User login
Breast MRI screening finds undetected cancers in 11 per 1,000 average-risk women
SAN ANTONIO – MRI screening of women who were at average risk of breast cancer and had a negative screening mammogram resulted in the diagnosis of 11 cases of cancer per 1,000 women screened, Dr. Simone Schrading said at the San Antonio Breast Cancer Symposium.
"The additional cancer detection rate is high, even in heavily prescreened women. In experienced hands, the positive predictive value of MRI screening in this average-risk cohort was comparable to that seen in mammographic screening programs or in MRI high-risk screening cohorts," said Dr. Schrading, of the University of Aachen, Germany.
While MRI is well established as a screening method for women at high familial risk of breast cancer, there have been no data to support its use in average-risk women.

Dr. Schrading reported on a prospective, single-center study evaluating the additional cancer yield and accuracy of breast MRI screening in 1,725 women at average risk for breast cancer. All had normal clinical breast examinations and digital screening mammograms. In addition, 89% of the women had undergone high-frequency breast ultrasound screening, which was normal in all cases. None of the subjects had a personal or family history of breast or ovarian cancer, and none had been diagnosed with breast proliferative changes or atypia. Their mean age was 55 years (range, 42-71 years).
MRI screening detected breast cancers in 18 of these patients, for a detection rate of 11 per 1,000 screened. Seven malignancies were ductal carcinoma in situ, and the other 11 were invasive breast cancer. The mean size of the invasive cancers was 11 mm. Five of the 7 ductal carcinomas in situ and 6 of 11 invasive cancers were high-grade cancers. On the other hand, the stage distribution of the invasive cancers was favorable: All were staged as pN0, M0.
Nearly 91% of screening MRIs were negative as defined by a BIRADS 1 or 2 rating. Another 5.9% were rated BIRADS 3; follow-up MRIs in this group of patients showed no breast cancers. Suspicious lesions – that is, BIRADS 4 or 5 – were noted in 54 patients, or 3.2% of the study group, and they were evaluated by MRI-guided biopsy. The lesions proved benign in 28 of 54 cases, high risk in 8, and malignant in 18.
Thus, the positive predictive value of breast MRI screening in this average-risk, extensively prescreened population was 33% if only BIRADS 4 and 5 cancers were defined as true positives, and 48% if BIRADS 4 and 5 high-risk lesions were also counted.
The age distribution of the patients with MRI-detected breast cancers was similar to that of the total study population. Mammographic breast density did not predict the likelihood of identifying breast cancer by MRI.
Dr. Laura J. Esserman rose from the audience to question the cost-benefit ratio of introducing MRI screening for the vast population of average-risk women.
The aggregate cost of breast cancer screening in the United States is already at least $8 billion annually. Utilizing MRI to screen average-risk women would push that figure up by an order of magnitude, observed Dr. Esserman, professor of surgery and of radiology and director of the Carol Franc Buck Breast Care Center at the University of California, San Francisco.
"MRI screening is still very expensive, it’s true," Dr. Schrading replied. "The main reason for the high cost of MRI is the long acquisition time and the long reading time. The long acquisition time is because the MRI protocols we have today are designed for diagnostic purposes, not for the purpose of screening. Our goal is to use a screening protocol for MRI, where the acquisition time is only 3 minutes and the reading time is less than 30 seconds. This might be a way to reduce the cost of MRI," she said.
The study was conducted free of commercial support. Dr. Schrading declared having no financial conflicts of interest.
SAN ANTONIO – MRI screening of women who were at average risk of breast cancer and had a negative screening mammogram resulted in the diagnosis of 11 cases of cancer per 1,000 women screened, Dr. Simone Schrading said at the San Antonio Breast Cancer Symposium.
"The additional cancer detection rate is high, even in heavily prescreened women. In experienced hands, the positive predictive value of MRI screening in this average-risk cohort was comparable to that seen in mammographic screening programs or in MRI high-risk screening cohorts," said Dr. Schrading, of the University of Aachen, Germany.
While MRI is well established as a screening method for women at high familial risk of breast cancer, there have been no data to support its use in average-risk women.
Dr. Schrading reported on a prospective, single-center study evaluating the additional cancer yield and accuracy of breast MRI screening in 1,725 women at average risk for breast cancer. All had normal clinical breast examinations and digital screening mammograms. In addition, 89% of the women had undergone high-frequency breast ultrasound screening, which was normal in all cases. None of the subjects had a personal or family history of breast or ovarian cancer, and none had been diagnosed with breast proliferative changes or atypia. Their mean age was 55 years (range, 42-71 years).
MRI screening detected breast cancers in 18 of these patients, for a detection rate of 11 per 1,000 screened. Seven malignancies were ductal carcinoma in situ, and the other 11 were invasive breast cancer. The mean size of the invasive cancers was 11 mm. Five of the 7 ductal carcinomas in situ and 6 of 11 invasive cancers were high-grade cancers. On the other hand, the stage distribution of the invasive cancers was favorable: All were staged as pN0, M0.
Nearly 91% of screening MRIs were negative as defined by a BIRADS 1 or 2 rating. Another 5.9% were rated BIRADS 3; follow-up MRIs in this group of patients showed no breast cancers. Suspicious lesions – that is, BIRADS 4 or 5 – were noted in 54 patients, or 3.2% of the study group, and they were evaluated by MRI-guided biopsy. The lesions proved benign in 28 of 54 cases, high risk in 8, and malignant in 18.
Thus, the positive predictive value of breast MRI screening in this average-risk, extensively prescreened population was 33% if only BIRADS 4 and 5 cancers were defined as true positives, and 48% if BIRADS 4 and 5 high-risk lesions were also counted.
The age distribution of the patients with MRI-detected breast cancers was similar to that of the total study population. Mammographic breast density did not predict the likelihood of identifying breast cancer by MRI.
Dr. Laura J. Esserman rose from the audience to question the cost-benefit ratio of introducing MRI screening for the vast population of average-risk women.
The aggregate cost of breast cancer screening in the United States is already at least $8 billion annually. Utilizing MRI to screen average-risk women would push that figure up by an order of magnitude, observed Dr. Esserman, professor of surgery and of radiology and director of the Carol Franc Buck Breast Care Center at the University of California, San Francisco.
"MRI screening is still very expensive, it’s true," Dr. Schrading replied. "The main reason for the high cost of MRI is the long acquisition time and the long reading time. The long acquisition time is because the MRI protocols we have today are designed for diagnostic purposes, not for the purpose of screening. Our goal is to use a screening protocol for MRI, where the acquisition time is only 3 minutes and the reading time is less than 30 seconds. This might be a way to reduce the cost of MRI," she said.
The study was conducted free of commercial support. Dr. Schrading declared having no financial conflicts of interest.
SAN ANTONIO – MRI screening of women who were at average risk of breast cancer and had a negative screening mammogram resulted in the diagnosis of 11 cases of cancer per 1,000 women screened, Dr. Simone Schrading said at the San Antonio Breast Cancer Symposium.
"The additional cancer detection rate is high, even in heavily prescreened women. In experienced hands, the positive predictive value of MRI screening in this average-risk cohort was comparable to that seen in mammographic screening programs or in MRI high-risk screening cohorts," said Dr. Schrading, of the University of Aachen, Germany.
While MRI is well established as a screening method for women at high familial risk of breast cancer, there have been no data to support its use in average-risk women.
Dr. Schrading reported on a prospective, single-center study evaluating the additional cancer yield and accuracy of breast MRI screening in 1,725 women at average risk for breast cancer. All had normal clinical breast examinations and digital screening mammograms. In addition, 89% of the women had undergone high-frequency breast ultrasound screening, which was normal in all cases. None of the subjects had a personal or family history of breast or ovarian cancer, and none had been diagnosed with breast proliferative changes or atypia. Their mean age was 55 years (range, 42-71 years).
MRI screening detected breast cancers in 18 of these patients, for a detection rate of 11 per 1,000 screened. Seven malignancies were ductal carcinoma in situ, and the other 11 were invasive breast cancer. The mean size of the invasive cancers was 11 mm. Five of the 7 ductal carcinomas in situ and 6 of 11 invasive cancers were high-grade cancers. On the other hand, the stage distribution of the invasive cancers was favorable: All were staged as pN0, M0.
Nearly 91% of screening MRIs were negative as defined by a BIRADS 1 or 2 rating. Another 5.9% were rated BIRADS 3; follow-up MRIs in this group of patients showed no breast cancers. Suspicious lesions – that is, BIRADS 4 or 5 – were noted in 54 patients, or 3.2% of the study group, and they were evaluated by MRI-guided biopsy. The lesions proved benign in 28 of 54 cases, high risk in 8, and malignant in 18.
Thus, the positive predictive value of breast MRI screening in this average-risk, extensively prescreened population was 33% if only BIRADS 4 and 5 cancers were defined as true positives, and 48% if BIRADS 4 and 5 high-risk lesions were also counted.
The age distribution of the patients with MRI-detected breast cancers was similar to that of the total study population. Mammographic breast density did not predict the likelihood of identifying breast cancer by MRI.
Dr. Laura J. Esserman rose from the audience to question the cost-benefit ratio of introducing MRI screening for the vast population of average-risk women.
The aggregate cost of breast cancer screening in the United States is already at least $8 billion annually. Utilizing MRI to screen average-risk women would push that figure up by an order of magnitude, observed Dr. Esserman, professor of surgery and of radiology and director of the Carol Franc Buck Breast Care Center at the University of California, San Francisco.
"MRI screening is still very expensive, it’s true," Dr. Schrading replied. "The main reason for the high cost of MRI is the long acquisition time and the long reading time. The long acquisition time is because the MRI protocols we have today are designed for diagnostic purposes, not for the purpose of screening. Our goal is to use a screening protocol for MRI, where the acquisition time is only 3 minutes and the reading time is less than 30 seconds. This might be a way to reduce the cost of MRI," she said.
The study was conducted free of commercial support. Dr. Schrading declared having no financial conflicts of interest.
AT SABCS 2013
Major finding: Breast MRI screening of women who were at average risk for breast cancer and already had a negative mammogram had a breast cancer detection rate of 11 cases per 1,000 women screened.
Data source: This was a prospective, uncontrolled, single-center study of breast MRI screening in 1,725 women with no personal or family history of breast or ovarian cancer, no diagnosis of proliferative changes, and a mean age of 55 years.
Disclosures: The study was conducted free of commercial support. Dr. Schrading declared having no financial conflicts of interest.

Add-on agents boost neoadjuvant chemo response in triple-negative disease
SAN ANTONIO – When added to standard neoadjuvant chemotherapy, carboplatin and bevacizumab each improve the odds of eradicating local disease in women with triple-negative breast cancer, but their impact on toxicity differs, based on findings from a randomized phase II trial.
Adding carboplatin to standard chemotherapy improved the odds of pathologic complete response (pCR) by 71%-76% with some increase in toxicity such as neutropenia and thrombocytopenia. Adding the antiangiogenic agent bevacizumab improved the odds of pCR by 58%, but with a considerable increase in toxicity such as hypertension and postoperative complications, based on results of the Cancer and Leukemia Group B (CALGB)/Alliance 40603 trial of 443 women with stage II or III triple-negative breast cancer. Dr. William M. Sikov reported the results in a session and at a press briefing at the San Antonio Breast Cancer Symposium.

Dr. Sikov of Warren Alpert Medical School of Brown University, Providence, R.I., acknowledged that the trial was not powered to assess recurrence-free and overall survivals. While it remains unclear whether pCR predicts improved survival, data from other trials and a meta-analysis suggest that pCR is a good surrogate endpoint and have prompted the Food and Drug Administration to consider this endpoint for new drug approval pending long-term data.
Based on the results from this trial and those of the similar GeparSixto trial reported at the 2013 ASCO annual meeting, he said, "if you have decided a patient with triple-negative breast cancer should receive neoadjuvant chemotherapy based on the size of the tumor, based on the desire to improve the chance of breast conservation, then I think it makes sense to add carboplatin to your neoadjuvant regimen, and that you can comfortably do so with acceptable additional toxicities."
Alternatively, Dr. Sikov said that bevacizumab "increased the pCR rate, but at the cost of significant toxicities, and I don’t think that [bevacizumab] should be routinely added to neoadjuvant chemotherapy."
In the CALGB/Alliance 40603 trial, which was funded in part by Genentech, about three-fourths of the women were white, and roughly two-thirds had clinical stage II disease; 55% had clinically positive nodes.
All of the women were treated with weekly paclitaxel followed by dose-dense AC (doxorubicin and cyclophosphamide).
In a 2-by-2 factorial design, patients were randomized to additionally receive carboplatin or not, and to additionally receive bevacizumab (Avastin) or not.
Adding carboplatin increased the rate of pCR in the breast only (60% vs. 46%; odds ratio, 1.76; P = .002) and pCR in both the breast and axilla (54% vs. 41%; odds ratio, 1.71; P = .003).
Similarly, adding bevacizumab increased the rate of pCR in the breast only (59% vs. 48%; odds ratio, 1.58; P = .009) but conferred only a trend toward an increased rate of pCR in both the breast and axilla (52% vs. 44%; odds ratio, 1.36; P = .057).
There was no significant interaction between the treatment effect of carboplatin and the treatment effect of bevacizumab, according to Dr. Sikov, who disclosed no conflicts of interest related to the trial.
In terms of toxicity, adding carboplatin increased rates of grade 3 or worse neutropenia and thrombocytopenia. Adding bevacizumab increased rates of grade 3 or worse hypertension, bleeding, and thrombosis. And adding both drugs increased rates of both sets of adverse events, with a higher rate of grade 3 or worse febrile neutropenia.
Serious adverse events were more common with added bevacizumab and with added carboplatin-bevacizumab. For example, 15% and 16% of patients in these arms, respectively, developed febrile neutropenia during receipt of the AC part of chemotherapy.
Also, addition of bevacizumab was associated with a higher rate of postsurgical complications (9% vs. 5%), most often hematoma or seroma, and a higher rate of delayed surgical complications (4% vs. 1%), such as wound healing issues.
Three randomized neoadjuvant studies – CALGB 40603, GeparSixto, and I-SPY 2 – have now established that inclusion of carboplatin increases pCR rate in triple-negative disease. This provides a valuable new treatment option for patients with high-risk triple-negative disease.
The impact on survival may be modest but real, I believe. Patient-level benefits other than survival also exist that can be derived from a more effective neoadjuvant chemotherapy, such as the potential for lesser surgery and tailored adjuvant therapy.
The variable and inconsistent results from the three randomized neoadjuvant studies [testing bevacizumab], including the CALGB 40603, and the disappointing survival results in both metastatic and adjuvant trials, indicate no current role for bevacizumab in the routine practice in breast cancer. However, this also suggests that a small and elusive subset of patients do benefit from this therapy, but their identification remains a challenge.
Dr. Lajos Pusztai is with the Yale Cancer Center and Smilow Cancer Hospital in New Haven, Conn. He was the discussant of the study at the meeting and had no relevant financial disclosures.
Three randomized neoadjuvant studies – CALGB 40603, GeparSixto, and I-SPY 2 – have now established that inclusion of carboplatin increases pCR rate in triple-negative disease. This provides a valuable new treatment option for patients with high-risk triple-negative disease.
The impact on survival may be modest but real, I believe. Patient-level benefits other than survival also exist that can be derived from a more effective neoadjuvant chemotherapy, such as the potential for lesser surgery and tailored adjuvant therapy.
The variable and inconsistent results from the three randomized neoadjuvant studies [testing bevacizumab], including the CALGB 40603, and the disappointing survival results in both metastatic and adjuvant trials, indicate no current role for bevacizumab in the routine practice in breast cancer. However, this also suggests that a small and elusive subset of patients do benefit from this therapy, but their identification remains a challenge.
Dr. Lajos Pusztai is with the Yale Cancer Center and Smilow Cancer Hospital in New Haven, Conn. He was the discussant of the study at the meeting and had no relevant financial disclosures.
Three randomized neoadjuvant studies – CALGB 40603, GeparSixto, and I-SPY 2 – have now established that inclusion of carboplatin increases pCR rate in triple-negative disease. This provides a valuable new treatment option for patients with high-risk triple-negative disease.
The impact on survival may be modest but real, I believe. Patient-level benefits other than survival also exist that can be derived from a more effective neoadjuvant chemotherapy, such as the potential for lesser surgery and tailored adjuvant therapy.
The variable and inconsistent results from the three randomized neoadjuvant studies [testing bevacizumab], including the CALGB 40603, and the disappointing survival results in both metastatic and adjuvant trials, indicate no current role for bevacizumab in the routine practice in breast cancer. However, this also suggests that a small and elusive subset of patients do benefit from this therapy, but their identification remains a challenge.
Dr. Lajos Pusztai is with the Yale Cancer Center and Smilow Cancer Hospital in New Haven, Conn. He was the discussant of the study at the meeting and had no relevant financial disclosures.
SAN ANTONIO – When added to standard neoadjuvant chemotherapy, carboplatin and bevacizumab each improve the odds of eradicating local disease in women with triple-negative breast cancer, but their impact on toxicity differs, based on findings from a randomized phase II trial.
Adding carboplatin to standard chemotherapy improved the odds of pathologic complete response (pCR) by 71%-76% with some increase in toxicity such as neutropenia and thrombocytopenia. Adding the antiangiogenic agent bevacizumab improved the odds of pCR by 58%, but with a considerable increase in toxicity such as hypertension and postoperative complications, based on results of the Cancer and Leukemia Group B (CALGB)/Alliance 40603 trial of 443 women with stage II or III triple-negative breast cancer. Dr. William M. Sikov reported the results in a session and at a press briefing at the San Antonio Breast Cancer Symposium.
Dr. Sikov of Warren Alpert Medical School of Brown University, Providence, R.I., acknowledged that the trial was not powered to assess recurrence-free and overall survivals. While it remains unclear whether pCR predicts improved survival, data from other trials and a meta-analysis suggest that pCR is a good surrogate endpoint and have prompted the Food and Drug Administration to consider this endpoint for new drug approval pending long-term data.
Based on the results from this trial and those of the similar GeparSixto trial reported at the 2013 ASCO annual meeting, he said, "if you have decided a patient with triple-negative breast cancer should receive neoadjuvant chemotherapy based on the size of the tumor, based on the desire to improve the chance of breast conservation, then I think it makes sense to add carboplatin to your neoadjuvant regimen, and that you can comfortably do so with acceptable additional toxicities."
Alternatively, Dr. Sikov said that bevacizumab "increased the pCR rate, but at the cost of significant toxicities, and I don’t think that [bevacizumab] should be routinely added to neoadjuvant chemotherapy."
In the CALGB/Alliance 40603 trial, which was funded in part by Genentech, about three-fourths of the women were white, and roughly two-thirds had clinical stage II disease; 55% had clinically positive nodes.
All of the women were treated with weekly paclitaxel followed by dose-dense AC (doxorubicin and cyclophosphamide).
In a 2-by-2 factorial design, patients were randomized to additionally receive carboplatin or not, and to additionally receive bevacizumab (Avastin) or not.
Adding carboplatin increased the rate of pCR in the breast only (60% vs. 46%; odds ratio, 1.76; P = .002) and pCR in both the breast and axilla (54% vs. 41%; odds ratio, 1.71; P = .003).
Similarly, adding bevacizumab increased the rate of pCR in the breast only (59% vs. 48%; odds ratio, 1.58; P = .009) but conferred only a trend toward an increased rate of pCR in both the breast and axilla (52% vs. 44%; odds ratio, 1.36; P = .057).
There was no significant interaction between the treatment effect of carboplatin and the treatment effect of bevacizumab, according to Dr. Sikov, who disclosed no conflicts of interest related to the trial.
In terms of toxicity, adding carboplatin increased rates of grade 3 or worse neutropenia and thrombocytopenia. Adding bevacizumab increased rates of grade 3 or worse hypertension, bleeding, and thrombosis. And adding both drugs increased rates of both sets of adverse events, with a higher rate of grade 3 or worse febrile neutropenia.
Serious adverse events were more common with added bevacizumab and with added carboplatin-bevacizumab. For example, 15% and 16% of patients in these arms, respectively, developed febrile neutropenia during receipt of the AC part of chemotherapy.
Also, addition of bevacizumab was associated with a higher rate of postsurgical complications (9% vs. 5%), most often hematoma or seroma, and a higher rate of delayed surgical complications (4% vs. 1%), such as wound healing issues.
SAN ANTONIO – When added to standard neoadjuvant chemotherapy, carboplatin and bevacizumab each improve the odds of eradicating local disease in women with triple-negative breast cancer, but their impact on toxicity differs, based on findings from a randomized phase II trial.
Adding carboplatin to standard chemotherapy improved the odds of pathologic complete response (pCR) by 71%-76% with some increase in toxicity such as neutropenia and thrombocytopenia. Adding the antiangiogenic agent bevacizumab improved the odds of pCR by 58%, but with a considerable increase in toxicity such as hypertension and postoperative complications, based on results of the Cancer and Leukemia Group B (CALGB)/Alliance 40603 trial of 443 women with stage II or III triple-negative breast cancer. Dr. William M. Sikov reported the results in a session and at a press briefing at the San Antonio Breast Cancer Symposium.
Dr. Sikov of Warren Alpert Medical School of Brown University, Providence, R.I., acknowledged that the trial was not powered to assess recurrence-free and overall survivals. While it remains unclear whether pCR predicts improved survival, data from other trials and a meta-analysis suggest that pCR is a good surrogate endpoint and have prompted the Food and Drug Administration to consider this endpoint for new drug approval pending long-term data.
Based on the results from this trial and those of the similar GeparSixto trial reported at the 2013 ASCO annual meeting, he said, "if you have decided a patient with triple-negative breast cancer should receive neoadjuvant chemotherapy based on the size of the tumor, based on the desire to improve the chance of breast conservation, then I think it makes sense to add carboplatin to your neoadjuvant regimen, and that you can comfortably do so with acceptable additional toxicities."
Alternatively, Dr. Sikov said that bevacizumab "increased the pCR rate, but at the cost of significant toxicities, and I don’t think that [bevacizumab] should be routinely added to neoadjuvant chemotherapy."
In the CALGB/Alliance 40603 trial, which was funded in part by Genentech, about three-fourths of the women were white, and roughly two-thirds had clinical stage II disease; 55% had clinically positive nodes.
All of the women were treated with weekly paclitaxel followed by dose-dense AC (doxorubicin and cyclophosphamide).
In a 2-by-2 factorial design, patients were randomized to additionally receive carboplatin or not, and to additionally receive bevacizumab (Avastin) or not.
Adding carboplatin increased the rate of pCR in the breast only (60% vs. 46%; odds ratio, 1.76; P = .002) and pCR in both the breast and axilla (54% vs. 41%; odds ratio, 1.71; P = .003).
Similarly, adding bevacizumab increased the rate of pCR in the breast only (59% vs. 48%; odds ratio, 1.58; P = .009) but conferred only a trend toward an increased rate of pCR in both the breast and axilla (52% vs. 44%; odds ratio, 1.36; P = .057).
There was no significant interaction between the treatment effect of carboplatin and the treatment effect of bevacizumab, according to Dr. Sikov, who disclosed no conflicts of interest related to the trial.
In terms of toxicity, adding carboplatin increased rates of grade 3 or worse neutropenia and thrombocytopenia. Adding bevacizumab increased rates of grade 3 or worse hypertension, bleeding, and thrombosis. And adding both drugs increased rates of both sets of adverse events, with a higher rate of grade 3 or worse febrile neutropenia.
Serious adverse events were more common with added bevacizumab and with added carboplatin-bevacizumab. For example, 15% and 16% of patients in these arms, respectively, developed febrile neutropenia during receipt of the AC part of chemotherapy.
Also, addition of bevacizumab was associated with a higher rate of postsurgical complications (9% vs. 5%), most often hematoma or seroma, and a higher rate of delayed surgical complications (4% vs. 1%), such as wound healing issues.
AT SABCS 2013
Major finding: Carboplatin improved the odds of pCR by 71%-76% with some additional toxicity; bevacizumab improved the odds of pCR by 58% with considerable additional toxicity.
Data Source: A randomized phase II trial testing addition of carboplatin and/or bevacizumab to neoadjuvant chemotherapy in 443 women with stage II or III triple-negative breast cancer (the CALGB/Alliance 40603 trial).
Disclosures: Dr. Sikov disclosed no conflicts of interest. The trial was funded in part by Genentech.

Meeting attendees identify top studies presented at SABCS
Live from the 2013 San Antonio Breast Cancer Symposium, our onsite reporters checked in with meeting attendees to find out the "most interesting thing" they had learned so far. From identifying predictive signatures via genomic data to treating postmenopausal women with bisphosphonates, passing oncologists shared their favorite, potentially practice-changing highlights.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Live from the 2013 San Antonio Breast Cancer Symposium, our onsite reporters checked in with meeting attendees to find out the "most interesting thing" they had learned so far. From identifying predictive signatures via genomic data to treating postmenopausal women with bisphosphonates, passing oncologists shared their favorite, potentially practice-changing highlights.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Live from the 2013 San Antonio Breast Cancer Symposium, our onsite reporters checked in with meeting attendees to find out the "most interesting thing" they had learned so far. From identifying predictive signatures via genomic data to treating postmenopausal women with bisphosphonates, passing oncologists shared their favorite, potentially practice-changing highlights.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
'Vogl, New York' offers San Antonio perspectives
In an interview with Frontline Medical News, New York oncologist and San Antonio Breast Cancer Symposium star gadfly Dr. Steven Vogl gives his quick take on several of the studies making news at this year's meeting.
In an interview with Frontline Medical News, New York oncologist and San Antonio Breast Cancer Symposium star gadfly Dr. Steven Vogl gives his quick take on several of the studies making news at this year's meeting.
In an interview with Frontline Medical News, New York oncologist and San Antonio Breast Cancer Symposium star gadfly Dr. Steven Vogl gives his quick take on several of the studies making news at this year's meeting.

Veliparib-carboplatin combo is first 'graduate' of I-SPY2 trial
SAN ANTONIO – The combination of veliparib and carboplatin is the first "graduate" of the I-SPY 2 trial, investigators reported at the San Antonio Breast Cancer Symposium.
The phase 2 trial uses an adaptive design to screen novel agents and regimens by assessing whether they improve response when added to neoadjuvant chemotherapy, with the aim of matching them to breast cancer biomarker signatures most likely to respond.
The novel agents or regimens graduate, or meet the bar for further testing, if there is a 85% probability or better that they will be superior to chemotherapy alone for at least one signature in a modestly sized phase 3 neoadjuvant trial.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
First results from 115 patients, reported in a session and press briefing by lead author Dr. Hope S. Rugo, showed that based on the estimated pathologic complete responses (pCRs) seen, there was a 90% probability that the combination of veliparib—an oral investigational inhibitor of poly-ADP-ribose, or PARP—and carboplatin added to chemotherapy would be superior to chemotherapy alone among patients with triple-negative disease.
In contrast, the probability in all patients with HER2-negative disease was only slightly better than a coin toss. And the probability in the subset with hormone receptor–positive, HER2-negative disease was less than one in 10.

"Veliparib and carboplatin has graduated with the triple-negative signature, the subset recommended for this drug’s subsequent development," said Dr. Rugo, who is a professor of medicine and director of breast oncology and clinical trials education at the UCSF Helen Diller Family Comprehensive Cancer Center in San Francisco.
"We identified a biomarker signature–drug pair for veliparib and carboplatin on the basis of a modest number of patients...This trial design will accelerate the process of identifying drugs that are effective for specific breast cancer subtypes and thereby reduce the cost, time, and numbers of patients needed to get effective drugs to market," she noted.
The trial was not designed to assess the contribution of each agent—veliparib (ABT-888, manufactured by AbbVie) and carboplatin—individually, Dr. Rugo acknowledged; regardless, their combination had a large effect size.
"I-SPY 2 is a biomarker-rich trial. Additional response predictors are under evaluation," such as BRCA status, she further noted.
"A lot of work has been done with the FDA [Food and Drug Administration] recently evaluating drugs for accelerated approval based on their response in the neoadjuvant setting. How this plays out in the future for other drugs [besides pertuzumab] remains to be seen," Dr. Rugo commented. "Clearly there needs to be a plan for outcome data that can correspond to the pCR rates in order for these drugs to obtain final approval. But there is the hope that this will be a mechanism for accelerated approval."
The trial has six other arms testing investigational regimens. Results for the arm that is testing neratinib (PB272, Puma Biotechnology), a tyrosine kinase inhibitor, are expected shortly.
Women are eligible for I-SPY 2 (Investigation of Serial Studies to Predict Your Therapeutic Response With Imaging And moLecular Analysis 2) if they have tumors measuring at least 2.5 cm. Those whose tumors have all of three favorable characteristics (hormone receptor positive, HER2 negative, and Low MammaPrint result) are excluded.
Eight biomarker signatures are created according to hormone receptor status, HER2 status, and MammaPrint result (High or Ultra High).
The trial uses adaptive randomization, whereby each patient’s MRI and pCR data are fed into an algorithm, affecting how the next patient is randomized. "This allows us to learn and adapt from each patient as we go along, and each new patient benefits from information obtained from the prior patient. In addition, this allows us to add and drop agents as we go along based on success of each agent or regimen," explained Dr. Rugo, who disclosed no conflicts of interest related to the trial.
Patients are randomized to receive weekly paclitaxel plus a novel agent/regimen or weekly paclitaxel alone—each followed by standard doxorubicin and cyclophosphamide (AC) chemotherapy and then surgery. The endpoint of pCR is defined as no residual cancer in the breast or lymph nodes at the time of surgery.
The results are used to predict the probability of superiority in a phase 3 neoadjuvant trial having just 300 patients and using pCR as its endpoint.
The findings that Dr. Rugo presented were based on 115 patients with HER2-negative disease: 71 randomized to veliparib-carboplatin plus chemotherapy and 44 randomized to chemotherapy alone.
Among patients with triple-negative disease, the estimated rate of pCR was 52% with veliparib-carboplatin and 26% without it. There was a 90% predictive probability that the combination with chemotherapy would be superior to chemotherapy alone in phase 3 testing in this subset.
In contrast, the difference in estimated pCR rates with addition of veliparib-carboplatin was much smaller among all patients with HER2-negative disease (33% vs. 22%) and in the opposite direction among the subset with hormone receptor–positive, HER2-negative disease (14% vs. 19%). The predictive probabilities that the combination with chemotherapy would be superior in phase 3 testing in these groups were just 55% and 9%, respectively.
"The toxicity was moderately increased as expected, but it was well managed with dose reduction and delay," Dr. Rugo reported.
Dr. Rugo disclosed no relevant conflicts of interest.
I would like to congratulate the first graduate from the I-SPY 2 trial.
The efficacy results with neoadjuvant carboplatin in the Cancer and Leukemia Group B (CALGB) 40603 trial, also presented at the symposium, are consistent with the I-SPY 2 prediction, with carboplatin really increasing pCR rates in triple-negative disease although direct cross-trial comparison is limited.
The rate of pCR was very similar, about 50%, in both trials with carboplatin-containing chemotherapy even though the former trial did not use veliparib. This suggests the contribution of veliparib is modest if any in this particular patient population.
What further complicates the interpretation is that the activity of veliparib is likely influenced by germline BRCA status and may also be dependent on the extent of somatic homologous DNA recombination defects in the tumor.
Two ongoing randomized trials will be especially important to clarifying the role of neoadjuvant veliparib in triple-negative breast cancer among BRCA carriers. Until these results are available, the value of veliparib to increase pCR rate in triple-negative disease remains uncertain.
Dr. Lajos Pusztai is with the Yale Cancer Center and Smilow Cancer Hospital in New Haven, Connecticut. He was the official discussant to the paper at the meeting.
I would like to congratulate the first graduate from the I-SPY 2 trial.
The efficacy results with neoadjuvant carboplatin in the Cancer and Leukemia Group B (CALGB) 40603 trial, also presented at the symposium, are consistent with the I-SPY 2 prediction, with carboplatin really increasing pCR rates in triple-negative disease although direct cross-trial comparison is limited.
The rate of pCR was very similar, about 50%, in both trials with carboplatin-containing chemotherapy even though the former trial did not use veliparib. This suggests the contribution of veliparib is modest if any in this particular patient population.
What further complicates the interpretation is that the activity of veliparib is likely influenced by germline BRCA status and may also be dependent on the extent of somatic homologous DNA recombination defects in the tumor.
Two ongoing randomized trials will be especially important to clarifying the role of neoadjuvant veliparib in triple-negative breast cancer among BRCA carriers. Until these results are available, the value of veliparib to increase pCR rate in triple-negative disease remains uncertain.
Dr. Lajos Pusztai is with the Yale Cancer Center and Smilow Cancer Hospital in New Haven, Connecticut. He was the official discussant to the paper at the meeting.
I would like to congratulate the first graduate from the I-SPY 2 trial.
The efficacy results with neoadjuvant carboplatin in the Cancer and Leukemia Group B (CALGB) 40603 trial, also presented at the symposium, are consistent with the I-SPY 2 prediction, with carboplatin really increasing pCR rates in triple-negative disease although direct cross-trial comparison is limited.
The rate of pCR was very similar, about 50%, in both trials with carboplatin-containing chemotherapy even though the former trial did not use veliparib. This suggests the contribution of veliparib is modest if any in this particular patient population.
What further complicates the interpretation is that the activity of veliparib is likely influenced by germline BRCA status and may also be dependent on the extent of somatic homologous DNA recombination defects in the tumor.
Two ongoing randomized trials will be especially important to clarifying the role of neoadjuvant veliparib in triple-negative breast cancer among BRCA carriers. Until these results are available, the value of veliparib to increase pCR rate in triple-negative disease remains uncertain.
Dr. Lajos Pusztai is with the Yale Cancer Center and Smilow Cancer Hospital in New Haven, Connecticut. He was the official discussant to the paper at the meeting.
SAN ANTONIO – The combination of veliparib and carboplatin is the first "graduate" of the I-SPY 2 trial, investigators reported at the San Antonio Breast Cancer Symposium.
The phase 2 trial uses an adaptive design to screen novel agents and regimens by assessing whether they improve response when added to neoadjuvant chemotherapy, with the aim of matching them to breast cancer biomarker signatures most likely to respond.
The novel agents or regimens graduate, or meet the bar for further testing, if there is a 85% probability or better that they will be superior to chemotherapy alone for at least one signature in a modestly sized phase 3 neoadjuvant trial.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
First results from 115 patients, reported in a session and press briefing by lead author Dr. Hope S. Rugo, showed that based on the estimated pathologic complete responses (pCRs) seen, there was a 90% probability that the combination of veliparib—an oral investigational inhibitor of poly-ADP-ribose, or PARP—and carboplatin added to chemotherapy would be superior to chemotherapy alone among patients with triple-negative disease.
In contrast, the probability in all patients with HER2-negative disease was only slightly better than a coin toss. And the probability in the subset with hormone receptor–positive, HER2-negative disease was less than one in 10.
"Veliparib and carboplatin has graduated with the triple-negative signature, the subset recommended for this drug’s subsequent development," said Dr. Rugo, who is a professor of medicine and director of breast oncology and clinical trials education at the UCSF Helen Diller Family Comprehensive Cancer Center in San Francisco.
"We identified a biomarker signature–drug pair for veliparib and carboplatin on the basis of a modest number of patients...This trial design will accelerate the process of identifying drugs that are effective for specific breast cancer subtypes and thereby reduce the cost, time, and numbers of patients needed to get effective drugs to market," she noted.
The trial was not designed to assess the contribution of each agent—veliparib (ABT-888, manufactured by AbbVie) and carboplatin—individually, Dr. Rugo acknowledged; regardless, their combination had a large effect size.
"I-SPY 2 is a biomarker-rich trial. Additional response predictors are under evaluation," such as BRCA status, she further noted.
"A lot of work has been done with the FDA [Food and Drug Administration] recently evaluating drugs for accelerated approval based on their response in the neoadjuvant setting. How this plays out in the future for other drugs [besides pertuzumab] remains to be seen," Dr. Rugo commented. "Clearly there needs to be a plan for outcome data that can correspond to the pCR rates in order for these drugs to obtain final approval. But there is the hope that this will be a mechanism for accelerated approval."
The trial has six other arms testing investigational regimens. Results for the arm that is testing neratinib (PB272, Puma Biotechnology), a tyrosine kinase inhibitor, are expected shortly.
Women are eligible for I-SPY 2 (Investigation of Serial Studies to Predict Your Therapeutic Response With Imaging And moLecular Analysis 2) if they have tumors measuring at least 2.5 cm. Those whose tumors have all of three favorable characteristics (hormone receptor positive, HER2 negative, and Low MammaPrint result) are excluded.
Eight biomarker signatures are created according to hormone receptor status, HER2 status, and MammaPrint result (High or Ultra High).
The trial uses adaptive randomization, whereby each patient’s MRI and pCR data are fed into an algorithm, affecting how the next patient is randomized. "This allows us to learn and adapt from each patient as we go along, and each new patient benefits from information obtained from the prior patient. In addition, this allows us to add and drop agents as we go along based on success of each agent or regimen," explained Dr. Rugo, who disclosed no conflicts of interest related to the trial.
Patients are randomized to receive weekly paclitaxel plus a novel agent/regimen or weekly paclitaxel alone—each followed by standard doxorubicin and cyclophosphamide (AC) chemotherapy and then surgery. The endpoint of pCR is defined as no residual cancer in the breast or lymph nodes at the time of surgery.
The results are used to predict the probability of superiority in a phase 3 neoadjuvant trial having just 300 patients and using pCR as its endpoint.
The findings that Dr. Rugo presented were based on 115 patients with HER2-negative disease: 71 randomized to veliparib-carboplatin plus chemotherapy and 44 randomized to chemotherapy alone.
Among patients with triple-negative disease, the estimated rate of pCR was 52% with veliparib-carboplatin and 26% without it. There was a 90% predictive probability that the combination with chemotherapy would be superior to chemotherapy alone in phase 3 testing in this subset.
In contrast, the difference in estimated pCR rates with addition of veliparib-carboplatin was much smaller among all patients with HER2-negative disease (33% vs. 22%) and in the opposite direction among the subset with hormone receptor–positive, HER2-negative disease (14% vs. 19%). The predictive probabilities that the combination with chemotherapy would be superior in phase 3 testing in these groups were just 55% and 9%, respectively.
"The toxicity was moderately increased as expected, but it was well managed with dose reduction and delay," Dr. Rugo reported.
Dr. Rugo disclosed no relevant conflicts of interest.
SAN ANTONIO – The combination of veliparib and carboplatin is the first "graduate" of the I-SPY 2 trial, investigators reported at the San Antonio Breast Cancer Symposium.
The phase 2 trial uses an adaptive design to screen novel agents and regimens by assessing whether they improve response when added to neoadjuvant chemotherapy, with the aim of matching them to breast cancer biomarker signatures most likely to respond.
The novel agents or regimens graduate, or meet the bar for further testing, if there is a 85% probability or better that they will be superior to chemotherapy alone for at least one signature in a modestly sized phase 3 neoadjuvant trial.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
First results from 115 patients, reported in a session and press briefing by lead author Dr. Hope S. Rugo, showed that based on the estimated pathologic complete responses (pCRs) seen, there was a 90% probability that the combination of veliparib—an oral investigational inhibitor of poly-ADP-ribose, or PARP—and carboplatin added to chemotherapy would be superior to chemotherapy alone among patients with triple-negative disease.
In contrast, the probability in all patients with HER2-negative disease was only slightly better than a coin toss. And the probability in the subset with hormone receptor–positive, HER2-negative disease was less than one in 10.
"Veliparib and carboplatin has graduated with the triple-negative signature, the subset recommended for this drug’s subsequent development," said Dr. Rugo, who is a professor of medicine and director of breast oncology and clinical trials education at the UCSF Helen Diller Family Comprehensive Cancer Center in San Francisco.
"We identified a biomarker signature–drug pair for veliparib and carboplatin on the basis of a modest number of patients...This trial design will accelerate the process of identifying drugs that are effective for specific breast cancer subtypes and thereby reduce the cost, time, and numbers of patients needed to get effective drugs to market," she noted.
The trial was not designed to assess the contribution of each agent—veliparib (ABT-888, manufactured by AbbVie) and carboplatin—individually, Dr. Rugo acknowledged; regardless, their combination had a large effect size.
"I-SPY 2 is a biomarker-rich trial. Additional response predictors are under evaluation," such as BRCA status, she further noted.
"A lot of work has been done with the FDA [Food and Drug Administration] recently evaluating drugs for accelerated approval based on their response in the neoadjuvant setting. How this plays out in the future for other drugs [besides pertuzumab] remains to be seen," Dr. Rugo commented. "Clearly there needs to be a plan for outcome data that can correspond to the pCR rates in order for these drugs to obtain final approval. But there is the hope that this will be a mechanism for accelerated approval."
The trial has six other arms testing investigational regimens. Results for the arm that is testing neratinib (PB272, Puma Biotechnology), a tyrosine kinase inhibitor, are expected shortly.
Women are eligible for I-SPY 2 (Investigation of Serial Studies to Predict Your Therapeutic Response With Imaging And moLecular Analysis 2) if they have tumors measuring at least 2.5 cm. Those whose tumors have all of three favorable characteristics (hormone receptor positive, HER2 negative, and Low MammaPrint result) are excluded.
Eight biomarker signatures are created according to hormone receptor status, HER2 status, and MammaPrint result (High or Ultra High).
The trial uses adaptive randomization, whereby each patient’s MRI and pCR data are fed into an algorithm, affecting how the next patient is randomized. "This allows us to learn and adapt from each patient as we go along, and each new patient benefits from information obtained from the prior patient. In addition, this allows us to add and drop agents as we go along based on success of each agent or regimen," explained Dr. Rugo, who disclosed no conflicts of interest related to the trial.
Patients are randomized to receive weekly paclitaxel plus a novel agent/regimen or weekly paclitaxel alone—each followed by standard doxorubicin and cyclophosphamide (AC) chemotherapy and then surgery. The endpoint of pCR is defined as no residual cancer in the breast or lymph nodes at the time of surgery.
The results are used to predict the probability of superiority in a phase 3 neoadjuvant trial having just 300 patients and using pCR as its endpoint.
The findings that Dr. Rugo presented were based on 115 patients with HER2-negative disease: 71 randomized to veliparib-carboplatin plus chemotherapy and 44 randomized to chemotherapy alone.
Among patients with triple-negative disease, the estimated rate of pCR was 52% with veliparib-carboplatin and 26% without it. There was a 90% predictive probability that the combination with chemotherapy would be superior to chemotherapy alone in phase 3 testing in this subset.
In contrast, the difference in estimated pCR rates with addition of veliparib-carboplatin was much smaller among all patients with HER2-negative disease (33% vs. 22%) and in the opposite direction among the subset with hormone receptor–positive, HER2-negative disease (14% vs. 19%). The predictive probabilities that the combination with chemotherapy would be superior in phase 3 testing in these groups were just 55% and 9%, respectively.
"The toxicity was moderately increased as expected, but it was well managed with dose reduction and delay," Dr. Rugo reported.
Dr. Rugo disclosed no relevant conflicts of interest.
AT SABCS 2013
Major finding: Among patients with triple-negative disease, there was a 90% predictive probability that veliparib-carboplatin added to chemotherapy would be superior to chemotherapy alone in a phase 3 neoadjuvant trial.
Data source: An analysis of 115 women with HER2-negative disease enrolled in an adaptive randomized phase 2 trial (I-SPY 2 trial).
Disclosures: Dr. Rugo disclosed no relevant conflicts of interest.

New mega-review underscores mammography’s benefits
SAN ANTONIO – The much-publicized wide disparities in the estimated value of mammographic screening for breast cancer reported in recent major reviews are overblown and largely an artifact of methodologic differences, according to a new examination of the evidence.
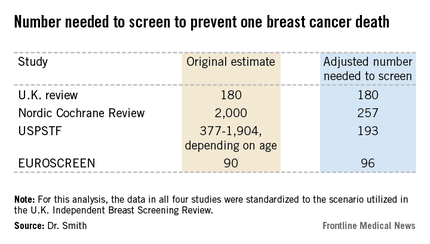
The four recent major reviews of the data regarding the absolute benefits of mammography came up with estimates ranging from 90-2,000 of the number of women who need to be screened (NNS) in order to prevent one death from breast cancer. That greater than 20-fold difference in estimated magnitude of benefit has done little to inspire public and physician confidence that mammography is a key tool in reducing cancer deaths.
But the two analyses with the least supportive outcomes – the Nordic Cochrane and U.S. Preventive Services Task Force (USPSTF-) analyses – used follow-up periods of 10 and 15 years, respectively. That follow-up is too short a time to assess the full value of mammographic screening, Robert A. Smith, Ph.D., asserted at the San Antonio Breast Cancer Symposium.
To illustrate: In a European mammographic screening study with a 30-year follow-up, the NNS after 10 years was 922 women. By 29 years of follow-up, the NNS had fallen to 414.
"At 10 years of follow-up, you haven’t even observed half of the deaths prevented. So follow-up of 20 years at a minimum is really critical to begin to see the full benefit of screening," according to Dr. Smith, senior director of cancer screening at the American Cancer Society in Atlanta.
Also, several of the major reviews estimated the absolute mortality benefit of screening by means of an intent-to-treat analysis based upon the number of women invited to screening in randomized trials. That approach, too, is highly problematic because commonly 30%-40% of women invited to breast cancer screening in randomized trials never actually present for mammography, he said.
"The difference between the number-needed-to-invite and number-needed-to-screen is quite a critical difference in these estimates of absolute benefit. If you want to measure the effectiveness, you have to appreciate that a letter of invitation doesn’t do anyone any good. You have to show up to get mammography in order to benefit from it," Dr. Smith observed.
All of the four recent major reviews – the Nordic Cochrane (Cochrane Database Syst. Rev. 2013;6:CD001877), the USPSTF (Ann. Intern. Med. 2009;151:727-37), the U.K. Independent Breast Screening Review (Br. J. Cancer 2013;108:2205-40), and the European Screening Network (EUROSCREEN) Review (J. Med. Screen. 2012;19 Suppl1:14-25) – painted different pictures of the benefits of mammographic screening because they focused on different age groups, with different screening and follow-up durations, and were inconsistent as to whether the appropriate yardstick was NNS or number-needed-to-invite.

Dr. Smith and his coinvestigators sought to level the playing field by reanalyzing each review, standardizing the data to the scenario utilized in the U.K. independent review. They picked the U.K. review as the reference because it was most recently published and it was led by renowned statistical experts who aren’t part of the debate over mammography’s value. The U.K. review scenario entailed screening every 3 years for 20 years starting at age 50 years, with a 20-year follow-up period and the endpoint being breast cancer mortality at ages 55-79 years. When the data were reanalyzed in this way, the magnitude of the difference between the high and low estimates of absolute benefit among the four major reviews dropped from more than 20-fold to less than 3-fold.
"The so-called controversy over the benefit of mammography screening as estimated from the trials is largely contrived," he declared. "In short, once you standardize the evidence to the same population, the same screening scenario, and the same duration of follow-up, then the differences in absolute benefit over 20 years in the reviews become really not so significant or important at all. They are hardly worth discussing, and are certainly not enough to question the value of mammography over a lifetime of screening."
The flip side of estimating the benefit of mammographic screening in terms of breast cancer deaths avoided is the harm from overdiagnosis of cancers that never would have been symptomatic during a woman’s lifetime and wouldn’t have been detected had screening mammography not been performed. Here again, the estimates reported in the four reviews differed widely because of the divergent analytic methods employed. The U.K. review concluded that for every death from breast cancer avoided via mammography, three people would be overdiagnosed, for an overdiagnosis rate of 19%. The Nordic Cochrane analysis estimated 10 cases of overdiagnosis for every breast cancer death avoided, for a 30% overdiagnosis rate. The USPSTF didn’t give an overdiagnosis estimate. The EUROSCREEN group calculated that for every two breast cancer deaths avoided there would be one case of overdiagnosis, for a 6.5% overdiagnosis rate.
Dr. Smith said the EUROSCREEN estimate of overdiagnosis is the one that rings true. The EUROSCREEN investigators have demonstrated that in estimating mammography overdiagnosis rates, it’s essential to adjust for trends over time in breast cancer incidence and for lead time bias. When that’s not done, estimated overdiagnosis rates run in the 30%-50% range. When adjustments are made, the overdiagnosis rates are in the 0%-10% range, with the EUROSCREEN estimate of 6.5% being representative (J. Med. Screen. 2012;19 Suppl 1:42-56).
The full details of the mega-review were recently published (Breast Cancer Management 2013;2:519-28 [doi:10.2217/bmt.13.53]). The mega-review was funded by the Center for Cancer Prevention, the Wolfson Institute of Preventive Medicine, Barts and the London School of Medicine and Dentistry, and Queen Mary University of London. Dr. Smith declared having no financial conflicts of interest.
I’m not a statistician, but the analysis presented by Dr. Smith makes common sense to me.
Basing benefit solely on those women invited to screen will clearly result in an underestimate of mammography’s true benefit if you’re going to count women who weren’t screened as being in the screened group. More and more, we are learning that breast cancer is a more indolent disease than we thought. Particularly in those with estrogen receptor–positive breast cancer, the most common subtype, many patients don’t recur and die for a decade or more. If you’re not following patients long enough to capture all of the recurrences and deaths from the disease, then you don’t get a full assessment of the value of screening earlier in the course of disease. Long-term follow-up is extremely important.
You’d think that point would be universally accepted in the world of breast cancer screening research, but it isn’t. Mammography is controversial. It takes on some of the same features as debates over global warming. Quite often we see that scientists are just as vulnerable to motivated reasoning as anybody else.
Dr. C. Kent Osborne is the SABCS codirector and director of the Dan L. Duncan Cancer Center and the Lester & Sue Smith Breast Center at Baylor College of Medicine, Houston. He made his comments during the post presentation discussion of the research.
I’m not a statistician, but the analysis presented by Dr. Smith makes common sense to me.
Basing benefit solely on those women invited to screen will clearly result in an underestimate of mammography’s true benefit if you’re going to count women who weren’t screened as being in the screened group. More and more, we are learning that breast cancer is a more indolent disease than we thought. Particularly in those with estrogen receptor–positive breast cancer, the most common subtype, many patients don’t recur and die for a decade or more. If you’re not following patients long enough to capture all of the recurrences and deaths from the disease, then you don’t get a full assessment of the value of screening earlier in the course of disease. Long-term follow-up is extremely important.
You’d think that point would be universally accepted in the world of breast cancer screening research, but it isn’t. Mammography is controversial. It takes on some of the same features as debates over global warming. Quite often we see that scientists are just as vulnerable to motivated reasoning as anybody else.
Dr. C. Kent Osborne is the SABCS codirector and director of the Dan L. Duncan Cancer Center and the Lester & Sue Smith Breast Center at Baylor College of Medicine, Houston. He made his comments during the post presentation discussion of the research.
I’m not a statistician, but the analysis presented by Dr. Smith makes common sense to me.
Basing benefit solely on those women invited to screen will clearly result in an underestimate of mammography’s true benefit if you’re going to count women who weren’t screened as being in the screened group. More and more, we are learning that breast cancer is a more indolent disease than we thought. Particularly in those with estrogen receptor–positive breast cancer, the most common subtype, many patients don’t recur and die for a decade or more. If you’re not following patients long enough to capture all of the recurrences and deaths from the disease, then you don’t get a full assessment of the value of screening earlier in the course of disease. Long-term follow-up is extremely important.
You’d think that point would be universally accepted in the world of breast cancer screening research, but it isn’t. Mammography is controversial. It takes on some of the same features as debates over global warming. Quite often we see that scientists are just as vulnerable to motivated reasoning as anybody else.
Dr. C. Kent Osborne is the SABCS codirector and director of the Dan L. Duncan Cancer Center and the Lester & Sue Smith Breast Center at Baylor College of Medicine, Houston. He made his comments during the post presentation discussion of the research.
SAN ANTONIO – The much-publicized wide disparities in the estimated value of mammographic screening for breast cancer reported in recent major reviews are overblown and largely an artifact of methodologic differences, according to a new examination of the evidence.
The four recent major reviews of the data regarding the absolute benefits of mammography came up with estimates ranging from 90-2,000 of the number of women who need to be screened (NNS) in order to prevent one death from breast cancer. That greater than 20-fold difference in estimated magnitude of benefit has done little to inspire public and physician confidence that mammography is a key tool in reducing cancer deaths.
But the two analyses with the least supportive outcomes – the Nordic Cochrane and U.S. Preventive Services Task Force (USPSTF-) analyses – used follow-up periods of 10 and 15 years, respectively. That follow-up is too short a time to assess the full value of mammographic screening, Robert A. Smith, Ph.D., asserted at the San Antonio Breast Cancer Symposium.
To illustrate: In a European mammographic screening study with a 30-year follow-up, the NNS after 10 years was 922 women. By 29 years of follow-up, the NNS had fallen to 414.
"At 10 years of follow-up, you haven’t even observed half of the deaths prevented. So follow-up of 20 years at a minimum is really critical to begin to see the full benefit of screening," according to Dr. Smith, senior director of cancer screening at the American Cancer Society in Atlanta.
Also, several of the major reviews estimated the absolute mortality benefit of screening by means of an intent-to-treat analysis based upon the number of women invited to screening in randomized trials. That approach, too, is highly problematic because commonly 30%-40% of women invited to breast cancer screening in randomized trials never actually present for mammography, he said.
"The difference between the number-needed-to-invite and number-needed-to-screen is quite a critical difference in these estimates of absolute benefit. If you want to measure the effectiveness, you have to appreciate that a letter of invitation doesn’t do anyone any good. You have to show up to get mammography in order to benefit from it," Dr. Smith observed.
All of the four recent major reviews – the Nordic Cochrane (Cochrane Database Syst. Rev. 2013;6:CD001877), the USPSTF (Ann. Intern. Med. 2009;151:727-37), the U.K. Independent Breast Screening Review (Br. J. Cancer 2013;108:2205-40), and the European Screening Network (EUROSCREEN) Review (J. Med. Screen. 2012;19 Suppl1:14-25) – painted different pictures of the benefits of mammographic screening because they focused on different age groups, with different screening and follow-up durations, and were inconsistent as to whether the appropriate yardstick was NNS or number-needed-to-invite.
Dr. Smith and his coinvestigators sought to level the playing field by reanalyzing each review, standardizing the data to the scenario utilized in the U.K. independent review. They picked the U.K. review as the reference because it was most recently published and it was led by renowned statistical experts who aren’t part of the debate over mammography’s value. The U.K. review scenario entailed screening every 3 years for 20 years starting at age 50 years, with a 20-year follow-up period and the endpoint being breast cancer mortality at ages 55-79 years. When the data were reanalyzed in this way, the magnitude of the difference between the high and low estimates of absolute benefit among the four major reviews dropped from more than 20-fold to less than 3-fold.
"The so-called controversy over the benefit of mammography screening as estimated from the trials is largely contrived," he declared. "In short, once you standardize the evidence to the same population, the same screening scenario, and the same duration of follow-up, then the differences in absolute benefit over 20 years in the reviews become really not so significant or important at all. They are hardly worth discussing, and are certainly not enough to question the value of mammography over a lifetime of screening."
The flip side of estimating the benefit of mammographic screening in terms of breast cancer deaths avoided is the harm from overdiagnosis of cancers that never would have been symptomatic during a woman’s lifetime and wouldn’t have been detected had screening mammography not been performed. Here again, the estimates reported in the four reviews differed widely because of the divergent analytic methods employed. The U.K. review concluded that for every death from breast cancer avoided via mammography, three people would be overdiagnosed, for an overdiagnosis rate of 19%. The Nordic Cochrane analysis estimated 10 cases of overdiagnosis for every breast cancer death avoided, for a 30% overdiagnosis rate. The USPSTF didn’t give an overdiagnosis estimate. The EUROSCREEN group calculated that for every two breast cancer deaths avoided there would be one case of overdiagnosis, for a 6.5% overdiagnosis rate.
Dr. Smith said the EUROSCREEN estimate of overdiagnosis is the one that rings true. The EUROSCREEN investigators have demonstrated that in estimating mammography overdiagnosis rates, it’s essential to adjust for trends over time in breast cancer incidence and for lead time bias. When that’s not done, estimated overdiagnosis rates run in the 30%-50% range. When adjustments are made, the overdiagnosis rates are in the 0%-10% range, with the EUROSCREEN estimate of 6.5% being representative (J. Med. Screen. 2012;19 Suppl 1:42-56).
The full details of the mega-review were recently published (Breast Cancer Management 2013;2:519-28 [doi:10.2217/bmt.13.53]). The mega-review was funded by the Center for Cancer Prevention, the Wolfson Institute of Preventive Medicine, Barts and the London School of Medicine and Dentistry, and Queen Mary University of London. Dr. Smith declared having no financial conflicts of interest.
SAN ANTONIO – The much-publicized wide disparities in the estimated value of mammographic screening for breast cancer reported in recent major reviews are overblown and largely an artifact of methodologic differences, according to a new examination of the evidence.
The four recent major reviews of the data regarding the absolute benefits of mammography came up with estimates ranging from 90-2,000 of the number of women who need to be screened (NNS) in order to prevent one death from breast cancer. That greater than 20-fold difference in estimated magnitude of benefit has done little to inspire public and physician confidence that mammography is a key tool in reducing cancer deaths.
But the two analyses with the least supportive outcomes – the Nordic Cochrane and U.S. Preventive Services Task Force (USPSTF-) analyses – used follow-up periods of 10 and 15 years, respectively. That follow-up is too short a time to assess the full value of mammographic screening, Robert A. Smith, Ph.D., asserted at the San Antonio Breast Cancer Symposium.
To illustrate: In a European mammographic screening study with a 30-year follow-up, the NNS after 10 years was 922 women. By 29 years of follow-up, the NNS had fallen to 414.
"At 10 years of follow-up, you haven’t even observed half of the deaths prevented. So follow-up of 20 years at a minimum is really critical to begin to see the full benefit of screening," according to Dr. Smith, senior director of cancer screening at the American Cancer Society in Atlanta.
Also, several of the major reviews estimated the absolute mortality benefit of screening by means of an intent-to-treat analysis based upon the number of women invited to screening in randomized trials. That approach, too, is highly problematic because commonly 30%-40% of women invited to breast cancer screening in randomized trials never actually present for mammography, he said.
"The difference between the number-needed-to-invite and number-needed-to-screen is quite a critical difference in these estimates of absolute benefit. If you want to measure the effectiveness, you have to appreciate that a letter of invitation doesn’t do anyone any good. You have to show up to get mammography in order to benefit from it," Dr. Smith observed.
All of the four recent major reviews – the Nordic Cochrane (Cochrane Database Syst. Rev. 2013;6:CD001877), the USPSTF (Ann. Intern. Med. 2009;151:727-37), the U.K. Independent Breast Screening Review (Br. J. Cancer 2013;108:2205-40), and the European Screening Network (EUROSCREEN) Review (J. Med. Screen. 2012;19 Suppl1:14-25) – painted different pictures of the benefits of mammographic screening because they focused on different age groups, with different screening and follow-up durations, and were inconsistent as to whether the appropriate yardstick was NNS or number-needed-to-invite.
Dr. Smith and his coinvestigators sought to level the playing field by reanalyzing each review, standardizing the data to the scenario utilized in the U.K. independent review. They picked the U.K. review as the reference because it was most recently published and it was led by renowned statistical experts who aren’t part of the debate over mammography’s value. The U.K. review scenario entailed screening every 3 years for 20 years starting at age 50 years, with a 20-year follow-up period and the endpoint being breast cancer mortality at ages 55-79 years. When the data were reanalyzed in this way, the magnitude of the difference between the high and low estimates of absolute benefit among the four major reviews dropped from more than 20-fold to less than 3-fold.
"The so-called controversy over the benefit of mammography screening as estimated from the trials is largely contrived," he declared. "In short, once you standardize the evidence to the same population, the same screening scenario, and the same duration of follow-up, then the differences in absolute benefit over 20 years in the reviews become really not so significant or important at all. They are hardly worth discussing, and are certainly not enough to question the value of mammography over a lifetime of screening."
The flip side of estimating the benefit of mammographic screening in terms of breast cancer deaths avoided is the harm from overdiagnosis of cancers that never would have been symptomatic during a woman’s lifetime and wouldn’t have been detected had screening mammography not been performed. Here again, the estimates reported in the four reviews differed widely because of the divergent analytic methods employed. The U.K. review concluded that for every death from breast cancer avoided via mammography, three people would be overdiagnosed, for an overdiagnosis rate of 19%. The Nordic Cochrane analysis estimated 10 cases of overdiagnosis for every breast cancer death avoided, for a 30% overdiagnosis rate. The USPSTF didn’t give an overdiagnosis estimate. The EUROSCREEN group calculated that for every two breast cancer deaths avoided there would be one case of overdiagnosis, for a 6.5% overdiagnosis rate.
Dr. Smith said the EUROSCREEN estimate of overdiagnosis is the one that rings true. The EUROSCREEN investigators have demonstrated that in estimating mammography overdiagnosis rates, it’s essential to adjust for trends over time in breast cancer incidence and for lead time bias. When that’s not done, estimated overdiagnosis rates run in the 30%-50% range. When adjustments are made, the overdiagnosis rates are in the 0%-10% range, with the EUROSCREEN estimate of 6.5% being representative (J. Med. Screen. 2012;19 Suppl 1:42-56).
The full details of the mega-review were recently published (Breast Cancer Management 2013;2:519-28 [doi:10.2217/bmt.13.53]). The mega-review was funded by the Center for Cancer Prevention, the Wolfson Institute of Preventive Medicine, Barts and the London School of Medicine and Dentistry, and Queen Mary University of London. Dr. Smith declared having no financial conflicts of interest.
EXPERT OPINION FROM SABCS 2013

No survival benefit to bisphosphonate in chemoresistant breast cancer
The bisphosphonate zolendronate didn't improve survival in patients with chemoresistant breast cancer, according to results from the phase III NATAN trial.
In an interview at the San Antonio Breast Cancer Symposium, Dr. Gunter von Minckwitz discusses the trial's results and clinical implications, and whether a role remains for bisphosphonates in postmenopausal patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The bisphosphonate zolendronate didn't improve survival in patients with chemoresistant breast cancer, according to results from the phase III NATAN trial.
In an interview at the San Antonio Breast Cancer Symposium, Dr. Gunter von Minckwitz discusses the trial's results and clinical implications, and whether a role remains for bisphosphonates in postmenopausal patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The bisphosphonate zolendronate didn't improve survival in patients with chemoresistant breast cancer, according to results from the phase III NATAN trial.
In an interview at the San Antonio Breast Cancer Symposium, Dr. Gunter von Minckwitz discusses the trial's results and clinical implications, and whether a role remains for bisphosphonates in postmenopausal patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Exercise dampens aromatase inhibitor–related joint pain
SAN ANTONIO – Adopting a standard exercise program resulted in a clinically meaningful 30% reduction in aromatase inhibitor-associated joint pain in breast cancer patients who participated in a year-long randomized trial.
The exercise prescription utilized in the HOPE (Hormones and Physical Exercise) trial was what’s recommended in national guidelines both for cancer survivors and healthy adults: 150 minutes per week of at least moderate-intensity aerobic activity, such as brisk walking, along with two strength-training sessions per week, Melinda L. Irwin, Ph.D., explained at the San Antonio Breast Cancer Symposium.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The HOPE studies enrolled 121 postmenopausal women who had stage 1-3, hormone receptor–positive breast cancers and were physically inactive and overweight yet physically able to exercise. At enrollment, they were experiencing moderate aromatase inhibitor (AI)–associated joint pain, defined as a score of 5-7 on the 0-10 Brief Pain Inventory (BPI), after about 18 months on the medication. Roughly two-thirds of participants had no history of joint pain prior to starting AI therapy; the rest reported the AI exacerbated their preexisting joint pain. Subjects were randomized to the exercise program or to usual care, which included written information about the importance of exercise.
The primary study endpoint was the 12-month change in BPI worst pain score, which dropped by an average of 30% among the exercise group. This translated to an improvement in pain level from moderate at baseline to mild at follow-up. In addition, BPI scores rating pain severity and pain interference improved by about 20%. In contrast, patients in the usual care control group experienced a slight increase in BPI scores in all three domains over time, added Dr. Irwin, co-leader of the cancer prevention and control research program at Yale University Cancer Center, New Haven, Conn.

This degree of improvement in joint pain is greater than reported in studies of glucosamine, acupuncture, or vitamin D supplementation, she noted.
The improvement in pain scores in the exercise group was greater at 12 months than at 3 or 6, suggesting that a year-long exercise program is probably necessary to see sustained reduction in joint pain.
At 12 months of follow-up, women in the exercise group averaged 159 minutes of physical activity per week, 110 minutes more than controls. Compliance with the supervised exercise program was notably good, with women attending an average of 70% of the twice-weekly small-group strength-training sessions.
In addition to the improvement in AI-related arthralgias, the exercise group experienced ancillary benefits: a mean 6.5% improvement in peak oxygen consumption, or VO2 max, compared with baseline, along with a 3% reduction in body weight.
HOPE was the first randomized trial to examine the effects of exercise on AI side effects in breast cancer patients. The impetus for the study was the recognition that arthralgias are the most common reason for poor adherence to and discontinuation of AI therapy. Up to 20% of breast cancer patients discontinue their AI within the first year. And both early discontinuation and poor adherence have been shown to be predictive of increased mortality risk.
The HOPE results received an enthusiastic audience reception. Physicians were particularly impressed with the 70% exercise adherence rate over the course of a year. They asked how they can keep their previously sedentary patients’ commitment to regular exercise from waning after an initial burst of enthusiasm, as so often happens.
Dr. Irwin replied that adherence to lifestyle change is always a challenge. Social support is quite helpful. The exercise group in HOPE received a paid gym membership and met in small groups with a personal trainer twice weekly.
"The women really bonded with each other. And there are now a growing number of free programs throughout the country, which give cancer survivors a start on an exercise program with a free gym membership for several months. For example, the Livestrong Foundation has partnered with the YMCA to offer free exercise programs for cancer survivors at local Ys," she said.
The HOPE trial was funded by the National Cancer Institute. Dr. Irwin reported having no financial conflicts of interest.
SAN ANTONIO – Adopting a standard exercise program resulted in a clinically meaningful 30% reduction in aromatase inhibitor-associated joint pain in breast cancer patients who participated in a year-long randomized trial.
The exercise prescription utilized in the HOPE (Hormones and Physical Exercise) trial was what’s recommended in national guidelines both for cancer survivors and healthy adults: 150 minutes per week of at least moderate-intensity aerobic activity, such as brisk walking, along with two strength-training sessions per week, Melinda L. Irwin, Ph.D., explained at the San Antonio Breast Cancer Symposium.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The HOPE studies enrolled 121 postmenopausal women who had stage 1-3, hormone receptor–positive breast cancers and were physically inactive and overweight yet physically able to exercise. At enrollment, they were experiencing moderate aromatase inhibitor (AI)–associated joint pain, defined as a score of 5-7 on the 0-10 Brief Pain Inventory (BPI), after about 18 months on the medication. Roughly two-thirds of participants had no history of joint pain prior to starting AI therapy; the rest reported the AI exacerbated their preexisting joint pain. Subjects were randomized to the exercise program or to usual care, which included written information about the importance of exercise.
The primary study endpoint was the 12-month change in BPI worst pain score, which dropped by an average of 30% among the exercise group. This translated to an improvement in pain level from moderate at baseline to mild at follow-up. In addition, BPI scores rating pain severity and pain interference improved by about 20%. In contrast, patients in the usual care control group experienced a slight increase in BPI scores in all three domains over time, added Dr. Irwin, co-leader of the cancer prevention and control research program at Yale University Cancer Center, New Haven, Conn.
This degree of improvement in joint pain is greater than reported in studies of glucosamine, acupuncture, or vitamin D supplementation, she noted.
The improvement in pain scores in the exercise group was greater at 12 months than at 3 or 6, suggesting that a year-long exercise program is probably necessary to see sustained reduction in joint pain.
At 12 months of follow-up, women in the exercise group averaged 159 minutes of physical activity per week, 110 minutes more than controls. Compliance with the supervised exercise program was notably good, with women attending an average of 70% of the twice-weekly small-group strength-training sessions.
In addition to the improvement in AI-related arthralgias, the exercise group experienced ancillary benefits: a mean 6.5% improvement in peak oxygen consumption, or VO2 max, compared with baseline, along with a 3% reduction in body weight.
HOPE was the first randomized trial to examine the effects of exercise on AI side effects in breast cancer patients. The impetus for the study was the recognition that arthralgias are the most common reason for poor adherence to and discontinuation of AI therapy. Up to 20% of breast cancer patients discontinue their AI within the first year. And both early discontinuation and poor adherence have been shown to be predictive of increased mortality risk.
The HOPE results received an enthusiastic audience reception. Physicians were particularly impressed with the 70% exercise adherence rate over the course of a year. They asked how they can keep their previously sedentary patients’ commitment to regular exercise from waning after an initial burst of enthusiasm, as so often happens.
Dr. Irwin replied that adherence to lifestyle change is always a challenge. Social support is quite helpful. The exercise group in HOPE received a paid gym membership and met in small groups with a personal trainer twice weekly.
"The women really bonded with each other. And there are now a growing number of free programs throughout the country, which give cancer survivors a start on an exercise program with a free gym membership for several months. For example, the Livestrong Foundation has partnered with the YMCA to offer free exercise programs for cancer survivors at local Ys," she said.
The HOPE trial was funded by the National Cancer Institute. Dr. Irwin reported having no financial conflicts of interest.
SAN ANTONIO – Adopting a standard exercise program resulted in a clinically meaningful 30% reduction in aromatase inhibitor-associated joint pain in breast cancer patients who participated in a year-long randomized trial.
The exercise prescription utilized in the HOPE (Hormones and Physical Exercise) trial was what’s recommended in national guidelines both for cancer survivors and healthy adults: 150 minutes per week of at least moderate-intensity aerobic activity, such as brisk walking, along with two strength-training sessions per week, Melinda L. Irwin, Ph.D., explained at the San Antonio Breast Cancer Symposium.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The HOPE studies enrolled 121 postmenopausal women who had stage 1-3, hormone receptor–positive breast cancers and were physically inactive and overweight yet physically able to exercise. At enrollment, they were experiencing moderate aromatase inhibitor (AI)–associated joint pain, defined as a score of 5-7 on the 0-10 Brief Pain Inventory (BPI), after about 18 months on the medication. Roughly two-thirds of participants had no history of joint pain prior to starting AI therapy; the rest reported the AI exacerbated their preexisting joint pain. Subjects were randomized to the exercise program or to usual care, which included written information about the importance of exercise.
The primary study endpoint was the 12-month change in BPI worst pain score, which dropped by an average of 30% among the exercise group. This translated to an improvement in pain level from moderate at baseline to mild at follow-up. In addition, BPI scores rating pain severity and pain interference improved by about 20%. In contrast, patients in the usual care control group experienced a slight increase in BPI scores in all three domains over time, added Dr. Irwin, co-leader of the cancer prevention and control research program at Yale University Cancer Center, New Haven, Conn.
This degree of improvement in joint pain is greater than reported in studies of glucosamine, acupuncture, or vitamin D supplementation, she noted.
The improvement in pain scores in the exercise group was greater at 12 months than at 3 or 6, suggesting that a year-long exercise program is probably necessary to see sustained reduction in joint pain.
At 12 months of follow-up, women in the exercise group averaged 159 minutes of physical activity per week, 110 minutes more than controls. Compliance with the supervised exercise program was notably good, with women attending an average of 70% of the twice-weekly small-group strength-training sessions.
In addition to the improvement in AI-related arthralgias, the exercise group experienced ancillary benefits: a mean 6.5% improvement in peak oxygen consumption, or VO2 max, compared with baseline, along with a 3% reduction in body weight.
HOPE was the first randomized trial to examine the effects of exercise on AI side effects in breast cancer patients. The impetus for the study was the recognition that arthralgias are the most common reason for poor adherence to and discontinuation of AI therapy. Up to 20% of breast cancer patients discontinue their AI within the first year. And both early discontinuation and poor adherence have been shown to be predictive of increased mortality risk.
The HOPE results received an enthusiastic audience reception. Physicians were particularly impressed with the 70% exercise adherence rate over the course of a year. They asked how they can keep their previously sedentary patients’ commitment to regular exercise from waning after an initial burst of enthusiasm, as so often happens.
Dr. Irwin replied that adherence to lifestyle change is always a challenge. Social support is quite helpful. The exercise group in HOPE received a paid gym membership and met in small groups with a personal trainer twice weekly.
"The women really bonded with each other. And there are now a growing number of free programs throughout the country, which give cancer survivors a start on an exercise program with a free gym membership for several months. For example, the Livestrong Foundation has partnered with the YMCA to offer free exercise programs for cancer survivors at local Ys," she said.
The HOPE trial was funded by the National Cancer Institute. Dr. Irwin reported having no financial conflicts of interest.
AT SABCS 20123
Major finding: Breast cancer patients experienced a 30% reduction in aromatase inhibitor–related joint pain, with pain scores going from moderate to mild, in response to a year-long exercise intervention.
Data source: The HOPE study was a 1-year randomized trial in which 121 postmenopausal breast cancer patients with significant pain from aromatase inhibitor–related arthralgias were randomized to a structured exercise program or to usual care.
Disclosures: The trial was funded by the National Cancer Institute. The presenter reported having no financial conflicts.

SABCS Roundtable with Dr. Howard Burris and Dr. William Gradishar
SAN ANTONIO – Perspectives on IBIS-II, dasatinib in combination with leutrozole, dual pathway blockade, CDK inhibitors, and more practice-changing trial results from the San Antonio Breast Cancer Symposium are discussed by Dr. Howard A. Burris, III, Chief Medical Officer and Director of Drug Development at the Sarah Cannon Research Institute, Nashville, Tenn.; and Dr. William A. Gradishar, Betsy Bramsen Professor of Breast Oncology at the Northwestern University Feinberg School of Medicine, Director of the Maggie Daley Center For Women's Cancer Care, and a member of the Robert H. Lurie Comprehensive Cancer Center, Chicago.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – Perspectives on IBIS-II, dasatinib in combination with leutrozole, dual pathway blockade, CDK inhibitors, and more practice-changing trial results from the San Antonio Breast Cancer Symposium are discussed by Dr. Howard A. Burris, III, Chief Medical Officer and Director of Drug Development at the Sarah Cannon Research Institute, Nashville, Tenn.; and Dr. William A. Gradishar, Betsy Bramsen Professor of Breast Oncology at the Northwestern University Feinberg School of Medicine, Director of the Maggie Daley Center For Women's Cancer Care, and a member of the Robert H. Lurie Comprehensive Cancer Center, Chicago.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – Perspectives on IBIS-II, dasatinib in combination with leutrozole, dual pathway blockade, CDK inhibitors, and more practice-changing trial results from the San Antonio Breast Cancer Symposium are discussed by Dr. Howard A. Burris, III, Chief Medical Officer and Director of Drug Development at the Sarah Cannon Research Institute, Nashville, Tenn.; and Dr. William A. Gradishar, Betsy Bramsen Professor of Breast Oncology at the Northwestern University Feinberg School of Medicine, Director of the Maggie Daley Center For Women's Cancer Care, and a member of the Robert H. Lurie Comprehensive Cancer Center, Chicago.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Surgery adds little after successful chemo in metastatic breast cancer
SAN ANTONIO – In patients with metastatic breast cancer who responded favorably to initial chemotherapy, radiotherapy and surgical removal of primary tumors failed to enhance overall survival, a new study has shown.
In an interview at the San Antonio Breast Cancer Symposium, study investigator Dr. Rajendra Badwe offers his perspectives on loco-regional treatment vs. chemotherapy alone, and he discusses why surgical removal of primary tumors might be linked to later spread of metastatic disease.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – In patients with metastatic breast cancer who responded favorably to initial chemotherapy, radiotherapy and surgical removal of primary tumors failed to enhance overall survival, a new study has shown.
In an interview at the San Antonio Breast Cancer Symposium, study investigator Dr. Rajendra Badwe offers his perspectives on loco-regional treatment vs. chemotherapy alone, and he discusses why surgical removal of primary tumors might be linked to later spread of metastatic disease.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – In patients with metastatic breast cancer who responded favorably to initial chemotherapy, radiotherapy and surgical removal of primary tumors failed to enhance overall survival, a new study has shown.
In an interview at the San Antonio Breast Cancer Symposium, study investigator Dr. Rajendra Badwe offers his perspectives on loco-regional treatment vs. chemotherapy alone, and he discusses why surgical removal of primary tumors might be linked to later spread of metastatic disease.
