User login
Racial Disparities in Treatment and Survival for Early-Stage Non-Small Cell Lung Cancer: Is Equal Access Health Care System the Answer?
Background
Survival for early-stage non-small cell lung cancer (NSCLC) has dramatically improved with advancement in surgical and radiation techniques over last two decades but there exists a disparity for African Americans (AA) having worse overall survival (OS) in recent studies on the general US population. We studied this racial disparity in Veteran population.
Methods
Data for 2589 AA and 14184 Caucasian Veterans diagnosed with early-stage (I, II) NSCLC between 2011-2017 was obtained from the Cancer Cube Registry (VACCR). IRB approval was obtained.
Results
The distribution of newly diagnosed cases of Stage I (73.92% AA vs 74.71% Caucasians) and Stage II (26.07% vs 25.29%) between the two races was comparable (p = .41). More Caucasians were diagnosed above the age of 60 compared to AA (92.22% vs 84.51%, p < .05). More AA were diagnosed with adenocarcinoma at diagnosis (56.01% vs 45.88% Caucasians, p < .05) for both Stage I and II disease. For the limited number of Veterans with reported performance status (PS), similar proportion of patients had a good PS defined as ECOG 0-2 among the two races (93.70% AA vs 93.97% Caucasians, p = .73). There was no statistically significant difference between 5-year OS for AA and Caucasians (69.81% vs 70.78%, p = .33) for both Stage I and II NSCLC. Both groups had similar rate of receipt of surgery as first line treatment or in combination with other treatments (58.90% AA vs 59.07% Caucasians, p = .90). Similarly, the rate of receiving radiation therapy was comparable between AA and Caucasians (42.4% vs 42.3%, p = .96). Although both races showed improved 5-year OS after surgery, there was no statistical difference in survival benefit between AA and Caucasians (69.8% vs 70.8%, p = .33).
Conclusion
In contrast to the studies assessing general US population trends, there was no racial disparity for 5-year OS in early-stage NSCLC for the Veteran population. This points to the inequities in access to treatment and preventive healthcare services as a possible contributing cause to the increased mortality in AA in general US population and a more equitable healthcare delivery within the VHA system.
Background
Survival for early-stage non-small cell lung cancer (NSCLC) has dramatically improved with advancement in surgical and radiation techniques over last two decades but there exists a disparity for African Americans (AA) having worse overall survival (OS) in recent studies on the general US population. We studied this racial disparity in Veteran population.
Methods
Data for 2589 AA and 14184 Caucasian Veterans diagnosed with early-stage (I, II) NSCLC between 2011-2017 was obtained from the Cancer Cube Registry (VACCR). IRB approval was obtained.
Results
The distribution of newly diagnosed cases of Stage I (73.92% AA vs 74.71% Caucasians) and Stage II (26.07% vs 25.29%) between the two races was comparable (p = .41). More Caucasians were diagnosed above the age of 60 compared to AA (92.22% vs 84.51%, p < .05). More AA were diagnosed with adenocarcinoma at diagnosis (56.01% vs 45.88% Caucasians, p < .05) for both Stage I and II disease. For the limited number of Veterans with reported performance status (PS), similar proportion of patients had a good PS defined as ECOG 0-2 among the two races (93.70% AA vs 93.97% Caucasians, p = .73). There was no statistically significant difference between 5-year OS for AA and Caucasians (69.81% vs 70.78%, p = .33) for both Stage I and II NSCLC. Both groups had similar rate of receipt of surgery as first line treatment or in combination with other treatments (58.90% AA vs 59.07% Caucasians, p = .90). Similarly, the rate of receiving radiation therapy was comparable between AA and Caucasians (42.4% vs 42.3%, p = .96). Although both races showed improved 5-year OS after surgery, there was no statistical difference in survival benefit between AA and Caucasians (69.8% vs 70.8%, p = .33).
Conclusion
In contrast to the studies assessing general US population trends, there was no racial disparity for 5-year OS in early-stage NSCLC for the Veteran population. This points to the inequities in access to treatment and preventive healthcare services as a possible contributing cause to the increased mortality in AA in general US population and a more equitable healthcare delivery within the VHA system.
Background
Survival for early-stage non-small cell lung cancer (NSCLC) has dramatically improved with advancement in surgical and radiation techniques over last two decades but there exists a disparity for African Americans (AA) having worse overall survival (OS) in recent studies on the general US population. We studied this racial disparity in Veteran population.
Methods
Data for 2589 AA and 14184 Caucasian Veterans diagnosed with early-stage (I, II) NSCLC between 2011-2017 was obtained from the Cancer Cube Registry (VACCR). IRB approval was obtained.
Results
The distribution of newly diagnosed cases of Stage I (73.92% AA vs 74.71% Caucasians) and Stage II (26.07% vs 25.29%) between the two races was comparable (p = .41). More Caucasians were diagnosed above the age of 60 compared to AA (92.22% vs 84.51%, p < .05). More AA were diagnosed with adenocarcinoma at diagnosis (56.01% vs 45.88% Caucasians, p < .05) for both Stage I and II disease. For the limited number of Veterans with reported performance status (PS), similar proportion of patients had a good PS defined as ECOG 0-2 among the two races (93.70% AA vs 93.97% Caucasians, p = .73). There was no statistically significant difference between 5-year OS for AA and Caucasians (69.81% vs 70.78%, p = .33) for both Stage I and II NSCLC. Both groups had similar rate of receipt of surgery as first line treatment or in combination with other treatments (58.90% AA vs 59.07% Caucasians, p = .90). Similarly, the rate of receiving radiation therapy was comparable between AA and Caucasians (42.4% vs 42.3%, p = .96). Although both races showed improved 5-year OS after surgery, there was no statistical difference in survival benefit between AA and Caucasians (69.8% vs 70.8%, p = .33).
Conclusion
In contrast to the studies assessing general US population trends, there was no racial disparity for 5-year OS in early-stage NSCLC for the Veteran population. This points to the inequities in access to treatment and preventive healthcare services as a possible contributing cause to the increased mortality in AA in general US population and a more equitable healthcare delivery within the VHA system.
Survival Analysis of Untreated Early-Stage Non-Small Cell Lung Cancer (NSCLC) in a Veteran Population
Introduction
Veterans with early-stage NSCLC who do not receive any form of treatment have been shown to have a worse overall survival compared to those who receive treatment. Factors that may influence the decision to administer treatment including age, performance status (PS), comorbidities, and racial disparity have not been assessed on a national level in recent years.
Methods
Data for 31,966 veterans diagnosed with early-stage (0, I) NSCLC between 2003-2017 was obtained from the Cancer cube registry (VACCR). IRB approval was obtained.
Results
Patients were divided into treatment (26,833/31,966, 83.16%) and no-treatment group (3096/31966, 9.68%). Of the no-treatment group, 3004 patients were stage I and 92 were stage 0 whereas in the treatment group, the distribution was 26,584 and 249 respectively. Gender, race, and histology distribution were comparable between the two. Patients with poor PS (defined as ECOG III and IV) received less treatment with any modality compared to those with good PS (ECOG I and II) (15.07% in no treatment group vs 4.03% in treatment group, p<0.05). The treatment group had a better 5-year overall survival (OS) as compared to no-treatment group (43.1% vs 14.7%, p<0.05). Regardless of treatment, patients above the age of 60 (41% vs 13.4%, p<0.05) and those with poor PS (19.6% vs 5.8%, p<0.05) had worse 5-year survival, with the effect being greater in the treatment group. Adenocarcinoma had a better 5-year survival compared to squamous cell carcinoma (SCC) in both groups (49.56% vs 39.1% p<0.05). There was no clinically significant OS difference in terms of race (Caucasian or African American) or tumor location (upper, middle, or lower lobe) in between the two groups. Our study was limited by lack of patient- level data including smoking status or reason why no treatment was given.
Conclusion
Patients with early-stage NSCLC who receive no treatment based on poor PS have a worse overall survival compared to the patients that receive treatment. Further investigation is required to assess what other criteria are used to decide treatment eligibility and whether these patients would be candidates for immunotherapy or targeted therapy in the future.
Introduction
Veterans with early-stage NSCLC who do not receive any form of treatment have been shown to have a worse overall survival compared to those who receive treatment. Factors that may influence the decision to administer treatment including age, performance status (PS), comorbidities, and racial disparity have not been assessed on a national level in recent years.
Methods
Data for 31,966 veterans diagnosed with early-stage (0, I) NSCLC between 2003-2017 was obtained from the Cancer cube registry (VACCR). IRB approval was obtained.
Results
Patients were divided into treatment (26,833/31,966, 83.16%) and no-treatment group (3096/31966, 9.68%). Of the no-treatment group, 3004 patients were stage I and 92 were stage 0 whereas in the treatment group, the distribution was 26,584 and 249 respectively. Gender, race, and histology distribution were comparable between the two. Patients with poor PS (defined as ECOG III and IV) received less treatment with any modality compared to those with good PS (ECOG I and II) (15.07% in no treatment group vs 4.03% in treatment group, p<0.05). The treatment group had a better 5-year overall survival (OS) as compared to no-treatment group (43.1% vs 14.7%, p<0.05). Regardless of treatment, patients above the age of 60 (41% vs 13.4%, p<0.05) and those with poor PS (19.6% vs 5.8%, p<0.05) had worse 5-year survival, with the effect being greater in the treatment group. Adenocarcinoma had a better 5-year survival compared to squamous cell carcinoma (SCC) in both groups (49.56% vs 39.1% p<0.05). There was no clinically significant OS difference in terms of race (Caucasian or African American) or tumor location (upper, middle, or lower lobe) in between the two groups. Our study was limited by lack of patient- level data including smoking status or reason why no treatment was given.
Conclusion
Patients with early-stage NSCLC who receive no treatment based on poor PS have a worse overall survival compared to the patients that receive treatment. Further investigation is required to assess what other criteria are used to decide treatment eligibility and whether these patients would be candidates for immunotherapy or targeted therapy in the future.
Introduction
Veterans with early-stage NSCLC who do not receive any form of treatment have been shown to have a worse overall survival compared to those who receive treatment. Factors that may influence the decision to administer treatment including age, performance status (PS), comorbidities, and racial disparity have not been assessed on a national level in recent years.
Methods
Data for 31,966 veterans diagnosed with early-stage (0, I) NSCLC between 2003-2017 was obtained from the Cancer cube registry (VACCR). IRB approval was obtained.
Results
Patients were divided into treatment (26,833/31,966, 83.16%) and no-treatment group (3096/31966, 9.68%). Of the no-treatment group, 3004 patients were stage I and 92 were stage 0 whereas in the treatment group, the distribution was 26,584 and 249 respectively. Gender, race, and histology distribution were comparable between the two. Patients with poor PS (defined as ECOG III and IV) received less treatment with any modality compared to those with good PS (ECOG I and II) (15.07% in no treatment group vs 4.03% in treatment group, p<0.05). The treatment group had a better 5-year overall survival (OS) as compared to no-treatment group (43.1% vs 14.7%, p<0.05). Regardless of treatment, patients above the age of 60 (41% vs 13.4%, p<0.05) and those with poor PS (19.6% vs 5.8%, p<0.05) had worse 5-year survival, with the effect being greater in the treatment group. Adenocarcinoma had a better 5-year survival compared to squamous cell carcinoma (SCC) in both groups (49.56% vs 39.1% p<0.05). There was no clinically significant OS difference in terms of race (Caucasian or African American) or tumor location (upper, middle, or lower lobe) in between the two groups. Our study was limited by lack of patient- level data including smoking status or reason why no treatment was given.
Conclusion
Patients with early-stage NSCLC who receive no treatment based on poor PS have a worse overall survival compared to the patients that receive treatment. Further investigation is required to assess what other criteria are used to decide treatment eligibility and whether these patients would be candidates for immunotherapy or targeted therapy in the future.
Metformin disappoints in two phase 2 lung cancer trials
Although well tolerated, metformin does not improve survival when given alongside chemoradiotherapy to patients with locally advanced non–small cell lung cancer (NSCLC), and may even make survival worse, suggest results from two recent phase 2 trials.
Epidemiologic studies have suggested that metformin is associated with a reduced incidence of cancer, while retrospective case studies have indicated that patients taking the drug have improved outcomes.
Moreover, preclinical data indicated that metformin has antineoplastic effects, with the drug showing both cytostatic and cytotoxic effects.
The current results cast doubt, however, over whether these benefits can be replicated in randomized controlled trials and thence brought to the clinic.
Despite this, “I don’t think metformin is dead,” commented Heath D. Skinner, MD, PhD, first author on one of the trials, published in JAMA Oncology.
He said in an interview there are “a few key areas where I think metformin could be of benefit” in lung cancer, such as in combination with tyrosine kinase inhibitors, or with immunotherapy.
Dr. Skinner also highlighted the unexpectedly good performance of standard chemoradiation, showing the “progress” that has been made in recent years in treatment delivery and quality.
No survival benefit
In the first trial, which was an open-label phase 2 study, NRG-LU001, patients with unresectable stage 3 NSCLC who did not have diabetes were randomized to carboplatin and paclitaxel-based chemoradiation either alone or with metformin.
Among the 167 patients eligible for analysis, 1-year progression-free survival (PFS) was 60.4% in the control group and 51.3% in the metformin group (P = .24) after a median follow-up of 27.7 months.
The only clinical factor associated with progression-free survival on multivariate analysis was clinical stage, at a hazard ratio of 1.79 (P = .05), reports Dr. Skinner, from the University of Pittsburgh Hillman Cancer Center, and colleagues.
With 1-year overall survival at 80.2% in the control group and 80.8% in the metformin arm, and no significant differences in rates of locoregional recurrence or distant metastasis, the team concluded that adding metformin to chemoradiation may have been “well tolerated but did not improve survival.”
Not recommended
The second randomized controlled trial, OCOG-ALMERA, involved patients with locally advanced NSCLC stratified into stages 3A and 3B, again without diabetes.
They were treated with platinum-based chemoradiotherapy, with chest radiotherapy with or without consolidation chemotherapy. They were randomized to metformin or no additional treatment for up to 12 months.
The trial had to be stopped early because of slow accrual, with only 54 patients randomized between 2014 and 2019, wrote the authors who were led by Theodoros Tsakiridis, MD, PhD, Juravinski Cancer Center, McMaster University, Hamilton, Ont.
The results revealed that treatment failure at 1 year was seen in 69.2% of metformin patients and 42.9% of those in the control arm.
The 1-year progression survival was markedly worse with metformin, at 34.8% versus 63.0% in the control arm and an HR for progression of 2.42, while overall survival was 47.4% versus 85.2% and an HR for death of 3.80.
With more than twice as many metformin than control patients reporting at least one grade 3 or higher adverse event, the researchers conclude the drug is “not recommended in patients with locally advanced non–small cell lung cancer who are candidates for chemoradiotherapy.”
Future research directions
Do these results sound the death knell for metformin in the treatment of lung cancer, or could lessons be learned from both studies that leave the door open for future research?
Chukwuka Eze, MD, of the University Hospital LMU Munich (Germany), thinks there may well be.
In an editorial accompanying the two studies, he and colleagues wrote: “Despite the negative results of both studies, invaluable information for the subsequent design of future trials could be extracted.”
For example, “there might yet be a role for metformin in selected patients with non–small cell lung cancer patients,” they continued, such as those with KRAS/LKB1-mutated tumors, or with tumors that have elevated fluorodeoxyglucose metabolism.
They also suggested that future studies should include continuous assessment of metabolic parameters and “comprehensive” analysis of responses on imaging, as well as biomarker analysis.
Moreover, in the era of immuno-oncology, “special attention to the immunomodulatory effects of metformin in the host and tumor are pertinent.”
Better-than-expected outcomes
Beyond that, both studies were hampered by limitations that make drawing conclusions difficult.
In the OCOG-ALMERA trial, the lack of double-blinding or placebo control, and limited accrual are identified by the authors as “weaknesses.”
The “much slower than anticipated” accrual may have been caused not only by exclusion of patients with diabetes, but also bias against the trial among physicians, who may have looked instead to immunotherapy trials for their patients.
On the other hand, the issue for NRG-LU001 was the “better-than-expected” performance of control arm, the researchers noted.
They make the comparison with the PACIFIC trial, which showed that giving durvalumab (Imfinzi, AstraZeneca) after platinum-based doublet chemotherapy and concurrent radiotherapy was associated with a doubling of progression-free survival over chemoradiation alone.
However, Dr. Skinner and colleagues pointed out that the 1-year progression-free survival achieved in PACIFIC with durvalumab after chemoradiotherapy was, at 55.9%, lower than that seen in the control arm of NRG-LU001.
“The PFS in NRG-LU001 remains striking, particularly as PACIFIC trial patients were randomized only when progression was not detected after concurrent chemoradiation,” the researchers wrote.
Dr. Skinner said in an interview they expected the control arm in their study “to do far worse than it actually did.”
He continued that they did not follow up chemoradiation with adjuvant immunotherapy, as would be the case nowadays, because it was “not the standard when we started the trial,” and did not become so “until the very end of accrual.”
Dr. Skinner warned that there are “many caveats” to comparing two different trials, but looking at the current results alongside those from PACIFIC, he said that, “for me, it seems like we have been making progress in the delivery of concurrent chemoradiation. I think that good quality concurrent chemoradiation and improvement in delivery really is one of the take-homes from this trial.”
NRG-LU001 was supported by grants from NRG Oncology and the National Cancer Institute. OCOG-ALMERA was funded by a grant from the Canadian Institutes of Health Research to Dr Tsakiridis. The Ontario Clinical Oncology Group assumed the role of the sponsor of this trial. Dr. Skinner reported receiving research funding from the National Cancer Institute and National Institute of Dental and Craniofacial Research outside the submitted work and has previously received a grant from the National Cancer Institute for a separate metformin-related clinical trial. Dr. Tsakiridis reported receiving a grant from Sanofi Canada for prostate cancer research outside the submitted work. Dr. Eze declares no relevant relationships.
Although well tolerated, metformin does not improve survival when given alongside chemoradiotherapy to patients with locally advanced non–small cell lung cancer (NSCLC), and may even make survival worse, suggest results from two recent phase 2 trials.
Epidemiologic studies have suggested that metformin is associated with a reduced incidence of cancer, while retrospective case studies have indicated that patients taking the drug have improved outcomes.
Moreover, preclinical data indicated that metformin has antineoplastic effects, with the drug showing both cytostatic and cytotoxic effects.
The current results cast doubt, however, over whether these benefits can be replicated in randomized controlled trials and thence brought to the clinic.
Despite this, “I don’t think metformin is dead,” commented Heath D. Skinner, MD, PhD, first author on one of the trials, published in JAMA Oncology.
He said in an interview there are “a few key areas where I think metformin could be of benefit” in lung cancer, such as in combination with tyrosine kinase inhibitors, or with immunotherapy.
Dr. Skinner also highlighted the unexpectedly good performance of standard chemoradiation, showing the “progress” that has been made in recent years in treatment delivery and quality.
No survival benefit
In the first trial, which was an open-label phase 2 study, NRG-LU001, patients with unresectable stage 3 NSCLC who did not have diabetes were randomized to carboplatin and paclitaxel-based chemoradiation either alone or with metformin.
Among the 167 patients eligible for analysis, 1-year progression-free survival (PFS) was 60.4% in the control group and 51.3% in the metformin group (P = .24) after a median follow-up of 27.7 months.
The only clinical factor associated with progression-free survival on multivariate analysis was clinical stage, at a hazard ratio of 1.79 (P = .05), reports Dr. Skinner, from the University of Pittsburgh Hillman Cancer Center, and colleagues.
With 1-year overall survival at 80.2% in the control group and 80.8% in the metformin arm, and no significant differences in rates of locoregional recurrence or distant metastasis, the team concluded that adding metformin to chemoradiation may have been “well tolerated but did not improve survival.”
Not recommended
The second randomized controlled trial, OCOG-ALMERA, involved patients with locally advanced NSCLC stratified into stages 3A and 3B, again without diabetes.
They were treated with platinum-based chemoradiotherapy, with chest radiotherapy with or without consolidation chemotherapy. They were randomized to metformin or no additional treatment for up to 12 months.
The trial had to be stopped early because of slow accrual, with only 54 patients randomized between 2014 and 2019, wrote the authors who were led by Theodoros Tsakiridis, MD, PhD, Juravinski Cancer Center, McMaster University, Hamilton, Ont.
The results revealed that treatment failure at 1 year was seen in 69.2% of metformin patients and 42.9% of those in the control arm.
The 1-year progression survival was markedly worse with metformin, at 34.8% versus 63.0% in the control arm and an HR for progression of 2.42, while overall survival was 47.4% versus 85.2% and an HR for death of 3.80.
With more than twice as many metformin than control patients reporting at least one grade 3 or higher adverse event, the researchers conclude the drug is “not recommended in patients with locally advanced non–small cell lung cancer who are candidates for chemoradiotherapy.”
Future research directions
Do these results sound the death knell for metformin in the treatment of lung cancer, or could lessons be learned from both studies that leave the door open for future research?
Chukwuka Eze, MD, of the University Hospital LMU Munich (Germany), thinks there may well be.
In an editorial accompanying the two studies, he and colleagues wrote: “Despite the negative results of both studies, invaluable information for the subsequent design of future trials could be extracted.”
For example, “there might yet be a role for metformin in selected patients with non–small cell lung cancer patients,” they continued, such as those with KRAS/LKB1-mutated tumors, or with tumors that have elevated fluorodeoxyglucose metabolism.
They also suggested that future studies should include continuous assessment of metabolic parameters and “comprehensive” analysis of responses on imaging, as well as biomarker analysis.
Moreover, in the era of immuno-oncology, “special attention to the immunomodulatory effects of metformin in the host and tumor are pertinent.”
Better-than-expected outcomes
Beyond that, both studies were hampered by limitations that make drawing conclusions difficult.
In the OCOG-ALMERA trial, the lack of double-blinding or placebo control, and limited accrual are identified by the authors as “weaknesses.”
The “much slower than anticipated” accrual may have been caused not only by exclusion of patients with diabetes, but also bias against the trial among physicians, who may have looked instead to immunotherapy trials for their patients.
On the other hand, the issue for NRG-LU001 was the “better-than-expected” performance of control arm, the researchers noted.
They make the comparison with the PACIFIC trial, which showed that giving durvalumab (Imfinzi, AstraZeneca) after platinum-based doublet chemotherapy and concurrent radiotherapy was associated with a doubling of progression-free survival over chemoradiation alone.
However, Dr. Skinner and colleagues pointed out that the 1-year progression-free survival achieved in PACIFIC with durvalumab after chemoradiotherapy was, at 55.9%, lower than that seen in the control arm of NRG-LU001.
“The PFS in NRG-LU001 remains striking, particularly as PACIFIC trial patients were randomized only when progression was not detected after concurrent chemoradiation,” the researchers wrote.
Dr. Skinner said in an interview they expected the control arm in their study “to do far worse than it actually did.”
He continued that they did not follow up chemoradiation with adjuvant immunotherapy, as would be the case nowadays, because it was “not the standard when we started the trial,” and did not become so “until the very end of accrual.”
Dr. Skinner warned that there are “many caveats” to comparing two different trials, but looking at the current results alongside those from PACIFIC, he said that, “for me, it seems like we have been making progress in the delivery of concurrent chemoradiation. I think that good quality concurrent chemoradiation and improvement in delivery really is one of the take-homes from this trial.”
NRG-LU001 was supported by grants from NRG Oncology and the National Cancer Institute. OCOG-ALMERA was funded by a grant from the Canadian Institutes of Health Research to Dr Tsakiridis. The Ontario Clinical Oncology Group assumed the role of the sponsor of this trial. Dr. Skinner reported receiving research funding from the National Cancer Institute and National Institute of Dental and Craniofacial Research outside the submitted work and has previously received a grant from the National Cancer Institute for a separate metformin-related clinical trial. Dr. Tsakiridis reported receiving a grant from Sanofi Canada for prostate cancer research outside the submitted work. Dr. Eze declares no relevant relationships.
Although well tolerated, metformin does not improve survival when given alongside chemoradiotherapy to patients with locally advanced non–small cell lung cancer (NSCLC), and may even make survival worse, suggest results from two recent phase 2 trials.
Epidemiologic studies have suggested that metformin is associated with a reduced incidence of cancer, while retrospective case studies have indicated that patients taking the drug have improved outcomes.
Moreover, preclinical data indicated that metformin has antineoplastic effects, with the drug showing both cytostatic and cytotoxic effects.
The current results cast doubt, however, over whether these benefits can be replicated in randomized controlled trials and thence brought to the clinic.
Despite this, “I don’t think metformin is dead,” commented Heath D. Skinner, MD, PhD, first author on one of the trials, published in JAMA Oncology.
He said in an interview there are “a few key areas where I think metformin could be of benefit” in lung cancer, such as in combination with tyrosine kinase inhibitors, or with immunotherapy.
Dr. Skinner also highlighted the unexpectedly good performance of standard chemoradiation, showing the “progress” that has been made in recent years in treatment delivery and quality.
No survival benefit
In the first trial, which was an open-label phase 2 study, NRG-LU001, patients with unresectable stage 3 NSCLC who did not have diabetes were randomized to carboplatin and paclitaxel-based chemoradiation either alone or with metformin.
Among the 167 patients eligible for analysis, 1-year progression-free survival (PFS) was 60.4% in the control group and 51.3% in the metformin group (P = .24) after a median follow-up of 27.7 months.
The only clinical factor associated with progression-free survival on multivariate analysis was clinical stage, at a hazard ratio of 1.79 (P = .05), reports Dr. Skinner, from the University of Pittsburgh Hillman Cancer Center, and colleagues.
With 1-year overall survival at 80.2% in the control group and 80.8% in the metformin arm, and no significant differences in rates of locoregional recurrence or distant metastasis, the team concluded that adding metformin to chemoradiation may have been “well tolerated but did not improve survival.”
Not recommended
The second randomized controlled trial, OCOG-ALMERA, involved patients with locally advanced NSCLC stratified into stages 3A and 3B, again without diabetes.
They were treated with platinum-based chemoradiotherapy, with chest radiotherapy with or without consolidation chemotherapy. They were randomized to metformin or no additional treatment for up to 12 months.
The trial had to be stopped early because of slow accrual, with only 54 patients randomized between 2014 and 2019, wrote the authors who were led by Theodoros Tsakiridis, MD, PhD, Juravinski Cancer Center, McMaster University, Hamilton, Ont.
The results revealed that treatment failure at 1 year was seen in 69.2% of metformin patients and 42.9% of those in the control arm.
The 1-year progression survival was markedly worse with metformin, at 34.8% versus 63.0% in the control arm and an HR for progression of 2.42, while overall survival was 47.4% versus 85.2% and an HR for death of 3.80.
With more than twice as many metformin than control patients reporting at least one grade 3 or higher adverse event, the researchers conclude the drug is “not recommended in patients with locally advanced non–small cell lung cancer who are candidates for chemoradiotherapy.”
Future research directions
Do these results sound the death knell for metformin in the treatment of lung cancer, or could lessons be learned from both studies that leave the door open for future research?
Chukwuka Eze, MD, of the University Hospital LMU Munich (Germany), thinks there may well be.
In an editorial accompanying the two studies, he and colleagues wrote: “Despite the negative results of both studies, invaluable information for the subsequent design of future trials could be extracted.”
For example, “there might yet be a role for metformin in selected patients with non–small cell lung cancer patients,” they continued, such as those with KRAS/LKB1-mutated tumors, or with tumors that have elevated fluorodeoxyglucose metabolism.
They also suggested that future studies should include continuous assessment of metabolic parameters and “comprehensive” analysis of responses on imaging, as well as biomarker analysis.
Moreover, in the era of immuno-oncology, “special attention to the immunomodulatory effects of metformin in the host and tumor are pertinent.”
Better-than-expected outcomes
Beyond that, both studies were hampered by limitations that make drawing conclusions difficult.
In the OCOG-ALMERA trial, the lack of double-blinding or placebo control, and limited accrual are identified by the authors as “weaknesses.”
The “much slower than anticipated” accrual may have been caused not only by exclusion of patients with diabetes, but also bias against the trial among physicians, who may have looked instead to immunotherapy trials for their patients.
On the other hand, the issue for NRG-LU001 was the “better-than-expected” performance of control arm, the researchers noted.
They make the comparison with the PACIFIC trial, which showed that giving durvalumab (Imfinzi, AstraZeneca) after platinum-based doublet chemotherapy and concurrent radiotherapy was associated with a doubling of progression-free survival over chemoradiation alone.
However, Dr. Skinner and colleagues pointed out that the 1-year progression-free survival achieved in PACIFIC with durvalumab after chemoradiotherapy was, at 55.9%, lower than that seen in the control arm of NRG-LU001.
“The PFS in NRG-LU001 remains striking, particularly as PACIFIC trial patients were randomized only when progression was not detected after concurrent chemoradiation,” the researchers wrote.
Dr. Skinner said in an interview they expected the control arm in their study “to do far worse than it actually did.”
He continued that they did not follow up chemoradiation with adjuvant immunotherapy, as would be the case nowadays, because it was “not the standard when we started the trial,” and did not become so “until the very end of accrual.”
Dr. Skinner warned that there are “many caveats” to comparing two different trials, but looking at the current results alongside those from PACIFIC, he said that, “for me, it seems like we have been making progress in the delivery of concurrent chemoradiation. I think that good quality concurrent chemoradiation and improvement in delivery really is one of the take-homes from this trial.”
NRG-LU001 was supported by grants from NRG Oncology and the National Cancer Institute. OCOG-ALMERA was funded by a grant from the Canadian Institutes of Health Research to Dr Tsakiridis. The Ontario Clinical Oncology Group assumed the role of the sponsor of this trial. Dr. Skinner reported receiving research funding from the National Cancer Institute and National Institute of Dental and Craniofacial Research outside the submitted work and has previously received a grant from the National Cancer Institute for a separate metformin-related clinical trial. Dr. Tsakiridis reported receiving a grant from Sanofi Canada for prostate cancer research outside the submitted work. Dr. Eze declares no relevant relationships.
FROM JAMA ONCOLOGY
A case is building for personalized, genome-based radiation dosing
A team of researchers from the Cleveland Clinic, the Moffitt Cancer Center in Tampa, and Case Western Reserve University in Cleveland is zeroing in on a way to personalize radiation therapy for cancer patients based on genomic profile, much as genomics is used to tailor oncologic drug therapy.
It’s called “genomic-adjusted radiation dose” (GARD), a dose tailored to a person’s radiosensitivity as determined by the expression of 10 genes, known as the radiosensitivity index (RSI), combined with a linear quadratic model to yield GARD, a prediction of risk and benefit at various radiation doses for a particular patient.
A recent report in The Lancet Oncology validated GARD in 1,615 patients with seven cancer types from 11 study cohorts. If it holds up in clinical trials set to start later this year, GARD should “allow us to predict the benefit of radiation for an individual patient and adjust their treatment strategy,” wrote the authors of an editorial that accompanied the study. “The efforts need to be applauded worldwide, because radiotherapy is considerably lagging, compared with the enormous progress done in the field of personalized medicine,” Orit Kaidar-Person, MD, a radiation oncologist at Sheba Medical Center in Ramat Gan, Israel, and colleagues wrote.
GARD was associated with time to first recurrence and overall survival for patients receiving radiotherapy and predicted radiotherapy benefit, while physical dose did not. The team found a relative 2% reduction in risk of first recurrence for each unit increase of GARD (P = .0017) and a relative 3% increase in overall survival for each unit increase in GARD (P = .0007), among those who got radiotherapy. Values of GARD run from 0 to over 100, with higher scores meaning more radiation benefit.
The radiosensitivity index, which was derived from genomic studies of cancer cell lines exposed to radiation, was previously validated by the team and other groups across several tumor types.
Currently, radiation dosing is generally uniform for a given disease site and stage, based on the assumption that a given dose of radiation results in the same clinical effect across patients. In fact, the biological effect of a given dose varies widely between individual patients. “Patients we treat uniformly do not have a uniform response” which is why a more personalized approach would help, said lead investigator and Cleveland Clinic radiation oncologist Jacob Scott, MD, DPhil.
One patient with a given tumor might benefit from 2 extra fractions, while the next might need an extra 15 for the same benefit. “You need to know about [a patient’s] tumor genomics to know how hard you have to work,” he said.
Dr. Scott and colleagues are working with a genomics company to commercialize the approach. The vision for now is that physicians would ship in biopsy samples to be analyzed; RSI and GARD would be calculated, and then a decision support report would be sent back to the treatment team outlining the risks and benefits of various doses for the patient.
Dr. Scott, who holds proprietary rights on the approach, is bullish. When asked if he anticipates GARD dosing to be standard of care in 10 years, he said that “I can’t imagine another world. Everything else in cancer is personalized. Why aren’t we? It just makes sense. I know there’s a better way” to prescribe radiation, “and I’m excited for the future when I can use it.”
When asked for comment, Brian Marples, PhD, a radiation oncology professor at the University of Rochester (N.Y.), said the data so far for GARD “seem very solid. I’m very excited by the concept.”
It’s been “the holy grail” of radiation researchers to find a biologic marker that predicts what dosages patients need and what can be given safely. “This strategy is a good way of doing that. Other groups are proposing similar strategies, but I think this group is ahead. I can see [GARD] being readily applied to the clinic because patients are [already] getting their tumors genomically characterized as part of care,” Dr. Marples said.
But many questions remain. For instance, the editorial writers questioned how GARD is “affected by tumor heterogeneity, response to systemic therapy, and changes in the tumor microenvironment.” Also, the approach is based on conventional 2 Gy fractions, but other fractionation regimens are becoming more common.
For Dr. Marples, the big caveat is that most cancer patients are treated with both radiation and chemotherapy. He said he would like to see GARD validated in patients who receive both.
They seven tumor types in the study included breast cancer, head and neck cancer, non–small cell lung cancer, pancreatic cancer, endometrial cancer, melanoma, and glioma. The majority of the subjects were treated with radiation, and each had the genomic data needed to calculate GARD.
Dr. Scott, senior author and Moffitt Center radiation oncologist Javier Torres-Roca, MD, and a third author hold intellectual property rights on RSI, GARD, and prescription dose base on RSI, plus equity in Cvergenx, a company that seeks to commercialize the approach. Dr. Torres-Roca and another author are cofounders. The editorial writers and Dr. Marples did not have any relevant disclosures.
A team of researchers from the Cleveland Clinic, the Moffitt Cancer Center in Tampa, and Case Western Reserve University in Cleveland is zeroing in on a way to personalize radiation therapy for cancer patients based on genomic profile, much as genomics is used to tailor oncologic drug therapy.
It’s called “genomic-adjusted radiation dose” (GARD), a dose tailored to a person’s radiosensitivity as determined by the expression of 10 genes, known as the radiosensitivity index (RSI), combined with a linear quadratic model to yield GARD, a prediction of risk and benefit at various radiation doses for a particular patient.
A recent report in The Lancet Oncology validated GARD in 1,615 patients with seven cancer types from 11 study cohorts. If it holds up in clinical trials set to start later this year, GARD should “allow us to predict the benefit of radiation for an individual patient and adjust their treatment strategy,” wrote the authors of an editorial that accompanied the study. “The efforts need to be applauded worldwide, because radiotherapy is considerably lagging, compared with the enormous progress done in the field of personalized medicine,” Orit Kaidar-Person, MD, a radiation oncologist at Sheba Medical Center in Ramat Gan, Israel, and colleagues wrote.
GARD was associated with time to first recurrence and overall survival for patients receiving radiotherapy and predicted radiotherapy benefit, while physical dose did not. The team found a relative 2% reduction in risk of first recurrence for each unit increase of GARD (P = .0017) and a relative 3% increase in overall survival for each unit increase in GARD (P = .0007), among those who got radiotherapy. Values of GARD run from 0 to over 100, with higher scores meaning more radiation benefit.
The radiosensitivity index, which was derived from genomic studies of cancer cell lines exposed to radiation, was previously validated by the team and other groups across several tumor types.
Currently, radiation dosing is generally uniform for a given disease site and stage, based on the assumption that a given dose of radiation results in the same clinical effect across patients. In fact, the biological effect of a given dose varies widely between individual patients. “Patients we treat uniformly do not have a uniform response” which is why a more personalized approach would help, said lead investigator and Cleveland Clinic radiation oncologist Jacob Scott, MD, DPhil.
One patient with a given tumor might benefit from 2 extra fractions, while the next might need an extra 15 for the same benefit. “You need to know about [a patient’s] tumor genomics to know how hard you have to work,” he said.
Dr. Scott and colleagues are working with a genomics company to commercialize the approach. The vision for now is that physicians would ship in biopsy samples to be analyzed; RSI and GARD would be calculated, and then a decision support report would be sent back to the treatment team outlining the risks and benefits of various doses for the patient.
Dr. Scott, who holds proprietary rights on the approach, is bullish. When asked if he anticipates GARD dosing to be standard of care in 10 years, he said that “I can’t imagine another world. Everything else in cancer is personalized. Why aren’t we? It just makes sense. I know there’s a better way” to prescribe radiation, “and I’m excited for the future when I can use it.”
When asked for comment, Brian Marples, PhD, a radiation oncology professor at the University of Rochester (N.Y.), said the data so far for GARD “seem very solid. I’m very excited by the concept.”
It’s been “the holy grail” of radiation researchers to find a biologic marker that predicts what dosages patients need and what can be given safely. “This strategy is a good way of doing that. Other groups are proposing similar strategies, but I think this group is ahead. I can see [GARD] being readily applied to the clinic because patients are [already] getting their tumors genomically characterized as part of care,” Dr. Marples said.
But many questions remain. For instance, the editorial writers questioned how GARD is “affected by tumor heterogeneity, response to systemic therapy, and changes in the tumor microenvironment.” Also, the approach is based on conventional 2 Gy fractions, but other fractionation regimens are becoming more common.
For Dr. Marples, the big caveat is that most cancer patients are treated with both radiation and chemotherapy. He said he would like to see GARD validated in patients who receive both.
They seven tumor types in the study included breast cancer, head and neck cancer, non–small cell lung cancer, pancreatic cancer, endometrial cancer, melanoma, and glioma. The majority of the subjects were treated with radiation, and each had the genomic data needed to calculate GARD.
Dr. Scott, senior author and Moffitt Center radiation oncologist Javier Torres-Roca, MD, and a third author hold intellectual property rights on RSI, GARD, and prescription dose base on RSI, plus equity in Cvergenx, a company that seeks to commercialize the approach. Dr. Torres-Roca and another author are cofounders. The editorial writers and Dr. Marples did not have any relevant disclosures.
A team of researchers from the Cleveland Clinic, the Moffitt Cancer Center in Tampa, and Case Western Reserve University in Cleveland is zeroing in on a way to personalize radiation therapy for cancer patients based on genomic profile, much as genomics is used to tailor oncologic drug therapy.
It’s called “genomic-adjusted radiation dose” (GARD), a dose tailored to a person’s radiosensitivity as determined by the expression of 10 genes, known as the radiosensitivity index (RSI), combined with a linear quadratic model to yield GARD, a prediction of risk and benefit at various radiation doses for a particular patient.
A recent report in The Lancet Oncology validated GARD in 1,615 patients with seven cancer types from 11 study cohorts. If it holds up in clinical trials set to start later this year, GARD should “allow us to predict the benefit of radiation for an individual patient and adjust their treatment strategy,” wrote the authors of an editorial that accompanied the study. “The efforts need to be applauded worldwide, because radiotherapy is considerably lagging, compared with the enormous progress done in the field of personalized medicine,” Orit Kaidar-Person, MD, a radiation oncologist at Sheba Medical Center in Ramat Gan, Israel, and colleagues wrote.
GARD was associated with time to first recurrence and overall survival for patients receiving radiotherapy and predicted radiotherapy benefit, while physical dose did not. The team found a relative 2% reduction in risk of first recurrence for each unit increase of GARD (P = .0017) and a relative 3% increase in overall survival for each unit increase in GARD (P = .0007), among those who got radiotherapy. Values of GARD run from 0 to over 100, with higher scores meaning more radiation benefit.
The radiosensitivity index, which was derived from genomic studies of cancer cell lines exposed to radiation, was previously validated by the team and other groups across several tumor types.
Currently, radiation dosing is generally uniform for a given disease site and stage, based on the assumption that a given dose of radiation results in the same clinical effect across patients. In fact, the biological effect of a given dose varies widely between individual patients. “Patients we treat uniformly do not have a uniform response” which is why a more personalized approach would help, said lead investigator and Cleveland Clinic radiation oncologist Jacob Scott, MD, DPhil.
One patient with a given tumor might benefit from 2 extra fractions, while the next might need an extra 15 for the same benefit. “You need to know about [a patient’s] tumor genomics to know how hard you have to work,” he said.
Dr. Scott and colleagues are working with a genomics company to commercialize the approach. The vision for now is that physicians would ship in biopsy samples to be analyzed; RSI and GARD would be calculated, and then a decision support report would be sent back to the treatment team outlining the risks and benefits of various doses for the patient.
Dr. Scott, who holds proprietary rights on the approach, is bullish. When asked if he anticipates GARD dosing to be standard of care in 10 years, he said that “I can’t imagine another world. Everything else in cancer is personalized. Why aren’t we? It just makes sense. I know there’s a better way” to prescribe radiation, “and I’m excited for the future when I can use it.”
When asked for comment, Brian Marples, PhD, a radiation oncology professor at the University of Rochester (N.Y.), said the data so far for GARD “seem very solid. I’m very excited by the concept.”
It’s been “the holy grail” of radiation researchers to find a biologic marker that predicts what dosages patients need and what can be given safely. “This strategy is a good way of doing that. Other groups are proposing similar strategies, but I think this group is ahead. I can see [GARD] being readily applied to the clinic because patients are [already] getting their tumors genomically characterized as part of care,” Dr. Marples said.
But many questions remain. For instance, the editorial writers questioned how GARD is “affected by tumor heterogeneity, response to systemic therapy, and changes in the tumor microenvironment.” Also, the approach is based on conventional 2 Gy fractions, but other fractionation regimens are becoming more common.
For Dr. Marples, the big caveat is that most cancer patients are treated with both radiation and chemotherapy. He said he would like to see GARD validated in patients who receive both.
They seven tumor types in the study included breast cancer, head and neck cancer, non–small cell lung cancer, pancreatic cancer, endometrial cancer, melanoma, and glioma. The majority of the subjects were treated with radiation, and each had the genomic data needed to calculate GARD.
Dr. Scott, senior author and Moffitt Center radiation oncologist Javier Torres-Roca, MD, and a third author hold intellectual property rights on RSI, GARD, and prescription dose base on RSI, plus equity in Cvergenx, a company that seeks to commercialize the approach. Dr. Torres-Roca and another author are cofounders. The editorial writers and Dr. Marples did not have any relevant disclosures.
FROM LANCET ONCOLOGY
Two patients with metastatic lung cancer are disease-free for 1.5 years after TILs
Adoptive cell therapy using tumor-infiltrating lymphocytes (TILs) led to complete and long-lasting responses in 2 of 16 patients with metastatic non-small cell lung cancer (NSCLC) who fully underwent the therapy in a phase 1 study.
The results are “very impressive, with two complete responses that are ongoing 1.5 years later, so it’s durable, and that’s encouraging,” Fred Hirsch, MD, PhD, director of the Center of Excellence for Thoracic Oncology at Mount Sinai’s Tisch Cancer Institute, New York, told this news organization.
Dr. Hirsch, who wasn’t involved in the research, also noted that this study is in immunotherapy-resistant metastatic lung cancer – “a situation where we actually don’t know exactly how best to treat it today.”
The study was published online in Nature Medicine.
A form of immunotherapy, TILs have been studied extensively in melanoma, as reported by this news organization, but this is the first test of the TIL therapy in metastatic NSCLC.
The single-arm, open-label phase 1 trial involved 20 patients who had TILs collected, including 16 who eventually received TILs. Median age was 54 years; all patients had metastatic NSCLC and disease progression after nivolumab monotherapy.
TILs cultured from an individual patient’s tumor were expanded ex vivo from minced tumors cultured with interleukin-2 (IL-2). Via this method, “billions of activated T cells can be produced and infused back into a patient,” explain the authors.
The full treatment regimen comprised cyclophosphamide and fludarabine lymphodepletion, TIL infusion and IL-2, followed by maintenance nivolumab.
“We found that infusion of TILs in combination with lymphodepletion and IL-2 had manageable toxicity and mediated tumor regressions in several patients, including complete responses,” report Benjamin Creelan, MD, of the Moffitt Cancer Center & Research Institute, Tampa, and colleagues.
The endpoint of safety was met according to the prespecified criteria of a rate of severe toxicity of 17% or less.
Among 13 evaluable patients, three had confirmed responses and 11 had reduction in tumor burden. Two patients achieved complete responses that were ongoing 1.5 years following TIL treatment.
One durable complete response occurred in a PD-L1-negative never-smoker, who had a low tumor mutation burden and who was refractory to nivolumab.
“This may be particularly encouraging for the large subset of never-smoker patients, for whom immune-checkpoint inhibitors have historically had limited efficacy,” the investigators say.
This complete responder had “features where you wouldn’t expect to see a response for immunotherapy,” Dr. Hirsch told this news organization.
“Low tumor mutation burden, negative PDL-1, and never-smoker are three factors which indicate some kind of resistance to immunotherapy, and despite that, there was a complete response with this specific therapy. That is fascinating,” he said.
In exploratory analyses, T cells recognizing multiple types of cancer mutations were detected after TIL treatment and were enriched in patients who responded to treatment.
The researchers say these early data indicate that TILs can mediate effective responses in tumor subtypes that are not sensitive to traditional immune-checkpoint-targeted therapy.
“Therefore, therapy with TILs may extend the scope and impact of immunotherapy into wider populations,” they write.
‘Yeoman’s effort’ paving the way forward
Also weighing in on the study, Philip Greenberg, MD, professor and head of immunology, Fred Hutchinson Cancer Center, Seattle, said, “In some respects, it’s quite promising and in other respects, actually more limited than you would hope for.”
“I think it’s a great demonstration that there is activity here, and there’s a world of things that can be done to improve the activity and no doubt that will be done. After this trial, I’m sure we will see next-generation trials,” said Dr. Greenberg.
He said key issues going forward are how cells are selected and manufactured: “That’s going to be a critical piece for making it better.”
“There is now a world of data that says T cells that recognize mutations in cancers can be effective in solid tumors,” Dr. Greenberg said.
“Sustaining that response is still a huge obstacle for achieving the kinds of therapeutic benefits we’d like to be achieved. And having that response be broad enough, particularly in the setting where most of the mutations are just passenger mutations, not driver oncogenes, is going to require a way of generating a large polyspecific population of cells that can persist for a long time,” he further commented.
All in all, this study was a “yeoman’s effort” and the researchers “deserve a lot of credit for pushing it forward,” Dr. Greenberg said.
The study was supported in part by grants from Stand Up to Cancer Foundation, the Barbara Bauer Prelude to a Cure Foundation, Iovance Biotherapeutics, and a Young Investigator award from Adaptive Biotechnologies. Nivolumab was supplied by Bristol-Myers Squibb. Aldesleukin (IL-2) was supplied by Clinigen Group. A complete list of author disclosures is available with the original article. Dr. Hirsch and Dr. Greenberg have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Adoptive cell therapy using tumor-infiltrating lymphocytes (TILs) led to complete and long-lasting responses in 2 of 16 patients with metastatic non-small cell lung cancer (NSCLC) who fully underwent the therapy in a phase 1 study.
The results are “very impressive, with two complete responses that are ongoing 1.5 years later, so it’s durable, and that’s encouraging,” Fred Hirsch, MD, PhD, director of the Center of Excellence for Thoracic Oncology at Mount Sinai’s Tisch Cancer Institute, New York, told this news organization.
Dr. Hirsch, who wasn’t involved in the research, also noted that this study is in immunotherapy-resistant metastatic lung cancer – “a situation where we actually don’t know exactly how best to treat it today.”
The study was published online in Nature Medicine.
A form of immunotherapy, TILs have been studied extensively in melanoma, as reported by this news organization, but this is the first test of the TIL therapy in metastatic NSCLC.
The single-arm, open-label phase 1 trial involved 20 patients who had TILs collected, including 16 who eventually received TILs. Median age was 54 years; all patients had metastatic NSCLC and disease progression after nivolumab monotherapy.
TILs cultured from an individual patient’s tumor were expanded ex vivo from minced tumors cultured with interleukin-2 (IL-2). Via this method, “billions of activated T cells can be produced and infused back into a patient,” explain the authors.
The full treatment regimen comprised cyclophosphamide and fludarabine lymphodepletion, TIL infusion and IL-2, followed by maintenance nivolumab.
“We found that infusion of TILs in combination with lymphodepletion and IL-2 had manageable toxicity and mediated tumor regressions in several patients, including complete responses,” report Benjamin Creelan, MD, of the Moffitt Cancer Center & Research Institute, Tampa, and colleagues.
The endpoint of safety was met according to the prespecified criteria of a rate of severe toxicity of 17% or less.
Among 13 evaluable patients, three had confirmed responses and 11 had reduction in tumor burden. Two patients achieved complete responses that were ongoing 1.5 years following TIL treatment.
One durable complete response occurred in a PD-L1-negative never-smoker, who had a low tumor mutation burden and who was refractory to nivolumab.
“This may be particularly encouraging for the large subset of never-smoker patients, for whom immune-checkpoint inhibitors have historically had limited efficacy,” the investigators say.
This complete responder had “features where you wouldn’t expect to see a response for immunotherapy,” Dr. Hirsch told this news organization.
“Low tumor mutation burden, negative PDL-1, and never-smoker are three factors which indicate some kind of resistance to immunotherapy, and despite that, there was a complete response with this specific therapy. That is fascinating,” he said.
In exploratory analyses, T cells recognizing multiple types of cancer mutations were detected after TIL treatment and were enriched in patients who responded to treatment.
The researchers say these early data indicate that TILs can mediate effective responses in tumor subtypes that are not sensitive to traditional immune-checkpoint-targeted therapy.
“Therefore, therapy with TILs may extend the scope and impact of immunotherapy into wider populations,” they write.
‘Yeoman’s effort’ paving the way forward
Also weighing in on the study, Philip Greenberg, MD, professor and head of immunology, Fred Hutchinson Cancer Center, Seattle, said, “In some respects, it’s quite promising and in other respects, actually more limited than you would hope for.”
“I think it’s a great demonstration that there is activity here, and there’s a world of things that can be done to improve the activity and no doubt that will be done. After this trial, I’m sure we will see next-generation trials,” said Dr. Greenberg.
He said key issues going forward are how cells are selected and manufactured: “That’s going to be a critical piece for making it better.”
“There is now a world of data that says T cells that recognize mutations in cancers can be effective in solid tumors,” Dr. Greenberg said.
“Sustaining that response is still a huge obstacle for achieving the kinds of therapeutic benefits we’d like to be achieved. And having that response be broad enough, particularly in the setting where most of the mutations are just passenger mutations, not driver oncogenes, is going to require a way of generating a large polyspecific population of cells that can persist for a long time,” he further commented.
All in all, this study was a “yeoman’s effort” and the researchers “deserve a lot of credit for pushing it forward,” Dr. Greenberg said.
The study was supported in part by grants from Stand Up to Cancer Foundation, the Barbara Bauer Prelude to a Cure Foundation, Iovance Biotherapeutics, and a Young Investigator award from Adaptive Biotechnologies. Nivolumab was supplied by Bristol-Myers Squibb. Aldesleukin (IL-2) was supplied by Clinigen Group. A complete list of author disclosures is available with the original article. Dr. Hirsch and Dr. Greenberg have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Adoptive cell therapy using tumor-infiltrating lymphocytes (TILs) led to complete and long-lasting responses in 2 of 16 patients with metastatic non-small cell lung cancer (NSCLC) who fully underwent the therapy in a phase 1 study.
The results are “very impressive, with two complete responses that are ongoing 1.5 years later, so it’s durable, and that’s encouraging,” Fred Hirsch, MD, PhD, director of the Center of Excellence for Thoracic Oncology at Mount Sinai’s Tisch Cancer Institute, New York, told this news organization.
Dr. Hirsch, who wasn’t involved in the research, also noted that this study is in immunotherapy-resistant metastatic lung cancer – “a situation where we actually don’t know exactly how best to treat it today.”
The study was published online in Nature Medicine.
A form of immunotherapy, TILs have been studied extensively in melanoma, as reported by this news organization, but this is the first test of the TIL therapy in metastatic NSCLC.
The single-arm, open-label phase 1 trial involved 20 patients who had TILs collected, including 16 who eventually received TILs. Median age was 54 years; all patients had metastatic NSCLC and disease progression after nivolumab monotherapy.
TILs cultured from an individual patient’s tumor were expanded ex vivo from minced tumors cultured with interleukin-2 (IL-2). Via this method, “billions of activated T cells can be produced and infused back into a patient,” explain the authors.
The full treatment regimen comprised cyclophosphamide and fludarabine lymphodepletion, TIL infusion and IL-2, followed by maintenance nivolumab.
“We found that infusion of TILs in combination with lymphodepletion and IL-2 had manageable toxicity and mediated tumor regressions in several patients, including complete responses,” report Benjamin Creelan, MD, of the Moffitt Cancer Center & Research Institute, Tampa, and colleagues.
The endpoint of safety was met according to the prespecified criteria of a rate of severe toxicity of 17% or less.
Among 13 evaluable patients, three had confirmed responses and 11 had reduction in tumor burden. Two patients achieved complete responses that were ongoing 1.5 years following TIL treatment.
One durable complete response occurred in a PD-L1-negative never-smoker, who had a low tumor mutation burden and who was refractory to nivolumab.
“This may be particularly encouraging for the large subset of never-smoker patients, for whom immune-checkpoint inhibitors have historically had limited efficacy,” the investigators say.
This complete responder had “features where you wouldn’t expect to see a response for immunotherapy,” Dr. Hirsch told this news organization.
“Low tumor mutation burden, negative PDL-1, and never-smoker are three factors which indicate some kind of resistance to immunotherapy, and despite that, there was a complete response with this specific therapy. That is fascinating,” he said.
In exploratory analyses, T cells recognizing multiple types of cancer mutations were detected after TIL treatment and were enriched in patients who responded to treatment.
The researchers say these early data indicate that TILs can mediate effective responses in tumor subtypes that are not sensitive to traditional immune-checkpoint-targeted therapy.
“Therefore, therapy with TILs may extend the scope and impact of immunotherapy into wider populations,” they write.
‘Yeoman’s effort’ paving the way forward
Also weighing in on the study, Philip Greenberg, MD, professor and head of immunology, Fred Hutchinson Cancer Center, Seattle, said, “In some respects, it’s quite promising and in other respects, actually more limited than you would hope for.”
“I think it’s a great demonstration that there is activity here, and there’s a world of things that can be done to improve the activity and no doubt that will be done. After this trial, I’m sure we will see next-generation trials,” said Dr. Greenberg.
He said key issues going forward are how cells are selected and manufactured: “That’s going to be a critical piece for making it better.”
“There is now a world of data that says T cells that recognize mutations in cancers can be effective in solid tumors,” Dr. Greenberg said.
“Sustaining that response is still a huge obstacle for achieving the kinds of therapeutic benefits we’d like to be achieved. And having that response be broad enough, particularly in the setting where most of the mutations are just passenger mutations, not driver oncogenes, is going to require a way of generating a large polyspecific population of cells that can persist for a long time,” he further commented.
All in all, this study was a “yeoman’s effort” and the researchers “deserve a lot of credit for pushing it forward,” Dr. Greenberg said.
The study was supported in part by grants from Stand Up to Cancer Foundation, the Barbara Bauer Prelude to a Cure Foundation, Iovance Biotherapeutics, and a Young Investigator award from Adaptive Biotechnologies. Nivolumab was supplied by Bristol-Myers Squibb. Aldesleukin (IL-2) was supplied by Clinigen Group. A complete list of author disclosures is available with the original article. Dr. Hirsch and Dr. Greenberg have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Pfizer recalls four more lots of smoking cessation drug Chantix
Pfizer has recalled four more lots of the smoking cessation drug varenicline (Chantix), according to an Aug. 16 update on the U.S. Food and Drug Administration website.

In a new FDA MedWatch, the agency notes that these 0.5 mg/1 mg tablets are being recalled because of the presence of N-nitroso-varenicline, a nitrosamine impurity, at a level higher than Pfizer’s acceptable intake limit.
On July 2, the FDA reported that Pfizer had voluntarily recalled nine lots of the drug for this reason. As reported by this news organization, the company added three more lots to the recall a few weeks later.
In the update, the FDA noted that, although long-term ingestion of the impurity “may be associated with a theoretical potential increased cancer risk in humans,” there is no immediate risk in taking this medication. The agency added that no related adverse events (AEs) have been reported.
The four additional lots included in the newest recall are as follows:
- 00018522 (expiration date: August 2021).
- 00018523 (expiration date: August 2021).
- 00018739 (expiration date: August 2021).
- 00018740 (expiration date: August 2021).
The recalled lots were distributed in the United States and Puerto Rico from June 2019 to June 2021.
As before, the FDA noted that the benefits of stopping smoking “outweigh the theoretical potential cancer risk” from varenicline’s impurity.
It added that, although the impurities may increase risk for cancer if a high level of exposure continues over a long period, the drug is intended as a short-term treatment to aid in smoking cessation.
For now, clinicians should report any AEs from varenicline to the FDA’s MedWatch program, and patients taking this treatment should consult with their health care practitioner or pharmacy, the update notes.
A version of this article first appeared on Medscape.com.
Pfizer has recalled four more lots of the smoking cessation drug varenicline (Chantix), according to an Aug. 16 update on the U.S. Food and Drug Administration website.
In a new FDA MedWatch, the agency notes that these 0.5 mg/1 mg tablets are being recalled because of the presence of N-nitroso-varenicline, a nitrosamine impurity, at a level higher than Pfizer’s acceptable intake limit.
On July 2, the FDA reported that Pfizer had voluntarily recalled nine lots of the drug for this reason. As reported by this news organization, the company added three more lots to the recall a few weeks later.
In the update, the FDA noted that, although long-term ingestion of the impurity “may be associated with a theoretical potential increased cancer risk in humans,” there is no immediate risk in taking this medication. The agency added that no related adverse events (AEs) have been reported.
The four additional lots included in the newest recall are as follows:
- 00018522 (expiration date: August 2021).
- 00018523 (expiration date: August 2021).
- 00018739 (expiration date: August 2021).
- 00018740 (expiration date: August 2021).
The recalled lots were distributed in the United States and Puerto Rico from June 2019 to June 2021.
As before, the FDA noted that the benefits of stopping smoking “outweigh the theoretical potential cancer risk” from varenicline’s impurity.
It added that, although the impurities may increase risk for cancer if a high level of exposure continues over a long period, the drug is intended as a short-term treatment to aid in smoking cessation.
For now, clinicians should report any AEs from varenicline to the FDA’s MedWatch program, and patients taking this treatment should consult with their health care practitioner or pharmacy, the update notes.
A version of this article first appeared on Medscape.com.
Pfizer has recalled four more lots of the smoking cessation drug varenicline (Chantix), according to an Aug. 16 update on the U.S. Food and Drug Administration website.
In a new FDA MedWatch, the agency notes that these 0.5 mg/1 mg tablets are being recalled because of the presence of N-nitroso-varenicline, a nitrosamine impurity, at a level higher than Pfizer’s acceptable intake limit.
On July 2, the FDA reported that Pfizer had voluntarily recalled nine lots of the drug for this reason. As reported by this news organization, the company added three more lots to the recall a few weeks later.
In the update, the FDA noted that, although long-term ingestion of the impurity “may be associated with a theoretical potential increased cancer risk in humans,” there is no immediate risk in taking this medication. The agency added that no related adverse events (AEs) have been reported.
The four additional lots included in the newest recall are as follows:
- 00018522 (expiration date: August 2021).
- 00018523 (expiration date: August 2021).
- 00018739 (expiration date: August 2021).
- 00018740 (expiration date: August 2021).
The recalled lots were distributed in the United States and Puerto Rico from June 2019 to June 2021.
As before, the FDA noted that the benefits of stopping smoking “outweigh the theoretical potential cancer risk” from varenicline’s impurity.
It added that, although the impurities may increase risk for cancer if a high level of exposure continues over a long period, the drug is intended as a short-term treatment to aid in smoking cessation.
For now, clinicians should report any AEs from varenicline to the FDA’s MedWatch program, and patients taking this treatment should consult with their health care practitioner or pharmacy, the update notes.
A version of this article first appeared on Medscape.com.
One in three cancer articles on social media has wrong info
Of the 200 most popular articles (50 each for prostate, lung, breast, and colorectal cancer), about a third (32.5%, n = 65) contained misinformation.
Among these articles containing misinformation, 76.9% (50/65) contained harmful information.
“The Internet is a leading source of health misinformation,” the study authors wrote. This is “particularly true for social media, where false information spreads faster and more broadly than fact-checked information,” they said, citing other research.
“We need to address these issues head on,” said lead author Skyler Johnson, MD, of the University of Utah’s Huntsman Cancer Institute in Salt Lake City.
“As a medical community, we can’t ignore the problem of cancer misinformation on social media or ask our patients to ignore it. We must empathize with our patients and help them when they encounter this type of information,” he said in a statement. “My goal is to help answer their questions, and provide cancer patients with accurate information that will give them the best chance for the best outcome.”
The study was published online July 22 in the Journal of the National Cancer Institute.
The study period ran from 2018 to 2019, and looked at articles posted on social media platforms Facebook, Reddit, Twitter, or Pinterest. Popularity was measured by engagement with readers, such as upvotes, comments, reactions, and shares.
Some of the articles came from long-established news entities such as CBS News, The New York Times, and medical journals, while others came from fleeting crowdfunding web pages and fledging nontraditional news sites.
One example of popular and harmful misinformation highlighted by Dr. Johnson in an interview was titled, “44-Year-Old Mother Claims CBD Oil Cured Her of Breast Cancer within 5 Months.” Posted on truththeory.com in February 2018, the article is tagged as “opinion” by the publisher and in turn links to another news story about the same woman in the UK’s Daily Mail newspaper.
The ideas and claims in such articles can be very influential, Jennifer L. Lycette, MD, suggested in a recent blog post.
“After 18 years as a cancer doctor, it sadly doesn’t come as a surprise anymore when a patient declines treatment recommendations and instead opts for ‘alternative’ treatment,” she wrote.
Sometimes, misinformation is not sensational but is still effective via clever wording and presentation, observed Brian G. Southwell, PhD, of Duke University, Durham, N.C., who has studied patients and misinformation.
“It isn’t the falsehood that is somehow magically attractive, per se, but the way that misinformation is often framed that can make it attractive,” he said in an interview.
Dr. Southwell recommends that clinicians be proactive about medical misinformation.
“Rather than expect patients to raise concerns without prompting, health care providers should invite conversations about potential misinformation with their patients,” he wrote in a recent essay in the American Journal of Public Health.
In short, ask patients what they know about the treatment of their cancer, he suggests.
“Patients don’t typically know that the misinformation they are encountering is misinformation,” said Dr. Southwell. “Approaching patients with compassion and empathy is a good first step.”
Study details
For the study, reported by Johnson et al., two National Comprehensive Cancer Network panel members were selected as content experts for each of the four cancers and were tasked with reviewing the primary medical claims in each article. The experts then completed a set of ratings to arrive at the proportion of misinformation and potential for harm in each article.
Of the 200 articles, 41.5% were from nontraditional news (digital only), 37.5% were from traditional news sources (online versions of print and/or broadcast media), 17% were from medical journals, 3% were from a crowdfunding site, and 1% were from personal blogs.
This expert review concluded that nearly one-third of the articles contained misinformation, as noted above. The misinformation was described as misleading (title not supported by text or statistics/data do not support conclusion, 28.8%), strength of the evidence mischaracterized (weak evidence portrayed as strong or vice versa, 27.7%) and unproven therapies (not studied or insufficient evidence, 26.7%).
Notably, the median number of engagements, such as likes on Twitter, for articles with misinformation was greater than that of factual articles (median, 2,300 vs. 1,600; P = .05).
In total, 30.5% of all 200 articles contained harmful information. This was described as harmful inaction (could lead to delay or not seeking medical attention for treatable/curable condition, 31.0%), economic harm (out-of-pocket financial costs associated with treatment/travel, 27.7%), harmful action (potentially toxic effects of the suggested test/treatment, 17.0%), and harmful interactions (known/unknown medical interactions with curative therapies, 16.2%).
The median number of engagements for articles with harmful information was statistically significantly greater than that of articles with correct information (median, 2,300 vs. 1,500; P = .007).
A limitation of the study is that it included only the most popular English language cancer articles.
This study was funded in part by the Huntsman Cancer Institute. Dr. Johnson, Dr. Lycette, and Dr. Southwell have disclosed no relevant financial relationships. Some study authors have ties to the pharmaceutical industry.
A version of this article first appeared on Medscape.com.
Of the 200 most popular articles (50 each for prostate, lung, breast, and colorectal cancer), about a third (32.5%, n = 65) contained misinformation.
Among these articles containing misinformation, 76.9% (50/65) contained harmful information.
“The Internet is a leading source of health misinformation,” the study authors wrote. This is “particularly true for social media, where false information spreads faster and more broadly than fact-checked information,” they said, citing other research.
“We need to address these issues head on,” said lead author Skyler Johnson, MD, of the University of Utah’s Huntsman Cancer Institute in Salt Lake City.
“As a medical community, we can’t ignore the problem of cancer misinformation on social media or ask our patients to ignore it. We must empathize with our patients and help them when they encounter this type of information,” he said in a statement. “My goal is to help answer their questions, and provide cancer patients with accurate information that will give them the best chance for the best outcome.”
The study was published online July 22 in the Journal of the National Cancer Institute.
The study period ran from 2018 to 2019, and looked at articles posted on social media platforms Facebook, Reddit, Twitter, or Pinterest. Popularity was measured by engagement with readers, such as upvotes, comments, reactions, and shares.
Some of the articles came from long-established news entities such as CBS News, The New York Times, and medical journals, while others came from fleeting crowdfunding web pages and fledging nontraditional news sites.
One example of popular and harmful misinformation highlighted by Dr. Johnson in an interview was titled, “44-Year-Old Mother Claims CBD Oil Cured Her of Breast Cancer within 5 Months.” Posted on truththeory.com in February 2018, the article is tagged as “opinion” by the publisher and in turn links to another news story about the same woman in the UK’s Daily Mail newspaper.
The ideas and claims in such articles can be very influential, Jennifer L. Lycette, MD, suggested in a recent blog post.
“After 18 years as a cancer doctor, it sadly doesn’t come as a surprise anymore when a patient declines treatment recommendations and instead opts for ‘alternative’ treatment,” she wrote.
Sometimes, misinformation is not sensational but is still effective via clever wording and presentation, observed Brian G. Southwell, PhD, of Duke University, Durham, N.C., who has studied patients and misinformation.
“It isn’t the falsehood that is somehow magically attractive, per se, but the way that misinformation is often framed that can make it attractive,” he said in an interview.
Dr. Southwell recommends that clinicians be proactive about medical misinformation.
“Rather than expect patients to raise concerns without prompting, health care providers should invite conversations about potential misinformation with their patients,” he wrote in a recent essay in the American Journal of Public Health.
In short, ask patients what they know about the treatment of their cancer, he suggests.
“Patients don’t typically know that the misinformation they are encountering is misinformation,” said Dr. Southwell. “Approaching patients with compassion and empathy is a good first step.”
Study details
For the study, reported by Johnson et al., two National Comprehensive Cancer Network panel members were selected as content experts for each of the four cancers and were tasked with reviewing the primary medical claims in each article. The experts then completed a set of ratings to arrive at the proportion of misinformation and potential for harm in each article.
Of the 200 articles, 41.5% were from nontraditional news (digital only), 37.5% were from traditional news sources (online versions of print and/or broadcast media), 17% were from medical journals, 3% were from a crowdfunding site, and 1% were from personal blogs.
This expert review concluded that nearly one-third of the articles contained misinformation, as noted above. The misinformation was described as misleading (title not supported by text or statistics/data do not support conclusion, 28.8%), strength of the evidence mischaracterized (weak evidence portrayed as strong or vice versa, 27.7%) and unproven therapies (not studied or insufficient evidence, 26.7%).
Notably, the median number of engagements, such as likes on Twitter, for articles with misinformation was greater than that of factual articles (median, 2,300 vs. 1,600; P = .05).
In total, 30.5% of all 200 articles contained harmful information. This was described as harmful inaction (could lead to delay or not seeking medical attention for treatable/curable condition, 31.0%), economic harm (out-of-pocket financial costs associated with treatment/travel, 27.7%), harmful action (potentially toxic effects of the suggested test/treatment, 17.0%), and harmful interactions (known/unknown medical interactions with curative therapies, 16.2%).
The median number of engagements for articles with harmful information was statistically significantly greater than that of articles with correct information (median, 2,300 vs. 1,500; P = .007).
A limitation of the study is that it included only the most popular English language cancer articles.
This study was funded in part by the Huntsman Cancer Institute. Dr. Johnson, Dr. Lycette, and Dr. Southwell have disclosed no relevant financial relationships. Some study authors have ties to the pharmaceutical industry.
A version of this article first appeared on Medscape.com.
Of the 200 most popular articles (50 each for prostate, lung, breast, and colorectal cancer), about a third (32.5%, n = 65) contained misinformation.
Among these articles containing misinformation, 76.9% (50/65) contained harmful information.
“The Internet is a leading source of health misinformation,” the study authors wrote. This is “particularly true for social media, where false information spreads faster and more broadly than fact-checked information,” they said, citing other research.
“We need to address these issues head on,” said lead author Skyler Johnson, MD, of the University of Utah’s Huntsman Cancer Institute in Salt Lake City.
“As a medical community, we can’t ignore the problem of cancer misinformation on social media or ask our patients to ignore it. We must empathize with our patients and help them when they encounter this type of information,” he said in a statement. “My goal is to help answer their questions, and provide cancer patients with accurate information that will give them the best chance for the best outcome.”
The study was published online July 22 in the Journal of the National Cancer Institute.
The study period ran from 2018 to 2019, and looked at articles posted on social media platforms Facebook, Reddit, Twitter, or Pinterest. Popularity was measured by engagement with readers, such as upvotes, comments, reactions, and shares.
Some of the articles came from long-established news entities such as CBS News, The New York Times, and medical journals, while others came from fleeting crowdfunding web pages and fledging nontraditional news sites.
One example of popular and harmful misinformation highlighted by Dr. Johnson in an interview was titled, “44-Year-Old Mother Claims CBD Oil Cured Her of Breast Cancer within 5 Months.” Posted on truththeory.com in February 2018, the article is tagged as “opinion” by the publisher and in turn links to another news story about the same woman in the UK’s Daily Mail newspaper.
The ideas and claims in such articles can be very influential, Jennifer L. Lycette, MD, suggested in a recent blog post.
“After 18 years as a cancer doctor, it sadly doesn’t come as a surprise anymore when a patient declines treatment recommendations and instead opts for ‘alternative’ treatment,” she wrote.
Sometimes, misinformation is not sensational but is still effective via clever wording and presentation, observed Brian G. Southwell, PhD, of Duke University, Durham, N.C., who has studied patients and misinformation.
“It isn’t the falsehood that is somehow magically attractive, per se, but the way that misinformation is often framed that can make it attractive,” he said in an interview.
Dr. Southwell recommends that clinicians be proactive about medical misinformation.
“Rather than expect patients to raise concerns without prompting, health care providers should invite conversations about potential misinformation with their patients,” he wrote in a recent essay in the American Journal of Public Health.
In short, ask patients what they know about the treatment of their cancer, he suggests.
“Patients don’t typically know that the misinformation they are encountering is misinformation,” said Dr. Southwell. “Approaching patients with compassion and empathy is a good first step.”
Study details
For the study, reported by Johnson et al., two National Comprehensive Cancer Network panel members were selected as content experts for each of the four cancers and were tasked with reviewing the primary medical claims in each article. The experts then completed a set of ratings to arrive at the proportion of misinformation and potential for harm in each article.
Of the 200 articles, 41.5% were from nontraditional news (digital only), 37.5% were from traditional news sources (online versions of print and/or broadcast media), 17% were from medical journals, 3% were from a crowdfunding site, and 1% were from personal blogs.
This expert review concluded that nearly one-third of the articles contained misinformation, as noted above. The misinformation was described as misleading (title not supported by text or statistics/data do not support conclusion, 28.8%), strength of the evidence mischaracterized (weak evidence portrayed as strong or vice versa, 27.7%) and unproven therapies (not studied or insufficient evidence, 26.7%).
Notably, the median number of engagements, such as likes on Twitter, for articles with misinformation was greater than that of factual articles (median, 2,300 vs. 1,600; P = .05).
In total, 30.5% of all 200 articles contained harmful information. This was described as harmful inaction (could lead to delay or not seeking medical attention for treatable/curable condition, 31.0%), economic harm (out-of-pocket financial costs associated with treatment/travel, 27.7%), harmful action (potentially toxic effects of the suggested test/treatment, 17.0%), and harmful interactions (known/unknown medical interactions with curative therapies, 16.2%).
The median number of engagements for articles with harmful information was statistically significantly greater than that of articles with correct information (median, 2,300 vs. 1,500; P = .007).
A limitation of the study is that it included only the most popular English language cancer articles.
This study was funded in part by the Huntsman Cancer Institute. Dr. Johnson, Dr. Lycette, and Dr. Southwell have disclosed no relevant financial relationships. Some study authors have ties to the pharmaceutical industry.
A version of this article first appeared on Medscape.com.
Cancer mortality continues to drop in females as breast cancer reversal looms
Overall cancer mortality in females continues to decrease in the United States, but “previous declining trends in death rates slowed” for breast cancer in recent years, according to an annual report by several national organizations.
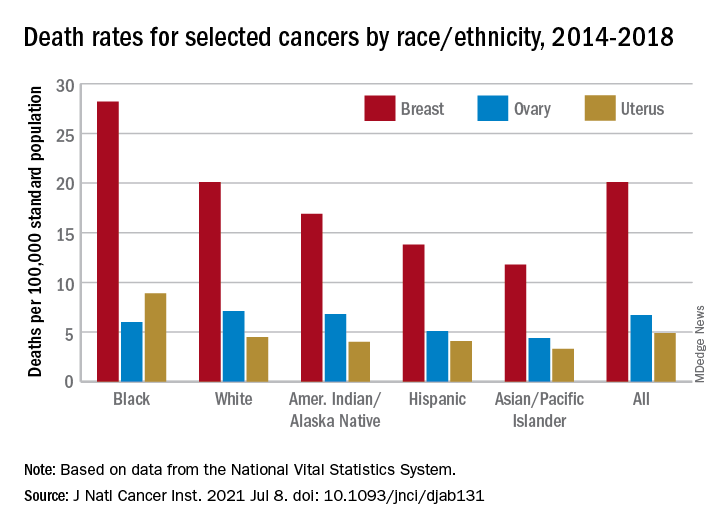
The analysis of long-term trends in cancer death rates shows that a decline of 1.4% per year from 2001 to 2016 accelerated to 2.1% per year in 2016-2018, the American Cancer Society, Centers for Disease Control and Prevention, National Cancer Institute, and the North American Association of Central Cancer Registries said.
Decreases in overall cancer mortality were seen in females of all races and ethnic groups over the most recent 5-year period included in the report, 2014-2018, varying from –1.6% per year in both non-Hispanic Blacks and Whites to –0.9% for non-Hispanic American Indians/Alaska Natives (AI/ANs), Farhad Islami, MD, PhD, of the American Cancer Society, Atlanta, and associates said in the Journal of the National Cancer Institute.
Over those 5 years, death rates fell for 14 of the 20 most common cancers in females; increased for liver, uterus, brain, pancreas, and soft tissue including heart; and remained stable for cancers of the oral cavity/pharynx, they reported.
Breast cancer was among those that declined, but the rate of that decline has been slowing. Mortality declined by an average of 2.3% per year in 2003-2007, by 1.6% a year in 2007-2014, and by just 1.0% annually during 2014-2018, based on data from the National Center for Health Statistics’ National Vital Statistics System.
Mortality from all cancers in 2014-2018 was 133.5 deaths per 100,000 standard population, with the racial/ethnic gap ranging from 85.4 per 100,000 (non-Hispanic Asian/Pacific Islander) to 154.9 (non-Hispanic Black), Dr. Islami and associates said.
Melanoma had the largest decline in mortality over that period among the 20 most common cancers in females, falling by an average of 4.4% per year, with lung cancer next at 4.3%. Among those with increased death rates, uterine cancer saw the largest rise at 2.0% a year, the research team said.
The deaths caused by cancer of the uterus were most common in non-Hispanic Black females, 8.9 per 100,000 population, followed by non-Hispanic White (4.5), Hispanic (4.1), non-Hispanic AI/AN (4.0), and non-Hispanic Asian/Pacific Islander (3.3), they reported.
“Long-term increasing trends in uterine cancer death rates parallel trends in incidence, although death rates are increasing at a somewhat faster rate. Increasing uterine cancer incidence has been attributed to increasing obesity prevalence and decreased use of combined hormone replacement therapy,” Dr. Islami and associates pointed out.
Breast cancer deaths also were most common among Blacks in 2014-2018, occurring at a rate of 28.2 per 100,000, as were deaths from cancer of the cervix (3.4 per 100,000), while ovarian cancers deaths were highest in White females (7.1 per 100,000), the researchers noted.
The continuing racial and ethnic disparity “largely reflects a combination of multiple intertwined factors” of tumor biology, diagnosis, treatment, and systemic discrimination, they wrote, adding that Black persons “are more likely to have a higher exposure to some cancer risk factors and limited access to healthy food, safe places for physical activity, and evidence-based cancer preventive services.”
The report was funded by the four participating groups. Six of the 12 investigators are employees of the American Cancer Society whose salaries are solely paid by the society; the other authors had no conflicts of interest to disclose.
Overall cancer mortality in females continues to decrease in the United States, but “previous declining trends in death rates slowed” for breast cancer in recent years, according to an annual report by several national organizations.
The analysis of long-term trends in cancer death rates shows that a decline of 1.4% per year from 2001 to 2016 accelerated to 2.1% per year in 2016-2018, the American Cancer Society, Centers for Disease Control and Prevention, National Cancer Institute, and the North American Association of Central Cancer Registries said.
Decreases in overall cancer mortality were seen in females of all races and ethnic groups over the most recent 5-year period included in the report, 2014-2018, varying from –1.6% per year in both non-Hispanic Blacks and Whites to –0.9% for non-Hispanic American Indians/Alaska Natives (AI/ANs), Farhad Islami, MD, PhD, of the American Cancer Society, Atlanta, and associates said in the Journal of the National Cancer Institute.
Over those 5 years, death rates fell for 14 of the 20 most common cancers in females; increased for liver, uterus, brain, pancreas, and soft tissue including heart; and remained stable for cancers of the oral cavity/pharynx, they reported.
Breast cancer was among those that declined, but the rate of that decline has been slowing. Mortality declined by an average of 2.3% per year in 2003-2007, by 1.6% a year in 2007-2014, and by just 1.0% annually during 2014-2018, based on data from the National Center for Health Statistics’ National Vital Statistics System.
Mortality from all cancers in 2014-2018 was 133.5 deaths per 100,000 standard population, with the racial/ethnic gap ranging from 85.4 per 100,000 (non-Hispanic Asian/Pacific Islander) to 154.9 (non-Hispanic Black), Dr. Islami and associates said.
Melanoma had the largest decline in mortality over that period among the 20 most common cancers in females, falling by an average of 4.4% per year, with lung cancer next at 4.3%. Among those with increased death rates, uterine cancer saw the largest rise at 2.0% a year, the research team said.
The deaths caused by cancer of the uterus were most common in non-Hispanic Black females, 8.9 per 100,000 population, followed by non-Hispanic White (4.5), Hispanic (4.1), non-Hispanic AI/AN (4.0), and non-Hispanic Asian/Pacific Islander (3.3), they reported.
“Long-term increasing trends in uterine cancer death rates parallel trends in incidence, although death rates are increasing at a somewhat faster rate. Increasing uterine cancer incidence has been attributed to increasing obesity prevalence and decreased use of combined hormone replacement therapy,” Dr. Islami and associates pointed out.
Breast cancer deaths also were most common among Blacks in 2014-2018, occurring at a rate of 28.2 per 100,000, as were deaths from cancer of the cervix (3.4 per 100,000), while ovarian cancers deaths were highest in White females (7.1 per 100,000), the researchers noted.
The continuing racial and ethnic disparity “largely reflects a combination of multiple intertwined factors” of tumor biology, diagnosis, treatment, and systemic discrimination, they wrote, adding that Black persons “are more likely to have a higher exposure to some cancer risk factors and limited access to healthy food, safe places for physical activity, and evidence-based cancer preventive services.”
The report was funded by the four participating groups. Six of the 12 investigators are employees of the American Cancer Society whose salaries are solely paid by the society; the other authors had no conflicts of interest to disclose.
Overall cancer mortality in females continues to decrease in the United States, but “previous declining trends in death rates slowed” for breast cancer in recent years, according to an annual report by several national organizations.
The analysis of long-term trends in cancer death rates shows that a decline of 1.4% per year from 2001 to 2016 accelerated to 2.1% per year in 2016-2018, the American Cancer Society, Centers for Disease Control and Prevention, National Cancer Institute, and the North American Association of Central Cancer Registries said.
Decreases in overall cancer mortality were seen in females of all races and ethnic groups over the most recent 5-year period included in the report, 2014-2018, varying from –1.6% per year in both non-Hispanic Blacks and Whites to –0.9% for non-Hispanic American Indians/Alaska Natives (AI/ANs), Farhad Islami, MD, PhD, of the American Cancer Society, Atlanta, and associates said in the Journal of the National Cancer Institute.
Over those 5 years, death rates fell for 14 of the 20 most common cancers in females; increased for liver, uterus, brain, pancreas, and soft tissue including heart; and remained stable for cancers of the oral cavity/pharynx, they reported.
Breast cancer was among those that declined, but the rate of that decline has been slowing. Mortality declined by an average of 2.3% per year in 2003-2007, by 1.6% a year in 2007-2014, and by just 1.0% annually during 2014-2018, based on data from the National Center for Health Statistics’ National Vital Statistics System.
Mortality from all cancers in 2014-2018 was 133.5 deaths per 100,000 standard population, with the racial/ethnic gap ranging from 85.4 per 100,000 (non-Hispanic Asian/Pacific Islander) to 154.9 (non-Hispanic Black), Dr. Islami and associates said.
Melanoma had the largest decline in mortality over that period among the 20 most common cancers in females, falling by an average of 4.4% per year, with lung cancer next at 4.3%. Among those with increased death rates, uterine cancer saw the largest rise at 2.0% a year, the research team said.
The deaths caused by cancer of the uterus were most common in non-Hispanic Black females, 8.9 per 100,000 population, followed by non-Hispanic White (4.5), Hispanic (4.1), non-Hispanic AI/AN (4.0), and non-Hispanic Asian/Pacific Islander (3.3), they reported.
“Long-term increasing trends in uterine cancer death rates parallel trends in incidence, although death rates are increasing at a somewhat faster rate. Increasing uterine cancer incidence has been attributed to increasing obesity prevalence and decreased use of combined hormone replacement therapy,” Dr. Islami and associates pointed out.
Breast cancer deaths also were most common among Blacks in 2014-2018, occurring at a rate of 28.2 per 100,000, as were deaths from cancer of the cervix (3.4 per 100,000), while ovarian cancers deaths were highest in White females (7.1 per 100,000), the researchers noted.
The continuing racial and ethnic disparity “largely reflects a combination of multiple intertwined factors” of tumor biology, diagnosis, treatment, and systemic discrimination, they wrote, adding that Black persons “are more likely to have a higher exposure to some cancer risk factors and limited access to healthy food, safe places for physical activity, and evidence-based cancer preventive services.”
The report was funded by the four participating groups. Six of the 12 investigators are employees of the American Cancer Society whose salaries are solely paid by the society; the other authors had no conflicts of interest to disclose.
FROM THE JOURNAL OF THE NATIONAL CANCER INSTITUTE
Key Presentations on Advanced Non–Small Cell Lung Cancer From ASCO 2021
Dr Mark A. Socinski, executive medical director of AdventHealth Cancer Institute in Orlando, Florida, highlights studies in advanced non–small cell lung cancer (NSCLC) presented at the 2021 annual meeting of the American Society of Clinical Oncology.
First, Dr Socinski reports on the updated results of the CheckMate 9LA study showing continued benefit of nivolumab and ipilimumab plus chemotherapy vs chemotherapy alone.
He also outlines an FDA pooled analysis of randomized controlled trials showing that patients with PD-L1 scores between 1% and 49% benefit most from immunotherapy plus chemotherapy compared with immunotherapy alone.
Dr Socinski then takes us through one of his own studies showing that immune-related adverse events are actually associated with better outcomes, and reports some sobering data from two studies suggesting that biomarker testing is lagging behind in NSCLC patients, especially among African Americans. He closes by reviewing updated results of the CodeBreak 100 trial which showed encouraging response to sotorasib among patients with G12C KRAS mutations.
--
Mark A. Socinski, MD, Executive Medical Director, AdventHealth Cancer Institute, Orlando, Florida.
Mark A. Socinski, MD, has disclosed the following relevant financial relationships:
Serve(d) as a speaker or a member of a speakers bureau for: Genentech; Novartis; Guardant; AstraZeneca; Eli Lilly and Company; Blueprint
Received research grant from: Genentech; AstraZeneca; Novartis; Spectrum; Cullinan.
Dr Mark A. Socinski, executive medical director of AdventHealth Cancer Institute in Orlando, Florida, highlights studies in advanced non–small cell lung cancer (NSCLC) presented at the 2021 annual meeting of the American Society of Clinical Oncology.
First, Dr Socinski reports on the updated results of the CheckMate 9LA study showing continued benefit of nivolumab and ipilimumab plus chemotherapy vs chemotherapy alone.
He also outlines an FDA pooled analysis of randomized controlled trials showing that patients with PD-L1 scores between 1% and 49% benefit most from immunotherapy plus chemotherapy compared with immunotherapy alone.
Dr Socinski then takes us through one of his own studies showing that immune-related adverse events are actually associated with better outcomes, and reports some sobering data from two studies suggesting that biomarker testing is lagging behind in NSCLC patients, especially among African Americans. He closes by reviewing updated results of the CodeBreak 100 trial which showed encouraging response to sotorasib among patients with G12C KRAS mutations.
--
Mark A. Socinski, MD, Executive Medical Director, AdventHealth Cancer Institute, Orlando, Florida.
Mark A. Socinski, MD, has disclosed the following relevant financial relationships:
Serve(d) as a speaker or a member of a speakers bureau for: Genentech; Novartis; Guardant; AstraZeneca; Eli Lilly and Company; Blueprint
Received research grant from: Genentech; AstraZeneca; Novartis; Spectrum; Cullinan.
Dr Mark A. Socinski, executive medical director of AdventHealth Cancer Institute in Orlando, Florida, highlights studies in advanced non–small cell lung cancer (NSCLC) presented at the 2021 annual meeting of the American Society of Clinical Oncology.
First, Dr Socinski reports on the updated results of the CheckMate 9LA study showing continued benefit of nivolumab and ipilimumab plus chemotherapy vs chemotherapy alone.
He also outlines an FDA pooled analysis of randomized controlled trials showing that patients with PD-L1 scores between 1% and 49% benefit most from immunotherapy plus chemotherapy compared with immunotherapy alone.
Dr Socinski then takes us through one of his own studies showing that immune-related adverse events are actually associated with better outcomes, and reports some sobering data from two studies suggesting that biomarker testing is lagging behind in NSCLC patients, especially among African Americans. He closes by reviewing updated results of the CodeBreak 100 trial which showed encouraging response to sotorasib among patients with G12C KRAS mutations.
--
Mark A. Socinski, MD, Executive Medical Director, AdventHealth Cancer Institute, Orlando, Florida.
Mark A. Socinski, MD, has disclosed the following relevant financial relationships:
Serve(d) as a speaker or a member of a speakers bureau for: Genentech; Novartis; Guardant; AstraZeneca; Eli Lilly and Company; Blueprint
Received research grant from: Genentech; AstraZeneca; Novartis; Spectrum; Cullinan.

HER3-targeted treatment demonstrates efficacy and safety in phase 1 lung cancer study
A HER3-targeted therapy has demonstrated clinically meaningful and durable efficacy in heavily pretreated patients with EGFR-mutant non–small cell lung cancer, according to results of a phase 1 study.
Patritumab deruxtecan, an antibody-drug conjugate targeting HER3, had an overall response rate (ORR) of 39% and median progression-free survival (PFS) of 8.2 months in a phase 1 study that included patients previously treated with tyrosine kinase inhibitors (TKIs) and chemotherapy, the results show.
The efficacy was seen across EGFR TKI resistance mechanisms in this very difficult-to-treat patient population, according to investigator Pasi A. Jänne, MD, PhD, of the Dana-Farber Cancer Institute, Boston.
“There is not one category of individuals that are having a response, or not having a response,” Dr. Jänne said in a presentation at the annual meeting of the American Society of Clinical Oncology (Abstract 9007).
“Responses are observed in patients with identifiable resistance mechanisms, and in patients that do not have an identifiable resistance mechanism, but have progressed on prior EGFR TKI therapy,” he added.
More than 80% of non–small cell lung cancer (NSCLC) tumors express HER3, and of note, HER3 alterations do not appear to confer resistance to EGFR TKIs in patients with EGFR-mutant NSCLC, according to Dr. Jänne.
Study details
Also known as HER3-DXd, patritumab deruxtecan consists of a fully human anti-HER3 monoclonal antibody linked to a topoisomerase inhibitor payload by a tetrapeptide-based cleavable linker.
The antibody-drug conjugate is also being evaluated in metastatic breast cancer and colorectal cancer, Dr. Jänne said.
In the present phase 1 dose escalation and dose expansion study, a total of 57 patients were treated with patritumab deruxtecan at 5.6 mg/kg, the recommended dose for the expansion phase.
The median age of these patients was 65 years, and the majority (63%) were women, Dr. Jänne reported. About half had a history of central nervous system metastases.
The median number of prior lines of systemic therapy was four, making this a heavily pretreated patient population, Dr. Jänne said. All patients had received prior EGFR TKI therapy, and 86% specifically had prior osimertinib. Ninety-one percent had prior platinum-based chemotherapy, and 40% had received immunotherapy.
Spectrum of responses
The confirmed ORR of 39% included 1 complete response (2%) and 21 partial responses (37%), Dr. Jänne reported. The disease control rate was 72%, and median duration of response was 6.9 months at a median follow-up of 10.2 months.
The median PFS was 8.2 months in 57 patients overall and in a subset of 44 patients who had received prior osimertinib and platinum-based chemotherapy, according to the report.
Activity of patritumab deruxtecan was seen not only across patients with diverse mechanisms of EGFR TKI resistance, but also regardless of prior number of treatments, and regardless of history of brain metastases, the investigator said.
In addition, clinical responses were seen across a spectrum of baseline HER3 expression by immunohistochemistry, the investigator added.
Safety was assessed in 81 patients treated at a range of doses in the phase 1 trial. The most common grade 3 or greater treatment-emergent adverse events, observed in 5% or more of patients, included thrombocytopenia, neutropenia, and anemia, while other side effects such as fatigue and dyspnea were observed, Dr. Jänne said. About 9% of the adverse events led to treatment discontinuation in the safety cohort.
Interstitial lung disease was observed in four patients, or 5% of the safety cohort. Three of these were grade 1-2 and one was grade 3, according to the report.
Questions to explore
The efficacy of patritumab deruxtecan was “high” in this phase 1 study, based on the reported response rate and median PFS, said discussant Nicolas Girard, MD, PhD, of Institut Curie in Paris.
However, the most striking finding of the study was the efficacy of the antibody-drug conjugate across all reported resistance mechanisms, Dr. Girard said in his remarks.
Questions that remains to be explored, according to Dr. Girard, include the impact of previous treatment sequencing with TKIs and chemotherapy on patient outcomes with patritumab deruxtecan, as well as the assessment of intracranial response and PFS for patients treated with the agent.
In addition, antitumor activity was seen across a wide range of baseline HER3 expression levels in this study, suggesting that a predictive biomarker remains to be identified, according to Dr. Girard.
“HER3 immunohistochemistry does not seem to be the candidate in this setting,” he said.
The study was sponsored by Daiichi Sankyo. Dr. Jänne reported disclosures related to Daiichi Sankyo, as well as Araxes Pharma, Astellas Pharma, AstraZeneca, and multiple other pharmaceutical companies. Dr. Jänne is also coinventor on a Dana Farber Cancer Institute–owned patent on EGFR mutations licensed to Labcorp and receives postmarketing royalties from this invention.
Dr. Girard reported disclosures related to AbbVie, AstraZeneca, Boehringer Ingelheim, and multiple other pharmaceutical companies.
A HER3-targeted therapy has demonstrated clinically meaningful and durable efficacy in heavily pretreated patients with EGFR-mutant non–small cell lung cancer, according to results of a phase 1 study.
Patritumab deruxtecan, an antibody-drug conjugate targeting HER3, had an overall response rate (ORR) of 39% and median progression-free survival (PFS) of 8.2 months in a phase 1 study that included patients previously treated with tyrosine kinase inhibitors (TKIs) and chemotherapy, the results show.
The efficacy was seen across EGFR TKI resistance mechanisms in this very difficult-to-treat patient population, according to investigator Pasi A. Jänne, MD, PhD, of the Dana-Farber Cancer Institute, Boston.
“There is not one category of individuals that are having a response, or not having a response,” Dr. Jänne said in a presentation at the annual meeting of the American Society of Clinical Oncology (Abstract 9007).
“Responses are observed in patients with identifiable resistance mechanisms, and in patients that do not have an identifiable resistance mechanism, but have progressed on prior EGFR TKI therapy,” he added.
More than 80% of non–small cell lung cancer (NSCLC) tumors express HER3, and of note, HER3 alterations do not appear to confer resistance to EGFR TKIs in patients with EGFR-mutant NSCLC, according to Dr. Jänne.
Study details
Also known as HER3-DXd, patritumab deruxtecan consists of a fully human anti-HER3 monoclonal antibody linked to a topoisomerase inhibitor payload by a tetrapeptide-based cleavable linker.
The antibody-drug conjugate is also being evaluated in metastatic breast cancer and colorectal cancer, Dr. Jänne said.
In the present phase 1 dose escalation and dose expansion study, a total of 57 patients were treated with patritumab deruxtecan at 5.6 mg/kg, the recommended dose for the expansion phase.
The median age of these patients was 65 years, and the majority (63%) were women, Dr. Jänne reported. About half had a history of central nervous system metastases.
The median number of prior lines of systemic therapy was four, making this a heavily pretreated patient population, Dr. Jänne said. All patients had received prior EGFR TKI therapy, and 86% specifically had prior osimertinib. Ninety-one percent had prior platinum-based chemotherapy, and 40% had received immunotherapy.
Spectrum of responses
The confirmed ORR of 39% included 1 complete response (2%) and 21 partial responses (37%), Dr. Jänne reported. The disease control rate was 72%, and median duration of response was 6.9 months at a median follow-up of 10.2 months.
The median PFS was 8.2 months in 57 patients overall and in a subset of 44 patients who had received prior osimertinib and platinum-based chemotherapy, according to the report.
Activity of patritumab deruxtecan was seen not only across patients with diverse mechanisms of EGFR TKI resistance, but also regardless of prior number of treatments, and regardless of history of brain metastases, the investigator said.
In addition, clinical responses were seen across a spectrum of baseline HER3 expression by immunohistochemistry, the investigator added.
Safety was assessed in 81 patients treated at a range of doses in the phase 1 trial. The most common grade 3 or greater treatment-emergent adverse events, observed in 5% or more of patients, included thrombocytopenia, neutropenia, and anemia, while other side effects such as fatigue and dyspnea were observed, Dr. Jänne said. About 9% of the adverse events led to treatment discontinuation in the safety cohort.
Interstitial lung disease was observed in four patients, or 5% of the safety cohort. Three of these were grade 1-2 and one was grade 3, according to the report.
Questions to explore
The efficacy of patritumab deruxtecan was “high” in this phase 1 study, based on the reported response rate and median PFS, said discussant Nicolas Girard, MD, PhD, of Institut Curie in Paris.
However, the most striking finding of the study was the efficacy of the antibody-drug conjugate across all reported resistance mechanisms, Dr. Girard said in his remarks.
Questions that remains to be explored, according to Dr. Girard, include the impact of previous treatment sequencing with TKIs and chemotherapy on patient outcomes with patritumab deruxtecan, as well as the assessment of intracranial response and PFS for patients treated with the agent.
In addition, antitumor activity was seen across a wide range of baseline HER3 expression levels in this study, suggesting that a predictive biomarker remains to be identified, according to Dr. Girard.
“HER3 immunohistochemistry does not seem to be the candidate in this setting,” he said.
The study was sponsored by Daiichi Sankyo. Dr. Jänne reported disclosures related to Daiichi Sankyo, as well as Araxes Pharma, Astellas Pharma, AstraZeneca, and multiple other pharmaceutical companies. Dr. Jänne is also coinventor on a Dana Farber Cancer Institute–owned patent on EGFR mutations licensed to Labcorp and receives postmarketing royalties from this invention.
Dr. Girard reported disclosures related to AbbVie, AstraZeneca, Boehringer Ingelheim, and multiple other pharmaceutical companies.
A HER3-targeted therapy has demonstrated clinically meaningful and durable efficacy in heavily pretreated patients with EGFR-mutant non–small cell lung cancer, according to results of a phase 1 study.
Patritumab deruxtecan, an antibody-drug conjugate targeting HER3, had an overall response rate (ORR) of 39% and median progression-free survival (PFS) of 8.2 months in a phase 1 study that included patients previously treated with tyrosine kinase inhibitors (TKIs) and chemotherapy, the results show.
The efficacy was seen across EGFR TKI resistance mechanisms in this very difficult-to-treat patient population, according to investigator Pasi A. Jänne, MD, PhD, of the Dana-Farber Cancer Institute, Boston.
“There is not one category of individuals that are having a response, or not having a response,” Dr. Jänne said in a presentation at the annual meeting of the American Society of Clinical Oncology (Abstract 9007).
“Responses are observed in patients with identifiable resistance mechanisms, and in patients that do not have an identifiable resistance mechanism, but have progressed on prior EGFR TKI therapy,” he added.
More than 80% of non–small cell lung cancer (NSCLC) tumors express HER3, and of note, HER3 alterations do not appear to confer resistance to EGFR TKIs in patients with EGFR-mutant NSCLC, according to Dr. Jänne.
Study details
Also known as HER3-DXd, patritumab deruxtecan consists of a fully human anti-HER3 monoclonal antibody linked to a topoisomerase inhibitor payload by a tetrapeptide-based cleavable linker.
The antibody-drug conjugate is also being evaluated in metastatic breast cancer and colorectal cancer, Dr. Jänne said.
In the present phase 1 dose escalation and dose expansion study, a total of 57 patients were treated with patritumab deruxtecan at 5.6 mg/kg, the recommended dose for the expansion phase.
The median age of these patients was 65 years, and the majority (63%) were women, Dr. Jänne reported. About half had a history of central nervous system metastases.
The median number of prior lines of systemic therapy was four, making this a heavily pretreated patient population, Dr. Jänne said. All patients had received prior EGFR TKI therapy, and 86% specifically had prior osimertinib. Ninety-one percent had prior platinum-based chemotherapy, and 40% had received immunotherapy.
Spectrum of responses
The confirmed ORR of 39% included 1 complete response (2%) and 21 partial responses (37%), Dr. Jänne reported. The disease control rate was 72%, and median duration of response was 6.9 months at a median follow-up of 10.2 months.
The median PFS was 8.2 months in 57 patients overall and in a subset of 44 patients who had received prior osimertinib and platinum-based chemotherapy, according to the report.
Activity of patritumab deruxtecan was seen not only across patients with diverse mechanisms of EGFR TKI resistance, but also regardless of prior number of treatments, and regardless of history of brain metastases, the investigator said.
In addition, clinical responses were seen across a spectrum of baseline HER3 expression by immunohistochemistry, the investigator added.
Safety was assessed in 81 patients treated at a range of doses in the phase 1 trial. The most common grade 3 or greater treatment-emergent adverse events, observed in 5% or more of patients, included thrombocytopenia, neutropenia, and anemia, while other side effects such as fatigue and dyspnea were observed, Dr. Jänne said. About 9% of the adverse events led to treatment discontinuation in the safety cohort.
Interstitial lung disease was observed in four patients, or 5% of the safety cohort. Three of these were grade 1-2 and one was grade 3, according to the report.
Questions to explore
The efficacy of patritumab deruxtecan was “high” in this phase 1 study, based on the reported response rate and median PFS, said discussant Nicolas Girard, MD, PhD, of Institut Curie in Paris.
However, the most striking finding of the study was the efficacy of the antibody-drug conjugate across all reported resistance mechanisms, Dr. Girard said in his remarks.
Questions that remains to be explored, according to Dr. Girard, include the impact of previous treatment sequencing with TKIs and chemotherapy on patient outcomes with patritumab deruxtecan, as well as the assessment of intracranial response and PFS for patients treated with the agent.
In addition, antitumor activity was seen across a wide range of baseline HER3 expression levels in this study, suggesting that a predictive biomarker remains to be identified, according to Dr. Girard.
“HER3 immunohistochemistry does not seem to be the candidate in this setting,” he said.
The study was sponsored by Daiichi Sankyo. Dr. Jänne reported disclosures related to Daiichi Sankyo, as well as Araxes Pharma, Astellas Pharma, AstraZeneca, and multiple other pharmaceutical companies. Dr. Jänne is also coinventor on a Dana Farber Cancer Institute–owned patent on EGFR mutations licensed to Labcorp and receives postmarketing royalties from this invention.
Dr. Girard reported disclosures related to AbbVie, AstraZeneca, Boehringer Ingelheim, and multiple other pharmaceutical companies.
REPORTING FROM ASCO 2021