User login
Lenvatinib/Pembrolizumab shows promise in previously treated metastatic NSCLC
WASHINGTON – (NSCLC), according to interim findings from a phase 1b/2 study.
Of note, the 21 patients enrolled in the multicenter, open-label study as of March 2018 were not preselected for programmed death-ligand 1 (PD-L1) tumor expression status, Marcia S. Brose, MD, reported at the annual meeting of the Society for the Immunotherapy of Cancer.
They were treated with 20 mg of oral lenvatinib daily and 200 mg of intravenous pembrolizumab every 3 weeks, and the overall response rate at 24 weeks – the primary endpoint of the study – was 33.3%, said Dr. Brose of Abramson Cancer Center of the University of Pennsylvania, Philadelphia.
One patient had a complete response, six had a partial response, 10 had stable disease, two progressed on treatment, and the outcome in two was unknown or not evaluable, for an overall clinical benefit rate of 66%, she said, adding that the median duration of response was 10.9 months and median progression-free survival (PFS) was 5.9 months.
All patients had good performance status (ECOG score of 0-1), and nine (43%) were PD-L1–positive as defined by a tumor proportion score of at least 1%, five (24%) were PD-L1-negative, and seven (33%) were not tested for PD-L1 status. Three (14%) were treatment naive, while seven (33%), 10 (48%), and one (5%) had received one, two, or three or more prior lines of systemic therapy, respectively. No prior nivolumab or pembrolizumab treatment was allowed.
“At least one of the patients who was PD-L1–negative remained on study after 40 weeks and still continuing to respond, and ... the PD-L1–positive patients were also doing well,” Dr. Brose said.
Tumor assessments were performed by study investigators using immune-related Response Evaluation Criteria in Solid Tumors (irRECIST).
Grade 3 or greater treatment-related adverse events occurred in 10 patients (48%), and mainly included hypertension, fatigue, and diarrhea, but only four were considered serious treatment-related adverse events. Nineteen patients had treatment adjustments because of adverse events, four discontinued treatment due to adverse events, and one patient died from a pulmonary hemorrhage that was thought to possibly be treatment related, Dr. Brose said.
“The toxicity is really what you would have expected from either of these drugs on their own; it didn’t seem like there was anything that happened in synergy from the two that was unexpected,” she noted.
Lenvatinib is a multikinase inhibitor of vascular endothelial growth factor (VEGF) receptors 1-3, fibroblast growth factor receptors (FGFR) 1-4, platelet-derived growth factor receptor (PDGFR) alpha, and the RET and c-KIT proto-oncogenes. Pembrolizumab is an anti–PD-1 antibody approved as a monotherapy for previously treated patients with metastatic PD-L1–positive NSCLC, and it has been shown to be associated with an overall response rate of 18%, she explained.
The current results are from the NSCLC cohort of an ongoing trial of lenvatinib plus pembrolizumab in patients with solid tumors.
“Further investigation of this study drug combination in patients is warranted, but we will have to think carefully about what point in the treatment paradigm these patients should be treated in order to maximize the benefit from this combination therapy,” she concluded.
Dr. Brose has received consulting fees, research grants, and honorarium from Eisai.
SOURCE: Brose M et al. SITC 2018, Abstract P392.
WASHINGTON – (NSCLC), according to interim findings from a phase 1b/2 study.
Of note, the 21 patients enrolled in the multicenter, open-label study as of March 2018 were not preselected for programmed death-ligand 1 (PD-L1) tumor expression status, Marcia S. Brose, MD, reported at the annual meeting of the Society for the Immunotherapy of Cancer.
They were treated with 20 mg of oral lenvatinib daily and 200 mg of intravenous pembrolizumab every 3 weeks, and the overall response rate at 24 weeks – the primary endpoint of the study – was 33.3%, said Dr. Brose of Abramson Cancer Center of the University of Pennsylvania, Philadelphia.
One patient had a complete response, six had a partial response, 10 had stable disease, two progressed on treatment, and the outcome in two was unknown or not evaluable, for an overall clinical benefit rate of 66%, she said, adding that the median duration of response was 10.9 months and median progression-free survival (PFS) was 5.9 months.
All patients had good performance status (ECOG score of 0-1), and nine (43%) were PD-L1–positive as defined by a tumor proportion score of at least 1%, five (24%) were PD-L1-negative, and seven (33%) were not tested for PD-L1 status. Three (14%) were treatment naive, while seven (33%), 10 (48%), and one (5%) had received one, two, or three or more prior lines of systemic therapy, respectively. No prior nivolumab or pembrolizumab treatment was allowed.
“At least one of the patients who was PD-L1–negative remained on study after 40 weeks and still continuing to respond, and ... the PD-L1–positive patients were also doing well,” Dr. Brose said.
Tumor assessments were performed by study investigators using immune-related Response Evaluation Criteria in Solid Tumors (irRECIST).
Grade 3 or greater treatment-related adverse events occurred in 10 patients (48%), and mainly included hypertension, fatigue, and diarrhea, but only four were considered serious treatment-related adverse events. Nineteen patients had treatment adjustments because of adverse events, four discontinued treatment due to adverse events, and one patient died from a pulmonary hemorrhage that was thought to possibly be treatment related, Dr. Brose said.
“The toxicity is really what you would have expected from either of these drugs on their own; it didn’t seem like there was anything that happened in synergy from the two that was unexpected,” she noted.
Lenvatinib is a multikinase inhibitor of vascular endothelial growth factor (VEGF) receptors 1-3, fibroblast growth factor receptors (FGFR) 1-4, platelet-derived growth factor receptor (PDGFR) alpha, and the RET and c-KIT proto-oncogenes. Pembrolizumab is an anti–PD-1 antibody approved as a monotherapy for previously treated patients with metastatic PD-L1–positive NSCLC, and it has been shown to be associated with an overall response rate of 18%, she explained.
The current results are from the NSCLC cohort of an ongoing trial of lenvatinib plus pembrolizumab in patients with solid tumors.
“Further investigation of this study drug combination in patients is warranted, but we will have to think carefully about what point in the treatment paradigm these patients should be treated in order to maximize the benefit from this combination therapy,” she concluded.
Dr. Brose has received consulting fees, research grants, and honorarium from Eisai.
SOURCE: Brose M et al. SITC 2018, Abstract P392.
WASHINGTON – (NSCLC), according to interim findings from a phase 1b/2 study.
Of note, the 21 patients enrolled in the multicenter, open-label study as of March 2018 were not preselected for programmed death-ligand 1 (PD-L1) tumor expression status, Marcia S. Brose, MD, reported at the annual meeting of the Society for the Immunotherapy of Cancer.
They were treated with 20 mg of oral lenvatinib daily and 200 mg of intravenous pembrolizumab every 3 weeks, and the overall response rate at 24 weeks – the primary endpoint of the study – was 33.3%, said Dr. Brose of Abramson Cancer Center of the University of Pennsylvania, Philadelphia.
One patient had a complete response, six had a partial response, 10 had stable disease, two progressed on treatment, and the outcome in two was unknown or not evaluable, for an overall clinical benefit rate of 66%, she said, adding that the median duration of response was 10.9 months and median progression-free survival (PFS) was 5.9 months.
All patients had good performance status (ECOG score of 0-1), and nine (43%) were PD-L1–positive as defined by a tumor proportion score of at least 1%, five (24%) were PD-L1-negative, and seven (33%) were not tested for PD-L1 status. Three (14%) were treatment naive, while seven (33%), 10 (48%), and one (5%) had received one, two, or three or more prior lines of systemic therapy, respectively. No prior nivolumab or pembrolizumab treatment was allowed.
“At least one of the patients who was PD-L1–negative remained on study after 40 weeks and still continuing to respond, and ... the PD-L1–positive patients were also doing well,” Dr. Brose said.
Tumor assessments were performed by study investigators using immune-related Response Evaluation Criteria in Solid Tumors (irRECIST).
Grade 3 or greater treatment-related adverse events occurred in 10 patients (48%), and mainly included hypertension, fatigue, and diarrhea, but only four were considered serious treatment-related adverse events. Nineteen patients had treatment adjustments because of adverse events, four discontinued treatment due to adverse events, and one patient died from a pulmonary hemorrhage that was thought to possibly be treatment related, Dr. Brose said.
“The toxicity is really what you would have expected from either of these drugs on their own; it didn’t seem like there was anything that happened in synergy from the two that was unexpected,” she noted.
Lenvatinib is a multikinase inhibitor of vascular endothelial growth factor (VEGF) receptors 1-3, fibroblast growth factor receptors (FGFR) 1-4, platelet-derived growth factor receptor (PDGFR) alpha, and the RET and c-KIT proto-oncogenes. Pembrolizumab is an anti–PD-1 antibody approved as a monotherapy for previously treated patients with metastatic PD-L1–positive NSCLC, and it has been shown to be associated with an overall response rate of 18%, she explained.
The current results are from the NSCLC cohort of an ongoing trial of lenvatinib plus pembrolizumab in patients with solid tumors.
“Further investigation of this study drug combination in patients is warranted, but we will have to think carefully about what point in the treatment paradigm these patients should be treated in order to maximize the benefit from this combination therapy,” she concluded.
Dr. Brose has received consulting fees, research grants, and honorarium from Eisai.
SOURCE: Brose M et al. SITC 2018, Abstract P392.
REPORTING FROM SITC 2018
Key clinical point: Lenvatinib/pembrolizumab shows promise in metastatic NSCLC.
Major finding: Overall response rate at 24 weeks was 33.3%.
Study details: Interim findings in 21 patients from a phase 1b/2 study.
Disclosures: Dr. Brose has received consulting fees, research grants, and honorarium from Eisai.Source: Brose M et al. SITC 2018, Abstract P392.
TMB measured by NGS may ID SCLC patients who will benefit from immunotherapy
WASHINGTON – and targeted next-generation sequencing may help identify those likely to benefit from immunotherapy, findings from a case series suggest.
Of 113 small cell lung cancer (SCLC) patients who had successful next-generation sequencing (NGS) with tumor mutational burden (TMB) assessment at the Dana-Farber Cancer Institute (DFCI) in Boston, 52 were treated with immune checkpoint inhibitors and 61 received chemotherapy but never received subsequent immunotherapy, Biagio Ricciuti, MD, of DFCI said at the annual meeting of the Society for the Immunotherapy of Cancer.
Median TMB for all patients was 9.68 mutations/megabase, with those with TMB above the median considered TMB high, and those with TMB below the median considered TMB low. Median progression-free survival (PFS) was significantly longer among TMB-high versus TMB-low patients (3.3 vs. 1.2 months; hazard ratio, 0.37), as was median overall survival (OS, 10.4 vs. 2.5 months; HR, 0.38), he said.
“To confirm that TMB was a predictive biomarker for immunotherapy only, we also looked at the outcome with chemotherapy according to tumor mutational burden, and as expected we found no difference in terms of median progression-free survival or median overall survival according to TMB-high versus TMB-low groups,” he said.
Additionally, patients with SCLC who were treated with immune checkpoint inhibitors and experienced at least one immune-related adverse event had significantly better median PFS and OS than did patients who experienced no immune-related adverse events (6.7 vs. 1.3 months; HR, 0.25; and 17.9 vs. 2.9 months; HR, 0.27, respectively), he said, noting that, in a 12-week landmark analysis, the differences in PFS and OS between the groups were “nearly double” but did not reach statistical significance.
TMB in the SCLC patients in this study was assessed using the DFCI NGS OncoPanel platform of more than 450 genes, and the TMB-high and TMB-low groups were similar with respect to baseline clinical and pathological features and known prognostic factors, Dr. Ricciuti said.
Prior studies have demonstrated that high TMB as assessed by whole exome sequencing correlates with benefits from immunotherapy. However, “whole exome sequencing is a very expensive technique, it’s challenging ... and it’s not really available to oncologists across countries,” he said.
Whether the more readily available targeted NGS could help identify the small fraction of SCLC patients who are likely to benefit from immunotherapy has been unclear, as has the relationship between the development of irAEs and immunotherapy response in SCLC; factors associated with clinical benefit from immunotherapy have not previously been well characterized, Dr. Ricciuti noted.
The current findings, though limited by the retrospective study design and small sample size, provide the first evidence for the use of targeted NGS panels to identify patients with advanced SCLC who are most likely to benefit from immunotherapy, he said, adding that, when compared with whole genome sequencing, TMB as assessed using targeted NGS “may offer a very useful tool for clinicians to optimize small cell lung cancer patient selection for immunotherapy.
“Our study also suggests that immune-related adverse events might be associated with improved efficacy of immunotherapy, although larger studies with longer follow-up are required to confirm this finding,” he concluded.
Dr. Ricciuti reported having no disclosures.
WASHINGTON – and targeted next-generation sequencing may help identify those likely to benefit from immunotherapy, findings from a case series suggest.
Of 113 small cell lung cancer (SCLC) patients who had successful next-generation sequencing (NGS) with tumor mutational burden (TMB) assessment at the Dana-Farber Cancer Institute (DFCI) in Boston, 52 were treated with immune checkpoint inhibitors and 61 received chemotherapy but never received subsequent immunotherapy, Biagio Ricciuti, MD, of DFCI said at the annual meeting of the Society for the Immunotherapy of Cancer.
Median TMB for all patients was 9.68 mutations/megabase, with those with TMB above the median considered TMB high, and those with TMB below the median considered TMB low. Median progression-free survival (PFS) was significantly longer among TMB-high versus TMB-low patients (3.3 vs. 1.2 months; hazard ratio, 0.37), as was median overall survival (OS, 10.4 vs. 2.5 months; HR, 0.38), he said.
“To confirm that TMB was a predictive biomarker for immunotherapy only, we also looked at the outcome with chemotherapy according to tumor mutational burden, and as expected we found no difference in terms of median progression-free survival or median overall survival according to TMB-high versus TMB-low groups,” he said.
Additionally, patients with SCLC who were treated with immune checkpoint inhibitors and experienced at least one immune-related adverse event had significantly better median PFS and OS than did patients who experienced no immune-related adverse events (6.7 vs. 1.3 months; HR, 0.25; and 17.9 vs. 2.9 months; HR, 0.27, respectively), he said, noting that, in a 12-week landmark analysis, the differences in PFS and OS between the groups were “nearly double” but did not reach statistical significance.
TMB in the SCLC patients in this study was assessed using the DFCI NGS OncoPanel platform of more than 450 genes, and the TMB-high and TMB-low groups were similar with respect to baseline clinical and pathological features and known prognostic factors, Dr. Ricciuti said.
Prior studies have demonstrated that high TMB as assessed by whole exome sequencing correlates with benefits from immunotherapy. However, “whole exome sequencing is a very expensive technique, it’s challenging ... and it’s not really available to oncologists across countries,” he said.
Whether the more readily available targeted NGS could help identify the small fraction of SCLC patients who are likely to benefit from immunotherapy has been unclear, as has the relationship between the development of irAEs and immunotherapy response in SCLC; factors associated with clinical benefit from immunotherapy have not previously been well characterized, Dr. Ricciuti noted.
The current findings, though limited by the retrospective study design and small sample size, provide the first evidence for the use of targeted NGS panels to identify patients with advanced SCLC who are most likely to benefit from immunotherapy, he said, adding that, when compared with whole genome sequencing, TMB as assessed using targeted NGS “may offer a very useful tool for clinicians to optimize small cell lung cancer patient selection for immunotherapy.
“Our study also suggests that immune-related adverse events might be associated with improved efficacy of immunotherapy, although larger studies with longer follow-up are required to confirm this finding,” he concluded.
Dr. Ricciuti reported having no disclosures.
WASHINGTON – and targeted next-generation sequencing may help identify those likely to benefit from immunotherapy, findings from a case series suggest.
Of 113 small cell lung cancer (SCLC) patients who had successful next-generation sequencing (NGS) with tumor mutational burden (TMB) assessment at the Dana-Farber Cancer Institute (DFCI) in Boston, 52 were treated with immune checkpoint inhibitors and 61 received chemotherapy but never received subsequent immunotherapy, Biagio Ricciuti, MD, of DFCI said at the annual meeting of the Society for the Immunotherapy of Cancer.
Median TMB for all patients was 9.68 mutations/megabase, with those with TMB above the median considered TMB high, and those with TMB below the median considered TMB low. Median progression-free survival (PFS) was significantly longer among TMB-high versus TMB-low patients (3.3 vs. 1.2 months; hazard ratio, 0.37), as was median overall survival (OS, 10.4 vs. 2.5 months; HR, 0.38), he said.
“To confirm that TMB was a predictive biomarker for immunotherapy only, we also looked at the outcome with chemotherapy according to tumor mutational burden, and as expected we found no difference in terms of median progression-free survival or median overall survival according to TMB-high versus TMB-low groups,” he said.
Additionally, patients with SCLC who were treated with immune checkpoint inhibitors and experienced at least one immune-related adverse event had significantly better median PFS and OS than did patients who experienced no immune-related adverse events (6.7 vs. 1.3 months; HR, 0.25; and 17.9 vs. 2.9 months; HR, 0.27, respectively), he said, noting that, in a 12-week landmark analysis, the differences in PFS and OS between the groups were “nearly double” but did not reach statistical significance.
TMB in the SCLC patients in this study was assessed using the DFCI NGS OncoPanel platform of more than 450 genes, and the TMB-high and TMB-low groups were similar with respect to baseline clinical and pathological features and known prognostic factors, Dr. Ricciuti said.
Prior studies have demonstrated that high TMB as assessed by whole exome sequencing correlates with benefits from immunotherapy. However, “whole exome sequencing is a very expensive technique, it’s challenging ... and it’s not really available to oncologists across countries,” he said.
Whether the more readily available targeted NGS could help identify the small fraction of SCLC patients who are likely to benefit from immunotherapy has been unclear, as has the relationship between the development of irAEs and immunotherapy response in SCLC; factors associated with clinical benefit from immunotherapy have not previously been well characterized, Dr. Ricciuti noted.
The current findings, though limited by the retrospective study design and small sample size, provide the first evidence for the use of targeted NGS panels to identify patients with advanced SCLC who are most likely to benefit from immunotherapy, he said, adding that, when compared with whole genome sequencing, TMB as assessed using targeted NGS “may offer a very useful tool for clinicians to optimize small cell lung cancer patient selection for immunotherapy.
“Our study also suggests that immune-related adverse events might be associated with improved efficacy of immunotherapy, although larger studies with longer follow-up are required to confirm this finding,” he concluded.
Dr. Ricciuti reported having no disclosures.
REPORTING FROM SITC 2018
Key clinical point: Next-generation sequencing may help identify small cell lung cancer patients who will benefit from immunotherapy.
Major finding: Median progression-free survival and overall survival were significantly better among tumor mutational burden–high versus tumor mutational burden–low patients (3.3 vs. 1.2 months; hazard ratio, 0.37; and 10.4 vs. 2.5 months; HR, 0.38, respectively).
Study details: A series of 113 patients.
Disclosures: Dr. Ricciuti reported having no disclosures.
Immunotherapy-related toxicities may be more common than reported in trials
SAN DIEGO – Certain immune-related adverse events related to PD1/PD-L1 treatment of patients with non–small cell lung cancer (NSCLC) may be more common than reported in clinical trials, a recent analysis of administrative claims data suggests.
Pneumonitis was seen in 10.9% of patients up to 60 days after the last dose of immunotherapy, according to the analysis of data from a large, U.S. commercial insurance database, presented at the Palliative and Supportive Care in Oncology Symposium.
By comparison, pneumonitis was reported in just 5.8% of NSCLC patients during treatment with the PD-1 (programmed cell death-1) inhibitor pembrolizumab in KEYNOTE-024, a pivotal randomized phase 3 clinical trial, said Elizabeth Jane Cathcart-Rake, MD, senior study author and an oncology fellow at the Mayo Clinic, Rochester, Minn.
Rates of immune-related adverse events in this study were generally higher than in clinical trials, both for common side effects and more rare conditions such as hypophysitis, according to Dr. Cathcart-Rake.
These new claims-based data might be considered complementary to clinical trial data, the researcher said.
“Together, they may give us a better sense of the broader implications of these adverse events,” she said in an interview.
Joe Rotella, MD, a board member of the American Academy for Hospice and Palliative Care Medicine, said results of this insurance database study provide a perspective on the real-world incidence of adverse events associated with immune checkpoint inhibitors.
“We’ve only been using these therapies for a few years, so this new analysis gives us more information on the prevalence of these side effects in patients as the therapies gain wider use,” Dr. Rotella said in a news release.
In the study, Dr. Cathcart-Rake and coinvestigators queried the OptumLabs Data Warehouse to identify 3,164 patients with NSCLC who received PD-1 or PD-L1 (programmed death-ligand 1) inhibitors between 2015 and 2017. They looked at incidence of adverse events both at the time of the last immunotherapy dose and at 60 days after the last dose.
The incidence of pneumonitis, just 4.9% on the last date of immunotherapy, increased to 10.9% at 60 days after the last dose, Dr. Cathcart-Rake reported.
Beyond pneumonitis, the most common immunotherapy-related toxicities at 60 days were hypothyroidism in 7.0%, arrhythmia in 6.1%, and nephritis or acute kidney injury in 5.4%, according to the investigators.
Dr. Cathcart-Rake also highlighted the incidence of some less common immunotherapy-related toxicities such as hypophysitis or hypothalamic-pituitary-adrenal axis toxicity, seen in 2.8% of patients by 60 days.
“That’s a small number, but hypophysitis can be really profound, and frequently leads to hospitalization,” she said. “I think this just gives us enough of a signal that providers really need to be on top of looking for these adverse events and to counsel patients beforehand.”
These data could also be helpful for advising hospitalists, emergency room physicians, and other providers who may not be attuned to the potential risks of cancer immunotherapy as compared with traditional cytotoxic chemotherapy, Dr. Cathcart-Rake said at the meeting cosponsored by AAHPM, ASCO, ASTRO, and MASCC.
“A patient with cancer may be on immunotherapy and their risk for infection is quite low, but they may be at a huge risk for pneumonitis, which is treated completely differently,” she said. “So I think this should just raise alarms that close clinical monitoring for these conditions is really important.”
Dr. Cathcart-Rake disclosed that her institution receives research funding from Novartis. One study coinvestigator reported consulting or advisory roles with Trovagene, Genentech, Bristol-Myers Squibb, and Abbvie.
SOURCE: Cathcart-Rake EJ et al. 2018 Palliative and Supportive Care in Oncology Symposium. Abstract 184.
SAN DIEGO – Certain immune-related adverse events related to PD1/PD-L1 treatment of patients with non–small cell lung cancer (NSCLC) may be more common than reported in clinical trials, a recent analysis of administrative claims data suggests.
Pneumonitis was seen in 10.9% of patients up to 60 days after the last dose of immunotherapy, according to the analysis of data from a large, U.S. commercial insurance database, presented at the Palliative and Supportive Care in Oncology Symposium.
By comparison, pneumonitis was reported in just 5.8% of NSCLC patients during treatment with the PD-1 (programmed cell death-1) inhibitor pembrolizumab in KEYNOTE-024, a pivotal randomized phase 3 clinical trial, said Elizabeth Jane Cathcart-Rake, MD, senior study author and an oncology fellow at the Mayo Clinic, Rochester, Minn.
Rates of immune-related adverse events in this study were generally higher than in clinical trials, both for common side effects and more rare conditions such as hypophysitis, according to Dr. Cathcart-Rake.
These new claims-based data might be considered complementary to clinical trial data, the researcher said.
“Together, they may give us a better sense of the broader implications of these adverse events,” she said in an interview.
Joe Rotella, MD, a board member of the American Academy for Hospice and Palliative Care Medicine, said results of this insurance database study provide a perspective on the real-world incidence of adverse events associated with immune checkpoint inhibitors.
“We’ve only been using these therapies for a few years, so this new analysis gives us more information on the prevalence of these side effects in patients as the therapies gain wider use,” Dr. Rotella said in a news release.
In the study, Dr. Cathcart-Rake and coinvestigators queried the OptumLabs Data Warehouse to identify 3,164 patients with NSCLC who received PD-1 or PD-L1 (programmed death-ligand 1) inhibitors between 2015 and 2017. They looked at incidence of adverse events both at the time of the last immunotherapy dose and at 60 days after the last dose.
The incidence of pneumonitis, just 4.9% on the last date of immunotherapy, increased to 10.9% at 60 days after the last dose, Dr. Cathcart-Rake reported.
Beyond pneumonitis, the most common immunotherapy-related toxicities at 60 days were hypothyroidism in 7.0%, arrhythmia in 6.1%, and nephritis or acute kidney injury in 5.4%, according to the investigators.
Dr. Cathcart-Rake also highlighted the incidence of some less common immunotherapy-related toxicities such as hypophysitis or hypothalamic-pituitary-adrenal axis toxicity, seen in 2.8% of patients by 60 days.
“That’s a small number, but hypophysitis can be really profound, and frequently leads to hospitalization,” she said. “I think this just gives us enough of a signal that providers really need to be on top of looking for these adverse events and to counsel patients beforehand.”
These data could also be helpful for advising hospitalists, emergency room physicians, and other providers who may not be attuned to the potential risks of cancer immunotherapy as compared with traditional cytotoxic chemotherapy, Dr. Cathcart-Rake said at the meeting cosponsored by AAHPM, ASCO, ASTRO, and MASCC.
“A patient with cancer may be on immunotherapy and their risk for infection is quite low, but they may be at a huge risk for pneumonitis, which is treated completely differently,” she said. “So I think this should just raise alarms that close clinical monitoring for these conditions is really important.”
Dr. Cathcart-Rake disclosed that her institution receives research funding from Novartis. One study coinvestigator reported consulting or advisory roles with Trovagene, Genentech, Bristol-Myers Squibb, and Abbvie.
SOURCE: Cathcart-Rake EJ et al. 2018 Palliative and Supportive Care in Oncology Symposium. Abstract 184.
SAN DIEGO – Certain immune-related adverse events related to PD1/PD-L1 treatment of patients with non–small cell lung cancer (NSCLC) may be more common than reported in clinical trials, a recent analysis of administrative claims data suggests.
Pneumonitis was seen in 10.9% of patients up to 60 days after the last dose of immunotherapy, according to the analysis of data from a large, U.S. commercial insurance database, presented at the Palliative and Supportive Care in Oncology Symposium.
By comparison, pneumonitis was reported in just 5.8% of NSCLC patients during treatment with the PD-1 (programmed cell death-1) inhibitor pembrolizumab in KEYNOTE-024, a pivotal randomized phase 3 clinical trial, said Elizabeth Jane Cathcart-Rake, MD, senior study author and an oncology fellow at the Mayo Clinic, Rochester, Minn.
Rates of immune-related adverse events in this study were generally higher than in clinical trials, both for common side effects and more rare conditions such as hypophysitis, according to Dr. Cathcart-Rake.
These new claims-based data might be considered complementary to clinical trial data, the researcher said.
“Together, they may give us a better sense of the broader implications of these adverse events,” she said in an interview.
Joe Rotella, MD, a board member of the American Academy for Hospice and Palliative Care Medicine, said results of this insurance database study provide a perspective on the real-world incidence of adverse events associated with immune checkpoint inhibitors.
“We’ve only been using these therapies for a few years, so this new analysis gives us more information on the prevalence of these side effects in patients as the therapies gain wider use,” Dr. Rotella said in a news release.
In the study, Dr. Cathcart-Rake and coinvestigators queried the OptumLabs Data Warehouse to identify 3,164 patients with NSCLC who received PD-1 or PD-L1 (programmed death-ligand 1) inhibitors between 2015 and 2017. They looked at incidence of adverse events both at the time of the last immunotherapy dose and at 60 days after the last dose.
The incidence of pneumonitis, just 4.9% on the last date of immunotherapy, increased to 10.9% at 60 days after the last dose, Dr. Cathcart-Rake reported.
Beyond pneumonitis, the most common immunotherapy-related toxicities at 60 days were hypothyroidism in 7.0%, arrhythmia in 6.1%, and nephritis or acute kidney injury in 5.4%, according to the investigators.
Dr. Cathcart-Rake also highlighted the incidence of some less common immunotherapy-related toxicities such as hypophysitis or hypothalamic-pituitary-adrenal axis toxicity, seen in 2.8% of patients by 60 days.
“That’s a small number, but hypophysitis can be really profound, and frequently leads to hospitalization,” she said. “I think this just gives us enough of a signal that providers really need to be on top of looking for these adverse events and to counsel patients beforehand.”
These data could also be helpful for advising hospitalists, emergency room physicians, and other providers who may not be attuned to the potential risks of cancer immunotherapy as compared with traditional cytotoxic chemotherapy, Dr. Cathcart-Rake said at the meeting cosponsored by AAHPM, ASCO, ASTRO, and MASCC.
“A patient with cancer may be on immunotherapy and their risk for infection is quite low, but they may be at a huge risk for pneumonitis, which is treated completely differently,” she said. “So I think this should just raise alarms that close clinical monitoring for these conditions is really important.”
Dr. Cathcart-Rake disclosed that her institution receives research funding from Novartis. One study coinvestigator reported consulting or advisory roles with Trovagene, Genentech, Bristol-Myers Squibb, and Abbvie.
SOURCE: Cathcart-Rake EJ et al. 2018 Palliative and Supportive Care in Oncology Symposium. Abstract 184.
REPORTING FROM PALLONC 2018
Key clinical point: In non–small cell lung cancer patients treated with PD-1/PD-L1 inhibitors, immune-related adverse events may occur more frequently than has been suggested by clinical trial data.
Major finding: Pneumonitis was seen in nearly 11% of patients up to 60 days after the last immunotherapy dose, which investigators said was higher than reported in a pivotal phase 3 study.
Study details: Analysis of administrative claims data for 3,164 NSCLC patients treated between 2015 and 2017.
Disclosures: Researchers reported institutional research funding from Novartis. One researcher reported consulting or advisory roles with Trovagene, Genentech, Bristol-Myers Squibb, and Abbvie.
Source: Cathcart-Rake EJ et al. Palliative and Supportive Care in Oncology Symposium. Abstract 184.
Early phase 2 data: Mocetinostat/durvalumab combo shows promise in mNSCLC
WASHINGTON, D.C. – (mNSCLC) – including patients who progressed on prior checkpoint inhibitor therapy (CIT), according to preliminary findings from a phase 2 trial.
Of 29 evaluable patients who progressed on prior checkpoint blockade, 12 had “some degree of tumor regression” and 5 achieved a confirmed partial response, Manish Patel, DO, reported at the annual meeting of the Society for Immunotherapy of Cancer.
“Some of these responses were quite durable. The longest response ... was a little over 1 year,” said Dr. Patel, of the University of Minnesota Masonic Cancer Center, Minneapolis.
Several patients continue to show objective responses, and the initial estimate of response duration is a median of more than 5 months, he added.
Of note, no differences have been seen to date with respect to clinical benefit in patients who did and did not have prior clinical benefit on checkpoint blockade, Dr. Patel said.
Overall, the combination was very well tolerated. The most common adverse events were fatigue, nausea, and diarrhea, with more than 10% of patients experiencing grade 3 or higher fatigue.
“Otherwise the toxicities were relatively minor,” he said, noting, however, that 8% of patients had cardiac events during the study, including atrial fibrillation, pericardial effusion, and a few cases of pericardial tamponade.
Such effects have been described in prior mocetinostat monotherapy trials, and all patients in the current study underwent pretreatment echocardiograms and did not have evidence of pericardial effusion at the start.
“So I think this is likely to be related to mocetinostat,” Dr. Patel said.
Mocetinostat is a spectrum-selective class I and class IV histone deacetylase inhibitor with multiple potential immunomodulatory features.
For example, the agent induces major histocompatibility complex Class I and Class II expression on tumor cells, enhances the function of T effector cells, and decreases the function of immunosuppressive cell subsets, including regulatory T cells and myeloid derived suppressor cells, Dr. Patel noted.
“It was hypothesized that because of these pleiotropic immune-supportive effects, that the combination of mocetinostat and checkpoint blockade might be a successful strategy for patients with non–small cell lung cancer,” he said.
In phase 1, doses of 50 mg, 70 mg, or 90 mg given three times weekly in combination with 1,500 mg of durvalumab were studied in patients with advanced solid tumors. Based on the safety data from that phase of the study, the recommended phase 2 dose of mocetinostat was 70 mg three times weekly with 1,500 mg of durvalumab on day 1 of each 28-day cycle.
Study subjects were patients with mNSCLC who had received at least one platinum-based doublet and whose most recent treatment prior to enrollment was with a checkpoint inhibitor, or who were immunotherapy naive.
The findings show promising clinical efficacy and safety, and enrollment in the study, which began in June 2016, is currently ongoing in the United States, he said.
Dr. Patel is an advisory board member for Nektar Therapeutics and has received research funding from Merck.
SOURCE: Patel M et al. SITC 2018, Abstract 027.
WASHINGTON, D.C. – (mNSCLC) – including patients who progressed on prior checkpoint inhibitor therapy (CIT), according to preliminary findings from a phase 2 trial.
Of 29 evaluable patients who progressed on prior checkpoint blockade, 12 had “some degree of tumor regression” and 5 achieved a confirmed partial response, Manish Patel, DO, reported at the annual meeting of the Society for Immunotherapy of Cancer.
“Some of these responses were quite durable. The longest response ... was a little over 1 year,” said Dr. Patel, of the University of Minnesota Masonic Cancer Center, Minneapolis.
Several patients continue to show objective responses, and the initial estimate of response duration is a median of more than 5 months, he added.
Of note, no differences have been seen to date with respect to clinical benefit in patients who did and did not have prior clinical benefit on checkpoint blockade, Dr. Patel said.
Overall, the combination was very well tolerated. The most common adverse events were fatigue, nausea, and diarrhea, with more than 10% of patients experiencing grade 3 or higher fatigue.
“Otherwise the toxicities were relatively minor,” he said, noting, however, that 8% of patients had cardiac events during the study, including atrial fibrillation, pericardial effusion, and a few cases of pericardial tamponade.
Such effects have been described in prior mocetinostat monotherapy trials, and all patients in the current study underwent pretreatment echocardiograms and did not have evidence of pericardial effusion at the start.
“So I think this is likely to be related to mocetinostat,” Dr. Patel said.
Mocetinostat is a spectrum-selective class I and class IV histone deacetylase inhibitor with multiple potential immunomodulatory features.
For example, the agent induces major histocompatibility complex Class I and Class II expression on tumor cells, enhances the function of T effector cells, and decreases the function of immunosuppressive cell subsets, including regulatory T cells and myeloid derived suppressor cells, Dr. Patel noted.
“It was hypothesized that because of these pleiotropic immune-supportive effects, that the combination of mocetinostat and checkpoint blockade might be a successful strategy for patients with non–small cell lung cancer,” he said.
In phase 1, doses of 50 mg, 70 mg, or 90 mg given three times weekly in combination with 1,500 mg of durvalumab were studied in patients with advanced solid tumors. Based on the safety data from that phase of the study, the recommended phase 2 dose of mocetinostat was 70 mg three times weekly with 1,500 mg of durvalumab on day 1 of each 28-day cycle.
Study subjects were patients with mNSCLC who had received at least one platinum-based doublet and whose most recent treatment prior to enrollment was with a checkpoint inhibitor, or who were immunotherapy naive.
The findings show promising clinical efficacy and safety, and enrollment in the study, which began in June 2016, is currently ongoing in the United States, he said.
Dr. Patel is an advisory board member for Nektar Therapeutics and has received research funding from Merck.
SOURCE: Patel M et al. SITC 2018, Abstract 027.
WASHINGTON, D.C. – (mNSCLC) – including patients who progressed on prior checkpoint inhibitor therapy (CIT), according to preliminary findings from a phase 2 trial.
Of 29 evaluable patients who progressed on prior checkpoint blockade, 12 had “some degree of tumor regression” and 5 achieved a confirmed partial response, Manish Patel, DO, reported at the annual meeting of the Society for Immunotherapy of Cancer.
“Some of these responses were quite durable. The longest response ... was a little over 1 year,” said Dr. Patel, of the University of Minnesota Masonic Cancer Center, Minneapolis.
Several patients continue to show objective responses, and the initial estimate of response duration is a median of more than 5 months, he added.
Of note, no differences have been seen to date with respect to clinical benefit in patients who did and did not have prior clinical benefit on checkpoint blockade, Dr. Patel said.
Overall, the combination was very well tolerated. The most common adverse events were fatigue, nausea, and diarrhea, with more than 10% of patients experiencing grade 3 or higher fatigue.
“Otherwise the toxicities were relatively minor,” he said, noting, however, that 8% of patients had cardiac events during the study, including atrial fibrillation, pericardial effusion, and a few cases of pericardial tamponade.
Such effects have been described in prior mocetinostat monotherapy trials, and all patients in the current study underwent pretreatment echocardiograms and did not have evidence of pericardial effusion at the start.
“So I think this is likely to be related to mocetinostat,” Dr. Patel said.
Mocetinostat is a spectrum-selective class I and class IV histone deacetylase inhibitor with multiple potential immunomodulatory features.
For example, the agent induces major histocompatibility complex Class I and Class II expression on tumor cells, enhances the function of T effector cells, and decreases the function of immunosuppressive cell subsets, including regulatory T cells and myeloid derived suppressor cells, Dr. Patel noted.
“It was hypothesized that because of these pleiotropic immune-supportive effects, that the combination of mocetinostat and checkpoint blockade might be a successful strategy for patients with non–small cell lung cancer,” he said.
In phase 1, doses of 50 mg, 70 mg, or 90 mg given three times weekly in combination with 1,500 mg of durvalumab were studied in patients with advanced solid tumors. Based on the safety data from that phase of the study, the recommended phase 2 dose of mocetinostat was 70 mg three times weekly with 1,500 mg of durvalumab on day 1 of each 28-day cycle.
Study subjects were patients with mNSCLC who had received at least one platinum-based doublet and whose most recent treatment prior to enrollment was with a checkpoint inhibitor, or who were immunotherapy naive.
The findings show promising clinical efficacy and safety, and enrollment in the study, which began in June 2016, is currently ongoing in the United States, he said.
Dr. Patel is an advisory board member for Nektar Therapeutics and has received research funding from Merck.
SOURCE: Patel M et al. SITC 2018, Abstract 027.
REPORTING FROM SITC 2018
Key clinical point: Mocetinostat/durvalumab shows clinical activity and manageable side effects in metastatic NSCLC.
Major finding: Five patients achieved a confirmed partial response.
Study details: A phase 2 study including 29 NSCLC patients.
Disclosures: Dr. Patel is an advisory board member for Nektar Therapeutics and has received research funding from Merck.
Source: Patel M et al. SITC 2018, Abstract 027.
Capmatinib active against NSCLC with MET exon 14 mutations
MUNICH – The experimental agent capmatinib was associated with a high response rate when used in the first line for patients with advanced non–small cell lung cancers bearing MET exon 14–skipping mutations, said investigators in the Geometry MONO-1 trial.

Among a cohort of 25 patients with treatment-naive, MET exon 14–mutated non–small cell lung cancer (NSCLC), the primary endpoint of overall response rate (ORR) as determined by blinded, independent reviewers was 72%.
In contrast, the ORR among 69 patients who had received one or more prior lines of therapy was 39.1%, reported Juergen Wolf, MD, of University Hospital Cologne (Germany).
“The differential benefit observed between patients treated in the first line and relapsed [settings] highlights the need of early diagnosis of this aberration, and prompt targeted treatment of this challenging patient population,” he said at the European Society for Medical Oncology Congress.
MET exon14–skipping mutations occur in approximately 3%-4% of NSCLC cases. The mutation is thought to be an oncogenic driver and has been shown to be a poor prognostic factor for patients with advanced NSCLC. Patients with this mutation have poor responses to conventional therapy and immune checkpoint inhibitors, even when their tumors have high levels of programmed death–ligand 1 (PD-L1) and high mutational burden, Dr. Wolf said.
Capmatinib (INC280) is an oral, reversible inhibitor of the MET receptor tyrosine kinase and is highly selective for MET, with particular affinity for MET exon 14 mutations. It is also capable of crossing the blood-brain barrier and has shown activity in the brain in preliminary studies.
The Geometry MONO-1 trial is a phase 2 study of capmatinib in patients with stage IIIB/IV NSCLC with tumors that demonstrate MET amplification and/or carry the MET exon 14 mutation. Three study cohorts of patients with MET amplification were closed for futility. Dr. Wolf reported results from two cohorts of patients with MET exon 14–skipping mutations regardless of gene copy number: one with treatment-naive patients and the other with patients being treated in the second or third line.
As noted, the ORR in 25 patients in the treatment-naive cohort after a median follow-up of 5.6 months was 72%, including 18 partial responses and no complete responses. In addition, six patients (24%) had stable disease, for a disease control rate of 96%.
In the pretreated cohort, however, there were no complete responses among 69 patients, and 27 patients (39.1%) had partial responses. In this cohort, an additional 26 patients (37.7%) had stable disease, for an ORR of 39.1% and disease-control rate of 78.3%.
Dr. Wolf also highlighted preliminary evidence of capmatinib activity in the brain. He noted that one patient, an 80-year-old woman with multiple untreated brain metastases as well as lesions in dermal lymph nodes, liver, and pleura, had complete resolution of brain metastases at the first postbaseline CT scan, 42 days after starting capmatinib. The duration of response was 11.3 months, at which point the patient discontinued the drug because of extracranial progressive disease.
Among all patients in all study cohorts (302) the most common grade 3 or 4 adverse events were peripheral edema, dyspnea, fatigue, nausea, vomiting, and decreased appetite. Adverse drug-related events (grade 3 or 4) included peripheral edema, nausea, vomiting, fatigue, and decreased appetite. In all, 10.3% of patients discontinued for adverse events suspected to be related to capmatinib.

Invited discussant James Chih-Hsin Yang, MD, PhD, from the National Taiwan University Hospital in Taipei, said that the study shows that the MET exon 14–skipping mutation is an oncogenic driver and that capmatinib is an effective tyrosine kinase inhibitor (TKI) for patients with NSCLC harboring this mutation.
Questions that still need to be answered, he said, include whether patients with the mutation are heterogeneous and may have differing response to TKIs, how long the duration of response is, how long it will take for resistance to capmatinib to occur, how it compares with other MET inhibitors, and if there are additional biomarkers that could help select patients for treatment with the novel agent.
The study was funded by Novartis. Dr. Wolf reported advisory board participation, institutional research support, and lecture fees from Novartis and others. Dr. Yang reported honoraria from advisory board participation and/or speaking from Novartis and others. His institution participated in the Geometry MONO-1 study, but he was not personally involved.
MUNICH – The experimental agent capmatinib was associated with a high response rate when used in the first line for patients with advanced non–small cell lung cancers bearing MET exon 14–skipping mutations, said investigators in the Geometry MONO-1 trial.
Among a cohort of 25 patients with treatment-naive, MET exon 14–mutated non–small cell lung cancer (NSCLC), the primary endpoint of overall response rate (ORR) as determined by blinded, independent reviewers was 72%.
In contrast, the ORR among 69 patients who had received one or more prior lines of therapy was 39.1%, reported Juergen Wolf, MD, of University Hospital Cologne (Germany).
“The differential benefit observed between patients treated in the first line and relapsed [settings] highlights the need of early diagnosis of this aberration, and prompt targeted treatment of this challenging patient population,” he said at the European Society for Medical Oncology Congress.
MET exon14–skipping mutations occur in approximately 3%-4% of NSCLC cases. The mutation is thought to be an oncogenic driver and has been shown to be a poor prognostic factor for patients with advanced NSCLC. Patients with this mutation have poor responses to conventional therapy and immune checkpoint inhibitors, even when their tumors have high levels of programmed death–ligand 1 (PD-L1) and high mutational burden, Dr. Wolf said.
Capmatinib (INC280) is an oral, reversible inhibitor of the MET receptor tyrosine kinase and is highly selective for MET, with particular affinity for MET exon 14 mutations. It is also capable of crossing the blood-brain barrier and has shown activity in the brain in preliminary studies.
The Geometry MONO-1 trial is a phase 2 study of capmatinib in patients with stage IIIB/IV NSCLC with tumors that demonstrate MET amplification and/or carry the MET exon 14 mutation. Three study cohorts of patients with MET amplification were closed for futility. Dr. Wolf reported results from two cohorts of patients with MET exon 14–skipping mutations regardless of gene copy number: one with treatment-naive patients and the other with patients being treated in the second or third line.
As noted, the ORR in 25 patients in the treatment-naive cohort after a median follow-up of 5.6 months was 72%, including 18 partial responses and no complete responses. In addition, six patients (24%) had stable disease, for a disease control rate of 96%.
In the pretreated cohort, however, there were no complete responses among 69 patients, and 27 patients (39.1%) had partial responses. In this cohort, an additional 26 patients (37.7%) had stable disease, for an ORR of 39.1% and disease-control rate of 78.3%.
Dr. Wolf also highlighted preliminary evidence of capmatinib activity in the brain. He noted that one patient, an 80-year-old woman with multiple untreated brain metastases as well as lesions in dermal lymph nodes, liver, and pleura, had complete resolution of brain metastases at the first postbaseline CT scan, 42 days after starting capmatinib. The duration of response was 11.3 months, at which point the patient discontinued the drug because of extracranial progressive disease.
Among all patients in all study cohorts (302) the most common grade 3 or 4 adverse events were peripheral edema, dyspnea, fatigue, nausea, vomiting, and decreased appetite. Adverse drug-related events (grade 3 or 4) included peripheral edema, nausea, vomiting, fatigue, and decreased appetite. In all, 10.3% of patients discontinued for adverse events suspected to be related to capmatinib.
Invited discussant James Chih-Hsin Yang, MD, PhD, from the National Taiwan University Hospital in Taipei, said that the study shows that the MET exon 14–skipping mutation is an oncogenic driver and that capmatinib is an effective tyrosine kinase inhibitor (TKI) for patients with NSCLC harboring this mutation.
Questions that still need to be answered, he said, include whether patients with the mutation are heterogeneous and may have differing response to TKIs, how long the duration of response is, how long it will take for resistance to capmatinib to occur, how it compares with other MET inhibitors, and if there are additional biomarkers that could help select patients for treatment with the novel agent.
The study was funded by Novartis. Dr. Wolf reported advisory board participation, institutional research support, and lecture fees from Novartis and others. Dr. Yang reported honoraria from advisory board participation and/or speaking from Novartis and others. His institution participated in the Geometry MONO-1 study, but he was not personally involved.
MUNICH – The experimental agent capmatinib was associated with a high response rate when used in the first line for patients with advanced non–small cell lung cancers bearing MET exon 14–skipping mutations, said investigators in the Geometry MONO-1 trial.
Among a cohort of 25 patients with treatment-naive, MET exon 14–mutated non–small cell lung cancer (NSCLC), the primary endpoint of overall response rate (ORR) as determined by blinded, independent reviewers was 72%.
In contrast, the ORR among 69 patients who had received one or more prior lines of therapy was 39.1%, reported Juergen Wolf, MD, of University Hospital Cologne (Germany).
“The differential benefit observed between patients treated in the first line and relapsed [settings] highlights the need of early diagnosis of this aberration, and prompt targeted treatment of this challenging patient population,” he said at the European Society for Medical Oncology Congress.
MET exon14–skipping mutations occur in approximately 3%-4% of NSCLC cases. The mutation is thought to be an oncogenic driver and has been shown to be a poor prognostic factor for patients with advanced NSCLC. Patients with this mutation have poor responses to conventional therapy and immune checkpoint inhibitors, even when their tumors have high levels of programmed death–ligand 1 (PD-L1) and high mutational burden, Dr. Wolf said.
Capmatinib (INC280) is an oral, reversible inhibitor of the MET receptor tyrosine kinase and is highly selective for MET, with particular affinity for MET exon 14 mutations. It is also capable of crossing the blood-brain barrier and has shown activity in the brain in preliminary studies.
The Geometry MONO-1 trial is a phase 2 study of capmatinib in patients with stage IIIB/IV NSCLC with tumors that demonstrate MET amplification and/or carry the MET exon 14 mutation. Three study cohorts of patients with MET amplification were closed for futility. Dr. Wolf reported results from two cohorts of patients with MET exon 14–skipping mutations regardless of gene copy number: one with treatment-naive patients and the other with patients being treated in the second or third line.
As noted, the ORR in 25 patients in the treatment-naive cohort after a median follow-up of 5.6 months was 72%, including 18 partial responses and no complete responses. In addition, six patients (24%) had stable disease, for a disease control rate of 96%.
In the pretreated cohort, however, there were no complete responses among 69 patients, and 27 patients (39.1%) had partial responses. In this cohort, an additional 26 patients (37.7%) had stable disease, for an ORR of 39.1% and disease-control rate of 78.3%.
Dr. Wolf also highlighted preliminary evidence of capmatinib activity in the brain. He noted that one patient, an 80-year-old woman with multiple untreated brain metastases as well as lesions in dermal lymph nodes, liver, and pleura, had complete resolution of brain metastases at the first postbaseline CT scan, 42 days after starting capmatinib. The duration of response was 11.3 months, at which point the patient discontinued the drug because of extracranial progressive disease.
Among all patients in all study cohorts (302) the most common grade 3 or 4 adverse events were peripheral edema, dyspnea, fatigue, nausea, vomiting, and decreased appetite. Adverse drug-related events (grade 3 or 4) included peripheral edema, nausea, vomiting, fatigue, and decreased appetite. In all, 10.3% of patients discontinued for adverse events suspected to be related to capmatinib.
Invited discussant James Chih-Hsin Yang, MD, PhD, from the National Taiwan University Hospital in Taipei, said that the study shows that the MET exon 14–skipping mutation is an oncogenic driver and that capmatinib is an effective tyrosine kinase inhibitor (TKI) for patients with NSCLC harboring this mutation.
Questions that still need to be answered, he said, include whether patients with the mutation are heterogeneous and may have differing response to TKIs, how long the duration of response is, how long it will take for resistance to capmatinib to occur, how it compares with other MET inhibitors, and if there are additional biomarkers that could help select patients for treatment with the novel agent.
The study was funded by Novartis. Dr. Wolf reported advisory board participation, institutional research support, and lecture fees from Novartis and others. Dr. Yang reported honoraria from advisory board participation and/or speaking from Novartis and others. His institution participated in the Geometry MONO-1 study, but he was not personally involved.
REPORTING FROM ESMO 2018
Key clinical point: Patients with non–small cell lung cancer bearing a MET exon 14–skipping mutation had high overall response rates to the MET inhibitor capmatinib.
Major finding: The overall response rate in treatment-naive patients was 72%.
Study details: A phase 2 trial with previously treated and untreated patients with advanced non–small cell lung cancers bearing MET exon 14–skipping mutations.
Disclosures: The study was funded by Novartis. Dr. Wolf reported advisory board participation and lecture fees from Novartis and others and institutional research support from Novartis and others. Dr. Yang reported honoraria from advisory board participation and/or speaking from Novartis and others. His institution participated in the Geometry MONO-1 study, but he was not personally involved.
Cigarette smoking at lowest level ever
“This new all-time low in cigarette smoking among U.S. adults is a tremendous public health accomplishment, and it demonstrates the importance of continued proven strategies to reduce smoking,” CDC Director Robert Redfield said in a written statement.
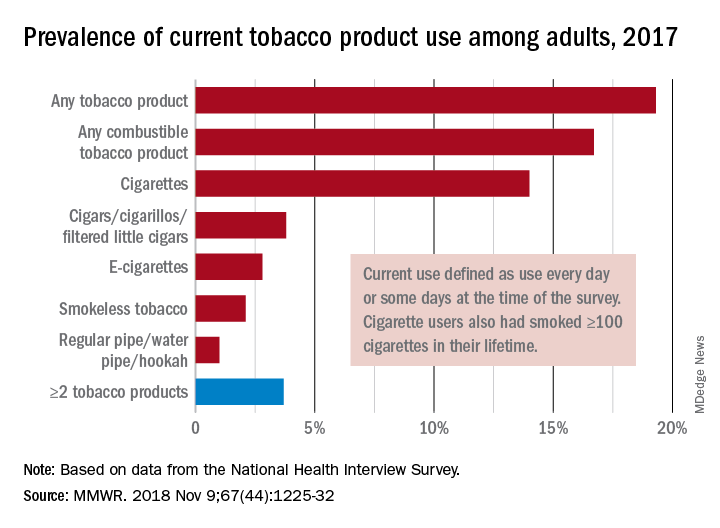
In 2017, 19.3% of adults aged 18 years and older – approximately 47.4 million Americans – reported current use of some type of tobacco product, and current use of combustible tobacco was 16.7%, Teresa W. Wang, PhD, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report. Current use was defined as use every day or some days, with an added requirement of at least 100 cigarettes in a lifetime added for cigarette smokers.
Data from the National Health Interview Survey showed that from 2016 to 2017, current use declined for any tobacco product, any combustible tobacco product, cigarettes, smokeless tobacco, and the combination of two or more tobacco products. The most common combination in 2017 was cigarettes and e-cigarettes, which was reported by 30.1% of the 9 million adults who used more than one product, Dr. Wang and her associates said.
Prevalence of current tobacco use was higher among men than women (24.8% vs. 14.2%), and adults aged 25-44 years (22.5%) had the highest level by age, followed by those aged 45-64 years (21.3%), 18-24 years (18.3%), and 65 years or older (11%). Use by race/ethnicity was highest among American Indian/Alaska Natives (29.8%), with the Midwest putting up the highest prevalence by region at 23.5%, they said.
“Although cigarette smoking among U.S. adults has declined considerably, tobacco products have evolved in recent years to include various combustible, noncombustible, and electronic products,” Dr. Wang and her associates wrote. “Implementation of evidence-based tobacco control interventions that address the diversity of tobacco products used by U.S. adults, in coordination with regulation of tobacco product manufacturing, marketing, and sales, can reduce tobacco-related disease and death in the United States.”
SOURCE: Wang TW et al. MMWR. 2018 Nov 9;67[44]:1225-32.
“This new all-time low in cigarette smoking among U.S. adults is a tremendous public health accomplishment, and it demonstrates the importance of continued proven strategies to reduce smoking,” CDC Director Robert Redfield said in a written statement.
In 2017, 19.3% of adults aged 18 years and older – approximately 47.4 million Americans – reported current use of some type of tobacco product, and current use of combustible tobacco was 16.7%, Teresa W. Wang, PhD, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report. Current use was defined as use every day or some days, with an added requirement of at least 100 cigarettes in a lifetime added for cigarette smokers.
Data from the National Health Interview Survey showed that from 2016 to 2017, current use declined for any tobacco product, any combustible tobacco product, cigarettes, smokeless tobacco, and the combination of two or more tobacco products. The most common combination in 2017 was cigarettes and e-cigarettes, which was reported by 30.1% of the 9 million adults who used more than one product, Dr. Wang and her associates said.
Prevalence of current tobacco use was higher among men than women (24.8% vs. 14.2%), and adults aged 25-44 years (22.5%) had the highest level by age, followed by those aged 45-64 years (21.3%), 18-24 years (18.3%), and 65 years or older (11%). Use by race/ethnicity was highest among American Indian/Alaska Natives (29.8%), with the Midwest putting up the highest prevalence by region at 23.5%, they said.
“Although cigarette smoking among U.S. adults has declined considerably, tobacco products have evolved in recent years to include various combustible, noncombustible, and electronic products,” Dr. Wang and her associates wrote. “Implementation of evidence-based tobacco control interventions that address the diversity of tobacco products used by U.S. adults, in coordination with regulation of tobacco product manufacturing, marketing, and sales, can reduce tobacco-related disease and death in the United States.”
SOURCE: Wang TW et al. MMWR. 2018 Nov 9;67[44]:1225-32.
“This new all-time low in cigarette smoking among U.S. adults is a tremendous public health accomplishment, and it demonstrates the importance of continued proven strategies to reduce smoking,” CDC Director Robert Redfield said in a written statement.
In 2017, 19.3% of adults aged 18 years and older – approximately 47.4 million Americans – reported current use of some type of tobacco product, and current use of combustible tobacco was 16.7%, Teresa W. Wang, PhD, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and her associates reported in the Morbidity and Mortality Weekly Report. Current use was defined as use every day or some days, with an added requirement of at least 100 cigarettes in a lifetime added for cigarette smokers.
Data from the National Health Interview Survey showed that from 2016 to 2017, current use declined for any tobacco product, any combustible tobacco product, cigarettes, smokeless tobacco, and the combination of two or more tobacco products. The most common combination in 2017 was cigarettes and e-cigarettes, which was reported by 30.1% of the 9 million adults who used more than one product, Dr. Wang and her associates said.
Prevalence of current tobacco use was higher among men than women (24.8% vs. 14.2%), and adults aged 25-44 years (22.5%) had the highest level by age, followed by those aged 45-64 years (21.3%), 18-24 years (18.3%), and 65 years or older (11%). Use by race/ethnicity was highest among American Indian/Alaska Natives (29.8%), with the Midwest putting up the highest prevalence by region at 23.5%, they said.
“Although cigarette smoking among U.S. adults has declined considerably, tobacco products have evolved in recent years to include various combustible, noncombustible, and electronic products,” Dr. Wang and her associates wrote. “Implementation of evidence-based tobacco control interventions that address the diversity of tobacco products used by U.S. adults, in coordination with regulation of tobacco product manufacturing, marketing, and sales, can reduce tobacco-related disease and death in the United States.”
SOURCE: Wang TW et al. MMWR. 2018 Nov 9;67[44]:1225-32.
FROM MMWR
FDA approves lorlatinib as second line for ALK-positive advanced NSCLC
The Food and Drug Administration has granted accelerated approval to lorlatinib for patients with anaplastic lymphoma kinase (ALK)–positive metastatic non–small cell lung cancer (NSCLC) whose disease has progressed on crizotinib and at least one other ALK inhibitor for metastatic disease or whose disease has progressed on alectinib or ceritinib as the first ALK inhibitor therapy for metastatic disease.

Approval of the next-generation ALK inhibitor was based on an overall response rate of 48% – with 4% complete and 44% partial – in a subgroup of 215 patients with ALK-positive metastatic NSCLC enrolled in a nonrandomized, phase 2 trial, the FDA said in a press announcement. All patients had been previously treated with one or more ALK kinase inhibitors.
The median response duration was 12.5 months (95% confidence interval, 8.4-23.7) and the intracranial overall response rate in 89 patients with measurable lesions in the CNS was 60% (95% CI, 49-70) with 21% complete and 38% partial responses.
Common adverse reactions in patients receiving lorlatinib were edema, peripheral neuropathy, cognitive effects, dyspnea, fatigue, weight gain, arthralgia, mood effects, and diarrhea. The most common laboratory abnormalities were hypercholesterolemia and hypertriglyceridemia, the FDA said.
The recommended dose of lorlatinib, to be marketed as Lorbrena by Pfizer, is 100 mg orally once daily.
The Food and Drug Administration has granted accelerated approval to lorlatinib for patients with anaplastic lymphoma kinase (ALK)–positive metastatic non–small cell lung cancer (NSCLC) whose disease has progressed on crizotinib and at least one other ALK inhibitor for metastatic disease or whose disease has progressed on alectinib or ceritinib as the first ALK inhibitor therapy for metastatic disease.
Approval of the next-generation ALK inhibitor was based on an overall response rate of 48% – with 4% complete and 44% partial – in a subgroup of 215 patients with ALK-positive metastatic NSCLC enrolled in a nonrandomized, phase 2 trial, the FDA said in a press announcement. All patients had been previously treated with one or more ALK kinase inhibitors.
The median response duration was 12.5 months (95% confidence interval, 8.4-23.7) and the intracranial overall response rate in 89 patients with measurable lesions in the CNS was 60% (95% CI, 49-70) with 21% complete and 38% partial responses.
Common adverse reactions in patients receiving lorlatinib were edema, peripheral neuropathy, cognitive effects, dyspnea, fatigue, weight gain, arthralgia, mood effects, and diarrhea. The most common laboratory abnormalities were hypercholesterolemia and hypertriglyceridemia, the FDA said.
The recommended dose of lorlatinib, to be marketed as Lorbrena by Pfizer, is 100 mg orally once daily.
The Food and Drug Administration has granted accelerated approval to lorlatinib for patients with anaplastic lymphoma kinase (ALK)–positive metastatic non–small cell lung cancer (NSCLC) whose disease has progressed on crizotinib and at least one other ALK inhibitor for metastatic disease or whose disease has progressed on alectinib or ceritinib as the first ALK inhibitor therapy for metastatic disease.
Approval of the next-generation ALK inhibitor was based on an overall response rate of 48% – with 4% complete and 44% partial – in a subgroup of 215 patients with ALK-positive metastatic NSCLC enrolled in a nonrandomized, phase 2 trial, the FDA said in a press announcement. All patients had been previously treated with one or more ALK kinase inhibitors.
The median response duration was 12.5 months (95% confidence interval, 8.4-23.7) and the intracranial overall response rate in 89 patients with measurable lesions in the CNS was 60% (95% CI, 49-70) with 21% complete and 38% partial responses.
Common adverse reactions in patients receiving lorlatinib were edema, peripheral neuropathy, cognitive effects, dyspnea, fatigue, weight gain, arthralgia, mood effects, and diarrhea. The most common laboratory abnormalities were hypercholesterolemia and hypertriglyceridemia, the FDA said.
The recommended dose of lorlatinib, to be marketed as Lorbrena by Pfizer, is 100 mg orally once daily.
FDA expands approval of pembrolizumab in NSCLC
The Food and Drug Administration .
The drug is now approved for use in combination with carboplatin and either paclitaxel or nanoparticle albumin–bound (nab) paclitaxel for the first-line treatment of NSCLC, regardless of PD-L1 expression status.
This makes pembrolizumab the first anti-PD-1 therapy approved in the first-line setting both as monotherapy and in combination treatment for certain patients with metastatic NSCLC. All appropriate patients with metastatic squamous NSCLC or metastatic nonsquamous NSCLC and no EGFR or ALK mutations are now eligible to receive pembrolizumab-based treatment first-line.
The FDA’s approval is based on results from the phase 3 KEYNOTE-407 trial. This randomized, double-blind study enrolled patients with metastatic squamous NSCLC, regardless of tumor PD-L1 expression status, who had received no prior systemic treatment for metastatic disease.
Patients in the pembrolizumab arm (n = 278) received pembrolizumab and carboplatin every 3 weeks for four cycles, plus paclitaxel every 3 weeks for four cycles or nab-paclitaxel on days 1, 8, and 15 of every 3-week cycle for four cycles, followed by pembrolizumab every 3 weeks.
Patients in the control arm (n = 281) received the same regimen of carboplatin and paclitaxel/nab-paclitaxel, but placebo instead of pembrolizumab.
There was a significant improvement in overall response rate, progression-free survival, and overall survival in patients who received pembrolizumab.
The overall response rate was 58% in the pembrolizumab arm and 35% in the placebo arm (P = .0008). The median duration of response was 7.2 months and 4.9 months, respectively.
The median progression-free survival was 6.4 months in the pembrolizumab arm and 4.8 months in the placebo arm (P less than .0001). The median overall survival was 15.9 months and 11.3 months, respectively (P = .0017).
Safety data are available for the first 203 patients treated on the trial, 101 of them in the pembrolizumab arm.
Fifteen percent of patients discontinued pembrolizumab because of adverse events (AEs), and 43% of patients on pembrolizumab experienced AEs leading to dose interruption.
The most common AEs leading to dose interruption in the pembrolizumab arm were thrombocytopenia, neutropenia, anemia, asthenia, and diarrhea. The most frequent serious AEs in the pembrolizumab arm were febrile neutropenia, pneumonia, and urinary tract infection.
Additional details on this trial are available in the prescribing information, which can be found on the Keytruda website.
The Food and Drug Administration .
The drug is now approved for use in combination with carboplatin and either paclitaxel or nanoparticle albumin–bound (nab) paclitaxel for the first-line treatment of NSCLC, regardless of PD-L1 expression status.
This makes pembrolizumab the first anti-PD-1 therapy approved in the first-line setting both as monotherapy and in combination treatment for certain patients with metastatic NSCLC. All appropriate patients with metastatic squamous NSCLC or metastatic nonsquamous NSCLC and no EGFR or ALK mutations are now eligible to receive pembrolizumab-based treatment first-line.
The FDA’s approval is based on results from the phase 3 KEYNOTE-407 trial. This randomized, double-blind study enrolled patients with metastatic squamous NSCLC, regardless of tumor PD-L1 expression status, who had received no prior systemic treatment for metastatic disease.
Patients in the pembrolizumab arm (n = 278) received pembrolizumab and carboplatin every 3 weeks for four cycles, plus paclitaxel every 3 weeks for four cycles or nab-paclitaxel on days 1, 8, and 15 of every 3-week cycle for four cycles, followed by pembrolizumab every 3 weeks.
Patients in the control arm (n = 281) received the same regimen of carboplatin and paclitaxel/nab-paclitaxel, but placebo instead of pembrolizumab.
There was a significant improvement in overall response rate, progression-free survival, and overall survival in patients who received pembrolizumab.
The overall response rate was 58% in the pembrolizumab arm and 35% in the placebo arm (P = .0008). The median duration of response was 7.2 months and 4.9 months, respectively.
The median progression-free survival was 6.4 months in the pembrolizumab arm and 4.8 months in the placebo arm (P less than .0001). The median overall survival was 15.9 months and 11.3 months, respectively (P = .0017).
Safety data are available for the first 203 patients treated on the trial, 101 of them in the pembrolizumab arm.
Fifteen percent of patients discontinued pembrolizumab because of adverse events (AEs), and 43% of patients on pembrolizumab experienced AEs leading to dose interruption.
The most common AEs leading to dose interruption in the pembrolizumab arm were thrombocytopenia, neutropenia, anemia, asthenia, and diarrhea. The most frequent serious AEs in the pembrolizumab arm were febrile neutropenia, pneumonia, and urinary tract infection.
Additional details on this trial are available in the prescribing information, which can be found on the Keytruda website.
The Food and Drug Administration .
The drug is now approved for use in combination with carboplatin and either paclitaxel or nanoparticle albumin–bound (nab) paclitaxel for the first-line treatment of NSCLC, regardless of PD-L1 expression status.
This makes pembrolizumab the first anti-PD-1 therapy approved in the first-line setting both as monotherapy and in combination treatment for certain patients with metastatic NSCLC. All appropriate patients with metastatic squamous NSCLC or metastatic nonsquamous NSCLC and no EGFR or ALK mutations are now eligible to receive pembrolizumab-based treatment first-line.
The FDA’s approval is based on results from the phase 3 KEYNOTE-407 trial. This randomized, double-blind study enrolled patients with metastatic squamous NSCLC, regardless of tumor PD-L1 expression status, who had received no prior systemic treatment for metastatic disease.
Patients in the pembrolizumab arm (n = 278) received pembrolizumab and carboplatin every 3 weeks for four cycles, plus paclitaxel every 3 weeks for four cycles or nab-paclitaxel on days 1, 8, and 15 of every 3-week cycle for four cycles, followed by pembrolizumab every 3 weeks.
Patients in the control arm (n = 281) received the same regimen of carboplatin and paclitaxel/nab-paclitaxel, but placebo instead of pembrolizumab.
There was a significant improvement in overall response rate, progression-free survival, and overall survival in patients who received pembrolizumab.
The overall response rate was 58% in the pembrolizumab arm and 35% in the placebo arm (P = .0008). The median duration of response was 7.2 months and 4.9 months, respectively.
The median progression-free survival was 6.4 months in the pembrolizumab arm and 4.8 months in the placebo arm (P less than .0001). The median overall survival was 15.9 months and 11.3 months, respectively (P = .0017).
Safety data are available for the first 203 patients treated on the trial, 101 of them in the pembrolizumab arm.
Fifteen percent of patients discontinued pembrolizumab because of adverse events (AEs), and 43% of patients on pembrolizumab experienced AEs leading to dose interruption.
The most common AEs leading to dose interruption in the pembrolizumab arm were thrombocytopenia, neutropenia, anemia, asthenia, and diarrhea. The most frequent serious AEs in the pembrolizumab arm were febrile neutropenia, pneumonia, and urinary tract infection.
Additional details on this trial are available in the prescribing information, which can be found on the Keytruda website.
Smoking neglected in patients with PAD
Patients with claudication consulting a peripheral arterial disease provider are often active smokers, rarely receive evidence-based cessation interventions, and frequently relapse if they do quit, according to a report published online in the Journal of the American Heart Association.

More than one-third of patients with claudication consulting PAD specialists are active smokers, as seen in a data analysis of an international registry, wrote Krishna K. Patel, MD, of the department of cardiology, University of Missouri–Kansas City, and her colleagues.
The authors assessed 1,272 patients with PAD and new or worsening claudication who were enrolled at 16 vascular specialty clinics from 2011 to 2015 in the PORTRAIT (Patient-Centered Outcomes Related to Treatment Practices in Peripheral Arterial Disease: Investigating Trajectories) registry, (Clinicaltrials.gov: NCT01419080).
In-person interviews obtained smoking status from the patients and information on cessation interventions at baseline and at 3, 6, and 12 months. At baseline, 474 (37%) patients were active, 660 (52%) were former, and 138 (11%) were never smokers.
Among active smokers, only 16% were referred to cessation counseling, and only 11% were prescribed pharmacologic treatment.
At 3 months, the probability of quitting smoking was 21%. Those who kept smoking had a probability of quitting during the next 9 months that varied between 11% and 12% (P less than .001). The probability of relapse was high, with more than one-third of initial quitters (36%) resuming smoking, and at 12 months; 72% of all original smokers continued to smoke, according to the authors.
The high level of initial smoking and the failed efforts at attempting cessation are clinically important because cigarette smoking is the most important and modifiable risk factor for PAD, and patients with PAD who smoke have higher rates of disease progression, according to Dr. Patel and her colleagues.
“Few patients receive formal cessation interventions. The dynamic nature of these patients’ smoking practices also underscores the need for ongoing assessment of smoking, even among those who report that they have quit, and consistent offering of evidence-based cessation support. Future research should focus on identifying optimal strategies for implementing consistent cessation support,” the researchers concluded.
The study was funded by grants from the Netherlands Organization for Scientific Research and an unrestricted grant from W. L. Gore & Associates. One of the authors owns the copyright for a Peripheral Artery Questionnaire used in the study and serves as a consultant to United Healthcare, Bayer, and Novartis, with research grants from Abbot Vascular and Novartis. Another author is supported by an unrestricted research grant by Merck and Boston Scientific. The remaining authors reported having no disclosures.
SOURCE: Patel KR et al. J Am Heart Assoc. 2018;7:e010076. doi: 10.1161/JAHA.118.010076.
Patients with claudication consulting a peripheral arterial disease provider are often active smokers, rarely receive evidence-based cessation interventions, and frequently relapse if they do quit, according to a report published online in the Journal of the American Heart Association.
More than one-third of patients with claudication consulting PAD specialists are active smokers, as seen in a data analysis of an international registry, wrote Krishna K. Patel, MD, of the department of cardiology, University of Missouri–Kansas City, and her colleagues.
The authors assessed 1,272 patients with PAD and new or worsening claudication who were enrolled at 16 vascular specialty clinics from 2011 to 2015 in the PORTRAIT (Patient-Centered Outcomes Related to Treatment Practices in Peripheral Arterial Disease: Investigating Trajectories) registry, (Clinicaltrials.gov: NCT01419080).
In-person interviews obtained smoking status from the patients and information on cessation interventions at baseline and at 3, 6, and 12 months. At baseline, 474 (37%) patients were active, 660 (52%) were former, and 138 (11%) were never smokers.
Among active smokers, only 16% were referred to cessation counseling, and only 11% were prescribed pharmacologic treatment.
At 3 months, the probability of quitting smoking was 21%. Those who kept smoking had a probability of quitting during the next 9 months that varied between 11% and 12% (P less than .001). The probability of relapse was high, with more than one-third of initial quitters (36%) resuming smoking, and at 12 months; 72% of all original smokers continued to smoke, according to the authors.
The high level of initial smoking and the failed efforts at attempting cessation are clinically important because cigarette smoking is the most important and modifiable risk factor for PAD, and patients with PAD who smoke have higher rates of disease progression, according to Dr. Patel and her colleagues.
“Few patients receive formal cessation interventions. The dynamic nature of these patients’ smoking practices also underscores the need for ongoing assessment of smoking, even among those who report that they have quit, and consistent offering of evidence-based cessation support. Future research should focus on identifying optimal strategies for implementing consistent cessation support,” the researchers concluded.
The study was funded by grants from the Netherlands Organization for Scientific Research and an unrestricted grant from W. L. Gore & Associates. One of the authors owns the copyright for a Peripheral Artery Questionnaire used in the study and serves as a consultant to United Healthcare, Bayer, and Novartis, with research grants from Abbot Vascular and Novartis. Another author is supported by an unrestricted research grant by Merck and Boston Scientific. The remaining authors reported having no disclosures.
SOURCE: Patel KR et al. J Am Heart Assoc. 2018;7:e010076. doi: 10.1161/JAHA.118.010076.
Patients with claudication consulting a peripheral arterial disease provider are often active smokers, rarely receive evidence-based cessation interventions, and frequently relapse if they do quit, according to a report published online in the Journal of the American Heart Association.
More than one-third of patients with claudication consulting PAD specialists are active smokers, as seen in a data analysis of an international registry, wrote Krishna K. Patel, MD, of the department of cardiology, University of Missouri–Kansas City, and her colleagues.
The authors assessed 1,272 patients with PAD and new or worsening claudication who were enrolled at 16 vascular specialty clinics from 2011 to 2015 in the PORTRAIT (Patient-Centered Outcomes Related to Treatment Practices in Peripheral Arterial Disease: Investigating Trajectories) registry, (Clinicaltrials.gov: NCT01419080).
In-person interviews obtained smoking status from the patients and information on cessation interventions at baseline and at 3, 6, and 12 months. At baseline, 474 (37%) patients were active, 660 (52%) were former, and 138 (11%) were never smokers.
Among active smokers, only 16% were referred to cessation counseling, and only 11% were prescribed pharmacologic treatment.
At 3 months, the probability of quitting smoking was 21%. Those who kept smoking had a probability of quitting during the next 9 months that varied between 11% and 12% (P less than .001). The probability of relapse was high, with more than one-third of initial quitters (36%) resuming smoking, and at 12 months; 72% of all original smokers continued to smoke, according to the authors.
The high level of initial smoking and the failed efforts at attempting cessation are clinically important because cigarette smoking is the most important and modifiable risk factor for PAD, and patients with PAD who smoke have higher rates of disease progression, according to Dr. Patel and her colleagues.
“Few patients receive formal cessation interventions. The dynamic nature of these patients’ smoking practices also underscores the need for ongoing assessment of smoking, even among those who report that they have quit, and consistent offering of evidence-based cessation support. Future research should focus on identifying optimal strategies for implementing consistent cessation support,” the researchers concluded.
The study was funded by grants from the Netherlands Organization for Scientific Research and an unrestricted grant from W. L. Gore & Associates. One of the authors owns the copyright for a Peripheral Artery Questionnaire used in the study and serves as a consultant to United Healthcare, Bayer, and Novartis, with research grants from Abbot Vascular and Novartis. Another author is supported by an unrestricted research grant by Merck and Boston Scientific. The remaining authors reported having no disclosures.
SOURCE: Patel KR et al. J Am Heart Assoc. 2018;7:e010076. doi: 10.1161/JAHA.118.010076.
FROM THE JOURNAL OF THE AMERICAN HEART ASSOCIATION
Key clinical point: Patients with PAD are often smokers, rarely receive cessation interventions, and frequently relapse if they quit.
Major finding: Only 16% of active smokers received cessation counseling, and at 3 months, the probability of quitting smoking was 21%.
Study details: Interview study of 1,272 patients with PAD and new or worsening claudication who were enrolled in the PORTRAIT registry.
Disclosures: Study funding included an unrestricted grant from W. L. Gore & Associates. One author owns the copyright for the Peripheral Artery Questionnaire used in the study and has ties to several pharmaceutical companies. Another author is supported by an unrestricted corporate research grant. The remaining authors reported having no disclosures.
Source: Patel KR et al. J Am Heart Assoc. 2018;7:e010076. doi: 10.1161/JAHA.118.010076.
Checkpoint inhibitor seems safe and effective for patients with HIV
MUNICH – Patients with HIV who are treated with nivolumab, a programmed death-1 (PD-1) inhibitor, appear to have similar safety and efficacy outcomes compared with HIV-negative patients treated with the same agent, investigators found.
The retrospective study also showed that viral load and CD4 status were largely unchanged by immunotherapy, lead author Aurélien Gobert, MD, of Groupe Hospitalier Pitié Salpêtrière, Paris, reported at the European Society for Medical Oncology Congress.
HIV increases risks of certain cancer types, Dr. Gobert said in a press release. “These patients are at higher risk for a number of cancers: AIDS-defining forms, the diagnosis of which results in the categorization of a person as suffering from AIDS, but also various other types that they are two to three times more likely to develop than in the general population, such as anal, skin, head and neck, and lung cancer,” he said.
Despite the increased risks, few studies have evaluated cancer treatments for patients with HIV due to exclusions from most clinical trials. As HIV is an immune-based disease, concerns have arisen surrounding the safety and efficacy of using anti-neoplastic immunotherapies for HIV-positive patients. Considering that millions of people worldwide are HIV positive, research in this area can have real-world consequences.
Dr. Gobert and his colleagues analyzed data from CANCERVIH, a French national database of patients with cancer and HIV. Since May 2014, nivolumab has been administered to 20 patients. Nineteen had metastatic non–small-cell lung cancer and 1 had metastatic melanoma. At diagnosis, the median CD4 count was 338.5 per cubic millimeter. Seventeen patients had undetectable viral load, two had fewer than 40 copies per millimeter, and one patient’s viral load was unknown. Dr. Gobert described the population as “demographically homogenous,” with “most patients being males around 60 years old.”
Analysis showed that nivolumab had little impact on CD4 count or viral load. One patient had a decreased CD4 count and an increased viral load, but this occurred during an interruption to antiretroviral therapy, which clouds potential associations with nivolumab. No immune-related adverse events or deaths due to drug toxicity occurred. Efficacy was assessed in 17 patients: Four (24%) showed a partial response, 2 (12%) had stable disease, and 11 (64%) had disease progression.
“Based on these preliminary data, treatment with anti-PD-1 ... seems to be feasible in people with HIV,” Dr. Gobert reported. He added that “antiretroviral therapy should not be interrupted.”
In a comment for ESMO, John Haanen, PhD, of the Netherlands Cancer Institute, Amsterdam, said that the results “confirm those of other, smaller cohorts in showing that while on antiretroviral therapy, cancer patients living with HIV can safely receive anti-PD-1 treatment. The efficacy data also suggests that the overall response rate of HIV-positive patients seems to be similar to that of other cancer patients. These promising results need to be confirmed in larger studies – ideally, in a prospective clinical trial.”
Principal investigator Jean-Philippe Spano, MD, PhD, disclosed relationships with Gilead, Roche, BMS, and others.
SOURCE: Gobert et al. ESMO 2018, Abstract 1213P_PR.
MUNICH – Patients with HIV who are treated with nivolumab, a programmed death-1 (PD-1) inhibitor, appear to have similar safety and efficacy outcomes compared with HIV-negative patients treated with the same agent, investigators found.
The retrospective study also showed that viral load and CD4 status were largely unchanged by immunotherapy, lead author Aurélien Gobert, MD, of Groupe Hospitalier Pitié Salpêtrière, Paris, reported at the European Society for Medical Oncology Congress.
HIV increases risks of certain cancer types, Dr. Gobert said in a press release. “These patients are at higher risk for a number of cancers: AIDS-defining forms, the diagnosis of which results in the categorization of a person as suffering from AIDS, but also various other types that they are two to three times more likely to develop than in the general population, such as anal, skin, head and neck, and lung cancer,” he said.
Despite the increased risks, few studies have evaluated cancer treatments for patients with HIV due to exclusions from most clinical trials. As HIV is an immune-based disease, concerns have arisen surrounding the safety and efficacy of using anti-neoplastic immunotherapies for HIV-positive patients. Considering that millions of people worldwide are HIV positive, research in this area can have real-world consequences.
Dr. Gobert and his colleagues analyzed data from CANCERVIH, a French national database of patients with cancer and HIV. Since May 2014, nivolumab has been administered to 20 patients. Nineteen had metastatic non–small-cell lung cancer and 1 had metastatic melanoma. At diagnosis, the median CD4 count was 338.5 per cubic millimeter. Seventeen patients had undetectable viral load, two had fewer than 40 copies per millimeter, and one patient’s viral load was unknown. Dr. Gobert described the population as “demographically homogenous,” with “most patients being males around 60 years old.”
Analysis showed that nivolumab had little impact on CD4 count or viral load. One patient had a decreased CD4 count and an increased viral load, but this occurred during an interruption to antiretroviral therapy, which clouds potential associations with nivolumab. No immune-related adverse events or deaths due to drug toxicity occurred. Efficacy was assessed in 17 patients: Four (24%) showed a partial response, 2 (12%) had stable disease, and 11 (64%) had disease progression.
“Based on these preliminary data, treatment with anti-PD-1 ... seems to be feasible in people with HIV,” Dr. Gobert reported. He added that “antiretroviral therapy should not be interrupted.”
In a comment for ESMO, John Haanen, PhD, of the Netherlands Cancer Institute, Amsterdam, said that the results “confirm those of other, smaller cohorts in showing that while on antiretroviral therapy, cancer patients living with HIV can safely receive anti-PD-1 treatment. The efficacy data also suggests that the overall response rate of HIV-positive patients seems to be similar to that of other cancer patients. These promising results need to be confirmed in larger studies – ideally, in a prospective clinical trial.”
Principal investigator Jean-Philippe Spano, MD, PhD, disclosed relationships with Gilead, Roche, BMS, and others.
SOURCE: Gobert et al. ESMO 2018, Abstract 1213P_PR.
MUNICH – Patients with HIV who are treated with nivolumab, a programmed death-1 (PD-1) inhibitor, appear to have similar safety and efficacy outcomes compared with HIV-negative patients treated with the same agent, investigators found.
The retrospective study also showed that viral load and CD4 status were largely unchanged by immunotherapy, lead author Aurélien Gobert, MD, of Groupe Hospitalier Pitié Salpêtrière, Paris, reported at the European Society for Medical Oncology Congress.
HIV increases risks of certain cancer types, Dr. Gobert said in a press release. “These patients are at higher risk for a number of cancers: AIDS-defining forms, the diagnosis of which results in the categorization of a person as suffering from AIDS, but also various other types that they are two to three times more likely to develop than in the general population, such as anal, skin, head and neck, and lung cancer,” he said.
Despite the increased risks, few studies have evaluated cancer treatments for patients with HIV due to exclusions from most clinical trials. As HIV is an immune-based disease, concerns have arisen surrounding the safety and efficacy of using anti-neoplastic immunotherapies for HIV-positive patients. Considering that millions of people worldwide are HIV positive, research in this area can have real-world consequences.
Dr. Gobert and his colleagues analyzed data from CANCERVIH, a French national database of patients with cancer and HIV. Since May 2014, nivolumab has been administered to 20 patients. Nineteen had metastatic non–small-cell lung cancer and 1 had metastatic melanoma. At diagnosis, the median CD4 count was 338.5 per cubic millimeter. Seventeen patients had undetectable viral load, two had fewer than 40 copies per millimeter, and one patient’s viral load was unknown. Dr. Gobert described the population as “demographically homogenous,” with “most patients being males around 60 years old.”
Analysis showed that nivolumab had little impact on CD4 count or viral load. One patient had a decreased CD4 count and an increased viral load, but this occurred during an interruption to antiretroviral therapy, which clouds potential associations with nivolumab. No immune-related adverse events or deaths due to drug toxicity occurred. Efficacy was assessed in 17 patients: Four (24%) showed a partial response, 2 (12%) had stable disease, and 11 (64%) had disease progression.
“Based on these preliminary data, treatment with anti-PD-1 ... seems to be feasible in people with HIV,” Dr. Gobert reported. He added that “antiretroviral therapy should not be interrupted.”
In a comment for ESMO, John Haanen, PhD, of the Netherlands Cancer Institute, Amsterdam, said that the results “confirm those of other, smaller cohorts in showing that while on antiretroviral therapy, cancer patients living with HIV can safely receive anti-PD-1 treatment. The efficacy data also suggests that the overall response rate of HIV-positive patients seems to be similar to that of other cancer patients. These promising results need to be confirmed in larger studies – ideally, in a prospective clinical trial.”
Principal investigator Jean-Philippe Spano, MD, PhD, disclosed relationships with Gilead, Roche, BMS, and others.
SOURCE: Gobert et al. ESMO 2018, Abstract 1213P_PR.
REPORTING FROM ESMO 2018
Key clinical point: Patients with HIV who are treated with nivolumab, a programmed death-1 (PD-1) inhibitor, appear to have similar safety and efficacy outcomes compared with HIV-negative patients treated with the same agent.
Major finding: No immune-related adverse events or deaths due to drug toxicity occurred.
Study details: A retrospective analysis of 20 patients with HIV who received nivolumab immunotherapy.
Disclosures: Jean-Philippe Spano, principal investigator, disclosed relationships with Gilead, Roche, BMS, and others.
Source: Gobert et al. ESMO 2018, Abstract 1213P_PR.