User login
What to do if an employee tests positive for COVID-19
An increasingly common question I’m receiving is:
As always, it depends, but here is some general advice: The specifics will vary depending on state/local laws, or your particular situation.
First, you need to determine the level of exposure, and whether it requires action. According to the Centers for Disease Control and Prevention, actionable exposure occurs 2 days prior to the onset of illness, and lasts 10 days after onset.
If action is required, you’ll need to determine who needs to quarantine and who needs to be tested. Vaccinated employees who have been exposed to suspected or confirmed COVID-19 are not required to quarantine or be tested if they are fully vaccinated and have remained asymptomatic since the exposure. Those employees should, however, follow all the usual precautions (masks, social distancing, handwashing, etc.) with increased diligence. Remind them that no vaccine is 100% effective, and suggest they self-monitor for symptoms (fever, cough, shortness of breath, etc.)
All other exposed employees should be tested. A negative test means an individual was not infected at the time the sample was collected, but that does not mean an individual will not get sick later. Some providers are retesting on days 5 and 7 post exposure.
Some experts advise that you monitor exposed employees (vaccinated or not) yourself, with daily temperature readings and inquiries regarding symptoms, and perhaps a daily pulse oximetry check, for 14 days following exposure. Document these screenings in writing. Anyone testing positive or developing a fever or other symptoms should, of course, be sent home and seek medical treatment as necessary.
Employees who develop symptoms or test positive for COVID-19 should remain out of work until all CDC “return-to-work” criteria are met. At this writing, the basic criteria include:
- At least 10 days pass after symptoms first appeared
- At least 24 hours pass after last fever without the use of fever-reducing medications
- Cough, shortness of breath, and any other symptoms improve
Anyone who is significantly immunocompromised may need more time at home, and probably consultation with an infectious disease specialist.
Your facility should be thoroughly cleaned after the exposure. Close off all areas used by the sick individual, and clean and disinfect all areas such as offices, doorknobs, bathrooms, common areas, and shared electronic equipment. Of course, the cleaners should wear gowns, gloves, masks, and goggles. Some practices are hiring cleaning crews to professionally disinfect their offices. Once the area has been disinfected, it can be reopened for use. Workers without close contact with the person who is sick can return to work immediately after disinfection.
If the potential infected area is widespread and cannot be isolated to a room or rooms where doors can be shut, it may be prudent to temporarily close your office, send staff home, and divert patients to other locations if they cannot be rescheduled. Once your facility is cleaned and disinfected and staff have been cleared, your office may reopen.
Use enhanced precautions for any staff or patients who are immunocompromised, or otherwise fall into the high-risk category, to keep them out of the path of potential exposure areas and allow them to self-quarantine if they desire.

You should continue following existing leave policies (paid time off, vacation, sick, short-term disability, leave of absence, Family and Medical Leave Act, and Americans with Disabilities Act). If the employee was exposed at work, contact your workers’ compensation carrier regarding lost wages. Unless your state laws specify otherwise, you are under no obligation to pay beyond your policies, but you may do so if you choose.
Of course, you can take proactive steps to prevent unnecessary exposure and avoid closures in the first place; for example:
- Call patients prior to their visit, or question them upon arrival, regarding fever, shortness of breath, and other COVID-19 symptoms.
- Check employees’ temperatures every morning.
- Check patients’ temperatures as they enter the office.
- Require everyone, patients and employees alike, to wear face coverings.
- Ask patients to leave friends and family members at home.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
An increasingly common question I’m receiving is:
As always, it depends, but here is some general advice: The specifics will vary depending on state/local laws, or your particular situation.
First, you need to determine the level of exposure, and whether it requires action. According to the Centers for Disease Control and Prevention, actionable exposure occurs 2 days prior to the onset of illness, and lasts 10 days after onset.
If action is required, you’ll need to determine who needs to quarantine and who needs to be tested. Vaccinated employees who have been exposed to suspected or confirmed COVID-19 are not required to quarantine or be tested if they are fully vaccinated and have remained asymptomatic since the exposure. Those employees should, however, follow all the usual precautions (masks, social distancing, handwashing, etc.) with increased diligence. Remind them that no vaccine is 100% effective, and suggest they self-monitor for symptoms (fever, cough, shortness of breath, etc.)
All other exposed employees should be tested. A negative test means an individual was not infected at the time the sample was collected, but that does not mean an individual will not get sick later. Some providers are retesting on days 5 and 7 post exposure.
Some experts advise that you monitor exposed employees (vaccinated or not) yourself, with daily temperature readings and inquiries regarding symptoms, and perhaps a daily pulse oximetry check, for 14 days following exposure. Document these screenings in writing. Anyone testing positive or developing a fever or other symptoms should, of course, be sent home and seek medical treatment as necessary.
Employees who develop symptoms or test positive for COVID-19 should remain out of work until all CDC “return-to-work” criteria are met. At this writing, the basic criteria include:
- At least 10 days pass after symptoms first appeared
- At least 24 hours pass after last fever without the use of fever-reducing medications
- Cough, shortness of breath, and any other symptoms improve
Anyone who is significantly immunocompromised may need more time at home, and probably consultation with an infectious disease specialist.
Your facility should be thoroughly cleaned after the exposure. Close off all areas used by the sick individual, and clean and disinfect all areas such as offices, doorknobs, bathrooms, common areas, and shared electronic equipment. Of course, the cleaners should wear gowns, gloves, masks, and goggles. Some practices are hiring cleaning crews to professionally disinfect their offices. Once the area has been disinfected, it can be reopened for use. Workers without close contact with the person who is sick can return to work immediately after disinfection.
If the potential infected area is widespread and cannot be isolated to a room or rooms where doors can be shut, it may be prudent to temporarily close your office, send staff home, and divert patients to other locations if they cannot be rescheduled. Once your facility is cleaned and disinfected and staff have been cleared, your office may reopen.
Use enhanced precautions for any staff or patients who are immunocompromised, or otherwise fall into the high-risk category, to keep them out of the path of potential exposure areas and allow them to self-quarantine if they desire.
You should continue following existing leave policies (paid time off, vacation, sick, short-term disability, leave of absence, Family and Medical Leave Act, and Americans with Disabilities Act). If the employee was exposed at work, contact your workers’ compensation carrier regarding lost wages. Unless your state laws specify otherwise, you are under no obligation to pay beyond your policies, but you may do so if you choose.
Of course, you can take proactive steps to prevent unnecessary exposure and avoid closures in the first place; for example:
- Call patients prior to their visit, or question them upon arrival, regarding fever, shortness of breath, and other COVID-19 symptoms.
- Check employees’ temperatures every morning.
- Check patients’ temperatures as they enter the office.
- Require everyone, patients and employees alike, to wear face coverings.
- Ask patients to leave friends and family members at home.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
An increasingly common question I’m receiving is:
As always, it depends, but here is some general advice: The specifics will vary depending on state/local laws, or your particular situation.
First, you need to determine the level of exposure, and whether it requires action. According to the Centers for Disease Control and Prevention, actionable exposure occurs 2 days prior to the onset of illness, and lasts 10 days after onset.
If action is required, you’ll need to determine who needs to quarantine and who needs to be tested. Vaccinated employees who have been exposed to suspected or confirmed COVID-19 are not required to quarantine or be tested if they are fully vaccinated and have remained asymptomatic since the exposure. Those employees should, however, follow all the usual precautions (masks, social distancing, handwashing, etc.) with increased diligence. Remind them that no vaccine is 100% effective, and suggest they self-monitor for symptoms (fever, cough, shortness of breath, etc.)
All other exposed employees should be tested. A negative test means an individual was not infected at the time the sample was collected, but that does not mean an individual will not get sick later. Some providers are retesting on days 5 and 7 post exposure.
Some experts advise that you monitor exposed employees (vaccinated or not) yourself, with daily temperature readings and inquiries regarding symptoms, and perhaps a daily pulse oximetry check, for 14 days following exposure. Document these screenings in writing. Anyone testing positive or developing a fever or other symptoms should, of course, be sent home and seek medical treatment as necessary.
Employees who develop symptoms or test positive for COVID-19 should remain out of work until all CDC “return-to-work” criteria are met. At this writing, the basic criteria include:
- At least 10 days pass after symptoms first appeared
- At least 24 hours pass after last fever without the use of fever-reducing medications
- Cough, shortness of breath, and any other symptoms improve
Anyone who is significantly immunocompromised may need more time at home, and probably consultation with an infectious disease specialist.
Your facility should be thoroughly cleaned after the exposure. Close off all areas used by the sick individual, and clean and disinfect all areas such as offices, doorknobs, bathrooms, common areas, and shared electronic equipment. Of course, the cleaners should wear gowns, gloves, masks, and goggles. Some practices are hiring cleaning crews to professionally disinfect their offices. Once the area has been disinfected, it can be reopened for use. Workers without close contact with the person who is sick can return to work immediately after disinfection.
If the potential infected area is widespread and cannot be isolated to a room or rooms where doors can be shut, it may be prudent to temporarily close your office, send staff home, and divert patients to other locations if they cannot be rescheduled. Once your facility is cleaned and disinfected and staff have been cleared, your office may reopen.
Use enhanced precautions for any staff or patients who are immunocompromised, or otherwise fall into the high-risk category, to keep them out of the path of potential exposure areas and allow them to self-quarantine if they desire.
You should continue following existing leave policies (paid time off, vacation, sick, short-term disability, leave of absence, Family and Medical Leave Act, and Americans with Disabilities Act). If the employee was exposed at work, contact your workers’ compensation carrier regarding lost wages. Unless your state laws specify otherwise, you are under no obligation to pay beyond your policies, but you may do so if you choose.
Of course, you can take proactive steps to prevent unnecessary exposure and avoid closures in the first place; for example:
- Call patients prior to their visit, or question them upon arrival, regarding fever, shortness of breath, and other COVID-19 symptoms.
- Check employees’ temperatures every morning.
- Check patients’ temperatures as they enter the office.
- Require everyone, patients and employees alike, to wear face coverings.
- Ask patients to leave friends and family members at home.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.

One-third of health care workers leery of getting COVID-19 vaccine, survey shows
Moreover, 54% of direct care providers indicated that they would take the vaccine if offered, compared with 60% of noncare providers.
The findings come from what is believed to be the largest survey of health care provider attitudes toward COVID-19 vaccination, published online Jan. 25 in Clinical Infectious Diseases.
“We have shown that self-reported willingness to receive vaccination against COVID-19 differs by age, gender, race and hospital role, with physicians and research scientists showing the highest acceptance,” Jana Shaw, MD, MPH, State University of New York, Syracuse, N.Y, the study’s corresponding author, told this news organization. “Building trust in authorities and confidence in vaccines is a complex and time-consuming process that requires commitment and resources. We have to make those investments as hesitancy can severely undermine vaccination coverage. Because health care providers are members of our communities, it is possible that their views are shared by the public at large. Our findings can assist public health professionals as a starting point of discussion and engagement with communities to ensure that we vaccinate at least 80% of the public to end the pandemic.”
For the study, Dr. Shaw and her colleagues emailed an anonymous survey to 9,565 employees of State University of New York Upstate Medical University, Syracuse, an academic medical center that cares for an estimated 1.8 million people. The survey, which contained questions intended to evaluate attitudes, belief, and willingness to get vaccinated, took place between Nov. 23 and Dec. 5, about a week before the U.S. Food and Drug Administration granted the first emergency use authorization for the Pfizer-BioNTech BNT162b2 mRNA vaccine.
Survey recipients included physicians, nurse practitioners, physician assistants, nurses, pharmacists, medical and nursing students, allied health professionals, and nonclinical ancillary staff.
Of the 9,565 surveys sent, 5,287 responses were collected and used in the final analysis, for a response rate of 55%. The mean age of respondents was 43, 73% were female, 85% were White, 6% were Asian, 5% were Black/African American, and the rest were Native American, Native Hawaiian/Pacific Islander, or from other races. More than half of respondents (59%) reported that they provided direct patient care, and 32% said they provided care for patients with COVID-19.
Of all survey respondents, 58% expressed their intent to receive a COVID-19 vaccine, but this varied by their role in the health care system. For example, in response to the statement, “If a vaccine were offered free of charge, I would take it,” 80% of scientists and physicians agreed that they would, while colleagues in other roles were unsure whether they would take the vaccine, including 34% of registered nurses, 32% of allied health professionals, and 32% of master’s-level clinicians. These differences across roles were significant (P less than .001).
The researchers also found that direct patient care or care for COVID-19 patients was associated with lower vaccination intent. For example, 54% of direct care providers and 62% of non-care providers indicated they would take the vaccine if offered, compared with 52% of those who had provided care for COVID-19 patients vs. 61% of those who had not (P less than .001).
“This was a really surprising finding,” said Dr. Shaw, who is a pediatric infectious diseases physician at SUNY Upstate. “In general, one would expect that perceived severity of disease would lead to a greater desire to get vaccinated. Because our question did not address severity of disease, it is possible that we oversampled respondents who took care of patients with mild disease (i.e., in an outpatient setting). This could have led to an underestimation of disease severity and resulted in lower vaccination intent.”
A focus on rebuilding trust
Survey respondents who agreed or strongly agreed that they would accept a vaccine were older (a mean age of 44 years), compared with those who were not sure or who disagreed (a mean age of 42 vs. 38 years, respectively; P less than .001). In addition, fewer females agreed or strongly agreed that they would accept a vaccine (54% vs. 73% of males), whereas those who self-identified as Black/African American were least likely to want to get vaccinated, compared with those from other ethnic groups (31%, compared with 74% of Asians, 58% of Whites, and 39% of American Indians or Alaska Natives).
“We are deeply aware of the poor decisions scientists made in the past, which led to a prevailing skepticism and ‘feeling like guinea pigs’ among people of color, especially Black adults,” Dr. Shaw said. “Black adults are less likely, compared [with] White adults, to have confidence that scientists act in the public interest. Rebuilding trust will take time and has to start with addressing health care disparities. In addition, we need to acknowledge contributions of Black researchers to science. For example, until recently very few knew that the Moderna vaccine was developed [with the help of] Dr. Kizzmekia Corbett, who is Black.”
The top five main areas of unease that all respondents expressed about a COVID-19 vaccine were concern about adverse events/side effects (47%), efficacy (15%), rushed release (11%), safety (11%), and the research and authorization process (3%).
“I think it is important that fellow clinicians recognize that, in order to boost vaccine confidence we will need careful, individually tailored communication strategies,” Dr. Shaw said. “A consideration should be given to those [strategies] that utilize interpersonal channels that deliver leadership by example and leverage influencers in the institution to encourage wider adoption of vaccination.”
Aaron M. Milstone, MD, MHS, asked to comment on the research, recommended that health care workers advocate for the vaccine and encourage their patients, friends, and loved ones to get vaccinated. “Soon, COVID-19 will have taken more than half a million lives in the U.S.,” said Dr. Milstone, a pediatric epidemiologist at Johns Hopkins University, Baltimore. “Although vaccines can have side effects like fever and muscle aches, and very, very rare more serious side effects, the risks of dying from COVID are much greater than the risk of a serious vaccine reaction. The study’s authors shed light on the ongoing need for leaders of all communities to support the COVID vaccines, not just the scientific community, but religious leaders, political leaders, and community leaders.”
Addressing vaccine hesitancy
Informed by their own survey, Dr. Shaw and her colleagues have developed a plan to address vaccine hesitancy to ensure high vaccine uptake at SUNY Upstate. Those strategies include, but aren’t limited to, institution-wide forums for all employees on COVID-19 vaccine safety, risks, and benefits followed by Q&A sessions, grand rounds for providers summarizing clinical trial data on mRNA vaccines, development of an Ask COVID email line for staff to ask vaccine-related questions, and a detailed vaccine-specific FAQ document.
In addition, SUNY Upstate experts have engaged in numerous media interviews to provide education and updates on the benefits of vaccination to public and staff, stationary vaccine locations, and mobile COVID-19 vaccine carts. “To date, the COVID-19 vaccination process has been well received, and we anticipate strong vaccine uptake,” she said.
Dr. Shaw acknowledged certain limitations of the survey, including its cross-sectional design and the fact that it was conducted in a single health care system in the northeastern United States. “Thus, generalizability to other regions of the U.S. and other countries may be limited,” Dr. Shaw said. “The study was also conducted before EUA [emergency use authorization] was granted to either the Moderna or Pfizer-BioNTech vaccines. It is therefore likely that vaccine acceptance will change over time as more people get vaccinated.”
The authors have disclosed no relevant financial relationships. Dr. Milstone disclosed that he has received a research grant from Merck, but it is not related to vaccines.
A version of this article first appeared on Medscape.com.
Moreover, 54% of direct care providers indicated that they would take the vaccine if offered, compared with 60% of noncare providers.
The findings come from what is believed to be the largest survey of health care provider attitudes toward COVID-19 vaccination, published online Jan. 25 in Clinical Infectious Diseases.
“We have shown that self-reported willingness to receive vaccination against COVID-19 differs by age, gender, race and hospital role, with physicians and research scientists showing the highest acceptance,” Jana Shaw, MD, MPH, State University of New York, Syracuse, N.Y, the study’s corresponding author, told this news organization. “Building trust in authorities and confidence in vaccines is a complex and time-consuming process that requires commitment and resources. We have to make those investments as hesitancy can severely undermine vaccination coverage. Because health care providers are members of our communities, it is possible that their views are shared by the public at large. Our findings can assist public health professionals as a starting point of discussion and engagement with communities to ensure that we vaccinate at least 80% of the public to end the pandemic.”
For the study, Dr. Shaw and her colleagues emailed an anonymous survey to 9,565 employees of State University of New York Upstate Medical University, Syracuse, an academic medical center that cares for an estimated 1.8 million people. The survey, which contained questions intended to evaluate attitudes, belief, and willingness to get vaccinated, took place between Nov. 23 and Dec. 5, about a week before the U.S. Food and Drug Administration granted the first emergency use authorization for the Pfizer-BioNTech BNT162b2 mRNA vaccine.
Survey recipients included physicians, nurse practitioners, physician assistants, nurses, pharmacists, medical and nursing students, allied health professionals, and nonclinical ancillary staff.
Of the 9,565 surveys sent, 5,287 responses were collected and used in the final analysis, for a response rate of 55%. The mean age of respondents was 43, 73% were female, 85% were White, 6% were Asian, 5% were Black/African American, and the rest were Native American, Native Hawaiian/Pacific Islander, or from other races. More than half of respondents (59%) reported that they provided direct patient care, and 32% said they provided care for patients with COVID-19.
Of all survey respondents, 58% expressed their intent to receive a COVID-19 vaccine, but this varied by their role in the health care system. For example, in response to the statement, “If a vaccine were offered free of charge, I would take it,” 80% of scientists and physicians agreed that they would, while colleagues in other roles were unsure whether they would take the vaccine, including 34% of registered nurses, 32% of allied health professionals, and 32% of master’s-level clinicians. These differences across roles were significant (P less than .001).
The researchers also found that direct patient care or care for COVID-19 patients was associated with lower vaccination intent. For example, 54% of direct care providers and 62% of non-care providers indicated they would take the vaccine if offered, compared with 52% of those who had provided care for COVID-19 patients vs. 61% of those who had not (P less than .001).
“This was a really surprising finding,” said Dr. Shaw, who is a pediatric infectious diseases physician at SUNY Upstate. “In general, one would expect that perceived severity of disease would lead to a greater desire to get vaccinated. Because our question did not address severity of disease, it is possible that we oversampled respondents who took care of patients with mild disease (i.e., in an outpatient setting). This could have led to an underestimation of disease severity and resulted in lower vaccination intent.”
A focus on rebuilding trust
Survey respondents who agreed or strongly agreed that they would accept a vaccine were older (a mean age of 44 years), compared with those who were not sure or who disagreed (a mean age of 42 vs. 38 years, respectively; P less than .001). In addition, fewer females agreed or strongly agreed that they would accept a vaccine (54% vs. 73% of males), whereas those who self-identified as Black/African American were least likely to want to get vaccinated, compared with those from other ethnic groups (31%, compared with 74% of Asians, 58% of Whites, and 39% of American Indians or Alaska Natives).
“We are deeply aware of the poor decisions scientists made in the past, which led to a prevailing skepticism and ‘feeling like guinea pigs’ among people of color, especially Black adults,” Dr. Shaw said. “Black adults are less likely, compared [with] White adults, to have confidence that scientists act in the public interest. Rebuilding trust will take time and has to start with addressing health care disparities. In addition, we need to acknowledge contributions of Black researchers to science. For example, until recently very few knew that the Moderna vaccine was developed [with the help of] Dr. Kizzmekia Corbett, who is Black.”
The top five main areas of unease that all respondents expressed about a COVID-19 vaccine were concern about adverse events/side effects (47%), efficacy (15%), rushed release (11%), safety (11%), and the research and authorization process (3%).
“I think it is important that fellow clinicians recognize that, in order to boost vaccine confidence we will need careful, individually tailored communication strategies,” Dr. Shaw said. “A consideration should be given to those [strategies] that utilize interpersonal channels that deliver leadership by example and leverage influencers in the institution to encourage wider adoption of vaccination.”
Aaron M. Milstone, MD, MHS, asked to comment on the research, recommended that health care workers advocate for the vaccine and encourage their patients, friends, and loved ones to get vaccinated. “Soon, COVID-19 will have taken more than half a million lives in the U.S.,” said Dr. Milstone, a pediatric epidemiologist at Johns Hopkins University, Baltimore. “Although vaccines can have side effects like fever and muscle aches, and very, very rare more serious side effects, the risks of dying from COVID are much greater than the risk of a serious vaccine reaction. The study’s authors shed light on the ongoing need for leaders of all communities to support the COVID vaccines, not just the scientific community, but religious leaders, political leaders, and community leaders.”
Addressing vaccine hesitancy
Informed by their own survey, Dr. Shaw and her colleagues have developed a plan to address vaccine hesitancy to ensure high vaccine uptake at SUNY Upstate. Those strategies include, but aren’t limited to, institution-wide forums for all employees on COVID-19 vaccine safety, risks, and benefits followed by Q&A sessions, grand rounds for providers summarizing clinical trial data on mRNA vaccines, development of an Ask COVID email line for staff to ask vaccine-related questions, and a detailed vaccine-specific FAQ document.
In addition, SUNY Upstate experts have engaged in numerous media interviews to provide education and updates on the benefits of vaccination to public and staff, stationary vaccine locations, and mobile COVID-19 vaccine carts. “To date, the COVID-19 vaccination process has been well received, and we anticipate strong vaccine uptake,” she said.
Dr. Shaw acknowledged certain limitations of the survey, including its cross-sectional design and the fact that it was conducted in a single health care system in the northeastern United States. “Thus, generalizability to other regions of the U.S. and other countries may be limited,” Dr. Shaw said. “The study was also conducted before EUA [emergency use authorization] was granted to either the Moderna or Pfizer-BioNTech vaccines. It is therefore likely that vaccine acceptance will change over time as more people get vaccinated.”
The authors have disclosed no relevant financial relationships. Dr. Milstone disclosed that he has received a research grant from Merck, but it is not related to vaccines.
A version of this article first appeared on Medscape.com.
Moreover, 54% of direct care providers indicated that they would take the vaccine if offered, compared with 60% of noncare providers.
The findings come from what is believed to be the largest survey of health care provider attitudes toward COVID-19 vaccination, published online Jan. 25 in Clinical Infectious Diseases.
“We have shown that self-reported willingness to receive vaccination against COVID-19 differs by age, gender, race and hospital role, with physicians and research scientists showing the highest acceptance,” Jana Shaw, MD, MPH, State University of New York, Syracuse, N.Y, the study’s corresponding author, told this news organization. “Building trust in authorities and confidence in vaccines is a complex and time-consuming process that requires commitment and resources. We have to make those investments as hesitancy can severely undermine vaccination coverage. Because health care providers are members of our communities, it is possible that their views are shared by the public at large. Our findings can assist public health professionals as a starting point of discussion and engagement with communities to ensure that we vaccinate at least 80% of the public to end the pandemic.”
For the study, Dr. Shaw and her colleagues emailed an anonymous survey to 9,565 employees of State University of New York Upstate Medical University, Syracuse, an academic medical center that cares for an estimated 1.8 million people. The survey, which contained questions intended to evaluate attitudes, belief, and willingness to get vaccinated, took place between Nov. 23 and Dec. 5, about a week before the U.S. Food and Drug Administration granted the first emergency use authorization for the Pfizer-BioNTech BNT162b2 mRNA vaccine.
Survey recipients included physicians, nurse practitioners, physician assistants, nurses, pharmacists, medical and nursing students, allied health professionals, and nonclinical ancillary staff.
Of the 9,565 surveys sent, 5,287 responses were collected and used in the final analysis, for a response rate of 55%. The mean age of respondents was 43, 73% were female, 85% were White, 6% were Asian, 5% were Black/African American, and the rest were Native American, Native Hawaiian/Pacific Islander, or from other races. More than half of respondents (59%) reported that they provided direct patient care, and 32% said they provided care for patients with COVID-19.
Of all survey respondents, 58% expressed their intent to receive a COVID-19 vaccine, but this varied by their role in the health care system. For example, in response to the statement, “If a vaccine were offered free of charge, I would take it,” 80% of scientists and physicians agreed that they would, while colleagues in other roles were unsure whether they would take the vaccine, including 34% of registered nurses, 32% of allied health professionals, and 32% of master’s-level clinicians. These differences across roles were significant (P less than .001).
The researchers also found that direct patient care or care for COVID-19 patients was associated with lower vaccination intent. For example, 54% of direct care providers and 62% of non-care providers indicated they would take the vaccine if offered, compared with 52% of those who had provided care for COVID-19 patients vs. 61% of those who had not (P less than .001).
“This was a really surprising finding,” said Dr. Shaw, who is a pediatric infectious diseases physician at SUNY Upstate. “In general, one would expect that perceived severity of disease would lead to a greater desire to get vaccinated. Because our question did not address severity of disease, it is possible that we oversampled respondents who took care of patients with mild disease (i.e., in an outpatient setting). This could have led to an underestimation of disease severity and resulted in lower vaccination intent.”
A focus on rebuilding trust
Survey respondents who agreed or strongly agreed that they would accept a vaccine were older (a mean age of 44 years), compared with those who were not sure or who disagreed (a mean age of 42 vs. 38 years, respectively; P less than .001). In addition, fewer females agreed or strongly agreed that they would accept a vaccine (54% vs. 73% of males), whereas those who self-identified as Black/African American were least likely to want to get vaccinated, compared with those from other ethnic groups (31%, compared with 74% of Asians, 58% of Whites, and 39% of American Indians or Alaska Natives).
“We are deeply aware of the poor decisions scientists made in the past, which led to a prevailing skepticism and ‘feeling like guinea pigs’ among people of color, especially Black adults,” Dr. Shaw said. “Black adults are less likely, compared [with] White adults, to have confidence that scientists act in the public interest. Rebuilding trust will take time and has to start with addressing health care disparities. In addition, we need to acknowledge contributions of Black researchers to science. For example, until recently very few knew that the Moderna vaccine was developed [with the help of] Dr. Kizzmekia Corbett, who is Black.”
The top five main areas of unease that all respondents expressed about a COVID-19 vaccine were concern about adverse events/side effects (47%), efficacy (15%), rushed release (11%), safety (11%), and the research and authorization process (3%).
“I think it is important that fellow clinicians recognize that, in order to boost vaccine confidence we will need careful, individually tailored communication strategies,” Dr. Shaw said. “A consideration should be given to those [strategies] that utilize interpersonal channels that deliver leadership by example and leverage influencers in the institution to encourage wider adoption of vaccination.”
Aaron M. Milstone, MD, MHS, asked to comment on the research, recommended that health care workers advocate for the vaccine and encourage their patients, friends, and loved ones to get vaccinated. “Soon, COVID-19 will have taken more than half a million lives in the U.S.,” said Dr. Milstone, a pediatric epidemiologist at Johns Hopkins University, Baltimore. “Although vaccines can have side effects like fever and muscle aches, and very, very rare more serious side effects, the risks of dying from COVID are much greater than the risk of a serious vaccine reaction. The study’s authors shed light on the ongoing need for leaders of all communities to support the COVID vaccines, not just the scientific community, but religious leaders, political leaders, and community leaders.”
Addressing vaccine hesitancy
Informed by their own survey, Dr. Shaw and her colleagues have developed a plan to address vaccine hesitancy to ensure high vaccine uptake at SUNY Upstate. Those strategies include, but aren’t limited to, institution-wide forums for all employees on COVID-19 vaccine safety, risks, and benefits followed by Q&A sessions, grand rounds for providers summarizing clinical trial data on mRNA vaccines, development of an Ask COVID email line for staff to ask vaccine-related questions, and a detailed vaccine-specific FAQ document.
In addition, SUNY Upstate experts have engaged in numerous media interviews to provide education and updates on the benefits of vaccination to public and staff, stationary vaccine locations, and mobile COVID-19 vaccine carts. “To date, the COVID-19 vaccination process has been well received, and we anticipate strong vaccine uptake,” she said.
Dr. Shaw acknowledged certain limitations of the survey, including its cross-sectional design and the fact that it was conducted in a single health care system in the northeastern United States. “Thus, generalizability to other regions of the U.S. and other countries may be limited,” Dr. Shaw said. “The study was also conducted before EUA [emergency use authorization] was granted to either the Moderna or Pfizer-BioNTech vaccines. It is therefore likely that vaccine acceptance will change over time as more people get vaccinated.”
The authors have disclosed no relevant financial relationships. Dr. Milstone disclosed that he has received a research grant from Merck, but it is not related to vaccines.
A version of this article first appeared on Medscape.com.
Survey: Most patients support teledermatology
Many medical practices turned to telemedicine when the pandemic shut down the economy last spring, but what do dermatology patients think about the socially distant approach?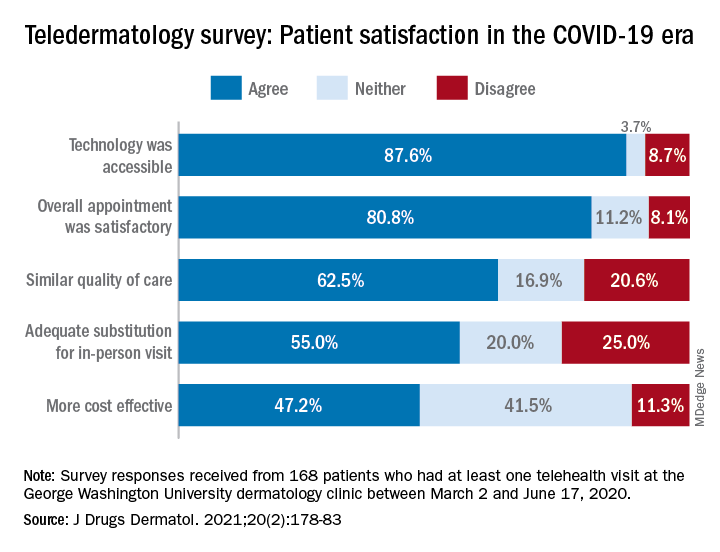
and 80% said that they would consider another such visit in the future, according to a survey conducted at George Washington University in Washington.
Although “telehealth is not without its drawbacks … it is clear from this study that the majority of patients feel positively towards teledermatology during the COVID-19 pandemic and [believe it] can be a suitable alternative for patients who are unable to meet with their providers in person,” Samuel Yeroushalmi, Sarah H. Millan, and associates at the university said in the Journal of Drugs in Dermatology.
When presented with a set of statements about the telehealth experience, the 168 survey respondents largely agreed that the overall appointment was satisfactory (80.8%), that minimal barriers were present (78.1%), and that the quality of care was similar to an in-person visit (62.5%), the investigators said.
Other factors, however, were not as well supported. Less than half (47.2%) of the respondents agreed that the telehealth appointments were more cost effective, and just over half (54.7%) agreed that they provided an adequate skin exam, they reported.
Of the set of 14 statements given to the patients – all of whom had at least one telehealth visit with the GW clinic between March 2 and June 17, 2020 – the one on the adequacy of the skin exam provided the largest share of disagreement at 27.1%, Mr. Yeroushalmi and Ms. Millan, medical students at the university and coauthors.
The lack of physical touch was mentioned most often (26.8%) when respondents were asked about their reasons for disliking telehealth visits, followed by the feeling that they had received an inadequate assessment (15.7%), they said.
Despite these drawbacks, “the convenience and efficacy of telehealth as well as its ability to maintain separation while social distancing recommendations are in place make it an effective way for dermatologists to continue to provide quality and safe care during the pandemics as well as during potential future public health crises,” the investigators concluded.
Many medical practices turned to telemedicine when the pandemic shut down the economy last spring, but what do dermatology patients think about the socially distant approach?
and 80% said that they would consider another such visit in the future, according to a survey conducted at George Washington University in Washington.
Although “telehealth is not without its drawbacks … it is clear from this study that the majority of patients feel positively towards teledermatology during the COVID-19 pandemic and [believe it] can be a suitable alternative for patients who are unable to meet with their providers in person,” Samuel Yeroushalmi, Sarah H. Millan, and associates at the university said in the Journal of Drugs in Dermatology.
When presented with a set of statements about the telehealth experience, the 168 survey respondents largely agreed that the overall appointment was satisfactory (80.8%), that minimal barriers were present (78.1%), and that the quality of care was similar to an in-person visit (62.5%), the investigators said.
Other factors, however, were not as well supported. Less than half (47.2%) of the respondents agreed that the telehealth appointments were more cost effective, and just over half (54.7%) agreed that they provided an adequate skin exam, they reported.
Of the set of 14 statements given to the patients – all of whom had at least one telehealth visit with the GW clinic between March 2 and June 17, 2020 – the one on the adequacy of the skin exam provided the largest share of disagreement at 27.1%, Mr. Yeroushalmi and Ms. Millan, medical students at the university and coauthors.
The lack of physical touch was mentioned most often (26.8%) when respondents were asked about their reasons for disliking telehealth visits, followed by the feeling that they had received an inadequate assessment (15.7%), they said.
Despite these drawbacks, “the convenience and efficacy of telehealth as well as its ability to maintain separation while social distancing recommendations are in place make it an effective way for dermatologists to continue to provide quality and safe care during the pandemics as well as during potential future public health crises,” the investigators concluded.
Many medical practices turned to telemedicine when the pandemic shut down the economy last spring, but what do dermatology patients think about the socially distant approach?
and 80% said that they would consider another such visit in the future, according to a survey conducted at George Washington University in Washington.
Although “telehealth is not without its drawbacks … it is clear from this study that the majority of patients feel positively towards teledermatology during the COVID-19 pandemic and [believe it] can be a suitable alternative for patients who are unable to meet with their providers in person,” Samuel Yeroushalmi, Sarah H. Millan, and associates at the university said in the Journal of Drugs in Dermatology.
When presented with a set of statements about the telehealth experience, the 168 survey respondents largely agreed that the overall appointment was satisfactory (80.8%), that minimal barriers were present (78.1%), and that the quality of care was similar to an in-person visit (62.5%), the investigators said.
Other factors, however, were not as well supported. Less than half (47.2%) of the respondents agreed that the telehealth appointments were more cost effective, and just over half (54.7%) agreed that they provided an adequate skin exam, they reported.
Of the set of 14 statements given to the patients – all of whom had at least one telehealth visit with the GW clinic between March 2 and June 17, 2020 – the one on the adequacy of the skin exam provided the largest share of disagreement at 27.1%, Mr. Yeroushalmi and Ms. Millan, medical students at the university and coauthors.
The lack of physical touch was mentioned most often (26.8%) when respondents were asked about their reasons for disliking telehealth visits, followed by the feeling that they had received an inadequate assessment (15.7%), they said.
Despite these drawbacks, “the convenience and efficacy of telehealth as well as its ability to maintain separation while social distancing recommendations are in place make it an effective way for dermatologists to continue to provide quality and safe care during the pandemics as well as during potential future public health crises,” the investigators concluded.
FROM JOURNAL OF DRUGS IN DERMATOLOGY
COVID-19: Helping patients overcome what might feel like an existential crisis
Way back in the spring of last year, I wrote about a pandemic of posttraumatic stress disorder that would descend upon us because of COVID-19. At the time, we were told that, by summer – June or July 2020 – all the steps we needed to take to stay ahead of the virus, including remaining socially distant, and yes, even wearing masks, would be over. Life would get back to normal.

Little did we know that a national plan for our safety, including making sure that we had enough masks and PPE, would not be forthcoming, and that so many thousands of Americans would perish, leaving millions of distraught families and friends.
So many people are suffering. Mothers, for example, are struggling to balance remote schooling with additional child care and domestic work. More than 2 million women left the U.S. workforce last year between February 2020 and October 2020, according to a report by the National Women’s Law Center. Even before COVID-19, loneliness among young adults was considered a domestic epidemic – and the social isolation forced by the pandemic has worsened those trends, research shows. These trends are creating so much more anxiety, depression, despair, and yes, even PTSD. As mental health professionals, we have a lot of work to do in educating people about coping skills and in providing treatments when appropriate.
Experiences take on new meaning
One day a friend and professional colleague called me, and he sounded quite distraught. He had not been able to reach his primary care physician and thought that, as a physician, I might have some insights about his symptoms. He began telling me that something really strange was happening whenever he walked around outside with his mask on. He couldn’t breathe with it on, he told me. In addition, his eyes teared up, his nose started running, and his eyeglasses fogged up so much that he couldn’t see where he was going. He was really anxious, nervous, and felt a great sense of despair – and disorientation. He did not fully understand what was happening and didn’t know whether those disorienting symptoms were mask-related or whether he was incubating some yet undiagnosed illness.
I addressed his concerns in the moment by assuring him that I, too, had been experiencing similar challenges with fogged-up glasses and a runny nose; many people were experiencing some of the same things. I explained that even I had called an allergist to find out whether I might be allergic to some component in the mask and whether he had seen those symptoms in his practice.
Albeit, those issues tied to masks are relatively minor, compared with the enormous psychological toll this pandemic has taken on some people. But it’s clear that different people suffer different effects in light of the marked changes in life and lifestyles caused by the pandemic.
‘It’s something else’
Two people I know, both professionals, recently told me that in their social lives they constantly feel tired and anxious, and that their concentration has diminished. They worry more about their futures, they told me separately. (They don’t know each other.) They reported going through daily life “like being on automatic.” Both said they were far too irritable and reported feeling that social isolation had dulled their thinking.
They said they were not depressed; “it’s something else.” I reassured them both that this would pass with time and suggested that they work at not socially isolating – to the extent that they can – during the pandemic. I also encouraged them to get vaccinated and to talk with a professional if their malaise was altering their level of functioning.
So far, more than 475,000 people in the United States have died of COVID-19, and thousands continue to suffer. People are saying goodbye to loved ones on iPads, and watching news stories about hospitals at overcapacity and refrigeration units storing bodies. Meanwhile, health care workers, many of whom are putting their lives and those of their families at risk, are reporting increased levels of burnout – and moral injury.
Value of relaxation techniques
We know that the latest mitigation measures advised by the Centers for Disease Control and Prevention must continue during the COVID-19 vaccination process. The new CDC guidelines on the value of double masking make sense and should be followed. However, even as we learn more about the virus and how to stop its spread, we must recognize that social distancing is not the same as social isolation. We must continue to do what we can to maintain social relationships and keep open the lines of communication, including the use of virtual tools. I am pleased to see the growth of telemedicine during the pandemic. When applicable, telemedicine allows greater medical and mental health care without the stress of travel and the risk of exposure to more people than necessary.
, whether it’s hypnosis, mindfulness, transcendental meditation, or deep breathing exercises. For the more advanced therapies, guided imagery can help patients develop a sense of calm and equanimity.
For those who are not skilled in relaxation techniques, YouTube offers some excellent programs that teach relaxation and mindfulness. Another thing I do is talk regularly with people I know and sometimes with people I know I’ll disagree with – just to keep my brain active. I also try to learn new things in my spare time to establish new brain pathways and stay mentally active.
The pain and grief tied to the pandemic are unlike anything we’ve ever experienced. Our training as psychiatrists, psychologists, and other mental health care professionals makes us all uniquely suited to assist patients as they process these traumatic times. We must step forward and do so.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (Kettlehole Publishing, 2019). He has no conflicts of interest.
Way back in the spring of last year, I wrote about a pandemic of posttraumatic stress disorder that would descend upon us because of COVID-19. At the time, we were told that, by summer – June or July 2020 – all the steps we needed to take to stay ahead of the virus, including remaining socially distant, and yes, even wearing masks, would be over. Life would get back to normal.
Little did we know that a national plan for our safety, including making sure that we had enough masks and PPE, would not be forthcoming, and that so many thousands of Americans would perish, leaving millions of distraught families and friends.
So many people are suffering. Mothers, for example, are struggling to balance remote schooling with additional child care and domestic work. More than 2 million women left the U.S. workforce last year between February 2020 and October 2020, according to a report by the National Women’s Law Center. Even before COVID-19, loneliness among young adults was considered a domestic epidemic – and the social isolation forced by the pandemic has worsened those trends, research shows. These trends are creating so much more anxiety, depression, despair, and yes, even PTSD. As mental health professionals, we have a lot of work to do in educating people about coping skills and in providing treatments when appropriate.
Experiences take on new meaning
One day a friend and professional colleague called me, and he sounded quite distraught. He had not been able to reach his primary care physician and thought that, as a physician, I might have some insights about his symptoms. He began telling me that something really strange was happening whenever he walked around outside with his mask on. He couldn’t breathe with it on, he told me. In addition, his eyes teared up, his nose started running, and his eyeglasses fogged up so much that he couldn’t see where he was going. He was really anxious, nervous, and felt a great sense of despair – and disorientation. He did not fully understand what was happening and didn’t know whether those disorienting symptoms were mask-related or whether he was incubating some yet undiagnosed illness.
I addressed his concerns in the moment by assuring him that I, too, had been experiencing similar challenges with fogged-up glasses and a runny nose; many people were experiencing some of the same things. I explained that even I had called an allergist to find out whether I might be allergic to some component in the mask and whether he had seen those symptoms in his practice.
Albeit, those issues tied to masks are relatively minor, compared with the enormous psychological toll this pandemic has taken on some people. But it’s clear that different people suffer different effects in light of the marked changes in life and lifestyles caused by the pandemic.
‘It’s something else’
Two people I know, both professionals, recently told me that in their social lives they constantly feel tired and anxious, and that their concentration has diminished. They worry more about their futures, they told me separately. (They don’t know each other.) They reported going through daily life “like being on automatic.” Both said they were far too irritable and reported feeling that social isolation had dulled their thinking.
They said they were not depressed; “it’s something else.” I reassured them both that this would pass with time and suggested that they work at not socially isolating – to the extent that they can – during the pandemic. I also encouraged them to get vaccinated and to talk with a professional if their malaise was altering their level of functioning.
So far, more than 475,000 people in the United States have died of COVID-19, and thousands continue to suffer. People are saying goodbye to loved ones on iPads, and watching news stories about hospitals at overcapacity and refrigeration units storing bodies. Meanwhile, health care workers, many of whom are putting their lives and those of their families at risk, are reporting increased levels of burnout – and moral injury.
Value of relaxation techniques
We know that the latest mitigation measures advised by the Centers for Disease Control and Prevention must continue during the COVID-19 vaccination process. The new CDC guidelines on the value of double masking make sense and should be followed. However, even as we learn more about the virus and how to stop its spread, we must recognize that social distancing is not the same as social isolation. We must continue to do what we can to maintain social relationships and keep open the lines of communication, including the use of virtual tools. I am pleased to see the growth of telemedicine during the pandemic. When applicable, telemedicine allows greater medical and mental health care without the stress of travel and the risk of exposure to more people than necessary.
, whether it’s hypnosis, mindfulness, transcendental meditation, or deep breathing exercises. For the more advanced therapies, guided imagery can help patients develop a sense of calm and equanimity.
For those who are not skilled in relaxation techniques, YouTube offers some excellent programs that teach relaxation and mindfulness. Another thing I do is talk regularly with people I know and sometimes with people I know I’ll disagree with – just to keep my brain active. I also try to learn new things in my spare time to establish new brain pathways and stay mentally active.
The pain and grief tied to the pandemic are unlike anything we’ve ever experienced. Our training as psychiatrists, psychologists, and other mental health care professionals makes us all uniquely suited to assist patients as they process these traumatic times. We must step forward and do so.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (Kettlehole Publishing, 2019). He has no conflicts of interest.
Way back in the spring of last year, I wrote about a pandemic of posttraumatic stress disorder that would descend upon us because of COVID-19. At the time, we were told that, by summer – June or July 2020 – all the steps we needed to take to stay ahead of the virus, including remaining socially distant, and yes, even wearing masks, would be over. Life would get back to normal.
Little did we know that a national plan for our safety, including making sure that we had enough masks and PPE, would not be forthcoming, and that so many thousands of Americans would perish, leaving millions of distraught families and friends.
So many people are suffering. Mothers, for example, are struggling to balance remote schooling with additional child care and domestic work. More than 2 million women left the U.S. workforce last year between February 2020 and October 2020, according to a report by the National Women’s Law Center. Even before COVID-19, loneliness among young adults was considered a domestic epidemic – and the social isolation forced by the pandemic has worsened those trends, research shows. These trends are creating so much more anxiety, depression, despair, and yes, even PTSD. As mental health professionals, we have a lot of work to do in educating people about coping skills and in providing treatments when appropriate.
Experiences take on new meaning
One day a friend and professional colleague called me, and he sounded quite distraught. He had not been able to reach his primary care physician and thought that, as a physician, I might have some insights about his symptoms. He began telling me that something really strange was happening whenever he walked around outside with his mask on. He couldn’t breathe with it on, he told me. In addition, his eyes teared up, his nose started running, and his eyeglasses fogged up so much that he couldn’t see where he was going. He was really anxious, nervous, and felt a great sense of despair – and disorientation. He did not fully understand what was happening and didn’t know whether those disorienting symptoms were mask-related or whether he was incubating some yet undiagnosed illness.
I addressed his concerns in the moment by assuring him that I, too, had been experiencing similar challenges with fogged-up glasses and a runny nose; many people were experiencing some of the same things. I explained that even I had called an allergist to find out whether I might be allergic to some component in the mask and whether he had seen those symptoms in his practice.
Albeit, those issues tied to masks are relatively minor, compared with the enormous psychological toll this pandemic has taken on some people. But it’s clear that different people suffer different effects in light of the marked changes in life and lifestyles caused by the pandemic.
‘It’s something else’
Two people I know, both professionals, recently told me that in their social lives they constantly feel tired and anxious, and that their concentration has diminished. They worry more about their futures, they told me separately. (They don’t know each other.) They reported going through daily life “like being on automatic.” Both said they were far too irritable and reported feeling that social isolation had dulled their thinking.
They said they were not depressed; “it’s something else.” I reassured them both that this would pass with time and suggested that they work at not socially isolating – to the extent that they can – during the pandemic. I also encouraged them to get vaccinated and to talk with a professional if their malaise was altering their level of functioning.
So far, more than 475,000 people in the United States have died of COVID-19, and thousands continue to suffer. People are saying goodbye to loved ones on iPads, and watching news stories about hospitals at overcapacity and refrigeration units storing bodies. Meanwhile, health care workers, many of whom are putting their lives and those of their families at risk, are reporting increased levels of burnout – and moral injury.
Value of relaxation techniques
We know that the latest mitigation measures advised by the Centers for Disease Control and Prevention must continue during the COVID-19 vaccination process. The new CDC guidelines on the value of double masking make sense and should be followed. However, even as we learn more about the virus and how to stop its spread, we must recognize that social distancing is not the same as social isolation. We must continue to do what we can to maintain social relationships and keep open the lines of communication, including the use of virtual tools. I am pleased to see the growth of telemedicine during the pandemic. When applicable, telemedicine allows greater medical and mental health care without the stress of travel and the risk of exposure to more people than necessary.
, whether it’s hypnosis, mindfulness, transcendental meditation, or deep breathing exercises. For the more advanced therapies, guided imagery can help patients develop a sense of calm and equanimity.
For those who are not skilled in relaxation techniques, YouTube offers some excellent programs that teach relaxation and mindfulness. Another thing I do is talk regularly with people I know and sometimes with people I know I’ll disagree with – just to keep my brain active. I also try to learn new things in my spare time to establish new brain pathways and stay mentally active.
The pain and grief tied to the pandemic are unlike anything we’ve ever experienced. Our training as psychiatrists, psychologists, and other mental health care professionals makes us all uniquely suited to assist patients as they process these traumatic times. We must step forward and do so.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (Kettlehole Publishing, 2019). He has no conflicts of interest.
Steroid and immunoglobulin standard of care for MIS-C
The combination of methylprednisolone and intravenous immunoglobulins works better than intravenous immunoglobulins alone for multisystem inflammatory syndrome in children (MIS-C), researchers say.
“I’m not sure it’s the best treatment because we have not studied every possible treatment,” François Angoulvant, MD, PhD, told this news organization, “but right now, it’s the standard of care.”
Dr. Angoulvant, a professor of pediatrics at University of Paris, and colleagues published a comparison of the two treatments in the Journal of the American Medical Association.
A small percentage of children infected with SARS-CoV-2 develop MIS-C about 2 to 4 weeks later. It is considered a separate disease entity from COVID-19 and is associated with persistent fever, digestive symptoms, rash, bilateral nonpurulent conjunctivitis, mucocutaneous inflammation signs, and frequent cardiovascular involvement. In more than 60% of cases, it leads to hemodynamic failure, with acute cardiac dysfunction.
Because MIS-C resembles Kawasaki disease, clinicians modeled their treatment on that condition and started with immunoglobulins alone, Dr. Angoulvant said.
Based on expert opinion, the National Health Service in the United Kingdom published a consensus statement in Sept. listing immunoglobulins alone as the first-line treatment.
But anecdotal reports have emerged that combining the immunoglobulins with a corticosteroid worked better. To investigate this possibility, Dr. Angoulvant and colleagues analyzed records of MIS-C cases in France, where physicians are required to report all suspected cases of MIS-C to the French National Public Health Agency.
Among the 181 cases they scrutinized, 111 fulfilled the World Health Organization criteria for MIS-C. Of these, the researchers were able to match 64 patients who had received immunoglobulins alone with 32 who had received the combined therapy and could be matched using propensity scores.
The researchers defined treatment failure as persistence of fever for 2 days after the start of therapy or recurrence of fever within a week. By this measure, the combination treatment failed in only 9% of cases while immunoglobulins alone failed in 38% of cases. The difference was statistically significant (P = .008). Most of those for whom these treatments failed received second-line treatments such as steroids or biological agents.
Patients treated with the combination therapy also had a lower risk of secondary acute left ventricular dysfunction (odds ratio, 0.20; 95% confidence interval, 0.06-0.66) and a lower risk of needing hemodynamic support (OR, 0.21; 95% CI, 0.06-0.76).
Those receiving the combination therapy spent a mean of 4 days in the pediatric intensive care unit compared with 6 days for those receiving immunoglobulins alone. (Difference in days, −2.4; 95% CI, −4.0 to −0.7; P = .005).
There are few drawbacks to the combination approach, Dr. Angoulvant said, as the side effects of corticosteroids are generally not severe and they can be anticipated because this class of medications has been used for many years.
The study raises the question of whether corticosteroids might work as well by themselves, but it could not be answered with this database as no one is using that approach in France, Dr. Angoulvant said. “I hope other teams around the world could bring us the answer.”
In the United States, most physicians appear to already be using the combination therapy, said David Teachey, MD, an associate professor of pediatrics at the Children’s Hospital of Philadelphia and the University of Pennsylvania, Philadelphia.
The reduction in time in pediatric intensive care and the reduced risk of cardiac dysfunction are important findings, he said.
This retrospective study falls short of the evidence provided by a randomized clinical trial, Dr. Teachey noted. But he acknowledged that few families would agree to participate in such a trial as they would have to take a chance that the sick children would receive a less effective therapy than what they would otherwise get. “It’s hard to [talk] about a therapy reduction,” he told this news organization.
Given that impediment, he agreed with Dr. Angoulvant that the current study and others like it may provide the best data available pointing to a treatment approach for MIS-C.
The study received an unrestricted grant from Pfizer. The French COVID-19 Paediatric Inflammation Consortium received an unrestricted grant from the Square Foundation (Grandir–Fonds de Solidarité pour L’Enfance). Dr. Angoulvant and Dr. Teachey have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The combination of methylprednisolone and intravenous immunoglobulins works better than intravenous immunoglobulins alone for multisystem inflammatory syndrome in children (MIS-C), researchers say.
“I’m not sure it’s the best treatment because we have not studied every possible treatment,” François Angoulvant, MD, PhD, told this news organization, “but right now, it’s the standard of care.”
Dr. Angoulvant, a professor of pediatrics at University of Paris, and colleagues published a comparison of the two treatments in the Journal of the American Medical Association.
A small percentage of children infected with SARS-CoV-2 develop MIS-C about 2 to 4 weeks later. It is considered a separate disease entity from COVID-19 and is associated with persistent fever, digestive symptoms, rash, bilateral nonpurulent conjunctivitis, mucocutaneous inflammation signs, and frequent cardiovascular involvement. In more than 60% of cases, it leads to hemodynamic failure, with acute cardiac dysfunction.
Because MIS-C resembles Kawasaki disease, clinicians modeled their treatment on that condition and started with immunoglobulins alone, Dr. Angoulvant said.
Based on expert opinion, the National Health Service in the United Kingdom published a consensus statement in Sept. listing immunoglobulins alone as the first-line treatment.
But anecdotal reports have emerged that combining the immunoglobulins with a corticosteroid worked better. To investigate this possibility, Dr. Angoulvant and colleagues analyzed records of MIS-C cases in France, where physicians are required to report all suspected cases of MIS-C to the French National Public Health Agency.
Among the 181 cases they scrutinized, 111 fulfilled the World Health Organization criteria for MIS-C. Of these, the researchers were able to match 64 patients who had received immunoglobulins alone with 32 who had received the combined therapy and could be matched using propensity scores.
The researchers defined treatment failure as persistence of fever for 2 days after the start of therapy or recurrence of fever within a week. By this measure, the combination treatment failed in only 9% of cases while immunoglobulins alone failed in 38% of cases. The difference was statistically significant (P = .008). Most of those for whom these treatments failed received second-line treatments such as steroids or biological agents.
Patients treated with the combination therapy also had a lower risk of secondary acute left ventricular dysfunction (odds ratio, 0.20; 95% confidence interval, 0.06-0.66) and a lower risk of needing hemodynamic support (OR, 0.21; 95% CI, 0.06-0.76).
Those receiving the combination therapy spent a mean of 4 days in the pediatric intensive care unit compared with 6 days for those receiving immunoglobulins alone. (Difference in days, −2.4; 95% CI, −4.0 to −0.7; P = .005).
There are few drawbacks to the combination approach, Dr. Angoulvant said, as the side effects of corticosteroids are generally not severe and they can be anticipated because this class of medications has been used for many years.
The study raises the question of whether corticosteroids might work as well by themselves, but it could not be answered with this database as no one is using that approach in France, Dr. Angoulvant said. “I hope other teams around the world could bring us the answer.”
In the United States, most physicians appear to already be using the combination therapy, said David Teachey, MD, an associate professor of pediatrics at the Children’s Hospital of Philadelphia and the University of Pennsylvania, Philadelphia.
The reduction in time in pediatric intensive care and the reduced risk of cardiac dysfunction are important findings, he said.
This retrospective study falls short of the evidence provided by a randomized clinical trial, Dr. Teachey noted. But he acknowledged that few families would agree to participate in such a trial as they would have to take a chance that the sick children would receive a less effective therapy than what they would otherwise get. “It’s hard to [talk] about a therapy reduction,” he told this news organization.
Given that impediment, he agreed with Dr. Angoulvant that the current study and others like it may provide the best data available pointing to a treatment approach for MIS-C.
The study received an unrestricted grant from Pfizer. The French COVID-19 Paediatric Inflammation Consortium received an unrestricted grant from the Square Foundation (Grandir–Fonds de Solidarité pour L’Enfance). Dr. Angoulvant and Dr. Teachey have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The combination of methylprednisolone and intravenous immunoglobulins works better than intravenous immunoglobulins alone for multisystem inflammatory syndrome in children (MIS-C), researchers say.
“I’m not sure it’s the best treatment because we have not studied every possible treatment,” François Angoulvant, MD, PhD, told this news organization, “but right now, it’s the standard of care.”
Dr. Angoulvant, a professor of pediatrics at University of Paris, and colleagues published a comparison of the two treatments in the Journal of the American Medical Association.
A small percentage of children infected with SARS-CoV-2 develop MIS-C about 2 to 4 weeks later. It is considered a separate disease entity from COVID-19 and is associated with persistent fever, digestive symptoms, rash, bilateral nonpurulent conjunctivitis, mucocutaneous inflammation signs, and frequent cardiovascular involvement. In more than 60% of cases, it leads to hemodynamic failure, with acute cardiac dysfunction.
Because MIS-C resembles Kawasaki disease, clinicians modeled their treatment on that condition and started with immunoglobulins alone, Dr. Angoulvant said.
Based on expert opinion, the National Health Service in the United Kingdom published a consensus statement in Sept. listing immunoglobulins alone as the first-line treatment.
But anecdotal reports have emerged that combining the immunoglobulins with a corticosteroid worked better. To investigate this possibility, Dr. Angoulvant and colleagues analyzed records of MIS-C cases in France, where physicians are required to report all suspected cases of MIS-C to the French National Public Health Agency.
Among the 181 cases they scrutinized, 111 fulfilled the World Health Organization criteria for MIS-C. Of these, the researchers were able to match 64 patients who had received immunoglobulins alone with 32 who had received the combined therapy and could be matched using propensity scores.
The researchers defined treatment failure as persistence of fever for 2 days after the start of therapy or recurrence of fever within a week. By this measure, the combination treatment failed in only 9% of cases while immunoglobulins alone failed in 38% of cases. The difference was statistically significant (P = .008). Most of those for whom these treatments failed received second-line treatments such as steroids or biological agents.
Patients treated with the combination therapy also had a lower risk of secondary acute left ventricular dysfunction (odds ratio, 0.20; 95% confidence interval, 0.06-0.66) and a lower risk of needing hemodynamic support (OR, 0.21; 95% CI, 0.06-0.76).
Those receiving the combination therapy spent a mean of 4 days in the pediatric intensive care unit compared with 6 days for those receiving immunoglobulins alone. (Difference in days, −2.4; 95% CI, −4.0 to −0.7; P = .005).
There are few drawbacks to the combination approach, Dr. Angoulvant said, as the side effects of corticosteroids are generally not severe and they can be anticipated because this class of medications has been used for many years.
The study raises the question of whether corticosteroids might work as well by themselves, but it could not be answered with this database as no one is using that approach in France, Dr. Angoulvant said. “I hope other teams around the world could bring us the answer.”
In the United States, most physicians appear to already be using the combination therapy, said David Teachey, MD, an associate professor of pediatrics at the Children’s Hospital of Philadelphia and the University of Pennsylvania, Philadelphia.
The reduction in time in pediatric intensive care and the reduced risk of cardiac dysfunction are important findings, he said.
This retrospective study falls short of the evidence provided by a randomized clinical trial, Dr. Teachey noted. But he acknowledged that few families would agree to participate in such a trial as they would have to take a chance that the sick children would receive a less effective therapy than what they would otherwise get. “It’s hard to [talk] about a therapy reduction,” he told this news organization.
Given that impediment, he agreed with Dr. Angoulvant that the current study and others like it may provide the best data available pointing to a treatment approach for MIS-C.
The study received an unrestricted grant from Pfizer. The French COVID-19 Paediatric Inflammation Consortium received an unrestricted grant from the Square Foundation (Grandir–Fonds de Solidarité pour L’Enfance). Dr. Angoulvant and Dr. Teachey have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
2021 ACIP adult schedule released
The Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention has updated its recommended immunization schedule for adults for 2021.
A summary of the annual update was published online Feb. 11 in the CDC’s Morbidity and Mortality Weekly Report and is available in Annals of Internal Medicine and on the CDC website.
It features a special section on vaccination during the pandemic as well as interim recommendations on administering the Pfizer-BioNtech and Moderna COVID-19 vaccines.
The authors, led by Mark S. Freedman, DVM, MPH, DACVPM, of the CDC’s National Center for Immunization and Respiratory Diseases, in Atlanta, note that this year’s recommendations for adults – persons aged 19 years and older – are largely the same as last year’s. “There have been very few changes,” Dr. Freedman said in an interview. “Changes to the schedule tables and notes were made to harmonize to the greatest extent possible the adult and child/adolescent schedules.”
Changes in the schedule include new or updated ACIP recommendations for influenza, hepatitis A, hepatitis B (Hep B), and human papillomavirus (HPV) as well as for meningococcal serogroups A, C, W, and Y (MenACYW) vaccines, meningococcal B (MenB) vaccines, and the zoster vaccine.
Vaccine-specific changes
Influenza
The schedule highlights updates to the composition of several influenza vaccines, which apply to components in both trivalent and quadrivalent formulations.
The cover page abbreviation for live attenuated influenza vaccine (LAIV) was changed to LAIV4. The abbreviation for live recombinant influenza vaccine (RIV) was changed to RIV4.
For individuals with a history of egg allergy who experience reactions other than hives, the following procedural warning has been added: “If using an influenza vaccine other than RIV4 or ccIIV4, administer in medical setting under supervision of health care provider who can recognize and manage severe allergic reactions.”
Zoster
The zoster vaccine live (Zostavax) has been removed from the schedule because it is no longer available in the United States. The recombinant zoster vaccine Shingrix remains available as a 2-dose regimen for adults aged 50 years or older.
HPV
As in previous years, HPV vaccination is routinely recommended for persons aged 11-12 years, with catch-up vaccination for those aged 26 or younger. Catch-up vaccination can be considered with shared decision making for those aged 27 through 45. In this year’s schedule, in the pregnancy column, the color pink, which formerly indicated “delay until after pregnancy,” has been replaced with red and an asterisk, indicating “vaccinate after pregnancy.”
HepB
ACIP continues to recommend vaccination of adults at risk for HepB; however, the text overlay has been changed to read, “2, 3, or 4 doses, depending on vaccine or condition.” Additionally, HepB vaccination is now routinely recommended for adults younger than 60 years with diabetes. For those with diabetes who are older than 60, shared decision making is recommended.
Meningococcal vaccine
ACIP continues to recommend routine vaccination with a quadrivalent meningococcal conjugate vaccine (MenACWY) for persons at increased risk for meningococcal disease caused by serogroups A, C, W, or Y. The MenQuadfi (MenACWY-TT) vaccine, which was first licensed in 2020, has been added to all relevant sections of MenACWY vaccines. For MenACWY booster doses, new text addresses special situations, including outbreaks.
Improvements have been made to text and layout, Dr. Freedman said. An example is the minimizing of specialized text. Other changes were made to ensure more consistent text structure and language. Various fine-tunings of color and positioning were made to the cover page and tables, and the wording of the notes sections was improved.
Vaccination in the pandemic
The updated schedule outlines guidance on the use of COVID-19 vaccines approved by the Food and Drug Administration under emergency use authorization, with interim recommendations for the Pfizer-BioNTech COVID-19 vaccine for people aged 16 and older and the Moderna COVID-19 vaccine for people aged 18 and older.
The authors stress the importance of receiving the recommended routine and catch-up immunizations notwithstanding widespread anxiety about visiting medical offices. Last spring, the CDC reported a dramatic drop in child vaccinations after the declaration of the national emergency in mid-March, a drop attributed to fear of COVID-19 exposure.
“ACIP continued to meet and make recommendations during the pandemic,” Dr. Freedman said. “Our recommendation remains that despite challenges caused by the COVID-19 pandemic, adults and their healthcare providers should follow the recommended vaccine schedule to protect against serious and sometimes deadly diseases.”
Regular vaccines can be safely administered even as COVID-19 retains its grasp on the United States. “Healthcare providers should follow the CDC’s interim guidance for the safe delivery of vaccines during the pandemic, which includes the use of personal protective equipment and physical distancing,” Dr. Freedman said.
Dr. Freedman has disclosed no relevant financial relationships. Coauthor Henry Bernstein, DO, is the editor of the Current Opinion in Pediatrics Office Pediatrics Series, is a Harvard School of Public Health faculty member, and is a member of the data safety and monitoring board for a Takeda study on intrathecal enzymes for Hunter and San Filippo syndromes. Coauthor Kevin Ault, MD, has served on the data safety and monitoring committee for ACI Clinical.
A version of this article first appeared on Medscape.com .
The Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention has updated its recommended immunization schedule for adults for 2021.
A summary of the annual update was published online Feb. 11 in the CDC’s Morbidity and Mortality Weekly Report and is available in Annals of Internal Medicine and on the CDC website.
It features a special section on vaccination during the pandemic as well as interim recommendations on administering the Pfizer-BioNtech and Moderna COVID-19 vaccines.
The authors, led by Mark S. Freedman, DVM, MPH, DACVPM, of the CDC’s National Center for Immunization and Respiratory Diseases, in Atlanta, note that this year’s recommendations for adults – persons aged 19 years and older – are largely the same as last year’s. “There have been very few changes,” Dr. Freedman said in an interview. “Changes to the schedule tables and notes were made to harmonize to the greatest extent possible the adult and child/adolescent schedules.”
Changes in the schedule include new or updated ACIP recommendations for influenza, hepatitis A, hepatitis B (Hep B), and human papillomavirus (HPV) as well as for meningococcal serogroups A, C, W, and Y (MenACYW) vaccines, meningococcal B (MenB) vaccines, and the zoster vaccine.
Vaccine-specific changes
Influenza
The schedule highlights updates to the composition of several influenza vaccines, which apply to components in both trivalent and quadrivalent formulations.
The cover page abbreviation for live attenuated influenza vaccine (LAIV) was changed to LAIV4. The abbreviation for live recombinant influenza vaccine (RIV) was changed to RIV4.
For individuals with a history of egg allergy who experience reactions other than hives, the following procedural warning has been added: “If using an influenza vaccine other than RIV4 or ccIIV4, administer in medical setting under supervision of health care provider who can recognize and manage severe allergic reactions.”
Zoster
The zoster vaccine live (Zostavax) has been removed from the schedule because it is no longer available in the United States. The recombinant zoster vaccine Shingrix remains available as a 2-dose regimen for adults aged 50 years or older.
HPV
As in previous years, HPV vaccination is routinely recommended for persons aged 11-12 years, with catch-up vaccination for those aged 26 or younger. Catch-up vaccination can be considered with shared decision making for those aged 27 through 45. In this year’s schedule, in the pregnancy column, the color pink, which formerly indicated “delay until after pregnancy,” has been replaced with red and an asterisk, indicating “vaccinate after pregnancy.”
HepB
ACIP continues to recommend vaccination of adults at risk for HepB; however, the text overlay has been changed to read, “2, 3, or 4 doses, depending on vaccine or condition.” Additionally, HepB vaccination is now routinely recommended for adults younger than 60 years with diabetes. For those with diabetes who are older than 60, shared decision making is recommended.
Meningococcal vaccine
ACIP continues to recommend routine vaccination with a quadrivalent meningococcal conjugate vaccine (MenACWY) for persons at increased risk for meningococcal disease caused by serogroups A, C, W, or Y. The MenQuadfi (MenACWY-TT) vaccine, which was first licensed in 2020, has been added to all relevant sections of MenACWY vaccines. For MenACWY booster doses, new text addresses special situations, including outbreaks.
Improvements have been made to text and layout, Dr. Freedman said. An example is the minimizing of specialized text. Other changes were made to ensure more consistent text structure and language. Various fine-tunings of color and positioning were made to the cover page and tables, and the wording of the notes sections was improved.
Vaccination in the pandemic
The updated schedule outlines guidance on the use of COVID-19 vaccines approved by the Food and Drug Administration under emergency use authorization, with interim recommendations for the Pfizer-BioNTech COVID-19 vaccine for people aged 16 and older and the Moderna COVID-19 vaccine for people aged 18 and older.
The authors stress the importance of receiving the recommended routine and catch-up immunizations notwithstanding widespread anxiety about visiting medical offices. Last spring, the CDC reported a dramatic drop in child vaccinations after the declaration of the national emergency in mid-March, a drop attributed to fear of COVID-19 exposure.
“ACIP continued to meet and make recommendations during the pandemic,” Dr. Freedman said. “Our recommendation remains that despite challenges caused by the COVID-19 pandemic, adults and their healthcare providers should follow the recommended vaccine schedule to protect against serious and sometimes deadly diseases.”
Regular vaccines can be safely administered even as COVID-19 retains its grasp on the United States. “Healthcare providers should follow the CDC’s interim guidance for the safe delivery of vaccines during the pandemic, which includes the use of personal protective equipment and physical distancing,” Dr. Freedman said.
Dr. Freedman has disclosed no relevant financial relationships. Coauthor Henry Bernstein, DO, is the editor of the Current Opinion in Pediatrics Office Pediatrics Series, is a Harvard School of Public Health faculty member, and is a member of the data safety and monitoring board for a Takeda study on intrathecal enzymes for Hunter and San Filippo syndromes. Coauthor Kevin Ault, MD, has served on the data safety and monitoring committee for ACI Clinical.
A version of this article first appeared on Medscape.com .
The Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention has updated its recommended immunization schedule for adults for 2021.
A summary of the annual update was published online Feb. 11 in the CDC’s Morbidity and Mortality Weekly Report and is available in Annals of Internal Medicine and on the CDC website.
It features a special section on vaccination during the pandemic as well as interim recommendations on administering the Pfizer-BioNtech and Moderna COVID-19 vaccines.
The authors, led by Mark S. Freedman, DVM, MPH, DACVPM, of the CDC’s National Center for Immunization and Respiratory Diseases, in Atlanta, note that this year’s recommendations for adults – persons aged 19 years and older – are largely the same as last year’s. “There have been very few changes,” Dr. Freedman said in an interview. “Changes to the schedule tables and notes were made to harmonize to the greatest extent possible the adult and child/adolescent schedules.”
Changes in the schedule include new or updated ACIP recommendations for influenza, hepatitis A, hepatitis B (Hep B), and human papillomavirus (HPV) as well as for meningococcal serogroups A, C, W, and Y (MenACYW) vaccines, meningococcal B (MenB) vaccines, and the zoster vaccine.
Vaccine-specific changes
Influenza
The schedule highlights updates to the composition of several influenza vaccines, which apply to components in both trivalent and quadrivalent formulations.
The cover page abbreviation for live attenuated influenza vaccine (LAIV) was changed to LAIV4. The abbreviation for live recombinant influenza vaccine (RIV) was changed to RIV4.
For individuals with a history of egg allergy who experience reactions other than hives, the following procedural warning has been added: “If using an influenza vaccine other than RIV4 or ccIIV4, administer in medical setting under supervision of health care provider who can recognize and manage severe allergic reactions.”
Zoster
The zoster vaccine live (Zostavax) has been removed from the schedule because it is no longer available in the United States. The recombinant zoster vaccine Shingrix remains available as a 2-dose regimen for adults aged 50 years or older.
HPV
As in previous years, HPV vaccination is routinely recommended for persons aged 11-12 years, with catch-up vaccination for those aged 26 or younger. Catch-up vaccination can be considered with shared decision making for those aged 27 through 45. In this year’s schedule, in the pregnancy column, the color pink, which formerly indicated “delay until after pregnancy,” has been replaced with red and an asterisk, indicating “vaccinate after pregnancy.”
HepB
ACIP continues to recommend vaccination of adults at risk for HepB; however, the text overlay has been changed to read, “2, 3, or 4 doses, depending on vaccine or condition.” Additionally, HepB vaccination is now routinely recommended for adults younger than 60 years with diabetes. For those with diabetes who are older than 60, shared decision making is recommended.
Meningococcal vaccine
ACIP continues to recommend routine vaccination with a quadrivalent meningococcal conjugate vaccine (MenACWY) for persons at increased risk for meningococcal disease caused by serogroups A, C, W, or Y. The MenQuadfi (MenACWY-TT) vaccine, which was first licensed in 2020, has been added to all relevant sections of MenACWY vaccines. For MenACWY booster doses, new text addresses special situations, including outbreaks.
Improvements have been made to text and layout, Dr. Freedman said. An example is the minimizing of specialized text. Other changes were made to ensure more consistent text structure and language. Various fine-tunings of color and positioning were made to the cover page and tables, and the wording of the notes sections was improved.
Vaccination in the pandemic
The updated schedule outlines guidance on the use of COVID-19 vaccines approved by the Food and Drug Administration under emergency use authorization, with interim recommendations for the Pfizer-BioNTech COVID-19 vaccine for people aged 16 and older and the Moderna COVID-19 vaccine for people aged 18 and older.
The authors stress the importance of receiving the recommended routine and catch-up immunizations notwithstanding widespread anxiety about visiting medical offices. Last spring, the CDC reported a dramatic drop in child vaccinations after the declaration of the national emergency in mid-March, a drop attributed to fear of COVID-19 exposure.
“ACIP continued to meet and make recommendations during the pandemic,” Dr. Freedman said. “Our recommendation remains that despite challenges caused by the COVID-19 pandemic, adults and their healthcare providers should follow the recommended vaccine schedule to protect against serious and sometimes deadly diseases.”
Regular vaccines can be safely administered even as COVID-19 retains its grasp on the United States. “Healthcare providers should follow the CDC’s interim guidance for the safe delivery of vaccines during the pandemic, which includes the use of personal protective equipment and physical distancing,” Dr. Freedman said.
Dr. Freedman has disclosed no relevant financial relationships. Coauthor Henry Bernstein, DO, is the editor of the Current Opinion in Pediatrics Office Pediatrics Series, is a Harvard School of Public Health faculty member, and is a member of the data safety and monitoring board for a Takeda study on intrathecal enzymes for Hunter and San Filippo syndromes. Coauthor Kevin Ault, MD, has served on the data safety and monitoring committee for ACI Clinical.
A version of this article first appeared on Medscape.com .
PPE protected critical care staff from COVID-19 transmission
, a new study has found.

“Other staff, other areas of the hospital, and the wider community are more likely sources of infection,” said lead author Kate El Bouzidi, MRCP, South London Specialist Virology Centre, King’s College Hospital NHS Foundation Trust, London.
She noted that 60% of critical care staff were symptomatic during the first wave of the coronavirus pandemic and 20% were antibody positive, with 10% asymptomatic. “Staff acquisition peaked 3 weeks before the peak of COVID-19 ICU admission, and personal protective equipment (PPE) was effective at preventing transmission from patients.” Working in other areas of the hospital was associated with higher seroprevalence, Dr. El Bouzidi noted.
The findings were presented at the Critical Care Congress sponsored by the Society of Critical Care Medicine.
The novel coronavirus was spreading around the world, and when it reached northern Italy, medical authorities began to think in terms of how it might overwhelm the health care system in the United Kingdom, explained Dr. El Bouzidi.
“There was a lot of interest at this time about health care workers who were particularly vulnerable and also about the allocation of resources and rationing of care, particularly in intensive care,” she said. “And this only intensified when our prime minister was admitted to intensive care. About this time, antibody testing also became available.”
The goal of their study was to determine the SARS-CoV-2 seroprevalence in critical care staff, as well as look at the correlation between antibody status, prior swab testing, and COVID-19 symptoms.
The survey was conducted at Kings College Hospital in London, which is a tertiary-care teaching center. The critical care department is one of the largest in the United Kingdom. The authors estimate that more than 800 people worked in the critical care units, and between March and April 2020, more than 2,000 patients with COVID-19 were admitted, of whom 180 required care in the ICU.
“There was good PPE available in the ICU units right from the start,” she said, “and staff testing was available.”
All staff working in the critical care department participated in the study, which required serum samples and completion of a questionnaire. The samples were tested via six different assays to measure receptor-binding domain, nucleoprotein, and tri-spike, with one antibody result determined for each sample.
Of the 625 staff members, 384 (61.4%) had previously reported experiencing symptoms and 124 (19.8%) had sent a swab for testing. COVID-19 infection had been confirmed in 37 of those health care workers (29.8%).
Overall, 21% were positive for SARS-CoV-2 antibodies, of whom 9.9% had been asymptomatic.
“We were surprised to find that 61% of staff reported symptoms they felt could be consistent with COVID-19,” she said, noting that fatigue, headache, and cough were the most common symptoms reported. “Seroprevalence was reported in 31% of symptomatic staff and in 5% of those without symptoms.”
Seroprevalence differed by role in a critical care unit, although it did not significantly differ by factors such as age, sex, ethnicity, or underlying conditions. Consultants, who are senior physicians, were twice as likely to test positive, compared with junior doctors. The reason for this finding is not clear, but it may lie in the nature of their work responsibilities, such as performing more aerosol-generating procedures in the ICU or in other departments.
The investigators looked at the timing of infections and found that they preceded peak of patient admissions by 3 weeks, with peak onset of staff symptoms in early March. At this time, Dr. El Bouzidi noted, there were very few patients with COVID-19 in the hospital, and good PPE was available throughout this time period.
“Staff were unlikely to be infected by ICU patients, and therefore PPE was largely effective,” she said. “Other sources of infection were more likely to be the cause, such as interactions with other staff, meetings, or contact in break rooms. Routine mask-wearing throughout the hospital was only encouraged as of June 15.”
There were several limitations to the study, such as the cross-sectional design, reliance on response/recall, the fact that antibody tests are unlikely to detect all previous infections, and no genomic data were available to confirm infections. Even though the study had limitations, Dr. El Bouzidi concluded that ICU staff are unlikely to contract COVID-19 from patients but that other staff, other areas of the hospital, and the wider community are more likely sources of infection.
These findings, she added, demonstrate that PPE was effective at preventing transmission from patients and that protective measures need to be maintained when staff is away from the bedside.

In commenting on the study, Greg S. Martin, MD, professor of medicine in the division of pulmonary, allergy, critical care and sleep medicine, Emory University, Atlanta, noted that, even though the study was conducted almost a year ago, the results are still relevant with regard to the effectiveness of PPE.
“There was a huge amount of uncertainty about PPE – what was most effective, could we reuse it, how to sterilize it, what about surfaces, and so on,” he said. “Even for people who work in ICU and who are familiar with the environment and familiar with the patients, there was 1,000 times more uncertainty about everything they were doing.”
Dr. Martin believes that the situation has improved. “It’s not that we take COVID more lightly, but I think the staff is more comfortable dealing with it,” he said. “They now know what they need to do on an hourly and daily basis to stay safe. The PPE had become second nature to them now, with all the other precautions.”
, a new study has found.
“Other staff, other areas of the hospital, and the wider community are more likely sources of infection,” said lead author Kate El Bouzidi, MRCP, South London Specialist Virology Centre, King’s College Hospital NHS Foundation Trust, London.
She noted that 60% of critical care staff were symptomatic during the first wave of the coronavirus pandemic and 20% were antibody positive, with 10% asymptomatic. “Staff acquisition peaked 3 weeks before the peak of COVID-19 ICU admission, and personal protective equipment (PPE) was effective at preventing transmission from patients.” Working in other areas of the hospital was associated with higher seroprevalence, Dr. El Bouzidi noted.
The findings were presented at the Critical Care Congress sponsored by the Society of Critical Care Medicine.
The novel coronavirus was spreading around the world, and when it reached northern Italy, medical authorities began to think in terms of how it might overwhelm the health care system in the United Kingdom, explained Dr. El Bouzidi.
“There was a lot of interest at this time about health care workers who were particularly vulnerable and also about the allocation of resources and rationing of care, particularly in intensive care,” she said. “And this only intensified when our prime minister was admitted to intensive care. About this time, antibody testing also became available.”
The goal of their study was to determine the SARS-CoV-2 seroprevalence in critical care staff, as well as look at the correlation between antibody status, prior swab testing, and COVID-19 symptoms.
The survey was conducted at Kings College Hospital in London, which is a tertiary-care teaching center. The critical care department is one of the largest in the United Kingdom. The authors estimate that more than 800 people worked in the critical care units, and between March and April 2020, more than 2,000 patients with COVID-19 were admitted, of whom 180 required care in the ICU.
“There was good PPE available in the ICU units right from the start,” she said, “and staff testing was available.”
All staff working in the critical care department participated in the study, which required serum samples and completion of a questionnaire. The samples were tested via six different assays to measure receptor-binding domain, nucleoprotein, and tri-spike, with one antibody result determined for each sample.
Of the 625 staff members, 384 (61.4%) had previously reported experiencing symptoms and 124 (19.8%) had sent a swab for testing. COVID-19 infection had been confirmed in 37 of those health care workers (29.8%).
Overall, 21% were positive for SARS-CoV-2 antibodies, of whom 9.9% had been asymptomatic.
“We were surprised to find that 61% of staff reported symptoms they felt could be consistent with COVID-19,” she said, noting that fatigue, headache, and cough were the most common symptoms reported. “Seroprevalence was reported in 31% of symptomatic staff and in 5% of those without symptoms.”
Seroprevalence differed by role in a critical care unit, although it did not significantly differ by factors such as age, sex, ethnicity, or underlying conditions. Consultants, who are senior physicians, were twice as likely to test positive, compared with junior doctors. The reason for this finding is not clear, but it may lie in the nature of their work responsibilities, such as performing more aerosol-generating procedures in the ICU or in other departments.
The investigators looked at the timing of infections and found that they preceded peak of patient admissions by 3 weeks, with peak onset of staff symptoms in early March. At this time, Dr. El Bouzidi noted, there were very few patients with COVID-19 in the hospital, and good PPE was available throughout this time period.
“Staff were unlikely to be infected by ICU patients, and therefore PPE was largely effective,” she said. “Other sources of infection were more likely to be the cause, such as interactions with other staff, meetings, or contact in break rooms. Routine mask-wearing throughout the hospital was only encouraged as of June 15.”
There were several limitations to the study, such as the cross-sectional design, reliance on response/recall, the fact that antibody tests are unlikely to detect all previous infections, and no genomic data were available to confirm infections. Even though the study had limitations, Dr. El Bouzidi concluded that ICU staff are unlikely to contract COVID-19 from patients but that other staff, other areas of the hospital, and the wider community are more likely sources of infection.
These findings, she added, demonstrate that PPE was effective at preventing transmission from patients and that protective measures need to be maintained when staff is away from the bedside.
In commenting on the study, Greg S. Martin, MD, professor of medicine in the division of pulmonary, allergy, critical care and sleep medicine, Emory University, Atlanta, noted that, even though the study was conducted almost a year ago, the results are still relevant with regard to the effectiveness of PPE.
“There was a huge amount of uncertainty about PPE – what was most effective, could we reuse it, how to sterilize it, what about surfaces, and so on,” he said. “Even for people who work in ICU and who are familiar with the environment and familiar with the patients, there was 1,000 times more uncertainty about everything they were doing.”
Dr. Martin believes that the situation has improved. “It’s not that we take COVID more lightly, but I think the staff is more comfortable dealing with it,” he said. “They now know what they need to do on an hourly and daily basis to stay safe. The PPE had become second nature to them now, with all the other precautions.”
, a new study has found.
“Other staff, other areas of the hospital, and the wider community are more likely sources of infection,” said lead author Kate El Bouzidi, MRCP, South London Specialist Virology Centre, King’s College Hospital NHS Foundation Trust, London.
She noted that 60% of critical care staff were symptomatic during the first wave of the coronavirus pandemic and 20% were antibody positive, with 10% asymptomatic. “Staff acquisition peaked 3 weeks before the peak of COVID-19 ICU admission, and personal protective equipment (PPE) was effective at preventing transmission from patients.” Working in other areas of the hospital was associated with higher seroprevalence, Dr. El Bouzidi noted.
The findings were presented at the Critical Care Congress sponsored by the Society of Critical Care Medicine.
The novel coronavirus was spreading around the world, and when it reached northern Italy, medical authorities began to think in terms of how it might overwhelm the health care system in the United Kingdom, explained Dr. El Bouzidi.
“There was a lot of interest at this time about health care workers who were particularly vulnerable and also about the allocation of resources and rationing of care, particularly in intensive care,” she said. “And this only intensified when our prime minister was admitted to intensive care. About this time, antibody testing also became available.”
The goal of their study was to determine the SARS-CoV-2 seroprevalence in critical care staff, as well as look at the correlation between antibody status, prior swab testing, and COVID-19 symptoms.
The survey was conducted at Kings College Hospital in London, which is a tertiary-care teaching center. The critical care department is one of the largest in the United Kingdom. The authors estimate that more than 800 people worked in the critical care units, and between March and April 2020, more than 2,000 patients with COVID-19 were admitted, of whom 180 required care in the ICU.
“There was good PPE available in the ICU units right from the start,” she said, “and staff testing was available.”
All staff working in the critical care department participated in the study, which required serum samples and completion of a questionnaire. The samples were tested via six different assays to measure receptor-binding domain, nucleoprotein, and tri-spike, with one antibody result determined for each sample.
Of the 625 staff members, 384 (61.4%) had previously reported experiencing symptoms and 124 (19.8%) had sent a swab for testing. COVID-19 infection had been confirmed in 37 of those health care workers (29.8%).
Overall, 21% were positive for SARS-CoV-2 antibodies, of whom 9.9% had been asymptomatic.
“We were surprised to find that 61% of staff reported symptoms they felt could be consistent with COVID-19,” she said, noting that fatigue, headache, and cough were the most common symptoms reported. “Seroprevalence was reported in 31% of symptomatic staff and in 5% of those without symptoms.”
Seroprevalence differed by role in a critical care unit, although it did not significantly differ by factors such as age, sex, ethnicity, or underlying conditions. Consultants, who are senior physicians, were twice as likely to test positive, compared with junior doctors. The reason for this finding is not clear, but it may lie in the nature of their work responsibilities, such as performing more aerosol-generating procedures in the ICU or in other departments.
The investigators looked at the timing of infections and found that they preceded peak of patient admissions by 3 weeks, with peak onset of staff symptoms in early March. At this time, Dr. El Bouzidi noted, there were very few patients with COVID-19 in the hospital, and good PPE was available throughout this time period.
“Staff were unlikely to be infected by ICU patients, and therefore PPE was largely effective,” she said. “Other sources of infection were more likely to be the cause, such as interactions with other staff, meetings, or contact in break rooms. Routine mask-wearing throughout the hospital was only encouraged as of June 15.”
There were several limitations to the study, such as the cross-sectional design, reliance on response/recall, the fact that antibody tests are unlikely to detect all previous infections, and no genomic data were available to confirm infections. Even though the study had limitations, Dr. El Bouzidi concluded that ICU staff are unlikely to contract COVID-19 from patients but that other staff, other areas of the hospital, and the wider community are more likely sources of infection.
These findings, she added, demonstrate that PPE was effective at preventing transmission from patients and that protective measures need to be maintained when staff is away from the bedside.
In commenting on the study, Greg S. Martin, MD, professor of medicine in the division of pulmonary, allergy, critical care and sleep medicine, Emory University, Atlanta, noted that, even though the study was conducted almost a year ago, the results are still relevant with regard to the effectiveness of PPE.
“There was a huge amount of uncertainty about PPE – what was most effective, could we reuse it, how to sterilize it, what about surfaces, and so on,” he said. “Even for people who work in ICU and who are familiar with the environment and familiar with the patients, there was 1,000 times more uncertainty about everything they were doing.”
Dr. Martin believes that the situation has improved. “It’s not that we take COVID more lightly, but I think the staff is more comfortable dealing with it,” he said. “They now know what they need to do on an hourly and daily basis to stay safe. The PPE had become second nature to them now, with all the other precautions.”
FROM CCC50
Inpatient psychiatrist? Maybe I’ll be a vaccinator instead
Now that completion of residency is fast approaching, I am asked regularly what I plan to do when I become a Real Doctor on July 1. It feels like it wasn’t so long ago I was trying to decide if I should even go to medical school, then later, if I should go into psychiatry, family medicine, or emergency medicine. And here I am at another decision point, another of the regular, 4-year milestones in my journey to full physicianhood.

A surprising thing happened to me during my psychiatry training: I fell in love with acute care. Instead of outpatient care, I preferred the longer hours with patients who insist they are Jesus Christ, believe deeply they are being actively pursued by the FBI, and sometimes eat their own feces. I was in awe of the remarkable capacity of the human brain to convince a graduate-school educated man with bipolar disorder that it is acceptable to call in bomb threats to a hospital. To lead a patient on a conservatorship to believe that I am not a doctor but, instead, a seamstress or leave socks full of feces as presents for Santa Claus (lots of feces in inpatient psychiatry). To believe their spouses are not humans or hear voices telling them they should jump off a bridge, sustaining near-lethal injuries. I was hooked.
Psychiatry as a field is not for those requiring instant gratification. Other than Ativan challenges and the remarkably quick response some patients have to ECT, outcomes of our treatments are usually modest, and they take time. We often delude ourselves into thinking that bumping a patient’s fluoxetine from 10 mg to 20 mg will be The Thing that changes a patient’s life. We address our own sense of helplessness as much as that of our patients, who are desperate for something, for someone, to do something that will alter the course of their lives.
Of course, what I can offer my patients usually falls short of their lofty expectations of my prowess. I offer them compassion, validation, empathy. I offer them medications for which we usually have meager data and meager results. I cannot find them shelter but for a few nights, perhaps a week. I rarely, in settings in which primary diagnoses of substance use and personality disorders are forbidden by insurance companies, can help them with their addiction to methamphetamine. I cannot cure their maladaptive characterological pathology stemming from childhood attachment trauma. To address my own sense of failure as a healer, I resort to the bottom of Maslow’s hierarchy of needs, providing their choice of juice box, more blankets. I slow-roll their discharges overnight so that they can stay in the ER hallway instead of spending the night outside in the rare Southern California rain.
In my 3rd year of residency, we were thrown into a pandemic. I felt both terrified of getting COVID-19 in the hospital and inadequate as a physician. I did not want to be intubating patients, but even more, I dreaded the potential “psychiatry-friendly” assignment of calling the family members of those who had perished from the disease. Rumors circulated that certain versions of surge planning had the inpatient psychiatry unit transitioned to a COVID unit and psychiatry residents “redeployed” to cover medicine floors. Fortunately, we did not have to (or have not yet had to) endure this apocalyptic episode of worst-case scenario. I remained a psychiatrist-in-training, seeing occasional COVID patients but with full personal protective equipment and the ability to maintain some physical distance to complete my examinations. Coming home to my apartment building in scrubs, now acceptable attire on inpatient units – it always should have been since, as we have established, our units are filled with feces – I early on felt like a leper. Later on, I was treated with dignity and respect, like a hero.
My position as a non–frontline-physician was personally challenging. I wanted to help, felt like I should and could help. I am a helper-in-recovery who has spent years learning to achieve a balance of service and loyalty to others and my own desires. The initial guilt I felt at feeling appreciated during the nightly celebration of health care workers downtown ultimately dissipated. I was no hero, nor did I claim to be one. I made peace with my pandemic hobbies of sourdough bread-baking, Moscow mule-making, jigsaw-puzzling, and, briefly, running (before a calcaneal stress fracture reminded me that I am not built for land exercise). I went to work; I came home. My cat was happy.
Then, in rapid succession, vaccines were approved and distributed. My hospital had partnered with the county to administer them at a new superstation, and they were in desperate need of licensed humans to be vaccinators. They cared not that I had given very few (n = 3) injections and only during medical school. I watched the YouTube videos on the Z-track technique for IMs, learned about needle gauges, and went off to the baseball stadium.
I loved this new gig, disproportionately. The 8+ hours flew by, 100 vaccines given to occupants of cars who had eagerly waited hours for the privilege of being vaccinated by an almost-psychiatrist. It was not the technical expertise of sticking a needle into someone’s arm that gave me a dopamine rush, nor the microstress of preparing the syringes with a flimsy needle and a slight caffeine-induced tremor while trying to flick air bubbles out of the syringe without dropping the precious vaccine vial. It was not the travel nurse asking me why anyone – especially an overworked resident – would volunteer to do this for free, while she and others were making “stupid amounts of money” to do the same job.
What drove me to keep volunteering for no pay, only Cheez-Its available as sustenance, minimal gratitude from my employer, long hours on my feet doing a task that was rote and at which I probably would never completely excel? On my second shift, I realized why I found it so gratifying to be a vaccinator: There was a perfect 1:1 correspondence in what patients wanted at that moment and in what I had to offer them. They did not want me to fix their lives, secure them housing, or go back in time and remove them from abusive homes so they could grow up to be more functional, happier adults. They merely wanted a shot. They were profusely grateful, hopeful that this was the Beginning of the End. Nobody spat on me; nobody called me obscene names. Nobody was upset with me for involuntarily holding them against their will. My services were welcome, appreciated. I had lovely, superficial conversations with dozens of people. I felt connected to strangers in a way that has been sorely lacking since March 2020. Understandably mistaken for a nurse throughout the day, I felt more like a bona fide physician than I had in over a year.
I know the adrenaline rush will fade, that volunteer-vaccinating in my free time will eventually become less exciting to me. I know I won’t be able to convince my colleagues indefinitely that volunteering together is a great, institution-sanctioned bonding opportunity. I know the initial enthusiasm over vaccine distribution will fade as the pandemic continues to transform our everyday lives and threaten the health of millions, the economy, and the sanctity of normal human interactions. The gratitude and hopefulness may well be replaced with frustration over waiting hours in a car to get an injection from a psychiatrist, with fear that this promised panacea may not restore normalcy anytime soon. But right now, 11 months into a pandemic that has left our profession exhausted and jaded, the coprophilia and catatonia have temporarily lost their allure. So, I’m adding “vaccinator” to my list of pandemic hobbies.
Dr. Stone is a chief resident in psychiatry at the University of California, San Diego. Before deciding to become a physician, she obtained a master’s degree in public health and worked in health policy research studying empathy and patient-doctor interactions. She has a passion for public psychiatry and acute care, and she dabbles in physician wellness, medical education, and the interface of psychiatry and primary care. Dr. Stone has no disclosures.
Now that completion of residency is fast approaching, I am asked regularly what I plan to do when I become a Real Doctor on July 1. It feels like it wasn’t so long ago I was trying to decide if I should even go to medical school, then later, if I should go into psychiatry, family medicine, or emergency medicine. And here I am at another decision point, another of the regular, 4-year milestones in my journey to full physicianhood.
A surprising thing happened to me during my psychiatry training: I fell in love with acute care. Instead of outpatient care, I preferred the longer hours with patients who insist they are Jesus Christ, believe deeply they are being actively pursued by the FBI, and sometimes eat their own feces. I was in awe of the remarkable capacity of the human brain to convince a graduate-school educated man with bipolar disorder that it is acceptable to call in bomb threats to a hospital. To lead a patient on a conservatorship to believe that I am not a doctor but, instead, a seamstress or leave socks full of feces as presents for Santa Claus (lots of feces in inpatient psychiatry). To believe their spouses are not humans or hear voices telling them they should jump off a bridge, sustaining near-lethal injuries. I was hooked.
Psychiatry as a field is not for those requiring instant gratification. Other than Ativan challenges and the remarkably quick response some patients have to ECT, outcomes of our treatments are usually modest, and they take time. We often delude ourselves into thinking that bumping a patient’s fluoxetine from 10 mg to 20 mg will be The Thing that changes a patient’s life. We address our own sense of helplessness as much as that of our patients, who are desperate for something, for someone, to do something that will alter the course of their lives.
Of course, what I can offer my patients usually falls short of their lofty expectations of my prowess. I offer them compassion, validation, empathy. I offer them medications for which we usually have meager data and meager results. I cannot find them shelter but for a few nights, perhaps a week. I rarely, in settings in which primary diagnoses of substance use and personality disorders are forbidden by insurance companies, can help them with their addiction to methamphetamine. I cannot cure their maladaptive characterological pathology stemming from childhood attachment trauma. To address my own sense of failure as a healer, I resort to the bottom of Maslow’s hierarchy of needs, providing their choice of juice box, more blankets. I slow-roll their discharges overnight so that they can stay in the ER hallway instead of spending the night outside in the rare Southern California rain.
In my 3rd year of residency, we were thrown into a pandemic. I felt both terrified of getting COVID-19 in the hospital and inadequate as a physician. I did not want to be intubating patients, but even more, I dreaded the potential “psychiatry-friendly” assignment of calling the family members of those who had perished from the disease. Rumors circulated that certain versions of surge planning had the inpatient psychiatry unit transitioned to a COVID unit and psychiatry residents “redeployed” to cover medicine floors. Fortunately, we did not have to (or have not yet had to) endure this apocalyptic episode of worst-case scenario. I remained a psychiatrist-in-training, seeing occasional COVID patients but with full personal protective equipment and the ability to maintain some physical distance to complete my examinations. Coming home to my apartment building in scrubs, now acceptable attire on inpatient units – it always should have been since, as we have established, our units are filled with feces – I early on felt like a leper. Later on, I was treated with dignity and respect, like a hero.
My position as a non–frontline-physician was personally challenging. I wanted to help, felt like I should and could help. I am a helper-in-recovery who has spent years learning to achieve a balance of service and loyalty to others and my own desires. The initial guilt I felt at feeling appreciated during the nightly celebration of health care workers downtown ultimately dissipated. I was no hero, nor did I claim to be one. I made peace with my pandemic hobbies of sourdough bread-baking, Moscow mule-making, jigsaw-puzzling, and, briefly, running (before a calcaneal stress fracture reminded me that I am not built for land exercise). I went to work; I came home. My cat was happy.
Then, in rapid succession, vaccines were approved and distributed. My hospital had partnered with the county to administer them at a new superstation, and they were in desperate need of licensed humans to be vaccinators. They cared not that I had given very few (n = 3) injections and only during medical school. I watched the YouTube videos on the Z-track technique for IMs, learned about needle gauges, and went off to the baseball stadium.
I loved this new gig, disproportionately. The 8+ hours flew by, 100 vaccines given to occupants of cars who had eagerly waited hours for the privilege of being vaccinated by an almost-psychiatrist. It was not the technical expertise of sticking a needle into someone’s arm that gave me a dopamine rush, nor the microstress of preparing the syringes with a flimsy needle and a slight caffeine-induced tremor while trying to flick air bubbles out of the syringe without dropping the precious vaccine vial. It was not the travel nurse asking me why anyone – especially an overworked resident – would volunteer to do this for free, while she and others were making “stupid amounts of money” to do the same job.
What drove me to keep volunteering for no pay, only Cheez-Its available as sustenance, minimal gratitude from my employer, long hours on my feet doing a task that was rote and at which I probably would never completely excel? On my second shift, I realized why I found it so gratifying to be a vaccinator: There was a perfect 1:1 correspondence in what patients wanted at that moment and in what I had to offer them. They did not want me to fix their lives, secure them housing, or go back in time and remove them from abusive homes so they could grow up to be more functional, happier adults. They merely wanted a shot. They were profusely grateful, hopeful that this was the Beginning of the End. Nobody spat on me; nobody called me obscene names. Nobody was upset with me for involuntarily holding them against their will. My services were welcome, appreciated. I had lovely, superficial conversations with dozens of people. I felt connected to strangers in a way that has been sorely lacking since March 2020. Understandably mistaken for a nurse throughout the day, I felt more like a bona fide physician than I had in over a year.
I know the adrenaline rush will fade, that volunteer-vaccinating in my free time will eventually become less exciting to me. I know I won’t be able to convince my colleagues indefinitely that volunteering together is a great, institution-sanctioned bonding opportunity. I know the initial enthusiasm over vaccine distribution will fade as the pandemic continues to transform our everyday lives and threaten the health of millions, the economy, and the sanctity of normal human interactions. The gratitude and hopefulness may well be replaced with frustration over waiting hours in a car to get an injection from a psychiatrist, with fear that this promised panacea may not restore normalcy anytime soon. But right now, 11 months into a pandemic that has left our profession exhausted and jaded, the coprophilia and catatonia have temporarily lost their allure. So, I’m adding “vaccinator” to my list of pandemic hobbies.
Dr. Stone is a chief resident in psychiatry at the University of California, San Diego. Before deciding to become a physician, she obtained a master’s degree in public health and worked in health policy research studying empathy and patient-doctor interactions. She has a passion for public psychiatry and acute care, and she dabbles in physician wellness, medical education, and the interface of psychiatry and primary care. Dr. Stone has no disclosures.
Now that completion of residency is fast approaching, I am asked regularly what I plan to do when I become a Real Doctor on July 1. It feels like it wasn’t so long ago I was trying to decide if I should even go to medical school, then later, if I should go into psychiatry, family medicine, or emergency medicine. And here I am at another decision point, another of the regular, 4-year milestones in my journey to full physicianhood.
A surprising thing happened to me during my psychiatry training: I fell in love with acute care. Instead of outpatient care, I preferred the longer hours with patients who insist they are Jesus Christ, believe deeply they are being actively pursued by the FBI, and sometimes eat their own feces. I was in awe of the remarkable capacity of the human brain to convince a graduate-school educated man with bipolar disorder that it is acceptable to call in bomb threats to a hospital. To lead a patient on a conservatorship to believe that I am not a doctor but, instead, a seamstress or leave socks full of feces as presents for Santa Claus (lots of feces in inpatient psychiatry). To believe their spouses are not humans or hear voices telling them they should jump off a bridge, sustaining near-lethal injuries. I was hooked.
Psychiatry as a field is not for those requiring instant gratification. Other than Ativan challenges and the remarkably quick response some patients have to ECT, outcomes of our treatments are usually modest, and they take time. We often delude ourselves into thinking that bumping a patient’s fluoxetine from 10 mg to 20 mg will be The Thing that changes a patient’s life. We address our own sense of helplessness as much as that of our patients, who are desperate for something, for someone, to do something that will alter the course of their lives.
Of course, what I can offer my patients usually falls short of their lofty expectations of my prowess. I offer them compassion, validation, empathy. I offer them medications for which we usually have meager data and meager results. I cannot find them shelter but for a few nights, perhaps a week. I rarely, in settings in which primary diagnoses of substance use and personality disorders are forbidden by insurance companies, can help them with their addiction to methamphetamine. I cannot cure their maladaptive characterological pathology stemming from childhood attachment trauma. To address my own sense of failure as a healer, I resort to the bottom of Maslow’s hierarchy of needs, providing their choice of juice box, more blankets. I slow-roll their discharges overnight so that they can stay in the ER hallway instead of spending the night outside in the rare Southern California rain.
In my 3rd year of residency, we were thrown into a pandemic. I felt both terrified of getting COVID-19 in the hospital and inadequate as a physician. I did not want to be intubating patients, but even more, I dreaded the potential “psychiatry-friendly” assignment of calling the family members of those who had perished from the disease. Rumors circulated that certain versions of surge planning had the inpatient psychiatry unit transitioned to a COVID unit and psychiatry residents “redeployed” to cover medicine floors. Fortunately, we did not have to (or have not yet had to) endure this apocalyptic episode of worst-case scenario. I remained a psychiatrist-in-training, seeing occasional COVID patients but with full personal protective equipment and the ability to maintain some physical distance to complete my examinations. Coming home to my apartment building in scrubs, now acceptable attire on inpatient units – it always should have been since, as we have established, our units are filled with feces – I early on felt like a leper. Later on, I was treated with dignity and respect, like a hero.
My position as a non–frontline-physician was personally challenging. I wanted to help, felt like I should and could help. I am a helper-in-recovery who has spent years learning to achieve a balance of service and loyalty to others and my own desires. The initial guilt I felt at feeling appreciated during the nightly celebration of health care workers downtown ultimately dissipated. I was no hero, nor did I claim to be one. I made peace with my pandemic hobbies of sourdough bread-baking, Moscow mule-making, jigsaw-puzzling, and, briefly, running (before a calcaneal stress fracture reminded me that I am not built for land exercise). I went to work; I came home. My cat was happy.
Then, in rapid succession, vaccines were approved and distributed. My hospital had partnered with the county to administer them at a new superstation, and they were in desperate need of licensed humans to be vaccinators. They cared not that I had given very few (n = 3) injections and only during medical school. I watched the YouTube videos on the Z-track technique for IMs, learned about needle gauges, and went off to the baseball stadium.
I loved this new gig, disproportionately. The 8+ hours flew by, 100 vaccines given to occupants of cars who had eagerly waited hours for the privilege of being vaccinated by an almost-psychiatrist. It was not the technical expertise of sticking a needle into someone’s arm that gave me a dopamine rush, nor the microstress of preparing the syringes with a flimsy needle and a slight caffeine-induced tremor while trying to flick air bubbles out of the syringe without dropping the precious vaccine vial. It was not the travel nurse asking me why anyone – especially an overworked resident – would volunteer to do this for free, while she and others were making “stupid amounts of money” to do the same job.
What drove me to keep volunteering for no pay, only Cheez-Its available as sustenance, minimal gratitude from my employer, long hours on my feet doing a task that was rote and at which I probably would never completely excel? On my second shift, I realized why I found it so gratifying to be a vaccinator: There was a perfect 1:1 correspondence in what patients wanted at that moment and in what I had to offer them. They did not want me to fix their lives, secure them housing, or go back in time and remove them from abusive homes so they could grow up to be more functional, happier adults. They merely wanted a shot. They were profusely grateful, hopeful that this was the Beginning of the End. Nobody spat on me; nobody called me obscene names. Nobody was upset with me for involuntarily holding them against their will. My services were welcome, appreciated. I had lovely, superficial conversations with dozens of people. I felt connected to strangers in a way that has been sorely lacking since March 2020. Understandably mistaken for a nurse throughout the day, I felt more like a bona fide physician than I had in over a year.
I know the adrenaline rush will fade, that volunteer-vaccinating in my free time will eventually become less exciting to me. I know I won’t be able to convince my colleagues indefinitely that volunteering together is a great, institution-sanctioned bonding opportunity. I know the initial enthusiasm over vaccine distribution will fade as the pandemic continues to transform our everyday lives and threaten the health of millions, the economy, and the sanctity of normal human interactions. The gratitude and hopefulness may well be replaced with frustration over waiting hours in a car to get an injection from a psychiatrist, with fear that this promised panacea may not restore normalcy anytime soon. But right now, 11 months into a pandemic that has left our profession exhausted and jaded, the coprophilia and catatonia have temporarily lost their allure. So, I’m adding “vaccinator” to my list of pandemic hobbies.
Dr. Stone is a chief resident in psychiatry at the University of California, San Diego. Before deciding to become a physician, she obtained a master’s degree in public health and worked in health policy research studying empathy and patient-doctor interactions. She has a passion for public psychiatry and acute care, and she dabbles in physician wellness, medical education, and the interface of psychiatry and primary care. Dr. Stone has no disclosures.
COVID-19 studies funded by rheumatology foundation
Five lines of research related to COVID-19 and people with rheumatic diseases will be explored with $1.65 million awarded recently by the Rheumatology Research Foundation.

Investigators will explore topics ranging from respiratory health to telemedicine with the awards, given by the foundation that is the largest private funding source for rheumatology research and training in the United States. The projects are an attempt to deepen the understanding about how people with rheumatic illnesses are affected by COVID-19.
“Our current understanding of why there are differences in severity of COVID-19 illness among rheumatology patients is limited,” Foundation President S. Louis Bridges, MD, PhD, said. “Additionally, there are many other gaps in our knowledge of the clinical aspects of SARS-CoV-2 infection in patients with rheumatic diseases, and how the pandemic has changed health care delivery. There is an urgent need to acquire new knowledge on COVID-19 in patients with [rheumatic and musculoskeletal diseases].”
These are the research projects funded:
- Scientist Development Award: Respiratory complications of coronavirus disease (COVID-19) in rheumatic diseases, led by Kristin D’Silva, MD, of Massachusetts General Hospital in Boston (3-year, $225,000 grant)
- Scientist Development Award: COVID-19 in patients with inflammatory arthritis: A prospective study on the effects of immunomodulatory therapy on susceptibility and clinical outcomes, by Rebecca Haberman, MD, of New York University (3-year, $225,000 grant)
- Innovative Research Award: Antiphospholipid antibodies in COVID-19, led by Jason Knight, MD, PhD, of the University of Michigan, Ann Arbor (2-year, $400,000 grant);
- Innovative Research Award: Effectiveness of telerheumatology for delivering high-quality rheumatology care during the COVID-19 crisis, led by Maria Danila, MD, MSc, MSPH, of University of Alabama at Birmingham (2-year, $400,000 grant)
- Norman B. Gaylis, MD, Clinical Research Award: Telehealth-delivered health care to improve care (THRIVE) in community-practice rheumatology, led by Swamy Venuturupalli, MD, of Beverly Hills, Calif.–based Attune Health (2-year, $400,000 grant)
Dr. Bridges said the foundation accepted submissions in basic science, translational science, clinical science, health services research, and patient- and practice-centered research.
“What differentiates these studies from our existing awards portfolio is they all explore the relationships between rheumatic and musculoskeletal diseases and SARS-CoV-2,” he said. “Ultimately, the outcomes of these projects will contribute to a more comprehensive knowledge base and advance avenues of patient care in the COVID-19 pandemic.”

Dr. Gaylis, a rheumatologist in private practice in Aventura, Fla., said he was pleased that a telehealth project was chosen as the award given in his name.
“From a COVID point of view, this has been extremely valuable in allowing us to continue to help out patients, connect with our patients, provide them treatment, even if it’s not hands on, at least guide them in how to deal with their chronic rheumatic illnesses,” he said.
This line of research can also help explore the feasibility of telemedicine in helping meet the needs of rural communities facing shortages of rheumatologists.
“Can telemedicine provide a source of rheumatologic access for people who really don’t have a live provider in close proximity?” he said. “I think that’s really why this particular award is very, very timely.”
“It’s so difficult for clinicians to get funding for their research, for their ideas and for the discoveries they were making on a day-to-day basis while they were practicing in a clinical community environment,” he said. “So for me it was really something that inspired me to really create this award.”
Five lines of research related to COVID-19 and people with rheumatic diseases will be explored with $1.65 million awarded recently by the Rheumatology Research Foundation.
Investigators will explore topics ranging from respiratory health to telemedicine with the awards, given by the foundation that is the largest private funding source for rheumatology research and training in the United States. The projects are an attempt to deepen the understanding about how people with rheumatic illnesses are affected by COVID-19.
“Our current understanding of why there are differences in severity of COVID-19 illness among rheumatology patients is limited,” Foundation President S. Louis Bridges, MD, PhD, said. “Additionally, there are many other gaps in our knowledge of the clinical aspects of SARS-CoV-2 infection in patients with rheumatic diseases, and how the pandemic has changed health care delivery. There is an urgent need to acquire new knowledge on COVID-19 in patients with [rheumatic and musculoskeletal diseases].”
These are the research projects funded:
- Scientist Development Award: Respiratory complications of coronavirus disease (COVID-19) in rheumatic diseases, led by Kristin D’Silva, MD, of Massachusetts General Hospital in Boston (3-year, $225,000 grant)
- Scientist Development Award: COVID-19 in patients with inflammatory arthritis: A prospective study on the effects of immunomodulatory therapy on susceptibility and clinical outcomes, by Rebecca Haberman, MD, of New York University (3-year, $225,000 grant)
- Innovative Research Award: Antiphospholipid antibodies in COVID-19, led by Jason Knight, MD, PhD, of the University of Michigan, Ann Arbor (2-year, $400,000 grant);
- Innovative Research Award: Effectiveness of telerheumatology for delivering high-quality rheumatology care during the COVID-19 crisis, led by Maria Danila, MD, MSc, MSPH, of University of Alabama at Birmingham (2-year, $400,000 grant)
- Norman B. Gaylis, MD, Clinical Research Award: Telehealth-delivered health care to improve care (THRIVE) in community-practice rheumatology, led by Swamy Venuturupalli, MD, of Beverly Hills, Calif.–based Attune Health (2-year, $400,000 grant)
Dr. Bridges said the foundation accepted submissions in basic science, translational science, clinical science, health services research, and patient- and practice-centered research.
“What differentiates these studies from our existing awards portfolio is they all explore the relationships between rheumatic and musculoskeletal diseases and SARS-CoV-2,” he said. “Ultimately, the outcomes of these projects will contribute to a more comprehensive knowledge base and advance avenues of patient care in the COVID-19 pandemic.”
Dr. Gaylis, a rheumatologist in private practice in Aventura, Fla., said he was pleased that a telehealth project was chosen as the award given in his name.
“From a COVID point of view, this has been extremely valuable in allowing us to continue to help out patients, connect with our patients, provide them treatment, even if it’s not hands on, at least guide them in how to deal with their chronic rheumatic illnesses,” he said.
This line of research can also help explore the feasibility of telemedicine in helping meet the needs of rural communities facing shortages of rheumatologists.
“Can telemedicine provide a source of rheumatologic access for people who really don’t have a live provider in close proximity?” he said. “I think that’s really why this particular award is very, very timely.”
“It’s so difficult for clinicians to get funding for their research, for their ideas and for the discoveries they were making on a day-to-day basis while they were practicing in a clinical community environment,” he said. “So for me it was really something that inspired me to really create this award.”
Five lines of research related to COVID-19 and people with rheumatic diseases will be explored with $1.65 million awarded recently by the Rheumatology Research Foundation.
Investigators will explore topics ranging from respiratory health to telemedicine with the awards, given by the foundation that is the largest private funding source for rheumatology research and training in the United States. The projects are an attempt to deepen the understanding about how people with rheumatic illnesses are affected by COVID-19.
“Our current understanding of why there are differences in severity of COVID-19 illness among rheumatology patients is limited,” Foundation President S. Louis Bridges, MD, PhD, said. “Additionally, there are many other gaps in our knowledge of the clinical aspects of SARS-CoV-2 infection in patients with rheumatic diseases, and how the pandemic has changed health care delivery. There is an urgent need to acquire new knowledge on COVID-19 in patients with [rheumatic and musculoskeletal diseases].”
These are the research projects funded:
- Scientist Development Award: Respiratory complications of coronavirus disease (COVID-19) in rheumatic diseases, led by Kristin D’Silva, MD, of Massachusetts General Hospital in Boston (3-year, $225,000 grant)
- Scientist Development Award: COVID-19 in patients with inflammatory arthritis: A prospective study on the effects of immunomodulatory therapy on susceptibility and clinical outcomes, by Rebecca Haberman, MD, of New York University (3-year, $225,000 grant)
- Innovative Research Award: Antiphospholipid antibodies in COVID-19, led by Jason Knight, MD, PhD, of the University of Michigan, Ann Arbor (2-year, $400,000 grant);
- Innovative Research Award: Effectiveness of telerheumatology for delivering high-quality rheumatology care during the COVID-19 crisis, led by Maria Danila, MD, MSc, MSPH, of University of Alabama at Birmingham (2-year, $400,000 grant)
- Norman B. Gaylis, MD, Clinical Research Award: Telehealth-delivered health care to improve care (THRIVE) in community-practice rheumatology, led by Swamy Venuturupalli, MD, of Beverly Hills, Calif.–based Attune Health (2-year, $400,000 grant)
Dr. Bridges said the foundation accepted submissions in basic science, translational science, clinical science, health services research, and patient- and practice-centered research.
“What differentiates these studies from our existing awards portfolio is they all explore the relationships between rheumatic and musculoskeletal diseases and SARS-CoV-2,” he said. “Ultimately, the outcomes of these projects will contribute to a more comprehensive knowledge base and advance avenues of patient care in the COVID-19 pandemic.”
Dr. Gaylis, a rheumatologist in private practice in Aventura, Fla., said he was pleased that a telehealth project was chosen as the award given in his name.
“From a COVID point of view, this has been extremely valuable in allowing us to continue to help out patients, connect with our patients, provide them treatment, even if it’s not hands on, at least guide them in how to deal with their chronic rheumatic illnesses,” he said.
This line of research can also help explore the feasibility of telemedicine in helping meet the needs of rural communities facing shortages of rheumatologists.
“Can telemedicine provide a source of rheumatologic access for people who really don’t have a live provider in close proximity?” he said. “I think that’s really why this particular award is very, very timely.”
“It’s so difficult for clinicians to get funding for their research, for their ideas and for the discoveries they were making on a day-to-day basis while they were practicing in a clinical community environment,” he said. “So for me it was really something that inspired me to really create this award.”
Burnout rates in ICU staff fueled by shortages, overtime
Health care professionals working in critical care settings have been overburdened because of the plethora of COVID-19 cases, which has led to symptoms of burnout in both physicians and nurses, findings from a new study show.

“Overburdening ICU professionals during an extended period of time leads to burnout,” said lead study author Niek Kok, MSc, of IQ healthcare, Radboud University Medical Center, Radboud Institute for Health Sciences, Nijmegen, the Netherlands. “All ICU professionals are at the risk of this, and in our study, the incidence of physicians experiencing burnout was significantly higher than that of nurses in June 2020.”
This burnout can be explained by conditions caused by the pandemic, he noted, such as the scarcity of staff and resources and having to work with colleagues who were not qualified to work in critical care but who were there out of necessity.
Mr. Kok presented the findings of the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine.
Burnout highest among critical care physicians
The ICU can be a stressful environment for both patients and health care personnel, and burnout is not uncommon among ICU clinicians. However, COVID-19 has amplified the degree of burnout being experienced by clinicians working in this setting. Critical care physicians now top the list of physicians experiencing burnout, at 51%, up from 44% last year, according to the Medscape report ‘Death by 1000 Thousand Cuts’: Physician Burnout and Suicide Report 2021.
The Medscape Nurse Career Satisfaction Report 2020, while not restricted to those working in critical care, also reported higher rates of burnout, compared with the prepandemic period. The percentage of nurses reporting being “very burned out” prior to the pandemic was 4%. Six months into the pandemic, that percentage soared to 18%.
In this study, Mr. Kok and colleagues examined the prevalence and incidence of burnout symptoms and moral distress in health care professionals working in the ICU, both before and during the COVID-19 pandemic.
“When the COVID-19 pandemic surfaced in the Netherlands, the health care professionals in our hospitals were motivated to do everything they could to provide the best care possible,” said Mr. Kok. “Many of the ICU professionals immediately realized that they would have to work longer hours.”
However, the health care professionals that he spoke with did have mixed feelings. Some were afraid of being infected with the virus, while others said that “it was very interesting times for them and that gave them extra motivation to do the work.
“Some physicians [and] the WHO warned that COVID-19 is not going to weathered by a heroic sprint – it is an arduous marathon that is going to go hand in hand with burnout symptoms,” Mr. Kok added. “It will eat away at our qualified ICU staff.”
Before and after data on burnout
It was widely believed that the COVID-19 pandemic would increase burnout symptoms, as had been demonstrated in studies of previous pandemics. However, Mr. Kok emphasized that there are no before and after measurements that transcend cross-sectional designs.
“The claim [has been] that it increases burnout – but there are no assessments of how it progresses in ICU professionals through time,” he said. “So what we really need is a comparison [of] before and after the pandemic.”
It is quite difficult to obtain this type of information because disruptive events like the COVID-19 pandemic cannot be predicted, he said. Thus, it is challenging to get a baseline measurement. But Mr. Kok pointed out that the study has both “before and after” measurements.
“By coincidence really, we had baseline data to measure the impact of the COVID-19 pandemic and had information that was collected before the pandemic,” he said.
In January 2020, a study began looking at the effects of ethics meetings on moral distress in ICU professionals. Data had been collected on moral distress and burnout on ICU professionals in December 2019. The first COVID-19 cases appeared in the Netherlands in February 2020.
A follow-up study was then conducted in May and June 2020, several months into the pandemic.
The longitudinal open cohort study included all ICU personnel who were working in five units within a single university medical center, plus another adult ICU that was based in a separate teaching hospital.
A total of 352 health care professionals responded to a baseline survey in October through December 2019, and then 233 responded to a follow-up survey sent in May and June 2020. The authors measured burnout symptoms and moral distress with the Maslach Burnout Inventory and the Moral Distress Scale, respectively.
Findings
The overall prevalence of burnout symptoms was 23.0% prior to the pandemic, and that jumped to 36.1% at post-peak time. Higher rates of burnout were reported by nurses (38.0%) than physicians (28.6%).
However, the incidence rate of new burnout cases was higher among physicians, compared with nurses (26.7% vs 21.9%). Not surprisingly, a higher prevalence of burnout symptoms was observed in the post-peak period for all clinicians (odds ratio, 1.83; 95% confidence interval, 1.32-2.53), and was higher for nurses (odds ratio, 1.77; 95% confidence interval, 1.03-3.04), for those working overtime (OR, 2.11; 95% CI, 1.48-3.02), and for personnel who directly engaged in patient care (OR, 1.87; 95% CI, 1.35-2.60).
Physicians in general were much more likely to develop burnout symptoms related to the pandemic, compared with nurses (OR, 3.56; 95% CI, 1.06-12.21).
When looking at findings on moral distress, Kok pointed out that it often arises in situations when the health care professional knows the right thing to do but is prevented from doing so. “Morally distressful situations all rose from December to June,” said Mr. Kok. “Scarcity was the most distressing. The other was where colleagues were perceived to be less skilled, and this had to do with the recruitment of people from outside of the ICU to provide care.”
Moral distress from scarcity and unskilled colleagues were both significantly related to burnout, he noted.
In the final model, working in a COVID-19 unit, stress from scarcity of resources and people, stress from unskilled colleagues, and stress from unsafe conditions were all related to burnout. “The stress of physicians was significantly higher,” said Kok. “Even though nurses had higher baseline burnout, it became less pronounced in June 2020. This indicates that burnout was significantly higher in physicians.”
Thus, Mr. Kok and colleagues concluded that overburdening ICU professionals during an extended period of time leads to burnout, and all ICU workers are at risk.
Burnout rates higher in physicians
Weighing in on the study, Greg S. Martin, MD, FCCP, professor of medicine in the division of pulmonary, allergy, critical care and sleep medicine, Emory University, Atlanta, noted that the differences observed between physicians and nurses may have to do with the fact that “nurses have been smoldering all along and experiencing higher rates of burnout.
“They may have adapted better to the pandemic conditions, since they are more used to working overtime and short staffed, and spending far more time at the bedside,” he said. “Because of the volume of patients, physicians may be spending more hours doing patient care and are experiencing more burnout.”
For physicians, this may be a more significant change in the workload, as well as the complexity of the situation because of the pandemic. “Many things layer into it, such as [the fact] that there are no families present to give patients support, the complexity of care of these patients, and things like lack of PPE,” Dr. Martin said.
The study did not differentiate among physician groups, so it is unclear if the affected physicians were residents, fellows, or more senior staff. “Residents are often quite busy already, and don’t usually have the capacity to add more to their schedules, and maybe attendings were having to spend more time doing patient care,” Dr. Martin said. “In the United States, at least some personnel were restricted from working with COVID-19 patients. Medical students were removed in many places as well as nonessential staff, so that may have also added to their burnout.”
The study was conducted in the Netherlands, so there may be differences in the work environment, responsibilities of nurses vs. physicians, staffing, and so on. “But it still shows that burnout is very real among doctors and nurses working in the ICU in pandemic conditions,” he said.
Health care professionals working in critical care settings have been overburdened because of the plethora of COVID-19 cases, which has led to symptoms of burnout in both physicians and nurses, findings from a new study show.
“Overburdening ICU professionals during an extended period of time leads to burnout,” said lead study author Niek Kok, MSc, of IQ healthcare, Radboud University Medical Center, Radboud Institute for Health Sciences, Nijmegen, the Netherlands. “All ICU professionals are at the risk of this, and in our study, the incidence of physicians experiencing burnout was significantly higher than that of nurses in June 2020.”
This burnout can be explained by conditions caused by the pandemic, he noted, such as the scarcity of staff and resources and having to work with colleagues who were not qualified to work in critical care but who were there out of necessity.
Mr. Kok presented the findings of the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine.
Burnout highest among critical care physicians
The ICU can be a stressful environment for both patients and health care personnel, and burnout is not uncommon among ICU clinicians. However, COVID-19 has amplified the degree of burnout being experienced by clinicians working in this setting. Critical care physicians now top the list of physicians experiencing burnout, at 51%, up from 44% last year, according to the Medscape report ‘Death by 1000 Thousand Cuts’: Physician Burnout and Suicide Report 2021.
The Medscape Nurse Career Satisfaction Report 2020, while not restricted to those working in critical care, also reported higher rates of burnout, compared with the prepandemic period. The percentage of nurses reporting being “very burned out” prior to the pandemic was 4%. Six months into the pandemic, that percentage soared to 18%.
In this study, Mr. Kok and colleagues examined the prevalence and incidence of burnout symptoms and moral distress in health care professionals working in the ICU, both before and during the COVID-19 pandemic.
“When the COVID-19 pandemic surfaced in the Netherlands, the health care professionals in our hospitals were motivated to do everything they could to provide the best care possible,” said Mr. Kok. “Many of the ICU professionals immediately realized that they would have to work longer hours.”
However, the health care professionals that he spoke with did have mixed feelings. Some were afraid of being infected with the virus, while others said that “it was very interesting times for them and that gave them extra motivation to do the work.
“Some physicians [and] the WHO warned that COVID-19 is not going to weathered by a heroic sprint – it is an arduous marathon that is going to go hand in hand with burnout symptoms,” Mr. Kok added. “It will eat away at our qualified ICU staff.”
Before and after data on burnout
It was widely believed that the COVID-19 pandemic would increase burnout symptoms, as had been demonstrated in studies of previous pandemics. However, Mr. Kok emphasized that there are no before and after measurements that transcend cross-sectional designs.
“The claim [has been] that it increases burnout – but there are no assessments of how it progresses in ICU professionals through time,” he said. “So what we really need is a comparison [of] before and after the pandemic.”
It is quite difficult to obtain this type of information because disruptive events like the COVID-19 pandemic cannot be predicted, he said. Thus, it is challenging to get a baseline measurement. But Mr. Kok pointed out that the study has both “before and after” measurements.
“By coincidence really, we had baseline data to measure the impact of the COVID-19 pandemic and had information that was collected before the pandemic,” he said.
In January 2020, a study began looking at the effects of ethics meetings on moral distress in ICU professionals. Data had been collected on moral distress and burnout on ICU professionals in December 2019. The first COVID-19 cases appeared in the Netherlands in February 2020.
A follow-up study was then conducted in May and June 2020, several months into the pandemic.
The longitudinal open cohort study included all ICU personnel who were working in five units within a single university medical center, plus another adult ICU that was based in a separate teaching hospital.
A total of 352 health care professionals responded to a baseline survey in October through December 2019, and then 233 responded to a follow-up survey sent in May and June 2020. The authors measured burnout symptoms and moral distress with the Maslach Burnout Inventory and the Moral Distress Scale, respectively.
Findings
The overall prevalence of burnout symptoms was 23.0% prior to the pandemic, and that jumped to 36.1% at post-peak time. Higher rates of burnout were reported by nurses (38.0%) than physicians (28.6%).
However, the incidence rate of new burnout cases was higher among physicians, compared with nurses (26.7% vs 21.9%). Not surprisingly, a higher prevalence of burnout symptoms was observed in the post-peak period for all clinicians (odds ratio, 1.83; 95% confidence interval, 1.32-2.53), and was higher for nurses (odds ratio, 1.77; 95% confidence interval, 1.03-3.04), for those working overtime (OR, 2.11; 95% CI, 1.48-3.02), and for personnel who directly engaged in patient care (OR, 1.87; 95% CI, 1.35-2.60).
Physicians in general were much more likely to develop burnout symptoms related to the pandemic, compared with nurses (OR, 3.56; 95% CI, 1.06-12.21).
When looking at findings on moral distress, Kok pointed out that it often arises in situations when the health care professional knows the right thing to do but is prevented from doing so. “Morally distressful situations all rose from December to June,” said Mr. Kok. “Scarcity was the most distressing. The other was where colleagues were perceived to be less skilled, and this had to do with the recruitment of people from outside of the ICU to provide care.”
Moral distress from scarcity and unskilled colleagues were both significantly related to burnout, he noted.
In the final model, working in a COVID-19 unit, stress from scarcity of resources and people, stress from unskilled colleagues, and stress from unsafe conditions were all related to burnout. “The stress of physicians was significantly higher,” said Kok. “Even though nurses had higher baseline burnout, it became less pronounced in June 2020. This indicates that burnout was significantly higher in physicians.”
Thus, Mr. Kok and colleagues concluded that overburdening ICU professionals during an extended period of time leads to burnout, and all ICU workers are at risk.
Burnout rates higher in physicians
Weighing in on the study, Greg S. Martin, MD, FCCP, professor of medicine in the division of pulmonary, allergy, critical care and sleep medicine, Emory University, Atlanta, noted that the differences observed between physicians and nurses may have to do with the fact that “nurses have been smoldering all along and experiencing higher rates of burnout.
“They may have adapted better to the pandemic conditions, since they are more used to working overtime and short staffed, and spending far more time at the bedside,” he said. “Because of the volume of patients, physicians may be spending more hours doing patient care and are experiencing more burnout.”
For physicians, this may be a more significant change in the workload, as well as the complexity of the situation because of the pandemic. “Many things layer into it, such as [the fact] that there are no families present to give patients support, the complexity of care of these patients, and things like lack of PPE,” Dr. Martin said.
The study did not differentiate among physician groups, so it is unclear if the affected physicians were residents, fellows, or more senior staff. “Residents are often quite busy already, and don’t usually have the capacity to add more to their schedules, and maybe attendings were having to spend more time doing patient care,” Dr. Martin said. “In the United States, at least some personnel were restricted from working with COVID-19 patients. Medical students were removed in many places as well as nonessential staff, so that may have also added to their burnout.”
The study was conducted in the Netherlands, so there may be differences in the work environment, responsibilities of nurses vs. physicians, staffing, and so on. “But it still shows that burnout is very real among doctors and nurses working in the ICU in pandemic conditions,” he said.
Health care professionals working in critical care settings have been overburdened because of the plethora of COVID-19 cases, which has led to symptoms of burnout in both physicians and nurses, findings from a new study show.
“Overburdening ICU professionals during an extended period of time leads to burnout,” said lead study author Niek Kok, MSc, of IQ healthcare, Radboud University Medical Center, Radboud Institute for Health Sciences, Nijmegen, the Netherlands. “All ICU professionals are at the risk of this, and in our study, the incidence of physicians experiencing burnout was significantly higher than that of nurses in June 2020.”
This burnout can be explained by conditions caused by the pandemic, he noted, such as the scarcity of staff and resources and having to work with colleagues who were not qualified to work in critical care but who were there out of necessity.
Mr. Kok presented the findings of the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine.
Burnout highest among critical care physicians
The ICU can be a stressful environment for both patients and health care personnel, and burnout is not uncommon among ICU clinicians. However, COVID-19 has amplified the degree of burnout being experienced by clinicians working in this setting. Critical care physicians now top the list of physicians experiencing burnout, at 51%, up from 44% last year, according to the Medscape report ‘Death by 1000 Thousand Cuts’: Physician Burnout and Suicide Report 2021.
The Medscape Nurse Career Satisfaction Report 2020, while not restricted to those working in critical care, also reported higher rates of burnout, compared with the prepandemic period. The percentage of nurses reporting being “very burned out” prior to the pandemic was 4%. Six months into the pandemic, that percentage soared to 18%.
In this study, Mr. Kok and colleagues examined the prevalence and incidence of burnout symptoms and moral distress in health care professionals working in the ICU, both before and during the COVID-19 pandemic.
“When the COVID-19 pandemic surfaced in the Netherlands, the health care professionals in our hospitals were motivated to do everything they could to provide the best care possible,” said Mr. Kok. “Many of the ICU professionals immediately realized that they would have to work longer hours.”
However, the health care professionals that he spoke with did have mixed feelings. Some were afraid of being infected with the virus, while others said that “it was very interesting times for them and that gave them extra motivation to do the work.
“Some physicians [and] the WHO warned that COVID-19 is not going to weathered by a heroic sprint – it is an arduous marathon that is going to go hand in hand with burnout symptoms,” Mr. Kok added. “It will eat away at our qualified ICU staff.”
Before and after data on burnout
It was widely believed that the COVID-19 pandemic would increase burnout symptoms, as had been demonstrated in studies of previous pandemics. However, Mr. Kok emphasized that there are no before and after measurements that transcend cross-sectional designs.
“The claim [has been] that it increases burnout – but there are no assessments of how it progresses in ICU professionals through time,” he said. “So what we really need is a comparison [of] before and after the pandemic.”
It is quite difficult to obtain this type of information because disruptive events like the COVID-19 pandemic cannot be predicted, he said. Thus, it is challenging to get a baseline measurement. But Mr. Kok pointed out that the study has both “before and after” measurements.
“By coincidence really, we had baseline data to measure the impact of the COVID-19 pandemic and had information that was collected before the pandemic,” he said.
In January 2020, a study began looking at the effects of ethics meetings on moral distress in ICU professionals. Data had been collected on moral distress and burnout on ICU professionals in December 2019. The first COVID-19 cases appeared in the Netherlands in February 2020.
A follow-up study was then conducted in May and June 2020, several months into the pandemic.
The longitudinal open cohort study included all ICU personnel who were working in five units within a single university medical center, plus another adult ICU that was based in a separate teaching hospital.
A total of 352 health care professionals responded to a baseline survey in October through December 2019, and then 233 responded to a follow-up survey sent in May and June 2020. The authors measured burnout symptoms and moral distress with the Maslach Burnout Inventory and the Moral Distress Scale, respectively.
Findings
The overall prevalence of burnout symptoms was 23.0% prior to the pandemic, and that jumped to 36.1% at post-peak time. Higher rates of burnout were reported by nurses (38.0%) than physicians (28.6%).
However, the incidence rate of new burnout cases was higher among physicians, compared with nurses (26.7% vs 21.9%). Not surprisingly, a higher prevalence of burnout symptoms was observed in the post-peak period for all clinicians (odds ratio, 1.83; 95% confidence interval, 1.32-2.53), and was higher for nurses (odds ratio, 1.77; 95% confidence interval, 1.03-3.04), for those working overtime (OR, 2.11; 95% CI, 1.48-3.02), and for personnel who directly engaged in patient care (OR, 1.87; 95% CI, 1.35-2.60).
Physicians in general were much more likely to develop burnout symptoms related to the pandemic, compared with nurses (OR, 3.56; 95% CI, 1.06-12.21).
When looking at findings on moral distress, Kok pointed out that it often arises in situations when the health care professional knows the right thing to do but is prevented from doing so. “Morally distressful situations all rose from December to June,” said Mr. Kok. “Scarcity was the most distressing. The other was where colleagues were perceived to be less skilled, and this had to do with the recruitment of people from outside of the ICU to provide care.”
Moral distress from scarcity and unskilled colleagues were both significantly related to burnout, he noted.
In the final model, working in a COVID-19 unit, stress from scarcity of resources and people, stress from unskilled colleagues, and stress from unsafe conditions were all related to burnout. “The stress of physicians was significantly higher,” said Kok. “Even though nurses had higher baseline burnout, it became less pronounced in June 2020. This indicates that burnout was significantly higher in physicians.”
Thus, Mr. Kok and colleagues concluded that overburdening ICU professionals during an extended period of time leads to burnout, and all ICU workers are at risk.
Burnout rates higher in physicians
Weighing in on the study, Greg S. Martin, MD, FCCP, professor of medicine in the division of pulmonary, allergy, critical care and sleep medicine, Emory University, Atlanta, noted that the differences observed between physicians and nurses may have to do with the fact that “nurses have been smoldering all along and experiencing higher rates of burnout.
“They may have adapted better to the pandemic conditions, since they are more used to working overtime and short staffed, and spending far more time at the bedside,” he said. “Because of the volume of patients, physicians may be spending more hours doing patient care and are experiencing more burnout.”
For physicians, this may be a more significant change in the workload, as well as the complexity of the situation because of the pandemic. “Many things layer into it, such as [the fact] that there are no families present to give patients support, the complexity of care of these patients, and things like lack of PPE,” Dr. Martin said.
The study did not differentiate among physician groups, so it is unclear if the affected physicians were residents, fellows, or more senior staff. “Residents are often quite busy already, and don’t usually have the capacity to add more to their schedules, and maybe attendings were having to spend more time doing patient care,” Dr. Martin said. “In the United States, at least some personnel were restricted from working with COVID-19 patients. Medical students were removed in many places as well as nonessential staff, so that may have also added to their burnout.”
The study was conducted in the Netherlands, so there may be differences in the work environment, responsibilities of nurses vs. physicians, staffing, and so on. “But it still shows that burnout is very real among doctors and nurses working in the ICU in pandemic conditions,” he said.
FROM CCC50