User login
Restrictive transfusion strategy superior for severe acute GI bleeding
For patients with severe acute GI bleeding, outcomes are significantly better when a restrictive transfusion strategy is used – limiting the hemoglobin threshold to 7 g/dL – rather than a liberal transfusion strategy allowing a 9 g/dL threshold, according to a report published online Jan. 2 in the New England Journal of Medicine.
In a single-center randomized controlled trial involving 889 patients, the restrictive transfusion strategy resulted in significantly lower mortality, lower rates of rebleeding, less frequent need for rescue therapy, fewer complications, and shorter hospitalizations than did the liberal transfusion strategy. "Our results suggest that in patients with acute GI bleeding, a strategy of not performing transfusion until the hemoglobin concentration falls below 7 g/dL is a safe and effective approach," said Dr. Càndid Villanueva of Hospital de Sant Pau, Barcelona, and his associates.
"Current international guidelines recommend decreasing the hemoglobin threshold level for transfusion ... from 10g/dL to 7 g/dL" in such patients, but these recommendations are based on trials involving critically ill patients with normovolemic anemia that did not include subjects with acute bleeding. "Transfusion requirements may be different for patients with acute hemorrhage due to factors such as hemodynamic instability or rapid onset of anemia" resulting from extremely low hemoglobin levels.
In particular, results of animal studies suggest that transfusion can be especially harmful in patients with bleeding from portal hypertension sources, "since restitution of blood volume after hemorrhage can lead to a rebound increase in portal pressure, which is associated with a risk of rebleeding," the investigators noted.
To examine the effects of different transfusion strategies in this setting, Dr. Villanueva and his colleagues enrolled adults who presented with hematemesis, melena, or both, randomly assigning 444 to receive restrictive transfusion (with a target range for the posttransfusion hemoglobin level of 7-9 g/dL) and 445 to receive liberal transfusion (with a target range of 9-11 g/dL).
The study protocol permitted transfusions to be administered at the discretion of the attending physician any time symptoms or signs of anemia developed, massive bleeding occurred, or surgical intervention was needed, as well as when hemoglobin levels dipped below the assigned threshold.
All the study subjects underwent emergency gastroscopy within 6 hours of presentation, with appropriate treatment when the source of the bleeding was identified. Diagnoses included peptic ulcer, esophageal varices, cirrhosis, portal hypertension, and nonvariceal lesions.
The primary outcome measure, mortality from any cause at 45 days, was significantly lower in the restrictive-strategy group (5%) than the liberal-strategy group (9%). Death resulted from uncontrolled bleeding in 0.7% vs 3.1% of the 2 groups, respectively, the researchers said (N. Engl. J. Med. 2013 Jan. 2 [doi:10.1056/NEJMoa1211801]).
The rate of rebleeding also was significantly lower with the restrictive strategy (10% vs. 16%), and length of hospital stay was significantly shorter. In addition, rescue therapy for esophageal varices with balloon tamponade or a transjugular intrahepatic portosystemic shunt was required less often in the restrictive-strategy group than in the liberal-strategy group, as was emergency surgery to control further bleeding from peptic ulcer.
The rate of overall complications was significantly lower with the restrictive strategy (40%) than with the liberal strategy (48%), as was the rate of serious adverse events. In addition, transfusion reactions and cardiac events such as pulmonary edema were more frequent with the liberal strategy.
"Our results are consistent with those from previous observational studies and randomized trials performed in other settings, which have shown that a restrictive transfusion strategy did not increase, and even decreased, the mortality observed with a liberal transfusion strategy," Dr. Villanueva and his associates said.
This important study "provides long-awaited evidence to guide practice and justify current recommendations for the management of upper GI bleeding," said Dr. Loren Laine.
A restrictive transfusion strategy reduced the relative risk of mortality at 45 days by 45%. Extrapolating the study findings, only 25 patients would have to be treated with a restrictive rather than a liberal transfusion strategy to avert one additional death.
Dr. Laine is at Yale University, New Haven, Conn., and the Veterans Affairs Connecticut Healthcare System, West Haven. He reported no financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Villanueva’s report (N. Engl. J. Med. 2013 Jan. 2 [doi:10.1056/NEJMe1212009]).
This important study "provides long-awaited evidence to guide practice and justify current recommendations for the management of upper GI bleeding," said Dr. Loren Laine.
A restrictive transfusion strategy reduced the relative risk of mortality at 45 days by 45%. Extrapolating the study findings, only 25 patients would have to be treated with a restrictive rather than a liberal transfusion strategy to avert one additional death.
Dr. Laine is at Yale University, New Haven, Conn., and the Veterans Affairs Connecticut Healthcare System, West Haven. He reported no financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Villanueva’s report (N. Engl. J. Med. 2013 Jan. 2 [doi:10.1056/NEJMe1212009]).
This important study "provides long-awaited evidence to guide practice and justify current recommendations for the management of upper GI bleeding," said Dr. Loren Laine.
A restrictive transfusion strategy reduced the relative risk of mortality at 45 days by 45%. Extrapolating the study findings, only 25 patients would have to be treated with a restrictive rather than a liberal transfusion strategy to avert one additional death.
Dr. Laine is at Yale University, New Haven, Conn., and the Veterans Affairs Connecticut Healthcare System, West Haven. He reported no financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Villanueva’s report (N. Engl. J. Med. 2013 Jan. 2 [doi:10.1056/NEJMe1212009]).
For patients with severe acute GI bleeding, outcomes are significantly better when a restrictive transfusion strategy is used – limiting the hemoglobin threshold to 7 g/dL – rather than a liberal transfusion strategy allowing a 9 g/dL threshold, according to a report published online Jan. 2 in the New England Journal of Medicine.
In a single-center randomized controlled trial involving 889 patients, the restrictive transfusion strategy resulted in significantly lower mortality, lower rates of rebleeding, less frequent need for rescue therapy, fewer complications, and shorter hospitalizations than did the liberal transfusion strategy. "Our results suggest that in patients with acute GI bleeding, a strategy of not performing transfusion until the hemoglobin concentration falls below 7 g/dL is a safe and effective approach," said Dr. Càndid Villanueva of Hospital de Sant Pau, Barcelona, and his associates.
"Current international guidelines recommend decreasing the hemoglobin threshold level for transfusion ... from 10g/dL to 7 g/dL" in such patients, but these recommendations are based on trials involving critically ill patients with normovolemic anemia that did not include subjects with acute bleeding. "Transfusion requirements may be different for patients with acute hemorrhage due to factors such as hemodynamic instability or rapid onset of anemia" resulting from extremely low hemoglobin levels.
In particular, results of animal studies suggest that transfusion can be especially harmful in patients with bleeding from portal hypertension sources, "since restitution of blood volume after hemorrhage can lead to a rebound increase in portal pressure, which is associated with a risk of rebleeding," the investigators noted.
To examine the effects of different transfusion strategies in this setting, Dr. Villanueva and his colleagues enrolled adults who presented with hematemesis, melena, or both, randomly assigning 444 to receive restrictive transfusion (with a target range for the posttransfusion hemoglobin level of 7-9 g/dL) and 445 to receive liberal transfusion (with a target range of 9-11 g/dL).
The study protocol permitted transfusions to be administered at the discretion of the attending physician any time symptoms or signs of anemia developed, massive bleeding occurred, or surgical intervention was needed, as well as when hemoglobin levels dipped below the assigned threshold.
All the study subjects underwent emergency gastroscopy within 6 hours of presentation, with appropriate treatment when the source of the bleeding was identified. Diagnoses included peptic ulcer, esophageal varices, cirrhosis, portal hypertension, and nonvariceal lesions.
The primary outcome measure, mortality from any cause at 45 days, was significantly lower in the restrictive-strategy group (5%) than the liberal-strategy group (9%). Death resulted from uncontrolled bleeding in 0.7% vs 3.1% of the 2 groups, respectively, the researchers said (N. Engl. J. Med. 2013 Jan. 2 [doi:10.1056/NEJMoa1211801]).
The rate of rebleeding also was significantly lower with the restrictive strategy (10% vs. 16%), and length of hospital stay was significantly shorter. In addition, rescue therapy for esophageal varices with balloon tamponade or a transjugular intrahepatic portosystemic shunt was required less often in the restrictive-strategy group than in the liberal-strategy group, as was emergency surgery to control further bleeding from peptic ulcer.
The rate of overall complications was significantly lower with the restrictive strategy (40%) than with the liberal strategy (48%), as was the rate of serious adverse events. In addition, transfusion reactions and cardiac events such as pulmonary edema were more frequent with the liberal strategy.
"Our results are consistent with those from previous observational studies and randomized trials performed in other settings, which have shown that a restrictive transfusion strategy did not increase, and even decreased, the mortality observed with a liberal transfusion strategy," Dr. Villanueva and his associates said.
For patients with severe acute GI bleeding, outcomes are significantly better when a restrictive transfusion strategy is used – limiting the hemoglobin threshold to 7 g/dL – rather than a liberal transfusion strategy allowing a 9 g/dL threshold, according to a report published online Jan. 2 in the New England Journal of Medicine.
In a single-center randomized controlled trial involving 889 patients, the restrictive transfusion strategy resulted in significantly lower mortality, lower rates of rebleeding, less frequent need for rescue therapy, fewer complications, and shorter hospitalizations than did the liberal transfusion strategy. "Our results suggest that in patients with acute GI bleeding, a strategy of not performing transfusion until the hemoglobin concentration falls below 7 g/dL is a safe and effective approach," said Dr. Càndid Villanueva of Hospital de Sant Pau, Barcelona, and his associates.
"Current international guidelines recommend decreasing the hemoglobin threshold level for transfusion ... from 10g/dL to 7 g/dL" in such patients, but these recommendations are based on trials involving critically ill patients with normovolemic anemia that did not include subjects with acute bleeding. "Transfusion requirements may be different for patients with acute hemorrhage due to factors such as hemodynamic instability or rapid onset of anemia" resulting from extremely low hemoglobin levels.
In particular, results of animal studies suggest that transfusion can be especially harmful in patients with bleeding from portal hypertension sources, "since restitution of blood volume after hemorrhage can lead to a rebound increase in portal pressure, which is associated with a risk of rebleeding," the investigators noted.
To examine the effects of different transfusion strategies in this setting, Dr. Villanueva and his colleagues enrolled adults who presented with hematemesis, melena, or both, randomly assigning 444 to receive restrictive transfusion (with a target range for the posttransfusion hemoglobin level of 7-9 g/dL) and 445 to receive liberal transfusion (with a target range of 9-11 g/dL).
The study protocol permitted transfusions to be administered at the discretion of the attending physician any time symptoms or signs of anemia developed, massive bleeding occurred, or surgical intervention was needed, as well as when hemoglobin levels dipped below the assigned threshold.
All the study subjects underwent emergency gastroscopy within 6 hours of presentation, with appropriate treatment when the source of the bleeding was identified. Diagnoses included peptic ulcer, esophageal varices, cirrhosis, portal hypertension, and nonvariceal lesions.
The primary outcome measure, mortality from any cause at 45 days, was significantly lower in the restrictive-strategy group (5%) than the liberal-strategy group (9%). Death resulted from uncontrolled bleeding in 0.7% vs 3.1% of the 2 groups, respectively, the researchers said (N. Engl. J. Med. 2013 Jan. 2 [doi:10.1056/NEJMoa1211801]).
The rate of rebleeding also was significantly lower with the restrictive strategy (10% vs. 16%), and length of hospital stay was significantly shorter. In addition, rescue therapy for esophageal varices with balloon tamponade or a transjugular intrahepatic portosystemic shunt was required less often in the restrictive-strategy group than in the liberal-strategy group, as was emergency surgery to control further bleeding from peptic ulcer.
The rate of overall complications was significantly lower with the restrictive strategy (40%) than with the liberal strategy (48%), as was the rate of serious adverse events. In addition, transfusion reactions and cardiac events such as pulmonary edema were more frequent with the liberal strategy.
"Our results are consistent with those from previous observational studies and randomized trials performed in other settings, which have shown that a restrictive transfusion strategy did not increase, and even decreased, the mortality observed with a liberal transfusion strategy," Dr. Villanueva and his associates said.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Mortality from any cause at 45 days was significantly lower in the restrictive-strategy group (5%) than in the liberal-strategy group (9%).
Data Source: A single-center randomized controlled trial of 889 patients.
Disclosures: This study was supported in part by the Fundacio Investigacio Sant Pau. Dr. Villanueva reported no financial conflicts of interest; one of his associates reported ties to Sequana Medical.
Laparoscopic diverticulitis surgery linked to fewer complications
PALM BEACH, FLA.– Using laparoscopic surgery for colectomy with primary anastomosis in patients with complicated diverticulitis linked with significantly fewer major complications compared with open surgical management in a review of more than 10,000 patients from a nationwide database.
However, the inherent biases at play when surgeons decide whether to manage a diverticulitis patient by a laparoscopic or open approach make it difficult to draw definitive conclusions from the findings, Dr. Edward E. Cornwell III said at the annual meeting of the Southern Surgical Association.

"If a surgeon did an operation laparoscopically, that by itself is an indicator of how sick the patient was. The surgeon selects an open operation for sicker patients, and laparoscopy for the less sick patients," he said in an interview. "Have we accounted for that difference [in the analysis]? That’s an open question," said Dr. Cornwell, professor and chairman of surgery at Howard University in Washington.
"Patients whom the surgeon deem well enough physiologically to sustain colectomy with primary anastomosis deserve strong consideration for the laparoscopic approach because those patients had the greatest difference in complications" compared with open surgery, he said.
The data Dr. Cornwell and his associates reviewed also showed a marked skewing in how surgeons used laparoscopy. Among the 10,085 patients included in the analysis, 7,562 (75%) underwent colectomy with primary anastomosis, and in this subgroup, 5,105 patients (68%) had their surgery done laparoscopically, while the remaining 2,457 (32%) were done with open surgery. In contrast, the 2,523 other patients in the series underwent a colectomy with colostomy, and within this subgroup, 2,286 patients (91%) had open surgery, with only 237 (9%) having laparoscopic surgery.
The overwhelming use of open surgery for the colostomy patients makes sense as it is a more complex operation, Dr. Cornwell said.
He and his associates used data collected during 2005-2009 at 237 U.S. hospitals by the National Surgical Quality Improvement Program of the American College of Surgeons on patients who underwent surgical management of complicated diverticulitis. The average age of the patients was 58 years, and overall 30-day mortality was 2%, while the overall postoperative complication rate during the 30 days following surgery was 23%.
Among the patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients, a statistically significant difference. Major complications included surgical site infections, dehiscence, transfusion, respiratory failure, sepsis, myocardial infarction, pulmonary embolism, stroke, renal failure or need for rehospitalization.
In a multivariate analysis that controlled for demographic parameters, body mass index, comorbidities, and functional status, patients who underwent laparoscopy had about half the number of total complications and major complications compared with patients who underwent open surgery – statistically significant differences. The laparoscopically-treated patients also had roughly half the rate of several individual major complications – wound infections, respiratory complications, and sepsis – compared with the open surgery patients, all statistically significant differences.
Thirty-day mortality was about 50% lower with laparoscopy compared with open surgery among patients who underwent a primary anastomosis, but this difference fell short of statistical significance.
The advantage of laparoscopy over open surgery was not nearly so clear among patients who underwent colectomy with colostomy. The data showed no significant difference between laparoscopy and open surgery in the rate of all major complications, although the number of major complications with laparoscopy was about 20% lower. The only individual complications significantly reduced in the laparoscopy group were wound infections, reduced by about 40% in the adjusted analysis, and respiratory complications, cut by about 50% by laparoscopy. The two surgical subgroups showed virtually no difference in 30-day mortality among patients who underwent a colectomy.
The results suggest that because of the broad reduction of major complications with laparoscopy, this approach "should be considered when primary anastomosis is deemed appropriate," Dr. Cornwell concluded.
Dr. Cornwell said that he had no disclosures.
This work falls somewhat short of actually comparing the efficacy of the laparoscopic approach and open surgery in patients with complicated diverticulitis. Without an adequate standardized description of the disease process itself, the patients’ comorbidities, and their physiologic perturbation at the time of presentation, it is exceedingly difficult to measure outcomes and the efficacy of therapeutic interventions.
I’m afraid the authors have not satisfactorily controlled for or analyzed the confounding factors so that plausible conclusions can be reached. The results are striking that mortality and complications were higher for patients treated with open surgery. I have watched the evolution of laparoscopic surgery over the past 25 years, and I am convinced that patients greatly benefit from this technology.
While the laparoscopic approach for treating diverticulitis resonates with my sensibility, the data do not support a clear recommendation. I urge surgeons to focus on this emergency, general-surgery population so that we can do important comparative effectiveness research and address some of these questions.
Dr. Michael F. Rotondo is professor and chairman of surgery at East Carolina University in Greenville, N.C. He had no disclosures. He made these comments as a designated discussant of the report.
This work falls somewhat short of actually comparing the efficacy of the laparoscopic approach and open surgery in patients with complicated diverticulitis. Without an adequate standardized description of the disease process itself, the patients’ comorbidities, and their physiologic perturbation at the time of presentation, it is exceedingly difficult to measure outcomes and the efficacy of therapeutic interventions.
I’m afraid the authors have not satisfactorily controlled for or analyzed the confounding factors so that plausible conclusions can be reached. The results are striking that mortality and complications were higher for patients treated with open surgery. I have watched the evolution of laparoscopic surgery over the past 25 years, and I am convinced that patients greatly benefit from this technology.
While the laparoscopic approach for treating diverticulitis resonates with my sensibility, the data do not support a clear recommendation. I urge surgeons to focus on this emergency, general-surgery population so that we can do important comparative effectiveness research and address some of these questions.
Dr. Michael F. Rotondo is professor and chairman of surgery at East Carolina University in Greenville, N.C. He had no disclosures. He made these comments as a designated discussant of the report.
This work falls somewhat short of actually comparing the efficacy of the laparoscopic approach and open surgery in patients with complicated diverticulitis. Without an adequate standardized description of the disease process itself, the patients’ comorbidities, and their physiologic perturbation at the time of presentation, it is exceedingly difficult to measure outcomes and the efficacy of therapeutic interventions.
I’m afraid the authors have not satisfactorily controlled for or analyzed the confounding factors so that plausible conclusions can be reached. The results are striking that mortality and complications were higher for patients treated with open surgery. I have watched the evolution of laparoscopic surgery over the past 25 years, and I am convinced that patients greatly benefit from this technology.
While the laparoscopic approach for treating diverticulitis resonates with my sensibility, the data do not support a clear recommendation. I urge surgeons to focus on this emergency, general-surgery population so that we can do important comparative effectiveness research and address some of these questions.
Dr. Michael F. Rotondo is professor and chairman of surgery at East Carolina University in Greenville, N.C. He had no disclosures. He made these comments as a designated discussant of the report.
PALM BEACH, FLA.– Using laparoscopic surgery for colectomy with primary anastomosis in patients with complicated diverticulitis linked with significantly fewer major complications compared with open surgical management in a review of more than 10,000 patients from a nationwide database.
However, the inherent biases at play when surgeons decide whether to manage a diverticulitis patient by a laparoscopic or open approach make it difficult to draw definitive conclusions from the findings, Dr. Edward E. Cornwell III said at the annual meeting of the Southern Surgical Association.
"If a surgeon did an operation laparoscopically, that by itself is an indicator of how sick the patient was. The surgeon selects an open operation for sicker patients, and laparoscopy for the less sick patients," he said in an interview. "Have we accounted for that difference [in the analysis]? That’s an open question," said Dr. Cornwell, professor and chairman of surgery at Howard University in Washington.
"Patients whom the surgeon deem well enough physiologically to sustain colectomy with primary anastomosis deserve strong consideration for the laparoscopic approach because those patients had the greatest difference in complications" compared with open surgery, he said.
The data Dr. Cornwell and his associates reviewed also showed a marked skewing in how surgeons used laparoscopy. Among the 10,085 patients included in the analysis, 7,562 (75%) underwent colectomy with primary anastomosis, and in this subgroup, 5,105 patients (68%) had their surgery done laparoscopically, while the remaining 2,457 (32%) were done with open surgery. In contrast, the 2,523 other patients in the series underwent a colectomy with colostomy, and within this subgroup, 2,286 patients (91%) had open surgery, with only 237 (9%) having laparoscopic surgery.
The overwhelming use of open surgery for the colostomy patients makes sense as it is a more complex operation, Dr. Cornwell said.
He and his associates used data collected during 2005-2009 at 237 U.S. hospitals by the National Surgical Quality Improvement Program of the American College of Surgeons on patients who underwent surgical management of complicated diverticulitis. The average age of the patients was 58 years, and overall 30-day mortality was 2%, while the overall postoperative complication rate during the 30 days following surgery was 23%.
Among the patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients, a statistically significant difference. Major complications included surgical site infections, dehiscence, transfusion, respiratory failure, sepsis, myocardial infarction, pulmonary embolism, stroke, renal failure or need for rehospitalization.
In a multivariate analysis that controlled for demographic parameters, body mass index, comorbidities, and functional status, patients who underwent laparoscopy had about half the number of total complications and major complications compared with patients who underwent open surgery – statistically significant differences. The laparoscopically-treated patients also had roughly half the rate of several individual major complications – wound infections, respiratory complications, and sepsis – compared with the open surgery patients, all statistically significant differences.
Thirty-day mortality was about 50% lower with laparoscopy compared with open surgery among patients who underwent a primary anastomosis, but this difference fell short of statistical significance.
The advantage of laparoscopy over open surgery was not nearly so clear among patients who underwent colectomy with colostomy. The data showed no significant difference between laparoscopy and open surgery in the rate of all major complications, although the number of major complications with laparoscopy was about 20% lower. The only individual complications significantly reduced in the laparoscopy group were wound infections, reduced by about 40% in the adjusted analysis, and respiratory complications, cut by about 50% by laparoscopy. The two surgical subgroups showed virtually no difference in 30-day mortality among patients who underwent a colectomy.
The results suggest that because of the broad reduction of major complications with laparoscopy, this approach "should be considered when primary anastomosis is deemed appropriate," Dr. Cornwell concluded.
Dr. Cornwell said that he had no disclosures.
PALM BEACH, FLA.– Using laparoscopic surgery for colectomy with primary anastomosis in patients with complicated diverticulitis linked with significantly fewer major complications compared with open surgical management in a review of more than 10,000 patients from a nationwide database.
However, the inherent biases at play when surgeons decide whether to manage a diverticulitis patient by a laparoscopic or open approach make it difficult to draw definitive conclusions from the findings, Dr. Edward E. Cornwell III said at the annual meeting of the Southern Surgical Association.
"If a surgeon did an operation laparoscopically, that by itself is an indicator of how sick the patient was. The surgeon selects an open operation for sicker patients, and laparoscopy for the less sick patients," he said in an interview. "Have we accounted for that difference [in the analysis]? That’s an open question," said Dr. Cornwell, professor and chairman of surgery at Howard University in Washington.
"Patients whom the surgeon deem well enough physiologically to sustain colectomy with primary anastomosis deserve strong consideration for the laparoscopic approach because those patients had the greatest difference in complications" compared with open surgery, he said.
The data Dr. Cornwell and his associates reviewed also showed a marked skewing in how surgeons used laparoscopy. Among the 10,085 patients included in the analysis, 7,562 (75%) underwent colectomy with primary anastomosis, and in this subgroup, 5,105 patients (68%) had their surgery done laparoscopically, while the remaining 2,457 (32%) were done with open surgery. In contrast, the 2,523 other patients in the series underwent a colectomy with colostomy, and within this subgroup, 2,286 patients (91%) had open surgery, with only 237 (9%) having laparoscopic surgery.
The overwhelming use of open surgery for the colostomy patients makes sense as it is a more complex operation, Dr. Cornwell said.
He and his associates used data collected during 2005-2009 at 237 U.S. hospitals by the National Surgical Quality Improvement Program of the American College of Surgeons on patients who underwent surgical management of complicated diverticulitis. The average age of the patients was 58 years, and overall 30-day mortality was 2%, while the overall postoperative complication rate during the 30 days following surgery was 23%.
Among the patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients, a statistically significant difference. Major complications included surgical site infections, dehiscence, transfusion, respiratory failure, sepsis, myocardial infarction, pulmonary embolism, stroke, renal failure or need for rehospitalization.
In a multivariate analysis that controlled for demographic parameters, body mass index, comorbidities, and functional status, patients who underwent laparoscopy had about half the number of total complications and major complications compared with patients who underwent open surgery – statistically significant differences. The laparoscopically-treated patients also had roughly half the rate of several individual major complications – wound infections, respiratory complications, and sepsis – compared with the open surgery patients, all statistically significant differences.
Thirty-day mortality was about 50% lower with laparoscopy compared with open surgery among patients who underwent a primary anastomosis, but this difference fell short of statistical significance.
The advantage of laparoscopy over open surgery was not nearly so clear among patients who underwent colectomy with colostomy. The data showed no significant difference between laparoscopy and open surgery in the rate of all major complications, although the number of major complications with laparoscopy was about 20% lower. The only individual complications significantly reduced in the laparoscopy group were wound infections, reduced by about 40% in the adjusted analysis, and respiratory complications, cut by about 50% by laparoscopy. The two surgical subgroups showed virtually no difference in 30-day mortality among patients who underwent a colectomy.
The results suggest that because of the broad reduction of major complications with laparoscopy, this approach "should be considered when primary anastomosis is deemed appropriate," Dr. Cornwell concluded.
Dr. Cornwell said that he had no disclosures.
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Among patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients.
Data Source: From 10,085 U.S. patients who had surgery for acute management of complicated diverticulitis during 2005-2009.
Disclosures: Dr. Cornwell said he had no disclosures.
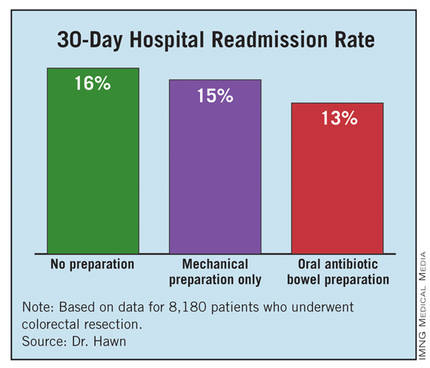
Antibiotic prophylaxis reduces colorectal surgery readmissions
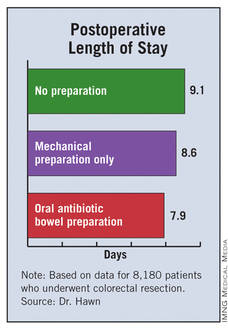
PALM BEACH, FLA. – Administering a brief oral antibiotic regimen preoperatively to colorectal surgery patients cut the average postoperative hospitalization by more than a day and reduced 30-day readmissions by about 3% compared with no presurgical bowel preparation, a review of more than 8,000 patients found.
The primary driver of these beneficial effects was a reduced rate of surgical site infections, Dr. Mary T. Hawn said at the annual meeting of the Southern Surgical Association.
"Efforts to improve adherence with the use of oral antibiotic preparation may improve the efficiency of care for colorectal surgery," said Dr. Hawn, chief of gastrointestinal surgery at the University of Alabama, Birmingham. "Further research is needed to determine the best protocol for bowel prep prior to colorectal surgery, and to prospectively monitor the rate of Clostridium difficile infection."
The findings by Dr. Hawn’s group also showed that oral antibiotic bowel preparation (OABP) led to a small but statistically significant increase in the rate of hospital readmissions among patients with a principal diagnostic code of colitis caused by C. difficile infection. The OABP patients had a 0.5% readmission rate, compared with a 0.1% rate among patients who received no presurgical bowel preparation.
The value of OABP as shown in this study is particularly important because the use of OABP before colorectal surgery has declined in the United States over the past 20 years, Dr. Hawn added.
Using data collected as part of the VA Surgical Quality Improvement Program, Dr. Hawn and her colleagues analyzed results for 8,180 patients who underwent elective colorectal resection at any of 112 participating VA hospitals during 2005-2009. Patients who had a partial or total colectomy, a rectal resection, or an ostomy were included. Patients were excluded if they had a preoperative stay of more than 2 days, a postoperative stay of more than 30 days, or an American Surgical Association 5 classification, or if they died before hospital discharge.
Most of the patients (83%) underwent surgery for neoplasms; the next most common reason for surgery was diverticulitis, in 6%. OABP was the most common form of presurgical preparation, used on 44% of patients; mechanical preparation only was used on 39%, and no preparation was done in 17%. Ninety percent of the OABP patients also underwent mechanical preparation, while the other 10% had OABP only.
The average postoperative length of stay was 9.1 days among those who received no preparation, 8.6 days for those who got mechanical preparation only, and 7.9 days for those who had OABP – a statistically significant advantage for OABP. In a multivariate regression analysis that controlled for indication, age, and wound class, OABP cut length of stay by an average of 12% compared with no preparation, a statistically significant reduction. In the same analysis, mechanical preparation cut length of stay by only 4% compared with no preparation, also a significant effect.
The hospital readmission rate was 16% with no preparation, 15% with mechanical preparation only, and 13% with OABP. In the multivariate regression analysis with adjustment for procedure, age, and wound class, OABP cut the readmission rate by 19% compared with no preparation, a statistically significant reduction. Mechanical preparation only did not have a statistically significant effect.

Further analyses showed that the most common reason for readmission among all patients studied was postoperative infection, in 18%, followed by digestive-system complications, in 10%. C. difficile infection caused 3% of readmissions.
In addition, infections were responsible for readmissions among 6% of patients who underwent no presurgical preparation and in 4% of those who underwent OABP, a statistically significant difference. In contrast, use of OABP produced no statistically significant decline in noninfectious causes of readmission. This rate ran 10% among patients with no preparation, and 9% in patients who underwent OABP.
Dr. Hawn said that she had no disclosures.
Surgical site infections (SSIs) remain a vexing problem despite the significant efforts by hospitals to increase compliance with measures of the Surgical Care Improvement Project. These efforts have so far failed to translate into improved outcomes. We need to identify additional processes that can be changed to improve surgical outcomes.
Elizabeth C. Wick |

At Johns Hopkins, we addressed SSIs by implementing the Comprehensive Unit-Based Safety Program for patients undergoing colorectal surgery. Interventions included standardization of skin preparation, administration of preoperative chlorhexidine showers, selective elimination of mechanical bowel preparation, warming of patients in the preanesthesia area, adoption of enhanced sterile techniques for skin and fascial closure, and addressing previously unrecognized lapses in antibiotic prophylaxis. The program was modeled on ICU processes designed to prevent central line bloodstream infections.
Our program improved the operating room culture by engaging and empowering front-line staff to address deficits and improve processes. A recent review of the rate of SSIs during the 12 months prior to and the 12 months after implementation of this program found that infection rates fell from 27% before implementation to 18% afterward – a 33% relative decrease (J. Am. Coll. Surg. 2012;215:193-200).
We are expanding this program to colon surgery programs at more than 100 U.S. hospitals. Hospitals want to institute new processes proven to improve patient outcomes. The report by Dr. Hawn and her associates is an important step toward identifying a new approach that might further reduce SSIs.
Dr. Elizabeth C. Wick is a colorectal surgeon at Johns Hopkins Hospital in Baltimore. She had no disclosures. She made these comments as a designated discussant for Dr. Hawn’s report.
Surgical site infections (SSIs) remain a vexing problem despite the significant efforts by hospitals to increase compliance with measures of the Surgical Care Improvement Project. These efforts have so far failed to translate into improved outcomes. We need to identify additional processes that can be changed to improve surgical outcomes.
Elizabeth C. Wick |
At Johns Hopkins, we addressed SSIs by implementing the Comprehensive Unit-Based Safety Program for patients undergoing colorectal surgery. Interventions included standardization of skin preparation, administration of preoperative chlorhexidine showers, selective elimination of mechanical bowel preparation, warming of patients in the preanesthesia area, adoption of enhanced sterile techniques for skin and fascial closure, and addressing previously unrecognized lapses in antibiotic prophylaxis. The program was modeled on ICU processes designed to prevent central line bloodstream infections.
Our program improved the operating room culture by engaging and empowering front-line staff to address deficits and improve processes. A recent review of the rate of SSIs during the 12 months prior to and the 12 months after implementation of this program found that infection rates fell from 27% before implementation to 18% afterward – a 33% relative decrease (J. Am. Coll. Surg. 2012;215:193-200).
We are expanding this program to colon surgery programs at more than 100 U.S. hospitals. Hospitals want to institute new processes proven to improve patient outcomes. The report by Dr. Hawn and her associates is an important step toward identifying a new approach that might further reduce SSIs.
Dr. Elizabeth C. Wick is a colorectal surgeon at Johns Hopkins Hospital in Baltimore. She had no disclosures. She made these comments as a designated discussant for Dr. Hawn’s report.
Surgical site infections (SSIs) remain a vexing problem despite the significant efforts by hospitals to increase compliance with measures of the Surgical Care Improvement Project. These efforts have so far failed to translate into improved outcomes. We need to identify additional processes that can be changed to improve surgical outcomes.
Elizabeth C. Wick |
At Johns Hopkins, we addressed SSIs by implementing the Comprehensive Unit-Based Safety Program for patients undergoing colorectal surgery. Interventions included standardization of skin preparation, administration of preoperative chlorhexidine showers, selective elimination of mechanical bowel preparation, warming of patients in the preanesthesia area, adoption of enhanced sterile techniques for skin and fascial closure, and addressing previously unrecognized lapses in antibiotic prophylaxis. The program was modeled on ICU processes designed to prevent central line bloodstream infections.
Our program improved the operating room culture by engaging and empowering front-line staff to address deficits and improve processes. A recent review of the rate of SSIs during the 12 months prior to and the 12 months after implementation of this program found that infection rates fell from 27% before implementation to 18% afterward – a 33% relative decrease (J. Am. Coll. Surg. 2012;215:193-200).
We are expanding this program to colon surgery programs at more than 100 U.S. hospitals. Hospitals want to institute new processes proven to improve patient outcomes. The report by Dr. Hawn and her associates is an important step toward identifying a new approach that might further reduce SSIs.
Dr. Elizabeth C. Wick is a colorectal surgeon at Johns Hopkins Hospital in Baltimore. She had no disclosures. She made these comments as a designated discussant for Dr. Hawn’s report.
PALM BEACH, FLA. – Administering a brief oral antibiotic regimen preoperatively to colorectal surgery patients cut the average postoperative hospitalization by more than a day and reduced 30-day readmissions by about 3% compared with no presurgical bowel preparation, a review of more than 8,000 patients found.
The primary driver of these beneficial effects was a reduced rate of surgical site infections, Dr. Mary T. Hawn said at the annual meeting of the Southern Surgical Association.
"Efforts to improve adherence with the use of oral antibiotic preparation may improve the efficiency of care for colorectal surgery," said Dr. Hawn, chief of gastrointestinal surgery at the University of Alabama, Birmingham. "Further research is needed to determine the best protocol for bowel prep prior to colorectal surgery, and to prospectively monitor the rate of Clostridium difficile infection."
The findings by Dr. Hawn’s group also showed that oral antibiotic bowel preparation (OABP) led to a small but statistically significant increase in the rate of hospital readmissions among patients with a principal diagnostic code of colitis caused by C. difficile infection. The OABP patients had a 0.5% readmission rate, compared with a 0.1% rate among patients who received no presurgical bowel preparation.
The value of OABP as shown in this study is particularly important because the use of OABP before colorectal surgery has declined in the United States over the past 20 years, Dr. Hawn added.
Using data collected as part of the VA Surgical Quality Improvement Program, Dr. Hawn and her colleagues analyzed results for 8,180 patients who underwent elective colorectal resection at any of 112 participating VA hospitals during 2005-2009. Patients who had a partial or total colectomy, a rectal resection, or an ostomy were included. Patients were excluded if they had a preoperative stay of more than 2 days, a postoperative stay of more than 30 days, or an American Surgical Association 5 classification, or if they died before hospital discharge.
Most of the patients (83%) underwent surgery for neoplasms; the next most common reason for surgery was diverticulitis, in 6%. OABP was the most common form of presurgical preparation, used on 44% of patients; mechanical preparation only was used on 39%, and no preparation was done in 17%. Ninety percent of the OABP patients also underwent mechanical preparation, while the other 10% had OABP only.
The average postoperative length of stay was 9.1 days among those who received no preparation, 8.6 days for those who got mechanical preparation only, and 7.9 days for those who had OABP – a statistically significant advantage for OABP. In a multivariate regression analysis that controlled for indication, age, and wound class, OABP cut length of stay by an average of 12% compared with no preparation, a statistically significant reduction. In the same analysis, mechanical preparation cut length of stay by only 4% compared with no preparation, also a significant effect.
The hospital readmission rate was 16% with no preparation, 15% with mechanical preparation only, and 13% with OABP. In the multivariate regression analysis with adjustment for procedure, age, and wound class, OABP cut the readmission rate by 19% compared with no preparation, a statistically significant reduction. Mechanical preparation only did not have a statistically significant effect.
Further analyses showed that the most common reason for readmission among all patients studied was postoperative infection, in 18%, followed by digestive-system complications, in 10%. C. difficile infection caused 3% of readmissions.
In addition, infections were responsible for readmissions among 6% of patients who underwent no presurgical preparation and in 4% of those who underwent OABP, a statistically significant difference. In contrast, use of OABP produced no statistically significant decline in noninfectious causes of readmission. This rate ran 10% among patients with no preparation, and 9% in patients who underwent OABP.
Dr. Hawn said that she had no disclosures.
PALM BEACH, FLA. – Administering a brief oral antibiotic regimen preoperatively to colorectal surgery patients cut the average postoperative hospitalization by more than a day and reduced 30-day readmissions by about 3% compared with no presurgical bowel preparation, a review of more than 8,000 patients found.
The primary driver of these beneficial effects was a reduced rate of surgical site infections, Dr. Mary T. Hawn said at the annual meeting of the Southern Surgical Association.
"Efforts to improve adherence with the use of oral antibiotic preparation may improve the efficiency of care for colorectal surgery," said Dr. Hawn, chief of gastrointestinal surgery at the University of Alabama, Birmingham. "Further research is needed to determine the best protocol for bowel prep prior to colorectal surgery, and to prospectively monitor the rate of Clostridium difficile infection."
The findings by Dr. Hawn’s group also showed that oral antibiotic bowel preparation (OABP) led to a small but statistically significant increase in the rate of hospital readmissions among patients with a principal diagnostic code of colitis caused by C. difficile infection. The OABP patients had a 0.5% readmission rate, compared with a 0.1% rate among patients who received no presurgical bowel preparation.
The value of OABP as shown in this study is particularly important because the use of OABP before colorectal surgery has declined in the United States over the past 20 years, Dr. Hawn added.
Using data collected as part of the VA Surgical Quality Improvement Program, Dr. Hawn and her colleagues analyzed results for 8,180 patients who underwent elective colorectal resection at any of 112 participating VA hospitals during 2005-2009. Patients who had a partial or total colectomy, a rectal resection, or an ostomy were included. Patients were excluded if they had a preoperative stay of more than 2 days, a postoperative stay of more than 30 days, or an American Surgical Association 5 classification, or if they died before hospital discharge.
Most of the patients (83%) underwent surgery for neoplasms; the next most common reason for surgery was diverticulitis, in 6%. OABP was the most common form of presurgical preparation, used on 44% of patients; mechanical preparation only was used on 39%, and no preparation was done in 17%. Ninety percent of the OABP patients also underwent mechanical preparation, while the other 10% had OABP only.
The average postoperative length of stay was 9.1 days among those who received no preparation, 8.6 days for those who got mechanical preparation only, and 7.9 days for those who had OABP – a statistically significant advantage for OABP. In a multivariate regression analysis that controlled for indication, age, and wound class, OABP cut length of stay by an average of 12% compared with no preparation, a statistically significant reduction. In the same analysis, mechanical preparation cut length of stay by only 4% compared with no preparation, also a significant effect.
The hospital readmission rate was 16% with no preparation, 15% with mechanical preparation only, and 13% with OABP. In the multivariate regression analysis with adjustment for procedure, age, and wound class, OABP cut the readmission rate by 19% compared with no preparation, a statistically significant reduction. Mechanical preparation only did not have a statistically significant effect.
Further analyses showed that the most common reason for readmission among all patients studied was postoperative infection, in 18%, followed by digestive-system complications, in 10%. C. difficile infection caused 3% of readmissions.
In addition, infections were responsible for readmissions among 6% of patients who underwent no presurgical preparation and in 4% of those who underwent OABP, a statistically significant difference. In contrast, use of OABP produced no statistically significant decline in noninfectious causes of readmission. This rate ran 10% among patients with no preparation, and 9% in patients who underwent OABP.
Dr. Hawn said that she had no disclosures.
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Oral antibiotic preparation before colorectal surgery cut hospital readmissions by 19% compared with no preparation.
Data Source: A review of 8,180 U.S. patients who underwent colorectal surgery during 2005-2009 at 112 VA hospitals.
Disclosures: Dr. Hawn said that she had no disclosures.

Colorectal SSIs Plummet After Targeted Improvement Project
Colorectal surgical site infections dropped by an average of 32% among hospitals that participated in a project designed to reduce facility-specific infection risk factors.
The project – co-sponsored by the Joint Commission Center for Transforming Healthcare and the American College of Surgeons – will result in a user-friendly online tool that can examine any hospital’s infections data and recommend detailed, site-specific interventions.

The commission’s Targeted Solutions Tool should be available by the middle of 2013.
"The hospitals we engaged have mastered these sophisticated change tools, and now we need to make sure this learning can be spread to others," Dr. Mark Chassin said during a press briefing. "[The new tool] will be a very easy-to-follow approach that applies all the lessons we learned – showing how to measure infection rates, figure out which contributing factors are present in their institution, and guiding them through implementations proven to address these factors."
The commission chose to tackle colorectal surgical site infections (SSIs) because they are common, dangerous, and expensive, said Dr. Chassin, president of the group. Unfortunately, risk factors don’t respond to a "one size fits all" prevention protocol. "These factors are highly variable across hospitals, suggesting that there are opportunities to improve performance."
The 2-year pilot project included seven hospitals of varying size and community demographics. The facilities tracked their colorectal SSI patterns using the American College of Surgeons National Surgical Quality Improvement Program. Each hospital then developed interventions targeted at their individual modifiable risk factors, implemented the changes, and recorded their results.
Overall, the protocol reduced colorectal SSIs by 32% – from an average of 16% to 11%. Superficial skin SSIs fell by an average of 45% over the entire study group.
The protocol improved other outcomes as well, Dr. Chassin said. The average length of stay for a colorectal surgery patient with a wound infection decreased from 15 to 13 days. Across the group, the changes were associated with a savings of almost $4 million.
The hospitals collectively identified 34 factors that greatly increased the risk of such infections. During the briefing, Dr. Jenna Lovely, the surgical pharmacotherapy manager at the Mayo Clinic, Rochester, Minn., shared some of their results (J. Am. Coll. Surg. 2011;213:83-92; 2012 [doi:10.1016/j.jamcollsurg.2012.09.009]).
Before implementation of the program, the colorectal SSI rate at Mayo was 10%. With a goal of reducing that number by at least 50%, the team examined risk factors in the preoperative, intraoperative, postoperative, and posthospitalization periods and made some changes, Dr. Lovely said.
Preoperatively, every patient now takes a shower with soap or with a chlorhexidine-based cleanser both the night before and the day of surgery.
Intraoperatively, the site is prepped with an antimicrobial cleansing agent, and the correct antibiotic is administered at 1 hour before the incision is made. If the surgery lasts more than 4 hours, a second dose of the same antibiotic is administered; cefazolin is given 24 hours after closing.
At fascia closing, the surgeon dons a complete change of gown, mask, and gloves. Closing is performed with the use of an entirely new set of instruments.
Postoperatively, everyone who comes in contact with the wound – including staff, the patient, and visitors – practices good hand hygiene. Reminder notes and hand cleanser are located prominently in rooms and all around the unit. Nurses are empowered to change dressings as needed. Wound probing occurs as needed to help expel any contaminated fluids.
Patients are discharged with infection control education and a bottle of chlorhexidine cleanser.
"These changes are embedded in the environment across the continuum of care. It’s part of the surgical unit’s culture, and this makes it easier to do the right thing. The changes also allow the surgeon to focus on doing what he does best – providing a timely and efficient surgery with the best possible outcome," Dr. Lovely said.
Implementation of these changes led to a reduction in SSI rate from 10% to 4%, and that rate has maintained this rate for 18 months.
Dr. Shirin Towfigh, a surgeon at Cedars-Sinai Medical Center in Los Angeles, said her unit experienced a similar improvement.
The project included 46 surgeons and all of the unit staff. Because the team didn’t want to dictate surgical technique, she said, their goal "was to come up with processes that would improve results independent of a surgeon’s practice. We wanted the changes to be effective, but also easy for surgeons to implement in their own practice."
By the end of the study period, the unit’s colorectal SSI rate had decreased by 50%. Since the project closed 6 months ago, that has further improved, with a total decrease of 65%.
"This is a problem colorectal surgeons have been struggling with for years," Dr. Chassin said. "We’ve always tried to get at it with the simple answer: ‘Here are 5 or 10 things everyone should do to decrease SSIs.’ That doesn’t work, because the critical factors that explain poor outcomes differ from one place to another. The best advice I can give is to look at all your contributing factors and assess where your organization falls short. Use these findings as a guide for where to focus your improvement efforts. The only way you know how to improve is to measure the cause of problems and target interventions right to them."
No disclosures were reported.
This is an innovative and exciting initiative that highlights our increasing sophistication about translating new knowledge and evidence into practice. In order to improve something, you must first document that there is a problem, establish a baseline, and set a goal.
The American College of Surgeons National Surgical Quality Improvement Program and similar initiatives allow for such a structured and standardized approach for data collection and reporting. Once the problem is characterized, interventions must be designed and tested in a variety of settings to determine under what conditions they are or are not effective.
No single intervention will be effective for a multifactorial problem like surgical site infections. In order to scale up and broadly disseminate such interventions, it is necessary to assess the facilitators and barriers to change that exist in a given environment to determine which interventions have the highest likelihood of success. The program described in this article, which allows such a tailored approach to quality improvement, potentially can have a profound impact on the quality and safety of the care that we provide.
Dr. Caprice C. Greenberg is an ACS Fellow, associate professor of surgery, and director of the Wisconsin Surgical Outcomes Research at the University of Wisconsin, Madison.
This is an innovative and exciting initiative that highlights our increasing sophistication about translating new knowledge and evidence into practice. In order to improve something, you must first document that there is a problem, establish a baseline, and set a goal.
The American College of Surgeons National Surgical Quality Improvement Program and similar initiatives allow for such a structured and standardized approach for data collection and reporting. Once the problem is characterized, interventions must be designed and tested in a variety of settings to determine under what conditions they are or are not effective.
No single intervention will be effective for a multifactorial problem like surgical site infections. In order to scale up and broadly disseminate such interventions, it is necessary to assess the facilitators and barriers to change that exist in a given environment to determine which interventions have the highest likelihood of success. The program described in this article, which allows such a tailored approach to quality improvement, potentially can have a profound impact on the quality and safety of the care that we provide.
Dr. Caprice C. Greenberg is an ACS Fellow, associate professor of surgery, and director of the Wisconsin Surgical Outcomes Research at the University of Wisconsin, Madison.
This is an innovative and exciting initiative that highlights our increasing sophistication about translating new knowledge and evidence into practice. In order to improve something, you must first document that there is a problem, establish a baseline, and set a goal.
The American College of Surgeons National Surgical Quality Improvement Program and similar initiatives allow for such a structured and standardized approach for data collection and reporting. Once the problem is characterized, interventions must be designed and tested in a variety of settings to determine under what conditions they are or are not effective.
No single intervention will be effective for a multifactorial problem like surgical site infections. In order to scale up and broadly disseminate such interventions, it is necessary to assess the facilitators and barriers to change that exist in a given environment to determine which interventions have the highest likelihood of success. The program described in this article, which allows such a tailored approach to quality improvement, potentially can have a profound impact on the quality and safety of the care that we provide.
Dr. Caprice C. Greenberg is an ACS Fellow, associate professor of surgery, and director of the Wisconsin Surgical Outcomes Research at the University of Wisconsin, Madison.
Colorectal surgical site infections dropped by an average of 32% among hospitals that participated in a project designed to reduce facility-specific infection risk factors.
The project – co-sponsored by the Joint Commission Center for Transforming Healthcare and the American College of Surgeons – will result in a user-friendly online tool that can examine any hospital’s infections data and recommend detailed, site-specific interventions.
The commission’s Targeted Solutions Tool should be available by the middle of 2013.
"The hospitals we engaged have mastered these sophisticated change tools, and now we need to make sure this learning can be spread to others," Dr. Mark Chassin said during a press briefing. "[The new tool] will be a very easy-to-follow approach that applies all the lessons we learned – showing how to measure infection rates, figure out which contributing factors are present in their institution, and guiding them through implementations proven to address these factors."
The commission chose to tackle colorectal surgical site infections (SSIs) because they are common, dangerous, and expensive, said Dr. Chassin, president of the group. Unfortunately, risk factors don’t respond to a "one size fits all" prevention protocol. "These factors are highly variable across hospitals, suggesting that there are opportunities to improve performance."
The 2-year pilot project included seven hospitals of varying size and community demographics. The facilities tracked their colorectal SSI patterns using the American College of Surgeons National Surgical Quality Improvement Program. Each hospital then developed interventions targeted at their individual modifiable risk factors, implemented the changes, and recorded their results.
Overall, the protocol reduced colorectal SSIs by 32% – from an average of 16% to 11%. Superficial skin SSIs fell by an average of 45% over the entire study group.
The protocol improved other outcomes as well, Dr. Chassin said. The average length of stay for a colorectal surgery patient with a wound infection decreased from 15 to 13 days. Across the group, the changes were associated with a savings of almost $4 million.
The hospitals collectively identified 34 factors that greatly increased the risk of such infections. During the briefing, Dr. Jenna Lovely, the surgical pharmacotherapy manager at the Mayo Clinic, Rochester, Minn., shared some of their results (J. Am. Coll. Surg. 2011;213:83-92; 2012 [doi:10.1016/j.jamcollsurg.2012.09.009]).
Before implementation of the program, the colorectal SSI rate at Mayo was 10%. With a goal of reducing that number by at least 50%, the team examined risk factors in the preoperative, intraoperative, postoperative, and posthospitalization periods and made some changes, Dr. Lovely said.
Preoperatively, every patient now takes a shower with soap or with a chlorhexidine-based cleanser both the night before and the day of surgery.
Intraoperatively, the site is prepped with an antimicrobial cleansing agent, and the correct antibiotic is administered at 1 hour before the incision is made. If the surgery lasts more than 4 hours, a second dose of the same antibiotic is administered; cefazolin is given 24 hours after closing.
At fascia closing, the surgeon dons a complete change of gown, mask, and gloves. Closing is performed with the use of an entirely new set of instruments.
Postoperatively, everyone who comes in contact with the wound – including staff, the patient, and visitors – practices good hand hygiene. Reminder notes and hand cleanser are located prominently in rooms and all around the unit. Nurses are empowered to change dressings as needed. Wound probing occurs as needed to help expel any contaminated fluids.
Patients are discharged with infection control education and a bottle of chlorhexidine cleanser.
"These changes are embedded in the environment across the continuum of care. It’s part of the surgical unit’s culture, and this makes it easier to do the right thing. The changes also allow the surgeon to focus on doing what he does best – providing a timely and efficient surgery with the best possible outcome," Dr. Lovely said.
Implementation of these changes led to a reduction in SSI rate from 10% to 4%, and that rate has maintained this rate for 18 months.
Dr. Shirin Towfigh, a surgeon at Cedars-Sinai Medical Center in Los Angeles, said her unit experienced a similar improvement.
The project included 46 surgeons and all of the unit staff. Because the team didn’t want to dictate surgical technique, she said, their goal "was to come up with processes that would improve results independent of a surgeon’s practice. We wanted the changes to be effective, but also easy for surgeons to implement in their own practice."
By the end of the study period, the unit’s colorectal SSI rate had decreased by 50%. Since the project closed 6 months ago, that has further improved, with a total decrease of 65%.
"This is a problem colorectal surgeons have been struggling with for years," Dr. Chassin said. "We’ve always tried to get at it with the simple answer: ‘Here are 5 or 10 things everyone should do to decrease SSIs.’ That doesn’t work, because the critical factors that explain poor outcomes differ from one place to another. The best advice I can give is to look at all your contributing factors and assess where your organization falls short. Use these findings as a guide for where to focus your improvement efforts. The only way you know how to improve is to measure the cause of problems and target interventions right to them."
No disclosures were reported.
Colorectal surgical site infections dropped by an average of 32% among hospitals that participated in a project designed to reduce facility-specific infection risk factors.
The project – co-sponsored by the Joint Commission Center for Transforming Healthcare and the American College of Surgeons – will result in a user-friendly online tool that can examine any hospital’s infections data and recommend detailed, site-specific interventions.
The commission’s Targeted Solutions Tool should be available by the middle of 2013.
"The hospitals we engaged have mastered these sophisticated change tools, and now we need to make sure this learning can be spread to others," Dr. Mark Chassin said during a press briefing. "[The new tool] will be a very easy-to-follow approach that applies all the lessons we learned – showing how to measure infection rates, figure out which contributing factors are present in their institution, and guiding them through implementations proven to address these factors."
The commission chose to tackle colorectal surgical site infections (SSIs) because they are common, dangerous, and expensive, said Dr. Chassin, president of the group. Unfortunately, risk factors don’t respond to a "one size fits all" prevention protocol. "These factors are highly variable across hospitals, suggesting that there are opportunities to improve performance."
The 2-year pilot project included seven hospitals of varying size and community demographics. The facilities tracked their colorectal SSI patterns using the American College of Surgeons National Surgical Quality Improvement Program. Each hospital then developed interventions targeted at their individual modifiable risk factors, implemented the changes, and recorded their results.
Overall, the protocol reduced colorectal SSIs by 32% – from an average of 16% to 11%. Superficial skin SSIs fell by an average of 45% over the entire study group.
The protocol improved other outcomes as well, Dr. Chassin said. The average length of stay for a colorectal surgery patient with a wound infection decreased from 15 to 13 days. Across the group, the changes were associated with a savings of almost $4 million.
The hospitals collectively identified 34 factors that greatly increased the risk of such infections. During the briefing, Dr. Jenna Lovely, the surgical pharmacotherapy manager at the Mayo Clinic, Rochester, Minn., shared some of their results (J. Am. Coll. Surg. 2011;213:83-92; 2012 [doi:10.1016/j.jamcollsurg.2012.09.009]).
Before implementation of the program, the colorectal SSI rate at Mayo was 10%. With a goal of reducing that number by at least 50%, the team examined risk factors in the preoperative, intraoperative, postoperative, and posthospitalization periods and made some changes, Dr. Lovely said.
Preoperatively, every patient now takes a shower with soap or with a chlorhexidine-based cleanser both the night before and the day of surgery.
Intraoperatively, the site is prepped with an antimicrobial cleansing agent, and the correct antibiotic is administered at 1 hour before the incision is made. If the surgery lasts more than 4 hours, a second dose of the same antibiotic is administered; cefazolin is given 24 hours after closing.
At fascia closing, the surgeon dons a complete change of gown, mask, and gloves. Closing is performed with the use of an entirely new set of instruments.
Postoperatively, everyone who comes in contact with the wound – including staff, the patient, and visitors – practices good hand hygiene. Reminder notes and hand cleanser are located prominently in rooms and all around the unit. Nurses are empowered to change dressings as needed. Wound probing occurs as needed to help expel any contaminated fluids.
Patients are discharged with infection control education and a bottle of chlorhexidine cleanser.
"These changes are embedded in the environment across the continuum of care. It’s part of the surgical unit’s culture, and this makes it easier to do the right thing. The changes also allow the surgeon to focus on doing what he does best – providing a timely and efficient surgery with the best possible outcome," Dr. Lovely said.
Implementation of these changes led to a reduction in SSI rate from 10% to 4%, and that rate has maintained this rate for 18 months.
Dr. Shirin Towfigh, a surgeon at Cedars-Sinai Medical Center in Los Angeles, said her unit experienced a similar improvement.
The project included 46 surgeons and all of the unit staff. Because the team didn’t want to dictate surgical technique, she said, their goal "was to come up with processes that would improve results independent of a surgeon’s practice. We wanted the changes to be effective, but also easy for surgeons to implement in their own practice."
By the end of the study period, the unit’s colorectal SSI rate had decreased by 50%. Since the project closed 6 months ago, that has further improved, with a total decrease of 65%.
"This is a problem colorectal surgeons have been struggling with for years," Dr. Chassin said. "We’ve always tried to get at it with the simple answer: ‘Here are 5 or 10 things everyone should do to decrease SSIs.’ That doesn’t work, because the critical factors that explain poor outcomes differ from one place to another. The best advice I can give is to look at all your contributing factors and assess where your organization falls short. Use these findings as a guide for where to focus your improvement efforts. The only way you know how to improve is to measure the cause of problems and target interventions right to them."
No disclosures were reported.
Major Finding: Implementation of a new protocol reduced colorectal surgical site infections by an average of 32% and average length of stay from 15 days to 13 days among participating hospitals.
Data Source: The results come from a pilot project co-sponsored by the Joint Commission Center for Transforming Healthcare and the American College of Surgeons.
Disclosures: No disclosures were reported.

Rapid Feedback Boosts Adherence to Oncology Quality Measures
SAN DIEGO – A Rapid Quality Reporting System significantly improved oncologists’ adherence to five measures of quality treatment for patients with breast and colon cancer during beta testing involving 64,129 patients at 64 cancer centers.
The system, developed by the American College of Surgeons’ Commission on Cancer, provides next-business-day feedback when centers submit data. Compliance rates climbed as high as 90% by the end of a 5-year period, according to researchers.

Erica J. McNamara and her associates reported the following gains at a symposium on quality care sponsored by the American Society of Clinical Oncology (ASCO):
• The proportion of patients receiving hormone therapy for hormone receptor–positive breast cancer increased from 47% in 2006 to 85% in 2011.
• Treatment with radiation following breast conserving surgery increased from 69% of patients to 90%.
• Use of multi-adjuvant chemotherapy for hormone receptor–negative breast cancer increased from 72% of patients to 90%,
• Treatment with adjuvant chemotherapy for lymph node–positive colon cancer increased from 68% to 86%.
• The proportion of patients with resected colon cancer who had at least 12 regional lymph nodes removed for pathological examination improved from 70% to 90%,
The study gathered data from the National Cancer Database in 2006-2007 for 18,151 patients with breast cancer and 6,369 patients with colon cancer and compared it with data reported to the Rapid Quality Reporting System (RQRS) in 2008-2011 for 31,590 patients with breast cancer and 11,338 patients with colon cancer.
The system monitors the five quality measures using reporting procedures similar to those that hospitals already use to submit patient data to cancer registries. Traditional registries generally report a hospital’s rate of performing quality measures 2 years after data submission, however, while the RQRS allows cancer programs to submit data whenever they want and sends feedback by the next business day, said Ms. McNamara, a quality improvement information analyst for the American College of Surgeons, Chicago.
With as little as a surgical or pathological report, cancer programs can submit a case to the RQRS to get alerts when quality care is not being provided. "What this does is it changes it from looking at retrospective cases to cases that are currently within their first course of therapy," she said in a press conference before the meeting.
Programs participating in the beta-test generally submitted data monthly, and new participants in the RQRS are required to submit data at least quarterly. The RQRS analyzes the data and returns a report in a variety of image formats, such as a year-to-date "dashboard" showing the program’s compliance rates for individual quality measures, and a list of every case submitted and whether the quality measures were applicable to the case or not, or if more information is needed.
The report also includes color-coded "case alerts" with the colors changing to orange and then red as a patient gets closer to the end of the first course of therapy with either no documentation of adjuvant therapy or no documentation that treatment decision has been made to not provide adjuvant therapy. Participants must log in to a password-protected site to view details of the case.
"For each of the adjuvant therapy measures, there’s a specific amount of time that each patient has to receive their adjuvant therapy," Ms. McNamara said. "We find that after about 6-9 months of using RQRS, about a third of programs tell us that they have seen RQRS prevent patients from slipping through the cracks or not receiving timely adjuvant care."
Breakdowns of the data by race, age, and type of insurance showed that quality care significantly improved in all subgroups. Disparities in quality adherence rates between patients of different races, ages, or insurance status were minimized or eliminated with use of the RQRS.
Two factors appeared to produce these improvements. Use of the RQRS improved the coordination of care and led to more complete reporting of adjuvant therapy data, she said.
More than 400 cancer programs now voluntarily use the RQRS. The American College of Surgeons is working on expanding the RQRS to include other measures of quality care for breast cancer and for lung, stomach, and esophageal cancers.
Ms. McNamara reported having no financial disclosures.
| This study is really noteworthy in that the development of this system significantly improved cancer care within a very short amount of time in more than 60 cancer centers nationally. This sort of innovative feedback system provides real-time improvement in care, so it’s very exciting.
Dr. Jyoti D. Patel is a thoracic oncologist at Northwestern University, Chicago, and a member of ASCO’s Cancer Communications Committee. |
|

| This study is really noteworthy in that the development of this system significantly improved cancer care within a very short amount of time in more than 60 cancer centers nationally. This sort of innovative feedback system provides real-time improvement in care, so it’s very exciting.
Dr. Jyoti D. Patel is a thoracic oncologist at Northwestern University, Chicago, and a member of ASCO’s Cancer Communications Committee. |
|
| This study is really noteworthy in that the development of this system significantly improved cancer care within a very short amount of time in more than 60 cancer centers nationally. This sort of innovative feedback system provides real-time improvement in care, so it’s very exciting.
Dr. Jyoti D. Patel is a thoracic oncologist at Northwestern University, Chicago, and a member of ASCO’s Cancer Communications Committee. |
|
SAN DIEGO – A Rapid Quality Reporting System significantly improved oncologists’ adherence to five measures of quality treatment for patients with breast and colon cancer during beta testing involving 64,129 patients at 64 cancer centers.
The system, developed by the American College of Surgeons’ Commission on Cancer, provides next-business-day feedback when centers submit data. Compliance rates climbed as high as 90% by the end of a 5-year period, according to researchers.
Erica J. McNamara and her associates reported the following gains at a symposium on quality care sponsored by the American Society of Clinical Oncology (ASCO):
• The proportion of patients receiving hormone therapy for hormone receptor–positive breast cancer increased from 47% in 2006 to 85% in 2011.
• Treatment with radiation following breast conserving surgery increased from 69% of patients to 90%.
• Use of multi-adjuvant chemotherapy for hormone receptor–negative breast cancer increased from 72% of patients to 90%,
• Treatment with adjuvant chemotherapy for lymph node–positive colon cancer increased from 68% to 86%.
• The proportion of patients with resected colon cancer who had at least 12 regional lymph nodes removed for pathological examination improved from 70% to 90%,
The study gathered data from the National Cancer Database in 2006-2007 for 18,151 patients with breast cancer and 6,369 patients with colon cancer and compared it with data reported to the Rapid Quality Reporting System (RQRS) in 2008-2011 for 31,590 patients with breast cancer and 11,338 patients with colon cancer.
The system monitors the five quality measures using reporting procedures similar to those that hospitals already use to submit patient data to cancer registries. Traditional registries generally report a hospital’s rate of performing quality measures 2 years after data submission, however, while the RQRS allows cancer programs to submit data whenever they want and sends feedback by the next business day, said Ms. McNamara, a quality improvement information analyst for the American College of Surgeons, Chicago.
With as little as a surgical or pathological report, cancer programs can submit a case to the RQRS to get alerts when quality care is not being provided. "What this does is it changes it from looking at retrospective cases to cases that are currently within their first course of therapy," she said in a press conference before the meeting.
Programs participating in the beta-test generally submitted data monthly, and new participants in the RQRS are required to submit data at least quarterly. The RQRS analyzes the data and returns a report in a variety of image formats, such as a year-to-date "dashboard" showing the program’s compliance rates for individual quality measures, and a list of every case submitted and whether the quality measures were applicable to the case or not, or if more information is needed.
The report also includes color-coded "case alerts" with the colors changing to orange and then red as a patient gets closer to the end of the first course of therapy with either no documentation of adjuvant therapy or no documentation that treatment decision has been made to not provide adjuvant therapy. Participants must log in to a password-protected site to view details of the case.
"For each of the adjuvant therapy measures, there’s a specific amount of time that each patient has to receive their adjuvant therapy," Ms. McNamara said. "We find that after about 6-9 months of using RQRS, about a third of programs tell us that they have seen RQRS prevent patients from slipping through the cracks or not receiving timely adjuvant care."
Breakdowns of the data by race, age, and type of insurance showed that quality care significantly improved in all subgroups. Disparities in quality adherence rates between patients of different races, ages, or insurance status were minimized or eliminated with use of the RQRS.
Two factors appeared to produce these improvements. Use of the RQRS improved the coordination of care and led to more complete reporting of adjuvant therapy data, she said.
More than 400 cancer programs now voluntarily use the RQRS. The American College of Surgeons is working on expanding the RQRS to include other measures of quality care for breast cancer and for lung, stomach, and esophageal cancers.
Ms. McNamara reported having no financial disclosures.
SAN DIEGO – A Rapid Quality Reporting System significantly improved oncologists’ adherence to five measures of quality treatment for patients with breast and colon cancer during beta testing involving 64,129 patients at 64 cancer centers.
The system, developed by the American College of Surgeons’ Commission on Cancer, provides next-business-day feedback when centers submit data. Compliance rates climbed as high as 90% by the end of a 5-year period, according to researchers.
Erica J. McNamara and her associates reported the following gains at a symposium on quality care sponsored by the American Society of Clinical Oncology (ASCO):
• The proportion of patients receiving hormone therapy for hormone receptor–positive breast cancer increased from 47% in 2006 to 85% in 2011.
• Treatment with radiation following breast conserving surgery increased from 69% of patients to 90%.
• Use of multi-adjuvant chemotherapy for hormone receptor–negative breast cancer increased from 72% of patients to 90%,
• Treatment with adjuvant chemotherapy for lymph node–positive colon cancer increased from 68% to 86%.
• The proportion of patients with resected colon cancer who had at least 12 regional lymph nodes removed for pathological examination improved from 70% to 90%,
The study gathered data from the National Cancer Database in 2006-2007 for 18,151 patients with breast cancer and 6,369 patients with colon cancer and compared it with data reported to the Rapid Quality Reporting System (RQRS) in 2008-2011 for 31,590 patients with breast cancer and 11,338 patients with colon cancer.
The system monitors the five quality measures using reporting procedures similar to those that hospitals already use to submit patient data to cancer registries. Traditional registries generally report a hospital’s rate of performing quality measures 2 years after data submission, however, while the RQRS allows cancer programs to submit data whenever they want and sends feedback by the next business day, said Ms. McNamara, a quality improvement information analyst for the American College of Surgeons, Chicago.
With as little as a surgical or pathological report, cancer programs can submit a case to the RQRS to get alerts when quality care is not being provided. "What this does is it changes it from looking at retrospective cases to cases that are currently within their first course of therapy," she said in a press conference before the meeting.
Programs participating in the beta-test generally submitted data monthly, and new participants in the RQRS are required to submit data at least quarterly. The RQRS analyzes the data and returns a report in a variety of image formats, such as a year-to-date "dashboard" showing the program’s compliance rates for individual quality measures, and a list of every case submitted and whether the quality measures were applicable to the case or not, or if more information is needed.
The report also includes color-coded "case alerts" with the colors changing to orange and then red as a patient gets closer to the end of the first course of therapy with either no documentation of adjuvant therapy or no documentation that treatment decision has been made to not provide adjuvant therapy. Participants must log in to a password-protected site to view details of the case.
"For each of the adjuvant therapy measures, there’s a specific amount of time that each patient has to receive their adjuvant therapy," Ms. McNamara said. "We find that after about 6-9 months of using RQRS, about a third of programs tell us that they have seen RQRS prevent patients from slipping through the cracks or not receiving timely adjuvant care."
Breakdowns of the data by race, age, and type of insurance showed that quality care significantly improved in all subgroups. Disparities in quality adherence rates between patients of different races, ages, or insurance status were minimized or eliminated with use of the RQRS.
Two factors appeared to produce these improvements. Use of the RQRS improved the coordination of care and led to more complete reporting of adjuvant therapy data, she said.
More than 400 cancer programs now voluntarily use the RQRS. The American College of Surgeons is working on expanding the RQRS to include other measures of quality care for breast cancer and for lung, stomach, and esophageal cancers.
Ms. McNamara reported having no financial disclosures.
AT THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY'S QUALITY CARE SYMPOSIUM
Major Finding: Compliance rates for five quality measures climbed to as high as 90% in centers that used RQRS.
Data Source: Data on 31,590 breast cancer cases and 11,338 colon cancer cases in the RQRS in 3008-2011 were compared with data from the National Cancer Database in 2006-2007 for 18,151 breast cancer cases and 6,369 colon cancer cases.
Disclosures: Ms. McNamara reported having no financial disclosures.

Teduglutide Trims Parenteral Support in Short Bowel Syndrome
Teduglutide significantly reduced the need for parenteral support in patients with short bowel syndrome and intestinal failure, based on data from 85 adults in a randomized, controlled multicenter trial. The findings were published in the December issue of Gastroenterology.
Patients with short bowel syndrome and intestinal failure (SBS-IF) have inadequate intestinal absorption and require parenteral support (PS) to maintain fluids, electrolytes, trace elements, vitamins, and nutrient balances, said Dr. Palle Bekker Jeppesen of Rigshospitalet in Copenhagen and colleagues.
Source: American Gastroenterological Association
Data from previous open-label studies suggest an association between teduglutide and clinically meaningful reductions in wet weight and energy, which may reduce the need for PS in these patients, the investigators noted.
The researchers randomized 86 adults with SBS-IF to either 0.05 mg/kg per day of teduglutide or a placebo. One patient was randomized in error; complete data were available for 42 teduglutide patients and 43 placebo patients.
Significantly more patients in the teduglutide group responded to treatment, compared with the placebo group (63% vs. 30%). This response was defined as sustaining a 20%-100% reduction from baseline in weekly PS volume during weeks 20-24. "Small bowel length did not appear to be a predictor of response," the researchers noted.
The high placebo response may be explained by examining the fluid composite effect, a measure of the combined effects of teduglutide on PS volume reduction as well as the ability to reduce oral fluid intake and increase urine output volume, the researchers noted.
"In the current study, where protocol modifications encouraged earlier and more aggressive PS reductions, significantly larger PS reductions were also achieved in patients receiving placebo, but subsequently these patients had to increase their oral fluid intake significantly to maintain urine production and hydration constant," they said.
After 24 weeks, overall PS volume was reduced by 32% from baseline in teduglutide patients, compared with 21% in placebo patients. Although no patients in either group were completely weaned from parenteral support at 24 weeks, the difference in PS volume reduction was significantly greater in the teduglutide group.
The average weekly PS volume in teduglutide patients decreased significantly from 12.5 L/wk at baseline to 8.1 L/wk at week 24. The placebo patients also had a significant decrease in average weekly PS volume, from 13.4 L/wk at baseline to 11.1 L/wk at week 24.
Treatment-ending adverse events were similar between the two groups; 5% of teduglutide patients and 7% of placebo patients discontinued treatment because of such events during the study period. The most frequently reported treatment-emergent adverse events included abdominal pain, abdominal distension, nausea, and gastrointestinal stoma complications.
Although the study did not specifically assess quality of life measures, significantly more teduglutide patients had at least 1 day off PS, compared with placebo patients, which could help to "liberate considerable time for unhindered daytime activities or undisturbed sleep," the researchers said.
The study did not address the possible benefit of teduglutide therapy earlier in the course of SBS, or the duration of effect after patients discontinued teduglutide, the researchers added.
However, the findings indicate that teduglutide was safe and well tolerated, and "could positively add to the limited treatment armamentarium" for patients with SBS-IF.
Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
Patients with short bowel syndrome whose absorption is insufficient to maintain nutritional or fluid autonomy have intestinal failure. These patients, particularly those with proximal jejunostomies, who may actually secrete more fluid than they ingest, are among the most complex and challenging to manage of patients with any gastrointestinal disease. Patients with short bowel syndrome and intestinal failure are dependent on parenteral nutrition and/or fluid support (PS) to maintain life. This therapy has substantial implications for employment, activities, sleep, and finances. Numerous, often life-threatening, complications develop.

|
|
A myriad of growth factors may be involved in the process of postresection intestinal adaptation, including glucagonlike peptide-2 (GLP-2), wherein intestinal epithelial growth is promoted. Teduglutide is a long-acting analog of native GLP-2 and is somewhat more resistant to enzymatic degradation in the enterocyte than is the native enzyme. Dr. Jeppesen and colleagues reported a sustained 20%-100% decrease in PS volume requirements during weeks 20-24 of treatment in 63% of patients who received teduglutide, compared with 30% of placebo-treated patients. The mean drop in weekly PS volume from baseline to week 24 totaled 4.4 L in patients who received teduglutide, which equates to a decrease of 1-2 nights of infusion weekly, a very profound improvement for individual patients. The PS weaning protocol used was similar to that used in most centers experienced in the care of these patients.
As would be expected in the SBS-IF patient population, there were many adverse events, although these were equally distributed across teduglutide and placebo groups. Stomal changes, primarily related to enlargement, were evident in a significant minority of patients in the teduglutide group, as would be expected given the hyperplastic effect of the medication on intestinal epithelial tissue.Concern has been raised about GLP-2’s potential to stimulate the development of colonic adenomas in rodent models. Although the risk for malignancy is hypothetical in humans, colonoscopy should be considered at baseline for those patients with residual colons and perhaps as frequently as annually while the patients are on therapy until more long-term safety data are available.
Is teduglutide a "game changer"? The only patients who will be able to discontinue PS completely will be those who are on the borderline between nutritional autonomy and PS dependence. It is important to realize that teduglutide should be used to augment, not replace conventional management. What happens when teduglutide is stopped? Preliminary evidence suggests the effects on adaptation may be persistent, although earlier study noted that histologic changes trended toward baseline within 4 weeks of discontinuation. Perhaps longer treatment or maintenance will be required. The real future is an artificially grown and harvested intestine; even intestinal transplantation represents a bridge at best.
Dr. Alan L. Buchman is a former professor of medicine and surgery at the Feinberg School of Medicine at Northwestern University, Chicago. Within the past 12 months he has consulted for Takeda Pharmaceuticals and NPS Pharmaceuticals.
Patients with short bowel syndrome whose absorption is insufficient to maintain nutritional or fluid autonomy have intestinal failure. These patients, particularly those with proximal jejunostomies, who may actually secrete more fluid than they ingest, are among the most complex and challenging to manage of patients with any gastrointestinal disease. Patients with short bowel syndrome and intestinal failure are dependent on parenteral nutrition and/or fluid support (PS) to maintain life. This therapy has substantial implications for employment, activities, sleep, and finances. Numerous, often life-threatening, complications develop.
|
|
|
A myriad of growth factors may be involved in the process of postresection intestinal adaptation, including glucagonlike peptide-2 (GLP-2), wherein intestinal epithelial growth is promoted. Teduglutide is a long-acting analog of native GLP-2 and is somewhat more resistant to enzymatic degradation in the enterocyte than is the native enzyme. Dr. Jeppesen and colleagues reported a sustained 20%-100% decrease in PS volume requirements during weeks 20-24 of treatment in 63% of patients who received teduglutide, compared with 30% of placebo-treated patients. The mean drop in weekly PS volume from baseline to week 24 totaled 4.4 L in patients who received teduglutide, which equates to a decrease of 1-2 nights of infusion weekly, a very profound improvement for individual patients. The PS weaning protocol used was similar to that used in most centers experienced in the care of these patients.
As would be expected in the SBS-IF patient population, there were many adverse events, although these were equally distributed across teduglutide and placebo groups. Stomal changes, primarily related to enlargement, were evident in a significant minority of patients in the teduglutide group, as would be expected given the hyperplastic effect of the medication on intestinal epithelial tissue.Concern has been raised about GLP-2’s potential to stimulate the development of colonic adenomas in rodent models. Although the risk for malignancy is hypothetical in humans, colonoscopy should be considered at baseline for those patients with residual colons and perhaps as frequently as annually while the patients are on therapy until more long-term safety data are available.
Is teduglutide a "game changer"? The only patients who will be able to discontinue PS completely will be those who are on the borderline between nutritional autonomy and PS dependence. It is important to realize that teduglutide should be used to augment, not replace conventional management. What happens when teduglutide is stopped? Preliminary evidence suggests the effects on adaptation may be persistent, although earlier study noted that histologic changes trended toward baseline within 4 weeks of discontinuation. Perhaps longer treatment or maintenance will be required. The real future is an artificially grown and harvested intestine; even intestinal transplantation represents a bridge at best.
Dr. Alan L. Buchman is a former professor of medicine and surgery at the Feinberg School of Medicine at Northwestern University, Chicago. Within the past 12 months he has consulted for Takeda Pharmaceuticals and NPS Pharmaceuticals.
Patients with short bowel syndrome whose absorption is insufficient to maintain nutritional or fluid autonomy have intestinal failure. These patients, particularly those with proximal jejunostomies, who may actually secrete more fluid than they ingest, are among the most complex and challenging to manage of patients with any gastrointestinal disease. Patients with short bowel syndrome and intestinal failure are dependent on parenteral nutrition and/or fluid support (PS) to maintain life. This therapy has substantial implications for employment, activities, sleep, and finances. Numerous, often life-threatening, complications develop.
|
|
|
A myriad of growth factors may be involved in the process of postresection intestinal adaptation, including glucagonlike peptide-2 (GLP-2), wherein intestinal epithelial growth is promoted. Teduglutide is a long-acting analog of native GLP-2 and is somewhat more resistant to enzymatic degradation in the enterocyte than is the native enzyme. Dr. Jeppesen and colleagues reported a sustained 20%-100% decrease in PS volume requirements during weeks 20-24 of treatment in 63% of patients who received teduglutide, compared with 30% of placebo-treated patients. The mean drop in weekly PS volume from baseline to week 24 totaled 4.4 L in patients who received teduglutide, which equates to a decrease of 1-2 nights of infusion weekly, a very profound improvement for individual patients. The PS weaning protocol used was similar to that used in most centers experienced in the care of these patients.
As would be expected in the SBS-IF patient population, there were many adverse events, although these were equally distributed across teduglutide and placebo groups. Stomal changes, primarily related to enlargement, were evident in a significant minority of patients in the teduglutide group, as would be expected given the hyperplastic effect of the medication on intestinal epithelial tissue.Concern has been raised about GLP-2’s potential to stimulate the development of colonic adenomas in rodent models. Although the risk for malignancy is hypothetical in humans, colonoscopy should be considered at baseline for those patients with residual colons and perhaps as frequently as annually while the patients are on therapy until more long-term safety data are available.
Is teduglutide a "game changer"? The only patients who will be able to discontinue PS completely will be those who are on the borderline between nutritional autonomy and PS dependence. It is important to realize that teduglutide should be used to augment, not replace conventional management. What happens when teduglutide is stopped? Preliminary evidence suggests the effects on adaptation may be persistent, although earlier study noted that histologic changes trended toward baseline within 4 weeks of discontinuation. Perhaps longer treatment or maintenance will be required. The real future is an artificially grown and harvested intestine; even intestinal transplantation represents a bridge at best.
Dr. Alan L. Buchman is a former professor of medicine and surgery at the Feinberg School of Medicine at Northwestern University, Chicago. Within the past 12 months he has consulted for Takeda Pharmaceuticals and NPS Pharmaceuticals.
Teduglutide significantly reduced the need for parenteral support in patients with short bowel syndrome and intestinal failure, based on data from 85 adults in a randomized, controlled multicenter trial. The findings were published in the December issue of Gastroenterology.
Patients with short bowel syndrome and intestinal failure (SBS-IF) have inadequate intestinal absorption and require parenteral support (PS) to maintain fluids, electrolytes, trace elements, vitamins, and nutrient balances, said Dr. Palle Bekker Jeppesen of Rigshospitalet in Copenhagen and colleagues.
Source: American Gastroenterological Association
Data from previous open-label studies suggest an association between teduglutide and clinically meaningful reductions in wet weight and energy, which may reduce the need for PS in these patients, the investigators noted.
The researchers randomized 86 adults with SBS-IF to either 0.05 mg/kg per day of teduglutide or a placebo. One patient was randomized in error; complete data were available for 42 teduglutide patients and 43 placebo patients.
Significantly more patients in the teduglutide group responded to treatment, compared with the placebo group (63% vs. 30%). This response was defined as sustaining a 20%-100% reduction from baseline in weekly PS volume during weeks 20-24. "Small bowel length did not appear to be a predictor of response," the researchers noted.
The high placebo response may be explained by examining the fluid composite effect, a measure of the combined effects of teduglutide on PS volume reduction as well as the ability to reduce oral fluid intake and increase urine output volume, the researchers noted.
"In the current study, where protocol modifications encouraged earlier and more aggressive PS reductions, significantly larger PS reductions were also achieved in patients receiving placebo, but subsequently these patients had to increase their oral fluid intake significantly to maintain urine production and hydration constant," they said.
After 24 weeks, overall PS volume was reduced by 32% from baseline in teduglutide patients, compared with 21% in placebo patients. Although no patients in either group were completely weaned from parenteral support at 24 weeks, the difference in PS volume reduction was significantly greater in the teduglutide group.
The average weekly PS volume in teduglutide patients decreased significantly from 12.5 L/wk at baseline to 8.1 L/wk at week 24. The placebo patients also had a significant decrease in average weekly PS volume, from 13.4 L/wk at baseline to 11.1 L/wk at week 24.
Treatment-ending adverse events were similar between the two groups; 5% of teduglutide patients and 7% of placebo patients discontinued treatment because of such events during the study period. The most frequently reported treatment-emergent adverse events included abdominal pain, abdominal distension, nausea, and gastrointestinal stoma complications.
Although the study did not specifically assess quality of life measures, significantly more teduglutide patients had at least 1 day off PS, compared with placebo patients, which could help to "liberate considerable time for unhindered daytime activities or undisturbed sleep," the researchers said.
The study did not address the possible benefit of teduglutide therapy earlier in the course of SBS, or the duration of effect after patients discontinued teduglutide, the researchers added.
However, the findings indicate that teduglutide was safe and well tolerated, and "could positively add to the limited treatment armamentarium" for patients with SBS-IF.
Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
Teduglutide significantly reduced the need for parenteral support in patients with short bowel syndrome and intestinal failure, based on data from 85 adults in a randomized, controlled multicenter trial. The findings were published in the December issue of Gastroenterology.
Patients with short bowel syndrome and intestinal failure (SBS-IF) have inadequate intestinal absorption and require parenteral support (PS) to maintain fluids, electrolytes, trace elements, vitamins, and nutrient balances, said Dr. Palle Bekker Jeppesen of Rigshospitalet in Copenhagen and colleagues.
Source: American Gastroenterological Association
Data from previous open-label studies suggest an association between teduglutide and clinically meaningful reductions in wet weight and energy, which may reduce the need for PS in these patients, the investigators noted.
The researchers randomized 86 adults with SBS-IF to either 0.05 mg/kg per day of teduglutide or a placebo. One patient was randomized in error; complete data were available for 42 teduglutide patients and 43 placebo patients.
Significantly more patients in the teduglutide group responded to treatment, compared with the placebo group (63% vs. 30%). This response was defined as sustaining a 20%-100% reduction from baseline in weekly PS volume during weeks 20-24. "Small bowel length did not appear to be a predictor of response," the researchers noted.
The high placebo response may be explained by examining the fluid composite effect, a measure of the combined effects of teduglutide on PS volume reduction as well as the ability to reduce oral fluid intake and increase urine output volume, the researchers noted.
"In the current study, where protocol modifications encouraged earlier and more aggressive PS reductions, significantly larger PS reductions were also achieved in patients receiving placebo, but subsequently these patients had to increase their oral fluid intake significantly to maintain urine production and hydration constant," they said.
After 24 weeks, overall PS volume was reduced by 32% from baseline in teduglutide patients, compared with 21% in placebo patients. Although no patients in either group were completely weaned from parenteral support at 24 weeks, the difference in PS volume reduction was significantly greater in the teduglutide group.
The average weekly PS volume in teduglutide patients decreased significantly from 12.5 L/wk at baseline to 8.1 L/wk at week 24. The placebo patients also had a significant decrease in average weekly PS volume, from 13.4 L/wk at baseline to 11.1 L/wk at week 24.
Treatment-ending adverse events were similar between the two groups; 5% of teduglutide patients and 7% of placebo patients discontinued treatment because of such events during the study period. The most frequently reported treatment-emergent adverse events included abdominal pain, abdominal distension, nausea, and gastrointestinal stoma complications.
Although the study did not specifically assess quality of life measures, significantly more teduglutide patients had at least 1 day off PS, compared with placebo patients, which could help to "liberate considerable time for unhindered daytime activities or undisturbed sleep," the researchers said.
The study did not address the possible benefit of teduglutide therapy earlier in the course of SBS, or the duration of effect after patients discontinued teduglutide, the researchers added.
However, the findings indicate that teduglutide was safe and well tolerated, and "could positively add to the limited treatment armamentarium" for patients with SBS-IF.
Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
FROM GASTROENTEROLOGY
Major Finding: Significantly more patients who received 0.05 mg/kg per day of teduglutide had a sustained response to treatment during weeks 20-24, compared with the placebo group (63% vs. 30%).
Data Source: The data come from a randomized, controlled multicenter trial of 85 adults with short bowel syndrome and intestinal failure.
Disclosures: Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
Early Oral Feeding Benefits Bowel Surgery Patients
CHICAGO – A total of 80% of bowel resection patients tolerated early fluids one day after surgery, based on data from 100 patients.
"Early oral feeding is an important part of fast-track surgery, which enhances recovery after surgery," but feeding in patients undergoing emergency bowel resection is often delayed until the resolution of ileus, Dr. Mohamed E. Shams of Suez Canal University in Ismailia, Egypt, said at the annual clinical congress of the American College of Surgeons.
Dr. Shams and colleagues randomized 100 adults who underwent small or large bowel resection into two groups. The early group comprised 50 patients who received fluid oral feedings on the first day after surgery. The late group comprised 50 patients who received oral feedings after the resolution of ileus.
Overall, 80% of patients in the early group tolerated the early oral feeding. In addition, patients in the early group averaged a significantly shorter time than did the late group to the passage of flatus (3.2 days vs. 0.8 days, respectively), and stool (4.4 days vs. 1.2 days, respectively).
Postoperative monitoring showed that the chest infections occurred in four patients in the early feeding group compared with 10 patients in the late feeding group, while wound infections occurred in 12 patients in the early group and 15 patients in the late group, Dr. Shams said. No incidents of a burst abdomen occurred in the early group, and three incidents occurred in the late group.
"Early oral feeding after emergency intestinal surgery is safe and well tolerated by the majority of patients, without an increase in mortality and morbidity risk," said Dr. Shams. "It also has a positive impact on reduction in hospital stay," he said.
The findings were limited by the small number of patients, but the results suggest that a majority of patients undergoing emergency intestinal surgery can benefit from early feeding, Dr. Shams noted.
Dr. Shams had no financial conflicts to disclose.
CHICAGO – A total of 80% of bowel resection patients tolerated early fluids one day after surgery, based on data from 100 patients.
"Early oral feeding is an important part of fast-track surgery, which enhances recovery after surgery," but feeding in patients undergoing emergency bowel resection is often delayed until the resolution of ileus, Dr. Mohamed E. Shams of Suez Canal University in Ismailia, Egypt, said at the annual clinical congress of the American College of Surgeons.
Dr. Shams and colleagues randomized 100 adults who underwent small or large bowel resection into two groups. The early group comprised 50 patients who received fluid oral feedings on the first day after surgery. The late group comprised 50 patients who received oral feedings after the resolution of ileus.
Overall, 80% of patients in the early group tolerated the early oral feeding. In addition, patients in the early group averaged a significantly shorter time than did the late group to the passage of flatus (3.2 days vs. 0.8 days, respectively), and stool (4.4 days vs. 1.2 days, respectively).
Postoperative monitoring showed that the chest infections occurred in four patients in the early feeding group compared with 10 patients in the late feeding group, while wound infections occurred in 12 patients in the early group and 15 patients in the late group, Dr. Shams said. No incidents of a burst abdomen occurred in the early group, and three incidents occurred in the late group.
"Early oral feeding after emergency intestinal surgery is safe and well tolerated by the majority of patients, without an increase in mortality and morbidity risk," said Dr. Shams. "It also has a positive impact on reduction in hospital stay," he said.
The findings were limited by the small number of patients, but the results suggest that a majority of patients undergoing emergency intestinal surgery can benefit from early feeding, Dr. Shams noted.
Dr. Shams had no financial conflicts to disclose.
CHICAGO – A total of 80% of bowel resection patients tolerated early fluids one day after surgery, based on data from 100 patients.
"Early oral feeding is an important part of fast-track surgery, which enhances recovery after surgery," but feeding in patients undergoing emergency bowel resection is often delayed until the resolution of ileus, Dr. Mohamed E. Shams of Suez Canal University in Ismailia, Egypt, said at the annual clinical congress of the American College of Surgeons.
Dr. Shams and colleagues randomized 100 adults who underwent small or large bowel resection into two groups. The early group comprised 50 patients who received fluid oral feedings on the first day after surgery. The late group comprised 50 patients who received oral feedings after the resolution of ileus.
Overall, 80% of patients in the early group tolerated the early oral feeding. In addition, patients in the early group averaged a significantly shorter time than did the late group to the passage of flatus (3.2 days vs. 0.8 days, respectively), and stool (4.4 days vs. 1.2 days, respectively).
Postoperative monitoring showed that the chest infections occurred in four patients in the early feeding group compared with 10 patients in the late feeding group, while wound infections occurred in 12 patients in the early group and 15 patients in the late group, Dr. Shams said. No incidents of a burst abdomen occurred in the early group, and three incidents occurred in the late group.
"Early oral feeding after emergency intestinal surgery is safe and well tolerated by the majority of patients, without an increase in mortality and morbidity risk," said Dr. Shams. "It also has a positive impact on reduction in hospital stay," he said.
The findings were limited by the small number of patients, but the results suggest that a majority of patients undergoing emergency intestinal surgery can benefit from early feeding, Dr. Shams noted.
Dr. Shams had no financial conflicts to disclose.
FROM THE ANNUAL CLINICAL CONGRESS OF THE AMERICAN COLLEGE OF SURGEONS
Major Finding: Eighty percent of patients who received oral fluids on the first day after surgery vs. delayed feeding had significantly shorter time to the passage of flatus (3.2 days vs. 0.8 days, respectively), and stool (4.4 days vs. 1.2 days, respectively).
Data Source: The data come from a randomized trial of 100 adults who underwent bowel resection.
Disclosures: Dr. Shams reported having no financial conflicts.
Withholding Warfarin After GI Bleed Raises Risk of Thrombosis, Death
Deciding not to resume warfarin therapy after an episode of gastrointestinal bleeding raises the risk of thrombosis by a factor of 10 and the risk of death threefold, according to a retrospective cohort study published online September 17 in Archives of Internal Medicine.
"For many patients who have experienced gastrointestinal bleeding, the benefits of resuming warfarin therapy will outweigh the risks," said Daniel M. Witt, Pharm.D., of the clinical pharmacy anticoagulation service at Kaiser Permanente of Colorado, Aurora, and his associates.

"Surprisingly little is known about warfarin therapy and resumption" following a GI bleed, and there is no consensus as to the optimal timing or the risks of restarting anticoagulation. Dr. Witt and his colleagues used Kaiser’s administrative and clinical databases to study the incidence of thrombosis, recurrent bleeding episodes, and death from any cause in 442 adults who presented to a hospital or emergency department with warfarin-associated GI bleeding in 2005-2009 and who were followed for 90 days.
The mean patient age was 74 years, and the study population was equally comprised of men and women. Half of the study subjects were taking warfarin to prevent atrial fibrillation–related stroke or systemic embolization. One-quarter of patients used it to treat or prevent a second venous thrombosis, 10% were on it to prevent thromboembolic complications from prosthetic heart valves, and the remainder took it for other indications.
After an index GI bleed, 260 patients (59%) resumed warfarin therapy, usually within a week. The median time to resumption of warfarin was 4 days. In 41 of these patients, warfarin therapy was never suspended. It was suspended and never resumed in the remaining 182 patients.
During the 90-day follow-up, 11 patients (2.5%) had a thrombotic event. There were six arterial events, including five strokes and one systemic embolus, and five venous events, including three pulmonary embolisms and two deep vein thromboses (DVTs).
The rate of thrombotic events was 0.4% among the patients who resumed warfarin therapy (one DVT), compared with 5.5% among those who did not resume warfarin (five strokes, one systemic embolus, three pulmonary embolisms, and one DVT), a significant difference, the investigators said (Arch. Intern. Med. 2012 [doi:10.1001/archinternmed.2012.5261]).
"Patients who either never interrupted warfarin therapy or resumed therapy within 14 days of the index GI bleed experienced no thromboses," they added.
GI bleeding recurred in 36 patients (8.4%) overall. A numerically higher proportion of patients who resumed warfarin therapy had recurrent GI bleeding (10%) than those who did not resume warfarin (5.5%), but this difference was not statistically significant.
In addition, a multivariable analysis that accounted for numerous possible confounders – including patient age, sex, propensity for complications; the INR at admission; acute treatment for the GI bleed; and location of GI bleed – also showed that the risk for rebleeding was not significantly greater in patients who resumed warfarin therapy than in those who did not.
Moreover, recurrent GI bleeding was never fatal. Fatal strokes did occur, however, in three patients with atrial fibrillation whose warfarin therapy was withdrawn and never resumed, Dr. Witt and his associates said.
A total of 52 patients (12%) died during follow-up. The most common cause of death was related to malignancy (29% of deaths), infection (19% of deaths), or cardiac disease (17%).
Resumption of warfarin therapy was strongly associated with a threefold decrease in the risk of death from any cause.
The investigators also performed a post hoc analysis excluding all patients who died within 1 week of the index GI bleed to rule out those who may not have had an opportunity to resume warfarin therapy. In this analysis, the strong association between resumption of warfarin and decreased mortality persisted.
Mortality was lowest among patients who resumed warfarin therapy within 15-90 days of the index GI bleed, the researchers said.
"Our results provide some guidance regarding the optimal timing of warfarin therapy resumption following GI bleeding, but clinical judgment remains a critical factor in this difficult decision," they noted.
This study was funded by CSL Behring. Dr. Witt’s associates, but not Dr. Witt, reported ties to numerous industry sources.
This study provides high-quality, real-world data showing that the risk of recurrent bleeding was acceptably low (10%), none of the episodes of recurrence were fatal, and most physicians and patients were willing to resume anticoagulation soon after GI bleeding, said Dr. Daniel J. Brotman and Dr. Amir K. Jaffer.
Dr. Amir K. Jaffer |

"We would hesitate to continue concurrent antiplatelet therapy in these patients without a compelling indication to do so (such as a recent coronary stent), and also would caution against extrapolating these findings to newer anticoagulants, such as dabigatran and rivaroxaban, that may be associated with more GI bleeding than warfarin when used long term and whose effects are not easily reversed," they said.
Dr. Brotman is with the hospitalist program at Johns Hopkins Hospital, Baltimore. Dr. Jaffer is with the division of hospital medicine at the University of Miami. Dr. Brotman reported ties to Gerson Lehrman Group, the Dunn Group, Quantia Communications, Siemens Healthcare Diagnostics, and Amerigroup Corporation. Dr. Jaffer reported ties to Sanofi-Aventis, Boehringer Ingelheim, Bristol Myers Squibb, Janssen Pharmaceuticals, Canyon Pharmaceuticals, and CSL. These remarks were taken from their invited commentary accompanying Dr. Witt’s report (Arch. Intern. Med. 2012 [doi:10.1001/archinternmed.2012.4309]).
This study provides high-quality, real-world data showing that the risk of recurrent bleeding was acceptably low (10%), none of the episodes of recurrence were fatal, and most physicians and patients were willing to resume anticoagulation soon after GI bleeding, said Dr. Daniel J. Brotman and Dr. Amir K. Jaffer.
Dr. Amir K. Jaffer |
"We would hesitate to continue concurrent antiplatelet therapy in these patients without a compelling indication to do so (such as a recent coronary stent), and also would caution against extrapolating these findings to newer anticoagulants, such as dabigatran and rivaroxaban, that may be associated with more GI bleeding than warfarin when used long term and whose effects are not easily reversed," they said.
Dr. Brotman is with the hospitalist program at Johns Hopkins Hospital, Baltimore. Dr. Jaffer is with the division of hospital medicine at the University of Miami. Dr. Brotman reported ties to Gerson Lehrman Group, the Dunn Group, Quantia Communications, Siemens Healthcare Diagnostics, and Amerigroup Corporation. Dr. Jaffer reported ties to Sanofi-Aventis, Boehringer Ingelheim, Bristol Myers Squibb, Janssen Pharmaceuticals, Canyon Pharmaceuticals, and CSL. These remarks were taken from their invited commentary accompanying Dr. Witt’s report (Arch. Intern. Med. 2012 [doi:10.1001/archinternmed.2012.4309]).
This study provides high-quality, real-world data showing that the risk of recurrent bleeding was acceptably low (10%), none of the episodes of recurrence were fatal, and most physicians and patients were willing to resume anticoagulation soon after GI bleeding, said Dr. Daniel J. Brotman and Dr. Amir K. Jaffer.
Dr. Amir K. Jaffer |
"We would hesitate to continue concurrent antiplatelet therapy in these patients without a compelling indication to do so (such as a recent coronary stent), and also would caution against extrapolating these findings to newer anticoagulants, such as dabigatran and rivaroxaban, that may be associated with more GI bleeding than warfarin when used long term and whose effects are not easily reversed," they said.
Dr. Brotman is with the hospitalist program at Johns Hopkins Hospital, Baltimore. Dr. Jaffer is with the division of hospital medicine at the University of Miami. Dr. Brotman reported ties to Gerson Lehrman Group, the Dunn Group, Quantia Communications, Siemens Healthcare Diagnostics, and Amerigroup Corporation. Dr. Jaffer reported ties to Sanofi-Aventis, Boehringer Ingelheim, Bristol Myers Squibb, Janssen Pharmaceuticals, Canyon Pharmaceuticals, and CSL. These remarks were taken from their invited commentary accompanying Dr. Witt’s report (Arch. Intern. Med. 2012 [doi:10.1001/archinternmed.2012.4309]).
Deciding not to resume warfarin therapy after an episode of gastrointestinal bleeding raises the risk of thrombosis by a factor of 10 and the risk of death threefold, according to a retrospective cohort study published online September 17 in Archives of Internal Medicine.
"For many patients who have experienced gastrointestinal bleeding, the benefits of resuming warfarin therapy will outweigh the risks," said Daniel M. Witt, Pharm.D., of the clinical pharmacy anticoagulation service at Kaiser Permanente of Colorado, Aurora, and his associates.
"Surprisingly little is known about warfarin therapy and resumption" following a GI bleed, and there is no consensus as to the optimal timing or the risks of restarting anticoagulation. Dr. Witt and his colleagues used Kaiser’s administrative and clinical databases to study the incidence of thrombosis, recurrent bleeding episodes, and death from any cause in 442 adults who presented to a hospital or emergency department with warfarin-associated GI bleeding in 2005-2009 and who were followed for 90 days.
The mean patient age was 74 years, and the study population was equally comprised of men and women. Half of the study subjects were taking warfarin to prevent atrial fibrillation–related stroke or systemic embolization. One-quarter of patients used it to treat or prevent a second venous thrombosis, 10% were on it to prevent thromboembolic complications from prosthetic heart valves, and the remainder took it for other indications.
After an index GI bleed, 260 patients (59%) resumed warfarin therapy, usually within a week. The median time to resumption of warfarin was 4 days. In 41 of these patients, warfarin therapy was never suspended. It was suspended and never resumed in the remaining 182 patients.
During the 90-day follow-up, 11 patients (2.5%) had a thrombotic event. There were six arterial events, including five strokes and one systemic embolus, and five venous events, including three pulmonary embolisms and two deep vein thromboses (DVTs).
The rate of thrombotic events was 0.4% among the patients who resumed warfarin therapy (one DVT), compared with 5.5% among those who did not resume warfarin (five strokes, one systemic embolus, three pulmonary embolisms, and one DVT), a significant difference, the investigators said (Arch. Intern. Med. 2012 [doi:10.1001/archinternmed.2012.5261]).
"Patients who either never interrupted warfarin therapy or resumed therapy within 14 days of the index GI bleed experienced no thromboses," they added.
GI bleeding recurred in 36 patients (8.4%) overall. A numerically higher proportion of patients who resumed warfarin therapy had recurrent GI bleeding (10%) than those who did not resume warfarin (5.5%), but this difference was not statistically significant.
In addition, a multivariable analysis that accounted for numerous possible confounders – including patient age, sex, propensity for complications; the INR at admission; acute treatment for the GI bleed; and location of GI bleed – also showed that the risk for rebleeding was not significantly greater in patients who resumed warfarin therapy than in those who did not.
Moreover, recurrent GI bleeding was never fatal. Fatal strokes did occur, however, in three patients with atrial fibrillation whose warfarin therapy was withdrawn and never resumed, Dr. Witt and his associates said.
A total of 52 patients (12%) died during follow-up. The most common cause of death was related to malignancy (29% of deaths), infection (19% of deaths), or cardiac disease (17%).
Resumption of warfarin therapy was strongly associated with a threefold decrease in the risk of death from any cause.
The investigators also performed a post hoc analysis excluding all patients who died within 1 week of the index GI bleed to rule out those who may not have had an opportunity to resume warfarin therapy. In this analysis, the strong association between resumption of warfarin and decreased mortality persisted.
Mortality was lowest among patients who resumed warfarin therapy within 15-90 days of the index GI bleed, the researchers said.
"Our results provide some guidance regarding the optimal timing of warfarin therapy resumption following GI bleeding, but clinical judgment remains a critical factor in this difficult decision," they noted.
This study was funded by CSL Behring. Dr. Witt’s associates, but not Dr. Witt, reported ties to numerous industry sources.
Deciding not to resume warfarin therapy after an episode of gastrointestinal bleeding raises the risk of thrombosis by a factor of 10 and the risk of death threefold, according to a retrospective cohort study published online September 17 in Archives of Internal Medicine.
"For many patients who have experienced gastrointestinal bleeding, the benefits of resuming warfarin therapy will outweigh the risks," said Daniel M. Witt, Pharm.D., of the clinical pharmacy anticoagulation service at Kaiser Permanente of Colorado, Aurora, and his associates.
"Surprisingly little is known about warfarin therapy and resumption" following a GI bleed, and there is no consensus as to the optimal timing or the risks of restarting anticoagulation. Dr. Witt and his colleagues used Kaiser’s administrative and clinical databases to study the incidence of thrombosis, recurrent bleeding episodes, and death from any cause in 442 adults who presented to a hospital or emergency department with warfarin-associated GI bleeding in 2005-2009 and who were followed for 90 days.
The mean patient age was 74 years, and the study population was equally comprised of men and women. Half of the study subjects were taking warfarin to prevent atrial fibrillation–related stroke or systemic embolization. One-quarter of patients used it to treat or prevent a second venous thrombosis, 10% were on it to prevent thromboembolic complications from prosthetic heart valves, and the remainder took it for other indications.
After an index GI bleed, 260 patients (59%) resumed warfarin therapy, usually within a week. The median time to resumption of warfarin was 4 days. In 41 of these patients, warfarin therapy was never suspended. It was suspended and never resumed in the remaining 182 patients.
During the 90-day follow-up, 11 patients (2.5%) had a thrombotic event. There were six arterial events, including five strokes and one systemic embolus, and five venous events, including three pulmonary embolisms and two deep vein thromboses (DVTs).
The rate of thrombotic events was 0.4% among the patients who resumed warfarin therapy (one DVT), compared with 5.5% among those who did not resume warfarin (five strokes, one systemic embolus, three pulmonary embolisms, and one DVT), a significant difference, the investigators said (Arch. Intern. Med. 2012 [doi:10.1001/archinternmed.2012.5261]).
"Patients who either never interrupted warfarin therapy or resumed therapy within 14 days of the index GI bleed experienced no thromboses," they added.
GI bleeding recurred in 36 patients (8.4%) overall. A numerically higher proportion of patients who resumed warfarin therapy had recurrent GI bleeding (10%) than those who did not resume warfarin (5.5%), but this difference was not statistically significant.
In addition, a multivariable analysis that accounted for numerous possible confounders – including patient age, sex, propensity for complications; the INR at admission; acute treatment for the GI bleed; and location of GI bleed – also showed that the risk for rebleeding was not significantly greater in patients who resumed warfarin therapy than in those who did not.
Moreover, recurrent GI bleeding was never fatal. Fatal strokes did occur, however, in three patients with atrial fibrillation whose warfarin therapy was withdrawn and never resumed, Dr. Witt and his associates said.
A total of 52 patients (12%) died during follow-up. The most common cause of death was related to malignancy (29% of deaths), infection (19% of deaths), or cardiac disease (17%).
Resumption of warfarin therapy was strongly associated with a threefold decrease in the risk of death from any cause.
The investigators also performed a post hoc analysis excluding all patients who died within 1 week of the index GI bleed to rule out those who may not have had an opportunity to resume warfarin therapy. In this analysis, the strong association between resumption of warfarin and decreased mortality persisted.
Mortality was lowest among patients who resumed warfarin therapy within 15-90 days of the index GI bleed, the researchers said.
"Our results provide some guidance regarding the optimal timing of warfarin therapy resumption following GI bleeding, but clinical judgment remains a critical factor in this difficult decision," they noted.
This study was funded by CSL Behring. Dr. Witt’s associates, but not Dr. Witt, reported ties to numerous industry sources.
FROM ARCHIVES OF INTERNAL MEDICINE
Major Finding: The rate of thrombotic events was 0.4% in patients who resumed warfarin therapy after an episode of GI bleeding, compared with 5.5% in those who did not resume warfarin.
Data Source: A retrospective cohort study compared outcomes between 260 patients who resumed warfarin therapy and 182 who did not, who were followed for 90 days.
Disclosures: This study was funded by CSL Behring. Dr. Witt’s associates, but not Dr. Witt, reported ties to numerous industry sources.

Transfusions Worsen Outcomes After Colorectal Cancer Surgery
The risks of death, postoperative infection, and other adverse clinical outcomes were significantly increased among patients undergoing colorectal cancer surgery who received perioperative allogeneic blood transfusions, according to a meta-analysis of 55 studies published in the August issue of Annals of Surgery.
Dr. Austin G. Acheson of the Nottingham (England) Digestive Disease Center at Queen’s Medical Centre and his associates reviewed 12 prospective studies and 43 retrospective cohort studies published between December 2004 and October 2010. The studies included 20,795 patients who were followed for a mean of about 5 years after undergoing surgery for colorectal cancer. Almost 60% (12,242) of these patients received a mean of three units of allogeneic red blood cells (Ann. Surg. 2012;256:235-44).
Patients who were transfused tended to be older, and the transfusion rate was significantly higher in women, those undergoing rectal surgery (compared with those undergoing right or left colon surgery), those with greater surgical blood loss, and those with worsening Duke's stage.
All associations between ABT and the adverse clinical outcomes described below were statistically significant.
The rates of all-cause mortality in the 29 studies that looked at this outcome were 45% among the patients who received blood transfusions vs. 35% of those who did not, a significant difference that represented a 72% increased risk. After adjusting for the duration of the observation period, the investigators found that the annual incidence of all-cause mortality was almost 9% among the transfused patients vs. 6.5% among those who were not transfused.
The rate of cancer-related mortality was 31% vs. 24% in the 17 studies that measured this outcome, a 71% increased risk. After adjusting for the length of observation, the investigators said the annual incidence of cancer-related mortality was 5.4% of those transfused and 4% of those who were not.
The rate of the combined end point of death resulting from recurrence/metastasis was 43% of those who were transfused vs. 33% of those who were not transfused – a 66% increase in risk – in the 19 studies that measured this outcome.
The risk of postoperative infections in the 12 studies that measured this outcome was 29% among those who were transfused vs. 11% of those who were not transfused, which was more than a threefold increased risk. In the two studies that measured the need for surgical reintervention, the risk was increased fourfold among those who were transfused.
In the four studies that measured the length of hospitalization, the hospital stay was a mean of almost 18 days among those who received transfusions, compared with 14 days among those who did not.
Based on evidence in this meta-analysis and other studies showing that preoperative anemia is an independent risk factor for a worse prognosis after colon surgery, and based on the association between ABTs and poorer clinical outcomes in this meta-analysis, the authors wrote that "appropriate blood management measures should, therefore, be given an important place in the care of patients with CRC [colorectal cancer] undergoing elective surgery."
The use of ABT has dropped over the past 25 years because of improvements in patient care, and the authors stated that they believe efforts should be made to further minimize ABT use. Well-designed studies are needed "to determine whether and in which patients preoperative corrective measures of anemia, other than ABTs, will contribute not only in the field of colorectal surgery but also to improve clinical outcomes," they added.
The study was supported by an unrestricted research grant from Vifor Pharma AG, a specialty pharmaceuticals company focused on the treatment of iron deficiency, according to its website. The authors disclosed receiving honoraria and/or travel support for consulting or lecturing for companies that include Vifor, Ethicon Endosurgery, Johnson & Johnson, and AstraZeneca AG; their research departments received grant support from companies that included Vifor.
The meta-analysis by Dr. Acheson and his colleagues and another recent publication using the American College of Surgeons National Surgical Quality Improvement Program (Surgery 2012;152:344-54) highlight concerns about the increased mortality associated with perioperative blood transfusions. Intraoperative transfusion is associated with higher rates of 30-day operative mortality, major complications, total number of complications, and prolonged length of stay.
In general, patients requiring transfusions tend to be older, more
anemic and debilitated, have more extensive disease, and often need
larger surgical procedures with attendant greater blood loss. Patients
with these characteristics should be relatively evenly distributed among hospitals performing colorectal cancer surgery, and one would expect the frequency of transfusion to be similar across institutions.
However, Dr. Acheson and his associates found that the transfusion rate varied from 17.4% to 82.2%, suggesting that the indications for transfusion were quite
variable. Furthermore, the National Surgical Quality Improvement Program noted that more than 60% of patients received only one to two units of blood. This
raises concerns about whether blood transfusions are being given appropriately.
Some of the steps can be taken to decrease the use of perioperative blood transfusions and prevent transfusion-related morbidity are:
• Correcting anemia prior to
surgery by giving iron with or with
out erythropoietin;
• Using blood conservation methods when extensive surgery is
planned;
• Educating anesthesiologists and
surgeons about the indications for
transfusion (there is no rigid “trans
fusion trigger”; each patient must be
assessed for the need to augment the
oxygen-carrying capacity of the
blood);
• Avoiding prospective donors alloimmunized to white cell antigens
and leuko-reduce blood products
(Blood 2009;113:3406-17);
• Avoiding the use of blood that has
undergone prolonged storage (new
blood is better than old) (N. Engl. J.
Med. 2008;20:358:1229-39; Blood
2011;118:6675-82); and
• Recognizing that acute illness after perioperative transfusions might be due to transfusion-transmitted infections or transfusion-associated lung injury (TRALI) (Blood 2012;119:1757-67).
Perioperative allogeneic blood transfusions can be life-saving, but must be used judiciously and with the recognition that they occasionally increase morbidity and mortality.
DAVID GREEN, M.D., PH.D., is in the
division of hematology/oncology in
the department of medicine at
Northwestern University Feinberg
School of Medicine, Chicago. He has
no relevant disclosures.
The meta-analysis by Dr. Acheson and his colleagues and another recent publication using the American College of Surgeons National Surgical Quality Improvement Program (Surgery 2012;152:344-54) highlight concerns about the increased mortality associated with perioperative blood transfusions. Intraoperative transfusion is associated with higher rates of 30-day operative mortality, major complications, total number of complications, and prolonged length of stay.
In general, patients requiring transfusions tend to be older, more
anemic and debilitated, have more extensive disease, and often need
larger surgical procedures with attendant greater blood loss. Patients
with these characteristics should be relatively evenly distributed among hospitals performing colorectal cancer surgery, and one would expect the frequency of transfusion to be similar across institutions.
However, Dr. Acheson and his associates found that the transfusion rate varied from 17.4% to 82.2%, suggesting that the indications for transfusion were quite
variable. Furthermore, the National Surgical Quality Improvement Program noted that more than 60% of patients received only one to two units of blood. This
raises concerns about whether blood transfusions are being given appropriately.
Some of the steps can be taken to decrease the use of perioperative blood transfusions and prevent transfusion-related morbidity are:
• Correcting anemia prior to
surgery by giving iron with or with
out erythropoietin;
• Using blood conservation methods when extensive surgery is
planned;
• Educating anesthesiologists and
surgeons about the indications for
transfusion (there is no rigid “trans
fusion trigger”; each patient must be
assessed for the need to augment the
oxygen-carrying capacity of the
blood);
• Avoiding prospective donors alloimmunized to white cell antigens
and leuko-reduce blood products
(Blood 2009;113:3406-17);
• Avoiding the use of blood that has
undergone prolonged storage (new
blood is better than old) (N. Engl. J.
Med. 2008;20:358:1229-39; Blood
2011;118:6675-82); and
• Recognizing that acute illness after perioperative transfusions might be due to transfusion-transmitted infections or transfusion-associated lung injury (TRALI) (Blood 2012;119:1757-67).
Perioperative allogeneic blood transfusions can be life-saving, but must be used judiciously and with the recognition that they occasionally increase morbidity and mortality.
DAVID GREEN, M.D., PH.D., is in the
division of hematology/oncology in
the department of medicine at
Northwestern University Feinberg
School of Medicine, Chicago. He has
no relevant disclosures.
The meta-analysis by Dr. Acheson and his colleagues and another recent publication using the American College of Surgeons National Surgical Quality Improvement Program (Surgery 2012;152:344-54) highlight concerns about the increased mortality associated with perioperative blood transfusions. Intraoperative transfusion is associated with higher rates of 30-day operative mortality, major complications, total number of complications, and prolonged length of stay.
In general, patients requiring transfusions tend to be older, more
anemic and debilitated, have more extensive disease, and often need
larger surgical procedures with attendant greater blood loss. Patients
with these characteristics should be relatively evenly distributed among hospitals performing colorectal cancer surgery, and one would expect the frequency of transfusion to be similar across institutions.
However, Dr. Acheson and his associates found that the transfusion rate varied from 17.4% to 82.2%, suggesting that the indications for transfusion were quite
variable. Furthermore, the National Surgical Quality Improvement Program noted that more than 60% of patients received only one to two units of blood. This
raises concerns about whether blood transfusions are being given appropriately.
Some of the steps can be taken to decrease the use of perioperative blood transfusions and prevent transfusion-related morbidity are:
• Correcting anemia prior to
surgery by giving iron with or with
out erythropoietin;
• Using blood conservation methods when extensive surgery is
planned;
• Educating anesthesiologists and
surgeons about the indications for
transfusion (there is no rigid “trans
fusion trigger”; each patient must be
assessed for the need to augment the
oxygen-carrying capacity of the
blood);
• Avoiding prospective donors alloimmunized to white cell antigens
and leuko-reduce blood products
(Blood 2009;113:3406-17);
• Avoiding the use of blood that has
undergone prolonged storage (new
blood is better than old) (N. Engl. J.
Med. 2008;20:358:1229-39; Blood
2011;118:6675-82); and
• Recognizing that acute illness after perioperative transfusions might be due to transfusion-transmitted infections or transfusion-associated lung injury (TRALI) (Blood 2012;119:1757-67).
Perioperative allogeneic blood transfusions can be life-saving, but must be used judiciously and with the recognition that they occasionally increase morbidity and mortality.
DAVID GREEN, M.D., PH.D., is in the
division of hematology/oncology in
the department of medicine at
Northwestern University Feinberg
School of Medicine, Chicago. He has
no relevant disclosures.
The risks of death, postoperative infection, and other adverse clinical outcomes were significantly increased among patients undergoing colorectal cancer surgery who received perioperative allogeneic blood transfusions, according to a meta-analysis of 55 studies published in the August issue of Annals of Surgery.
Dr. Austin G. Acheson of the Nottingham (England) Digestive Disease Center at Queen’s Medical Centre and his associates reviewed 12 prospective studies and 43 retrospective cohort studies published between December 2004 and October 2010. The studies included 20,795 patients who were followed for a mean of about 5 years after undergoing surgery for colorectal cancer. Almost 60% (12,242) of these patients received a mean of three units of allogeneic red blood cells (Ann. Surg. 2012;256:235-44).
Patients who were transfused tended to be older, and the transfusion rate was significantly higher in women, those undergoing rectal surgery (compared with those undergoing right or left colon surgery), those with greater surgical blood loss, and those with worsening Duke's stage.
All associations between ABT and the adverse clinical outcomes described below were statistically significant.
The rates of all-cause mortality in the 29 studies that looked at this outcome were 45% among the patients who received blood transfusions vs. 35% of those who did not, a significant difference that represented a 72% increased risk. After adjusting for the duration of the observation period, the investigators found that the annual incidence of all-cause mortality was almost 9% among the transfused patients vs. 6.5% among those who were not transfused.
The rate of cancer-related mortality was 31% vs. 24% in the 17 studies that measured this outcome, a 71% increased risk. After adjusting for the length of observation, the investigators said the annual incidence of cancer-related mortality was 5.4% of those transfused and 4% of those who were not.
The rate of the combined end point of death resulting from recurrence/metastasis was 43% of those who were transfused vs. 33% of those who were not transfused – a 66% increase in risk – in the 19 studies that measured this outcome.
The risk of postoperative infections in the 12 studies that measured this outcome was 29% among those who were transfused vs. 11% of those who were not transfused, which was more than a threefold increased risk. In the two studies that measured the need for surgical reintervention, the risk was increased fourfold among those who were transfused.
In the four studies that measured the length of hospitalization, the hospital stay was a mean of almost 18 days among those who received transfusions, compared with 14 days among those who did not.
Based on evidence in this meta-analysis and other studies showing that preoperative anemia is an independent risk factor for a worse prognosis after colon surgery, and based on the association between ABTs and poorer clinical outcomes in this meta-analysis, the authors wrote that "appropriate blood management measures should, therefore, be given an important place in the care of patients with CRC [colorectal cancer] undergoing elective surgery."
The use of ABT has dropped over the past 25 years because of improvements in patient care, and the authors stated that they believe efforts should be made to further minimize ABT use. Well-designed studies are needed "to determine whether and in which patients preoperative corrective measures of anemia, other than ABTs, will contribute not only in the field of colorectal surgery but also to improve clinical outcomes," they added.
The study was supported by an unrestricted research grant from Vifor Pharma AG, a specialty pharmaceuticals company focused on the treatment of iron deficiency, according to its website. The authors disclosed receiving honoraria and/or travel support for consulting or lecturing for companies that include Vifor, Ethicon Endosurgery, Johnson & Johnson, and AstraZeneca AG; their research departments received grant support from companies that included Vifor.
The risks of death, postoperative infection, and other adverse clinical outcomes were significantly increased among patients undergoing colorectal cancer surgery who received perioperative allogeneic blood transfusions, according to a meta-analysis of 55 studies published in the August issue of Annals of Surgery.
Dr. Austin G. Acheson of the Nottingham (England) Digestive Disease Center at Queen’s Medical Centre and his associates reviewed 12 prospective studies and 43 retrospective cohort studies published between December 2004 and October 2010. The studies included 20,795 patients who were followed for a mean of about 5 years after undergoing surgery for colorectal cancer. Almost 60% (12,242) of these patients received a mean of three units of allogeneic red blood cells (Ann. Surg. 2012;256:235-44).
Patients who were transfused tended to be older, and the transfusion rate was significantly higher in women, those undergoing rectal surgery (compared with those undergoing right or left colon surgery), those with greater surgical blood loss, and those with worsening Duke's stage.
All associations between ABT and the adverse clinical outcomes described below were statistically significant.
The rates of all-cause mortality in the 29 studies that looked at this outcome were 45% among the patients who received blood transfusions vs. 35% of those who did not, a significant difference that represented a 72% increased risk. After adjusting for the duration of the observation period, the investigators found that the annual incidence of all-cause mortality was almost 9% among the transfused patients vs. 6.5% among those who were not transfused.
The rate of cancer-related mortality was 31% vs. 24% in the 17 studies that measured this outcome, a 71% increased risk. After adjusting for the length of observation, the investigators said the annual incidence of cancer-related mortality was 5.4% of those transfused and 4% of those who were not.
The rate of the combined end point of death resulting from recurrence/metastasis was 43% of those who were transfused vs. 33% of those who were not transfused – a 66% increase in risk – in the 19 studies that measured this outcome.
The risk of postoperative infections in the 12 studies that measured this outcome was 29% among those who were transfused vs. 11% of those who were not transfused, which was more than a threefold increased risk. In the two studies that measured the need for surgical reintervention, the risk was increased fourfold among those who were transfused.
In the four studies that measured the length of hospitalization, the hospital stay was a mean of almost 18 days among those who received transfusions, compared with 14 days among those who did not.
Based on evidence in this meta-analysis and other studies showing that preoperative anemia is an independent risk factor for a worse prognosis after colon surgery, and based on the association between ABTs and poorer clinical outcomes in this meta-analysis, the authors wrote that "appropriate blood management measures should, therefore, be given an important place in the care of patients with CRC [colorectal cancer] undergoing elective surgery."
The use of ABT has dropped over the past 25 years because of improvements in patient care, and the authors stated that they believe efforts should be made to further minimize ABT use. Well-designed studies are needed "to determine whether and in which patients preoperative corrective measures of anemia, other than ABTs, will contribute not only in the field of colorectal surgery but also to improve clinical outcomes," they added.
The study was supported by an unrestricted research grant from Vifor Pharma AG, a specialty pharmaceuticals company focused on the treatment of iron deficiency, according to its website. The authors disclosed receiving honoraria and/or travel support for consulting or lecturing for companies that include Vifor, Ethicon Endosurgery, Johnson & Johnson, and AstraZeneca AG; their research departments received grant support from companies that included Vifor.
FROM THE ANNALS OF SURGERY
Major Finding: Adverse clinical outcomes including mortality were significantly increased among patients who had an allogeneic blood transfusion around the time of undergoing colorectal cancer surgery, compared with those who were not transfused.
Data Source: A meta-analysis of 55 mostly retrospective cohort studies evaluated mortality and other clinical outcomes associated with the use of allogeneic red blood cell transfusions in almost 21,000 patients undergoing colorectal cancer surgery, 60% of whom were transfused.
Disclosures: The study was supported by an unrestricted research grant from Vifor Pharma AG. The authors disclosed receiving honoraria and/or travel support for consulting or lecturing from companies that include Vifor, Ethicon Endosurgery, Johnson & Johnson, and AstraZeneca AG; their research departments received grant support from companies including Vifor.
'Weekend Effect' Seen for Diverticulitis Procedures
Patients who were admitted for emergency surgery on a weekend to treat left-sided diverticulitis experience more short-term complications and are markedly more likely to undergo a Hartmann procedure than are those admitted on weekdays, according to results from a large population-based study.
Longer hospital stays, significantly higher treatment costs, and higher rates of reoperations were also associated with weekend admission. However, no differences in mortality were observed between the patient groups.
Previous studies have shown worse outcomes for patients with gastrointestinal hemorrhage, kidney injury, myocardial infarction, pulmonary embolism, and intracerebral hemorrhage when they were admitted on weekends. Although the current study, led by Dr. Mathias Worni of Duke University Medical Center in Durham, N.C., and Bern (Switzerland) University Hospital, was not designed to isolate the cause of the "weekend effect" for left-sided diverticulitis patients, the authors noted that hospital staffing tends to be reduced on weekends – especially among specialists such as colorectal surgeons.
Dr. Worni and his colleagues looked at records from the Nationwide Inpatient Sample between January 2002 and December 2008. Of the 31,832 patients who were treated surgically for left-sided diverticulitis, 7,066 (22.2%) were admitted on weekends and 24,766 (77.8%) on weekdays. Patients’ mean age was 60.8 years, and more than half were women.
Among patients who were admitted on a Saturday or Sunday, a Hartmann procedure was performed on 64.8% (n = 4,580), compared with only 53.9% (n = 13,351) for those admitted on a weekday (Arch. Surg. 2012;147:649-55). The Hartmann procedure – which involves formation of a colostomy – has long been the standard surgery for people presenting with left-sided diverticulitis, but is associated with long-term complications and a low rate of reversals.
Primary anastomosis, in which colostomy is avoided, is increasingly preferred, but only 35.2% of patients who were admitted on weekends underwent primary anastomosis, compared with 46.1% of patients admitted on weekdays.
The investigators found that patients admitted on weekends had significantly higher risk for any postoperative complication (odds ratio, 1.10; P = .005), compared with patients admitted on weekdays. Risk of reoperation was also higher among weekend admissions (OR, 1.50; P less than .001).
Furthermore, median total hospital charges were $3,734 higher among patients treated on weekends, and the median length of hospital stay was 0.5 days longer (P less than .001). The authors observed that these findings should motivate improvements in the quality of weekend care.
"Physicians working on weekends are thought to be less experienced than teams working during the week," they wrote. Experienced and specialized colorectal surgeons have been shown to perform more primary anastomoses, compared with trainees or general surgeons (Arch. Surg. 2010;145:79-86; Dis. Colon Rectum 2003;46:1461-8).
Limitations of the study include the fact that it did not capture long-term outcomes or severity of disease at presentation. The latter could be of potential importance: "Some patients, especially those with milder symptoms, may prefer weekend or weekday admission and may time their admission accordingly," the investigators noted.
In an invited critique that accompanied the article, Dr. Juerg Metzger, a surgeon at Lucerne (Switzerland) Cantonal Hospital, wrote that a disparity in experience among weekday and weekend surgical staff likely accounted for the higher rate of Hartmann procedures and complications following weekend admissions.
"Work-hour restrictions do not seem to have a negative influence on mortality and morbidity in surgical patients," Dr. Metzger wrote. "However, reduced experience owing to restricted working hours may negatively influence the practical skills of younger surgeons, resulting in more limited surgery [for example, a Hartmann procedure being performed instead of a primary anastomosis] and an increase in complications related to that surgery."
In the end, Dr. Metzger wrote, "quality is expensive, and our society has to decide if it is desirable and necessary to have the best surgical quality available all the time, especially when considering that health care costs will dramatically increase. It would be relevant to analyze additional large databases, asking similar questions about the outcomes of other common diseases [for example, appendicitis, cholecystitis, and strangulated hernias] and studying the effect of weekend admission on these illnesses."
Dr. Worni’s and colleagues’ was funded by a grant from the Swiss National Science Foundation. None of the investigators declared conflicts of interest. Dr. Metzger declared that he had no conflicts of interest related to his critique.
Patients who were admitted for emergency surgery on a weekend to treat left-sided diverticulitis experience more short-term complications and are markedly more likely to undergo a Hartmann procedure than are those admitted on weekdays, according to results from a large population-based study.
Longer hospital stays, significantly higher treatment costs, and higher rates of reoperations were also associated with weekend admission. However, no differences in mortality were observed between the patient groups.
Previous studies have shown worse outcomes for patients with gastrointestinal hemorrhage, kidney injury, myocardial infarction, pulmonary embolism, and intracerebral hemorrhage when they were admitted on weekends. Although the current study, led by Dr. Mathias Worni of Duke University Medical Center in Durham, N.C., and Bern (Switzerland) University Hospital, was not designed to isolate the cause of the "weekend effect" for left-sided diverticulitis patients, the authors noted that hospital staffing tends to be reduced on weekends – especially among specialists such as colorectal surgeons.
Dr. Worni and his colleagues looked at records from the Nationwide Inpatient Sample between January 2002 and December 2008. Of the 31,832 patients who were treated surgically for left-sided diverticulitis, 7,066 (22.2%) were admitted on weekends and 24,766 (77.8%) on weekdays. Patients’ mean age was 60.8 years, and more than half were women.
Among patients who were admitted on a Saturday or Sunday, a Hartmann procedure was performed on 64.8% (n = 4,580), compared with only 53.9% (n = 13,351) for those admitted on a weekday (Arch. Surg. 2012;147:649-55). The Hartmann procedure – which involves formation of a colostomy – has long been the standard surgery for people presenting with left-sided diverticulitis, but is associated with long-term complications and a low rate of reversals.
Primary anastomosis, in which colostomy is avoided, is increasingly preferred, but only 35.2% of patients who were admitted on weekends underwent primary anastomosis, compared with 46.1% of patients admitted on weekdays.
The investigators found that patients admitted on weekends had significantly higher risk for any postoperative complication (odds ratio, 1.10; P = .005), compared with patients admitted on weekdays. Risk of reoperation was also higher among weekend admissions (OR, 1.50; P less than .001).
Furthermore, median total hospital charges were $3,734 higher among patients treated on weekends, and the median length of hospital stay was 0.5 days longer (P less than .001). The authors observed that these findings should motivate improvements in the quality of weekend care.
"Physicians working on weekends are thought to be less experienced than teams working during the week," they wrote. Experienced and specialized colorectal surgeons have been shown to perform more primary anastomoses, compared with trainees or general surgeons (Arch. Surg. 2010;145:79-86; Dis. Colon Rectum 2003;46:1461-8).
Limitations of the study include the fact that it did not capture long-term outcomes or severity of disease at presentation. The latter could be of potential importance: "Some patients, especially those with milder symptoms, may prefer weekend or weekday admission and may time their admission accordingly," the investigators noted.
In an invited critique that accompanied the article, Dr. Juerg Metzger, a surgeon at Lucerne (Switzerland) Cantonal Hospital, wrote that a disparity in experience among weekday and weekend surgical staff likely accounted for the higher rate of Hartmann procedures and complications following weekend admissions.
"Work-hour restrictions do not seem to have a negative influence on mortality and morbidity in surgical patients," Dr. Metzger wrote. "However, reduced experience owing to restricted working hours may negatively influence the practical skills of younger surgeons, resulting in more limited surgery [for example, a Hartmann procedure being performed instead of a primary anastomosis] and an increase in complications related to that surgery."
In the end, Dr. Metzger wrote, "quality is expensive, and our society has to decide if it is desirable and necessary to have the best surgical quality available all the time, especially when considering that health care costs will dramatically increase. It would be relevant to analyze additional large databases, asking similar questions about the outcomes of other common diseases [for example, appendicitis, cholecystitis, and strangulated hernias] and studying the effect of weekend admission on these illnesses."
Dr. Worni’s and colleagues’ was funded by a grant from the Swiss National Science Foundation. None of the investigators declared conflicts of interest. Dr. Metzger declared that he had no conflicts of interest related to his critique.
Patients who were admitted for emergency surgery on a weekend to treat left-sided diverticulitis experience more short-term complications and are markedly more likely to undergo a Hartmann procedure than are those admitted on weekdays, according to results from a large population-based study.
Longer hospital stays, significantly higher treatment costs, and higher rates of reoperations were also associated with weekend admission. However, no differences in mortality were observed between the patient groups.
Previous studies have shown worse outcomes for patients with gastrointestinal hemorrhage, kidney injury, myocardial infarction, pulmonary embolism, and intracerebral hemorrhage when they were admitted on weekends. Although the current study, led by Dr. Mathias Worni of Duke University Medical Center in Durham, N.C., and Bern (Switzerland) University Hospital, was not designed to isolate the cause of the "weekend effect" for left-sided diverticulitis patients, the authors noted that hospital staffing tends to be reduced on weekends – especially among specialists such as colorectal surgeons.
Dr. Worni and his colleagues looked at records from the Nationwide Inpatient Sample between January 2002 and December 2008. Of the 31,832 patients who were treated surgically for left-sided diverticulitis, 7,066 (22.2%) were admitted on weekends and 24,766 (77.8%) on weekdays. Patients’ mean age was 60.8 years, and more than half were women.
Among patients who were admitted on a Saturday or Sunday, a Hartmann procedure was performed on 64.8% (n = 4,580), compared with only 53.9% (n = 13,351) for those admitted on a weekday (Arch. Surg. 2012;147:649-55). The Hartmann procedure – which involves formation of a colostomy – has long been the standard surgery for people presenting with left-sided diverticulitis, but is associated with long-term complications and a low rate of reversals.
Primary anastomosis, in which colostomy is avoided, is increasingly preferred, but only 35.2% of patients who were admitted on weekends underwent primary anastomosis, compared with 46.1% of patients admitted on weekdays.
The investigators found that patients admitted on weekends had significantly higher risk for any postoperative complication (odds ratio, 1.10; P = .005), compared with patients admitted on weekdays. Risk of reoperation was also higher among weekend admissions (OR, 1.50; P less than .001).
Furthermore, median total hospital charges were $3,734 higher among patients treated on weekends, and the median length of hospital stay was 0.5 days longer (P less than .001). The authors observed that these findings should motivate improvements in the quality of weekend care.
"Physicians working on weekends are thought to be less experienced than teams working during the week," they wrote. Experienced and specialized colorectal surgeons have been shown to perform more primary anastomoses, compared with trainees or general surgeons (Arch. Surg. 2010;145:79-86; Dis. Colon Rectum 2003;46:1461-8).
Limitations of the study include the fact that it did not capture long-term outcomes or severity of disease at presentation. The latter could be of potential importance: "Some patients, especially those with milder symptoms, may prefer weekend or weekday admission and may time their admission accordingly," the investigators noted.
In an invited critique that accompanied the article, Dr. Juerg Metzger, a surgeon at Lucerne (Switzerland) Cantonal Hospital, wrote that a disparity in experience among weekday and weekend surgical staff likely accounted for the higher rate of Hartmann procedures and complications following weekend admissions.
"Work-hour restrictions do not seem to have a negative influence on mortality and morbidity in surgical patients," Dr. Metzger wrote. "However, reduced experience owing to restricted working hours may negatively influence the practical skills of younger surgeons, resulting in more limited surgery [for example, a Hartmann procedure being performed instead of a primary anastomosis] and an increase in complications related to that surgery."
In the end, Dr. Metzger wrote, "quality is expensive, and our society has to decide if it is desirable and necessary to have the best surgical quality available all the time, especially when considering that health care costs will dramatically increase. It would be relevant to analyze additional large databases, asking similar questions about the outcomes of other common diseases [for example, appendicitis, cholecystitis, and strangulated hernias] and studying the effect of weekend admission on these illnesses."
Dr. Worni’s and colleagues’ was funded by a grant from the Swiss National Science Foundation. None of the investigators declared conflicts of interest. Dr. Metzger declared that he had no conflicts of interest related to his critique.
FROM ARCHIVES OF SURGERY
Major Finding: Weekend admission to the hospital for diverticulitis posed a significantly higher risk for any postoperative complication (OR, 1.10; P = .005) and risk of reoperation (OR, 1.50; P less than .001), compared with weekday admission.
Data Source: The findings are based on an analysis of NIS records for 31,832 patients who were treated surgically for left-sided diverticulitis.
Disclosures: Dr. Worni’s and colleagues’ study was funded by a grant from the Swiss National Science Foundation. None of the investigators declared conflicts of interest. Dr. Metzger declared that he had no conflicts of interest related to his critique.