User login
More tools for the COVID toolbox
I was recently asked to see a 16-year-old, unvaccinated (against COVID-19) adolescent with hypothyroidism and obesity (body mass index 37 kg/m2) seen in the pediatric emergency department with tachycardia, O2 saturation 96%, urinary tract infection, poor appetite, and nausea. Her chest x-ray had low lung volumes but no infiltrates. She was noted to be dehydrated. Testing for COVID-19 was PCR positive.1

She was observed overnight, tolerated oral rehydration, and was being readied for discharge. Pediatric Infectious Diseases was called about prescribing remdesivir.
Remdesivir was not indicated as its current use is limited to inpatients with oxygen desaturations less than 94%. Infectious Diseases Society of America guidelines do recommend the use of monoclonal antibodies against the SARS-CoV-2 spike protein for prevention of COVID disease progression in high-risk individuals. Specifically, the IDSA guidelines say, “Among ambulatory patients with mild to moderate COVID-19 at high risk for progression to severe disease, bamlanivimab/etesevimab, casirivimab/imdevimab, or sotrovimab rather than no neutralizing antibody treatment.”
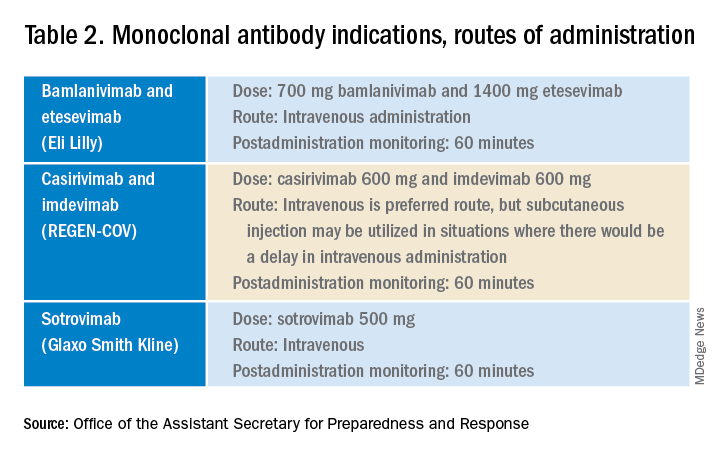
The Food and Drug Administration’s Emergency Use Authorization (EUA) allowed use of specific monoclonal antibodies (casirivimab/imdevimab in combination, bamlanivimab/etesevimab in combination, and sotrovimab alone) for individuals 12 years and above with a minimum weight of 40 kg with high-risk conditions, describing the evidence as moderate certainty.2
Several questions have arisen regarding their use. Which children qualify under the EUA? Are the available monoclonal antibodies effective for SARS-CoV-2 variants? What adverse events were observed? Are there implementation hurdles?
Unlike the EUA for prophylactic use, which targeted unvaccinated individuals and those unlikely to have a good antibody response to vaccine, use of monoclonal antibody for prevention of progression does not have such restrictions. Effectiveness may vary by local variant susceptibility and should be considered in the choice of the most appropriate monoclonal antibody therapy. Reductions in hospitalization and progression to critical disease status were reported from phase 3 studies; reductions were also observed in mortality in some, but not all, studies. Enhanced viral clearance on day 7 was observed with few subjects having persistent high viral load.
Which children qualify under the EUA? Adolescents 12 years and older and over 40 kg are eligible if a high risk condition is present. High-risk conditions include body mass index at the 85th percentile or higher, immunosuppressive disease, or receipt of immunosuppressive therapies, or baseline (pre-COVID infection) medical-related technological dependence such as tracheostomy or positive pressure ventilation. Additional high-risk conditions are neurodevelopmental disorders, sickle cell disease, congenital or acquired heart disease, asthma, or reactive airway or other chronic respiratory disease that requires daily medication for control, diabetes, chronic kidney disease, or pregnancy.3
Are the available monoclonal antibodies effective for SARS-CoV-2 variants? Of course, this is a critical question and relies on knowledge of the dominant variant in a specific geographic location. The CDC data on which variants are susceptible to which monoclonal therapies were updated as of Oct. 21 online (see Table 1). Local departments of public health often will have current data on the dominant variant in the community. Currently, the dominant variant in the United States is Delta and it is anticipated to be susceptible to the three monoclonal treatments authorized under the EUA based on in vitro neutralizing assays.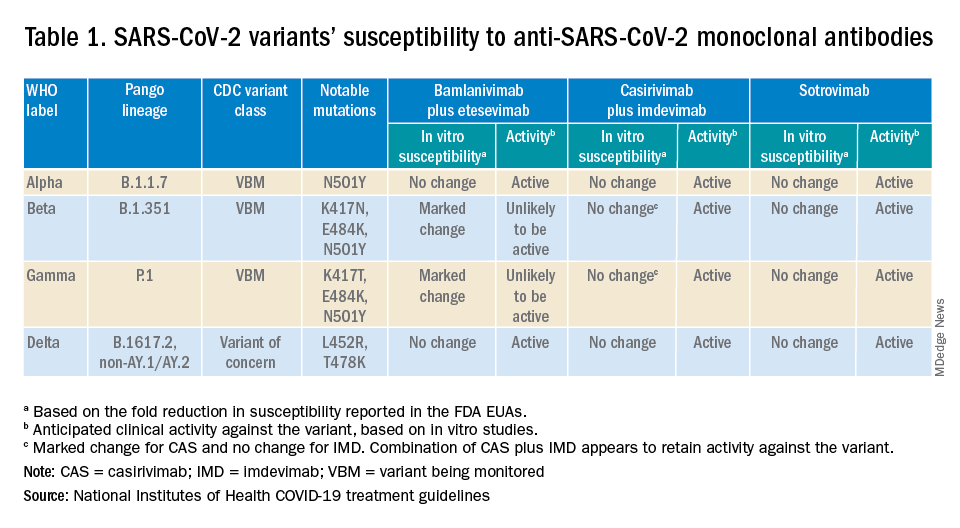
What adverse events were observed? Monoclonal antibody infusions are in general safe but anaphylaxis has been reported. Other infusion-related adverse events include urticaria, pruritis, flushing, pyrexia, shortness of breath, chest tightness, nausea, vomiting, and rash. Nearly all events were grade 1, mild, or grade 2, moderate. For nonsevere infusion-related reactions, consider slowing the infusion; if necessary, the infusion should be stopped.
Implementation challenges
The first challenge is finding a location to infuse the monoclonal antibodies. Although they can be given subcutaneously, the dose is large and little, if any, time is saved as the recommendation is for observation post administration for 1 hour. The challenge we and other centers may face is that the patients are COVID PCR+ and therefore our usual infusion program, which often is occupied by individuals already compromised and at high risk for severe COVID, is an undesirable location. We are planning to use the emergency department to accommodate such patients currently, but even that solution creates challenges for a busy, urban medical center.
Summary
Anti–SARS-CoV-2 monoclonal antibodies are an important part of the therapeutic approach to minimizing disease severity. Clinicians should review high-risk conditions in adolescents who are PCR+ for SARS-CoV-2 and have mild to moderate symptoms. Medical care systems should implement programs to make monoclonal infusions available for such high-risk adolescents.4 Obesity and asthma reactive airways or requiring daily medication for control are the two most common conditions that place adolescents with COVID-19 at risk for progression to hospitalization and severe disease in addition to the more traditional immune-compromising conditions and medical fragility.
Dr. Pelton is professor of pediatrics and epidemiology at Boston University schools of medicine and public health and senior attending physician in pediatric infectious diseases, Boston Medical Center. Email him at pdnews@mdedge.com.
References
1. Federal Response to COVID-19: Monoclonal Antibody Clinical Implementation Guide. U.S. Department of Health and Human Services. 2021 Sep 2.
2. Bhimraj A et al. IDSA Guidelines on the Treatment and Management of Patients with COVID-19. Last updated 2021 Nov 9.
3. Anti-SARS-CoV-2 Monoclonal Antibodies. National Institutes of Health’s COVID 19 Treatment Guidelines. Last updated 2021 Oct 19.
4. Spreading the Word on the Benefits of Monoclonal Antibodies for COVID-19, by Hannah R. Buchdahl. CDC Foundation, 2021 Jul 2.
I was recently asked to see a 16-year-old, unvaccinated (against COVID-19) adolescent with hypothyroidism and obesity (body mass index 37 kg/m2) seen in the pediatric emergency department with tachycardia, O2 saturation 96%, urinary tract infection, poor appetite, and nausea. Her chest x-ray had low lung volumes but no infiltrates. She was noted to be dehydrated. Testing for COVID-19 was PCR positive.1
She was observed overnight, tolerated oral rehydration, and was being readied for discharge. Pediatric Infectious Diseases was called about prescribing remdesivir.
Remdesivir was not indicated as its current use is limited to inpatients with oxygen desaturations less than 94%. Infectious Diseases Society of America guidelines do recommend the use of monoclonal antibodies against the SARS-CoV-2 spike protein for prevention of COVID disease progression in high-risk individuals. Specifically, the IDSA guidelines say, “Among ambulatory patients with mild to moderate COVID-19 at high risk for progression to severe disease, bamlanivimab/etesevimab, casirivimab/imdevimab, or sotrovimab rather than no neutralizing antibody treatment.”
The Food and Drug Administration’s Emergency Use Authorization (EUA) allowed use of specific monoclonal antibodies (casirivimab/imdevimab in combination, bamlanivimab/etesevimab in combination, and sotrovimab alone) for individuals 12 years and above with a minimum weight of 40 kg with high-risk conditions, describing the evidence as moderate certainty.2
Several questions have arisen regarding their use. Which children qualify under the EUA? Are the available monoclonal antibodies effective for SARS-CoV-2 variants? What adverse events were observed? Are there implementation hurdles?
Unlike the EUA for prophylactic use, which targeted unvaccinated individuals and those unlikely to have a good antibody response to vaccine, use of monoclonal antibody for prevention of progression does not have such restrictions. Effectiveness may vary by local variant susceptibility and should be considered in the choice of the most appropriate monoclonal antibody therapy. Reductions in hospitalization and progression to critical disease status were reported from phase 3 studies; reductions were also observed in mortality in some, but not all, studies. Enhanced viral clearance on day 7 was observed with few subjects having persistent high viral load.
Which children qualify under the EUA? Adolescents 12 years and older and over 40 kg are eligible if a high risk condition is present. High-risk conditions include body mass index at the 85th percentile or higher, immunosuppressive disease, or receipt of immunosuppressive therapies, or baseline (pre-COVID infection) medical-related technological dependence such as tracheostomy or positive pressure ventilation. Additional high-risk conditions are neurodevelopmental disorders, sickle cell disease, congenital or acquired heart disease, asthma, or reactive airway or other chronic respiratory disease that requires daily medication for control, diabetes, chronic kidney disease, or pregnancy.3
Are the available monoclonal antibodies effective for SARS-CoV-2 variants? Of course, this is a critical question and relies on knowledge of the dominant variant in a specific geographic location. The CDC data on which variants are susceptible to which monoclonal therapies were updated as of Oct. 21 online (see Table 1). Local departments of public health often will have current data on the dominant variant in the community. Currently, the dominant variant in the United States is Delta and it is anticipated to be susceptible to the three monoclonal treatments authorized under the EUA based on in vitro neutralizing assays.
What adverse events were observed? Monoclonal antibody infusions are in general safe but anaphylaxis has been reported. Other infusion-related adverse events include urticaria, pruritis, flushing, pyrexia, shortness of breath, chest tightness, nausea, vomiting, and rash. Nearly all events were grade 1, mild, or grade 2, moderate. For nonsevere infusion-related reactions, consider slowing the infusion; if necessary, the infusion should be stopped.
Implementation challenges
The first challenge is finding a location to infuse the monoclonal antibodies. Although they can be given subcutaneously, the dose is large and little, if any, time is saved as the recommendation is for observation post administration for 1 hour. The challenge we and other centers may face is that the patients are COVID PCR+ and therefore our usual infusion program, which often is occupied by individuals already compromised and at high risk for severe COVID, is an undesirable location. We are planning to use the emergency department to accommodate such patients currently, but even that solution creates challenges for a busy, urban medical center.
Summary
Anti–SARS-CoV-2 monoclonal antibodies are an important part of the therapeutic approach to minimizing disease severity. Clinicians should review high-risk conditions in adolescents who are PCR+ for SARS-CoV-2 and have mild to moderate symptoms. Medical care systems should implement programs to make monoclonal infusions available for such high-risk adolescents.4 Obesity and asthma reactive airways or requiring daily medication for control are the two most common conditions that place adolescents with COVID-19 at risk for progression to hospitalization and severe disease in addition to the more traditional immune-compromising conditions and medical fragility.
Dr. Pelton is professor of pediatrics and epidemiology at Boston University schools of medicine and public health and senior attending physician in pediatric infectious diseases, Boston Medical Center. Email him at pdnews@mdedge.com.
References
1. Federal Response to COVID-19: Monoclonal Antibody Clinical Implementation Guide. U.S. Department of Health and Human Services. 2021 Sep 2.
2. Bhimraj A et al. IDSA Guidelines on the Treatment and Management of Patients with COVID-19. Last updated 2021 Nov 9.
3. Anti-SARS-CoV-2 Monoclonal Antibodies. National Institutes of Health’s COVID 19 Treatment Guidelines. Last updated 2021 Oct 19.
4. Spreading the Word on the Benefits of Monoclonal Antibodies for COVID-19, by Hannah R. Buchdahl. CDC Foundation, 2021 Jul 2.
I was recently asked to see a 16-year-old, unvaccinated (against COVID-19) adolescent with hypothyroidism and obesity (body mass index 37 kg/m2) seen in the pediatric emergency department with tachycardia, O2 saturation 96%, urinary tract infection, poor appetite, and nausea. Her chest x-ray had low lung volumes but no infiltrates. She was noted to be dehydrated. Testing for COVID-19 was PCR positive.1
She was observed overnight, tolerated oral rehydration, and was being readied for discharge. Pediatric Infectious Diseases was called about prescribing remdesivir.
Remdesivir was not indicated as its current use is limited to inpatients with oxygen desaturations less than 94%. Infectious Diseases Society of America guidelines do recommend the use of monoclonal antibodies against the SARS-CoV-2 spike protein for prevention of COVID disease progression in high-risk individuals. Specifically, the IDSA guidelines say, “Among ambulatory patients with mild to moderate COVID-19 at high risk for progression to severe disease, bamlanivimab/etesevimab, casirivimab/imdevimab, or sotrovimab rather than no neutralizing antibody treatment.”
The Food and Drug Administration’s Emergency Use Authorization (EUA) allowed use of specific monoclonal antibodies (casirivimab/imdevimab in combination, bamlanivimab/etesevimab in combination, and sotrovimab alone) for individuals 12 years and above with a minimum weight of 40 kg with high-risk conditions, describing the evidence as moderate certainty.2
Several questions have arisen regarding their use. Which children qualify under the EUA? Are the available monoclonal antibodies effective for SARS-CoV-2 variants? What adverse events were observed? Are there implementation hurdles?
Unlike the EUA for prophylactic use, which targeted unvaccinated individuals and those unlikely to have a good antibody response to vaccine, use of monoclonal antibody for prevention of progression does not have such restrictions. Effectiveness may vary by local variant susceptibility and should be considered in the choice of the most appropriate monoclonal antibody therapy. Reductions in hospitalization and progression to critical disease status were reported from phase 3 studies; reductions were also observed in mortality in some, but not all, studies. Enhanced viral clearance on day 7 was observed with few subjects having persistent high viral load.
Which children qualify under the EUA? Adolescents 12 years and older and over 40 kg are eligible if a high risk condition is present. High-risk conditions include body mass index at the 85th percentile or higher, immunosuppressive disease, or receipt of immunosuppressive therapies, or baseline (pre-COVID infection) medical-related technological dependence such as tracheostomy or positive pressure ventilation. Additional high-risk conditions are neurodevelopmental disorders, sickle cell disease, congenital or acquired heart disease, asthma, or reactive airway or other chronic respiratory disease that requires daily medication for control, diabetes, chronic kidney disease, or pregnancy.3
Are the available monoclonal antibodies effective for SARS-CoV-2 variants? Of course, this is a critical question and relies on knowledge of the dominant variant in a specific geographic location. The CDC data on which variants are susceptible to which monoclonal therapies were updated as of Oct. 21 online (see Table 1). Local departments of public health often will have current data on the dominant variant in the community. Currently, the dominant variant in the United States is Delta and it is anticipated to be susceptible to the three monoclonal treatments authorized under the EUA based on in vitro neutralizing assays.
What adverse events were observed? Monoclonal antibody infusions are in general safe but anaphylaxis has been reported. Other infusion-related adverse events include urticaria, pruritis, flushing, pyrexia, shortness of breath, chest tightness, nausea, vomiting, and rash. Nearly all events were grade 1, mild, or grade 2, moderate. For nonsevere infusion-related reactions, consider slowing the infusion; if necessary, the infusion should be stopped.
Implementation challenges
The first challenge is finding a location to infuse the monoclonal antibodies. Although they can be given subcutaneously, the dose is large and little, if any, time is saved as the recommendation is for observation post administration for 1 hour. The challenge we and other centers may face is that the patients are COVID PCR+ and therefore our usual infusion program, which often is occupied by individuals already compromised and at high risk for severe COVID, is an undesirable location. We are planning to use the emergency department to accommodate such patients currently, but even that solution creates challenges for a busy, urban medical center.
Summary
Anti–SARS-CoV-2 monoclonal antibodies are an important part of the therapeutic approach to minimizing disease severity. Clinicians should review high-risk conditions in adolescents who are PCR+ for SARS-CoV-2 and have mild to moderate symptoms. Medical care systems should implement programs to make monoclonal infusions available for such high-risk adolescents.4 Obesity and asthma reactive airways or requiring daily medication for control are the two most common conditions that place adolescents with COVID-19 at risk for progression to hospitalization and severe disease in addition to the more traditional immune-compromising conditions and medical fragility.
Dr. Pelton is professor of pediatrics and epidemiology at Boston University schools of medicine and public health and senior attending physician in pediatric infectious diseases, Boston Medical Center. Email him at pdnews@mdedge.com.
References
1. Federal Response to COVID-19: Monoclonal Antibody Clinical Implementation Guide. U.S. Department of Health and Human Services. 2021 Sep 2.
2. Bhimraj A et al. IDSA Guidelines on the Treatment and Management of Patients with COVID-19. Last updated 2021 Nov 9.
3. Anti-SARS-CoV-2 Monoclonal Antibodies. National Institutes of Health’s COVID 19 Treatment Guidelines. Last updated 2021 Oct 19.
4. Spreading the Word on the Benefits of Monoclonal Antibodies for COVID-19, by Hannah R. Buchdahl. CDC Foundation, 2021 Jul 2.
High-dose fish oil: ‘Intriguing’ results in COVID-19
A high dose of the purified form of eicosapentaenoic acid, icosapent ethyl (Vascepa, Amarin), failed to significantly reduce hospitalizations or death in patients infected with COVID-19 in the PREPARE-IT 2 study.
The study did, however, show a favorable trend, with a 16% reduction in the primary endpoint of death or an indication for hospitalization. All secondary endpoints were also numerically reduced, but none reached statistical significance.
The product was also well tolerated over the 28 days of the study period, even though a new high-loading dose was used, with no increase in atrial fibrillation or bleeding or other adverse events versus placebo, although there was a slightly higher rate of discontinuation.
The trial was presented at the American Heart Association scientific sessions on Nov. 15 by Rafael Díaz, MD, director of Estudios Clínicos Latinoamérica in Rosario, Argentina.
“Larger, randomized trials powered for a relative risk reduction of around 15% with icosapent ethyl are needed to establish whether or not this product may have a role in the management of COVID-positive outpatients,” Dr. Diaz concluded.
‘Intriguing signals’
Commenting on the study, Manesh Patel, MD, chief of the division of cardiology and codirector of the Heart Center at Duke University, Durham, N.C., and chair of the Scientific Sessions scientific program, said that: “Certainly there are some intriguing signals.”
“I think the trend is valuable, but do we need a larger trial to confirm a benefit? I will leave that to the clinical community to decide,” Dr. Patel added. “But it is hard to power a trial to get that answer, and the world of COVID has changed since this trial started with vaccines now available and new therapeutics coming. So, there’s going to be a competing landscape.”
Discussing the trial at an AHA news briefing, Erin Michos, MD, associate professor of medicine within the division of cardiology at Johns Hopkins University, Baltimore, said: “Results showed that everything trended in the right direction, but did not reach statistical significance largely because there were fewer events than anticipated. COVID hospitalizations are going down because of the broad adoption of vaccines, which meant that this study didn’t quite meet its endpoint.”
But, she added: “Reassuringly, even with the higher loading dose, there was no increased risk of [atrial fibrillation] when used for just 28 days, and no increased risk in bleeding, so there was very good safety.”
“We need a larger trial to really definitely show whether icosapent ethyl can or cannot help COVID-positive outpatients, but I think a better prevention strategy would be the broad adoption of vaccinations globally,” Dr. Michos concluded.
‘A pretty big ask’
Donald Lloyd-Jones, MD, AHA president and designated discussant at the late-breaking science session, congratulated the investigators on conducting “a very nice pragmatic trial in the midst of the COVID pandemic.”
Dr. Lloyd-Jones concluded that the broad range of potentially beneficial actions of icosapent ethyl – including antitriglyceride, anti-inflammatory, antioxidant, and antithrombotic effects – leads to the possibility of it helping in COVID, but he added that “this is a pretty big ask for a fish oil supplement given short term.”
Presenting the study, Dr. Diaz noted that there are limited options for the outpatient treatment of patients with COVID-19 infection, and it is believed that inflammation plays a major role in worsening the severity of the infection.
He pointed out that previous data support a potential role of omega-3 fatty acids in reducing inflammation and infection, and that icosapent ethyl has shown a reduction in major cardiovascular events in the REDUCE-IT trial, with the mechanism thought to involve anti-inflammatory effects.
In the first trial to investigate the role of icosapent ethyl in COVID-19, PREPARE-IT, the product did not prevent uninfected individuals at risk from COVID from becoming infected with the virus, but there was no increase in side effects versus placebo with use over a 60-day period.
A small study last year in 100 COVID-positive patients showed icosapent ethyl reduced C-reactive protein, an inflammatory marker, and also improved symptoms.
PREPARE-IT 2, a pragmatic web-based trial, was conducted to investigate whether icosapent ethyl in nonhospitalized patients with a positive diagnosis of COVID-19 could reduce hospitalization rates and complications.
The trial enrolled 2,052 patients (mean age, 50 years), of whom 1,010 were allocated to the active group and 1,042 to the placebo group. Inclusion criteria included individuals aged 40 years or older with a confirmed COVID-19 diagnosis and no more than 7 days from the onset of symptoms and without a clear indication for hospitalization.
Patients who were allocated to the active arm received icosapent ethyl at a dose of 8 g (four capsules every 12 hours, morning and evening) for the first 3 days, followed by 4 g (two capsules every 12 hours) thereafter (days 4-28).
The primary outcome, COVID-19–related hospitalization (indication for hospitalization or hospitalization) or death at 28 days, occurred in 11.16% of the active group and 13.69% of the placebo group, giving a hazard ratio of 0.84 (95% confidence interval, 0.65-1.08; P = .166)
Secondary outcomes showed similar positive trends, but none were significant. These included: death or still hospitalized at 28 days (HR, 0.74), major events (MI, stroke, death; HR, 0.38), and total mortality (HR, 0.52).
In terms of safety, there was no significant difference in total adverse events between the two groups (16.5% in the active group vs. 14.8% in the placebo group). The most common adverse effects were constipation (2.7%), diarrhea (7.2%), and nausea (4%), but these were not significantly different from placebo. There were, however, more discontinuations in the active group (7% vs. 4%).
Dr. Diaz pointed out that the PREPARE-IT 2 trial was started in May 2020, when there wasn’t much known about the COVID-19 condition, and there were no vaccines or treatments, so hospitalization rates were high.
“We were hoping to see a 25%-30% reduction in hospitalizations with icosapent ethyl, and the trial was powered for that sort of reduction, but today we know we can expect a more modest reduction of about 15%,” Dr. Diaz concluded. “But to show that, we need a much larger trial with 8,000 or 9,000 patients, and that will be much more difficult to conduct.”
The PREPARE-IT 2 study was funded by Amarin. Dr. Diaz has received grants from Dalcor, Amarin, PHRI, and Lepetit.
A version of this article first appeared on Medscape.com.
A high dose of the purified form of eicosapentaenoic acid, icosapent ethyl (Vascepa, Amarin), failed to significantly reduce hospitalizations or death in patients infected with COVID-19 in the PREPARE-IT 2 study.
The study did, however, show a favorable trend, with a 16% reduction in the primary endpoint of death or an indication for hospitalization. All secondary endpoints were also numerically reduced, but none reached statistical significance.
The product was also well tolerated over the 28 days of the study period, even though a new high-loading dose was used, with no increase in atrial fibrillation or bleeding or other adverse events versus placebo, although there was a slightly higher rate of discontinuation.
The trial was presented at the American Heart Association scientific sessions on Nov. 15 by Rafael Díaz, MD, director of Estudios Clínicos Latinoamérica in Rosario, Argentina.
“Larger, randomized trials powered for a relative risk reduction of around 15% with icosapent ethyl are needed to establish whether or not this product may have a role in the management of COVID-positive outpatients,” Dr. Diaz concluded.
‘Intriguing signals’
Commenting on the study, Manesh Patel, MD, chief of the division of cardiology and codirector of the Heart Center at Duke University, Durham, N.C., and chair of the Scientific Sessions scientific program, said that: “Certainly there are some intriguing signals.”
“I think the trend is valuable, but do we need a larger trial to confirm a benefit? I will leave that to the clinical community to decide,” Dr. Patel added. “But it is hard to power a trial to get that answer, and the world of COVID has changed since this trial started with vaccines now available and new therapeutics coming. So, there’s going to be a competing landscape.”
Discussing the trial at an AHA news briefing, Erin Michos, MD, associate professor of medicine within the division of cardiology at Johns Hopkins University, Baltimore, said: “Results showed that everything trended in the right direction, but did not reach statistical significance largely because there were fewer events than anticipated. COVID hospitalizations are going down because of the broad adoption of vaccines, which meant that this study didn’t quite meet its endpoint.”
But, she added: “Reassuringly, even with the higher loading dose, there was no increased risk of [atrial fibrillation] when used for just 28 days, and no increased risk in bleeding, so there was very good safety.”
“We need a larger trial to really definitely show whether icosapent ethyl can or cannot help COVID-positive outpatients, but I think a better prevention strategy would be the broad adoption of vaccinations globally,” Dr. Michos concluded.
‘A pretty big ask’
Donald Lloyd-Jones, MD, AHA president and designated discussant at the late-breaking science session, congratulated the investigators on conducting “a very nice pragmatic trial in the midst of the COVID pandemic.”
Dr. Lloyd-Jones concluded that the broad range of potentially beneficial actions of icosapent ethyl – including antitriglyceride, anti-inflammatory, antioxidant, and antithrombotic effects – leads to the possibility of it helping in COVID, but he added that “this is a pretty big ask for a fish oil supplement given short term.”
Presenting the study, Dr. Diaz noted that there are limited options for the outpatient treatment of patients with COVID-19 infection, and it is believed that inflammation plays a major role in worsening the severity of the infection.
He pointed out that previous data support a potential role of omega-3 fatty acids in reducing inflammation and infection, and that icosapent ethyl has shown a reduction in major cardiovascular events in the REDUCE-IT trial, with the mechanism thought to involve anti-inflammatory effects.
In the first trial to investigate the role of icosapent ethyl in COVID-19, PREPARE-IT, the product did not prevent uninfected individuals at risk from COVID from becoming infected with the virus, but there was no increase in side effects versus placebo with use over a 60-day period.
A small study last year in 100 COVID-positive patients showed icosapent ethyl reduced C-reactive protein, an inflammatory marker, and also improved symptoms.
PREPARE-IT 2, a pragmatic web-based trial, was conducted to investigate whether icosapent ethyl in nonhospitalized patients with a positive diagnosis of COVID-19 could reduce hospitalization rates and complications.
The trial enrolled 2,052 patients (mean age, 50 years), of whom 1,010 were allocated to the active group and 1,042 to the placebo group. Inclusion criteria included individuals aged 40 years or older with a confirmed COVID-19 diagnosis and no more than 7 days from the onset of symptoms and without a clear indication for hospitalization.
Patients who were allocated to the active arm received icosapent ethyl at a dose of 8 g (four capsules every 12 hours, morning and evening) for the first 3 days, followed by 4 g (two capsules every 12 hours) thereafter (days 4-28).
The primary outcome, COVID-19–related hospitalization (indication for hospitalization or hospitalization) or death at 28 days, occurred in 11.16% of the active group and 13.69% of the placebo group, giving a hazard ratio of 0.84 (95% confidence interval, 0.65-1.08; P = .166)
Secondary outcomes showed similar positive trends, but none were significant. These included: death or still hospitalized at 28 days (HR, 0.74), major events (MI, stroke, death; HR, 0.38), and total mortality (HR, 0.52).
In terms of safety, there was no significant difference in total adverse events between the two groups (16.5% in the active group vs. 14.8% in the placebo group). The most common adverse effects were constipation (2.7%), diarrhea (7.2%), and nausea (4%), but these were not significantly different from placebo. There were, however, more discontinuations in the active group (7% vs. 4%).
Dr. Diaz pointed out that the PREPARE-IT 2 trial was started in May 2020, when there wasn’t much known about the COVID-19 condition, and there were no vaccines or treatments, so hospitalization rates were high.
“We were hoping to see a 25%-30% reduction in hospitalizations with icosapent ethyl, and the trial was powered for that sort of reduction, but today we know we can expect a more modest reduction of about 15%,” Dr. Diaz concluded. “But to show that, we need a much larger trial with 8,000 or 9,000 patients, and that will be much more difficult to conduct.”
The PREPARE-IT 2 study was funded by Amarin. Dr. Diaz has received grants from Dalcor, Amarin, PHRI, and Lepetit.
A version of this article first appeared on Medscape.com.
A high dose of the purified form of eicosapentaenoic acid, icosapent ethyl (Vascepa, Amarin), failed to significantly reduce hospitalizations or death in patients infected with COVID-19 in the PREPARE-IT 2 study.
The study did, however, show a favorable trend, with a 16% reduction in the primary endpoint of death or an indication for hospitalization. All secondary endpoints were also numerically reduced, but none reached statistical significance.
The product was also well tolerated over the 28 days of the study period, even though a new high-loading dose was used, with no increase in atrial fibrillation or bleeding or other adverse events versus placebo, although there was a slightly higher rate of discontinuation.
The trial was presented at the American Heart Association scientific sessions on Nov. 15 by Rafael Díaz, MD, director of Estudios Clínicos Latinoamérica in Rosario, Argentina.
“Larger, randomized trials powered for a relative risk reduction of around 15% with icosapent ethyl are needed to establish whether or not this product may have a role in the management of COVID-positive outpatients,” Dr. Diaz concluded.
‘Intriguing signals’
Commenting on the study, Manesh Patel, MD, chief of the division of cardiology and codirector of the Heart Center at Duke University, Durham, N.C., and chair of the Scientific Sessions scientific program, said that: “Certainly there are some intriguing signals.”
“I think the trend is valuable, but do we need a larger trial to confirm a benefit? I will leave that to the clinical community to decide,” Dr. Patel added. “But it is hard to power a trial to get that answer, and the world of COVID has changed since this trial started with vaccines now available and new therapeutics coming. So, there’s going to be a competing landscape.”
Discussing the trial at an AHA news briefing, Erin Michos, MD, associate professor of medicine within the division of cardiology at Johns Hopkins University, Baltimore, said: “Results showed that everything trended in the right direction, but did not reach statistical significance largely because there were fewer events than anticipated. COVID hospitalizations are going down because of the broad adoption of vaccines, which meant that this study didn’t quite meet its endpoint.”
But, she added: “Reassuringly, even with the higher loading dose, there was no increased risk of [atrial fibrillation] when used for just 28 days, and no increased risk in bleeding, so there was very good safety.”
“We need a larger trial to really definitely show whether icosapent ethyl can or cannot help COVID-positive outpatients, but I think a better prevention strategy would be the broad adoption of vaccinations globally,” Dr. Michos concluded.
‘A pretty big ask’
Donald Lloyd-Jones, MD, AHA president and designated discussant at the late-breaking science session, congratulated the investigators on conducting “a very nice pragmatic trial in the midst of the COVID pandemic.”
Dr. Lloyd-Jones concluded that the broad range of potentially beneficial actions of icosapent ethyl – including antitriglyceride, anti-inflammatory, antioxidant, and antithrombotic effects – leads to the possibility of it helping in COVID, but he added that “this is a pretty big ask for a fish oil supplement given short term.”
Presenting the study, Dr. Diaz noted that there are limited options for the outpatient treatment of patients with COVID-19 infection, and it is believed that inflammation plays a major role in worsening the severity of the infection.
He pointed out that previous data support a potential role of omega-3 fatty acids in reducing inflammation and infection, and that icosapent ethyl has shown a reduction in major cardiovascular events in the REDUCE-IT trial, with the mechanism thought to involve anti-inflammatory effects.
In the first trial to investigate the role of icosapent ethyl in COVID-19, PREPARE-IT, the product did not prevent uninfected individuals at risk from COVID from becoming infected with the virus, but there was no increase in side effects versus placebo with use over a 60-day period.
A small study last year in 100 COVID-positive patients showed icosapent ethyl reduced C-reactive protein, an inflammatory marker, and also improved symptoms.
PREPARE-IT 2, a pragmatic web-based trial, was conducted to investigate whether icosapent ethyl in nonhospitalized patients with a positive diagnosis of COVID-19 could reduce hospitalization rates and complications.
The trial enrolled 2,052 patients (mean age, 50 years), of whom 1,010 were allocated to the active group and 1,042 to the placebo group. Inclusion criteria included individuals aged 40 years or older with a confirmed COVID-19 diagnosis and no more than 7 days from the onset of symptoms and without a clear indication for hospitalization.
Patients who were allocated to the active arm received icosapent ethyl at a dose of 8 g (four capsules every 12 hours, morning and evening) for the first 3 days, followed by 4 g (two capsules every 12 hours) thereafter (days 4-28).
The primary outcome, COVID-19–related hospitalization (indication for hospitalization or hospitalization) or death at 28 days, occurred in 11.16% of the active group and 13.69% of the placebo group, giving a hazard ratio of 0.84 (95% confidence interval, 0.65-1.08; P = .166)
Secondary outcomes showed similar positive trends, but none were significant. These included: death or still hospitalized at 28 days (HR, 0.74), major events (MI, stroke, death; HR, 0.38), and total mortality (HR, 0.52).
In terms of safety, there was no significant difference in total adverse events between the two groups (16.5% in the active group vs. 14.8% in the placebo group). The most common adverse effects were constipation (2.7%), diarrhea (7.2%), and nausea (4%), but these were not significantly different from placebo. There were, however, more discontinuations in the active group (7% vs. 4%).
Dr. Diaz pointed out that the PREPARE-IT 2 trial was started in May 2020, when there wasn’t much known about the COVID-19 condition, and there were no vaccines or treatments, so hospitalization rates were high.
“We were hoping to see a 25%-30% reduction in hospitalizations with icosapent ethyl, and the trial was powered for that sort of reduction, but today we know we can expect a more modest reduction of about 15%,” Dr. Diaz concluded. “But to show that, we need a much larger trial with 8,000 or 9,000 patients, and that will be much more difficult to conduct.”
The PREPARE-IT 2 study was funded by Amarin. Dr. Diaz has received grants from Dalcor, Amarin, PHRI, and Lepetit.
A version of this article first appeared on Medscape.com.
FROM AHA 2021
The Sobering Medical, Emotional, Psychological Challenge of Covid-19

Cheryl K. Lee, MD, an Assistant Professor of Medicine at Northwestern Feinberg School of Medicine, practices internal medicine and pediatrics at Northwestern Memorial and the Ann & Robert H. Lurie Children's Hospital, both in Chicago, IL. She also serves on the Northwestern Medicine Covid Quality Committee and as core clinical faculty in the Internal Medicine Residency.
Is it fair to say that for hospitalists, the pandemic has been a sobering experience, why so?
Dr. Lee: There are several reasons; one stems from the increasing impact of Covid on children. Early in the pandemic, young children, teens, and young adults were not infected or hospitalized at the rate of older adults.1 For those of us who care for hospitalized patients, that early finding was somewhat of a relief, knowing at least one portion of the population wasn’t as heavily affected. In fact, I normally split my time as a pediatric and adult hospitalist, and I was reassigned to work full-time in the adult hospital because so few children had been admitted. But all that changed with the arrival of the highly transmissible Delta variant and the loosening of social distancing and masking guidelines and other regulations. The American Academy of Pediatrics2 reported that, as of October, 8,364 of every 100,000 children have been infected by Covid, largely driven by the summer surge. Furthermore, pediatric Covid hospitalizations increased five-fold in August 2021 as compared to the prior 6 weeks. And these numbers likely underestimate the true impact, as several states did not release complete reports and did not account for long-term sequelae from milder infections.
What other issues were far-reaching for hospitalists?
Dr. Lee: Early in 2020, we were scrambling to learn about a novel, deadly, highly transmissible disease. Some groups in our population were experiencing a high fatality rate, and the medical community had no proven treatments. We felt helpless in caring for these patients who pleaded for our help and ultimately died. When data proved that medications like steroids were effective and the vaccines arrived, I had hoped that the pandemic would be ending. But now with the quick dissemination of false information and the evolution of new variants, we are left caring for seriously ill, unvaccinated patients along with younger patients. The heartbreaking thing is that these are largely preventable tragedies now that we have effective vaccines.
What medications have changed the course of Covid in the hospital?
Dr. Lee: Steroids are interesting; they are a good reminder that Covid has different stages and that we should be mindful of how we treat patients within those particular stages. Simply, Covid infection begins with a phase of viral replication characterized by fevers, cough, loss of taste and smell, and gastrointestinal symptoms. In time, this is followed by a second phase of high inflammation and immune response, sometimes causing hypoxemia and respiratory failure. What we know is that steroids such as dexamethasone reduce mortality, but they are only effective during this second phase, and only in those whose oxygen levels are low enough to require oxygen. This was not an intuitive finding, since steroids do not help, and may harm, those with other viral pneumonias, such as influenza. Steroid use in severe, hypoxemic Covid, however, is life-saving and the mainstay of inpatient care which might include antivirals and interleukin-6 inhibitors3 in select patients. As with steroid use in other patients, physicians should watch their Covid patients for hyperglycemia4 and delirium. That said, steroids provide a mortality benefit that strongly supports their continued use -- in tandem with management of those expected side effects. Last, it is important to note that steroid use has been associated with possible harm when given to those with mild Covid,5 so its use should be avoided, in light of its expected side effects, unless a patient requires supplemental oxygen.
That said, although steroids can be helpful for our sickest patients, vaccines are the best medicine of all because they can allow patients to avoid hospitalization and death -- outcomes that far outweigh what steroids or any other medication can do for the gravely ill.
Given the complexity of the evidence surrounding the treatments for Covid in the hospital, no wonder some people are confused about which medicines work.
Dr. Lee: First, let me say that I have yet to encounter a patient or family member whose motivation to ask questions or question a loved one’s treatment wasn’t grounded in concern and fear for their loved one.
What do they ask about?
Dr. Lee: They ask about alternative treatments, anti-parasitics, even vitamins. I agree with them that there is so much out there about Covid that it is difficult for anyone to know what is true or false. I then explain what therapies are proven – medications such as steroids and supportive care such as oxygen and prone positioning. I also review the lack of good evidence for the alternative treatments that they ask about. It is sometimes surprising to folks that all research isn’t conducted with equal rigor, and that false conclusions can be made based on faulty evidence. A good example is how providers used hydroxychloroquine early in the pandemic, but ultimately it didn’t prove to be helpful. Although we are always hopeful and looking for new therapies, I say, those specific alternatives haven’t worked out. And I end with a promise that I will continue to keep up with the literature and let them know when something new does look promising.
Your responses to the above questions prompts this one: How do physicians who are treating Covid-19 stay on top of what is being learned about Covid-19? At last count, there were 191,968 results in PubMed, found using that sole keyword.
Dr. Lee: One of the amazing things about the Covid era is that members of the scientific community dropped everything to research Covid. But on the flip side, there is now a lot of research out there, and it frankly has become difficult to keep up with it. Our hospital system identified a core group of collaborators with backgrounds such as pharmacy, nursing, infectious disease, pulmonary, and hospital medicine to regularly review the evidence and identify anything that has strong enough evidence to change our system’s clinical practice. Furthermore, I regularly tap consultants in various specialties to help me contextualize new research. And I’ve found it helpful to review the living practice guidelines from the Infectious Disease Society of America and the NIH.3,6
What else has been remarkable about the last 19 months?
Dr. Lee: I have never spent this much time talking with patients and their caregivers. I’ve always been one to talk a lot with families, but it feels like the pandemic has created another level. My guess is that many colleagues are experiencing the same thing. Caring for hospitalized Covid patients is not only intense from a medical standpoint, but also from a psychosocial vantage point. Patients are ill and usually scared, and they are supported by friends and family who are equally afraid for them, who furthermore can’t visit because of isolation needs. And I often forget that, besides Covid, families have gone through immense social and financial changes. Sometimes communication can be fraught because of that stress. I am trying to be mindful that patients and families come into the hospital with a lot of these burdens, so that, if the conversation takes a tense turn, I will try not to take it personally. Some days are harder than others.
What you are describing isn’t necessarily an innate skill.
Dr. Lee: Absolutely. As have many others, our medical school and residency program has been incorporating communication skills into the standard curriculum, analogous to teaching anatomy or heart failure treatments. We are more aware that handling a difficult conversation isn’t an instinctive thing; that it must be modeled and learned. But I was surprised at how communication in a pandemic, when caretakers can’t see their loved ones, is truly a unique challenge. It is challenging for me despite being in practice for several years.
What will happen when the pandemic subsides? How much of the impact of Covid will stay with you, when dealing with a broken leg, or a patient with osteoporosis?
Dr. Lee: There will be lasting effects of this era on the health-care workforce, but I honestly can’t predict how severe that impact will be or how long-lasting. Already we are seeing health-care workers drop out of the workforce, driven by effects of the pandemic itself, increased workload, or being underpaid.7 This is occurring alongside a national conversation that cannot agree on life-saving interventions such as vaccines. I worry that the current environment will lead to many more dropping out.
What can hospital administrators do now to put stop gaps in place? What advice would you give to them?
Dr. Lee: Workers in each hospital will have unique needs and stressors, so it makes sense that the first step is to provide an opportunity to make their opinions heard. It may be tempting for hospitals to jump on quick fixes such as offering classes in “resilience training,” but that may not be a data-driven solution, particularly if burnout is being driven by an ever increasing workload.
References
- L. Shekerdemian, N. Mahmood, K.Wolfe, et al. Characteristics and Outcomes of Children With Coronavirus Disease 2019 (Covid-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr. 2020 Sep; 174(9): 1–6.
- Children and Covid-19: State-Level Data Report. American Academy of Pediatrics. Published Oct. 25, 2021. https://www.aap.org/en/pages/2019-novel-coronavirus-Covid-19-infections/children-and-Covid-19-state-level-data-report/
- NIH. Therapeutic Management of Hospitalized Adults with Covid-19. Last updated August 25, 2021. https://www.Covid19treatmentguidelines.nih.gov/management/clinical-management/hospitalized-adults--therapeutic-management/
- Sosale A, Sosale B, Kesavadev J, et al. Steroid use during Covid-19 infection and hyperglycemia - What a physician should know. Diabetes Metab Syndr. 2021;15(4):102167. doi:10.1016/j.dsx.2021.06.004
- The RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384:693-704.
- IDSA. IDSA Guidelines on the Treatment and Management of Patients with Covid-19. Last updated November 1, 2021. https://www.idsociety.org/practice-guideline/Covid-19-guideline-treatment-and-management/
- Galvin, G. “Nearly 1 in 5 Health Care Workers Have Quit Their Jobs During the Pandemic.” Morning Consult. https://morningconsult.com/2021/10/04/health-care-workers-series-part-2-workforce/ Accessed November 1, 2021.
Cheryl K. Lee, MD, an Assistant Professor of Medicine at Northwestern Feinberg School of Medicine, practices internal medicine and pediatrics at Northwestern Memorial and the Ann & Robert H. Lurie Children's Hospital, both in Chicago, IL. She also serves on the Northwestern Medicine Covid Quality Committee and as core clinical faculty in the Internal Medicine Residency.
Is it fair to say that for hospitalists, the pandemic has been a sobering experience, why so?
Dr. Lee: There are several reasons; one stems from the increasing impact of Covid on children. Early in the pandemic, young children, teens, and young adults were not infected or hospitalized at the rate of older adults.1 For those of us who care for hospitalized patients, that early finding was somewhat of a relief, knowing at least one portion of the population wasn’t as heavily affected. In fact, I normally split my time as a pediatric and adult hospitalist, and I was reassigned to work full-time in the adult hospital because so few children had been admitted. But all that changed with the arrival of the highly transmissible Delta variant and the loosening of social distancing and masking guidelines and other regulations. The American Academy of Pediatrics2 reported that, as of October, 8,364 of every 100,000 children have been infected by Covid, largely driven by the summer surge. Furthermore, pediatric Covid hospitalizations increased five-fold in August 2021 as compared to the prior 6 weeks. And these numbers likely underestimate the true impact, as several states did not release complete reports and did not account for long-term sequelae from milder infections.
What other issues were far-reaching for hospitalists?
Dr. Lee: Early in 2020, we were scrambling to learn about a novel, deadly, highly transmissible disease. Some groups in our population were experiencing a high fatality rate, and the medical community had no proven treatments. We felt helpless in caring for these patients who pleaded for our help and ultimately died. When data proved that medications like steroids were effective and the vaccines arrived, I had hoped that the pandemic would be ending. But now with the quick dissemination of false information and the evolution of new variants, we are left caring for seriously ill, unvaccinated patients along with younger patients. The heartbreaking thing is that these are largely preventable tragedies now that we have effective vaccines.
What medications have changed the course of Covid in the hospital?
Dr. Lee: Steroids are interesting; they are a good reminder that Covid has different stages and that we should be mindful of how we treat patients within those particular stages. Simply, Covid infection begins with a phase of viral replication characterized by fevers, cough, loss of taste and smell, and gastrointestinal symptoms. In time, this is followed by a second phase of high inflammation and immune response, sometimes causing hypoxemia and respiratory failure. What we know is that steroids such as dexamethasone reduce mortality, but they are only effective during this second phase, and only in those whose oxygen levels are low enough to require oxygen. This was not an intuitive finding, since steroids do not help, and may harm, those with other viral pneumonias, such as influenza. Steroid use in severe, hypoxemic Covid, however, is life-saving and the mainstay of inpatient care which might include antivirals and interleukin-6 inhibitors3 in select patients. As with steroid use in other patients, physicians should watch their Covid patients for hyperglycemia4 and delirium. That said, steroids provide a mortality benefit that strongly supports their continued use -- in tandem with management of those expected side effects. Last, it is important to note that steroid use has been associated with possible harm when given to those with mild Covid,5 so its use should be avoided, in light of its expected side effects, unless a patient requires supplemental oxygen.
That said, although steroids can be helpful for our sickest patients, vaccines are the best medicine of all because they can allow patients to avoid hospitalization and death -- outcomes that far outweigh what steroids or any other medication can do for the gravely ill.
Given the complexity of the evidence surrounding the treatments for Covid in the hospital, no wonder some people are confused about which medicines work.
Dr. Lee: First, let me say that I have yet to encounter a patient or family member whose motivation to ask questions or question a loved one’s treatment wasn’t grounded in concern and fear for their loved one.
What do they ask about?
Dr. Lee: They ask about alternative treatments, anti-parasitics, even vitamins. I agree with them that there is so much out there about Covid that it is difficult for anyone to know what is true or false. I then explain what therapies are proven – medications such as steroids and supportive care such as oxygen and prone positioning. I also review the lack of good evidence for the alternative treatments that they ask about. It is sometimes surprising to folks that all research isn’t conducted with equal rigor, and that false conclusions can be made based on faulty evidence. A good example is how providers used hydroxychloroquine early in the pandemic, but ultimately it didn’t prove to be helpful. Although we are always hopeful and looking for new therapies, I say, those specific alternatives haven’t worked out. And I end with a promise that I will continue to keep up with the literature and let them know when something new does look promising.
Your responses to the above questions prompts this one: How do physicians who are treating Covid-19 stay on top of what is being learned about Covid-19? At last count, there were 191,968 results in PubMed, found using that sole keyword.
Dr. Lee: One of the amazing things about the Covid era is that members of the scientific community dropped everything to research Covid. But on the flip side, there is now a lot of research out there, and it frankly has become difficult to keep up with it. Our hospital system identified a core group of collaborators with backgrounds such as pharmacy, nursing, infectious disease, pulmonary, and hospital medicine to regularly review the evidence and identify anything that has strong enough evidence to change our system’s clinical practice. Furthermore, I regularly tap consultants in various specialties to help me contextualize new research. And I’ve found it helpful to review the living practice guidelines from the Infectious Disease Society of America and the NIH.3,6
What else has been remarkable about the last 19 months?
Dr. Lee: I have never spent this much time talking with patients and their caregivers. I’ve always been one to talk a lot with families, but it feels like the pandemic has created another level. My guess is that many colleagues are experiencing the same thing. Caring for hospitalized Covid patients is not only intense from a medical standpoint, but also from a psychosocial vantage point. Patients are ill and usually scared, and they are supported by friends and family who are equally afraid for them, who furthermore can’t visit because of isolation needs. And I often forget that, besides Covid, families have gone through immense social and financial changes. Sometimes communication can be fraught because of that stress. I am trying to be mindful that patients and families come into the hospital with a lot of these burdens, so that, if the conversation takes a tense turn, I will try not to take it personally. Some days are harder than others.
What you are describing isn’t necessarily an innate skill.
Dr. Lee: Absolutely. As have many others, our medical school and residency program has been incorporating communication skills into the standard curriculum, analogous to teaching anatomy or heart failure treatments. We are more aware that handling a difficult conversation isn’t an instinctive thing; that it must be modeled and learned. But I was surprised at how communication in a pandemic, when caretakers can’t see their loved ones, is truly a unique challenge. It is challenging for me despite being in practice for several years.
What will happen when the pandemic subsides? How much of the impact of Covid will stay with you, when dealing with a broken leg, or a patient with osteoporosis?
Dr. Lee: There will be lasting effects of this era on the health-care workforce, but I honestly can’t predict how severe that impact will be or how long-lasting. Already we are seeing health-care workers drop out of the workforce, driven by effects of the pandemic itself, increased workload, or being underpaid.7 This is occurring alongside a national conversation that cannot agree on life-saving interventions such as vaccines. I worry that the current environment will lead to many more dropping out.
What can hospital administrators do now to put stop gaps in place? What advice would you give to them?
Dr. Lee: Workers in each hospital will have unique needs and stressors, so it makes sense that the first step is to provide an opportunity to make their opinions heard. It may be tempting for hospitals to jump on quick fixes such as offering classes in “resilience training,” but that may not be a data-driven solution, particularly if burnout is being driven by an ever increasing workload.
Cheryl K. Lee, MD, an Assistant Professor of Medicine at Northwestern Feinberg School of Medicine, practices internal medicine and pediatrics at Northwestern Memorial and the Ann & Robert H. Lurie Children's Hospital, both in Chicago, IL. She also serves on the Northwestern Medicine Covid Quality Committee and as core clinical faculty in the Internal Medicine Residency.
Is it fair to say that for hospitalists, the pandemic has been a sobering experience, why so?
Dr. Lee: There are several reasons; one stems from the increasing impact of Covid on children. Early in the pandemic, young children, teens, and young adults were not infected or hospitalized at the rate of older adults.1 For those of us who care for hospitalized patients, that early finding was somewhat of a relief, knowing at least one portion of the population wasn’t as heavily affected. In fact, I normally split my time as a pediatric and adult hospitalist, and I was reassigned to work full-time in the adult hospital because so few children had been admitted. But all that changed with the arrival of the highly transmissible Delta variant and the loosening of social distancing and masking guidelines and other regulations. The American Academy of Pediatrics2 reported that, as of October, 8,364 of every 100,000 children have been infected by Covid, largely driven by the summer surge. Furthermore, pediatric Covid hospitalizations increased five-fold in August 2021 as compared to the prior 6 weeks. And these numbers likely underestimate the true impact, as several states did not release complete reports and did not account for long-term sequelae from milder infections.
What other issues were far-reaching for hospitalists?
Dr. Lee: Early in 2020, we were scrambling to learn about a novel, deadly, highly transmissible disease. Some groups in our population were experiencing a high fatality rate, and the medical community had no proven treatments. We felt helpless in caring for these patients who pleaded for our help and ultimately died. When data proved that medications like steroids were effective and the vaccines arrived, I had hoped that the pandemic would be ending. But now with the quick dissemination of false information and the evolution of new variants, we are left caring for seriously ill, unvaccinated patients along with younger patients. The heartbreaking thing is that these are largely preventable tragedies now that we have effective vaccines.
What medications have changed the course of Covid in the hospital?
Dr. Lee: Steroids are interesting; they are a good reminder that Covid has different stages and that we should be mindful of how we treat patients within those particular stages. Simply, Covid infection begins with a phase of viral replication characterized by fevers, cough, loss of taste and smell, and gastrointestinal symptoms. In time, this is followed by a second phase of high inflammation and immune response, sometimes causing hypoxemia and respiratory failure. What we know is that steroids such as dexamethasone reduce mortality, but they are only effective during this second phase, and only in those whose oxygen levels are low enough to require oxygen. This was not an intuitive finding, since steroids do not help, and may harm, those with other viral pneumonias, such as influenza. Steroid use in severe, hypoxemic Covid, however, is life-saving and the mainstay of inpatient care which might include antivirals and interleukin-6 inhibitors3 in select patients. As with steroid use in other patients, physicians should watch their Covid patients for hyperglycemia4 and delirium. That said, steroids provide a mortality benefit that strongly supports their continued use -- in tandem with management of those expected side effects. Last, it is important to note that steroid use has been associated with possible harm when given to those with mild Covid,5 so its use should be avoided, in light of its expected side effects, unless a patient requires supplemental oxygen.
That said, although steroids can be helpful for our sickest patients, vaccines are the best medicine of all because they can allow patients to avoid hospitalization and death -- outcomes that far outweigh what steroids or any other medication can do for the gravely ill.
Given the complexity of the evidence surrounding the treatments for Covid in the hospital, no wonder some people are confused about which medicines work.
Dr. Lee: First, let me say that I have yet to encounter a patient or family member whose motivation to ask questions or question a loved one’s treatment wasn’t grounded in concern and fear for their loved one.
What do they ask about?
Dr. Lee: They ask about alternative treatments, anti-parasitics, even vitamins. I agree with them that there is so much out there about Covid that it is difficult for anyone to know what is true or false. I then explain what therapies are proven – medications such as steroids and supportive care such as oxygen and prone positioning. I also review the lack of good evidence for the alternative treatments that they ask about. It is sometimes surprising to folks that all research isn’t conducted with equal rigor, and that false conclusions can be made based on faulty evidence. A good example is how providers used hydroxychloroquine early in the pandemic, but ultimately it didn’t prove to be helpful. Although we are always hopeful and looking for new therapies, I say, those specific alternatives haven’t worked out. And I end with a promise that I will continue to keep up with the literature and let them know when something new does look promising.
Your responses to the above questions prompts this one: How do physicians who are treating Covid-19 stay on top of what is being learned about Covid-19? At last count, there were 191,968 results in PubMed, found using that sole keyword.
Dr. Lee: One of the amazing things about the Covid era is that members of the scientific community dropped everything to research Covid. But on the flip side, there is now a lot of research out there, and it frankly has become difficult to keep up with it. Our hospital system identified a core group of collaborators with backgrounds such as pharmacy, nursing, infectious disease, pulmonary, and hospital medicine to regularly review the evidence and identify anything that has strong enough evidence to change our system’s clinical practice. Furthermore, I regularly tap consultants in various specialties to help me contextualize new research. And I’ve found it helpful to review the living practice guidelines from the Infectious Disease Society of America and the NIH.3,6
What else has been remarkable about the last 19 months?
Dr. Lee: I have never spent this much time talking with patients and their caregivers. I’ve always been one to talk a lot with families, but it feels like the pandemic has created another level. My guess is that many colleagues are experiencing the same thing. Caring for hospitalized Covid patients is not only intense from a medical standpoint, but also from a psychosocial vantage point. Patients are ill and usually scared, and they are supported by friends and family who are equally afraid for them, who furthermore can’t visit because of isolation needs. And I often forget that, besides Covid, families have gone through immense social and financial changes. Sometimes communication can be fraught because of that stress. I am trying to be mindful that patients and families come into the hospital with a lot of these burdens, so that, if the conversation takes a tense turn, I will try not to take it personally. Some days are harder than others.
What you are describing isn’t necessarily an innate skill.
Dr. Lee: Absolutely. As have many others, our medical school and residency program has been incorporating communication skills into the standard curriculum, analogous to teaching anatomy or heart failure treatments. We are more aware that handling a difficult conversation isn’t an instinctive thing; that it must be modeled and learned. But I was surprised at how communication in a pandemic, when caretakers can’t see their loved ones, is truly a unique challenge. It is challenging for me despite being in practice for several years.
What will happen when the pandemic subsides? How much of the impact of Covid will stay with you, when dealing with a broken leg, or a patient with osteoporosis?
Dr. Lee: There will be lasting effects of this era on the health-care workforce, but I honestly can’t predict how severe that impact will be or how long-lasting. Already we are seeing health-care workers drop out of the workforce, driven by effects of the pandemic itself, increased workload, or being underpaid.7 This is occurring alongside a national conversation that cannot agree on life-saving interventions such as vaccines. I worry that the current environment will lead to many more dropping out.
What can hospital administrators do now to put stop gaps in place? What advice would you give to them?
Dr. Lee: Workers in each hospital will have unique needs and stressors, so it makes sense that the first step is to provide an opportunity to make their opinions heard. It may be tempting for hospitals to jump on quick fixes such as offering classes in “resilience training,” but that may not be a data-driven solution, particularly if burnout is being driven by an ever increasing workload.
References
- L. Shekerdemian, N. Mahmood, K.Wolfe, et al. Characteristics and Outcomes of Children With Coronavirus Disease 2019 (Covid-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr. 2020 Sep; 174(9): 1–6.
- Children and Covid-19: State-Level Data Report. American Academy of Pediatrics. Published Oct. 25, 2021. https://www.aap.org/en/pages/2019-novel-coronavirus-Covid-19-infections/children-and-Covid-19-state-level-data-report/
- NIH. Therapeutic Management of Hospitalized Adults with Covid-19. Last updated August 25, 2021. https://www.Covid19treatmentguidelines.nih.gov/management/clinical-management/hospitalized-adults--therapeutic-management/
- Sosale A, Sosale B, Kesavadev J, et al. Steroid use during Covid-19 infection and hyperglycemia - What a physician should know. Diabetes Metab Syndr. 2021;15(4):102167. doi:10.1016/j.dsx.2021.06.004
- The RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384:693-704.
- IDSA. IDSA Guidelines on the Treatment and Management of Patients with Covid-19. Last updated November 1, 2021. https://www.idsociety.org/practice-guideline/Covid-19-guideline-treatment-and-management/
- Galvin, G. “Nearly 1 in 5 Health Care Workers Have Quit Their Jobs During the Pandemic.” Morning Consult. https://morningconsult.com/2021/10/04/health-care-workers-series-part-2-workforce/ Accessed November 1, 2021.
References
- L. Shekerdemian, N. Mahmood, K.Wolfe, et al. Characteristics and Outcomes of Children With Coronavirus Disease 2019 (Covid-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr. 2020 Sep; 174(9): 1–6.
- Children and Covid-19: State-Level Data Report. American Academy of Pediatrics. Published Oct. 25, 2021. https://www.aap.org/en/pages/2019-novel-coronavirus-Covid-19-infections/children-and-Covid-19-state-level-data-report/
- NIH. Therapeutic Management of Hospitalized Adults with Covid-19. Last updated August 25, 2021. https://www.Covid19treatmentguidelines.nih.gov/management/clinical-management/hospitalized-adults--therapeutic-management/
- Sosale A, Sosale B, Kesavadev J, et al. Steroid use during Covid-19 infection and hyperglycemia - What a physician should know. Diabetes Metab Syndr. 2021;15(4):102167. doi:10.1016/j.dsx.2021.06.004
- The RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384:693-704.
- IDSA. IDSA Guidelines on the Treatment and Management of Patients with Covid-19. Last updated November 1, 2021. https://www.idsociety.org/practice-guideline/Covid-19-guideline-treatment-and-management/
- Galvin, G. “Nearly 1 in 5 Health Care Workers Have Quit Their Jobs During the Pandemic.” Morning Consult. https://morningconsult.com/2021/10/04/health-care-workers-series-part-2-workforce/ Accessed November 1, 2021.
Sleep-related hypoxia and COVID-19 outcomes
Key clinical point: Sleep-related hypoxia is associated with worse outcomes in patients with COVID-19.
Major finding: Sleep-related hypoxia was associated with an increased risk for COVID-19-related hospitalization and mortality (adjusted hazard ratio, 1.31; 95% CI, 1.08-1.57; P = .005).
Study details: The data come from a case-control study involving 5,402 individuals who had previously participated in a sleep study, of whom 1,935 tested positive for SARS-CoV-2.
Disclosures: The study was supported by the Neuroscience Transformative Research Resource Development Award (R Mehra). A Milinovich reported ties with various pharmaceutical companies and research organizations. L Aboussouan, L Jehi, R Mehra, and C Pena Orbea reported ties with research organizations and/or publishing companies. The remaining authors declared no competing interests.
Source: Pena Orbea C et al. JAMA Netw Open. 2021 Nov 10. doi: 10.1001/jamanetworkopen.2021.34241.
Key clinical point: Sleep-related hypoxia is associated with worse outcomes in patients with COVID-19.
Major finding: Sleep-related hypoxia was associated with an increased risk for COVID-19-related hospitalization and mortality (adjusted hazard ratio, 1.31; 95% CI, 1.08-1.57; P = .005).
Study details: The data come from a case-control study involving 5,402 individuals who had previously participated in a sleep study, of whom 1,935 tested positive for SARS-CoV-2.
Disclosures: The study was supported by the Neuroscience Transformative Research Resource Development Award (R Mehra). A Milinovich reported ties with various pharmaceutical companies and research organizations. L Aboussouan, L Jehi, R Mehra, and C Pena Orbea reported ties with research organizations and/or publishing companies. The remaining authors declared no competing interests.
Source: Pena Orbea C et al. JAMA Netw Open. 2021 Nov 10. doi: 10.1001/jamanetworkopen.2021.34241.
Key clinical point: Sleep-related hypoxia is associated with worse outcomes in patients with COVID-19.
Major finding: Sleep-related hypoxia was associated with an increased risk for COVID-19-related hospitalization and mortality (adjusted hazard ratio, 1.31; 95% CI, 1.08-1.57; P = .005).
Study details: The data come from a case-control study involving 5,402 individuals who had previously participated in a sleep study, of whom 1,935 tested positive for SARS-CoV-2.
Disclosures: The study was supported by the Neuroscience Transformative Research Resource Development Award (R Mehra). A Milinovich reported ties with various pharmaceutical companies and research organizations. L Aboussouan, L Jehi, R Mehra, and C Pena Orbea reported ties with research organizations and/or publishing companies. The remaining authors declared no competing interests.
Source: Pena Orbea C et al. JAMA Netw Open. 2021 Nov 10. doi: 10.1001/jamanetworkopen.2021.34241.
Real-world effectiveness of J&J's COVID-19 vaccine
Key clinical point: Johnson & Johnson's (J&J) adenoviral vector COVID-19 vaccine (Ad26.COV) was effective in preventing COVID-19 and severe outcomes in a real-world setting.
Major finding: The incidence rate ratio of COVID-19 in the Ad26.COV-vaccinated vs unvaccinated cohort was 0.26 (95% CI, 0.20-0.34), corresponding to an effectiveness of 73.6% (95% CI, 65.9%-79.9%). Ad26.COV recipients also had a lower risk for hospitalization (odds ratio [OR], 0.32; P = .00028) and ICU admissions (OR, 0.00; P = .001) compared with unvaccinated individuals.
Study details: The data come from an analysis of 8,889 individuals vaccinated with Ad26.COV and 88,898 unvaccinated matched controls.
Disclosures: No information on funding was available. J Corchado-Garcia, D Zemmour, T Hughes, P Lenehan, C Pawlowski, JC O’Horo, AD Badley, MD Swift, T Wagner, and V Soundararajan reported relationships with various pharmaceutical companies. The remaining authors declared no conflict of interests.
Source: Corchado-Garcia J et al. JAMA Netw Open. 2021 Nov 2. doi: 10.1001/jamanetworkopen.2021.32540.
Key clinical point: Johnson & Johnson's (J&J) adenoviral vector COVID-19 vaccine (Ad26.COV) was effective in preventing COVID-19 and severe outcomes in a real-world setting.
Major finding: The incidence rate ratio of COVID-19 in the Ad26.COV-vaccinated vs unvaccinated cohort was 0.26 (95% CI, 0.20-0.34), corresponding to an effectiveness of 73.6% (95% CI, 65.9%-79.9%). Ad26.COV recipients also had a lower risk for hospitalization (odds ratio [OR], 0.32; P = .00028) and ICU admissions (OR, 0.00; P = .001) compared with unvaccinated individuals.
Study details: The data come from an analysis of 8,889 individuals vaccinated with Ad26.COV and 88,898 unvaccinated matched controls.
Disclosures: No information on funding was available. J Corchado-Garcia, D Zemmour, T Hughes, P Lenehan, C Pawlowski, JC O’Horo, AD Badley, MD Swift, T Wagner, and V Soundararajan reported relationships with various pharmaceutical companies. The remaining authors declared no conflict of interests.
Source: Corchado-Garcia J et al. JAMA Netw Open. 2021 Nov 2. doi: 10.1001/jamanetworkopen.2021.32540.
Key clinical point: Johnson & Johnson's (J&J) adenoviral vector COVID-19 vaccine (Ad26.COV) was effective in preventing COVID-19 and severe outcomes in a real-world setting.
Major finding: The incidence rate ratio of COVID-19 in the Ad26.COV-vaccinated vs unvaccinated cohort was 0.26 (95% CI, 0.20-0.34), corresponding to an effectiveness of 73.6% (95% CI, 65.9%-79.9%). Ad26.COV recipients also had a lower risk for hospitalization (odds ratio [OR], 0.32; P = .00028) and ICU admissions (OR, 0.00; P = .001) compared with unvaccinated individuals.
Study details: The data come from an analysis of 8,889 individuals vaccinated with Ad26.COV and 88,898 unvaccinated matched controls.
Disclosures: No information on funding was available. J Corchado-Garcia, D Zemmour, T Hughes, P Lenehan, C Pawlowski, JC O’Horo, AD Badley, MD Swift, T Wagner, and V Soundararajan reported relationships with various pharmaceutical companies. The remaining authors declared no conflict of interests.
Source: Corchado-Garcia J et al. JAMA Netw Open. 2021 Nov 2. doi: 10.1001/jamanetworkopen.2021.32540.
Single-dose levilimab safe and effective in severe COVID-19
Key clinical point: A single subcutaneous dose of levilimab (LVL) was safe and effective in severely ill patients with COVID-19 not requiring mechanical ventilation.
Major finding: 63.1% of patients in the LVL group vs 42.7% in the placebo group achieved sustained clinical improvement on day 14 (P = .0017). Adverse event frequency was comparable between the groups.
Study details: In the phase 3 CORONA trial, 206 patients were randomly assigned (1:1) to receive either LVL+standard of care (SOC) vs placebo+SOC.
Disclosures: This study was funded by JSC BIOCAD. MY Gilyarov reported ties with various pharmaceutical companies. AI Seleznev, YN Linkova, EA Dokukina, PS Pukhtinskaia, AV Eremeeva, MA Morozova, AV Zinkina-Orikhan, and AA Lutckii are employees of JSC BIOCAD.
Source: Lomakin NV et al. Inflamm Res. 2021 Sep 29. doi: 10.1007/s00011-021-01507-5.
Key clinical point: A single subcutaneous dose of levilimab (LVL) was safe and effective in severely ill patients with COVID-19 not requiring mechanical ventilation.
Major finding: 63.1% of patients in the LVL group vs 42.7% in the placebo group achieved sustained clinical improvement on day 14 (P = .0017). Adverse event frequency was comparable between the groups.
Study details: In the phase 3 CORONA trial, 206 patients were randomly assigned (1:1) to receive either LVL+standard of care (SOC) vs placebo+SOC.
Disclosures: This study was funded by JSC BIOCAD. MY Gilyarov reported ties with various pharmaceutical companies. AI Seleznev, YN Linkova, EA Dokukina, PS Pukhtinskaia, AV Eremeeva, MA Morozova, AV Zinkina-Orikhan, and AA Lutckii are employees of JSC BIOCAD.
Source: Lomakin NV et al. Inflamm Res. 2021 Sep 29. doi: 10.1007/s00011-021-01507-5.
Key clinical point: A single subcutaneous dose of levilimab (LVL) was safe and effective in severely ill patients with COVID-19 not requiring mechanical ventilation.
Major finding: 63.1% of patients in the LVL group vs 42.7% in the placebo group achieved sustained clinical improvement on day 14 (P = .0017). Adverse event frequency was comparable between the groups.
Study details: In the phase 3 CORONA trial, 206 patients were randomly assigned (1:1) to receive either LVL+standard of care (SOC) vs placebo+SOC.
Disclosures: This study was funded by JSC BIOCAD. MY Gilyarov reported ties with various pharmaceutical companies. AI Seleznev, YN Linkova, EA Dokukina, PS Pukhtinskaia, AV Eremeeva, MA Morozova, AV Zinkina-Orikhan, and AA Lutckii are employees of JSC BIOCAD.
Source: Lomakin NV et al. Inflamm Res. 2021 Sep 29. doi: 10.1007/s00011-021-01507-5.
Higher risk for COVID-19-related hospitalization, death in HIV-positive individuals
Key clinical point: HIV-positive individuals are more likely to be hospitalized for or die from COVID-19 compared with non-HIV individuals.
Major finding: The HIV-positive vs non-HIV group had a higher risk for COVID-19-related hospitalization (adjusted odds ratio [aOR], 1.20; 95% CI, 1.15-1.26) and mortality (aOR, 1.29; 95% CI, 1.16-1.44). The risk was pronounced for older patients, male sex, and Black race.
Study details: The data come from a US population-based surveillance study involving 1,436,622 COVID-19 cases, of which 13,170 were HIV positive.
Disclosures: The study was funded by National Center for Advancing Translational Sciences, National Institute of Allergy and Infectious Diseases, and National Institutes of Health, USA. The authors declared no competing interests.
Source: Yang X et al. Lancet HIV. 2021 Oct 13. doi: 10.1016/S2352-3018(21)00239-3.
Key clinical point: HIV-positive individuals are more likely to be hospitalized for or die from COVID-19 compared with non-HIV individuals.
Major finding: The HIV-positive vs non-HIV group had a higher risk for COVID-19-related hospitalization (adjusted odds ratio [aOR], 1.20; 95% CI, 1.15-1.26) and mortality (aOR, 1.29; 95% CI, 1.16-1.44). The risk was pronounced for older patients, male sex, and Black race.
Study details: The data come from a US population-based surveillance study involving 1,436,622 COVID-19 cases, of which 13,170 were HIV positive.
Disclosures: The study was funded by National Center for Advancing Translational Sciences, National Institute of Allergy and Infectious Diseases, and National Institutes of Health, USA. The authors declared no competing interests.
Source: Yang X et al. Lancet HIV. 2021 Oct 13. doi: 10.1016/S2352-3018(21)00239-3.
Key clinical point: HIV-positive individuals are more likely to be hospitalized for or die from COVID-19 compared with non-HIV individuals.
Major finding: The HIV-positive vs non-HIV group had a higher risk for COVID-19-related hospitalization (adjusted odds ratio [aOR], 1.20; 95% CI, 1.15-1.26) and mortality (aOR, 1.29; 95% CI, 1.16-1.44). The risk was pronounced for older patients, male sex, and Black race.
Study details: The data come from a US population-based surveillance study involving 1,436,622 COVID-19 cases, of which 13,170 were HIV positive.
Disclosures: The study was funded by National Center for Advancing Translational Sciences, National Institute of Allergy and Infectious Diseases, and National Institutes of Health, USA. The authors declared no competing interests.
Source: Yang X et al. Lancet HIV. 2021 Oct 13. doi: 10.1016/S2352-3018(21)00239-3.
Heart rate variability predicts COVID-19 outcomes
Key clinical point: Heart rate variability (HRV) is a predictor of survival and intensive care unit (ICU) admission in older adults hospitalized with COVID-19.
Major finding: After adjusting for age and chronic heart disease, HRV was a significant predictor of survival (adjusted hazard ratio [aHR] with low vs high HRV, 0.51; 95% CI, 0.27-0.97). This association was primarily driven by patients aged ≥70 years (aHR with low vs high HRV, 0.28; 95% CI, 0.12-0.66). HRV also predicted ICU admission within the first week of hospitalization (adjusted HR, 0.51; 95% CI, 0.29-0.90), independent of age and chronic heart disease.
Study details: The data come from a retrospective cohort study involving 271 consecutive adults hospitalized with COVID-19 between March 2020 and May 2020.
Disclosures: The study did not receive any specific funding. The authors declared no competing interests.
Source: Mol MBA et al. PLoS One. 2021 Oct 28. doi: 10.1371/journal.pone.0258841.
Key clinical point: Heart rate variability (HRV) is a predictor of survival and intensive care unit (ICU) admission in older adults hospitalized with COVID-19.
Major finding: After adjusting for age and chronic heart disease, HRV was a significant predictor of survival (adjusted hazard ratio [aHR] with low vs high HRV, 0.51; 95% CI, 0.27-0.97). This association was primarily driven by patients aged ≥70 years (aHR with low vs high HRV, 0.28; 95% CI, 0.12-0.66). HRV also predicted ICU admission within the first week of hospitalization (adjusted HR, 0.51; 95% CI, 0.29-0.90), independent of age and chronic heart disease.
Study details: The data come from a retrospective cohort study involving 271 consecutive adults hospitalized with COVID-19 between March 2020 and May 2020.
Disclosures: The study did not receive any specific funding. The authors declared no competing interests.
Source: Mol MBA et al. PLoS One. 2021 Oct 28. doi: 10.1371/journal.pone.0258841.
Key clinical point: Heart rate variability (HRV) is a predictor of survival and intensive care unit (ICU) admission in older adults hospitalized with COVID-19.
Major finding: After adjusting for age and chronic heart disease, HRV was a significant predictor of survival (adjusted hazard ratio [aHR] with low vs high HRV, 0.51; 95% CI, 0.27-0.97). This association was primarily driven by patients aged ≥70 years (aHR with low vs high HRV, 0.28; 95% CI, 0.12-0.66). HRV also predicted ICU admission within the first week of hospitalization (adjusted HR, 0.51; 95% CI, 0.29-0.90), independent of age and chronic heart disease.
Study details: The data come from a retrospective cohort study involving 271 consecutive adults hospitalized with COVID-19 between March 2020 and May 2020.
Disclosures: The study did not receive any specific funding. The authors declared no competing interests.
Source: Mol MBA et al. PLoS One. 2021 Oct 28. doi: 10.1371/journal.pone.0258841.
COVID-19: Sotrovimab may prevent disease progression
Key clinical point: Sotrovimab significantly reduced the risk for complications, hospitalization, or mortality in patients with mild-to-moderate COVID-19.
Major finding: 1% of patients in the sotrovimab group vs 7% in the placebo group experienced disease progression leading to hospitalization (relative risk reduction, 85%; P = .002). Grade 3/4 adverse events were reported in 2% of patients in the sotrovimab group vs 6% of patients in the placebo group.
Study details: The data come from a prespecified, interim analysis of the ongoing, double-blind, placebo-controlled phase 3 COMET-ICE trial assessing the efficacy and safety of sotrovimab in patients with high-risk, ambulatory, mild-to-moderate COVID-19.
Disclosures: The COMET-ICE trial was funded by Vir Biotechnology and GlaxoSmithKline. The COMET-ICE Investigators reported relationships with Vir Biotechnology and GlaxoSmithKline.
Source: Gupta A et al. N Engl J Med. 2021 Oct 27. doi: 10.1056/NEJMoa2107934.
Key clinical point: Sotrovimab significantly reduced the risk for complications, hospitalization, or mortality in patients with mild-to-moderate COVID-19.
Major finding: 1% of patients in the sotrovimab group vs 7% in the placebo group experienced disease progression leading to hospitalization (relative risk reduction, 85%; P = .002). Grade 3/4 adverse events were reported in 2% of patients in the sotrovimab group vs 6% of patients in the placebo group.
Study details: The data come from a prespecified, interim analysis of the ongoing, double-blind, placebo-controlled phase 3 COMET-ICE trial assessing the efficacy and safety of sotrovimab in patients with high-risk, ambulatory, mild-to-moderate COVID-19.
Disclosures: The COMET-ICE trial was funded by Vir Biotechnology and GlaxoSmithKline. The COMET-ICE Investigators reported relationships with Vir Biotechnology and GlaxoSmithKline.
Source: Gupta A et al. N Engl J Med. 2021 Oct 27. doi: 10.1056/NEJMoa2107934.
Key clinical point: Sotrovimab significantly reduced the risk for complications, hospitalization, or mortality in patients with mild-to-moderate COVID-19.
Major finding: 1% of patients in the sotrovimab group vs 7% in the placebo group experienced disease progression leading to hospitalization (relative risk reduction, 85%; P = .002). Grade 3/4 adverse events were reported in 2% of patients in the sotrovimab group vs 6% of patients in the placebo group.
Study details: The data come from a prespecified, interim analysis of the ongoing, double-blind, placebo-controlled phase 3 COMET-ICE trial assessing the efficacy and safety of sotrovimab in patients with high-risk, ambulatory, mild-to-moderate COVID-19.
Disclosures: The COMET-ICE trial was funded by Vir Biotechnology and GlaxoSmithKline. The COMET-ICE Investigators reported relationships with Vir Biotechnology and GlaxoSmithKline.
Source: Gupta A et al. N Engl J Med. 2021 Oct 27. doi: 10.1056/NEJMoa2107934.
History of diphtheria or tetanus vaccination linked to lower risk for severe COVID-19
Key clinical point: Individuals who had received diphtheria or tetanus vaccinations in the last 10 years were less likely to develop severe COVID-19 compared with those who had not received them.
Major finding: The study included 103,049 participants (mean age, 71.5 years; 54.2% women) with vaccination records for the past 10 years and data on COVID-19 testing.
Study details: Individuals who had been vaccinated against diphtheria (odds ratio [OR], 0.47; 95% CI, 0.33-0.68; P = .000053) and tetanus (OR, 0.52; 95% CI, 0.37-0.72; P = .00012) in the last 10 years had a lower likelihood of developing severe COVID-19 symptoms compared with those who had not received them.
Disclosures: The study was funded by the Research Council of Norway, the South-Eastern Norway Regional Health Authority, Stiftelsen Kristian Gerhard Jebsen, The European Research Council under the European Union’s Horizon 2020 research and innovation programme, and National Institutes of Health. O Andreassen and J Pinzón-Espinosa reported relationships with various pharmaceutical companies. The remaining authors declared no conflict of interests.
Source: Monereo-Sánchez J et al. Front Immunol. 2021 Oct 7. doi: 10.3389/fimmu.2021.749264.
Key clinical point: Individuals who had received diphtheria or tetanus vaccinations in the last 10 years were less likely to develop severe COVID-19 compared with those who had not received them.
Major finding: The study included 103,049 participants (mean age, 71.5 years; 54.2% women) with vaccination records for the past 10 years and data on COVID-19 testing.
Study details: Individuals who had been vaccinated against diphtheria (odds ratio [OR], 0.47; 95% CI, 0.33-0.68; P = .000053) and tetanus (OR, 0.52; 95% CI, 0.37-0.72; P = .00012) in the last 10 years had a lower likelihood of developing severe COVID-19 symptoms compared with those who had not received them.
Disclosures: The study was funded by the Research Council of Norway, the South-Eastern Norway Regional Health Authority, Stiftelsen Kristian Gerhard Jebsen, The European Research Council under the European Union’s Horizon 2020 research and innovation programme, and National Institutes of Health. O Andreassen and J Pinzón-Espinosa reported relationships with various pharmaceutical companies. The remaining authors declared no conflict of interests.
Source: Monereo-Sánchez J et al. Front Immunol. 2021 Oct 7. doi: 10.3389/fimmu.2021.749264.
Key clinical point: Individuals who had received diphtheria or tetanus vaccinations in the last 10 years were less likely to develop severe COVID-19 compared with those who had not received them.
Major finding: The study included 103,049 participants (mean age, 71.5 years; 54.2% women) with vaccination records for the past 10 years and data on COVID-19 testing.
Study details: Individuals who had been vaccinated against diphtheria (odds ratio [OR], 0.47; 95% CI, 0.33-0.68; P = .000053) and tetanus (OR, 0.52; 95% CI, 0.37-0.72; P = .00012) in the last 10 years had a lower likelihood of developing severe COVID-19 symptoms compared with those who had not received them.
Disclosures: The study was funded by the Research Council of Norway, the South-Eastern Norway Regional Health Authority, Stiftelsen Kristian Gerhard Jebsen, The European Research Council under the European Union’s Horizon 2020 research and innovation programme, and National Institutes of Health. O Andreassen and J Pinzón-Espinosa reported relationships with various pharmaceutical companies. The remaining authors declared no conflict of interests.
Source: Monereo-Sánchez J et al. Front Immunol. 2021 Oct 7. doi: 10.3389/fimmu.2021.749264.