User login
Oral antibiotics successfully treat community-acquired pneumonia with empyema
MADRID – Outpatient oral antibiotics were more successful than outpatient parenteral antibiotic therapy at treating children with community-acquired pneumonia complicated by empyema, in a study presented at the annual meeting of the European Society for Paediatric Infectious Diseases.
Thirty-five percent of the patients were culture positive, a typically low rate that makes treatment of this disease particularly challenging, Lauren Kushner, a medical student at the University of California, Irvine, and one of the study’s authors, said at the meeting.
The treatment success rates, which were defined as improvement with no change in treatment, were 93% for the patients taking oral antibiotics and 58% in the patients on outpatient parenteral antibiotic therapy.
This retrospective observational study included 149 patients under age 18 years hospitalized for community-acquired pneumonia complicated by empyema, at Children’s Hospital of Orange County, Calif. Only 12 of the patients were treated with parenteral antibiotic therapy and none of the study participants had comorbid chronic medical conditions. As in other studies, Streptococcus pneumoniae was the most commonly identified pathogen.
Laboratory markers of inflammation are useful in guiding oral antibiotic therapy for children with CAP complicated by empyema, reported Ms. Kushner.
“A rapid drop in C-reactive protein [CRP] in combination with a decrease in white blood cell count [WBC] can be used acutely in the hospitalization phase to tell you the patient is improving on the selected antibiotic and also to help dictate when the patient might be able to go home, whereas improvement in the erythrocyte sedimentation rate [ESR] does not happen until much later in the course of treatment but can be used to tell you when a patient has been adequately treated,” said Ms. Kushner.
One hundred thirty-seven patients were discharged on oral antibiotic therapy, as is strongly recommended in Infectious Diseases Society of America guidelines for postdischarge treatment of complicated pneumonia, even though there are no randomized clinical trials demonstrating it to be superior or even noninferior to outpatient parenteral antibiotics. An aminopenicillin was the most frequently prescribed type of oral antibiotic, while ceftriaxone was the top choice for outpatient parenteral therapy.
The average total duration of antibiotic therapy, inpatient plus outpatient, was similar in the two groups: 30.4 days in the oral antibiotic group and 33.2 days in children on outpatient IV therapy.
The transition to oral therapy occurred a median of 6 days after admission. At that point, CRP levels had dropped sharply by a mean of 204 mg/L from a baseline of more than 250 mg/L at admission. In the same time frame, mean WBC dropped by 6,400 cells/mcL from close to 20,000/mcL at admission. Thus, sharp declines in these two inflammatory markers while a patient is still in the hospital provide reassurance that antibiotic therapy is on the right track. Their rate of decline slowed considerably after the switch to oral therapy: for example, mean CRP decreased by only another 44 mg/L from switch to discharge, and by a further 19 mg/L from discharge to end of treatment.
In contrast, the mean ESR remained elevated at a level approaching 100 mm/hour with little fluctuation from admission through discharge. Weekly monitoring of ESR post discharge showed that this inflammatory marker improved only late in the course of oral therapy. A drop to less than 30 mm/hour indicates the infection has resolved, Ms. Kushner said.
She noted that in contrast to her study findings, a recent multicenter, 2,123-patient study by the Pediatric Research in Inpatient Settings Network found that treatment failure rates didn’t differ significantly between the two treatment strategies (Pediatrics. 2016 Dec;138[6]. pii: e20161692). Similarly, a retrospective study of 391 children with empyema admitted to Primary Children’s Hospital in Salt Lake City found closely similar rates of treatment failure and other complications regardless of whether the patients were placed on outpatient oral or parenteral antibiotic therapy (Hosp Pediatr. 2015 Dec;5[12]:605-12).
Ms. Kushner reported having no financial conflicts of interest regarding the study.
MADRID – Outpatient oral antibiotics were more successful than outpatient parenteral antibiotic therapy at treating children with community-acquired pneumonia complicated by empyema, in a study presented at the annual meeting of the European Society for Paediatric Infectious Diseases.
Thirty-five percent of the patients were culture positive, a typically low rate that makes treatment of this disease particularly challenging, Lauren Kushner, a medical student at the University of California, Irvine, and one of the study’s authors, said at the meeting.
The treatment success rates, which were defined as improvement with no change in treatment, were 93% for the patients taking oral antibiotics and 58% in the patients on outpatient parenteral antibiotic therapy.
This retrospective observational study included 149 patients under age 18 years hospitalized for community-acquired pneumonia complicated by empyema, at Children’s Hospital of Orange County, Calif. Only 12 of the patients were treated with parenteral antibiotic therapy and none of the study participants had comorbid chronic medical conditions. As in other studies, Streptococcus pneumoniae was the most commonly identified pathogen.
Laboratory markers of inflammation are useful in guiding oral antibiotic therapy for children with CAP complicated by empyema, reported Ms. Kushner.
“A rapid drop in C-reactive protein [CRP] in combination with a decrease in white blood cell count [WBC] can be used acutely in the hospitalization phase to tell you the patient is improving on the selected antibiotic and also to help dictate when the patient might be able to go home, whereas improvement in the erythrocyte sedimentation rate [ESR] does not happen until much later in the course of treatment but can be used to tell you when a patient has been adequately treated,” said Ms. Kushner.
One hundred thirty-seven patients were discharged on oral antibiotic therapy, as is strongly recommended in Infectious Diseases Society of America guidelines for postdischarge treatment of complicated pneumonia, even though there are no randomized clinical trials demonstrating it to be superior or even noninferior to outpatient parenteral antibiotics. An aminopenicillin was the most frequently prescribed type of oral antibiotic, while ceftriaxone was the top choice for outpatient parenteral therapy.
The average total duration of antibiotic therapy, inpatient plus outpatient, was similar in the two groups: 30.4 days in the oral antibiotic group and 33.2 days in children on outpatient IV therapy.
The transition to oral therapy occurred a median of 6 days after admission. At that point, CRP levels had dropped sharply by a mean of 204 mg/L from a baseline of more than 250 mg/L at admission. In the same time frame, mean WBC dropped by 6,400 cells/mcL from close to 20,000/mcL at admission. Thus, sharp declines in these two inflammatory markers while a patient is still in the hospital provide reassurance that antibiotic therapy is on the right track. Their rate of decline slowed considerably after the switch to oral therapy: for example, mean CRP decreased by only another 44 mg/L from switch to discharge, and by a further 19 mg/L from discharge to end of treatment.
In contrast, the mean ESR remained elevated at a level approaching 100 mm/hour with little fluctuation from admission through discharge. Weekly monitoring of ESR post discharge showed that this inflammatory marker improved only late in the course of oral therapy. A drop to less than 30 mm/hour indicates the infection has resolved, Ms. Kushner said.
She noted that in contrast to her study findings, a recent multicenter, 2,123-patient study by the Pediatric Research in Inpatient Settings Network found that treatment failure rates didn’t differ significantly between the two treatment strategies (Pediatrics. 2016 Dec;138[6]. pii: e20161692). Similarly, a retrospective study of 391 children with empyema admitted to Primary Children’s Hospital in Salt Lake City found closely similar rates of treatment failure and other complications regardless of whether the patients were placed on outpatient oral or parenteral antibiotic therapy (Hosp Pediatr. 2015 Dec;5[12]:605-12).
Ms. Kushner reported having no financial conflicts of interest regarding the study.
MADRID – Outpatient oral antibiotics were more successful than outpatient parenteral antibiotic therapy at treating children with community-acquired pneumonia complicated by empyema, in a study presented at the annual meeting of the European Society for Paediatric Infectious Diseases.
Thirty-five percent of the patients were culture positive, a typically low rate that makes treatment of this disease particularly challenging, Lauren Kushner, a medical student at the University of California, Irvine, and one of the study’s authors, said at the meeting.
The treatment success rates, which were defined as improvement with no change in treatment, were 93% for the patients taking oral antibiotics and 58% in the patients on outpatient parenteral antibiotic therapy.
This retrospective observational study included 149 patients under age 18 years hospitalized for community-acquired pneumonia complicated by empyema, at Children’s Hospital of Orange County, Calif. Only 12 of the patients were treated with parenteral antibiotic therapy and none of the study participants had comorbid chronic medical conditions. As in other studies, Streptococcus pneumoniae was the most commonly identified pathogen.
Laboratory markers of inflammation are useful in guiding oral antibiotic therapy for children with CAP complicated by empyema, reported Ms. Kushner.
“A rapid drop in C-reactive protein [CRP] in combination with a decrease in white blood cell count [WBC] can be used acutely in the hospitalization phase to tell you the patient is improving on the selected antibiotic and also to help dictate when the patient might be able to go home, whereas improvement in the erythrocyte sedimentation rate [ESR] does not happen until much later in the course of treatment but can be used to tell you when a patient has been adequately treated,” said Ms. Kushner.
One hundred thirty-seven patients were discharged on oral antibiotic therapy, as is strongly recommended in Infectious Diseases Society of America guidelines for postdischarge treatment of complicated pneumonia, even though there are no randomized clinical trials demonstrating it to be superior or even noninferior to outpatient parenteral antibiotics. An aminopenicillin was the most frequently prescribed type of oral antibiotic, while ceftriaxone was the top choice for outpatient parenteral therapy.
The average total duration of antibiotic therapy, inpatient plus outpatient, was similar in the two groups: 30.4 days in the oral antibiotic group and 33.2 days in children on outpatient IV therapy.
The transition to oral therapy occurred a median of 6 days after admission. At that point, CRP levels had dropped sharply by a mean of 204 mg/L from a baseline of more than 250 mg/L at admission. In the same time frame, mean WBC dropped by 6,400 cells/mcL from close to 20,000/mcL at admission. Thus, sharp declines in these two inflammatory markers while a patient is still in the hospital provide reassurance that antibiotic therapy is on the right track. Their rate of decline slowed considerably after the switch to oral therapy: for example, mean CRP decreased by only another 44 mg/L from switch to discharge, and by a further 19 mg/L from discharge to end of treatment.
In contrast, the mean ESR remained elevated at a level approaching 100 mm/hour with little fluctuation from admission through discharge. Weekly monitoring of ESR post discharge showed that this inflammatory marker improved only late in the course of oral therapy. A drop to less than 30 mm/hour indicates the infection has resolved, Ms. Kushner said.
She noted that in contrast to her study findings, a recent multicenter, 2,123-patient study by the Pediatric Research in Inpatient Settings Network found that treatment failure rates didn’t differ significantly between the two treatment strategies (Pediatrics. 2016 Dec;138[6]. pii: e20161692). Similarly, a retrospective study of 391 children with empyema admitted to Primary Children’s Hospital in Salt Lake City found closely similar rates of treatment failure and other complications regardless of whether the patients were placed on outpatient oral or parenteral antibiotic therapy (Hosp Pediatr. 2015 Dec;5[12]:605-12).
Ms. Kushner reported having no financial conflicts of interest regarding the study.
AT ESPID 2017
Key clinical point:
Major finding: The treatment success rate with outpatient oral antibiotic therapy for pediatric community-acquired pneumonia with empyema was 93% in a retrospective study, significantly better than the 58% rate in a much smaller group of patients discharged with outpatient parenteral antibiotic therapy.
Data source: This retrospective single-center study included 149 patients under age 18 years hospitalized for community-acquired pneumonia complicated by empyema and later sent home on either oral or parenteral antibiotic therapy.
Disclosures: The study presenter reported having no financial conflicts of interest.
When families participate in rounds, errors decrease
NASHVILLE, TENN. – When families are actively included in pediatric hospital rounds, preventable adverse events drop 38% and families report better hospital experiences, with no negative impact on rounds duration or teaching, according to a prospective investigation on inpatient pediatric units of seven North American hospitals.

“We always talk about how parents know their children better than anyone else; empowering the family to know what we are looking for can have downstream safety implications,” she said. In the study, families often caught problems before medical staff, such as IV infiltrations. They also reported delays in diagnoses and conflicting information, among other things, Dr. Khan explained at the Pediatric Hospital Medicine meeting.
There’s not much data on family-centered rounds in pediatric medicine, so Dr. Khan and her team decided to investigate. They modified the I-PASS resident handoff model (illness severity; patient summary; action list; situation awareness and contingency planning; and synthesis by receiver) to be more family friendly.
Families were given a short form before rounds that asked if their child was better, worse, or about the same as the day before, and what questions and items they wanted to address. There was also space for them to take notes during the presentation about what had changed overnight, what still needed to be done, and what to look out for.
Families were given the opportunity to speak first during rounds, and medical staff used plain language: “has a fever” instead of “febrile,” for instance. At the end of the presentation, families were asked to read back their take-aways.
The investigators compared baseline data from the 3 months before implementation with data for the 3 months afterward. The study included more than 1,500 patients and more than 300 rounds in both the pre- and postimplementation arms. The children were general inpatients; surgery and ICU patients were excluded.
Harmful errors/preventable AEs dropped from 20.7/1,000 patients days to 12.9/1,000 after implementation, a 38% reduction (P = .01). There was also a reduction in overall AEs from 34 to 18.5/1,000 patient-days (P = .002).
Compared with baseline data, after implementation, families were more likely to report that they understood the medical plan and what was said on rounds. They also were more likely to report that nurses had addressed their concerns and made them feel like an important member of the team.
Direct observation of pre- and postimplementation rounds showed that family and nursing engagement improved and families more often got written updates. There were no statistically significant differences in rounds duration or decreases in teaching.
“Congratulations. This is very impressive work, and also the right thing to do,” an audience member said after Dr. Khan’s presentation at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
The work was funded by the Patient-Centered Outcomes Research Institute and the Agency for Healthcare Research and Quality. Dr. Khan had no disclosures.
NASHVILLE, TENN. – When families are actively included in pediatric hospital rounds, preventable adverse events drop 38% and families report better hospital experiences, with no negative impact on rounds duration or teaching, according to a prospective investigation on inpatient pediatric units of seven North American hospitals.
“We always talk about how parents know their children better than anyone else; empowering the family to know what we are looking for can have downstream safety implications,” she said. In the study, families often caught problems before medical staff, such as IV infiltrations. They also reported delays in diagnoses and conflicting information, among other things, Dr. Khan explained at the Pediatric Hospital Medicine meeting.
There’s not much data on family-centered rounds in pediatric medicine, so Dr. Khan and her team decided to investigate. They modified the I-PASS resident handoff model (illness severity; patient summary; action list; situation awareness and contingency planning; and synthesis by receiver) to be more family friendly.
Families were given a short form before rounds that asked if their child was better, worse, or about the same as the day before, and what questions and items they wanted to address. There was also space for them to take notes during the presentation about what had changed overnight, what still needed to be done, and what to look out for.
Families were given the opportunity to speak first during rounds, and medical staff used plain language: “has a fever” instead of “febrile,” for instance. At the end of the presentation, families were asked to read back their take-aways.
The investigators compared baseline data from the 3 months before implementation with data for the 3 months afterward. The study included more than 1,500 patients and more than 300 rounds in both the pre- and postimplementation arms. The children were general inpatients; surgery and ICU patients were excluded.
Harmful errors/preventable AEs dropped from 20.7/1,000 patients days to 12.9/1,000 after implementation, a 38% reduction (P = .01). There was also a reduction in overall AEs from 34 to 18.5/1,000 patient-days (P = .002).
Compared with baseline data, after implementation, families were more likely to report that they understood the medical plan and what was said on rounds. They also were more likely to report that nurses had addressed their concerns and made them feel like an important member of the team.
Direct observation of pre- and postimplementation rounds showed that family and nursing engagement improved and families more often got written updates. There were no statistically significant differences in rounds duration or decreases in teaching.
“Congratulations. This is very impressive work, and also the right thing to do,” an audience member said after Dr. Khan’s presentation at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
The work was funded by the Patient-Centered Outcomes Research Institute and the Agency for Healthcare Research and Quality. Dr. Khan had no disclosures.
NASHVILLE, TENN. – When families are actively included in pediatric hospital rounds, preventable adverse events drop 38% and families report better hospital experiences, with no negative impact on rounds duration or teaching, according to a prospective investigation on inpatient pediatric units of seven North American hospitals.
“We always talk about how parents know their children better than anyone else; empowering the family to know what we are looking for can have downstream safety implications,” she said. In the study, families often caught problems before medical staff, such as IV infiltrations. They also reported delays in diagnoses and conflicting information, among other things, Dr. Khan explained at the Pediatric Hospital Medicine meeting.
There’s not much data on family-centered rounds in pediatric medicine, so Dr. Khan and her team decided to investigate. They modified the I-PASS resident handoff model (illness severity; patient summary; action list; situation awareness and contingency planning; and synthesis by receiver) to be more family friendly.
Families were given a short form before rounds that asked if their child was better, worse, or about the same as the day before, and what questions and items they wanted to address. There was also space for them to take notes during the presentation about what had changed overnight, what still needed to be done, and what to look out for.
Families were given the opportunity to speak first during rounds, and medical staff used plain language: “has a fever” instead of “febrile,” for instance. At the end of the presentation, families were asked to read back their take-aways.
The investigators compared baseline data from the 3 months before implementation with data for the 3 months afterward. The study included more than 1,500 patients and more than 300 rounds in both the pre- and postimplementation arms. The children were general inpatients; surgery and ICU patients were excluded.
Harmful errors/preventable AEs dropped from 20.7/1,000 patients days to 12.9/1,000 after implementation, a 38% reduction (P = .01). There was also a reduction in overall AEs from 34 to 18.5/1,000 patient-days (P = .002).
Compared with baseline data, after implementation, families were more likely to report that they understood the medical plan and what was said on rounds. They also were more likely to report that nurses had addressed their concerns and made them feel like an important member of the team.
Direct observation of pre- and postimplementation rounds showed that family and nursing engagement improved and families more often got written updates. There were no statistically significant differences in rounds duration or decreases in teaching.
“Congratulations. This is very impressive work, and also the right thing to do,” an audience member said after Dr. Khan’s presentation at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
The work was funded by the Patient-Centered Outcomes Research Institute and the Agency for Healthcare Research and Quality. Dr. Khan had no disclosures.
AT PHM 2017
Key clinical point:
Major finding: Harmful errors/preventable AEs dropped from 20.7/1,000 patients days to 12.9 after implementation of a program to engage families in pediatric rounds, a 38% reduction (P = .01).
Data source: More than 600 pediatric inpatient rounds at seven North American hospitals.
Disclosures: The work was funded by the Patient-Centered Outcomes Research Institute and the Agency for Healthcare Research and Quality. The lead investigator had no disclosures.
New genetic causes of ichthyoses likely to emerge
CHICAGO– The way Keith Choate, MD, PhD, sees it, he and other clinicians are only beginning to scratch the surface on their understanding of the genetic causes of ichthyosis and ichthyosis syndromes.
“Despite the fact that we now understand that there are about 21,000 genes in the genome, we have very superficial understanding and functions known for only about 4,000 genes,” Dr. Choate of the departments of dermatology and genetics at Yale University, New Haven, Conn., said at the World Congress of Pediatric Dermatology. “Clinical insight is what’s driving all of the discovery. We continue to find new disorders, and these next-generation technologies really permit us to find the genetic basis for those disorders. I like to say that it’s the disorders that we don’t read about in the textbook that end up being the ones that are most interesting.”
Ichthyoses are cardinal disorders that occur when the normal pattern of epidermal differentiation is disrupted and leads to compensatory hyperproliferation. Clinically, ichthyoses present in a variety of ways, and more than 50 genes can cause them.

Dr. Choate is the principal investigator of the National Registry for Ichthyosis and Related Skin Types, which has been recruiting kindreds of ichthyosis patients within the United States and internationally. To date, they have provided genetic diagnoses for 674 of the 880 cases enrolled. The process involves phenotyping with a clinical history and photography, obtaining DNA from blood or saliva, and prescreening the DNA samples for mutations in 51 genes currently implicated in ichthyosis. Subjects without known mutations undergo whole exome or genome sequencing.
“We have created a unique resource in doing this,” he said. “Genotyped/phenotyped patients provide a resource for clinical and translational studies in disorders of keratinization.”
When the researchers examined patients from the registry who have epidermolytic presentations, 100% had mutations in the known genes, “so the biopsy is diagnostic,” Dr. Choate said. “About 80% have mutations in keratin 10, about 13% have mutations in keratin 1, and another 6% have mutations in keratin 2.”
About 85% of patients with recessive and syndromic disorders have mutations in this same 51-gene panel; 15% of cases don’t have mutations in those genes. “This is a similar fraction to what my colleagues have found at a variety of institutions around the world,” Dr. Choate said. “What’s fascinating is that this 15% has been the source of remarkable discovery.”
He then discussed three cases of a novel erythrokeratoderma phenotype that were referred to the registry. In one case, a boy had pervasive intellectual disability, congenital alopecia, and absence of the eyebrows. “Within the first days of life, he developed a significant erythroderma with copious scaling of the skin that persisted throughout life and that was unresponsive to a variety of different therapeutic interventions, including immunosuppressant medications,” Dr. Choate said. “He had nail dystrophy and progressive enamel decay with severe caries, leading to loss of all of his teeth by the age of 6.”
Another case was a child who died of cardiomyopathy at about 3 years of age. He had congenital absence of the eyebrows and eyelashes, nail dystrophy, and scaling. “About 2 weeks before his death, he had a skin biopsy that we would ultimately repurpose to identify a new genetic cause of what we would call the erythrokeratodermia-cardiomyopathy syndrome,” Dr. Choate said. “It included features of congenital erythroderma, defective dental enamel, abnormal nails, and progressive and lethal cardiomyopathy. When we did exome sequencing, we found that all three of these patients showed tightly clustered de novo mutations in a gene called desmoplakin (DSP). Other DSP mutations do not cause erythrokeratoderma.”
Electron microscopy showed aggregates of desmosomes, normal corneodesmosomes, widening of intercellular spaces, and abnormal lipid secretion. The finding led the researchers to conclude that clustered DSP mutations cause a novel cutaneous phenotype with erythrokeratoderma and progressive cardiomyopathy. “The next time an insurer refuses to do genetic testing for you in a patient who has erythrokeratoderma, this is the disorder that you want to cite as the reason why you need to do genetic testing,” he said.
In a recent study, Dr. Choate and his associates identified the genetic cause for a rare subtype of progressive symmetric erythrokeratoderma (PSEK), a disorder that features thick facial plaques and thickened palms and soles (Am J Hum Genet. 2017 Jun 1;100[6]:978-84). Histology reveals a thickened epidermis, loss of granular layer, and retention of nuclei in the stratum corneum. They discovered that PSEK was caused by mutations in 3-ketodihydrosphingosine reductase (KDSR), an enzyme that is central to de novo ceramides in skin.
“Ceramides are secreted by keratinocytes with cholesterol and free fatty acids to form the cutaneous lipid barrier,” he explained. “They also regulate cutaneous proliferation and differentiation. One of the things this story in particular told us was, when you find just one mutation and a compelling candidate gene and can’t find the other, it’s often because of how you’re approaching detection. In two of our cases, genome sequencing was necessary to find a large inversion, which disrupted the encoded protein. Finally, the challenge of studying ceramides is that it’s hard to get cells in culture to produce them. Therefore, we had to work with collaborators in yeast biology to prove pathogenesis.”
Dr. Choate cited other recent developments, including the discovery that familial pityriasis rubra pilaris is caused by mutations in CARD14, which is a known activator of nuclear factor kappa B signaling (Am J Hum Genet. 2012 Jul 13;91[1]:163-70). This led to the subsequent use of ustekinumab for patients with familial pityriasis rubra pilaris. Another group of researchers found that SULT2B1 encodes sulfotransferase family 2B member 1 and is central to epidermal cholesterol metabolism (Am J Hum Genet. 2017 Jun 1;100[6]:926-39).
“There are still new genetic causes of ichthyosis to be found, particularly cases that don’t meet the textbook criteria for the disorder,” he concluded. “Severe, dominant disorders primarily due to de novo mutations are fertile ground for discovery. Genetic investigation is critical to our understanding of disease biology and biology of the skin. It’s also potentially relevant to outcomes of therapy. [Erythrokeratodermia-cardiomyopathy syndrome] highlights the potential for comorbidities, and the efficacy of ustekinumab in familial [pityriasis rubra pilaris] highlights the therapeutic importance of understanding the pathway underlying the disease.”
Dr. Choate reported having no financial disclosures.
CHICAGO– The way Keith Choate, MD, PhD, sees it, he and other clinicians are only beginning to scratch the surface on their understanding of the genetic causes of ichthyosis and ichthyosis syndromes.
“Despite the fact that we now understand that there are about 21,000 genes in the genome, we have very superficial understanding and functions known for only about 4,000 genes,” Dr. Choate of the departments of dermatology and genetics at Yale University, New Haven, Conn., said at the World Congress of Pediatric Dermatology. “Clinical insight is what’s driving all of the discovery. We continue to find new disorders, and these next-generation technologies really permit us to find the genetic basis for those disorders. I like to say that it’s the disorders that we don’t read about in the textbook that end up being the ones that are most interesting.”
Ichthyoses are cardinal disorders that occur when the normal pattern of epidermal differentiation is disrupted and leads to compensatory hyperproliferation. Clinically, ichthyoses present in a variety of ways, and more than 50 genes can cause them.
Dr. Choate is the principal investigator of the National Registry for Ichthyosis and Related Skin Types, which has been recruiting kindreds of ichthyosis patients within the United States and internationally. To date, they have provided genetic diagnoses for 674 of the 880 cases enrolled. The process involves phenotyping with a clinical history and photography, obtaining DNA from blood or saliva, and prescreening the DNA samples for mutations in 51 genes currently implicated in ichthyosis. Subjects without known mutations undergo whole exome or genome sequencing.
“We have created a unique resource in doing this,” he said. “Genotyped/phenotyped patients provide a resource for clinical and translational studies in disorders of keratinization.”
When the researchers examined patients from the registry who have epidermolytic presentations, 100% had mutations in the known genes, “so the biopsy is diagnostic,” Dr. Choate said. “About 80% have mutations in keratin 10, about 13% have mutations in keratin 1, and another 6% have mutations in keratin 2.”
About 85% of patients with recessive and syndromic disorders have mutations in this same 51-gene panel; 15% of cases don’t have mutations in those genes. “This is a similar fraction to what my colleagues have found at a variety of institutions around the world,” Dr. Choate said. “What’s fascinating is that this 15% has been the source of remarkable discovery.”
He then discussed three cases of a novel erythrokeratoderma phenotype that were referred to the registry. In one case, a boy had pervasive intellectual disability, congenital alopecia, and absence of the eyebrows. “Within the first days of life, he developed a significant erythroderma with copious scaling of the skin that persisted throughout life and that was unresponsive to a variety of different therapeutic interventions, including immunosuppressant medications,” Dr. Choate said. “He had nail dystrophy and progressive enamel decay with severe caries, leading to loss of all of his teeth by the age of 6.”
Another case was a child who died of cardiomyopathy at about 3 years of age. He had congenital absence of the eyebrows and eyelashes, nail dystrophy, and scaling. “About 2 weeks before his death, he had a skin biopsy that we would ultimately repurpose to identify a new genetic cause of what we would call the erythrokeratodermia-cardiomyopathy syndrome,” Dr. Choate said. “It included features of congenital erythroderma, defective dental enamel, abnormal nails, and progressive and lethal cardiomyopathy. When we did exome sequencing, we found that all three of these patients showed tightly clustered de novo mutations in a gene called desmoplakin (DSP). Other DSP mutations do not cause erythrokeratoderma.”
Electron microscopy showed aggregates of desmosomes, normal corneodesmosomes, widening of intercellular spaces, and abnormal lipid secretion. The finding led the researchers to conclude that clustered DSP mutations cause a novel cutaneous phenotype with erythrokeratoderma and progressive cardiomyopathy. “The next time an insurer refuses to do genetic testing for you in a patient who has erythrokeratoderma, this is the disorder that you want to cite as the reason why you need to do genetic testing,” he said.
In a recent study, Dr. Choate and his associates identified the genetic cause for a rare subtype of progressive symmetric erythrokeratoderma (PSEK), a disorder that features thick facial plaques and thickened palms and soles (Am J Hum Genet. 2017 Jun 1;100[6]:978-84). Histology reveals a thickened epidermis, loss of granular layer, and retention of nuclei in the stratum corneum. They discovered that PSEK was caused by mutations in 3-ketodihydrosphingosine reductase (KDSR), an enzyme that is central to de novo ceramides in skin.
“Ceramides are secreted by keratinocytes with cholesterol and free fatty acids to form the cutaneous lipid barrier,” he explained. “They also regulate cutaneous proliferation and differentiation. One of the things this story in particular told us was, when you find just one mutation and a compelling candidate gene and can’t find the other, it’s often because of how you’re approaching detection. In two of our cases, genome sequencing was necessary to find a large inversion, which disrupted the encoded protein. Finally, the challenge of studying ceramides is that it’s hard to get cells in culture to produce them. Therefore, we had to work with collaborators in yeast biology to prove pathogenesis.”
Dr. Choate cited other recent developments, including the discovery that familial pityriasis rubra pilaris is caused by mutations in CARD14, which is a known activator of nuclear factor kappa B signaling (Am J Hum Genet. 2012 Jul 13;91[1]:163-70). This led to the subsequent use of ustekinumab for patients with familial pityriasis rubra pilaris. Another group of researchers found that SULT2B1 encodes sulfotransferase family 2B member 1 and is central to epidermal cholesterol metabolism (Am J Hum Genet. 2017 Jun 1;100[6]:926-39).
“There are still new genetic causes of ichthyosis to be found, particularly cases that don’t meet the textbook criteria for the disorder,” he concluded. “Severe, dominant disorders primarily due to de novo mutations are fertile ground for discovery. Genetic investigation is critical to our understanding of disease biology and biology of the skin. It’s also potentially relevant to outcomes of therapy. [Erythrokeratodermia-cardiomyopathy syndrome] highlights the potential for comorbidities, and the efficacy of ustekinumab in familial [pityriasis rubra pilaris] highlights the therapeutic importance of understanding the pathway underlying the disease.”
Dr. Choate reported having no financial disclosures.
CHICAGO– The way Keith Choate, MD, PhD, sees it, he and other clinicians are only beginning to scratch the surface on their understanding of the genetic causes of ichthyosis and ichthyosis syndromes.
“Despite the fact that we now understand that there are about 21,000 genes in the genome, we have very superficial understanding and functions known for only about 4,000 genes,” Dr. Choate of the departments of dermatology and genetics at Yale University, New Haven, Conn., said at the World Congress of Pediatric Dermatology. “Clinical insight is what’s driving all of the discovery. We continue to find new disorders, and these next-generation technologies really permit us to find the genetic basis for those disorders. I like to say that it’s the disorders that we don’t read about in the textbook that end up being the ones that are most interesting.”
Ichthyoses are cardinal disorders that occur when the normal pattern of epidermal differentiation is disrupted and leads to compensatory hyperproliferation. Clinically, ichthyoses present in a variety of ways, and more than 50 genes can cause them.
Dr. Choate is the principal investigator of the National Registry for Ichthyosis and Related Skin Types, which has been recruiting kindreds of ichthyosis patients within the United States and internationally. To date, they have provided genetic diagnoses for 674 of the 880 cases enrolled. The process involves phenotyping with a clinical history and photography, obtaining DNA from blood or saliva, and prescreening the DNA samples for mutations in 51 genes currently implicated in ichthyosis. Subjects without known mutations undergo whole exome or genome sequencing.
“We have created a unique resource in doing this,” he said. “Genotyped/phenotyped patients provide a resource for clinical and translational studies in disorders of keratinization.”
When the researchers examined patients from the registry who have epidermolytic presentations, 100% had mutations in the known genes, “so the biopsy is diagnostic,” Dr. Choate said. “About 80% have mutations in keratin 10, about 13% have mutations in keratin 1, and another 6% have mutations in keratin 2.”
About 85% of patients with recessive and syndromic disorders have mutations in this same 51-gene panel; 15% of cases don’t have mutations in those genes. “This is a similar fraction to what my colleagues have found at a variety of institutions around the world,” Dr. Choate said. “What’s fascinating is that this 15% has been the source of remarkable discovery.”
He then discussed three cases of a novel erythrokeratoderma phenotype that were referred to the registry. In one case, a boy had pervasive intellectual disability, congenital alopecia, and absence of the eyebrows. “Within the first days of life, he developed a significant erythroderma with copious scaling of the skin that persisted throughout life and that was unresponsive to a variety of different therapeutic interventions, including immunosuppressant medications,” Dr. Choate said. “He had nail dystrophy and progressive enamel decay with severe caries, leading to loss of all of his teeth by the age of 6.”
Another case was a child who died of cardiomyopathy at about 3 years of age. He had congenital absence of the eyebrows and eyelashes, nail dystrophy, and scaling. “About 2 weeks before his death, he had a skin biopsy that we would ultimately repurpose to identify a new genetic cause of what we would call the erythrokeratodermia-cardiomyopathy syndrome,” Dr. Choate said. “It included features of congenital erythroderma, defective dental enamel, abnormal nails, and progressive and lethal cardiomyopathy. When we did exome sequencing, we found that all three of these patients showed tightly clustered de novo mutations in a gene called desmoplakin (DSP). Other DSP mutations do not cause erythrokeratoderma.”
Electron microscopy showed aggregates of desmosomes, normal corneodesmosomes, widening of intercellular spaces, and abnormal lipid secretion. The finding led the researchers to conclude that clustered DSP mutations cause a novel cutaneous phenotype with erythrokeratoderma and progressive cardiomyopathy. “The next time an insurer refuses to do genetic testing for you in a patient who has erythrokeratoderma, this is the disorder that you want to cite as the reason why you need to do genetic testing,” he said.
In a recent study, Dr. Choate and his associates identified the genetic cause for a rare subtype of progressive symmetric erythrokeratoderma (PSEK), a disorder that features thick facial plaques and thickened palms and soles (Am J Hum Genet. 2017 Jun 1;100[6]:978-84). Histology reveals a thickened epidermis, loss of granular layer, and retention of nuclei in the stratum corneum. They discovered that PSEK was caused by mutations in 3-ketodihydrosphingosine reductase (KDSR), an enzyme that is central to de novo ceramides in skin.
“Ceramides are secreted by keratinocytes with cholesterol and free fatty acids to form the cutaneous lipid barrier,” he explained. “They also regulate cutaneous proliferation and differentiation. One of the things this story in particular told us was, when you find just one mutation and a compelling candidate gene and can’t find the other, it’s often because of how you’re approaching detection. In two of our cases, genome sequencing was necessary to find a large inversion, which disrupted the encoded protein. Finally, the challenge of studying ceramides is that it’s hard to get cells in culture to produce them. Therefore, we had to work with collaborators in yeast biology to prove pathogenesis.”
Dr. Choate cited other recent developments, including the discovery that familial pityriasis rubra pilaris is caused by mutations in CARD14, which is a known activator of nuclear factor kappa B signaling (Am J Hum Genet. 2012 Jul 13;91[1]:163-70). This led to the subsequent use of ustekinumab for patients with familial pityriasis rubra pilaris. Another group of researchers found that SULT2B1 encodes sulfotransferase family 2B member 1 and is central to epidermal cholesterol metabolism (Am J Hum Genet. 2017 Jun 1;100[6]:926-39).
“There are still new genetic causes of ichthyosis to be found, particularly cases that don’t meet the textbook criteria for the disorder,” he concluded. “Severe, dominant disorders primarily due to de novo mutations are fertile ground for discovery. Genetic investigation is critical to our understanding of disease biology and biology of the skin. It’s also potentially relevant to outcomes of therapy. [Erythrokeratodermia-cardiomyopathy syndrome] highlights the potential for comorbidities, and the efficacy of ustekinumab in familial [pityriasis rubra pilaris] highlights the therapeutic importance of understanding the pathway underlying the disease.”
Dr. Choate reported having no financial disclosures.
AT WCPD 2017
CDC: 3.4 million Americans have epilepsy
Epilepsy estimates available for the first time for every state show that the disorder is widespread, with at least 3.4 million people affected, according to the Centers for Disease Control and Prevention.
The CDC data also show that the number of people with epilepsy is increasing, probably as a result of population growth. The number of affected adults went from 2.3 million in 2010 to 3 million in 2015, and the number of children with epilepsy rose from 450,000 in 2007 to 470,000 in 2015, CDC investigators reported (MMWR. 2017 Aug 11;66[31]:821-5).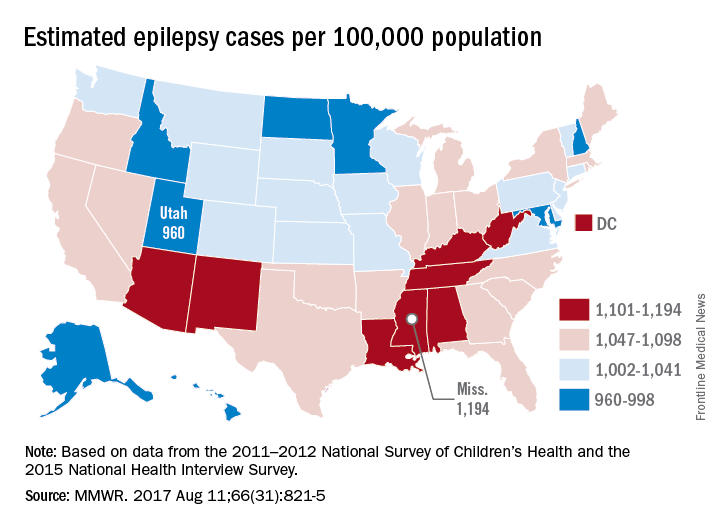
“Millions of Americans are impacted by epilepsy, and unfortunately, this study shows cases are on the rise,” CDC Director Brenda Fitzgerald said in a separate statement. “Proper diagnosis is key to finding an effective treatment – and at CDC we are committed to researching, testing, and sharing strategies that will improve the lives of people with epilepsy.”
The CDC investigators based their estimates for children under age 18 years on data from the 2011-2012 National Survey of Children’s Health; estimates for those age 18 and over are based on data from the 2015 National Health Interview Survey.
Epilepsy estimates available for the first time for every state show that the disorder is widespread, with at least 3.4 million people affected, according to the Centers for Disease Control and Prevention.
The CDC data also show that the number of people with epilepsy is increasing, probably as a result of population growth. The number of affected adults went from 2.3 million in 2010 to 3 million in 2015, and the number of children with epilepsy rose from 450,000 in 2007 to 470,000 in 2015, CDC investigators reported (MMWR. 2017 Aug 11;66[31]:821-5).
“Millions of Americans are impacted by epilepsy, and unfortunately, this study shows cases are on the rise,” CDC Director Brenda Fitzgerald said in a separate statement. “Proper diagnosis is key to finding an effective treatment – and at CDC we are committed to researching, testing, and sharing strategies that will improve the lives of people with epilepsy.”
The CDC investigators based their estimates for children under age 18 years on data from the 2011-2012 National Survey of Children’s Health; estimates for those age 18 and over are based on data from the 2015 National Health Interview Survey.
Epilepsy estimates available for the first time for every state show that the disorder is widespread, with at least 3.4 million people affected, according to the Centers for Disease Control and Prevention.
The CDC data also show that the number of people with epilepsy is increasing, probably as a result of population growth. The number of affected adults went from 2.3 million in 2010 to 3 million in 2015, and the number of children with epilepsy rose from 450,000 in 2007 to 470,000 in 2015, CDC investigators reported (MMWR. 2017 Aug 11;66[31]:821-5).
“Millions of Americans are impacted by epilepsy, and unfortunately, this study shows cases are on the rise,” CDC Director Brenda Fitzgerald said in a separate statement. “Proper diagnosis is key to finding an effective treatment – and at CDC we are committed to researching, testing, and sharing strategies that will improve the lives of people with epilepsy.”
The CDC investigators based their estimates for children under age 18 years on data from the 2011-2012 National Survey of Children’s Health; estimates for those age 18 and over are based on data from the 2015 National Health Interview Survey.
FROM MMWR
Researchers identify ‘congenital NAD deficiency disorders’
Mutations that disrupt de novo synthesis of nicotinamide adenine dinucleotide (NAD) were associated with multiple congenital malformations in humans and mice, and supplementing niacin during gestation prevented these malformations in mice, new research suggests.
The malformations include vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, renal anomalies, and limb abnormalities (VACTERL), “a nonrandom combination of congenital defects without a known cause,” wrote Hongjun Shi, PhD, of Victor Chang Cardiac Research Institute, New South Wales, Australia, and colleagues (N Engl J Med. 2017;377:544-52).
Numerous genetic and environmental factors can potentially cause NAD deficiency during gestation and the investigators suggested collectively referring to the resulting malformations as “congenital NAD deficiency disorders.”
Congenital defects can occur together in newborns more often than would be expected by chance, but “in many such cases, it has proved difficult to identify a genetic cause,” the investigators noted. Using genomic sequencing, they looked for possible pathogenic gene variants within four unrelated families in which a person was born with multiple congenital malformations. Next, they evaluated the function of the variants by testing in vitro enzyme activity and measuring relevant plasma metabolites. Finally, they used the CRISPR (clustered regularly interspaced short palindromic repeats)–Cas9 system to create mouse models with similar variants.
This approach identified variants in two genes encoding enzymes of the kynurenine pathway: 3-hydroxyanthranilic acid 3,4-dioxygenase (HAAO) and kynureninase (KYNU). Three patients had homozygous variants associated with loss-of-function changes in these proteins. A fourth patient had heterozygous variants in the gene encoding KYNU.
“The mutant enzymes had greatly reduced activity in vitro,” the researchers wrote. Patients had decreased circulating levels of NAD, which tryptophan synthesizes through the kynurenine pathway. Notably, mouse embryos lacking the mouse equivalents of HAAO or KYNU also had congenital defects associated with NAD deficiency. Preventing NAD deficiency during gestation averted these defects in mice.
“The NAD de novo synthesis pathway catabolizes tryptophan,” the researchers added. “Although metabolite levels upstream of the block are elevated, and the metabolites have postnatal functions, we found that it is the deficiency in embryonic NAD, downstream of the block, that is disrupting embryogenesis.”
The study was supported by the Australian and New South Wales governments and foundations. The investigators reported having no other financial disclosures.
Shi et al. report that a deficiency of nicotinamide adenine dinucleotide (NAD) causes congenital malformations, suggesting that interventions to raise NAD levels during fetal and early postnatal development might further reduce the incidence of congenital anomalies.
Regardless of how NAD depletion leads to congenital malformations (whether by compromising the detection of DNA damage by PARP proteins, reducing the supply of nucleotides, or both), dietary supplementation with NAD precursors merits further study. At high doses, niacin can cause flushing and gastrointestinal symptoms, but it has few side effects at lower doses.
Nicotinamide mononucleotide, nicotinamide riboside, and nicotinamide itself are better tolerated than niacin and are generally considered to be safe as dietary supplements, but the doses of NAD precursors required to reduce the risk of congenital malformations in humans are not known. Also unknown is the extent to which raising dietary levels of NAD would limit cognitive impairment in infants with congenital malformations.
Matthew G. Vander Heiden, MD, PhD, is with the Massachusetts Institute of Technology, Cambridge, Mass., and the Dana Farber Cancer Center, Boston. He reported receiving personal fees from Agios Pharmaceuticals and Aeglea Biotherapeutics outside the submitted work. These comments are adapted from an editorial (N Engl J Med. 2007;377:509-11).
Shi et al. report that a deficiency of nicotinamide adenine dinucleotide (NAD) causes congenital malformations, suggesting that interventions to raise NAD levels during fetal and early postnatal development might further reduce the incidence of congenital anomalies.
Regardless of how NAD depletion leads to congenital malformations (whether by compromising the detection of DNA damage by PARP proteins, reducing the supply of nucleotides, or both), dietary supplementation with NAD precursors merits further study. At high doses, niacin can cause flushing and gastrointestinal symptoms, but it has few side effects at lower doses.
Nicotinamide mononucleotide, nicotinamide riboside, and nicotinamide itself are better tolerated than niacin and are generally considered to be safe as dietary supplements, but the doses of NAD precursors required to reduce the risk of congenital malformations in humans are not known. Also unknown is the extent to which raising dietary levels of NAD would limit cognitive impairment in infants with congenital malformations.
Matthew G. Vander Heiden, MD, PhD, is with the Massachusetts Institute of Technology, Cambridge, Mass., and the Dana Farber Cancer Center, Boston. He reported receiving personal fees from Agios Pharmaceuticals and Aeglea Biotherapeutics outside the submitted work. These comments are adapted from an editorial (N Engl J Med. 2007;377:509-11).
Shi et al. report that a deficiency of nicotinamide adenine dinucleotide (NAD) causes congenital malformations, suggesting that interventions to raise NAD levels during fetal and early postnatal development might further reduce the incidence of congenital anomalies.
Regardless of how NAD depletion leads to congenital malformations (whether by compromising the detection of DNA damage by PARP proteins, reducing the supply of nucleotides, or both), dietary supplementation with NAD precursors merits further study. At high doses, niacin can cause flushing and gastrointestinal symptoms, but it has few side effects at lower doses.
Nicotinamide mononucleotide, nicotinamide riboside, and nicotinamide itself are better tolerated than niacin and are generally considered to be safe as dietary supplements, but the doses of NAD precursors required to reduce the risk of congenital malformations in humans are not known. Also unknown is the extent to which raising dietary levels of NAD would limit cognitive impairment in infants with congenital malformations.
Matthew G. Vander Heiden, MD, PhD, is with the Massachusetts Institute of Technology, Cambridge, Mass., and the Dana Farber Cancer Center, Boston. He reported receiving personal fees from Agios Pharmaceuticals and Aeglea Biotherapeutics outside the submitted work. These comments are adapted from an editorial (N Engl J Med. 2007;377:509-11).
Mutations that disrupt de novo synthesis of nicotinamide adenine dinucleotide (NAD) were associated with multiple congenital malformations in humans and mice, and supplementing niacin during gestation prevented these malformations in mice, new research suggests.
The malformations include vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, renal anomalies, and limb abnormalities (VACTERL), “a nonrandom combination of congenital defects without a known cause,” wrote Hongjun Shi, PhD, of Victor Chang Cardiac Research Institute, New South Wales, Australia, and colleagues (N Engl J Med. 2017;377:544-52).
Numerous genetic and environmental factors can potentially cause NAD deficiency during gestation and the investigators suggested collectively referring to the resulting malformations as “congenital NAD deficiency disorders.”
Congenital defects can occur together in newborns more often than would be expected by chance, but “in many such cases, it has proved difficult to identify a genetic cause,” the investigators noted. Using genomic sequencing, they looked for possible pathogenic gene variants within four unrelated families in which a person was born with multiple congenital malformations. Next, they evaluated the function of the variants by testing in vitro enzyme activity and measuring relevant plasma metabolites. Finally, they used the CRISPR (clustered regularly interspaced short palindromic repeats)–Cas9 system to create mouse models with similar variants.
This approach identified variants in two genes encoding enzymes of the kynurenine pathway: 3-hydroxyanthranilic acid 3,4-dioxygenase (HAAO) and kynureninase (KYNU). Three patients had homozygous variants associated with loss-of-function changes in these proteins. A fourth patient had heterozygous variants in the gene encoding KYNU.
“The mutant enzymes had greatly reduced activity in vitro,” the researchers wrote. Patients had decreased circulating levels of NAD, which tryptophan synthesizes through the kynurenine pathway. Notably, mouse embryos lacking the mouse equivalents of HAAO or KYNU also had congenital defects associated with NAD deficiency. Preventing NAD deficiency during gestation averted these defects in mice.
“The NAD de novo synthesis pathway catabolizes tryptophan,” the researchers added. “Although metabolite levels upstream of the block are elevated, and the metabolites have postnatal functions, we found that it is the deficiency in embryonic NAD, downstream of the block, that is disrupting embryogenesis.”
The study was supported by the Australian and New South Wales governments and foundations. The investigators reported having no other financial disclosures.
Mutations that disrupt de novo synthesis of nicotinamide adenine dinucleotide (NAD) were associated with multiple congenital malformations in humans and mice, and supplementing niacin during gestation prevented these malformations in mice, new research suggests.
The malformations include vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, renal anomalies, and limb abnormalities (VACTERL), “a nonrandom combination of congenital defects without a known cause,” wrote Hongjun Shi, PhD, of Victor Chang Cardiac Research Institute, New South Wales, Australia, and colleagues (N Engl J Med. 2017;377:544-52).
Numerous genetic and environmental factors can potentially cause NAD deficiency during gestation and the investigators suggested collectively referring to the resulting malformations as “congenital NAD deficiency disorders.”
Congenital defects can occur together in newborns more often than would be expected by chance, but “in many such cases, it has proved difficult to identify a genetic cause,” the investigators noted. Using genomic sequencing, they looked for possible pathogenic gene variants within four unrelated families in which a person was born with multiple congenital malformations. Next, they evaluated the function of the variants by testing in vitro enzyme activity and measuring relevant plasma metabolites. Finally, they used the CRISPR (clustered regularly interspaced short palindromic repeats)–Cas9 system to create mouse models with similar variants.
This approach identified variants in two genes encoding enzymes of the kynurenine pathway: 3-hydroxyanthranilic acid 3,4-dioxygenase (HAAO) and kynureninase (KYNU). Three patients had homozygous variants associated with loss-of-function changes in these proteins. A fourth patient had heterozygous variants in the gene encoding KYNU.
“The mutant enzymes had greatly reduced activity in vitro,” the researchers wrote. Patients had decreased circulating levels of NAD, which tryptophan synthesizes through the kynurenine pathway. Notably, mouse embryos lacking the mouse equivalents of HAAO or KYNU also had congenital defects associated with NAD deficiency. Preventing NAD deficiency during gestation averted these defects in mice.
“The NAD de novo synthesis pathway catabolizes tryptophan,” the researchers added. “Although metabolite levels upstream of the block are elevated, and the metabolites have postnatal functions, we found that it is the deficiency in embryonic NAD, downstream of the block, that is disrupting embryogenesis.”
The study was supported by the Australian and New South Wales governments and foundations. The investigators reported having no other financial disclosures.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: Major congenital defects affecting unrelated families were associated with variants in genes encoding 3-hydroxyanthranilic acid 3,4-dioxygenase (HAAO) and kynureninase (KYNU).
Data source: Genomic sequencing of four unrelated families in which a person was born with multiple congenital malformations, plus in vitro measurements of enzyme activity and plasma metabolites and studies of mouse models created with the CRISPR–Cas9 system.
Disclosures: The study was supported by the Australian and New South Wales governments and foundations. The investigators reported having no other financial disclosures.
Childhood poverty sets stage for adult heart disease
Children from the poorest families show signs of thicker carotid artery walls that may raise their risk for heart attack and stroke as adults, according to data from a longitudinal study of more than 1,000 families in Australia.
“Understanding when associations between SEP [socioeconomic position] and CVD [cardiovascular disease] first appear may help address the increasing social gradients in CVD outcomes and risk factors,” wrote Richard S. Liu, MD, of the Murdoch Children’s Research Institute, Parkville, Australia, and colleagues.
The researchers reviewed data from 1,477 families in Australia. Socioeconomic position of the children’s families was measured biennially at age 0-1 year and onward, and the researchers used imaging to measure the right carotid arteries of children between age 11 and 12 years. Overall, children in the lowest socioeconomic quartile at age 11-12 years were 46% more likely than those in the highest quartile to have thicker carotid arteries (defined as greater than the 75th percentile).
“In univariable analyses, each quartile increment higher of family SEP was associated with a 3.7-micrometer thicker carotid intima-media thickness [IMT],” and the association remained significant in a multivariate analysis controlling for cardiovascular risk factors including secondhand smoke, body weight, and blood pressure, the researchers wrote.
The socioeconomic status of the family had a greater impact than that of the neighborhood, they noted.
In addition, low socioeconomic status of a child’s family at age 2-3 years was associated with thickness in carotid artery measurements at age 11-12 years.
The study findings were limited by several factors, including a lack of data on the clinical consequences of increased carotid thickness in children, as well as the need for investigation of other signs of subclinical atherosclerosis, the researchers said. However, “consistent evidence showed an association between SEP from early life and midchildhood carotid IMT,” and additional research is needed to explore the impact of household factors on childhood health, they emphasized.
The findings were published online Aug. 9 in the Journal of the American Heart Association (J Am Heart Assoc. 2017;6:e0059255).
The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
Children from the poorest families show signs of thicker carotid artery walls that may raise their risk for heart attack and stroke as adults, according to data from a longitudinal study of more than 1,000 families in Australia.
“Understanding when associations between SEP [socioeconomic position] and CVD [cardiovascular disease] first appear may help address the increasing social gradients in CVD outcomes and risk factors,” wrote Richard S. Liu, MD, of the Murdoch Children’s Research Institute, Parkville, Australia, and colleagues.
The researchers reviewed data from 1,477 families in Australia. Socioeconomic position of the children’s families was measured biennially at age 0-1 year and onward, and the researchers used imaging to measure the right carotid arteries of children between age 11 and 12 years. Overall, children in the lowest socioeconomic quartile at age 11-12 years were 46% more likely than those in the highest quartile to have thicker carotid arteries (defined as greater than the 75th percentile).
“In univariable analyses, each quartile increment higher of family SEP was associated with a 3.7-micrometer thicker carotid intima-media thickness [IMT],” and the association remained significant in a multivariate analysis controlling for cardiovascular risk factors including secondhand smoke, body weight, and blood pressure, the researchers wrote.
The socioeconomic status of the family had a greater impact than that of the neighborhood, they noted.
In addition, low socioeconomic status of a child’s family at age 2-3 years was associated with thickness in carotid artery measurements at age 11-12 years.
The study findings were limited by several factors, including a lack of data on the clinical consequences of increased carotid thickness in children, as well as the need for investigation of other signs of subclinical atherosclerosis, the researchers said. However, “consistent evidence showed an association between SEP from early life and midchildhood carotid IMT,” and additional research is needed to explore the impact of household factors on childhood health, they emphasized.
The findings were published online Aug. 9 in the Journal of the American Heart Association (J Am Heart Assoc. 2017;6:e0059255).
The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
Children from the poorest families show signs of thicker carotid artery walls that may raise their risk for heart attack and stroke as adults, according to data from a longitudinal study of more than 1,000 families in Australia.
“Understanding when associations between SEP [socioeconomic position] and CVD [cardiovascular disease] first appear may help address the increasing social gradients in CVD outcomes and risk factors,” wrote Richard S. Liu, MD, of the Murdoch Children’s Research Institute, Parkville, Australia, and colleagues.
The researchers reviewed data from 1,477 families in Australia. Socioeconomic position of the children’s families was measured biennially at age 0-1 year and onward, and the researchers used imaging to measure the right carotid arteries of children between age 11 and 12 years. Overall, children in the lowest socioeconomic quartile at age 11-12 years were 46% more likely than those in the highest quartile to have thicker carotid arteries (defined as greater than the 75th percentile).
“In univariable analyses, each quartile increment higher of family SEP was associated with a 3.7-micrometer thicker carotid intima-media thickness [IMT],” and the association remained significant in a multivariate analysis controlling for cardiovascular risk factors including secondhand smoke, body weight, and blood pressure, the researchers wrote.
The socioeconomic status of the family had a greater impact than that of the neighborhood, they noted.
In addition, low socioeconomic status of a child’s family at age 2-3 years was associated with thickness in carotid artery measurements at age 11-12 years.
The study findings were limited by several factors, including a lack of data on the clinical consequences of increased carotid thickness in children, as well as the need for investigation of other signs of subclinical atherosclerosis, the researchers said. However, “consistent evidence showed an association between SEP from early life and midchildhood carotid IMT,” and additional research is needed to explore the impact of household factors on childhood health, they emphasized.
The findings were published online Aug. 9 in the Journal of the American Heart Association (J Am Heart Assoc. 2017;6:e0059255).
The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF THE AMERICAN HEART ASSOCIATION
Key clinical point: Low socioeconomic status of families was significantly linked with thicker carotid arteries in children at age 11-12 years, which could increase the risk of stroke in adulthood.
Major finding: Children in the lowest socioeconomic group at age 11-12 years were 46% more likely to have carotid intima-media thickness at a level above the 75th percentile.
Data source: A longitudinal study of children from 1,477 families in Australia.
Disclosures: The study was funded by the National Health and Medical Research Council of Australia and several research institutions. The researchers had no financial conflicts to disclose.
HPV vaccination rose after ACA implementation
Human papillomavirus vaccination in girls and women has increased significantly since the implementation of the Affordable Care Act (ACA), according an analysis of federal survey data.
Overall, girls and women were 3.3 times more likely to receive the vaccine (95% confidence interval, 2.0, 5.5; P less than .0001) in the post–ACA implementation period, compared with the pre-ACA period. They were 5.8 times more likely to receive all three doses of the vaccine (95% CI, 2.5-13.6; P = .0001) post ACA, compared with one dose during that period, according to Rosemary Corriero of the University of Georgia, Athens, who is also a fellow at the Centers for Disease Control and Prevention, and her coauthors (J Pediatr Adolesc Gynecol. 2017 Jul 26. doi: 10.1016/j.jpag.2017.07.002).
The cross-sectional analysis included four waves of data from 2007-2008, 2009-2010, 2011-2012, and 2013-2014 – two waves before the ACA and two waves after. The data comes from the National Health and Nutrition Examination Survey (NHANES) questionnaire. In the pre-ACA surveys, 2,452 teenage girls and women were included, compared with 2,147 in the post-ACA years. The majority of participants were white, and analysis was limited to those aged 9-33 years.
The increase in vaccination could be due to the ACA’s provision requiring coverage of preventive health services without patient cost sharing in most health plans, but the investigators couldn’t say for sure.
Vaccination uptake was significantly higher for those with insurance coverage in both pre- and post-ACA groups (P = .0007 and P = .01, respectively).
Despite these increases, vaccination rates are still low. There has been progress, but “physicians and public health professionals could assist in the acceleration of HPV vaccination uptake by increasing communication of HPV vaccination importance and by utilizing campaigns and materials that are readily available,” the investigators wrote.
The study was limited by a lack of data for teenage boys and men before implementation of the ACA and by the overlap in pre- and post-ACA data in the 2009-2010 wave because of the timing of the provision. Additionally, the data was self-reported.
The investigators reported having no relevant financial disclosures.
Human papillomavirus vaccination in girls and women has increased significantly since the implementation of the Affordable Care Act (ACA), according an analysis of federal survey data.
Overall, girls and women were 3.3 times more likely to receive the vaccine (95% confidence interval, 2.0, 5.5; P less than .0001) in the post–ACA implementation period, compared with the pre-ACA period. They were 5.8 times more likely to receive all three doses of the vaccine (95% CI, 2.5-13.6; P = .0001) post ACA, compared with one dose during that period, according to Rosemary Corriero of the University of Georgia, Athens, who is also a fellow at the Centers for Disease Control and Prevention, and her coauthors (J Pediatr Adolesc Gynecol. 2017 Jul 26. doi: 10.1016/j.jpag.2017.07.002).
The cross-sectional analysis included four waves of data from 2007-2008, 2009-2010, 2011-2012, and 2013-2014 – two waves before the ACA and two waves after. The data comes from the National Health and Nutrition Examination Survey (NHANES) questionnaire. In the pre-ACA surveys, 2,452 teenage girls and women were included, compared with 2,147 in the post-ACA years. The majority of participants were white, and analysis was limited to those aged 9-33 years.
The increase in vaccination could be due to the ACA’s provision requiring coverage of preventive health services without patient cost sharing in most health plans, but the investigators couldn’t say for sure.
Vaccination uptake was significantly higher for those with insurance coverage in both pre- and post-ACA groups (P = .0007 and P = .01, respectively).
Despite these increases, vaccination rates are still low. There has been progress, but “physicians and public health professionals could assist in the acceleration of HPV vaccination uptake by increasing communication of HPV vaccination importance and by utilizing campaigns and materials that are readily available,” the investigators wrote.
The study was limited by a lack of data for teenage boys and men before implementation of the ACA and by the overlap in pre- and post-ACA data in the 2009-2010 wave because of the timing of the provision. Additionally, the data was self-reported.
The investigators reported having no relevant financial disclosures.
Human papillomavirus vaccination in girls and women has increased significantly since the implementation of the Affordable Care Act (ACA), according an analysis of federal survey data.
Overall, girls and women were 3.3 times more likely to receive the vaccine (95% confidence interval, 2.0, 5.5; P less than .0001) in the post–ACA implementation period, compared with the pre-ACA period. They were 5.8 times more likely to receive all three doses of the vaccine (95% CI, 2.5-13.6; P = .0001) post ACA, compared with one dose during that period, according to Rosemary Corriero of the University of Georgia, Athens, who is also a fellow at the Centers for Disease Control and Prevention, and her coauthors (J Pediatr Adolesc Gynecol. 2017 Jul 26. doi: 10.1016/j.jpag.2017.07.002).
The cross-sectional analysis included four waves of data from 2007-2008, 2009-2010, 2011-2012, and 2013-2014 – two waves before the ACA and two waves after. The data comes from the National Health and Nutrition Examination Survey (NHANES) questionnaire. In the pre-ACA surveys, 2,452 teenage girls and women were included, compared with 2,147 in the post-ACA years. The majority of participants were white, and analysis was limited to those aged 9-33 years.
The increase in vaccination could be due to the ACA’s provision requiring coverage of preventive health services without patient cost sharing in most health plans, but the investigators couldn’t say for sure.
Vaccination uptake was significantly higher for those with insurance coverage in both pre- and post-ACA groups (P = .0007 and P = .01, respectively).
Despite these increases, vaccination rates are still low. There has been progress, but “physicians and public health professionals could assist in the acceleration of HPV vaccination uptake by increasing communication of HPV vaccination importance and by utilizing campaigns and materials that are readily available,” the investigators wrote.
The study was limited by a lack of data for teenage boys and men before implementation of the ACA and by the overlap in pre- and post-ACA data in the 2009-2010 wave because of the timing of the provision. Additionally, the data was self-reported.
The investigators reported having no relevant financial disclosures.
FROM THE JOURNAL OF PEDIATRIC & ADOLESCENT GYNECOLOGY
Key clinical point:
Major finding: Girls and women were 3.3 times more likely to receive the HPV vaccine in the period after the ACA was implemented (95% confidence interval, 2.0-5.5; P less than .0001).
Data source: A cross-sectional analysis of the NHANES questionnaire that included responses from more than 4,500 girls and women aged 9-33 years.
Disclosures: The investigators reported having no relevant financial disclosures.
Improving children’s sleep may reduce internalizing problems long term
SAN FRANCISCO – , new research showed.
“Interventions addressing externalizing difficulties may lead to improvements in sleep, but addressing internalizing difficulties are unlikely to lead to benefits for children’s sleep,” concluded Jon Quach, PhD, of the University of Melbourne and Murdoch Children’s Research Institute, Victoria, Australia, and his colleagues.
Although they also conclude that “addressing sleep problems at earlier time points may reduce both internalizing and externalizing difficulties,” the researchers said the data are inconsistent, only weakly suggesting that sleep influences later externalizing problems at only two different age points, Dr. Quach said when presenting the findings at the Pediatric Academic Societies meeting.

Data collection every 2 years included parent-reported sleep problems and child behavior. Behavior assessment came from the parent-reported Strengths and Difficulties Questionnaire for externalizing and internalizing difficulties. Parents reported severity of sleep difficulties and presence of specific problems at least 4 nights a week: difficulty falling asleep, night waking, sleep restlessness, and not wanting to sleep alone.
The researchers investigated the direction of influence – potential but unproven causation – between sleep problems and internalizing and externalizing problems. The analysis also assessed the extent of the associations. The first pair of analyses examined the relationship between sleeping and either externalizing or internalizing problems, independently assessed.
The findings revealed that sleeping problems were primarily associated with later internalizing difficulties, strongly suggesting that sleeping issues may cause or contribute to internalizing issues 2 years later.
With externalizing problems, however, the effect of poor sleep was inconsistent: Only at one point did it appear that sleeping difficulties contributed to externalizing difficulties. Instead, externalizing problems appeared to contribute to sleeping difficulties at three out of four time points. (The exception was that externalizing problems at ages 8-9 years did not appear to affect sleep at ages 10-11 years.) Though inconsistent, the results suggest that externalizing problems likely affect difficulty sleeping much more so than the other way around.
Then the researchers assessed the interacting associations between all three factors together. At all ages, poor sleep appeared to lead to internalizing difficulties 2 years later. Only once – at ages 6-7 years – did internalizing problems appear to influence sleep 2 years later.
The relationship between sleeping problems and externalizing problems was more complex and less consistent. Externalizing problems often, but not always, were positively associated with sleeping problems 2 years later. And only at ages 4-5 years did difficulty sleeping appear to lead to externalizing problems at ages 6-7 years.
In addition, independent of any interaction with sleeping problems, externalizing difficulties appeared to lead to internalizing problems at all time points.
Although this type of analysis can strongly suggest a direction of causality, Dr. Quach noted, the associations remain subject to the limitations of any observational data, where clearly determining causation or its direction is not possible.
The Australian Research Council and the National Health Medical Research Council in Australia funded the research. The authors did not report any conflicts of interest.
SAN FRANCISCO – , new research showed.
“Interventions addressing externalizing difficulties may lead to improvements in sleep, but addressing internalizing difficulties are unlikely to lead to benefits for children’s sleep,” concluded Jon Quach, PhD, of the University of Melbourne and Murdoch Children’s Research Institute, Victoria, Australia, and his colleagues.
Although they also conclude that “addressing sleep problems at earlier time points may reduce both internalizing and externalizing difficulties,” the researchers said the data are inconsistent, only weakly suggesting that sleep influences later externalizing problems at only two different age points, Dr. Quach said when presenting the findings at the Pediatric Academic Societies meeting.
Data collection every 2 years included parent-reported sleep problems and child behavior. Behavior assessment came from the parent-reported Strengths and Difficulties Questionnaire for externalizing and internalizing difficulties. Parents reported severity of sleep difficulties and presence of specific problems at least 4 nights a week: difficulty falling asleep, night waking, sleep restlessness, and not wanting to sleep alone.
The researchers investigated the direction of influence – potential but unproven causation – between sleep problems and internalizing and externalizing problems. The analysis also assessed the extent of the associations. The first pair of analyses examined the relationship between sleeping and either externalizing or internalizing problems, independently assessed.
The findings revealed that sleeping problems were primarily associated with later internalizing difficulties, strongly suggesting that sleeping issues may cause or contribute to internalizing issues 2 years later.
With externalizing problems, however, the effect of poor sleep was inconsistent: Only at one point did it appear that sleeping difficulties contributed to externalizing difficulties. Instead, externalizing problems appeared to contribute to sleeping difficulties at three out of four time points. (The exception was that externalizing problems at ages 8-9 years did not appear to affect sleep at ages 10-11 years.) Though inconsistent, the results suggest that externalizing problems likely affect difficulty sleeping much more so than the other way around.
Then the researchers assessed the interacting associations between all three factors together. At all ages, poor sleep appeared to lead to internalizing difficulties 2 years later. Only once – at ages 6-7 years – did internalizing problems appear to influence sleep 2 years later.
The relationship between sleeping problems and externalizing problems was more complex and less consistent. Externalizing problems often, but not always, were positively associated with sleeping problems 2 years later. And only at ages 4-5 years did difficulty sleeping appear to lead to externalizing problems at ages 6-7 years.
In addition, independent of any interaction with sleeping problems, externalizing difficulties appeared to lead to internalizing problems at all time points.
Although this type of analysis can strongly suggest a direction of causality, Dr. Quach noted, the associations remain subject to the limitations of any observational data, where clearly determining causation or its direction is not possible.
The Australian Research Council and the National Health Medical Research Council in Australia funded the research. The authors did not report any conflicts of interest.
SAN FRANCISCO – , new research showed.
“Interventions addressing externalizing difficulties may lead to improvements in sleep, but addressing internalizing difficulties are unlikely to lead to benefits for children’s sleep,” concluded Jon Quach, PhD, of the University of Melbourne and Murdoch Children’s Research Institute, Victoria, Australia, and his colleagues.
Although they also conclude that “addressing sleep problems at earlier time points may reduce both internalizing and externalizing difficulties,” the researchers said the data are inconsistent, only weakly suggesting that sleep influences later externalizing problems at only two different age points, Dr. Quach said when presenting the findings at the Pediatric Academic Societies meeting.
Data collection every 2 years included parent-reported sleep problems and child behavior. Behavior assessment came from the parent-reported Strengths and Difficulties Questionnaire for externalizing and internalizing difficulties. Parents reported severity of sleep difficulties and presence of specific problems at least 4 nights a week: difficulty falling asleep, night waking, sleep restlessness, and not wanting to sleep alone.
The researchers investigated the direction of influence – potential but unproven causation – between sleep problems and internalizing and externalizing problems. The analysis also assessed the extent of the associations. The first pair of analyses examined the relationship between sleeping and either externalizing or internalizing problems, independently assessed.
The findings revealed that sleeping problems were primarily associated with later internalizing difficulties, strongly suggesting that sleeping issues may cause or contribute to internalizing issues 2 years later.
With externalizing problems, however, the effect of poor sleep was inconsistent: Only at one point did it appear that sleeping difficulties contributed to externalizing difficulties. Instead, externalizing problems appeared to contribute to sleeping difficulties at three out of four time points. (The exception was that externalizing problems at ages 8-9 years did not appear to affect sleep at ages 10-11 years.) Though inconsistent, the results suggest that externalizing problems likely affect difficulty sleeping much more so than the other way around.
Then the researchers assessed the interacting associations between all three factors together. At all ages, poor sleep appeared to lead to internalizing difficulties 2 years later. Only once – at ages 6-7 years – did internalizing problems appear to influence sleep 2 years later.
The relationship between sleeping problems and externalizing problems was more complex and less consistent. Externalizing problems often, but not always, were positively associated with sleeping problems 2 years later. And only at ages 4-5 years did difficulty sleeping appear to lead to externalizing problems at ages 6-7 years.
In addition, independent of any interaction with sleeping problems, externalizing difficulties appeared to lead to internalizing problems at all time points.
Although this type of analysis can strongly suggest a direction of causality, Dr. Quach noted, the associations remain subject to the limitations of any observational data, where clearly determining causation or its direction is not possible.
The Australian Research Council and the National Health Medical Research Council in Australia funded the research. The authors did not report any conflicts of interest.
AT PAS 17
Key clinical point: Improving children’s sleep may reduce internalizing problems 2 years later.
Major finding: Externalizing problems were associated with sleep problems later on, and sleeping difficulties were linked to later internalizing problems.
Data source: The findings are based on analysis of four longitudinal, biennial questionnaires from parents of 4,983 Australian children aged 4-5 years, starting in 2004.
Disclosures: The Australian Research Council and the National Health Medical Research Council in Australia funded the research. The authors did not report any conflicts of interest.
Cardiovascular risk factors more common in girls
Girls were more likely than boys to have cardiovascular disease risk factors such as poor aerobic capacity and a high percentage of body fat in a study involving almost 1,800 elementary school students.
Using the FITNESSGRAM Healthy Fitness Zone (HFZ) standards in 1,775 fourth- and fifth-grade students (879 boys, 896 girls) from an urban, predominantly black population, investigators found that significantly more girls than boys did not meet the HFZ for aerobic capacity (71% vs. 42%), percent body fat (53% vs. 30%), and body mass index (44% vs. 34%). Those who did not meet the HFZ for each measure were classified as “needs improvement” or “needs improvement – health risk.”
Overall, more than 66% of the study sample “had metabolic syndrome risk factors based on FITNESSGRAM assessments,” said Susan B. Racette, PhD, of Washington University, St. Louis, and her associates (Prev Med. 2017. doi: 10.1016/j.ypmed.2017.07.032).
More than half of the girls (51%) didn’t meet the HFZ for aerobic capacity and one of the body composition measures, compared with 32% of the boys, and 38% of the girls failed to meet the HFZ for all three measures, compared with 21% of the boys. The reverse side of that coin – those who did meet the HFZ for all three – favored the boys, 46% to 21%, the investigators reported.
“The presence of these cardiovascular disease risk factors in girls, in particular, highlights an important need for creative strategies to mitigate the long-term health and societal consequences of these modifiable risk factors,” Dr. Racette and her associates wrote.
This work was supported by the U.S. Department of Education and the Washington University division of biostatistics. The investigators said that they had no conflicts of interest.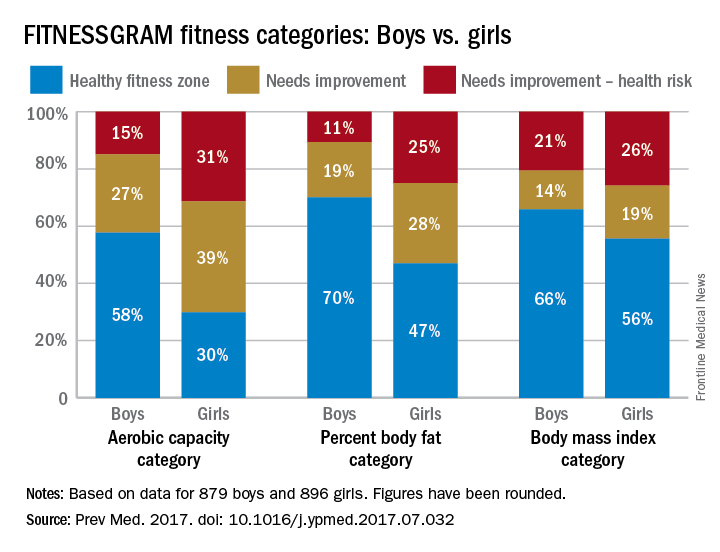
Girls were more likely than boys to have cardiovascular disease risk factors such as poor aerobic capacity and a high percentage of body fat in a study involving almost 1,800 elementary school students.
Using the FITNESSGRAM Healthy Fitness Zone (HFZ) standards in 1,775 fourth- and fifth-grade students (879 boys, 896 girls) from an urban, predominantly black population, investigators found that significantly more girls than boys did not meet the HFZ for aerobic capacity (71% vs. 42%), percent body fat (53% vs. 30%), and body mass index (44% vs. 34%). Those who did not meet the HFZ for each measure were classified as “needs improvement” or “needs improvement – health risk.”
Overall, more than 66% of the study sample “had metabolic syndrome risk factors based on FITNESSGRAM assessments,” said Susan B. Racette, PhD, of Washington University, St. Louis, and her associates (Prev Med. 2017. doi: 10.1016/j.ypmed.2017.07.032).
More than half of the girls (51%) didn’t meet the HFZ for aerobic capacity and one of the body composition measures, compared with 32% of the boys, and 38% of the girls failed to meet the HFZ for all three measures, compared with 21% of the boys. The reverse side of that coin – those who did meet the HFZ for all three – favored the boys, 46% to 21%, the investigators reported.
“The presence of these cardiovascular disease risk factors in girls, in particular, highlights an important need for creative strategies to mitigate the long-term health and societal consequences of these modifiable risk factors,” Dr. Racette and her associates wrote.
This work was supported by the U.S. Department of Education and the Washington University division of biostatistics. The investigators said that they had no conflicts of interest.
Girls were more likely than boys to have cardiovascular disease risk factors such as poor aerobic capacity and a high percentage of body fat in a study involving almost 1,800 elementary school students.
Using the FITNESSGRAM Healthy Fitness Zone (HFZ) standards in 1,775 fourth- and fifth-grade students (879 boys, 896 girls) from an urban, predominantly black population, investigators found that significantly more girls than boys did not meet the HFZ for aerobic capacity (71% vs. 42%), percent body fat (53% vs. 30%), and body mass index (44% vs. 34%). Those who did not meet the HFZ for each measure were classified as “needs improvement” or “needs improvement – health risk.”
Overall, more than 66% of the study sample “had metabolic syndrome risk factors based on FITNESSGRAM assessments,” said Susan B. Racette, PhD, of Washington University, St. Louis, and her associates (Prev Med. 2017. doi: 10.1016/j.ypmed.2017.07.032).
More than half of the girls (51%) didn’t meet the HFZ for aerobic capacity and one of the body composition measures, compared with 32% of the boys, and 38% of the girls failed to meet the HFZ for all three measures, compared with 21% of the boys. The reverse side of that coin – those who did meet the HFZ for all three – favored the boys, 46% to 21%, the investigators reported.
“The presence of these cardiovascular disease risk factors in girls, in particular, highlights an important need for creative strategies to mitigate the long-term health and societal consequences of these modifiable risk factors,” Dr. Racette and her associates wrote.
This work was supported by the U.S. Department of Education and the Washington University division of biostatistics. The investigators said that they had no conflicts of interest.
FROM PREVENTIVE MEDICINE
Acute otitis media: Which children to treat
Children whose ear infections involve severe bulging of the eardrum are likely to benefit from antibiotic treatment, while children with a peaked tympanogram pattern are likely to recover from the infections without the use of antibiotics, according to results from a new study.
The findings, published online Aug. 8 (Pediatrics. 2017), may help restrict pediatricians’ use of antibiotics to the patients who are most likely to benefit. For their research, Paula A. Tähtinen, MD, PhD, of Turku (Finland) University Hospital, and her colleagues, analyzed results from a previous placebo-controlled trial of 319 children in Finland with acute otitis media. Subjects were aged 6-35 months (median age 14 months; 57% boys; 99% white). The children in the cohort were evenly randomized to treatment with amoxicillin or placebo for 7 days. In the antibiotic arm, about 19% of patients failed to respond to treatment, while about 45% in the placebo arm did.
Dr. Tähtinen and her colleagues noted that in their study, severe bulging was an important prognostic factor irrespective of the number of ears affected or the severity of other common symptoms such as pain or fever. In this study, involvement of both ears and severity of other symptoms such as pain or fever were not seen affecting risk of treatment failure. Though only a minority of children in the study had a peaked tympanogram, failure rates for these were low in both treatment and placebo groups, and the number needed to treat to prevent treatment failure was 1 in 29.
“The evaluation of otoscopic signs is always subjective and prone to interobserver bias,” the researchers wrote. “Severe bulging is, however, a sign that is difficult to miss even for a less experienced otoscopist, and therefore this prognostic factor as an indication for antimicrobial treatment could be easily applied into clinical practice.”
Dr. Tähtinen and her colleagues’ research was supported by grants from the European Society for Pediatric Infectious Diseases and several other foundations. The study authors disclosed no financial conflicts of interest.
Children whose ear infections involve severe bulging of the eardrum are likely to benefit from antibiotic treatment, while children with a peaked tympanogram pattern are likely to recover from the infections without the use of antibiotics, according to results from a new study.
The findings, published online Aug. 8 (Pediatrics. 2017), may help restrict pediatricians’ use of antibiotics to the patients who are most likely to benefit. For their research, Paula A. Tähtinen, MD, PhD, of Turku (Finland) University Hospital, and her colleagues, analyzed results from a previous placebo-controlled trial of 319 children in Finland with acute otitis media. Subjects were aged 6-35 months (median age 14 months; 57% boys; 99% white). The children in the cohort were evenly randomized to treatment with amoxicillin or placebo for 7 days. In the antibiotic arm, about 19% of patients failed to respond to treatment, while about 45% in the placebo arm did.
Dr. Tähtinen and her colleagues noted that in their study, severe bulging was an important prognostic factor irrespective of the number of ears affected or the severity of other common symptoms such as pain or fever. In this study, involvement of both ears and severity of other symptoms such as pain or fever were not seen affecting risk of treatment failure. Though only a minority of children in the study had a peaked tympanogram, failure rates for these were low in both treatment and placebo groups, and the number needed to treat to prevent treatment failure was 1 in 29.
“The evaluation of otoscopic signs is always subjective and prone to interobserver bias,” the researchers wrote. “Severe bulging is, however, a sign that is difficult to miss even for a less experienced otoscopist, and therefore this prognostic factor as an indication for antimicrobial treatment could be easily applied into clinical practice.”
Dr. Tähtinen and her colleagues’ research was supported by grants from the European Society for Pediatric Infectious Diseases and several other foundations. The study authors disclosed no financial conflicts of interest.
Children whose ear infections involve severe bulging of the eardrum are likely to benefit from antibiotic treatment, while children with a peaked tympanogram pattern are likely to recover from the infections without the use of antibiotics, according to results from a new study.
The findings, published online Aug. 8 (Pediatrics. 2017), may help restrict pediatricians’ use of antibiotics to the patients who are most likely to benefit. For their research, Paula A. Tähtinen, MD, PhD, of Turku (Finland) University Hospital, and her colleagues, analyzed results from a previous placebo-controlled trial of 319 children in Finland with acute otitis media. Subjects were aged 6-35 months (median age 14 months; 57% boys; 99% white). The children in the cohort were evenly randomized to treatment with amoxicillin or placebo for 7 days. In the antibiotic arm, about 19% of patients failed to respond to treatment, while about 45% in the placebo arm did.
Dr. Tähtinen and her colleagues noted that in their study, severe bulging was an important prognostic factor irrespective of the number of ears affected or the severity of other common symptoms such as pain or fever. In this study, involvement of both ears and severity of other symptoms such as pain or fever were not seen affecting risk of treatment failure. Though only a minority of children in the study had a peaked tympanogram, failure rates for these were low in both treatment and placebo groups, and the number needed to treat to prevent treatment failure was 1 in 29.
“The evaluation of otoscopic signs is always subjective and prone to interobserver bias,” the researchers wrote. “Severe bulging is, however, a sign that is difficult to miss even for a less experienced otoscopist, and therefore this prognostic factor as an indication for antimicrobial treatment could be easily applied into clinical practice.”
Dr. Tähtinen and her colleagues’ research was supported by grants from the European Society for Pediatric Infectious Diseases and several other foundations. The study authors disclosed no financial conflicts of interest.
FROM PEDIATRICS
Key clinical point: Severe bulging of the eardrum, or a peaked tympanogram pattern, can inform the administration or withholding of antibiotic treatment in AOM.
Major finding: The number needed to treat using antibiotics among children presenting with severe eardrum bulging was 1.9.
Data source: Analysis of results from a randomized, placebo controlled trial (n = 319) of children younger than 3 with AOM conducted in Finland during 2006-2008.
Disclosures: Study authors disclosed research support from several foundations but no commercial conflicts of interest.