User login
FDA advisory panel backs approval of neoadjuvant pertuzumab for breast cancer
SILVER SPRING, MD. – Pertuzumab is likely to be approved for the neoadjuvant treatment of breast cancer in the preoperative setting, based on the recommendation of a Food and Drug Administration advisory panel.
At a meeting on Sept. 12, the FDA’s Oncologic Drugs Advisory Committee panel voted 13-0, with 1 abstention, that treatment with pertuzumab, a human epidermal growth factor receptor 2 (HER2)-targeted monoclonal antibody, had a favorable benefit-to-risk profile as a neoadjuvant treatment in combination with trastuzumab and docetaxel before surgery in patients with locally-advanced, inflammatory, or early-stage breast cancers greater than 2 cm in diameter. The neoadjuvant approach would be part of a complete early breast cancer treatment regimen containing fluorouracil, epirubicin, and cyclophosphamide or carboplatin.
The drug is being reviewed under the accelerated approval process, a mechanism that makes drugs available to fill an unmet medical need in patients with serious diseases. Historically, the usual sequence of the FDA approvals for breast cancer agents starts with approval for metastatic disease, followed by approval for early-stage disease years later after the results of large studies with long follow-up periods are available. Pertuzumab, marketed as Perjeta by Genentech, was just approved in 2012 as a first-line treatment for metastatic HER2-positive breast cancer in women who have not received prior anti-HER2 therapy or chemotherapy for metastatic disease.
Accelerated approvals are based on a surrogate endpoint that is considered “reasonably likely” to predict clinical benefit. In this instance, pathologic complete response rate (pCR) was used in the phase II NeoSphere study. For this trial, pertuzumab was added to trastuzumab (Herceptin) – another HER2 receptor antagonist – and docetaxel, and was given before surgery to women with HER-2-positive, locally advanced, inflammatory or early-stage breast cancer. The comparator group was patients treated preoperatively with trastuzumab and docetaxel.
The women who received the three-drug neoadjuvant regimen had an 18% improvement in pCR as compared to women given trastuzumab and docetaxel only.
In addition to the NeoSphere study, the panel also considered the body of data on pertuzumab in metastatic breast cancer, the known biology of the pertuzumab, and the activity of HER-2 targeted therapies in breast cancer.
Should pertuzumab receive the accelerated approval, its full approval will be contingent on the final results of APHINITY, a confirmatory study. If the APHINITY results do not confirm the NeoSphere results, the FDA can withdraw the approval for this indication.
The vote to support the first approval of a drug for the neoadjuvant treatment of breast cancer is “a historic moment,” said the panel chair, Dr. Mikkael A. Sekeres of the Cleveland Clinic. “In so doing, we are supporting the rapid movement of a highly active drug for metastatic breast cancer to the first-line setting with the hope that women with earlier stages of breast cancer will live longer and better.”
However, he added, “all eyes will be on the confirmatory APHINITY trial” and on Genentech, to “verify this initial signal of efficacy and to confirm the bandwidth of safety we have seen so far.” If the results are negative, he and other panelists urged the company to voluntarily remove the drug for this indication, and avoid what happened with another Genentech drug, bevacizumab (Avastin), which was granted an accelerated approval as a first-line treatment in combination with paclitaxel for metastatic breast cancer in 2008. The FDA decided to withdraw approval of this indication after studies failed to confirm the benefit. The company appealed the decision, however, delaying the FDA’s withdrawal of the approval until 2011.
NeoSphere, a randomized study conducted outside of the United States, compared four treatment regimens in 417 women newly diagnosed with locally advanced, inflammatory or operable HER2-positive early breast cancer, with tumors greater than 2 cm, treated for four cycles before surgery. The median tumor size was about 5 cm, and two-thirds were node positive.
Based on the pCR definition used by Genentech (the absence of invasive cancer in the breast), almost 46% of those on the combination of pertuzumab, trastuzumab, and docetaxel reached the primary endpoint, compared with 29% of those on trastuzumab and docetaxel – a statistically significant difference of nearly 17%. Based on the FDA-preferred definition of pCR definition (the absence of invasive cancer in the breast and lymph nodes), the pCR rate was almost 18% higher with the three-drug regimen (39.3% vs. 21.5%).
The FDA considers pCR as “reasonably likely” to predict outcomes in HER2-positive breast cancer.
The treatment has the potential to cure more patients in this high risk population, said Dr. Suparna Wedam, a medical officer in FDA’s Office of Hematology and Oncology Products. Yet, still to be determined are whether the regimen has long-term safety and results in improvements in overall survival, progression-free survival, and other improvements in long-term outcomes.
Genentech also provided results from the TRYPHAENA phase II study that compared three neoadjuvant treatment regimens before surgery; as well as the CLEOPATRA phase III study, the basis of the 2012 approval of trastuzumab. In TRYPHAENA, 225 women with HER2-positive, locally advanced, operable or inflammatory breast cancer, received one of three neoadjuvant treatment regimens. The pCR rates, a secondary endpoint, ranged from about 55% to 64% when pertuzumab was added to trastuzumab and chemotherapy. CLEOPATRA enrolled 808 women with HER2-positive, locally recurrent, unresectable or metastatic breast cancer previously untreated with a biologic or chemotherapy for metastatic disease. In that trial, pertuzumab in combination with trastuzumab and docetaxel resulted in significant improvements in progression-free survival and overall survival.
The most common adverse events with the three-drug regimen in the NeoSphere study were neutropenia, diarrhea, nausea, fatigue, mucosal inflammation, and rash, according to the company. No unexpected safety signals were observed with the addition of pertuzumab. The addition of pertuzumab did not appear to increase symptomatic cardiac toxicity when added to trastuzumab-based neoadjuvant or metastatic treatment regimens.
The FDA reviewers noted, however, that the rate of left ventricular dysfunction (mostly asymptomatic) was higher with neoadjuvant pertuzumab treatment. Cardiac toxicity appeared to be reversible, however.
Panel member Deborah Armstrong of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, said that there were “some hints of increased cardiac toxicity.” She encouraged the company to closely evaluate patients on longer-term pertuzumab in trials for cardiac toxicity. Dr. Armstrong voted in favor of the benefit risk profile, but like other panelists, was concerned about the potential for approval “opening the floodgates” to the use of this drug in treating patients for whom it may not yet be appropriate.
Citing the clear potential benefit in the intended population, Dr. Michael Menefee of the division of hematology and oncology at the Mayo Clinic, Jacksonville, Fla., also shared his concerns about the potential for toxicity and overuse of the drug. “My hope is that the FDA is very clear in the ultimate labeling so practitioners have clear guidance as to how to use this drug best and most safely.”
Genentech has completed enrollment in the confirmatory, phase III APHINITY study, which will compare chemotherapy plus trastuzumab with or without pertuzumab before surgery in about 4,800 patients with HER-2 positive early breast cancer. The patients will be followed for 10 years, and the study will evaluate invasive disease-free survival. Results are expected to be first available in 2016.
Panel members have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
Genentech also markets trastuzumab.
SILVER SPRING, MD. – Pertuzumab is likely to be approved for the neoadjuvant treatment of breast cancer in the preoperative setting, based on the recommendation of a Food and Drug Administration advisory panel.
At a meeting on Sept. 12, the FDA’s Oncologic Drugs Advisory Committee panel voted 13-0, with 1 abstention, that treatment with pertuzumab, a human epidermal growth factor receptor 2 (HER2)-targeted monoclonal antibody, had a favorable benefit-to-risk profile as a neoadjuvant treatment in combination with trastuzumab and docetaxel before surgery in patients with locally-advanced, inflammatory, or early-stage breast cancers greater than 2 cm in diameter. The neoadjuvant approach would be part of a complete early breast cancer treatment regimen containing fluorouracil, epirubicin, and cyclophosphamide or carboplatin.
The drug is being reviewed under the accelerated approval process, a mechanism that makes drugs available to fill an unmet medical need in patients with serious diseases. Historically, the usual sequence of the FDA approvals for breast cancer agents starts with approval for metastatic disease, followed by approval for early-stage disease years later after the results of large studies with long follow-up periods are available. Pertuzumab, marketed as Perjeta by Genentech, was just approved in 2012 as a first-line treatment for metastatic HER2-positive breast cancer in women who have not received prior anti-HER2 therapy or chemotherapy for metastatic disease.
Accelerated approvals are based on a surrogate endpoint that is considered “reasonably likely” to predict clinical benefit. In this instance, pathologic complete response rate (pCR) was used in the phase II NeoSphere study. For this trial, pertuzumab was added to trastuzumab (Herceptin) – another HER2 receptor antagonist – and docetaxel, and was given before surgery to women with HER-2-positive, locally advanced, inflammatory or early-stage breast cancer. The comparator group was patients treated preoperatively with trastuzumab and docetaxel.
The women who received the three-drug neoadjuvant regimen had an 18% improvement in pCR as compared to women given trastuzumab and docetaxel only.
In addition to the NeoSphere study, the panel also considered the body of data on pertuzumab in metastatic breast cancer, the known biology of the pertuzumab, and the activity of HER-2 targeted therapies in breast cancer.
Should pertuzumab receive the accelerated approval, its full approval will be contingent on the final results of APHINITY, a confirmatory study. If the APHINITY results do not confirm the NeoSphere results, the FDA can withdraw the approval for this indication.
The vote to support the first approval of a drug for the neoadjuvant treatment of breast cancer is “a historic moment,” said the panel chair, Dr. Mikkael A. Sekeres of the Cleveland Clinic. “In so doing, we are supporting the rapid movement of a highly active drug for metastatic breast cancer to the first-line setting with the hope that women with earlier stages of breast cancer will live longer and better.”
However, he added, “all eyes will be on the confirmatory APHINITY trial” and on Genentech, to “verify this initial signal of efficacy and to confirm the bandwidth of safety we have seen so far.” If the results are negative, he and other panelists urged the company to voluntarily remove the drug for this indication, and avoid what happened with another Genentech drug, bevacizumab (Avastin), which was granted an accelerated approval as a first-line treatment in combination with paclitaxel for metastatic breast cancer in 2008. The FDA decided to withdraw approval of this indication after studies failed to confirm the benefit. The company appealed the decision, however, delaying the FDA’s withdrawal of the approval until 2011.
NeoSphere, a randomized study conducted outside of the United States, compared four treatment regimens in 417 women newly diagnosed with locally advanced, inflammatory or operable HER2-positive early breast cancer, with tumors greater than 2 cm, treated for four cycles before surgery. The median tumor size was about 5 cm, and two-thirds were node positive.
Based on the pCR definition used by Genentech (the absence of invasive cancer in the breast), almost 46% of those on the combination of pertuzumab, trastuzumab, and docetaxel reached the primary endpoint, compared with 29% of those on trastuzumab and docetaxel – a statistically significant difference of nearly 17%. Based on the FDA-preferred definition of pCR definition (the absence of invasive cancer in the breast and lymph nodes), the pCR rate was almost 18% higher with the three-drug regimen (39.3% vs. 21.5%).
The FDA considers pCR as “reasonably likely” to predict outcomes in HER2-positive breast cancer.
The treatment has the potential to cure more patients in this high risk population, said Dr. Suparna Wedam, a medical officer in FDA’s Office of Hematology and Oncology Products. Yet, still to be determined are whether the regimen has long-term safety and results in improvements in overall survival, progression-free survival, and other improvements in long-term outcomes.
Genentech also provided results from the TRYPHAENA phase II study that compared three neoadjuvant treatment regimens before surgery; as well as the CLEOPATRA phase III study, the basis of the 2012 approval of trastuzumab. In TRYPHAENA, 225 women with HER2-positive, locally advanced, operable or inflammatory breast cancer, received one of three neoadjuvant treatment regimens. The pCR rates, a secondary endpoint, ranged from about 55% to 64% when pertuzumab was added to trastuzumab and chemotherapy. CLEOPATRA enrolled 808 women with HER2-positive, locally recurrent, unresectable or metastatic breast cancer previously untreated with a biologic or chemotherapy for metastatic disease. In that trial, pertuzumab in combination with trastuzumab and docetaxel resulted in significant improvements in progression-free survival and overall survival.
The most common adverse events with the three-drug regimen in the NeoSphere study were neutropenia, diarrhea, nausea, fatigue, mucosal inflammation, and rash, according to the company. No unexpected safety signals were observed with the addition of pertuzumab. The addition of pertuzumab did not appear to increase symptomatic cardiac toxicity when added to trastuzumab-based neoadjuvant or metastatic treatment regimens.
The FDA reviewers noted, however, that the rate of left ventricular dysfunction (mostly asymptomatic) was higher with neoadjuvant pertuzumab treatment. Cardiac toxicity appeared to be reversible, however.
Panel member Deborah Armstrong of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, said that there were “some hints of increased cardiac toxicity.” She encouraged the company to closely evaluate patients on longer-term pertuzumab in trials for cardiac toxicity. Dr. Armstrong voted in favor of the benefit risk profile, but like other panelists, was concerned about the potential for approval “opening the floodgates” to the use of this drug in treating patients for whom it may not yet be appropriate.
Citing the clear potential benefit in the intended population, Dr. Michael Menefee of the division of hematology and oncology at the Mayo Clinic, Jacksonville, Fla., also shared his concerns about the potential for toxicity and overuse of the drug. “My hope is that the FDA is very clear in the ultimate labeling so practitioners have clear guidance as to how to use this drug best and most safely.”
Genentech has completed enrollment in the confirmatory, phase III APHINITY study, which will compare chemotherapy plus trastuzumab with or without pertuzumab before surgery in about 4,800 patients with HER-2 positive early breast cancer. The patients will be followed for 10 years, and the study will evaluate invasive disease-free survival. Results are expected to be first available in 2016.
Panel members have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
Genentech also markets trastuzumab.
SILVER SPRING, MD. – Pertuzumab is likely to be approved for the neoadjuvant treatment of breast cancer in the preoperative setting, based on the recommendation of a Food and Drug Administration advisory panel.
At a meeting on Sept. 12, the FDA’s Oncologic Drugs Advisory Committee panel voted 13-0, with 1 abstention, that treatment with pertuzumab, a human epidermal growth factor receptor 2 (HER2)-targeted monoclonal antibody, had a favorable benefit-to-risk profile as a neoadjuvant treatment in combination with trastuzumab and docetaxel before surgery in patients with locally-advanced, inflammatory, or early-stage breast cancers greater than 2 cm in diameter. The neoadjuvant approach would be part of a complete early breast cancer treatment regimen containing fluorouracil, epirubicin, and cyclophosphamide or carboplatin.
The drug is being reviewed under the accelerated approval process, a mechanism that makes drugs available to fill an unmet medical need in patients with serious diseases. Historically, the usual sequence of the FDA approvals for breast cancer agents starts with approval for metastatic disease, followed by approval for early-stage disease years later after the results of large studies with long follow-up periods are available. Pertuzumab, marketed as Perjeta by Genentech, was just approved in 2012 as a first-line treatment for metastatic HER2-positive breast cancer in women who have not received prior anti-HER2 therapy or chemotherapy for metastatic disease.
Accelerated approvals are based on a surrogate endpoint that is considered “reasonably likely” to predict clinical benefit. In this instance, pathologic complete response rate (pCR) was used in the phase II NeoSphere study. For this trial, pertuzumab was added to trastuzumab (Herceptin) – another HER2 receptor antagonist – and docetaxel, and was given before surgery to women with HER-2-positive, locally advanced, inflammatory or early-stage breast cancer. The comparator group was patients treated preoperatively with trastuzumab and docetaxel.
The women who received the three-drug neoadjuvant regimen had an 18% improvement in pCR as compared to women given trastuzumab and docetaxel only.
In addition to the NeoSphere study, the panel also considered the body of data on pertuzumab in metastatic breast cancer, the known biology of the pertuzumab, and the activity of HER-2 targeted therapies in breast cancer.
Should pertuzumab receive the accelerated approval, its full approval will be contingent on the final results of APHINITY, a confirmatory study. If the APHINITY results do not confirm the NeoSphere results, the FDA can withdraw the approval for this indication.
The vote to support the first approval of a drug for the neoadjuvant treatment of breast cancer is “a historic moment,” said the panel chair, Dr. Mikkael A. Sekeres of the Cleveland Clinic. “In so doing, we are supporting the rapid movement of a highly active drug for metastatic breast cancer to the first-line setting with the hope that women with earlier stages of breast cancer will live longer and better.”
However, he added, “all eyes will be on the confirmatory APHINITY trial” and on Genentech, to “verify this initial signal of efficacy and to confirm the bandwidth of safety we have seen so far.” If the results are negative, he and other panelists urged the company to voluntarily remove the drug for this indication, and avoid what happened with another Genentech drug, bevacizumab (Avastin), which was granted an accelerated approval as a first-line treatment in combination with paclitaxel for metastatic breast cancer in 2008. The FDA decided to withdraw approval of this indication after studies failed to confirm the benefit. The company appealed the decision, however, delaying the FDA’s withdrawal of the approval until 2011.
NeoSphere, a randomized study conducted outside of the United States, compared four treatment regimens in 417 women newly diagnosed with locally advanced, inflammatory or operable HER2-positive early breast cancer, with tumors greater than 2 cm, treated for four cycles before surgery. The median tumor size was about 5 cm, and two-thirds were node positive.
Based on the pCR definition used by Genentech (the absence of invasive cancer in the breast), almost 46% of those on the combination of pertuzumab, trastuzumab, and docetaxel reached the primary endpoint, compared with 29% of those on trastuzumab and docetaxel – a statistically significant difference of nearly 17%. Based on the FDA-preferred definition of pCR definition (the absence of invasive cancer in the breast and lymph nodes), the pCR rate was almost 18% higher with the three-drug regimen (39.3% vs. 21.5%).
The FDA considers pCR as “reasonably likely” to predict outcomes in HER2-positive breast cancer.
The treatment has the potential to cure more patients in this high risk population, said Dr. Suparna Wedam, a medical officer in FDA’s Office of Hematology and Oncology Products. Yet, still to be determined are whether the regimen has long-term safety and results in improvements in overall survival, progression-free survival, and other improvements in long-term outcomes.
Genentech also provided results from the TRYPHAENA phase II study that compared three neoadjuvant treatment regimens before surgery; as well as the CLEOPATRA phase III study, the basis of the 2012 approval of trastuzumab. In TRYPHAENA, 225 women with HER2-positive, locally advanced, operable or inflammatory breast cancer, received one of three neoadjuvant treatment regimens. The pCR rates, a secondary endpoint, ranged from about 55% to 64% when pertuzumab was added to trastuzumab and chemotherapy. CLEOPATRA enrolled 808 women with HER2-positive, locally recurrent, unresectable or metastatic breast cancer previously untreated with a biologic or chemotherapy for metastatic disease. In that trial, pertuzumab in combination with trastuzumab and docetaxel resulted in significant improvements in progression-free survival and overall survival.
The most common adverse events with the three-drug regimen in the NeoSphere study were neutropenia, diarrhea, nausea, fatigue, mucosal inflammation, and rash, according to the company. No unexpected safety signals were observed with the addition of pertuzumab. The addition of pertuzumab did not appear to increase symptomatic cardiac toxicity when added to trastuzumab-based neoadjuvant or metastatic treatment regimens.
The FDA reviewers noted, however, that the rate of left ventricular dysfunction (mostly asymptomatic) was higher with neoadjuvant pertuzumab treatment. Cardiac toxicity appeared to be reversible, however.
Panel member Deborah Armstrong of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, said that there were “some hints of increased cardiac toxicity.” She encouraged the company to closely evaluate patients on longer-term pertuzumab in trials for cardiac toxicity. Dr. Armstrong voted in favor of the benefit risk profile, but like other panelists, was concerned about the potential for approval “opening the floodgates” to the use of this drug in treating patients for whom it may not yet be appropriate.
Citing the clear potential benefit in the intended population, Dr. Michael Menefee of the division of hematology and oncology at the Mayo Clinic, Jacksonville, Fla., also shared his concerns about the potential for toxicity and overuse of the drug. “My hope is that the FDA is very clear in the ultimate labeling so practitioners have clear guidance as to how to use this drug best and most safely.”
Genentech has completed enrollment in the confirmatory, phase III APHINITY study, which will compare chemotherapy plus trastuzumab with or without pertuzumab before surgery in about 4,800 patients with HER-2 positive early breast cancer. The patients will be followed for 10 years, and the study will evaluate invasive disease-free survival. Results are expected to be first available in 2016.
Panel members have been cleared of potential conflicts of interest related to the topic of the meeting. Occasionally, a panelist may be given a waiver, but not at this meeting.
Genentech also markets trastuzumab.
MammoSite has comparatively high long-term complication rate
The rate of long-term complications such as palpable masses and telangiectasias was nearly five times higher in women who had MammoSite therapy, compared with those who underwent whole breast radiation therapy, results from a retrospective study showed.
Dr. Kari Rosenkranz and her associates at Dartmouth Hitchcock Medical Center, Hanover, N.H., analyzed the data charts of all women who met criteria for brachytherapy and underwent MammoSite (n = 71) or whole breast radiation therapy (WBRT) (n = 245) at the center between 2003 and 2008.

The incidence of palpable masses at the site of the lumpectomy, telangiectasias, and local recurrence were the studied endpoints. No significant differences existed between the study groups regarding age (average was 63.5 years), mean size of tumor (average was 1.1 cm), the percentage of patients with estrogen receptor–positive tumors (92% in total), or the length of follow-up (median was 4 years).
In the MammoSite cohort with hormone receptor–positive tumors, 83% received adjuvant endocrine therapy; 94% of the WBRT group with hormone receptor–positive tumors had endocrine therapy. No significant difference was found in systemic chemotherapy rates.
The rate of long-term complications such as palpable masses, telangiectasias, or both were found to have occurred in 42% of MammoSite patients, compared with 9% in the WBRT group (J. Am. Coll. Surg. 2013;217:497-502).
During follow-up in the MammoSite group, the incidence rate of palpable mass detection at the lumpectomy site was nearly 27%; for the WBRT group, the rate was approximately 7%. MammoSite patients were three times more likely to require a core biopsy of the mass to rule out malignancy than were WBRT patients (16.9% vs. 4.9%, respectively). Telangiectasia was six times more likely to develop in MammoSite patients than in WBRT patients (24% vs. 4%).
Dr. Rosenkranz and her colleagues reported that a prospective, randomized clinical trial which began in 2005, sponsored by the National Surgical Adjuvant Breast and Bowel Project (NSABP)/Radiation Therapy Oncology Group (RTOG), is currently underway to compare WBRT with partial radiation therapies such as MammoSite. The primary endpoint of this study in women who have had surgery for ductal carcinoma in situ or stage I or stage II breast cancer, is breast tumor recurrence; secondary endpoints include toxicity. The study is expected to end in 2015, according to the researchers.
"Until this prospective, randomized trial reports, the increased rate of long-term local toxicity found in our institution’s experience with MammoSite brachytherapy should be considered when counseling women on options for adjuvant radiation therapy after breast-conserving surgery," concluded Dr. Rosenkranz and her associates.
The researchers reported no relevant disclosures.
The rate of long-term complications such as palpable masses and telangiectasias was nearly five times higher in women who had MammoSite therapy, compared with those who underwent whole breast radiation therapy, results from a retrospective study showed.
Dr. Kari Rosenkranz and her associates at Dartmouth Hitchcock Medical Center, Hanover, N.H., analyzed the data charts of all women who met criteria for brachytherapy and underwent MammoSite (n = 71) or whole breast radiation therapy (WBRT) (n = 245) at the center between 2003 and 2008.
The incidence of palpable masses at the site of the lumpectomy, telangiectasias, and local recurrence were the studied endpoints. No significant differences existed between the study groups regarding age (average was 63.5 years), mean size of tumor (average was 1.1 cm), the percentage of patients with estrogen receptor–positive tumors (92% in total), or the length of follow-up (median was 4 years).
In the MammoSite cohort with hormone receptor–positive tumors, 83% received adjuvant endocrine therapy; 94% of the WBRT group with hormone receptor–positive tumors had endocrine therapy. No significant difference was found in systemic chemotherapy rates.
The rate of long-term complications such as palpable masses, telangiectasias, or both were found to have occurred in 42% of MammoSite patients, compared with 9% in the WBRT group (J. Am. Coll. Surg. 2013;217:497-502).
During follow-up in the MammoSite group, the incidence rate of palpable mass detection at the lumpectomy site was nearly 27%; for the WBRT group, the rate was approximately 7%. MammoSite patients were three times more likely to require a core biopsy of the mass to rule out malignancy than were WBRT patients (16.9% vs. 4.9%, respectively). Telangiectasia was six times more likely to develop in MammoSite patients than in WBRT patients (24% vs. 4%).
Dr. Rosenkranz and her colleagues reported that a prospective, randomized clinical trial which began in 2005, sponsored by the National Surgical Adjuvant Breast and Bowel Project (NSABP)/Radiation Therapy Oncology Group (RTOG), is currently underway to compare WBRT with partial radiation therapies such as MammoSite. The primary endpoint of this study in women who have had surgery for ductal carcinoma in situ or stage I or stage II breast cancer, is breast tumor recurrence; secondary endpoints include toxicity. The study is expected to end in 2015, according to the researchers.
"Until this prospective, randomized trial reports, the increased rate of long-term local toxicity found in our institution’s experience with MammoSite brachytherapy should be considered when counseling women on options for adjuvant radiation therapy after breast-conserving surgery," concluded Dr. Rosenkranz and her associates.
The researchers reported no relevant disclosures.
The rate of long-term complications such as palpable masses and telangiectasias was nearly five times higher in women who had MammoSite therapy, compared with those who underwent whole breast radiation therapy, results from a retrospective study showed.
Dr. Kari Rosenkranz and her associates at Dartmouth Hitchcock Medical Center, Hanover, N.H., analyzed the data charts of all women who met criteria for brachytherapy and underwent MammoSite (n = 71) or whole breast radiation therapy (WBRT) (n = 245) at the center between 2003 and 2008.
The incidence of palpable masses at the site of the lumpectomy, telangiectasias, and local recurrence were the studied endpoints. No significant differences existed between the study groups regarding age (average was 63.5 years), mean size of tumor (average was 1.1 cm), the percentage of patients with estrogen receptor–positive tumors (92% in total), or the length of follow-up (median was 4 years).
In the MammoSite cohort with hormone receptor–positive tumors, 83% received adjuvant endocrine therapy; 94% of the WBRT group with hormone receptor–positive tumors had endocrine therapy. No significant difference was found in systemic chemotherapy rates.
The rate of long-term complications such as palpable masses, telangiectasias, or both were found to have occurred in 42% of MammoSite patients, compared with 9% in the WBRT group (J. Am. Coll. Surg. 2013;217:497-502).
During follow-up in the MammoSite group, the incidence rate of palpable mass detection at the lumpectomy site was nearly 27%; for the WBRT group, the rate was approximately 7%. MammoSite patients were three times more likely to require a core biopsy of the mass to rule out malignancy than were WBRT patients (16.9% vs. 4.9%, respectively). Telangiectasia was six times more likely to develop in MammoSite patients than in WBRT patients (24% vs. 4%).
Dr. Rosenkranz and her colleagues reported that a prospective, randomized clinical trial which began in 2005, sponsored by the National Surgical Adjuvant Breast and Bowel Project (NSABP)/Radiation Therapy Oncology Group (RTOG), is currently underway to compare WBRT with partial radiation therapies such as MammoSite. The primary endpoint of this study in women who have had surgery for ductal carcinoma in situ or stage I or stage II breast cancer, is breast tumor recurrence; secondary endpoints include toxicity. The study is expected to end in 2015, according to the researchers.
"Until this prospective, randomized trial reports, the increased rate of long-term local toxicity found in our institution’s experience with MammoSite brachytherapy should be considered when counseling women on options for adjuvant radiation therapy after breast-conserving surgery," concluded Dr. Rosenkranz and her associates.
The researchers reported no relevant disclosures.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Major finding: Forty-two percent of MammoSite patients had long-term complications, vs. 9% of those who had whole breast radiation therapy.
Data source: Retrospective study of 71 women who underwent MammoSite brachytherapy and 245 who had whole breast radiation therapy at a single academic medical center between 2003 and 2008.
Disclosures: Dr. Rosenkranz and her associates reported no relevant disclosures.

Response-guided neoadjuvant chemotherapy may boost survival
Response-guided neoadjuvant chemotherapy may improve disease-free and overall survival in patients with early breast cancer, particularly in those patients with hormone receptor–positive tumors, findings from an exploratory analysis of data from the phase III GeparTrio trial suggest.
"Our exploratory analyses of this prospective trial strongly suggest that the various breast cancer phenotypes require different chemotherapy approaches and show that even patients with luminal tumors can derive greater benefit from response-guided chemotherapy," Dr. Gunter von Minckwitz of the German Breast Group, Neu-Isenburg, and his colleagues reported, noting that the findings must be tested prospectively but can be used to guide the design of future trials.
After treating 2,072 patients with two cycles of docetaxel, doxorubicin, and cyclophosphamide (TAC), the researchers randomized 1,390 early responders to receive either four or six additional TAC cycles, and randomized 622 early nonresponders either to four additional TAC cycles or to non-cross-resistant treatment with vinorelbine and capecitabine (TAC-NX) before surgery. TAC cycles included 75 mg/m2 of docetaxel, 50 mg/m2 of doxorubicin, and 500 mg/m2 of cyclophosphamide on day 1 every 3 weeks. NX included 25 mg/m2 of vinorelbine on days 1 and 8 plus 1,000 mg/m2 of capecitabine given orally twice daily on days 1-14 every 3 weeks. Sixty patients did not continue in the study after the initial TAC cycles.
Disease-free survival was better in the 686 early responders who received a total of eight TAC cycles, compared with the 704 patients who received six TAC cycles (hazard ratio, 0.78), and in 301 early nonresponders who received TAC-NX, compared with 321 early nonresponders who received six TAC cycles (HR, 0.59), the investigators reported online Sept. 3 in the Journal of Clinical Oncology.
An exploratory analysis demonstrated that both disease-free survival and overall survival were longer following either eight TAC cycles or TAC-NX, as compared with conventional chemotherapy with six TAC cycles (HRs, 0.71 and 0.79, respectively), the investigators reported (J. Clin. Oncol. 2013 Sept. 3 [doi: 10.1200/JCO.2012.45.0940]).
"Treatment effects on overall survival were less pronounced. Responders receiving TAC x 8 showed only a trend toward longer overall survival compared with those receiving TAC x 6 (hazard ratio, 0.76), whereas nonresponders receiving TAC-NX showed no improvement in overall survival compared with those receiving TAC x 6 (hazard ratio, 0.85). Response-guided chemotherapy provided significant but marginal overall survival benefit over conventional chemotherapy (hazard ratio, 0.79)," they said.
Of note, the effects of response-guided therapy on disease-free survival were apparent in all hormone receptor–positive tumors but not in hormone receptor–negative tumors, they noted (HRs for luminal A, luminal B HER2-negative, and luminal B HER2-positive tumors were 0.55, 0.40, and 0.56, respectively; HRs for nonluminal HER2-positive and triple-negative tumors were 1.01 and 0.87, respectively).
Pathological complete response (pCR) did not predict long-term outcomes; a comparison of pCR rates based on treatment strategy showed that "survival in patients with hormone receptor–positive tumors did not depend on pCR but was improved by response-guided therapy, whereas survival in patients with hormone receptor–negative tumors did depend on pCR but was not improved by response-guided therapy," they said. pCR predicted improved disease-free survival in triple-negative, nonluminal HER2-positive, and luminal B HER2-negative tumors (HRs, 6.67, 5.24, and 3.74, respectively), they reported.
Patients included in the study had unilateral or bilateral primary breast cancer confirmed by core biopsy, and had at least one additional risk factor, including age under 36, clinical tumor size more than 5 cm, estrogen receptor and progesterone receptor negativity, clinical axillary node involvement, or undifferentiated tumor grade.
The findings from the GeparTrio study demonstrate the advantage of neoadjuvant versus adjuvant chemotherapy. Response-guided treatment can only be conducted when the tumor is available for the monitoring of response, the investigators noted.
This study was supported by Amgen, Chugai, Roche, and Sanofi-Aventis. Dr. von Minckwitz and multiple coauthors reported serving as a consultant or advisor for, owning stock in, and/or receiving honoraria or research funding from Amgen, Roche, Sanofi-Aventis, and other companies.
The GeparTrio study represents an enormous effort that tests an interesting strategy of response-guided chemotherapy treatment, but prospective testing is needed before this strategy is ready for routine clinical practice in hormone-responsive breast cancer.

|
| Dr. Melinda Telli |
An important question to consider is whether we have the collective resources and fortitude to move forward with a prospective evaluation of this strategy in hormone receptor–positive breast cancer. If this approach were pursued, long-term results would not be expected for nearly a decade and we need to consider what the landscape of breast cancer will look like at that time.
Given the lack of early pCR readout for such a strategy, and given that it is more challenging to control for postneoadjuvant systemic therapy, this neoadjuvant model is not as attractive as our current pCR-based model as a platform for drug development and correlative biology.
Several large efforts are underway to evaluate a new model of postneoadjuvant therapy in patients who have high-risk triple-negative and HER2-positive breast cancers and have residual disease after standard neoadjuvant therapy.
This type of approach is response-guided in principle and synergizes with the current neoadjuvant model based on pCR. As we look to the future, my bias is that advancing neoadjuvant models with the greatest potential to accelerate the pace of progress in early-stage high-risk breast cancer should remain our priority.
Dr. Melinda L. Telli is with Stanford (Calif.) University. She made her remarks in an editorial (J. Clin. Oncol. 2013 Sept 3 [doi: 10.1200/JCO.2013.51.0313]) that accompanied the published study. Dr. Telli reported having no disclosures.
The GeparTrio study represents an enormous effort that tests an interesting strategy of response-guided chemotherapy treatment, but prospective testing is needed before this strategy is ready for routine clinical practice in hormone-responsive breast cancer.
|
|
| Dr. Melinda Telli |
An important question to consider is whether we have the collective resources and fortitude to move forward with a prospective evaluation of this strategy in hormone receptor–positive breast cancer. If this approach were pursued, long-term results would not be expected for nearly a decade and we need to consider what the landscape of breast cancer will look like at that time.
Given the lack of early pCR readout for such a strategy, and given that it is more challenging to control for postneoadjuvant systemic therapy, this neoadjuvant model is not as attractive as our current pCR-based model as a platform for drug development and correlative biology.
Several large efforts are underway to evaluate a new model of postneoadjuvant therapy in patients who have high-risk triple-negative and HER2-positive breast cancers and have residual disease after standard neoadjuvant therapy.
This type of approach is response-guided in principle and synergizes with the current neoadjuvant model based on pCR. As we look to the future, my bias is that advancing neoadjuvant models with the greatest potential to accelerate the pace of progress in early-stage high-risk breast cancer should remain our priority.
Dr. Melinda L. Telli is with Stanford (Calif.) University. She made her remarks in an editorial (J. Clin. Oncol. 2013 Sept 3 [doi: 10.1200/JCO.2013.51.0313]) that accompanied the published study. Dr. Telli reported having no disclosures.
The GeparTrio study represents an enormous effort that tests an interesting strategy of response-guided chemotherapy treatment, but prospective testing is needed before this strategy is ready for routine clinical practice in hormone-responsive breast cancer.
|
|
| Dr. Melinda Telli |
An important question to consider is whether we have the collective resources and fortitude to move forward with a prospective evaluation of this strategy in hormone receptor–positive breast cancer. If this approach were pursued, long-term results would not be expected for nearly a decade and we need to consider what the landscape of breast cancer will look like at that time.
Given the lack of early pCR readout for such a strategy, and given that it is more challenging to control for postneoadjuvant systemic therapy, this neoadjuvant model is not as attractive as our current pCR-based model as a platform for drug development and correlative biology.
Several large efforts are underway to evaluate a new model of postneoadjuvant therapy in patients who have high-risk triple-negative and HER2-positive breast cancers and have residual disease after standard neoadjuvant therapy.
This type of approach is response-guided in principle and synergizes with the current neoadjuvant model based on pCR. As we look to the future, my bias is that advancing neoadjuvant models with the greatest potential to accelerate the pace of progress in early-stage high-risk breast cancer should remain our priority.
Dr. Melinda L. Telli is with Stanford (Calif.) University. She made her remarks in an editorial (J. Clin. Oncol. 2013 Sept 3 [doi: 10.1200/JCO.2013.51.0313]) that accompanied the published study. Dr. Telli reported having no disclosures.
Response-guided neoadjuvant chemotherapy may improve disease-free and overall survival in patients with early breast cancer, particularly in those patients with hormone receptor–positive tumors, findings from an exploratory analysis of data from the phase III GeparTrio trial suggest.
"Our exploratory analyses of this prospective trial strongly suggest that the various breast cancer phenotypes require different chemotherapy approaches and show that even patients with luminal tumors can derive greater benefit from response-guided chemotherapy," Dr. Gunter von Minckwitz of the German Breast Group, Neu-Isenburg, and his colleagues reported, noting that the findings must be tested prospectively but can be used to guide the design of future trials.
After treating 2,072 patients with two cycles of docetaxel, doxorubicin, and cyclophosphamide (TAC), the researchers randomized 1,390 early responders to receive either four or six additional TAC cycles, and randomized 622 early nonresponders either to four additional TAC cycles or to non-cross-resistant treatment with vinorelbine and capecitabine (TAC-NX) before surgery. TAC cycles included 75 mg/m2 of docetaxel, 50 mg/m2 of doxorubicin, and 500 mg/m2 of cyclophosphamide on day 1 every 3 weeks. NX included 25 mg/m2 of vinorelbine on days 1 and 8 plus 1,000 mg/m2 of capecitabine given orally twice daily on days 1-14 every 3 weeks. Sixty patients did not continue in the study after the initial TAC cycles.
Disease-free survival was better in the 686 early responders who received a total of eight TAC cycles, compared with the 704 patients who received six TAC cycles (hazard ratio, 0.78), and in 301 early nonresponders who received TAC-NX, compared with 321 early nonresponders who received six TAC cycles (HR, 0.59), the investigators reported online Sept. 3 in the Journal of Clinical Oncology.
An exploratory analysis demonstrated that both disease-free survival and overall survival were longer following either eight TAC cycles or TAC-NX, as compared with conventional chemotherapy with six TAC cycles (HRs, 0.71 and 0.79, respectively), the investigators reported (J. Clin. Oncol. 2013 Sept. 3 [doi: 10.1200/JCO.2012.45.0940]).
"Treatment effects on overall survival were less pronounced. Responders receiving TAC x 8 showed only a trend toward longer overall survival compared with those receiving TAC x 6 (hazard ratio, 0.76), whereas nonresponders receiving TAC-NX showed no improvement in overall survival compared with those receiving TAC x 6 (hazard ratio, 0.85). Response-guided chemotherapy provided significant but marginal overall survival benefit over conventional chemotherapy (hazard ratio, 0.79)," they said.
Of note, the effects of response-guided therapy on disease-free survival were apparent in all hormone receptor–positive tumors but not in hormone receptor–negative tumors, they noted (HRs for luminal A, luminal B HER2-negative, and luminal B HER2-positive tumors were 0.55, 0.40, and 0.56, respectively; HRs for nonluminal HER2-positive and triple-negative tumors were 1.01 and 0.87, respectively).
Pathological complete response (pCR) did not predict long-term outcomes; a comparison of pCR rates based on treatment strategy showed that "survival in patients with hormone receptor–positive tumors did not depend on pCR but was improved by response-guided therapy, whereas survival in patients with hormone receptor–negative tumors did depend on pCR but was not improved by response-guided therapy," they said. pCR predicted improved disease-free survival in triple-negative, nonluminal HER2-positive, and luminal B HER2-negative tumors (HRs, 6.67, 5.24, and 3.74, respectively), they reported.
Patients included in the study had unilateral or bilateral primary breast cancer confirmed by core biopsy, and had at least one additional risk factor, including age under 36, clinical tumor size more than 5 cm, estrogen receptor and progesterone receptor negativity, clinical axillary node involvement, or undifferentiated tumor grade.
The findings from the GeparTrio study demonstrate the advantage of neoadjuvant versus adjuvant chemotherapy. Response-guided treatment can only be conducted when the tumor is available for the monitoring of response, the investigators noted.
This study was supported by Amgen, Chugai, Roche, and Sanofi-Aventis. Dr. von Minckwitz and multiple coauthors reported serving as a consultant or advisor for, owning stock in, and/or receiving honoraria or research funding from Amgen, Roche, Sanofi-Aventis, and other companies.
Response-guided neoadjuvant chemotherapy may improve disease-free and overall survival in patients with early breast cancer, particularly in those patients with hormone receptor–positive tumors, findings from an exploratory analysis of data from the phase III GeparTrio trial suggest.
"Our exploratory analyses of this prospective trial strongly suggest that the various breast cancer phenotypes require different chemotherapy approaches and show that even patients with luminal tumors can derive greater benefit from response-guided chemotherapy," Dr. Gunter von Minckwitz of the German Breast Group, Neu-Isenburg, and his colleagues reported, noting that the findings must be tested prospectively but can be used to guide the design of future trials.
After treating 2,072 patients with two cycles of docetaxel, doxorubicin, and cyclophosphamide (TAC), the researchers randomized 1,390 early responders to receive either four or six additional TAC cycles, and randomized 622 early nonresponders either to four additional TAC cycles or to non-cross-resistant treatment with vinorelbine and capecitabine (TAC-NX) before surgery. TAC cycles included 75 mg/m2 of docetaxel, 50 mg/m2 of doxorubicin, and 500 mg/m2 of cyclophosphamide on day 1 every 3 weeks. NX included 25 mg/m2 of vinorelbine on days 1 and 8 plus 1,000 mg/m2 of capecitabine given orally twice daily on days 1-14 every 3 weeks. Sixty patients did not continue in the study after the initial TAC cycles.
Disease-free survival was better in the 686 early responders who received a total of eight TAC cycles, compared with the 704 patients who received six TAC cycles (hazard ratio, 0.78), and in 301 early nonresponders who received TAC-NX, compared with 321 early nonresponders who received six TAC cycles (HR, 0.59), the investigators reported online Sept. 3 in the Journal of Clinical Oncology.
An exploratory analysis demonstrated that both disease-free survival and overall survival were longer following either eight TAC cycles or TAC-NX, as compared with conventional chemotherapy with six TAC cycles (HRs, 0.71 and 0.79, respectively), the investigators reported (J. Clin. Oncol. 2013 Sept. 3 [doi: 10.1200/JCO.2012.45.0940]).
"Treatment effects on overall survival were less pronounced. Responders receiving TAC x 8 showed only a trend toward longer overall survival compared with those receiving TAC x 6 (hazard ratio, 0.76), whereas nonresponders receiving TAC-NX showed no improvement in overall survival compared with those receiving TAC x 6 (hazard ratio, 0.85). Response-guided chemotherapy provided significant but marginal overall survival benefit over conventional chemotherapy (hazard ratio, 0.79)," they said.
Of note, the effects of response-guided therapy on disease-free survival were apparent in all hormone receptor–positive tumors but not in hormone receptor–negative tumors, they noted (HRs for luminal A, luminal B HER2-negative, and luminal B HER2-positive tumors were 0.55, 0.40, and 0.56, respectively; HRs for nonluminal HER2-positive and triple-negative tumors were 1.01 and 0.87, respectively).
Pathological complete response (pCR) did not predict long-term outcomes; a comparison of pCR rates based on treatment strategy showed that "survival in patients with hormone receptor–positive tumors did not depend on pCR but was improved by response-guided therapy, whereas survival in patients with hormone receptor–negative tumors did depend on pCR but was not improved by response-guided therapy," they said. pCR predicted improved disease-free survival in triple-negative, nonluminal HER2-positive, and luminal B HER2-negative tumors (HRs, 6.67, 5.24, and 3.74, respectively), they reported.
Patients included in the study had unilateral or bilateral primary breast cancer confirmed by core biopsy, and had at least one additional risk factor, including age under 36, clinical tumor size more than 5 cm, estrogen receptor and progesterone receptor negativity, clinical axillary node involvement, or undifferentiated tumor grade.
The findings from the GeparTrio study demonstrate the advantage of neoadjuvant versus adjuvant chemotherapy. Response-guided treatment can only be conducted when the tumor is available for the monitoring of response, the investigators noted.
This study was supported by Amgen, Chugai, Roche, and Sanofi-Aventis. Dr. von Minckwitz and multiple coauthors reported serving as a consultant or advisor for, owning stock in, and/or receiving honoraria or research funding from Amgen, Roche, Sanofi-Aventis, and other companies.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Major finding: Disease-free survival and overall survival were longer with response-guided neoadjuvant chemotherapy vs. conventional chemotherapy (hazard ratios, 0.71 and 0.79, respectively).
Data source: An exploratory analysis of data from a phase III study of 2,072 patients.
Disclosures: This study was supported by Amgen, Chugai, Roche, and Sanofi-Aventis. Dr. von Minckwitz and multiple coauthors reported serving as a consultant or advisor for, owning stock in, and/or receiving honoraria or research funding from Amgen, Roche, Sanofi-Aventis, and other companies.

Abbreviated MRI breast cancer screening protocol accurate
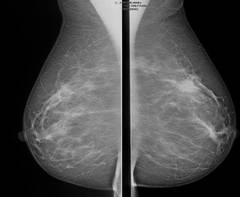
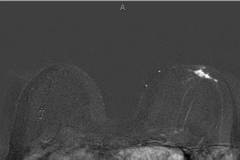
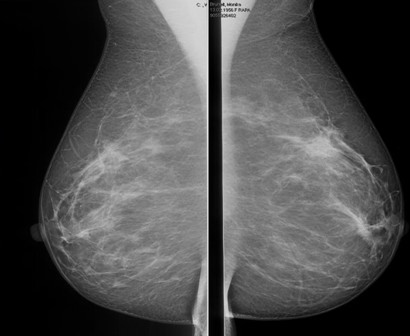
SAN FRANCISCO – A 3-minute MRI allowed a radiologist to rule out breast cancer with 99% accuracy in a prospective study of 443 women at a slightly increased or intermediate lifetime risk of breast cancer.
Extending the expert’s reading time to no more than 30 seconds to also interpret the first postcontrast subtracted (FAST) images provided the same sensitivity and specificity as a full diagnostic MRI protocol that had patients on the MRI table for 21 minutes on average, Dr. Christiane K. Kuhl reported at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
Conventional breast MRI protocols are time consuming and more expensive, because they are designed for diagnosis, not screening, said Dr. Kuhl, director of the department of diagnostic and interventional radiology at Rheinisch-Westfälische Technische Hochschule Aachen (Germany) University. The study aimed to trade some of the high sensitivity of MRI in detecting breast cancer for faster image acquisition and interpretation, perhaps eventually leading to lower cost and greater accessibility to MRI.
For the study, experienced breast radiologists were asked to review the maximum intensity projection (MIP) of the FAST images to determine whether there was significant enhancement. They then examined the FAST images for possible further categorization of any enhancement seen on the MIP, and analyzed the MRI under the full diagnostic protocol.
The prospective proof-of-concept study included patients who had imaging done between January 2009 and June 2010 and who were followed for 2 years to validate negative diagnoses. These were asymptomatic women with an intermediate risk with less than a 25% estimated lifetime risk of breast cancer. All of the women had a normal or benign mammogram and, if they had dense breasts, a normal or benign ultrasound result.
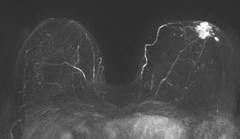
Acquiring the MIP and FAST images took less than 3 minutes with the patient on the MRI table. Reading the maximum intensity projection averaged 3 seconds, and reading the MIP plus FAST image averaged 28 seconds.
MRI screening identified 11 cancers, for an additional yield of 18 cancers per 1,000 examinations beyond what could be detected by mammography. Reading the MIP alone had a negative predictive value of 99%; the maximum intensity projection plus FAST readings and the full MRI protocol had negative predictive values just under 100%, Dr. Kuhl reported. The sensitivity of the MIP was close to 95% compared with 100% for MIP plus FAST or the full protocol. The specificity and positive predictive value could not be calculated for the MIP because the MIP reading detected only the presence or absence of significant enhancement. Evaluating the MIP plus FAST or the full MRI protocol produced similar specificities (in the mid-90% range) and positive predictive values (in the low 20% range).
All 11 breast cancers were intermediate- or high-grade cancers; 4 were ductal carcinoma in situ (DCIS) and 7 were invasive cancers. The median tumor size was 8 mm, and the mean age of the women with cancer was 51 years.
Conventional breast cancer screening using mammography picks up cancers that may be prognostically irrelevant, which add to potential overdiagnosis of breast cancer, she noted. In 11 studies that compared screening with breast MRI and mammography, MRI detected two to four times as many cancers as did mammography or ultrasound. Finding more DCIS and invasive cancers via MRI doesn’t necessarily add to the problem of overdiagnosis, she said, because the issue is as much underdiagnosis of prognostically relevant disease as it is overdiagnosis of relevant disease.
The technology of mammography favors detection of slowly growing cancers because of its focus on architectural distortions, spiculations, and calcifications that reflect regressive changes, while MRI technology detects angiogenic and protease activity that is biased toward biologically active disease, she said.
Previous data from her institution show that the sensitivity of MRI for detecting DCIS increases from 80% with low-grade DCIS to 98% with high-grade DCIS, but the sensitivity of mammography decreases as DCIS grade increases, dropping from 61% with low-grade DCIS to 35% with high-grade DCIS without necrosis*.
The symposium was cosponsored by the American Society of Breast Disease, the American Society of Breast Surgeons, the National Consortium of Breast Centers, the Society of Surgical Oncology, and the American Society for Radiation Oncology.
Dr. Kuhl has been a consultant to Bayer. She reported no other relevant financial disclosures.
*This story was updated 10/16/2013.
On Twitter @sherryboschert
SAN FRANCISCO – A 3-minute MRI allowed a radiologist to rule out breast cancer with 99% accuracy in a prospective study of 443 women at a slightly increased or intermediate lifetime risk of breast cancer.
Extending the expert’s reading time to no more than 30 seconds to also interpret the first postcontrast subtracted (FAST) images provided the same sensitivity and specificity as a full diagnostic MRI protocol that had patients on the MRI table for 21 minutes on average, Dr. Christiane K. Kuhl reported at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
Conventional breast MRI protocols are time consuming and more expensive, because they are designed for diagnosis, not screening, said Dr. Kuhl, director of the department of diagnostic and interventional radiology at Rheinisch-Westfälische Technische Hochschule Aachen (Germany) University. The study aimed to trade some of the high sensitivity of MRI in detecting breast cancer for faster image acquisition and interpretation, perhaps eventually leading to lower cost and greater accessibility to MRI.
For the study, experienced breast radiologists were asked to review the maximum intensity projection (MIP) of the FAST images to determine whether there was significant enhancement. They then examined the FAST images for possible further categorization of any enhancement seen on the MIP, and analyzed the MRI under the full diagnostic protocol.
The prospective proof-of-concept study included patients who had imaging done between January 2009 and June 2010 and who were followed for 2 years to validate negative diagnoses. These were asymptomatic women with an intermediate risk with less than a 25% estimated lifetime risk of breast cancer. All of the women had a normal or benign mammogram and, if they had dense breasts, a normal or benign ultrasound result.
Acquiring the MIP and FAST images took less than 3 minutes with the patient on the MRI table. Reading the maximum intensity projection averaged 3 seconds, and reading the MIP plus FAST image averaged 28 seconds.
MRI screening identified 11 cancers, for an additional yield of 18 cancers per 1,000 examinations beyond what could be detected by mammography. Reading the MIP alone had a negative predictive value of 99%; the maximum intensity projection plus FAST readings and the full MRI protocol had negative predictive values just under 100%, Dr. Kuhl reported. The sensitivity of the MIP was close to 95% compared with 100% for MIP plus FAST or the full protocol. The specificity and positive predictive value could not be calculated for the MIP because the MIP reading detected only the presence or absence of significant enhancement. Evaluating the MIP plus FAST or the full MRI protocol produced similar specificities (in the mid-90% range) and positive predictive values (in the low 20% range).
All 11 breast cancers were intermediate- or high-grade cancers; 4 were ductal carcinoma in situ (DCIS) and 7 were invasive cancers. The median tumor size was 8 mm, and the mean age of the women with cancer was 51 years.
Conventional breast cancer screening using mammography picks up cancers that may be prognostically irrelevant, which add to potential overdiagnosis of breast cancer, she noted. In 11 studies that compared screening with breast MRI and mammography, MRI detected two to four times as many cancers as did mammography or ultrasound. Finding more DCIS and invasive cancers via MRI doesn’t necessarily add to the problem of overdiagnosis, she said, because the issue is as much underdiagnosis of prognostically relevant disease as it is overdiagnosis of relevant disease.
The technology of mammography favors detection of slowly growing cancers because of its focus on architectural distortions, spiculations, and calcifications that reflect regressive changes, while MRI technology detects angiogenic and protease activity that is biased toward biologically active disease, she said.
Previous data from her institution show that the sensitivity of MRI for detecting DCIS increases from 80% with low-grade DCIS to 98% with high-grade DCIS, but the sensitivity of mammography decreases as DCIS grade increases, dropping from 61% with low-grade DCIS to 35% with high-grade DCIS without necrosis*.
The symposium was cosponsored by the American Society of Breast Disease, the American Society of Breast Surgeons, the National Consortium of Breast Centers, the Society of Surgical Oncology, and the American Society for Radiation Oncology.
Dr. Kuhl has been a consultant to Bayer. She reported no other relevant financial disclosures.
*This story was updated 10/16/2013.
On Twitter @sherryboschert
SAN FRANCISCO – A 3-minute MRI allowed a radiologist to rule out breast cancer with 99% accuracy in a prospective study of 443 women at a slightly increased or intermediate lifetime risk of breast cancer.
Extending the expert’s reading time to no more than 30 seconds to also interpret the first postcontrast subtracted (FAST) images provided the same sensitivity and specificity as a full diagnostic MRI protocol that had patients on the MRI table for 21 minutes on average, Dr. Christiane K. Kuhl reported at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
Conventional breast MRI protocols are time consuming and more expensive, because they are designed for diagnosis, not screening, said Dr. Kuhl, director of the department of diagnostic and interventional radiology at Rheinisch-Westfälische Technische Hochschule Aachen (Germany) University. The study aimed to trade some of the high sensitivity of MRI in detecting breast cancer for faster image acquisition and interpretation, perhaps eventually leading to lower cost and greater accessibility to MRI.
For the study, experienced breast radiologists were asked to review the maximum intensity projection (MIP) of the FAST images to determine whether there was significant enhancement. They then examined the FAST images for possible further categorization of any enhancement seen on the MIP, and analyzed the MRI under the full diagnostic protocol.
The prospective proof-of-concept study included patients who had imaging done between January 2009 and June 2010 and who were followed for 2 years to validate negative diagnoses. These were asymptomatic women with an intermediate risk with less than a 25% estimated lifetime risk of breast cancer. All of the women had a normal or benign mammogram and, if they had dense breasts, a normal or benign ultrasound result.
Acquiring the MIP and FAST images took less than 3 minutes with the patient on the MRI table. Reading the maximum intensity projection averaged 3 seconds, and reading the MIP plus FAST image averaged 28 seconds.
MRI screening identified 11 cancers, for an additional yield of 18 cancers per 1,000 examinations beyond what could be detected by mammography. Reading the MIP alone had a negative predictive value of 99%; the maximum intensity projection plus FAST readings and the full MRI protocol had negative predictive values just under 100%, Dr. Kuhl reported. The sensitivity of the MIP was close to 95% compared with 100% for MIP plus FAST or the full protocol. The specificity and positive predictive value could not be calculated for the MIP because the MIP reading detected only the presence or absence of significant enhancement. Evaluating the MIP plus FAST or the full MRI protocol produced similar specificities (in the mid-90% range) and positive predictive values (in the low 20% range).
All 11 breast cancers were intermediate- or high-grade cancers; 4 were ductal carcinoma in situ (DCIS) and 7 were invasive cancers. The median tumor size was 8 mm, and the mean age of the women with cancer was 51 years.
Conventional breast cancer screening using mammography picks up cancers that may be prognostically irrelevant, which add to potential overdiagnosis of breast cancer, she noted. In 11 studies that compared screening with breast MRI and mammography, MRI detected two to four times as many cancers as did mammography or ultrasound. Finding more DCIS and invasive cancers via MRI doesn’t necessarily add to the problem of overdiagnosis, she said, because the issue is as much underdiagnosis of prognostically relevant disease as it is overdiagnosis of relevant disease.
The technology of mammography favors detection of slowly growing cancers because of its focus on architectural distortions, spiculations, and calcifications that reflect regressive changes, while MRI technology detects angiogenic and protease activity that is biased toward biologically active disease, she said.
Previous data from her institution show that the sensitivity of MRI for detecting DCIS increases from 80% with low-grade DCIS to 98% with high-grade DCIS, but the sensitivity of mammography decreases as DCIS grade increases, dropping from 61% with low-grade DCIS to 35% with high-grade DCIS without necrosis*.
The symposium was cosponsored by the American Society of Breast Disease, the American Society of Breast Surgeons, the National Consortium of Breast Centers, the Society of Surgical Oncology, and the American Society for Radiation Oncology.
Dr. Kuhl has been a consultant to Bayer. She reported no other relevant financial disclosures.
*This story was updated 10/16/2013.
On Twitter @sherryboschert
AT THE ASCO BREAST CANCER SYMPOSIUM
Major finding: MRI screening identified 11 cancers, for an additional yield of 18 cancers per 1,000 examinations beyond what could be detected by mammography.
Data source: A prospective proof-of-concept study of MRI screening in 443 women with slightly increased or intermediate risk for breast cancer and negative mammograms.
Disclosures: Dr. Kuhl has been a consultant to Bayer. She reported no other relevant financial disclosures.
Perioperative MRI fails to reduce recurrence risk in women with ductal carcinoma in situ
Routine use of magnetic resonance imaging does not improve outcomes in women undergoing lumpectomy for ductal carcinoma in situ, according to the results of a retrospective cohort study conducted at the Memorial Sloan-Kettering Cancer Center in New York.
A team led by Dr. Melissa L. Pilewskie studied 2,321 patients who underwent lumpectomy for ductal carcinoma in situ (DCIS) between 1997 and 2010. A quarter had breast MRI before or immediately after their surgery, in addition to conventional imaging with mammography and/or ultrasound.

Study results, being reported in full later this week at the breast cancer symposium sponsored by the American Society of Clinical Oncology, showed that the 5-year rate of locoregional recurrence was about 8%, with no significant difference between the groups who did and did not have MRI.
The findings were the same after adjustment for potential confounders and also when analyses were restricted to the subset of patients who did not receive radiation therapy, according to Dr. Pilewskie, a breast surgeon at Sloan-Kettering.
In addition, perioperative MRI did not reduce the rate of contralateral breast cancer, which stood at about 4% in each group.
"In the absence of evidence that MRI is improving our surgical management or – as we showed here – long-term outcomes, the routine use of this test for DCIS should be questioned," Dr. Pilewskie commented in a related press briefing.
She outlined circumstances that may justify this additional testing. "I think that MRI can be a useful adjunct if there are discrepancies or still clinical questions when someone comes in, between the imaging that they have on their mammogram or ultrasound and their physical exam or their presentation," she said. "The majority of women who present with DCIS have a normal exam and calcifications or changes on a mammogram. So when there are differences, and someone has a palpable mass or nipple discharge or a different presentation that wasn’t answered by their imaging, I think MRI can help give additional information. But that again is not the routine woman who presents with DCIS."
With a median 59-month follow-up, the groups who did and did not receive MRI were statistically indistinguishable in terms of the actuarial rate of locoregional recurrence at 5 years (8.5% vs. 7.2%) and at 8 years (14.6% vs. 10.2%).
"When comparing the MRI and no-MRI groups, there were some differences between them in that the women who had an MRI had more high-risk features," Dr. Pilewskie noted, and those features might have influenced the decision to obtain this additional imaging and outcomes.
However, MRI was not a significant predictor of locoregional recurrence in a multivariate analysis that adjusted for these and other potential confounders: age, family history, mode of presentation, tamoxifen or other hormonal therapy, margin status, number of excisions, and year of surgery.
On the other hand, receipt of radiation therapy, receipt of endocrine therapy, and negative margins were all significantly associated with a lower risk of locoregional recurrence.
In a subset analysis, MRI also failed to reduce the risk of locoregional recurrence in the roughly one-third of patients who did not receive radiation therapy.
Similarly, patients who did and did not receive MRI were statistically indistinguishable in terms of the actuarial rate of contralateral breast cancer at 5 years (3.5% vs. 3.5%) and at 8 years (3.5% vs. 5.1%). Again, results were essentially the same in the subset who did not receive radiation therapy.
Dr. Steven O’Day, director of clinical research at the Beverly Hills Cancer Institute in California and moderator of the press briefing, commented, "There has been a tremendous increase in the use of MRI perioperatively and postoperatively in invasive as well as noninvasive breast cancer. And this [study] I think just grounds us to continue to – as new technologies, new imaging is used – be sure that we are actually" improving outcomes.
He concurred that the added sensitivity of MRI may be helpful in challenging cases. "But its routine use certainly in DCIS from this large retrospective study has not been shown as an independent predictor to improve locoregional or contralateral breast outcomes," he said. "So I think this is an important study" and leads us to want "to study MRI further prospectively both in DCIS and invasive cancer."
Giving some background to the research, Dr. Pilewskie noted that current guidelines do not address when MRI should be used in the work-up of patients with DCIS.
"However, about 30% of physicians currently obtain a perioperative MRI to look for areas of additional disease in patients with DCIS, and theoretically, treating this additional disease found by MRI could result in a lower risk of local recurrence or contralateral breast cancer down the road," she said. "And, again theoretically, this effect could be most pronounced in women treated with excision alone, meaning just having lumpectomy and no radiation therapy."
Overall, 26% of the patients studied had breast MRI near the time of surgery, most commonly preoperatively, to assess disease extent.
Dr. Pilewskie and Dr. O’Day disclosed no relevant conflicts of interest.
Routine use of magnetic resonance imaging does not improve outcomes in women undergoing lumpectomy for ductal carcinoma in situ, according to the results of a retrospective cohort study conducted at the Memorial Sloan-Kettering Cancer Center in New York.
A team led by Dr. Melissa L. Pilewskie studied 2,321 patients who underwent lumpectomy for ductal carcinoma in situ (DCIS) between 1997 and 2010. A quarter had breast MRI before or immediately after their surgery, in addition to conventional imaging with mammography and/or ultrasound.
Study results, being reported in full later this week at the breast cancer symposium sponsored by the American Society of Clinical Oncology, showed that the 5-year rate of locoregional recurrence was about 8%, with no significant difference between the groups who did and did not have MRI.
The findings were the same after adjustment for potential confounders and also when analyses were restricted to the subset of patients who did not receive radiation therapy, according to Dr. Pilewskie, a breast surgeon at Sloan-Kettering.
In addition, perioperative MRI did not reduce the rate of contralateral breast cancer, which stood at about 4% in each group.
"In the absence of evidence that MRI is improving our surgical management or – as we showed here – long-term outcomes, the routine use of this test for DCIS should be questioned," Dr. Pilewskie commented in a related press briefing.
She outlined circumstances that may justify this additional testing. "I think that MRI can be a useful adjunct if there are discrepancies or still clinical questions when someone comes in, between the imaging that they have on their mammogram or ultrasound and their physical exam or their presentation," she said. "The majority of women who present with DCIS have a normal exam and calcifications or changes on a mammogram. So when there are differences, and someone has a palpable mass or nipple discharge or a different presentation that wasn’t answered by their imaging, I think MRI can help give additional information. But that again is not the routine woman who presents with DCIS."
With a median 59-month follow-up, the groups who did and did not receive MRI were statistically indistinguishable in terms of the actuarial rate of locoregional recurrence at 5 years (8.5% vs. 7.2%) and at 8 years (14.6% vs. 10.2%).
"When comparing the MRI and no-MRI groups, there were some differences between them in that the women who had an MRI had more high-risk features," Dr. Pilewskie noted, and those features might have influenced the decision to obtain this additional imaging and outcomes.
However, MRI was not a significant predictor of locoregional recurrence in a multivariate analysis that adjusted for these and other potential confounders: age, family history, mode of presentation, tamoxifen or other hormonal therapy, margin status, number of excisions, and year of surgery.
On the other hand, receipt of radiation therapy, receipt of endocrine therapy, and negative margins were all significantly associated with a lower risk of locoregional recurrence.
In a subset analysis, MRI also failed to reduce the risk of locoregional recurrence in the roughly one-third of patients who did not receive radiation therapy.
Similarly, patients who did and did not receive MRI were statistically indistinguishable in terms of the actuarial rate of contralateral breast cancer at 5 years (3.5% vs. 3.5%) and at 8 years (3.5% vs. 5.1%). Again, results were essentially the same in the subset who did not receive radiation therapy.
Dr. Steven O’Day, director of clinical research at the Beverly Hills Cancer Institute in California and moderator of the press briefing, commented, "There has been a tremendous increase in the use of MRI perioperatively and postoperatively in invasive as well as noninvasive breast cancer. And this [study] I think just grounds us to continue to – as new technologies, new imaging is used – be sure that we are actually" improving outcomes.
He concurred that the added sensitivity of MRI may be helpful in challenging cases. "But its routine use certainly in DCIS from this large retrospective study has not been shown as an independent predictor to improve locoregional or contralateral breast outcomes," he said. "So I think this is an important study" and leads us to want "to study MRI further prospectively both in DCIS and invasive cancer."
Giving some background to the research, Dr. Pilewskie noted that current guidelines do not address when MRI should be used in the work-up of patients with DCIS.
"However, about 30% of physicians currently obtain a perioperative MRI to look for areas of additional disease in patients with DCIS, and theoretically, treating this additional disease found by MRI could result in a lower risk of local recurrence or contralateral breast cancer down the road," she said. "And, again theoretically, this effect could be most pronounced in women treated with excision alone, meaning just having lumpectomy and no radiation therapy."
Overall, 26% of the patients studied had breast MRI near the time of surgery, most commonly preoperatively, to assess disease extent.
Dr. Pilewskie and Dr. O’Day disclosed no relevant conflicts of interest.
Routine use of magnetic resonance imaging does not improve outcomes in women undergoing lumpectomy for ductal carcinoma in situ, according to the results of a retrospective cohort study conducted at the Memorial Sloan-Kettering Cancer Center in New York.
A team led by Dr. Melissa L. Pilewskie studied 2,321 patients who underwent lumpectomy for ductal carcinoma in situ (DCIS) between 1997 and 2010. A quarter had breast MRI before or immediately after their surgery, in addition to conventional imaging with mammography and/or ultrasound.
Study results, being reported in full later this week at the breast cancer symposium sponsored by the American Society of Clinical Oncology, showed that the 5-year rate of locoregional recurrence was about 8%, with no significant difference between the groups who did and did not have MRI.
The findings were the same after adjustment for potential confounders and also when analyses were restricted to the subset of patients who did not receive radiation therapy, according to Dr. Pilewskie, a breast surgeon at Sloan-Kettering.
In addition, perioperative MRI did not reduce the rate of contralateral breast cancer, which stood at about 4% in each group.
"In the absence of evidence that MRI is improving our surgical management or – as we showed here – long-term outcomes, the routine use of this test for DCIS should be questioned," Dr. Pilewskie commented in a related press briefing.
She outlined circumstances that may justify this additional testing. "I think that MRI can be a useful adjunct if there are discrepancies or still clinical questions when someone comes in, between the imaging that they have on their mammogram or ultrasound and their physical exam or their presentation," she said. "The majority of women who present with DCIS have a normal exam and calcifications or changes on a mammogram. So when there are differences, and someone has a palpable mass or nipple discharge or a different presentation that wasn’t answered by their imaging, I think MRI can help give additional information. But that again is not the routine woman who presents with DCIS."
With a median 59-month follow-up, the groups who did and did not receive MRI were statistically indistinguishable in terms of the actuarial rate of locoregional recurrence at 5 years (8.5% vs. 7.2%) and at 8 years (14.6% vs. 10.2%).
"When comparing the MRI and no-MRI groups, there were some differences between them in that the women who had an MRI had more high-risk features," Dr. Pilewskie noted, and those features might have influenced the decision to obtain this additional imaging and outcomes.
However, MRI was not a significant predictor of locoregional recurrence in a multivariate analysis that adjusted for these and other potential confounders: age, family history, mode of presentation, tamoxifen or other hormonal therapy, margin status, number of excisions, and year of surgery.
On the other hand, receipt of radiation therapy, receipt of endocrine therapy, and negative margins were all significantly associated with a lower risk of locoregional recurrence.
In a subset analysis, MRI also failed to reduce the risk of locoregional recurrence in the roughly one-third of patients who did not receive radiation therapy.
Similarly, patients who did and did not receive MRI were statistically indistinguishable in terms of the actuarial rate of contralateral breast cancer at 5 years (3.5% vs. 3.5%) and at 8 years (3.5% vs. 5.1%). Again, results were essentially the same in the subset who did not receive radiation therapy.
Dr. Steven O’Day, director of clinical research at the Beverly Hills Cancer Institute in California and moderator of the press briefing, commented, "There has been a tremendous increase in the use of MRI perioperatively and postoperatively in invasive as well as noninvasive breast cancer. And this [study] I think just grounds us to continue to – as new technologies, new imaging is used – be sure that we are actually" improving outcomes.
He concurred that the added sensitivity of MRI may be helpful in challenging cases. "But its routine use certainly in DCIS from this large retrospective study has not been shown as an independent predictor to improve locoregional or contralateral breast outcomes," he said. "So I think this is an important study" and leads us to want "to study MRI further prospectively both in DCIS and invasive cancer."
Giving some background to the research, Dr. Pilewskie noted that current guidelines do not address when MRI should be used in the work-up of patients with DCIS.
"However, about 30% of physicians currently obtain a perioperative MRI to look for areas of additional disease in patients with DCIS, and theoretically, treating this additional disease found by MRI could result in a lower risk of local recurrence or contralateral breast cancer down the road," she said. "And, again theoretically, this effect could be most pronounced in women treated with excision alone, meaning just having lumpectomy and no radiation therapy."
Overall, 26% of the patients studied had breast MRI near the time of surgery, most commonly preoperatively, to assess disease extent.
Dr. Pilewskie and Dr. O’Day disclosed no relevant conflicts of interest.
FROM THE ASCO BREAST CANCER SYMPOSIUM
Major finding: Women who received MRI in addition to conventional imaging did not have a lower 5-year rate of locoregional recurrence when compared with women who received conventional imaging alone (8.5% vs. 7.2%).
Data source: A retrospective cohort study of 2,321 patients who underwent lumpectomy for DCIS.
Disclosures: Dr. Pilewskie and Dr. O’Day disclosed no relevant conflicts of interest.

Most women misestimate their breast cancer risk
Most women do not have an accurate understanding of their breast cancer risk – a finding that has important implications for prevention and early detection, as well as psychological well-being, according to a survey of nearly 10,000 women undergoing mammography screening.
When asked to estimate their lifetime personal breast cancer risk, just 9.4% of the women gave a value that was within 10% of their actual calculated risk, according to data reported in a press briefing held in advance of the breast cancer symposium sponsored by the American Society of Clinical Oncology, where the study will be presented in full.
"Despite all the ongoing media attention, awareness campaigns, pink ribbons, breast cancer walks, and breast cancer month, most women lack accurate knowledge of their own breast cancer risk," maintained first author Dr. Jonathan D. Herman, an ob.gyn. at Hofstra University, New Hyde Park, N.Y. This tells us that "our education messaging is far off and we should change the way breast cancer awareness is presented."
"We began to think: What happens to women when they underestimate their risk of breast cancer? Well, they probably don’t get the necessary or most accurate treatment," he said. In particular, this group could benefit from a tailored plan of chemoprevention and early detection. On the other hand, "we think that women who overestimate their risk are worrying about getting breast cancer more than they really have to."
In the study, the investigators surveyed 9,873 women aged 35-70 years who were about to undergo screening at 21 Long Island mammography centers. The anonymous questionnaire included many questions adapted from the National Cancer Institute’s Breast Cancer Risk Assessment Tool, which is available online and typically used by physicians.
The women’s subjective estimate of risk was compared with their risk as calculated with the tool. Their estimate was considered inaccurate if it differed from their calculated risk by more than 10%.
Most of the women were at average calculated risk, with 35% having a 5%-10% lifetime risk and 40% having a 10%-15% lifetime risk.
Just 9.4% of the women, however, accurately estimated their risk, while 46% overestimated their risk and 45% underestimated their risk.
The predominant direction of estimation error varied by race/ethnicity. Of the white women, 10% accurately estimated their risk, 39% underestimated, and 51% overestimated their risk. Women of other ethnicities were more likely to underestimate their breast cancer risks. Just 9% of African American women were in line with their risk, with 58% underestimating and 34% overestimating. Asian women had similar assessments. Hispanic women’s inaccurate assessments were more balanced, with 50% underestimating and 41% overestimating risk. Although these differences were statistically significant, it is more important to note that the overall level of understanding was very low, Dr. Herman said.
Ideally, patients should learn of their breast cancer risk from their physician, he said, but the study data told another story. "All of these women were about to have mammography, so they obviously had some interest in their breast health," but when asked when they last spoke to their doctor about their personal breast cancer risk, "we were shocked to find that 40% of women said they never ever had a conversation with a health care provider," he reported.
The findings suggest a need to improve communication about risk by primary care providers, especially as the U.S. Preventive Services Task Force is now putting greater emphasis on informed decision making, Dr. Herman acknowledged.
But patients could be spurred to action as well, by moving beyond the pink ribbons and asking their physician, "What are my breast cancer numbers? I need to know that," he proposed.
Dr. Steven O’Day, director of clinical research at the Beverly Hills (Calif.) Cancer Institute and moderator of the press briefing, noted that the study has important implications for making use of guidelines for women at elevated risk. "To make decisions about chemoprevention, an accurate understanding of prognosis and risk both from the patient’s perspective and the physician’s is going to be essential to making good decisions in terms of surveillance and chemoprevention," he said.
A follow-up study planned by Dr. Herman will be important for informing efforts to improve risk communication, according to Dr. O’Day. "It’s a huge hurdle, yet how we are going to implement this [in primary care], as well as the tertiary-care oncology setting?" he commented. "If we don’t, the implications are huge; interventions by increased surveillance or chemoprevention are not trivial in terms of cost as well as potential side effects and morbidity. And these are difficult decisions even with accurate information. And without the information, you really can’t make any decision, in my mind."
Dr. Herman disclosed no relevant conflicts of interest. Dr. O’Day disclosed no relevant conflicts of interest.
Most women do not have an accurate understanding of their breast cancer risk – a finding that has important implications for prevention and early detection, as well as psychological well-being, according to a survey of nearly 10,000 women undergoing mammography screening.
When asked to estimate their lifetime personal breast cancer risk, just 9.4% of the women gave a value that was within 10% of their actual calculated risk, according to data reported in a press briefing held in advance of the breast cancer symposium sponsored by the American Society of Clinical Oncology, where the study will be presented in full.
"Despite all the ongoing media attention, awareness campaigns, pink ribbons, breast cancer walks, and breast cancer month, most women lack accurate knowledge of their own breast cancer risk," maintained first author Dr. Jonathan D. Herman, an ob.gyn. at Hofstra University, New Hyde Park, N.Y. This tells us that "our education messaging is far off and we should change the way breast cancer awareness is presented."
"We began to think: What happens to women when they underestimate their risk of breast cancer? Well, they probably don’t get the necessary or most accurate treatment," he said. In particular, this group could benefit from a tailored plan of chemoprevention and early detection. On the other hand, "we think that women who overestimate their risk are worrying about getting breast cancer more than they really have to."
In the study, the investigators surveyed 9,873 women aged 35-70 years who were about to undergo screening at 21 Long Island mammography centers. The anonymous questionnaire included many questions adapted from the National Cancer Institute’s Breast Cancer Risk Assessment Tool, which is available online and typically used by physicians.
The women’s subjective estimate of risk was compared with their risk as calculated with the tool. Their estimate was considered inaccurate if it differed from their calculated risk by more than 10%.
Most of the women were at average calculated risk, with 35% having a 5%-10% lifetime risk and 40% having a 10%-15% lifetime risk.
Just 9.4% of the women, however, accurately estimated their risk, while 46% overestimated their risk and 45% underestimated their risk.
The predominant direction of estimation error varied by race/ethnicity. Of the white women, 10% accurately estimated their risk, 39% underestimated, and 51% overestimated their risk. Women of other ethnicities were more likely to underestimate their breast cancer risks. Just 9% of African American women were in line with their risk, with 58% underestimating and 34% overestimating. Asian women had similar assessments. Hispanic women’s inaccurate assessments were more balanced, with 50% underestimating and 41% overestimating risk. Although these differences were statistically significant, it is more important to note that the overall level of understanding was very low, Dr. Herman said.
Ideally, patients should learn of their breast cancer risk from their physician, he said, but the study data told another story. "All of these women were about to have mammography, so they obviously had some interest in their breast health," but when asked when they last spoke to their doctor about their personal breast cancer risk, "we were shocked to find that 40% of women said they never ever had a conversation with a health care provider," he reported.
The findings suggest a need to improve communication about risk by primary care providers, especially as the U.S. Preventive Services Task Force is now putting greater emphasis on informed decision making, Dr. Herman acknowledged.
But patients could be spurred to action as well, by moving beyond the pink ribbons and asking their physician, "What are my breast cancer numbers? I need to know that," he proposed.
Dr. Steven O’Day, director of clinical research at the Beverly Hills (Calif.) Cancer Institute and moderator of the press briefing, noted that the study has important implications for making use of guidelines for women at elevated risk. "To make decisions about chemoprevention, an accurate understanding of prognosis and risk both from the patient’s perspective and the physician’s is going to be essential to making good decisions in terms of surveillance and chemoprevention," he said.
A follow-up study planned by Dr. Herman will be important for informing efforts to improve risk communication, according to Dr. O’Day. "It’s a huge hurdle, yet how we are going to implement this [in primary care], as well as the tertiary-care oncology setting?" he commented. "If we don’t, the implications are huge; interventions by increased surveillance or chemoprevention are not trivial in terms of cost as well as potential side effects and morbidity. And these are difficult decisions even with accurate information. And without the information, you really can’t make any decision, in my mind."
Dr. Herman disclosed no relevant conflicts of interest. Dr. O’Day disclosed no relevant conflicts of interest.
Most women do not have an accurate understanding of their breast cancer risk – a finding that has important implications for prevention and early detection, as well as psychological well-being, according to a survey of nearly 10,000 women undergoing mammography screening.
When asked to estimate their lifetime personal breast cancer risk, just 9.4% of the women gave a value that was within 10% of their actual calculated risk, according to data reported in a press briefing held in advance of the breast cancer symposium sponsored by the American Society of Clinical Oncology, where the study will be presented in full.
"Despite all the ongoing media attention, awareness campaigns, pink ribbons, breast cancer walks, and breast cancer month, most women lack accurate knowledge of their own breast cancer risk," maintained first author Dr. Jonathan D. Herman, an ob.gyn. at Hofstra University, New Hyde Park, N.Y. This tells us that "our education messaging is far off and we should change the way breast cancer awareness is presented."
"We began to think: What happens to women when they underestimate their risk of breast cancer? Well, they probably don’t get the necessary or most accurate treatment," he said. In particular, this group could benefit from a tailored plan of chemoprevention and early detection. On the other hand, "we think that women who overestimate their risk are worrying about getting breast cancer more than they really have to."
In the study, the investigators surveyed 9,873 women aged 35-70 years who were about to undergo screening at 21 Long Island mammography centers. The anonymous questionnaire included many questions adapted from the National Cancer Institute’s Breast Cancer Risk Assessment Tool, which is available online and typically used by physicians.
The women’s subjective estimate of risk was compared with their risk as calculated with the tool. Their estimate was considered inaccurate if it differed from their calculated risk by more than 10%.
Most of the women were at average calculated risk, with 35% having a 5%-10% lifetime risk and 40% having a 10%-15% lifetime risk.
Just 9.4% of the women, however, accurately estimated their risk, while 46% overestimated their risk and 45% underestimated their risk.
The predominant direction of estimation error varied by race/ethnicity. Of the white women, 10% accurately estimated their risk, 39% underestimated, and 51% overestimated their risk. Women of other ethnicities were more likely to underestimate their breast cancer risks. Just 9% of African American women were in line with their risk, with 58% underestimating and 34% overestimating. Asian women had similar assessments. Hispanic women’s inaccurate assessments were more balanced, with 50% underestimating and 41% overestimating risk. Although these differences were statistically significant, it is more important to note that the overall level of understanding was very low, Dr. Herman said.
Ideally, patients should learn of their breast cancer risk from their physician, he said, but the study data told another story. "All of these women were about to have mammography, so they obviously had some interest in their breast health," but when asked when they last spoke to their doctor about their personal breast cancer risk, "we were shocked to find that 40% of women said they never ever had a conversation with a health care provider," he reported.
The findings suggest a need to improve communication about risk by primary care providers, especially as the U.S. Preventive Services Task Force is now putting greater emphasis on informed decision making, Dr. Herman acknowledged.
But patients could be spurred to action as well, by moving beyond the pink ribbons and asking their physician, "What are my breast cancer numbers? I need to know that," he proposed.
Dr. Steven O’Day, director of clinical research at the Beverly Hills (Calif.) Cancer Institute and moderator of the press briefing, noted that the study has important implications for making use of guidelines for women at elevated risk. "To make decisions about chemoprevention, an accurate understanding of prognosis and risk both from the patient’s perspective and the physician’s is going to be essential to making good decisions in terms of surveillance and chemoprevention," he said.
A follow-up study planned by Dr. Herman will be important for informing efforts to improve risk communication, according to Dr. O’Day. "It’s a huge hurdle, yet how we are going to implement this [in primary care], as well as the tertiary-care oncology setting?" he commented. "If we don’t, the implications are huge; interventions by increased surveillance or chemoprevention are not trivial in terms of cost as well as potential side effects and morbidity. And these are difficult decisions even with accurate information. And without the information, you really can’t make any decision, in my mind."
Dr. Herman disclosed no relevant conflicts of interest. Dr. O’Day disclosed no relevant conflicts of interest.
Major Finding: Overall, 44.7% of women underestimated their risk and 45.9% overestimated their risk, while just 9.4% gave an accurate estimate.
Data Source: A survey of 9,873 women undergoing breast cancer screening at Long Island mammography centers.
Disclosures: Dr. Herman disclosed no relevant conflicts of interest. Dr. O’Day disclosed no relevant conflicts of interest.
No increase in cardiovascular risk seen after radiation therapy for DCIS
Women who receive radiation therapy as part of their treatment for very early breast cancer do not have an elevated risk of developing or dying from cardiovascular disease later in life, new data suggest.
In a population-based cohort study, researchers assessed cardiovascular outcomes among 10,468 women in the Netherlands given a diagnosis of ductal carcinoma in situ (DCIS) before the age of 75 years during 1989-2004.
Overall, 28% of the cohort received radiation therapy after their surgery (lumpectomy or mastectomy), lead investigator Naomi B. Boekel reported in a press briefing held in advance of the breast cancer symposium sponsored by the American Society of Clinical Oncology, where the findings will be presented in full.
During a median follow-up of 10 years, about 9% of the patients received a diagnosis of cardiovascular disease.
There was no significant difference in the rate between patients who did vs. did not receive radiation, or between patients who received left-sided radiation (in which the heart gets a low direct dose) vs. right-sided radiation (in which the heart gets only a scatter dose).
Specifically, the rate of cardiovascular disease diagnosis was 9% in patients who received surgery alone, compared with 8% in patients who received surgery plus radiation, a nonsignificant difference. The CVD rate was 7% in patients who received left-sided radiation therapy vs. 8% in their counterparts who received right-sided radiation therapy, another nonsignificant difference.
Furthermore, DCIS survivors as a whole had a 23% lower risk of dying from cardiovascular disease, compared with peers in the general Dutch population.
"This lower risk might be due to lifestyle adaption after DCIS diagnosis," proposed Ms. Boekel, a doctoral student at the Netherlands Cancer Institute in Amsterdam. "It could be due to conflicting risk factors between DCIS and cardiovascular disease, such as age at menopause. Or it could also be due to differences in health consciousness in that DCIS patients are probably more health conscious than the general population."
The risk of all-cause mortality was essentially the same between the DCIS cohort and the general population.
"We also looked at this for specific cardiovascular diseases and there were similar results, so there is no risk difference between these treatment groups," Ms. Boekel reported.
"Although these results are reassuring, longer follow-up is necessary before definitive conclusions can be drawn," she commented.
There is no established upper limit for such follow-up, she said. "But other studies have shown that the increased risk of cardiovascular disease starts after 5 to 10 years. ... We do have half of the cohort at more than 10 years, but [estimates] are less precise. So we need another 5 to 10 years before we are sure."
Strengths of the study, according to Dr. Steven O’Day, director of clinical research at the Beverly Hills (Calif.) Cancer Institute and moderator of the press briefing, included its occurrence in a time period in which more modern radiation therapy techniques were used. Also, the follow-up was fairly lengthy, although he agreed that more is needed.
"This is an important study that allows us to feel comfortable continuing our aggressive treatment of DCIS, with screening and trying to reduce overall mortality from breast cancer," Dr. O’Day maintained.
Ms. Boekel disclosed no relevant conflicts of interest. Dr. O’Day disclosed no relevant conflicts of interest.
Women who receive radiation therapy as part of their treatment for very early breast cancer do not have an elevated risk of developing or dying from cardiovascular disease later in life, new data suggest.
In a population-based cohort study, researchers assessed cardiovascular outcomes among 10,468 women in the Netherlands given a diagnosis of ductal carcinoma in situ (DCIS) before the age of 75 years during 1989-2004.
Overall, 28% of the cohort received radiation therapy after their surgery (lumpectomy or mastectomy), lead investigator Naomi B. Boekel reported in a press briefing held in advance of the breast cancer symposium sponsored by the American Society of Clinical Oncology, where the findings will be presented in full.
During a median follow-up of 10 years, about 9% of the patients received a diagnosis of cardiovascular disease.
There was no significant difference in the rate between patients who did vs. did not receive radiation, or between patients who received left-sided radiation (in which the heart gets a low direct dose) vs. right-sided radiation (in which the heart gets only a scatter dose).
Specifically, the rate of cardiovascular disease diagnosis was 9% in patients who received surgery alone, compared with 8% in patients who received surgery plus radiation, a nonsignificant difference. The CVD rate was 7% in patients who received left-sided radiation therapy vs. 8% in their counterparts who received right-sided radiation therapy, another nonsignificant difference.
Furthermore, DCIS survivors as a whole had a 23% lower risk of dying from cardiovascular disease, compared with peers in the general Dutch population.
"This lower risk might be due to lifestyle adaption after DCIS diagnosis," proposed Ms. Boekel, a doctoral student at the Netherlands Cancer Institute in Amsterdam. "It could be due to conflicting risk factors between DCIS and cardiovascular disease, such as age at menopause. Or it could also be due to differences in health consciousness in that DCIS patients are probably more health conscious than the general population."
The risk of all-cause mortality was essentially the same between the DCIS cohort and the general population.
"We also looked at this for specific cardiovascular diseases and there were similar results, so there is no risk difference between these treatment groups," Ms. Boekel reported.
"Although these results are reassuring, longer follow-up is necessary before definitive conclusions can be drawn," she commented.
There is no established upper limit for such follow-up, she said. "But other studies have shown that the increased risk of cardiovascular disease starts after 5 to 10 years. ... We do have half of the cohort at more than 10 years, but [estimates] are less precise. So we need another 5 to 10 years before we are sure."
Strengths of the study, according to Dr. Steven O’Day, director of clinical research at the Beverly Hills (Calif.) Cancer Institute and moderator of the press briefing, included its occurrence in a time period in which more modern radiation therapy techniques were used. Also, the follow-up was fairly lengthy, although he agreed that more is needed.
"This is an important study that allows us to feel comfortable continuing our aggressive treatment of DCIS, with screening and trying to reduce overall mortality from breast cancer," Dr. O’Day maintained.
Ms. Boekel disclosed no relevant conflicts of interest. Dr. O’Day disclosed no relevant conflicts of interest.
Women who receive radiation therapy as part of their treatment for very early breast cancer do not have an elevated risk of developing or dying from cardiovascular disease later in life, new data suggest.
In a population-based cohort study, researchers assessed cardiovascular outcomes among 10,468 women in the Netherlands given a diagnosis of ductal carcinoma in situ (DCIS) before the age of 75 years during 1989-2004.
Overall, 28% of the cohort received radiation therapy after their surgery (lumpectomy or mastectomy), lead investigator Naomi B. Boekel reported in a press briefing held in advance of the breast cancer symposium sponsored by the American Society of Clinical Oncology, where the findings will be presented in full.
During a median follow-up of 10 years, about 9% of the patients received a diagnosis of cardiovascular disease.
There was no significant difference in the rate between patients who did vs. did not receive radiation, or between patients who received left-sided radiation (in which the heart gets a low direct dose) vs. right-sided radiation (in which the heart gets only a scatter dose).
Specifically, the rate of cardiovascular disease diagnosis was 9% in patients who received surgery alone, compared with 8% in patients who received surgery plus radiation, a nonsignificant difference. The CVD rate was 7% in patients who received left-sided radiation therapy vs. 8% in their counterparts who received right-sided radiation therapy, another nonsignificant difference.
Furthermore, DCIS survivors as a whole had a 23% lower risk of dying from cardiovascular disease, compared with peers in the general Dutch population.
"This lower risk might be due to lifestyle adaption after DCIS diagnosis," proposed Ms. Boekel, a doctoral student at the Netherlands Cancer Institute in Amsterdam. "It could be due to conflicting risk factors between DCIS and cardiovascular disease, such as age at menopause. Or it could also be due to differences in health consciousness in that DCIS patients are probably more health conscious than the general population."
The risk of all-cause mortality was essentially the same between the DCIS cohort and the general population.
"We also looked at this for specific cardiovascular diseases and there were similar results, so there is no risk difference between these treatment groups," Ms. Boekel reported.
"Although these results are reassuring, longer follow-up is necessary before definitive conclusions can be drawn," she commented.
There is no established upper limit for such follow-up, she said. "But other studies have shown that the increased risk of cardiovascular disease starts after 5 to 10 years. ... We do have half of the cohort at more than 10 years, but [estimates] are less precise. So we need another 5 to 10 years before we are sure."
Strengths of the study, according to Dr. Steven O’Day, director of clinical research at the Beverly Hills (Calif.) Cancer Institute and moderator of the press briefing, included its occurrence in a time period in which more modern radiation therapy techniques were used. Also, the follow-up was fairly lengthy, although he agreed that more is needed.
"This is an important study that allows us to feel comfortable continuing our aggressive treatment of DCIS, with screening and trying to reduce overall mortality from breast cancer," Dr. O’Day maintained.
Ms. Boekel disclosed no relevant conflicts of interest. Dr. O’Day disclosed no relevant conflicts of interest.
FROM THE ASCO BREAST CANCER SYMPOSIUM
Major finding: The rate of CVD diagnosis did not differ between patients treated with surgery alone and patients treated with surgery plus radiation therapy (9% vs. 8%).
Data source: A population-based cohort study of 10,468 women in the Netherlands treated for DCIS
Disclosures: Ms. Boekel disclosed no relevant conflicts of interest. Dr. O’Day disclosed no relevant conflicts of interest.
Minimizing cancer’s impact on bone with denosumab: current and future perspectives
Bone metastasis is a serious complication of advanced cancer. It is most commonly observed in patients with metastatic breast and prostate cancers, but also occurs in most other metastatic solid cancers. Without treatment, patients may experience complications including intractable bone pain, hypercalcemia, fracture, spinal cord compression and/or a requirement for surgical or radiotherapeutic intervention. In 2010, denosumab, a fully human monoclonal antibody that inhibits RANK ligand (RANKL) and subsequent osteoclast-mediated bone destruction, was approved by the Food and Drug Administration for the prevention of skeletal-related events (SREs) in patients with bone metastases from solid tumors. This article reviews the role of denosumab in preventing SREs due to bone metastases, treating bone loss due to hormone-ablative cancer therapies, and describes denosumab’s safety profile and potential future indications under investigation.
Click on the PDF icon at the top of this introduction to read the full article.
Bone metastasis is a serious complication of advanced cancer. It is most commonly observed in patients with metastatic breast and prostate cancers, but also occurs in most other metastatic solid cancers. Without treatment, patients may experience complications including intractable bone pain, hypercalcemia, fracture, spinal cord compression and/or a requirement for surgical or radiotherapeutic intervention. In 2010, denosumab, a fully human monoclonal antibody that inhibits RANK ligand (RANKL) and subsequent osteoclast-mediated bone destruction, was approved by the Food and Drug Administration for the prevention of skeletal-related events (SREs) in patients with bone metastases from solid tumors. This article reviews the role of denosumab in preventing SREs due to bone metastases, treating bone loss due to hormone-ablative cancer therapies, and describes denosumab’s safety profile and potential future indications under investigation.
Click on the PDF icon at the top of this introduction to read the full article.
Bone metastasis is a serious complication of advanced cancer. It is most commonly observed in patients with metastatic breast and prostate cancers, but also occurs in most other metastatic solid cancers. Without treatment, patients may experience complications including intractable bone pain, hypercalcemia, fracture, spinal cord compression and/or a requirement for surgical or radiotherapeutic intervention. In 2010, denosumab, a fully human monoclonal antibody that inhibits RANK ligand (RANKL) and subsequent osteoclast-mediated bone destruction, was approved by the Food and Drug Administration for the prevention of skeletal-related events (SREs) in patients with bone metastases from solid tumors. This article reviews the role of denosumab in preventing SREs due to bone metastases, treating bone loss due to hormone-ablative cancer therapies, and describes denosumab’s safety profile and potential future indications under investigation.
Click on the PDF icon at the top of this introduction to read the full article.
Occult cancer: suspected breast and BRCA gene mutations
Currently, the best means of managing and preventing breast cancer is through early detection and identification of women who are at significantly increased risk for the disease. Those who are at increased risk are candidates for genetic testing involving the BRCA1 and BRCA2 genes. However, those who present with an occult cancer present a significant challenge in regard to etiology, which can have an impact on decisions about cancer risk management. We report here on two cases demonstrating an association between occult cancer, with suspected breast primary, and the presence of a BRCA gene mutation. These cases draw attention to the fact that occurrences of occult cancer, in particular those with a suspected breast primary, warrant consideration of genetic testing for possible mutations in the BRCA1 and BRCA2 genes. This is especially important as identification of a mutation will impact secondary cancer risk and medical management decisions.
Click on the PDF icon at the top of this introduction to read the full article.
Currently, the best means of managing and preventing breast cancer is through early detection and identification of women who are at significantly increased risk for the disease. Those who are at increased risk are candidates for genetic testing involving the BRCA1 and BRCA2 genes. However, those who present with an occult cancer present a significant challenge in regard to etiology, which can have an impact on decisions about cancer risk management. We report here on two cases demonstrating an association between occult cancer, with suspected breast primary, and the presence of a BRCA gene mutation. These cases draw attention to the fact that occurrences of occult cancer, in particular those with a suspected breast primary, warrant consideration of genetic testing for possible mutations in the BRCA1 and BRCA2 genes. This is especially important as identification of a mutation will impact secondary cancer risk and medical management decisions.
Click on the PDF icon at the top of this introduction to read the full article.
Currently, the best means of managing and preventing breast cancer is through early detection and identification of women who are at significantly increased risk for the disease. Those who are at increased risk are candidates for genetic testing involving the BRCA1 and BRCA2 genes. However, those who present with an occult cancer present a significant challenge in regard to etiology, which can have an impact on decisions about cancer risk management. We report here on two cases demonstrating an association between occult cancer, with suspected breast primary, and the presence of a BRCA gene mutation. These cases draw attention to the fact that occurrences of occult cancer, in particular those with a suspected breast primary, warrant consideration of genetic testing for possible mutations in the BRCA1 and BRCA2 genes. This is especially important as identification of a mutation will impact secondary cancer risk and medical management decisions.
Click on the PDF icon at the top of this introduction to read the full article.
Adjuvant ibandronate adds no benefit in early stage, node-positive breast cancer
Two years of adjuvant treatment with ibandronate after dose-dense chemotherapy did not improve survival in a study of more than 3,000 German patients with early stage, node-positive breast cancer.
The results were published online Aug. 26 in the Journal of Clinical Oncology.
Bisphosphonates have been shown to prevent skeletal-related events in patients with metastatic breast cancer, but their effectiveness has not been demonstrated in early breast cancer.
No differences in disease-free survival or overall survival were noted in the GAIN (German Adjuvant Intergroup Node-Positive) study, an open-label, randomized, controlled phase III trial (NCT00196872), reported Dr. Gunter von Minckwitz of the German Breast Group, along with his colleagues in the German Breast Group/Gynecologic Oncology Working Group/North-Eastern Germany Society of Gynecologic Oncology study groups.
In patients randomly assigned to 2 years of ibandronate or observation, there was no difference in disease-free survival (HR, 0.945; 95% CI, 0.768 to 1.161; P equals .589) or in overall survival (HR, 1.040; 95% CI, 0.763 to 1.419; P equals .803). Metastasis to the bone was documented in 31% in the ibandronate arm and in 38% in the observation arm.
Post hoc subgroup analyses of the study data imply that the benefit of adjuvant bisphosphonates was restricted to patients with low estrogen levels, either because of medical ovarian suppression or definite menopause. Future meta-analyses on an individual patient data level may reliably reveal subgroups of early-stage, high-risk breast cancer patients who might benefit from adjuvant bisphosphonates, the researchers noted (J. Clin. Oncol. 2013 Aug. 26 [doi:10.1200/JCO.2012.47.2167]).
In GAIN, patients with node-positive early breast cancer were randomly assigned within 4 weeks after surgery to two different dose-dense chemotherapy regimens and then in 2:1 fashion to ibandronate 50 mg per day orally starting within 4 weeks after last administration of chemotherapy and continuing for 2 years (2,015 patients) or to observation (1,008 patients).
Randomly assigned chemotherapy consisted of three courses of epirubicin 150 mg/m2 followed by three courses of paclitaxel 225 mg/m2 followed by three courses of cyclophosphamide 2,500 mg/m2 (reduced to 2,000 mg/m2 after recruitment of approximately 1,200 patients), all given at 2-week intervals (iddETC regimen) or epirubicin 112.5 mg/m2 and cyclophosphamide 600 mg/m2 for four 2-week courses followed by 10 courses of paclitaxel 67.5 mg/m2 given once per week with capecitabine 2,000 mg/m2 given days 1-14 every 3 weeks (EC-TX regimen).
Radiotherapy, endocrine treatment, and trastuzumab were indicated according to AGO guidelines and, if appropriate, were given in parallel with ibandronate after the end of chemotherapy. All patients received radiotherapy to the affected breast if breast-conserving surgery was performed, the researchers wrote.
Patients with endocrine-sensitive disease received endocrine treatment for 5 years with an aromatase inhibitor either alone or in sequence with tamoxifen if they were postmenopausal. Tamoxifen alone was given for 5 years in some patients together with a luteinizing hormone-releasing hormone (LHRH) analog if they were premenopausal after the end of chemotherapy. Patients with human epidermal growth factor receptor 2–overexpressing tumors received 1 year of adjuvant trastuzumab treatment.
Patients were evaluated every 12 weeks during the first 2 years of treatment and then every 6 months.
A total of 1,421 patients (78.2%) completed ibandronate treatment as planned, 5.8% discontinued treatment due to progression or death, and 16% discontinued treatment for various reasons. There were 405 events, including 186 deaths, after a median of 38.7 months (range, 0-73 months) with a completeness of follow-up of 76.8%.
The study was supported by Amgen, Germany; Bristol-Myers Squibb, Germany; and Roche, Germany, which also provided drugs for the study. Dr. von Minckwitz reported ties with Roche. His colleagues noted ties with numerous drug companies.
Two years of adjuvant treatment with ibandronate after dose-dense chemotherapy did not improve survival in a study of more than 3,000 German patients with early stage, node-positive breast cancer.
The results were published online Aug. 26 in the Journal of Clinical Oncology.
Bisphosphonates have been shown to prevent skeletal-related events in patients with metastatic breast cancer, but their effectiveness has not been demonstrated in early breast cancer.
No differences in disease-free survival or overall survival were noted in the GAIN (German Adjuvant Intergroup Node-Positive) study, an open-label, randomized, controlled phase III trial (NCT00196872), reported Dr. Gunter von Minckwitz of the German Breast Group, along with his colleagues in the German Breast Group/Gynecologic Oncology Working Group/North-Eastern Germany Society of Gynecologic Oncology study groups.
In patients randomly assigned to 2 years of ibandronate or observation, there was no difference in disease-free survival (HR, 0.945; 95% CI, 0.768 to 1.161; P equals .589) or in overall survival (HR, 1.040; 95% CI, 0.763 to 1.419; P equals .803). Metastasis to the bone was documented in 31% in the ibandronate arm and in 38% in the observation arm.
Post hoc subgroup analyses of the study data imply that the benefit of adjuvant bisphosphonates was restricted to patients with low estrogen levels, either because of medical ovarian suppression or definite menopause. Future meta-analyses on an individual patient data level may reliably reveal subgroups of early-stage, high-risk breast cancer patients who might benefit from adjuvant bisphosphonates, the researchers noted (J. Clin. Oncol. 2013 Aug. 26 [doi:10.1200/JCO.2012.47.2167]).
In GAIN, patients with node-positive early breast cancer were randomly assigned within 4 weeks after surgery to two different dose-dense chemotherapy regimens and then in 2:1 fashion to ibandronate 50 mg per day orally starting within 4 weeks after last administration of chemotherapy and continuing for 2 years (2,015 patients) or to observation (1,008 patients).
Randomly assigned chemotherapy consisted of three courses of epirubicin 150 mg/m2 followed by three courses of paclitaxel 225 mg/m2 followed by three courses of cyclophosphamide 2,500 mg/m2 (reduced to 2,000 mg/m2 after recruitment of approximately 1,200 patients), all given at 2-week intervals (iddETC regimen) or epirubicin 112.5 mg/m2 and cyclophosphamide 600 mg/m2 for four 2-week courses followed by 10 courses of paclitaxel 67.5 mg/m2 given once per week with capecitabine 2,000 mg/m2 given days 1-14 every 3 weeks (EC-TX regimen).
Radiotherapy, endocrine treatment, and trastuzumab were indicated according to AGO guidelines and, if appropriate, were given in parallel with ibandronate after the end of chemotherapy. All patients received radiotherapy to the affected breast if breast-conserving surgery was performed, the researchers wrote.
Patients with endocrine-sensitive disease received endocrine treatment for 5 years with an aromatase inhibitor either alone or in sequence with tamoxifen if they were postmenopausal. Tamoxifen alone was given for 5 years in some patients together with a luteinizing hormone-releasing hormone (LHRH) analog if they were premenopausal after the end of chemotherapy. Patients with human epidermal growth factor receptor 2–overexpressing tumors received 1 year of adjuvant trastuzumab treatment.
Patients were evaluated every 12 weeks during the first 2 years of treatment and then every 6 months.
A total of 1,421 patients (78.2%) completed ibandronate treatment as planned, 5.8% discontinued treatment due to progression or death, and 16% discontinued treatment for various reasons. There were 405 events, including 186 deaths, after a median of 38.7 months (range, 0-73 months) with a completeness of follow-up of 76.8%.
The study was supported by Amgen, Germany; Bristol-Myers Squibb, Germany; and Roche, Germany, which also provided drugs for the study. Dr. von Minckwitz reported ties with Roche. His colleagues noted ties with numerous drug companies.
Two years of adjuvant treatment with ibandronate after dose-dense chemotherapy did not improve survival in a study of more than 3,000 German patients with early stage, node-positive breast cancer.
The results were published online Aug. 26 in the Journal of Clinical Oncology.
Bisphosphonates have been shown to prevent skeletal-related events in patients with metastatic breast cancer, but their effectiveness has not been demonstrated in early breast cancer.
No differences in disease-free survival or overall survival were noted in the GAIN (German Adjuvant Intergroup Node-Positive) study, an open-label, randomized, controlled phase III trial (NCT00196872), reported Dr. Gunter von Minckwitz of the German Breast Group, along with his colleagues in the German Breast Group/Gynecologic Oncology Working Group/North-Eastern Germany Society of Gynecologic Oncology study groups.
In patients randomly assigned to 2 years of ibandronate or observation, there was no difference in disease-free survival (HR, 0.945; 95% CI, 0.768 to 1.161; P equals .589) or in overall survival (HR, 1.040; 95% CI, 0.763 to 1.419; P equals .803). Metastasis to the bone was documented in 31% in the ibandronate arm and in 38% in the observation arm.
Post hoc subgroup analyses of the study data imply that the benefit of adjuvant bisphosphonates was restricted to patients with low estrogen levels, either because of medical ovarian suppression or definite menopause. Future meta-analyses on an individual patient data level may reliably reveal subgroups of early-stage, high-risk breast cancer patients who might benefit from adjuvant bisphosphonates, the researchers noted (J. Clin. Oncol. 2013 Aug. 26 [doi:10.1200/JCO.2012.47.2167]).
In GAIN, patients with node-positive early breast cancer were randomly assigned within 4 weeks after surgery to two different dose-dense chemotherapy regimens and then in 2:1 fashion to ibandronate 50 mg per day orally starting within 4 weeks after last administration of chemotherapy and continuing for 2 years (2,015 patients) or to observation (1,008 patients).
Randomly assigned chemotherapy consisted of three courses of epirubicin 150 mg/m2 followed by three courses of paclitaxel 225 mg/m2 followed by three courses of cyclophosphamide 2,500 mg/m2 (reduced to 2,000 mg/m2 after recruitment of approximately 1,200 patients), all given at 2-week intervals (iddETC regimen) or epirubicin 112.5 mg/m2 and cyclophosphamide 600 mg/m2 for four 2-week courses followed by 10 courses of paclitaxel 67.5 mg/m2 given once per week with capecitabine 2,000 mg/m2 given days 1-14 every 3 weeks (EC-TX regimen).
Radiotherapy, endocrine treatment, and trastuzumab were indicated according to AGO guidelines and, if appropriate, were given in parallel with ibandronate after the end of chemotherapy. All patients received radiotherapy to the affected breast if breast-conserving surgery was performed, the researchers wrote.
Patients with endocrine-sensitive disease received endocrine treatment for 5 years with an aromatase inhibitor either alone or in sequence with tamoxifen if they were postmenopausal. Tamoxifen alone was given for 5 years in some patients together with a luteinizing hormone-releasing hormone (LHRH) analog if they were premenopausal after the end of chemotherapy. Patients with human epidermal growth factor receptor 2–overexpressing tumors received 1 year of adjuvant trastuzumab treatment.
Patients were evaluated every 12 weeks during the first 2 years of treatment and then every 6 months.
A total of 1,421 patients (78.2%) completed ibandronate treatment as planned, 5.8% discontinued treatment due to progression or death, and 16% discontinued treatment for various reasons. There were 405 events, including 186 deaths, after a median of 38.7 months (range, 0-73 months) with a completeness of follow-up of 76.8%.
The study was supported by Amgen, Germany; Bristol-Myers Squibb, Germany; and Roche, Germany, which also provided drugs for the study. Dr. von Minckwitz reported ties with Roche. His colleagues noted ties with numerous drug companies.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Major finding: In patients randomly assigned to 2 years of ibandronate or observation, there was no difference in disease-free survival (HR, 0.945; 95% CI, 0.768 to 1.161; P equals .589) or in overall survival (HR, 1.040; 95% CI, 0.763 to 1.419; P equals .803).
Data source: GAIN (German Adjuvant Intergroup Node-Positive) study, an open-label, randomized, controlled phase III trial comprising more than 3,000 patients.
Disclosures: The study was supported by Amgen, Germany; Bristol-Myers Squibb, Germany; and Roche, Germany which also provided drugs for the study. Dr. von Minckwitz reported ties with Roche. His colleagues noted ties with numerous drug companies.