User login
Sun Protection for Infants: Parent Behaviors and Beliefs in Miami, Florida
Sun exposure and sunburns sustained during childhood are linked to an increased risk for development of skin cancers in adulthood. In infants, the skin is particularly vulnerable and is considered to be at increased risk for UV radiation damage,1 even as early as the first 6 months of life.2 Sun-safe behaviors instituted from a young age may help reduce the risk for future skin cancers.3 To effectively teach parents proper sun-safe practices, it is essential to understand their existing perceptions and behaviors. This study sought to examine differences in infant sun-safety practices during the first 6 months of life among black, Hispanic, and non-Hispanic white (NHW) parents in Miami, Florida.
Methods
Parents presenting to the University of Miami general pediatrics clinic from February 2015 through April 2015 with a child younger than 5 years were administered a 15-item questionnaire that included items on demographics, sun-safety strategies, sunburns and tanning, beliefs and limitations regarding sunscreen, and primary information source regarding sun safety (eg, physician, Internet, media, instincts). Parents were approached by the investigators consecutively for participation in scheduled blocks, with the exception of those who were otherwise engaged in appointment-related tasks (eg, paperwork). The study was approved by the University of Miami Miller School of Medicine institutional review board. The primary objective of this study was to determine the sun protection behaviors that black and Hispanic parents in Miami, Florida, employ in infants younger than 6 months. Secondary objectives included determining if this patient population is at risk for infant sunburns and tanning, beliefs among parents regarding sunscreen's efficacy in the prevention of skin cancers, and limitations of sunscreen use.
All data were analyzed using SAS software version 9.3. Wilcoxon signed rank test, Kruskal-Wallis test, Fisher exact test, and proportional-odds cumulative logit model were used to compare nonparametric data. Parents reporting on the full first 6 months of life (ie, the child was older than 6 months at the time of study completion) were included for analysis of sun-safety strategies. All survey respondents were included for analysis of secondary objectives. Responses from parents of infants of mixed racial and ethnic backgrounds were excluded from applicable subgroup analyses.
Results
Ninety-eight parents were approached for participation in the study; 97 consented to participate and 95 completed the survey. Seventy parents had children who were at least 6 months of age and were included for analysis of the primary objectives (ie, sun-protection strategies in the first 6 months of life). The cohort included 49 Hispanic parents, 26 black parents, and 9 NHW parents; 5 parents indicated their child was of mixed racial and ethnic background. Six respondents indicated another minority group (eg, Native American, Pacific Islander). Eighty-three respondents were mothers, 72 were educated beyond high school, and 14 were Spanish-speaking only. Four reported a known family history of skin cancer.
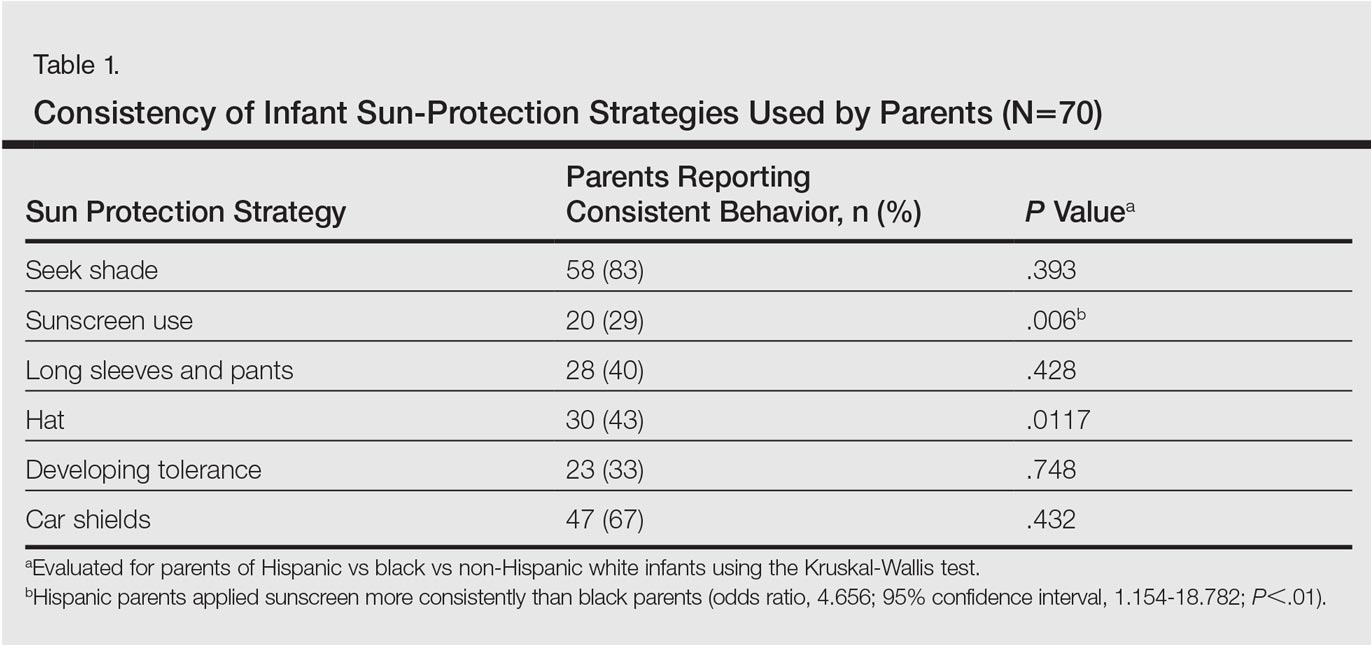
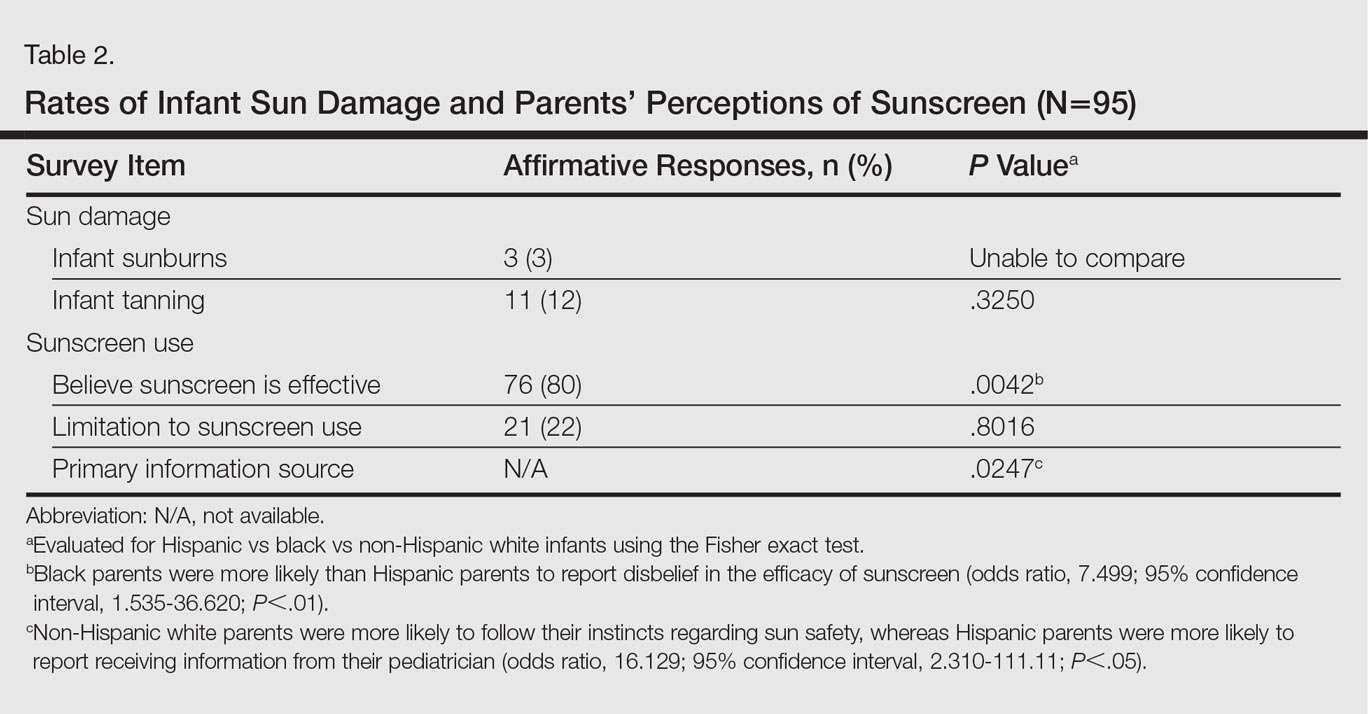
There were notable differences in application of sunscreen, belief in the efficacy of sunscreen, and primary source of information between parents (Tables 1 and 2). Hispanic parents reported applying sunscreen more consistently than black parents (odds ratio, 4.656; 95% confidence interval, 1.154-18.782; P<.01). Hispanic parents also were more likely than black parents to believe sunscreen is effective in the prevention of skin cancers (odds ratio, 7.499; 95% confidence interval, 1.535-36.620; P<.01). Hispanic parents were more likely to report receiving information regarding sun-safety practices for infants from their pediatrician, whereas NHW parents were more likely to follow their instincts regarding how and if infants should be exposed to the sun (P<.05). No significant differences were found in the reported primary source of information in black versus Hispanic parents or in black versus NHW parents. Three percent (3/95) of respondents reported a sunburn in the infant's first 6 months of life, and 12% (11/95) reported tanning of infants' skin from sun exposure. Tanning was associated with inconsistent shade (P<.01), inconsistent clothing coverage (P<.01), and consistently allowing infants to "develop tolerance to the sun's rays by slowly increasing sun exposure each day" (P<.05).
Comment
The survey results indicated suboptimal sun-protection practices among parents of black and Hispanic infants in Miami. Although the majority of respondents (83% [58/70]) reported keeping their infants in the shade, less than half of parents consistently covered their infants adequately with clothing and hats (40% [28/70] and 43% [30/70], respectively). More alarmingly, one-third of parents reported intentionally increasing their infant's level of sun exposure to develop his/her tolerance to the sun. A minority of parents reported sunburns (3%) and tanning (12%) within the first 6 months of life. Twenty-nine percent of parents (20/70) reported consistently applying sunscreen to their infants who were younger than 6 months despite limited safety data available for this age group.
Although our study included a limited sample size and represents a narrow geographic distribution, these results suggest that shortcomings in current practices in sun protection for black and Hispanic infants younger than 6 months may be a widespread problem. Black and Hispanic patients have a lower incidence of skin cancer, but the diagnosis often is delayed and the mortality is higher when skin cancer does occur.4 The common perception among laypeople as well as many health care providers that black and Hispanic individuals are not at risk for skin cancer may limit sun-safety counseling as well as the overall knowledge base of this patient demographic. As demonstrated by the results of this study, there is a need for counseling on sun-safe behaviors from a young age among this population.
Conclusion
This study highlights potential shortcomings in current sun-protection practices for black and Hispanic infants younger than 6 months. Sun-safe behaviors instituted from a young age may help reduce the risk for future skin cancers.3 Additional studies are needed to further define sun-safety behaviors in black and Hispanic children across the United States. Further, additional studies should focus on developing interventions that positively influence sun-safety behaviors in this patient population.
- Paller AS, Hawk JL, Honig P, et al. New insights about infant and toddler skin: implications for sun protection. Pediatrics. 2011;128:92-102.
- Benjes LS, Brooks DR, Zhang Z, et al. Changing patterns of sun protection between the first and second summers for very young children. Arch Dermatol. 2004;140:925-930.
- Oliveria SA, Saraiya M, Geller AC, et al. Sun exposure and risk of melanoma. Arch Dis Child. 2006;91:131-138.
- Wu XC, Eide MJ, King J, et al. Racial and ethnic variations in incidence and survival of cutaneous melanoma in the United States, 1999-2006. J Am Acad Dermatol. 2011;65(5 suppl 1):S26-S37.
Sun exposure and sunburns sustained during childhood are linked to an increased risk for development of skin cancers in adulthood. In infants, the skin is particularly vulnerable and is considered to be at increased risk for UV radiation damage,1 even as early as the first 6 months of life.2 Sun-safe behaviors instituted from a young age may help reduce the risk for future skin cancers.3 To effectively teach parents proper sun-safe practices, it is essential to understand their existing perceptions and behaviors. This study sought to examine differences in infant sun-safety practices during the first 6 months of life among black, Hispanic, and non-Hispanic white (NHW) parents in Miami, Florida.
Methods
Parents presenting to the University of Miami general pediatrics clinic from February 2015 through April 2015 with a child younger than 5 years were administered a 15-item questionnaire that included items on demographics, sun-safety strategies, sunburns and tanning, beliefs and limitations regarding sunscreen, and primary information source regarding sun safety (eg, physician, Internet, media, instincts). Parents were approached by the investigators consecutively for participation in scheduled blocks, with the exception of those who were otherwise engaged in appointment-related tasks (eg, paperwork). The study was approved by the University of Miami Miller School of Medicine institutional review board. The primary objective of this study was to determine the sun protection behaviors that black and Hispanic parents in Miami, Florida, employ in infants younger than 6 months. Secondary objectives included determining if this patient population is at risk for infant sunburns and tanning, beliefs among parents regarding sunscreen's efficacy in the prevention of skin cancers, and limitations of sunscreen use.
All data were analyzed using SAS software version 9.3. Wilcoxon signed rank test, Kruskal-Wallis test, Fisher exact test, and proportional-odds cumulative logit model were used to compare nonparametric data. Parents reporting on the full first 6 months of life (ie, the child was older than 6 months at the time of study completion) were included for analysis of sun-safety strategies. All survey respondents were included for analysis of secondary objectives. Responses from parents of infants of mixed racial and ethnic backgrounds were excluded from applicable subgroup analyses.
Results
Ninety-eight parents were approached for participation in the study; 97 consented to participate and 95 completed the survey. Seventy parents had children who were at least 6 months of age and were included for analysis of the primary objectives (ie, sun-protection strategies in the first 6 months of life). The cohort included 49 Hispanic parents, 26 black parents, and 9 NHW parents; 5 parents indicated their child was of mixed racial and ethnic background. Six respondents indicated another minority group (eg, Native American, Pacific Islander). Eighty-three respondents were mothers, 72 were educated beyond high school, and 14 were Spanish-speaking only. Four reported a known family history of skin cancer.
There were notable differences in application of sunscreen, belief in the efficacy of sunscreen, and primary source of information between parents (Tables 1 and 2). Hispanic parents reported applying sunscreen more consistently than black parents (odds ratio, 4.656; 95% confidence interval, 1.154-18.782; P<.01). Hispanic parents also were more likely than black parents to believe sunscreen is effective in the prevention of skin cancers (odds ratio, 7.499; 95% confidence interval, 1.535-36.620; P<.01). Hispanic parents were more likely to report receiving information regarding sun-safety practices for infants from their pediatrician, whereas NHW parents were more likely to follow their instincts regarding how and if infants should be exposed to the sun (P<.05). No significant differences were found in the reported primary source of information in black versus Hispanic parents or in black versus NHW parents. Three percent (3/95) of respondents reported a sunburn in the infant's first 6 months of life, and 12% (11/95) reported tanning of infants' skin from sun exposure. Tanning was associated with inconsistent shade (P<.01), inconsistent clothing coverage (P<.01), and consistently allowing infants to "develop tolerance to the sun's rays by slowly increasing sun exposure each day" (P<.05).
Comment
The survey results indicated suboptimal sun-protection practices among parents of black and Hispanic infants in Miami. Although the majority of respondents (83% [58/70]) reported keeping their infants in the shade, less than half of parents consistently covered their infants adequately with clothing and hats (40% [28/70] and 43% [30/70], respectively). More alarmingly, one-third of parents reported intentionally increasing their infant's level of sun exposure to develop his/her tolerance to the sun. A minority of parents reported sunburns (3%) and tanning (12%) within the first 6 months of life. Twenty-nine percent of parents (20/70) reported consistently applying sunscreen to their infants who were younger than 6 months despite limited safety data available for this age group.
Although our study included a limited sample size and represents a narrow geographic distribution, these results suggest that shortcomings in current practices in sun protection for black and Hispanic infants younger than 6 months may be a widespread problem. Black and Hispanic patients have a lower incidence of skin cancer, but the diagnosis often is delayed and the mortality is higher when skin cancer does occur.4 The common perception among laypeople as well as many health care providers that black and Hispanic individuals are not at risk for skin cancer may limit sun-safety counseling as well as the overall knowledge base of this patient demographic. As demonstrated by the results of this study, there is a need for counseling on sun-safe behaviors from a young age among this population.
Conclusion
This study highlights potential shortcomings in current sun-protection practices for black and Hispanic infants younger than 6 months. Sun-safe behaviors instituted from a young age may help reduce the risk for future skin cancers.3 Additional studies are needed to further define sun-safety behaviors in black and Hispanic children across the United States. Further, additional studies should focus on developing interventions that positively influence sun-safety behaviors in this patient population.
Sun exposure and sunburns sustained during childhood are linked to an increased risk for development of skin cancers in adulthood. In infants, the skin is particularly vulnerable and is considered to be at increased risk for UV radiation damage,1 even as early as the first 6 months of life.2 Sun-safe behaviors instituted from a young age may help reduce the risk for future skin cancers.3 To effectively teach parents proper sun-safe practices, it is essential to understand their existing perceptions and behaviors. This study sought to examine differences in infant sun-safety practices during the first 6 months of life among black, Hispanic, and non-Hispanic white (NHW) parents in Miami, Florida.
Methods
Parents presenting to the University of Miami general pediatrics clinic from February 2015 through April 2015 with a child younger than 5 years were administered a 15-item questionnaire that included items on demographics, sun-safety strategies, sunburns and tanning, beliefs and limitations regarding sunscreen, and primary information source regarding sun safety (eg, physician, Internet, media, instincts). Parents were approached by the investigators consecutively for participation in scheduled blocks, with the exception of those who were otherwise engaged in appointment-related tasks (eg, paperwork). The study was approved by the University of Miami Miller School of Medicine institutional review board. The primary objective of this study was to determine the sun protection behaviors that black and Hispanic parents in Miami, Florida, employ in infants younger than 6 months. Secondary objectives included determining if this patient population is at risk for infant sunburns and tanning, beliefs among parents regarding sunscreen's efficacy in the prevention of skin cancers, and limitations of sunscreen use.
All data were analyzed using SAS software version 9.3. Wilcoxon signed rank test, Kruskal-Wallis test, Fisher exact test, and proportional-odds cumulative logit model were used to compare nonparametric data. Parents reporting on the full first 6 months of life (ie, the child was older than 6 months at the time of study completion) were included for analysis of sun-safety strategies. All survey respondents were included for analysis of secondary objectives. Responses from parents of infants of mixed racial and ethnic backgrounds were excluded from applicable subgroup analyses.
Results
Ninety-eight parents were approached for participation in the study; 97 consented to participate and 95 completed the survey. Seventy parents had children who were at least 6 months of age and were included for analysis of the primary objectives (ie, sun-protection strategies in the first 6 months of life). The cohort included 49 Hispanic parents, 26 black parents, and 9 NHW parents; 5 parents indicated their child was of mixed racial and ethnic background. Six respondents indicated another minority group (eg, Native American, Pacific Islander). Eighty-three respondents were mothers, 72 were educated beyond high school, and 14 were Spanish-speaking only. Four reported a known family history of skin cancer.
There were notable differences in application of sunscreen, belief in the efficacy of sunscreen, and primary source of information between parents (Tables 1 and 2). Hispanic parents reported applying sunscreen more consistently than black parents (odds ratio, 4.656; 95% confidence interval, 1.154-18.782; P<.01). Hispanic parents also were more likely than black parents to believe sunscreen is effective in the prevention of skin cancers (odds ratio, 7.499; 95% confidence interval, 1.535-36.620; P<.01). Hispanic parents were more likely to report receiving information regarding sun-safety practices for infants from their pediatrician, whereas NHW parents were more likely to follow their instincts regarding how and if infants should be exposed to the sun (P<.05). No significant differences were found in the reported primary source of information in black versus Hispanic parents or in black versus NHW parents. Three percent (3/95) of respondents reported a sunburn in the infant's first 6 months of life, and 12% (11/95) reported tanning of infants' skin from sun exposure. Tanning was associated with inconsistent shade (P<.01), inconsistent clothing coverage (P<.01), and consistently allowing infants to "develop tolerance to the sun's rays by slowly increasing sun exposure each day" (P<.05).
Comment
The survey results indicated suboptimal sun-protection practices among parents of black and Hispanic infants in Miami. Although the majority of respondents (83% [58/70]) reported keeping their infants in the shade, less than half of parents consistently covered their infants adequately with clothing and hats (40% [28/70] and 43% [30/70], respectively). More alarmingly, one-third of parents reported intentionally increasing their infant's level of sun exposure to develop his/her tolerance to the sun. A minority of parents reported sunburns (3%) and tanning (12%) within the first 6 months of life. Twenty-nine percent of parents (20/70) reported consistently applying sunscreen to their infants who were younger than 6 months despite limited safety data available for this age group.
Although our study included a limited sample size and represents a narrow geographic distribution, these results suggest that shortcomings in current practices in sun protection for black and Hispanic infants younger than 6 months may be a widespread problem. Black and Hispanic patients have a lower incidence of skin cancer, but the diagnosis often is delayed and the mortality is higher when skin cancer does occur.4 The common perception among laypeople as well as many health care providers that black and Hispanic individuals are not at risk for skin cancer may limit sun-safety counseling as well as the overall knowledge base of this patient demographic. As demonstrated by the results of this study, there is a need for counseling on sun-safe behaviors from a young age among this population.
Conclusion
This study highlights potential shortcomings in current sun-protection practices for black and Hispanic infants younger than 6 months. Sun-safe behaviors instituted from a young age may help reduce the risk for future skin cancers.3 Additional studies are needed to further define sun-safety behaviors in black and Hispanic children across the United States. Further, additional studies should focus on developing interventions that positively influence sun-safety behaviors in this patient population.
- Paller AS, Hawk JL, Honig P, et al. New insights about infant and toddler skin: implications for sun protection. Pediatrics. 2011;128:92-102.
- Benjes LS, Brooks DR, Zhang Z, et al. Changing patterns of sun protection between the first and second summers for very young children. Arch Dermatol. 2004;140:925-930.
- Oliveria SA, Saraiya M, Geller AC, et al. Sun exposure and risk of melanoma. Arch Dis Child. 2006;91:131-138.
- Wu XC, Eide MJ, King J, et al. Racial and ethnic variations in incidence and survival of cutaneous melanoma in the United States, 1999-2006. J Am Acad Dermatol. 2011;65(5 suppl 1):S26-S37.
- Paller AS, Hawk JL, Honig P, et al. New insights about infant and toddler skin: implications for sun protection. Pediatrics. 2011;128:92-102.
- Benjes LS, Brooks DR, Zhang Z, et al. Changing patterns of sun protection between the first and second summers for very young children. Arch Dermatol. 2004;140:925-930.
- Oliveria SA, Saraiya M, Geller AC, et al. Sun exposure and risk of melanoma. Arch Dis Child. 2006;91:131-138.
- Wu XC, Eide MJ, King J, et al. Racial and ethnic variations in incidence and survival of cutaneous melanoma in the United States, 1999-2006. J Am Acad Dermatol. 2011;65(5 suppl 1):S26-S37.
Practice Points
- Infants of all racial and ethnic backgrounds need protection from the sun's rays. Remember to counsel parents on the importance of sun protection.
- Instruct parents to keep infants in the shade when outdoors and to dress infants in a long-sleeved shirt, pants, and a hat. Intentional sun exposure for infants is not recommended.
- The American Academy of Dermatology currently recommends that parents begin sunscreen application when their child reaches 6 months of age. Broad-spectrum barrier sunscreens containing zinc oxide or titanium dioxide are preferred and should provide a sun protection factor of 30 or greater.

Declining bullying rates in Maryland study contradict common misconception
Rates of bullying among students in grades 4-12 decreased over the past 10 years in a state study, contradicting a common perception of a rising trend in schools, according to a study.
The rate of self-reported, frequent bullying victimization fell from 28% in 2005 to 13% in 2014, reported Tracy Evian Waasdorp, PhD, at the Children’s Hospital of Philadelphia and the Center for the Prevention of Youth Violence at the Johns Hopkins Bloomberg School of Public Health, Baltimore, and her associates. “These findings do contradict the public’s [mis]perception that bullying is increasing.”
Data collected through a survey of 246,306 students in grades 4-12 from 109 schools in Maryland in 2005-2014 found significant decreases in 10 of 13 bullying indicators (Pediatrics. 2017. doi: 10.1542/peds.2016-2615).
In the survey, students anonymously reported if they had been a frequent victim of bullying – two or more times within the past month – as defined by the World Health Organization and Center for Disease Control and Prevention’s definition: “A person is bullied when he or she is exposed, repeatedly and over time, to negative actions on the part of one or more other persons. Bullying often occurs in situations where there is a power or status difference. Bullying includes actions like threatening, teasing, name-calling, ignoring, rumor spreading, sending hurtful emails and text messages, and leaving someone out on purpose.”
The investigators found victimization decreased across indicators including pushing (beta = –0.03), hitting (beta = –0.03), threats (beta = –0.02), cyberbullying (beta = –0.01), and rumors (beta = –0.02), according to the researchers. All values were determined with a P value less than .001.
“It was hypothesized that cyberbullying might increase, but consistent with the other forms of bullying, cyberbullying also decreased,” the researchers wrote. “However, given the rapid change of technology and new social media platforms used by youth and increasingly at younger ages, the nature and quality of cyberbullying may change.”
Dr. Waasdorp and her colleagues also had children report if and how often they had participated in bullying or had witnessed bullying, both of which also declined, from 21% to 7% of students and 66% to 43% of students, respectively.
Along with bullying, students were asked how safe they felt in school and if adults in their school were doing enough to prevent bullying, both of which sentiments increased over the course of the study. While 80% of students reported feeling safe in the school, the number of those who felt as though they belonged remained relatively unchanged.
While decreases in each category were relatively small from year to year, “some of these changes were fairly substantial across 10 years, as indicated by the effect size estimates comparing the first and last years (average difference = 0.325),” according to the researchers.
In fact, Dr. Waasdorp and her peers found the final year of the study to have the greatest improvement, which they estimate may come from more comprehensive bullying laws and school practices.
Looking across grade levels, Dr. Waasdorp and her colleagues found greater declines in witnessing bullying and school safety in high schoolers than middle schoolers, which they say may indicate more support in middle school systems, where bullying peaks.
Because of the large number of outcomes, significant associations between school levels and bullying indicators were limited. The anonymous nature of the survey limited the ability of the researchers to link student data across years. The investigators also did not collect data on why changes to the bullying indicators occurred.
During the study, the researchers were supported in part by grants from the U.S. Department of Education, the William T. Grant Foundation, and the National Institute of Justice. The authors reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
The Waasdorp et al. study is a comprehensive one using a sophisticated longitudinal design and a number of covariates to give a better comprehension of current bullying trends.
While it is encouraging to hear of the declining trends across many forms of bullying, it is important to remember 48% of children still reported bullying as an issue in their lives, with nearly as many reporting witnessing bullying against others.
We must be watchful for instances of bullying and active in getting rid of it both in and out of the classroom.
This means calling on educators to implement programs that not only sound like they will work, but have been tested and proven to be the best choice for the entire community. Programs that build empathy and encourage students to figure out productive conflict-management solutions often are good choices.
The responsibility to end bullying is not just with educators, but with pediatricians as well. Bullying can have serious mental and physical ramifications for patients, and clinicians must be vigilant for signs of victimization, such as anxiety, depression, or social withdrawal. If it seems as though a patient has been the victim or is the perpetrator of bullying, clinicians may want to talk with the child and their parents about finding a counselor at school where bullying might occur most often, encourage the child to talk with his or her parents about any problems at school, build a stronger communication between parents and the school, and help to support at least one peer friendship, which has been found to be a strong buffer against peer victimization.
This study is a good example of the progress made so far, but there is still plenty of work to be done.
Stephen S. Leff, PhD, is a psychologist in the department of child and adolescent psychiatry and behavioral sciences and codirector of the Violence Prevention Initiative at the Children’s Hospital of Philadelphia and Chris Feudtner, MD, PhD, is director of the department of medical ethics at the hospital. This a summary of their comments from an editorial accompanying the report by Waasdorp et al. (Pediatrics. 2017. doi: 10.1542/peds.2017-0504 ) Neither Dr. Leff nor Dr. Feudtner reported any relevant disclosures.
The Waasdorp et al. study is a comprehensive one using a sophisticated longitudinal design and a number of covariates to give a better comprehension of current bullying trends.
While it is encouraging to hear of the declining trends across many forms of bullying, it is important to remember 48% of children still reported bullying as an issue in their lives, with nearly as many reporting witnessing bullying against others.
We must be watchful for instances of bullying and active in getting rid of it both in and out of the classroom.
This means calling on educators to implement programs that not only sound like they will work, but have been tested and proven to be the best choice for the entire community. Programs that build empathy and encourage students to figure out productive conflict-management solutions often are good choices.
The responsibility to end bullying is not just with educators, but with pediatricians as well. Bullying can have serious mental and physical ramifications for patients, and clinicians must be vigilant for signs of victimization, such as anxiety, depression, or social withdrawal. If it seems as though a patient has been the victim or is the perpetrator of bullying, clinicians may want to talk with the child and their parents about finding a counselor at school where bullying might occur most often, encourage the child to talk with his or her parents about any problems at school, build a stronger communication between parents and the school, and help to support at least one peer friendship, which has been found to be a strong buffer against peer victimization.
This study is a good example of the progress made so far, but there is still plenty of work to be done.
Stephen S. Leff, PhD, is a psychologist in the department of child and adolescent psychiatry and behavioral sciences and codirector of the Violence Prevention Initiative at the Children’s Hospital of Philadelphia and Chris Feudtner, MD, PhD, is director of the department of medical ethics at the hospital. This a summary of their comments from an editorial accompanying the report by Waasdorp et al. (Pediatrics. 2017. doi: 10.1542/peds.2017-0504 ) Neither Dr. Leff nor Dr. Feudtner reported any relevant disclosures.
The Waasdorp et al. study is a comprehensive one using a sophisticated longitudinal design and a number of covariates to give a better comprehension of current bullying trends.
While it is encouraging to hear of the declining trends across many forms of bullying, it is important to remember 48% of children still reported bullying as an issue in their lives, with nearly as many reporting witnessing bullying against others.
We must be watchful for instances of bullying and active in getting rid of it both in and out of the classroom.
This means calling on educators to implement programs that not only sound like they will work, but have been tested and proven to be the best choice for the entire community. Programs that build empathy and encourage students to figure out productive conflict-management solutions often are good choices.
The responsibility to end bullying is not just with educators, but with pediatricians as well. Bullying can have serious mental and physical ramifications for patients, and clinicians must be vigilant for signs of victimization, such as anxiety, depression, or social withdrawal. If it seems as though a patient has been the victim or is the perpetrator of bullying, clinicians may want to talk with the child and their parents about finding a counselor at school where bullying might occur most often, encourage the child to talk with his or her parents about any problems at school, build a stronger communication between parents and the school, and help to support at least one peer friendship, which has been found to be a strong buffer against peer victimization.
This study is a good example of the progress made so far, but there is still plenty of work to be done.
Stephen S. Leff, PhD, is a psychologist in the department of child and adolescent psychiatry and behavioral sciences and codirector of the Violence Prevention Initiative at the Children’s Hospital of Philadelphia and Chris Feudtner, MD, PhD, is director of the department of medical ethics at the hospital. This a summary of their comments from an editorial accompanying the report by Waasdorp et al. (Pediatrics. 2017. doi: 10.1542/peds.2017-0504 ) Neither Dr. Leff nor Dr. Feudtner reported any relevant disclosures.
Rates of bullying among students in grades 4-12 decreased over the past 10 years in a state study, contradicting a common perception of a rising trend in schools, according to a study.
The rate of self-reported, frequent bullying victimization fell from 28% in 2005 to 13% in 2014, reported Tracy Evian Waasdorp, PhD, at the Children’s Hospital of Philadelphia and the Center for the Prevention of Youth Violence at the Johns Hopkins Bloomberg School of Public Health, Baltimore, and her associates. “These findings do contradict the public’s [mis]perception that bullying is increasing.”
Data collected through a survey of 246,306 students in grades 4-12 from 109 schools in Maryland in 2005-2014 found significant decreases in 10 of 13 bullying indicators (Pediatrics. 2017. doi: 10.1542/peds.2016-2615).
In the survey, students anonymously reported if they had been a frequent victim of bullying – two or more times within the past month – as defined by the World Health Organization and Center for Disease Control and Prevention’s definition: “A person is bullied when he or she is exposed, repeatedly and over time, to negative actions on the part of one or more other persons. Bullying often occurs in situations where there is a power or status difference. Bullying includes actions like threatening, teasing, name-calling, ignoring, rumor spreading, sending hurtful emails and text messages, and leaving someone out on purpose.”
The investigators found victimization decreased across indicators including pushing (beta = –0.03), hitting (beta = –0.03), threats (beta = –0.02), cyberbullying (beta = –0.01), and rumors (beta = –0.02), according to the researchers. All values were determined with a P value less than .001.
“It was hypothesized that cyberbullying might increase, but consistent with the other forms of bullying, cyberbullying also decreased,” the researchers wrote. “However, given the rapid change of technology and new social media platforms used by youth and increasingly at younger ages, the nature and quality of cyberbullying may change.”
Dr. Waasdorp and her colleagues also had children report if and how often they had participated in bullying or had witnessed bullying, both of which also declined, from 21% to 7% of students and 66% to 43% of students, respectively.
Along with bullying, students were asked how safe they felt in school and if adults in their school were doing enough to prevent bullying, both of which sentiments increased over the course of the study. While 80% of students reported feeling safe in the school, the number of those who felt as though they belonged remained relatively unchanged.
While decreases in each category were relatively small from year to year, “some of these changes were fairly substantial across 10 years, as indicated by the effect size estimates comparing the first and last years (average difference = 0.325),” according to the researchers.
In fact, Dr. Waasdorp and her peers found the final year of the study to have the greatest improvement, which they estimate may come from more comprehensive bullying laws and school practices.
Looking across grade levels, Dr. Waasdorp and her colleagues found greater declines in witnessing bullying and school safety in high schoolers than middle schoolers, which they say may indicate more support in middle school systems, where bullying peaks.
Because of the large number of outcomes, significant associations between school levels and bullying indicators were limited. The anonymous nature of the survey limited the ability of the researchers to link student data across years. The investigators also did not collect data on why changes to the bullying indicators occurred.
During the study, the researchers were supported in part by grants from the U.S. Department of Education, the William T. Grant Foundation, and the National Institute of Justice. The authors reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
Rates of bullying among students in grades 4-12 decreased over the past 10 years in a state study, contradicting a common perception of a rising trend in schools, according to a study.
The rate of self-reported, frequent bullying victimization fell from 28% in 2005 to 13% in 2014, reported Tracy Evian Waasdorp, PhD, at the Children’s Hospital of Philadelphia and the Center for the Prevention of Youth Violence at the Johns Hopkins Bloomberg School of Public Health, Baltimore, and her associates. “These findings do contradict the public’s [mis]perception that bullying is increasing.”
Data collected through a survey of 246,306 students in grades 4-12 from 109 schools in Maryland in 2005-2014 found significant decreases in 10 of 13 bullying indicators (Pediatrics. 2017. doi: 10.1542/peds.2016-2615).
In the survey, students anonymously reported if they had been a frequent victim of bullying – two or more times within the past month – as defined by the World Health Organization and Center for Disease Control and Prevention’s definition: “A person is bullied when he or she is exposed, repeatedly and over time, to negative actions on the part of one or more other persons. Bullying often occurs in situations where there is a power or status difference. Bullying includes actions like threatening, teasing, name-calling, ignoring, rumor spreading, sending hurtful emails and text messages, and leaving someone out on purpose.”
The investigators found victimization decreased across indicators including pushing (beta = –0.03), hitting (beta = –0.03), threats (beta = –0.02), cyberbullying (beta = –0.01), and rumors (beta = –0.02), according to the researchers. All values were determined with a P value less than .001.
“It was hypothesized that cyberbullying might increase, but consistent with the other forms of bullying, cyberbullying also decreased,” the researchers wrote. “However, given the rapid change of technology and new social media platforms used by youth and increasingly at younger ages, the nature and quality of cyberbullying may change.”
Dr. Waasdorp and her colleagues also had children report if and how often they had participated in bullying or had witnessed bullying, both of which also declined, from 21% to 7% of students and 66% to 43% of students, respectively.
Along with bullying, students were asked how safe they felt in school and if adults in their school were doing enough to prevent bullying, both of which sentiments increased over the course of the study. While 80% of students reported feeling safe in the school, the number of those who felt as though they belonged remained relatively unchanged.
While decreases in each category were relatively small from year to year, “some of these changes were fairly substantial across 10 years, as indicated by the effect size estimates comparing the first and last years (average difference = 0.325),” according to the researchers.
In fact, Dr. Waasdorp and her peers found the final year of the study to have the greatest improvement, which they estimate may come from more comprehensive bullying laws and school practices.
Looking across grade levels, Dr. Waasdorp and her colleagues found greater declines in witnessing bullying and school safety in high schoolers than middle schoolers, which they say may indicate more support in middle school systems, where bullying peaks.
Because of the large number of outcomes, significant associations between school levels and bullying indicators were limited. The anonymous nature of the survey limited the ability of the researchers to link student data across years. The investigators also did not collect data on why changes to the bullying indicators occurred.
During the study, the researchers were supported in part by grants from the U.S. Department of Education, the William T. Grant Foundation, and the National Institute of Justice. The authors reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
FROM PEDIATRICS
Key clinical point:
Major finding: Reports of victimization overall among Maryland students in grades 4-12 decreased from 28% to 13% over a decade, with decreases in 10 of 13 bullying indicators in the study.
Data source: Self-reported survey of 246,306 students in grades 4-12 from 109 Maryland schools in 2005-2014, analyzed using a longitudinal hierarchical linear model.
Disclosures: During the study, researchers were supported in part by grants from the U.S. Department of Education, the William T. Grant Foundation, and the National Institute of Justice. The authors reported no relevant financial disclosures.
SJS, TEN occur less frequently in children than adults
Although incidences of Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are lower in children than in adults, the increased costs, lengths of stay, and mortality still pose a substantial health burden, said Derek Y. Hsu, of Northwestern University, Chicago, and his associates.
Using data from the 2009-2012 Nationwide Inpatient Sample of 1,687,172 pediatric admissions, “estimated frequencies per million children ranged from 4.3 to 5.8 for SJS, 0.6 to 1.4 for SJS/TEN, and 0 to 0.7 for TEN,” the study researchers reported. In adults, those numbers are 9.3, 1.9, and 1.6 per million adults per year, according to a 2016 study by the authors (J Invest Dermatol. 2016 Jul;136[7]:1387-97).
Pediatric SJS, SJS/TEN, and TEN mean hospital costs were $24,947, $63,787, and $102,243, respectively, compared with $10,496 for the control group.
The mean length of stay for patients with SJS, SJS/TEN, and TEN was 9.4 days, 15.7 days, and 20.4 days, compared with 4.6 days in children without these disorders, respectively, and they most often were discharged to their home or to other self-care.
“One in 10 children with SJS, SJS/TEN, and TEN underwent mechanical ventilation,” Mr. Hsu and his associates reported.
Mortality was 0% for SJS, 4% for SJS/TEN, and 16% for TEN.
Read more at the Journal of the American Academy of Dermatology (2017 May;76[5]:811-7).
Although incidences of Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are lower in children than in adults, the increased costs, lengths of stay, and mortality still pose a substantial health burden, said Derek Y. Hsu, of Northwestern University, Chicago, and his associates.
Using data from the 2009-2012 Nationwide Inpatient Sample of 1,687,172 pediatric admissions, “estimated frequencies per million children ranged from 4.3 to 5.8 for SJS, 0.6 to 1.4 for SJS/TEN, and 0 to 0.7 for TEN,” the study researchers reported. In adults, those numbers are 9.3, 1.9, and 1.6 per million adults per year, according to a 2016 study by the authors (J Invest Dermatol. 2016 Jul;136[7]:1387-97).
Pediatric SJS, SJS/TEN, and TEN mean hospital costs were $24,947, $63,787, and $102,243, respectively, compared with $10,496 for the control group.
The mean length of stay for patients with SJS, SJS/TEN, and TEN was 9.4 days, 15.7 days, and 20.4 days, compared with 4.6 days in children without these disorders, respectively, and they most often were discharged to their home or to other self-care.
“One in 10 children with SJS, SJS/TEN, and TEN underwent mechanical ventilation,” Mr. Hsu and his associates reported.
Mortality was 0% for SJS, 4% for SJS/TEN, and 16% for TEN.
Read more at the Journal of the American Academy of Dermatology (2017 May;76[5]:811-7).
Although incidences of Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are lower in children than in adults, the increased costs, lengths of stay, and mortality still pose a substantial health burden, said Derek Y. Hsu, of Northwestern University, Chicago, and his associates.
Using data from the 2009-2012 Nationwide Inpatient Sample of 1,687,172 pediatric admissions, “estimated frequencies per million children ranged from 4.3 to 5.8 for SJS, 0.6 to 1.4 for SJS/TEN, and 0 to 0.7 for TEN,” the study researchers reported. In adults, those numbers are 9.3, 1.9, and 1.6 per million adults per year, according to a 2016 study by the authors (J Invest Dermatol. 2016 Jul;136[7]:1387-97).
Pediatric SJS, SJS/TEN, and TEN mean hospital costs were $24,947, $63,787, and $102,243, respectively, compared with $10,496 for the control group.
The mean length of stay for patients with SJS, SJS/TEN, and TEN was 9.4 days, 15.7 days, and 20.4 days, compared with 4.6 days in children without these disorders, respectively, and they most often were discharged to their home or to other self-care.
“One in 10 children with SJS, SJS/TEN, and TEN underwent mechanical ventilation,” Mr. Hsu and his associates reported.
Mortality was 0% for SJS, 4% for SJS/TEN, and 16% for TEN.
Read more at the Journal of the American Academy of Dermatology (2017 May;76[5]:811-7).
Hidradenitis suppurativa diagnosis typically delayed in children
WASHINGTON – Children with hidradenitis suppurativa (HS) may suffer with symptoms for an average of 7 years before they are diagnosed, according to pediatric dermatologist Anna Yasmine Kirkorian, MD.
Data from a 2015 study showed that 73% of pediatric patients with HS were diagnosed more than 2 years after the onset of symptoms, said Dr. Kirkorian of the department of dermatology at Children’s National Health System and George Washington University, Washington. (Br J Dermatol. 2015 Dec;173[6]:1546-9).

Genetics can play a role in HS, likely via mutations in the gamma-secretase protein that leads to epidermal differentiation and immune regulation, Dr. Kirkorian said. Most of her patients with HS are black, and a recent study described a gamma-secretase mutation in a black family of a proband and four family members, she noted (JAMA Dermatol. 2015 Jun;151[6]:668-70). Gamma-secretase mutations also have been identified in Han Chinese populations, she said.

HS also is associated with precocious puberty. However, defining the age of onset of puberty can be difficulty because pubertal onset may vary between different ethnicities, noted Dr. Kirkorian. “Prepubertal children presenting with HS warrant an endocrinologic evaluation,” she said.
Dr. Kirkorian added that more research is needed to pinpoint the possible genetic component of HS and to identify genetic susceptibility that could lead to targeted treatment strategies.
The optimal treatment plan for pediatric HS is multimodal and addresses the comorbidities common with the condition, she said, and she predicted that specialized clinic or treatment centers that bring together areas, including psychiatry, wound care, pain management, surgery, endocrinology, and genetics, will evolve to serve these patients. To support these collaborative efforts, Dr. Kirkorian is a member of the Pediatric Dermatology Research Alliance (PeDRA), an organization formed to accelerate research on skin diseases in children.
The symposium was sponsored by AbbVie. Dr. Kirkorian had no financial conflicts to disclose. She is on the editorial board of Dermatology News.
WASHINGTON – Children with hidradenitis suppurativa (HS) may suffer with symptoms for an average of 7 years before they are diagnosed, according to pediatric dermatologist Anna Yasmine Kirkorian, MD.
Data from a 2015 study showed that 73% of pediatric patients with HS were diagnosed more than 2 years after the onset of symptoms, said Dr. Kirkorian of the department of dermatology at Children’s National Health System and George Washington University, Washington. (Br J Dermatol. 2015 Dec;173[6]:1546-9).
Genetics can play a role in HS, likely via mutations in the gamma-secretase protein that leads to epidermal differentiation and immune regulation, Dr. Kirkorian said. Most of her patients with HS are black, and a recent study described a gamma-secretase mutation in a black family of a proband and four family members, she noted (JAMA Dermatol. 2015 Jun;151[6]:668-70). Gamma-secretase mutations also have been identified in Han Chinese populations, she said.
HS also is associated with precocious puberty. However, defining the age of onset of puberty can be difficulty because pubertal onset may vary between different ethnicities, noted Dr. Kirkorian. “Prepubertal children presenting with HS warrant an endocrinologic evaluation,” she said.
Dr. Kirkorian added that more research is needed to pinpoint the possible genetic component of HS and to identify genetic susceptibility that could lead to targeted treatment strategies.
The optimal treatment plan for pediatric HS is multimodal and addresses the comorbidities common with the condition, she said, and she predicted that specialized clinic or treatment centers that bring together areas, including psychiatry, wound care, pain management, surgery, endocrinology, and genetics, will evolve to serve these patients. To support these collaborative efforts, Dr. Kirkorian is a member of the Pediatric Dermatology Research Alliance (PeDRA), an organization formed to accelerate research on skin diseases in children.
The symposium was sponsored by AbbVie. Dr. Kirkorian had no financial conflicts to disclose. She is on the editorial board of Dermatology News.
WASHINGTON – Children with hidradenitis suppurativa (HS) may suffer with symptoms for an average of 7 years before they are diagnosed, according to pediatric dermatologist Anna Yasmine Kirkorian, MD.
Data from a 2015 study showed that 73% of pediatric patients with HS were diagnosed more than 2 years after the onset of symptoms, said Dr. Kirkorian of the department of dermatology at Children’s National Health System and George Washington University, Washington. (Br J Dermatol. 2015 Dec;173[6]:1546-9).
Genetics can play a role in HS, likely via mutations in the gamma-secretase protein that leads to epidermal differentiation and immune regulation, Dr. Kirkorian said. Most of her patients with HS are black, and a recent study described a gamma-secretase mutation in a black family of a proband and four family members, she noted (JAMA Dermatol. 2015 Jun;151[6]:668-70). Gamma-secretase mutations also have been identified in Han Chinese populations, she said.
HS also is associated with precocious puberty. However, defining the age of onset of puberty can be difficulty because pubertal onset may vary between different ethnicities, noted Dr. Kirkorian. “Prepubertal children presenting with HS warrant an endocrinologic evaluation,” she said.
Dr. Kirkorian added that more research is needed to pinpoint the possible genetic component of HS and to identify genetic susceptibility that could lead to targeted treatment strategies.
The optimal treatment plan for pediatric HS is multimodal and addresses the comorbidities common with the condition, she said, and she predicted that specialized clinic or treatment centers that bring together areas, including psychiatry, wound care, pain management, surgery, endocrinology, and genetics, will evolve to serve these patients. To support these collaborative efforts, Dr. Kirkorian is a member of the Pediatric Dermatology Research Alliance (PeDRA), an organization formed to accelerate research on skin diseases in children.
The symposium was sponsored by AbbVie. Dr. Kirkorian had no financial conflicts to disclose. She is on the editorial board of Dermatology News.

VIDEO: SHM seeks sites to test pediatric transition tool
Would you like to help the Society of Hospital Medicine translate its award-winning Project BOOST® Mentored Implementation Program into the pediatric setting?
“We’re hoping to get six sites to help us implement this project so we can collect data and see how well it works for pediatrics,” James O’Callaghan, MD, medical director, EvergreenHealth, Seattle Children’s, said in an interview.
In this video, recorded during HM17 , Dr. O’Callaghan describes how Pedi-BOOST is intended to work, and what types of pediatric transition concerns it is intended to address.
For more information, please visit the SHM website.
Dr. O’Callaghan had no relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Would you like to help the Society of Hospital Medicine translate its award-winning Project BOOST® Mentored Implementation Program into the pediatric setting?
“We’re hoping to get six sites to help us implement this project so we can collect data and see how well it works for pediatrics,” James O’Callaghan, MD, medical director, EvergreenHealth, Seattle Children’s, said in an interview.
In this video, recorded during HM17 , Dr. O’Callaghan describes how Pedi-BOOST is intended to work, and what types of pediatric transition concerns it is intended to address.
For more information, please visit the SHM website.
Dr. O’Callaghan had no relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Would you like to help the Society of Hospital Medicine translate its award-winning Project BOOST® Mentored Implementation Program into the pediatric setting?
“We’re hoping to get six sites to help us implement this project so we can collect data and see how well it works for pediatrics,” James O’Callaghan, MD, medical director, EvergreenHealth, Seattle Children’s, said in an interview.
In this video, recorded during HM17 , Dr. O’Callaghan describes how Pedi-BOOST is intended to work, and what types of pediatric transition concerns it is intended to address.
For more information, please visit the SHM website.
Dr. O’Callaghan had no relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

In sickle cell disease, osteomyelitis is a tough call
MONTREAL – Osteomyelitis is an especially challenging diagnosis in children with sickle cell disease (SCD) because the bone and joint signs, elevated white cell counts, and C-reactive protein levels that are commonly used to diagnose bone infection are frequently features of SCD as well.
As a result, most patients with SCD and suspected osteomyelitis are treated without a confirmation of the diagnosis.

Among 30 patients with SCD who were followed at a single center over a decade, 29 patients had elevated ESR, but only 13 patients had leukocytosis, and only 13 had elevated CRP.
“Prior studies on sickle cell disease have shown that it is very difficult to differentiate between osteoarticular infection and bone infarction. Therefore, oftentimes, this diagnosis is very difficult to make,” Dr. Weisman said at the annual meeting of the American Society of Pediatric Hematology/Oncology.
Laboratory findings for osteomyelitis in SCD are often nonspecific, including leukocytosis, elevated CRP and ESR, and blood cultures positive for Staphylococcus aureus (the predominant pathogen in children with osteomyelitis), or, in children with hemoglobinopathies, salmonella.
In children with SCD, CRP levels can vary from normal to elevated. ESR is similarly variable, as low hematocrit values can result in higher ESR values. Additionally, sickle erythrocytes can fail to aggregate, which can lead to lower ESR values.
A decade of data
The researchers set out to get a better handle on the characteristics and outcomes of osteomyelitis in patients with SCD and to see which laboratory and imaging findings might prove most useful for diagnosing osteomyelitis in this population. They reviewed data on 59 patients who were identified with indeterminate or likely osteomyelitis over a 10-year span. Of those, 30 were diagnosed and treated for osteomyelitis, and 29 were tentatively diagnosed but not treated. The latter group likely had symptoms caused by a bone infarction or vaso-occlusive crisis, Dr. Weisman said.
Among the 30 treated patients, osteomyelitis was confirmed by bone biopsy in 3, and an organism was isolated from blood or an abscess in 6. In the other 21, osteomyelitis was presumed based on clinical, laboratory, and MRI findings.
The median patient age was 12 years (range, 8 months to 18 years), 18 were male, and all but three patients have the HbSS genotype. Of the remaining patients, two had the HbSC and one the HbSF genotypes.
Infections occurred in the lower extremities in 11 patients, in the upper extremities in 10, in the pelvis or vertebrae in 2 each, and in the scapula, clavicle, hand, rib, or mandible in 1 patient each.
Just 13 of the 30 patients (43%) had lab findings of leukocytosis (more than 15,000 cells/mm2), and an equal number had elevated CRP (greater than 10 mg/L).
In contrast, 29 patients had an ESR above 20 mm/hour, and, in three of these patients, the rate was higher than 100 mm/hour.
When the researchers compared white blood cell counts and CRP levels between the treated patients and the 29 untreated controls, they found no significant differences for either measure of inflammation. In contrast, ESR was significantly higher among treated patients (P = .03).
Looking at the receiver operating characteristic curve for ESR, they found that an ESR of more than 100 mm/hour had 100% specificity for osteomyelitis in this group of patients.
Only 6 of the 30 (20%) had bacteremia. In 9 patients, nontyphoidal salmonella was isolated from cultures of either bone biopsy (3), abscess (3), or blood (6), but no possible causative organism could be isolated in the remaining 21 patients.
All patients were treated with prolonged antibiotic therapy. Surgical drainage and/or debridement were required in 6 patients. Two patients developed chronic osteomyelitis, but infection eventually resolved in all patients.
Recommendations
Dr. Weisman recommended early consultation with infectious disease experts and orthopedists; labs studies with complete blood counts, CRP, and ESR; and imaging studies with MRI when there is clinical suspicion of osteomyelitis in patients with SCD.
When an SCD patient has indeterminate findings, a blood culture can be performed. If it is positive for salmonella and the ESR is above 100 mm/hour, the patient can then go on to treatment. If the blood culture is negative and the ESR is below 100 mm hour but the suspicion of osteomyelitis remains high, a bone biopsy can be considered, they concluded.
The study was internally funded. Dr. Weisman reported no conflicts of interest to disclose.
MONTREAL – Osteomyelitis is an especially challenging diagnosis in children with sickle cell disease (SCD) because the bone and joint signs, elevated white cell counts, and C-reactive protein levels that are commonly used to diagnose bone infection are frequently features of SCD as well.
As a result, most patients with SCD and suspected osteomyelitis are treated without a confirmation of the diagnosis.
Among 30 patients with SCD who were followed at a single center over a decade, 29 patients had elevated ESR, but only 13 patients had leukocytosis, and only 13 had elevated CRP.
“Prior studies on sickle cell disease have shown that it is very difficult to differentiate between osteoarticular infection and bone infarction. Therefore, oftentimes, this diagnosis is very difficult to make,” Dr. Weisman said at the annual meeting of the American Society of Pediatric Hematology/Oncology.
Laboratory findings for osteomyelitis in SCD are often nonspecific, including leukocytosis, elevated CRP and ESR, and blood cultures positive for Staphylococcus aureus (the predominant pathogen in children with osteomyelitis), or, in children with hemoglobinopathies, salmonella.
In children with SCD, CRP levels can vary from normal to elevated. ESR is similarly variable, as low hematocrit values can result in higher ESR values. Additionally, sickle erythrocytes can fail to aggregate, which can lead to lower ESR values.
A decade of data
The researchers set out to get a better handle on the characteristics and outcomes of osteomyelitis in patients with SCD and to see which laboratory and imaging findings might prove most useful for diagnosing osteomyelitis in this population. They reviewed data on 59 patients who were identified with indeterminate or likely osteomyelitis over a 10-year span. Of those, 30 were diagnosed and treated for osteomyelitis, and 29 were tentatively diagnosed but not treated. The latter group likely had symptoms caused by a bone infarction or vaso-occlusive crisis, Dr. Weisman said.
Among the 30 treated patients, osteomyelitis was confirmed by bone biopsy in 3, and an organism was isolated from blood or an abscess in 6. In the other 21, osteomyelitis was presumed based on clinical, laboratory, and MRI findings.
The median patient age was 12 years (range, 8 months to 18 years), 18 were male, and all but three patients have the HbSS genotype. Of the remaining patients, two had the HbSC and one the HbSF genotypes.
Infections occurred in the lower extremities in 11 patients, in the upper extremities in 10, in the pelvis or vertebrae in 2 each, and in the scapula, clavicle, hand, rib, or mandible in 1 patient each.
Just 13 of the 30 patients (43%) had lab findings of leukocytosis (more than 15,000 cells/mm2), and an equal number had elevated CRP (greater than 10 mg/L).
In contrast, 29 patients had an ESR above 20 mm/hour, and, in three of these patients, the rate was higher than 100 mm/hour.
When the researchers compared white blood cell counts and CRP levels between the treated patients and the 29 untreated controls, they found no significant differences for either measure of inflammation. In contrast, ESR was significantly higher among treated patients (P = .03).
Looking at the receiver operating characteristic curve for ESR, they found that an ESR of more than 100 mm/hour had 100% specificity for osteomyelitis in this group of patients.
Only 6 of the 30 (20%) had bacteremia. In 9 patients, nontyphoidal salmonella was isolated from cultures of either bone biopsy (3), abscess (3), or blood (6), but no possible causative organism could be isolated in the remaining 21 patients.
All patients were treated with prolonged antibiotic therapy. Surgical drainage and/or debridement were required in 6 patients. Two patients developed chronic osteomyelitis, but infection eventually resolved in all patients.
Recommendations
Dr. Weisman recommended early consultation with infectious disease experts and orthopedists; labs studies with complete blood counts, CRP, and ESR; and imaging studies with MRI when there is clinical suspicion of osteomyelitis in patients with SCD.
When an SCD patient has indeterminate findings, a blood culture can be performed. If it is positive for salmonella and the ESR is above 100 mm/hour, the patient can then go on to treatment. If the blood culture is negative and the ESR is below 100 mm hour but the suspicion of osteomyelitis remains high, a bone biopsy can be considered, they concluded.
The study was internally funded. Dr. Weisman reported no conflicts of interest to disclose.
MONTREAL – Osteomyelitis is an especially challenging diagnosis in children with sickle cell disease (SCD) because the bone and joint signs, elevated white cell counts, and C-reactive protein levels that are commonly used to diagnose bone infection are frequently features of SCD as well.
As a result, most patients with SCD and suspected osteomyelitis are treated without a confirmation of the diagnosis.
Among 30 patients with SCD who were followed at a single center over a decade, 29 patients had elevated ESR, but only 13 patients had leukocytosis, and only 13 had elevated CRP.
“Prior studies on sickle cell disease have shown that it is very difficult to differentiate between osteoarticular infection and bone infarction. Therefore, oftentimes, this diagnosis is very difficult to make,” Dr. Weisman said at the annual meeting of the American Society of Pediatric Hematology/Oncology.
Laboratory findings for osteomyelitis in SCD are often nonspecific, including leukocytosis, elevated CRP and ESR, and blood cultures positive for Staphylococcus aureus (the predominant pathogen in children with osteomyelitis), or, in children with hemoglobinopathies, salmonella.
In children with SCD, CRP levels can vary from normal to elevated. ESR is similarly variable, as low hematocrit values can result in higher ESR values. Additionally, sickle erythrocytes can fail to aggregate, which can lead to lower ESR values.
A decade of data
The researchers set out to get a better handle on the characteristics and outcomes of osteomyelitis in patients with SCD and to see which laboratory and imaging findings might prove most useful for diagnosing osteomyelitis in this population. They reviewed data on 59 patients who were identified with indeterminate or likely osteomyelitis over a 10-year span. Of those, 30 were diagnosed and treated for osteomyelitis, and 29 were tentatively diagnosed but not treated. The latter group likely had symptoms caused by a bone infarction or vaso-occlusive crisis, Dr. Weisman said.
Among the 30 treated patients, osteomyelitis was confirmed by bone biopsy in 3, and an organism was isolated from blood or an abscess in 6. In the other 21, osteomyelitis was presumed based on clinical, laboratory, and MRI findings.
The median patient age was 12 years (range, 8 months to 18 years), 18 were male, and all but three patients have the HbSS genotype. Of the remaining patients, two had the HbSC and one the HbSF genotypes.
Infections occurred in the lower extremities in 11 patients, in the upper extremities in 10, in the pelvis or vertebrae in 2 each, and in the scapula, clavicle, hand, rib, or mandible in 1 patient each.
Just 13 of the 30 patients (43%) had lab findings of leukocytosis (more than 15,000 cells/mm2), and an equal number had elevated CRP (greater than 10 mg/L).
In contrast, 29 patients had an ESR above 20 mm/hour, and, in three of these patients, the rate was higher than 100 mm/hour.
When the researchers compared white blood cell counts and CRP levels between the treated patients and the 29 untreated controls, they found no significant differences for either measure of inflammation. In contrast, ESR was significantly higher among treated patients (P = .03).
Looking at the receiver operating characteristic curve for ESR, they found that an ESR of more than 100 mm/hour had 100% specificity for osteomyelitis in this group of patients.
Only 6 of the 30 (20%) had bacteremia. In 9 patients, nontyphoidal salmonella was isolated from cultures of either bone biopsy (3), abscess (3), or blood (6), but no possible causative organism could be isolated in the remaining 21 patients.
All patients were treated with prolonged antibiotic therapy. Surgical drainage and/or debridement were required in 6 patients. Two patients developed chronic osteomyelitis, but infection eventually resolved in all patients.
Recommendations
Dr. Weisman recommended early consultation with infectious disease experts and orthopedists; labs studies with complete blood counts, CRP, and ESR; and imaging studies with MRI when there is clinical suspicion of osteomyelitis in patients with SCD.
When an SCD patient has indeterminate findings, a blood culture can be performed. If it is positive for salmonella and the ESR is above 100 mm/hour, the patient can then go on to treatment. If the blood culture is negative and the ESR is below 100 mm hour but the suspicion of osteomyelitis remains high, a bone biopsy can be considered, they concluded.
The study was internally funded. Dr. Weisman reported no conflicts of interest to disclose.
Key clinical point: ESR may be a better lab marker for osteomyelitis in sickle cell disease than either WBC or CRP.
Major finding: An ESR greater than 100 mm/hr was 100% specific for osteomyelitis in this study.
Data source: A retrospective review of data on 59 patients with sickle cell disease and suspected or probable osteomyelitis.
Disclosures: The study was internally funded. Dr. Weisman reported having no conflicts of interest to disclose.

Cord blood/placental cell combo induces rapid immune recovery
MONTREAL – A combination of placenta-derived stem cells and umbilical cord blood was associated with early engraftment and high degrees of cord blood donor chimerism in the treatment of children with both malignant and nonmalignant hematologic conditions requiring stem cell transplantation, updated results of a pilot study show.
Among 16 children treated with the combination, the probability of neutrophil engraftment was 87.5%, and all patients who had neutrophil engraftment went on to have platelet engraftment. The probability of 12-month overall survival was 81.2%, reported Allyson Flower, MD, from Boston Children’s Health Physicians in Hawthorne, N.Y. “The probability of grade II-IV acute graft vs. host disease was 12.5%, compared with 32.5% seen with unrelated cord blood in our group’s previous studies. Cellular immune reconstitution was robust,” she said at the annual meeting of the American Society of Pediatric Hematology/Oncology.

Augmenting cord blood
Although unrelated donor cord blood transplantation expands the donor pool, is rapidly available, and is associated with decreases in both severe acute graft vs. host disease (GVHD) and chronic GVHD, compared with other stem cell sources, the technique is hampered by limited cell doses, prolonged immune reconstitution time, delays in hematopoietic recovery, and a higher incidence of graft failure.
Early studies of myeloablative conditioning followed by unrelated umbilical or placental blood transplantation showed a median of 22-24 days to neutrophil engraftment (Blood 1996 88:795-802; N Engl J Med. 1996;335:157-66), Dr. Flower noted.
More recently, a multivariate analysis of patients who underwent reduced-intensity conditioning followed by hematopoietic stem cell transplant with unrelated cord blood showed that graft failure was an independent risk factor for worse overall survival (Biol Blood Marrow Transplant. 2013 Apr;19:4;552-61).
Multiple groups have shown that adding human placenta–derived stem cells (HPDSC) to cord blood transplantation can facilitate more rapid hematopoietic engraftment by increasing the number of stem cells, increasing the proportion of hematopoietic progenitor cells, and providing additional, immature CD34+/CD45– progenitor cells.
In a single-arm, nonrandomized study, the investigators enrolled 16 patients ranging in age from 0.3 to 15.7 years with inborn errors of metabolism, marrow failure syndromes, severe immunodeficiency states, or hematologic malignancies.
Malignant conditions included B-cell precursor acute lymphoblastic leukemia (B-ALL; four patients), acute myeloid leukemia (AML; two), and T-cell ALL (one) in first complete remission, and T-cell lymphoblastic lymphoma following induction failure (one). Nonmalignant conditions included adrenoleukodystrophy (two patients), amegakaryotic thrombocytopenia (one), severe combined immunodeficiency (SCID; two), dyskeratosis congenita (one), chronic granulomatous disease (one), and severe congenital neutropenia (one).
The patients first underwent either myeloablative or reduced-intensity conditioning, followed 10 days later by infusion of unrelated cord blood and HPDSCs. Prior to HPDSC infusion, patients were medicated with diphenhydramine and hydrocortisone to prevent or reduce potential sensitivity reactions. HPDSCs were infused no sooner than 4 hours after the end of the cord blood infusion.
Patients received GVHD prophylaxis with either tacrolimus or cyclosporine, plus mycophenolate mofetil.
The combination appeared to be safe, with no cases of grade 3 or 4 toxicity secondary to HPDSC infusion.
The probability of neutrophil engraftment was 87.5%, with engraftment occurring at a median of 23 days (range 13-53). As noted before, all patients who had neutrophil engraftment had platelet engraftment, which was achieved at a median of 47 days (range, 20-98). In the group’s previous studies, median time to platelet engraftment was 53 days for patients who had undergone reduced-intensity conditioning, and 118 days for patients who had undergone myeloablation.
The probability of grade 2-4 acute GVHD within 100 days was 12.5%, and there were no cases of chronic GVHD.
Respective percentages of cord blood donor chimerism at days 30, 60, 100, and 180 were 88%, 98%, 99%, and 99%.
Immune reconstitution was strong, with normalization of mean CD3+, CD19+, and CD56+ cells occurring by day 100, CD8+ cells by day 180, and CD4+ cells by day 270.
There were three patient deaths: one from adenoviremia in a patient with B-ALL and CNS relapse, who had neutrophil engraftment at day 21; one in a patient with SCID, from adenoviremia and multiple system organ failure, who did not have engraftment before death; and one in a patient with severe congenital neutrophilia, who also did not have neutrophil engraftment.
None of the eight patients with malignant disease have experienced relapse to date, Dr. Flower noted.
The study was funded by a grant from Celgene Cellular Therapeutics. Dr. Flower reported having no conflicts of interest.
MONTREAL – A combination of placenta-derived stem cells and umbilical cord blood was associated with early engraftment and high degrees of cord blood donor chimerism in the treatment of children with both malignant and nonmalignant hematologic conditions requiring stem cell transplantation, updated results of a pilot study show.
Among 16 children treated with the combination, the probability of neutrophil engraftment was 87.5%, and all patients who had neutrophil engraftment went on to have platelet engraftment. The probability of 12-month overall survival was 81.2%, reported Allyson Flower, MD, from Boston Children’s Health Physicians in Hawthorne, N.Y. “The probability of grade II-IV acute graft vs. host disease was 12.5%, compared with 32.5% seen with unrelated cord blood in our group’s previous studies. Cellular immune reconstitution was robust,” she said at the annual meeting of the American Society of Pediatric Hematology/Oncology.
Augmenting cord blood
Although unrelated donor cord blood transplantation expands the donor pool, is rapidly available, and is associated with decreases in both severe acute graft vs. host disease (GVHD) and chronic GVHD, compared with other stem cell sources, the technique is hampered by limited cell doses, prolonged immune reconstitution time, delays in hematopoietic recovery, and a higher incidence of graft failure.
Early studies of myeloablative conditioning followed by unrelated umbilical or placental blood transplantation showed a median of 22-24 days to neutrophil engraftment (Blood 1996 88:795-802; N Engl J Med. 1996;335:157-66), Dr. Flower noted.
More recently, a multivariate analysis of patients who underwent reduced-intensity conditioning followed by hematopoietic stem cell transplant with unrelated cord blood showed that graft failure was an independent risk factor for worse overall survival (Biol Blood Marrow Transplant. 2013 Apr;19:4;552-61).
Multiple groups have shown that adding human placenta–derived stem cells (HPDSC) to cord blood transplantation can facilitate more rapid hematopoietic engraftment by increasing the number of stem cells, increasing the proportion of hematopoietic progenitor cells, and providing additional, immature CD34+/CD45– progenitor cells.
In a single-arm, nonrandomized study, the investigators enrolled 16 patients ranging in age from 0.3 to 15.7 years with inborn errors of metabolism, marrow failure syndromes, severe immunodeficiency states, or hematologic malignancies.
Malignant conditions included B-cell precursor acute lymphoblastic leukemia (B-ALL; four patients), acute myeloid leukemia (AML; two), and T-cell ALL (one) in first complete remission, and T-cell lymphoblastic lymphoma following induction failure (one). Nonmalignant conditions included adrenoleukodystrophy (two patients), amegakaryotic thrombocytopenia (one), severe combined immunodeficiency (SCID; two), dyskeratosis congenita (one), chronic granulomatous disease (one), and severe congenital neutropenia (one).
The patients first underwent either myeloablative or reduced-intensity conditioning, followed 10 days later by infusion of unrelated cord blood and HPDSCs. Prior to HPDSC infusion, patients were medicated with diphenhydramine and hydrocortisone to prevent or reduce potential sensitivity reactions. HPDSCs were infused no sooner than 4 hours after the end of the cord blood infusion.
Patients received GVHD prophylaxis with either tacrolimus or cyclosporine, plus mycophenolate mofetil.
The combination appeared to be safe, with no cases of grade 3 or 4 toxicity secondary to HPDSC infusion.
The probability of neutrophil engraftment was 87.5%, with engraftment occurring at a median of 23 days (range 13-53). As noted before, all patients who had neutrophil engraftment had platelet engraftment, which was achieved at a median of 47 days (range, 20-98). In the group’s previous studies, median time to platelet engraftment was 53 days for patients who had undergone reduced-intensity conditioning, and 118 days for patients who had undergone myeloablation.
The probability of grade 2-4 acute GVHD within 100 days was 12.5%, and there were no cases of chronic GVHD.
Respective percentages of cord blood donor chimerism at days 30, 60, 100, and 180 were 88%, 98%, 99%, and 99%.
Immune reconstitution was strong, with normalization of mean CD3+, CD19+, and CD56+ cells occurring by day 100, CD8+ cells by day 180, and CD4+ cells by day 270.
There were three patient deaths: one from adenoviremia in a patient with B-ALL and CNS relapse, who had neutrophil engraftment at day 21; one in a patient with SCID, from adenoviremia and multiple system organ failure, who did not have engraftment before death; and one in a patient with severe congenital neutrophilia, who also did not have neutrophil engraftment.
None of the eight patients with malignant disease have experienced relapse to date, Dr. Flower noted.
The study was funded by a grant from Celgene Cellular Therapeutics. Dr. Flower reported having no conflicts of interest.
MONTREAL – A combination of placenta-derived stem cells and umbilical cord blood was associated with early engraftment and high degrees of cord blood donor chimerism in the treatment of children with both malignant and nonmalignant hematologic conditions requiring stem cell transplantation, updated results of a pilot study show.
Among 16 children treated with the combination, the probability of neutrophil engraftment was 87.5%, and all patients who had neutrophil engraftment went on to have platelet engraftment. The probability of 12-month overall survival was 81.2%, reported Allyson Flower, MD, from Boston Children’s Health Physicians in Hawthorne, N.Y. “The probability of grade II-IV acute graft vs. host disease was 12.5%, compared with 32.5% seen with unrelated cord blood in our group’s previous studies. Cellular immune reconstitution was robust,” she said at the annual meeting of the American Society of Pediatric Hematology/Oncology.
Augmenting cord blood
Although unrelated donor cord blood transplantation expands the donor pool, is rapidly available, and is associated with decreases in both severe acute graft vs. host disease (GVHD) and chronic GVHD, compared with other stem cell sources, the technique is hampered by limited cell doses, prolonged immune reconstitution time, delays in hematopoietic recovery, and a higher incidence of graft failure.
Early studies of myeloablative conditioning followed by unrelated umbilical or placental blood transplantation showed a median of 22-24 days to neutrophil engraftment (Blood 1996 88:795-802; N Engl J Med. 1996;335:157-66), Dr. Flower noted.
More recently, a multivariate analysis of patients who underwent reduced-intensity conditioning followed by hematopoietic stem cell transplant with unrelated cord blood showed that graft failure was an independent risk factor for worse overall survival (Biol Blood Marrow Transplant. 2013 Apr;19:4;552-61).
Multiple groups have shown that adding human placenta–derived stem cells (HPDSC) to cord blood transplantation can facilitate more rapid hematopoietic engraftment by increasing the number of stem cells, increasing the proportion of hematopoietic progenitor cells, and providing additional, immature CD34+/CD45– progenitor cells.
In a single-arm, nonrandomized study, the investigators enrolled 16 patients ranging in age from 0.3 to 15.7 years with inborn errors of metabolism, marrow failure syndromes, severe immunodeficiency states, or hematologic malignancies.
Malignant conditions included B-cell precursor acute lymphoblastic leukemia (B-ALL; four patients), acute myeloid leukemia (AML; two), and T-cell ALL (one) in first complete remission, and T-cell lymphoblastic lymphoma following induction failure (one). Nonmalignant conditions included adrenoleukodystrophy (two patients), amegakaryotic thrombocytopenia (one), severe combined immunodeficiency (SCID; two), dyskeratosis congenita (one), chronic granulomatous disease (one), and severe congenital neutropenia (one).
The patients first underwent either myeloablative or reduced-intensity conditioning, followed 10 days later by infusion of unrelated cord blood and HPDSCs. Prior to HPDSC infusion, patients were medicated with diphenhydramine and hydrocortisone to prevent or reduce potential sensitivity reactions. HPDSCs were infused no sooner than 4 hours after the end of the cord blood infusion.
Patients received GVHD prophylaxis with either tacrolimus or cyclosporine, plus mycophenolate mofetil.
The combination appeared to be safe, with no cases of grade 3 or 4 toxicity secondary to HPDSC infusion.
The probability of neutrophil engraftment was 87.5%, with engraftment occurring at a median of 23 days (range 13-53). As noted before, all patients who had neutrophil engraftment had platelet engraftment, which was achieved at a median of 47 days (range, 20-98). In the group’s previous studies, median time to platelet engraftment was 53 days for patients who had undergone reduced-intensity conditioning, and 118 days for patients who had undergone myeloablation.
The probability of grade 2-4 acute GVHD within 100 days was 12.5%, and there were no cases of chronic GVHD.
Respective percentages of cord blood donor chimerism at days 30, 60, 100, and 180 were 88%, 98%, 99%, and 99%.
Immune reconstitution was strong, with normalization of mean CD3+, CD19+, and CD56+ cells occurring by day 100, CD8+ cells by day 180, and CD4+ cells by day 270.
There were three patient deaths: one from adenoviremia in a patient with B-ALL and CNS relapse, who had neutrophil engraftment at day 21; one in a patient with SCID, from adenoviremia and multiple system organ failure, who did not have engraftment before death; and one in a patient with severe congenital neutrophilia, who also did not have neutrophil engraftment.
None of the eight patients with malignant disease have experienced relapse to date, Dr. Flower noted.
The study was funded by a grant from Celgene Cellular Therapeutics. Dr. Flower reported having no conflicts of interest.
Key clinical point: A combination of donor cord blood and human placenta–derived stem cells induced more rapid engraftment than cord blood alone.
Major finding: The probability of 12-month overall survival was 81%.
Data source: Open-label single-arm study in 16 children with severe malignant and nonmalignant diseases requiring hematopoietic stem cell transplants.
Disclosures: The study was funded by a grant from Celgene Cellular Therapeutics. Dr. Flower reported having no conflicts of interest.

Routine surveillance adds cost but little benefit following a pediatric tumor
MONTREAL – It can be a tough sell to worried patients or their caregivers, but surveillance imaging in children with a history of some treated solid tumors may not add anything to care except costs, a team of investigators suggested.
A study of the relationship between surveillance imaging and outcomes in patients who were followed after therapy for solid tumors found that “off therapy surveillance imaging did not affect outcomes in our relapsed solid tumor patients,” wrote Jacob Zimmerli and his coinvestigators at the University of Utah Huntsman Cancer Institute, Salt Lake City.
“In the case of rhabdomyosarcoma, we had a 31% relapse rate of our 39 unique cancer diagnoses that we looked at over a 10-year period. We had 12 relapses, and, of those relapses, 10 were found through nonroutine imaging,” Mr. Zimmerli said in an interview.
Survival rates for patients with rhabdomyosarcoma were identical whether their relapsed disease was detected via surveillance imaging or imaging performed when relapse was directly suspected because of clinical or physical findings, he said.
Surveillance imaging also came at a significant financial cost. Of the $345,000 total expenditure for imaging of rhabdomyosarcoma, $223,000 was spent on imaging for patients who never experienced a relapse. Additionally, $95,000 was spent on imaging for patients who had a relapse but whose relapses were not detected by routine surveillance imaging. Therefore, the investigators calculated, 92% of costs associated with surveillance did not lead to a relapse diagnosis.
“This finding in itself will lead us to look at a few more specific cancer subgroups and maybe do more cost analysis to see if there is a better way to treat these patients,” Mr. Zimmerli said.
To see whether surveillance imaging was associated with outcomes, the investigators performed a retrospective review of data on 292 patients treated at Primary Children’s Hospital in Salt Lake City for osteosarcoma, Wilms’ tumor, neuroblastoma, hepatoblastoma, Ewing sarcoma , or rhabdomyosarcoma.
All patients had either completed a minimum of 2 years of posttherapy follow-up or had a disease relapse within 2 years of completing therapy.
The investigators found that 8 of 10 osteosarcoma relapses, five of seven Wilms’ tumor relapses, and 9 of 15 neuroblastoma relapses were detected on routine imaging.
In contrast, only two of four hepatoblastoma relapses, three of nine Ewings sarcoma relapses, and 2 of 12 rhabdomyosarcoma relapses were found on routine imaging.
The overall survival rate for patients with relapses diagnosed on routine imaging was 51.72%, compared with 50% for patients whose relapses were diagnosed on imaging following the appearance of symptoms. The difference represented only one patient and was not statistically significant.
Mr. Zimmerli acknowledged that many routine posttherapy imaging studies are performed to assuage patient concerns and that it may be difficult to convince parents of children with a history of cancer that routine imaging of some tumors may not offer the assurances of relapse-free survival that they seek.
The study was supported by Intermountain Healthcare. The investigators reported no conflicts of interest.
MONTREAL – It can be a tough sell to worried patients or their caregivers, but surveillance imaging in children with a history of some treated solid tumors may not add anything to care except costs, a team of investigators suggested.
A study of the relationship between surveillance imaging and outcomes in patients who were followed after therapy for solid tumors found that “off therapy surveillance imaging did not affect outcomes in our relapsed solid tumor patients,” wrote Jacob Zimmerli and his coinvestigators at the University of Utah Huntsman Cancer Institute, Salt Lake City.
“In the case of rhabdomyosarcoma, we had a 31% relapse rate of our 39 unique cancer diagnoses that we looked at over a 10-year period. We had 12 relapses, and, of those relapses, 10 were found through nonroutine imaging,” Mr. Zimmerli said in an interview.
Survival rates for patients with rhabdomyosarcoma were identical whether their relapsed disease was detected via surveillance imaging or imaging performed when relapse was directly suspected because of clinical or physical findings, he said.
Surveillance imaging also came at a significant financial cost. Of the $345,000 total expenditure for imaging of rhabdomyosarcoma, $223,000 was spent on imaging for patients who never experienced a relapse. Additionally, $95,000 was spent on imaging for patients who had a relapse but whose relapses were not detected by routine surveillance imaging. Therefore, the investigators calculated, 92% of costs associated with surveillance did not lead to a relapse diagnosis.
“This finding in itself will lead us to look at a few more specific cancer subgroups and maybe do more cost analysis to see if there is a better way to treat these patients,” Mr. Zimmerli said.
To see whether surveillance imaging was associated with outcomes, the investigators performed a retrospective review of data on 292 patients treated at Primary Children’s Hospital in Salt Lake City for osteosarcoma, Wilms’ tumor, neuroblastoma, hepatoblastoma, Ewing sarcoma , or rhabdomyosarcoma.
All patients had either completed a minimum of 2 years of posttherapy follow-up or had a disease relapse within 2 years of completing therapy.
The investigators found that 8 of 10 osteosarcoma relapses, five of seven Wilms’ tumor relapses, and 9 of 15 neuroblastoma relapses were detected on routine imaging.
In contrast, only two of four hepatoblastoma relapses, three of nine Ewings sarcoma relapses, and 2 of 12 rhabdomyosarcoma relapses were found on routine imaging.
The overall survival rate for patients with relapses diagnosed on routine imaging was 51.72%, compared with 50% for patients whose relapses were diagnosed on imaging following the appearance of symptoms. The difference represented only one patient and was not statistically significant.
Mr. Zimmerli acknowledged that many routine posttherapy imaging studies are performed to assuage patient concerns and that it may be difficult to convince parents of children with a history of cancer that routine imaging of some tumors may not offer the assurances of relapse-free survival that they seek.
The study was supported by Intermountain Healthcare. The investigators reported no conflicts of interest.
MONTREAL – It can be a tough sell to worried patients or their caregivers, but surveillance imaging in children with a history of some treated solid tumors may not add anything to care except costs, a team of investigators suggested.
A study of the relationship between surveillance imaging and outcomes in patients who were followed after therapy for solid tumors found that “off therapy surveillance imaging did not affect outcomes in our relapsed solid tumor patients,” wrote Jacob Zimmerli and his coinvestigators at the University of Utah Huntsman Cancer Institute, Salt Lake City.
“In the case of rhabdomyosarcoma, we had a 31% relapse rate of our 39 unique cancer diagnoses that we looked at over a 10-year period. We had 12 relapses, and, of those relapses, 10 were found through nonroutine imaging,” Mr. Zimmerli said in an interview.
Survival rates for patients with rhabdomyosarcoma were identical whether their relapsed disease was detected via surveillance imaging or imaging performed when relapse was directly suspected because of clinical or physical findings, he said.
Surveillance imaging also came at a significant financial cost. Of the $345,000 total expenditure for imaging of rhabdomyosarcoma, $223,000 was spent on imaging for patients who never experienced a relapse. Additionally, $95,000 was spent on imaging for patients who had a relapse but whose relapses were not detected by routine surveillance imaging. Therefore, the investigators calculated, 92% of costs associated with surveillance did not lead to a relapse diagnosis.
“This finding in itself will lead us to look at a few more specific cancer subgroups and maybe do more cost analysis to see if there is a better way to treat these patients,” Mr. Zimmerli said.
To see whether surveillance imaging was associated with outcomes, the investigators performed a retrospective review of data on 292 patients treated at Primary Children’s Hospital in Salt Lake City for osteosarcoma, Wilms’ tumor, neuroblastoma, hepatoblastoma, Ewing sarcoma , or rhabdomyosarcoma.
All patients had either completed a minimum of 2 years of posttherapy follow-up or had a disease relapse within 2 years of completing therapy.
The investigators found that 8 of 10 osteosarcoma relapses, five of seven Wilms’ tumor relapses, and 9 of 15 neuroblastoma relapses were detected on routine imaging.
In contrast, only two of four hepatoblastoma relapses, three of nine Ewings sarcoma relapses, and 2 of 12 rhabdomyosarcoma relapses were found on routine imaging.
The overall survival rate for patients with relapses diagnosed on routine imaging was 51.72%, compared with 50% for patients whose relapses were diagnosed on imaging following the appearance of symptoms. The difference represented only one patient and was not statistically significant.
Mr. Zimmerli acknowledged that many routine posttherapy imaging studies are performed to assuage patient concerns and that it may be difficult to convince parents of children with a history of cancer that routine imaging of some tumors may not offer the assurances of relapse-free survival that they seek.
The study was supported by Intermountain Healthcare. The investigators reported no conflicts of interest.
FROM ASPHO
Key clinical point: Routine surveillance was less effective at detecting relapse of some pediatric solid tumors than imaging performed to confirm a clinical finding.
Major finding: Using imaging performed after symptoms appeared, 10 of 12 rhabdomyosarcoma relapses were detected.
Data source: A retrospective review of outcomes following routine and nonroutine imaging among children followed after treatment for one of six solid tumor types.
Disclosures: The study was supported by Intermountain Healthcare. The investigators reported no conflicts of interest.
FDA approves first ready-to-use oral solution of methotrexate

The US Food and Drug Administration (FDA) has approved a ready-to-use oral solution of methotrexate (Xatmep) for use in certain pediatric patients.
The drug is approved as part of a multi-phase, combination chemotherapy maintenance regimen to treat pediatric patients with acute lymphoblastic leukemia.
Xatmep is also approved for use in pediatric patients with active polyarticular juvenile idiopathic arthritis who have had an insufficient response to, or cannot tolerate, an adequate trial of first-line therapy, including full-dose non-steroidal anti-inflammatory agents.
Xatmep is the first ready-to-use oral solution of methotrexate to be approved by the FDA.
There was previously no such formulation of the drug approved for use in pediatric patients requiring body surface area dosing (mg/m2), patients who have difficulty swallowing or cannot consume tablets, or those with needle-phobia.
Xatmep (methotrexate) Oral Solution, 2.5 mg/mL, requires no preparation. It eliminates the need for needles, crushing or splitting tablets, or for compounding tablets into a liquid formulation.
Xatmep requires refrigeration but may be stored at room temperature for 60 days after dispensing.
For more on Xatmep, see the prescribing information, which includes a boxed warning detailing the risk of severe toxic reactions, including embryo-fetal toxicity.
Xatmep is available through pharmacies and a qualified mail-order service. For information on how to obtain the drug, call 1-855-379-0382.
Xatmep is a product of Silvergate Pharmaceuticals, Inc. ![]()
The US Food and Drug Administration (FDA) has approved a ready-to-use oral solution of methotrexate (Xatmep) for use in certain pediatric patients.
The drug is approved as part of a multi-phase, combination chemotherapy maintenance regimen to treat pediatric patients with acute lymphoblastic leukemia.
Xatmep is also approved for use in pediatric patients with active polyarticular juvenile idiopathic arthritis who have had an insufficient response to, or cannot tolerate, an adequate trial of first-line therapy, including full-dose non-steroidal anti-inflammatory agents.
Xatmep is the first ready-to-use oral solution of methotrexate to be approved by the FDA.
There was previously no such formulation of the drug approved for use in pediatric patients requiring body surface area dosing (mg/m2), patients who have difficulty swallowing or cannot consume tablets, or those with needle-phobia.
Xatmep (methotrexate) Oral Solution, 2.5 mg/mL, requires no preparation. It eliminates the need for needles, crushing or splitting tablets, or for compounding tablets into a liquid formulation.
Xatmep requires refrigeration but may be stored at room temperature for 60 days after dispensing.
For more on Xatmep, see the prescribing information, which includes a boxed warning detailing the risk of severe toxic reactions, including embryo-fetal toxicity.
Xatmep is available through pharmacies and a qualified mail-order service. For information on how to obtain the drug, call 1-855-379-0382.
Xatmep is a product of Silvergate Pharmaceuticals, Inc. ![]()
The US Food and Drug Administration (FDA) has approved a ready-to-use oral solution of methotrexate (Xatmep) for use in certain pediatric patients.
The drug is approved as part of a multi-phase, combination chemotherapy maintenance regimen to treat pediatric patients with acute lymphoblastic leukemia.
Xatmep is also approved for use in pediatric patients with active polyarticular juvenile idiopathic arthritis who have had an insufficient response to, or cannot tolerate, an adequate trial of first-line therapy, including full-dose non-steroidal anti-inflammatory agents.
Xatmep is the first ready-to-use oral solution of methotrexate to be approved by the FDA.
There was previously no such formulation of the drug approved for use in pediatric patients requiring body surface area dosing (mg/m2), patients who have difficulty swallowing or cannot consume tablets, or those with needle-phobia.
Xatmep (methotrexate) Oral Solution, 2.5 mg/mL, requires no preparation. It eliminates the need for needles, crushing or splitting tablets, or for compounding tablets into a liquid formulation.
Xatmep requires refrigeration but may be stored at room temperature for 60 days after dispensing.
For more on Xatmep, see the prescribing information, which includes a boxed warning detailing the risk of severe toxic reactions, including embryo-fetal toxicity.
Xatmep is available through pharmacies and a qualified mail-order service. For information on how to obtain the drug, call 1-855-379-0382.
Xatmep is a product of Silvergate Pharmaceuticals, Inc. ![]()
Pediatric psoriasis may have a distinct presentation
Children may have a distinctive presentation of psoriasis, compared with adults, Dr. Wynnis Tom said at a pediatric dermatology meeting sponsored by Rady Children’s Hospital–San Diego and UC San Diego School of Medicine.
Infants may present with diaper involvement, also known as “napkin psoriasis,” which may be confused with irritant dermatitis or perineal infections. Moreover, guttate psoriasis, which can be preceded by infectious triggers such as Streptococcus and appears as small, salmon-pink bumps on the skin, is more frequent in children than adults, said Dr. Tom, associate professor of dermatology and pediatrics at the university.

Patients with psoriasis are at higher risk for psychiatric disorders, especially depression and anxiety. A study by Varni et al. discussed QOL ratings by 208 children aged 4-17 years with moderate to severe plaque disease. The study demonstrated a significant negative QOL impact in patients with plaque psoriasis, comparable to the impairment of QOL from arthritis or asthma (Eur J Pediatr. 2011 Sep 30;171[3]485-92).
Dr. Tom talked about other comorbidities associated with psoriasis, including psoriatic arthritis, and encouraged physicians to inquire about morning stiffness, joint pains, swelling, and gait abnormalities. “Psoriatic arthritis occurs in about 10% of children, and it is essential to detect early to prevent permanent joint damage,” she said. “Over the past decade, psoriasis has resurfaced as a systemic disorder as it may be associated with obesity, metabolic syndrome, and inflammatory bowel disease.” Psoriasis also entails an increased risk for cardiovascular disease, myocardial infarction, and stroke.
Dr. Tom emphasized, “because of these risks, we need to extend comorbidity screening to the pediatric population.”
Management of pediatric psoriasis has focused on topical and systemic therapies, in addition to phototherapies. Most systemic agents are used off-label on the basis of experience rather than evidence. Clinical trials are currently underway to extend indications for systemic therapy to the pediatric age group, she said.
Dr. Tom disclosed she is an investigator for Promius Pharma, Celgene, and Janssen.
Children may have a distinctive presentation of psoriasis, compared with adults, Dr. Wynnis Tom said at a pediatric dermatology meeting sponsored by Rady Children’s Hospital–San Diego and UC San Diego School of Medicine.
Infants may present with diaper involvement, also known as “napkin psoriasis,” which may be confused with irritant dermatitis or perineal infections. Moreover, guttate psoriasis, which can be preceded by infectious triggers such as Streptococcus and appears as small, salmon-pink bumps on the skin, is more frequent in children than adults, said Dr. Tom, associate professor of dermatology and pediatrics at the university.
Patients with psoriasis are at higher risk for psychiatric disorders, especially depression and anxiety. A study by Varni et al. discussed QOL ratings by 208 children aged 4-17 years with moderate to severe plaque disease. The study demonstrated a significant negative QOL impact in patients with plaque psoriasis, comparable to the impairment of QOL from arthritis or asthma (Eur J Pediatr. 2011 Sep 30;171[3]485-92).
Dr. Tom talked about other comorbidities associated with psoriasis, including psoriatic arthritis, and encouraged physicians to inquire about morning stiffness, joint pains, swelling, and gait abnormalities. “Psoriatic arthritis occurs in about 10% of children, and it is essential to detect early to prevent permanent joint damage,” she said. “Over the past decade, psoriasis has resurfaced as a systemic disorder as it may be associated with obesity, metabolic syndrome, and inflammatory bowel disease.” Psoriasis also entails an increased risk for cardiovascular disease, myocardial infarction, and stroke.
Dr. Tom emphasized, “because of these risks, we need to extend comorbidity screening to the pediatric population.”
Management of pediatric psoriasis has focused on topical and systemic therapies, in addition to phototherapies. Most systemic agents are used off-label on the basis of experience rather than evidence. Clinical trials are currently underway to extend indications for systemic therapy to the pediatric age group, she said.
Dr. Tom disclosed she is an investigator for Promius Pharma, Celgene, and Janssen.
Children may have a distinctive presentation of psoriasis, compared with adults, Dr. Wynnis Tom said at a pediatric dermatology meeting sponsored by Rady Children’s Hospital–San Diego and UC San Diego School of Medicine.
Infants may present with diaper involvement, also known as “napkin psoriasis,” which may be confused with irritant dermatitis or perineal infections. Moreover, guttate psoriasis, which can be preceded by infectious triggers such as Streptococcus and appears as small, salmon-pink bumps on the skin, is more frequent in children than adults, said Dr. Tom, associate professor of dermatology and pediatrics at the university.
Patients with psoriasis are at higher risk for psychiatric disorders, especially depression and anxiety. A study by Varni et al. discussed QOL ratings by 208 children aged 4-17 years with moderate to severe plaque disease. The study demonstrated a significant negative QOL impact in patients with plaque psoriasis, comparable to the impairment of QOL from arthritis or asthma (Eur J Pediatr. 2011 Sep 30;171[3]485-92).
Dr. Tom talked about other comorbidities associated with psoriasis, including psoriatic arthritis, and encouraged physicians to inquire about morning stiffness, joint pains, swelling, and gait abnormalities. “Psoriatic arthritis occurs in about 10% of children, and it is essential to detect early to prevent permanent joint damage,” she said. “Over the past decade, psoriasis has resurfaced as a systemic disorder as it may be associated with obesity, metabolic syndrome, and inflammatory bowel disease.” Psoriasis also entails an increased risk for cardiovascular disease, myocardial infarction, and stroke.
Dr. Tom emphasized, “because of these risks, we need to extend comorbidity screening to the pediatric population.”
Management of pediatric psoriasis has focused on topical and systemic therapies, in addition to phototherapies. Most systemic agents are used off-label on the basis of experience rather than evidence. Clinical trials are currently underway to extend indications for systemic therapy to the pediatric age group, she said.
Dr. Tom disclosed she is an investigator for Promius Pharma, Celgene, and Janssen.