to me on three medications – one for each of her significant romantic break-ups. She, too, was depressively self-diminishing, beginning therapy by letting me know all the things she could think of that might make me think less of her. Understanding some of the reasons for her self-deprecation helped her toward better romantic relationships but did not give her the courage to get off her medications. Pregnancy, however, led her to promptly and successfully discontinue an antidepressant and a mood stabilizer (she has never had any symptoms suggestive of manic depression). She remained on a low dose of a selective serotonin reuptake inhibitor, had an uneventful pregnancy, and then fell in love with a charming baby.
Principles for consideration
• Psychiatrists (and other mental health professionals and primary care physicians treating mental illness) should always make a dynamic, and not merely a descriptive, diagnosis. Even with a more clearly biologically driven problem, such as bipolar disorder, the patient’s personality and conflicts matter.
• Psychiatrists should be very judicious about prescribing medications in adolescence and young adulthood, especially for difficulties adapting to the typical events of those phases of life. Expert psychotherapy should be the first choice in these instances.
• Medication, when necessary, should be prescribed for as limited a time as possible. It is important for young people to advance their own development, not feel needlessly beholden to medications, not get iatrogenically dependent on them, and not feel that they have “diseases” they don’t have.
Amphetamines for misdiagnosed ADHD
When Ms. D’s family moved to a new house, she, her brother, and her sister, each attended a new school. Unlike her siblings, Ms. D, who was in high school, had a difficult adjustment. Her grades fell. She was taken to a psychiatrist who diagnosed ADHD and prescribed amphetamines. The psychiatrist paid little attention to her prior lack of difficulty in school or her struggles making new friends. Nor did the psychiatrist learn that Ms. D had to ward off the seductive advances of an older teacher (although Ms. D would likely not have been immediately forthcoming about this at the time).
When Ms. D came to me as a college student, for troubles with anger, anxiety, and some depression, she was religiously taking 70 mg of amphetamines daily. After I learned a bit about her and raised the question of whether she actually had ADHD, and whether it might make sense to consider tapering the amphetamines, she was appalled and looked like a toddler who was afraid I was about to steal her candy. Helping her to get off the unneeded medication was a multiyear process.
First, she had to recognize that it was prescribed to treat a problem she probably didn’t have, and second, that it was failing to help her with the problems she did have. As we attended to some of her actual emotional conflicts, she became willing to experiment with lower doses. She was able to see that her work was little changed as the dose was lowered, and that her difficulties with school had more to do with feelings toward classmates and teachers than with the presence or absence of amphetamines. After a protracted struggle, finally off the medication, she felt in charge of her life and no longer believed there was something inherently wrong with her mind or her brain.
Mr. E was the only son in a high-powered academic family. His older sisters were all intellectual standouts. Early in high school, he received his first B as a grade in a course. He was taken to a pediatrician, diagnosed with ADHD, and put on stimulants. Like Ms. D, he came to believe that he needed them. In college, he began to develop some magical aspects to his thinking, a potential side effect of the stimulants. It was very difficult to help him see either that he had a problem with his thinking or that it might be attributable to the medication.
Principles to consider
• If the ADHD wasn’t there in elementary school or before, it is unlikely that an adolescent or young adult has new-onset ADHD. A new or newly amplified conflict is occurring in the person’s mind and life A dynamic diagnosis, as always, is essential.
• When medication is prescribed for actual ADHD, as with anything else, the question of how long it will be taken must be asked. For life? Until other means of adaptation are accomplished? Until adequate outcome studies of long-term use of the medication are performed?
Helping patients to get off unneeded, or no longer needed, medications can be a difficult task. Their emotional attachments to the medications can be intense and varied. For some, the prescription is a sign of being loved and cared for. For others, it represents a certification of a deficit, appeases guilt about success, and/or attests to the need for special consideration. Insofar as the medication has been helpful, it may have come to be regarded as a dearly loved friend, or even a part of the self.
When medication has been helpful, there is also, of course, concern about the potential return of the difficulties for which it was prescribed. Few patients are told at the time of first prescription that there is potential risk of habituation and return of, or potential exaggeration of, symptoms with discontinuation. This type of discussion is more difficult to have in situations in which a prescription is urgently needed and the patient is reluctant, but is still not often done in those instances in which a prescription is more optional than essential. The picture is seldom simple.
These few comments only scratch the surface of the difficulties doctors and patients face in helping patients to discontinue their medications. Residency programs pay a lot of attention to helping trainees learn to prescribe medications; rarely do they sufficiently educate residents how to help patients discontinue them. The fact that so many residencies currently pay limited attention to interventions apart from medication contributes further to the difficulty.
Medications have saved the life of many a psychiatric patient. Some patients need medication for life. But some end up on medication for life, even in some instances when the medication may not have been needed in the first place. Although it is often a difficult task, we need to do a better job of distinguishing which patients are which.
Dr. Blum is a psychiatrist and psychoanalyst in private practice in Philadelphia. He teaches in the departments of anthropology and psychiatry at the University of Pennsylvania and at the Psychoanalytic Center of Philadelphia.
Some areas of psychiatry would benefit from more controversy. One of them is the prescription of antidepressants to young people dealing with romantic disappointments.
I have seen many young men and women given an antidepressant for the very painful, but ordinary, romantic break-ups characteristic of this phase of life, who then become habituated to the drug. They take the medication indefinitely, their brains accommodate neurophysiologically to the presence of the chemical, and they become unable to discontinue it without intolerable withdrawal symptoms that look like an underlying illness. A parallel phenomenon occurs not infrequently with the use of amphetamines (and other stimulants) for attention-deficit hyperactivity disorder that is at times mistakenly diagnosed in this age group.
Antidepressants for early romantic disappointments
Mr. A, now in his 30s, became sullen and withdrawn at age 16 after a girl refused his romantic approaches. His well-intentioned parents took him to a psychiatrist, who, after a brief evaluation, prescribed fluoxetine. Mr. A is now well adjusted and happily married but unable to get off fluoxetine. Even when it is carefully tapered, 2 or 3 months after it is discontinued, he becomes anxious and depressed. This is an iatrogenic problem. It is not related to goings-on in his mind or his life; rather it is the result of his brain’s accommodation to a medication, producing a serious withdrawal syndrome.
His original psychiatrist made only a descriptive diagnosis. He did not inquire about what was going on in Mr. A’s mind and thus could not make a dynamic diagnosis (that is, a diagnosis of a patient’s central emotional conflicts, ability to function in relation to other people, strengths, and weaknesses). Mr. A, like many adolescents, had a lot of anxiety and guilt about sexual and romantic involvement, and potential success. He defended against his anxiety and guilt by assuring himself life would never work out for him. When the girl he admired rebuffed him, he immediately concluded this would perpetually be his fate, so the girl’s refusal was particularly painful. Mr. A feels that had this dynamic been discussed with him at the time, he may well not have needed medication at all.
Ms. B, like Mr. A, was prescribed antidepressants for depressive reactions to early romantic disappointments. Likewise, she self-punitively convinced herself, despite easily attracting men’s attentions, that these disappointments meant a lifetime alone. Ms. B has a family history of depression (although neither of her brothers struggles with it), and she felt that she needed the medications to help negotiate difficult periods. But should she have been on them for extended periods of time? Therapeutic attention to her emotional conflicts helped her to form lasting relationships, marry, and have children. Unable to get off the medications, she had to deal with the risks of their use during pregnancy, which she then subjected to the same sort of guilty self-accusations as she previously had used to limit her romantic prospects.
Ms. C came to me on three medications – one for each of her significant romantic break-ups. She, too, was depressively self-diminishing, beginning therapy by letting me know all the things she could think of that might make me think less of her. Understanding some of the reasons for her self-deprecation helped her toward better romantic relationships but did not give her the courage to get off her medications. Pregnancy, however, led her to promptly and successfully discontinue an antidepressant and a mood stabilizer (she has never had any symptoms suggestive of manic depression). She remained on a low dose of a selective serotonin reuptake inhibitor, had an uneventful pregnancy, and then fell in love with a charming baby.
Principles for consideration
• Psychiatrists (and other mental health professionals and primary care physicians treating mental illness) should always make a dynamic, and not merely a descriptive, diagnosis. Even with a more clearly biologically driven problem, such as bipolar disorder, the patient’s personality and conflicts matter.
• Psychiatrists should be very judicious about prescribing medications in adolescence and young adulthood, especially for difficulties adapting to the typical events of those phases of life. Expert psychotherapy should be the first choice in these instances.
• Medication, when necessary, should be prescribed for as limited a time as possible. It is important for young people to advance their own development, not feel needlessly beholden to medications, not get iatrogenically dependent on them, and not feel that they have “diseases” they don’t have.
Amphetamines for misdiagnosed ADHD
When Ms. D’s family moved to a new house, she, her brother, and her sister, each attended a new school. Unlike her siblings, Ms. D, who was in high school, had a difficult adjustment. Her grades fell. She was taken to a psychiatrist who diagnosed ADHD and prescribed amphetamines. The psychiatrist paid little attention to her prior lack of difficulty in school or her struggles making new friends. Nor did the psychiatrist learn that Ms. D had to ward off the seductive advances of an older teacher (although Ms. D would likely not have been immediately forthcoming about this at the time).
When Ms. D came to me as a college student, for troubles with anger, anxiety, and some depression, she was religiously taking 70 mg of amphetamines daily. After I learned a bit about her and raised the question of whether she actually had ADHD, and whether it might make sense to consider tapering the amphetamines, she was appalled and looked like a toddler who was afraid I was about to steal her candy. Helping her to get off the unneeded medication was a multiyear process.
First, she had to recognize that it was prescribed to treat a problem she probably didn’t have, and second, that it was failing to help her with the problems she did have. As we attended to some of her actual emotional conflicts, she became willing to experiment with lower doses. She was able to see that her work was little changed as the dose was lowered, and that her difficulties with school had more to do with feelings toward classmates and teachers than with the presence or absence of amphetamines. After a protracted struggle, finally off the medication, she felt in charge of her life and no longer believed there was something inherently wrong with her mind or her brain.
Mr. E was the only son in a high-powered academic family. His older sisters were all intellectual standouts. Early in high school, he received his first B as a grade in a course. He was taken to a pediatrician, diagnosed with ADHD, and put on stimulants. Like Ms. D, he came to believe that he needed them. In college, he began to develop some magical aspects to his thinking, a potential side effect of the stimulants. It was very difficult to help him see either that he had a problem with his thinking or that it might be attributable to the medication.
Principles to consider
• If the ADHD wasn’t there in elementary school or before, it is unlikely that an adolescent or young adult has new-onset ADHD. A new or newly amplified conflict is occurring in the person’s mind and life A dynamic diagnosis, as always, is essential.
• When medication is prescribed for actual ADHD, as with anything else, the question of how long it will be taken must be asked. For life? Until other means of adaptation are accomplished? Until adequate outcome studies of long-term use of the medication are performed?
Helping patients to get off unneeded, or no longer needed, medications can be a difficult task. Their emotional attachments to the medications can be intense and varied. For some, the prescription is a sign of being loved and cared for. For others, it represents a certification of a deficit, appeases guilt about success, and/or attests to the need for special consideration. Insofar as the medication has been helpful, it may have come to be regarded as a dearly loved friend, or even a part of the self.
When medication has been helpful, there is also, of course, concern about the potential return of the difficulties for which it was prescribed. Few patients are told at the time of first prescription that there is potential risk of habituation and return of, or potential exaggeration of, symptoms with discontinuation. This type of discussion is more difficult to have in situations in which a prescription is urgently needed and the patient is reluctant, but is still not often done in those instances in which a prescription is more optional than essential. The picture is seldom simple.
These few comments only scratch the surface of the difficulties doctors and patients face in helping patients to discontinue their medications. Residency programs pay a lot of attention to helping trainees learn to prescribe medications; rarely do they sufficiently educate residents how to help patients discontinue them. The fact that so many residencies currently pay limited attention to interventions apart from medication contributes further to the difficulty.
Medications have saved the life of many a psychiatric patient. Some patients need medication for life. But some end up on medication for life, even in some instances when the medication may not have been needed in the first place. Although it is often a difficult task, we need to do a better job of distinguishing which patients are which.
Dr. Blum is a psychiatrist and psychoanalyst in private practice in Philadelphia. He teaches in the departments of anthropology and psychiatry at the University of Pennsylvania and at the Psychoanalytic Center of Philadelphia.
Some areas of psychiatry would benefit from more controversy. One of them is the prescription of antidepressants to young people dealing with romantic disappointments.
I have seen many young men and women given an antidepressant for the very painful, but ordinary, romantic break-ups characteristic of this phase of life, who then become habituated to the drug. They take the medication indefinitely, their brains accommodate neurophysiologically to the presence of the chemical, and they become unable to discontinue it without intolerable withdrawal symptoms that look like an underlying illness. A parallel phenomenon occurs not infrequently with the use of amphetamines (and other stimulants) for attention-deficit hyperactivity disorder that is at times mistakenly diagnosed in this age group.
Antidepressants for early romantic disappointments
Mr. A, now in his 30s, became sullen and withdrawn at age 16 after a girl refused his romantic approaches. His well-intentioned parents took him to a psychiatrist, who, after a brief evaluation, prescribed fluoxetine. Mr. A is now well adjusted and happily married but unable to get off fluoxetine. Even when it is carefully tapered, 2 or 3 months after it is discontinued, he becomes anxious and depressed. This is an iatrogenic problem. It is not related to goings-on in his mind or his life; rather it is the result of his brain’s accommodation to a medication, producing a serious withdrawal syndrome.
His original psychiatrist made only a descriptive diagnosis. He did not inquire about what was going on in Mr. A’s mind and thus could not make a dynamic diagnosis (that is, a diagnosis of a patient’s central emotional conflicts, ability to function in relation to other people, strengths, and weaknesses). Mr. A, like many adolescents, had a lot of anxiety and guilt about sexual and romantic involvement, and potential success. He defended against his anxiety and guilt by assuring himself life would never work out for him. When the girl he admired rebuffed him, he immediately concluded this would perpetually be his fate, so the girl’s refusal was particularly painful. Mr. A feels that had this dynamic been discussed with him at the time, he may well not have needed medication at all.
Ms. B, like Mr. A, was prescribed antidepressants for depressive reactions to early romantic disappointments. Likewise, she self-punitively convinced herself, despite easily attracting men’s attentions, that these disappointments meant a lifetime alone. Ms. B has a family history of depression (although neither of her brothers struggles with it), and she felt that she needed the medications to help negotiate difficult periods. But should she have been on them for extended periods of time? Therapeutic attention to her emotional conflicts helped her to form lasting relationships, marry, and have children. Unable to get off the medications, she had to deal with the risks of their use during pregnancy, which she then subjected to the same sort of guilty self-accusations as she previously had used to limit her romantic prospects.
Ms. C came to me on three medications – one for each of her significant romantic break-ups. She, too, was depressively self-diminishing, beginning therapy by letting me know all the things she could think of that might make me think less of her. Understanding some of the reasons for her self-deprecation helped her toward better romantic relationships but did not give her the courage to get off her medications. Pregnancy, however, led her to promptly and successfully discontinue an antidepressant and a mood stabilizer (she has never had any symptoms suggestive of manic depression). She remained on a low dose of a selective serotonin reuptake inhibitor, had an uneventful pregnancy, and then fell in love with a charming baby.
Principles for consideration
• Psychiatrists (and other mental health professionals and primary care physicians treating mental illness) should always make a dynamic, and not merely a descriptive, diagnosis. Even with a more clearly biologically driven problem, such as bipolar disorder, the patient’s personality and conflicts matter.
• Psychiatrists should be very judicious about prescribing medications in adolescence and young adulthood, especially for difficulties adapting to the typical events of those phases of life. Expert psychotherapy should be the first choice in these instances.
• Medication, when necessary, should be prescribed for as limited a time as possible. It is important for young people to advance their own development, not feel needlessly beholden to medications, not get iatrogenically dependent on them, and not feel that they have “diseases” they don’t have.
Amphetamines for misdiagnosed ADHD
When Ms. D’s family moved to a new house, she, her brother, and her sister, each attended a new school. Unlike her siblings, Ms. D, who was in high school, had a difficult adjustment. Her grades fell. She was taken to a psychiatrist who diagnosed ADHD and prescribed amphetamines. The psychiatrist paid little attention to her prior lack of difficulty in school or her struggles making new friends. Nor did the psychiatrist learn that Ms. D had to ward off the seductive advances of an older teacher (although Ms. D would likely not have been immediately forthcoming about this at the time).
When Ms. D came to me as a college student, for troubles with anger, anxiety, and some depression, she was religiously taking 70 mg of amphetamines daily. After I learned a bit about her and raised the question of whether she actually had ADHD, and whether it might make sense to consider tapering the amphetamines, she was appalled and looked like a toddler who was afraid I was about to steal her candy. Helping her to get off the unneeded medication was a multiyear process.
First, she had to recognize that it was prescribed to treat a problem she probably didn’t have, and second, that it was failing to help her with the problems she did have. As we attended to some of her actual emotional conflicts, she became willing to experiment with lower doses. She was able to see that her work was little changed as the dose was lowered, and that her difficulties with school had more to do with feelings toward classmates and teachers than with the presence or absence of amphetamines. After a protracted struggle, finally off the medication, she felt in charge of her life and no longer believed there was something inherently wrong with her mind or her brain.
Mr. E was the only son in a high-powered academic family. His older sisters were all intellectual standouts. Early in high school, he received his first B as a grade in a course. He was taken to a pediatrician, diagnosed with ADHD, and put on stimulants. Like Ms. D, he came to believe that he needed them. In college, he began to develop some magical aspects to his thinking, a potential side effect of the stimulants. It was very difficult to help him see either that he had a problem with his thinking or that it might be attributable to the medication.
Principles to consider
• If the ADHD wasn’t there in elementary school or before, it is unlikely that an adolescent or young adult has new-onset ADHD. A new or newly amplified conflict is occurring in the person’s mind and life A dynamic diagnosis, as always, is essential.
• When medication is prescribed for actual ADHD, as with anything else, the question of how long it will be taken must be asked. For life? Until other means of adaptation are accomplished? Until adequate outcome studies of long-term use of the medication are performed?
Helping patients to get off unneeded, or no longer needed, medications can be a difficult task. Their emotional attachments to the medications can be intense and varied. For some, the prescription is a sign of being loved and cared for. For others, it represents a certification of a deficit, appeases guilt about success, and/or attests to the need for special consideration. Insofar as the medication has been helpful, it may have come to be regarded as a dearly loved friend, or even a part of the self.
When medication has been helpful, there is also, of course, concern about the potential return of the difficulties for which it was prescribed. Few patients are told at the time of first prescription that there is potential risk of habituation and return of, or potential exaggeration of, symptoms with discontinuation. This type of discussion is more difficult to have in situations in which a prescription is urgently needed and the patient is reluctant, but is still not often done in those instances in which a prescription is more optional than essential. The picture is seldom simple.
These few comments only scratch the surface of the difficulties doctors and patients face in helping patients to discontinue their medications. Residency programs pay a lot of attention to helping trainees learn to prescribe medications; rarely do they sufficiently educate residents how to help patients discontinue them. The fact that so many residencies currently pay limited attention to interventions apart from medication contributes further to the difficulty.
Medications have saved the life of many a psychiatric patient. Some patients need medication for life. But some end up on medication for life, even in some instances when the medication may not have been needed in the first place. Although it is often a difficult task, we need to do a better job of distinguishing which patients are which.
Dr. Blum is a psychiatrist and psychoanalyst in private practice in Philadelphia. He teaches in the departments of anthropology and psychiatry at the University of Pennsylvania and at the Psychoanalytic Center of Philadelphia.
Aortic repair in Loeys-Dietz syndrome requires close follow-up
The knowledge about Loeys-Dietz syndrome has evolved quickly since Hal Dietz, MD, and Bart Loeys, MD, at Johns Hopkins University, Baltimore, first reported on it in 2005. Now, another team of Johns Hopkins investigators have reported that an aggressive approach with aortic root replacement coupled with valve-sparing whenever possible produces favorable results, but that clinicians must follow these patients closely with cardiovascular imaging.
“Growing experience with Loeys-Dietz syndrome has confirmed early impressions of its aggressive nature and proclivity toward aortic catastrophe,” Nishant D. Patel, MD, and his coauthors said in the February issue of the Journal of Thoracic and Cardiovascular Surgery (2017;153:406-12). They reported on results of all 79 patients with Loeys-Dietz syndrome (LDS) who had cardiovascular surgery at Johns Hopkins. There were two (3%) deaths during surgery and eight (10%) late deaths.
Patients with LDS are at risk for dissection early when the aortic root reaches 4 cm. Despite what they termed “favorable” outcomes of surgery, Dr. Patel and his coauthors acknowledged that reintervention rates for this population are high – 19 patients (24%) had subsequent operations. That suggests cardiac surgeons must closely monitor these patients. “Meticulous follow-up with cardiovascular surveillance imaging remains important for management, particularly as clinical LDS subtypes are characterized and more tailored treatment is developed,” Dr. Patel and his coauthors reported.
They advise echocardiography every 3 to 6 months for the first year after surgery and then every 6 to 12 months afterward. Full-body imaging should occur at least every 2 years.
“In particular, patients with type B dissections should be monitored aggressively for aneurysm growth,” Dr. Patel and his coauthors said. They recommend imaging at seven to 14 days after dissection, then repeat imaging at 1, 3, 6, and 12 months, and then yearly thereafter.
They noted that four LDS subtypes have been identified. Although those with LDS1 and 2 subtypes are prone to aortic rupture at an earlier age and at smaller aortic diameters than other connective tissue disorders, the medical and surgical management for all subtypes are similar, Dr. Patel and his coauthors indicated.
“Certain congenital heart defects are more common among patients with LDS, compared with the normal population, including patent ductus arteriosus and mitral valve prolapse/insufficiency,” they said. Genotype is one factor that determines the need for surgery in LDS patients, Dr. Patel and his coauthors said. Others are growth rate, aortic valve function, family history, and severity of noncardiac phenotype.
The 79 patients in the study were divided almost evenly between gender, and the average age at first operation was 24.9 years; 38 were children younger than 18 years and 20 had a previous sternotomy.
Aortic root replacement represented the predominant operation in the group, accounting for 65 operations (82.3%), of which 52 (80%) were valve-sparing procedures and the remainder were composite valve-graft procedures. The other procedures the researchers performed were nine aortic arch replacements (11.4%), three open thoracoabdominal repairs (3.8%) and two ascending aorta replacements (2.5%).
“Valve-sparing root replacement has become a safe and reliable option for appropriately selected younger patients with LDS,” Dr. Patel and his coauthors wrote. Five patients needed a second operation on the aortic valve or root; three of them had a Florida sleeve procedure. “Based on these initial outcomes with the Florida sleeve at our institution, we have abandoned this procedure in favor of conventional valve-sparing root replacement,” Dr. Patel and his coauthors stated.
Dr. Patel and his coauthors had no financial relationships to disclose.
This report by Dr. Patel and his coauthors confirms the need for close surveillance of individuals with Loeys-Dietz syndrome who have had aortic operations, John S. Ikonomidis, MD, PhD, of the Medical University of South Carolina, Charleston, said in his invited commentary (J Thorac Cardiovasc Surg. 2017;153:413-4).
Dr. Ikonomidis noted this study is important because of its population size. “This is probably the largest single-center surgical report of this kind in the world,” he said.
The study highlighted a number of issues germane to LDS patients who have cardiovascular surgery, among them a critical need for genetic testing to help cardiac surgeons determine the disease genotype and what operation to perform, Dr. Ikonomidis said.
But Dr. Ikonomidis also pointed out the variation in aortic root size in the study patients. The smallest root in the series was 2 cm and 21 of 65 patients with a maximum root diameter smaller than 4 cm had root surgery. “This is a testament to the fact that surgical decision making in this population is dependent not just on the known genotype and aortic dimensions, but also on the rate of growth, aortic valve function, severity of noncardiac phenotype, and family history,” Dr. Ikonomidis said.
Dr. Ikonomidis had no financial relationships to disclose.
This report by Dr. Patel and his coauthors confirms the need for close surveillance of individuals with Loeys-Dietz syndrome who have had aortic operations, John S. Ikonomidis, MD, PhD, of the Medical University of South Carolina, Charleston, said in his invited commentary (J Thorac Cardiovasc Surg. 2017;153:413-4).
Dr. Ikonomidis noted this study is important because of its population size. “This is probably the largest single-center surgical report of this kind in the world,” he said.
The study highlighted a number of issues germane to LDS patients who have cardiovascular surgery, among them a critical need for genetic testing to help cardiac surgeons determine the disease genotype and what operation to perform, Dr. Ikonomidis said.
But Dr. Ikonomidis also pointed out the variation in aortic root size in the study patients. The smallest root in the series was 2 cm and 21 of 65 patients with a maximum root diameter smaller than 4 cm had root surgery. “This is a testament to the fact that surgical decision making in this population is dependent not just on the known genotype and aortic dimensions, but also on the rate of growth, aortic valve function, severity of noncardiac phenotype, and family history,” Dr. Ikonomidis said.
Dr. Ikonomidis had no financial relationships to disclose.
This report by Dr. Patel and his coauthors confirms the need for close surveillance of individuals with Loeys-Dietz syndrome who have had aortic operations, John S. Ikonomidis, MD, PhD, of the Medical University of South Carolina, Charleston, said in his invited commentary (J Thorac Cardiovasc Surg. 2017;153:413-4).
Dr. Ikonomidis noted this study is important because of its population size. “This is probably the largest single-center surgical report of this kind in the world,” he said.
The study highlighted a number of issues germane to LDS patients who have cardiovascular surgery, among them a critical need for genetic testing to help cardiac surgeons determine the disease genotype and what operation to perform, Dr. Ikonomidis said.
But Dr. Ikonomidis also pointed out the variation in aortic root size in the study patients. The smallest root in the series was 2 cm and 21 of 65 patients with a maximum root diameter smaller than 4 cm had root surgery. “This is a testament to the fact that surgical decision making in this population is dependent not just on the known genotype and aortic dimensions, but also on the rate of growth, aortic valve function, severity of noncardiac phenotype, and family history,” Dr. Ikonomidis said.
Dr. Ikonomidis had no financial relationships to disclose.
The knowledge about Loeys-Dietz syndrome has evolved quickly since Hal Dietz, MD, and Bart Loeys, MD, at Johns Hopkins University, Baltimore, first reported on it in 2005. Now, another team of Johns Hopkins investigators have reported that an aggressive approach with aortic root replacement coupled with valve-sparing whenever possible produces favorable results, but that clinicians must follow these patients closely with cardiovascular imaging.
“Growing experience with Loeys-Dietz syndrome has confirmed early impressions of its aggressive nature and proclivity toward aortic catastrophe,” Nishant D. Patel, MD, and his coauthors said in the February issue of the Journal of Thoracic and Cardiovascular Surgery (2017;153:406-12). They reported on results of all 79 patients with Loeys-Dietz syndrome (LDS) who had cardiovascular surgery at Johns Hopkins. There were two (3%) deaths during surgery and eight (10%) late deaths.
Patients with LDS are at risk for dissection early when the aortic root reaches 4 cm. Despite what they termed “favorable” outcomes of surgery, Dr. Patel and his coauthors acknowledged that reintervention rates for this population are high – 19 patients (24%) had subsequent operations. That suggests cardiac surgeons must closely monitor these patients. “Meticulous follow-up with cardiovascular surveillance imaging remains important for management, particularly as clinical LDS subtypes are characterized and more tailored treatment is developed,” Dr. Patel and his coauthors reported.
They advise echocardiography every 3 to 6 months for the first year after surgery and then every 6 to 12 months afterward. Full-body imaging should occur at least every 2 years.
“In particular, patients with type B dissections should be monitored aggressively for aneurysm growth,” Dr. Patel and his coauthors said. They recommend imaging at seven to 14 days after dissection, then repeat imaging at 1, 3, 6, and 12 months, and then yearly thereafter.
They noted that four LDS subtypes have been identified. Although those with LDS1 and 2 subtypes are prone to aortic rupture at an earlier age and at smaller aortic diameters than other connective tissue disorders, the medical and surgical management for all subtypes are similar, Dr. Patel and his coauthors indicated.
“Certain congenital heart defects are more common among patients with LDS, compared with the normal population, including patent ductus arteriosus and mitral valve prolapse/insufficiency,” they said. Genotype is one factor that determines the need for surgery in LDS patients, Dr. Patel and his coauthors said. Others are growth rate, aortic valve function, family history, and severity of noncardiac phenotype.
The 79 patients in the study were divided almost evenly between gender, and the average age at first operation was 24.9 years; 38 were children younger than 18 years and 20 had a previous sternotomy.
Aortic root replacement represented the predominant operation in the group, accounting for 65 operations (82.3%), of which 52 (80%) were valve-sparing procedures and the remainder were composite valve-graft procedures. The other procedures the researchers performed were nine aortic arch replacements (11.4%), three open thoracoabdominal repairs (3.8%) and two ascending aorta replacements (2.5%).
“Valve-sparing root replacement has become a safe and reliable option for appropriately selected younger patients with LDS,” Dr. Patel and his coauthors wrote. Five patients needed a second operation on the aortic valve or root; three of them had a Florida sleeve procedure. “Based on these initial outcomes with the Florida sleeve at our institution, we have abandoned this procedure in favor of conventional valve-sparing root replacement,” Dr. Patel and his coauthors stated.
Dr. Patel and his coauthors had no financial relationships to disclose.
The knowledge about Loeys-Dietz syndrome has evolved quickly since Hal Dietz, MD, and Bart Loeys, MD, at Johns Hopkins University, Baltimore, first reported on it in 2005. Now, another team of Johns Hopkins investigators have reported that an aggressive approach with aortic root replacement coupled with valve-sparing whenever possible produces favorable results, but that clinicians must follow these patients closely with cardiovascular imaging.
“Growing experience with Loeys-Dietz syndrome has confirmed early impressions of its aggressive nature and proclivity toward aortic catastrophe,” Nishant D. Patel, MD, and his coauthors said in the February issue of the Journal of Thoracic and Cardiovascular Surgery (2017;153:406-12). They reported on results of all 79 patients with Loeys-Dietz syndrome (LDS) who had cardiovascular surgery at Johns Hopkins. There were two (3%) deaths during surgery and eight (10%) late deaths.
Patients with LDS are at risk for dissection early when the aortic root reaches 4 cm. Despite what they termed “favorable” outcomes of surgery, Dr. Patel and his coauthors acknowledged that reintervention rates for this population are high – 19 patients (24%) had subsequent operations. That suggests cardiac surgeons must closely monitor these patients. “Meticulous follow-up with cardiovascular surveillance imaging remains important for management, particularly as clinical LDS subtypes are characterized and more tailored treatment is developed,” Dr. Patel and his coauthors reported.
They advise echocardiography every 3 to 6 months for the first year after surgery and then every 6 to 12 months afterward. Full-body imaging should occur at least every 2 years.
“In particular, patients with type B dissections should be monitored aggressively for aneurysm growth,” Dr. Patel and his coauthors said. They recommend imaging at seven to 14 days after dissection, then repeat imaging at 1, 3, 6, and 12 months, and then yearly thereafter.
They noted that four LDS subtypes have been identified. Although those with LDS1 and 2 subtypes are prone to aortic rupture at an earlier age and at smaller aortic diameters than other connective tissue disorders, the medical and surgical management for all subtypes are similar, Dr. Patel and his coauthors indicated.
“Certain congenital heart defects are more common among patients with LDS, compared with the normal population, including patent ductus arteriosus and mitral valve prolapse/insufficiency,” they said. Genotype is one factor that determines the need for surgery in LDS patients, Dr. Patel and his coauthors said. Others are growth rate, aortic valve function, family history, and severity of noncardiac phenotype.
The 79 patients in the study were divided almost evenly between gender, and the average age at first operation was 24.9 years; 38 were children younger than 18 years and 20 had a previous sternotomy.
Aortic root replacement represented the predominant operation in the group, accounting for 65 operations (82.3%), of which 52 (80%) were valve-sparing procedures and the remainder were composite valve-graft procedures. The other procedures the researchers performed were nine aortic arch replacements (11.4%), three open thoracoabdominal repairs (3.8%) and two ascending aorta replacements (2.5%).
“Valve-sparing root replacement has become a safe and reliable option for appropriately selected younger patients with LDS,” Dr. Patel and his coauthors wrote. Five patients needed a second operation on the aortic valve or root; three of them had a Florida sleeve procedure. “Based on these initial outcomes with the Florida sleeve at our institution, we have abandoned this procedure in favor of conventional valve-sparing root replacement,” Dr. Patel and his coauthors stated.
Dr. Patel and his coauthors had no financial relationships to disclose.
Key clinical point: Outcomes for aortic surgery in Loeys-Dietz syndrome are favorable, but reintervention rates are high.
Major finding: Patients require close postoperative follow-up with cardiovascular imaging.
Data source: Retrospective review of 79 patients who had cardiovascular surgery for LDS over 26 years at Johns Hopkins University.
Disclosure: Dr. Patel and his coauthors reported having no relevant financial disclosures.
CDC: More preterm births after fertility treatments
Infants conceived through assisted reproductive technology (ART) represented less than 2% of all children born in the United States in 2014, but they experienced disproportionately large shares of adverse perinatal outcomes, according to the Centers for Disease Control and Prevention.
Of the 4.02 million children born in the United States in 2014, a total of 65,296 (1.6%) were conceived with ART procedures. ART-conceived children, however, represented 5.5% of all low-birth-weight infants (less than 2,500 g) and 5.6% of all very-low-birth-weight infants (less than 1,500 g). ART-conceived children also represented 4.7% of all preterm births (less than 37 weeks) in 2014 and 5.0% of all very preterm (less than 32 weeks) infants nationally, the CDC reported (MMWR Surveill Summ. 2017;66[SS-6]:1-24).
These poor outcomes are related, at least in part, to the effect of infertility treatment on multiple births. The percentage of triplets or higher-order infants among ART-conceived infants has decreased since 2000, but “the percentage of twin infants has remained persistently high,” the CDC noted. Multiple-birth infants represent 39.4% of all ART infants but only 3.5% of all infants, and ART-conceived multiple-birth infants represent 18.3% of all multiple-birth infants, the CDC said.
The multiple-birth effect varied considerably by state, however. In Hawaii, ART-conceived multiple-birth infants accounted for 37.3% of all multiple births in 2014, while Alaska and West Virginia both had rates of 5.5%. Poor outcomes also varied by state: In Massachusetts, ART infants represented 14.2% of all low-birth-weight infants, compared with 1.2% in West Virginia. Massachusetts had the highest rate of ART preterm infants to all infants, 13.4%, and Puerto Rico had the lowest, 1.2%, according to the CDC report, which was based on data from the National ART Surveillance System.
Puerto Rico’s rate of 364 ART procedures per 1 million women aged 15-44 years was the lowest in the country, and the highest rate belonged to Massachusetts at 6,726 per 1 million women aged 15-44 years.
Infants conceived through assisted reproductive technology (ART) represented less than 2% of all children born in the United States in 2014, but they experienced disproportionately large shares of adverse perinatal outcomes, according to the Centers for Disease Control and Prevention.
Of the 4.02 million children born in the United States in 2014, a total of 65,296 (1.6%) were conceived with ART procedures. ART-conceived children, however, represented 5.5% of all low-birth-weight infants (less than 2,500 g) and 5.6% of all very-low-birth-weight infants (less than 1,500 g). ART-conceived children also represented 4.7% of all preterm births (less than 37 weeks) in 2014 and 5.0% of all very preterm (less than 32 weeks) infants nationally, the CDC reported (MMWR Surveill Summ. 2017;66[SS-6]:1-24).
These poor outcomes are related, at least in part, to the effect of infertility treatment on multiple births. The percentage of triplets or higher-order infants among ART-conceived infants has decreased since 2000, but “the percentage of twin infants has remained persistently high,” the CDC noted. Multiple-birth infants represent 39.4% of all ART infants but only 3.5% of all infants, and ART-conceived multiple-birth infants represent 18.3% of all multiple-birth infants, the CDC said.
The multiple-birth effect varied considerably by state, however. In Hawaii, ART-conceived multiple-birth infants accounted for 37.3% of all multiple births in 2014, while Alaska and West Virginia both had rates of 5.5%. Poor outcomes also varied by state: In Massachusetts, ART infants represented 14.2% of all low-birth-weight infants, compared with 1.2% in West Virginia. Massachusetts had the highest rate of ART preterm infants to all infants, 13.4%, and Puerto Rico had the lowest, 1.2%, according to the CDC report, which was based on data from the National ART Surveillance System.
Puerto Rico’s rate of 364 ART procedures per 1 million women aged 15-44 years was the lowest in the country, and the highest rate belonged to Massachusetts at 6,726 per 1 million women aged 15-44 years.
Infants conceived through assisted reproductive technology (ART) represented less than 2% of all children born in the United States in 2014, but they experienced disproportionately large shares of adverse perinatal outcomes, according to the Centers for Disease Control and Prevention.
Of the 4.02 million children born in the United States in 2014, a total of 65,296 (1.6%) were conceived with ART procedures. ART-conceived children, however, represented 5.5% of all low-birth-weight infants (less than 2,500 g) and 5.6% of all very-low-birth-weight infants (less than 1,500 g). ART-conceived children also represented 4.7% of all preterm births (less than 37 weeks) in 2014 and 5.0% of all very preterm (less than 32 weeks) infants nationally, the CDC reported (MMWR Surveill Summ. 2017;66[SS-6]:1-24).
These poor outcomes are related, at least in part, to the effect of infertility treatment on multiple births. The percentage of triplets or higher-order infants among ART-conceived infants has decreased since 2000, but “the percentage of twin infants has remained persistently high,” the CDC noted. Multiple-birth infants represent 39.4% of all ART infants but only 3.5% of all infants, and ART-conceived multiple-birth infants represent 18.3% of all multiple-birth infants, the CDC said.
The multiple-birth effect varied considerably by state, however. In Hawaii, ART-conceived multiple-birth infants accounted for 37.3% of all multiple births in 2014, while Alaska and West Virginia both had rates of 5.5%. Poor outcomes also varied by state: In Massachusetts, ART infants represented 14.2% of all low-birth-weight infants, compared with 1.2% in West Virginia. Massachusetts had the highest rate of ART preterm infants to all infants, 13.4%, and Puerto Rico had the lowest, 1.2%, according to the CDC report, which was based on data from the National ART Surveillance System.
Puerto Rico’s rate of 364 ART procedures per 1 million women aged 15-44 years was the lowest in the country, and the highest rate belonged to Massachusetts at 6,726 per 1 million women aged 15-44 years.
FROM MMWR SURVEILLANCE SUMMARIES
Steroid use in adolescents
Anabolic androgenic steroid (AAS) use in athletes is not a new topic. In fact, many teens can relate a story involving a famous athlete and use of a performance-enhancing drug and the consequences associated with it. Although published data do not support a significant increase in use of performance-enhancing drugs among adolescents,1 more recent studies show that anabolic steroids are being found in nonprescription supplements, and their use among adolescents may be substantially underestimated.
Supplements are not regulated by the Food and Drug Administration, so many of these products are easily found on the Internet and sold in local stores.2,3 Some of these are marketed for increasing muscle mass, strength, and performance, which is appealing to the young athlete. Much of the marketing of these products minimize the side effects associated with their use and, therefore, most users are unaware of their harmful effects.

Approximately 5%-11% of teen athletes use AAS to improve physique and performance.3 Given its promotion for improved physique, many nonathletes also are turning to AAS for weight loss in both males and females. Side effects of steroid use are extrapolated from the data of therapeutic use, but most adolescents using steroids are not using under medical supervision. The dosing for building muscle mass uses a pyramid type dosing over a 6- to 12-week period and can be up to forty times the therapeutic dosing; therefore, the side effects can be greater than reported.4,5 Common side effects of AAS are hypogonadism, gynecomastia, decreased sperm count and infertility, acne, and aggressiveness. Liver tumors and psychosis have been reported, and increased depressed mood have been identified with discontinuation of use.4,6 Studies suggest that these side effects are reversible with discontinuation, but more studies are needed.4,6
Given that many of the side effects are not identifiable on physical exam, pediatricians must be proactive in questioning adolescents about their knowledge and use of AAS. Testing for steroid use is difficult and not very sensitive. Urine test for carbon isotopes 13/12 is the most common test, but if not done within hours of ingestion it will not be detected. T/E test (testosterone/epitestosterone glucuronide) is another test, but also limited by the timing of the test.6 Home screening also is available but the American Academy of Pediatrics 2014 guidelines warns against parents using these given the high false positive rate and risk of confrontation.7
Home and school screening may function more to deter athletes from using steroids to avoid consequences of being caught more than actually identifying use. If an athlete is suspected of using steroids, a test should be done. If negative, it should be repeated another time, as repeated testing is more likely to identify use. Studies have shown a correlation between steroid use and use of other illicit drugs so further screening should be done to identify if other drugs are being used.8
Widespread screening has not been shown to be cost effective and, therefore, should not be encouraged. Educating the patient on the risk of use and potential side effects along with healthy alternatives that improve performance and physique is much more effective.9 Being observant to signs and symptoms of AAS use helps to initiate conversation on the risk of using anabolic steroids.
References
1. Arch Pediatr Adolesc Med. 1997 Dec;151(12):1197-206.
2. Subst Use Misuse. 2012 Feb; 47(3):329-41.
3. Am J Clin Nutr. 2000 Feb;71(2):399-400.
4. J Sports Sci Med. 2006 Jun 1;5(2):182-93.
5. Br J Sports Med. 2006 Jul; 40(Suppl 1): i21-24.
6. J Athl Train. 1994 Mar; 29(1):60-4.
7. Pediatrics. 2014;133:e1798-1807.
8. Pediatrics. 1995 Jul;96(1 Pt 1):23-8.
9. Pediatrics. 1997 Jun;99(6):904-8.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Anabolic androgenic steroid (AAS) use in athletes is not a new topic. In fact, many teens can relate a story involving a famous athlete and use of a performance-enhancing drug and the consequences associated with it. Although published data do not support a significant increase in use of performance-enhancing drugs among adolescents,1 more recent studies show that anabolic steroids are being found in nonprescription supplements, and their use among adolescents may be substantially underestimated.
Supplements are not regulated by the Food and Drug Administration, so many of these products are easily found on the Internet and sold in local stores.2,3 Some of these are marketed for increasing muscle mass, strength, and performance, which is appealing to the young athlete. Much of the marketing of these products minimize the side effects associated with their use and, therefore, most users are unaware of their harmful effects.
Approximately 5%-11% of teen athletes use AAS to improve physique and performance.3 Given its promotion for improved physique, many nonathletes also are turning to AAS for weight loss in both males and females. Side effects of steroid use are extrapolated from the data of therapeutic use, but most adolescents using steroids are not using under medical supervision. The dosing for building muscle mass uses a pyramid type dosing over a 6- to 12-week period and can be up to forty times the therapeutic dosing; therefore, the side effects can be greater than reported.4,5 Common side effects of AAS are hypogonadism, gynecomastia, decreased sperm count and infertility, acne, and aggressiveness. Liver tumors and psychosis have been reported, and increased depressed mood have been identified with discontinuation of use.4,6 Studies suggest that these side effects are reversible with discontinuation, but more studies are needed.4,6
Given that many of the side effects are not identifiable on physical exam, pediatricians must be proactive in questioning adolescents about their knowledge and use of AAS. Testing for steroid use is difficult and not very sensitive. Urine test for carbon isotopes 13/12 is the most common test, but if not done within hours of ingestion it will not be detected. T/E test (testosterone/epitestosterone glucuronide) is another test, but also limited by the timing of the test.6 Home screening also is available but the American Academy of Pediatrics 2014 guidelines warns against parents using these given the high false positive rate and risk of confrontation.7
Home and school screening may function more to deter athletes from using steroids to avoid consequences of being caught more than actually identifying use. If an athlete is suspected of using steroids, a test should be done. If negative, it should be repeated another time, as repeated testing is more likely to identify use. Studies have shown a correlation between steroid use and use of other illicit drugs so further screening should be done to identify if other drugs are being used.8
Widespread screening has not been shown to be cost effective and, therefore, should not be encouraged. Educating the patient on the risk of use and potential side effects along with healthy alternatives that improve performance and physique is much more effective.9 Being observant to signs and symptoms of AAS use helps to initiate conversation on the risk of using anabolic steroids.
References
1. Arch Pediatr Adolesc Med. 1997 Dec;151(12):1197-206.
2. Subst Use Misuse. 2012 Feb; 47(3):329-41.
3. Am J Clin Nutr. 2000 Feb;71(2):399-400.
4. J Sports Sci Med. 2006 Jun 1;5(2):182-93.
5. Br J Sports Med. 2006 Jul; 40(Suppl 1): i21-24.
6. J Athl Train. 1994 Mar; 29(1):60-4.
7. Pediatrics. 2014;133:e1798-1807.
8. Pediatrics. 1995 Jul;96(1 Pt 1):23-8.
9. Pediatrics. 1997 Jun;99(6):904-8.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Anabolic androgenic steroid (AAS) use in athletes is not a new topic. In fact, many teens can relate a story involving a famous athlete and use of a performance-enhancing drug and the consequences associated with it. Although published data do not support a significant increase in use of performance-enhancing drugs among adolescents,1 more recent studies show that anabolic steroids are being found in nonprescription supplements, and their use among adolescents may be substantially underestimated.
Supplements are not regulated by the Food and Drug Administration, so many of these products are easily found on the Internet and sold in local stores.2,3 Some of these are marketed for increasing muscle mass, strength, and performance, which is appealing to the young athlete. Much of the marketing of these products minimize the side effects associated with their use and, therefore, most users are unaware of their harmful effects.
Approximately 5%-11% of teen athletes use AAS to improve physique and performance.3 Given its promotion for improved physique, many nonathletes also are turning to AAS for weight loss in both males and females. Side effects of steroid use are extrapolated from the data of therapeutic use, but most adolescents using steroids are not using under medical supervision. The dosing for building muscle mass uses a pyramid type dosing over a 6- to 12-week period and can be up to forty times the therapeutic dosing; therefore, the side effects can be greater than reported.4,5 Common side effects of AAS are hypogonadism, gynecomastia, decreased sperm count and infertility, acne, and aggressiveness. Liver tumors and psychosis have been reported, and increased depressed mood have been identified with discontinuation of use.4,6 Studies suggest that these side effects are reversible with discontinuation, but more studies are needed.4,6
Given that many of the side effects are not identifiable on physical exam, pediatricians must be proactive in questioning adolescents about their knowledge and use of AAS. Testing for steroid use is difficult and not very sensitive. Urine test for carbon isotopes 13/12 is the most common test, but if not done within hours of ingestion it will not be detected. T/E test (testosterone/epitestosterone glucuronide) is another test, but also limited by the timing of the test.6 Home screening also is available but the American Academy of Pediatrics 2014 guidelines warns against parents using these given the high false positive rate and risk of confrontation.7
Home and school screening may function more to deter athletes from using steroids to avoid consequences of being caught more than actually identifying use. If an athlete is suspected of using steroids, a test should be done. If negative, it should be repeated another time, as repeated testing is more likely to identify use. Studies have shown a correlation between steroid use and use of other illicit drugs so further screening should be done to identify if other drugs are being used.8
Widespread screening has not been shown to be cost effective and, therefore, should not be encouraged. Educating the patient on the risk of use and potential side effects along with healthy alternatives that improve performance and physique is much more effective.9 Being observant to signs and symptoms of AAS use helps to initiate conversation on the risk of using anabolic steroids.
References
1. Arch Pediatr Adolesc Med. 1997 Dec;151(12):1197-206.
2. Subst Use Misuse. 2012 Feb; 47(3):329-41.
3. Am J Clin Nutr. 2000 Feb;71(2):399-400.
4. J Sports Sci Med. 2006 Jun 1;5(2):182-93.
5. Br J Sports Med. 2006 Jul; 40(Suppl 1): i21-24.
6. J Athl Train. 1994 Mar; 29(1):60-4.
7. Pediatrics. 2014;133:e1798-1807.
8. Pediatrics. 1995 Jul;96(1 Pt 1):23-8.
9. Pediatrics. 1997 Jun;99(6):904-8.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.